Embed Size (px)
Citation preview

EMPIRICAL RESEARCH
Help-Negation and Suicidal Ideation: The Role of Depression,Anxiety and Hopelessness
Coralie J. Wilson • Frank P. Deane
Received: 19 July 2009 / Accepted: 20 November 2009 / Published online: 2 December 2009
� Springer Science+Business Media, LLC 2009
Abstract Help-negation is expressed behaviorally by the
refusal or avoidance of available help and cognitively by
the inverse relationship between self-reported symptoms of
psychological distress and help-seeking intentions. The
current study examined the association between suicidal
ideation and intentions to seek help from friends, family
and professional mental health sources in a sample of 302
Australian university students. Participants were 77.5%
female and aged from 18–25 years old, with 85.4% aged
21 years or younger. Higher levels of suicidal ideation
were related to lower help-seeking intentions for family,
friends, and professional mental health care, and higher
intentions to seek help from no one. Moderation effects
indicated that higher levels of depressive symptoms
strengthen the help-negating effect of suicidal ideation for
seeking help from friends, family and no one. The results
indicate that, even at subclinical levels, suicidal ideation
impedes the cognitive help-seeking process at the decision
making stage. The results also highlight the importance of
improving our understanding of why young people become
reluctant to seek help as their levels of suicidal ideation and
depressive symptoms increase. Raising awareness that the
experience of suicidal ideation and depressive symptoms
can promote intentions to avoid help might reduce the help-
negation effect when symptoms are first recognized.
Keywords Help-seeking � Help-negation � Suicidal
ideation � Depression � Anxiety � Hopelessness
Introduction
Suicide is a concern for a number of cultures and countries.
Internationally, suicide is the third leading cause of death in
the 15–24-year age-group (Belfer 2008). In 2005, approx-
imately 10% of deaths amongst Americans aged 15–24-
years were by suicide, and in Australia between 2004 and
2006, 20% (n = 266) of all deaths in the 16–24 age-group
were by suicide (Australian Bureau of Statistics [ABS]
2008). Suicide is not an impulsive act, but lies on a con-
tinuum from suicidal ideation to attempt and completion
(Brown et al. 2006). Suicidal ideation refers to people’s
thoughts about death, suicide, and serious self-injurious
behaviors, and is an independent estimate of risk for suicide
completion (Beck et al. 1999; Brown et al. 2000; Reynolds
1988). For example, using a sample of 3,701 outpatients
seeking psychiatric treatment, Beck et al. (1999) found that
suicidal ideation at its worst point predicted suicide com-
pletion at a rate 14 times higher than ideation in a lower risk
category. Unfortunately, suicidal ideation is also relatively
common in young people. Epidemiological studies con-
verge to suggest that, at any point in time, almost one
quarter of young people worldwide are experiencing sui-
cidal thoughts (e.g., Goldney et al. 1989; Reinherz et al.
1995; Swanson et al. 1992). These sobering statistics indi-
cate that seeking appropriate help, before suicidal ideation
C. J. Wilson (&) � F. P. Deane
Illawarra Institute for Mental Health, Wollongong,
NSW, Australia
e-mail: [email protected]
F. P. Deane
e-mail: [email protected]
C. J. Wilson
Graduate School of Medicine, University of Wollongong,
Wollongong, NSW, Australia
F. P. Deane
School of Psychology, University of Wollongong,
Wollongong, NSW, Australia
123
J Youth Adolescence (2010) 39:291–305
DOI 10.1007/s10964-009-9487-8

is at its worst point, may be crucial for interrupting the
development of ideation to completion. The statistics also
underscore the need to identify and better understand vari-
ables that exacerbate suicide risk, together with those that
protect against the development of suicidal ideation and
consequent completion (Graham et al. 2000).
Appropriate Help-Seeking
Appropriate help-seeking refers to a match between prob-
lem type, severity and help source. For example, low levels
of distress following transitory stressful experiences may
only require support from a family member. More severe
and traumatic experiences might require professional
mental health treatment. A productive help-seeking expe-
rience might also facilitate problem-solving or access to a
more appropriate help provider. Accessing appropriate help
can successfully reduce the long-term impact of many
mental health problems and protect against the develop-
ment of psychological distress (Rickwood et al. 2007). In
turn, appropriate help can reduce the risk for suicide
completion when ideation is experienced or when suicidal
behaviors are exhibited (Greenberg et al. 2001; Kalafat
1997). However, epidemiological studies indicate that only
about a quarter of young people with a mental health
problem seek professional care (e.g., Zachrisson et al.
2006). This means that, globally, up to three quarters of the
young people who would likely benefit from mental health
care are not seeking or engaging in this type of help when
they are psychologically distressed or suicidal.
In Australia, even after a decade of universal and tar-
geted initiatives to improve mental health help-seeking,
preliminary results from 2007 National Survey of Mental
Health and Wellbeing suggest that only 23.3% of young
people, aged 16–24 years, who had common forms of
psychological distress during the last year, sought or
engaged in professional help for their condition (Burgess
et al. 2009). In the general population, 41% of those with
serious thoughts of suicide during the last year did not seek
or engage in professional help for their suicidality (John-
ston et al. 2009). Even more concerning are the preliminary
results from the 2007 Survey which suggest that 86% of
those who did not seek help for their common mental
disorders thought that they didn’t need any type of mental
health care (Meadows and Burgess 2009; age specific
results were not available). Although we still don’t know
why people with mental health problems do not want help
(Henderson et al. 2009), the 2007 Survey raises the pos-
sibility that a lack of perceived need for treatment
(Meadows and Burgess 2009) or incomplete mental health
literacy (Whiteford and Groves 2009) is implicated in low
service use. It is also possible that the gap between service
need and use is partially explained by the help-negation
process (Wilson and Deane 2009).
Help-Negation for Suicidal Thoughts in Clinical
Samples
Help-negation was first described in the literature as the
unique pattern shown by acutely suicidal clients who have
‘‘reached a state of utter hopelessness concerning treat-
ment, [to] soundlessly abandon, politely terminate, or
angrily reject treatment’’ (Clark and Fawcett 1992, p. 40).
As the research area has developed, help-negation has been
indicated behaviorally as the refusal or avoidance of
available help (e.g., Rudd et al. 1995), and cognitively, as
the inverse relationship between the cognitive response to
an episode of psychological distress (e.g., self-reported
suicidal ideation or depressive symptoms) and help-seeking
intention (i.e., the planning and action component of the
individual’s decision to seek help; e.g., Deane et al. 2001;
Wilson et al. 2005a, 2007, 2009). Help-negation differen-
tiates those who are at high risk for suicide completion
from those who are at low or moderate risk (Clark and
Fawcett 1992), and thus, provides an independent indica-
tion of risk for suicide completion (Stellrecht et al. 2006).
Help-negation suggests that people at the highest risk for
suicide completion are those who are most likely to avoid
seeking help for their potentially lethal thoughts and
behaviors (Wilson et al. 2009).
In one of the first empirical studies of help-negation,
Rudd et al. (1995) followed a group of 45 clients, aged
18–26 years old, who withdrew prematurely from treat-
ment. The researchers continued to assess the client’s
levels of suicidal ideation and behavior, and examined
whether suicidal clients who drop out of treatment feel
hopeless about the potential efficacy of treatment or whe-
ther help-negation might reflect personal characteristics
underpinning the suicidal state, that is, poor: judgment,
decision making, problem solving, and overall adaptive
coping. The study revealed that those clients who with-
drew from treatment prematurely shared similar sympto-
mology across diagnoses, personality characteristics, and
levels of psychological distress. Both groups exhibited
similar levels of hopelessness and negative expectancies
about the future, and neither group considered themselves
to be effective problem solvers. Yet, one group withdrew
from treatment and the other did not. Rudd et al. con-
cluded that, although help-negation seemed to be at least
in part a function of hopelessness in clinical samples, it is
‘‘most likely not unique to the therapeutic situation or
immediate crisis, but indicative of the individual’s general
adaptive coping and interpersonal style’’ (p. 503). The
researchers suggested that help-negation might be a
292 J Youth Adolescence (2010) 39:291–305
123

function of a general coping style that is avoidant, nega-
tivistic, and passive-aggressive, and which is exacerbated
by situational stress, associated symptomology, and resul-
tant Axis I diagnoses (i.e., clinical disorders, such as mood
and anxiety disorders, and other conditions that may be the
focus of clinical treatment).
Other studies have indicated that suicidal ideation itself
might be a factor associated with help-refusal. Studies also
suggest that the help-negation effect might exist for infor-
mal help-sources, such as friends and family, as it does for
formal professional mental health sources. For example, a
case-controlled study of one hundred and fifty-three 13–34-
year-old ‘‘nearly lethal’’ suicide attempters found that this
group was significantly less likely to seek help from any
source, either formal or informal, than the non-suicidal
controls (odds ratio = 0.50, p \ .05, 95% confidence
intervals = 0.3–0.8; Barnes et al. 2001). Importantly,
young people are more likely to seek help when they rec-
ognize that they have a mental health problem and have the
knowledge, skills and encouragement to seek help (Rick-
wood et al. 2006; Zwaanswijk et al. 2003a). This encour-
agement often comes from parents, friends, and family
doctors, who have a significant role in the pathway to pro-
fessional mental health care (Zwaanswijk et al. 2003b).
Parents are particularly important for younger adoles-
cents because they facilitate access to professional help
sources. While the capacity for self-referral develops over
adolescence into young adulthood, as independence and
autonomy from parents develops, parents continue to play a
significant role in the help-seeking process, particularly
until young people are financially independent (Rickwood
et al. 2006). As young people progress through adoles-
cence, the role of friends becomes prominent in help-
seeking pathways (Kramer and Garralda 2000; Rickwood
et al. 2005). For young adults, intimate relationships
become an important source of support, particularly for
males. Intimate partners have been shown to exert a strong
influence on men who seek specialist psychological ser-
vices (Cusack et al. 2004). Thus, indications that the help-
negation effect might extend to informal help sources are
particularly concerning. It means that suicidal young peo-
ple, who are most in need of professional help, may not
receive professional care because they simultaneously
reject help from the people they are often closest to.
Friends and family are often those who are most likely to
recognize a young person’s need for help (Wilson and
Deane 2001). Consequently, young people who are at risk
for suicide might not receive the support they need to
facilitate access to appropriate mental health services.
These possibilities underscore the importance of identify-
ing and addressing the variables that promote reluctance to
seek help from both formal and informal sources for sui-
cidal thinking.
Help-Negation for Suicidal Thoughts in Subclinical
Samples
Since help-negation may not be unique to the therapeutic
situation, or completely explained as a function of hope-
lessness, it is noteworthy that there is evidence of the help-
negation process in subclinical (i.e., non-acutely suicidal)
samples. A large American study, which examined suicidal
ideation as a predictor of formal help-seeking behavior in
17,193 adolescents, found that those with high levels of
suicidal ideation were less likely to obtain help than those
with less severe ideation (odds ratio = .90, p \ .05) or no
suicidal ideation (odds ratio = .81, p \ .001). It was con-
cluded that ‘‘substantial barriers to seeking help are
associated with suicidality’’ (Saunders et al. 1994, p. 727).
Two Australian studies have since confirmed that an
inverse relationship between suicidal ideation and help-
seeking intentions occurs in subclinical samples of ado-
lescents and young adults (Deane et al. 2001; Wilson et al.
2005a). Help-seeking intentions and levels of suicidal
ideation were measured because these variables proximate
help-seeking behavior and suicide completion (Martin
2002; Webb and Sheeran 2006; Wilson et al. 2005b). In
both studies, even with the developmental differences that
exist between adolescents and young adults (i.e., differ-
ences in brain development, developmental tasks and social
expectations), a help-negation effect was found for formal
and informal help-sources. As levels of suicidal ideation
increased, intentions to seek help from a range of formal
help-sources, such as a mental health professional and a
family doctor, decreased. Similarly, help-seeking inten-
tions for informal sources, such as friends and family, also
decreased as suicidal ideation increased. In addition, in
both studies as levels of suicidal ideation increased, stu-
dents became increasingly likely to report that they would
not seek help from anyone for managing their suicidal
thoughts (Deane et al. 2001; Wilson et al. 2005a). Toge-
ther, the behavioral and cognitive help-negation results
raise an important implication for suicide prevention ini-
tiatives that rely on young people to proactively seek and
access help. How successful can these initiatives be if a
consequence of experiencing suicidal ideation, even in its
very early stages of development, is a tendency to with-
draw both behaviorally and cognitively from specific
helping opportunities, or to avoid help altogether?
Help-Negation for Symptoms of General Psychological
Distress
Suicidal ideation without other psychological disturbance
is rare in young people (Marttunen et al. 1991). In an
Australian study of 590 adolescents, higher levels of
self-reported suicidal ideation and symptoms of general
J Youth Adolescence (2010) 39:291–305 293
123

psychological distress were both related significantly to
lower intentions to seek help from a family doctor for
suicidal and physical health problems (Wilson et al. 2009).
These results extend our understanding of the help-nega-
tion effect by indicating that, at subclinical levels, increases
in general psychological distress symptoms, as well as
suicidal ideation, can lead to intentions to avoid help.
Depression and anxiety are two of the most frequent
mental health problems experienced by young people
(ABS 2008). Research has shown that people can experi-
ence acutely clinical levels of depressive symptoms,
hopelessness and suicidality as independent mental health
problems (Fairweather-Schmidt et al. 2009; Stellrecht et al.
2006), or together, in what appears to be a subtype of
depression, called suicidal depression, which is particularly
chronic and treatment resistant (Shahar et al. 2006). It is
also common for people to experience co-occurring
symptoms of depression and anxiety when these symptoms
are at both acutely clinical and subclinical levels (Sheffield
et al. 2004; Thompson et al. 2004). The extent to which
symptoms of depression, hopelessness, and/or anxiety
influence the help-negating effect of suicidal ideation is a
question that is yet to be answered. Another question is
whether help-negation is a phenomenon that occurs for
different symptom clusters in subclinical samples of young
adults rather than just in subclinical samples of adolescents.
Depressive Symptoms
Almost 50% of young people who complete suicide have a
diagnosable mood disorder, such as depression (Cheung
and Dewa 2007). Several large-scale studies also point to
symptoms of depression having a help-negation effect that
is independent of suicidal ideation. A 20-year prospective
study of 6,891 psychiatric outpatients found that current
suicidal ideation, together with major depression, were two
of four unique and modifiable risk factors for eventual
suicide (Brown et al. 2000). Two population-based epide-
miological studies also suggest that young people with
higher levels of depressive symptoms are often more
reluctant to seek help than those with low levels of
depression. In a study that examined the coping and help-
seeking strategies of 2,419 American adolescents, one
quarter of those who participated in the study, who also had
depressive symptoms, indicated that they would keep their
feelings to themselves (Gould et al. 2004). Similarly, when
the relationship between depressive symptoms and the
help-seeking behavior of 9,000 American adolescents was
examined, higher levels of depressive symptoms were
related to ‘‘not seeking help from anyone’’ (Sen 2004).
Aspects of depression, which have been linked theoreti-
cally to the help-negation process, include the loss of
motivation and apathy (Wilson et al. 2007). It is possible
that even when levels of suicidal ideation are not acute, as
levels of depressive symptoms increase, young people
might experience increased levels of apathy and indiffer-
ence towards help-seeking, which subsequently reduce
their motivation to seek help for suicidal thinking. It is also
possible that, even in samples with subclinical levels of
suicidal ideation, the help-negation effect might be a
function of co-occurring processes that are either explained
by, or associated with, depressive symptoms.
Hopelessness
Hopelessness is a cognitive-emotional process that is wor-
thy of further consideration in relation to help-seeking.
Although studies that have controlled for hopelessness have
found that it does not fully account for the help-negating
effect of suicidal ideation in subclinical samples (Deane
et al. 2001; Wilson et al. 2005a), there are indications that
hopelessness, together with depressive symptoms, might
have a role in help-negation. An epidemiological study of
364 currently symptomatic 40-year-olds with affective
disorders found that hopelessness and self-criticism were
the only affective symptoms that predicted future help-
seeking (Burns et al. 2003). The researchers observed that
these cognitions were essentially pessimistic appraisals
about the individual’s emotional state rather than somatic
manifestations of depression (e.g., insomnia, anhedonia).
This suggests that global pessimistic self-judgments (i.e.,
the individual’s cognitive response to their distressed state)
may be more overwhelming, and may consequently have a
greater influence on help-seeking, than the immediate
extent of distress (Burns et al. 2003). Thus, hopelessness,
when it co-occurs with depressive symptoms, might
decrease help-seeking intentions and promote the help-
negation relationship.
Anxiety Symptoms
Although suicidal ideation and depressive symptoms have
been associated with help negation, the relationship
between symptoms of anxiety and help-seeking is unclear.
A study of 233 clients at an Australian specialist anxiety
clinic found that increased illness severity was the primary
prompt for clients’ actual help-seeking (Thompson et al.
2004). The researchers concluded that higher levels of
anxiety symptoms act as an ‘‘approach’’ factor for help-
seeking in that, as they experience increased levels of
anxiety, individuals become more likely to recognize that
they have a problem needing help, then seek help for it
(Thompson et al. 2004). If anxiety symptoms are approach
factors for help-seeking, then those who are suicidal and
have accompanying symptoms of anxiety may be more
likely to seek help than those without anxiety symptoms.
294 J Youth Adolescence (2010) 39:291–305
123

However, a large school-based survey of 15–16-year-old
Norwegian young people (n = 11,154) found that even at
the highest symptom levels for anxiety and depression,
only a third of adolescents had sought professional help for
their condition (Zachrisson et al. 2006). A clearer under-
standing of the relationship between levels of anxiety
symptoms and seeking help from different sources is
warranted.
A Theoretical Framework for Studying Help-Negation
Mental health help-seeking in emerging adults requires a
dynamic interaction between the individual, often their
family, and always their cultural values, beliefs about
mental health and help-seeking, and contextual or sys-
tematic factors, such as the availability of services and
social networks (e.g., Cauce et al. 2002; Issakidis and
Andrews 2002; Liang et al. 2005; Mechanic 1995; Pesc-
osolido and Boyer 1999). Unlike other social interactions,
the objective in mental health help-seeking is intensely
personal. The decision to seek help for symptoms of psy-
chological distress is at the nexus of the individual’s per-
sonal experience of their distress and their interpersonal
expression of this experience. Consequently, the individ-
ual’s cognitive, affective and behavioral responses to their
symptoms of psychological distress are implicated in
explaining the gap between mental health need and service
use (Rickwood et al. 2005).
Help-seeking models, which focus on the individual’s
cognitive processes, converge to provide a useful frame-
work for examining the cognitive aspects of help-negation
in subclinical samples (e.g., Ajzen 1991; Anderson 1995;
Leventhal et al. 1998; Prochaska et al. 1992). Most models
of the cognitive aspects of help-seeking include similar
constructs under different labels (e.g., Bandura 1998; Nigg
et al. 2002; Noar and Zimmerman 2004). Common ele-
ments across cognitive help-seeking models are: beliefs
about seeking help (attitudinal, self-efficacy, normative,
risk-related) and help-seeking intention (Schreiber et al.
2009). Across cognitive help-seeking models, it is gener-
ally agreed that beliefs and intention are embedded within
a non-linear help-seeking process, which comprises three
broad stages: problem recognition, deciding to seek help,
and selecting a help provider. It is also generally agreed
that these stages lie within a context that includes indi-
vidual, interpersonal and sociocultural variables, which
both promote and support help-seeking (e.g., Cauce et al.
2002; Fox et al. 2001; Greenlay and Mullen 1990; Liang
et al. 2005; Pescosolido 1992).
Although these models are helpful for guiding our
understanding of the cognitive help-seeking process, they
don’t contribute to our understanding of how suicidal ide-
ation and other symptoms of psychological distress might
influence the decision to seek help. A major weakness of
many well-established social-cognitive help-seeking mod-
els is the assumption that making a decision to seek help is
a solely rational process, which, in turn, determines
behavior (Wills and Gibbons 2009). Few models pay any
attention to the influence of the individual’s affective state
or their cognitive response to their affective state (Henshaw
and Freedman-Doan 2009). Yet, in order to seek help, an
individual needs to recognize their symptoms and need for
help (i.e., have good mental health literacy and perceive
their need for help), but at the same time, the individual’s
psychological state can cause a lack of awareness of their
state (anosognosia; Shad et al. 2007), which, in turn,
impairs the individual’s cognitive awareness of their need
for help (Saunders and Bowersox 2007). Adolescents have
explained that they usually don’t know that they are
experiencing elevated levels of psychological distress until
a friend or family member points out their symptoms or
behavioral changes (Wilson and Deane 2001).
Suicidal ideation is the individual’s cognitive response
to their experience of the suicidal state, which is charac-
terized by cognitive and affective restriction (Clark and
Fawcett 1992). Symptoms of depression and anxiety are
also associated with cognitive distortion and altered cog-
nitive and affective function (e.g., Weishaar 1996). While
people who recognize their psychological symptoms and
need for help will seek it, elevated levels of cognitive
impairment impede the process (Saunders and Bowersox
2007). This suggests that the help-negating effecting of
suicidal ideation might be a function of impaired capacity
to make a help-seeking decision. It also suggests that
psychological symptoms, which commonly co-occur with
suicidal ideation (e.g., depression, hopelessness, and anxi-
ety), will exacerbate the individual’s cognitive impairment
and consequently strengthen the help-negating effect of
suicidal ideation.
Study Aims and Hypotheses
The first aim of the current study was to examine the extent
to which levels of suicidal ideation are related to help-
seeking intentions for a range of formal and informal
sources, as well as no one. We hypothesized that a sig-
nificant inverse relationship would be found between levels
of suicidal ideation and intentions to seek help from
informal and formal sources for suicidal thoughts. We also
hypothesized that higher levels of suicidal ideation would
be associated significantly with higher intentions to seek
help from no one for suicidal thinking.
The second aim of the current study was to examine the
extent to which symptoms of depression, anxiety, and
hopelessness, both individually and together, account for,
J Youth Adolescence (2010) 39:291–305 295
123

or strengthen, the help-negating effect of suicidal ideation
in the subclinical sample. We hypothesized that higher
levels of depressive symptoms, anxiety symptoms and
hopelessness would, individually and together, explain the
help-negating effect of suicidal ideation for suicidal
thoughts. We also predicted that the strength of the help-
negating effect of suicidal ideation would be increased by
higher levels of depressive symptoms and hopelessness,
and reduced by higher levels of anxiety symptoms.
We expected that the results from the current study would
clarify whether aspects of subclinical suicidal ideation itself
act as help-seeking barriers, or whether the help-negating
effect of subclinical suicidal ideation appears to be a func-
tion of co-occurring symptoms of depression, anxiety, and
hopelessness. We also expected the results to clarify whether
the help-negating effect of suicidal ideation appears to be a
global effect that exists across all help sources or for only
some sources when symptoms of depression, anxiety, and
hopelessness are controlled. Through this clarification, we
anticipate that the current study will provide timely direc-
tions for further developments in universal and targeted
youth suicide prevention and early intervention initiatives.
Method
Participants and Procedure
The research received approval from the University of
Wollongong Human Ethics Committee. The study was
described in an advertisement on a Department of Psychol-
ogy research project sign-up board. Participants voluntarily
signed up for inclusion in the study to gain additional course
credit. A total of 302 psychology undergraduates completed
the anonymous study questionnaire, individually and under
the supervision of a postgraduate research assistant. Sample
characteristics are presented in Table 1.
Measures
Help-Seeking Intentions
The General Help-seeking Questionnaire (GHSQ; Wilson
et al. 2005b) measures participants’ intentions by asking
them to rate the likelihood that they would seek help for
suicidal thoughts from a variety of specific help sources.
Help sources were: intimate partner, friend, parent, non-
parent family member, mental health professional (e.g.,
counselor, psychologist, and psychiatrist), doctor/GP, tele-
phone helpline (e.g., Lifeline), and ‘‘would not seek help
from anyone’’. The following problem prompt was used: ‘‘If
you were having suicidal thoughts, how likely is it that you
would seek help from the following people?’’ Participants
rated their intentions to seek help from each of the eight
help-source items on a 7-point scale (1 = ‘‘Extremely
unlikely’’, 7 = ‘‘Extremely likely’’). Higher scores indicate
higher help-seeking intentions and are related to prospec-
tive help-seeking behavior, as well as inverse associations
with negative beliefs about seeking professional psycho-
logical help (Wilson et al. 2005b). For ease of expression,
‘‘Non-parent relative’’ was relabeled ‘‘Family’’, ‘‘Telephone
helpline’’ was relabeled ‘‘Phone counseling’’ and ‘‘Would
not seek help from anyone’’ was relabeled ‘‘No-one’’.
‘‘Friend’’, ‘‘Mental health professional’’, and ‘‘Doctor’’ were
left unchanged (as listed in Table 2).
Suicidal Ideation
The Suicidal Ideation Questionnaire (SIQ; Reynolds 1988)
comprises 30 items reflecting suicidal thoughts that are
self-rated on a 7-point scale (0 = ‘‘I never had this thought
before’’, 6 = ‘‘Almost every day’’). Items are scored to
indicate the frequency with which each suicidal thought
has occurred in the preceding month. Scores range from 0
to 180. Scores of 41 or above are considered to indicate
potentially significant psychopathology and acute suicidal
risk (Reynolds 1988). The SIQ is supported by sound
reliability and construct validity data in high school sam-
ples, aged 12–18 years-old, and university samples, aged
18–21 years-old (Reynolds 1987, 1988). The measure has
been found to relate positively to adolescent depression,
adult depression, hopelessness, anxiety, and negative life
events, and correlates negatively with self-esteem (Reynolds
1987). In the present study, Cronbach’s alpha was .96, sug-
gesting good reliability for the measure.
Table 1 Sample characteristics
Total sample Level of suicidal ideation
Minimal-
moderate
Criticala
ntotal (% Total Sample) 302 (100%) 279 (92.4%) 23 (7.6%)
nfemale (% Total Sample) 234 (77.5%) 215 (91.9%) 19 (8.1%)
nmale (% Total Sample) 68 (22.5%) 64 (94.1%) 4 (5.9%)
M(SD)age in years 19.78 (1.59)b 19.81 (1.59) 19.48 (1.62)
Rangeage in years 18–25 18–25 18–24
M(SD)SIQ 19.61 (21.24) 14.82 (10.62) 77.70 (30.48)
RangeSIQ scores 0–145 0–40 41–145
a A sum score of 41 or above indicates a level of suicidal ideation in
need of further investigation (Suicidal Ideation Questionnaire [SIQ];
Reynolds 1988)b 85.4% of the sample was 21 years or younger (n = 258)
296 J Youth Adolescence (2010) 39:291–305
123

Depressive Symptoms
The Depression, Anxiety and Stress Survey (DASS;
Lovibond and Lovibond 1995) consists of 42 statements
that measure symptoms of depression, anxiety and stress
experienced in the past week (14 statements per scale).
Items included in the depression scale are: ‘‘I couldn’t
seem to experience any positive feeling at all’’, ‘‘I was
unable to become enthusiastic about anything’’, and ‘‘I felt
I wasn’t worth much as a person’’. Each statement is rated
on a 4-point scale (0 = ‘‘Did not apply to me at all’’,
3 = ‘‘Applied to me very much, or most of the time’’).
Scores for each scale are summed to indicate participants’
levels of depressive, anxiety or stress symptoms, and can
range from 0 to 42 per scale. The DASS has shown good
discriminant and concurrent validity (e.g., Antony et al.
1998; Lovibond and Lovibond 1995). In previous studies
with clinical samples, the DASS has shown excellent factor
structure that supports the independent use of each scale
(e.g., Antony et al. 1998). In the current study, the DASS
depression scale had a Cronbach’s alpha of .94 and was
used to measure depressive symptoms.
Anxiety Symptoms
The DASS anxiety scale (Lovibond and Lovibond 1995)
was used to measure anxiety symptoms. Items included in
the anxiety scale are: ‘‘I experienced breathing difficulty
(e.g., excessively rapid breathing, breathlessness in the
absence of physical exertion)’’, ‘‘I was aware of the action
of my heart in the absence of physical exertion (e.g., sense
of heart rate increase, heart missing a beat)’’, and ‘‘I felt
scared without any good reason’’. In the current study, the
DASS anxiety scale also demonstrated acceptable reli-
ability with a Cronbach’s alpha .82.
Hopelessness
The Beck Hopelessness Scale (BHS; Beck et al. 1974)
comprises 20 true–false items that reflect hopelessness and
appear to assess the general hopelessness construct (e.g.,
‘‘My future seems dark to me’’). Items are scored to indi-
cate the existence of hopelessness and the extent to which
an individual holds negative attitudes about the future.
Possible scores range from 0 to 20. The BHS is supported
by sound reliability and construct validity data across
samples (e.g., Metalsky and Joiner 1992). The measure has
been found to associate positively with suicidal ideation
and attempt, single-episode major depression, recurrent-
episode major depression, dysthymia, drug and alcohol
misuse (Beck and Steer 1988), and other self-report mea-
sures of hopelessness (Beck et al. 1974). In the present
study, Cronbach’s alpha for the scale was .81, indicating
acceptable reliability for the measure.
Results
Preliminary Analyses
The mean score and standard deviation for the raw SIQ data
are reported in Table 1. Only 80% (n = 23) of the sample
reported a level of suicidal ideation similar to that of
suicidal attempters with chronic psychiatric problems
(Reynolds 1987). This result, together with the mean
scores and standard deviations for depression (M = 8.59,
SD = 8.80), anxiety (M = 4.46, SD = 4.29), and hope-
lessness (M = 3.27, SD = 3.21), indicate that in the current
study, the majority of participants were in the normal range
on all measures of psychological distress. The mean scores
and standard deviations for help-seeking intentions for each
help-source are reported in Table 2. Frequencies of help-
seeking intention scores, indicating whether students were
generally unlikely (scores of 1, 2, or 3) or likely to seek help
(scores of 5, 6 or 7), are also reported in Table 2 for each
help-source.
To correct for positive skew, loglinear transformation
was applied to SIQ scores prior to analysis. Log SIQ was
used in all reported analyses (unless otherwise specified as
raw SIQ data). For ease of expression, log SIQ is described
as suicidal ideation in the results.
Given the substantial difference in group size for males
versus females in the total sample, we examined the pos-
sibility of sex effects in the following main analyses.
Additional calculations found that the mean SIQ scores for
Table 2 Frequencies (listed with approximate % of the sample),
means, standard deviations, and factor loadings (as reported in the
pattern matrix with a Direct Oblimin rotation) for intentions to seek
help for suicidal thoughts by help-source
Help-source Frequency M SD Factors
Unlikelya Likelyb 1 2
Partner 68 (23%) 207 (69%) 5.14 2.08 .84 -.13
Friend 75 (25%) 198 (66%) 5.02 2.04 .81 -.03
Parent 118 (39%) 156 (52%) 4.34 2.34 .82 .07
Family 159 (53%) 108 (36%) 3.40 2.18 .66 .12
Mental health 117 (39%) 150 (50%) 4.07 2.17 .08 .81
Phone counseling 176 (58%) 90 (30%) 3.08 2.05 -.14 .86
Doctor 194 (64%) 74 (25%) 2.87 1.98 .15 .74
No-one 190 (63%) 69 (23%) 2.68 2.19 – –
n = 302a Includes intentions scores of 1 = ‘‘extremely unlikely’’, 2 =
‘‘unlikely’’, and 3 = ‘‘somewhat unlikely’’b Includes intentions scores of 5 = ‘‘somewhat likely’’, 6 =
‘‘likely’’, and 7 = ‘‘extremely likely’’
J Youth Adolescence (2010) 39:291–305 297
123

females and males were not significantly different
(p = .572), the correlation between sex and suicidal idea-
tion was non-significant (p = .722), and there were no sex
differences on measures for intentions to seek help from
any sources for suicidal thoughts, or for depressive symp-
toms and hopelessness (all ps [ .05). Being female had
only a small correlation with higher levels of anxiety
symptoms (r = .13, p \ .05). Consequently, sex is not
included in further analyses.
Next, we examined whether categories of help-source
could be identified that would allow us to combine help-
source items to form subscales for use in the main analyses.
We submitted the seven sources of actual help to an
exploratory principle component analysis (PCA). Seeking
help from no one was not included in the PCA since ‘‘no
one’’ is not an actual source. We uncovered two factors with
eigenvalues greater than 1, which explained 65.61% of the
variance (Keiser–Meyer–Olkin measure of sampling ade-
quacy = .746; Bartlett’s test of sphericity: Approx
v2 = 677.470, df = 21, p \ .001). Factor loadings are
presented in Table 2. Based on this factor analysis, new
variables for different help-source categories were formed
by averaging group items with factor loadings that were
greater than .65. The new help-source variables were labeled
‘‘Family and friends’’ (4 items: M = 4.48, SD = 1.72,
a = .81) and ‘‘Professional care’’ (3 items: M = 3.34,
SD = 1.69, a = .75). The mean difference between the new
subscales revealed that intentions to seek help from family/
friends were significantly higher (p \ .001) than from
sources of professional care. The new help-seeking variables
were used in the main analysis, together with the single item
measuring intentions to seek help from no one.
Main Analyses
Intercorrelations between measures are reported in Table 3.
Evidence for help negation is indicated by significant
inverse correlations between suicidal ideation and help
seeking intentions. Higher levels of suicidal ideation were
significantly associated with lower intentions to seek help
from family/friends and health care professionals, and
higher intentions to seek help from no one, for suicidal
thoughts (Table 3). It is noteworthy that the magnitude of
the help-negation effect was strongest for seeking help
from no one. It is also noteworthy that depressive symp-
toms and hopelessness had significant inverse correlations
with intentions to seek help, and significant positive cor-
relations with intentions to seek no help, for suicidal
thoughts.
To test the hypotheses that university students with
higher levels of suicidal ideation might negate help because
they feel generally hopeless, depressed, or anxious, we
conducted three hierarchical regression analyses, one for
each intentions variable, with suicidal ideation and hope-
lessness entered in Step 1, depressive symptoms in Step 2
and anxiety symptoms in Step 3. As reported in Table 4,
with hopelessness, depressive symptoms and anxiety
symptoms controlled, suicidal ideation remained associated
significantly with lower intentions to seek help from fam-
ily/friends and health care professionals, and higher
intentions to seek help from no one for suicidal thoughts
(Step 3: Friends and family, F(4, 298) = 8.65, p \ .001;
Professional sources, F(4, 298) = 5.26, p \ .001; No one,
F(4, 298) = 9.77, p \ .001). Contrary to expectations, hope-
lessness, depressive symptoms and anxiety symptoms,
neither individually nor together, were able to fully account
for the help-negation effect for family and friends or
seeking help from no one for suicidal thoughts. For
intentions to seek help from a mental health professional,
the inclusion of depressive symptoms at Step 2 meant that
the inverse relationship between suicidal ideation and
intentions became non-significant. However, the extent to
which depressive symptoms explain the help-negating
effect of suicidal ideation for mental health professionals is
Table 3 Intercorrelations between measures
Measure 2 3 4 5 6 7
1 Suicidal ideation(SIQ) .62*** .50*** .55*** -.32*** -.20*** .37***
2 Depression(DASS) .68*** .52*** -.20*** -.18** .31***
3 Anxiety(DASS) .38*** -.10 -.06 .19**
4 Hopelessness(BHS) -.23*** -.22*** .29***
Help-seeking intentions for suicidal thoughts(GHSQ)
5 Friends and family .37*** -.46***
6 Professional carea -.29***
7 No one
n = 302; SIQ = Suicidal Ideation Questionnaire; DASS = Depression, Anxiety, Stress Scales; GHSQ = General Help-Seeking Questionnairea Professional care includes mental health specialists as well as general medical practitioners (family doctors)
*** p \ .001, ** p \ .01
298 J Youth Adolescence (2010) 39:291–305
123
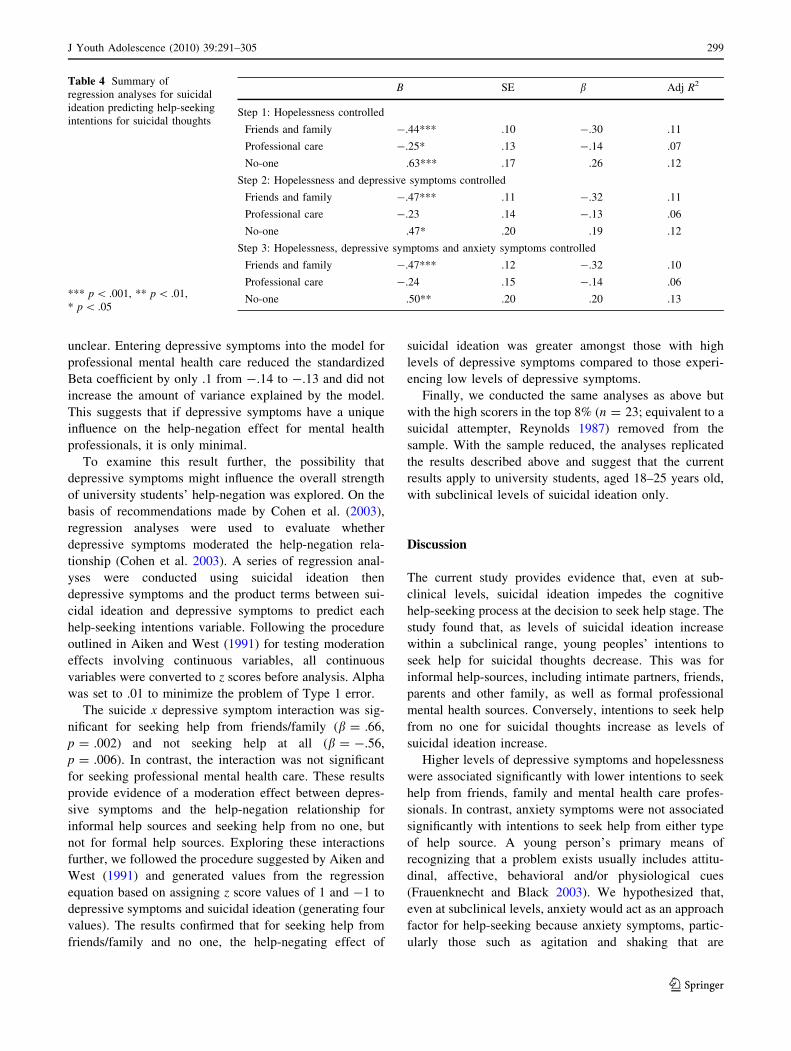
unclear. Entering depressive symptoms into the model for
professional mental health care reduced the standardized
Beta coefficient by only .1 from -.14 to -.13 and did not
increase the amount of variance explained by the model.
This suggests that if depressive symptoms have a unique
influence on the help-negation effect for mental health
professionals, it is only minimal.
To examine this result further, the possibility that
depressive symptoms might influence the overall strength
of university students’ help-negation was explored. On the
basis of recommendations made by Cohen et al. (2003),
regression analyses were used to evaluate whether
depressive symptoms moderated the help-negation rela-
tionship (Cohen et al. 2003). A series of regression anal-
yses were conducted using suicidal ideation then
depressive symptoms and the product terms between sui-
cidal ideation and depressive symptoms to predict each
help-seeking intentions variable. Following the procedure
outlined in Aiken and West (1991) for testing moderation
effects involving continuous variables, all continuous
variables were converted to z scores before analysis. Alpha
was set to .01 to minimize the problem of Type 1 error.
The suicide x depressive symptom interaction was sig-
nificant for seeking help from friends/family (b = .66,
p = .002) and not seeking help at all (b = -.56,
p = .006). In contrast, the interaction was not significant
for seeking professional mental health care. These results
provide evidence of a moderation effect between depres-
sive symptoms and the help-negation relationship for
informal help sources and seeking help from no one, but
not for formal help sources. Exploring these interactions
further, we followed the procedure suggested by Aiken and
West (1991) and generated values from the regression
equation based on assigning z score values of 1 and -1 to
depressive symptoms and suicidal ideation (generating four
values). The results confirmed that for seeking help from
friends/family and no one, the help-negating effect of
suicidal ideation was greater amongst those with high
levels of depressive symptoms compared to those experi-
encing low levels of depressive symptoms.
Finally, we conducted the same analyses as above but
with the high scorers in the top 8% (n = 23; equivalent to a
suicidal attempter, Reynolds 1987) removed from the
sample. With the sample reduced, the analyses replicated
the results described above and suggest that the current
results apply to university students, aged 18–25 years old,
with subclinical levels of suicidal ideation only.
Discussion
The current study provides evidence that, even at sub-
clinical levels, suicidal ideation impedes the cognitive
help-seeking process at the decision to seek help stage. The
study found that, as levels of suicidal ideation increase
within a subclinical range, young peoples’ intentions to
seek help for suicidal thoughts decrease. This was for
informal help-sources, including intimate partners, friends,
parents and other family, as well as formal professional
mental health sources. Conversely, intentions to seek help
from no one for suicidal thoughts increase as levels of
suicidal ideation increase.
Higher levels of depressive symptoms and hopelessness
were associated significantly with lower intentions to seek
help from friends, family and mental health care profes-
sionals. In contrast, anxiety symptoms were not associated
significantly with intentions to seek help from either type
of help source. A young person’s primary means of
recognizing that a problem exists usually includes attitu-
dinal, affective, behavioral and/or physiological cues
(Frauenknecht and Black 2003). We hypothesized that,
even at subclinical levels, anxiety would act as an approach
factor for help-seeking because anxiety symptoms, partic-
ularly those such as agitation and shaking that are
Table 4 Summary of
regression analyses for suicidal
ideation predicting help-seeking
intentions for suicidal thoughts
*** p \ .001, ** p \ .01,
* p \ .05
B SE b Adj R2
Step 1: Hopelessness controlled
Friends and family -.44*** .10 -.30 .11
Professional care -.25* .13 -.14 .07
No-one .63*** .17 .26 .12
Step 2: Hopelessness and depressive symptoms controlled
Friends and family -.47*** .11 -.32 .11
Professional care -.23 .14 -.13 .06
No-one .47* .20 .19 .12
Step 3: Hopelessness, depressive symptoms and anxiety symptoms controlled
Friends and family -.47*** .12 -.32 .10
Professional care -.24 .15 -.14 .06
No-one .50** .20 .20 .13
J Youth Adolescence (2010) 39:291–305 299
123

physiological and often visible, would improve problem
recognition and, in turn, enable the cognitive help-seeking
process. However, we found no evidence to support this
hypothesis. Since anxiety symptoms are associated with
help-seeking in acutely anxious patients (Thompson et al.
2004), it is possible that anxiety acts as an approach factor
only when symptoms are acute. There may be a critical
level that anxiety symptoms need to reach before a young
person will respond to them by seeking help. Further
research needs to examine this possibility.
With symptoms of depression, anxiety and hopelessness
controlled, higher levels of suicidal ideation predicted lower
help-seeking intentions for friends and family, and higher
intentions to seek no help from anyone. The covariates were
unable to fully account for the help-negating effect of sui-
cidal ideation for seeking help from friends, family and no
one. In contrast, for mental health professionals, the sig-
nificant inverse relationship between suicidal ideation and
intentions became non-significant once depressive symp-
toms were controlled. Entering depressive symptoms into
the regression equation reduced the standardized Beta
coefficient by .1 and did not increase the amount of variance
explained by the model. This suggests that the role of
depressive symptoms in explaining the help-negation rela-
tionship for mental health professionals is, at best, minimal.
Instead, these results suggest that before suicidal ideation
reaches levels that would be considered acute and clinically
significant, there are variables over and above the symptom
clusters examined in the current study, which might explain
the help-negation process. The results also confirm that
suicidal ideation itself is both a significant barrier to seeking
help and a general help-avoidance factor, which impedes
the cognitive help-seeking process by reducing help-seek-
ing intentions that are located in the decision making stage.
Saunders and Bowersox (2007) have outlined a 7-step
cognitive process model for seeking professional mental
health care. After problem recognition (Step 1) and before
selecting a help source (Step 7), the model suggests that
five steps are involved in deciding to seek treatment:
deciding the problem is mental health related (Step 2),
deciding change is needed (Step 3), deciding to make
efforts to effect change (Step 4), deciding professional help
is needed to effect change (Step 5), and deciding to seek
professional mental health care (Step 6). Since Steps 4–6
are planning and action steps, and thus, the intention steps
involved in making a mental health help-seeking decision,
the model suggests that suicidal ideation has the greatest
impact on Steps 4–6.
Saunders and Bowersox’ (2007) model also suggests
that each intention step (Steps 4–6) relates to specific
barriers, which are prominent at these steps and which
impede the mental health help-seeking process. At Step 4,
the prominent barrier that promotes treatment delay or
help-avoidance is the preference for solving one’s own
problems. At Step 5, doubting the need for treatment,
having negative attitudes about treatment, distrusting
mental health professionals, and fearing stigma, others’
reactions to seeking treatment and vulnerability through
self-disclosure in treatment are the prominent barriers. At
Step 6, the prominent barrier is the real or perceived
inadequate availability of services. It is notable that most
barriers, which are related to Steps 4–6, are beliefs that
might influence help-negation for mental health sources.
Even at low levels, suicidal ideation might exacerbate these
beliefs and consequently reduce the individual’s intention
and decision to seek treatment for their suicidal thinking.
Further research needs to examine this possibility. Whether
these specific beliefs have a role in the help-negation
process for informal sources or generally avoiding help
also needs to be clarified.
Although depressive symptoms couldn’t fully explain
the help-negation relationship for informal sources and no
one, the current study found evidence that depressive
symptoms moderate help-negation for seeking help from
family, friends, and seeking no help at all. This suggests
that at least some depressive symptoms have a role in
strengthening the help-negating effect of suicidal ideation
for friends and family, as well as in promoting general
reluctance to seek help from everyone. These results are
also consistent with a study of over 1,700 adolescents and
young adults which found that higher levels of depressive
symptoms were related significantly to lower help-seeking
intentions for informal sources for personal-emotional
problems (Wilson et al. 2007). Wilson et al. found that the
help-negating effect of depressive symptoms was strongest
for parents when compared to other help sources, but that
young people with the highest levels of depression were
also those who were most likely to avoid help altogether.
This trend is particularly concerning given the major role
that friends and parents often have in providing support and
access to professional help sources (e.g., Burns et al. 2003;
Cusack et al. 2004).
Other aspects of depression that might be of interest
include the loss of motivation or apathy that is part of the
depressive symptom spectrum. As levels of depressive
symptoms increase, young people might experience
increased levels of apathy and indifference towards help-
seeking, which subsequently reduce their motivation to
seek help (Wilson et al. 2007). Limited cognitive aware-
ness of one’s psychological state, which is associated with
the experience of different types of psychological symp-
toms, is also implicated in help-negation (Saunders and
Bowersox 2007). Further research needs to identify the
specific aspects of depression that contribute to the help-
negation process, together with the ways that these aspects
function to reduce help-seeking intentions when depressive
300 J Youth Adolescence (2010) 39:291–305
123

symptoms are at subclinical levels. Answers to these
questions might explain why almost 90% of Australians
who didn’t seek help for their common mental disorders in
the last year did not think that they needed any type of
mental health care (Meadows and Burgess 2009).
There are several variables that might influence the help-
negation process specifically for family and friends, some of
which are consistent with the barriers that are related to
treatment seeking by Saunders and Bowersox (2007).
Firstly, it is possible that individuals who are experiencing
suicidal ideation or increased levels of depressive symptoms
become reluctant to seek support or advice from informal
sources because they do not think these sources can help.
Help-negation in acutely suicidal and depressed individuals
‘‘involves the belief that one’s problems are so severe or so
complicated that others are unlikely to understand them or
even be capable of providing assistance’’ (Stellrecht et al.
2006, p. 1131). The belief that ‘‘nothing could help’’ was the
second most endorsed barrier (18%) to seeking help for
symptoms of psychological distress in the 1997 Australian
National Survey of Mental Health and Well-being (Sawyer
et al. 2000). Past experiences where seeking help is not
perceived as helpful by the young person may also contribute
to help avoidance (Wilson et al. 2007). This can include
experiences where the young person felt that they were not
listened to or that their problems were not taken seriously
(Rickwood et al. 2005; Stellrecht et al. 2006). It also seems
likely that help-avoidance would be exacerbated in families
and friendships that are experiencing dysfunction or inter-
personal distance.
Secondly, it is possible that suicidal or depressed young
people strive to maintain an appearance of strength,
believing that to tell family or friends about their distress
might ‘‘let their friends or family down’’. Prior research has
identified several belief-based barriers to help-seeking that
support this possibility. The beliefs: ‘‘I think it is important
to remain strong and silent in the face of hardship, even if
you are hurting inside’’ and ‘‘I work hard to prevent people
from seeing my vulnerable side’’ have both been found to
impede help-seeking (Burns et al. 2003; Kuhl et al. 1997).
Alternatively, young people have described their concern
about unduly worrying their friends and family if they talk
about a distressing problem, and particularly if that prob-
lem relates to suicide (Wilson and Deane 2001). For friends
and family, this suggests that the help-negating effect of
suicidal ideation might be underpinned by a fear that tell-
ing one’s friends and family about suicidal thoughts would
place too great a burden on these loved ones.
Another possibility is that the meaning that a young
person associates with their psychological distress symp-
toms might contribute to help-seeking reluctance (Wilson
et al. 2009). Young people are particularly concerned about
being seen as ‘‘mental’’ by their friends and others
(Wisdom et al. 2006). Stigma is associated with different
types of mental health problems and is a major barrier to
health service use (e.g., Samargia et al. 2006; Saunders and
Bowersox 2007; Vogel et al. 2007). Young people who are
experiencing suicidal ideation, even at subclinical levels,
might avoid help because they predict negative conse-
quences if they tell their friends or family about their
problem (e.g., Barney et al. 2005). The extent to which
each of these hypotheses can explain the help-negation
effect is unknown and requires further research.
In the meantime, the current results suggest that help-
seeking promotion programs would do well to place further
attention on the role of parents and friends, as well as other
gatekeepers such as coaches and teachers, in the pathway
to professional mental health care. Australia provides
several examples of how this might be done. Beyondblue—
the Australian national depression initiative—runs a tele-
vision and radio advertising campaign that teaches friends
how to support friends who are depressed. The Motor
Trade Association of Australia promotes the slogan ‘‘mates
help mates’’ through its readthesigns website. The website
also teaches strategies for colleagues, friends and family
members to recognize and facilitate access to professional
mental health care for signs of depression, anxiety and
suicidality; in employees, peers and loved ones. The Aus-
tralian national headspace PASS!—Promoting Access and
Support Seeking—program uses classroom presentations to
promote the value of help-seeking from a range of avail-
able sources. It also implements a range of rehearsal
activities to teach young people how to seek help and what
they can do when they find the response of others, to their
initial help-seeking advances, to be unhelpful. Similar
initiatives are also implemented internationally (Gould
et al. 2003). Help-seeking programs such as these would
also benefit from preparation of helpers or ‘‘gatekeepers’’
(i.e., the support people in a young person’s community
who are not trained mental health professionals). For
example, gatekeepers might benefit from assistance in
recognizing the signs of mental disorders, reducing stigma,
and recognizing their own personal barriers to help-seek-
ing. This would serve the dual purpose of modeling healthy
behavior for young people, as well as maintaining gate-
keepers’ own mental health and their ability to function
effectively as help-providers (Cartmill et al. 2009). Such
initiatives should also emphasize teaching skills to young
people and their gatekeepers, which involve practicing the
specific steps involved in seeking help. By rehearsing the
steps involved in help-seeking when people are not dis-
tressed, it might be possible to improve their use of these
steps when they are distressed and needing appropriate
support and good advice.
At a policy level, the current study reinforces the need
for Governments to fund suicide prevention strategies that
J Youth Adolescence (2010) 39:291–305 301
123

focus on reducing barriers to help-seeking, paying particu-
lar attention to the help-negation process and the ways in
which this trend might differ for different indicators of
mental health problems, different help sources, and for each
of the five systems of interaction within an individual’s
bioecological system (i.e., their Microsystem, Mesosystem,
Exasystem, Macrosystem, and Chronosystem; Bronfen-
brenner 2005). There is also a need for Governments to fund
longitudinal epidemiological research that maps help-
seeking pathways for different types of psychiatric symp-
toms, together with the impact of co-morbidity between
these symptoms, across cultures and countries. For exam-
ple, there is evidence that different forms of mood disorder
are equally severe in young people but that they may have
different patterns of associated factors that might influence
help-seeking (Flament et al. 2001). Such research might
make it possible to address help-avoidance early, and con-
sequently, reduce the high prevalence of mental illness that
currently exists among young people the world over (Belfer
2008).
Limitations
There are several limitations to the current study that should
be considered when reviewing these results. It is encour-
aging that the help-negation effect, as found in the current
results, appears consistent with the pattern of results found
in previous behavioral help-negation studies using acutely
suicidal samples, as well as in large-scale help-seeking
studies using subclinical community samples. Nonetheless,
the use of university students as the only source of data in
the current study means that the extent to which these
results generalize to young adults at the community- or
population-level is not known. Similarly, the use of cross-
sectional data, collected at one time-point, does not allow
for unequivocal causal conclusions. The extent to which the
results were influenced by shared sources of method vari-
ance in self-report data is also not known.
In addition to the limitations above, the current study
used a measure of help-seeking intentions (GHSQ) that
asked participants about problems that might be experi-
enced hypothetically. It is unclear to what extent partici-
pants were actually able to identify with the problem when
making their ratings. Subsequent studies might address this
issue by supplementing the GHSQ with aspects of Hinson
and Swanson’s (1993) methodology for assessing willing-
ness to seek help. Their method used two personal-emo-
tional problem vignettes (one with high severity and one
with low severity) to examine participants’ help-seeking
intentions. Future studies might be improved by obtaining
behavioral data (e.g., via observer rating or diary) to sup-
port self-report ratings, from participants who are recruited
from a wide range of contexts.
Ultimately, there is a need for prospective epidemio-
logical studies to more clearly define the causal relation-
ships between different forms of psychological distress,
particularly suicidal ideation and depressive symptoms,
and subsequent help-seeking cognitions and behaviors. In
the meantime, less expensive cross-sectional studies, which
have stronger correlational designs than used in the current
study, are needed to identify modifiable variables that show
promise for explaining the help-negation process. In future
studies, the directions of relationships between variables
might be examined by using a prospective-longitudinal,
cross-lagged, multi-wave design (Shahar et al. 2006).
Future studies would also benefit by the guidance of a
person-centered model, which is framed by a person-in-
context model, and which accounts for both the actual and
perceived availability of support that exists across the
developmental course of an individual’s life.
Conclusion
The current study provides evidence that, even at sub-
clinical levels, suicidal ideation impedes the cognitive
help-seeking process at the decision to seek help stage in
18–25-year-old university students. Higher levels of sui-
cidal ideation predicted lower intentions to seek help from
formal and informal help sources, and higher intentions to
seek no help, for suicidal thoughts. Depressive symptoms
moderated the help-negation relationship for seeking help
from friends, family and no one. Thus, it appears that
higher levels of depressive symptoms have a role in
strengthening the help-negating effect of suicidal ideation
for informal sources and seeking help from no one.
Although the identification of the specific variables that
account for these results remains for further research, the
current results highlight the importance of improving our
understanding of why young people become reluctant to
seek help as their levels of suicidal ideation and depressive
symptoms increase. Future research would do well to
examine the impact of suicidal ideation on the other stages
of the cognitive help-seeking process (i.e., problem rec-
ognition and selecting a help provider). Future research
also needs to identify the determinants of help-negation for
suicidal ideation and depressive symptoms, whether the
effect occurs for symptom clusters other than those
examined in the current study, and whether the effect
occurs for different symptom clusters across groups with a
range of demographic and developmental characteristics.
In the meantime, mental health promotion strategies should
continue to focus on promoting appropriate help-seeking,
as well as to alert young people, and their families, friends
and mental health care clinicians, about the help-negation
effect for suicidal ideation and depressive symptoms. By
302 J Youth Adolescence (2010) 39:291–305
123

raising awareness, it might be possible to reverse this effect
when symptoms of depression and suicidal thoughts are
first recognized.
Acknowledgments The study was funded by the National Health
and Medical Council of Australia (Grant YS060). The authors wish to
thank Greg Scott and Associate Professor Joseph Ciarrochi for their
contribution to data collection and entry.
References
Aiken, L. S., & West, S. G. (1991). Multiple regression: Testing andinterpreting interactions. Thousand Oaks, CA: Sage.
Ajzen, I. (1991). The theory of planned behavior. OrganizationalBehavior and Human Decision Processes, 50, 179–211.
Anderson, R. M. (1995). Revisiting the behavioral model and access
to medical care: Does it matter? Journal of Health and SocialBehavior, 36, 1–10.
Antony, M. M., Bieling, P. J., Cox, B. J., Enns, M. W., & Swinson,
R. P. (1998). Psychometric properties of the 42-item and 21-
items versions of the Depression anxiety stress scales in clinical
groups and a community sample. Psychological Assessment, 10,
176–181.
Australian Bureau of Statistics. (2008). Australian social trends.Canberra; ABS (ABS Catalogue No. 4102.0).
Bandura, A. (1998). Health promotion from the perspective of social
cognitive theory. Psychology and Health, 13, 623–649.
Barnes, L. S., Ikeda, R. M., & Kresnow, M. (2001). Help seeking
behavior prior to nearly lethal suicide attempts. Suicide and LifeThreatening Behavior, 32(Supplement), 68–75.
Barney, L. J., Griffiths, K. M., Jorm, A. F., & Christensen, H. (2005).
Stigma about depression and its impact on help-seeking inten-
tions. Australian and New Zealand Journal of Psychiatry, 40,
51–54.
Beck, A. T., Brown, G. K., Steer, R. A., Dahlsgaard, K. K., &
Grisham, J. R. (1999). Suicide ideation at its worst point: A
predictor of eventual suicide in psychiatric outpatients. Suicideand Life-Threatening Behavior, 29, 1–9.
Beck, A. T., & Steer, R. A. (1988). Manual for the beck hopelessnessscale. Odessa, FL: Psychological Assessment Resources.
Beck, A. T., Weissman, A., Lester, D., & Trexler, L. (1974). The
measurement of pessimism: The hopelessness scale. Journal ofConsulting and Clinical Psychology, 42, 862–865.
Belfer, M. L. (2008). Child and adolescent mental disorders: The
magnitude of the problem across the globe. Journal of ChildPsychology and Psychiatry, 49, 226–236.
Bronfenbrenner, U. (2005). Making human beings human: Bioeco-logical perspectives on human development. Thousand Oaks.
CA: Sage.
Brown, G. K., Beck, A. T., Steer, R. A., & Grisham, J. R. (2000). Risk
factors for suicide in psychiatric outpatients: A 20-year pro-
spective study. Journal of Consulting and Clinical Psychology,68, 371–377.
Brown, G. K., Jeglic, E., Henriques, G. R., & Beck, A. T. (2006).
Cognitive therapy, cognition, and suicidal behaviour. In T. E.
Ellis (Ed.), Cognition and suicide: Theory, research, and therapy(pp. 53–74). Washington: American Psychological Association.
Burgess, P. M., Pirkis, J. E., Slade, T. N., Johnston, A. K., Meadows,
G. N., & Gunn, J. M. (2009). Service use for mental health
problems: Findings from the 2007 National Survey of Mental
Health and Wellbeing. Australian and New Zealand Journal ofPsychiatry, 43, 615–623.
Burns, T., Eichenberger, A., Eich, D., Ajdacic-Gross, V., Angst, J., &
Rossler, W. (2003). Which individuals with affective symptoms
seek help? Results from the Zurick epidemiology study. ActaPsychiatrica Scandinavica, 108, 419–426.
Cartmill, T. K., Deane, F. P., & Wilson, C. J. (2009). Gatekeeper
training for youth workers: Impact on mental health help-seeking
and referral skill. Youth Studies Australia, 28, 5–12.
Cauce, A. M., Domenech-Rodriguez, M., Paradise, M., Cochran,
B. N., Shea, J. M., Srebnik, D., et al. (2002). Cultural and
contextual influences in mental health help seeking: A focus on
ethnic minority youth. Journal of Consulting and ClinicalPsychology, 70, 44–55.
Cheung, A. H., & Dewa, C. S. (2007). Mental health service use
among adolescents and young adults with Major Depressive
Disorder and suicidality. La Revue Canadienne de Psychiatrie,52, 228–232.
Clark, D., & Fawcett, B. (1992). Review of empirical risk factors for
evaluation of the suicidal patient. In B. Bongar (Ed.), Suicide:Guidelines for assessment, management, and treatment (pp. 16–48).
New York, NY: Oxford University Press.
Cohen, J., Cohen, P., West, S. G., & Aiken, L. S. (2003). Appliedmultiple regression/correlation analysis for the behavioralsciences (3rd ed.). Mahwah, NJ: Lawrence Erlbaum Associates.
Cusack, J., Deane, F. P., Wilson, C. J., & Ciarrochi, J. (2004). Who
influence men to go to therapy? Reports from men attending
psychological services. Journal for the Advancement of Coun-selling, 26, 271–283.
Deane, F. P., Wilson, C. J., & Ciarrochi, J. (2001). Suicidal ideation
and help-negation: Not just hopelessness or prior help. Journalof Clinical Psychology, 57, 1–14.
Fairweather-Schmidt, K., Anstey, K., & Mackinnon, A. J. (2009). Is
suicidality distinguishable from depression? Evidence from a
community-based sample. Australian and New Zealand Journalof Psychiatry, 43, 208–215.
Flament, M. F., Cohen, D., Choquet, M., Jeammet, P., & Ledoux, S.
(2001). Phenomenology, psychosocial correlates, and treatment
seeking in major depression and dysthymia of adolescence.
Journal of the American Academy of Child and AdolescentPsychiatry, 40, 1070–1078.
Fox, J. C., Blank, M., Rovnyak, V. G., & Barnett, R. Y. (2001).
Barriers to help-seeking for mental disorders in a rural impov-
erished population. Community Mental Health Journal, 37,
421–436.
Frauenknecht, M., & Black, D. R. (2003). The social problem solvinginventory for adolescents (SPSI-A): A manual for application,interpretation, and psychometric evaluation. Morgantown WV:
PNG Publications.
Goldney, R. D., Smith, S., Winefield, A. H., Tiggemann, M., &
Winefield, H. R. (1989). Suicidal ideation: Its enduring nature
and associated morbidity. Acta Psychiatrica Scandinavica, 83,
115–120.
Gould, M. S., Greenberg, T., Velting, D. M., & Shaffer, D. (2003).
Youth suicide risk and preventative interventions: A review of
the past 10 years. Journal of the American Academy for Childand Adolescent Psychiatry, 42, 386–405.
Gould, M. S., Velting, D., Kleinman, M., Lucas, C., Thomas, J. G., &
Chung, M. (2004). Teenagers’ attitudes about coping strategies
and help-seeking behavior for suicidality. Journal of theAmerican Academy of Child and Adolescent Psychiatry, 43,
1124–1133.
Graham, A., Reser, J., Scuderi, C., Zubrick, S., Smith, M., & Turley,
B. (2000). Suicide: An Australian psychological society discus-
sion paper. Australian Psychologist, 35, 1–28.
Greenberg, M. T., Domitrovich, C., & Bumbarger, B. (2001). The
prevention of mental disorders in school-aged children: Current
state of the field. Prevention & Treatment, 4, 1–58.
J Youth Adolescence (2010) 39:291–305 303
123

Greenlay, R., & Mullen, A. (1990). Help-seeking and the use of
mental health services. Research in Community Mental Health,6, 325–350.
Henderson, S., Andrews, A., & Hall, W. (2009). State of the nation’s
mental health 2007. Australian and New Zealand Journal ofPsychiatry, 43, 591–593.
Henshaw, E. J., & Freedman-Doan, C. R. (2009). Conceptualizing
mental health care utilization using the Health Belief Model.
Clinical Psychology: Science and Practice, 16, 420–439.
Hinson, J. A., & Swanson, J. L. (1993). Willingness to seek help as a
function of self-disclosure and problem severity. Journal ofCounseling & Development, 71, 465–470.
Issakidis, C., & Andrews, G. (2002). Service utilization for anxiety in
an Australian community sample. Social Psychiatry and Psy-chiatric Epidemiology, 37, 153–163.
Johnston, A. K., Pirkis, J. E., & Burgess, P. M. (2009). Suicidal
thoughts and behaviours among Australian adults: Findings from
the 2007 National Survey of Mental Health and Wellbeing.
Australian and New Zealand Journal of Psychiatry, 43, 635–643.
Kalafat, J. (1997). Prevention of youth suicide. In R. P. Weissberg &
T. P. Gullotta (Eds.), Healthy children 2010: Enhancingchildren’s wellness. Issues in children’s and families’ lives, 8(pp. 175–213). Thousand Oaks: Sage.
Kramer, T., & Garralda, M. E. (2000). Child and adolescent mental
health problems in primary care. Advances in PsychiatricTreatment, 6, 287–294.
Kuhl, J., Jarkon-Horlick, L., & Morrissey, R. F. (1997). Measuring
barriers to help-seeking behavior in adolescents. Journal ofYouth and Adolescence, 26, 637–650.
Leventhal, H., Leventhal, E., & Contrada, R. J. (1998). Self-regulation,
health and behavior: A perceptual-cognitive approach. Psychol-ogy and Health, 13, 717–733.
Liang, B., Goodman, L., Tummala-Narra, P., & Weintraub, S. (2005).
A theoretical framework for understanding help-seeking pro-
cesses among survivors of intimate partner violence. AmericanJournal of Community Psychology, 36, 71–84.
Lovibond, S. H., & Lovibond, P. F. (1995). Manual for the depressionanxiety stress scales (2nd ed.). Sydney, Australia: Psychology
Foundation.
Martin, G. (2002). The prevention of suicide through lifetime mental
health promotion: Healthy, happy young people don’t suicide, do
they? In L. Rowling, G. Martin, & L. Walker (Eds.), Mentalhealth promotion and young people: Concepts and practice(pp. 245–257). Sydney: McGraw-Hill.
Marttunen, M. J., Hillevi, M. A., Hendriksson, M. M., & Lonnqvist,
J. K. (1991). Mental disorders in adolescent suicide DSM III-R-
Axes I and II diagnoses in suicide among 13 to 19 year olds in
Finland. Archives of General Psychiatry, 48, 834–839.
Meadows, G. N., & Burgess, P. M. (2009). Perceived need for mental
health care: Findings from the 2007 Australian Survey of Mental
Health and Wellbeing. Australian and New Zealand Journal ofPsychiatry, 43, 624–634.
Mechanic, D. (1995). Sociological dimensions of illness behavior.
Social Science and Medicine, 41, 1207–1216.
Metalsky, G. I., & Joiner, T. E., Jr. (1992). Vulnerability to depressive
symptomatology: A prospective test of the diathesis-stress and
causal mediation components of the Hopelessness Theory of
Depression. Journal of Personality and Social Psychology, 63,
667–675.
Nigg, C. R., Allegrante, J. P., & Ory, M. (2002). Theory-comparison
and multiple-behavior research: Common themes advancing
health behavior research. Health Education Research, 20,
275–290.
Noar, S. M., & Zimmerman, R. S. (2004). Health behavior theory and
cumulative knowledge regarding health behavior: Are we
moving in the right direction? Health Education Research, 20,
275–290.
Pescosolido, B. A. (1992). Beyond rational choice: The social
dynamics of how people seek help. American Journal ofSociology, 97, 1096–1138.
Pescosolido, B. A., & Boyer, C. A. (1999). How do people come to
use mental health services? In A. V. Horwitz & T. L. Scheid
(Eds.), A handbook for the study of mental health: Socialcontexts, theories and systems. Cambridge, UK: Cambridge
University Press.
Prochaska, J. O., DiClemente, C. C., & Norcross, J. C. (1992). In
search of how people change. American Psychologist, 47, 1102–
1114.
Reinherz, H. Z., Giaconia, R. M., Silverman, A. B., Friedman, A.,
Pakiz, B., Frost, A. K., et al. (1995). Early psychosocial risks for
adolescent suicidal ideation and attempts. Journal of theAmerican Academy of Child and Adolescent Psychiatry, 34,
559–561.
Reynolds, W. M. (1987). Reynolds adolescent depression scale:Professional manual. Odessa, FL: Psychological Assessment
Resources.
Reynolds, W. M. (1988). Suicidal ideation questionnaire: Profes-sional manual. Odessa, FL: Psychological Assessment
Resources.
Rickwood, D. J., Deane, F. P., & Wilson, C. J. (2007). When and how
do young people seek professional help for mental health
problems? The Medical Journal of Australia, 187, S35–S39.
Rickwood, D., Deane, F. P., Wilson, C. J., & Ciarrochi, J.
(2005). Help seeking for mental health problems in adolescence
and early adulthood. Australian e-Journal for the Advancementof Mental Health, 4 (Supplement). www.auseinet.com/journal/
vol4iss3suppl/rickwood.pdf.
Rickwood, D., Wilson, C. J., & Deane, F. P. (2006). Supporting
young people to seek professional help for mental health
problems: Cover Feature. InPsyc: Bulletin of the AustralianPsychological Society, 28, August. http://www.psychology.org.
au/publications/inpsych/support_youth/
Rudd, M. D., Joiner, T. E., Jr., & Rajab, M. H. (1995). Help-negation
after acute suicidal crisis. Journal of Consulting and ClinicalPsychology, 63, 499–503.
Samargia, L. A., Saewyc, E. M., & Elliott, B. A. (2006). Foregone
mental health care and self-reported access barriers among
adolescents. The Journal of School Nursing, 22, 17–24.
Saunders, S., & Bowersox, N. (2007). The process of seeking
treatment for mental health problems. Mental Health andLearning Disabilities Research and Practice, 4, 99–123.
Saunders, S. M., Resnick, M. D., Hoberman, H. M., & Blum, R. W.
(1994). Formal help seeking behavior of adolescents identifying
themselves as having mental health problems. Journal of theAmerican Academy of Child and Adolescent Psychiatry, 33,
718–728.
Sawyer, M. G., Arney, F. M., Baghurst, P. A., Clark, J. J., Graetz,
B. W., Kosky, R. J., et al. (2000). The mental health of youngpeople in Australia. Canberra: Mental Health and Special
Programs Branch, Commonwealth Department of Health and
Aged Care.
Schreiber, V., Renneberg, B., & Maercker, A. (2009). Seeking
psychosocial care after interpersonal violence: An integrative
model. Violence and Victims, 24, 322–336.
Sen, B. (2004). Adolescent propensity for depressed mood and help
seeking: Race and gender differences. Journal of Mental HealthPolicy and Economics, 7, 133–145.
Shad, M. U., Keshavan, M. S., Tamminga, C. A., Cullum, C. M., &
David, A. (2007). Neurobiological underpinnings of insight
deficits in schizophrenia. International Review of Psychiatry, 19,
439–448.
304 J Youth Adolescence (2010) 39:291–305
123

Shahar, G., Bareket, L., Joiner, T., & Rudd, M. D. (2006). In severely
suicidal young adults, hopelessness, depressive symptoms, and
suicidal ideation constitute a single syndrome. PsychologicalMedicine, 36, 913–922.
Sheffield, J. K., Fiorenza, E., & Sofronoff, K. (2004). Adolescents’
willingness to seek psychological help: Promoting and prevent-
ing factors. Journal of Youth and Adolescence, 33, 495–507.
Stellrecht, N. E., Joiner, T. E., & Rudd, M. D. (2006). Responding to
and treating negative interpersonal processes in suicidal depres-
sion. Journal of Clinical Psychology, 62, 1129–1140.
Swanson, J. W., Linskey, A. O., Quintero-Salinas, R., Pumariega,
A. J., & Holzer, C. E. (1992). A binational school survey of
depressive symptoms, drug use and suicidal ideation. Journal ofthe American Academy of Child and Adolescent Psychiatry, 31,
669–778.
Thompson, A., Hunt, C., & Issakidis, C. (2004). Why wait? Reasons
for delay and prompts to seek help for mental health problems in
an Australian clinical sample. Social Psychiatry and PsychiatricEpidemiology, 39, 810–817.
Vogel, D. L., Wade, N. G., & Hackler, A. J. (2007). Perceived public
stigma and the willingness to seek counseling: The mediating
roles of self-stigma and attitudes toward counseling. Journal ofCounseling Psychology, 54, 40–50.
Webb, T. L., & Sheeran, P. (2006). Does changing behavioral
intentions engender behavior change? A meta-analysis of the
experimental evidence. Psychological Bulletin, 132, 249–268.
Weishaar, M. E. (1996). Cognitive risk factors in suicide. In
P. Salkorskis (Ed.), Frontiers of cognitive therapy (pp. 226–249).
New York: Guilford Press.
Whiteford, H., & Groves, A. (2009). Policy implications of the 2007
Australian National Survey of Mental Health and Wellbeing.
Australian and New Zealand Journal of Psychiatry, 43, 644–651.
Wills, T. A., & Gibbons, F. X. (2009). Using psychological theory in
help-seeking research. Clinical Psychology: Science and Prac-tice, 16, 440–444.
Wilson, C. J., & Deane, F. P. (2001). Adolescent opinions about
reducing help-seeking barriers and increasing engagement.
Journal of Educational and Psychological Consultation, 12,
345–364.
Wilson, C. J., & Deane, F. P. (2009). Help-negation. Australian andNew Zealand Journal of Psychiatry.
Wilson, C. J., Deane, F. P., & Ciarrochi, J. (2005a). Can hopelessness
and adolescents’ beliefs about seeking help account for help-
negation? Journal of Clinical Psychology, 61, 1525–1539.
Wilson, C. J., Deane, F. P., Ciarrochi, J., & Rickwood, D. (2005b).
Measuring help-seeking intentions: Properties of the General
Help-seeking Questionnaire. Canadian Journal of Counselling,39, 15–28.
Wilson, C. J., Deane, F. P., Marshall K. L., & Dalley, A. (2009).
Adolescents’ suicidal thinking and reluctance to consult general
medical practitioners. Journal of Youth and Adolescence. doi:
10.1007/s10964-009-9436-6.
Wilson, C. J., Rickwood, D., & Deane, F. P. (2007). Depressive
symptoms and help-seeking intentions in young people. ClinicalPsychologist, 11, 98–107.
Wisdom, J. P., Clarke, G. N., & Green, C. A. (2006). What teens
want: barriers to seeking care for depression. Administration andPolicy in Mental Health and Mental Health Research Services,33, 133–145.
Zachrisson, H. D., Rodje, K., & Mykletun, A. (2006). Utilization of
health services in relation to mental health problems in
adolescents: A population based survey. BMC Public Health,6, 34–40.
Zwaanswijk, M., Van der Ende, J., Verhaak, P. F. M., Bensing, J. M.,
& Verhulst, F. C. (2003a). Factors associated with adolescent
mental health service need and utilization. Journal of theAmerican Academy of Child and Adolescent Psychiatry, 42,
692–700.
Zwaanswijk, M., Verhaak, P. F. M., Bensing, J. M., Van der Ende, J.,
& Verhulst, F. C. (2003b). Help seeking for emotional and
behavioral problems in children and adolescents: A review of
recent literature. European Child and Adolescent Psychiatry, 12,
153–161.
Author Biographies
Dr. Coralie Wilson is the Academic Leader for the Professional and
Personal Development Curriculum Theme and a Senior Lecturer in
Behavioral Health Sciences in the Graduate School of Medicine at the
University of Wollongong. She is also Co-Chair of the Graduate
School of Medicine Research Themes. Coralie received her PhD in
clinical psychology research from the University of Wollongong, has
professional training in both teaching and psychology, and has major
research interests in help-seeking and behavioral psychological
medicine.
Dr. Frank Deane is a Clinical Psychologist, Professor of Psychology
and Director of the Illawarra Institute for Mental Health at the
University of Wollongong. He received his PhD from Massey
University and has major research interests in the areas of mental
health and drug & alcohol service use, medication alliance, the use of
homework in clinical practice and help-seeking.
J Youth Adolescence (2010) 39:291–305 305
123





























