Embed Size (px)
Citation preview
Examination of the Equine Foot
Andrew Parks, MA, Vet MB, MRCVS, Diplomate ACVS
Author’s address: College of Veterinary Medicine, University of Georgia, Athens, Georgia 30602;e-mail: [email protected]. © 2010 AAEP.
1. Introduction
There are excellent journal articles and book chap-ters that describe the examination of the foot, someof which are listed as references.1–8 Reviewingthem reveals that each clinician performs their ex-amination in their own style, and they emphasizedifferent aspects of the examination; however, theyall have a method, and all describe an effective pro-cess to diagnose as effectively as possible the variousconditions that affect the equine foot. This articledescribes the author’s approach to examination ofthe foot, which is a synthesis of formal educationreceived, personal experience, and experience of oth-ers. It is a reductionist rather than proceduralapproach.
The majority of disease processes originating inthe foot that cause lameness are associated withinflammation, usually related to trauma or infec-tion. Disease processes associated with a markedfocus of inflammation, typically associated withacute onset of lameness, are most likely to be iden-tified with a basic examination, whereas diseaseprocesses associated with subtle symptoms andlonger duration may require much more extensiveexamination of the limb and ancillary diagnostictests. Furthermore, even the best examination inconjunction with ancillary diagnostic tests may notalways obtain a definitive diagnosis, but the infor-mation gained may suggest an approach for symp-
tomatic treatment. The latter is particularlyimportant when access to advanced diagnostic tech-nology, such as magnetic resonance imaging, is lim-ited. Therefore, the following discussion is dividedinto two parts, the basic examination and a moredetailed examination. The detailed examination isfurther divided into three main sections that providedifferent types of information.
All examinations begin by gathering the present-ing complaint, signalment, and history. With mostfoot problems, the presenting complaint is lameness.However, presenting complaint may also be the ap-pearance of the foot. The signalment for any horsedoes not give specific information about the present-ing complaint, but it does contain risk factors forcertain conditions, which must then be correlatedwith information obtained from the history andphysical examination.
There are three main time points of importance inhistory taking: the date of the examination, thedate that the problem was first noticed, and the datethat the owner first knew/owned the horse. Thesecond date gives an indication of the duration of theproblem, and the length of time between the secondand third dates gives the clinician an indication ofhow much history before this problem is known; thismay lead to further enquiry about this time. Notwo sets of questions asked during a history takingare the same, because so many questions are pred-
AAEP PROCEEDINGS � Vol. 56 � 2010 485
FARRIER PROGRAM
NOTES
icated on the answer to a previous question; how-ever, there is a common set of starting questions.After ascertaining the duration of the problem,questions should be directed at determining the na-ture of the onset—acute or chronic—and whether aspecifically identifiable event can be linked to it.The clinician needs to know the progression of thedisease, whether it has been constant, becomeworse, become better, or varied over the course ofthe history. Additionally, it is important to see ifany treatment measures have already been takenand if so, what effect they have had. If the horse isable to work, what is the influence of exercise on theproblem, and how does it change with the surfacethat the horse is worked on? Furthermore for feetproblems, it is also important to determine the shoe-ing history if the horse is shod: when was the horselast shod, have there been changes in the shoeingtechnique, has the farrier changed before or duringthe course of the problem, etc. More general ques-tions may need to be asked about the health andmanagement of the horse, including questions aboutany other problems that the horse has had in thepast, the husbandry of the horse, and disease-pre-vention management.
2. The Basic Examination
1. Examination of the HorseIt is important to examine the horse as a whole andnot rush to examine an extremity. The body condi-tion of the horse should be assessed. Chronic painrelated to lameness can cause weight loss. Pres-sure sores indicate that a horse has spent an exces-sive amount of time lying down. A horses posturemay not only indicate which limb is lame, but it may
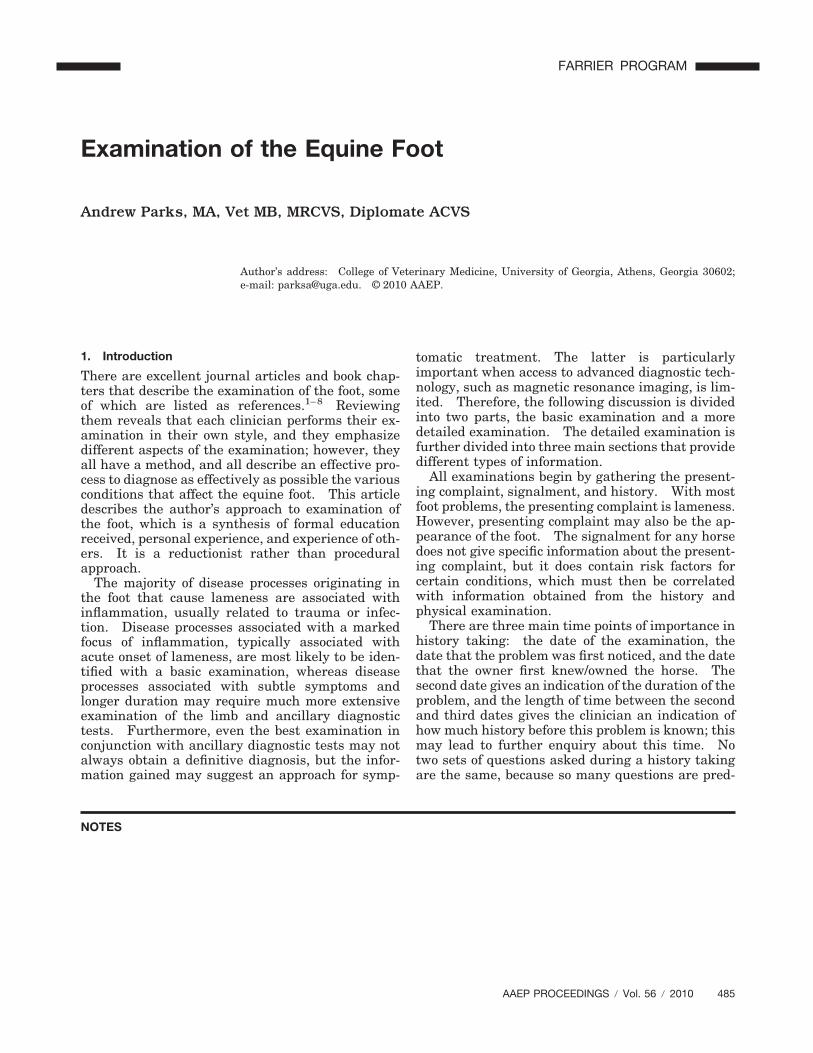
also provide information about the nature of theproblem, the classic example of which is the rocking-back stance seen with bilateral forelimb laminitis(Fig. 1). If one heel is persistently held off theground, it suggests that tension in a structure on theflexor surface is causing pain.
2. Basic Examination of the Foot
Gross Examination of the Shape of the FootIt is important to have some appreciation for the sizeand shape of normal feet when conducting the ex-amination, and although most observations on thesize and shape of feet are subjective, values for thelength and angle of the toe and the size of the foot inrelation to the weight of the horse have been pub-lished.1,9,10 The forefeet are more circular in shapewhen viewed from the ground surface, whereas thehindfeet may appear to be shaped like a diamond inwhich one end has been cut off.
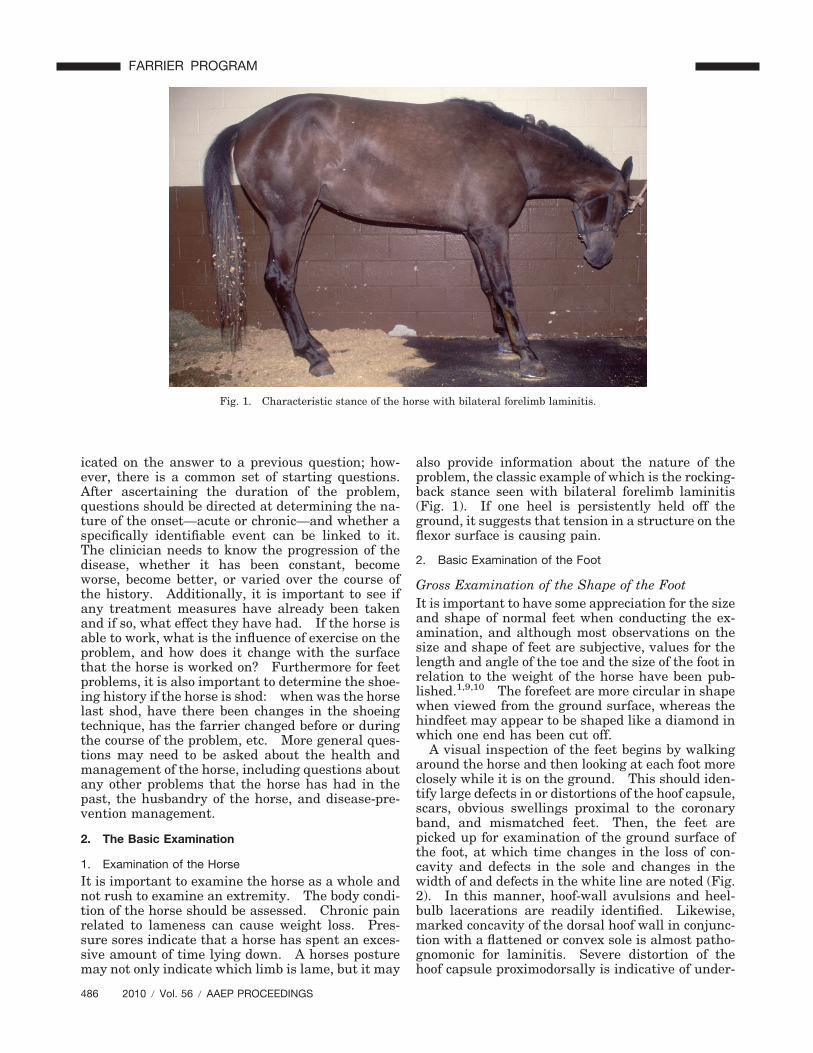
A visual inspection of the feet begins by walkingaround the horse and then looking at each foot moreclosely while it is on the ground. This should iden-tify large defects in or distortions of the hoof capsule,scars, obvious swellings proximal to the coronaryband, and mismatched feet. Then, the feet arepicked up for examination of the ground surface ofthe foot, at which time changes in the loss of con-cavity and defects in the sole and changes in thewidth of and defects in the white line are noted (Fig.2). In this manner, hoof-wall avulsions and heel-bulb lacerations are readily identified. Likewise,marked concavity of the dorsal hoof wall in conjunc-tion with a flattened or convex sole is almost patho-gnomonic for laminitis. Severe distortion of thehoof capsule proximodorsally is indicative of under-
Fig. 1. Characteristic stance of the horse with bilateral forelimb laminitis.
486 2010 � Vol. 56 � AAEP PROCEEDINGS
FARRIER PROGRAM
lying proliferation of bone on the surface of the ex-tensor process of the distal phalanx, often referred toas buttress foot. When in doubt about a question-able finding in one foot, examining the contralateralfoot may determine whether or not it is abnormal.It should be borne in mind that some mild asymme-try between feet is within normal limits.
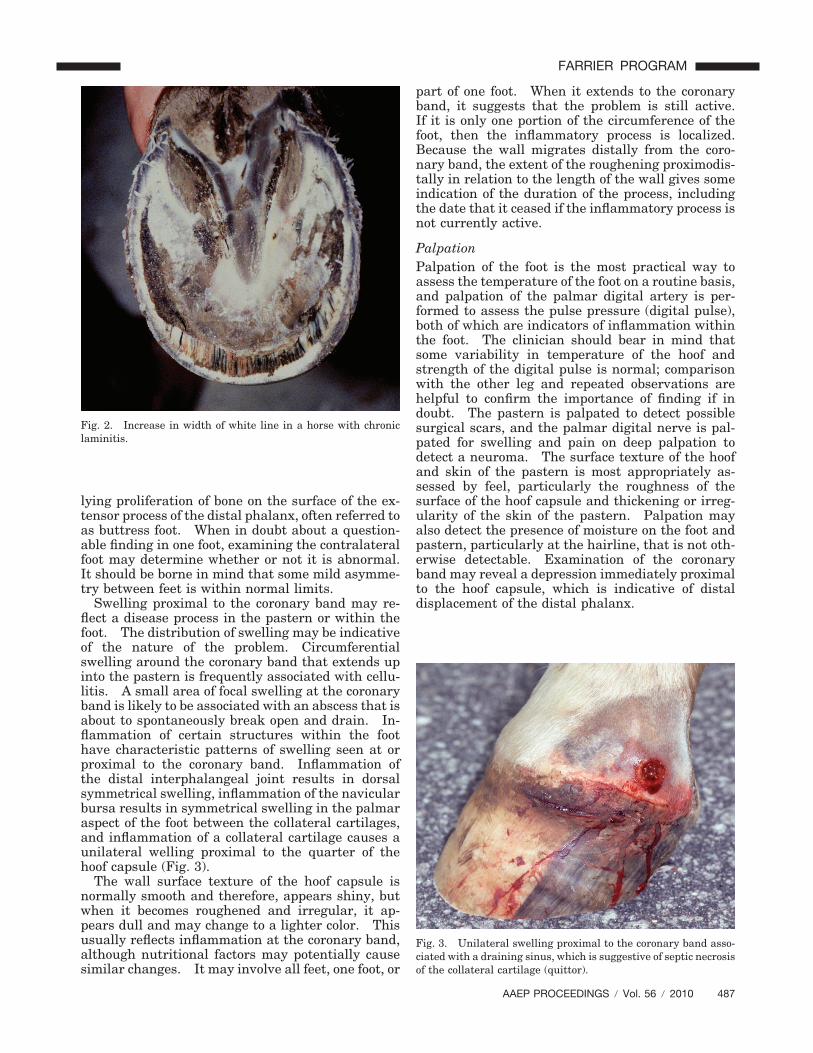
Swelling proximal to the coronary band may re-flect a disease process in the pastern or within thefoot. The distribution of swelling may be indicativeof the nature of the problem. Circumferentialswelling around the coronary band that extends upinto the pastern is frequently associated with cellu-litis. A small area of focal swelling at the coronaryband is likely to be associated with an abscess that isabout to spontaneously break open and drain. In-flammation of certain structures within the foothave characteristic patterns of swelling seen at orproximal to the coronary band. Inflammation ofthe distal interphalangeal joint results in dorsalsymmetrical swelling, inflammation of the navicularbursa results in symmetrical swelling in the palmaraspect of the foot between the collateral cartilages,and inflammation of a collateral cartilage causes aunilateral welling proximal to the quarter of thehoof capsule (Fig. 3).
The wall surface texture of the hoof capsule isnormally smooth and therefore, appears shiny, butwhen it becomes roughened and irregular, it ap-pears dull and may change to a lighter color. Thisusually reflects inflammation at the coronary band,although nutritional factors may potentially causesimilar changes. It may involve all feet, one foot, or
part of one foot. When it extends to the coronaryband, it suggests that the problem is still active.If it is only one portion of the circumference of thefoot, then the inflammatory process is localized.Because the wall migrates distally from the coro-nary band, the extent of the roughening proximodis-tally in relation to the length of the wall gives someindication of the duration of the process, includingthe date that it ceased if the inflammatory process isnot currently active.
PalpationPalpation of the foot is the most practical way toassess the temperature of the foot on a routine basis,and palpation of the palmar digital artery is per-formed to assess the pulse pressure (digital pulse),both of which are indicators of inflammation withinthe foot. The clinician should bear in mind thatsome variability in temperature of the hoof andstrength of the digital pulse is normal; comparisonwith the other leg and repeated observations arehelpful to confirm the importance of finding if indoubt. The pastern is palpated to detect possiblesurgical scars, and the palmar digital nerve is pal-pated for swelling and pain on deep palpation todetect a neuroma. The surface texture of the hoofand skin of the pastern is most appropriately as-sessed by feel, particularly the roughness of thesurface of the hoof capsule and thickening or irreg-ularity of the skin of the pastern. Palpation mayalso detect the presence of moisture on the foot andpastern, particularly at the hairline, that is not oth-erwise detectable. Examination of the coronaryband may reveal a depression immediately proximalto the hoof capsule, which is indicative of distaldisplacement of the distal phalanx.
Fig. 3. Unilateral swelling proximal to the coronary band asso-ciated with a draining sinus, which is suggestive of septic necrosisof the collateral cartilage (quittor).
Fig. 2. Increase in width of white line in a horse with chroniclaminitis.
AAEP PROCEEDINGS � Vol. 56 � 2010 487
FARRIER PROGRAM

Palpation is used to determine whether a swellingproximal to the coronary band is firm, edematous, orfluctuant. Digital pressure is applied, at firstgently and then more firmly, to identify a focus ofpain, if present. Structures proximal to the coro-nary band that may be palpated directly through theskin include the proximodorsal distal interphalan-geal joint capsule, proximal aspect of the distal in-terphalalangeal joint collateral ligaments, proximalinterphalangeal joint collateral ligaments, middleand proximal phalanges, common digital extensortendon, deep digital flexor tendon and sheath, col-lateral cartilages, and digital cushion. Pressuremay be applied to the navicular area through the deepdigital flexor tendon and digital cushion. Deep sulcimay need to be palpated for discomfort with the aidof a tongue depressor. The flexibility of the collat-eral cartilages may also be determined by palpation.
ManipulationThe distal limb should be flexed and extended todetermine if it elicits a pain response or if there is areduced range of motion. In general, structuresthat are associated with flexion/extension duringnormal locomotion, such as the tendons and theirsheath, ligaments, joints, and navicular bursa, arelikely to elicit a painful response. Usually, painassociated with the hoof capsule and non-articularportions of the distal phalanx are unlikely to do so.However, manipulation should be interpreted cau-tiously, because instability between two parts of thehoof capsule or instability between the hoof capsuleand underlying distal phalanx may also be stressedby such handling.
Rotation of the foot in relation to the remainder ofthe digit shows a remarkable degree of mobility innormal horses, which should not be interpreted asabnormal. Marked sprains of collateral ligamentsmight be expected to elicit a painful response aftermanipulation in this manner.
Compression and PercussionDetection of pain within the foot is difficult withpalpation because of the rigidity of the hoof capsule.Therefore, compression and percussion are used toidentify and localize pain within the foot. Hooftesters are used to compress the foot. They shouldbe applied in a systematic manner, typically startingat one heel, progressing around the quarter, toe,opposite quarter, and heel and followed by compres-sion across both heels and from each side of the frogto the opposite heel. In addition to progressingaround the foot, systematic application of hooftesters must also evaluate the sole at different dis-tances from the white line. When the initial with-drawal response is mild, consistency with repetitionand comparison with the contralateral limb isneeded to determine if the response is clinically sig-nificant. In addition to eliciting a pain response,compression of the foot may also cause moisture tobe expressed from defects in the hoof capsule and
identify instability of fissures in the hoof capsule.Flexion of sole with hoof testers gives some indica-tion as to its thickness. When applying hooftesters, it is frequently assumed that any pain re-sponse identified is coming from the solar aspect ofthe foot. Although this is frequently the case, itshould be borne in mind that hoof testers mightelicit a painful response from any of the tissuesbetween their jaws. For example, when hooftesters are applied across the toe, the tissues af-fected include the integument of the wall as well asthe integument of the sole and the distal phalanx.
Percussion of the hoof capsule with a shoeinghammer is not performed as frequently as compres-sion, but it occasionally yields information that hooftesters do not give. Additionally, it is useful when nohoof testers are available. Although the foot mustbe elevated off the ground to percuss the sole, thewall may be percussed with the foot on or off theground, but the latter is easier.
Paring With a Hoof KnifeThe ground surface of the foot provides clues regard-ing the quality of the sole, evidence of past trauma,and defects that are potential entry sites for infec-tion. Defects in the ground surface of the stratummedium of the wall and the white line cannot beidentified if a shoe is present. The manner inwhich paring is performed and when it is performedis related to the presenting clinical symptom. Inhorses that present with an acute marked onset oflameness in which an abscess is the most likelydiagnosis, paring the foot is usually performedpromptly. However, removal of shoes and paring ofthe ground surface of the foot is not recommendedfor horses with mild lameness and no obvious abnor-malities of the ground surface of the foot until afterthe horse has been exercised and all pertinent diag-nostic analgesia has been performed. Not all lame-ness originating in the foot requires paring of thesole, and when it is done, caution should be exer-cised to preserve the thickness of the sole wheneverpossible. In particular, if a horse is suspected ofhaving laminitis, preservation of the sole thicknessis very important, and therefore, paring should bevery limited in extent or avoided. The frog mayrequire trimming to expose the sulci or investigateprimary diseases of the frog, such as thrush andcanker.
The ground surface of the foot in horses withmarked lameness of abrupt onset is explored forpuncture wounds and defects in the sole that arelikely entry sites for infection. Both usually appearas dark marks. Naturally occurring defects aremost likely to be present in the white line. Punc-ture wounds in the frog are frequently difficult toidentify, because the elastic nature of the frogcauses the entry wound to close over (Fig. 4); punc-tures in the collateral sulci are difficult to identify,because the exposure is poor. In horses in whichthe most likely diagnosis is an abscess, paring
488 2010 � Vol. 56 � AAEP PROCEEDINGS
FARRIER PROGRAM
should be very focal and should extend through thefull thickness of the hoof capsule until either puru-lent exudates or pinpoint hemorrhage is encoun-tered. If the likely entry site is in the white line, itis preferable to explore the defect by enlarging theside adjacent to the wall rather than the sole, ineffect creating a notch in the distal wall that extendsproximally to the junction with the inner surface ofthe sole. In horses with milder but more chroniclameness, paring the sole is kept to a minimum.Lightly debriding of the surface of the sole fre-quently reveals hemorrhage related to bruising.Blood that extravasates into the sole maintains itsred coloration, and it can further be distinguishedfrom pigmentation, because it has a stippled patternas it migrates down and around the horn tubules.
Evaluation of Shoes and ShoeingThe shoes should be evaluated to determine that thesize of the shoe is appropriate for the size of the footand that the type of shoe is appropriate for the typeof work that the horse is performing. Uneven wearon the ground surface of the shoe may indicate areasof excessive weight-bearing. If a shoe has been ontoo long, it moves forward in relation to the heelsand is likely to put pressure on the angles of the sole.Additionally, shoes that have been on too long mayloosen and shift.
3. The Detailed Examination
1. Morphological Examination of the HoofThe goal of examination of the detailed morphologyof the hoof is to identify deformation of the hoofcapsule and changes in the growth pattern of thehoof that may indicate the presence of abnormaldistribution of stresses within the foot. Increasedstress or weight-bearing by a portion of the wall hasthree consequences that may be detected on physical
examination: it may cause deviation of the walloutward or inward from its normal position, it maycause the wall to move proximally, or it may causethe growth of the wall to decelerate. A reduction instress or weight-bearing, for the most part, has theopposite effect. In contrast to the situation wherestress can retard hoof growth, there are occasionswhen hoof growth is accelerated in one part of thefoot in relation to another; the best examples of thiswould be the growth pattern associated with inflam-mation or tumors.
To accomplish a more detailed morphological ex-amination of the foot, the foot should be viewed fromall sides when it is on the ground, and then, theground surface should be examined with the foot offthe ground. Additionally, small changes in theshape of the hoof capsule may be better appreciatedby careful palpation of the foot than by visualinspection.
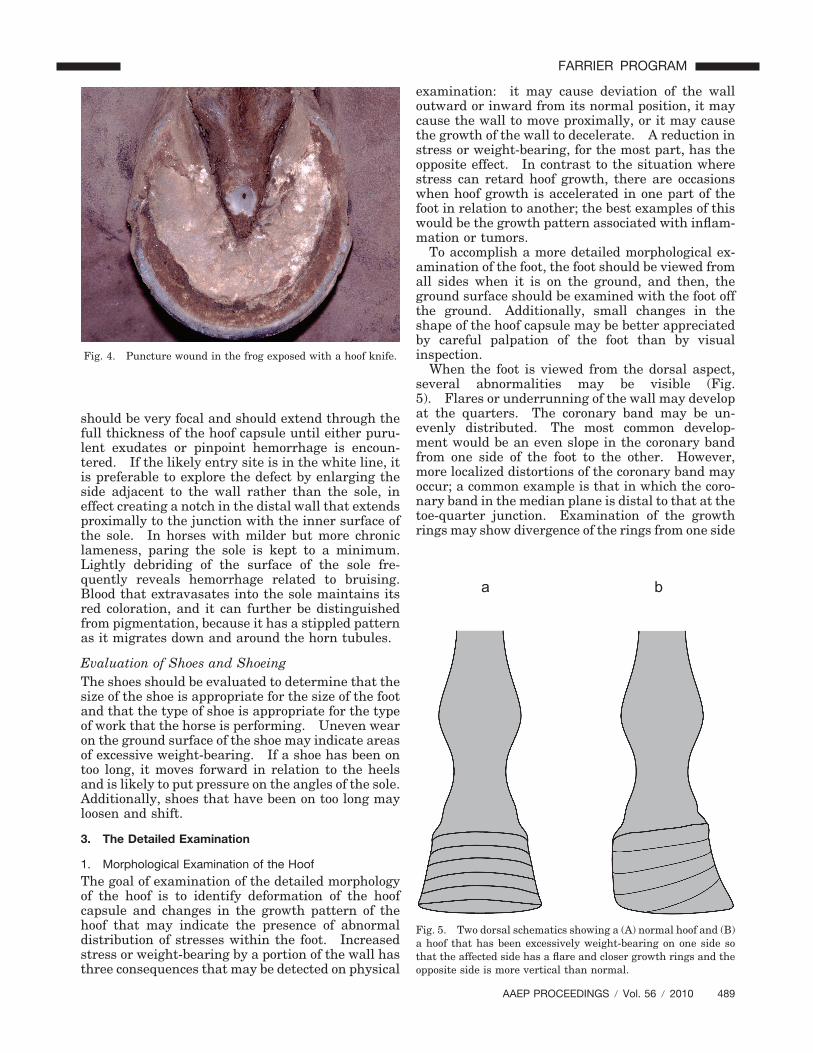
When the foot is viewed from the dorsal aspect,several abnormalities may be visible (Fig.5). Flares or underrunning of the wall may developat the quarters. The coronary band may be un-evenly distributed. The most common develop-ment would be an even slope in the coronary bandfrom one side of the foot to the other. However,more localized distortions of the coronary band mayoccur; a common example is that in which the coro-nary band in the median plane is distal to that at thetoe-quarter junction. Examination of the growthrings may show divergence of the rings from one side
a b
Fig. 5. Two dorsal schematics showing a (A) normal hoof and (B)a hoof that has been excessively weight-bearing on one side sothat the affected side has a flare and closer growth rings and theopposite side is more vertical than normal.
Fig. 4. Puncture wound in the frog exposed with a hoof knife.
AAEP PROCEEDINGS � Vol. 56 � 2010 489
FARRIER PROGRAM
to the other. The angle of the dorsal-horn tubulesto the saggital plane should be noted; normally, theyshould be parallel, and therefore, when they appeartilted medially or laterally, it suggests that thewhole hoof capsule may be tilted.
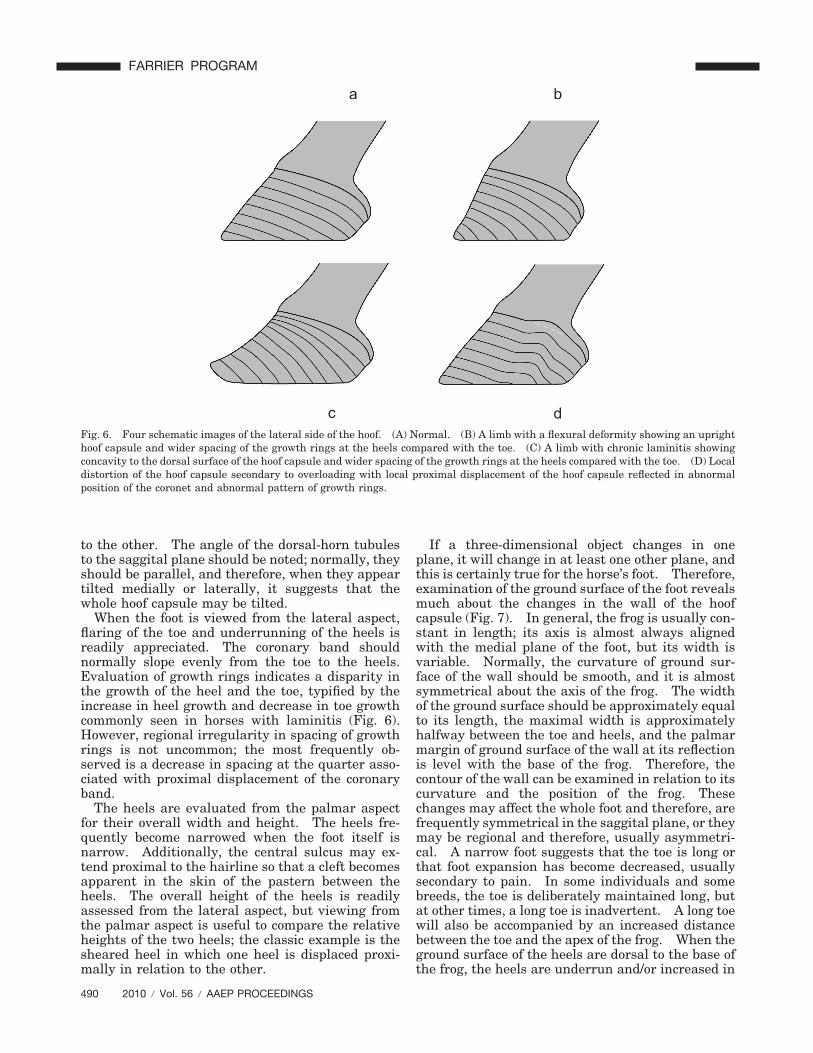
When the foot is viewed from the lateral aspect,flaring of the toe and underrunning of the heels isreadily appreciated. The coronary band shouldnormally slope evenly from the toe to the heels.Evaluation of growth rings indicates a disparity inthe growth of the heel and the toe, typified by theincrease in heel growth and decrease in toe growthcommonly seen in horses with laminitis (Fig. 6).However, regional irregularity in spacing of growthrings is not uncommon; the most frequently ob-served is a decrease in spacing at the quarter asso-ciated with proximal displacement of the coronaryband.
The heels are evaluated from the palmar aspectfor their overall width and height. The heels fre-quently become narrowed when the foot itself isnarrow. Additionally, the central sulcus may ex-tend proximal to the hairline so that a cleft becomesapparent in the skin of the pastern between theheels. The overall height of the heels is readilyassessed from the lateral aspect, but viewing fromthe palmar aspect is useful to compare the relativeheights of the two heels; the classic example is thesheared heel in which one heel is displaced proxi-mally in relation to the other.
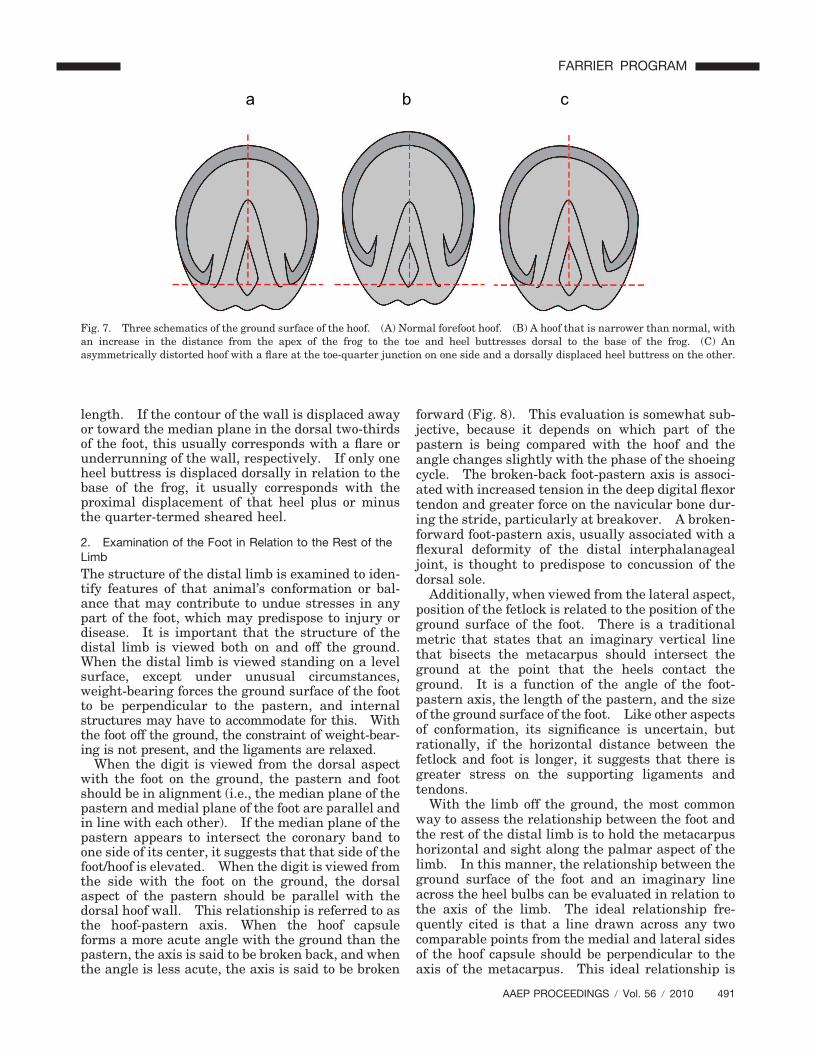
If a three-dimensional object changes in oneplane, it will change in at least one other plane, andthis is certainly true for the horse’s foot. Therefore,examination of the ground surface of the foot revealsmuch about the changes in the wall of the hoofcapsule (Fig. 7). In general, the frog is usually con-stant in length; its axis is almost always alignedwith the medial plane of the foot, but its width isvariable. Normally, the curvature of ground sur-face of the wall should be smooth, and it is almostsymmetrical about the axis of the frog. The widthof the ground surface should be approximately equalto its length, the maximal width is approximatelyhalfway between the toe and heels, and the palmarmargin of ground surface of the wall at its reflectionis level with the base of the frog. Therefore, thecontour of the wall can be examined in relation to itscurvature and the position of the frog. Thesechanges may affect the whole foot and therefore, arefrequently symmetrical in the saggital plane, or theymay be regional and therefore, usually asymmetri-cal. A narrow foot suggests that the toe is long orthat foot expansion has become decreased, usuallysecondary to pain. In some individuals and somebreeds, the toe is deliberately maintained long, butat other times, a long toe is inadvertent. A long toewill also be accompanied by an increased distancebetween the toe and the apex of the frog. When theground surface of the heels are dorsal to the base ofthe frog, the heels are underrun and/or increased in
ba
dcFig. 6. Four schematic images of the lateral side of the hoof. (A) Normal. (B) A limb with a flexural deformity showing an uprighthoof capsule and wider spacing of the growth rings at the heels compared with the toe. (C) A limb with chronic laminitis showingconcavity to the dorsal surface of the hoof capsule and wider spacing of the growth rings at the heels compared with the toe. (D) Localdistortion of the hoof capsule secondary to overloading with local proximal displacement of the hoof capsule reflected in abnormalposition of the coronet and abnormal pattern of growth rings.
490 2010 � Vol. 56 � AAEP PROCEEDINGS
FARRIER PROGRAM
length. If the contour of the wall is displaced awayor toward the median plane in the dorsal two-thirdsof the foot, this usually corresponds with a flare orunderrunning of the wall, respectively. If only oneheel buttress is displaced dorsally in relation to thebase of the frog, it usually corresponds with theproximal displacement of that heel plus or minusthe quarter-termed sheared heel.
2. Examination of the Foot in Relation to the Rest of theLimbThe structure of the distal limb is examined to iden-tify features of that animal’s conformation or bal-ance that may contribute to undue stresses in anypart of the foot, which may predispose to injury ordisease. It is important that the structure of thedistal limb is viewed both on and off the ground.When the distal limb is viewed standing on a levelsurface, except under unusual circumstances,weight-bearing forces the ground surface of the footto be perpendicular to the pastern, and internalstructures may have to accommodate for this. Withthe foot off the ground, the constraint of weight-bear-ing is not present, and the ligaments are relaxed.
When the digit is viewed from the dorsal aspectwith the foot on the ground, the pastern and footshould be in alignment (i.e., the median plane of thepastern and medial plane of the foot are parallel andin line with each other). If the median plane of thepastern appears to intersect the coronary band toone side of its center, it suggests that that side of thefoot/hoof is elevated. When the digit is viewed fromthe side with the foot on the ground, the dorsalaspect of the pastern should be parallel with thedorsal hoof wall. This relationship is referred to asthe hoof-pastern axis. When the hoof capsuleforms a more acute angle with the ground than thepastern, the axis is said to be broken back, and whenthe angle is less acute, the axis is said to be broken
forward (Fig. 8). This evaluation is somewhat sub-jective, because it depends on which part of thepastern is being compared with the hoof and theangle changes slightly with the phase of the shoeingcycle. The broken-back foot-pastern axis is associ-ated with increased tension in the deep digital flexortendon and greater force on the navicular bone dur-ing the stride, particularly at breakover. A broken-forward foot-pastern axis, usually associated with aflexural deformity of the distal interphalanagealjoint, is thought to predispose to concussion of thedorsal sole.
Additionally, when viewed from the lateral aspect,position of the fetlock is related to the position of theground surface of the foot. There is a traditionalmetric that states that an imaginary vertical linethat bisects the metacarpus should intersect theground at the point that the heels contact theground. It is a function of the angle of the foot-pastern axis, the length of the pastern, and the sizeof the ground surface of the foot. Like other aspectsof conformation, its significance is uncertain, butrationally, if the horizontal distance between thefetlock and foot is longer, it suggests that there isgreater stress on the supporting ligaments andtendons.
With the limb off the ground, the most commonway to assess the relationship between the foot andthe rest of the distal limb is to hold the metacarpushorizontal and sight along the palmar aspect of thelimb. In this manner, the relationship between theground surface of the foot and an imaginary lineacross the heel bulbs can be evaluated in relation tothe axis of the limb. The ideal relationship fre-quently cited is that a line drawn across any twocomparable points from the medial and lateral sidesof the hoof capsule should be perpendicular to theaxis of the metacarpus. This ideal relationship is
a b c
Fig. 7. Three schematics of the ground surface of the hoof. (A) Normal forefoot hoof. (B) A hoof that is narrower than normal, withan increase in the distance from the apex of the frog to the toe and heel buttresses dorsal to the base of the frog. (C) Anasymmetrically distorted hoof with a flare at the toe-quarter junction on one side and a dorsally displaced heel buttress on the other.
AAEP PROCEEDINGS � Vol. 56 � 2010 491
FARRIER PROGRAM

thought to provide optimal distribution of weightwithin the foot and therefore, is frequently used as aguide for trimming the foot. Unfortunately, thisrelationship varies with rotation within the meta-carpus and pastern and angulation at the metacar-pophalangeal joint. Therefore, it is important thatit is interpreted in conjunction with the appearanceof the distal limb when placed on the ground and themorphology of the hoof capsule.
3. Examination of the Foot in MotionObservation of the distal limbs in motion should beperformed at both a walk and trot, if possible, andshould be performed from in front, to the side, andfrom behind the horse as it moves. It is only re-cently that advances in technology have allowed usto better understand the manner in which the footmoves at breakover, during flight, and on landing.It is now known that most horses land laterally atthe heel or quarter and less commonly, land flat.Breakover is normally slightly lateral to or at thecenter of the toe. However, landing and breakoverare rapid events that are difficult to discern bywatching a horse at a trot, and therefore, they arebest observed at a walk. A toe-first landing or me-dial first landing are both abnormal events at a walkand warrant further investigation. Additionally,excessive lateral-first or heel-first landing is likely tobe abnormal. When mediolateral asymmetricallanding can be detected at a trot, it is likely to besignificant. Although the implications of abnormallanding and breakover are not fully understood, it ismost likely because of one or more of the followingreasons. It could be because of the horse’s confor-mation. It could be because of the horse’s attemptsto ameliorate pain in the foot. It could also be thatthe normal range of the stride is altered, usuallybecause of a more proximal focus of pain, and there-
fore, an earlier or later breakover or landing mayinfluence what part of the foot contacts and leavesthe ground first. In addition to changing the waythat the foot lands and leaves the ground, the horsemay place its limb farther to or away from the me-dian plane to redistribute weight, which would beaccompanied by associated changes in flight afterbreakover or before landing. This is most likely tobe seen when a horse positions its foot farther fromthe median plane to reduce lateral weight-bearing orvice versa. Flexion tests and toe/heel elevationtests are designed to stretch a set of structures be-fore trotting to make an occult lameness apparent ora mild lameness more obvious.
4. Ancillary Diagnostic Aids
There are three main objectives to ancillary diagnos-tic tests: exploration of an injury, usually with aflexible metal probe, diagnostic analgesia to localizethe source of pain, and diagnostic imaging to iden-tify discrete pathology. Their discussion is beyondthe scope of this article.
5. Summary
The manner in which the parts of the exam havebeen described is a reductionist approach because itis often easier to understand the significance of anindividual finding in isolation. However, the exam-ination is performed in the most clinically efficientmanner so that several characteristics of the limbare being observed at one time. For example, whenobserving the distal limb on the ground from eitherthe dorsal or lateral aspect, the morphology of thehoof capsule and the relationship between the footand remainder of the distal limb when weight-bear-ing are evaluated concurrently.
The basic examination is likely to provide a diag-nosis for many common and simple disorders, such
a b c
Fig. 8. Three lateral schematics depicting (A) a straight foot-pastern axis, (B) a broken-back foot-pastern axis, and (C) a broken-forward foot-pastern axis.
492 2010 � Vol. 56 � AAEP PROCEEDINGS
FARRIER PROGRAM

as a foot abscess. The detailed examination may,under some circumstances, provide a definitive di-agnosis but is as likely or more likely to direct theclinicians attention to risk factors for injury andindicators of abnormal stresses. The three mainareas that are assessed provide different types ofinformation as described previously. In brief, themorphology of the hoof capsule reveals deformationand changes in growth that occur after increased orreduced force, and the relationship between the limband the foot indicates conformations that may pre-dispose to abnormal weight-bearing. Observingthe limb in motion is most helpful to corroboratewith findings identified when the horse is examinedat rest; however, because there are limited dataavailable for comparison of the landing and break-over patterns with different disease states, it is moreof an art than a science at present.
The correlation of the clinical findings to suggest aprobable diagnosis may be good. However, at othertimes, the clinical findings may have conflicting im-plications; this may point to two separate clinicalproblems or a break in our understanding of thepathogenesis of the changes in structure of functionobserved. The latter is particularly importantwhen attempting symptomatic treatment in the ab-sence of a definitive diagnosis for whatever reason.In this instance, a measure of trial and error iswarranted, and it is based on the preponderance ofthe evidence rather than the total evidence.
Lastly, it should be remembered that, for somepurposes, the hindfeet can be considered very simi-lar in structure and function to the forefeet (forexample, in the diagnosis of abscesses, avulsions,and distal phalanx fractures). However, when dis-
eases such as those that can be attributed to hoofimbalance are considered, then the structure andfunction of the hindfoot should be considered sepa-rately from the forelimb. This is because thestresses associated with locomotion are sufficientlydifferent (and less well-understood) that changes inthe hoof capsule should not necessarily be inter-preted in the same manner as they would be in theforelimbs.
References1. Hickman J. Lameness and its diagnosis. In: Hickman J,
ed. Veterinary orthopaedics. Edinburgh, Scotland: Oliverand Boyd, 1964;1–8.
2. Adams OR. Diagnosis of lameneness. In: Lameness inhorses, 2nd ed. Philadelphia, PA: Lea & Febiger, 1966;89–113.
3. Moyer W. Clinical examination of the equine foot. Vet ClinNorth Am [Equine Pract] 1989;5:29–46.
4. Stashak TS. Examination for lameness. In: Stashak TS,ed. Adams’ lameness in horses, 5th ed. Philadelphia, PA:Lippincott Williams & Wilkins, 2002;113–183.
5. Keegan K, Dyson SJ. Clinical investigation of foot pain.In: Ross MW, Dyson SJ, eds. Diagnosis and management oflameness in the horse. Philadelphia, PA: Saunders, 2003;242–249.
6. Turner TA. Examination of the equine foot. Vet Clin NorthAm [Equine Pract] 2003;19:309–332.
7. Hunt RJ. Clinical evaluation and diagnosis of palmar footpain, in Proceedings. 52nd Annual American Association ofEquine Practitioners Convention 2006;198–202.
8. Moyer WA, GK Carter. Examination of the equine foot.In: Floyd AE, Mannsman RA, eds. Equine podiatry. Phi-ladelphia, PA: W. B. Saunders, 2007;112–127.
9. Balch O, White K, Butler D. Factors involved in the balanc-ing of equine hooves. J Am Vet Med Assoc 1980;198:1991–1989.
10. Turner TA. Hoof abnormalities and their relation to lame-ness, in Proceedings. 34th Annual American Association ofEquine Practitioners Convention 1988;293–297.
AAEP PROCEEDINGS � Vol. 56 � 2010 493
FARRIER PROGRAM





























