Embed Size (px)
Citation preview

REVIEW
Generation and maintenance of human memory cellsduring viral infection
Rabih Halwani & Mehrnoosh Doroudchi &Bader Yassine-Diab & Loury Janbazian & Yu Shi &Elias A. Said & Elias K. Haddad & Rafick-Pierre Sékaly
Received: 17 March 2006 /Accepted: 30 March 2006 / Published online: 12 September 2006# Springer-Verlag 2006
Abstract Long-term maintenance of memory T cell re-sponse is the hallmark of immune protection and hence theholy grail of most vaccine development studies. Persistentmemory cells, developed after either viral infection orvaccination, ensure the generation of an antiviral responseupon reexposure to the pathogen. During acute viralinfections, as in the case of measles and influenza viruses,strong T cell effector functions, which eradicate the virusand protect patients against reexposure, are achieved by thegeneration of persistent protective memory cells. However,in chronic infections, T cells drastically lose effectorfunctions before acquiring a memory phenotype. Chronicinfections can be categorized into infections where viremiais controlled and protective memory cells are maintained asin the case of EBV and CMV infections, or where the viruspersists and memory cells are exhausted and disrupted as inthe case of human immunodeficiency virus infection. In thisreview, we will discuss the different phenotypical andfunctional characteristics of memory cells subsets, theimportance of the role they play during acute and chronicinfections, and the mechanisms behind their effectivenessand persistence.
Keywords Effector memory Tcells .
Central memory Tcells . Acute viral infection .
Chronic viral infections
Memory: historical perspective and relevance
The major function of the immune system is to defend thehost against the invasion of microbial pathogens. Genera-tion of antiviral immunity and maintenance of recallresponses against various viruses results from the highlycontrolled interactions between the two arms of immunity,the innate and the adaptive immune systems. The innateimmune system can recognize pathogen-associated molec-ular patterns through pattern recognition receptors andmount a highly coordinated cascade of molecular inter-actions, which not only activate but also heighten thepotential to bias the ensuing adaptive phenotype [54]. Therecognition of antigens, their proper presentation andprocessing, will lead to the activation of specific adaptiveimmune responses that would control the infection. One ofthe hallmarks of the adaptive immune response is still itscapacity to develop memory against infectious pathogens.The central feature of immune memory is the ability ofmemory T cells to mediate faster, stronger, and moreeffective responses to secondary pathogen challenges thannaïve T cells [15]. Immunological memory-mediatedprotection was first described by the Greek historianThucydides. When describing the Peloponnesian war in430 B.C., he mentioned that the deadly plague of Athensnever attacked the same man twice [60]. This observationconstituted the basis of vaccination. The concept ofvaccination was first applied in China in the 16th century.Inoculation with dried smallpox pustules obtained from
Springer Semin Immun (2006) 28:197–208DOI 10.1007/s00281-006-0027-2
R. Halwani :M. Doroudchi :B. Yassine-Diab : L. Janbazian :Y. Shi : E. A. Said : E. K. Haddad : R.-P. SékalyLaboratoire d’Immunologie, Centre de Recherche du CHUM,Campus St.-Luc, Pavillon Edouard-Asselin, 264 Boulevard ReneLevesque Est, #1370D,Montréal, Québec H3C 3J7, Canada
R.-P. Sékaly (*)Centre de recherche du CHUM, Hôpital Saint-Luc,264, René-Lévesque est, Bureau 1317,Montréal, Québec H2X 1P1, Canadae-mail: [email protected]

infected individuals was used to protect from the disease[28]. The first scientific proof of vaccination was providedby Edward Jenner [32] in the late 1700s who demonstratedthat individuals immunized with the cowpox virus wereprotected from the disease caused by smallpox virus.Protective immune memory can persist for many yearsafter the initial antigenic exposure and in the absence ofreexposure to antigen. Measles immunity on the FaroeIslands (65 years ago) [52] and yellow fever immunity inVirginia (75 years ago) [64] are two such examples. Thisreview will be focused on the development of memoryT cells and their persistence in acute and chronic viralinfections. We will provide evidence on how latent virusesare able to subvert the immune system by interfering withthe development and persistence of memory T cells. One ofthe major obstacles in understanding the development ofmemory T cells was the incapacity to identify those cellsand to have molecular markers that allow us to track theirdevelopment and persistence. This topic will also beaddressed in this review.
Memory T cell homeostasis in healthy individuals
Subsets of memory T cells
Memory T cell population are subdivided into centralmemory and effector memory [25] cells based on: (1) theexpression of homing receptors that allow cells to migrateto secondary lymphoid organs vs nonlymphoid tissues and(2) their functional characteristics.
Phenotypes of subsets of memory T cells
Multiparametric flow cytometry has provided a major toolto facilitate the characterization of memory T cellssubsets. Naïve T cells are characterized by the expressionof CD45RA, CCR7, the costimulatory receptors CD28and CD27, and the lack of expression of cytolyticmolecules (granzyme, perforin, and CD107a). “Central”memory T cells (TCM), which home preferentially tolymph nodes, share several phenotypic properties withnaïve cells, except that they do not express CD45RA.As opposed to naïve cells, TCM can rapidly mediateeffector functions after restimulation and upregulateCD40L to a greater extent. Moreover, TCM cells arecharacterized by their ability to proliferate and to secretehigh levels of IL-2. “Effector” memory T cells (TEM) [25]migrate preferentially to peripheral tissues and do notexpress CD45RA nor CCR7 and depending on their stateof differentiation, they may or may not express CD27/CD28. TEM cells possess immediate effector functions(cytotoxicity and IFN-γ secretion) but have reduced ability
to proliferate and to secrete IL-2. Another subset termed “late”or “terminally” differentiated TEM, which is mostly found inCD8 T cells, express CD45RA but lack expression of CCR7,CD27, and CD28. These cells have potent effector functionsbut have limited proliferative capacity and fail to produce IL-2 (Fig. 1). TEM cells are thus subdivided into two subsets:CD45RA− [25] and CD45RA+ (TEMRA). The presence of theCD8 TEMRA subset is well established; however, CD4TEMRA subset existence is debatable. It must be noted thatthe phenotypic classification of TCM and TEM applies to onlyresting cells, as cells engaged in antigenic stimulation maymodify the expression of many distinctive memory subsetsmarkers.
Furthermore, IL-7 and the expression of CD127 (IL-7Rα) chain were recently shown to identify the memoryprecursors at early time points. These cells were IL-7Rhi,expressed high levels of antiapoptotic molecules, andconferred protective immunity upon adaptive transfer [36].In addition, Madakamutil et al. [43] demonstrated thatexpression of the homotypic form of CD8, which uses theα chain of the CD8 molecule (CD8αα), enhanced thesurvival of CD8 memory T cell precursors. Several othercell surface markers were proposed to delineate thememory T cell function. It is, however, very important tocorrelate the expression of the cell surface markers withthe cellular function and survival capacity as one of thehallmarks of TCM is still their capacity to survive for long-term intervals.
Function of subsets of memory T cells
A distinctive feature of TCM is their ability to produce IL-2and to undergo multiple rounds of proliferation uponantigenic stimulation. After proliferation, those cells effi-ciently differentiate into effector cells and produce largeamounts of IFN-γ (Th1) or IL-4 (Th2). Initial experiments,on the other hand, suggested that TEM were better producersof IFN-γ and TNF-α after stimulation than TCM [63]. CD8TEM carries large amounts of perforin, and both CD4 andCD8 produce IFN-γ, IL-4, and IL-5 within hours afterantigenic stimulation. On the contrary, recent studies inboth humans [57] and mice [76] have found that whenstimulated with similar antigen, both subsets producedcomparable levels of IFN-γ and TNF-α. However, TCM,not TEM, produced IL-2 and have a greater proliferativecapacity compared to TEM [79]. Needless to say, adaptivetransfer experiments, while can only be performed in themurine system, clearly show the distinction between thedifferent subsets of memory T cells. Indeed, the antigen-specific protection of TCM (CD44+ CD62L+) can betransferred after residing for more than 3 months inimmunized or virus-challenged mice while TEM function
198 Springer Semin Immun (2006) 28:197–208

and activity is more transient. The availability of suchreadout in mice provides the true evaluation of Tcell memory.
Lineage relationship between memory subsets
In the past few years, progress was made in understandingthe basis for the generation and maintenance of memoryT cells. Many issues, however, are still controversial. It iswell established that the T cell response is divided into threedistinct phases: the expansion phase, the contraction ordeath phase, and the memory phase. In the expansionphase, the initial activation and clonal expansion of T cellsoccur. This is followed by the contraction or death phasewhere 90–95% of the activated effector T cells die viaapoptosis. The 5–10% effector cells that survive this phaseenter into the final phase where the establishment andmaintenance of memory T cell take place. Programming ofall three phases was suggested to happen shortly afterantigenic stimulation [33].
Determining the lineage relationship between TCM andTEM memory subsets was the focus of several studies,although this relation is still controversial. Using the mouselymphocytic choriomeningitis system, Wherry et al. [79]were able to directly track the lineage of TCM and TEM CD8T cells in the memory compartment using the adaptivetransfer approach. They noticed that after the clearance of
antigen during acute infections, there was a gradualconversion from TEM to TCM within the memory CD8T cell pool [79]. This approach cannot exclude thepossibility that a small number of TCM, which are endowedwith strong proliferation potential, could eventually outgrowand differentiate into other subsets. These findings led to theinitial conclusion that in mice TCM and TEM do notrepresent distinct subsets, but are part of a linear naïve▶effector▶TEM▶TCM progressive differentiation pathway[69]. In accordance with this model, stimulation of sortedhuman immunodeficiency virus (HIV)-specific CD8 TEM
cells induced their CCR7 expression [11] although, again,one cannot exclude a few contaminant TCM outgrowingother cells. Similarly, stimulation of CD4 TEM cells fromhealthy individuals induced a transient expression of CCR7[62]. These findings, however, were challenged by severalgroups [9].
Indeed, human CD4 and CD8 TEM, in contrast to themouse TEM, were detected several years after priming [5]and failed to regain the constitutive CCR7 expression invitro [40]. This implies that TEM cells are either stable orcontinuously replenished through cytokine-driven differen-tiation of TCM, a model very different from the oneoriginally proposed by Ahmed and colleagues.Lanzavecchia and coworkers proposed a signal-strengthprogressive differentiation model for memory T cells and
ILILILIL----22227+457+457+457+45----
27+28+27+28+27+28+27+28+
ILILILIL----2 2 2 2 IFNIFNIFNIFN 7777----45454545----
27+28+27+28+27+28+27+28+
IFNIFNIFNIFN 7777----45454545----
27272727----28282828----57575757----
IFNIFNIFNIFN 7777----45+45+45+45+27272727----28282828----57+ 57+ 57+ 57+
CMV CMV
LowViremia
High Viremia
HIV HIVHIV HIV
ILILILIL----22227777----45454545----
27+28+ 27+28+ 27+28+ 27+28+
IFNIFNIFNIFN 7777----45454545----
27272727----28+28+28+28+57575757----
ILILILIL----2 2 2 2 IFNIFNIFNIFN 7777----45454545----
27272727----28+28+28+28+
IFNIFNIFNIFN 7777----45454545----
27+28+27+28+27+28+27+28+
ILILILIL----2 2 2 2 IFNgIFNgIFNgIFNg7+457+457+457+45----
27+28+27+28+27+28+27+28+
Chronic Stimulation
Low viremia
Chronic Stimulation
High viremia
Early HARRT Treated
Low viremia
ILILILIL----22227+457+457+457+45----
27+28+27+28+27+28+27+28+
ILILILIL----2 2 2 2 IFNIFNIFNIFN γ γ γ γ γ 7777----45454545----
27+28+27+28+27+28+27+28+
IFNIFNIFNIFN γ γ γ γ γ 7777----45454545----
27272727----28282828----57575757----
IFNIFNIFNIFN γ γ γ γ γ 7777----45+45+45+45+27272727----28282828----57+ 57+ 57+ 57+
CMV CMV
LowViremia
High Viremia
HIV HIVHIV HIV
ILILILIL----22227777----45454545----
27+28+ 27+28+ 27+28+ 27+28+
IFNIFNIFNIFN γ γ γ γ γ 7777----45454545----
27272727----28+28+28+28+57575757----
ILILILIL----2 2 2 2 IFNIFNIFNIFN γ γ γ γ γ 7777----45454545----
27272727----28+28+28+28+
IFNIFNIFNIFN γ γ γ γ 7777----45454545----
27+28+27+28+27+28+27+28+
ILILILIL----2 2 2 2 IFNgIFNgIFNgIFNg7+457+457+457+45----
27+28+27+28+27+28+27+28+
Chronic Stimulation
Low viremia
Chronic Stimulation
High viremia
Early HARRT Treated
Low viremia
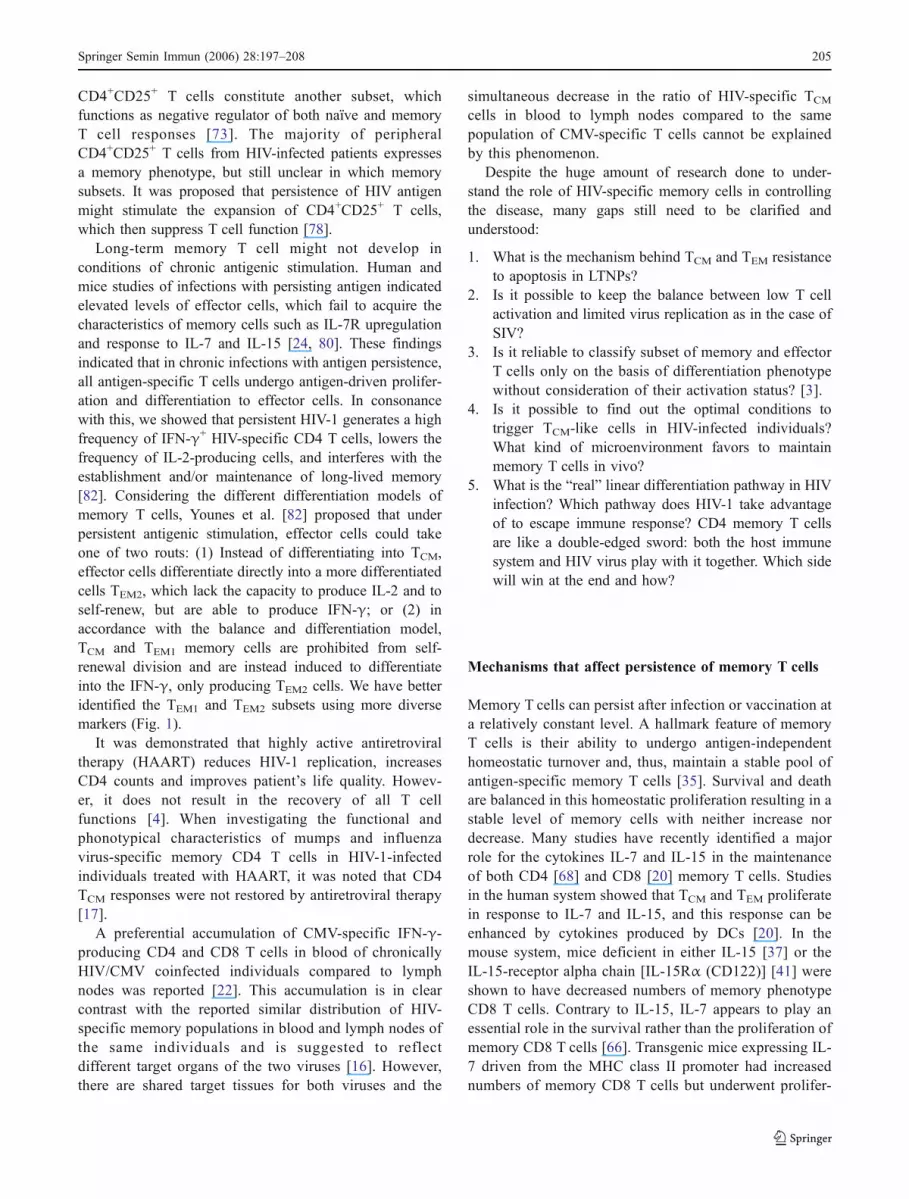
Fig. 1 Proposed model for the differentiation and maturation of CD4 Tcells. This model is based on the use of multicolor flow cytometry assaysincluding CD3, CD4, CD45RA, CCR7, CD27, CD28, CD57, IL-2, andIFN-γ antibodies. TCM are defined as CD45RA−CCR7+CD27+, TEM as
CD45RA−CCR7−CD27−, and TEMRA as CD45RA+CCR7−CD27−.CMV- or HIV-specific CD4 T cell were monitored by IL-2 and IFN-γsecretion and their correlation with surface markers in different viralinfection diseases
Springer Semin Immun (2006) 28:197–208 199

placed TCM between naïve and TEM cells. In this model,TCM are generated by subthreshold stimulation and arrestedat intermediate stages of differentiation preceding TEM.Differences between the human and mouse species mayaccount for this inconsistency.
Antigen-specific CD8 TCM and TEM cells can persist forlong time, although their relative proportion depends on theimpact each viral infection can exert on the memory T cellpool. For example, HIV-specific T cells are largely TEM,whereas CMV-specific T cells are predominantly TEMRA
[11]. Because they are localized in peripheral tissues, TEM
could constitute the first line of defense against invadingpathogens. However, due to its ability to generate a largereffector population as a consequence of its greaterproliferative capacity, TCM may provide a better long-termprotective immunity after both a systemic or peripheralinfections [79].
Molecular requirements for the induction of memory T cells
Several studies showed that stimulation with antigen for24 h is sufficient to set a developmental program foreffector and memory CD8 T cells associated withchanges in gene expression [34]. This program wassignificantly shown to pass on to daughter cells instructingthem to undergo at least 7–10 rounds of division withoutfurther antigenic stimulation. Furthermore, the properdevelopment and survival of functional memory cellsrequires signaling not only through the T cell receptor(TCR) but also via costimulatory molecule such as CD28and cytokines such as IL-7 [68]. Signaling through CD27,CD40, 4-1BB, and ICOS was shown to promote continuedexpansion, survival, or memory differentiation of CD8 Tcells [12]. On the other hand, recent studies havedemonstrated that help from CD4 T cells during activationalso plays an important role in the formation of competentCD8 T cell memory [29].
Role of the innate immune system
Toll-like receptors (TLRs) are one of the links that bridgeinnate and adaptive immune responses. TLRs activate theinnate and adaptive immunity through the upregulation ofcostimulatory molecules, enhancing antigen presentation tonaïve T cells, induction of inflammatory cytokines produc-tion, and activation of antigen-specific adaptive immuneresponses [58]. TLR-induced signals are required for thedevelopment of memory CD4 T cell and their differentia-tion, but once memory T cells are generated, theirpersistence and subsequent maturation does not requireTLR signaling [53]. In addition, direct evidence of the roleof TLR in the establishment of memory responses comesfrom the work of Delale et al. [13]. They showed that TLR9
is required to ensure rapid antiviral memory responses incoordination with other TLR-dependent and TLR-indepen-dent events that are sufficient to establish adaptiveimmunity [13]. Moreover, T cell clonal conditioning, thetime period after antigen presentation but before clonalexpansion where T cells communicate with cells of theinnate immune system, is affected by TLR stimulation. Thisphase of T cell activation was suggested to determinewhether T cells are conditioned to survive, differentiate intomemory cells, or are deleted [46].
Importance of memory T cells in the control of viralinfections
In general, T cell responses to acute infections arecharacterized by strong effector functions that eradicatethe virus and the generation of persistent memory cells,which ensure the generation of an antiviral response uponreexposure. This is in contrast to chronic infections whereT cells lose effector functions drastically before acquiring amemory phenotype. Chronic infections can be categorizedinto infections where viremia is controlled and memorycells are maintained as is the case for Epstein–Barr virus(EBV) and cytomegalovirus (CMV) infection, or where thevirus persists and memory cells are exhausted anddisrupted as in the case of HIV infection. In the followingsection, we will discuss the state of memory T cells duringthese infections, their importance, and the means by whichthis powerful tool of the immune system could beenhanced in an attempt to rescue immune function. Wewill focus on three types of infections:
1. Acute infections [measles virus (MV) and flu] that arewell controlled and where most, if not all, infected cellsare eradicated.
2. Latent chronic (EBV and CMV) infections where theimmune system is capable of eliminating most infectedcells after the acute phase. The immune system isfurther capable of preventing latently infected cellsfrom disseminating into the infected host.
3. Persistent chronic infections (HIV) where in mostinfected individuals, the immune system is incapable,on its own, to control viremia and the concomitantdestruction of the virus.
Memory T cells and acute infections (MV, flu)
Memory T cell responses to MV
MV, a single-stranded negative-sense RNA virus, is ahighly contagious respiratory pathogen causing measles in
200 Springer Semin Immun (2006) 28:197–208

humans. Effective vaccines against MV need to be furtherinvestigated because mortality from measles is still beingreported annually. MV causes transient lymphopenia andimmunosuppression, which can persist months after virusclearance. Patients with MV infection can be categorizedinto those who suffered the severe complications ofmeasles infection vs agammaglobulinemic patients whosuccessfully recovered and developed immunity againstthe virus [48]. This provides a very nice model todetermine the impact of MV on the activation of memorywith the idea that the memory T cells pool is notestablished in patients who fail to recover. The immuno-suppression of peripheral blood mononuclear cells(PBMCs) by MV was a major obstacle in studying thedevelopment of memory T cells in MV individuals.PBMCs from acute measles and in vitro infected PBMCsexhibit a state of unresponsiveness to mitogenic stimula-tion [47]. Nanan et al. [48] described a novel method forquantifying MV-specific memory T cells by stimulatingPBMCs with MV-infected autologous B-lymphoblastoidcell lines or dendritic cells (DCs), and performingintracellular staining and interferon (INF)-γ production.Using this approach, they could measure frequencies aslow as 0.01% for MV-specific CD4 and CD8 T cells.Moreover, using the ELISPOT assays, Nanan et al. [48]also reported the high frequency of CD4 and CD8 Tcells against MV, thus suggesting the long-lived MV-specific memory response. In addition, other groupsused the same method to measure the frequency of MV-specific CD4 and CD8 T cells in patients who areseronegative and seropositive for MV vaccine. Anassociation was evident between MV-specific CD4 andCD8 T cells frequency and antibody seropositivity,which persisted for a long time after immunization [48].
In 2003, Jaye et al. [30] reported the MV-specificcytotoxic T-lymphocyte (CTL) response against the immu-nodominant HLA-A*0201-restricted peptide KLWESPQEIof the MV nonstructural C protein. INF-γ responses againstthis epitope were analyzed in Gambian patients during andafter measles infection (41 to 231 days to measure memoryresponses). Massive INF-γ responses were observed in themajority of HLA-A*0201 patients (eight out of ten patientswith acute infection) during infection, but were undetectedby restimulation after the clearance of the virus. The use ofthe tetramer assays can help explain whether this epitopefails to establish a memory pool after virus is eradicated orwhether established memory cells are exhausted. More suchimmunodominant epitopes may aid in the elucidation of theimmunopathogenesis of measles [30].
CD4 T cells are crucial in the generation of antibodyresponses and in the generation and maintenance of CD8T cell cytotoxicity. Naniche et al. [49] reported decreasinglevels of MV-specific CD4 T memory cells after vaccina-
tion, while MV-specific CD8 T cells and antibody titersremained constant. Differences in MV-specific memoryCD4 T cell responses were also noted between subjectswho were vaccinated and those who had a natural history ofmeasles infection. This could stem from differences in thedynamics of T cell responses that exist between vaccinatedand naturally infected subjects. This issue, while predict-able, is still difficult to address. It is likely that impropervaccination strategies might result in the observed dispro-portion of CD4 T cell dynamics between vaccinated andinfected subjects. By assessing individuals who hadcontracted MV 23–47 years earlier (as controls), the MV-specific CD4 T cell levels were in the same range as inthose vaccinated more than 21 years earlier. By extrapola-tion to earlier time points, it could be estimated thatfrequencies of MV-specific CD4 cells are higher innaturally infected than in vaccinated individuals. Therefore,it remains enigmatic how the MV-specific IgG antibodylevels and memory CD8 T cells are maintained after thedecrease in memory CD4 T cell numbers.
So far, the hemagglutinin (H) and fusion (F) proteinsof MV were identified as antigens for long-lived memoryT cells in macaques [50]. Further research should focus onthe characterization of MV-specific epitopes that elicitstrong cytotoxic activity in the implication of futurevaccine designs. Moreover, new vaccine strategiesexploiting Sindbis virus replicon particles expressingMV-derived H and F were used in macaques [51]. Theinvestigators reported a biphasic appearance of H- and F-specific INF-γ-producing CD4 and CD8 T cells, afterchallenge in vaccinated macaques, with peaks at approx-imately 1 and 3–4 months later, respectively. This couldbe explained by the fact that new T cell subsets arerecruited due to the persistence of viral antigens. Furtherstudies aiming at both phenotypic and functional charac-terization of memory MV-specific CD4 and CD8 T cellswill enlighten future vaccination strategies.
Memory T cell responses to influenza virus
The influenza virus is a negative sense RNA virus causingacute respiratory infection. Different subtypes of influenzaexist, a fact that hampers the development of successfulvaccination strategies. The use of tetramer–peptide com-plexes in the context of MHC restricting HLA has helpedin the elucidation of different memory T cell responsesagainst influenza virus. Indeed, Lucas et al. [42] havecharacterized the frequency and phenotype of influenza-specific CD4 memory T cells ex vivo. They reported thatinfluenza virus-specific memory CD4 and CD8 T cellswere maintained at low frequencies in the peripheral bloodof healthy individuals. Moreover, because influenza is anacute infection, one would expect that the phenotypic
Springer Semin Immun (2006) 28:197–208 201

markers on the memory CD4 T cells somehow have“stem-like” properties for self-renewal and further protec-tion against reinfection. In fact, this was supported byfindings of the above group who reported the presence ofmarkers distinctive to TCM. Furthermore, functionalcharacterization of the virus-specific memory CD4 T cellsyielded production of INF-γ and IL-2 at frequenciessimilar to those detected with tetramer in the absence ofantigen. However, these specific CD4 T cells lacked a lateor effector phenotype.
Since data supporting the fact that influenza derivedantigens persist even after viral clearance, the impact ofthe kinetics of antigen presentation was proposed to play arole in the priming of T cells. Recently, Jelley-Gibbs et al.[31] studied the impact of kinetics of influenza antigenpresentation on CD4 T cell differentiation and the impactof the latter on the maintenance of memory. They showedthat naïve CD4 T cells injected into infected mice at theearly stages of antigen presentation resulted in T cellexpansion and differentiation, but generated low numbersof memory cells. On the other hand, the injection of naïveCD4 T cells in infected mice at late phases of antigenpresentation resulted in a less drastic T cell expansion,which had an intermediate phenotype that gave rise to amemory pool. This indicated that late phases of antigenpresentation are less effective in T cell expansion but moreeffective in the persistence of memory CD4 T cellpopulations. Therefore, the design of vaccines againstacute infections could be efficient if focused on thegeneration of intermediately differentiated (effectors thatare not completely differentiated and that can contribute tothe generation of IL-2 producing memory subsets) cells[31].
Memory T cells in resolving chronic infections(EBV, CMV)
Infection with the two members of the herpesvirus family,namely, EBV, a gamma herpesvirus, and CMV, a betaherpesvirus, is very common in the human population.After a period of acute viral replication, both viruses initiatea latency period in immunocompetent individuals. Theinfection remains asymptomatic until reactivation mainlydue to transplantation, immunodeficiency, and pregnancy.The biphasic and prolonged nature of these infectionsprovide powerful models to study memory T cell responsesin acute and chronic infections. In addition, as both virusesmostly cause morbidity and mortality in immunocompro-mised hosts, comparison of the memory response in EBVand CMV infections with more life-threatening viralinfections such as HIV can shed light on the unresolvedaspects of skewed memory development. Moreover, delin-
eating memory responses to EBVand CMVantigens will bepromising in the development of effective vaccines forindividuals at risk.
CD4 and CD8 T cell responses in primary and persistentEBV infection
The mean of EBV-specific CD4 T cells dropped from 1.4%during the primary phase of infection to 0.22% in a 4-monthperiod, which further reached 0.34% during the persistentphase of infection [2]. The phenotype of the majority of CD4T cells in the primary phase of infection was that of effectorcells. This phenotype significantly did not change during thepersistent phase of the infection. However, expression ofCCR7 was preserved on a fraction of EBV-specific T cells,which are major producers of IL-2. This upregulation ofCCR7 expression enabled them to recirculate to lymphoidtissues [2].
During the acute phase of primary EBV infection, ahighly expanded CD8 T cell population dominates inresponse to lytic epitopes [27]. Most of the expandedcells, however, are subjected to apoptosis and theremaining population consists of CD8 T cells specificfor both lytic and latent viral antigens. Although thebreadth of CD4 and CD8 T cell responses to lytic andlatent EBV-specific epitopes was shown to be similar inacute and persistent infections [81], longitudinal study ofphenotype and function of epitope-specific CD8 T cellshas revealed different phenotypic and functional evolutionof lytic vs latent epitope-specific CD8 T cells. In thisregard, higher levels of CD62L and CCR7 expression canbe detected on latent compared to lytic protein-specificCD8 T cells [26]. Moreover, the CD8 T cells in the twophases of the EBV infection show qualitative differencesin their composition [27]. Hence, the CD8 T cell responseto EBV latent antigens is enriched in TCM cells while theCD8 T cell response to lytic proteins is enriched in bothTEM and TEMRA cells [26, 27]. Therefore, different viral loadsin the lytic and latent phases of infection may result inqualitatively different phenotypes of CD8 memory T cells.Cytotoxic CD8 T cells with specificity to latent and lytic EBVantigens are reported to be CD69−CD38− and can be traced tothe CD45RA+, CD45RO+, CD28+, and CD28− subpopulations,which are able to produce IFN-γ and TNF-α [26]. However,no information exists on the phenotype of IL-2-producing cellsin these studies.
Clonality of the response to EBV
In a study by Silins et al. [70], TCRVβ sequence analysisof CTL clones against two epitopes of EBNA-3 antigenarouse during acute infectious mononucleosis revealed abroad polyclonotypic response, which remained intact
202 Springer Semin Immun (2006) 28:197–208

during the 6 months course of their study. Moreover,cytotoxic CD8 T cell response to different HLA–A11-restricted epitopes of an EBV antigen (EBNA4) in seropos-itive carriers encompasses a number of TCR clonotypes withdifferent diversities and affinities [10]. In this regard,studying Vβ gene usage of 21 clones specific for animmunodominant epitope of EBNA4 (IVT; 208 clones) infour donors has revealed a broad CD8 T cell response ofdiverse clonotypes. However, a subdominant epitope (AVF;92 clones) of the same protein generated a very restrictedresponse with limited Vβ usage and CDR3 diversity. Asubstantial similarity in nucleotide sequences of the CDR3region was also observed for AVF-specific but not IVT-specific clones [10]. Therefore, apart from antigenic load,the level of immunogenicity and structure of peptide canaffect the clonality of the CD8 T cell repertoire in EBVinfection.
CD4 and CD8 T cells responses in primary and chronicCMV infection
Previous studies showed the expansion of IFN-γ-producingeffector CD4 T cells during primary CMV infection.Moreover, the delayed appearance of IFN-γ-producingCMV-specific CD4 T cells in symptomatic patients resultedin failure to control the infection early in disease reactiva-tion [19]. During chronic CMV infection, the lack of IL-2-secreting CD4 T cell responses in bone marrow transplantrecipients compared to asymptomatic individuals wasreported [67]. In addition, although the majority of CMV-specific CD4 T cells in primary infection are CD45RA−
cells, CMV-specific CD4 T cells in chronic infection areenriched in terminally differentiated TEMRA cells [23].Moreover, CMV-specific CD4 T cells do not expressCCR7 and CD62L in both phases of infection (primaryand latent), but express CD11a and VLA-4, which enablesthem to enter peripheral tissues [18]. The IL-2-secretingfunction, on the other hand, resides, as expected, in theCMV-specific TCM CD4 T cell population [22]. Similar tomany other viruses, expansion of CD8 memory T cells andtheir subsequent differentiation into effector cells play acrucial role in controlling CMV viremia at the beginning ofinfection. The loss of immune control of the virus by CMV-specific CD8 T cells is concomitant with the reactivation ofseveral clinical symptoms, including retinitis, enteritis,interstitial pneumonia, and a mononucleosis-like syndrome.This is specially evidenced by reduced cytokine productionand proliferative responses in such patients [67]. The65 kDa late phosphoprotein (pp65) and the 72 kDa earlyantigen (IE-1) of human CMV are known to be theimmunodominant targets of CD8 T cells. The relativefrequency of CD8 T cells in asymptomatic carriers and renaltransplant patients is higher for pp65 compared to IE-1
epitope [38]. The pp65 protein can also induce animmunodominant CD4 T cell response [7]. Differentepitopes of pp65 were shown to be restricted by more thanone HLA allele, which makes them favorable targets forimmune therapy or vaccination [56].
During primary CMV infection, virus-specific CD8T cells are shown to have TEM phenotype andeffectively express granzyme B and perforin [18]. How-ever, accumulation of both subpopulations of CMV-specific TEM and TEMRA CD8 T cells are reported inasymptomatic seropositive individuals [39]. Almanzar etal. [1] reported that in response to CMV-pp65 epitope,more proliferation could be detected in CD45RA−CD28+
population in spite of the higher frequency of peptide-specific cells in the CD28− population. In their assay, theproliferation potential of the CD45RA−CD28− andCD45RA+CD28− populations could not be restored evenin the presence of exogenous IL-2 [1]. It was also reportedthat both populations of TCM and TEM CD8 T cells arecapable of producing IFN-γ while high levels of perforincan only be found in the TEMRA subpopulation [63].
Clonality of the response to CMV
A very limited Vβ gene usage and high degree ofclonality in both CD4 and CD8 T cell responses toCMV pp65 matrix protein was reported in chronicallyinfected individuals. The clonal structure of the reper-toire was reported to include phenotypic heterogeneityin clones that originated from a single maternal clone.In this regard, Weekes et al. [77] have reported thatCMV pp65-specific CD4 T cell clones are distributed inboth CD45RAhi CD45ROlo and CD45RAlo CD45ROhi
subpopulations and were particularly enriched within theCD28−CD45RAhi subpopulation in one individual [77].However, the extent of clonality in response to differentCMV antigens remains to be elucidated [8].
CMV-driven polarization of the immune system
CMV infection was suggested to decrease the size ofnaïve CD8 T cell pool and increase the IFN-γ-producing CD8 effector T cells, which drive theimmune system toward Th1 polarization. Contrary tothe CMV seronegative healthy age-matched individuals,no increase in IL-2-producing CD8 T cell populationcan be observed in middle-aged and elderly CMVcarriers [44]. In addition, a different phenotypic patternof CMV-pp65 epitope-specific CD8 T cells was observedover time. Accordingly, a shift from effector to memoryphenotype in CMV-pp65-specific CD8 T cells wasreported [1].
Springer Semin Immun (2006) 28:197–208 203

Comparison of CMV and EBV memory T cells
In EBV infection, the predominant CD8 memory T cellspopulation is TEM while the majority of CMV-specific CD8memory T cells are TEMRA. This suggests that CD8 T cellsin EBV infection are less differentiated than their counter-parts in CMV-infected hosts [44, 75]. Furthermore, amongthe memory CD8 T cell population, the majority of CMV-specific T cells are reported to be TEM while the majority ofEBV-specific cells are detected as TCM [75]. In addition,investigation of cytokine production profile of ex vivoCMV- and EBV-specific responses in CD8 T cells showedthat while no exclusive production of IL-2 could bedetected, IFN-γ synthesis was seen in a majority oftetramer-specific cells. A lower percentage of IL-2+ IFN-γ+ CD8 T cells compared to IFN-γ+ T cells was reported inthese infections suggesting that both populations of effectorT cells and TEM are more likely to produce IFN-γ than IL-2[44]. Moreover, the percentage of CD8 T cells producingboth cytokines was higher in CMV-specific compared toEBV-specific cells [44].
On the other hand, higher frequencies of EBV IL-2-producing CD4 memory T cells compared to CMV IL-2were observed in HIV patients. Comparison of the IL-2,IFN-γ, and IL-2/IFN-γ-secreting CD4 T cells in response toEBV, CMV, and HIV in these patients indicated differencesin cellular functionality. Whereas the majority of EBV CD4Tcells are IL-2-secreting, CMV- and HIV-specific CD4 cellsproduce mainly IFN-γ. However, in response to CMVantigens a high percentage of cells also produced both IFN-γ and IL-2 [24]. Evaluation of the CD4 memory T cells inprimary CMV infection has revealed that the majority ofIL-2-secreting cells are TCM while the majority of IFN-γ-producing cells are TEM. However, in chronic CMV andEBV infections, IL-2-secreting cells are shown to belong toTCM and TEM populations, while TEM and TEMRA popula-tions produce IFN-γ [23]. Therefore, a specific profile ofcytokine production cannot be simply attributed to expres-sion of a specific phenotype as the infective agent andstimulatory antigen load might affect the phenotype ofcytokine-secreting cells [23].
Memory T cells in nonresolving chronic infections (HIV)
HIV pathogenesis is well known as a chronic infection,which leads to slow degradation of immunity that ulti-mately develops to AIDS. HIV infects CD4 T cells as targetcells, meanwhile CD4 and CD8 cells leads the antiviralimmune responses. Many factors have involved in thecomplex interaction between HIV and T cells. Understand-ing the function and mechanisms of memory T cells under
infection should facilitate the development of effective andsafe vaccines against HIV.
The hallmark of immune protection is the long-termmaintenance of memory T cell response. When comparingmemory T cells among HIV-exposed uninfected individuals(ESN) and HIV-infected patients, Gag-specific T cellspresented in ESN mainly secrete IL-2 while IFN-γ inHIV-infected patients. Both central and effector memoryCD4 and CD8 T cells are more abundant in ESN than HIVpatients [65], indicating the importance of memory T cellson controlling the virus.
It was demonstrated that during acute infection,enormous viral replication and extensive CD4 memoryT cell destruction make the baseline for further immunefailure. On the other hand, chronic infection end up withbystander apoptosis, functional exhaustion, and gradualloss of T cell regenerative capabilities and a microenvi-ronment, which ultimately lead to whole immune systemfailure [55]. Douek et al. [14] showed that HIV preferen-tially infects HIV-specific CD4 T cells. The questionabout how mass CD4 T cells are destroyed has then beenraised. More and more evidences suggested that HIV-specific CD4 cells in individuals with persistent HIVinfection were not simply deleted by HIV virus but havealso lost their ability to produce IL-2 and to proliferate.Furthermore, it was shown that the rate of CD4 T celldecline is linked better with markers of immune activationthan viral load [71]. In addition, increased activation-induced apoptosis of CD4 and CD8 T cells may be onereason for T cells death. Yue et al. [83] recently suggestedthat compared with CMV infection, ex vivo HIV-1-specific memory CD4 T cells have greater apoptoticpotential and this potential directly correlated with viralload and disease progression. Bcl-2 was expressedsignificantly low within HIV-1-infected individuals withchronic progression. Rethi et al. [59] reported that in HIV-infected patients, a decrease in the expression of IL-7Rαwas found on TEM cells. Downregulation of IL-7Rα wasshown to be linked with CD4 T cell depletion and mightimpair effects of IL-7 on survival and homeostaticproliferation of T cells.
Harari et al. [22] indicated that different disease progressstages have functionally distinct CD4 T cell populations. Intheir study, HIV-specific CD4 T cells were shown to havesingle IL-2, IL-2/IFN-γ, and single IFN-γ-secreting mem-ory cells. However, IL-2/IFN-γ-producing cells wereabsent only in progressors [22]. Moreover, they havesuggested that phenotypic and functional heterogeneity ofmemory CD4 T cells is regulated by Ag load andpersistence. They have also noticed that monophenotypicmemory CD4 T cell responses typical to the case of chronicand progressive HIV infections was absent in long-termnonprogressors (LTNPs) [23]. On the other hand,
204 Springer Semin Immun (2006) 28:197–208
CD4+CD25+ T cells constitute another subset, whichfunctions as negative regulator of both naïve and memoryT cell responses [73]. The majority of peripheralCD4+CD25+ T cells from HIV-infected patients expressesa memory phenotype, but still unclear in which memorysubsets. It was proposed that persistence of HIV antigenmight stimulate the expansion of CD4+CD25+ T cells,which then suppress T cell function [78].
Long-term memory T cell might not develop inconditions of chronic antigenic stimulation. Human andmice studies of infections with persisting antigen indicatedelevated levels of effector cells, which fail to acquire thecharacteristics of memory cells such as IL-7R upregulationand response to IL-7 and IL-15 [24, 80]. These findingsindicated that in chronic infections with antigen persistence,all antigen-specific T cells undergo antigen-driven prolifer-ation and differentiation to effector cells. In consonancewith this, we showed that persistent HIV-1 generates a highfrequency of IFN-γ+ HIV-specific CD4 T cells, lowers thefrequency of IL-2-producing cells, and interferes with theestablishment and/or maintenance of long-lived memory[82]. Considering the different differentiation models ofmemory T cells, Younes et al. [82] proposed that underpersistent antigenic stimulation, effector cells could takeone of two routs: (1) Instead of differentiating into TCM,effector cells differentiate directly into a more differentiatedcells TEM2, which lack the capacity to produce IL-2 and toself-renew, but are able to produce IFN-γ; or (2) inaccordance with the balance and differentiation model,TCM and TEM1 memory cells are prohibited from self-renewal division and are instead induced to differentiateinto the IFN-γ, only producing TEM2 cells. We have betteridentified the TEM1 and TEM2 subsets using more diversemarkers (Fig. 1).
It was demonstrated that highly active antiretroviraltherapy (HAART) reduces HIV-1 replication, increasesCD4 counts and improves patient’s life quality. Howev-er, it does not result in the recovery of all T cellfunctions [4]. When investigating the functional andphonotypical characteristics of mumps and influenzavirus-specific memory CD4 T cells in HIV-1-infectedindividuals treated with HAART, it was noted that CD4TCM responses were not restored by antiretroviral therapy[17].
A preferential accumulation of CMV-specific IFN-γ-producing CD4 and CD8 T cells in blood of chronicallyHIV/CMV coinfected individuals compared to lymphnodes was reported [22]. This accumulation is in clearcontrast with the reported similar distribution of HIV-specific memory populations in blood and lymph nodes ofthe same individuals and is suggested to reflectdifferent target organs of the two viruses [16]. However,there are shared target tissues for both viruses and the
simultaneous decrease in the ratio of HIV-specific TCM
cells in blood to lymph nodes compared to the samepopulation of CMV-specific T cells cannot be explainedby this phenomenon.
Despite the huge amount of research done to under-stand the role of HIV-specific memory cells in controllingthe disease, many gaps still need to be clarified andunderstood:
1. What is the mechanism behind TCM and TEM resistanceto apoptosis in LTNPs?
2. Is it possible to keep the balance between low T cellactivation and limited virus replication as in the case ofSIV?
3. Is it reliable to classify subset of memory and effectorT cells only on the basis of differentiation phenotypewithout consideration of their activation status? [3].
4. Is it possible to find out the optimal conditions totrigger TCM-like cells in HIV-infected individuals?What kind of microenvironment favors to maintainmemory T cells in vivo?
5. What is the “real” linear differentiation pathway in HIVinfection? Which pathway does HIV-1 take advantageof to escape immune response? CD4 memory T cellsare like a double-edged sword: both the host immunesystem and HIV virus play with it together. Which sidewill win at the end and how?
Mechanisms that affect persistence of memory T cells
Memory T cells can persist after infection or vaccination ata relatively constant level. A hallmark feature of memoryT cells is their ability to undergo antigen-independenthomeostatic turnover and, thus, maintain a stable pool ofantigen-specific memory T cells [35]. Survival and deathare balanced in this homeostatic proliferation resulting in astable level of memory cells with neither increase nordecrease. Many studies have recently identified a majorrole for the cytokines IL-7 and IL-15 in the maintenanceof both CD4 [68] and CD8 [20] memory T cells. Studiesin the human system showed that TCM and TEM proliferatein response to IL-7 and IL-15, and this response can beenhanced by cytokines produced by DCs [20]. In themouse system, mice deficient in either IL-15 [37] or theIL-15-receptor alpha chain [IL-15Rα (CD122)] [41] wereshown to have decreased numbers of memory phenotypeCD8 T cells. Contrary to IL-15, IL-7 appears to play anessential role in the survival rather than the proliferation ofmemory CD8 T cells [66]. Transgenic mice expressing IL-7 driven from the MHC class II promoter had increasednumbers of memory CD8 T cells but underwent prolifer-
Springer Semin Immun (2006) 28:197–208 205

ation at a comparable rate to normal cells [45]. Expressionof high level of IL-7Rα was shown to be a hallmark ofsurvival effector cells that enter the memory CD8 T cellpool [36]. One way by which IL-7 enhances the survivalof memory T cells is by inducing the sustained expressionof antiapoptotic molecules such as Bcl-2 [45]. Moreover,CD4 T cells could also contribute to the maintenance oflong-lived memory CD8+ T cells. This might be throughthe control of the expression or presentation of homeo-static cytokines such as IL-15 to CD8 T cells [72].
On the other hand, it is likely that CD4 cells alsorequire cytokines for their survival. However, cytokinesthat signal through the shared gamma chain such as IL-2,IL-4, IL-9, and IL-15 may not be required for themaintenance of CD4 memory cells [74]. In spite of this,Seddon et al. [68] provided evidence that IL-7 may indeedbe important in sustaining the survival of memory CD4T cells. In addition, IL-12 may enhance the maintenance ofCD4 memory cells, as IL-12 was shown to increase thepotency and the durability of a leishmanial protein vaccinein mice [21]. Molecules such as OX-40 and OX-40 ligandmay also play a role in sustaining CD4 T cell survival[61].
Conclusions
During HIV infection, effective CD8 T cell responses areassociated with an initial drop in viremia, and in somecases, with long-term control of viral replication. Strategieslike therapeutic vaccination that would boost immuneresponses and enhance viral control during chronic viralinfection are of great interest. This could slow down diseaseprogress and lower viral transmission. Therefore, it isimportant to determine how to elicit the most successfulimmune responses after therapeutic intervention. Currentapproaches of therapeutic vaccination have failed todemonstrate sustained recovery of T cell function and moreimportantly of clinical recovery.
It was proposed that effector memory cells present animmediate, but not sustained, defense at pathogen sites ofentry, whereas TCM maintain the response by proliferatingin the secondary lymphoid organs and producing a supplyof new effectors. When protection relies on a secondaryresponse, TCM would be more efficient in mediatingprotection than TEM. In other conditions, however, protec-tion might require preexisting levels of competent effectorT cells. During leishmania major infection, protectiveimmunity was mediated by either short-lived pathogen-dependent effector cells [6] or long-lived pathogen-independent TCM capable, upon secondary infection, ofdifferentiating into tissue-homing effector cells [84]. On
the other hand, the ability to manipulate the number ofeffector CD8 T cells that will ultimately differentiate intospecific memory subsets would be a powerful tooltoward a protective vaccine. Determining which type ofmemory cells provides protective immunity against aspecific infection (e.g., TEM at the site of infection, TCM
for systemic infections) would enlighten the way forrationally designing vaccines that induce protective,long-lasting cellular immunity against persistent viralinfections.
References
1. Almanzar G, Schwaiger S, Jenewein B et al (2005) Long-termcytomegalovirus infection leads to significant changes in thecomposition of the CD8+ T-cell repertoire, which may be thebasis for an imbalance in the cytokine production profile in elderlypersons. J Virol 79:3675–3683
2. Amyes E, Hatton C, Montamat-Sicotte D et al (2003) Character-ization of the CD4+ T cell response to Epstein–Barr virus duringprimary and persistent infection. J Exp Med 198:903–911
3. Appay V, Dunbar PR, Callan M et al (2002) Memory CD8+T cells vary in differentiation phenotype in different persistentvirus infections. Nat Med 8:379–385
4. Autran B, Carcelain G, Li TS et al (1997) Positive effects ofcombined antiretroviral therapy on CD4+ T cell homeostasis andfunction in advanced HIV disease. Science 277:112–116
5. Baron V, Bouneaud C, Cumano et al (2003) The repertoires ofcirculating human CD8(+) central and effector memory T cellsubsets are largely distinct. Immunity 18:193–204
6. Belkaid Y, Piccirillo CA, Mendez S et al (2002) CD4+CD25+regulatory T cells control leishmania major persistence andimmunity. Nature 420:502–507
7. Beninga J, Kropff B, Mach M (1995) Comparative analysis offourteen individual human cytomegalovirus proteins for helperT cell response. J Gen Virol 76(Pt 1):153–160
8. Bitmansour AD, Douek DC, Maino VC et al (2002) Direct exvivo analysis of human CD4(+) memory T cell activationrequirements at the single clonotype level. J Immunol 169:1207–1218
9. Brenchley JM, Price DA, Douek DC (2006) HIV disease: falloutfrom a mucosal catastrophe? Nat Immunol 7:235–239
10. Campos-Lima PO, Levitsky V, Imreh MP et al (1997) Epitope-dependent selection of highly restricted or diverse T cell receptorrepertoires in response to persistent infection by Epstein–Barrvirus. J Exp Med 186:83–89
11. Champagne P, Ogg GS, King AS et al (2001) Skewedmaturation of memory HIV-specific CD8 T lymphocytes. Nature410:106–111
12. Curtsinger JM, Johnson CM, Mescher MF (2003) CD8 T cellclonal expansion and development of effector function requireprolonged exposure to antigen, costimulation, and signal 3cytokine. J Immunol 171:5165–5171
13. Delale T, Paquin A, Asselin-Paturel C et al (2005) MyD88-dependent and -independent murine cytomegalovirus sensingfor IFN-alpha release and initiation of immune responses in vivo.J Immunol 175:6723–6732
14. Douek DC, Brenchley JM, Betts MR et al (2002) HIV preferen-tially infects HIV-specific CD4+ T cells. Nature 417:95–98
15. Dutton RW, Bradley LM, Swain SL (1998) T cell memory. AnnuRev Immunol 16:201–223
206 Springer Semin Immun (2006) 28:197–208

16. Ellefsen K, Harari A, Champagne P et al (2002) Distribution andfunctional analysis of memory antiviral CD8 T cell responses inHIV-1 and cytomegalovirus infections. Eur J Immunol 32:3756–3764
17. Elrefaei M, McElroy MD, Preas CP et al (2004) Central memoryCD4+ T cell responses in chronic HIV infection are not restoredby antiretroviral therapy. J Immunol 173:2184–2189
18. Gamadia LE, Remmerswaal EB, Weel JF et al (2003) Primaryimmune responses to human CMV: a critical role for IFN-gamma-producing CD4+ T cells in protection against CMV disease. Blood101:2686–2692
19. Gamadia LE, Rentenaar RJ, van Lier RA et al (2004) Properties ofCD4(+) T cells in human cytomegalovirus infection. HumImmunol 65:486–492
20. Geginat J, Lanzavecchia A, Sallusto F (2003) Proliferation anddifferentiation potential of human CD8+ memory T-cell subsets inresponse to antigen or homeostatic cytokines. Blood 101:4260–4266
21. Gurunathan S, Prussin C, Sacks DL et al (1998) Vaccinerequirements for sustained cellular immunity to an intracellularparasitic infection. Nat Med 4:1409–1415
22. Harari A, Petitpierre S, Vallelian F et al (2004) Skewedrepresentation of functionally distinct populations of virus-specific CD4 T cells in HIV-1-infected subjects with progres-sive disease: changes after antiretroviral therapy. Blood 103:966–972
23. Harari A, Vallelian F, Pantaleo G (2004) Phenotypic heterogeneityof antigen-specific CD4 T cells under different conditions ofantigen persistence and antigen load. Eur J Immunol 34:3525–3533
24. Harari A, Vallelian F, Meylan PR et al (2005) Functionalheterogeneity of memory CD4 T cell responses in differentconditions of antigen exposure and persistence. J Immunol174:1037–1045
25. Hazenberg MD, Otto SA, Hamann D et al (2003) Depletion ofnaive CD4 T cells by CXCR4-using HIV-1 variants occursmainly through increased T-cell death and activation. Aids17:1419–1424
26. Hislop AD, Gudgeon NH, Callan MF et al (2001) EBV-specificCD8+ T cell memory: relationships between epitope specificity,cell phenotype, and immediate effector function. J Immunol167:2019–2029
27. Hislop AD, Annels NE, Gudgeon NH et al (2002) Epitope-specific evolution of human CD8(+) T cell responses fromprimary to persistent phases of Epstein–Barr virus infection. JExp Med 195:893–905
28. Hume E (1040) The Chinese way in medicine. John HopkinsUniversity Press, Baltimore
29. Janssen EM, Lemmens EE, Wolfe T et al (2003) CD4+ T cells arerequired for secondary expansion and memory in CD8+ Tlymphocytes. Nature 421:852–856
30. Jaye A, Herberts CA, Jallow S et al (2003) Vigorous but short-term gamma interferon T-cell responses against a dominantHLA-A*02-restricted measles virus epitope in patients withmeasles. J Virol 77:5014–5016
31. Jelley-Gibbs DM, Brown DM, Dibble JP et al (2005)Unexpected prolonged presentation of influenza antigenspromotes CD4 T cell memory generation. J Exp Med 202:697–706
32. Jenner E (1798) An inquiry into the causes and effects of thevariolae vaccinae. Low, London
33. Kaech SM, Ahmed R (2001) Memory CD8+ T cell differentiation:initial antigen encounter triggers a developmental program innaive cells. Nat Immunol 2:415–422
34. Kaech SM, Hemby S, Kersh E et al (2002) Molecular andfunctional profiling of memory CD8 T cell differentiation. Cell111:837–851
35. Kaech SM, Wherry EJ, Ahmed R (2002) Effector and memoryT cell differentiation: implications for vaccine development. NatRev Immunol 2:251–262
36. Kaech SM, Tan JT, Wherry EJ et al (2003) Selective expression ofthe interleukin 7 receptor identifies effector CD8 T cells that giverise to long-lived memory cells. Nat Immunol 4:1191–1198
37. Kennedy MK, Glaccum M, Brown SN et al (2000) Reversibledefects in natural killer and memory CD8 T cell lineages ininterleukin 15-deficient mice. J Exp Med 191:771–780
38. Kern F, Faulhaber N, Frommel C et al (2000) Analysis of CD8T cell reactivity to cytomegalovirus using protein-spanning poolsof overlapping pentadecapeptides. Eur J Immunol 30:1676–1682
39. Khan N, Shariff N, Cobbold M et al (2002) Cytomegalovirusseropositivity drives the CD8 T cell repertoire toward greaterclonality in healthy elderly individuals. J Immunol 169:1984–1992
40. Langenkamp A, Nagata K, Murphy K et al (2003) Kinetics andexpression patterns of chemokine receptors in human CD4+ Tlymphocytes primed by myeloid or plasmacytoid dendritic cells.Eur J Immunol 33:474–482
41. Lodolce JP, Boone DL, Chai S et al (1998) IL-15 receptormaintains lymphoid homeostasis by supporting lymphocytehoming and proliferation. Immunity 9:669–676
42. Lucas M, Day CL, Wyer JR et al (2004) Ex vivo phenotype andfrequency of influenza virus-specific CD4 memory T cells. J Virol78:7284–7287
43. Madakamutil LT, Christen U, Lena CJ et al (2004) CD8alpha-alpha-mediated survival and differentiation of CD8 memory T cellprecursors. Science 304:590–593
44. Mallard E, Vernel-Pauillac F, Velu T et al (2004) IL-2 productionby virus- and tumor-specific human CD8 T cells is determined bytheir fine specificity. J Immunol 172:3963–3970
45. Maraskovsky E, O’Reilly LA, Teepe M et al (1997) Bcl-2 canrescue T lymphocyte development in interleukin-7 receptor-deficient mice but not in mutant rag-1−/−mice. Cell 89:1011–1019
46. Maxwell JR, Rossi RJ, McSorley SJ et al (2004) T cell clonalconditioning: a phase occurring early after antigen presentationbut before clonal expansion is impacted by Toll-like receptorstimulation. J Immunol 172:248–259
47. McChesney MB, Oldstone MB (1989) Virus-induced immuno-suppression: infections with measles virus and human immuno-deficiency virus. Adv Immunol 45:335–380
48. Nanan R, Rauch A, Kampgen E et al (2000) A novel sensitiveapproach for frequency analysis of measles virus-specific memoryT-lymphocytes in healthy adults with a childhood history ofnatural measles. J Gen Virol 81:1313–1319
49. Naniche D, Garenne M, Rae C et al (2004) Decrease in measlesvirus-specific CD4 T cell memory in vaccinated subjects. J InfectDis 190:1387–1395
50. Pahar B, Li J, McChesney MB (2005) Detection of T cellmemory to measles virus in experimentally infected rhesusmacaques by cytokine flow cytometry. J Immunol Methods304:174–183
51. Pan CH, Valsamakis A, Colella T et al (2005) Inaugural article:modulation of disease, T cell responses, and measles virusclearance in monkeys vaccinated with H-encoding alphavirusreplicon particles. Proc Natl Acad Sci USA 102:11581–11588
52. Panum P (1939) Observations made during the epidemic ofmeasles on the Faroe Islands in the year 1846. Med Classics3:839–886
53. Pasare C, Medzhitov R (2004) Toll-dependent control mecha-nisms of CD4 T cell activation. Immunity 21:733–741
54. Pasare C, Medzhitov R (2004) Toll-like receptors: linking innateand adaptive immunity. Microbes Infect 6:1382–1387
55. Picker LJ, Watkins DI (2005) HIV pathogenesis: the first cut is thedeepest. Nat Immunol 6:430–432
Springer Semin Immun (2006) 28:197–208 207

56. Provenzano M, Lim JB, Mocellin S et al (2003) The matrix proteinpp65(341–350): a peptide that induces ex vivo stimulation and invitro expansion of CMV-specific CD8+ T cells in subjects bearingeither HLA-A*2402 or A*0101 allele. Transfusion 43:1567–1574
57. Ravkov EV, Myrick CM, Altman JD (2003) Immediate earlyeffector functions of virus-specific CD8+CCR7+ memory cells inhumans defined by HLA and CC chemokine ligand 19 tetramers.J Immunol 170:2461–2468
58. Reis e Sousa C (2004) Toll-like receptors and dendritic cells: forwhom the bug tolls. Semin Immunol 16:27–34
59. Rethi B, Fluur C, Atlas A et al (2005) Loss of IL-7Ralpha isassociated with CD4 T-cell depletion, high interleukin-7 levels andCD28 down-regulation in HIV infected patients. Aids 19:2077–2086
60. Retief FP, Cilliers L (1998) The epidemic of Athens, 430–426 BC.S Afr Med J 88:50–53
61. Rogers PR, Song J, Gramaglia I et al (2001) OX40 promotes Bcl-xL and Bcl-2 expression and is essential for long-term survival ofCD4 T cells. Immunity 15:445–455
62. Sallusto F, Kremmer E, Palermo B et al (1999) Switch inchemokine receptor expression upon TCR stimulation revealsnovel homing potential for recently activated T cells. Eur JImmunol 29:2037–2045
63. Sallusto F, Lenig D, Forster R et al (1999) Two subsets of memoryT lymphocytes with distinct homing potentials and effectorfunctions. Nature 401:708–712
64. Sawyer W (1930) Persistence of yellow fever immunity. J PrevMed 5:413–428
65. Schenal M, Lo Caputo S, Fasano F et al (2005) Distinct patternsof HIV-specific memory T lymphocytes in HIV-exposed unin-fected individuals and in HIV-infected patients. Aids 19:653–661
66. Schluns KS, Kieper WC, Jameson SC et al (2000) Interleukin-7mediates the homeostasis of naive and memory CD8 T cells invivo. Nat Immunol 1:426–432
67. Scholz M, Doerr HW, Cinatl J (2003) Human cytomegalovirusretinitis: pathogenicity, immune evasion and persistence. TrendsMicrobiol 11:171–178
68. Seddon B, Tomlinson P, Zamoyska R (2003) Interleukin 7 and Tcell receptor signals regulate homeostasis of CD4 memory cells.Nat Immunol 4:680–686
69. Seder RA, Ahmed R (2003) Similarities and differences in CD4+and CD8+ effector and memory T cell generation. Nat Immunol4:835–842
70. Silins SL, Cross SM, Elliott SL et al (1996) Development ofEpstein–Barr virus-specific memory T cell receptor clonotypes inacute infectious mononucleosis. J Exp Med 184:1815–1824
71. Sousa AE, Carneiro J, Meier-Schellersheim M et al (2002) CD4T cell depletion is linked directly to immune activation in the
pathogenesis of HIV-1 and HIV-2 but only indirectly to the viralload. J Immunol 169:3400–3406
72. Sun JC, Williams MA, Bevan MJ (2004) CD4+ T cells arerequired for the maintenance, not programming, of memory CD8+T cells after acute infection. Nat Immunol 5:927–933
73. Suvas S, Kumaraguru U, Pack CD et al (2003) CD4+CD25+T cells regulate virus-specific primary and memory CD8+ T cellresponses. J Exp Med 198:889–901
74. Tan JT, Ernst B, Kieper WC et al (2002) Interleukin (IL)-15 andIL-7 jointly regulate homeostatic proliferation of memoryphenotype CD8+ cells but are not required for memory phenotypeCD4+ cells. J Exp Med 195:1523–1532
75. Tomiyama H, Matsuda T, Takiguchi M (2002) Differentiation ofhuman CD8(+) T cells from a memory to memory/effectorphenotype. J Immunol 168:5538–5550
76. Unsoeld H, Krautwald S, Voehringer D et al (2002) Cutting edge:CCR7+ and CCR7- memory T cells do not differ in immediateeffector cell function. J Immunol 169:638–641
77. Weekes MP, Wills MR, Sissons JG et al (2004) Long-term stableexpanded human CD4+ T cell clones specific for humancytomegalovirus are distributed in both CD45RAhigh andCD45ROhigh populations. J Immunol 173:5843–5851
78. Weiss L, Donkova-Petrini V, Caccavelli L et al (2004) Humanimmunodeficiency virus-driven expansion of CD4+CD25+ regu-latory T cells, which suppress HIV-specific CD4 T-cell responsesin HIV-infected patients. Blood 104:3249–3256
79. Wherry EJ, Teichgraber V, Becker TC et al (2003) Lineagerelationship and protective immunity of memory CD8 T cellsubsets. Nat Immunol 4:225–234
80. Wherry EJ, Barber DL, Kaech SM et al (2004) Antigen-independent memory CD8 T cells do not develop duringchronic viral infection. Proc Natl Acad Sci USA 101:16004–16009
81. Woodberry T, Suscovich TJ, Henry LM et al (2005) Differen-tial targeting and shifts in the immunodominance of Epstein–Barr virus-specific CD8 and CD4 T cell responses during acuteand persistent infection. J Infect Dis 192:1513–1524
82. Younes SA, Yassine-Diab B, Dumont AR et al (2003) HIV-1viremia prevents the establishment of interleukin 2-producingHIV-specific memory CD4+ T cells endowed with proliferativecapacity. J Exp Med 198:1909–1922
83. Yue FY, Kovacs CM, Dimayuga RC et al (2005) Preferentialapoptosis of HIV-1-specific CD4+ T cells. J Immunol 174:2196–2204
84. Zaph C, Uzonna J, Beverley SM et al (2004) Central memoryT cells mediate long-term immunity to leishmania major in theabsence of persistent parasites. Nat Med 10:1104–1110
208 Springer Semin Immun (2006) 28:197–208































