Embed Size (px)
Citation preview

REVIEW ARTICLE
Gastric cancer: surgery in 2011
Katja Ott & Florian Lordick & Susanne Blank &
Markus Büchler
# Springer-Verlag 2011
AbstractBackground Treatment of gastric cancer is more and morebecoming an individualized decision. The choice of theoptimal approach is based on prognostic factors, on theanatomic site of the tumor, and on expectations about theresponse to neoadjuvant treatment. Early gastric cancerthat is limited to the mucosal layer is the domain ofendoscopic resections. As soon as the submucosal layeris invaded, surgical strategies with adequate lymphade-nectomy become necessary.Discussion In many East Asian Centers and some othercenters in the world, these tumors are resected by alaparoscopic approach. With a high experience, this canbe done with excellent quality and outcome. In locallyadvanced gastric cancer, multimodal treatment can improvesurvival in comparison to surgery alone. However, thestrategies differ significantly around the world. Whileadjuvant chemoradiotherapy is standard in the USA, inEurope, perioperative chemotherapy is the first choice, andin Japan, adjuvant chemotherapy is recommended. InEurope, three randomized phase III studies on the valueof preoperative chemotherapy have been performed. Two ofthem have shown that perioperative chemotherapy doessignificantly improve the survival of patients with adeno-carcinoma of the stomach and of the esophagogastricjunction. The one including only preoperative chemother-
apy failed to show a survival benefit for the combinedtreatment arm but showed excellent outcomes in both thesurgery alone and the preoperative chemotherapy arms.Based on these studies, patients with stage II or stage IIIdisease are now treated with perioperative chemotherapy.Additionally, it is generally accepted for more than 10 yearsnow that responding patients have a significantly improvedprognosis compared to nonresponding patients. The per-centage of responding patients varies depending on theapplied regimen between 20% and 45%. Therefore, earlyresponse evaluation or response prediction is an utmostimportant field of research. Proximal tumors are treatedwith a transhiatal extended gastrectomy, tumors in themiddle third with a total gastrectomy, and distal tumorswith a subtotal gastrectomy, if possible. Modified D2lymphadenectomy avoiding splenectomy is now acceptedas the standard procedure, providing improved prognosisfor certain subgroups of patients. Individualized resectionand lymphadenectomy techniques for early tumor stagesand response-based neoadjuvant concepts for locallyadvanced tumors are the challenge for the future.
Keywords Gastric cancer . Surgery . Treatment
Introduction
Tumor stage, growth pattern, and tumor site are majorfactors determining the extent of resection and lympha-denectomy in gastric cancer [1, 2]. For pretherapeuticstaging, endoscopy with biopsy, and CT scan of thethorax, abdomen and pelvis should be performed [3, 4].The clinical value of EUS for initial staging is discussedcontroversially at the moment, but EUS predicts accu-rately the clinical T stage and may help to select patients
K. Ott (*) : S. Blank :M. BüchlerDepartment of Surgery, University of Heidelberg,INF 110,69120 Heidelberg, Germanye-mail: [email protected]
F. LordickDepartment of Medicine, Klinikum Braunschweig,Hannover Medical School,Hannover, Germany
Langenbecks Arch Surg (2011) 396:743–758
DOI 10.1007/s00423-010-0738-7
Received: 7 December 2010 /Accepted: 20 December 2010 /Published online: 14 January 2011

for neoadjuvant treatment [5]. 18F-Fluorodeoxyglucosepositron emission tomography (FDG-PET) scan cannotgenerally be recommended for staging in gastric cancerbecause more than 50% of the diffuse type gastric canceris not avid for the principal tracer which is FDG [6–8]. Astaging laparoscopy may add important information toconventional staging even in earlier stages [9]. In locallyadvanced tumors, about 20% occult peritoneal carcino-matosis can be detected by laparoscopy [10]. In patientswith neoadjuvant chemotherapy, sequential pretherapeu-tic and preoperative laparoscopy helps for risk stratifica-tion of the patients. Neoadjuvant chemotherapy appearsto be a risky strategy for about 20% of the patientsdeveloping free peritoneal tumor cells during therapy[11].
In patients with early tumor stages, endoscopically oranatomically orientated limited resection techniques areincreasingly important, probably in combination with theconcept of the sentinel lymph node detection [2, 12, 13]. Atthe moment, uT1m gastric cancer, which is cancer limitedto the mucosal layer of the stomach, is treated mostlyendoscopically. Gastric cancer staged uT1sm/2 is treatedwith surgery with adequate lymphadenectomy [14]. InJapan and some other countries and specialized centers,for these tumor categories, laparoscopic resections areprovided with high experience and excellent oncologicalquality [2]. In locally advanced gastric cancer, multimodaltreatment can improve the outcome in comparison tosurgery alone [15]. However, the strategies differ signifi-cantly around the world. In the USA since the SWOG/Intergroup Study 0116, an adjuvant chemoradiotherapy isstandard [16], in Europe since the MAGIC study aperioperative chemotherapy [15], and in Japan an adjuvantchemotherapy [17] is the preferred treatment. However, allstudies have their specific limitations. In Europe, threerandomized studies have been performed. Only the MAGICstudy [15] and the EORTC 40954 [18] have beenpublished, and the other study (French FFCD 9703 trial)has been presented as American Society of ClinicalOncology (ASCO) abstracts. Two of them (MAGIC andFFCD 9703) have shown that perioperative chemotherapydoes significantly improve the survival of patients withadenocarcinoma of the stomach and of the esophagogastricjunction (5-year survival: MAGIC 36% versus 23% p=0.009; FFCD 9703 38% versus 24% p=0.003). TheEORTC study 40095 [19] applied only preoperativechemotherapy but failed to show a survival benefit for thecombined treatment arm. On the other side, this studyshowed excellent outcomes in both treatment arms (mediansurvival 64.6 versus 52.5 months; 2-year survival 72.7%versus 69.9%). Based on these studies, patients with stageII or stage III disease are now treated with perioperativechemotherapy [15]. Additionally, it is generally accepted
for more than 10 years now that responding patients have asignificant improved prognosis compared to nonrespondingpatients [20]. The percentage of responding patients variesdepending on the used regimen and is reported to be 20–45% [3, 4, 21, 22]. Therefore, (early) response evaluationor response prediction is of utmost importance [8, 23–31].
The surgical strategy is discussed controversially fortumors of the proximal third, especially adenocarcinomaof the esophagogastric junction (AEG) type II accordingto Siewerts classification [32], in which either a transhia-tal extended gastrectomy [32] or an Ivor Lewis procedure(right transthoracic esophagectomy with a gastric pull upand intrathoracic anastomosis) [33] can be performed. Toachieve a safety margin of 5 cm in situ as requested by thegroup from Sloan Kettering, an abdominothoracic ap-proach may be superior to a transhiatal extended gastrec-tomy [34]. Tumors in the middle third are resected by totalgastrectomy and distal tumors by subtotal gastrectomy, ifpossible [35, 36], otherwise with a total gastrectomy. Aftertotal gastrectomy, reconstruction with a pouch seems toimprove quality of life within the first months after theresection and reduces the risk of a leakage of theesophagojejunostomy.
The most controversially discussed issue over the lasttwo decades in gastric cancer was the type of lymphade-nectomy [37–41]. The D2 lymphadenectomy is nowbroadly accepted as a standard procedure, providingimproved prognosis for certain subgroups of patients [39].Individualized resection and lymphadenectomy techniquesfor early tumor stages and response-based neoadjuvantconcepts for locally advanced tumors are the challenge ofthe future.
Staging
The goal of pretherapeutic staging is to define tumorstage and the patient’s prognosis and to identify patientswho may need and benefit from preoperative treatment[5]. Furthermore, the assessment of local tumor infiltra-tion (T category) and regional lymph node involvement(N category) is necessary in patients with resectable diseaseranging from early gastric cancer to locally advanced gastriccancer in order to decide whether a complete tumor resection(R0) is feasible, which is one of the most accepted andindependent prognostic factors in gastric cancer [14, 34].Local tumor infiltration (T category) and nodal involvement(N category) are also frequently used for therapystratification. While patients with c/uT1a are treatedendoscopically and c/uT1b tumors without lymph nodesmetastases are treated by primary resection and lymphnode dissection, patients with c/uT2-4 tumors arefrequently offered multimodal treatment to improve the
Langenbecks Arch Surg (2011) 396:743–758744

rate of curative resections and overall survival [15].Based on the data of the MAGIC study, in which alimited pretherapeutic staging was performed, onlypatients with a c/uT1 category or without lymph nodemetastases should be primarily resected. Endoscopicendoluminal ultrasound for early tumor categories andCT scan for more advanced tumor categories are therequired examinations for exact definition of the prether-apeutic c/uT category [5, 42].
In contrast to the c/uT category, the prediction of thecorrect c/uN category remains difficult because a certainsize or diameter is not obligatory correlated with malig-nancy [1]. Endoluminal ultrasound reaches a diagnosticaccuracy of 65–87%. FDG-PET offers a low sensitivity of51% and a sufficient specificity of 84% for the locoregionallymph node staging [42–45]. In gastric cancer, a strongcorrelation between T category and number and localizationof the lymph nodes was shown. In patients with a pT3category, the probability for lymph node metastases is morethan 70% [46].
Today in resectable tumors, the removal of the primarytumor together with a systematic lymphadenectomy isnecessary for the histopathological lymph node stagingand is the accepted standard therapy [40, 41, 46–50]. A CTscan of the thorax, abdomen, and pelvis should beobligatory for staging in locally advanced gastric cancerto exclude distant metastases. Patients with distant metas-tases should not undergo primary resection, only inindividual selected cases. These patients should receive asystemic medical treatment. A resection may make sense ifthe patient responded to the treatment and if a completeresection is likely to be reached. The specificity of the CTscan for the prediction of the TNM categories could beimproved in only one study by FDG-PET [43]. In general,FDG-PET cannot be recommended for staging gastriccancer [51]. Interestingly, approximately 1/3 of patientswith gastric cancer, even with locally advanced tumors,have initially insufficient FDG uptake for quantificationand are called FDG non-avid tumors [6–8, 45, 52].Especially gastric tumors localized in the distal third withdiffuse growth pattern are FDG non-avid [8].
In gastric cancer, additionally to the conventional stagingmodalities, a staging laparoscopy can be performed. Thedetection of free peritoneal tumor cells is associated withpoor prognosis, even in early gastric cancer, e.g., tumorstage IB [9, 53]. Therefore, a pretherapeutic laparoscopywith lavage cytology can be used for risk stratification ofthe patients. Additionally, there is evidence that a diagnos-tic laparoscopy adds relevant information to the conven-tional staging techniques in up to 20% [10]. In these cases,an upstaging occurs [10]. An extended diagnostic laparos-copy is superior to all staging techniques in detecting aperitoneal carcinomatosis [10, 11].
Surgery
Type of surgery is dependent on the infiltration depth,growth pattern, and localization of the tumor. Early gastriccancer staged u/cT1a is treated endoscopically. Tumorsmore advanced than c/uT1a are treated surgically due to thepossibility of lymph node metastases. The pT category isstrongly association with the probability of lymph nodemetastases (Fig. 1). Figure 1 demonstrates the highprobability of lymph node metastases already in early pTcategories in gastric cancer and underlines the importanceof an adequate lymphadenectomy. The type of resection ismainly based on the localization of the tumor (Fig. 2). Thelocalization of the primary tumor influences also thelymphatic spread (Fig. 3a). The Maruyama computerprogram can predict the localization of lymph nodemetastases with high accuracy (Fig. 3b), even after transferto the Western world [54, 55]. The stomach is divided intothree parts: the distal, the middle, and the proximal third.
Type of resection for proximal tumors
In proximal gastric cancer, the surgical strategy wasdiscussed controversially because AEG II and III wereintegrated until 2009 [32, 34]. Based on the 2009 TNMclassification, these tumor types are now classified asesophageal cancer. However, the type of operation forAEG II has to be discussed with caution. A Japanese studyhas shown no survival benefit for a left abdominothoracicapproach compared to a transhiatal extended gastrectomy in167 patients [56]. The 5-year survival rate of 52% versus38%, the complication rate of 34% versus 49% (p=0.06),and the mortality of 0% versus 4% favor clearly thetranshiatal extended gastrectomy [56].
A retrospective analysis on 505 patients with AEGfrom the Sloan Kettering Cancer Center has shown thatin primarily resected patients, a safety margin of at least5 cm in situ (3.8 cm ex situ) and a dissection of at least15 lymph nodes are necessary to improve the prognosisof the patients [34, 48]. Based on these data, anabdominothoracic approach (Ivor Lewis procedure) hasto be discussed for AEG II and III to guarantee anadequate safety margin and a more radical lymph nodedissection [33]. A randomized study comparing a tran-shiatal extended gastrectomy with a right abdominothora-cic approach does not exist so far.
Based on the 2009 TNM classification with exclusion ofAEG II and III from gastric cancer, the standard procedureis nowadays a transhiatal extended gastrectomy for proxi-mal gastric cancer [32] (Fig. 2). A transhiatal extendedgastrectomy should start with the esophageal resection withan intraoperative frozen section to provide a proximaltumor free proximal resection margin.
Langenbecks Arch Surg (2011) 396:743–758 745

For carcinomas of the proximal third, a D2 lymph nodedissection is standard. Due to the retroperitoneal lymph nodedrainage (see Fig. 3), additionally the lymph node stations 11,12, and 16 should be dissected [32]. In early proximal tumorsstaged c/uT1sm/pT2a, a limited resection with a pedicledjejunal interposition (Merendino procedure) can be performed[57, 58]. For this individualized therapy stratification, anexact pretherapeutic staging is of utmost importance [5].
Type of resection for tumors in the middle third
Tumors localized in the middle third are in general resectedby a total gastrectomy including a D2 lymphadenectomywith the lymph node stations 1–6 and 7–1 (Fig. 2).
Type of resection for distal tumors
Method of choice for distal gastric cancer, irrespective ofthe Lauren classification, is a subtotal gastrectomy [35, 36].
The study of the Italian gastrointestinal tumor study grouprandomized a total of 618 patients. Three hundred fifteenpatients underwent a subtotal gastrectomy and 303 patients atotal gastrectomy. In both study groups, a D2 lymphadenec-tomy was performed. The 5-year survival was 65.3% in thegroup with subtotal gastrectomy and 62.4% in the groupwith total gastrectomy [35] (Table 1). In patients withtumors localized close to the pylorus additionally to theD2 lymph node resection, the lymph node stations 12(ligamentum hepatoduodenale), 13 (retroduodenal), and16 (right paraaortic) should be harvested (Fig. 2).
Own unpublished nonrandomized data show even animproved survival after a subtotal gastrectomy compared toa total gastrectomy (Table 1). Even in locally advancedtumors after neoadjuvant chemotherapy, a subtotal gastrec-tomy with D2 lymphadenectomy can be recommended.
In distal tumors infiltrating the duodenum, the extensionof a subtotal or total gastrectomy to an additionalpancreaticoduodenectomy should be considered with cau-
proximal
middle
distal
Without AEGII/III based on new TNM 2009:Transhiatal extended gastrectomy with D2-lymphadenectomy including lymph node station10 (retroperitoneal left paraaortic)
Total gastrectomy with D2 lymphadenectomy:Lymph nodes stations 1-6 and 7-12
Subtotal gastrectomy: D2 lymphadenectomy(lymphnode station 2 remains in situ) includinglymph node stations 12 (Lig. hepatoduodenale),13 (retroduodenal) and 16 (right paraaortic)
Fig. 2 Type of resection and lymphadenectomy in respect of the localization of the primary tumor
pT-CategoryTNM UICC 2002
Probability of lymph-node metastases
Mucosa
Submucosa
Fig. 1 Correlation of pT category and probability of lymph node metastases
Langenbecks Arch Surg (2011) 396:743–758746

tion and should only be performed if a complete tumorresection can be achieved [59].
Lymphadenectomy: D1 or D2 or D3
The type of lymphadenectomy is discussed controversially.Despite the negative data from two European randomizedtrials (D1 versus D2 lymphadenectomy; Fig. 4a) [37, 38],the D2 lymphadenectomy is standard in Japan and inWestern centers [46]. A subgroup analysis of the Dutchstudy shows a significant survival benefit for patients withpN2 category after a D2 resection [39]. In neoadjuvantlytreated patients with a high probability of lymph nodemetastases, a D2 lymphadenectomy should be performed.Recently published data from Korea and Japan show thesuperiority of a D2 or even D3 lymphadenectomy. Bothprocedures were performed with extremely low morbidityand mortality [40, 41, 60] (Table 2). As compared with aD2 lymph node dissection alone, an additional paraaorticlymph node dissection does not improve the survival rate incurable gastric cancer [40]. The randomized study fromKorea on 221 patients comparing D1 and D3 lymph noderesection shows a significantly improved overall survival(Fig. 4b), but no improved recurrence-free survival [41](Table 2). The large Japanese study on 523 patientscomparing a D2 lymphadenectomy with a D2 lymphade-
nectomy with an additional paraaortic lymphadenectomy(PAND) shows no benefit after additional PAND [40](Table 2; Fig. 4c). Both mortality (0.8% in both arms) andcomplication rate (20.9% after D2 and 28.1% after D2+PAND) are excellent and cannot be reproduced in Westernmulticenter trials. Also the survival data presented aresuperior to those in the Western world (5-year survival of69.2% for the patients with D2 and 70.3% for the patientswith D2+PAND) [40] (Table 2).
Multimodal treatment
In the Western world, at least 70% of gastric cancers arediagnosed in locally advanced stages. Those patients are nomore candidates for primary surgery. Those patients benefitfrom preoperative chemotherapy due to the followingtheoretical advantages:
1. Medical treatment can be more intensive due to a bettercondition compared to the postoperative approach.2. Blood and lymphatic vessels, which may be importantfor the chemotherapy-induced cell kill, are not altered bythe operation3. Downsizing of the tumor offers the possibility of highercomplete resection rates.4. Micrometastases can be treated at an early time point.
Author Resection Number Morbidity (%) Med. survival 5-year survival (%) p
Gouziet [36] TG 93 32 – 48 n.s
SG 76 34 – 48
Bozzetti [35] TG 303 13 – 62 n.s
SG 315 9 – 65
Heidelberg TG 93 n.s 33 months – 0.045
SG 126 n.s Not reached –
Table 1 Randomized studiescomparing total gastrectomyand subtotal gastrectomy andnon randomized data fromHeidelberg
TG total gastrectomy, SG subto-tal gastrectomy, Med. median
Fig. 3 a Typical lymphaticspread of a proximal gastriccarcinoma. b Prediction oflymph node metastases for alocally advanced gastric cancerlocalized in the proximal thirdby the Maruyama computerprogram
Langenbecks Arch Surg (2011) 396:743–758 747

Fig. 4 a Dutch study: D1 ver-sus D2 [39]: no survival benefitfor D2 lymphadenectomy inoverall survival. b Koreanstudy: D1 versus D3 [41]: sig-nificant survival benefit for D3lymphadenectomy in overallsurvival. c Japanese study: D2versus D2 with paraaortic lym-phadenectomy (PAND) [40]: nosurvival benefit for D2 + PAND
Langenbecks Arch Surg (2011) 396:743–758748
5. Reduced contamination of the abdominal cavity with freetumor cells due to “tumor sterilization”6. Preoperative treatment offers the possibility of an “invivo testing” of the therapy applied.7. The postoperative therapy can be adjusted according tothe individual preoperative response.
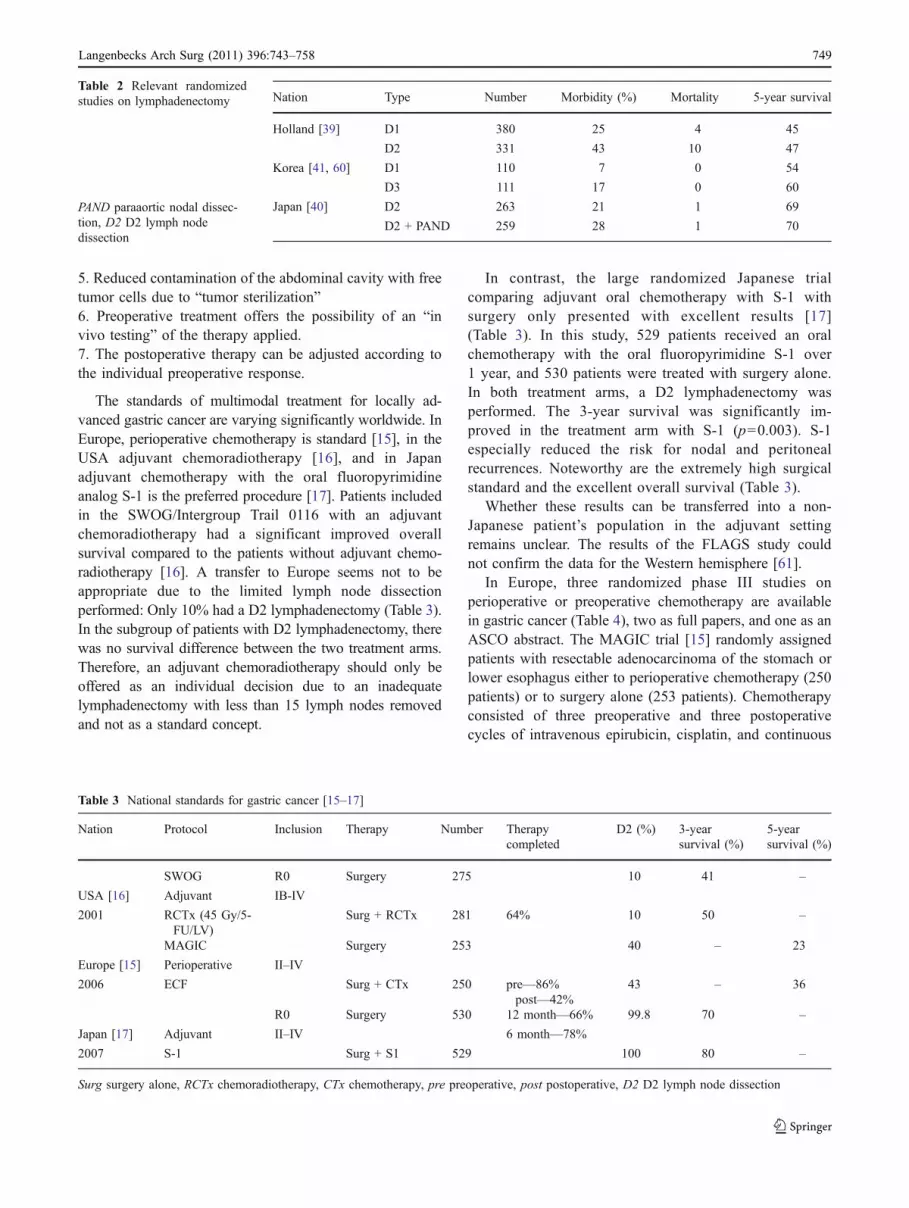
The standards of multimodal treatment for locally ad-vanced gastric cancer are varying significantly worldwide. InEurope, perioperative chemotherapy is standard [15], in theUSA adjuvant chemoradiotherapy [16], and in Japanadjuvant chemotherapy with the oral fluoropyrimidineanalog S-1 is the preferred procedure [17]. Patients includedin the SWOG/Intergroup Trail 0116 with an adjuvantchemoradiotherapy had a significant improved overallsurvival compared to the patients without adjuvant chemo-radiotherapy [16]. A transfer to Europe seems not to beappropriate due to the limited lymph node dissectionperformed: Only 10% had a D2 lymphadenectomy (Table 3).In the subgroup of patients with D2 lymphadenectomy, therewas no survival difference between the two treatment arms.Therefore, an adjuvant chemoradiotherapy should only beoffered as an individual decision due to an inadequatelymphadenectomy with less than 15 lymph nodes removedand not as a standard concept.
In contrast, the large randomized Japanese trialcomparing adjuvant oral chemotherapy with S-1 withsurgery only presented with excellent results [17](Table 3). In this study, 529 patients received an oralchemotherapy with the oral fluoropyrimidine S-1 over1 year, and 530 patients were treated with surgery alone.In both treatment arms, a D2 lymphadenectomy wasperformed. The 3-year survival was significantly im-proved in the treatment arm with S-1 (p=0.003). S-1especially reduced the risk for nodal and peritonealrecurrences. Noteworthy are the extremely high surgicalstandard and the excellent overall survival (Table 3).
Whether these results can be transferred into a non-Japanese patient’s population in the adjuvant settingremains unclear. The results of the FLAGS study couldnot confirm the data for the Western hemisphere [61].
In Europe, three randomized phase III studies onperioperative or preoperative chemotherapy are availablein gastric cancer (Table 4), two as full papers, and one as anASCO abstract. The MAGIC trial [15] randomly assignedpatients with resectable adenocarcinoma of the stomach orlower esophagus either to perioperative chemotherapy (250patients) or to surgery alone (253 patients). Chemotherapyconsisted of three preoperative and three postoperativecycles of intravenous epirubicin, cisplatin, and continuous
Table 3 National standards for gastric cancer [15–17]
Nation Protocol Inclusion Therapy Number Therapycompleted
D2 (%) 3-yearsurvival (%)
5-yearsurvival (%)
SWOG R0 Surgery 275 10 41 –
USA [16] Adjuvant IB-IV
2001 RCTx (45 Gy/5-FU/LV)
Surg + RCTx 281 64% 10 50 –
MAGIC Surgery 253 40 – 23
Europe [15] Perioperative II–IV
2006 ECF Surg + CTx 250 pre—86%post—42%
43 – 36
R0 Surgery 530 12 month—66% 99.8 70 –
Japan [17] Adjuvant II–IV 6 month—78%
2007 S-1 Surg + S1 529 100 80 –
Surg surgery alone, RCTx chemoradiotherapy, CTx chemotherapy, pre preoperative, post postoperative, D2 D2 lymph node dissection
Nation Type Number Morbidity (%) Mortality 5-year survival
Holland [39] D1 380 25 4 45
D2 331 43 10 47
Korea [41, 60] D1 110 7 0 54
D3 111 17 0 60
Japan [40] D2 263 21 1 69
D2 + PAND 259 28 1 70
Table 2 Relevant randomizedstudies on lymphadenectomy
PAND paraaortic nodal dissec-tion, D2 D2 lymph nodedissection
Langenbecks Arch Surg (2011) 396:743–758 749

infusional 5-FU. Postoperative complications and 30-daymortality did not differ significantly in both treatment arms(46% versus 45% and 5.6% versus 5.9%, respectively).Downstaging occurred in terms of lower ypT and Ncategories in the group with preoperative chemotherapy.One hundred forty-nine patients in the group with peri-operative chemotherapy have died compared to 170patients in the surgery only group. Patients with perioper-ative chemotherapy had a significantly improved overall(p=0.009) and progression free survival (p<0.001) com-pared to patients with surgery alone (Fig. 5a). The 5-yearsurvival rate was 36% for patients with perioperativechemotherapy and 23% for patients with surgery alone[15]. In 2007, the French presented their FNLCC AC-CORD07 FFCD 9703 trial at ASCO which confirmedbasically the results of the MAGIC trial (Table 4). In theFrench trial, a combination of infusional 5-FU and cisplatinfor two to three cycles preoperatively was delivered inresectable patients with gastric or esophageal adenocarci-noma. Postoperative chemotherapy was recommended incase of response to preoperative chemotherapy or in stabledisease with positive lymph nodes. A total of 224 patients111 patients with surgery alone and 113 patients withperioperative chemotherapy were included. The rate ofcomplete resections (R0) was significantly higher afterpreoperative chemotherapy (84% versus 73%, p=0.04).After chemotherapy, the disease free (p=0.003) and overallsurvival (p=0.02) were improved. The reported 5-yearsurvival rates of 38% with chemotherapy and 24% withsurgery alone (Fig. 5b) are in line with the MAGIC trial. Inboth studies, only a small percentage (MAGIC trial 42%and FFDC 9703 50%) of patients completed both pre- andpostoperative chemotherapy, whereas in 86% and 87% ofthe patients, preoperative chemotherapy was administered.However, it is not possible to attribute the survival benefitto preoperative chemotherapy only because both studiesevaluated perioperative chemotherapy. Both studies havebeen criticized due to the long recruitment period (8 yearseach), the insufficient preoperative staging, the inaccuratehistopathological workup, and the high dropout rate in thepostoperative treatment arm and the low surgical quality. Inboth studies, neither a clinical nor a histopathologicalresponse evaluation was performed. However, these pointsof criticism have probably been balanced on both arms dueto randomization. Therefore, in the Western world, theseresults are widely accepted, even if some questions remainopen and perioperative chemotherapy is standard at themoment in Europe for locally advanced gastric cancer. TheEORTC study 40954 [18], which started in 1999, wasdesigned to answer open questions. This study examinedthe value of purely preoperative neoadjuvant chemotherapywith cisplatin, infusional 5-FU, and leucovorin in a phaseIII trial with sophisticated preoperative staging including
endoscopy, EUS, CT, and staging laparoscopy and strictsurgical resection guidelines including a D2 lymphadenec-tomy. Patients with locally advanced adenocarcinoma of thestomach or esophagogastric junction (AEG II and III) wereincluded and randomized to preoperative chemotherapyfollowed by surgery or to surgery alone. The study wasdesigned to detect an improvement in median survival from17 months with surgery alone to 24 months with preoper-ative chemotherapy. To reach an 80% power, 282 deathswould have been required. Due to the low accrual, thestudy was stopped after 144 patients, and 72 patients wereallocated to each arm. Tumors in the proximal third werepredominant with 52.8% including AEG types II and III. Incontrast to the two other European randomized studies, thecompletion of two cycles of preoperative chemotherapywas relatively low with 65.2%. Downsizing (ypT0-2) wasmore frequent in the neoadjuvant group (65.7% versus50%) but did not reach statistical significance (p=0.113) incontrast to the MAGIC trial. The complete resection ratewas higher with 81.9% after neoadjuvant chemotherapycompared to 66.7% with surgery alone (p=0.036). Thechemotherapy followed by surgery group had less frequentlymph node metastases than the surgery alone group(38.6% versus 19.1%; p=0.018). Postoperative complica-tions (27.1% vs. 16.2%; p=0.09) and mortality (4.3%versus 1.5%) occurred more often in the neoadjuvant arm.Based on 67 deaths, a survival benefit for the preoperativetreatment could not be shown (HR=0.84; 95% CI 0.52 to1.35; p=0.466). The median survival for both arms wasexcellent and far better than expected. The overall survivalin the chemotherapy followed by surgery group was64.6 months compared to 52.5 months in the surgery onlygroup (p=0.466; Fig. 5c). There was a trend toward longertime to progression in the group with neoadjuvant chemo-therapy (p=0.065; Table 4). Interestingly, this study failedto demonstrate a survival benefit despite a significantlyincreased R0 resection rate and lower rate of lymph nodemetastases in the neoadjuvant arm, most likely due to thesmall number of included patients. The excellent outcomeafter radical surgery alone can be explained by the high rateof D2 resections, by the inclusion of 75% of the patients inonly two centers with high experience in upper GI surgery,and by the exclusion of patients with occult peritonealcarcinomatosis by a pretherapeutic staging laparoscopy.
Severe chemotherapy-related complications inhibitingresection after chemotherapy are relatively rare. In theMAGIC study, 212 of 250 patients were resected, in theFFCD 109 of 113, and in the EORTC study 69 of 72.
Postoperative mortality was similar in both treatmentarms in the three randomized phase III studies. Mortalityranges from 1.5% to 6% in the patients without chemo-therapy and from 4.3% to 6% in patients with chemother-apy. The reported complication rate was the highest in the
Langenbecks Arch Surg (2011) 396:743–758750

MAGIC trial (45.3 for surgery alone, 45.7 for perioperativechemotherapy) followed by the French trial (19% forsurgery alone and 26% for perioperative chemotherapy)and the EORCT trial (16.2% for surgery alone and 27.1%for neoadjuvant chemotherapy). This imbalance betweenthe studies might be due to an inclusion of minorcomplications into the analysis.
In conclusion, effectiveness and superiority of perioper-ative chemotherapy followed by surgery compared tosurgery alone was proven by two randomized phase IIIstudies. The third study with preoperative chemotherapyonly failed to show a survival benefit for the neoadjuvanttreatment arm most likely due to the excellent results in thesurgery alone arm and the low accrual rate. There is nosignificant difference in morbidity, mortality, hospital stay,and incidence or type of complications between the twotreatment groups in all three randomized trials. Histopath-ological results seem to be improved significantly bypreoperative chemotherapy (Table 4).
Response evaluation
It is generally accepted that patients who respond topreoperative chemotherapy have a significantly improvedsurvival compared to patients who do not respond [20].Recent data even suggest that patients who do not profitfrom neoadjuvant treatment have even an impairedprognosis to patients with primary resection [62]; there-fore, the pretherapeutic selection of nonrespondingpatients would be of utmost importance. Until today, nostandardized concepts for response evaluation have been
established so far to make studies easier comparable.Clinical, histopathological, and metabolic response classi-fications have been reported for gastric cancer [3, 4, 8, 21,25, 63].
Clinical response
Clinical response evaluation by morphologic imagingtechniques has limitations especially in gastric cancer andis judged to be investigator dependent. For example, thewall thickness is critically dependent on the distension ofthe stomach during the examination. Criteria from theResponse Evaluation Criteria in Solid Tumor (RECIST)Group ratings, which use one-dimensional measurements,are in principle applicable for gastric cancer [64].
Only in few phase II trials with induction therapyRECIST criteria have been used so far [64–66]. Carefulclinical response evaluation by a combination of endolu-minal ultrasound, endoscopy, and CT scan used forrestaging is predictive of histopathological regression andprognosis in experienced centers [3, 4, 8, 21, 25].
Histopathological regression
The histopathological response is often called “goldstandard” for response evaluation. However, we have tobe aware that even histopathological response evaluation isinvestigator and experience dependent as well. Further-more, not in all patients the histopathological response willbe translated into an excellent prognosis. If the residualtumor is localized in the subserosal layer, patients maysuffer from an early recurrence and a poor prognosis due to
Table 4 Randomized studies for gastric cancer in Europe
Parameter MAGIC [15] p FFCD 9703 p EORTC 40954 [18] p
+CTx S +CTx S +CTx S
Patients 250 253 113 111 72 72
Resected 212 232 n.s. 109 110 n.s. 69 68 n.s.
R0 category 79% 70% 0.018 84% 73% 0.04 82% 67% 0.036
According to the surgeon Histopathologically Histopathologically
pT012 52% 37% 0.002 42% 32% 0.16 66% 50% 0.113
pN0 31% 27% n.s 33% 20% 0.054 39% 19% 0.018
Preoperative CTx 86% 87% 65.2%
CTx completed 42% 50% 65.2%
Mortality 6% 6% n.s 5% 4% n.s 4.3% 1.5% n.s
OS months (log rank) 0.009 0.021 64.6 52.5 0.466
PFS (log rank) <0.001 0.0033 0.200
2-year survival 72.7% 69.9%
5-year survival 36% 23% 38% 24%
CTx chemotherapy, S surgery alone, p p values, n.s. not significant, pT pT category, pN pN category, OS overall survival, PFS progression freesurvival
Langenbecks Arch Surg (2011) 396:743–758 751

an advanced ypT category despite of less than 10% residualtumor.
Although similar criteria for histopathological regressionhave been used in several studies, histopathological
response is not standardized so far. A modified regressionscore of Mandard et al. [67], who described first histopath-ological regression for esophageal cancer after chemo-radiotherapy, was published by Becker et al. for gastric
a
b
(years)
0 1 2 3 4 5 6 7
0
10
20
30
40
50
60
70
80
90
100
O N Number of patients at risk : Treatment35 72 58 48 34 20 11 4
32 72 61 49 41 29 15 6
Surgery alone
CT and surgery
Overall Logrank test: p=0.466
c
Fig. 5 a MAGIC study [15]:ECF perioperative versus sur-gery alone (p=0.009; 5-yearsurvival 36% versus 23%).b FFCD 9703 study: 5-Fu/cis-platin perioperative versus sur-gery alone (p=0.021, 5-yearsurvival 38% versus 24%).c EORTC 40954 [18]: 5-FU/cisplatin/leucovorin preoperativeversus surgery alone (p=0.466,2-year survival 64.6% versus52.5%)
Langenbecks Arch Surg (2011) 396:743–758752

cancer after chemotherapy (Fig. 6) [63]. Applying thisscoring system patients with less than 10% residual tumorcells after neoadjuvant treatment is classified as histopath-ological responders (score 1a: complete response and score1b: less than 10% residual tumor cells). In contrast, Shah etal. defined even patients with less than 50% residual tumorcells as histopathological responders [68]. Both regressionscores are strongly correlated with prognosis. However, ahomogenization of the scoring systems used for clinical andhistopathological response evaluation would be desirable inthe future to make studies with preoperative chemotherapyeasier comparable with each other.
Early response evaluation
Since no pretherapeutic molecular markers for the predic-tion of response and/or prognosis are available for clinicalroutine so far, FDG-PET has been tested for the predictionof response and prognosis in esophageal cancer since 1998at the Technische Universität München [69]. Measurementsof early changes in tumor glucose uptake after only 2 weeksof induction therapy by the use of FDG-PET have shownreproducible results that can be used for the prediction ofclinical and histopathological response after the end ofneoadjuvant treatment in adenocarcinomas of the esoph-agogastric junction types I and II[69, 70] (Fig. 7). Thecutoff value of a decrease of more than 35% of the initialSUV after only 2 weeks of induction therapy whichpredicted clinical and histopathological response andprognosis of the patients was prospectively validated [70].
This cutoff was chosen to predict nonresponding patientswith high accuracy to avoid toxic, expensive, and ineffec-tive treatment. After the prospective validation of thiscutoff, metabolic response after 2 weeks was used to tailortreatment to the individual patient within the MetabolicResponse Evaluation for Individualisation of NeoadjuvantChemotherapy in Oesophageal and Oesophagogastric Ad-enocarcinoma trial [62]. In metabolic nonrespondingpatients in which neoadjuvant treatment was stopped afteronly 2 weeks of chemotherapy, the median survival was28 months [62] compared to 18 months in the historicalcontrol with chemotherapy over 3 months [70]. Theseresults have to be interpreted with caution, but stoppingchemotherapy in nonresponding patients seems not toimpair the outcome of those patients. However, in gastriccancer, the early response assessment with FDG-PET ismore challenging than in esophageal cancer of the
Fig. 6 Patients prognosis inrespect of histopathologicalresponse [63] to the neoadjuvanttreatment (p<0.001). Blue,regression 1a, no residual tumor,n=17. Red, regression 1b, <10%residual tumor, n=73. Brown,regression 2, 10–50% residualtumor, n=107. Purple, regres-sion 3, >50% residual tumor,n=177
PET
Zeit (Wochen)
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Cycle 1 Cycle 2
Resection
Staging CT/EGD/EUS
CTx
-1
Prospective evaluation: Cut-off: –35%
PET: Change of SUV during CTx
Fig. 7 Schedule for early response evaluation by metabolic imagingin adenocarcinomas of the esophagus and stomach [8, 25, 62, 69, 70,76, 80]
Langenbecks Arch Surg (2011) 396:743–758 753

esophagogastric junction types I and II because a relativelyhigh percentage of diffuse type gastric cancer is not FDGavid [43, 44, 52, 71, 72]. In 2003, Ott et al. showed, usingthe same methods as in AEG I and II for gastric cancer, thatthe prediction of response and prognosis seems to befeasible in gastric cancer if the tumor is FDG avid. Thecutoff of 35% decrease of the initial FDG uptake after2 weeks of CTx was a surrogate for response and improvedprognosis in this patients’ population [73]. However, morethan 50% of the tumors was localized in the proximal third,and the patient’s number was relatively small. Thisprospectively established cutoff was further validated in alarger patient cohort with almost 30% FDG non-avidtumors [74]. Interestingly, survival data suggested threeindependent prognostic groups: metabolic responders,metabolic non-responders, and non-FDG avid patients, thuscomplicating the early response assessment with FDG [74].The prognosis of FDG non-avid tumors was in-betweenmetabolic responding and nonresponding tumors (Fig. 8),but the prospective results were less convincing than inadenocarcinomas of the esophagogastric junction types Iand II. Tailoring of treatment in gastric cancer seems not tobe possible by FDG-PET. A tracer that may complementthe information of FDG in gastric cancer is the proliferationmarker 18F-fluorothymidine (FLT) [7, 75]. FLT-PET had ahigher sensitivity than FDG and could visualize all locallyadvanced gastric cancers with sufficient contrast, even insignet ring cell carcinomas in two recently publishedstudies [7, 75]. Not yet published data on 45 patientsrevealed only the FLT mean value after 2 weeks and theLauren classification as independent prognostic factors. Incontrast to the studies presented above, a decrease of more
than 35% of the FDG uptake compared to baseline afteronly 2 weeks of chemotherapy was neither predictive forresponse nor prognosis [73, 74]. None of the other analyzedparameters of FDG or FLT-PET at any time point wasassociated with either clinical or histopathological response.
Response prediction
Tumor-dependent parameters as well as constitutionalfactors like polymorphisms have been investigated for theirpredictive value in neoadjuvantly treated gastric cancer.None of the tumor-related factors like p53 [31], micro-satellite instability [26, 31], or methylation [28] is prospec-tively tested and feasible for response prediction in clinicalroutine. A risk stratification for patients responding tochemotherapy might be possible by the histone deacetylasetype I [27]. Some polymorphisms in chemotherapy-relatedgenes are associated with prognosis, not with response [29,30, 76], but are far away from clinical relevance.
Incomplete (R1) resections
The question how to treat patients best with residual tumor(R1 resection) cannot clearly be answered based on theliterature [77]. The decision on an additive chemoradio-therapy is based on the localization of the residual tumor,the postoperative performance status of the patient, and hisrisk factors for systemic and local tumor progression.
Patterns of recurrence
Knowledge about time and patterns of recurrence facilitatespostoperative treatment and follow-up of the patients. Ingastric cancer, three main types of recurrence exist:
& Locoregional recurrence& Distant metastases and& Peritoneal carcinomatosis
Locoregional recurrences can occur in three localizations:
& Intraluminal at the anastomosis (consequence of aninadequate proximal or distal safety margin)
& Extraluminal (“third dimension”; insufficient radicalityoften due to anatomical reasons such as vicinity to theceliac trunk, etc.)
& Recurrence of the lymphatic drainage (“fourth dimen-sion”; to avoid this type of recurrence, a high number oflymph nodes removed is necessary)
An interesting analysis was performed by the group ofSloan Kettering [78]. Recurrence after complete resection
Fig. 8 Prognosis of patients with locally advanced gastric canceraccording to metabolic response. Only metabolic responder andnonresponder have a statistically significant different prognosis (p=0.037) [8]. NE FDG non-avid, R metabolic responder, NR metabolicnonresponder
Langenbecks Arch Surg (2011) 396:743–758754
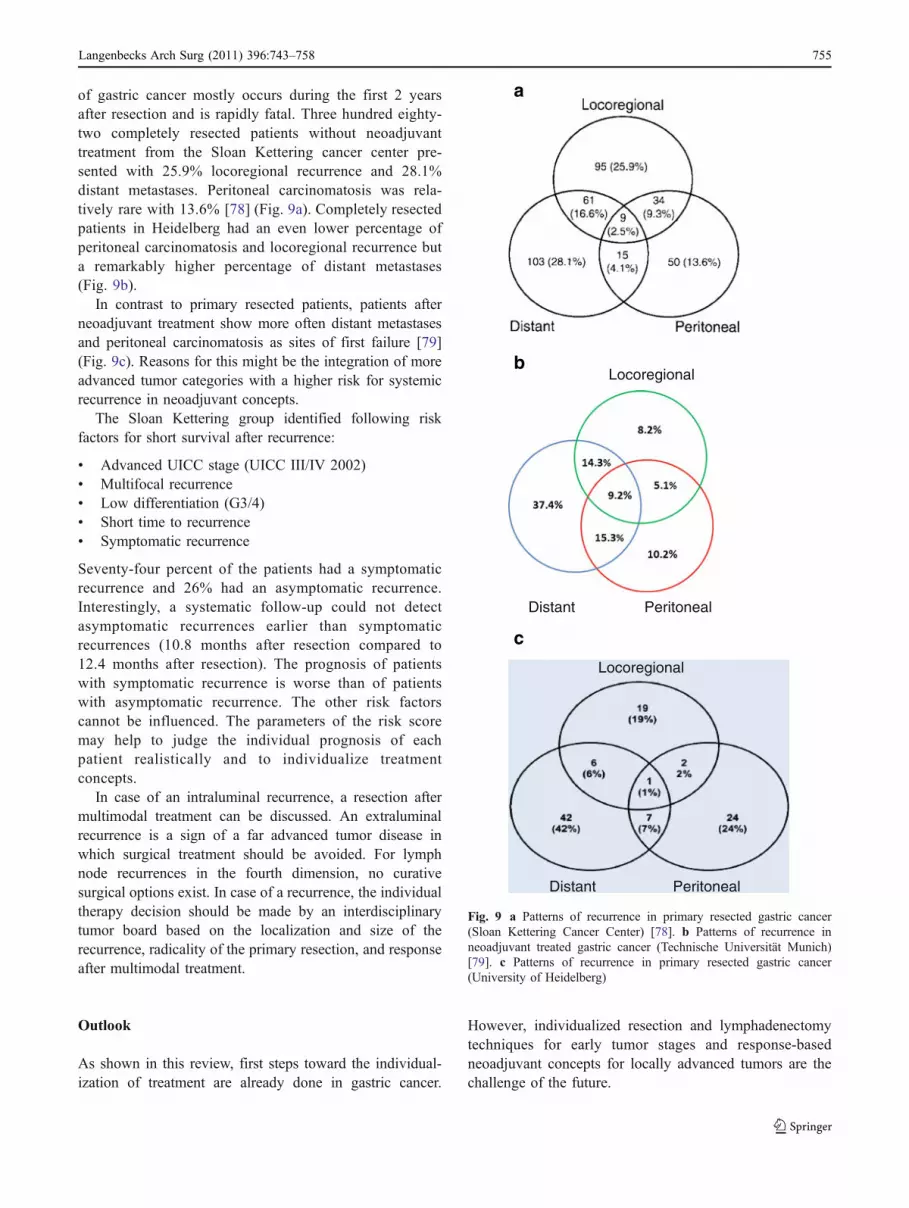
of gastric cancer mostly occurs during the first 2 yearsafter resection and is rapidly fatal. Three hundred eighty-two completely resected patients without neoadjuvanttreatment from the Sloan Kettering cancer center pre-sented with 25.9% locoregional recurrence and 28.1%distant metastases. Peritoneal carcinomatosis was rela-tively rare with 13.6% [78] (Fig. 9a). Completely resectedpatients in Heidelberg had an even lower percentage ofperitoneal carcinomatosis and locoregional recurrence buta remarkably higher percentage of distant metastases(Fig. 9b).
In contrast to primary resected patients, patients afterneoadjuvant treatment show more often distant metastasesand peritoneal carcinomatosis as sites of first failure [79](Fig. 9c). Reasons for this might be the integration of moreadvanced tumor categories with a higher risk for systemicrecurrence in neoadjuvant concepts.
The Sloan Kettering group identified following riskfactors for short survival after recurrence:
& Advanced UICC stage (UICC III/IV 2002)& Multifocal recurrence& Low differentiation (G3/4)& Short time to recurrence& Symptomatic recurrence
Seventy-four percent of the patients had a symptomaticrecurrence and 26% had an asymptomatic recurrence.Interestingly, a systematic follow-up could not detectasymptomatic recurrences earlier than symptomaticrecurrences (10.8 months after resection compared to12.4 months after resection). The prognosis of patientswith symptomatic recurrence is worse than of patientswith asymptomatic recurrence. The other risk factorscannot be influenced. The parameters of the risk scoremay help to judge the individual prognosis of eachpatient realistically and to individualize treatmentconcepts.
In case of an intraluminal recurrence, a resection aftermultimodal treatment can be discussed. An extraluminalrecurrence is a sign of a far advanced tumor disease inwhich surgical treatment should be avoided. For lymphnode recurrences in the fourth dimension, no curativesurgical options exist. In case of a recurrence, the individualtherapy decision should be made by an interdisciplinarytumor board based on the localization and size of therecurrence, radicality of the primary resection, and responseafter multimodal treatment.
Outlook
As shown in this review, first steps toward the individual-ization of treatment are already done in gastric cancer.
However, individualized resection and lymphadenectomytechniques for early tumor stages and response-basedneoadjuvant concepts for locally advanced tumors are thechallenge of the future.
Locoregional
Distant Peritoneal
Locoregional
Distant Peritoneal
a
b
c
Fig. 9 a Patterns of recurrence in primary resected gastric cancer(Sloan Kettering Cancer Center) [78]. b Patterns of recurrence inneoadjuvant treated gastric cancer (Technische Universität Munich)[79]. c Patterns of recurrence in primary resected gastric cancer(University of Heidelberg)
Langenbecks Arch Surg (2011) 396:743–758 755

Conflicts of interest None.
References
1. Monig SP, SchroderW, Baldus SE, Holscher AH (2002) Preoperativelymph-node staging in gastrointestinal cancer—correlation betweensize and tumor stage. Onkologie 25(4):342–344
2. Kitagawa Y, Kitajima M (2006) Gastroesophageal carcinoma:individualized surgical therapy. Surg Oncol Clin N Am 15(4):793–802. doi:10.1016/j.soc.2006.07.010
3. Schuhmacher CP, Fink U, Becker K, Busch R, Dittler HJ, MuellerJ, Siewert JR (2001) Neoadjuvant therapy for patients with locallyadvanced gastric carcinoma with etoposide, doxorubicin, andcisplatinum. Closing results after 5 years of follow-up. Cancer 91(5):918–927. doi:10.1002/1097-0142(20010301)91:5<918::AID-CNCR1081>3.0.CO;2-W
4. Ott K, Sendler A, Becker K, Dittler HJ, Helmberger H, Busch R,Kollmannsberger C, Siewert JR, Fink U (2003) Neoadjuvantchemotherapy with cisplatin, 5-FU, and leucovorin (PLF) inlocally advanced gastric cancer: a prospective phase II study.Gastric Cancer 6(3):159–167. doi:10.1007/s10120-003-0245-4
5. Barbour AP, Rizk NP, Gerdes H, Bains MS, Rusch VW, BrennanMF, Coit DG (2007) Endoscopic ultrasound predicts outcomes forpatients with adenocarcinoma of the gastroesophageal junction. JAm Coll Surg 205(4):593–601. doi:10.1016/j.jamcollsurg.2007.05.010
6. Stahl A, Ott K, Weber WA, Becker K, Link T, Siewert JR,Schwaiger M, Fink U (2003) FDG PET imaging of locallyadvanced gastric carcinomas: correlation with endoscopic andhistopathological findings. Eur J Nucl Med Mol Imaging 30(2):288–295. doi:10.1007/s00259-002-1029-5
7. Herrmann K, Ott K, Buck AK, Lordick F, Wilhelm D, SouvatzoglouM, Becker K, Schuster T, Wester HJ, Siewert JR, Schwaiger M,Krause BJ (2007) Imaging gastric cancer with PET and theradiotracers 18 F-FLT and 18 F-FDG: a comparative analysis. J NuclMed 48(12):1945–1950. doi:10.2967/jnumed.107.044867
8. Ott K, Herrmann K, Lordick F, Wieder H, Weber WA, Becker K,Buck AK, Dobritz M, Fink U, Ulm K, Schuster T, Schwaiger M,Siewert JR, Krause BJ (2008) Early metabolic response evaluationby fluorine-18 fluorodeoxyglucose positron emission tomographyallows in vivo testing of chemosensitivity in gastric cancer: long-term results of a prospective study. Clin Cancer Res 14(7):2012–2018. doi:10.1158/1078-0432.CCR-07-0934
9. Rosenberg R, Nekarda H, Bauer P, Schenck U, Hoefler H, SiewertJR (2006) Free peritoneal tumour cells are an independentprognostic factor in curatively resected stage IB gastric carcinoma.Br J Surg 93(3):325–331. doi:10.1002/bjs.5196
10. Feussner H, Hartl F (2006) Staging laparoscopy in oncology.Chirurg 77(11):971–980. doi:10.1007/s00104-006-1259-3
11. Lorenzen S, Panzram B, Rosenberg R, Nekarda H, Becker K,Schenk U, Hofler H, Siewert JR, Jager D, Ott K (2010) Prognosticsignificance of free peritoneal tumor cells in the peritoneal cavitybefore and after neoadjuvant chemotherapy in patients with gastriccarcinoma undergoing potentially curative resection. Ann SurgOncol 17(10):2733–2739. doi:10.1245/s10434-010-1090-4
12. Burian M, Stein HJ, Sendler A, Feith M, Siewert JR (2004)Sentinel lymph node mapping in gastric and esophageal carcino-mas. Chirurg 75(8):756–760. doi:10.1007/s00104-004-0909-6
13. Burian M, Stein HJ, Sendler A, Piert M, Nahrig J, Feith M,Siewert JR (2004) Sentinel node detection in Barrett’s and cardiacancer. Ann Surg Oncol 11(3 Suppl):255S–258S
14. Roder JD, Bottcher K, Siewert JR, Busch R, Hermanek P, MeyerHJ (1993) Prognostic factors in gastric carcinoma. Results of theGerman Gastric Carcinoma Study 1992. Cancer 72(7):2089–2097
15. Cunningham D, Allum WH, Stenning SP, Thompson JN, Van deVelde CJ, Nicolson M, Scarffe JH, Lofts FJ, Falk SJ, Iveson TJ,Smith DB, Langley RE, Verma M, Weeden S, Chua YJ,Participants MT (2006) Perioperative chemotherapy versus sur-gery alone for resectable gastroesophageal cancer. N Engl J Med355(1):11–20. doi:10.1056/NEJMoa055531
16. Macdonald JS, Smalley SR, Benedetti J, Hundahl SA, Estes NC,Stemmermann GN, Haller DG, Ajani JA, Gunderson LL, JessupJM, Martenson JA (2001) Chemoradiotherapy after surgerycompared with surgery alone for adenocarcinoma of the stomachor gastroesophageal junction. N Engl J Med 345(10):725–730.doi:10.1056/NEJMoa010187
17. Sakuramoto S, Sasako M, Yamaguchi T, Kinoshita T, Fujii M,Nashimoto A, Furukawa H, Nakajima T, Ohashi Y, Imamura H,Higashino M, Yamamura Y, Kurita A, Arai K (2007) Adjuvantchemotherapy for gastric cancer with S-1, an oral fluoropyrimi-dine. N Engl J Med 357(18):1810–1820. doi:10.1056/NEJMoa072252
18. Schuhmacher C, Gretschel S, Lordick F, Reichardt P, HohenbergerW, Eisenberger CF, Haag C, Mauer ME, Hasan B, Welch J, Ott K,Hoelscher A, Schneider PM, Bechstein W, Wilke H, Lutz MP,Nordlinger B, Van Cutsem E, Siewert JR, Schlag PM (2010)Neoadjuvant chemotherapy compared with surgery alone for locallyadvanced cancer of the stomach and cardia: European Organisationfor research and treatment of cancer randomized trial 40954. J ClinOncol 28:5210–5218. doi:10.1200/JCO. 2009.26.6114
19. Siewert JR, Schuhmacher C, Fink U (1998) The German EORTCStudy of neoadjuvant therapy of stomach carcinoma. LangenbecksArch Chir Suppl Kongressbd 115:717–719
20. Lowy AM, Mansfield PF, Leach SD, Pazdur R, Dumas P, AjaniJA (1999) Response to neoadjuvant chemotherapy best predictssurvival after curative resection of gastric cancer. Ann Surg 229(3):303–308
21. Fink U, Schuhmacher C, Stein HJ, Busch R, Feussner H, DittlerHJ, Helmberger A, Bottcher K, Siewert JR (1995) Preoperativechemotherapy for stage III–IV gastric carcinoma: feasibility,response and outcome after complete resection. Br J Surg 82(9):1248–1252
22. Shah MA, Ramanathan RK, Ilson DH, Levnor A, D’Adamo D,O’Reilly E, Tse A, Trocola R, Schwartz L, Capanu M, SchwartzGK, Kelsen DP (2006) Multicenter phase II study of irinotecan,cisplatin, and bevacizumab in patients with metastatic gastric orgastroesophageal junction adenocarcinoma. J Clin Oncol 24(33):5201–5206. doi:10.1200/JCO.2006.08.0887
23. Becker K, Fink U, Ott K, Busch R, Siewert JR, Hofler H (2001)How can the effectiveness of multimodality therapy concepts beevaluated? From the viewpoint of the pathologist. KongressbdDtsch Ges Chir Kongr 118:58–62
24. Fink U, Ott K, Weber W, Siewert JR (2002) Neoadjuvanttherapeutic principles guided by response prediction and evalua-tion. Kongressbd Dtsch Ges Chir Kongr 119:829–833
25. Ott K, Fink U, Becker K, Stahl A, Dittler HJ, Busch R, Stein H,Lordick F, Link T, Schwaiger M, Siewert JR, Weber WA (2003)Prediction of response to preoperative chemotherapy in gastriccarcinoma by metabolic imaging: results of a prospective trial. JClin Oncol 21(24):4604–4610. doi:10.1200/JCO.2003.06.574
26. Grundei T, Vogelsang H, Ott K, Mueller J, Scholz M, Becker K,Fink U, Siewert JR, Hofler H, Keller G (2000) Loss ofheterozygosity and microsatellite instability as predictive markersfor neoadjuvant treatment in gastric carcinoma. Clin Cancer Res 6(12):4782–4788
27. Mutze K, Langer R, Becker K, Ott K, Novotny A, Luber B,Hapfelmeier A, Gottlicher M, Hofler H, Keller G (2010) Histonedeacetylase (HDAC) 1 and 2 expression and chemotherapy ingastric cancer. Ann Surg Oncol 17:3336–3343. doi:10.1245/s10434-010-1182-1
Langenbecks Arch Surg (2011) 396:743–758756

28. Napieralski R, Ott K, Kremer M, Becker K, Boulesteix AL,Lordick F, Siewert JR, Hofler H, Keller G (2007) Methylation oftumor-related genes in neoadjuvant-treated gastric cancer: relationto therapy response and clinicopathologic and molecular features.Clin Cancer Res 13(17):5095–5102. doi:10.1158/1078-0432.CCR-07-0241
29. Ott K, Lordick F, Becker K, Ulm K, Siewert J, Hofler H, Keller G(2008) Glutathione-S-transferase P1, T1 and M1 genetic poly-morphisms in neoadjuvant-treated locally advanced gastric cancer:GSTM1-present genotype is associated with better prognosis incompletely resected patients. Int J Colorectal Dis 23(8):773–782.doi:10.1007/s00384-008-0490-4
30. Ott K, Vogelsang H, Marton N, Becker K, Lordick F, Kobl M,Schuhmacher C, Novotny A, Mueller J, Fink U, Ulm K, SiewertJR, Hofler H, Keller G (2006) The thymidylate synthase tandemrepeat promoter polymorphism: a predictor for tumor-relatedsurvival in neoadjuvant treated locally advanced gastric cancer.Int J Cancer 119(12):2885–2894. doi:10.1002/ijc.22235
31. Ott K, Vogelsang H, Mueller J, Becker K, Muller M, Fink U,Siewert JR, Hofler H, Keller G (2003) Chromosomal instabilityrather than p53 mutation is associated with response to neo-adjuvant cisplatin-based chemotherapy in gastric carcinoma. ClinCancer Res 9(6):2307–2315
32. Siewert JR, Bottcher K, Stein HJ, Roder JD, Busch R (1995)Problem of proximal third gastric carcinoma. World J Surg 19(4):523–531
33. Ott K, Bader FG, Lordick F, Feith M, Bartels H, Siewert JR(2009) Surgical factors influence the outcome after Ivor-Lewisesophagectomy with intrathoracic anastomosis for adenocarcino-ma of the esophagogastric junction: a consecutive series of 240patients at an experienced center. Ann Surg Oncol 16(4):1017–1025. doi:10.1245/s10434-009-0336-5
34. Barbour AP, Rizk NP, Gonen M, Tang L, Bains MS, Rusch VW,Coit DG, Brennan MF (2007) Adenocarcinoma of the gastro-esophageal junction: influence of esophageal resection margin andoperative approach on outcome. Ann Surg 246(1):1–8.doi:10.1097/01.sla.0000255563.65157.d2
35. Bozzetti F, Marubini E, Bonfanti G, Miceli R, Piano C, Gennari L(1999) Subtotal versus total gastrectomy for gastric cancer: five-year survival rates in a multicenter randomized Italian trial. ItalianGastrointestinal Tumor Study Group. Ann Surg 230(2):170–178
36. Gouzi JL, Huguier M, Fagniez PL, Launois B, Flamant Y, LacaineF, Paquet JC, Hay JM (1989) Total versus subtotal gastrectomy foradenocarcinoma of the gastric antrum. A French prospectivecontrolled study. Ann Surg 209(2):162–166
37. Bonenkamp JJ, Songun I, Hermans J, Sasako M, Welvaart K,Plukker JT, van Elk P, Obertop H, Gouma DJ, Taat CW et al(1995) Randomised comparison of morbidity after D1 and D2dissection for gastric cancer in 996 Dutch patients. Lancet 345(8952):745–748
38. Cuschieri A, Weeden S, Fielding J, Bancewicz J, Craven J,Joypaul V, Sydes M, Fayers P (1999) Patient survival after D1 andD2 resections for gastric cancer: long-term results of the MRCrandomized surgical trial. Surgical Co-operative Group. Br JCancer 79(9–10):1522–1530. doi:10.1038/sj.bjc.6690243
39. Hartgrink HH, van de Velde CJ, Putter H, Bonenkamp JJ, KleinKranenbarg E, Songun I, Welvaart K, van Krieken JH, Meijer S,Plukker JT, van Elk PJ, Obertop H, Gouma DJ, van Lanschot JJ,Taat CW, de Graaf PW, von Meyenfeldt MF, Tilanus H, Sasako M(2004) Extended lymph node dissection for gastric cancer: whomay benefit? Final results of the randomized Dutch gastric cancergroup trial. J Clin Oncol 22(11):2069–2077. doi:10.1200/JCO.2004.08.026
40. Sasako M, Sano T, Yamamoto S, Kurokawa Y, Nashimoto A,Kurita A, Hiratsuka M, Tsujinaka T, Kinoshita T, Arai K,Yamamura Y, Okajima K (2008) D2 lymphadenectomy alone or
with para-aortic nodal dissection for gastric cancer. N Engl J Med359(5):453–462. doi:10.1056/NEJMoa0707035
41. Wu CW, Hsiung CA, Lo SS, Hsieh MC, Chen JH, Li AF, Lui WY,Whang-Peng J (2006) Nodal dissection for patients with gastriccancer: a randomised controlled trial. Lancet Oncol 7(4):309–315.doi:10.1016/S1470-2045(06)70623-4
42. Yun M, Lim JS, Noh SH, Hyung WJ, Cheong JH, Bong JK, ChoA, Lee JD (2005) Lymph node staging of gastric cancer using (18)F-FDG PET: a comparison study with CT. J Nucl Med 46(10):1582–1588
43. Chen J, Cheong JH, Yun MJ, Kim J, Lim JS, Hyung WJ, Noh SH(2005) Improvement in preoperative staging of gastric adenocar-cinoma with positron emission tomography. Cancer 103(11):2383–2390. doi:10.1002/cncr.21074
44. Kim SK, Kang KW, Lee JS, Kim HK, Chang HJ, Choi JY, LeeJH, Ryu KW, Kim YW, Bae JM (2006) Assessment of lymphnode metastases using 18F-FDG PET in patients with advancedgastric cancer. Eur J Nucl Med Mol Imaging 33(2):148–155.doi:10.1007/s00259-005-1887-8
45. Mukai K, Ishida Y, Okajima K, Isozaki H, Morimoto T,Nishiyama S (2006) Usefulness of preoperative FDG-PET fordetection of gastric cancer. Gastric Cancer 9(3):192–196.doi:10.1007/s10120-006-0374-7
46. Siewert JR, Bottcher K, Stein HJ, Roder JD (1998) Relevantprognostic factors in gastric cancer: ten-year results of the GermanGastric Cancer Study. Ann Surg 228(4):449–461
47. Siewert JR, Bottcher K, Roder JD, Busch R, Hermanek P, MeyerHJ (1993) Prognostic relevance of systematic lymph nodedissection in gastric carcinoma. German Gastric Carcinoma StudyGroup. Br J Surg 80(8):1015–1018
48. Barbour AP, Rizk NP, Gonen M, Tang L, Bains MS, Rusch VW,Coit DG, Brennan MF (2007) Lymphadenectomy for adenocarci-noma of the gastroesophageal junction (GEJ): impact of adequatestaging on outcome. Ann Surg Oncol 14(2):306–316.doi:10.1245/s10434-006-9166-x
49. Marchet A, Mocellin S, Ambrosi A, Morgagni P, Garcea D,Marrelli D, Roviello F, de Manzoni G, Minicozzi A, Natalini G,De Santis F, Baiocchi L, Coniglio A, Nitti D (2007) The ratiobetween metastatic and examined lymph nodes (N ratio) is anindependent prognostic factor in gastric cancer regardless of thetype of lymphadenectomy: results from an Italian multicentricstudy in 1853 patients. Ann Surg 245(4):543–552. doi:10.1097/01.sla.0000250423.43436.e1
50. Schuhmacher C, Novotny A, Ott K, Feith M, Siewert JR (2007)[Lymphadenectomy with tumors of the upper gastrointestinaltract]. Chirurg 78(3):203–206. doi:10.1007/s00104-007-1307-7,208–212, 214–206
51. Ott K, Lordick F, Herrmann K, Krause BJ, Schuhmacher C,Siewert JR (2008) The new credo: induction chemotherapy inlocally advanced gastric cancer: consequences for surgicalstrategies. Gastric Cancer 11(1):1–9. doi:10.1007/s10120-007-0448-1
52. Yoshioka T, Yamaguchi K, Kubota K, Saginoya T, Yamazaki T,Ido T, Yamaura G, Takahashi H, Fukuda H, Kanamaru R (2003)Evaluation of 18F-FDG PET in patients with advanced, meta-static, or recurrent gastric cancer. J Nucl Med 44(5):690–699
53. Bonenkamp JJ, Songun I, Hermans J, van de Velde CJ (1996)Prognostic value of positive cytology findings from abdominalwashings in patients with gastric cancer. Br J Surg 83(5):672–674
54. Hundahl SA, Peeters KC, Kranenbarg EK, Hartgrink H, van deVelde CJ (2007) Improved regional control and survival with “lowMaruyama Index” surgery in gastric cancer: autopsy findings fromthe Dutch D1-D2 Trial. Gastric Cancer 10(2):84–86. doi:10.1007/s10120-007-0426-7
55. Peeters KC, Hundahl SA, Kranenbarg EK, Hartgrink H, van deVelde CJ (2005) Low Maruyama index surgery for gastric cancer:
Langenbecks Arch Surg (2011) 396:743–758 757

blinded reanalysis of the Dutch D1-D2 trial. World J Surg 29(12):1576–1584. doi:10.1007/s00268-005-7907-9
56. Sasako M, Sano T, Yamamoto S, Sairenji M, Arai K, Kinoshita T,Nashimoto A, Hiratsuka M (2006) Left thoracoabdominalapproach versus abdominal-transhiatal approach for gastric cancerof the cardia or subcardia: a randomised controlled trial. LancetOncol 7(8):644–651. doi:10.1016/S1470-2045(06)70766-5
57. Stein HJ, Feith M, Siewert JR (2000) Cancer of the esophago-gastric junction. Surg Oncol 9(1):35–41. doi:S0960-7404(00)00021-9
58. Stein HJ, Feith M, Mueller J, Werner M, Siewert JR (2000)Limited resection for early adenocarcinoma in Barrett’s esopha-gus. Ann Surg 232(6):733–742
59. Wang XB, Yang LT, Zhang ZW, Guo JM, Cheng XD (2008)Pancreaticoduodenectomy for advanced gastric cancer withpancreaticoduodenal region involvement. World J Gastroenterol14(21):3425–3429
60. Wu CW, Chang IS, Lo SS, Hsieh MC, Chen JH, Lui WY, Whang-Peng J (2006) Complications following D3 gastrectomy: post hocanalysis of a randomized trial. World J Surg 30(1):12–16.doi:10.1007/s00268-005-7951-5
61. Ajani JA, Rodriguez W, Bodoky G, Moiseyenko V, Lichinitser M,Gorbunova V, Vynnychenko I, Garin A, Lang I, Falcon S (2010)Multicenter phase III comparison of cisplatin/S-1 with cisplatin/infusional fluorouracil in advanced gastric or gastroesophagealadenocarcinoma study: the FLAGS trial. J Clin Oncol 28(9):1547–1553. doi:10.1200/JCO.2009.25.4706
62. Lordick F, Ott K, Krause BJ, Weber WA, Becker K, Stein HJ,Lorenzen S, Schuster T, Wieder H, Herrmann K, Bredenkamp R,Hofler H, Fink U, Peschel C, Schwaiger M, Siewert JR (2007)PET to assess early metabolic response and to guide treatment ofadenocarcinoma of the oesophagogastric junction: the MUNICONphase II trial. Lancet Oncol 8(9):797–805. doi:10.1016/S1470-2045(07)70244-9
63. Becker K, Mueller JD, Schulmacher C, Ott K, Fink U, Busch R,Bottcher K, Siewert JR, Hofler H (2003) Histomorphology andgrading of regression in gastric carcinoma treated with neo-adjuvant chemotherapy. Cancer 98(7):1521–1530. doi:10.1002/cncr.11660
64. Park JO, Lee SI, Song SY, Kim K, Kim WS, Jung CW, Park YS,Im YH, Kang WK, Lee MH, Lee KS, Park K (2003) Measuringresponse in solid tumors: comparison of RECIST and WHOresponse criteria. Jpn J Clin Oncol 33(10):533–537
65. Yoshida S, Miyata Y, Ohtsu A, Boku N, Shirao K, Shimada Y(2000) Significance of and problems in adopting responseevaluation criteria in solid tumor RECIST for assessing anticancereffects of advanced gastric cancer. Gastric Cancer 3(3):128–133
66. Burge ME, Smith D, Topham C, Jackson DP, Anthoney DA,Halstead F, Seymour MT (2006) A phase I and II study of 2-weekly irinotecan with capecitabine in advanced gastroesophagealadenocarcinoma. Br J Cancer 94(9):1281–1286. doi:10.1038/sj.bjc.6603084
67. Mandard AM, Dalibard F, Mandard JC, Marnay J, Henry-AmarM, Petiot JF, Roussel A, Jacob JH, Segol P, Samama G et al(1994) Pathologic assessment of tumor regression after preoper-ative chemoradiotherapy of esophageal carcinoma. Clinicopatho-logic correlations. Cancer 73(11):2680–2686
68. Shah MA, Yeung H, Coit D, Trocola R, Ilson D, Randazzo J,Tang L, Brennan M, Divgi C, Kelsen DP (2007) A phase IIstudy of preoperative chemotherapy with irinotecan (CPT) and
cisplatin (CIS) for gastric cancer(NCI 5917): FDG-PET/CTpredicts patient outcome. ASCO Meeting Abstracts 25(18_suppl):4502
69. Weber WA, Ott K, Becker K, Dittler HJ, Helmberger H, Avril NE,Meisetschlager G, Busch R, Siewert JR, Schwaiger M, Fink U(2001) Prediction of response to preoperative chemotherapy inadenocarcinomas of the esophagogastric junction by metabolicimaging. J Clin Oncol 19(12):3058–3065
70. Ott K, Weber WA, Lordick F, Becker K, Busch R, Herrmann K,Wieder H, Fink U, Schwaiger M, Siewert JR (2006) Metabolicimaging predicts response, survival, and recurrence in adenocar-cinomas of the esophagogastric junction. J Clin Oncol 24(29):4692–4698. doi:10.1200/JCO.2006.06.7801
71. Berger AC, Farma J, Scott WJ, Freedman G, Weiner L, Cheng JD,Wang H, Goldberg M (2005) Complete response to neoadjuvantchemoradiotherapy in esophageal carcinoma is associated withsignificantly improved survival. J Clin Oncol 23(19):4330–4337.doi:10.1200/JCO.2005.05.017
72. Mochiki E, Kuwano H, Katoh H, Asao T, Oriuchi N, Endo K(2004) Evaluation of 18F-2-deoxy-2-fluoro-D-glucose positronemission tomography for gastric cancer. World J Surg 28(3):247–253. doi:10.1007/s00268-003-7191-5
73. Arnott SJ, Duncan W, Gignoux M, Hansen HS, Launois B,Nygaard K, Parmar MK, Rousell A, Spilopoulos G, Stewart G,Tierney JF, Wang M, Rhugang Z (2005) Preoperative radiotherapyfor esophageal carcinoma. Cochrane Database Syst Rev (4):CD001799. doi:10.1002/14651858.CD001799.pub2
74. Bader FG, Lordick F, Fink U, Becker K, Hofler H, Busch R,Siewert JR, Ott K (2008) Paclitaxel in the neoadjuvant treatmentfor adeno carcinoma of the distal esophagus (AEG I). Acomparison of two phase II trials with long-term follow-up.Onkologie 31(7):366–372. doi:10.1159/000135515
75. Kameyama R, Yamamoto Y, Izuishi K, Takebayashi R, HagiikeM, Murota M, Kaji M, Haba R, Nishiyama Y (2009) Detection ofgastric cancer using 18F-FLT PET: comparison with 18F-FDGPET. Eur J Nucl Med Mol Imaging 36(3):382–388. doi:10.1007/s00259-008-0970-3
76. Lorenzen S, Panzram B, Keller G, Lordick F, Herrmann K,Becker K, Langer R, Schwaiger M, Siewert JR, Ott K (2010)Association of the VEGF 936C> T polymorphism with FDGuptake, clinical, histopathological, and metabolic response inpatients with adenocarcinomas of the esophagogastric junction.Mol Imaging Biol. doi:10.1007/s11307-010-0330-0
77. Lordick F, Ott K, Novotny A, Schuhmacher C, Siewert JR (2007)R1 resection in the surgery of upper gastrointestinal tumors:relevance and therapeutic consequences. Chirurg 78(9):792–801.doi:10.1007/s00104-007-1381-x
78. D’Angelica M, Gonen M, Brennan MF, Turnbull AD, Bains M,Karpeh MS (2004) Patterns of initial recurrence in completelyresected gastric adenocarcinoma. Ann Surg 240(5):808–816.doi:00000658-200411000-00012
79. Siewert JR, Lordick F, Ott K, Brucher BL, Rosenberg R (2006)Curative vs palliative strategies in locoregional recurrence ofgastrointestinal malignancies. Chirurg 77(3):227–235.doi:10.1007/s00104-006-1163-x
80. Siewert JR, Lordick F, Ott K, Stein HJ, Weber WA, Becker K,Peschel C, Fink U, Schwaiger M (2007) Induction chemotherapy inBarrett cancer: influence on surgical risk and outcome. Ann Surg 246(4):624–628. doi:10.1097/SLA.0b013e318155a7d1, discussion628–631
Langenbecks Arch Surg (2011) 396:743–758758





























