Embed Size (px)
Citation preview

RAPID COMMUNICATION
Experience after the Evaluation of 700 Potential Donorsfor Living Donor Liver Transplantation in
a Single CenterCamino Valentın-Gamazo,1 Massimo Malago,1 Marc Karliova,2 Juergen T. Lutz,3
Andrea Frilling,1 Silvio Nadalin,1 Giuliano Testa,7 Stefan G. Ruehm,5
Yesim Erim,4 Andreas Paul,1 Hauke Lang,1 Guido Gerken,2 andChristoph E. Broelsch1
Adequate selection of donors is a major prerequisite forliving donor liver transplantation (LDLT). Few centersreport on the entire number of potential donors consid-ered or rejected for living donation. From April 1998 toJuly 2003, a total of 111 living donor liver transplanta-tions were performed at our institution, with 622 poten-tial donors for 297 adult recipients and 78 potentialdonors for 52 pediatric recipients evaluated. In the adultgroup, only 89 (14%) potential donors were consideredsuitable, with a total of 533 (86%) potential donorsrejected. Of these, 67% were excluded either at initialscreening or during the first and second steps of the eval-uation procedure. In 31% of all cases, the evaluation ofdonors was canceled because of recipient issues. In thepediatric group, 22 (28%) donors were selected, with theother 56 (72%) rejected. Costs of the complete evaluationprocess accounted for 4,589 Euro (€) per donor. The eval-uation of a potential living donor is a complex and expen-sive process. We present the results on the evaluation ofthe largest group of potential donors for adults reported inthe literature. Only 14% of potential donors in our serieswere considered suitable candidates. It has not yet beenestablished who should cover the expenses of the evalua-tion of all rejected donors. In conclusion, all efforts shouldbe made in order to develop an effective screening proto-col for the evaluation of donors with the aim of savingtime and resources for a liver transplantation program.(Liver Transpl 2004;10:1087–1096.)
One of the most important problems facing thetransplant community is the growing discrepancy
between the number of patients listed for liver trans-plantation and the availability of donor organs. As aresult, the median waiting time for transplantation andthe number of patients that die awaiting a donor liverincreases every year. This situation has led to an increas-ing number of transplant teams pursuing an interest inthe use of living donors for adult liver transplantation asa way to cope with the shortage of cadaveric organsfrom cadaver sources.
The application of living donor liver transplantation(LDLT) is associated with several theoretical advan-tages for the recipient: transplantation can be per-
formed electively before serious decompensation in therecipient occurs, complications associated with organpreservation are minimized, and grafts of optimal qual-ity are provided.1,2 Additionally, LDLT offers the pos-sibility of liver replacement to selected patients whomay be ineligible for cadaveric organ transplantation.3
The drawback of this technique is the potential risk ofdeath or serious complications in the donor and agreater incidence of technical complications in recipi-ents. Ethical concerns have subsequently arisen and thesuccess of this procedure will depend ultimately on 2critical issues: donor morbidity and mortality should bereduced to a minimum and graft and recipient survivalshould be similar to that of conventional liver trans-plantation.4–6 Therefore, an adequate and thoughtfulselection of donors is a major prerequisite for LDLT.Exhaustive medical and psychological evaluation and aprecise anatomical study of the liver should be per-formed in order to guarantee the safety of the donor andprovide good results for the recipient.
Most reports in the literature have focused on theevaluation protocol, morbidity, and mortality indonors or the ethical aspects of living donation. The
Abbreviations: LDLT, living donor liver transplantation;ALDLT, adult living donor liver transplantation; €, Euro.
From the 1Departments of General Surgery and Transplantation,2Gastroenterology and Hepatology, 3Anesthesiology and Intensive CareMedicine, and 4Psychotherapy and Psychosomatics, and the 5Institute ofDiagnostic and Interventional Radiology, University Hospital Essen,Essen, Germany; and the 6Department of Surgery, Division of Trans-plantation, University of Illinois, Chicago, IL.
Address reprint requests to Camino Valentın-Gamazo, MD, Depart-ment of General Surgery and Transplantation, University HospitalEssen, Hufelandstr. 55, 45122 Essen, Germany. Telephone: 0049-201-723-1101; FAX: 0049-201-723-5946; E-mail: [email protected]
Copyright © 2004 by the American Association for the Study ofLiver Diseases
Published online in Wiley InterScience (www.interscience.wiley.com).DOI 10.1002/lt.20223
1087Liver Transplantation, Vol 10, No 9 (September), 2004: pp 1087–1096

majority of reports concerning the results of the evalu-ation of living donors present data of only pediatric orboth adult and pediatric LDLT together.7–12 However,these data may not be directly applicable to adult LDLT(ALDLT). Some other reports have been recently pub-lished about the evaluation of potential donors forALDLT.1,13–17 Though the evaluation protocols aresimilar, the population of donors considered differs sig-nificantly in most centers: some series include only indi-viduals who qualify for donation, but not those whowere rejected on the initial screening. In other series,donors whose evaluation was canceled because of recip-ient issues were also excluded. Thus, while it is difficultto compare the results presented in those reports andcomprehensive data about the real number of potentialdonors evaluated, reasons for rejection and costs of theevaluation procedure in centers performing ALDLT arestill missing.
We present our experience with the development ofan evaluation protocol for potential donors forALDLT, which was adapted from our pediatric proto-col. Specific criteria for the selection of donors are sug-gested, and the costs of the evaluation procedure arealso analyzed. Results after the evaluation of a large poolof donors for ALDLT (including all screened and eval-
uated donors) are presented in detail and compared tothe ones reported in the literature by other centers.
Patients and Methods
The policy of our program is to present the possibility ofLDLT to all potential adult recipients at the time of evalua-tion for liver transplantation. In our pediatric program, par-ents are informed about this alternative. Donors should shareeither a genetic or significant emotional relationship with therecipient. A first interview with the potential donor(s) and therecipient is always performed by a transplant physician. Thiscolloquium is important to inform the parties about thedetails of the surgery, postoperative care, complications, andreported outcomes associated with ALDLT. During this ses-sion, the initial screening of potential donors is performed.Exclusion criteria for donors include being under 18 years ofage, obesity (body mass index �30 kg/m2) and medicalcomorbidity. The first step of the evaluation (Table 1) isperformed for candidates considered initially suitable. Theprocess of evaluation of donors can run parallel to theevaluation of the recipient, sometimes performed once therecipient has been fully evaluated. For patients with extendedoncologic indications, the identification of a live donoris a prerequisite before proceeding with the recipient evalua-tion.
Table 1. Evaluation Protocol for Potential Living Liver Donors
Step 1 Clinical evaluation: history and physical examinationLab tests: blood group, hematological tests, chemistry, coagulation profile, C-reactive protein, and pregnancy testSerology: hepatitis A, B and C, HIV, CMV, HSV, EBVFirst informed consent
Step 2 Imaging studies: “all in one” CT scanHistology: liver biopsyFirst psychological evaluationHepatitis B vaccination (1° doses)
Step 3 Special studies: ECG, chest x-ray, pulmonary function test, echocardiography, stress testLaboratory: thyroid function tests (TSH, T3, T4), immunoglobulines IgA, IgG, IgM, iron, transferrin, ferritin,
�-1-antitrypsin, ceruloplasmin, tumor markers (CEA, AFP, Ca19-9), factors V, VII and VIII, protein C and S,APCR, and urine sediment
Liver function tests: galactose, indocyanine, lidocaineFirst autologous blood donationSelected consultations
Step 4 Second psychological evaluation (donor and recipient together)Hepatologist consultationSecond autologous blood donation
Step 5 HLA typing, cross-matchHepatitis B vaccination (2° doses)Anesthesiological consultationEthical board evaluationFinal informed consent
Abbreviations: HIV, human immunodeficiency virus; CMV, cytomegalovirus; HSV, herpes simplex virus; EBV, Epstein-Barr virus; CT,computed tomography; ECG, electrocardiogram; TSH, thyroid-stimulating hormone; T3, triiodothyronin; T4, thyroxin; CEA, carci-noembryonic antigen; AFP, alpha-fetoprotein; APCR, activated protein C resistance.
1088 Valentın-Gamazo et al.

The protocol for evaluation of donors for ALDLTincludes 5 steps (Table 1).
Step 1
The first step in the evaluation consists of a medical work-up.Blood group identity is the optimal condition, but compati-bility is also accepted. We consider positive serology for hep-atitis C an absolute contraindication for living donation, evenin the case of a recipient with hepatitis C cirrhosis. Donorswith positive core antibody for hepatitis B were initiallyrejected, but at present are considered for hepatitis B infectedrecipients. These donors should have normal liver enzymes,normal liver histology and negative hepatitis B virus in serumand in the liver detected by quantitative polymerase chainreaction assay with the Amplicor HBV Monitor test (RocheDiagnostic Systems, Grenzach-Wyhlen, Germany). This testis a standardized assay for quantifying hepatitis B virus vire-mia levels in the range from 102 to 107 copies/mL.
Step 2
Examinations performed in this phase evaluate the volumetry,anatomy and quality of the graft. Computed tomographyscan was used for the first series of donors and seemed to besufficiently accurate to estimate the volume of the graft. Addi-tionally, a celiac angiography was performed to define thevascular anatomy. Since November 1999, magnetic reso-nance imaging has been implemented as a standard techniquein our program. Initially, this exam was still supplementedwith the performance use of a celiac angiography. SinceNovember 2000, simultaneous performance use of magneticresonance angiography reliably defined the vascular anatomy,eliminating the use of the angiography. Nevertheless, a gooddefinition of the arterial blood supply and the anatomy of thebiliary tract were not achieved until the introduction of the“all-in-one” protocol with multidetector row computedtomography scan in May 2001 (Fig. 1). The protocol includesacquisition of 3 subsequent scans after the intravenous admin-istration of both a biliary contrast agent and a conventionaliodinated contrast agent. This technique allows a detailedanalysis of the vascular and biliary anatomy and accuratemeasurement of the total volume of the liver and the graftvolume. Results obtained with the use of this techniqueshowed a good correlation between the radiological and intra-operative findings.18,19 We consider a graft-to-recipient bodyweight ratio �.8% a safe lower limit for adults, with a maxi-mal percentage of resection in the donor liver of 60 to 65%.The ratio between residual liver volume and the donor’sweight is also calculated, and a ratio of .8% is considered as asafe lower limit.
Liver biopsy was initially performed only in case of mar-ginal percentage of resection (resection of �60% of livertissue) or when findings that might indicate pathologic liverconditions were disclosed in advance. After the loss of a donordue to congenital lipodystrophy not diagnosed preopera-
tively, a liver biopsy became a mandatory part of the evalua-tion. In donors for children liver biopsy is only performed inselected cases. We consider a 20% or more degree of steatosisas an absolute contraindication for donation. In case of ratesbetween 10 and 20% we recommend diet and the perfor-mance of a second biopsy after weight reduction. Results of10% or less of fat infiltration are accepted when the percent-age of resection of the donor liver is less than 50%.
In the psychosomatic evaluation, there are two relevantaspects: one is the psychological stability of the potentialdonor and the second is the verification of informed consent.In case of donors for ALDLT, this evaluation is performedtwice, first for the donor and in a second session for bothdonor and recipient together.
Step 3
During this phase, an assessment of the general operative riskis performed, including a pulmonary function test, echocar-diography, and stress test. Laboratory tests are also performed(Table 1). Additional tests deemed necessary are obtained ona selective basis (e.g., colonoscopy, mammography) depend-ing on the individual donor. The first autologous blood dona-tion also takes place in this phase. In donors for ALDLT, weconsider 2 units of autologous blood sufficient. In the case ofdonation for pediatric recipients, this does not seem to bemandatory. In order to perform the liver function test, poten-tial donors are admitted to the hospital for 1 day.
Figure 1. Three-dimensional computed tomographyarteriogram and cholangiogram obtained with the “all-in-one” protocol. The protocol includes acquisition of threesubsequent scans (cholangiogram, arteriogram, and por-tal-hepatic venous phases) after the intravenous adminis-tration of both a biliary contrast agent and a conventionaliodinated contrast agent.
1089Donor Evaluation for Living Liver Transplantation
Step 4
At the beginning of our experience, celiac angiography wasperformed during this step, but this has now been practicallyabandoned after the introduction of the “all-in-one” com-puted tomography scan. In this phase, the second autologousblood donation, the second psychological assessment indonors for ALDLT, and the consultation by our hepatologistare performed.
Step 5
German transplantation law establishes that living donorsshould be first or second degree relatives of recipients orshould have close emotional ties with them. This condition,and the absence of any financial interest for donation, areevaluated by the ethical board, which was created in Germanyafter the first cases of ALDLT were performed, completelyindependent of the hospital evaluation team. It meets once ortwice per month; however, an extra session can be called forurgent cases (i.e., fulminant hepatic failure) within 24 hours.The consultation by the anesthesiologist and the final consentfrom both donor and recipient are also obtained in this phase.Donors who are not native Germans are required to providean independent translator for the consent procedures.
For the complete evaluation, candidates are scheduled for4 to 5 appointments in the outpatient clinic and 1-day admis-sion to perform the liver function test. Liver biopsy is alsoperformed in the outpatient clinic, including a 3-hour periodfor observation after the procedure. We do not proceed in thedonors evaluation process until acceptable findings are con-firmed in the previous step. Potential donors are explicitlyinformed that they can withdraw their consent at any time.Decisions of donors to abort the donation process are keptconfidential and are ascribed to medical or anatomical con-straints. Once the donor evaluation is completed, both donorand recipient are presented at the interdisciplinary transplan-tation conference and either approved or rejected for LDLT.If they are deemed appropriate for LDLT, transplantation isscheduled.
In the case of patients with fulminant hepatic failure weperform a “quick” evaluation of the potential donor, includ-ing blood tests, electrocardiogram, chest x-ray, pulmonaryfunction test, echocardiography, imaging study of the liverwith “all-in-one” computed tomography scan, psychologicalassessment, and evaluation by the ethical board. The evalua-tion can be completed in a 24- to 48-hour time period.
Results
From April 1998 to July 2003, a total of 111 livingdonor liver transplantations were performed at ourinstitution (89 cases involving a right lobe, 3 with a leftlobe, and 19 cases with a left lateral lobe). In this period,a total of 700 potential living donors were consideredfor 349 recipients. We included in this series not onlythe donors who were evaluated following the stepwiseprocedure but also the ones who were rejected after aninitial screening (through an interview with the trans-plant physician) and the ones whose evaluation wascanceled for recipient issues. Potential donors weredivided into 2 groups: Group A included donors foradult recipients, and group B consisted of donors forpediatric patients.
Group A
This group included 622 potential donors for 297recipients (Table 2). Only 89 (14%) were suitable forliving donation, with a total of 533 (86%) potentialdonors rejected. Out of these, 104 (20%) were refusedon initial screening, 265 (49%) were rejected during theevaluation and in 164 (31%) cases the evaluation wascanceled because of recipient-related reasons (Table 3and 4).
On initial screening, most of the donors wereexcluded for obesity (body mass index �30 kg/m2),documented previous illness, or the presence of morethan 2 risk factors (e.g., age, nicotine abuse, alcoholabuse, hypertension). These potential donors were con-sidered unsuitable after the first interview with the
Table 2. Demographics of Donors and RelationshipWith Recipients
Group A Group B
Total potential donors 622 78Gender (M/F) 340 / 282 39 / 39Age (yr) 37 � 11 (17–75) 35 � 6 (22–59)
RelationOffspring 231 (38%) 1 (1%)Siblings 127 (20%) 0 (0%)Parents 52 (8%) 73 (94%)2nd degree 51 (8%) 3 (4%)Spouse 86 (14%) 0 (0%)Unrelated 75 (12%) 1 (1%)
Table 3. Global Results of Evaluated Donors
Group A Group B Total
Total potentialdonors 622 78 700
Potential recipients 297 52 349Ratio 2.1 1.5 2Accepted 89 (14%) 22 (28%) 111 (16%)Excluded 533 (86%) 56 (72%) 589 (84%)
1090 Valentın-Gamazo et al.
transplant physician. No further medical tests were per-formed.
A total of 265 potential donors presented a contra-indication for donation during the evaluation and wereconsequently excluded. Of these, 12 (42%) donorswere excluded in the first step, with incompatible bloodgroup or positive hepatitis serology being the most fre-quent reasons for rejection.
A total of 139 (53%) donors were rejected in thesecond step. Of these, 82 donors were excluded due toinappropriate liver volumetry. The most frequent rea-son (70 cases) was a small remnant liver for the donor(residual liver volume to donor body weight ratio �.8).In 5 cases, both graft and remnant liver were insuffi-cient. A total of 5 donors were excluded because ofalternative donors with more suitable volumetric find-ings. In only 2 cases was the reason for rejection a “smallfor size” graft for the recipient (graft-to-recipient bodyweight ratio �.8).
In 22 potential donors, the reason for exclusion wasa pathological histology of the liver: 14 cases of steatosisdegree �20%, 4 cases of hepatitis, 2 cases of hemochro-matosis, 1 case of schistosomiasis in a donor originatingfrom Egypt, and another 1 with liver fibrosis.
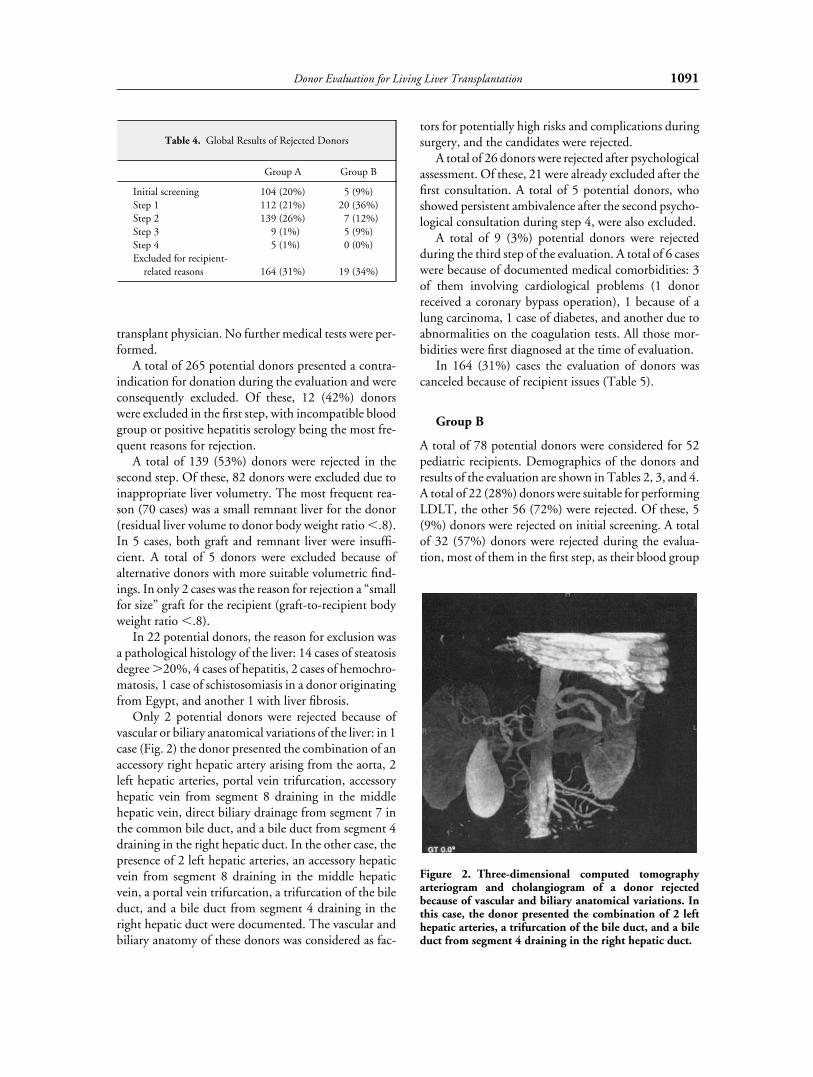
Only 2 potential donors were rejected because ofvascular or biliary anatomical variations of the liver: in 1case (Fig. 2) the donor presented the combination of anaccessory right hepatic artery arising from the aorta, 2left hepatic arteries, portal vein trifurcation, accessoryhepatic vein from segment 8 draining in the middlehepatic vein, direct biliary drainage from segment 7 inthe common bile duct, and a bile duct from segment 4draining in the right hepatic duct. In the other case, thepresence of 2 left hepatic arteries, an accessory hepaticvein from segment 8 draining in the middle hepaticvein, a portal vein trifurcation, a trifurcation of the bileduct, and a bile duct from segment 4 draining in theright hepatic duct were documented. The vascular andbiliary anatomy of these donors was considered as fac-
tors for potentially high risks and complications duringsurgery, and the candidates were rejected.
A total of 26 donors were rejected after psychologicalassessment. Of these, 21 were already excluded after thefirst consultation. A total of 5 potential donors, whoshowed persistent ambivalence after the second psycho-logical consultation during step 4, were also excluded.
A total of 9 (3%) potential donors were rejectedduring the third step of the evaluation. A total of 6 caseswere because of documented medical comorbidities: 3of them involving cardiological problems (1 donorreceived a coronary bypass operation), 1 because of alung carcinoma, 1 case of diabetes, and another due toabnormalities on the coagulation tests. All those mor-bidities were first diagnosed at the time of evaluation.
In 164 (31%) cases the evaluation of donors wascanceled because of recipient issues (Table 5).
Group B
A total of 78 potential donors were considered for 52pediatric recipients. Demographics of the donors andresults of the evaluation are shown in Tables 2, 3, and 4.A total of 22 (28%) donors were suitable for performingLDLT, the other 56 (72%) were rejected. Of these, 5(9%) donors were rejected on initial screening. A totalof 32 (57%) donors were rejected during the evalua-tion, most of them in the first step, as their blood group
Figure 2. Three-dimensional computed tomographyarteriogram and cholangiogram of a donor rejectedbecause of vascular and biliary anatomical variations. Inthis case, the donor presented the combination of 2 lefthepatic arteries, a trifurcation of the bile duct, and a bileduct from segment 4 draining in the right hepatic duct.
Table 4. Global Results of Rejected Donors
Group A Group B
Initial screening 104 (20%) 5 (9%)Step 1 112 (21%) 20 (36%)Step 2 139 (26%) 7 (12%)Step 3 9 (1%) 5 (9%)Step 4 5 (1%) 0 (0%)Excluded for recipient-
related reasons 164 (31%) 19 (34%)
1091Donor Evaluation for Living Liver Transplantation

was incompatible or a positive virus serology wasdetected. In 19 (34%) cases, the evaluation of the donorwas canceled for recipient-related reasons (Table 5).
Fulminant Hepatic Failure
From April 1998 to July 2003, a total of 71 patientswho were intensive care unit–bound because of fulmi-nant hepatic failure were put on a high-urgency list forliver transplantation in our institution. In 55 (77%)patients, no family member volunteered as a livingdonor: 15 died awaiting donor organs and 40 received acadaveric graft. A total of 16 (23%) patients (11 ingroup A and 5 in group B) had 40 candidates whovolunteered as living donors. Before the evaluation ofthe potential donors was completed, 5 patients receiveda cadaveric transplantation and 3 patients died. LDLTcould not be performed in 5 patients because of with-drawal of the donor. Of these 5 patients, 2 died and theother 3 received a cadaveric graft. One patient with liverfailure due to a syndrome including hemolysis, elevatedliver enzymes, and low platelet counts improved rapidlywithout transplantation. LDLT was performed in 2cases: a child with fulminant hepatic failure ofunknown etiology and a 17-year-old patient with acuteMorbus Wilson who received a right lobe from hermother.
For those patients who received a cadaveric graft,mean time from listing by Eurotransplant to transplan-tation was 2.6 days.
Complications during the Evaluation Procedure
A total of 116 liver biopsies were performed in donorsin group A and 6 in group B. Complications were
observed in 2 cases (1.6%). One donor developed asubcapsular hematoma in the right liver lobe, which wastreated conservatively; however it required blood trans-fusion. After 7 months, the hematoma was resolved andthe donor was reconsidered for ALDLT. During thistime, the recipient was still waiting for a cadaveric graftand unfortunately died before the transplantationcould be performed. Another potential donor alsodeveloped a subcapsular hematoma with hemobilia,requiring blood transfusion and the performance of anendoscopic retrograde cholangiography with papil-lotomy. The recipient in this case, diagnosed with pri-mary biliary cirrhosis and hepatocellular carcinoma,died 5 months later. No complications were observed indonors related to the performance of celiac angiogra-phy.
Costs of the Evaluation
We analyzed the costs of the examinations performed inevery step of the evaluation procedure: costs of step 1were 567 € (Euro), for step 2 794 €, step 3 accountedfor 1,462 €, step 4 for 185 € (costs of celiac angiographywere not included) and step 5 for 1,581 €. Costs of thecomplete evaluation procedure were 4,589 €. Profes-sional fees were not included, which would increase thecosts significantly. The cost of the evaluation of all“failed donors” must be accounted for in a cost analysisof LDLT. We divided the sum of all costs associatedwith donor evaluations, including “failed donors,” bythe total number of LDLT recipients. This numberreflects the “donor acquisition fee,” which accountedfor 10,619 € in the adult group and 8,644 € in thepediatric group. The “costs per recipient” reflect thesum of all costs of the evaluation of potential donorsdivided by the total number of potential recipients(Table 6). Costs of the evaluation of donors, hospitaladmission, surgical procedure, and follow-up examina-tions are covered by the insurance company of therecipient when LDLT is performed. It is not yet defin-itively established who should cover the expenses of theevaluation of all rejected donors or donors whose eval-uation was canceled because of recipient issues.
Outcome of Potential Recipients Evaluated forLDLT
A total of 349 potential recipients were considered forLDLT. A total of 107 (36%) adult and 12 (23%) pedi-atric patients were not able to find a suitable donor. Atotal of 101 (34%) patients in the adult group and 18(35%) in the pediatric group were excluded for recipi-
Table 5. Donors Rejected for Recipient-Related Reasons(Recipients Between Parenthesis)
Group A Group B
Donors rejected (no. recipients) 164 (101) 19 (18)Recipient reasons
Exitus 60 (37) 1 (1)Tumor stage 40 (20) 1 (1)Medical comorbidity 27 (17) 0Cadaveric LT 20 (15) 15 (14)Fear of recipient 13 (8) 0Resectable tumor 3 (3) 2 (2)Recovery after FHF 1 (1) 0
Abbreviations: LT, liver transplantation; FHF, fulminanthepatic failure.
1092 Valentın-Gamazo et al.

ent issues. LDLT was performed in 89 (30%) adult and22 (42%) pediatric recipients.
Discussion
Living donors undergo some degree of suffering with-out the compensation of a direct therapeutic benefit.For ethical reasons, adequate and thoughtful selectionof donors is a major prerequisite for LDLT. The maingoal of the evaluation process is to assure the safety ofthe donor and to provide better quality grafts for therecipients. This can only be achieved by first, an exhaus-tive medical and psychological evaluation of the donorand second, a precise study of the size, anatomy, andquality of the liver graft.
In the initial experience with ALDLT, most centerssimply adopted the evaluation protocols used for pedi-atric LDLT. In time, the remarkable differences in theevaluation of donors for adult and pediatric recipientsbecame obvious: first, the operation consists of a largerresection with potentially higher risk for the donor.Second, most pediatric donor candidates are young,healthy parents, whereas adult-to-adult donor candi-dates cover a wide age range (range in our series was17–75 years) and are usually at higher risk of present-ing medical problems. Finally, there is a larger numberof potential donors (ratio between number of donorsand recipients was 2.2 for adults and 1.5 for children inour series) and they are mostly professionals, whosetime schedule is limited and psychological motivationand relationship with the donor is also quite differentcompared to the pediatric program (26% nonrelateddonors in our adult group, 1% in our pediatric group ).That means there is a need for more precise anatomicalinformation, more exhaustive medical work-up, and amore refined psychological evaluation in ALDLT.Modifications introduced in the selection protocolshave already been well described by most centers. Theprocess of evaluation of donors starts with an initial
screening, which in some centers is performed througha brief telephone interview conducted by a transplantcoordinator. This screening sometimes includes theassessment of liver function and blood group by theprimary care physician. The evaluation itself is a step-wise procedure, consisting of a series of blood tests andcardiopulmonary and radiological examinations, com-bined with an intensive interaction between donor andtransplant staff (including hepatologists, surgeons,anesthesiologists, and psychiatrists). The Achilles heelin the evaluation of donors is definitively the assessmentof the anatomy and quality of the graft, and differentreports1,2,17,20,21 have confirmed that there is still a greatdeal of variability among centers, mainly regardingmainly 3 diagnostic studies: liver biopsy, hepaticangiography, and cholangiography.
Most reports in the literature have been focused on adescription of the evaluation protocol, but comprehen-sive data about the total number of donors evaluated,reasons for rejection, or costs of the evaluation proce-dure are still missing. Initial reports were made on theevaluation of donors for LDLT in children.7–12 How-ever, this data may not be directly applicable to ALDLTdue to the vastly different surgical procedure and thediversity of potential donors. Trotter et al.13 publishedthe first detailed report on the outcome of potentialrecipients and donors evaluated for ALDLT. Only 3other groups have recently reported their experience onthe evaluation of candidates for ALDLT.1,15,16
We show the results of the selection process of allpotential donors for LDLT. Comparison between ourresults and the ones previously published is difficultbecause of the lack of uniform criteria on the presenta-tion of the data.
In our study, 86% of potential donors for ALDLTwere rejected; Pomfret et al.16 and Pascher et al.15
reported a lower rejection rate of 69%, but donorsrejected on initial screening were not included. Trotter
Table 6. Costs (€) of the Evaluation Program for LDLT
Donors Adult Costs (€) Pediatric Costs (€)
Rejected on initial screening 104 10,400 5 500Rejected during evaluation 265 293,130 32 34,982Rejected for recipients reasons 164 233,172 19 53,746Total donors rejected 533 536,702 56 89,228Total donors accepted 89 408,421 22 100,958Total 945,123 190,186Costs per recipient 3,182 3,657Costs per LDLT-donor acquisition fee 10,619 8,644
1093Donor Evaluation for Living Liver Transplantation

et al.13 reported a significantly lower rejection rate of35%, but donors excluded for recipient-reasons anddonors excluded on initial screening were not consid-ered.
In the pediatric group in our series, 72% of donorswere rejected, which represents a significantly higherrate compared with other pediatric series: 29% by Ster-neck et al.10; 28% by Hashikura et al.7; 11% by Mori-moto et al.8; and 57% by Baker et al.11 The differencecan be explained because most of the candidates werereferred to these centers after a previous selection pro-cess.
The reality is that with an increasing number ofpotential candidates being evaluated and a more strin-gent selection criteria, the evaluation of donors forALDLT has become a costly, labor-intensive, and time-consuming procedure. In Germany, the costs of theevaluation, hospital admission, surgical procedure, andfollow-up examinations of donors are paid by the recip-ient’s insurance when LDLT is performed. The costs ofevaluation of potential donors who are rejected for anyreason during selection are neither covered by donor’snor by the recipient’s insurance. In these cases,the hospital budget is burdened with high expenses(Table 6).
The sequence of the examinations performed duringthe evaluation procedure is typically based on a progres-sion from least to most invasive, but the key factor isalso to determine which examinations identify a higherproportion of unsuitable candidates. Consequently, aperson with no real chance of donation could beexcluded as soon as possible during the selection pro-cess, saving considerable time and expenses for theLDLT program. In our series, 67% of donors in theadult group and 64% in the pediatric group wererejected on initial screening and during the first andsecond steps of the evaluation. The costs of initialscreening are minimal, since no medical tests are per-formed. Costs of examinations performed during thefirst and second steps of the evaluation are 566 € and793 €, respectively, being the most expensive proce-dures included in the final steps of the selection (1,427€ for step 3 and 1,579 € for step 5). Thus, our evalua-tion protocol is effective in detecting a high percentageof unsuitable donors early in the evaluation process,saving substantial time and resources. A very importantissue is the flexibility of the evaluation protocol, whichshould always be adapted to the characteristics of thedonor (i.e., for a nonrelated donor, the psychosomaticevaluation has priority over the other examinations, fora donor older than 60 years of age, the cardiopulmonaryevaluation takes place before the liver biopsy).
In our center, patients with extended indications arealso considered candidates for LDLT. For this reason,we found a lower rejection rate of potential recipients(34% in the adult and 35% in the pediatric group)when compared with other series (51% by Trotter etal.13). For these patients, the identification of a livingdonor is a prerequisite to proceed with the recipientevaluation. This results in a large population of donorswho are excluded for recipient contraindications: 31%in the adult group and 34% in the pediatric group. Thecosts of the evaluation of this group of donors representone-half of the costs of all rejected donors in our pro-gram (Table 6). In order to cut the costs, we wouldrecommend not to proceed with the evaluation ofdonors until the suitability of those potentially criticalrecipients is established.
In the pediatric group, most of the potential donorswere excluded on the first step, whereas in the adultgroup, a similar proportion of donors were rejectedduring steps 1 and 2. That means once we have a suit-able medical and blood group donor, the volume of theleft lateral graft is almost always adequate for a pediatricrecipient. Inadequate liver volume was one of the mainreasons for exclusion in the adult group (31% of evalu-ated donors). We observed that the volume of the rightgraft is mostly suitable for an adult patient; however ahigh percentage of resection and / or a low residual livervolume (residual liver volume to donor body weightratio �.8) in the donor was the most frequent reasonfor rejection. No similar data have been reported: in theseries of Pascher et al.15 and Trotter et al.,13 no donorwas rejected because of inadequate liver volumetry; byMarcos,1 this rate was 3%; only in the series of Pomfretet al.16 were 19.5% of donors excluded for this reason.We consider this relevant data in order to avoid a “smallfor size” residual liver in the donor.
A total of 8% of potential donors evaluated in ouradult group were rejected because of abnormal liverbiopsy. In 16 out of 26 donors, Pascher et al.15 found asteatosis �10%; Marcos1 and Pomfret et al.16 alsoreport relatively high rates (17 and 22%, respectively)of donors rejected for the same reason. Liver biopsy isnot routinely performed in all centers for the evaluationof donors, but an estimation of steatosis of the liverseems to be essential in the selection process.1,22 Clini-cal, imaging, and biochemical parameters do not seemto be accurate enough to judge the extent of hepaticsteatosis.23 We observed serious complications in 2donors (1.6%) related to a liver biopsy; however, we stillconsider this risk to be low, taking into account that animportant proportion of donors are rejected for abnor-mal histological findings. After the loss of a donor due
1094 Valentın-Gamazo et al.

to congenital lipodystrophy not diagnosed preopera-tively, a liver biopsy is performed routinely in all poten-tial donors for adult patients in our center.
Preoperative imaging studies should be able to accu-rately detect most anatomical variations of the donorliver, which enables preparation and may aid the surgi-cal dissection. In very few cases, however, variations ofthe vascular or biliary anatomy represent a contraindi-cation for donation in our series (2%) and in the onesreported by other authors (1% by Marcos1 and 4% byPascher et al.15).
The relationship between donor and recipient and,consequently, the psychological motivation of potentialdonors, is quite different in adult versus pediatricLDLT, implicating special considerations during theselection process. In the adult group, 10% of donorswere rejected after the first or second psychologicalassessment, with only one nonrelated donor excluded inthe pediatric group (in this case no significant emo-tional relationship with the recipient was found). In thereport of Pascher et al.15 psychological contraindica-tions were the second most frequent cause of rejectionof donors (7 out of 26). In the series of Marcos1 andPomfret et al.,16 lower rates were reported (2 and 2.4%,respectively). The most important aspect is to establisha process of fully informed consent to protect thedonor.24 The informational process starts in our centerat the first interview between donor, recipient, and thephysician responsible for the evaluation of donors. Atthis time, complete information is provided, withdetails about the evaluation process, surgery, complica-tions, and outcomes, for donors and recipients, includ-ing the possible impact of donation on work andfinances. Furthermore, a booklet with extensive infor-mation on LDLT is also provided. It cannot be ruledout that the physician may be “priming” the potentialdonors and in a way even manipulating them. To avoidthis, the candidates are asked not to respond immedi-ately but rather to think for some time before makingthe decision. Another question is to what extentpatients understand the information provided and ifthey are aware of the risks and benefits of the procedure.In this sense, the role of the psychiatrist is essential,evaluating the “competence of the donors to make adecision” and finding out whether this decision wasmade voluntarily or whether it was influenced by anykind of internal or external coercion.25,26
In our study, 30% of the potential transplant recip-ients in the adult group and 42% in the pediatric groupfound a suitable donor. Trotter et al.13 also reported a30% rate and Brown et al.20 46%, both in ALDLT. Thepercentage of recipients with suitable donors in reports
from pediatric series7,10,11 was higher, varying between50 and 85%. As previously mentioned, patients werereferred specifically for LDLT at these centers; in addi-tion, screening criteria for pediatric LDLT are less strin-gent than for right-lobe donation. Data on the percent-age of patients with suitable donors are not comparablewith the ones from countries without brain-death laws.Also, differences in values, ideals, religious beliefs, andfamily structure vary across ethnic groups and thesedifferences may also explain variations in the donationrates.27
Emergency adult-to-adult living donor liver trans-plantation for fulminant hepatic failure raises seriousethical, medical, logistic, and economic concerns. It hasbeen strongly criticized that the evaluation in this emer-gency situation places the donor in a very compromis-ing medical and psychological situation.28–30 In ourexperience, there was excellent cooperation betweendepartments and personnel, making it possible togather all needed tests and information from donorswithin 24 hours. Lack of voluntarism from familymembers (only 23% of patients had potential livingdonors) and the high rate of rejection of donors werethe main reasons that limited the applicability of emer-gency LDLT in our program. A high mortality ratepretransplantation was observed, even though the aver-age time to receive a cadaveric organ was 2.6 days.
In summary, an adequate and thoughtful selectionof donors is a major prerequisite for LDLT. The maingoal of the evaluation process is to assure the safety ofthe donor and to provide grafts of better quality for therecipients. The selection of candidates for ALDLT rep-resents a complex, time-consuming, and expensive pro-cedure. All efforts should be made to develop an effec-tive screening protocol for the evaluation of donors,with the aim of saving substantial time and resources fora LDLT program. It should be definitively establishedwho should cover the expenses of the evaluation of allrejected donors. We encourage all centers performingALDLT to develop a registry to retrieve comprehensivedata on the evaluation of donors. These data will con-stitute the scientific base to answer many questions thatare still unresolved.
References1. Marcos A. Right lobe living donor liver transplantation: a review.
Liver Transpl 2000;6:3–20.2. Trotter JF, Wachs M, Everson GT, Kam I. Adult-to-adult trans-
plantation of the right hepatic lobe from a living donor. N EnglJ Med 2002;346:1074–1082.
3. Malago M, Testa G, Frilling A, Nadalin S, Valentin-Gamazo C,Paul A, et al. Right living donor liver transplantation: an option
1095Donor Evaluation for Living Liver Transplantation

for adult patients: single institution experience with 74 patients.Ann Surg 2003;238:853–862 [Discussion 862–853].
4. Caplan AL. Proceed with caution: live living donation of lobes ofliver for transplantation. Liver Transpl 2001;7:494–495.
5. Shiffman ML, Brown RS Jr, Olthoff KM, Everson G, Miller C,Siegler M, et al. Living donor liver transplantation: summary ofa conference at the National Institutes of Health. Liver Transpl2002;8:174–188.
6. Malago M, Testa G, Marcos A, Fung JJ, Siegler M, Cronin DC,et al. Ethical considerations and rationale of adult-to-adult livingdonor liver transplantation. Liver Transpl 2001;7:921–927.
7. Hashikura Y, Kawasaki S, Miyagawa S, Terada M, Ikegami T,Nakazawa Y, et al. Donor selection for living-related liver trans-plantation. Transplant Proc 1997;29:3410–3411.
8. Morimoto T, Ichimiya M, Tanaka A, Ikai I, Yamamoto Y, Naka-mura Y, et al. Guidelines for donor selection and an overview ofthe donor operation in living related liver transplantation.Transpl Int 1996;9:208–213.
9. Renz JF, Mudge CL, Heyman MB, Tomlanovich S, KingsfordRP, Moore BJ, et al. Donor selection limits use of living-relatedliver transplantation. Hepatology 1995;22(Pt 1):1122–1126.
10. Sterneck MR, Fischer L, Nischwitz U, Burdelski M, Kjer S, LattaA, et al. Selection of the living liver donor. Transplantation1995;60:667–671.
11. Baker A, Dhawan A, Devlin J, Mieli-Vergani G, O’Grady J,Williams R, et al. Assessment of potential donors for livingrelated liver transplantation. Br J Surg 1999;86:200–205.
12. Hashikura Y, Kawasaki S, Miyagawa S, Terada M, Ikegami T,Nakazawa Y, et al. Recent advance in living donor liver trans-plantation. World J Surg 2002;26:243–246.
13. Trotter JF, Wachs M, Trouillot T, Steinberg T, Bak T, EversonGT, et al. Evaluation of 100 patients for living donor liver trans-plantation. Liver Transpl 2000;6:290–295.
14. Schiano TD, Kim-Schluger L, Gondolesi G, Miller CM. Adultliving donor liver transplantation: the hepatologist’s perspective.Hepatology 2001;33:3–9.
15. Pascher A, Sauer IM, Walter M, Lopez-Haeninnen E, TheruvathT, Spinelli A, et al. Donor evaluation, donor risks, donor out-come, and donor quality of life in adult-to-adult living donorliver transplantation. Liver Transpl 2002;8:829–837.
16. Pomfret EA, Pomposelli JJ, Gordon FD, Erbay N, Lyn Price L,Lewis WD, et al. Liver regeneration and surgical outcome indonors of right-lobe liver grafts. Transplantation 2003;76:5–10.
17. Chen YS, Cheng YF, De Villa VH, Wang CC, Lin CC, HuangTL, et al. Evaluation of living liver donors. Transplantation2003;75(Suppl):S16–S19.
18. Schroeder T, Nadalin S, Stattaus J, Debatin JF, Malago M,
Ruehm SG. Potential living liver donors: evaluation with anall-in-one protocol with multi-detector row CT. Radiology2002;224:586–591.
19. Schroeder T, Malago M, Debatin JF, Testa G, Nadalin S, Bro-elsch CE, et al. Multidetector computed tomographic cholan-giography in the evaluation of potential living liver donors.Transplantation 2002;73:1972–1973.
20. Brown RS Jr, Russo MW, Lai M, Shiffman ML, RichardsonMC, Everhart JE, et al. A survey of liver transplantation fromliving adult donors in the United States. N Engl J Med 2003;348:818–825.
21. Brandhagen D, Fidler J, Rosen C. Evaluation of the donor liverfor living donor liver transplantation. Liver Transpl 2003;9(Suppl 2):S16–S28.
22. Ryan CK, Johnson LA, Germin BI, Marcos A. One hundredconsecutive hepatic biopsies in the workup of living donors forright lobe liver transplantation. Liver Transpl 2002;8:1114–1122.
23. Rinella ME, Alonso E, Rao S, Whitington P, Fryer J, AbecassisM, et al. Body mass index as a predictor of hepatic steatosis inliving liver donors. Liver Transpl 2001;7:409–414.
24. Singer PA, Siegler M, Whitington PF, Lantos JD, Emond JC,Thistlethwaite JR, et al. Ethics of liver transplantation with livingdonors. N Engl J Med 1989;321:620–622.
25. Karliova M, Malago M, Trippler M, Valentin-Gamazo C, Roth-aar T, Broelsch CE, et al. Seroconversion in patients with acutehepatitis B reinfection after liver transplantation with a com-bined treatment of lamivudine and hepatitis B immune globulin.Transplant Proc 2002;34:3319–3322.
26. Erim Y, Malago M, Valentin-Gamazo C, Senf W, Broelsch CE.Guidelines for the psychosomatic evaluation of living liverdonors: analysis of donor exclusion. Transplant Proc 2003;35:909–910.
27. Rudow DL, Russo MW, Hafliger S, Emond JC, Brown RS Jr.Clinical and ethnic differences in candidates listed for liver trans-plantation with and without potential living donors. LiverTranspl 2003;9:254–259.
28. Abouna GJ. Emergency adult to adult living donor liver trans-plantation for fulminant hepatic failure—is it justifiable? Trans-plantation 2001;71:1498–1500.
29. Lo CM, Fan ST, Liu CL, Wei WI, Chan JK, Lai CL, et al.Applicability of living donor liver transplantation to high-ur-gency patients. Transplantation 1999;67:73–77.
30. Liu CL, Fan ST, Lo CM, Wong J. Living-donor liver transplan-tation for high-urgency situations. Transplantation 2003;75(Suppl):S33–S36.
1096 Valentın-Gamazo et al.





























