Embed Size (px)
Citation preview

At the Intersection of Health, Health Care and Policy
doi: 10.1377/hlthaff.18.5.89
, 18, no.5 (1999):89-105Health Affairspractices
Evidence-based care for depression in managed primary careMinnium, M L Pearson and K B Wells
L V Rubenstein, M Jackson-Triche, J Unutzer, J Miranda, KCite this article as:
http://content.healthaffairs.org/content/18/5/89
information and services, is available at: The online version of this article, along with updated
For Reprints, Links & Permissions: http://healthaffairs.org/1340_reprints.php
http://content.healthaffairs.org/subscriptions/etoc.dtlE-mail Alerts :
http://content.healthaffairs.org/subscriptions/online.shtmlTo Subscribe:
from the Publisher. All rights reserved.information storage or retrieval systems, without prior written permission
byor by any means, electronic or mechanical, including photocopying or may be reproduced, displayed, or transmitted in any formHealth Affairs
provided by United States copyright law (Title 17, U.S. Code), no part of by Project HOPE - The People-to-People Health Foundation. As1999
Georgetown Road, Suite 600, Bethesda, MD 20814-6133. Copyright © is published monthly by Project HOPE at 7500 OldHealth Affairs
Not for commercial use or unauthorized distribution
by guest on January 21, 2016Health Affairs by content.healthaffairs.orgDownloaded from
by guest on January 21, 2016Health Affairs by content.healthaffairs.orgDownloaded from

Evidence-Based Care ForDepression In ManagedPrimary Care PracticesAcollaborative approach shows promise in improvingcare ofdepression in a variety of sites.
by Lisa V. Rubenstein, Maga Jackson-Triche, Jürgen Unützer, JeanneMiranda, Katy Minnium, Marjorie L. Pearson, and Kenneth B. Wells
PROLOGUE: The gap between theory and practice in health carecan be daunting. Researchers armed with massive amounts ofoutcomes data face the problem of translating their findingsinto workable interventions in the practice setting. This paperreports on an attempt to bridge the gap, taking advantage ofthe administrative capabilities of managed care organizations.The authors designed, implemented, and tracked acollaborative-care program of treatment for patients withsymptoms of depression. The results presented here highlightthe program’s success in creating a “partnership betweenhealth care organizations and researchers.”
Lisa Rubenstein is a practicing geriatrician and internist atthe University of California, Los Angeles (UCLA), School ofMedicine and Veterans Administration Medical Center(VAMC), Sepulveda, California; a senior natural scientist atRAND; and director of the VA/RAND/UCLA Center for theStudy of Healthcare Provider Behavior. Maga Jackson-Triche isdirector of the Psychiatry Consultation and Liaison Services atthe Sepulveda VAMC, and the psychiatric administrator forthe PACE (Primary Care and Education) program there. JürgenUnützer is a geriatric psychiatrist and health servicesresearcher at the UCLA Neuropsychiatric Institute (NPI).Jeanne Miranda, a psychologist, is an associate professor ofpsychiatry at Georgetown University Medical Center inWashington, D.C. Katy Minnium is a research associate in thedepartment of psychiatry at UCLA. Marjorie Pearson is ahealth policy analyst at RAND. Ken Wells isprofessor-in-residence of psychiatry and biobehavioral sciencesat UCLA-NPI and a senior scientist at RAND.
© 1999 The People-to-People Health Foundation, Inc.
QUALITY 89& VALUE
H E A L T H A F F A I R S ~ S e p t e m b e r / O c t o b e r 1 9 9 9
D E P R E S S I O N C A R E
by guest on January 21, 2016Health Affairs by content.healthaffairs.orgDownloaded from

ABSTRACT: This paper evaluates whether externally designed, evidence-basedinterventions for improving care for depression can be locally implemented inmanaged care organizations. The interventions were carried out as part of arandomized trial involving forty-six practices within six diverse, nonacademicmanaged care plans. Based on evaluation of adherence to the interventionprotocol, we determined that local practice leaders are able to implementpredesigned interventions for improving depression care. Adherence rates formost key intervention activities were above 70 percent, and many were near100 percent. Three intervention activities fell short of the goal of 70 percentimplementation and should be targets for future improvement.
Imp rov in g c are fo r de p re ss io n in primary care practices isa national mental health goal.1 Over the next decade depression isexpected to become the second-leading cause of disability
worldwide.2 National clinical guidelines define appropriate treat-ment strategies for this highly treatable condition, but studies overthe past decade have consistently found low rates of detection andappropriate treatment in primary care, the setting from which mostdepressed persons seek care, if they seek it at all.3
Simple interventions to improve depression care have not beeneffective. Interventions to increase providers’ knowledge and atti-tudes about depression, such as dissemination of national guide-lines, have not changed what providers do about depression.4 Feed-back of information to clinicians about their patients’ moods hashad some impact but has not improved major depression outcomes.5
Recent studies suggest that current attitudes among primary careclinicians are favorable to treating depression and that these clini-cians have good basic knowledge about antidepressant use, but careis still inadequate.6
It is tempting to attribute this lack of progress to the stubborn-ness or callousness of primary care clinicians, managed care plans,and insurance companies. In reality, the poor response is predict-able. Social science theory and empirical clinical studies agree thatknowledge-based interventions are ineffective in improving prob-lems for which the solutions require complex behavior change.7
Successful depression care requires a proactive and systematicapproach to detection and management, more so than is required forcare of other chronic conditions. First, depressed patients are lesscapable than nondepressed patients are of acting as assertive, in-formed consumers. Patients with chest pain complain of this symp-tom to their physicians and expect treatment; patients with depres-sion rarely complain of it directly and often need to be convinced ofthe need for treatment. This is because depression induces fatigueand low self-confidence, is not easily recognized by patients, and isassociated with the stigma attached to having a mental illness. Sec-
90 DEPRESSIONCARE
H E A L T H A F F A I R S ~ V o l u m e 1 8 , N u m b e r 5
Q u a l i t y & V a l u e
by guest on January 21, 2016Health Affairs by content.healthaffairs.orgDownloaded from

ond, once symptoms are detected by a clinician, patients with de-pression require at least a half-hour of initial assessment and educa-tion followed by active treatment and monitoring for up to a year.8
Carrying out all of these tasks is daunting for primary care clini-cians, whose typical appointment slot is fifteen minutes. Finally,mental health specialists are less integrated into primary care prac-tices than medical subspecialists are, so primary care cliniciansoften must struggle with difficult cases of on their own.
A specific type of disease-management program, collaborativecare, is specifically designed to overcome these barriers and has beenevaluated and proven to be effective.9 Collaborative care is a team-based approach that transfers assessment, education, and treat-ment-monitoring activities for depression to nonphysicians andprovides mechanisms for improved primary care/mental health spe-cialty partnerships.10 Unfortunately, collaborative-care models haveproved to be difficult to disseminate outside of the research settingsin which they were first tested. One might expect, for example, thatlocal quality-improvement teams would design collaborative-careinterventions when asked to improve depression care, but they donot.11 Such teams likely lack the time and expertise required to fullydesign the protocols, training sessions, and materials required forimplementing such complex interventions. They also might not bein a good position to demand the changes in staffing and resourcesrequired for improving depression care. On the other hand, wide-spread dissemination of care improvements cannot occur withoutlocal clinical leadership and staff involvement.
The approaches tested in the study presented here combine someof the benefits of local social influence and knowledge of the prac-tice with the benefits of external expertise and resources to developinterventions. 12 The study postulates that improving care on a broadscale for complex chronic illnesses such as depression will requirenew, population-oriented disease-management approaches that in-corporate provider behavior-change strategies. The approachestested entail (1) external expert intervention design based on pre-viously tested strategies and premarket assessment of potential cus-tomers; (2) dissemination of the interventions by the designers tomedical care organizations through appropriate marketing, negotia-tion, training, and materials; and (3) implementation of the inter-ventions by trained local clinical leaders and staff. This paper exam-ines the development, final features, and extent and variability ofimplementation of two evidence-based interventions to improve de-pression care that were designed and disseminated using a popula-tion- oriented approach. Results describing the modifications incollaborative care asked for by managed care plans show the relative
QUALITY 91& VALUE
H E A L T H A F F A I R S ~ S e p t e m b e r / O c t o b e r 1 9 9 9
D E P R E S S I O N C A R E
by guest on January 21, 2016Health Affairs by content.healthaffairs.orgDownloaded from
acceptability of various collaborative-care features. Our findings aboutthe degree to which the interventions were actually carried out canbe used to improve depression-care models for managed care.
Overview Of The StudyThe Partners in Care (PIC) study is an Agency for Health CarePolicy and Research (AHCPR) Patient Outcomes Research Team(PORT) II study.13 It is a randomized trial comparing quality im-provement for medications in one experimental group arm (QI-meds) and for psychotherapy in a second experimental group arm(QI-therapy), with treatment as usual in the third arm (usual-carecontrol). The study randomized forty-six practices within six di-verse, nonacademic managed care organizations into the threeequal-size arms. Patient outcomes are not yet available.
n Developing intervention components. The interventions forthis study were based on a review of the literature on providerbehavior change, quality improvement, and depression-care im-provement.14 Potential intervention strategies then were discussedwith managed care organizations to determine which features, andwhat level of resource commitment, they would accept. Before thestudy, managed care organizations emphasized as motivations forparticipation their wish to improve care, a belief that improvingdepression care might lower costs, the possibility of improved per-formance among enrollees, the opportunity to be responsive to un-ion pressures, and the potential for improved enrollees’ satisfactionwith care. Given these modest but compelling motivations, we de-signed low-intensity interventions (low cost as well as modest intheir demands for change) that nevertheless incorporated the keyintervention elements shown in prior literature to be effective.
To reduce costs in comparison to previously tested collaborative-care models, we substituted nurses’ time for physicians’ and doc-toral-level psychologists’ time whenever possible (mostly in theform of a depression nurse specialist, or DNS, who was a primarycare nurse trained by the study). We also eliminated some collabo-rative-care components. In QI-therapy we eliminated nurse follow-up of patients on antidepressants but spent an equivalent amounton reduced copayments for short-term cognitive behavioral therapy(CBT), which has been shown to be as effective as medications forthe majority of depressed patients. In QI-meds we eliminated re-duced psychotherapy copayments but spent an equivalent amounton nurse follow-up of patients on antidepressants. To make theinterventions realistic, our training and materials encouraged clini-cians to base treatment choices on clinical considerations so that,for example, a patient in the QI-therapy arm with severe vegetative
92 DEPRESSIONCARE
H E A L T H A F F A I R S ~ V o l u m e 1 8 , N u m b e r 5
Q u a l i t y & V a l u e
by guest on January 21, 2016Health Affairs by content.healthaffairs.orgDownloaded from

symptoms would be expected to receive antidepressants. Finally,although all participating organizations were required to imple-ment the basic intervention plans, we encouraged flexibility andcreativity in adapting the basic plan to local conditions.
Enrolling managed care organizations. To participate in this study,managed care organizations had to agree to hire the number ofnurses required by the study protocol and to reduce copayments forpsychotherapy in the QI-therapy arm. They also had to be willing toidentify local primary care, mental health, and nurse “expert leaders”and agree to allow them to attend two days of off-site training.Organizations were offered honoraria, ranging from $30,000 to$70,000 depending on the size of the study populations at theirsites. Honoraria equaled about half of the cost of participation.
We approached about thirty U.S. managed care organizationsfrom diverse geographic areas to assess their interest in and suitabil-ity for the project. We sought to enroll public and private network-and staff-model organizations, particularly those that care for poorand Hispanic patients. After detailed negotiations with ten organi-zations, six were deemed suitable and agreed to enroll.
Intervention plans and flow. Exhibit 1 shows the key components ofthe interventions. Before the intervention began, local expert leaderswere identified by each managed care organization and trained cen-trally during a two-day training session. A primary care, a nursing,and a mental health specialty expert leader were required for eachexperimental group within each managed care organization; onelarge organization was divided into two halves and required twosets of expert leaders. Primary care expert leaders hired DNSs tocarry out the initial assessment of study patients (in both QI-medsand QI-therapy) and case management (QI-meds only). Thesenurses attended a one-day training session. In QI-therapy only theseleaders also identified or hired study psychotherapists to be trainedin short-term psychotherapy (CBT). Study psychotherapists wereprovided with at least two days of training in CBT for depression, adetailed manual for the group and individual treatments, andweekly telephone supervision of a first treatment case. The psycho-therapists were expected to use study forms to provide feedbackabout the patient to the referring primary care clinician. Every oneto two months study investigators called the primary care expertleaders and the DNSs to review the intervention progress.
Once the DNSs and psychotherapists were in place, the studyteam began screening patients for depression as they came for ap-pointments with study clinicians. The DNSs then called all patientswho screened positive for depression on the Composite Interna-tional Diagnostic Interview (CIDI) depression screen to schedule an
QUALITY 93& VALUE
H E A L T H A F F A I R S ~ S e p t e m b e r / O c t o b e r 1 9 9 9
D E P R E S S I O N C A R E
by guest on January 21, 2016Health Affairs by content.healthaffairs.orgDownloaded from
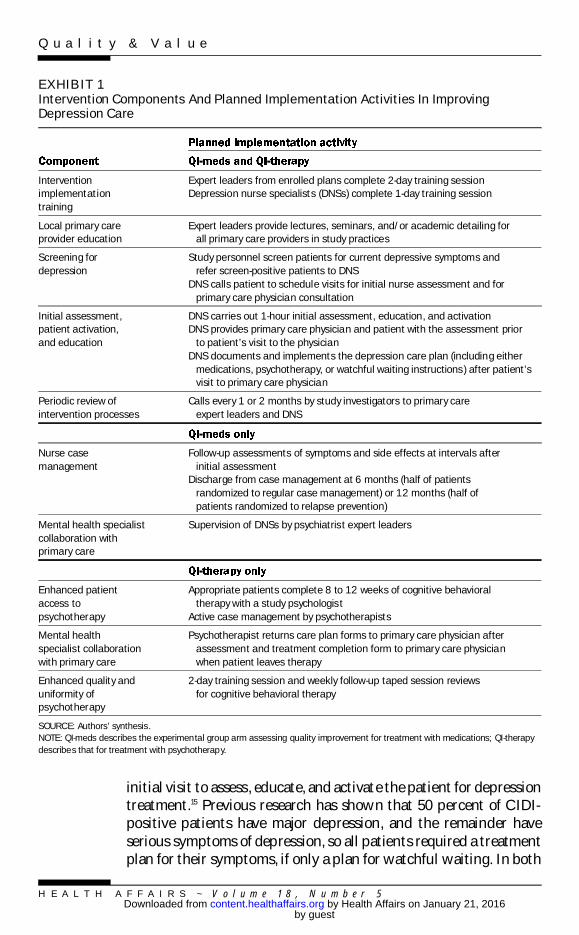
initial visit to assess, educate, and activate the patient for depressiontreatment.15 Previous research has shown that 50 percent of CIDI-positive patients have major depression, and the remainder haveserious symptoms of depression, so all patients required a treatmentplan for their symptoms, if only a plan for watchful waiting. In both
EXHIBIT 1Intervention Components And Planned Implementation Activities In ImprovingDepression Care
Interventionimplementationtraining
Expert leaders from enrolled plans complete 2-day training sessionDepression nurse specialists (DNSs) complete 1-day training session
Local primary careprovider education
Expert leaders provide lectures, seminars, and/or academic detailing forall primary care providers in study practices
Screening fordepression
Study personnel screen patients for current depressive symptoms andrefer screen-positive patients to DNS
DNS calls patient to schedule visits for initial nurse assessment and forprimary care physician consultation
Initial assessment,patient activation,and education
DNS carries out 1-hour initial assessment, education, and activationDNS provides primary care physician and patient with the assessment prior
to patient’s visit to the physicianDNS documents and implements the depression care plan (including either
medications, psychotherapy, or watchful waiting instructions) after patient’svisit to primary care physician
Periodic review ofintervention processes
Calls every 1 or 2 months by study investigators to primary careexpert leaders and DNS
Nurse casemanagement
Follow-up assessments of symptoms and side effects at intervals afterinitial assessment
Discharge from case management at 6 months (half of patientsrandomized to regular case management) or 12 months (half ofpatients randomized to relapse prevention)
Mental health specialistcollaboration withprimary care
Supervision of DNSs by psychiatrist expert leaders
Enhanced patientaccess topsychotherapy
Appropriate patients complete 8 to 12 weeks of cognitive behavioraltherapy with a study psychologist
Active case management by psychotherapists
Mental healthspecialist collaborationwith primary care
Psychotherapist returns care plan forms to primary care physician afterassessment and treatment completion form to primary care physicianwhen patient leaves therapy
Enhanced quality anduniformity ofpsychotherapy
2-day training session and weekly follow-up taped session reviewsfor cognitive behavioral therapy
SOURCE: Authors’ synthesis.NOTE: QI-meds describes the experimental group arm assessing quality improvement for treatment with medications; QI-therapydescribes that for treatment with psychotherapy.
H E A L T H A F F A I R S ~ V o l u m e 1 8 , N u m b e r 5
Q u a l i t y & V a l u e
by guest on January 21, 2016Health Affairs by content.healthaffairs.orgDownloaded from

intervention arms, nurses strove to elicit patients’ treatment prefer-ences as an important consideration in choosing psychotherapy ormedications for initial treatment. The nurse passed his or her assess-ment on to the primary care clinician, who met with the patient ifpossible the same day and decided on treatment. For those patientsin clinics assigned to QI-meds, the nurse followed any patients be-gun on antidepressants to monitor symptoms, side effects, and ad-herence. The nurse encouraged continued treatment, if treatmentwas successful, or worked with the primary care clinician and psy-chiatrist to change the therapy if need be. Length of nurse follow-upwas randomly assigned to be either six (usual-case-managementgroup) or twelve (relapse-prevention group) months. In addition, apsychiatrist was available at each site to supervise the nurses and toprovide on-site consultation for difficult-to-treat patients. For pa-tients in clinics assigned to QI-therapy, the nurse helped patientswhose care plan called for entering CBT to reach a study-trainedmental health care provider.
n Design of study materials. Both written and videotaped edu-cational materials were developed; these included overheads for ex-pert leaders for giving lectures on depression, pocket-size cardswith an algorithm for diagnosing and treating depression and adetailed algorithm-based clinician guide for all primary care clini-cians and expert leaders, and training manuals for nurses and psy-chotherapists. In addition, these latter groups received detailed log-ging and tracking materials for ensuring accurate patient follow-up.Materials were developed with input from patients and providers.Leaders from the National Alliance for the Mentally Ill (NAMI), aconsumer group, and five members of the AHCPR depression-careguideline panel reviewed all final study materials.
n Implementation evaluation methods. The implementationevaluation relies on data from both study records and study surveys.Two types of study records are involved: information on all trainingactivities undertaken during the project; and data from the struc-tured records and logs kept by the nurses and psychotherapists.
Several surveys provide implementation information. At the endof the intervention, all thirteen expert leaders completed a survey toevaluate the extent to which each component had been completed.In addition, primary care providers were surveyed at baseline andeighteen months later, regarding their background and the extent oftheir participation in the study. The response rate for the one-yearfollow-up survey used in these analyses was 94 percent.
Throughout the study patients completed a variety of surveys,including a brief screening for depression; a diagnostic interview;and baseline, six-month, and twelve-month questionnaires. Sam-
QUALITY 95& VALUE
H E A L T H A F F A I R S ~ S e p t e m b e r / O c t o b e r 1 9 9 9
D E P R E S S I O N C A R E
by guest on January 21, 2016Health Affairs by content.healthaffairs.orgDownloaded from

pling and enrollment methods have been reported elsewhere.16 Ofpatients who were eligible and read the study’s informed-consentform, 79 percent (1,356) enrolled; the remaining 21 percent eitherrefused or left the clinic. The completion rate for baseline survey was85 percent at six months and 83 percent at twelve months.
n Data analysis. For the expert leader survey, study records, andnurse records, we used descriptive statistics. For the clinician back-ground questionnaire we evaluated significance based on chi-squaretests. For patient survey data we weighted the data for nonresponseusing patients’ demographic and clinical factors and randomizationblock as predictors. Analysis was carried out in STATA.
Study ResultsOverall, 100 percent of those scheduled for initial training completedthe training (Exhibit 2). The total of sixty-two persons reflects someoverlap of roles because a few expert-leader nurses also acted asDNSs and a few expert-leader mental health specialists also acted astherapists; these persons received both types of training. Elevenpercent of expert leaders, 24 percent of CBT therapists, and 31 per-cent of DNSs left the study. Most were replaced.
Based on the expert-leader survey, about 80 percent of 112 localprimary care clinicians participated in an expert leader–led seminar;about 48 percent received outreach visits (academic detailing)either instead of or in addition to a seminar; and 66 percent weregiven some level of feedback about study patients (audit and feed-back). Across practices, 100 percent of on-site primary care physi-cians received study clinician guides and quick-reference pocketcards for diagnosis. Rates were similar in QI-meds and QI-therapy.
Looking at training for cognitive behavioral therapists, nine (40percent) submitted all twelve session tapes for monitoring by thestudy CBT expert, and all were reviewed. Seven (30 percent) sentbetween three and nine tapes and had between three and twelvesupervision sessions. The remaining seven (30 percent) submittedno tapes and received no supervision; five of these left the study, onewas an expert leader only and did not see patients, and one refused.
Exhibit 3 shows the degree to which patients actually got theservices we expected them to get from the DNSs. The enrolled sam-ple of intervention patients who should have been sent to the DNSsfor assessment was 913. Seven patients who were not fully eligiblealso were referred to the DNSs, for a total of 920 intervention pa-tients. According to DNS records, study nurses called 96 percent ofthese patients to try to schedule an initial visit, but this did notalways result in an actual visit. Among the 920 intervention pa-tients, only 73 percent (675) had a recorded initial assessment visit
96 DEPRESSIONCARE
H E A L T H A F F A I R S ~ V o l u m e 1 8 , N u m b e r 5
Q u a l i t y & V a l u e
by guest on January 21, 2016Health Affairs by content.healthaffairs.orgDownloaded from

with the DNS. Within this visit, patients did not always get theassessments and educational interventions that we trained theDNSs to give. DNSs virtually always assessed for depression diagno-sis and assessed a Beck score for depression symptoms. They werenearly as thorough about completing a care plan with the participa-tion of the primary care clinician (89 percent). On the other hand,adherence to patient education and activation activities was lowerand was highly variable between sites. DNSs assessed treatmentpreferences among 74 percent of patients overall, with a range of 42percent to 96 percent among sites. They recorded handing out edu-cational materials to 67 percent of initially assessed patients, with a
EXHIBIT 2Overall Adherence To The Depression-Care Intervention Protocol, By Data Source
Intervention implementation trainingb
Regional expert leadersLocal depression nurse specialists (DNSs)Local cognitive behavioral therapists 100% 62
Local primary care provider educationc
Lectures or seminarsAcademic detailingAudit and feedback
804866
905474
ScreeningReferral to DNS for screener-positive patientsb
Patients called by DNS to schedule first visitd100
96920883
Initial assessment, patient activation, and educationd
1-hour initial assessment, education, and activation 73 577
Periodic review of intervention progressb
Calls every 1 to 2 months by study investigators 100 14
Nurse case management of patients on medicationsd
Any follow-up assessments of symptoms, side effects 71 302
Mental health specialist collaboration with primary careDNS contacts with expert-leader psychiatristsPsychotherapist returns care plan to primary care physician
–e
–e–e–e
Enhanced patient access to psychotherapyPatients referred to study psychotherapyd,f 40 197
Enhanced quality and uniformity of psychotherapyWeekly follow-up sessions for therapy reviewedb 70 16
SOURCE: Authors’ analysis of data from Partners in Care study.a The ideal score for all measures reported here is 100 percent, except for enhanced patient access to psychotherapy. No idealscore can be specified for this item.b Based on study records.c Based on expert-leader survey.d Based on nurse records.e No record.f Not all patients would be appropriate to refer.
H E A L T H A F F A I R S ~ S e p t e m b e r / O c t o b e r 1 9 9 9
D E P R E S S I O N C A R E
by guest on January 21, 2016Health Affairs by content.healthaffairs.orgDownloaded from
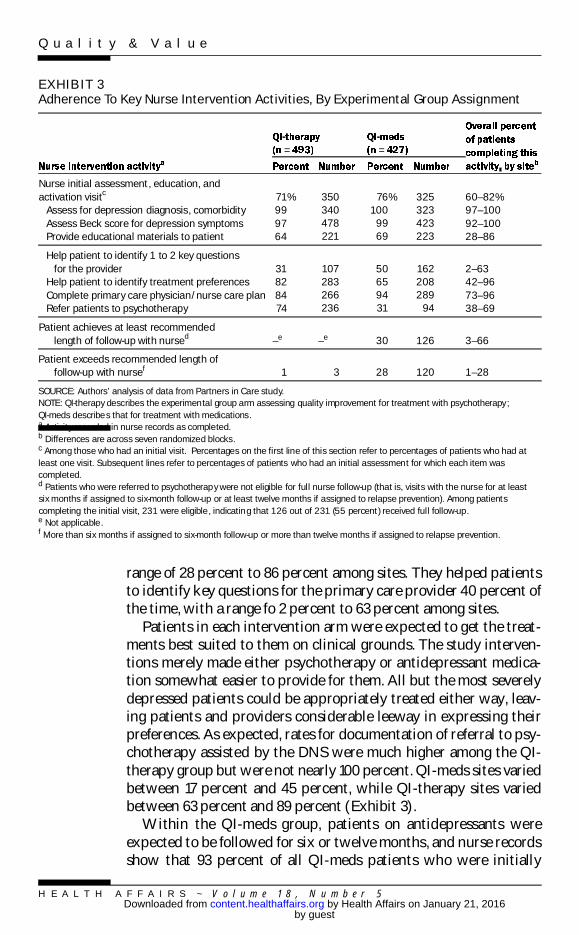
range of 28 percent to 86 percent among sites. They helped patientsto identify key questions for the primary care provider 40 percent ofthe time, with a range fo 2 percent to 63 percent among sites.
Patients in each intervention arm were expected to get the treat-ments best suited to them on clinical grounds. The study interven-tions merely made either psychotherapy or antidepressant medica-tion somewhat easier to provide for them. All but the most severelydepressed patients could be appropriately treated either way, leav-ing patients and providers considerable leeway in expressing theirpreferences. As expected, rates for documentation of referral to psy-chotherapy assisted by the DNS were much higher among the QI-therapy group but were not nearly 100 percent. QI-meds sites variedbetween 17 percent and 45 percent, while QI-therapy sites variedbetween 63 percent and 89 percent (Exhibit 3).
Within the QI-meds group, patients on antidepressants wereexpected to be followed for six or twelve months, and nurse recordsshow that 93 percent of all QI-meds patients who were initially
EXHIBIT 3Adherence To Key Nurse Intervention Activities, By Experimental Group Assignment
= =
Nurse initial assessment, education, andactivation visitc
Assess for depression diagnosis, comorbidityAssess Beck score for depression symptomsProvide educational materials to patient
71%999764
350340478221
76%100
9969
325323423223
60–82%97–10092–10028–86
Help patient to identify 1 to 2 key questionsfor the provider
Help patient to identify treatment preferencesComplete primary care physician/nurse care planRefer patients to psychotherapy
31828474
107283266236
50659431
162208289
94
2–6342–9673–9638–69
Patient achieves at least recommendedlength of follow-up with nursed –e –e 30 126 3–66
Patient exceeds recommended length offollow-up with nursef 1 3 28 120 1–28
SOURCE: Authors’ analysis of data from Partners in Care study.NOTE: QI-therapy describes the experimental group arm assessing quality improvement for treatment with psychotherapy;QI-meds describe s that for treatment with medications.a Activity recorded in nurse records as completed.b Differences are across seven randomized blocks.c Among those who had an initial visit. Percentages on the first line of this section refer to percentages of patients who had atleast one visit. Subsequent lines refer to percentages of patients who had an initial assessment for which each item wascompleted.d Patients who were referred to psychotherapy were not eligible for full nurse follow-up (that is, visits with the nurse for at leastsix months if assigned to six-month follow-up or at least twelve months if assigned to relapse prevention). Among patientscompleting the initial visit, 231 were eligible , indicating that 126 out of 231 (55 percent) received full follow-up.e Not applicable.f More than six months if assigned to six-month follow-up or more than twelve months if assigned to relapse prevention.
H E A L T H A F F A I R S ~ V o l u m e 1 8 , N u m b e r 5
Q u a l i t y & V a l u e
by guest on January 21, 2016Health Affairs by content.healthaffairs.orgDownloaded from

assessed received follow-up care beyond the initial assessment.However, only 30 percent of them were followed by nurses for thefull six months (usual-case-management group) or twelve months(relapse-prevention group) anticipated by the protocol. Completionof follow-up varied greatly among sites. To understand these resultsbetter, we note that 22 percent of QI-meds patients were referredfor psychotherapy and thus were eligible only for one follow-up callat eight weeks (Exhibit 1). Another 24 percent did not complete theinitial nurse assessment. The remaining patients are those whoshould have completed the full nurse follow-up (55 percent did).
The mean number of follow-up sessions, either by telephone or inperson, for which DNSs completed a structured follow-up form was1.8 for QI-therapy and 5.1 for QI-meds. Some patients were followedlonger than their scheduled time window (about 1 percent of QI-therapy patients and 30 percent of QI-meds patients). The meanduration of excess follow-up was thirty-six days among the 30 per-cent of patients who exceeded follow-up expectations in QI-meds.
Based on a survey done eighteen months after the beginning of theintervention, we found that clinicians at the intervention-groupstudy sites were significantly more likely to report having partici-pated in educational sessions led by local experts than were primarycare providers in the usual-care group (Exhibit 4). They also were
EXHIBIT 4Clinicians’ Self-Reported Participation In Depression-Care Improvement Activities, ByExperimental Group Assignment
= = =Read clinical practice
guidelines or manualsAttended clinician education or
training sessions by local experts
70%
68
66%
77
56%
57**
50–81%
42–88
Received feedback onpatient outcomes
Experienced nursingassessment and follow-up ofdepressed patients
75
61
72
81
61
41* * * *
57–92
36–69
Gave depressed patientsdepression brochures orvideotapes
Referred depressed patients tomental health specialists
55
96
54
98
57
94
71–100
86–100
SOURCE: Authors’ analysis of data from Partners in Care study.NOTES: QI-therapy describes the experimental group arm assessing quality improvement for treatment with psychotherapy;QI-meds describe s that for treatment with medications. Measures of significance compare the intervention groups to usual care.* * p < .05 * * * * p < .001
QUALITY 99& VALUE
H E A L T H A F F A I R S ~ S e p t e m b e r / O c t o b e r 1 9 9 9
D E P R E S S I O N C A R E
by guest on January 21, 2016Health Affairs by content.healthaffairs.orgDownloaded from

more likely to have experienced nursing assessment and follow-upof depressed patients. As would be expected, since guidelines wereprovided to both intervention and usual-care groups, there were nosignificant group differences in the more than half of clinicians whoreported having read clinical practice guidelines for depression.There also were no significant differences in the proportion of clini-cians who received feedback on patient outcomes, which was highin all groups, or in having referred any depressed patients to mentalhealth specialists. A little more than half of providers in each grouphad given their patients depression-education materials; we wouldnot have expected a difference between experimental-group andusual-care clinicians in this activity because DNSs were chargedwith performing it.
Exhibit 5 looks for evidence that the DNSs’ educational andfollow-up activities or materials were received by patients andwhether the activities or materials were perceived as helpful whenthey were received. The survey upon which this exhibit is basedoccurred one year after the intervention began and asked about careover the past six months, so most patients would have received their
EXHIBIT 5Patients’ Self-Reported Participation In Depression-Care Improvement Activities, ByExperimental Group Assignment
= = =
Receiving telephonecalls from nurses 12.9% 1.7 22.2% * * * * 2.3 15.0% 2.0 4–21% 8–35%
Reviewing written materialsabout depression
Materials somewhat orvery helpful
36.8* *
32.0* *
2.6
2.4
38.0* * *
32.0* *
2.7
2.6
27.6
24.0
2.4
2.2
22–51
22–43
31–43
25–40
Reviewing a videotape ondepression
Materials somewhat orvery helpful
23.0* * * *
17.0* *
2.3
2.0
22.5* * * *
17.0* *
2.2
2.0
7.8
4.0
1.4
1.0
27–30
11–24
10–33
7–27
Talking with a nurse aboutdepression
Talk was somewhat orvery helpful
14.9
11.0* *
1.8
1.5
26.1* * * *
24.0* *
2.3
2.2
9.7
6.0
1.5
1.2
4–25
6–19
21–40
10–36
SOURCE: Authors’ analysis of data from Partners in Care study.NOTES: QI-therapy describes the experimental group arm assessing quality improvement for treatment with psychotherapy;QI-meds describe s that for treatment with medications. Measures of significance compare the intervention groups to usual care.a As patients recalled twelve months after enrollment.b Differences are across seven randomized blocks.* * p < .05 * * * p < .01 * * * * p < .001
H E A L T H A F F A I R S ~ V o l u m e 1 8 , N u m b e r 5
Q u a l i t y & V a l u e
by guest on January 21, 2016Health Affairs by content.healthaffairs.orgDownloaded from

study intervention at least three months before the time windowreferenced. We thus would not expect a high proportion of positiveresponses. Nevertheless, significantly more patients in both experi-mental groups than in usual care remembered having received edu-cational materials. Significantly more QI-meds patients remem-bered being called by nurses and talking with them aboutdepression materials. Experimental-group patients who receivedwritten materials, brochures, or telephone calls were significantlymore likely to have found them helpful than were control-grouppatients who had received similar materials or calls.
Discussion And Policy ImplicationsThis implementation evaluation of an expert-designed but locallyadapted and executed program to improve depression care is en-couraging. Managed care organizations were able to comply 100percent with the basic elements of the interventions, such as identi-fying local expert leaders, hiring nurses, and reducing copaymentsfor psychotherapy. Our target adherence level for considering imple-mentation successful was 70 percent, and for most interventionactivities at least 70 percent of the target group participated. Plan-ning for training clearly needs to account for retraining in responseto turnover among intervention participants, which was significant.
Three important areas had adherence rates lower than 70 percent.One was for length of nurse follow-up for patients on antidepres-sants: Only 55 percent of patients eligible for follow-up (and 30percent of the entire QI-meds group) were followed for the fullexpected duration. Nurse case management proved challenging,particularly in sites that were geographically dispersed, and nursesvaried in the creativity with which they pursued elusive patients.Setting up a meeting between nurse and patient, either in person orby telephone, typically required many telephone calls. Improve-ments in our case management strategy, such as giving nurses accessto computerized tracking, should be evaluated. The other two areaswith lower adherence rates were for participation in academic de-tailing and audit and feedback, perhaps because these activities arelabor-intensive for the expert leaders. More detailed training, mate-rials, and instructions for these purposes might have improved ad-herence. Referral rates to psychotherapy were lower than 70 per-cent; this was by design, because not all patients were appropriateto refer. Intervention activities by expert leaders and nurses wereremembered by both primary care clinicians and patients long afterthey occurred and produced significant differences between experi-mental and control groups for both clinicians and patients. Thesefindings are strong enough that effects on the process and outcomes
QUALITY 101& VALUE
H E A L T H A F F A I R S ~ S e p t e m b e r / O c t o b e r 1 9 9 9
D E P R E S S I O N C A R E
by guest on January 21, 2016Health Affairs by content.healthaffairs.orgDownloaded from

of care for depression can realistically be anticipated.These findings are a feasibility test of the kinds of changes re-
quired for successful management of depression. Because the studytargeted both public and private network- and staff-model managedcare plans as well as practices with large numbers of poor andHispanic patients, its results are potentially generalizable across abroad spectrum of health care settings. Most previous high-qualityresearch on improving primary care practices has been carried out inacademically affiliated organizations; none of the practices studiedhere was so affiliated.17 Furthermore, study investigators had noprior relationship or familiarity with the participating organizationsbut nevertheless were able to market the interventions to them.These findings suggest that, particularly if appropriate policy incen-tives were in place, evidence-based interventions such as these thatare tailored to customers’ needs will be marketable to diverse man-aged care or practice organizations.
The interventions’ effects on process and outcomes of care will belimited by the major across-site differences in adherence to thenurse interventions that are apparent in our results. For example,there is a twenty-two-percentage-point difference between thehighest and the lowest site in completing the initial assessmentvisit, a cornerstone of the entire intervention, and a fifty-eight-percentage-point difference in provision of educational materials.There is even greater discrepancy among sites in completion of pa-tient education and activation activities.
Because all major resource commitments by study practices wereadhered to (such as giving reduced copayment for therapy and hir-ing nurses), we suspect that differences in implementation acrosssites were related to other factors. For example, some of the organi-zations experienced major changes during the study, such as merg-ers, buy-outs, and financial distress; these changes resulted in turn-over of key expert leaders, which may have affected the site’senthusiasm for the study. In addition, the personalities, skills, andcommitment of nurses and psychotherapists varied widely. We planto carry out analyses to assess the path from intervention implemen-tation to differences in treatments and in outcomes among sites andthe direct and indirect costs of the interventions in each site.255
n Study limitations. This study has limitations. First are thelimitations of each data source. For example, we used self-reports by
“These findings are a feasibility test of the kinds of changesrequired for successful management of depression.”
102 DEPRESSIONCARE
H E A L T H A F F A I R S ~ V o l u m e 1 8 , N u m b e r 5
Q u a l i t y & V a l u e
by guest on January 21, 2016Health Affairs by content.healthaffairs.orgDownloaded from

expert leaders for some information, and social-desirability biasesmay have affected their responses in our favor. On the other hand,we assessed patients’ and physicians’ recall of intervention activitieslong after they would have occurred, making our estimates of impacton these measures extremely conservative. For nurse data we de-pended on written records, which may not have reflected the fullextent of actual activities. Nevertheless, the multiple data sourceswe used confirmed one another in terms of relative rates of adher-ence in most cases, and we suspect that our overall picture of theintervention process is accurate.
Another limitation is that our findings are based on results in onlysix managed care organizations. However, while these organiza-tions were volunteers and thus were self-selected, we identifiedthem based on geographic, structural, and patient-diversity consid-erations in combination with the organization’s willingness to par-ticipate, rather than on any criteria related to factors that mightpredict the intervention’s success. Finally, it is important to empha-size that the usefulness of our approach depends upon the availabil-ity of prior research that convincingly identifies successful interven-tion models. Broad dissemination of untested models would bepotentially wasteful. On the other hand, not moving to this assisteddissemination step when dissemination has not occurred naturallymeans that the social investment in basic research to find efficacioustreatments, and in the development and initial testing of models forimproving the effectiveness of use of the treatments, may be lost.
Ou r r e s u l t s h i g h l i g h t the process of translating re-search into practice for a complex chronic illness. They pro-vide cause for optimism that partnerships between health
care organizations and researchers can be successful in the long runin affecting health care across the nation. Policy-level involvement iscritical for several reasons. First, although we have not yet analyzedthe costs of our intervention, it seems clear that support for in-creased depression care will require either new resources or shiftingof resources from other purposes. Typical primary care clinics donot provide the type of service we have described. Managed careorganizations would find it easier to shift resources toward im-proved depression care if their competitors were doing the same.
Our results also illustrate the complexity of depression care im-provement. Resource shifts of the kinds described are more likely toimprove care if they are carefully designed and evaluated. Achievingthis depends upon fostering collaborations among researchers,health care organizations, quality-improvement organizations, andprivate-sector companies interested in improving care. Thus, policy
QUALITY 103& VALUE
H E A L T H A F F A I R S ~ S e p t e m b e r / O c t o b e r 1 9 9 9
D E P R E S S I O N C A R E
by guest on January 21, 2016Health Affairs by content.healthaffairs.orgDownloaded from

interventions such as tax breaks for implementing mentalhealth–oriented primary care improvements; funding opportunitiesthat encourage pairing of health services researchers and health careorganizations; public education about seeking high-quality depres-sion care; and mandates to track rates of detection, care, and out-comes for depression might all be considered. We hope that policy-makers and clinical managers will bring their own expertise to theproblem of improving care for depression and will create mecha-nisms for supporting the improvement of mental health care in pri-mary care settings.
This work was funded by the Agency for Health Care Policy and Research, Grantno. R01-HS08349; the National Institute on Mental Health (NIMH), ResearchScientist Award MH01170-05, and the Research Center on Managed Care forPsychiatric Disorders, Grant no. P50 MH54623; and the John D. and Catherine T.MacArthur Foundation, Grant no. 96-42901A-HE. The authors acknowledge thenumerous contributions of Mary Abdun-Nur and Alissa Simon for the creation ofintervention materials; Manhal Weiland for her management of intervention de-sign; Maureen Carney for her design and implementation of study evaluation pro-cedures across the country; and Bernadette Benjamin for her meticulous program-ming support. The Veterans Affairs (VA) Center for the Study of Healthcare ProviderBehavior, VA Greater Los Angeles Healthcare System, Sepulveda AmbulatoryCare Center, in Sepulveda, California, supported educational materials develop-ment, as did American Medical Productions and the Biomedical Foundation ofSouth Texas. The Hogg Foundation for Mental Health supported production anddistribution of the Spanish version of the videotape. This study is a companionstudy to the NIMH Cooperative Agreement to Test Depression Practice Guide-lines (Lisa Rubenstein, Kathryn Rost, and Daniel Ford, principal investigators),and investigators from that project helped to design the quality-of-care and healthmeasures. The authors acknowledge the participating managed care organiza-tions, which provided access to their expertise and patients, implemented interven-tions, and provided in-kind resources: Allina Medical Group (Twin Cities, Minne-sota), Columbia Medical Plan (Maryland), Humana Health Care Plans and Pacifi-Care of Texas (San Antonio), MedPartners (Los Angeles, California), and Valley-Wide Health Services (Colorado); and their internal behavioral health organiza-tions and participating contract behavioral health organizations: Alamo MentalHealth Group (San Antonio), San Luis Valley Mental Health/Colorado HealthNetworks (Colorado), and GreenSpring Mental Health Services (Maryland).
NOTES1. R.M.A. Hirschfeld et al., “The National Depressive and Manic-Depressive As-
sociation Consensus Statement on the Undertreatment of Depression,” Journalof the American Medical Associatio n 277, no. 4 (1995): 333–340.
2. C.J. Murray and A.D. Lopez, “Global Mortality, Disability, and the Contribu-tion of Risk Factors: Global Burden or Disease Study,” Lancet 349, no. 9063
104 DEPRESSIONCARE
H E A L T H A F F A I R S ~ V o l u m e 1 8 , N u m b e r 5
Q u a l i t y & V a l u e
by guest on January 21, 2016Health Affairs by content.healthaffairs.orgDownloaded from

(1997): 1436–1442.3. K.B. Wells et al., Caring for Depression (Cambridge, Mass.: Harvard University
Press, 1996); K.B. Wells et al., “Quality of Care for Depressed Primary CarePatients,” Archives of Family Medicine (forthcoming); and W. Katon et al., “Ade-quacy of Duration of Antidepressant Treatment in Primary Care,” Medical Care30, no. 1 (1992): 67–76.
4. Depression Guidelines Panel, Depression in Primary Care, Volume 1: Detection andDiagnosis, Pub. no. 93-0550 (Rockville, Md.: AHCPR, 1993); and Volume 2:Treatment of Major Depression, Pub. no. 93-0551 (1993).
5. L. Lynn and J. Yager, “The Effect of Screening, Sensitization, and Feedback onNotation of Depression,” Journal of Medical Education 55, no. 11 (1980): 942–949;and L.V. Rubenstein et al., “Improving Patient Quality of Life with Feedback toPhysicians about Functional Status,” Journal of General Internal Medicine 10, no. 11(1995): 607–614.
6. L.S. Meredith et al., “Treating Depression in Staff-Model versus Network-Model Managed Care Organizations,” Journal of General Internal Medicine 14, no. 1(1999): 39–49; and Wells et al., “Quality of Care.”
7. D.A. Davis et al., “Changing Physician Performance: A Systematic Review ofthe Effect of Continuing Medical Education Strategies,” Journal of the AmericanMedical Associatio n 274, no. 9 (1995): 700–705; and A.D. Oxman et al., “No MagicBullets: A Systematic Review of 102 Trials of Interventions to Improve Profes-sional Practice,” Canadian Medical Associatio n Journal 153, no. 10 (1995):1423–1431.
8. L. Rubenstein et al., Partners in Care Clinician Guide to Depression and Management inPrimary Care Settings (Santa Monica, Calif.: RAND, 1996).
9. W. Katon et al., “Collaborative Management to Achieve Treatment Guide-lines: Impact on Depression in Primary Care,” Journal of the American MedicalAssociation 273, no. 6 (1995): 1026–1031; and H.C. Schulberg et al., “TreatingMajor Depression in Primary Care Practice: Eight-Month Clinical Outcomes,”Archives of General Psychiatry 53, no. 10 (1996): 913–919.
10. W. Katon et al., “A Multifaceted Intervention to Improve Treatment of De-pression in Primary Care,” Archives of General Psychiatry 53, no. 10 (1996):924–932.
11. H.I. Goldberg et al., “A Randomized Controlled Trial of CQI Terms and Aca-demic Detailing: Can They Alter Compliance with Guidelines?” Journal of Qual-ity Improvement 24, no. 3 (1998): 130–142.
12. B.S. Mittman, X. Tonesh, and P.D. Jacobson, “Implementing Clinical PracticeGuidelines: Social Influence Strategies and Practitioner Behavior Change,”Quality Review Bulletin 18, no. 12 (1992): 413–422.
13. H.I. Goldberg et al., “Deliberations on the Dissemination of PORT Products:Translating Research Findings into Improved Patient Outcomes,” Medical Care32, no. 7 (1994): JS90–JS110.
14. L.V. Rubenstein et al., “From Understanding Health Care Provider Behavior toImproving Health Care: A Framework for Quality Improvement,” Medical Care(forthcoming).
15. Composite International Diagnostic Interview (CIDI), Core Version 2.1 Interviewer’sManual (Geneva: World Health Organization, 1997).
16. K.B. Wells, “The Design of Partners in Care: Evaluating the Cost-Effectivenessof Improving Care for Depression in Primary Care,” Social Psychiatry and Psychi-atric Epidemiology 34, no. 1 (1999): 20–29.
17. E.M. Yano et al., “Helping Practices Reach Primary Care Goals: Lessons fromthe Literature,” Archives of Internal Medicine 155, no. 11 (1995): 1146–1156.
QUALITY 105& VALUE
H E A L T H A F F A I R S ~ S e p t e m b e r / O c t o b e r 1 9 9 9
D E P R E S S I O N C A R E
by guest on January 21, 2016Health Affairs by content.healthaffairs.orgDownloaded from





























