Embed Size (px)
Citation preview

C
CE: Tripti; JCM-D-14-00422; Total nos of Pages: 8;
JCM-D-14-00422
Original article
Heart surgery for immigrants in Italy: burden ofcardiovascular disease, adherence to treatmentand outcomesAntonio Grimaldi, Anna Chiara Vermi, Valeria Cammalleri,Alessandro Castiglioni, Federico Pappalardo, Maurizio Taramasso,Francesca Baratto and Ottavio Alfieri
Aim Italy is a country with high rates of immigration and the
knowledge of immigrant health is very fragmentary. We
provide a current picture of cardiovascular disease causes
and clinical outcomes following heart surgery.
Methods A clinical and echocardiographic survey was
conducted on 154 consecutive immigrants referred for
heart surgery to San Raffaele Hospital in Milan between
2003 and 2011.
Results Major causes of heart disease were rheumatic
heart disease (RHD) (n U 64, 41%), nonrheumatic
valvulopathies (n U 41, 27%), ischemic heart disease (IHD)
(n U 25, 16%), congenital heart disease (n U 13, 9%) and
miscellaneous (n U 11, 7%). Median age was 49 years
[interquartile range (IQR) 7–81]; 55% of patients were male.
Among valvulopathies, rheumatic mitral disease was
predominant (n U 56, 53%) as both single and multivalvular
disease (n U 46, 73%); myxomatous prolapse emerged as
the second main pattern of mitral disease (n U 30, 33%).
Among patients with IHD, 72% had a high cardiovascular
risk. Surgery was scheduled in 138 patients (90%).
Clinical follow-up was available in 96 patients (62%)
[median time 62 months (IQR 15–123)], among whom 92
opyright © Italian Federation of Cardiology. Una
1558-2027 � 2014 Italian Federation of Cardiology
(96%) were alive, four patients (4%) had died and 58 (38%)
were lost.
Conclusion Cardiovascular diseases represent a major
health topic among immigrants in developed countries.
RHD still is the predominant cause of hospitalization for
heart surgery, nonrheumatic valvulopathies and IHD
emerging as second and third causes, respectively. Data
underline the need of reinforcement of prevention and care
strategies in the matter of immigrant health and warrant the
urgent attention of the international public health and
research communities.
J Cardiovasc Med 2014, 15:000–000
Keywords: heart surgery, immigration and health, rheumatic heart disease,valvular heart disease
Cardiovascular and Thoracic Department, San Raffaele Scientific Institute andUniversita Vita-Salute, Milan, Italy
Correspondence to Antonio Grimaldi, Cardiovascular and Thoracic Department,San Raffaele Scientific Institute, via Olgettina 60, 20132 Milan, ItalyTel: +390226437124; e-mail: [email protected]
Received 24 July 2014 Revised 10 September 2014Accepted 16 September 2014
IntroductionMovement of people between countries has become an
essential part of contemporary society and approximately
175 million people, up to 2.9% of the world’s population,
currently live outside their countries of origin, spurred by
poverty, political and social conflicts (http://publication-
s.iom.int/bookstore/free/WMR_2003.pdf). The widening
economic gap between the European Union and other
regions continues to prompt people to move elsewhere
and the need for more data on immigrants’ health has
definitely been recognized by the WHO.1 Italy is no
exception to this and the movement in and around the
country is unlikely to diminish in the foreseeable future
(http://www.istat.it/en/archive/40658). Cardiovascular
diseases (CVDs) account for the largest proportion of
all-cause mortality and up to 48% of all deaths in Europe,2
but estimating CVDs in immigrants is complicated and
should take into consideration net migration, morbidity
and ethnic identity. Mass population movements fre-
quently produce a mishmash between the diseases
inherently linked to the native country [e.g. rheumatic
heart disease (RHD), and other communicable diseases]
and acquired risk factors (e.g. smoking, alcohol abuse,
obesity).3–5 The population-based study aimed to pro-
vide a current picture of major heart diseases in immi-
grants referred for heart surgery to a tertiary care centre.
Ethnic provenance, noncommunicable risk factors,
adherence to treatment and outcomes are the major
issues addressed in a community in epidemiologic transi-
tion.
Materials and methodsStudy cohortWe prospectively analysed the demographic and
clinical characteristics of 159 consecutive indivi-
duals [median age 48 years, interquartile range (IQR)
7–81 years; male/female ratio ¼ 1,1)] referred for heart
disease to the Department of Cardiac Surgery of San
Raphael Hospital (Milan, Italy) between 2003 and 2011.
Patients were systematically evaluated by clinical and
uthorized reproduction of this article is prohibited.
DOI:10.2459/JCM.0000000000000228

Co
CE: Tripti; JCM-D-14-00422; Total nos of Pages: 8;
JCM-D-14-00422
2 Journal of Cardiovascular Medicine 2014, Vol 00 No 00
echocardiographic examination based on transthoracic
echocardiography (TTE) and transoesophageal echocar-
diography (TEE). Among the 159 individuals, 154 (97%)
presented with clinical symptoms related to structural
heart disease and constituted the study cohort (Fig. 1).
Clinical assessmentRHD was diagnosed on the basis of medical history of
acute rheumatic fever, clinical evaluation and echocar-
diographic features according to WHO/WHF guidelines
(http://whqlibdoc.who.int/trs/WHO_TRS_923.pdf).6
Single and multiple valve diseases were quantified
according to EAE/ASE criteria7; patients with trivial
mitral regurgitation and no structural valve changes were
excluded. TTE and TEE were performed in all patients
aimed to assess the degree of valvular regurgitations and
other associated valvulopathies; valve area planimetry;
left ventricular dimensions and ejection fraction and right
ventricular systolic function; suitability for repair surgery;
and to rule out embolic sources in patients with atrial
fibrillation.
Statistical analysisWe performed descriptive statistics for the more fre-
quently observed heart diseases and the results are
pyright © Italian Federation of Cardiology. Unau
Fig. 1
Patientsstructura
diseaN = 1
RHDN = 64
Nonrheumaticvalvulopathies
N = 41N
Surgery pe
YesN = 138
Lost to FUN = 50 (36%)
Mortality at FUN = 4 (5%)
Alive to FUN = 84 (100% NYHA 1/2)
Flow chart, surgical treatment and outcomes in the overall study population
reported as median and IQR, or as numbers and percen-
tages, as appropriate.
ResultsAll causes of heart disease in the whole studypopulationThe clinical and echocardiographic characteristics of
patients are depicted in Table 1. The study group con-
stitutes a cohort of 154 patients; the median age was
49 years (IQR 7–81) and 85 patients (55%) were male. All
patients were symptomatic [New York Heart Association
(NYHA)¼ 2.3� 0.7; class II¼ 60%; class III/IV¼ 40%]
under optimized medical treatment and 25 patients
(16%) were in permanent atrial fibrillation at the time
of admission. The ethnic provenance included 61
Eastern Europeans (40%), 51 black Africans (33%), 19
Asians (12%), 19 Latin Americans (12%) and four Middle
Easterners (3%); all immigrants lived in urban and sub-
urban areas of Milan in Lombardy and were regularly
registered with the Italian NHS. A previous heart surgery
was reported in 25 patients (16%) and included mitral
(n¼ 8, 32%) and aortic valve replacement (n¼ 4, 16%),
mitral commissurotomy (n¼ 6, 24%), atrial septal
defect(s) (ASD) closure (n¼ 4, 16%), tricuspid annulo-
plasty (n¼ 2, 8%) and surgery for ascending aortic disease
(n¼ 1, 4%).
thorized reproduction of this article is prohibited.
with l heartse54
IHD = 25
CHDN = 13
VariousN = 11
rformed
NoN = 16
Lost to FUN = 8 (50%)
Mortality at FUN = 0
Alive to FUN = 8 (88% NYHA 1/2)
.
C
CE: Tripti; JCM-D-14-00422; Total nos of Pages: 8;
JCM-D-14-00422
Heart surgery in immigrants Grimaldi et al. 3
Table 1 Clinical and echocardiographic characteristics of 154 patients with structural heart disease
Main cause of heart disease RHD Nonrheumatic valvulpathies IHD CHD Various Total
No. of cases (%) 64 (41) 41 (27) 25 (16) 13 (9) 11 (7) 154 (100)Age (years) median (IQR) 44 (7–68) 52 (10–81) 57 (36–77) 43 (8–63) 43 (30–69) 49 (7–81)Male sex, n (%) 26 (40) 23 (56) 23 (92) 6 (46) 7 (64) 85 (55)Ethnic provenance, n (%)
Eastern Europe 19 (30) 20 (49) 10 (40) 6 (46) 6 (54) 61 (40)Africa (north/sub-Saharian) 28 (44) 12 (29) 7 (28) 2 (15) 2 (18) 51 (33)Central/South America 11 (17) 2 (5) 2 (8) 3 (23) 1 (9) 19 (12)Asia 6 (9) 6 (15) 6 (24) 0 (0) 1 (9) 19 (12)Middle East 0 (0) 1 (2) 0 (0) 2 (15) 1 (9) 4 (3)
CVD risk factors, n (%)Hypertension 12 (19) 13 (32) 20 (80) 7 (54) 2 (18) 54 (35)Hypercholesterolaemia 10 (16) 11 (27) 20 (80) 3 (23) 3 (27) 47 (31)Type 2 diabetes 3 (5) 1 (2) 11 (44) 1 (8) 1 (9) 17 (11)Smoking 6 (9) 6 (15) 7 (28) 1 (8) 3 (27) 23 (15)Overweight 9 (14) 18 (44) 12 (48) 1 (8) 4 (36) 44 (29)
NYHA (mean�SD) 2.6�0.7 2.2�0.7 2.2�0.6 1.8�0.5 2.4�0.9 2.3�0.7LV systolic dysfunction, n (%) 17 (26) 10 (24) 12 (48) 1 (8) 6 (54) 46 (30)LVEF % median (IQR) 60 (25–66) 60 (20–70) 50 (20–64) 60 (55–70) 50 (25–70) 60 (20–70)LV dilatation
�, n (%) 28 (44) 21 (51) 12 (48) 1 (8) 3 (27) 65 (42)
LA dilatation��
, n (%) 62 (97) 38 (93) 23 (92) 11 (85) 11 (100) 145 (94)AF 22 (34) 0 (0) 1 (4) 0 (0) 2 (18) 25 (16)Moderate-to-severe MR, n (%) 33 (51) 32 (78) 8 (32) 1 (8) 4 (36) 78 (51)PH, n (%)
���52 (81) 22 (54) 11 (44) 4 (31) 5 (45) 94 (61)
Moderate-to-severe RV dysfunction, n (%) 11 (17) 4 (10) 2 (8) 2 (15) 5 (45) 23 (16)Coronary artery disease, n (%) 1 (1) 8 (20) 25 (100) 0 (0) 2 (18) 36 (23)Surgical treatment 54 (35) 39 (25) 24 (16) 12 (8) 9 (6) 138 (90)
Valve surgery 54 (100) 37 (95) 5 (21) 9 (75) 3 (33) 108 (70)CABG 1 (2) 6 (15) 21 (88) 0 (0) 1 (11) 29 (19)Complex aorta surgery 0 (0) 2 (5) 0 (0) 7 (58) 0 (0) 9 (6)Others 0 (0) 3 (8) 3 (13) 6 (50) 6 (67) 18 (12)
AF, atrial fibrillation; CABG, coronary artery bypass graft; CHD, congenital heart disease; CVD, cardiovascular disease; IHD, ischemic heart disease; IQR, interquartilerange; LA, left atrium; LV, left ventricular; LVEF, left ventricular ejection fraction; MR, mitral regurgitation; MVD, multivalvular disease; PH, pulmonary hypertension; RHD,rheumatic heart disease; RV, right ventricular; SVD, single-vessel disease.
�end-diastolic diameter >55 mm.
��volume >40 ml.
���systolic pulmonary artery pressure
>35mmHg.
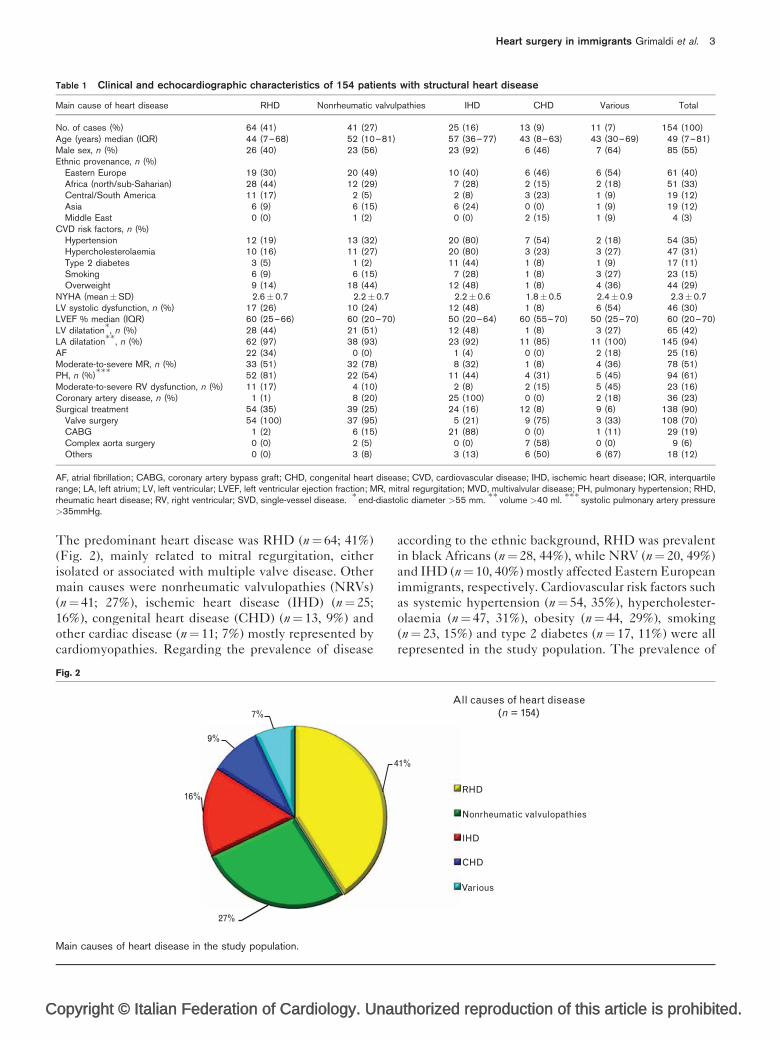
The predominant heart disease was RHD (n¼ 64; 41%)
(Fig. 2), mainly related to mitral regurgitation, either
isolated or associated with multiple valve disease. Other
main causes were nonrheumatic valvulopathies (NRVs)
(n¼ 41; 27%), ischemic heart disease (IHD) (n¼ 25;
16%), congenital heart disease (CHD) (n¼ 13, 9%) and
other cardiac disease (n¼ 11; 7%) mostly represented by
cardiomyopathies. Regarding the prevalence of disease
opyright © Italian Federation of Cardiology. Una
Fig. 2
7%
9%
16%
27%
Main causes of heart disease in the study population.
according to the ethnic background, RHD was prevalent
in black Africans (n¼ 28, 44%), while NRV (n¼ 20, 49%)
and IHD (n¼ 10, 40%) mostly affected Eastern European
immigrants, respectively. Cardiovascular risk factors such
as systemic hypertension (n¼ 54, 35%), hypercholester-
olaemia (n¼ 47, 31%), obesity (n¼ 44, 29%), smoking
(n¼ 23, 15%) and type 2 diabetes (n¼ 17, 11%) were all
represented in the study population. The prevalence of
uthorized reproduction of this article is prohibited.
41%
RHD
Nonrheumatic valvulopathies
IHD
CHD
Various
All causes of heart disease(n = 154)

Co
CE: Tripti; JCM-D-14-00422; Total nos of Pages: 8;
JCM-D-14-00422
4 Journal of Cardiovascular Medicine 2014, Vol 00 No 00
coronary artery disease (CAD) in the overall population
study (n¼ 36, 23%) was higher than that from the single
IHD group, as 11 additional patients (17%) had subcli-
nical CAD at preoperative angiography. Left ventricular
ejection fraction (LVEF) was reduced in 46 cases (30%);
moderate-to-severe right ventricular dysfunction was
found in 23 (15%) cases.
Rheumatic heart diseaseRHD (n¼ 64) was the main cause of hospitalization for
heart surgery. The median age of patients was 44 years
(IQR 7–68) with a female/male ratio of 1.5/1. The
distinctive valvular patterns of RHD are depicted in
Table 2. Multivalvular disease (MVD) was prevalent
(n¼ 46, 72%) and mitral involvement was preferably
associated with tricuspid and aortic valve disease
(n¼ 24/46, 52%); two patients were affected by rheumatic
involvement of four valves (n¼ 2, 4%). Single valve
disease (SVD) (n¼ 17, 26%) affected the mitral valve
(n¼ 10/17, 59%) and the aortic valve (n¼ 7/17, 41%) with
a higher prevalence in female in both groups (MVD
n¼ 26; 26/46¼ 57%, SVD n¼ 12; 12/17¼ 70%). The
pyright © Italian Federation of Cardiology. Unau
Table 2 Clinical and echocardiographic characteristics of patientswith rheumatic and nonrheumatic valvulopathies
Main cause of heartdisease RHD
Nonrheumaticvalvulopathies
No. of cases (%) 64 (41) 41 (27)Age (years) median (IQR) 44 (7–68) 52 (10–81)Male sex (M), n (%) 26 (40) 23 (56)SVD, n (%) 18 (28) 24 (59)MVD, n (%) 46 (72) 17 (41)Mitral valve disease, n (%) 56 (88) 35 (85)
MS 8 (14) 0 (0)MR 15 (27) 35 (100)Combined 34 (61) 0 (0)Valve prolapse 7 (13) 30 (86)Ruptured cordae 3 (5) 12 (34)Infective endocarditis 2 (4) 4 (11)Prosthesis dysfunction 8 (14) 0 (0)
Aortic valve disease, n (%) 40 (63) 12 (29)AS 1 (3) 0 (0)AR 26 (67) 6 (50)Combined 13 (33) 6 (50)Infective endocarditis 0 (0) 1 (8)Prosthesis dysfunction 4 (10) 0 (0)Ascending aorta dilatation 4 (10) 6 (50)
Tricuspid valve disease, n (%) 37 (58) 13 (32)Annular dilatation 36 (97) 10 (77)Leaflet thickening/fibrosis 11 (30) 2 (15)Valve prolapse 0 (0) 3 (23)Infective endocarditis 0 (0) 2 (15)
LA dilatation�
(ml, mean�SD) 110�52 78�24Atrial thrombi, n (%) 8 (12,5) 1 (2)Coronary artery disease, n (%) 1 (1) 8 (20)sPAP (mean�SD) 52�16 38�7Surgical treatment 54 (35) 39 (25)
Valve replacement 49 (91) 12 (31)Valve repair 5 (9) 25 (64)AF ablation 15 (28) 0 (0)Redo operation 6 (11) 1 (3)CABG 1 (2) 6 (15)Ascending aorta surgery 0 (0) 2 (5)Others 0 (0) 3 (8)
AF, atrial fibrillation; AR, aortic regurgitation; AS, aortic stenosis; IHD, ischemicheart disease; IQR, interquartile range; MVD, multivalvular disease; RHD, rheu-matic heart disease; sPAP, systolic pulmonary artery pressure; SVD, single-vesseldisease.
�volume >40 ml.
mitral valve was affected in 57 patients (89%) and mitral
regurgitation was the most common lesion (49/64 cases,
77%). Mitral stenosis was severe in 21 patients (33%) and
combined disease (MS-MR) affected 34 patients (61%).
Interestingly, 13% of rheumatic mitral valves also showed
an associated myxomatous valve prolapse. We observed
different patterns of rheumatic mitral regurgitation: sym-
metrical leaflet restriction with annular dilatation;
posterior leaflet restriction and anterior leaflet pseudo-
prolapse; and leaflet restriction associated with commis-
sural fusion and valve stenosis. Calcified lesions were
deemed not suitable for surgical repair.
Pulmonary hypertension (i.e. pulmonary artery systolic
pressures >35 mmHg) was present in 58 patients [81%;
median 50 (30–100 mmHg)] and moderate-to-severe right
ventricular dysfunction in 11 patients (17%). Moderate-to-
severe tricuspid regurgitation, mostly due to functional
annular dilatation, was present in 28 patients (44%).
Nonrheumatic valvulopathiesNRV (n¼ 41) was the second referring cause for heart
surgery in the population study. The median age of
patients was 52 years (IQR 10–81) with a male/female
ratio of 1.3/1. Mitral regurgitation was the most common
lesion observed (n¼ 35/41, 85%) (Table 2) and the
degree of mitral regurgitation was often severe (n¼ 32/
41, 78%). Among mitral valve disease, mitral regurgita-
tion was mostly related to myxomatous prolapse (n¼ 30,
86%) with associated ruptured chordae tendinae in 12
individuals (34%). Overall, among all (rheumatic and
nonrheumatic) valvulopathies, myxomatous prolapse
emerged as the second main pattern of mitral disease
(n¼ 30/91, 33%) following rheumatic mitral regurgitation
(n¼ 49/91, 54%).
Aortic valve disease (n¼ 12, 29%) was prevalent as aortic
insufficiency (n¼ 6, 50%) or combined disease (n¼ 6,
50%). Isolated Aortic Regurgitation was related to
intrinsic valve disease (n¼ 3) or functional involvement
secondary to aortic root disease (two hypertensive indi-
viduals and one with Takayasu’s arteritis). One out the
patients affected by severe calcified aortic stenosis (AS)
(n 4/12, 33%) also had severe porcelain aorta deemed not
suitable for opern heart surgery. Infective endocarditis
affected 17% of nonrheumatic mitral valves.
Ischemic heart diseaseIHD presenting with coronary syndromes affected 16%
(n¼ 25) of patients in the survey. The clinical profile is
depicted in Table 3. The median age of patients was
57 years (IQR 36–77) with a male/female ratio of 11.5/1.
Chest pain (80%) and shortness of breath (20%) were the
main symptoms at the time of admission to hospital.
Overall, a high cardiovascular risk profile (more than
two risk factors) was observed in 72% of patients.
Cigarette smoking was reported in 28% of patients,
and high blood pressure, dyslipidemia, obesity and
thorized reproduction of this article is prohibited.

C
CE: Tripti; JCM-D-14-00422; Total nos of Pages: 8;
JCM-D-14-00422
Heart surgery in immigrants Grimaldi et al. 5
Table 3 Cardiovascular risk factors and clinical profile ofimmigrants with ischemic heart disease
CVD risk factors IHD
No. of cases (%) 25 (16)Age (years) median (IQR) 57 (36–77)Male sex (M), n (%) 23 (92)Multiple risk factors (>2 of the following), n (%) 18 (72)
Hypertension 20 (80)Hypercholesterolaemia 16 (64)Type 2 diabetes 8 (32)Smoking 9 (36)Overweight/obesity 12 (48)
History of IHD, n (%) 10 (40)Previous coronary intervention, n (%) 4 (16)Reason for referral, n (%)
Chest pain 20 (80)SOB 5 (20)
Echocardiographic patterns, n (%)No WMA 8 (32)WMA (hypokinesis/akinesis) 17 (68)LV aneurysm 4 (16)
LA size (mean�SD) 65�15LV dimension (mean�SD) 55�7EF, n (mean�SD) 49�12sPAP (mmHg) (mean�SD) 36�6Angiographic patterns of CAD, n (%)
Single-vessel disease 3 (12)Double-vessel disease 5 (20)Multivessel disease (�3 coronary arteries) 17 (68)a
Valvular heart disease associated with coronary Sdrs 6 (24)Severe AS 4 (67)Severe MR 2 (33)
Treatment options, n (%) 24 (96)CABG alone 13 (54)CABG and LV aneurysmectomy 3 (13)CABG and valvular surgery 5 (21)PTCA 3 (13)TAVI 1 (4)
AS, aortic stenosis; CABG, coronary artery bypass graft (or grafting); CAD,coronary artery disease; CVD, cardiovascular disease; IHD, ischemic heart dis-ease; IQR, interquartile range; LA, left atrium; LV, left ventricular; MR, mitralregurgitation; PTCA, percutaneous transluminal coronary angioplasty; SOB, short-ness of breath; sPAP, systolic pulmonary artery pressure; TAVI, transcatheteraortic valve implanation; WMA, wall motion abnormality; a Included two patientswith 4-vessel coronary artery disease.
type 2 diabetes affected 80, 80, 48 and 44% of patients,
respectively. All patients suffered from CAD in the
following proportion: 68% with severe multivessel dis-
ease, 20% with double-vessel disease and 12% with
single-vessel disease. Six patients (24%) were found to
be also affected by severe valvular disease (four patients
with severe calcified AS and two with ischemic mitral
regurgitation). Subclinical CAD (n¼ 8, 20%) also affected
four patients (50%) with degenerative mitral disease, two
patients (25%) with aortic valve disease, one (13%) with
Takayasu’s arteritis and one (13%) with tricuspid valve
infective endocarditis. Regarding the angiographic
patterns of CAD in the overall population (including
patients with subclinical CAD), 56% of patients had
severe multivessel disease, 22% had double-vessel disease
and 22% had single-vessel disease.
Congenital heart diseaseCHD (n¼ 13) affected 9% of the study population
(Table 1). The median age of patients was 43 years
(IQR 8–63) with a female/male ratio of 1.2/1. Briefly,
six patients (46%) suffered from valvular heart disease
opyright © Italian Federation of Cardiology. Una
related to bicuspid aortic valve and associated ascen-
ding aorta aneurysm (n¼ 4/6, 67%) or aortic coartaction
(n¼ 2/6, 33%); five patients had type II ASDs (including
one patient with associated severe pulmonic stenosis),
one patient (8%) had a ventricular septal defect(s) with
associated aortic regurgitation and one patient (8%) had
aortic insufficiency in dysplastic valve and supravalvular
stenosis.
Other diseasesOther cardiac diseases (n¼ 11, 7%) were mostly
represented by eight cases of cardiomyopathies (73%),
one case of constrictive pericarditis (9%), one case of
pulmonary hypertension related to sarcoidosis (9%)
and one case of penetrating cardiac trauma caused by
stab (9%). Median age was 43 years (IQR 30–69) with a
male/female ratio of 1.7/1. Among cardiomyopathies,
four patients (36%) had obstructive hypertrophic cardio-
myopathy (including one patient with associated CAD),
two patients (18%) had secondary CMP related to CAD
and valvular heart disease, respectively, and two patients
(9%) had primary CMP (including one case of with
peripartum cardiomyopathy).
Treatment optionsAmong the study population, 138 patients (90%) with an
indication of heart surgery were deemed fit for interven-
tion and 16 patients (10%) underwent clinical follow-up
(including one patient with severe mitral valve disease
who refused the intervention) (Fig. 1). Surgery was
scheduled in 54 patients with RHD (n¼ 54/138, 39%),
in 39 patients with NRVs (n¼ 39/138, 28%), in 24 patients
with IHD (n¼ 24/138, 17%), in 12 patients with CHD
(n¼ 12/138, 9%) and in nine patients with various dis-
eases (n¼ 9/138, 6%). Treatment options included valv-
ular surgery in 108 patients (n¼ 108/138, 78%), Coronary
Artery Bypass Graft (CABG) in 29 patients (n¼ 29/138,
21%), surgery of ascending aortic disease in nine patients
(n¼ 9/138, 6%) and various interventions in 18 patients
(n¼ 18/138, 13%) (including septal miectomy in five
patients and surgical correction of congenital defects in
six patients).
Clinical follow-up and outcomesData concerning main outcomes measures and surgical
follow-up are depicted in Fig. 1. Clinical follow-up was
available in 96 patients (62%) [median time 62 months
(IQR 15–123)], among whom 92 patients (96%) survived
during the study period and four patients (4%) had died.
The mortality rate among patients who did undergo
surgery included one perioperative death during redo
operation for tetralogy of Fallot and three late postopera-
tive deaths (one mitral prosthesis thrombosis and two
patients with severe CAD and heart failure). Fifty-eight
patients (38%) were lost to follow-up due to logistical
difficulties (i.e. incorrect phone numbers, transfer to
other countries). All patients (n¼ 84) who had undergone
cardiac surgery reverted to NYHA class I/II; patients who
uthorized reproduction of this article is prohibited.

Co
CE: Tripti; JCM-D-14-00422; Total nos of Pages: 8;
JCM-D-14-00422
6 Journal of Cardiovascular Medicine 2014, Vol 00 No 00
did not undergo surgery (n¼ 8) did not report significant
clinical deterioration during the study period.
DiscussionImmigration will be the driving force in accounting for
the future growth of the European Union countries where
there is a growing interest in improving the primary care
health systems and in assessing the burden of CVD.8
Recent studies on migrants to Europe4,5,9 have attempted
to define the cardiovascular profile by comparing indi-
vidual risk factors among different ethnic groups of
immigrants. Health disparities seem to be inherently
related to the primordial ethnic identities, but they also
reflect new environmental factors: stress, depression and
uptake of western lifestyle10 may rapidly reverse the
immigrants’ ‘coronary disease (CHD) advantage’. Italy
seems to follow the epidemiological transition (OECD
2011)11 witnessed in many European countries and CVD
accounts for 36.6% of the deaths among immigrants.12
Demographics of immigrants in ItalyItaly is one of the most important destination countries
for migrants to Europe accounting for up to 5 000 000
regular migrants (8% of the total population) living in the
country, and shares with Spain the highest annual growth
of the European Union (http://www.iom.int/cms/en/sites/
pyright © Italian Federation of Cardiology. Unau
Fig. 3
Non-European Union citizens holding a residence permit, Italian provinces: 1place of issue/renewal of the permit. Source: Istat on data of Ministry of In
iom/home/where-we-work/europa/european-economic
area/italy.html). The phenomenon is progressively grow-
ing. In 2011, the burden of immigrants was 335 000 more
than the previous year (þ7.9%) and non-European Union
foreigners holding a residence permit in Italy were over
3 500 000;13 from 2008 to 2011, there was an increase of
35%. The most relevant citizenships are Morocco,
Albania, China, Ukraine and Moldova. The distribution
of resident foreigners in Italy continues to be uneven:
86.5% live in the North (64.5%) and Central Italy (22%),
with the remaining 13.5% in the South (Fig. 3); however,
in 2010, the largest increases were seen in the South
(þ11.5%) and the Islands (þ11.9%) (http://www.istat.it/
en/archive/40658). The foreigners account for up to 85%
of the global growth rate of population in northwest Italy
and Lombardy is the region that hosts the largest number
of regular foreigners (26.6%), followed by Emilia-
Romagna (12.6%), and by Veneto (12.1%) where the
highest percentage of long-term permits is registered.
Italy and Japan share the record for longevity of the
population, being the countries in which demographic
pressure is most perceived as a result of the increase life
expectancy. In Italy, the ‘Ageing Population’ would have
been even bigger without the migratory flow: in 2008,
there were 19 000 newborns from migrants vs. 79 000
thorized reproduction of this article is prohibited.
Less than 9001
From 9001 to 18 500From 18 501 to 35 000From 35 001 to 70 000More than 70 000
January 2012. Data are expressed in absolute values and referred to theterior.

C
CE: Tripti; JCM-D-14-00422; Total nos of Pages: 8;
JCM-D-14-00422
Heart surgery in immigrants Grimaldi et al. 7
newborns from Italians recorded in Lombardy, whereas
in 2002, there were 9000 vs. 77 000, respectively (http://
www.ismu.org/ISMUnews-notizia.php?id_notizia=201).
Most immigration has been illegal, although a series of
regulation has granted many immigrants legal status.14
Clear legislation was enacted as of 1998 to regulate the
immigrant population’s access to services provided under
the Italian National Health System (NHS) on a par with
Italian citizens; regular immigrants register with the NHS
in the same way as Italian citizens, as they have access to
primary and hospital care, rehabilitation and emergency
care.15 Italy has currently declared a state of emergency
over the recent surge in illegal immigrants flooding into
the country: most of the displaced populations arrive from
the Maghreb area and sub-Saharan Africa. Currently,
Sicily is the hub for Mediterranean migrants, the majority
of whom arrive through Lampedusa (http://www.euro.
who.int/__data/assets/pdf_file/0010/184465/e96796.pdf).
Trends in heart diseaseWe report here the first hospital-based series of immi-
grants referred to one of the highest-volume national
cardiac surgery centres, which shows that RHD still
prevails among the adult population and that more
Western patterns of diseases such as IHD and NRVs
progressively emerge. RHD represents a major health
topic by affecting 15 million people and leading to
200 000 deaths per annum worldwide,16 and despite
the significant decline over the last century,17 the disease
also persists among industrialized countries, primarily
because health-related resources may be unbalanced
between immigrants and not enough to provide full
protection. Furthermore, some outbreaks of RHD have
been reported in middle-class children in the USA in the
1990s17,18 and more recently in Italy19,20 where a worri-
some resurgence of the disease is expected to increase
according to migratory flows. Data from our survey
emphasize the need for reinforcement of primordial,
primary and secondary prevention strategies in order to
tackle re-emerging RHD from immigrants. As in other
series, the rheumatic patterns are similar to those recur-
ring in the developing countries such as higher pre-
valence among women from the third decade of life,
predominant mitral disease and severity of MVD; how-
ever, where more expertise exists, echocardiography
focused on anatomic details before surgery also allows
the identification of mixed patterns of rheumatic valves
associated with degenerative prolapse (13%). NRVs, in
fact, emerged as the second main cause of heart failure,
and interestingly, mixomatous mitral prolapse affected
73% of patients. More than half patients (53%; 16/30)
affected by mitral prolapse were Eastern European immi-
grants, both European Union and non-European Union
citizens, possibly reflecting different socio-economic and
ethnic background and environmental exposure com-
pared with black Africans suffering from RHD.
opyright © Italian Federation of Cardiology. Una
According to the epidemiologic transition of their country
of origin, Eastern Europeans exhibit the most hetero-
geneous picture of heart disease in the survey: rheumatic
and nonrheumatic valvuopathies, IHD and hypertrophic
cardiomyopathies were all represented.
CAD played a central role in the study. The prevalence of
CAD in the whole population was even higher than that
observed in the IHD group, due to the subclinical CAD
detected at preoperative angiography in the other groups
(n¼ 11, 17%); furthermore, the extension of coronary
burden was significantly high, 68% of patients being
affected from severe multivessel disease and 72% of
them having more than two risk factors. The lower
prevalence of IHD among immigrants than the Italian
citizens previously reported21 seems to be related to an
initial ‘healthy immigrant effect’, whereas the higher
prevalence of type 2 diabetes is inherently related to
ethnic differences.22 Over the time, the decline of the
‘CHD advantage’ after the arrival2,23,24 can be attributed
to the adoption of unhealthy lifestyles: physical inactivity
and dietary changes can result in higher overweight
rates among migrants than in native residents. Obesity
is thought to be the fastest growing health problem
worldwide and a strong risk factor for CVD and other
illnesses.14 Although the time of stay and the duration of
exposure were not datable in our survey, the overall
burden of risk factors among immigrants was high:
systemic hypertension, dyslipidemia, tobacco smoking,
type 2 diabetes and obesity (29%) were all represented.
As a well recognized cause of heart failure,25 systemic
hypertension affected 35% (n¼ 54) of the overall popu-
lation and 80% (n¼ 20) of IHD patients and it was also
associated with target organ damage as witnessed by the
dilatation of ascending aorta affecting 11% of patients.
The use of simple algorithms aimed to assess the cardio-
vascular risk and promote salt intake reduction among
immigrants should therefore become a priority.
Adherence to treatment and outcomesImmigrants to Italy are heterogeneous and differences
among the subgroups may address health issues. Most
Latinos have a common ancestry in people speaking the
Italian or Spanish languages or emigrating from Latin
America; eastern Europeans formed the largest subgroup,
including Romanians, Albanians and Ukrainians; black
Africans mostly came from Maghreb and sub-Saharan
Africa; Asians were mainly from the Philippines, Pakistan
and Sri Lanka. Recent immigration, family-oriented
cultural values and poverty are common and shared
features among the various subgroups. There is a wide
range of socio-economic characteristics in communities,
including reluctance to seek care when symptoms occur-
red, and different explanations for delays. In addition,
most patients from Albania and Romania were not
familiar with the Italian language and unaware of the
underlying illness. All these factors might explain the
uthorized reproduction of this article is prohibited.

Co
CE: Tripti; JCM-D-14-00422; Total nos of Pages: 8;
JCM-D-14-00422
8 Journal of Cardiovascular Medicine 2014, Vol 00 No 00
percentage of patients lost to follow-up (n¼ 58, 38%) due
to logistical difficulties (incorrect phone numbers, trans-
fer to other countries). Nevertheless, the adherence to
surgical treatment and clinical follow-up was acceptable
(Fig. 1) and the clinical predictors such as proper timing
for surgery, early recovery and lack of complications from
late presentation were all similar to the standards
reported among Italian citizens.
LimitationsOur study has some limitations. First of all, data were
insufficient to investigate the relative relevance of push–
pull factors behind the migration such as the presence of
relatives already here, the political circumstances sur-
rounding departure, the time of stay in Italy and the
overall exposure time to risk factors. Moreover, a drop-
out from the cohort follow-up was recorded for 58
patients, including those needing to stick to the second-
ary prevention programmes following heart surgery;
migrants might decide to leave the area without inform-
ing or giving incorrect personal information. More
effort is needed to guarantee adequate support for vulner-
able groups and improve their access to healthcare
services (http://www.who.int/hac/events/consultation_
report_health_migrants_colour_web.pdf). Finally, the
small cohort of study was limited to patients referred
for heart surgery, regardless of the burden of patients with
missed diagnoses and nonsurgical follow-up.
Conclusion and perspectivesMigration and health are two processes inherently related
to each other. Poverty, despair and lack of employment
opportunities will continue to trigger migration flows
allowing an increase in the burden of CVD among the
industrialized nations. In order to design appropriate
public health policies and health promotion interven-
tions, greater consideration of the cultural environment
should be warranted. Migrants will form an increasing
proportion of the workforce in many European countries
and the demographic trends suggest that the health status
of immigrants and their descendants will play a central
role in shaping health outcomes of the developed
countries’ people. The current survey confirms that they
represent a high-risk group for which targeted CVD risk
reduction is needed and that the outcomes from surgical
treatment can be satisfactory if health-related pro-
grammes are adequately strengthened. It is therefore
of great importance to address these issues.
AcknowledgementsThere were no external funding sources for this study.
There is no potential conflict of interest in this article.
References1 World Health Assembly. Health of Migrants, Resolution 61.17. Geneva:
World Health Organization; 2008.
pyright © Italian Federation of Cardiology. Unau
2 Allender S, Scarborough P, Peto V et al. European cardiovascular diseasestatistics, 2008 edition. British Heart Foundation Health PromotionResearch Group; HYPERLINK "http://www.biomedcentral.com/sfx_links?ui¼1471-2458-12-864&bibl¼B1"2008. Available from URL:http://www.bhf.org.uk/publications/view-publication.aspx?ps¼1001443(Accessed 23 April, 2014).
3 Carlsson AC, Wandell PE, de Faire U, Hellenius ML. Prevalence ofhypertension in immigrants and Swedish-born individuals, a cross-sectionalstudy of 60-year-old men and women in Sweden. J Hypertens 2008;26:2295–2302.
4 Yusuf S, Hawken S, Ounpuu S, et al., INTERHEART Study Investigators.Effect of potentially modifiable risk factors associated with myocardialinfarction in 52 countries (the INTERHEART study): case–control study.Lancet 2004; 364:937–952.
5 Glenday K, Kumar BN, Tverdal A, Meyer. Cardiovascular disease risk factorsamong five major ethnic groups in Oslo, Norway: the Oslo Immigrant HealthStudy. Eur J Cardiovasc Prev Rehabil 2006; 13:348–355.
6 Remenyi B, Wilson N, Steer A, et al. World Heart Federation criteria forechocardiographic diagnosis of rheumatic heart disease: an evidence-based guideline. Nat Rev Cardiol 2012; 9:297–309.
7 Baumgartner H, Hung J, Bermejo J, et al., EAE/ASE. Echocardiographicassessment of valve stenosis: EAE/ASE recommendations for clinicalpractice. Eur J Echocardiogr 2009; 10:1–25.
8 Anand SS, Yusuf S. Stemming the global tsunami of cardiovasculardisease. Lancet 2011; 377:529–532.
9 Gadd M, Johansson SE, Sundquist J, Wandell P. The trend ofcardiovascular disease in immigrants in Sweden. Eur J Epidemiol 2005;20:755–760.
10 Rosengren A, Hawken S, Ounpuu S, et al., INTERHEART investigators.Association of psychosocial risk factors with risk of acute myocardialinfarction in 11119 cases and 13648 controls from 52 countries (theINTERHEART study): case–control study. Lancet 2004; 364:953–962.
11 Azzolini D, Schnell P, Palmer J. Educational achievement gaps betweenimmigrant and native students in two ‘new immigration countries’: Italy andSpain in comparison. Ann Am Acad Pol Soc Sci 2012; 643:46–77.
12 Cacciani L, Baglio G, Rossi L, et al. Hospitalisation among immigrants inItaly. Emerg Themes Epidemiol 2006; 3:4.
13 Bonifazi C, Heins F, Strozza S, Vitiello M. The Italian transition from anemigration to immigration country: citizens and governance in knowledge-based society. Italy: EU; 2009. http://www.idea6fp.uw.edu.pl/pliki/WP5_Italy.pdf. (Accessed 01 March, 2014).
14 Gualdi-Russo E, Zironi A, Dallari GV, Toselli S. Migration and health in Italy:a multiethnic adult sample. J Travel Med 2009; 16:88–95.
15 Lo Scalzo A, Donatini A, Orzella L, Cicchetti A, Profili S, Maresso A. Italy:health system review. Health Syst Transit 2009; 11:1–216.
16 Marijon E, Mirabel M, Celermajer DS, Jouven X. Rheumatic heart disease.Lancet 2012; 379:953–964.
17 Stollerman GH. Rheumatic fever. Lancet 1997; 349:935–942.18 Miyake CY, Gauvreau K, Tani LY, Sundel RP, Newburger JW.
Characteristics of children discharged from hospitals in the United Statesin 2000 with the diagnosis of acute rheumatic fever. Pediatrics 2007;120:503–508.
19 Breda L, Marzetti V, Gaspari S, Del Torto M, Chiarelli F, Altobelli E.Population-based study of incidence and clinical characteristics ofrheumatic fever in Abruzzo, central Italy, 2000–2009. J Pediatr 2012;160:832–836.
20 Pastore S, De Cunto A, Benettoni A, Berton E, Taddio A, Lepore L. Theresurgence of rheumatic fever in a developed country area: the role ofechocardiography. Rheumatology (Oxf) 2011; 50:396–400.
21 Buja A, Gini R, Visca M, et al. Valore Project. Prevalence of chronicdiseases by immigrant status and disparities in chronic diseasemanagement in immigrants: a population-based cohort study, ValoreProject. BMC Public Health 2013; 13:504.
22 Centers for Disease Control and Prevention. National Diabetes Fact Sheet:general information and national estimates on diabetes in the United States,2005. http://www.cdc.gov/diabetes/pubs/factsheet05.htm. (AccessedFebruary 17, 2007).
23 Koya DL, Egede LE. Association between length of residence andcardiovascular disease risk factors among an ethnically diverse group ofUnited States immigrants. J Gen Intern Med 2007; 22:841–846.
24 Alkerwi A, Sauvageot N, Pagny S, Beissel J, Delagardelle C, Lair ML.Acculturation, immigration status and cardiovascular risk factors amongPortuguese immigrants to Luxembourg: findings from ORISCAV-LUXstudy. BMC Public Health 2012; 12:864.
25 Lloyd-Jones DM, Larson MG, Leip EP, et al., Framingham Heart Study.Lifetime risk for developing congestive heart failure: the Framingham HeartStudy. Circulation 2002; 106:3068–3072.
thorized reproduction of this article is prohibited.





























