Embed Size (px)
Citation preview

q
ELSEVIER Biochimica et Biophysica Acta 1241 (1995) 215-268
Btt Biochi f ic~a et Biophysica A~ta
Hepatobiliary secretion of organic compounds; molecular mechanisms of
membrane transport
Ronald P.J. Oude Elferink a,*, Dirk K.F. Meijer b, Folkert Kuipers c, Peter L.M. Jansen d,
Albert K. Groen a, Geny M.M. Groothuis b
Department of Gastrointestinal and Lit'er Diseases, Center for Lit'er and Intestinal Research, Academic Medical Center F0-116, Meibergdreef 9, 1105
AZ Amsterdam, The Netherlands b . . .
Department of Pharmacokmetws and Drug Dehvery, Universi~ Centre for Pharmacy, Groningen Institute for Drug Studies, Groningen , The
Netherlands
c Department of Pediatrics, UniL'ersio' ofGroningen, Groningen, The Netherlands
d Department of Gastroenterology and Hepatology, Uniuersity ofGroningen, Groningen, The Netherlands
Received 21 December 1994; revised 15 Febuari 1995; accepted 23 Febuari 1995
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 216
2. Methods for studying hepatic transport processes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 216
2.1. In vivo studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 216
2.2. In vitro studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 217
2.3. Methods used for isolation of transport proteins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 219
2.4. The use of animal models . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 221
3. Hepatobiliary transport of organic anions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 221
3.1. Sinusoidal uptake of organic anions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 222
3.2. Transcellular transport of organic anions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 225
3.3. Canalicular transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 226
4. Hepatobil iary6 transport of organic cations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 235
4.1. Sinusoidal uptake of organic cations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 235
4.2. Intracellular sequestration of organic cations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 239
4.3. Canalicular transport of organic cations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 241
4.4. The role of P-glycoproteins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 242
5. Hepatobiliary transport of lipids . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 247
5. I. Composi t ion and physical form of biliary lipids . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 247
5.2. The origin and precursor pools of biliary lipids . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 248
5.3. Intracellular trafficking of biliary lipids . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 249
5.4. Regulation of biliary lipid secretion: the role of bile salts . . . . . . . . . . . . . . . . . . . . . . . . . 250
5.5. Regulation of biliary l ipid secretion: the role of mdr2 P-glycoprotein . . . . . . . . . . . . . . . . . . . 251
5.6. Functional aspects of biliary lipid secretion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 253
* Corresponding author. Fax: +31 20 6917033.
0 3 0 4 - 4 1 5 7 / 9 5 / $ 0 9 . 5 0 © 1995 Elsevier Science B.V. All rights reserved
SSDI 0 3 0 4 - 4 1 5 7 ( 9 5 ) 0 0 0 0 6 - 2

216 R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215 268
6. Regulation of canalicular transport and its consequence for development of cholestasis . . . . . . . . . . . . 254
6.1. Regulation of transport . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 254
6.2. Cholestasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 255
7. Perspectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 257
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 258
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 258
1. Introduction
One of the main functions of the liver, the formation of
bile, involves the vectorial transport of compounds such as
bile salts, phospholipids, cholesterol and other organic
compounds. Bile flow is critically dependent on the trans-
port of bile salts and organic anions because it is an
osmotically driven process; the secretion of bile salts
provides an osmotic gradient between canalicular lumen
and plasma, which causes a water flow through the tight
junctions sealing the adjacent hepatocytes. Thus any im-
pairment of the transport of major biliary components will
lead to compromised bile flow, i.e., cholestasis. It is
therefore important to understand the complex series of
events responsible for the uptake of compounds into the
hepatocyte, transport through the cell and secretion into the
canalicular lumen. Once these processes are delineated one
can try to understand the etiology of diverse forms of
intrahepatic cholestasis. Due to the critical dependence of
bile formation on transport processes it is conceivable that,
in most cases, intrahepatic cholestasis will be the conse-
quence of a disturbance in one or more steps of hepatobil-
iary transport.
Besides the maintenance of bile flow, transport pro-
cesses are of importance for the disposition of a wide array
of endo-and xenobiotics. The disposition of drugs from the
body as reflected by plasma clearance may largely depend
on their hepatic metabolism and biliary clearance. The
elucidation of the mechanisms of hepatic uptake and bil-
iary disposition will therefore contribute to a better defini-
tion of the plasma disappearance profiles of existing and
newly developed pharmaceuticals. In addition, proper un-
derstanding of hepatic transport may lead to the develop-
ment of compounds that can be specifically targeted to
various cell types in the liver.
In this review we will give an overview of the present
knowledge of the processes involved in biliary secretion of
organic solutes. In order to limit the scope of this review
we will only deal with transport of 'cholephilic' com-
pounds, i.e., those compounds that undergo significant
hepatic uptake and are secreted into bile in high concentra-
tions. In this respect, three classes of compounds can be
discerned: organic anions (including bile salts), organic
cations and lipids. Furthermore, our aim is primarily to
discuss the present knowledge of the mechanisms involved
in these transport processes, rather than to extensively
describe the behavior of individual compounds. Evidently,
emphasis will be put on recent developments in this field;
many excellent reviews have been devoted to this subject
in the past [ 1 - 11 ].
2. Methods for studying hepatic transport processes
Hepatobiliary transport can be studied using various in
vivo and in vitro techniques. Because each of these tech-
niques has its own requirements, possibilities and limita-
tions, a proper insight in the process studied often requires
their combined use.
2.1. In vivo studies
In the intact organism the hepatobiliary transport of
drugs or endogenous cholephils should ideally be evalu-
ated by taking an adequate number plasma, urine and bile
samples after intravenous injection of the compound of
interest. Subsequent compartmental analyses of the con-
centrations will provide data on the rate constants for
uptake and excretion, thereby assessing quantitatively the
involvement of the liver in the clearance of the compound
under study under optimal conditions of liver function. For
obvious ethical and toxicological reasons, the majority of
the in vivo studies on drug transport are performed in
laboratory animals, mostly the rat. Under anesthesia a
limited number of blood samples can be obtained together
with bile samples via a cannula in the common bile duct
and urine samples using a cannula in the urinary bladder.
Although these experiments allow the study of drug trans-
port under optimal liver function they are limited to a time
period of about 4 - 6 hours. In addition, effects of anesthe-
sia on drug transport can seriously influence the results
[12]. Therefore, techniques were developed to study hepa-
tobiliary transport of drugs in the unrestrained, non-
anesthetized rat using permanent cannulas in the jugular
vein and the common bile duct and in the urine bladder,
although the latter is technically more difficult [13-16].
When a permanent cannula of the bile duct is combined
with cannulation of the duodenum, bile secretion into the
duodenum is maintained. In this way bile samples can be
collected without long-term interruption of the enterohep-
atic circulation.

R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268 217
In man, pharmacokinetic studies are usually limited to
analysis of plasma disappearance curves and urinary excre-
tion data.This implies that the involvement of the liver
cannot be rigorously assessed, due to the unknown extra-
hepatic distribution and elimination. Sampling bile directly
from the bile duct can only be performed in patients with
temporarily implanted bile catheters after major liver or
gallbladder surgery. This limits these kinetic studies to
patients, who may have abnormal liver function due to
their disease, to surgery and/or concomitant medication
[17,18]. In addition, only incomplete recovery of bile can
be achieved. Balloon-occludable multilumen duodenal
tubes [19] and triple-lumen-tubes [20] were used to mea-
sure biliary excretion in normal subjects. Recently novel
techniques were developed to quantify biliary excretion in
healthy, unanesthetised humans: Vonk et al. [21] used an
encapsulated nylon thread, swallowed by a fasting subject.
After dissolution of the capsule the thread extends into the
duodenum and duodenal bile can be sampled upon recov-
ery of the thread. With this technique relative concentra-
tions of bile components can be measured [22,23] but
absolute excretion rates can not be measured. Using the
'duodenal-marker-perfusion technique' developed by An-
gelin et al. [24] more quantitative data on biliary excretion
can be obtained, and the kinetic interactions of digitoxine
with verapamil [25] and with quinine and quinidine [26]
were established.
In vivo hepatic transport studies in man are complex,
due to the influence of extrabepatic elimination and the
impossibility to study the influence of blood and bile flow.
Therefore, in vitro studies are necessary to obtain more
detailed kinetic data on the mechanisms involved in uptake
and excretion processes by the liver.
2.2. In uitro studies
The isolated perfused liuer
Studying drug transport in the isolated perfused liver
[27-31] combines the advantages of excluding extrahep-
atic influences, maintaining an intact liver structure along
with the opportunity to manipulate medium flow, composi-
tion and temperature as well as perfusion direction. This
allows, for example, studies on the influence of protein
binding [28,32,33], on the acinar heterogeneity of hepato-
cytes with regard to transport functions [34-36], on flow-
dependency of drug clearance [37] and on the influence of
temperature on hepatic clearance [38]. Multiple samples
can be taken from both the inflow and the outflow medium,
allowing pharmacokinetic analysis by compartmental mod-
els [39] and multiple indicator dilution studies [31,40].
Adequate oxygen supply to the liver can be achieved with
Krebs solutions supplied at high perfusion rates [27,41].
Addition of washed (human or rat) red blood cells to the
medium allows studies under more physiological flow
rates [42,43]. This is, however, technically more compli-
cated and results may be influenced by drug binding to the
blood cells. As alternative oxygen carriers, fluorocarbons
have been added to the medium, but toxic effects such as
ballooning of the sinusoids [44] and depression of cy-
tochrome P-450 activity were reported [45]. Livers can be
perfused in a single pass fashion, allowing optimal control
of the inflowing medium composition. Alternatively, the
medium can be recirculated, which mimicks the in vivo
situation and allows simple kinetic compartmental analy-
sis. The latter method is less expensive when costly sub-
strates or medium components are to be used [46].
Usually livers are perfused through the portal vein only.
As a consequence the biliary plexus, which in vivo is
mainly supplied with blood via the arteria hepatica, is not
adequately perfused. This does not, however, seem to
influence biliary transport function to a large extent, be-
cause in the combined arterial-portal venous perfusion
[47,48] only a modestly increased bile flow is reported
[48]. Whether the denervation of the perfused liver influ-
ences transport processes has not been estabfished yet.
The limited number of experiments thal~ can be per-
formed with a single perfused liver preparation and the
constraints of an acceptable liver viability of about 3 -4 h
initiated the development of other techniques, such as
isolated liver cells, hepatocyte couplets, plasma membrane
vesicles, and, more recently, the precision-cut liver slices.
Liter slices
The use of liver slices to study liver function was
virtually abandoned when the succesfull isolation of viable
hepatocytes was reported by Berry and Friend in 1968
[49]. Technical limitations in the preparation of slices thin
enough to allow sufficient oxygen and substrate supply to
the inner cell layers have led to alternative approaches.
The recent development of the Krumdieck tissue slicer,
allows a reproducible production of 200-300 /zm thin
slices [50]. Cell damage as result of the slicing procedure
seems rather limited. This technique initiated a revival in
the use of liver slices in research on hepatic metabolism
and transport. The advantages of this method are evident:
the liver structure with the various parenchymal and sinu-
soidal liver cells remains intact and the hepatocytes retain
their polarity,as in the isolated perfused liver, but now
many experiments can be performed in one liver. In addi-
tion, the localisation of periportal and perivenous cells in
the acinus is maintained. However, in contrast to the intact
liver, where acinar gradients of substrates are inevitable
due to the unidirectional blood flow, all cells in the slices
are exposed to the same substrate concentrations [36].
Potentially deleterious enzymes, present in collagenase
preparations, are not needed for the preparation of the
slices, in contrast to the usual hepatocyte preparation tech-
niques. Most importantly, the technique is easily applica-
ble to the livers of various species including that of man,
which renders this technique very useful to study drug
transport in human liver in vitro and to assess interspecies
differences in drug metabolism and transport [51,52]. The

218 R.P..I. Oude Elferink et aL / Biochirnica et Biophysica Acta 1241 (1995) 215-268
cells of the inner cell-layers seem to be adequately sup-
plied with oxygen and substrates [53] and the slices can be
cultured for at least 24 h. The slices can still be conve-
niently used after 24 h of cold storage in UW ('University
of Wisconsin'; [54,55]) organ preservation solution (Olinga,
to be published). As with isolated hepatocytes, cryopreser-
vation results in appreciable loss in metabolic function. Up
to now liver slices are mainly employed for drug
metabolism and toxicity studies [56,57], and studies on
drug transport until now are limited to the excretion of bile
salts [58].
The applicability of this technique to the study on
mechanisms of drug transport in man makes it an attractive
experimental tool. Human liver slices can be succesfully
prepared from pieces of livers that are discarded after
tranplantation of a part of a donor liver and from liver
tissue obtained after partial hepatectomy. The liver tissue
may be stored for up to 24 h in an adequate storage
solution before slicing without loss of viability. Using
human liver slices drug metabolism rates have been ob-
tained which were comparable to those in isolated cells
[57,59], but detailed transport studies with human liver
slices have not been published yet.
Isolated hepatocytes
Isolated hepatocytes are widely used to investigate the
mechanisms of hepatic transport and often isolated cells
show transport characteristics similar to those in isolated
perfused livers [39,60-62]. Nevertheless, damage to plasma
membrane proteins during perfusion with collagenase (that
often contains variable amounts of trypsin) cannot be
excluded. The ease of performing experiments with multi-
ple identical cell samples, excluding the influence of other
liver cell types, makes this technique very versatile in
determining the K m and Vma ~ as well as the driving forces
for uptake of a compound under study. Competition by
other compounds and the influence of protein binding can
be easily defined [61,63-65].
The loss of cell polarity and the redistribution of
canalicular membrane proteins over the entire cell surface
[66,67] creates a problem for the study of canalicular
transport processes and makes this model less suitable for
such experiments. It has, nevertheless, been demonstrated
that under the proper conditions canalicular transport func-
tions can be measured in freshly isolated hepatocytes
[68,69].
Uptake studies are usually performed with freshly iso-
lated cells. Although the cell polarity is partly recovered
during culture [67], the uptake rate in cultured hepatocytes
may rapidly decrease during culturing of the cells [70,71].
In the case of bile salt uptake this has been shown to be, at
least partly, due to a decrease in the mRNA levels of the
Na-taurocholate transporter during culture [72]. Possibly
also the loss of available membrane area as a result of
spreading and attachment of the cells to the culture dish
may play a role here [73]. Coculturing the cells with a liver
epithelial cell-line [74], or addition of tocopherol and
dexamethasone [75], retards this loss in transport rate.
Such experimental conditions may enable studies on
chronic effects of drugs and on mechanisms and regulation
of transport [65].
Isolated hepatocytes can be stored for at least 24 h in
organ preservation solution, i.e., the University of Wiscon-
sin (UW) solution or modifications thereof [54,55], without
loss of transport functions. Cryopreservation of liver cells
generally leads to a considerable loss of metabolically
viable cells after thawing [76].
Separation of isolated rat hepatocytes into fractions
enriched in periportal and perivenous cells can be achieved
by a brief, zone-selective perfusion with digitonin [77,78]
or by fluorescence activated cell sorting after selective
labelling of one of the zones [79]. The obtained cell
fractions can be used for studies into the zonal distribution
of metabolic functions including transport [36,80].
Hepatocytes can be isolated from human donor liver
tissue and from liver tissue obtained after partial hepatec-
tomy. The reproducibility of the isolation procedure how-
ever, with respect to yield and viability is generally less
than with rat liver. This seems to be mainly due to the
variability in the human liver tissue specimens [81]. How-
ever, after removal of non-viable cells by Percoll density
separation, human hepatocytes have been used for drug
metabolism and toxicity studies [81,82]. Published drug
transport studies with human hepatocytes are still scarce,
but the available data show that these cells are an appropri-
ate model to study interspecies differences and the mecha-
nisms of hepatic transport in man [81,83].
In the past, hepatocyte derived cell-lines have been
tested as a model to study drug transport, but with little
success due to decreased or even absent transport functions
[84,85]. More recently, cell lines have been obtained which
display a higher differentiation state. An important exam-
ple is the WIF-B cell, a hepatoma-derived hybrid cell line.
The majority of these cells (> 70%) form large canalicular
spaces in which organic anions like fluorescein and FITC-
labeled glycocholate are concentrated, suggesting that tran-
scellular transport of organic anions is functional in these
cells [86]. Similar results were obtained by Petzinger et al.
[87,88] who produced hybrid cells by fusion of primary rat
hepatocytes with Reuber hepatoma cells. These cells too
form canaliculi into which NBD-labeled cholate is concen-
trated. Analysis of the bile salt uptake revealed, however,
that these cells lack the sodium-dependent taurocholate
uptake system that is expressed in normal hepatocytes.
Thus, although for some purposes such cells can be highly
valuable, the expression of the various transport systems
cannot be predicted.
Canalicular secretion is successfully being studied in
couplets of hepatocytes: pairs of cells that are not sepa-
rated from each other during collagenase treatment, and
that have conserved a bile canalicular vacuole. Cell prepa-
rations can be enriched in couplets by limiting the collage-

R.P.J. Oude EIferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215 268 219
membranes seems to be inevitable with the presently avail-
able techniques [103]. Recently, conventionally purified
canalicular membranes [104] were further purified by free
flow electrophoresis [105]. Despite its limitations the use
of hepatocyte plasma membrane vesicles has been invalu-
able to the characterization of hepatic transport mecha-
nisms. Interference of intracellular events such as toxic
influence on liver cell function, metabolism and binding to
intracellular binding proteins and organelles is excluded. In
additon, both the internal and external medium can be
manipulated and this enables the study on the electrogenic
features, the energy dependency and the ion requirements
of transport [ 106].
Plasma membrane vesicles can also be prepared from
human livers [107-109] and sodium-dependent transport
of taurocholate was demonstrated in human basolateral
vesicles in accordance with isolated human cells [81] and
rat basolateral vesicles [110] and hepatocytes [111].
Fig. 1. The use of hepatocyte couplets for functional characterization of organic anion transport. Hepatocyte couplets from TR- rats (see Section 3.3) were analysed by phase contrast (panel A). Subsequently the cells were incubated with carboxydichlorofluorescein diacetate and analysed by confocal scanning laser microscopy. Note that no secretion of fluores- cence is observed in the canalicular vacuole due to the defect in organic anion secretion (panel B). As a control the couplets were also incubated with the fluorescent bile salt, FITC-glycocholate. Line scanning reveals concentrative secretion of the bile salt in the canalicular vacuole (panel C). From Ref. [124]
nase digestion and subsequent centrifugal elutriation of the
obtained cell suspension [89,90]. These couplets are espe-
cially suitable to study biliary excretion processes using
fluorescence microscopy [91,92], confocal microscopy (see
Fig. 1) [93,94] and time lapse video recording [95]. Using
such techniques the contractile nature of the canaliculi,
comparable to the canaliculi in vivo, has been demon-
strated [96,97]. Even the separation of periportal and
perivenous couplets was reported recently using elutriation
centrifugation [98]. Another important advantage of cou-
plets is the possibility to study routing and localization of
canalicular (transport) proteins. A beginning has been made
with studies into the influence of various conditions, like
hormones and second messengers, on these processes
[99,100].
Plasma membrane vesicles
The development of techniques to prepare sealed mem-
brane vesicles from the sinusoidai (basolateral) and
canalicular domains of the plasma membrane, allowed the
study of transport mechanisms at both poles of the hepato-
cyte separately [ 101,102]. For a proper interpretation of the
data care must be taken to define the origin and the
orientation (right side out or inside out) of the vesicles.
Cross contamination with the mutual domain specific
plasma membrane elements as well as other (intracellular)
2.3. Methods" used fi)r isolation ~?f" transport proteins
AffiniO' chromatography
In the past many groups have approached the isolation
of hepatic transport proteins by affinity chromatography
[112-114]. Suitable ligands were immobilized to a matrix
and solubilized fractions of hepatic membranes were ap-
plied to such columns and eluted by addition of the free
ligand. In the case of transport proteins this approach may
be hindered by a number of intrinsic problems.
Firstly, one has to be sure that the solubilized protein is
still functionally active, c.q. able to bind its ligand properly
with a low dissociation constant. It is a well known fact
that many integral membrane proteins lose their activity
upon complete solubilization. It is crucial for this approach
that the putative transporter protein is completely solubi-
lized. If solubilization is not complete, membrane frag-
ments may be formed that contain more than one protein.
Then, if the desired protein binds to the column due to its
affinity for the ligand, other (abundant) proteins may be
also retained by 'piggy-back' isolation due to their ubiqui-
tous presence in membrane vesicles. In the past this effect
has probably led to erroneous assignment of a transport
function to major binding proteins present in hepatic mem-
brane preparations.
Secondly, amphipathic ligands, like bil~rubin and bile
salts, have often been used for affinity chromatography.
The inherent problem of such compounds is that they also
aspecifically bind to hydrophobic sites on proteins. Since
the purification involves membrane proteins, many of such
sites will be present in the preparations. Therefore the
chance of aspecific binding of proteins to these columns is
considerable.
Thirdly, a problem arises that is general to any form of
purification of transport proteins; the purification process
can only be evaluated by reconstitution of the protein into
liposomes followed by the measurement ,of its transport

220 R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268
capacity. In many cases this represents an insensitive assay
for which too little protein is obtained to get correct data.
With these problems in mind it is not surprising that in
the past 'carrier' proteins have been isolated that later
turned out to have either another cellular localization than
the plasma membrane or exhibited another enzymatic func-
tion rather than the transport of cholephilic compounds.
Although well known examples exist of proteins which
have multiple localizations within the cell or have multiple
enzymic functions, the finding of bifunctional proteins
must be approached with great care and suspicion in view
of the pitfalls mentioned above.
Photoaffinity labeling of putative transport proteins Photo-reactive, radioactive, derivatives of ligands that
are transported across the hepatic membrane have been
synthesized in the past to identify proteins involved in the
transport process [115]. When incubated with membranes
in a sufficiently low concentration, proteins that specifi-
cally bind these compounds (among which must be the
carrier proteins) will bind the radioactive ligand to a higher
extent than other proteins. Upon illumination, the specific
binding proteins will therefore be labeled ro a relatively
higher extent than other proteins and this may help in the
purification and identification of these proteins. Although
elegant, this technique also suffers from significant prob-
lems. Transport proteins may indeed be labeled to higher
specific radioactivity, but their abundancy may be too low
to recognize them among other binding proteins. Con-
versely, aspecific binding proteins may reach only low
specific radioactivity but, due to their abundancy, they still
may come out as the most prominent labeled species. In
addition, similar to the situation with affinity chromatog-
raphy, often ligands are used with amphipathic properties.
Such substrates tend to bind aspecifically to proteins or
even may insert into membranes. In this context it is
important to note that in the past photo-affinity labeling
with radioactive 7,7 azo-derivative of taurocholate has led
to the assignment of a canalicular 100 kDa protein as the
protein involved in taurocholate transport across the
canalicular membrane [116]. However, when total proteins
from the canalicular membrane are analyzed by SDS-PAGE
it is clear that multiple 100 kDa proteins are abundantly
present in this membrane. Indeed, many proteins in this
molecular mass region have been identified in the canalic-
ular membrane at present among which are the ecto-ATPase
and dipeptidylpeptidase IV. Therefore labeling of this 100
kDa protein could in fact represent aspecific binding to
one or more highly abundant proteins. Although the pro-
tein preparation, upon purification and reconstitution gave
rise to potential-dependent taurocholate transport, it has
recently become clear that in highly purified canalicular
membranes no potential-dependent taurocholate transport
can be observed in spite of the fact that the particular 100
kDa protein was exclusively present in this fraction [105]
(see also Section 3). In view of the problems mentioned
above the assignment of a transport function to these
proteins on basis of photo-affinity labeling must be ap-
proached with caution.
Expression cloning with Xenopus laevis oocytes
The recognized capacity of Xenopus laevis oocytes to
efficiently translate foreign genetic information combined
with their ability to assemble oligomeric receptor/channel
complexes and insert them into the plasma membrane, has
greatly stimulated the cloning of plasma membrane recep-
tors and transport proteins [117]. Recently, this technique
has also been implemented in the field of hepatic trans-
porters and within a relative short period several cDNAs
have been isolated, the RNA of which upon injection in
oocytes give rise to transport functions.
In this approach the oocytes are used as an expression
system, while the actual cloning of a cDNA is achieved by
standard procedures. As a preliminary step in cloning
studies, the microinjection of total poly(A) + mRNA from
liver homogenate into the oocytes serves to provide evi-
dence for the presence of translatable mRNA encoding the
desired transport function while establishing the ability of
the oocyte to express the biologically active protein. At
this important stage several possibilities exist: injection of
total mRNA gives a transport signal above the background
and this means that after size fractionation, establishment
of a cDNA library and testing of pools of clones from the
library can only increase the signal due to the higher
abundancy of the signal. Thus, if a transport signal is
obtained with total poly(A) + mRNA further strategies for
cloning are straightforward, though laborious. However,
for several reasons a signal may be absent. The assay used
to assess transport activity is of crucial importance: it must
be sensitive enough to monitor activity in a few oocytes
and it must be rapid and simple enough to handle large
numbers when clones are to be tested. It is clear that a
transport assay involving uptake into the cells is consider-
ably easier to perform than an assay that exclusively
reflects a secretory process. Another important problem is
that the endogenous transport activity of the oocytes must
be low; otherwise the signal derived from the injected
mRNA will disappear in the background [118,119]. The
latter problem has clearly impeded the cloning of some
transport functions, like bile salt secretion, of which con-
siderable background is already present in the oocyte
[119]. Bile salt secretion as well as the secretion of non-bile
salt organic anions seems to be a function that is ubiqui-
tously expressed in many cell types including plants and
bacteria [ 120-122].
Once a cDNA encoding a putative transporter is ob-
tained, the sequence can be used to produce antibodies so
that the plasma membrane localization can be verified. In
addition the cDNA can be expressed in more suitable
mammalian cell types to verify its function [123]. Even at
this stage one has to be careful with interpretation of the
results. Using the suitable vectors and cell types one may

R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268 221
obtain extremely high expression levels of a single protein
and this may derange the target cell. Therefore the demon-
stration of a transport function by expression of a cDNA
per se is not sufficient and has to be accompanied by a
certain assessment of the specific activity of the protein
and this specific activity has to be in the same order of
magnitude as that in the normal hepatocyte.
2.4. The use o f animal models
Animal models have proven to be invaluable for studies
into hepatic transport processes. The advantage of animal
models is that transport can be studied in an integrated
model that is defined by the absence, malfunction or
overexpression of a single gene. These animal models are
especially valuable for the study of canalicular transport
mechanisms. Two types of animal models can be discerned
in this respect; animal strains with a spontanous mutation
that gives rise to disturbances in transport and transgenic
animal models. The TR rat (Section 3.3) and the LEC rat
(Section 3.3.6) are examples of the first group. These
animals exist within the population of control rats (like the
Wistar and Sprague Dawley colonies) and have been dis-
covered by serendipitous observation of phenotypic abnor-
malities. Even in models where the relevant gene and its
mutation are not known, as is the case in the TR- and the
LEC rat, a host of information can be obtained by compar-
ison of transport processes in control and mutated animals.
Using hepatocytes and plasma membrane vesicles from
TR- rats it was discovered that canalicular organic anion
transport is a primary active, ATP-dependent mechanism
[68,124]; the protein(s) involved in this process have,
however, still not been characterized. The mdr2 knockout
mouse (Section 5.3.2) is an example of a transgenic animal
model. In this model the situation is quite reverse in that
the mdr2 gene had been isolated and characterized already
more than ten years ago. Its function remained elusive
until the phenotype of the mdr2 knockout mouse demon-
strated the involvement of mdr2 Pgp in canalicular secre-
tion of phosphatidylcholine [125]. This gene was inacti-
vated in embryonic stem cells by homologous recombina-
tion of the normal mdr2 gene with a construct that lacked
the promotor region and the first two exons of the gene
(see Ref. [126] for this technique). After selection of
clones with an inactivated gene the embryonic stem cells
were injected into blastocysts which gave rise to chimeric
mice. Chimers in which the inactivated gene had under-
gone gerrnline transmission were used to breed hetero-
zygotes and these were in turn used to breed homozygotes.
Although these procedures are more and more becoming
standard techniques, it must be born in mind that the
production of such mouse models is laborious and is only
successful if a number of criteria is met with: the protein
involved should not have a vital function during embryo-
genesis and fetal development because otherwise no viable
animals will be obtained. Preferably, the gene to be dis-
rupted must have a single tissue-specific function; if the
protein has a ubiquitous expression and if its function is
vital in several tissues, the animal will suffer from a severe
pathology or even not be viable. In such cases primary and
secondary consequences of gene disruption will not be
easily discriminated. In addition, the function to be charac-
terized must preferably be mediated by a single gene
product. Thus if the function is mediated by a number of
homologous proteins with overlapping substrate specifici-
ties, the disruption of the gene of one of these proteins is
not likely to give rise to a characteristic phenotype. As an
example, knockout mice have also been produced for the
m d r l a gene in the mouse [127]. Because the m d r l a and
the m d r l b gene have a strongly overlapping substrate
specificity for amphipatic neutral and cationic compounds,
double knockouts for both genes will have to be produced
before information can be obtained about the involvement
of these P-glycoproteins in hepatobiliary transport of these
compounds. The mentioned criteria certainly hold for a
number of hepatocyte-specific (transport) functions so that
in the future more knockout mouse models may be ex-
pected in this field of research.
3. Hepatobiliary transport of organic anions
As far as transhepatic transport is concerned the cate-
gory of organic anions has to be divided into bile salts and
non-bile salt organic anions. Bile salts, quantitatively, are
by far the most important organic anions in bile and, in
addition, are transported by mechanisms different from
that of most other organic anions. Although the term
'organic anions' may suggest a homogenous group of
compounds, this notion is incorrect: compounds that are
traditionally included in this group vary widely in their
physicochemical characteristics and it is very difficult to
describe common features apart from their anionic groups,
Bile salts, in most mammalian species conjugated to glycine
or to taurine, display a single negative charge at physio-
logical pH. The presence of one, two or three hydroxyl
groups at different positions of the bile salt molecule lead
to a considerable difference in hydrophilicity of the vari-
ous bile salt species identified. Taurocholate, a trihydroxy
bile salt abundant in human and rat bile, has been used
mainly in transport studies. Most, but not all, cholephilic
non-bile salt organic anions have more than one negative
charge at physiological pH and are, to a certain extent,
amphiphilic. The latter feature seems to be important for
hepatic uptake while the multianionic ,character of a
molecule increases the efficiency of canalicular secretion.
Examples of endogenous non-bile salt organic anions are
bilirubin glucuronides, (oxidized and reduced) glutathione,
glucuronides of estrogens, leukotrienes, and sulfate and
glucuronide conjugates of thyroid hormone. Many exoge-
nous organic anions or anionic conjugates are secreted into

222 R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268
bile too; examples include some cefalosporins, glu- ou t
curonidated, sulfated and glutathione-conjugated farmaca S" . . . . . ...a
like the conjugates of aminacetophen.
3.1. Sinusoidal uptake of organic anions
Bile salts
Functionally, two different mechanisms have been dis-
cerned for uptake of organic anions: a Na+-dependent and
a Na+-independent system. The Na+-dependent system is
driven by the sodium gradient that is built up by the
activity of Na÷K+-ATPase which is exclusively present in
the basolateral membrane of the hepatocyte [128].
There is ample evidence that taurocholate is taken up by
hepatocytes in a Na+-dependent fashion [129-131]. How-
ever, non-bile salt compounds like bumetanide, phalloidin
are also substrates for sodium-dependent uptake [131,132].
Hepatic uptake of bile salts is affected by the length and
charge of the side chain as well as the number of hydroxyl
groups [131,133-135]. Conjugation of bile salts with tau-
rine increases the affinity for the uptake system. Reduction
of the number of hydroxyl groups on the steroid moiety
increases the inhibitory potency on taurocholate transport,
although the actual sodium-dependent uptake of unconju-
gated mono- and dihydroxy bile salts might be much less
efficient than that of taurocholate. Several compounds like
cyclosporin A and BSP were reported to inhibit tauro-
cholate transport non-competitively with low K i [131,136].
Conflicting data have been obtained as to whether the
sodium-dependent uptake involves an electroneutral or an
electrogenic mechanism. Neutral cotransport was sug-
gested by comparisons of sodium and taurocholate fluxes
in isolated hepatocytes [137], by the absence of a stimula-
tory effect of valinomycin and an outwardly directed K +-
gradient on the Na+-dependent uptake of taurocholate into
sinusoidal membrane vesicles [138] and by the lack of an
effect of taurocholate on membrane voltages and resis-
tances in hepatocytes [139]. Electrogenic transport is sup-
ported by the finding of Hill coefficients for sodium of
about 2 in isolated hepatocytes [129,140,141] and the
observation in sinusoidal membrane vesicles that permeant
anions stimulate the uptake of taurocholate [110]. More
recently, Lidofsky et al. added evidence to this by demon-
strating both in the perfused liver and in isolated and
cultured hepatocytes that uptake of taurocholate leads to
depolarization of the membrane potential [142]. Using
microelectrode impalement, Weinman and Weeks provided
additional evidence for the electrogenic character of sinu-
soidal taurocholate uptake. They observed taurocholate
induced depolarization under conditions of minimized cor-
recting K ÷ and C1- conductances in isolated rat hepato-
cytes [143]. Wehner [144], however, suggested from his
results that the depolarization observed in cultured hepato-
cytes is caused by an induced Na ÷ conductance. Using
microelectrode impalement in 24 h cultured hepatocytes he
observed that taurocholate-induced depolarization was not
in
cytosol
photoaffinity labeling
48 - 54 kDa
epoxide hydrolase
48 kDa 6 transmembrane
domains
1 Ntcp
39 kDa
7 transmsmbrane domains
Fig. 2. Postulated sinusoidal sodium-dependent uptake systems for tauro-
cholate (TC). The upper transporter represents protein(s) that were identi-
fied by photoaffinity labeling with azido-derivatives of taurocholate and
which have a molecular mass between 48 and 54 kDa [145-147]. A
transport function has never been directly demonstrated for these proteins
(stippled arrow for transport). The middle transporter represents the
protein isolated by the group of Levy [ 114,148-150], which has sequence
identity with micrsornal epoxide hydrolase. This putative transporter was
reconstituted but did not display strict Na + dependency (as indicated by
the stippled arrow for Na+-transport. The third transporter represents
Ntcp, which was recently cloned by the group of Meier [152,153,669].
Upon expression in oocytes this transporter displays strict Na+-depend -
ency. In vitro translation of the mRNA in the presence of microsomes
yields a protein of 39 kDa. However, it was shown very recently [669]
that this gene product has an apparent molecular mass of 51 kDa in rat
liver, probably due to more extensive glycosylation.
reversible upon withdrawal of the bile salt from the culture
medium.
At the protein level several basolateral candidate pro-
teins have been isolated and postulated to catalyze the
sodium-dependent uptake of taurocholate Fig. 2. Firstly,
photoaffinity labeling with reactive taurocholate deriva-
tives have lighted up protein(s) in the molecular mass
range of 48 to 54 kDa which were postulated (subunits of)
taurocholate transporting proteins [145-147]. These pro-
teins have, however, never been isolated and reconstituted
to demonstrate transporting activity in proteoliposomes.
The group of Levy et al. [114] has isolated a sinusoidal
membrane protein of 48 kDa by means of affinity chro-
matography on a glycocholate-column. Upon reconstitu-
tion this protein preparation gave rise to both Na+-depen -
dent and Na+-independent transport suggesting that trans-
port through this protein is not strictly dependent on
sodium cotransport. Subsequently, a monoclonal antibody
was generated against this preparation [148]. Immunopu-

R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268 223
rification of the 49 kDa protein from sinusoidal rat liver
membranes followed by reconstitution also demonstrated
taurocholate transport [149]. More recently, this group
discovered that the protein which reacts with this antibody
is similar if not identical to the microsomal epoxide hydro-
lase [150]. Although the extent of similarity has to be
further delineated these findings pose problems on the
interpretation of previous results. Evidently, it may be
postulated that epoxide hydrolase is localized both on the
plasma membrane and in the endoplasmic reticulum, which
has been demonstrated for other proteins. However, at the
same time two entirely different functions have to be
assigned to the protein, i.e., stereospecific hydration of
alkene and arene oxides to trans-dihydrols vs. Na+-depen -
dent transmembrane transport of bile salts. Epoxide hydro-
lase is a member of a group of very abundant + 50 kDa
proteins in the endoplasmic reticulum. Thus plasma mem-.
brane preparations may well be contaminated with this
protein and so may a glycocholate affinity purified prepa-
ration from such membranes. This may in turn indicate
that the antibody reacts with epoxide hydrolase instead of
the bile salt transporter. It remains to be explained why the
immunoaffinity purified protein displays bile salt transport-
ing properties. As has been demonstrated for a similar
situation in canalicular preparations, immunopurified
preparations may not be absolutely pure and may, probably
depending on the conditions of solubilization, contain con-
taminating proteins of similar molecular mass. Since the
microsomal epoxide hydrolase has been cloned [151],
transfection of of cells with this cDNA will reveal the
possible bile salt transporting capacities of this protein in
near future.
Recently, a Na+-dependent taurocholate uptake system
from rat liver has been expressed in Xenopus laeuis
oocytes [152] and a full-length cDNA was subsequently
cloned using this expression system [153]. This cDNA
encodes for a protein (called Ntcp for Na+/taurocholate
cotransport polypeptide) that has an (unglycosylated)
molecular mass of 33-35 kDa. Hydrophobicity analysis
reveals seven putative transmembrane domains and the
cDNA shows no homology with epoxide hydrolase. High
stringency blotting of several rat tissues only revealed
expression in the liver. Recently, the ileal Na+-dependent
bile salt transporter from the hamster was cloned and this
cDNA displays considerable amino acid sequence identity
and predicted structural similarity with Ntcp. When trans-
lated in the presence of microsomes, Ntcp cDNA gives rise
to a glycosylated polypeptide of about 39 kDa. This is
significantly lower than the molecular mass of the putative
transporters that were identified by photoaffinity labeling,
which are in the region of 48 kDa. The difference may be
explained by a more extensive glycosylation of Ntcp in
hepatocytes giving rise to a higher molecular mass. Indeed,
using recently developed antibodies against this protein,
Stieger er al. [669] demonstrated that the molecular mass
of the gene product in rat liver is 51 kDa. They also
demonstrated that the protein is specifically localized in
the sinusoidal membrane [669]. Taurocholate transport into
oocytes that had been injected with Ntcp cDNA was found
to be strictly Na+-dependent and was inhibited by tau-
rochenodeoxycholate and BSP, but not by taurodehydro-
cholate. Inhibition by the loop-diuretic bumetanide which
was also thought to be a substrate for the Na+-dependent
transporter [154] was relatively weak [15211. This adds
evidence to the results from Honscha et al. [155] who
showed that different fractions from size-fractionated rat
liver poly(A*)-RNA give rise to taurocholate and
bumetanide transport, respectively, when injected into
Xenopus oocytes. These results suggest that bumetanide
and taurocholate are taken up via separate Na+-dependent
transporters.
Using a probe complementary to the rat Ntcp, Hagen-
buch et al. [156] also cloned the homologous human cDNA
(NTCP) and mRNA from this clone injected in Xenopus
oocytes also gave rise to Na÷-dependent taurocholate up-
take in these cells. There is 88% similarity between the
human and rat amino acid sequences. The gene for NTCP
was localized on chromosome 14. The human transporter
has a distinctly higher affinity for taurocholate than the rat
protein (Kms 6.3 /xM and 25 #M respectively). The
inhibition pattern of a number of bile salts confirmed the
earlier observation that taurine-and glycine-conjugated bile
salts are better substrates than unconjugated bile salts
[156].
In an ontogenic study, Boyer et al. [157] showed that
the mRNA for Ntcp is absent through most of gestation
and is first detected toward the end of gestation on fetal
days 18-21. The expression of Ntcp further increased after
birth up to a 5-told higher level at adulthood compared to
the expression just before birth. This perinatal develop-
ment coincides with earlier transport studies by Suchy et
al. [158] who only found Na+-dependent bile salt transport
in basolateral plasma membranes prepared from fetal rat
livers just before birth. It was furthermore shown that Ntcp
mRNA is absent from HepG2 cells [157] and from dedif-
ferentiated primary hepatocytes (i.e., rat hepatocytes alter
three days culture [159]). These cells also lack functional
Na+-dependent taurocholate uptake. Altogether these data
suggest that Ntcp/NTCP is a major determinant of bile
salt uptake into hepatocytes.
Non-bile salt organic anions
Many non-bile salt organic anions such as bilirubin,
bromosulphthalein (BSP), indocyanine green (ICG),
pravastatin and dinitrophenylglutathione, are substrates for
one or more Na+-independent uptake mechanisms
[11,160-162]. For an extensive review on the uptake of
individual cholephilic organic anions see [I,10]. In many
studies BSP was used as a model compound for sinusoidal
uptake. The transport of this compound into rat liver
plasma membrane vesicles was shown to be Na~-indepen -
dent and electrogenic [163,164]. At present it appears that

224 R.P.J. Oude El/Prink et al. / Biochimica et Biophysica Acta 1241 (1995) 215 268
out in
• ' c-'oso'yt, s in t
BBBP O A ss kDa
OABP OA 8-subunit mitochondrial
F1 -ATPase
55 kDa
OA BTL 37 kDa
o a t p
O A 71 kDa
10 transmambrana domains
CI"
Fig. 3. Postulated uptake systems for sinusoidal sodium-independem
uptake of organic anions. The first two proteins (BBBP [ 113,154,165,166]
and OABP [112,168,169]) have never been reconstituted to demonstrate a
transport function. Bilitranslocase (BTL; [ 1 I, 174-176]) has been reconsti-
tuted and mediates electrogenic transport of BSP, but its sequence is
unknown. The last protein (oatp) has been cloned from both rat [177,178]
and human [670,671] liver and upon expression this 71 kDa protein
mediates high affinity, Na+-independent transport of BSP and bile salts.
Transport via this protein can be stimulated by CI-.
the assumption of a single Na+-independent system for
uptake of organic anions is an oversimplification. The
number of polypeptides involved in the uptake of non-bile
salt organic anions may very well be more than one and
overlapping substrate specificities may further confuse the
situation.
Several groups have postulated the identification of
polypeptides involved in basolateral transport of organic
anions (see Fig. 3). Using affinity chromatography with
immobilized bilirubin and BSP as ligands, a 55 kDa
protein was isolated from rat liver plasma membranes
[113,154]. Antibodies raised against this BSP/bilirubin
binding protein (BBBP) inhibited uptake of BSP and
bilirubin into isolated rat hepatocytes [165] as well as
HepG2 cells [166]. Thus far the protein has, however, not
been reconstituted to test its capacity for organic anion
transport.
Wolkoff et al. [112] also isolated a 55 kDa protein by
affinity chromatography on BSP-glutathione-agarose and
raised an antiserum against this organic anion binding
protein (OABP). Immunological studies with this anti-
serum revealed expression of the protein in many tissues
like heart, brain and intestine. Comparison of BBBP and
OABP by immunochemical techniques suggested that these
preparations represent different proteins [167]. Subse-
quently, anti-OABP was used for cloning of the cDNA for
this protein [168]. The sequence of the isolated cDNA
clone turned out to be identical to the /3-subunit of mito-
chondrial FrATPase. Though unexpected, this finding was
explained by demonstrating in an immunofluorescence
study that an antibody against the /3-subunit of mitochon-
drial FrATPase also reacted with the hepatocyte plasma
membrane. In HepG2 cells, however, only intracellular
localization of immunoreactive material was observed;
these cells were shown to lack chloride-sensitive, high
affinity uptake of BSP [169]. The OABP protein prepara-
tion has not been reconstituted to verify its transporting
capacity.
More or less independent from the characterization of
this polypeptide the same group characterized the mecha-
nism of BSP transport into cultured primary rat hepato-
cytes. They observed that uptake is chloride-dependent
[170], but not driven by a chloride-gradient [171,172]. The
presence of chloride ions strongly increased the affinity of
BSP binding to the cells [172]. Micromolar concentrations
of ATP in the medium rapidly and reversibly inhibited
BSP uptake by more than 60%, suggesting that this trans-
port is subject to regulation via purinergic receptors [173].
A third protein, termed bilitranslocase (BTL), has been
purified from rat liver plasma membranes. This prepara-
tion, which contains a single polypeptide of 37 kDa upon
SDS-PAGE, was used to raise monoclonal and polyclonal
antibodies. Furthermore, the protein was reconstituted in
liposomes. The proteoliposomes were shown to transport
BSP by an electrogenic mechanism [11,174]. BTL was
furthermore shown to be present in HepG2 cells by
Marchegiano et al. [175] who also observed saturable BSP
uptake in these cells.
The relative role of these proteins (BBBP, OABP and
BTL) in the uptake of organic anions by hepatocytes has
still to be demonstrated. In an attempt to address this
question, Torres et al, [176] recently measured the effect of
anti-BBBP and anti-BTL antibodies on BSP uptake into rat
liver plasma membrane vesicles. Transport was measured
both in the presence and absence of an inside-positive
membrane potential and it was observed that anti-BTL
antibodies inhibited the electrogenic uptake while anti-
BBBP antibodies inhibited the electroneutral uptake of
BSP. They extrapolated their results and calculated that
both BTL and BBBP are important for transport, the
relative importance being determined by the prevailing
BSP concentration (Km, BT L 5 /zM and Km,BBBP 20 /zM). This calculation does, however, not take into account the
fact that the hepatocyte membrane potential is negative
inside ( + 36 mY) and the possible presence of at least one
other transport system (see below).
Finally, a cDNA was recently isolated from a rat liver
library by Jacquemin et al. [177,178] encoding an organic
anion transporting polypeptide (OATP). Upon injection in
Xenopus laevis oocytes, mRNA derived from this clone
gave rise to Na+-independent BSP transport into these

R.P.J. Oude EIferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215 268 225
cells. Similar to what was noted with isolated hepatocytes
[172], BSP uptake in these transfected oocytes was Cl--de-
pendent: however, this dependency was only noted when
albumin-bound BSP was used as substrate and the effect of
chloride was only observed at low BSP concentrations
[178]. Maximal uptake velocity was identical in the pres-
ence and absence of albumin but the K m for BSP de-
creased more than ten-fold by the omission of albumin.
The effect of chloride may actually represent a stimulation
of the extraction of BSP from albumin. In addition to BSP,
OATP was capable of mediating Na+-independent
(tauro)cholate uptake. Surprisingly, this cDNA encoded a
polypeptide with a substantially higher molecular mass
than the putative transporters mentioned above. Cell-free
translation yielded a protein of 59 kDa and in the presence
of canine pancreatic microsomes a glycosylated product of
71 kDa was observed. Northern blot analysis of mRNA
from different tissues revealed expression in liver and
kidney. Low stringency blotting conditions also revealed
that multiple forms of OATP may be present in this tissue,
indicating that a family of homologous polypeptides could
be involved in the uptake process.
3.2. Transcellular transport of organic anions
lntracellular binding proteins and interaction with mem-
branes
After uptake across the basolateral membrane, organic
anions have to be directed to the canaliculus in order to
achieve vectorial secretion. Pharmacokinetic studies have
shown that the hepatocyte cytosol constitutes a storage
compartment for many organic anions [179]. This is due to
the presence of proteins with high affinity for organic
compounds. Three classes of proteins should be mentioned
in this context: glutathione S-transferases (including lig-
andins), 3-c~-hydroxysteroid dehydrogenase ( Y ' - b i n d i n g
protein) and fatty acid binding proteins [180]. Glutathione
S-transferase is present in the cytosol in concentrations up
to 0.2 mM and is the most important intracellular binding
protein for non-bile salt organic anions; Y'-binding protein
or 3-c~-hydroxysteroid dehydrogenase is an important
binder of bile salts. Binding of organic anions to these
cytosolic binding proteins may reduce the efflux rate from
the cells at both the sinusoidal and canalicular level and
also may reduce accumulation in intracellular membranes
and organelles.
Besides binding to proteins, bile salts and more hy-
drophobic organic anions can interact with intracellular
membranes. This may constitute an additional storage
compartment. Unconjugated bilirubin, which is very hy-
drophobic due to internal hydrogen bonding of the car-
boxyl groups, has been demonstrated to rapidly associate
with unilamellar phospholipid vesicles [181]. It was sug-
gested that lhe transfer of bilirubin and similar hydropho-
bic organic anions between intracellular membranes may
actually be an important mechanism of transport through
the cell [181].
Intracellular L'esicular transport
Vesicles play a role in a number of different hepatic
transport processes. The best characterized vesicular trans-
port through the hepatocyte is that of polymeric IgA.
Vesicular transport has, however, also been implicated for
biliary lipids, bile salts and a variety of other organic
amphipaths. Several groups have shown that secretion of
phospholipid and cholesterol in bile can be inhibited by
high doses of the microtubule assembly inhibitors
colchicine and vinblastine [182-188]. This issue will be
extensively discussed in Section 5.
A number of groups has demonstrated sensitivity of bile
salt and organic anion secretion to microtubule poisons
and this has been used as indirect evidence for the involve-
ment of intracellular vesicles [188-190]. Mori et al. [191]
have demonstrated that the canalicular secretion of indo-
cyanine green is inhibited by colchicine treatment, whereas
sulfobromophtalein secretion was unaffected. Dumont et
al. [192] reported that the biliary secretion of the glu-
tathione conjugate of diethylmaleate after peritoneal ad-
ministration of high doses of diethylmaleate is inhibited by
pretreatment of the rats with colchicine. A general conclu-
sion from these data must be, however, that the sensitivity
of bile salt and organic anion transport to colchicine
appears to occur only at high fluxes of these compounds.
Using an elegant approach with antibodies against bile salt,
the group of Erlinger [193,194] demonstrated the associa-
tion of bile salt with vesicles inside hepatocytes. Ayoma et
al. [ 195,196] reported the presence of several vesicle-medi-
ated pathways for organic anions. Notably phenol red in
their studies was transported by a colchicine-insensitive
but monensin-sensitive pathway [196]. At sufficiently low
concentrations, monensin rather selectively disrupts the
Golgi network [197]. Since this machinery is certainly
involved in the assembly of transport proteins destined for
the canalicular membrane, the results of Ayoma et al. [196]
could very well be explained by a primary effect on the
amount of transport protein. In view of the fact that phenol
red is highly soluble and the inhibitory effect was greater
at a high dose of the organic anion, which obviously
requires a higher capacity of transport protein, this expla-
nation seems plausible. By incubating hepatocytes with
monochlorobimane, which, after intracellular conversion to
glutathione-bimane, is an excellent substrate for the
canalicular multispecific organic anion transporler (see
Section 3.3), Oude Elferink et al. [198] demonstrated the
presence of intracellular vesicles that accumulate this fluo-
rescent organic anion. Since this phenomenon was virtu-
ally absent in the hepatocytes from TR- rats it was
concluded that this vesicular accumulation involves the
canalicular organic anion transporter. They hypothesized
that these vesicles are involved in regulation of the amount

226 R.P.J. Oude Elf erink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268
of canalicular organic anion transporters on the membrane
rather than in vectorial transport of organic anions to bile.
It cannot be excluded that data which suggest a vesicu-
lar pathway actually represent translocation of bile salt or
organic anions into vesicles by de novo synthesized or
endocytosed carrier proteins which can be transported to
the plasma membrane. For the housekeeping of proteins
and lipids in the different cellular compartments cells have
extremely active vesicle trafficking. According to the group
of Hubbard [199-203] proteins which eventually end up in
the canalicular membrane first travel by a vesicular path-
way to the sinusoidal membrane where they are sorted,
endocytosed and transported to the canalicular membrane.
It is not yet clear whether all proteins take this route and
recent data suggests that even the proteins that do follow
this pathway do not all travel at the same rate and thus
could be present in different kinds of vesicles [199]. When
proteins such as the canalicular bile salt carrier also first
travel to the sinusoidal membrane then, depending on the
rates of vesicular transport, the proteins must be present
inside the cell for an appreciable period. It is therefore not
surprising that the presence of bile salts can be demon-
strated in vesicular structures. In addition it may be that a
fraction of the canalicular transport proteins is stored in
intracellular compartments for recruitment during in-
creased need for secretory capacity (see Section 6.1.1)
The conclusion from the data available on putative
intracellular transport of organic anions and bile salts via
intracellular vesicles must be that under physiological con-
ditions this represents at best a minor pathway for the
secretion of these compounds.
Sinusoidal effiux o f organic anions
Subsequent to their uptake into the hepatocyte, com-
pounds can be secreted back into the sinusoidal space.
Especially in the absence of substantial canalicular secre-
tion this is an evident process. Sinusoidal effiux has been
demonstrated for compounds like bilirubin [170], DBSP
[38] and harmol-sulfate [204]. It may be mediated by the
same carrier that catalyzes uptake of these compounds but
indirect evidence exists that it may involve separate mech-
anisms [38]. Plasma albumin strongly binds a large amount
of organic anions and thereby stimulates sinusoidal efflux
[205]. This phenomenon may at least partly explain the
predominant sinusoidal secretion of sulfate conjugates:
compared to glucuronide conjugates, sulfate conjugates
bind more avidly to albumin than the glucuronides [206].
Sinusoidal effiux of GSH is a physiologically highly
relevant process. Over 90% of GSH in the circulation
originates from the liver [207] and this plays an important
role in detoxification and protection against oxidative stress
[208]. GSH effiux can be inhibited by a number of organic
anions including BSP-glutathione and bilirubin [209]. Si-
nusoidal GSH transport is bidirectional and driven by the
plasma membrane potential [210-212]. Recently, Fernan-
dez-Checa et al. [213] isolated a mRNA size fraction from
rat liver which, upon injection in Xenopus laevis oocytes,
gives rises to GSH transport with sinusoidal character-
istics.
3.3. Canalicular transport
The secretion across the canalicular membrane is rate-
limiting in the overall secretion of many cholephilic com-
pounds and represents the most important concentrative
step. Indeed, for all classes of organic compounds (cations,
anions and bile salts) this step creates a larger concentra-
tion gradient than that observed over the sinusoidal/baso-
lateral membrane. For example, for organic anions like
dibromosulphthalein (DBSP) a bile/l iver concentration ra-
tio of 100-1000 can be reached [179]. It was assumed for
many years that canalicular transport of both bile salts and
organic anions was primarily driven by the plasma mem-
brane potential [214-216] The concentration gradients are,
however, too large to be accounted for only by the mem-
brane potential difference over the canalicular membrane,
even when a micellar sink in the biliary compartment is
postulated [217]. For amphiphilic compounds this sink
could be constituted by the biliary lipids. In recent years it
has become clear that for most classes of compounds
primary active (i.e., ATP-dependent) transport systems are
present in the canalicular membrane [2,182,218,219]. The
characterization of these transport systems has been im-
peded for a long time, primarily by the inaccessibility of
this small membrane domain. The purification of canalicu-
lar membrane vesicles [104,220] made direct transport
experiments possible. Finally, the discovery of mutant
animals with defective canalicular organic anion secretion
has stimulated the characterization of separate transporters
for organic anions and bile salts [221]
Distinct canalicular transport mechanisms fo r bile salts
and organic anions
Early studies have suggested that separate canalicular
secretion routes may exist for bile salts and organic anions.
The evidence was mostly based on studies employing
techniques such as competitive inhibition in either whole
animals or isolated perfused liver preparations. However,
interpretation of the data was often difficult because inter-
actions may occur at many levels when transport is mea-
sured in the whole organ or animal. Interaction occurs at
the level of sinusoidal/basolateral uptake and at the level
of intracellular binding, intracellular metabolism and
canalicular secretion (for extensive review of these studies
see Ref. [l ]).
The first direct evidence for distinct canalicular trans-
port systems for bile salts and non-bile salt organic anions
came with the recognition of the human Dubin-Johnson
syndrome; this is a rare congenital chronic conjugated
hyperbilirubinemia [222,223]. The hepatic clearance of
bilirubin and other cholephilic organic anions, like BSP
and indocyanine green, is impaired in these patients [224],

R.P.J. Oude Elferink et al. /Biochimica et Biophysica Acta 1241 (1995) 215-268 227
whereas bile salt clearance is normal [225]. Mutant Cor-
riedale sheep have an inherited defect that closely resem-
bles the Dubin Johnson syndrome: these animals also show
a decreased secretion of conjugated bilirubin, BSP,
iopanoic acid and indocyanine green, while taurocholate
transport is normal [226,227]. The discovery of a more
suitable experimental animal model for the Dubin-Johnson
syndrome, the GY or TR- rat, made it possible to charac-
terize this system at the biochemical level. These animals
have a phenotype which strongly resembles that of the
Corriedale sheep and the Dubin-Johnson syndrome.
G Y / T R - rats have impaired biliary secretion of bilirubin
glucuronides, BSP, ICG and many other organic anions
(see below), while taurocholate secretion is almost normal
[221,228-230].
Canalicular bile salt transport (Fig. 4)
Until recently canalicular bile salt transport was charac-
terized as a membrane potential-driven process [138]. A
protein of 100 kDa was partially purified from canalicular
rat membranes that, upon reconstitution, gave rise to po-
tential dependent taurocholate transport into proteo-
liposomes [116,231 ]. It was, however, clear that the magni-
tude of the membrane potential over the canalicular mem-
brane ( _ 35 mV) is not high enough to explain the high
bile salt concentration gradient that is actually observed in
vivo. Adachi et al. [106] were the first to demonstrate that
uptake of taurocholate into rat canalicular membrane vesi-
cles could strongly be stimulated by the addition of ATP.
This observation was soon confirmed by a number of other
groups in rat [232-234] and human liver membranes [108].
These studies point to a system that is specific for bile
salts with a K m for taurocholate in the low micromolar
range. No other nucleotides than ATP can drive transport
and vanadate inhibits transport at low concentrations (90%
inhibition at 50 p~M) suggesting z-phosphate transfer from
ATP to the transporter-polypeptide. ATP-dependent tauro-
cholate transport could be inhibited by glycocholate and by
unconjugated as well as taurine-conjugated di-and trihy-
droxy bile salts but not by (tauro)dehydrocholate [233,234].
The more recent detection of considerable ATP-depen-
dent taurocholate transport in canalicular membrane vesi-
cles questions the physiological role of the previously
demonstrated electrogenic transport. It could be that the
latter experiments have demonstrated the residual electro-
genic transport of the ATP-dependent transporter in the
absence of ATP. On the other hand it is possible that two
distinct bile salt transporters are present in the canalicular
membrane. A recent study by the group of Meier [105] has
brought considerable clarity in this confusing situation.
Using free flow electrophoresis they have further purified
the conventional canalicular membrane preparation which
still contains considerable amounts of endoplasmatic retic-
ulum. In this way two subfractions were obtained one of
which was 2-3-fold depleted of markers of the endoplas-
mic reticulum and 2.5-fold further enriched in the canalicu-
lar marker alkaline phosphatase. The other subfraction was
further enriched for ER-markers and virtually devoid of
canalicular enzyme activity. Removal of contaminating ER
resulted in a complete loss of electrogenic taurocholate
transport activity from the enriched canalicular membrane
fraction. In contrast, ATP-dependent transport activity re-
(~) ER
~ kDa ?
o TC
cytosol
T C --------_____ ?
ATP
T C - -
ADP
canaliculus
, ATP
i
ecto-
ATPase
ADP
cBAT
polypept ide
u n k n o w n
Fig. 4. Postulated transporters involved in canalicular secretion and intracellular sequestration of taurocholate. In the canalicular membrane an
ATP-dependent taurocholate transport activity is present [106,232-234], which has not been characterized at the protein level. It is distinct from the
previously characterized 100 kDa protein, which transports taurocholate in an ATP-independent, electrogenic mechanism [116,231]. The latter protein is
now thought to be localized in intracellular membranes, notably endoplasmic reticulum [105]. In addition Sippel et al. [240-242] have purified a putative
ATP-dependent bile salt transporter which turned out to be identical with ecto-ATPase. This protein is thought to mediate ATP-dependent bile salt
transport, but this function is not dependent on the ecto-ATPase function.

228 R.P.J. Oude Elferink et a l . / Biochimica et Biophysica Acta 1241 (1995) 215-268
mained associated with both the ER and the canalicular
membrane fraction. These data suggest that the electro-
genic transport activity is a distinct entity which is absent
from the canalicular membrane and resides in the endo-
plasmic reticulum, whereas the ATP-dependent transport
system appears to be the primary mediator of canalicular
taurocholate transport. Strikingly, substantial ATP-depen-
dent transport was also present in the fraction that was
de-enriched for canalicular membranes. This strongly sug-
gests that ATP-dependent transport is also present in intra-
cellular compartments. This observation may shed light on
the discussion of regulation of transport by recruitment of
transporters from intracellular stores (see Section 6). The
experiments by Kast et al. [105] must lead to reinterpreta-
tion of previous experiments from the same group concern-
ing a 100 kDa protein that would be responsible for
canalicular bile salt secretion. This protein was purified
from conventional canalicular membrane preparations and
gave rise to potential-dependent taurocholate transport upon
reconstitution in liposomes [116,231]. The conclusion from
the most recent results must be that this protein is not a
canalicular bile salt transporter.
Several groups have attempted to identify the canalicu-
lar protein that is responsible for ATP-dependent tauro-
cholate transport. Muller et al. [232] have attributed this
primary active transport to a 110 kDa protein which is
recognized by an antiserum against gp110. Immunoprecip-
itation of solubilized canalicular membranes with this anti-
serum gave rise to a fraction that, upon reconstitution,
catalyzed ATP-dependent taurocholate transport. Using this
antiserum for purification of this heavily glycosylated pro-
tein from rat liver, Becker et al. [235] demonstrated by
sequencing of ten internal peptides that the protein was
identical or at least highly similar to the cloned rat liver
ecto-ATPase [236]. Surprisingly, however, immunoprecip-
itation of this protein was not associated with removal of
any ATPase activity. Moreover the purified gp110 did not
display ATPase activity although it had been characterized
as an ATP-dependent bile salt transporter [232]. The pro-
tein displayed considerable microheterogeneity, probably
due to differences in glysosylation. Complete deglycosyla-
tion yielded a polypeptide of 48 kDa and these character-
istics strongly resemble those of canalicular proteins that
had been identified with antibodies raised in a similar
fashion: HA4 [237], C-CAMI05 [238], and another gp110
[239]).
More recently, Sippel et al. purified a 110 kDa protein
from rat canalicular membrane vesicles by bile salt affinity
chromatography. Sequencing of this protein revealed iden-
tity with the cloned ecto-ATPase. This was surprising
since the sequence of this protein predicts a single mem-
brane-spanning domain [236], which is unlikely for a
transporter protein. In order to determine its function as a
bile salt transporter, the cDNA for ecto-ATPase was trans-
fected into COS cells and these cells were used to demon-
strate taurocholate efflux [240]. Using a truncated cDNA
the authors furthermore observed that the cytoplasmic tail
of the protein is essential for its transport function. In a
subsequent report the same group [241] showed, using
modified cDNA constructs, that the exoplasmic ATPase
function of the protein was not essential for transport.
Nevertheless extracellular ATP stimulated taurocholate ef-
flux. In addition, depletion of intracellular ATP abrogated
efflux. On the other hand protein kinase C-dependent
phosphorylation of the cytoplasmic tail appeared to be
essential for activity and tyrosine kinase dependent phos-
phorylation would regulate the activity [242]. On the basis
of these results Sippel et al. [241] suggested that the
mechanism of taurocholate transport involves secretion of
ATP into the canaliculus (e.g., by the putative ATP-chan-
nel function of mdrl P-glycoprotein [243]) followed by
subsequent energization of transport by the protein that
does not involve the ecto-ATPase activity. It is difficult to
envisage how this function, which needs the presence of
ATP in the canalicular lumen, should be combined with
the massive ATPase activity that is present on the canalic-
ular membrane. As mentioned above, all these studies rely
on an assay of taurocholate transport in transfected COS
cells. In this assay radioactive taurocholate is allowed to
associate with the cells and subsequently release of label
from the cell is measured. It is difficult to envision how a
substantial amount of the added taurocholate can enter
cells by simple diffusion. Specific transport was defined by
the difference in taurocholate release in the presence and
absence of DIDS, but the obtained data in absence and
presence of DIDS were never shown. The assay that was
used did not unequivocally demonstrate transmembrane
transport of taurocholate using criteria like saturability,
time-dependency and temperature-sensitive efflux in the
presence and absence of DIDS. A further concern is that
the data conflict with the observation that ATP-dependent
taurocholate transport is only observed in inside-out vesi-
cles in the presence of ATP. In addition, the study of Kast
et al. [105], described above, demonstrated that subfrac-
tionation of canalicular plasma membranes dissociated the
immunodetectable presence of ecto-ATPase from ATP-de-
pendent taurocholate transport indicating that ecto-ATPase
at best represents a minor component of canalicular ATP-
dependent bile salt transport. Altogether it is, as yet, quite
unclear which polypeptide(s) are responsible for the ATP-
dependent translocation of bile salts into the canaliculus.
The canalicular multispecO~c organic anion transporter:
cMOAT
Using the TR rat as a standard model for the defi-
ciency of canalicular organic anion transport it was possi-
ble to define a group of substrates that is transported into
bile via a putative transport system that is absent or
inactive in this animal. Although this transport system has
not yet been characterized at the protein level nor at the
cDNA level, it has been termed canalicular multispecific
organic anion transporter (cMOAT). The characteristics

R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268 229
and substrate specificity are thus far entirely defined by its
absence in the TR rat. Upon description of the TR- rat,
two other rat strains, the GY [244] and the EHBR rat [245],
have independently been discovered and characterized by
two laboratories. These groups have initially investigated
different aspects of the secretory defect. Fortunately, cross
breeding experiments with the different strains have shown
that the offspring is always jaundiced and therefore the
conclusion can be drawn that the mutation in these animals
is either identical or at least allelic [246,247]. Thus, results
concerning phenotypical characteristics of these different
strains may be highly interchangable, except that the dif-
ferent genetic backgrounds may cause different observa-
tions between the EHBR rat (from the Sprague-Dawley
strain) and the TR and GY strains (from the same
original Wistar colony). Using model organic anions like
dinitrophenyl-glutathione (GS-DNP) and BSP, which are
poorly secreted by the G Y / T R rat, the mechanism of
transport has been studied in different experimental sys-
tems ranging from the intact animal [221,228,244,248,249],
isolated perfused liver [229], isolated hepatocytes
[246,250.251], hepatocyte couplets [252] and isolated
canalicular membrane vesicles [247,252-254].
Kobayashi et al. [255] were the first to show that
transport of GS-DNP in mixed rat liver plasma membrane
vesicles could be stimulated by ATP. The kinetics of
transport (linear over a period of two hours) strongly
deviated from that observed in later studies using more
purified canalicular vesicles, in which it was shown that
ATP-dependent transport can only be measured for a short
period ( < 10 rain) due to high rate of ATP hydrolysis in
these membranes, even in the presence of a regenerating
system. ATP-dependent GS-DNP transport was subse-
quently observed in freshly isolated hepatocytes [251] and
purified canalicular membranes [256] Similarly, the uptake
of cysteinyl-leukotriene [253], bilirubin-glucuronide [254],
BSP [247], and p-nitrophenyl-glucuronide [257] could
strongly be stimulated by the addition of ATP. Nishida et
al. [247] directly demonstrated that enrichment of inside-out
oriented vesicles by antibody induced density perturbation
increased the specific ATP-dependent transport activity of
the preparation with BSP as substrate. This strongly sug-
gests that the observed ATP-dependent transport acts as an
extrusion system in the canalicular membrane.
The work of several groups [247,252-254,256-258]
has demonstrated that the putative transport system
cMOAT, as studied in membrane vesicles, is temperature
dependent, osmotically sensitive and saturable with Km'S
for the organic anions in the low micromolar range (BSP:
31 /zM; GS-DNP: 71 /zM; cysteinyl-leukotriene C4:0.25
/.tM; p-nitrophenyl-glucuronide: 20 /zM; and bilirubin
glucuronide: 71 /zM). When transport is measured in
canalicular plasma membrane vesicles, the K m for GS-
DNP (71 #M) was found to be about 15-fold lower than
the apparent K m that was observed in transport experi-
ments with isolated hepatocytes (0.9 mM [250]). This
suggests that in the intact cell almost all GS-DNP is
present in a (protein-)bound form.
The transport is ATP-dependent and no other nu-
cleotides are able to drive the transport nor could this be
achieved with non-hydrolyzable analogues of ATP. Trans-
port could be inhibited by DIDS, vanadate and probenecid.
Furthermore the addition of protonophore (CCCP) or the
ionophore valinomycin did not inhibit transport [247,254]
indicating that transport was not secondarily driven by
ATP-induced H+-or K+-gradients. In fact, valinomycin
further induced ATP-stimulated uptake of bilirubin glu-
curonide suggesting that transport is electrogenic.
Nishida et al. [254] demonstrated that normal canalicu-
lar plasma membrane vesicles transport bilirubin glu-
curonide by both an ATP-and a membrane potential-de-
pendent mechanism. In TR- membrane vesicles the ATP-
dependent mechanism was absent, but the membrane po-
tential-dependent mechanism was retained. The observa-
tions of Nishida et al. are confirmed by more recent
experiments in TR rats and perfused livers [228], which
indicate that for some organic anions, like bilirubin ditau-
rate, a low affinity secretion pathway is preserved in TR
rats. It is, as yet, not clear whether these two secretory
systems represent separate systems of which apparently
only one is defective in the TR rat. Another plausible
explanation is that one system (the putative cMOAT) can
transport compounds both in an ATP-and a membrane
potential-dependent fashion and that in the TR rat the
protein is mutated in such a way that only the ATP-hy-
drolysing modality is defective. In this respect it is also of
importance to note that~ in the in vivo situation, the biliary
output of bilirubin in TR / G Y rats is only mildly de-
creased [221,259]. Apparently these animals are capable of
significant bilirubin excretion, albeit at strongly increased
serum bilirubin concentration. This also suggests that a
low affinity secretion pathway for bilirubin is still present
in the canalicular membrane of these animals. The studies
mentioned above concerning ATP-dependent bilirubin
transport contrast with Adachi et al. [260] who reported
that uptake of bilirubin-glucuronide in canalicular vesicles
is not ATP-but bicarbonate-dependent. This group also
recently reported that transport of bilirubin glucuronides in
canalicular membrane vesicles l¥om the EHBR rat is nor-
mal in contrast to the data from other groups [261], At
present it is difficult to reconcile these findings.
Studies with transport deficient rats clearly demon-
strated that the ATP-dependent transport of the compounds
described above is mediated by the same transporter or by
members of the same family of transporters. The particular
transport processes could be related to the findings of
Nicotera et al, [262,263] who had demonstrated earlier that
both GSSG and GS-DNP are able to stimulate an ATP-hy-
drolyzing activity in isolated rat liver plasma membranes.
Zimniak et al. [264] showed that this activity could be
purified as a 37 kDa protein from canalicular membranes,
using antibodies directed against affinity-purified GS-

230 R.P.J. Oude Elferink et a l . / Biochimica et Biophysica Acta 1241 (1995) 215-268
DNP-stimulated ATPase from erythrocyte membranes
[265]. However, this polypeptide was found to be normally
present in TR-rat liver plasma membranes and this makes
a relation, if any, between this ATPase and cMOAT
hypothetical. A possible explanation could be that the
isolated polypeptide may represent a subunit with ATPase
activity that is part of a larger complex necessary for
transport. It was suggested by Zimniak and Awasthi [218]
that the 37 kDa polypeptide may be a proteolytic fragment
of a larger 85-90 kDa protein. Very recently, the group of
Zimniak [266,267] reported that the above-mentioned puri-
fied 90 kDa protein displays organic anion transport capac-
ity upon reconstitution in liposomes. They furthermore
found that transport could be stimulated 2-fold by protein
kinase C-mediated phosphorylation. This would be in line
with the observation of Roelofsen et al. [268] that canalicu-
iar organic anion transport in hepatocytes can be either
directly or indirectly stimulated by protein kinase C.
In transport studies with isolated canalicular plasma
membrane vesicles little or no inhibition of bilirubin glu-
curonide or BSP transport could be observed by the addi-
tion of 10-100 /zM taurocholate [247,254]. Furthermore,
bile salt transport is not defective in canalicular membrane
preparations from TR- rats [247] (see Fig. 5). In contrast,
o e o E
0 u) (/) 40
(0
"6 E " 2 0
8O
131 E " " 60 O. z a
d) 40
E o. 20
0
20
15 ¢D
E
"3 E Q.
G
Wistar . A
, 0
0 S 10 IS 20
Wi . ~ t
--,-o
0 $ 10 15 20 4o
• m
6o
B
70
Wistar C
0 5 10 1S 20 50 60
T i m e ( ra in)
5o
o o
TR-
40
30
2O
10
o
o s lo
6o T R
4O
0
TF Jo
Io
!o
A
_ _ - - - - !
| , * -
1 S 20 60 70
r . j
B
0 S 10 IS 20 40 50
e j
C
o 5 1o 1§ 20 ,so 60
T i m e (ra in)
Fig. 5. ATP-dependent transport of organic anions (GSSG and GS-DNP) and bile salt (taurocholate) in canalicular membrane vesicles from Wistar (left)
and T R - (right) rats. Vesicles were incubated with the radioactive ligand (upper panel: 3H-GSSG; middle panel: 3H-GS-DNP; lower panel:
3H-taurocholate) and an ATP-regenerating system. Note that organic anion uptake is completely absent in TR- membranes while taurocholate transport is
fully functional. The apparent overshoot in the uptake of various compunds is caused by the depletion of ATP in the incubation medium. Data from Ref.
[667]

R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268 231
Table 1 Organic anions (or anionic complexes) of which biliary transport is reduced in GY/TR- rats
Number of Reference negative charges
Endogenous compounds conjugated bilirubin 2 [229] glutathione GSH 2 [250] glutathione GSSG 4 [251] cysteinyl-leukotrienes 2/3 [248] triiodothyronine-glucuronide 2 [652] coproporphyrin 1 2 [221 ] Bile salt conjugates cholate 3-O-glucuronide 2 [270] lithocholate 3-O-glucuronide 2 [270] nordeoxycholate 3-O-glucuronide 2 [249] tauro/glycolithocholate 3-sulfate 2 [244] taurochenodeoxycholate 3-sulfate 2 [244] nordeoxycholate-3-sulfate 2 [249] Exogenous compounds ceftriaxone 2 [653] ampicillin 2 [275] carboxydichlorofluorescein 2 [ 124] dibromosulfophthalein 2 [229] bromosulfophthalein-glutathione 4 [229l dinitrophenyl-glutathione 2 [250] glutathionyl-bromoisovalerylurea 2 [654] naphtol- 1-glucuronide 1 [332] indocyanine green 2 [228] gadolinium-ethoxybenzyl-DTPA 2 [655] Metals zinc [295] copper (acute i.v. administation) [295] manganese [296]
basis of the reduced secretion these compounds are consid-
ered as substrates for the putative cMOAT. Compounds
from this list which deserve special attention will be
discussed below.
Bilirubin. The most prominent substrate for cMOAT is
conjugated bilirubin. In the absence of active cMOAT,
bilirubin accumulates in the blood and its removal is partly
by renal secretion [269]. It should be noted that in the
absence of active ATP-dependent cMOAT the accumula-
tion of conjugated bilirubin in serum is relatively moderate
(33 p~M). This is caused by renal secretion and by a
considerable residual biliary secretion of bilirubin-
glucuronide. Recently Jansen et al. [228] have studied the
biliary secretion of a number of organic anions at different
infusion rates in the TR . It was observed that the residual
secretion in TR rats of some putative cMOAT substrates,
like bilirubin-ditaurate is quite high when high infusion
doses are applied and that reduced secretion is only ob-
served at low doses. It is possible that this residual biliary
secretion is caused by an alternative organic anion trans-
porter. This could be related to the observed ATP-indepen-
dent transport in TR-ra ts that may be driven by the
membrane potential [254]. Alternatively, the mutation in
the transport system in TR- rats may be such that only the
affinity for substrates like bilirubin ditaurate is strongly
decreased. This residual activity apparently cannot be used
to transport glutathione-conjugates because the secretion of
these compounds is low at all doses in the TR- rat
[228,250].
many studies demonstrated mutual transport inhibition of
several non-bile salt organic anions and in some cases this
inhibition was competitive. This suggests that cMOAT has
a rather broad substrate specificity. Since in T R - rats the
canalicular taurocholate transporter operates normally and
the secretion of compounds like bilirubin-glucuronide and
BSP is severely impaired, one can draw the conclusion that
the bile salt transporter does not accommodate these non-
bile salts as substrates. Whether the converse is also true,
unconjugated bile salts as substrates for cMOAT, is more
difficult to prove since an animal model with absent
canalicular bile salt transport is not available. It should be
stressed that the separation between bile salt and organic
anion is probably not complete. Inhibition of bilirubin-dig-
lucuronide [254] and GS-DNP [256] transport by high
concentrations of taurocholate (500-600 /zM) in canalicu-
lar membrane vesicles have been observed.
Substrates for the canalicular multispecific organic anion
transporter
Table 1 shows a list of compounds of which biliary
secretion is significantly reduced in G Y / T R - rats. On
Divalent anionic bile salt conjugates. Bile salts can be
sulfated or glucuronidated at the 3-OH position. In particu-
lar for the secondary, more hydrophobic bile salts like
lithocholate this may represent a detoxification route. This
conjugation adds an additional negative charge to the
molecule as to make it considerably more hydrophilic.
Strong evidence exists that in contrast to the monovalent
bile salts, the secretion of these divalent anionic bile salts
occurs via cMOAT. The secretion of sulfated taurolitho-
cholic acid, sulfated glycolithocholic acid and sulfated
taurochenodeoxycholic acid is considerably impaired in
the G Y / T R rat, whereas the secretion of their unsulfated
counterparts is normal [244]. The secretion of sulfated
taurocholate, however was almost normal It was also
shown that the 3-OH glucuronide of nordeoxycholic acid,
which is a divalent anion, is severely impaired in the
G Y / T R - rat, in contrast to the carboxyl-linked glu-
curonide which is a monovalent anion [249]. Similarly, the
3-OH glucuronide of lithocholate undergoes little biliary
secretion in the G Y / T R rat whereas the respective car-
boxyl-linked glucuronides are efficiently removed via bile
[270]. These data have led to the hypothesis that a sub-
strate for cMOAT must have at least two negative charges
to be transported by this system [230,246,250,270]. Fur-
thermore, in view of the fact that the more hydrophilic

232 R.P.J. Oude Elferink et al. / Biochimica et Biophysica A cta 1241 (1995) 215-268
divalent anionic bile salts are almost normally transported
in the TR- rat, the substrate apparently should also have a
core with a certain hydrophobicity. Indeed almost all
molecules of which transport is impaired in the TR- rat
have at least two negative charges (see Table 1).
Anionic antibiotics. The third generation cephalosporin,
ceftriaxone, is rapidly secreted into bile of both man and
rat [271,272]. The biliary secretion of ceftriaxone in the rat
is inhibited by ursodeoxycholate and this has led Xia et ai.
[273] to the suggestion that ceftriaxone may be secreted
via the canalicular bile salt transporter. However, secretion
of ceftriaxone is virtually absent in TR rats. In the
normal rat about 75% of the infused dose of ceftriaxone
was recovered in bile and no competition could be ob-
served by simultanous infusion of taurocholate. From this
it may be concluded that for its hepatobiliary secretion
ceftriaxone is not transported by the bile salt transporter
but via cMOAT [274]. An explanation for the inhibitory
effect of ursodeoxycholate may be that at high dose of
ursodeoxycholate divalent anionic metabolites like the 3-
O-sulfate or the 3-O-glucuronide are formed that may
inhibit ceftriaxone secretion. Verkade et al. [275] have
shown that biliary secretion of ampicillin is strongly im-
paired in the G Y / T R - rat indicating that this antibiotic is
most probably also secreted via cMOAT. Many other
antibiotics like rifamycin and amoxycillin are concentrated
into bile [276] but the responsible transport system has not
been characterized yet. It is interesting, however, to com-
pare the pharmacokinetic properties of a large group of
related compounds like the cephalosporins. Bergan [277]
described that from a group of 30 cephalosporins only 5
(cefotiam, cefoperazone, cefbuperazone, ceftriaxone and
latamoxef) were secreted into bile for more than 10%.
There was no clear relation between the extent of binding
to serum proteins and biliary secretion; high serum binding
only tended to increase the serum half-life of the
cephalosporin. This may indicate that the specificity of
hepatic carriers involved in uptake and secretion may play
a crucial role in the choice between renal and biliary
secretion. Interestingly, most of the cephalosporins that
undergo biliary secretion have two negative charges on the
molecule suggesting that this may be an important deter-
mining parameter. However, several of the compounds that
are secreted via the kidney exclusively also bear a double
negative charge, indicating that the prerequisites for biliary
secretion are clearly more complex.
The physiological role o f biliary GSSG secretion
When the liver is subjected to oxidative stress intra-
cellular GSH is rapidly oxidized to GSSG. This can occur
under conditions of reperfusion after ischemia or when
certain oxidants like paraquat or t-butylhydroperoxide reach
the liver in sufficiently high concentrations [278]. The
formation of GSSG is accompanied by its concentrative
secretion into bile and this transport competes with that of
glutathione-conjugates like GS-DNP [279]. Furthermore
this secretion is ATP-dependent and absent in TR rats
suggesting that this transport occurs via cMOAT [251].
The paradoxical consequence of high affinity canalicular
GSSG transport is that the hepatocyte extrudes GSH-
equivalents (in the form of GSSG) under conditions of
increased need. Indeed, inhibition of GSSG secretion ap-
pears to protect hepatocytes from injury during oxidative
stress. It was demonstrated that incubation of hepatocytes
in 10 mM fructose inhibits GSSG extrusion by a drastic
reduction of the cellular ATP level [251]. Silva et al. [280]
showed that this treatment prevented nitrofurantoin-in-
duced cytotoxicity in isolated hepatocytes, suggesting that
the extrusion of thiol equivalents is deleterious for the
cells. Therefore, questions arise concerning the function of
biliary GSSG secretion. It is well known that GSSG may
form mixed disulfides with thiol groups in proteins thereby
influencing their activity [281]. In this respect the extrusion
may function to eliminate potentially toxic GSSG to pre-
vent inactivation of enzyme activities. However, the activ-
ity of the GSSG-reductase cycle in hepatocytes, which
reduces GSSG at the expense of NADPH, is much higher
than the activity of GSSG secretion [282,283]. As a conse-
quence, the G S H / G S S G ratio in the hepatocyte under
normal conditions and during oxidative stress will be
determined by the balance between GSSG formation and
reduction by GSSG-reductase while canalicular efflux will
have little or no influence. Recently, Chung et al. [284]
reported that GSH under normal conditions inhibits the
activity of the GSSG reductase. They hypothesized that the
efflux of GSSG during oxidative stress principally serves
to decrease the total glutathione content of the cell, thereby
relieving GSH-mediated inhibition of the GSSG-reductase.
In this way the actual activity of the reductase would be
increased by net extrusion of thiol equivalents. At the same
time this mechanism may protect the cell from too high
NADPH consumption through the GSSG-reductase cycle
which would be needed to restore the G S H / G S S G ratio at
high total glutathione contents. Further evidence lbr this
hypothesis has as yet to be produced.
The secretion of GSH and GSH-associated compounds
Reduced glutathione (GSH) is present in millimolar
concentrations in bile of rats and a number of other species
[285]. Since the GSH concentration in plasma is in the
micromolar range, there is a large concentration gradient
from plasma to bile and this may drive water flux through
the tight junctions of the hepatocytes. A number of elegant
studies by Ballatori et al. [286,287] have indeed demon-
strated that GSH is a major determinant of the bile salt-in-
dependent bile flow in rats. In contrast to normal rats,
reduced glutathione is virtually absent from TR- bile. This
may explain the significant reduction of the bile salt
independent bile flow in this mutant animal [221]. The

R.P.J. Oude ElJerink et al. / Biochimica et Biophysica Acre 1241 (1995) 215-268 233
absence of GSH in TR bile may lead to the suggestion
that GSH secretion into bile occurs via cMOAT. There are,
however, arguments contradicting this suggestion.
Firstly, in contrast to all other organic anions that are
secreted into bile via cMOAT, there is no uphill gradient
for GSH from hepatocyte to bile. The intracellular concen-
tration of GSH in the rat varies between 5 and l0 mM and
that in bile between 1 and 5 mM [285]. However, this
probably represents an underestimation of the amount of
GSH that is secreted by the hepatocyte. Gamma-gluta-
myltranspeptidase, which is an apical ectoenzyme, is pre-
sent on the canalicular membrane and on the apical mem-
brane of bile duct epithelial cells. Thus, GSH present in
bile is actively degraded during its passage through the
biliary tree. Indeed, inhibition of gamma-GT by treatment
of rats with acivicin leads to a substantial increase in the
biliary GSH concentration, but never exceeds that of the
hepatocyte cytosol [288].
Secondly, several groups [289,290] have demonstrated
that the transport of GSH into canalicular membrane vesi-
cles is not stimulated by ATP but driven by the membrane
potential. Furthermore, Fernandez-Checa et al. [289]
showed that GSH transport is not deficient in canalicular
membrane vesicles from the EHBR ( ~ G Y / T R - ) rat.
Thirdly. several reports on organic anion transport in
canalicular membrane vesicles demonstrate that millimolar
concentrations of GSH do not, or hardly, inhibit the
(cMOAT-mediated) transport of typical organic anions like
BSP [247], GS-DNP [256] and bilirubin-glucuronide [254].
Although these arguments seem straightforward indica-
tions for the existence of a GSH transport system that is
distinct from ATP-dependent cMOAT it remains to be
demonstrated why GSH is completely absent from TR rat
bile. Fernandez-Checa showed that GS-conjugates in rather
low concentrations cis-inhibit GSH uptake in canalicular
vesicles. Therefore, they hypothesized that GSH secretion
in T R rats may be inhibited by certain endogenous
cMOAT substrates that have accumulated in TR- rat
hepatocytes [289].
The mechanism of canalicular GSH secretion may be
elucidated in the near future by the recent isolation of a
cDNA for the putative canalicular GSH transporter. With
Xenopus oocytes as expression system Yi et al. [291] were
able to isolate a 4 kb cDNA which gives rise to a 96 kDa
polypeptide that catalyzes GS-BSP insensitive effiux of
GSH from the oocytes. In previous studies this group had
already shown that sinusoidal GSH effiux can be inhibited
by BSP-glutathione whereas canalicular GSH transport is
insensitive to this compound. Furthermore, canalicular GSH
efflux could be induced by phenobarbital treatment
[210,289,292]. Northern blot analysis revealed that the
mRNA for this protein is present in liver, kidney, brain,
intestine and lung but not in heart. In addition, the mRNA
level could be induced by phenobarbital treatment. On
basis of these characteristics the authors conclude that
isolated cDNA probably represents the canalicular GSH
transporter. In an earlier study Femandez-Checa et al.
[213] had shown that, in addition to 4 kb mRNA for the
putative canalicular transporter, a 2.5kb mRNA is present
in liver that encodes for a BSP-glutathione inhibitable
GSH transporter. This mRNA may represent the sinusoidal
GSH transporter.
Healey metal ions as complexes with GSH. A number of
(heavy) metals has been shown to undergo substantial
biliary secretion. Since some of these appear to be depen-
dent on biliary secretion of glutathione they will be dis-
cussed in this section; for extensive review see [293].
It has been postulated that copper is secreted into bile as
a GSH-complex. Alexander and Aaseth [294] proposed this
mechanism on basis of the observation that depletion of
hepatic GSH leads to a marked decrease in biliary copper
secretion. However, in G Y / T R rats, which do not se-
crete GSH in their bile, secretion of endogenous copper
into bile is not impaired [295,296], implying that the
secretion of endogenous copper is independent of GSH
secretion. On the other hand, such a GSH-dependent path-
way may be of importance for the removal of copper
during i.v. copper administration [295,296]. In this model
of acute copper loading, a rapid and a slow phase of
elimination can be discerned in normal rats; the rapid
phase is absent in the mutant animals. These findings
indicate that at least two pathways must exist for biliary
copper secretion, one GSH-independent and another one
GSH-dependent and responsible for elimination of acutely
administered copper. The latter pathway does not accom-
modate copper that accumulates in the liver during dietary,
chronic copper overload. Data from several studies
[297,298] have suggested that biliary copper secretion, in
particular during hepatic copper overload, involves lysoso-
mal sequestration and subsequent exocytosis into bile. It
was very recently shown by Dijkstra et al. (J. Clin. Invest.,
in press) that rat liver membranes contain an ATP-depen-
dent, saturable, high affinity transport system 10r copper.
Its cellular localization remains, however, to be estab-
lished. In patients with Wilson's disease hepatobiliary
copper elimination is impaired and copper accumulates in
the liver. Recently, a candidate gene for Wilson's disease
was discovered and this gene encodes a P-type ATPase.
The cellular localization of this protein is not yet known
but this will shed light on the sequence of events in biliary
copper secretion. Also the characterization of a rat model
(the LEC rat, see Ref. [299]) will be of great value in the
near future in this field. This inbred mutant strain of rats
was originally isolated from a closed colony ,of Long-Evans
rats. This strain, associated with spontaneous hepatitis,
exhibits excessive hepatic copper accumulation and low
copper incorporation into ceruloplasmin [2!)9]. It was re-
cently shown that biliary copper secretion is also impaired
in these rats [300]. Thus, these rats have a phenotype
highly similar to that of patients with Wilson's disease.
Very recently, it was also shown that the defective gene in

234 R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268
this strain cosegregates with the rat homologue of the
human ' Wilson gene' [301 ].
There are indications that the canalicular secretion of
zinc also involves a GSH-dependent mechanism. Alexan-
der et al. [294,302] demonstrated that hepatic GSH-deple-
tion leads to a reduction in biliary zinc elimination. Fur-
thermore Houwen et al. [295] showed that biliary zinc
secretion is severely decreased in the G Y / T R - rat. The
biliary secretion route, however, does not play an impor-
tant role in the overall homeostasis of this metal [293].
There is ample evidence that the biliary secretion of
mercury and methylmercury is a GSH-dependent process
[303-305]. Recently, Dutczak et al. [306] substantiated this
contention by looking at the transport of a glutathione-
methylmercury complex in canalicular plasma membrane
vesicles. They demonstrated temperature-sensitive trans-
port into an osmotically active space. Transport was elec-
trogenic but could not be stimulated by ATP. The transport
was cis-inhibited and trans-stimulated by GSH. In con-
trast, inhibition by GSSG and a number of GS-conjugates
was very weak or absent. These data suggest that glu-
tathione-methylmercury is secreted into bile by a GSH-
specific carrier and not by cMOAT. It is interesting to note
in this respect that this complex is monovalent. Other
metal-GSH complexes like those of inorganic mercury,
lead [307] and cadmium [308] are thought to form multiva-
lent GSH-complexes and these complexes may reach bile
via cMOAT.
Oxoanions. When arsenite is injected into rats about 24-
37% of the drug is recovered in bile within 2 h [309]. This
is accompanied by a very strong (20-30-fold) increase in
the secretion of GSH in bile [310,311]. Upon administra-
tion of radioactive arsenite to the isolated perfused rat liver
Anundi et al. [312] analysed the secreted arsenite by thin
layer chromatography and found that the major part of the
radioactive arsenite was associated with a ninhydrin posi-
tive spot eluting together with glutathione. This is in
accordance with a recent NMR study by Delnomdedieu et
al. [313] in which the spontaneous in vitro association
between 3 molecules GSH with 1 molecule arsenite was
demonstrated. Similarly, the metabolite dimethylarsinite
formed a 1:1 complex with GSH. It was also demonstrated
that organic anions like BSP and indocyanine green (ICG)
are able to inhibit biliary arsenite secretion [310-312].
Recently Gyurasics et al. [314] reported similar results for
bismuth and antimony. Taken together, these results sug-
gest that arsenite (and bismuth and antimony) may un-
dergo canalicular secretion as a GSH complex, possibly
via cMOAT.
Ubiquitous expression o f organic anion secretion
Although the efficient concentrative secretion of amphi-
pathic anions seems to be a dedicated function of the
hepatocanalicular membrane, there is ample evidence that
highly similar transport systems are present in a wide
variety of cell types. It is already known for a long time
that GSSG [315] and GS-DNP [316] are pumped out of
erythrocytes and erythrocyte ghosts and it was demon-
strated that this process is ATP-dependent [317]. Similarly,
GS-DNP tranport can be observed in erythrocyte mem-
brane vesicles and this transport is competitively inhibited
by GSSG [318]. Thus, there are striking similarities in
transport characteristics between hepatocanalicular and
erythrocyte organic anion transport systems. The GSSG-
dependent ATPase activity in the rat liver plasma mem-
brane demonstrated by Nicotera et al. [262,263] had simi-
lar characteristics as that in the erythrocyte membrane
[319]. Furthermore Heijn et al. [320] demonstrated that
transport of GSSG in erythrocyte membrane vesicles is
inhibited by a very similar spectrum of organic anions
(including divalent sulfated and glucuronidated bile salts)
as the canalicular organic anion transport in hepatocytes
[246]. GS-DNP transport in erythrocytes from TR rats
was studied by two groups and it was found that the
activity was only slightly [320] or not [321] reduced as
compared to normal rats. Similarly, Board et al. [321]
detected no difference in the GS-DNP transport between
erythrocyte membranes from Dubin-Johnson patients and
normal subjects. Thus, it may be suggested that, although
the transporters in erythrocyte and liver canalicular mem-
branes resemble each other quite strongly functionally,
they may be derived from different genes. Nevertheless, it
is interesting to follow the achievements in the purification
of the erythrocyte transporter. A comprehensive review
concerning this subject has been published [218]. Unfortu-
nately, the results so far are rather confusing: the group of
Kondo et al. [322] reported the purification of a het-
erodimer consisting of a 62 kDa and 82 kDa protein which
has ATPase activity and is able to transport GSSG upon
reconstitution. On the other hand, the group of Awasthi et
al. has isolated a GS-DNP stimulated ATPase with a
postulated molecular mass of 38 kDa. Therefore, in con-
trast to what one would expect, GSSG and GS-DNP seem
to be transported by entirely different transport systems in
erythrocytes, although mutual inhibition of transport by
these substrates has been demonstrated in both liver [279]
and erythrocytes [320]. The interpretation of the putative
role of the GS-DNP-ATPase was further complicated by
the recent observation [323] that GS-DNP ATPase isolated
from human erythrocytes is also capable of transporting a
typical 'mdrl P-glycoprotein substrate', doxorubicin. It
was also shown that various other amphipathic substrates,
that are transported by mdrl P-glycoprotein, were able to
stimulate the ATPase activity of this isolated protein. From
these observations it was concluded that this putative
organic anion transporter actually translocates an even
broader spectrum of compounds including uncharged and
cationic amphipaths [323]. These data contrast with obser-
vations made with liver canalicular membrane vesicles
where no inhibition of ATP-dependent GS-DNP transport
is observed by compounds like doxorubicin [247,254].

R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268 235
Similarly, daunomycin does not inhibit canalicular GS-
DNP secretion by intact hepatocytes [246].
ATP-dependent transport of GSSG has also been re-
ported in the isolated perfused rat heart [324,325] and that
of GSSG and GS-conjugates, including leukotriene C 4, in
heart sarcolemma vesicles [326]. In a comparative study
with heart sarcolemma and liver plasma membrane vesi-
cles very similar K ms (150 nM and 250 nM respectively)
were found for LTC 4 transport in addition to a very similar
inhibition of LTC 4 transport by a spectrum of glutathione-
conjugates [326]. Since LTC 4 is synthesized by mast cells
(as well as several other blood cell types) Schaub et al.
[327] investigated transport in plasma membrane vesicles
of a mastocytoma cell line. They described a transport
system for LTC 4 that could be inhibited by GS-DNP and
that had a K m for LTC 4 similar as that in liver cell
membranes but with a much lower K m for ATP. More
recently, this group attempted to identify the polypeptide
that is responsible for LTC 4 transport in mastocytoma cells
by photoaffinity labeling with radioactive LTC 4. They
observed incorporation of radioactivity in a 190 kDa mem-
brane glycoprotein and speculated that the transporter might
be related to MRP (for multidrug resistance related pro-
tein; see Section 4) which has a similar molecular mass.
This contention was recently further substantiated by
showing that membrane vesicles from HL60 /ADR cells
which overexpress MRP display strongly increased trans-
port activity for LTC 4 and GS-DNP [328]. Very recently,
MiJller et al. [329] reported very similar results with an-
other MRP-overexpressing cell line as well as with MRP-
transfected cells. Zaman et al. [330] showed that MRP is
also ubiquitously expressed in normal human tissues, but
particularly low in liver. Thus endogenous MRP expres-
sion may be responsible for organic anion secretion in
many tissues, but it is unclear whether the low MRP
expression in liver could explain the very active organic
anion secretion into bile.
It was also reported that GS-DNP is secreted by CaCo 2
cells. This cell line represents a model for polarized intesti-
nal epithelium. It was observed that, in analogy with
hepatocytes, the secretion of the glutathione-conjugate was
highly assymetrical and dependent on the intracellular
ATP concentration. However, in contrast to the situation in
liver, secretion was detected both at the apical and basolat-
eral pole of the cell [331]. This is in accordance with a
study by de Vries et al. [332] who showed in the isolated
perfused rat small intestine that secretion of the organic
anion, 1-naphthol-/3-glucuronide, occurs both at the lumi-
nal and at the serosal side. Furthermore, they found that
the secretion of this compound was normal in the isolated
intestine of the TR rat whereas biliary secretion was
strongly reduced.
Taken together, it may be concluded from these obser-
vations that although highly similar organic anion secre-
tion systems are present in a wide variety of cell types, it is
not very likely that these transporters are derived from the
same gene as that encoding the putative canalicular multi-
specific organic anion transporter.
4. Hepatobiliary transport of organic cations
During evolution, organisms have been exposed to many
cationic food components. Examples are plant alkaloids of
which many are readily absorbed and can be extremely
toxic due to interaction with neural and hormonal receptor
systems and/or genetic material. In the evolutionary pro-
cesses, excretory organs such as kidney, gut and liver
became adequately equipped with detoxifying mecha-
nisms~ These include metabolic conversion processes and
secretory systems for cationic compounds to remove such
potential life-threatening agents from the body [333,334].
At the same time, selective cationic transport mecha-
nisms for essential nutrients such as choline, certain vita-
mins, and nucleosides are necessary to maintain hepatic
cell function and the production of vital physiological
substrates. Against this background, it is not surprising that
multiple carrier-mediated transport systems for cationic
compounds evolved at the hepatic uptake and excretion
level.
Apart from the many transport processes in the sinu-
soidal and canalicular domains of the hepatocyte plasma
membrane, intracellular transport sites have been identified
in organelles such as endosomes, lysosomes, mitochondria
and probably the cell nucleus [333,335].
Classical physiology postulates organic: cations as a
homogenous class of agents that are transported by single
transport systems at the uptake and secretory level [334]. It
became clear however in the past two decades that organic
cations encompass a very heterogenous group of agents. At
least five different uptake mechanisms have been postu-
lated to date for exogenous cationic compounds (mostly
drugs) and at least two different translocation processes are
supposed to be present at the excretion level [333,335,336].
In addition, multiple transport processes have been identi-
fied for the abovementioned endogenous cations. The latter
systems, in general, poorly accommodate the exogenous
organic cations, although overlapping substrate specificity
may exist. The relative contribution of these multiple
cation transporters to the overall uptake and secretion rate
of a given compound is depending on the (unbound)
concentration of the particular agent in relation to the
affinity for the various transporting modalities.
4.1. Sinusoidal uptake o[ organic cations
The overall picture emerging from many studies using a
variety of experimental systems is that multiple mecha-
nisms exist for the hepatic uptake of organic cations.
Widely overlapping substrate specificity may exist and,
depending on the concentration of the organic cation stud-
ied, often more than one system will contribute to the

236 R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268
Type TT compounds ~ N C H 3 0"'~''*~ 0 ~ :~c.~
- . . . - , A t . . c._c. . o ' y . . r , .o.3
i0 I . . . . 0 i ~ ! v HOH2C-CH CH I
; i N ~ CH?. OH 0 H3C-C-O H H3C-C-O H CH =CH-CH2- H ~ N ~
PANCURONIUM ORG 6368 2 I I H3C~ ALCURONIUM OCH3
T y p e I" c o m p o u n d s
CH3 Q CH~ N-CH-CH-CH-N-CH S / ~ N +1
2 Z 2 3 --CH-CH-N-CH CH 2 I I 3
N-METHYLJMIPRAMINE THIAZINAMIUM
0
CH 3 CH 3
d-TUSOCURARINE
~7"-~CN3 CH 3 ~ ' ~ I I
~,,L_yc% c%
HEXAFLUORENIUM N-METHYLDEPTROPINE
C2H 5 C'H7 C4H9 O / C 2 H ' ' +, +1 +1 __O._11 :N , -CzH 5 C2Hs-~-C2H5 C3H7-~ -CH3 C4H9-~ -CH3 H2N C-NH-CHz-CH2 i
CH 3 C3H7 C4H9 'CzH 5
TRIETHYLMETHYLAMMONIUM TRIPROPYLMETHYLAMMONIUM /RIBUTYLMETHYLAMMONIUM PROCAINAMIDE ETHOBROMIDE
Fig, 6. Chemical structure of cationic drugs that are taken up in the liver by two separate (type 1 and type 2) transport systems. Type 1 compounds are
either hydrophilic/aliphatic organic cations or aromatic compounds with a clear separation of ring strucures and the positively charged nitrogen group.
Type 2 compounds are generally more bulky molecules with one or two cationic groups enclosed in (or close to) ring structures.
overall uptake rate of given compound. Nevertheless, the
individual transport systems exhibit quite different features
with regard to maximal transport rate, energization and
ion-dependency as well as to the influence of inhibitors.
Non-carrier-mediated mechanisms in hepatic uptake
Although carrier mediated transport is the major mecha-
nism for uptake of organic cations, it should be empha-
sized that passive uptake can occur for very lipophilic
organic cations. Examples are the fluorescent probe rho-
damine B [337,338] and the anticholinergic drug dep-
tropine [339] (see for structure Figs.Fig. 6 and Fig. 7 7).
As the consequence of its passive transfer mechanism,
uptake rate of rhodamine B is not inhibited by other
cationic compounds [340]. Due to the efficient uptake
process of rhodamine B, sharp tissue concentration gradi-
ents are observed for this agent in whole liver. The initially
observed periportal to perivenous concentration gradient
reverses in time due to a time-dependent redistribution and
a higher binding capacity for dye in the pericentral (zone
3) hepatocytes [337,338]. In contrast, the hydrophilic fluo-
rescent compound lucigenin (see Fig. 7), that cannot pass
the sinusoidal plasma membrane by passive transport or
carrier-mediated mechanisms, is probably internalized via
a vesicular uptake process [341,342]. This was inferred
from fluorescence-microscopy studies showing a clustered
intracellular distribution of lucigenin with dots of fluores-
cence close to the plasma membrane. Partial inhibition by
microfilament inhibitors such as cytochalasin B and noco-
dazole, as well as by competitors for membrane adsorption
such as poly(L-lysine) [341] indicated a process of adsorp-
ORGANIC CATIONS
CH3 (~)JC2 H 5
. ~ C O O H Rhodamine B
~ (lipophilic)
CH3 I
Lucigenin
[hydrophilie)
i CH 3
O II
H3C-C-O c ®
II
O (lip o pl~ilic/hydr ophilic)
Fig. 7. Bulky organic cations that largely differ in lipophi]icity and are
taken up in the liver by entirely different mechanisms: rhodamine B is
sufficiently lipohilic to pass membranes by lipoid diffusion [337]. In
contrast, two quarternary nitrogen centers make lucigenin much more
hydrophilic and this compound can only be taken up by an endocytic
mechanism [341,342]. Vecuronium has an intermediate lipophilicity and
in the deprotonized form is an amphipathic organic cation that is trans-
ported via caiTier-mediated mechanisms [336].

R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268 237
Sinusoid
03 OC ~
Cl', HC~
0 OC~_~
© OC:---'
Bile canaliculus
© ©
~h Sinusoid . - . _ i _ ~ . _ . . ~
4Tp 7
®
OC ~
OC"
@ Pgp CI-
Fig. 8. Tentative scheme depicting carrier-mediated transport of organic
cations at the sinuoidal and the canalicular level of the hepatocyte. Five
uptake systems are indicated for exogenous cations: type 1 carrier system
(1), type 2 carrier system (2), absorptive endocytosis (3), passive lipoid
diffusion (4) and paracellular permeation (5). Transport processes for
choline and thiamine exhibit Na+-dependency in cells and for NMN a
H+-dependency in basolateral membranes was shown. Sinusoidal mem-
branes contain the N a + / K + pump and the Na+/H+-antiporter. The
canalicular membrane possesses a CI- /HCO~- antiporter and at least
two organic cation carriers: mdrl P-glycoprotein and a carrier for rela-
tively hydrophilic organic cations.
tive endocytosis. Such a phenomenon has also been de-
scribed for basic drugs at the renal tubular level [343].
Carrier-mediated uptake systems for organic cations With regard to saturable hepatic uptake of endogenous
cations (see Fig. 8Fig. 8), various carrier-mediated trans-
port processes have been described, in studies in whole
(isolated perfused) liver and isolated hepatocytes. In some
of these studies it is difficult to distinguish the membrane
transport process from further metabolic steps since many
of these compounds are rapidly converted within the hepa-
tocyte. Yet, in most of these studies evidence was obtained
that carrier-mediated uptake and accumulation of the par-
ent compounds in the cells can occur in the absence of
sequential metabolic steps [336]. Kinetic analysis often
demonstrated the presence of high and low affinity uptake
processes for the individual compounds. The outcome of
inhibition studies with metabolic inhibitors or structurally
related cationic compounds is therefore dependent on the
range of substrate concentrations tested.
Choline uptake in hepatocytes was claimed to be (at
least partly) Na + dependent, could not be inhibited by
tetra-ethyl-ammonium but was strongly inhibited by hemi-
cholinium-3 [344]. Although thiamine seemed to competi-
tively inhibit choline transport, choline inhibited thiamine
uptake in a non-competitive manner [345]. Three indepen-
dent studies with isolated hepatocytes clearly showed
Na+-dependency of (high affinity) thiamine uptake [346-
348]. This process that was poorly inhibited by tetrameth-
ylammonium but in contrast strongly decreased by diben-
zyl-dimethyl ammonium [345,349] as well as other more
lipophilic ammonium and phosphonium derivatives
[349,350]. A study with the thiamine derivative dimethal-
lium [351], in which replacement of the hydroxyethyl
group by a methyl group prevents phosphorylation, showed
carrier-mediatedneur uptake dissociable from the phospho-
rylation step.
In general, caution should be exercised with regard to
such ion-dependency studies: replacement of Na + by
potassium, lithium or choline can produce many other
effects. These may include a direct influence on the cell
membrane, plasma membrane depolarization (high K+),
and substrate competition (choline).
In a more recent study on thiamine transport with
hepatocyte basolateral membrane vesicles Na+-depend -
ency of thiamine uptake could not be dete, cted [352]. In
contrast an electroneutral thiamine/H + exchange system
was demonstrated. This process was inhibitable by ammo-
nium ions, choline and imipramine but not by the endoge-
nous cations N-methylnicotinamide (NMN) and exogenous
cations such as PAEB, TBuMA and vecuronium [352]. An
electroneutral H+-antiport system was also detected for
NMN in the same membrane preparation [353] (see Fig.
8). Choline, TBuMA, PAEB and vecuronium did not
significantly affect pH-dependent transport of NMN [354],
whereas acetylcholine, spermine, hamaline and imipramine
were clearly inhibitory [353].
With regard to cartier-mediated uptake of exogenous
compounds studies have been focused around a number of
model cations. Tetraethylammonium (TEA)uptake in ba-
solateral membrane vesicles was claimed to be pH-inde-
pendent in one study [352] and found to be stimulated by a
negative membrane potential [352]. The uptake rate of
TEA was cis-inhibited by PAEB, TBuMA and vecuronium
[354] but interestingly not by NMN [354,355]. Contrasting
observations were made in two uptake studies in basolat-
eral plasma membrane vesicles with TEA [355] and TBuMa
[356] from which involvement of an electroneutral proton-
antiport translocation mechanism was concluded.
Transstimulation of TEA transport was demonstrated for
thiamine while cimetidine and quinidine inhibited this
counter transport [357]. Since thiamine showed cis-inhibi-
tion and trans-stimulation, involvement of the earlier men-
tioned thiamine transporter might play a role. Alterna-
tively, cross-contamination of the basolateral plasma mem-

238 R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268
brane fraction with endosomal/lysosomal membranes may
have occurred. In these organelles H+-antiport of quater-
nary drugs has been reported [358].
It is important to note here that cis-inhibifion does not
necessarily prove that a common carrier system is in-
volved: cationic substrates could inhibit TEA transport
without being transported by the same carrier. Such a
phenomenon also explains that uptake of small (type I)
cations is strongly inhibited by bulky (type II) organic
cations but not vice versa [336]. Only cis inhibition com-
bined with trans stimulation may give a clue for a com-
mon transporter. The abovementioned vesicle studies indi-
cate that at least two cation transporters are involved in
uptake of TEA and TBuMa in basolateral plasma mem-
brane vesicles. For TEA an electrogenic cation/cation
exchanger is operating [354,355] along with an electroneu-
tral H+-antiport system [355].
The characteristics of TEA transport in basolateral
membrane vesicles are only partially in line with hepato-
cyte uptake studies for the cationic drugs, azido-PAEB
[357], TBuMa [359] and vecuronium [360]. For all of these
compounds at least two uptake systems could be kineti-
cally demonstrated. These studies showed no Na+-or pH-
dependency of uptake; neither was evidence for membrane
potential driven uptake found. For TBuMA uptake the
latter observations was corroborated by direct microelec-
trode studies [359]. In the abovementioned basolateral
membrane vesicle studies, a negative membrane (diffusion
potential) did not drive uphill TEA transport [354,357].
The stimulatory effect of an intravesicular negative mem-
brane potential was therefore interpreted with the involve-
ment of a conductive pathway [354,355]. Whether such a
mechanism does also operate for larger organic cations
remains to be established.
In a study in isolated hepatocytes it was shown that
various classical metabolic inhibitors clearly affect ATP
synthesis and largely lower cellular ATP content [358].
These agents significantly (but not completely) inhibited
initial uptake rate of TBuMA [358,359] and vecuronium
[360]. Part of the effects of metabolic inhibitors on uptake
rate may also be due to interference with cellular seques-
tration steps such as electrogenic uptake into mitochondria
and proton antiport in endosomes and lysosomes (see
Section 4.2). The lack of influence of ATP and ATP-gen-
erating systems on uptake of TBuMa in basolateral plasma
membrane vesicles suggests that this transport is not di-
rectly ATP-dependent [356].
In conclusion: hepatic uptake of cationic drugs seems to
occur by at least two facilitated diffusion carrier processes
that are Na+-independent and of which one may be stimu-
lated by proton gradients. The latter process is not identical
to thiamine and NMN proton antiporters. The electrogenic-
ity of the uptake systems for exogenous cations currently
remains unresolved. ATP dependency could not be demon-
strated and facilitated (carrier-mediated) diffusion mecha-
nisms are the most likely candidates.
Heterogeneity in uptake systems for cationic drugs
The cationic drugs as a whole also show clear hetero-
geneity in hepatocyte uptake mechanisms. The relatively
small cations such as TEA [354,355], TBuMA [359], PAEB
[336] and its azido analogue APM [357] are transported by
a system that is inhibited by choline and lipophilic (amphi-
pathic) cations but not by cardiac glycosides and bile salts
[336,361,362]. They were categorized as type 1 organic
cations and comprise either aliphatic quaternary ammo-
nium compounds or molecules in which the cationic amine
group is at some distance from the aromatic ring structure.
Larger cationic drugs with the positively charged group
included in or situated close to large, aromatic ring struc-
tures (called type II compounds) behave differently: hep-
atic uptake is not affected by a large excess of choline or
the type I compounds but can be largely blocked by
cardiac glycosides and bile salts. This is explained by
competitive inhibition for a multispecific system that rec-
ognized bulky amphipathic compounds independent on
their charge [361 ]. It is of interest that hepatocyte uptake of
both type I and type II organic cations is stimulated by
inorganic counter anions [359,360] such as HCO 3 and I-.
This effect was speculated to be due to an improved
presentation of the cations to the membrane carriers via
ion-pair formation rather than to facilitation through
cation/anion symport [359].
Photoaffinity labeling and expression cloning of potential
carriers for uptake of organic cations
Preliminary photo affinity labeling studies with azido-
procainamide methyliodide (APM) [357,363] showed in
plasma membrane fraction of rat liver predominant label-
ing of 50 kDa and 72 kDa proteins while labeling studies
with the bulky type II compound azo-N-pentyl-deoxy-
ajmalinium (APDA) showed labeling of 48 kDa and 50
kDa proteins [364]. Incorporation of label in the APM
studies was inhibited by type II compounds (an interaction
also found in isolated hepatocytes) while labeling of poten-
tial carrier proteins with APDA was strongly reduced by
cardiac glycosides and bile salts (see above). Prior photo-
affinity labeling of hepatocytes with APDA reduced the
Vmax without changing the K m of N-propyl-deoxy ajma-
linium (NPDA) uptake into hepatocytes indicating that part
of the carriers was inactivated through covalent labeling.
More definitive identification of the putative carrier pro-
teins for organic cations is awaited.
Expression cloning of organic cation uptake carrier
protein has recently be attempted independently by two
groups [365,366] in studies with TEA and TBuMA respec-
tively. A 1.8-3.0 KB mRNA fraction seems to encode for
proteins that mediate TEA uptake in Xenopus laevis
oocytes. However, enrichment compared with total m-RNA
is only 5-fold and the transport signal compared to controls
is quite weak. Consequently complete sequencing of the
genetic code was not yet feasible. Cloning, sequencing and
large scale synthesis of such proteins may enable reconsti-

R.P.J. Oude Elf'erink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268 239
tution and further characterization at the molecular level.
Among others, ATP-dependency and potential regulation
mechanisms could be studied with such techniques.
4.2. Intracellular sequestration of organic cations
Following uptake at the sinusoidal domain of the hepa-
tocyte, organic cations can reach high concentrations in the
cytoplasmic compartments [333-336,367]. Transmem-
brane concentration gradients of 15-fold and more have
been calculated, both for monovalent [368] and bivalent
positively charged model compounds [369]. For many
compounds this value largely exceeds the gradient that
would occur by passive equilibration of cations according
to the membrane potential ( - 35 mV in hepatocytes). It is
important to note that cytoplasma/bloodplasma concentra-
tion gradients under steady state conditions, even corrected
for extracellular and intracellular protein binding, do not
merely reflect the uptake process since they are the resul-
tant of the relative rates of uptake, biliary excretion and
sequestration into organelles [369]. The latter processes
may provide sink conditions especially if hepatic uptake
rate is relatively low. For some organic cations the sinu-
soidal uptake process is rate limiting in overall hepatobil-
iary transport [368,369]. In such cases cytoplasma/blood
plasma concentration gradients below unity have indeed
been reported [368,369]. Real uphill transport against an
electrochemical gradient of the cationic species however,
is difficult to prove since many of these studies rely on
subcellular distribution studies after whole liver homoge-
nization. Since considerable accumulation of organic
cations in various types of organelles can occur, the cyto-
plasmic cytosol concentrations are overestimated, at least
to some extent, since redistribution from particulate frac-
tion to the cytosol fractions cannot entirely be prevented.
Uptake of cationic drugs in endosomes / lysosomes
Cell fractionation studies of livers taken from animals
that were injected with organic cations in vivo revealed
subce]lular distribution patterns that are entirely different
from the patterns obtained after addition of these com-
pounds to homogenized livers in vitro [368-372]. In par-
ticular, enrichment of the mitochondrial and lysosomal
fractions was detected after in vivo administration of the
cations [368,372]. Lysosomal/endosomal accumulation
was confirmed by electronmicroscopy of electron-dense
precipitates of such agents [373] as well as by more recent
uptake studies in acidified multivesicular membrane prepa-
ration [370]. It was shown that organic cation transport is
partly ATP-dependent (see Fig. 9Fig. 9) and sensitive to
proton-dissipating agents such as monensin as well as to
H+-ATPase inhibitors, These data suggest two possible
mechanisms of uptake. Similar to the accumulation of
chloroquine and other lysosomotropic agents, weakly basic
compounds can diffuse across the membrane, become
protonated in the acidic interior and thereby trapped in the
~ , ~ uptake by MVB
6 0 0
0 CYTOPLASM~'~'- ~ ~ wll h alp
, o o . . . . . , , o
400
"~ 3 0 0
I11 200
or , , l
,OOoo ,Q~ 0
= 0 20 40 60 80 100 120 140 160
Time (min) Fig. 9. Uptake of of the permanently charged tubocurarine in muhivesicular bodies isolated from rat liver, representing a model lot endosomal and
lysosomal sequestration. Vesicles were incubated with the radioactive ligand in the presence or absence of an ATP-regenerating system. The inset shows
intravesicular acidification through an ATP-driven proton pump while CI- cations follow passively. Organic cations (quarternary amines) can be taken up
by proton/cation antiport. In contrast, tertiary amines such as chloroquine pass the membrane in the uncharged form and accumulate through intravesicular
protonation (from Ref. [370]).

240 R.P.J. Oude E!ferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268
organelle. Alternatively, compounds can be taken up by a
putative proton-cation antiporter. The first mechanism
could be operable for compounds with tertiary amine
moieties, like tubocurarine or vecuronium, if it is assumed
that the singly charged species is permeable. This mecha-
nism is unlikely to occur with the permanently charged
quarternary amine, TBuMA. Therefore, an ATP driven
proton-antiport or a cation/hydroxyl symporter was pro-
posed [370].
Storage of organic cations in acidified organelles can be
partly prevented by prior administration of basic drugs
such as primaquin both in vitro and in the intact organ
[372]. The resulting displacement of organic cations from
the acidified compartment, however, did not lead to an
increased biliary excretion rate [370,372]. A decrease in
biliary output was observed for d-tubocurarine [372] as
well as TBuMA and vecuronium [370] after administration
of primaquin. This lack of stimulation may be explained
by the relatively small functional size of this displaceable
organelle compartment [370]. In addition, competitive inhi-
bition of the protonized tertiary amine with the quaternary
agents at the level of carrier transport in the canalicular
membrane may well have occurred. An alternative expla-
nation for the lower biliary output would be a decreased
intracellular (vesicular) transport of the organic cations to
the canalicular pole of the cell [370]. In such a process
biliary excretion of the cations would occur through fusion
of cation-containing vesicles with the canalicular plasma
membrane followed by exocytosis. However, such a pro-
cess remains to be demonstrated. In this respect it is of
interest that a proton-antiport system for TEA was detected
in canalicular plasma membrane vesicles [354]. This trans-
port of TEA, however, was not ATP-dependent, in contrast
to that in endosomes.
Uptake and binding of organic cations in mitochondria
Mitochondrial sequestration of organic cations consti-
tutes another major storage compartment in the hepatocyte
[333,358,369]. Since the lysosomal sequestration process
has a limited capacity, especially at high doses of organic
cations, association with mitochondria may become a
quantitatively important process [369]. A number of factors
determine mitochondrial sequestration: (a) the considerable
intracellular volume of mitochondria; (b) the presence of
mitochondrial DNA, to which the cationic drugs can bind;
(c) the sizeable negative membrane potential of the or-
ganelle ( - 2 2 0 mV) that drives the uptake process
[358,374]. Fluorescent cationic probes are widely used for
measurement of the organelle membrane potential [375].
Initial uptake rate of various organic cations into isolated
rat liver mitochondria was shown to be highly sensitive to
agents that dissipate the mitochondrial membrane potential
such as lipophilic cationic dyes and to ionophores such as
CCCP and valinomycin [358]. Electrogenic transport into
the inner mitochondrial space was found to be (at least
partly) carrier-mediated and mutual competitive inhibition
was demonstrated for various model organic cations [376].
Apart from electrogenic uptake an electroneutral proton
antiport (or OH- symport) systems has been identified
[377].
Uptake rate into the mitochondria was positively corre-
lated with the lipophilicity of the cationic model com-
pounds [376]. This was supposed to be due to the relative
affinity for putative carriers in the mitochondrial mem-
branes. It is of interest that many cationic agents that
avidly enter mitochondria are also substrate for the MDR
(P-glycoprotein) system [378,379]. P-glycoproteins how-
ever, have not been detected in mitochondria and lyso-
somes. Yet, the apparent accumulation of cationic drugs in
these organelles in expense of the cytoplasmic concentra-
tion may contribute to drug resistance in non-steady state
conditions. On the other hand intercalation of some or-
ganic cations such as ethidium bromide with mitochondrial
DNA is a central aspect of cytotoxicity and efficient
cellular extrusion by P-glycoprotein may therefore lead to
drug resistance [378,380].
Carrier-mediated mitochondrial transport processes were
described for choline and quinidine [381] as well as sper-
midine [382]. Saturable and electrophoretic choline trans-
port was competitively inhibited by hemicholiniums, quini-
dine and quinine, the latter agent being a 10-fold stronger
inhibitor than the first [381]. The polyvalent polyamines
are also transported via a uniport system or channel that is
membrane potential dependent [336] and indirectly cou-
pled to transport of inorganic phosphate. Interestingly,
photoaffinity labeling studies with lipophilic (type 2) or-
ganic cations in hepatocytes consistently reveal labeling of
the mitochondrial protein carbamoyl synthetase that is
localized inside the mitochondrial matrix, suggesting an
intra-organelle localization of the probe [115,383].
As indicated above, the mitochondrial pool of organic
cations can be largely mobilized by addition of inhibitors
of mitochondrial function. In isolated perfused livers, addi-
tion of CCCP or valinomycin leads to massive efflux of
the hepatically stored organic cations back into the perfu-
sion medium. This confirms that mitochondria constitute a
major component of the hepatic storage compartment for
organic cations.
Various organic cations including d-tubocurarine [384],
adriamycin, spermine, and related anticancer agents as
well as alkyl guanidines inhibit respiratory chain activities
of isolated mitochondria [379,385]. Cytotoxic effects of
such agents have been, at least partly, attributed to inhibi-
tion of oxidative phosporylation [379,384]. Conclusion:
although the outer membrane of mitochondria provides
some barriers against the effects of especially hydrophilic
cationic agents [379], more lipophilic basic drugs may
easily reach these potential sites of toxicity [386]. Both
passive membrane potential driven uptake [358,374] and
carrier-mediated transport across both the outer and inner
mitochondrial membranes [374,376,381] may occur;
choline may play a role in this process.

R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268 241
Binding of cationic drugs to the cell nucleus
Apart from the lysosomal/endosomal and mitocbon-
drial sequestration of organic cations, the cell nuclear
material may bind considerable amounts of these agents.
Nuclear staining with fluorescent cations such as propid-
ium, ethidium and acridine dyes is generally used in
cytofluorometric analysis [387-389]. The relative amount
of cationic drugs in the cell nucleus is dependent on the
liver load [369]. The extent of nuclear binding of cationic
drugs therefore does not only depend on the inherent
affinity of the cationic drugs for the polyanionic DNA but
also on 'saturation' of the lysosomal and mitochondrial
pools. It is assumed that quaternary probes such as ethid-
ium passively pass pores in the nuclear envelope and bind
to the polyanionic polynucleotides through electrostatic
forces. The strong intercalation of some cytostatic drugs
with double-strain DNA is partly explained by their cationic
character.
4.3. Canalicular transport of organic cations
Excretion of organic cations into bile occurs under quite
different conditions compared with renal tubular secretion:
major H+-gradients as present in the renal tubuli probably
do not exist at the bile canaliculus. Proton-antiport, as
described for several cationic probes in the kidney [390], is
therefore less likely to occur at the hepatic excretory level.
Another major difference with urinary excretion is the
presence of biliary micelles and vesicles in bile that can
avidly bind hydrophilic and lipophilic organic cations [391 ].
Passive transport of cationic drug across the canaliculus
followed by binding to biliary micelles could in principle
lead to biliary 'sink' conditions and net output of cations
into bile. Excretion of organic cations into the canalicular
lumen occurs against the negative membrane potential.
However, the membrane potential 'hill' could be taken via
electroneutral exchange with organic or inorganic cations
or be facilitated by formation of ion-pairs with suitable
counter anions. Marked stimulation of transport of cationic
probes across liver plasma membranes by lipophilic anions
has been demonstrated [392]. This was explained by dissi-
pation of the intramembrane potential hill in the lipid
bilayer and/or ion-pair transport of the uncharged
cation/anion complex. In this respect it has been shown
that tetrapbenylborate completely blocks the biliary excre-
tion of TBuMA at an unchanged bile flow in isolated
perfused livers [393]. The lipophilic anion might have
favored electrogenic reabsorbtion of the organic cation or
could have facilitated intracellular binding/sequestration
to macromolecules and organelles.
Evidence was obtained for heterogeneity of organic
cation transport from studies with canalicular liver plasma
membrane vesicles (cLPM). Intravesicular accumulation
and initial uptake rate of TEA in inside-out canalicular
vesicles showed no apparent ATP-dependency. The pres-
ence of an electroneutral T E A / H + exchange mechanism
exhibiting trans-stimulation was shown. PAEB, vecuro-
nium and tributylmethyl ammonium cis-inhibited this pro-
cess [354]. The choice of the transport model compound
TEA seems less appropriate since it is unlikely to be
excreted in bile [394]. Similar results were found, however,
for the tributyl-methyl analogue, which is strongly secreted
into bile (Moseley, pers. communication). In contrast, the
accumulation of NMN in cLPM did not show a pH-gradi-
ent dependent mechanism [353]. Earlier observations
showed that inside-out cLPM manifest ATP-dependent
accumulation of daunomycin [395]. Accumulation in cLPM
was shown to be inhibited by other cytostatic (basic) drugs
such as vinblastine, vincristine and andriamycin as well as
by other lipohilic drugs with a tertiary amine function such
as verapamil and quinidine [395]. More recently, vinblas-
tine accumulation in cLPM was reported which exhibited
temperature dependency and osmotic sensitivity [396].
Daunomycin avidly binds to membranes ,~o that actual
transmembrane transport of the drug in vesicles is quite
difficult to prove. Therefore the relation of these in vitro
cation studies with the biliary excretion in the intact liver
remains to be clarified.
Evidence ~ r carrier-mediated transport in the biliarv
excretion of cationic antineoplastic drugs
In the isolated perfused organ and in the,, liver in vivo,
daunomycin is extensively metabolized and converted to
glucuronide conjugates among other metabolites [397].
Yet, abundant biliary excretion of unchanged doxorubicin
was also observed [398]. Elimination of the anthracyclin
into bile can be completely blocked by verapamil at an
unchanged bile flow (see Fig. 10Fig. 10). In this experi-
ment verapamil was added at the moment that most of the
added doxorubicin was taken up in the liver, excluding
potential interaction at the uptake level [398]. Two other
liver perfusion studies showed a profound inhibition of
colchicine excretion into bile by the lipoph~lic cyclic pep-
tide cyclosporin [399,400]. Biliary excretion of the basic
fluorescent dye acridine orange is also largely affected by
cyclosporin [401]. Finally, an inhibitory effect of vera-
pamil on the biliary excretion of 3H-vincristine was found
by Watanabe et al. [402]. Daunomycin, vincristine,
colchicine and acridine orange are known substrates for
P-glycoprotein and verapamil and cyclosporin are strong
inhibitors of this pump [403,404]. These studies therefore
are suggestive for the involvement of P-glycoprotein
and/or related ATP-dependent translocator(s) in the bil-
iary excretion process of organic cations. The ATP-depen-
dent vesicular accumulation of cationic drugs in isolated
canalicular membrane vesicles [395,396] as well as the
canalicular localization of P-glycoproteins (mdrla, mdrlb,
mdr2), that was demonstrated by immunochemistry and
photoaffinity labeling [405-408], may support such a hy-
pothesis.
In the light of the interesting hypothesis of involvement
of P-glycoprotein in biliary secretion of organic corn-

242 R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268
10
E O
E
t~
O
X LU
0 .1 ,
0.01 -
0.001
/ /
/ /
/
/
Addition
J i
/
/ ' 'o ' 0 20 4 6O
Time (min)
i i
80 1 O0
Fig. 10. Inhibition of biliary excretion of doxorubicin by verapamil in the isolated perfused rat liver. Doxorubicin was allowed to be taken up from the perfusate during 20 rain. Subsequently verapamil was administered to the perfusate in a single dose. Verapamil did not affect bile flow but reduced biliary excretion rate of unchanged (HPLC assayed) doxorubicin temporarily for more than 90%. At t = 40 rain biliary excretion of doxorubicin is restored due to metabolic inactivation of verapamil in the liver (from Ref. [398]).
pounds more detailed information on this peculiar trans-
port system will be provided and recent findings on its
possible function in organic cation transport will be inte-
grated.
4.4. The role o f P-glycoproteins
P-glycoproteins (Pgps) are members of the super family
of transporter proteins that contain ATP-binding cassettes,
also called ABC proteins or traffick ATPases [403,409-
413]. The proteins consist of about 1200 amino acids that
constitute two homologous halves each with one nu-
cleotide binding segment and 6 transmembrane domains.
The apparent MW varies from 130-190 kDa, dependent
on species and cellular origin. Murine species exhibit three
gene products: mdrla, mdr lb and mdr2 while in the
human two variants MDR1 and MDR3 were identified.
MDR1 and mdr la or b confer drug resistance whereas
MDR3 and the related murine protein mdr2 do not.
M D R 1 / m d r l a / l b compared with M D R 3 / m d r 2 have
very different tissue localization and are also differently
induced [405,414-418]. M D R 3 / m d r 2 is particularly ex-
pressed in the canalicular domain of the hepatocyte and
may function as a phospholipid translocator or flippase
[419,420] (see also Section 5.3). In contrast,
M D R I / m d r l a / l b display a more general body distribu-
tion, being highly expressed at the apical domains of cells
in colon, small intestine, liver, adrenal glands and to a
lesser extent in choroid plexus, placenta, testis and bone
marrow [403,409]. Recent studies showed its presence in
peripheral blood lymphocytes [421,422]. The strategic body
localization points to an active protective function towards
potentially toxic agents and/or an essential role in trans-
port of endogenous substrates.
The multidrug resistant tumor phenotype, characterized
by a decreased cellular drug accumulation of cationic
drugs, is directly related to overproduction of this naturally
occurring protein via gene-amplification [403,409,411,423].
It was recently demonstrated that this resistance is achieved
by ATP-dependent extrusion of drugs from cells by P-
glycoprotein [424-426]. The genes responsible for the
various MDR modalities have been cloned and sequenced
[423,427-429]. Although the transport function can be
reconstituted in artificial systems [424,425,429] or trans-
fected in M D R ( - ) cell lines, insufficient quantities are
available to date for structural analysis. Yet, mutational
analysis enabled further characterization at the molecular
level [403,409].
Mechanisms o f P-glycoprotein mediated membrane
translocation ~1 ~ drugs
At least two potential drug binding sites, one in each
half of the molecule, have been detected through photo-
affinity labeling/proteolytic digestion studies and by site
directed mutagenesis [403,409]. Subtle changes in amino
acid composition in the transmembrane domains 3 and 11
can change the relative binding affinity of various sub-
strates but can also differently affect the rate of dissocia-
tion of various drugs from the protein. It should be realized
that both association and dissociation are essential for
membrane translocation of organic compounds. The inter-
relation of the above mentioned binding sites in the func-
tional transport structure of Pgp is not exactly known, but
recent studies support a single channel model in which the
two binding sites somehow cooperate [403]. P-gp variants
have been proposed to function as volume regulated CI-
channels [430] and even as ATP channels [431]. However,
it is difficult to explain how all these functions would be
incorporated in a single transmembrane protein.
In addition, a proton pump activity has been claimed
since Pgp(+) cell lines exhibit an increased (cytoplasmic)
pH [432-437]. Chloride and proton (or cation) fluxes
could be somehow linked in the sense that ATP-hydrolysis
leads to binding of the cationic species that for vectorial
transport is either passively followed by C1 or exchanged
for H +. A recent study does not support the idea that
changes in intra-or extracellular pH mediate Pgp-depen-
dent multidrug resistance [438].
With regard to drug transport, it remains to be estab-
lished whether the P-glycoprotein really functions as a

R.P.J. Oude EIferink et al./ Biochimica et Biophysica Acta 1241 (1995) 215-268 243
conventional transporter or, alternatively, acts as a mem-
brane extruder that merely expels amphiphilic compounds
that entered the membrane by non-ionic lipoid diffusion
[439]. The latter concept has been called the 'hydrophobic
vacuum cleaner' model and may bear resemblance with
phospholipid flippase-type of translocation [419]. The lat-
ter modality implies that access of substrate to the trans-
port protein occurs directly from the lipid phase and that
the drug is flipped from the inner leaflet of the bilayer to
the outer. This model also predicts that the P-glycoproteins
could decrease the initial uptake rate of the substrate in
cells in vitro since it would not differentiate between drug
entering the membrane from the inner or outer cellular
space [440]. Homolya et al. [441] have tried to substantiate
this concept by looking at the uptake of acetoxymethyl
esters of fluorescent (anionic) dyes. Due to their hydropho--
bic character these compounds diffuse through the plasma
membrane and are extremely rapidly hydrolysed by abun-
dant intracellular hydrolases. It was shown that cells over.-
expressing mdrl Pgp accumulate the hydrolysed com-
pounds much less than control cells, suggesting that the
acetoxymethyl esters are extruded by Pgp from the mem-
brane before they can reach the intracellular space.
Stein et al. [442] studied the behavior of a variant of
MDR1 in which a glycine at position 185 is replaced by
valine. On basis of the differential effect of this mutation
on the initial uptake vs. efflux rates of various substrates
they proposed that Pgp can extract drugs from the internal
as well as from the external leaflet of the membrane by
different paths.
In an alternative model, Gottesman and Pastan [443]
have tried to combine the different reported transport
functions of Pgp for protons, chloride and amphipathic
compounds. In this hypothetical model ATP hydrolysis is
linked to the transport of protons into the transporter, with
chloride following passively. Once within the transporter
these ions will draw water osmotically into the pump out
of the membrane. Amphipathic drugs within the membrane
then: "should follow the water, and drugs will be removed
from the membrane just as a scrubber on a smokestack
removes water-soluble materials from smoke". Although
this model (like the vacuum-cleaner model) would explain
the broad specificity for amphipathic compounds it is not
in line with the observation that the chloride channel
activity, if indeed an inherent feature of Pgp, could be
dissociated from its drug transporter activity [430]
Substrate specifici~ o f P-glycoprotein
A central feature of multidrug resistance is the phe-
nomenon of cross-resistance: persistent exposure to an
amphiphilic cytostatic compound leads to overexpression
of the 170 kDa protein. The overproduced protein accom-
modates such a broad range of substrates that resistance
occurs for many related antineoplastic drugs [403]. How-
ever, it is highly unlikely that evolution has resulted in a
P-glycoprotein that is specific for anti-tumor agents alone.
Indeed, it can bind and may transport a wealth of naturally
occurring as well as therapeutic and diagnostic agents
[404 ,~ ,445] . Many of these agents stimulate ATP hydro-
lysis by purified and reconstituted Pgp [424-426] and are
likely candidates for vectorial transport. Some compounds
may only bind to Pgp but do so with high affinity. Such
inhibitors may have value as so called 'reversal agents'
that can antagonize the MDR phenotype.
Structure-transport relation o f P-glycoprotein
The wide variety of organic compounds that seems to
be accommodated by P-glycoprotein (at least the
MDR 1 / m d r l a / mdr lb Pgps) raises the question what the
common physicochemical and structural features of such
substrates are. Many systematic structure-kinetic studies
have been performed, including three-dimensional struc-
tural analysis [404,444-452]. Most of these studies con-
firm a general picture that comprises a number of struc-
tural features:
(a) The presence of at least one but preferentially several
planar aromatic ring structures enabling interaction
with a supposedly 'flat ' hydrophobic structure in the
P-glycoprotein drug-binding domains
(b) In relation to this, a partition coefficient (octanol-aque-
ous buffer) higher than 1 but preferentially exceeding
2
(c) Preferentially a cationic charge at physiological pH,
for instance through a protonable nitrogen center in the
molecule
(d) A proper molar refractivity reflecting the 'space fill-
ing' molecular volume, indicating that a minimal
'bulky' structure is a necessary prerequisite for a
proper MDR substrate.
The fact that the molecular mass of MDR substrates
mostly exceeds 400 Da is in line with such a structure. The
latter characteristic is a necessary element since a combi-
nation of aromatic rings and protonatable nitrogens in
itself is not sufficient to modulate pump activity [404,453].
The importance of a nitrogen centre in MDR
modulators/substrates was demonstrated for the acetamide
group of colchicine [453] and is also supported by the
finding that removal of the basic center from doxorubicin
partially destroys its feature of a MDR substrate [454].
Nevertheless some steroidal compounds without a basic
center have been shown to be transported by the MDRI
gene product. These include certain steroidal hormones
and cardiac glycosides such as digoxin.
At least two drug binding sites seem to be present in
P-glycoprotein [403,411,455]. A model was, proposed in
which both halves of the transporter, each with one bind-
ing site, come together to form a single transport channel
[403,456]. This in spite of the fact that the binding sites of
verapamil and vinblastin are not identical [45'7]. The differ-
ing abilities of various drugs that can reverse MDR to
inhibit other drug or drug analogue binding also indicates

244 R.P.Z Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268
that P-glycoprotein has multiple drug-binding sites (see
[423,458]. Recent evidence indicates a dihydropyridine
selective acceptor site that is allosterically coupled to a
vinca-alkaloid-selective binding site [459]. Aliosterically
coupled drug binding domains have also been reported for
other channel/pump and receptor proteins [459]. The im-
plication of the latter aspect is that both negative and
positive allosteric effects (synergism) may occur in the
presence of more than one MDR-substrates/inhibitor. It
also means that Pgp-directed bifunctional modulators could
be developed for counteraction of drug resistance. Other
types of 'bifunctional' MDR-modulators that are in the
stage of development comprise compounds that both in-
hibit nucleoside transport and MDR1 [460] or consist of
agents that simultaneously inhibit P-glycoprotein and non-
Pgp carrier system(s) (see below).
Non P-glycoprotein related MDR phenomena
A number of laboratories have independently observed
that reduced accumulation of drugs in tumor cell lines can
occur without mdrl gene overexpression while multidrug
resistance in such cells is poorly reversed by chemosensi-
tizers that are effective in cells overexpressing MDR1
[330,461-465]. Recently, a potential carrier channel pro-
tein has been cloned: the MDR-related protein (MRP) that
like P-glycoprotein belongs to the ABC protein superfam-
ily [462]. MRP overexpression results in high levels of a
190 kDa ATP-binding plasma membrane protein
[330,462,464]. However, MRP is only distantly related to
the characterized members of the superfamily. The amino
acid identity with human MDRI is only 14% and predomi-
nantly confined to the ATP binding site [462]. The MRP-
gene is ubiquitously expressed in human tissues, but its
expression in liver is relatively low [330]. Although the
protein is mainly localized on the plasma membrane, sub-
stantial amounts may be present in the endoplasmic reticu-
lum and other intracellular organelles [464]. Cell-type spe-
cific variation in MRP distribution between plasma mem-
brane and intracellular compartments may explain why
decreases in cytoplasmic drug accumulation are in some
cases due to drug extrusion and in others related to intra-
cellular drug sequestration [462]. Recent studies [465] indi-
cate that the specific tyrosine kinase inhibitor genestein
highly influences intracellular distribution of cationic drugs
in cells with MRP overexpression but fails to do so in Pgp
(MDR1) cell lines. Tyrosine kinase may be involved in
deactivation or down regulation of the MRP pump. In
contrast, P-glycoproteins seem to be regulated via protein
kinase C (see 4.4.6).
In a recent study by Jedlitschky et al. [328] it was
demonstrated that plasma membrane vesicles of MRP-
overexpressing cells display increased ATP-dependent
transport of leukotriene C 4 and dinitrophenyl-
glutathione,which both are typical organic anions. These
experiments suggest that MRP is a primary active organic
anion pump. In order to explain the (relatively low) resis-
tance of MRP-overexpressing cells towards cationic cyto-
toxic drugs like daunomycin, one has to assume that this
transporter accommodates both organic anions and neutral
or cationic cytotoxic drugs. Alternatively, it may be that
metabolism of daunomycin and other drugs into anionic
species, like glutathione conjugates, is sufficient in these
cells to give rise to increased efflux via an organic anion
transporter. Very recently, Miiller et al. [329] reported very
similar results with another MRP-overexpressing cell line
as well as with MRP-transfected cells.
Interestingly, another protein of 110 kDa is also overex-
pressed in some non-Pgp MDR cell lines. In normal tissues
with a secretory/excretory function such as the liver, this
protein is highly expressed and predominantly present in
intracellular vesicles [466]. From a recent study [330] it
was indeed concluded that MRP overexpression can not
account for all lbrms of non-Pgp MDR. In non-steady state
conditions the activity of such an intracellular pump could
lead to MDR via lowering of the cytoplasmic drug concen-
tration.
Regulation o f P-glycoprotein expression and activ~v in the
liver
In a number of pathologic and experimental conditions
major fluctuations in Pgp activity have been demonstrated.
Increased MDRI RNA levels have been demonstrated in
hepatocellular carcinoma (HCC) [418], in cirrhotic non-
tumorous tissue in HCC patients but not in other patients
with liver cirrhosis [418]. In contrast Teeter et al. [467,468]
found no consistent elevation or even a lowered expression
of MDRI gene in metastatic colon tumors and HCC while
MDR2 was clearly underexpressed in metastatic tumors.
In rodents mdr genes are induced in preneoplastic and
especially neoplastic liver nodules, in the later stages of
carcinogenesis. However, the underlying molecular mecha-
nisms are unresolved [414,469,470]. During regeneration
of mouse liver both mdr2 and mdrla are induced whereas
in mouse HCC only mdr la is elevated [414,417]. In-
creased levels of mdrla and l b have also been reported in
hepatoma derived cell lines and hepatocytes treated with
acetyl aminofluorene (AAF) [417].
P-glycoprotein is also overexpressed in canalicular
structures that are formed between adult rat hepatocytes in
primary culture [471-473]. During regeneration of rat
liver, after partial hepatectomy, and following tetrachloride
[416] and colchicine treatment [474], hepatic mdrl and
mdr2 are largely but differently induced. After CC14 and
colchicine, increased levels of mdrl Pgp are already found
at 3 h after treatment, remaining increased for up to 5
days. A 5-to 10-fold increase in transcription rate is found.
Mdr2 expression after CCL4 increased only after 48 h and
is back to normal after 72 h. Increased expression of mdr2
was found especially in the canalicular domain, initially in
the periportal zone and subsequently spreading to pericen-
tral cells. Both obstructive-and a-naphthyl isothiocyanate-
induced cholestasis in rats and monkeys increase mdrla

R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268 245
and mdrlb gene expression in liver [415]. In the latter
study a possible correlation with biliary excretory function
was found: treatment of rats with AAF led both to in-
creased mdrl mRNA levels and vinblastine excretion into
bile. However, the causal relationship of these phenomena
remains to be established. In a recent study of Lee et al.
[473], the differential expression of P-glycoprotein genes
in primary rat hepatocytes cultures was studied; mdrlb
was only moderately elevated. Expression of mdr2 Pgp,
which is most abundant in rat liver even decreased and a
reciprocal relation step between mdrlb and mdr2 seems to
be present. The level of mdrlb was strongly correlated
with actin mRNA, suggesting a common regulation of
gene expression. Microtubuli and microfilament inhibitors
(colchicine, cytochalasin B) inhibited the normal mdrlb
overexpression. A similar differential activation was ob-
served during liver regeneration and hepatocarcinogenesis:
mdrlb expression was much more increased than that of
the mdrla and mdr2 gene [414].
Apart from variations in P-glycoprotein levels, also the
intrinsic activity of the pump seems to be regulated (see
Fig. l lFig. 11) [475]. There is abundant evidence that
basal activity of P-glycoprotein is modulated through phos-
phorylation/dephosphorylation reactions mediated through
protein kinase C (PKC) and probably other kinases
[465,476]. In most cell lines stimulation of PKC by phor-
bol esters leads to an increased phosphorylation of Pgp and
increased drug effiux from cell lines with overexpression
of P-glycoprotein [477-484]. Analysis of the primary se-
quence of Pgp indicates 37 potential phosporylation sites
of which 14 are probably accommodated by PKC. Other
kinases such as cAMP dependent kinases as well as an
unidentified kinase that is neither identical to PKC nor to
protein kinase A [485] mediates phosphorylation of Pgp.
PKC is a family of at least 10 closely related phospholipid
and thiol dependent isoenzymes of which some are also
Ca2+-dependent. Most of the isotorms are activated by
diacylglycerol (DAG) (see Fig. 11) [486]. Among the most
selective PKC inhibitors are synthetic peptide substrate
analogs [487]. It is of interest that many PgP substrates can
activate phospholipase-C and thereby can stimulate the
pump activity via DAG release. The positive regulation by
PKC of mdr-encoded PgP was elegantly demonstrated in
cotransfection studies using the human MDR1 gene and
PKCa cDNA [488]. Staurosporin and its more selective
7-hydroxy derivative are inhibitors of PKC that bind to its
catalytic domains [489] and reverse the phorbol ester ef-
fects [490]. However, staurosporins are cationic drugs and
bind to P-glycoprotein directly [491]. Indeed, it has been
shown that staurosporin and some derivatives can reverse
drug resistance irrespective of their PKC inhibitory activity
[492]. However, two other more specific inhibitors of PKC
exhibited similar effects on phosphorylation of P-glyco-
protein and its pumping activity: sodium butyrate [485]
that decreases Pgp phosphorylation and calphostin C that
binds to the regulatory domain of PKC [493,494]. The dual
SINUSOID
÷ ¢X::-- bile acids q
c a r d d ~
El>
CANALJCULUS
I
5 3 .'z.kq
0¢ HCO~
CI-
Fig. 1 I. Intracellular sequestrat ion sites o f organic cat ions and potential
regulat ion mechan i sms for transport . O C * = organic cations: 1 = type I
uptake system; 2 = type 2 uptake system: M = multispecific uptake sys-
tem; VP = vasopressin; R = receptor: G = GTP-b ind ing protein: D A G =
diacylglycerol ; P K C = protein kinase C,
inhibition of Pgp by staurosporins through direct binding
and lowering its phosphorylation is probably true for many
'reversal agents' and have been demonstrated for vera-
pamil, phenothiazines, cyclosporins and tamoxifen (see
[476,495]) among others. Interestingly, treatment of some
colon cancer cell lines with butyrate leads to decreased
transport of vinblastine and adriamycin but not of
colchicine [485]. This indicates that the PKC influence on
MDR-mediated translocation may be drug-class specific.
PKC mediated phosphorylation of P-glycoprotein also
modifies the efficacy of reversal agents [494]. How drug
transport via P-glycoprotein is changed by phosphorylation
is presently unclear. In general, decreased phosphorylation
does not affect binding of substrates to the MDR1 proteins
[494] although azidopine is a remarkable exception [494].
In relation to P-glycoprotein, activity of PKC plays a
dual role: it modulates the intrinsic activity of the pump
but also regulates its cellular expression. PKC agonists
activate P-glycoprotein gene expression whereas stau-

246 R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268
rosporin and other PKC antagonists lower its cellular
expression [496,497].
Protein kinase C and biliary excretion of drugs
PKC may also be involved in the regulation of canalicu-
lar drug transport. Organic anion efflux from isolated
hepatocytes, that likely reflects the bile canalicular excre-
tion process via cMOAT, is increased by vasopressin and
phorbol esters and inhibited by staurosporin [268]. A re-
cent study demonstrates that such agents also affect the
biliary excretion rate of the monovalent organic cation
TBuMA [498]. A dose-dependent stimulation was found
for PMA. Vasopressin also increased biliary output of the
quaternary amine whereas staurosporin blocked these ef-
fects and also lowered the basal excretion rate. These
effects were observed in the intact (isolated perfused) liver
and were unrelated to moderate changes in bile flow and
uptake rate of the organic cation [498]. Whether the effects
on cation transport are related to P-glycoprotein activity
remains to be demonstrated. Preliminary studies indicate
that high TBuMA concentrations fail to inhibit dauno-
mycin transport in canalicular membrane vesicles and do
not affect the biliary excretion of classical MDR substrates
in the perfused liver [398]. Yet a number of reversal agents
such as verapamil and quinidine strongly inhibit TBuMA
excretion into bile at an unchanged bile flow [398]. These
observations point to multiplicity in hepatic excretory
mechanisms for organic cations and also indicate that the
effects of verapamil may not be specific for MDR-media-
ted transport.
Current evidence for the involvement of P-glycoprotein in
hepatobiliary cation transport
Recent studies in highly purified right-side out canalicu-
lar membrane vesicles confirm the earlier observation
[395,396] of ATP-dependent cation transport. In these
studies the quaternary amines N-pentyl-quinidinium (NPG)
and N-pentyl-deoxyajmalinum (NPDA) were used [499].
Especially the quinidium derivative has the advantage of
low aspecific binding to the plasma membranes, a phe-
nomenon that endangers proper experimentation with
daunomycin and vincristine. The pentyl analogue of quini-
dine with a permanent positive charge exhibited a 10-fold
higher uptake compared with the tertiary compound.
Photoaffinity labeling of the canalicular membranes with
N-azo-pentyl-deoxyajmalinum revealed polypeptides of
143 and 108 kDa [499]. Transport in vesicles was in-
hibitable by verapamil and daunomycin but not by tauro-
cholate. N-pentyl-quinidinum transport could also be ele-
gantly demonstrated in Sf9 insect cells transfected with the
mdrlb gene product via a recombinant baculovirus vector
[500]. ATP-dependent transport of NPG, NPDA and
daunomycin as well as quinidine was clearly demonstrated
and interestingly the differences in K m of transport of
these agents in the mdr-transfected cells was almost identi-
cal to the ones observed in the canalicular membrane
vesicle experiments. Photoaffinity labeling of the Sf9
membrane vesicles again revealed a 140 kDa protein that
probably represents a non-glycosylated form of P-glyco-
protein [500].
In summary, a number of indirect observations support
the hypothesis that P-glycoprotein is one of the putative
cation carriers responsible for biliary excretion of bulky
(amphiphilic) organic cations:
(a) ATP-dependent transport in canalicular membrane
vesicles and in plasma membrane vesicles of MDR
transfected cells of various amphiphilic basic drugs
such as daunomycin [395,396] as well as quinidine,
deoxyajmalinum and their quaternary N-pentyl deriva-
tives [499,500]
(b) Excretion of cationic antineoplastic agents in bile in
the intact organ is highly inhibited by verapamil and
other so-called reversal agents [398,400-402]
(c) Induction of mdrla through partial hepatectomy and
regeneration leads to an increased biliary clearance of
vinblastine [415]
(d) Excretion rate into bile of unchanged doxorubicin is
increased by phorbol esters suggesting PKC regulation
[3981.
Some, more hydrophilic, quaternary ammonium com-
pounds such as TBuMA, PAEB and d-tubocurarine do not
affect doxorubicin excretion into bile even when used at
extremely high doses [398]. Nevertheless TBuMA excre-
tion is highly influenced by PKC modulators [398,498].
These observations point to at least one additional organic
cation transport system at the canalicular level that might
be ATP-dependent, PKC stimulated but not identical to
mdrla or mdrlb. A non-P glycoprotein (MRP) type of
carrier could be responsible or alternatively transport activ-
ity might be related to a 110 kDa protein that apart from
the abovementioned 140 kDa polypeptide is consistently
photolabeled in these canalicular membrane preparations
[364].
The supposed cation transport systems in the canalicu-
lus likely display overlapping substrate specificity depend-
ing on the hydrophobicity/hydrophilicity balance in the
particular molecules. Hydrophobic bile salts and other
lipophilic organic anions such as estradiol glucuronide
[501,502] may inhibit both transport systems [503].
Whether hormonal steroids, cardiac glycosides and their
metabolites are also accommodated by these ATP-depen-
dent carrier systems in the canaliculus is presently un-
known. It is of interest that evidence is accumulating for a
role of P-glycoprotein in transmembrane transport of
steroidal compounds such as corticosterone [504], cortisol
[505] and digoxin [506-508] in renal tubular monolayers
[509], adrenal gland, kidney in vivo [510], multidrug resis-
tant tumor cell lines [505,510] and perfused rat kidney
[507,508].

R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268 247
5. Hepatobiliary transport of lipids
Hepatocytes secrete substantial amounts of lipids, both
at their basolateral (sinusoidal) side into the blood and at
their apical (canalicular) pole into the bile. The first pro-
cess involves the packaging of triglycerides, cholesterol
(ester) and phospholipids together with apolipoprotein B
into nascent Very Low Density Lipoproteins (VLDL) in
the endoplasmic reticulum, as well as processing of the
particles in the Golgi complex and secretion by exocytotic
mechanFig. 12Fig. 12isms [511]. Nascent High Density
Lipoproteins (HDL), in the form of discoidal apolipo-
protein-phospholipid complexes containing apolipoprotein
A-I, A-II and/or A-IV, are also secreted into the blood by
the liver cells [512]. The apical route, i.e., the movement
of free cholesterol and phospholipids from hepatocytes
into the bile, occurs via clearly different, but as yet
incompletely understood mechanisms. Data from a large
amount of studies published during the past two decades,
suggest that the secretion of cholesterol and phospholipid
is coupled. Thus, in general, fluctuations in bile secretion
of phospholipid induced by experimental means, e.g., by
feeding choline-deficient diets to rats [513], result in paral-
lel alterations in the cholesterol secretion pattern. It has,
however, been recognized that under certain metabolic
conditions deviations can occur [514-516]. It is also evi-
dent that the secretion of cholesterol and phospholipids is,
at least in part, governed by bile salts. How and where in
the sequence of events leading to the secretion of lipids the
bile salts exert their regulatory function is still a matter of
debate. Basically, the relationship between bile salt secre-
tion and that of cholesterol and phospholipids is described
by a hyperbolic function, i.e., lipid secretion plateaus at
high bile salt secretion, in all animal species studied so far.
However, in different species marked quantitative differ-
ences exist in the amounts of lipids secreted per amount of
bile salt [517] as well as in the maximal secretion rates of
phospholipids and cholesterol [517]. This may, in part, be
related to interspecies differences in the bile formation
process, or, according to the model of Mazer and Carey
3£
%
-4
~, o o o ° ° ~ ~ , o o o o ° °
o ~ \Theory o o ° o o o o o o o o O O O o o o o ° ~ o o o o o o o O O o o ° ° ° °
- - I I I ] I
50 ioo 15o 20o 25o 300
BS~ (#mol.kg -I. hr -I)
Fig. 12. The relation between biliary bile salt secretion (BS~e c) and biliary
phospholipid secretion (L~e c). The data represent a compilation of several
studies with different animal species. These data were used by Mazer and
Carey for a mathematical model of bile salt-induced phospholipid secre-
tion. (from Ref. [518]).
[518], by interspecies differences in hepatic phospholipid
synthesis rate (see Section 5.2 and Fig. 12). It is also
well-established that the capacity of the individual bile
salts to induce lipid secretion correlates with its relative
hydropbobicity [519-521] as reflected in its so-called criti-
cal micellar concentration (CMC). However, intracanalicu-
lar bile salt micelle formation alone can not be responsible
for regulation of biliary lipid secretion. This would not be
in line with the observed presence of cholesterol-phospho-
lipid vesicles in native bile samples [522-524], with obser-
vations such as the isolated hypo-or hypersecretion of
phospholipids [516] and of cholesterol [514,515] under
certain experimental conditions and with the highly
species-specific coupling of lipid-to-bile salts [517] There-
tore, alternative modes of regulation must exist. Recent
work indicates the presence of (an) additional regulatory
mechanism(s) involving canalicular membrane proteins,
specifically the mdr2 P-glycoprotein [125]. The issues that
will be addressed in this Section concern the origin of the
biliary lipids and the factors involved in the regulation of
their secretion. In addition, some considerations on the
potential physiological function(s) of biliary lipids will be
presented. In view of the scope of this review, emphasis
will be on recent developments in this field of research; for
a more complete overview of available literature the reader
is referred to a number of excellent reviews on this subject
[5,517,525,526].
5.1. Composition and physical.h~rm o[ bilia~ lipids
Cholesterol and phospholipids comprise a major part of
the organic fraction of bile in quantitative terms; their
secretion into the bile amounts up to 0.8-1.2 g /day and
3-4 g/day, respectively, in humans [517] and to 15 m g /
day and 200 rag/day, respectively, in the rat [527]. Con-
sidering the large differences in lipid composition that
exist between liver and bile, it is evident that secretion
does not occur in a random fashion but rather involves an
advanced level of 'sorting'. Bile phospholipids consist
almost exclusively of phosphatidylcholine (PC) of specific,
relatively hydrophilic, fatty acid composition in all animal
species studied. The sn 1 position of biliary PC usually is
occupied by the saturated fatty acid species palmitate
(16:0) whereas the sn 2 position invariably contains an
unsaturated species, predominantly oleate (18:1) or
linoleate (18:2). This contrasts with PC of the canalicular
membrane which has a high content of arachidonate (20:4)
in the sn 2 position. Using state-of-the-art analytical tech-
niques, however, approximately 25 additional PC species
could be identified in normal human [528] and rat [529]
bile, albeit in small proportions. Fatty acid composition
can be influenced by diet, e.g., diets rich in n - 3 fatty
acid-containing fish oils lead to enrichment of biliary PC
species with these specific fatty acids [530] and, in the
perfused rat liver, by acute administration of hydrophilic
fatty acids such as 16:1 [529]. Only minor amounts of

248 R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268
sphingomyelin and phosphatidylethanolamine, both major
constituents of hepatic membranes, are present in the bile
under normal conditions. Thus, the hepatocyte selectively
recruits specific PC species for secretion into bile and/or
effectively excludes other phospholipids from entering this
pathway. Cholesterol appears to be present in bile exclu-
sively in its unesterified form under any condition.
It is well established that lipids are present in bile in the
form of aggregates, of which the size, shape and composi-
tion are primarily determined by the concentration of these
lipids relative to that of the biliary bile salts as well as by
the physicochemical characteristics of the phospholipids
and bile salts present. A large body of evidence is avail-
able to indicate that simple micelles, consisting of bile
salts and cholesterol, mixed micelles, containing bile salts,
cholesterol and phospholipids, and unilamellar vesicles,
consisting of cholesterol and phospholipids and trace
amounts of bile salts, can co-exist as biliary lipid carriers
in a dynamic, i.e., interchangeable, fashion [531]. In addi-
tion, multilamellar vesicles (liquid crystals) may be present
in lithogenic-supersaturated bile [53 l]. The vesicular struc-
tures contain a characteristic and constant pattern of (glyco)
proteins, with the canalicular transmembrane glycoprotein
aminopeptidase N as an important representative [532].
The term 'bile lipoprotein complexes' has been proposed
for vesicular structures containing a 7 kDa apoprotein
designated as anionic polypeptide fraction (APF) [533,534].
Whether these structures represent a distinct entity within
the population of vesicular carriers and whether they have
specific physiological importance remains unclear. It has
also been claimed that 'lamellae', composed of stretched
membrane-like bilayers, comprise the major cholesterol-
carrying particles in human bile [535,536]. However, as
recently discussed in great detail [531], these structures
may represent artifacts of the microscopic technique em-
ployed.
A key question concerning the regulation of biliary lipid
secretion relates to the form in which the lipids actually
enter the bile canaliculus. This question is difficult to
approach directly because of the inaccesibility of the
canalicular lumen for direct bile sampling at the site of its
formation. In the 'traditional' view (see further below),
based on the pioneering studies of Kay and Entenman
[537], Hardison and Apter [538] and Wheeler and King
[539], solubilization of bile-specific lipids from intra-
cellular or canalicular membranes into mixed micelles
reflects the initial event in the secretory process. More
recent concepts, generated by the physicochemical analysis
of freshly collected bile by quasi-elastic light scattering
and electronmicroscopic techniques [522-524], postulate a
form of vesicular secretion. This form of secretion has
been proposed to result from an exocytotic process or from
membrane-shedding or budding, and is, under physio-
logical conditions, followed by micellar dissolution of the
vesicles. As bile salts rapidly dissolve the PC-cholesterol
vesicles in unsaturated bile, only simple and mixed mi-
celles are found after equilibration, i.e., the situation that
usually occurs under experimental conditions when bile is
collected for prolonged periods of time after creation of a
bile fistula. Clearly, the different mechanisms of secretion
are by nature not mutually exclusive and may even occur
simultaneously, perhaps contributing to a variable extent to
total lipid secretion under different conditions.
5.2. The origin and precursor pools of biliary lipids
Considerable efforts have been made to define the
origin of biliary lipids. Concerning the question to what
extent de novo synthesis contributes to biliary cholesterol
secretion, recent studies employing tritiated water as a
precursor yielded values in the order of 7-16% [540,541 ]
under control conditions in the rat. The observation that
the specific activity of cholesterol in bile under these
experimental conditions is much higher than in the liver
[540,542] has led to the speculation that newly synthetized
cholesterol is preferentially secreted from the liver into the
bile or, alternatively, is derived from a specific hepatic
pool. As elegantly shown by Robins et al. [543], this
observation may in fact reflect the secretion of (newly
synthetized) cholesterol by a specific subpopulation of
hepatocytes. It is known that HMG-CoA reductase, which
is considered to be the rate-limiting enzyme in cholesterol
biosynthesis, is sharply localized to the periportal region of
the liver acinus [544]. From other studies [34] it is known
that this region of hepatocytes is primarily involved in bile
salt transport during normal enterohepatic cycling. The
relative amount of newly synthetized cholesterol can ex-
perimentally be altered to a considerable degree by manip-
ulation of hepatic cholesterogenesis [540,545]. Recent
studies [546,547] indicate that, under certain circum-
stances, the rate of hepatic cholesterol synthesis may co-
regulate the total amount of cholesterol secreted into the
bile. Nevertheless, the major part of biliary cholesterol is
derived from preformed sources, including cholesterol in
membranes of liver cells, cholesterol released from hepatic
cholesterylester pools and cholesterol originating from
lipoproteins taken up by the hepatocytes from the blood
compartment. With respect to the latter, numerous studies
on the contribution of lipoprotein cholesterol(ester) em-
ploying radiolabeled tracers have suggested the existence
of a metabolically active cholesterol pool that is replen-
ished from lipoprotein cholesterol, with HDL cholesterol
possibly as an important contributor, but interpretation of
these studies is hampered by the rapidity and extent of
cholesterol exchange that occurs in vivo. Recent work by
the group of Robins [548] indicates that all of the pre-
formed free cholesterol in the liver should be considered as
a single kinetic pool, potentially available for biliary secre-
tion. From a functional point of view, there seems to be an
interrelationship between pools available for VLDL pro-
duction and bile secretion or, alternatively, there may be a
single pool present for both secretory pathways; in general,

R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268 249
experimental procedures resulting in increased or de-
creased secretion of VLDL cholesterol have an opposing
effect on bile cholesterol secretion [514,515,530].
A number of studies from different laboratories have
shown that biliary PC is mainly derived from preformed
hepatic and extrahepatic pools. From recent work by Portal
et al. [549] it was concluded that in rats, under basal
conditions, choline-labeled HDL-PC contributes 38% of
total biliary PC as compared to 44% from a preformed
hepatic microsomal pool. It should be stressed, however,
that the relatively large contribution of HDL-PC reported
by these authors may reflect an unique feature of hepatic
HDL metabolism: i.e., of the way that HDL surface lipid is
handled by the liver. It has been shown that liposomal
bile-type PC, that enters the endosomal-lysosomal pathway
after uptake by hepatocytes, is extensively degraded and
remodeled and only to a limited extent secreted into the
bile [550]. De novo synthesis, mainly via the CDP-choline
pathway, contributes only to a limited extent to biliary PC:
values in the order of 3-14% have been reported for rats
using [J4C]choline as a precursor [551]. This relatively
small proportion is surprising considering the fact that
bile-salt induced PC secretion was dramatically reduced in
rats when PC synthesis was impaired by feeding choline-
deficient diets, while total hepatic PC content was not
altered by the experimental diets [513]. In this respect,
there seems to be an analogy to VLDL secretion, a process
that is also critically dependent upon the synthesis of PC
[552] and therefore is inhibited by feeding choline-defi-
cient diets to rats [552,553]. It thus seems that specific de
novo synthetized phospholipids, selected on the basis of
their biosynthetic routes, are required for both secretory
processes. Coenzyme labeling with [l,l-2H]ethanol, that
does not discriminate between both synthetic routes for
PC, suggested that liver, bile and plasma are supplied from
a common pool [554]. The high specific activity found in
bile compared to liver found in [14C]choline-labeling stud-
ies, on the other hand, were suggested to indicate that
newly synthetized biliary PC originates from a small hep-
atic pool with high turnover [555] although secretion by a
subset of hepatocytes should also be considered. In this
respect it is of interest to note that HDL particles, newly
synthetized and secreted by the perfused rat liver, were
found to have a PC composition very similar to that of
bile, whereas the PC composition of VLDL exactly mir-
rored that of whole liver [556]. In addition, secretion of
bile-type PC in HDL was stimulated by bile salts, suggest-
ing that PC of bile and HDL originates from the same pool
with both pathways of secretion susceptible to regulation
by bile salts [556].
5.3. Intracellular trafficking of biliary lipids
As can be inferred from the data discussed, the
'anatomical' localization of the putative precursor pool(s)
for biliary lipids within the liver cells has not been defined,
but probably includes components of the plasma mem-
brane, endoplasmic reticulum and Golgi network. Attempts
to identify these pools by extensive subcellular fractiona-
tion of livers during increased phospholipid flux, followed
by comparison of phospholipid composition and choles-
terol/phospholipid content of the fractions with that of
bile, have been unsuccessful [516]. Based on the knowl-
edge of lipid trafficking obtained with non-hepatic cell-
types [557], on studies demonstrating increased numbers of
vesicles in the pericanalicular region during high lipid
secretion [558,559] and on studies employing inhibitors of
intracellular vesicular transport [ 182,186], it has been in-
ferred that biliary lipids derived from (specific) areas of
the endoplasmic reticulum are transported towards the
canaliculus by vesicle movement, as discussed in detail in
a recent review by Coleman and Rahman [5]. The Golgi
apparatus and the trans Golgi network have been suggested
to play an important role in the sorting of the lipids,
analogous to their function in sorting and processing of
proteins. This is mainly based on the observation that it
shows transient localisation of fluorescent lipid precursors
[560] and of bile salts [193]. In 1975 Gregory et ai. [184]
suggested that phospholipid transport, probably together
with cholesterol, is vesicular. In the presence of micro-
tubule poisons phospholipid transport is inhibited by about
40-60%. Complete inhibition has not been reported. In
some studies cholesterol transport seems to be more sus-
ceptible to the inhibitory effect of these compounds than
lecithin [183]. Studies in which the effects of monensin, a
N a+ /K + ionophore interfering with Golgi function, on
lipid secretion were evaluated yielded conflicting results
[561,562], indicating that the role of the Golgi apparatus is
by no means clear at the moment. Nevertheless, in the
general view, endosomal (and Golgi-derived) vesicles are
transferred to the bile canaliculus in a microtubule-depen-
dent, i.e., colchicine and vinblastine-sensitive, fashion. The
nature of the vesicles, e.g., whether they transport bile-de-
stined lipids only or also carry other bile-destined com-
pounds to the canaliculus, whether they are remodelled
during their transport to the canaliculus by the action of
phospholipid transfer proteins and, most importantly, by
what mechanism they are targeted to the canaliculus, re-
mains unclear at the moment and awaits their isolation and
further characterization. Several groups have attempted to
isolate the vesicles involved taking advantage of the fact
that these vesicles should be enriched in phosphatidyl-
choline (PC) of the typical biliary PC type; 16:0, 18:2 and
16:0, 18:1. Graham et al. [563] reported the isolation of
these vesicles. They fractionated cells on gradients and
found biliary type vesicles in a fraction enriched in
canalicular markers. However, others (R. Coleman, per-
sonal communication) have not been able to confirm these
results and further studies are required to characterize the
putative biliary lipid transport vesicles. The question arises
why it is so difficult to isolate these vesicles. There are

250 R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268
two rather obvious reasons. Firstly, it can not be excluded
that they simply do not exist. Secondly, the vesicles may
be so short-lived that during the isolation procedures they
fuse rapidly with intracellular membranes. At high bile salt
fluxes accumulation of vesicles in the pericanalicular re-
gion of the hepatocyte has been observed [564]. It is not
yet clear whether these vesicles do indeed consist of lipids
destined for secretion into bile. Under normal, physio-
logical, conditions it appears to be difficult to visualize
such vesicles.
The vesicular pathway is most probably not the only
pathway mediating lipid secretion. Stein et al. [565] could
not demonstrate the inhibitory effect of microtubule poi-
sons at low rates of lipid secretion. Although these results
have to be confirmed they suggest that alternative path-
ways are operating as well. Recently Cohen et al. [566]
suggested a role for PC transfer protein, which is abun-
dantly present in the hepatocyte [567], in transport of PC
from ER to canalicular membrane. In an in vitro model,
employing the naturally fluorescent PC (i.e., 1-palmitoyl,
2-parinaroyl PC), they demonstrated a rapid transfer of this
phospholipid from small unilamellar vesicles modelling
endoplasmic reticulum to model canalicular membranes
(devoid of PC) which could be induced by submicellar
concentrations of bile salts (BS). Though submicellar,
these concentrations were still at least one order of magni-
tude higher than the estimated intracellular concentration
of bile salts. Furthermore, support for this hypothesis from
in vivo studies is, as yet, still lacking.
Non-vesicular transport to the bile canaliculus by lateral
diffusion has also been considered for delivery of lipids to
the bile canaliculus. In line with the first option, Robins et
al. [542] reported marked kinetic differences when hepatic
newly synthetized cholesterol and preformed cholesterol
were separately labeled and traced into the bile. The
specific activity of preformed cholesterol in the canalicular
membrane was closer to that in bile than in any other
organelle immediately after isotope administration, which
they explained by direct transport of these cholesterol
molecules from the blood through the plasma membrane to
the canaliculus, without entering the interior of the cell.
Although other interpretations of the data are possible, this
is a very intruiging possibility. Lateral diffusion of PC
through the inner leaflet of the plasma membrane may also
supply PC to the canalicular membrane. This could explain
the higher specific activity of canalicular membrane PC
compared to microsomal PC after injection of [3H]PC-
labeled HDL in rats. It could also explain the very marked
increase in canalicular membrane PC specific activity rela-
tive to that of the microsomes when phospolipid secretion
was inhibited by dehydrocholate under the above-men-
tioned conditions [549]. Lateral diffusion of (fluorescently
labeled) phospholipids from the basolateral membrane to
the apical pole, passing the tight junctional barrier via the
inner leaflet of the plasma membrane, has been reported to
occur in cultured polarized MDCK cells [557].
5.4. Regulation of bilia~ lipid secretion: the role of bile
salts
Although, as mentioned earlier, the stimulatory effects
of bile salts on lipid secretion have been known for more
than three decades, the fundamental issues of where and
how these compounds exert their effects still are controver-
sial. Concerning the localization of the bile salt action, the
discussion has been focused on the question whether it is
exerted at the intracellular as opposed to the canalicular
level, or, in other words, whether it is a matter of 'push-
ing' or of 'pulling'. It is evident that the processes of
supply and of actual secretion must occur coordinately to
maintain ongoing secretion, but, as will be discussed in
this section, available evidence strongly indicates that the
quantitative regulation takes place at the level of the bile
canaliculus. With respect to the intracellular bile salt ef-
fects, it has been suggested that intracellular mixed micelle
formation may occur by interaction of bile salts, during
their passage through the hepatocyte, with intracellular
membranes [568]. However, this assumption probably is
incorrect, not in the least because the intracellular bile salt
concentration is far below CMC. A large number of stud-
ies have been devoted to the interactions of bile salts with
the endoplasmic reticulum and the Golgi complex to evalu-
ate the role of these organelles in transcellular bile salt
transport and to provide a background for the intracellular
flow of lipids required to maintain bile salt-induced biliary
lipid secretion. As indicated in Section 5.2, and discussed
in detail by Coleman and Rahman [5], a number of these
studies have provided evidence that, en route from the
sinusoidal to the canalicular membrane, bile salts mobilize
the bile-destined lipids from their intracellular sources for
transport towards the canaliculus. The findings that bile
salt administration leads to (i) an increased abundance and
altered morphology of vesicles in the pericanalicular re-
gion in vivo [558,559], (ii) acceleration of the translocation
of Golgi-derived phospholipid analogues to the peri-
canalicular region in hepatocyte couplets and stimulation
of their biliary secretion in isolated perfused rat liver [560],
and (iii) an increase in vesicular transcytosis of compounds
such as horseradish peroxidase [569] and inulin [570], have
been interpreted to suggest that bile salts are able to direct
vesicular transport towards the bile canaliculus. The in-
volvement of microtubuli in the movement of bile-destined
vesicles was revealed in studies showing impaired lipid
secretion after colchicine or vinblastine treatment, although
the role of microtubuli-dependent (vesicular) transport was
only appreciable under the condition of high bile salt load
[186]. Furthermore, recent studies by Katagiri et al. [571]
demonstrated that colchicine does not inhibit lipid secre-
tion as induced by /3-muricholate and tauroursodeoxy-
cholate, implying that the cholchicine-effect may be spe-
cific for more hydrophobic bile salts, such as taurocholate.
The importance of proper functioning of another part of
the cytoskeleton, i.e., the actin filaments surrounding the

R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268 251
canaliculus, for lipid secretion was suggested by the
demonstration of reduced biliary lipid secretion after phal-
loidin treatment [572]. However, the question how bile
salts actually affect cytoskeleton-dependent vesicular trans-
port has remained unanswered until now. It is clear, on the
other hand, that bile salts are secreted into the bile unac-
companied by lipids: (i) bile salts are secreted in the form
of monomers (see Section 3), (ii) 'kinetic' studies in the
isolated perfused rat liver with very low endogenous bile
salt output showed that the secretion of (radiolabeled)
taurocholate preceeded the induced peak in lipid secretion
by minutes [573], and (iii) it is well known that several
hydrophilic organic anions are able to inhibit biliary lipid
secretion without affecting that of bile salts [574-576].
This latter phenomenon, usually referred to as 'uncou-
pling', has recently been used to provide evidence that,
under physiological conditions, quantitative regulation of
bile salt-induced lipid secretion is exerted at the level of
the canaliculus and not at some site within the hepatocyte.
In these studies, reviewed by Verkade et al. [577], it was
first shown that hydrophilic organic anions, that avidly
interact with biliary bile salts, are unable to uncouple
lipid-from-bile salt secretion in mutant ( G Y / T R - ) rats
[221,244]. These rats lack canalicular ATP-dependent or-
ganic anion transport and therefore show impaired bile
secretion and increased intracellular concentrations of the
uncoupling agents [259,275]. This observation demon-
strates that uncoupling takes place within the canaliculus
and this strongly suggests that the quantitative regulation
of lipid secretion by bile salts is exerted after secretion of
the bile salts across the bile canalicular membrane
[259,275].
As discussed in Section 3, bile salts build up extremely
high concentrations in the canalicular lumen, largely ex-
ceeding their CMC values. These bile salts subsequently
are able to induce the secretion from the canalicular mem-
brane of cholesterol and specific PC as a function of their
concentration and their hydrophobicity. It was recently
demonstrated that the residence time of the bile salts inside
the canaliculus represents an additional parameter in the
quantitative regulation of bile salt mediated lipid secretion
[578]. The specificity of the process at canalicular level is
documented very clearly by the release of bile-specific PC
species from isolated rat liver canalicular membranes in
vitro [579] as well as by retrograde, intrabiliary injection of
taurocholate and taurochenodeoxycholate in rats in vivo
[580]. In these latter studies, the detergent CHAPS induced
the instantaneous release of lipid with a general membrane
profile [580]. It has been suggested that the hydrophilic-hy-
drophobic balance of biliary bile salts, at least in part,
determines the selective composition of bile PC. More
hydrophobic bile salts stimulate the secretion of arachi-
donic-and stearic-rich PC in humans, implying a physical-
chemical mechanism for selective secretion [581-583].
Recent work [584], on the other hand, showed that in rats
selectivity was greatest at unphysiologically low secretion
rates and that selectivity was already partially lost when
PC secretion was in the physiological range. In these
experiments, bile salt hydrophobicity had no acute effects
on the selection of biliary PC species. The results of the
latter studies are in line with the well-known change in
biliary phospholipid composition to a more aspecific pat-
tern that occurs during the course of administration of bile
salts to rats at supraphysiological rates, eventually leading
to cholestasis [585,586]. The occurence of this type of
cholestasis has been explained by inadequate lipid supply
during excessive secretion leading to a depleted, function-
ally impaired, canalicular membrane. Under normal condi-
tions, the canalicular domain is the most rigid domain of
the hepatocytic plasma membrane, relatively enriched in
cholesterol and sphingomyelin. It has been suggested that
the canalicular membrane contains microdomains of higher
fluidity containing the bile-destined lipids, possibly repre-
senting fusion points of the supplying vesicles, that would
allow for a more easy interaction with the bile salts.
Although never demonstrated in canalicular membranes up
to now, such microdomains have been observed in other.
in vitro systems [587]. Bile salts have been shown to
induce the pinching-off of membrane lipids from red blood
cell membranes in the form of vesicles [588]. Accordingly,
it has been suggested that intercalation of bile salts into the
canalicular membrane (microdomains) would cause out-
ward curving and budding of the membrane at this point,
ultimately causing it to be pinched off as a vesicle of
specific, relatively hydrophilic lipid composition. Although
attractive, direct proof for such a mechanism of secretion
has not been provided.
5.5. Regulation of biliar3, lipid secretion: the role of mdr2
P-glycoprotein
Recent studies demonstrate that the process of lipid
secretion in the mouse is critically depending upon the
presence of the canalicular mdr2 P-glycoproteins
[125,672]. This dependency was revealed by the observa-
tion that bile of mice in which the gene encoding this
protein was disrupted by homologous recombination did
not contain measurable amounts of phospholipids in the
presence of normal bile salt output [125]. As phospholipid
secretion was the only function that was completely abol-
ished in the homozygous ( - / - ) mice and also the only
one that was substantially reduced, by 40%, in the het-
erozygous ( + / - ) mice, it is very likely that an inability
to deliver phospholipids to the bile represents the primary
defect in the mdr2 P-glycoprotein knock-out mice. Thus,
not included in any of the proposed mechanisms of biliary
lipid secretion sofar, it turns out that the delivery of PC
from the hepatocytes into the bile requires the active
participation of a canalicular membrane protein, which, of
course, is fully in line with a quantitative regulation of the
process at this level. Apparently, mdr2 P-glycoprotein
activity and canalicular bile salts cooperate functionally in

252 R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268
the lipid secretion process. Cholesterol secretion was re-
duced by about 90% in the ( - / - ) mice but virtually
normal in the heterozygotes, again underscoring the depen-
dency of cholesterol secretion on (a minimal level) of
phospholipid secretion. Bile salt composition in mice is
very hydrophilic ( + 60% muricholate with the remainder
taurocholate). When a more hydrophobic bile salt, tauro-
cholate, was infused into ( - / - ) mice cholesterol secre-
tion could be partly restored [672]. Thus, cholesterol and
phospholipid secretion can be partly uncoupled.
The mechanism of the mdr2 P-glycoprotein action re-
mains speculative at the moment. As discussed by Smit et
al. [125], it may facilitate the entry of (bile-specific)
phospholipids into the membrane, the translocation of
these phospholipids through the membrane as well as their
actual exit into the bile. An attractive model, in view of
recently published work on phospholipid translocation in
rat liver canalicular membranes by Berr et al. [589] as well
as the proposed mode of action of other P-glycoproteins
[590], involves the action of the protein as a 'flippase', i.e.,
translocating bile-specific PC from the inner to the outer
leaflet of the membrane. This process could result in a
local protrusion of PC-enriched buds into the canalicular
lumen that subsequently, under the influence of bile salts,
pinch off to form biliary vesicles. The data of Berr et al.
[589] suggest the presence of a flippase activity in the
canalicular membrane of rat liver with kinetic properties
similar to those of the system identified previously in
microsomes by Bishop and Bell [591]. In these studies the
transport of the water-soluble short chain PC analogue
L-a-dibutyroyl-glycero-3-PC was used as a measure of
flippase activity. Saturable uptake of the radiolabeled com-
pound was observed in microsomes as well as in canalicu-
lar membrane vesicles, with similar K m values but two-fold
higher Vma x values in the ¢analicular membranes compared
to microsomal membranes. This transport was not affected
by taurocholate and ATP-independent, and its relation to
bile-specific (long-chain) PC translocation remains to be
established. How this activity relates to mdr2 P-glyco-
protein, which on the basis of its relationship to other
MDR proteins would be expected to act in an ATP-depen-
dent manner, remains to be established. Very recently,
cytosol ~ canaliculus
~ -- -- - - ~ ~ biliary
~ - - - - " ~ ' ~ vesicles
E ~ m dr 2 ~ bile salt J ~ (rnicelles)
PHOSPHATIDYLCHOLINE CHOLESTEROL
"APICAL OUTER LEAFLET PHOSPHOLIPIDS" ~ "INNER LEAFLET PHOSPHOLIPIDS"
GLYCOSPHINGOLIPIDS PHOSPHATIDYLETHANOLAMINE SPHINGOMYELIN PHOSPHATIDYLSERINE
Fig. 13. Hypothetical model of the mechanism of mdr2 Pgp-mediated lipid secretion. Phosphatidylcboline is mainly supplied to the membrane via
phosphatidylcholine-transfer protein which inserts PC into the inner leaflet, mdr2 Pgp translocates PC to the outer leaflet into PC-rich microdomains and
this ATP-dependent process leads to phospholipid imbalance in the membrane. Luminal bile salt micelles or monomers further destabilize these domains
and this leads (via an unknown mechanism) to the formation and release of vesicular structures. In the absence of PC-rich domains luminal bile salt
micelles are unable to extract phospholipids from the (outer leaflet of the) membrane [125]. This may be caused by a high proportion of
glycosphingolipids, sphingomyelin and cholesterol in the outer leaflet. Luminal bile salts can, however, extract cholesterol directly from the outer leaflet
[672]. This extraction is more efficient when mixed micelles of bile salts and PC are present because these have a higher affinity for cholesterol.

R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268 253
Ruetz and Gros [420] provided experimental data which
support the model of mdr2 Pgp as a primary active
flippase. They transfected the mdr2 gene into the yeast
sec6-4 mutant which has a defect in the secretory appara-
tus. This mutation leads to the accumulation of plasma
membrane proteins in secretory vesicles. After isolation,
these vesicles were used to demonstrate translocation of
fluorescent NBD-PC from the inner to the outer leaflet.
The translocation was strictly ATP-dependent and specific,
based on the observation that vesicles from yeast trans-
fected with the mdrla gene were inactive. Interestingly,
verapamil inhibited this translocation while colchicine and
vinblastine were without effect. Further evidence support-
ing the flippase function of mdr2 Pgp was provided by
Smith et al. [673] who used fibroblasts from transgenic
mice that express MDR3, the human homologue of mdr2
Pgp. After metabolic labeling of intracellular phosphatidyl-
choline with radioactive choline, translocation from the
inner to the outer leaflet was assayed and this was com-
pared with normal mouse fibroblasts which do not express
mdr2. Translocation of radioactive phosphphatidylcholine
to the outer leaflet was measured by the possibility to
exchange with phosphatidylcholine-transfer protein and li-
posomes in the medium. In MDR3 expressing fibroblasts a
more rapid translocation of PC was observed than in
control fibroblasts.
In conclusion, these data suggest that mdr2 Pgp may
indeed be a primary active PC translocator. The passive
flippase described by Berr et al. [589] probably represents
another function. Since it was demonstrated that conven-
tionally purified canalicular membrane fractions contain
significant amounts of intracellular membranes [105] this
flippase activity may also have an intracellular localiza-
tion.
The inclusion of PC-flipping in a model describing the
mechanism of biliary PC secretion assumes that lipid
asymmetry of the canalicular membrane is an important
parameter and clearly imposes restraints on the mechanism
of lipid supply to the membrane. If PC is supplied via
phosphatidylcholine transfer protein to the inner leaflet
there is an obvious role for mdr2 Pgp in the translocation
of PC from the inner to the outer leaflet of the membrane.
If, however, vesicular supply is the major mechanism, a
substantial amount of PC molecules will already be present
in the outer leaflet of the membrane because PC may be
expected to be present in both leaflets of such vesicles. In
that case a substantial amount of PC is already present in
the outer leaflet of the canalicular membrane and therefore
available for bile salt-mediated secretion without the need
for a flippase. By virtue of its primary active transport of
PC, mdr2 Pgp may induce a surplus of phospholipid
molecules in the outer leaflet compared to the inner leaflet
of the canalicular membrane. Such a lipid imbalance can
create localized instable structures in the membrane (mi-
crodomains) and these strucures may be especially vulner-
able to bile salt-mediated extraction. Under the influence
of bile salts these instable structures may pinch off as
vesicles, since it has been observed that lipids in primary
bile exist as vesicles [592] (see Fig. 13Fig. 13). How this
happens is, however, as yet, completely unclear. Perhaps
new emerging rapid-fixation techniques will solve this
urgent problem. Recently, Crawford et al. [593] employing
an ultra-rapid freezing technique have succeeded in visual-
izing vesicular structures attached to the canalicular mem-
brane. Whether these vesicles represent intermediate struc-
tures in the biliary lipid secretion process is not yet clear.
5.6. Functional aspects o( biliar 3, lipid secretion
A number of physiological functions for the biliary
lipids can be discerned, some of them well-recognized and
some appreciated to a lesser extent. Apart from conversion
into bile salts, nature has not provided an enzymic machin-
ery for the breakdown of cholesterol molecules. Therefore,
the biliary pathway represents first and foremost the major
route for the removal of cholesterol from the body and
functions as a crucial factor in the maintenance of choles-
terol homeostasis [594]. Somewhat paradoxically, it ap-
pears that a large part of the secreted molecules are
reabsorbed from the intestine [595], which may, however,
reflect the presence of a control mechanism in cholesterol
metabolism at the intestinal level.
In bile, the presence of cholesterol and phospholipids
may protect the hepatocytes and the cell lining of the bile
ductules from the cytotoxic effects of the (detergent) bile
salts. This function is probably best examplified by the
development of liver disease in the mdr2 P-glycoprotein
knock-out mice produced by Smit et al. [125] which is
mild directly after birth but progresses to severe liver
disease during lifetime and ends with the development of
hepatocellular carcinoma. Liver histology showed degener-
ative features (of hepatocytes) throughout the lobule, irreg-
ular size with nuclear polymorphism, and focal necrosis
with formation of eosinophilic bodies. Upon electronmi-
croscopic examination, a prominent widening and turtuos-
ity of the canaliculi with Loss of microvilli was observed.
In these mice, the bile ducts were affected as well, with
extensive portal expansion owing to ductular proliferation.
This pathology may be the result of prolonged exposure of
apical membranes along the biliary tree to the detergent
action of lipid-free bile salt micelles [596].
Another (potential) function of the biliary lipids may
involve the hepatobiliary transport of certain hydrophobic
organic anions. As shown initially by Tazuma et al.
[597,598], several hydrophobic organic anions show a very
high affinity for the (vesicular) lipid fraction in bile and it
has been suggested that these vesicular structures act as
carriers of these compounds during their transit from the
liver to the intestine. To what extent the presence/absence
of biliary lipids actually affects the transport kinetics of the
organic anions remains to be established.

254 R.P.J. Oude Elferink et aL / Biochimica et Biophysica Acta 1241 (1995) 215-268
Finally, biliary phospholipids play an important role in
the absorption of dietary lipids from the intestine, addi-
tional to the well-established function of bile salts in this
process. Studies by Davidson et al. [599] have provided
evidence for a physiologic role of biliary phospholipids in
the regulation of intestinal apolipoprotein B48 expression,
an apolipoprotein essential for proper assembly and secre-
tion of chylomicrons containing the absorbed dietary fats.
6. Regulation of canalicular transport and its conse-
quence for development of cholestasis
As outlined in the introductory section, the generation
of bile flow critically depends upon (active) transport of a
number of organic solutes from hepatocytes into the
canalicular lumen. Consequently, disturbances of these
transport processes may lead to impairment of bile forma-
tion; i.e., cholestasis.
6.1. Regulation o f transport
Bile flow is not a continuous process. It is subject to
diurnal variations and depends on the delivery of bile salts
and non-bile salt organic anions and cations to the canalic-
ular lumen. For example, in many species, but not in the
rat, the bile salt flux to the liver is greatly enhanced after
gallbladder contraction. The gallbladder contains 60% of
the total bile salt pool. It contracts after each meal and
several times per day during the spontaneous phases of
gastrointestinal motitility. These fluxes in substrate supply
need to be modulated in order to dampen intracellular bile
salt concentration changes. Enhanced secretion at high
concentration and decreased efflux during situations of low
concentration could be of importance here. The liver as
part of the digestive system is under the control of gastro-
intestinal hormones. For example, secretin not only stimu-
lates bicarbonate secretion [600] but also enhances biliru-
bin secretion [601-603]. Gastrointestinal hormones may be
candidates for the fine tuning of the secretory processes in
the liver as part of the digestive process. Against this
background regulation of canalicular transport processes
may be relevant and it is even possible that some forms of
cholestasis may result from a disordered regulation of bile
secretion.
Regulation by recruitment o f transporters f rom intra-
cellular stores
Canalicular cartier proteins that are involved in hepato-
biliary transport are synthesized in the endoplasmic reticu-
lum and are then transported through the Golgi network to
the basolateral membranes of the hepatocyte [604]. From
there they are directed to the canalicular domains by way
of a microtubule-dependent transcytotic pathway [199].
Canalicular transport activity depends on synthesis and
processing of the carder proteins in the ER and Golgi, and
on transport and removal of the carrier proteins to and
from the canalicular membranes. Regulation at the level of
transcription and translation represents long-term regula-
tion. For example, in primary rat hepatocyte cultures, the
sodium-dependent taurocholate cotransporting polypeptide
is down-regulated at the mRNA level [159]. In addition to
this type of regulation, canalicular transport activity can be
decreased during cholestasis by a redistribution of the bile
salt and organic anion transporters from the canalicular
either to intracellular compartments or to the basolateral
domains [605,606]. Whether, and if so to what extent, such
processes actually contribute to the etiology of (certain
forms of) cholestasis remains to be established.
Intracellular storage of transporter proteins represents a
flexible type of regulation, whereby a cell can rapidly
respond to fluctuations of hormones. The existence of this
type of regulation has been extensively described for the
glucose transporter GLUT4. Adipocytes and muscle cells
respond to insulin by recruitment of glucose transporters
from intracellular vesicles to the plasma membrane. In this
way the hormone prepares the cell for increased glucose
transport [607]. Also the hepatic receptor for epithelial
growth factor responds in this way [608]. There are indi-
rect indications that canalicular carrier proteins are also
present in intracellular vesicles [105,609]. For example,
evidence was found for MOAT activity in small intra-
cellular organelles in isolated hepatocytes. This activity
was absent in hepatocytes of TR rat livers [609]. Using
free flow electrophoresis, Kast et al. isolated three subcel-
lular fractions: endoplasmic reticulum with electrogenic,
ATP-independent, taurocholate transport; canalicular mem-
branes with both ATP-dependent taurocholate transport
and ecto-ATPase activity; and an as yet unidentified frac-
tion with ATP-dependent taurocholate transport but devoid
of ecto-ATPase [105]. These results provide circumstantial
evidence for the presence of a pool of subcellular or-
ganelles with canalicular ATP-dependent transport activity.
Apparently these organelles do not simply represent re-
trieved or endocytosed canalicular membranes since they
probably contain a selective repertoire of canalicular mark-
ers and, for example, lack canalicular ecto-ATPase. This
subfraction may represent a reservoir of canalicular bile
salt transporters, waiting for a signal to be inserted into the
canaliculus. This potential intracellular pool of transporters
may be recruited by certain stimuli and this would allow
short-term regulation of canalicular transport. Whether this
is indeed the case needs to be proven. However, it is
evident that hormones and intracellular messengers can
modulate canalicular transport activity. For example,
canalicular and ductular C1- /HCO 3 exchange activity
mediates biliary bicarbonate secretion. The canalicular ac-
tivity can be stimulated by cyclic-AMP [99]. This increase
can be blocked by colchicine. The colchicine effect sug-
gests that a C1 / H C O 3 exchanger is targeted from a
pre-formed pool of exchanger proteins to the canalicular
domain via a microtubule-dependent pathway.
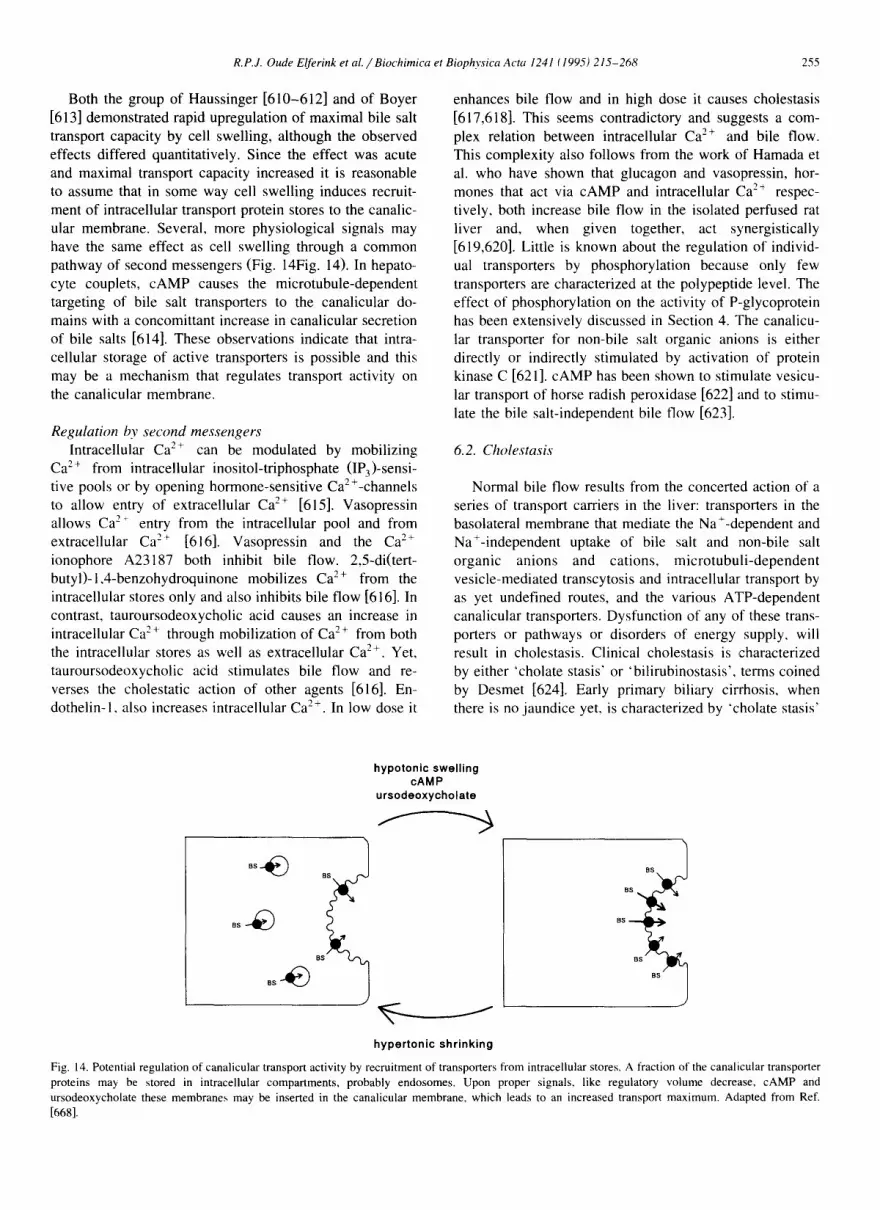
R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268 255
Both the group of Haussinger [610-612] and of Boyer
[613] demonstrated rapid upregulation of maximal bile salt
transport capacity by cell swelling, although the observed
effects differed quantitatively. Since the effect was acute
and maximal transport capacity increased it is reasonable
to assume that in some way cell swelling induces recruit-
ment of intracellular transport protein stores to the canalic-
ular membrane. Several, more physiological signals may
have the same effect as cell swelling through a common
pathway of second messengers (Fig. 14Fig. 14). In hepato-
cyte couplets, cAMP causes the microtubule-dependent
targeting of bile salt transporters to the canalicular do-
mains with a concomittant increase in canalicular secretion
of bile salts [614]. These observations indicate that intra-
cellular storage of active transporters is possible and this
may be a mechanism that regulates transport activity on
the canalicular membrane.
Regu la t ion by s e c o n d m e s s e n g e r s
Intracellular Ca 2+ can be modulated by mobilizing
Ca 2+ from intracellular inositol-triphosphate (IP3)-sensi-
tive pools or by opening hormone-sensitive Ca2+-channels
to allow entry of extracellular Ca 2+ [615]. Vasopressin
allows Ca-'" entry from the intracellular pool and from
extracellular Ca z~ [616]. Vasopressin and the Ca 2+
ionophore A23187 both inhibit bile flow. 2,5-di(tert-
butyl)-l,4-benzohydroquinone mobilizes C a 2+ from the
intracellu[ar stores only and also inhibits bile flow [616]. In
contrast, tauroursodeoxycholic acid causes an increase in
intracellular Ca 2 ~ through mobilization of Ca 2 + from both
the intracellular stores as well as extracellular Ca 2+. Yet,
tauroursodeoxycholic acid stimulates bile flow and re.-
verses the cho[estatic action of other agents [616]. En-
dothelin-1, also increases intracellular Ca 2+. In low dose it
enhances bile flow and in high dose it causes cholestasis
[617,618]. This seems contradictory and suggests a com-
plex relation between intracellular Ca 2+ and bile flow.
This complexity also follows from the work of Hamada et
al. who have shown that glucagon and vasopressin, hor-
mones that act via cAMP and intracellular Ca 2÷ respec-
tively, both increase bile flow in the isolated perfused rat
liver and, when given together, act synergistically
[619,620]. Little is known about the regulation of individ-
ual transporters by phosphorylation because only few
transporters are characterized at the polypeptide level. The
effect of phosphorylation on the activity of P-glycoprotein
has been extensively discussed in Section 4. The canalicu-
lar transporter for non-bile salt organic anions is either
directly or indirectly stimulated by activation of protein
kinase C [621]. cAMP has been shown to stimulate vesicu-
lar transport of horse radish peroxidase [622] and to stimu-
late the bile salt-independent bile flow [623].
6.2. Choles tas i s
Normal bile flow results from the concerted action of a
series of transport carriers in the liver: transporters in the
basolateral membrane that mediate the Na%dependent and
Na+-independent uptake of bile salt and non-bile salt
organic anions and cations, microtubuli-dependent
vesicle-mediated transcytosis and intracellular transport by
as yet undefined routes, and the various ATP-dependent
canalicular transporters. Dysfunction of any of these trans-
porters or pathways or disorders of energy supply, will
result in cholestasis. Clinical cholestasis is characterized
by either 'cholate stasis' or 'bilirubinostasis', terms coined
by Desmet [624]. Early primary bi[iary cirrhosis, when
there is no jaundice yet, is characterized by "cholate stasis'
hypotonic swelling cAMP
ursodeoxycholate
0 BS
BS
hypertonic shrinking
Fig. 14. Potential regulation of canalicular transport activity by recruitment of transporters from intracellular stores. A traction of the canalicular transporter proteins may be stored in intracellular compartments, probably endosomes. Upon proper signals, like regulatory volume decrease, cAMP and ursodeoxycholate these membranes may be inserted in the canalicular membrane, which leads to an increased transport maximum. Adapted from Ref. [668].

256 R.P.J. Oude Elferink et al./Biochimica et Biophysica Acta 1241 (1995) 215-268
Table 2 Cholestatic drugs and agents
Cholestatic agent Animal Reference
Taurocholate rat [656] Taurolithocholate rat,hamster [657,658] Glycolithocholate-3 a-O-sulfate rat [659.660] Lithocholate-3 ot-O-glucuronide rat [661] Ethinylestradiol rat [636,662] Estradiol- 17B-glucuronide rat [641 ] Chlorpromazine rat [663] Cyclosporin rat [664,665] Manganese-bilirubin rat [643,666] a-Naphthylisothiocyanate rat,mouse [645] Phalloidin rat [629]
with elevated serum bile salt levels and increased alkaline
phosphatase. Byler's disease may be the best example of
'cholate stasis' marked by high serum bile salt levels and
only very mild jaundice. Examples of 'bilirubinostasis' are
leptospirosis, with greatly elevated serum bilirubin levels
caused by a combination of decreased biliary secretion and
increased supply because of hemolysis, Dubin-Johnson and
Rotor syndromes with elevated serum levels of conjugated
bilirubin and normal alkaline phosphatase activity and
normal bile salt levels. Most cases of cholestasis are
mixtures of 'cholate stasis' and 'bilirubinostasis'.
Experimental models of cholestasis include drug-induced
cholestasis
Table 2 gives an overview of various drugs and chemi-
cals that cause cholestasis in animals. Major actions of
some of these agents include: a decrease of N a + / K +
ATPase activity and an increase of membrane viscosity of
predominantly the sinusoidal membrane [625]; an increase
of tight-junctional permeability [626]; an increase of intra-
cellular calcium [627]; changes of the microcirculation
[628]; effects on the cytoskeleton with irreversible poly-
merization of microfilaments, which has consequences for
both transcellular transport as well as junctional permeabil-
ity [629]. Apart from reduced transport activities cholesta-
sis can be induced or aggravated by the disappearance of
the canalicular contractions. These contractions are Ca 2 +-
dependent and agents that block Ca 2+ release from IP 3-
sensitive stores, also inhibit canalicular contractions, cGMP
generated by nitric oxide is such an agent [614]. Canalicu-
lar contractions represent a major propulsive force for the
bile flow. The pathophysiological importance of these
contractions is not well understood but one could imagine
a sort of canalicular 'ileus', similar to intestinal ileus, in
their absence. Phalloidin-induced cholestasis is most prob-
ably caused by its irreversible polymerisation of actin into
microfilaments [629].
Chronic administration of cyclosporin A reduces the
hepatic excretory function in man and causes cholestasis in
the rat [630,631]. Cyclosporin is an important immuno-
suppressive drug, used e.g., after organ transplantation. It
is metabolized and secreted by the liver. Cyclosporin A
inhibits ATP-dependent uptake of bile salts, leukotriene
C 4, and daunomycin in human and rat liver canalicular
membrane vesicles [632,633]. In addition, the drug inhibits
Na+-dependent taurocholate uptake in sinusoidal mem-
brane vesicles [634]. Also in cultured rat hepatocytes,
cyclosporin reduces both taurocholate uptake and effiux
[635]. However, ATP-dependent canalicular transport of
bile salts shows the most potent inhibition suggesting that
inhibition of biliary bile salt secretion is the main cause of
cyclosporin-induced cholestasis [632,633].
Ethinyl estradiol is also a cholestatic agent which in the
rat reduces bile flow [636]. In isolated rat hepatocytes it
reduces the uptake of taurocholate [637]. Further proof that
ethinyl estradiol causes alterations in the sinusoidal mem-
brane and in sinusoidal membrane function came from
Berr et al. and Rosario et al. [625,638]. They showed that
the drug decreases Na+-K + ATPase activity and tauro-
cholate uptake in isolated rat hepatocytes and that alter-
ations of sinusoidal membrane fluidity may play a role.
Bossard et al. confirmed this effect by showing a reduction
of taurocholate uptake in sinusoidal membrane vesicles but
they also showed that the most dramatic change is a
decrease of ATP-dependent canalicular bile salt transport,
as measured in canalicular rat liver membrane vesicles
[605]. In addition the ATP-dependent transport of the
glutathione-conjugate, GS-DNP, in canalicular membranes
from ethinyl estradiol-treated rats is reduced [605]. As was
seen with cyclosporin, ethinyl estradiol-induced cholestasis
mainly results from an inhibition of the main concentrative
step in hepatobiliary secretion, the ATP-dependent canalic-
utar secretion of bile salts.
Estradiol- 17/3(/3-D-glucuronide) causes a reversible type
of cholestasis by inhibiting the hepatobiliary secretion of
taurocholate and non-bile salt organic anions [639,640].
This steroid inhibits the biliary excretion not the hepatic
uptake of taurocholate [639]. In addition, it increases the
tight-junctional permeability [626]. Estradiol-3/3(/3-D-
glucuronide) and estriol-3/3(/3-o-glucuronide) are not
cholestatic [641]. Estriol 17/3(/3-D-glucuronide), estriol-
16a( /3-D-glucuronide) and testosterone-17/3(/3-D-
glucuronide) show intermediate cholestatic potency [642].
Infusion of manganese together with bilirubin induces
cholestasis probably by precipitation of manganese-biliru-
bin in the biliary tree [643,644]. Similarly, c~-naphthyli-
sothiocyanate (ANIT) [645] causes severe necrosis of bil-
iary epithelial cells which leads to obstruction of the
biliary tree and subsequent cholestasis. In addition it in-
creases tight junction permeability.
Expression and localization of transporters during extra-
hepatic cholestasis
Bile duct ligation, as an experimental model for extra-
hepatic cholestasis, leads to dramatic changes in the ex-
pression and domain-specific localization of plasma mem-

R.P.Z Oude Elferink et al. /Biochimica et Biophysica Acta 1241 (1995) 215-268 257
brane proteins. In general it appears to induce a shift of
canalicular membrane proteins from their specific apical to
a basolateral or random localization. This was shown in
several immunocytochemical studies using antibodies
against canalicular antigens [646,647], but also by means
of functional studies [606]. It was also shown that transcy-
tosis, both fluid phase and receptor-mediated, is abrogated
during complete cholestasis [199,647,648] and impaired
during reduced bile flow [649]. Several mechanisms may
be proposed for the altered localization of canalicular
membrane proteins. Firstly, the impaired transcytosis can
be due to a compromised fusion process of transcytotic
vesicles with the canalicular membrane. This may also
hold for the fusion of vesicles containing de novo synthe-
sized canalicular membrane proteins. Indeed, accumulation
of canalicular antigens in pericanalicular vesicles was ob-
served during bile duct ligation [647] very similar to what
was demonstrated for the transcytotic marker, polymeric
IgA [199]. If fusion of such vesicles with the basolateral
plasma membrane is not impaired this will lead to a net
redistribution of proteins. It was shown that after release of
the bile duct ligation the pericanalicular vesicles rapidly
disappear, probably by fusion with the canalicular mem-
brane [647]. Secondly, canalicular membrane proteins may
be retro-endocytosed during bile duct obstruction and redi-
rected to the basolateral domain. Thirdly, the increase in
paracellular permeability that was reported to occur during
bile duct ligation [647] indicates that the barrier function of
the tight junction is drastically decreased. This may lead to
lateral redistribution of canalicular proteins over the entire
plasma membrane including the basolateral domain.
Bile duct ligation also affects the expression of trans-
port proteins. In a preliminary report Gartung et al. [650]
showed that it leads to down-regulation of the basolateral
Na+-dependent bile salt co-transporter. Similarly, Kothe et
al. [651] found a strong decrease in the activity of the
canalicular organic anion transporter as well as a complete
abrogation of the canalicular GSH secretion. The latter
may, however, be due to increased gamma-glutamyltrans-
peptidase activity. Reconstruction of bile flow led to a
slow recovery of cMOAT activity, which may reflect the
rate of synthesis of this transporter.
7. Perspectives
In the past decades a vast amount of research has been
invested by many groups in unraveling the mechanisms of
hepatobiliary transport. Although this taught us much about
the physiology of several transport processes, this work
had not led to the unequivocal assignment of transport
functions to specific membrane proteins. In the past few
years, however, this situation is dramatically changing and
several candidate proteins have now been cloned which
play a function in uptake of organic compounds by the
liver. The introduction of molecular biology and more
specifically that of expression cloning has caused a break-
through in this deadlock situation. It may be expected that
in the near future many more transporters, including those
of the canaliculus, will be recognized. This represents an
important advance in hepatology because the use of cDNA
probes will allow the analysis of expression of these
transporters under different physiological and pathological
conditions. This opens possibilities to analyse the molecu-
lar mechanism of action of these transporters and the
definition of the multiplicity of transport proteins involved
in the secretion of very diverse compounds. Only then one
can start to explain the different conditions of intrahepatic
cholestasis that are presently not understood. The exact
molecular description of transport mechanisms will also be
of importance to pharmacology; it will give a clue to the
diverse forms of drug-induced liver disease, and it will
eventually also open the way to a rational design of drugs
that are specifically delivered to parenchymal and non-
parenchymal cells, to hepatocellular carcinomas and to
cells of the biliary tree. It may be that eventually a
similarly impressive collection of gene products for trans-
port will be known as now already exists for drug
metabolism.
Because of the high ultrastructural complexity of the
liver as an organ it will always remain essential to study
hepatobiliary transport processes in the intact organ and
animal. Unfortunately, until now no model system has
been developed that can properly mimick biliary transport.
The canaliculus is unique in its membrane composition
and localization in the cell and in the organ. Even the
hepatocyte couplet that partially retains its polarity and is
generally seen as an attractive model system, has no free
flowing primary bile. It may therefore under many condi-
tions share more properties with a cholestatic hepatocyte
than with a normal hepatocyte. The need for intact animals
is well exemplified by the discovery of the function of
mdr2 P-glycoprotein. Although this protein and its gene
were well characterized it has taken many years before a
(putative) function in phospholipid secretion could be pro-
posed; no other model system than the intact liver exists in
which bile salt mediated phospholipid secretion can be
studied. It was therefore not until a transgenic knockout
animal was available that the involvement of mdr2 P-
glycoprotein in this complex process could be observed.
Mutant and transgenic animals will therefore remain in-
valuable for studies into hepatobiliary transport.
The complexity of the hepatocyte also explains why cell
biology of the hepatocyte as an epithelial cell lags behind
that of other epithelia like enterocytes and proximal tubule
cells. Relatively little is known about the exact biosyn-
thetic routing of canalicular (transport) proteins, let alone
about its possible defects. Nevertheless, the use of polariz-
ing hepatocyte cell lines will open a new, exciting area of
research.

258 R.P.Z Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268
Acknowledgements
The authors acknowledge the support from the EEC
program BIOMED I, project #BMHI-CT93-1436; 'Design
and development of therapeutic and diagnostic agents for
the treatment of diseases of the liver and biliary tract'.
References
[1] Klaassen, C.D. and Watkins III, J.B. (1984) Pharmacol. Rev. 36,
1-67.
[2] Arias, I.M., Che, M.X., Gatmaitan, Z., Leveille, C., Nishida, T. and
Stpierre, M. (1993)Hepatology 17, 318-329.
[3] Boyer, J.L., Graf, J. and Meier, P.J. (1992) Annu. Rev. Physiol. 54,
415-438.
[4] Nathanson, M.H. and Boyer, J.L. (1991) Hepatology 14, 551-566.
[5] Coleman, R. and Rahman, K. (1992) Biochim. Biophys. Acta 1125,
113-133.
[6] Coleman, R. (1987) Biochem. J. 244, 249-261.
[7] Erlinger, S. (1987) in Physiology of the Gastrointestinal Tract
(Johnson, L.R., ed.), pp. 1557-1580, Raven Press, New York.
[8] Anwer, M.S., Berk, P.D., Suchy, F.J. and Wolkoff, A.W. (1992)
Hepatology 15, 1179-1193.
[9] Crawford, J.M., Strahs, D.C.J., Crawford, A.R. and Barnes, S.
(1994) J. Lipid Res. 35, 1738-1748.
[10] Petzinger, E. (1994) Rev. Physiol. Biochem. Pharmacol. 123, 47-
211.
[11] Tiribelli, C. (1992) J. Hepatol. 14, 385-390.
[12] Kuipers, F., Dijkstra, T., Havinga, R., Van Asselt, W. and Vonk,
R.J. (1985) Biochem. Pharmacol. 34, 1731 - 1736.
[13] Kuipers, F., Havinga, R., Bossenieter, H., Toorop, G.P., Hindriks,
F.R. and Vonk, R.J. (1985) Gastroenterology 88, 403-411.
[14] Remie, R., Rensema, J.W. and Kuipers, F. (1991) in Biliary
Excretion of Drugs and Other Chemicals (Siegers, C.P. and
Watkins, J.B., eds.), pp. 127-145, G. Fisher Verlag, Stuttgart.
[15] Mulder, G.J., Scholtens, E. and Meijer, D.K.F. (1981) in Methods
in Enzymology, Vol. 77 (Jakoby, W.B., ed.), pp. 21-30, Academic
Press, New York.
[16] Accatino, L., Hono, J., Koenig, C., Pizarro, M. and Rodriguez, L.
(1993) J. Hepatol. 19, 95-104.
[17] Meijer, D,K.F., Weitering, J.G. and Vermeer, G.A. (1983) Eur. J.
Clin. Pharmacol. 24, 549-556.
[18] Herman, R.H., Redinger, R.N. and Small, D.M. (1971) Surgery
Forum 22, 378-380.
[19] Askin, J.R., Lyon, D.I., Shull, S.D., Wagner, C.I. and Soloway,
R.D. (1978) Gastroenterology 74, 560-565.
[20] Dujovne, C.A., Gustafson, J.H. and Dickey, R.A. (1982) Clin.
Pharmacol. Ther. 31, 187-194.
[21] Vonk, R.J., Kneepkens, C.M.F., Havinga, R., Kuipers, F. and
Bijleveld, C.M.A. (1986) J. Lipid. Res. 27, 901-904.
[22] Bijleveld, C.M.A., Vonk, R.J., Kuipers, F., Havinga, R., Boverhof,
R., Koopman, B.J., Wolthers, B.G. and Fernandes, J. (1989)
Gastroenterology 97, 427-432.
[23] van der Meer, R., Welberg, J.W.M., Kuipers, F., Kleibeuker, J.H.,
Mulder, N.H., Termont, D.S.M.L., Vonk, R.J., De Vries, H.T. and
De Vries, E.G.E. (1990) Gastroenterology 99, 1653-1659.
[24] Angelin, B., Arvidsson, A., Dahlqvist, R., Hedman, A. and
Schenk-Gustafsson, K. (1987) Eur. J. Clin. Invest. 17, 262-265.
[25] Hedman, A., Angelin, B., Arvidsson, A., Beck, O., Dahlqvist, R.,
Nilsson, B., Olsson, M. and Schenck-Gustafsson, K. (1991) Clin.
Pharmacol. Ther. 49, 256-262.
[26] Hedman, A., Angelin, B., Arvidsson, A., Dahlqvist, R. and Nils-
son, B. (1990) Clin. Pharmacol. Ther. 47, 20-26.
[27] Meijer, D.K.F. and Nijssen, H.M.J. (1991) in Perfused Liver:
Clinical and Basic Applications (Ballet, F. and Thurman, R.G.,
eds.), pp. 165-208, John Libbey, London.
[28] Nijssen, H.M.J., Pijning, T., Meijer, D.K.F. and Groothuis, G.M.M.
(1992) Hepatology 15, 302-309.
[29] Meijer, D.K.F., Keulemans, K. and Mulder, G.J. (1981) Methods
Enzymol. 77, 81-94.
[30] Reichen, J. (1991) in Research in Perfused Liver (Ballet, F. and
Thurman, R.G., eds.), pp. 149-163, John Libbey, London.
[31] Pang, K.S., Goresky, C.A. and Schwab, A.J. (1991) in Research in
Perfused Liver (Ballet, F. and Thurman, R.G., eds.), pp. 259-302,
John Libbey, London.
[32] Meijer, D.K.F., Vonk, R.J., Keulemans, K. and Weitering, J.G.
(1977) J. Pharmacol. Exp. Ther. 202, 8-21.
[33] Proost, J.H., Nijssen, H.M.J.. Strating, C.B., Meijer, D.K.F. and
Groothuis, G.M.M. (1993)J. Pharmacokinet. Biopharm. 21, 375-
394.
[34] Groothuis, G.M.M., Hardonk, M.J., Keulemans, K.T.P., Nieuwen-
huis, P. and Meijer, D.K.F. (1982) Am. J. Physiol. 243. G455-
G462.
[35] Groothuis, G.M.M., Hardonk, M.J. and Meijer, D.K.F. (1985)
Trends Pharmacol. Sci. 6, 322-327.
[36] Groothuis, G.M.M. and Meijer, D.K.F. (1992) Enzyme 46, 94-138.
[37] Pang, K.S., Lee, W.F., Cherry, W.F., Yuen, V., Accaputo, J.,
Schab, A.J. and Goresky, C.A. (1988) J. Pharmacokinet. Biopharm.
16, 595-632.
[38] Nijssen, H.MJ., Pijning, T., Meijer, D.K.F. and Groothuis, G.MM.
(1991 ) Biochem. Pharmacol. 42, 1997-2002.
[39] Blom, A., Scaf, A.H.J. and Meijer, D.K.F. (1982) Biochem. Phar-
macol. 31, 1553-1565.
[40] Goreski, C.A., Ziegler, W.H. and Bach, G.G. (1970) Circ. Res. 27,
739-764.
[41] Mischinger, HJ., Walsh, T.R., Liu, T., Rao, P.N., Rubin, R..
Nakamura, K., Todo, S. and Starzl, T.E. (1992) J. Surg. Res. 53,
158-165.
[42] Riedel, G.L., Scholle, J.L. and Shepherd, A.P. (1983) Am. J.
Physiol. 245, 769-774.
[43] Palmen, N.G.M., Evelo, C.T.A., Borm, PJ.A. and Henderson, P.T.
(1992) Toxicol. In Vitro 6, 357-365.
[44] Pang, K.S. (1919) in Drug Metabolism and Drug Toxicity (Mitchell,
J.R. and Homing, M.G., eds.), pp. 331-352, Raven Press. New
York.
[45] Ullrich, V. and Diehl, H. (1971) Eur. J. Biochem. 20, 509-512.
[46] Evans, A.M., Hussein, Z. and Rowland, M. (1993) J. Pharm. Sci.
82, 421-428. [47] Pang, K.S., Cherry, W.F., Accaputo, J., Schwab, A. and Goresky,
C.A. (1988)J. Pharmacol. Exp. Ther. 247, 690-700.
[48] Reichen, J. (1988) J. Clin. Invest. 81, 1462-1469.
[49] Berry, M.N. and Friend, D.S. (1969)J. Cell. Biol. 43. 506-520.
[50] Krumdieck, C.L., Dos Santon, J.E. and Ho, K.J. (1980) Anal.
Biochem. 104, 118-123.
[51] Connors, S., Ramlin, D., Gandolfi, A.J., Krumdieck, C.L., Koep,
L.J. and Brendel, K. (1990) Toxicology 61, 171-183.
[52] Dogterom. P. and Rothuizen, J. (1993) Drug. Metab. Dispos. 21,
705-709.
[53] Smith, P.F., Krack, G. and McKee, R.L. (1986) Biol. Cell. 22,
706-712.
[54] Saadker, G.W., Slooff, MJH. and Groothuis, G.MM. (1992)
Biochern. Pharmacol. 43, 1479-1485.
[55] Sandker, G.W., Weert, B., Olinga, P., Wolters, H., Slooff, MJ.H.,
Meijer, D.K.F. and Groothuis, G.M.M. (1994) Biochem. Pharma-
col. accepted,
[56] Brendel, K., Gandolfi, A.J., Krumdieck, C.L. and Smith, P.F.
(1987) Science 8, 11-15.

R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268 259
[57] Powis, G. (1989) Drug Metab. Rev. 20, 379-394.
[58] Thompson, M.B., Davis, D.G. and Morris, R.W. (1993) J. Lipid.
Res. 34, 553-561.
[59] Olinga, P., Merema, M.T., Meijer, D.K.F., Slooff, MJ.H. and
Groothuis, G.M.M. (1993) ATLA-Altern. Lab. Anim. 21,466-468.
[60] Schwenk, M. (1980) Arch, Toxicol. 44, 113-126.
[61] Berry, M.N., Halls, H.J. and Grivell, M.B. (1992) Life, Sci. 51,
1-16. [62] Miyanchi, S., Sawada, Y., Iga, T., Hanano, M. and Sugiyama, Y.
(1993) Pharm. Res. 10, 434-440.
[63] Klaassen, C.D. and Watkins, LB.,Ill (1984) Pharmacol. Rev. 36,
1-67.
[64] Berry, M.N., Edwards, A.M. and Berritt, G.J. (1991) in Isolated
Hepatocytes Preparation, Properties and Applications (Burdon R.H.,
ed.), pp. 182-184, Elsevier, Amsterdam.
[65] Wolkoff, A.W., Samuelson, A.C., Johansen, K.L., Nakata, R.,
Withers, D.M. and Sosiak, A. (1987) J. Clin. Invest. 79, 1259-1268.
[66] Groothuis, G.M.M., Hulstaert, C.E., Kalicharan, D. and Hardonk,
M.J. (1981) Eur. J. Cell. Biol. 26, 43-51.
[67] Gebhardt, R. (1986) in Research in Isolated and Cultured Hepato-
cytes (Guillouzo, A. and Guguen-Guillouzo, C., eds.), pp. 353-376,
John Libbey Eurotext Ltd./INSERM,
[68] Oude Elferink, R.P.J., Ottenhoff, R., Liefting, W.G.M., Schoen-
maker, B., Groen, A.K. and Jansen, P.L.M. (1990) Am. J. Physiol.
258, G699-G706.
[69] Tarao, K., Clinger, E.J., Ostrow, D. and Balistreri, W.F. (1982)
Am. J. Physiol. 243, G253-G258.
[70] Kwekkeboom, J., Princen, H.M.G., Van Voorthuizen, E.M., Mei-
jer, P. and Kempen, H.J.M. (1989) Biochem. Biophys. Res. Com-
mun. 162, 619-625.
[71] Petzinger, E. and Frimmer, M. (1988) Biochim. Biophys. Acta 937,
135-144.
[72] Liang, D., Hagenbuch, B., Stieger, B. and Meijer, P.J. (1993)
Hepatology 18, 1163-1166.
[73] F~511mann, W., Petzinger, E. and Kinne, R.K.H. (1990) Am..1.
Physiol. 258, C700-C712.
[74] Foliot, A.. Glaise, D., Erlinger, S. and Guguen-Guillonzo, C.
(1985) Hepatology 5, 215-219.
[75] Galivan, J. (1982) Arch. Biochem. Biophys. 214, 850-852.
[76] Chesn6, C., Guyomard, C., Grislain, L., Clerc, C., Fautrel, A. and
Guillouzo, A. (1991) Toxicol. In Vitro 5, 479-482.
[77] Quistorff, B. and Grunnet, N. (1985) Biochem. J. 229, 221-226.
[78] Lindros, K.O. and Penttil~i, K.E. (1985) Biochem. J. 228, 757-760.
[79] Braakman, I., Keij, J., Hardonk, M.J., Meijer, D.K.F. and Groothuis,
G.M.M. (1991) Hepatology 13, 73-82.
[80] Buscher, H.P., Fricker, G., Gerok, W,, Kurz, G., Miiller, M.,
Schneider, S., Schramm, U. and Schreyer, A. (1987) in Bile Acids
and the Liver (Paumgartner, G., Stiehl, A. and Gerok, W., eds.),
pp. 95-110, MTP Press, Lancaster, England.
[81] Rogiers, V. (1992) in Human Cells in In Vitro Pharmaco-toxicol-
ogy (Rogiers, V., Sonck, W., Shephard, E. and Vercruysse, A.,
eds.), pp. 77-115, VUB Press. Brussels.
[82] Sandker, G.W., Vos, R.M.E., Delbressine, L.P.C., Slooff, M.J.H.,
Meijer, D.K.F. and Groothuis, G.M.M. (1994) Xenobiotica 24.
143-155.
[83] Azer, S.A. and Stacey, NH. (1993) Biochem. Pharmacol. 46,
813-819.
[84] Day, J.F., Thorpe, S.R. and Baynes, J.W. (1979) J. Biol. Chem.
254, 595-597.
[85] Chalmers, D.K., Scholz, G.H., Topliss, D.J., Kolliniatis, E., Munro,
S.L.A., Craik, D.J., Iskander, M.N. and Stockigt, J.R. (1993) J.
Med. Chem. 36, 1272-1277.
[86] Ihrke, G., Neufeld, E.B., Meads, T., Shanks, M.R., Cassio, D.,
Laurent, M., Schroer, T.A., Pagano, R.E. and Hubbard, A.L.
(1993) J. Cell Biol. 123, 1761-1775.
[87] Petzinger, E., Follmann, W., Blumrich, M., Walther, P., Hentschel,
J., Bette, P., Maurice, M. and Feldmann, G. (1994) Eur. J. Cell.
Biol. 64, 328-338. [88] Blumrich, M., Zeyenblumrich, U., Pagels, P. and Petzinger, E.
(1994) Eur. J. Cell. Biol. 64, 339-347.
[89] Bayer, J.L., Philips, J.M. and Graf, J. (1990) Methods Enzymol.
192, 501-516.
[90] Wilton, J.C., Williams, D.E., Strain, A.J., Parslow, R.A., Chipman,
J.K. and Coleman, R. (1991) Hepatology 14, 180-183.
[91] Verkade, H.J., Zaal, K.J., Derksen, J.T., Vonk, R.J., Hoekstra, D.,
Kuipers, F. and ScherphoL G.L. (1992)Biochem. J. 284, 259-265.
[92] Fentem, J.H., Foster, B., Mills, C.O., Coleman, R. and Chipman,
J.K. (1990) Toxicol. In Vitro 4, 452-457.
[93] Nathanson, M.H. and Burgstahler, A.D. (1992) Cell. Calcium. 13,
89-98.
[94] GraL J. and Boyer, J.L. (1990) J. Hepatol. 10, 387-394.
[95] Watanabe, N., Tsukada, N., Smith, C.R. and Phillips, M.J. (1991)
J. Cell. Biol. 113, 1069-1080.
[96] Watanabe, N., Tsukada, N., Smith, C.R., Edwards, V. and Phillips,
M.J. (1991) Lab. Invest. 65, 203-213.
[97] Thibault, N., Claude, J.R. and Ballet, F. (1992) Toxicology 73,
269-279.
[98] Wilton, J.C., Chipman, J.K., Lawson, C.J., Strain, A.J. and Cole-
man, R. (1993) Biochem. J. 292, 773-779.
[99] Benedetti, A., Strazzabosco, M., Ng, O.C. and Boyer, J.L. (1994)
Proc. Natl. Acad. Sci. USA 91,792-796.
[100] Bruck, R., Nathanson, M.H., Roelofsen, H. and Boyer, J.L. (1994)
Hepatology 20, 1032-1040.
[101] Blitzer, B.L. and Donovan, C.B. (1984) J. Biol. Chem. 259,
9295-9301. [102] Meier, P.J., Meier-Abt, A.S., Barrett, C. and Boyer. ,I.L. (1984) J.
Biol. Chem. 259, 10614-10622.
[103] Hardikar, W. and Suchy, F.J. (1993) Hepatology 18, 1278-1279.
[104] Meier, P.J., Sztul, E.S., Reuben, A. and Boyer, J.L. (1984) J. Cell.
Biol. 98, 991-1000.
[105] Kast, C., Stieger, B., Winterhalter, K.H. and Meier, P.J. (1994)J.
Biol. Chem. 269, 5179-5186.
[106] Adachi, Y., Kobayashi, H., Kurumi, Y., Shouji, M., Kitano, M. and
Yamamoto, T. (1991) Hepatology 14, 655-659.
[107] Novak, D.A., Ryckman, F.C. and Suchy, F.J. (1989) Hepatology
10, 447-453.
[108] Wolters, H., Kuipers, F., Slooff, M.J.H. and Vonk, R.J. (1992) J.
Clin. Invest. 90, 2321-2326.
[109] Wolters, H., Spiering, M., Gerding, A., Slooff, M.JH., Kuipers, F.,
Hardonk, M.J. and Vonk, R.J. (1991) Biochirn. Biophys. Acta
1069, 61-69.
[110] lnoue, M., Kinne, R., Tran, T. and Arias, I.M. (1982) Hepatology
2, 572-579.
[111] Bear, C.E., Davison, J.S. and Shaffer, E.A. (1987) Biochim. Bio-
phys. Acta 903, 388-394.
[112] Wolkoff, A.W. and Chung. C.T. (1980) J. Clin. ]Invest. 65, 1152-
1169.
[113] Stremmel, W., Gerber, M.A., Glezerov, V., Thung, S.N., Kochwa,
S. and Berk, P.D. (1983) J. Clin. Invest. 71, 1796-1805.
[114] yon Dippe, P., Ananthanarayanan, M. and Levy, D. (1986) Biochim.
Biophys. Acta 862, 352-360.
[115] Buscher, H.-P., Fricker, G., Gerok, W., Kramer, W., Kurz, G.,
Miiller, M. and Schneider, S. (1986) in Receptor-Mediated Uptake
in the Liver (Greten, H., Windier, E. and Beisiegel, U., eds.), pp.
189-199, Springer Verlag, Berlin Heidelberg.
[116] Ruetz, S., Fricker, G., Hugentobler, G., Winterhalter, K., Kurz, G.
and Meier, P.J. (1987) J. Biol. Chem. 262, 11324-11330.
[117] Soreq, H. and Seidman, S. (1992) Methods Enzymol. 207,225-231.
[118] Mori, M., Izumi, T. and Shimizu, T. (1993) Biochim. Biophys.
Acta 1168, 23-29.
[119] Shneider, B.L. and Moyer, M.S. (1993) J. Biol. Chem. 268,
6985-6988.

260 R.P.J. Oude Elferink et a l . / Biochimica et Biophysica Acta 1241 (1995) 215-268
[120] Hortensteiner, S., Vogt, E., Hagenbuch, B., Meier, P.J., Amrhein,
N. and Martinoia, E. (1993) J. Biol. Chem. 268, 18446-18449.
[121] Martinoia, E., Grill, E., Tommasini, R., Kreuz, K. and Amrhein, N.
(1993) Nature 364, 247-249.
[122] Molenaar, D., Bolhuis, H., Abee, T., Poolman, B. and Konings,
W.N. (1992)J. Bacteriol. 174, 3118-3124.
[123] Boyer, J.L., Ng, O.C., Ananthanarayanan, M., Hofmann, A.F.,
Schteingart, C.D., Hagenbuch, B., Stieger, B. and Meier, P.J.
(1994) Am, J. Physiol. 266, G382-G387.
[124] Kitamura, T., Jansen, P.L.M., Hardenbrook, C., Kamimoto, Y.,
Gatmaitan, Z. and Arias, I.M. (1990) Proc. Natl. Acad. Sci. USA
87, 3557-3561.
[125] Smit, J.J.M., Schinkel, A.H., Oude Elferink, R.P.J., Groen, A.K.,
Wagenaar, E., Van Deemter, L., Mol, C.A.A.M., Ottenhoft, R.,
Van der Lugt, N.M.T., van Roon, M.A., Van der Valk, M.A.,
Offerhaus, G.J.A., Berns, A.J.M. and Borst, P. (1993) Cell 75,
451-462.
[126] Capecchi, M.R. (1994) Scientific American March, 34-41.
[127] Schinkel, A.H., Smit, J.J.M., Vantellingen, O., Beijnen, J.H., Wa-
genaar, E., Vandeemter, L., Mol, C.A.A.M., Vandervalk, M.A.,
Robanusmaandag, E.C., Teriele, H.P.J., Berns, A.J.M. and Borst,
P. (1994) Cell 77, 491-502.
[128] Hammerton, R.W., Krzeminski, K.A., Mays, R.W., Ryan, T.A.,
Wollner, D.A. and Nelson, W.J. (1991) Science 254, 847-850.
[129] Anwer, M.S. and Hegner, D. (1978) Hoppe-Seyler. 's. Z. Physiol.
Chem. 359, 181-192.
[130] Meier, P.J. (1989) J, Hepatol. 9, 124-129.
[131] Zimmerli, B., Valantinas, J. and Meier, P.J. (1989) J. Pharmacol.
Exp. Ther. 250, 301-308.
[132] Petzinger, E., Muller, N., Follmann, W., Dentscher, J. and Kinne,
R.K.H. (1989) Am. J. Physiol. 256, G78-G86.
[133] Anwer, M.S., O'Maille, E.RL., Hofmann, A.F., DiPietro, R.A. and
Michelotti, E. (1985) Am. J. Physiol. 249, G479-G488.
[134] Hardison, W.G.M., Bellentani, S., Heasley, V. and Sbelhamer, D.
(1984) Am. J. Physiol. 246, G477-G483.
[135] Bellentani, S., Hardison, W.G.M., Marchegiano, P., Zanasi, G. and
Manenti, F. (1987) Am. J. Physiol. 252, G339-G344.
[136] Stacey, N. and Koteckex, B. (1988) Gastroenterology 95,780-786.
[137] Scharschmidt, B.F. and Stephens, J.E. (1981) Proc. Natl. Acad. Sci.
USA 78, 986-990.
[138] Meier, P.J., Meier-Abt A, S.T., Barrett, C. and Boyer, J.L. (1984)
J. Biol. Chem. 259, 10614-10622.
[139] Weinman, S., Graf, J. and Boyer, J.L. (1989) Am. J. Physiol. 256,
G826-G832.
[140] Nunez, L., Amigo, L., Rigotti, A., Puglielli, L., Mingrone, G.,
Greco, A.V. and Nervi, F. (1993) FEBS Lett. 329, 84-88.
[141] Reference deleted.
[142] Lidofsky, S.D., Fitz, J.G., Weisiger, R.A. and Scharschmidt, B.F.
(1993) Am. J. Physiol. 264, G478-G485.
[143] Weinman, S.A. and Weeks, R.P. (1993) Am. J. Physiol. 265,
G73-G80.
[144] Wehner, F. (1993) Pflugers. Arch-Eur. J. Physiol. 424, 145-151.
[145] Kramer, W., Bickel, U., Buscher, H.P., Gerok, W. and Kurz, G.
(1982) Eur. J. Biochem. 129, 13-24.
[146] Von Dippe, P. and Levy, D. (1983) J. Biol. Chem. 258, 8896-8901.
[147] Wieland, T., Nassal, M., Kramer, W., Fricker, G., Bickel, U. and
Kurz, G. (1984) Proc. Natl. Acad. Sci. USA 81, 5232-5236.
[148] Ananthanarayanan, M., Von Dippe, P. and Levy, D. (1988) J. Biol.
Chem. 263, 8338-8343.
[149] Von Dippe, P. and Levy, D. (1990) J. Biol. Chem. 265, 14812-
14816.
[150] Von Dippe, P., Amoui, M., Alves, C. and Levy, D. (1993) Am. J.
Physiol. 264, G528-G534.
[151] Porter, T.D., Beck, T.W. and Kasper, C.B. (1986) Arch. Biochem.
Biophys. 248, 121-129,
[152] Hagenbuch, B., Lubbert, H., Stieger, B. and Meier, P.J. (1990) J.
Biol. Chem. 265, 5357-5360,
[153] Hagenbuch, B,, Stieger, B., Foguet, M., Lubbert, H. and Meier,
P.J. (1991) Proc. Natl. Acad. Sci. USA 88, 10629-10633.
[154] Reichen, J. and Berk, P.D. (1979) Biochem. Biophys. Res. Com-
mun. 91,484-489.
[155] Honscha, W., Schulz, K., Muller, D. and Petzinger, E. (1993) Ear.
J. Pharmacol. Mol. Pharmacol. 246, 227-232.
[156] Hagenbuch, B. and Meier, P.J. (1994) J. Clin. Invest. 93, 1326-
1331.
[157] Boyer, J.L., Hagenbuch, B., Ananthanarayanan, M., Suchy, F.,
Stieger, B. and Meier, P.J. (1993) Proc. Natl. Acad. Sci. USA 90,
435-438.
[158] Ananthanarayanan, M., Bucuvalas, J.C., Shneider, L., Sippel, C.J.
and Suchy, F.J, (1991) Am. J. Physiol. 261, G810-G817.
[159] Liang, D., Hagenbuch, B., Stieger, B. and Meier, P.J. (1993)
Hepatology 18, 1162-1166.
[160] Hsu, S.M., Waldron, J.W., Hsu, P.L. and Hough, A.J. (1993) Hum.
Pathol. 24, 1040-1057.
[161] Yamazaki, M., Suzuki, H., Hanano, M., Tokui, T., Komai, T. and
Sugiyama, Y. (1993) Am. J. Physiol. 264, G36-G44.
[162] Hinchman, C.A., Truong, A.T. and Ballatori, N. (1993) Am. J.
Physiol. 265, G547-G554.
[163] Baldini, G., Passamonti, S., Lunazzi, G.C., Tiribelli, C. and Sotto-
casa, G.L. (1986) Biochim. Biophys. Acta 856, 1-10.
[164] Persico, M. and Sottocasa, G.L. (1987) Biochim. Biophys. Acta
930, 129-134.
[165] Stremmel, W. and Berk, P.D. (1986) J. Clin. Invest. 78, 822-826.
[166] Stremmel, W. and Diede, H.E. (1990) J. Hepatol. 10, 99-104.
[167] WolkofL A.W.. Sosiak, A., Greenblatt, H.C., Van Renswoude, J.
and Stockert, R.J. (1985) J. Clin. Invest. 76, 454-459.
[168] Goeser, T., Nakata, R., Braly, L.F., Sosiak, A., Campbell, C.G.,
Dermietzel, R., Novikoff, P.M., Stockert, R.J., Burk, R.D. and
Wolkoff, A.W. (1990) J. Clin. Invest. 86, 220-227.
[169] Min, A.D.. Goeser, T., Liu, R., Campbell, C.G., Novikoff, P.M.
and Wolkoff, A.W. (1991) Hepatology 14, 1217-1223.
[170] Wolkoff, A.W., Samuelson, A,C., Johansen, K.L., Nakata, R.,
Withers, D.M. and Sosiak, A. (1987) J. Clin. Invest. 79, 1259-1268.
[171] Wolkoff, A.W. (1989) in Hepatic transport of organic substances
(Petzinger, E., Kinne, R.K.H. and Sies, H., eds.), pp. 221-232,
Springer Verlag, Berlin.
[172] Min, A.D., Johansen, K.L., Campbell, C.G. and Wolkoff, A.W,
(1991) J. Clin. Invest. 87, 1496-1502.
[173] Campbell, C.G., Spray, D.C. and Wolkoff, A.W. (1993) J. Biol.
Chem. 268. 15399-15404.
[174] Sottocasa, G.L., Baldini, G., Sandi, G., Lunazzi, G. and Tribelli, C.
(1982) Biochim. Biophys. Acta 685, 123-128.
[175] Marchegiano, P., Carubbi, F., Tiribelli, C., Amarri, S., Stebel, M.,
Lunazzi, G.C., Levy, D. and Bellentani, S. (1992) Biochem. Bio-
phys. Res. Commun. 183, 1203-1208.
[176] Torres, A.M., Lunazzi, G.C., Stremmel, W. and Tiribelli, C. (1993)
Proc. Natl. Acad. Sci. USA 90, 8136-8139.
[177] Jacquemin, E., Hagenbuch, B., Stieger, B., Wolkofl-; A.W. and
Meier, P.J. (1991) J. Clin. Invest. 88, 2146-2149.
[178] Jacquemin, E., Hagenbnch, B., Stieger, B., Wolkoff, A.W. and
Meier, P.J. (1994) Proc. Natl. Acad. Sci. USA 91, 133-137.
[179] Meijer, D.K.F. (1989) in Handbook of Physiology Section 6, vol
III (pp. 717-758,
[180] Stolz, A., Takikawa, H., Ookhtens, M. and Kaplowitz, N. (1989)
Annu. Rev. Physiol. 51, 161-176.
[181] Zucker, S.D., Storch, J., Zeidel, M.L. and Gollan, J.L. (1992)
Biochemistry. 31, 3184-3192.
[182] Barnwell, S.G., Lowe, P.J. and Coleman, R. (1984) Biochem. J.
220, 723-731.
[183] Rao, C.V. and Mehendale, H.M. (1991) Biochem. Pharmacol. 42,
2323-2332.
[184] Gregory, D.H., Vlahcevic, Z.R., Prugh, M.F. and Swell, L. (1978)
Gastroenterology 74, 93-100.

R.P.J. Oude Elferink et a l . / Biochimica et Biophysica Acta 1241 (1995) 215-268 261
[185] Crawford, J.M. and Gollan, J.L. (1988) Am. J. Physiol. 255,
GI21-GI31.
[186] Crawford, J.M., Berken, C.A. and Gollan, J.L. (1988) J. Lipid Res.
29, 144-156.
[187] Nakai, T., Katagiri, K., Hoshino, M., Hayakawa, T, and Ohiwa, T.
(1992) Biochem. J. 288, 613-617.
[188] Crawford, J.M., Crawford, A.R. and Strahs, D.CJ. (1993) Hepatol-
ogy 18, 903-911.
[189] Crawford, J.M. and Gollan, J.L. (1991) Hepatology 14, 192-197.
[190] Crawford, J. and Gollan, J.L. (1988) Am. J. Physiol. 255, GI21-
GI31,
[191] Mori, M., Oyamada, M., Sakauchi, F. and Ogawa, K. (1987)
Virchows. Arch. 53, 37-43.
[192] Dumont, M,, Dhont, C., Durandschneider, A.M., Legranddefretin,
V., Feldmann, G. and Erlinger, S. (1991) Hepatology 14, 10-15.
[193] Lamri, Y., Roda, A., Dumont, M., Feldmann, G. and Erlinger, S.
(1988) J. Clin. Invest. 82, 1173-1182.
[194] Lamri, Y., Erlinger, S., Dumont, M., Roda, A. and Feldmann, G.
(1992) Liver 12, 351-354.
[195] Aoyama, N., Ohya, T., Chandler, K., Gresky, S. and Holzbach.
R.T. (1991)Hepatology 14, I-9.
[196] Aoyama, N., Tokumo, H., Ohya, T., Chandler, K. and Holzbach,
R.T. (1991) Am. J. Physiol. 261, G305-G311.
[197] Melby, E.L,, Prydz, K., Olsnes, S. and Sandvig, K. (1991) J. Cell
Biochem. 47, 251-260.
[198] Oude Elferink. R.P.J., Bakker, C.T.M,, Roelofsen, H., Middelkoop,
E., Ottenhoff, R.. Heijn, M. and Jansen, P.L.M. (1993) Hepatology
17, 434-444.
[199] Barr, V.A. and Hubbard, A.L. (1993) Gastroenterology 105, 554-
571.
[200] Scott, L.J. and Hubbard, A.L. (1993) J. Biol. Chem. 268, 19160.
[201] Weisz, O.A., Machamer, C.E. and Hubbard. A.L, (1992) J. Biol.
Chem. 267, 22282-22288.
[202] Schell, M.J., Maurice, M., Stieger, B. and Hubbard, A.L. (1992) J.
Cell Biol. 119, 1173-1182.
[203] Bortles, J.R., Feracci, H.M., Stieger, B. and Hubbard, A.L. (1987)
J. Biol. Chem. 105, 1241-1251.
[204] de Vries. M.H., Groothuis, G.M.M., Mulder, G.J., Nguyen, H. and
Meijer, D.K.F. (1985) Biochem. Pharmacol. 34, 2129-2135.
[205] Proost, J.H., Nijssen, H.MJ.. Strating, C.B., Meijer, D.K.F. and
Groothuis. G.MM. (1993)J. Pharmacokinet. Biopharm. 21, 375-
394.
[206] Mizuma, T., Komori, M., Ueno, M. and Horikoshi, I. (1991) J.
Pharm. Pharmacol. 43, 446-448.
[207] Lauterburg, B.H., Adams, J.D. and Mitchell, J.R. (1984) Hepatol-
ogy 4, 586-590.
[208] Deleve, L.D. and Kaplowitz, N. (1991) Pharmacol. Ther. 52,
287-305.
[209] Ookhtens, M., Lyon, L, Fernandez-Checa, J. and Kaplowitz, N.
(1988) J. Clin. Invest. 82, 608-616.
[210] Garciaruiz, C., Fernandezcheca, J.C. and Kaplowitz, N, (1992) J.
Biol. Chem. 267, 22256-22264.
[211] Aw, T.Y., Ookhtens. M., Kuhlenkamp, J.F. and Kaplowitz, N.
(1987) Biochem. Biophys. Res. Commun. 143, 377-382.
[212] Fernandez-Checa, J.C., Ren, C., Yee aw, T., Ookhtens, M. and
Kaplowitz, N. (1988) Am. J. Physiol. 255, g403-g408.
[213] Fernandez-Checa, J.C., Yi, J.R., Garciaruiz, C., Knezic, Z., Tahara,
S.M. and Kaplowitz, N, (1993) J. Biol. Chem. 268, 2324-2328.
[214] Meier. P.J., Meier-Abt A, S.T. and Boyer, J.L. (1987) Biochem. J.
242, 465-469.
[215] Inoue, M., Akerboom, T.P.M., Sies, H., Kinne, R., Thao, T. and
Arias, I.M. (1984) J. Biol. Chem. 259, 4998-5002.
[216] Akerboom, T., lnoue, M., Sies, H., Kinne, R. and Arias, I.M.
(19831Eur. J. Biochem. 141,211-215.
[217] Scharschmidt, B.F. and Schmid, R. (1978) J. Clin. Invest. 62,
1121-1131.
[218] Zimniak, P. and Awasthi, Y.C. (1993) Hepatology 17, 330-339.
[219] Larkin, J.M. (1993) Gastroenterology 105, 594-597.
[220] Inoue, M., Kinne, R., Tran, T. and Arias, I.M. (1983) Eur. J.
Biochem. 134, 467-471.
[221] Jansen, P.L.M., Peters. W.H. and Lamers, W.H. (1985) Hepatology
5, 573-579.
[222] Dubin, I.N. and Johnson, F.B. (1954)Medicine 33, 155-197.
[223] Sprintz, H. and Nelson, R.S. (1954) Ann. Intern. Med. 41,952-960.
[224] Arias, I.M. (1961) Am. J. Med. 31, 510-518.
[225] Javitt, N.B., Kondo, T. and Kuchiba, K. (1978) Gastroenterology
75, 931-932.
[226] Cornelius, C.E., Arias, I.M. and Osburn, B.I (1965) J. Am. Vet.
Med. Ass. 146, 709-713.
[227] Alpert, S., Mosher, M., Shanske, A. and Arias. I.M. (1969) J. Gen.
Physiol. 53, 238-247.
[228] Jansen, P.L.M., Vanklinken, J.W., Vangelder, M., Ottenhoff, R.
and Oude Elferink, R.PJ. (1993) Am. J. Physiol. 265, G445-G452.
[229] Jansen, P.L.M., Groothuis, G.MM., Peters. W,HM. and Meijer,
D.K.F. (1987) Hepatology 7, 71-76.
[230] Jansen, P,L.M. and Oude Elferink, R.P.J. (1993) in Hepatic Trans-
port and Bile Secretion: Physiology and Pathophysiology (Tavoloni,
N. and Berk, P.D., eds.), pp. 721-731, Raven Press, New York.
[231] Ruetz, S., Hugentobler, G. and Meier, P.J. (1988) Proc. Natl. Acad.
Sci. USA 85, 6147-6151.
[232] Muller, M., Ishikawa, T., Berger, U., Klunemann, C., Lucka, L.,
Schreyer, A., Kannicht, C., Reutter, W., Kurz, G. and Keppler, D.
(1991) J. Biol. Chem. 266, 18920-18926.
[233] Nishida, T., Gatmaitan, Z., Che, M.X. and Arias, I.M. (1991) Proc.
Natl. Acad. Sci. USA 88, 6590-6594.
[234] Stieger, B., Oneill, B. and Meier, P.J. (1992) Biochem. J. 284,
67-74.
[235] Becker, A., Lucka, L., Kiliam C., Kannicht, C. and Reutter, W.
(1993) Eur. J. Biochem. 214, 539-548.
[236] Lin. S.H. and Guidotti, G. (1989) J. Biol. Chem. 264, 14408-14414.
[237] Bartles, J.R.. Braiterman, L.T. and Hubbard, A.L. (1985) J. Biol.
Chem. 260, 12792-12802.
[238] Culic, O,, Huang, Q.H., Flanagan, D., Hixson. D. and Lin, S.H.
(1992) Biochem. J. 285, 47-53.
[239] Petell, J.K., Diamond, M., Hong, W., Bujanover, Y., Amarri, S.,
Pittschieler, K. and Doyle, D. (1987) J. Biol. Chem. 262, 14753-
14765.
[240] Sippel, C.J., Suchy, FJ., Ananthanarayanan, M. and Perlmutter,
D.H. (1993)J. Biol. Chem. 268, 2083-2091.
[241] Sippel, C.J., Mccollum. M.J. and Perlmutter, D.tt. (1994)J. Biol.
Chem. 269. 2820-2826.
[242] Sippel, CJ., Fallon, R.J. and Perlmutter, D.H. (1994) J. Biol.
Chem. 269, 19539-19545.
[243] Abraham, E.H., Prat, A.G.. Gerweck, L., Seneverame, T., Arceci,
R.J., Kramer, R., Guidotti, G. and Cantiello, H.F. (1993) Proc.
Natl. Acad. Sci. USA 90, 312-316.
[244] Kuipers, F., Enserink, M., Havinga, R., Van de, r Steen, A.B.M.,
Hardonk, M.J., Fevery, J. and Vonk, R.J. (1988) J. Clin. Invest. 81,
1593-1599.
[245] Takikawa, H., Sano, N., Narita, T., Uchida, Y., Yamanaka, M.,
Horie, T., Mikami, T. and Tagaya, O. (1991~ Hepatology 14,
352-360.
[246] Oude Elferink, R.P.J., Ottenhoff, R., Radominska, A., Hofmann,
A.F., Kuipers, F. and Jansen, P,L.M. (1991) Biochem. J. 274,
281-286.
[247] Nishida, T., Hardenbrook, C., Gatmaitan, Z. and Arias, I.M. (1992)
Am. J. Physiol. 262. G629-G635.
[248] Huber, M., Guhlmann, A., Jansen, P.L.M. and Keppler, D. (1987)
Hepatology 7, 224-228.
[249] Oude Elferink, R.P.J., Haan de, J., Lambert, K., Hofmann, A.F.
and Jansen, P.L.M. (1987) Hepatology 7, 1109.
[250] Oude Elferink, R.PJ., Ottenhoff, R., Liefting, W., De haan. J. and
Jansen, P.L.M. (1989) J. Clin. Invest. 84, 476-483.
[251] Oude Elferink, R.P.J., Ottenhoff, R., Liefting, W., Schoemaker, B.,

262 R,P.Z Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268
Groen, A.K. and Jansen, P.L.M. (1990) Am. J. Physiol. 258,
G699-G706.
[252] Kitamura, T., Alroy, J., Gatmaitan, Z., Inoue, M., Mikami, T.,
Jansen, P.L.M. and Arias, I.M. (1992) Hepatology 15, 1154-1159.
[253] Ishikawa, T., Muller, M., Klunemann, C., Schaub, T. and Keppler,
D. (1990) J. Biol. Chem. 265, 19279-19286.
[254] Nishida, T., Gatmaitan, Z., Roychowdhry, J. and Arias, I.M. (1992)
J. Clin. Invest. 90, 2130-2135.
[255] Kobayashi, K., Sogame, Y., Hayashi, K., Nicotera, P. and Orre-
nius, S. (1988) FEBS Lett. 240, 55-58.
[256] Akerboom, T.P.M., Narayanaswami, V., Kunst, M. and Sies, H.
(1991) J. Biol. Chem. 266, 13147-13152.
[257] Kobayashi, K., Komatsu, S., Nishi, T., Hara, H. and Hayashi, K.
(1991) Biochem. Biophys. Rese. Commun. 176, 622-626.
[258] Kobayashi, K., Sogame, Y., Hara, H. and Hayashi, K. (1990) J.
Biol. Chem. 265, 7737-7741.
[259] Verkade, H.J., Havinga, R., Gerding, A., Vonk, R.J. and Kuipers,
F. (1993) Am. J. Physiol. 264, G462-G469.
[260] Adachi, Y., Kobayashi, H., Kurumi, Y., Shouji, M., Kitano, M. and
Yamamoto, T. (1991) Hepatology 14, 1251-1258.
[261] Adachi, Y., Kobayashi, H., Shouji, M., Kitano, M., Okuyama, Y.
and Yamamoto, T. (1993) Life. Sci. 52, 777-784.
[262] Nicotera, P., Moore, M., Bellomo, G., Mirabelli, F. and Orrenius,
S. (1985) J. Biol. Chem. 260, 1999-2002.
[263] Nicotera, P., Moore, M., Bellomo, G., Mirabelli, F. and Orrenius,
S. (1985) FEBS Lett. 187, 121-125.
[264] Zimniak, P., Ziller, S.A, Panfil, I., Radominska, A., Wolters, H.,
Kuipers, F., Sharma, R., Saxena, M., Moslen, M.T., Vore, M..
Vonk, R., Awasthi, Y.C. and Lester, R. (1992) Arch. Biochem.
Biophys. 292, 534-538.
[265] Sharma, R., Gupta, S., Singh, S.V., Medh, R.D., Ahmad, H.,
Labelle, E.F. and Awasthi, Y.C. (1990) Biochem. Biophys. Res.
Commun. 171, 155-161.
[266] Pikula, S., Hayden, J.B., Awasthi, S., Awasthi, Y.C. and Zimniak,
P. (1994) J. Biol. Chem. 269, 27566-27573.
[267] Pikula, S., Hayden, J.B., Awasthi, S., Awasthi, Y.C. and Zimniak,
P. (1994) J. Biol. Chem. 269, 27574-27579.
[268] Roelofsen, H., Ottenhoff, R., Oude Elferink, R.P.J. and Jansen,
P.L.M. (1991) Biochem. J. 278, 637-641.
[269] Okuda, H., Tavoloni, N., Blaschke, T.F., Kiang, C.L., Jones,
M.JT., Waggoner, J.G., Sardana, M.K., Sassa, S., Shrager, R.I. and
Berk, P.D. (1991) Hepatology 14, 1153-1160.
[270] Kuipers, F., Radominska, A., Zimniak, P., Little, J.M., Havinga,
R., Vonk, R.J. and Lester, R. (1989) J. Lipid Res. 30, 1835-1845.
[271] Maudgal, D.P., Maxwell, J.D., Lees, L.J. and Wild, R.N. (1982)
Br. J. Clin. Pharrnacol. 14, 213-217.
[272] Arvidsson, A., Leijd, B., Nord, C.E. and Angelin, B. (1988) Eur. J.
Clin. Invest. 18, 261-266.
[273] Xia, Y., Lambert, K. and Hofmann, A.F. (1988) Gastroenterology
94, A606.
[274] Oude Elferink, R.P.J. (1989) in Bile Duct and Bile Duct Abnormal-
ities (Tytgat, G.N.J. and Huibregtse, K., eds.), pp. 9-14, Thieme
Verlag, New York.
[275] Verkade, H.J., Wolbers, M.J., Havinga, R., Uges, D.R., Vonk, R.J.
and Kuipers, F. (1990) Gastroenterology 99, 1485-1492.
[276] Levine, W.G. (1978)Ann. Rev. Pharmacol. Toxicol. 18, 81-96.
[277] Bergan, T. (1987) Drugs 34, 89-104.
[278] Akerboom, T.P.M. and Sies, H. (1989) Methods Enzymol. 173,
523-535.
[279] Akerboom, T.P.M., Bilzer, M. and Sies, H. (1982) FEBS Lett. 140,
73-76.
[280] Silva, J.M., Mcgirr, L. and Obrien, P.J. (1991) Arch. Biochem.
Biophys. 289, 313-318.
[281] Gilbert, H.F. (1982) J. Biol. Chem. 2, 12086-12091.
[282] Chance, B., Sies, H. and Boveris, A. (1979) Physiol. Rev. 59,
527-605.
[283] Smith, P.F., Alberts, D.W. and Rush, G.F. (1987) Toxicol. Appl.
Pharmacol. 89, 190-201.
[284] Chung, P.M, Cappel, R.E. and Gilbert, H.F. (1991) Arch. Biochem.
Biphys. 288, 48-53.
[285] Stein, A.F., Gregus, Z. and Klaassen, C.D. (1988) Toxicol. Appl.
Pharmacol. 93, 351-359.
[286] Ballatori, N. and Truong, A.T. (1989) Am. J. Physiol. 256, G22-
G30.
[287] Ballatori, N. and Truong, A.T. (1992) Am. J. Physiol. 263, G617-
G624.
[288] Ballatoil, N., Jacob, R. and Boyer, J.L. (1986) J. Biol. Chem. 261,
7860-7865.
[289] Fernandezcheca, J.C., Takikawa, H., Horie, T., Ookhtens, M. and
Kaplowitz, N. (1992) J. Biol. Chem. 267, 1667-1673.
[290] Ballatori, N. and Dutczak, W.J. (1994)J. Biol. Chem. 269, 19731- 19737.
[291] Yi, J.R., Lu, S.L., Fernandezcheca, J. and Kaplowitz, N. (1994)J.
Clin. Invest. 93, 1841-1845.
[292] Fernandezcheca, J.C., Ookhtens, M. and Kaplowitz, N. (1993) J.
Biol. Chem. 268, 10836-10841.
[293] Ballatori, N. (1991)Drug Metab. Rev. 23, 83-132,
[294] Alexander, J. and Aaseth, J. (1980) Biochem. Pharmacol. 29, 2129-2133.
[295] Houwen, R., Dijkstra, M., Kuipers, F., Smit, E., Havinga, R. and
Vonk, R.J. (1990) Biochem. Pharmacol. 39, 1039-1044.
[296] Dijkstra, M., Kuipers, F., Havinga, R., Smit, E.P. and Vonk, R.J.
(1990) Pediatr. Res. 28, 339-343.
[297] Gross, J.B., Myers, B.., Kost, L.., Kuntz, S.. and La Russo, N.
(1989) J. Clin. Invest. 83, 30-39.
[298] Kressner, M.S., Stockert, R.J., Morell, A.G. and Sternlieb, I.
(1984) Hepatology 4, 867-870.
[299] Moil, M., Hattori, A., Sawaki, M., Tsuzuki, N., Sawada, N.,
Oyamada, M., Sugawara, N. and Enomoto, K. (1994) Am. J. Pathol. 144, 200-204.
[300] Suzuki, M. and Aoki, T. (1994) Pediatr. Res. 35, 598-601.
[301] Muramatsu, Y., Yamada, T., Miura, M., Sakai, T., Suzuki, Y.,
Serikawa, T., Tanzi, R.E. and Matsumoto, K. (1994)Gastroenterol-
ogy 107, 1189-1192.
[302] Alexander, J., Aaseth, J. and Refsvik, T. (1981) Acta Pharmacol.
Toxicol, 49, 190-194.
[303] Ballatori, N. and Clarkson, T.W. (1982) Science 216, 61-62.
[304] Ballatori, N. and Clarkson, T.W. (1983) Am. J. Physiol. 244, G435-G441.
[305] Ballatori, N. and Clarkson, T.W. (1984) Biochem. Pharmacol. 33,
1087-1092.
[306] Dutczak, W.J. and Ballatori, N. (1994) J. Biol. Chem. 269, 9746- 9751.
[307] Alexander, J., Aaseth, J. and Mikalsen, A. (1986) Acta Pharmacol.
Toxicol. 59, 486-489.
[308] Gregus, Z. and Varga, F. (1985) Acta Pharmacol. Toxicol. 56,
398-403.
[309] Klaassen, C.D. (1974) Toxicol. Appl. Pharmacol. 29, 447-457.
[310] Gyurasics, A., Varga, F. and Gregus, Z. (1991) Biochem. Pharma-
col. 42, 465-468.
[311] Gyurasics, A., Varga, F. and Gregus, Z. (1991) Biochem. Pharma- col. 41,937-944.
[312] Anundi, I., Hogberg, J. and Vahter, M. (1982) FEBS Lett. 145, 285-288.
[313] Delnomdedieu, M., Basti, M.M., Otvos, J.D. and Thomas, D.J.
(1994) Chem. Biol Interact. 90, 139-155,
[314] Gyurasics, A., Koszorus, L., Varga, F. and Gregus, Z. (1992)
Biochem. Pharrnacol. 44, 1275-1281.
[315] Srivastava, S.K. and Beutler, E. (1969) J. Biol. Chem. 244, 9-16. [316] Board, P.G. (1981) FEBS Lett. 124, 163-165.
[317] Prchal, J., Srivastava, S.K. and Beutler, E. (1975) Blood 46, 111-117.
R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268 263
[318] Kondo, T., Murao, M. and Taniguchi, N. (1982) Eur. J. Biochem.
125, 551-554.
[319] Kondo, T., Kawakami, Y., Taniguchi, N. and Beutler, E. (1987)
Proc. Natl. Acad. Sci. USA 84, 7373-7377.
[320] Heijn, M., Oude Elferink, R.P.J. and Jansen, P.L.M. (1992) Am. J.
Physiol. 262, C104-C110.
[321] Board, P., Nishida, T., Gatmaitan, Z., Che, M.X. and Arias, I.M.
(1992) Hepatology 15, 722-725.
[322] Kondo, T., Miyamoto, K., Gasa, S., Taniguchi, N. and Kawakami,
Y. (1989) Biochem. Biophys. Res. Commun. 162, 1-8.
[323] Awasthi, S., Singhal, S.S., Srivastava, S.K, Zimniak, P., Bajpai.
K.K., Saxena, M., Sharma, R., Ziller, S.A., Frenkel, E.P., Singh,
S.V., He, N.G. and Awasthi, Y.C. (1994) J. Clin. Invest. 93,
958-965.
[324] Ishikawa, T., Zimmer, M. and Sies, H. (1986) FEBS Lett. 200,
128-132.
[325] Ishikawa, T. and Sies, H. (1984) J. Biol. Chem. 259, 3838-3843.
[326] Ishikawa, T. (1989) J. Biol. Chem. 264, 17343-17348.
[327] Schaub, T., lshikawa, T. and Keppler, D. (1991) FEBS Lett. 279,
83-86.
[328] Jedlitschky, G., Leier, 1., Buchholz, U., Center, M. and Keppler, D.
(1994) Cancer Res. 54, 4833-4836.
[329] Muller, M., Meijer, C., Zaman, G.J.R., Borst, P,, Scheper, R.J.,
Mulder, N.H., De Vries, E.G.E. and Jansen, P.L.M. (1994) Proc.
Natl. Acad. Sci. USA 91, 13033-13037
[330] Zaman, G.JR., Versantw)ort, C.HM., Smit, J.JM., Eijdems,
E.WHM., de Haas, M., Smith, A.J., Broxterman, H.J., Mulder,
N.H., De Vries, E.GE., Baas. F. and Borst, P. (1993) Cancer Res.
53. 1747-1750.
[331] Oude Elferink, R.P.J., Bakker, C.T.M. and Jansen, P.L.M. (1993)
Biochem. J. 290, 759-764.
[332] de Vries, M.H., Redegeld, F.A.M., Koster, A.S., Noordhoek, J., de
Haan, J.G., Oude Elferink, R.P.J. and Jansen, P.L.M. (1989)
Naunyn-Schmied. Arch. Pharmacol. 340, 588-592.
[333] Meijer, D.K.F. and Groothuis, G.M.M. (1991) in Oxford Textbook
of Clinical Hepatology, Volume 1 (Mclntyre, N., Benhamou, J.P.,
Bircher, J.. Rizzetto, M. and Rodes, J., eds.), pp. 40-78, Oxford
University Press, Oxford, New York, Tokyo.
[334] Meijer. D.K.F. (1989) in Handbook of Physiology, Sect. 6, Vol. III
(Schuhz, S.G., Forte, J.G. and Rauner, B.B., eds.), pp. 717-758.
Oxford University Press, New York.
[335] Meijer. D.K.F., Mol, W.EM., Miiller, M. and Kurz, G. (1990) J.
Pharmacokinet. Biopharm. 18, 35-70.
[336] Steen, H. and Meijer, D.K.F. (1991) Prog. Pharmacol. Clin. Phar-
macol. 8. 239-272.
[337] Braakman, I.. Groothuis, G.MM. and Meijer, D.K.F. (1987) Hepa-
tology 7, 849-855.
[338] Braakman, I., Groothuis, G.MM. and Meijer, D.K.F. (1989) J.
Pharmacol. Exp. Ther. 249. 869-873.
[339] Van der, Sluijs P., Spanjer, H.H. and Meijer, D.K.F. (1987) J.
Pharmacol. Exp. Ther. 240, 668-673.
[340] Braakman, 1. (1988) Hepatocyte heterogeneity in organic cation
transport, Thesis, Rijksuniversiteit Groningen.
[341] Braakman, I.. Verest, O., Pijning, T., Meijer, D.K.F. and Groothuis,
G.MM. (1990)Mol. Pharmacol, 36, 532-536.
[342] Braakman, 1., Pijning, T., Verest, O., Weert, B., Meijer, D.K.F. and
Groothuis, G.MM. (1989) Mol. Pharmacol. 36, 537-542.
[343] Tulkens, P.M. (1991) Eur. J. Clin. Microbiol. 10, 100-106.
[344] Yoshioka, K. and Nishimura, H. (1988) Experientia 44, 889-892.
[345] Yoshioka, K., Nishimura, H., Himukai, M. and Iwashima, A.
(1985) Biochim. Biophys. Acta 815, 499-504.
[346] Lumeng, L., Edmondson, J.W., Schenker, S. and Li, T.-K. (1979)
J. Biol. Chem. 254, 7265-7268.
[347] Chen. C.P. (1978)J. Nutr. Sci. Vitaminol. 24, 351-362.
[348] Yoshioka, K. (1984) Biochim. Biophys. Acta 778, 201-209.
[349] Yoshioka, K., Nishimura, H. and Hasegawa, T. (1985) Biochim.
Biophys. Acta 819, 263-266.
[350] Yoshioka, K. and Nishimura, H. (1986) Experientia 42, 1022-1023.
[351] Yoshioka, K., Nishimura, H. and Iwashima, A. (1983) Biochim.
Biophys. Acta 732, 308-311.
[352] Moseley, R.H., Vashi, P.G., Jarose, S.M., Dickinson, C.J. and
Permoad, P.A. (1992) Gastroenterology 103, 1056-1065.
[353] Moseley, R.H., Morrissette. J. and Johnson, T.R. (1990) Am. J.
Physiol. 259, G973-G982.
[354] Moseley, R.H., Jarose, S.M. and Permoad, P. (1992) Am. J.
Physiol. 263, G775-G785.
[355] Mckinney, T.D. and Hosford, M.A. (1992) Am. J. Physiol. 263,
G939-G946.
[356] King, P.D. and Cai, Z.-S. (1993) Gastroenterology 104, A927.
[357] Mol, W.EM., Miiller, M., Kurz, G. and Meijer, D.K.F. (1992)
Biochem. Pharrnacol. 43, 2217-2226.
[358] Steen, H., Maring, J.G. and Meijer, D.K.F. (1993) Biochem.
Pharmacol. 45, 809-818.
[359] Steen, H., Oosting, R. and Meijer, D.K.F. (1991) J. Pharmacol.
Exp. Ther. 258, 537-543.
[360] Mol, W.EM., Fokkema, G.N., Weert, B. and Meijer, D.K.F. (1988)
J. Pharmacol. Exp. Ther. 244, 268-275.
[361] Steen, H., Merema, M. and Meijer, D.K.F. (1992) Biochem. Phar-
macol, 44, 2323-2331.
[362] Faraji-Shadan, F., Stubbs, J.D. and Bowman, P.D. (1990) Med.
Hypotheses 32, 81-84.
[363] Mol, W.EM., Miiller, M. and Meijer, D.K.F. (1989) Arch. Pharm.
322, 613-615.
[364] Miiller, M., Mol, W.EM., Meijer, D.K.F. and Kurz, G. (1994)
submitted.
[365] Xie, M.-H., Cochran, M., Lidofsky, S.D. and Scharschmidt, B.F.
(1992) Hepatology 16, 147A.
[366] Moseley, R.H., Smit, H., van Solkema, B.G.H., Wang, W. and
Meijer, D.K.F. (1994) Hepatology 20, 261A.(Abstract)
[367] Meijer, D.K.F. (1976) in Intestinal permeation (Kramer, M. and
Lauterbach, F., eds.), pp. 196-207, Excerpta Medica, Amsterdam.
[368] Meijer, D.K.F., Wester, J. and Gunnik, M. (1972) Naunyn.
Schmiedebergs. Arch. Pharmacol. 273, 179-192.
[369] Mol, W.EM. and Meijer, D.K.F. (1990) Biochem. Pharmacol. 39,
383-390.
[370] Van Dyke, R.W., Faber. E.D. and Meijer, D.K.F. (1992) J. Phar-
macol. Exp. Ther. 261, 1-11.
[371] Meijer, D.K.F., Weltering, J.G. and Vonk. R.J. (1976) J. Pharma-
col. Exp. Ther. 198, 229-239.
[372] Weltering, J.G., Lammers, W., Meijer, D.K.F. and Mulder, G.J.
(1977) Naunyn. Schmiedebergs. Arch. Pharmacol. 299, 277-281.
[373] Weltering, J.G., Mulder, G.J., Meijer, D.K.F., Lammers, W., Veen-
huis, M. and Wendelaar Bonga, S.E. (1975)Naunyn. Schmiede-
bergs, Arch. Pharmacol. 289, 251-256.
[374] Woolley, G.A., Kapral, M.K. and Deber, C.M. (1987)FEBS Lett.
224, 337-342.
[375] Bunting, J.R., Phan, T.V., Kamali, E. and Dowben, R.M. (1989)
Biophys. J. 56, 979-993.
[376] Steen, H. (1992) Mechanisms for the hepatic disposition of organic
cations. Molecular aspects of membrane transport in the hepato-
cyte, Thesis, Rijksuniversiteit Groningen.
[377] Kr~imer, R., Mayr, U., Heberger, C. and Tsompanidou, S. (1986)
Biochim. Biophys. Acta 855, 201-210.
[378] Singh, G., Sharkey, S.M. and Moorehead, R. (1992) Pharmacol.
Ther. 54, 217-230.
[379] Diwan, J.J., Yune, H.H., Bawa, R., Haley, T. and Mannella, C.A.
(1988) Biochem. Pharmacol. 37, 957-961.
[380] Berman, J.J. (1988) Cell Biol. Toxicol. 4, 325-332.
[381] Porter, R.K., Scott, J.M. and Brand, M.D. (1992) J. Biol, Chem.
267, 14637-14646.

264 R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268
[382] Toninello, A., Dalla Via, L., Siliprandi, D. and Garlid, K.D. (1992)
J. Biol. Chem. 267, 18393-18397.
[383] Miiller, M. (1988) Membrantransport von organischen kationen in
hepatocyten. Ein beitrag zur aufkl~rung von hepatischen trans-
portvorg~ingen, Dissertation, Universitiit von Freiburg.
[384] Koch, J.K. and Gallagher, C.H. (1960) Biochem. Pharrnacol. 3,
231-243.
[385] Meier, P.J., Knickelbein, R., Moseley, R.H., Dobbins, J.W. and
Boyer, J.L. (1985) J. Clin. Invest. 75, 1256-1263.
[386] Mannella, C.A. and Wang, Q. (1989) Biochim. Biophys. Acta 981,
363-366.
[387] Zimmermann, H.W. (1986) Angew. Chem. [Int Ed.] 25, 115-130.
[388] Yeh, C.G., Hsi, B. and Faulk, W.P. (1981) J. Immunol. 43,
269-275. [389] Ronot, X., Benel, L., Adolphe, M. and Mounolou, J.C. (1986) Biol
Cell. 57, 1-8.
[390] Ullrich, K.J. and Rumrich, G. (1993) Clin. Investig. 71, 843-848.
[391] Vonk, R.J., Scholtens, E., Keulemans, G.TP. and Meijer, D.K.F,
(1978) Naunyn. Schmiedebergs. Arch. Pharmacol. 302, 1-9.
[392] Ruifrok, P.G. (1982) Biochem. Pharmacol. 31, 1431-1435.
[393] Neef, C., Keulemans, K.TP. and Meijer, D.K.F. (1984) Biochem.
Pharmacol. 33, 3991-4002.
[394] Neef, C., Keulemans, K.TP. and Meijer, D.K.F. (1984) Biochem.
Pharmacol. 33, 3977-3990.
[395] Kamimoto, Y.. Gatmaitan, Z., Hsu, J. and Arias, I.M. (1989) J.
Biol. Chem. 264, 11693-11698.
[396] Sinicrope, F.A., Dudeja, P.K., Bissonnette, B.M., Safa, A.R. and
Brasitus, T.A. (1992) J. Biol. Chem. 267, 24995-25002.
[397] Ballet, F., Vrignaud, P., Robert, J., Rey, C. and Poupon, R. (1987)
Cancer Chemother. Pharmacol. 19, 240-245.
[398] Smit, J.W., Steen, H. and Meijer, D.K.F. (1994) in Transport in the
Liver (Keppler, D. and Jungermann, K., eds.), pp. Abstract-Abno.
27, Falk Symposium No. 74, Heidelberg.
[399] Speeg, K.V. and Maldonado, A.L. (1993) Cancer Chemother.
Pharmacol. 32, 434-436.
[400] Speeg, K.V., Maldonado, A.L., Liaci, J. and Muirhead, D. (1992)
Hepatology 15, 899-903.
[401] Thalhammer, T., Stapf, V., Gajdzik, L. and Graf, J. (1994) Eur. J.
Pharmacol. 270, 213-220.
[402] Watanabe, T., Miyauchi, S., Sawada, Y., Iga, T., Hanano, M.,
Inaba, M. and Sugiyarna, Y. (1992) J. Hepatol. 16, 77-88.
[403] Gottesman, M.M. and Pastan, I. (1993) Annu. Rev. Biochem. 62,
385-427. [404] Zamora, J.M., Pearce, H.L. and Beck, W.T. (1988) Mol. Pharma-
col. 33, 454-462.
[405] Buschman, E., Arceci, R.J., Croop, J.M., Che, M.X., Arias, 1.M.,
Housman, D.E. and Gros, P. (1992) J. Biol. Chem. 267, 18093-
18099.
[406] Thiebaut, F., Tsuruo, T., Hamada, H., Gottesman, M.M., Pastan, I.
and WiUingham, M.C. (1987) Proc. Natl. Acad. Sci. USA 84.
7735-7738. [407] Bradley, G., Georges, E. and Ling, V. (1990) J. Cell. Physiol. 145,
398-408.
[408] Fojo, A.T., Ueda, K., Slamon, D.J., Poplack, D.G., Gottesman,
M.M. and Pastan, I. (1987) Proc. Natl. Acad. Sci. USA 84,
265 -269. [409] Germann, U.A., Pastan, I. and Gottesman, M.M. (1993) Semin.
Cell Biol. 4, 63-76.
[410] Doige, C.A. and Ames, G.FL. (1993) Annu. Rev. Microbiol. 47,
291-319.
[411] Roninson, I.B. (1992) Biochem. Pharmacol. 43, 95-102.
[412] Schinkel, A.H. and Borst, P. (1991) Semin. Cancer Biol. 2, 213-
226.
[413] Borst, P. (1991) Acta Oncol. 30, 87-105. [414] Teeter, L.D., Estes, M., Chan, J.Y., Atassi, H., Sell, S., Becker,
F.F. and Kuo, M.T. (1993) Mol. Carcinog. 8, 67-73.
[415] Schrenk, D., Gant, T,W., Preisegger, K.-H., Silverman, J.A.,
Marino, P.A. and Thorgeirsson, S.S. (1993) Hepatology 17, 854-
860.
[416] Nakatsukasa, H., Silverman, J.A., Gant, T.W., Evarts, R.P. and
Thorgeirsson, S.S. (1993) Hepatology 18, 1202-1207.
[417] Kuo, M.T. (1993) Mol. Carcinog. 7, 73-75.
[418] Chenivesse, X., Franco, D. and Br&hot, C. (1993) J. Hepatol. 18,
168-172.
[419] Smit, J.J.M., Schinkel, A.H., Oude Elferink, R.P.J., Groen, A.K.,
Wagenaar, E., Van Deemter, L., Mol, C.A.A.M., Ottenhoff, R.,
Van der Lugt, N.M.T., Van Roon, M., Van der Valk, M.A.,
Offerhaus, G.J.A., Berns, A.J.M. and Borst, P. (1993) Cell 75,
451-462.
[420] Ruetz, S. and Gros, P. (1994) Cell 77, 1071-1082.
[421] Chaudhary, P.M., Mechetner, E.B. and Roninson, I.B. (1992)
Blood 80, 2735-2739.
[422] Gupta, S. and Gollapudi, S. (1993) J. Clin. Immunol. 13, 289-301.
[423] Endicott, J.A. and Ling, V. (1989) Annu. Rev. Biochem. 58,
137-171.
[424] Ambudkar, S.V., Lelong, I.H., Zhang, J.P., Cardarelli, C.O.,
Gottesman, M.M. and Pastan, I. (1992) Proc. Natl. Acad. Sci. USA
89, 8472-8476.
[425] Sharom, F.J., Yu, X.H. and Doige, C.A. (1993) J. Biol. Chem. 268,
24197-24202.
[426] Garrigos, M., Belehradek, J.,Jr., Mir, L.M. and Orlowski, S. (1993)
Biochem. Biophys. Res. Commun. 196, 1034-1041.
[427] Hammond, J.R., Johnstone, R.M. and Gros, P. (1989) Cancer Res.
49, 3867-3871.
[428] Gros, P., Croop, J. and Housman, D, (1986) Cell 47, 371-380.
[429] Ueda, K., Cardarelli, C., Gottesman, M.M. and Pastan. I. (1987)
Proc. Natl. Acad. Sci. USA 84, 3004-3008.
[430] Gill, D.R., Hyde, S.C., Higgins, C.F., Valverde, M.A., Mintenig,
G.M. and Sepfilveda, F.V. (1992) Cell 71, 23-32.
[431] Abraham, E.H., Prat, A.G., Gerweck, L., Seneveratne, T., Arceci,
R.J., Kramer, R.. Guidotti, G. and Cantiello, H.F. (1993) Proc.
Natl. Acad. Sci. USA 90, 312-316.
[432] Roepe, P.D., Wei, L.Y., Cruz, J. and Carlson, D. (1993) Biochem-
istry. 32, 11042-11056.
[433] Boscoboinik, D., Gupta, R.S. and Epand, R.M. (1990) Br. J.
Cancer. 61,568-572.
[434] Keizer, H.G. and Joenje, H. (1989) J. Natl. Cancer Inst. 81,
706-709.
[435] Thiebaut, F.. Currier, S.J., Whitaker, J., Haugland, R.P., Gottes-
man, M.M., Pastan, I. and Willingham, M.C. (1990) J. Histochem.
Cytochem. 38, 685-690.
[436] Speeg, K.V.,Jr., Deleon, C. and Mcguire, W.L. (1992) Cancer Res.
52, 3539-3546.
[437] Skovsgaard, T. (1989) in Anticancer drugs (Tapiero, H., Robert, J.
and Lampidis, T.J., eds.), pp. 233-244, Colloque INSERM/John
Libbey Eurotext Ltd.
[438] Altenberg, G.A., Young, G., Horton, J.K., Glass, D., Belli, J.A.
and Reuss, L. (1993) Proc. Natl. Acad. Sci. USA 90, 9735-9738.
[439] Higgins, C.F. and Gottesman, M.M. (1992) Trends Biochem. Sci.
17, 18-21.
[440] Shalinsky, D.R., Jekunen, A.P., Alcaraz, J.E., Christen, R.D., Kim,
S., Khatibi, S. and Howell, S.B. (1993) Br. J. Cancer. 67, 30-36.
[441] Homolya, L., Hollo, Z., Germann, U.A., Pastan, I., Gottesman,
M.M. and Sarkadi, B. (1993) J. Biol. Chem. 268, 21493-21496.
[442] Stein, W.D., Cardarelli, C., Pastan, I. and Gottesman, M.M. (1994)
Mol. Pharmacol 45, 763-772.
[443] Gottesman, M.M. and Pastan, I. (1993) Annu. Rev. Biochem. 284,
278-284.
[444] Klopman, G., Srivastava, S., Kolossvary, I., Epand, R.F., Ahmed,
N. and Epand, R.M. (1992) Cancer Res. 52, 4121-4129,
[445] Selassie, C.D., Hansch, C. and Khwaja, T.A. (1990) J. Med. Chem.
33, 1914-1919. [446] Pearce, H.L., Safa, A.R., Bach, N.J., Winter, M.A., Cirtain, M.C.
and Beck, W.T. (1989) Proc. Natl. Acad. Sci. USA 86, 5128-5132.

R.P.Z Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268 265
[447] Ford, J.M., Bruggemann, E.P., Pastan, I., Gottesman, M.M. and
Hait, W.N. (1990) Cancer Res. 50, 1748-1756.
[448] Nogae, I., Kohno, K., Kikuchi, J., Kuwano, M., Akiyama, S.I.,
Kiue, A., Suzuki, K.I., Yoshida, Y., Cornwell, M.M., Pastan, I. and
Gottesman, M.M. (1989) Biochem. Pharmacol. 38, 519-527.
[449] Hofsli, E. and Nissen-Meyer, J. (1990) Cancer Res. 50, 3997-4002.
[450] Dellinger, M., Pressman, B.C., Calderon-Higginson, C., Savarai,
N., Tapiero, H., Kolonias, D. and Lampidis, T.J. (1992) Cancer
Res. 52, 6385-6389.
[451] Ramu, A. and Ramu, N. (1992) Cancer Chemother. Pharmacol. 30,
165-173.
[452] Piwnica-Worms, D., Chiu, M.L., Budding, M., Kronauge, J.F.,
Kramer, R.A. and Croop, J.M. (1993) Cancer Res. 53, 977-984.
[453] Tang-Wai, D.F., Brossi, A., Arnold, L.D. and Gros, P. (1993)
Biochemistry 32, 6470-6476.
[454] Priebe, W., Van, N.T., Burke, T.G. and Perez-Soler, R. (1993)
Anti-Cancer. Drugs 4, 37-48.
[455] Sehested, M., Skoosgaard, T., Van Deurs, B. and Winther-Nielsen,
H. (1987) Br. J. Cancer. 56, 747-751.
[456] Bruggemann, E.P., Currier, S.J., Gottesman, M.M. and Pastan, I.
(1992) J. Biol. Chem. 267, 21020-21026.
[457] Tamai, I. and Sara, A.R. (1991) J. Biol. Chem. 266, 16796-16800.
[458] Loo, T.W. and Clarke, D.M. (1993) J. Biol. Chem. 268, 19965-
19972.
[459] Ferry, D.R., Russell, M.A. and Cullen, M.H. (1992) Biochem.
Biophys. Res. Commun. 188, 440-445.
[460] Chen, H.-X., Bamberger, U., Heckel, A., Guo, X. and Cheng,
Y.-C. (1993) Cancer Res. 53, 1974-1977.
[461] Gruber, A., Briese, B., Arestrtim, I., Vitols, S., BjiSrkholm, M. and
Peterson, C. (1993) Leuk. Res. 17, 353-358.
[462] Grant, C.E., Valdimarsson, G., Hipfner, D.R., Almquist, K.C.,
Cole, S.PC. and Deeley, R.G. (1994)Cancer Res. 54, 357-361.
[463] Miilder, H.S., van Grondelle, R., Westerhoff, H.V. and Lankelma,
J. (1993) Eur. J. Biochem. 218, 871-882.
[464] Krishnamachary, N. and Center, M.S. (1993) Cancer Res. 53,
3658-3661.
[465] Versantvoort, C.HM., Schuurhuis, G.J., Pinedo, H.M., Eekman,
C.A., Kuiper, C.M., Lankelma, J. and Broxterman, H.J. (1993) Br.
J. Cancer 68, 939-946.
[466] Scheper, R.J., Broxterman, H.J., Scheffer, G.L., Kaaijk, P., Dalton,
W.S., Van Heijningen, T.HM., Van Kalken, C.K., Slovak, M.L.,
De Vries, E.GE., Van der, V.alk P., Meijer, C.JLM. and Pinedo,
H.M. (1993) Cancer Res. 53, 1475-1479.
[467] Teeter, L.D., Hsu, H.-C., Curley, S.A., Tong, M.J. and Kuo, M.T.
(1993) Int. J. Oncol. 2, 73-80.
[468] Kuo, M.T., Zhao, J.Y., Teeter, L.D., Ikeguchi, M. and Chisari,
F.V. (1992) Cell Growth Differ. 3, 531-540.
[469] Nakatsukasa, H., Evarts, R.P., Burt, R.K., Nagy, P. and Thorgeirs-
son, S.S. (1992) Mol. Carcinog. 6, 190-198.
[470] Bradley, G.. Sharma, R., Rajalakshmi, S. and Ling, V. (1992)
Cancer Res. 52, 5154-5161.
[471] Fardel, O., Ratanasavanh, D., Loyer, P., Ketterer, B. and Guil-
louzo, A. (1992) Eur. J. Biochem. 205, 847-852.
[472] Fardel, O., Morel, F. and Guillouzo, A. (1993) Carcinogenesis 14,
781-783.
[473] Lee, C.H.. Bradley, G., Zhang, J.-T. and Ling, V. (1993) J. Cell.
Physiol. 157, 392-402.
[474] Acufia, C., Vollrath, V., Wielandt, A., Andrade, L., Duarte, I. and
Chianale, J. (1994) submitted.
[475] Hait, W.N. and Aftab, D.T. (1992) Biochem. Pharmacol. 43, 103-107.
[476] Grunicke, H. and Hofmann, J. (1992) Pharmacol. Ther. 55, 1-30.
[477] Chambers, T.C., Chalikonda, I. and Eilon, G. (1990) Biochem.
Biophys. Res. Commun. 169, 253-259.
[478] Chambers, T.C., McAvoy, E.M., Jacobs, J.W. and Eilon, G. (1990) J. Biol. Chem. 265, 7679-7686.
[479] Ford, J.M. and Hait, W.N. (1990) Pharmacol. Rev. 42, 155-199.
[480] Fine, R.L., Patel, J., Hamilton, T.C., Cowan, K., Curt, G.A.,
Friedman, M.A. and Chabner, B.A. (1986) Proc. Am. Assoc.
Cancer Res. 27, 271. [481] Hamada, H., Hagiwara, K., Jakajima, T. and Tsuruo, T. (1987)
Cancer Res. 47, 2860-2865.
[482] Mellado, W. and Horwitz, S.B. (1987) Biochemistry. 26, 6900-
6904.
[483] Center, M.S. (1983) Biochem. Biophys. Res. Commun. 115, 159-
166. [484] Mickley, L.A., Bates, S.E., Richert, N.D., Currier, S., Tanaka, S.,
Foss, F., Rosen, N. and Fojo, A.T. (1989) J. Biol. Chem. 264,
18031-18040.
[485] Bates, S.E., Currier, S.J., Alvarez, M. and Fojo, A.T. (1992)
Biochemistry 31, 6366-6372.
[486] Nishizuka, Y. (1988)Nature 334, 661-665.
[487] Ward, N.E. and O'Brian, C.A. (1993) Biochemistry 32, 11903-
11909.
[488] Yu, G., Ahmad, S., Aquino, A., Fairchild, C.R., Trepel, J.B., Ohno,
S., Suzuki, K., Tsuruo, T., Cowan, K.H. and Glazer, R.I. (1991)
Cancer Commun. 3, 181 - 189.
[489] Tamaoki, T., Nomoto, H., Takahashi, I., Kato, Y., Morimoto, M.
and Tomita, F. (1986) Biochem. Biophys. Res. Commun. 135,
397-402.
[490] Hidaka, H. and Kobayashi, R. (1992) Annu. Rev. Pharmacol.
Toxicol. 32, 377-397.
[491] Sato, W., Yusa, K., Naito, M. and Tsuruo, T. (1990) Biochem.
Biophys. Res. Commun. 173, 1252-1257.
[492] Wakusawa, S., lnoko, K., Miyamoto, K., Kajita, S., Hasegawa, T.,
Harimaya, K. and Koyama, M. (1993) J. Antibiot. 46, 353-355.
[493] Kobayashi, E., Nakano, H., Morimoto, M. and Tamaoki, T. (1989)
Biochem. Biophys. Res. Commun. 159, 548-553.
[494] Bates, S.E., Lee, J.S., Dickstein, B., Spolyar, M. and Fojo, A.T.
(1993) Biochemistry 32, 9156-9164.
[495] Brunton, V.G. and Workman, P. (1993) Cancer Chemother. Phar-
macol. 32, 1-19.
[496] Chaudhary, P.M. and Roninson, I.B. (1993)J. Natl. Cancer Inst.
85, 632-639.
[497] Chaudhary, P.M. and Roninson, I.B. (1992) Oncol. Res. 4, 281-
290.
[498] Steen, H., Smit, H., Nijholt, A., Merema, M. and Meijer, D.K.F.
(1993) Hepatology 18, 1208-1215.
[499] Mtiller, M., Mayer, R., Hero, U. and Keppler, D. (1994) FEBS
Lett.
[500] Mittenbiihler, K., Miiller, M., Wallstab, A.. Biichter, M,, Hero, U.,
Spiess, E., Silverman, J.A., Thorgeirsson, S.S. and Keppler, D.
(1994) J. Biol. Chem.
[501] Gosland, M., Tsuboi, C., Hoffman, T., Goodin, S. and Vore, M.
(1993) Cancer Res. 53, 5382-5385.
[502] Vore, M. (1993)Toxicol. Appl. Pharmacol. 118, 2-7.
[503] Arias, I.M. (1993) Hepatology 18, 216-217.
[504] Wolf, D.C. and Horwitz, S.B. (1992) Int J. Cancer 52, 141-146.
[505] Van Kalken, C,K., Broxterman, H.J., Pinedo, H.M., Feller, N.,
Dekker, H., Lankelma, J. and Giaccone, G. (1993) Br. J. Cancer
67, 284-289.
[506] De Lannoy, I.AM. and Silverman, M. (1992) Biochem. Biophys.
Res. Commun. 189, 551-557.
[507] Hori, R., Okamura, N., Aiba, T. and Tanigawara, Y. (1993) J.
Pharmacol. Exp. Ther. 266, 1620-1625.
[508] Okamura, N., Hirai, M., Tanigawara, Y., Tanaka, K., Yasuhara,
M., Ueda, K., Komano, T. and Hori, R. (1993) J. Pharmacol. Exp.
Ther. 266, 1614-1619.
[509] Ito, S., Koren, G., Harper, P.A. and Silverman, M. (1993) Can. J.
Physiol. Pharmacol. 71, 40-47.
[510] Becker, K.F., Allmeier, H. and HiSllt, V. (1992) lqiorm. Metab. Res.
24, 210-213.

266 R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268
[511] Gibbons, G.F. (1990)Biochem. J. 268, 1-13.
[512] Eisenberg, S. (1984) J. Lipid. Res. 25, 1017-1058.
[513] Robins, S.J. and Armstrong, M.J. (1976) Gastroenterology 70,
397-402.
[514] Marzolo, M.P., Amigo, L. and Nervi, F. (1993) J. Lipid Res. 34,
807-814.
[515] Smit, M.J., Temmerman, A.M., Wolters, H., Kuipers, F., Beynen,
A.C. and Vonk, R.J. (1991) J. Clin. Invest. 88, 943-951.
[516] Hardison, W.G.M. and Evans, W.H. (1986) J. Hepatol. 3, 318-327.
[517] Lanzini, A. and Northfield, T.C. (1991) Eur. J. Clin. Invest. 21,
259-272.
[518] Mazer, N.A. and Carey, M.C. (1984) J. Lipid Res. 25, 932-953.
[519] Gurantz, D. and Hofmann, A.F. (1984) Am. J. Physiol. 247,
G736-G748.
[520] Carulli, N., Loria, P., Bertolotti, M., Ponz de Leon, M., Menozzi,
D., Medici, G. and Piccagli, I. (1984) J. Clin. Invest. 74, 614-624.
[521] Alvaro, D., Cantafora, A., Attili, A.F., Ginanni Corradini, S., De
Luca, C., Minervini, G., Di Biase, A. and Angelico, A. (1986)
Comp. Biochem. Physiol. [B]. 83, 551-554.
[522] Somjen, G.J. and Gilat, T. (1983) FEBS Lett. 156, 265-268.
[523] Ulloa, N., Garrido, J. and Nervi, F. (1987) Hepatology 7, 235-244.
[524] Cohen, D.E., Angelico, M. and Carey, M.C. (1989) Am. J. Physiol.
257, G1-G8.
[525] Hofmann, A.F. (1990) Hepatology 12, 17S-25S.
[526] Hay, D.W. and Carey, M.C. (1990) Hepatology 12, 6S-14S.
[527] Smit, M.J., Temmerman, A.M., Havinga, R., Kuipers, F. and
Vonk, R.J. (1990) Biochem. J. 269, 781-788.
[528] Hay, D.W., Cahalane, M.J., Timofeyeva, N. and Carey, M.C.
(1993) J. Lipid Res. 34, 759-768.
[529] Robins, S.J., Fasulo, J.M., Robins, V.F. and Patton, G.M. (1991) J.
Lipid Res. 32, 985-992.
[530] Smit, M.J., Verkade, H.J., Havinga, R., Vonk, R.J., Scherphof,
G.L., Tveld, G.I. and Kuipers, F. (1994)J. Lipid. Res. 35, 301-310.
[531] Cohen, D.E., Kaler, E.W. and Carey, M.C. (1993) Hepatology 18,
1522-1531.
[532] Rigotti, A., Nunez, L., Amigo, L., Puglielli, L., Garrido, J., Santos,
M., Gonzalez, S., Mingrone, G., Greco, A. and Nervi, F. (1993) J.
Lipid Res. 34, 1883-1894.
[533] Domingo, N., Chanussot, F., Botta, D., Reynier, M.O., Crotte, C.,
Hauton, J. and Lafont, H. (1993) Lipids 28, 883-887.
[534] Chanussot, F., Domingo, N., Tuchweber, B., Lafont, H. and Yousef,
I. (1992) Scand. J. Gastroenterol. 27, 238-242.
[535] S~imjen, G.J., Marikovsky, Y., Wachtel, E., Harvey, P.R.C., Rosen-
berg, R., Strasberg, S.M. and Gilat, T. (1990) Biochim. Biophys.
Acta 1042, 28-35.
[536] Somjen, G.J., Coleman, R., Koch, M.HJ., Wachtel, E., Billington,
D., Townsandrews, E. and Gilat, T. (1991) FEBS Lett. 289,
163-166. [537] Kay, R.E. and Entenman, C. (1961) Am. J. Physiol. 200, 855-859.
[538] Hardison, W.G.M. and Apter, J.T. (1972) Am. J. Physiol. 222,
61-67.
[539] Wheeler, H.O. and King, K.K. (1972) J. Clin. Invest. 51, 1337-
1350.
[540] Turley, S.D. and Dietschy, J.M. (1981) J. Biol. Chem. 256, 2438-
2446. [541] Scheibner, J., Fuchs, M., Schiemann, M., Tauber, G., H6rmann, E.
and Stange, E.F. (1993) Hepatology 17, 1095-1102.
[542] Robins, S.J., Fasulo, J.M., Collins, M.A. and Patton, G.M. (1985)
J. Biol. Chem. 260, 6511-6513.
[543] Robins, S.J., Fasulo, J.M., Lessard, P.D. and Patton, G.M. (1993)
Biochem. J. 289, 41-44.
[544] Singer, I.I., Kawka, D.W., Kazazis, D.M., Alberts, A.W., Chen,
J.S., Huff, J.W. and Ness, G.C. (1984) Proc. Natl. Acad. Sci. USA
81, 5556-5560.
[545] Stone, B.G., Eridison, S.K., Graig, W.Y. and Copper, A.D. (1985)
J. Clin. Invest. 76, 1773-1781.
[546] Robins, S.J., Fasulo, J.M., Lessard, P.D. and Patton, G.M. (1993) J.
Lipid Res. 34, 1445-1450.
[547] Bilhartz, L.E., Spady, D.K. and Dietschy, J.M. (1989) J. Clin.
Invest. 84, 1181-1187.
[548] Robins, S.J., Fasulo, J.M., Leduc, R. and Patton, G.M. (1989)
Biochim. Biophys. Acta 1004, 327-331.
[549] Portal, I., Clerc, T., Sbarra, V., Portugal, H., Pauli, A.M., Lafont,
H., Tuchweber, B., Yousef, I. and Chanussot, F. (1993) Am. J.
Physiol. 264, GI052-GI056.
[550] Verkade, H.J., Derksen, J.T.P., Gerding, A., ScherphoE G.L.,
Vonk, R.J. and Kuipers, F. (1991) Biochem. J. 275, 139-144.
[551 ] Robins, S.J. and Brunengraber, H. (1982) J. Lipid Res. 23,604-608.
[552] Yao, Z.M. and Vance, D.E. (1988)J. Biol. Chem. 263, 2998-3004.
[553] Verkade, H.J., Fast, D.G., Rusinol, A.E., Scraba, D.G. and Vance,
D.E. (1993)J. Biol. Chem. 268, 24990-24996.
[554] Cronholm, T., Curstedt, T. and Sj6vall, J. (1983) Biochim. Bio-
phys. Acta 753. 276-279.
[555] Kawamoto, T., Akino, T., Nakamura, M. and Mori, M. (1980)
Biochim. Biophys. Acta 619, 35-47.
[556] Robins, S.J., Fasulo, J.M. and Patton, G.M. (1990) Am. J. Physiol.
259, G205-G211.
[557] Simons, K. and Van Meer, G. (1988)Biochemistry. 27, 6197-6202.
[558] Goldsmith, M.A., Huling, S. and Jones, A.L. (1983) Gastroenterol-
ogy 84, 978-986.
[559] Jones, A.L., Schmucker, D.L., Mooney, J.S., Ockner, R.K. and
Adler, R.D. (1979) Lab. Invest. 40, 512-517.
[560] Crawford, J.M., Vinter, D.W. and Gollan, J.L. (1991) Am. J.
Physiol. 260, G119-G132.
[561] Casu, A. and Camogliano, L. (1990) Biochim. Biophys. Acta 1043,
113-115.
[562] Reynier, M.O., Abouhashieh, I., Crotte, C., Carbuccia, N., Richard,
B. and Gerolami, A. (1992) Gastroenterology 102, 2024-2032.
[563] Graham, J., Ahmed, H. and Northfield, T.C. (1989) in Trends in
Bile Acid Research (Paumgartner, G., Stiehl, A. and Gerok, W.,
eds.), pp. 177-188, Kluwer Academic Publishers, Lancaster.
[564] Sakisaka, S., Cheng, N.OI. and Boyer, J. (1988) Gastroenterology
95, 793-804.
[565] Stein, O., Sanger, L. and Stein, Y. (1974) J. Cell Biol. 62,
390-405.
[566] Cohen, D.E., Leonard, M.R. and Carey, M.C. (1994) Biochemistry
33, 9975-9980.
[567] Wirtz, K.WA. (1991) Annu. Rev. Biochem. 60, 73-99.
[568] Reuben, A, and Allen, R.M. (1986) Biochim. Biophys. Acta 876,
1-12.
[569] Hayakawa, T., Cheng, O., Ma, A. and Boyer, J.L. (1990) Gastro-
enterology 99, 216-228.
[570] Lorenzini, I., Sakisaka, S., Meier, P.J. and Boyer, J.L (1986)
Gastroenterology 91, 1278-1288.
[571] Katagiri, K., Nakai, T. and Hoshino, M. (1992) Gastroenterology
102, 1660-1667.
[572] Dubin, M. and Erlinger, S. (1980) Clin. Sci. 58, 545-548.
[573] Lowe, P.J., Barnwell, S.G. and Coleman, R. (1984) Biochem. J.
222, 631-637.
[574] Kuipers, F., Derksen, J.PT., Gerding, A., ScherphoL G.L. and
Vonk, R.J. (1987)Biochim. Biophys. Acta 922, 136-144.
[575] Apstein, M.D. (1984) Gastroenterology 87, 634-638.
[576] Pattinson, N.R., Willis, K.E. and Chapman, B.A. (1987) Dig. Dis.
Sci. 32, 615-619. [577] Verkade, H.J., Vonk, R.J. and Kuipers, F. (1994) Hepatology 17,
1074-1080. [578] Verkade, H.J., Wolters, H., Gerding, A., Havinga, R., Fidler, V.,
Vonk, R.J. and Kuipers, F. (1993) Hepatology 17, 1074-1080.
[579] Yousef, I.M. and Fisher, M.M. (1976) Can. J. Biochem. 54,
1040-1046.
[580] Coleman, R., Rahman, K., Kan, K.S. and Parslow, R.A. (1989)
Biochem. J. 258, 17-22.

R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268 267
[581] Van-Berge-Henegouwen, G.P., VanderWerf, S.DJ. and Ruben, A.T.
(1987) Clin. Chim. Acta 165, 27-37.
[582] Salvioli, G., Romani, M., Loria, P., Carulli, N. and Pradelli, J.M.
(1985) J. Hepatol. 1, 291-300.
[583] Ben-, F., Schreiber, E. and Frick, U. (1992) Hepatology 16, 71-81.
[584] Shamburek, R.D. and Schwartz, C.C. (1993) J. Lipid Res. 34,
1833-1842.
[585] Yousef, I.M., BarnwelL S., Gratton, F., Tuchweber, B., Weber, A.
and Roy, C.C. (1987) Am. J. Physiol. 252, G84-G91.
[586] Hardison, W.G.M., Hatoff, D.E., Miyai, K. and Weiner, R.G.
(1981) Am. J. Physiol. 241, G337-G343.
[587] Coleman, R., Rahman, K., Bellringer, M.E., Kan, K. and Hamlin,
S. (1989) in Trends in Bile Acid Research (Paumgartner, G., Stiehl,
A. and Gerok, W., eds.), pp. 161-176, Kluwer Academic Publish-
ers, Lancaster.
[588] Billington, D. and Coleman, R. (1978) Biochim. Biophys. Acta
509, 33-47.
[589] Berr, F., Meier, P.J. and Stieger, B. (1993) J. Biol. Chem. 268,
3976-3979.
[590] Higgins. C.F. and Gottesman, M.M. (1992)Trends Biochem. Sci.
17, 18-21.
[591] Bishop, W.R. and Bell, R.M. (1985) Cell 42, 51-60.
[592] Ulloa, N., Garrido, J. and Nervi, F. (1987) Hepatology 7, 235-244.
[593] Crawford, J.M., Barnes, S., Stearns, R.C., Hastings, C.L. and
Godleski, J.L. (1994) Lab. Invest.
[594] Dietschy, J.M., Turley, S.D. and Spady, D.K. (1993) J. Lipid Res.
34, 1637- 1659.
[595] Grundy, S.M. (1983) Ann. Rev. Nutr. 3, 71-96.
[596] Mauad, T.H., van Nieuwkerk, C.M.J., Dingemans, K.P., Smit,
J.J.M.. Schinkel, A.H., Notenboom, R.G.E., van den Bergh Weer-
man, M.A., Verkruisen, R.P., Groen, A.K., Oude Elferink, R.P.J.,
Van der Valk, M.A., Borst, P. and Offerhaus, G.J.A. (1994) Am J.
Pathol. 145, 1237-1245.
[597] Tazuma, S., Barnhart, R.L., Reeve, L.E., Tokumo, H. and Holzbach,
R.T. (1988) Am. J. Physiol. 255,
[598] Tazuma, S. and Holzbach, R.T. (1987) Proc. Natl. Acad. Sci. USA
84, 2052- 2056.
[599] Davidson. N.O., Drewek, M.J., Gordon, J.I. and Elovson, J. (1988)
J. Clin. Invest. 82, 300-308.
[600] Wheeler, H.O. and Mancusi-Ungaro, P.L. (1966) Am. J. Physiol.
210, 1153-1159.
[601] Kountouras, J., McKavanagh, S., Burmicky, M. and Billing, B.H.
(1987) J. Hepatol. 4, 198-205.
[602] Ricci, G.L. and Fevery, J. (1989) Gut 30, 1266-1269.
[603] Ricci, G.L.. Michiels, R. and Fevery, J. (1984) Hepatology 4,
651-657.
[604] Bartles, JR., Feracci, H.M., Stieger, B. and Hubbard, A.H. (1987)
J. Cell. Biol. 105. 1241-1251.
[605] Bossard, R., Stieger, B., Oneill, B., Fricker, G. and Meier, P.J.
(1993) J. Clin. Invest. 91, 2714-2720.
[606] Fricker, G., Landmann, L. and Meier, P.J. (1989) J. Clin. Invest.
84, 876-885.
[607] Silverman, M. (1991) Annu. Rev. Biochem. 60, 757-794.
[608] Gladhaug, I.P. and Christoffersen, T. (1988) J. Biol. Chem. 263,
12199-12203.
[609] Oude Elferink, R.P.J., Bakker, C.T.M., Roelofsen, H., Middelkoop,
E., Ottenhoff, R., Heijn, M. and Jansen, P.L.M. (1993) Hepatology
17,434-444.
[610] Hallbrucker, C., Lang, F., Gerok, W. and Haussinger, D. (1992)
Biochem. J. 281,593-595.
[611] Haussinger, D., Saha, N., Hallbrucker, C., Lang, F. and Gerok, W.
(1993) Biochem. J. 291, 355-360.
[612] Haussinger, D., Hallbrucker, C., Saha, N., Lang, F. and Gerok, W.
(1992) Biochem. J. 288, 681-689.
[613] Bruck, R., Haddad, P., Graf, J. and Boyer, J.L. (1992) Am. J.
Physiol. 262, G806-G812.
[614] Boyer, J.L., McGrath, J.W. and Ng, O.C. (1993) Hepatology 18,
107A.(Abstract)
[615] Rasmussen, H. (1990) Hoppe-Seyler's. Z. Physiol. Chem. 371,
191-206.
[616] Nathanson, M.H., Gautam, A.. Bruck, R., Isales, C.M. and Boyer,
J.L. (1992) Hepatology 15, 107-116.
[617] Tanaka, A., Katagiri, K., Hoshino, M., Hayakawa, T., Tsukada, K.
and Takeuchi, T. (1994) Am. J. Physiol. 266, G324-G329.
[618] Isales, C.M., Nathanson, M.H. and Bruck. R. (1993) Biochem.
Biophys. Res. Commun. 191, 1244-1251.
[619] Hamada, Y., Karjalainen, A., Setchell, B., Millard, J. and Bygrave,
F.L. (1992) Biochem. J. 281, 387-392.
[620] Hamada, Y., Karjalainen, A., Setchell, B., Millard. J. and Bygrave,
F.L. (1992) Biochem. J. 283, 575-581.
[621] Roelofsen, H., Ottenhoff, R., Oude Elferink, R.P.J. and Jansen,
P.L.M. (1991) Biochem. J. 278, 637-641.
[622] Hayakawa, T., Bruck, R., Ng, O.C. and Boyer, J.L. (1990) Am. J.
Physiol. 259, G727-G735.
[623] Lenzen, R., Hruby, V,J. and Tavoloni, N. (1990) Am. J. Physiol.
259, G736-G745.
[624] Desmet, V.J. (1987) in Pathology of the Liver (MacSween, R.N.M.,
Anthony, P.P. and Scheuer, P.J., eds.), pp. 364-423, Churchill
Livingstone, Edinburgh.
[625] Rosario, J., Sutherland, E., Zaccaro, L. and Simon, F.R. (1987)
Biochemistry 27, 3939-3946.
[626] Kan, K.S., Monte, M.J., Parslow, R.A. and Coleman, R. (1989)
Biochem. J. 261,297-300.
[627] Combettes, L., Dumont, M., Berthon, B., Erlinger, S. and Claret,
M. (1988)J. Biol. Chem. 263. 2299-2303.
[628] Akerboom, T.P.M., Schneider, I.. Vom Dahl, S. and Sies, H.
(1991 ) Hepatology 13, 216-221.
[629] Dubin, M., Maurice, M., Feldmann, G. and Erlinger, S. (1978)
Gastroenterology 75,450-455.
[630] Cadranel, J.F., Erlinger, S., Desruenne, M., Luciani, J., Lunel, F.,
Grippon, P.. Cabrol. A. and Opolon, P. (1992) Dig. Dis. Sci. 37,
1473-1476.
[631] Stone, B.G., Udani, M., Sanghvi, A., Warty, V., Plocki, K.,
Bedetti, C.D. and Van Thiel, D.H. (1987) Gastroenterology 93,
344-351.
[632] Bohme, M., Buchler, M., Muller, M. and Keppler, D. (1993) FEBS
Lett. 333, 193-196.
[633] Kadmon, M., Klunemann, C., Bohme, M., Ishikawa, T., Gorgas,
K., Otto, G., Herfarth, C. and Keppler, D. (1993) Gastroenterology
104, 1507-1514.
[634] Moseley, R.H., Johnson, T.R. and Morisette, J.M. (1990) J. Phar-
macol. Exp. Ther. 253, 974-980.
[635] Kukongviriyapan, V.. and Stacey, N.H. (1988) J. Pharmacol. Exp.
Ther. 247, 685-689.
[636] Heikel, T.A.J. and Lathe. G.H. (1970) Br. J. Pharmacol. 38,
593-601.
[637] Stacey, N.H. (1986) Biochem. Pharmacol. 35, 2495-2500.
[638] Ben-, F., Simon, F.R. and Reichen, J. (1984) Am. J. Physiol. 247,
G437-G443.
[639] Vore, M., Durham, S., Yeh. S. and Ganguly, T. (1991) Biochem.
Pharmacol. 41, 431-437.
[640] Kitamura, T., Brauneis, U., Gatmaitan, Z. and Arias, I.M. (1991)
Hepatology 14, 640-647.
[641] Cohen, D.E., Leonard, M.R. and Carey, M.C. (1992) Hepatology
16, 90a.
[642] Meyers, M., Slikker, W. and Vore, M. (1981) J. Pharmacol. Exp.
Ther. 218, 63-73.
[643] Boyce, W. and Witzleben, C.L. (1973) Am. J. Pathol. 72, 427-432.
[644] Ayotte, P. and Plaa, G.L. (1988) Hepatology 8, 1069-1078.
[645] Becker, B.A. and Plaa, G.L. (1965) Toxicol. Appl. Pharmacol. 7,
708-718.
[646] Durand-Schneider, A.M., Maurice. M., Dumont, M. and Feldmann,
G. (1987) Hepatology 7, 1239-1248.
[647] Stieger, B., Meier, P.J. and Landmann, L. (1994) Hepatology 20,
201-212.
[648] Larkin, J.M. and Palade, G.E. (1991) J. Cell Sci. 98, 205-216.

268 R.P.J. Oude Elferink et al. / Biochimica et Biophysica Acta 1241 (1995) 215-268
[649] Rank, J. and Wilson, I.D. (1983) Hepatology 3, 241-247.
[650] Gartung, C., Ananthanarayanan, M., Rahman, M.A., Stolz, A,,
Suchy, F.J. and Boyer, J.L. (1993) Hepatology 18, 139A.(Abstract)
[651] Kothe, M.J.C., Bakker, C.T.M., De haan, J., Maas, A., Jansen,
P.L.M. and Oude Elferink, R.P.J. (1993) Hepatology 18,
138A.(Abstract)
[652] De Herder, W.W., Van der Hul, R.L., Bonthuis, F., Jansen, P.L.M.,
Oude Elferink, R.P.J. and Visser, T.J. (1989) Ann. Endocrinol. 50,
98. [653] Oude Elferink, R.P.J. and Jansen, P.L.M. (1994) Pharmacol. Ther.
64, 77-97.
[654] Polhuis, M., Kuipers, F., Vonk, R.J. and Mulder, G.J. (1989) J.
Pharmacol. Exp. Ther. 249, 874-878.
[655] Muhler, A., Oude Elferink, R.P.J. and Weinmann, H.J. (1993)
MAGMA 1, 134-139.
[656] Herz, R., Paumgartner, G. and Preisig, R. (1976) Scand. J. Gas-
troenterol. 11,741-746.
[657] Javitt, N.B. (1966) Nature 210, 1262-1263.
[658] King, J.E. and Schoenfield, L.J. (1971) J. Clin. Invest. 50, 2305-
2312.
[659] Yousef, I.M., Tuchweber, B., Vonk, R.J., Masse, D., Audet, M.
and Roy, C.C. (1981) Gastroenterology 80, 233-241.
[660] Van der Meer, R., Vonk, R.J. and Kuipers, F. (1988) Am. J.
Physiol. 254, G644-G649.
[661] Oelberg, D.G., Chari, M.V., Little, J.M., Adcock, E.W. and Lester,
R. (1984) J. Clin. Invest. 73, 1507-1514.
[662] Gumucio, J.J. and Valdivieso, V.D. (1971) Gastroenterology 61,
339-344.
[663] Tavoloni, N., Reed, J.S. and Boyer, J.L. (1982) Proc. Soc. Exp.
Biol. Med. 170, 486-492.
[664] Farthing, M.J.G. and Clark, M.L. (1981) Biochem. Pharmacol. 30,
3311-3316.
[665] Rotolo, F.S., Branum, G.D., Browers, B.A. and Meyers, W.C.
(1986) Am. J. Surg. 151, 35-40.
[666] Witzleben, C.L. (1971) Am. J. Pathol. 62, 181-194.
[667] Heijn, M. (1994) Characterization of ATP-dependent organic anion
transport, PhD. Thesis, Amsterdam.
[668] Haussinger, D. (1994) in Transport in the Liver (Keppler, D. and
Jungermann, K., eds.), pp. 97-116, Kluwer Academic Publ., Dor-
drecht/Boston/London.
[669] Stieger, B., Hagenbuch, B., Landmann, L., HSchli, M., Schroeder,
A. and Meier, P.J. (1994) Gastroenterology 107, 1781-1787.
[670] Kullak-Ublick, G.A., Hagenbuch, B., Stieger, B., Wolkoff, A.W.
and Meier, P.J. (1994) Hepatology 20, 411-416.
[671] Boyer, J.L., Ng, O.C., Ananthanarayanan, M., Hofmann, A.F.,
Schteingart, C.D., Hagenbuch, B., Stieger, B., and Meier, P.J.
(1994) Am. J. Physiol. 266: G382-G387.
[672] Oude Elferink, R.P.J., Ottenhoff, R. van Wijland, M., Smit, J.J.M.,
Schinkel, A.H. and Groen, A.K. (1995) J. Clin. Invest. 95, 31-38.
[673] Smith, A.J., Timmermans-Hereijgers, J.L.P.M., Roelofsen, B.,
Wirtz, K.W.A., van Blitterswijk, W.J., Smit, J.J.M., Schinkel, A.H.
and Borst, P. (1994) FEBS Lett. 354, 263-266.





























