Embed Size (px)
Citation preview

Gross Enamel Hypoplasia in Molars From Subadultsin a 16th–18th Century London Graveyard
A.R. Ogden,1* R. Pinhasi,2 and W.J. White3
1Biological Anthropology Research Centre (BARC), Archaeological Sciences, University of Bradford,West Yorkshire BD7 1DP, UK2School of Human and Life Sciences, Roehampton University, Whiteland’s College, Holybourne Avenue,London SW15 4JD, UK3Centre for Human Bioarchaeology, Museum of London, 150 London Wall, London EC2Y 5HN, UK
KEY WORDS enamel defects; dental development; childhood health; molar incisalhypomineralisation (MIH); cuspal enamel hypoplasia (CEH)
ABSTRACT Dental Enamel Hypoplasia has longbeen used as a common nonspecific stress indicator inteeth from archaeological samples. Most researchersreport relatively minor linear and pitted hypoplasticdefects on tooth crown surfaces. In this work we report ahigh prevalence and early age of onset of extensiveenamel defects in deciduous and permanent molars inthe subadults from the post-medieval cemetery of Broad-gate, east central London. Analysis of the dentition of all45 subadults from the cemetery, using both macroscopicand microscopic methods, reveals disturbed cusp pat-terns and pitted, abnormal and arrested enamel forma-tion. Forty-one individuals from this group (93.2%)showed some evidence of enamel hypoplasia, 28 of themshowing moderate or extensive lesions of molars, deciduous
or permanent (63.6% of the sample). Scanning ElectronMicroscope images reveal many molars with grosslydeformed cuspal architecture, multiple extra cusps andlarge areas of exposed Tomes’ process pits, where theameloblasts have abruptly ceased matrix production,well before normal completion. This indented, rough andpoorly mineralized surface facilitates both bacterial ad-hesion and tooth wear, and when such teeth erupt fullyinto the mouth they are likely to wear and decay rapidly.We suggest that this complex combination of pitted andplane-form lesions, combined with disruption of cusppattern and the formation of multiple small cusps,should henceforth be identified as ‘‘Cuspal EnamelHypoplasia.’’ Am J Phys Anthropol 133:957–966, 2007.VVC 2007 Wiley-Liss, Inc.
Dental enamel hypoplasia (DEH) has long been usedas a nonspecific indicator of systemic physiological stressduring early life (Goodman and Rose, 1990; Gautelli-Steinberg and Lukacs, 1999). Bouts of malnutrition, dis-ease, and fever are known to depress the activity of theenamel-forming ameloblasts and to result in the forma-tion of a thin and poorly calcified enamel matrix, withthe formation of linearly distributed pits or grooves ofdefective enamel. Nearly 100 systemic conditions havebeen associated with DEH, but most are rare (Cutressand Suckling, 1982).Enamel is not remodeled during life and every individ-
ual’s enamel is a record of the first 8 or 9 years of theirlife when their crowns are formed (Smith, 1991; Skinnerand Goodman, 1992; Hillson and Bond, 1997). However,the DEH in archaeological individuals is often underesti-mated, as the very high level of tooth wear in past popu-lations has removed evidence of hypoplasia from thefirst-formed regions of each tooth (the enamel-dentinejunction beneath the cusp tips) in those individuals whodie in adolescence or adult life (Hillson, 2005). On thevertical surfaces of the teeth, where most linear hypopla-sia occurs, enamel layers overlap (the imbricationalzone). However, under the cusps of the teeth the domedlayers are piled upon one another, forming the apposi-tional zone (Dean and Beynon, 1991). Incisors and can-ines have 15–20% of enamel layers buried in this region.Molars, however, have a large proportion (40–50%)within this appositional zone. It is with major defects inthis region that we are concerned in this article.
A large cemetery was uncovered in 1985 in east cen-tral London during the demolition of Broad StreetRailway station and the building of the Broadgate devel-opment (White, 1987; Harding, 2002). The ‘‘New Grave-yard’’ was founded in 1569 by the City as an overflowcemetery to relieve the congestion occurring in London’sparish burial grounds and it continued in use until themid 18th century (Harding, 2002). Nonparochial grave-yards were often seen as ‘‘last-resort’’ burial places andthe relatively low fees charged encouraged householdersto bury servants and dependents there, along withfoundlings and ‘‘stranger paupers". In contrast, nonparo-chial graveyards were attractive to dissenters andFrench and Dutch immigrants as the rituals used wereout of the detailed control of the Church of England(Harding, 2002). The cemetery contained many primaryuncoffined burials at a high density of 8/cubic metre(Schofield and Maloney, 1998; Harding, 2002). Only asmall part of this cemetery was excavated during the de-velopment and some 388 individuals, of whom 45 were
*Correspondence to: A.R. Ogden, Biological Anthropology ResearchCentre, Archaeological Sciences, University of Bradford, BradfordBD7 1DP, UK. E-mail: [email protected]
Received 26 April 2006; accepted 15 February 2007
DOI 10.1002/ajpa.20608Published online 9 May 2007 in Wiley InterScience
(www.interscience.wiley.com).
VVC 2007 WILEY-LISS, INC.
AMERICAN JOURNAL OF PHYSICAL ANTHROPOLOGY 133:957–966 (2007)

subadults, were retrieved and stored at the Museum ofLondon (White, 1987).Examination of these subadults has revealed a quite
exceptional level of disturbed enamel formation, not onlyin prevalence, but in extent, compared with otherarchaeological populations (Saunders et al., 2000). Someof this enamel hypoplasia is of the expected linear or pit-ted character, but much of this disruption of enamel isfar more extensive and profound than is usually found(Hillson, 2005).
MATERIALS AND METHODS
This study is a follow-up of our investigation of theeffects of rickets on long-bone growth patterns in the 45subadults retrieved from the Broadgate cemetery (Pinhasiet al., 2006). We examined the dentitions of all subadultsusing standard macroscopic methods and systematicallyrecorded each dentition. A total of 557 teeth were exam-ined with a *5 lens and photographed. Ages of the indi-viduals were estimated from their dental crown and rootdevelopment stages and not from charts that combinetooth eruption with development stages (cf. Ubelaker,1989), as it is known that one of the key signs of ricketsis delayed eruption (Stuart-Macadam, 1989; Wharton andBishop, 2003). The dental age of the individual and theapproximate age of onset of hypoplasia was then calcu-lated based on the chronological sequence of incrementaldeposition and calcification of the enamel matrix (Moor-rees, et al., 1963a,b; Smith, 1991; Hillson, 1992). Thesecharts suggest the approximate ages at which disturbanceof enamel formation began, and after which, in most indi-viduals, amelogenesis appeared to return to relativenormality.The hypoplasia on many molars, both deciduous and
permanent, was on such a scale that none of the conven-tional methods of assessment which are used to record thecommon linear and pitted lesions on canines and incisorswere applicable (Hargreaves et al., 1989; Federation Den-taire International, 1992; Ensor and Irish, 1995; Blakeyand Armelagos, 1997). For the purposes of this prelimi-nary study to establish the extent of the problem, thehypoplasia was coarsely graded visually as:Mild: <30% of the tooth’s enamel surface area visibly
disrupted (this encompasses the entire range reported inmost other studies).Moderate: 31–49% of the tooth’s enamel surface area
visibly disrupted.Extensive: >50% of the tooth’s enamel surface area
visibly disrupted.As all the individuals had died in early life it was pos-
sible to detect hypoplasia on the cusps of their relativelyunworn deciduous or permanent molars. Many uner-upted teeth were also visible because of the disintegra-tion of the bone. Selected teeth were examined,uncoated, with scanning electron microscopy (SEM),under low vacuum, using an FEI Quanta 400. Histologi-cal examination was not attempted at this stage as the
methods are inherently destructive and very time-consuming, but with so many molars affected, this willbe possible and it should answer many of the questionsposed in this article.
RESULTS
Forty-one individuals from this group (93.2%) showedevidence of enamel hypoplasia, 28 of them showing mod-erate or severe lesions of molars, deciduous or perma-nent (63.6% of the sample) (Table 1; Fig. 1). Incisors andcanines, though surviving very much less often, showedepisodes of linear hypoplasia.Fourteen of these individuals (34.1%) showed evidence
of dental malformations probably starting before birth.The deformations of 22 (53.8%) probably started betweenbirth and 6 months. Five individuals (12.2%) showed theonset of hypoplasia as occurring at 6–12 months.Ten of these children (24.4%) also had cavitated cari-
ous lesions opening into dentine, even in permanentteeth, although they had not long been erupted beforedeath supervened. It is known that malnutrition leads toincreased caries, certainly in the deciduous dentition,though its effect on caries of the permanent dentitionhas essentially not yet been studied (Psoter et al., 2005).However it is known that the pattern of caries develop-ment as a function of age is significantly altered in indi-viduals with rickets, as a consequence of the delay in theeruption and exfoliation of the deciduous teeth (Alvarez,1995; Psoter et al., 2005).SEM images of the teeth (not impressions or epoxy
replicas) clearly show grossly deformed cuspal architec-ture (Fig. 2). Large areas of Tomes’ process pits, wherethe ameloblasts evidently ceased matrix productionabruptly, are exposed between islands of more normalenamel (Figs. 3–5). As soon as such teeth erupt into themouth they will rapidly decay, as bacteria can readilylodge on the rough and incompletely mineralizedenamel. With all affected molars it was striking that thecervical third of the crowns was uninvolved, often with aclear demarcation between the cuspal and the cervicalenamel (Figs. 2–5).
DISCUSSION
Enamel development
Amelogenesis takes place in two stages; matrix pro-duction, and maturation. Matrix production involves theformation of an organic gel matrix and the seeding intoit of thin, ribbon-like crystallites of hydroxyapatite fromthe tapering Tomes’ Process of the ameloblast. This ma-trix is only about one third mineral, one third proteinand one third water. Maturation involves removing theprotein and water and increasing the size of the crystal-lites, to produce the heavily mineralized and matureenamel (<1% organic material). The Tomes’ Processshrinks and flattens as enamel formation ends and mat-uration begins, leaving a smooth enamel surface (Nanci,
TABLE 1. Enamel hypoplasia in the broadgate subadults
Commencement Mild Moderate Extensive Total
Before birth (deciduous molars) 7 3 4 14Birth–6 months (deciduous andpermanent molars)
5 9 8 22
6–12 months (permanent molars) 1 2 2 5Total 13 14 14 41
958 A.R. OGDEN ET AL.
American Journal of Physical Anthropology—DOI 10.1002/ajpa

2003, 171–175). The overlapping layers of enamel form-ing the final surface of a tooth crown hide a considerableproportion of the earlier enamel deposition. Many earlylayers do not appear at all on the surface of the com-pleted crown. For anterior teeth, the surface hides some10–20% of crown formation time. For molars, up to one-half of crown formation time may be hidden from viewbeneath the molar cusps (Hillson, 1992).Each ameloblast is involved in all stages of amelogene-
sis, with matrix production for up to 1 year and thenmaturation, which may take up to 5 years in the case ofcanines (Boyde, 1989; Sasaki et al., 1997). The incremen-tal structures in enamel, the brown Striae of Retzius,represent matrix formation only: they appear to be simi-lar in both immature and mature enamel (Hillson, 2005)and persist throughout mineralization. The time of for-mation of the defective enamel is crucial to suggestingpossible aetiology. Important factors to consider are thephase of ameloblastic activity and the severity and dura-tion of the insult (Hillson, 2005).Mineralization of enamel does not progress as a single
simple wave. It progresses on several fronts: from theenamel-dentine junction toward the surface; from the outerenamel surface inwards; from the cusp tips to the root; andthin enamel mineralizes before thick (Boyde, 1989; Smith,1998). It is also possible that all the enamel on a tooth maygo into the maturation process at the same time (Robinsonet al., 1981).Suga (1989) suggested that ameloblasts are very sensi-
tive to disorders at an early stage of maturation, and if acell is damaged by a systemic or local disorder at thisstage, it cannot easily recover from dysfunction duringthe long period of maturation. He stated that amelo-blasts affected during the matrix secretion stage, alter or
even terminate the physiochemical conditions for thecommencement of maturation. Suga also claimed thatthe sensitivity to systemic disorders and the mode ofreaction of the ameloblasts are not the same for each ofthe stages of enamel development. In some cases, cellsat the matrix formation stage when the disorderoccurred, afterwards form a highly mineralized andsound enamel, whereas enamel disturbed at a very earlystage of maturation remains permanently hypomineral-ized.Suckling (1989) described three main phases of amelo-
blast activity, secretory, maturation, and regression.Based on changes in appearance and hardness values,the maturation phase can be divided into an early and alate stage. In the early stage, the enamel is dull andwhite, and relatively soft. In the late-maturation phase,the deeper enamel is well mineralized, but the thin sur-face layer is still incompletely mineralized.The common types of hypoplasia usually recorded are
linear or pitted lesions in the mid-crown region of teeth(Fig. 6). However rarer and more complex forms of hypo-plasia appear in the teeth from Broadgate. ‘‘Plane-form’’defects represent a whole band of ameloblasts that hasceased matrix secretion and are very difficult to inter-pret (Hillson and Bond, 1997). The exposed planeappears to be the surface of just one growth layer. Thewidth of the band may bear no relationship to the dura-tion of the defect and even wide bands probably repre-sent very short disruptions. The initial disturbance mayonly have been of a short duration, affecting ameloblastsat a critical stage of development. As to the severity ofthe insult, it is possible that two or more interacting fac-tors are required to produce the lesions (Hillson, 2005).Hillson and Bond (1997) in their major paper on enamel
Fig. 1. Barchart showing the teeth examined and the incidence of moderate to extensive enamel hypoplasia. As would beexpected, molars, both deciduous and permanent, have survived best as they are larger and multi-rooted, compared with the single-rooted incisors and canines: mandibular teeth have survived better than maxillary as they are embedded in much denser bone. Thehypoplasia occurred most frequently in the deciduous second molars and the first permanent molars.
959ENAMEL HYPOPLASIA IN MOLARS
American Journal of Physical Anthropology—DOI 10.1002/ajpa
hypoplasia and crown growth included only a singleclose-up showing a plane-form defect on a molar. Whatmakes the Broadgate subadults unusual is the sheernumber of individuals (14 or 31.8%) whose molars showlarge areas of defective enamel. This population there-fore provides a unique opportunity to investigate themanifestations of enamel hypoplasia, but also poses aquestion of why they appear so much worse than otherequivalent groups.
New categories of enamel hypoplasia?
The lesions seen on many of the Broadgate molarsare too extensive and complex to be adequatelydescribed as simply ‘‘pitted’’ or ‘‘plane-form’’. The onlymolar illustrated in the literature to also show thisextreme degree of malformation appears in Jenkins,
1978: 262), and is simply labeled by him as ‘‘gross hy-poplasia’’. The combination of pitted and plane-formlesions, combined with the disruption of cusp patternand the formation of multiple small cusps, suggeststhat this nonlinear hypoplasia should be identified as‘‘Cuspal Enamel Hypoplasia, CEH’’ (Fig. 6). Thisappearance, although very rare, is certainly not uniqueto the Broadgate subadults. One of the authors (ARO)has many times been consulted about molars fromother collections, which show this appearance. Unlikeconventional linear or pitted hypoplasia which brieflyinterferes with a process that is already set in motion,CEH develops at the very outset of a tooth’s develop-ment, when the pattern of the cusps is being laid out,and should be designated as a distinct entity. Whateverthe cause, however, in all cases the disturbance toenamel formation seems to have ceased, leading to an
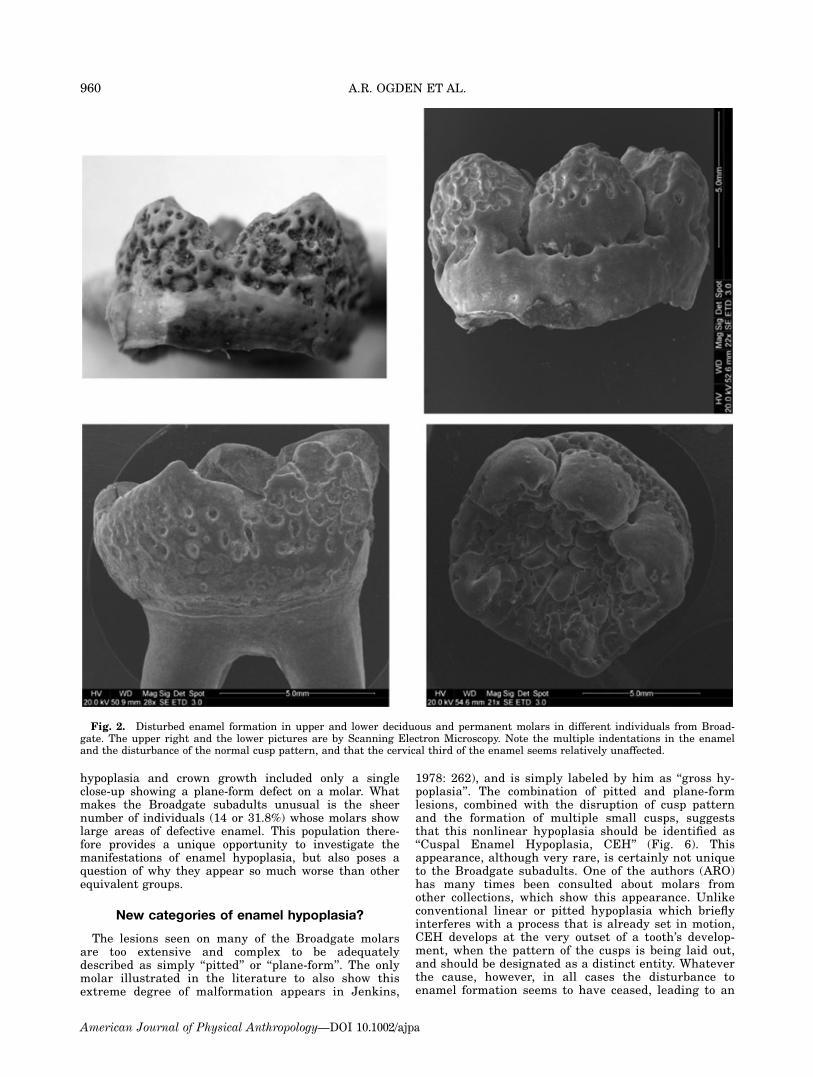
Fig. 2. Disturbed enamel formation in upper and lower deciduous and permanent molars in different individuals from Broad-gate. The upper right and the lower pictures are by Scanning Electron Microscopy. Note the multiple indentations in the enameland the disturbance of the normal cusp pattern, and that the cervical third of the enamel seems relatively unaffected.
960 A.R. OGDEN ET AL.
American Journal of Physical Anthropology—DOI 10.1002/ajpa

eventual resumption in the production of enamel, ofnormal thickness and appearance.Clinically another new type of hypoplasia has recently
been identified: so-called ‘‘cheese molars’’ or Molar Inci-sor Hypomineralisation (MIH) (Weerheijm, 2003; Weer-heijm et al., 2003). MIH is characterized by demarcateddefects in those regions of molar and incisor enamelwhich develop during the same time period, involving analteration in the translucency of the enamel, with thearea being white, yellow, or brown in color. Until recentyears dental caries rates in developed countries wereextremely high, with many first permanent molarsdecaying so rapidly during eruption that there was nopossibility of diagnosing the initial state of the tooth orthe cause of this rampant caries. With the decline indental caries it has become possible clinically to identifyand study erupting molars showing signs of hypoplasia,hypomineralisation, or hypomaturation and this has ledto the identification of MIH (Beentjes, 2003; Weerheijm,2003). There are no good clinical photographs of this con-dition in the literature because such molars have alwaysbeen grossly carious or heavily restored by the time theywere recognized. SEM studies of such molars show theenamel bordering carious lesions to be poorly organizedand porous (Jalevik et al., 2005).Available modern clinical prevalence data for MIH,
mostly from Northern Europe, ranges from 3.6 to 25%,with the highest rates apparently occurring in childrenfrom low fluoride areas whose mothers had been encour-aged to practice extensive and prolonged breast-feeding(Weerheijm, 2003). Histologically the disturbed enamel
shows a severely hypomineralized enamel in the cuspalpart of the tooth with a clearly defined border betweenhypomineralized and normal enamel. It is characteristictoo that the cervical third of the enamel always has anormal appearance (Jalevik et al., 2001, 2005). Thispresent-day condition, when better understood, mayturn out to be related to CEH, but will be difficult toidentify in archaeological teeth, because of the naturaldiscoloration that can occur in the soil.
Comparison with other sites
Lewis (2002b) examined the prevalence of enamelhypoplasia among Anglo-Saxon, early medieval and post-medieval cemetery English populations from St. Helen-on-the-Walls, Christ Church Spitalfields or Raunds Fur-nells, respectively. She reports no DEH among infantsyounger than 6 months from any of these sites. At theage intervals of 0.5–2.5 years DEH was absent amonginfants from Raunds, low in frequency among those fromSt. Helen-on-the-Walls (5%) and moderate among infantsfrom Spitalfields (20%). However the investigator mayhave been looking for conventional clearly demarcatedlinear or pitted enamel hypoplasia in otherwise soundand erupted teeth. Severe hypoplasia may have beenmasked by occlusal destruction from caries and wear.King et al. (2005) examined the onset, frequency, and
duration of linear enamel hypoplasia episodes among 30specimens from the relatively privileged populations ofChrist Church Spitalfields and St Bride’s London. Theyfound that the earliest age at which enamel defects first
Fig. 3. (a, b) Views showing the distorted occlusal architecture of the enamel seen on a developing upper left second deciduousmolar. (c) Developing permanent upper central incisor, showing stepped Plane-form cuspal enamel. This individual also displayedCEH in their permanent first molars. The magnification and scale of each picture are shown at the margins.
961ENAMEL HYPOPLASIA IN MOLARS
American Journal of Physical Anthropology—DOI 10.1002/ajpa

occurred was at 1.2 years and the highest frequencies ofenamel growth disruptions occur between ages 2 and 4years. However these investigators were also looking forlinear or pitted enamel hypoplasia and again caries andattrition may have masked nonlinear hypoplasia. Ourfindings therefore point to a sharp contrast between theage of onset and highest prevalence of enamel hypo-plasias in Broadgate and Christ Church, Spitalfields.
Systemic or local causes?
It is evident that equivalent teeth in the other quad-rants of the mouth were all affected to a varying extentand the systemic disorder must have occurred duringthe first 2 years of life (Moorrees et al., 1963 a,b; Smith,1991). It is also reasonable to assume that the amelo-blasts have been affected by a systemic or local disorderduring a very specific stage of their development.The reason why the first molars were more affected
than the canines and incisors may be that first molarcrowns form in 3.8 years, i.e. half the time that canines take,and so are more vulnerable to short systemic disturbances
(Ensor and Irish, 1995; Fitzgerald, 1998). As the cervicalpart of the enamel on all teeth was relatively unaffectedit could be that the insult only had potential to seriouslydisturb the ameloblasts during the child’s early years.Hillson and Bond (1997) suggested that this may be dueto the abrupt change from widely-spaced and shallowperikymata occlusally to narrowly-spaced perikymatacervically, where defects would be less extensive andobvious. Another possible explanation is that the thick-ness of the enamel influences the ability of the amelo-blasts to resist the insult (Jalevik and Noren, 2000).A Dutch pilot study of medical records from children
with first molars with developmental defects found that48% of the cases had problems related to birth and 67%suffered from respiratory disease (van Amerongen andKreulen, 1995). These figures were higher than normal,and the authors hypothesized that oxygen shortagemight influence the mineralization of the enamel.Chronic diarrhea or environmental toxins, dioxins inparticular, taken up directly with food or via breast milkhave also been suggested as possible causes (Alaluusuaet al., 1996).
Fig. 4. Lower right first permanent molar that was partially erupted, showing arrested development of enamel over the cuspalregions of the crown. Caries has already attacked the first erupted cusp. The close-ups reveal the presence of incompletely mineral-ised enamel with deep Tomes’pits exposed above the rolled enamel margin. The lower left first permanent molar showed a very sim-ilar appearance. The magnification and scale of each picture are shown at the margins.
962 A.R. OGDEN ET AL.
American Journal of Physical Anthropology—DOI 10.1002/ajpa

Was vitamin D deficiency rickets involved? Children incrowded sunless alleys are unable to synthesize vitaminD and we now know this was made even worse in thepast by the ability of a polluted atmosphere to absorbwhat little ultra-violet light there was (David, 1991;Wharton and Bishop, 2003; Mays, 2003; Mays et al.,2006). In recent years there have even been reports fromScandinavia and North America of the reappearance ofrickets (Welch et al., 2000). These are mild cases result-ing however from maternal vitamin D deficiency orprolonged breastfeeding without sufficient vitamin D sup-plementation. Kunzel (2003) has even suggested thatsuch deficiency might cause the appearance of MIH with-out the classical skeletal signs of rickets.It is of significance that Purvis et al. (1973) reporting
on enamel hypoplasia in deciduous incisors, canines andmolars in individuals known to have suffered from neo-natal tetany, described and illustrated the presence of acervical hump separating the normal enamel at the basefrom the thinner enamel nearer the tip. Neonatal tetany,
due to low blood calcium, is a brief, self-limiting bio-chemical disturbance of only a few days duration, yet ithad apparently led to major enamel disruption in 63individuals out of the 112 reviewed.Pinhasi et al. (2006) examined the effect of vitamin D
deficiency rickets on long bone growth in two postme-dieval populations from London: this low socioeconomicstatus population from Broadgate and the middle socioe-conomic status population from Spitalfields. They inves-tigated whether rickets causes growth faltering by com-paring long bone growth curves of individuals withrickets to those without the condition in these two popu-lations. Seven out of the 35 (20%) of the analyzed Broad-gate subadults whose long bones could be measuredwere diagnosed with rickets; in comparison to the 14 outof the 95 subadults from Christ Church Spitalfields(14.7%) reported by Lewis (2002a,b). No statistically sig-nificant difference in long bone growth pattern wasdetected when comparing individuals with rickets tothose without the condition in these skeletal samples.
Fig. 5. Upper and lower developing first permanent molars from different individuals. The abnormalities of cusp pattern and(in close-up) poorly mineralised enamel with Tomes’ pits in the crevices, reveal how vulnerable these teeth would be to rapiddestruction by caries once erupted. It is for this reason that such teeth have seldom survived to attract attention as being hypoplas-tic. The magnification and scale of each picture are shown at the margins.
963ENAMEL HYPOPLASIA IN MOLARS
American Journal of Physical Anthropology—DOI 10.1002/ajpa

However, a cross-population diachronic analysis ofgrowth variation during infancy (0–3 years of age) andearly childhood (3–7 years of age) of these two post-medieval English populations in relation to two medievalpopulations (Raunds Furnells and St-Helens-on-the-Walls) indicated pronounced variations in long bonegrowth attainment between the four populations duringinfancy. This contrasts with nonsignificant variationbetween the populations during early childhood. Themost significant difference in growth during infancy wasbetween two post medieval populations from CentralLondon, as the Broadgate growth curves indicate thatthese infants had significantly lower diaphyseal lengthdimensions per age from birth until the age of four. Atthe age of four this population displays a remarkable‘‘catch-up’’ (in the cross-sectional sense) so that the appa-rent differences between the curves of Broadgate andSpitalfields diminish during childhood. These resultssuggest that the very low socioeconomic status of Broad-gate must have played a significant role in the diet andhealth status of the subadults from this population (Pin-hasi et al., 2006).Seow et al. (2005) studying primary dental enamel
from modern preterm children have reported that theincisal enamel is 20% thinner than in full-term children,but none of the teeth they examined showed visible hy-poplasia, although 52% showed minor defects underSEM. This suggests that the massive disruptions seen inthe teeth of the Broadgate subadults were not related topremature birth.The period of weaning is especially precarious for
infants, with an increase in nutritional stress because ofthe sudden loss of nutrients provided by human milk,and a decrease in immunity because of the decreased im-munoglobulin levels as well as the loss of immunity pro-vided by the mother’s milk. The child is subjected also tothe first real extramaternal contact with the environ-ment and new pathogens (Larsen, 1987). Historicalsources suggest that during the 17th–18th centuries,mean weaning age in Britain dropped from 18 months to7 months (Lewis, 2002a). While weaning at ChristChurch Spitalfields probably occurred around the age of
7 months, there are no indications of growth faltering af-ter this age (Lewis, 2002b). The high prevalence of DEHon the deciduous dentition of Broadgate infants at 0–6months of age suggests that growth faltering startedfrom birth or even in utero. It is therefore likely that theinfants’ mothers were immunodeficient and malnour-ished to the extent that their colostrum could not bufferthese infants from severe environmental stress and thatthe high prevalence of DEH in this population is not dueto post-weaning stress.The apparently unique severity and frequency of
severe hypoplasia in the Broadgate population leads usto ask whether these lesions were perhaps the result ofsome infection, in combination with the likely malnutri-tion of this population. The appearance of many of theseteeth, with multiple small cusps is certainly reminiscentof that of the ‘‘Mulberry molars’’ of congenital syphilis.However in CEH the channels of exposed poorly miner-alized enamel between the islands of more normalsmooth enamel are very different, as in congenital syphi-lis the enamel layer appears intact and smooth, even inthe crevices, and only cusp architecture is affected(Hillson et al., 1998: 175).Industrialization is associated with malnourishment,
poor health and low stature (Floud and Wachter, 1982).During the Industrial Revolution large European citiesbecame a magnet to people from diverse ethnic and soci-oeconomic backgrounds. The variations in socioeconomicstress among urban populations are associated with var-iations in nutrition, living conditions, child labor andother factors (Bogin, 1998). By 1695, residential differen-tiation within London was no longer characterized byoccupation but rather the city became geographically di-vided according to wealth, and people of similar meanswere living in proximity to each other (Finlay, 1981).Thus, 17th–18th century London was an economicallyand socially stratified city with a widening difference inhealth profile among its inhabitants that was associatedto a large extent with the parish in which they dwelled.Inwood (1998) asserts that by 1650 East London had al-ready acquired a working class complexion when newneighborhoods of shacks were erected outside the citywalls. The residents of these shacks lived in high den-sity, without sufficient heating and with poor sanitation,environmental conditions that likely affected their over-all growth status as well as their dental development.The New Graveyard’s peripheral location turned it froman amenity to a refuse burial dump within a mere hun-dred years (Harding, 2002).In modern populations minor hypoplasias and hypomi-
neralizations can appear with surprising frequency inapparently healthy children’s teeth, being present in afrequency as high as 43–64% (Suckling and Pearce,1984; Suckling et al., 1985; Dummer et al., 1986). Thesheer severity and incidence of enamel hypoplasia andcaries in this archaeological population appears to berare. However, it is difficult to compare these figureswith other work, as most published archaeological stud-ies have reported on adults as well, when caries andattrition have destroyed much of the hypoplastic enameland the deciduous teeth have been lost (Palumbeckaiteet al., 2002). An important aspect of this present paperis to alert others to look for evidence of CEH and MIHand to suspect it, if molars are unexpectedly carious orworn for the age of the individual in their population.The teeth examined in this study provide us with a
unique opportunity to examine gross developmental
Fig. 6. The different types of enamel hypoplasia seen onmolars. Pits and furrows (Linear enamel hypoplasias) are welldescribed in the literature. Plane-form hypoplasia is much rarerand is usually bounded and overlapped by an irregular borderof relatively normal enamel, but occasionally all the occlusalenamel is thin and there may be only a cervical border of rela-tively normal enamel. Cuspal enamel hypoplasia is a combina-tion of irregular plane-form defects with extensive and irregularnonlinear pitting, but commences at the very onset of tooth de-velopment when the cusps are being mapped out, with a disrup-tion of normal cusp formation and the formation of additionalsmall cusps on the occlusal surface. Note that with all types ofhypoplasia the cervical third of the enamel, demarcated herewith a dotted line, is relatively little effected.
964 A.R. OGDEN ET AL.
American Journal of Physical Anthropology—DOI 10.1002/ajpa

disruption of the early stages of crown formation. Con-centrated effort will be required to make the most of thisunusual population. Image analysis will help more pre-cisely quantify the surface area of enamel involved. His-tological analysis using ground sections of the Broadgatemolars will enable us to clarify the formation andsequence of these lesions. By examination of their rela-tionship to the Striae of Retzius, neo-natal lines andevidence of weaning, and by measurement using thechronology by Reid and Dean (2006), we hope to betterunderstand these lesions and to further our understand-ing of their aetiology.
CONCLUSIONS
This group of subadults displays a high prevalence ofmoderate-to-extensive enamel defects never previouslyreported in a subadult sample. Molars, both deciduous andpermanent, were affected with large areas of incompletelymineralized enamel with disruption of the normal cusppattern. The enamel that is formed is often pitted andabnormal in morphology. The lesions seen on many ofthese molars are too extensive and complex to be simplydescribed as a combination of ‘‘pitted’’ or ‘‘plane-form".With disruption of normal cusp pattern, and the formationof multiple additional small cusps, we suggest that a newpattern of nonlinear hypoplasia should be described as‘‘CEH". Research will further investigate the structure ofthese teeth and the formation and possible causes of CEH,and should shed light on why this condition was so dra-matically present in this archaeological population.
ACKNOWLEDGMENTS
The authors thank Professor Martin Curzon of LeedsDental Institute for supplying a clinical perspective andStuart Fox of the Department of Archaeological Sciences,University of Bradford for his advice on SEM technique.
LITERATURE CITED
Alaluusua S, Lukinmaa PL, Koskimies M, Pirinen S, Holtta P,Kallio M, Holttinen T Salmenpera L. 1996. Developmentaldental defects associated with long breast feeding. Eur J OralSci 104:493–197.
Alvarez JA. 1995. Nutrition, tooth development, and dentalcaries. Am J Clin Nutr 61(Suppl):410S–416S.
Beentjes VE, Weerheim KL, Groen HJ. 2003. Factors involvedin the aetiology of molar-incisor hypomineralisation (MIH).Eur J Paediatr Dent 3:9–13.
Blakey ML, Armelagos GJ. 1997. Comment on ‘‘Hypoplastic areamethod for analyzing enamel hypoplasia’’ B.E. Ensor and J.D.Irish, American Journal of Physical Anthropology (1995) 98:507–517. Am J Phys Anthropol 102:295–299.
Bogin B. 1998. Social and economic class. In: Ulijaszek, SJ,Johnston, FE, Preece, MA, editors. The Cambridge encyclo-paedia of human growth and development. Cambridge: Cam-bridge University Press. p 399–401.
Boyde A. 1989. Enamel. In: Berkovitz BKB, editor. Handbook ofmicroscopic anatomy: teeth, Vol.V/6. Berlin: Springer-Verlag.p 309–473.
Cutress TW, Suckling GW. 1982. The assessment of noncariousdefects of enamel. Int Dent J 32:117–22.
David L. 1991. Common vitamin D-deficiency rickets. In: Glori-eux FH, editor. Rickets, Vol. 21. New York: Raven. p 107–122.Nestle Nutrition Workshop Series.
Dean MC, Beynon AD. 1991. Histological reconstruction ofcrown formation times and initial root formation times in amodern human child. Am J Phys Anthropol 86:215–228.
Dummer PM, Kingdon A, Kingdon R. 1986. Distribution of de-velopmental defects of tooth enamel by tooth type in 11-12year-old children in South Wales. Comm Dent Oral Epidemiol14:341–344.
Ensor BE, Irish JD. 1995. Hypoplastic area method for analyz-ing dental enamel hypoplasia. Am J Phys Anthropol 98:507–517.
Federation Dentaire International. 1992. A review of the devel-opmental defects of enamel index (DDE Index). Commissionon oral health, research & epidemiology: report of an FDIworking group. Int Dent J 42:411–426.
Finlay R. 1981. Population and metropolis: the demography ofLondon 1580–1650. Cambridge: Cambridge University Press.
FitzGerald CM. 1998. Do enamel microstructures have regulartime dependency? Conclusions from the literature and alarge-scale study. J Hum Evol 35:371–386.
Floud R, Wachter K. 1982. Poverty and physical stature: evi-dence on the standard of living in London boys, 1770–1870.Soc Sci Hist 6:422–452.
Gautelli-Steinberg D, Lukacs JR. 1999. Interpreting sex differen-ces in enamel hypoplasia in human and non-human primates:developmental, environmental, and cultural considerations.Yrbk Phys Anthropol 42:78–126.
Goodman AH, Rose JC. 1990. Assessment of systemic physiolog-ical perturbations from dental enamel hypoplasias and associ-ated histological structures. Yrbk Phys Anthropol 33:59–110.
Harding V. 2002. The dead and the living in Paris and London1500–1670. Cambridge: Cambridge University Press.
Hargreaves JA, Cleaton-Jones PE, Williams SD. 1989. Hypocal-cification and hypoplasia in permanent teeth of children fromdifferent ethnic groups in South Africa assessed with a newindex. Adv Dent Res 3:126–131.
Hillson S. 1992. Studies of growth in dental tissues. J Hum Ecol3(Special Issue 2):7–23.
Hillson S. 2005. Teeth, 2nd ed. Cambridge: Cambridge Univer-sity Press. p 169–176.
Hillson S, Bond S. 1997. Relationship of enamel hypoplasia tothe pattern of tooth crown growth: a discussion. Am J PhysAnthropol 104:89–103.
Hillson S, Grigson C, Bond S. 1998. Dental defects of congenitalsyphilis. Am J Phys Anthropol 107:25–40.
Inwood S. 1998. A history of London. London: Macmillan.Jalevik B, Noren JG. 2000. Enamel hypomineralisation of
permanent first molars: a morphological study and survey ofpossible aetiological factors. Int J Paediatr Dent 10:278–289.
Jalevik B, Klingberg G, Barregard L Noren JG. 2001. The prev-alence of demarcated opacities in permanent first molars in agroup of Swedish children. Acta Odontol Scand 59:255–260.
Jalevik B, Dietz W, Noren JG. 2005. Scanning electron micro-graph analysis of hypomineralised enamel in permanent firstmolars. Int J Paediatr Dent 15:233–240.
Jenkins GN. 1978. The physiology and biochemistry of themouth. Oxford: Blackwell.
King T, Humphrey LT, Hillson S. 2005. Linear enamel hypopla-sias as indicators of systemic physiological stress: evidencefrom two known age-at-death and sex populations from post-medieval London. Am J Phys Anthropol 128:547–559.
Kunzel W. 2003. Die hypomineralisation bei molaren und inci-siven. Zahnarztl Mitt 93:1626–1629.
Larsen CS. 1987. Bioarchaeological interpretations of subsist-ence economy and behavior from human skeletal remains.Adv Archaeol Method Theory 10:339–445.
Lewis ME. 2002a. The impact of industrialisation: comparativestudy of child health in four sites from medieval and post-medi-eval England (850–1859). Am J Phys Anthropol 119:211–223.
Lewis ME. 2002b. Urbanisation and child health in medievaland post-medieval England. Oxford: BAR. BAR British Series339.
Mays S. 2003. The rise and fall of rickets in England. In: Mur-phy P, Wiltshire PEJ, editors. The environmental archaeologyof industry. Oxford: Oxbow. p 144–153.
Mays S, Brickley M, Ives R. 2006. Skeletal manifestations ofrickets in infants and young children in an historic populationfrom England. Am J Phys Anthropol 129:518–528.
965ENAMEL HYPOPLASIA IN MOLARS
American Journal of Physical Anthropology—DOI 10.1002/ajpa

Moorrees CFA, Fanning EA, Hunt EE. 1963a. Age variation offormation stages for ten permanent teeth. J Dent Res 42:1490–1502.
Moorrees CFA, Fanning EA, Hunt EE. 1963b. Formation andresorption of three deciduous teeth in children. Am J PhysAnthropol 21:205–213.
Nanci A. 2003. Ten cate’s oral histology: development, structureand function. St Louis: Mosby. p 145–191.
Palumbeckaite Z, Jankausas R, Boldsen J. 2002. Enamel hypo-plasia in Danish and lithuanian late medieval/early modernsamples: a possible reflection of child morbidity and mortalitypatterns. Int J Osteoarch 12:189–201.
Pinhasi R, Shaw P, White B, Ogden AR. 2006. Morbidity, rick-ets, and long-bone growth in post-medieval Britain—a cross-population analysis. Ann Hum Biol 33:372–389.
Psoter WJ, Reid BC, Katz RV. 2005. Malnutrition and dentalcaries: a review of the literature. Caries Res 39:441–447.
Purvis RJ, Barrie WJ, MacKay GS, Wilkinson EM, Cockburn FBelton NR. 1973. Enamel hypoplasia of the teeth associatedwith neonatal tetany: a manifestation of maternal vitamin-Ddeficiency. Lancet 2:811–814.
Reid DJ, Dean MC. 2006. Variation in modern human enamelformation times. J Hum Evol 50:329–346.
Robinson C, Briggs HD, Atkinson PJ, Weatherell JA. 1981.Chemical changes during formation and maturation of humandeciduous enamel. Arch Oral Biol 26:1027–1033.
Sasaki T, Takagi M, Yanagisawa T. 1997. Structure and func-tion of secretory ameloblasts in enamel formation. In: Chad-wick DJ, Carew G, editors. Dental enamel. Proceedings ofthe Ciba Foundation Symposium 205. Chichester: Wiley. p32–50.
Saunders SR, Hoppa RD, Macchiarelli R, Bondioli L. 2000.Investigating variability in human dental development in thepast. Anthropologie 38:101–107.
Schofield J, Maloney C, editors. 1998. Archaeology in the cityof London, 1907–1991: a guide to records of excavations bythe museum of London and its predecessors. The archaeologi-cal Gazetteer Series, Vol. 1. London: Museum of London.
Seow WK, Young WG, Tsang AK, Daley T. 2005. A study of pri-mary dental enamel from preterm and full-term childrenusing light and scanning electron microscopy. Pediatr Dent27:374–379.
Skinner M, Goodman AH. 1992. Anthropological uses of devel-opmental defects in enamel. In: Saunders SR, Katzenberg
MA, editors. Skeletal biology of past people: research meth-ods. New York: Wiley-Liss. p 153–174.
Smith BH. 1991. Standards of human tooth formation and dentalage assessment. In: Kelley MA, Larsen CS, editors. Advancesin dental anthropology. New York: Wiley-Liss. p 143–168.
Smith CE. 1998. Cellular and chemical events during enamelmaturation. Crit Rev Oral Biol Med 9:128–161.
Stuart-Macadam PL. 1989. Nutritional deficiency diseases: asurvey of scurvy, rickets, and iron-deficiency anaemia. In:Iscan MY, Kennedy KAR, editors. Reconstruction of life fromthe skeleton. New York: Wiley-Liss.
Suckling GW. 1989. Developmental defects of enamel—historicaland present-day perspectives of their pathogenesis. Adv DentRes 3:87–94.
Suckling GW, Brown RH, Herbison GP. 1985. The prevalence ofdevelopmental defects of enamel in 696 nine-year-old NewZealand children participating in a health and developmentstudy. Community Dent Health 2:303–313.
Suckling GW, Pearce EI. 1984. Developmental defects of enamelin a group of New Zealand children: their prevalence andsome associated etiological factors. Community Dent Oral Epi-demiol 12:177–184.
Suga S. 1989. Enamel hypomineralisation viewed from the pat-tern of progressive mineralisation of human and monkeydeveloping enamel. Adv Dent Res 3:188–198.
Ubelaker DH. 1989. Human skeletal remains, 2nd ed. Washing-ton: Taraxacum Press.
van Amerongen WE, Kreulen CM. 1995. Cheese molars: a pilotstudy of the etiology of hypocalcifications in first permanentmolars. ASDC J Dent Child 62:266–269.
Weerheijm KL. 2003. Molar incisor hypomineralisation (MIH).Eur J Paediatr Dent 4:114–120.
Weerheijm KL, Duggal M, Mejare I, Papagiannoulis L, Koch G,Martens LC, Hallonsten AL. 2003. Judgement criteria formolar incisor hypomineralisation MIH in epidemiologic stud-ies: a summary of the European meeting on MIH held in Ath-ens, 2003. Eur J Paediatr Dent 4:110–113.
Welch TR, Bergstrom WH, Tsang RC. 2000. Vitamin D-deficientrickets: the re-emergence of a once conquered-disease. J Pae-diatr 137:143–145.
Wharton B, Bishop N. 2003. Rickets. Lancet 362:1389–1394.White WJ. 1987. The human skeletal remains from the broad-
gate site LSS85. Museum of London archaeological serviceMOLAS unpublished report HUM/REP/87/01.
966 A.R. OGDEN ET AL.
American Journal of Physical Anthropology—DOI 10.1002/ajpa





























