Embed Size (px)
Citation preview

~ Y 4 ~ ? f
~ ' 6 F -
ELSEVIER
JOURNAL OF C L I N I C A L VIROLOGY
Journal of Chmcal Virology 34 Suppl 2 (2005) $33 $38 www elsevier corn locate jcv
Hepatitis C virus seroprevalence in multi-transfused patients in Colombia
Maur ic io Beltrfin a' *, Maria-Cris t ina Navas b, Fernando D e la H o z a' 1, Maria M e r c e d e s M u f i o z c, Sergio Jaramillo d, Cecilia Estrada e, Lucia del Pilar Cort6s f, Maria Patricia Arbelfiezg,
Jorge Donado b'd, Gloria Barco e, Martha Luna e, Gustavo Adolfo Uribe c, Amalia de Maldonado b, Juan Carlos Restrepo b, Gonzalo Correa b, Paula Borda a, Gloria Rey a, Marlen de Neira a,
Angela Estrada d, Sandra Yepes d, Oscar Beltrfin c, Javier Pacheco f, Ivfin Villegas h, Jorge Boshell a' 2 alnstttuto Nactonal de Sahut. Calle 26 # 51-60 CAN Zona 6. Bogotd D C. Colomhta
t'GHtpo de Gczs'tlohepatolog{a. Facultad de Medtcma. Untc'elsutad de Anttoquta. C1 51D # 62-29. Medell[n. Colomhta ~Instttuto de los Segutos Soctales. Cl{ntca San Pe~ho Clac, et. Ct 10 # 64-28. Bogotd D C. Colomhta
dHospttal Pahlo Toh6n Ut the. Cl 78 B # 69-240. 3Iedell{n. Colomhta elnstttuto de los Segwos Soctales. Cl[ntca Le6n XIIL C1 52 # 69-16. Medell[n. Colomhta
tlnstttuto Nactonal de Cancelolog[a Cl 1 # 9-85. Bogotd D C. Colomhta ~Gtupo de Eptdemtolog{a. Untc'etstdad de Anttoquta. Cl 62 # 52-59. 3Iedell{n. Colomhta
IZlnstttuto del Rt~6n. Cl l i b S # 44-103. Medell[n. Colomhta
Abstract Background: Hepatitis C Vtrus (HCV) refection is a public health problem worldwide, with particular relevance m multi-transfused
patients given that HCV is principally transmitted by exposure to infected blood Study design: Between February and September 2003 a cross-sectional study was carried out m four hospital centres m Bogotfi and
Medellln, Colombia, to determine the risk factors for HCV refection m 500 multi-transfused patients Results: The study population was distributed in five groups haemophlha, haemodyahsls, acute bleeding, oncologlcal illnesses and
sickle cell disease or thalassemla Serum samples from patients were tested for HCV aXltlbodles (Asxym TM, Abbott) An overall prevalence (9 0%, 95% confidence interval (CI) 6 4 11 6) (45/500) of HCV infection was found Antl-HCV aXltlbodles were detected m 32 2% of patients with haemophlha, 6 1% of patients undergoing haemodlalysls, 7 1% of patients with sickle cell disease or thalassemla, 2 6% of patients with acute bleeding and 3 4% of patients with oncologlcal or hematological diseases
The mare risk t;actors associated with refection by HCV were to be hemophdlc (odds ratio, OR 18 03, 95% CI 3 96 114 17), having received transfusions before 1995 (OR 12 27, 95% CI 5 57 27 69), and having received more than 48 units of blood components (OR 6 08, 95% CI 3 06 12 1) In the multlwxlate axmlysls, only the year of transfusions (before 1995) remained significantly associated with risk of infection by HCV
Conclusions: The data show a 3-fold reduction m the refection risk between 1993 and 1995, when the serological screening for HCV in blood donors was being introduced A reduction greater than 90% was achteved by 1995 when the screening coverage reached 99% '4' 2005 Elsevier B V All rights reserved
Kevwolds HCV, prevalence, Multi-transfused patients, Colombm
1. Introduct ion
Hepatitis C Virus (HCV) is a positive-strand RNA virus, be- longing to the Flavtvtrtdae family, whose genome encodes a polyproteln that is cleaved into 4 structural proteins (Core, E 1, E2, p7) and 6 non-structural proteins (NS2, NS3, NS4A, NS5A, NS4B, NS5B) (Penin et al., 2004).
* Corresponding author Tel fax 0 57 1 220 77 00 E-mad a&h ess mbeltrand(a'ms gov co (M Beltran)
HCV is the main cause of morbidity and mortality associ- ated with chronic liver diseases, cirrhosis and hepatocelullar carcinoma (Albertl and Benvegnu, 2003). According to the World Health Organization (WHO), approximately 170 million people are infected with HCV worldwide. In Latin America, WHO estimates a prevalence of infection of 1-2.5"/,, in most of the countries, except in Brazil and Bolivia where prevalences of 2.5-10% and >10%, respectively, have been estimated (WHO, 2000, 2002).
1 Present address Programa Clencla y Tecnologla de la Salud, Colclenclas, Tr 9 a- # 133-28, Bogotfi D C, Colombia 2 Present address Secretana de Salud del Meta, Calle 37 # 41-80, Vlllavlcenclo, Colombia
1590-8658 $ see front matter ,c, 2005 Flsevler B V All rights reserved

$34 3I Beltldn et a l / loulnal o/'Chntcal l'tlologv 34 Suppl 2 (2005) $33 $38
This public health problem is of particular relevance in multi-transfused patients given that HCV is principally transmitted by exposure to infected blood, indeed, the incidence of HCV infection in this group is directly related to the amount of blood products received (Lal et al., 1993, Flnk et al., 1993). Since HCV screening of blood donors became mandatory in 1990, the incidence of post- transfusion HCV has continued to decline in developed countries (Barrera et al., 1991, Donahue et al., 1992). In developing countries some difficulties remain in the safety of blood supply, however the risk of transfusion-transmitted infectious diseases tends to be minimized by strategies such as promoting altruistic voluntary repeat donation, improving serologic screening, and restraining transfusions according to good standards of medical practice (Schmums et al., 1998,2001 ). In addition, the use of improperly steril- ized needles and syringes is related to HCV transmission in some parts of the world (Luby et al., 1997, Slmonsen et al., 1999, Kane et al., 1999).
The estimates of HCV prevalence in Colombia corre- spond to data collected from blood donors, since there is no study of prevalence in the general population. According to the National Blood Banks Unit of the Colombian National Institute of Health, seroprevalence of HCV in blood donors was 0.7-1.0% from 1993 to 1996, and 0.5% in 2002 (Beltrfin et al., 1997a,b, Cortes et al., 1999a, unpublished data). Studies carried out in high-risk populations have reported HCV prevalences of 60% and 35"/,, in patients subjected to haemodlalysls, 32"/,, to 6.5"/,, in hemophiliac patients, 49"/,, to 21% in patients with a history of renal transplant, and 45"/,, in patients with chronic liver disease (Echavarna, 1992, De la Hoz, 2000, Consenso Colomblano de Hepatitis C, 2002).
The alms of this study were to determine the frequency of the HCV serological marker and to explore the risk factors for infection in a population of 500 multi-transfused patients recruited in the two largest cities in Colombia, Bogotfi and Medellfn.
2. Materials and methods
2 l PatlenL~'
The population included in this cross-sectional study was recruited using the data from four hospital blood banks. The inclusion criteria were, first, diagnosis of hemophilia, sickle cell disease, thalassemla, acute bleeding, oncologlcal illnesses or renal failure requiring haemodlalysls, and second, no less than 10 units of allogenelc blood or blood components, transfused on at least two different occasions. The exclusion cntenon was previous diagnosis of HCV infection.
The population was recruited in two hospitals in Bogotfi (Clfmca San Pedro Claver and Inshtuto Naclonal de Cancerologfa) and two hospitals in Medellfn (Clfmca
Ledn XIII and Hospital Pablo Tobdn Unbe) from February to September 2003.
Informed consent was obtained from patients accord- ing to requirements of the School of Medicine Ethical Committee, Antloqma University. Patients who agreed to participate were informed of the risks and benefits, advised of their rights, and given a copy of the informed consent form. A standardized form was used to collect data on demographic and transfusion variables and other risk factors for HCV infection, obtained from patient interviews and clinical records. The quality of the information was assured by training the interviewers in each hospital. All questionnaires were reviewed and validated by the team epldemlologlsts at the Instltuto Naclonal de Salud and the Umversldad de Antloqma.
2 2 Blood samples a , d detectlo, o fa , t lbodtes
Blood samples were collected m vacuum tubes by venop- uncture, centrifuged and sera stored m ahquots at -70°C. Biological specimens were tested for HCV antibodies using commercially available kits (HCV version 3, Asxym TM, Abbott), at the Hospital Pablo Tobdn Unbe blood bank. This laboratory participates in the external quality program of the Colombian National Institute of Health.
All methods, procedures as well as consent forms were approved by the institutional review boards of the Panamencan Health Organization (PAHO), the Instltuto Naclonal de Salud, the Umversldad de Antloqma and the Instltuto Naclonal de Cancerologla.
2 3 Stattstlcal anah,ms
Statistical analysis was done using Epflnfo (version 6.04) and SPSS (version 11.0). Two identical databases were constructed and checked for inconsistencies assuring the quality of data entry. X 2 test was used to compare proportions among patients positive or negative for HCV. Prevalence ratios (PR) and odds ratios (OR) with their 95% confidence intervals (CI) were used to analyse the association between the variables and HCV infection.
3. Results
Five hundred multi-transfused patients participated m the study, of whom 279 (55.8"/,,) came from Bogotfi and the rest from Medellin, 303 (60.6%) were males. The mean age was 43 years, and 375 (75"/,,) of them were older than 28 years. Two hundred and twenty-one (44.2"/,,) patients reported some level of formal education, such as primary, secondary or university. Of these, 94 (42.5"/,,) completed primary school, 89 (40.27%) secondary and 38 (17.19"/,,) had a university degree.
The majority of the population entered the study because they had oncologlcal or haematologlcal illnesses (OHI, n = 236), the others were patients with haemophflla (PWH,
M Beltldn et a l / Ioulnal qfChntcal l'tlolog3' 34 Suppl 2 (2005) $33 $38
Table 1 S u m m a r y o f risks factors for H C V Infection
$35
Factor n H C V + H C V O R O R 9 5 % CI
n % n %
Groups
Hemoph lhacs 90 29
Renal dialysis 82 5
Sickle cell disease or tha lassemla 14 1
OncologIcal hematological 236 8
Acute bleeding 78 2
N u m b e r of units
>48 units 125 28
48 units 375 17
Exposure to transfusions
1 yea r 266 9
>1 year 234 36
Transfused components
Whole hlood
Yes 13 8
No 487 37
Red Blood CelLs'
Yes 439 32
No 61 13
Blood plasma
Yes 134 20
No 366 25
Platelets
Yes 187 13
No 313 32
Ct3'opt ec tpttate and Lvophthzed Both Cryop and Lyoph 67 27
Cryop only 23 2
Eyoph only 8 0
None 402 16
Year of transfusion
Before 1993 122 34
1993 1995 14 1
Af ter 1995 364 10
3 2 2 61 6 7 8 18 03 3 9 6 114 17
6 1 77 9 3 9 2 4 7 0 4 1 1 9 0 0
7 1 13 9 2 9 2 9 2 0 0 0 46 40
3 4 228 9 6 6 1 3 3 0 2 5 9 3 0
2 56 76 97 4 1 0
2 2 4 97 77 60 6 8 3 0 6 121
4 53 358 95 47 1 0
3 38 257 96 62
1 5 3 8 198 4 6 2 5 2 2 3 1 1 9
61 53 5 38 47 19 46 5 3 6 73 57
7 60 450 92 40 1 0
7 29 407 92 71 0 29 0 13 0 63
21 31 48 78 69 1 0
1 4 9 7 114 8 5 0 7 2 3 9 1 2 2 4 7 0
6 83 341 93 17 1 0
6 95 174 93 05 0 66 0 31 1 35
10 22 281 89 78 1 0
40 30 40 59 70 16 28 7 6 8 34 82
8 6 9 21 91 31 2 3 0 0 0 0 1 1 5 2
0 0 8 100
3 98 386 96 02 1 0
27 87 88 72 13 13 68 6 2 0 30 86
7 14 13 92 86 2 72
2 75 354 97 25 1 0
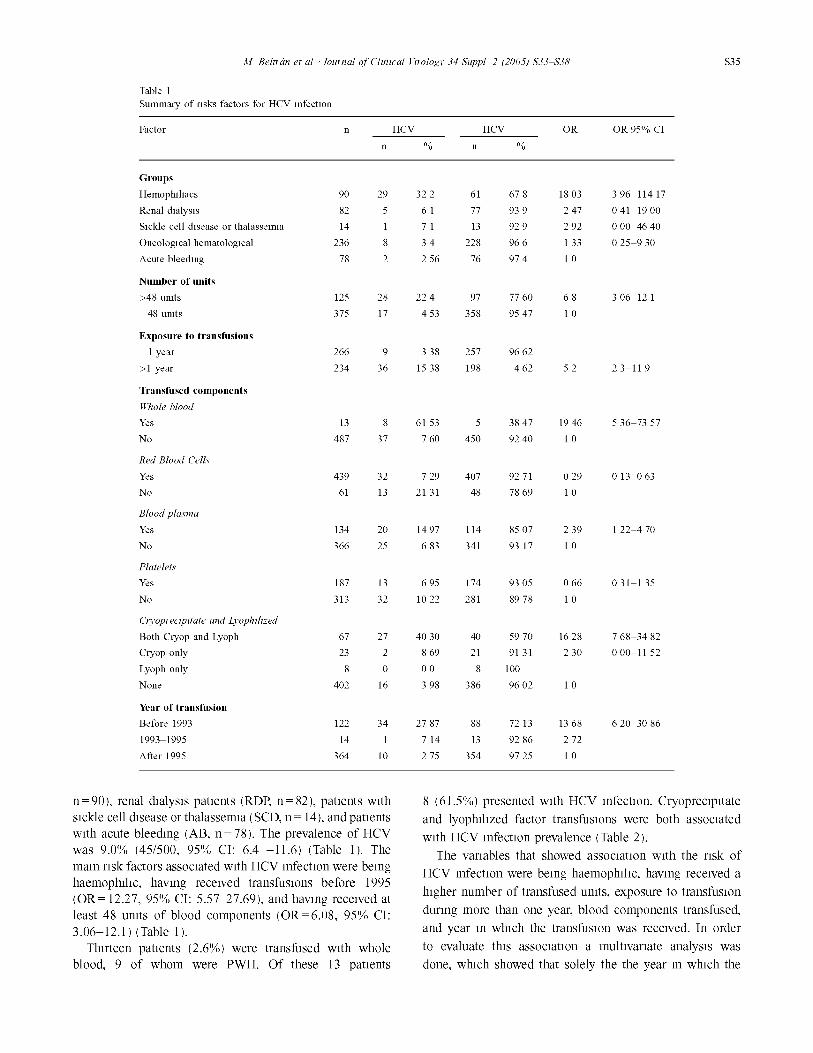
n=90) , renal dmlys~s patients (RDR n = 82), patients w~th sickle cell d~sease or thalassemm (SCD, n = 14), and patients w~th acute bleeding (AB, n = 78). The prevalence of HCV was 9.0% (45/500, 95"/,, CI: 6.4 -11.6) (Table 1). The mare risk factors assocmted w~th HCV mfect~on were being haemophd~c, hawng received transfusions before 1995 (OR = 12.27, 95"/,, CI: 5.57~7.69), and hawng received at least 48 umts of blood components (OR=6.08, 95"/,, CI: 3.06-12.1 ) (Table 1 ).
Thirteen patients (2.6"/,,) were transfused w~th whole blood, 9 of whom were PWH. Of these 13 patients
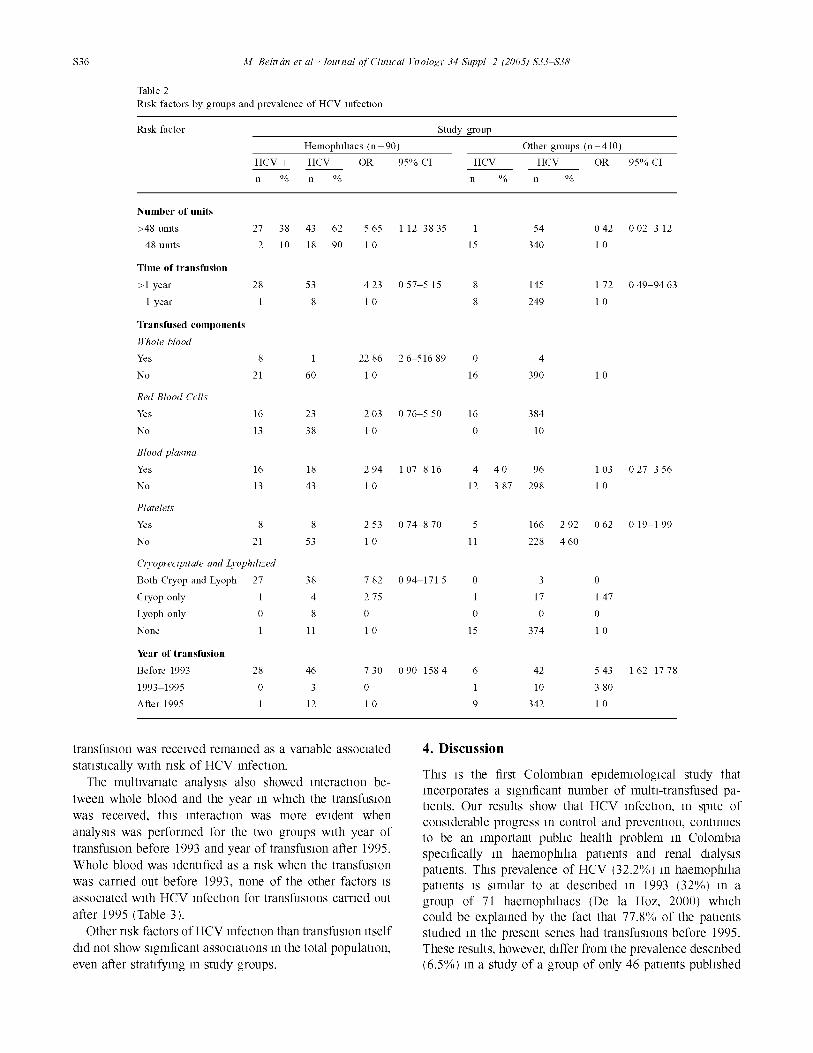
8 (61.5"/,,) presented with HCV mfect~on. Cryoprec~p~tate and lyophdlzed factor transfusions were both assocmted w~th HCV refection prevalence (Table 2).
The variables that showed assocmt~on w~th the risk of HCV mfect~on were being haemophdlc, hawng received a h~gher number of transfused umts, exposure to transfusion during more than one year, blood components transfused, and year m which the transfusion was received. In order to evaluate th~s assocmt~on a multivariate analys~s was done, which showed that solely the the year m which the
$36 3I Beltldn et al / Iomnal o/'Chntcal Vtlolog3' 34 Suppl 2 (2005) $33 $38
Table 2 RJsk factors by groups and prevalence o f H C V mfec tmn
Rask fac tor Study group
Hemophf lmcs ( n = 9 0 )
H C V + H C V O R
n % n %
Other groups ( n = 4 1 0 )
95% CI H C V + H C V O R 9 5 % CI
n % n %
N u m b e r o f units
>48 umts 27 38 43 62 5 65 1 12 38 35 1 54 0 42 0 02 3 12
48 umts 2 10 18 90 1 0 15 340 1 0
T i m e o f transfus ion
> l y e a r 28 53 4 2 3 0 5 7 5 15 8 145 1 7 2 0 4 9 94 63
1 year 1 8 1 0 8 249 1 0
Transfused c o m p o n e n t s
Whole hlood
Yes 8 1 22 86 2 6 516 89 0 4
No 21 60 1 0 16 390 1 0
Red Blood Cells'
Yes 16 23 2 03 0 76 5 50 16 384
No 13 38 1 0 0 10
Blood plasma
Yes 16 18 2 9 4 1 0 7 8 1 6 4 4 0 96 1 0 3 0 2 7 3 5 6
No 13 43 1 0 12 3 87 298 1 0
Platelets
Yes 8 8 2 53 0 74 8 70 5 166 2 92 0 62 0 19 1 99
No 21 53 1 0 11 228 4 60
C13'opl ectpttate and Lvophthzed
Both Cryop and Lyoph 27 38 7 82 0 94 171 5 0 3 0
Cryop only 1 4 2 75 1 17 1 47
Lyoph only 0 8 0 0 0 0
None 1 11 1 0 15 374 1 0
Year o f transfus ion
Before 1993 28 46 7 30 0 90 158 4 6 42 5 43
1993 1995 0 3 0 1 10 3 80
Af ter 1995 1 12 1 0 9 342 1 0
1 62 17 78
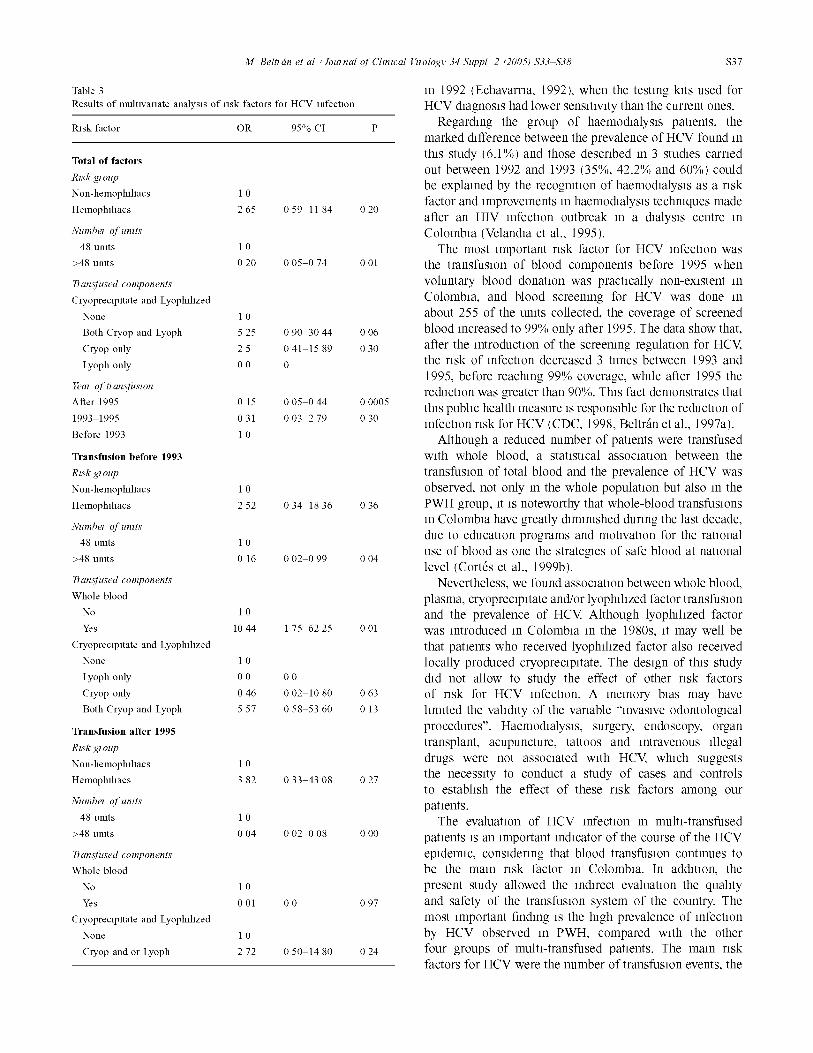
transfusion was received remained as a variable assocmted stahshcally w~th risk of HCV mfechon.
The multivariate analysis also showed interaction be- tween whole blood and the year m which the transfusion was received, th~s mterachon was more evident when analys~s was performed for the two groups w~th year of transfusion before 1993 and year of transfusion after 1995. Whole blood was ldenhfied as a risk when the transfusion was carried out before 1993, none of the other factors is assocmted w~th HCV mfect~on for transfusions carried out after 1995 (Table 3 ).
Other risk factors of HCV mfechon than transfusion ~tself d~d not show s~gmficant assocmt~ons m the total populat~om even after stratifying m study groups.
4. Discussion
Tins is the first Colombmn ep~dem~olog~cal study that incorporates a slgmficant number of multi-transfused pa- hents. Our results show that HCV mfechon, m sp~te of considerable progress m control and preventlom continues to be an ~mportant pubhc health problem m Colombm specifically m haemopinha patients and renal dmlys~s pahents. Th~s prevalence of HCV (32.2"/,,) m haemophflm patients ~s s~mflar to at described m 1993 (32"/,,) m a group of 71 haemopinhacs (De la Hoz, 2000) which could be explained by the fact that 77.8"/,, of the pahents stud~ed m the present series had transfusions before 1995. These results, however, differ from the prevalence described (6.5"/,,) m a study of a group of only 46 patients pubhshed
M Belttdn et a l / Ioulnal ofChntcal l'tlolog3' 34 Suppl 2 (2005) $33 $38 $37
Table 3 Results of multivariate analysis of risk factors for HCV Infection
Rask factor OR 95% CI P
Total o f factors
Rtsk El oup Non-hemophlhacs 1 0
Hemophlhacs 2 65 0 59 11 84 0 20
Numhel of'tlmts
48 umts 1 0 > 4 8 u n i t s 0 2 0 0 0 5 0 7 4 001
Tl an,yfused components Cryopreclpltate and Lyophdlzed
None 1 0 Both Cryop and Lyoph 5 25 0 90 30 44 0 06
Cryop only 2 5 0 41 15 89 0 30
Lyoph only 0 0 0
Year o/'tl an,~/'uston After 1995 0 15 0 05 0 44 0 0005
1993 1995 031 0 0 3 2 7 9 0 3 0
Before 1993 1 0
Transfusion before 1993
Rtsk gl oup
Non-hemophdmcs 1 0
Hemophil iacs 2 52 0 34 18 36 0 36
Number qf umts 48 umts 1 0
>48 umts 0 16 0 02 0 99 0 04
Tl an,y/'used components
Whole blood No 1 0
Yes 1044 175 62 25 001 Cryopreclpltate and Lyophdlzed
None 1 0
Lyoph only 0 0 0 0 Cryop only 0 46 0 02 10 80 0 63 Both Cryop and Lyoph 5 57 0 58 53 60 0 13
Transfusion after 1995
Rtsk gl oup
Non-hemophdmcs 1 0 Hemophdmcs 3 82 0 33 43 08 0 27
Number qf umts
48 umts 1 0
>48 umts 0 04 0 02 0 08 0 00
Tl an,y/'used components
Whole blood
No 1 0
Yes 0 01 0 0 0 97 Cryopreclpltate and Lyophdlzed
None 1 0 Cryop and or Lyoph 2 72 0 50 14 80 0 24
in 1992 (Echavarrla, 1992), when the testing kits used for HCV diagnosis had lower sensitivity than the current ones.
Regarding the group of haemodlalysls patients, the marked difference between the prevalence of HCV found in this study (6.1%) and those described in 3 studies carried out between 1992 and 1993 (35"/,,, 42.2"/,, and 60%) could be explained by the recognition of haemodlalysls as a risk factor and improvements in haemodlalysls techniques made after an HIV infection outbreak in a dialysis centre in Colombia (Velandla et al., 1995).
The most important risk factor for HCV infection was the transfusion of blood components before 1995 when voluntary blood donation was practically non-existent in Colombia, and blood screening for HCV was done in about 255 of the units collected, the coverage of screened blood increased to 99"/,, only after 1995. The data show that, after the introduction of the screening regulation for HCV, the risk of infection decreased 3 times between 1993 and 1995, before reaching 99"/,, coverage, while after 1995 the reduction was greater than 90%. This fact demonstrates that this pubhc health measure is responsible for the reduction of infection risk for HCV (CDC, 1998, Beltrfin et al., 1997a).
Although a reduced number of patients were transfused with whole blood, a statistical association between the transfusion of total blood and the prevalence of HCV was observed, not only in the whole population but also in the PWH group, it is noteworthy that whole-blood transfusions in Colombia have greatly diminished during the last decade, due to education programs and motivation for the rational use of blood as one the strategies of safe blood at national level (Cortes et al., 1999b).
Nevertheless, we found association between whole blood, plasma, cryopreclpltate and/or lyophlhzed factor transfusion and the prevalence of HCV. Although lyophlhzed factor was introduced in Colombia in the 1980s, it may well be that patients who received lyophlhzed factor also received locally produced cryopreclpltate. The design of this study did not allow to study the effect of other risk factors of risk for HCV infection. A memory bias may have hmlted the vahdlty of the variable "lnvaslve odontologlcal procedures". Haemodlalysls, surgery, endoscopy, organ transplant, acupuncture, tattoos and intravenous illegal drugs were not associated with HCV, which suggests the necessity to conduct a study of cases and controls to estabhsh the effect of these risk factors among our patients.
The evaluation of HCV infection in multi-transfused patients is an important indicator of the course of the HCV epidemic, consldenng that blood transfusion continues to be the main risk factor in Colombia. In addition, the present study allowed the indirect evaluation the quahty and safety of the transfusion system of the country. The most important finding is the high prevalence of infection by HCV observed in PWH, compared with the other four groups of multi-transfused patients. The main risk factors for HCV were the number of transfusion events, the

$38 M Beltldn et al / lomnal q/'Chntcal Vtlologv 34 Suppl 2 (2005) $33 $38
amount of transfused blood components, and hawng had transfusions before 1995. The fact that the risk of HCV mfect~on dlmm~shed drastically after 1995 demonstrates the value of the strategies that the national blood program ~mplemented m 1993, by m~tlat~ve of the Mm~steno de Salud Instltuto Nac~onal de Salud (Mmlsteno de Salud, 2002) w~th the support of the PAHO.
Acknowledgements
The authors wish to thank Drs. Joss Ramlro Cruz and Serge Xueref for crmcal reading of the manuscript and helpful dlscuss~on. This study was supported by PAHO thanks to a grant from by the Bill and Mehnda Gates Foundation.
References Albertl A, Benvegnu ML Management of hepatitis C J Hepatol 2003,38
S104 18 Barrera JM, Bruguera M, Ercllla MG, Sanchez-Taplas JM, Gll MP, Costa J,
et al Incidence of non-A, non-B hepatitis after screening blood donors for antibodies to hepatitis C virus and surrogate markers Ann Intern Med 1991,115(8) 596 600
BeltrAn M, Ayala M, Chmg R Sltuacl6n actual del tanuzaje en bancos de sangre Blom~dlca 1997a,16(2) 51 2
BeltrAn M, Raad J, Ayala M, Chmg R Tamlzaje de enfermedades mfecclosas en bancos de sangre, Colombia, 1995 Blom~dlca 1997b,17(2) 137 42
CDC Recommendations for Prevention and Control of Hepatitis C Virus (HCV) Infection and HCV-related chronic disease MMWR, 1998,47(RR19), 1 39
Consenso Colomblano de Hepatitis C Repertono de medlcma y clrugla 2002,11 8 38
Cortes A, Beltrfin M, Olaya B, Hernfindez M, Raesgo de enfermedades mfecclosas transmltldas por transfusldn en el Valle del Cauca Colombia M~dlca 1999a,30 13 8
Cortes A, Beltrfin M, Olaya B, Hernfindez M Fpldemlologia de la coleccldn, proceso y uso de la sangre y componentes sangulneos en el Valle del Cauca Colombia Colombia M~dlca 1999b,30(1) 29~5
De la Hoz FP Hepatitis C epldemlology m Latin America and Colombia BlomSdlca 2000,20(1) 66 72
Donahue JG, Munoz A, Ness PM, Brown Jr DE, Yawn DH, McAlhster Jr HA, et al The dechnmg risk of post-transfusion hepatitis C virus refection N Engl J Med 1992,327(6) 369 73
Echavarna E Estudlos de antlcuerpos contra el virus de la Hepatitis C en donantes de sangre y gmpos alto nesgo Acta MSdlca Colomblana 1992,17 11 5
Fmk FM, Hocker-Schulz S, Mot W, Puchhammer-Stockl E, Hofmann H, Zoubek A, et al Association of hepatitis C virus refection with chromc hver m pedlatnc cancer patients Eur J Pedlatr 1993,152 490 2
Kane A, Lloyd J, Zaffran M, Slmonsen L, Kane M Transmission of hepatitis B, hepatitis C and human lmmunodeficlency viruses through unsafe reJections m the developing world model-based regional estimates Bull WHO 1999,77(10) 801 7
Lal ME, De Vlrglhs S, Arglolu F, Farcl P, Mazzolem AP, Llscl V, et al Evaluation of antibodies to hepatitis C virus m a long- term prospective study of posttransfuslon hepatitis among thalassenuc children companson between first- and second-generation assay J Pedlatr Gastroenterol Nutr 1993,16(4) 458 64
Luby SP, Qamruddm K, Shah AA, Omalr A, Pahsa O, Khan A J, et al The relationship between therapeutic Injections and high prevalence of hepatitis C Infection m Hafizabad, Pakistan Epldemlol Infect 1997, 119(3) 349 56
Mmlsteno de Salud Instltuto Naclonal de Salud Boletm epldemlol6glco SIVIGILA 2002,42 2 3
Penm F, Dubmsson J, Rey FA, Moradpour D, Pawlotsky JM Structural biology of hepatitis C vires Hepatology 2004,39(1) 5 19
Schmums GA, Zlcker F, Pmhelro F, Brandhng-Bennett D Rask for transfuslon-transnutted Infectious diseases m Central and South Amenca Emerg Infect Dis 1998,4(1) 5 11
Schmums GA, Zlcker F, Cruz JR, Cuchl P Safety of blood supply for Infectious diseases m Latin Amencan countnes, 1994 1997 Am J Trop Med Hyg 2001,65(6) 924 30
Slmonsen L, Kane A, Lloyd J, Zaffran M, Kane M Unsafe Injections m the developing world and transmission of bloodborne pathogens a review Bull WHO 1999,77(10) 789 800
Velandla M, Fndkm SK, Cardenas V Transmission of HIV m dialysis center Lancet 1995,345 1417 22
WHO (World Health Organization) Hepatitis C-Global prevalence (update) Wkly Epldemlol Rec 2000,75 18 9
WHO (World Health Organization) Global dlstnbutlon of hepatitis A, B and C, 2001 Wkly Epldemlol Rec 2002,77(6) 45 7





























