Embed Size (px)
Citation preview

http://cjp.sagepub.com/Criminal Justice Policy Review
http://cjp.sagepub.com/content/23/1/40The online version of this article can be found at:
DOI: 10.1177/0887403410392026
2012 23: 40 originally published online 10 January 2011Criminal Justice Policy ReviewRiane N. Miller and Joseph B. Kuhns
Self-Reported Marijuana Use Among Juvenile Arrestees Over TimeExploring the Impact of Medical Marijuana Laws on the Validity of
Published by:
http://www.sagepublications.com
On behalf of:
Department of Criminlogy at Indiana University of Pennsylvania
can be found at:Criminal Justice Policy ReviewAdditional services and information for
http://cjp.sagepub.com/cgi/alertsEmail Alerts:
http://cjp.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://cjp.sagepub.com/content/23/1/40.refs.htmlCitations:
What is This?
- Jan 10, 2011 OnlineFirst Version of Record
- Mar 18, 2012Version of Record >>
by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from by guest on October 11, 2013cjp.sagepub.comDownloaded from
CJP392026CJP23110.1177/0887403410392026Miller and KuhnsCriminal Justice Policy Review
1University of South Carolina, Columbia2University of North Carolina at Charlotte, Charlotte
Corresponding Author:Joseph B. Kuhns, Department of Criminal Justice and Criminology, University of North Carolina at Charlotte, 9201 University City Blvd, Charlotte, NC 28223 Email: [email protected]
Exploring the Impact of Medical Marijuana Laws on the Validity of Self-Reported Marijuana Use Among Juvenile Arrestees Over Time
Riane N. Miller1 and Joseph B. Kuhns2
Abstract
Past studies have found that underreporting of marijuana use is particularly high. The present study extends previous research that examined the temporal validity of self-reported marijuana use among juvenile arrestees. Furthermore, the present study explores whether the passage of medical marijuana laws in some states have affected the validity of self-reported marijuana use among juvenile arrestees. Using existing juvenile offender interview and urinalysis data from the Arrestee Drug Abuse Monitoring Program (ADAM) for the years 1998 to 2002, we find that the validity of self-reported marijuana use was low, but quite stable, over time even after the threshold for a positive test was changed. However, study sites in states that had passed medical marijuana laws had significantly higher validity levels than states that had not, suggesting that the passage of medical marijuana laws may affect validity of self-reported marijuana use.
Keywords
marijuana use, urinalysis, validity, juvenile arrestees, medicalized marijuana
Criminal Justice Policy Review23(1) 40 –66
© 2012 SAGE PublicationsReprints and permission: http://www. sagepub.com/journalsPermissions.nav
DOI: 10.1177/0887403410392026http://cjp.sagepub.com

Miller and Kuhns 41
Introduction
For more than 30 years, marijuana has been the most widely used illicit drug among adolescents (Johnston, O’Malley, Bachman, & Schulenberg, 2009). Specifically, according to the 2007 Monitoring the Future, 19% of 12th graders reported having used marijuana during their lifetime (Johnston et al., 2009). Past research studies have also found that the extent of underreporting illicit drug use, including marijuana, is particularly high within the criminal justice system (Gray & Wish, 1999; Johnson, Baumler, Yacoubian, Peters, & Ross, 2001; Lu, Taylor, & Riley, 2001). For exam-ple, Johnson et al. (2001) conducted a longitudinal analysis of drug user reporting among Houston adult arrestees surveyed through the Arrestee Drug Abuse Monitoring Program (ADAM) between 1990 and 1997 and found that some partici-pants were consistently unwilling to report use over time. Several factors have pre-dicted underreporting including race (Johnson et al., 2001; Kim, Fendrich, & Wislar, 2000; Rosay, Najaka, & Hertz, 2007), gender (Kim et al., 2000), interviewer charac-teristics (Fendrich, Johnson, Shaligram, & Wislar, 1999; Lord, Friday, & Brennan, 2005), type of substance (Mieczkowski, 1990; Wish, Hoffman, & Nemes, 1997), time frame use (Kim et al., 2000), prior treatment experience (Gray & Wish, 1999), and type of offense (Gray & Wish, 1999). However, no studies have explored the validity of self-reported marijuana use over time and across locations with different marijuana policies.
The purpose of the present study is to further explore the validity of self-reported marijuana use over time and examine whether the passage of medical marijuana laws in some states has affected the validity of self-reported marijuana use among juvenile arrestees. We expand on Yacoubian’s (2001) study, which examined the validity of self-reported marijuana use among juvenile arrestees for the years 1991 to 1997. We use existing juvenile offender interview and urinalysis data from ADAM for the years 1998 to 2002 in five of the original 23 ADAM sites to conduct our analyses. Specifically, the study tests the following research questions:
Research Question 1: Does the temporal validity of self-reported 30-day mari-juana use among juvenile arrestees, based on self-report and urinalysis data, change over time?
Research Question 2: Is the average rate of validity of self-reported 30-day marijuana use among juvenile arrestees similar in study sites located in states that have legalized medical marijuana compared to those that have not?
Findings from this research will help provide a further understanding of whether the validity of self-reported marijuana use among juveniles changes over time and across locations, and perhaps offer some explanations as to why such changes (if apparent) do occur.

42 Criminal Justice Policy Review 23(1)
Justification for the Current Study
Yacoubian’s (2001) study improved our understanding about the limitations of juvenile arrestee self-reported drug use. However, further investigation is merited for several reasons. First, Yacoubian’s (2001) study focused on data collected between 1991 and 1997. Juvenile arrestee data were collected through ADAM up until 2002; therefore, 5 more years of ADAM juvenile arrestee data are available. Importantly, the threshold for testing for marijuana in urine changed in 1996 in the ADAM study. Prior to 1996, the threshold level for marijuana was 100 ng/ml. From 1996 until 2002, the threshold level was lowered to 50 ng/ml. This change was based on recommendations made by the federal workplace testing program and new guidelines that were issued by the Substance Abuse and Mental Health Services Administration (National Institute of Justice, 1997). Following this change, it was expected that more marijuana users would be identified, particularly among those who were occasional to moderate users. It is therefore possible that the change in testing threshold could have an impact on validity estimates.
A final reason for supplementing Yacoubian’s (2001) study is because major changes in the law regarding medical marijuana began to occur in 1996. On November 5, 1996, California voters passed a ballot that legalized the use of medical marijuana. Between 1996 and 2002, several other states with ADAM sites (e.g., Alaska, 1998; Washington, 1998; Nevada, 2000; and Colorado, 2000) enacted similar medical marijuana laws (ProCon.org, 2010). With the implementation of these laws, it is important to examine whether these changes have had any effect on the validity of self-reported marijuana use. The examination is further justified because several researchers have studied marijuana use and found that states that have decriminalized marijuana have slightly higher use rates than other states (Chaloupka, Grossman, & Tauras, 1999; Model, 1993; Saffer & Chaloupka, 1999). Thus a change in drug policy will likely have some initial or delayed effect on societal use and acceptance of drugs, specifically marijuana.
Literature ReviewLegalization of Marijuana
The debate over the legal status of marijuana has been ongoing for more than 40 years now. The debate began in the mid-1960s when enforcement of marijuana laws by police became lax and public perceptions of the risks of regular marijuana use declined (Joffe & Yancy, 2004). Proponents of legalization argued that marijuana is a safe drug and that criminal sanctions against possession and personal use represent excessively harsh and unnecessary punishment. They also noted that morbidity, mor-tality, and economic costs to society associated with tobacco and alcohol use in the United States far outweigh those associated with marijuana use (Joffe & Yancy, 2004; Katel, 2009; Marshall, 2005).

Miller and Kuhns 43
Opponents, on the other hand, argued that marijuana is not a benign substance, pointing to psychopharmacological information demonstrating that marijuana has many of the same features as other illicit drugs. They also called attention to the sig-nificant neuropharmacological, cognitive, behavioral, and somatic consequences that have been documented among long-term acute marijuana users. Furthermore, oppo-nents asserted that legalization or decriminalization would likely generate a substan-tial increase in use, particularly among adolescents and youth, with probable increases in social, economic, and health costs similar to tobacco and alcohol (Joffe & Yancy, 2004; Marshall, 2005). So far, opponents have been successful in maintaining the illegal status of marijuana, but not without persistent challenges.
In 1977, attempting to take advantage of the promarijuana movement, President Jimmy Carter endorsed legislation to remove criminal penalties for possession of an ounce or less of marijuana. However, plagued by scandal, the proposal for marijuana decriminalization was ultimately terminated. This largely put an end to the legaliza-tion argument for the foreseeable future. President Regan paved the way for a decade of zero tolerance, including mandatory minimums for marijuana possession. These tough sentencing laws renewed the decriminalization movement. Opposition over the zero tolerance sentencing schemes caused many state legislatures to reduce pen-alties for marijuana possession, particularly for first time offenders. Into the 1990s, the medical-marijuana movement added further fuel to the fire (Joffe & Yancy, 2004; Katel, 2009).
Medical Marijuana MovementAlthough the therapeutic qualities of cannabis were discovered nearly 5,000 years ago, it was not until 1842 that doctors in the United States began prescribing mari-juana for various ailments. Marijuana as a medicine remained popular from 1840 to 1900. As the 20th century approached, the use of medical marijuana declined in part because of the variation in the potency of marijuana and the unpredictability of the effects of orally ingested marijuana. Furthermore, more chemically stable drugs had been developed for pain relief (Koch, 1999; Marshall, 2005).
During the 1930s, marijuana was still prescribed by some doctors. However, after the Marihuana Tax Act, doctors found the tax and registration system to be too com-plex, stressful, and time consuming and many eventually quit prescribing marijuana altogether. Throughout the 1960s, marijuana use dramatically increased and users once again began to recognize the possible medicinal benefits. However, the excite-ment over the medicinal benefits of marijuana was short-lived due to the Uniform Controlled Substance Act of 1970, which placed marijuana in the Schedule 1 category thereby making it unavailable for doctors to prescribe (Koch, 1999; Marshall, 2005). In 1972, the National Organization for the Reform of Marijuana Laws (NORML), the first Washington-based prolegalization lobbying group, filed a petition to have marijuana downgraded to a Schedule II drug, which would make it available by prescription. The result was years of legal maneuvering with ultimately no victory for advocates of medicalization (Katel, 2009; Marshall, 2005).

44 Criminal Justice Policy Review 23(1)
During the 1980s, scientists were interested in conducting research on the effective-ness of marijuana as a form of treatment. Six states (New Mexico, California, New York, Tennessee, Michigan, and Georgia) were granted federal permission to conduct research. Thousands of critically ill patients received marijuana for medicinal purposes from the federal government. The results from these studies mostly suggested that marijuana had some medicinal value including relief from pain and chemotherapy-induced nau-sea. Despite the positive results, the program was nevertheless discontinued in 1992 (Katel, 2009; Koch, 1999).
Despite federal prohibitions, in 1996, California became the first state to legalize marijuana for medical purposes. Voters passed a referendum authorizing anyone to grow or possess marijuana if a physician recommended it for medical reasons. By 2010, there were 13 other states (and the District of Columbia) that had enacted medi-cal marijuana laws: Alaska, Oregon, Washington, Maine, Colorado, Hawaii, Nevada, Montana, Vermont, Rhode Island, New Mexico, Michigan, and New Jersey (Cooper, 2000; Katel, 2009; Koch, 1999; Marshall, 2005; Pro-Con.org, 2010). Furthermore, in October 2009, the Department of Justice announced that it would no longer prosecute individuals who use or distribute marijuana for medical purposes. This announce-ment represented a small victory for decriminalization and legalization proponents (Stout & Moore, 2009).
Trends in Marijuana Use and Drug Arrests in AmericaAs marijuana policies changed over time, trends in use and marijuana-related arrests have also fluctuated. According to the Monitoring the Future (MTF) project, reported lifetime marijuana use among 12th graders peaked in 1979 at 60.4%. Since then, reported lifetime use among 12th graders gradually declined until 1992, but from 1993 to 1997, use rates doubled. Reported use then continued to decline from 1997 to 2007, reaching 19% in 2007 (Johnston et al., 2009). These trends tend to be consistent across prevalence rates (annual, 30-day, daily) and age groups (8th and 10th graders). Research also suggests that the MTF trends are comparable for older populations as well. For example, the National Household Survey on Drug Abuse found that past month reported use for those aged 18 to 25 peaked in 1979 at 35.6%; for those aged 26 to 34 reported use also peaked in 1979 at 19.7%.
Trends in juvenile drug abuse arrests tend to follow a similar pattern as juvenile self-reported drug use. According to data collected and compiled from the FBI’s Uniform Crime Report, in 1983 juvenile drug arrests reached an all-time low with less than 300 arrests per 100,000 juveniles between the ages of 10 and 17. Between 1983 and 1990, drug arrests among juveniles fluctuated from more than 400 arrests per 100,000 juveniles in 1989 to a low of 300 juvenile drug arrests per 100,000 in 1990. Juvenile drug arrests increased between 1990 and 1996 before peaking in 1997 with approxi-mately 725 arrests per 100,000 juveniles (Puzzanchera, 2009). Since 1997, the juvenile arrest rate for drug abuse violations has trended downward similar to self-reported juve-nile drug use (Johnston et al., 2009; Puzzanchera, 2009). One could reasonably con-clude that juvenile drug use rates affect juvenile drug arrests.

Miller and Kuhns 45
Societal Approval of Marijuana Use
Several studies have suggested that trends in reported drug use also coincide with society’s approval of the use of certain drugs (Johnson et al., 2001; Kim et al., 2000; Wish et al., 1997). For example, Johnson et al. (2001) found that Houston arrestees were more willing to acknowledge heroin and marijuana use than cocaine use. One explanation for this finding was that marijuana and heroin had become so immersed in the local society that disapproval of use had dropped.
The MTF also provides an opportunity to examine trends in use and disapproval. An increase in personal disapproval of regular marijuana use among 8th, 10th, and 12th graders coincided with a decrease in last 12-month reported marijuana use and vice versa (Johnston et al., 2009). Based on this information, it appears as if personal disapproval of marijuana use and self-reported marijuana use are inversely associated. These results are typically based on self-reported drug use data.
Validity of Self-Reported Drug Use DataResearchers most often rely on self-reported measures of drug use because of the advantages over indirect measures such as treatment admissions, arrests, emergency room visits, and drug seizures (Harrison, 1997; Johnston et al., 2009; Substance Abuse and Mental Health Services Administration [SAMHSA], 2008). One such study is the National Survey on Drug Use and Health, the major source of information on the patterns and prevalence of illegal drug use and abuse within the noninstitution-alized population in the United States. The MTF study also collects self-reported drug use data annually from a nationally representative sample of public and private school students in 8th, 10th, and 12th grades (Johnston et al., 2009).
Some scholars have suggested that the validity of self-report studies is threatened because drug use estimates are dependent on the accuracy of self-reported drug use (Golub, Liberty, & Johnson, 2005; Harrell, 1985; Harrell, 1997; Rosay et al., 2007). There are several reasons why self-reported drug use data may be inaccurate. First, the accuracy of the data may be affected by respondent’s memory or comprehension (Harrison, Martin, Enev, & Harrington, 2007; Johnson et al., 2001). Harrison et al. (2007) examined this question by asking respondents if they thought they, and oth-ers, would have difficulty understanding or remembering drug-related information. Most respondents stated that they would have “no difficulty” understanding (73%) and remembering (58%) drug-related questions. However, respondents were not as confident in the ability of others to understand and remember drug-related informa-tion. Specifically, only 42% of respondents believed that others would have “no difficulty” in understanding drug-related questions while only 25% stated that others would have “no difficulty” in remembering drug-related questions. In an attempt to avoid the possibility of individuals misunderstanding questions, some studies, including MTF, have hired trained staff members to administer questionnaires to

46 Criminal Justice Policy Review 23(1)
students so that they can provide clarity if respondents do not understand a question (Johnston et al., 2009).
Two other potential threats to the validity of self-reported drug use are fear of embarrassment and threat of potential sanctions (Guardiola, 1985; Harrell, 1997; Rosay et al., 2007; SAMHSA, 2009). Researchers try to counter these threats by promising confidentiality during data collection. For example, administrators of the National Survey on Drug Use and Health try to reduce inaccurate self-reports by con-ducting face-to-face interviews with respondents in their home, so that the respondents can be assured that their information will remain confidential and their identity will not be revealed (SAMHSA, 2009).
Yet another factor that affects the validity of self-reported drug use is social desir-ability (Heeb & Gmel, 2001; Lord et al., 2005). An individual may tailor his or her response based on the perceived acceptability of the use of particular illicit drugs. Again, Johnson et al. (2001) found that Houston arrestees were more willing to admit heroin and marijuana use than crack or powder cocaine use, arguing that this may be based on the notion that marijuana carries less of a social stigma (in Houston) than crack or powder cocaine and heroin has become more ingrained in the local arrestee population.
Lord et al. (2005) examined the applicability of the Social Distance Theory and the Social Attribution Theory in predicting arrestee participation in a drug use survey. Social Distance Theory suggests that respondents will be more willing to participate when they share common characteristics with the interviewer. Social Attribution Theory suggests that respondents choose to participate based on the respondent’s per-ception about the norms and expectations of an interviewer. To examine the applica-bility of these theories, data from the Charlotte, North Carolina Arrestee Drug Abuse Monitoring (ADAM) site were used. The study found that the Social Attribution Theory was statistically supported with significant main effects of race, gender, and age on a respondents’ willingness to consent to a drug use survey. Although not statis-tically supported, Lord et al. (2005) argued that the results also supported the applica-bility of the Social Distance. For instance, while African Americans were more likely to gain arrestee consent, two thirds of the arrestees were African Americans thus lend-ing support for the Social Distance Theory.
Because of these various validity threats, studies that rely solely on self-reported drug use data have consistently been criticized (Guardiola, 1985). In response to these concerns, some researchers have been engaged in validation studies, with urinalysis being the most often used technique for validating self-reported drug use.
Urinalysis TestingDrug testing programs have been widely used within the criminal justice system over the past few decades. The purpose of the programs vary, but the most common reasons include screening for recent drug use, identifying chronic users, monitoring and deterring

Miller and Kuhns 47
use, and tracking national and local trends. Validating self-reported drug use is another reason for drug testing. The most common technique used for drug use screening within the criminal justice system is urinalysis because of the many advantages it has over other techniques like blood tests and hair analyses (Wish & Gropper, 1990).
The advantages and disadvantages of urine tests for testing criminal justice populations for drug use vary according to the particular type of test used. There are four categories of urine tests available: screening by thin-layer chromatography, screening by immuno-assays, confirmation by gas chromatography, and confirmation by gas chromatography/mass spectrometry (GC/MS). One’s desired combination of sensitivity, specificity, and cross-reactivity helps determine which of these tests are most appropriate.
ADAM utilized the Enzyme Multiplied Immune Test (EMIT) to conduct urinalysis tests for arrestees. One advantage of the EMIT test is that it is still relatively inexpen-sive. A second advantage of the EMIT test is that it is highly sensitive; thus a small concentration of a drug can be consistently detected in a urine sample. Furthermore, minimal training is required to facilitate and evaluate the test results. One last major advantage is that facilities may be able to establish on-site testing programs because of the simplicity of the EMIT process.
Immunoassay tests also have some major disadvantages. First, immunoassay tests have reduced specificity. Thus the test has a limited ability to differentiate between crack cocaine and powder cocaine. Second, there is the possibility of cross-reactivity. In other words, a substance other than the drug in question could produce a positive effect and thereby generate a false positive result. Thus it may be necessary to use a different test to verify the results. Furthermore, while cross-reactivity can occur and create a false positive outcome, adulteration of an individual’s specimen can also lead to false negative results (Golub et al., 2005; Wish & Gropper, 1990).
All urinalysis tests have one common disadvantage—a limited time frame for drug detection. Many of the major drugs of abuse, such as cocaine, heroin, and amphetamines, are quickly metabolized and excreted. The time frame for detection for most drugs, with the exception of marijuana, is 2 to 3 days although this is dependent on purity of the drug taken, the rate of individual use, the test cutoff, and retention of the drug in the body (Mieczkowski, 2002; National Institute of Justice, 2003; Wish & Gropper, 1990) This general disadvantage has led some to speculate on whether a different type of analysis should be used. For now, urinalysis continues to be the primary technique used to vali-date self-reported drug use (Mieczkowski, 2002; Wish et al., 1997).
The Validity of Self-Reported Drug UsePrior to the 1980s, self-report data were generally perceived to be reasonably valid. Studies that examined validity unanimously reported validity as “good” or “very good.” However, in 1986, Eric Wish challenged the validity of self-report drug use. More recent validity studies, particularly within treatment facilities and the criminal justice system, have verified these concerns by concluding that underreporting is a common occurrence (Fendrich et al., 1999; Hser, Maglione, & Boyle, 1999; Johnson

48 Criminal Justice Policy Review 23(1)
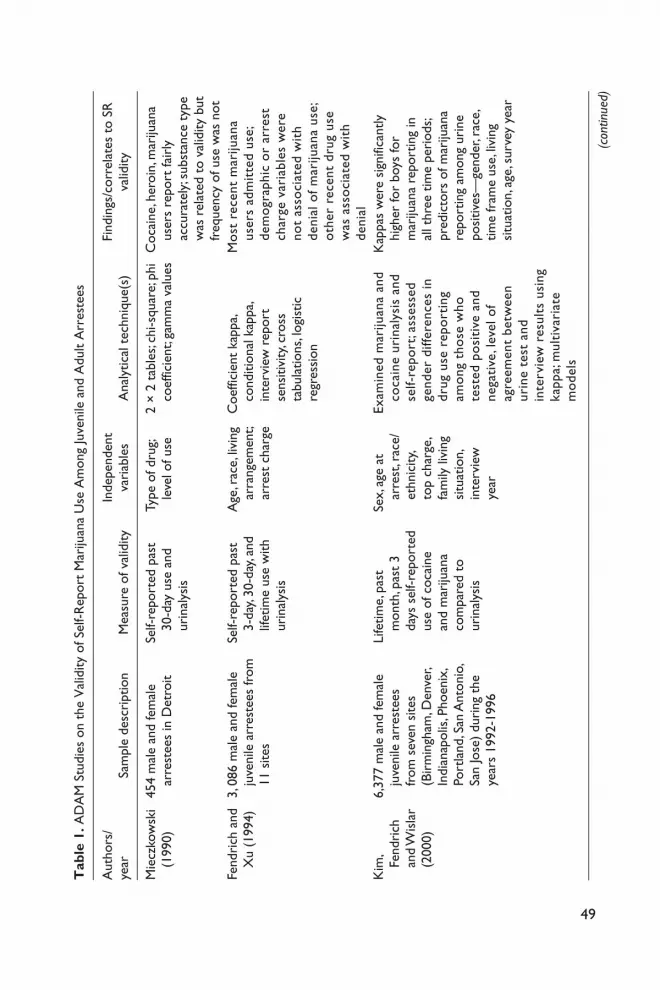
et al., 2001; Lu et al., 2001; Wish et al., 1997). Table 1 presents a compilation of stud-ies that have explored characteristics and variables that are related to underreporting. Some of these include gender, race, type of drug, offense seriousness, education, fam-ily structure, gang membership, interviewer characteristics, marital status, amount of drug use, intensity, frequency of use, location, employment status and age. A number of studies have examined the validity of self-reported drug use among juveniles, including juvenile offenders.
A couple of these studies are particularly relevant here. First, Mensch and Kandel (1988) examined the extent of underreporting among youth with data from the National Longitudinal Survey of Youth (NLSY), a longitudinal survey of young adults con-ducted since 1979. To validate the results from the NLSY, the self-report data were compared with MTF data and the General Household Survey (GHS) data. Mensch and Kandel (1988) found that underreporting of lifetime prevalence use in the NLSY study was considerable for illicit drugs other than marijuana.
Meanwhile, Feucht, Stephens, and Walker (1994) examined the validity of self-reported drug use data from Cleveland juvenile arrestees surveyed through the Drug Use Forecasting program (which was an earlier iteration of the ADAM program). Over a 2-month period, 169 male juvenile arrestees were asked to participate in the study and provide hair and urine samples. Eighty-eight juveniles provided both a hair and urine sample. Feucht et al. determined that self-reports of drug use appear to severely underestimate the prevalence of cocaine in juvenile arrestee populations. Only 6 of 88 juvenile arrestees admitted to ever using cocaine, while hair assay tests revealed that 50 had used cocaine. Meanwhile, urinalysis tests only identified 7 cocaine users, which is not particularly surprising due to the limited time frame in which cocaine can be detected in urine.
Longitudinal Validity of Self-Reported Marijuana Use among Juvenile ArresteesOnly a small number of studies have examined longitudinal trends in the validity of self-reported drug use, particularly among arrestees. Those that have examined valid-ity trends have mainly focused on adult populations (Golub et al., 2005; Johnson et al., 2001). For example, Johnson et al. (2001) conducted a longitudinal analysis of drug user reporting among Houston adult arrestees surveyed through ADAM between 1990 and 1997. Utilizing kappa statistics,1 Johnson et al. (2001) found that some partici-pants were consistently unwilling to report use over time. Despite the low agreement, it was found that the proportion of drug-positive adult arrestees who self-reported drug use remained relatively stable over time.
Yacoubian (2001) explored the temporal validity of self-reported drug use among juvenile arrestees using the ADAM data by comparing urinalysis results and self-reported 30-day marijuana use from 33,313 juvenile arrestees who were interviewed between 1991 and 1997 in 12 of the original 23 sites.2 Using Cohen’s kappa to com-pare marijuana urinalysis results to self-reported 30-day marijuana use, Yacoubian
49
Tab
le 1
. AD
AM
Stu
dies
on
the
Val
idity
of S
elf-R
epor
t M
ariju
ana
Use
Am
ong
Juve
nile
and
Adu
lt A
rres
tees
Aut
hors
/ye
arSa
mpl
e de
scri
ptio
nM
easu
re o
f val
idity
Inde
pend
ent
vari
able
sA
naly
tical
tec
hniq
ue(s
)Fi
ndin
gs/c
orre
late
s to
SR
va
lidity
Mie
czko
wsk
i (1
990)
454
mal
e an
d fe
mal
e ar
rest
ees
in D
etro
itSe
lf-re
port
ed p
ast
30-d
ay u
se a
nd
urin
alys
is
Type
of d
rug;
leve
l of u
se2
× 2
tab
les;
chi-s
quar
e; p
hi
coef
ficie
nt; g
amm
a va
lues
Coc
aine
, her
oin,
mar
ijuan
a us
ers
repo
rt fa
irly
ac
cura
tely
; sub
stan
ce t
ype
was
rel
ated
to
valid
ity b
ut
freq
uenc
y of
use
was
not
Fend
rich
and
X
u (1
994)
3, 0
86 m
ale
and
fem
ale
juve
nile
arr
este
es fr
om
11 s
ites
Self-
repo
rted
pas
t 3-
day,
30-d
ay, a
nd
lifet
ime
use
with
ur
inal
ysis
Age
, rac
e, li
ving
ar
rang
emen
t; ar
rest
cha
rge
Coe
ffici
ent
kapp
a, co
nditi
onal
kap
pa,
inte
rvie
w r
epor
t se
nsiti
vity
, cro
ss
tabu
latio
ns, l
ogis
tic
regr
essi
on
Mos
t re
cent
mar
ijuan
a us
ers
adm
itte
d us
e;
dem
ogra
phic
or
arre
st
char
ge v
aria
bles
wer
e no
t as
soci
ated
wit
h de
nial
of m
ariju
ana
use;
ot
her
rece
nt d
rug
use
was
ass
ocia
ted
wit
h de
nial
Kim
, Fe
ndri
ch
and
Wis
lar
(200
0)
6,37
7 m
ale
and
fem
ale
juve
nile
arr
este
es
from
sev
en s
ites
(Bir
min
gham
, Den
ver,
Indi
anap
olis
, Pho
enix
, Po
rtla
nd, S
an A
nton
io,
San
Jose
) du
ring
the
ye
ars
1992
-199
6
Life
time,
pas
t m
onth
, pas
t 3
days
sel
f-rep
orte
d us
e of
coc
aine
an
d m
ariju
ana
com
pare
d to
ur
inal
ysis
Sex,
age
at
arre
st, r
ace/
ethn
icity
, to
p ch
arge
, fa
mily
livi
ng
situ
atio
n,
inte
rvie
w
year
Exam
ined
mar
ijuan
a an
d co
cain
e ur
inal
ysis
and
se
lf-re
port
; ass
esse
d ge
nder
diff
eren
ces
in
drug
use
rep
orti
ng
amon
g th
ose
who
te
sted
pos
itiv
e an
d ne
gati
ve, l
evel
of
agre
emen
t be
twee
n ur
ine
test
and
in
terv
iew
res
ults
usi
ng
kapp
a; m
ulti
vari
ate
mod
els
Kap
pas
wer
e si
gnifi
cant
ly
high
er fo
r bo
ys fo
r m
ariju
ana
repo
rtin
g in
al
l thr
ee t
ime
peri
ods;
pred
icto
rs o
f mar
ijuan
a re
port
ing
amon
g ur
ine
posi
tives
—ge
nder
, rac
e,
time
fram
e us
e, li
ving
si
tuat
ion,
age
, sur
vey
year
(con
tinue
d)

50
Aut
hors
/ye
arSa
mpl
e de
scri
ptio
nM
easu
re o
f val
idity
Inde
pend
ent
vari
able
sA
naly
tical
tec
hniq
ue(s
)Fi
ndin
gs/c
orre
late
s to
SR
va
lidity
Yaco
ubia
n (2
001)
33,3
13 m
ale
and
fem
ale
juve
nile
arr
este
es
from
199
1 to
199
7 in
12
sit
es (
Birm
ingh
am,
Cle
vela
nd, D
enve
r, In
dian
apol
is, L
os
Ang
eles
, Pho
enix
, Po
rtla
nd, S
an A
nton
io,
San
Die
go, S
an Jo
se,
St. L
ouis
, Was
hing
ton,
D
C)
Self-
repo
rted
30-
day
mar
ijuan
a us
e an
d ur
inal
ysis
Year
, loc
atio
n,
age,
sex
, ra
ce, p
rim
ary
char
ge
Des
crip
tive
stat
istic
s; ka
ppa
stat
istic
sSt
reng
th o
f agr
eem
ent
betw
een
the
two
mea
sure
s (s
elf-
repo
rt a
nd u
rina
lysi
s)
vari
es b
y ju
risd
ictio
n;
intr
ajur
isdi
ctio
nal
agre
emen
ts a
re c
onsi
sten
t ov
er t
ime
John
son
et a
l. (2
001)
11,0
95 m
ale
and
fem
ale
adul
t ar
rest
ees
in
Hou
ston
199
0 to
199
7
Mar
ijuan
a, co
cain
e,
and
hero
in s
elf-
repo
rted
pas
t 72
-hr
use
and
urin
alys
is
Rac
e, g
ende
r, ye
arD
escr
iptiv
e st
atis
tics;
kapp
a st
atis
tics
Mar
ijuan
a—ag
reem
ent
is lo
w b
ut s
tabl
e ov
er
time;
sta
bilit
y w
ithin
bot
h ge
nder
gro
ups;
tem
pora
l va
riat
ion
amon
g Whi
tes
and
His
pani
csSl
oan,
Bo
dapa
ti,
and
Tuck
er
(200
4)
479
mal
e an
d fe
mal
e ad
ult
arre
stee
s in
Bi
rmin
gham
in 1
995
Self-
repo
rted
pas
t 30
-day
mar
ijuan
a us
e an
d ur
inal
ysis
; se
lf-re
port
ed p
ast
3-da
y co
cain
e us
e an
d ur
inal
ysis
Age
, sex
, rac
e,
mar
ital s
tatu
s, em
ploy
men
t st
atus
, in
com
e,
mon
ey s
pent
on
dru
gs
per
wee
k,
educ
atio
n
Biva
riat
e an
alys
es, l
ogis
tic
regr
essi
onSo
cial
des
irab
ility
the
ory
supp
orte
d; a
ge, l
egal
and
ill
egal
inco
me,
res
pond
ent
arre
sted
with
or
with
out
a w
arra
nt, m
ore
rece
ntly
ar
rest
ed, a
nd m
oney
spe
nt
on d
rugs
pre
dict
ed u
ser’s
lik
elin
ess
of m
isre
port
ing
use
Tabl
e 1.
(co
ntin
ued)
(con
tinue
d)

51
Aut
hors
/ye
arSa
mpl
e de
scri
ptio
nM
easu
re o
f val
idity
Inde
pend
ent
vari
able
sA
naly
tical
tec
hniq
ue(s
)Fi
ndin
gs/c
orre
late
s to
SR
va
lidity
leve
l, se
veri
ty
of c
harg
e,
type
of
crim
e, a
rres
t w
ith(o
ut)
war
rant
, typ
e of
dru
g, ag
e at
firs
t us
e,
inte
rvie
wer
ra
ceG
olub
, Li
bert
y, an
d Jo
hnso
n (2
005)
335,
940
adul
t m
ale
and
fem
ale
arre
stee
s co
llect
ed b
etw
een
1988
an
d 20
01 in
23
AD
AM
si
tes
Self-
repo
rted
pas
t 30
-day
use
and
ur
inal
ysis
Loca
tion,
typ
e of
dru
gT
ime
vari
atio
n; r
egre
ssio
n;
and
grap
hica
l tre
nds
Vari
atio
n in
rep
orte
d us
e re
flect
ed c
hang
es
in d
etec
ted
use;
Fa
ctor
s co
ntri
buti
ng t
o di
verg
ence
: % m
ariju
ana
user
s th
at d
iscl
osed
ac
tivi
ty c
hang
ed o
ver
tim
e, a
ccur
acy
of A
DA
M
urin
alys
is t
est
incr
ease
d w
ith
tim
e, p
erce
ntag
e of
in
freq
uent
use
rs c
hang
ed
over
tim
eW
ebb,
K
atz,
and
Dec
ker
(200
6)
939
mal
e an
d fe
mal
e ju
veni
le a
rres
tees
co
llect
ed b
etw
een
1999
an
d 20
03 in
Pho
enix
, M
esa,
& T
ucso
n, A
Z
Self-
repo
rted
pas
t 72
-hr
use
and
urin
alys
is
Type
of
drug
, gan
g m
embe
rshi
p,
race
, age
, sc
hool
Mul
tinom
ial l
ogis
tic
regr
essi
onD
iscl
osur
e ra
tes
of g
ang
mem
bers
did
not
diff
er
from
non
gang
mem
bers
; ag
e an
d pr
ior
arre
st
pred
icte
d di
sclo
sure
s of
Tabl
e 1.
(co
ntin
ued)
(con
tinue
d)

52
Tabl
e 1.
(co
ntin
ued)
Aut
hors
/ye
arSa
mpl
e de
scri
ptio
nM
easu
re o
f val
idity
Inde
pend
ent
vari
able
sA
naly
tical
tec
hniq
ue(s
)Fi
ndin
gs/c
orre
late
s to
SR
va
lidity
stat
us, t
ype
of c
rim
e,
prio
r ar
rest
s
mar
ijuan
a us
e; a
ge, p
rior
ar
rest
, and
rac
e pr
edic
ted
disc
losu
re o
f coc
aine
use
Ros
ay,
Naj
aka,
and
Her
tz
(200
7)
4,89
9 W
hite
and
Bla
ck
adul
t m
ale
and
fem
ale
arre
stee
s fr
om In
dian
apol
is, F
t. La
uder
dale
, Pho
enix
, an
d D
alla
s in
199
4
Self-
repo
rted
pas
t 72
-hr
use
and
urin
alys
is
Type
of d
rug,
age,
offe
nse
seri
ousn
ess,
race
, gen
der
Des
crip
tive
stat
istic
s; H
iera
rchi
cal l
oglin
ear,
logi
t, an
d lo
gist
ic
regr
essi
on m
odel
s
Rac
e in
fluen
ces
the
valid
ity
of s
elf-r
epor
t dr
ug u
se;
no d
iffer
ence
s w
ere
foun
d ac
ross
gen
der,
age,
or
offe
nse
seri
ousn
ess

Miller and Kuhns 53
found only slight agreement between the two raters (urinalysis and self-report); how-ever, the relationship between the two measures of drug use was fairly consistent intrajurisdictionally over the 7-year time period.
MethodHistory of Arrestee Drug Abuse Monitoring Program
The present study uses data from five different sites (Birmingham, AL, Cleveland, OH, Phoenix, AZ, San Antonio, TX, and San Diego, CA) that collected juvenile information as part of the ADAM program during the years 1998-2002. The ADAM Program—formerly the Drug Use Forecasting (DUF) Program—was established in 1987 by the National Institute of Justice to conduct research on drug use among urban adult and juvenile arrestees in the jail setting (National Institute of Justice, 1999; National Institute of Justice, 2000). The primary goals of the program were to track changes in drug use patterns, determine what drugs were being used in various juris-dictions, alert local officials to trends in use and availability of new drugs, supply data to help study the drug-crime connection, and serve as a research base for policymak-ers (Johnson et al., 2001; National Institute of Justice, 2000; Yacoubian, 2000). ADAM operations across the country were postponed in 2004 because of federal spending constraints. Before the cessation of ADAM, however, data were collected on hundreds of thousands of recently booked arrestees in 35 sites across the country. The information continues to be used to help communities make educated decisions on the distribution of funds to law and enforcement and drug treatment programs (National Institute of Justice, 2003; Webb, Katz, & Decker, 2006).
Data Collection ProcessAs mentioned above, the data used in this study are from the years 1998-2002.3 During these years, for no more than 2 weeks in a single facility every calendar quarter, data were collected on convenience samples of juvenile arrestees. Juveniles who had been arrested within the past 48 hours were approached and asked to participate in the study. Potential participants were read an informed consent form, which stated that no identifying information would be collected and that a urine specimen would be requested at the end of the interview. All juveniles were free to refuse to participate. However, in most sites, more than 80% of individuals approached agreed to be interviewed, and of those participants, more than 80% also agreed to give a urine specimen (National Institute of Justice [NIJ], 1999, 2000, 2003). If the participant agreed to be interviewed, a trained, nonuniformed interviewer would ask the individual a series of questions regarding demographics, past and present drug use, perception of one’s drug problem, and involvement in past and present drug treatment.

54 Criminal Justice Policy Review 23(1)
Once the interview was completed, participants were asked to provide a urine sam-ple. Drug testing is of particular importance to the ADAM program because it helps analysts to obtain a measure of recent drug use and to assess the validity of self-report data (Johnson et al., 2001; NIJ, 1999). The ADAM program uses the Enzyme Multiplied Immunoassay Testing (EMIT) system to screen for the presence of 10 different drugs (amphetamines, barbiturates, benzodiazepines, cocaine, marijuana, methadone, meth-aqualone, opiates, PCP, and propoxyphene) in urine. A laboratory conducts all testing and the specificity and accuracy for most drugs is higher than 95% (NIJ, 1999). If a particular drug is present in the urine sample at a level above or equal to a specified cutoff point then the result is considered to be positive for that particular drug. Again, from 1996 to 2002, the cutoff level for marijuana was 50 ng/ml. Prior to 1996, a higher cutoff level (100 ng/ml) was used (NIJ, 1997).
One methodological limitation should be noted in regard to the ADAM data collec-tion process between 1998 and 2002. In all years, there was a relatively high level of missing data for self-reported marijuana use and 2 years, 2001 and 2002, had substan-tial missing data for urine specimens. Across all 5 years, missing data constituted 32.7% of the sample for self-reported marijuana use and 8.4% of the sample for uri-nalysis results. Smaller percentages of the urinalysis data were missing because indi-viduals had either refused to participate, were unable to use the bathroom, or did not provide a sufficient quantity to be tested. However, a vast majority of the missing data were simply not obtained during data collection. The proportion of missing data for marijuana urinalysis tests was similar for other drugs. Conversely, percentages of missing data for self-reported use of other drugs varied. Self-reported marijuana use actually had the least amount of missing data, relative to other drugs, in terms of past 30-day use. We discuss the implications of this missing data later.
ResultsData analysis was accomplished in two phases. First, descriptive statistics were calcu-lated to summarize the study sample. Second, kappa statistics were computed to exam-ine the relationship between marijuana urinalysis and self-reported 30-day marijuana use at each of the five sites from 1998 to 2002. Cohen’s kappa is used to measure the agreement between the evaluation of two raters (in this case, urinalysis and self-report) when both are rating the same object (i.e., recent drug use). This measure of agreement is considered to be appropriate when the time periods covered by the self-report and the criterion measure are similar and when both variables have the same number of categories and use the same category values. Perfect agreement is indicated by a value of one; a value of zero indicates that agreement is no better than chance (Johnson et al., 2001; Magura & Kang, 1996; Yacoubian, 2001). Furthermore, to determine whether there were any changes in the level of agreement between each of the years, as well as across the 5-year time period, z tests were performed.4 A 30-day self-report measure was used, even though the ADAM program also collects data on 3-day self-report use,

Miller and Kuhns 55
because marijuana can be detected in urine for up to 30 days depending on the fre-quency of use and the potency of the marijuana (NIJ, 1999).
Description of the Study SampleA total of 7,487 juvenile arrestees were originally surveyed in the five selected sites (Birmingham, AL, Cleveland, OH, Phoenix, AZ, San Antonio, TX, and San Diego, CA) between 1998 and 2002. However, only 7,484 were used in these analyses because three arrestees who were interviewed were older than 18 thus disqualifying them as juveniles. The majority of the sample was male (83%). Hispanics (39%) had the largest racial representation followed by African Americans (31%) and Whites (26%). Almost half of the juvenile arrestees were aged 13 to 15 (49%) followed by those aged 16 to 18 (49%) and 9 to 12 (4%). Felonies (51%) made up the majority of the offenses for which the participants were arrested. Furthermore, 75% of the juvenile arrestees were still in school. As shown in Table 2, the demographic characteristics within each indi-vidual year are similar to those for the overall sample across all 5 years.
Temporal Comparison of Urinalysis Results to Self-Reported 30-day Marijuana Use by SiteAcross the 5-year time period within each site, some variations in level of agreement were found.5 As shown in Table 3, on average, Birmingham had the strongest level of agreement (.42), whereas San Antonio had the lowest level of agreement (.21). Despite the rather low strength of agreement, the kappa statistics remained relatively stable across the 5-year period for each site with the exception of Birmingham. The
Table 2. Sample Demographic Characteristics by Year (N = 7,484)
1998 (N = 1,603)
1999 (N = 1,555)
2000 (N = 1,517)
2001 (N = 1,767)
2002(N = 1,042)
1998-2002 (N = 7,484)
% % % % % %
Male 87 85 82 80 80 83Black 34 29 31 32 30 31White 23 26 27 27 28 26Hispanic 38 42 39 39 39 39Other 5 3 3 2 3 4Ages 9-12 4 4 5 4 3 413-15 46 46 46 48 49 4716-18 50 50 49 48 48 49Felony 50 53 51 51 51 51Misdemeanor 46 41 42 43 44 43Status 4 6 7 6 5 6Still in school 74 73 78 74 74 75

56 Criminal Justice Policy Review 23(1)
Table 3. Kappa Statistics for Marijuana Urinalysis (50 ng) Results and Self-Reported 30-day Marijuana Use by Site (standard errors in parentheses)
1998 1999 2000 2001 2002 Mean Range
All .29 .31 .37 .34 .35 .33 .08Birmingham .25 (.08) .22 (.10) .60 (.12) .41 (.10) .62 (.20) .42 .40Cleveland .35 (.07) .24 (.06) .23 (.06) .37 (.06) .49 (.10) .34 .26Phoenix .28 (.06) .40 (.05) .44 (.05) .34 (.05) .35 (.07) .36 .16San Antonio .15 (.04) .28 (.06) .27 (.06) .24 (.06) .11 (.07) .21 .17San Diego .40 (.06) .34 (.06) .36 (.06) .35 (.06) .39 (.09) .37 .06
range of agreement extended from a low of .06 in San Diego to a high of .40 in Birmingham. Only one site, San Antonio, experienced any significant changes over the 5-year time period at the standard level of p < .05. After a slight increase from 1998 to 1999, San Antonio experienced a significant decrease (p < .01) in level of agreement between 1999 and 2002. Birmingham, Cleveland, and Phoenix also expe-rienced changes, but these changes were not significant (p < .10). Furthermore, when examining yearly changes in level of agreement San Antonio was the only site to experience a significant change. From 2001 to 2002, San Antonio experienced a sig-nificant decrease (p < .05) in level of agreement.
When examining the entire sample over the 5-year time period, the kappa statistics were all relatively low, but remained fairly consistent with a range of .08. There was no significant change in agreement from year to year within sites or across the 5-year time period when considering the overall sample. Thus, based on these results, it does not appear that validity of self-reported 30-day marijuana use among juvenile arrestees changed over time across these five locations. Furthermore, the validity is rather low overall among the entire sample.
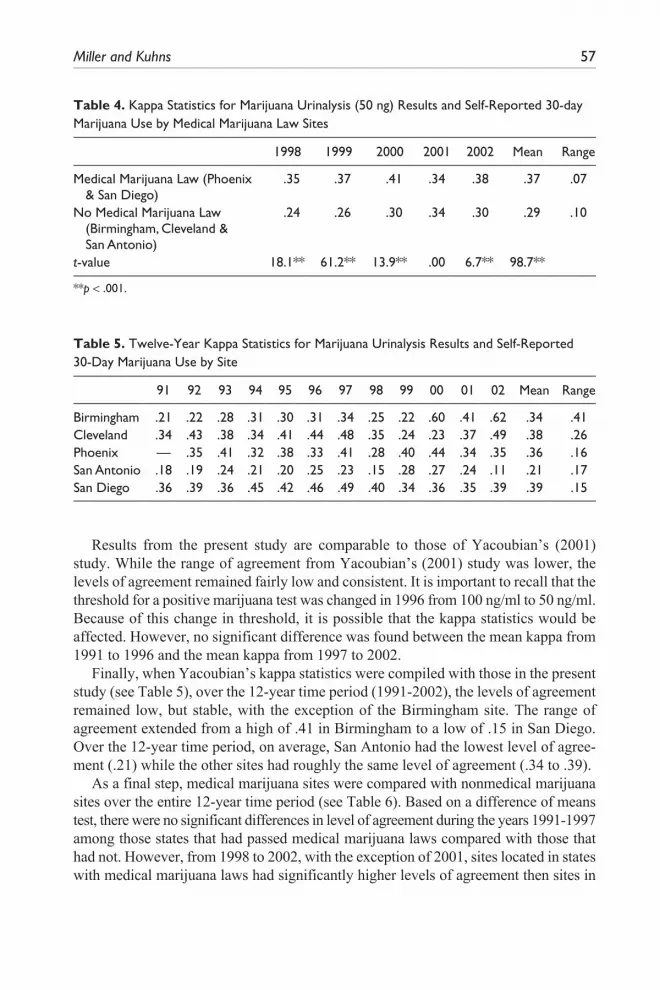
Temporal Comparison of Urinalysis Results to Self-Reported 30-day Marijuana Use by Sites with Medical Marijuana LawsAs shown in Table 4, the strength of agreement remained low, but consistent, for the two sites that were located in states with medical marijuana laws (Phoenix6 and San Diego) and the three sites without such laws (Birmingham, Cleveland, and San Antonio). The average kappa was significantly higher in sites located in states that passed medical marijuana laws compared to those sites located in states that had not passed such a law. Furthermore, over the 5-year time period, the two sites with medical marijuana laws consistently had significantly higher agreement than the three sites without such laws, with the exception of 2001 when the level of agreement was essentially the same. Therefore, it appears that the passage of medical marijuana laws in some states may affect the validity of self-reported marijuana use among juvenile arrestees.
Miller and Kuhns 57
Table 4. Kappa Statistics for Marijuana Urinalysis (50 ng) Results and Self-Reported 30-day Marijuana Use by Medical Marijuana Law Sites
1998 1999 2000 2001 2002 Mean Range
Medical Marijuana Law (Phoenix & San Diego)
.35 .37 .41 .34 .38 .37 .07
No Medical Marijuana Law (Birmingham, Cleveland & San Antonio)
.24 .26 .30 .34 .30 .29 .10
t-value 18.1** 61.2** 13.9** .00 6.7** 98.7**
**p < .001.
Table 5. Twelve-Year Kappa Statistics for Marijuana Urinalysis Results and Self-Reported 30-Day Marijuana Use by Site
91 92 93 94 95 96 97 98 99 00 01 02 Mean Range
Birmingham .21 .22 .28 .31 .30 .31 .34 .25 .22 .60 .41 .62 .34 .41Cleveland .34 .43 .38 .34 .41 .44 .48 .35 .24 .23 .37 .49 .38 .26Phoenix — .35 .41 .32 .38 .33 .41 .28 .40 .44 .34 .35 .36 .16San Antonio .18 .19 .24 .21 .20 .25 .23 .15 .28 .27 .24 .11 .21 .17San Diego .36 .39 .36 .45 .42 .46 .49 .40 .34 .36 .35 .39 .39 .15
Results from the present study are comparable to those of Yacoubian’s (2001) study. While the range of agreement from Yacoubian’s (2001) study was lower, the levels of agreement remained fairly low and consistent. It is important to recall that the threshold for a positive marijuana test was changed in 1996 from 100 ng/ml to 50 ng/ml. Because of this change in threshold, it is possible that the kappa statistics would be affected. However, no significant difference was found between the mean kappa from 1991 to 1996 and the mean kappa from 1997 to 2002.
Finally, when Yacoubian’s kappa statistics were compiled with those in the present study (see Table 5), over the 12-year time period (1991-2002), the levels of agreement remained low, but stable, with the exception of the Birmingham site. The range of agreement extended from a high of .41 in Birmingham to a low of .15 in San Diego. Over the 12-year time period, on average, San Antonio had the lowest level of agree-ment (.21) while the other sites had roughly the same level of agreement (.34 to .39).
As a final step, medical marijuana sites were compared with nonmedical marijuana sites over the entire 12-year time period (see Table 6). Based on a difference of means test, there were no significant differences in level of agreement during the years 1991-1997 among those states that had passed medical marijuana laws compared with those that had not. However, from 1998 to 2002, with the exception of 2001, sites located in states with medical marijuana laws had significantly higher levels of agreement then sites in

58
Tab
le 6
. Tw
elve
-Yea
r K
appa
Sta
tistic
s fo
r M
ariju
ana
Uri
naly
sis
(50
ng)
Res
ults
and
Sel
f-Rep
orte
d 30
-Day
Mar
ijuan
a U
se, b
y M
edic
al
Mar
ijuan
a La
w S
ites
(Sta
ndar
d Er
rors
in P
aren
thes
es)
9192
9394
9596
9798
9900
0102
Med
ical
Mar
ijuan
a L
aw (
Phoe
nix
&
San
Die
go)
.29
(11)
.31
(.12)
.32
(.06)
.38
(.10)
.36
(.08)
.39
(.11)
.42
(.11)
.35
(.01)
.37
(.04)
.41
(.06)
.34
(.01)
.38
(.01)
No
Med
ical
M
ariju
ana
Law
(
Birm
ingh
am,
Cle
vela
nd, &
San
A
nton
io)
.26
(.11)
.32
(.12)
.34
(.09)
.29
(.07)
.33
(.11)
.34
(.10)
.37
(.13)
.24
(.10)
.26
(.03)
.30
(.22)
.34
(.09)
.30
(.30)
t-va
lue
.27
−.08
−.25
1.0
.30
.45
.42
22.8
**61
.2**
13.9
**.0
06.
7**
**p
< .0
01.

Miller and Kuhns 59
states without such laws. Again, it appears that the passage of medical marijuana laws may affect the validity of self-reported marijuana use among juvenile arrestees.
DiscussionIn the current study, self-reported marijuana use was validated using urinalysis test results within a sample of 7,484 juvenile arrestees who were interviewed between 1998 and 2002 in five locations. Based on the premise that a kappa statistic below .7 indicates poor agreement (Johnson et al., 2001; Magura & Kang, 1996), the temporal analyses illustrate a consistent unwillingness of juvenile arrestees to accurately self-report marijuana use over the 5-year time period within the full sample. Site-specific temporal analyses also revealed a consistent unwillingness to accurately report mari-juana use within all five sites examined here.
The results were generally similar when comparing two sites located in states that enacted medical marijuana laws (Phoenix and San Diego) with three sites located in states that did not adopt medical marijuana laws (Birmingham, Cleveland, and San Antonio). Although juveniles interviewed in sites with medical marijuana laws and those without generally reported low agreement, the medical marijuana law sites had significantly higher levels of agreement (as measured via kappa statistics) than those without such laws.
General Policy ImplicationsIt is rather alarming that two measures of drug use (urinalysis and self-report) used by ADAM have such a low level of agreement among juveniles over a 12-year time period. Golub et al. (2005) found similar inconsistencies between self-reported drug use and urinalysis results among adult arrestees. These findings call into question the reliance on self-report (and urinalysis data) among arrestee populations to formulate drug policy decisions. These findings also raise concerns about the validity of other self-report studies that examine trends in drug use among juveniles and adults. In the absence of biological verification, it remains uncertain whether changes in drug use trends are because of actual changes in use levels or to changes in respondents’ will-ingness (or lack thereof) to report use. It may also be the case that validity of self- reported drug use would be higher within other nonincarcerated populations (e.g., school samples). This seems to be a particularly important question that warrants further review given the costs associated with annual data collection processes.
It may be impractical, however, to conduct biological tests due to costs and other concerns (privacy, for example). Based on the present findings, as well as Yacoubian’s (2001), collecting urinalysis specimens each year is unnecessary given that the level of agreement between urinalysis and self-reported use, while low, does remain consis-tent over time. A more cost effective solution would be to simply collect fewer urine specimens or collect specimens perhaps every 2 or 3 years.

60 Criminal Justice Policy Review 23(1)
Furthermore, it is important to note that this study examined data from the medical marijuana sites fairly recently after new laws had been enacted. At most, there were 6 years of data available to determine whether validity rates had changed since these laws were enacted. Based on this relatively short time frame, it would be useful to replicate this study using a longer time frame to better determine whether the introduc-tion of medical marijuana laws resulted in the higher level of agreement or whether other factors can account for the change. In addition, as of 2010, 14 states had passed medical marijuana laws. Therefore, this study could be improved by including a larger number of sites located in states with medical marijuana laws although these sites would have to focus on adult arrestees if the ADAM data were used.
Implications for ADAM/ADAM IIAgain, ADAM stopped collecting data on juvenile arrestees in 2003 and had to fully postpone its operations across the country in 2004 because of federal spending con-straints (NIJ, 2003). However, in 2007, ADAM was revitalized under the Office of National Drug Control Policy under the name of ADAM II. ADAM II continues to utilize the same methodology as the original ADAM, but data collection is limited to Atlanta, GA, Charlotte, NC, Denver, CO, Indianapolis, IN, Minneapolis, MN, New York, NY, Portland, OR, Sacramento, CA, and Washington, D.C., and is restricted to male arrestees only (Office of National Drug Control Policy [ONDCP], 2009). Based on the findings from this study, two recommendations might be useful for ADAM II. First, it would be beneficial to begin collecting data specifically on juveniles again. ADAM has a major advantage over traditional self report surveys due to the fact that it collects self-report and urinalysis data, which allows for validating self-reported use and more accurately monitoring trends in arrestee populations (ONDCP, 2009). Second, several ADAM II sites are located in states where medical marijuana laws have been passed (e.g., Denver, Portland, and Sacramento—ProCon.org, 2010). A longitudinal study would better determine whether the changing marijuana laws have truly affected self reporting processes. Since ADAM II is one of the only studies that uses a biological test to validate self-reported use, more states with medical marijuana laws need to be examined through ADAM II.
The Impact of Medical Marijuana Laws on Marijuana Use and Self ReportingPast research suggests that the use of substances rises and falls, to some degree, with societal acceptance of those substances, particularly since societal acceptance, to some degree, influences laws and law enforcement practices. The free-spirited decade of the 1960s included extensive substance use and greater societal acceptance and tolerance. In the 1980s societal disapproval of drug use increased with the “just say no” message. However, in the past four decades, and particularly since 1990, societal
Miller and Kuhns 61
approval and acceptance of both the medical use and legalization of marijuana has steadily increased (Pew Research Center, 2010). In fact, Californians will have an opportunity to vote on the legalization of Marijuana in November 2010 (California Proposition 19, 2010). As marijuana laws move from prohibition to decriminalization (many law enforcement agencies give citations, in lieu of arrests, for simple posses-sion) to restricted legalization (e.g., medical) to legalization, the illicit stigma associ-ated with marijuana will erode and users, including juveniles, will become more comfortable with acknowledging use. As a result, the use and subsequent validity of self reported marijuana use will likely rise in the future. This study provides an early indication that that may be already occurring in two sites that are located in states that adopted medical marijuana laws.
Limitations of the Current StudyThe present study was affected by certain limitations that need to be noted. First, the study was limited to juvenile arrestees in five sites across the United States who were selected based on a convenience sampling procedure. It is highly unlikely that each site used the same standards for processing juvenile arrestees, and therefore, the samples are probably not representative of all juvenile arrestees within each city. Furthermore, because only five sites were examined the results are not representative of juvenile arrestees in other geographic locations.
Second, along the same lines, ADAM focuses only on arrestees. Therefore, it can-not be assumed that the results from this study extend to other criminal/deviant popu-lations or noncriminal/nondeviant populations. Future research would benefit from studies examining the temporal validity of self-reported drug use among juveniles, within both deviant and nondeviant populations, based on a probability sample in vari-ous locations to assess the broader implications of drug-reporting trends.
Third, as we discussed above, missing data were a particular concern with the ADAM project. This concern may be a function of the convenience sampling approach used or of variations in arrestee processing, data collection protocols, or site manage-ment overall. Regardless, ADAM II should seek to reduce missing data to the extent possible. As a reminder, Social Distance Theory suggests that respondents might be more willing to participate when they share common characteristics with the inter-viewer. Social Attribution Theory suggests that respondents choose to participate based on the respondent’s perception about the norms and expectations of an inter-viewer. ADAM II should consider these two perspectives when selecting interviewers and within the context of their data collection protocols and questionnaire language. It might even be useful to test variations in protocols across locations.
Fourth, in this study only the validity of self-reported marijuana use was explored. The rationale for choosing marijuana was that the laws governing this particular drug have been rapidly changing in the past few decades. Specifically, since 1996, the use of medical marijuana has been legalized in at least 14 states with many others consid-ering legalization (ProCon.org, 2010). Therefore, since these changes in law have been

62 Criminal Justice Policy Review 23(1)
highly publicized it was assumed that such changes could potentially affect societal approval to marijuana use and subsequently affect validity rates. However, it cannot be assumed that changes in laws regarding other drugs of abuse will have similar effects (or any effect for that matter). For that reason, future research should further examine how changes in drug laws, beyond marijuana, affect the validity of self-reported drug use within and outside of correctional settings.
Appendix
Direction of Disagreement Among Juvenile Arrestees
Year% Reported use, tested positive
% Reported use, tested negative
% Denied use, tested positive
% Denied use, tested negative
1998 70.6 29.4 20.4 79.61999 73.5 26.5 20.7 79.32000 71.8 28.2 13.0 87.02001 69.2 30.8 18.9 81.12002 74.2 25.8 18.4 81.6Mean 71.8 28.2 18.3 81.7
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.
Notes
1. Cohen’s kappa is used to measure the agreement between the evaluation of two raters (in this case, urinalysis and self-report) when both are rating the same object (i.e., recent drug use). This measure of agreement is appropriate when the time periods covered by the self-report and the criterion measures are similar and when both variables have the same number of categories and use the same category values. Perfect agreement is indicated by a value of one and a value of zero indicates that agreement is no better than chance (Johnson et al., 2001; Magura & Kang, 1996; Yacoubian, 2001).
2. The following sites were included in Yacoubian’s (2001) study: Birmingham, AL; Cleve-land, OH; Denver, CO; Indianapolis, IN; Los Angeles, CA; Phoenix, AZ; Portland, OR; San Antonio, TX; San Diego, CA; San Jose, CA; St. Louis, MO; and Washington, D.C.
3. These years were selected because Yacoubian’s study had examined the validity of self-reported marijuana use among juvenile arrestees for the previous years in which juveniles

Miller and Kuhns 63
were interviewed. Furthermore, data collection for juveniles was suspended in 2002, so this was the last year that data were available for juveniles.
4. z test = k1-k2/se (k1-k2)5. Over the 5 years of study, an average of 28% of juveniles who reported using marijuana in
the last 30 days tested negative, while an average of 18% of those who denied use tested positive. Considering the latter figure, it appears that nearly 1 in 5 juvenile arrestees may have misrepresented their use. See appendix for an annual breakdown.
6. In 1996, Arizona passed a law which allowed physicians to prescribe marijuana. The law did not, however, actually legalize medical marijuana (ProCon.org, 2010).
References
California Proposition 19. (2010). The Regulate, Control and Tax Cannabis Act of 2010. Retrieved from http://ballotpedia.org/wiki/index.php/Text_of_Proposition_19,_the_%22Regulate, _Control_and_Tax_Cannabis_Act_of_2010%22_(California)
Chaloupka, F. J., Grossman, M., & Tauras, J. A. (1999). The demand for cocaine and marijuana by youth. In F. Chaloupka, M. Grossman, W. K. Bickel, & H. Saffer (Eds.), The economic analysis of substance use and abuse (pp. 133-155). Chicago, IL: The University of Chicago Press.
Cooper, M. H. (2000). Drug-policy debate: Is there too much emphasis on law enforcement? CQ Research, 10, 593-624.
Fendrich, M., Johnson, T., Shaligram, C., & Wislar, J. (1999). The impact of interviewer char-acteristics on drug use reporting by male juvenile arrestees. Journal of Drug Issues, 29(1), 37-58.
Fendrich, M., & Xu, Y. (1994). The validity of drug use reports from juvenile arrestees. Inter-national Journal of the Addictions, 29, 971-985.
Feucht, T., Stephens, R., & Walker, M. L. (1994). Drug use among juvenile arrestees: A com-parison of self-report, urinalysis, and hair assay. Journal of Drug Issues, 24(1-2), 99-116.
Golub, A., Liberty, H. J., & Johnson, B. D. (2005). Inaccuracies in self-reports and urinalysis tests: Impacts on monitoring marijuana use trends among arrestees. Journal of Drug Issues, 35, 944-945.
Gray, T. A., & Wish, E.D. (1999). Correlates of underreporting recent drug use by female arrest-ees. Journal of Drug Issues, 29(1), 91-106.
Guardiola, D. (April, 1985). A study on the validity of self-reports: Follow-up research on the Puerto Rican treated drug user. Paper presented at the National Symposium on Doctoral Research and Social Work Practice. Columbus, Ohio: The Ohio State University.
Harrell, A. (1985). Validation of self-report: The research record. In B. Rouse, N. Kozel, & L. Richards (Eds.), Self-reported methods of estimating drug use: Meeting current chal-lenges to validity (pp. 12-21). [NIDA Research Monograph, 57]. Rockville, MD: U.S. Department of Health and Human Services.
Harrell, A. (1997). The validity of self-reports of drug use data: The accuracy of responses on confidential self-administered answered sheets. In L. Harrison & A. Hughes (Eds.), The validity of self-reported drug use: Improving the accuracy of survey estimates (pp. 37-58). Washington, DC: National Institute of Drug Abuse.

64 Criminal Justice Policy Review 23(1)
Harrison, L. (1997). The validity of self-reports of drug use in survey research: An overview and critique of research methods. In L. Harrison & A. Hughes (Eds.), The validity of self-reported drug use: Improving the accuracy of survey estimates (pp. 17-36). Washington, DC: National Institute of Drug Abuse.
Harrison, L., Martin, S., Enev, T., & Harrington, D. (2007). Comparing drug testing and self-report of drug use among youths and young adults in the general population (DHHS Pub-lication No. (SMA) 07-4249, Methodology Series M-7). Rockville, MD: Substance Abuse and Mental Health Services Administration, Office of Applied Studies.
Heeb, J., & Gmel, G. (2001, July). Interviewers’ and respondents’ effects on self-reported alco-hol consumption in a Swiss health survey. Journal of Studies on Alcohol, 62, 434-442.
Hser, Y., Maglione, M., & Boyle, K. (1999). Validity of self-report of drug use among STD patients, ER patients, and arrests. American Journal of Drug and Alcohol Abuse, 25(1), 81-91.
Joffe, A., & Yancy, W. S. (2004). Legalization of marijuana: Potential impact on youth. Pedi-atrics, 113, 632-638.
Johnson, R. J., Baumler, E. R., Yacoubian, G. S., Peters, R. J., & Ross, M. W. (2001). A lon-gitudinal analysis of drug use reporting among Houston arrestees. Journal of Drug Issues, 31, 757-766.
Johnston, L. D., O’Malley, P. M., Bachman, J. G., & Schulenberg, J. E. (2009). Monitoring the Future national survey results on drug use, 1975-2008: Volume I, Secondary school students (NIH Publication No. 09-7402). Bethesda, MD: National Institute on Drug Abuse.
Katel, P. (2009). Legalizing marijuana: Should pot be treated like alcohol and taxed? CQ Researcher, 19, 525-548.
Kim, J. Y. S., Fendrich, M., & Wislar, J. S. (2000). The validity of juvenile arrestees’ drug use reporting: A gender comparison. Journal of Research in Crime and Delinquency, 37, 419-432.
Koch, K. (1999). Medical marijuana: Should doctors be able to prescribe the drug? CQ Researcher, 9, 705-728.
Lord, V. B., Friday, P. C., & Brennan, P. K. (2005). The effects of interviewer characteristics on arrestees’ responses to drug-related questions. Applied Psychology in Criminal Justice, 1(1), 36- 55.
Lu, N. T., Taylor, B. C., & Riley, K. J. (2001). The validity of adult arrestee self-reports of crack cocaine use. American Journal of Drug & Alcohol Abuse, 27, 399-419.
Magura, S., & Kang, S. (1996). Validity of self-reported drug use in high risk populations: A meta-analytical review. Substance Use & Misuse, 31, 1131-1153.
Marshall, P. (2005). Marijuana laws: Should state and federal marijuana laws be reformed? CQ Researcher, 15(6), 125-148.
Mensch, B. S., & Kandel, D. B. (1988). Underreporting of substance use in a national longi-tudinal youth cohort: Individual and interviewer effects. Public Opinion Quarterly, 52(1), 100-124.
Mieczkowski, T. (1990). The accuracy of self-reported drug use: An evaluation and analysis of new data. In R. Weisheit (Ed.), Drugs, crime, and the criminal justice system. Cincinnati, OH: Anderson.
Mieczkowski, T. (2002). Does ADAM need a haircut? A pilot study of self-reported drug use and hair analysis in an arrestee sample. Journal of Drug Issues, 32(1), 91-118.
Miller and Kuhns 65
Model, K. E. (1993). The effect of marijuana decriminalization on hospital emergency room drug episodes: 1975-1978. Journal of the American Statistical Association, 88, 737-747.
National Institute of Justice. (1997). Drug Use Forecasting: Annual Report on Adult and Juvenile Arrestees, 1996 (National Institute of Justice, NCJ 176800). Washington, DC: U.S. Depart-ment of Justice.
National Institute of Justice. (1999). 1998 Annual Report on Drug Use Among Adult and Juvenile Arrestees (Office of Justice Programs, NCJ No. 175656). Washington, DC: U.S. Department of Justice.
National Institute of Justice. (2000). 1999 Annual Report on Drug Use Among Adult and Juvenile Arrestees (Office of Justice Programs, NCJ No. 181426). Washington, DC: U.S. Department of Justice.
National Institute of Justice. (2003). 2000 Arrestee Drug Abuse Monitoring Program: Annual Report (Office of Justice Programs, NCJ No. 193013). Washington, DC: U.S. Department of Justice.
Office of National Drug Control Policy. (2009). 2008 Arrestee Drug Abuse Monitoring Pro-gram: Annual Report. Washington, DC: Executive Office of the President.
Pew Research Center. (2010, April 1). Public Support for Legalizing Medical Marijuana: Mod-est Rise in Percentage Favoring General Legalization. Retrieved from http://people-press .org/report/602/marijuana
ProCon.org. (2010). Medical Marijuana: 14 Legal Medical Marijuana States. Retrieved from http://medicalmarijuana.procon.org/view.resource.php?resourceID=000881
Puzzanchera, C. (2009). Juvenile Arrests 2008. Juvenile Justice Bulletin. (NCJ 228479) Washington, DC: U.S. Department of Justice, Office of Juvenile Justice and Delinquency Prevention.
Rosay, A. B., Najaka, S. S., & Hertz, D. C. (2007). Differences in the validity of self-reported drug use across five factors: Gender, race, age, type of drug, and offender seriousness. Jour-nal of Quantitative Criminology, 23(1), 41-58.
Saffer, H., & Chaloupka, F. (1999). The demand for illicit drugs. Economic Inquiry, 37, 401-411.
Sloan, J. J., Bodapati, M. R., & Tucker, T. A. (2004). Respondent misreporting of drug use in self-reports: Social desirability and other correlates. Journal of Drug Issues, 34, 269-292.
Stout, D., & Moore, S. (2009, October 19). U.S. won’t prosecute in states that allow medi-cal marijuana. The New York Times. Retrieved from http://www.nytimes.com/2009/10/20/us/20cannabis.html
Substance Abuse and Mental Health Services Administration. (2008). Drug Abuse Warning Net-work, 2006: National Estimates of Drug-Related Emergency Department Visits (Office of Applied Sciences, DAWN Series D-30, DHHS Publication No. SMA 08-4339). Rockville, MD: U.S. Department of Health and Human Services.
Substance Abuse and Mental Health Services Administration. (2009). Results from the 2008 National Survey on Drug Use and Health: National Findings (Office of Applied Studies, NSDUH Series H-36, HHS Publication No. SMA 09-4434). Rockville, MD: U.S. Depart-ment of Health and Human Services.

66 Criminal Justice Policy Review 23(1)
Webb, V. J., Katz, C. M., & Decker, S. H. (2006). Assessing the validity of self-reports by gang members: Results from the Arrestee Drug Abuse Monitoring Program. Crime & Delin-quency, 52, 232-252.
Wish, E. D., & Gropper, B. A. (1990). Drug testing by the criminal justice system: Methods, research, and applications. In M. Tonry & J. Wilson (Eds.), Drugs and Crime (pp. 321-391). Chicago, IL: University of Chicago Press.
Wish, E. D., Hoffman, J. A., & Nemes, S. (1997). The validity of self-reports of drug use at treatment admission and at follow up: Comparisons with urinalysis and hair assays. In L. Harrison & A. Hughes (Eds.), The validity of self-reported drug use: Improving the accu-racy of survey estimates (pp. 200-226). Rockville, MD: National Institute of Drug Abuse.
Yacoubian, G. (2000, Spring). Assessing ADAM’s domain: Past problems and future prospects. Contemporary Drug Problems, 27, 121-135.
Yacoubian, G. (2001). Exploring the temporal validity of self-reported marijuana use among juvenile arrestees. Journal of Alcohol and Drug Education, 46(3), 34-42.
Bios
Riane N. Miller is a doctoral student at the University of South Carolina (USC). Her current research interests focus on juvenile delinquency and drug use among juveniles.
Joseph B. Kuhns is an Associate Professor at the University of North Carolina at Charlotte (UNCC). Prior to arriving at UNCC, Dr. Kuhns served as a Senior Policy Analyst at the U.S. Department of Justice (Office of Community Oriented Policing Services). He recently co-edited Police Use of Force: A Global Perspective which explores police use of force, firearms, and non-lethal weapons in various countries around the world. Dr. Kuhns continues to explore the relationship between drug use and violent behavior by analyzing toxicology data within and outside of the United States.





























