Embed Size (px)
Citation preview

EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
FINAL REPORT

IIEVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015

IIIEVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
FOREWORD
The Government of Sudan, represented by the Humanitarian Aid Commissioner Secretary Gen-eral (HAC) and UNICEF Representative in Sudan, are pleased to present and communicate a final and comprehensive report of an independent evaluation of the effectiveness and impact of the Humanitarian Action in North Darfur. The humanitarian action was a joint initiative between the Sudanese Government, UNICEF, other UN agencies and partners, with the financial support of various donors from 2010 through 2015. The report primarily focused on interventions for Child Survival (Health, Nutrition and Water, Sanitation and Hygiene) in Sudan.
This evaluation provides, for the first time in 13 years, evidence towards the learning of good practices, achieved results and explanatory factors for shortfalls. Subsequently, better informed developments of adequate policies, strategies, appropriate programmes as well as partnerships in improving humanitarian effectiveness and impact in Sudan, are then facilitated. The Government, Local Authorities, Communities, UNICEF and Partners, among other stakeholders, will find this report extremely beneficial.
The objective of UNICEF’s and the Government’s commitment to completing this first independent and transparent evaluation of the benefit to vulnerable children and families of the humanitarian interventions in North Darfur is part of UNICEF’s readiness and accountability to ensuring greater impact for saving the lives of vulnerable children affected by conflicts, natural disasters, poverty and inequalities in North Darfur. Several questions were also addressed such as:
� What did we learn from multi-sector interventions and multi partnerships?
� What could we do better to improve the lives of the lost generation of children who were born and raised in IDP camps since 2003 and amongst host communities?
� Are we addressing the needs and rights of children?
� What are some of the examples of strategic gaps?
� What are the key bottlenecks that hinder effective service delivery and impact to change the situation?
� How do we ensure the sustainability of gains for children’s wellbeing that aim to achieve the SDG 2030 in Sudan?
Under the leadership of the HAC Secretary General and UNICEF, Sudan’s EHA Country Team and a multi-sector Technical Committee of the evaluation was established. This evaluation process

IVEVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
involved sector line Ministries of Health, WASH, Education and Social Welfare and 3 consultants recruited by UNICEF (one international team leader and two national consultants). The National Team has designed the evaluation ToR that has guided the design by the consultant team of the methodology, the field assessment and the reporting, benefiting from the timely adequate technical guidance and logistical support of UNICEF at all levels and the HAC including support of Line Ministries and State Governor at federal and state levels. We appreciate the technical support provided by the Central Bureau of Statistics (CBS) regarding the sampling and the field data collection. We are also grateful for the technical assistance provided by UNICEF Regional Office in Amman and UNICEF Headquarters in New York, particularly regarding quality assurance of technical tools, including the final report.
We thank all Sector Line Ministries, States, Local Authorities in North and South Darfur, and our wide range of partners for their roles during the implementation of this evaluation from March through July 2016.
We would also like to further acknowledge UNICEF for the technical and financial support provided for the completion of this evaluation. We are grateful to the financial support provided by DFID at global level. In the same vein, we thank the team of consultants for the quality assessment and analytical nature of the report they have delivered.
In light of the above, we encourage all policy makers and development partners, academic insti-tutions and indeed the people of Sudan to make effective use of this report to plan, monitor and evaluate relevant goals and objectives addressing the advancement and prosperity of the population and children affected by emergency in North Darfur and other areas.
Signed on …………………………31 March 2017, by:
For the Government of Sudan For the United Nations Children’s Fund (UNICEF)
Signature______________________
H.E. Mr Ahmed MohamedHumanitarian Aid Commissioner Secretary General
Signature______________________
Mr Abdullah FadilUNICEF Representative in Sudan

VEVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
ACKNOWLEDGEMENTS
The Evaluation Team expresses its gratitude to Mr. Geert Cappelaere, former UNICEF Repre-sentative in Sudan, Mr Abdullah Fadil, current UNICEF Representative, and the Humanitarian Aid Commissioner Secretary General H.E. Mr Ahmed Mohamed, who approved this evalua-tion and provided strong support as part of the Government, UNICEF and partners’ mutual re-sponsibility towards child wellbeing in Sudan and accountability to Donors.
The team also extends its thanks to the UNICEF evaluation office in Khartoum head by Mr Rob-ert Ndamobissi, Chief of Planning, Monitoring and Evaluation assisted by Mrs Aala Mahmoud, Monitoring and Evaluation Specialist and Mr Tarig Mekkawi, Nutrition Officer, all of whom provided invaluable technical direction, guidance, management and quality assurance during the evaluation. The evaluation team is grateful to the multi variate statistical analysis that has been performed by Mr Robert Ndamobissi using the EHA Household survey raw data as key added value contribution to this evidence generation related to assessing the impact on child survival.
The evaluation team also worked in close col-laboration with the Emergency Chief Stephane Pichette, and the UNICEF Field Offices in North Darfur and South Darfur.
The team is extremely grateful to Mrs Mona, the Planning Officer at the HAC, and Imadeldin Abdel-rahim Mohamed, the Director of Programmes at Sudan’s Red Crescent, who worked tirelessly to provide adequate support towards the comple-tion of this evaluation. These officers also worked in close collaboration with UNICEF PME team,
Line Ministries and State Authorities taking lead in coordination, facilitating the acquisition of travel permits and mobilisation of communities and key informants. The officers also provided their ser-vices for the facilitation of access to information related to EHA and their assistance to the field data collection in selected communities.
The Evaluation team also wishes to highlight the efforts of all those who took part in this work in one way or another, and would like to acknowl-edge their invaluable contributions to its improve-ment. From the early days of the elaboration of the Terms of Reference by the Country Team, the methodological design fieldwork planning to the final evaluation report, many individuals were involved through a variety of approaches that made it possible to complete this assignment.
We would also like to highlight the contribution of the experts at the Central Bureau of Statis-tics (CBS), data collectors and enumerators from Sudan Red Crescent volunteers in North Darfur and South Darfur, who have played a critical role in the field data collection. This team reviewed the survey questionnaire making it compatible with the field language, helped in the selection of the sites within each locality and organised expert and qualified teams to collect, compile and summarise data.
We would further like to thank the UNICEF Regional Office M&E team in Amman and the Evaluation Office in New York (particularly Ms Laura Olsen coordinator of the global project of Evaluation of Humanitarian action in partnership DFID/UNICEF), for the timely technical support to all steps of the evaluation.

VIEVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015

VIIEVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
CONTENTS
FOREWORD ............................................................................................................................... III
ACKNOWLEDGEMENTS ...........................................................................................................V
TABLE OF CONTENTS .............................................................................................................VII
LIST OF FIGURES ...................................................................................................................... X
LIST OF TABLES ....................................................................................................................... XI
ACRONYMS ............................................................................................................................ XII
EXECUTIVE SUMMARY ........................................................................................................ XIII
INTRODUCTION AND BACKGROUND ................................................................................. XIII
Purpose of the Evaluation ..............................................................................................xiiiSpecific objectives of the Evaluation: ............................................................................xiiiKey evaluation questions: ..............................................................................................xivScope of the Evaluation .................................................................................................xiv
METHODOLOGY .....................................................................................................................XV
Evaluation Limitation and Challenges ............................................................................ xv
SUMMARY OF FINDINGS ....................................................................................................XVII
The summary of the findings on best practices (what worked) and for whom ............xviiThe summary of the findings on challenges (what did not work – shortfall in results) ...xviiiThe summary of the findings on the impact of Lifesaving Humanitarian Action for children ...................................................................xixRecommendations to UNICEF ....................................................................................... xxRecommendations to the Government of Sudan ..........................................................xxiRecommendations to Partners .....................................................................................xxii

VIIIEVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
1. INTRODUCTION AND BACKGROUND .........................................................................1
1.1 HUMANITARIAN SITUATION IN NORTH DARFUR ..............................................21.2 UNICEF INTERVENTIONS IN NORTH DARFUR ..................................................4
1.2.1 Nutrition ....................................................................................................41.2.2 Health ........................................................................................................41.2.3 Water, Sanitation and Hygiene ..................................................................4
2. PURPOSE OF THE EVALUATION ...................................................................................6
2.1 OBJECTIVES OF THE EVALUATION ....................................................................72.2 KEY EVALUATION QUESTIONS ..........................................................................82.3 THEORY OF CHANGE AND CONCEPTUAL FRAMEWORK FOR THE EVALUATION ........................................................................................82.4 SCOPE OF THE EVALUATION .............................................................................9
3. METHODOLOGY .......................................................................................................... 11
3.1 DATA COLLECTION TOOLS ............................................................................... 133.1.1 Desk Review ........................................................................................... 133.1.2 Key informant interviews ........................................................................ 133.1.3 Focus group discussions ......................................................................... 143.1.4 Significant Stories of Change .................................................................. 143.1.5 Household questionnaire ........................................................................ 143.1.6 Observation of WASH, Nutrition and Health Facilities ............................. 15
3.2 SAMPLING AND DATA COLLECTION ............................................................... 153.2.1 Sampling for administration of household questionnaires ...................... 153.2.2 Quality assurance and ethical considerations ......................................... 163.2.2 Limitations of the evaluation ................................................................... 17
4. EVALUATION FINDINGS AND DISCUSSIONS ........................................................... 19
4.1 RELEVANCE AND APPROPRIATENESS ............................................................204.2 COORDINATION ................................................................................................234.3 EFFICIENCY .......................................................................................................24
4.3.1 Efficiency of WASH Programme .............................................................254.3.2 Efficiency of Nutrition Programme ..........................................................314.3.3 Efficiency of Health Programme .............................................................36

IXEVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
4.4 EFFECTIVENESS ................................................................................................424.4.1 Effectiveness of WASH Programme ........................................................424.4.2 Effectiveness of Nutrition Programme ....................................................474.4.3 Effectiveness of Health Programme .......................................................49
4.5 IMPACT ..............................................................................................................524.5.1 Impact of WASH Programme ..................................................................524.5.2 Impact of Nutrition Programme...............................................................534.5.3 Impact of Health Programme ..................................................................574.5.4 Impact on Child Survival ..........................................................................59
4.6 SUSTAINABILITY ...............................................................................................66
4.7 LESSONS LEARNED .........................................................................................66
5. CONCLUSION AND RECOMMENDATIONS ...............................................................69
5.1 CONCLUSION ....................................................................................................70The summary of the findings on best practices (what worked) and for whom .... 70The summary of the findings on challenges (what did not work – shortfall in results) ..............................................................................................71The summary of the findings on the impact of Lifesaving Humanitarian Action for children .......................................................72
5.2 RECOMMENDATIONS TO UNICEF....................................................................72
5.3 RECOMMENDATIONS TO THE GOVERNMENT OF SUDAN ............................. 74
5.4. RECOMMENDATIONS TO PARTNERS .............................................................. 74

XEVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
List of Figures
Figure 1: Administrative boundary of North DarfurFigure 2: Evaluation conceptual framework adapted from Tremolet et al.Figure 3: Comparison of funding for WASH programmes by UNICEF and other donorsFigure 4: Number of people reached through the provision of clean water in North Darfur Figure 5: Outputs of water in South Darfur Figure 6: Progress towards WASH in North Darfur schools Figure 7: Provision cost for water and sanitation service per person (household survey)Figure 8: Funding for nutrition humanitarian programmes for 2010–2015 Figure 9: Admission of children with SAMFigure 10: Children aged 6–59 months having received two doses of vitamin A Figure 11: Cost per life saved through UNICEF nutrition Interventions as calculated from UNICEF financial reports.Figure 12: Comparison of distributed Plumpy’Nut and the number of under-five children admitted for SAM treatment Figure 13: Funding of the health humanitarian programmeFigure 14: Number of children receiving BCG vaccine against the target Figure 15: Number of children receiving measles immunization in North DarfurFigure 16: Number of children receiving measles immunization in South Darfur Figure 17: Number of children receiving pentavalent immunization in North Darfur Figure 18: Number of children receiving pentavalent immunization in South DarfurFigure 19: Cost of delivering one dose of a vaccine Figure 20: Distance of the household to the nearest water sourceFigure 21: Presentation of the time taken at the water pointFigure 22: Presentation of household water treatment optionsFigure 23: Presentation of under-five children suffering from wasting Figure 24: Main source of household food Figure 25: Illustration of under-five children sleeping under a bed net Figure 26: Responses from caregivers on whether children under 5 suffered from malaria in the past six months Figure 27: Trends in the under-five mortality rate (per 1,000) in North DarfurFigure 28: Prevalence of wasting – MAM and SAM (%) by stateFigure 29: Presentation of trends of childhood diseases between 2006 and 2014 Figure 30: Visual diagram for factorial plans of determinants of under-five child deaths

XIEVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
List of Tables
Table 1: Distribution of the sample size within the localitiesTable 2: Representation of the new cases from 2010–2015 by disaster type Table 3: Presentation of the cost of a 20-litre Jerry can of water Table 4: Source of household income for the internally displaced persons for households with under-five children Table 5: Presentation of child illness cases in North Darfur as reported by the State Ministry of Health Table 6: Presentation of child illness in South Darfur as reported by the State Ministry of Health

XIIEVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
ACRONYMS
BCG Bacillus Calmette-Guérin
CMAM Community Management of Acute Malnutrition
EHA Evaluation of Humanitarian Action
EPI Expanded Programme on Immunization
GAM global acute malnutrition
HAC Humanitarian Aid Commission
IDP internally displaced person
IMCI Integrated Management of Childhood Illness
MAM moderate acute malnutrition
MICS Multiple Indicator Cluster Survey
NGO non-governmental organization
SAM severe acute malnutrition
WASH water, sanitation and hygiene
WES Water Environment and Sanitation
WFP World Food Programme
WHO World Health Organization

XIIIEVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
EXECUTIVE SUMMARY
1 Annual Humanitarian Strategic Plans is a UN mechanism which pools resources for all UN agencies for humanitarian programming within North Darfur
2 Annual Humanitarian Strategic Plans is a UN mechanism which pools resources for all UN agencies for humanitarian programming within North Darfur
INTRODUCTION AND BACKGROUND
UNICEF’s humanitarian interventions in North Darfur focused on supporting the affected people with immediate lifesaving assistance and pro-tection crucial to their survival, in a sustainable manner. UNICEF targeted more than 517,000 IDPs , (including 180,950 men, 232,650 women, and 103,400 children) between 2010 and 2015, for provision of water and sanitation services under its WASH Humanitarian Programming. The goal was to contribute to a reduction of diarrheal cases through provisions of safe drinking water and sanitation facilities. The Nutrition Humanitar-ian Programme focused on the integration of the new CMAM services into the existing Primary Health Care facilities targeting up to 163,420 chil-dren with Severe Acute Malnutrition. Regarding the Health Humanitarian Programming, UNICEF targeted the strengthening of the IMCI program reaching some 628,566 individuals, representing 33 percent of children under five in North Dar-fur, and capacity building state level health care workers.
Purpose of the EvaluationThe Government of Sudan, represented by Hu-manitarian Aid Commission (HAC) and UNICEF, agreed to undertake an independent evaluation to assess the effectiveness of UNICEF human-
itarian interventions from 2010 through 2015 in North Darfur. One of the primary targets was to learn from the outcome and impact of the interventions in promoting child survival. Evi-dence generated on the intervention strengths and weakness will be used by the Government of Sudan (Federal, State and Locality level), UNICEF, Donors, and other UN agencies to im-prove humanitarian programming for the greater wellbeing of children.
Specific objectives of the Evaluation: To measure the achievement of expected chain of results (efficiency/coverage, effectiveness and impacts) of the implementation of the Annual Humanitarian Strategic Plans1 funded through emergency funds and implemented in North Darfur from 2010 to 2015. Furthermore:
1. Measure the achievement of expected chain of results (efficiency/coverage, effec-tiveness and impacts) of the implementa-tion of the Annual Humanitarian Strategic Plans2 funded through emergency funds and implemented in North Darfur from 2010 to 2015.
2. To document the relevance, coordination, and sustainability of the UNICEF Humani-tarian Programme in North Darfur.
3. To generate explanations to the possible

XIVEVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
reasons for the increased under five mortal-ity despite all efforts exhausted in the state.
4. To assess how well humanitarian pro-grammes address host community needs in the same way they address humanitarian needs to the affected population.
5. To assess the institutional, financial and op-erational capacities for better coordination, planning, implementation, management and M&E of Humanitarian Action at national level, state, locality and community levels, both from Government and UN Agencies (UNICEF).
6. To develop a Theory of Change of the inter-ventions implemented in North Darfur and identify the gaps.
7. To document good practices, intervention challenges, bottlenecks and solutions ap-plied to overcome the intervention challeng-es by documenting lessons learnt on what works for whom, what does not work for whom, and why.
Key evaluation questions:1. Relevance/Appropriateness: To what extent
is UNICEF’s humanitarian programmes aligned with National humanitarian policies and the needs of the affected population?
2. Coordination: To what extent has adequate humanitarian programme coordination been implemented among various actors/sectors in order to avoid gaps or duplications at community level?
3. Efficiency: To what extent did UNICEF mo-bilise for adequate financial and operational capacities to offer rapid delivery of services to the affected under 5 children in compli-ance with UNICEF’s Core Commitment to Children (CCC).
4. Effectiveness: What were the achievements of expected outcomes of the implementa-tion of the Annual Humanitarian Strategic Plans?
5. Impact: What significant changes (positive and negative) happened to children lifesav-ing and communities as a result of UNICEF and partners interventions? What are the main determinant factors of increasing child mortality observed in North Darfur during the last five years 2010-2015?
6. Sustainability: To what extent are the inter-ventions and their impact likely to contin-ue when UNICEF and Partners’ support is withdrawn?
Scope of the EvaluationThe evaluation focused on UNICEF child survival programming (Health, Nutrition, Water, Sanita-tion and Hygiene humanitarian programmes) between 2010 and 2015 in addressing the main question related to the effectiveness and impact of humanitarian service delivery. The focus on multi-sectoral responses in North Darfur also included the analysis of conflict effects, promo-tion of social cohesion and building resilience (empowerment of communities and families). The evaluation applied the universal criteria of OECD/DAC, adapted for the particularity of evaluation of humanitarian action: i) relevance (appropriateness), (ii) coordination/coherence (iii) effectiveness, (iv) efficiency/cost-effective-ness/value for money/coverage, (v) impact and (vii) sustainability/ connectedness (as it con-cerns protracted emergency) of humanitarian responses in North Darfur.
The Geographical focus of the evaluation of humanitarian action was on North Darfur, with targeted six localities including Elfasher, Kabk-abia, Kutum, Mellit, Saraf Omra and Tawila, in North Darfur state.

XVEVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
METHODOLOGY
3 DFID Approach to Value for Money, July 2011.
The evaluation was an ex-post outcomes and impact evaluation of the humanitarian action delivered by UNICEF and partners in addressing the needs of the population affected by emer-gencies in North Darfur. The evaluation used the utilization- focused approach where the intend-ed users of the evaluation were identified and engaged in the design of the evaluation TOR and tools from the onset. This was enhanced by putting in place a technical committee from the ministry of education, Health, Nutrition, water and social services from the Government side. While from UNICEF there was engagement of UNICEF PME and Senior management team in the evaluation process. The quantitative analy-sis is built on the already existing reports from previous Household Surveys conducted during the period under review (2010 – 2015) mainly MICS 2014, S3M 2013, SHHS 2010, Routine Statistics of Sector MIS (for example, routine data related to health services) and Community Village Survey Data. Data on programme imple-mentation related to Services Delivery (Supply and Cash) and achieved Outputs were extracted from UNICEF internal financial reports. Trends Analysis was conducted in order to assess progress made vis-à-vis base line indicators as captured in UNICEF annual work plans. Quali-tative data was collected from various project stakeholders through individual interviews, Fo-cus Group Discussions with key beneficiaries (children aged 8 - 12, parents, caregivers and service providers), and community members. The cost effectiveness analysis focused on the cost of achieving the intended programme ac-tual outcomes. The analysis of financial data,
including budget allocation, utilisation by out-comes and sector result area was initiated to compute the cost effective analysis as outlined in the DFID value for money framework3.
Evaluation Limitation and Challenges1. The initial scope of the evaluation included
education and child protection program-ming, but this was excluded from the evaluation in a revised TOR. The new TOR focused mainly on child survival and cau-sality of under 5 child mortality rather than on overall humanitarian programming of UNICEF in North Darfur.
2. Since this was a multi-stakeholder pro-gramme in a high-risk area, politically sen-sitive and a complex operating context, it was at times challenging to get a consen-sus on the evaluation from all stakeholders, both at federal and state levels. However, an agreement was finally reached in moving forward with this independent evaluation for the purpose of learning.
3. With the change of the UNICEF financial management system from “PROMS” to “VISION”, the performance data both finan-cial and programmatic in terms of reports, could not be accessed easily. Therefore, the assessment of progress between 2011 and 2012, were completed with difficulty. UNICEF should link the old IT system and the new IT system to ensure that future analysis more focused on financial audits against programmes can be undertaken effectively.

XVIEVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
4. The consultant had envisaged availability of routine data at locality level, but the rele-vant Government and UNICEF offices in El Fasher were unable to provide the data at locality level. Most routine data collected are at state level, hence the team analysed data generated from both the household questionnaire and the Focus Group Discus-sions (FGDs) in the different localities.
5. The prevailing circumstances of the emer-gency in these regions are characterised by conflict, hence respondents and FGD par-ticipants required the utmost confidentiality. The team found it prudent not to take the names of the some community members
who participated in the FGDs, but kept the cumulative number of the participants for accountability purposes only.
6. During the data collection exercise mainly for FGD and household (HH) questionnaire, some households which experienced the death of a child before the exercise and therefore did not have an under 5 child present, were excluded. The risk of this ex-clusion is a potential underestimation of the number of child deaths during the five years covered by the evaluation – however 14% of HH have experienced at least one case of U5 child death within the HH during the last five years.

XVIIEVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
SUMMARY OF FINDINGS
The details of findings presented for each uni-versal evaluation’s criteria are well developed within the content of the report. The following are the important points highlighted around those criteria, for easier learning about strength-ens and weakness (shortfalls) of the Humanitar-ian Action for child survival during the last five years (2010-2015).
The summary of the findings on best practices (what worked) and for whom 1. UNICEF WASH, Nutrition and Health hu-
manitarian programmes are relevant and ap-propriate to the needs of targeted displaced and affected population. The programmes contributed to the Sudan Government’s poli-cies in humanitarian programming, focusing on Health, Nutrition, Water and Sanitation at sub national level (state and community).
2. In terms of coordination, UNICEF ensured that it effectively met its obligation as a clus-ter lead for WASH and Nutrition by ensuring that there were strategic engagements in planning at the North Darfur state level. This ensured that there was no duplication of activities among the humanitarian actors. UNICEF led and coordinated inter-agency needs assessment mainly for WASH, while for Nutrition there were periodic nutrition-al status assessments to inform program-ming. UNICEF led the contingency planning process, which is a key preparedness tool for the WASH and Nutrition Clusters at the state level.
3. Regarding efficiency, UNICEF demonstrated the comparative advantage of being pres-ent on the ground through the existence of a fully functional field office (staff and logistics), the pre-positioning of supplies at state level within the warehouses of line ministries and UNAMID team sites, strong partnership with Government counterparts and existing signed agreements with NGOs/implementing partners.
4. UNICEF in 2016 strengthened its capacity for programme field monitoring at the field office (FO) level, through the establishment of Third Party Monitoring. This ensured in-dependent assessment of the effectiveness of service delivery, due diligence and im-plementation of financial risk management through HACT at state level, while capaci-ties for information management in support to sector cluster coordination was strength-ened in Khartoum. However, there is a gap in North Darfur.
5. Efficiency of the UNICEF humanitarian programme between 2010 and 2015 was achieved for vaccination and nutrition treat-ment services for acute malnutrition - re-sulting in about 85 percent achievement of the planned outputs.
6. On effectiveness, UNICEF has been able to ensure increased coverage of nutrition services for treatment of SAM over the last five years, including screening and referral of cases to nutrition services centers.

XVIIIEVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
7. The effectiveness of UNICEF’s humanitarian programming in terms of ensuring a sus-tained outcome was observed in health services for preventable diseases, mainly in urban and peri-urban areas, as well as in the increased number of children admitted for the treatment of SAM.
8. Concerning impact, health programming contributed to the reduction of vaccine pre-ventable diseases by ensuring increased immunization coverage of up to 90 percent in North Darfur. Nutrition programming con-tributed to the stabilization of the Global Acute Malnutrition and Severe Acute Mal-nutrition rates, though the malnutrition bur-den remains at double the 15 percent WHO emergency threshold.
The summary of the findings on challenges (what did not work – shortfall in results)1. In terms of relevance, UNICEF’s interven-
tions in the state focused mostly on IDPs, refugees and populations affected by disas-ters and did not cover the needs of host communities, which represents an equity gap for children living in the poorest and most vulnerable communities.
2. The inter-cluster coordination (for example, WASH and Nutrition) was found to be weak at state and community levels. Joint plan-ning for these clusters were carried out on a quarterly basis in North Darfur while in South Darfur, joint planning was implement-ed on a monthly basis. At the community level, there was no evidence of contingency planning processes or a joint inter-cluster implementation plan in North Darfur. In ad-dition, the situation monitoring and infor-mation management is weak at state level. If strengthened, it could potentially ensure
adequate sector cluster coordination and multi-sector integrations as seen in Khar-toum.
3. UNICEF was found to be efficient in supply delivery. However, partners, both Govern-ment and NGOs expressed concern about UNICEF’s delay in the finalization of part-nerships and cash disbursement, especially within the context of the agility of response required within 72 hours after the occur-rence of an emergency.
4. The leakage of humanitarian supplies due to the lack of an effective supply chain man-agement and end-user monitoring, the low coverage of basic services to all the affected areas, poor cold chain management prac-tices, and low involvement of the affected population in programming to promote ownership, constitute high risk barriers to achieve expected outcomes and impact for children. The continuous leak of UNICEF’s plumpy nut into the local market has affect-ed the efficiency and effectiveness of the Nutrition programme’s ability to reduce mal-nutrition cases in a cost effective manner. The evaluation also recorded the leakage of WASH supply items based on the ben-eficiaries and partners’ comments. Part of the distributed soap, water jerry cans and tarpaulins were being sold in the local mar-kets in North Darfur.
5. High administrative costs of up to 48.5 per cent (including operating cost of partner-ships with NGOs) has challenged value for money and results for children within the health and nutrition programmes in North Darfur, as compared to the improved child health indicators in South Darfur with less investment, due to a number of factors in-cluding lower administrative costs.

XIXEVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
6. Due to the lack of funding for capital invest-ments in new WASH facilities, the planned expectation with WASH and preventive Nu-trition programming recorded low perfor-mance, (less than 50 percent), in terms of translating the planned supply-based inputs into outputs. There is more investment in South Darfur in term of WASH programming (but WASH interventions are weak in North Darfur) however, investment in health and nutrition are higher in North Darfur. WASH humanitarian programming between 2010 to 2015 were largely below expectations in terms of ensuring adequate coverage and sustained access to water and sanitation services both in schools and among the af-fected population. UNICEF staffing for the effective delivery of Nutrition and WASH in North Darfur was low. For instance, one in-ternational staff supported Nutrition, Health and WASH programming, resulting in poor supervision of the implementing partners.
7. Low coverage and poor quality of health ser-vices in rural areas resulted in the outbreak of measles within hard to reach commu-nities and localities in 2014 and 2015. The poor cold chain management practices at the peri-urban and rural areas affected the sustained control of vaccine preventable diseases.
8. The weak linkage between the programme management of child severe acute malnutri-tion and moderate acute malnutrition, high open defecation practices and high number of diarrhea cases and malaria, contributed to continued high prevalence of child mal-nutrition in North Darfur.
9. The humanitarian action did not show any contribution in terms of the reduction of malaria cases and the uptake of the use of
long lasting insecticide treated nets among children under the age of five. Weak pro-cesses for the provision of quality vaccines and enhancement systems, particularly cold chain equipment that were substandard in rural areas of North Darfur, contributed to concerns about the effectiveness of the vaccines being used in those areas against diseases.
The summary of the findings on the impact of Lifesaving Humanitarian Action for children1. On the impact of lifesaving Humanitarian
Action on children, persistent insecurity, high levels of wasting prevalence among under-five children in North Darfur, high prevalence of diarrhea and increasing cases of childhood illnesses, provided evidence of high mortality risk for children over the last five years.
2. Despite efforts by UNICEF to achieve sup-ply-based outputs, the increase of under-five mortality in North Darfur over the last five years (2010-2015) represents a result gap in humanitarian action to improve the situ-ation of children in the state. Key contrib-uting factors include protracted conflicts/insecurity, weak health systems and inade-quate adoption of family practices for child care. The current strategies and narrow scale emergency focused supply-based in-vestment from Government, UNICEF and partners are inadequate to ensure tangible life-saving impact for children because of the sheer magnitude of displacements, food insecurity, child morbidity caused by persistent conflicts, increased child mal-nutrition, outbreak of diarrhea (due to poor hygiene practices), pneumonia, drought or other public health-related hazard.

XXEVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
3. Concerning sustainability, due to limited human and financial resource capacity of UNICEF, inadequate technical capacity of implementing partners to effectively ensure the delivery of quality services to the affect-ed population, declining donor funding and the poor involvement of the affected popula-tion, UNICEF’s current humanitarian actions within the protracted emergency crisis (13 years) in North Darfur, are not sustainable.
Recommendations for UNICEF 1. The current administrative cost of up to 48.5
percent is on the high side and UNICEF should institute innovative strategies of partnerships in order to minimize the ad-ministrative/ overheads costs.
2. Institute an independent audit to examine and document the extent of the leakage of plumpy nut, water jerry can and soap, and UNICEF must take immediate measures closely with the Government to eliminate the leakage of supplies and commodities in order to increase the effects of outcomes for children.
3. Strengthen and extend the supply chain management system beyond the state lev-el by ensuring the delivery of commodity to beneficiaries at community and locality level complemented with an effective recording and documentation system.
a. UNICEF needs to explore the engage-ment with private shop owners as av-enues for distribution of therapeutic plumpy nut, mainly in the hard to reach areas where the shops are the first point of reference for assistance at the com-munity level.
b. Branding and visibility of relief items mainly water jerry cans and plumpy nut
should be explored to minimize the leak-age of such items.
c. c. As noted in South Darfur where there is an elaborate policy framework in han-dling humanitarian leakage, UNICEF should lobby North Darfur state Govern-ment and the national Government to enact policies criminalizing the sale of therapeutic relief items.
4. Promote a multi-sector integrated pack-age of interventions at the community lev-el starting from the programme planning stage. UNICEF should promote equity in delivering basic services (Health, Nutrition and WASH) to affected populations and host communities.
5. Revise the supply-based strategy focus of humanitarian actions and explore the introduction of cash-based programming (safety nets) and the strengthening of so-cial protection systems, in order to enable the affected population effective use of Health, Water and Nutritional Services and assure the sustainability of gains of results. UNICEF must also clearly outline its roles of evidence-based policy advocacy to leverage adequate Government investments to scale up the equitable coverage/access and the quality of social services.
6. Strengthen the State Ministry of Health’s capacity to ensure effective and efficient management of vaccine cold chain at the locality level in order to secure the preven-tive strategy.
7. Strengthen the capacities of communities to ensure the maintenance and sustainabil-ity of basic services with a clear capacity building strategy.

XXIEVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
8. Strengthen the primary health preventive and care systems through adequate tech-nical and financial support to scaling up MNCH and IMCI, which could contribute to improving the quality and demand of health services and reduce child morbidity and deaths – beyond humanitarian or emer-gency response.
9. Enhance inter-sector/cluster coordination within UNICEF, mainly at implementation level, focusing on the community/locality level. UNICEF should also strengthen the situation monitoring and information man-agement at state level to better prioritise the agility of response to emerging vulnerable situations.
10. Strengthen Communication for Develop-ment in order to address the magnitude of inadequate practices of sanitations and hy-giene; UNICEF should sensitize the affect-ed population, specifically the mothers and caregivers on not referring to plumpy nuts as “Biscuit”, but as a therapeutic product for treating Severe Acute Malnutrition.
11. Strengthen the documentation and infor-mation management within UNICEF key Sections.
Recommendations to the Government of Sudan1. The Government is recommended to accel-
erate the recruitment of medical doctors, nurses and midwifes or clinical officers for community level health facilities that will en-sure the quality and use of health services.
2. The Federal and State Ministry of Health should improve the health early warning system for North Darfur to reduce disease detection time and establish a robust anal-ysis mechanism.
3. The Federal and State Ministry of Health should assess and improve on cold chain management in North Darfur.
4. State Government officials should establish a legislation that criminalises any sale of hu-manitarian supplies and commodities, par-ticularly those used for therapeutic needs of the children (Plumpy nut) using the best legal practices in place in South Darfur;
5. The Federal and State Ministry of Health should explore ways to improve access to the vulnerable population by humanitarian agencies mainly for the hard to reach areas where the humanitarian need is high.
6. Government and all other parties in conflict should continue with the ongoing efforts to end conflicts, establish a final peace agree-ment for the restoration of hope for human well-being and dignity of the deprived pop-ulation and vulnerable children of North Darfur, and break down the vicious circle of violence.
7. The Government of Sudan and state Gov-ernment, as well as other stakeholders in-cluding UNICEF, should develop a mecha-nism for the establishment of a safe corridor for delivery of humanitarian services and goods to the affected population in crisis prone regions and areas.
8. The engagement of Government and stake-holders in favour of durable solutions for peaceful social cohesion, recovery and de-velopment, represents the hopes of the population of North Darfur and the gen-eration of children that have had to live in camps for many years without any perspec-tive (unfortunately, many cases of suicides are recorded).

XXIIEVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
Recommendations to Partners1. The achievement of the global transforma-
tive agenda of SDG 2030 n Sudan “no one left behind prosperity; dignity and access to basic human needs” requires an increase of financial investments for scaling up multi-sector interventions. Donors should reverse the decline curb of financial assis-tance to humanitarian action in Sudan to avoid any additional loss of children’s lives as observed during the last five years in North Darfur, for reasons such as child malnutrition and preventable diseases.
2. The establishment of durable solutions to ensure sustainable gains in the context of protracted emergency, represent the new direction of strategic reflection and invest-ments of partners to ensure the continuum of Humanitarian to Development (building resilience, recovery and development).
3. Donor support for ending conflicts and achieving the Peace agreement in Sudan is the ultimate hope for the vulnerable popu-lation affected by a protracted 13 year con-flict, which represents a source of external emigrations and persistent violence.

1EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
1. INTRODUCTION AND BACKGROUND
© U
NIC
EF/U
NI1
6579
8

2EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
1. INTRODUCTION AND BACKGROUND
4 Food and Agriculture Organization, Land Cover Atlas of Sudan, FAO, Rome, 2012.
5 The National Council for Strategic Planning General Secretariat, ‘The Twenty-Five-Year National Strategy 2007-2031’.
6 United Nations Office for Disaster Risk Reduction, ‘Sudan: Basic Country Statistics and Indicators (2014)’, PreventionWeb, UNISDR, <www.preventionweb.net/countries/sdn/data/>, accessed 8 March 2017.
The Sudan is a semi-arid country situated in the Sahel region that is characterized by low precip-itation, water scarcity and a short agricultural season (three to four months). It is one of the largest economies and most populous coun-tries in Africa, with 37,964,306 million people. However, drought in the country is a recursive phenomenon, with frequent cycles that extend over two to three year periods. Out of the coun-try’s total area (1.87 million square kilometres), 1.13 million square kilometres (60.2 per cent) is desert and semi-desert, while the remain-ing 0.687 million square kilometres (39.8 per cent) is divided between low-rainfall savannah (300–500 millimetres of annual rainfall) and rich savannah (more than 500 millimetres of annual rainfall).4
The impacts of climate change are evident throughout the Sudan. Rainfall records from El Fasher, North Darfur, show a marked drop be-ginning with the 1972 drought. This is a more compelling indication that droughts have be-come more frequent, with 16 of the 20 driest years recorded in the region occurring since 1972. Various climate change models also pre-dict a reduction of more than 20 per cent in the length of the growing period between 2000 and 2020.
Apart from the drought, the Sudan continues to experience humanitarian challenges due to armed conflict that has led to displacement and food insecurity. The country also grapples with an influx of refugees from neighbouring and regional countries, and international economic sanctions have hindered the achievement of the 25-year National Development Plan.5 Addi-tional hazards that have increased disaster risk within the Sudan include flooding (73.2 per cent frequency of occurrence), earthquakes (4.9 per cent) and storms (4.9 per cent).6 Outbreaks of animal and human diseases are also among the key natural hazards affecting the Sudan.
1.1 Humanitarian situation in North Darfur
Darfur is a region affected by conflict and secu-rity concerns. Simmering tensions throughout the 1990s exploded into conflict in 2003, as self-defence groups militarized into armed re-sistance and initiated a significant conflict that affected Darfur for more than 12 years. This re-sulted not only in the internal displacement of some 1.7 million people, but also caused the influx of 280,000 refugees from western Darfur into Chad. The entire population of Darfur—ap-proximately 8 million people—were affected

3EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
l
l
l
l
!!!
!!!!
!!!!
!!!!
!!!!
!!!!
!!!!
!!!
!!!
!!!
!!!!
!!
EL TINA
EL MALHA
KUTUM
MELLIT
EL FASHER
EL TAWEISHA
EL KUMA
UMM KEDDADA
KALIMENDO
EL SIREAF
KEBKABIYA
DAR EL SALAM
SARAF OMRA
Anka
Gabir
Tabit
Sabun
Galgi
Bahia
Khamis
Kulkul
MuzbatBamina
Wakhaim
El Lait
Um Lyon
Um Sidir
Sarafaya
Furawiya
Ana Bagi
Abu Delek
Um Eshera
Abu Sakin
Saq AlnyamAbu Zerega
Sani Karaw
Abu Sufyan
Ed Al Beada
Tarny North
Shegeg Karo
Baashim/tina
Abdel Shakur
Um Gullah Haj
Sigeir Umm Sa Shaqq Al Huja
Hashaba North
Kuma
Tina
Malha
Korma
Kutum
Tawila
Saiyah
Mellit
Karnoi
Umm Baru
El Sireaf
Kebkabiya
Fata Borno
Saraf Omra
Umm Keddada
El Taweisha
Ed Al Nagab
Dar El Salam
Birkat Seira
Kafod
Burush
Wada`ah
Shangil Tobay
El FasherOm
Ogr
Ali
Mou
Kur
Kom
Kil
Ali
UruUru
Ini
Sir
Dus
Zur
Eijo
Argi
Jaur
Asad Gaal
DifaTulu
Fado
Geri
Kosa
Juma
Debs
Dady
Saby
Tora
Tina
Tega
Mara
DugoDali
Kona
Tega
DaliNima
Madu
Fazi
Uama
Wiza
Sita
Meli
Madu
Gawa
Elwi
Ebni
Atri
Arid
Idda
Deen
Mado
NairSaya
Fonu
Dawa
Buly
Amou
Sole
Neni
Disa
Naro
Miki
Jaco
Fazy
Wama
Golo
Kamu
Tuji
Treh
AmboLill
Eima
Luti
Kuri
Jung
Boba
Dade
Hara
Wadi
Dibl
OwryNumu
Bouo
Kury
Giri
Eima
Auro
Maya
Zonar
Surgi
Da Ud
Hatan
Tulul
Adrur
Lugdi
Alhja
Magun
Imeka
BeeizGaour
Turug
Tahir
Usban
Zirug
Godat
Kadja
Gragf
Finga
Timoa
Katur
Jense
Habir
Nijou
AraraDally
Abiat
Dalil
Dirma
MaralUtashKullu
Toftu
Grida
Ashab
Tosal
Warta
Sersa
LabdaKraty
FasorEkibo
Deldi
Amara
SindyHasan
Birto
Malet
Kenin
Janga
Kursi
Karka
Jabir
Hamra
Eldah
Durum
Dobbe
Bumyu
Kuron
MadelBiery
Wedja
Dekly
Elong
Masri
Bauri
YunisTurdi
Kunga
Irgie
Gerfu
Ahmar
Yonka
TurraGanbu
Jafal
Nimra
Miski
Laban
DarmaDabai
Arnap
Basao
Turba
Oriri
Murha
Matar
Lukka
Lauda
Kolbe
Harun
HajarGirbu
Gedil
Ebbei
AmmarMaylo
Shoba
Farik
Kingo
Fajaj
Dadee
Conya
Souko
Birmo
Affia
Talha
Gelli
BerdySenjo
KaiguFaggu
Ghetis
Tindil
Kenana
Angero
Marega
Mugran
Sereif
Batran
Bulgar
Zarafa YafilaSheiga
Satiha
Safaye
Tagali
Hafara
EfeeinKorbat
Shadad HafaraUm Dul
Martei
Hazama
DubakhLayuna
Karkur
Humayr
Hazeil
Hazama
Daqqaq
MonjarSa`dan
Fagarg
Bonsor
BasigaKabire
Faguri
KurulaKegilo
Khalil
Bashem
Lakadi
Katkoq
Harmal
Bashum
Watoto
Umraha
Selibo
MinnerMellit
Bomadi
Hariga
Bakhit
Baabai
DeremaOstani
KumbudKhitir
Insuru
Deleba
Jeffom
Birdik Diyori
Gadara
Um Rai
KuwaynGibsra
Al Dor
Dirrah
Bilala
Djenge
Jakoha
Fyresh
Alf Mr
Lwabit
Zamzam
Um DamKasanm
Shagra
Djenge
Mirkan
Kornoi
Naeima
Tululu
Azawia Karzwa
Tamaru
Kobbai
Kutuba
HamrahSangor
Kurbia
Qumqum
Orschi
Nagoba
Komora
Hajjak
Geidri
Gabera
Kalkal
Aramba
Kallah
Kaoura
Taurei
Morgeh
Konjar
Bisaron
Hdadyat
El Hara
Kendira
Marsoos
El Foda
Dogeshi
Al Biri
Sheshat
Um Gafa
Kharlif
Kerfees
El Naim
Saffaha
Um Kuda Kharrat
Farshah
Dardaqa
Alawana
Layon E
Keybeir
Kalmena
Monguri
Fingyar
Khamsat
Gambara
Um Atam
Firaiwa
Al Alim
ShalkhaHarhasa
Umsiyal ShekaraMassala
Laskeny
Gadarib
Jawahir
Siladop Masimbo
Marmedi
Bakhita
Wertiba
Wargean
Umbella
Markisi
Elnusub
MartagoMajetti
Siladop
Gosappa
Birmaza
Bakaore
Serreih
MukhtarGerasam
Manzula
AbuzaraShagera
Jakho I
Majdoub
Um Lyun
Manzula
Helelia
Shabaki
GasimbaKerwagi
Kaorika
Kirinik
Furawia
Juktora
SibiggaShigaibLobbodo
Gurbura
Golabai
Gassana
Gantura
Tombare
Deley 1
Tuilliu
Heijliej
Shahakha
El Helif
Bandarbi
Al Atrun
Abu Giri
Um Ridim
Um Araba
Um Freha
Um Kitra
Abu Odam
Wad Kota
HulaylahDubaybah
Taweisha
Umm Hosh
Abu Doma
Um Hawsh
Meshawar
Umm UrufUmm Gola
Um Laota
Taradona
Markassa
KerkarelKarkersa
Barakara
Tebeldia
Qawz Nai
Al Arais
Jakho Ii
Moubabel
Um Dalil
Munyiner
Al Dirra
Al Kiber
Kabkabia
Khudayra
Abu-liha
HilaliyaJurajeew
JarbokeyKirekise
Hirikula MatbettiBetbethi
Hamar Fa
Abu Leha
Ternowda
Um Haraz
Shibarni
Musteria
Kaidebba
Tilingue
Fiabuggu
Wadigarad
HainassurElnazehin
Targambot
Jam Bagly
Tamoleika
Dar Deifa
Um Bayada
Umm SidraEl Abyiad
Um KereinUm Habila
Um Gafala
Um EreidaSadenahamHegeir Fo
Um Muherr
Um Hashab
Umm DarbaUm Tartar
Ghannamah
At Tulayh
Um Daraba
Haskanita
Um Fanato Um DarabaGhubeisha
Um Kafall
Hilla Que
Abu Tango
Sari Town
Um Silelo
Um Haglig
Al Jazera
Sany Haya
Um HegligAbu Kuraa
Sangerfut
Boshareia
Garrah Za
Um Kitoro
Abu Gamra
Niarshige
Misteriya
Birijango
Ein Bessar
Helif Sany
Jabel Eisa
Wadi Osher
Wadi Hadid
El Mashura
Um Shanqah
Widn BaridUm Higeina
Umm Katkut
Eiyal Amin
Umm Shawir
Um Qantura
Um Hijarah
Um Gurraba
Dar Hammad
Umm Kagaya
El Mashrot
Hillet AliWad Balila
Um Qawzayn
Korma Bier
Amushadiga
Abu Shakor
Daym Qarad
Abu Sikkin
Um SumeimaUm Marahik
Al Sheriff
Dangulolbe
Gubarshige
Bi'r Sindi
Adam Bawsh
Amar Gedit
Jebel Hilla
Sag El Naam
Um Burayrah
Fadl Es Sid
Wadi Gellab
Abu Gileiha
Jebel Banat
Hillet Omar
Um Khutayla
Deleba Bowa
Bowa Turmes
Debus Weiki
Ed El Kheir Um Mahareik
Tui Village
Karoya LabanUm Ghabeisha
Abu Kulaywat
Zarqa Hadida
Unknown Name
Kahsab Donky
Donki Shatta
Terh (miski)
Unknown Name
Unknown Name
Damra Siriba
Wahat An Nukh
Shag El SimiaShag El SimiaShaqq An Nimr
Qawz Adh Dhi'
Bahar Um DurmTebeldiya Wan
Tawm Bisharah
Shaqq El Khad
Birish Malyan
Al Higair AliHashaba South
Umm El Hussie
Shaq El Gamous
Jajuor (aluna)
Bobayi Tawiesha
Ali Shams Eldin
Abu Gau Al Hillet
Serief Ben Hussein
Nyala
Zalingei
El Geneina
Dei
Arid
Duma
Limo
Kalu Dilu
Arga
Suni
Silo
Tono
Dago
Murr
Diri
Kuka
Madi
Luma
Agra
Dauro
Qubba
Tumbo
Dashi
Seilo
Tumko
Buddu
Kaira
Kurgo
Seyeh
Korei
GudaiNureiGuldo
Kurbi Gyaga
Gulli
Balla
Oubbe
Nyama
Kulme
Djiri
Dalia
Kagko
Kurto
Lerwa
Gafalu
SineitBuhera
Karbab
Zulata
Tangya
Shurab
Labado
Taisha
Baddal
Ludung
Ballah
Seingo
Keikei Baraka
Saheib
Mogara
KubbumNurlei
Sigiba
Dankud
Djedid
Kourro
Korare
Dogoum
Godoba
DeleigBurburTanako
ArtalaDeimboAmbara
Tetene
Shearia
Um Boim
Gulobei
Garoula
Solwong
Shuwayy
Girgira
Bardani
Gosmino
Kondobe
Derjeil
Korgusa
KirarowBuronga
Lasirei
Gartaga
Gertobak
Beringil
Kalamboa
Mabrouka
Bajouggi
Um Sarir
Goldober Singeiwa
Falankei
Taziriba
Mingyeir
MargibbaDuraysah
DeirirroFongfong
Kasoleri
Uraydimah
Tebeldina
Gostoweir
Abu Gheid
Manawashi
Qawz Baya
Um Kurdus
Damba Agi
Istereina
Abd Allah
Asandalou
Futajiggi
Wad Hassib
Muhajiriya
Tandubayah
Abu Rumayl
Gami Filli
Burbu Basi
Amar Gedid
Wad Bandah
Umm Shalkha
Kazanjedeed
Al Muturwed
Nyangadoula
Zulumingtong
Hagar Jembuh
Shaqq Al Gawa
Abd Allah Bas
Ghubaysh
Abou Adid
Hamrat El Sheikh
Wadi How
ar
Wadi el-Ku
Wadi Azum
Wadi Barei
W
adi Simdu
Wadi Al Khadari
Wadi S a lih
Wad
i Tarai
Wadi Gimri
Wadi Bulbul
Wadi el-Qubbah
Wadi Kej
Wadi Samir
Wad
i Mur
raya
Wadi Hawar
Wad i Fug
ama
Wadi Gweira
Wad
i alG
halla
h
Wad i Mah
ba
s
Wadi Derrion
Wadi Aradeib
W
adi Kolongei
Wadi U
mmSaqqat
Wadi Bugbug
Wadi Bahai
Wad i Abu Sant
Wadi E
l Malik
Bah
r Azoum
Wadi Debarei
Ouadi Kadja
Wadi Hawar
Wadi Bulbul
Wad i Bulbul
Wad
i How
ar
Wad
i Fug
ama
Um
Tuu Aya
Nur
Bom
UmaOda
Mob
Aro
Umu
UluKia
Aja
Tay
Dur
Sow
Tulu
SumoSebi
MoroKude
Kara
KairBoga
King
TaluLugi Jawa
Gubu
Doal
Kuka
Arto
AtulBadi
Kuma
DumaYara
Adwa
Uyer
YoyoAmer
Alda
Ehda
DulaMila
Dugu
Yara
MusiMora
Madu
Firo
Erli
Dami
Bori
Dugo
Guba
TuwaLuko
Kebe
NimaDogi
BuliMaow
Aybo
Fidi
Tiru Nari
Miro
Kudu
Juba
Muku
Diri
Arwa
AdarAabu
Sani
Ieta
Giya Buri
LimaAtro
FogiSisi
Krow
JetaHabi
Atia
Kure
Ryad
Oyur
Lita
Gale
Buli
MariMari
Daya
Wara
Towa
OlowDayaSisi
Abun
Saga
Kuda
Thur
Kuja
DomoMali
TuluToraTolo
KosaDalw
UrdiSuluMara
Gara
Fufu
SobaMisa
DodoMali
Gara
Fura
Uyur
Sala
Gobe
Zare
SojaSede
Kulo
Firi
Fere
Faya Baja
AndiOrdoBela
Beja
Gusa
Fosa
Komo
Amar
YuyuYoya
Buru
Dasa
Buru
Bala
Dina
LulaKure
KoreFado
Tama
TiroSigi
Roto
Saka
ManaMamo
Holi
Eina
Buta
DomiAris
Foga
TumboTolly
Tabla
Norma
Golol
DueruBarri
AbbasSarra
Kutee
Koyee
Auwla YiodiRodotMerla
Dumay
RhyllDerar
DomaiHalaf
OtashZawia
TaggaKurru
SuraaKarko
Dubah
Agara
Baide
Telua
Wanjo
Sulba
Manga
Ganjo
Tangi
Sarah
Endur
SlethHeger
BagerChawa
TarriNango
Jukka
GideiGhula
Debla
Ishma
Anoor
Dibis
Sulil
Fedwa
Kalmo
Abrum
Turri
Terta
Tarli
Sulli
Meija
Komda
Tebol
Kirwa
Nyama
Daura
Turba
MortoBeldo
Leiba
Teiga
MalamKeila
Hijer
Galdi
Kalma
Yuruf
Tomat
Domia
Afona
Mayok
Hajer
DwanaCookaRahma
SeleaKasib
Barka
Jibal
Mansi
JogarKerli
Wadmi
Kosti
Misig
Shano
Murer
Gandy
Mukku
Buddu
Gandi
SaniaTawil
BardiBatro
Birdi
Ma`unChref
AtmurAbaka
Selea
Agara
KorniJeruf
Diiba
Falko
Arafa
SirbaKouta
Kosti
Zeina
Kongi
Dadei
Borta
Adarr
TirtoLiria
Gokar
KalgoAmara
FassiDuana
Tella
Kurra
KulaiTurra
Kurra
Kongi
Mandi
Arkis
Rouko
FunduGorne
Dungo
Senga
Kibli
Bokoj
Bardo
TulusTulus
KoukeKolmeKarti
Morai
TerejLulan
Dorty
Fohab
Salca
Iriji
Jakok
AmedaAmara
Targo
Sunga
OmeriNyima
Borda
Niesa
Barda
Korun
TouroMindo
Zelou
IuourDebee
BarsaTamorDelli
Sirri
Tamer
Soujo
Kenyo
JagniWeigoDeiro
Darsa
Nurly
Bogog
FortoDenow
Sarow
TendyMorol
Balda
Kubuk
Geger
Tulil
Enene
Karbi
Erbee
Kirbi
Babel
Wadaa
Hamar
Barud
AmaraAdila
Gamal
Dagma
Lingu
Sagha
KanklyFuguli
Torray
Faluja
Negeha
Salama
MusaliJiddie
DapkarWasata
Warral
Sereif
Gabrok
El QozDangia
BarangYa`qub
Breiga
Um Rab
KornukBakrem
Kilkil
Ardeba
Futaha
Hamada
Tululu
Morgei
Halouf
Tibrei
BulbulMoraya
LabadoKudmel
Kalajo
Mujabi
Ashaba
Arbaha
Al Moj
SuneitQardud
OmareiKhummi
Fudulu Ereida
Daraba
Barkaz
Zaiafa
Kalagi
Bashom
Dukali
Barkaz
LajeitSeegayKidada
Zaleda
TawangLagaro
TergamLabada
Kalaha
Diyeir
Konjar
Edermi
Bumuye
BobajaDahaba
BielelYogoga
Hasaba
ZalataAmburu
Araok_
Kalkaf
Sakali
Tambra
Takaro
Dwonky
JogoteSeleahZerafa
Madany
Tutuma
Teirab
SakiniSakini
Moumou
Garess
Hereiz
Amasho
Bulbul
Talila
Loeiya
Merrih
Erenda
HabobaHaboba
Sinsin
Ambalu
Kasita
Shagug
Kurnye HarazaAdarib
Sangir
Daraba
Dankis
HarubaArafar
Ushara
Habila
HabilaDressaGafura
Artega
Rufeid
Karrak
GreidaKubuki
Fajara
Gadeir
Kafani
AgouraKakari
Celila
Aramta
Kirkir Andrew
Ballas
Ruvata
GurmulUrtula GreasaJaboun
Duroti
Ardebe Boldon
Talama
Tululu
Sauria
Tululu
Abinay
Kongye
Atomor
RevinaTaweng
Kabira
Nyango
Kolnge
Kirila
Brungo
Sambat
Durmei Boubou
Korney
Forsah
Fagora
Kordul
Keylis
Gangar
Jingev
Arumba
Gambra
Safary
Kajang
Denger
Ma'mun
Bonbol Sondol
Anbara
Bookoj
Dangai
Iseina Ardiba
Tundur
Bornal
Rosoli
Juguma
Kododo
En Nur
FaiyukMajrur
Kulayl
Hugeir
Humayr
Hamdan
Fofaya
Fanyer
El Ait
Dardog
DirrahTuwayr
Maarka
Galusa
Zankor
Shaluf
Tuluba
Kulwat
Kortula
Guilibi
Kurunji
SheariaKindiwa
Kilikil
GarnayaKamirah Bwaytel
KunjariHamouda
Ta'albaEl Nair
Shadidi
Korgati
Rimella
Khataba
ManansaGashtir
Dul Dul
Tergung
Taringa
Nyaldir
Wastani
KoronliDouggou
ShawaraHashaba
Banyala
Um Drua
Karonia
Durduma
Shadani Amabila
Touboum
Seldiro
Nyerlei
Aradeib
FigengaMabruka
SambalaSirsira
Dagrase
Tartura
Kafandu
Umm Jod
Ereredi
Gimmeza
Mastura
SitteibQanatir
Manjura MalalisKernoya
JucutumMourkou
Mararit
Habilah
Goronei
MukjajaKagolei
Khirban
Wastani
Girleli
Burunga
MardugaRumalia Waranga
Debenga
KabareiMurundu
Bugulay
Selenyi
Masmaja
Ambleng
Kafunga
Megatya
Korenga
Balbaso
El Daba
WustaniDamirge
ArdannaTuktuka
EldroutEl Umda
Tebeldi
SheheitManasraMaaglia
GhabishEl Amin
Abu Dik
Bernawi
Serambe
Khashum
Zakfero
Sharafa
Shalluf
Hanatir
Umm Bel
Kinyeir
Baldanga
Shanabla
Babu Nou
Um Luwai
El Erada
El Bobai
El Sahab
Morafata
Mershing
Tabajour
FergulliBurusini
El Melem
Um Gasum
Abardana
TokomayaAmranamaUm Ganah
Ed Debba
Rangatos
Qaradaya
Assibeit
Al Mairl
Sheigiba
Kushkush
Amrikena
KhashabaDar Zubi
Faragene
Majmeray Melmelli
Fujungur
Tongfuka
Fogadiko
Semongha Kammbuna
GaradaiaTirkeldi
Qawz Fil
Birganga
GallabatGallabatKolongei
Amjemena
Kaskeidi
Owha Awo
KosokaraQuarangaKorofata
Taykanga
Namatala
Jalkasim
Tigilden
Humaydan
Hujaylij
Duwaynah
Abbasiya
Umm Busa
Wad Bahr
Kileigau
GamaniyaUmm Sunt
Sarariya
Sakramoj
Umm Badr
Idd Agha
Kolo Bari
Khorsilla
Yourtobek
Dabanaira
Hela Dabl
Um Burins
Umm SerirWad Belal
Helakenin
Umm Ushar
Um Hojane
Ali Shumu
Tebeldina
DimlalaliDeleibiya
Kidingeer
Birkatuli
Fulenwara
Kusu West
El Kebiuo
Karo Karo
Muhajryia
Um Dursoh
Dar Marra
Koukoudja
Mouhaggir
Tougougou
Sina Sine
Baril Fur
Masteriha
Twil Dajo El HamariEd Dereis
Wad Murdi
As Samhat
Umm Shiba
Umm Ginah
Umm Dobia
Ritreirit
Eshangyei
Abu Dazza
Dam Gamad
Wad Salim
Umm Eidam
Umm Sunta
Umm Gerfa
Jubeil Tin
Abu Dangal
Sheq Jorab
Hillet ZumSheq Albur
Amarjadeed
Tingilanei
Gassa Sail
Shagabashi
Taha Tahan
Sheq Ahmed
Hila Beida
Dor Waning
Amarjadeed
Nyangadulo
Kaja-bagol
Bata Nasim
KeregkeregBurbur Fur
Ahmad Badw
Ingliterra
Ahmad Jabr
Abu Shatat
Umm Lebana
Umm Sayyal
Wad Ashqar
Foga Wells
Abu Gezira
Junga Jura
Abu Shawag
Ermil Post
Abu Shanab
Umm Leyuna
Umm HabilaAbu Kabisa
Umm Sughra
Umm Berbit
Tung Kittir
Surrmanjago
Taua Duldul
Um CardoussDangur Gebi
Idd As Sami
Kosormungia
Hillet Nuga
Nur Elsalam
Hajar Bagar
Abu Fawaghi
Umm Sagaaun
Umm Geleima
Wad An Naim
Ummat Arifa
Idd Al Arat
Zalat Jalil
Abou Shibeid
Domaya Temed
Saidah Aisha
Alban Jadeed
Hajar Jenadi
Idd Al Khala
Fatima Karol
Helat Hissen
Fag El Halla
Umm Aradeiba
Humayr Sibil
Tuleih Wells
Qawz Ar Rayy
Habisa Hills
Shaqq Hamura
Umm Inderaba
Bakkit En Nur
Kafran Kaulah Shaqq Al Bash
Dobo Madrassa
Debba En Nair
El Assir WestEl Assir East
Noor El-salam
Humayr Dirrah
Suqa El Gamal
Qoz El Merakh
Burg El Hizam El Bereigwiat
Qalat Al Wish
Zalat Al Hadd
Dalso( Kabeer)
Saraf El Saada
Sugat Al Jamal
Umm Gernanchok
Shaqq Al Qalti
Idd Abu Sufyan
Burg Er Riyasa
Qalti Al Adusa
Laqiya Arba'in
Talila Village1
Borbor Kajakssa
Humayr Ar Ru'us
Qurun El Ugeimi
Rahad Al Humrat
Qalat Al Hamra'
Ruhud Al Maykah
Sheinat Al Agha
Yaganang Musalit
Hamir Ath Thiran
Shabakati Ireida
Quraynat An Nimr
Hamrat El Sheikh
El Heitan Plateau
Ibrahim Wad Arabi
Qalti Umm Tasawir
Zarqa Gamal Ed Din
Qalti Al Khudayra'
Barqat Walad Hawal
Quraynat Umm Inderab
28°E27°E26°E25°E24°E23°E
20°N
19°N
18°N
17°N
16°N
15°N
14°N
13°N
12°N
SUDAN:September 2012
North Darfur State - Administrative Map
CHAD
NORTH KORDOFAN
SOUTHDARFUR
EAST DARFUR
CENTRALDARFUR
WESTDARFUR
NORTHERN
Disclaimer: The designations employed and the presentation of material on this map do notimply the expression of any opinion whatsoever on the part of the Secretariat of the UnitedNations concerning the legal status of any country, territory, city or area or of its authorities,or concerning the delimitation of its frontiers or boundaries.Final boundary between Sudan and South Sudan has not yet been determined.Final status of Abyei area is not yet determined.Production date: 16 September 2012 (VU,CIS, KRT).
State Capital
Principal Town
Administrative Center
Secondary Town
Village
Airf eld
Airport
River
Gully (Wadi)
Operational Railway
Non-Operational Railway
Primary Road
Secondary Road
Locality Boundary
State Boundary
International Boundary
Undetermined Boundary
N
Legend
SOUTH SUDAN
ETHIOPIA
ERITREA
CENTRALAFRICANREPUBLIC
CHAD
LIBYAEGYPT
SAUDIARABIA
Northern
Nile
North Darfur
Red Sea
North Kordofan
SouthDarfur
South Kordofan
Gedaref
Kassala
Sennar
Blue Nile
WestDarfur
WhiteNile
Khartoum
El Gezira
Red Sea
CentralDarfur
EastDarfur
AbyeiArea
Data Sources: Locality boundaries 2012 (Work in progress)Bureau of Local Government, El Fashir & Nyala, State Ministry of Physical Planningand Survey, El Geneina.State boundaries, 2012: Census 2009, www.sudan.gov.sd. Unverifed betweenWest-Central and South-East Darfur states.International boundaries 2007: Sudan Information Management Group IMWG.Settlements: OCHA, UNMIS, CBS. Hydrology: UNMIS. Transportation Network: UNJLC.
0 30 6015
Kilometers
Figure 1: Administrative boundary of North DarfurSource: Office for the Coordination of Humanitarian Affairs (OCHA)

4EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
by the conflict. Eighty per cent of refugees lost nearly everything they owned, and the liveli-hoods and social cohesion of other community members such as sedentary rural farmers, no-madic pastoralists, public sector workers and urban dwellers, were affected. Approximately 38 per cent of the total population of Darfur (3 million people) have received some form of monthly food aid in the past decade.7
1.2 UNICEF interventions in North Darfur
UNICEF has been working in North Darfur for the past 12 years, with a specific focus on pro-viding technical and financial assistance to the affected populations in six locations. Through the United Nations common humanitarian ap-proach, UNICEF has conducted its operations in close collaboration with other United Nations agencies, state officials, local authorities and host communities.
1.2.1 NutritionUNICEF nutrition management in North Darfur focuses on the integration of community-based management of acute malnutrition (CMAM) ser-vices into existing primary health care facilities to provide a full package of health and nutrition services (outpatient therapeutic feeding, sta-bilization centres and targeted supplementary feeding programmes) in one centre. This allows all beneficiaries, including those with severe acute malnutrition (SAM) and moderate acute malnutrition (MAM), to receive services in one place. To ensure an effective implementation process that will improve the quality of services for malnourished children at facility and commu-
7 2013-2019-Developping Darfur: A recovery and reconstruction Strategy; UNDP, Sudan 2013.
nity levels, the programme has enrolled State Ministry of Health staff, implementing partners and community-based workers in various skills enhancement efforts.
1.2.2 HealthUNICEF’s health interventions focus on tackling under-five mortality and morbidity by supporting the Government to adopt new implementation models designed to reach all vulnerable chil-dren, including those in inaccessible areas. The primary focus is on sustaining and monitoring interventions. In North Darfur, UNICEF provided financial and technical support to 97 health facil-ities (34 per cent) to implement the Integrated Management of Childhood Illness (IMCI) pro-gramme, which reached 33 per cent of children under 5. UNICEF supported the training of 240 health workers from 20 health facilities, includ-ing five from rural hospitals who were selected across the 18 localities. Through the training of community health workers in community IMCI, 42 per cent of selected communities in targeted localities initiated integrated community case management. UNICEF also supported the im-munization of 68,624 children (68 per cent), with each child receiving three doses of pentavalent vaccine and 59,542 children (59 per cent) re-ceiving the first dose of the measles vaccine. To strengthen Expanded Programme on Immu-nization (EPI) coverage, UNICEF supported six rounds of acceleration campaigns and two polio campaigns targeting 546,432 children.
1.2.3 Water, sanitation and hygieneWorking through implementing partners, UNICEF provided water, sanitation and hygiene (WASH) support to 422,650 internally displaced persons (IDPs) (82 per cent of the 517,000

5EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
people targeted, which includes 180,950 men, 232,650 women and 103,400 children). UNICEF support incorporates the construction of new water sources, the rehabilitation of dysfunction-al sources, and the operation and maintenance of motorized schemes and water trucking in emergency-affected hotspot areas. UNICEF also provided safe water supply sources to basic schools. WASH sector partners provided access to safe drinking water supply to 111,400 internally displaced persons (50,130 women, 38,990 men and 22,280 children). To prevent outbreaks of diarrhoea, in 2015, UNICEF assis-tance enabled the construction of 3,036 new la-trines and the replacement of damaged latrines (including the rehabilitation of 803 latrines) for displaced populations of North Darfur. With UNICEF support, 591,475 people (50 per cent women) in vulnerable areas, more than 100 per cent of the 270,000 people targeted, benefited from hygiene promotion messages.

6EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
2. PURPOSE OF THE EVALUATION
© U
NIC
EF/U
NI1
6585
3

7EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
2. PURPOSE OF THE EVALUATION
8 ‘Annual humanitarian strategic plans’ refers to a United Nations mechanism that pools resources for all United Nations agencies for humanitarian programming in North Darfur
The protracted nature of humanitarian program-ming in North Darfur, which spans more than 13 years, calls for more attention to the structural causes of malnutrition and ill-health. Underly-ing causes such as the ongoing conflict lead to continuous crises since they determine the amount, control and use of human, econom-ic and organizational resources that are avail-able to households and communities. As such, this evaluation of humanitarian action provides evidence-based results on the effectiveness, efficiency, impact and sustainability of WASH, health and nutrition interventions. The evalua-tion aims to contribute to an understanding of the root causes of child survival in North Darfur in the context of integrated malnutrition man-agement.
The purpose of the evaluation was to take stock of UNICEF humanitarian interventions from 2010 through 2015 to learn from the outcomes and impact and highlight the strengths and weaknesses of its contribution to reducing child mortality in North and South Darfur. The evalua-tion will contribute to evidence-based judgment and explanations for the met and unmet needs, as well as lessons learned from multi-sector interventions implemented in North Darfur and South Darfur between 2010 and 2015 in regards to saving children’s lives.
2.1 Objectives of the evaluation
1. Measure the achievement of the expected chain of results (efficiency/coverage, effec-tiveness and impacts) of the implementa-tion of the annual humanitarian strategic plans8 funded through emergency funds and implemented in North Darfur from 2010 to 2015.
2. Document the relevance, coordination and sustainability of the UNICEF humanitarian programme in North Darfur.
3. Generate explanations for the possible reasons for the sustained increased of un-der-five mortality, despite all efforts exhaust-ed in the state.
4. Assess how humanitarian programmes ad-dress the needs of host communities and internally displaced populations.
5. Assess the institutional, financial and op-erational capacities for better coordination, planning, implementation, management and monitoring and evaluation of humani-tarian action at national, state, locality and community levels, both of the Government and United Nations agencies (UNICEF).
6. Develop a theory of change of the inter-ventions implemented in North Darfur and identify the gaps.
2. PURPOSE OF THE EVALUATION

8EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
7. Document good practices, intervention chal-lenges, bottlenecks and solutions applied to overcome the intervention challenges by documenting lessons learned on what works for whom, what does not work for whom and why.
2.2 Key evaluation questions
Relevance/appropriateness
1. To what extent are UNICEF’s humanitarian programmes aligned to national humanitar-ian policies and the humanitarian response strategic plan?
2. To what extent does UNICEF’s humanitar-ian programme address the needs of the affected population?
Coordination
1. What is the extent of humanitarian pro-gramme coordination among various actors/sectors to avoid gaps or duplications at the community level?
Efficiency and coverage
1. Did UNICEF and partners have adequate financial and operational capacities to offer rapid delivery of services to affected un-der-five children in compliance to UNICEF’s Core Commitments for Children in Human-itarian Action?
2. Are the actions being undertaken cost effec-tively (best approach economically)?
Effectiveness
1. What were the achievements against the expected outcomes of the implementation of the annual humanitarian strategic plans
funded through emergency funds and im-plemented in North Darfur from 2010 to 2015?
2. What were the good practices, challenges, bottlenecks and solutions that contributed to the achievements or that hindered the realization of the expected outcomes?
Impact
1. What are the significant changes (positive and negative) that happened to children and communities because of UNICEF interven-tions?
Sustainability
1. To what extent are the interventions and their impact likely to continue when UNICEF and partners’ support is withdrawn?
2.3 Theory of change and conceptual framework for the evaluation
The evaluation of humanitarian action in North and South Darfur was based on the theory of change (see Annexes 1–3), which was devel-oped after review of UNICEF partnership agree-ments, UNICEF rolling work plans and UNICEF annual work plans, which are the key account-ability tools for humanitarian programming. Due to the integrated nature of WASH, health and nutrition programming, the theory of change had a common impact level indicator of reduc-ing child mortality to improve child survival in North and South Darfur.
The development of this theory of change also took note of the nutrition conception pro-gramme developed by UNICEF in 1990. This

9EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
concept outlined the key programmatic link-ages of sectors contributing to the manage-ment of malnutrition at the community level. The analysis of the continuum of progress and the UNICEF humanitarian delivery system, is
9 This conceptual framework was adapted from a value for money analysis for WASH programming is available at: <http://vfm-wash.org/wp-content/uploads/2015/08/OPM-2015-Synthesis-report-of-6-VFM-WASH-studies.pdf>, accessed 8 March 2017. Key definitions are as follows: a) cost: the financial costs of inputs as captured in the annual UNICEF financial estimations; b) input: the resources used, in terms of finance and staff time (capital and labour); c) process: the process by which inputs are transformed into results; d) output: the direct deliverables of the programme (number of water and sanitation facilities built, number of activities implemented such as borehole construction, etc; e) assumed outcome: resulting from the outputs, for example, the number of beneficiaries assumed to have gained access to WASH services because of the outputs of the programme’s interventions; f) sustained actual outcome: the actual change in the affected population’s lives over time, such as the number of new people moving from using an unimproved water point to an improved one. The key difference with ‘assumed outcomes’ is that ‘sustained actual outcomes’ was measured based on household survey data; g) impact: the impact of the WASH programme, including the impact on health and education, for example, reduced cases of diarrhoea, malnutrition and vaccine-preventable diseases over the past five years, as presented by the UNICEF Strategic Plan for the Sudan; h) equity: although equity was not a major area of focus, it was considered during various levels of the results chain, including at the level of inputs, outputs, outcomes and impacts. The affected population groups vary in many ways, depending on how inequity manifests itself, such as through differences in income, gender or social groups (e.g. agro pastoralist, pastoralist, urban dwellers, rural dwellers, children, etc.).
aligned to the United Kingdom Department for International Development value for money con-ceptual framework presented in Figure 2.
Figure 2: Evaluation conceptual framework adapted from Tremolet et al.9
2.4 Scope of the evaluation
The evaluation focused on UNICEF child survival programming (health, nutrition and WASH hu-
manitarian programmes) to address the main question related to the effectiveness of human-itarian service delivery in the 2010 and 2015 humanitarian programme cycle. The focus on
COST (US$)
• Amount allocated
INPUT
• WASH supplies• Nutrition
supplies• Health supplies• Labour
PROCESS
• Drilling boreholes
• Latrine construction
• Establishing a stabilization center
• Orgnizing immunization campaigns
OUTPUT
• Water facilities constructed
• Sanitation facilities constructed
• Stabilization centers initiated
• Health facilities offering immunization services
SUSTAINED ACTUAL OUTCOME
• Number of people receving water
• Number of people with safe excretal disposal option
• Number of children immunized
• Number of children treated of SAM
IMPACT
• Rreduced child mortality, reduced child wasting and stunting
• Reduce water related diseases
• Reduced malnutrition cases
• Reduced vaccine preventable illness cases among children

10EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
multi-sectoral responses in North Darfur also included the analysis of conflict effects, promo-tion of social cohesion and building resilience (empowerment of communities and families). The evaluation applied the Organisation for Economic Co-operation and Development-De-velopment Assistance Committee criteria, adapted for humanitarian action: 1) relevance (appropriateness); 2) coordination/coherence; 3) effectiveness; 4) efficiency/cost-effectiveness/value for money/coverage; 5) impact; and 6) sustainability/connectedness of humanitarian responses in North Darfur (as it relates to pro-tracted emergencies).
The geographic focus of the evaluation was on North Darfur state, targeting six localities (El Fasher, Kabkabiya, Kutum, Mellit, Saraf Omra and Tawila).

11EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
3. METHODOLOGY
© U
NIC
EF/U
NI1
6657
0

12EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
3. METHODOLOGY
10 The Development Assistance Committee criteria is available at: <www.oecd.org/dac/evaluation/daccriteriaforevaluatingdevelopment assistance.htm>, accessed 8 March 2017.
The evaluation was an ex-post outcomes and impact evaluation of the humanitarian action delivered by UNICEF and partners to address the needs of the population affected by emer-gencies in North Darfur. Thus, a retrospective evaluative design involving both qualitative and quantitative analysis was adopted. The evalu-ation employed both qualitative and quantita-tive methodologies to collect data from the stakeholders and communities targeted in the programme. It also took account of the Devel-opment Assistance Committee criteria10 and the United Nations Evaluation Group/UNICEF standards for evaluation. This approach focused on the relevance, effectiveness, efficiency, sus-tainability and impact of the programme, includ-ing its latent effects. It used a participatory eval-uation design, which involved a comparison of various groups drawn from localities that were not part of the UNICEF intervention in North Darfur (Umkadada locality) and South Darfur (Kass locality), to ensure the reliability and va-lidity of the evaluation data. In so doing, the consultants analysed the inter-locality dynamics on targeting at the community/village levels.
To test the contribution of the inputs to the impacts of the programme, the consultants developed a theory of change to provide a log-ical analysis of causality and the effects of the programmes that UNICEF supported. The basis for the application of the theory was the consul-
tants’ understanding of UNICEF’s results-based framework for its operation in the Sudan, with emphasis on the factors contributing to the reduction of child mortality at the community level, as presented in the UNICEF nutritional framework (1990). The indicators used in the theory of change were derived from UNICEF partnership agreements and its annual work plan for humanitarian interventions in North Darfur.
The quantitative analysis is built on existing re-ports from household surveys conducted during the period under review (2010–2015), mainly the Multiple Indicator Cluster Survey (MICS) 2014, the Simple Spatial Sampling Survey 2013, the Sudan Household Health Survey 2010, routine statistics of sector management information systems (e.g. routine data related to health services) and community village survey data. Data on programme implementation related to service delivery (supply and cash) and achieved outputs were generated from UNICEF internal financial reports. Trends analysis was conducted to assess the progress made vis-à-vis baseline indicators, as captured in UNICEF annual work plans.
Qualitative analysis on the opinions of the var-ious project stakeholders was applied through individual interview and focus group discussions with key beneficiaries (adolescents, parents and

13EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
service providers), implementing partners, Unit-ed Nations and non-governmental organization (NGO) stakeholders and community members.
The cost-effectiveness analysis focused on the cost of achieving the intended programme out-comes. The analysis of financial data, including budget allocation and utilization by outcomes and sector results areas was initiated to com-pute the cost-effective analysis as outlined in the Department for International Development value for money framework.11 The WASH pro-gramme analysis was based on cost per ac-tual sustainable water and sanitation service beneficiary, both at the community level and in schools. The nutrition programme analysis was based on the cost per life saved in terms of children admitted and cured of SAM. Finally, the health programme cost-effective analysis was based on the cost per under-five child saved through the administration of vaccines. The computation of the ratio was done using the financial resources that were mobilized within the year of review against the outcomes, as per the UNICEF thematic sector.
The evaluation employed a utilization-focused approach, whereby the intended users of the evaluation were identified and engaged from the outset in the development of the evaluation terms of reference (see Annex 22) and tools. This was enhanced by establishing a techni-cal committee with representatives from the Ministry of Education, health, nutrition, water and social services from the Government. From UNICEF, the Planning, Monitoring and Evalua-tion (PME) and senior management team en-gaged in the evaluation process.
11 Department for International Development, ‘DFID’s Approach to Value for Money’, DFID, July 2011.
3.1 Data collection tools
3.1.1 Desk reviewThe evaluation involved a desk review of key documents related to humanitarian interven-tions in North Darfur (analysis of the Strate-gic Response Plan Document for 2010–2015), including partner annual work plans; project proposals; studies/reviews; project agreement documents; partner, donor and annual reports; UNICEF and partner financial records; and field monitoring reports (see Annex 13). Analysis was carried out using the routine data analysis tool, which provided a framework for the systematic analysis of the progress made by UNICEF, as recorded by UNICEF and the Government of the Sudan, which is the major implementing partner.
3.1.2 Key informant interviewsThe evaluator conducted 82 key informant inter-views with staff from UNICEF, the Government of the Sudan and United Nations agencies in North and South Darfur who had registered a considerable presence in the programme since 2010 or earlier (see Annex 14). The selection of these organizations was made based on a list captured during the coordination meetings, as well as the UNICEF partner database for pro-grammes in North and South Darfur. The main objective of the interviews was to document the progress made so far and issues related to humanitarian action in North and South Darfur. The interviews were conducted based on an elaborate interview guide (see Annex 18) that ensured the consistency and reliability of feed-back received from interviewees. The analysis involved mapping of feedback based on related themes.

14EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
3.1.3 Focus group discussionsUsing a systematic approach, the team gath-ered information from community members through group discussions, using a discussion guide. The consulting team held such conver-sations with 22 groups that were purposively sampled for the evaluation within the eight lo-calities from which a total of 252 respondents (90 male and 162 female) were consulted. The selection of the communities was based on a random selection of the administrative units within the eight localities. Both the internally displaced communities living in camps and host communities were involved in the development of the selection criteria. The key criterion for the selection of the participants in the focus group discussions was their stay or residence in the selected areas for at least five years (see Annex 16).
The discussion process was four-fold. First, the team initiated discussions with primary health-care personnel to formulate a basic understand-ing of the primary healthcare situation in the locality, as well as challenges and priorities. Second, the team held mixed and represen-tative discussions with community develop-ment committees to explore prospects, verify answers and reach a common consensus on the health, WASH and nutrition situations within the areas of intervention. Third, the team con-ducted group discussions with mothers and caregivers at health facility waiting rooms, wa-ter points and markets. Fourth, the team held a series of discussions with children at various water points. Up to two focus group discus-sions targeted groups of children aged 8–12 years in Kass Camp and Zam Zam Camp. The
12 The calculation of the sample size was done using the UNICEF MICS formula, available at: <www.childinfo.org/files/MICS3_Chapter_4_-_Designing_and_Selecting_the_Sample_060219.pdf>, accessed 8 March 2017.
focus group discussion analysis, however, in-volved the identification of related themes or sub-themes based on the discussions’ basic guidelines and findings, but with a bias for the WASH, child health and nutrition programmes.
3.1.4 Significant stories of change The consultants collected significant stories of change from 22 community members that documented the progress of the programme in regards to the quality of life of the target popula-tion. The process followed a prescribed format, while the selection of community members de-pended on the community member having a child under age 5 and a resident in the area for the past five years (see Annex 15). The most successful aspect of this approach was the ability to document and capture real changes, as well as the programme’s contributions to ad-dressing the needs of the affected population. During this process, information was exchanged in Arabic and national consultants later translat-ed the transcripts into English.
3.1.5 Household questionnaireThe consulting team tasked local enumerators with administering the household question-naire to 764 households.12 The main criterion for household selection was the presence of a child aged 5 years or younger and the presence of the household in that locality before 2010 (see Annex 20). The consultants had previously developed a criterion for sampling households, including randomization at household level, which involved listing all households within the locality. In addition, the team developed a lot criterion, in which all administrative units within El Fasher, Saraf Omra, Mellit, Kutum, Kabkabiya,

15EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
Umkadada and Kass were listed on a roster. Pa-pers with the name of the administrative units written on them were then folded, after which the equivalent number of the administrative unit based on the sample size above were picked randomly from the folded papers.
In the subsequent selection of villages and households, the consultants repeated the above randomization process. During the actual administration of the household questionnaire, the determination of the first household was based on its location (the first on the right-hand side of the enumerator upon their arrival at a village) and having a child who was 5 years old. The subsequent households were selected by ensuring a sampling interval of nine13 between the former and the next household with a child who is 5 years old. In the absence of a five-year-old child in the next household, the enumerator was required to get to the household with a five-year-old child or below.
3.1.6 Observation of WASH, nutrition and health facilitiesObservation played a complementary role, es-pecially observation of practices and core areas
13 The questionnaire used for the household survey is attached as Appendix 20.
14 The formula used for the sample size calculation was adapted from: <www.childinfo.org/files/MICS3_Chapter_4_-_Designing_and_Selecting_the_Sample_060219.pdf>, accessed 8 March 2017. In the formula, n is the required sample size, expressed as number of households, for the key indicator (see following section on determining the key indicator); 4 is a factor to achieve the 95 per cent level of confidence; r is the predicted or anticipated prevalence (coverage rate) for the indicator being estimated (rate of 44.9 per cent is the underweight prevalence rate as reported in the MICS 2014 report for North Darfur) is the factor necessary to raise the sample size by 10 per cent for non-response; f is the shortened symbol for deff which as 1.5; 0.12r is the margin of error to be tolerated at the 95 per cent level of confidence, defined as 12 per cent of r (12 per cent thus represents the relative sampling error of r); p is the proportion of the total population upon which the indicator, r, is based which has been taken as 0.15; nh is the average household size taken as 5.9 (as reported in MICS 2014 report).
of intervention (WASH, health and nutrition). At-tention was paid to how community members and target groups (e.g. children and caregivers) practice or use the trainings and knowledge they acquired from the trainers. The team also closely observed the health facilities, including payment of services, functionality, manage-ment and physical accessibility. They also ob-served under-five children accessing services at the nutritional centres (see Annex 17).
3.2 Sampling and data collection
3.2.1 Sampling for administration of household questionnairesThe calculation of sample size for the admin-istration of the household questionnaire used the formula proposed by the MICS sample size calculation shown below.14
([4 (r)(1-r)(f)(1.1)])
([(0.12r)2 (p) (nh)])
This translates into 763 households after includ-ing 20 per cent non-responsive. Table 1 elabo-rates on the target populations per locality.
n =

16EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
Table 1: Distribution of the sample size within the localities
LocalityTarget population
Number of households
Households to be sampled
Focus group discussions
El Fasher, North Darfur 220,297 44,059 232 6
Umkadada, North Darfur 105,846 17,641 93 4
Kass, South Darfur 292,548 48,758 257 5
Other localities* 171691 34,338 181 7
Total 790,382 144,796 763 22
15 Focus group discussion leaders led discussions in line with: Graham, A. et al., ‘Ethical Research Involving Children’, UNICEF Office of Research – Innocenti, Florence, 2013.
The enumerators recorded impressive high response rates with all targeted households responding to the questionnaire. Considerations were made to not collect data on information that was considered sensitive based on the situation.
3.2.2 Quality assurance and ethical considerations This evaluation upheld the respect and protec-tion of the rights and welfare of the affected population. While many of the quality stan-dards relating to aspects of evaluation design and management were under the control of the evaluation team, some of the key focus issues aimed at ensuring the quality and accountabil-ity of the evaluation process are listed below. The confidentiality of information collected from communities, households, children’s groups (aged 8–12) and key informants was observed. While collecting information from children, spe-cial emphasis was placed on ensuring that the children, guardians and parents had consent-ed to the process.15 A briefing was prepared for the children to explain the purpose of the
discussions and how the information collect-ed from them would be used. In addition, the female national consultants who were tasked with collecting information and all enumerators were fully vetted against having any records of child exploitation or any other abuses in regards to children.
a. Humanitarian action principles: The con-sultant ensured that the evaluation process adhered to the following principles for ac-countability to affected populations:
� Humanity: The process ensured the protection of life, health and respect for human beings.
� Neutrality: The evaluation consultants did not take sides in hostilities or en-gage in controversies of a political, ra-cial, religious or ideological nature.
� Impartiality: The evaluation was carried out taking into account the needs of the affected population and made no distinc-tions on the basis of race, gender, reli-gious belief, class or political opinions.
* Other localities where sampling was done include Kabkabiya, Saraf Omra, Tawila and Kutum localities

17EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
� Independence: The evaluation process was autonomous of the political, eco-nomic, military or other objectives of the client or any other interested party.
b. Evaluation ethics: The consultants were fully cognizant of the principles and chal-lenges of conducting evaluations in an eth-ical and respectful manner. The consultant ensured that team members adhered to the ethical protocols as highlighted in the data collection tools during the evaluation process. Informed consent was collect-ed through signed consent forms for the household interviews and individual stories of significant change, while verbal consent was accepted for the focus group discus-sions and key informant interviews.
c. Timeliness and relevance: The consultant proposed a utilization-focused approach to the evaluation, starting with a detailed stakeholder analysis and continuing with the participatory involvement of stakeholders in the validation and sharing of evaluation findings.
d. Process quality: The methodology de-signed for the evaluation ensured that quality was embedded in the evaluation pro-cess. This included the use of Development Assistance Committee quality criteria for evaluation design; an evaluation framework, which lists the main evaluation questions, based on the criteria, and clearly describes the methodology for data collection, trian-gulation and analysis; detailed questions, tools and reporting formats based on the evaluation framework; and standard check-lists and reporting forms.
e. Timely delivery: The methods and tools used fit within the scope of the evaluation
and the resources available, as well as the deadlines for the deliverables.
f. Do no harm: The evaluation ensured that the process of data collection, interviews with key informants and with the affected population did not contribute to any mis-understandings of the main objectives and outcomes of the evaluation process.
Limitations of the evaluationThe initial scope of the evaluation included ed-ucation and child protection programming, but excluded this from the evaluation in a revised terms of reference. The new terms of reference focused mainly on child survival and causality of under-five child mortality rather than on overall UNICEF humanitarian programming in North Darfur.
Since this was a multi-stakeholder programme in a high-risk area, politically sensitive and taking place in a complex operating context, it was at times challenging to get a consensus on the evaluation from all stakeholders, both at federal and state levels. However, an agreement was finally reached to move forward with this inde-pendent evaluation for the purpose of learning.
The lack of reliable and accurate data for 2010–2011 contributed to weaknesses in the analy-sis of value for money and the effectiveness of the humanitarian programme during the period 2010–2011.
The consultant had envisaged the availability of routine data at the locality level, but the relevant government and UNICEF offices in El Fasher were unavailable. Given that most routine data are collected at the state level, the team an-alysed data generated from both household questionnaires from different localities and the

18EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
findings of the focus group discussions.
Given that the prevailing emergency contexts in the target regions are characterized by conflict, respondents and focus group discussions par-ticipants required the utmost confidentiality. The team found it prudent not to take the names of some community members who participat-ed in the focus group discussions, but tracked
the cumulative number of the participants for accountability purposes only.
Due to the focus on surviving under-five children during the data collection exercise (primarily the focus group discussions and household ques-tionnaire), some households without children under 5, in which children had died before the exercise, were excluded.

19EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
4. EVALUATION FINDINGS AND DISCUSSION
©UN
ICEF
Sud
an/N
orth
Dar
fur F
O

20EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
4. EVALUATION FINDINGS AND DISCUSSIONS
16 Details of the Sudan’s Humanitarian Response Plan are available at: <www.humanitarianresponse.info/en/operations/sudan>, accessed 8 March 2017.
17 ‘United Nations Development Assistance Framework for the Republic of Sudan’, Khartoum, May 2012.
The presentation of the evaluation results is based on the UNICEF nutrition conceptual framework, which outlined the association be-tween food security, health, nutrition, water and sanitation, as the key factors contributing to un-der-five child mortality in North Darfur. This chap-ter discusses key related areas, including the relevance, impact, effectiveness and efficiency of humanitarian action, as well as coordination, sustainability and recommendations.
4.1 Relevance and appropriateness
At the policy level, UNICEF humanitarian pro-grammes are aligned with various international, national and state policy documents that aim to improve quality of life in North and South Darfur. As a result, these interventions contributed to the Government’s policy on disaster manage-ment by responding to the needs of its citizens in North Darfur, as outlined in the annual Su-dan humanitarian response plans (2010–2015).16 Moreover, UNICEF’s focus on basic emergen-cy service delivery (i.e. water, health, nutrition and sanitation) contributed to the Sudan United Nations Development Assistance Framework 2013–2016,17 specifically to Pillar 2, Outcome 4, which states, “People in Sudan [sic], with special emphasis on populations in need, have access to equitable and sustainable quality ba-
sic services.” UNICEF also supported the en-hancement of the Humanitarian Aid Commis-sion (HAC) mandate through sector and cluster coordination systems, while its design relied on inter-agency needs assessment conducted after community members reported these emergen-cies (i.e. conflict, floods and drought).
The following is a quote from a mother in Al-salam Camp in North Darfur that illustrates the relevance of UNICEF interventions and the impact that these interventions have had on her life: “I have arrived to Alsalam Camp from Korma on 2006. At that time, it was the raining season, I have used clothes in order to build a shelter in order to protect us from the rain. The number of the people was very high, people help each other and shared together the food and the shelters. The organizations available was Oxfam America and UNICEF, who partici-pated in distributing mosquito net, Jerry cans, soaps, chlorine and bed covers. In 2015, I par-ticipated in health awareness for the mothers at their houses in addition to covering the water pots and cleaning practices.”
At the programme level, UNICEF humanitarian interventions succeeded in specific programme areas. Under the health programme, UNICEF humanitarian interventions adhered to two of the five commitments made on health. UNICEF

21EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
personnel attended to and supported links for other cluster/sector coordination mechanisms on critical and inter-sectoral issues evident in the EPI. This created a strong inter-agency co-ordination mechanism in line with Commitment 1 (“Inter-agency coordination mechanisms in the health sector are supported and enhanced with links to other cluster coordination mech-anisms”). Similarly, children and women ac-cessed life-saving interventions through popu-lation- and community-based activities such as campaigns and child health days, in line with Commitment 2 (“Children and women access life-saving interventions through population and community-based activities”).
After a hard work I arrived to the camp after 28 days of giving birth by a cae-sarean operation. But I thank God that by the time we arrived to the Camp the services provided by UNICEF, whether for the mothers or for our children at schools. And in addition to the aware-ness programmes, workshops and health services provided at the hospi-tals. Furthermore, UNICEF has distribut-ed free treatment, built a kindergarten, provided notebooks for schools and tents for the displaced people. I per-sonally thank UNICEF for helping and rescuing people and guiding the people by distributing health awareness post-ers and brochures that was very easy to understand because it has photos and pictures. Now I am working as a health-care awareness provider in the Camp. I disseminate awareness pictures and photos to the people in the camp ‘Moth-ers, at the water points’ and this to teach them with the basics to preserve food and water from getting contaminated.
What I have learned from UNICEF I was able to deliver to other people especially the mothers about health and hygiene and how to prevent our children from getting infected and if they got ill, how would they manage to control the situ-ation not to get worse and this can give the mother enough time to get to the hospital.— Samira Mohammed Yousif, Community Health Worker Zam Zam Camp, North Darfur
Under the WASH programme, UNICEF humani-tarian interventions adhered to three of the five commitments made previously on WASH, in-cluding effective leadership for WASH cluster/inter-agency coordination under Commitment 1 (“Effective leadership is established for WASH cluster / interagency coordination”). It also ensured that children and women access sufficient volumes of safe drinking water for cooking and maintaining personal hygiene un-der Commitment 2 (“Children and women ac-cess sufficient water of appropriate quality and quantity for drinking, cooking and maintaining personal hygiene”). In addition, it ensured that children and women access secure, sanitary, user-friendly and culturally and gender-appro-priate toilets and washing facilities under the Commitment 3.
Under the nutrition programme, UNCEF’s hu-manitarian commitment was evident through its contribution to the affected women and children who were able to access the programme as part of Commitment 3, “Support for appropriate infant and young child feeding is accessed by affected women and children”, and Commitment 4, “Children and women with acute malnutrition access appropriate management services”.

22EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
In terms of targeting affected populations, UNICEF designed the humanitarian interven-tions after conducting a community level needs assessment with the State Ministry of Health, United Nations agencies and National NGOs. This resulted in some 1,004,840 people in North Darfur and 864,416 people in South Darfur, in-cluding 153,338 children under 5, being priori-tized for humanitarian assistance between 2010 and 2015. Cumulatively, humanitarian action tar-geted 1,333,700 people in 2011, 1,430,000 in 2012, 1,759,155 in 2013, 2,500,000 in 2014, and 2,733,000 in 2015,18 illustrating the protracted nature of the crisis in North and South Darfur, as reflected in Table 2.
UNICEF and its humanitarian partners provid-ed much-needed life-saving services to affect-ed populations. Feedback from community members during the focus group discussions confirmed that the WASH interventions—the provision of water and sanitation facilities and hygiene promotion—contributed to addressing their needs. Immunization and nutrition pro-grammes also contributed immensely to the improvement and sustainability of the health
18 OCHA weekly humanitarian bulletins 2010–2015.
statuses of children under 5 within affected communities in North and South Darfur, as captured in routine data collected by the State Ministry of Health and discussions with care-givers at the community level.
The changes that was done by UNICEF was very good at the beginning regard-ing education and water supply resourc-es, since UNICEF with coordination with Oxfam America participated in estab-lishing wells, pumps and this was the major benefit we have received from UNICEF since the clean drinking water has become available. We also had train-
ing courses in education; UNICEF has also provided us with books, teaching equipment and has implemented toilets. I would like to thank UNICEF for what they have provided us with awareness programme we all came from differ-ent places most of us don’t have basic knowledge about health and hygiene practices, but UNICEF has taught us about these issues. We would like to re-
Table 2: Representation of the new cases from 2010–2015 by disaster type
Shock/hazard New number of people displaced ( 2010–2015)
North Darfur South Darfur
Dry spell 500,051 489,080
Conflict 454,084 328,236
Floods 44,735 47,000
Health shocks (measles, dengue fever, yellow fever)
422 100
Source: OCHA weekly humanitarian bulletins 2010–2015

23EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
quest UNICEF to be the one who imple-ment the activities and not let the NGOs take the lead on this.— Community leader, Alsalam Camp, North Darfur
Feedback from community members, key in-formant interviews and review of assessment reports show that the time it took for humani-tarian services to be delivered far exceeded the stipulated 72 hours after an emergency strikes. For a period of two to three months, between 2013 and 2015, UNICEF delayed actual delivery of humanitarian relief due to security concerns and slow clearance of humanitarian action by the Government of the Sudan, even after an emergency needs assessment was conducted within 24 hours. Despite the delay, the Gov-ernment and communities responded to the crisis quickly. Though the contingency planning process was designed to mitigate this, lack of pre-positioned stocks at the locality level com-bined with access challenges, further delayed humanitarian assistance.
The appropriateness of capacity building was another major area of concern for the evalua-tion. After the sudden 2009 withdrawal of inter-national NGOs from North Darfur which led to the destabilization of services, UNICEF humani-tarian action fell short of filling the gap left by hu-manitarian agencies by providing capacity to line ministries, mainly the Ministry of Health and The Ministry of Water, Resources, Irrigation and Electricity. The humanitarian agencies focused mainly on delivering humanitarian programmes through local community-based organizations, which ensured that the capacities of various organizations to deliver humanitarian services were enhanced in line with agreed global stan-dards, for example the Sphere standards.
4.2 Coordination
In regards to coordination, UNICEF efforts de-pend on the organization’s ability to support ser-vice delivery internally and externally with other humanitarian agencies. Such coordination en-sures that the platform functions under agreed strategic priorities to eliminate duplication of ser-vice delivery, and supports the management of needs assessment, stakeholder gap analysis, joint contingency planning processes and ac-countability to affected populations.
Based on the key informant interviews and review of minutes, the evaluation established that an active coordination system existed in North Darfur and South Darfur, at both internal and external levels, between 2010 and 2015. UNICEF’s internal coordination involved regular monthly programme and emergency coordina-tion meetings to ensure that the WASH, health and nutrition sections addressed humanitarian service delivery, contingency planning and needs assessment at both North and South Darfur state levels. In some instances, however, WASH-spe-cific activities were implemented by the edu-cation section, which did not fully achieve the targeted outputs such as delivering sanitation and water facilities without the technical support of the WASH section.
In contrast, while OCHA leads the external coordination of 11 United Nations clusters in a number of humanitarian intervention areas, UNICEF’s mandate focuses on WASH, nutrition, child protection and education programmes that operate under the sectoral coordination forum. The respective line ministries chair these forums, including health, WASH and education.
The HAC also made considerable effort to ensure

24EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
smooth humanitarian programme operations in both North and South Darfur, though this was affected by late and delayed approvals. Between 2010 and 2015, although the coordination of humanitarian action registered considerable success with active sectors/clusters at the state level, its applicability at the camp level continued to experience targeting challenges. This area therefore requires strengthening in the future. Its applicability at the camp level was measured based on sector-specific coordination verses an integrated coordination forum, where clusters are grouped together for easier admin-istration of humanitarian action and promotion of inter-cluster harmony.
In practice, clusters and inter-cluster meetings occur interchangeably. In North Darfur, the for-mer occurs on a weekly basis and the latter occurs on a quarterly basis. In South Darfur, however, the former occurs weekly and the latter occurs biweekly. At the state level, such meetings have enhanced inter-cluster coordina-tion among humanitarian agencies, though this is more the case in South Darfur than in North Darfur. State level coordination forums effec-tively brought together agencies and minimized duplication, though inter-sectoral coordination was weak. Such inherent weakness led to the duplication of nutrition, health and sanitation programming activities at the State Ministry of Health in North Darfur. In contrast, South Dar-fur inter-sectoral and intra-sectoral coordination highlighted clear roles and activity planning.
At the community level, coordination efforts weakened in most affected communities. For example, feedback from community members in Zam Zam Camp, Dar es Salaam camp and Kass Camp indicated that UNICEF’s coordina-tion was disjointed. Unlike at the state level,
coordination at the community level is largely ad hoc with limited engagement of the different sectors/clusters. Each cluster/sector is focusing on their respective sector/cluster-specific activ-ities even though all have a common focus on affected communities.
The HAC Planning Unit, the Ministry of Finance and National Economy, the Ministry of Welfare and Social Security and the Ministry of Interna-tional Cooperation were barely involved in the integration of early recovery into emergency programming. The HAC Planning Unit neither integrated nor mainstreamed early recovery processes into humanitarian programming, though the Ministry of Finance and National Economy Planning Division has recognized this gap. Though this division was not significant-ly involved in the humanitarian programme, it should have initiated early recovery program-ming focusing on the sustainability of humani-tarian programming. However, at the state and locality levels, it is difficult to identify the inte-gration of early recovery programming initia-tives in the context of the protracted emergency situations in North and South Darfur, which have lasted for more than 13 years.
4.3 Efficiency
The analysis of efficiency focused on how well UNICEF humanitarian inputs were converted into their respective outputs; that is, whether the planned outputs were achieved and wheth-er implementation challenges such as program-matic, logistical and financial challenges were documented. The efficiency analysis reviewed the operation of the monitoring systems, while the cost-effective analysis for key output indica-tors examined the representativeness of each

25EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
thematic area vis-à-vis the financial allocation. The financial allocation relied on the mone-tary resources that UNICEF had mobilized for humanitarian action for 2010 through 2015. It should be noted, however, that the design of the UNICEF monitoring and reporting system fo-cused mainly on the results/outcome level indi-cators, but not on input/output indicators. Thus, the efficiency analysis (presented below) was derived from indicators taken from the UNICEF annual work plans and partnership agreements and reflected in the theory of change developed by the evaluation team.
4.3.1 WASH programme efficiency UNICEF invested US$16,166,439 in North Darfur and US$19,834,180 in South Darfur, with varying annual allocations. For North Darfur, US$4,055,887 was allocated in 2010, US$2,953,351 was allocated in 2014 and US$4,430,423 was allocated in 2015. For South Darfur, US$3,780,394 was allocated in 2010, US$6,356,210 was allocated in 2013 and US$2,224,899 was allocated in 2015, as shown in Figure 3 (see Annex 4). These investments in new water sources translated into access to safe water for 38 per cent of the affected
0
5,000,000
Amou
nt (U
S$)
10,000,000
15,000,000
20,000,000
25,000,000
30,000,000
2010 2011 2012 2013 2014 2015
UNICEF Allocated Budget, USD, (South Darfur
3,780,394 4,041,421 2,638,367 1,726,000
UNICEF Allocated Budget, USD (North Darfur)
4,055,887 801,617 1,289,118 3,787,784
SHRP Planned, USD, (South Darfur)
27,288,247 22,857,330 12,373,975 13,845,914
SHRP Planned Budget, USD (North Darfur)
25,852,024 20,486,688 11,371,005 11,215,430
SHRP Allocated funds, USD, (South Darfur)
12,202,064 11,101,892 5,779,351 4,725,225 5,607,465 5,464,461
SHRP Allocated funds, USD, (North Darfur)
11,559,850 7,550,614 6,695,032 5,016,272 2,884,213 4,736,211
Figure 3: Comparison of funding for WASH programmes by UNICEF and other donors
Source: UNICEF financial records 2010–2015 and OCHA financial records 2010–2015

26EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
population in North Darfur and 36 per cent of the affected population in South Darfur. Through the rehabilitation of water sources, 55 per cent of the affected population in North Darfur and 76 per cent of the affected population in South Darfur gained access to safe water.
UNICEF spent US$588,003 and US$468,561 on the procurement of generators in North Darfur and South Darfur, respectively. An additional US$545,992 and US$1,118,244 was spent to procure soap between 2010 and 2015 in North Darfur and South Darfur, respectively. UNICEF used US$472,152 and US$344,410 to procure chlorine tablets in North Darfur and South Dar-fur, respectively. Expenditure on hand pump spare kits was US$312,574 and US$347,415 for North Darfur and South Darfur, respectively, while US$4,570 and US$82,717 was used for the procurement of complete hand pump equip-ment in North Darfur and South Darfur, respec-tively. An additional US$83,984 and US$44,343 was spent on vent pipe valves in North Darfur and South Darfur, respectively, as presented in Figures 4 and 5.
UNICEF spent US$420,450 and US$298,240 on latrine plastic slabs in North Darfur and South Darfur, respectively. An additional US$256, 678 and US$124,192 was used to purchase plastic sheets/tarpaulins in North Darfur and South Darfur, respectively. For water quali-ty enhancement, UNICEF spent US$137,593 and US$68,199 on pool testing equipment and US$25,272 and US$11,640 on bacteriological test equipment in North Darfur and South Dar-fur, respectively. UNICEF spent US$178,655 on water trucking in South Darfur, compared with US$67,701 on water trucking in North Darfur. UNICEF spent 10 times more on water blad-ders in South Darfur (US$109,073) than it did
in North Darfur (US$13,164). The expenditure on water Jerry cans was unusually low in North Darfur (US$4,848) compared with South Darfur (US$196,950), a nearly 15-fold difference.
During this period, UNICEF focused on devel-oping a functional community management of operation and maintenance system that re-vamped 89 per cent and 84 per cent of water facilities that had broken down in North Darfur and South Darfur, respectively. The organiza-tion also trained 63 per cent and 34 per cent of water yard operators in North Darfur and South Darfur, respectively. As a result, UNICEF ser-viced 63 per cent and 60 per cent of hand pump operated boreholes in North Darfur and South Darfur, respectively, while increasing access to water for the affected population in the same proportion. UNICEF also trained a number of chlorinators across North and South Darfur, but there is no available data on the chlorination of various water sources in North Darfur. Available data from UNICEF shows that the organization last chlorinated 74 per cent of planned water sources in South Darfur in 2010.
UNICEF made a significant effort to strength-en the capacities of the affected population through Community Approaches to Total Sanita-tion trainings targeting WASH sector members, natural leaders and village health committees, but the achievement was ultimately minimal—only 45 per cent and 15 per cent of the targeted cadre were trained in North Darfur and South Darfur, respectively. However, UNICEF didn’t build capacity of Water Environment and Sani-tation (WES) Department to conduct state-wide water quality assessment, since there are no records documenting this undertaking. Rou-tine water quality assessment at various water points show that this programme tested 97 per

27EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
0
100000
200000
300000
400000
500000
Num
ber o
f Peo
ple
2010 2011 2012 2013 2014 2015
New
Wat
erSo
urce
Reha
bilit
ated
Wat
er S
ourc
e
New
Wat
erSo
urce
Reha
bilit
ated
Wat
er S
ourc
e
New
Wat
erSo
urce
Reha
bilit
ated
Wat
er S
ourc
e
New
Wat
erSo
urce
Reha
bilit
ated
Wat
er S
ourc
e
New
Wat
erSo
urce
Reha
bilit
ated
Wat
er S
ourc
e
New
Wat
erSo
urce
Reha
bilit
ated
Wat
er S
ourc
e
Planned Target Achieved Output
1475
00
8660
0
1947
50
1732
00 2000
00
1469
54
2000
00
1395
00
3500
00
1800
0
2385
00
1400
00
1000
00
2750
0
4000
00
2028
41
1200
00
2700
0
4390
00
1745
00
1350
00
5650
0
2700
00
6450
0
0
100000
200000
300000
400000
500000
600000
700000
800000
Num
ber o
f Peo
ple
2010 2011 2012 2013 2014 2015
New
Wat
erSo
urce
Reha
bilit
ated
Wat
er S
ourc
e
New
Wat
erSo
urce
Reha
bilit
ated
Wat
er S
ourc
e
New
Wat
erSo
urce
Reha
bilit
ated
Wat
er S
ourc
e
New
Wat
erSo
urce
Reha
bilit
ated
Wat
er S
ourc
e
New
Wat
erSo
urce
Reha
bilit
ated
Wat
er S
ourc
e
New
Wat
erSo
urce
Reha
bilit
ated
Wat
er S
ourc
e
Planned Target Achieved Output
2315
00
1768
00
1305
00
1130
00
1220
00 7200
0
1460
00
2247
93
2385
00
3275
0 2120
00
1320
00
1500
00
8000
0
6000
00 6400
00
4000
00 4550
00
4000
00
1215
00 7125
0
3120
2600
00
4975
0
Figure 4: Number of people reached through the provision of clean water in North Darfur
Source: Routine data from UNICEF annual reports 2010–2015
Figure 5: Outputs of water in South Darfur
Source: Routine data from UNICEF annual reports 2010–2015

28EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
cent of the water sources in North Darfur and 44 per cent in South Darfur, though it is yet to deliver urban water assessment at IDP-host-ing centres. Key informant interviews with the State Water Corporation in North and South Darfur confirmed these routine assessments. Although the WASH sector registered consid-erable progress in regards to preparedness by developing a WASH contingency plan and en-suring the availability of emergency WASH sup-plies for up to 20,000 people for all years under review, feedback from community members and key informant interviews confirmed that the activation of the contingency plan within 72 Hours was largely not achieved.
WES in coordination with UNICEF has implemented a number of water pumps, most of them are not working now due to the dryness of the seasons, because they mostly depend on the rains and groundwater. And another reasons is that they have also broke and aren’t working anymore.—Focus group discussion participant, Zam Zam Camp, North Darfur
To contribute to the promotion of personal hygiene and the reduction of diarrheal cases, UNICEF distributed soap to 43 per cent of the targeted affected population in North Darfur and 51 per cent in South Darfur. In addition, though UNICEF planned to distribute garbage collec-tion equipment to the affected population, only 13 per cent in North Darfur and 31 per cent in South Darfur were reached. Hygiene promotion activities supported by UNICEF reached 43 per cent of the targeted affected population in North Darfur and 47 per cent in South Darfur.
Although the WASH and education sections have a cordial intra-relationship at the state level, these sections were unable to achieve WASH programming outputs in schools. As a result, UNICEF WASH programmes ensured access to clean and safe water for 43 per cent of targeted schoolchildren and the provision of sanitation and handwashing facilities in 39 per cent of the schools in North Darfur, as shown in the figure below. In North Darfur, however, WASH programmes ensured access to clean and safe water for 47 per cent of targeted schoolchildren and the provision of sanitation and handwashing facilities in 43 per cent and 56 per cent of school, respectively, as shown in Figure 6.
Regarding monitoring, UNICEF developed a functional WASH monitoring system for track-ing achievement against the targets. However, there is a disconnect between the WASH mon-itoring system and the implementing partner monitoring system with different indicators and activities being undertaken by UNICEF, under-scoring the utility of the system. For example, critical process indicators showed the number of people targeted for specific activities was largely missing, hence tracking of achievement against actual versus planned results was not possible. This was also evident through the ab-sence of harmonized indicators in school pro-gramming for water in 2013–2014 and for WASH in 2014–2015.
In regards to programme planning and budgeting, the UNICEF/WASH procurement policy outlines appropriate quality and prices for humanitarian supplies to ensure compliance with UNICEF’s quality standards. However, the evaluation ver-ified that the WASH planning and budgeting

29EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
process has poor bookkeeping practices, and that as a result, WASH inputs, including physical supplies for water point construction (e.g. soap, water Jerry can and hand pumps) and staff in-puts, did not have any itemized breakdown for how the WASH supplies were procured, though the UNICEF supply system captures all of this information for other sections.
The delineation of the WASH supply chain from the UNICEF central supply system created an opaque operating system. UNICEF cannot au-thoritatively confirm the quantities and the cost of the supplies that were distributed to North Darfur and South Darfur without going through an external WES Department supply chain sys-
tem. This affected the accountability mecha-nisms by the implementing partner (WES) to UNICEF.
UNICEF’s cost-effective analysis focused on the WASH programme costs per actual beneficiary in terms of both water and sanitation services accessed between 2010 and 2015. This analysis considered the amount of funds that UNICEF al-located for WASH programming within UNICEF and to implementing partners, as shown in An-nex 4. Figure 7 shows that the per-person cost of providing clean water and sanitation to one person varied from US$14 (in 2010) to US$25 (in 2015) in North Darfur, and from US$13 (in 2010) to US$34 (in 2015) in South Darfur.
0
5000
10000
15000
20000
25000
30000
Num
ber o
f Peo
ple
2010 2011 2012 2013 2014 2015
Scho
ol W
ater
Scho
ol L
atrin
e
Hand
Was
hing
Faci
lity
Scho
ol W
ater
Scho
ol L
atrin
e
Hand
Was
hing
Faci
lity
Scho
ol W
ater
Scho
ol L
atrin
e
Hand
Was
hing
Faci
lity
Scho
ol W
ater
Scho
ol L
atrin
e
Hand
Was
hing
Faci
lity
Scho
ol W
ater
Scho
ol L
atrin
e
Hand
Was
hing
Faci
lity
Scho
ol W
ater
Scho
ol L
atrin
e
Hand
Was
hing
Faci
lity
Planned Target Achieved Output
3000
0
3000
0
3000
0
6800
6800
6800
6400
6400
6400
1000
0
1000
0
1000
0
7500
7500
7500
7500
7500
3000
3000
300014
85
1485
1485 25
00
2500
2500
0 0 0
6000 74
70
7470
7470
6000
6000
Figure 6: Progress towards WASH in North Darfur schools
Source: UNICEF 2010–2015 annual reports

30EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
Figure 7: Provision cost for water and sanitation service per person (household survey)
Financial analysis and feedback from the key informant interviews at both the national and state levels showed a variation in administrative and overhead costs in terms of percentages deducted from the mobilized WASH humani-tarian funds. At the global level, the fund ad-ministrative agent deducts 1 per cent of the total amount mobilized before the funds are transferred to UNICEF. At UNICEF Headquar-ters in New York, between 7 and 8 per cent is deducted as overhead costs, while at UNICEF Sudan, 15 per cent of the mobilized funds are deducted as overhead costs before implement-ing partners deduct an additional 7 per cent. At the state level, however, the overhead costs range from 20 to 30 per cent, depending on the implementing partner. In total, these administra-tive or overhead costs range from 50 to 61 per cent of allocated humanitarian funds. Further computations reduce the total overhead cost to
48.5 per cent, which is broken down as follows:
� Fund administrative agent: 1 per cent
� UNICEF Headquarters in New York: 15 per cent
� UNICEF Sudan (Khartoum): 7.5 per cent
� Implementing partners at Khartoum level: 7 per cent
� Implementing partners at state level: 25 per cent
Despite the considerable progress mentioned above, WASH programming was encumbered by numerous challenges. Feedback from com-munity members who participated in the focus group discussion confirmed the lack of an ac-countability mechanism for the distribution of WASH supplies at the community level. They also confirmed an apparent selling of UNICEF/
0
20
40
60
80
100
North Darfur
Num
ber o
f Peo
ple
2010 2011 2012 2013 2014 2015
South Darfur
B
14 13
4 7
4235 34
84
58
25
63
5

31EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
WASH supplies, mainly water Jerry cans and soap supplies, for the targeted affected popula-tion. Records from the WES Department show the amount of WASH supplies distributed to North and South Darfur, but there is no docu-mentation at the UNICEF level of whether the beneficiaries received the supplies.
The other evident challenge is in the use of var-ious forms of indicators, as presented in the UNICEF rolling work plan and the WASH section annual work plans. For example, in 2013–2014 annual work plans, the water and sanitation targets referred to communities (e.g. 15 com-munities) whereas in 2015–2016 annual work plans, the targets referred to the actual number of people reached.
The relatively high administrative and operation costs of the WASH programme have increased the focus on physical water and sanitation struc-tures than software components, mainly train-ings. This has led to low outputs; that is, the programme achieved 43 percent and 17 percent of planned trainings in North Darfur and South Darfur, respectively.
The available human resources (one staff mem-ber in North Darfur and three staff members in South Darfur) is not commensurate with the demand for WASH humanitarian programming at the state and community levels. Hence, ad-ditional focus is placed on the coordination and procurement of WASH supplies and minimal effort is made to ensure the implementation of the programmes at the community level. UNICEF staff serve more supervisory and mon-itoring roles.
4.3.2 Nutrition programme efficiency The efficiency analysis for nutrition program-ming was based on the translation of the inputs outlined in the theory of change (see Annex 1) to the planned outputs. The key outputs anal-ysed included the number of children who re-ceived therapeutic feeding (Plumpy’Nut, F-100 and F-75) and vitamin A supplementation; the number of children who adopted the infant and young child feeding plan; and the capacity build-ing activities conducted, particularly training for the State Ministry of Health and implementing partner staff on SAM treatment and logistics management.
UNICEF mobilized resources to ensure that the planned nutrition activities and outputs were achieved. It increased funding for nutri-tion programming from US$651,000 in 2012 to US$5,991,555 in 2015 in North Darfur, and from US$2,412,464 in 2013 to US$2,850,899 in 2015 in South Darfur. The variation of these allo-cations was due to the difference in needs be-tween North and South Darfur, in terms of the susceptibility of under-five children to SAM. The Sudan Humanitarian Fund also reduced its fund-ing significantly from US$12,159,449 in 2010 to US$8,872,444 in 2015 for North Darfur and from US$12,834,974 in 2010 to US$8,214,029 in 2015 for South Darfur. Figure 8 highlights the variation in funding from 2010 to 2015 (additional figures are captured in Annex 5).

32EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
According to routine data analysis from the State Ministry of Health and UNICEF, the num-ber of children cured of SAM increased signifi-cantly from 12,838 in 2010 to 35,485 in 2015 in North Darfur, corresponding to increased SAM rates in that region. In South Darfur, the num-ber of under-five children treated for SAM in-
creased from 15,788 in 2010 to 21,275 in 2015. The procurement of therapeutic foods, mainly Plumpy’Nut correspond to the increased num-ber of children who were admitted with SAM. The conversion rate against the children’s ad-mission increased from 25 per cent in 2012 to 150 per cent in 2015 for Plumpy’Nut, while for
Amou
nt (U
S$)
20,000,000
18,000,000
16,000,000
14,000,000
12,000,000
10,000,000
8,000,000
6,000,000
4,000,000
2,000,000
2010 2011 2012 2013 2014 20150
2010 2011 2012 2013 2014 2015
UNICEF Allocated Budget, USD, (South Darfur)
2,412,464 3,469,287 2,850,899
UNICEF Allocated Budget, USD (North Darfur)
651,000 3,686,184 4,143,548 5,991,555
SHRP Planned, USD, (South Darfur)
17,340,300 12,782,227 11,886,844 18,689,390
SHRP Planned Budget, USD (North Darfur)
16,427,652 11,456,622 10,923,359 15,138,728
SHRP Allocated funds, USD, (South Darfur)
12,159,449 2,142,853 5,948,750 5,799,981 9,637,746 8,872,444
SHRP Allocated funds, USD, (North Darfur)
12,834,974 3,720,280 5,313,843 5,463,463 12,417,706
Figure 8: Funding for nutrition humanitarian programmes for 2010–2015
Source: UNICEF and OCHA financial reports 2010–2015

33EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
F-75, the rate increased from 222 per cent to 300 per cent for North Darfur. In South Darfur, the rate for Plumpy’Nut increased from 96 per cent to 113 per cent, while for F-75, the rate in-creased from 6 per cent to 257 per cent. Based on planning and programming logic, the conver-sion rate for Plumpy’Nut vis-à-vis the number of children admitted for SAM should be in a ratio of 1:1 and thus a 100 per cent score should re-flect high efficiency in UNICEF’s contribution to SAM management. Given that the rates exceed 100 per cent, it’s clear that UNICEF is spending more resources on purchasing Plumpy’Nut and other therapeutic food for SAM management, which indicates inefficiency. This is illustrated in Figure 9.
The purchase of therapeutic food was carried out using a competitive process to ensure the procurement of high quality products at a rea-sonable price in line with UNICEF procurement guidelines. The UNICEF supply system regis-tered variations in the price of 150 sachets that ranged from US$49 to US$51. There was also a disparity in the actual number of procured nu-trition items by the UNICEF supply unit and the nutrition section. The absence of a reconciliation report of the therapeutic supplements sent to the state level made it impossible to make an authoritative conclusion as to whether the un-der-five children suffering from SAM were the sole recipients of Plumpy’Nut.
0
5000
10000
15000
20000
25000
30000
35000
40000
Num
ber o
f Chi
ldre
n
2010 2011 2012 2013 2014 2015
Nor
th D
arfu
r
Sout
h Da
rfur
Nor
th D
arfu
r
Sout
h Da
rfur
Nor
th D
arfu
r
Sout
h Da
rfur
Nor
th D
arfu
r
Sout
h Da
rfur
Nor
th D
arfu
r
Sout
h Da
rfur
Nor
th D
arfu
r
Sout
h Da
rfur
Planned Target Achieved Output
2293
0
2365
4
2293
0
2440
2
1800
0
2517
3
1800
0
3363
1
3363
1
2293
0
2293
0
18000251731800033631229303363122930
2293
0
1505
2
1654
0
1610
8
2024
1
1651
1 1956
1
2109
7
2136
8
2937
2
2207
5
3987
1
2437
0
Figure 9: Admission of children with SAM

34EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
UNICEF’s key implementing partners—the fed-eral and state ministries of health—adopted the Infant and Young Child Feeding Plan at the na-tional level, though the plan was not adopted at the locality level. As a result, there was no data consolidation due to the absence of a nutrition database for CMAM, vitamin A supplementa-tion and infant and young child feeding. In this regard, UNICEF contributed to the realization of 84 per cent and 99 per cent of children aged 6–59 months in North and South Darfur respec-tively receiving two annual doses of vitamin A supplementation, as shown in Figure 10.
The cost-effectiveness analysis relied on the analysis of the financial cost of the UNICEF CMAM programme. It pegged the unit of ef-fectiveness as the number of children cured of SAM. However, the absence of financial records for 2010–2011 made it impossible to calculate the cost-effective ratio for the UNICEF human-itarian nutrition programme. The cost-effective ratio for North Darfur decreased from US$206 per life saved in 2014 to US$169 per life saved in 2015. In South Darfur the cost per life saved was US$138 in 2014 and US$134 in 2015, as presented in Figure 11.
0
100000
200000
300000
400000
500000
600000
700000
800000
4144
96
7242
87
4397
01
6151
07
4636
88
6487
20
4636
88
6523
87
4917
89
6523
87
3897
43
6949
44
4597
01
6311
85
4787
45
6148
15
4767
02
6562
06
4932
94
6749
46
Num
ber o
f Chi
ldre
n
2010 2011 2012 2013 2014 2015
Nor
th D
arfu
r
Sout
h Da
rfur
Nor
th D
arfu
r
Sout
h Da
rfur
Nor
th D
arfu
r
Sout
h Da
rfur
Nor
th D
arfu
r
Sout
h Da
rfur
Sout
h Da
rfur
Nor
th D
arfu
r
Nor
th D
arfu
r
Sout
h Da
rfur
Planned Target Achieved Output
Figure 10: Children aged 6–59 months having received two doses of vitamin A
Source: UNICEF routine data

35EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
Regarding the UNICEF Core Commitments of Children operational commitment for human resources, the posting of competent UNICEF nutrition staff to support implementing partners for both nutrition programming and supervision was inadequate. In the North Darfur office, for example, only one international staff member supported both nutrition and health program-ming, which is below the cluster role require-ment for UNICEF. This led to poor supervision of implementing partners.
Feedback from the key informant interviews with State Ministry of Health officials and the community-based organizations depicted high logistical costs for the delivery of nutrition-re-lated supplies (mainly Plumpy’Nut), and as a result, low performance in the coverage of
children at risk for MAM and SAM. Nutrition treatment centres are not an integral part of health facilities due to the nature of their design. Access to the most vulnerable children in villag-es far from the nutrition treatment centres has also led to missing output targets since not all vulnerable children were met within the period of evaluation (2010–2015).
The continuous leakage of UNICEF’s Plumpy’Nut into the local market affected the efficiency and effectiveness of the nutrition programme’s abil-ity to reduce malnutrition cases in a cost-ef-fective manner. There are no records to verify whether the procured Plumpy’Nut reached the affected children, but it was possible to verify the sale of Plumpy’Nut in the market.
Figure 11: Cost per life saved through UNICEF nutrition Interventions as calculated from UNICEF financial reports.
0
50
100
150
200
250
CER (UNICEF) – SAM ADMISSION CER (UNICEF) – SAM CURED
US$
2010 2011 2012 2013 2014 2015
Nor
th D
arfu
r
Sout
h Da
rfur
Nor
th D
arfu
r
Sout
h Da
rfur
Nor
th D
arfu
r
Sout
h Da
rfur
Nor
th D
arfu
r
Sout
h Da
rfur
Sout
h Da
rfur
Nor
th D
arfu
r
Nor
th D
arfu
r
Sout
h Da
rfur
$39$48
$141
$157$150
$117
$175
$113
$138
$162
$189
$169
$134
$206

36EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
In South Darfur, the HAC issued a directive to immediately halt NGO peacebuilding activities19
after verifying the diversion of nutrition items to markets in 2011. In North Darfur, however, there was no action from the HAC or a similar author-ity on the reports of the leakage of Plumpy’Nut into the local market. As presented in Figure 12, there is a significant difference in the number of under-five children admitted for SAM and the amount of Plumpy’Nut distributed.
19 Office for the Coordination of Humanitarian Affairs, ‘Sudan Weekly Humanitarian Bulletin 12-18 August 2011’, OCHA, 18 August 2011, available at: <http://reliefweb.int/sites/reliefweb.int/files/resources/Full_Report_2189.pdf>, accessed 9 March 2017.
4.3.3 Health programme efficiency The health efficiency analysis was also based on the theory of change, developed from the UNICEF rolling work plan and UNICEF partner-ship agreements. The cost of the humanitarian health programme was computed based on UNICEF financial reports. From these reports, funding for humanitarian health programmes declined significantly for both UNICEF-fund-ed programmes and the Sudan Humanitarian
0
10000
20000
30000
40000
50000
60000
SAM (Admission) Plumpy Nut (Distributed)
Num
ber o
f ite
ms
2010 2011 2012 2013 2014 2015
Nor
th D
arfu
r
Sout
h Da
rfur
Nor
th D
arfu
r
Sout
h Da
rfur
Nor
th D
arfu
r
Sout
h Da
rfur
Nor
th D
arfu
r
Sout
h Da
rfur
Sout
h Da
rfur
Nor
th D
arfu
r
Nor
th D
arfu
r
Sout
h Da
rfur
1505
2
1654
0
1610
8 2024
1
1651
1
1956
1
2109
7
2136
8
2937
2
2207
5
2328
2
3987
1
2437
0
6193
2460
4
1732
4
3329
1
2509
6
5040
2
000 00
Figure 12: Comparison of distributed Plumpy’Nut and the number of under-five children admitted for SAM treatment
Source: UNICEF nutrition and supply reports

37EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
Response Plan funding system. In the latter programme, the planned budget decreased be-tween 2010 and 2015 in both states, while allo-cation decreased from US$13,320,139 in 2010 to US$9,482, 975 in 2015 for South Darfur and from US$12,619, 079 in 2010 to US$8671,075
in 2015 for North Darfur. In the former, there was slight variation between funds allocated to both states over the five-year period. In South Darfur, UNICEF allocation decreased between
2010 and 2015, but there was a significant drop in 2011. In North Darfur, funds dropped sharply in 2011 and 2012, increased with a major allo-cation of US$5,389,317 in 2013 and dropped again in subsequent years, as shown in Figure 13 and Annex 6.
The vaccine procurement process, mainly for Bacillus Calmette-Guérin (BCG), measles and pentavalent vaccines, adhered to UNICEF pro-curement regulations. The unit cost for the
2010 2011 2012 2013 2014 2015
UNICEF Allocated Budget, USD, (South Darfur
4,246,068 121,698 265,584 1,588,174 1,629,613 1,537,962
UNICEF Allocated Budget, USD (North Darfur)
4,238,290 104,833 235,839 5,389,317 2,597,897 1,877,249
SHRP Planned, USD, (South Darfur)
24,417,510 19,615,241 14,040,608 11,485,685
SHRP Planned Budget, USD (North Darfur)
23,132,378 17,580,851 12,902,549 9,303,603
SHRP Allocated funds, USD, (South Darfur)
13,320,139 9,935,480 7,230,137 5,712,529 6,861,466 9,482,975
SHRP Allocated funds, USD, (North Darfur)
12,619,079 5,578,939 8,377,332 6,066,041 3,685,805 8,671,075
2010 2011 2012 2013 2014 20150
5,000,000
10,000,000
15,000,000
20,000,000
25,000,000
30,000,000
Figure 13: Funding of the health humanitarian programme
Source: UNICEF financial Reports and OCHA financial reports

38EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
BCG vaccine was US$0.1134, for measles was US$0.3069 and for pentavalent was US$0.1733, including their delivery in state level capitals in South and North Darfur. In general, immuniza-tion procurement achieved between 85 per cent and 101 per cent of the planned targets for both North Darfur and South Darfur, respectively. The UNICEF immunization programme contributed to an increase in the uptake of the BCG vaccine in North Darfur from 82 per cent in 2010 to 87 per cent in 2015, while in South Darfur uptake increased from 79 per cent to 87 per cent over the same period, as shown in Figure 14. In addi-tion, UNICEF procured various medical supplies to strengthen health service delivery. This in-cluded a total of 536,400 doses of 500-millilitre ringers lactate, 1,135,000 sachets of oral rehy-dration salts, 372,100 tablets of zinc sulphate, 17,893 bed nets and 874 primary health care kits for North Darfur. In South Darfur, 65,000 doses of 500-millilitre ringers lactate, 715,000 sachets
of oral rehydration salt, 511,000 zinc sulphate tablets, 7,000 bed nets and 10 primary health kits were distributed.
The uptake of the first dose of measles vaccine decreased from 78 per cent to 72 per cent in North Darfur and from 74 per cent to 80 per cent in South Darfur. There was low uptake of the second dose of measles in both North and South Darfur compared with the uptake of the first dose. However, UNICEF contributed to the increase in uptake of the second dose through sustained community mobilization to create awareness of the need for children under 5 re-ceiving the second dose of measles as shown in Figure 15 and Figure 16 below. This saw the uptake increase from 26 per cent in 2012 to 63 per cent in 2015 for North Darfur. While in South Darfur, the uptake increased from 26 per cent in 2012 to 65 per cent in 2015.
Figure 14: Number of children receiving BCG vaccine against the target
0
50000
100000
150000
200000
Num
ber o
f Chi
ldre
n
2010 2011 2012 2013 2014 2015
Nor
th D
arfu
r
Sout
h Da
rfur
Nor
th D
arfu
r
Sout
h Da
rfur
Nor
th D
arfu
r
Sout
h Da
rfur
Nor
th D
arfu
r
Sout
h Da
rfur
Sout
h Da
rfur
Nor
th D
arfu
r
Nor
th D
arfu
r
Sout
h Da
rfur
Planned Target Achieved Output
9222
2
1786
54
9513
6
1105
07
1028
24
1429
18
1060
75
1477
92
1194
25
1528
31
1128
84
1580
43
7594
3
1402
57
7581
9 1023
71
8503
0
1323
85
9450
1
1436
59
9177
4
1503
30
9859
4
1373
09
Source: UNICEF immunization reports

39EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
Figure 15: Number of children receiving measles immunization in North Darfur
0
20000
40000
60000
80000
100000
120000
Num
ber o
f Chi
ldre
n
2010 2011 2012 2013 2014 2015
Firs
t Dos
e
Seco
nd D
ose
Firs
t Dos
e
Seco
nd D
ose
Firs
t Dos
e
Seco
nd D
ose
Firs
t Dos
e
Seco
nd D
ose
Firs
t Dos
e
Seco
nd D
ose
Firs
t Dos
e
Seco
nd D
ose
Planned Target Achieved Output
8244
6
8505
2 9192
5
9192
5
9482
9
9482
9
9782
7
9782
7
1009
18
1009
18
6418
3 7223
9
6773
2
2367
5
6911
8
4768
2
6339
8
4464
3
7311
5
6343
2
0
50000
100000
150000
200000
Num
ber o
f Chi
ldre
n
2010 2011 2012 2013 2014 2015
Firs
t Dos
e
Seco
nd D
ose
Firs
t Dos
e
Seco
nd D
ose
Firs
t Dos
e
Seco
nd D
ose
Firs
t Dos
e
Seco
nd D
ose
Firs
t Dos
e
Seco
nd D
ose
Firs
t Dos
e
Seco
nd D
ose
Planned Target Achieved Output
1587
34
9818
6 1269
83
1269
83
1313
13
1313
13
1359
71
1359
71
4041
2
4041
2
1173
11
8260
4 1036
56
3313
0
1203
41
8606
8
1199
51
9479
4 1121
93
9112
6
Source: UNICEF immunization reports
Figure 16: Number of children receiving measles immunization in South Darfur
Source: UNICEF immunization reports

40EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
Between 2010 and 2015, the targets for pen-tavalent immunization were higher; and in South Darfur, the targets were nearly double what they were in North Darfur. However, in both states, these targets were neither surpassed nor met, save for a few cases in the administra-
tion of first doses. In North Darfur, targets were surpassed for the administration of first doses in 2011, 2012 and 2013, while in South Darfur targets were surpassed for the administration of first doses in 2012, 2013 and 2014, as show in Figures 17 and 18.
Figure 17: Number of children receiving pentavalent immunization in North Darfur
Figure 18: Number of children receiving pentavalent immunization in South Darfur
Source: UNICEF immunization reports
0
20000
40000
60000
80000
100000
120000
Planned Target Achieved Output
Num
ber o
f Chi
ldre
n
2010 2011 2012 2013 2014 2015
Firs
t Dos
e
Seco
nd D
ose
Third
Dos
e
Firs
t Dos
e
Seco
nd D
ose
Third
Dos
e
Firs
t Dos
e
Seco
nd D
ose
Third
Dos
e
Firs
t Dos
e
Seco
nd D
ose
Third
Dos
e
Firs
t Dos
e
Seco
nd D
ose
Third
Dos
e
Firs
t Dos
e
Seco
nd D
ose
Third
Dos
e
8244
6
8244
6
8244
6
8505
2
8505
2
8505
2
9192
5
9192
5
9192
5
9482
9
9482
9
9482
9
9728
7
9728
7
9728
7
1009
18
1009
18
1009
18
8161
5
7696
3
7152
4
8910
9
8371
4
8142
6 9430
9
8807
7
8462
0 9746
2
9395
9
9162
5
9318
0
8760
9
8362
0 9344
0
8979
0
8924
7
0
20000
40000
60000
80000
100000
120000
Planned Target Achieved Output
Num
ber o
f Chi
ldre
n
2010 2011 2012 2013 2014 2015
Firs
t Dos
e
Seco
nd D
ose
Third
Dos
e
Firs
t Dos
e
Seco
nd D
ose
Third
Dos
e
Firs
t Dos
e
Seco
nd D
ose
Third
Dos
e
Firs
t Dos
e
Seco
nd D
ose
Third
Dos
e
Firs
t Dos
e
Seco
nd D
ose
Third
Dos
e
Firs
t Dos
e
Seco
nd D
ose
Third
Dos
e
8244
6
8244
6
8244
6
8505
2
8505
2
8505
2
9192
5
9192
5
9192
5
9482
9
9482
9
9482
9
9728
7
9728
7
9728
7
1009
18
1009
18
1009
18
8161
5
7696
3
7152
4
8910
9
8371
4
8142
6 9430
9
8807
7
8462
0 9746
2
9395
9
9162
5
9318
0
8760
9
8362
0 9344
0
8979
0
8924
7
Source: UNICEF immunization reports

41EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
In regards to cost-effective analysis, and in ref-erence to the UNICEF nutritional framework, the humanitarian health programmes contribut-ed to improving the health status of under-five children and mitigated risks of malnourish-ment. As a result, UNICEF achieved its goal of reducing vaccine-preventable diseases. The cost-effective analysis therefore examined the number of vaccine shots administered to un-der-five children. Based on the calculations, the cost-effective ration for the health programme was US$6.91 in 2010 and US$1.04 in 2015, per vaccine administered to a child in North Darfur, while in South Darfur the cost per vaccine ad-ministered was US$6.19 in 2010 and US$0.88 in 2015 as shown in Figure 19.
20 The WHO Health Resource Availability Monitoring System is a rapid online system for monitoring health facilities, services and resource availability in emergencies. More details available at: <www.who.int/hac/herams/en/>, accessed 9 March 2017.
After the withdrawal of international NGO ser-vices in 2010, most health facilities became dys-functional due to the limited resources of the Government of the Sudan to facilitate and sup-port various health operations. Such funding gaps led to intermittent procurement and distribution of essential drugs as well as administrative costs for health personnel. This also affected the provi-sion of quality vaccines and the enhancement of systems, particularly cold chain equipment, which were substandard in rural areas in North Darfur.
Although the World Health Organization (WHO) Health Resource Availability Monitoring Sys-tem20 highlights a progressive increase in the number of health facilities providing IMCI, this
Figure 19: Cost of delivering one dose of a vaccine
Source: UNICEF financial reports
$0.00
$1.00
$2.00
$3.00
$4.00
$5.00
$6.00
$7.00
$8.00
North Darfur
Amou
nt (U
S$)
2010 2011 2012 2013 2014 2015
South Darfur
$6.91
$4.77
$0.18 $0.20
$3.18
$1.21
$2.04
$0.88
$0.21$0.15
$6.19
$1.04

42EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
is not evident in the coverage of under-five dis-eases, particularly the management of diarrheal and vaccine-preventable diseases in North and South Darfur. As such, this signalled additional challenges in regards to the quality of service provisions in rural/locality level health facilities. In addition, the unavailability of qualified health workers in health facilities continued to contrib-ute to this disparity, as confirmed during the key informant interviews with health personnel.
Though there are weekly coordination forums chaired by the State Ministry of Health, feed-back from health personnel confirm cases of duplication of activities that focus on the EPI activities in North Darfur. South Darfur has, however, outlined, the roles and responsibil-ities of all stakeholders, with WHO playing a distinct role in ensuring the quality of vaccines and related services in terms of EPI.
UNICEF contributed by fighting against harmful habits such as for measles. In the past, people didn’t know that im-munization is important; organizations have raised the awareness of the people about the importance of immunization and vaccination. UNICEF has also im-plemented awareness campaigns and awareness programmes, such as for female genital mutilation, health and sanitation and the malaria campaign. When the awareness campaign have started and it is usually done by the health committee assigned by what-ever organization, people who attend usually bring what they have learned to the other people in the camp who didn’t have the chance to attend; they raise the awareness of the other people. It’s youth who usually do this activity.
— Community leader, Zam Zam Camp, North Darfur
The leakage of long-lasting insecticide-treated nets, as reported during the focus group dis-cussions and the key informant interviews, led to the low coverage of under-five children, thus increasing their risk of malaria.
4.4 Effectiveness
The assessment of the effectiveness of humani-tarian action between 2010 and 2015 was based on UNICEF’s monitoring and evaluation frame-work indicators (Country Programme Document/Country Programme Action Plan Result Matrix, the Annual Work Plan and the theory of change) against the achievements made at the state level. Thus, the analysis was based on how the humanitarian programmes translated outputs into sustained outcomes at the community level.
4.4.1 WASH programme effectiveness UNICEF’s WASH programme focused on the af-fected population, schools and the sustained de-velopment of the operation and maintenance of water and sanitation facilities. In this regard, the evaluation established that the UNICEF WASH section set an ambitious target of 50 per cent, although only 6.19 per cent of the population had access to an improved drinking water source in North Darfur and 4.92 per cent had access in South Darfur. From the sampled households, the respondents indicated that they obtained water that was piped into their yard/plot/compound (5.2 per cent) or through public taps (21.4 per cent), an open public well (23.5 per cent) or boreholes (34.7 per cent). A small proportion of these wa-ter sources (7.1 per cent) only provide water for a maximum of six months, while another 10.6

43EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
per cent of water sources have water for up to nine months and the other 70.4 per cent of water sources have water throughout the year (see Annex 7). This was further confirmed through the focus group discussions.
WES, in coordination with UNICEF, has implemented a number of water pumps in our area, though most of them are not working in the dry season. In our Zam Zam Camp, only 15 out of the 72 water pumps are working. — Community leader, Zam Zam Camp
Water facilities supported by UNICEF in North Darfur. Operation time for the water facility is between 8 a.m. and 11 a.m.
A man drawing water from the commercial water vendors in Zam Zam Camp
One of the key Sphere standards in the pro-vision of water is ensuring that the maximum distance from any household to the nearest water point is no more than 500 meters. From the sampled household respondents, it was observed that:
� 26 per cent of the target population ac-cessed water within a 500-metre radius
� 31.3 per cent walked up to 1 kilometre to access water
� 20.9 per cent walked 2 kilometres to access water
� 17.5 per cent walked for more than 3 kilo-metres to access water
These distances have not changed significantly since 2010. Only 12.8 per cent reported some changes in the distance to and from the water sources. In addition, 69 per cent of the sampled households reported that they wait for more than 31 minutes at the water point, which is above the recommended 30 minutes in Sphere standards. The analysis of distances to various water sources was corroborated through the community mapping tool during the focus group discussion, which confirmed the community walked up to five kilometres to access water, as illustrated in Figure 20.
©UN
ICEF
Sud
an/E
valu
atio
n Te
am©
UNIC
EF S
udan
/Eva
luat
ion
Team

44EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
Although a significant number of people could access water within a 1-kilometre radius, they also spent more than 31 minutes queuing at the water sources, as presented in Figure 21. This shows that either more people are using the same water facility or the discharge rate of the water facilities is slow. The slow discharge,
primarily during dry seasons, is one of the ma-jor causes of delay at the water sources. As a result, most water providers dispense water only for a few hours per a day to manage the recharge of the water levels in the various bore-holes in North and South Darfur.
0
3
6
9
12
15
Perc
ent o
f Hou
seho
lds
Less than500 m
501m – Lessthan 1 km
1.1 km – Lessthan 2 km
2.1 km – Lessthan 3 km
More than3.1 km
Don’t know
9.4%
3.4%
9.9%
11.1%
1.0%1.4%
0.5%
8.9%
6.0%
4.5%
1.8%
2.9%
5.5%
3.3% 3.3%
1.8%2.2%1.3%
0.7%
13.6%
1.6% 1.7%
3.9%
0.1%
El Fasher Umkadada Kass Other
0
5
10
15
20
25
30
35
El Fasher
Perc
ent o
f Hou
seho
lds
Under 5min
6-10 mins Over 11-20mins
21-30 mins Over 31 mins
Umkadada Kass Other
0.5%
3.0%
5.7%3.2%
13.0%
0.5% 1.3% 1.3%3.5%
21.3%
0.2% 0.3% 0.8% 1.2%
7.3%
0.3% 0.7% 0.5%
4.8%
30.6%
Figure 20: Distance of the household to the nearest water source
Source: Evaluation of Humanitarian Action (EHA) 2016 Household Survey
Figure 21: Presentation of the time taken at the water point
Source: EHA 2016 Household Survey

45EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
As confirmed during the focus group discus-sions, in stressed areas, the majority of rural and poor urban communities use surface holes from streambeds, open wells and hand pumps if available, given that these sources are free (however, the price is at least 12 to 15 Sudanese Pounds21 for one barrel per day per household from commercial wells). From the sampled household respondents, 92.1 per cent spend less than 1 Sudanese Pound to purchase a 20-li-tre Jerry can; 6.5 per cent spend between 2 and 5 Sudanese Pounds; 1 per cent spend between 6 and 10 Sudanese Pounds; and 0.5 per cent get water for free, as shown in Table 3.
21 US$1 = 6.5 Sudanese Pounds
A review of UNICEF WASH supply indicated that it contributed to ensuring the continuity of water treatment using chlorinators who chlo-rinated water in camps and within host com-munities. However, feedback from the sample household showed that there is a weakness in household water treatment, with only 13.9 per cent (in 2015) and 18.8 per cent (in 2010) of households having treated their drinking water. As shown in Figure 22, 12 per cent of house-holds use chlorine-based compounds, 0.1 per cent use sunlight, 3 per cent use alum stones, 4 per cent use all treatment options, and 6 per cent prefer to boil water.
Table 3: Presentation of the cost of a 20-litre Jerry can of water
El Fasher Umkadada Kass Others Total
Less than 1 Sudanese Pound 50.0% 21.9% 5.3% 14.9% 92.1%
2–5 Sudanese Pound 1.9% 1.2% 0.5% 2.9% 6.5%
6–10 Sudanese Pound 0.0% 0.0% 0.0% 1.0% 1.0%
No payment 0.0% 0.0% 0.0% 0.5% 0.5%
Total 51.9% 23.1% 5.8% 19.2% 100.0%
Source: EHA 2016 Household Survey
0
5
10
15
20
25
30
35
Perc
ent o
f Hou
seho
lds
Boiling Addingchlorine/PUR
Alumstones
Traditionalleaves
Ash Sunlight Don’t treat
El Fasher Umkadada Kass Other
1.9%3.7%
0%1.0% 0.2% 0.2%
24.1%
5.9% 5.4%
0.3%2.4%
0% 0%
28.5%
0% 0% 0% 0.8% 0% 0%
15.3%
0.3%
6.2%
0% 0.2% 0.2% 0%
32.2%
Figure 22: Presentation of household water treatment options
Source: EHA 2016 Household Survey

46EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
Key informant interviews with laboratory ana-lysts in North and South Darfur confirmed that up to 85 per cent of the water from various sources is polluted.
What we need is instead of UNICEF and its partners digging and implementing wells and after a few months it be-comes dry, it’s better for us that they dig wells that mostly depends on the groundwater. As you see here in Zam Zam Camp, we only have two ground-water wells. We have already request-ed this from UNICEF before, ‘we need wells’; at least six or seven wells in Zam Zam will be enough for us. Generally pumps dry due to sand.—Community leader, Zam Zam Camp
The provision of safe excreta disposal was a key activity for UNICEF during the evaluation period. UNICEF reached 67 per cent of the tar-geted affected population in North Darfur and 64 per cent of the targeted affected popula-tion in South Darfur with safe excreta disposal. However, the number of community members within the population that is open defecation free and using improved sanitation facilities was 33 per cent in North Darfur and 60 per cent in South Darfur, within UNICEF-targeted areas. From sampled household respondents in North and South Darfur, 50 per cent (n=381) of the af-fected population use traditional pit latrines,22 2 per cent (n=16) use an open pit that is dug some distance away from their households, 1 per cent (n=4) use ventilated improved pit latrines, 1 per cent (n=4) use flush toilets, and the remaining 46 per cent (n=360) practice open defecation.
22 The traditional pit latrine refers to a structure that collects human faeces in a hole covered with a slab. The structure is then surrounded by a shelter with no ventilation pipe.
The toilets are shared between all peo-ple in this area, women, men, boys and girls. These toilets were built by Oxfam America and they used to dig a big hole to empty these toilets and then bury this hole. Now it is the people who do this job and they rarely do it since it is not hygienic and comfortable anymore.—Community member
Temporary sanitation facilities erected by UNICEF in Zam Zam Camp
UNICEF has made significant contributions to hygiene behaviour change. The number of peo-ple sampled from households who confirmed that they wash their hands after visiting the toilet, before feeding a child and before eating has increased over the past five years. Among those who wash their hands after visiting the toilet, 89 per cent (n= 678) in the last five years and 98 per cent (n=751) in the last six months, while those who occasionally and did not wash their hands declined by 11 per cent (n=86) and 0.2 per cent (n=13), respectively. Before feed-ing a child, 92 per cent (n=702) in the last five years and 98 per cent (n=752) in the last six months washed their hands with soap, while those who occasionally and did not wash their
©UN
ICEF
Sud
an/E
valu
atio
n Te
am

47EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
hands before feeding a child declined by 3.1 per cent (n=24) and 2 per cent (n=6), respectively. Before eating, 94 per cent (n=715) in the last five years and 99.6 per cent (n=761) in the last six months washed their hands, while those who occasionally and did not wash their hands declined by 6.4 per cent (n=49) and 0.3 per cent (n=3), respectively.
Based on the focus group discussion analysis and the key informant interviews, lack of ad-equate implementation and enforcement of environmental health laws and protocols was due to poor resource allocation for sanitation activities by the Ministry of Health, local au-thorities and the community. Discussion with children’s groups confirmed that hygiene educa-tion was put into practice in Grade 6, while for the lower grades, parents and caregivers orient the children on personal hygiene practices. The children, who doubled up as caregivers for chil-dren under 5, were not targeted with sanitation messages early enough.
In conflict areas of the western part of North Darfur, UNICEF supported the implementation sanitation and vector control activities to limit disease transfer in urban and peri-urban areas, as confirmed by communities during the focus group discussions. Rural populations, however, especially nomads, have poor environmental health education due to their continuous relo-cation in search of pasture and water.
WASH programming in schools is a key UNICEF strategy aimed at controlling diarrheal diseases among affected populations. UNICEF has en-abled 39 per cent of targeted school children to benefit of access to safe drinking water in North Darfur and 43 per cent in South Darfur. Seventy-six per cent of children interviewed in
focus group discussions confirmed that they accessed water from taps and perceived the water to be clean.
In addition, 39 per cent and 56 per cent of schoolchildren targeted by UNICEF were pro-vided with adequate sanitary latrines in North Darfur and South Darfur, respectively. Focus group discussions with children confirmed that they wash their hands with soap. This assertion was further corroborated through observation of children washing their hands with soap.
In terms of challenges, heavy investment in the operation and maintenance of water sources due to water drawdown led to already drilled water sources drying up, and high operation costs for drilling new water sources to provide water to affected populations. In addition, fol-lowing the departure of international NGOs in 2010, target local communities and local author-ities could not continue with operations and maintenance due to the lack of a clear hando-ver process, lack of spare parts, lack of main-tenance skills, and the absence of dedicated entrepreneurs in the community. In all five local-ities, however, the local community’s capacity to manage water supply continued to improve through assigned water committees, though the quality of leadership and coordination of efforts was lacking.
4.4.2 Nutrition programme effectiveness The main UNICEF nutritional programme out-come envisaged in the theory of change was the management of Severe Acute Malnutrition (SAM). The performance indicators of manage-ment of SAM targeted a cure rate of at least 75 per cent of admitted severe acute malnourished children. But the default rate and death rate are high: i) around 15 per cent of children admitted

48EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
for SAM management default from treatment, ii) 5 per cent of the children admitted do not respond to treatment and iii) about 5 per cent of the admitted children die due to SAM (see Annex 9 and Annex 10).
The number of children under 5 admitted for SAM treatment increased from 66 per cent in 2010 to 119 per cent in 2015 in North Darfur. Admissions in South Darfur increased from 72 per cent in 2010 to 106 per cent in 2015 against planned targets. The share of primary health care facilities providing SAM treatment was 40 per cent in North Darfur and 24 per cent in South Darfur. Thus, most admissions by UNICEF for SAM treatment were at stabilization centres. The analysis of the UNICEF and State Ministry of Health reports recorded an increase in the percentage of under-five children cured of SAM between 2011 and 2015, from 79.7 per cent to 89 per cent in North Darfur and from 78 per cent to 87 per cent in South Darfur. The default rate declined over that same period, from 12.3 per cent to 8 per cent in North Darfur and from 6 per cent to 4 per cent in South Darfur. The non-response rate decreased from 7 per cent to 2.5 per cent in North Darfur, while in South Darfur the rate decreased from 6 per cent to 4 per cent. The death rate for both North Darfur and South Darfur remained below 1 per cent.
In an effort to prevent MAM, the World Food Programme (WFP) supported the Blanket Sup-plementary Feeding Programme for four to five months during the lean season for all children under 5. This was followed by strong collab-oration between UNICEF and WFP targeting the most vulnerable children at risk of malnu-trition—a priority for the intervention as high-lighted in the Nutrition Cluster minutes in El Fasher for the periods under review. Similarly,
there was significant action on the Integrated Blanket Supplementary Feeding Programme initiated in 2011 for MAM prevention, targeting children under 3 years and in response to rising malnutrition rates among children under 5 years in both North and South Darfur.
The number of children who were covered with two annual doses of vitamin A increased from 94 to 100 per cent in North Darfur and from 96 to 103 per cent in South Darfur. The achieve-ment of the vitamin A target was closely tied to the immunization programmes at the communi-ty level, thus corresponding to high EPI cover-age, and illustrating an example of inter-section collaboration at the community level. Feedback from the sampled households shows a higher uptake of breastfeeding practices by mothers and caregivers as a result of UNICEF’s continu-ous promotion of breastfeeding practices at the community level. Within the first three months after the child is born, up to 87 per cent of the sampled respondents breastfed their children. This decreased to 80 per cent for those who breastfed for up to six months and 77 per cent for those who breastfed for up to 12 months.
Bottleneck analysis (factor analysis) for nutrition programmeFrom the key informant interviews with the State Ministry of Health officials and commu-nity-based organizations, the high logistical cost for the delivery of nutrition-related supplies, mainly Plumpy’Nut, contributed to low perfor-mance in regards to covering children at risk for MAM and SAM.
The supplementary food of flour mix provided by WFP in the past has par-ticipated mainly in supporting the child health but now it has stopped; there

49EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
were available drugs for treatments of diseases, now the situation has changed.”—Mother from El Fasher IDP Camp
In the design of the nutrition programme, how-ever, nutrition treatment centres were not an integral part of health facilities. As such, there are health facilities that provided other curative services for the under-five children alongside nutritional services, while others did not.
Limited access to the most vulnerable children residing in villages far away from the nutrition treatment centres undermined achievement against the targets, since not all vulnerable chil-dren were met within the period of evaluation (2010–2015). This also arose from an inadequate number of functional nutrition centres within affected communities, since only 42 per cent of functional health facilities (288 health facili-ties out of 422 health facilities in North Darfur) offer the IMCI services that include nutritional services or packages. The nutrition and health education also did not cover some hard-to-reach areas where the vulnerable population is found; innovative ways to reach these areas should be devised.
4.4.3 Health programme effectiveness UNICEF’s health programme endeavoured to increase oral rehydration salt uptake among children with diarrhoea by 65 per cent; the per-centage uptake of recommended vaccines at stipulated ages; the number of newborns ben-efiting from essential newborn and postnatal care at the community level; and the number of births attended by skilled birth attendants .
UNICEF health interventions contributed to the treatment of 40 per cent of children with diar-
rhoea in North Darfur, and up to 66 per cent in South Darfur. Routine data from the State Ministry of Health and UNICEF show that ap-propriate management of diarrhoea using oral rehydration salts is unavailable; hence monitor-ing report figures are missing from the years 2012 and 2013 (see Annex 11 and Annex 12).
The UNICEF vaccine programme recorded am-bivalent results during the period under review. UNICEF contributed to an increase in the uptake of the BCG vaccine in North Darfur from 82 per cent in 2010 to 87 per cent in 2015, and in South Darfur from 79 per cent to 87 per cent. The uptake of the first dose of measles decreased from 78 per cent to 72 per cent in North Darfur, and increased from 74 per cent to 80 per cent in South Darfur. There was low uptake of the sec-ond dose of measles in both North and South Darfur compared with uptake of the first dose. However, uptake of the second dose increased tremendously from 26 per cent in 2012 to 63 per cent in 2015 for North Darfur and from 26 per cent in 2012 to 65 per cent in 2015 for South Darfur. These changes resulted from sustained community mobilization to create awareness of the need for children under 5 to receive the second dose of measles vaccination.
Both the measles and pentavalent vaccine re-gimes illustrated interesting trends in access to routine immunization programmes and ser-vice utilization. A significant variation is evident in regards to coverage of measles vaccination among the one-year-old children in North Darfur compared with South Darfur. Coverage of the first dose of measles vaccination is lower than coverage of the second dose in North Darfur, though the administration of these two doses were on par in 2015. Thus, UNICEF and partners made impressive efforts to increase the second

50EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
dose coverage through accelerated immuniza-tion exercises.
Uptake of the first dose of pentavalent vaccine in North Darfur decreased from 99 per cent in 2010 to 93 per cent in 2015. The UNICEF inter-vention realized an increased uptake of up to 105 per cent between 2011 and 2013 due to a rise in demand at the community level. In South Darfur, however, uptake decreased from 97 per cent to 94 per cent, showing a decline in the demand from community members.
The uptake of vaccines differs between the states. In North Darfur, the uptake of the first dose of oral polio vaccine was 66 per cent, for the second dose was 62 per cent and for the third dose was 75 per cent. The disparity be-tween the first and third doses points to the accuracy of the data in North Darfur. In South Darfur, however, the uptake of the first dose was 78 per cent, the second dose was 73 per cent and the third dose was 71 per cent. It was evident through key informant interviews and observations that the investments in immuni-zation services in North Darfur are weak com-pared with in South Darfur, which had a reliable and functional EPI information management system.
UNICEF investment in maternal and neonatal health programmes contributed to up to 81 per cent of skilled attendants supporting births in North Darfur, but except for 2010, data are un-available for South Darfur from 2011 through 2015. In 2010, only 46 per cent of births involved skilled attendants. UNICEF’s IMCI in primary health facilities increased from 13 per cent to 67 per cent in North Darfur and from 28 per cent to 40 per cent in South Darfur, but this fell short of its 60 per cent targets, with an overall
achievement of 38 per cent and 34 per cent in North Darfur and South Darfur, respectively. This programme also supplied midwifery kits to health centres in South Darfur, but did not deliver any to North Darfur.
Bottleneck analysis (factor analysis) for the health programmeAlthough UNICEF’s IMCI strategy is in line with the Ministry of Health’s commitment to improve child health, it failed to realize set objectives due lack of technical and logistical capacity. The strategy promoted health activities, mainly at the health facility level, as well as at the com-munity/village levels. Challenges included poor child identification, irregular child referrals and low adherence to children’s various treatment regimens. Information recording and report-ing mechanisms are available for IMCI within community component reporting—including for reporting on the causes of under-five deaths, neonatal deaths and maternal deaths—but have remained fragile and non-informative.
The inconsistent functionality of the cold chain management system, which is primarily due to the absence of reliable power sources in rural-based health facilities, impedes vaccine quality assurance.
The cultural reliance of Darfurian households on women’s income, despite the limited liveli-hood opportunities for women, has led caregiv-ers to spend most of the day outside of their households for daily earning. This has a major impact on maternal health, child health and the level of care practice provided to children at the household level. However, poor environmental and health conditions, especially in rural areas, have considerably worsened children’s health after the departure of international NGOs. These

51EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
challenges have dramatically affected utiliza-tion rates of health services and increased the popularity of preliminary management by tradi-tional healers with their aggressive treatment approaches (curettage, superficial skin cutting, etc.), which has aggravated children’s condi-tions, delayed their treatment and made them more prone to death.
The annual review does not recognize the par-ticipation of health technical expertise from Lo-cality Level, including in planning activities with partners (UNICEF and implementing partners) at the state level to raise specific issues per locality. These representatives participate only in annual meetings with the Ministry of Health in El Fasher.
The majority of the affected population, includ-ing children with multiple sicknesses, cannot access health services due to security issues, high transportation fees and health facility
fees. Moreover, the limited financial, human and physical capacity of the Ministry of Health, communities and local authorities, makes them unable to run an adequate health service in ur-ban and rural areas. The complicated delivery of health services has continued to raise concerns from various audiences.
Feedback from community members and key informant interviews with health staff highlight-ed challenges such as the inadequacy and stock outs of essential drugs, mosquito nets—and sometimes vaccines—for several months; com-plex drug/supply delivery from El Fasher due to the long distance; lack of budget for drug trans-portation; and insecurity. Drugs are available in commercial drug stores but are too expensive for beneficiaries and in some cases do not meet safety and quality standards. The presence of commercial drug stores has encouraged some caregivers to buy drugs directly without ade-quate medical management.
Mothers and caregivers wait to receive treatment from a community dispensary in Saraf Omra locality.
©UN
ICEF
Sud
an/N
orth
Dar
fur F
O
©UN
ICEF
Sud
an/N
orth
Dar
fur F
O

52EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
UNICEF used to spray pesticides and distributes mosquito nets for eradica-tion of malaria in the area in addition of distribution of Jerry cans, this was done in 2010; However, since that time in 2010, there is no Mosquito nets dis-tributed.—Community leader, Alsalam Camp
4.5 Impact
The impact analysis was based on documenta-tion of the positive and negative changes evi-dent at the community level, specifically on im-pact indicators for WASH, nutrition and health, to which UNICEF humanitarian programmes contributed. The WASH analysis focused on the changes in regards to diarrheal diseases as an indicator of the quality of water and san-itation services. It also analysed changes in global acute malnutrition (GAM) rates and the accompanying factors that contributed to the reduction or increase in GAM rates, mainly liveli-hood options and access to food by the affected population, as presented in the UNICEF nutri-tion conceptual framework. The responses from the caregivers, sampled households and focus group discussion participants on whether the child had suffered from marasmus were proxy indicators for wasting. The health impact analy-sis was based on the reduction of vaccine-pre-ventable diseases and the prevalence of malaria among children under 5, but also documented responses on the number of children who had died of those diseases.
4.5.1 Impact of the WASH programme The WASH impact analysis was based on the reduction of diarrheal disease incidence due to the provision of safe water and sanitation op-
Community Voice:
“I arrived in Kabkabiya in 2007 when Médecins Sans Frontières and Oxfam GB were operational. Water was available but we were asked to dig a toilet hole and we received cement platform. Our house and toilet clean were without flies. There were women who taught my mother how to breastfeed my little brother and when my sister got married they came to examine her during her pregnancy. They taught us how to triage garbage and dig a hole to burn it at home.
I fill five Jerry cans a day and if I have laundry I fill eight ones. The hand pump is slow and people are a lot.
I have two kids at 3 and 5 years old who always fall sick with chest infections and diarrhoea. Drugs are expensive but I give them water with salt and sugar for diarrhoea and I’ve never taken them to nutrition centre. Once some people came to our neighbourhood and measure their arms and said they are okay.”
Halima from Kabkabiya Locality
tions in accordance with the WASH Sphere stan-dards. The changes documented included the adoption of personal hygiene practices, noted through observation of the affected population washing their hands after using a toilet, before eating, before preparing food and after clean-ing a baby. The responses from the sampled households indicated that 37 per cent believed that UNICEF WASH programming is contribut-

53EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
ing to improved hygiene, sanitation and health status among the affected population. About 70 per cent of the focus group discussion partici-pants also confirmed that water and sanitation standards have deteriorated immediately after the withdrawal of the international NGOs from North and South Darfur.
Community members among the sampled re-spondents reported their previous experience of fewer diarrhoea cases in 2010 (33 per cent) than in 2015 (36 per cent). Up to 6 per cent of sampled respondents from El Fasher reported suffering from diarrhoea, while 18 per cent re-ported similar cases in Kass locality in 2015. This difference between the 2010 scenario, where up to 12 per cent reported cases of diarrhoea in El Fasher and 10 per cent reported cases of diarrhea in Kass locality, is consistent with UNICEF’s investment in WASH programming in North Darfur compared with South Darfur.
In line with UNICEF’s hygiene promotion strate-gies, there are a considerable number of house-holds that sought professional medical services mainly at the health facilities for the manage-ment of diarrheal cases among children under 5 years. However, a significant number sought no treatment due to lack of money to pay for the recovery costs at various health facilities and unreliable transport to dispensaries located far away from their area.
23 The 10 per cent WHO GAM emergency threshold is outlined in the Sphere standards published on 2014.
4.5.2 Impact of the nutrition programmeThe GAM rate for North Darfur increased from 22 per cent in 2010 to 28 per cent in 2014, and in South Darfur, decreased from 15 per cent in 2010 to 14 per cent in 2015, as captured in the routine statistics reports conducted by UNICEF in collaboration with the State Ministry of Health for North Darfur and South Darfur. These fig-ures are relatively high compared with the WHO emergency threshold of 10 per cent GAM.23 Feedback from key informant interviews with State Ministry of Agriculture officials in both states confirmed that access to food among the affected population contributed to increased GAM rates in North and South Darfur.
A mother in El Salam Camp, North Darfur passing a dry water tap in search of water
©UN
ICEF
Sud
an/E
valu
atio
n Te
am
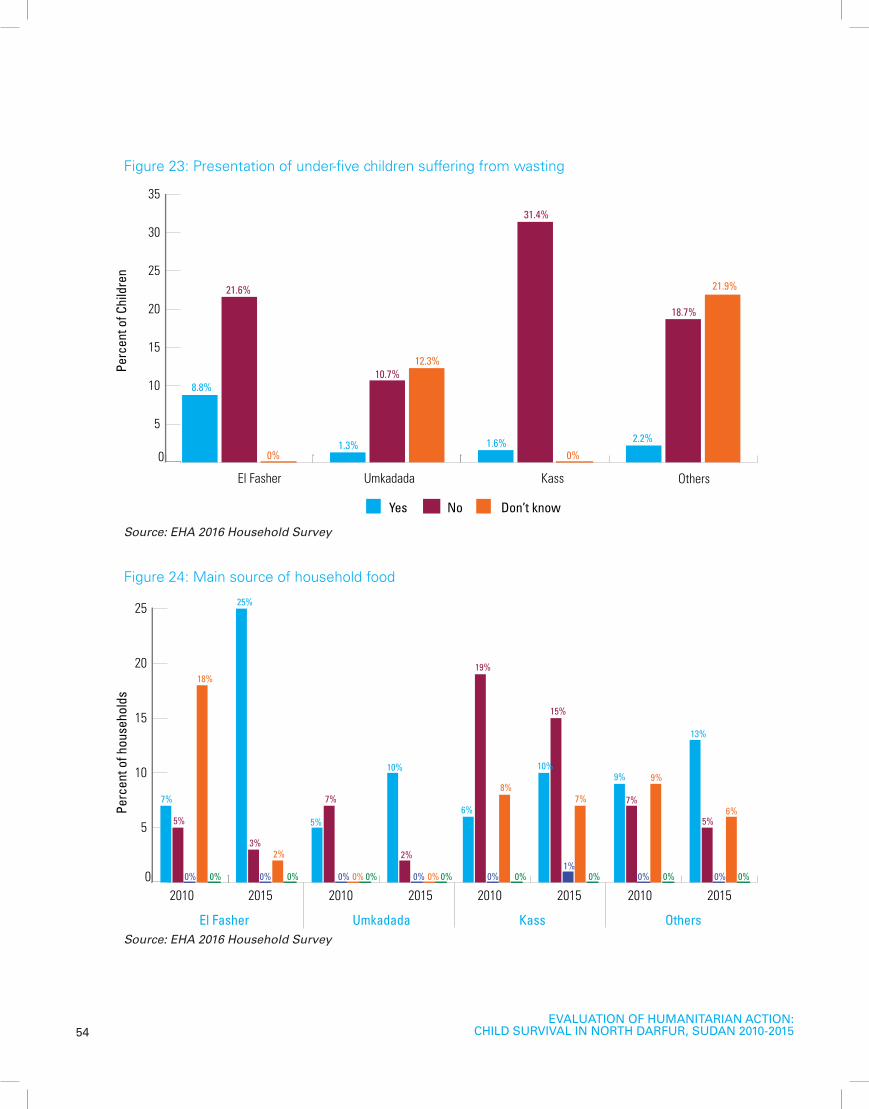
54EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
0
5
10
15
20
25
30
35
Yes
Perc
ent o
f Chi
ldre
n
El Fasher Umkadada Kass Others
No Don’t know
0%
12.3%
0%
21.9%21.6%
10.7%
31.4%
18.7%
8.8%
1.3% 1.6% 2.2%
Figure 23: Presentation of under-five children suffering from wasting
Source: EHA 2016 Household Survey
0
5
10
15
20
25
Purchase from market From the family farmland Kitchen garden
Food ration from WFP Donation food from community members
Perc
ent o
f hou
seho
lds
2010 2015 2010 2015 2010 2015 2010 2015
El Fasher Umkadada Kass Others
7%
25%
5%
10%
6%
10%9%
13%
5%
3%
7%
2%
19%
15%
7%
5%
0% 0%0% 0% 0% 0% 0%0% 0% 0% 0% 0% 0% 0% 0% 0%1%
0%
18%
2%
8%7%
9%
6%
Figure 24: Main source of household food
Source: EHA 2016 Household Survey

55EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
Fourteen per cent (n=106) of households sam-pled reported a child suffered from marasmus (an indicator of wasting). More cases of child wasting were reported in El Fasher (9 per cent) compared with other localities, as presented in Figure 23.
Wasting in North and South Darfur occurred due to varied food insecurities and dietary diversity weaknesses in these two states, as confirmed by the focus group discussions with the com-munity in Kass locality. The frequent displace-ments in North Darfur compared with South Darfur due to the conflict continued to affect the major food sources among the affected, signalling an over-dependence on relief food, which declined between the review years of 2010 and 2015.
Responses from households sampled in the community indicated that in 2015, purchase from the market is the main source of food for 59 per cent of households (n=447), followed by family farmland at 25 per cent (n=194) and WFP food rations at 14 per cent (n=109). Kitchen gar-den and community food donations constituted the lowest sources. Five years ago, however, family farmland (38 per cent) was the main source of food for most households, followed by WFP food rations (34 per cent), purchase from the market (27 per cent), NGOs (0.7 per cent) and kitchen gardens (0.1 per cent).
The availability of food rations and sources have declined. For example, the WFP food ration de-creased significantly from 34 per cent (n=261) in 2010 to 14 per cent in 2015. Similarly, food from family farmland declined from 38 per cent (n=288) in 2010 to 25 per cent (n=194) in 2015. Feedback from key informant interviews and focus group discussions with the affected
community corroborated the changes in the WFP food ration and the increased demand for food among the affected population. WFP has therefore begun profiling the affected popula-tion in terms of their capacity and ability to buy food depending on their economic situation, in order to develop a more sustainable food distribution strategy. Despite the reduction of WFP food rations, up to 86.5 per cent of the sampled households consume between two and three meals in one day. Feedback from the focus group discussion supported this eating pattern, with tea and porridge being the main types of food given to children under 5.
WFP stopped supporting 63 per cent of the population. Of the 40 per cent of the population who have the food vouchers, this support will stop in the next one year. Out of 237,000 people in the camp, 107,000 have the WFP food vouchers. From this number, 37,000 have stopped getting the food vouch-ers, 23,000 will be phased out after six months and 40,000 will stop getting the food voucher in the next 12 months—Community member, Zam Zam IDP Camp
Since the purchase of food from the market is the most preferred option for food acquisition, it formed the basis for conducting an analysis of the livelihood options of targeted household. The main economic activities in these regions over the past five years are casual labour (19 per cent), agriculture (19 per cent), small-scale projects (19 per cent), and selling dried farmed produce (18 per cent). The minor activities constituting less than 5 per cent include shop keeping, livestock keeping, formal employment, livestock trade and teaching religious books.

56EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
Respondents from the household survey in El Fasher are predominantly small-scale project executers (12 per cent), agriculturalists (8 per cent) and casual labourers (5 per cent), com-pared with Umkadada and Kass residents. Kass has more sellers of dried farm produce (6 per cent) than Umkadada (5 per cent) and El Fash-er (0.4 per cent). These residents sell fresher farm products (2.4 per cent) than El Fasher (0.5 per cent) and other localities (2 per cent). Sentiments from the community focus group discussions corroborated these data as the community member notes in the quote below.
The UNICEF nutrition programme did not take into consideration the livelihood component to enhance access to food for the affected popu-lation. Feedback from the sampled households indicated that the average household income per month varied between 1 and 800 Sudanese Pounds, while in the majority of localities, aver-age household income was between 201 and 400 Sudanese Pounds. Within the 201 and 400 Pounds income cluster, the most households came from El Fasher (12 per cent), followed
by Kass (7.8 per cent), Umkadada (4 per cent) and other localities (7.8 per cent). Within the 1 and 200 Pound income cluster, the most households came from El Fasher (5 per cent), followed by Kass (4 per cent) and Umkadada (2 per cent), but not other localities put together (6.5 per cent). Most of the residents of inter-nally displaced persons had no income (35 per cent), while 12 per cent depended on farming, small-scale projects, casual labour, trade and organizational support. Among the residents of IDP camps without income, there were more residents of El Fasher without income (18 per cent) than Kass (12.7 per cent) and other lo-calities (4.3 per cent); Umkadada did not have residents in camps.
“Local farming outputs and crops exchange with neighbouring localities are the main food sources. The main crops we trade for include millet, okra, dark green vegetables, groundnuts, mangoes, pigeon peas and other fruits. Livestock and poultry were one of the main food sources in the locality but for the past five years they became threats for the household by attracting violent livestock thieves.”
El Fashir-Rural, Community Member
Community Voice:
“Asil is my daughter’s baby, she is always sick since her mother weaned her after she got pregnant. Her feeding is poor and we don’t have milk to give her. When she gets sick I bring her to the hospital and stay with her. She lives with her mother in Umkdada but I live in Zarafa. Her mother did not bring her to the nutrition clinic before and after she got admitted by the doctor the first time she followed up at the clinic but never received the food ration after because her mother could not bring her. Now her mother has delivered and Asil got sick again. We brought her drugs from the pharmacy with no improvement. Now she has been admitted for two weeks and takes only hospital milk but she doesn’t eat because of her oral sores.”
Halima from Umkadada Locality

57EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
This low-level income and change in food distri-bution modalities contributed to affected pop-ulations accessing less nutritious food due to minimal buying capacity, which played a role in the increase in GAM rates in North Darfur. The increased number of displaced people due to conflict further exacerbated the cases of wasting with more IDPs in El Fasher reporting more wasting among children under 5.
The economy of the target population relies entirely on agricultural and livestock production, while dietary diversity varies among many urban and rural communities. Millet grain, pulses and dark green vegetables are available for most of the population. Meat, fresh milk, poultry and eggs, however, are considered luxury commodi-ties. Over the past five years, livestock and poul-try keeping have precipitated threats and violent robberies. In Umkadada, for example, food is available but at a higher price due to poor crop production over the years and limited range-lands for animals, which lead to threats similar to those seen in conflict zones.
4.5.3 Impact of the health programme Although the evaluation recognizes that the UNICEF health programming goes beyond EPI and IMCI, the evaluation focuses on key health areas that contribute to reducing child mortality in North and South Darfur, within the humani-tarian context and as captured in UNICEF roll-ing work plans. Fourteen per cent of sampled households confirmed that a child under age 5 from that household had died between 2010 and 2015. More deaths were reported in 2015 compared with other years. In El Fasher, 5 per cent of sampled households confirmed a child death, in Kass, 4 per cent confirmed a child death, and in Umkadada, 2 per cent confirmed a child death. The distribution of these deaths shows that children aged 0–12 months were the ones who died in higher numbers, overall accounting for 69 per cent of all child deaths. On the other hand, children aged 0–24 months accounted for 83 per cent of all deaths.
From the routine data analysis, the affected population’s compliance with EPI services in-
Table 4: Source of household income for the internally displaced persons for households with under-five children
Source of income El Fasher (%) Umkadada (%) Kass (%) Others (%) Total (%)
Farmer 2.09 0.00 0.26 1.05 3.40
Small-scale projects 2.23 0.00 0.39 0.26 2.88
Trade 0.65 0.00 0.13 1.18 1.96
No income 17.93 0.00 12.70 4.32 34.95
Full-time employment 0.00 0.00 0.00 0.13 0.13
Casual labour 0.13 0.00 0.00 3.14 3.27
Cash transfers from organizations 0.00 0.00 0.00 0.39 0.39
Not IDPs 7.33 12.57 19.50 13.61 53.01
Total 30.37 12.57 32.98 24.08 100.00 Source: EHA 2016 Household survey

58EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
creased between 2010 and 2015 within the immunization regimes for BCG, measles, polio and pentavalent. However, there were cases of measles that were reported by community members from sample households and during focus group discussions. Regarding the utili-zation of long-lasting insecticide treated nets by children under 5, 49 per cent (n=377) slept under a treated bed net the night before the survey and 41 per cent (n=315) did not sleep under a treated bed net the night before the
survey (see Figure 25). Feedback from 85 per cent (n=282) of the sampled households shows that most children under 5 did not sleep under a bed net because they did not have one.
Reported cases of malaria among children un-der 5 was proportionate to the number of un-der-five children who had never slept under a bed net. A total of 53 per cent (n=407) of sam-ple households reported malaria cases within the past six months (see Figure 26).
0
5
10
15
20
Yes
Perc
ent o
f Chi
ldre
n
El Fasher Umkadada Kass Others
No Don’t know
17%
7%
15%
9%
13%
3%
17%
9%
1%3%
1%
5%
0
5
10
15
20
Perc
ent o
f Car
egiv
ers
18%
4%
18%
13%13%
7%
14%
8%
0%2%
1%3%
Yes
El Fasher Umkadada Kass Others
No Don’t know
Figure 25: Illustration of under-five children sleeping under a bed net
Figure 26: Responses from caregivers on whether children under 5 suffered from malaria in the past six months
Source: EHA 2016 Household Survey
Source: EHA 2016 Household Survey
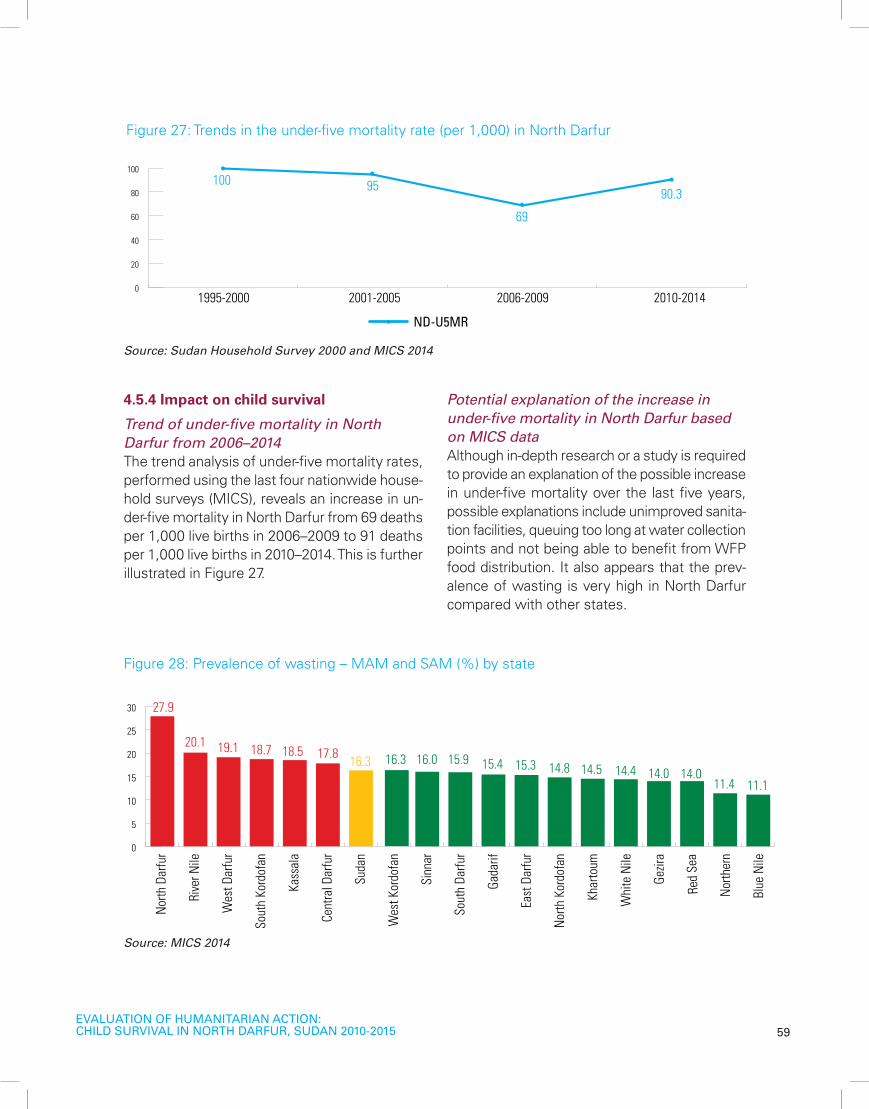
59EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
4.5.4 Impact on child survival
Trend of under-five mortality in North Darfur from 2006–2014 The trend analysis of under-five mortality rates, performed using the last four nationwide house-hold surveys (MICS), reveals an increase in un-der-five mortality in North Darfur from 69 deaths per 1,000 live births in 2006–2009 to 91 deaths per 1,000 live births in 2010–2014. This is further illustrated in Figure 27.
Potential explanation of the increase in under-five mortality in North Darfur based on MICS dataAlthough in-depth research or a study is required to provide an explanation of the possible increase in under-five mortality over the last five years, possible explanations include unimproved sanita-tion facilities, queuing too long at water collection points and not being able to benefit from WFP food distribution. It also appears that the prev-alence of wasting is very high in North Darfur compared with other states.
100 95
69
90.3
1995-2000
ND-U5MR
2001-2005 2006-2009 2010-20140
20
40
60
80
100
Figure 27: Trends in the under-five mortality rate (per 1,000) in North Darfur
Source: Sudan Household Survey 2000 and MICS 2014
Source: MICS 2014
Figure 28: Prevalence of wasting – MAM and SAM (%) by state
0
5
10
15
20
25
30
Nor
th D
arfu
r
Rive
r Nile
Wes
t Dar
fur
Sout
h Ko
rdof
an
Kass
ala
Cent
ral D
arfu
r
Suda
n
Wes
t Kor
dofa
n
Sinn
ar
Sout
h Da
rfur
Gada
rif
East
Dar
fur
Nor
th K
ordo
fan
Khar
toum
Whi
te N
ile
Gezir
a
Red
Sea
Nor
ther
n
Blue
Nile
27.9
20.1 19.1 18.7 18.5 17.8 16.3 16.3 16.0 15.9 15.4 15.3 14.8 14.5 14.4 14.0 14.011.4 11.1

60EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
A trend analysis of data from the MICS (2006–2014) (see Figure 29) confirmed the deteriora-tion in health outcome indicators in North Dar-fur over the past 10 years, as captured in the following charts. The increase in the prevalence of diarrhoea was accompanied by a decrease in children’s access to oral rehydration salts for
treatment, and the decrease in the treatment of pneumonia was accompanied by an increase in the prevalence of Acute Respiratory Infec-tion. These trends are consistent with UNICEF’s weak focus on providing health facilities with medical supplies (see Figure 29).
68.4
82.6
69.473.4
65.2 65.4
39.9
55.3
43.4
65.259.5
6.1 6.410.5
66.1
24 24.2
37.328.2
24.1
11.4 1115.9
30.9
80.3
65.3
18.3
0
10
20
30
40
50
60
70
80
90
100
0
10
20
30
40
50
60
70
80
90
100
0
10
20
30
40
50
60
70
80
90
100
0
10
20
30
40
50
60
70
80
90
100
ANC once assisted by skilled staff
Assisted ANC & Birth Delivery (%) Immunization Coverage (%)
MICS 2006 MICS 2010 MICS 2014 MICS 2006 MICS 2010 MICS 2014
MICS 2006 MICS 2010 MICS 2014 MICS 2006 MICS 2010 MICS 2014
Delivery in Health Facility
Measles
Full immunization
Birth delivery assisted by skilled staff
Preval Diarrhea
Trend of Prevalence & Treatment of Child Diarrhea-Use of ORS Packet in North Darfur (%)
Trend of Prevalence & Treatment of Child Pneumonia-Use of Antibiotic in North Darfur (%)
Use of ORS Packet
Preval of ARI-Pneumonia
Antibiotic Treatment
Figure 29: Presentation of trends of childhood diseases between 2006 and 2014
Source: UNICEF

61EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
Potential explanations of the increase in under-five mortality based on routine data from the Ministry of HealthTables 5 and 6 present trends in child illness at the state level between 2010 and 2014, using routine statistics compiled by the Ministry of Health. The number of malaria cases reported by health facilities decreased by 60 per cent and the number of reported deaths dropped by 53 per cent, largely due to the increased availability and use of insecticide-treated nets (available for free) and the use of the Artemisia combi-nation treatment. Antenatal care attendance, including one attendance by skilled personnel, improved from 74.3 per cent in 2010 to 79 per cent in 2014, while skilled assistance at delivery increased from 73 per cent in 2010 to 78 per cent in 2014.24
24 Ministry of Cabinet Central Bureau of Statistics, ‘Sudan Multiple Indicator Cluster Survey 2014: Key findings’, April 2015.
In South Darfur, there was a gradual reduction in the number of diarrheal cases between 2010 and 2015, from 6,796 cases to 3,467. The same trend applies to malaria and pneumonia cases as shown Table 6.
Multivariate statistical in-depth causal analysis of determinant factors of under-five mortality
Using the Statistical Package for the Social Sci-ences (SPSS) raw database of the household survey completed in the eight localities, the evaluation team performed a multivariate sta-tistical analysis to determine the factors that explain under-five child deaths over the last five years in the conflict-affected areas of North and South Darfur. This in-depth analysis intends to provide additional evidence to respond to the
Table 5: Presentation of child illness cases in North Darfur as reported by the State Ministry of Health.
Cases of child illness 2010 2011 2012 2013 2014 2015
Measles cases 32 3 15 70 16
Diarrheal cases 643 335 6,773 18,945 14,448 18,928
Malaria cases 1,992 525 6,310 8,448 6,969 10,723
Pneumonia cases 1,813 1,022 3,434 4,862 6,135 7,639
Table 6: Presentation of child illness in South Darfur as reported by the State Ministry of Health
Cases of child illness 2010 2011 2012 2013 2014 2015
Measles cases 1 4 19 5 13 5
Diarrheal cases 6,796 2,222 1,601 4,514 3,974 3,467
Malaria cases 3,259 1,301 759 2,163 3,869 2,539
Pneumonia cases 7,489 1,650 2,256 3,231 2,319 3,369

62EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
evaluation question: “What are the main causes of the increasing under-five mortality observed during the last five years based on the two MICS surveys?”
During the household survey, the head of the household has been asked to respond ‘yes’ or ‘no’ to whether a case of child death has occurred in the household during the last five years. In total, 14 per cent of the interviewed households confirmed a case of child death. The hypothesis is that the current contextual factors of household access (or no access) to basic services probably contributed to the level of risk of child death. This means that children who are living in the current situation are exposed to the same risk of death if there is no improved change that happened in their environment or life. This assumption is limited, however, due to the evolving environment of conflict and di-saster.
This causal analysis is undertaken based on the conceptual model elaborated by Mosley and Chen for the explanation of under-five mortali-ty.25 The information available in the database was limited, however. This model considers communities/systems, households and indi-vidual level determinants of child survival.
Three methods of analysis were performed: 1) the bivariate analysis of test of correlation using the chi-squared test and Cramer’s V test, which enabled the identification of relevant indepen-dent variables; 2) the analysis of multiple com-ponents, which established the associations of relations between the dependant variable (death of child recorded in the household) and
25 W. Henry Mosley et Lincoln C. Chen: ‘’An analytical framework for the study of child survival in developing countries”, Population and Development Reviews, 1984 (25-45).
independent explicative factors shown through the figure number 30 named (factorial plan); and 3) the logistic regression which determined the effective explicative factors using the odd ratios (the probability or degree of risk for a child to die taking many factors into consideration).
Analysis in Multiple Components (AMC) – factorial schematic plans of household profiles at high-risk of child deathsFigure 30 indicates two categories of household profiles at risk or at less risk of child death:
1. Profile of households at risk of child death: Over the past five years, frequent cases of child deaths occurred in the El Fasher IDP Camp in North Darfur. Those households had low monthly income of under 200 Sudanese Pounds or between 200-399 Sudanese Pounds; they did not benefit from WFP food distribution (they purchased their food at the market or re-ceived food donations from the communi-ty); they could not afford water payments; they had to queue for a long time to collect water; they lacked an improved sanitation facility (latrine); children of these house-holds did not benefit from child protection services; and children had been affected by child illnesses such as malaria and diarrhoea. This profile of households in North Darfur at risk of child death is presented on the left axis of the graph in Figure 30.
2. Profile of households at low risk of child death: These households were located in Umkadada in North Darfur, as well as Mellit, Kutum, Kabkabiya, Tawila and Saraf Omra

63EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
in rural North Darfur and Kass IDP Camp in South Darfur. Their financial situations were good (monthly income above 400 Su-danese Pounds); they benefited from WFP food distribution; they had family land and a kitchen garden as a food source; they could afford water payments; time was not spent queuing to collect water; they had access
to an improved sanitation facility (latrine); household children were benefiting from child protection services; and children had not been affected by child illnesses such as malaria and diarrhoea. This profile of a household with low risk of child death in North and South Darfur is presented on the right axis of the graph in Figure 30.
Source: Multivariate statistical analysis generated using SPSS and household survey raw data
Figure 30: Visual diagram for factorial plans of determinants of under-five child deaths
Umkadada in North Darfur
Yes water afford
Yes Latrine No Child DiarrheaNo Child Malaria
No water queueNo Child Death
Food NGOsNot Benefit CP Services200-399 SDG
Donate Community
Yes Child Death
Yes water queueAt least 600 SDG per month
Food WFP
400-599 SDG
Benefit CP Services
Kitchen GardenFamily Farm Land
KASS Camp-Comparison Locality in South Darfur
No latrineYes Child Diarrhea
Yes Child Malaria
Less than 200 SDG
1.5
1.0
0.5
0.0
-0.5
-1.0
-1.5-1.5 -1.0 -0.5 0.0
Dimension 1
HH at high risk of child death
HH at low risk of child death
Dim
ensi
on 2
0.5 1.0 1.5
Water not afford
El Fasher in North DarfurOther localities Mellit-Kutum-Kabkabiya- Tawila-Saraf Omra in North Darfur
Purchase Market
Recent Cases of Children Death in the HH
Grouping 8 Localities into 4 Comparable Zones
Household Monthly Income in SDG
Yes queue before access to water
Yes water price affordable
Yes HH has Latrine
Yes Case of Child Diarrhea
Current source of HH food supply
Yes Case of Child Malaria
Yes Beneficiary of CP Services

64EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
Statistical logistic regression of determinant factors of child deaths in North DarfurThe multivariate statistical logistic regression causal analysis performed by the evaluation team identified the following high-risk determi-nant factors of child death that occurred during the past five years in North Darfur compared with South Darfur in the surveyed 764 house-holds using the odds ratios. Findings reveal that households living in Umkadada locality in North Darfur had a two-times higher risk of death (odds ratio of 2.15) than children living in other localities in North Darfur that are considered as reference for the analysis (Mellit, Kutum, Kab-kabiya, Tawila, Saraf Omra) and compared with the low risk of death (0.99) for children living in Kass Camp in South Darfur.
The inequity of household income also impact-ed the risk of child death: Households with a monthly income under 200 Sudanese Pounds had a high risk of child death (1.5) compared with children living in households earning more than 600 Sudanese Pounds per month (1.00). The time it took to collect water was also a risk factor of child death: children living in house-holds that spent a long time queuing for water collection had a two-time higher risk of death (odds ratio of 2.02) compared with children in households that do not queue to collect wa-ter. The unavailability of improved latrines for a household caused a higher risk of child death (odds ratio of 1.34) than for children living in households with improved latrines.
Households for which children did not benefit from child protection services had a 2.5-time higher risk (odds ratio of 2.52) of under-five child deaths than households for which children had access to child protection services. Regarding the impact of child illness on child deaths in North and South Darfur, malaria represented a high risk of child death: households that had reported cases of malaria among children had an odds ratio of 1.93 for child death compared with households that did not experience recent cases of malaria among children. Finally, house-holds that reported cases of diarrhoea among children were exposed to a 3 per cent greater risk of child death compared with households for which there were no cases of diarrhoea among children.
The multivariate statistical causal analysis of risk of child death provided solid evidence for child survival in the protracted emergency sit-uation in North Darfur by revealing a number of risk factors such as: i) living in Umkadada in North Darfur; ii) living in the poorest families; iii) facing long queues for collecting water; iv) lacking access to adequate sanitation facilities; v) not benefiting from access to child protection services; vi) exposure to malaria; vii) and not benefiting from WFP food distribution.

65EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
Independent variables/factorsOdds ratio
risksP value
(significance)
Geographic area
�� El Fasher camp in North Darfur 0.9936 0.988
�� Umkadada in North Darfur 2.1455 0.071 (7%)
�� Kass Camp – comparison locality in South Darfur 0.9377 0.871
�� Other localities (reference) 1.0000 -
Household monthly income
�� Less than 200 Sudanese Pounds 1.4573 0.705
�� 200–399 Sudanese Pounds 0.8339 0.461
�� 400–599 Sudanese Pounds 0.59961 0.299
�� 600 Sudanese Pounds + (reference) 1.0000 -
Quantity of water drinking
�� Sufficient quantity of water (reference) 1.0000 -
�� Insufficient quantity of water 0.999 0.998
Long time in queue for collecting water
�� Yes – queue for water 2.0220 0.021 (2%)
�� No queue for water (reference) 1.0000 -
Financial payment of water
�� Yes – household is paying water 0.9993 0.998
�� Do not pay – free access to water as reference (reference) 1.0000 -
Access to improved sanitation
�� Yes – household has improved latrine as (reference) 1.0000 -
�� No – household does not have improved latrine 1.3450 0.238
Children have benefited from child protection services
�� Yes – children have benefited from child protection services (reference.) 1.0000 -
�� No – children have not benefited from child protection services 2.528 0.000 (0%)
Household children are affected by diarrhoea
�� Yes – children suffered from diarrhoea 1.0264 0.620
�� No cases of diarrhoea affecting children (reference) 1.0000 -
Household children are affected by malaria
�� Yes – children suffered from malaria 1.9256 0.009 (0%)
�� No cases of malaria affecting children (reference) 1.0000 -
Table 7: Net risk effects on child deaths of household living conditions and access to social services in North Darfur vs. South Darfur using the logistic regression statistical analysis (Stata software)
Number of observations = 715; LR Chi2 (13) = 0.0001; Pseudo R2 = 0.0736
Source: Statistical logistic regression analysis performed using the EHA household survey raw data

66EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
4.6 Sustainability
For continued sustainability, the Government of the Sudan and development partners em-barked on the long-term development of Darfur through the improvement of the Darfur Devel-opment Strategy and the Intergovernmental Authority on Development Drought Disaster Resilience and Sustainability Initiative. Howev-er, there is still weak and lack of integration of early recovery26 programming within the emer-gency phase of the crisis, which has affected the already meagre infrastructure within host communities, even though the integration of early recovery and emergencies are key pillars of the Darfur Development Strategy and the Development Drought Disaster Resilience and Sustainability Initiative.
The current aid delivery system based on blan-ket targeting of beneficiaries is unsustainable; a more systematic classification of the bene-ficiary is required. All of the newly arriving in-ternally displaced persons might be in need of life-saving assistance, but this should cover an initial period of between 3–6 months after the agreed emergency phase cycle. Subsequent programming, should examine vulnerability assessment of the affected population and ca-pacity assessment the programming based on real needs at the household level. The use of the voucher system or targeted unconditional cash will ensure that the most vulnerable population is reached.
The leakage of therapeutic foods (Plumpy’Nut), WASH supplies (water Jerry cans and soap) and
26 The UNICEF Core Commitments for Children state: “Early recovery actions in the Core Commitments for Children are actions and approaches that should be applied immediately and in parallel with immediate response.”
mosquito nets has meant that UNICEF human-itarian programming—mainly the reduction of malnutrition, malaria and diarrheal cases among affected populations—is unsustainable.
Poor participation and involvement of affected populations in programming will lead to lack of ownership and community contributions to the humanitarian programme in North Darfur. There-fore, implementing partners will be tasked with key activities on WASH operations and mainte-nance, since it is a perceived responsibility of the humanitarian agencies, thereby increasing the financial requirements for UNICEF program-ming. This weak involvement of the community was evident in the collapse of service delivery after the withdrawal of humanitarian agencies in 2009.
WES, in coordination with UNICEF has implemented a number of water pumps; most of them are not working now due to the dryness of the seasons because they mostly depend on the rains and groundwater. And another reason is that they have also broke and aren’t working any more.—Focus group discussion participant, Zam Zam Camp, North Darfur.
4.7 Lessons learned
1. Multi-sectoral interventions at both state and community levels contributed signifi-cantly to addressing the immediate needs to the affected population. This approach ensured that there was no duplication of

67EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
activities, that efforts were complementary and leveraged the various technical, logis-tic and financial capacities of organizations within the target areas.
2. UNICEF’s presence in operations and in the field, as well as the availability of human resources and emergency financing, en-sured a response within the recommend-ed 72 hours, after supporting stakeholders to develop actionable contingency plans in both North and South Darfur.
3. Investment in multi-hazard contingency planning has improved emergency services and timely responses in both slow onset emergencies (floods) and rapid onset emer-gencies that involve targeting displaced communities due to conflict.
4. The focus on humanitarian intervention in the context of protracted crisis led to weak emphasis on investment in long-term strengthening of primary health care services, water service provision and liveli-hood programming at the community level to improve resilience among the affected population.
5. Long-term, supply-based humanitarian ser-vice delivery in a protracted emergency has limitations in regards to transforming out-puts into impact in the context of recurrent insecurity due to ongoing conflict, tribal ten-sions, household poverty and vulnerability, food insecurity and poor quality of basic services. New and innovative programme strategies such as the introduction of cash transfers for income generation and comple-mentary roles of actors are required.
6. Investment by the Government of the Su-dan is key to ensuring the availability of hu-man resources for basic service provisions,
mainly the absence of primary health care services, which increases dependence on volunteers for service provision.
7. Improved preparedness of emergency re-sponses and the low cost of immunization supplies contributed to the reduction of the cost of emergency response without elimi-nating preventable diseases outbreak (e.g. the 2014 measles outbreak in North Darfur).
8. The concept of early recovery needs to be more nuanced within emergency response programmingas reflected in disaster man-agement policies. Strong progress was made in regards to capacity building for early recovery programming and outlining early recovery in UNICEF humanitarian pro-gramming, but the lack of an enabling envi-ronment has undermined the realization of this programming in practice.
9. Although UNICEF has invested significantly in humanitarian programmes in both North and South Darfur, community members did not clearly recognize UNICEF support ver-sus implementing partner support. On the one hand, this will make it easy to imple-ment an exit strategy for UNICEF; on the other hand, it will undermine the realization of UNICEF’s communications / visibility ob-jectives.
10. The enactment of South Darfur state justice policy and criminalization measures regard-ing the management of leaked humanitarian items is a good practice that should be repli-cated not only in North Darfur, but also in all major humanitarian operations in the Sudan. Branding of the relief items as a strategy for minimizing leakage is a key lesson learned from other humanitarian operations (e.g. Somalia, Kenya and Ethiopia) and should

68EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
be explored.
11. Coordination among stakeholders (i.e. the HAC, UNICEF and federal and state min-istries) at both the state and community levels is a prerequisite for timely and ef-fective humanitarian response. Clear roles and responsibilities should be captured in contingency plans to avoid confusion and duplication of programming during the hu-manitarian response.
12. Strengthening water and sanitation systems as part of a long-term development strategy ensures that the affected population has access to a sustainable water supply. Cost recovery strategies with balanced vulnera-bility mappings of the affected population on the affordability of water services should be explored further.
13. For effectiveness and efficiency monitor-ing, a good financial and programme level monitoring system needs to be in place. In addition, UNICEF’s focus on results, a system is needed to capture outputs and in-puts in respective humanitarian programme areas that the organization is supporting. The achievement of results depends on several external factors that might not be in UNICEF’s control, thus measurements of effectiveness and efficiency might be skewed.
14. UNICEF investment since October 2015 in establishing an independent third-party monitoring and verification system of ser-vice delivery through long-term agreements with a consulting firm and strengthening the human capacity of eight field offices for reg-ular field programme monitoring within the recruitment of 23 national United Nations Volunteer monitoring officers and six Na-
tional Fixed Term professional programme monitoring officers represents good prac-tice in regards to managing humanitarian action for equity and results. These ef-forts must be capitalized on through the establishment of adequate accountability management responses to the volume of information generated on bottlenecks and persistent challenges for children on the ground.
15. Strong Information management and docu-mentation of data among the stakeholders is a key factor that ensures the validity of progress indicators from various stakehold-ers who are involved in humanitarian action. The current information management and documentation system needs should be harmonized among all stakeholders, which can be done by developing a robust cluster information management and documenta-tion system.
16. The end of conflicts and the realization of a sustainable peace agreement for devel-opment are the only long-term sustainable solutions that will facilitate human well-be-ing and dignity for vulnerable children in North Darfur.

69EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
5. CONCLUSIONS AND RECOMMENDATIONS
© U
NIC
EF/U
NI1
6580
0

70EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
5. CONCLUSIONS AND RECOMENDATIONS
5.1 Conclusions
The summary of the findings on best practices (what worked) and for whom 1. UNICEF WASH, Nutrition and Health hu-
manitarian programmes are relevant and ap-propriate to the needs of targeted displaced and affected population. The programmes contributed to the Sudan Government’s poli-cies in humanitarian programming, focusing on Health, Nutrition, Water and Sanitation at sub national level (state and community).
2. In terms of coordination, UNICEF ensured that it effectively met its obligation as a clus-ter lead for WASH and Nutrition by ensuring that there were strategic engagements in planning at the North Darfur state level. This ensured that there was no duplication of activities among the humanitarian actors. UNICEF led and coordinated inter-agency needs assessment mainly for WASH, while for Nutrition there were periodic nutrition-al status assessments to inform program-ming. UNICEF led the contingency planning process, which is a key preparedness tool for the WASH and Nutrition Clusters at the state level.
3. Regarding efficiency, UNICEF demonstrated the comparative advantage of being pres-ent on the ground through the existence of a fully functional field office (staff and logistics), the pre-positioning of supplies at state level within the warehouses of line ministries and UNAMID team sites, strong
partnership with Government counterparts and existing signed agreements with NGOs/implementing partners.
4. UNICEF in 2016 strengthened its capacity for programme field monitoring at the field office (FO) level, through the establishment of Third Party Monitoring. This ensured in-dependent assessment of the effectiveness of service delivery, due diligence and im-plementation of financial risk management through HACT at state level, while capaci-ties for information management in support to sector cluster coordination was strength-ened in Khartoum. However, there is a gap in North Darfur.
5. Efficiency of the UNICEF humanitarian programme between 2010 and 2015 was achieved for vaccination and nutrition treat-ment services for acute malnutrition - re-sulting in about 85 percent achievement of the planned outputs.
6. On effectiveness, UNICEF has been able to ensure increased coverage of nutrition services for treatment of SAM over the last five years, including screening and referral of cases to nutrition services centers.
7. The effectiveness of UNICEF’s humanitarian programming in terms of ensuring a sus-tained outcome was observed in health services for preventable diseases, mainly in urban and peri-urban areas, as well as in the increased number of children admitted for the treatment of SAM.

71EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
8. Concerning impact, health programming con-tributed to the reduction of vaccine prevent-able diseases by ensuring increased immuni-zation coverage of up to 90 percent in North Darfur. Nutrition programming contributed to the stabilization of the Global Acute Malnu-trition and Severe Acute Malnutrition rates, though the malnutrition burden remains at double the 15 percent WHO emergency threshold.
The summary of the findings on challenges (what did not work – shortfall in results)1. In terms of relevance, UNICEF’s interven-
tions in the state focused mostly on IDPs, refugees and populations affected by disas-ters and did not cover the needs of host com-munities, which represents an equity gap for children living in the poorest and most vulnerable communities.
2. The inter-cluster coordination (for example, WASH and Nutrition) was found to be weak at state and community levels. Joint plan-ning for these clusters were carried out on a quarterly basis in North Darfur while in South Darfur, joint planning was implemented on a monthly basis. At the community level, there was no evidence of contingency planning processes or a joint inter-cluster implemen-tation plan in North Darfur. In addition, the situation monitoring and information man-agement is weak at state level. If strength-ened, it could potentially ensure adequate sector cluster coordination and multi-sector integrations as seen in Khartoum.
3. UNICEF was found to be efficient in supply delivery. However, partners, both Govern-ment and NGOs expressed concern about UNICEF’s delay in the finalization of part-nerships and cash disbursement, especially within the context of the agility of response
required within 72 hours after the occurrence of an emergency.
4. The leakage of humanitarian supplies due to the lack of an effective supply chain man-agement and end-user monitoring, the low coverage of basic services to all the affected areas, poor cold chain management prac-tices, and low involvement of the affected population in programming to promote own-ership, constitute high risk barriers to achieve expected outcomes and impact for children. The continuous leak of UNICEF’s plumpy nut into the local market has affected the efficiency and effectiveness of the Nutrition programme’s ability to reduce malnutrition cases in a cost effective manner. The eval-uation also recorded the leakage of WASH supply items based on the beneficiaries and partners’ comments. Part of the distributed soap, water jerry cans and tarpaulins were being sold in the local markets in North Dar-fur.
5. High administrative costs of up to 48.5 per cent (including operating cost of partnerships with NGOs) has challenged value for mon-ey and results for children within the health and nutrition programmes in North Darfur, as compared to the improved child health indi-cators in South Darfur with less investment, due to a number of factors including lower administrative costs.
6. Due to the lack of funding for capital invest-ments in new WASH facilities, the planned expectation with WASH and preventive Nu-trition programming recorded low perfor-mance, (less than 50 percent), in terms of translating the planned supply-based inputs into outputs. There is more investment in South Darfur in term of WASH programming (but WASH interventions are weak in North

72EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
Darfur) however, investment in health and nutrition are higher in North Darfur. WASH humanitarian programming between 2010 to 2015 were largely below expectations in terms of ensuring adequate coverage and sustained access to water and sanitation ser-vices both in schools and among the affected population. UNICEF staffing for the effective delivery of Nutrition and WASH in North Dar-fur was low. For instance, one international staff supported Nutrition, Health and WASH programming, resulting in poor supervision of the implementing partners.
7. Low coverage and poor quality of health ser-vices in rural areas resulted in the outbreak of measles within hard to reach communities and localities in 2014 and 2015. The poor cold chain management practices at the peri-ur-ban and rural areas affected the sustained control of vaccine preventable diseases.
8. The weak linkage between the programme management of child severe acute malnutri-tion and moderate acute malnutrition, high open defecation practices and high number of diarrhea cases and malaria, contributed to continued high prevalence of child malnutri-tion in North Darfur.
9. The humanitarian action did not show any contribution in terms of the reduction of ma-laria cases and the uptake of the use of long lasting insecticide treated nets among chil-dren under the age of five. Weak processes for the provision of quality vaccines and en-hancement systems, particularly cold chain equipment that were substandard in rural areas of North Darfur, contributed to con-cerns about the effectiveness of the vaccines being used in those areas against diseases.
The summary of the findings on the impact of Lifesaving Humanitarian Action for children1. On the impact of lifesaving Humanitarian
Action on children, persistent insecurity, high levels of wasting prevalence among under-five children in North Darfur, high prevalence of diarrhea and increasing cases of childhood illnesses, provided evidence of high mortality risk for children over the last five years.
2. Despite efforts by UNICEF to achieve sup-ply-based outputs, the increase of under-five mortality in North Darfur over the last five years (2010-2015) represents a result gap in humanitarian action to improve the situation of children in the state. Key contributing fac-tors include protracted conflicts/insecurity, weak health systems and inadequate adop-tion of family practices for child care. The current strategies and narrow scale emer-gency focused supply-based investment from Government, UNICEF and partners are inadequate to ensure tangible life-sav-ing impact for children because of the sheer magnitude of displacements, food insecuri-ty, child morbidity caused by persistent con-flicts, increased child malnutrition, outbreak of diarrhea (due to poor hygiene practices), pneumonia, drought or other public health-re-lated hazard.
3. Concerning sustainability, due to limited human and financial resource capacity of UNICEF, inadequate technical capacity of im-plementing partners to effectively ensure the delivery of quality services to the affected population, declining donor funding and the poor involvement of the affected population, UNICEF’s current humanitarian actions with-in the protracted emergency crisis (13 years) in North Darfur, are not sustainable.

73EVALUATION OF HUMANITARIAN ACTION: CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
5.2 Recommendations for UNICEF
1. The current administrative cost of up to 48.5 percent is on the high side and UNICEF should institute innovative strategies of part-nerships in order to minimize the administra-tive/ overheads costs.
2. Institute an independent audit to examine and document the extent of the leakage of plumpy nut, water jerry can and soap, and UNICEF must take immediate measures closely with the Government to eliminate the leakage of supplies and commodities in order to increase the effects of outcomes for children.
3. Strengthen and extend the supply chain management system beyond the state lev-el by ensuring the delivery of commodity to beneficiaries at community and locality level complemented with an effective recording and documentation system.
a. UNICEF needs to explore the engage-ment with private shop owners as av-enues for distribution of therapeutic plumpy nut, mainly in the hard to reach areas where the shops are the first point of reference for assistance at the com-munity level.
b. Branding and visibility of relief items mainly water jerry cans and plumpy nut should be explored to minimize the leak-age of such items.
c. c. As noted in South Darfur where there is an elaborate policy framework in han-dling humanitarian leakage, UNICEF should lobby North Darfur state Govern-ment and the national Government to enact policies criminalizing the sale of therapeutic relief items.
4. Promote a multi-sector integrated package of
interventions at the community level start-ing from the programme planning stage. UNICEF should promote equity in delivering basic services (Health, Nutrition and WASH) to affected populations and host communi-ties.
5. Revise the supply-based strategy focus of humanitarian actions and explore the intro-duction of cash-based programming (safety nets) and the strengthening of social protec-tion systems, in order to enable the affected population effective use of Health, Water and Nutritional Services and assure the sustain-ability of gains of results. UNICEF must also clearly outline its roles of evidence-based policy advocacy to leverage adequate Gov-ernment investments to scale up the equita-ble coverage/access and the quality of social services.
6. Strengthen the State Ministry of Health’s capacity to ensure effective and efficient management of vaccine cold chain at the locality level in order to secure the preventive strategy.
7. Strengthen the capacities of communities to ensure the maintenance and sustainability of basic services with a clear capacity building strategy.
8. Strengthen the primary health preventive and care systems through adequate techni-cal and financial support to scaling up MNCH and IMCI, which could contribute to improv-ing the quality and demand of health services and reduce child morbidity and deaths – be-yond humanitarian or emergency response.
9. Enhance inter-sector/cluster coordination within UNICEF, mainly at implementation lev-el, focusing on the community/locality level. UNICEF should also strengthen the situation monitoring and information management at

74EVALUATION OF HUMANITARIAN ACTION:
CHILD SURVIVAL IN NORTH DARFUR, SUDAN 2010-2015
state level to better prioritise the agility of response to emerging vulnerable situations.
10. Strengthen Communication for Develop-ment in order to address the magnitude of inadequate practices of sanitations and hy-giene; UNICEF should sensitize the affect-ed population, specifically the mothers and caregivers on not referring to plumpy nuts as “Biscuit”, but as a therapeutic product for treating Severe Acute Malnutrition.
11. Strengthen the documentation and infor-mation management within UNICEF key Sections.
5.3 Recommendations to the Government of the Sudan
1. The Government should accelerate the re-cruitment of medical doctors or clinical of-ficers for community level health facilities.
2. The federal and state ministries of health should improve the health early warning system for North Darfur to reduce disease detection time and establish robust analysis mechanisms.
3. The federal and state ministries of health should assess and improve on cold chain management in North Darfur.
4. State Government officials should establish legislation that criminalizes the sale of hu-manitarian supplies and commodities, partic-ularly those used for the therapeutic needs of children (i.e. Plumpy’Nut) using the best legal practices in place in South Darfur.
5. The federal and state ministries of health should explore ways of improving the access of humanitarian agencies to vulnerable popu-lations, mainly for hard-to-reach areas where humanitarian needs are high.
6. The Government and all other parties to con-flict should continue with ongoing efforts to end conflicts, establish a final peace agree-ment for the restoration of hope for human well-being and dignity of the deprived popu-lation and vulnerable children of North Darfur, and break down the vicious cycle of violence.
7. The federal and state governments, as well as other stakeholders, including UNICEF, should develop a mechanism for the establishment of a safe corridor for the delivery of human-itarian services and goods to the affected population in crisis-prone regions and areas.
5.4. Recommendations to partners
1. The achievement of the 2030 transformative agenda for sustainable development in the Sudan (“no one left behind prosperity; dignity and access to basic human needs”) requires an increase in financial investments in scaling up multi-sector interventions. Donors should reverse the decline in financial assistance to humanitarian action in the Sudan to avoid any additional loss of children’s lives, as observed over the last five years in North Darfur, for reasons such as child malnutrition and pre-ventable diseases.
2. The establishment of durable solutions to en-sure sustainable gains in the context of pro-tracted emergency represent the new direc-tion of strategic reflection and investments by partners in ensuring work across the human-itarian to development continuum (building resilience, recovery and development).
3. Donor support for ending conflicts and achieving the peace agreement in the Su-dan represents the ultimate hope for the vul-nerable population affected by a protracted 13-year conflict, which has led to external emigration and persistent violence.





























