Embed Size (px)
Citation preview

Addictive Behaviors 32 (2007) 1769–1786
Evaluation of an Internet virtual world chat roomfor adolescent smoking cessation
Susan I. Woodruff a,⁎, Terry L. Conway a, Christine C. Edwards a,Sean P. Elliott a, Jim Crittenden b
a Graduate School of Public Health, San Diego State University, 9245 Sky Park Ct, Ste 120, San Diego,CA 92123, United States
b San Diego County Office of Education, Safe Schools Unit, 5404 Napa St., San Diego, CA 92110, United States
Abstract
The goal of this longitudinal study was to test an innovative approach to smoking cessation that might beparticularly attractive to adolescent smokers. The study was a participatory research effort between academic andschool partners. The intervention used an Internet-based, virtual reality world combined with motivationalinterviewing conducted in real-time by a smoking cessation counselor. Participants were 136 adolescent smokersrecruited from high schools randomized to the intervention or a measurement-only control condition. Those whoparticipated in the program were significantly more likely than controls to report at the immediate post-interventionassessment that they had abstained from smoking during the past week (p≤ .01), smoked fewer days in the pastweek (p≤ .001), smoked fewer cigarettes in the past week (p≤ .01), and considered themselves a former smoke(p≤ .05). Only the number of times quit was statistically significant at a one-year follow-up assessment (p≤ .05).The lack of longer-term results is discussed, as are methodological challenges in conducting a cluster-randomizedsmoking cessation study.© 2006 Elsevier Ltd. All rights reserved.
Keywords: Smoking cessation; Adolescents; Health behavior; Trial; Chat room; Internet
1. Introduction
Smoking among adolescents has significant public health importance. Onset of smoking occurs primarilyin adolescence, and because tobacco is highly addictive, regular use in adolescence develops into nicotine
⁎ Corresponding author. Tel.: +1 619 594 2787; fax: +1 619 594 3143.E-mail address: [email protected] (S.I. Woodruff).
0306-4603/$ - see front matter © 2006 Elsevier Ltd. All rights reserved.doi:10.1016/j.addbeh.2006.12.008
1770 S.I. Woodruff et al. / Addictive Behaviors 32 (2007) 1769–1786
dependency. Smoking among adolescents is likely to continue into the adult years, increasing the risk ofnumerous long-term negative health consequences (USDHHS, 2000a). Yet, after three decades of efforts toprevent smoking among children, rates of adolescent smoking remain unacceptably high. Adult smokingrates have declined steadily over the last several decades; however, smoking rates among adolescents havenot shown a comparable pattern of steady decline (Johnston, O'Malley, & Bachman, 2003).
Smoking cessation clearly has major and immediate health benefits (USDHHS, 2000a,b). Even amongadolescent smokers, most report they would like to quit smoking (Lantz et al., 2000; Mermelstein, 2003;Vuckovic, Polen, & Hollis, 2003). Although many adolescents attempt to quit, most relapse quickly(Prokhorov, Hudmon, & Stancic, 2003), probably in part because they lack effective support and skills(Vuckovic et al., 2003). Previous research has shown that adolescent smokers trying to quit experiencewithdrawal symptoms that parallel those experienced by adults, suggesting addictive processes inadolescent smoking in addition to well-documented social factors (O'Loughlin et al., 2003; Prokhorovet al., 2003; Vuckovic et al., 2003). Also, as for many adults, adolescent smokers appear to benefit fromsocial support in the quitting process (Vuckovic et al., 2003). However, other findings indicate uniqueaspects of adolescent smoking and cessation. Adolescents may be more influenced by (a) social–psychological cues to smoke, (b) tobacco advertising, (c) self-perceptions and low self-efficacy related tocessation, (d) perceptions of invulnerability to smoking's health effects, (e) perceived advantages ofsmoking including those related to coping and stress reduction, and (f) lack of recognition of the benefitsof cessation (Pallonen et al., 1990; Turner, Mermelstein, & Flay, 2004; Vuckovic et al., 2003).
Most school-based tobacco use programs have been classroom-based prevention programs designed toreduce the incidence of adolescent tobacco use. Whereas some have realized positive effects especially indelaying the initiation of smoking, the results are somewhat limited and less likely to reach minority andhigh-risk adolescents (Spruijt-Metz et al., 2004; Unger et al., 2000). Further, these programs have notbeen successful in smoking reduction or cessation among adolescents who have already begun to smoke(Backinger et al., 2003). A few studies have evaluated programs designed specifically for adolescentsmoking cessation, although findings have been mixed (Mermelstein, 2003; Rohde et al., 2001).Cognitive-behaviorally oriented cessation interventions that have been effective with adults, when triedwith adolescents in clinics and classrooms, have not shown much promise (USDHHS, 2000a).Furthermore, adolescents are difficult to recruit and retain in smoking cessation interventions(Mermelstein, 2003; USDHHS, 2000a). The absence of effective intervention for young smokers iscause for concern, as adolescent smokers will likely continue on to become adult smokers. Innovativeinterventions are needed to engage teen smokers and to motivate interest in making quit attempts (DuRant& Smith, 1999; Sussman et al., 1999). Many believe that advances in health among young people willfocus on use of interesting technologies, such as computer information and communication (Borzekowski& Rickert, 2001; Fotheringham, Owies, Leslie, & Owen, 2000; McTavish et al., 1995; Rhodes, Fishbein,& Reis, 1997; Stivers, Bentley, & Meccouri, 1995; Weinberg, Schmale, Uken, & Wessel, 1996).
Computer technology has been used for smoking cessation by creating tailored, cessation materials basedon individual data (Escoffery, McCormick, & Bateman, 2004; Strecher, 1999; Strecher, Shiffman, & West,2005; Velicer & Prochaska, 1999;Walters,Wright, & Shegog, 2006), and by building powerful, compelling,and flexible learning environments in which users interact with “smart” programs or are free to interact withone another from remote sites (Burling, Seidner, & Gaither, 1994; Lenert et al., 2003; Pallonen et al., 1998;Schneider, Walter, & O'Donnell, 1990; Scott & McIlvain, 2000; Takahashi, Satomura, Miyagishima, &Nakahara, 1999). Computer-based smoking cessation support to date has primarily employed educationalwebsites, expert systems, games on CD-ROM, or electronic bulletin boards.

1771S.I. Woodruff et al. / Addictive Behaviors 32 (2007) 1769–1786
Although some of these programs are interactive in that they involve the user and can tailor supportbased on the user's needs, they typically have not used real-time discussion. Real-time interactivediscussion (between smokers and professional change agents, and among smokers themselves) couldpotentiate the effectiveness of computerized communication for smoking cessation. For example,numerous studies have validated the assumptions that high school students look to their peers foremotional and social support and believe that their peers are capable of providing help (Mattey, 2003;Valente et al., 2003; Whiist, 2004). Other studies have well documented the positive effects of socialsupport on smoking cessation outcomes both for adults and adolescents (Chassin, Presson, & Sherman,1985; Cohen & Lichtenstein, 1990; Fisher, Lichtenstein, Haire-Joshu, Morgan, & Rehberg, 1993; Gruderet al., 1993; Lacey et al., 1993; Myers, 1999). The use of a trained smoking cessation counselor orfacilitator has also been shown to be associated with cessation and long-term abstinence (Fisher et al.,1993; Lichtenstein & Glasgow, 1992; Viswesvaran & Schmidt, 1992) and may be more successful thanself-help programs alone specifically among adolescents and young adults (Charlton, Melia, & Moyer,1990; Viswesvaran & Schmidt, 1992).
The rationale for this study derived from the fact that traditional school-based programs (e.g., clinic-based, face-to-face, and classroom-based prevention programs) have had limited success in helpingadolescent smokers quit, and new strategies and technologies need to be explored. The present studytested a web-based counseling program, Breathing Room, in which young smokers interacted with atrained cessation counselor and other teen smokers in real-time in an Internet “virtual world.” Theeffectiveness of the real-time Breathing Room Internet intervention for smoking cessation was evaluatedby comparing intervention participants with teens who participate in a measurement-only control group.
2. Methods
2.1. Design
The primary goal of this study was to test an innovative approach to smoking cessation that might beparticularly attractive to adolescent smokers. The intervention used an Internet-based, virtual reality worldcombined with motivational interviewing conducted by a smoking cessation counselor. Participants wereadolescent smokers recruited from high schools in San Diego County. Participants in the interventioncondition were recruited to participate in seven 45-minute virtual world sessions over a 7-week period,and complete 4 online surveys. Participants recruited into the measurement-only condition were askedonly to complete the 4 online surveys. Participants in both conditions were surveyed at baseline, post-intervention, 3-months post-intervention, and 12-months post-intervention. Randomization to conditionwas done by school to avoid contamination between intervention and control groups, to facilitaterecruitment and intervention implementation, and because the program, if broadly disseminated, wouldlikely be applied at the school level (Edwards, Braunholtz, Lilford, & Stevens, 1999).
2.2. Recruitment and program implementation
From October 2002 through April 2004, teenage smokers were recruited from 14 local high schoolsites to participate in the Breathing Room study. Schools included traditional high schools, continuationhigh schools, and schools from the Juvenile Court and Community School system. Seven schools

1772 S.I. Woodruff et al. / Addictive Behaviors 32 (2007) 1769–1786
participated in the control arm of the study, and seven in the intervention arm. Six of the 14 schools werecontinuation/alternative high schools, and 8 were regular high schools.
Numerous strategies were employed at the school sites to recruit participants including classroompresentations, lunch-hour sign-up tables, flyers, posters, school newspaper ads and articles, school-wideannouncements, and school liaison referrals.
At the suggestion of school personnel, the recruitment approach and materials were different forintervention and control schools. At the control schools, Breathing Room was promoted as a researchproject about teen smoking. Potential participants were asked to help researchers “learn more about teensmoking” by completing 4 online surveys over a 15-month period, for which participants would receiveup to $50.00. Recruitment for participants at the intervention schools advertised a virtual reality Internet-based program to help students quit smoking. Materials and presentations promoted spending about45 min per week for 7 weeks online in a virtual reality world with other teenagers and a counselor toexplore quitting smoking. Similar to control group recruitment, intervention recruitment publicizedearning up to $50 for completing 4 online surveys over a 15-month period. Participants at the controlschools were recruited on an ongoing basis; participants at the intervention schools were recruited onceeach semester to accommodate the 7-week online counseling schedule.
To participate in the study, a student must have smoked at least one cigarette within the past 30 days.Eligible participants were given a Breathing Room project folder that contained a brief project description,contact information, assent form, parent consent form, survey schedule, and an instruction sheet forlogging onto the Breathing Room website (to complete surveys only, or to participate in the virtual worldchat room and complete surveys). Parental consent forms described the study as a teen health project, anddid not reveal that participants necessarily were smokers. Per school liaison request, the parental consentforms were individualized for control or intervention schools, describing specifically what would berequired by the adolescent. Completed consent and assent forms were collected by the school liaisons andforwarded to research staff who would then set up a secure password protected account for the participant.Intervention participants were also given instructions for logging onto and using the Breathing Roomvirtual world. All procedures had full University Institutional Review Board approval.
A new Dell computer dedicated to the Breathing Room project was donated to each school, and housedin a location where participants could take a survey or participate in the virtual world intervention withoutinterruption. Breathing Room surveys also could be completed at home or elsewhere with Internet access.
Each semester at the intervention schools the Breathing Room virtual world counseling was availableMonday through Thursday at four different times throughout the day for 7 weeks. Slots were availablebefore school, during lunch hour, and after school. All intervention participants were asked to sign up fora specific time slot during the week for their virtual world intervention session with the counselor.Although participants were strongly encouraged to choose a counseling time and adhere to it, they werealso told they could “drop in” on another session if they needed to make up a session.
School liaisons were an integral part of implementing the program on campus, encouraging completion ofcounseling sessions and surveys, andmaintaining the cohort. Liaisons were given an intervention session listfor participants, and asked to remind students to attend their assigned sessions. Participants who did not showup for their initial intervention session were contacted by research staff by phone and reminded to attend thenext session. At the close of each week, liaisons were faxed an updated list indicating the number of sessionsparticipants had attended, number of sessions remaining, and when surveys were due.
Intervention and control participants were provided the same stipend amounts for completing eachsurvey. Stipends were tied to survey completion (not intervention sessions). Stipend amounts were $5.00

1773S.I. Woodruff et al. / Addictive Behaviors 32 (2007) 1769–1786
for the baseline survey, $10.00 for the immediate post-test, $15.00 for the 3-month follow-up, and $20.00for the 12-month follow-up survey for a total of $50.00 if all surveys were completed. Upon signing up forthe study each participant was given the choice of receiving their stipends as a check or a gift card. Oncean online survey was completed, the participant was mailed the stipend, a thank you letter, and a reminderof when the next survey was due.
2.3. Appearance and content of the Breathing Room virtual world
The Breathing Room website allowed secure entry into the online surveys (for control participants),and to surveys and the virtual world chat room (for intervention participants). The Breathing Room virtualworld used powerful, proprietary interactive software known as ActiveWorlds that allows moreinteresting features than the usual text-based chat rooms. ActiveWorlds is a virtual environment in whichparticipants can see each other as 3-dimensional figures (i.e., avatars) on their computer screens, movearound in the “world,” and have real-time discussions with each other. ActiveWorlds softwareautomatically provided approximately 20 avatars that differed in gender, race, and clothing. Avatars couldrun, jump, fly, and dance at the click of a button, enabling a participant to express emotions. Althougheasily changed with a click of a button, most participants chose the same avatar each session.
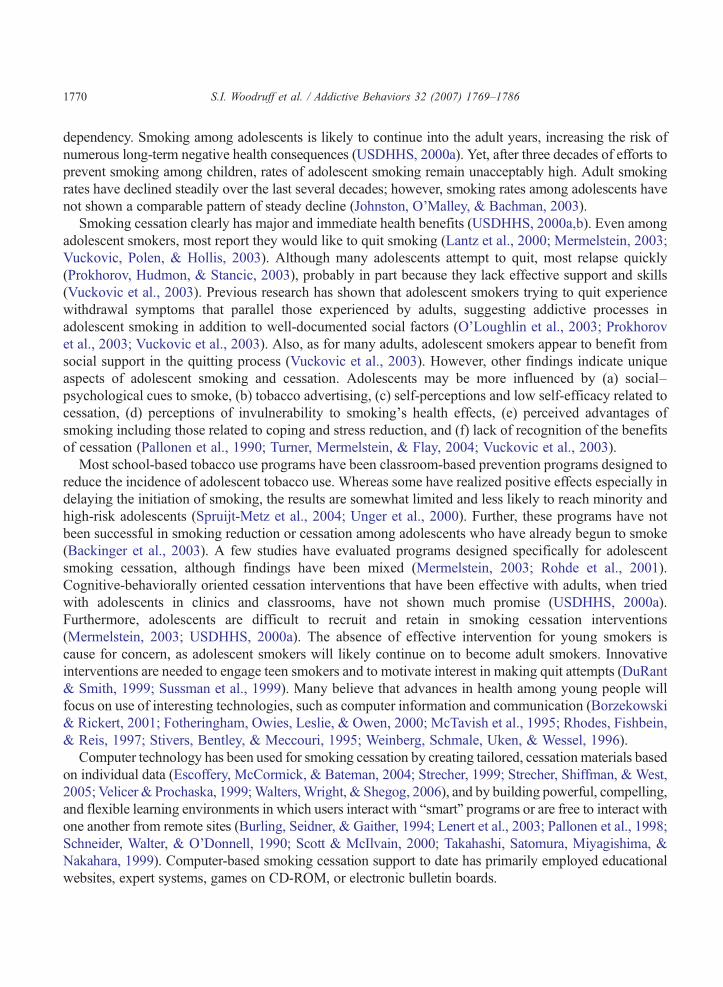
The Breathing Room virtual world was developed by the research staff and a graphics software engineer.A sky mall was chosen as the setting because malls frequently serve as meeting places for teens. Within thesky mall, there were various virtual storefronts that supported the content of the counseling. For example, apathology lab showing pictures of diseased organs and premature aging, provided a backdrop for discussingthe short- and long-term health effects of smoking (see Fig. 1). An art gallery facilitated discussion of theeffects of tobacco advertising, as well as appreciation of anti-tobacco art. Billboards throughout the virtualworld allowed the counselor to display topics of interest to be addressed (e.g., “Dealing with Cravings”) and
Fig. 1. Scene from pathology lab in the Breathing room virtual world.
1774 S.I. Woodruff et al. / Addictive Behaviors 32 (2007) 1769–1786
individualize messages to participants (e.g., “Guero's been quit for a month!”). Avirtual pharmacy was usedto discuss biological responses to smoking and quitting, as well as pharmacological aids to quitting. Astorefront called “The Man,” pejoratively referring to the heads of the large tobacco corporations, containedlinks to incriminating tobacco industry documents released as part of the Master Settlement Agreement. Agraveyard outside the sky mall displayed tombstones of celebrities and sports figures that have died fromsmoking-related disease, and provided an opportunity to discuss health risks. A teen dance club and a fastfood restaurant provided settings to discuss social influences to smoke and relapse, and an amphitheater wasavailable for additional virtual meetings and discussions. The participants' chat content appeared real-time ina box below the virtual world. An early version of the virtual world chat roomwas pilot tested with rural teensmokers to collect their comments for refining the world and preliminary information about its effectiveness(Woodruff, Edwards, Conway, & Elliott, 2001).
In the virtual world, up to four adolescent smokers interacted with each other as well as with thecounselor, capitalizing on the benefits of peer-to-peer interaction. All sessions were conducted by thesame counselor, an experienced smoking cessation advisor who had an undergraduate degree inpsychology. During the sessions, participants were required to stay with the group and participate in thediscussion. The counselor had the authority to “pull” participants back to the group, or to eject themtemporarily or permanently for inappropriate behavior.
Session 1 was an introductory session devoted to familiarizing participants with moving and chatting inthe virtualworld, and reviewing the rules of conduct. The nature and content of the subsequent six counselingsessions was somewhat fluid and partly driven by the participants, although the counselor worked from anoutline and attempted to cover key topics considered effective in motivating adolescents to quit smoking.Social Learning Theory concepts (Bandura, 1986, 1997), behavioral principles and relapse preventionconcepts (Marlatt & Gordon, 1985), stage of change theory (Dino et al., 2004; Prochaska & Velicer, 1997),and social support/group interaction (Lancaster, Stead, Silagy, & Sowden, 2000) provided guidance for thecontent of these semi-structured sessions. Topics covered includedmotivation to quit (e.g., weighing the prosand cons of smoking/quitting), self-efficacy for quitting, sharing experiences of quitting with each other,identifying barriers to quitting and ideas for overcoming those barriers, setting sub-goals for quitting andstrategies for handling cravings, handling social situations and other temptations to relapse, developing aplan for a quit attempt, peer influences and social support, cues to smoke (e.g., personal stress, tobaccoadvertising), and tobacco industry tactics. Relevant practical and health issues such as smoking effects onemployability, sports performance, short-term health problems, long-term health problems (e.g., impotence,fertility), and economics of smoking were addressed throughout the sessions.
The smoking cessation counselor used motivational interviewing techniques when chatting withparticipants. Motivational interviewing is a technique and style of brief intervention derived from socialcognitive theory that is a “client-centered” non-confrontational approach to behavior change (Miller &Rollnick, 1991; Rollnick & Miller, 1995). Motivational interviewing may be particularly effective withadolescent smokers who might resist more “didactic” approaches to behavior change (Lawendowski,1998; Myers, 1999). In line with this approach, the counselor explored ambivalence about behaviorchange, and elicited personal goals and self-motivational statements from participants.
2.4. Participatory nature of the research study
The ultimate goal of health-related research is to improve the lives of people in the community studied.However, in traditional research, the community (e.g., churches, neighborhoods, schools) is not actively

1775S.I. Woodruff et al. / Addictive Behaviors 32 (2007) 1769–1786
involved in designing or conducting the projects. In addition, community members, who frequently givetheir time and energy for no compensation discover that they are left without information about theoutcome of the research or any findings that can benefit the community. Participatory research countersthese shortcomings by making the researchers and community groups partners from the early stages of theresearch and throughout the process (Israel, Schulz, Parker, & Becker, 1998).
The Breathing Room study was funded by the California Tobacco-related Disease Research Program(TRDRP) as a School and Academic Research Award (SARA). TRDRP SARAs are participatory researchstudies that involve an academic/university partner and a school community partner. The primary schoolpartner (author J.C.) is a specialist with the San Diego County Office of Education, and additional schoolpartners at the district levels and schools levels were instrumental in developing and implementing theBreathing Room study. School partners, or liaisons, played a direct role in the design and conduct of theresearch study. For example, the liaisons recommended a web-based approach for evaluation surveys tomatch the web-based intervention approach, determined the times and most of the logistics of the onlinecounseling sessions, suggested and often implemented recruitment strategies, suggested appropriateincentives for schools and students participating in the control arm of the study, and brainstormedapproaches to disseminate research findings and garner funds for institutionalization of the BreathingRoom program. This involvement not only helped carry out the study, but also ensured that schoolpriorities were addressed and improved the relevance of the study to the school community.
2.5. Measures
The self-report online surveys consisted of items measuring demographic characteristics, smokingstatus, smoking behavior, quitting history, and readiness to quit. Most measures were standard items usedelsewhere, particularly those from the National Youth Tobacco Survey/American Legacy Foundation, andthe California Youth Tobacco Survey.
Sociodemographic information included gender and age in years computed from birth date.Participants reported their race/ethnic group as Hispanic, White/Non-Hispanic, African–American,Asian/Pacific Islander, or Other.
Seven outcome variables were examined in the present study: (a) past-week abstinence (yes versus no);(b) number of days smoked in the past 7 days ranging from 0 (0 days) to 7 (all 7 days); (c) numbercigarettes smoked per day during the past 7 days with response options of 0 (0 cigarettes), 1 (less than1 cigarette per day), 2 (1 cigarette per day), 3 (2–5 cigarettes), 4 (6–10 cigarettes), 5 (11–15 cigarettes) 6(16–20 cigarettes), 7 (21–25 cigarettes), 8 (26–30 cigarettes), 9 (31–35 cigarettes), 10 (36–40 cigarettes),and 11 (more than 40 cigarettes per day); (d) number of lifetime quit attempts measured on a scale rangingfrom 0 (none) to 5 (10 or more times); (e) latency to first cigarette of the day assessed on a scale rangingfrom 1 (immediately after waking) to 6 (more than 2 h after waking); (f) readiness/intentions to quitmeasured on an ordinal scale with the options of 1 (I don't intend to quit smoking in the next 6 months), 2(I intend to quit smoking in the next 6 months), 3 (I intend to quit smoking in the next 30 days), and 4 (Ihave already quit smoking); and (g) participant's self-described Current Smoking Category(experimenter, occasional smoker, daily smoker, or former smoker).
For describing the smoking and quitting experience of the sample by condition, several additionalsmoking/quitting history baseline variables were examined: (a) the age one started smoking regularlymeasured on a scale ranging from 1 (11 years of age or younger) to 8 (18 years of age or older), (b) the lasttime one smoked a cigarette ranged from 1 (Today) to 8 (5 or more years ago), (c) length of longest quit

1776 S.I. Woodruff et al. / Addictive Behaviors 32 (2007) 1769–1786
attempt ranging from 1 (less than 24 h) to 8 (1 year or more), and (d) the last time one tried to quit rangingfrom 1 (1 to 7 days ago) to 7 (5 or more years ago).
Participation in sessions and satisfaction with the virtual world chat room was assessed for interventionparticipants. The counselor recorded the number of sessions each participant completed. Interventionparticipants were asked to complete 5 items assessing their satisfaction with the program at the end of thepost-test assessment. Ease of use of the virtual world chat room was rated on a scale ranging from 1 (verydifficult to use) to 5 (very easy to use). Similarly, liking of the chat room was rated on a 5-point scaleranging from 1 (disliked it very much) to 5 (liked it very much). Usefulness of the chat room for “helpingyou quit” smoking and for helping “other teen smokers quit” was measured on a 3-point scale rangingfrom 1 (not at all useful) to 3 (very useful). A final item asked about whether the participant wouldrecommend the chat room program to other teen smokers (yes vs. no).
2.6. Statistical analysis
Because school was the unit of randomization rather than individuals, it was necessary to assess thedegree to which results could be affected by clustering within schools (Bland, 2004). To assess thedependence in the data accounted for by school, design effects were computed based on baselinevariables' intraclass correlations and average cluster sizes. Intraclass correlations were generally small(.10 or less), and the magnitude of the effect sizes was below 2, indicating that school-level clustering wassmall (Hox, 2002; Muthen & Satorra, 1995). Therefore, analyses were conducted at the individual levelwithout a school-level cluster term.
Analyses were based on intention to treat. Differential rate of change in abstinence rates and othermeasures of smoking/abstinence relied on analysis of repeated measures over time. We analyzed theeffects of Breathing Room using the generalized estimating equations approach (SAS version 6.12).Modeling procedures in GEE (Liang & Zeger, 1986; Zeger & Liang, 1986) are superior to models basedon analysis of variance in that they do not require repeated measures to be equally spaced from oneanother, and they retain cases with missing data on one or more variables. We first modeled differentialchange from baseline to post-intervention to assess an immediate intervention effect. We then repeated theGEE analysis using all 4 repeated assessments to assess the overall and long-term effect of theintervention.
3. Results
Over 300 students showed interest in the program by contacting school liaisons or project staff. About200 eligible smokers completed and returned consent/assent forms, although only 136 took the baselinesurvey. Of these 136 actual participants, 77 participated as intervention subjects and 59 as controlsubjects. The number of participants at individual schools ranged from 2 to 36, with a mean of 9.7participants (mean of 11 participants per intervention school, and 8.4 per control school).
3.1. Sample characteristics and equivalence of groups at baseline
Approximately 54% of the sample was male (n=73) and 46% was female (n=63). The average age ofthe sample was 16, with a range of 14 to 19 years. The racial/ethnic composition was varied: 51% were

1777S.I. Woodruff et al. / Addictive Behaviors 32 (2007) 1769–1786
Hispanic, 28% were White non-Hispanic, 5% were African–American, 7% were Asian/Pacific Islander,and 9% were of Other ethnic groups. Forty-one percent of participants were from continuation/alternativehigh schools, while the remaining 59% were from regular high schools. On average, participants had beensmoking about two years, smoked 2–5 cigarettes a day, and smoked about 5 days a week. Three-fourthshad ever tried to quit. Additional characteristics of the overall sample are reported elsewhere (Woodruff,Lee, & Conway, 2006).
Table 1 presents demographic and baseline smoking-related characteristics of the sample by condition.The two conditions did not differ significantly in their gender, ethnic, and age characteristics, although asignificantly greater proportion of intervention subjects were alternative/continuation high schoolstudents. The groups differed significantly on several baseline smoking variables. Compared to controlsubjects, intervention participants had started smoking at a younger age, had smoked more cigarettes perday during the previous week, and had smoked more days in the previous week. Group differences werenot statistically significant for self-described current smoking category, the last time one smoked a
Table 1Comparison of intervention and control groups on demographic, smoking, and quitting variables
Variable % or mean category
Intervention Control χ2 or t
(n=77) (n=59)
Gender (%)Male 51 58Female 49 42 0.65
Ethnic group (%)Hispanic 51 50White non-Hispanic 27 28African American 3 5Asian/Pacific Islander 10 7Other 9 11 0.94
Age in years (mean) 16.5 16.1 −1.86Alternative/continuation students (%) 50 17 16.46⁎⁎⁎
Age first started smoking regularly (mean category) 3.79 2.97 −2.41⁎⁎Self-described current smoking category (%)Experimented 25 15Occasional 34 30Daily 32 45Former 9 11 3.68
No. of cigarettes smoked per day in past week (mean category) 2.97 2.29 −2.14⁎No. of days smoked in past week (mean category) 4.63 3.47 −2.40⁎⁎Latency to first cigarette of the day (mean category) 4.44 4.78 1.05Last time one smoked a cigarette (mean category) 2.00 2.22 1.37No. of times ever quit (mean) 1.66 1.50 0.56Longest time ever quit (mean category) 3.49 3.17 −0.81Last time one tried to quit (mean category) 4.06 4.78 1.70Readiness/intentions to quit (mean category) 2.42 2.18 −1.27⁎p≤ .05.⁎⁎p≤ .01.⁎⁎⁎p≤ .001.

Fig. 2. Past-week abstinence rates by condition.
Table 2Estimates from Generalized Estimating Equations (GEE) assessing main effects and condition-by-time interactions
GEE estimate
Condition Time Condition-by-timeinteraction
Outcome Main effect Main effect
Past-week abstinencePre-post 2.292⁎⁎ 1.797⁎ −1.401⁎⁎4 time periods .516 − .111 − .106
No. cigarettes smoked per day/past weekPre-post 1.675⁎⁎ 1.271⁎ − .989⁎⁎4 time periods .577 .035 − .155
No. days smoked in past weekPre-post 2.915⁎⁎ 1.763⁎⁎ −1.753⁎⁎⁎4 time periods .940 − .081 − .249
No. times ever quitPre-post .086 − .014 .0844 time periods − .031 − .097 .170⁎
Latency to first cigarettePre-post − .555 − .020 .2174 time periods − .290 .144 .065
Readiness/intentions to quitPre-post − .018 − .353 .2554 time periods .389 .273⁎ − .063
Self-described former smoker3 time periods 2.550⁎ 1.110⁎ − .720⁎
⁎p≤ .05.⁎⁎p≤ .01.
1778 S.I. Woodruff et al. / Addictive Behaviors 32 (2007) 1769–1786
cigarette, or latency to first cigarette of the day. The groups did not differ significantly in their baselinequitting history, including number of times quit, longest time ever quit, last time one tried to quit, and theirreadiness/intentions to quit.

Fig. 4. Days smoked in the past week by condition.
Fig. 3. Amount smoked in the past week by condition.
1779S.I. Woodruff et al. / Addictive Behaviors 32 (2007) 1769–1786
3.2. Intervention effects
Fig. 2 presents past week abstinence rates by condition at the four assessments. Table 2 presents the GEEestimates for the condition main effect, time main effect, and of particular interest, condition-by-timeinteractions. Although intervention participants had lower past-week abstinence rates than controls at baseline,at the post-assessment, they had significantly higher abstinence rates than controls (significant condition-by-time interaction). The interaction term considering all 4 assessments was not significant (see Table 2). At thefinal 12-month follow-up, the two conditions were nearly identical in their past-week abstinence rates.
A similar pattern was seen for the amount smoked per day in the past week (Fig. 3). Interventionparticipants smoked more than controls at baseline, but by the post-intervention assessment, reportedsmoking less than controls. This statistically significant condition-by-time interaction seen for the pre-to-post change did not hold when considering all 4 repeated assessments (see Table 2).
Fig. 4 shows changes in the number of days smoked in the past week by condition. Interventionparticipants showed greater change than controls at the intervention phase (i.e., pre-to-post intervention),as indicated by a statistically significant interaction. However, the analysis using all 4 time periods was

Fig. 5. Number of times quit by condition.
Fig. 6. Percent of baseline smokers describing themselves as a former smoker.
1780 S.I. Woodruff et al. / Addictive Behaviors 32 (2007) 1769–1786
not statistically significant. Fig. 5 presents changes in the number of times ever tried to quit by condition.The number of times quit increased more steeply over the study period for intervention participants thancontrols. Unlike other outcomes, the condition-by-time interaction for times quit was significant using all4 assessments, and not for pre-post changes.
Latency to first cigarette of the day and readiness/intentions to quit did not change differentially bycondition either in the pre-post analysis or the analysis using all four assessments. However, there was asignificant time main effect for readiness/intentions to quit using all assessments, with both groupsimproving over time.
Although adolescents had to have said they smoked in the past month to be eligible for the study, 9.6%described their current smoking category on the baseline survey as “former” smoker (i.e., they quitbetween volunteering to participate and going online to complete the baseline survey). Fig. 6 presents thepercent of baseline smokers (i.e., excluding baseline former smokers) who described themselves asformer smokers at the post-intervention and follow-up assessments. The GEE condition-by-timeinteraction using all 3 assessments was statistically significant (Table 2), indicating differential group

1781S.I. Woodruff et al. / Addictive Behaviors 32 (2007) 1769–1786
change over time. Follow-up chi-square analysis showed that at the post-intervention assessment, asignificantly higher percent of intervention participants than controls described themselves as a formersmoker (χ2(1)=3.64, p=.05). However, differences at the 3- and 12-month assessments were notstatistically significant. The percent of intervention participants considering themselves former smokershad declined by the 12-month assessment, while the percent of control participants describing themselvesas former smokers increased over time.
3.3. Attrition analysis
Cohort maintenance strategies included contacting the school liaison with a list of students due tocomplete surveys, multiple telephone contact attempts to the participant to remind them of surveys,mailed personalized reminder letters, and mailing surveys to the participant's home if he/she had movedand had no computer available. Overall non-response or loss to follow-up was 25% for the post-intervention survey, 21% for the 3-month follow-up survey, and 27% for the 12-month follow-up survey.There was tendency for survey non-response to be higher among intervention participants than amongcontrols. For example, at the post-intervention assessment, 15% of controls did not respond compared to33% of intervention participants. However, those who responded did not differ greatly from those whodropped out in terms of their demographic characteristics, baseline smoking history, or baseline quittinghistory. Furthermore, the characteristics of those who dropped out or remained did not differ by condition.
3.4. Participation in and satisfaction with the Breathing Room program
The 77 intervention participants averaged about 3 online sessions. About 19% (n=15) never logged onto any session, and 9% (n=7) received all 7 sessions. Sixty-eight percent (n=52) of interventionparticipants completed the 5 items assessing their satisfaction with the program immediately after thepost-test assessment. Participants rated the ease of use of the chat room a 4.2 (SD=.89) on a 5-point scale.Similarly, liking of the program averaged 4.0 (SD=.98) on a 5-point scale. Usefulness of the virtual worldchat room for both “helping you quit” smoking and for helping “other teen smokers quit” was 2.2 on a 3-point scale (SDs= .69 and .67). A large percent of participants (89%) reported they would recommend theprogram to another smoker.
4. Discussion
Expert smoking cessation guidance via the Internet holds promise because of its accessibility, visualappeal, use of multiple media, potential anonymity, interactivity, and nonreliance on school classroomtime or resources (Parlove, Cowdery, & Hoerauf, 2004; Woodruff et al., 2001). Results of this innovativestudy suggest that the Internet virtual world real-time counseling intervention was effective in helpingadolescent smokers stay off cigarettes or reduce their consumption, at least in the short-term. Those whoparticipated in the program were more likely than controls to report at the post-intervention assessmentthat they abstained from smoking during the past week, smoked fewer days in the past week, smokedfewer cigarettes in the past week, and considered themselves a former smoker. This pattern of findings isnotable, given the intervention group's worse smoking profile at baseline. The positive results of theintervention, however, were generally not maintained at the follow-up assessments, a fairly consistent

1782 S.I. Woodruff et al. / Addictive Behaviors 32 (2007) 1769–1786
finding that has been documented by other researchers (Walters et al., 2006). These results suggest thatcontinued support, perhaps in the form of online booster sessions, is needed to reinforce what the smokerhas learned and to help deal with relapse. Booster sessions are an integral part of most adult smokingcessation programs, and are an important component for effective tobacco use prevention programs foryouth (Pentz, 1999). Some of our own research (author S.I.W.) shows that boosters or further applicationof the program have been effective in helping to maintain prevention intervention effects (Eckhardt,Woodruff, & Elder, 1997; Elder et al., 1993). Less is known about the importance of boosters onmaintaining cessation among adolescents, although it makes sense that additional contact and activitywith participants may help to maintain abstinence or spur a quit attempt if the participant has relapsed.
Of the seven outcomes examined, only the number of times quit was statistically significant long-term(i.e., one year post intervention). It may be that the intervention, while not resulting in protractedabstinence or reduction in smoking, may have helped adolescent smokers continue to make quit attemptslong after the program ended. Multiple quit attempts are associated with eventual cessation successamong adult smokers, and therefore, this finding may be a positive outcome. However, experience withquitting may not be a particularly strong predictor of eventual cessation among adolescents (Sargent,Mott, & Stevens, 1998). The association of multiple quit attempts with cessation among young smokers isan area needing further research.
In the present study, control participants generally improved over time, probably due to the type ofsmokers that comprised the control group. Compared to intervention subjects, control participants werelighter and less frequent smokers at baseline, an unintended difference that was likely the result of thedifferent recruitment methods used for the two conditions. This type of recruitment bias is common intrials in which clusters rather than individuals are randomly assigned to treatment groups. Different typesof participants are selected into the various arms of the trial, resulting in nonequivalent groups (Torgerson,2000). One solution is to ask for informed consent to participate in a study (rather than participation inspecific intervention or evaluation activities) and to collect baseline measures prior to notice ofrandomization. However, logistical and practical considerations and suggestions of the schools led us toinform participants of the specific intervention or evaluation activities that would be asked of them priorto the baseline assessment. The result was that regular, “hard core” smokers were more likely to volunteerfor the intervention, and occasional, less frequent smokers were more likely to participate in the controlarm. In a related vein, a higher percent of intervention participants than controls were from alternative/continuation high schools. These types of students are likely to have different characteristics (beyondsmoking behavior) than regular high school students (Sussman, Dent, Severson, Burton, & Flay, 1998),that may have impacted the long-term effects of the intervention. The control group's exposure to othertobacco programs, or reaction to simply being measured may have also contributed to their improvementover time.
It may be that the Internet virtual world chat room may have been more effective as an adjunct to atraditional face-to-face counseling program. The question of whether Internet technology can be usedsuccessfully as an alternative stand-alone intervention medium is still difficult to judge (Christensen &Griffiths, 2003).
The level of participation in the intervention was somewhat disappointing, given the advantages of theInternet approach, and the participants' generally positive ratings of its appeal and usefulness. We believethat there may have been barriers (e.g., counseling times) that prevented more complete participation.Perhaps allowing participation during school hours (rather than before and after school), or allowing classcredit for participation would have improved involvement.

1783S.I. Woodruff et al. / Addictive Behaviors 32 (2007) 1769–1786
There were several positive aspects of the study, including the multiethnic group of smokers, theparticipatory relationship with school partners, the satisfaction of the participants with the approach, andthe inclusion of all data points in the analyses. Although the attrition rate differed by condition, thecharacteristics of those who dropped out did not differ greatly by condition. However, there are limitationsof the study, including the differential recruitment strategies that resulted in nonequivalent groups atbaseline. In addition, there was no objective validation of smoking/quitting, although collection of thistype of information was not feasible or desirable in the context of an Internet-based study. Despite thelimitations, this study suggests that real-time Internet communication may be an appealing and effectiveapproach to help young smokers quit or reduce smoking in the short term, but that additional support isprobably needed for longer-term success. One area of interest to us is the relative impact of the virtualworld chat room technology compared to a more traditional chat room. In addition, we are interested inhow interactive chat room approaches compare to lower-cost, education-oriented smoking cessationwebsites for teen smokers.
Acknowledgements
This research was funded by California's Tobacco-related Disease Research Program (TRDRP), grantnumber 11HT-3301.
The authors wish to acknowledge the invaluable contribution of Dr. Lynn Covarrubias, SummerLambert, Chellie Stoffel, Elizabeth “Liz” Garcia, Dr. Sharon Snyder, and Dr. Phil Gardiner.
References
Backinger, C. L., Fagan, P., Matthews, E., & Grana, R. (2003). Adolescent and young adult tobacco prevention and cessation:Current status and future directions. Tobacco Control, 12(Supp I), iv46−iv53.
Bandura, A. (1997). Self-efficacy: The exercise of control. New York: W.H. Freeman.Bandura, A. (1986). Social foundations of thought and action. Englewood Cliffs, NJ: Prentice-Hall.Bland, M. (2004). Clustered randomized trails in the medical literature: Two bibliometric surveys. BMC Medical Research
Methodology, 4, 21.Borzekowski, D. L. G., & Rickert, V. I. (2001). Adolescents, the internet, and health issues of access and content. Applied
Developmental Psychology, 22, 49−59.Burling, T. A., Seidner, A. L., & Gaither, D. E. (1994). A computer-directed program for smoking cessation treatment. Journal of
Substance Abuse, 6, 427−431.Charlton, A., Melia, P., & Moyer, C. (1990). A manual on tobacco and young people for the industrialized world. Geneva:
International Union Against Cancer (UICC).Chassin, L., Presson, C., & Sherman, S. (1985). Cognitive and social influence factors in adolescent smoking cessation.
Addictive Behaviors, 9, 383−390.Christensen, H., & Griffiths, K. (2003). The internet and mental health practice. Evidence Based Mental Health Notebook, 6,
66−69.Cohen, S., & Lichtenstein, E. (1990). Partner behaviors that support quitting smoking. Journal of Consulting and Clinical
Psychology, 58, 304−309.Dino, G., Kamal, K., Horn, K., Kalsekar, I., & Fernandes, A. (2004). Stage of change and smoking cessation outcomes among
adolescents. Addictive Behaviors, 29(5), 935−940.DuRant, R. H., & Smith, J. A. (1999). Adolescent tobacco use and cessation. Primary Care, 26, 553−575.Eckhardt, L., Woodruff, S. I., & Elder, J. P. (1997). Relative effectiveness of continued, lapsed, and delayed smoking prevention
intervention in senior high school students. American Journal of Health Promotion, 11(6), 418−421.Edwards, S., Braunholtz, D., Lilford, R., & Stevens, A. (1999). Ethical issues in the design and conduct of cluster randomised
controlled trials. British Medical Journal, 318, 1407−1409.

1784 S.I. Woodruff et al. / Addictive Behaviors 32 (2007) 1769–1786
Elder, J. P., Wildey, M., de Moor, C., Sallis, J. F., Eckhardt, L., Edwards, C., et al. (1993). The long-term prevention of tobaccouse among junior high school students: Classroom and telephone interventions. American Journal of Public Health, 83(9),1239−1244.
Escoffery, C., McCormick, L., & Bateman, K. (2004). Development and process evaluation of a web-based smoking cessationprogram for college smokers: Innovative tool for education. Patient Education and Counseling, 53, 217−225.
Fisher, E. B., Lichtenstein, E., Haire-Joshu, D., Morgan, G. D., & Rehberg, H. R. (1993). Methods, successes, and failures ofsmoking cessation programs. Annual Review of Medicine, 44, 481−513.
Fotheringham, M. J., Owies, D., Leslie, E., & Owen, N. (2000). Interactive health communication in preventive medicine:Internet-based strategies in teaching and research. American Journal of Preventive Medicine, 19(2), 113−120.
Gruder, C. L., Mermelstein, R. J., Kirkendol, S., Hedeker, D., Wong, S. C., Schreckengost, J., et al. (1993). Effects ofsocial support and relapse prevention training as adjuncts to a televised smoking-cessation intervention. Journal ofConsulting and Clinical Psychology, 61(1), 113−120.
Hox, J. J. (2002). Multilevel analysis: Techniques and applications. Mahwah, NJ: Lawrence Erlbaum Associates.Israel, B., Schulz, A., Parker, E., & Becker, A. (1998). Review of community-based research: Assessing partnership approaches
to improve public health. Annual Review of Public Health, 19, 173−202.Johnston, L. D., O'Malley, P. M., & Bachman, J. G. (2003).Monitoring the Future national survey results on drug use, 1975–2002.
Volume I: Secondary school students (NIH Publication No. 03-5375) Bethesda, MD: National Institute on Drug Abuse.Lacey, L. P., Manfredi, C., Balch, G., Warnecke, R. B., Allen, K., & Edwards, C. (1993). Social support in smoking cessation
among black women in Chicago public housing. Public Health Reports, 108(3), 387−394.Lancaster, T., Stead, L., Silagy, C., & Sowden, A. (2000). Effectiveness of interventions to help people stop smoking: Findings
from the Cochrane Library. British Medical Journal, 321, 355−358.Lantz, P. M., Jacobson, P. D., Warner, K. E., Wasserman, J., Pollack, H. A., Berson, J., et al. (2000). Investing in youth tobacco
control: A review of smoking prevention and control strategies. Tobacco Control, 9, 47−63.Lawendowski, L. A. (1998). A motivational intervention for adolescent smokers. Preventive Medicine, 27, A39−A46 (Article
No. PM980424).Lenert, L., Munoz, R. F., Stoddard, J., Delucchi, K., Bansod, A., Skoczen, S., et al. (2003). Design and pilot evaluation of an
Internet smoking cessation program. Journal of the American Medical Informatics Association, 10(1), 16−20.Liang, K. Y., & Zeger, S. L. (1986). Longitudinal data analysis using generalized linear models. Biometrika, 73, 13−22.Lichtenstein, E., & Glasgow, R. E. (1992). Smoking cessation: What have we learned over the past decade? Journal of
Consulting and Clinical Psychology, 60(4), 518−527.Marlatt, G. A., & Gordon, J. R. (Eds.) (1985). Relapse prevention: Maintenance strategies in the treatment of addictive
behaviors. New York: Guilford Press.Mattey, E.A. (2003). Knights Against Tobacco: teens lead the charge to prevent tobacco use among adolescents. Pediatric
Nursing, 29 (5), 390, 393–396.McTavish, F. M., Gustafson, D. H., Owens, B. H., Wise, M., Taylor, J. O., Apantaku, F. M., et al. (1995). CHESS
(Comprehensive Health Enhancement Support System): An interactive computer system for women with breast cancerpiloted with an underserved population. Journal of Ambulatory Care Management, 18(3), 35−41.
Mermelstein, R. (2003). Teen smoking cessation. Tobacco Control, 12(Supp I), i25−i34.Miller, W. R., & Rollnick, S. (1991). Motivational interviewing: Preparing people to change addictive behavior. New York:
Guilford Publications.Muthen, B., & Satorra, A. (1995). Complex sample data in structural equation modeling. In P. V. Marsden (Ed.), Sociological
Methodology (pp. 267−316). Washington D.C.: The American Sociological Association.Myers, M. G. (1999). Smoking intervention with adolescent substance abusers. Journal of Substance Abuse Treatment, 16(4),
289−298.O'Loughlin, J., DiFranza, J., Tyndale, R. F., Meshefedjian, G., McMillan-Davey, E., Clarke, P. B. S., et al. (2003). Nicotine-
dependence symptoms are associated with smoking frequency in adolescents. American Journal of Preventive Medicine, 25(3), 219−225.
Pallonen, U., Murray, D., Schmid, L., et al. (1990). Patterns of self-initiated smoking cessation among young adults. HealthPsychology, 9, 418−426.
Pallonen, U. E., Velicer, W. F., Prochaska, J. O., Rossi, J. S., Bellis, J. M., Tsoh, J. Y., et al. (1998). Computer-based smokingcessation interventions in adolescents: Description, feasibility, and six-month follow-up findings. Substance Use and Misuse,33(4), 935−965.

1785S.I. Woodruff et al. / Addictive Behaviors 32 (2007) 1769–1786
Parlove, A. E., Cowdery, J. E., & Hoerauf, S. L. (2004). Acceptability and appeal of web-based smoking prevention interventionfor adolescents. The International Electronic Journal of Health Education, 7, 1−8.
Pentz, M. A. (1999). Effective prevention programs for tobacco use. Nicotine and Tobacco Research, 1(Suppl 2),S99−S107.
Prochaska, J. O., & Velicer, W. F. (1997). The transtheoretical model of health behavior change. American Journal of HealthPromotion, 12(1), 31−33.
Prokhorov, A. V., Hudmon, K. S., & Stancic, M. (2003). Adolescent smoking: Epidemiology and approaches for achievingcessation. Paediatric Drugs, 5(1), 1−10.
Rhodes, F., Fishbein, M., & Reis, J. (1997). Using behavioral theory in computer-based health promotion and appraisal. HealthEducation and Behavior, 24(1), 20−34.
Rohde, K., Pizacani, B., Stark, M., Pietrukowicz, M., Mosbaek, C., Romoli, C., et al. (2001). Effectiveness of school-basedprograms as a component of a statewide tobacco control initiative—Oregon, 1999–2000. Morbidity and Mortality WeeklyReport, 50(31), 663−666.
Rollnick, S., & Miller, W. R. (1995). What is motivational interviewing? Behavioral and Cognitive Psychotherapy, 23,325−334.
Sargent, J. D., Mott, L. A., & Stevens, M. (1998). Predictors of smoking cessation in adolescents. Archives of Pediatrics &Adolescent Medicine, 152(4), 388−393.
Schneider, S. J., Walter, R., & O'Donnell, R. (1990). Computerized communication as a medium for behavioral smokingcessation treatment: Controlled evaluation. Computers in Human Behavior, 6, 141−151.
Scott, W. J., & McIlvain, H. (2000). Interactive software: An educational/behavioural approach to smoking cessation forpregnant women and their families. Tobacco Control, 9(Suppl III), 56−57.
Spruijt-Metz, D., Gallaher, P. E., Unger, J. B., & Anderson-Johnson, C. (2004). Meanings of smoking and adolescent smokingacross ethnicities. Journal of Adolescent Health, 35(3), 197−205.
Stivers, C., Bentley, M. K., & Meccouri, L. L. (1995). Internet: The contemporary health educator's most versatile tool. Journalof Health Education, 26(4), 196−199.
Strecher, V. J. (1999). Computer-tailored smoking cessation materials: A review and discussion. Patient Education andCounseling, 36, 107−117.
Strecher, V. J., Shiffman, S., & West, R. (2005). Randomized controlled trial of a web-based computer-tailored smokingcessation program as a supplement to nicotine patch therapy. Addiction, 100, 682−688.
Sussman, S., Dent, C. W., Severson, H., Burton, D., & Flay, B. R. (1998). Self-initiated quitting among adolescent smokers.Preventive Medicine, 27, A19−A28.
Sussman, S., Lichtman, K., Ritt, A., & Pallonen, U. E. (1999). Effects of thirty-four adolescent tobacco use cessation andprevention trials on regular users of tobacco products. Substance Use and Misuse, 34, 1469−1503.
Takahashi, Y., Satomura, K., Miyagishima, K., & Nakahara, T. (1999). A new smoking cessation programme using the internet.Tobacco Control, 8, 109−110.
Torgerson, D. J. (2000). Contamination in trials: Is cluster randomization the answer? British Medical Journal, 322, 355−357.Turner, L., Mermelstein, R., & Flay, B. (2004). Individual and contextual influences on adolescent smoking. Annals of the New
York Academy of Sciences, 1021, 175−197.Unger, J. B., Palmer, P. H., Dent, C. W., Rohrbach, L. A., & Johnson, C. A. (2000). Ethnic differences in adolescent smoking
prevalence in California: Are multi-ethnic youth at higher risk? Tobacco Control, 9(Supp II), ii9−ii14.US Department of Health and Human Services-USDHHS. (2000a). Reducing Tobacco Use: A Report of the Surgeon General.
Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, NationalCenter for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2000.
US Department of Health and Human Services-USDHHS (2000, November). Healthy People 2010: Understanding andImproving Health, 2nd. ed. Washington, DC: U.S. Government Printing Office.
Valente, T. W., Hoffman, B. R., Ritt-Olsen, A., Lichtman, K., & Johnson, A. (2003). Effects of a social-network method forgroup assignment strategies on peer-led tobacco prevention programs in school. American Journal of Public Health, 93(11),1837−1843.
Velicer, W. F., & Prochaska, J. O. (1999). An expert system intervention for smoking cessation. Patient Education andCounseling, 36, 119−129.
Viswesvaran, C., & Schmidt, F. L. (1992). A meta-analytic comparison of the effectiveness of smoking cessation methods.Journal of Applied Psychology, 77(4), 554−561.

1786 S.I. Woodruff et al. / Addictive Behaviors 32 (2007) 1769–1786
Vuckovic, N., Polen, M. R., & Hollis, J. F. (2003). The problem is getting us to stop: What teens say about smoking cessation.Preventive Medicine, 37, 209−218.
Walters, S. T., Wright, J. A., & Shegog, R. (2006). A review of computer and Internet-based interventions for smoking behavior.Addictive Behaviors, 31(2), 264−277.
Weinberg, N., Schmale, J., Uken, J., & Wessel, K. (1996). Online help: Cancer patients participate in a computer-mediatedsupport group. National Association of Social Workers, 21, 24−29.
Whiist, W. H. (2004). Social networks and peer education. American Journal of Public Health, 94(8), 1293.Woodruff, S. I., Edwards, C. C., Conway, T. L., & Elliott, S. P. (2001). Pilot test of an internet virtual world chat room for rural
teen smokers. Journal of Adolescent Health, 29, 239−243.Woodruff, S. I., Lee, J., & Conway, T. L. (2006). Smoking and quitting history correlates of readiness to quit in multiethnic
adolescents. American Journal of Health Behavior, 30(6), 663−674.Zeger, S. L., & Liang, K. Y. (1986). Longitudinal data analysis for discrete and continuous outcomes. Biometrics, 42, 121−130.










![[Smoking cessation in smokers with chronic obstructive pulmonary disease.]](https://img.pdfslide.net/doc/110x75/635f7df0ac0cd8fcb10e3773/smoking-cessation-in-smokers-with-chronic-obstructive-pulmonary-disease.jpg)


















