Embed Size (px)
Citation preview

RBMOnline - Vol 19. No 3. 2009 326-336 Reproductive BioMedicine Online; www.rbmonline.com/Article/4002 on web 4 August 2009
326
© 2009 Published by Reproductive Healthcare Ltd, Duck End Farm, Dry Drayton, Cambridge CB23 8DB, UK
Patricia Fauque graduated in 2003 from the medical school of Besançon, France. She is currently an embryologist in the Reproductive Biology laboratory of Cochin Hospital, Paris where she is participating in the assisted reproduction programme. Her areas of interest include the assessment of embryo quality and ovarian cryopreservation and her work of PhD degree concerned early epigenetic modifications observed in mice after in-vitro fertilization and embryo culture.
Dr Patricia Fauque
Patricia Fauque1–4,8, Martine Albert5, Catherine Serres3,4, Vivian Viallon2,3,6, Céline Davy2,3,7, Sylvie Epelboin2,3,7, Céline Chalas1, Pierre Jouannet1, Catherine Patrat1
1Centre Hospitalier de Cochin-Saint-Vincent de Paul, Paris, France; 2Assistance Publique, Hôpitaux de Paris; 3Université Paris Descartes, Paris, France; 4Laboratoire d’Histologie – Embryologie – Biologie de la Reproduction, Groupe hospitalier Cochin, Paris, France; 5Biologie de la Reproduction et Génétique Médicale, CHIPS, UVSQ, Poissy, France; 6Département de Biostatistiques, Groupe hospitalier Cochin, Paris, France; 7Service de Gynécologie–Obstétrique II, Groupe hospitalier Cochin, Paris, France8Correspondence: e-mail: [email protected]
Abstract
The objective of this retrospective study was to describe a population of patients displaying impaired sperm motility due to ultrastructural flagellar defects and to analyse the intracytoplasmic sperm injection (ICSI) results and neonatal outcomes in this population. The fertilization rate, embryo quality, clinical pregnancy rate, implantation rate, birth rate and perinatal health of babies were determined. Patients (n = 20) were divided into seven categories according to ultrastructural flagellar abnormalities. The type of flagellar abnormality significantly affected the fertilization rate (P <0.025). Two types of flagellar abnormalities showed slower early embryo cleavage kinetics (P <0.001) when axonemal central structures and periaxonemmal columns were abnormal or absent. Of 53 ICSI attempts, 14 resulted in clinical pregnancies (26.4% per cycle) after fresh and frozen embryo transfer. Three (21.4%) of these pregnancies ended in miscarriages and, in the remaining, 12 infants were born (7.2% of transferred embryos). The outcomes differed according to the ultrastructural defect. This study demonstrates that a high proportion of patients could father a child (45.0%). However, flagellar abnormalities appear to influence ICSI results and fetal development.
Keywords: embryo quality, flagella, ICSI, pregnancy outcome, sperm ultrastructure
Sperm motility is essential for successful fertilization, and decreased motility is a frequent cause of male infertility (Curi et al., 2003). In most cases, asthenozoospermia is associated with oligozoospermia and/or teratozoospermia and corresponds to a variable degree of spermatogenesis impairment. However, in some rare situations, asthenozoospermia is the only abnormal sperm parameter and can be related to primary movement abnormality (Inaba, 2003). In such cases, structural defects of the sperm tail can be detected by transmission electron microscopy. To date, numerous flagellar abnormalities have been identified in humans, in the axonemal and/or peri-axonemal structures (Zamboni, 1992). One example is the absence of external and/or internal dynein arms or other axonemal abnormalities, known
as immotile cilia syndromes (Escalier and David, 1984). Clinical manifestations associated with male infertility in this syndrome can include chronic pansinusitis, respiratory tract infections and bronchiectases. Approximately 50% of immotile cilia syndrome patients have alterations in the visceral rotation (situs inversus) with dextrocardia, known as Kartagener’s syndrome (Afzelius, 1998). A variant of immotile cilia syndrome is dysplasia of the fibrous sheath, which is characterized by serious disturbances in the organization of the fibrous sheath and identified by electron microscopic examination. Dysplasia of the fibrous sheath is generally included in the so-called stump tail or short
tail syndrome (Chemes et al., 1987; Escalier and Albert, 2006). Other abnormalities include defects in the mitochondrial sheath
Article
From ultrastructural flagellar sperm defects to the health of babies conceived by ICSI
Introduction

and in the attachment of the flagellum to the nucleus (Chemes and Rawe, 2003).
In the past, such infertile patients were unable to conceive naturally; however, the advances in subzonal insemination (SUZI) (Wolf et al., 1993; Nijs et al., 1996) and intracytoplasmic sperm injection (ICSI) have allowed some of these individuals to become fathers using their own spermatozoa (Olmedo et al., 1997, 2000; Chemes et al., 1998; von Zumbusch et al., 1998; Okada et al., 1999; Cayan et al., 2001; Alosilla Fonttis et al., 2002; Westlander et al., 2003; Peeraer et al., 2004). However, the use of spermatozoa from patients with a primary flagellar anomaly may pose two different but related problems. The first is the genetic risk of passing some anomaly to the progeny, possibly resulting in births defects (Rives et al., 2005). The second is a lower fertilization rate and impairment of embryo development with decreased rate of pregnancy. Previous studies have explored ICSI outcomes for men with absent dynein arms (Stalf et al., 1995; Olmedo et al., 1997, 2000; Papadimas et al., 1997; von Zumbusch et al., 1998; Cayan et al., 2001; Westlander et al., 2003; Peeraer et al., 2004), absent central microtubules (Vandervorst et al., 1997; Okada et al., 1999), dysplasia of the fibrous sheath (Chemes et al., 1998) or partial absence of inner dynein arms and dysplasia of the fibrous sheath (Olmedo et al., 2000). However, these studies were limited by their small samples size (between one and six patients) (Chemes et al., 1998; Okada et al., 1999; Olmedo et al., 2000). Only one recent study was carried out on a larger series of 21 patients (Mitchell et al., 2006). Therefore, firm conclusions concerning ICSI results and outcomes cannot be drawn.
This retrospective study reports the outcome of ICSI attempts with information on early embryo development using spermatozoa of 20 infertile men whose specific flagellar phenotypes were evaluated by electron microscope, and who had requested assisted reproduction treatment. Moreover, the analysis is extended to pregnancy outcome, live birth rate and neonatal health.
Materials and methods
Patients
The men participating in the study were recruited from the assisted reproductive technology centre of Cochin–Saint-Vincent de Paul hospital between 1994 and 2003. Patient history and clinical data, including testis volume, were collected. Semen analyses were performed according to World Health Organization (1999) recommendations. Sperm morphology was evaluated by the identification of normal spermatozoa and of various sperm abnormalities according to the classification of David et al. (1975). Hormonal status (serum FSH, testosterone) and lymphocyte karyotype were also analysed. Transmission electron microscopy was performed on semen samples from selected patients having normal semen volume (≥2 ml), normal sperm concentration (≥20 × 106/ml), normal viability (≥40%), motility grade a ≤5% and/or grades a+b ≤30% and absence of sperm penetration in female partner’s and control ovulatory cervical mucus.
Only patients whose ultrastructural flagellar sperm defects were diagnosed as described below were included in this retrospective study.
Transmission electron microscopy study
Spermatozoa were fixed in 2.5% v/v glutaraldehyde in 0.1 mol/l phosphate buffer, washed for 15 min in fresh phosphate buffer containing 4% w/v sucrose and embedded in 2% agar. Post-fixation lasted 1 h in 1% w/v osmic acid in phosphate buffer. After dehydration in a graded series of ethanol, small pieces of agar containing spermatozoa were embedded in Epon resin (Polysciences, Warrington, PA, USA). Sections were cut on a Reichert OmU2 ultramicrotome (Reichert-Jung, Vienna, Austria) using a diamond knife (70 nm). They were then collected on nickel grids and stained with uranyl acetate (4% in 70% ethanol, 20 min) and Reynolds lead citrate (10 min), and examined using a JEOL JEM100 CXII transmission electron microscope (Jeol, Tokyo, Japan) operated at 80 kV.
Seven types of flagellar abnormalities were defined (Figure 1 and Table 1): type I, absence of inner dynein arms regardless of the presence of axonemal doublets; type II absence of outer dynein arms regardless of the presence of axonemal doublets; type III, absence of outer and inner dynein arms; type IV, absence of or abnormal axonemal central structures; type V, variable abnormalities of axonemal structures; type VI, disorganized axoneme and periaxoneme; type VII, absence of or abnormal columns.
In this study, only men with monomorphic flagellar abnormalities in at least 50% of their spermatozoa were included, as already stated (Mitchell et al., 2006) except in one case (patient 18). Before ICSI, all couples selected for the study underwent genetic counselling to inform them of the potential defect transmission risk.
Ovarian stimulation and ICSI procedures
Multiple follicular growth was induced by various protocols as described elsewhere (Papageorgiou et al., 2002). The procedures involved desensitization with GnRH analogues and subsequent administration of exogenous gonadotrophins. Oocyte retrieval was performed under vaginal ultrasound guidance, 36 h after human chorionic gonadotrophin administration.
Motile spermatozoa were selected through a two-step 90–45% density gradient (Puresperm; JCD, Lyon, France). When the progressive motility was low (≤5%), a simple sperm washing with Ferticult medium of the ejaculate was performed (JCD). Assisted fertilization by ICSI was performed 1–3 h following oocyte collection on morphologically intact metaphase II (MII) oocytes, with freshly ejaculated spermatozoa.
Fertilization was assessed 18 h after injection, and normal fertilization was defined as the presence of two distinct pronuclei and a second polar body. The fertilization rate per attempt was defined as the ratio between the number of zygotes and the mature retrieved injected oocytes. Embryo cleavage was assessed 24 h later and embryo quality evaluated according to the number of blastomeres and the degree of fragmentation (Fauque et al., 2007). Blastomeric fragmentation was scored as follows: A = no fragmentation; B = 1–20% by volume of anucleated fragments; C = 21–50% by volume of anucleated fragments; and D = ≥51% by volume of anucleated fragments. The cleavage rate per attempt was defined as the ratio between the number of 327
Article - Flagellar defects, pregnancy and birth outcome after ICSI - P Fauque et al.
RBMOnline®

Article - Flagellar defects, pregnancy and birth outcome after ICSI - P Fauque et al.
328
RBMOnline®
Figure 1. Ultrastructure of sperm flagellum and main ultrastructural abnormalities. The sperm flagellum was transversely sectioned at the level of the principal piece. Schematic representation (left panel) and ultrastructural overview (right panel) of periaxonemal and axonemal structures of a normal sperm flagellum (A) and abnormal sperm flagella (B–E). (A) Normal flagellum. The axonemal complex is formed from nine peripheral and two central microtubule doublets. Peripheral doublets are linked by nexin link. Each peripheral microtubule is composed of two microtubules, A and B. Microtubule A is complete, with outer and inner dynein arms spreading towards microtubule B of the adjacent doublet and radial spoke towards the fibrous sheath around the central microtubule doublets. Microtubule B is incomplete. Nine dense fibres, with variable length, are disposed in regard to the peripheral doublets. The fibrous sheath surrounds the axonemal structure and the dense fibres. It presents two bulges, called longitudinal columns, next to dense fibres 3 and 8. (B–E) Examples of abnormalities of the axonemal and/or periaxonemal structures with: (B) absence of inner and outer arms; (C) absence of axonemal central structures; (D) disorganized axoneme and periaxoneme; and (E) unique and mislocated column. Bar = 0.1 µm.

embryos and the number of MII injected oocytes. Up to three embryos were transferred to the uterus on day 2 or 3 following ICSI, and the remaining high-grade embryos (Fauque et al., 2007) were cryopreserved. High-grade embryos had less than 20% of fragmentation and were at least at the four-cell stage at day 2 after ICSI (Fauque et al., 2007).
Outcomes
A pregnancy was detected by rising serum human chorionic gonadotrophin concentration in two consecutive assays at least 12 days after embryo transfer and was defined later as clinical if one or more gestational sacs were visualized by ultrasonography in week 7 of gestation and embryo heartbeat was confirmed. Early spontaneous abortion was defined as an embryo loss before 12 completed weeks of gestation and late spontaneous abortion as a pregnancy loss after 12 weeks.
The clinical pregnancy rate per attempt was defined as the ratio between the number of clinical pregnancies per cycle. The implantation rate was defined as the ratio between the number of gestational sacs and the number of transferred embryos. The birth rate was calculated as the ratio between the number of children born and the number of transferred embryos. The cumulative pregnancy rate and cumulative birth rate took into account all clinical pregnancies or births obtained to date after fresh and frozen embryo transfers.
Statistics
Fisher’s exact test was used to compare the different rates. The statistical analyses were conducted using SAS software (SAS
Institute, Cary, NC, USA). A P-value of <0.05 was considered significant.
Results
Description of patients
A total of 20 men were included in this retrospective study and were classified into seven groups according to the ultrastructural flagellar abnormality of their spermatozoa (Table 1). They were 39.3 ± 1.0 years old (ranging from 29 to 48). Each suffered from primary infertility for at least 2 years, except two men (13 and 15) who reported a previous pregnancy. None had a history of cryptorchidism. Varicocele was noted in two patients (1 and 13). Three patients suffered from respiratory symptoms, i.e. bronchitis and/or bronchectasis (rhino-sinusitis), from early childhood (4, 6 and 10) and one had a situs inversus (7). Among the 20 patients, four patients (20.0%) were born from consanguineous, first-cousin unions (1, 12, 15 and 16). Fourteen patients (70.0%) were Caucasian (2–11, 13, 17, 18, 20) and six (30.0%) from North Africa (1, 12, 15 and 16), Mali (14) and Egypt (19). A familial history of infertility was present in four patients (3, 14, 15 and 16); each of them had an infertile brother, but unfortunately the semen parameters of these relatives could not be analysed. All patients presented a normal XY karyotype and normal concentrations of FSH and testosterone (means 6.6 IU/l and 4.8 ng/ml, respectively).
Semen analysis
Semen volume, sperm concentration and viability were normal for all patients with a mean of 3.8 ± 0.3 ml (range 1.5–6), 329
Article - Flagellar defects, pregnancy and birth outcome after ICSI - P Fauque et al.
RBMOnline®
Table 1. Ultrastructural flagellar abnormalities of the patients.
Type of Patient Main axonemal and/or flagellar number periaxonemal structure defects abnormality
I 1 100% absence of inner dynein arms II 2 100% absence of outer dynein arms 3 100% absence of outer dynein arms 4 100% absence of outer dynein arms 5 100% absence of outer dynein arms III 6 100% absence of outer + inner dynein arms 7 100% absence of outer + inner dynein armsIV 8 90% absence of central structures and radial spokes 9 100% absence of central structures + dysplasia of the fibrous sheath 10 100% abnormal central structures and radial spokes V 11 84% variable abnormalities of axonemal structures VI 12 100% disorganized axoneme and periaxoneme 13 53% disorganized axoneme and periaxoneme 14 95% disorganized axoneme and periaxoneme VII 15 100% absence or abnormal columns 16 100% absence or abnormal columns 17 > 50% absence or abnormal columns 18 40% absence or abnormal columns 19 54% absence or abnormal columns 20 > 50% absence or abnormal columns

Article - Flagellar defects, pregnancy and birth outcome after ICSI - P Fauque et al.
71.6 ± 13.9 × 106/ml (4.2- 280) and 62.5 ± 2.7% (41–86), respectively. Other semen characteristics are summarized in Table 2. Progressive motility varied from 0 to 30% and was very low (grade a ≤5%) for 10 (50.0%) patients (1, 5–7, 10–14, 16). The severity of motility alteration was related to the type of flagellar abnormality and was major for patients from types I, III, V and VI. The mean percentage of spermatozoa with normal morphology was 21.6 ± 3.0% and was normal for nine patients (1, 3, 5, 6, 12, 16–19). The sum of sperm head abnormalities on sperm head was the same for all types. In this series, patients exhibited a high number of flagellar abnormalities detectable by light microscopy: short or absent flagella for seven patients (6, 8, 9, 12–15) and coiled flagella for six patients (2–4, 11–13). Numerous flagellar abnormalities were observed mainly for types IV and VI.
ICSI results and outcomes
A total of 53 ICSI cycles were performed, all with ejaculated spermatozoa. For the two cycles performed for the patient 14, a hypo-osmotic swelling test was associated. The mean number of attempts was 2.6 ± 0.3 (1–6). The results are described in Table 3. The mean age of the female partner was 33.2 ± 0.5 years (26–40). Only one female partner had high FSH concentration at day 3 (>12 IU/ml), explaining the low number of mature oocytes (n = 3) retrieved for this patient.
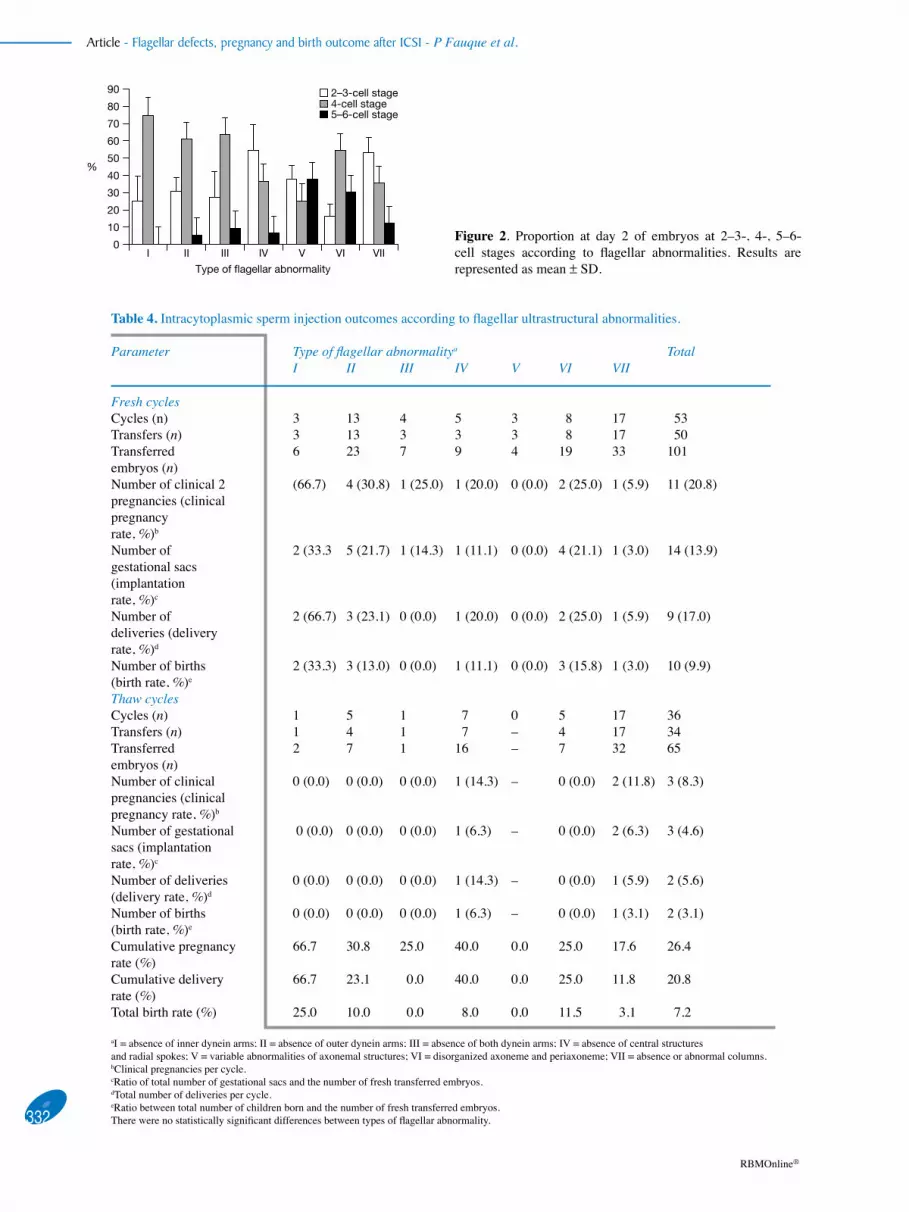
The mean fertilization rate was 48.8% ± 0.4 (22.2–60.0) and was significantly different according to the type of flagellar abnormality (P < 0.025). The embryo cleavage rate was low (50.6 ± 0.4%). When evaluated 2 days after ICSI, the percentage of embryos with few or no fragmentation was above 60.0% for all the types, except for one type (V) corresponding to a single couple. The proportion of embryos at four-cell stage was above 50% except in types IV, V and VII (36.4%, 25.0% and 35.2%, respectively). This modification in cleavage kinetics was explained by a significantly higher proportion of embryos at 2–3-cell stages in types IV and VII as compared with other types (54.7% and 54.2% versus 24.8% respectively, P < 0.001; Figure 2) and by an important number of embryos at five-cell stage in type V. The percentage of good embryos (four cells, <20% fragmentation at day 2) was lower in types IV, V and VII (24.2%, 0.0% and 26.4%, respectively) than in the remaining types.
A fresh embryo transfer was performed in 50 cases with a mean of 2 ± 0.1 transferred embryos (Table 4). No transfer could be performed in three cases corresponding to two couples (5, 9) due to ovarian hyperstimulation syndrome in the first case, female hyperthermia in the second case and fertilization failure in the third case. Eleven clinical pregnancies were obtained (20.8% clinical pregnancy per cycle, Table 4). The implantation rate was 13.9%. No significant difference in implantation rate was observed between types (Fisher test, Table 4); however, it 330
RBMOnline®
Table 2. Patient and sperm characteristics according to type of flagellar abnormality.
Abnor- Patient characteristics Sperm characteristics malitya No. Age Originb Consan- ICSI Motility Viab- Normal Total number of Detailed number of (years) guinity attempts (%) ility sperm- morphological flagellar abnormalities* (n) a:b:c:d (%) atozoa abnormalitiesc Short/ Irre- Coiled (%) Heads Mid- Flag- absent gular pieces ella
I 1 42.7 NA Yes 3 0:0:8:92 60 33 52 21 18 6 6 6II 2 38.2 C No 2 0:30:5:65 78 19 75 25 20 0 1 19II 3 37.9 C No 3 0:30:10:60 59 30 71 14 34 8 4 22II 4 40.4 C No 3 0:10:10:80 78 19 94 15 25 5 1 19II 5 32.1 C No 5 0:5:20:75 68 42 83 23 8 2 1 5III 6 42.7 C No 3 0:0:1:99 67 35 60 19 37 30 1 6III 7 29.0 C No 2 0:1:2:97 70 17 119 10 31 9 17 5IV 8 40.9 C No 2 0:10:10:80 56 10 124 20 40 18 16 6IV 9 40.1 C No 2 5:5:10:80 45 3 84 18 94 65 23 6IV 10 32.4 C No 1 0:0:5:95 52 10 139 11 12 2 2 8V 11 40.0 C No 3 0:1:1:98 45 7 145 32 36 16 3 17VI 12 43.5 NA Yes 4 0:4:8:88 52 28 89 10 43 18 5 20VI 13 40.5 C No 2 0:1:2:97 47 0 102 44 124 55 32 37VI 14 48.0 M No 2 0:0:0:100 60 10 119 8 63 50 3 10VII 15 37.4 NA Yes 2 0:10:15:75 58 18 80 20 50 35 6 9VII 16 38.3 NA Yes 2 0:1:9:90 62 28 97 17 4 2 0 2VII 17 37.8 C No 6 15:10:10:65 71 38 99 23 9 0 1 8VII 18 33.8 C No 3 10:15:10:65 79 40 79 5 4 2 2 0VII 19 48.2 E No 3 2:13:10:75 86 37 74 21 18 8 4 6VII 20 32.0 C No 1 0:25:10:65 61 7 155 35 19 6 7 6
aI = absence of inner dynein arms; II = absence of outer dynein arms; III = absence of both dynein arms; IV = absence of central structures and radial spokes; V = variable abnormalities of axonemal structures; VI = disorganized axoneme and periaxoneme; VII = absence or abnormal columns. bC = Caucasian, E = Egyptian; M = Malian; NA = North African. cMeasured in 100 spermatozoa, several morphological abnormalities may be associated in the same cell.

was null or very low for groups V (0.0%) and VII (3.0%). Two pregnancies resulted in a miscarriage (one an early spontaneous abortion and the other a late spontaneous abortion). One vanishing twin syndrome, defined as a first-trimester missed abortion of one of the twins, was observed. Of nine deliveries (17.0% per cycle, one twin and eight single), a total of 10 infants were born. Thirty-six additional transfers of frozen–thawed embryos led to three pregnancies, resulting in one miscarriage and two single deliveries. The cumulative pregnancy and delivery rates, taking into account the pregnancies obtained from fresh and frozen–thawed embryos transfers, were 20.8% and 26.4% per cycle respectively (Table 4). No significant differences in cumulative pregnancy or cumulative delivery rates were observed when comparing the seven types. However, the cumulative birth rate for types III, V and VII was null or very low (0.0%, 0.0% and 3.1% respectively).
To date, a total of nine out of 20 couples (45.0%) have delivered 12 babies, including eight boys and four girls. Obstetrical and neonatal data, including pregnancy term (36.3 ± 0.3 gestational weeks at birth), delivery, birth weight (3027 ± 210.9g) and Apgar score were not abnormal. After 1 year, the developmental outcome, i.e. cognitive and motor development, was normal in all but two babies. The son of patient 10 had Menkes disease, which is a rare X-linked recessive inherited disorder of copper metabolism characterized by neurodegeneration. This infant
died at 1 year of age. A girl born from patient 1 had severe deafness, which was diagnosed early after the delivery. No information on the cause of the defect could be identified.
In summary, 53 ICSI attempts were performed for 20 couples; six couples obtained one child and three couples two children.
Discussion
Asthenozoospermia is a frequent cause of male infertility. Many andrological conditions diminishing sperm motility, such as varicocele, various testicular pathologies, infections of the male genital tract, anti-spermatozoa antibodies, etc., can be identified and treated. But in some cases the reasons for motility disorders remain obscure to the andrologist. Moreover, the ultrastructural examination of spermatozoa is not frequently used in the diagnosis of asthenozoospermia. Thus, the link between ICSI results such as fertilization ability, early and late embryo development potential or perinatal baby health and spermatozoa with ultrastructural flagellar abnormalities is poorly understood since most published articles have been case reports (Table 5). This series of infertile men with specific ultrastructural flagellar defects reports the ICSI outcomes based not only on the fertilization rate and early embryo development but also with detailed results concerning the cumulative rates of
331
Article - Flagellar defects, pregnancy and birth outcome after ICSI - P Fauque et al.
RBMOnline®
Table 3. Fertilization rate and embryo quality at day 2 after intracytoplasmic sperm injection (ICSI) according to flagellar ultrastructural abnormalities.
Parameter Abnormalitya TotalI II III IV V VI VII
No. of patients 1 4 2 3 1 3 6 20Age of woman (years)
31.0 33.1 ± 1.0 33.1 ± 7.0 34.8 ± 2.0 35.0 35.0 ± 2.0 33.0 ± 2.0 33.2 ± 0.5
No. of cycles (mean ± SD)
3 (3.0 ± 0) 13 (3.2 ± 0.4)
4 (2.0 ± 0.7)
5 (1.7 ± 0.2)
3 (3.0 ± 0)
8 (2.7 ± 0.4)
17 (2.8 ± 0.4)
53 (2.6 ± 0.3)
No. of MII oocytes injected (mean ± SD)
15 (5.0 ± 2.0) 119 (9.2 ± 1.3)
36 (9.0 ± 2.1)
53 (10.6 ± 2.8)
18 (6.0 ± 0.6)
92 (11.5 ± 1.2)
175 (10.3 ± 1.3)
508 (9.6 ± 0.7)
No. of 2PN (fertilization rate, %)
9 (60.0) 57 (47.9) 10 (27.8) 30 (56.6) 4 (22.2) 48 (52.2) 90 (51.4) 248 (48.8)
Number of embryos (embryo cleavage rate, %)b
8 (53.3) 56 (47.1) 11 (30.6) 33 (62.3) 8 (44.4) 50 (54.3) 91 (52.0) 257 (50.6)
Mean no. of A and B embryos ± SD (%)
2.7 ± 0.7 (100.0)
3.5 ± 0.5 (75.0)
2.3 ± 0.3 (63.6)
6.0 ± 1.1 (90.9)
1.6 ± 0.3 (62.5)
4.1 ± 0.7 (66.0)
4.5 ± 0.8 (83.5)
3.9 ± 0.4 (78.2)
Mean no. of embryos at 4-cell stage ± SD (%)
2.0 ± 0.6 (75.0)
2.8 ± 0.5 (60.7)
2.3 ± 0.3 (63.6)
2.4 ± 0.4 (36.4)
2.0 (25.0) 3.3 ± 0.6 (54.0)
2.0 ± 0.5 (35.2)
2.7 ± 0.2 (46.7)
Mean no. of ‘good embryos’ ± SD (%)c
2.0 ± 0.6 (75.0)
2.7 ± 0.4 (48.2)
1.7 ± 0.3 (45.5)
1.6 ± 0.4 (24.2)
0.0 2.6 ± 0.4 (42.0)
2.2 ± 0.4 (26.4)
2.3 ± 0.2 (35.4)
aI = absence of inner dynein arms; II = absence of outer dynein arms; III = absence of both dynein arms; IV = absence of central structures and radial spokes; V = variable abnormalities of axonemal structures; VI = disorganized axoneme and periaxoneme; VII = absence or abnormal columns. bThe cleavage rate per attempt was defined as the ratio between the number of embryos and the number of metaphase II injected oocytes. cNumber of embryos at 4-cell stage, A and B; Good embryos = four blastomeres and <20% fragmentation 2 days after ICSI.
Article - Flagellar defects, pregnancy and birth outcome after ICSI - P Fauque et al.
332
RBMOnline®
0
90
80
70
60
50
40
30
20
10
I II III IV V VI VII
Type of flagellar abnormality
2–3-cell stage4-cell stage5–6-cell stage
%
Figure 2. Proportion at day 2 of embryos at 2–3-, 4-, 5–6-cell stages according to flagellar abnormalities. Results are represented as mean ± SD.
Table 4. Intracytoplasmic sperm injection outcomes according to flagellar ultrastructural abnormalities.
Parameter Type of flagellar abnormalitya Total I II III IV V VI VII
Fresh cycles Cycles (n) 3 13 4 5 3 8 17 53Transfers (n) 3 13 3 3 3 8 17 50Transferred 6 23 7 9 4 19 33 101 embryos (n)Number of clinical 2 (66.7) 4 (30.8) 1 (25.0) 1 (20.0) 0 (0.0) 2 (25.0) 1 (5.9) 11 (20.8) pregnancies (clinical pregnancy rate, %)b Number of 2 (33.3 5 (21.7) 1 (14.3) 1 (11.1) 0 (0.0) 4 (21.1) 1 (3.0) 14 (13.9) gestational sacs (implantation rate, %)c Number of 2 (66.7) 3 (23.1) 0 (0.0) 1 (20.0) 0 (0.0) 2 (25.0) 1 (5.9) 9 (17.0) deliveries (delivery rate, %)d Number of births 2 (33.3) 3 (13.0) 0 (0.0) 1 (11.1) 0 (0.0) 3 (15.8) 1 (3.0) 10 (9.9) (birth rate, %)e Thaw cycles Cycles (n) 1 5 1 7 0 5 17 36 Transfers (n) 1 4 1 7 – 4 17 34 Transferred 2 7 1 16 – 7 32 65 embryos (n) Number of clinical 0 (0.0) 0 (0.0) 0 (0.0) 1 (14.3) – 0 (0.0) 2 (11.8) 3 (8.3) pregnancies (clinical pregnancy rate, %)b Number of gestational 0 (0.0) 0 (0.0) 0 (0.0) 1 (6.3) – 0 (0.0) 2 (6.3) 3 (4.6) sacs (implantation rate, %)c Number of deliveries 0 (0.0) 0 (0.0) 0 (0.0) 1 (14.3) – 0 (0.0) 1 (5.9) 2 (5.6) (delivery rate, %)d Number of births 0 (0.0) 0 (0.0) 0 (0.0) 1 (6.3) – 0 (0.0) 1 (3.1) 2 (3.1) (birth rate, %)e Cumulative pregnancy 66.7 30.8 25.0 40.0 0.0 25.0 17.6 26.4 rate (%) Cumulative delivery 66.7 23.1 0.0 40.0 0.0 25.0 11.8 20.8 rate (%) Total birth rate (%) 25.0 10.0 0.0 8.0 0.0 11.5 3.1 7.2
aI = absence of inner dynein arms; II = absence of outer dynein arms; III = absence of both dynein arms; IV = absence of central structures and radial spokes; V = variable abnormalities of axonemal structures; VI = disorganized axoneme and periaxoneme; VII = absence or abnormal columns. bClinical pregnancies per cycle. cRatio of total number of gestational sacs and the number of fresh transferred embryos. dTotal number of deliveries per cycle. eRatio between total number of children born and the number of fresh transferred embryos. There were no statistically significant differences between types of flagellar abnormality.

pregnancy, delivery and birth, taking into account transfers of fresh and frozen–thawed embryos.
Contrary to non-specific flagellar anomalies, the ultrastructural flagellar modifications reported in this study are known as primary and monomorphic sperm anomalies. They are stable in time, even following numerous treatments. These
abnormalities are not secondary to any andrological disorder and are effectively untreatable since they do not respond to medical therapies (Chemes et al., 2000). In this series, it should be noted that the phenotypes of ultrastructural flagellar sperm defects of all patients were very severe. In 12 patients, the defects were found in 100% of spermatozoa so it was clear that the injected spermatozoa were carrying the ultrastructural 333
Article - Flagellar defects, pregnancy and birth outcome after ICSI - P Fauque et al.
RBMOnline®
Table 5. Literature summary of all reported intracytoplasmic sperm injection cases (with or without subzonal sperm injection) for patients having immotile cilia syndrome, Kartagener’s syndrome, mitochondrial sheath anomalies and dysplasia of fibrous sheath.
Authors Patients (n)
ICS/KS/DFS Cycles (n)
Fertili- zation rate (%)
Clinical pregnancies (n)
Miscarriages (n)
Deliveries (n)
Children (n)
Outcomea
Wolf et al. (1993)
5 ICS SUZI 47.1 3 1 1 and 1 ongoing pregnancy
1 1 healthy baby (g)
Nijs et al. (1996)
1 KS 1+1
SUZIa25.0 0, 1 nd 1 1 1 healthy
baby (b)Olmedo et al. (1997)
1 DFS 1 75.0 1 nd 1 1 1 healthy baby (g)
Papadimas et al. (1997)
1 ICS 2 42.8 0
Chemes et al. (1998)
5 DFS – – 1 1 ongoing pregnancy
von Zumbusch et al. (1998)
2 KS 2 67.0 2 2 (1 twin) 3 3 healthy babies (2 g and 1 b)
Okada et al. (1999)
4 ICS 5 38.6 0
Olmedo et al. (2000)
6 DFS 10 73.4 4 1 3 (1 triplet) 5 5 healthy babies (2b and 3g)
Cayan et al. (2001)
2 KS/ICS 5 40.4 1 nd 1 1 1 healthy baby (g)
Alosilla Fonttis et al. (2002)
1 MS 1 40.0 1 nd 1 ongoing pregnancy
Westandler et al. (2003)
2 KS 3 45.4 2 nd 1 (1 twin) and 1 ongoing pregnancy
2 2 healthy babies
Peeraer et al. (2004)
1 ICS 1 66 2 1 1 ongoing pregnancy
Mitchell et al. (2006)
21 ICS/DFS/MS 53 61.8 14 3 11 nd nd
Rawe et al. (2007)
2 MS 3 1 1
Current study
20 ICS/DFS 53 48.8 14 11 (1 twin) 12 12 babies (8 b and 4 g)b
Total 74 ICS/KS/DFS/MS
142 58.2 47 7 32 and 5 ongoing pregnancies
26 26 babies (12 b and 12 g)
DFS = dysplasia of fibrous sheath; ICS = immotile cilia syndrome; KS = Kartagener’s syndrome; MS = mitochondrial sheath anomalies; SUZI = subzonal sperm injection; nd: not documented.ag = girl; b = boy. bTwo babies with congenital pathologies.

Article - Flagellar defects, pregnancy and birth outcome after ICSI - P Fauque et al.
defect. Five of these patients were able to conceive a child. In the other cases, the selected spermatozoa were motile and the possibility that they did not carry the defect cannot be excluded. The distribution of sperm ultrastructural defects in this series was different compared with the series previously reported by Mitchell et al. (2006). In the above-mentioned study, the great majority of patients displayed axonemal abnormalities, whereas in this series, a high number of patients exhibited periaxonemal defects. Indeed, in this study, type VII defined by column abnormalities was the most frequent (six patients), and type VI characterized by disorganization of axoneme and periaxoneme was described in three patients. This difference is important because the effect of the ultrastructural abnormality on the fertilization rate varies significantly according to the type. The fertilization rate was not dramatically diminished (52.1%) when the axoneme was disorganized or when the columns were abnormal and was similar to those found for three patients with fibrous sheath column mislocation (Mitchell et al., 2006). Only case reports of patients with sperm without inner dynein arms have been described to date (Neustein et al., 1980; Antonelli et al., 1982; Vevaina et al., 1987; Zamboni, 1992; Tanaka et al., 2007) and fertilization potential and embryo development and pregnancy results for these patients were not available in the literature. In the present series, the patient with sperm lacking inner and outer arms had two children, one of whom was severely deaf. Sperm lacking outer arms with or without axonemal defects were observed in four patients in this series. The fertilization rate in this group was 47.9 ± 3.5% after ICSI, similar to 42.8% and 43.2% previously reported (Papadimas et al., 1997; Mitchell et al., 2006). The fertilization rate after ICSI with ejaculated spermatozoa of two patients with absence of outer and inner dynein arms (type III) was particularly low (27.7%), as found in most reports (Papadimas et al., 1997; Abu-Musa et al., 1999; Westlander et al., 2003). However, in the literature, three patients with Kartagener’s syndrome (von Zumbusch et al., 1998; Peeraer et al., 2004) had normal fertilization rates with or without hypo-osmotic swelling test prior to ICSI. The fertilization rate obtained for patients whose spermatozoa had flagella with central structure defects, defining type IV, was not affected (above 55%), as previously found (Mitchell et al., 2006).
In this series, the embryo fragmentation rate appeared uninfluenced by the ultrastructural defects. However, the kinetics of early embryo cleavage were slower, and the implantation rates were lower than that of the total mean of all attempts when the central axonemal structures were missing or when there were column abnormalities. Since axonemal structures and sperm aster in the oocyte come from the sperm centriole, one explanation could be a possible dysfunction causing abnormal sperm aster formation in the oocyte, pronuclear movement, thus abnormal first embryo cleavage (Palermo et al., 1994) and aberrant embryonic development (Palermo et al., 1997; Rawe et al., 2002). These findings have been supported by studies showing a greater incidence of centriolar abnormalities or absence of centrioles in immotile or non-progressively motile spermatozoa of infertile men when compared with normally motile sperm cells (Sathananthan, 1994). The pathology of the sperm centriole has also been cited as the cause of fertilization failure and early abortions for a patient with abnormalities in head–neck attachment and with dysplasia of the fibrous sheath (Rawe et al., 2002). In addition, the involvement of sperm centrosomal dysfunction in aberrant embryonic development
was proposed by a study reporting a low sperm aster formation rate following heterologous ICSI into bovine eggs with abnormal spermatozoa (dysplasia of fibrous sheath) (Terada, 2004) or after micro-injection of dissected spermatozoa (Moomjy et al., 1999). In animal models, centrosomes have been proven necessary for normal embryonic development (Li et al., 2006; Yabe et al., 2007; Zhang and Megraw, 2007). Moreover, IVF experiments in a mouse model lacking dynein heavy chain (MDHC7–/–) and associated with a dramatic reduced flagellar motility had a retarded rate of early embryo development (Neesen et al., 2001). Therefore, it can be speculated that fertilization by spermatozoa with structural flagella defects could disturb early embryonic development.
In this study, the ICSI outcome varies according to the type of ultrastructural abnormality. But the number of patients included in the different types was small, except in types II and VII, and,
consequently, it is difficult to draw any firm conclusion about embryo development potential after implantation. Overall, the rate of miscarriage in this study was higher than that reported in the entire population treated by ICSI with ejaculated spermatozoa in the study centre (21.4% and 12%, respectively). A male genetic cause of miscarriage has yet to be demonstrated, although spermatozoa with flagellar abnormalities have an increased incidence of aneuploidy (Lewis-Jones et al., 2003; Rives et al., 2005).
This series highlighted the consequences of consanguineous unions since 20.0% of patients were born from consanguineous parents, which is in accordance with a previous report (Baccetti et al., 2001). Given the high proportion of African men with flagellar defects of the fibrous sheath, geographic background could have an impact on the incidence of ultrastructural flagellar defects, as also previously reported (Chemes, 2000). The existence of a genetic component to structural disorders of sperm flagellum, as found in brothers or consanguineous men, was first suggested in 1978 (Alexandre et al., 1978; Baccetti et al., 2001; Latini et al., 2004; Escalier and Albert, 2006; Ravel et al., 2006). Most genetic ultrastructural sperm defects are probably due to a recessive autosomal mutation as suggested in ‘dynein arm deficiency syndromes’, stunted tail syndrome (Chemes et al., 1998; Latini et al., 2004; Ravel et al., 2006) and in an anomaly of the fibrous sheath’s assembly (Escalier and Albert, 2006). The genes involved in these various complex disease phenotypes are just beginning to be identified. To date, five genes have been implicated in primary ciliary dyskinesia: a human dynein sequence DNAI1 (Pennarun et al., 1999; Guichard et al., 2001; Zariwala et al., 2001), a gene encoding a dynein arm DNAH5 (Omran et al., 2000), the RPGR gene (Omran et al., 2000), DNHA11 (Bartoloni et al., 2002) and TXNDC3 (Duriez et al., 2007). Moreover, a genetic linkage between autosomal dominant polycystic kidney disease and the axonemal defect was suggested, but to date has not been investigated (Okada et al., 1999). Several knockout mouse models have been developed to identify potential candidate genes for infertile men with other specific sperm flagellum anomalies (Escalier, 2006). Therefore, a genetic factor could be involved in most sperm flagellum defects. Furthermore, even if most children were healthy after 1 year, two of them presented pathology. No evidence was found of a genetic risk linked to flagellar defects in Menkes disease, which is an X-linked recessive disorder of copper transport metabolism. To date, no information was available concerning the genetic risk of deafness when fertilization was obtained from 334
RBMOnline®

spermatozoa with flagellar anomalies. Besides an increased risk of chromosomal abnormalities, especially those of sex chromosomes found correlated to the motility of the father’s spermatozoa (Bonduelle et al., 2002) or in a patient with dysplasia of the fibrous sheath (Baccetti et al., 2005), a possible genetic risk for the descendants cannot be excluded (Baccetti et al., 2001). No Y microdeletion testing was performed as all but one patient (14), had normal sperm count. Therefore, genetic counselling is necessary to inform couples of potential risks for children born from ICSI when the male has severe sperm flagellar defects. Unfortunately, accurate genetic counselling, taking into account the genetic origin of primary defects, will not be possible until the genes involved and the mode of inheritance are fully understood. For this reason, the study centre has established a multidisciplinary network, including assisted reproductive technology practitioners, embryologists and geneticists, to detect ultrastructural flagellar abnormalities in well-targeted patients, to look for genes that could be implicated in these abnormalities and to give appropriate advice on the risk of potential problems in the childhood. For instance, human outer dynein arm genes and candidates for primary ciliary dyskinesia, have been identified (Pazour et al., 2006). By screening for mutations in these candidates, the centre will be able to formally identify genes responsible for specific pathologies and to precisely counsel patients.
In conclusion, although a previous study focused on the ICSI outcome of 21 patients with ultrastructural flagellar anomalies (Mitchell et al., 2006), the anomaly pattern reported in the present series was not the same and the analysis was extended to the health of babies. The results in this report lead to the recommendation that transmission electron microscopy is performed for patients with isolated abnormal sperm motility or increased abnormalities at the flagellar level using light microscopy to precisely define the ultrastructural defect. As most flagellar defects are likely to have a genetic basis, or may occur in men exhibiting some degree of consanguinity, any mutations present in the spermatozoa could be transmitted to the offspring through the ICSI technique. To date, series in the literature, including the present study, are too small to claim that ICSI parameters, including fertilization rate, embryo quality or outcome, are impaired in patients with ultrastructural flagellar defects or that there is an increased risk of offspring abnormalities in such patients. But there are doubts to be aware of and explore further. It is therefore necessary to inform patients of potential genetic risks for their descendants, even if they are only presumptions at present. A better characterization of male infertility linked to sperm ultrastructural flagellar defects and reports of data on ICSI outcome in such patients should contribute to improve the quality of enrolment to assisted reproduction treatment.
Acknowledgements
The authors would like to thank Jérôme Terribile for technical assistance and Kristen Ben for English correction.
References
Abu-Musa A, Hannoun A, Khabbaz A et al. 1999 Failure of fertilization after intracytoplasmic sperm injection in a patient with Kartagener’s syndrome and totally immotile spermatozoa: case report. Human Reproduction 14, 2517–2518.
Afzelius BA 1998 Genetics and pulmonary medicine. 6. Immotile cilia syndrome: past, present, and prospects for the future. Thorax 53, 894–897.
Alexandre C, Bisson JP, David G 1978 [Total asthenospermia with an ultrastructural anomaly of the flagellum in two sterile brothers.] Journal de Gynécologie, Obstétrique et Biologie de la Reproduction 7, 31–38.
Alosilla Fonttis A, Napolitano R, Tomas MA 2002 Successful ICSI in a case of severe asthenozoospermia due to 93% non-specific axonemal alterations and 90% abnormal or absent mitochondrial sheaths. Reproductive BioMedicine Online 5, 270–272.
Antonelli M, Bravo E, Quattrucci S et al. 1982 [The absence of the internal arms of dynein as a cause of the immotile cilia syndrome.] La Pediatria Medica e Chirurgica: Medical and Surgical Pediatrics 4, 639–641.
Baccetti B, Collodel G, Estenoz M et al. 2005 Gene deletions in an infertile man with sperm fibrous sheath dysplasia. Human Reproduction 20, 2790–2794.
Baccetti B, Capitani S, Collodel G et al. 2001 Genetic sperm defects and consanguinity. Human Reproduction 16, 1365–1371.
Bartoloni L, Blouin JL, Pan Y et al. 2002 Mutations in the DNAH11 (axonemal heavy chain dynein type 11) gene cause one form of situs inversus totalis and most likely primary ciliary dyskinesia. Proceedings of the National Academy of Sciences of the United States of America 99, 10282–10286.
Bonduelle M, Van Assche E, Joris H et al. 2002 Prenatal testing in ICSI pregnancies: incidence of chromosomal anomalies in 1586 karyotypes and relation to sperm parameters. Human Reproduction 17, 2600–2614.
Cayan S, Conaghan J, Schriock ED et al. 2001 Birth after intracytoplasmic sperm injection with use of testicular sperm from men with Kartagener/immotile cilia syndrome. Fertility and Sterility 76, 612–614.
Chemes HE 2000 Phenotypes of sperm pathology: genetic and acquired forms in infertile men. Journal of Andrology 21, 799–808.
Chemes EH, Rawe YV 2003 Sperm pathology: a step beyond descriptive morphology. Origin, characterization and fertility potential of abnormal sperm phenotypes in infertile men. Human Reproduction Update 9, 405–428.
Chemes HE, Olmedo SB, Carrere C et al. 1998 Ultrastructural pathology of the sperm flagellum: association between flagellar pathology and fertility prognosis in severely asthenozoospermic men. Human Reproduction 13, 2521–2526.
Chemes HE, Brugo S, Zanchetti F et al. 1987 Dysplasia of the fibrous sheath: an ultrastructural defect of human spermatozoa associated with sperm immotility and primary sterility. Fertility and Sterility 48, 664–669.
Curi SM, Ariagno JI, Chenlo PH et al. 2003 Asthenozoospermia: analysis of a large population. Archives of Andrology 49, 343–349.
David G, Bisson JP, Czyglik F et al. 1975 Anomalies morphologiques du spermatozoïde humain. 1) Propositions pour un système de classification. Journal de Gynécologie, Obstétrique et Biologie de la Reproduction 4 (Suppl. 1), 17–36.
Duriez B, Duquesnoy P, Escudier E et al. 2007 A common variant in combination with a nonsense mutation in a member of the thioredoxin family causes primary ciliary dyskinesia. Proceedings of the National Academy of Sciences of the United States of America 104, 3336–3341.
Escalier D 2006 Knockout mouse models of sperm flagellum anomalies. Human Reproduction Update 12, 449–461.
Escalier D, Albert M 2006 New fibrous sheath anomaly in spermatozoa of men with consanguinity. Fertility and Sterility 86, 219 e1–9.
Escalier D, David G 1984 Pathology of the cytoskeleton of the human sperm flagellum: axonemal and peri-axonemal anomalies. Biology of Cell 50, 37–52.
Fauque P, Leandri R, Merlet F et al. 2007 Pregnancy outcome and live birth after IVF and ICSI according to embryo quality. Journal of Assisted Reproduction and Genetics 24, 159–165.
Guichard C, Harricane MC, Lafitte JJ et al. 2001 Axonemal dynein intermediate-chain gene (DNAI1) mutations result in situs inversus 335
Article - Flagellar defects, pregnancy and birth outcome after ICSI - P Fauque et al.
RBMOnline®

Article - Flagellar defects, pregnancy and birth outcome after ICSI - P Fauque et al.
and primary ciliary dyskinesia (Kartagener syndrome). American Journal of Human Genetics 68, 1030–1035.
Inaba K 2003 Molecular architecture of the sperm flagella: molecules for motility and signaling. Zoological Science 20, 1043–1056.
Latini M, Gandini L, Lenzi A, Romanelli F 2004 Sperm tail agenesis in a case of consanguinity. Fertility and Sterility 81, 1688–1691.
Lewis-Jones I, Aziz N, Seshadri S et al. 2003 Sperm chromosomal abnormalities are linked to sperm morphologic deformities. Fertility and Sterility 79, 212–215.
Li X, Qin Y, Wilsher S, Allen WR 2006 Centrosome changes during meiosis in horse oocytes and first embryonic cell cycle organization following parthenogenesis, fertilization and nuclear transfer. Reproduction 131, 661–667.
Mitchell V, Rives N, Albert M et al. 2006 Outcome of ICSI with ejaculated spermatozoa in a series of men with distinct ultrastructural flagellar abnormalities. Human Reproduction 21, 2065–2074.
Moomjy M, Colombero LT, Veeck LL et al. 1999 Sperm integrity is critical for normal mitotic division and early embryonic development. Molecular Human Reproduction 5, 836–844.
Neesen J, Kirschner R, Ochs M et al. 2001 Disruption of an inner arm dynein heavy chain gene results in asthenozoospermia and reduced ciliary beat frequency. Human Molecular Genetics 10, 1117–1128.
Neustein HB, Nickerson B, O’Neal M 1980 Kartagener’s syndrome with absence of inner dynein arms of respiratory cilia. American Review of Respiratory Disease 122, 979–981.
Nijs M, Vanderzwalmen P, Vandamme B et al. 1996 Fertilizing ability of immotile spermatozoa after intracytoplasmic sperm injection. Human Reproduction 11, 2180–2185.
Okada H, Fujioka H, Tatsumi N et al. 1999 Assisted reproduction for infertile patients with 9 + 0 immotile spermatozoa associated with autosomal dominant polycystic kidney disease. Human Reproduction 14, 110–113.
Olmedo SB, Rawe VY, Nodar FN et al. 2000 Pregnancies established through intracytoplasmic sperm injection (ICSI) using spermatozoa with dysplasia of fibrous sheath. Asian Journal of Andrology 2, 125–130.
Olmedo SB, Nodar F, Chillik C, Chemes HE 1997 Successful intracytoplasmic sperm injection with spermatozoa from a patient with dysplasia of the fibrous sheath and chronic respiratory disease. Human Reproduction 12, 1497–9149.
Omran H, Haffner K, Volkel A et al. 2000 Homozygosity mapping of a gene locus for primary ciliary dyskinesia on chromosome 5p and identification of the heavy dynein chain DNAH5 as a candidate gene. American Journal of Respiratory Cell and Molecular Biology 23, 696–702.
Palermo GD, Colombero LT, Rosenwaks Z 1997 The human sperm centrosome is responsible for normal syngamy and early embryonic development. Reviews of Reproduction 2, 19–27.
Palermo G, Munné S, Cohen J 1994 The human zygote inherits its mitotic potential from the male gamete. Human Reproduction 9, 1220–1225.
Papadimas J, Tarlatzis BC, Bili H et al. 1997 Therapeutic approach of immotile cilia syndrome by intracytoplasmic sperm injection: a case report. Fertility and Sterility 67, 562–565.
Papageorgiou T, Guibert J, Goffinet F et al. 2002 Percentile curves of serum estradiol levels during controlled ovarian stimulation in 905 cycles stimulated with recombinant FSH show that high estradiol is not detrimental to IVF outcome. Human Reproduction 17, 2846–2850.
Pazour GJ, Agrin N, Walker BL, Witman GB 2006 Identification of predicted human outer dynein arm genes: candidates for primary ciliary dyskinesia genes. Journal of Medical Genetics 43, 62–73.
Peeraer K, Nijs M, Raick D, Ombelet W 2004 Pregnancy after ICSI with ejaculated immotile spermatozoa from a patient with immotile cilia syndrome: a case report and review of the literature. Reproductive BioMedicine Online 9, 659–663.
Pennarun G, Escudier E, Chapelin C et al. 1999 Loss-of-function mutations in a human gene related to Chlamydomonas reinhardtii dynein IC78 result in primary ciliary dyskinesia. American Journal of Human Genetics 65, 1508–1519.
Ravel C, Chantot-Bastaraud S, Siffroi JP et al. 2006 Tail stump syndrome associated with chromosomal translocation in two brothers attempting intracytoplasmic sperm injection. Fertility and Sterility 86, 719 e1–7.
Rawe VY, Hermes R, Nodar FN et al. 2007 Results of intracytoplasmic sperm injection in two infertile patients with abnormal organization of sperm mitochondrial sheaths and severe asthenoteratozoospermia. Fertility and Sterility 88, 649-653.
Rawe VY, Terada Y, Nakamura S et al. 2002 A pathology of the sperm centriole responsible for defective sperm aster formation, syngamy and cleavage. Human Reproduction 17, 2344–2349.
Rives N, Mousset-Simeon N, Mazurier S, Mace B 2005 Primary flagellar abnormality is associated with an increased rate of spermatozoa aneuploidy. Journal of Andrology 26, 61–69.
Sathananthan AH 1994 Functional competence of abnormal spermatozoa. Baillière’s Clinical Obstetrics and Gynaecology 8, 141–156.
Stalf T, Sanchez R, Kohn FM et al. 1995 Pregnancy and birth after intracytoplasmic sperm injection with spermatozoa from a patient with tail stump syndrome. Human Reproduction 10, 2112–2114.
Tanaka K, Sutani A, Uchida Y et al. 2007 Ciliary ultrastructure in two sisters with Kartagener’s syndrome. Medical Molecular Morphology 40, 34–39.
Terada Y 2004 Human sperm centrosomal function during fertilization, a novel assessment for male sterility. Human Cell 17, 181–186.
Vandervorst M, Tournaye H, Camus M et al. 1997 Patients with absolutely immotile spermatozoa and intracytoplasmic sperm injection. Human Reproduction 12, 2429–2433.
Vevaina JR, Teichberg S, Buschman D, Kirkpatrick CH 1987 Correlation of absent inner dynein arms and mucociliary clearance in a patient with Kartagener’s syndrome. Chest 91, 91–95.
von Zumbusch A, Fiedler K, Mayerhofer A et al. 1998 Birth of healthy children after intracytoplasmic sperm injection in two couples with male Kartagener’s syndrome. Fertility and Sterility 70, 643–646.
Westlander G, Barry M, Petrucco O, Norman R 2003 Different fertilization rates between immotile testicular spermatozoa and immotile ejaculated spermatozoa for ICSI in men with Kartagener’s syndrome: case reports. Human Reproduction 18, 1286–1288.
Wolf JP, Feneux D, Escalier D et al. 1993 Pregnancy after subzonal insemination with spermatozoa lacking outer dynein arms. Journal of Reproduction and Fertility 97, 487–492.
World Health Organization 1999 Laboratory Manual for the Examination of Human Semen and Sperm-Cervical Mucus Interaction 4th edn. Cambridge University Press, Cambridge.
Yabe T, Ge X, Pelegri F 2007 The zebrafish maternal-effect gene cellular atoll encodes the centriolar component sas-6 and defects in its paternal function promote whole genome duplication. Developmental Biology 312, 44–60.
Zamboni L 1992 Sperm structure and its relevance to infertility. An electron microscopic study. Archives of Pathology and Laboratory Medicine 116, 325–344.
Zariwala M, Noone PG, Sannuti A et al. 2001 Germline mutations in an intermediate chain dynein cause primary ciliary dyskinesia. American Journal of Respiratory Cell and Molecular Biology 25, 577–583.
Zhang J, Megraw TL 2007 Proper recruitment of gamma-tubulin and D-TACC/Msps to embryonic Drosophila centrosomes requires Centrosomin Motif 1. Molecular Biology of the Cell 18, 4037–4049.
Declaration: The authors report no financial or commercial conflicts of interest.
Received 17 October 2008; refereed 18 December 2008; accepted 29 April 2009.
336
RBMOnline®





























