Embed Size (px)
Citation preview
ARTICLE IN PRESS
0021-9290/$ - se
doi:10.1016/j.jb
�CorrespondE-mail addr
Journal of Biomechanics 38 (2005) 2311–2316
www.elsevier.com/locate/jbiomech
Short communication
Excessive compression of the human tibio-femoral joint causesACL rupture
Eric G. Meyer, Roger C. Haut�
Orthopaedic Biomechanics Laboratories, College of Osteopathic Medicine, Michigan State University, A-414 East Fee Hall, East Lansing,
MI 48824, USA
Accepted 7 October 2004
www.JBiomech.com
Abstract
The knee is one of the most frequently injured joints in the human body. A recent study suggests that axial compressive loads on
the knee may play a role in injury to the anterior cruciate ligament (ACL) for the flexed knee, because of an approximate 101
posterior tilt in the tibial plateau (J. Orthop. Res. 16 (1998) 122–127). The hypothesis of the current study was that excessive axial
compressive loads in the human tibio-femoral (TF) joint would cause relative displacement and rotation of the tibia with respect to
the femur, and result in isolated injury to the ACL when the knee is flexed to 601, 901 or 1201. Sixteen isolated knees from eleven
fresh cadaver donors (74.3710.5 yr) were exposed to repetitive TF compressive loads increasing in intensity until catastrophic
injury. ACL rupture was documented in 14/16 cases. The maximum TF joint compressive force for ACL failure was 5.172.1 kN for
all flexion angles combined. For the 901 flexed knee, the injury occurred with a relative anterior displacement of 5.473.8mm, a
lateral displacement of 4.171.4mm, and a 7.877.01 internal rotation of the tibia with respect to the femur.
r 2004 Elsevier Ltd. All rights reserved.
Keywords: Anterior cruciate ligament rupture; Knee impact; Tibio-femoral compression
1. Introduction
The knee is one of the most frequently injured jointsin the human body. Epidemiological studies have shownthere are approximately 80,000 anterior cruciate liga-ment (ACL) tears in the United States each year with atotal cost nearly 1 billion dollars (Griffin et al., 2000).This study also reports that 70% of ACL tears are dueto ‘‘non-contact’’ types of injury. In a study of highschool soccer, volleyball and basketball players for oneseason, six of eight serious ACL injuries were ‘‘non-contact’’ (Hewett et al., 1999). Many studies haveinvestigated the loading mechanisms that cause injuryto the ACL. Boden et al. (2000) suggest that ACLinjuries frequently occur in landing from a jump on oneor both legs. In jump landings the knee may be flexed
e front matter r 2004 Elsevier Ltd. All rights reserved.
iomech.2004.10.003
ing author. Tel.: +517 355 0320; fax: +517 353 0789.
ess: [email protected] (R.C. Haut).
60–801 (Hewett et al., 1996). ACL injury is also commonin skiing with 25–30% of all ski-related knee injuriesinvolving the ACL (Speer et al., 1995). These injuries aremainly associated with twisting or a hard landing from ajump with a flexed knee (Ettlinger et al., 1995).The ACL functions as the primary restraint to limit
anterior tibial displacements for both 301 and 901 ofknee flexion (Butler et al., 1980; Fukubayashi et al.,1982; Torzilli et al., 1994). It provides approximately85% of the total ligamentous restraining force duringanterior tibial displacement. Fleming et al. (2001)confirm this notion by showing that normal, in vivoweight bearing in the knee induces tensile strain in theACL due to anterior position shift of the tibia relative tothe femur. This study also supports earlier investigationsshowing that tensile forces develop in the ACL underphysiological levels of tibio-femoral (TF) joint compres-sive loading (Li et al., 1998; Markolf et al., 1981).Torzilli et al. (1994) show that physiological levels of
ARTICLE IN PRESS
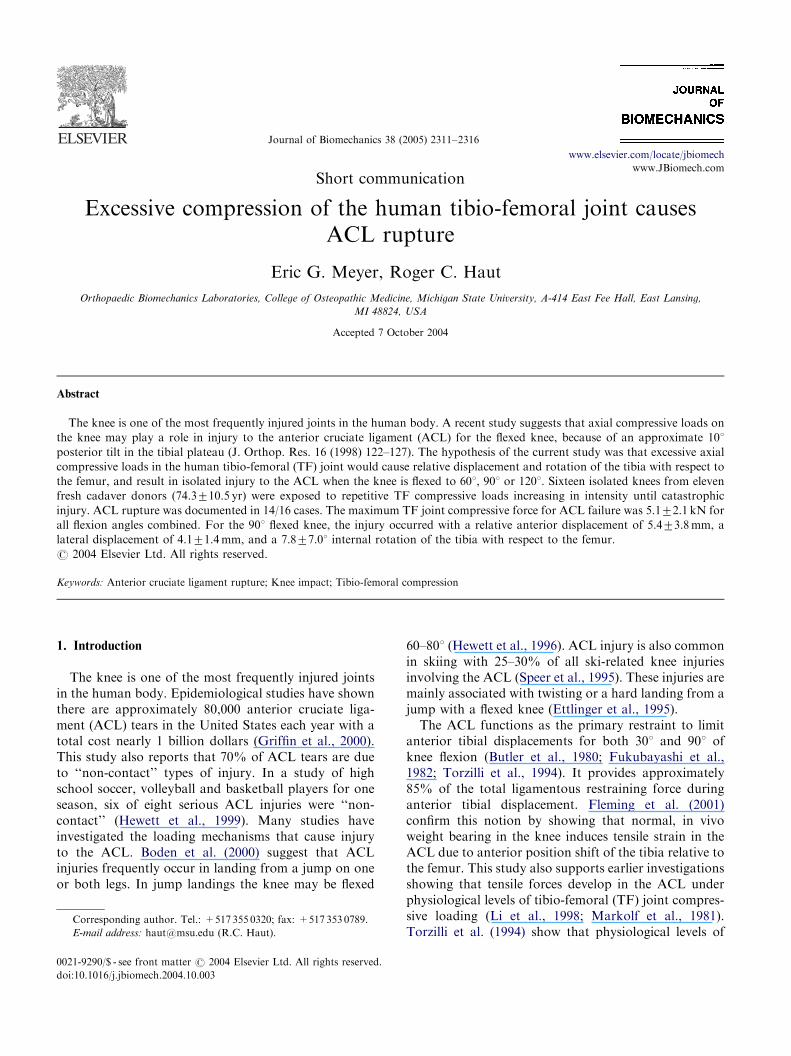
Fig. 1. Anterior neutral-position shift, which is attributed to the
inherent tilt of the tibial plateau, may cause an anterior translation of
the tibia during TF joint loading.
E.G. Meyer, R.C. Haut / Journal of Biomechanics 38 (2005) 2311–23162312
compressive loading on the human TF joint generatesanterior tibial translation with respect to the femur inthe ACL-deficient knee for all flexion angles greaterthan 151. This response is primarily thought to be due tothe inherent posterior tilt of the tibial plateau of 10–151(Li et al., 1998) (Fig. 1). This study further suggests‘‘that excessive compressive loads caused by impactloads along the tibial shaft (e.g., load from a jumplanding) may contribute to injury of the ACL, especiallywhen the knee is flexed’’.The hypothesis of the current study was that the
primary injury outcome for a flexed, isolated humanknee joint under excessive TF compression would beACL rupture. This study was designed to document thecompressive loads required to cause an ACL ruptureand the associated TF joint displacements and rotationswhen the knee is at 901 of flexion. Additional datashowing the same injury in knees flexed to 601 and 1201will also be documented in the study.
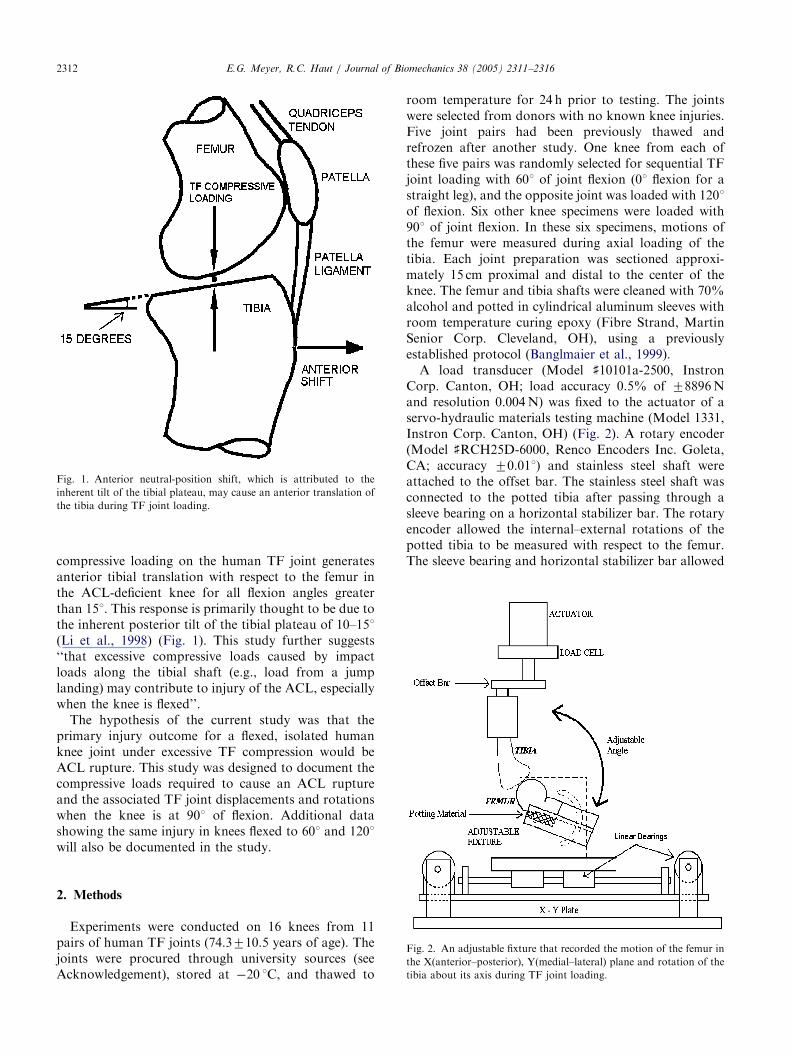
Fig. 2. An adjustable fixture that recorded the motion of the femur in
the X(anterior–posterior), Y(medial–lateral) plane and rotation of the
tibia about its axis during TF joint loading.
2. Methods
Experiments were conducted on 16 knees from 11pairs of human TF joints (74.3710.5 years of age). Thejoints were procured through university sources (seeAcknowledgement), stored at �20 1C, and thawed to
room temperature for 24 h prior to testing. The jointswere selected from donors with no known knee injuries.Five joint pairs had been previously thawed andrefrozen after another study. One knee from each ofthese five pairs was randomly selected for sequential TFjoint loading with 601 of joint flexion (01 flexion for astraight leg), and the opposite joint was loaded with 1201of flexion. Six other knee specimens were loaded with901 of joint flexion. In these six specimens, motions ofthe femur were measured during axial loading of thetibia. Each joint preparation was sectioned approxi-mately 15 cm proximal and distal to the center of theknee. The femur and tibia shafts were cleaned with 70%alcohol and potted in cylindrical aluminum sleeves withroom temperature curing epoxy (Fibre Strand, MartinSenior Corp. Cleveland, OH), using a previouslyestablished protocol (Banglmaier et al., 1999).A load transducer (Model ]10101a-2500, Instron
Corp. Canton, OH; load accuracy 0.5% of 78896Nand resolution 0.004N) was fixed to the actuator of aservo-hydraulic materials testing machine (Model 1331,Instron Corp. Canton, OH) (Fig. 2). A rotary encoder(Model ]RCH25D-6000, Renco Encoders Inc. Goleta,CA; accuracy 70.011) and stainless steel shaft wereattached to the offset bar. The stainless steel shaft wasconnected to the potted tibia after passing through asleeve bearing on a horizontal stabilizer bar. The rotaryencoder allowed the internal–external rotations of thepotted tibia to be measured with respect to the femur.The sleeve bearing and horizontal stabilizer bar allowed
ARTICLE IN PRESSE.G. Meyer, R.C. Haut / Journal of Biomechanics 38 (2005) 2311–2316 2313
axial forces in the tibia to compress the TF joint with aminimal bending moment applied to the load transdu-cer. The potted femur was secured to a fixture thatallowed knee joint flexion angles of 601, 901 and 1201. Abed of epoxy was added to the anterior surface of thefemur to help distribute compressive loads over theproximal end of the femur. The fixture was attached toan X–Y translational plate that had linear encoders(Model ]X00Z01A, Renishaw, Hoffman Estates, IL;accuracy 71 mm) attached to record anterior–posteriorand medial–lateral motions of the femur relative to thetibia during tests on the 901 flexed joints. All joints wererepeatedly loaded using a protocol in which a preload of6–8N was applied, followed by a single 10Hz haversineload waveform that simulated the time to peak groundreaction loads in a typical jump landing (Richards et al.,
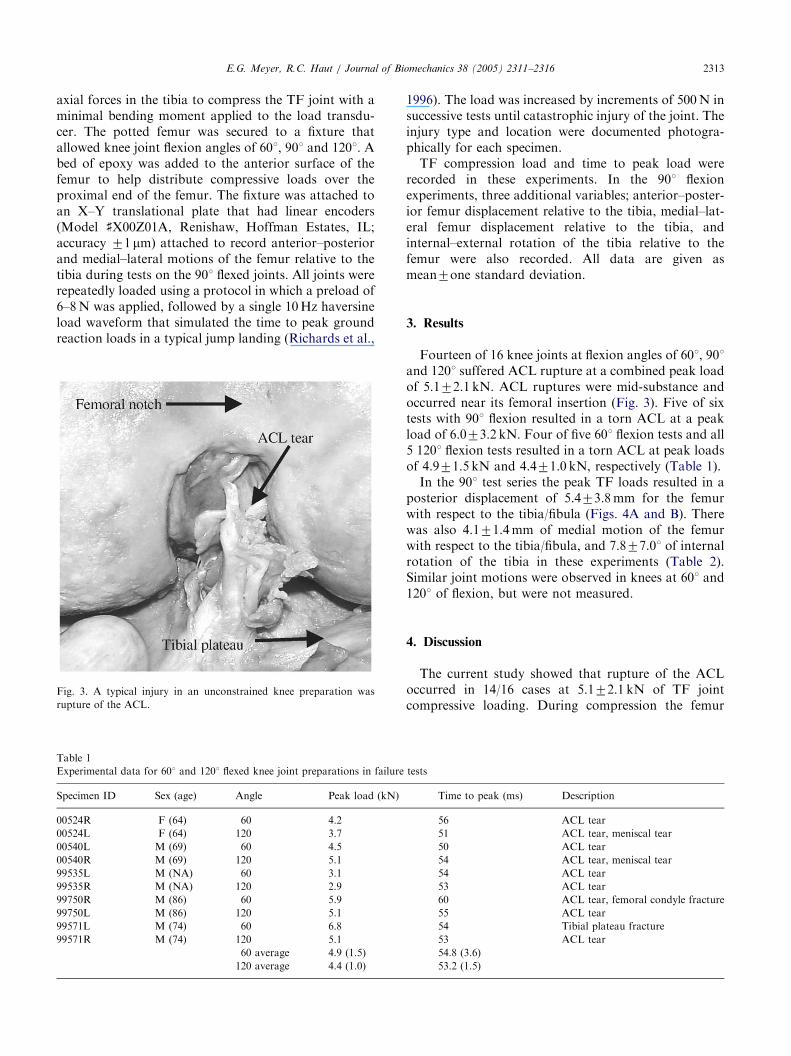
Fig. 3. A typical injury in an unconstrained knee preparation was
rupture of the ACL.
Table 1
Experimental data for 601 and 1201 flexed knee joint preparations in failure
Specimen ID Sex (age) Angle Peak load (kN)
00524R F (64) 60 4.2
00524L F (64) 120 3.7
00540L M (69) 60 4.5
00540R M (69) 120 5.1
99535L M (NA) 60 3.1
99535R M (NA) 120 2.9
99750R M (86) 60 5.9
99750L M (86) 120 5.1
99571L M (74) 60 6.8
99571R M (74) 120 5.1
60 average 4.9 (1.5)
120 average 4.4 (1.0)
1996). The load was increased by increments of 500N insuccessive tests until catastrophic injury of the joint. Theinjury type and location were documented photogra-phically for each specimen.TF compression load and time to peak load were
recorded in these experiments. In the 901 flexionexperiments, three additional variables; anterior–poster-ior femur displacement relative to the tibia, medial–lat-eral femur displacement relative to the tibia, andinternal–external rotation of the tibia relative to thefemur were also recorded. All data are given asmean7one standard deviation.
3. Results
Fourteen of 16 knee joints at flexion angles of 601, 901and 1201 suffered ACL rupture at a combined peak loadof 5.172.1 kN. ACL ruptures were mid-substance andoccurred near its femoral insertion (Fig. 3). Five of sixtests with 901 flexion resulted in a torn ACL at a peakload of 6.073.2 kN. Four of five 601 flexion tests and all5 1201 flexion tests resulted in a torn ACL at peak loadsof 4.971.5 kN and 4.471.0 kN, respectively (Table 1).In the 901 test series the peak TF loads resulted in a
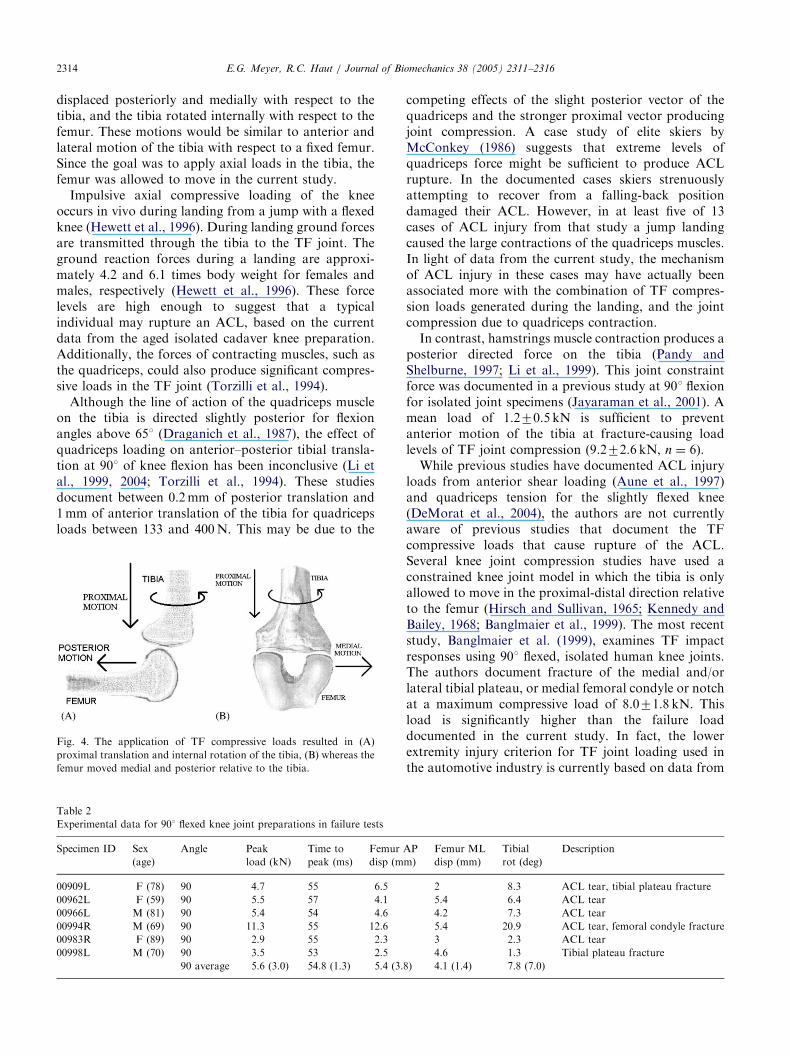
posterior displacement of 5.473.8mm for the femurwith respect to the tibia/fibula (Figs. 4A and B). Therewas also 4.171.4mm of medial motion of the femurwith respect to the tibia/fibula, and 7.877.01 of internalrotation of the tibia in these experiments (Table 2).Similar joint motions were observed in knees at 601 and1201 of flexion, but were not measured.
4. Discussion
The current study showed that rupture of the ACLoccurred in 14/16 cases at 5.172.1 kN of TF jointcompressive loading. During compression the femur
tests
Time to peak (ms) Description
56 ACL tear
51 ACL tear, meniscal tear
50 ACL tear
54 ACL tear, meniscal tear
54 ACL tear
53 ACL tear
60 ACL tear, femoral condyle fracture
55 ACL tear
54 Tibial plateau fracture
53 ACL tear
54.8 (3.6)
53.2 (1.5)
ARTICLE IN PRESSE.G. Meyer, R.C. Haut / Journal of Biomechanics 38 (2005) 2311–23162314
displaced posteriorly and medially with respect to thetibia, and the tibia rotated internally with respect to thefemur. These motions would be similar to anterior andlateral motion of the tibia with respect to a fixed femur.Since the goal was to apply axial loads in the tibia, thefemur was allowed to move in the current study.Impulsive axial compressive loading of the knee
occurs in vivo during landing from a jump with a flexedknee (Hewett et al., 1996). During landing ground forcesare transmitted through the tibia to the TF joint. Theground reaction forces during a landing are approxi-mately 4.2 and 6.1 times body weight for females andmales, respectively (Hewett et al., 1996). These forcelevels are high enough to suggest that a typicalindividual may rupture an ACL, based on the currentdata from the aged isolated cadaver knee preparation.Additionally, the forces of contracting muscles, such asthe quadriceps, could also produce significant compres-sive loads in the TF joint (Torzilli et al., 1994).Although the line of action of the quadriceps muscle
on the tibia is directed slightly posterior for flexionangles above 651 (Draganich et al., 1987), the effect ofquadriceps loading on anterior–posterior tibial transla-tion at 901 of knee flexion has been inconclusive (Li etal., 1999, 2004; Torzilli et al., 1994). These studiesdocument between 0.2mm of posterior translation and1mm of anterior translation of the tibia for quadricepsloads between 133 and 400N. This may be due to the
Fig. 4. The application of TF compressive loads resulted in (A)
proximal translation and internal rotation of the tibia, (B) whereas the
femur moved medial and posterior relative to the tibia.
Table 2
Experimental data for 901 flexed knee joint preparations in failure tests
Specimen ID Sex
(age)
Angle Peak
load (kN)
Time to
peak (ms)
Femur
disp (m
00909L F (78) 90 4.7 55 6.5
00962L F (59) 90 5.5 57 4.1
00966L M (81) 90 5.4 54 4.6
00994R M (69) 90 11.3 55 12.6
00983R F (89) 90 2.9 55 2.3
00998L M (70) 90 3.5 53 2.5
90 average 5.6 (3.0) 54.8 (1.3) 5.4 (3.
competing effects of the slight posterior vector of thequadriceps and the stronger proximal vector producingjoint compression. A case study of elite skiers byMcConkey (1986) suggests that extreme levels ofquadriceps force might be sufficient to produce ACLrupture. In the documented cases skiers strenuouslyattempting to recover from a falling-back positiondamaged their ACL. However, in at least five of 13cases of ACL injury from that study a jump landingcaused the large contractions of the quadriceps muscles.In light of data from the current study, the mechanismof ACL injury in these cases may have actually beenassociated more with the combination of TF compres-sion loads generated during the landing, and the jointcompression due to quadriceps contraction.In contrast, hamstrings muscle contraction produces a
posterior directed force on the tibia (Pandy andShelburne, 1997; Li et al., 1999). This joint constraintforce was documented in a previous study at 901 flexionfor isolated joint specimens (Jayaraman et al., 2001). Amean load of 1.270.5 kN is sufficient to preventanterior motion of the tibia at fracture-causing loadlevels of TF joint compression (9.272.6 kN, n ¼ 6).While previous studies have documented ACL injury
loads from anterior shear loading (Aune et al., 1997)and quadriceps tension for the slightly flexed knee(DeMorat et al., 2004), the authors are not currentlyaware of previous studies that document the TFcompressive loads that cause rupture of the ACL.Several knee joint compression studies have used aconstrained knee joint model in which the tibia is onlyallowed to move in the proximal-distal direction relativeto the femur (Hirsch and Sullivan, 1965; Kennedy andBailey, 1968; Banglmaier et al., 1999). The most recentstudy, Banglmaier et al. (1999), examines TF impactresponses using 901 flexed, isolated human knee joints.The authors document fracture of the medial and/orlateral tibial plateau, or medial femoral condyle or notchat a maximum compressive load of 8.071.8 kN. Thisload is significantly higher than the failure loaddocumented in the current study. In fact, the lowerextremity injury criterion for TF joint loading used inthe automotive industry is currently based on data from
AP
m)
Femur ML
disp (mm)
Tibial
rot (deg)
Description
2 8.3 ACL tear, tibial plateau fracture
5.4 6.4 ACL tear
4.2 7.3 ACL tear
5.4 20.9 ACL tear, femoral condyle fracture
3 2.3 ACL tear
4.6 1.3 Tibial plateau fracture
8) 4.1 (1.4) 7.8 (7.0)

ARTICLE IN PRESSE.G. Meyer, R.C. Haut / Journal of Biomechanics 38 (2005) 2311–2316 2315
these constrained knee joint studies (Kuppa, 2002). Thecurrent study would suggest that the current injurycriterion should be re-examined using unconstrainedknee joint preparations.A study by Woo et al. (1991) documents that
approximately 6mm of tensile deformation and6587129N of load is required to rupture the 60–97-year-old ACL mid-substance in its anatomic orienta-tion. Since the ACL is oriented approximately 71 withrespect to the tibial plateau in the 901 flexed knee(Herzog and Reed, 1993), it seems reasonable thattensile failure of the ACL occurred at 5.473.8mm ofposterior translation of the femur in the current study.Yet this does not take into account internal rotation ofthe tibia, which may further strain the ACL and medialtranslation of the femur, which may partially unload theACL during TF joint compression. Because of differ-ences in test methodologies between Woo et al. (1991)and the current study (tension versus compression)failure loads could not be directly compared.There were a number of limitations in the current
study that need to be addressed in the future. Sinceisolated knee preparations were used, the potentialeffects of muscle forces acting across the knee were notincluded. Since documented loads in jump landings mayapproach those causing ACL rupture in the currentstudy with aged cadaver specimens, these data suggestmuscle action is essential in preventing ACL injuries.Because of their ages these specimens only represent asmall portion of today’s population, and not that of thepopulation active in sports. Additional studies arerequired on a younger population of human knees toaddress the potential for ACL injuries in sports relatedjump landings. Additionally, the repetitive nature of thetests in the current study may be a limitation. Thepotential consequence of accumulated microdamages insoft tissue structures, such as the ACL, must beconsidered in future studies. Microdamages are knownto occur prior to gross rupture in other ACL models(Yahia et al., 1990).In summary, this study showed that ACL rupture
occurred in the human knee via excessive TF compres-sive loading. Since the peak compressive loads were inthe range that could regularly be generated during ajump landing, the role of muscle forces in preventinganterior translation, lateral displacement and internalrotation of the tibia are essential constraints andtherefore must be investigated in future studies usingyounger human cadaver specimens that represent thepopulation involved in sports today.
Acknowledgement
This study was supported by a Grant from theCenters for Disease Control and Prevention, National
Center for Injury Prevention and Control (R49/CCR503607). Its contents are the sole responsibility ofthe authors and do not necessarily represent the officialviews of the Centers for Disease Control and Preven-tion. The authors wish to gratefully acknowledge CliffBeckett, Vijay Jayaraman, Eric Sevensma, MasayaKitagawa and Chris O’Neill for technical assistanceduring this study. We also thank Mr. R.S. Wade,Director of the Anatomical Services Division/StateAnatomy Board, University of Maryland, for helpprocuring these test specimens.
References
Aune, A.K., Cawley, P.W., Ekeland, A., 1997. Quadriceps muscle
contraction protects the anterior cruciate ligament during anterior
tibial translation. American Journal of Sports Medicine 25 (2),
187–190.
Banglmaier, R., Dvoracek-Driksna, D., Oniang’o, T., Haut, R.C.,
1999. Axial compressive load response of the 901 flexed human
tibio-femoral joint. 43rd Stapp Car Crash Conference. pp. 127–140.
Boden, B.P., Dean, G.S., Feagen Jr., J.A., 2000. Mechanisms of
anterior cruciate ligament injury. Orthopedics 23 (6), 573–578.
Butler, D.L., Noyes, F.R., Grood, E.S., 1980. Ligamentous restraints
to anterior-posterior drawer in the human knee. Journal of Bone &
Joint Surgery 62A, 259–270.
DeMorat, G., Weinhold, P., Blackburn, T., Chudik, S., Garrett, W.,
2004. Aggressive quadriceps loading can induce noncontact
anterior cruciate ligament injury. American Journal of Sports
Medicine 32 (2), 477–483.
Draganich, L.F., Andriacchi, T.P., Anderson, G.B.J., 1987. Interac-
tion between intrinsic knee mechanics and the knee extensor
mechanism. Journal of Orthopaedic Research 5, 539–547.
Ettlinger, C.F., Johnson, R.J., Shealy, J.E., 1995. A method to help
reduce the risk of serious knee sprains incurred in alpine skiing.
American Journal of Sports Medicine 23 (5), 531–537.
Fleming, B., Renstrom, P., Beynnon, B., 2001. The effect of weight-
bearing and external loading on anterior cruciate ligament strain.
Journal of Biomechanics 34, 163–170.
Fukubayashi, T., Torzilli, P.A., Sherman, M.F., Warren, R.F., 1982.
An in vitro biomechanical evaluation of anterior-posterior motion
of the knee, tibial displacement, rotation and torque. Journal of
Bone & Joint Surgery 64A, 258–264.
Griffin, L.Y., Agel, J., Albohm, M.J., et al., 2000. Noncontact anterior
cruciate ligament injuries: risk factors and prevention strategies.
Journal of American Academy of Orthopedic Surgery 8 (3), 141–150.
Herzog, W., Reed, L.J., 1993. Lines of action and moment arms of the
major force-carrying structures crossing the human knee joint.
Journal of Anatomy 182 (Pt 2), 213–230.
Hewett, T.E., Stroupe, A.L., Nance, T.A., Noyes, F.R., 1996.
Plyometric training in female athletes: decreased impact forces
and increased hamstrings torques. American Journal of Sports
Medicine 24 (6), 765–773.
Hewett, T.E., Lindenfeld, T.N., Riccobene, J.V., Noyes, F.R., 1999.
The effect of neuromuscular training on the incidence of knee
injury in female athletes: a prospective study. American Journal of
Sports Medicine 27 (6), 699–705.
Hirsch, G., Sullivan, L., 1965. Experimental knee-joint fractures. Acta
Orthopaedica Scandinavica 36, 391–399.
Jayaraman, V.M., Sevensma, E.T., Kitagawa, M., Haut, R.C., 2001.
Effects of anterior-posterior constraint on injury patterns in the
human knee during tibio-femoral joint loading from axial forces
through the tibia. Stapp Car Crash Journal 45, 449–468.

ARTICLE IN PRESSE.G. Meyer, R.C. Haut / Journal of Biomechanics 38 (2005) 2311–23162316
Kennedy, J.C., Bailey, W.H., 1968. Experimental tibial-plateau
fractures: studies of the mechanism and a classification. Journal
of Bone & Joint Surgery 50 (A), 1522–1534.
Kuppa, S., 2002. An overview of knee-thigh-hip injuries in frontal
crashes in the United States. 17th ESV.
Li, G., Rudy, T., Allen, C., 1998. Effect of combined axial compressive
and anterior tibial loads on in situ forces in the anterior cruciate
ligament: a porcine study. Journal of Orthopaedic Research 16,
122–127.
Li, G., Rudy, T.W., Sakane, M., Kanamori, A., Ma, C.B., Woo, S.L.-
Y., 1999. The importance of quadriceps and hamstring muscle
loading on knee kinematics and in-situ forces in the ACL. Journal
of Biomechanics 32, 395–400.
Li, G., DeFrate, L.E., Zayontz, S., Park, S.E., Gill, T.J., 2004. The
effect of tibiofemoral joint kinematics on patellofemoral contact
pressures under simulated muscle loads. Journal of Orthopaedic
Research 22, 801–806.
Markolf, K.L., Bargar, W.L., Shoemaker, S.C., Amstutz, H.C., 1981.
The role of joint load in knee stability. Journal of Bone & Joint
Surgery 63, 570–585.
McConkey, J.P., 1986. Anterior cruciate ligament rupture in skiing: a
new mechanism of injury. American Journal of Sports Medicine 14
(2), 160–164.
Pandy, M.G., Shelburne, K.B., 1997. Dependence of cruciate-ligament
loading on muscle forces and external load. Journal of Biomecha-
nics 30 (10), 1015–1024.
Richards, D.P., Ajemian, S.V., Wiley, J.P., Zernicke, R.F., 1996.
Knee joint dynamics predict patellar tendonitis in elite
volleyball players. American Journal of Sports Medicine 24 (5),
676–683.
Speer, K.P., Warren, R.F., Wickiewicz, T.L., Horowitz, L., Hender-
son, L., 1995. Obeservations on the injury mechanism of anterior
cruciate ligament tears in skiers. American Journal of Sports
Medicine 23 (1), 77–81.
Torzilli, P., Deng, X., Warren, R., 1994. The effect of joint-
compression load and quadreceps muscle force on knee motion
in the intact and the anterior cruciate ligament-sectioned knee.
American Journal of Sports Medicine 22, 105–112.
Woo, S.L., Hollis, J.M., Adams, D.J., Lyon, R.M., Takai, S., 1991.
Tensile properties of the human femur-anterior cruciate
ligament–tibia complex: the effects of specimen age and
orientation. American Journal of Sports Medicine 19 (3),
217–225.
Yahia, L., Brunet, J., Labella, S., Rivard, C.H., 1990. A scanning
electron microscopic study of rabbit ligaments under strain. Matrix
10, 58–66.





























