Embed Size (px)
Citation preview
Home intravenous antibiotics in children:
determining the population, efficacy, safety and
cost-‐effectiveness using cellulitis as a paradigm
Laila Farah Binti Ibrahim
Submitted in total fulfillment of the requirements of the degree of
Doctor of Philosophy
January 2019
Department of Paediatrics Melbourne Medical School
Faculty of Medicine, Dentistry and Health Sciences
The University of Melbourne

i
Abstract
Admission to hospital has a negative impact on quality of life in children, carries
the risk of hospital-‐acquired infections and is associated with higher costs. The
alternative to hospital admission for intravenous antibiotics is outpatient
parenteral antimicrobial therapy (OPAT). There has been increasing use of OPAT
in children but evidence supporting its use remains scarce. Although OPAT is
usually used for children who are deemed stable after a period of hospitalisation,
there has been increasing interest in avoiding admission completely by using
OPAT for acute infections directly from the Emergency Department (ED). In this
thesis, cellulitis, a common infection in children, is used as a paradigm to
determine the efficacy and safety of home treatment. The main aim of this thesis
was to investigate the clinical and non-‐clinical outcomes of intravenous
antibiotic treatment at home compared to hospital, for children presenting to the
ED with moderate/severe cellulitis.
A series of studies were planned and undertaken to accomplish this aim. The first
phase aimed to better understand current practice, through a baseline
observational study of treatment at home directly from the ED and a clinician
survey about broader cellulitis management. This was followed by two
foundation studies that aimed to increase current knowledge and inform a
planned randomised controlled trial (RCT). The first foundation study was a non-‐
randomised cohort study of home versus hospital treatment and the second
foundation study investigated the impact of antibiotics on nasal colonisation
with Staphylococcus aureus. The subsequent study aimed to determine which
patients with cellulitis need intravenous antibiotics. Finally, the first ever RCT in
children that aimed to determine the efficacy and safety of home versus hospital
treatment for cellulitis, was undertaken, accompanied by a comprehensive cost-‐
effectiveness analysis.
The baseline study showed that treatment of cellulitis with once daily
ceftriaxone under Hospital-‐in-‐the-‐Home care appeared to have low risks of

ii
treatment failure, complications and adverse events although numbers were
small and predominantly included older children with limb cellulitis without
systemic symptoms. The clinician survey identified barriers for OPAT, which
included the perceived high risk of bacteraemia and concern of children
deteriorating at home, particularly younger children and those with periorbital
cellulitis. The foundation studies found that treatment failure and complication
rates for children treated at home were no different to those treated in hospital,
despite including a wider population. The RCT was informed by the foundation
studies in several ways. These included a clinically relevant primary outcome of
treatment failure, and the need for a cost-‐effectiveness analysis. The nasal
colonisation study showed low prevalence of methicillin resistant Staphylococcus
aureus (MRSA) in this population, and that the administration of ceftriaxone at
home was not associated with the development of MRSA. It confirmed the
importance, due to the broad spectrum of ceftriaxone, of investigating resistant
bacterial acquisition as an outcome of the RCT. To determine which children
need intravenous antibiotics for this common infection, a score using clinical
features of patients presenting with cellulitis was derived and validated: the
Melbourne ASSET score. The crux of the thesis was the RCT, which showed that
treatment at home was non-‐inferior to treatment in hospital, in children with
uncomplicated moderate/severe cellulitis. In the per-‐protocol analysis,
treatment failure was significantly lower with home treatment and there were
fewer adverse events. There was no difference in acquisition of resistant nasal or
stool bacteria. The health economic analysis showed that home intravenous
antibiotic treatment for children with moderate/severe cellulitis was
emphatically more cost-‐effective with significantly higher quality of life than
hospital admission, and costs to families were significantly lower.
This thesis provides novel evidence for policy, practice and future research for
the use of intravenous antibiotics at home to avoid hospital admission.
iii
Declaration
The material presented in this thesis is principally my original work, although
many people contributed to the conception, design and final published
manuscripts included in Chapters 2, 3, 4, 5 and 6. All manuscript co-‐authors
provided advice and suggestions in the initial stage of the study design and on
the manuscript. All co-‐authors have authorised the inclusion of these
publications within this thesis. Professional editor Minn Stewart provided
document formatting guidance according to standards D and E of the Australian
Standards for Editing Practice and the Guidelines for Editing Research Theses
from the Institute of Professional Editors.
Study 1: a baseline observational study that describes the current OPAT practice
in treating cellulitis at a tertiary paediatric hospital after the initial introduction
of a direct-‐from-‐ED pathway. This study has been published.
I was the project coordinator for this study. I prepared a protocol and ethics
submission to the Royal Children’s Hospital Human Research and Ethics
Committee (RCH HREC) for this project. Patients for this study were
predominately recruited by myself with assistance from Emergency Research
staff. I also conducted the statistical analyses, interpretation of data and
produced the final tables and figures as presented in this chapter. I wrote the
initial draft of the published manuscript and performed the subsequent editing.
Study 2: a survey of clinicians’ practice in hospital with regards to the
management of cellulitis. This study has been submitted and is under review.
I was the project coordinator for this study. I prepared a protocol and ethics
submission to the RCH HREC for this project. Participants for this study were
predominately recruited by myself with assistance from the Emergency
Research staff. I also conducted the statistical analyses, interpretation of data
iv
and produced the final tables and figures as presented in this chapter. I wrote the
initial draft of the published manuscript and performed the subsequent editing.
Study 3: a prospective cohort study comparing the outcomes of children treated
at home versus hospital, and assessing the feasibility and informing the
methodology of the RCT. This study has been published.
I was the project coordinator for this study. I prepared a protocol and ethics
submission to the RCH HREC for this project. Patients for this study were
predominately recruited by myself, with assistance from Emergency Research
staff. I also conducted the statistical analyses, with guidance from A/Prof
Penelope Bryant, interpretation of data and produced the final tables and figures
as presented in this chapter. I wrote the initial draft of the published manuscript
and performed the subsequent editing.
Study 4: a longitudinal study on the same cohort of children comparing
acquisition of nasal carriage of Staphylococcus aureus. This study has been
submitted and is under review.
I was the project coordinator for this study. Patients for this study were
predominately recruited by myself; while Dr. Alex Scrivener performed the
majority of the 1 year follow up nasal swabs. I also conducted the statistical
analyses, interpretation of data and produced the final tables and figures as
presented in this chapter. I wrote the initial draft of the submitted manuscript
and performed the subsequent editing.
Study 5: the development and validation of a clinical scoring system to determine
whether intravenous or oral antibiotics are needed to treat cellulitis. This study
has been published.
I was the project coordinator for this study. Patients for this study were
predominately recruited by myself, with assistance from the Emergency
v
Research group research nurses. I also conducted the statistical analyses, with
guidance from A/Prof Susan Donath, interpretation of data and produced the
final tables and figures as presented in this chapter. I wrote the initial draft of the
published manuscript and performed the subsequent editing.
Study 6: RCT of home versus hospital intravenous antibiotics for children with
uncomplicated moderate/severe cellulitis. This study has been accepted and is in
press.
I was the project coordinator for this study. I prepared the protocol and full
ethics submission to the RCH HREC for this project. Patients for this study were
predominately recruited by myself, with assistance from the Emergency
Research group research nurses. I collected all the microbiology samples which
were processed by the RCH microbiology laboratory. I also conducted the
statistical analyses, with guidance from Ms. Francesca Orsini, the initial
interpretation of data and produced the final tables and figures as presented in
this chapter. I wrote the initial draft of the published manuscript and performed
the subsequent editing.
Study 7: a health economic analysis of home versus hospital intravenous
antibiotics for children with uncomplicated moderate/severe cellulitis. This
study has been submitted and is under review.
The institutional costs were obtained from the Clinical Decision Support Unit at
RCH. I performed the statistical analyses, with guidance from Dr. Li Huang,
interpretation of data and produced the final tables and figures as presented in
this chapter. I wrote the initial draft of the published manuscript and performed
the subsequent editing.
This work has not been submitted for any other qualification.
vi
Acknowledgement
The work described in this PhD was done over nearly 3 and a half years, with 2
of my 3 children born during this time. I could not have made it to this stage
without the practical and moral support of a great number of people.
I would like to express my sincere gratitude to my primary supervisor, A/Prof
Penelope Bryant, who has not been just a supervisor but a mentor, a friend and
life coach. I can never thank you enough for all that you have done for me. I am so
lucky to have you as my supervisor and am finally now ready to share you with
others. I hope the rest of our research journey together will be just as fun!
My gratitude to Prof Franz Babl, for planting the seed that I could complete a
higher degree, followed by persistent reminders for me to enrol with the
University of Melbourne and the rest is history. Although a giant in the research
world, you have always made time for me. Thank you for your guidance, your
wisdom, for fighting my corner, for making me a priority to the very end. You
inspire me to be a better researcher!
Thank you Prof Nigel Curtis, without your support I wouldn’t have been able to
start this PhD, I am immensely grateful. Throughout this journey you have
provided constant guidance and as always, a wealth of knowledge.
My advisory committee members, Dr Tom Connell and A/Prof Andrew Davidson,
thank you for teaching me, for your words of encouragement and support. I am
indebted to all my co-‐authors – especially the CHOICE team, A/Prof Sandy
Hopper, Ms Francesca Orsini, Dr Andrew Daley, and others A/Prof Susan Donath,
Dr Alex Scrivener, Dr Bennett Salvin, A/Prof Kim Dalziel and Dr Li Huang.
I am especially thankful to the staff of the Emergency Department and the
Emergency Research group (MCRI), Hospital-‐In-‐The-‐Home, Dolphin ward and
Microbiology at The Royal Children’s Hospital, Melbourne. Without your support,
vii
this thesis would not have been possible. Thank you for taking the time to
identify appropriate patients for the study and liaise with the study team, despite
your busy workload.
Thank you to the patients and families of The Royal Children’s Hospital. It is
always a stressful time in the life of a family when a child is admitted to hospital.
Agreeing to be part of research at this time is truly altruistic, thank you for your
generosity.
To my friends in Melbourne, Nisa and Rahman, Michelle and Gerald, Cathy and
Nigel, being far from family in Malaysia meant I got to find new family here in
Melbourne, couldn’t have done it without your support. Thank you to my coffee
and research buddy, Barry, without whom this journey would have been quite
lonely. My sincere gratitude to the educators at the RCH crèche (Bouchra, Manjot,
Harshee, Shamalie, Angela, Daryl, Hetal, Hayley) without whom the last 3 years
would not have been possible, seeing you every morning made everything better.
Thank you for showering my babies with love while I had to work on this PhD, I
will always remember your warmth and kindness.
To my family in Malaysia, especially my parents, thank you for raising me to be a
strong and determined person, for your unwavering support and love, for always
being there and for the many travels to help care for your daughter and
grandchildren. My parents-‐in-‐law, thank you for your prayers, understanding
and support to start this journey. My brothers and sisters, thank you for your
encouragement and always having my back. I can always count on you and hope
to spend more time with you with the completion of this work.
To my husband Andy, thank you for giving me the opportunity to develop my
career and passion (and depleting all of our savings over the past 3 years), for
supporting me through the best and worst parts of these last few years. Knowing
you were there for our family, no matter what, made this work possible. To my
gorgeous boys, you are my source of resilience. When things got tough, all I had
to do was think of you and I would find my strength again.

viii
ix
Preface
This is to certify that:
(i) the thesis comprises only my original work towards the PhD degree except
where indicated in the preface
(ii) due acknowledgement has been made in the text to all other material used
(iii) the thesis is fewer than 100,000 words in length, exclusive of tables,
bibliography and appendices.
Laila Ibrahim 11/1/19
x
Table of Contents
Abstract ...................................................................................................................................................................................... i Declaration ............................................................................................................................................................................. iii Acknowledgement ............................................................................................................................................................... vi Preface ...................................................................................................................................................................................... ix Abbreviations ...................................................................................................................................................................... xiv
Chapter 1 Outpatient parenteral antimicrobial therapy, cellulitis and antibiotic resistance in children ................................... 1 1.1 Introduction ...................................................................................................................... 1 1.2 Background ....................................................................................................................... 2 1.3 Out-‐of-‐hospital settings ................................................................................................ 3 1.4 Benefits of out-‐of-‐hospital treatment ...................................................................... 3 1.4.1 Hospital-‐acquired infections ................................................................................................. 3 1.4.2 Parental satisfaction and preference ................................................................................. 5 1.4.3 Quality of life ................................................................................................................................ 6 1.4.4 Cost-‐effectiveness ...................................................................................................................... 8 1.4.5 Disadvantages of out-‐of-‐hospital settings .................................................................... 10
1.5 Infections suitable for ambulatory treatment .................................................... 11 1.5.1 Observational OPAT studies ............................................................................................... 12 1.5.2 Home versus hospital studies ............................................................................................ 14
1.6 Cellulitis and treatment .............................................................................................. 16 1.7 Cellulitis treatment: who needs intravenous antibiotics? .............................. 18 1.8 Cellulitis treatment: what is a suitable antibiotic for OPAT? ......................... 19 1.9 Acquisition of resistant bacteria and other pathogens .................................... 21 1.9.1 Extended spectrum beta lactamase (ESBL)-‐producing Enterobacteriaceae 22
1.10 Vancomycin-‐resistant enterococci (VRE) .......................................................... 24 1.11 Clostridium difficile .................................................................................................... 26 1.12 Staphylococcus aureus .............................................................................................. 27 1.13 Conclusion and research questions ..................................................................... 29 1.14 Aims of the project ..................................................................................................... 30 1.15 Thesis structure .......................................................................................................... 30
Chapter 2 Current practice in home intravenous antibiotic management of cellulitis ......................................................................... 33 2.1 Introduction to current practice .............................................................................. 33 2.2 Management of cellulitis – how and why? ............................................................ 34
xi
2.3 Study 1: Clinician practice and opinions about antibiotic management of cellulitis in children .................................................................................................. 35
2.4 Current practice of home treatment of cellulitis with intravenous antibiotics – a baseline study ................................................................................ 56
2.5 Study 2: Management of children with cellulitis with intravenous antibiotics at home ................................................................................................... 58
2.5.1 Additional data ......................................................................................................................... 65 2.6 Implications of studies on current practice ......................................................... 66
Chapter 3 Foundation studies ............................................................ 69 3.1 Introduction to foundation studies ......................................................................... 69 3.2 Home versus hospital cohort .................................................................................... 70 3.3 Study 3: Home versus hospital cohort ................................................................... 73 3.4 Nasal colonisation in cellulitis .................................................................................. 81 3.5 Study 4: Nasal colonisation ........................................................................................ 83 3.6 Implication of foundation studies ........................................................................ 113
Chapter 4 Determining who needs intravenous antibiotics in cellulitis – a clinical scoring system .................................................. 117 4.1 Introduction to the clinical scoring system ....................................................... 117 4.2 Study 5: Clinical scoring system ............................................................................ 119 4.3 Implications of the Melbourne ASSET score ..................................................... 131
Chapter 5 Randomised controlled trial ........................................ 134 5.1 Introduction to the randomised controlled trial of home versus hospital
...................................................................................................................................... 134 5.2 Study 6a: RCT protocol ............................................................................................. 136 5.3 Study 6b: RCT .............................................................................................................. 145 5.3.1 Additional data ...................................................................................................................... 191
5.4 Implications of the RCT ............................................................................................ 192
Chapter 6 Health economic analysis .............................................. 195 6.1 Economic evaluation – comparison of alternative courses of actions ..... 195 6.2 Cost-‐effectiveness analysis ..................................................................................... 195 6.3 Study 7: Cost-‐effectiveness of home versus hospital treatment of children
with moderate/severe cellulitis ........................................................................ 199 6.4 Implications of the cost-‐effectiveness analysis ................................................ 235
Chapter 7 Discussion ........................................................................... 238 7.1 Introduction to key findings ................................................................................... 238 7.2 Home versus hospital for intravenous antibiotics ......................................... 239
xii
7.3 Is home treatment as efficacious as in hospital? ............................................. 239 7.4 Is home treatment as safe as in hospital? .......................................................... 241 7.5 Do home intravenous antibiotics have different implications on
acquisition of bacterial resistance than in hospital? ................................. 244 7.6 What is the impact of home treatment on satisfaction and quality of life?
...................................................................................................................................... 247 7.7 Which patients with cellulitis need intravenous antibiotics? .................... 250 7.8 Cost-‐effectiveness of home versus hospital ...................................................... 252 7.9 Future directions ....................................................................................................... 254 7.9.1 Management of cellulitis – impact analysis of the Melbourne ASSET score254 7.9.2 Microbiology – OPAT, resistant and colonising bacteria, and the microbiome
255 7.9.3 Hospital-‐In-‐The-‐Home – future RCTs of home versus hospital using the same
platform .................................................................................................................................... 256 7.9.4 Translating evidence into practice ............................................................................... 258
7.10 Conclusions ................................................................................................................ 259
Bibliography ............................................................................................. 268
Appendix 1 RCT Protocol ...................................................................... 291
Appendix 2 Blood Cultures in Cellulitis are not cost effective and should prompt investigation for an alternative focus ................ 335
Appendix 3 Clinician survey questionnaire ................................... 337
xiii
List of Figures
Figure 1.2 Lower limb cellulitis (photo by author) ........................................................... 16 Figure 1.3 Extended spectrum beta lactamase (ESBL) -‐ producing
Enterobacteriaceae ................................................................................................... 22 Figure 1.4 Vancomycin-‐resistant enterococci (VRE) ....................................................... 24
Figure 1.5 Clostridium diificile ..................................................................................................... 26
Figure 1.6 Staphylococcus aureus .............................................................................................. 27 Figure 6.1 Cost-‐effectiveness plane ....................................................................................... 198
List of Tables
Table 2.1 Details of patients whose empirical antibiotics were changed ............. 65
xiv
Abbreviations
CDI Clostridium difficile infection CHOICE Cellulitis at Home Or Inpatient in Children from the Emergency
ED Emergency Department ESBL extended spectrum beta lactamase
HAI hospital-‐acquired infections
HITH Hospital-‐In-‐The-‐Home ICER incremental cost-‐effectiveness ratio
MRSA methicillin resistant Staphylococcus aureus
MSSA methicillin sensitive Staphylococcus aureus OPAT outpatient parenteral antimicrobial therapy
PPI proton pump inhibitor QOL quality of life
RCT randomised controlled trial
RSV respiratory syncytial virus UK United Kingdom
UTI urinary tract infections VAS visual analogue scale
VRE vancomycin resistant enterococci

1
Chapter 1 Outpatient parenteral antimicrobial therapy, cellulitis and antibiotic resistance in children
1.1 Introduction
In the last decade, the treatment of children in an out-‐of-‐hospital setting as an
alternative to hospitalisation has become increasingly popular.1-‐4 This practice
initially began as an option for prolonged courses of intravenous antibiotics
administration, for the cystic fibrosis population in the 1970s.5 Several different
types of hospital alternative settings have been described such as ambulatory
centres,1 daily visits to the emergency department (ED)6 and medical care in the
patients’ home.4 The terminology in the literature also varies according to the
setting such as ‘ambulatory care’, ‘Hospital-‐At-‐Home’, ‘Hospital-‐In-‐The-‐Home’ or
outpatient parenteral antimicrobial therapy (OPAT). Regardless of the setting,
the studies show benefits such as increased quality of life (QOL),7,8 higher
parental satisfaction9 and avoidance of hospital-‐acquired infections10. With this
awareness, this practice has extended to acute conditions such as cellulitis and
urinary tract infections (UTI). It is this area of short-‐term home management of
acute conditions that triggered the clinical interest and research questions for
this thesis.
Despite its increasing popularity, the evidence for treatment of acute conditions
is lacking. There are no randomised trials of the efficacy of home versus hospital
management in infections in children. As such, this home/ambulatory pathway is
still not widely adopted as standard practice. Without the gold standard
randomised evidence, it is often hard to implement change. The initial plan for
this thesis was therefore to conduct a randomised controlled trial (RCT) of home
versus hospital intravenous antibiotics in children, the first to compare the
efficacy of home versus standard hospital treatment for an acute infection.
Cellulitis was chosen as a paradigm being one of the most common acute
infections treated on OPAT.3,11,12 During the literature review it became apparent
that there were large gaps in knowledge and that some of these needed to be
addressed prior to undertaking the RCT. The review of the literature described
herein, provides the background to the thesis of what was known, and not
2
known, at the start of the project. It provides the context both for the first half of
this thesis which was focused on obtaining a clearer understanding of current
management of cellulitis, and the second half of this thesis which was an RCT to
answer questions about efficacy, safety, acquisition of bacterial resistance, QOL
and cost-‐effectiveness of home versus hospital intravenous antibiotics in
cellulitis.
1.2 Background
In 1974, Rucker et al first described a cohort of 127 patients with cystic fibrosis,
aged between 7 and 27 who completed their course of intravenous antibiotics
for infective pulmonary exacerbation at home.5 Even then, it was recognised that
hospital avoidance resulted in ‘savings in medical costs, lack of disruption to
family routine, as well as in some cases continuation in school or employment’
which were all deemed important considerations by the author. Fast forward to
nearly half a century later, and medical treatment in a home/ambulatory setting
has not progressed rapidly. The standard treatment for infections requiring
antibiotics is still hospitalisation rather than home treatment.
To better understand the context in which the background research for this
thesis was conducted, several areas of the published literature were reviewed as
detailed below:
• The different types of out-‐of-‐hospital settings that exist.
• The advantages and disadvantages of treatment in these settings
• The management of cellulitis and the criteria for using intravenous antibiotics
• The effect of antibiotics on the acquisition of resistant bacteria, which is the
concern with using broad-‐spectrum intravenous antibiotics, a frequent choice
for home antibiotic therapy.
3
1.3 Out-‐of-‐hospital settings
A few types of alternative settings to hospitalisation are described in the
literature. The term used most widely and frequently is OPAT.3,12,13 However
OPAT services vary in the way the care is delivered, specifically in the location
where the antibiotic is administered. OPAT can occur in an outpatient centre 1, in
the ED 11 or in patients’ homes 12. The service at home can be delivered by
visiting nurses or by patients and families who are taught how to administer the
antibiotics themselves. With such a variation in practice it is not surprising that
outcomes have differed, with some studies documenting higher complication and
readmission rates compared to others. Although there is a wide variation in
practice, all these models of care serve the purpose of avoiding hospital
admission.
1.4 Benefits of out-‐of-‐hospital treatment
1.4.1 Hospital-‐acquired infections
The hospital environment is known to be a reservoir for transmission of
infections or asymptomatic carriage of potential pathogens. The literature on
hospital-‐acquired infections (HAI) largely consists of studies on patient
populations who would not be treated on OPAT anyway, for example paediatric
and neonatal intensive care units.14-‐16
However, general medical wards are not exempted from HAI, and since patients
on these wards are more likely to be amenable to an out-‐of-‐hospital pathway, the
focus of this review is for patients on general wards. It is not uncommon for
general medical wards to have patients with a variety of conditions, such as
those with respiratory, gastrointestinal and skin and soft tissue infections. One of
the most common diagnoses found on the general wards are infants with
respiratory syncytial virus (RSV) bronchiolitis who are admitted for
supplementary oxygen, rehydration or simply for monitoring in those at high
risk of deterioration. One study in the United Kingdom (UK) found that the air
(measured up to 5 metres from the index case) surrounding infants with RSV
4
bronchiolitis contained high numbers of particles containing the infectious
virus.17 In addition, RSV particles continued to be measured up to two hours
after the patients were discharged, potentially putting the next occupant at risk
of contracting this virus. Hospital-‐acquired diarrhea is also a common
occurrence. In thirty-‐one French paediatric wards, the incidence of hospital-‐
acquired diarrhoea was as high as 3.6%.18 Of these episodes, 2.5% were
rotavirus-‐related infections. This French study aimed to investigate which
hygienic measures reduced the incidence of hospital-‐acquired diarrhoea, based
on ward self-‐reported surveys. Worryingly, the authors found that standard
hospital precautions such as isolating patients, gowning, and emphasis on hand
washing did not demonstrate significant prevention. In a separate UK study,
69/157 (44%) of hospital-‐acquired diarrhoea occurred on general acute medical
and surgical wards.10 This study identified five different viral pathogens, with
rotavirus and norovirus being the two most common. These highly contagious
gastrointestinal infections have significant morbidity.19
Staphylococcus aureus (S. aureus) is also implicated as a HAI, most commonly
causing skin and soft tissue infections and bacteraemia. This was shown in a
study of 242 patients in a childrens’ hospital in Texas, USA. Although the
majority of patients in this study had a chronic underlying medical condition, 9%
had no underlying diagnoses, suggesting healthy children with no previous
diagnoses are also at risk.20 In this study, 42% of patients had a hospital stay of
equal to or less than 10 days, before the hospital-‐acquired S. aureus infection. In
addition to HAI, there is also evidence of colonisation of potential pathogens
occurring on hospital wards. For instance current hospitalisation or
hospitalisation of a family member is known to be a risk factor for S. aureus
colonisation.21
The literature on HAI on medical wards highlights a risk of contracting many
types of infections such as a respiratory tract infection, gastroenteritis or even
bacteraemia. Therefore clinicians should consider an alternate setting if feasible
and safe. However, it is unknown whether these risks extend to children who are
admitted for a short period, for instance up to 48 hours on a short stay ward. It is
5
likely that these risks remain although there are no studies specifically
investigating the risk of HAI in children with acute infections who are admitted
for a short period.
1.4.2 Parental satisfaction and preference
In studies of home/ambulatory treatment that have attempted to assess the
experience from the child or family’s point of view, the majority have used
simple measures of patient/parent preference or satisfaction with the treatment
location rather than using validated QOL tools.1,6 There are multiple studies
where patients and/or parents have expressed satisfaction with a home
pathway, but without any comparison with hospital treatment.1,6 It is perhaps
reassuring that there has never been a study showing participant dissatisfaction
with home/ambulatory treatment. In a study of families of children with cancer
who were offered hypothetical home and hospital treatment strategies for febrile
neutropenia, most families stated they would prefer total inpatient antibiotic
therapy.22 However, this may not reflect what families would prefer when
actually faced with this situation. This finding was confounded by the fact that
these families had never experienced any other treatment pathway other than
inpatient care and 50% of the children in the study had never experienced an
episode of febrile neutropenia.
In contrast to the above, in a study of 14 patients who received nurse-‐
administered chemotherapy infusions and parent-‐administered antibiotics at
home for one course of chemotherapy, preference for treatment location was
obtained. Only 1 of the 14 patients who had received home care, preferred future
care in hospital.23 The 1 patient who preferred future care in hospital had doubts
about his mother’s competence although the authors did not give further details.
The authors did not measure satisfaction with care. Another study of 36 children
who received ambulatory ceftriaxone in an ED for various acute infections such
as cellulitis, lymphadenitis and UTI surveyed parental preference for treatment
location. Of the 32 sets of parents who participated in the survey, 30/32 (94%)
would choose ambulatory treatment if faced with similar circumstances.6 One
6
parent who preferred hospitalisation had a child who was subsequently
admitted to hospital for worsening lymphadenitis and the other felt that
ambulatory treatment was an ‘overly stressful experience’.
There are two randomised trials of home versus hospital care in children that
included an outcome of satisfaction and only one assessed parental preference.
In the RCT on children with febrile neutropenia, satisfaction level for the hospital
group compared to the home group were no different.7 In this trial families were
not asked for preference of treatment location for subsequent episodes. In the
second RCT, which compared home versus hospital care for acute medical
conditions that require nursing observations or would require at least 24 hours
of ward observations, such as asthma, croup and gastroenteritis, a subset of 40
patients participated in a semi-‐structured interview to assess satisfaction and
preference.24 The findings were that 90% of families in both the home and
hospital groups would prefer home treatment for subsequent similar illnesses.
There was high satisfaction and no difference between treatment groups. The
only significant difference between the two groups was in disruption to family
life: 55% of the hospital group reported great disruption compared to 5% of the
home group (p<0.001).
In summary, although there is some evidence for parental preference for
treatment at home/ambulatory pathway, there is only one RCT, which
investigated this as an outcome and in this study, antibiotics were not
administered. Findings may have been different in a randomised study where
patients required antibiotics.
1.4.3 Quality of life
Specific evaluations of QOL in the literature that compare home to hospital
treatment is limited to the oncology 7,23,25 and cystic fibrosis populations.26 One
reason for this may be a lack of validated QOL tool specifically designed to
compare home versus hospital care.7,23 To overcome this problem, a QOL tool
was designed specifically in the study investigating the QOL in children receiving
7
chemotherapy infusions at home compared to hospital.23 The outcomes
measured seven domains for a child’s QOL including schoolwork, mood and
appetite, and four domains of parents’ QOL including time spent with spouse and
other children. Each of these domains were rated on a Likert scale from 0 to 6. In
this study, QOL was significantly better at home compared to hospital care for
both children and parents in the majority of domains measured. However there
was no difference between the two treatment locations for the amount of time
out of bed or duration of sleep. This scale was then replicated in another RCT
investigating children with cancer diagnosed with febrile neutropenia where the
primary outcome was QOL.7 The results from this trial showed a higher QOL was
reported for the home group on parental questionnaire in terms of time spent
with partner, other children and keeping up with household tasks. In the patient
questionnaire, children in the home group had better appetite and sleep
compared to the hospital group. Cheng et al investigated the anticipated QOL for
the treatment of children with febrile neutropenia utilizing a visual analogue
scale (VAS) if given 4 different treatment options which were: 1) total inpatient
antibiotic therapy, 2) inpatient antibiotic therapy followed by early discharge
with outpatient oral antibiotics, 3) total outpatient intravenous antibiotics and 4)
total outpatient oral antibiotics. The VAS scores were measured out of a
maximum of 10 points (0 worst, 10 perfect). From a parental perspective,
outpatient oral antibiotic management had the lowest median VAS score
(4.7/10) while median VAS scores for early discharge and outpatient
intravenous antibiotics (5.9/10 each) had the highest score. However, the
limitation of this study, which likely had a large impact on the finding, was that
the participants and parents were not actually receiving treatment or care at the
time of the interview. Instead, they were asked to imagine hypothetical scenarios
which the study authors noted may or may not be applicable to the participants.
Although VAS scores are a quick and simple way to measure QOL, they are prone
to bias and therefore have a limited role in measuring QOL.27
In a prospective non-‐randomised study where parents of children with cystic
fibrosis were given the option to complete antibiotic treatment at home or
hospital , a validated QOL tool for children called the DISABKIDS questionnaire
8
for chronic illness was utilised, which contains 37 questions on seven different
domains including independence, physical and emotional well-‐being.26 This
study found that for the home group, there were significant improvements in all
of the seven measured QOL domains after treatment. This is in contrast to the
hospital group where an improvement was only seen in two of the seven
parameters. Whether QOL for children with acute infections and their families is
better with home or hospital treatment remains unanswered.
1.4.4 Cost-‐effectiveness
Although there are several comparative studies of home versus hospital care
comparing costs, very few have actually performed a comprehensive economic
evaluation.23,28 There is only one study whereby a cost analysis using a cost-‐
utility modeling method was performed, using clinical and cost data from
previous randomised trials. Home intravenous treatment was found to be the
most cost-‐effective strategy for managing low risk febrile neutropenia.29 In this
study, a home intravenous treatment strategy was compared to three others:
hospital intravenous treatment, outpatient oral antibiotic treatment and hospital
intravenous treatment with early discharge (48 hours hospital intravenous
treatment followed by oral antibiotics at home). Hospital intravenous treatment
was found to be the least cost-‐effective strategy. However, there were several
limitations to this study such as the use of secondary data, costs being based on
an analytical model and not actual patients, as well as the use of hypothetical
scenarios to obtain utility scores to measure QOL. The authors concluded that
prospective randomised trials are needed to establish reliability and validity of
their findings.22 In a randomised trial of home versus hospital care, in children
who required nursing observations, a cost minimization approach was taken
rather than a cost-‐effectiveness analysis.30 In order to justify this type of
economic evaluation, the authors surmised that there would be no significant
difference in terms of clinical effectiveness between home and hospital care.
Therefore there were no measurements of QOL for patients in this study. With
regards to cost, the total National Health Service costs per patient in the study
was documented as £130/AUD230 greater for the home group compared to the
9
hospital group (£870/AUD1542 versus £741/AUD1313), with staffing salaries
being the main driver of costs. The interpretation of this finding must be taken
with caution though because at the time of the study, the Hospital-‐At-‐Home
service had been very recently established and was therefore, not at full capacity,
increasing the cost per patient. Additionally, the patients in the home group were
not directly discharged home from the ED, but had a period of hospitalisation,
thereby increasing ‘home group’ costs. This study is the only study in children to
compare home with hospital costs from the patient/family perspective. Direct
costs (travel, food, childcare) borne by families were reduced by 41% for home
patients (£23/AUD40 versus £14/AUD25, p=0.001). There were no differences
in the proportion of families who needed absence from work (and therefore
income lost) between the groups (76% versus 73%, p=0.84). However, in this
study, randomisation occurred at two time points, either early randomisation
(within 6 hours of presentation) or late randomisation (after 24 hours of
admission). For the subgroup of patients who were randomised to home
treatment early, there were fewer absences than those who went home later
(43% versus 90%, p<0.001), and parents appeared to take fewer days off work
(0.98 versus 2.32 days, p=0.09). A comparison of demographics and clinical
features between the group who went home early and the hospital group would
have been informative but was not provided. In a study of patients with cystic
fibrosis, a simple cost comparison was performed which resulted in the finding
that the home intervention was less costly, EUR2100/AUD3363 versus EUR
3360/AUD5381, p<0.001.26 However, this study did not document a breakdown
of these costs or how these costs were estimated making it unclear to the reader
how these figures were derived. Additionally, only healthcare institutional costs
were considered. A few other studies on the oncology population with febrile
neutropenia reported a limited economic evaluation.23,28 In one study, a simple
cost comparison was performed and the results showed that that home
treatment was cheaper by USD500/AUD695. However, the authors
acknowledged that without investigating costs to families one could not be
certain whether there was a transfer of burden of costs from the healthcare
provider to families.28 A cost analysis was also performed in a study on children
who received one course of nurse-‐administered chemotherapy infusions and

10
parent-‐administered antibiotics at home, with the conclusion that home was less
costly.23 However, in this pre and post home intervention study, absence from
work was not documented because the authors believed this to be similar for
treatment at home or hospital.
Most of the published literature comparing the costs of home to hospital
treatment have gaps in data such as lack of transparency of sources of data, use
of hypothetical cohorts, lack of a utility tool to measure effectiveness or do not
consider costs incurred by patients and their families. Overall, studies have
reported that home/ambulatory pathways are less costly, but a comprehensive
cost-‐effectiveness analysis has never before been conducted for home versus
hospital in children.
1.4.5 Disadvantages of out-‐of-‐hospital settings
For patients and families who are suitable for treatment outside the hospital
setting, there are potential disadvantages to consider. Firstly, there are several
comparative home versus hospital studies that report a longer duration under
medical care for the OPAT group.4,31 For example, in 63 children treated for
febrile neutropenia, the home group were treated for 7.6 days while the hospital
group were treated for 6.3 days, p=0.008.31 This may be due to a more cautious
approach by physicians for those patients who are not physically in the hospital,
resulting in a prolonged duration of care. Another reason may be a result of
selection bias: that those who are selected by physicians to receive OPAT
treatment are those who require a longer course of antibiotics or medical care
anyway, which is a limitation of non-‐randomised studies. However, it is possible
that this is due to an artifactual reason. For instance, in some healthcare settings
nurses who travel to administer treatments at several locations are not able to
‘discharge’ patients until they physically return to hospital, which leads to a
falsely increased duration of care. These studies do not report precisely how the
duration of medical care or length of stay was calculated for those on OPAT.
11
Another disadvantage for the outpatient pathway is the small percentage of
families who would still prefer hospital treatment.1,7 Orme et al reported that
families were anxious about caring for their children with febrile neutropenia in
the home.7 For some parents, being in hospital may offer a physical ‘burden-‐
sharing’ option, especially for those with complex and chronic illnesses such as
the oncology population. The constant presence of medical staff may be a source
of comfort for some families, particularly those who are very sick or frequently
in hospital. Another reason why families may prefer hospital admission is if they
are required to travel for OPAT care.1,6 In a study of cellulitis treatment at a ‘day
treatment centre’, approximately 30% of families reported preference for
hospital admission should their child have the same condition again. Although
reasons were not specifically documented, the authors mentioned travel time
and care of other siblings as possible reasons. However, most families still prefer
to commute rather than have their child hospitalised.
Lastly, one of the biggest downsides for those treated on OPAT is the risk of
readmission due to complications or treatment failure. Although most
comparative studies report a similar complication rate32,33, having a
complication for those outside the hospital requires the onerous process of re-‐
presenting to hospital and waiting for a hospital bed. Only those who have
infections where there is a reasonable chance of OPAT being successful should be
treated via this pathway. What constitutes ‘a reasonable chance of success’ is
likely to differ between infections and even individuals.
1.5 Infections suitable for ambulatory treatment
Studies of infections treated via a home/ambulatory pathway can be broadly
divided into two types: 1) observational or descriptive studies; and 2)
comparative studies of home versus hospital. Infections treated by
home/ambulatory services can also be classed into prolonged and short-‐course
antibiotic therapy. As defined by the Infectious Diseases Society of America
(IDSA) guidelines on OPAT, short-‐course antibiotics are defined as antibiotic
therapy of less than one week duration.34 Prolonged antibiotics are given for
12
infections such as osteomyelitis, septic arthritis, meningitis and cystic fibrosis
respiratory exacerbations.3,35 Shorter course antibiotics are given for cellulitis1
and UTI36,37. In addition, febrile neutropenia 7 and post-‐operative complicated
appendicitis have also been reported to be amenable to home treatment 32,33,38,
although these conditions may be either short-‐course or prolonged antibiotic
therapy. The majority of these studies are descriptive, observational studies
where a selected group of patients deemed to be less unwell are treated at home
or ambulatory pathway.
1.5.1 Observational OPAT studies
Observational studies of OPAT all comprise single centre studies describing their
management of a range of infections 3,35 or focusing on a single infection.1
Patients are pre-‐selected and high rates of success and low rates of
complications are usually reported. The issue with these non-‐comparative
studies is the lack of benchmarking to allow readers to judge whether or not
patients treated via the ambulatory pathway are disadvantaged compared to
standard care. Most OPAT studies include children that have had at least a brief
hospital admission during the worst of their infection, but often much longer
with many inpatient bed days before a final period of OPAT to finish a long
course of intravenous antibiotics. There are, however a handful of studies where
OPAT is commenced from the ED, so that the patient is never admitted to an
inpatient bed and avoids hospital altogether. A prospective Canadian study
investigated the outcomes of children with cellulitis requiring intravenous
antibiotics treated at a day treatment centre. 1 In this study, 224 children aged 3
months to 18 years presented to the ED with moderate/severe cellulitis, defined
in this study as those requiring intravenous antibiotics, over a 2 year period. Of
224 children, 92 (41%) were treated at a day treatment centre with once daily
intravenous ceftriaxone, while the remaining 59% of patients received standard
care in hospital. Referral to the day treatment centre was offered as an
alternative to conventional hospitalisation, according to the judgement of the ED
physicians. However this study did not clarify of those offered this treatment
option, how many patients had declined. Exclusion criteria for treatment were
13
complicated cellulitis such as those associated with toxicity (lethargy,
cardiovascular instability), immunosuppression and presence of significant
comorbidity. These patients received a single dose of ceftriaxone in the ED
administered through a peripheral intravenous access that was heparinised daily
throughout treatment duration. This day treatment centre was opened 7 days a
week and was staffed by paediatricians. Ceftriaxone was continued until the
fever disappeared and the cellulitis improved by 75%. Subsequently, the patient
was prescribed oral cephalexin. The success rate was reported as 79%, defined
as those not readmitted to hospital during treatment. However, the remainder
required hospitalization for concerns regarding emerging complications. The
mean duration of antibiotics was 2.5 days. The authors did not report the
duration of antibiotics or rate of complications for the hospital group, therefore
the interpretation of the purported success of this home pathway is unclear. If,
for example, the proportion of those in the hospital group who developed
complications was also around 20%, then clearly, those that had ambulatory
treatment did not suffer a disadvantage.
In another observational study, the use of ambulatory ceftriaxone in the ED
setting to treat a variety of infections such as cellulitis, lymphadenitis, UTI and
tonsillitis in 36 children was described prospectively, without a comparison to
standard of care.6 Only one child with a diagnosis of lymphadenitis was
considered as having failed treatment which led to hospitalisation. The criteria
for treatment failure was not reported, therefore it was possible that this child
just required a longer duration of antibiotics as commonly seen in lymphadenitis.
Other studies retrospectively report their experiences as an OPAT service with a
focus on the appropriateness of antibiotics prescribed.3,35 Although these studies
contribute to the growing body of literature on ambulatory care, they may give
the inaccurate impression to those not familiar with OPAT, of a generally high
rate of readmission and complications. This impression may have come about as
many of the patients commonly treated via OPAT were those requiring
prolonged antibiotics, as shown in two studies from the United States reporting
a median treatment length of 11 and 12 days respectively.3,35 As a result, this
14
patient population is at risk for not only complications of the disease they are
being treated for, but also the side effects of prolonged antibiotics such as
abnormal biochemistry and haematological status and the complications
associated with central venous catheter. In the two US studies, antibiotic or
catheter related complication rates of 24% and 29%, were reported.3,35 In both
studies, the most commonly used antibiotic was ceftriaxone at 18% and 25%
respectively. Despite the high rate of complications, when prolonged antibiotics
are required, ambulatory treatment is attractive in order to avoid prolonged
hospitalisation.
1.5.2 Home versus hospital studies
Comparative studies of home versus hospital care are more informative than
descriptions of a home service alone. When key outcomes such as duration of
antibiotics and length of stay are reported for both ambulatory and hospital
cohorts, readers are able to better discern the benefits and risks of ambulatory
treatment. One of the earliest comparative studies was reporting on post-‐
operative complicated appendicitis in a small study of 16 children.32 Eight
children were treated at home with insertion of a peripherally inserted central
catheter while the remaining eight were treated in hospital. The number of total
care days was no different between the groups. However, the authors did not
report how treatment location was assigned, whether by self-‐selection or
physician selection, an important factor in deciding which patients would be
suitable for this pathway based on this study. Additionally, although the authors
stated that families had no difficulties accepting the insertion of a peripherally
inserted central catheter, this appears to have been inserted at the same time as
surgery for appendectomy. It is difficult to imagine families accepting additional
anaesthetic or sedation for their child for a shorter antibiotic duration, which is
likely to be necessary for many children requiring central catheters or cannulas.
Another study also comparing home versus hospital in post-‐operative
complicated appendicitis, also found no difference in key outcomes or rate of
complications.38 This study reported a list of selection criteria for home
treatment suitability, divided into medical and social criteria. Medical criteria

15
included being afebrile >24 hours, normal gastrointestinal function and
tolerating oral analgesics. Social criteria included having a functioning home
telephone, insurance coverage for home care and continuous caretaker
availability. By having a list of criteria both medical and social, other services are
able to use this information to establish their own service or for those with
existing pathways, these criteria can be compared with their own protocol. There
is one retrospective study comparing the outcomes of 42 children with
periorbital cellulitis who received ambulatory treatment and the 21 children
treated in hospital.2 In this retrospective chart review, the criteria that clinicians
used to decide on route of treatment, intravenous antibiotics versus oral
antibiotics, or location of treatment, ambulatory versus hospital care, was not
documented. There was no significant difference in duration of treatment in days
between those on ambulatory management and those admitted (mean 2.8 days
in both groups) and the rate of complications were also similar.
All of these studies suffer from selection bias, and for many, the source of bias is
often unknown, due to lack of clarity around patient selection for OPAT. There is
a single RCT of home versus hospital intravenous antibiotics in children with
febrile neutropenia.7 In 36 children randomised to treatment at home or
hospital, the primary outcome was QOL, not efficacy or safety. The authors state
that families were anxious about supporting their unwell children outside of the
hospital setting despite the fact that the literature suggests likely superior QOL
with outpatient treatment. The main finding of this study that treatment at home
was associated with a higher QOL, although important, is unlikely to convince
clinicians to change their practice. There were a few complications, but the study
was not powered to investigate efficacy, which is crucial to change practice. It is
unclear why a clinical outcome was not chosen by the investigators, for example
persistence of fever beyond 48 hours or requiring additional antibiotics, but is
potentially related to the numbers required for a trial with a clinical outcome.
Despite the inertia to changing practice, it is important to note that even in
conditions such as post complicated appendicitis or febrile neutropenia, there
have been no reported fatalities in those treated at home. Serious adverse events

16
are even less likely in other less serious infections such as cellulitis. This,
therefore, seems like a good infection to use as a paradigm for home intravenous
antibiotic use, to develop evidence that would inform practice. In the following
section, the literature on the ambulatory treatment of cellulitis, as the focus of
this thesis is explored in more detail.
1.6 Cellulitis and treatment
In Australia in 2002, the rate of
hospitalisation for the skin infection
cellulitis was 11.5 episodes per 10,000
people with a mean duration of 5.9 days.39
In the United States, skin and soft tissue
infections which include cellulitis account
for over 74,000 pediatric hospital
admissions per year.40 Clinically, cellulitis
is manifested by rapidly spreading areas
of oedema, redness and heat, sometimes
accompanied by lymphangitis and
inflammation of the regional lymph nodes,
Figure 1.1 Lower limb cellulitis
(image source: author)
with or without systemic features.41 This infection when uncomplicated, typically
responds to antibiotics targeting Group A Streptococci and S. aureus. Although
mild cellulitis is treated with oral antibiotics, parenteral antibiotics are used for
more severe cellulitis or cases where oral antibiotics fail.42,43 In children and
adults, catastrophic outcomes for cellulitis are very unlikely and the risk of
bacteraemia is low.44,45 Due to these reasons, it is an ideal condition to treat with
OPAT. In fact, the most common acute infection treated with OPAT in adults is
cellulitis, increasingly directly from the ED.46-‐48
17
At the start of the work leading to this thesis there were only three home or
ambulatory studies in children specifically investigating the treatment of
cellulitis. Although all three treated children directly from the ED with the goal of
admission avoidance, only one was a prospective study and two were
retrospective chart reviews.1,2,43 In the prospective Canadian study1, 92 children
with cellulitis were treated at a day treatment centre, returning once daily for
intravenous ceftriaxone. In this study the treatment failure rate, defined as
readmission to hospital, was 20%.1 However, the authors did not compare the
outcomes of these children to those treated in hospital. Similarly, in a UK study,
ambulatory treatment of periorbital cellulitis has also been shown to be feasible
in 42 children.2
Although these studies describe the use of intravenous antibiotics to treat
cellulitis, none of these studies set out clear inclusion criteria for those who
require intravenous treatment. In the prospective Canadian study,
moderate/severe cellulitis was defined as ‘cellulitis that would have traditionally
required intravenous antibiotics according to the physician’s judgement and
would then have required inpatient admission’. Similarly in an adult RCT of
home versus hospital treatment for moderate/severe cellulitis, the decision to
commence intravenous antibiotics was ‘left to the attending doctors in the
emergency.’46 However one study did compare severity of symptoms and found
that those who were commenced on intravenous antibiotics were more likely to
have systemic symptoms.43
With regards to treatment, the recommended intravenous antibiotics are
dicloxacillin, flucloxacillin or nafcillin 6-‐hourly, cefazolin 8-‐hourly or cephalothin
6-‐hourly.49 However, the frequency of these antibiotics, makes administration
incompatible with OPAT unless the patient or family were to self-‐administer.
However, there are several problems with this option. Firstly, not all families are
comfortable with administering medication. Secondly, assuming some families
are keen, the time it would take to train the family to administer medication
would probably equate to the whole duration of the hospital admission. Thirdly,

18
extra resources would be required to fund a training program for families, which
is unlikely to be cost-‐effective for a once off episode of cellulitis.
During review of the literature on the ambulatory treatment of cellulitis, it
became apparent there were two questions to address: 1) Which children
presenting with cellulitis need intravenous antibiotics? 2) Which intravenous
antibiotic is suitable for an ambulatory or OPAT pathway?
1.7 Cellulitis treatment: who needs intravenous antibiotics?
The Infectious Diseases Society of America (IDSA) guideline for the diagnosis and
management of skin and soft tissue infection recommends intravenous
antibiotics for cellulitis with systemic signs of infection.34 However, children with
systemic signs such as pyrexia, are commonly treated at home with oral
antibiotics.43,50,51 The IDSA guideline is intended for both adults and children but
is not necessarily applicable to children. The Clinical Resource Efficiency Support
Team (CREST) guidelines for the management of cellulitis recommend
intravenous antibiotics for those with underlying co-‐morbidities such as varicose
veins or peripheral vascular disease, again clearly not applicable to children.52
Even our institutional guidelines are unclear, recommending intravenous
treatment for those with ‘severe/extensive, systemically unwell or not
responding to oral treatment’, without any specific clinical details to guide these
definitions. In this situation intravenous antibiotics are recommended and
potentially investigations.53
Although the majority of patients with cellulitis will respond to oral antibiotics, a
proportion of children require intravenous antibiotics.1,6 A study from over three
decades ago showed that clinicians have tried to stratify children with cellulitis
according to severity.54 However guidelines for the recommendation of when to
start intravenous antibiotics for cellulitis in children do not exist. None of the
previous studies on children with cellulitis requiring antibiotics have described
clear criteria for commencing intravenous treatment.1,2,43 There are studies
providing evidence to support guidelines for cellulitis affecting the periorbital
19
region.51,55,56 However, the purpose of the resulting guidelines is to differentiate
orbital from periorbital cellulitis, to guide which investigations and specialists
should be involved, but they do not aid the primary care or emergency clinician
to determine whether to commence oral or intravenous treatment.57
The absence of clear guidelines for the management of cellulitis in children is not
unique to this condition. Other common childhood infections also lack clear
evidence-‐based recommendations on when intravenous treatment is necessary,
such as UTI and pneumonia. Several clinical prediction rules have been
established for common childhood illnesses and trauma such as the Westley
croup score58, the Pediatric Respiratory Assessment Measure (PRAM) for
asthma59, the Paediatric Appendicitis Score (PAS) for acute appendicitis60 and
the Children's Head Injury Algorithm for the prediction of Important Clinical
Events (CHALICE) for head injuries61. Although clinical scores still require a
clinician’s judgment and cannot be used on their own to determine the best
course of action for patients62, they provide an aid for clinicians, particularly
more junior clinicians, when making decisions and are valuable tools in clinical
research. It is clear from the literature that there is a gap for a clinical scoring
system or a clinical prediction rule for cellulitis in children.
1.8 Cellulitis treatment: what is a suitable antibiotic for OPAT?
In order for an antibiotic to be used in OPAT, it needs to be one with a long half-‐
life, only requiring ideally once or at most twice daily administration. This would
mean that patients would only be required to travel to a treatment centre once
or twice daily or a home visiting nurse would be required to visit patients once
or twice a day. One way around this is to insert a central venous catheter to allow
the administration of a continuous infusion over 24 hours. This would mean
many types of antibiotics could be given, including intravenous flucloxacillin, the
antibiotic used in our centre to treat moderate/severe cellulitis. However the
risks of inserting and maintaining a central catheter which would usually require
a general anaesthetic or sedation in children, is not justified for infections in
children where the antibiotic duration is usually less than 5 days.1 Another

20
alternative is to administer cefazolin with oral probenecid to increase its half-‐
life. This alternative has been shown to be a viable option in adults with
cellulitis.47,63 Only one study in paediatrics has investigated the use of cefazolin
with probenecid for the outpatient treatment of cellulitis.43 This study was a
retrospective chart review investigating the outpatient treatment of patients
with cellulitis, by dividing patients into three groups, those treated with oral
antibiotics, those treated with cefazolin 8 hourly and those treated with cefazolin
twice a day with oral probenicid. There were 39 patients who had to return to
ED every 8 hours for a dose of cefazolin compared to another group of 85
patients, who returned to ED twice a day for cefazolin while taking oral
probenecid. The treatment failure rate for the cefazolin only group was 31%
compared to the cefazolin with probenecid group which was 8%. They attributed
this difference to potentially a clinically more severe patient cohort in the
cefazolin only group and lack of compliance with frequency of dosing due to the
need to return to hospital three times a day. The study documented 5/85 (6%)
patients with side effects secondary to probenecid which were nausea, vomiting,
abdominal pain, difficulty swallowing, and refusal of the child to take probenecid.
However, given that this was retrospective, the proportion of patients who
actually had side effects was likely higher. One of the most commonly used
antibiotics on OPAT is the broad spectrum cephalosporin, ceftriaxone.1,2,13,34,35
Bradley et al first described ceftriaxone as a once daily antibiotic suitable for
outpatient treatment of serious infections.64 This antibiotic is administered once
daily, compatible with OPAT services.1,2 It can be administered over a five minute
short intravenous infusion. However, the association of ceftriaxone with
resistant organisms in predominantly adult literature causes concern for
widespread OPAT use.65 An RCT in adults comparing once daily ceftriaxone to
once daily cefazolin with probenecid found that although equivalent in terms of
effectiveness, nausea was significantly more common in the cefazolin with
probenecid group.46 The other two paediatric studies of OPAT for cellulitis both
used ceftriaxone without comparison. Although the evidence is therefore not
strong, ceftriaxone can reasonably be considered the best clinical option for
OPAT management of cellulitis. This leads to the next question: how strong is the
21
association of ceftriaxone with the acquisition or colonisation of resistant
organisms and other potential pathogens?
1.9 Acquisition of resistant bacteria and other pathogens
The association between third generation cephalosporins, including ceftriaxone,
and resistance arose initially from its use in adults. Although all antibiotic use
has the potential to drive resistance, third-‐generation cephalosporins raise
particular concern because of their broad spectrum nature. These resistant
bacteria not only have the ability to colonise the human body but more
concerning is their potential to become pathogenic and cause infections,
resistant to multiple antibiotics.
This had led to a warning for cautious use of ceftriaxone aimed at adult OPAT
services66 despite the difficulty in establishing specific evidence for the
association of commensal overgrowth with ceftriaxone alone due to the many
confounding factors in studies. Resistant bacteria that have published evidence
suggesting an association with third-‐generation cephalosporin use include
cephalosporin-‐resistant extended spectrum beta lactamase (ESBL)-‐producing
Enterobacteriaceae, vancomycin resistant enterococci (VRE), and methicillin
resistant S. aureus (MRSA).67-‐69 In addition to colonisation with resistant
bacteria, the use of ceftriaxone is often associated with Clostridium difficile
infections.70 The focus of my review of the literature in this area is evidence of
the association of ceftriaxone with these organisms specifically in children.

22
1.9.1 Extended spectrum beta lactamase (ESBL)-‐producing
Enterobacteriaceae
Figure 1.2 Extended spectrum beta lactamase (ESBL) -‐ producing Enterobacteriaceae
(image source: downloaded from http://media3.picsearch.com/is IbbANfZSzo, in June 2018)
Enterobacteriaceae are Gram negative bacteria that colonise the gastrointestinal
tract and include potential pathogens such as Escherichia coli and Klebsiella
pneumoniae. The Enterobacteriaceae can cause multiple types of infections, for
instance, E. coli is a common pathogen in UTI, while Klebsiella spp are known to
cause pneumonia. All of the Enterobacteriaceae have been implicated in
bloodstream infections and intra-‐abdominal infections such as peritonitis and
cholangitis. Resistance to third-‐generation cephalosporins in this family is
commonly associated with the expression of extended spectrum beta lactamases
(ESBLs), a family of enzymes that are able to inactivate beta lactam antibiotics,
including ceftriaxone. These enzymes are mostly produced by the bacteria E. coli
and K. pneumoniae.71 They are of particular concern due to their increased
activity against the third generation cephalosporins, which includes cefotaxime,
ceftriaxone and ceftazidime in addition to resistance against penicillins and first
and second generation cephalosporins. Another mechanism of antibiotic
resistance for this group of bacteria is the ability to pass on the plasmid encoding
resistance between bacterial strains and species which poses challenges in terms
of infection control.72 Infections caused by ESBL producing bacteria have a
higher mortality and morbidity in adults than those not producing ESBL.73 Most
of the paediatric literature on ESBL-‐producing bacteria involve hospitalised
children but more recent literature suggest these organisms are rising in the
community.74 A Swedish study investigating the prevalence of ESBL-‐producing

23
bacteria in 313 healthy children aged 1-‐5 years in the community documented a
stool carriage rate of 2.9%.75 However, a Spanish study documented a much
higher carriage rate of 24% in healthy toddlers aged between 8 to 16 months.76
This difference may have been attributed to the difference in geographical region
between these studies although the author of the latter study noted their finding
was the highest found in Europe. In a study that compared children with UTI
caused by ESBL-‐producing bacteria to those whose UTI were caused by non
ESBL-‐producing bacteria, risk factors for the former were identified as previous
hospitalisation and previous antibiotic use.77 There are several studies that
specifically associate third-‐generation cephalosporin use with ESBL-‐producing
bacteria although most of these studies are in the neonatal population, known to
be high risk with multiple confounding risk factors. For instance, in a neonatal
intensive care unit in Taiwan where 47/1106 (4%) episodes of bacteremia were
due to ESBL-‐producing organisms, exposure to cefotaxime was significantly
associated with acquisition of multi-‐drug resistant bacteremia (odds ratio [OR]
6.0, 95% confidence interval [CI]: 2.4–15.1; p<0.001).78 The most common
mechanism of resistance was ESBL production, mostly by K. pneumoniae.
However, in this non-‐randomised prospective cohort study, the group with
multi-‐drug resistant bacteremia had higher overall antibiotic exposure
suggesting other contributing factors. The most convincing study of third
generation cephalosporin use and its association with resistance was a
prospective cross-‐over interventional study of a change in antibiotic neonatal
unit policy by De Man et al.79 This study showed that an antibiotic policy
including cefotaxime was associated with colonisation with cefotaxime-‐resistant
Enterobacteriaceae (although it did not specifically address ESBL bacteria)
which reduced when the policy changed to one that did not include cefotaxime.
There is a single case control study showing an association between cefotaxime
use and cefotaxime resistance in older children with cancer, although patients
had also received more aminoglycosides reflecting an increase in overall
antibiotic exposure.80 There are no studies addressing the association between
third generation cephalosporin use and ESBL in healthy children and no studies
in those treated with home/ambulatory antibiotics in the existing literature.
24
1.10 Vancomycin-‐resistant enterococci (VRE)
Figure 1.3 Vancomycin-‐resistant enterococci (VRE)
(image source: downloaded from
https://www.publichealthontario.ca/en/BrowseByTopic/InfectiousDiseases/PublishingImages/VRE.png,
in June 2018)
Enterococci are Gram positive bacteria which colonise the gastrointestinal tract.
The two most important species which can cause infections of the urinary tract,
endocardium, meninges or in the bloodstream are Enterococcus faecalis (E.
faecalis) and Enterococcus faecium (E. faecium). These bacteria were first
reported as important pathogens in both the hospital and community in the
1980s.81 This was followed by the detection of vancomycin resistance, primarily
in E. faecium. VRE have been reported primarily as a nosocomial pathogen in
adults and children, commonly in the context of an outbreak.82-‐84 VRE
bloodstream infections are a major cause of morbidity and mortality for
hospitalized patients.82
Enterococci are inherently resistant to cephalosporins and are able to colonise
gastrointestinal sites previously populated by cephalosporin-‐susceptible
organisms.85 The association between VRE and cephalosporin use has been
reported in the context of a reduction in VRE with limiting use of cephalosporins.
However, outbreaks of VRE are not restricted to units where third generation
cephalosporins are used. For example, a study investigating risk factors for VRE
colonisation in a neonatal intensive care unit found that antimicrobial therapy
use for second line empiric treatment of late onset neonatal sepsis

25
(glycopeptides, ciprofloxacin, azithromycin, meropenem and cefepime) was a
significant risk factor for VRE colonisation.84 In a paediatric oncology unit where
a VRE outbreak occurred, successful control of the incident was attributed to an
overall restriction in the use of cephalosporins (ceftazidime) and
glycopeptides.83 The authors found risk factors for VRE colonisation to include
previous antibiotic use, amikacin exposure and ceftazidime exposure with a
prevalence of 14/73 (19%) amongst inpatients in the oncology unit. However,
the successful eradication of VRE was attributed to several factors which were
institution of infection control measures, coupled with a comprehensive
educational program in addition to modification of antibiotic policy. The same
group of authors later conducted a study to investigate the prevalence of VRE
colonisation in children of hospital staff members as a ‘community cohort’. In
116 children who had a faecal sample tested, none were colonised with VRE.86
Similarly, a Swedish study that investigated the prevalence of ESBL in healthy
children attending preschools used faeces from the same cohort to investigate
the prevalence of VRE. They found none of the children to be VRE carriers.87
There are no other studies in children showing direct association between
ceftriaxone and VRE. In contrast to the paediatric population, studies in adults
have reported VRE to be directly associated with ceftriaxone use.82 However this
was a retrospective analysis where ceftriaxone use in the prior month was
related to the incidence of VRE bloodstream infection, so other potential risk
factors may have been overlooked. The concern for the association between
ceftriaxone use in children contributing to the development of VRE does not
appear to be evidence-‐based.
26
1.11 Clostridium difficile
Figure 1.4 Clostridium difficile
(image source: downloaded from https://si.wsj.net/public/resources/images/HEAA179_CDIFFI_P_20160129144116.jpg, in June 2018)
C. difficile is a Gram positive spore forming anaerobic bacillus that colonises the
gastrointestinal tract. They were first described as part of the intestinal flora in
neonates.88 C. difficile is associated with a range of clinical diseases, from mild
antibiotic-‐associated diarrhoea to pseudomembranous colitis, bowel perforation,
sepsis and death.89 Overgrowth of C. difficile, with or without clinical symptoms,
is not exclusively associated with cephalosporins and has been reported
following administration of many other antibiotics.90 C. difficile infections (CDI)
can be hospital-‐acquired or community-‐acquired.91 Although in adults, CDI is
strongly associated with antibiotic use, in children the role of antibiotics is less
clear as CDI can occur in them without recent use of antibiotics.92 Samady et al
performed a retrospective case-‐control study in hospitalised children, they found
cephalosporin use within the previous 90 days as a risk factor for CDI but also
found many other associations such as recent hospitalisation, immunodeficiency
and proton pump inhibitor (PPI) use to be significant risk factors.93 Furthermore,
they found that in 8% of CDI cases, there was no previous antibiotic use, recent
hospitalisation or past history of CDI suggesting other factors playing a role.93
Amongst hospitalised children with cancer, one retrospective study found third
and fourth generation cephalosporins which includes ceftriaxone use in the
previous 21 days to be a significant risk factor for CDI. 94 They also found PPI use
to be a significant risk factor in this population. In another study, also on
hospitalised children, exposure to multiple (three or more) antibiotic classes to
was associated with severe CDI.95 Although one of the antibiotic classes was the

27
third generation cephalosporins, the authors did not find any significant
association of severe CDI with any one or two classes of antibiotic use,
suggesting it may not be the type of antibiotic but the overall burden of antibiotic
exposure in addition to the vulnerability of the patient if they are exposed to
multiple antibiotics. In another retrospective study on patients with
inflammatory bowel disease from outpatient clinics, 134 patients were evaluated
and 47% had CDI.96 The previously noted risk factors such as antibiotic
exposure, previous hospitalisation and PPI use were not found to be a significant
association. The only risk factors identified in this study were the age of the
patient and disease severity. The other factor to be aware of in children is the
high burden of colonisation without infection, especially in those under 2 years,
at a rate of about 50%.97 This not only means that detection may not be
associated with any risk factors, but also that they may act as a silent reservoir
for infection in more vulnerable patients.
In summary, the literature in C. difficile in the paediatric population mainly
reports on vulnerable groups of hospitalised patients using retrospective
methods, where there may be an association with third generation
cephalosporins but there are likely a number of contributing factors. In addition
in children who are not hospitalised, antibiotics may not be a risk factor at all.
1.12 Staphylococcus aureus
Figure 1.5 Staphylococcus aureus
(image source: downloaded from https://encryptedtbn0.gstatic.com/images?q=tbn:ANd9GcSeafrGXdR3aHwHx9W0ZrYVooOKEkT1HjdHXk5iAdSC3nvu1gPQ, in June 2018)

28
S. aureus is a Gram positive bacteria that colonises the human respiratory tract
and skin. Nasal colonisation with S. aureus plays a key role in the pathogenesis of
invasive infection including cellulitis and bacteremia98-‐100 and is also associated
with non-‐infectious conditions such as asthma101, eczema102 and epistaxis103. In
1960, MRSA was first reported in clinical practice and has been a rising global
challenge. One of the earliest reports of an association between third generation
cephalosporin use and MRSA was by Washio et al in Japan.69 This study
conducted in a geriatric hospital, showed that the use of third generation
cephems; cephalosporins, monobactam and carbapanem was a significant
association with MRSA infections in the elderly. However, in children, there is
conflicting evidence on the importance of antibiotic exposure as a risk factor for
MRSA colonisation or infection. It has been shown that MRSA-‐colonised children
are 24 times more likely to have MRSA infections compared to non-‐colonised
patients, therefore risk factors for carriage are equally important.104 Reported
risk factors for colonisation by both MSSA and MRSA in children include prior
antibiotic use, hospitalisation, maternal colonisation, colonisation in other
household members, hospitalisation of a household member and older age.21,105-‐
107 Lo et al showed that antibiotic use in the previous 12 months was a significant
risk factor for colonisation with MRSA in healthy children recruited from
kindergartens and health visits. However the authors found that there was
variability in risk factors depending on age and gender. For instance, in girls aged
1 to 5 year olds, antibiotic use in the preceding 12 months was not a significant
risk factor, a finding which underlines the complex pathophysiology involved in
determining MRSA carriage status. 108 Another study that also demonstrated a
significant association was by Rodriguez et al where beta-‐lactamase inhibitor use
in the previous six months was shown to have a significant association with
MRSA carriage. 105 The biggest limitation for both these studies investigating risk
factors for MRSA carriage is having to rely on parental recall with regards to
antibiotic use.
In contrast to these findings, a number of studies suggest that antibiotics reduce
the risk of colonisation with MRSA. An Italian cross-‐sectional study on children
admitted to the general paediatric ward found antibiotic use in the previous six
29
months was a protective factor for both MRSA colonisation.109 Similarly, a 3-‐year
surveillance study in children with congenital heart disease admitted to the
paediatric intensive care unit (PICU) also found that previous antibiotic use
reduced the risk of being colonised with S. aureus by 81%.110 The conflicting
evidence with regards to the role of antibiotics in nasal colonisation most likely
relates to the type of antibiotics used and the duration of therapy which most of
these studies do not report. There is one prospective study of healthy pre-‐school
children that showed antibiotic use in the previous three months did not
increase nasal colonisation with MSSA or MRSA. However,
amoxicillin/clavulanate use was found to increase the proportion of MSSA that
produced penicillinase, a potential early step towards resistance.111
Overall the evidence is conflicting about whether there is an association in
children between antibiotic and specifically ceftriaxone use and either MSSA or
MRSA carriage or infection. It is important to consider the effects on MSSA
carriage as well as MRSA, because in children MSSA causes a much higher
proportion of invasive infection. No study has prospectively compared the effect
of different antibiotics on colonization with MSSA or MRSA.
1.13 Conclusion and research questions
After reviewing the literature, the paucity of good evidence for the safety and
efficacy of home/ambulatory pathways was clear. Cellulitis was the condition
chosen as a model, as it is a common infection in children and the most common
acute infection treated in adult OPAT services. In support of this, there were a
few studies suggesting that a home management pathway directly from the ED
may be a feasible option, at least in some children. The best way to answer the
question of whether intravenous antibiotics at home was as good as those
administered in hospital for cellulitis would be through the gold standard of a
randomised controlled trial. However, the review of the literature showed
substantial gaps in knowledge and several issues that needed addressing before
an RCT was undertaken.
30
1.14 Aims of the project
1) To better understand current practice in the management of
moderate/severe cellulitis.
2) To develop and validate a system for determining which patients with
cellulitis need intravenous antibiotics.
3) To investigate clinical and non-‐clinical outcomes of home versus hospital
intravenous treatment in children presenting to the emergency department
with uncomplicated moderate/severe cellulitis.
1.15 Thesis structure
Chapter 1 is a review of the literature encompassing treatment for children in a
home/ambulatory setting, management of cellulitis including who should be
treated with intravenous antibiotics and acquisition of resistance, focusing on
children and home/ambulatory management when a broad spectrum antibiotic
is used.
Chapter 2 addresses current practice at the author’s institution with regards to
the management of cellulitis, particularly focusing on OPAT (chapter with
publication and submitted manuscript).
• Study 1: a baseline observational study that describes the current
OPAT practice in treating cellulitis at a tertiary paediatric hospital after
the initial introduction of a direct-‐from-‐ED pathway. This study has
been published.
• Study 2: a survey of clinicians’ practice in hospital with regards to the
management of cellulitis. This study has been submitted and is under
review.
Chapter 3 details the preliminary research that formed the foundation for the
design of the RCT (chapter with publication and submitted manuscript)
31
• Study 3: a prospective cohort study comparing the outcomes of
children treated at home versus hospital, and assessing the feasibility
and informing the methodology of the RCT. This study has been
published.
• Study 4: a longitudinal study on the same cohort of children comparing
acquisition of nasal carriage of Staphylococcus aureus. This study has
been published.
Chapter 4 describes the preliminary research to determine the criteria for using
intravenous antibiotics to treat cellulitis in children (chapter with accepted
manuscript).
• Study 5: the development and validation of a clinical scoring system to
determine whether intravenous or oral antibiotics are needed to treat
cellulitis. This study has been published.
Chapter 5 describes the RCT that is the focus of this thesis comparing home and
hospital intravenous antibiotics. It includes two manuscripts, the first is the RCT
protocol which has been published and secondly the RCT paper which has been
accepted (chapter with submitted manuscript).
• Study 6: RCT of home versus hospital intravenous antibiotics for
children with uncomplicated moderate/severe cellulitis. This study has
been accepted and is in press.
Chapter 6 provides details of a secondary outcome from the main RCT, a detailed
report on a quality of life assessment during the RCT and a cost-‐effectiveness
analysis (chapter with submitted manuscript)
• Study 7: a heath economic analysis of home versus hospital
intravenous antibiotics for children with uncomplicated
moderate/severe cellulitis. This study has been submitted and under
review.
32
Chapter 7 contains a discussion on the overall findings within the context of the
previously published literature and subsequent developments. I present my
conclusions with an outline on future directions for the treatment of acute
infections in children at home
33
Chapter 2 Current practice in home intravenous antibiotic management of cellulitis
2.1 Introduction to current practice
Cellulitis is a common skin infection in children presenting to the ED.112 Despite
the common nature of the infection, there appears to be wide variation in
management including which, if any, investigations are needed, via which route
antibiotics should be administered, whether the patient should be treated in
hospital or at home. Therefore, the first step was to better understand current
management at our institution by surveying paediatricians’ opinions on their
beliefs and practices around cellulitis, specifically with regards to 1) indications
for the use of intravenous antibiotics in cellulitis, 2) the use of investigations and
3) barriers to treating children at home via OPAT.
The practice of treating children who require prolonged intravenous antibiotics
in the home, such as patients with acute exacerbations of cystic fibrosis, has been
described for decades.5,28 The OPAT pathway has been available at the RCH since
2001, to provide for these patients. Recently there has been increasing interest
in using this pathway directly from the ED.1,6 By transferring patients directly
from the ED, patients are more likely to avoid the risks associated with hospital
admissions such as nosocomial infections and psychological effects.7,25 At the
first stage of this PhD, in addition to understanding clinician’s opinions, it was
necessary to understand actual current practice specifically in regard to patients
with cellulitis who have used this pathway from the ED and their outcomes.
This chapter contains two manuscripts, the clinician survey which investigates
clinicians’ beliefs and practice in the management of cellulitis and a published
baseline study describing the current practice of an OPAT pathway for the
intravenous antibiotic management of cellulitis.

34
2.2 Management of cellulitis – how and why?
Although the general clinical approach to cellulitis is widely available in
textbooks42, the literature113 and local guidelines53, the subjective features of this
pathology such as erythema, warmth and tenderness, coupled with the
variability in presentation, renders it difficult to standardise management. For
instance, to investigate cellulitis, the guideline at RCH recommends a full blood
count (FBC) and blood culture if systemic symptoms are present, although these
investigations are acknowledged in the literature to be of low yield.45
Additionally, a swab for Gram stain and culture is advised if pus discharge is
present. For treatment, oral flucloxacillin or cephalexin are recommended for
mild cellulitis but ‘if severe or systemically unwell’, intravenous flucloxacillin is
recommended.53 The definition of severe is not defined in the guideline, allowing
subjective interpretation according to clinicians’ knowledge and beliefs.
With these guidelines open to interpretation, there is a likelihood that variation
exists in the management of cellulitis, and some of this may be unwarranted. This
led to the need to understand how clinicians manage cellulitis based on their
knowledge and beliefs about the infection. Senior and junior clinicians who treat
children with cellulitis at our institution were invited to participate in a survey
about their knowledge, beliefs and practice around this condition. The
hypothesis was that clinicians at RCH were practicing in alignment with the
recommendations of the hospital clinical practice guidelines. The survey was
designed to provide insight into clinicians’ knowledge and beliefs around
cellulitis and how these guidelines were being interpreted.
In designing the survey, questions were carefully designed to provide
information on the following issues:
• Differentiating between mild and moderate/severe cellulitis
• Investigations performed in cellulitis
• Antibiotics (choice and route) used to treat cellulitis
• Attitudes towards OPAT for the treatment of cellulitis

35
2.3 Study 1: Clinician practice and opinions about antibiotic management of cellulitis in children
Ibrahim LF, Hopper SM, Babl FE, Bryant PA. Cellulitis Management: Clinicians
Opinions and Practice. Under review Archives of Disease in Childhood
(The following manuscript is a Word version of the submitted work instead of
the PDF version from Archives of Disease in Childhood due to a large
watermark.)
Management of cellulitis in children: how do beliefs impact on practice?
Laila F Ibrahim1,2,3, Franz E Babl1,4,5, Sandy M Hopper1,4,5, Penelope A Bryant1,2,3,6
Affiliations:
1 Department of Pediatrics, University of Melbourne, Melbourne, Australia
2 Hospital-‐-‐-‐In-‐-‐-‐The-‐-‐-‐Home Department
3 Clinical Pediatrics Group, Murdoch Children’s Research Institute
4 Emergency Department
5 Emergency Research Group, Murdoch Children’s Research Institute
6 Infectious Diseases Unit, Department of General Medicine
The Royal Children’s Hospital, 50 Flemington Road, Parkville, Victoria 3052,
Australia
Key words:
Cellulitis, antibiotics, intravenous, hospital-‐-‐-‐in-‐-‐-‐the-‐-‐-‐home, OPAT
Abbreviated title: Cellulitis: beliefs and practice
Running head title: Management of cellulitis
Correspondence:
A/Prof. Franz Babl
Emergency Department, The Royal Children’s Hospital Melbourne
50 Flemington Road, Parkville, VIC 3052, Australia
Email: [email protected]
Tel: +613 93455522 Fax: +613 9345 6667
Disclosure:
The authors listed above certify that they have no affiliations with any organization or
36

entity with any financial or non financial interest on the materials discussed in this
manuscript. The authors declare there are no competing interests of note.
37
Abstract
Background
There are no evidence-‐-‐-‐based guidelines for the management of cellulitis and use of
outpatient parenteral antimicrobial therapy (OPAT) in particular, in children. This can lead
to variation in practice with implications on resources and patient care. An important
component to reducing variation is to understand physicians’ beliefs and practice. The aim
of this study was to determine pediatricians’ opinions about the management of cellulitis.
Methods This survey was undertaken in a tertiary teaching hospital. Participants were trainee and
senior pediatricians who manage cellulitis. The survey was based on two case vignettes
relating to investigations and management as well as their underlying beliefs around
cellulitis.
Results The response rate was 106/138 (77%), of whom 61% were senior physicians. There was
variability of which clinical features were used to decide when to use intravenous
antibiotics, the most common being lymphangitis (90%), functional impairment (82%) and
systemic features (78%). Trainee physicians were more likely to organise investigations in
moderate/severe cellulitis (92% versus 71%, p=0.02). 60% physicians would take a blood
culture, although there was a wide variation in the perceived risk of bacteremia, with 46%
believing it to be <=5% and 15% believing it to be >50%. In moderate/severe cellulitis,
52% would use OPAT although 93% believed it was psychologically better.
38
Conclusion
Although physicians agree on what constitutes mild or moderate/severe cellulitis, this
survey highlights the variation in how physicians use investigations and antibiotics in
cellulitis – amenable to education, guidelines and a clinical score. Barriers for using OPAT
in cellulitis were identified.
39
Introduction There are a lack of evidence-‐-‐-‐based guidelines for the management of cellulitis in children.
The Practice Guidelines For The Diagnosis And Management Of Skin And Soft Tissue
Infection by the Infectious Diseases Society of America (IDSA), the only published
guidelines for skin and soft tissue infections, are aimed at adults and some of the outlined
recommendations are not applicable to children.1 For example, the IDSA guidelines
recommend intravenous (IV) antibiotics for those with any systemic symptoms, but
children often present with fever and can still be safely treated with oral antibiotics. Lack
of standardized guidelines for children can result in variation in pediatricians’ practice,
which has implications on resources and patient care.
The institutional guidelines at the Australian study hospital state that cellulitis should be
treated with oral antibiotics unless ‘severe/extensive, systemically unwell or not
responding to oral treatment’, without any specific clinical details to guide these
definitions.2 In this situation IV antibiotics are recommended and potentially
investigations. For those deemed to require IV antibiotics, an outpatient parenteral
antibiotic therapy (OPAT) pathway exists at our institution.3 To avoid hospitalization,
patients who require IV antibiotics can receive treatment at home directly from the
Emergency Department (ED) under the care of the Hospital-‐-‐-‐in-‐-‐-‐the-‐-‐-‐Home (HITH) program,
using daily ceftriaxone through a peripheral cannula. However, there was no clarity about
the decisions for IV versus oral antibiotics, or hospital versus home treatment, with most
children still being admitted to hospital if they needed IV antibiotics.3 4
An important component to reducing variation in care is to determine the clinical
reasoning in the management of cellulitis – the way in which beliefs impact on practice.
40
The aim of this study was to ascertain hospital pediatricians’ opinions on the management
of cellulitis, specifically with regards to 1) indications for the use of IV antibiotics in
cellulitis, 2) use of investigations and 3) barriers to treating children at home via HITH.
Methods Study setting and participants This survey was undertaken over a period of 4 weeks, at a tertiary children’s hospital (Royal
Children’s Hospital (RCH)), with an annual ED census of 90,000 attendances. In the ED, 1-‐-‐-‐2
children with cellulitis are managed every day.5 Acute care pediatricians who would be
expected to diagnose and manage cellulitis in their regular practice were identified as those
in the following departments: ED, General Medicine, Infectious Diseases, Adolescent
Medicine and Developmental Medicine. All doctors in these departments were initially
contacted through their hospital-‐-‐-‐based email address and every participant was given a link
to the survey online via Research Electronic Data Capture (REDCap) hosted at the Murdoch
Children’s Research Institute 6. Each participant was informed of an investigator’s contact
email should they prefer to complete a paper-‐-‐-‐based survey, and if requested, this was
provided. Neither mode of survey compelled participants to answer every question. This
survey was anonymous to obtain the most candid answers from physicians. Data entered by
accessing the electronic link to the survey were autopopulated onto REDCap, and paper-‐
-‐-‐based surveys were entered onto the same database by a research assistant.
Study questions and analyses The first section of the survey focused on the management of cellulitis in the form of two
clinical scenarios, with questions relating to clinical symptoms, investigations and
41
antibiotic management. The second section related to treating children with
moderate/severe cellulitis on HITH. The final section related to beliefs of physicians that
serve to underpin and explain their practice. Data analyses was performed using Stata/IC
version 15.0 (StataCorp, College Station, TX). The analysis was primarily descriptive with
chi-‐-‐-‐square testing of comparisons where appropriate. Denominators presented differ due
to different numbers of participants answering some of the questions.
This study received approval from the RCH Human Research Ethics Committee no. 32291A. Box 1 Scenario 1 A 12-‐-‐-‐year-‐-‐-‐old previously well boy, presents to the Emergency Department with a 1 day history
of localized redness on his leg after grazing his leg in the playground. On examination he is
alert, interactive and afebrile with an area of localised erythema, mild swelling and
tenderness measuring 7 x 4 cm on his lower left shin. He does not have a limp.
Scenario 2 A 3-‐-‐-‐year-‐-‐-‐old previously well girl presents to the Emergency Department with swelling and
tenderness on her left shin after grazing her leg in the park when she fell. On examination, she
has a temperature of 38.5C but is systemically well, with an area of erythema, swelling and
tenderness measuring 20 x 10 cm on her lower left shin. She has tracking lymphangitis going
up 10cm to above knee level. She can weight bear but has a limp.
Results
42
The survey was sent to 138 hospital physicians who would be expected to manage children
with cellulitis and 106 (77%) participated. Of these, 65 (61%) were senior physicians
(consultant or fellow) and 41 (39%) were trainee trainees (registrar or resident). The
majority of physicians worked in either the General Medicine Department (54 respondents,
45%), or ED (53, 44%). There was no difference between specialty in responses.
With regards to the severity of cellulitis, 103/104 (99%) classified the episode in scenario
1 as mild, and 98/98, (100%) classified the episode in scenario 2 as moderate/severe.
Regarding investigations in the two scenarios, only 10/103 (10%) would perform any in
mild cellulitis, while 76/96 (79%) would do further investigations in moderate/severe
cellulitis (OR 35, 95% CI 16-‐-‐-‐80, p<0.001). Trainee physicians were more likely than senior
physicians to do any investigations in moderate/severe cellulitis (92% versus 71%, OR 4.6
95% CI (1.3-‐-‐-‐15.8), p=0.02)(table 1). For moderate/severe cellulitis, all participants were
asked about risk of bacteremia and methicillin-‐-‐-‐resistant Staphylococcus aureus (MRSA), and
if specific investigations were selected, they were asked how an abnormal result would
affect management (table 2). 76/95 (83%) responded that the risk of bacteremia was
moderate or high or at the very least important to exclude. When asked to quantify this risk,
64/96 (67%) physicians estimated that it was <=10%, with 44 (46%) <=5%. However, one
third (32, 33%) estimated the risk as >10%, with 14/96 (15%) deemed the risk as
>50%. Of the 64 respondents who would perform a blood culture, a positive result would
affect antibiotic duration for 48 (75%).
When asked to quantify the risk of MRSA as the causative pathogen, 69/96 (72%)
physicians estimated that it was <=10%, with 49 (51%) <=5%. 11/96 (11%) deemed the
43
risk as >20%. Of the 37 respondents who would perform a skin swab, a positive result
would affect the need for MRSA eradication for 28 (75%).
In mild cellulitis, 100/103 (97%) would use oral antibiotics, whereas in moderate/severe
cellulitis 97/98 (99%) would use the IV route. The most common clinical features used to
determine when to treat with IV antibiotics were lymphangitis or ‘tracking’ for 94/104
(90%) physicians, functional impairment of the affected area for 85 (82%) and systemic
features, including fever, for 81 (78%)(table 3). When asked if they believed a clinical score
would be helpful to guide decision-‐-‐-‐making between oral or IV antibiotics, 70 (67%)
physicians believed it would be useful to decrease variation in practice, and 32 (31%)
neutral. Of just trainee doctors, 31/40 (78%) responded that a clinical score would be
useful.
For moderate/severe cellulitis, the first line IV choice was flucloxacillin for 78/95 (82%),
ceftriaxone for 14 (15%), and cephazolin for 3 (3%). No respondent selected an anti-‐-‐-‐MRSA
antibiotic first line, despite 11% deeming the risk of MRSA to be >20%. When asked for
how many days they would prescribe antibiotics, any number of days could be chosen, but
respondents only selected three durations: 7 days: 43/71 (61%), 5 days: 23 (32%) or 10
days: 4 (6%). Regarding the location of treatment with IV antibiotics, proportions were similar between
choosing hospital admission (46/98, 47%) and home with OPAT (51, 52%). The reasons
for choosing hospitalization in preference to OPAT were frequently the same as those for
using IV antibiotics in preference to oral (table 3). Of those that were different, features
that were used in deciding between IV and oral antibiotics were fever,
44
lymphangitis/tracking and having already received oral antibiotics for 24 hours. The
feature used in deciding between hospitalization versus OPAT was family preference.
Potential barriers to OPAT were investigated further regarding age, clinical features and
complications (table 4). The most likely reasons to make physicians hesitate to use OPAT
were: age under <6m (92/96, 96%), periorbital cellulitis (57, 60%) and sunburn-‐-‐-‐like rash
(52, 54%). When specifically asked if they would use the ED-‐-‐-‐to-‐-‐-‐OPAT pathway for
periorbital cellulitis, 60 (60%) physicians responded ‘never’ or ‘unlikely’, with 37 (39%)
believing that at least 1 in 10 of these children actually have orbital cellulitis either due to
progression of disease and/or incorrect initial diagnosis. When compared to the narrower
antibiotic flucloxacillin, 74 (77%) responded that ceftriaxone is more likely to cause
anaphylaxis than flucloxacillin, although 60 (63%) thought less likely to cause other short-‐-‐-‐
term side effects (e.g. gastrointestinal symptoms). With regards to the association between
ceftriaxone with potential long-‐-‐-‐term side effects of acquisition of resistance, 40 (42%)
believed there was a stronger association than with flucloxacillin, 25 (26%) thought a
weaker association and 31 (32%) did not know. Regarding safety of OPAT, 24 (25%)
responded that the risk of a child deteriorating unnoticed was high/very high (table 4).
However, 89/96 (93%) also believed it was beneficial for the child’s psychology, 95 (99%)
for family functioning and 79 (83%) believed it would reduce the cost to the family. The
majority of physicians (81, 84%) believed that more than 60% parents would prefer
treatment at home, although a sizeable minority (15, 16%) thought that this was only true
for 50% or fewer parents. Participants were asked if their patients were treated using
OPAT directly from ED, what percentage they would accept re-‐-‐-‐presenting to hospital and
still consider this a useful pathway for patients. Although responses ranged from 0-‐-‐-‐100%,
45
66/92 (72%) of responses fell in the 10-‐-‐-‐30% range, with the median 20% of patients re-‐-‐-‐
presenting still considered acceptable.
Engagement with families in decision-‐-‐-‐making was variable. When asked whether a child
should complete a course of antibiotics as prescribed, 54/104 (52%) advise always to
complete the course, 28 (27%) advise to attend their general practitioner for clinical
review and a final decision on antibiotic duration and 12 (12%) had no specific advice. A
further 10 (10%) physicians advise to stop the antibiotics earlier if the cellulitis resolves,
but when asked if parents can be trusted to make the decision, only 5/59 (9%) stated yes,
14 (24%) stated no, while 40 (68%) stated it depended on the parents. Only 23/97 (24%)
physicians would ‘frequently’ involve the parents in deciding between hospital and home
with OPAT and only 2 (2%) in the decision between IV and oral antibiotics.
Discussion The survey shows that physicians agree about the severity of cellulitis from the clinical
vignettes. The scenarios were deliberately designed to reflect less and more severe clinical
cases as institutional and other guidelines make this distinction, although often in non-‐-‐-‐
specific terms. Physicians, especially those with less experience, were positive about the
concept of a clinical score for cellulitis that incorporates various clinical features they
usually use to improve the determination of severity and guide the route of antibiotics.
It is not surprising that more physicians would undertake investigations in
moderate/severe than mild cellulitis, due to the higher risk of complications. It is perhaps
surprising that any blood investigations were suggested at all in mild cellulitis given the
invasiveness and lack of utility of blood tests. That two-‐-‐-‐thirds would do a blood culture in
46
moderate/severe cellulitis reflects that over half of physicians perceive the risk of
bacteremia as over 5%, and one-‐-‐-‐third over 10%, although studies have consistently shown
this risk to be less than 1%.7 8 Taking a blood culture in patients with cellulitis has
conversely been associated with an increased length of stay related to spurious results.9 A
raised CRP has previously been found to correlate with severity of symptoms and more
severe sonographic findings.10 However, of those who would request a CRP, only one-‐-‐-‐third
of physicians would use it to decide on the route of treatment. The majority stated they
would use CRP to monitor clinical improvement, which is surprising since a clinical
response in this condition is clearly observable. One previous study of soft tissue infections
in children found a correlation between raised CRP and prolonged duration of stay.11
Although the authors argued the raised CRP was a sign of more serious infection, it is
possible that the raised CRP led to the decision to prolong admission. This practice may
therefore have implications on resources, while providing minimal benefit.12
There was high consistency in responses for antibiotic first-‐-‐-‐line choice (flucloxacillin) and
duration (5-‐-‐-‐7 days), both recommended in the local institutional guideline. This guideline
reflects the low prevalence of MRSA in children in our region at approximately 6%, of
which most physicians appeared to be aware.13 The recommended duration of antibiotics,
aligns with recent recommendations of a systematic review.14 However, physicians’
opinions on cessation of an oral antibiotic course were divided. The lack of willingness to
involve parents in deciding on stopping oral antibiotics was striking, with fewer than 10%
trusting parents to be involved. This lack of engagement was also apparent when
determining whether a child with moderate/severe cellulitis was appropriate for OPAT
with only about a quarter involving parents in this decision. This is despite the emphasis
47
on patient and family-‐-‐-‐centred care at our institution, and the benefits, popularity and
effectiveness of this approach.15
Where IV antibiotics are needed, only half of physicians would choose treatment at home in
preference to hospitalisation despite the fact that cellulitis is a condition with low
morbidity,16 there is a rapidly responsive ED-‐-‐-‐to-‐-‐-‐OPAT service at our institution17 and that the
majority acknowledged that most parents would prefer treatment at home. The preference
for hospitalisation may be explained by the unwarranted perception of the high risk of
bacteremia, also reflected by hesitancy with this pathway if there is fever18, risk of unnoticed
deterioration, and difficulty in distinguishing orbital from periorbital cellulitis despite low
rates of complications when ambulatory treatment is used for periorbital cellulitis.3 19 For
this reason, in our published algorithm for management of cellulitis via OPAT/HITH, we
recommended that a child with periorbital cellulitis should be reviewed by a senior
physician prior to being sent home.3 In developing an OPAT/HITH service, it is important to
understand physician risk aversion to use it, so that real clinical concerns can be separated
from perceived concerns about degree of oversight or monitoring which are amendable to
education. It is also useful to know that physicians accept a rate of re-‐-‐-‐ presentation in
patients treated with OPAT, and still consider this a valuable treatment pathway.
This is the first time that pediatricians’ attitudes towards the management of cellulitis have
been surveyed, and although there was a high response rate there are several limitations.
Firstly, it was conducted in a single tertiary centre and may not reflect the opinions of
physicians in other settings. Secondly, it was an electronic survey which does not provide
the full opportunity to understand details of beliefs compared to interviews with
48
physicians, which may be valuable in future. Thirdly, it is possible that how people
responded may not reflect their actual practice, although we tried to mitigate this by having
an anonymous survey. Lastly, our institution has a well-‐-‐-‐established HITH/OPAT service
which is not universal, but the information obtained from this survey may be useful for
institutions that are considering establishing a similar pathway.
This study provides important insights into how beliefs may impact on management of
children with cellulitis. The clinical features used to decide on whether to use IV antibiotics
could fill a gap in current guidelines or contribute to the development of a clinical score.
There appears to be overuse of investigations and over-‐-‐-‐perception of risk in this condition.
A study on the variation in how physicians use investigations in cellulitis could identify low
value care amenable to quality improvement interventions. Barriers for pediatricians using
the HITH/OPAT pathway were identified and will inform future studies to address these.
Acknowledgements We are grateful to all the physicians for their participation in the survey. Funding This study was funded in part by grants from the RCH Foundation, the Murdoch Children's
Research Institute (MCRI), the Victorian Department of Health, Melbourne Australia. LFI
was supported in part by a scholarship from AVANT Mutual Group Ltd, Melbourne, the
Melbourne Children’s Campus Postgraduate Health Research Scholarship and the Doctor
Nicholas Collins Fellowship. PAB was in part supported by a Melbourne Campus Physician
49
Scientist Fellowship, Melbourne, Australia. FEB was supported in part by a grant from the
RCH Foundation and a Melbourne Campus Physician Scientist Fellowship, Melbourne,
Australia and a National Health and Medical Research Council (NHMRC) Practitioner
Fellowship, Canberra, Australia. The emergency research group, MCRI, is in part supported
by an NHMRC Centre for Research Excellence Grant for Pediatric Emergency Medicine,
Canberra, Australia and the Victorian government infrastructure support program.
References 1. Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and
management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin Infect Dis 2014;59(2):e10-52. doi: 10.1093/cid/ciu444
2. The Royal Children's Hospital M, Australia. Cellulitis and skin infections [cited 2015 7 June]. Available from: https://wwww.rch.org.au/clinicalguide/.
3. Ibrahim LF, Hopper SM, Babl FE, et al. Who Can Safely Have Antibiotics at Home? A Prospective Observational Study in Children with Moderate/Severe Cellulitis. Pediatr Infect Dis J 2015 doi: 10.1097/INF.0000000000000992
4. Gouin S, Chevalier I, Gauthier M, et al. Prospective evaluation of the management of moderate to severe cellulitis with parenteral antibiotics at a paediatric day treatment centre. Journal of paediatrics and child health 2008;44(4):214-8. doi: 10.1111/j.1440- 1754.2007.01236.x
5. Ibrahim LF, Hopper SM, Connell TG, et al. Evaluating an admission avoidance pathway for children in the emergency department: outpatient intravenous antibiotics for moderate/severe cellulitis. Emergency medicine journal : EMJ 2017 doi: 10.1136/emermed-2017-206829
6. Harris PA, Taylor R, Thielke R, et al. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009;42(2):377-81. doi: 10.1016/j.jbi.2008.08.010
7. Bryant PA, Babl FE, Daley AJ, et al. Blood Cultures in Cellulitis are not Cost Effective and Should Prompt Investigation for an Alternative Focus. The Paediatric Infectious Disease Journal 2016;35(1)(January 2016):118. doi: 10.1097/INF.0000000000000938
8. Trenchs V, Hernandez-Bou S, Bianchi C, et al. Blood Cultures are not Useful in the Evaluation of Children with Uncomplicated Superficial Skin and Soft Tissue Infections. Pediatr Infect Dis J 2015 doi: 10.1097/INF.0000000000000768
9. Malone JR, Durica SR, Thompson DM, et al. Blood cultures in the evaluation of uncomplicated skin and soft tissue infections. Pediatrics 2013;132(3):454-9. doi: 10.1542/peds.2013-1384
10. Chao HC, Lin SJ, Huang YC, et al. Sonographic evaluation of cellulitis in children. J Ultrasound Med 2000;19(11):743-9.
11. Tanir G, Tonbul A, Tuygun N, et al. Soft tissue infections in children: a retrospective analysis of 242 hospitalized patients. Jpn J Infect Dis 2006;59(4):258-60.
50
12. Greenberg J, Green JB. Over-testing: why more is not better. Am J Med 2014;127(5):362-3. doi: 10.1016/j.amjmed.2013.10.024
13. Wolf J, Daley AJ, Tilse MH, et al. Antibiotic susceptibility patterns of Staphylococcus aureus isolates from Australian children. Journal of paediatrics and child health 2010;46(7-8):404-11. doi: 10.1111/j.1440-1754.2010.01751.x
14. McMullan BJ, Andresen D, Blyth CC, et al. Antibiotic duration and timing of the switch from intravenous to oral route for bacterial infections in children: systematic review and guidelines. The Lancet Infectious diseases 2016;16(8):e139-52. doi: 10.1016/S1473- 3099(16)30024-X
15. Laila Ibrahim SH, Francesca Orsini, Franz Babl, Penelope Bryant. A Randomised Controlled Trial Comparing Home To Hospital In Children With Moderate/Severe Cellulitis. HITH Society Conference 2017. Melbourne, Australia, 2017.
16. Ginsberg MB. Cellulitis: analysis of 101 cases and review of the literature. South Med J 1981;74(5):530-3.
17. Hodgson KA, Huynh J, Ibrahim LF, et al. The use, appropriateness and outcomes of outpatient parenteral antimicrobial therapy. Archives of disease in childhood 2016;101(10):886-93. doi: 10.1136/archdischild-2015-309731
18. Teach SJ, Fleisher GR. Duration of fever and its relationship to bacteremia in febrile outpatients three to 36 months old. The Occult Bacteremia Study Group. Pediatric emergency care 1997;13(5):317-9.
19. Brugha RE, Abrahamson E. Ambulatory intravenous antibiotic therapy for children with preseptal cellulitis. Pediatric emergency care 2012;28(3):226-8. doi: 10.1097/PEC.0b013e318248b19b
51
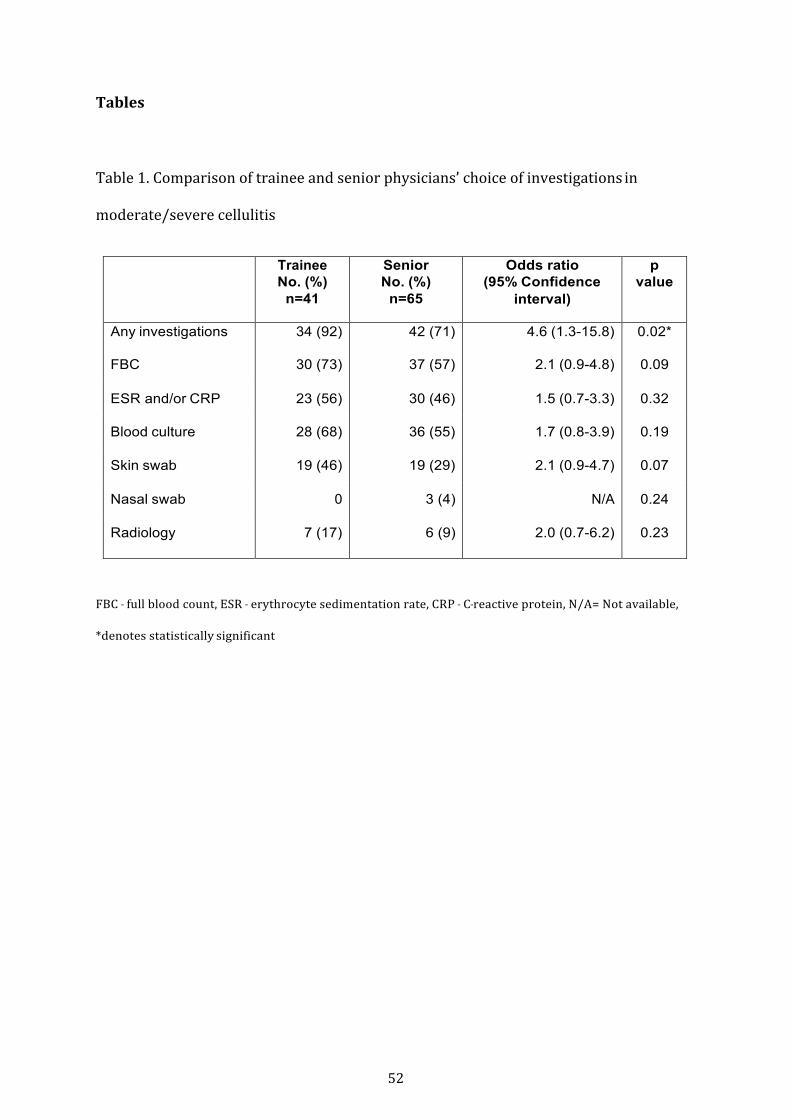
Tables Table 1. Comparison of trainee and senior physicians’ choice of investigations in
moderate/severe cellulitis
Trainee
No. (%) n=41
Senior No. (%)
n=65
Odds ratio (95% Confidence
interval)
p value
Any investigations 34 (92) 42 (71) 4.6 (1.3-15.8) 0.02*
FBC 30 (73) 37 (57) 2.1 (0.9-4.8) 0.09
ESR and/or CRP 23 (56) 30 (46) 1.5 (0.7-3.3) 0.32
Blood culture 28 (68) 36 (55) 1.7 (0.8-3.9) 0.19
Skin swab 19 (46) 19 (29) 2.1 (0.9-4.7) 0.07
Nasal swab 0 3 (4) N/A 0.24
Radiology 7 (17) 6 (9) 2.0 (0.7-6.2) 0.23
FBC -‐-‐-‐ full blood count, ESR -‐-‐-‐ erythrocyte sedimentation rate, CRP -‐-‐-‐ C-‐-‐-‐reactive protein, N/A= Not available, *denotes statistically significant
52
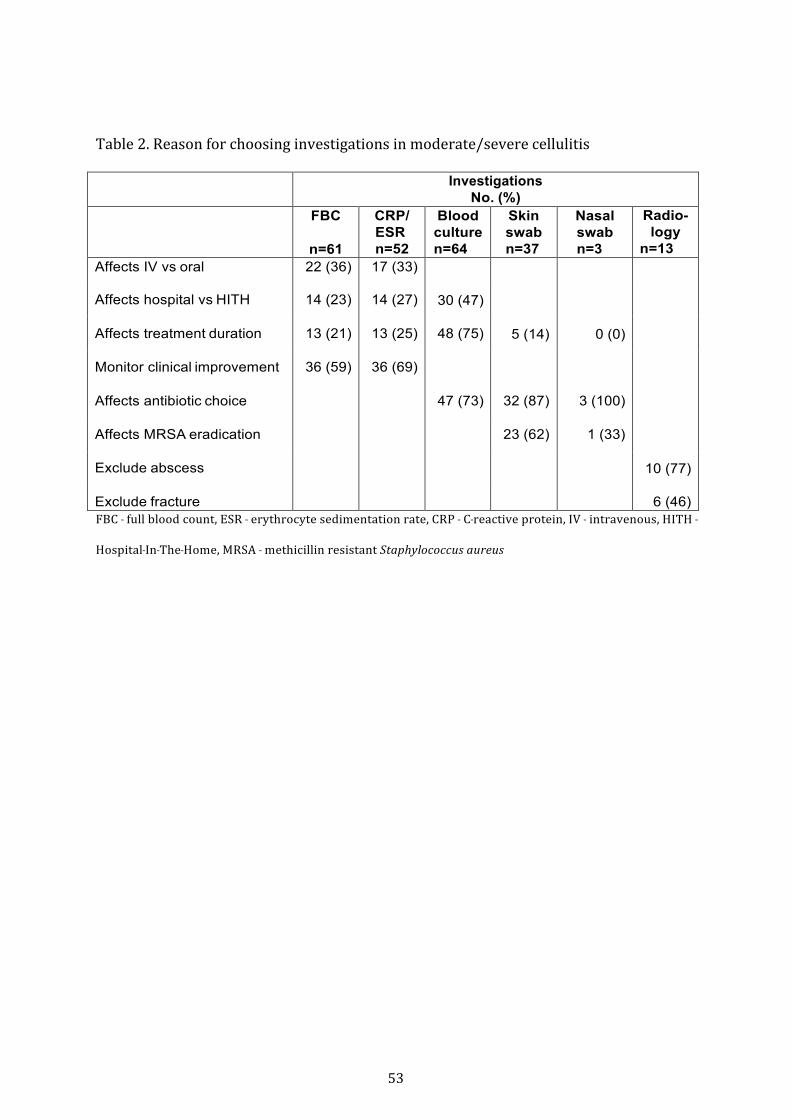
Table 2. Reason for choosing investigations in moderate/severe cellulitis
Investigations
No. (%) FBC
n=61
CRP/ ESR n=52
Blood culture n=64
Skin swab n=37
Nasal swab n=3
Radio- logy
n=13 Affects IV vs oral 22 (36) 17 (33)
30 (47)
5 (14)
0 (0)
10 (77)
Affects hospital vs HITH 14 (23) 14 (27)
Affects treatment duration 13 (21) 13 (25) 48 (75)
Monitor clinical improvement 36 (59) 36 (69)
Affects antibiotic choice 47 (73) 32 (87) 3 (100)
Affects MRSA eradication 23 (62) 1 (33)
Exclude abscess
Exclude fracture 6 (46) FBC -‐-‐-‐ full blood count, ESR -‐-‐-‐ erythrocyte sedimentation rate, CRP -‐-‐-‐ C-‐-‐-‐reactive protein, IV -‐-‐-‐ intravenous, HITH -‐-‐-‐
Hospital-‐-‐-‐In-‐-‐-‐The-‐-‐-‐Home, MRSA -‐-‐-‐ methicillin resistant Staphylococcus aureus
53
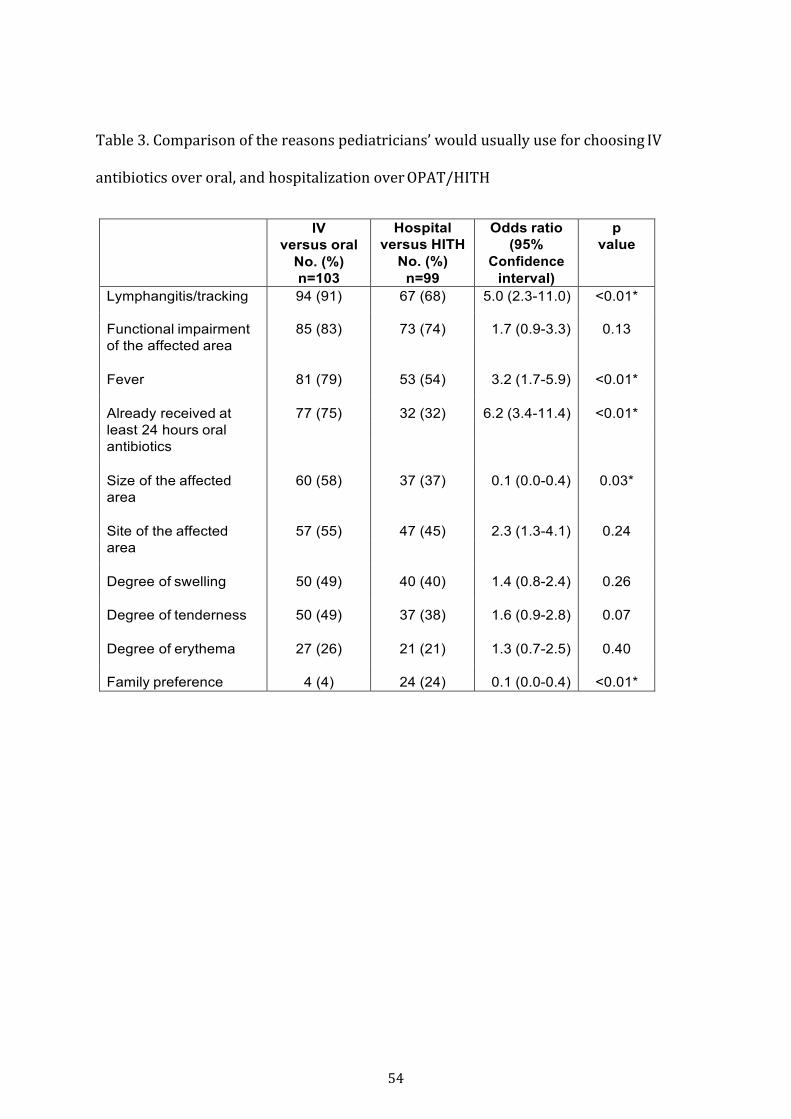
Table 3. Comparison of the reasons pediatricians’ would usually use for choosing IV
antibiotics over oral, and hospitalization over OPAT/HITH
IV
versus oral No. (%) n=103
Hospital versus HITH
No. (%) n=99
Odds ratio (95%
Confidence interval)
p value
Lymphangitis/tracking 94 (91) 67 (68) 5.0 (2.3-11.0) <0.01*
Functional impairment 85 (83) 73 (74) 1.7 (0.9-3.3) 0.13 of the affected area
Fever 81 (79) 53 (54) 3.2 (1.7-5.9) <0.01*
Already received at 77 (75) 32 (32) 6.2 (3.4-11.4) <0.01* least 24 hours oral antibiotics
Size of the affected 60 (58) 37 (37) 0.1 (0.0-0.4) 0.03* area
Site of the affected 57 (55) 47 (45) 2.3 (1.3-4.1) 0.24 area
Degree of swelling 50 (49) 40 (40) 1.4 (0.8-2.4) 0.26
Degree of tenderness 50 (49) 37 (38) 1.6 (0.9-2.8) 0.07
Degree of erythema 27 (26) 21 (21) 1.3 (0.7-2.5) 0.40
Family preference 4 (4) 24 (24) 0.1 (0.0-0.4) <0.01*
54
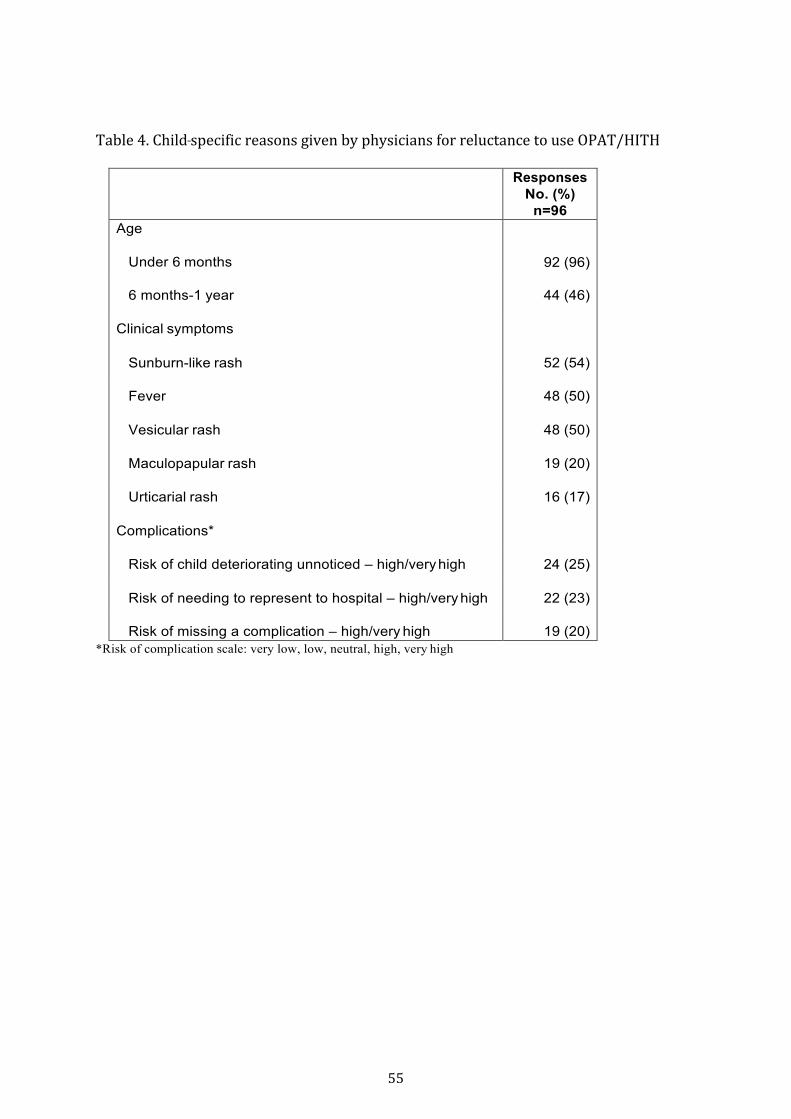
Table 4. Child-‐-‐-‐specific reasons given by physicians for reluctance to use OPAT/HITH
Responses No. (%)
n=96 Age
92 (96) Under 6 months
6 months-1 year 44 (46)
Clinical symptoms
Sunburn-like rash 52 (54)
Fever 48 (50)
Vesicular rash 48 (50)
Maculopapular rash 19 (20)
Urticarial rash 16 (17)
Complications*
Risk of child deteriorating unnoticed – high/very high 24 (25)
Risk of needing to represent to hospital – high/very high 22 (23)
Risk of missing a complication – high/very high 19 (20) *Risk of complication scale: very low, low, neutral, high, very high
55

56
2.4 Current practice of home treatment of cellulitis with intravenous antibiotics – a baseline study
Parallel to the investigation into clinicians’ knowledge and beliefs around
cellulitis management, another study was carried out to investigate the current
practice of cellulitis treatment, with a focus on the home pathway at our
institution. The RCH has an established OPAT service since 2001 known as
Hospital-‐in-‐the-‐Home (HITH).12 The HITH service at RCH is nurse-‐led with
medical oversight. In addition to highly experienced nursing staff who conduct
home visits to administer treatment, a full time consultant paediatrician and a
full time senior paediatric trainee are allocated to this department. This service
provides home care for multiple interventions that traditionally would be
provided in hospital. Specifically regarding OPAT, the majority at the start of this
PhD was for children requiring long-‐term antibiotics after being on a hospital
ward. Patients were predominantly from oncology, cystic fibrosis and
orthopaedic populations. These patients were initially admitted to hospital for a
number of days, before being considered stable enough for transfer home via
HITH to finish the course of intravenous antibiotics overseen by the initial team
overseeing their care.
More recently and infrequently, patients were referred directly from the ED to
HITH with acute conditions such as cellulitis and UTI for antibiotic treatment at
home.1 6 Patients who were referred directly from the ED to HITH, would receive
the first dose of intravenous antibiotics in the ED and be discharged home with a
peripherally inserted cannula in situ. The HITH nurse would visit the patient at
home daily for subsequent doses of antibiotics and medical review. In these
cases, the HITH medical staff would oversee their treatment and medical care.
To better understand how this pathway was being used to treat cellulitis, a
baseline study was needed to investigate the characteristics of patients who use
this pathway and to assess the safety and efficacy of home treatment for these
patients. Although the focus was on patients treated at home, it became apparent
at the start of this study that the majority of patients needing intravenous
57
antibiotics for cellulitis were still treated in hospital. Therefore the
characteristics of patients treated in hospital were also collected to determine
whether there were features that make these patients unsuitable for home
management.

58
2.5 Study 2: Management of children with cellulitis with intravenous antibiotics at home
Ibrahim LF, Hopper SM, Babl FE, Bryant PA. Who Can Have Parenteral
Antibiotics at Home? A Prospective Observational Study in Children with
Moderate/Severe Cellulitis. Pediatr Infect Dis J. 2016 Mar;35(3):269-‐74

www.pidj.com | 269
Original StudieS
Background: The benefits of treating children at home or in an ambulatory setting have been well documented. We aimed to describe the characteris-tics and evaluate the outcomes of children with moderate/severe cellulitis treated at home with intravenous (IV) ceftriaxone via direct referral from the Emergency Department to a hospital-in-the-home (HITH) program.Methods: Patients aged 3 months to 18 years with moderate/severe cellulitis referred from a tertiary pediatric Emergency Department to HITH from Sep-tember 2012 to January 2014 were prospectively identified. Data collection included demographics, clinical features, microbiological characteristics and outcomes. To ensure home treatment did not result in inferior outcomes, these patients were retrospectively compared with patients who were hospitalized for IV flucloxacillin, the standard-of-care over the same period. The primary out-come was home treatment failure necessitating hospital admission. Secondary outcomes included antibiotic changes, complications, length of stay and cost.Results: Forty-one (28%) patients were treated on HITH and 103 (72%) were hospitalized. Compared with hospitalized patients, HITH patients were older (P < 0.01) and less likely to have periorbital cellulitis (P = 0.01) or fever (P = 0.04). There were no treatment failures under HITH care. The rate of antibiotic changes was similar in both groups (5% vs. 7%, P = 0.67), as was IV antibiotic duration (2.3 vs. 2.5 days, P = 0.23).Conclusion: Older children with moderate/severe limb cellulitis without systemic symptoms can be treated at home. To ascertain if this practice can be applied more widely, a comparative prospective, ideally randomized, study is needed.
Key Words: antibiotics, intravenous, hospital-in-the-home, ambulatory, cellulitis
(Pediatr Infect Dis J 2016;35:269–274)
Cellulitis is a common infection in children, but while adultswho require intravenous (IV) antibiotics for moderate or severe
cellulitis commonly receive it under an outpatient parenteral anti-microbial treatment (OPAT) model, children are usually admitted to hospital.1,2 In comparison with hospital admission, children treated
at home do better psychologically and physically, have fewer inves-tigations, are at decreased risk of hospital-acquired infections and have subsequent decreased use of healthcare resources.3–6 It is also cheaper and psychologically better for their families.6,7 Previous randomized trials in adults with cellulitis show OPAT is a safe and efficient model of care.8,9 OPAT may be delivered as an outpatient returning daily to the hospital, or via a hospital-in-the-home (HITH) program whereby nurses visit the patient’s home daily to administer IV antibiotics. Although OPAT has been used in children since the 1970s for those requiring long-term antibiotics, it is less commonly used for acute infections requiring short-term antibiotics.10,11
When IV treatment is required for cellulitis, a semisynthetic penicillin or first-generation cephalosporin are the usual choices because they are effective against Staphylococcus aureus and group A streptococci (Streptococcus pyogenes), the main pathogens caus-ing cellulitis.12 However, they are not suitable for OPAT because of their frequent dosing with the majority of OPAT services only able to deliver once daily interventions. Although probenecid can overcome this problem for adults on cefazolin, there are no pharmacokinetic studies of its use children, and the side effect of vomiting may prevent probenecid use.9 Ceftriaxone has anti-staphylococcal activity and can be administered once daily.13 There are only a few studies in children in which ceftriaxone has been used to treat cellulitis either in hospital or OPAT, and although promising, none have compared outcomes to children treated with the standard-of-care inpatient therapy.11,13–16
Increasingly hospitals are developing programs where patients who have traditionally been treated as inpatients are treated at home under the care of hospital doctors and nurses in HITH programs. The Royal Children’s Hospital (RCH) Melbourne has the largest pediatric HITH program in Australia. As an alternative to hospital admission for IV flucloxacillin, RCH HITH recently developed a direct-from-the Emergency Department (ED) pathway for moderate/severe cel-lulitis, using once daily ceftriaxone and medical review at home. However, currently, there are no guidelines about which patients can be transferred to HITH to receive treatment at home. Therefore, the decision between hospital-based and home-based treatment is made variably by ED clinicians. A new pathway should be as safe and as effective as the current standard of care, so evaluating clinical fea-tures and outcomes provides evidence to inform guidelines.17
The aim of this study was to describe the demographics, clinical and microbiological features, outcomes and cost of a cohort of patients with moderate/severe cellulitis who were treated with IV ceftriaxone at home. Additionally, we aimed to compare these with patients concurrently admitted to hospital with the same diagnosis, to determine the differences between these 2 groups at presentation and whether treatment via HITH affected outcomes unfavorably. Based on our findings, we aimed to propose a guideline for which patients with cellulitis can safely receive IV antibiotics at home.
METHODS
SettingThis was a prospective observational study of children pre-
senting to the ED at the RCH Melbourne over a 17-month period
Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.ISSN: 0891-3668/16/3503-0269DOI: 10.1097/INF.0000000000000992
Who Can Have Parenteral Antibiotics at Home?
A Prospective Observational Study in Children with Moderate/Severe Cellulitis
Laila F. Ibrahim, MB BCh, BAO,*†‡ Sandy M. Hopper MB BS,‡§ Franz E. Babl, MD,†‡§ and Penelope A. Bryant, PhD*†‡¶
Accepted for publication September 4, 2015.From the *RCH@Home Department, The Royal Children’s Hospital; † Murdoch
Children’s Research Institute; ‡Department of Pediatrics, University of Melbourne; §Emergency Department, and ¶Infectious Diseases Unit, Department of General Medicine, The Royal Children’s Hospital, Parkville, Victoria, Australia.
This study is funded in part by grants from the RCH Foundation, the Murdoch Children's Research Institute and the Victorian Department of Health, Mel-bourne Australia. F.E.B. was supported in part by a grant from the RCH Foundation. The emergency research group, MCRI, is in part supported by a Centre for Research Excellence Grant for Paediatric Emergency Medicine from the National Health and Medical Research Council, Canberra, Austra-lia and the Victorian government infrastructure support program. The fund-ing bodies do not have any authority in collection, management, analysis and interpretation of data. The authors have no conflict of interest to disclose.
Address for correspondence: Penelope A Bryant, PhD, Department of General Medicine, The Royal Children’s Hospital Melbourne, 50 Flemington Road, Parkville, VIC 3052, Australia. E-mail: [email protected].
59

Ibrahim et al The Pediatric Infectious Disease Journal • Volume 35, Number 3, March 2016
270 | www.pidj.com © 2015 Wolters Kluwer Health, Inc. All rights reserved.
from September 1, 2012 to January 31, 2014 with uncomplicated moderate/severe cellulitis and treated at home. As there is no vali-dated or objective score for distinguishing moderate/severe from mild cellulitis, this was defined in the study as those assessed by ED physicians as requiring IV antibiotics because of any of the follow-ing clinical features: rapidly spreading redness (from history), sig-nificant swelling/redness/pain, systemic symptoms/signs (eg, fever, lethargy) or failed oral therapy (not improving despite at least 24 hours oral antibiotics).
Inclusion CriteriaPatients aged 3 months to 18 years with moderate/severe
cellulitis who were referred by ED clinicians directly to the HITH program for IV ceftriaxone were included.
Exclusion CriteriaChildren younger than 3 months, those with mild or com-
plicated cellulitis and those where the initial antibiotic choice within HITH was not ceftriaxone were excluded. Complicated cellulitis included cellulitis associated with abscess requiring surgical drainage, lymphadenitis, underlying soft-tissue mal-formation, bite or penetrating injury, foreign body, fracture, lymphedema, orbital cellulitis, medical comorbidities or immu-nosuppression.
Study ProcedureChildren with moderate/severe cellulitis were identified
by ED clinicians and assessed for HITH suitability at presen-tation. They were referred to the HITH program directly from ED. This involved the ED clinician filling an online referral form and calling the admitting HITH nurse to hand over the patient. After receiving the first dose of ceftriaxone 50 mg/kg once daily in the ED, the patient went home with the peripheral cannula in situ. The HITH nurse visited the child the following day and administered IV ceftriaxone at home. This was followed by daily nursing review and daily ceftriaxone until the child was deemed suitable for oral therapy. The HITH doctor reviewed the child at least once during the course of treatment in person, via telecon-ferencing or by reviewing digital photographs taken by nursing staff. The decision to cease IV antibiotics was made by the HITH doctor. The HITH nurse removed the cannula upon cessation of IV therapy in the patient’s home.
Hospitalized GroupThe standard of care for moderate/severe cellulitis at RCH
is hospitalization with at least daily medical review and IV flu-cloxacillin 50 mg/kg every 6 hours. Patients who received the standard-of-care therapy were identified retrospectively from the ED electronic database (Emergency Department Information Sys-tem for Oracle Version EDISAPAC 12.1 1B5). The same inclusion and exclusion criteria were applied when identifying these patients retrospectively, except for the decision to refer to HITH. Patients who did not receive IV flucloxacillin as their empiric antibiotic were excluded to enable comparison with standard recommended management.
Data CollectionData for HITH patients were collected prospectively
including demographic data and clinical information: age, sex, systemic symptoms at presentation (reported or documented fever >38°C, vomiting, tachycardia or hypotension), prior use of oral antibiotics, results from skin swab and/or blood culture if taken and timing of IV ceftriaxone administration. For all patients who were hospitalized, case notes and microbiology results were reviewed retrospectively.
Outcome MeasuresThe primary outcome was treatment failure, defined as
admission from HITH back to hospital because of inadequate improvement at home as determined by the treating clinician.
Secondary outcomes were change of antibiotic because of poor clinical improvement, septic complications or recurrence during use or within 48 hours of ceasing empiric IV antibiotics, adverse events and readmission to hospital for the same diagno-sis or death within 28 days of discharge, length of stay, duration of IV antibiotics and subsequent oral antibiotic duration. A cost analysis was also done which included the average costs of beds, consumables and overhead costs, such as administrative time, information technology, and use of hospital cars. Antibiotic costs were included but were low. A vial of ceftriaxone costs Australian Dollar (AUD) 0.60 [United States Dollar (USD) 0.46], whereas a vial of flucloxacillin costs AUD 0.94 (USD 0.72).
Data AnalysisStudent t test was used to compare continuous data between
the 2 groups and χ2-square test for categorical data, with a P value of <0.05 considered statistically significant.
EthicsThis study received approval from the RCH Human
Research Ethics Committee (32291A).
RESULTSOver the 17 months of the study, 700 children presented to
the ED with cellulitis, of which 396 (57%) were discharged home on oral antibiotics. Of the 304 children treated with IV antibiotics, 120 were excluded from the analysis because of being younger than 3 months or having complicated cellulitis, and 40 patients were excluded for being treated with nonstandard antibiotics (Fig. 1). One hundred and forty-four children were treated for uncomplicated moderate/severe cellulitis. Forty-one were treated at home via HITH, and 103 were hospitalized, receiving the RCH standard of care. In terms of the primary outcome, none of the 41 HITH patients had treatment failure at home necessitating admis-sion to hospital. Demographic, clinical and microbiological data were compared with those from the hospitalized patients to deter-mine differences that might explain their different treatment loca-tion choices. Secondary outcomes were compared with determine whether treatment under HITH affected outcomes unfavorably.
Demographics and Clinical FeaturesPatients had similar sex distribution, but HITH patients
were older than hospitalized patients (9.0 vs. 5.9 years; P < 0.01; Table 1). Of patients younger than 5 years, 58 (83%) were hospital-ized. Patients treated under HITH had a higher rate of prior oral antibiotic treatment than hospitalized patients (59% vs. 40%; P = 0.04) and a lower rate of systemic symptoms, in particular fever (22% vs. 37%; P = 0.04). Only 1 patient received a fluid bolus, and no patient in either group was hypotensive. Fewer HITH patients than hospitalized patients had a blood culture taken (27% vs. 41%; P < 0.01), but no cultures were truly positive for a pathogen in either group. Patients with periorbital cellulitis were less likely to be treated under HITH than hospitalized (10% vs. 30%; P = 0.01), whereas a higher proportion of HITH patients than hospitalized patients had lower limb cellulitis (56% vs. 37%; P = 0.03). A total of 59 skin swabs were taken. The 2 most common pathogens iso-lated were S. aureus in 31 (22%) children and S. pyogenes in 9 (6%) children. Methicillin-resistant S. aureus (MRSA) was identified in 6 children, accounting for 10% of pathogens where a skin swab was taken.
60
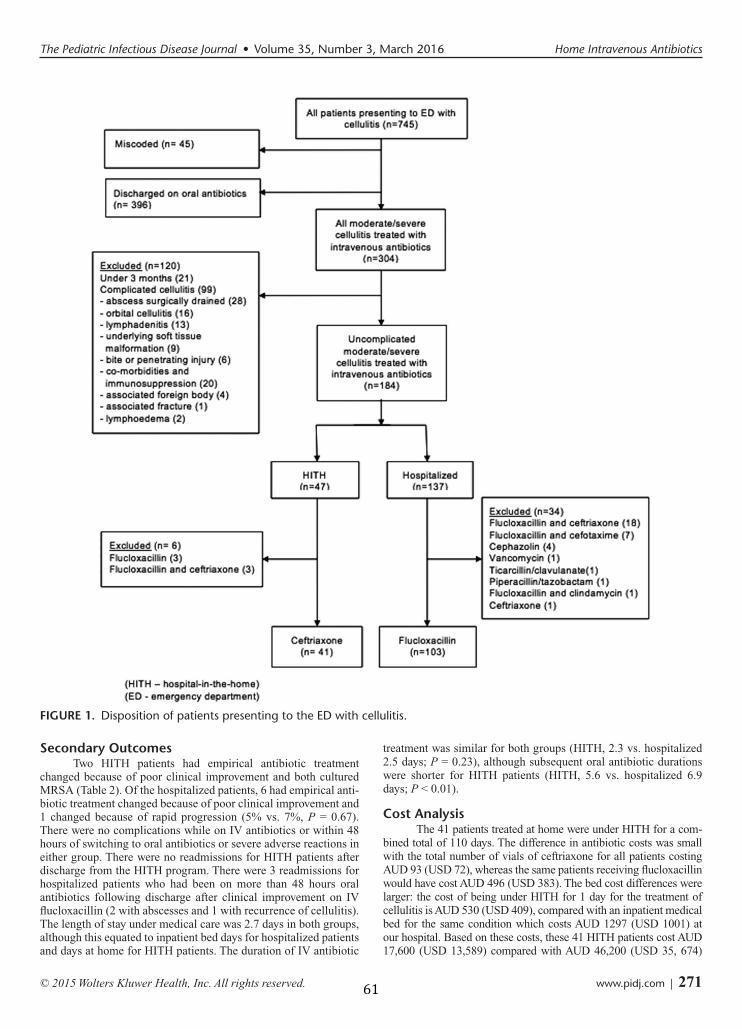
The Pediatric Infectious Disease Journal • Volume 35, Number 3, March 2016 Home Intravenous Antibiotics
© 2015 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | 271
Secondary OutcomesTwo HITH patients had empirical antibiotic treatment
changed because of poor clinical improvement and both cultured MRSA (Table 2). Of the hospitalized patients, 6 had empirical anti-biotic treatment changed because of poor clinical improvement and 1 changed because of rapid progression (5% vs. 7%, P = 0.67). There were no complications while on IV antibiotics or within 48 hours of switching to oral antibiotics or severe adverse reactions in either group. There were no readmissions for HITH patients after discharge from the HITH program. There were 3 readmissions for hospitalized patients who had been on more than 48 hours oral antibiotics following discharge after clinical improvement on IV flucloxacillin (2 with abscesses and 1 with recurrence of cellulitis). The length of stay under medical care was 2.7 days in both groups, although this equated to inpatient bed days for hospitalized patients and days at home for HITH patients. The duration of IV antibiotic
treatment was similar for both groups (HITH, 2.3 vs. hospitalized 2.5 days; P = 0.23), although subsequent oral antibiotic durations were shorter for HITH patients (HITH, 5.6 vs. hospitalized 6.9 days; P < 0.01).
Cost AnalysisThe 41 patients treated at home were under HITH for a com-
bined total of 110 days. The difference in antibiotic costs was small with the total number of vials of ceftriaxone for all patients costing AUD 93 (USD 72), whereas the same patients receiving flucloxacillin would have cost AUD 496 (USD 383). The bed cost differences were larger: the cost of being under HITH for 1 day for the treatment of cellulitis is AUD 530 (USD 409), compared with an inpatient medical bed for the same condition which costs AUD 1297 (USD 1001) at our hospital. Based on these costs, these 41 HITH patients cost AUD 17,600 (USD 13,589) compared with AUD 46,200 (USD 35, 674)
FIGURE 1. Disposition of patients presenting to the ED with cellulitis.
61

Ibrahim et al The Pediatric Infectious Disease Journal • Volume 35, Number 3, March 2016
272 | www.pidj.com
if they had been treated in hospital, a real cost saving AUD 28,600 (USD 22,083). If all of the hospitalized patients had been treated under HITH (combined total of 275 days), the estimated cost saving would have been AUD 210,925 (USD 163,072).
DISCUSSIONThis is the first study describing demographics, clinical and
microbiological characteristics and outcomes of children with uncom-plicated moderate/severe cellulitis treated at home. Home treatment of cellulitis under HITH appears both feasible and efficacious, particu-larly for older children with limb cellulitis without systemic symptoms.
The reason to compare HITH patients with inpatients is not to suggest that the 2 groups are necessarily equivalent, but to
identify features associated with safe treatment under HITH and to evaluate whether the benefits of treatment at home come at a cost in any outcome measures. The measured outcomes, duration of IV antibiotics and length of stay were the same in the 2 groups analyzed. Given that the outcomes were not inferior, referral of these patients to HITH resulted in significant cost savings. As this was a new pathway, it is likely that there were other patients who could have been treated via HITH with additional cost savings. This would need to be evaluated in a prospective study.
There were differences between HITH patients and hospitalized patients. First, HITH patients were older, possibly because of concern about higher likelihood of bacteremia in younger children. This is also reflected in a higher proportion of blood cultures taken in the hospital-ized group. Another difference was that hospitalized patients had more systemic symptoms (almost exclusively fever), although this did not reflect bacteremia or risk of progression to sepsis. A higher proportion of HITH patients received prior oral antibiotics, which may indicate that they had more indolent presentations rather than rapidly progres-sive cellulitis. Children with periorbital cellulitis were more likely to be hospitalized (only 11% were admitted under HITH). The most likely reason is uncertainty in distinguishing periorbital from orbital cellulitis at presentation especially in an uncooperative young child. One previ-ous study of periorbital cellulitis described 42 children treated on an ambulatory basis with low rates of complications.16 However, the clini-cal characteristics of these patients were not specified. Other previous studies using outpatient ceftriaxone in children have either excluded or not reported on periorbital cellulitis.11,14,18
Ceftriaxone is the antibiotic of choice for home-based treat-ment of cellulitis because it can be administered once daily via a peripheral cannula. Use of peripheral cannula is usual practice for patients on HITH receiving short-term OPAT because these are the easiest IV access devices to insert, do not require general anes-thesia and have low complication rates. Flucloxacillin at home would need to be infused over 24 hours via a central venous cath-eter (CVC). As the mean duration of IV antibiotics in our patient population was only 2.5 days, CVC insertion would not be justified. The only adverse event in either group in our study was a single patient with a rash secondary to cannula fixation tape. No patients needed their cannula resiting, but even if they had, the benefits still outweigh the disadvantages of a CVC.
As a novel intervention, it is important to consider whether ceftriaxone is an appropriate antibiotic regarding its effective-ness for the treatment of S. aureus infection and the potential for adverse ecological effects due its broad spectrum. Regarding effectiveness, the literature suggests a rate of <3% ceftriaxone resistance in methicillin-sensitive S. aureus.19 The few studies in
TABLE 1. Comparison of Characteristics of HITH Patients and Hospitalized Patients for Uncomplicated Moderate/Severe Cellulitis
HITH, No. (%)
Hospitalized, No. (%)
P Value
Demographics Total patients 41 (28) 103 (72) Sex, female:male 16:25 52:51 0.21 Age (yr), mean (range) 9.0 (1–17) 5.9 (0.5–17) <0.01*
Clinical features Prior oral antibiotic 24 (59) 41 (40) 0.04* Systemic symptoms 9 (22) 38 (37) 0.08
Fever 8 (20) 38 (37) 0.04* Vomiting 1 (1) 2 (2) 0.85 Tachycardia 0 (0) 1 (1) 0.41
Hypotension 0 (0) 0 (0) Site
Periorbital 4 (10) 31 (30) 0.01* Lower limb 23 (56) 38 (37) 0.03* Upper limb 8 (20) 17 (17) 0.66
Head and neck 1 (2) 12 (12) 0.08 Trunk and abdomen 5 (12) 4 (4) 0.06
Microbiology Skin swab (total) 14 (34) 45 (44) 0.29
Methicillin-sensitive Staphylococcus aureus
8 (57) 17 (38) 0.20
Streptococcus pyogenes 1 (7) 8 (18) 0.33 MRSA 2 (14) 4 (9) 0.55 No growth 1 (7) 11 (24) 0.16
Blood culture taken (total) 11 (27) 42 (41) <0.01* Positive culture 1 (2) 0 (0) 0.03* Contaminant 1 (2) 0 (0) 0.03*
*Significant at P <0.05.
TABLE 2. Outcomes of HITH Patients and Hospitalized Patients for Uncomplicated Moderate/Severe Cellulitis
HITH, No. (%) Hospitalized, No. (%) P Value
Primary outcome Treatment failure 0 (0) Not applicableSecondary outcomes
Change of antibiotic 2 (5) 7 (7) 0.67 Sepsis/complications 0 (0) 0 (0) Adverse events 0 (0) 0 (0) Readmission 0 (0) 3 (3) 0.14 Length of stay (d), mean (range)
In hospital 0 2.7 (1–8) <0.001* Under medical care 2.7 (1–10) 2.7 (1–8) 0.96 Duration of IV antibiotics (d), mean (range) 2.3 (1–6) 2.5 (1–5) 0.23 Duration of oral antibiotics (d), mean (range) 5.6 (4–10) 6.9 (4–14) <0.01*
*Significant at P <0.05.
62
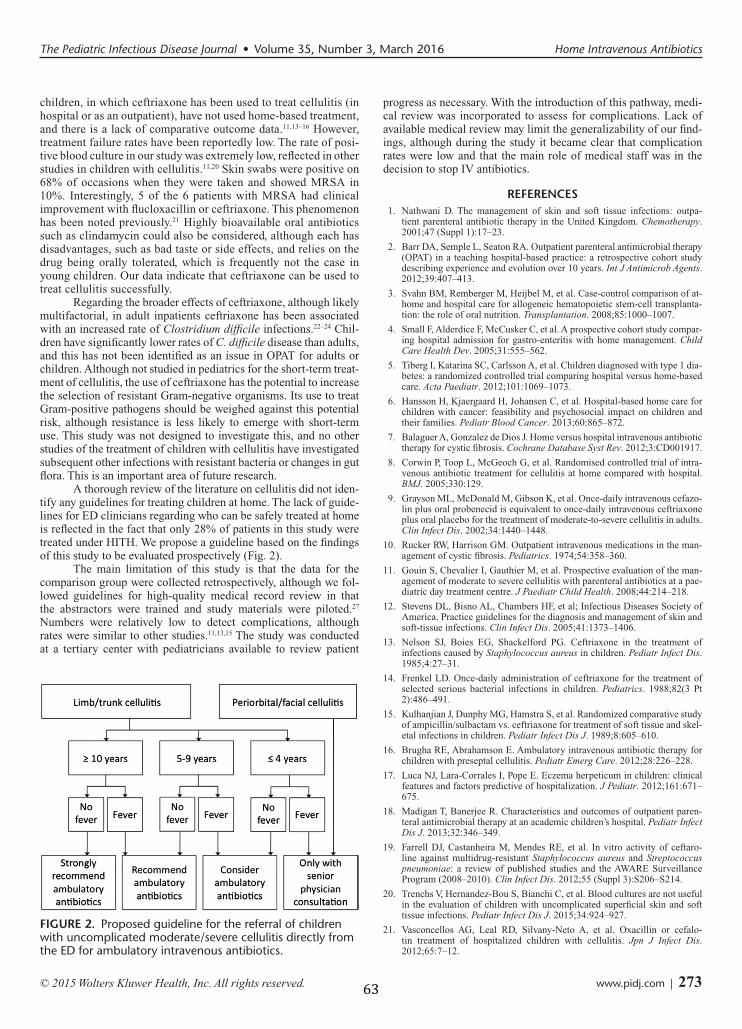
The Pediatric Infectious Disease Journal • Volume 35, Number 3, March 2016 Home Intravenous Antibiotics
© 2015 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | 273
children, in which ceftriaxone has been used to treat cellulitis (in hospital or as an outpatient), have not used home-based treatment, and there is a lack of comparative outcome data.11,13–16 However, treatment failure rates have been reportedly low. The rate of posi-tive blood culture in our study was extremely low, reflected in other studies in children with cellulitis.11,20 Skin swabs were positive on 68% of occasions when they were taken and showed MRSA in 10%. Interestingly, 5 of the 6 patients with MRSA had clinical improvement with flucloxacillin or ceftriaxone. This phenomenon has been noted previously.21 Highly bioavailable oral antibiotics such as clindamycin could also be considered, although each has disadvantages, such as bad taste or side effects, and relies on the drug being orally tolerated, which is frequently not the case in young children. Our data indicate that ceftriaxone can be used to treat cellulitis successfully.
Regarding the broader effects of ceftriaxone, although likely multifactorial, in adult inpatients ceftriaxone has been associated with an increased rate of Clostridium difficile infections.22–24 Chil-dren have significantly lower rates of C. difficile disease than adults, and this has not been identified as an issue in OPAT for adults or children. Although not studied in pediatrics for the short-term treat-ment of cellulitis, the use of ceftriaxone has the potential to increase the selection of resistant Gram-negative organisms. Its use to treat Gram-positive pathogens should be weighed against this potential risk, although resistance is less likely to emerge with short-term use. This study was not designed to investigate this, and no other studies of the treatment of children with cellulitis have investigated subsequent other infections with resistant bacteria or changes in gut flora. This is an important area of future research.
A thorough review of the literature on cellulitis did not iden-tify any guidelines for treating children at home. The lack of guide-lines for ED clinicians regarding who can be safely treated at home is reflected in the fact that only 28% of patients in this study were treated under HITH. We propose a guideline based on the findings of this study to be evaluated prospectively (Fig. 2).
The main limitation of this study is that the data for the comparison group were collected retrospectively, although we fol-lowed guidelines for high-quality medical record review in that the abstractors were trained and study materials were piloted.27 Numbers were relatively low to detect complications, although rates were similar to other studies.11,13,15 The study was conducted at a tertiary center with pediatricians available to review patient
progress as necessary. With the introduction of this pathway, medi-cal review was incorporated to assess for complications. Lack of available medical review may limit the generalizability of our find-ings, although during the study it became clear that complication rates were low and that the main role of medical staff was in the decision to stop IV antibiotics.
REFERENCES1. Nathwani D. The management of skin and soft tissue infections: outpa-
tient parenteral antibiotic therapy in the United Kingdom. Chemotherapy. 2001;47 (Suppl 1):17–23.
2. Barr DA, Semple L, Seaton RA. Outpatient parenteral antimicrobial therapy (OPAT) in a teaching hospital-based practice: a retrospective cohort studydescribing experience and evolution over 10 years. Int J Antimicrob Agents. 2012;39:407–413.
3. Svahn BM, Remberger M, Heijbel M, et al. Case-control comparison of at-home and hospital care for allogeneic hematopoietic stem-cell transplanta-tion: the role of oral nutrition. Transplantation. 2008;85:1000–1007.
4. Small F, Alderdice F, McCusker C, et al. A prospective cohort study compar-ing hospital admission for gastro-enteritis with home management. Child Care Health Dev. 2005;31:555–562.
5. Tiberg I, Katarina SC, Carlsson A, et al. Children diagnosed with type 1 dia-betes: a randomized controlled trial comparing hospital versus home-basedcare. Acta Paediatr. 2012;101:1069–1073.
6. Hansson H, Kjaergaard H, Johansen C, et al. Hospital-based home care forchildren with cancer: feasibility and psychosocial impact on children andtheir families. Pediatr Blood Cancer. 2013;60:865–872.
7. Balaguer A, Gonzalez de Dios J. Home versus hospital intravenous antibiotic therapy for cystic fibrosis. Cochrane Database Syst Rev. 2012;3:CD001917.
8. Corwin P, Toop L, McGeoch G, et al. Randomised controlled trial of intra-venous antibiotic treatment for cellulitis at home compared with hospital.BMJ. 2005;330:129.
9. Grayson ML, McDonald M, Gibson K, et al. Once-daily intravenous cefazo-lin plus oral probenecid is equivalent to once-daily intravenous ceftriaxoneplus oral placebo for the treatment of moderate-to-severe cellulitis in adults. Clin Infect Dis. 2002;34:1440–1448.
10. Rucker RW, Harrison GM. Outpatient intravenous medications in the man-agement of cystic fibrosis. Pediatrics. 1974;54:358–360.
11. Gouin S, Chevalier I, Gauthier M, et al. Prospective evaluation of the man-agement of moderate to severe cellulitis with parenteral antibiotics at a pae-diatric day treatment centre. J Paediatr Child Health. 2008;44:214–218.
12. Stevens DL, Bisno AL, Chambers HF, et al; Infectious Diseases Society ofAmerica. Practice guidelines for the diagnosis and management of skin and soft-tissue infections. Clin Infect Dis. 2005;41:1373–1406.
13. Nelson SJ, Boies EG, Shackelford PG. Ceftriaxone in the treatment ofinfections caused by Staphylococcus aureus in children. Pediatr Infect Dis. 1985;4:27–31.
14. Frenkel LD. Once-daily administration of ceftriaxone for the treatment ofselected serious bacterial infections in children. Pediatrics. 1988;82(3 Pt2):486–491.
15. Kulhanjian J, Dunphy MG, Hamstra S, et al. Randomized comparative study of ampicillin/sulbactam vs. ceftriaxone for treatment of soft tissue and skel-etal infections in children. Pediatr Infect Dis J. 1989;8:605–610.
16. Brugha RE, Abrahamson E. Ambulatory intravenous antibiotic therapy forchildren with preseptal cellulitis. Pediatr Emerg Care. 2012;28:226–228.
17. Luca NJ, Lara-Corrales I, Pope E. Eczema herpeticum in children: clinicalfeatures and factors predictive of hospitalization. J Pediatr. 2012;161:671–675.
18. Madigan T, Banerjee R. Characteristics and outcomes of outpatient paren-teral antimicrobial therapy at an academic children’s hospital. Pediatr Infect Dis J. 2013;32:346–349.
19. Farrell DJ, Castanheira M, Mendes RE, et al. In vitro activity of ceftaro-line against multidrug-resistant Staphylococcus aureus and Streptococcus pneumoniae: a review of published studies and the AWARE SurveillanceProgram (2008–2010). Clin Infect Dis. 2012;55 (Suppl 3):S206–S214.
20. Trenchs V, Hernandez-Bou S, Bianchi C, et al. Blood cultures are not useful in the evaluation of children with uncomplicated superficial skin and softtissue infections. Pediatr Infect Dis J. 2015;34:924–927.
21. Vasconcellos AG, Leal RD, Silvany-Neto A, et al. Oxacillin or cefalo-tin treatment of hospitalized children with cellulitis. Jpn J Infect Dis. 2012;65:7–12.
FIGURE 2. Proposed guideline for the referral of children with uncomplicated moderate/severe cellulitis directly from the ED for ambulatory intravenous antibiotics.
63

Ibrahim et al The Pediatric Infectious Disease Journal • Volume 35, Number 3, March 2016
274 | www.pidj.com
22. Owens RC Jr, Donskey CJ, Gaynes RP, et al. Antimicrobial-associated risk factorsfor Clostridium difficile infection. Clin Infect Dis. 2008;46 (Suppl 1):S19–S31.
23. Chapman AL, Dixon S, Andrews D, et al. Clinical efficacy and cost-effec-tiveness of outpatient parenteral antibiotic therapy (OPAT): a UK perspec-tive. J Antimicrob Chemother. 2009;64:1316–1324.
24. Matthews PC, Conlon CP, Berendt AR, et al. Outpatient parenteral antimi-crobial therapy (OPAT): is it safe for selected patients to self-administer athome? A retrospective analysis of a large cohort over 13 years. J Antimicrob Chemother. 2007;60:356–362.
25. Choi SH, Lee JE, Park SJ, et al. Emergence of antibiotic resistance duringtherapy for infections caused by Enterobacteriaceae producing AmpC beta-lactamase: implications for antibiotic use. Antimicrob Agents Chemother. 2008;52:995–1000.
26. Spritzer R, vd Kamp HJ, Dzoljic G, et al. Five years of cefotaxime use in aneonatal intensive care unit. Pediatr Infect Dis J. 1990;9:92–96.
27. Gilbert EH, Lowenstein SR, Koziol-McLain J, et al. Chart reviews inemergency medicine research: where are the methods? Ann Emerg Med. 1996;27:305–308.
64
65
2.5.1 Additional data
Table 2.1 Details of patients whose empirical antibiotics were changed
GAS (Group A Streptococci), MRSA (Methicillin resistant Staphylococcus aureus)
MSSA (Methicillin sensitive Staphylococcus aureus)
Empirical antibiotic
Duration of empirical antibiotic (hours)
Reason for change
Second line antibiotic choice Organism isolated from skin swab
Flucloxacillin 72 Slow to improve Ticarcillin/clavulanate Nil
Flucloxacillin 48 Slow to improve Vancomycin Nil
Flucloxacillin 48 Slow to improve Ticarcillin/clavulanate Nil
Flucloxacillin <12 Rapidly spreading, fever
Ticarcillin/clavulanate + vancomycin + clindamycin
GAS
Flucloxacillin 24 Slow to improve Vancomycin + clindamycin Nil
Flucloxacillin 24 Slow to improve Vancomycin + clindamycin Nil
Flucloxacillin 48 Slow to improve Vancomycin + ceftriaxone MSSA
Ceftriaxone 72 Slow to improve, skin swab result
Trimethoprim/sulfamethoxazole MRSA
Ceftriaxone 48 Poor improvement, skin swab result
Trimethoprim/sulfamethoxazole MRSA
66
2.6 Implications of studies on current practice
The studies in this chapter (the clinician survey and the baseline study) provided
invaluable insight into the management of cellulitis at our institution and
specifically the outcomes of patients treated at home with intravenous
antibiotics.114 The survey showed that nearly all clinicians treated mild cellulitis
with oral antibiotics and moderate/severe cellulitis with intravenous antibiotics,
as recommended by our local guideline.53 Through the survey, clinicians were
found to be concerned with using the home pathway, which had an impact on the
proportion of patients treated at home. The baseline study then clearly found
that the majority of patients with moderate/severe cellulitis were still being
admitted to hospital.
One major concern clinicians expressed was the risk of bacteraemia in
moderate/severe cellulitis. This risk was believed to be more than 10% by a
third of clinicians or even as high as 50% by a sizeable minority of clinicians.
This belief was inconsistent with the findings of the baseline study, where
bacteraemia did not occur at all, although only 53/144 (36%) patients had a
blood culture taken. This finding is in line with a previous study of
moderate/severe cellulitis that found the risk of bacteraemia to be less than
1%.45 In addition, there were no complications in the baseline study, contrary to
clinicians’ belief that there was substantial risk of a child deteriorating unnoticed
in the home.
A reasonable concern that clinicians had when managing cellulitis was the risk of
MRSA. The baseline study revealed for 4% of patients, skin swabs of the cellulitis
area was positive for MRSA. Therefore, in future studies it would be important to
investigate how consistent this risk was, particularly if the empiric antibiotic
used in hospital or at home, does not cover MRSA. However, in the baseline
study, even if a child with cellulitis caused by MRSA was sent home on
ceftriaxone which does not cover it, the worst outcome was readmission rather
than a more serious adverse outcome. An unexpected finding was that clinicians
were willing to accept up to 20% of readmissions from a home treatment
67
pathway because of the perceived benefits of being at home, However, from the
baseline study, the rate of readmission was actually much lower at 2%. The
survey also showed the variation in factors believed to be important for starting
intravenous antibiotics. This may mean it would be challenging to standardise
the indications for intravenous antibiotics for clinicians in the ED.
The baseline study added to the existing literature on the practice of home
treatment with intravenous antibiotics, showed that a select group of children,
predominantly older children with limb cellulitis and no systemic features, can
be safely and effectively treated at home with no clear difference in outcomes
from those treated in hospital.114 With this initial evidence for home intravenous
antibiotic treatment directly from the ED, there was increasing clinician interest
in using this pathway. This led to the question of whether all children with
uncomplicated moderate/severe cellulitis, not just those who are carefully
selected, can be treated at home. It was determined that the most robust way to
address this would be an RCT of home versus hospital intravenous antibiotics for
the management of cellulitis. However, the clinician survey showed that
confidence to use home intravenous antibiotics was very variable, with the
majority of clinicians concerned about treating children with periorbital cellulitis
or systemic features at home, and high levels of concern about bacteraemia and
unnoticed clinical deterioration.
Prior to undertaking an RCT it was therefore decided that a prospective
comparative study was necessary for two main reasons. The first reason was to
engage clinicians in the research while allowing them to retain choice of
treatment location, to provide additional prospectively-‐gathered evidence. The
aim was to reach equipoise on the question of whether home treatment is as
good as hospital treatment, ensuring clinician engagement and patient
enrolment in a subsequent definitive RCT. The second reason was that a number
of elements key to undertaking an RCT needed either additional information or
an assessment of feasibility prior to starting, including inclusion and exclusion
criteria, sample size calculation, antibiotic choice based on prevailing bacteria
and collection of microbiological samples. A prospective cohort study of children

68
managed at home and in hospital based on clinician choice was therefore
planned as a foundation study, and this is detailed in chapter 3.

69
Chapter 3 Foundation studies
3.1 Introduction to foundation studies
Although the baseline study (Chapter 2) showed the efficacy and safety of
treating a select group of children with moderate/severe cellulitis using an
ambulatory pathway, there were still some concerns and key questions that
needed to be addressed before embarking on an RCT.115 Clinicians were still
reluctant to use the home pathway, reflected by both the clinician survey and
baseline study that showed that only 28% of potentially eligible patients were
treated at home. For there to be genuine equipoise – the ethical basis for an RCT
–regarding treatment at home for moderate/severe cellulitis, more evidence was
needed for this treatment pathway particularly for younger patients and children
with periorbital cellulitis.
Additionally, a number of key elements to undertaking an RCT were unknown.
Specifically, we needed to investigate whether outcomes such as treatment
failure rates and readmissions would be similar to the previous study, when
including a wider, more generic population. The clinician survey and baseline
study provided invaluable information about the state of current practice and
the reasons for clinicians’ hesitation regarding OPAT for cellulitis which included
complications such as bacteraemia as well as the concern with the risk of MRSA
in this population. In addition, we wanted to assess the practicality of the study
design for the RCT, which include the primary outcome of change in empiric
antibiotic used, cost analysis and collection of microbiology samples.
This chapter contains two foundation studies. The first is a published manuscript
of a prospective cohort study that investigated the clinical outcomes of home
treatment compared to hospital care, for children with cellulitis. The patients
were not randomised but represented a broader cohort than the baseline study,
with both arms having data collected prospectively, and the study incorporated
aspects to address practicality and acceptability for the subsequent planned RCT.
The second manuscript describes the investigation of nasal colonisation with S.
70
aureus in children with cellulitis to better understand the role of MSSA and
MRSA, in our cohort and to inform the RCT.
3.2 Home versus hospital cohort
The were two main aims of the home versus hospital foundation study: 1) to
develop more evidence comparing home with hospital treatment to address the
clinical concerns of clinicians thereby engaging them in the research in
preparation for the RCT; and 2) to determine factors to inform the design of the
RCT. Evidence was needed to determine whether the outcomes of the home care
pathway were comparable to standard care in hospital, if the home pathway was
available to a wider patient population, including younger children, those with
periorbital cellulitis and those with fever, and to investigate the risk of
bacteraemia in this population. In order to engage ED clinicians in this research
while addressing their concerns, treatment location would be determined by
clinician choice.
In addition, key design issues needed to be addressed at this stage, which
included calculation of the sample size, inclusion and exclusion criteria,
practicality of the primary outcome of the RCT, determining the population of
those who required intravenous antibiotics and conducting a cost analysis. The
microbiology aspects will be addressed in the foundation colonisation study in
the next section of this chapter.
In the previous baseline study, outcomes for the home group were reassuring
but patients were older and had uncomplicated lower limb cellulitis.114 We
considered the age group that could be included in this study and although the
mean age of patients treated at home was 9 years old in the baseline study, the
youngest child to be treated at home was only a year old and a previous
ambulatory treatment study also had children as young as six months with no
adverse outcomes.6 To be consistent with previous ambulatory studies, we
determined the inclusion criteria to be children aged as young as 6 months to 18
years old in the foundation cohort.1
71
In determining the criteria for which patients with moderate/severe cellulitis
required intravenous antibiotics, we had obtained from the clinician survey the
features clinicians usually used when deciding route of antibiotic administration
as follows: lymphangitis/tracking (86%), functional impairment (76%), systemic
features (78%), whether the patient had received prior oral antibiotics (70%),
the size of the affected area (63%), whether the site affected was periorbital
(52%), swelling (52%) and tenderness (48%). However, these data were
insufficient to allow us to narrow down the population that required antibiotics.
As the study was designed specifically for the treating clinician to determine
whether to start intravenous antibiotics and where to treat the patient, the
reasons for using intravenous antibiotics and for clinicians’ choice in treatment
location needed to be documented in this study.
The clinician survey showed that one reason for clinicians’ hesitation with
treating children outside the hospital was their perception of the high risk of
bacteraemia. There are very few studies in children that have attempted to
determine the risk of bacteraemia in cellulitis. Those that have, show low risk of
bacteraemia and that taking a blood culture may be associated with an increase
in length of stay in hospital.44,45 When a blood culture is initially flagged as
positive, patients are frequently kept in hospital to continue intravenous
antibiotics until the organism is identified, or confirmed as a contaminant, which
may prolong length of stay in hospital. This was found in the baseline study, with
no true bacteraemia in any patient.114 Given the importance of this factor to
clinicians and the paucity of studies on this, it was determined that further
investigation of this phenomenon was warranted as a foundation to the planned
RCT.
Another key design issue to address was the primary outcome. In the baseline
study, the primary outcome was readmission from home during treatment.
Although important, this outcome was not applicable to the hospital cohort and
therefore not applicable for a comparative study of both treatment locations. In
previous studies in adults with cellulitis, primary outcomes used were ‘days to
no advancement of erythema’46 and in another study ‘clinical cure’, which was
72
defined as complete resolution of all signs and symptoms of cellulitis116. The
outcome of no advancement of erythema is not useful and was previously shown
to have poor association with clinical improvement.1 Clinical cure based on signs
and symptoms can vary for each child and is a subjective measurement. In order
to have a robust and objective outcome, we decided on treatment failure defined
as a change in empiric antibiotics due to inadequate clinical improvement or
serious adverse events. If this outcome was feasible in this foundation cohort
study, it would be used in the RCT.
Lastly, we aimed to assess the practicality of collecting cost data, which are
important for impact, with previous studies showing that treatment at home was
less costly.23,28 However, we needed to investigate if this finding was similar in
our setting, and determine what would comprise the components of calculating
the institutional costs. By collecting these data for the foundation cohort study,
we would be in a better position to design the economic analysis for the RCT.
We hypothesized that in a non-‐randomised cohort, children selected by
clinicians for treatment at home with intravenous ceftriaxone, would have
similar outcomes to those treated in hospital with flucloxacillin. In summary, the
foundation cohort study aimed to determine the following:
• The efficacy and safety of home versus hospital care measured by the rate
of treatment failure, complications and adverse events for a broad cohort
of children with uncomplicated moderate/severe cellulitis
• The underlying reasons for clinicians’ decisions for commencing
intravenous antibiotics and choice of treatment location
• Sample size calculation, practicality of the primary outcome and obtaining
costing data

73
3.3 Study 3: Home versus hospital cohort
Ibrahim LF, Hopper SM, Daley A, Connell T, Babl FE, Bryant PA. Home versus
Hospital: A Prospective Cohort of Children with Moderate/Severe Cellulitis.
Emerg Med J. 2017 Dec;34(12):780-‐785. doi: 10.1136/emermed-‐2017-‐206829.
Epub 2017 Oct 4

780
AbstrActObjective Children with moderate/severe cellulitis requiring intravenous antibiotics are usually admitted to hospital. Admission avoidance is attractive but there are few data in children. We implemented a new pathway for children to be treated with intravenous antibiotics at home and aimed to describe the characteristics of patients treated on this pathway and in hospital and to evaluate the outcomes.Methods This is a prospective, observational cohort study of children aged 6 months–18 years attending the ED with uncomplicated moderate/severe cellulitis in March 2014–January 2015. Patients received either intravenous ceftriaxone at home or intravenous flucloxacillin in hospital based on physician discretion. Primary outcome was treatment failure defined as antibiotic change within 48 hours due to inadequate clinical improvement or serious adverse events. Secondary outcomes include duration of intravenous antibiotics and complications.results 115 children were included: 47 (41%) in the home group and 68 (59%) in the hospital group (59 hospital-only, 9 transferred home during treatment). The groups had similar clinical features. 2/47 (4%) of the children in the home group compared with 8/59 (14%) in the hospital group had treatment failure (P=0.10). Duration of intravenous antibiotics (median 1.9 vs 1.8 days, P=0.31) and complications (6% vs 10%, P=0.49) were no different between groups. Home treatment costs less, averaging $A1166 (£705) per episode compared with $A2594 (£1570) in hospital.conclusions Children with uncomplicated cellulitis may be able to avoid hospital admission via a home intravenous pathway. This approach has the potential to provide cost and other benefits of home treatment.
IntrOductIOnSkin and soft tissue infections are common in chil-dren and the majority are treated with oral anti-biotics. A significant minority are treated with intravenous antibiotics for more acute clinical features, including rapid spreading of cellulitis, systemic features or if symptoms are progressing despite oral antibiotics. These infections usually require short-course intravenous antibiotics and in adults are commonly treated without hospital admission in an ambulatory setting (home, outpa-tient clinic or physician’s office).1–3 The well-doc-umented benefits of avoiding hospital admission include psychological benefits, reduced risk of
hospital-acquired infections and decreased use of healthcare resources.4–9 In contrast to adults, chil-dren with cellulitis are usually admitted to hospital due to a lack of evidence for outpatient intravenous treatment for skin and soft tissue infection even though they rarely have serious complications such as bacteraemia.10–12
To enable children to be treated in an outpatient setting, an antibiotic with a long half-life is ideal. First-line antibiotics for cellulitis (flucloxacillin, cephazolin) treat Staphylococcus aureus and group A streptococci (GAS) in settings of low prevalence of methicillin-resistant S. aureus (MRSA). However, they are dosed several times a day so are unsuit-able for outpatient treatment, and bioavailable oral alternatives are often unsuitable in children due to taste and side effects.13–15 The third-generation cephalosporin ceftriaxone has antistaphylococcal activity and can be administered once a day.16 17 While in some studies ceftriaxone was used to treat cellulitis, none of these studies have compared outcomes with first-line antibiotics, and none have been administered at home.16–20
Our institution has a home outreach programme whereby nurses administer antibiotics to children in
Original article
Evaluating an admission avoidance pathway for children in the emergency department: outpatient intravenous antibiotics for moderate/severe cellulitisLaila F Ibrahim,1,2,3 Sandy M Hopper,2,4 Tom G Connell,3,5 Andrew J Daley,5,6 Penelope A Bryant,1,2,3,5 Franz E Babl2,3,4
to cite: Ibrahim LF, Hopper SM, Connell TG, et al. Emerg Med J 2017;34:780–785.
► Additional material is published online only. To view please visit the journal online (http:// dx. doi. org/ 10. 1136/ emermed- 2017- 206829).1Department of RCH@Home, The Royal Children’s Hospital, Parkville, Victoria, Australia2Murdoch Childrens Research Institute, Parkville, Victoria, Australia3Department of Pediatrics, University of Melbourne, Parkville, Victoria, Australia4Department of Emergency, The Royal Children’s Hospital, Parkville, Victoria, Australia5Department of General Medicine, Infectious Diseases Unit, The Royal Children’s Hospital, Parkville, Victoria, Australia6Department of Microbiology, The Royal Children’s Hospital, Parkville, Victoria, Australia
correspondence toDr Penelope A Bryant, Department of General Medicine, The Royal Children’s Hospital Melbourne, Parkville, VIC 3052, Australia; penelope. bryant@ rch. org. au
PAB and FEB contributed equally.
Received 18 April 2017Revised 22 August 2017Accepted 31 August 2017Published Online First 4 October 2017
Key messages
What is already known on this subject? ► Children, their families and healthcaresystems all benefit from home versus hospitaltreatment, where possible.
► Children with moderate/severe cellulitisrequiring intravenous antibiotics are usuallytreated in hospital.
What this study adds? ► In a prospective, observational study ofmoderate/severe cellulitis, we comparedoutcomes of children treated at home withdaily ceftriaxone with those treated in hospital.
► Children selected by ED physicians to be treatedat home had low rates of treatment failureand complications. In addition, treatment athome was associated with cost savings for thehealthcare institution.
► Home treatment of moderate/severe cellulitiswith intravenous ceftriaxone may avoidhospital admission altogether.
74

781Ibrahim LF, et al. Emerg Med J 2017;34:780–785. doi:10.1136/emermed-2017-206829
Original article
the home with medical staff oversight. This model uses once-daily ceftriaxone via a peripheral intravenous catheter, the venous access recommended by the Infectious Diseases Society of America practice guidelines for short-course outpatient intra-venous therapy.3 Following a preliminary study, we formulated and implemented guidelines in the ED that allowed children with uncomplicated moderate/severe cellulitis requiring intra-venous antibiotic therapy to be treated either at home or in hospital.21 While the benefits of being at home are not disputed, it is important to ensure that home intravenous treatment in chil-dren does not put them at risk, and therefore prospective evalua-tion of this new pathway is necessary to provide confidence that the guidelines are appropriate.
This study aimed to describe the characteristics of children treated via the direct-to-home from the ED pathway and to prospectively evaluate the outcomes of these children. We hypothesised that there would be a low treatment failure rate at home and the duration of treatment would be comparable to standard hospital care.
MethOdsstudy design and settingThis is a prospective, observational cohort study at the Royal Children’s Hospital (RCH) Melbourne, a tertiary paediatric hospital.
selection of participantsInclusion criteriaChildren aged 6 months–18 years attending ED with uncompli-cated moderate/severe cellulitis from March 2014 to January 2015 were eligible. As there is no validated objective score for distinguishing moderate/severe from mild cellulitis, this was defined in the study as including any of following clin-ical features: rapidly spreading erythema, significant swelling/redness/pain, systemic symptoms/signs (eg, fever, lethargy) or failed oral therapy leading to treatment with intravenous antibiotics.
Exclusion criteriaPatients with complicated cellulitis (orbital cellulitis, undrained abscess, large animal/human bite, penetrating injury, foreign body, suspected fasciitis, toxicity) and comorbidities (immuno-compromise, varicella, any condition receiving different anti-biotic treatment) were excluded. Patients with mild cellulitis (treated with oral antibiotics) were excluded.
InterventionsStudy procedureED physicians were educated on the guidelines for the referral of children with cellulitis to the home intravenous antibiotic pathway (online supplementary figure). They were informed of the benefits and risks of the treatment locations for managing cellulitis prior to starting the study. If a patient was eligible, the ED physician followed an algorithm of inclusion and exclusion criteria, and after discussion with the family decided whether to treat the patient at home or in hospital. Physicians were asked for their reasons for treating with intravenous versus oral antibiotics and their reason for choosing home versus hospital. Patients meeting inclusion criteria were consented and recruited. Patients had cultures of blood, nose and the affected skin if indicated.
Home groupTo receive antibiotics at home, a referral was made to the home intravenous programme with handover to the home nursing team. After receiving the first dose of ceftriaxone 50 mg/kg in ED, the patient went home with the peripheral intravenous catheter in situ until intravenous antibiotics were ceased. On leaving the ED, families were provided with a contact telephone number for a (home intravenous programme) nurse available 24 hours a day, 7 days a week if they had any concerns about their child, while they were at home. A nurse visited the child daily at home and administered intravenous ceftriaxone until the child was deemed suitable for oral therapy. The medical staff overseeing patients at home aimed to review the child at least once during the course of treatment in person, and subsequently daily by teleconferencing or by reviewing digital photographs. The decision to cease intravenous antibiotics was made by the home programme medical staff.
Hospital groupThe standard of care for moderate/severe cellulitis at RCH is admission to the short stay unit for intravenous flucloxacillin 50 mg/kg six hourly. There is at least daily review by medical staff and at least four hourly nursing observations.
In all patients, whether in hospital or at home intravenous antibiotics were ceased when clinically appropriate to switch to oral antibiotics. Any patient deemed to require a further obser-vation period or ongoing interventions (eg, wound dressing) remained under medical care until these were no longer needed.
sample size and data collectionSample size calculation Sample size was calculated based on a treatment failure rate of approximately 3% with standard treatment; a home treatment failure rate of 25% (ie, three of four children treated at home successfully) that was considered acceptable by a panel of senior ED physicians, based on the other advantages of home; and a power of 80%—47 children in each arm. We continued recruit-ment for all eligible patients until we had reached at least this sample size for each group.
Data collectionData collected included age, sex, clinical features, systemic symp-toms at presentation (fever >38°C reported or documented at home or in the ED, vomiting, tachycardia or hypotension) and prior oral antibiotics. Physicians were asked their reason for intravenous versus oral antibiotics and hospital versus home treatment.
OutcomesThe primary outcome was measured as treatment failure defined as any change of initial empiric antibiotics within 48 hours due to inadequate clinical improvement or serious adverse events (anaphylaxis, suspected allergic reaction, sepsis). Secondary outcomes were readmission after discharge, rates of repeat intravenous catheterisation, complications, length of stay in ED, duration of intravenous antibiotics and length of stay under medical care (from the time of arrival in ED to the time of offi-cial discharge from medical care from the home or ward team). A cost comparison between home and hospital, provided by our institution’s business department, included the cost of nursing and medical resources, consumable items, and indirect overhead costs including administrative time, information technology and use of hospital vehicles for visiting patients.
75
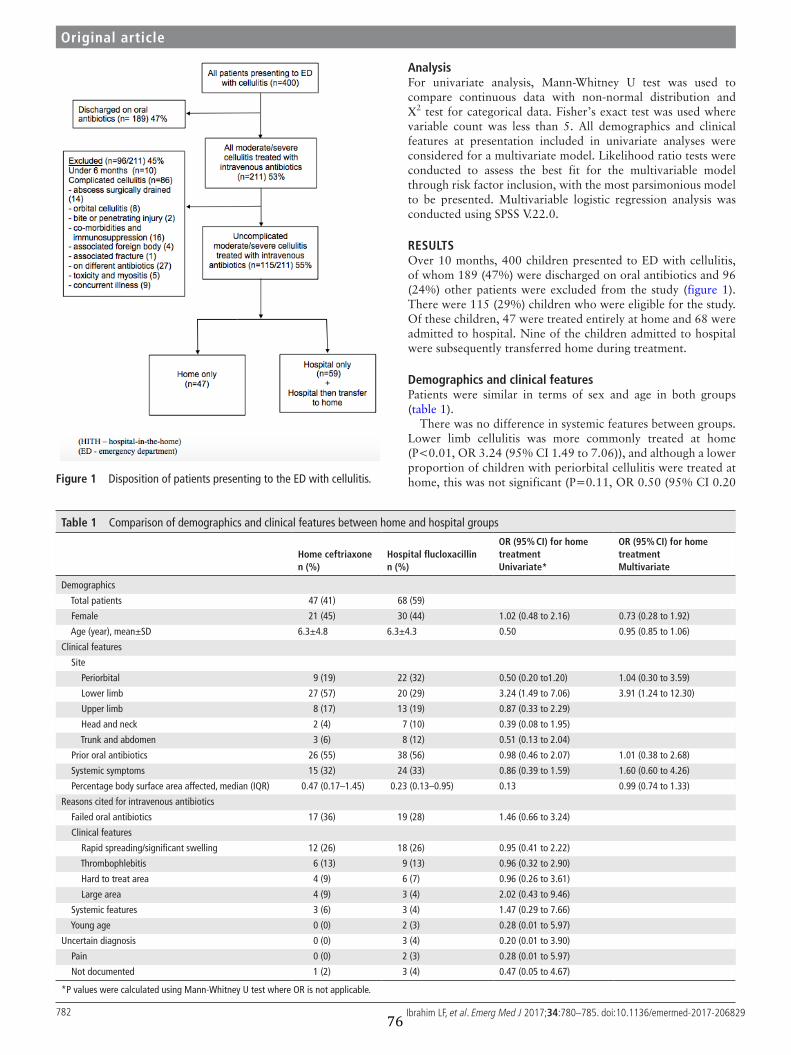
782 Ibrahim LF, et al. Emerg Med J 2017;34:780–785. doi:10.1136/emermed-2017-206829
Figure 1 Disposition of patients presenting to the ED with cellulitis.
table 1 Comparison of demographics and clinical features between home and hospital groups
home ceftriaxonen (%)
hospital flucloxacillinn (%)
Or (95% cI) for home treatmentunivariate*
Or (95% cI) for home treatmentMultivariate
Demographics
Total patients 47 (41) 68 (59)
Female 21 (45) 30 (44) 1.02 (0.48 to 2.16) 0.73 (0.28 to 1.92)
Age (year), mean±SD 6.3±4.8 6.3±4.3 0.50 0.95 (0.85 to 1.06)
Clinical features
Site
Periorbital 9 (19) 22 (32) 0.50 (0.20 to1.20) 1.04 (0.30 to 3.59)
Lower limb 27 (57) 20 (29) 3.24 (1.49 to 7.06) 3.91 (1.24 to 12.30)
Upper limb 8 (17) 13 (19) 0.87 (0.33 to 2.29)
Head and neck 2 (4) 7 (10) 0.39 (0.08 to 1.95)
Trunk and abdomen 3 (6) 8 (12) 0.51 (0.13 to 2.04)
Prior oral antibiotics 26 (55) 38 (56) 0.98 (0.46 to 2.07) 1.01 (0.38 to 2.68)
Systemic symptoms 15 (32) 24 (33) 0.86 (0.39 to 1.59) 1.60 (0.60 to 4.26)
Percentage body surface area affected, median (IQR) 0.47 (0.17–1.45) 0.23 (0.13–0.95) 0.13 0.99 (0.74 to 1.33)
Reasons cited for intravenous antibiotics
Failed oral antibiotics 17 (36) 19 (28) 1.46 (0.66 to 3.24)
Clinical features
Rapid spreading/significant swelling 12 (26) 18 (26) 0.95 (0.41 to 2.22)
Thrombophlebitis 6 (13) 9 (13) 0.96 (0.32 to 2.90)
Hard to treat area 4 (9) 6 (7) 0.96 (0.26 to 3.61)
Large area 4 (9) 3 (4) 2.02 (0.43 to 9.46)
Systemic features 3 (6) 3 (4) 1.47 (0.29 to 7.66)
Young age 0 (0) 2 (3) 0.28 (0.01 to 5.97)
Uncertain diagnosis 0 (0) 3 (4) 0.20 (0.01 to 3.90)
Pain 0 (0) 2 (3) 0.28 (0.01 to 5.97)
Not documented 1 (2) 3 (4) 0.47 (0.05 to 4.67)
*P values were calculated using Mann-Whitney U test where OR is not applicable.
Original article
AnalysisFor univariate analysis, Mann-Whitney U test was used to compare continuous data with non-normal distribution and Χ2 test for categorical data. Fisher’s exact test was used where variable count was less than 5. All demographics and clinical features at presentation included in univariate analyses were considered for a multivariate model. Likelihood ratio tests were conducted to assess the best fit for the multivariable model through risk factor inclusion, with the most parsimonious model to be presented. Multivariable logistic regression analysis was conducted using SPSS V.22.0.
resultsOver 10 months, 400 children presented to ED with cellulitis, of whom 189 (47%) were discharged on oral antibiotics and 96 (24%) other patients were excluded from the study (figure 1). There were 115 (29%) children who were eligible for the study. Of these children, 47 were treated entirely at home and 68 were admitted to hospital. Nine of the children admitted to hospital were subsequently transferred home during treatment.
demographics and clinical featuresPatients were similar in terms of sex and age in both groups (table 1).
There was no difference in systemic features between groups. Lower limb cellulitis was more commonly treated at home (P<0.01, OR 3.24 (95% CI 1.49 to 7.06)), and although a lower proportion of children with periorbital cellulitis were treated at home, this was not significant (P=0.11, OR 0.50 (95% CI 0.20
76
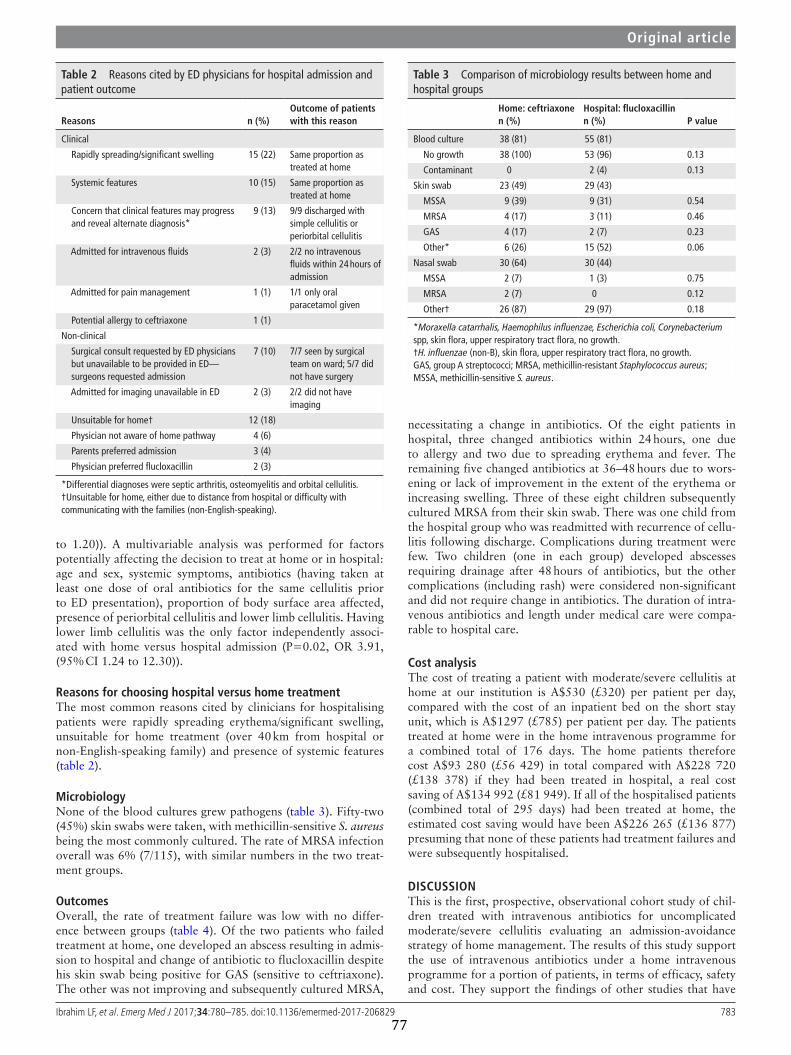
783Ibrahim LF, et al. Emerg Med J 2017;34:780–785. doi:10.1136/emermed-2017-206829
table 2 Reasons cited by ED physicians for hospital admission and patient outcome
reasons n (%)Outcome of patients with this reason
Clinical
Rapidly spreading/significant swelling 15 (22) Same proportion as treated at home
Systemic features 10 (15) Same proportion as treated at home
Concern that clinical features may progress and reveal alternate diagnosis*
9 (13) 9/9 discharged with simple cellulitis or periorbital cellulitis
Admitted for intravenous fluids 2 (3) 2/2 no intravenous fluids within 24 hours of admission
Admitted for pain management 1 (1) 1/1 only oral paracetamol given
Potential allergy to ceftriaxone 1 (1)
Non-clinical
Surgical consult requested by ED physicians but unavailable to be provided in ED—surgeons requested admission
7 (10) 7/7 seen by surgical team on ward; 5/7 did not have surgery
Admitted for imaging unavailable in ED 2 (3) 2/2 did not have imaging
Unsuitable for home† 12 (18)
Physician not aware of home pathway 4 (6)
Parents preferred admission 3 (4)
Physician preferred flucloxacillin 2 (3)
*Differential diagnoses were septic arthritis, osteomyelitis and orbital cellulitis.†Unsuitable for home, either due to distance from hospital or difficulty with communicating with the families (non-English-speaking).
table 3 Comparison of microbiology results between home and hospital groups
home: ceftriaxonen (%)
hospital: flucloxacillinn (%) P value
Blood culture 38 (81) 55 (81)
No growth 38 (100) 53 (96) 0.13
Contaminant 0 2 (4) 0.13
Skin swab 23 (49) 29 (43)
MSSA 9 (39) 9 (31) 0.54
MRSA 4 (17) 3 (11) 0.46
GAS 4 (17) 2 (7) 0.23
Other* 6 (26) 15 (52) 0.06
Nasal swab 30 (64) 30 (44)
MSSA 2 (7) 1 (3) 0.75
MRSA 2 (7) 0 0.12
Other† 26 (87) 29 (97) 0.18
*Moraxella catarrhalis, Haemophilus influenzae, Escherichia coli, Corynebacterium spp, skin flora, upper respiratory tract flora, no growth.†H. influenzae (non-B), skin flora, upper respiratory tract flora, no growth.GAS, group A streptococci; MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-sensitive S. aureus.
Original article
to 1.20)). A multivariable analysis was performed for factors potentially affecting the decision to treat at home or in hospital: age and sex, systemic symptoms, antibiotics (having taken at least one dose of oral antibiotics for the same cellulitis prior to ED presentation), proportion of body surface area affected, presence of periorbital cellulitis and lower limb cellulitis. Having lower limb cellulitis was the only factor independently associ-ated with home versus hospital admission (P=0.02, OR 3.91, (95% CI 1.24 to 12.30)).
reasons for choosing hospital versus home treatmentThe most common reasons cited by clinicians for hospitalising patients were rapidly spreading erythema/significant swelling, unsuitable for home treatment (over 40 km from hospital or non-English-speaking family) and presence of systemic features (table 2).
MicrobiologyNone of the blood cultures grew pathogens (table 3). Fifty-two (45%) skin swabs were taken, with methicillin-sensitive S. aureus being the most commonly cultured. The rate of MRSA infection overall was 6% (7/115), with similar numbers in the two treat-ment groups.
OutcomesOverall, the rate of treatment failure was low with no differ-ence between groups (table 4). Of the two patients who failed treatment at home, one developed an abscess resulting in admis-sion to hospital and change of antibiotic to flucloxacillin despite his skin swab being positive for GAS (sensitive to ceftriaxone). The other was not improving and subsequently cultured MRSA,
necessitating a change in antibiotics. Of the eight patients in hospital, three changed antibiotics within 24 hours, one due to allergy and two due to spreading erythema and fever. The remaining five changed antibiotics at 36–48 hours due to wors-ening or lack of improvement in the extent of the erythema or increasing swelling. Three of these eight children subsequently cultured MRSA from their skin swab. There was one child from the hospital group who was readmitted with recurrence of cellu-litis following discharge. Complications during treatment were few. Two children (one in each group) developed abscesses requiring drainage after 48 hours of antibiotics, but the other complications (including rash) were considered non-significant and did not require change in antibiotics. The duration of intra-venous antibiotics and length under medical care were compa-rable to hospital care.
cost analysisThe cost of treating a patient with moderate/severe cellulitis at home at our institution is A$530 (£320) per patient per day, compared with the cost of an inpatient bed on the short stay unit, which is A$1297 (£785) per patient per day. The patients treated at home were in the home intravenous programme for a combined total of 176 days. The home patients therefore cost A$93 280 (£56 429) in total compared with A$228 720 (£138 378) if they had been treated in hospital, a real cost saving of A$134 992 (£81 949). If all of the hospitalised patients (combined total of 295 days) had been treated at home, the estimated cost saving would have been A$226 265 (£136 877) presuming that none of these patients had treatment failures and were subsequently hospitalised.
dIscussIOnThis is the first, prospective, observational cohort study of chil-dren treated with intravenous antibiotics for uncomplicated moderate/severe cellulitis evaluating an admission-avoidance strategy of home management. The results of this study support the use of intravenous antibiotics under a home intravenous programme for a portion of patients, in terms of efficacy, safety and cost. They support the findings of other studies that have
77

784 Ibrahim LF, et al. Emerg Med J 2017;34:780–785. doi:10.1136/emermed-2017-206829
table 4 Outcomes of home and hospital groups
home: ceftriaxonen=47
hospital: flucloxacillinn=59* Or (95% cI)†
Treatment failure, n (%) 2 (4) 8 (14) 0.28 (0.00 to 1.25)
Complications, n (%) 3 (6) 6 (10) 0.74 (0.18 to 2.97)
Abscess after 48 hours 1 (2) 1 (2)
Phlebitis at catheter site 0 1 (2)
Rash 1 (2) 2 (3)
Vomiting 1 (2) 2 (3)
Required intravenous catheter insertion more than once, n (%) 2 (4) 8 (14) 0.28 (0.00 to 1.25)
Readmission (after discharge), n (%) 0 1 (2) 0
Home transfer to hospital (during treatment) 2 (4) N/A N/A
Duration of intravenous antibiotics (days), median (IQR) 1.9 (1.0–2.6) 1.8 (1.3–2.6) 0.31
Length of stay under medical care (days), median (IQR) 2.2 (1.8–3.0) 2.0 (1.6–3.1) 0.39
Duration of stay in ED (hours), median (IQR) 3.3 (2.6–4.4) 4.0 (3.1–5.7) <0.01
*Nine patients transferred during treatment from hospital to home under home intravenous programme excluded from outcome comparisons.†P values were calculated using Mann-Whitney U test where OR is not applicable.N/A denotes not applicable as outcome only available for the home group.
Original article
either been retrospective or did not collect data from the hospi-talised group.18 20 21
In our previous study we concluded that older children with lower limb cellulitis can be treated at home based on the patient cohort that had predominantly been treated via this model to date.21 We hypothesised that this model could be applicable to all patients with uncomplicated moderate/severe cellulitis. We formulated and implemented a guideline that included a wider age range with different sites of cellulitis and prospectively evaluated this. The success of the guideline implementation is reflected in the increase in the proportion of all eligible patients referred via the home intravenous pathway, from 28% in the previous period studied to 41% in this study. In addition, in the previous study only 24% of children treated at home were aged under 4 years old compared with 53% in this study. Although the guideline was cautious with periorbital cellulitis, requiring discussion with senior clinicians, the proportion of these cases referred for home intravenous antibiotics increased from 11% in the previous study to 29%.
In the current study the success rate was high for patients treated at home with intravenous ceftriaxone (96%). However, despite the introduction of guidelines, 59% of patients were still hospitalised. Reasons for hospitalisation were clinical in 56% of admitted patients. Almost all of the remaining hospitalised patients could potentially have been treated at home. We had excluded patients with complicated cellulitis/comorbidities. Reasons for physician hesitation may relate to lack of confidence with this relatively novel home treatment approach or a gener-ally conservative approach.
Regarding efficacy, ceftriaxone is not the usual first-line treat-ment for cellulitis, but it is suitable for home-based treatment because it can be administered once daily via a peripheral cath-eter. The short intravenous duration for cellulitis would not have warranted central venous catheter insertion, and peripheral cath-eter use at home was safe and acceptable to parents. However, uncertainties have remained around the efficacy of ceftriaxone against S. aureus. Although one study suggested high rates of resis-tance to ceftriaxone in methicillin-sensitive S. aureus (MSSA),22 it was subsequently retracted due to methodological flaws.23 24 A more recent study found 99% of MSSA isolates were ceftri-axone-susceptible.25 The in vitro findings are borne out by our study, which had a high clinical success rate. This corroborates
clinical studies where ceftriaxone has been effective for skin and soft tissue infection.17 26
Regarding the broader effects of ceftriaxone, although emer-gence of resistance is a concern for broad-spectrum antibiotics, this has never been shown for short-course antibiotics in children or for patients receiving outpatient/home intravenous antibiotics.21 While antibiotic resistance is a global problem, it is important not to extrapolate effects of longer duration broad-spectrum antibiotics administered in hospital into every situation, partic-ularly where there are other benefits of home treatment such as avoidance of hospital-acquired infections. Further studies in this area are urgently needed and should encompass the impact of short-term antibiotic use on the microbiome.
Although this study was not designed to assess the use of oral antibiotics, it is possible that some of these patients could have been treated with oral antibiotics with high oral bioavailability (eg, clindamycin, high-dose flucloxacillin). However, even disre-garding taste and adherence issues, data collected on reasons for the decision to treat with intravenous antibiotics are hard to refute: failed oral antibiotics (31%), severe clinical features of rapid spreading, significant swelling, thrombophlebitis or systemic features (44%) and large or hard to treat areas (15%), leaving 10% (only 4% of all patients with uncomplicated cellu-litis) where patients could potentially have been treated with oral antibiotics. As there are no comparative safety data for treating moderate/severe cellulitis at home via any route, this study provides valuable evidence that hospital admission may not always be required for this condition.
The strength of this study is its systematic evaluation after formulating and implementing a novel pathway to treating moderate/severe cellulitis in children. Implementation of this new pathway was considered successful with the increase in the proportion of admissions avoided. Our data suggest that increasing ED physician education and awareness of this new pathway may improve the proportion of referrals.
The main potential limitation of this study is that this pathway is specific to institutions that have a home intravenous team. For institutions without a home outreach programme, the antibi-otics could be delivered via an outpatient clinic or in the ED, but returning to the hospital daily may be less acceptable to patients. Second, as this study was not a randomised trial, other unknown factors which may have influenced the treatment location could
78

785Ibrahim LF, et al. Emerg Med J 2017;34:780–785. doi:10.1136/emermed-2017-206829
Original article
not be fully addressed. In addition, this study took place in a locale with low MRSA prevalence, so the results may not be externally valid to MRSA-prevalent regions. Lastly, although our study used the actual costs from our institution’s operational budget to compare the cost of home versus hospital treatment, a thorough assessment of cost-effectiveness to include patient returns was not performed.
In summary, children with uncomplicated moderate/severe cellulitis may be successfully treated at home with intravenous ceftriaxone directly from the ED, avoiding hospital admission altogether. Applying the results across other ambulatory/outpa-tient settings should include physician oversight until there is evidence to the contrary. Even though we found no signifi-cant differences in patient characteristics between the groups, because this study was not randomised, at this stage physicians prescribing intravenous antibiotics for children with cellulitis can select patients for home/outpatient treatment with daily review based on the home cohort in this study. Evaluation of this novel pathway has provided sufficient feasibility, efficacy and safety cohort data to recommend a randomised controlled trial to answer this question for all children presenting to ED with uncomplicated moderate/severe cellulitis.
Acknowledgements We would like to acknowledge the participation of patients and families.
contributors LFI conceptualised, designed and coordinated the study, carried out the initial data analysis, drafted the initial manuscript, and approved the final manuscript as submitted. PAB, FEB and SMH were involved in the design of the study, data analysis, reviewed and revised the manuscript, and approved the final draft. TGC and AJD were involved in the design of the study, reviewed and revised the manuscript, and approved the final draft. PAB had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This study is funded in part by grants from the RCH Foundation, the Murdoch Childrens Research Institute (MCRI) and the Victorian Department of Health, Melbourne, Australia. LFI was supported in part by a scholarship from Avant Mutual Group. PAB was in part supported by a Clinician Scientist Fellowship from the MCRI. FEB was supported in part by a grant from the RCH Foundation. The emergency research group, MCRI, is in part supported by a Centre for Research Excellence Grant for Paediatric Emergency Medicine from the National Health and Medical Research Council, Canberra, Australia, and the Victorian government infrastructure support programme.
competing interests None declared.
ethics approval The Royal Children’s Hospital Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
RefeRences 1 Chambers S, Gallagher K, Metcalf S, et al. Home intravenous antimicrobial service--
twelve months experience in Christchurch. N Z Med J 2002;115:216–8. 2 Barr DA, Semple L, Seaton RA. Outpatient parenteral antimicrobial therapy (OPAT) in
a teaching hospital-based practice: a retrospective cohort study describing experience and evolution over 10 years. Int J Antimicrob Agents 2012;39:407–13.
3 Tice AD, Rehm SJ, Dalovisio JR, et al. Practice guidelines for outpatient parenteral antimicrobial therapy. IDSA guidelines. Clin Infect Dis 2004;38:1651–71.
4 Svahn BM, Remberger M, Heijbel M, et al. Case-control comparison of at-home and hospital care for allogeneic hematopoietic stem-cell transplantation: the role of oral nutrition. Transplantation 2008;85:1000–7.
5 Small F, Alderdice F, McCusker C, et al. A prospective cohort study comparing hospital admission for gastro-enteritis with home management. Child Care Health Dev 2005;31:555–62.
6 Tiberg I, Katarina SC, Carlsson A, et al. Children diagnosed with type 1 diabetes: a randomized controlled trial comparing hospital versus home-based care. Acta Paediatr 2012;101:1069–73.
7 Hansson H, Kjaergaard H, Johansen C, et al. Hospital-based home care for children with cancer: feasibility and psychosocial impact on children and their families. Pediatr Blood Cancer 2013;60:865–72.
8 Orme LM, Babl FE, Barnes C, et al. Outpatient versus inpatient IV antibiotic management for pediatric oncology patients with low risk febrile neutropenia: a randomised trial. Pediatr Blood Cancer 2014;61:1427–33.
9 Sarvis A, Mathison D. 188 inpatient versus outpatient management of infants 29-60 days with presumed pyelonephritis at low risk for bacteremia: a cost analysis. Ann Emerg Med 2016;68:S74.
10 Bryant PA, Babl FE, Daley AJ, et al. Blood cultures in cellulitis are not cost effective and should prompt investigation for an alternative focus. Pediatr Infect Dis J 2016;35:118.
11 Trenchs V, Hernandez-Bou S, Bianchi C, et al. Blood cultures are not useful in the evaluation of children with uncomplicated superficial skin and soft tissue infections. Pediatr Infect Dis J 2015;34:924–7.
12 Malone JR, Durica SR, Thompson DM, et al. Blood cultures in the evaluation of uncomplicated skin and soft tissue infections. Pediatrics 2013;132:454–9.
13 Grayson ML, McDonald M, Gibson K, et al. Once-daily intravenous cefazolin plus oral probenecid is equivalent to once-daily intravenous ceftriaxone plus oral placebo for the treatment of moderate-to-severe cellulitis in adults. Clin Infect Dis 2002;34:1440–8.
14 Steele RW, Russo TM, Thomas MP. Adherence issues related to the selection of antistaphylococcal or antifungal antibiotic suspensions for children. Clin Pediatr 2006;45:245–50.
15 Gee SC, Hagemann TM. Palatability of liquid anti-infectives: clinician and student perceptions and practice outcomes. J Pediatr Pharmacol Ther 2007;12:216–23.
16 Nelson SJ, Boies EG, Shackelford PG. Ceftriaxone in the treatment of infections caused by staphylococcus aureus in children. Pediatr Infect Dis 1985;4:27–31.
17 Frenkel LD. Once-daily administration of ceftriaxone for the treatment of selected serious bacterial infections in children. Pediatrics 1988;82(3 Pt 2):486–91.
18 Gouin S, Chevalier I, Gauthier M, et al. Prospective evaluation of the management of moderate to severe cellulitis with parenteral antibiotics at a paediatric day treatment centre. J Paediatr Child Health 2008;44:214–8.
19 Kulhanjian J, Dunphy MG, Hamstra S, et al. Randomized comparative study of ampicillin/sulbactam vs. ceftriaxone for treatment of soft tissue and skeletal infections in children. Pediatr Infect Dis J 1989;8:605–10.
20 Brugha RE, Abrahamson E. Ambulatory intravenous antibiotic therapy for children with preseptal cellulitis. Pediatr Emerg Care 2012;28:226–8.
21 Ibrahim LF, Hopper SM, Babl FE, et al. Who can safely have antibiotics at home? a prospective observational study in children with moderate/severe cellulitis. Pediatr Infect Dis J 2015.
22 Pickering AJ HR, Harrison LH, et al. Common occurrence of ceftriaxone-resistant, methicillin-sensitive Staphylococcus aureus at a community teaching hospital. Clin Infect Dis 2014;59:e72.
23 Limbago BM, Pierce VM, Lonsway DR, et al. Elevated Staphylococcus ceftriaxone MICs are an Etest artifact. Clin Infect Dis 2015;60:162–3.
24 Phe K, Dao D, Palmer HR, et al. In vitro ceftriaxone susceptibility in methicillin-susceptible staphylococcus aureus. Antimicrob Agents Chemother 2015;59:1370.
25 Greenwood-Quaintance KE, Kohner P, Osmon DR, et al. Ceftriaxone susceptibility of oxacillin-susceptible staphylococcus aureus from patients with prosthetic joint infection. Diagn Microbiol Infect Dis 2015;82:177–8.
26 Vinen J, Hudson B, Chan B, et al. A randomised comparative study of once-daily ceftriaxone and 6-hourly flucloxacillin in the treatment of moderate to severe cellulitis - Clinical efficacy, safety and pharmacoeconomic implications. Clinical Drug Investigation 1996;12:221–5.
79
moderate/severe cellulitisoutpatient intravenous antibiotics forfor children in the emergency department: Evaluating an admission avoidance pathway
Penelope A Bryant and Franz E BablLaila F Ibrahim, Sandy M Hopper, Tom G Connell, Andrew J Daley,
doi: 10.1136/emermed-2017-2068292017
2017 34: 780-785 originally published online October 4,Emerg Med J
http://emj.bmj.com/content/34/12/780Updated information and services can be found at:
These include:
References http://emj.bmj.com/content/34/12/780#ref-list-1
This article cites 25 articles, 3 of which you can access for free at:
serviceEmail alerting
box at the top right corner of the online article. Receive free email alerts when new articles cite this article. Sign up in the
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
80
81
3.4 Nasal colonisation in cellulitis
Skin and soft tissue infections, including cellulitis, are associated with nasal
colonisation with S. aureus.105,107 The strain of S. aureus that colonises the
anterior nares has been shown to be concordant with the strain that causes skin
infection.117 Therefore investigating prevalence of S. aureus nasal colonisation in
children presenting with cellulitis has the potential to improve our
understanding of this condition in several ways.
Primary amongst these is the prevalence of MRSA in our patient population as
this directly informs choice of empiric antibiotics. According to the clinician
survey, clinicians believed the risk of MRSA to be as high as 20% in children
presenting to ED with cellulitis. In an Australia-‐wide study of S. aureus,
susceptibility patterns for isolates from children attending tertiary paediatric
hospitals, the rates of MRSA were between 6-‐14%, varying in different states.118
MRSA-‐colonised children are 24 times more likely to have MRSA infections
compared to non-‐colonised patients.104 In the baseline study (Chapter 2) 6/59
(10%) patients had skin swabs positive for MRSA. However, skin swabs were
only performed when clinically indicated, for example if the clinician suspected
MRSA due to past history. Therefore, 59% of the study cohort did not have a skin
swab, obscuring the actual proportion of those with MRSA colonisation.
Determining prevalence of MRSA colonisation would be an important
determinant of empiric antibiotic choice for the RCT. Although MRSA has
received more attention in the literature, MSSA is more prevalent in most
populations, both as a colonising organism and as a cause of invasive infections.
Since there are few studies investigating risk factors and the effect of antibiotics
on MSSA, we determined that this was an opportunity to investigate both MSSA
and MRSA in children with cellulitis.
Although there is increasing use of ceftriaxone for ambulatory/home treatment
in children with cellulitis, there have never been any studies prospectively
investigating the impact of short-‐course ambulatory ceftriaxone on bacterial
82
colonisation and development of resistance. In a study in a geriatric hospital, use
of third generation cephalosporins, monobactam and carbapanem was
significantly associated with MRSA infections.69 However, in children, there is
conflicting evidence on the importance of antibiotic exposure as a risk factor for
MRSA colonisation or infection. Reported risk factors for colonisation by both
MSSA and MRSA in children include prior antibiotic use, hospitalisation,
maternal colonisation, colonisation in other household members, hospitalisation
of a household member and older age.21,105-‐107 This study, using the same cohort
of patients in the previous foundation study, was therefore an opportunity to
investigate the risk factors for colonisation with S. aureus at baseline to compare
our population with those in other studies, and for the first time prospectively to
investigate the longitudinal impact of antibiotics on nasal colonisation with
MSSA and MRSA. It also enabled us to determine the feasibility of longitudinal
microbiological sample collection for the RCT.
Thirdly, the effect of S. aureus colonisation status on the severity of cellulitis has
never been investigated. This study was an opportunity to determine whether
nasal colonisation affects outcomes such as duration of treatment or
complications such as abscess.119
In summary, the nasal colonisation study aimed to investigate the following:
• The risk of nasal colonisation with both MSSA and MRSA in children
presenting with moderate/severe cellulitis
• The risk factors for nasal colonisation with MSSA and MRSA at baseline
and the longitudinal impact of ceftriaxone on colonisation
• The effect of S. aureus colonisation status on the severity of cellulitis and
outcomes

83
3.5 Study 4: Nasal colonisation
Ibrahim LF, Scrivener A, Hopper SM, Babl FE, Bryant PA. Does Hospitalisation Of
Children With Cellulitis Increase Nasal Carriage Of Methicillin-‐Sensitive And
Resistant Staphylococcus aureus. Under review with Journal of Pediatric
Infectious Diseases Society.
(The following manuscript is a Word version of the submitted work instead of
the PDF version from Journal of Pediatric Infectious Diseases Society due to a
large watermark.)
The impact of antibiotics on colonization with Staphylococcus aureus in children
with cellulitis
Laila F Ibrahim MB BCh BAOa,d,e, Alexander Scrivener MDe, Sandy M Hopper
MBBSb,d, Andrew J Daley MMedc,f, Nigel Curtis PhDc,d,e , Franz E Babl MDb,d,e ,
Penelope A Bryant PhDa,c,d,e
Affiliations:
a Hospital-In-The-Home Department, The Royal Children’s Hospital
b Emergency Department, The Royal Children’s Hospital
c Infectious Diseases Unit, Department of General Medicine, The Royal Children’s
Hospital
d Murdoch Children’s Research Institute
e Department of Pediatrics, University of Melbourne
f Department of Microbiology, The Royal Children’s Hospital
50 Flemington Road, Parkville, Victoria 3052, Australia
Corresponding author:
A/Prof. Penelope A Bryant
Department of General Medicine, The Royal Children’s Hospital Melbourne
50 Flemington Road, Parkville, VIC 3052, Australia
Email: [email protected]
Tel: +613 93455522 Fax: +613 9345 6667
Key words: Staphylococcus aureus, antibiotics, cellulitis
Word count 2, 704
84
Abbreviated title: Antibiotic impact on Staphylococcus aureus colonization
Running head title: Staphylococcus aureus colonization and antibiotics
Key points:
• In children treated with intravenous antibiotics for cellulitis, there was an
increase in nasal colonization of Staphylococcus aureus 12-months post-
antibiotic treatment for those who received flucloxacillin in hospital.
• In contrast those who received ambulatory ceftriaxone did not have increased
colonization.
85
Abstract
Background
Staphylococcus aureus is a major cause of invasive infection in children, with nasal
colonization playing a key role in pathogenesis. We aimed to: 1) compare
colonization with nasal S. aureus (methicillin-sensitive (MSSA) and methicillin-
resistant (MRSA)) in children with cellulitis treated with either intravenous
flucloxacillin in hospital or ambulatory ceftriaxone at home; 2) assess other risk
factors for colonization; 3) evaluate the effect of colonization on cellulitis severity.
Methods
A prospective cohort study from 2014-2015 in patients with cellulitis treated with
intravenous antibiotics. Patients had a nasal swab at baseline and 12 months post
antibiotics, which was cultured for S. aureus. Risk factors and clinical features were
collected.
Results
90 children had at least one swab, with 50 sampled at both time points. Forty-five
(50%) received flucloxacillin in hospital and 45 (50%) ceftriaxone at home. Between
baseline and 12 months, S. aureus colonization increased in the flucloxacillin group
(12% versus 40%, p=0.01), but did not in the ceftriaxone group (18% versus 19%,
p=1.00). The difference in post-antibiotic acquisition between flucloxacillin and
ceftriaxone was 42% versus 12% (p=0.02). Only 4 patients were colonized with
MRSA at baseline and none at 12 months. The only additional risk factor for
colonization with MSSA was having a large area of cellulitis. S. aureus colonization
did not affect severity of cellulitis.
86

Conclusions
The unexpected increase in S. aureus acquisition may be attributable to either
hospitalization or flucloxacillin use. The use of short-course ceftriaxone at home was
not associated with an increase in colonization with S. aureus.
87
Introduction
Staphylococcus aureus is a major cause of invasive infection in children, and
bacteremia is associated with 4% mortality.(1) Nasal colonization with S. aureus
plays a key role in the pathogenesis of invasive infection including cellulitis and
bacteremia(2-5) and is associated with non-infectious conditions such as asthma(6),
eczema(7) and epistaxis(8). In adults, much is known about the risk factors for nasal
colonization with methicillin-resistant S. aureus (MRSA), with fewer studies
investigating children.(9) Less still is known about risk factors for methicillin-
sensitive S. aureus (MSSA) colonization, which in many settings causes a higher
proportion of invasive infections than MRSA and is associated with a similar
mortality.(1, 10)
Reported risk factors for colonization by both MSSA and MRSA in children include
prior antibiotic use, hospitalization, maternal colonization, colonization in other
household members, hospitalization of a household member and older age.(11-14)
However these findings are from a relatively small number of studies, relying on
recollection of antibiotic use, predominantly screening healthy children, and there is
conflicting evidence on the importance of antibiotic exposure as a risk factor. No
study with prospective antibiotic administration, has compared the effect of different
antibiotics on colonization and no study has related colonization to the severity of
concurrent infection.
The most common infection caused by S. aureus in children is cellulitis. At our
institution we developed a treatment pathway to avoid admission for children with
moderate/severe cellulitis requiring intravenous (IV) treatment.(15) Patients can
receive ceftriaxone at home as outpatient parenteral antimicrobial therapy (OPAT) as
88
an alternative to standard admission to hospital for flucloxacillin. Although the
advantage of ceftriaxone is its once daily administration allowing ambulatory use, a
potential disadvantage is that third-generation cephalosporins have been associated
with resistance in colonizing bacteria, including MRSA in adults, although the latter
has not been clearly identified in children.(9, 16-20) There are many centres
worldwide using ceftriaxone for ambulatory/home treatment without any prospective
studies documenting the impact on nasal colonization, compared to those receiving
standard care in hospital.(15, 21-23)
We therefore undertook a prospective study of children with moderate/severe
cellulitis with the following aims: 1) to compare the rates of colonization and
acquisition of nasal S. aureus in children treated for cellulitis between intravenous
flucloxacillin in hospital and ambulatory ceftriaxone at home; 2) to identify risk
factors for both MSSA and MRSA nasal colonization in this setting, in particular the
impact of antibiotics; and 3) to determine whether nasal S. aureus colonization at
presentation affects the severity of cellulitis.
Methods
Design and setting: A prospective cohort study recruiting from March 2014 to Jan
2015 in the Emergency Department (ED) at the Royal Children’s Hospital (RCH)
Melbourne, a tertiary pediatric hospital.
Inclusion/exclusion criteria: Children aged 6 months to 18 years treated for
uncomplicated moderate/severe cellulitis with IV antibiotics were eligible. Patients
with complicated cellulitis (orbital cellulitis, undrained abscess, large animal/human
bite, penetrating injury, foreign body, suspected fasciitis, toxicity) and co-morbidities
89
(immunocompromise, varicella, any condition receiving different antibiotic treatment)
were excluded. Patients with mild cellulitis (treated with oral antibiotics) were also
excluded.
Recruitment: ED clinicians received education about the home pathway and they then
decided whether to treat a child with moderate/severe cellulitis with standard care of
IV flucloxacillin 50 mg/kg 6 hourly in hospital or IV ceftriaxone 50 mg/kg once daily
at home. For completion with oral antibiotics, patients in both groups were switched
to cephalexin 25 mg/kg 8 hourly, unless they cultured MRSA from a skin swab for
which they received trimethoprim/sulfamethoxazole (8/40 mg per mL – 0.5 ml/kg).
Intervention: Patients in either group had a peripheral cannula inserted in the ED
using standard cannulation techniques. The first dose of antibiotic was administered in
the ED. For home patients, after the first dose of ceftriaxone, they were discharged
home with the peripheral cannula in situ followed by once daily visits at home from
the OPAT nurse for assessment and further doses of ceftriaxone. For the hospital
patients, after commencing the first dose of flucloxacillin, they were transferred to a
medical ward followed by routine medical ward care. For both groups of patients,
decision to cease IV antibiotics were made by the treating clinician (either OPAT
clinician or ward clinician of at least senior registrar level)
Data and sample collection: Data collected included demographics, features of
cellulitis, oral antibiotic use, duration of IV antibiotics and length of stay in hospital.
At baseline prior to IV antibiotics, a nasal sample was collected using a dry sterile
Amies charcoal swab (Copan,USA) by rotating two to three times in the vestibule of
both anterior nares and placing immediately in Amies charcoal transport medium.
90
After 12 months, a second swab was collected and a questionnaire was administered
to collect information on the clinical history between the two time points, including
antibiotic use, other infections and hospitalizations. Colonization was defined as a
positive nasal swab at either baseline or 12 months. Acquisition was defined as those
who had a negative nasal swab at baseline and subsequently had a positive swab at 12
months.
Bacterial culture: The nasal swab was processed in the microbiology laboratory at
RCH within 24 hours of collection. The swab was inoculated on to mannitol salt agar,
horse blood agar and MacConkey agar, incubated at 35°C and reviewed at 24 and 48
hours. Colonies with mannitol-salt fermentation and morphology suggestive of S.
aureus were tested with Prolex Staph Xtra latex (Pro-Lab Diagnostics, Canada) from
non-selective media, followed by a DNase test. Isolates that were both staphylococcal
latex and DNase positive were identified as S. aureus. Antibiotic susceptibility testing
was done by Vitek AST card (bioMérieux, France). The results were interpreted
according to the 2014 Clinical & Laboratory Standards Institute (CLSI) guideline.
Statistical analysis: For univariate analysis, the Student t test was used to compare
continuous data and chi-square or Fisher’s exact test for categorical data (where
frequency of variables are <5) using Stata statistics (Stata/IC 15.0). All risk factors
included in univariate analyses were considered for a multivariate model. Likelihood
ratio tests were conducted to assess the best fit for the multivariate model through risk
factor inclusion, with the most parsimonious model presented.
Ethics: This study received approval from the RCH human research ethics committee
(No. HREC 34018).
91
Results
Over a 10-month period, 90 children with moderate/severe cellulitis were recruited
who had at least one nasal swab taken: 68 at presentation (baseline), 72 at 12 months
post antibiotics and 50 sampled at both time points. The patients treated with inpatient
flucloxacillin or ambulatory ceftriaxone were of similar age, sex and most clinical
characteristics, with 45 (50%) in each group (table 1). There was a higher proportion
of children in the inpatient flucloxacillin group who had eczema although overall
numbers were small and statistically this was not significant: 9 (20%) versus 2 (4%)
(OR 5.37, 95% CI 1.09 to 26.48, p=0.05). Of those colonised at baseline, there were
2/10 patients who had eczema, 1 from the home group and the other from the hospital
group. At 12 months, of those colonised only 1/21 had eczema, this patient was from
the hospital group.
Nasal colonization with S. aureus
At the time of presentation with cellulitis, 10/68 (15%) children had nasal
colonization with S. aureus (table 2), of which 4 (6%) had MRSA. At 12 months post
IV antibiotics for treatment of cellulitis, 21/72 (29%) children were colonized with S.
aureus, of which no (0%) patients had MRSA (table 3). There was a significant
difference 12 months after antibiotics between the two groups: 14/35 (40%) were
colonized in the flucloxacillin group and 7/37 (19%) in the ceftriaxone group (OR
0.35, 95% CI 0.12 to 1.00, p=0.049). Since there was no difference between the
groups at baseline, this represents an increase in proportion of colonization in the
flucloxacillin group between presentation and 12 months later (4 (12%) versus 14
(40%) patients colonized (OR 5.0, 95% CI 1.44 to 17.34, p=0.01). This was
investigated further for patients who had both baseline and 12 month swabs: overall
92
13/50 (26%) acquired nasal S. aureus colonization post IV antibiotics, 7 (14%) were
no longer colonized and 1 (2%) had persistent colonization. Acquisition of S. aureus
occurred in 10 (42%) patients treated with flucloxacillin in hospital, significantly
more than the 3 (12%) of those treated with ceftriaxone at home (OR 5.48, 95% CI
1.35 to 21.63, p=0.02).
Risk factors for acquisition of S. aureus
We assessed the impact of antibiotics and multiple other risk factors on both
colonization (MRSA and MSSA) and acquisition of S. aureus after treatment for
cellulitis (all MSSA) (table 4). No risk factors investigated prior to the cellulitis
episode were associated with colonization status at baseline or acquisition by 12
months. In addition to the treatment pathway (home versus hospital) being associated
with a difference in acquisition of S. aureus as previously stated, we also found that if
children had a large area of cellulitis (body surface area >1%), a significantly higher
proportion acquired S. aureus than did not: 7/13 (54%) versus 7/36 (19%), OR 4.8
95% CI 1.3-18.4, p=0.02. No other clinical features of cellulitis were associated with
colonization at 12 months or acquisition, nor were any other factors that were
investigated in the 12 months post treatment (table 4). Upon adding each potential risk
factor for S. aureus colonization to the multivariate model, likelihood ratio tests did
not identify model improvement, so a multivariate analysis was not required.
Impact of colonization on severity of cellulitis
The only significant clinical correlation between nasal S. aureus colonization and
severity of cellulitis or outcomes was abscess formation: 4 (40%) patients who were
colonized developed an abscess, compared to 6 (10%) who were not colonized (OR
5.78, 95% CI 1.36 to 25.2, p=0.01). Of those with MRSA colonization, 3 (75%)
93
patients developed an abscess, compared to 1 (17%) with MSSA (OR 15, 95% CI 0.7
to 339, p=0.11). All patients with MSSA colonization at presentation had
improvement in their cellulitis regardless of whether they were treated with
flucloxacillin or ceftriaxone. Of the 4 with MRSA colonization, 2 improved on
ceftriaxone and were subsequently switched to oral trimethoprim/sulfamethoxazole
with the culture result, and 2 did not improve on empiric IV treatment until antibiotics
were changed to vancomycin.
Discussion
This is the first study comparing nasal colonization in children with cellulitis before
and after antibiotic use. The most important finding was that short course IV
ceftriaxone administered via an ambulatory pathway at home did not result in
increased nasal colonization with S. aureus, either MSSA or MRSA, when measured
after 12 months. This is a key finding to add support to the use of ceftriaxone in this
specific setting. Non-inpatient treatment has advantages both for the patient in terms
of psychological outcomes and reduced hospital-associated risks, and for the
healthcare institution in terms of patient flow and costs.(24-26)
An unexpected finding was that IV flucloxacillin in hospital was associated with a 4-
fold increase in the likelihood of nasal S. aureus colonization – all MSSA – after 12
months. There are three possible reasons for the significant difference in S. aureus
colonization between the groups: difference in antibiotic choice, difference in
treatment location or another difference. As both antibiotic and location were different
between the two treatment pathways, we are unable to determine whether the
difference is due to flucloxacillin use or hospital admission. Both are possible based
on hypothesis and supporting literature. Hospital admission is a known risk for
94
pathogen transmission and it has been reported in one previous study as a risk factor
for S. aureus nasal colonization.(11) However, the only other study to investigate
hospitalization as a risk factor found no association, with the authors suggesting that
antibiotic use in previous hospitalizations may have negated the effect.(14) In our
study, neither prior hospitalization nor hospitalization in the 12 months after the
cellulitis were independent risks for acquisition, which therefore questions hospital
admission as the sole risk factor, unless it is a marker for severity of the cellulitis
episode.
We therefore considered aspects of the episode relating to severity that may have been
different between the groups and that may have resulted in hospital admission rather
than the home treatment pathway. However, there was no difference between the
groups in local cellulitis features (large size, rapid spreading, severe swelling),
presence of systemic clinical features or duration of antibiotics.
This leaves the difference in antibiotics between the groups. It might seem unexpected
that flucloxacillin, an anti-staphylococcal antibiotic, would increase nasal colonization
with MSSA. However, we hypothesize that flucloxacillin has an immediate effect
reducing nasal S. aureus colonization but it may additionally cause collateral decrease
in other Gram-positive commensal bacteria. This effect may be greater than
with ceftriaxone due to the high efficacy of flucloxacillin against certain Gram-
positive bacteria. Several studies have shown an inverse relationship between S.
aureus and the presence of other colonising bacteria including Corynebacterium spp,
Staphylococcus epidermidis, Lactobacillus spp and Propionibacterium spp.(27-30)
The absence of these other bacteria competing for space and nutrients may allow S.
aureus to take over the microbiological niche. This hypothesis would also explain the
95
conflicting results of the four retrospective studies in children that have investigated
antibiotics as a risk factor for nasal S. aureus colonization. Three studies showed no
association with antibiotic use over the previous two(31) and three months(14, 32)
whereas the other study investigating antibiotic use in the previous six months showed
increased S. aureus colonization.(11) Time post antibiotics, and therefore time for S.
aureus to take over the newly unoccupied niche, is potentially the factor explaining
the difference. Although in our study a few patients had received subsequent
antibiotics, numbers are too small to draw conclusions from either type or time since
the most recent course.
MRSA rates were low in this study and there was no increase in nasal colonization
after antibiotics contrary to studies in adults(33, 34). There are several possibilities for
this. First, the prevalence of MRSA in our population is low and second, it may be
related to the relatively short antibiotic duration in the study. However, importantly
the results show that in contrast to previous reports of ceftriaxone use in adults in
hospitals(9, 19) short course ceftriaxone use at home in children is not associated with
acquiring MRSA.(9, 19)
Nasal colonization was not associated with a more severe episode of cellulitis, or its
outcomes, apart from the recognized association between MRSA colonization and
soft tissue abscesses.(35) A previous study relating nasal S. aureus colonization to
incidence of bacteremia raises the possibility that colonization may be related to
incidence of cellulitis rather than severity or outcome, although this study was not
designed to answer that.(5)
Limitations of our study include that we are unable to separate IV antibiotic and
96
treatment location as risk factors, but this was a necessary study design based on
assessing the ambulatory pathway and the findings are reassuring regarding that. Also,
as treatment location was decided by the ED clinician, it is possible that other
unknown risk factors may have affected colonization. We mitigated this by
investigating risk factors that other studies have investigated, although numbers of
patients with each risk factor were small and a larger randomized study would be
required to definitively answer this question. We only investigated colonization in the
nose as this is the main reservoir for S. aureus colonization and allows comparison
with other studies; however, it is possible that higher rates may have been found if
other body sites had also been tested for colonization.
In conclusion, use of short-course ceftriaxone at home in this study was not associated
with increased rates of S. aureus colonization. It also did not appear to affect MRSA
acquisition, although this study should be replicated where MRSA has higher
prevalence. These findings provide some reassurance that the widespread use of short-
course ceftriaxone for OPAT in children is not contributing to acquisition or
colonization of S. aureus. That we unexpectedly found that hospitalization with a
narrow spectrum antibiotic appears to be a greater risk factor for colonization than
home administration of a broader spectrum antibiotic needs further study. Future
studies should also investigate the impact of ceftriaxone on gastrointestinal bacteria
given its broader effects against Gram-negative bacteria.
Funding: This study is funded in part by grants from the RCH Foundation, the
Murdoch Children's Research Institute (MCRI), the Victorian Department of Health,
Melbourne Australia. LFI was supported in part by a scholarship from AVANT
Mutual Group Ltd, Melbourne, the Melbourne Children’s Campus Postgraduate
97
Health Research Scholarship and the Doctor Nicholas Collins Fellowship. PAB was
in part supported by a Melbourne Campus Clinician Scientist Fellowship, Melbourne,
Australia. FEB was supported in part by a grant from the RCH Foundation and a
Melbourne Campus Clinician Scientist Fellowship, Melbourne, Australia and a
National Health and Medical Research Council (NHMRC) Practitioner Fellowship,
Canberra, Australia. The emergency research group, MCRI, is in part supported by an
NHMRC Centre for Research Excellence Grant for Pediatric Emergency Medicine,
Canberra, Australia and the Victorian government infrastructure support program.
Acknowledgements: We would like to acknowledge the participation of patients and
families. We would also like to thank the staff of the Department of Microbiology at
the Royal Children’s Hospital.
Transparency declarations: All authors have indicated they have no financial
relationships relevant to this article to disclose. The funding bodies do not have any
authority in design and conduct of the study; collection, management, analysis, and
interpretation of the data; and preparation, review, or approval of the manuscript.
Conflicts of Interest: The authors listed above certify that they have no affiliations
with any organization or entity with any financial or non-financial interest on the
materials discussed in this manuscript. The authors declare there are no competing
interests of note.
Transparency declarations: All authors have indicated they have no financial
relationships relevant to this article to disclose. The funding bodies do not have any
authority in design and conduct of the study; collection, management, analysis, and
98

interpretation of the data; and preparation, review, or approval of the manuscript.
99
References
1. McMullan BJ, Bowen A, Blyth CC, Van Hal S, Korman TM, Buttery J, et al.
Epidemiology and Mortality of Staphylococcus aureus Bacteremia in Australian
and New Zealand Children. JAMA pediatrics. 2016;170(10):979-‐86. doi:
10.1001/jamapediatrics.2016.1477. PubMed PMID: 27533601.
2. von Eiff C, Becker K, Peters G. Nasal carriage of Staphylococcus aureus.
Reply. New Engl J Med. 2001;344(18):1400-‐1. PubMed PMID:
WOS:000168413500019.
3. Almeida GC, dos Santos MM, Lima NG, Cidral TA, Melo MC, Lima KC.
Prevalence and factors associated with wound colonization by Staphylococcus
spp. and Staphylococcus aureus in hospitalized patients in inland northeastern
Brazil: a cross-‐sectional study. BMC infectious diseases. 2014;14:328. doi:
10.1186/1471-‐2334-‐14-‐328. PubMed PMID: 24925025; PubMed Central PMCID:
PMC4065078.
4. Rocha LA, Marques Ribas R, da Costa Darini AL, Gontijo Filho PP.
Relationship between nasal colonization and ventilator-‐associated pneumonia
and the role of the environment in transmission of Staphylococcus aureus in
intensive care units. American journal of infection control. 2013;41(12):1236-‐40.
doi: 10.1016/j.ajic.2013.04.009. PubMed PMID: 23890377.
5. von Eiff C, Becker K, Machka K, Stammer H, Peters G. Nasal carriage as a
source of Staphylococcus aureus bacteremia. Study Group. The New England
journal of medicine. 2001;344(1):11-‐6. doi: 10.1056/NEJM200101043440102.
PubMed PMID: 11136954.
100
6. Davis MF, Peng RD, McCormack MC, Matsui EC. Staphylococcus aureus
colonization is associated with wheeze and asthma among US children and
young adults. The Journal of allergy and clinical immunology. 2015;135(3):811-‐3
e5. doi: 10.1016/j.jaci.2014.10.052. PubMed PMID: 25533526; PubMed Central
PMCID: PMC4955790.
7. Lebon A, Labout JA, Verbrugh HA, Jaddoe VW, Hofman A, van Wamel WJ,
et al. Role of Staphylococcus aureus nasal colonization in atopic dermatitis in
infants: the Generation R Study. Archives of pediatrics & adolescent medicine.
2009;163(8):745-‐9. doi: 10.1001/archpediatrics.2009.117. PubMed PMID:
19652107.
8. Whymark AD, Crampsey DP, Fraser L, Moore P, Williams C, Kubba H.
Childhood epistaxis and nasal colonization with Staphylococcus aureus.
Otolaryngology-‐-‐head and neck surgery : official journal of American Academy of
Otolaryngology-‐Head and Neck Surgery. 2008;138(3):307-‐10. doi:
10.1016/j.otohns.2007.10.029. PubMed PMID: 18312876.
9. Washio M, Mizoue T, Kajioka T, Yoshimitsu T, Okayama M, Hamada T, et al.
Risk factors for methicillin-‐resistant Staphylococcus aureus (MRSA) infection in
a Japanese geriatric hospital. Public health. 1997;111(3):187-‐90. doi:
10.1016/S0033-‐3506(97)00581-‐7. PubMed PMID: 9175465.
10. Dolapo O, Dhanireddy R, Talati AJ. Trends of Staphylococcus aureus
bloodstream infections in a neonatal intensive care unit from 2000-‐2009. BMC
pediatrics. 2014;14:121. doi: 10.1186/1471-‐2431-‐14-‐121. PubMed PMID:
24886471; PubMed Central PMCID: PMC4024190.
11. Rodriguez EA, Correa MM, Ospina S, Atehortua SL, Jimenez JN. Differences
in epidemiological and molecular characteristics of nasal colonization with
101
Staphylococcus aureus (MSSA-‐MRSA) in children from a university hospital and
day care centers. PloS one. 2014;9(7):e101417. doi:
10.1371/journal.pone.0101417. PubMed PMID: 24987854; PubMed Central
PMCID: PMC4079298.
12. Jimenez-‐Truque N, Tedeschi S, Saye EJ, McKenna BD, Langdon W, Wright
JP, et al. Relationship between maternal and neonatal Staphylococcus aureus
colonization. Pediatrics. 2012;129(5):e1252-‐9. doi: 10.1542/peds.2011-‐2308.
PubMed PMID: 22473373; PubMed Central PMCID: PMC3340589.
13. Fritz SA, Hogan PG, Hayek G, Eisenstein KA, Rodriguez M, Krauss M, et al.
Staphylococcus aureus colonization in children with community-‐associated
Staphylococcus aureus skin infections and their household contacts. Archives of
pediatrics & adolescent medicine. 2012;166(6):551-‐7. doi:
10.1001/archpediatrics.2011.900. PubMed PMID: 22665030; PubMed Central
PMCID: PMC3596005.
14. Datta F, Erb T, Heininger U, Gervaix A, Schaad UB, Berger C, et al. A
multicenter, cross-‐sectional study on the prevalence and risk factors for nasal
colonization with Staphylococcus aureus in patients admitted to children's
hospitals in Switzerland. Clinical infectious diseases : an official publication of
the Infectious Diseases Society of America. 2008;47(7):923-‐6. doi:
10.1086/591700. PubMed PMID: 18715155.
15. Ibrahim LF, Hopper SM, Connell TG, Daley AJ, Bryant PA, Babl FE.
Evaluating an admission avoidance pathway for children in the emergency
department: outpatient intravenous antibiotics for moderate/severe cellulitis.
Emergency medicine journal : EMJ. 2017. doi: 10.1136/emermed-‐2017-‐206829.
PubMed PMID: 28978652.
102
16. Heikkinen T, Saeed KA, McCormick DP, Baldwin C, Reisner BS,
Chonmaitree T. A single intramuscular dose of ceftriaxone changes
nasopharyngeal bacterial flora in children with acute otitis media. Acta
paediatrica. 2000;89(11):1316-‐21. PubMed PMID: 11106042.
17. Conus P, Francioli P. Relationship between ceftriaxone use and resistance
of Enterobacter species. Journal of clinical pharmacy and therapeutics.
1992;17(5):303-‐5. PubMed PMID: 1464634.
18. Banerjee T, Bhattacharjee A, Upadhyay S, Mishra S, Tiwari K, Anupurba S,
et al. Long-‐term outbreak of Klebsiella pneumoniae& third generation
cephalosporin use in a neonatal intensive care unit in north India. The Indian
journal of medical research. 2016;144(4):622-‐9. doi: 10.4103/0971-‐
5916.200900. PubMed PMID: 28256474; PubMed Central PMCID: PMC5345312.
19. Schentag JJ, Hyatt JM, Carr JR, Paladino JA, Birmingham MC, Zimmer GS, et
al. Genesis of methicillin-‐resistant Staphylococcus aureus (MRSA), how
treatment of MRSA infections has selected for vancomycin-‐resistant
Enterococcus faecium, and the importance of antibiotic management and
infection control. Clinical infectious diseases : an official publication of the
Infectious Diseases Society of America. 1998;26(5):1204-‐14. PubMed PMID:
9597254.
20. de Man P, Verhoeven BA, Verbrugh HA, Vos MC, van den Anker JN. An
antibiotic policy to prevent emergence of resistant bacilli. Lancet.
2000;355(9208):973-‐8. PubMed PMID: 10768436.
21. Gouin S, Chevalier I, Gauthier M, Lamarre V. Prospective evaluation of the
management of moderate to severe cellulitis with parenteral antibiotics at a
paediatric day treatment centre. Journal of paediatrics and child health.
103
2008;44(4):214-‐8. doi: 10.1111/j.1440-‐1754.2007.01236.x. PubMed PMID:
17944880.
22. Smith JK, Alexander S, Abrahamson E. Ambulatory intravenous
ceftriaxone in paediatric A&E: a useful alternative to hospital admission?
Emergency medicine journal : EMJ. 2011;28(10):877-‐81. doi:
10.1136/emj.2010.093443. PubMed PMID: 21325012.
23. Brugha RE, Abrahamson E. Ambulatory intravenous antibiotic therapy for
children with preseptal cellulitis. Pediatric emergency care. 2012;28(3):226-‐8.
doi: 10.1097/PEC.0b013e318248b19b. PubMed PMID: 22344208.
24. Hansson H, Kjaergaard H, Johansen C, Hallstrom I, Christensen J, Madsen
M, et al. Hospital-‐based home care for children with cancer: feasibility and
psychosocial impact on children and their families. Pediatr Blood Cancer.
2013;60(5):865-‐72. doi: 10.1002/pbc.24474. PubMed PMID: 23335455.
25. Small F, Alderdice F, McCusker C, Stevenson M, Stewart M. A prospective
cohort study comparing hospital admission for gastro-‐enteritis with home
management. Child Care Health Dev. 2005;31(5):555-‐62. doi: 10.1111/j.1365-‐
2214.2005.00550.x. PubMed PMID: 16101651.
26. Svahn BM, Remberger M, Heijbel M, Martell E, Wikstrom M, Eriksson B, et
al. Case-‐control comparison of at-‐home and hospital care for allogeneic
hematopoietic stem-‐cell transplantation: the role of oral nutrition.
Transplantation. 2008;85(7):1000-‐7. doi: 10.1097/TP.0b013e31816a3267.
PubMed PMID: 18408581.
27. Yan M, Pamp SJ, Fukuyama J, Hwang PH, Cho DY, Holmes S, et al. Nasal
microenvironments and interspecific interactions influence nasal microbiota
complexity and S. aureus carriage. Cell host & microbe. 2013;14(6):631-‐40. doi:
104
10.1016/j.chom.2013.11.005. PubMed PMID: 24331461; PubMed Central
PMCID: PMC3902146.
28. Bessesen MT, Kotter CV, Wagner BD, Adams JC, Kingery S, Benoit JB, et al.
MRSA colonization and the nasal microbiome in adults at high risk of
colonization and infection. The Journal of infection. 2015;71(6):649-‐57. doi:
10.1016/j.jinf.2015.08.008. PubMed PMID: 26335708.
29. Frank DN, Feazel LM, Bessesen MT, Price CS, Janoff EN, Pace NR. The
human nasal microbiota and Staphylococcus aureus carriage. PloS one.
2010;5(5):e10598. doi: 10.1371/journal.pone.0010598. PubMed PMID:
20498722; PubMed Central PMCID: PMC2871794.
30. Liu CM, Price LB, Hungate BA, Abraham AG, Larsen LA, Christensen K, et al.
Staphylococcus aureus and the ecology of the nasal microbiome. Science
advances. 2015;1(5):e1400216. doi: 10.1126/sciadv.1400216. PubMed PMID:
26601194; PubMed Central PMCID: PMC4640600.
31. Lee GM, Huang SS, Rifas-‐Shiman SL, Hinrichsen VL, Pelton SI, Kleinman K,
et al. Epidemiology and risk factors for Staphylococcus aureus colonization in
children in the post-‐PCV7 era. BMC infectious diseases. 2009;9:110. doi:
10.1186/1471-‐2334-‐9-‐110. PubMed PMID: 19594890; PubMed Central PMCID:
PMC2716346.
32. Guillemot D, Bonacorsi S, Blanchard JS, Weber P, Simon S, Guesnon B, et al.
Amoxicillin-‐clavulanate therapy increases childhood nasal colonization by
methicillin-‐susceptible Staphylococcus aureus strains producing high levels of
penicillinase. Antimicrobial agents and chemotherapy. 2004;48(12):4618-‐23.
doi: 10.1128/AAC.48.12.4618-‐4623.2004. PubMed PMID: 15561834; PubMed
Central PMCID: PMC529192.
105
33. Hidron AI, Kourbatova EV, Halvosa JS, Terrell BJ, McDougal LK, Tenover
FC, et al. Risk factors for colonization with methicillin-‐resistant Staphylococcus
aureus (MRSA) in patients admitted to an urban hospital: emergence of
community-‐associated MRSA nasal carriage. Clinical infectious diseases : an
official publication of the Infectious Diseases Society of America.
2005;41(2):159-‐66. doi: 10.1086/430910. PubMed PMID: 15983910.
34. Graffunder EM, Venezia RA. Risk factors associated with nosocomial
methicillin-‐resistant Staphylococcus aureus (MRSA) infection including previous
use of antimicrobials. The Journal of antimicrobial chemotherapy.
2002;49(6):999-‐1005. PubMed PMID: 12039892.
35. Britton PN, Andresen DN. Paediatric community-‐associated
Staphylococcus aureus: a retrospective cohort study. Journal of paediatrics and
child health. 2013;49(9):754-‐9. doi: 10.1111/jpc.12255. PubMed PMID:
23721234.
106
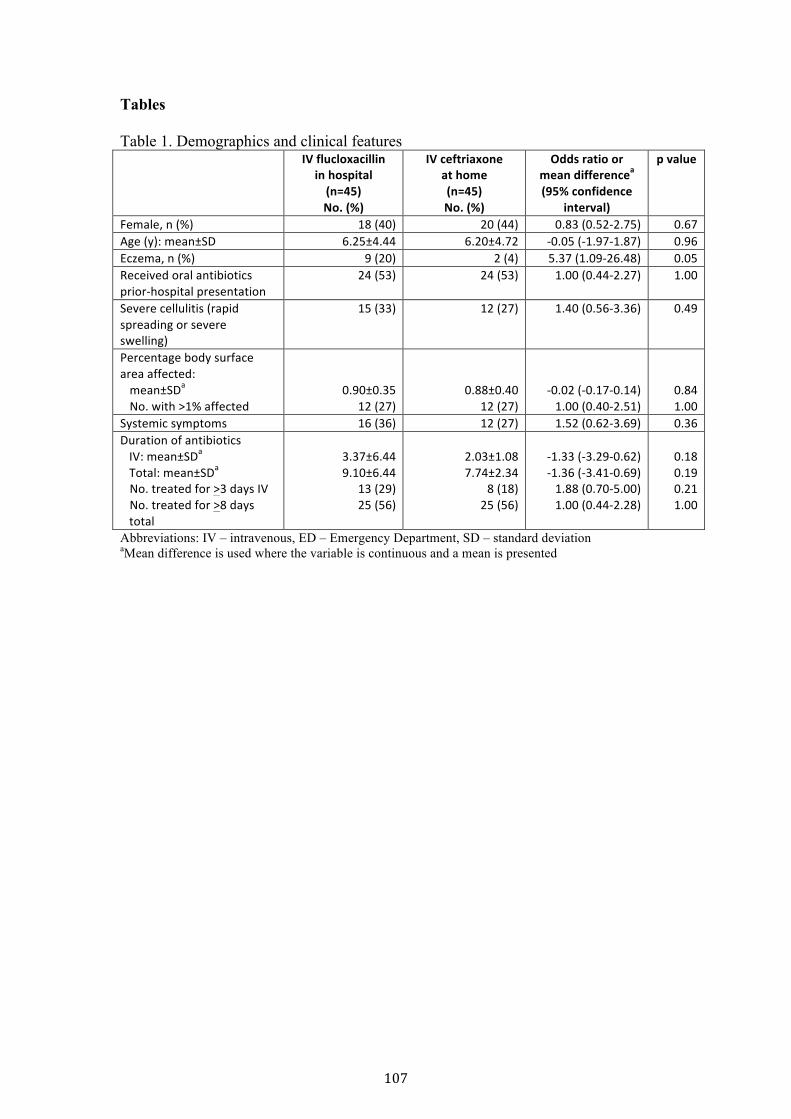
Tables Table 1. Demographics and clinical features IV flucloxacillin
in hospital (n=45) No. (%)
IV ceftriaxone at home (n=45) No. (%)
Odds ratio or mean differencea (95% confidence
interval)
p value
Female, n (%) 18 (40) 20 (44) 0.83 (0.52-‐2.75) 0.67 Age (y): mean±SD 6.25±4.44 6.20±4.72 -‐0.05 (-‐1.97-‐1.87) 0.96 Eczema, n (%) 9 (20) 2 (4) 5.37 (1.09-‐26.48) 0.05 Received oral antibiotics prior-‐hospital presentation
24 (53) 24 (53) 1.00 (0.44-‐2.27) 1.00
Severe cellulitis (rapid spreading or severe swelling)
15 (33) 12 (27) 1.40 (0.56-‐3.36) 0.49
Percentage body surface area affected: mean±SDa No. with >1% affected
0.90±0.35 12 (27)
0.88±0.40 12 (27)
-‐0.02 (-‐0.17-‐0.14) 1.00 (0.40-‐2.51)
0.84 1.00
Systemic symptoms 16 (36) 12 (27) 1.52 (0.62-‐3.69) 0.36 Duration of antibiotics IV: mean±SDa Total: mean±SDa No. treated for >3 days IV No. treated for >8 days total
3.37±6.44 9.10±6.44
13 (29) 25 (56)
2.03±1.08 7.74±2.34
8 (18) 25 (56)
-‐1.33 (-‐3.29-‐0.62) -‐1.36 (-‐3.41-‐0.69) 1.88 (0.70-‐5.00) 1.00 (0.44-‐2.28)
0.18 0.19 0.21 1.00
Abbreviations: IV – intravenous, ED – Emergency Department, SD – standard deviation aMean difference is used where the variable is continuous and a mean is presented
107
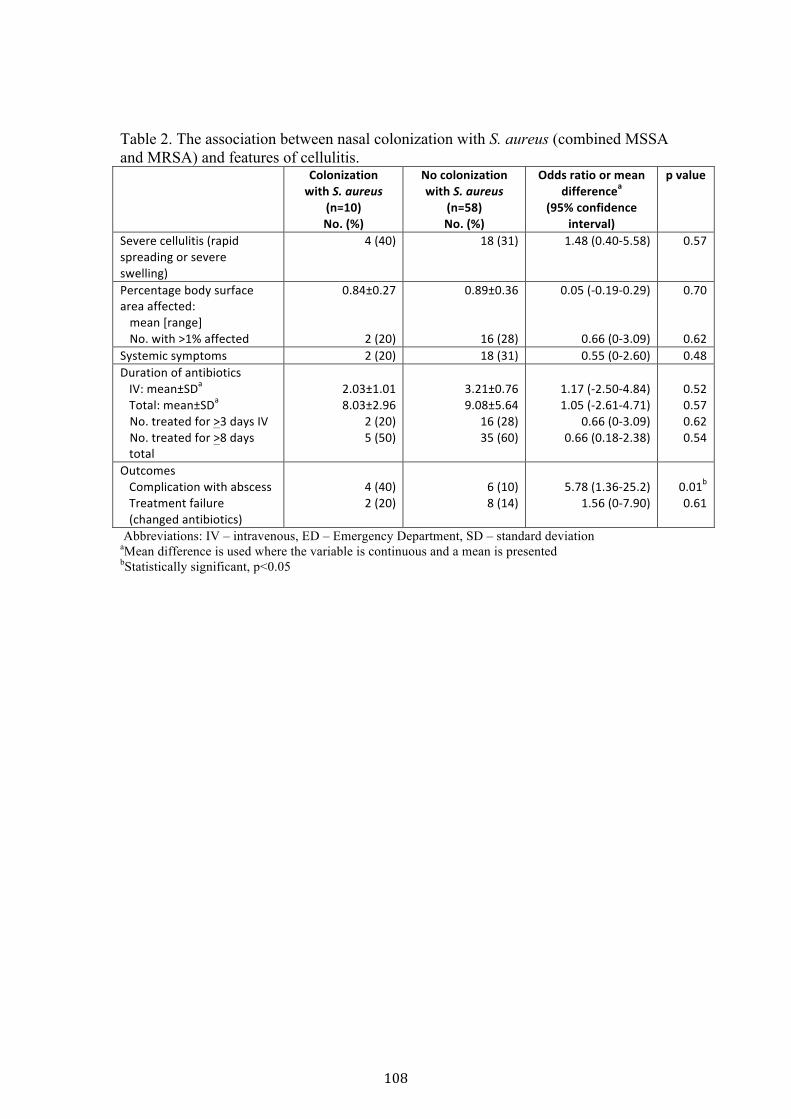
Table 2. The association between nasal colonization with S. aureus (combined MSSA and MRSA) and features of cellulitis.
Colonization with S. aureus
(n=10) No. (%)
No colonization with S. aureus
(n=58) No. (%)
Odds ratio or mean differencea
(95% confidence interval)
p value
Severe cellulitis (rapid spreading or severe swelling)
4 (40) 18 (31) 1.48 (0.40-‐5.58) 0.57
Percentage body surface area affected: mean [range] No. with >1% affected
0.84±0.27
2 (20)
0.89±0.36
16 (28)
0.05 (-‐0.19-‐0.29)
0.66 (0-‐3.09)
0.70
0.62 Systemic symptoms 2 (20) 18 (31) 0.55 (0-‐2.60) 0.48 Duration of antibiotics IV: mean±SDa Total: mean±SDa No. treated for >3 days IV No. treated for >8 days
total
2.03±1.01 8.03±2.96
2 (20) 5 (50)
3.21±0.76 9.08±5.64
16 (28) 35 (60)
1.17 (-‐2.50-‐4.84) 1.05 (-‐2.61-‐4.71)
0.66 (0-‐3.09) 0.66 (0.18-‐2.38)
0.52 0.57 0.62 0.54
Outcomes Complication with abscess Treatment failure (changed antibiotics)
4 (40) 2 (20)
6 (10) 8 (14)
5.78 (1.36-‐25.2) 1.56 (0-‐7.90)
0.01b 0.61
Abbreviations: IV – intravenous, ED – Emergency Department, SD – standard deviation aMean difference is used where the variable is continuous and a mean is presented bStatistically significant, p<0.05
108
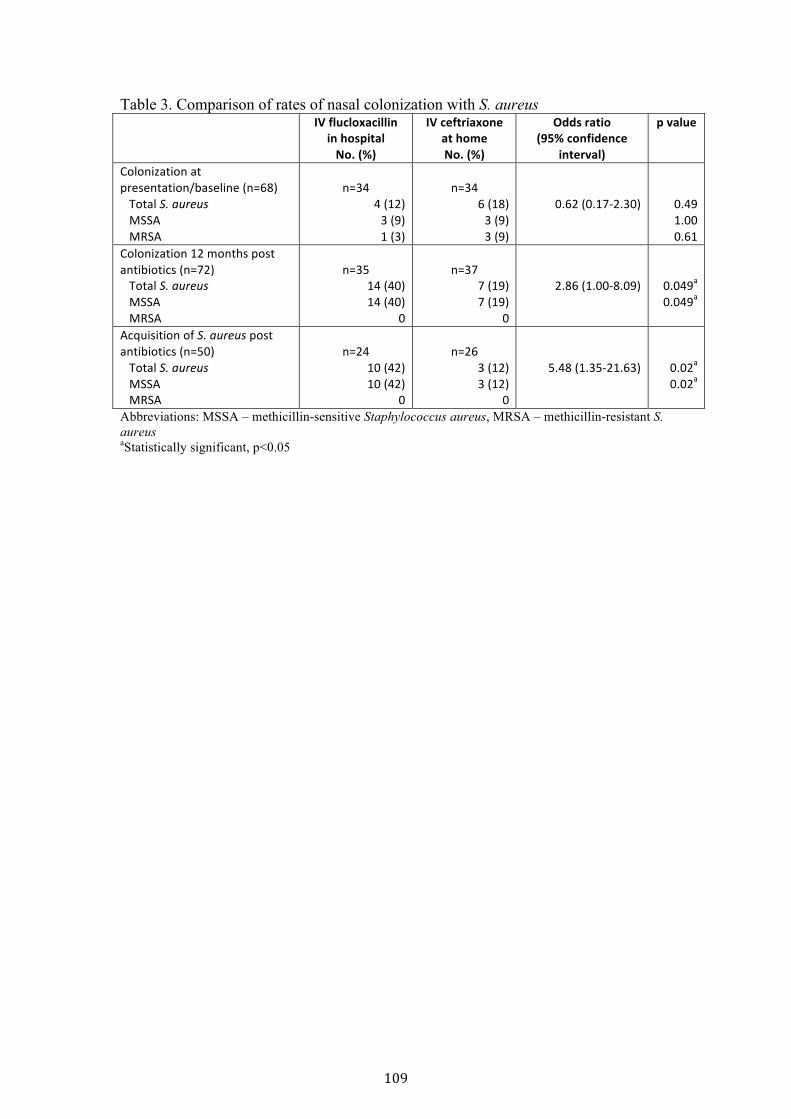
Table 3. Comparison of rates of nasal colonization with S. aureusIV flucloxacillin in hospital No. (%)
IV ceftriaxone at home No. (%)
Odds ratio (95% confidence
interval)
p value
Colonization at presentation/baseline (n=68) Total S. aureus MSSA MRSA
n=34 4 (12) 3 (9) 1 (3)
n=34 6 (18) 3 (9) 3 (9)
0.62 (0.17-‐2.30) 0.49 1.00 0.61
Colonization 12 months post antibiotics (n=72) Total S. aureus MSSA MRSA
n=35 14 (40) 14 (40)
0
n=37 7 (19) 7 (19)
0
2.86 (1.00-‐8.09) 0.049a 0.049a
Acquisition of S. aureus post antibiotics (n=50) Total S. aureus MSSA MRSA
n=24 10 (42) 10 (42)
0
n=26 3 (12) 3 (12)
0
5.48 (1.35-‐21.63) 0.02a 0.02a
Abbreviations: MSSA – methicillin-sensitive Staphylococcus aureus, MRSA – methicillin-resistant S. aureus aStatistically significant, p<0.05
109
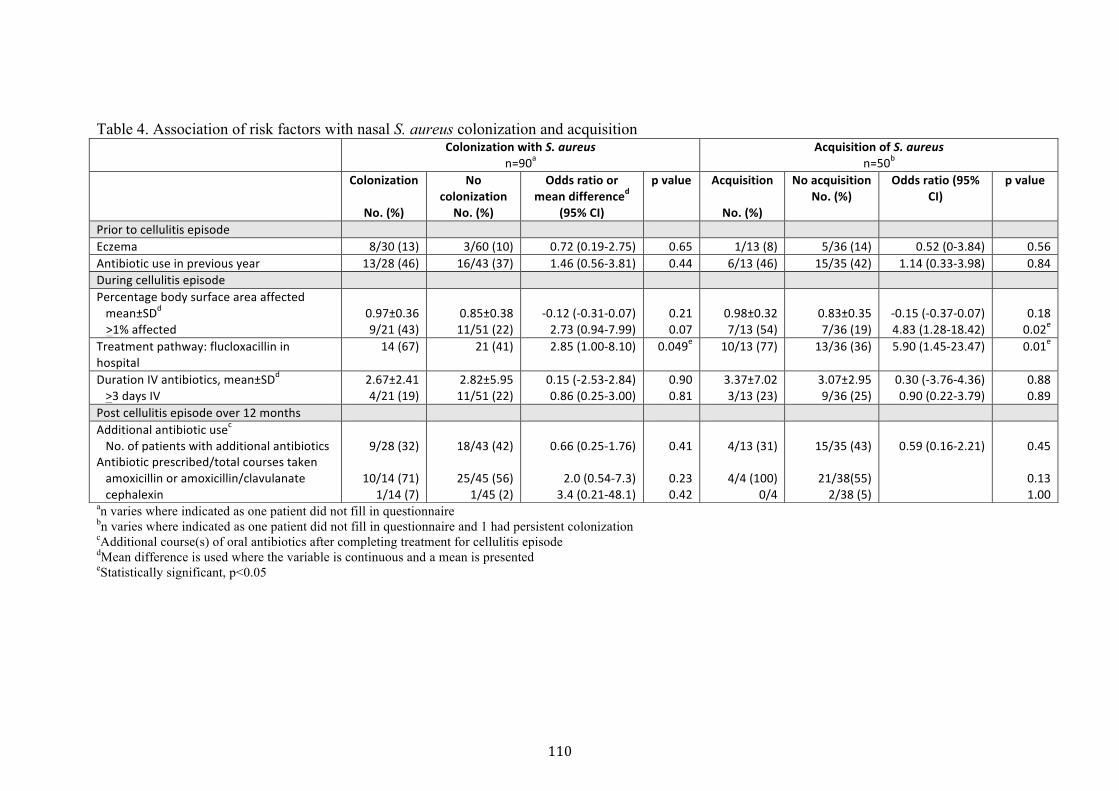
Table 4. Association of risk factors with nasal S. aureus colonization and acquisition
an varies where indicated as one patient did not fill in questionnaire bn varies where indicated as one patient did not fill in questionnaire and 1 had persistent colonization cAdditional course(s) of oral antibiotics after completing treatment for cellulitis episode dMean difference is used where the variable is continuous and a mean is presented eStatistically significant, p<0.05
Colonization with S. aureus n=90a
Acquisition of S. aureus n=50b
Colonization
No. (%)
No colonization
No. (%)
Odds ratio or mean differenced
(95% CI)
p value Acquisition
No. (%)
No acquisition No. (%)
Odds ratio (95% CI)
p value
Prior to cellulitis episode Eczema 8/30 (13) 3/60 (10) 0.72 (0.19-‐2.75) 0.65 1/13 (8) 5/36 (14) 0.52 (0-‐3.84) 0.56 Antibiotic use in previous year 13/28 (46) 16/43 (37) 1.46 (0.56-‐3.81) 0.44 6/13 (46) 15/35 (42) 1.14 (0.33-‐3.98) 0.84 During cellulitis episode Percentage body surface area affected mean±SDd >1% affected
0.97±0.36 9/21 (43)
0.85±0.38 11/51 (22)
-‐0.12 (-‐0.31-‐0.07) 2.73 (0.94-‐7.99)
0.21 0.07
0.98±0.32 7/13 (54)
0.83±0.35 7/36 (19)
-‐0.15 (-‐0.37-‐0.07) 4.83 (1.28-‐18.42)
0.18 0.02e
Treatment pathway: flucloxacillin in hospital
14 (67) 21 (41) 2.85 (1.00-‐8.10) 0.049e 10/13 (77) 13/36 (36) 5.90 (1.45-‐23.47) 0.01e
Duration IV antibiotics, mean±SDd >3 days IV
2.67±2.41 4/21 (19)
2.82±5.95 11/51 (22)
0.15 (-‐2.53-‐2.84) 0.86 (0.25-‐3.00)
0.90 0.81
3.37±7.02 3/13 (23)
3.07±2.95 9/36 (25)
0.30 (-‐3.76-‐4.36) 0.90 (0.22-‐3.79)
0.88 0.89
Post cellulitis episode over 12 months Additional antibiotic usec No. of patients with additional antibiotics Antibiotic prescribed/total courses taken amoxicillin or amoxicillin/clavulanate cephalexin
9/28 (32)
10/14 (71) 1/14 (7)
18/43 (42)
25/45 (56) 1/45 (2)
0.66 (0.25-‐1.76)
2.0 (0.54-‐7.3) 3.4 (0.21-‐48.1)
0.41
0.23 0.42
4/13 (31)
4/4 (100) 0/4
15/35 (43)
21/38(55) 2/38 (5)
0.59 (0.16-‐2.21) 0.45
0.13 1.00
110
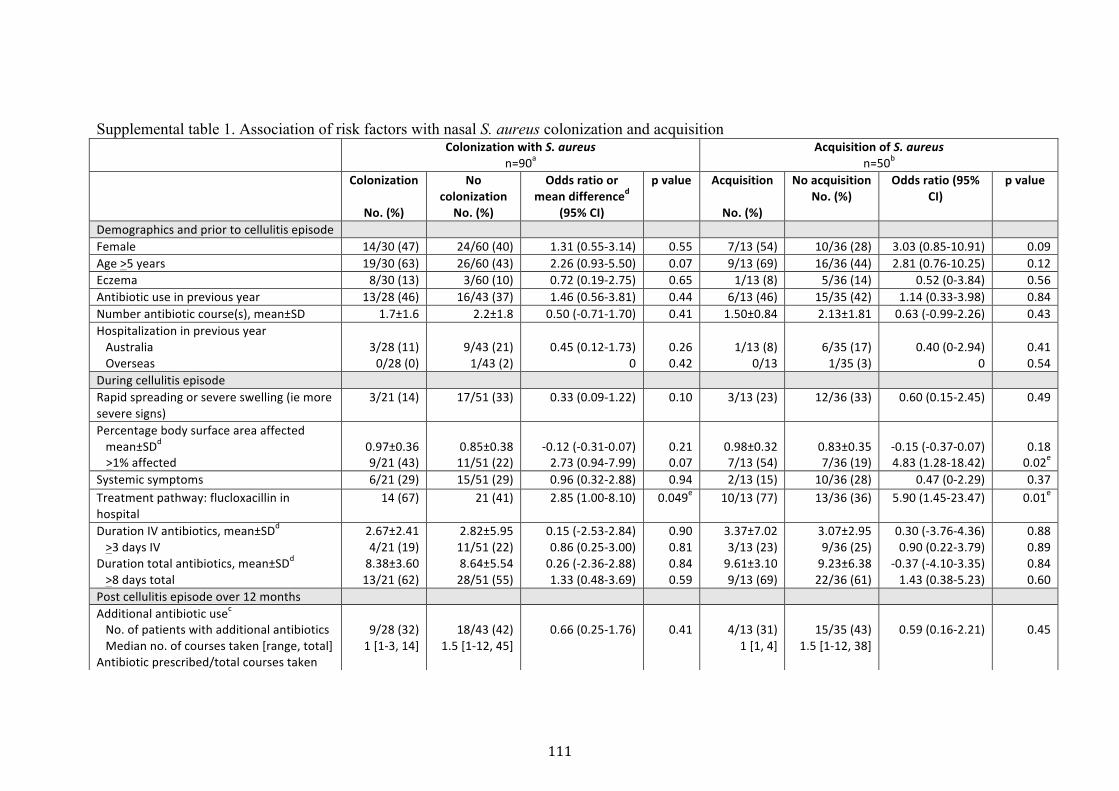
Supplemental table 1. Association of risk factors with nasal S. aureus colonization and acquisition Colonization with S. aureus
n=90a Acquisition of S. aureus
n=50b Colonization
No. (%)
No colonization
No. (%)
Odds ratio or mean differenced
(95% CI)
p value Acquisition
No. (%)
No acquisition No. (%)
Odds ratio (95% CI)
p value
Demographics and prior to cellulitis episode Female 14/30 (47) 24/60 (40) 1.31 (0.55-‐3.14) 0.55 7/13 (54) 10/36 (28) 3.03 (0.85-‐10.91) 0.09 Age >5 years 19/30 (63) 26/60 (43) 2.26 (0.93-‐5.50) 0.07 9/13 (69) 16/36 (44) 2.81 (0.76-‐10.25) 0.12 Eczema 8/30 (13) 3/60 (10) 0.72 (0.19-‐2.75) 0.65 1/13 (8) 5/36 (14) 0.52 (0-‐3.84) 0.56 Antibiotic use in previous year 13/28 (46) 16/43 (37) 1.46 (0.56-‐3.81) 0.44 6/13 (46) 15/35 (42) 1.14 (0.33-‐3.98) 0.84 Number antibiotic course(s), mean±SD 1.7±1.6 2.2±1.8 0.50 (-‐0.71-‐1.70) 0.41 1.50±0.84 2.13±1.81 0.63 (-‐0.99-‐2.26) 0.43 Hospitalization in previous year Australia Overseas
3/28 (11) 0/28 (0)
9/43 (21) 1/43 (2)
0.45 (0.12-‐1.73) 0
0.26 0.42
1/13 (8) 0/13
6/35 (17) 1/35 (3)
0.40 (0-‐2.94) 0
0.41 0.54
During cellulitis episode Rapid spreading or severe swelling (ie more severe signs)
3/21 (14) 17/51 (33) 0.33 (0.09-‐1.22) 0.10 3/13 (23) 12/36 (33) 0.60 (0.15-‐2.45) 0.49
Percentage body surface area affected mean±SDd >1% affected
0.97±0.36 9/21 (43)
0.85±0.38 11/51 (22)
-‐0.12 (-‐0.31-‐0.07) 2.73 (0.94-‐7.99)
0.21 0.07
0.98±0.32 7/13 (54)
0.83±0.35 7/36 (19)
-‐0.15 (-‐0.37-‐0.07) 4.83 (1.28-‐18.42)
0.18 0.02e
Systemic symptoms 6/21 (29) 15/51 (29) 0.96 (0.32-‐2.88) 0.94 2/13 (15) 10/36 (28) 0.47 (0-‐2.29) 0.37 Treatment pathway: flucloxacillin in hospital
14 (67) 21 (41) 2.85 (1.00-‐8.10) 0.049e 10/13 (77) 13/36 (36) 5.90 (1.45-‐23.47) 0.01e
Duration IV antibiotics, mean±SDd >3 days IV
Duration total antibiotics, mean±SDd >8 days total
2.67±2.41 4/21 (19) 8.38±3.60 13/21 (62)
2.82±5.95 11/51 (22) 8.64±5.54 28/51 (55)
0.15 (-‐2.53-‐2.84) 0.86 (0.25-‐3.00) 0.26 (-‐2.36-‐2.88) 1.33 (0.48-‐3.69)
0.90 0.81 0.84 0.59
3.37±7.02 3/13 (23) 9.61±3.10 9/13 (69)
3.07±2.95 9/36 (25) 9.23±6.38 22/36 (61)
0.30 (-‐3.76-‐4.36) 0.90 (0.22-‐3.79)
-‐0.37 (-‐4.10-‐3.35) 1.43 (0.38-‐5.23)
0.88 0.89
0.84 0.60
Post cellulitis episode over 12 months Additional antibiotic usec No. of patients with additional antibiotics Median no. of courses taken [range, total] Antibiotic prescribed/total courses taken
9/28 (32) 1 [1-‐3, 14]
18/43 (42) 1.5 [1-‐12, 45]
0.66 (0.25-‐1.76) 0.41 4/13 (31) 1 [1, 4]
15/35 (43) 1.5 [1-‐12, 38]
0.59 (0.16-‐2.21) 0.45
111
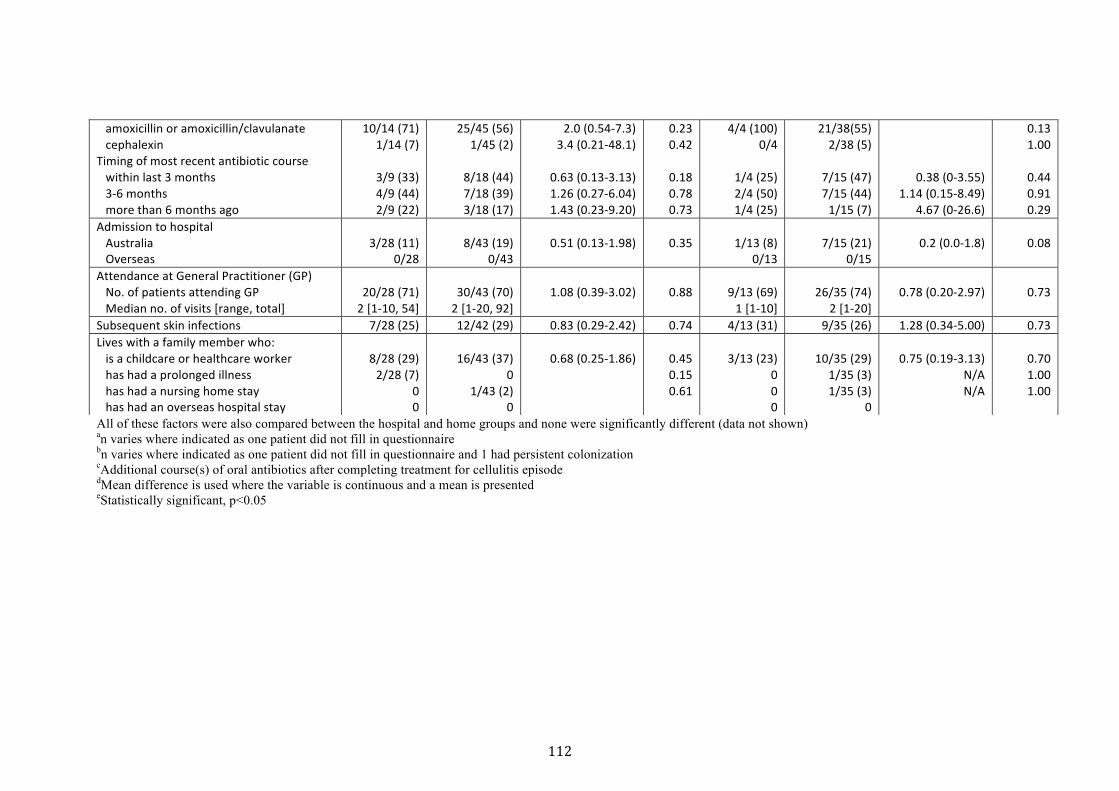
All of these factors were also compared between the hospital and home groups and none were significantly different (data not shown) an varies where indicated as one patient did not fill in questionnaire bn varies where indicated as one patient did not fill in questionnaire and 1 had persistent colonization cAdditional course(s) of oral antibiotics after completing treatment for cellulitis episode dMean difference is used where the variable is continuous and a mean is presented eStatistically significant, p<0.05
amoxicillin or amoxicillin/clavulanate cephalexin Timing of most recent antibiotic course within last 3 months 3-‐6 months more than 6 months ago
10/14 (71) 1/14 (7)
3/9 (33) 4/9 (44) 2/9 (22)
25/45 (56) 1/45 (2)
8/18 (44) 7/18 (39) 3/18 (17)
2.0 (0.54-‐7.3) 3.4 (0.21-‐48.1)
0.63 (0.13-‐3.13) 1.26 (0.27-‐6.04) 1.43 (0.23-‐9.20)
0.23 0.42
0.18 0.78 0.73
4/4 (100) 0/4
1/4 (25) 2/4 (50) 1/4 (25)
21/38(55) 2/38 (5)
7/15 (47) 7/15 (44) 1/15 (7)
0.38 (0-‐3.55) 1.14 (0.15-‐8.49)
4.67 (0-‐26.6)
0.13 1.00
0.44 0.91 0.29
Admission to hospital Australia Overseas
3/28 (11) 0/28
8/43 (19) 0/43
0.51 (0.13-‐1.98) 0.35 1/13 (8) 0/13
7/15 (21) 0/15
0.2 (0.0-‐1.8) 0.08
Attendance at General Practitioner (GP) No. of patients attending GP Median no. of visits [range, total]
20/28 (71) 2 [1-‐10, 54]
30/43 (70) 2 [1-‐20, 92]
1.08 (0.39-‐3.02) 0.88 9/13 (69) 1 [1-‐10]
26/35 (74) 2 [1-‐20]
0.78 (0.20-‐2.97) 0.73
Subsequent skin infections 7/28 (25) 12/42 (29) 0.83 (0.29-‐2.42) 0.74 4/13 (31) 9/35 (26) 1.28 (0.34-‐5.00) 0.73 Lives with a family member who: is a childcare or healthcare worker has had a prolonged illness has had a nursing home stay has had an overseas hospital stay
8/28 (29) 2/28 (7)
0 0
16/43 (37) 0
1/43 (2) 0
0.68 (0.25-‐1.86) 0.45 0.15 0.61
3/13 (23) 0 0 0
10/35 (29) 1/35 (3) 1/35 (3)
0
0.75 (0.19-‐3.13) N/A N/A
0.70 1.00 1.00
112

113
3.6 Implication of foundation studies
The foundation studies were crucial for developing more evidence for clinicians
and determining factors to inform the RCT methodology. The increased
engagement in the home pathway was clear from the increase in children treated
at home, from 28% in the baseline study to 41% in this study. Reasons provided
by clinicians in the study for choosing hospitalisation, rather than home
treatment appeared to be clinically valid reasons in 56% of admitted patients.
However, the remaining hospitalised patients could potentially have been
treated at home. It was clear from the outcomes of this study that there was
clinical equipoise and that clinicians would engage in the RCT, a crucial factor in
patient recruitment.
The effect of broadening the population base for inclusion in the home treatment
pathway and educating clinicians about this was clear. In the baseline study only
24% of children treated at home were aged under 4 years old compared with
53% in the foundation cohort. Although clinicians remained cautious with
periorbital cellulitis, the proportion of children with this condition referred for
home intravenous antibiotic increased from 11% in the baseline study to 29% in
this study.
Despite this broader patient cohort, while accepting that this was not a
randomised study, the primary outcome of treatment failure and safety as
reflected by complications and adverse events, were not significantly different
between home and hospital care.115 The treatment failure rate at home in this
foundation cohort study, defined as requiring a change in antibiotics, was still
reassuringly low at 4%, no different to the hospital group. The combined risk of
complications and adverse events was 6% for the home group, also similar to the
hospital group. The risk of bacteraemia was investigated in 93/115 (81%) of the
study population and none were bacteraemic, resolving this concern. With the
results of the baseline and foundation studies, and acknowledging that there was
still clinician choice in the decision to admit children to hospital, we anticipated
114
that when children were randomised in the RCT, the treatment failure rate for
the home group would potentially be higher. However, we hypothesised that
both efficacy and safety would still be within a sufficiently similar margin to
hospital treatment so that other benefits of home treatment would also be
relevant.
In terms of determining the criteria for which patients have moderate/severe
cellulitis requiring intravenous antibiotics, we found that clinicians had various
reasons for starting intravenous antibiotics, which were similar to the reasons in
the clinician survey (Chapter 2). Often, clinicians had more than one reason for
choosing the intravenous route. The most common reason was failed oral
antibiotics, followed by rapid spreading or significant swelling. No previous
studies of cellulitis have investigated the reasons or criteria for clinicians
commencing intravenous antibiotics.1,43,120 While evidence-‐based criteria for the
decision to use intravenous antibiotics would therefore not be in place for the
RCT, this was an identified gap that warranted further research.
The study on nasal colonisation showed that there did not appear to be an
increased risk of acquisition of MRSA with ceftriaxone use in this non-‐
randomised cohort. Although this was preliminarily reassuring, we determined
that collecting microbiology samples to assess the effect of ceftriaxone on the
development of resistance would be crucial in the study of treatment of children
at home with this antibiotic. Providing evidence for the safety of this home
pathway should also encompass investigating the association of ceftriaxone with
the development of not just nasal MRSA, but other pathogens of concern,
specifically the stool pathogens ESBL-‐producing bacteria, VRE and C. difficile.
In the nasal colonisation study, nasal swabs were only obtained at baseline and 1
year, so whether there was a transient increase in colonisation between that
time period was unknown. We decided for the RCT, that to obtain a complete
picture of the dynamics of colonisation, samples should be obtained at the
following time points: baseline, 1 week after starting antibiotics (maximal
antibiotic pressure) and at 3 months (after a washout period), as well as at 1
115
year to determine the short and medium term risks. Nasal colonisation was not
associated with a more severe episode of cellulitis, or its outcomes, apart from
the recognised association between MRSA colonisation and soft tissue
abscesses.119 There was no association found with any other clinical features at
presentation or clinical outcomes when investigated.
With regards other RCT design issues to address, the sample size calculation was
informed by all of the three previous studies (baseline study, clinician survey,
foundation cohort study) and the literature. According to the survey, clinicians
will accept approximately 20-‐25% failure of treatment at home. This resulted
from a combination of the benefits for children of being treated at home, and that
treatment failure for moderate/severe cellulitis is not a rapidly dangerous
outcome. In the study by Gouin et al on cellulitis treatment at a day treatment
centre, 79% were deemed successfully treated, adding to the information that
this was an appropriate approximate proportion. Although in both the baseline
study and the foundation cohort study, treatment failure rates at home were low
at 2-‐4%, we anticipated this to be higher in a randomised non pre-‐selected
cohort. We estimated a hospital failure rate of around 5-‐7%, based on the
baseline study. The margin of acceptable difference between home and hospital
treatment arms was therefore 13-‐20%. Given the inherent inaccuracy of all of
these numbers and our belief that a 20% margin was too wide, we determined
based on the above factors that it was reasonable and clinically relevant to use a
15% margin of acceptable difference between the home and hospital arms, given
the other benefits of home treatment.
The primary outcome of treatment failure defined as a change in antibiotics due
to a lack of clinical improvement or an adverse event was determined as an
appropriate outcome for the RCT. Clinicians were observed to consistently
diagnose treatment failure within the first 48 hours of commencing empiric
intravenous antibiotics. This would then lead to a change in intravenous
antibiotic. It was crucial, however, to ensure that doctors making this assessment
received training and recorded the clinical progress objectively using daily
116
photographs as well as an objective scale of rating for the different features of
cellulitis.
In this study a simple cost analysis was done by obtaining the average cost for
treating a patient with a diagnosis of cellulitis at home and hospital from the
clinical costing unit in our institution. However, it was determined that we
should be more precise in the RCT and that the best method for doing this was to
obtain institutional individual patient level cost data. Additionally although in
this study only institutional costs were obtained, for the RCT we determined that
understanding the burden of costs to families was also very important. We
determined that a comprehensive cost-‐effectiveness analysis should be done that
incorporated both the cost differences of these two interventions and
effectiveness in terms of quality of life, the key reason for treating children at
home.
As a result of these foundation studies, there were sufficient data to inform the
methodology for the RCT, clinicians were engaged to participate, and crucially,
we believed there was equipoise in the question of whether home or hospital
treatment was better for patients with uncomplicated moderate/severe cellulitis.
At the same time, through the baseline and foundation studies, we identified a
gap in evidence regarding which patients with cellulitis require intravenous
antibiotics, and the research to provide that evidence will be presented in the
next chapter.
117
Chapter 4 Determining who needs intravenous antibiotics in cellulitis – a clinical scoring system
4.1 Introduction to the clinical scoring system
Through the previous studies in this thesis, (clinician survey: Chapter 2, baseline
study: Chapter 2, foundation studies: Chapter 3), the absence of standardised
guidelines for commencing intravenous antibiotics in children with cellulitis was
highlighted.114,115 In our centre and in others described in the literature, the
criteria for starting intravenous antibiotics in cellulitis was based on clinician
judgement.1,2,43 This results in inconsistencies in the management of cellulitis,
with unwarranted variation in care known to be associated with poorer
outcomes.121 Not treating patients with intravenous antibiotics when they
require it leads to slower recovery and the potential for increased complications.
Unwarranted use of intravenous antibiotics can expose children to unnecessary
side effects, hospitalisation with its associated risks, and complications of
intravenous catheters. It also places an additional financial burden on healthcare
institutions. Use of a standardised method to guide route of initial treatment
would limit the inappropriate use of intravenous antibiotics. In addition,
research in cellulitis would be more robust if there was a standardised way of
describing the severity of the infection.114
The findings from the previous two chapters were that clinicians base their
decision to start intravenous antibiotics on multiple different clinical features.
However, the clinician survey showed that there appeared to be several features
that the majority of clinicians recognised as representing moderate/severe
cellulitis requiring intravenous antibiotics. In the foundation cohort study, the
reasons for clinicians commencing intravenous antibiotics included clinical
features such as significant swelling and systemic features.115 With the
groundwork for this study already carried out, the next study in this PhD was to
attempt to develop a clinical scoring system to aid clinician decision-‐making
when deciding which patient with moderate/severe cellulitis require
intravenous antibiotics.
118
There are four stages of developing a clinical score122:
1. Derivation – deriving the score from a cohort of patients by identifying the
predictors of the intervention of interest: intravenous antibiotics for cellulitis.
2. Validation – using the derived score and applying it to a separate cohort of
patients to test the reliability of the score.
3. Impact analysis – investigating the impact of the score in real practice, in terms
of its usefulness for clinical outcomes, cost-‐effectiveness and patient and
clinician satisfaction.
4. Refinement and implementation – once the impact is investigated, the score
may need to be refined to improve its impact prior to more widespread
implementation of the score.
The scope of this PhD was to achieve the first two stages with a view to
completing the final two steps in the postdoctoral phase.

119
4.2 Study 5: Clinical scoring system
Ibrahim LF, Hopper SM, Donath S, Salvin B, Babl FE, Bryant PA. Development
and Validation of a Cellulitis Risk Score: The Melbourne ASSET Score.
Pediatrics 2019.

ARTICLE
Development and Validation of a Cellulitis Risk Score: The Melbourne ASSET ScoreLaila F. Ibrahim, MB, BCh, BAO, a, b Sandy M. Hopper, FRACP, FACEM, a, b, c Susan Donath, MA, b Bennett Salvin, MD, a Franz E. Babl, MD, a, b, c Penelope A. Bryant, PhDa, b, d, e
BACKGROUND: The evidence is unclear about the optimal route of treatment for children with cellulitis, specifically how to assess the risk of moderate-to-severe cellulitis requiring intravenous (IV) antibiotics. We aimed to derive and validate a cellulitis risk assessment scoring system to guide providers as to which patients require IV antibiotics.METHODS: This was a prospective cohort study of children presenting to the emergency department aged 6 months to 18 years diagnosed with cellulitis from January 2014 to August 2017. Patients were divided into 2 groups based on route of antibiotics at 24 hours (the predetermined gold standard). Demographics and clinical features were compared. Clinicians were surveyed about which features they used to decide whether to start IV antibiotics. Combinations of differentiating features were plotted on receiver operating characteristic curves.RESULTS: There were 285 children in the derivation cohort used to create the Melbourne Area, Systemic features, Swelling, Eye, Tenderness (ASSET) Score, which has a maximum score of 7. The area under the curve was 0.86 (95% confidence interval 0.83–0.91). Using a cutoff score of 4 to start IV antibiotics yielded the highest correct classification of 80% of patients (sensitivity 60%; specificity 93%). This score was validated in 251 children and maintained a robust area under the curve of 0.83 (95% confidence interval 0.78–0.89).CONCLUSIONS: The Melbourne ASSET Score was derived and validated for cellulitis in children to guide clinicians regarding when to start IV antibiotics. Although intended for widespread use, if limitations exist in other settings, it is designed to allow for refinement and is amenable to local impact analysis.
abstract
aDepartment of Paediatrics, University of Melbourne, Parkville, Australia; and bMurdoch Children’s Research Institute, cEmergency Department, dInfectious Diseases Unit, Department of General Medicine, and eHospital-In-The-Home Department, The Royal Children’s Hospital, Parkville, Australia
Dr Ibrahim conceptualized, designed, and coordinated the study, conducted the initial and subsequent data analyses, drafted the initial manuscript, and revised subsequent drafts; Drs Bryant, Babl, and Hopper were involved in the design of the study, provided input into data analysis, and reviewed and revised the manuscript; Ms Donath was involved in the design of the study, advised on statistical analysis, and revised the final manuscript; Dr Salvin was involved in the design of the study, coordinated parts of the study, and revised the final manuscript; and all authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
DOI: https:// doi. org/ 10. 1542/ peds. 2018- 1420
Accepted for publication Oct 29, 2018
WHAT’S KNOWN ON THIS SUBJECT: Cellulitis is a common childhood skin infection. However, there is no clear evidence to guide clinicians treating this condition regarding which patients need intravenous antibiotics. This poses risks for both undertreatment and overtreatment, resulting in unnecessary hospitalization.
WHAT THIS STUDY ADDS: The Melbourne ASSET Score is proposed to aid in decision-making regarding the route of antibiotics for treating cellulitis. This score involves 5 easily assessed clinical features (area, systemic features, swelling, eye involvement, and tenderness) and is adaptable to different clinical environments.
To cite: Ibrahim LF, Hopper SM, Donath S, et al. Develop-ment and Validation of a Cellulitis Risk Score: The Melbourne ASSET Score. Pediatrics. 2019;143(2):e20181420
120

Cellulitis is a superficial skin and soft tissue infection that is a common cause of presentation to emergency departments (EDs) and primary care physicians.1 – 4 Although many children with cellulitis are successfully treated with oral antibiotics, up to 60% are treated with intravenous (IV) antibiotics.5 – 8 In the UnitedStates alone, skin and soft tissueinfections account for >74 000pediatric hospital admissions peryear.9 However, despite the fact thatcellulitis is common, the evidence isunclear about the optimal route oftreatment for children with cellulitis,specifically how to assess the riskof moderate-to-severe cellulitisrequiring IV antibiotics. Since theearly 1980s, clinicians have tried tostratify the severity of cellulitis inchildren, but to date, there are noexisting evidence-based guidelines.10
This is likely due to an absence ofobjective, universally agreed oncriteria or a gold standard for theassessment of cellulitis that requiresIV antibiotics.
The authors of the Infectious Diseases Society of America guidelines for the diagnosis and management of skin and soft tissue infections recommend IV antibiotics for cellulitis with systemic signs of infection.1 However, many children with systemic signs (such as pyrexia, which commonly accompanies cellulitis) can be safely and effectively treated with oral antibiotics.8, 11, 12 These guidelines were intended for a broad population, including adults; therefore, recommendations are not necessarily applicable to children. Attempts to establish guidelines for treating cellulitis affecting the eye serve to differentiate periorbital from orbital cellulitis (to avoid the risk of missing orbital cellulitis) rather than help the primary care or emergency clinician decide between oral or IV treatment for uncomplicated periorbital cellulitis.12 – 15 The local institutional
guideline recommends treatment with oral flucloxacillin or cephalexin unless a case is severe and/or extensive, a patient is systemically unwell, or a patient is not responding to oral treatment, in which case IV flucloxacillin is recommended. These clinical scenarios for when to use the IV route are open to different interpretations and therefore practices.
The absence of standardized practice means that some children are unnecessarily admitted to the hospital and administered IV antibiotics, putting them at risk for hospital-acquired infections, iatrogenic adverse events, and negative psychosocial impacts.16, 17 Several clinical scoring systems have been established for common childhood illnesses, for example, the Westley Croup Score, 18 the Pediatric Respiratory Assessment Measure for asthma, 19 and the Pediatric Appendicitis Score for acute appendicitis.20, 21 Such clinical scores are not intended to be used in isolation to stratify patients, 22, 23 but having a practical guideline for a common condition, such as cellulitis, can improve patient flow and be an important tool in clinical research.24 For a clinical score to be useful in the acute decision-making process, it needs to (1) have as few features as possible while remaining accurate and (2) be unambiguous and easily assessable by junior clinical staff.25
In this study, we had 2 aims: (1) to derive a pediatric cellulitis risk assessment scoring system for use by clinicians in EDs or primary care to guide the decision to start IV antibiotics and (2) to validate this scoring system on a separate cohort of children.
METHODS
Study Design and Population
This was a prospective cohort study in a convenience sample of children
presenting with cellulitis to the ED at the Royal Children’s Hospital in Melbourne. Recruitment occurred over a 15-month period from January 2014 to May 2015. Children aged 6 months to 18 years were eligible if an ED clinician made a diagnosis of cellulitis. The decision to treat with oral or IV antibiotics was made by an experienced ED physician (at least at the registrar and/or fellow level). Per routine institutional practice, patients who were treated with oral antibiotics were discharged from the ED, whereas those who were started on IV antibiotics were admitted to the hospital. Exclusion criteria were children with complicated cellulitis or associated toxicity. Complicated cellulitis was defined as cellulitis associated with the following conditions: orbital cellulitis, undrained abscess, penetrating injury, immunosuppression, fasciitis or foreign body, or cellulitis caused by large animal or human bite. Toxicity was defined as those with signs or symptoms of hypotension, resting tachycardia, or poor central perfusion.
Procedures
We correlated clinical features and outcomes to derive a cellulitis scoring system and, when appropriate, take into account clinicians’ opinions and practice on the basis of a survey. This study was approved by the institutional human research ethics committee (HREC34018).
Data Collection of Clinical Features
Data collection occurred in real time as patients were being assessed in the ED after written consent was obtained. This included demographics, whether previous oral antibiotics were taken before presenting to the ED, and clinical features at presentation. Clinical features were collected from ED clinicians on a standardized proforma and consisted of the size of the area affected (longest diameters
IBRAHIM et al2
121
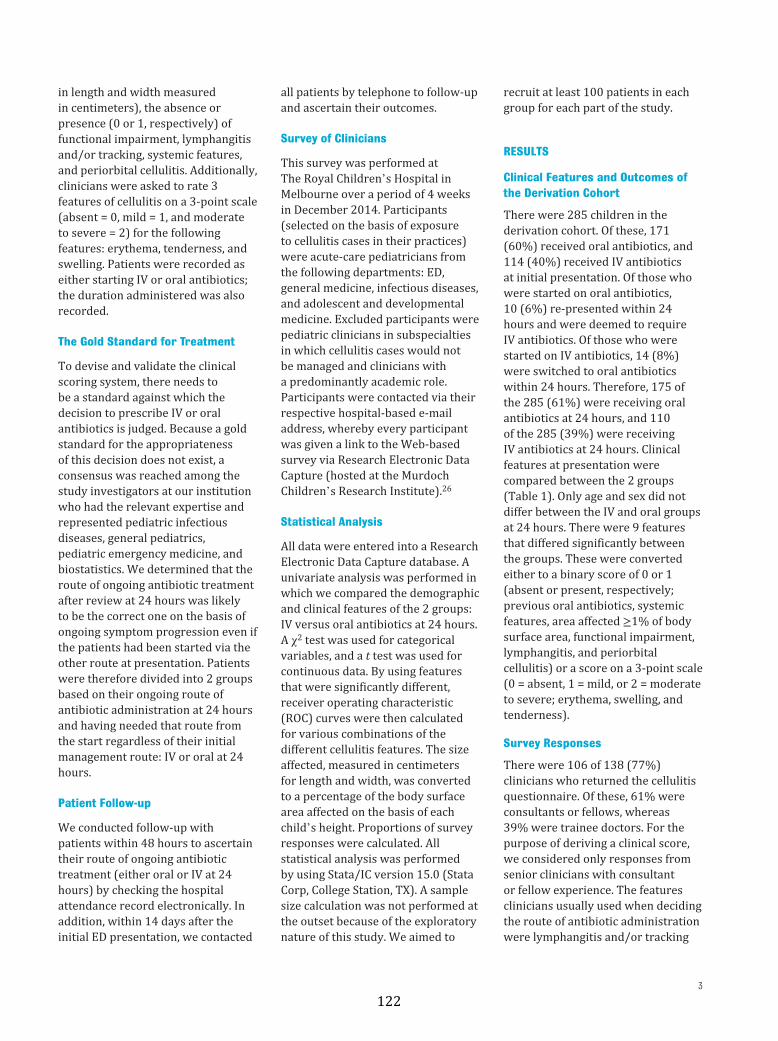
in length and width measured in centimeters), the absence or presence (0 or 1, respectively) of functional impairment, lymphangitis and/or tracking, systemic features, and periorbital cellulitis. Additionally, clinicians were asked to rate 3 features of cellulitis on a 3-point scale (absent = 0, mild = 1, and moderate to severe = 2) for the following features: erythema, tenderness, and swelling. Patients were recorded as either starting IV or oral antibiotics; the duration administered was also recorded.
The Gold Standard for Treatment
To devise and validate the clinical scoring system, there needs to be a standard against which the decision to prescribe IV or oral antibiotics is judged. Because a gold standard for the appropriateness of this decision does not exist, a consensus was reached among the study investigators at our institution who had the relevant expertise and represented pediatric infectious diseases, general pediatrics, pediatric emergency medicine, and biostatistics. We determined that the route of ongoing antibiotic treatment after review at 24 hours was likely to be the correct one on the basis of ongoing symptom progression even if the patients had been started via the other route at presentation. Patients were therefore divided into 2 groups based on their ongoing route of antibiotic administration at 24 hours and having needed that route from the start regardless of their initial management route: IV or oral at 24 hours.
Patient Follow-up
We conducted follow-up with patients within 48 hours to ascertain their route of ongoing antibiotic treatment (either oral or IV at 24 hours) by checking the hospital attendance record electronically. In addition, within 14 days after the initial ED presentation, we contacted
all patients by telephone to follow-up and ascertain their outcomes.
Survey of Clinicians
This survey was performed at The Royal Children’s Hospital in Melbourne over a period of 4 weeks in December 2014. Participants (selected on the basis of exposure to cellulitis cases in their practices) were acute-care pediatricians from the following departments: ED, general medicine, infectious diseases, and adolescent and developmental medicine. Excluded participants were pediatric clinicians in subspecialties in which cellulitis cases would not be managed and clinicians with a predominantly academic role. Participants were contacted via their respective hospital-based e-mail address, whereby every participant was given a link to the Web-based survey via Research Electronic Data Capture (hosted at the Murdoch Children’s Research Institute).26
Statistical Analysis
All data were entered into a Research Electronic Data Capture database. A univariate analysis was performed in which we compared the demographic and clinical features of the 2 groups: IV versus oral antibiotics at 24 hours. A χ2 test was used for categorical variables, and a t test was used for continuous data. By using features that were significantly different, receiver operating characteristic (ROC) curves were then calculated for various combinations of the different cellulitis features. The size affected, measured in centimeters for length and width, was converted to a percentage of the body surface area affected on the basis of each child’s height. Proportions of survey responses were calculated. All statistical analysis was performed by using Stata/IC version 15.0 (Stata Corp, College Station, TX). A sample size calculation was not performed at the outset because of the exploratory nature of this study. We aimed to
recruit at least 100 patients in each group for each part of the study.
RESULTS
Clinical Features and Outcomes of the Derivation Cohort
There were 285 children in the derivation cohort. Of these, 171 (60%) received oral antibiotics, and 114 (40%) received IV antibiotics at initial presentation. Of those who were started on oral antibiotics, 10 (6%) re-presented within 24 hours and were deemed to require IV antibiotics. Of those who were started on IV antibiotics, 14 (8%) were switched to oral antibiotics within 24 hours. Therefore, 175 of the 285 (61%) were receiving oral antibiotics at 24 hours, and 110 of the 285 (39%) were receiving IV antibiotics at 24 hours. Clinical features at presentation were compared between the 2 groups (Table 1). Only age and sex did not differ between the IV and oral groups at 24 hours. There were 9 features that differed significantly between the groups. These were converted either to a binary score of 0 or 1 (absent or present, respectively; previous oral antibiotics, systemic features, area affected ≥1% of body surface area, functional impairment, lymphangitis, and periorbital cellulitis) or a score on a 3-point scale (0 = absent, 1 = mild, or 2 = moderate to severe; erythema, swelling, and tenderness).
Survey Responses
There were 106 of 138 (77%) clinicians who returned the cellulitis questionnaire. Of these, 61% were consultants or fellows, whereas 39% were trainee doctors. For the purpose of deriving a clinical score, we considered only responses from senior clinicians with consultant or fellow experience. The features clinicians usually used when deciding the route of antibiotic administration were lymphangitis and/or tracking
3
122
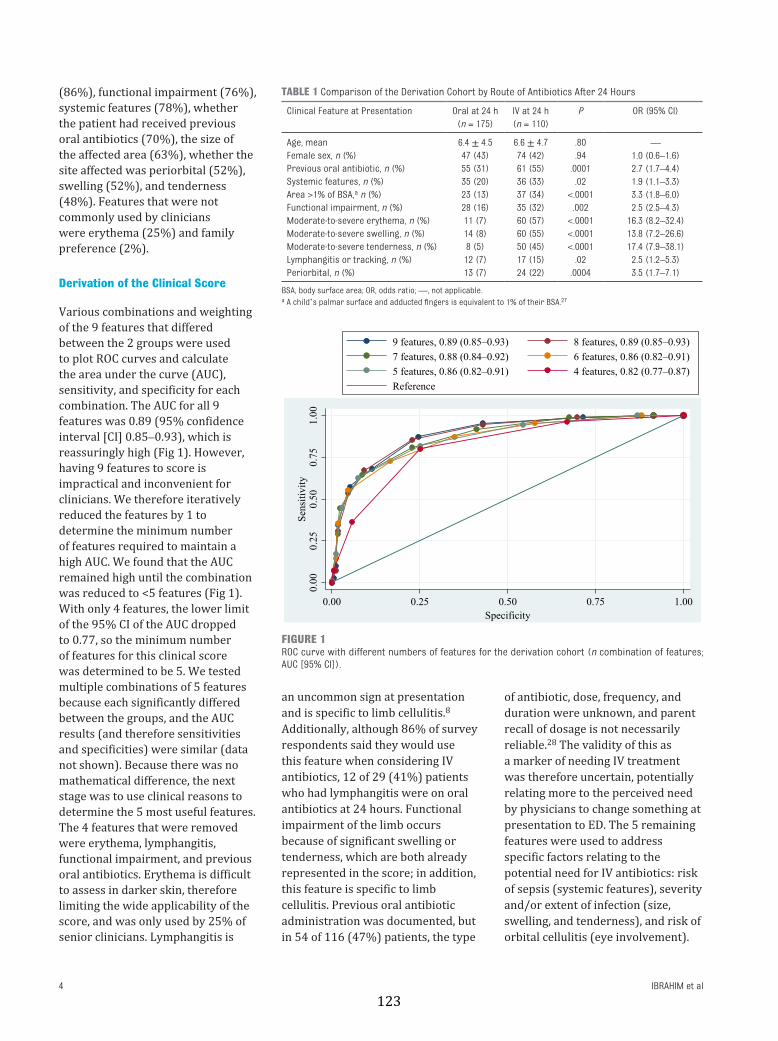
(86%), functional impairment (76%), systemic features (78%), whether the patient had received previous oral antibiotics (70%), the size of the affected area (63%), whether the site affected was periorbital (52%), swelling (52%), and tenderness (48%). Features that were not commonly used by clinicians were erythema (25%) and family preference (2%).
Derivation of the Clinical Score
Various combinations and weighting of the 9 features that differed between the 2 groups were used to plot ROC curves and calculate the area under the curve (AUC), sensitivity, and specificity for each combination. The AUC for all 9 features was 0.89 (95% confidence interval [CI] 0.85–0.93), which is reassuringly high (Fig 1). However, having 9 features to score is impractical and inconvenient for clinicians. We therefore iteratively reduced the features by 1 to determine the minimum number of features required to maintain a high AUC. We found that the AUC remained high until the combination was reduced to <5 features (Fig 1). With only 4 features, the lower limit of the 95% CI of the AUC dropped to 0.77, so the minimum number of features for this clinical score was determined to be 5. We tested multiple combinations of 5 features because each significantly differed between the groups, and the AUC results (and therefore sensitivities and specificities) were similar (data not shown). Because there was no mathematical difference, the next stage was to use clinical reasons to determine the 5 most useful features. The 4 features that were removed were erythema, lymphangitis, functional impairment, and previous oral antibiotics. Erythema is difficult to assess in darker skin, therefore limiting the wide applicability of the score, and was only used by 25% of senior clinicians. Lymphangitis is
an uncommon sign at presentation and is specific to limb cellulitis.8 Additionally, although 86% of survey respondents said they would use this feature when considering IV antibiotics, 12 of 29 (41%) patients who had lymphangitis were on oral antibiotics at 24 hours. Functional impairment of the limb occurs because of significant swelling or tenderness, which are both already represented in the score; in addition, this feature is specific to limb cellulitis. Previous oral antibiotic administration was documented, but in 54 of 116 (47%) patients, the type
of antibiotic, dose, frequency, and duration were unknown, and parent recall of dosage is not necessarily reliable.28 The validity of this as a marker of needing IV treatment was therefore uncertain, potentially relating more to the perceived need by physicians to change something at presentation to ED. The 5 remaining features were used to address specific factors relating to the potential need for IV antibiotics: risk of sepsis (systemic features), severity and/or extent of infection (size, swelling, and tenderness), and risk of orbital cellulitis (eye involvement).
IBRAHIM et al4
TABLE 1 Comparison of the Derivation Cohort by Route of Antibiotics After 24 Hours
Clinical Feature at Presentation Oral at 24 h (n = 175)
IV at 24 h (n = 110)
P OR (95% CI)
Age, mean 6.4 ± 4.5 6.6 ± 4.7 .80 —Female sex, n (%) 47 (43) 74 (42) .94 1.0 (0.6–1.6)Previous oral antibiotic, n (%) 55 (31) 61 (55) .0001 2.7 (1.7–4.4)Systemic features, n (%) 35 (20) 36 (33) .02 1.9 (1.1–3.3)Area >1% of BSA, a n (%) 23 (13) 37 (34) <.0001 3.3 (1.8–6.0)Functional impairment, n (%) 28 (16) 35 (32) .002 2.5 (2.5–4.3)Moderate-to-severe erythema, n (%) 11 (7) 60 (57) <.0001 16.3 (8.2–32.4)Moderate-to-severe swelling, n (%) 14 (8) 60 (55) <.0001 13.8 (7.2–26.6)Moderate-to-severe tenderness, n (%) 8 (5) 50 (45) <.0001 17.4 (7.9–38.1)Lymphangitis or tracking, n (%) 12 (7) 17 (15) .02 2.5 (1.2–5.3)Periorbital, n (%) 13 (7) 24 (22) .0004 3.5 (1.7–7.1)
BSA, body surface area; OR, odds ratio; —, not applicable.a A child’s palmar surface and adducted fingers is equivalent to 1% of their BSA.27
FIGURE 1ROC curve with different numbers of features for the derivation cohort (n combination of features; AUC [95% CI]).
123
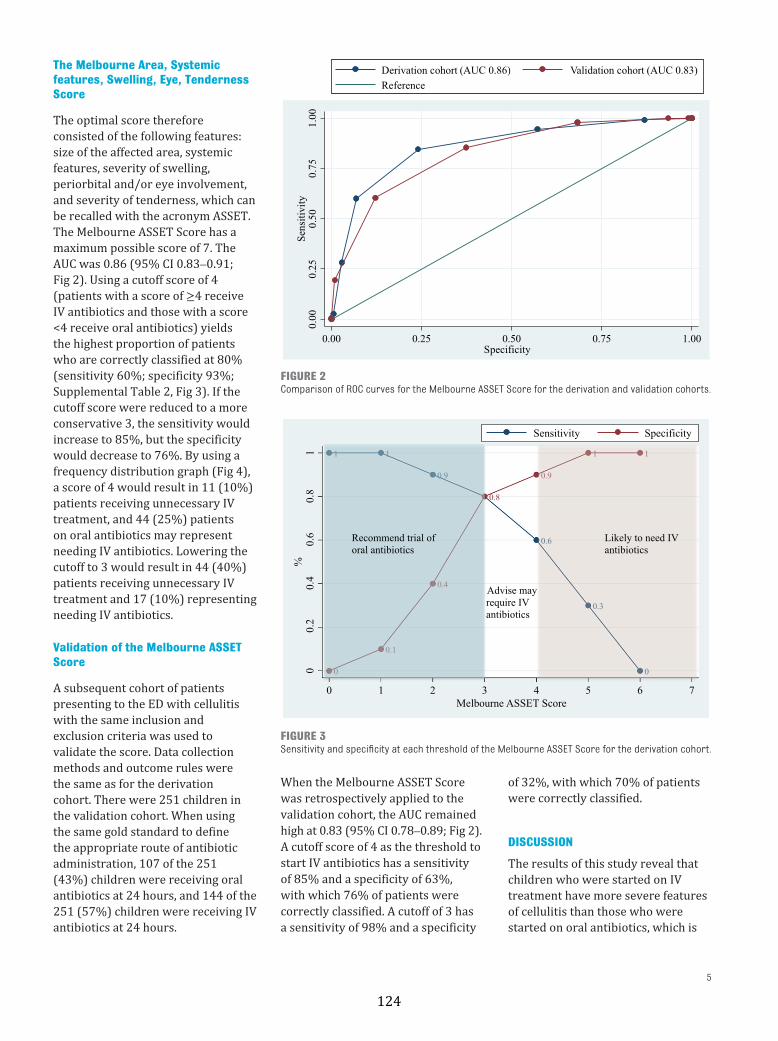
The Melbourne Area, Systemic features, Swelling, Eye, Tenderness Score
The optimal score therefore consisted of the following features: size of the affected area, systemic features, severity of swelling, periorbital and/or eye involvement, and severity of tenderness, which can be recalled with the acronym ASSET. The Melbourne ASSET Score has a maximum possible score of 7. The AUC was 0.86 (95% CI 0.83–0.91; Fig 2). Using a cutoff score of 4 (patients with a score of ≥4 receive IV antibiotics and those with a score <4 receive oral antibiotics) yields the highest proportion of patients who are correctly classified at 80% (sensitivity 60%; specificity 93%; Supplemental Table 2, Fig 3). If the cutoff score were reduced to a more conservative 3, the sensitivity would increase to 85%, but the specificity would decrease to 76%. By using a frequency distribution graph (Fig 4), a score of 4 would result in 11 (10%) patients receiving unnecessary IV treatment, and 44 (25%) patients on oral antibiotics may represent needing IV antibiotics. Lowering the cutoff to 3 would result in 44 (40%) patients receiving unnecessary IV treatment and 17 (10%) representing needing IV antibiotics.
Validation of the Melbourne ASSET Score
A subsequent cohort of patients presenting to the ED with cellulitis with the same inclusion and exclusion criteria was used to validate the score. Data collection methods and outcome rules were the same as for the derivation cohort. There were 251 children in the validation cohort. When using the same gold standard to define the appropriate route of antibiotic administration, 107 of the 251 (43%) children were receiving oral antibiotics at 24 hours, and 144 of the 251 (57%) children were receiving IV antibiotics at 24 hours.
When the Melbourne ASSET Score was retrospectively applied to the validation cohort, the AUC remained high at 0.83 (95% CI 0.78–0.89; Fig 2). A cutoff score of 4 as the threshold to start IV antibiotics has a sensitivity of 85% and a specificity of 63%, with which 76% of patients were correctly classified. A cutoff of 3 has a sensitivity of 98% and a specificity
of 32%, with which 70% of patients were correctly classified.
DISCUSSION
The results of this study reveal that children who were started on IV treatment have more severe features of cellulitis than those who were started on oral antibiotics, which is
5
FIGURE 2Comparison of ROC curves for the Melbourne ASSET Score for the derivation and validation cohorts.
FIGURE 3Sensitivity and specificity at each threshold of the Melbourne ASSET Score for the derivation cohort.
124
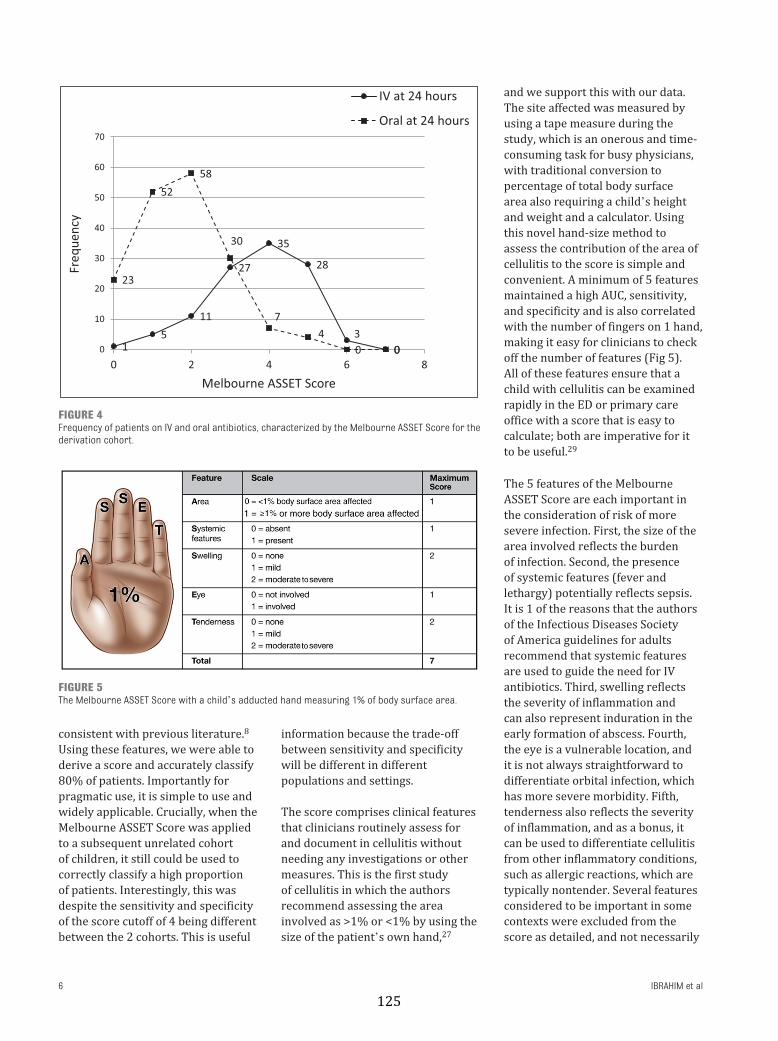
consistent with previous literature.8 Using these features, we were able to derive a score and accurately classify 80% of patients. Importantly for pragmatic use, it is simple to use and widely applicable. Crucially, when the Melbourne ASSET Score was applied to a subsequent unrelated cohort of children, it still could be used to correctly classify a high proportion of patients. Interestingly, this was despite the sensitivity and specificity of the score cutoff of 4 being different between the 2 cohorts. This is useful
information because the trade-off between sensitivity and specificity will be different in different populations and settings.
The score comprises clinical features that clinicians routinely assess for and document in cellulitis without needing any investigations or other measures. This is the first study of cellulitis in which the authors recommend assessing the area involved as >1% or <1% by using the size of the patient’s own hand, 27
and we support this with our data. The site affected was measured by using a tape measure during the study, which is an onerous and time-consuming task for busy physicians, with traditional conversion to percentage of total body surface area also requiring a child’s height and weight and a calculator. Using this novel hand-size method to assess the contribution of the area of cellulitis to the score is simple and convenient. A minimum of 5 features maintained a high AUC, sensitivity, and specificity and is also correlated with the number of fingers on 1 hand, making it easy for clinicians to check off the number of features (Fig 5). All of these features ensure that a child with cellulitis can be examined rapidly in the ED or primary care office with a score that is easy to calculate; both are imperative for it to be useful.29
The 5 features of the Melbourne ASSET Score are each important in the consideration of risk of more severe infection. First, the size of the area involved reflects the burden of infection. Second, the presence of systemic features (fever and lethargy) potentially reflects sepsis. It is 1 of the reasons that the authors of the Infectious Diseases Society of America guidelines for adults recommend that systemic features are used to guide the need for IV antibiotics. Third, swelling reflects the severity of inflammation and can also represent induration in the early formation of abscess. Fourth, the eye is a vulnerable location, and it is not always straightforward to differentiate orbital infection, which has more severe morbidity. Fifth, tenderness also reflects the severity of inflammation, and as a bonus, it can be used to differentiate cellulitis from other inflammatory conditions, such as allergic reactions, which are typically nontender. Several features considered to be important in some contexts were excluded from the score as detailed, and not necessarily
IBRAHIM et al6
FIGURE 4Frequency of patients on IV and oral antibiotics, characterized by the Melbourne ASSET Score for the derivation cohort.
FIGURE 5The Melbourne ASSET Score with a child’s adducted hand measuring 1% of body surface area.
125

because they have no value in individual patients. In addition to those mentioned above, the age of the child is an important consideration in any pediatric condition. However, whether analyzed on a continuum or stratified by different age categories, age was not different between the groups.
A hurdle for us in this study, like for many others attempting to devise a clinical score, is the absence of a gold standard for cellulitis against which to assess the true requirement for IV antibiotics. The rationale behind using the status at 24 hours is that if a change in route has already been made within 24 hours, the features at presentation could likely be used to predict this. It is possible that clinicians who treat children with IV antibiotics may unnecessarily treat beyond 24 hours simply because there is IV access in situ. This would result in a slightly more conservative gold standard than true need, which is similar to other scoring systems.18 If found to be too conservative when validated in a different setting, the score cutoff can be refined.30, 31 Similarly, if using this score in settings in which patients live farther from the hospital,
minimizing ED reattendance may be more important, so the cutoff could be lowered.
Our study has some limitations. Firstly, it was conducted in a tertiary pediatric hospital with experienced pediatric ED clinicians, and a more conservative approach may be required in a different setting. However, we have been able to use the expertise of these clinicians in the absence of a gold standard to derive and validate a clinical score for cellulitis in children for the first time. If a more conservative approach is desired, the cutoff threshold for IV treatment can be lowered. Second, our region has a low prevalence of methicillin-resistant Staphylococcus aureus, which is similar to many other pediatric populations. However, although we would recommend external validation of the score in high-prevalence areas, there is no reason to suspect that this score would not be applicable because it is the defining route, not choice, of antibiotic. Lastly, with this clinical score, we do not aim to replace clinical assessment for each individual patient but to aid in decision-making.22
CONCLUSIONS
The Melbourne ASSET Score is the first risk assessment scoring system for pediatric cellulitis that is proposed to aid clinicians in deciding whether to treat with IV or oral antibiotics. It is simple, easy to use, applicable, and reliable. Although intended for widespread use, if limitations exist in other settings, it is designed to allow for refinement and is amenable to local impact analysis. We propose an impact analysis of this score, ideally in a different setting and population.
ACKNOWLEDGMENTS
We acknowledge the participation of the patients and families.
ABBREVIATIONS
ASSET: Area, Systemic features, Swelling, Eye, Tenderness
AUC: area under the curveCI: confidence intervalED: emergency departmentIV: intravenousROC: receiver operating
characteristic
7
Address correspondence to Franz E. Babl, MD, Emergency Department, Murdoch Children’s Research Institute, The Royal Children’s Hospital, Flemington Rd, Parkville, VIC 3052, Australia. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2019 by the American Academy of Pediatrics
All authors hereby declare there has been no support from any organization for the submitted work. There have been no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years. There are no other relationships or activities that could appear to have influenced the submitted work.
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Funded in part by grants from The Royal Children’s Hospital Foundation, the Murdoch Children’s Research Institute, and the Victorian Department of Health and Human Services in Melbourne, Australia. Ms Ibrahim was supported in part by a scholarship from Avant Mutual Group Ltd (Melbourne), the Melbourne Children’s Campus Postgraduate Health Research Scholarship, and the Doctor Nicholas Collins Fellowship. Dr Bryant was supported in part by a Melbourne Campus Clinician Scientist Fellowship (Melbourne, Australia). Dr Babl was supported in part by a grant from The Royal Children’s Hospital Foundation, a Melbourne Campus Clinician Scientist Fellowship (Melbourne, Australia), and a National Health and Medical Research Council Practitioner’s Fellowship (Canberra, Australia). The Emergency Research Group at Murdoch Children’s Research Institute is supported in part by a National Health and Medical Research Council Centre for Research Excellence grant for pediatric emergency medicine (Canberra, Australia) and the Victorian government’s Operational Infrastructure Support Program. The funding bodies do not have any authority in design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
126

REFERENCES
1. Stevens DL, Bisno AL, Chambers HF,et al; Infectious Diseases Society ofAmerica. Practice guidelines for thediagnosis and management of skinand soft tissue infections: 2014 updateby the Infectious Diseases Societyof America [published correctionappears in Clin Infect Dis. 2014;59:147–159]. Clin Infect Dis. 2014;59(2):e10–e52
2. Pallin DJ, Egan DJ, Pelletier AJ,Espinola JA, Hooper DC, Camargo CA Jr.Increased US emergency departmentvisits for skin and soft tissueinfections, and changes in antibioticchoices, during the emergence ofcommunity-associated methicillin-resistant Staphylococcus aureus. AnnEmerg Med. 2008;51(3):291–298
3. Pallin DJ, Espinola JA, LeungDY, Hooper DC, Camargo CA Jr.Epidemiology of dermatitis and skininfections in United States physicians’offices, 1993-2005. Clin Infect Dis.2009;49(6):901–907
4. Schuler CL, Courter JD, Conneely SE,et al. Decreasing duration of antibioticprescribing for uncomplicated skinand soft tissue infections. Pediatrics.2016;137(2):e20151223
5. Ibrahim LF, Hopper SM, Connell TG,Daley AJ, Bryant PA, Babl FE. Evaluatingan admission avoidance pathway forchildren in the emergency department:outpatient intravenous antibiotics formoderate/severe cellulitis. Emerg MedJ. 2017;34(12):780–785
6. Gouin S, Chevalier I, Gauthier M,Lamarre V. Prospective evaluationof the management of moderateto severe cellulitis with parenteralantibiotics at a paediatric daytreatment centre. J Paediatr ChildHealth. 2008;44(4):214–218
7. Smith JK, Alexander S, Abrahamson E.Ambulatory intravenous ceftriaxonein paediatric A&E: a useful alternativeto hospital admission? Emerg Med J.2011;28(10):877–881
8. Khangura S, Wallace J, Kissoon N,Kodeeswaran T. Management ofcellulitis in a pediatric emergencydepartment. Pediatr Emerg Care.2007;23(11):805–811
9. Lopez MA, Cruz AT, KowalkowskiMA, Raphael JL. Trends in resource
utilization for hospitalized children with skin and soft tissue infections. Pediatrics. 2013;131(3). Available at: www. pediatrics. org/ cgi/ content/ full/ 131/ 3/ e718
10. Fleisher G, Ludwig S, Henretig F,Ruddy R, Henry W. Cellulitis: initialmanagement. Ann Emerg Med.1981;10(7):356–359
11. Moran GJ, Krishnadasan A, MowerWR, et al. Effect of cephalexin plustrimethoprim-sulfamethoxazolevs cephalexin alone on clinicalcure of uncomplicated cellulitis:a randomized clinical trial. JAMA.2017;317(20):2088–2096
12. Goldman RD, Dolansky G, RogovikAL. Predictors for admission ofchildren with periorbital cellulitispresenting to the pediatric emergencydepartment. Pediatr Emerg Care.2008;24(5):279–283
13. Vu BL, Dick PT, Levin AV, Pirie J.Development of a clinical severityscore for preseptal cellulitis inchildren. Pediatr Emerg Care.2003;19(5):302–307
14. Crosbie RA, Nairn J, Kubba H.Management of paediatric periorbitalcellulitis: our experience of 243children managed according to astandardised protocol 2012-2015.Int J Pediatr Otorhinolaryngol.2016;87:134–138
15. Reynolds DJ, Kodsi SR, Rubin SE,Rodgers IR. Intracranial infectionassociated with preseptal and orbitalcellulitis in the pediatric patient. JAAPOS. 2003;7(6):413–417
16. Hultén KG, Kaplan SL, Lamberth LB, etal. Hospital-acquired Staphylococcusaureus infections at Texas Children’sHospital, 2001-2007. Infect ControlHosp Epidemiol. 2010;31(2):183–190
17. Cunliffe NA, Booth JA, Elliot C, etal. Healthcare-associated viralgastroenteritis among childrenin a large pediatric hospital,United Kingdom. Emerg Infect Dis.2010;16(1):55–62
18. Westley CR, Cotton EK, Brooks JG.Nebulized racemic epinephrine byIPPB for the treatment of croup: adouble-blind study. Am J Dis Child.1978;132(5):484–487
19. Ducharme FM, Chalut D, PlotnickL, et al. The pediatric respiratoryassessment measure: a valid clinicalscore for assessing acute asthmaseverity from toddlers to teenagers. JPediatr. 2008;152(4):476–480, 480.e1
20. Samuel M. Pediatric appendicitisscore. J Pediatr Surg.2002;37(6):877–881
21. Kharbanda AB, Vazquez-BenitezG, Ballard DW, et al. Developmentand validation of a novel PediatricAppendicitis Risk Calculator (pARC).Pediatrics. 2018;141(4):e20172699
22. Babl FE, Borland ML, Phillips N, et al;Paediatric Research in EmergencyDepartments InternationalCollaborative (PREDICT). Accuracyof PECARN, CATCH, and CHALICE headinjury decision rules in children: aprospective cohort study. Lancet.2017;389(10087):2393–2402
23. Mandeville K, Pottker T, Bulloch B,Liu J. Using appendicitis scores inthe pediatric ED. Am J Emerg Med.2011;29(9):972–977
24. Barata I, Brown KM, Fitzmaurice L,Griffin ES, Snow SK; American Academyof Pediatrics Committee on PediatricEmergency Medicine; American Collegeof Emergency Physicians PediatricEmergency Medicine Committee;Emergency Nurses AssociationPediatric Committee. Best practices for improving flow and care of pediatricpatients in the emergency department.Pediatrics. 2015;135(1). Available at:www. pediatrics. org/ cgi/ content/ full/ 135/ 1/ e273
25. Stiell IG, Bennett C. Implementationof clinical decision rules in theemergency department. Acad EmergMed. 2007;14(11):955–959
26. Harris PA, Taylor R, Thielke R, PayneJ, Gonzalez N, Conde JG. Researchelectronic data capture (REDCap)–ametadata-driven methodology andworkflow process for providingtranslational research informaticssupport. J Biomed Inform.2009;42(2):377–381
27. Nagel TR, Schunk JE. Using the handto estimate the surface area of aburn in children. Pediatr Emerg Care.1997;13(4):254–255
IBRAHIM et al8
127

28. Dasanayake AP, Macaluso M,Roseman JM, Caufield PW. Validityof the mother’s recall of her child’santibiotic use. ASDC J Dent Child.1995;62(2):118–122
29. Moons KG, Kengne AP, Grobbee DE,et al. Risk prediction models: II.External validation, model updating,
and impact assessment. Heart. 2012;98(9):691–698
30. Kharbanda AB, Dudley NC, Bajaj L,et al; Pediatric Emergency MedicineCollaborative Research Committee ofthe American Academy of Pediatrics.Validation and refinement of aprediction rule to identify children
at low risk for acute appendicitis. Arch Pediatr Adolesc Med. 2012;166(8):738–744
31. Reilly BM, Evans AT. Translatingclinical research into clinical practice:impact of using prediction rules tomake decisions. Ann Intern Med.2006;144(3):201–209
9
128

originally published online January 3, 2019; Pediatrics Penelope A. Bryant
Laila F. Ibrahim, Sandy M. Hopper, Susan Donath, Bennett Salvin, Franz E. Babl andScore
Development and Validation of a Cellulitis Risk Score: The Melbourne ASSET
ServicesUpdated Information &
018-1420http://pediatrics.aappublications.org/content/early/2019/01/02/peds.2including high resolution figures, can be found at:
References
018-1420#BIBLhttp://pediatrics.aappublications.org/content/early/2019/01/02/peds.2This article cites 31 articles, 7 of which you can access for free at:
Subspecialty Collections
bhttp://www.aappublications.org/cgi/collection/infectious_diseases_suInfectious Diseasesubhttp://www.aappublications.org/cgi/collection/emergency_medicine_Emergency Medicinefollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
129
originally published online January 3, 2019; Pediatrics Penelope A. Bryant
Laila F. Ibrahim, Sandy M. Hopper, Susan Donath, Bennett Salvin, Franz E. Babl andScore
Development and Validation of a Cellulitis Risk Score: The Melbourne ASSET
http://pediatrics.aappublications.org/content/early/2019/01/02/peds.2018-1420located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2019/01/02/peds.2018-1420.DCSupplementalData Supplement at:
1073-0397. ISSN:60007. Copyright © 2019 by the American Academy of Pediatrics. All rights reserved. Print
the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
130

131
4.3 Implications of the Melbourne ASSET score
The Melbourne ASSET score is anticipated to have a significant impact on clinical
practice, to both patients and clinicians.123 Clinical predictive rules that explicitly
recommend a decision, such as the ASSET score, will have greater impact
compared to an assistive prediction rule which provide probabilities without
recommending decisions.124,125 For patients, the risk of being overtreated or
undertreated with intravenous antibiotics will likely be reduced as
recommendations are more standardised. For clinicians, firstly, this method
allows for a rapid, easy-‐to-‐use, evidence-‐based method to aid decision-‐making.
Secondly, this ensures consistency in practice, regardless of bed capacity or
parental social circumstances, factors that potentially play a role in decision-‐
making under pressure. Lastly, with further impact analysis and refinement of
this score, the proposed clinical score has the potential to be more accurate than
clinician judgement, as has been shown in previous clinical prediction
rules.126,127
The obstacle for determining a standardised pathway for children with cellulitis
has been the absence of a gold standard against which to assess the true
requirement for intravenous antibiotics. Therefore, the next best method was
used to establish a ‘gold standard’, which was a consensus amongst clinicians
who had the relevant expertise and represented paediatric infectious diseases,
general paediatrics, paediatric emergency medicine and biostatistics. This was
based on the work in the first part of this thesis, the clinician survey and the
foundation cohort study, both of which ascertained prospectively the reasons
clinicians start intravenous antibiotics.115
The consensus of the expert clinicians was that the route of treatment at 24
hours after ED presentation was likely the correct one, based on the availability
of additional observations about infection progress and patient status. If within
24 hours of initial presentation a child is started on intravenous antibiotics, the
clinical features the child had at presentation were determined as the criteria for
132
requiring intravenous treatment. If within 24 hours of initial presentation, a
child was switched from intravenous to oral antibiotics, meaning the child
received less than a day of intravenous antibiotics, the clinical features the child
had at initial presentation was determined as the criteria for requiring oral
antibiotics. It is possible that clinicians may unnecessarily treat beyond 24 hours
simply because there is intravenous access in situ. This would result in a slightly
more conservative gold standard than ‘true need’, which is similar to other
clinical scores.58
In assessing the impact of the ASSET score, there are several potential clinical
outcomes for patients. The proportion of patients who are started on
intravenous antibiotics can be measured. The baseline and foundation studies
showed that 26-‐29% of children who present to the ED with uncomplicated
cellulitis were commenced on intravenous treatment.114,115 With the
introduction of the score, a decline in this proportion is anticipated. Secondly, the
number of patients discharged home on oral antibiotics is expected to increase
while the number of patients with complications should remain the same. Other
outcomes include changes in length of stay in ED for patients with cellulitis and
the impact on cost of treatment.
The ASSET score also has the potential to impact future research in cellulitis.
Previous research studies investigating patients with cellulitis differentiated
mild from moderate/severe based on clinician judgement.1,43,120 This score
would allow an objective method of classifying patients that has the potential to
reduce selection bias in future studies. In addition, the methodology of this
clinical score can be used as a platform to develop similar scores for other
childhood infections.
The Melbourne ASSET score was derived and validated parallel to the RCT
(Chapter 5) and therefore recruitment of patients into the trial and later analysis
did not incorporate the ASSET score. The decision to commence intravenous
antibiotics in the RCT was based on several clinical criteria along with clinical
judgement, resulting in the potential inclusion of patients who may not have
133
required intravenous antibiotics. However, in a randomised study, these patients
should have been equally assigned to both study groups. The Melbourne ASSET
score will prevent further studies investigating children with cellulitis from
having to use clinical judgement to determine their study population, thereby
reducing bias.
The derivation and validation of the Melbourne ASSET score represent an
important first step in standardising antibiotic management for cellulitis. The
next stages of implementation and impact analysis now need to be undertaken to
encourage widespread use of this score.122

134
Chapter 5 Randomised controlled trial
5.1 Introduction to the randomised controlled trial of home versus hospital
The concept of intravenous antibiotic administration in a non-‐inpatient setting,
has been previously reported in the literature.1,3,6 Patients usually receive OPAT
after a period of hospital admission when they are deemed sufficiently stable to
receive further intravenous antibiotics in an outpatient ambulatory unit or the
patient’s home.5,38 A more recent concept in acute care has been to use OPAT for
patients directly from the ED, avoiding hospital admission altogether.1,6,114
However, widespread uptake of this hospital admission avoidance pathway for
intravenous antibiotics in children with acute infections is limited, despite
benefits such as higher quality of life for patients and families and lower costs.7,38
The reason for this is likely due at least in part to the absence of high quality
evidence supporting that treatment at home is as good as standard care in
hospital.
To definitively answer the question about the efficacy and safety of treatment at
home compared to hospital care, a randomised study was needed. As a common
condition in children with low risk of severe morbidity or mortality, cellulitis
was suitable to be used as a paradigm to answer the broader question regarding
the safety and efficacy of treating children at home with intravenous
antibiotics.1,128 The treatment comparison for the two locations was carefully
considered for the RCT with a deliberate design decision to ensure a combination
of best practice and translatability. The choice of intravenous ceftriaxone for
home treatment was made due to its once daily administration making it a
pragmatic choice for ambulatory services, which may only have capacity to
provide a service to patients once a day. Despite ceftriaxone being the most
commonly used antibiotic in OPAT, there have been no prospective studies to
answer the question of ceftriaxone efficacy or its association with the
development of bacterial resistance.2,3,6 The aims of the RCT were to investigate
the efficacy, safety, microbiological outcomes, quality of life and cost-‐
135
effectiveness of the treatment of moderate/severe cellulitis at home compared to
standard care in hospital using flucloxacillin.
This chapter contains two manuscripts, the published protocol of the RCT, and
the manuscript of the RCT itself containing the primary and clinical secondary
outcomes, and simple cost analysis. The quality of life outcomes and associated
comprehensive cost-‐effectiveness analysis are in the next chapter.

136
5.2 Study 6a: RCT protocol
Ibrahim LF, Babl FE, Orsini F, Hopper SM, Bryant PA. Cellulitis: Home Or
Inpatient in Children from the Emergency Department (CHOICE): protocol for a
randomised controlled trial. BMJ open 2016; 6(1): e009606.
Cellulitis: Home Or Inpatient inChildren from the EmergencyDepartment (CHOICE): protocolfor a randomised controlled trial
Laila F Ibrahim,1,2,3 Franz E Babl,2,3,4 Francesca Orsini,5 Sandy M Hopper,2,4
Penelope A Bryant6,1,2,3
To cite: Ibrahim LF, Babl FE,
Orsini F, et al. Cellulitis:
Home Or Inpatient in Children
from the Emergency
Department (CHOICE):
protocol
for a randomised controlled
trial. BMJ Open 2016;6:
e009606. doi:10.1136/
bmjopen-2015-009606
▸ Prepublication history for
this paper is available online.
To view these files please
visit the journal online
(http://dx.doi.org/10.1136/
bmjopen-2015-009606).
PAB and FEB contributed
equally to this study.
Received 3 August 2015
Revised 28 September 2015
Accepted 19 October 2015
For numbered affiliations see
end of article.
Correspondence to
Dr Franz E Babl;
ABSTRACTIntroduction: Children needing intravenous antibiotics
for cellulitis are usually admitted to hospital, whereasadults commonly receive intravenous treatment athome. This is a randomised controlled trial (RCT) ofintravenous antibiotic treatment of cellulitis in childrencomparing administration of ceftriaxone at home withstandard care of flucloxacillin in hospital. The studyaims to compare (1) the rate of treatment failure athome versus hospital (2) the safety of treatment athome versus hospital; and (3) the effect of exposure toshort course ceftriaxone versus flucloxacillin on nasaland gut micro-organism resistance patterns and theclinical implications.
Methods and analysis: Inclusion criteria: childrenaged 6 months to <18 years with uncomplicatedmoderate/severe cellulitis, requiring intravenousantibiotics. Exclusions: complicated cellulitis (eg,orbital, foreign body) and immunosuppressed or toxicpatients. The study is a single-centre, open-label, non-inferiority RCT. It is set in the emergency department(ED) at the Royal Children’s Hospital (RCH) inMelbourne, Australia and the Hospital-in-the-Home(HITH) programme; a home-care programme, whichprovides outreach from RCH. Recruitment will occur inED from January 2015 to December 2016. Participantswill be randomised to either treatment in hospital, ortransfer home under the HITH programme. Thecalculated sample size is 188 patients (94 per group)and data will be analysed by intention-to-treat. Primary
outcome: treatment failure defined as a change intreatment due to lack of clinical improvement accordingto the treating physician or adverse events, within 48 hSecondary outcomes: readmission to hospital,representation, adverse events, length of stay,microbiological results, development of resistance,cost-effectiveness, patient/parent satisfaction. Thisstudy has started recruitment.
Ethics and dissemination: This study has beenapproved by the Human Research Ethics Committee ofthe RCH Melbourne (34254C) and registered with theClinicalTrials.gov registry (NCT02334124). We aim todisseminate the findings through international peer-reviewed journals and conferences.
Clinical trial: Pre-results.
INTRODUCTIONChildren with cellulitis receiving intravenousantibiotics are usually admitted to hospital,whereas adults commonly receive intraven-ous treatment at home. Various reasons havebeen cited including parental anxiety andthe acute nature of the infection in children.However, in comparison to hospital admis-sion, children treated at home do better psy-chologically and physically, have fewerinvestigations, are at decreased risk ofhospital-acquired infections, and have subse-quent decreased use of healthcareresources.1 2 It is also less expensive (time offwork and transport costs) and disruptive forfamilies.1 3 Some children with moderate/severe cellulitis may be safely treated athome, but criteria for this are unclear.4
There are no randomised trials comparinghome versus hospital treatment in childrenfor cellulitis. In a recent study at our institu-tion of children presenting with cellulitis tothe emergency department (ED), 57% weredischarged on oral antibiotics and 43% weretreated with intravenous antibiotics due toextensive, rapidly spreading or complicated
Strengths and limitations of this study
▪ Randomisation of a novel home-care interventionversus standard hospital care.
▪ Primary outcome relevant to clinical practice.▪ First investigation of differential impact of short
course antibiotics on the acquisition of resistantorganisms.
▪ Key assessment of parental preference of treat-ment location.
▪ The antibiotics in the two arms are unavoidablydifferent.
▪ Decisions to start or stop intravenous antibioticsare based on a subjective clinical opinion reflect-ing real clinical practice.
Ibrahim LF, et al. BMJ Open 2016;6:e009606. doi:10.1136/bmjopen-2015-009606 1
Open Access Protocol
137

cellulitis or worsening features despite oral antibiotics.Forty-five per cent of those with uncomplicated moder-ate/severe cellulitis had been started on oral therapyand cellulitis had progressed despite this.5 Of those dis-charged on oral antibiotics, 10% re-presented with wor-sening cellulitis, suggesting there is a culture of tryingoral antibiotics first and not starting intravenous antibio-tics unnecessarily (unpublished data).When intravenous treatment is required for cellulitis,
flucloxacillin or cephazolin are the usual choicesbecause they are effective against Staphylococcus aureus
and group A streptococci, the main pathogens causingcellulitis.6 However, they are not suitable for outpatientparenteral antibiotic therapy (OPAT) due to their fre-quent dosing. The majority of paediatric OPAT servicesare only able to deliver once daily interventions.Ceftriaxone has antistaphylococcal activity and can beadministered once daily.7 There are only a few studies inchildren in which ceftriaxone has been used to treat cel-lulitis either in hospital or OPAT, but none have com-pared outcomes to children treated with otherrecommended antibiotics.4 7–10 There are no studies inchildren with cellulitis who require intravenous treat-ment comparing administration at home and in hos-pital. A study of children with moderate/severe cellulitiswho were treated with ceftriaxone at a day treatmentcentre had an 80% success rate, but no comparison wasmade with children treated in hospital.4 Other studiesthat have included ceftriaxone for the treatment of cel-lulitis in children have had cure rates of 91–96%, buthave had small numbers, no comparison group and/orunclear methodology.8 9 A small study in adults com-pared ceftriaxone with flucloxacillin, and while ceftriax-one resulted in a higher success rate than flucloxacillin(96% vs 70%), this was not statistically significant.11 Thedifferential effect of ceftriaxone and flucloxacillin onthe microbiota of children has also never previouslybeen described.Increasingly, hospitals are developing programmes
where patients who have traditionally been treated on ahospital ward are treated at home under the care of hos-pital doctors and nurses in Hospital-in-the-Home(HITH) programmes. While attractive in terms ofresource use, it is unclear to what extent HITH care isefficacious and safe. The Royal Children’s Hospital(RCH) Melbourne has the largest paediatric HITH pro-gramme in Australia. As an alternative to admission forintravenous flucloxacillin, RCH HITH developed adirect-from-the ED pathway for cellulitis, using oncedaily ceftriaxone and medical review at home. SinceSeptember 2012, more than 70 children at RCH withmoderate/severe cellulitis have been treated successfullyat home, with outcomes similar to children treated inhospital, although there may be unappreciated differ-ences in selection criteria.12 13
We therefore plan to randomly assign patients with cel-lulitis requiring intravenous antibiotics to either betreated at home (intravenous ceftriaxone) or to the
hospital ward (intravenous flucloxacillin). The studyaims to compare (1) the rate of treatment failure ofhome treatment with intravenous ceftriaxone versus hos-pital treatment with intravenous flucloxacillin; (2) thesafety of treatment at home versus treatment in hospital;and (3) the effect of exposure to short course ceftriax-one versus flucloxacillin on nasal and gut micro-organism resistance patterns and the clinical implica-tions of this. The main outcome is treatment failure;defined as a change in treatment due to lack of clinicalimprovement or the occurrence of adverse events.
METHODSDesignThis is a single-centre, open-label, non-inferiority rando-mised controlled trial (RCT). This pragmatic trial aimsto determine whether treatment for cellulitis adminis-tered at home is non-inferior to (ie, no worse than)treatment in hospital. It has two parallel arms with 1:1allocation of children with moderate/severe cellulitis.
SettingPatients will be recruited from the ED at the RCH, a ter-tiary paediatric hospital in Melbourne, Australia fromJanuary 2015 to December 2016.
Inclusion criteria▸ Children aged 6 months to <18 years.▸ Children presenting to RCH ED with moderate/
severe cellulitis, that is, those assessed as needingintravenous antibiotics. Currently, there is no vali-dated scoring system on which to base the choicebetween intravenous or oral antibiotics, thereforeclinician judgement is the current gold standard.Although reasons may differ between clinicians, thiswill be accounted for by randomisation. Reasons forstarting intravenous antibiotics include:
A. Failed oral antibiotics (no improvement despite 24 horal antibiotics).
B. Rapidly spreading redness (patient/parent history).C. Significant swelling/redness/pain.D. Systemic symptoms/signs (eg, fever, lethargy).E. Difficult to treat areas (eg, face, ear, toe).
Exclusion criteriaChildren will be excluded if they have:1. Complicated cellulitis defined as follows: orbital cellu-
litis or unable to exclude orbital cellulitis, penetrat-ing injury/bites, suspected/confirmed foreign body,suspected fasciitis or myositis, varicella, undrainedabscess including dental abscess.
2. Toxicity: tachycardia when afebrile or hypotension(both as per the limits from the ‘Development ofheart and respiratory rate percentile curves for hospi-talised children’14), poor central perfusion (capillaryrefill >2 s).
2 Ibrahim LF, et al. BMJ Open 2016;6:e009606. doi:10.1136/bmjopen-2015-009606
Open Access
138
3. Underlying comorbidities: immunosuppression, liverdisease.
4. Any concurrent infection necessitating different anti-biotic treatment to intravenous flucloxacillin or cef-triaxone monotherapy, for example, concurrentsinusitis or otitis media or lymphadenitis.
5. Other medical diagnoses necessitating admission tohospital for observation or treatment relating to theknown medical condition.
6. Unable to obtain intravenous access.7. Age <6 months old.8. With mild cellulitis (ie, can be treated with oral
antibiotics).Non-English speakers will be included so long as at
the time of obtaining consent, an interpreter is avail-able. At our centre, an interpreter is available in personduring normal working hours Monday to Friday and viatelephone 24 h a day. An interpreter service will also beused for subsequent phone calls and clinic visits similarto routine clinical practice involving non-Englishspeakers.
Primary outcomeThe primary outcome is treatment failure defined as achange in treatment due to lack of clinical improvementaccording to the treating physician or adverse events,within 48 h (i,e by Day 3) from the start of the first anti-biotic dose administered in the ED (Day 1). Clinicalimprovement is assessed by the treating physician dailyand includes: reduction in fever (if fever source is cellu-litis and not concurrent illness; reduction in frequencyor degree of temperature), reduction in the cellulitisarea (measured by the largest diameter of erythema),reduction in the severity of swelling ( judged by clinicianas mild, moderate or severe) and reduction in the inten-sity of erythema ( judged by clinician on a scale of 0=noerythema to 5=severe erythema).
Secondary outcomes1. Time to no progression of cellulitis: number of days
(including fractions of days—to one decimal point)from the start of the first dose in ED to the time atwhich the cellulitis stops spreading past the markedarea.
2. Time to discharge: number of days (including frac-tions of days) from the time of arrival in ED to thetime the patient no longer needs hospital-basedinterventions/care, whether in hospital or at home.
3. Readmission rate: proportion of children readmit-ted to hospital within 14 days of discharge date dueto the same cellulitis.
4. Representation to ED: proportion of children repre-senting to ED within 14 days of discharge due to thesame cellulitis.
5. Length of stay in ED: from triage time in ED to thetime the patient leaves ED to go either home or toward.
6. Duration of intravenous antibiotics: in days.
7. Rates of intravenous cannula needing at least oneresiting.
8. Complications of cellulitis: development of abscessrequiring drainage after starting intravenous antibio-tics, bacteraemia.
9. Adverse events: anaphylaxis; allergic reaction (sus-pected or confirmed) necessitating change ofempiric antibiotic; sepsis; death.
10. Microbiology:▸ Rate of ceftriaxone susceptibility in bacteria iso-
lated from a nasal or skin swab of the affectedarea.
▸ Rate of Staphylococcus aureus nasal carriage(methicillin-sensitive and methicillin-resistant)collected within 48 h, after 7–14 days, 3 monthsand 1 year after starting antibiotics.
▸ Rate of resistant bacteria present in stool samplescollected within 48 h, after 7–14 days, 3 monthsand 1 year after starting antibiotics. Rates of clin-ical infection with resistant organisms up to1 year after starting antibiotics.
11. Costs of hospital versus HITH treatment: includingcosts of beds, consumables, nursing and medicaltime and overheads including administrative time,information technology, use of hospital cars.
12. Patient and parent satisfaction (measured byanonymous survey) including questions from a pub-lished quality of life (QOL) tool.15
Patient recruitment, study procedure and data collectionED clinicians (senior doctors, junior doctors or nursepractitioners) will identify patients with moderate/severecellulitis presenting to RCH ED at triage or during clin-ical assessment (figure 1). The patient or parents ofpatients meeting inclusion criteria will be invited to par-ticipate in the study. Consent will be obtained for ran-domisation, data collection and follow-up that is notroutine practice. Data collection includes: age, sex, siteof cellulitis, size of area affected, prior antibiotics, under-lying comorbidity not affecting inclusion, systemic symp-toms and signs. In addition, consent will be requestedfor nasal swab samples and stool samples.Randomisation will be performed after consent isobtained by a study investigator or the ED clinician.Patients who are randomised to HITH will be prescribedintravenous ceftriaxone (50 mg/kg once daily) andthose randomised to the ward will be prescribed intra-venous flucloxacillin (50 mg/kg 6 hourly). A bloodculture, nasal swab and where relevant a skin swab (onlyin the presence of discharge from the site of cellulitis)will be collected at presentation. A stool specimen willbe collected within 48 h of the first dose of antibiotics.Parents will be asked to take two photos of the cellu-
litis area using their own camera/phone (if available)after the affected area is demarcated with indelible inkwith a tape measure placed alongside the area affected.If parents do not have a camera/phone, permission willbe sought from the parent to use a hospital camera to
Ibrahim LF, et al. BMJ Open 2016;6:e009606. doi:10.1136/bmjopen-2015-009606 3
Open Access
139
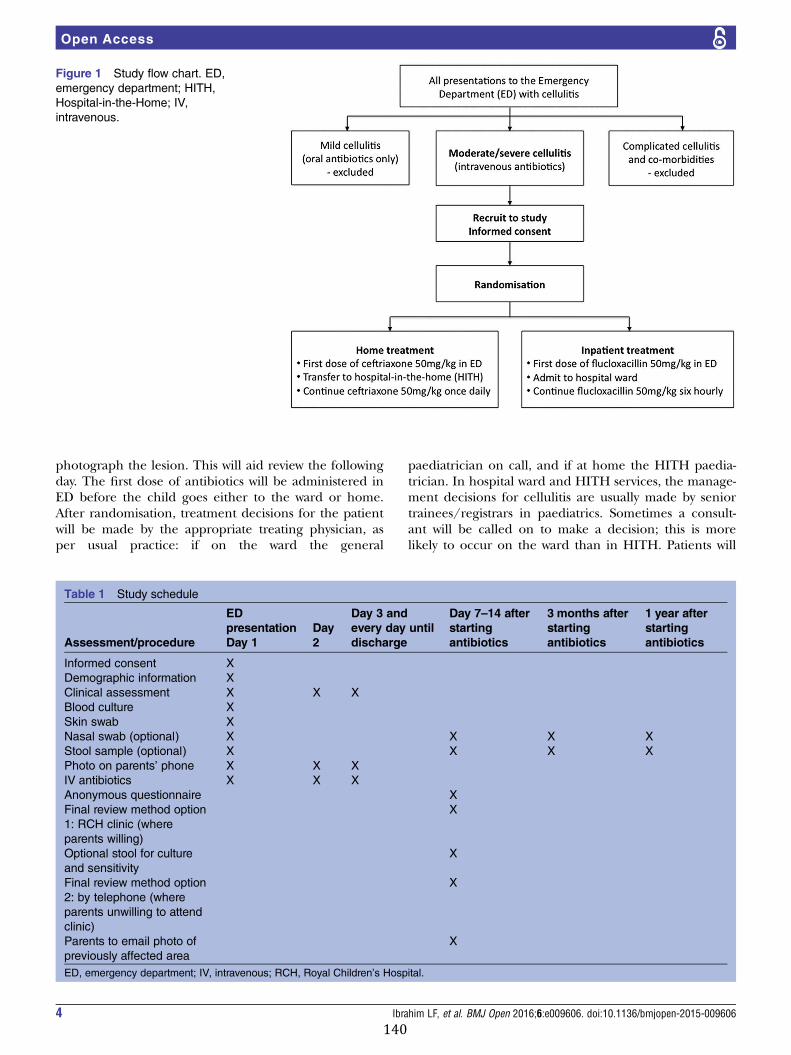
photograph the lesion. This will aid review the followingday. The first dose of antibiotics will be administered inED before the child goes either to the ward or home.After randomisation, treatment decisions for the patientwill be made by the appropriate treating physician, asper usual practice: if on the ward the general
paediatrician on call, and if at home the HITH paedia-trician. In hospital ward and HITH services, the manage-ment decisions for cellulitis are usually made by seniortrainees/registrars in paediatrics. Sometimes a consult-ant will be called on to make a decision; this is morelikely to occur on the ward than in HITH. Patients will
Figure 1 Study flow chart. ED,emergency department; HITH,Hospital-in-the-Home; IV,intravenous.
Table 1 Study schedule
Assessment/procedure
EDpresentationDay 1
Day2
Day 3 andevery day untildischarge
Day 7–14 afterstartingantibiotics
3 months afterstartingantibiotics
1 year afterstartingantibiotics
Informed consent XDemographic information XClinical assessment X X XBlood culture XSkin swab XNasal swab (optional) X X X XStool sample (optional) X X X XPhoto on parents’ phone X X XIV antibiotics X X XAnonymous questionnaire XFinal review method option1: RCH clinic (whereparents willing)
X
Optional stool for cultureand sensitivity
X
Final review method option2: by telephone (whereparents unwilling to attendclinic)
X
Parents to email photo ofpreviously affected area
X
ED, emergency department; IV, intravenous; RCH, Royal Children’s Hospital.
4 Ibrahim LF, et al. BMJ Open 2016;6:e009606. doi:10.1136/bmjopen-2015-009606
Open Access
140

be switched to oral therapy when there is clinicalimprovement of the cellulitis as judged by the treatingclinician. Oral antibiotics will be cephalexin 25 mg/kg 6hourly (as per RCH guidelines), or the most appropriateantibiotic based on microbiology results. Althoughpatients are usually not followed up any further in hos-pital, in this study, all participants will be followed up asper the study schedule (table 1). If parents decline thefirst follow-up visit at clinic, a review will be conductedby telephone and the parents will be requested to emailphotos of the area previously affected with cellulitis orgive a verbal report (to ensure clinical resolution). Theanonymous patient/parent satisfaction survey will beposted out to the parents at Day 7–14 after startingantibiotics.The nasal swab and stool sample will be requested at
four different time points: (1) within 48 h of the firstantibiotic dose; (2) 7–14 days after starting antibiotics;(3) 3 months after starting antibiotics; and (4) 1 yearafter starting antibiotics. At each time point, additionalinformation will be collected: previous overseas travel,previous hospital admissions, household member whohas been admitted to hospital overseas, other antibioticuse, other infections, medical visits or hospital admis-sions. These samples are optional and do not affect par-ticipation in the study.
STATISTICAL METHODSSample size and power calculation:Previous data collection at RCH has shown a failure rateof standard treatment of cellulitis with flucloxacillin inhospital of approximately 5%.16 Based on the literatureand discussion with clinicians, we have determined thatthe intervention would be deemed acceptable if 80% ofchildren can be successfully treated at home ,that is, amaximum difference of 15%. For a non-inferiority studydesign with a 15% difference, 89 patients are needed ineach treatment arm (based on 80% power). Allowing for5% dropout rate, a total of 188 are therefore required(94 in each treatment arm). Based on our previous data,we will be able to recruit this number over a 2-yearperiod if this study remains within RCH.12 16 However,once this study starts at RCH, depending on recruit-ment, we may expand this study to other centres, whichwould shorten the length of time to complete the study.
RandomisationThe randomisation schedule will be provided by theClinical Epidemiology and Biostatistics Unit atthe Murdoch Children’s Research Institute (MCRI). Therandomisation will be in randomly permuted blocks ofvariable length, stratified by age (6 months to less than9 years and 9 years to 18 years) and by the presence ofperiorbital cellulitis. Randomisation will be enabledthrough the REDCap (Research electronic Data Capture,REDCap Software—V.6.6.2—copyright 2015 VanderbiltUniversity) web-based application housed at MCRI.
Statistical analysisStatistical analysis will follow standard methods for ran-domised controlled trials and the primary analysis willbe primarily by intention to treat. We will also conduct aper protocol analysis, including all randomised partici-pants where outcome data are available. For the primaryoutcome Pearson’s χ
2 test will be used to compare theproportion of participants who fail treatment within48 h from the first dose. Non-inferiority will determinedby calculating difference in treatment failure (risk differ-ence and 95% two-sided CI between the failure rates inthe home and hospital groups. For the home arm to benon-inferior to treatment in the hospital, the upperlimit of the 95% CI must be less than 15% (as we haveprespecified this as the non-inferiority margin). As a sec-ondary analysis on the primary outcome a logistic regres-sion model will be used to investigate whether inclusionof the stratification factor (age at randomisation) as pre-dictor modifies the estimated effect (and 95%CI) oftreatment group on the primary outcome.Secondary continuous outcomes will be compared
between the two groups using unadjusted linear regres-sion while binary outcomes will be compared usingunadjusted logistic regression. Furthermore, as explora-tive analyses, regression models (or logistic modelsaccording to the nature of the outcome) will also befitted to the primary and secondary outcomes adjustingfor age (as used in the randomisation), presence offever at baseline and any other baseline and demo-graphic variables where an imbalance is found. Theappropriate survival analysis models will be used tocompare time to event outcomes between the treatmentgroups. The statistician performing data analysis for theprimary and secondary outcomes will be blinded to thetreatment allocation.
Ethical issues and disseminationPrior to starting of the study and on an on-going basis,ED clinicians have had education sessions to informthem about the study. The appropriate informationsheet will be given to the parent and/or child, the studyexplained and written consent requested. Where parentsdo not give consent, the ED clinician will make the deci-sion about treatment location. Photos will be identifiedonly by the subject unique identifier assigned for thestudy and will be stored in a password-protected data-base. Data will be entered into a password-protecteddatabase enabled through the REDCap (Research elec-tronic Data Capture, REDCap Software—V.6.6.2—copy-right 2015 Vanderbilt University) web-based applicationhoused at MCRI. The case report forms will be kept in alocked filing cabinet, accessible only by the researchers.Consent to collect information will be sought from parti-cipants who deviate from the protocol. All data will beretained until 7 years after last contact with patients oronce all patients involved in the study have reached25 years of age (whichever is longer) as per the ethicsrequirements for our institution.
Ibrahim LF, et al. BMJ Open 2016;6:e009606. doi:10.1136/bmjopen-2015-009606 5
Open Access
141

We aim to disseminate the findings through inter-national peer-reviewed journals and international con-ferences either as an oral or a poster presentation.At the end of the study a summary of the results will
also be posted to the participants. Results will bereported as an analysis of group data rather than individ-ual data and will contain only de-identified information.
Risk management, adverse events and patient safetyThere are no foreseeable additional risks to patients ortheir families by participating in this study. HITH hasbeen shown to be a safe programme under which chil-dren can be treated at home for many conditions, andthere will be daily medical review of all patients. Familieson the HITH programme have direct access via tele-phone to an experienced nurse 24 h a day and thisnurse is supported by a medical team. Potential adverseevents in this study would be an allergic reaction toeither of the antibiotics used, and these will be reportedto the study’s independent data safety monitoringboard. Serious adverse events such as overwhelmingsepsis or death are not expected in this study as cellulitisin children is a condition not associated with such mor-bidity and mortality. None of the patients in our pro-spective study of home treatment of cellulitis developedsepsis or any other serious adverse event.16
Independent safety and data monitoring committeeAn Independent Safety and Data Monitoring Committee(ISDMC) have been established. The ISDMC consists oftwo independent clinicians and a biostatistician whom,collectively, have experience in the management ofpaediatric patients with cellulitis and in the conduct andmonitoring of randomised controlled trials. The ISDMCwill function independently of all other individuals andbodies associated with the conduct of the study. TheISDMC will review all data by treatment arm every 6 to10 months. The first planned ISDMC review is inOctober 2015.
Time planWe have thus far recruited 52 of the planned 188patients. We plan to complete recruitment by the end of2016.
DISCUSSIONOur study will be the first RCT to evaluate the effective-ness and safety of home intravenous antibiotics for chil-dren directly from ED. If treatment at home is found tobe non-inferior, the benefits for children/families andcost-effectiveness for healthcare constitutions will lead tothis pathway (direct-from-the ED to home) becomingstandard care.Our study design has some unavoidable limitations.
Although the main aim is to compare standard care inhospital with the novel intervention of home treatment,the antibiotics in the two arms are also necessarily
different. Intravenous flucloxacillin or cephazolin (usualstandard care) require dosing 3–4 times a day in chil-dren, which is not feasible for home treatment. Thealternative of administering these via a continuous infu-sion would require a form of central line access, whichin children may require sedation or anaesthesia, withassociated increased risks and time in hospital. The onlyintravenous antibiotic viable for home use in this acutedirect-from-ED context is therefore once daily ceftriax-one, and from our previous study we do not anticipatedifferences in antibiotic efficacy.16 Although longer termuse of ceftriaxone has been associated with increasedacquisition of resistant organisms in adults, this has notbeen shown in healthy children or for very short coursesas anticipated in this study. To address the potentialissues of resistance development this study is specificallydesigned to detect any changes in the nasal and gutmicro-organisms and any clinically relevant conse-quences of such changes. Another limitation of thisstudy is that this is a single site, single city study.Antibiotic resistance is geographically influenced, andthe availability/skills of home-based care programmesfor children may not be available to many centres.These factors may limit applicability to other areas.This study will likely have a high impact on clinical
practice not only in our own clinical institution but alsoon a wider global scale. The successful use of home anti-biotics is the tip of the iceberg, as it can be expanded toinclude many common medical conditions ensuringchildren can go home directly to be treated under theHITH programme and avoid hospitalisation. We antici-pate that this would ultimately impact on health policy.
Author affiliations1RCH@Home Department, The Royal Children’s Hospital, Parkville, Victoria,
Australia2Murdoch Children’s Research Institute, Parkville, Victoria, Australia3Department of Paediatrics, University of Melbourne, Melbourne, Victoria,
Australia4Emergency Department, The Royal Children’s Hospital, Parkville, Victoria,
Australia5Clinical Epidemiology and Biostatistics Unit, Murdoch Children’s Research
Institute, Parkville, Victoria, Australia6Infectious Diseases Unit, Department of General Medicine, The Royal
Children’s Hospital, Parkville, Victoria, Australia
Acknowledgements The authors would like to thank participating families,
emergency department staff and HITH staff. This study is funded in part by
grants from the RCH Foundation, the Murdoch Children’s Research Institute
and the Victorian Department of Health, Melbourne Australia. LFI was
supported in part by a scholarship from Avant Mutual Group Limited. FEB
was supported in part by a grant from the RCH Foundation. The emergency
research group, MCRI, is in part supported by a Centre for Research
Excellence Grant for Paediatric Emergency Medicine from the National Health
and Medical Research Council, Canberra, Australia and the Victorian
government infrastructure support program.
Contributors LFI, PAB and FEB were responsible for identifying the research
question and the design of the study. SMH and FO were responsible for
refining the design and developing the research protocol. All authors have
contributed to the development of the protocol, the implementation of the
study and enrolment of patients. LFI was responsible for the drafting of this
paper. All authors provided comments on the drafts and have read and
6 Ibrahim LF, et al. BMJ Open 2016;6:e009606. doi:10.1136/bmjopen-2015-009606
Open Access
142

approved the final version. PAB and FEB contributed equally to this study.
FEB takes responsibility for the manuscript as a whole.
Funding Victorian Department of Health, The Royal Childrens Hospital
Foundation, Murdoch Childrens Research Institute.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Human Research Ethics Committee of The Royal Children’s
Hospital Melbourne.
Provenance and peer review Not commissioned; externally peer reviewed.
Open Access This is an Open Access article distributed in accordance with
the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license,
which permits others to distribute, remix, adapt, build upon this work non-
commercially, and license their derivative works on different terms, provided
the original work is properly cited and the use is non-commercial. See: http://
creativecommons.org/licenses/by-nc/4.0/
REFERENCES1. Svahn BM, Remberger M, Heijbel M, et al. Case-control comparison
of at-home and hospital care for allogeneic hematopoietic stem-celltransplantation: the role of oral nutrition. Transplantation2008;85:1000–7.
2. Small F, Alderdice F, McCusker C, et al. A prospective cohort studycomparing hospital admission for gastro-enteritis with homemanagement. Child Care Health Dev 2005;31:555–62.
3. Balaguer A, Gonzalez de Dios J. Home versus hospital intravenousantibiotic therapy for cystic fibrosis. Cochrane Database Syst Rev2012;(3):CD001917.
4. Gouin S, Chevalier I, Gauthier M, et al. Prospective evaluation of themanagement of moderate to severe cellulitis with parenteralantibiotics at a paediatric day treatment centre. J Paediatr ChildHealth 2008;44:214–18.
5. Ibrahim LF, Hopper SM, Babl FE, et al. Who can safely haveantibiotics at home? A prospective observational study in children
with moderate/severe cellulitis. Pediatr Infect Dis J 13 Nov 2015.[Epub ahead of print] www.ncbi.nlm.nih.gov/pubmed/26569189
6. Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines forthe diagnosis and management of skin and soft-tissue infections.Clin Infect Dis 2005;41:1373–406.
7. Nelson SJ, Boies EG, Shackelford PG. Ceftriaxone in the treatmentof infections caused by Staphylococcus aureus in children. PediatrInfect Dis 1985;4:27–31.
8. Frenkel LD. Once-daily administration of ceftriaxone for the treatmentof selected serious bacterial infections in children. Pediatrics1988;82(3 Pt 2):486–91.
9. Kulhanjian J, Dunphy MG, Hamstra S, et al. Randomizedcomparative study of ampicillin/sulbactam vs. ceftriaxone fortreatment of soft tissue and skeletal infections in children. PediatrInfect Dis J 1989;8:605–10.
10. Brugha RE, Abrahamson E. Ambulatory intravenous antibiotictherapy for children with preseptal cellulitis. Pediatr Emerg Care2012;28:226–8.
11. Vinen J, Hudson B, Chan B, et al. A randomised comparative studyof once-daily ceftriaxone and 6-hourly flucloxacillin in the treatmentof moderate to severe cellulitis—Clinical efficacy, safety andpharmacoeconomic implications. Clin Drug Investig 1996;12:221–5.
12. Ibrahim LF, Hopper SM, Sacks B, et al. Pilot study of the safety andacceptability of parenteral antibiotics in children referred from theEmergency Department directly to Hospital-In-The-Home. The 8thWorld Congress of the World Society for Pediatric Infectious Disease(WSPID 2013); Cape Town, South Africa, 2013.
13. Ibrahim LF, Hopper SM, Babl FE, et al. A comparison of treatment athome or in hospital for moderate/severe cellulitis in children.Australasian Society for Infectious Diseases Annual ScientificMeeting; Adelaide, Australia, 2014.
14. Bonafide CP, Brady PW, Keren R, et al. Development of heart andrespiratory rate percentile curves for hospitalized children. Pediatrics2013;131:e1150–7.
15. Orme LM, Babl FE, Barnes C, et al. Outpatient versus inpatient IVantibiotic management for pediatric oncology patients with low riskfebrile neutropenia: a randomised trial. Pediatr Blood Cancer2014;61:1427–33.
16. Ibrahim LF, Hopper SM, Babl FE, et al. The CHOICE study: Cellulitistreatment at Home Or Inpatient in Children from Emergency.Australasian College for Emergency Medicine Annual ScientificMeeting; Melbourne, Australia, 2014.
Ibrahim LF, et al. BMJ Open 2016;6:e009606. doi:10.1136/bmjopen-2015-009606 7
Open Access
143

protocol for a randomised controlled trialthe Emergency Department (CHOICE): Cellulitis: Home Or Inpatient in Children from
Penelope A BryantLaila F Ibrahim, Franz E Babl, Francesca Orsini, Sandy M Hopper and
doi: 10.1136/bmjopen-2015-0096062016 6: BMJ Open
http://bmjopen.bmj.com/content/6/1/e009606Updated information and services can be found at:
These include:
References #BIBLhttp://bmjopen.bmj.com/content/6/1/e009606
This article cites 11 articles, 2 of which you can access for free at:
Open Access
http://creativecommons.org/licenses/by-nc/4.0/non-commercial. See: provided the original work is properly cited and the use isnon-commercially, and license their derivative works on different terms, permits others to distribute, remix, adapt, build upon this workCommons Attribution Non Commercial (CC BY-NC 4.0) license, which This is an Open Access article distributed in accordance with the Creative
serviceEmail alerting
box at the top right corner of the online article. Receive free email alerts when new articles cite this article. Sign up in the
CollectionsTopic Articles on similar topics can be found in the following collections
(648)Paediatrics (582)Infectious diseases
(302)Emergency medicine
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
144

145
5.3 Study 6b: RCT
Ibrahim LF, Hopper SM, Daley A, Orsini F, Babl FE, Bryant PA. Home versus
Hospital Intravenous Antibiotics for Children with Moderate/Severe Cellulitis a
Randomised Controlled Non-‐inferiority Trial. The Lancet Infectious Diseases.
Accepted – In press.
Elsevier Editorial System(tm) for The Lancet
Infectious Diseases
Manuscript Draft
Manuscript Number: THELANCETID-D-18-01041R1
Title: Randomised controlled trial of intravenous antibiotics on OPAT
versus hospital for cellulitis in children: comparison of efficacy and
safety
Article Type: Article (Clinical Trials)
Keywords: Antibiotics; intravenous; hospital-in-the-home; ambulatory;
skin and soft tissue; OPAT
Corresponding Author: Dr. Laila F Ibrahim, MBBCHBAO
Corresponding Author's Institution: The Royal Children's Hospital
Melbourne
First Author: Laila F Ibrahim, MBBCHBAO
Order of Authors: Laila F Ibrahim, MBBCHBAO; Sandy Hopper; Francesca
Orsini; Andrew Daley; Franz Babl; Penelope Bryant
Manuscript Region of Origin: AUSTRALIA
Abstract: Summary
Background
Outpatient parenteral antimicrobial therapy (OPAT) in children, commonly
using ceftriaxone, has no trial-based evidence to support it. We aimed to
compare the efficacy and safety of intravenous antibiotic therapy at home
versus standard treatment in hospital, in children with moderate/severe
cellulitis.
Methods
In a randomised non-inferiority trial, children aged 6 months-18 years
with uncomplicated moderate/severe cellulitis were randomised to receive
either intravenous ceftriaxone at home or intravenous flucloxacillin in
hospital. Patients were randomised 1:1, using web-based randomisation,
stratified by age and periorbital cellulitis. The primary outcome was
treatment failure defined as lack of clinical improvement or adverse
event, resulting in change of antibiotics within 48 hours. For home
treatment to be non-inferior, the difference was designated as less than
15%, with a sample size of 188 providing 80% power. ClinicalTrials.gov:
NCT02334124.
Findings
188 children were randomised, 93 to home and 95 to hospital treatment. By
intention-to-treat, 2 (2%) patients in the home group had treatment
failure compared to 7 (7%) in the hospital group (risk difference [RD] -
5·2%; 95% confidence interval [CI] -11·3 to 0·8, p=0·09). In the per-
protocol analysis, the difference was significantly higher in favour of
the home group. The findings significantly reject the null hypothesis
that home treatment is inferior to hospital treatment. Adverse events
occurred less with home treatment (2% vs 10%, p=0·048). As a secondary
outcome, there was no difference in the rates of acquisition of nasal
methicillin-resistant Staphylococcus aureus, or gastrointestinal extended
146

spectrum beta-lactamase-producing bacteria or Clostridium difficile after
3 months.
Interpretation
Home treatment of cellulitis in children with intravenous ceftriaxone is
not inferior to treatment in hospital with intravenous flucloxacillin.
Ceftriaxone at home did not show a signal of increased acquisition of
resistant bacteria, although larger studies are needed.
Funding
RCH Foundation, MCRI, Victorian Department of Health.
147
Randomised controlled trial of intravenous antibiotics on OPAT versus hospital for
cellulitis in children: comparison of efficacy and safety
Laila F Ibrahim MB BCh BAOa,b, Sandy M Hopper MBBSa,b,c, Francesca Orsini MScb,d,
Andrew J Daley MBBSe,f, *Prof Franz E Babl MDa,b,c,d,*Penelope A Bryant PhDa,b,e,g
*Contributed equally
Affiliations
a Department of Paediatrics, University of Melbourne
b Murdoch Children’s Research Institute
c Emergency Department, The Royal Children’s Hospital
d Melbourne Children's Trials Centre
e Infectious Diseases Unit, Department of General Medicine, The Royal Children’s
Hospital
f Microbiology Department, The Royal Children’s Hospital
g Hospital-In-The-Home Department, The Royal Children’s Hospital
50 Flemington Road, Parkville, Victoria 3052, Australia
Corresponding author
A/Prof. Penelope A Bryant
Department of General Medicine, The Royal Children’s Hospital Melbourne
50 Flemington Road, Parkville, VIC 3052, Australia
Email: [email protected]
Tel: +613 93455522 Fax: +613 9345 6667
148

Key words
Antibiotics; intravenous; hospital-in-the-home; ambulatory; skin and soft tissue; OPAT
Financial Disclosure
All authors have indicated they have no financial relationships relevant to this article to
disclose. The funding bodies did not have any authority in design and conduct of the study;
collection, management, analysis, and interpretation of the data; and preparation, review, or
approval of the manuscript.
149
Research in context
Evidence before this study
A search was performed on MEDLINE 1946 to October 2nd 2018 and EMBASE 1974 to
October 3rd 2018 using the search terms ‘cellulitis/ or soft tissue infections/’, ‘ceftriaxone’
‘outpatient’, ‘home care/’ ‘ambulatory care/’ and limited to ‘all child (0-18years)’ with no
language restrictions. This produced no randomised controlled trials (RCT) and there is no
Cochrane review on home/ambulatory management of cellulitis. The only RCT comparing
home versus hospital care primarily investigated quality of life. However a number of
published retrospective and observational studies were identified indicating widespread use
of home/ambulatory care in children, despite the lack of robust evidence of efficacy and
safety of home treatment. These studies suggest that some children with moderate/severe
cellulitis can be successfully treated via a home or ambulatory pathway, with a readmission
rate ranging from 0-20%. Ceftriaxone is the most common antibiotic used in this setting
because it can be administered once daily. However, no study using ambulatory ceftriaxone
has investigated the broader potential association of ceftriaxone use with resistant bacteria
and opportunistic pathogens such as Clostridium difficile.
Added value of this study
This is the first randomised controlled trial of any acute infection requiring intravenous
antibiotics in children to compare efficacy and safety of home/ambulatory treatment
directly from the Emergency Department to standard management in hospital. Findings
from our study provide robust evidence that children with moderate to severe cellulitis can
be effectively treated at home without the need for hospital admission. In addition, we have
shown that this management pathway is highly acceptable to families and has cost-saving
benefits to the hospital. Of equal importance to clinicians, for uptake of ceftriaxone use for
150
OPAT, there was no signal of increased colonisation with resistant nasal or gastrointestinal
bacteria.
Implications of all the available evidence
Our study provides the first unbiased evidence to support the existing literature and
increasing practice of treating childhood infections with intravenous antibiotics outside the
hospital environment. It promotes the broader uptake of home/ambulatory management of
moderate to severe cellulitis so that children can avoid hospital admission. For centres
without a pre-existing home care or ambulatory service, these findings enable advocacy for
resources for a similar treatment pathway. For those with existing services this study acts as
a platform to be replicated in other acute infections to increase the evidence for
home/ambulatory care.
151
Summary
Background
Outpatient parenteral antimicrobial therapy (OPAT) in children, commonly using
ceftriaxone, has no trial-based evidence to support it. We aimed to compare the efficacy
and safety of intravenous antibiotic therapy at home versus standard treatment in hospital,
in children with moderate/severe cellulitis.
Methods
In a randomised non-inferiority trial, children aged 6 months-18 years with uncomplicated
moderate/severe cellulitis were randomised to receive either intravenous ceftriaxone at
home or intravenous flucloxacillin in hospital. Patients were randomised 1:1, using web-
based randomisation, stratified by age and periorbital cellulitis. The primary outcome was
treatment failure defined as lack of clinical improvement or adverse event, resulting in
change of antibiotics within 48 hours. For home treatment to be non-inferior, the difference
was designated as less than 15%, with a sample size of 188 providing 80% power.
Secondary outcomes included adverse events and acquisition of resistant organisms.
ClinicalTrials.gov: NCT02334124.
Findings
188 children were randomised, 93 to home and 95 to hospital treatment. By intention-to-
treat, 2 (2%) patients in the home group had treatment failure compared to 7 (7%) in the
hospital group (risk difference [RD] -5·2%; 95% confidence interval [CI] -11·3 to 0·8,
p=0·09). In the per-protocol analysis, the difference was significantly higher in favour of
the home group. The findings significantly reject the null hypothesis that home treatment is
inferior to hospital treatment. Adverse events occurred less with home treatment (2 [2%] vs
10 [11]%, p=0·048). There was no difference in the rates of acquisition of nasal
152
methicillin-resistant Staphylococcus aureus, or gastrointestinal extended spectrum beta-
lactamase-producing bacteria or Clostridium difficile after 3 months.
Interpretation
Home treatment of cellulitis in children with intravenous ceftriaxone is not inferior to
treatment in hospital with intravenous flucloxacillin. Ceftriaxone at home did not show a
signal of increased acquisition of resistant bacteria, although larger studies are needed.
Funding
RCH Foundation, MCRI
153
Introduction
There has been a dramatic increase in children in the use of intravenous antibiotics in non-
inpatient settings, known as outpatient parenteral antimicrobial therapy (OPAT).1,2 This is
due to increased awareness that admission to hospital has a negative impact on quality of
life in children, carries the risk of hospital-acquired infections and is associated with higher
costs.3-5 Given the choice, children and caregivers choose treatment at home, an important
factor as we aim to move towards truly patient-centred care.6,7 As such, OPAT has shifted
rapidly from being a novel concept to an accepted model of care. However, published
evidence for its use in children has not kept pace. A recent systematic review found only a
single randomised controlled trial (RCT) of OPAT in children, and its primary outcome
was quality of life.8 The review found that evidence for efficacy and safety were lacking.
The inability to blind patients and clinicians to treatment location may have discouraged
trials in this field. The standard in hospital versus home care RCTs for other conditions in
adults is an open-label approach.9 This should therefore be adopted in OPAT because the
lack of randomised trial evidence is hindering a possible change in practice.
This has not stopped medical practitioners from using OPAT, with an increasing number of
reports of institutional practice, including the recent concept of OPAT for patients directly
from the emergency department (ED), completely avoiding admission to hospital.4,10,11-13
This increase in practice without robust evidence for efficacy and safety has created an
unresolved debate, as the antibiotic most frequently used in paediatric OPAT, and
particularly in admission avoidance management pathways, is ceftriaxone, a broad
spectrum cephalosporin.1,2,13 The reasons for using ceftriaxone are that it can be
administered once daily, it is a single dose so a peripheral cannula can be inserted in ED,
and it has efficacy against many pathogens causing common childhood infections.14
154
However, the argument against using ceftriaxone is that broad spectrum cephalosporin use
in predominantly adult inpatient studies has been temporally associated with the isolation
of resistant bacteria.15,16,17 Although this has not been shown for ceftriaxone use at home,
the current global crisis in antibiotic resistance raises legitimate concerns which have not
been addressed in OPAT in children. The question is therefore whether the benefits of
OPAT outweigh the disadvantages of ceftriaxone use in this setting, and we currently lack
the data to answer this.
We therefore designed the first RCT of OPAT for admission avoidance in children, using
ceftriaxone to treat moderate to severe cellulitis as a paradigm. While the majority of
children with cellulitis can be treated with oral antibiotics, a significant proportion who
have moderate/severe cellulitis, defined as those who require intravenous antibiotics, with
skin and soft tissue infections accounting for over 74,000 US paediatric hospitalisations
annually.18 Cellulitis in hospitalised children is usually managed with narrow spectrum
intravenous antibiotics such as flucloxacillin, but this is administered 6 hourly so is not
compatible with ambulatory use through a peripheral cannula, with ceftriaxone the only
viable alternative. For a trial of OPAT to have useful outcomes that are translatable to
clinical practice, it needs to compare a feasible OPAT option to standard hospital treatment.
Our aim was to compare the efficacy, safety, satisfaction and institutional costs of
treatment at home using intravenous ceftriaxone with standard treatment in hospital using
intravenous flucloxacillin. We hypothesized that children treated at home with intravenous
antibiotics (by necessity ceftriaxone) would not have inferior outcomes to those treated in
hospital (with flucloxacillin). We also specifically aimed to investigate the association
between ceftriaxone use and colonisation with resistant bacteria to provide the first
microbiological evidence for or against its use in the OPAT setting.
155
Methods
Study Design and participants
The Cellulitis at Home or Inpatient in Children from the Emergency Department
(CHOICE) trial was a single centre, randomised, open label non-inferiority trial. Patients
were enrolled from The Royal Children’s Hospital Melbourne (RCH), a tertiary paediatric
hospital in Melbourne, Australia. Ethics approval was obtained from the institutional
human research and ethics committee. The study protocol was previously published.19
Children and adolescents aged 6 months to 18 years who presented to the RCH ED with
moderate to severe cellulitis were eligible. The inclusion criteria included a diagnosis of
cellulitis requiring intravenous antibiotics by an experienced Emergency clinician (senior
trainee). Reasons for intravenous antibiotics included failed oral antibiotics (no
improvement despite 24 hours of oral antibiotics), rapidly spreading redness, significant
swelling or erythema or pain, systemic symptoms or signs, and difficult to treat areas (eg
facial, periorbital). Children were excluded if they had complicated cellulitis which
includes an undrained abscess, toxicity, underlying comorbidities, unable to obtain
intravenous access, age <6 months old, and with mild cellulitis (appendix). Written
informed consent was obtained from a parent or guardian and from the child when
appropriate, by a study investigator or a research nurse. Ethics approval was obtained from
the institutional human research and ethics committee, at the RCH, reference number
HREC34254. All participants gave informed consent before taking part.
Randomisation and masking
After obtaining written informed consent, eligible patients were randomly assigned in a 1:1
ratio using a web-based randomisation procedure to receive either standard care, which was
156
hospitalisation for treatment with intravenous flucloxacillin (50 mg/kg, every 6 hours) or
the intervention care, which was treatment at home with intravenous ceftriaxone (50 mg/kg,
once a day). The randomisation was in randomly permuted blocks of variable length,
stratified by a) age (6 months to 8 years versus 9 to 18 years) and b) presence of periorbital
cellulitis. These stratification factors, young age and presence of periorbital involvement,
were previously identified as reasons for clinicians’ hesitation in using OPAT. Preparation
of the randomisation sequence was completed by a data management coordinator
independent of the research team and had no further role in the trial. The trial statistician
was blinded to treatment assignment until the primary outcome was analysed. Home care
and hospital medical and nursing staff were not blinded to group assignment.
Procedures
Regardless of the study arm, the child had an intravenous peripheral cannula inserted, and
the first dose of antibiotic administration in ED. None of the patients received intravenous
antibiotics pre-randomisation. The patient had a blood culture collected and a skin swab if
there was discharge from the infected area. A line was drawn on the skin to demarcate the
cellulitis in the ED.
Hospital group: The patient received further doses of intravenous flucloxacillin every 6
hours on the ward in hospital. There was at least daily review by a hospital ward medical
registrar (senior trainee) and at least 4 hourly nursing observations. All of the children in
the hospital group had a continuous infusion of normal saline through their intravenous
cannula between antibiotic doses as per standard practice.
Home group: A referral was made from the ED to the home care team (available 24/7).
After receiving the first dose of ceftriaxone in the ED and meeting a home care nurse, the
patient went home with the peripheral cannula in situ until intravenous antibiotics were
157
ceased. Families were provided with a contact telephone number for a home care nurse
available 24 hours a day. A nurse visited the child at home and administered intravenous
ceftriaxone 50 mg per kilogram over a period of 3 to 5 minutes once daily until the child
was deemed suitable for oral therapy. A home care medical registrar (senior trainee)
reviewed the child in person at least once during the course of treatment, and daily by
teleconferencing and, where necessary, reviewing digital photographs.
In all patients, the decision to cease intravenous antibiotics was made when deemed
clinically appropriate by the hospital or home care doctors respectively, reflecting the real
clinical situation.
Outcomes
The primary outcome was treatment failure defined as lack of clinical improvement of
cellulitis or an adverse event, resulting in a change of initial empiric antibiotics within 2
days (48 hours) of treatment from the start of the first antibiotic dose given in the ED.
Clinical improvement was an objective measure: either continuous or binary assessments as
per the trial protocol (reduction in fever i.e. temperature, cellulitis area, severity of swelling
and erythema). Treatment failure was identified when there were no improvements in any
of the clinical features documented at baseline or an adverse event. Additionally, daily
photographs were taken for comparison, with the first taking place in the ED as baseline.
Secondary outcomes, assessed for 14 days for all patients after discharge, were length of
stay in ED, cessation of erythema spread within 24 hours (by observing spread of erythema
from demarcated line), duration of intravenous antibiotics, the number of intravenous
catheterisations during treatment, length of stay under medical care, re-presentation to ED,
readmission, safety measures (adverse events and complications). The hospital and home
158
care registrars were trained to perform assessments in a standardized way, documented
their assessment of the child daily with regards to clinical improvement, adverse events,
complications and cessation of spread of cellulitis.
Microbiology outcomes were collected for a subgroup of patients who consented. Samples
were used for the investigation of the potential acquisition of resistant colonizing
organisms (extended-spectrum beta-lactamase (ESBL) producing bacteria, vancomycin-
resistant enterococci (VRE) and methicillin-resistant S. aureus (MRSA) and Clostridium
difficile (C. difficile). This was optional and not providing samples did not preclude them
from the study. Parents were also asked to anonymously rate their experience (1 to 5 Likert
scale, 1=very poor, 5=very good), their routine disruption (1=no disruption, 2=slight
disruption, 3=a lot of disruption) and state their preference for either hospital or home
treatment 7 to 14 days after discharge from medical care. An institutional cost comparison
was conducted between the home and hospital groups including the cost of nursing and
medical resources (which includes 24/7 availability for referral and calls), consumable
items, indirect overhead costs including administrative time, information technology and
use of hospital vehicles for visiting patients. A full cost-effectiveness analysis was planned
and conducted alongside this trial, which will be published separately.
Statistical Analysis
Previous data collection at RCH showed a failure rate of standard treatment of cellulitis
with flucloxacillin in hospital of 5-7%.11 The premise for the sample size calculation of this
trial was a treatment failure rate in hospital of approximately 7% and an estimated
treatment failure rate at home of about 10%. We specified that for the home group to be
non-inferior (and clinically acceptable based on the literature and in discussion with ED
159
clinicians), the upper margin of the two-sided 95% confidence interval of the difference in
proportions of treatment failure between the home and the hospital group should be no
greater than 15% difference. In other words, OPAT would be deemed acceptable to
clinicians and families if 80% of children can be successfully treated at home.13 With this
premise, 89 subjects per group were required to provide a statistical power of 80%. Thus,
allowing for a dropout rate and/or cross over between treatments of 5%, 94 participants
were required in each treatment arm, or 188 in total.
The risk difference (RD) between the failure rates in the home and the hospital groups and
its 95% two-sided confidence interval (CI) was obtained by running a binomial regression
model on the primary outcome, adjusted by the stratification factors (age at randomisation
and presence of periorbital cellulitis) as predictors. Binary secondary outcomes were
compared between the two groups using the same adjusted binomial regression used for the
primary outcome. Continuous secondary outcomes were compared between the two groups
using a linear regression model adjusted by the stratification factors. When investigating
acquisition of post-intravenous antibiotic resistant organisms, samples were analysed only
from the per-protocol analysis. Acquisition was documented if a sample at 7 to 14 days or 3
month time point was positive for ESBL, VRE, C. difficile in stool or MRSA in nasal
swabs with a preceding sample that was negative. Microbiology laboratory methodology is
detailed separately (appendix).
As this was a non-inferiority trial, the analyses of the primary and secondary outcomes was
done via intention-to-treat and per-protocol analyses, since participants not following the
protocol were likely to bias the estimated treatment effect towards zero (figure 1).
Participants who were found to be randomised in error were excluded from the analysis and
replaced. An independent data and safety monitoring committee provided trial oversight
160
and reviewed data including adverse events and protocol violations by treatment arm every
six months for the duration of the recruitment period. All analyses were done using Stata
version 15·0. This trial was registered at ClinicalTrials.gov, registry number
NCT02334124.
Role of the funding source
The funder of the study had no role in study design, data collection, data analysis, data
interpretation, or writing of the report. The first and corresponding author had full access to
all the data in the study and had final responsibility for the decision to submit for
publication.
Results
Between 9th January 2015 and 15th June 2017, 1135 children who presented to ED with
cellulitis were screened (figure 1). Of 190 randomised, two patients were found to be
ineligible after randomisation and were therefore replaced. This resulted in 188 study
participants with 93 randomised to the home arm and 95 to the hospital arm. All study
participants had a primary outcome and 100% were followed up at 7 to 14 days after initial
presentation to document secondary outcomes. Forty-two percent of patients presented with
systemic features, which was primarily fever.(table 1) When systemic features were
explored in more detail, the proportion of patients febrile in the ED was significantly lower
in the home group than the hospital group (3% vs 18%). Fifty-two percent of participants
had received prior oral antibiotics, with a median number of 4 doses (interquartile range 3
to 8).
In the intention-to-treat analysis, there were 2 patients in the home group who had
treatment failure compared to 7 patients in the hospital group (2% vs 7%, RD -5·3%; 95%
161
CI -11·3 to 0·8) (table 2). Therefore the pre-specified criteria for non-inferiority for the
home group were met. In other words, the results of this non-inferiority randomised trial
significantly reject the null hypothesis that home treatment is inferior to hospital treatment.
Further, in the per-protocol analysis of the primary outcome, treatment failure was
significantly lower in the home group [1 (1%) of 89 vs 7 (8%) of 91, RD -6·5%; 95% CI -
12·4 to -0·7]. In the intention-to-treat analysis, the 2 patients who had treatment failure in
the home group were as follows: 1 patient developed a localised abscess a day after initial
ED presentation. At this point, a family history of MRSA infection was elicited, so this
patient was admitted to hospital for intravenous vancomycin and her skin swab
subsequently cultured MRSA. The second patient who had treatment failure in the
intention-to-treat home group was actually treated in hospital with intravenous
flucloxacillin after randomisation. This patient developed a rash consistent with
flucloxacillin allergy after 24 hours and was therefore switched to intravenous ceftriaxone.
In the hospital group, 5 of the 7 patients with treatment failure had no clinical
improvement, which prompted an additional antibiotic to be added to the treatment regimen
within 48 hours (ceftriaxone n=3, vancomycin n=1, oral clindamycin n=1). The remaining
2 of 7 patients were changed to a different antibiotic: one to benzylpenicillin due to lack of
clinical improvement after 47 hours and to ceftriaxone after 24 hours when he developed a
rash consistent with flucloxacillin allergy. All patients eventually fully recovered.
The proportion of children in the intention-to-treat analysis with adverse events were lower
in the home group (2% vs 11%, p=0·048, table 3). These comprised the following: home:
(n=2); rash (n=1), dosing error (n=1); hospital: (n=10), diarrhea or vomiting (n=7),
headache (n=1), vasovagal episode (n=1), and hypotension (n=1). The patient with
hypotension had intermittent low blood pressure (lowest reading 85/56 with normal blood
162
pressure in between, without associated tachycardia) and looked clinically well throughout.
Six percent of children in both groups had complications during treatment (p=0·99). These
comprised the following: home: drainage of abscess or blister (n=6); hospital: drainage of
abscess or blister (n=5) and removal of foreign body (n=1).
Secondary outcomes favoring the home group were shorter length of stay in ED and lower
rate of re-catheterisation, while outcomes favoring the hospital group were shorter duration
of intravenous antibiotics and medical care (table 3). Two percent of children in both
groups re-presented to the ED after discharge (p=0·98). The per-protocol analysis of all
secondary clinical outcomes yielded similar results (appendix). An exploratory analysis
compared those who had failed prior antibiotics to those who had not received any
antibiotics previously and this did not show any differences (appendix).
Of 170 (90%) patients who had a blood culture taken, only 1 (1%) isolated a pathogenic
organism. A single positive blood culture for Staphylococcus aureus occurred in a patient
in the home group who was subsequently diagnosed with osteomyelitis. This patient
remained at home on ceftriaxone as he was already clinically well by the time the culture
flagged as positive; repeat blood culture was negative. Of 159 (85%) patients who provided
at least one microbiological sample, approximately 50% of patients provided longitudinal
stool and nasal swab samples for evaluation of acquisition of resistance. Those who
provided stool samples were slightly younger than those who did not (baseline:
5.8±4.3versus 8.5±4.5, p=0.0001, 7-14 days: 6.0±4.8 versus 8.1±4.5, p=0.001, 3 months:
5.6±4.4 versus 8.1±4.5, p=0.001) and those with treatment failure were less likely to
provide follow up stool samples than those without (7-14 days: 1/81 versus 7/99, p=0.045,
3 months: 0/79 versus 8/101, p<0.001)(appendix). In stool samples at baseline, the
prevalence of ESBL and C. difficile were similar between the home and hospital groups
163
and no patient isolated VRE (table 4). After antibiotics there was no difference between
groups in the proportion of acquisition of ESBL at 7-14 days (home 6% vs hospital 0%,
p=0·13) or at 3 months (11% vs 8%, p=0.64). Likewise there was no difference in
acquisition of C. difficile at 7-14 days (home 6% vs hospital 8%, p=0·94) or at 3 months
(11% vs 10%, p=0·95). No patient acquired VRE at either time point. The rate of MRSA
nasal carriage was 0% in both groups, although one patient cultured MRSA from abscess
pus as above. After antibiotics no patient acquired MRSA.
With regards to quality of life during treatment, 69/73 (95%) of the home group rated the
experience of care as very good compared to 45/62 (73%) of the hospital group
(p=0·001)(table 3). Disruption to parental and child routine were both significantly greater
in the hospital group, and more parents in the home than hospital group would choose
treatment for their child in the same location again (p<0·001).
At our institution, the average cost of treating a patient with moderate to severe cellulitis at
home is AUD530 (GBP308) per day, compared to the cost of a hospital bed on a medical
ward which is AUD1,297 (GBP752) per day. The patients treated at home in the intention-
to-treat analysis were under medical care for a combined total of 242 days. Including the
cost of hospital stay for the 2 patients who were assigned home treatment but had treatment
failure and subsequently required hospitalisation, (6 hospitalised days), the home patients
cost AUD1463 (GBP849) per patient per day. The patients in the hospital group in the
intention-to-treat analysis were admitted for a total of 190 days which cost AUD 2594
(GBP1505) per patient per day, amounting to an excess cost of AUD110,387 (GBP64,052)
compared to the home group. The cost analysis of the per-protocol population yielded a
cost difference of AUD122,104, (GBP70,884) in favor of the home group.
164
Discussion
In this randomised trial of home versus hospital for the treatment of cellulitis in children,
the rate of treatment failure at home with intravenous ceftriaxone was non-inferior to
standard treatment in hospital of intravenous flucloxacillin. In addition, the per-protocol
analysis showed home treatment had lower treatment failure than hospital treatment.
Failing to improve meant there was no improvement at all in all four of the assessment
criteria compared to baseline. This resulted in a team discussion between at least the
registrar and consultant (and usually other members of the team) which led to a discussion
with parents/guardian of the child before changing the antibiotic. Although there were more
children febrile in ED in the hospital group, only 2 of the 18 febrile children had treatment
failure, both in the hospital group.
This study also found that treatment of cellulitis at home with ceftriaxone, appeared to be
safe, as measured by low rates of adverse events, complications and readmissions, although
it was not powered for rare serious events. Although the frequency of formal reporting of
adverse events was daily for both groups, hospital patients had more opportunities to report
any adverse events in face-to-face encounters with medical or nursing staff compared to the
home group. It is very unlikely that symptomatic adverse events such as vasovagal
syncope, diarrhoea or vomiting occurring in patients of the home group would not have
been reported by parents. The worst outcome for a patient at home was return to hospital
for drainage of an abscess. No patient with moderate to severe cellulitis developed sepsis,
consistent with previous studies.11,20,21
With antimicrobial resistance increasing globally, investigating acquisition of resistant
organisms is as important as clinical efficacy and safety. In our study, there was no
165
increased risk of acquisition of resistant nasal or gastrointestinal bacteria or C. difficile in
those treated with ceftriaxone at home compared to those treated with flucloxacillin in
hospital; in particular there was zero acquisition of MRSA. We propose that these findings
are due to a) a different population and b) different antibiotic duration. The association
between third-generation cephalosporin use and colonisation with resistant organisms in
children is less strong than in adults and is predominantly from neonatal studies of unit
antibiotic policy. While most are retrospective or observational making confounding
factors difficult to exclude, there is a single prospective cross-over intervention trial
showing that an antibiotic policy including cefotaxime is associated with colonisation with
cefotaxime-resistant Enterobacteriaceae 22 However, a recent neonatal unit study showed a
steady increase over 25 years in third-generation cephalosporin resistance despite the
absence of third-generation cephalosporin use.23 The same is true with VRE, C. difficile
and nasal colonisation with MRSA: studies have either been in sick or inpatient populations
with prolonged use15, or have not shown a relationship16. No previous studies associating
ceftriaxone with increased bacterial resistance were in previously healthy children
receiving OPAT at home and none investigated short-course use.17,23-26 Other factors to
consider include that our region has low prevalence of resistance in children, particularly
MRSA, although this reflects many paediatric populations worldwide, applicability of the
trial's findings may be limited in regions with high prevalence. Only approximately half of
patients provided longitudinal samples for resistance analysis, so this result may not be
representative of the whole population. However, the tested patients were for the most part,
clinically indistinguishable from those that did not provide a sample (appendix). Our
findings suggest therefore that short-term ceftriaxone use in the OPAT setting in previously
healthy children does not appear to be associated with acquisition of resistance in children.
166
However, as our study was powered for efficacy and not microbiological outcomes, larger
studies are now needed of longer-term use in the outpatient/home setting.
Length of stay in ED was longer in the hospital group, likely reflecting the wait for a
hospital bed, an important finding with ever-increasing pressure to reduce ED waiting
times.27 Intravenous cannulation was also repeated more often in the hospital group. This
may be related to the use in hospital of low volume continuous infusion to keep the vein
open, or possibly the direct irritant effect of intravenous flucloxacillin.28 The duration of
intravenous treatment and consequent length of medical care were longer in the home
group by half a day, likely reflecting that the home care staff only had one opportunity per
day to stop treatment or discharge the patient - a result of the antibiotic dosing interval.
Our study reported high satisfaction rates with home management, and significantly lower
disruption for both parents and patients. While previous studies have shown satisfaction for
children treated via ambulatory pathways, this is the first study to compare satisfaction
between home and hospital groups in non pre-selected patients.4,13
The strengths of this study are that it is the first randomised study of OPAT in children
directly from the ED. It is powered for clinical efficacy, with as low a risk of bias as is
possible in an OPAT RCT. It is also the first to attempt to answer the question about the
microbiological effects of ceftriaxone for short-term OPAT. The main limitation of our
study is applicability to other centers without a home care visiting team. However, studies
have shown that other modes of ambulatory pathways (eg day treatment centres, patients
returning to a physician’s rooms) are also cost effective and preferred by patients to
hospitalisation. We therefore designed this study to be as widely applicable as possible to
other healthcare systems, for example by administering a daily rather than twice daily
167
antibiotic in the home arm, by having more junior doctors make the daily assessments and
by having multiple doctors actually working on the job rather than study doctors assessing
the patients, so our results could be translated to other management pathways. Additionally,
patients who required abscess drainage were directed to the ED, with minimal waiting time
as they already had a management pathway identified. Secondly, there is no gold standard
for the diagnosis of cellulitis requiring intravenous antibiotics. However, the proportion of
children at RCH that receive intravenous antibiotics for uncomplicated cellulitis is lower
than at other institutions.29 Additionally it has reduced from 184 (26%) of 700 in an earlier
observational study11 to 190 (22%) of 881 in this trial and our data showed more than half
had already failed oral antibiotic treatment; this reflects the pragmatic reality of decision-
making by clinicians. Thirdly, due to the deliberate design of this study comparing two
locations with two different antibiotics, the findings of this study cannot be attributed
solely to the location of treatment or to the different antibiotics. For example, the increased
adverse events in hospital compared to home could be due to location or antibiotic or a
combination of the two, so the trial results must be examined in detail when drawing
conclusions. This decision was made to ensure a combination of best practice and
translatability and the only comparison of clinical relevance in the real world. Lastly,
clinicians assessing the primary outcome could not be blinded to home versus hospital care.
While not having blinded assessors has the potential to introduce bias, we determined that
for translatability into clinical practice it was important that it was the ‘on the ground’
clinicians assessing the patients in front of them in real time. We believe we have
minimised the risk of bias by having both pre-determined criteria for ceasing intravenous
antibiotics and multiple clinicians in both arms making the assessments.
168
For children who require intravenous antibiotics for cellulitis, this study provides evidence
that treatment at home with short-course ceftriaxone is efficacious, safe, preferred by
patients and less costly, allowing children to avoid hospital admission with all of its
attendant benefits. In previously healthy children, the use of ceftriaxone at home did not
show a signal of increased acquisition of resistant organisms investigated, although larger
studies are now needed. Regardless, this finding should not be extrapolated to longer
courses of ceftriaxone and robust antimicrobial stewardship should remain a mainstay of
OPAT programs.
Contributors
LFI conceptualized, designed and coordinated the study, carried out the initial and
subsequent data analysis, drafted the initial manuscript, revised subsequent drafts and
approved the final manuscript as submitted. PAB, FEB, and SMH, were involved in the
design of the study, provided input into data analysis, reviewed and revised the manuscript
and approved the final draft. FO was involved in the design of the study, planned the
statistical analysis, carried out the initial data analysis, revised and approved the final
manuscript as submitted. AJD was involved in the design of the microbiology part of the
study, reviewed and revised the manuscript and approved the final draft. All authors
approved the final manuscript.
Declaration of interests
The authors listed above certify that they have no affiliations with any organisation or
entity with any financial or non-financial interest on the materials discussed in this
manuscript. The authors declare there are no competing interests of note. Funding
169
organisations had no role in study design, data collection, data analysis, data interpretation,
or writing of the report.
Acknowledgments
We would like to acknowledge the participation of patients and families and the RCH
Microbiology laboratory staff.
Funding
This study was funded in part by grants from the RCH Foundation, the Murdoch Children's
Research Institute (MCRI), the Victorian Department of Health, Melbourne Australia. LFI
was supported in part by a scholarship from AVANT Mutual Group Ltd, Melbourne, the
Melbourne Children’s Campus Postgraduate Health Research Scholarship and the Doctor
Nicholas Collins Fellowship. PAB was in part supported by a Melbourne Campus Clinician
Scientist Fellowship, Melbourne, Australia. FEB was supported in part by a grant from the
RCH Foundation and a Melbourne Campus Clinician Scientist Fellowship, Melbourne,
Australia and a National Health and Medical Research Council (NHMRC) Practitioner
Fellowship, Canberra, Australia. The emergency research group, MCRI, is in part
supported by an NHMRC Centre for Research Excellence Grant for Paediatric Emergency
Medicine, Canberra, Australia and the Victorian government infrastructure support
program.
References
1. Fernandes P, Milliren C, Mahoney-West HM, Schwartz L, Lachenauer CS,
Nakamura MM. Safety of Outpatient Parenteral Antimicrobial Therapy in Children.
Pediatr Infect Dis J 2017.
170
2. Hodgson KA, Huynh J, Ibrahim LF, et al. The use, appropriateness and outcomes of
outpatient parenteral antimicrobial therapy. Archives of disease in childhood 2016;
101(10): 886-93.
3. Elema A, Zalmstra TA, Boonstra AM, Narayanan UG, Reinders-Messelink HA,
AA VDP. Pain and hospital admissions are important factors associated with quality of life
in nonambulatory children. Acta paediatrica 2016; 105(9): e419-25.
4. Orme LM, Babl FE, Barnes C, Barnett P, Donath S, Ashley DM. Outpatient versus
inpatient IV antibiotic management for pediatric oncology patients with low risk febrile
neutropenia: a randomised trial. Pediatr Blood Cancer 2014; 61(8): 1427-33.
5. Hulten KG, Kaplan SL, Lamberth LB, et al. Hospital-acquired Staphylococcus
aureus infections at Texas Children's Hospital, 2001-2007. Infection control and hospital
epidemiology 2010; 31(2): 183-90.
6. Sartain SA, Maxwell MJ, Todd PJ, Haycox AR, Bundred PE. Users' views on
hospital and home care for acute illness in childhood. Health Soc Care Community 2001;
9(2): 108-17.
7. Hansson H, Kjaergaard H, Johansen C, et al. Hospital-based home care for children
with cancer: feasibility and psychosocial impact on children and their families. Pediatr
Blood Cancer 2013; 60(5): 865-72.
8. Bryant PA, Katz NT. Inpatient versus outpatient parenteral antibiotic therapy at
home for acute infections in children: a systematic review. The Lancet Infectious diseases
2017.
9. Caplan GA. A meta-analysis of "hospital in the home". Med J Aust 2013; 198(4):
195-6.
171
10. Sartain SA, Maxwell MJ, Todd PJ, et al. Randomised controlled trial comparing an
acute paediatric hospital at home scheme with conventional hospital care. Archives of
disease in childhood 2002; 87(5): 371-5.
11. Ibrahim LF, Hopper SM, Babl FE, Bryant PA. Who Can Safely Have Antibiotics at
Home? A Prospective Observational Study in Children with Moderate/Severe Cellulitis.
Pediatr Infect Dis J 2015.
12. Brugha RE, Abrahamson E. Ambulatory intravenous antibiotic therapy for children
with preseptal cellulitis. Pediatric emergency care 2012; 28(3): 226-8.
13. Gouin S, Chevalier I, Gauthier M, Lamarre V. Prospective evaluation of the
management of moderate to severe cellulitis with parenteral antibiotics at a paediatric day
treatment centre. Journal of paediatrics and child health 2008; 44(4): 214-8.
14. Frenkel LD. Once-daily administration of ceftriaxone for the treatment of selected
serious bacterial infections in children. Pediatrics 1988; 82(3 Pt 2): 486-91.
15. Washio M, Mizoue T, Kajioka T, et al. Risk factors for methicillin-resistant
Staphylococcus aureus (MRSA) infection in a Japanese geriatric hospital. Public health
1997; 111(3): 187-90.
16. McKinnell JA, Kunz DF, Chamot E, et al. Association between vancomycin-
resistant Enterococci bacteremia and ceftriaxone usage. Infection control and hospital
epidemiology 2012; 33(7): 718-24.
17. Meletiadis J, Turlej-Rogacka A, Lerner A, et al. Amplification of Antimicrobial
Resistance in Gut Flora of Patients Treated with Ceftriaxone. Antimicrobial agents and
chemotherapy 2017.
18. Lopez MA, Cruz AT, Kowalkowski MA, Raphael JL. Trends in resource utilization
for hospitalized children with skin and soft tissue infections. Pediatrics 2013; 131(3): e718-
25.
172
19. Ibrahim LF, Babl FE, Orsini F, Hopper SM, Bryant PA. Cellulitis: Home Or
Inpatient in Children from the Emergency Department (CHOICE): protocol for a
randomised controlled trial. BMJ open 2016; 6(1): e009606.
20. Bryant PA, Babl FE, Daley AJ, Hopper SM, Ibrahim LF. Blood Cultures in
Cellulitis are not Cost Effective and Should Prompt Investigation for an Alternative Focus.
The Paediatric Infectious Disease Journal 2016; 35(1)(January 2016): 118.
21. Malone JR, Durica SR, Thompson DM, Bogie A, Naifeh M. Blood cultures in the
evaluation of uncomplicated skin and soft tissue infections. Pediatrics 2013; 132(3): 454-9.
22. de Man P, Verhoeven BA, Verbrugh HA, Vos MC, van den Anker JN. An
antibiotic policy to prevent emergence of resistant bacilli. Lancet 2000; 355(9208): 973-8.
23. Carr D, Barnes EH, Gordon A, Isaacs D. Effect of antibiotic use on antimicrobial
antibiotic resistance and late-onset neonatal infections over 25 years in an Australian
tertiary neonatal unit. Archives of disease in childhood Fetal and neonatal edition 2017;
102(3): F244-F50.
24. Knudsen PK, Brandtzaeg P, Hoiby EA, et al. Impact of extensive antibiotic
treatment on faecal carriage of antibiotic-resistant enterobacteria in children in a low
resistance prevalence setting. PloS one 2017; 12(11): e0187618.
25. Prevot MH, Andremont A, Sancho-Garnier H, Tancrede C. Epidemiology of
intestinal colonization by members of the family Enterobacteriaceae resistant to cefotaxime
in a hematology-oncology unit. Antimicrobial agents and chemotherapy 1986; 30(6): 945-
7.
26. Adams DJ, Eberly MD, Rajnik M, Nylund CM. Risk Factors for Community-
Associated Clostridium difficile Infection in Children. The Journal of pediatrics 2017; 186:
105-9.
173
27. Melo MR, Ferreira-Magalhaes M, Flor-Lima F, et al. Dedicated Pediatricians in
Emergency Department: Shorter Waiting Times and Lower Costs. PloS one 2016; 11(8):
e0161149.
28. Paquet F, Marchionni C. What Is Your KVO? Historical Perspectives, Review of
Evidence, and a Survey About an Often Overlooked Nursing Practice. Journal of infusion
nursing : the official publication of the Infusion Nurses Society 2016; 39(1): 32-7.
29. Khangura S, Wallace J, Kissoon N, Kodeeswaran T. Management of cellulitis in a
pediatric emergency department. Pediatric emergency care 2007; 23(11): 805-11.
174
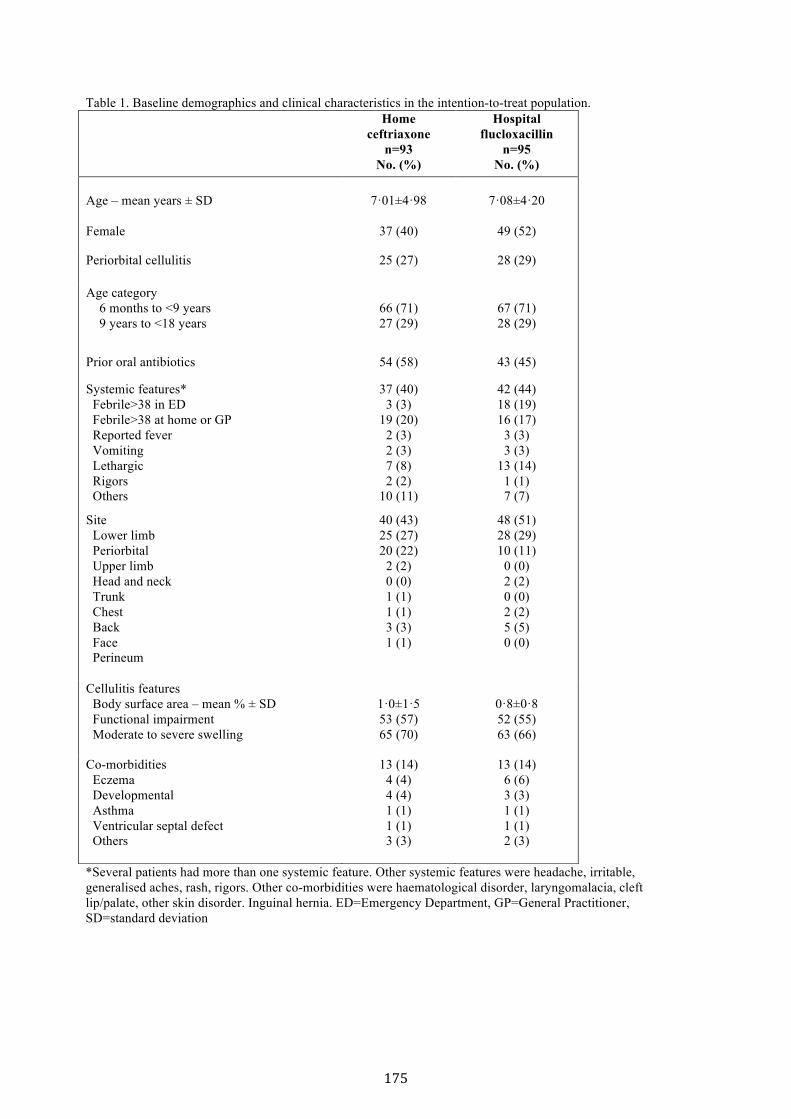
Table 1. Baseline demographics and clinical characteristics in the intention-to-treat population.
*Several patients had more than one systemic feature. Other systemic features were headache, irritable, generalised aches, rash, rigors. Other co-morbidities were haematological disorder, laryngomalacia, cleft lip/palate, other skin disorder. Inguinal hernia. ED=Emergency Department, GP=General Practitioner, SD=standard deviation
Home ceftriaxone
n=93 No. (%)
Hospital flucloxacillin
n=95 No. (%)
Age – mean years ± SD
7·01±4·98
7·08±4·20
Female 37 (40) 49 (52)
Periorbital cellulitis 25 (27) 28 (29)
Age category 6 months to <9 years 9 years to <18 years
66 (71) 27 (29)
67 (71) 28 (29)
Prior oral antibiotics 54 (58) 43 (45)
Systemic features* Febrile>38 in ED Febrile>38 at home or GP Reported fever Vomiting Lethargic Rigors Others
37 (40) 3 (3)
19 (20) 2 (3) 2 (3) 7 (8) 2 (2)
10 (11)
42 (44) 18 (19) 16 (17)
3 (3) 3 (3)
13 (14) 1 (1) 7 (7)
Site Lower limb Periorbital Upper limb Head and neck Trunk Chest Back Face Perineum
40 (43) 25 (27) 20 (22)
2 (2) 0 (0) 1 (1) 1 (1) 3 (3) 1 (1)
48 (51) 28 (29) 10 (11)
0 (0) 2 (2) 0 (0) 2 (2) 5 (5) 0 (0)
Cellulitis features Body surface area – mean % ± SD Functional impairment Moderate to severe swelling
1·0±1·5 53 (57) 65 (70)
0·8±0·8 52 (55) 63 (66)
Co-morbidities Eczema Developmental Asthma Ventricular septal defect Others
13 (14) 4 (4) 4 (4) 1 (1) 1 (1) 3 (3)
13 (14) 6 (6) 3 (3) 1 (1) 1 (1) 2 (3)
175
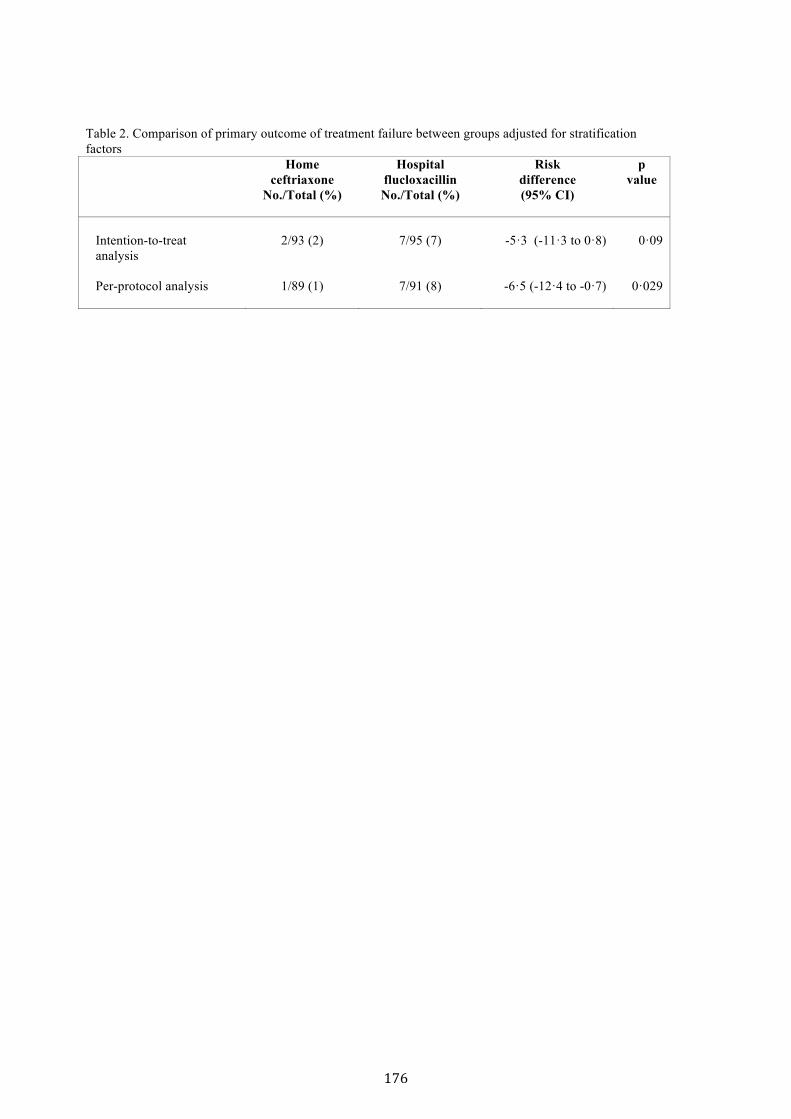
Table 2. Comparison of primary outcome of treatment failure between groups adjusted for stratification factors Home
ceftriaxone No./Total (%)
Hospital flucloxacillin No./Total (%)
Risk difference (95% CI)
p value
Intention-to-treat analysis Per-protocol analysis
2/93 (2)
1/89 (1)
7/95 (7)
7/91 (8)
-5·3 (-11·3 to 0·8)
-6·5 (-12·4 to -0·7)
0·09
0·029
176
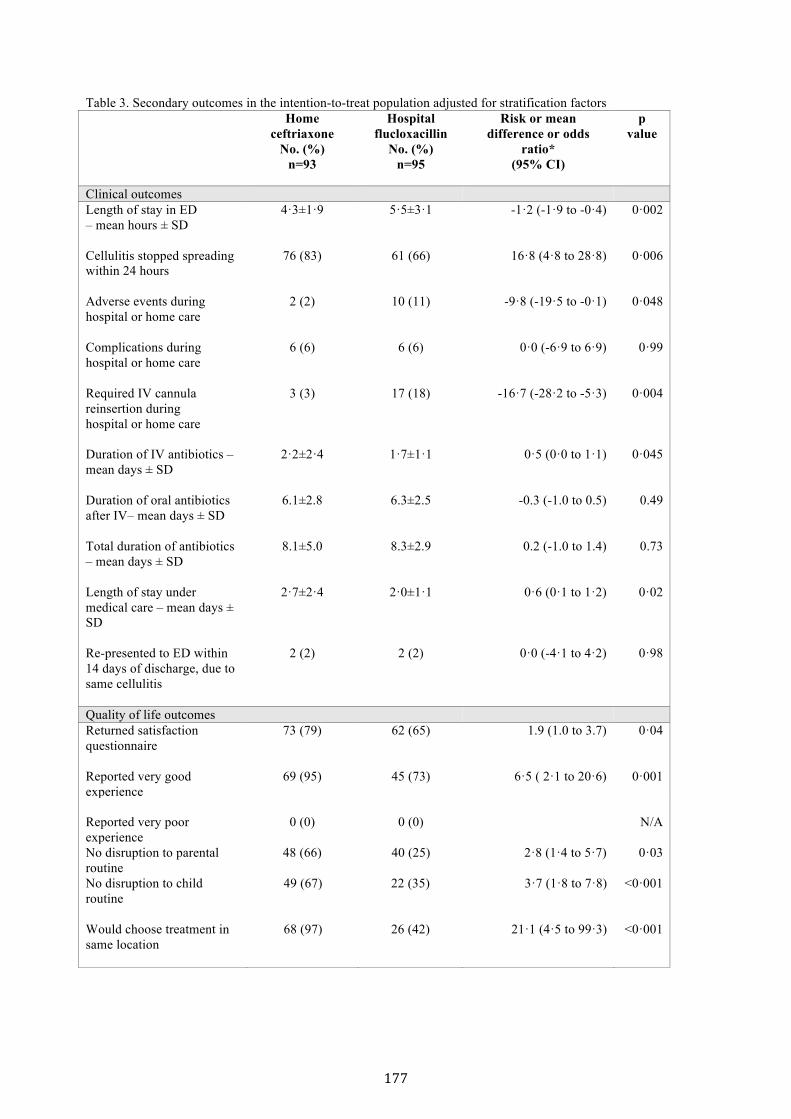
Table 3. Secondary outcomes in the intention-to-treat population adjusted for stratification factors
Home ceftriaxone
No. (%) n=93
Hospital flucloxacillin
No. (%) n=95
Risk or mean difference or odds
ratio* (95% CI)
p value
Clinical outcomes Length of stay in ED – mean hours ± SD
4·3±1·9 5·5±3·1 -1·2 (-1·9 to -0·4) 0·002
Cellulitis stopped spreading within 24 hours
76 (83) 61 (66) 16·8 (4·8 to 28·8) 0·006
Adverse events during hospital or home care
2 (2) 10 (11) -9·8 (-19·5 to -0·1) 0·048
Complications during hospital or home care
6 (6) 6 (6) 0·0 (-6·9 to 6·9) 0·99
Required IV cannula reinsertion during hospital or home care
3 (3) 17 (18) -16·7 (-28·2 to -5·3) 0·004
Duration of IV antibiotics – mean days ± SD
2·2±2·4 1·7±1·1 0·5 (0·0 to 1·1) 0·045
Duration of oral antibiotics after IV– mean days ± SD
6.1±2.8 6.3±2.5 -0.3 (-1.0 to 0.5) 0.49
Total duration of antibiotics – mean days ± SD
8.1±5.0 8.3±2.9 0.2 (-1.0 to 1.4) 0.73
Length of stay under medical care – mean days ± SD
2·7±2·4 2·0±1·1 0·6 (0·1 to 1·2) 0·02
Re-presented to ED within 14 days of discharge, due to same cellulitis
2 (2) 2 (2) 0·0 (-4·1 to 4·2) 0·98
Quality of life outcomes Returned satisfaction questionnaire
73 (79) 62 (65) 1.9 (1.0 to 3.7) 0·04
Reported very good experience
69 (95)
45 (73)
6·5 ( 2·1 to 20·6)
0·001
Reported very poor experience
0 (0)
0 (0)
N/A
No disruption to parental routine
48 (66)
40 (25) 2·8 (1·4 to 5·7) 0·03
No disruption to child routine
49 (67) 22 (35) 3·7 (1·8 to 7·8)
<0·001
Would choose treatment in same location
68 (97)
26 (42)
21·1 (4·5 to 99·3) <0·001
177

*Risk difference is reported for binary outcomes and mean difference for continuous outcomes, odds ratios are presented for questionnaire responses. Percentages for satisfaction questionnaire are based on those who returned the questionnaires (questionnaire responses are not corrected for stratification factors). ED=Emergency Department, IV=intravenous, SD=standard deviation
178
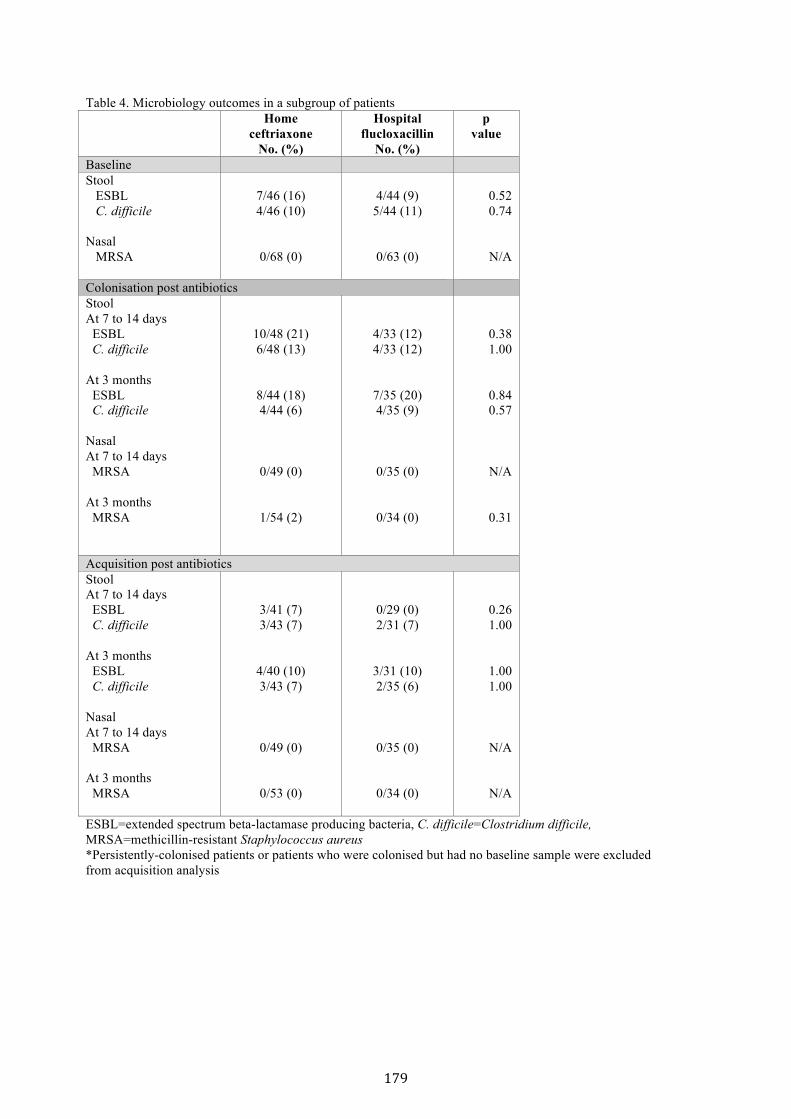
Table 4. Microbiology outcomes in a subgroup of patients Home
ceftriaxone No. (%)
Hospital flucloxacillin
No. (%)
p value
Baseline Stool ESBL C. difficile Nasal MRSA
7/46 (16) 4/46 (10)
0/68 (0)
4/44 (9)
5/44 (11)
0/63 (0)
0.52 0.74
N/A
Colonisation post antibiotics Stool At 7 to 14 days ESBL C. difficile At 3 months ESBL C. difficile Nasal At 7 to 14 days MRSA At 3 months MRSA
10/48 (21) 6/48 (13)
8/44 (18) 4/44 (6)
0/49 (0)
1/54 (2)
4/33 (12) 4/33 (12)
7/35 (20) 4/35 (9)
0/35 (0)
0/34 (0)
0.38 1.00
0.84 0.57
N/A
0.31
Acquisition post antibiotics Stool At 7 to 14 days ESBL C. difficile At 3 months ESBL C. difficile Nasal At 7 to 14 days MRSA At 3 months MRSA
3/41 (7) 3/43 (7)
4/40 (10) 3/43 (7)
0/49 (0)
0/53 (0)
0/29 (0) 2/31 (7)
3/31 (10) 2/35 (6)
0/35 (0)
0/34 (0)
0.26 1.00
1.00 1.00
N/A
N/A
ESBL=extended spectrum beta-lactamase producing bacteria, C. difficile=Clostridium difficile, MRSA=methicillin-resistant Staphylococcus aureus *Persistently-colonised patients or patients who were colonised but had no baseline sample were excluded from acquisition analysis
179
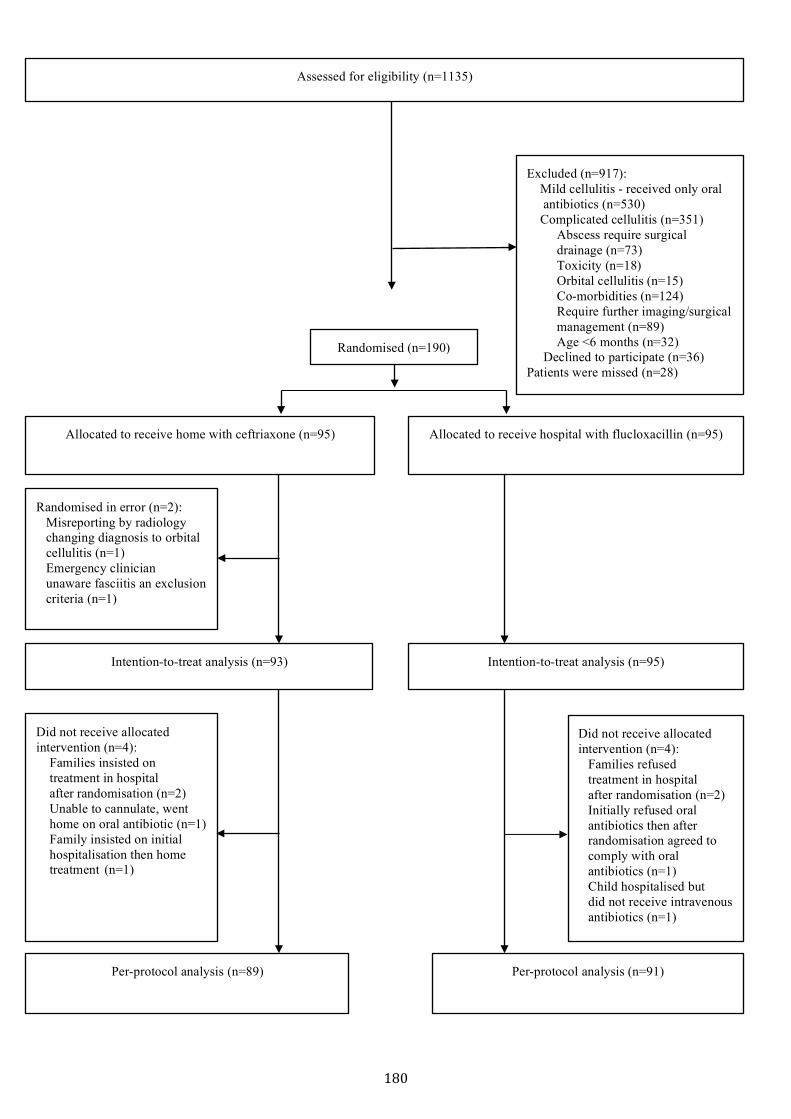
Excluded (n=917): Mild cellulitis - received only oral antibiotics (n=530) Complicated cellulitis (n=351) Abscess require surgical drainage (n=73) Toxicity (n=18) Orbital cellulitis (n=15) Co-morbidities (n=124) Require further imaging/surgical management (n=89) Age <6 months (n=32) Declined to participate (n=36) Patients were missed (n=28)
Randomised (n=190)
Randomised in error (n=2): Misreporting by radiology changing diagnosis to orbital cellulitis (n=1) Emergency clinician unaware fasciitis an exclusion criteria (n=1)
Allocated to receive home with ceftriaxone (n=95)
Assessed for eligibility (n=1135)
Allocated to receive hospital with flucloxacillin (n=95)
Per-protocol analysis (n=89)
Per-protocol analysis (n=91)
Did not receive allocated intervention (n=4): Families insisted on treatment in hospital after randomisation (n=2) Unable to cannulate, went home on oral antibiotic (n=1) Family insisted on initial hospitalisation then home treatment (n=1)
Did not receive allocated intervention (n=4): Families refused treatment in hospital after randomisation (n=2) Initially refused oral antibiotics then after randomisation agreed to comply with oral antibiotics (n=1) Child hospitalised but did not receive intravenous antibiotics (n=1)
Intention-to-treat analysis (n=93)
Intention-to-treat analysis (n=95)
180

Legend Figure 1. Trial profile The intention-to-treat analysis included all randomised participants where outcome data were available, regardless of treatment received. The per-protocol analysis included all individuals that received treatment as per randomised allocation and did not encounter any major protocol violation such as: received treatment in the hospital if randomised to the home group, or received treatment at home if randomised to hospital group or did not receive any study treatment.
181
Appendix Table of Contents
Exclusion criteria ...................................................................................................................................... 2
Supplementary microbiology methodology .............................................................................................. 2 Stool specimen .................................................................................................................................... 2 Nasal specimen .................................................................................................................................... 2
Supplementary tables ................................................................................................................................ 3 Supplementary table 1. Secondary outcomes in the per-protocol analyses adjusted for stratification factors ................................................................................................................................................... 3 Supplementary table 2. Comparison of baseline characteristics and clinical outcomes between patients who provided nasal samples and those who did not at baseline, 7-14 days and 3 months ..... 4 Supplementary table 3. Comparison of baseline characteristics and outcomes of patients who provided stool samples and those who did not at baseline, 7-14 days and 3 months .......................... 5 Supplementary table 4. Comparison of baseline characteristics and outcomes between those who failed prior oral antibiotics and those who did not receive any adjusted for stratification factors ...... 6 Supplementary table 5. Comparison of primary and secondary outcomes for those with periorbital cellulitis ................................................................................................................................................ 7 Supplementary table 6. Comparison of primary and secondary outcomes for those aged 6 months to 9 years ..................................................................................................................................................... 8 Supplementary table 7. Comparison of primary and secondary outcomes for those aged more than 9 years ..................................................................................................................................................... 9
182
Exclusion criteria Children were excluded if they had complicated cellulitis (orbital cellulitis or unable to exclude orbital cellulitis, penetrating injury/bites, suspected/confirmed foreign body, suspected fasciitis or myositis, varicella, undrained abscess including dental abscess), toxicity (tachycardia when afebrile or hypotension, poor central perfusion), underlying comorbidities (immunosuppression, liver, disease, any concurrent infection necessitating different antibiotic treatment to intravenous flucloxacillin or ceftriaxone monotherapy), other medical diagnoses necessitating admission to hospital for observation or treatment relating to the known medical condition, unable to obtain intravenous access, age <6 months old, with mild cellulitis (i.e. can be treated with oral antibiotics)
Supplementary microbiology methodology
Stool specimen Participants were provided with stool jars and provided with verbal and written instructions. Once stool was obtained using the attached spatula, the stool jars were refrigerated and collected within 12 hours and transported to the hospital laboratory where they were processed within 24 hours.
C. difficile detection: Three steps: 1) Qualitative enzyme immunoassay screening of stool usingglutamate dehydrogenase to detect C. difficile antigen (ImmunoCard C. difficile GDH (MeridianBioscience, Inc.)); 2) Positive results confirmed by PCR testing for toxigenic genes Toxin B, binarytoxin and the tcdC deletion (Xpert C.difficile assay Cepheid). 3) Culture: Samples are inoculated ontochromogenic C. difficile agar plate (chromID™ Biomerieux) and incubated anaerobically for 24 hours.Suspected C.difficile colonies are subcultured onto horse blood agar for 24-48 hours. Anaerobiccolonies are Gram stained and sent for Maldi-TOF identification.
ESBL detection: Samples are plated on ESBL screening agar plates producing 1 µg/ml cefotaxime and 3 µg/ml vancomycin for detection of ESBL-producing organisms and incubated overnight in air at 35°C. An oxidase test is done for any Gram-negative bacillus cultured. If it is oxidase positive, the screen is negative. If oxidase negative, VITEK 2 GN AST (Biomerieux) cards are set up for identification, sensitivity assays and ESBL detection.
VRE detection: Samples are inoculated directly onto chromogenic agar plates, Brilliance VRE (Oxoid) and incubated at 37°C in air for 24-48 hours. Plates were inspected for suspicious colonies at 24 hours then at 28 hours. Suspicious colonies were followed up by performing Streptococcal grouping. If group D is identified, a VITEK 2 GN AST (Biomerieux) cards are set up for identification sensitivity testing.
Nasal specimen A nasal swab was gently twirled in both anterior nares and immediately placed in Amies charcoal transport medium and processed in the microbiology laboratory within 12 hours of sampling.
MRSA detection: Nasal swabs are inoculated onto mannitol salt agar, horse blood agar (HBA) and MacConkey agar, and incubated at 35°C in air for 2 days. Colonies suggestive of Staphylococcus have Staph latex (Prolex) testing and are subcultured on DNase agar for S. aureus confirmation. Antibiotic susceptibility testing is done on a VITEK 2 GN AST (Biomerieux) and interpreted per the CLSI guideline.
183
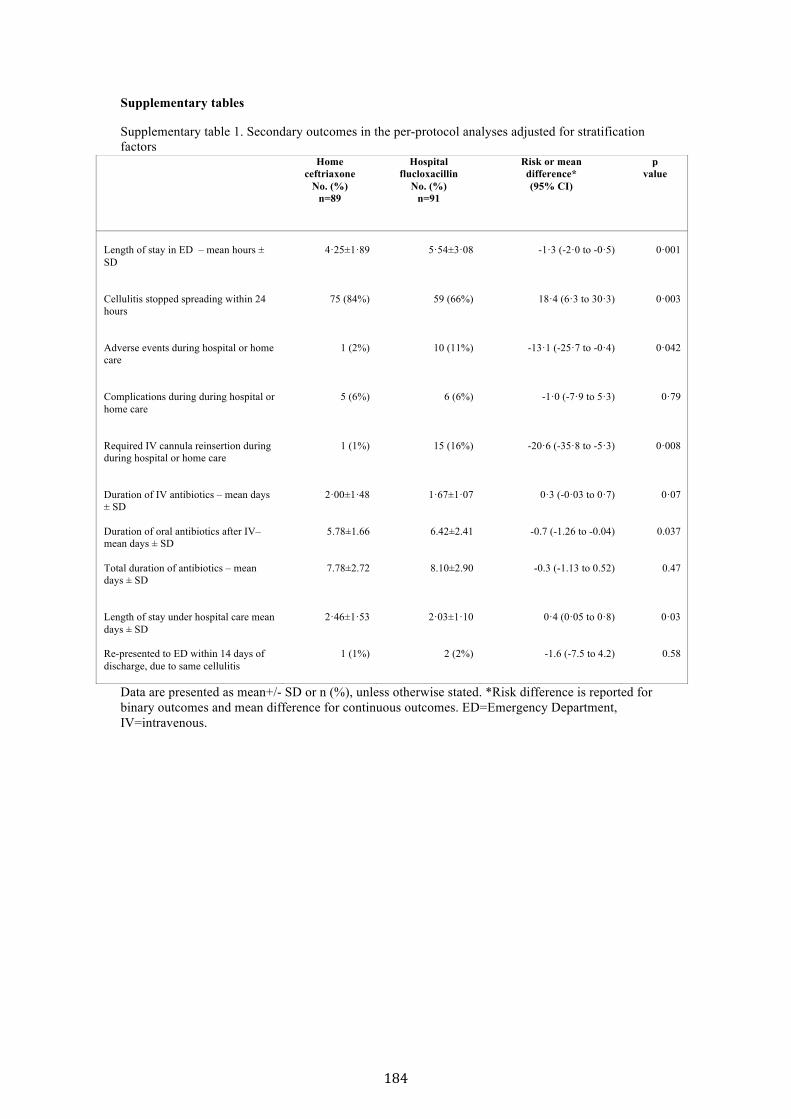
Supplementary tables
Supplementary table 1. Secondary outcomes in the per-protocol analyses adjusted for stratification factors
Data are presented as mean+/- SD or n (%), unless otherwise stated. *Risk difference is reported for binary outcomes and mean difference for continuous outcomes. ED=Emergency Department, IV=intravenous.
Home ceftriaxone
No. (%) n=89
Hospital flucloxacillin
No. (%) n=91
Risk or mean difference* (95% CI)
p value
Length of stay in ED – mean hours ± SD
4·25±1·89
5·54±3·08
-1·3 (-2·0 to -0·5)
0·001
Cellulitis stopped spreading within 24 hours
75 (84%)
59 (66%)
18·4 (6·3 to 30·3)
0·003
Adverse events during hospital or home care
1 (2%)
10 (11%)
-13·1 (-25·7 to -0·4)
0·042
Complications during during hospital or home care
5 (6%)
6 (6%)
-1·0 (-7·9 to 5·3)
0·79
Required IV cannula reinsertion during during hospital or home care
1 (1%)
15 (16%)
-20·6 (-35·8 to -5·3)
0·008
Duration of IV antibiotics – mean days ± SD Duration of oral antibiotics after IV– mean days ± SD Total duration of antibiotics – mean days ± SD
2·00±1·48
5.78±1.66
7.78±2.72
1·67±1·07
6.42±2.41
8.10±2.90
0·3 (-0·03 to 0·7)
-0.7 (-1.26 to -0.04)
-0.3 (-1.13 to 0.52)
0·07
0.037
0.47
Length of stay under hospital care mean days ± SD Re-presented to ED within 14 days of discharge, due to same cellulitis
2·46±1·53
1 (1%)
2·03±1·10
2 (2%)
0·4 (0·05 to 0·8)
-1.6 (-7.5 to 4.2)
0·03
0.58
184
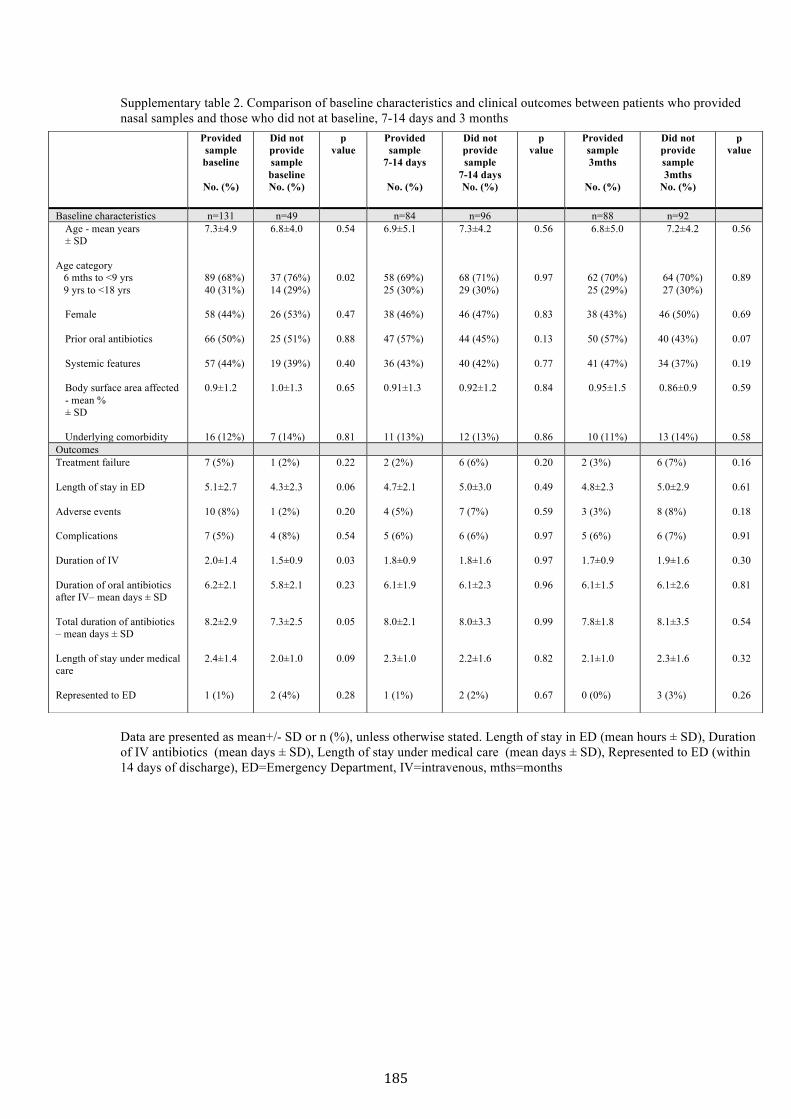
Supplementary table 2. Comparison of baseline characteristics and clinical outcomes between patients who provided nasal samples and those who did not at baseline, 7-14 days and 3 months
Data are presented as mean+/- SD or n (%), unless otherwise stated. Length of stay in ED (mean hours ± SD), Duration of IV antibiotics (mean days ± SD), Length of stay under medical care (mean days ± SD), Represented to ED (within 14 days of discharge), ED=Emergency Department, IV=intravenous, mths=months
Provided sample baseline
No. (%)
Did not provide sample baseline No. (%)
p value
Provided sample
7-14 days
No. (%)
Did not provide sample
7-14 days No. (%)
p value
Provided sample 3mths
No. (%)
Did not provide sample 3mths
No. (%)
p value
Baseline characteristics n=131 n=49 n=84 n=96 n=88 n=92 Age - mean years ± SD
Age category 6 mths to <9 yrs 9 yrs to <18 yrs
Female Prior oral antibiotics Systemic features Body surface area affected - mean % ± SD Underlying comorbidity
7.3±4.9 89 (68%) 40 (31%) 58 (44%) 66 (50%) 57 (44%) 0.9±1.2 16 (12%)
6.8±4.0 37 (76%) 14 (29%) 26 (53%) 25 (51%) 19 (39%) 1.0±1.3 7 (14%)
0.54
0.02 0.47 0.88 0.40 0.65 0.81
6.9±5.1 58 (69%) 25 (30%) 38 (46%) 47 (57%) 36 (43%) 0.91±1.3 11 (13%)
7.3±4.2 68 (71%) 29 (30%) 46 (47%) 44 (45%) 40 (42%) 0.92±1.2 12 (13%)
0.56 0.97 0.83 0.13 0.77 0.84 0.86
6.8±5.0
62 (70%) 25 (29%)
38 (43%)
50 (57%)
41 (47%)
0.95±1.5
10 (11%)
7.2±4.2
64 (70%) 27 (30%)
46 (50%)
40 (43%)
34 (37%)
0.86±0.9
13 (14%)
0.56 0.89 0.69 0.07 0.19 0.59 0.58
Outcomes Treatment failure Length of stay in ED Adverse events Complications Duration of IV Duration of oral antibiotics after IV– mean days ± SD Total duration of antibiotics – mean days ± SD Length of stay under medical care Represented to ED
7 (5%) 5.1±2.7 10 (8%) 7 (5%) 2.0±1.4 6.2±2.1 8.2±2.9
2.4±1.4 1 (1%)
1 (2%) 4.3±2.3 1 (2%) 4 (8%) 1.5±0.9 5.8±2.1 7.3±2.5
2.0±1.0 2 (4%)
0.22 0.06 0.20 0.54 0.03 0.23 0.05
0.09 0.28
2 (2%) 4.7±2.1 4 (5%) 5 (6%) 1.8±0.9 6.1±1.9 8.0±2.1
2.3±1.0 1 (1%)
6 (6%) 5.0±3.0 7 (7%)
6 (6%) 1.8±1.6 6.1±2.3 8.0±3.3
2.2±1.6
2 (2%)
0.20 0.49 0.59 0.97 0.97 0.96 0.99
0.82 0.67
2 (3%) 4.8±2.3 3 (3%) 5 (6%) 1.7±0.9 6.1±1.5 7.8±1.8
2.1±1.0 0 (0%)
6 (7%) 5.0±2.9 8 (8%) 6 (7%) 1.9±1.6 6.1±2.6 8.1±3.5
2.3±1.6
3 (3%)
0.16 0.61 0.18 0.91 0.30 0.81 0.54
0.32 0.26
185
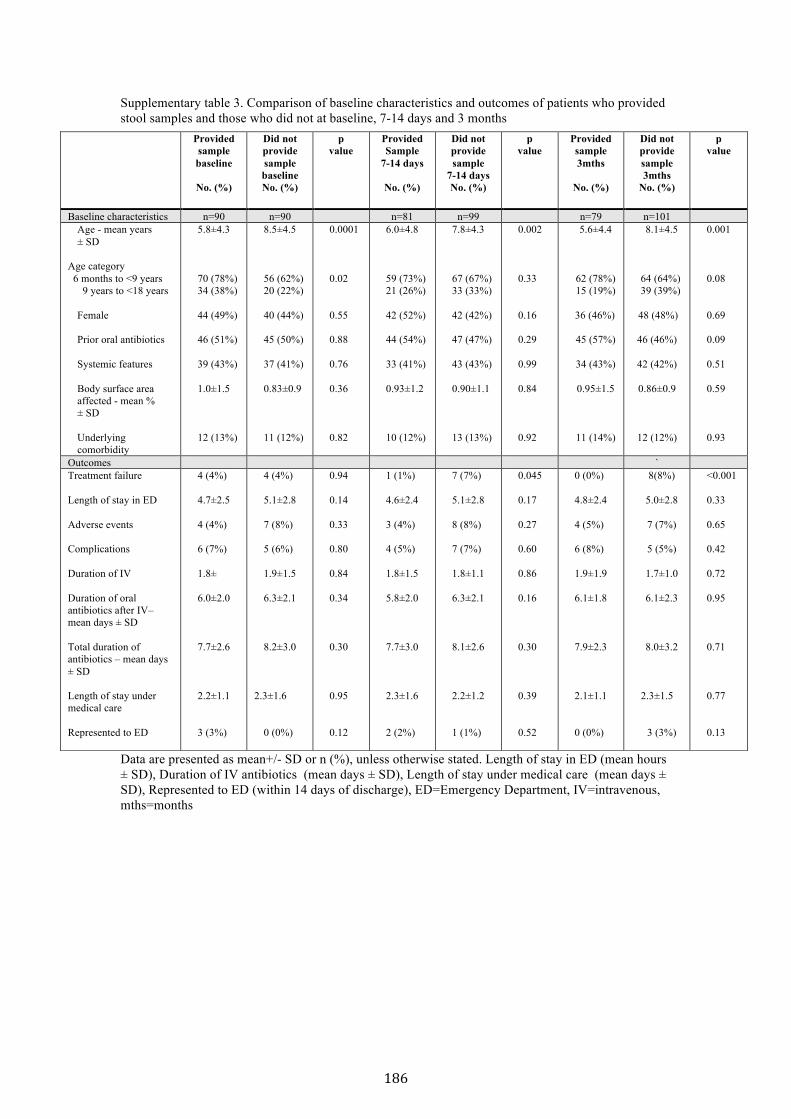
Supplementary table 3. Comparison of baseline characteristics and outcomes of patients who provided stool samples and those who did not at baseline, 7-14 days and 3 months
Data are presented as mean+/- SD or n (%), unless otherwise stated. Length of stay in ED (mean hours ± SD), Duration of IV antibiotics (mean days ± SD), Length of stay under medical care (mean days ± SD), Represented to ED (within 14 days of discharge), ED=Emergency Department, IV=intravenous, mths=months
Provided sample baseline
No. (%)
Did not provide sample baseline No. (%)
p value
Provided Sample
7-14 days
No. (%)
Did not provide sample
7-14 days No. (%)
p value
Provided sample 3mths
No. (%)
Did not provide sample 3mths
No. (%)
p value
Baseline characteristics n=90 n=90 n=81 n=99 n=79 n=101 Age - mean years ± SD
Age category 6 months to <9 years
9 years to <18 years Female Prior oral antibiotics Systemic features Body surface area affected - mean % ± SD Underlying comorbidity
5.8±4.3 70 (78%) 34 (38%) 44 (49%) 46 (51%) 39 (43%) 1.0±1.5 12 (13%)
8.5±4.5 56 (62%) 20 (22%) 40 (44%) 45 (50%) 37 (41%) 0.83±0.9 11 (12%)
0.0001
0.02 0.55 0.88 0.76 0.36 0.82
6.0±4.8 59 (73%) 21 (26%) 42 (52%) 44 (54%) 33 (41%) 0.93±1.2 10 (12%)
7.8±4.3 67 (67%) 33 (33%) 42 (42%) 47 (47%) 43 (43%) 0.90±1.1 13 (13%)
0.002 0.33 0.16 0.29 0.99 0.84 0.92
5.6±4.4
62 (78%) 15 (19%)
36 (46%)
45 (57%)
34 (43%)
0.95±1.5
11 (14%)
8.1±4.5
64 (64%) 39 (39%)
48 (48%)
46 (46%)
42 (42%)
0.86±0.9
12 (12%)
0.001 0.08 0.69 0.09 0.51 0.59 0.93
Outcomes ` Treatment failure Length of stay in ED Adverse events Complications Duration of IV Duration of oral antibiotics after IV– mean days ± SD Total duration of antibiotics – mean days ± SD Length of stay under medical care Represented to ED
4 (4%) 4.7±2.5 4 (4%) 6 (7%) 1.8± 6.0±2.0 7.7±2.6 2.2±1.1 3 (3%)
4 (4%) 5.1±2.8 7 (8%) 5 (6%) 1.9±1.5 6.3±2.1 8.2±3.0
2.3±1.6
0 (0%)
0.94 0.14 0.33 0.80 0.84 0.34 0.30 0.95 0.12
1 (1%) 4.6±2.4 3 (4%) 4 (5%) 1.8±1.5 5.8±2.0 7.7±3.0 2.3±1.6 2 (2%)
7 (7%) 5.1±2.8 8 (8%)
7 (7%) 1.8±1.1 6.3±2.1 8.1±2.6 2.2±1.2 1 (1%)
0.045 0.17 0.27 0.60 0.86 0.16 0.30 0.39 0.52
0 (0%) 4.8±2.4 4 (5%) 6 (8%) 1.9±1.9 6.1±1.8 7.9±2.3 2.1±1.1 0 (0%)
8(8%)
5.0±2.8
7 (7%)
5 (5%)
1.7±1.0
6.1±2.3
8.0±3.2
2.3±1.5
3 (3%)
<0.001 0.33 0.65 0.42 0.72 0.95 0.71 0.77 0.13
186
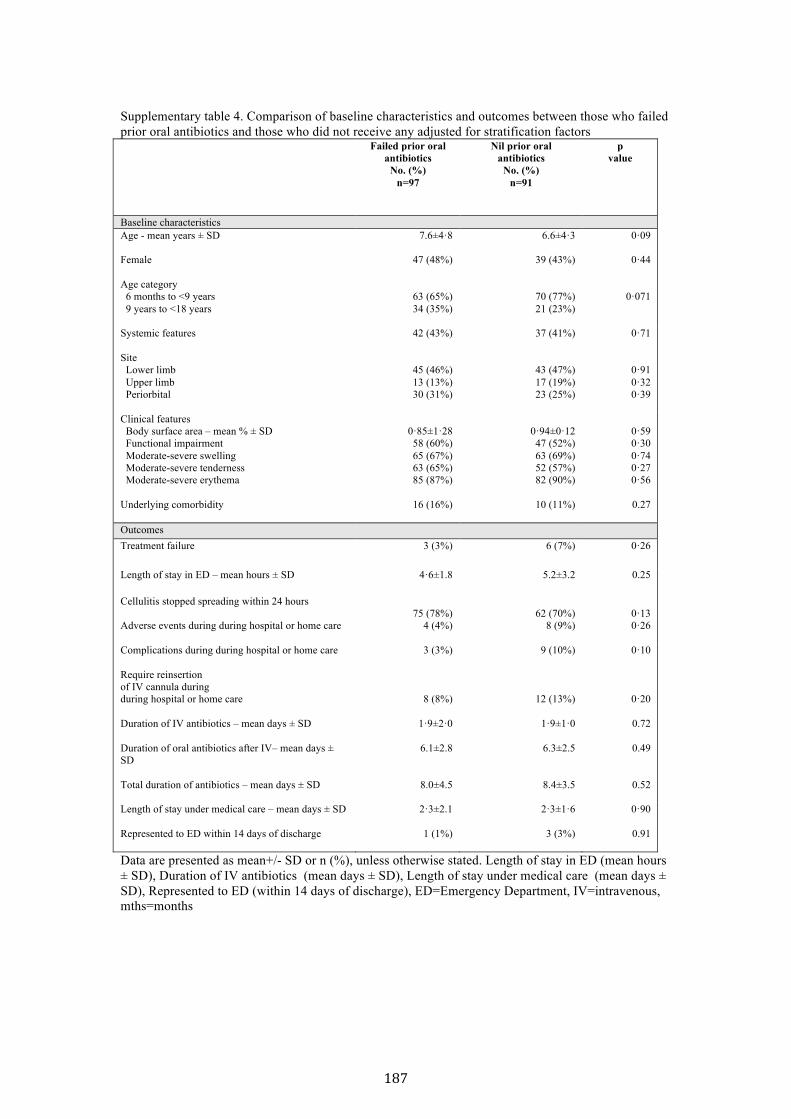
Supplementary table 4. Comparison of baseline characteristics and outcomes between those who failed prior oral antibiotics and those who did not receive any adjusted for stratification factors
Failed prior oral antibiotics
No. (%) n=97
Nil prior oral antibiotics
No. (%) n=91
p value
Baseline characteristics Age - mean years ± SD
7.6±4·8 6.6±4·3 0·09
Female 47 (48%)
39 (43%)
0·44
Age category 6 months to <9 years 9 years to <18 years
63 (65%) 34 (35%)
70 (77%) 21 (23%)
0·071
Systemic features
42 (43%)
37 (41%)
0·71
Site Lower limb Upper limb Periorbital
45 (46%) 13 (13%) 30 (31%)
43 (47%) 17 (19%) 23 (25%)
0·91 0·32 0·39
Clinical features Body surface area – mean % ± SD Functional impairment Moderate-severe swelling Moderate-severe tenderness Moderate-severe erythema Underlying comorbidity
0·85±1·28 58 (60%) 65 (67%) 63 (65%) 85 (87%)
16 (16%)
0·94±0·12 47 (52%) 63 (69%) 52 (57%) 82 (90%)
10 (11%)
0·59 0·30 0·74 0·27 0·56
0.27
Outcomes Treatment failure 3 (3%) 6 (7%) 0·26
Length of stay in ED – mean hours ± SD 4·6±1.8 5.2±3.2 0.25
Cellulitis stopped spreading within 24 hours
75 (78%)
62 (70%)
0·13
Adverse events during during hospital or home care
4 (4%) 8 (9%) 0·26
Complications during during hospital or home care
3 (3%) 9 (10%) 0·10
Require reinsertion of IV cannula during during hospital or home care
8 (8%)
12 (13%)
0·20
Duration of IV antibiotics – mean days ± SD Duration of oral antibiotics after IV– mean days ± SD Total duration of antibiotics – mean days ± SD
1·9±2·0
6.1±2.8
8.0±4.5
1·9±1·0
6.3±2.5
8.4±3.5
0.72
0.49
0.52
Length of stay under medical care – mean days ± SD
2·3±2.1 2·3±1·6 0·90
Represented to ED within 14 days of discharge
1 (1%) 3 (3%) 0.91
Data are presented as mean+/- SD or n (%), unless otherwise stated. Length of stay in ED (mean hours ± SD), Duration of IV antibiotics (mean days ± SD), Length of stay under medical care (mean days ± SD), Represented to ED (within 14 days of discharge), ED=Emergency Department, IV=intravenous, mths=months
187
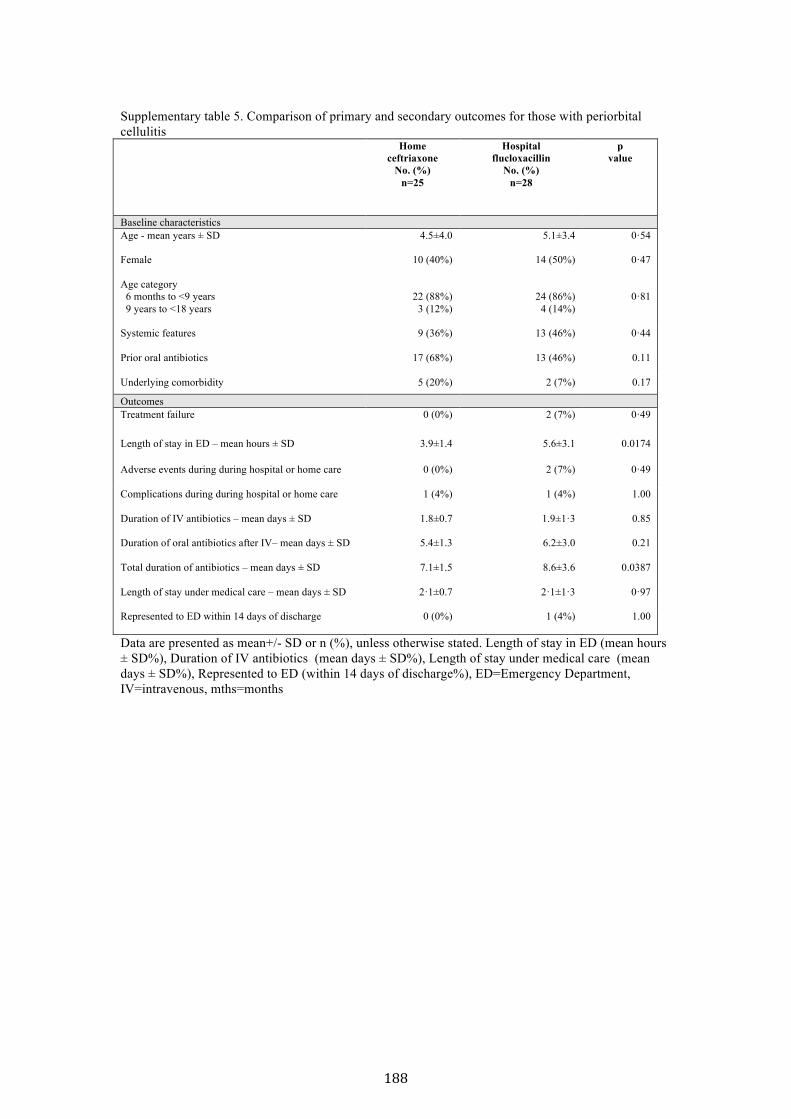
Supplementary table 5. Comparison of primary and secondary outcomes for those with periorbital cellulitis
Home ceftriaxone
No. (%) n=25
Hospital flucloxacillin
No. (%) n=28
p value
Baseline characteristics Age - mean years ± SD
4.5±4.0 5.1±3.4 0·54
Female 10 (40%)
14 (50%)
0·47
Age category 6 months to <9 years 9 years to <18 years
22 (88%)
3 (12%)
24 (86%)
4 (14%)
0·81
Systemic features Prior oral antibiotics
9 (36%)
17 (68%)
13 (46%)
13 (46%)
0·44
0.11
Underlying comorbidity 5 (20%) 2 (7%) 0.17
Outcomes Treatment failure 0 (0%) 2 (7%) 0·49
Length of stay in ED – mean hours ± SD 3.9±1.4 5.6±3.1 0.0174
Adverse events during during hospital or home care
0 (0%) 2 (7%) 0·49
Complications during during hospital or home care
1 (4%) 1 (4%) 1.00
Duration of IV antibiotics – mean days ± SD Duration of oral antibiotics after IV– mean days ± SD Total duration of antibiotics – mean days ± SD
1.8±0.7
5.4±1.3
7.1±1.5
1.9±1·3
6.2±3.0
8.6±3.6
0.85
0.21
0.0387
Length of stay under medical care – mean days ± SD
2·1±0.7 2·1±1·3 0·97
Represented to ED within 14 days of discharge
0 (0%) 1 (4%) 1.00
Data are presented as mean+/- SD or n (%), unless otherwise stated. Length of stay in ED (mean hours ± SD%), Duration of IV antibiotics (mean days ± SD%), Length of stay under medical care (mean days ± SD%), Represented to ED (within 14 days of discharge%), ED=Emergency Department, IV=intravenous, mths=months
188
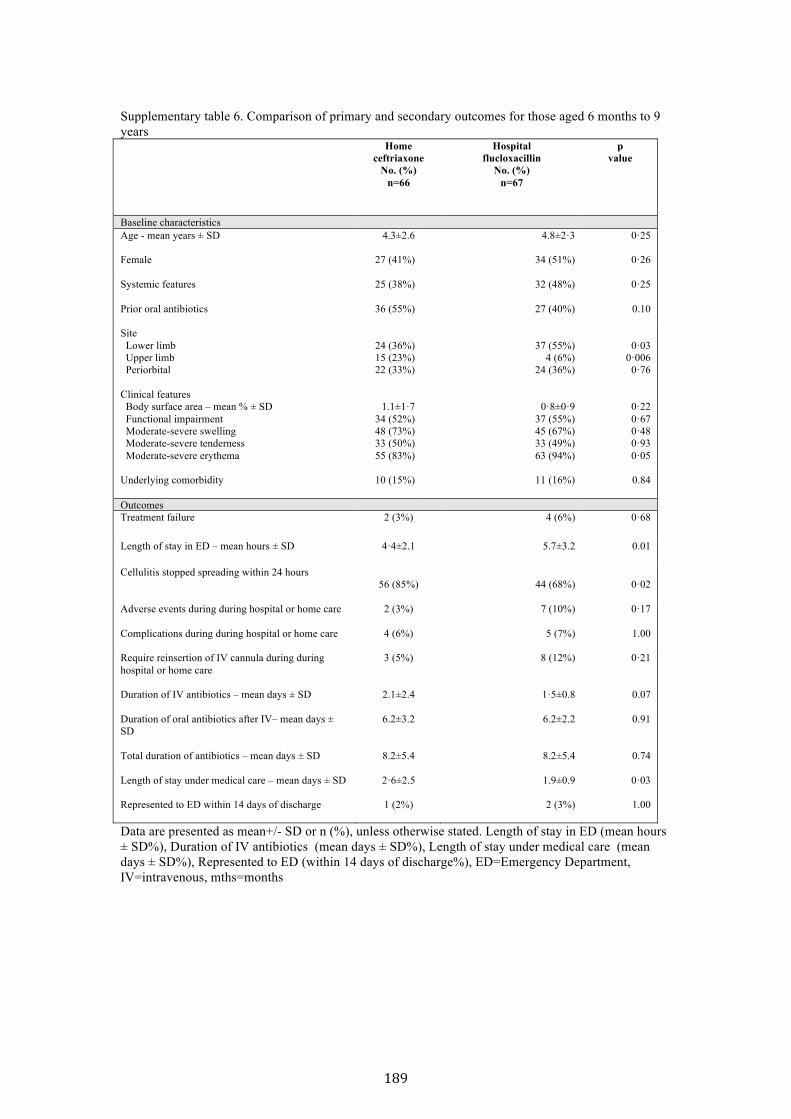
Supplementary table 6. Comparison of primary and secondary outcomes for those aged 6 months to 9 years
Home ceftriaxone
No. (%) n=66
Hospital flucloxacillin
No. (%) n=67
p value
Baseline characteristics Age - mean years ± SD
4.3±2.6 4.8±2·3 0·25
Female 27 (41%)
34 (51%)
0·26
Systemic features Prior oral antibiotics
25 (38%)
36 (55%)
32 (48%)
27 (40%)
0·25
0.10
Site Lower limb Upper limb Periorbital
24 (36%) 15 (23%) 22 (33%)
37 (55%)
4 (6%) 24 (36%)
0·03
0·006 0·76
Clinical features Body surface area – mean % ± SD Functional impairment Moderate-severe swelling Moderate-severe tenderness Moderate-severe erythema Underlying comorbidity
1.1±1·7
34 (52%) 48 (73%) 33 (50%) 55 (83%)
10 (15%)
0·8±0·9
37 (55%) 45 (67%) 33 (49%) 63 (94%)
11 (16%)
0·22 0·67 0·48 0·93 0·05
0.84
Outcomes Treatment failure 2 (3%) 4 (6%) 0·68
Length of stay in ED – mean hours ± SD 4·4±2.1 5.7±3.2 0.01
Cellulitis stopped spreading within 24 hours
56 (85%)
44 (68%)
0·02
Adverse events during during hospital or home care
2 (3%) 7 (10%)
0·17
Complications during during hospital or home care
4 (6%) 5 (7%) 1.00
Require reinsertion of IV cannula during during hospital or home care
3 (5%) 8 (12%) 0·21
Duration of IV antibiotics – mean days ± SD Duration of oral antibiotics after IV– mean days ± SD Total duration of antibiotics – mean days ± SD
2.1±2.4
6.2±3.2
8.2±5.4
1·5±0.8
6.2±2.2
8.2±5.4
0.07
0.91
0.74
Length of stay under medical care – mean days ± SD
2·6±2.5 1.9±0.9 0·03
Represented to ED within 14 days of discharge
1 (2%) 2 (3%) 1.00
Data are presented as mean+/- SD or n (%), unless otherwise stated. Length of stay in ED (mean hours ± SD%), Duration of IV antibiotics (mean days ± SD%), Length of stay under medical care (mean days ± SD%), Represented to ED (within 14 days of discharge%), ED=Emergency Department, IV=intravenous, mths=months
189
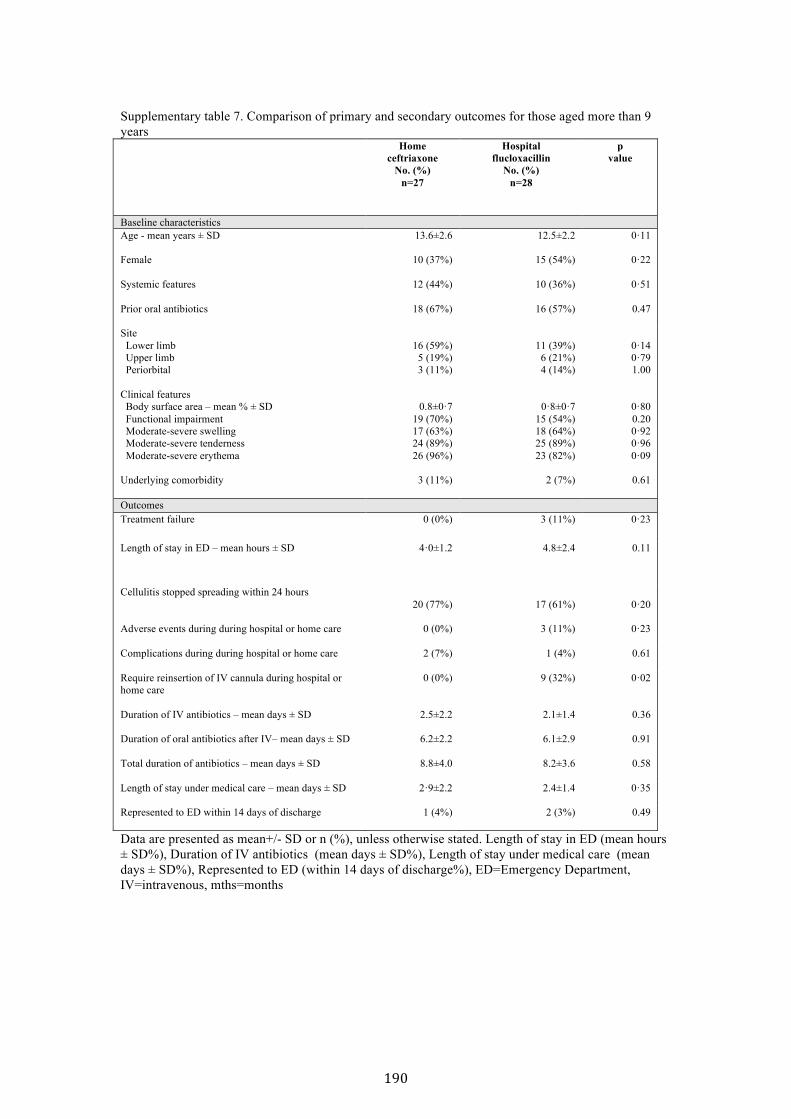
Supplementary table 7. Comparison of primary and secondary outcomes for those aged more than 9 years
Home ceftriaxone
No. (%) n=27
Hospital flucloxacillin
No. (%) n=28
p value
Baseline characteristics Age - mean years ± SD
13.6±2.6 12.5±2.2 0·11
Female 10 (37%)
15 (54%)
0·22
Systemic features Prior oral antibiotics
12 (44%)
18 (67%)
10 (36%)
16 (57%)
0·51
0.47
Site Lower limb Upper limb Periorbital
16 (59%)
5 (19%) 3 (11%)
11 (39%)
6 (21%) 4 (14%)
0·14 0·79 1.00
Clinical features Body surface area – mean % ± SD Functional impairment Moderate-severe swelling Moderate-severe tenderness Moderate-severe erythema Underlying comorbidity
0.8±0·7
19 (70%) 17 (63%) 24 (89%) 26 (96%)
3 (11%)
0·8±0·7
15 (54%) 18 (64%) 25 (89%) 23 (82%)
2 (7%)
0·80 0.20 0·92 0·96 0·09
0.61
Outcomes Treatment failure 0 (0%) 3 (11%) 0·23
Length of stay in ED – mean hours ± SD
4·0±1.2 4.8±2.4 0.11
Cellulitis stopped spreading within 24 hours
20 (77%)
17 (61%)
0·20
Adverse events during during hospital or home care
0 (0%) 3 (11%)
0·23
Complications during during hospital or home care
2 (7%) 1 (4%) 0.61
Require reinsertion of IV cannula during hospital or home care
0 (0%) 9 (32%) 0·02
Duration of IV antibiotics – mean days ± SD Duration of oral antibiotics after IV– mean days ± SD Total duration of antibiotics – mean days ± SD
2.5±2.2
6.2±2.2
8.8±4.0
2.1±1.4
6.1±2.9
8.2±3.6
0.36
0.91
0.58
Length of stay under medical care – mean days ± SD
2·9±2.2 2.4±1.4 0·35
Represented to ED within 14 days of discharge
1 (4%) 2 (3%) 0.49
Data are presented as mean+/- SD or n (%), unless otherwise stated. Length of stay in ED (mean hours ± SD%), Duration of IV antibiotics (mean days ± SD%), Length of stay under medical care (mean days ± SD%), Represented to ED (within 14 days of discharge%), ED=Emergency Department, IV=intravenous, mths=months
190

191
5.3.1 Additional data
Results
Parental quality of life was measured using a modified rating scales which had
been used in two previous studies comparing home to hospital care.7,23 There
were 135/188 (72%) parental questionnaires were returned: 73/93 (79%) from
home-‐treated patients and 62/95 (65%) from hospitalised patients. With
regards to experience of care during treatment, 95% of the home group rated the
experience as very good compared to 73% of the hospital group (OR 6.5, 95% CI
2.1 to 20.6, p=0.001). None of the patients rated their experience as very poor.
When asked how much disruption the treatment caused to parental daily
routine, 66% of the home group experienced no disruption compared to 40% of
the hospital group (OR 2.8, 95% CI 1.4 to 5.7, p=0.03). With regards to disruption
to the child’s routine, 67% in the home group reported that their child had no
disruption compared to 35% of the hospital group (OR 3.7, 95% CI 1.8 to 7.8,
p<0.001). Parents were asked at the end of treatment if they would choose
hospital or home treatment if faced with the same situation again. Of the home
group, 58 (79%) stated a preference for home treatment, 2 (3%) for hospital
treatment and 13 (18%) had no preference. Of the hospital group, 22 (35%)
stated a preference for home treatment, 16 (26%) for hospital treatment and 24
(39%) had no preference. In other words, for parents with a clear preference for
treatment location, 97% of the home group and 42% of the hospital group would
choose treatment for their child in the same location (OR 21.1, 95% CI 4.5 to
99.3, p<0.001).
192
5.4 Implications of the RCT
In this non-‐inferiority RCT of home versus hospital care in children with
moderate to severe cellulitis, home treatment was found to be as good as
hospital treatment. The outcomes of efficacy and safety of home treatment in this
RCT confirmed the findings of the two previous non-‐randomised studies
described in this thesis, the baseline (Chapter 2) and foundation (Chapter 3)
studies.114,115 However, given that treatment at home was shown to result in
higher quality of life for patients and their families and preferred by most
families, this RCT provides evidence for the home pathway to be the standard of
care for the treatment of children with moderate/severe cellulitis.
There are several design issues that warrants further discussion. First is the
decision to use two different antibiotics for the two arms. We were very mindful
of the translatability of this trial from the outset. If intravenous ceftriaxone at
home had been compared with ceftriaxone in hospital, we would not have been
comparing against the current standard of care, which in our centre is
intravenous flucloxacillin in hospital. If this design had been chosen simply based
on a direct comparison of ceftriaxone at home and in hospital, the results may
have had limited implications on clinical care, as inpatient narrow spectrum
antibiotic use would still have been viewed as the gold standard.
Comparing intravenous flucloxacillin in hospital with intravenous flucloxacillin
at home would also have been a more straightforward comparison. However,
four times a day dosing of flucloxacillin is not feasible for OPAT, so a 24-‐hour
infusion via a central line would have likely been requested. Inserting a central
line for most children requires sedation or a general anaesthetic, which does not
appear to be an ethical prospect (nor one that parents would agree to) when
there is a once daily alternative that can be delivered via a peripheral cannula.
Likewise, although we considered the possibility of a 24-‐hour flucloxacillin
infusion via a peripheral cannula, it is not considered acceptable practice for
OPAT in children because of the high chance of extravasation being unrecognised
due to the slow infusion rate and inclusion of pre-‐verbal infants. We are unaware

193
of any paediatric OPAT service that would do this. Therefore in addition to
pragmatic reasons, for ethical and translatability reasons, having two different
antibiotics was the only viable comparison between the two arms.
Other antibiotics considered for the treatment of cellulitis were cefazolin and
clindamycin.46,129 Cefazolin has similar activity against bacteria causing cellulitis
as flucloxacillin. Cefazolin could have been used for both the home and hospital
group, although that would have meant changing our current hospital guidelines.
However, cefazolin has a short half-‐life requiring 8 hourly dose frequency. In
adult OPAT, cefazolin is used in combination with oral probenecid to increase its
half-‐life, but oral probenecid is poorly tolerated in children.43,46 In order to use
cefazolin in the trial, it would have been necessary to first conduct a study on
pharmacokinetics and pharmacodynamics of once daily cefazolin with
probenecid in children, which we considered. However, many OPAT services
around the world already use ceftriaxone.3,13 Therefore there was a more urgent
need to find the evidence for or against the use of this antibiotic. Clindamycin
was also considered as it has the advantage of high oral bioavailability.130
However this antibiotic is not considered first line treatment in most parts of the
world for skin and soft tissue infection and is usually reserved for suspected or
confirmed MRSA.131 In regions with lower rates of MRSA than the US, such as
ours, it is not used in young children because of its low taste tolerance and its
role in the acquisition of C. difficile.132-‐134
The second methodological issue which required careful consideration was the
unblinded assessment of the primary outcome. Ideally, clinicians assessing the
primary outcome would be blinded to treatment location. Using central
adjudication by assessors not involved in the delivery of care (prospective
randomised open blinded endpoint -‐ PROBE design) was considered, but this
would mean having the hospital as the location of assessment for all patients.
This would place a skewed burden on only the home patients, with a substantial
risk of affecting secondary outcomes such as quality of life measures.135 Likewise
photos were taken to aid assessment, but they do not give the full clinical picture
of the patient and frequently had clues to the location inadvertently caught in the
194
frame. There are no blinded comparative home versus hospital care studies in
the literature, likely at least in part for these reasons.
However, we attempted to mitigate any potential bias by designing the
assessments of the primary outcome to be as objective as possible as either
continuous or binary outcomes as per our published protocol.136 These clinical
assessments were performed in addition to taking daily photographs of the
affected area, with the first taking place in the ED at baseline.
Since the completion of this RCT, the impact of this research has already been
seen. It has already changed practice at RCH and is has great potential to change
the way we manage this and other acute infections in Australia and beyond.
However, the biggest factor determining the enthusiasm with which institutions
will implement this pathway on a wider scale will be the cost-‐effectiveness of
treatment at home. This is addressed in the next chapter.
195
Chapter 6 Health economic analysis
6.1 Economic evaluation – comparison of alternative courses of actions
Economic evaluations are used to inform decision-‐making in healthcare in
Australia and many other countries.137 An economic evaluation is defined as the
comparative analysis of the costs and consequences of alternative programs or
interventions.138 RCTs commonly incorporate an economic evaluation such as a
cost-‐effectiveness analysis as part of the study design.139,140 In fact, research
funders commonly request that RCTs also assess the cost-‐effectiveness of any
intervention investigated.141
6.2 Cost-‐effectiveness analysis
A cost-‐effectiveness analysis, the most common type of health economic
evaluation is always a comparison of two interventions. For example for the RCT
(Chapter 5), the home treatment program was compared with the standard of
care, in hospital management.142 The two components of a cost-‐effectiveness
analysis are calculations of costs and measurement of effectiveness.138 New
healthcare interventions are often more effective, for example a new drug or a
new health program, but are frequently more costly than the current care.
Therefore, a decision is made about the threshold for which the cost is
considered worth spending for the extra benefit of the new intervention, which
is also known as the ‘willingness to pay’ threshold.137
Calculation of costs in a health economic evaluation takes into account a
specified pre-‐determined perspective.138 This could be the health institution
perspective, taking into consideration costs to the hospital or it could be the
patient perspective, taking into consideration costs incurred by patients. Ideally
a societal perspective is considered, taking into account both the costs to the
healthcare provider and to the patients and their families. The advantage of a
societal perspective is the ability to exclude any ‘cost shifting’, the transfer of cost
burden to the other party, for example, from the healthcare institution to the

196
patient.143 For this cost-‐effectiveness analysis, a societal perspective was chosen,
incorporating both the costs to our institution and costs to families of having
their child treated in each location.
Measurement of effectiveness can be done in different ways, and to some degree
depends on the priorities and perspective of the investigators. Clinical
researchers often use a clinical outcome as a measure of effectiveness, based on
the study design to answer a clinical question and impact on clinicians’ decision-‐
making. The downside of this is that clinical outcomes vary between studies,
even in those investigating the same condition.139 The preferred method by
health economists, policymakers and funders, is to use quality adjusted life years
(QALY) as a measure of effectiveness.27 The QALY combines and summarises into
a single measure the effects of health interventions on mortality and morbidity.
This provides a ‘common currency’ in a standardised format to enable
comparisons between different diseases and interventions.144,145 QALY is valued
with a number between 0 and 1, with 0 representing death and 1 representing
perfect health for one whole year. QALY are ideally obtained using validated
tools, usually in the form of questionnaires that ascertain the respondent’s
quality of life. These questions usually relate to domains of health such as sleep,
appetite and social activities.146 Some studies employ less robust methods for
measuring quality of life such as visual analogue scales, which are less time-‐
consuming to complete.147 QALY are calculated using utility scores that measure
a health state over a specified period of time: the ‘time horizon’. For this cost-‐
effectiveness analysis, the Child Health Utility 9D (CHU9D) questionnaire, a
validated quality of life tool, was used to measure the utility scores based on
activities of daily living, which are then converted into QALY.
Once the cost and effectiveness of the two compared interventions are obtained,
they can then be averaged across all patients in the study. In the RCT, the cost for
each patient in the home treatment program (h) and each patient who received
standard care of hospital admission (s) were obtained and averaged to obtain the
mean cost C for each group.141 Likewise individual measurements of
effectiveness for each patient were obtained and averaged to obtain the mean
197
effectiveness E for each group. The differences of the mean cost and mean
effectiveness, between the two interventions can be summarised as a single
index measure, called the incremental cost-‐effectiveness ratio (ICER).148 The
ICER is the difference in cost of the two interventions divided by the difference in
effectiveness of the two interventions:
ICER=Ch-‐Cs/Eh-‐Es
The ICER can be depicted as a cost-‐effectiveness plane. (Figure 6.1) The ideal
health intervention would plot in the right lower quadrant of this plane,
reflecting that it is both more effective and less costly. For this cost-‐effectiveness
analysis, two effectiveness measures were used: the primary clinical outcome of
the RCT for clinical relevance, and QALY as a standardised measure comparable
with other studies.
Lastly, a key concept in a cost-‐effectiveness analysis is the uncertainty around
the measures of cost and effectiveness.149 Determining the uncertainty
surrounding cost-‐effectiveness requires investigation of the joint distribution of
costs and effectiveness, termed a sensitivity analysis.150 It allows varying the
input of the costs and effectiveness to hypothetically reflect what the cost-‐
effectiveness of the intervention may be in other settings or under different
circumstances. One method of sensitivity analysis that is typically used to
represent the uncertainty in the costs and effectiveness associated with an
intervention is a scatter plot of simulated (by bootstrapping or probabilistic
modeling) incremental cost and effectiveness plots on the incremental cost-‐
effectiveness plane, whereby incremental cost is plotted on the y axis and
incremental effectiveness is plotted on the x axis.151,152
To summarise, the key components of a cost-‐effectiveness analysis are costs,
effectiveness, calculation of the ICER and a sensitivity analysis. The cost-‐
effectiveness analysis was incorporated into the RCT study design, crucial to the
success of the analysis.
This chapter contains one manuscript, which has been submitted for publication.
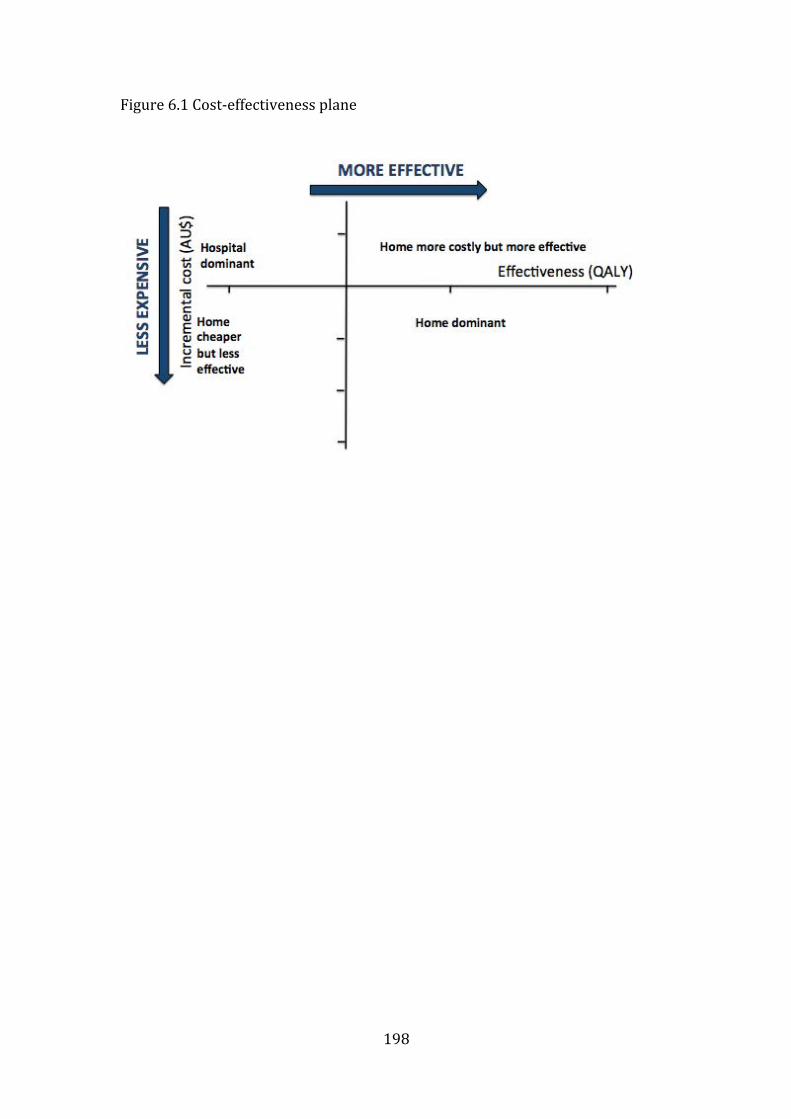
198
Figure 6.1 Cost-‐effectiveness plane

199
6.3 Study 7: Cost-‐effectiveness of home versus hospital treatment of children with moderate/severe cellulitis
Ibrahim LF, Huang L, Hopper SM, Dalziel K, Babl FE, Bryant PA. Cost-‐
effectiveness of admission avoidance with moderate/severe cellulitis. Submitted
to The Lancet Infectious Diseases Dec 2018.
Elsevier Editorial System(tm) for The Lancet
Infectious Diseases
Manuscript Draft
Manuscript Number:
Title: Cost-effectiveness of admission avoidance with outpatient
parenteral antibiotic therapy for children with moderate/severe
cellulitis'
Article Type: Article (Original Research)
Keywords: Cost-effectiveness, QALY, OPAT, antibiotics, intravenous,
hospital-in-the-home
Corresponding Author: Dr. Laila F Ibrahim, MBBCHBAO
Corresponding Author's Institution: The Royal Children's Hospital
Melbourne
First Author: Laila F Ibrahim, MBBCHBAO
Order of Authors: Laila F Ibrahim, MBBCHBAO; Li Huang; Sandy Hopper; Kim
Dalziel; Franz Babl; Penelope Bryant
Manuscript Region of Origin: AUSTRALIA
Abstract: Background
Outpatient parenteral antibiotic therapy (OPAT) following hospital
admission is increasingly popular, but its use to avoid admission to
hospital altogether by treating wholly as an outpatient, remains uncommon
in children. One reason for this is the lack of evidence for the cost-
effectiveness of this strategy. We aimed to assess the cost-effectiveness
of an admission avoidance pathway compared to standard hospital care for
the intravenous treatment of moderate/severe cellulitis in children.
Methods
A cost-effectiveness analysis of home versus hospital treatment was
undertaken for 180 children aged 6 months-18 years with moderate/severe
cellulitis enrolled in randomised controlled trial. Costs were included
from two sources: institutional costs at patient level and expenses
incurred by families. Effectiveness was measured in two ways: quality
adjusted life years (QALYs) derived from the Child Health Utility 9D, a
validated quality of life assessment tool, and a clinical outcome of
treatment failure which was the primary outcome of the trial.
Findings
The institutional cost per patient per episode was significantly lower
for the home group compared to the hospital group (AUD1965 versus
AUD3775, p<0·001). The mean cost incurred per family was AUD182 for the
home group and AUD593 for the hospital group (p<0·001). Both measures of
effectiveness were significantly better in the home group than the
hospital group. The utility score was higher in the home group (0·86
versus 0·75, p<0·001), as were the QALYs (0·005 versus 0·004, p<0·001).
Treatment failure was lower in the home group (1% versus 7%, p=0·03).
OPAT was therefore less costly and more effective than standard hospital
care and is the dominant treatment choice.

Interpretation
Home intravenous antibiotic treatment for children with moderate/severe
cellulitis is more cost-effective compared to hospital admission, and
costs to families are substantially lower. These finding support
institutions to develop this admission avoidance pathway.
Funding
RCH Foundation
Cost-effectiveness of admission avoidance with outpatient parenteral antibiotic
therapy for children with moderate/severe cellulitis
Laila F Ibrahim MB BCh BAOa,b Li Huang PhDc, Sandy M Hopper MBBSa,b,d, Kim
Dalziel PhDc, Franz E Babl MDa,b,d, Penelope A Bryant PhDa,b,d,e
Affiliations
a Department of Paediatrics, University of Melbourne
b Murdoch Children’s Research Institute
c Centre for Health Policy, the University of Melbourne
d Emergency Department, The Royal Children’s Hospital
e Infectious Diseases Unit, Department of General Medicine, The Royal Children’s
Hospital
e Hospital-In-The-Home Department, The Royal Children’s Hospital
Corresponding author
A/Prof. Penelope A Bryant
Department of General Medicine, The Royal Children’s Hospital, Melbourne,
50 Flemington Road, Parkville, VIC 3052, Australia
Email: [email protected]
Tel: +613 93455522 Fax: +613 9345 6667
Key words
Cost-effectiveness, QALY, OPAT, antibiotics, intravenous, hospital-in-the-home
202
Financial Disclosure
All authors have indicated they have no financial relationships relevant to this article
to disclose. The funding bodies do not have any authority in design and conduct of the
study; collection, management, analysis, and interpretation of the data; and
preparation, review, or approval of the manuscript.
203
Research in context
Evidence before this study
A search was performed on MEDLINE and EMBASE for articles published between
1946 to November 30, 2018 using the search terms ‘cost-effectiveness’ and
‘outpatient’ limited to ‘all child (0-18years)’ with no language restrictions. There
were no cost-effectiveness analyses in randomised studies comparing outpatient
versus hospital treatment either using antibiotics, or where patients avoided
hospitalisation completely. Non-randomised outpatient versus hospital studies have
used secondary or retrospective data or hypothetical cohorts, and these have
suggested that outpatient treatment is less costly. Additionally, a systematic review of
the literature on the economic evaluation of outpatient parenteral antimicrobial
therapy (OPAT) in adults did not identify any cost-effectiveness analyses in
randomised cohorts, and only two economic evaluations studies were considered of
high quality.
Added value of this study
This is the first cost-effectiveness study to compare outpatient with hospital treatment
in a randomised cohort in children, either requiring intravenous antibiotics, or
avoiding hospital admission completely. This study considered costs from the
healthcare provider perspective as well as the patients’ and families’ perspective.
Findings from our study provide robust evidence that treatment of children with
moderate to severe cellulitis at home is more cost-effective compared to standard
admission to hospital. In addition, we have shown that families incur a three-fold
burden of cost when their child is treated in hospital compared to at home, a factor
204
often overlooked by clinicians. This is the first study of outpatient versus hospital care
to measure the incremental cost-effectiveness ratio, using both clinical effectiveness
specific to cellulitis as well as in terms of quality adjusted life years, a widely used
and standardised measure in economic evaluations.
Implications of all the available evidence
This economic analysis, together with the findings of clinical efficacy, safety and
patient preference of intravenous antibiotics at home, provides strong evidence for
avoiding hospitalisation altogether through a home or ambulatory pathway for
children with moderate/severe cellulitis. This study provides the evidence for
policymakers and stakeholders to resource outpatient/ambulatory pathways that are
immediately responsive to children attending emergency departments. The design and
outcomes also act as a platform for the evaluation of outpatient pathways for other
acute infections.
205
Summary
Background
Outpatient parenteral antibiotic therapy (OPAT) following hospital admission is
increasingly popular, but its use to avoid admission to hospital altogether by treating
wholly as an outpatient, remains uncommon in children. One reason for this is the
lack of evidence for the cost-effectiveness of this strategy. We aimed to assess the
cost-effectiveness of an admission avoidance pathway compared to standard hospital
care for the intravenous treatment of moderate/severe cellulitis in children.
Methods
A cost-effectiveness analysis of home versus hospital treatment was undertaken for
180 children aged 6 months-18 years with moderate/severe cellulitis enrolled in
randomised controlled trial. Costs were included from two sources: institutional costs
at patient level and expenses incurred by families. Effectiveness was measured in two
ways: quality adjusted life years (QALYs) derived from the Child Health Utility 9D, a
validated quality of life assessment tool, and a clinical outcome of treatment failure
which was the primary outcome of the trial.
Findings
The institutional cost per patient per episode was significantly lower for the home
group compared to the hospital group (AUD1965 versus AUD3775, p<0·001). The
mean cost incurred per family was AUD182 for the home group and AUD593 for the
hospital group (p<0·001). Both measures of effectiveness were significantly better in
the home group than the hospital group. The utility score was higher in the home
group (0·86 versus 0·75, p<0·001), as were the QALYs (0·005 versus 0·004,
p<0·001). Treatment failure was lower in the home group (1% versus 7%, p=0·03).
206
OPAT was therefore less costly and more effective than standard hospital care and is
the dominant treatment choice.
Interpretation
Home intravenous antibiotic treatment for children with moderate/severe cellulitis is
more cost-effective compared to hospital admission, and costs to families are
substantially lower. These finding support institutions to develop this admission
avoidance pathway.
Funding
RCH Foundation
207
Introduction
Outpatient parenteral antibiotic therapy (OPAT) following a hospital admission has
become a widely endorsed model of care worldwide in the last decade.1-3 Its use
reduces hospital-acquired infections, negative psychosocial impact and the
inconvenience of hospital admission.4,5 There is increasing interest in its use to avoid
admission to hospital altogether by treating directly from the emergency department
(ED) or outpatient practice, but this has yet to gain traction in children. One reason for
this is concern regarding the acuity of infections in children and the potential for rapid
deterioration. Consequently, while OPAT has been shown to be less costly than
inpatient treatment,6 the lack of evidence for effectiveness in children and concern
about readmission has resulted in admission to hospital remaining the default
pathway.7,8 Additionally, widespread implementation has been limited by studies pre-
selecting patients for success, with no cost-effectiveness analysis in either adults or
children of an admission avoidance pathway on randomised patients.
The ideal cost-effectiveness analysis uses patient-level data, taking into account both
institutional costs and expenses incurred by patients and families, to inform a societal
perspective. In addition, for results to have impact, the economic analysis needs to
incorporate intervention outcomes that are meaningful to patients and clinicians, and
comparable for healthcare institutions. Effectiveness in economic evaluations is
commonly reported as quality adjusted life years (QALY).9 The advantage of using
the standardised measure of QALY is the ability to compare between the values of
different options for allocating healthcare resources. QALY are calculated using
utility scores that measure a health state over a specified period of time: the ‘time
horizon’. Despite QALY being the most widely used measure of disease burden in
208
assessing the value of medical interventions, the few studies to date of OPAT and
admission avoidance have relied on disaggregated measures of cost and effect and
without the use of QALY.10,11
One of the most common acute infections treated with OPAT is cellulitis2,12, a skin
infection with a rate in children of 20 per 1000 person years.13 Moderate/severe
cellulitis requiring intravenous antibiotics has been shown in a few previous studies to
be effectively and safely treated at home directly from the ED, although none have
evaluated cost-effectiveness.14,15 The first randomised controlled trial (RCT) to
compare efficacy and safety of OPAT versus hospital treatment in children was
undertaken in the management of moderate/severe cellulitis directly from the ED.16
An economic evaluation was planned for this trial, using patient-level costs and
QALY. The aim of this study was to analyse the cost-effectiveness of an admission
avoidance pathway versus hospital treatment for moderate/severe cellulitis requiring
intravenous antibiotics in children.
Methods
Setting and outcomes
The economic evaluation was undertaken for children enrolled in the Cellulitis at
Home Or Inpatient in Children from Emergency (CHOICE) RCT.17 The CHOICE
trial was a single centre, randomized, open label non-inferiority trial, at The Royal
Children’s Hospital Melbourne, Australia. The trial recruited children aged 6 months
to 18 years from the ED from January 2015 to June 2017, who were diagnosed with
moderate/severe uncomplicated cellulitis and excluded those with complicated
cellulitis, immunosuppression, toxicity or serious co-morbidities. Eligible children
209
who consented were randomised to either standard care in hospital or care at home
under the Hospital-In-The-Home (HITH) program, an alternative care pathway
provided for by the same hospital (figure 1). The primary outcome of the trial was
treatment failure defined as lack of clinical improvement of cellulitis or an adverse
event, resulting in a change of initial empiric antibiotics within 2 days (48 hours) of
treatment from the start of the first antibiotic dose given in the ED. The full details of
the trial protocol and outcomes have been published elsewhere.16,17 The intravenous
antibiotics used for the two arms were necessarily different: the empiric antibiotic at
our institution for moderate/severe cellulitis is flucloxacillin administered every six
hours, while for the home program the once daily antibiotic ceftriaxone is used.
The cost-effectiveness analysis of home versus hospital was conducted from a societal
perspective, taking into account the burden of costs to the healthcare institutions and
to patients and families, and the time horizon was from the initial ED presentation to
the point of discharge from medical care. All children in the per protocol analysis
were included, rather than the intention to treat population due to patients crossing
arms which would lead to a mismatch between resources used and outcomes
achieved.
Determining resources and costs
The costs of the home intervention and standard hospital care were obtained from the
hospital administrative costing unit, which included direct and indirect costs of
medical care including medications, staff time, and overheads. Drug costs were
obtained from the institutional pharmacy and costs of distance travelled were obtained
from the Australian Taxation Office, using figures for car expenses. In Australian
210
tertiary hospitals, the standard reporting of patient level cost data combines direct and
indirect costs associated with the hospital admission.18 The total cost for each
individual patient comprise the total sum of cost ‘buckets’ such as medical, nursing,
allied health, imaging, pathology, pharmacy, theatre, emergency department and
allied health.19 Costs to the patients and their families were collected using self-
reported questionnaires completed by parents or carers. These included the costs
incurred by families for food, transport or parking, medication or any other expenses
during treatment as well as number of days absent from paid or unpaid work from the
time they presented to ED to the end of treatment. The costs used to calculate the
earnings loss from work leave were obtained from the Australian Bureau of Statistics,
specifically the average weekly total earnings for all employees. All costs were
recorded in Australian dollars (AUD).
Measurement of effectiveness
Effectiveness was measured in two ways: the clinical primary outcome of treatment
failure, and QALY measurements derived from utility scores. The latter were
obtained from the Child Health Utility 9 (CHU9) questionnaire, a widely used
validated quality of life assessment tool for children20,21, which was collected within
24-48 hours of admission, reflecting the quality of life during treatment. For those
under 6 years of age these were parent-reported, for those above 6 years of age these
were child-reported. A second CHU9D was administered at 14 days after resolution
of the infection (cellulitis) and cessation of treatment reflecting the quality of life after
resolution of infection. For those with missing utility scores, a random score was
generated using the mean and standard error of available utility data. To obtain the
QALY figures during treatment, utility scores obtained from the questionnaires were
211
multiplied by two days (0·0056), the mean duration that study participants were in
receipt of the care intervention (home or hospital). To obtain the QALY figures after
resolution of infection, utility scores were multiplied by 14 days (0·04).
Analytic methods
The incremental cost-effectiveness ratio, defined as the difference in total cost (home
versus hospital) divided by the difference in effectiveness (home versus hospital), was
reported firstly as the cost per additional treatment failure observed in the OPAT
group compared to standard hospital care, and secondly as the cost per QALY gained.
Chi-square test and Student’s t-test (2-sided) were used to compare dichotomous and
continuous outcomes between groups respectively. Analysis was performed by
StataIC version 15·1.
Sensitivity analysis
To account for uncertainty, a series of one way and two-way sensitivity analyses were
conducted varying the costs and the effectiveness for four different scenarios: 1)
Double the distance of the actual catchment area from 50 to 100 kilometres from the
hospital; 2) Double the readmission rate using utility data from a previous study;22 3)
Inflation of doctors’ salaries by 50% to reflect applicability of this study to places
where doctors are paid at a higher rate; 4). Double the number of nursing visits to
twice daily, for a different medical condition. The results were presented in a
summary table and using cost-effectiveness planes.
The economic evaluation follows the International Society for Pharmacoeconomics
and Outcomes Research (ISPOR) guideline for trial-based cost-effectiveness
212
analysis23 and reports using the ISPOR consolidated health economic evaluation
reporting standards guideline.24 This trial was registered at ClinicalTrials.gov, registry
number NCT02334124. The trial and cost-effectiveness analysis were approved by
the institutional ethics committee.
Role of the funding source
The funder of the study had no role in study design, data collection, data analysis,
data interpretation, or writing of the report. The first and corresponding author had
full access to all the data in the study and had final responsibility for the decision to
submit for publication.
Results
There were 180 children in the per protocol analysis, 89 assigned to the home group
and 91 to the hospital group (supplementary figure 1). There were no differences in
demographics or clinical features at presentation between the two groups (table 1).
Costs
The actual individual institutional cost was available for every patient in the trial. The
costs to family questionnaires were returned by 68/89 (76%) of the home group and
69/91 (76%) of the hospital group. The demographics, clinical features, outcomes and
Socioeconomic Index for Areas (SEIFA) scores for those who returned questionnaires
and those who did not showed no significant differences (table 1).
The mean cost to our institution of treating a patient with moderate/severe cellulitis at
home was AUD970 (GBP548) per day, compared to the cost of treating a patient in
213
an inpatient medical bed which was AUD2388 (GBP1348) per day (table 2). The
highest component of cost incurred was medical and nursing staff salaries. The mean
cost to the ED for a patient treated at home was AUD623 and for those treated as an
inpatient, the mean cost was AUD850 (-227 (95% CI -106 to -347), p=0·0003). The
total mean cost to families who had a child treated at home was AUD182 (GBP104)
per patient episode, compared to the cost of having a child treated in an inpatient bed
which was AUD593 (GBP338) per patient episode (table 3). The highest cost incurred
by families was attributed by absence from paid work which was a mean of 0·7 days
for the home group and a mean of 2·0 days for parents of hospitalised children,
p<0·001. The cost to families for absence from both paid and unpaid work, was
significantly less (AUD171 versus AUD542, p<0·001) for children in the home
group.
The total cost savings to our hospital for these 180 patients over the 29 months of the
study were AUD325,620. If all 252 patients who were eligible during that time
period16 had been treated via the home pathway, the potential cost savings would have
been AUD455,868 (AUD188,136 per year, 95%CI 137,696-238,680). For the
families of the 180 patients in this study the total savings were AUD73,800. If every
eligible child had been treated via the home pathway, the potential cost savings for
families would have been AUD103,320 (AUD42,640 per year, 95%CI 32,448-
52,832). This represents a potential total cost saving per year of AUD230,776 (95%CI
170,144-291,512).
Effectiveness
214
Of the patients in the home group, 1/89 (1%) had treatment failure, compared to 7/91
(8%) in the hospital group (risk difference [RD] -6·5 %; 95% confidence interval [CI]
-12·4 to -0·7, p=0·03). The home patient who had treatment failure was admitted to
hospital for 3 days. Length of stay under medical care and duration of intravenous
antibiotics were longer for the home group by half a day (table 1).
The CHU9D questionnaires were returned by 68/89 (76%) of the home group and
68/91 (75%) of the hospital group during treatment. Baseline characteristics and
clinical outcomes between those who returned the questionnaires and those who did
not, were the same (supplemental table 1). The mean utility score – the ability to carry
out activities of daily living – was higher in the home group (0.86) compared to the
hospital group (0·75)(p<0·001). When converted into QALY, the QALY for the
home group (0·005) was higher than the hospital group (0·004) (p<0·001). After 2
weeks, at the point of resolution of the cellulitis, the utility score was no different
between home (0·95) versus hospital (0·93) (difference -0·02; 95%CI -0·04 to 0·00,
p=0·06).
Cost-effectiveness
Treatment at home was therefore less costly (for the institution and families) and
more effective (using either the clinical outcome or QALY), which means it is
dominant in health economic terms: both cost saving and clinically superior.
Therefore, calculating the incremental cost-effectiveness ratio is redundant because
there is no extra cost for home treatment compared to hospital care to achieve the
reported effectiveness. The cost-effectiveness plane (figure 2a and 2b) shows that
treatment at home is cost-effective using either measure of effectiveness with a high
215
level of certainty – the proportion of data points in the bottom right quadrant. With
QALY there was 100% certainty of the findings, and with treatment failure there was
a 98·3% certainty (1·7% data points in the bottom left quadrant). In the sensitivity
analysis, despite varying different components of care to determine the effects of
making the travel or staff costs more expensive or the treatment failure rate worse, the
home intervention remained dominant (table 4, figure 3).
Discussion
In this first comprehensive economic evaluation of home versus hospital treatment for
any condition in children,25 home treatment for cellulitis was shown to be
convincingly dominant. There is published evidence that children with
moderate/severe cellulitis can be safely and effectively treated at home12,15,26 and this
study now provides the cost-effectiveness evidence. Our results are in contrast to the
findings of the only other cost comparison study in randomised children. In a United
Kingdom RCT of children requiring nursing observations in hospital versus home,
costs to the healthcare provider (NHS) were not significantly different (GBP870 per
patient at home versus GBP741 per hospitalised patient).25 This is likely explained by
patients in the home group in that study being initially hospitalised, incurring a
hospital cost in addition to the home cost, and the home service under-recruiting
patients resulting in a higher ratio of nurses to patients and higher costs per patient.
In considering the generalisability of the cost-effectiveness findings under different
care pathways and resource contexts, the sensitivity analyses were reassuring. Factors
were chosen that would adversely affect either a) costs of home treatment (catchment
distance, number of visits), b) costs and effectiveness of home treatment (readmission
216
rate from home during treatment), or c) costs of both treatment locations (medical
staff costs). The increase in catchment area (increasing nursing time and travel
resources) provides relevance to services in more rural areas where patients may live
further from the hospital. Doubling the readmission rate during treatment at home did
not affect the dominance of the outcome and reassures that even if a patient has to
return to hospital, there are benefits in initiating a home treatment pathway. Finally,
although increasing doctors’ salaries was somewhat tongue in cheek, it shows that the
cost-effectiveness benefits still stand even in differently-resourced situations.
Although all analyses were specific to management of cellulitis, they should be
broadly applicable to comparison of home versus hospital treatment of other medical
conditions. The findings of a dominant home intravenous pathway in our study was
similar to the only previous cost-effectiveness analysis of OPAT in children with
febrile neutropenia, supporting the generalisability of these results.22 The variation of
two visits per day was included to consider the home needs in other conditions such
as the management of a newly diagnosed diabetes mellitus where glucose monitoring
may be required twice a day. The benefits of treating infections at home in children
with underlying chronic conditions necessitating frequent admissions to hospital, such
as cystic fibrosis or cancer, may have even stronger benefits in terms of QALY.
These findings inform clinicians for the first time of the costs that families incur when
children are hospitalised for cellulitis: AUD593 per family for an admission lasting
two days, a substantial cost for the average family. This compares unfavourably to the
AUD182 for home treatment for the same condition. Most clinicians would likely not
consider this when admitting a child to hospital. Most of that cost is from parental or
carer’s absence from work, which was significantly higher in the hospital group by a
217
mean difference of AUD410 per admission. Two previous studies have also found
that parents/guardians of children treated with OPAT were less likely to have absence
from work.25,27 This may be attributed to parents being more likely to stay with their
child when their child is hospitalised, whereas other carers or extended family may
care for a child treated at home. Additionally, one parent may stay with a child in
hospital while the other looks after siblings at home, whereas if a child is treated at
home, one parent can do all child-caring activities. This would be an especially
important factor to consider for single parent families.
The economic implications across the whole of Australia are currently unrealised. In
2016 to 2017 there were 85,991 ED attendances at our hospital, and approximately
1,997,606 ED attendances in children aged 18 years and under across the whole of
Australia.28 Over the 29 months of the CHOICE trial, 252 children at our hospital
were eligible, ie 104/year.16 With a conservative estimate that a similar proportion of
paediatric attendances are due moderate/severe cellulitis across Australia (although it
is likely to be higher in tropical northern regions), this equates to 2,415 children
attending ED with this infection per year who would be eligible for ambulatory
intravenous treatment. The cost savings across Australia would therefore be
AUD4,368,735 (95%CI 3,197,460-5,542,425) per year for hospitals and AUD990,150
(95%CI 753,480-1,226,820) per year for families. Although the total potential societal
cost saving of AUD5,358,885 (95%CI 3,950,940-6,769,245) seems perhaps not
dramatic, this is for a two-day admission for the severe end of a single infection. If
this could be replicated in multiple infections needing antibiotics such as urinary tract
infection29 and febrile neutropenia4, and even viral infections needing nursing
observations30, then savings would rapidly accrue.
218
The strengths of this study include that children were randomised reducing the bias of
self-selection or a highly selected patient group, patient-level cost data with real
outcomes were used, and that the cost-effectiveness analysis was comprehensive. The
study has several limitations. Firstly, it was conducted in a single tertiary centre with
the largest paediatric home care team in Australia.3 This team has strong medical
oversight and skilled nurses, which contribute to low complication and readmission
rates. However, when the readmission rates were hypothetically increased, the home
treatment pathway was still dominant. Secondly, the questionnaires to families were
anonymous (to obtain candid answers from families), prohibiting the ability to relate
the burden of costs incurred by families to specific patient outcomes. The utility data
was provided by only 75% of families, although when compared the baseline
characteristics and clinical outcomes were the same.
Conclusion
Home intravenous antibiotic treatment for moderate/severe cellulitis directly from the
ED is cost-effective compared to standard care of admission to a hospital ward. These
findings, in addition to the RCT showing clinical efficacy, fewer adverse events and
higher patient/parent satisfaction, provide strong evidence to stakeholders and
policymakers in support of a direct-from-ED-to-home pathway for this condition. It
highlights the value of a comprehensive cost-effectiveness analysis in the allocation
of resources for developing new models of care, although each condition should be
analysed independently as there may be unrecognised differences.
219
Contributors' Statement
LFI conceptualized, designed and coordinated the study, carried out the initial and
subsequent data analysis, drafted the initial manuscript, revised subsequent drafts and
approved the final manuscript as submitted. PAB, FEB, and SMH, were involved in
the design of the study, provided input into data analysis, reviewed and revised the
manuscript and approved the final draft. LH was involved in the design of the study,
guided the statistical analysis, revised and approved the final manuscript as submitted.
KD was involved in the design of the family questionnaire part of the study, reviewed
and revised the manuscript and approved the final draft. All authors approved the
final manuscript.
Declaration of interests
All authors hereby declare there has been no support from any organisation for the
submitted work; no financial relationships with any organisations that might have an
interest in the submitted work in the previous three years; no other relationships or
activities that could appear to have influenced the submitted work.
Acknowledgements
We would like to acknowledge the participation of patients and families.
Funding
This study was funded in part by grants from the RCH Foundation, the Murdoch
Children's Research Institute (MCRI), the Victorian Department of Health,
Melbourne Australia. LFI was supported in part by a scholarship from AVANT
Mutual Group Ltd, Melbourne, the Melbourne Children’s Campus Postgraduate
220
Health Research Scholarship and the Doctor Nicholas Collins Fellowship. PAB was
in part supported by a Melbourne Campus Clinician Scientist Fellowship, Melbourne,
Australia. FEB was supported in part by a grant from the RCH Foundation and a
Melbourne Campus Clinician Scientist Fellowship, Melbourne, Australia and a
National Health and Medical Research Council (NHMRC) Practitioner Fellowship,
Canberra, Australia. The emergency research group, MCRI, is in part supported by an
NHMRC Centre for Research Excellence Grant for Paediatric Emergency Medicine,
Canberra, Australia and the Victorian government infrastructure support program.
1. Fernandes P, Milliren C, Mahoney-‐West HM, Schwartz L, Lachenauer CS, Nakamura MM. Safety of Outpatient Parenteral Antimicrobial Therapy in Children. Pediatr Infect Dis J 2017. 2. Madigan T, Banerjee R. Characteristics and outcomes of outpatient parenteral antimicrobial therapy at an academic children's hospital. Pediatr Infect Dis J 2013; 32(4): 346-‐9. 3. Hodgson KA, Huynh J, Ibrahim LF, et al. The use, appropriateness and outcomes of outpatient parenteral antimicrobial therapy. Archives of disease in childhood 2016; 101(10): 886-‐93. 4. Orme LM, Babl FE, Barnes C, Barnett P, Donath S, Ashley DM. Outpatient versus inpatient IV antibiotic management for pediatric oncology patients with low risk febrile neutropenia: a randomised trial. Pediatr Blood Cancer 2014; 61(8): 1427-‐33. 5. Balaguer A, Gonzalez de Dios J. Home versus hospital intravenous antibiotic therapy for cystic fibrosis. Cochrane Database Syst Rev 2012; 3: CD001917. 6. Bryant PA, Katz NT. Inpatient versus outpatient parenteral antibiotic therapy at home for acute infections in children: a systematic review. The Lancet Infectious diseases 2017.
221
7. Chrysochoou EA, Hatziagorou E, Kirvassilis F, Tsanakas J. Home intravenous antibiotic therapy in children with cystic fibrosis: clinical outcome, quality of life and economic benefit. Hippokratia 2016; 20(4): 279-‐83. 8. Wiernikowski JT, Rothney M, Dawson S, Andrew M. Evaluation of a home intravenous antibiotic program in pediatric oncology. The American journal of pediatric hematology/oncology 1991; 13(2): 144-‐7. 9. IMPROVE Trial Investigators. Comparative clinical effectiveness and cost effectiveness of endovascular strategy v open repair for ruptured abdominal aortic aneurysm: three year results of the IMPROVE randomised trial. Bmj 2017; 359: j4859. 10. Chapman AL, Dixon S, Andrews D, Lillie PJ, Bazaz R, Patchett JD. Clinical efficacy and cost-‐effectiveness of outpatient parenteral antibiotic therapy (OPAT): a UK perspective. The Journal of antimicrobial chemotherapy 2009; 64(6): 1316-‐24. 11. Wai AO, Frighetto L, Marra CA, Chan E, Jewesson PJ. Cost analysis of an adult outpatient parenteral antibiotic therapy (OPAT) programme. A Canadian teaching hospital and Ministry of Health perspective. PharmacoEconomics 2000; 18(5): 451-‐7. 12. Gouin S, Chevalier I, Gauthier M, Lamarre V. Prospective evaluation of the management of moderate to severe cellulitis with parenteral antibiotics at a paediatric day treatment centre. Journal of paediatrics and child health 2008; 44(4): 214-‐8. 13. Ellis Simonsen SM, van Orman ER, Hatch BE, et al. Cellulitis incidence in a defined population. Epidemiology and infection 2006; 134(2): 293-‐9. 14. Ibrahim LF, Hopper SM, Babl FE, Bryant PA. Who Can Safely Have Antibiotics at Home? A Prospective Observational Study in Children with Moderate/Severe Cellulitis. Pediatr Infect Dis J 2015. 15. Ibrahim LF, Hopper SM, Connell TG, Daley AJ, Bryant PA, Babl FE. Evaluating an admission avoidance pathway for children in the emergency department: outpatient intravenous antibiotics for moderate/severe cellulitis. Emergency medicine journal : EMJ 2017. 16. Ibrahim LF, Hopper SM, Orsini F, Daley AJ, Babl FE, Bryant PA. Randomised controlled trial of intravenous antibiotics on OPAT versus hospital for cellulitis in children: comparison of efficacy and safety. In press The Lancet Infectious diseases 2018. 17. Ibrahim LF, Babl FE, Orsini F, Hopper SM, Bryant PA. Cellulitis: Home Or Inpatient in Children from the Emergency Department (CHOICE): protocol for a randomised controlled trial. BMJ open 2016; 6(1): e009606. 18. Independent Hospital Pricing Authority. National Hospital Cost Data Collection: Australian Public Hospitals Cost Report 2013-‐2014 Round 18. https://www.ihpa.gov.au/sites/g/files/net636/f/publications/nhcdc-round18.pdf. (accessed 15 June 2018). 19. Department of Health and Ageing. Australian Hospital Patient Costing Standards, version 2.0 – 1 March 2011. https://www.ihpa.gov.au/publications/australianhospital-patient-costing-standards-version-20. (accessed 26 April 2018). 20. Stevens K. Valuation of the Child Health Utility 9D Index. PharmacoEconomics 2012; 30(8): 729-‐47.
222
21. Stevens K, Ratcliffe J. Measuring and valuing health benefits for economic evaluation in adolescence: an assessment of the practicality and validity of the child health utility 9D in the Australian adolescent population. Value in health : the journal of the International Society for Pharmacoeconomics and Outcomes Research 2012; 15(8): 1092-‐9. 22. Teuffel O, Amir E, Alibhai SM, Beyene J, Sung L. Cost-‐effectiveness of outpatient management for febrile neutropenia in children with cancer. Pediatrics 2011; 127(2): e279-‐86. 23. Ramsey S, Willke R, Briggs A, et al. Good research practices for cost-‐effectiveness analysis alongside clinical trials: the ISPOR RCT-‐CEA Task Force report. Value in health : the journal of the International Society for Pharmacoeconomics and Outcomes Research 2005; 8(5): 521-‐33. 24. Husereau D, Drummond M, Petrou S, et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS)-‐-‐explanation and elaboration: a report of the ISPOR Health Economic Evaluation Publication Guidelines Good Reporting Practices Task Force. Value in health : the journal of the International Society for Pharmacoeconomics and Outcomes Research 2013; 16(2): 231-‐50. 25. Bagust A, Haycox A, Sartain SA, Maxwell MJ, Todd P. Economic evaluation of an acute paediatric hospital at home clinical trial. Archives of disease in childhood 2002; 87(6): 489-‐92. 26. Brugha RE, Abrahamson E. Ambulatory intravenous antibiotic therapy for children with preseptal cellulitis. Pediatric emergency care 2012; 28(3): 226-‐8. 27. Pena A, Zambrano A, Alvarado M, Cerda J, Vergara R. [Evaluation of the effectiveness, safety and costs of outpatient intravenous antimicrobial treatment (OPAT) vs hospitalized in urinary infection in pediatrics]. Revista chilena de infectologia : organo oficial de la Sociedad Chilena de Infectologia 2013; 30(4): 426-‐34. 28. Australian Institute of Health Welfare. Emergency department care 2016–17: Australian hospital statistics. https://www.aihw.gov.au/reports/hospitals/ahs-2016-17-emergency-department-care/contents/table-of-contents (accessed 15 May 2018). 29. Scanlan BT, Ibrahim LF, Hopper SM, Babl FE, Davidson A, Bryant PA. Selected Children with Complicated Acute Urinary Tract Infection May be Treated with Outpatient Parenteral Antibiotic Therapy at Home Directly from the Emergency Department. Pediatr Infect Dis J 2018. 30. Sartain SA, Maxwell MJ, Todd PJ, et al. Randomised controlled trial comparing an acute paediatric hospital at home scheme with conventional hospital care. Archives of disease in childhood 2002; 87(5): 371-‐5.
223
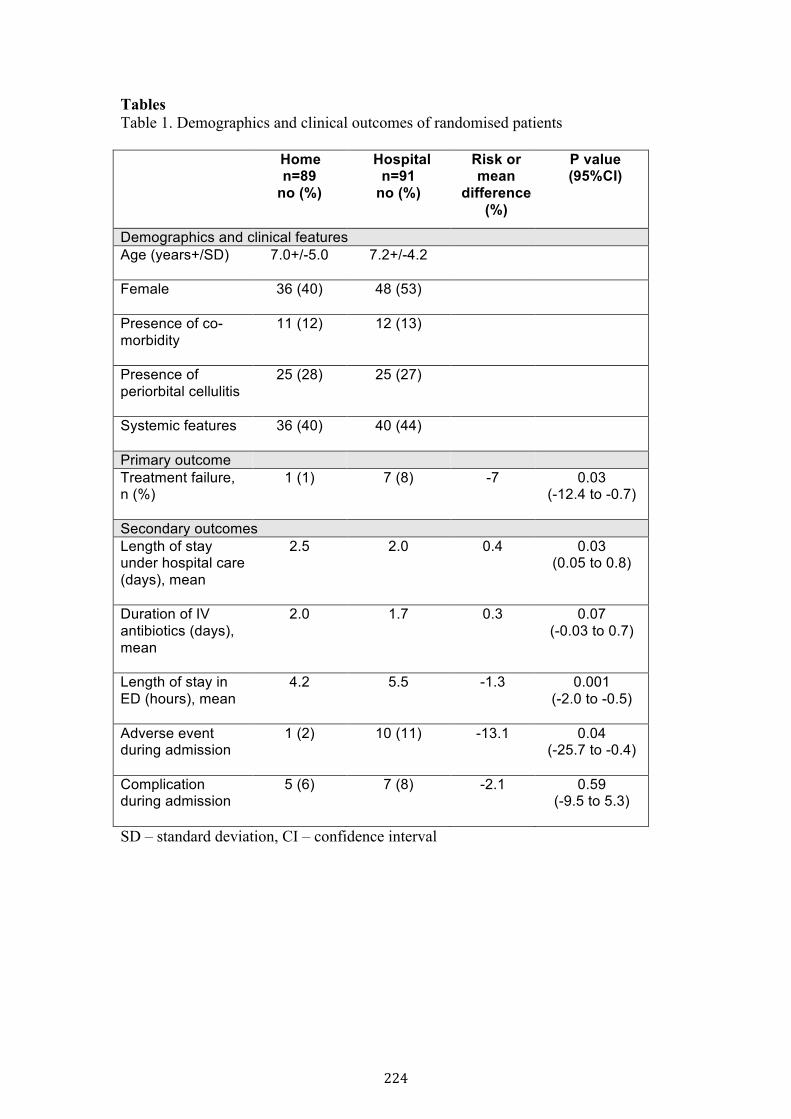
Tables Table 1. Demographics and clinical outcomes of randomised patients
Home n=89
no (%)
Hospital n=91
no (%)
Risk or mean
difference (%)
P value (95%CI)
Demographics and clinical features Age (years+/SD)
7.0+/-5.0 7.2+/-4.2
Female
36 (40) 48 (53)
Presence of co-morbidity
11 (12) 12 (13)
Presence of periorbital cellulitis
25 (28) 25 (27)
Systemic features
36 (40) 40 (44)
Primary outcome Treatment failure, n (%)
1 (1) 7 (8) -7 0.03 (-12.4 to -0.7)
Secondary outcomes Length of stay under hospital care (days), mean
2.5 2.0 0.4 0.03 (0.05 to 0.8)
Duration of IV antibiotics (days), mean
2.0 1.7 0.3 0.07 (-0.03 to 0.7)
Length of stay in ED (hours), mean
4.2 5.5 -1.3 0.001 (-2.0 to -0.5)
Adverse event during admission
1 (2) 10 (11) -13.1 0.04 (-25.7 to -0.4)
Complication during admission
5 (6) 7 (8) -2.1 0.59 (-9.5 to 5.3)
SD – standard deviation, CI – confidence interval
224
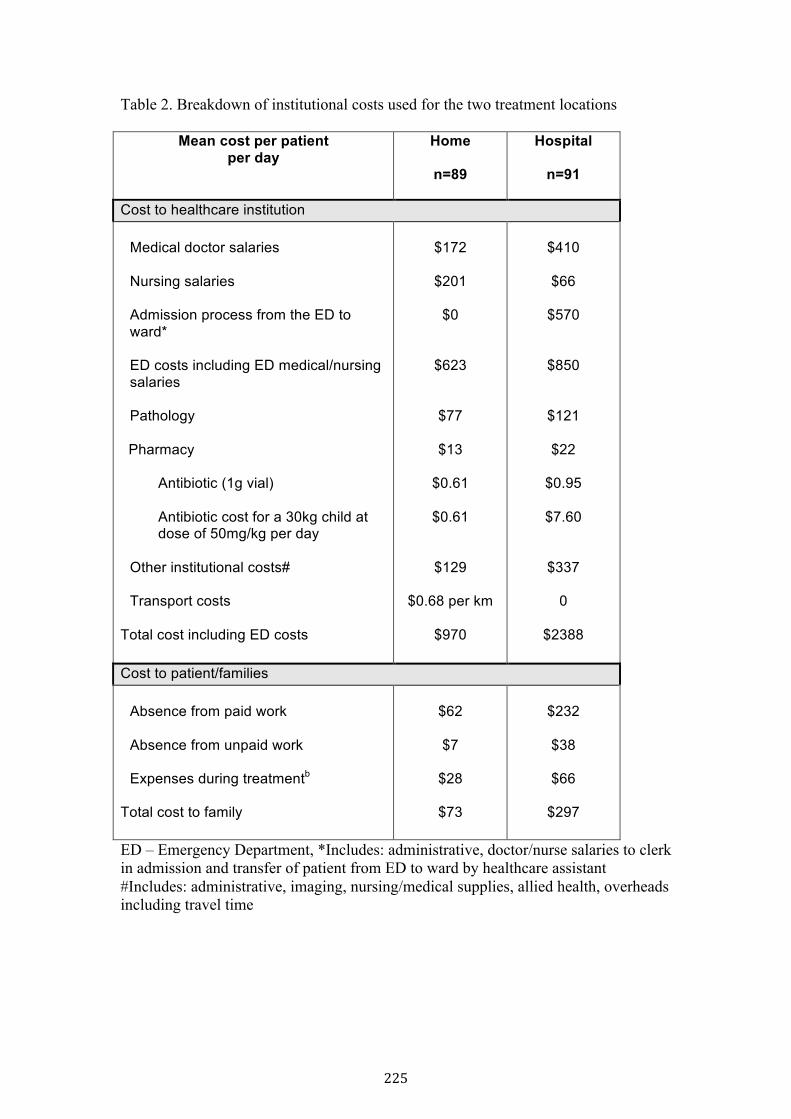
Table 2. Breakdown of institutional costs used for the two treatment locations
Mean cost per patient per day
Home
n=89
Hospital
n=91
Cost to healthcare institution
Medical doctor salaries
Nursing salaries
Admission process from the ED to ward*
ED costs including ED medical/nursing salaries Pathology
Pharmacy
Antibiotic (1g vial)
Antibiotic cost for a 30kg child at dose of 50mg/kg per day
Other institutional costs# Transport costs
Total cost including ED costs
$172
$201
$0
$623
$77
$13
$0.61
$0.61
$129 $0.68 per km
$970
$410
$66
$570
$850
$121
$22
$0.95
$7.60
$337
0
$2388
Cost to patient/families
Absence from paid work
Absence from unpaid work
Expenses during treatmentb
Total cost to family
$62
$7
$28
$73
$232
$38
$66
$297
ED – Emergency Department, *Includes: administrative, doctor/nurse salaries to clerk in admission and transfer of patient from ED to ward by healthcare assistant #Includes: administrative, imaging, nursing/medical supplies, allied health, overheads including travel time
225
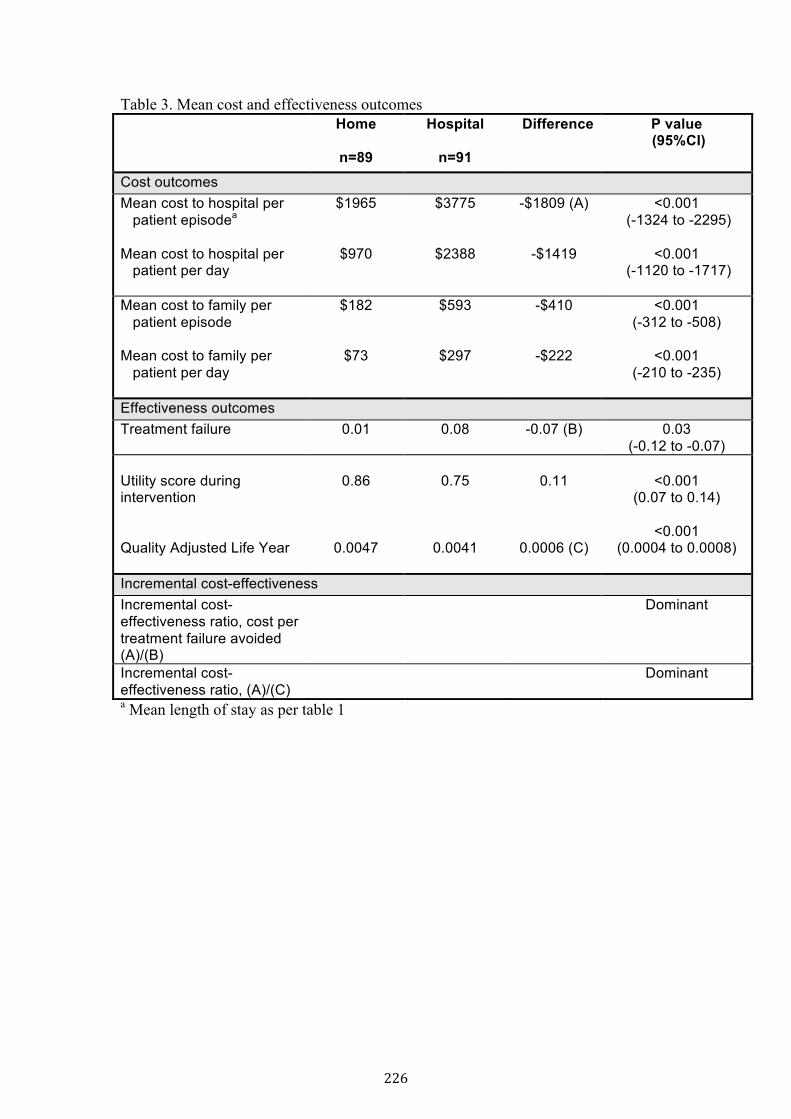
Table 3. Mean cost and effectiveness outcomes Home
n=89
Hospital
n=91
Difference P value (95%CI)
Cost outcomes Mean cost to hospital per patient episodea Mean cost to hospital per patient per day
$1965
$970
$3775
$2388
-$1809 (A)
-$1419
<0.001 (-1324 to -2295)
<0.001
(-1120 to -1717)
Mean cost to family per patient episode Mean cost to family per patient per day
$182
$73
$593
$297
-$410
-$222
<0.001 (-312 to -508)
<0.001
(-210 to -235)
Effectiveness outcomes Treatment failure
0.01 0.08 -0.07 (B) 0.03 (-0.12 to -0.07)
Utility score during intervention Quality Adjusted Life Year
0.86
0.0047
0.75
0.0041
0.11
0.0006 (C)
<0.001
(0.07 to 0.14)
<0.001 (0.0004 to 0.0008)
Incremental cost-effectiveness Incremental cost-effectiveness ratio, cost per treatment failure avoided (A)/(B)
Dominant
Incremental cost-effectiveness ratio, (A)/(C)
Dominant
a Mean length of stay as per table 1
226
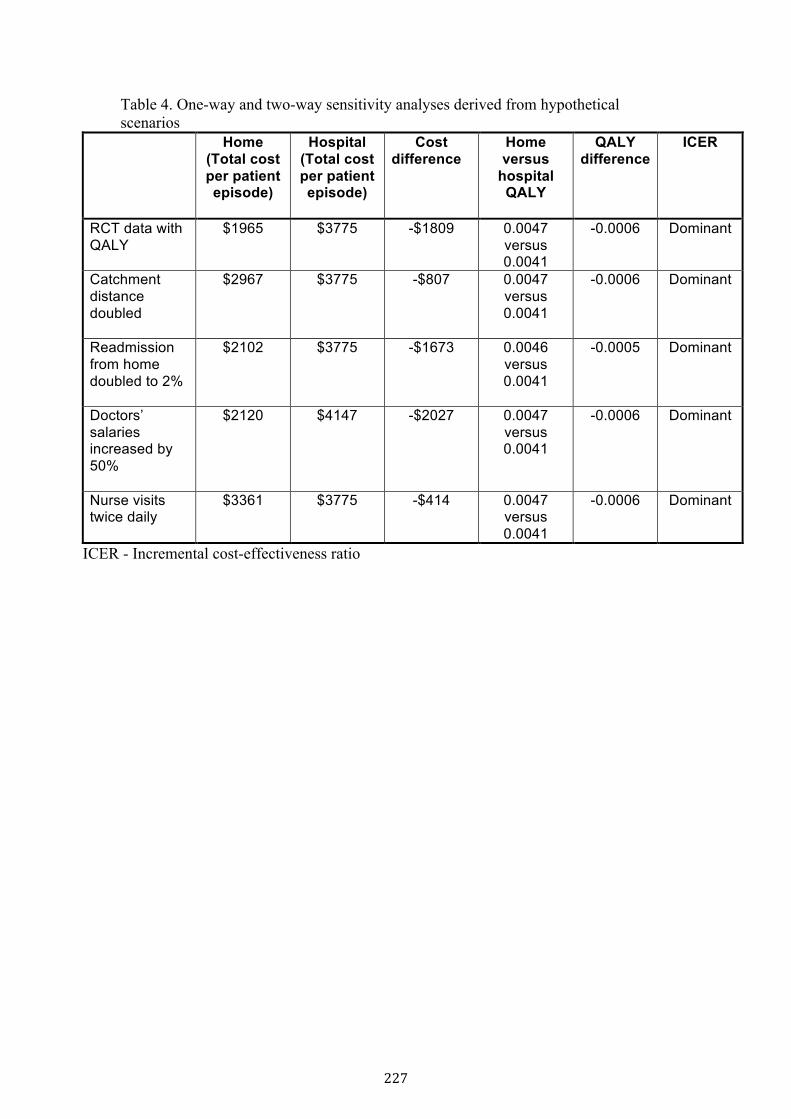
Table 4. One-way and two-way sensitivity analyses derived from hypothetical scenarios
Home (Total cost per patient episode)
Hospital (Total cost per patient episode)
Cost difference
Home versus
hospital QALY
QALY difference
ICER
RCT data with QALY
$1965 $3775 -$1809 0.0047 versus 0.0041
-0.0006 Dominant
Catchment distance doubled
$2967 $3775 -$807 0.0047 versus 0.0041
-0.0006 Dominant
Readmission from home doubled to 2%
$2102 $3775 -$1673 0.0046 versus 0.0041
-0.0005 Dominant
Doctors’ salaries increased by 50%
$2120
$4147
-$2027
0.0047 versus 0.0041
-0.0006 Dominant
Nurse visits twice daily
$3361 $3775 -$414 0.0047 versus 0.0041
-0.0006 Dominant
ICER - Incremental cost-effectiveness ratio
227
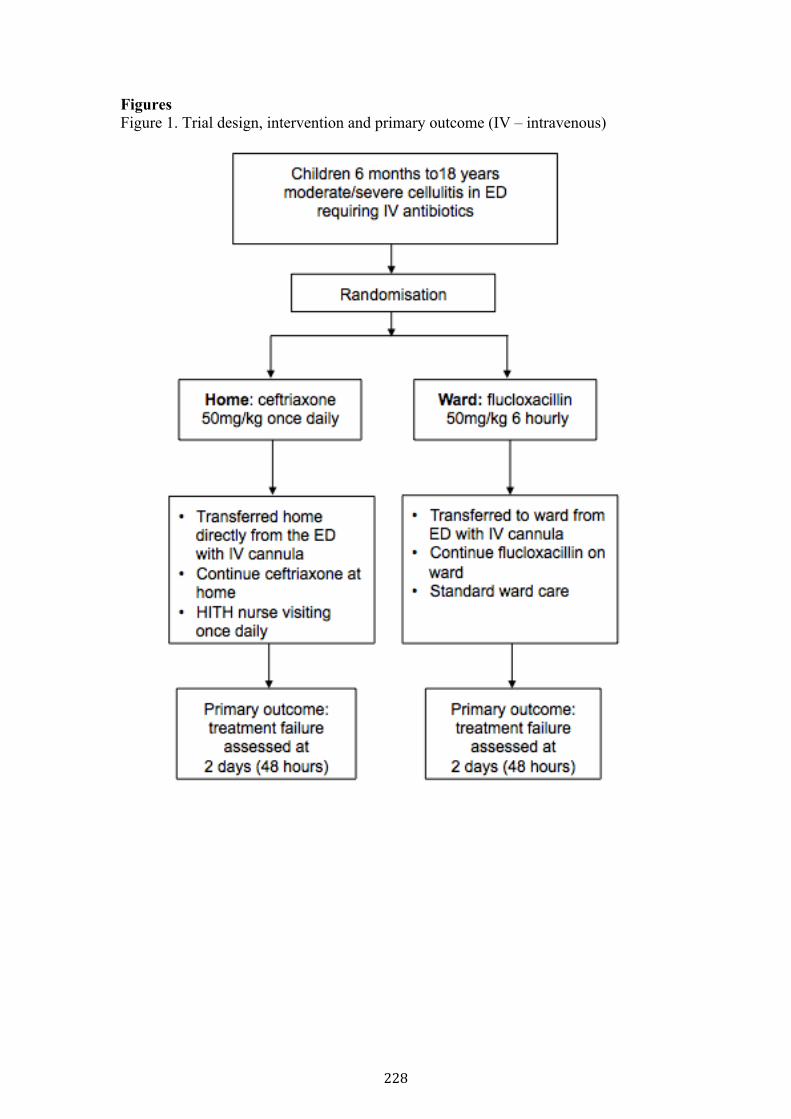
Figures Figure 1. Trial design, intervention and primary outcome (IV – intravenous)
228
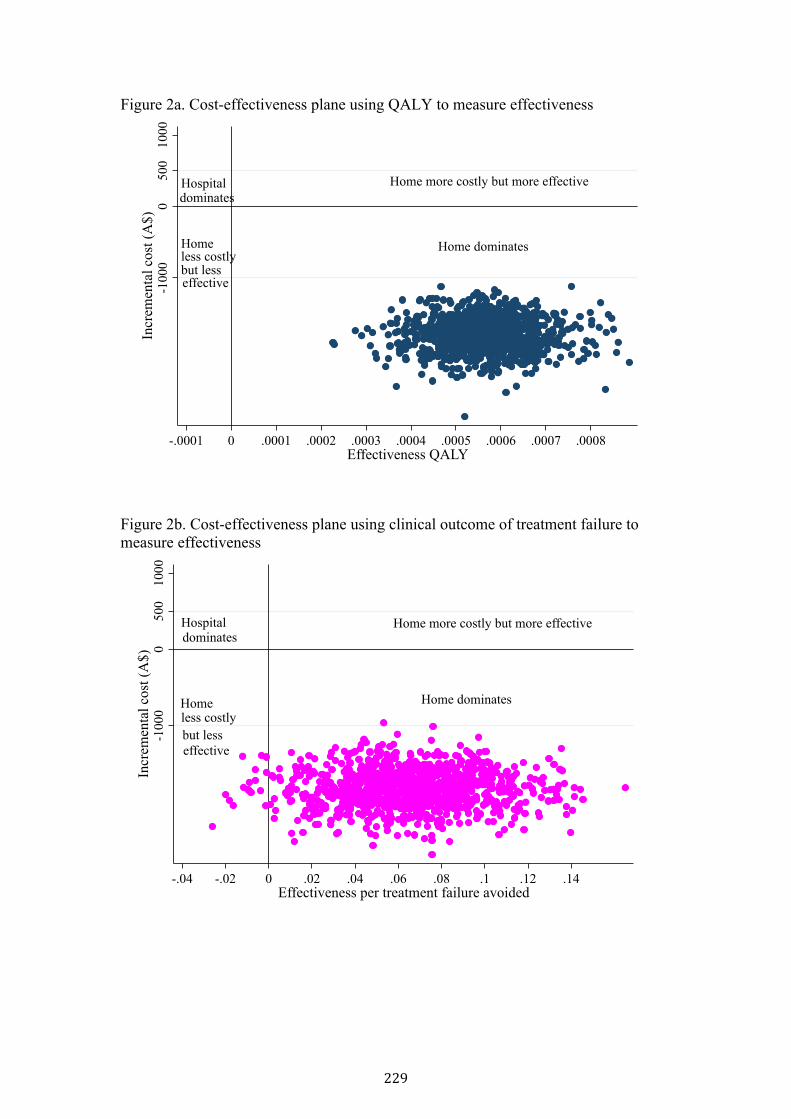
Figure 2a. Cost-effectiveness plane using QALY to measure effectiveness
Figure 2b. Cost-effectiveness plane using clinical outcome of treatment failure to measure effectiveness
Home more costly but more effective
Home
Hospitaldominates
less costlybut lesseffective-1
000
05001000
Incr
emen
tal c
ost (
A$)
-.0001 0 .0001 .0002 .0003 .0004 .0005 .0006 .0007 .0008Effectiveness QALY
Home dominates
Home more costly but more effectiveHospitaldominates
Homeless costlybut lesseffective
-1000
0500
1000
Incr
emen
tal c
ost (
A$)
-.04 -.02 0 .02 .04 .06 .08 .1 .12 .14Effectiveness per treatment failure avoided
Home dominates
229
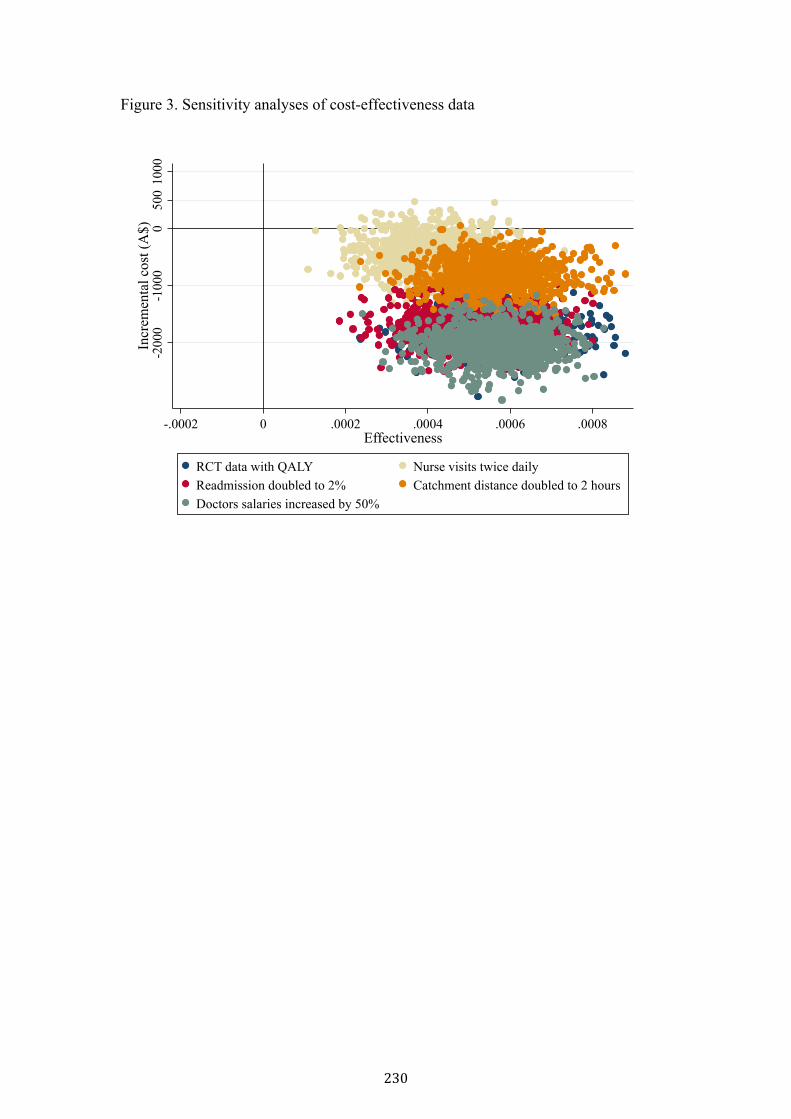
Figure 3. Sensitivity analyses of cost-effectiveness data
-200
0-1
000
050
010
00In
crem
enta
l cos
t (A
$)
-.0002 0 .0002 .0004 .0006 .0008Effectiveness
RCT data with QALY Nurse visits twice dailyReadmission doubled to 2% Catchment distance doubled to 2 hoursDoctors salaries increased by 50%
230
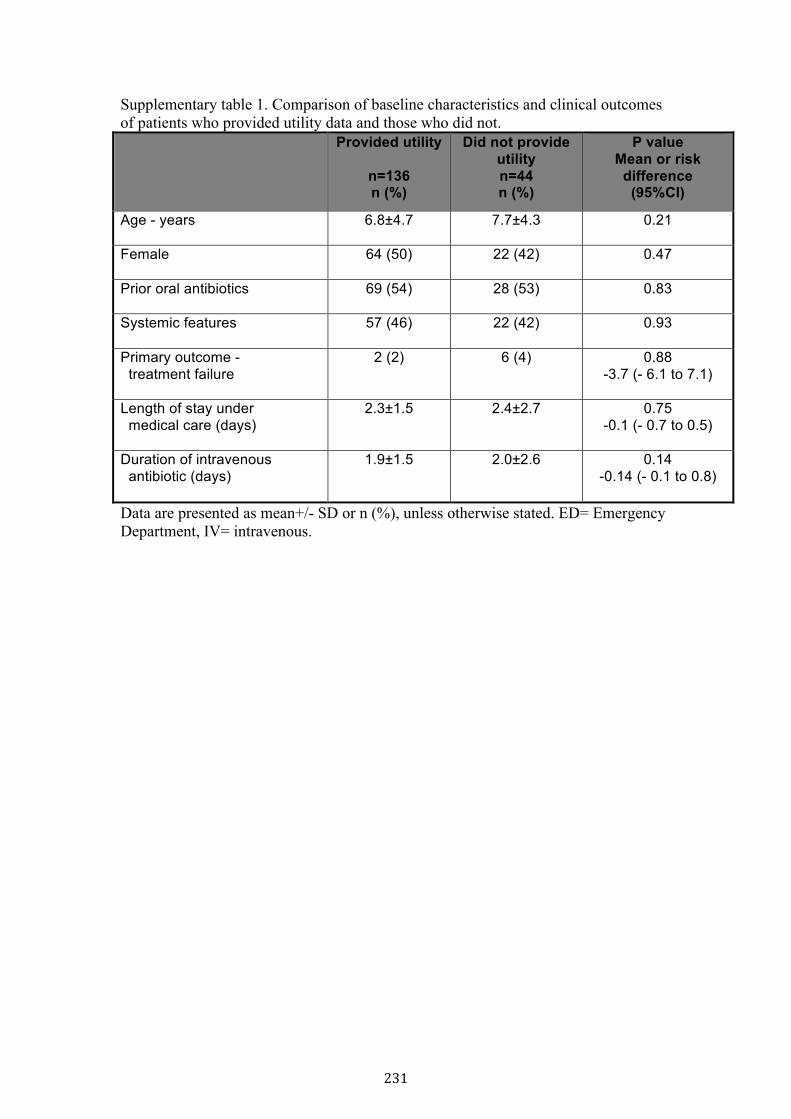
Supplementary table 1. Comparison of baseline characteristics and clinical outcomes of patients who provided utility data and those who did not.
Provided utility
n=136 n (%)
Did not provide utility n=44 n (%)
P value Mean or risk
difference (95%CI)
Age - years 6.8±4.7 7.7±4.3 0.21
Female 64 (50) 22 (42) 0.47
Prior oral antibiotics 69 (54) 28 (53) 0.83
Systemic features 57 (46) 22 (42) 0.93
Primary outcome - treatment failure
2 (2) 6 (4) 0.88 -3.7 (- 6.1 to 7.1)
Length of stay under medical care (days)
2.3±1.5 2.4±2.7 0.75 -0.1 (- 0.7 to 0.5)
Duration of intravenous antibiotic (days)
1.9±1.5 2.0±2.6 0.14 -0.14 (- 0.1 to 0.8)
Data are presented as mean+/- SD or n (%), unless otherwise stated. ED= Emergency Department, IV= intravenous.
231
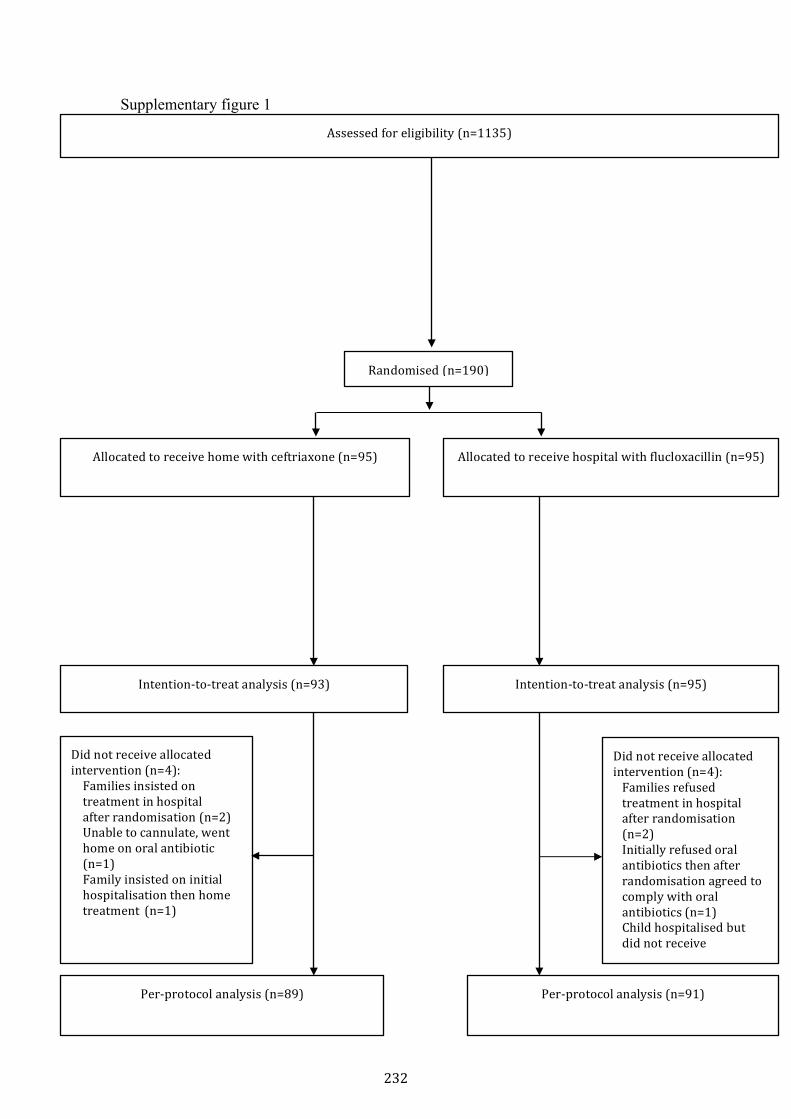
Supplementary figure 1
Randomised (n=190)
Allocated to receive home with ceftriaxone (n=95)
Assessed for eligibility (n=1135)
Allocated to receive hospital with flucloxacillin (n=95)
Per-‐protocol analysis (n=89)
Per-‐protocol analysis (n=91)
Did not receive allocated intervention (n=4): Families insisted on treatment in hospital after randomisation (n=2) Unable to cannulate, went home on oral antibiotic (n=1) Family insisted on initial hospitalisation then home treatment (n=1)
Did not receive allocated intervention (n=4): Families refused treatment in hospital after randomisation (n=2) Initially refused oral antibiotics then after randomisation agreed to comply with oral antibiotics (n=1) Child hospitalised but did not receive intravenous
Intention-‐to-‐treat analysis (n=93)
Intention-‐to-‐treat analysis (n=95)
232

Legend Figure 1. Trial profile The intention-to-treat analysis included all randomised participants where outcome data were available, regardless of treatment received. The per-protocol analysis included all individuals that received treatment as per randomised allocation and did not encounter any major protocol violation such as: received treatment in the hospital if randomised to the home group, or received treatment at home if randomised to hospital group or did not receive any study treatment.
233

234
235
6.4 Implications of the cost-‐effectiveness analysis
Previous studies suggest that children and their families benefit from avoiding
hospital admission where feasible. A number of non-‐randomised studies suggest
that the ambulatory or OPAT pathway is less costly than standard hospital
care.38,147 In this first comprehensive economic evaluation of home versus
hospital treatment for any condition in children,30 home treatment for cellulitis
was shown to be convincingly dominant. There is published evidence that
children with moderate/severe cellulitis can be safely and effectively treated at
home1,2,115 and this study now provides the cost-‐effectiveness evidence.
The strength of this study, planned meticulously alongside the RCT, are that the
costs to the institution were obtained for each individual patient in the study,
enabled by liaising with the institutional clinical costing unit. Previous studies
have used the method of diagnosis related grouping (DRG) to calculate costs to
the institution.26,115 The DRG is based on the average cost for a number of
patients with a particular diagnosis, in this case, cellulitis. However, this average
is likely to be inaccurate due to this diagnosis being recorded by junior clinicians
or by non-‐clinicians in many places. For example using the DRG method in the
foundation cohort study, to estimate cost to the institution resulted in a mean
cost for the home group to be AUD530 versus AUD1297 for the hospital group. In
contrast, patient level data reflect the real costs involved during the intervention,
resulting in a mean cost for the home group to be AUD970 versus AUD2388 for
the hospital group. The 45% difference in costs obtained using two different
methods, particularly when extrapolating for a larger population has a
substantial impact. The same is true for modeling studies.147 Cost-‐modeling
studies estimate costs using secondary data, whereas real individual patient level
data adds to the precision of a cost-‐effectiveness analysis.
Of equal importance in this study was obtaining the burden of costs to families
usually not considered in previous studies.31 This may be because of an
assumption that costs of home or hospital treatment is no different for families,
236
that these data are considered hard to gather accurately, or because this is not
considered important. One previous study on children with cancer receiving
chemotherapy infusions at home, stated that data on parental absence from
work was not gathered due to the assumption that regardless of treatment
location, absence from work would not differ.23 As shown in our study, the cost
to families for absence from both paid and unpaid work, was significantly less
(AUD171 versus AUD542, p<0·001) for children in the home group. This also
highlights how much less disruption there is to daily family routine with home
treatment, previously shown in the RCT.142 We were thorough with measuring
the burden of costs to families, taking into account paid and unpaid employment,
medical expenses as well as other expenditure such as childcare, food,
accommodation and travelling.
To measure effectiveness in the RCT, the CHU9D was chosen due to this
questionnaire having low response burden.153 This quality of life tool was
developed using research in children, is brief and simply worded and is available
in proxy and self-‐report forms.146 It uses a shortened reference time frame
(‘today’) suitable for an acute illness. The nine domains which include daily
routine, social activities, sleep and pain are relevant in comparing home versus
hospital care and the tool has been validated in Australia and the UK. Due to the
many appealing features, the tool has been used widely in the literature in many
different populations.154,155 This tool allows rapid conversion of the answers
obtained to utility scores by using an algorithm. Utility scores can then be
conveniently converted to QALY by multiplying the utility scores with the time
horizon.
QALY are considered to be the cornerstone of economic analysis, which
combines both morbidity gains and the mortality impact of a treatment.145 QALY,
through the incorporation of utilities as measured using the CHU9, aid decision-‐
making in healthcare in order to prioritise limited resources. In addition to use
for economic evaluations, quality of life data can also be useful in monitoring an
individual patient's health status, the measurement of population health or the
effect of therapies in clinical studies.144 Although health economists are familiar
237
with terms such as QALYs and ICER, ultimately, clinicians would interpret
effectiveness from a clinical perspective. Many studies present the effectiveness
data using clinical outcomes, the disadvantage being how highly specific this
outcome is to the disease.139 This limits the ability to compare the ICER with
other interventions. Therefore, to be relevant to all stakeholders and to provide
robustness to the results, it was important to calculate the ICER using both
effectiveness measures: the clinical outcome from the RCT and QALY.
This is the first time that a cost-‐effectiveness analysis has been performed using
a randomised cohort in the literature of either paediatric or adult OPAT. It has
the potential to act as a platform for societal and resource analysis for all
admission avoidance and home management. In addition to supporting the
hypothesis that treatment at home is cost-‐effective compared to hospital care,
we found that families incur three-‐fold higher costs when their child is treated in
hospital compared to at home – a factor often forgotten when deciding to admit
patients to hospital. These findings are crucial in the risk/benefit conversation of
home versus hospital management.

238
Chapter 7 Discussion
7.1 Introduction to key findings
This thesis was driven by the belief that home is a better place to treat children
than hospital, if it is feasible and appropriate to deliver care there. Unfortunately,
a lack of evidence has hampered universal implementation of this practice, as it
has remained unclear for which children and which treatments this is a suitable
option. This evidence vacuum led to a number of research questions addressed
in separate phases of work, represented by the different chapters in this thesis.
At the beginning of the PhD journey was a detailed interrogation of the literature
to identify the current evidence for the use of intravenous antibiotics in children
outside the hospital setting, and the management of cellulitis as a paradigm,
including efficacy, safety, quality of life, cost, hospital-‐acquired infections, and
antibiotic resistance (Chapter 1). Identifying the gaps led to the research aims
outlined at the beginning of this thesis, which were: 1) to better understand
current practice in the management of moderate/severe cellulitis; 2) to develop
and validate a system for determining which patients with cellulitis need
intravenous antibiotics; and 3) most importantly, to investigate clinical and non-‐
clinical outcomes of home versus hospital intravenous treatment in children
presenting to the emergency department with uncomplicated moderate/severe
cellulitis. The overarching goal was to improve the evidence to improve the
practice.
The research encompassed in this thesis addressed and achieved these aims in
three parts: 1) studies to better understand current practice and the reasons
behind it (Chapter 2); 2) studies to assess the feasibility and inform the key
design elements of the RCT (Chapters 3 and 4); and 3) the RCT which included
outcomes of efficacy, safety, antibiotic resistance, quality of life and
incorporating a cost-‐effectiveness analysis of home versus hospital care (Chapter
5 and 6).
239
The aim of this chapter is to summarise the overall key findings of the work in
this thesis and place them in context of the existing literature, and then to
discuss the implications of these findings on practice and future research. Each
study described in the thesis already has a thorough discussion in the
manuscript included in the chapters. This discussion chapter is exploring a
broader perspective.
7.2 Home versus hospital for intravenous antibiotics
The RCT that forms the crux of this thesis remains the only randomised trial in
children investigating a pathway completely avoiding hospital admission. In
addition to the studies described at the beginning of this thesis, the studies that
have been published since the start of this PhD include a systematic review of
OPAT in acute infections.156 In this thorough review, the authors emphasised the
lack of randomised trials that would clarify which patient populations are
amenable to OPAT. Only two other studies of home versus hospital care have
been published since Chapter 1 was written: both of these studies were based on
OPAT in the same institutional (hospital) setting as this thesis, the RCH, and
investigated the outcomes of patients with UTI and meningitis.157,158 In addition,
three other OPAT studies which describe the patient characteristics and
outcomes of those treated on OPAT, have been published but do not have a
hospital comparison group.12,13,159 The following sections will describe the key
findings of this thesis in the context of the literature to date.
7.3 Is home treatment as efficacious as in hospital?
Efficacy is often measured by the proportion of treatment failure in comparative
home versus hospital care studies.31,115 In the three studies in this thesis
(baseline: Chapter 2, foundation: Chapter 3, RCT: Chapter 5) comparing home
versus hospital for the treatment of moderate/severe cellulitis, ceftriaxone at
home was as efficacious as in hospital. Efficacy measured by the rate of
treatment failure in all three studies was no different between home and hospital
care. In the first baseline study, this was 2/41 (5%) versus 7/103 (7%)
240
respectively, OR 1.4, (95% CI 0.3 to 7.1), p=0.67, whereas in the foundation
cohort study, the treatment failure rates were 2/47 (4%) versus 8/59 (14%), OR
0.28 (95% CI 0.0 to 1.3), p=0.10. These initial findings, despite not being
randomised, were consistent with the subsequent findings of the RCT (Chapter
5), which had treatment failure rates of 2/93 (2%) versus 7/95 (7%)
respectively, risk difference 5.3 (95% CI -‐11.3 to 0.8), p=0.09. The consistency of
these findings is reassuring and adds to the weight of the evidence.
The findings of treatment failure in these three studies (baseline, foundation,
RCT) cannot be directly compared with other studies on moderate/severe
cellulitis due to the difference in the definition of efficacy. In particular, the two
other studies within the literature on moderate/severe cellulitis measured
efficacy by the rate of readmission to hospital during treatment and did not have
a comparator group.1,2 Nevertheless, in the Canadian study, the rate of
readmission to hospital during treatment was quite high at 21%, compared to
4% in the foundation cohort study and 1% in the RCT. There were no
readmissions during home treatment in the baseline study. One possible reason
for this is the ability to consult other specialist teams at the institution where the
RCT was conducted. For example, in cases where there was suspicion of a joint
involvement, orthopaedic surgeons were contacted to obtain an opinion or
advice over the phone or as part of an unscheduled outpatient review. It was also
possible to organise imaging such as ultrasonography without admission to
hospital. This represented an institutional level support to keep children out of
hospital whenever feasible. Another reason to explain the high rate of
readmission in the Canadian study was the location of the day treatment centre
which being close to or even a part of the hospital potentially makes it easier for
clinicians to decide to readmit patients whereas when the patient was at home,
asking patients to return to hospital was a burden to families, encouraging
clinicians to consider the decision to readmit only when absolutely necessary. In
addition, 11% of those treated at the day treatment centre lived further than 50
kilometres from the centre. This would likely lead to a far more cautious
approach and a lower threshold to direct patients to hospitalisation.
241
In a study of children treated for pyelonephritis, where a comparison was made
between OPAT and hospital in acute conditions, the readmission rate was no
different between the home and hospital group.157 Other comparative studies
had different measures of efficacy. In the only previous randomised study of
home versus hospital care, comparing the treatment of febrile neutropenia in
children with cancer, the primary outcome was not efficacy but quality of life.
With only 36 patients in this trial, it was not powered for clinical outcomes7.
Despite the majority of studies showing no difference in efficacy for home versus
hospital care in patients with cystic fibrosis, several studies160,161 have
documented a significantly greater clinical improvement in the hospital group
than in the home group, even though all studies showed an improvement in
forced expiratory volume in 1 second (FEV1) for both the home and hospital
patients. The reason for this is most likely due to the hospital group receiving
more physiotherapy due to increased resources and adherence. Another possible
explanation may be that hospital-‐based patients may have had access to a
multidisciplinary team for example, a dietitian and endocrinologist. If more
resources were available to the home patients, results may have been different.
For example, physiotherapy and consultations with a multidisciplinary team
could be delivered virtually via telehealth while the patient is at home.162
In summary, the findings of treatment at home being as efficacious as hospital in
this thesis may be extended to other patient populations.
7.4 Is home treatment as safe as in hospital?
In order to expand and increase the uptake of the home pathway, it is equally
important to document safety, with hospital treatment being the standard
against which OPAT should be compared. In the clinician survey (Chapter 3), a
quarter of clinicians revealed their reluctance to use OPAT due to the perceived
risk of a child deteriorating unnoticed. If anything, treatment at home needs to
be safer than hospital treatment because of the lack of clinical support available
if an adverse event occurs at home.

242
In addition to adverse events, considerations of safety also include complications
of the disease occurring at home. In the survey, 20% of clinicians expressed
concern with the risk of missing a complication with home treatment.
Complications are generally disease-‐specific, and for cellulitis, this is most
commonly development of an abscess that requires drainage. For the baseline
study, there were no complications documented for those who received home
treatment. In the subsequent foundation cohort study, the combined risk of
complications and adverse events were no different between home and hospital,
3/47 (6%) versus 6/59 (10%), OR 0.74 (95% CI 0.2 to 3.0), p>0.05. In the RCT,
the complication rate of abscess formation was no different between the home
and hospital group at 6% in each arm. This finding was very similar to a previous
Canadian study investigating the outcomes for the treatment of moderate/severe
cellulitis at a day treatment centre with a 7% abscess formation rate. This low
overall complication rate is expected, as cellulitis is not associated with major
complications compared to other conditions, for instance, post complicated
appendicectomy or febrile neutropenia where complications could potentially be
more serious.38,112
In a study of antibiotic treatment post complicated appendicectomy, there were
52/150 patients treated at home for the last 5 days of a 10-‐day piperacillin-‐
tazobactam course through a peripherally inserted central catheter (PICC) line.38
After treatment, 4/52 (8%) patients from the home group while 5/98 (5%) from
the hospital group required readmission to the hospital for complications
including phlegmon, abscess, bowel obstruction, fever or abdominal pain. (no
statistical analysis in the published paper).38 Two other studies on complicated
appendicectomy described either the absence of complications, or no difference
between home and hospital-‐based patients on the subsequent development of an
intraabdominal abscess.32,163 However, none of these studies are completely
reassuring as they are not randomised studies.
In a randomised trial of 37 episodes of febrile neutropenia comparing
intravenous cefepime administered twice per day in hospital or at home,
complications were defined as a change in antimicrobial treatment. Six out of
243
eighteen (33%) home patients required a change in antimicrobial treatment
because of positive blood cultures, prolonged fever, or clinical change, whereas
only 3/19 (16%) inpatients required a change because of positive blood cultures
or clinical change. Although the proportion was higher in the home group, the
small number of patients in this trial makes it difficult to interpret. Additionally,
there was no specified objective way to decide on change of treatment, with
potentially many different clinicians involved with differing management
approaches. With the parameters for treatment change being subjective, medical
staff might have been more cautious with home-‐based patients resulting in the
higher proportion of change in antimicrobial treatment.
Regarding adverse events, in the RCT (Chapter 5), an unexpected finding was
that adverse events occurred more frequently with hospital care than at home:
2/93 (2%) versus 10/95 (11%), OR -‐9.8, (95% CI -‐19.5 to -‐0.1), p=0.048. These
comprised the following: home: rash (1), dosing error (1); hospital; diarrhea or
vomiting (7), headache (1), vasovagal episode (1), and hypotension (1). The
patient with hypotension had intermittent low blood pressure and looked
clinically well throughout. Of note, diarrhea and vomiting occurred only in the
hospital group. This may have been attributed to treatment location, a result of
hospital-‐acquired gastroenteritis or it may have been a side effect of the
antibiotic in hospital, flucloxacillin. Regardless of the cause, this did not occur for
those assigned home treatment. Another unexpected outcome was the higher
need for repeat peripheral cannula insertion in the hospital group, compared to
the home group. A concern that parents have previously expressed when
receiving home treatment is that the peripheral intravenous cannula could be
accidentally pulled out at home, by the patient or siblings. The findings in this
RCT can be reassuring to the parents whose children are treated via this
pathway in future. In other patient populations, adverse events were assessed in
five studies on cystic fibrosis, but were found to be similarly low or absent.26,164-‐
167 In the RCT of children with febrile neutropenia, there were no adverse events
due to cefepime or outpatient management.7
244
The findings from studies of this thesis have shown that the risks of adverse
events and complications at home are likely to be similar to the risks in hospital.
Importantly, there have been no serious adverse events or mortality in children
treated at home, although these studies were not powered for these safety
outcomes. Nevertheless, this finding is reassuring that even when patients are
not pre-‐selected to have treatment at home, as was the case in the RCT,
treatment at home appears to be just as safe as standard care.
7.5 Do home intravenous antibiotics have different implications on acquisition of bacterial resistance than in hospital?
There is no other study to date investigating the impact of acquisition or
colonisation of bacterial resistance with the use of intravenous ceftriaxone.
Despite the almost universal concern that third generation cephalosporin use
induces resistance and that studies of paediatric OPAT invariably show that the
most frequently used antibiotic is ceftriaxone, this association has never been
investigated.3,13,159 One reason for this, which was experienced in the RCT, may
be the difficulty in collecting stool samples from children who are continent,
relying on both parents and children, and the rapid processing needed to ensure
optimal culture results.168 There may also be reluctance to investigate this in
case ceftriaxone, a very useful OPAT drug, is found to cause a major problem. We
believed that it was important to be informed about this potential risk and
therefore be able to balance the advantages and disadvantages of OPAT, rather
than continue to ignore the issue. The findings in this RCT provide the most
robust evidence to date that short course ceftriaxone at home is not associated
with an increase in the risk of ESBL, VRE, C. difficile and MRSA carriage,
compared to treatment with flucloxacillin in hospital.
There is in fact not that much evidence that ceftriaxone use causes an increase in
antimicrobial resistance in children. Most published studies on this topic are
time associations, without strong causal links, and at least one time series in
neonates showed ESBL-‐producing bacteria increased despite no increase in third
generation cephalosporin use.169 During 25 years in a tertiary neonatal unit, an
increase in colonising cephalosporin-‐resistant Gram-‐negative organisms was
245
documented, despite this unit intentionally not using broad-‐spectrum antibiotics
such as meropenem and third generation cephalosporins. The authors propose
that their finding highlights the complex relationship between antimicrobial use
and drug resistance, with other factors including increasing travel by families
with overseas acquisition of resistant organisms.
Although VRE has emerged as a major healthcare problem in Australia, with
numbers higher than in any European country, in the RCT, there were no
samples that cultured VRE, at baseline or subsequently.170 This is in keeping with
a low rate of colonisation of VRE in an otherwise healthy community cohort.87
One retrospective study described a direct association between ceftriaxone use
and VRE bacteraemia in the following month after ceftriaxone use, in a
population consisting of hospitalised adults with multiple co-‐morbidities.
However, this study did not take into account the severity of illness or co-‐
administration of antibiotics, which may have confounded the results.
C. difficile colonisation and acquisition in our RCT was also not different between
the two groups. The baseline carriage rate for C. difficile was 10/90 (11%) of
children in the RCT. In the literature, colonisation rates in healthy children from
outpatient settings have been documented to be 3.5% in children aged more
than 12 months and as high as 44% in children aged 1 to 12 months.97,171
Asymptomatic C. difficile colonisation can be detected in the absence of
symptoms of infection.172 None of the patients in the trial reported symptoms to
suggest C. difficile infection (CDI). However, asymptomatic C. difficile colonised
patients potentially act as an infection reservoir and may present a risk to
others.173,174 Hospitalisation is a known risk factor for colonisation with C.
difficile.175-‐177 In one epidemiological study to investigate risk factors for
healthcare-‐associated C. difficile colonisation, hospitalisation within the previous
12 months, exposure to corticosteroids, history of CDI and presence of antibody
against toxin B were significantly associated with C. difficile colonisation. In the
RCT, neither the hospitalised children nor those treated at home developed an
increased risk of C. difficile colonisation or acquisition. This is likely due to the
fact that children in the hospital group had a mean length of stay of only 1.7 days.
246
Additionally children who were hospitalised were admitted to the short stay
unit, mainly consisting of generally healthy children with short-‐term illnesses.
Regarding MRSA, in the RCT, the baseline risk of colonisation in those who
present with cellulitis was low in our region.142 The prevalence of MRSA
colonisation in the community is estimated to be between 0.2% and 7.4%.178
Nasal colonisation with MRSA was consistently low in the foundation cohort and
the RCT. More importantly, there was no increase in nasal colonisation after
antibiotics up to 1 year later, as investigated in the foundation nasal colonisation
study (Chapter 3). Several studies in adults have shown antibiotic use to be a risk
factor for colonisation with MRSA,179,180 but in our nasal colonisation study there
were no cases of acquisition in either antibiotic group, even if they also had
additional antibiotics in the ensuing 12 months.142 The prevalence of MRSA in
our population is low to begin with, and the absence of new acquisition may be
related to the relatively short antibiotic duration in the study. In a study of
healthy pre-‐school children, antibiotic use in the previous three months did not
increase nasal colonisation with MSSA or MRSA, but amoxicillin/clavulanate use
increased the proportion of MSSA that produced penicillinase, a potential early
step towards resistance.111 In our studies, short course ceftriaxone use at home
in children is not associated with acquiring MRSA, unlike in studies in
adults.69,181
Nasal colonisation with S. aureus plays a key role in the pathogenesis of invasive
infection including cellulitis and bacteremia98-‐100,182 Few studies explore the risk
factors for methicillin-‐sensitive S. aureus (MSSA) colonisation, which in many
settings causes a higher proportion of invasive infections than MRSA and is
associated with a similar mortality.183,184 Reported risk factors for colonisation
by both MSSA and MRSA in children include prior antibiotic use and
hospitalisation.21,105-‐107 However these findings are from a relatively small
number of studies, relying on recollection of antibiotic use, predominantly
screening healthy children, and there is conflicting evidence on the importance
of antibiotic exposure as a risk factor. For the first time the effect of different
antibiotics was investigated prospectively, which found that reassuringly,
247
ceftriaxone at home did not increase the risk of nasal colonisation. Additionally,
the nasal colonisation study showed that colonisation was not significantly
associated with the severity of concurrent infection.
We accept that considering only 50% of patients provide samples in the RCT, the
other possibility for our finding is that the results were biased and reflect a
skewed sample of only the children who were not colonised by the organisms
discussed above. However, a detailed analysis comparing demographics, clinical
features and outcomes showed that the tested patients were for the most part,
clinically indistinguishable from those that did not provide a sample. In fact, the
only differences was that those who provided stool samples were slightly
younger than those who did not and those with treatment failure were less likely
to provide follow up stool samples than those without. Previous studies
suggesting the role of third generation cephalosporin in the rise of resistance
have been in hospitalised adult or neonatal patients with multiple comorbidities
and risk factors.80,82 None of the previous studies in the literature have
investigated healthy children treated with short course ceftriaxone. It is likely
that ceftriaxone can cause increase in resistance but that short-‐term use has low
risk for this. Therefore the risk benefit ratio needs to be weighed up rather than
to persist with dogmatic assertions that ceftriaxone use will universally lead to
increased resistance. On this subject it is important to know the risks of
treatment in hospital compared to home and the RCT is the first attempt to
provide an assessment of risks of home treatment. The findings from this thesis
points to a multifactorial causation for bacterial resistance and stresses the
importance of detailed interrogation of the literature before a blanket policy on
the use of antibiotics.
7.6 What is the impact of home treatment on satisfaction and quality of life?
The literature on OPAT investigating the patient’s or family’s perspective
consists of three aspects. Firstly, satisfaction with the service or care provided,
secondly preference for either OPAT or hospital, and lastly, quality of life has
been addressed, with the latter rarely assessed in studies.1,6,7,147 With regards to
248
satisfaction, parents of children enrolled in the RCT rated their experience with
the service provided on a scale of 0 to 5. A higher proportion (95%) of parents of
children in the home group reported having very good experience during
treatment than parents of children in the hospital group (73%). This finding is
similar to a Canadian study where patients with cellulitis were treated at a day
treatment centre, where 95% of families rated their experience as very good to
excellent.1 However, our study is the first study to compare satisfaction between
home and hospital groups in non pre-‐selected patients.
In the clinician survey (Chapter 2), the majority of physicians at RCH 81/96
(84%) believed that more than 60% parents would prefer treatment at home. In
the foundation cohort study (Chapter 3), 60% of all parents, regardless of where
their child was treated, stated that they would prefer home-‐based treatment, and
no parents of children treated at home would have preferred to be in hospital.
Sixteen percent of parents preferred hospital treatment (all of whom had
received treatment in hospital). In the RCT, when patients were not pre-‐selected,
97% of the home group and 42% of the hospital group would choose treatment
for their child in the same location. Preference for ambulatory treatment was not
limited to treatment at home. In the Canadian study of children with cellulitis,
despite having to travel for treatment at a day treatment centre for daily
ceftriaxone, 69% would prefer future treatments via the same pathway.1 In a
different study of 36 children with a variety of acute infections such as cellulitis,
UTI and lymphadenitis, parents travelled daily to the ED for medical review and
intravenous ceftriaxone. Despite having to travel, 94% of families would choose
the same method of ambulatory treatment again.6 This emphasises the fact that
parents appear to be willing to accept some degree of inconvenience, in order to
avoid hospitalisation for their child.
Quality of life for both parents and children were measured in the RCT. Parental
quality of life was measured using a modified rating scale which was based on a
two previous studies comparing home to hospital care.7,23 Questions were
around the ability for parents to maintain their daily routine, despite having a
child who requires treatment with intravenous antibiotics. Parents from the

249
home group were significantly more able to keep up with household tasks, spend
time with their partner and spend time with their children compared to parents
from the hospital group. Similar to our finding, in another randomised study of
children with cancer presenting to the ED with febrile neutropenia, the authors
found that parents in the home group were significantly more able than those in
the hospital group, to keep up with household tasks and spend time with their
partner and children. Although the patient cohort in the RCT were healthy
children, experiencing acute infection, the similar findings in the study on
children with cancer, suggest that parental perception of higher quality of life at
home, is not predicated on having children who are chronically unwell with
frequent hospitalisation episodes.7 Even in acute illness, quality of life is better
for parents with treatment at home.
There are no previous OPAT or ambulatory care studies that have measured
utility scores with a validated quality of life questionnaire. In the RCT, children’s
quality of life was measured using the CHU9D. This provides an objective
measure of quality of life that provides robust evidence to support the widely
held perception that children have better quality of life with treatment at home.
Additionally, this questionnaire allows calculation of quality of life in terms of
utility scores for conversion to cost-‐effectiveness measures, such as QALY. The
CHU9D has been validated in multiple languages and in various medical
conditions.185,186 This tool enables a single score to be given to a combination of 9
domains assessed, which are sleep, appetite, routine, pain, schoolwork, activities,
worry, tiredness and sadness. The difference found between the home and
hospital group was highly significant, 0.86 versus 0.75, mean difference 0.11,
(95% CI 0.07 to 0.14), p<0.001. There is one previous comparative study that has
measured utility scores by using visual analogue scales. Parents of children with
cancer were asked to imagine a scenario where their child had febrile
neutropenia and could receive one of four possible treatment options. In this
study, the utility score obtained for home intravenous treatment was 0.70
compared to 0.67 for treatment in hospital, a mean difference of 0.03 (OR or p
value not reported in study). Our finding of a larger mean difference between
home and hospital treatment is more likely to be accurate considering the fact
250
that we measured quality of life in patients actually undergoing treatment as
opposed to a hypothetical cohort.
The RCT as well as the preceding foundation cohort study contributes to the
literature by showing that parents and children have a significantly higher
satisfaction and quality of life with treatment at home. If given the choice, most
families would prefer to avoid hospitalisation.
7.7 Which patients with cellulitis need intravenous antibiotics?
In all of the previous studies investigating cellulitis, the criteria for diagnosis of
moderate/severe cellulitis requiring intravenous antibiotics were based on
‘clinical judgement’.1,6,43 This is likely due to the absence of standardised
guidelines. The implication of this is potential unwarranted variation in care,
which may lead to over-‐ or under-‐use of intravenous antibiotics.
The RCT in this thesis similarly relied on the ED doctor to make a clinical
judgement to decide who needed intravenous antibiotics. Although senior
clinicians make the decisions about intravenous antibiotic use in the ED at our
institution, and we have relatively low rates of intravenous antibiotic use for
cellulitis compared to other centres, differences in judgement and variation in
care may have resulted in a few patients being enrolled in the RCT who could
have been treated with oral antibiotics.43,120 Even though in a randomised study
these patients should be distributed equally in both groups, we realised that a
more objective standardised method of determining the need for intravenous
antibiotics would be useful clinically and in research settings. This led to the
derivation and validation of the Melbourne ASSET score.
When appropriately developed and validated, clinical risk scores such as the
Melbourne ASSET score likely have inherent advantages over human clinical
decision-‐making. Firstly, the statistical models can accommodate many more
factors than the human brain is capable of taking into consideration.126 Secondly,
if given identical data, a statistical model will always give the same result,
whereas human clinical judgment has been shown to result in both inconsistency
251
and disparity, especially with less experienced clinicians and when other factors
such as tiredness are involved.126,187 Of the trainee doctors in the clinician survey
(Chapter 3), 31/ 40 (78%) responded that a clinical score would be useful.
Finally, and perhaps most importantly, several prediction models have been
shown to be more accurate than clinical judgment alone.126,127,187,188 Despite
these advantages, many clinical risk scores do not gain traction.62,189 One reason
for low implementation of clinical prediction rules is the sheer number of models
available, for instance there are multiple different predictive rules for paediatric
head injury.190 If many prediction rules exist for the same problem, identifying
the best one is difficult.190 Not only is this potentially time consuming but also
differences in the methods used in the studies on which they are based, may
make reliable comparison impossible.191,192
The Melbourne ASSET score was designed with applicability in mind.123 Firstly,
the acronym ASSET stands for the features required to make the assessment.
Secondly, the five features that make up this score, correlate with the number of
fingers on one hand, making it easy for clinicians to check the number of features
off while also using the hand-‐size measure. The incorporated hand-‐size method
to assess the contribution of the area of cellulitis to the score, is simple and
convenient. Additionally it is a score based solely on clinical features, with no use
of invasive or delaying tests. All of these features ensure that a child with
cellulitis can be examined rapidly in ED or primary care with a score that is easy
to calculate. In the clinician survey, when asked if clinicians believed a clinical
score would be helpful to guide decision-‐making between oral or intravenous
antibiotics, 70/102 (67%) physicians believed it would be useful to decrease
variation in practice. Although the impact of this score is yet to be tested, it can
already be used in the research setting to classify patients with cellulitis. Since
the development of the Melbourne ASSET score, the same methodology has been
used as a platform to develop a clinical score to address the uncertainty of
intravenous versus oral antibiotics in UTI. Although this work is still in progress,
it aims to be another clinical score that has the potential to standardise practice
and assist in future research in the ED and primary care.
252
7.8 Cost-‐effectiveness of home versus hospital
Most studies on OPAT in children have found that the OPAT pathway is less
costly to the healthcare institution than standard hospital care. Previous studies
have documented a cost saving of 30–75% with home treatment compared to
standard care in hospital, although there are differences in study methodology
and patient populations.32,33,38,157 Despite the heterogeneity in terms of the
population and geographical variation in the studies that analysed cost,
differences between home and hospital care were significant.
In the foundation cohort study, the cost per patient per day was AUD580,
compared to AUD1290, a 55% cost saving per patient. This cost was based on
patients who received a diagnosis of cellulitis in the hospital administration
system, this is also known as a diagnosis related grouping (DRG) cost. Although
many studies use DRG costs and this is a valid method of obtaining cost
estimates, inevitably some patients who do not actually have cellulitis will be
included in this group introducing inaccuracies.28 On the other hand, data for the
cost-‐effectiveness analysis within the RCT was obtained for actual patients in the
study with a definite diagnosis. Using these costs, home treatment cost AUD940
per patient per day, 60% less than standard hospital care, which cost AUD2388
patient per day, with medical and nursing staff salaries being the predominant
drivers in the cost differences.
For the first time in a paediatric OPAT study, costs to families were investigated
to ensure the burden of cost did not transfer from the healthcare institution to
families. The finding that families incurred a significant burden if their child has
even a short admission to hospital with a mean cost of AUD593 for a 2-‐day stay
in hospital, three-‐fold the financial cost of treatment at home, was unexpected.
This burden to families is driven by parental or carer’s absence from work,
which was significantly higher in the hospital group, by a mean difference of
AUD371 per admission. Two previous studies have also found that
parents/guardians of children treated with OPAT were less likely to have
absence from work.30,193 Parents may be more comfortable leaving children with
253
other carers or extended family with treatment at home, whereas parents are
more likely to stay with their child when their child is hospitalised. Additionally,
if there are other children at home, having the patient at home may allow one
parent to do all the child care rather than two parents needing to split between
hospital and home.
With regards to cost-‐effectiveness, only one other OPAT study has calculated the
aggregated measure of cost and effectiveness, the ICER.29 In this cost-‐modelling
study four strategies for the management of children with febrile neutropenia
were compared, namely: hospital with intravenous antibiotics, home with
intravenous antibiotics, home with oral antibiotics and hospital followed by early
discharge on oral antibiotics. Treatment at home with intravenous antibiotics
was found to be the dominant strategy, meaning it was more effective and less
costly. The model predicted that the costs of ‘home with intravenous antibiotics’
(USD2732/AUD3785 per person per episode) would be lowest of the four
strategies. When the prevalence of treatment failure and hospital readmission
was taken into account, home with intravenous antibiotic was still less costly
than home with oral antibiotics. The authors found an 81% difference in the cost
between hospital with intravenous antibiotics and home with intravenous
antibiotics. As far as it is possible to tell in the published study, there was no
medical staff salary apportioned to the home intravenous strategy, driving the
cost down. Although it is possible to have a home intravenous program without
medical oversight, studies of OPAT treatment of febrile neutropenia, have
described medical staff involvement.7 In the setting of the home pathway of the
RCT, medical oversight is a prominent feature which likely contributed to low
treatment failure rates and readmissions. This does, however, increase the costs
of this service. One possible way to reduce the cost of OPAT is to apply a daily
clinical score, such as the Melbourne ASSET score, which may result in less need
for a medical review and consequently reduce the cost per patient.
254
7.9 Future directions
7.9.1 Management of cellulitis – impact analysis of the Melbourne ASSET
score
The Melbourne ASSET score was derived and validated on patients attending the
RCH.123 The objective of this clinical score is to improve consistency of care for
children with cellulitis, ultimately ensuring the best possible outcomes for
affected children. The next step is to implement the score in the RCH ED to
determine the impact of applying this score prospectively at our institution on
the proportion of children commenced on intravenous antibiotics. An impact
analysis will assess whether the implementation of this clinical score in clinical
practice is better than usual care for the patient, process of care and cost
outcomes.194,195
Once the impact has been assessed, refinement of this score may be needed. The
next step would be to implement the Melbourne ASSET score in a multi-‐centre
study. The prospectively-‐validated version of the Melbourne ASSET score could
then be disseminated and used internationally. If the findings from the original
study in this thesis are replicated, the impact of the score would be that the
proportion of children treated with intravenous antibiotics could be reduced
without an increased number of complications or re-‐presentations to ED.
Implementation of the Melbourne ASSET score is anticipated to improve the flow
in the ED, hospital and outpatient management through improved efficiency in
the ED, reduced intravenous antibiotic use and cost-‐effectiveness.
Additionally, the introduction and subsequent application of the score could
contribute to the development of risk stratification tools to standardise
treatment for other common illnesses such as UTI and set the agenda and
platform for future projects.
255
7.9.2 Microbiology – OPAT, resistant and colonising bacteria, and the
microbiome
Despite concerns about resistance as a result of broad spectrum antibiotic use
associated with OPAT, the RCT is the first study of OPAT of any kind in either
adults or children, to investigate this concern by collecting microbiology
samples. Collecting nasal and faecal samples longitudinally was challenging and
resulted in only achieving 50% sample collection.142 In future, all OPAT studies
should incorporate this as an outcome and data on acquisition and colonisation
of the organisms of concern, ESBL, VRE, MRSA and C. difficile should be
considered as a key performance indicator for all OPAT programs. Although this
study has found no increased risk with the use of ceftriaxone at home, we would
encourage other centres with different baseline resistance patterns to
investigate this outcome.
In addition to the above, it is increasingly being understood that resistant and
commonly invasive bacteria are not the only colonising bacteria that have
implications on the long-‐term health of children. The community of
microorganisms that inhabit our bodies, predominantly the gastrointestinal
tract, but including other niches such as the nose and pharynx, are collectively
known as the microbiome. The way that these microorganisms interact with our
body can affect the development of the immune system in infancy, and our
metabolism.196 197Disruption of this community with antibiotics may have long-‐
term health implications.
Studies in adults have shown that treatment with antibiotics can be followed by
substantial changes in the microbiome that may influence diseases such as
colorectal cancer and ulcerative colitis.198,199 There are scarcely any microbiome
studies in healthy children. The only study to assess the effect of prior antibiotic
use on the healthy childhood microbiome used the national Finnish prescription
database and stool samples from 142 children to show that macrolide use in the
previous 6 months was associated with microbiome changes.200,201 The study
also showed a correlation between macrolide use under the age of 2 years and
256
both asthma and obesity. There is only one study that has prospectively
evaluated the effect of antibiotics on the microbiome. This compared 9 neonates
treated with ampicillin and gentamicin with 9 healthy controls, with stool
samples collected 4 and 8 weeks after antibiotics (although not at baseline).201
Both of these studies show that changes occur in the microbiome of children
receiving antibiotics that persist long after antibiotics have ceased. However
patients were not randomised so confounding is possible.
There have been no studies assessing the microbiome in children colonised with
either C. difficile or ESBL-‐producing bacteria. Stool samples collected during the
RCT had their DNA extracted and stored. These samples will allow the
identification of the longitudinal effect and persistence of changes of short term
antibiotics on the microbiome over 12 months to determine whether there is a
microbiome signature associated with colonisation with C. difficile and resistant
gastrointestinal bacteria. If a certain pattern or signature is found to be
associated with colonisation or acquisition with these organisms, future
strategies could include avoidance of risk factors or preventative treatment for a
targeted cohort.
7.9.3 Hospital-‐In-‐The-‐Home – future RCTs of home versus hospital using
the same platform
With the success of the RCT in this thesis, other acute infections amenable to
home treatment could also be investigated. Infections amenable for home
treatment directly from ED include UTI, pneumonia, and lymphadenitis.
Although cellulitis was used as a model in the RCT, the same approach can be
used to investigate these other conditions. We would propose a baseline study to
understand current practice, followed by preliminary foundation studies to
inform key aspects of a subsequent RCT for these different conditions.114,136,142
We would hypothesize that quality of life and cost-‐effectiveness are likely to be
improved at home for these other infections too, but efficacy and safety would
need to be individually compared to hospital care.
257
There are several studies on the ambulatory treatment of UTI in children
worldwide, but it is still an uncommon practice.37,158,193 UTI is particularly
suitable for OPAT considering the antibiotic commonly used for treatment in
several countries including Australia, is once daily gentamicin.158 One reason for
this maybe because of vomiting that frequently accompanies this condition, but
this could be managed for instance by a period of observation in the ED prior to
discharge home to observe oral intake after administration of anti-‐emetics.
Other conditions amenable for home treatment may be children diagnosed with
pneumonia which requires intravenous treatment.202 However, patients
potentially need oxygen therapy which is still feasible at home but may be
perceived as too complex or risky. There is a subgroup of patients with extensive
disease or small pleural effusions requiring intravenous antibiotics but not
oxygen. This selected population could be amenable to OPAT. Lymphadenitis is
another condition which often requires several days of intravenous antibiotics.
However, clinicians may prefer to admit patients due to the potential
development of an abscess and need for ultrasound imaging. A way to avoid this
perceived need for hospitalisation would be to ensure easy access to outpatient
ultrasound imaging for those receiving treatment under OPAT.
Other infections that are not commonly documented from studies describing an
OPAT patient cohort are those with surgical infections, such as post complicated
appendicitis or post-‐mastoidectomy.3,12 OPAT could also be better used for acute
infections after a short hospital admission for these surgical infections. The first
study on antibiotic treatment at home for post complicated appendicitis was
published in 1994 and yet very few patients in this category are treated at
home32. The reason for this is unclear but likely attributable to the complexity of
this condition and the lack of randomised evidence.38
The challenges faced by service providers to treat other medical condition such
as UTI or post complicated appendicitis at home include the lack of clear
guidelines with regards to who should receive intravenous antibiotics and when
the right time is to be transferred home.

258
7.9.4 Translating evidence into practice
The research described in this thesis, the RCT and two non-‐randomised studies,
provides evidence for the treatment of moderate/severe cellulitis via
OPAT.114,136,142 The next logical step is translating this evidence into widespread
practice. However, strong evidence alone is often insufficient for change in
practice and getting new ideas adopted in a healthcare service is often
challenging despite being shown to be beneficial.203
With the RCT showing the efficacy, safety and cost-‐effectiveness of treating
moderate/severe cellulitis at home, the next question for widespread
implementation is whether the same results would apply if implemented in a
different centre and in a different population. In order to test whether the results
of the efficacy trial (RCT, Chapter 5) would translate on a larger scale, ideally a
“real-‐world” effectiveness trial would be conducted. The gold standard would be
a multi-‐centre cluster randomised trial of home versus hospital in
moderate/severe cellulitis with intravenous ceftriaxone. However, this would be
time and resource consuming. An interrupted time series analysis is arguably the
“next best” approach for dealing with interventions when randomisation is not
possible.204 The approach usually involves constructing a time series of
population-‐level rates for a particular quality improvement focus (home
treatment of moderate/severe cellulitis at home) and testing statistically for a
change in the outcome rate in the time periods before and time periods after
implementation of a policy/program designed to change the outcome.205
Multisite with capacity for a home/ambulatory service, could be recruited for
this next phase. Sites could be identified through the existing emergency
research network. These sites would first undergo a pre-‐intervention period of
data collection to reflect standard practice. Outcome data would include
treatment failure rate, adverse events, complications, quality of life and cost-‐
effectiveness measures. Then implementation of a home program would follow,
with data collection of outcomes. We would anticipate the efficacy and safety of
home pathways in other centres to still be non-‐inferior to standard care in
259
hospitals but the risk difference may not be as large as the results of the RCT
described in Chapter 5, which has been previously shown to occur when
translating single centre efficacy trials into a multicentre effectiveness trial.206
Barriers for this study would be the variation in practice that exists in multiple
sites and a need to engage local practitioners to change attitudes and behaviours.
However with careful planning and the experience gained during the PhD
studies, these challenges can be addressed.
7.10 Conclusions
The literature review at the beginning of this thesis revealed the absence of any
randomised trial of home versus hospital treatment for any acute infection in
childhood. This lack of crucial evidence in an increasingly evidence-‐hungry world
is at least part of the reason why hospitalisation remains the standard of care for
many children with infections amenable to home treatment. This is despite the
fact that paediatricians know that children in general are better off at home with
their families. For this thesis, cellulitis was the acute infection chosen as a
paradigm to answer the key question of whether intravenous antibiotic
treatment at home is as good as hospital treatment. This condition is common
and is associated with low morbidity and mortality in children. Definitively
confirming the findings in the literature and from the studies in the first half of
this thesis, the RCT showed that home treatment with ceftriaxone is as good as
hospital treatment with flucloxacillin in terms of efficacy, complications and
microbiological outcomes. It showed that treatment was in favour of home care
in terms of adverse events, child quality of life, parental satisfaction and cost-‐
effectiveness. This represents a significant contribution to the field, but should
be seen as a first step of many. At the end of this candidature, this remains the
only RCT to compare an admission avoidance pathway to hospitalisation in
children. In addition to the RCT, the derivation and validation of the Melbourne
ASSET score for cellulitis in children, has the potential both to make an impact on
clinical practice and on future research in cellulitis. The studies contained in this
thesis will act as a platform for future research on admission avoidance
pathways in children.

260
268
Bibliography
1. Gouin S, Chevalier I, Gauthier M, Lamarre V. Prospective evaluation of the management of moderate to severe cellulitis with parenteral antibiotics at a paediatric day treatment centre. Journal of paediatrics and child health 2008; 44(4): 214-‐8.
2. Brugha RE, Abrahamson E. Ambulatory intravenous antibiotic therapy for children with preseptal cellulitis. Pediatric emergency care 2012; 28(3): 226-‐8.
3. Madigan T, Banerjee R. Characteristics and outcomes of outpatient parenteral antimicrobial therapy at an academic children's hospital. Pediatr Infect Dis J 2013; 32(4): 346-‐9.
4. Sartain SA, Maxwell MJ, Todd PJ, et al. Randomised controlled trial comparing an acute paediatric hospital at home scheme with conventional hospital care. Archives of disease in childhood 2002; 87(5): 371-‐5.
5. Rucker RW, Harrison GM. Outpatient intravenous medications in the management of cystic fibrosis. Pediatrics 1974; 54(3): 358-‐60.
6. Smith JK, Alexander S, Abrahamson E. Ambulatory intravenous ceftriaxone in paediatric A&E: a useful alternative to hospital admission? Emergency medicine journal : EMJ 2011; 28(10): 877-‐81.
7. Orme LM, Babl FE, Barnes C, Barnett P, Donath S, Ashley DM. Outpatient versus inpatient IV antibiotic management for pediatric oncology patients with low risk febrile neutropenia: a randomised trial. Pediatr Blood Cancer 2014; 61(8): 1427-‐33.
8. Svahn BM, Remberger M, Heijbel M, et al. Case-‐control comparison of at-‐home and hospital care for allogeneic hematopoietic stem-‐cell transplantation: the role of oral nutrition. Transplantation 2008; 85(7): 1000-‐7.
9. Tiberg I, Katarina SC, Carlsson A, Hallstrom I. Children diagnosed with type 1 diabetes: a randomized controlled trial comparing hospital versus home-‐based care. Acta paediatrica 2012; 101(10): 1069-‐73.
269
10. Cunliffe NA, Booth JA, Elliot C, et al. Healthcare-‐associated viral gastroenteritis among children in a large pediatric hospital, United Kingdom. Emerging infectious diseases 2010; 16(1): 55-‐62.
11. Xu M, Doan Q. Outpatient Parenteral Antimicrobial Therapy and Judicious Use of Pediatric Emergency Resources. Pediatric emergency care 2017.
12. Hodgson KA, Huynh J, Ibrahim LF, et al. The use, appropriateness and outcomes of outpatient parenteral antimicrobial therapy. Archives of disease in childhood 2016; 101(10): 886-‐93.
13. Fernandes P, Milliren C, Mahoney-‐West HM, Schwartz L, Lachenauer CS, Nakamura MM. Safety of Outpatient Parenteral Antimicrobial Therapy in Children. Pediatr Infect Dis J 2017.
14. Fisher D, Cochran KM, Provost LP, et al. Reducing central line-‐associated bloodstream infections in North Carolina NICUs. Pediatrics 2013; 132(6): e1664-‐71.
15. Ortega HW, Cutler G, Dreyfus J, Flood A, Kharbanda A. Hospital-‐acquired pneumonia among pediatric trauma patients treated at national trauma centers. The journal of trauma and acute care surgery 2015; 78(6): 1149-‐54.
16. Sohn AH, Garrett DO, Sinkowitz-‐Cochran RL, et al. Prevalence of nosocomial infections in neonatal intensive care unit patients: Results from the first national point-‐prevalence survey. The Journal of pediatrics 2001; 139(6): 821-‐7.
17. Kulkarni H, Smith CM, Lee Ddo H, Hirst RA, Easton AJ, O'Callaghan C. Evidence of Respiratory Syncytial Virus Spread by Aerosol. Time to Revisit Infection Control Strategies? American journal of respiratory and critical care medicine 2016; 194(3): 308-‐16.
18. Jusot JF, Vanhems P, Benzait F, et al. Reported measures of hygiene and incidence rates for hospital-‐acquired diarrhea in 31 French pediatric wards: is there any relationship? Infection control and hospital epidemiology 2003; 24(7): 520-‐5.
270
19. Ruuska T, Vesikari T. Rotavirus disease in Finnish children: use of numerical scores for clinical severity of diarrhoeal episodes. Scandinavian journal of infectious diseases 1990; 22(3): 259-‐67.
20. Hulten KG, Kaplan SL, Lamberth LB, et al. Hospital-‐acquired Staphylococcus aureus infections at Texas Children's Hospital, 2001-‐2007. Infection control and hospital epidemiology 2010; 31(2): 183-‐90.
21. Datta F, Erb T, Heininger U, et al. A multicenter, cross-‐sectional study on the prevalence and risk factors for nasal colonization with Staphylococcus aureus in patients admitted to children's hospitals in Switzerland. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 2008; 47(7): 923-‐6.
22. Cheng S, Teuffel O, Ethier MC, et al. Health-‐related quality of life anticipated with different management strategies for paediatric febrile neutropaenia. British journal of cancer 2011; 105(5): 606-‐11.
23. Close P, Burkey E, Kazak A, Danz P, Lange B. A prospective, controlled evaluation of home chemotherapy for children with cancer. Pediatrics 1995; 95(6): 896-‐900.
24. Sartain SA, Maxwell MJ, Todd PJ, Haycox AR, Bundred PE. Users' views on hospital and home care for acute illness in childhood. Health Soc Care Community 2001; 9(2): 108-‐17.
25. Hansson H, Kjaergaard H, Johansen C, et al. Hospital-‐based home care for children with cancer: feasibility and psychosocial impact on children and their families. Pediatr Blood Cancer 2013; 60(5): 865-‐72.
26. Chrysochoou EA, Hatziagorou E, Kirvassilis F, Tsanakas J. Home intravenous antibiotic therapy in children with cystic fibrosis: clinical outcome, quality of life and economic benefit. Hippokratia 2016; 20(4): 279-‐83.
27. Torrance GW, Feeny D, Furlong W. Visual analog scales: do they have a role in the measurement of preferences for health states? Med Decis Making 2001; 21(4): 329-‐34.
271
28. Wiernikowski JT, Rothney M, Dawson S, Andrew M. Evaluation of a home intravenous antibiotic program in pediatric oncology. The American journal of pediatric hematology/oncology 1991; 13(2): 144-‐7.
29. Teuffel O, Amir E, Alibhai SM, Beyene J, Sung L. Cost-‐effectiveness of outpatient management for febrile neutropenia in children with cancer. Pediatrics 2011; 127(2): e279-‐86.
30. Bagust A, Haycox A, Sartain SA, Maxwell MJ, Todd P. Economic evaluation of an acute paediatric hospital at home clinical trial. Archives of disease in childhood 2002; 87(6): 489-‐92.
31. Raisch DW, Holdsworth MT, Winter SS, Hutter JJ, Graham ML. Economic comparison of home-‐care-‐based versus hospital-‐based treatment of chemotherapy-‐induced febrile neutropenia in children. Value in health : the journal of the International Society for Pharmacoeconomics and Outcomes Research 2003; 6(2): 158-‐66.
32. Stovroff MC, Totten M, Glick PL. PIC lines save money and hasten discharge in the care of children with ruptured appendicitis. Journal of pediatric surgery 1994; 29(2): 245-‐7.
33. Warner BW, Kulick RM, Stoops MM, Mehta S, Stephan M, Kotagal UR. An evidenced-‐based clinical pathway for acute appendicitis decreases hospital duration and cost. Journal of pediatric surgery 1998; 33(9): 1371-‐5.
34. Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin Infect Dis 2014; 59(2): e10-‐52.
35. Akar A, Singh N, Hyun DY. Appropriateness and safety of outpatient parenteral antimicrobial therapy in children: opportunities for pediatric antimicrobial stewardship. Clinical pediatrics 2014; 53(10): 1000-‐3.
36. Sannier N, Le Masne A, Sayegh N, Gaillard JL, Cheron G. Ambulatory management of acute pyelonephritis in children. Acta paediatrica 2000; 89(3): 372-‐3.
272
37. Gauthier M, Chevalier I, Sterescu A, Bergeron S, Brunet S, Taddeo D.Treatment of urinary tract infections among febrile young children with dailyintravenous antibiotic therapy at a day treatment center. Pediatrics 2004;114(4): e469-‐76.
38. Fishman SJ, Pelosi L, Klavon SL, O'Rourke EJ. Perforated appendicitis:prospective outcome analysis for 150 children. Journal of pediatric surgery 2000;35(6): 923-‐6.
39. Australian Institute of Health Welfare. Emergency department care 2016–2017: Australian hospital statistics.https://www.aihw.gov.au/reports/hospitals/ahs-‐2016-‐17-‐emergency-‐department-‐care/contents/table-‐of-‐contents (accessed 15 May 2018).
40. Lopez MA, Cruz AT, Kowalkowski MA, Raphael JL. Trends in resourceutilization for hospitalized children with skin and soft tissue infections.Pediatrics 2013; 131(3): e718-‐25.
41. Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for thediagnosis and management of skin and soft-‐tissue infections. Clin Infect Dis 2005;41(10): 1373-‐406.
42. Isaacs D. Evidence-‐Based Pediatric Infectious Diseases. Victoria, Australia:Blackwell Publishing; 2007.
43. Khangura S, Wallace J, Kissoon N, Kodeeswaran T. Management ofcellulitis in a pediatric emergency department. Pediatric emergency care 2007;23(11): 805-‐11.
44. Trenchs V, Hernandez-‐Bou S, Bianchi C, Arnan M, Gene A, Luaces C. BloodCultures are not Useful in the Evaluation of Children with UncomplicatedSuperficial Skin and Soft Tissue Infections. Pediatr Infect Dis J 2015.
45. Malone JR, Durica SR, Thompson DM, Bogie A, Naifeh M. Blood cultures inthe evaluation of uncomplicated skin and soft tissue infections. Pediatrics 2013;132(3): 454-‐9.
273
46. Corwin P, Toop L, McGeoch G, et al. Randomised controlled trial ofintravenous antibiotic treatment for cellulitis at home compared with hospital.Bmj 2005; 330(7483): 129.
47. Garrett T, Harbort Y, Trebble M, Docherty T. Once or twice-‐daily,algorithm-‐based intravenous cephazolin for home-‐based cellulitis treatment.Emergency medicine Australasia : EMA 2012; 24(4): 383-‐92.
48. Barr DA, Semple L, Seaton RA. Outpatient parenteral antimicrobialtherapy (OPAT) in a teaching hospital-‐based practice: a retrospective cohortstudy describing experience and evolution over 10 years. International journal ofantimicrobial agents 2012; 39(5): 407-‐13.
49. Pickering LK BC, Kimberlin DW, Long SS. Red Book: 2012 Report of theCommittee on Infectious Diseases Elk Grove Village, IL: American Academy ofPediatrics.
50. Moran GJ, Krishnadasan A, Mower WR, et al. Effect of Cephalexin PlusTrimethoprim-‐Sulfamethoxazole vs Cephalexin Alone on Clinical Cure ofUncomplicated Cellulitis: A Randomized Clinical Trial. Jama 2017; 317(20):2088-‐96.
51. Goldman RD, Dolansky G, Rogovik AL. Predictors for admission ofchildren with periorbital cellulitis presenting to the pediatric emergencydepartment. Pediatric emergency care 2008; 24(5): 279-‐83.
52. Koerner R, Johnson AP. Changes in the classification and management ofskin and soft tissue infections. The Journal of antimicrobial chemotherapy 2011;66(2): 232-‐4.
53. The Royal Children's Hospital Melbourne Clinical Practice Guideline:Cellulitis and skin infections.https://www.rch.org.au/clinicalguide/guideline_index/cellulitis_and_skin_infections/ (accessed 7 June 2015).
54. Fleisher G, Ludwig S, Henretig F, Ruddy R, Henry W. Cellulitis: initialmanagement. Ann Emerg Med 1981; 10(7): 356-‐9.
274
55. Vu BL, Dick PT, Levin AV, Pirie J. Development of a clinical severity scorefor preseptal cellulitis in children. Pediatric emergency care 2003; 19(5): 302-‐7.
56. Crosbie RA, Nairn J, Kubba H. Management of paediatric periorbitalcellulitis: Our experience of 243 children managed according to a standardisedprotocol 2012-‐2015. International journal of pediatric otorhinolaryngology 2016;87: 134-‐8.
57. Reynolds DJ, Kodsi SR, Rubin SE, Rodgers IR. Intracranial infectionassociated with preseptal and orbital cellulitis in the pediatric patient. Journal ofAAPOS : the official publication of the American Association for PediatricOphthalmology and Strabismus / American Association for PediatricOphthalmology and Strabismus 2003; 7(6): 413-‐7.
58. Westley CR, Cotton EK, Brooks JG. Nebulized racemic epinephrine by IPPBfor the treatment of croup: a double-‐blind study. American journal of diseases ofchildren 1978; 132(5): 484-‐7.
59. Ducharme FM, Chalut D, Plotnick L, et al. The Pediatric RespiratoryAssessment Measure: a valid clinical score for assessing acute asthma severityfrom toddlers to teenagers. The Journal of pediatrics 2008; 152(4): 476-‐80, 80e1.
60. Samuel M. Pediatric appendicitis score. Journal of pediatric surgery 2002;37(6): 877-‐81.
61. Dunning J, Daly JP, Lomas JP, et al. Derivation of the children's head injuryalgorithm for the prediction of important clinical events decision rule for headinjury in children. Archives of disease in childhood 2006; 91(11): 885-‐91.
62. Mandeville K, Pottker T, Bulloch B, Liu J. Using appendicitis scores in thepediatric ED. The American journal of emergency medicine 2011; 29(9): 972-‐7.
63. Grayson ML, McDonald M, Gibson K, et al. Once-‐daily intravenouscefazolin plus oral probenecid is equivalent to once-‐daily intravenousceftriaxone plus oral placebo for the treatment of moderate-‐to-‐severe cellulitis inadults. Clin Infect Dis 2002; 34(11): 1440-‐8.
275
64. Bradley JS. Once-‐daily ceftriaxone in the outpatient treatment of paediatric infections. Chemotherapy 1991; 37 Suppl 3: 3-‐6.
65. Chapman AL. Outpatient parenteral antimicrobial therapy. Bmj 2013; 346: f1585.
66. Chapman AL, Dixon S, Andrews D, Lillie PJ, Bazaz R, Patchett JD. Clinical efficacy and cost-‐effectiveness of outpatient parenteral antibiotic therapy (OPAT): a UK perspective. The Journal of antimicrobial chemotherapy 2009; 64(6): 1316-‐24.
67. Bamberger DM, Dahl SL. Impact of voluntary vs enforced compliance of third-‐generation cephalosporin use in a teaching hospital. Arch Intern Med 1992; 152(3): 554-‐7.
68. Bradley SJ, Wilson AL, Allen MC, Sher HA, Goldstone AH, Scott GM. The control of hyperendemic glycopeptide-‐resistant Enterococcus spp. on a haematology unit by changing antibiotic usage. The Journal of antimicrobial chemotherapy 1999; 43(2): 261-‐6.
69. Washio M, Mizoue T, Kajioka T, et al. Risk factors for methicillin-‐resistant Staphylococcus aureus (MRSA) infection in a Japanese geriatric hospital. Public health 1997; 111(3): 187-‐90.
70. Ambrose NS, Johnson M, Burdon DW, Keighley MR. The influence of single dose intravenous antibiotics on faecal flora and emergence of Clostridium difficile. The Journal of antimicrobial chemotherapy 1985; 15(3): 319-‐26.
71. Sturenburg E, Mack D. Extended-‐spectrum beta-‐lactamases: implications for the clinical microbiology laboratory, therapy, and infection control. The Journal of infection 2003; 47(4): 273-‐95.
72. Livermore DM. Defining an extended-‐spectrum beta-‐lactamase. Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases 2008; 14 Suppl 1: 3-‐10.
73. Schwaber MJ, Carmeli Y. Mortality and delay in effective therapy associated with extended-‐spectrum beta-‐lactamase production in
276
Enterobacteriaceae bacteraemia: a systematic review and meta-‐analysis. The Journal of antimicrobial chemotherapy 2007; 60(5): 913-‐20.
74. Fan NC, Chen HH, Chen CL, et al. Rise of community-‐onset urinary tract infection caused by extended-‐spectrum beta-‐lactamase-‐producing Escherichia coli in children. J Microbiol Immunol Infect 2014; 47(5): 399-‐405.
75. Kaarme J, Molin Y, Olsen B, Melhus A. Prevalence of extended-‐spectrum beta-‐lactamase-‐producing Enterobacteriaceae in healthy Swedish preschool children. Acta paediatrica 2013; 102(6): 655-‐60.
76. Fernandez-‐Reyes M, Vicente D, Gomariz M, et al. High rate of fecal carriage of extended-‐spectrum-‐beta-‐lactamase-‐producing Escherichia coli in healthy children in Gipuzkoa, northern Spain. Antimicrobial agents and chemotherapy 2014; 58(3): 1822-‐4.
77. Megged O. Extended-‐spectrum beta-‐lactamase-‐producing bacteria causing community-‐acquired urinary tract infections in children. Pediatric nephrology 2014; 29(9): 1583-‐7.
78. Tsai MH, Chu SM, Hsu JF, et al. Risk factors and outcomes for multidrug-‐resistant Gram-‐negative bacteremia in the NICU. Pediatrics 2014; 133(2): e322-‐9.
79. de Man P, Verhoeven BA, Verbrugh HA, Vos MC, van den Anker JN. An antibiotic policy to prevent emergence of resistant bacilli. Lancet 2000; 355(9208): 973-‐8.
80. Prevot MH, Andremont A, Sancho-‐Garnier H, Tancrede C. Epidemiology of intestinal colonization by members of the family Enterobacteriaceae resistant to cefotaxime in a hematology-‐oncology unit. Antimicrobial agents and chemotherapy 1986; 30(6): 945-‐7.
81. Moellering RC, Jr. Emergence of Enterococcus as a significant pathogen. Clin Infect Dis 1992; 14(6): 1173-‐6.
277
82. McKinnell JA, Kunz DF, Chamot E, et al. Association between vancomycin-‐resistant Enterococci bacteremia and ceftriaxone usage. Infection control and hospital epidemiology 2012; 33(7): 718-‐24.
83. Nourse C, Murphy H, Byrne C, et al. Control of a nosocomial outbreak of vancomycin resistant Enterococcus faecium in a paediatric oncology unit: risk factors for colonisation. European journal of pediatrics 1998; 157(1): 20-‐7.
84. Iosifidis E, Evdoridou I, Agakidou E, et al. Vancomycin-‐resistant Enterococcus outbreak in a neonatal intensive care unit: epidemiology, molecular analysis and risk factors. American journal of infection control 2013; 41(10): 857-‐61.
85. Edlund C, Barkholt L, Olsson-‐Liljequist B, Nord CE. Effect of vancomycin on intestinal flora of patients who previously received antimicrobial therapy. Clin Infect Dis 1997; 25(3): 729-‐32.
86. Nourse C, Byrne C, Murphy H, Kaufmann ME, Clarke A, Butler K. Eradication of vancomycin resistant Enterococcus faecium from a paediatric oncology unit and prevalence of colonization in hospitalized and community-‐based children. Epidemiology and infection 2000; 124(1): 53-‐9.
87. Kaarme J, Hasan B, Rashid M, Olsen B. Zero prevalence of vancomycin-‐resistant enterococci among Swedish preschool children. Microbial drug resistance 2015; 21(1): 65-‐8.
88. Hall IC OTE. Intestinal flora in new-‐born infants: with a description of a new pathogenic anaerobe, Bacillus difficilis. Am J Dis Child 1935; 49(2): 390-‐402.
89. Rupnik M, Wilcox MH, Gerding DN. Clostridium difficile infection: new developments in epidemiology and pathogenesis. Nat Rev Microbiol 2009; 7(7): 526-‐36.
90. Riley TV. Nosocomial diarrhoea due to Clostridium difficile. Curr Opin Infect Dis 2004; 17(4): 323-‐7.
278
91. Crews JD, Koo HL, Jiang ZD, Starke JR, DuPont HL. A hospital-‐based study of the clinical characteristics of Clostridium difficile infection in children. Pediatr Infect Dis J 2014; 33(9): 924-‐8.
92. Kociolek LK, Gerding DN. Is pediatric Clostridium difficile infection associated with prior antibiotic exposure? Future Microbiol 2014; 9(7): 825-‐8.
93. Samady W, Bush R, Pong A, Andrews A, Fisher ES. Predictors of Clostridium difficile infections in hospitalized children. J Hosp Med 2014; 9(2): 94-‐8.
94. de Blank P, Zaoutis T, Fisher B, Troxel A, Kim J, Aplenc R. Trends in Clostridium difficile infection and risk factors for hospital acquisition of Clostridium difficile among children with cancer. The Journal of pediatrics 2013; 163(3): 699-‐705 e1.
95. Kim J, Shaklee JF, Smathers S, et al. Risk factors and outcomes associated with severe clostridium difficile infection in children. Pediatr Infect Dis J 2012; 31(2): 134-‐8.
96. Banaszkiewicz A, Kowalska-‐Duplaga K, Pytrus T, Pituch H, Radzikowski A. Clostridium difficile infection in newly diagnosed pediatric patients with inflammatory bowel disease: prevalence and risk factors. Inflamm Bowel Dis 2012; 18(5): 844-‐8.
97. Cooperstock M, Riegle L, Woodruff CW, Onderdonk A. Influence of age, sex, and diet on asymptomatic colonization of infants with Clostridium difficile. J Clin Microbiol 1983; 17(5): 830-‐3.
98. von Eiff C, Becker K, Peters G. Nasal carriage of Staphylococcus aureus. Reply. New Engl J Med 2001; 344(18): 1400-‐1.
99. Almeida GC, dos Santos MM, Lima NG, Cidral TA, Melo MC, Lima KC. Prevalence and factors associated with wound colonization by Staphylococcus spp. and Staphylococcus aureus in hospitalized patients in inland northeastern Brazil: a cross-‐sectional study. BMC infectious diseases 2014; 14: 328.
279
100. Rocha LA, Marques Ribas R, da Costa Darini AL, Gontijo Filho PP. Relationship between nasal colonization and ventilator-‐associated pneumonia and the role of the environment in transmission of Staphylococcus aureus in intensive care units. American journal of infection control 2013; 41(12): 1236-‐40.
101. Davis MF, Peng RD, McCormack MC, Matsui EC. Staphylococcus aureus colonization is associated with wheeze and asthma among US children and young adults. The Journal of allergy and clinical immunology 2015; 135(3): 811-‐3 e5.
102. Lebon A, Labout JA, Verbrugh HA, et al. Role of Staphylococcus aureus nasal colonization in atopic dermatitis in infants: the Generation R Study. Archives of pediatrics & adolescent medicine 2009; 163(8): 745-‐9.
103. Whymark AD, Crampsey DP, Fraser L, Moore P, Williams C, Kubba H. Childhood epistaxis and nasal colonization with Staphylococcus aureus. Otolaryngology-‐-‐head and neck surgery : official journal of American Academy of Otolaryngology-‐Head and Neck Surgery 2008; 138(3): 307-‐10.
104. Zervou FN, Zacharioudakis IM, Ziakas PD, Mylonakis E. MRSA colonization and risk of infection in the neonatal and pediatric ICU: a meta-‐analysis. Pediatrics 2014; 133(4): e1015-‐23.
105. Rodriguez EA, Correa MM, Ospina S, Atehortua SL, Jimenez JN. Differences in epidemiological and molecular characteristics of nasal colonization with Staphylococcus aureus (MSSA-‐MRSA) in children from a university hospital and day care centers. PloS one 2014; 9(7): e101417.
106. Jimenez-‐Truque N, Tedeschi S, Saye EJ, et al. Relationship between maternal and neonatal Staphylococcus aureus colonization. Pediatrics 2012; 129(5): e1252-‐9.
107. Fritz SA, Hogan PG, Hayek G, et al. Staphylococcus aureus colonization in children with community-‐associated Staphylococcus aureus skin infections and their household contacts. Archives of pediatrics & adolescent medicine 2012; 166(6): 551-‐7.
280
108. Lo WT, Wang CC, Lin WJ, et al. Changes in the nasal colonization with methicillin-‐resistant Staphylococcus aureus in children: 2004-‐2009. PloS one 2010; 5(12): e15791.
109. Gesualdo F, Onori M, Bongiorno D, et al. Methicillin-‐resistant Staphylococcus aureus nasal colonization in a department of pediatrics: a cross-‐sectional study. Ital J Pediatr 2014; 40: 3.
110. Wells S, Anderson T, Tiemieier A, et al. Methicillin-‐resistant Staphylococcus aureus in patients with congenital heart disease in the pediatric intensive care unit. World J Pediatr Congenit Heart Surg 2013; 4(4): 344-‐8.
111. Guillemot D, Bonacorsi S, Blanchard JS, et al. Amoxicillin-‐clavulanate therapy increases childhood nasal colonization by methicillin-‐susceptible Staphylococcus aureus strains producing high levels of penicillinase. Antimicrobial agents and chemotherapy 2004; 48(12): 4618-‐23.
112. Ellis Simonsen SM, van Orman ER, Hatch BE, et al. Cellulitis incidence in a defined population. Epidemiology and infection 2006; 134(2): 293-‐9.
113. Drews SJ, Richardson SE, Wray R, et al. An outbreak of vancomycin-‐resistant Enterococcus faecium in an acute care pediatric hospital: Lessons from environmental screening and a case-‐control study. The Canadian journal of infectious diseases & medical microbiology = Journal canadien des maladies infectieuses et de la microbiologie medicale / AMMI Canada 2008; 19(3): 233-‐6.
114. Ibrahim LF, Hopper SM, Babl FE, Bryant PA. Who Can Safely Have Antibiotics at Home? A Prospective Observational Study in Children with Moderate/Severe Cellulitis. Pediatr Infect Dis J 2015.
115. Ibrahim LF, Hopper SM, Connell TG, Daley AJ, Bryant PA, Babl FE. Evaluating an admission avoidance pathway for children in the emergency department: outpatient intravenous antibiotics for moderate/severe cellulitis. Emergency medicine journal : EMJ 2017.
116. Vinen J, Hudson B, Chan B, Fernandes C. A randomised comparative study of once-‐daily ceftriaxone and 6-‐hourly flucloxacillin in the treatment of moderate
281
to severe cellulitis -‐ Clinical efficacy, safety and pharmacoeconomic implications. Clinical Drug Investigation 1996; 12(5): 221-‐5.
117. Ellis MW, Schlett CD, Millar EV, et al. Prevalence of nasal colonization and strain concordance in patients with community-‐associated Staphylococcus aureus skin and soft-‐tissue infections. Infection control and hospital epidemiology 2014; 35(10): 1251-‐6.
118. Wolf J, Daley AJ, Tilse MH, et al. Antibiotic susceptibility patterns of Staphylococcus aureus isolates from Australian children. Journal of paediatrics and child health 2010; 46(7-‐8): 404-‐11.
119. Britton PN, Andresen DN. Paediatric community-‐associated Staphylococcus aureus: a retrospective cohort study. Journal of paediatrics and child health 2013; 49(9): 754-‐9.
120. Kam AJ, Leal J, Freedman SB. Pediatric cellulitis: success of emergency department short-‐course intravenous antibiotics. Pediatric emergency care 2010; 26(3): 171-‐6.
121. Hiscock H, Perera P, McLean K, et al. Variation in paediatric clinical practice: A review of care in inpatient, outpatient and emergency department settings. Journal of paediatrics and child health 2016; 52(7): 691-‐3.
122. Adams ST, Leveson SH. Clinical prediction rules. Bmj 2012; 344: d8312.
123. Ibrahim LF, Hopper SM, Donath S, Salvin B, Babl FE, Bryant PA. Development and Validation of a Cellulitis Risk Score: The Melbourne ASSET Score. Pediatrics 2019.
124. Michie S, Johnston M. Changing clinical behaviour by making guidelines specific. Bmj 2004; 328(7435): 343-‐5.
125. Grol R, Dalhuijsen J, Thomas S, Veld C, Rutten G, Mokkink H. Attributes of clinical guidelines that influence use of guidelines in general practice: observational study. Bmj 1998; 317(7162): 858-‐61.
282
126. Liao L, Mark DB. Clinical prediction models: are we building better mousetraps? J Am Coll Cardiol 2003; 42(5): 851-‐3.
127. Bandiera G, Stiell IG, Wells GA, et al. The Canadian C-‐spine rule performs better than unstructured physician judgment. Ann Emerg Med 2003; 42(3): 395-‐402.
128. Ginsberg MB. Cellulitis: analysis of 101 cases and review of the literature. South Med J 1981; 74(5): 530-‐3.
129. Miller LG, Daum RS, Creech CB, et al. Clindamycin versus trimethoprim-‐sulfamethoxazole for uncomplicated skin infections. N Engl J Med 2015; 372(12): 1093-‐103.
130. MacGregor RR, Graziani AL. Oral administration of antibiotics: a rational alternative to the parenteral route. Clin Infect Dis 1997; 24(3): 457-‐67.
131. Dillon HC, Derrick CW. Clinical experience with clindamycin hydrochloride: I. Treatment of streptococcal and mixed streptococcal-‐staphylococcal skin infections. Pediatrics 1975; 55(2): 205-‐12.
132. Buffie CG, Jarchum I, Equinda M, et al. Profound alterations of intestinal microbiota following a single dose of clindamycin results in sustained susceptibility to Clostridium difficile-‐induced colitis. Infect Immun 2012; 80(1): 62-‐73.
133. Gee SC, Hagemann TM. Palatability of liquid anti-‐infectives: clinician and student perceptions and practice outcomes. The journal of pediatric pharmacology and therapeutics : JPPT : the official journal of PPAG 2007; 12(4): 216-‐23.
134. Steele RW, Russo TM, Thomas MP. Adherence issues related to the selection of antistaphylococcal or antifungal antibiotic suspensions for children. Clinical pediatrics 2006; 45(3): 245-‐50.
135. Smith DH, Neutel JM, Lacourciere Y, Kempthorne-‐Rawson J. Prospective, randomized, open-‐label, blinded-‐endpoint (PROBE) designed trials yield the
283
same results as double-‐blind, placebo-‐controlled trials with respect to ABPM measurements. J Hypertens 2003; 21(7): 1291-‐8.
136. Ibrahim LF, Babl FE, Orsini F, Hopper SM, Bryant PA. Cellulitis: Home Or Inpatient in Children from the Emergency Department (CHOICE): protocol for a randomised controlled trial. BMJ open 2016; 6(1): e009606.
137. Wang S, Gum D, Merlin T. Comparing the ICERs in Medicine Reimbursement Submissions to NICE and PBAC-‐Does the Presence of an Explicit Threshold Affect the ICER Proposed? Value in health : the journal of the International Society for Pharmacoeconomics and Outcomes Research 2018; 21(8): 938-‐43.
138. Drummond MF, Mooney GH. Essentials of health economics: Part V. Assessing the cost and benefits of treatment alternatives. Br Med J (Clin Res Ed) 1982; 285(6355): 1638-‐9 contd.
139. Huang L, Roberts CT, Manley BJ, Owen LS, Davis PG, Dalziel KM. Cost-‐Effectiveness Analysis of Nasal Continuous Positive Airway Pressure Versus Nasal High Flow Therapy as Primary Support for Infants Born Preterm. The Journal of pediatrics 2018; 196: 58-‐64 e2.
140. de Bruin M, Oberje EJM, Viechtbauer W, et al. Effectiveness and cost-‐effectiveness of a nurse-‐delivered intervention to improve adherence to treatment for HIV: a pragmatic, multicentre, open-‐label, randomised clinical trial. The Lancet Infectious diseases 2017; 17(6): 595-‐604.
141. Petrou S, Gray A. Economic evaluation alongside randomised controlled trials: design, conduct, analysis, and reporting. Bmj 2011; 342: d1548.
142. Ibrahim LF, Hopper SM, Orsini F, Daley AJ, Babl FE, Bryant PA. Randomised controlled trial of intravenous antibiotics on OPAT versus hospital for cellulitis in children: comparison of efficacy and safety. In press The Lancet Infectious diseases 2018.
143. Briggs A. Economics notes: handling uncertainty in economic evaluation. Bmj 1999; 319(7202): 120.
284
144. Kind P. Cost-‐effectiveness analysis: a view into the abyss. Appl Health Econ Health Policy 2015; 13(3): 269-‐71.
145. Whitehead SJ, Ali S. Health outcomes in economic evaluation: the QALY and utilities. Br Med Bull 2010; 96: 5-‐21.
146. Stevens K. Valuation of the Child Health Utility 9D Index. PharmacoEconomics 2012; 30(8): 729-‐47.
147. Teuffel O, Amir E, Alibhai S, Beyene J, Sung L. Cost effectiveness of outpatient treatment for febrile neutropaenia in adult cancer patients. British journal of cancer 2011; 104(9): 1377-‐83.
148. Torrance GW, Blaker D, Detsky A, et al. Canadian guidelines for economic evaluation of pharmaceuticals. Canadian Collaborative Workshop for Pharmacoeconomics. PharmacoEconomics 1996; 9(6): 535-‐59.
149. Weinstein MC. Economic assessments of medical practices and technologies. Med Decis Making 1981; 1(4): 309-‐30.
150. Fenwick E, Claxton K, Sculpher M. Representing uncertainty: the role of cost-‐effectiveness acceptability curves. Health Econ 2001; 10(8): 779-‐87.
151. Cohen DJ, Reynolds MR. Interpreting the results of cost-‐effectiveness studies. J Am Coll Cardiol 2008; 52(25): 2119-‐26.
152. Drummond M, Sculpher M. Common methodological flaws in economic evaluations. Med Care 2005; 43(7 Suppl): 5-‐14.
153. Ratcliffe J, Stevens K, Flynn T, Brazier J, Sawyer M. An assessment of the construct validity of the CHU9D in the Australian adolescent general population. Qual Life Res 2012; 21(4): 717-‐25.
154. Boyer NR, Miller S, Connolly P, McIntosh E. Paving the way for the use of the SDQ in economic evaluations of school-‐based population health interventions: an empirical analysis of the external validity of SDQ mapping algorithms to the CHU9D in an educational setting. Qual Life Res 2016; 25(4): 913-‐23.
285
155. Furber G, Segal L. The validity of the Child Health Utility instrument (CHU9D) as a routine outcome measure for use in child and adolescent mental health services. Health Qual Life Outcomes 2015; 13: 22.
156. Bryant PA, Katz NT. Inpatient versus outpatient parenteral antibiotic therapy at home for acute infections in children: a systematic review. The Lancet Infectious diseases 2017.
157. Hensey CC, Sett A, Connell TG, Bryant PA. A Comparison of Hospital Versus Outpatient Parenteral Antibiotic Therapy at Home for Pyelonephritis and Meningitis. Pediatr Infect Dis J 2017; 36(9): 827-‐32.
158. Scanlan BT, Ibrahim LF, Hopper SM, Babl FE, Davidson A, Bryant PA. Selected Children with Complicated Acute Urinary Tract Infection May be Treated with Outpatient Parenteral Antibiotic Therapy at Home Directly from the Emergency Department. Pediatr Infect Dis J 2018.
159. Patel S, Burzio V, Green H, et al. The Impact of Pediatric Outpatient Parenteral Antibiotic Therapy Implementation at a Tertiary Children's Hospital in the United Kingdom. Pediatr Infect Dis J 2018; 37(12): e292-‐e7.
160. Nazer D, Abdulhamid I, Thomas R, Pendleton S. Home versus hospital intravenous antibiotic therapy for acute pulmonary exacerbations in children with cystic fibrosis. Pediatr Pulmonol 2006; 41(8): 744-‐9.
161. Collaco JM, Green DM, Cutting GR, Naughton KM, Mogayzel PJ, Jr. Location and duration of treatment of cystic fibrosis respiratory exacerbations do not affect outcomes. American journal of respiratory and critical care medicine 2010; 182(9): 1137-‐43.
162. van Egmond MA, van der Schaaf M, Vredeveld T, et al. Effectiveness of physiotherapy with telerehabilitation in surgical patients: a systematic review and meta-‐analysis. Physiotherapy 2018; 104(3): 277-‐98.
163. Warner BW, Rich KA, Atherton H, Andersen CL, Kotagal UR. The sustained impact of an evidenced-‐based clinical pathway for acute appendicitis. Seminars in pediatric surgery 2002; 11(1): 29-‐35.
286
164. Donati MA, Guenette G, Auerbach H. Prospective controlled study of homeand hospital therapy of cystic fibrosis pulmonary disease. The Journal ofpediatrics 1987; 111(1): 28-‐33.
165. Riethmueller J, Busch A, Damm V, Ziebach R, Stern M. Home and hospitalantibiotic treatment prove similarly effective in cystic fibrosis. Infection 2002;30(6): 387-‐91.
166. Strandvik B, Hjelte L, Malmborg AS, Widen B. Home intravenous antibiotictreatment of patients with cystic fibrosis. Acta paediatrica 1992; 81(4): 340-‐4.
167. Proesmans M, Heyns L, Moons P, Havermans T, De Boeck K. Real lifeevaluation of intravenous antibiotic treatment in a paediatric cystic fibrosiscentre: outcome of home therapy is not inferior. Respir Med 2009; 103(2): 244-‐50.
168. Heida A, Dijkstra A, Dantuma SK, van Rheenen PF. A Cross-‐Sectional Studyon the Perceptions and Practices of Teenagers With Inflammatory Bowel DiseaseAbout Repeated Stool Sampling. J Adolesc Health 2016; 59(4): 479-‐81.
169. Carr D, Barnes EH, Gordon A, Isaacs D. Effect of antibiotic use onantimicrobial antibiotic resistance and late-‐onset neonatal infections over 25years in an Australian tertiary neonatal unit. Archives of disease in childhood Fetaland neonatal edition 2017; 102(3): F244-‐F50.
170. ACSQHC. AURA 2017: Second Australian report on antimicrobial use andresistance in human health. 2017. https://www.safetyandquality.gov.au/wp-‐content/uploads/2018/01/AURA-‐2017-‐Second-‐Australian-‐report-‐on-‐Antimicrobial-‐Use-‐and-‐Resistance-‐in-‐human-‐health.pdf (accessed 5 Dec 2018).
171. Vernacchio L, Vezina RM, Mitchell AA, Lesko SM, Plaut AG, Acheson DW.Diarrhea in American infants and young children in the community setting:incidence, clinical presentation and microbiology. Pediatr Infect Dis J 2006;25(1): 2-‐7.
172. Furuya-‐Kanamori L, Marquess J, Yakob L, et al. Asymptomatic Clostridiumdifficile colonization: epidemiology and clinical implications. BMC Infect Dis2015; 15: 516.
287
173. Riggs MM, Sethi AK, Zabarsky TF, Eckstein EC, Jump RL, Donskey CJ. Asymptomatic carriers are a potential source for transmission of epidemic and nonepidemic Clostridium difficile strains among long-‐term care facility residents. Clin Infect Dis 2007; 45(8): 992-‐8.
174. McFarland LV, Mulligan ME, Kwok RY, Stamm WE. Nosocomial acquisition of Clostridium difficile infection. N Engl J Med 1989; 320(4): 204-‐10.
175. Loo VG, Bourgault AM, Poirier L, et al. Host and pathogen factors for Clostridium difficile infection and colonization. N Engl J Med 2011; 365(18): 1693-‐703.
176. Kong LY, Dendukuri N, Schiller I, et al. Predictors of asymptomatic Clostridium difficile colonization on hospital admission. American journal of infection control 2015; 43(3): 248-‐53.
177. Leekha S, Aronhalt KC, Sloan LM, Patel R, Orenstein R. Asymptomatic Clostridium difficile colonization in a tertiary care hospital: admission prevalence and risk factors. American journal of infection control 2013; 41(5): 390-‐3.
178. Salgado CD, Farr BM, Calfee DP. Community-‐acquired methicillin-‐resistant Staphylococcus aureus: a meta-‐analysis of prevalence and risk factors. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 2003; 36(2): 131-‐9.
179. Hidron AI, Kourbatova EV, Halvosa JS, et al. Risk factors for colonization with methicillin-‐resistant Staphylococcus aureus (MRSA) in patients admitted to an urban hospital: emergence of community-‐associated MRSA nasal carriage. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 2005; 41(2): 159-‐66.
180. Graffunder EM, Venezia RA. Risk factors associated with nosocomial methicillin-‐resistant Staphylococcus aureus (MRSA) infection including previous use of antimicrobials. The Journal of antimicrobial chemotherapy 2002; 49(6): 999-‐1005.
288
181. Schentag JJ, Hyatt JM, Carr JR, et al. Genesis of methicillin-‐resistant Staphylococcus aureus (MRSA), how treatment of MRSA infections has selected for vancomycin-‐resistant Enterococcus faecium, and the importance of antibiotic management and infection control. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 1998; 26(5): 1204-‐14.
182. von Eiff C, Becker K, Machka K, Stammer H, Peters G. Nasal carriage as a source of Staphylococcus aureus bacteremia. Study Group. The New England journal of medicine 2001; 344(1): 11-‐6.
183. McMullan BJ, Bowen A, Blyth CC, et al. Epidemiology and Mortality of Staphylococcus aureus Bacteremia in Australian and New Zealand Children. JAMA pediatrics 2016; 170(10): 979-‐86.
184. Dolapo O, Dhanireddy R, Talati AJ. Trends of Staphylococcus aureus bloodstream infections in a neonatal intensive care unit from 2000-‐2009. BMC pediatrics 2014; 14: 121.
185. Stevens K, Ratcliffe J. Measuring and valuing health benefits for economic evaluation in adolescence: an assessment of the practicality and validity of the child health utility 9D in the Australian adolescent population. Value in health : the journal of the International Society for Pharmacoeconomics and Outcomes Research 2012; 15(8): 1092-‐9.
186. Poder TG, Carrier N, Mead H, Stevens KJ. Canadian French translation and linguistic validation of the child health utility 9D (CHU9D). Health Qual Life Outcomes 2018; 16(1): 168.
187. Gandara E, Wells PS. Diagnosis: use of clinical probability algorithms. Clin Chest Med 2010; 31(4): 629-‐39.
188. Gardner W, Lidz CW, Mulvey EP, Shaw EC. Clinical versus actuarial predictions of violence of patients with mental illnesses. J Consult Clin Psychol 1996; 64(3): 602-‐9.
189. Gao H, McDonnell A, Harrison DA, et al. Systematic review and evaluation of physiological track and trigger warning systems for identifying at-‐risk patients on the ward. Intensive Care Med 2007; 33(4): 667-‐79.
289
190. Babl FE, Borland ML, Phillips N, et al. Accuracy of PECARN, CATCH, and CHALICE head injury decision rules in children: a prospective cohort study. Lancet 2017; 389(10087): 2393-‐402.
191. Stiell IG, Wells GA. Methodologic standards for the development of clinical decision rules in emergency medicine. Ann Emerg Med 1999; 33(4): 437-‐47.
192. Yealy DM, Auble TE. Choosing between clinical prediction rules. N Engl J Med 2003; 349(26): 2553-‐5.
193. Pena A, Zambrano A, Alvarado M, Cerda J, Vergara R. [Evaluation of the effectiveness, safety and costs of outpatient intravenous antimicrobial treatment (OPAT) vs hospitalized in urinary infection in pediatrics]. Revista chilena de infectologia : organo oficial de la Sociedad Chilena de Infectologia 2013; 30(4): 426-‐34.
194. Wallace E, Uijen MJ, Clyne B, et al. Impact analysis studies of clinical prediction rules relevant to primary care: a systematic review. BMJ open 2016; 6(3): e009957.
195. Moons KG, Altman DG, Vergouwe Y, Royston P. Prognosis and prognostic research: application and impact of prognostic models in clinical practice. Bmj 2009; 338: b606.
196. Teo SM, Mok D, Pham K, et al. The infant nasopharyngeal microbiome impacts severity of lower respiratory infection and risk of asthma development. Cell host & microbe 2015; 17(5): 704-‐15.
197. Vrieze A, Out C, Fuentes S, et al. Impact of oral vancomycin on gut microbiota, bile acid metabolism, and insulin sensitivity. J Hepatol 2014; 60(4): 824-‐31.
198. Boursi B, Haynes K, Mamtani R, Yang YX. Impact of antibiotic exposure on the risk of colorectal cancer. Pharmacoepidemiol Drug Saf 2015; 24(5): 534-‐42.
199. Koido S, Ohkusa T, Kajiura T, et al. Long-‐term alteration of intestinal microbiota in patients with ulcerative colitis by antibiotic combination therapy. PloS one 2014; 9(1): e86702.
290
200. Korpela K, Salonen A, Virta LJ, et al. Intestinal microbiome is related to lifetime antibiotic use in Finnish pre-‐school children. Nat Commun 2016; 7: 10410.
201. Fouhy F, Guinane CM, Hussey S, et al. High-‐throughput sequencing reveals the incomplete, short-‐term recovery of infant gut microbiota following parenteral antibiotic treatment with ampicillin and gentamicin. Antimicrob Agents Chemother 2012; 56(11): 5811-‐20.
202. Glackin L, Flanagan F, Healy F, Slattery DM. Outpatient parenteral antimicrobial therapy: a report of three years experience. Ir Med J 2014; 107(4): 110-‐2.
203. Doran DM, Sidani S. Outcomes-‐focused knowledge translation: a framework for knowledge translation and patient outcomes improvement. Worldviews Evid Based Nurs 2007; 4(1): 3-‐13.
204. Kontopantelis E, Doran T, Springate DA, Buchan I, Reeves D. Regression based quasi-‐experimental approach when randomisation is not an option: interrupted time series analysis. Bmj 2015; 350: h2750.
205. Penfold RB, Zhang F. Use of interrupted time series analysis in evaluating health care quality improvements. Acad Pediatr 2013; 13(6 Suppl): S38-‐44.
206. Costa ML, Griffin XL, Parsons N, et al. Efficacy versus effectiveness in clinical trials. Bone Joint J 2017; 99-‐B(4): 419-‐20.

291
Appendix 1 RCT Protocol
This supplement contains the following items: 1. Final protocol and summary of changes from original protocol2. Original statistical analysis plan which has never been
changed
292
PROTOCOL
CHOICE Trial: Cellulitis at Home Or Inpatient in Children from ED
Protocol Number: HREC34254 Date: 18/04/2017
Investigator/s: Dr Laila Ibrahim, Paediatric Fellow, PI Dr Penelope Bryant, Paediatric Infectious Diseases and HITH Physician Ms Francesca Orsini, CEBU Biostatistician Murdoch Children’s Research Institute Dr Franz Babl, Paediatric Emergency Physician, Director of Emergency Research Dr Sandy Hopper, Paediatric Emergency Physician
293

Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 2 of 26
CONFIDENTIAL
This document is confidential and the property of The Royal Children’s Hospital Melbourne. No part of it may be transmitted, reproduced, published, or used without prior written
authorization from the institution.
Statement of Compliance
This document is a protocol for a research project. This study will be conducted in compliance with all stipulation of this protocol, the conditions of the ethics committee
approval, the NHMRC National Statement on ethical Conduct in Human Research (2007) and the Note for Guidance on Good Clinical Practice (CPMP/ICH-‐135/95).
294
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 3 of 26
TABLE OF CONTENTS
Table of Contents 3 1. Study Sites 6 1.1 Study Location 6
2. Funding and Resources 6 2.1 Sources of Funding 6
3. Introduction/Background Information 6 3.1 Lay Summary 6 3.2 Introduction and Background 7
4. Study Objectives 8 4.1 Research Question 8 4.2 Primary Objective 10 4.3 Secondary Objectives 10 4.4 Outcome Measures 11
5. Study Design 13 5.1 Study Design Diagram 13 5.2 Study Type & Design & Schedule 14 5.3 Randomisation 16 5.4 Study methodology 16
6. Study Population 18 6.1 Recruitment Procedure 18 6.2 Interventions 18 6.3 Inclusion and Exclusion criteria 19 6.4 Consent 19
7. Participant Safety and Withdrawal 20 7.1 Risk Management and Safety 20 7.2 Handling of Withdrawals 20 7.3 Independent Safety and Data Monitoring Committee 21
8. Statistical Methods 21 8.1 Sample Size Estimation & Justification 21 8.2 Statistical Methods 21
9. Storage of Blood and Tissue Samples 22 10. Data Security & Handling 23 10.1 Details of where records will be kept & How long will they be stored 23 10.2 Confidentiality and Security 23 10.3 Ancillary data 23
11. References 23
295
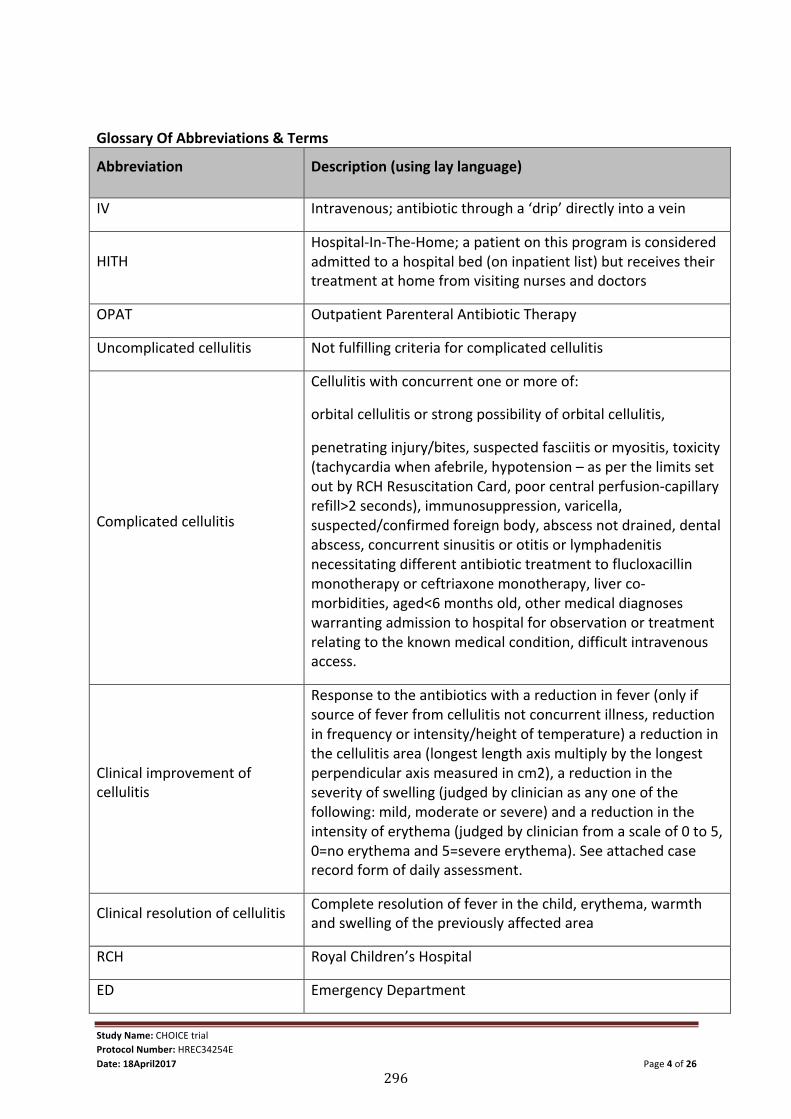
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 4 of 26
Glossary Of Abbreviations & Terms
Abbreviation Description (using lay language)
IV Intravenous; antibiotic through a ‘drip’ directly into a vein
HITH Hospital-‐In-‐The-‐Home; a patient on this program is considered admitted to a hospital bed (on inpatient list) but receives their treatment at home from visiting nurses and doctors
OPAT Outpatient Parenteral Antibiotic Therapy
Uncomplicated cellulitis Not fulfilling criteria for complicated cellulitis
Complicated cellulitis
Cellulitis with concurrent one or more of:
orbital cellulitis or strong possibility of orbital cellulitis,
penetrating injury/bites, suspected fasciitis or myositis, toxicity (tachycardia when afebrile, hypotension – as per the limits set out by RCH Resuscitation Card, poor central perfusion-‐capillary refill>2 seconds), immunosuppression, varicella, suspected/confirmed foreign body, abscess not drained, dental abscess, concurrent sinusitis or otitis or lymphadenitis necessitating different antibiotic treatment to flucloxacillin monotherapy or ceftriaxone monotherapy, liver co-‐morbidities, aged<6 months old, other medical diagnoses warranting admission to hospital for observation or treatment relating to the known medical condition, difficult intravenous access.
Clinical improvement of cellulitis
Response to the antibiotics with a reduction in fever (only if source of fever from cellulitis not concurrent illness, reduction in frequency or intensity/height of temperature) a reduction in the cellulitis area (longest length axis multiply by the longest perpendicular axis measured in cm2), a reduction in the severity of swelling (judged by clinician as any one of the following: mild, moderate or severe) and a reduction in the intensity of erythema (judged by clinician from a scale of 0 to 5, 0=no erythema and 5=severe erythema). See attached case record form of daily assessment.
Clinical resolution of cellulitis Complete resolution of fever in the child, erythema, warmth and swelling of the previously affected area
RCH Royal Children’s Hospital
ED Emergency Department
296
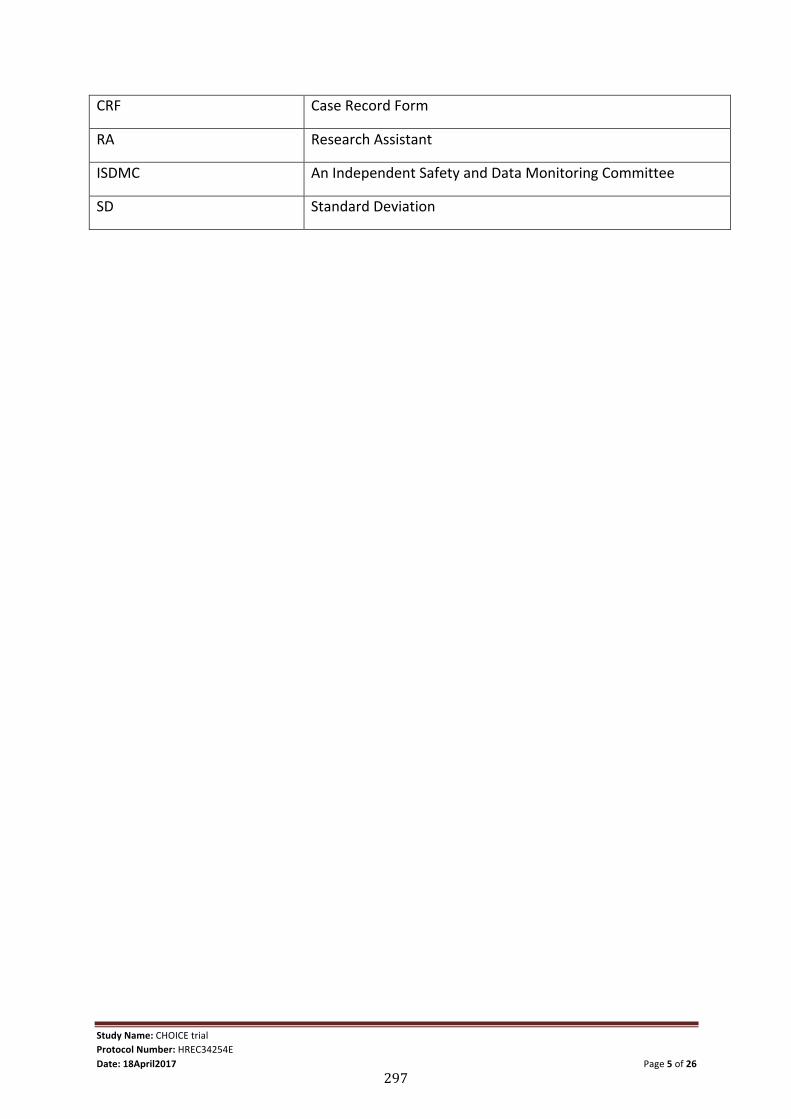
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 5 of 26
CRF Case Record Form
RA Research Assistant
ISDMC An Independent Safety and Data Monitoring Committee
SD Standard Deviation
297
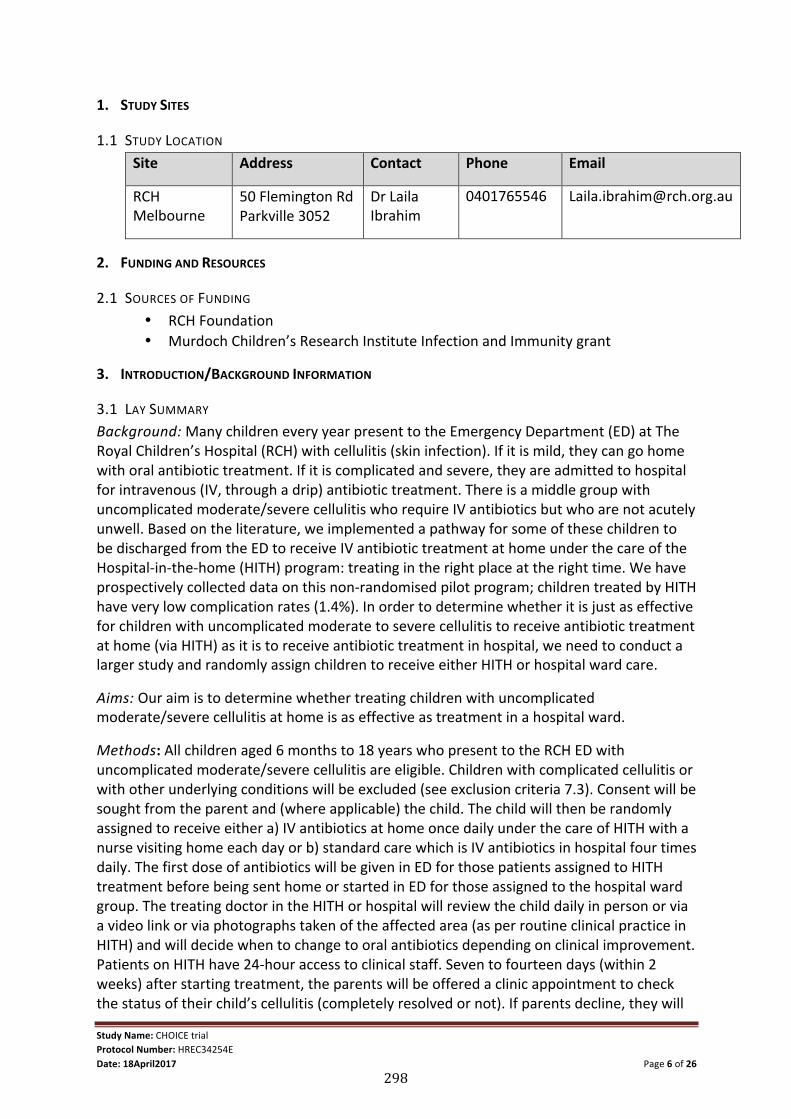
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 6 of 26
1. STUDY SITES
1.1 STUDY LOCATION Site Address Contact Phone Email
RCH Melbourne
50 Flemington Rd Parkville 3052
Dr Laila Ibrahim
0401765546 [email protected]
2. FUNDING AND RESOURCES
2.1 SOURCES OF FUNDING • RCH Foundation • Murdoch Children’s Research Institute Infection and Immunity grant
3. INTRODUCTION/BACKGROUND INFORMATION
3.1 LAY SUMMARY Background: Many children every year present to the Emergency Department (ED) at The Royal Children’s Hospital (RCH) with cellulitis (skin infection). If it is mild, they can go home with oral antibiotic treatment. If it is complicated and severe, they are admitted to hospital for intravenous (IV, through a drip) antibiotic treatment. There is a middle group with uncomplicated moderate/severe cellulitis who require IV antibiotics but who are not acutely unwell. Based on the literature, we implemented a pathway for some of these children to be discharged from the ED to receive IV antibiotic treatment at home under the care of the Hospital-‐in-‐the-‐home (HITH) program: treating in the right place at the right time. We have prospectively collected data on this non-‐randomised pilot program; children treated by HITH have very low complication rates (1.4%). In order to determine whether it is just as effective for children with uncomplicated moderate to severe cellulitis to receive antibiotic treatment at home (via HITH) as it is to receive antibiotic treatment in hospital, we need to conduct a larger study and randomly assign children to receive either HITH or hospital ward care.
Aims: Our aim is to determine whether treating children with uncomplicated moderate/severe cellulitis at home is as effective as treatment in a hospital ward.
Methods: All children aged 6 months to 18 years who present to the RCH ED with uncomplicated moderate/severe cellulitis are eligible. Children with complicated cellulitis or with other underlying conditions will be excluded (see exclusion criteria 7.3). Consent will be sought from the parent and (where applicable) the child. The child will then be randomly assigned to receive either a) IV antibiotics at home once daily under the care of HITH with a nurse visiting home each day or b) standard care which is IV antibiotics in hospital four times daily. The first dose of antibiotics will be given in ED for those patients assigned to HITH treatment before being sent home or started in ED for those assigned to the hospital ward group. The treating doctor in the HITH or hospital will review the child daily in person or via a video link or via photographs taken of the affected area (as per routine clinical practice in HITH) and will decide when to change to oral antibiotics depending on clinical improvement. Patients on HITH have 24-‐hour access to clinical staff. Seven to fourteen days (within 2 weeks) after starting treatment, the parents will be offered a clinic appointment to check the status of their child’s cellulitis (completely resolved or not). If parents decline, they will
298
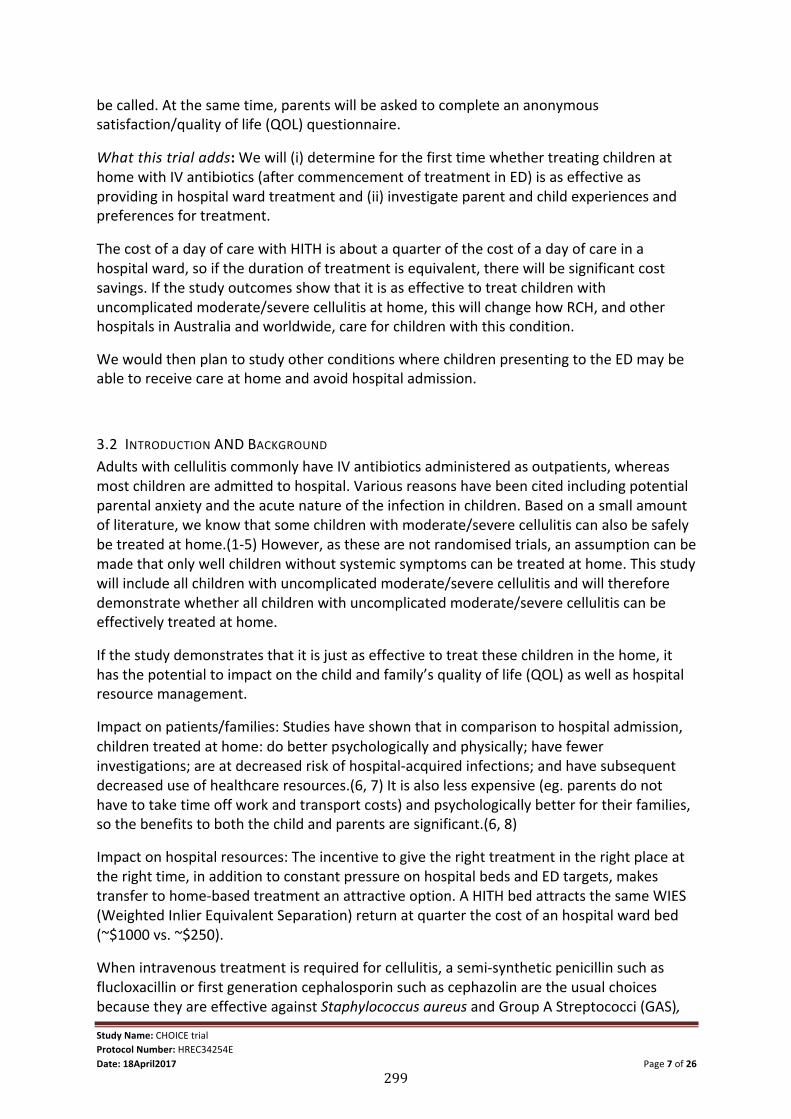
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 7 of 26
be called. At the same time, parents will be asked to complete an anonymous satisfaction/quality of life (QOL) questionnaire.
What this trial adds: We will (i) determine for the first time whether treating children at home with IV antibiotics (after commencement of treatment in ED) is as effective as providing in hospital ward treatment and (ii) investigate parent and child experiences and preferences for treatment.
The cost of a day of care with HITH is about a quarter of the cost of a day of care in a hospital ward, so if the duration of treatment is equivalent, there will be significant cost savings. If the study outcomes show that it is as effective to treat children with uncomplicated moderate/severe cellulitis at home, this will change how RCH, and other hospitals in Australia and worldwide, care for children with this condition.
We would then plan to study other conditions where children presenting to the ED may be able to receive care at home and avoid hospital admission.
3.2 INTRODUCTION AND BACKGROUND Adults with cellulitis commonly have IV antibiotics administered as outpatients, whereas most children are admitted to hospital. Various reasons have been cited including potential parental anxiety and the acute nature of the infection in children. Based on a small amount of literature, we know that some children with moderate/severe cellulitis can also be safely be treated at home.(1-‐5) However, as these are not randomised trials, an assumption can be made that only well children without systemic symptoms can be treated at home. This study will include all children with uncomplicated moderate/severe cellulitis and will therefore demonstrate whether all children with uncomplicated moderate/severe cellulitis can be effectively treated at home.
If the study demonstrates that it is just as effective to treat these children in the home, it has the potential to impact on the child and family’s quality of life (QOL) as well as hospital resource management.
Impact on patients/families: Studies have shown that in comparison to hospital admission, children treated at home: do better psychologically and physically; have fewer investigations; are at decreased risk of hospital-‐acquired infections; and have subsequent decreased use of healthcare resources.(6, 7) It is also less expensive (eg. parents do not have to take time off work and transport costs) and psychologically better for their families, so the benefits to both the child and parents are significant.(6, 8)
Impact on hospital resources: The incentive to give the right treatment in the right place at the right time, in addition to constant pressure on hospital beds and ED targets, makes transfer to home-‐based treatment an attractive option. A HITH bed attracts the same WIES (Weighted Inlier Equivalent Separation) return at quarter the cost of an hospital ward bed (~$1000 vs. ~$250).
When intravenous treatment is required for cellulitis, a semi-‐synthetic penicillin such as flucloxacillin or first generation cephalosporin such as cephazolin are the usual choices because they are effective against Staphylococcus aureus and Group A Streptococci (GAS),
299
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 8 of 26
the main pathogens causing cellulitis. (13) However they are not suitable for OPAT due to their frequent dosing with the majority of paediatric Outpatient Parenteral Antibiotic Therapy (OPAT) services only able to deliver once daily interventions. Whilst probenecid can overcome this problem for adults on cephazolin, there are no pharmacokinetic studies of the use of probenecid with cephazolin in children, and the side effect of vomiting may prevent probenecid use.(14) Ceftriaxone has anti-‐staphylococcal activity and can be administered once daily.(15) There are only a few studies in children in which ceftriaxone has been used to treat cellulitis either in hospital or OPAT, but none have compared outcomes to children treated with other recommended antibiotics.(5, 15-‐18) There are no studies in children with cellulitis who require intravenous treatment comparing administration at home and in hospital. In a study of 224 children with moderate/severe cellulitis, 92 were treated with ceftriaxone at a day treatment centre with an 80% success rate, but no contrast was made with the group treated in hospital.(5) Other studies that have included ceftriaxone for the treatment of cellulitis in children have had cure rates of 91-‐96%, but have had small numbers, no comparison group and/or unclear methodology.(16, 17) The only study comparing ceftriaxone with flucloxacillin has been in adults, and while ceftriaxone resulted in a higher success rate than flucloxacillin (96% vs 70%), numbers were not clinically significant.(19) The differential effect of ceftriaxone and flucoxacillin on the microbiome of children has also never previously been described. One of the secondary aims of this study is to investigate whether there is any effect of antibiotics on the identification of resistant organisms in stool samples of children in both groups. None of the studies described above have used home-‐based treatment.
Increasing numbers of hospitals are developing programs where patients who have traditionally been treated as hospital ward patients are treated at home under the care of hospital doctors and nurses in HITH programs. While attractive in terms of resource use, it is unclear to what extent HITH care is efficacious and safe. The Royal Children’s Hospital (RCH) Melbourne has the largest paediatric HITH program in Australia. As an alternative to admission for intravenous flucloxacillin, RCH HITH developed a direct-‐from-‐the Emergency Department (ED) pathway for cellulitis based on ED clinician assessment and decision, using once daily ceftriaxone and medical review at home. Since September 2012 to date at RCH, more than 70 children with moderate/severe cellulitis have been treated successfully at home.(1-‐4) The outcomes of these children are similar to the children treated in hospital. We now plan to randomly assign patients with cellulitis requiring IV antibiotics to either be treated at home (iv ceftriaxone) or to the hospital ward (iv flucloxacillin) and compare the success/failure rates in the two groups. The plan for this randomized trial has been discussed extensively with the Melbourne Clinical Trials Centre (MCTC) and presented at the MCTC forum attended by established researchers. The response to the trial was overwhelmingly positive with many experienced clinicians agreeing to the pragmatic approach and the need to find evidence for a pathway that is becoming routine practice.
4. STUDY OBJECTIVES
4.1 RESEARCH QUESTION The primary research question to be addressed is:
300
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 9 of 26
• In children with moderate/severe uncomplicated cellulitis, is the failure rate at 2 days following the first dose of antibiotic non-‐inferior for children treated with IV antibiotics at home compared to the failure rate at 2 days following the first dose for children treated with IV antibiotics in hospital?
The secondary research questions to be addressed are: • In children with moderate/severe uncomplicated cellulitis, is time to non-‐
progression of cellulitis in children treated with iv antibiotics at home at least the same as the time to non-‐progression of cellulitis in children treated with iv antibiotics in the hospital?
• In children with moderate/severe uncomplicated cellulitis, is time to discharge of children treated with iv antibiotics at home at least the same as the time to discharge of cellulitis children treated with iv antibiotics in the hospital?
• In children with moderate/severe uncomplicated cellulitis, is the rate of readmission of children treated with iv antibiotics at home different from the rate to readmission of children treated with iv antibiotics in the hospital?
• In children with moderate/severe uncomplicated cellulitis, is the rate of re-‐presentation to ED of children treated with iv antibiotics at home different from the rate of re-‐presentation of children treated with iv antibiotics in the hospital?
• In children with moderate/severe uncomplicated cellulitis, is the duration of iv antibiotics administration of children treated with iv antibiotics at home at least the same as duration of iv antibiotics administration to children treated with iv antibiotics in the hospital?
• Is treating children with cellulitis with iv antibiotics at home at least the same as treating them with iv antibiotics in the hospital, in terms of rates of complications, adverse events and allergic reactions?
• In children with moderate/severe uncomplicated cellulitis, is the rate of resistant organisms in children at home the same as children treated in hospital?
• Are quality of life indicators of children treated with iv antibiotics at home at least the same as quality of life indicators of children treated with iv antibiotics in the hospital?
• Is the assessment of cellulitis features in terms of : § presence of systemic features § surface area affected (longest length axis multiply by the longest
perpendicular axis measured in cm2) § severity of swelling (judged by clinician as any one of the following: mild,
moderate or severe) § intensity of erythema (judged by clinician from a scale of 0 to 5, 0=no
erythema and 5=severe erythema) § impairment of function of affected area § tenderness of cellulitis area (judged by clinician from a scale of 0 to 5, 0=not
tender and 5=very tender) helpful in tracking the progress of all children with uncomplicated moderate/severe cellulitis? See attached case record form of daily assessment.
301
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 10 of 26
4.2 PRIMARY OBJECTIVE To compare the failure rate of IV antibiotic treatment of children treated at home (iv ceftriaxone) with those treated in hospital (iv flucloxacillin) in the first 2 days of treatment following the first dose given in the ED in children with moderate/severe cellulitis (Moderate/severe: defined in this study, as those assessed by ED doctor to need iv antibiotics)
4.3 SECONDARY OBJECTIVES To compare: 1. Time to no progression of cellulitis 2. Time to discharge 3. Readmission rate 4. Representation to ED rate 5. Length of stay in ED 6. Duration of iv antibiotics administration, 7. Rates of IV cannula needing at least one resiting 8. Complications 9. Adverse events 10. Microbiology and microbiome 11. HITH and hospital patient costs 12. Quality of life indicators 13. The clinical assessment in terms of presence of systemic features, surface area affected
(longest length axis multiply by the longest perpendicular axis measured in cm2), severity of swelling (judged by clinician as any one of the following: mild, moderate or severe), intensity of erythema (judged by clinician from a scale of 0 to 5, 0=no erythema and 5=severe erythema), impairment of function of affected area, tenderness of cellulitis area (judged by clinician from a scale of 0 to 5, 0=not tender and 5=very tender) In children treated with iv antibiotics at home (iv ceftriaxone) with children treated with iv antibiotics (iv flucloxacillin) in the hospital during the study period.
302
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 11 of 26
4.4 OUTCOME MEASURES Primary outcome: The primary outcome is treatment failure defined as lack of clinical improvement of cellulitis or an adverse event, resulting in a change of initial empiric antibiotics within 2 days (48 hours) of treatment from the start of the first antibiotic dose given in the ED. The features contributing to clinical improvement are assessed and recorded daily in the CRF by the treating clinician and include: reduction in fever (reduction in fever frequency or degree of temperature, if fever source is cellulitis and not concurrent illness), reduction in the cellulitis area (measured by largest diameter of erythema), reduction in the severity of swelling (judged as mild, moderate or severe) and a reduction in the intensity of erythema (judged on a scale of 0 to 5, 0=no erythema and 5=severe erythema).
Secondary outcomes: 1. Time to no progression of cellulitis: number of days (including fractions of days) elapsed
from the start of the first dose in ED (Day 1) to the time at which the cellulitis stops spreading past the marked area, judged during daily assessment of cellulitis
2. Time to discharge: number of days (including fractions of days) elapsed from the time of arrival in ED to the moment the patient is discharged. (Discharge is defined as when patients admitted to hospital are deemed not to require any hospital funded care/intervention from a hospital based nurse/doctor. The time and date is registered on the electronic hospital database IBA. Admission to hospital is defined as patients who are deemed to need hospital funded care/intervention from a hospital based nurse/doctor)
3. Readmission rate: Number of children readmitted to hospital within 14 days of discharge date due to the same cellulitis
4. Representation to ED: Number of children representing to ED within 14 days of discharge and diagnosed to have incomplete resolution or recurrence of same cellulitis
5. Length of stay in ED (from first presentation in ED to time the patient leaves ED to go either home or to ward)
6. Duration of iv antibiotics 7. Rates of iv cannula needing at least one resiting 8. Complications of cellulitis: development of abscess requiring drainage after starting IV
antibiotics and bacteremia 9. Adverse events: occurrences of anaphylaxis, allergic reaction (suspected or confirmed)
necessitating change of empiric antibiotic, sepsis, death 10. Microbiology:
a. Any cultured isolate (bacteria) from a skin swab of the affected area will have susceptibility testing performed against ceftriaxone to document the rate of organism susceptibility to ceftriaxone
b. Rate of Staphylococcus aureus nasal carriage collected within 48 hours, 14 days, 3 months and 1 year of initial presentation to hospital
c. Any cultured isolate (bacteria) from a nasal swab will have susceptibility testing performed against ceftriaxone to document the rate of organism susceptibility to ceftriaxone
d. Any resistant bacteria present in stool sample collected within 48 hours, 14 days, 3 months and 1 year of initial presentation to hospital (This outcome may be published separately as require longer follow up.)
303
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 12 of 26
e. Any microbiome changes in the nasal and stool sample collected within 48 hours, 14 days, 3 months and 1 year of initial presentation to hospital (This outcome may be published separately as require longer follow up.)
11. Hospital ward patient costs and HITH patient costs 12. Quality of life (QOL) indicators (through survey asking parents how much admission to
hospital or HITH disrupt their routine as well as a validated Quality of Life tool -‐Child Health Utility 9)
13. Clinical assessment in all study participants in terms of presence of systemic features, surface area affected (longest length axis multiply by the longest perpendicular axis measured in cm2), severity of swelling (judged by clinician as any one of the following: mild, moderate or severe), intensity of erythema (judged by clinician from a scale of 0 to 5, 0=no erythema and 5=severe erythema), impairment of function of affected area, tenderness of cellulitis area (judged by clinician from a scale of 0 to 5, 0=not tender and 5=very tender).
304
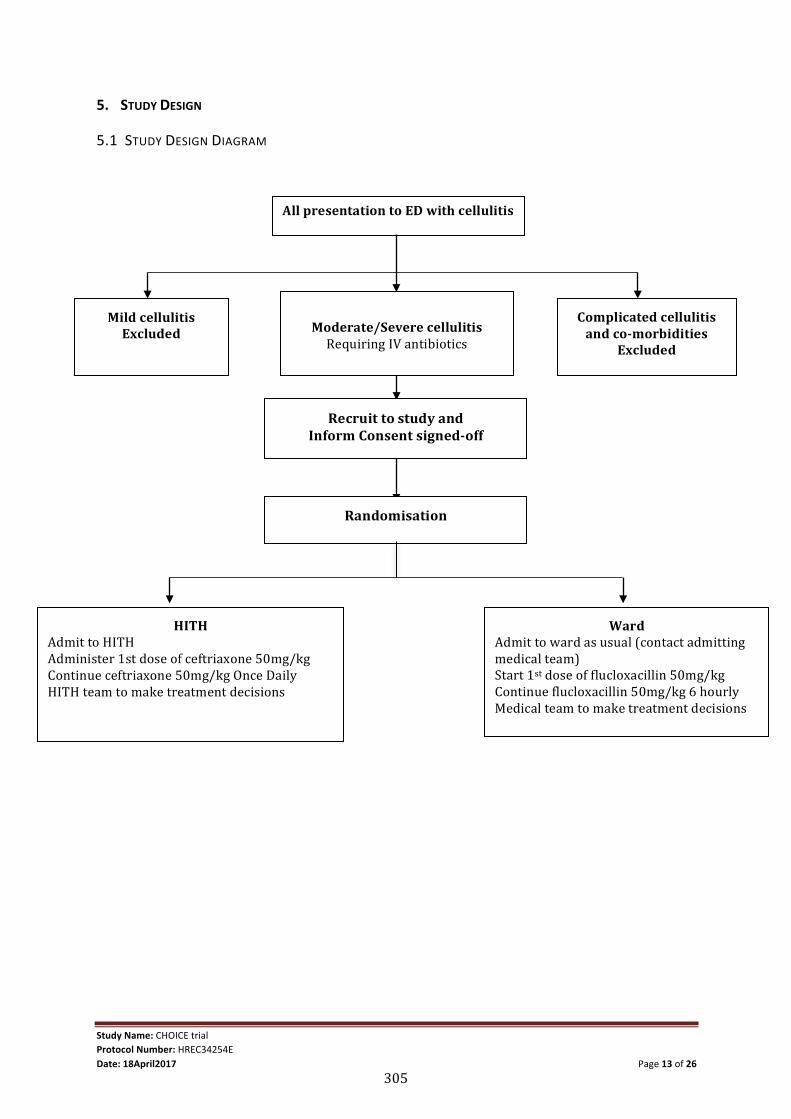
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 13 of 26
5. STUDY DESIGN
5.1 STUDY DESIGN DIAGRAM
All presentation to ED with cellulitis
Complicated cellulitis and co-‐morbidities
Excluded
Moderate/Severe cellulitis Requiring IV antibiotics
Mild cellulitis Excluded
HITH Admit to HITH Administer 1st dose of ceftriaxone 50mg/kg Continue ceftriaxone 50mg/kg Once Daily HITH team to make treatment decisions
Ward Admit to ward as usual (contact admitting medical team) Start 1st dose of flucloxacillin 50mg/kg Continue flucloxacillin 50mg/kg 6 hourly Medical team to make treatment decisions
Recruit to study and Inform Consent signed-‐off
Randomisation
305

Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 14 of 26
5.2 STUDY TYPE & DESIGN & SCHEDULE Study design: This study is a pragmatic, prospective, single-‐centre, open label non-‐inferiority randomised controlled trial with economic analysis. This pragmatic trial aims to determine whether cellulitis treatment given at home is non-‐inferior to (at least as good as) cellulitis treatment in the hospital, to inform decisions about practice. It will incorporate a two-‐arm, non-‐inferiority design with parallel groups and 1:1 allocation of children with moderate/severe cellulitis presenting to the RCH ED.
306
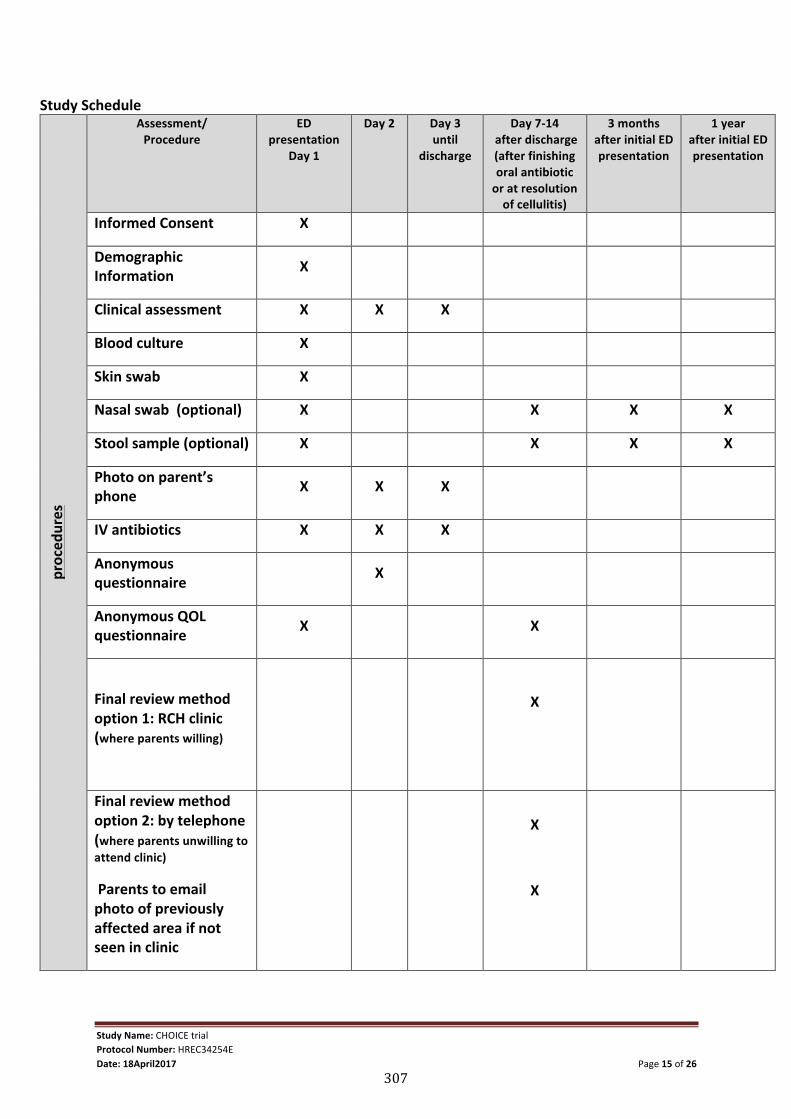
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 15 of 26
Study Schedule
proced
ures
Assessment/ Procedure
ED presentation
Day 1
Day 2 Day 3 until
discharge
Day 7-‐14 after discharge (after finishing oral antibiotic or at resolution of cellulitis)
3 months after initial ED presentation
1 year after initial ED presentation
Informed Consent X
Demographic Information X
Clinical assessment X X X
Blood culture X
Skin swab X
Nasal swab (optional) X X X X
Stool sample (optional) X X X X
Photo on parent’s phone X X X
IV antibiotics X X X
Anonymous questionnaire X
Anonymous QOL questionnaire X X
Final review method option 1: RCH clinic (where parents willing)
X
Final review method option 2: by telephone (where parents unwilling to attend clinic)
Parents to email photo of previously affected area if not seen in clinic
X
X
307

Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 16 of 26
5.3 RANDOMISATION After a baseline assessment is performed, the parent/guardian will be given information about the study and have the opportunity to discuss the study with the researcher/clinician. After a written consent is obtained, children will be randomised to either HITH group or treatment at hospital group with an allocation ratio of 1:1, using a web-‐based randomisation procedure. The randomisation schedule and web-‐based service will be provided by the Clinical Epidemiology and Biostatistics Unit (CEBU) at the Murdoch Childrens Research Institute. The randomisation will be in randomly permuted blocks of variable length, stratified by age (6 months to <9 years and 9 to 18 years) and presence of periorbital cellulitis. Web randomisation will be enabled through the Redcap (Research electronic Data Capture) web based application. A study icon labelled ‘Choice Trial’ will be visible on all desktops in both the ED pods. This will take clinicians directly to the Redcap log in page. Any ED clinician can use a generic username and password which can be found on a lanyard stuck onto to the desktops. Then the clinician will enter the child’s date of birth and whether or not the area affected is periorbital (stratification factors). This will then generate a randomisation assignment which will be displayed as ‘HITH’ or ‘Ward’ along with a randomisation sequential number.
5.4 STUDY METHODOLOGY Clinical management after randomization is as per routine clinical practice. In addition, we will take a nasal swab to determine the rate of nasal carriage of Staphylococcus aureus in patients with cellulitis and to identify methicillin resistant S. aureus (MRSA) carriers. This may be used to guide treatment if the patient is not clinically improving and MRSA is present: if a patient fails treatment and they are found to have a positive skin or nasal swab with MRSA the treating doctor may change their treatment appropriately. If, in addition, they have had multiple infections with MRSA patients will be offered the current usual practice in this situation which is to decolonize (eradicate MRSA) all household members with the explanation that it is only 50% effective at 3 months. Decolonization or eradication process involves using an antiseptic body wash, a mouthwash and nasal ointment for 5 days. Parents who are interested in submitting a stool specimen are provided with a standard hospital stool collection jar. They are advised to place a disposable container in the toilet bowl to catch a stool specimen. In addition, they are instructed to use the spatula that forms part of the lid to obtain a small pea-‐sized stool sample for testing and the remaining stool can be disposed of. Once stool samples are available, parents can notify a research team member (phone number provided on the information statements) for the stool specimen to be transported to the pathology lab. The jar containing the stool sample should be kept in the fridge or freezer until a member of the study team collects the sample.
If there is skin breakdown, a skin swab would be done as per routine clinical practice. Prior to commencing IV antibiotics. In addition, the researcher or ED clinician will ask parents to take 2 photos of the cellulitis area using their own camera/phone (if available) after the affected area is demarcated with indelible ink (Sharpie) with a tape measure placed along side the area affected. If parents do not have a camera/phone, permission will be sought by researcher/clinician to use a HITH tablet to photograph the lesion. This tablet will be stored in the ED research drawer in the main ED pod and is available 24 hours a day. This will be
308
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 17 of 26
helpful for the reviewing doctor the following day to judge whether there is an improvement. Prior to starting this study, the ED physicians have been deciding whether patients are admitted to ward or HITH based on ill-‐defined factors including time of day and familiarity with the HITH program. In our data collection to date all of the patients admitted to hospital could have been admitted to HITH and would not have been excluded from this study. The only new intervention is randomization process and data collection. Data collection will begin once consent has been obtained in ED. The ED clinician will be asked to fill in a CRF and then the treating clinician (HITH or Ward clinician) will record the assessment findings on the CRF on a daily basis (CRF will be available in the ED research drawers, these are clearly marked as ‘Research drawer-‐blank CRF’ .ED clinicians will be informed of where these can be found in education sessions). A member of the research team will obtain the CRF from the research drawer and ask the treating clinician to fill in the daily assessment details. They will be reminded on a daily basis. Other information collected will be from the medical records. In the first 2 days of admission, the parent and where applicable the child will be given a parental/patient satisfaction questionnaire and a quality of life questionnaire. The questionnaires will be given on the ward or at home after recruitment. The questionnaires would remain anonymous by de-‐identification and providing a stamped envelope to conceal answers when returned to the investigators. A child aged 7 years old or older will be given the ‘child complete’ version and if younger, the parent will be given the ‘parent complete’ version of the quality of life questionnaire (Child Health Utility 9). As per normal practice, patients will be switched to oral therapy after 2-‐4 days of IV antibiotics, when there is clinical improvement of the cellulitis. Based on the current prospective study, both HITH patients and ward patients are switched to oral antibiotics when there is a reduction in fever, swelling, erythema and improvement of function of affected area (eg. Previously limping, now walking). Once changed to oral antibiotics (as per RCH clinical practice guidelines; cephalexin 25mg/kg 6 hourly, total dose may be combined and divided to twice daily), patients are usually discharged from hospital care and normally not followed up any further in hospital. In this study, we would like to offer all participants a follow up in clinic 7-‐14 days (by the RA who is a paediatric registrar) after discharge from hospital. Parents will be requested to bring a stool sample from the patient to the clinic review but this is not mandatory. A separate consent will not be sought for attendance at clinic or provision of stool sample as consent will be implied with parents’ attendance at clinic and provision of stool sample. If parents decline the follow-‐up visit at clinic, a follow up review will be conducted by telephone and the parent will be requested to email photos of the area previously affected with cellulitis (to ensure clinical resolution). Photos will be identified only by the subject unique identifier assigned for the study and will be stored in a password protected database accessible only to the researchers. If parents are unable to provide photographic evidence of clinical resolution, as per routine practice parental verbal report will be accepted .The same parental/patient satisfaction and quality of life questionnaires will be posted out to the parents at Day 7-‐14 after discharge for completion by the parent and, where applicable, the child. At about 3 months and 1 year after initial admission to hospital, parents will be contacted and asked if interested in providing a nasal swab and stool sample.
309
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 18 of 26
6. STUDY POPULATION
6.1 RECRUITMENT PROCEDURE Prior to the study commencing, ED clinicians will have education sessions to inform them about the study. These education sessions will be integrated into a pre-‐existing ED staff education morning which usually takes place every fortnight. A member of the research team will explain the study in detail to ED doctors. These education sessions will continue every fortnight until all doctors in ED have attended a session. Names of those already attended will be obtained and stored in the study binder. Participation is voluntary.
ED clinicians (senior doctors, junior doctors or nurse practitioners) will identify patients with moderate/severe cellulitis presenting to RCH ED, at the point of triage or during clinical assessment. At this stage, the ED clinician may decide to enrol the patient or if uncertain, the clinicians are encouraged to make contact with a member of the research team. The parents of patients (and where applicable the patient) in the moderate/severe group meeting inclusion criteria will be invited by the researcher or treating ED clinician to provide their consent to participate in the study. The consent will be for randomization, data collection and follow up which is not part of routine practice. In addition, patients will be asked for their consent to provide a nasal swab sample and a stool sample. Both of these samples (nasal swab and stool) will be requested at four different time points, firstly in the first 48 hours of admission, secondly a week to 14 days after starting antibiotics, thirdly about 3 months after initial ED presentation and lastly a year after initial presentation to ED. At these time points, parents will be asked if there have there been any recent antibiotic use, any other recent infections, GP visits or hospital admissions to correlate with findings of nasal swabs and stool samples. These samples are optional and does not affect participation in the study. Randomisation to the location of treatment is the essential difference from normal clinical practice. The researcher or ED clinician will give the appropriate information sheet to parent and/or child, explain the study and request written consent. These will be stored at the research office (RCH@home department) in a locked storage cabinet. Where parents do not give consent, the ED clinician will make the decision on where the patient should be treated.
6.2 INTERVENTIONS Patients who are randomised to HITH will be prescribed IV ceftriaxone (50mg/kg once daily) as per current practice and those randomised to the ward will be prescribed IV flucloxacillin (50mg/kg 6 hourly). On insertion of the IV cannula, the ED clinician will obtain a blood culture.
The first dose of antibiotics will be commenced in ED. For children assigned to hospital ward treatment, the child will be transferred to the ward and the IV infusion continued. Children assigned to the HITH will complete their first dose in ED before going home. The management after this point will be as per usual practice. The responsible ward doctor will review and make all management decisions for patients admitted to the ward whereas the HITH registrar will review the patients on HITH. The research assistant (RA) (a paediatric registrar) will meet with the child and their parent(s) within 24 hours of consent being obtained to answer any further questions parents or participants may have about the study.
310
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 19 of 26
Currently, there are no guidelines on when to start IV antibiotic in cellulitis. The authors’ recommendation is provided under Section 6.3 (Inclusion criteria) and this reflects consensus among RCH ED clinicians. Some patients who did not require IV antibiotics may be recruited but they will exist in both groups. This randomised study will determine whether treatment at home is effective for children with uncomplicated moderate/severe cellulitis and therefore applicable to all children with uncomplicated moderate/severe cellulitis.
6.3 INCLUSION AND EXCLUSION CRITERIA
Inclusion Criteria 1. Children aged 6 months to 18 years 2. Children presenting to RCH ED with moderate/severe cellulitis 3. Moderate/severe: defined in this study, as those assessed by ED clinician to
need IV antibiotics 4. Reasons for starting IV antibiotics include:
a. Failed oral therapy (not improving despite 24h of oral therapy) b. Rapidly spreading redness (from patient/parent history) c. Significant swelling/redness/pain d. Systemic symptoms/signs (eg. fever, lethargy) e. Difficult to treat areas (eg. face, ear, toe)
Exclusion Criteria
1. With orbital cellulitis or unable to exclude orbital cellulitis, 2. With penetrating injury/bites, 3. With suspected fasciitis or myositis, 4. With toxicity: tachycardia when afebrile or hypotension (both as per the
limits set out by RCH Resuscitation Card), poor central perfusion (capillary refill >2 seconds)
5. With immunosuppression, 6. With varicella, 7. With suspected/confirmed foreign body, 8. With abscess not drained, 9. With dental abscess, 10. With concurrent sinusitis or otitis media or lymphadenitis necessitating
different antibiotic treatment to flucloxacillin monotherapy or ceftriaxone monotherapy,
11. With liver co-‐morbidities 12. With other medical diagnoses warranting admission to hospital for
observation or treatment relating to the known medical condition 13. With difficult intravenous access, 14. Age <6 months old, 15. 15. Who could be managed on oral antibiotics (ie assessed as mild cellulitis)
6.4 CONSENT
311
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 20 of 26
Parents will be given a parent/guardian information sheet (PGIS) and participants will be given, where applicable, a participant information sheet (PIS). Participation in the study will be discussed with any members of the research team who will be available 24 hours a day, 7 days a week. The contact details can be found on the CRF. This will happen in the ED. The principal investigator, associate investigators and research officer may be involved in the clinical care of the patient. Parents/participants will be assured that if they do not wish to participate this will in no way affect their care. This is also stated in the PIS and PGIS.
7. PARTICIPANT SAFETY AND WITHDRAWAL
7.1 RISK MANAGEMENT AND SAFETY There are no foreseeable additional risks to patients or their families by participating in this study. HITH has been shown to be a safe program under which children can be treated at home for many conditions, and there will be daily medical review of all patients. Families on the HITH program have direct access via telephone to an experienced nurse who is available 24 hours a day every day and this nurse is supported by a medical team. Only 1 out of 70 children (1.4%) with uncomplicated moderate/severe cellulitis treated on the HITH program developed an abscess. This child was assessed at home by a HITH clinician to have developed an abscess and appropriately referred to ED for drainage of the abscess. After drainage was completed, this child continued treatment at home. This compares to 3 out of 130 children (2.3%) treated on the hospital ward who developed abscesses requiring drainage.
Adverse Event Reporting For the purposes of this study the treating clinician is responsible for recording in the medical record and following up on all Adverse Events. For patients at home this will be the HITH consultant and registrar; for hospital ward patients it will be the treating medical team. The investigators will also record and report adverse events in the database.
The adverse effects possible in this study would be an allergic reaction to either of the registered drugs used (flucloxacillin or ceftriaxone). Serious adverse events such as overwhelming sepsis or death are not expected in this study as cellulitis in children is a condition not associated with such morbidity and mortality. Patients may develop an abscess (pus under skin) while on treatment which would require drainage but this would be the natural progression of this medical condition in some cases.
7.2 HANDLING OF WITHDRAWALS Participants will be informed at the time of obtaining consent that they may withdraw from the study at any stage and that this will not affect the treatment or management of their medical condition or their relationship with RCH. Once consent is withdrawn, no more data or samples will be collected. Data, photos and samples collected prior to withdrawal of consent will be retained. Withdrawals will not be replaced. Patients who are found to not meet the inclusion/exclusion criteria after being randomised (randomised in error) will be replaced by further recruitment to maintain the required sample size.
312
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 21 of 26
7.3 INDEPENDENT SAFETY AND DATA MONITORING COMMITTEE An Independent Safety and Data Monitoring Committee (ISDMC) will be established. The ISDMC will consist of three independent clinicians and/or biostatisticians that, collectively, have experience in the management of paediatric patients with cellulitis and in the conduct and monitoring of randomised controlled trials. The ISDMC will function independently of all other individuals and bodies associated with the conduct of the study. The ISDMC will review all data by treatment arm every six months. At each meeting a report will be prepared by the trial statistician based on the participants recruited so far which will be presented to the ISDMC by the trial statistician. A descriptive summary of status of accrual, reasons for not randomising, withdrawals, protocol violations, serious adverse events and non-‐serious adverse events thought to be related to the study drugs will be provided. The first meeting of the ISDMC will be after 6 months. The interim report at this time will present a descriptive analysis of primary outcome data only, with no formal comparison of the treatment groups. Subsequent reports will include a formal interim analysis of the primary outcome. All information presented in the interim report will be by presented by study arm, but will be labelled treatment “X” and “Y” to ensure that the trial statistician remains blinded to treatment allocation. The key to identify the treatment regimen will be supplied separately by an independent statistician if requested by the ISDMC.
8. STATISTICAL METHODS
8.1 SAMPLE SIZE ESTIMATION & JUSTIFICATION The retrospective data collected in 2013 and the prospective data in 2014 showed a failure rate of treatment in hospital of approximately 5%. We have determined based on the literature and discussion with clinicians that the maximum amount by which the failure rate in the HITH group could exceed the failure rate in the hospital treatment group before it is considered to be inferior is 15% ie. clinical acceptability if 80% of children can be successfully treated at home. With a study design of a ‘non-‐inferiority’ trial, and assuming the failure rate in the Hospital-‐In-‐The-‐Home group is equal to 10% and the failure rate in the treatment at hospital group is equal to 7%, if the maximum amount by which the failure rate in the Hospital-‐In-‐The-‐Home group could exceed the failure rate in the hospital treatment group before it is considered to be inferior is 15%, 89 subjects in each treatment group gives a power to the study of approximately 81%. Thus, allowing for 5% dropout and cross over between treatments rates, a total of 188 are required (94 in each treatment arms). Based on the retrospective and prospective study, we would be able to recruit this number over a 2 year period if this study remains within RCH. However, once this study commences in RCH, we would look to expand this study to other centers which would shorten length of time to complete this study.
8.2 STATISTICAL METHODS
313
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 22 of 26
Data analysis for the study will be performed by CEBU at MCRI. Statistical analysis will follow both intention to treat (ITT) and per-‐protocol (PP) approaches, which is common for non-‐inferiority randomised controlled trials. If both approaches support non-‐inferiority is the trial considered positive.
The ITT population will include all randomised participants where outcome data are available.
Baseline characteristics (such as patient demographics, underlying diagnosis, presence of systemic symptoms, site of cellulitis, characteristics of the cellulitis) will be presented separately for participants in the groups using means and standard deviations (SD) for continuous data (or medians and inter-‐quartile ranges for non-‐normal data) and proportions for categorical data.
Primary analysis The number and proportion of participants who will be assessed as treatment failures by the treating clinician within two days from the first dose will be summarized by treatment group, using frequency tabulations. Pearson’s Chi-‐Square test will be used to compare the proportion of participants who fail treatment at 2 days from the first dose. Non-‐inferiority will determined by calculating the risk difference and its one-‐sided 97.5% confidence interval [CI] (or equivalently a 95% two-‐sided confidence interval) between the failure rates in the HITH and in hospital groups. We have pre-‐specified the margin of non-‐inferiority for HITH as 15% above the treatment in hospital failure rate. For the HITH to be non-‐inferior to treatment in the hospital, the upper limit of the 95% CI must be less than 15%.
Secondary analyses As a secondary analysis on the primary outcome a logistic regression model will be used to investigate whether inclusion of the stratification factor (age at randomisation) as predictor modifies the estimated effect (and 95%CI) of treatment group on the primary outcome.
Secondary continuous outcomes will be compared between the two groups using unadjusted linear regression whilst binary outcomes will be compared using unadjusted logistic regression. Furthermore, as explorative analyses, regression models (or logistic models according to the nature of the outcome) will also be fitted to the primary and secondary outcomes adjusting for age (as used in the randomisation), presence of fever at baseline and any other baseline and demographic variables where an imbalance is found. The appropriate survival analysis models will be used to compare time to event outcomes between the treatment groups.
9. STORAGE OF BLOOD AND TISSUE SAMPLES Samples taken may include a blood culture and a skin swab which would all be directed to the microbiology lab. As written above, a blood culture would be obtained on insertion of the IV cannula. This will be sent for culture and sensitivity testing to ensure children do not have any bacteremia. All samples would then be processed as per routine practice as follows: for blood cultures, if the sample is culture-‐negative, it will be discarded after 7 days. If the sample is culture-‐positive, the organism will be purified and frozen and kept for 1 month after the collection date. For skin swabs, all swabs are discarded after 1 week of the
314
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 23 of 26
finalized report. Process of discarding samples is in line with routine laboratory practice. Samples will not be entered into a biobank and consent to use samples will only be for this study. None of the samples will be used for genetic testing.
10. DATA SECURITY & HANDLING
10.1 DETAILS OF WHERE RECORDS WILL BE KEPT & HOW LONG WILL THEY BE STORED All study participants will be assigned a unique study number (Subject ID) for the study. The document linking the Subject ID with personal identifiers will be accessible only to the researchers. The unique study identifier will be used to identify all CRFs. It will also be used to identify the clinical and laboratory data entered into the password protected study database from RCH clinical and laboratory databases.
Consent forms along with Subject ID coded paper study records will be stored in locked storage in the RCH@home department. All electronic participant study records will be stored in the password protected study database, accessible to the researchers only.
As per guidelines, all health information will be kept until a participant reaches 25 years of age.
10.2 CONFIDENTIALITY AND SECURITY Confidentiality will be ensured by storing data in a password-‐protected database for which only the research team will have the password.
The questionnaire will be completely anonymous. Any patient data published will not allow personal identification.
Group data only will be published.
10.3 ANCILLARY DATA Images will be stored in a password protected database in the RCH@Home department local drive and will be identified by the unique subject identifier only. Only the researchers will have access to the photos.
11. REFERENCES 1. Ibrahim LF, Hodgson KA, Sacks B, Golshevsky D, Layley M, Spagnolo M, Bryant PA. Once daily ceftriaxone for moderate/severe cellulitis at home in children referred from the Emergency Department. World Society for Pediatric Infectious Diseases Congress, Cape Town, Nov 2013
315
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 24 of 26
2. Ibrahim L, Hopper S, Babl F, Bryant PA. A comparison of treatment at home or in hospital for the treatment of moderate/severe cellulitis in children. Australasian Society of Infectious Diseases Conference, Adelaide, Mar 2014 3. Ibrahim L, Hopper S, Babl F, Bryant PA. Ceftriaxone at home versus flucloxacillin in hospital for moderate/severe cellulitis. Emergency Medicine Journal under review, Oct 2014. 4. Ibrahim L, Bryant PA, Babl F, Hopper S. A prospective comparison of home versus hospital IV treatment for cellulitis. Submitted to Australasian College for Emergency Medicine Annual Conference, Melbourne, Dec 2014 5. Gouin S, Chevalier I, Gauthier M, Lamarre V. Prospective evaluation of the management of moderate to severe cellulitis with parenteral antibiotics at a paediatric day treatment centre. Journal of paediatrics and child health. 2008;44(4):214-‐8. 6. Svahn BM, Remberger M, Heijbel M, Martell E, Wikstrom M, Eriksson B, et al. Case-‐control comparison of at-‐home and hospital care for allogeneic hematopoietic stem-‐cell transplantation: the role of oral nutrition. Transplantation. 2008;85(7):1000-‐7. 7. Small F, Alderdice F, McCusker C, Stevenson M, Stewart M. A prospective cohort study comparing hospital admission for gastro-‐enteritis with home management. Child: care, health and development. 2005;31(5):555-‐62. 8. Balaguer A, Gonzalez de Dios J. Home versus hospital intravenous antibiotic therapy for cystic fibrosis. The Cochrane database of systematic reviews. 2012;3:CD001917. 9. Tiberg I, Katarina SC, Carlsson A, Hallstrom I. Children diagnosed with type 1 diabetes: a randomized controlled trial comparing hospital versus home-‐based care. Acta paediatrica. 2012;101(10):1069-‐73. 10. Hansson H, Kjaergaard H, Johansen C, Hallstrom I, Christensen J, Madsen M, et al. Hospital-‐based home care for children with cancer: feasibility and psychosocial impact on children and their families. Pediatric blood & cancer. 2013;60(5):865-‐72. 11. Laupland KB, Valiquette L. Outpatient parenteral antimicrobial therapy. The Canadian journal of infectious diseases & medical microbiology = Journal canadien des maladies infectieuses et de la microbiologie medicale / AMMI Canada. 2013;24(1):9-‐11. 12. Rucker RW, Harrison GM. Outpatient intravenous medications in the management of cystic fibrosis. Pediatrics. 1974;54(3):358-‐60. 13. Stevens DL, Bisno AL, Chambers HF, Everett ED, Dellinger P, Goldstein EJ, et al. Practice guidelines for the diagnosis and management of skin and soft-‐tissue infections. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2005;41(10):1373-‐406. 14. Grayson ML, McDonald M, Gibson K, Athan E, Munckhof WJ, Paull P, et al. Once-‐daily intravenous cefazolin plus oral probenecid is equivalent to once-‐daily intravenous ceftriaxone plus oral placebo for the treatment of moderate-‐to-‐severe cellulitis in adults. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2002;34(11):1440-‐8. 15. Nelson SJ, Boies EG, Shackelford PG. Ceftriaxone in the treatment of infections caused by Staphylococcus aureus in children. Pediatric infectious disease. 1985;4(1):27-‐31. 16. Frenkel LD. Once-‐daily administration of ceftriaxone for the treatment of selected serious bacterial infections in children. Pediatrics. 1988;82(3 Pt 2):486-‐91. 17. Kulhanjian J, Dunphy MG, Hamstra S, Levernier K, Rankin M, Petru A, et al. Randomized comparative study of ampicillin/sulbactam vs. ceftriaxone for treatment of soft
316
Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 25 of 26
tissue and skeletal infections in children. The Pediatric infectious disease journal. 1989;8(9):605-‐10. 18. Brugha RE, Abrahamson E. Ambulatory intravenous antibiotic therapy for children with preseptal cellulitis. Pediatric emergency care. 2012;28(3):226-‐8. 19. Vinen J, Hudson B, Chan B, Fernandes C. A randomised comparative study of once-‐daily ceftriaxone and 6-‐hourly flucloxacillin in the treatment of moderate to severe cellulitis -‐ Clinical efficacy, safety and pharmacoeconomic implications. Clin Drug Invest. 1996;12(5):221-‐5.
317

Study Name: CHOICE trial Protocol Number: HREC34254E Date: 18April2017 Page 26 of 26
318
Summary of protocol amendments Primary outcome: no changes Secondary outcomes: -‐ majority no changes -‐ one secondary outcome (microbiology follow up) was expanded twice: 1) June 2015 (ClinicalTrials.gov updated Aug 2015): inclusion of nasal swab collection (skin swabs already being collected) and clarification of time points for stool sample collection (already being collected for analysis of resistant bacteria) 2) Dec 2016 (ClinicalTrials.gov updated Dec 2016) to include microbiome analysis of stored stool and nasal swabs after we received competitive funding to do this Personnel change: April 2017: The Principal Investigator was amended from the supervising researcher and senior author Dr. Penelope Bryant to Dr. Laila Ibrahim, the PhD student undertaking this RCT for her thesis. This was specifically to allow a competitive scholarship application, but it was also appropriate for Dr Ibrahim to take on this responsibility at this stage in the trial which she had been co-‐ordinating since the outset. Other changes were minor and included clarification of the type of QOL instrument being used and reordering of outcomes to align with order of objectives.
319
HREC34254E CHOICE Statistical Analysis Plan Page 1 of 15
HREC34254E
CHOICE Trial:
Cellulitis at Home Or Inpatient in Children from ED
Investigator/s: Dr Laila Ibrahim, Paediatric Fellow, PI Dr Penelope Bryant, Paediatric Infectious Diseases and HITH Physician Ms Francesca Orsini, CEBU Biostatistician Murdoch Children’s Research Institute Dr Franz Babl, Paediatric Emergency Physician, Director of Emergency Research Dr Sandy Hopper, Paediatric Emergency Physician
320
HREC34254E CHOICE Statistical Analysis Plan Page 2 of 15
TABLE OF CONTENTS
LIST OF ABBREVIATIONS .......................................................................................................... 4 1. STUDY OBJECTIVES ....................................................................................................... 5 1.1. PRIMARY OBJECTIVE ..................................................................................................... 5 1.2. SECONDARY OBJECTIVES ............................................................................................... 5
2. BACKGROUND/INTRODUCTION .................................................................................... 5 2.1. STUDY DESIGN ............................................................................................................. 5 2.2. TREATMENT GROUPS .................................................................................................... 6 2.3. STUDY POPULATION ..................................................................................................... 7 2.4. SAMPLE SIZE ................................................................................................................ 8 2.5. STUDY PROCEDURE ...................................................................................................... 8
3. DEFINITION OF PROTOCOL VIOLATIONS, STUDY POPULATIONS AND STATISTICAL ANALYSIS ............................................................................................................................... 9 3.1. MISRANDOMISATION ................................................................................................... 9 3.2. HANDLING OF STRATIFICATION ERROR ........................................................................... 9 3.3. PROTOCOL VIOLATIONS ................................................................................................ 9 3.4. DEFINITIONS OF STUDY POPULATIONS AND ANALYSIS SETS ............................................. 9
4. OUTCOME VARIABLES ................................................................................................ 10 4.1. PRIMARY OUTCOME ................................................................................................... 10 4.2. SECONDARY PARAMETERS OUTCOMES ........................................................................ 10 4.3. OTHER PARAMETERS .................................................................................................. 11
5. STATISTICAL METHODOLOGY ...................................................................................... 12 5.1. GENERAL METHODOLOGY ........................................................................................... 12 5.2. PRIMARY DATA ANALYSES ........................................................................................... 13 5.3. SECONDARY DATA ANALYSES ...................................................................................... 14
321

HREC34254E CHOICE Statistical Analysis Plan Page 3 of 15
322
HREC34254E CHOICE Statistical Analysis Plan Page 4 of 15
(FORM-STAT-04A-01/Version 1.0)
LIST OF ABBREVIATIONS
AE Adverse Event
CRF Case Report Form
ED Emergency Department
GCP Good Clinical Practice
HITH Hospital-‐In-‐The-‐Home; a patient on this program is considered admitted to a hospital bed (on inpatient list) but receives their treatment at home from visiting nurses and doctors
ITT Intent-‐To-‐Treat
IV Intravenous; antibiotic through a ‘drip’ directly into a vein
OPAT Outpatient Parenteral Antibiotic Therapy
PP Per Protocol
RA Research Assistant
RCH Royal Children’s Hospital
SAE Serious Adverse Event
SD Standard Deviation
323
HREC34254E CHOICE Statistical Analysis Plan Page 5 of 15
(FORM-STAT-04A-01/Version 1.0)
1. STUDY OBJECTIVES This study is a prospective, open label non-‐inferiority randomised controlled trial of intravenous treatment for children with moderate/severe cellulitis. Participants are randomised to receive treatment either at home or in hospital. 1.1. PRIMARY OBJECTIVE
To compare the failure rate of IV antibiotic treatment of children treated at home (IV ceftriaxone) with those treated in hospital (IV flucloxacillin) in the first 48 hours of treatment following the first dose given in the ED in children with moderate/severe cellulitis (moderate/severe defined in this study as those assessed by a senior ED physician to need IV antibiotics)
1.2. SECONDARY OBJECTIVES To compare: § time to no progression of cellulitis § duration of IV antibiotic administration § time to discharge i.e. length of stay under clinical care § length of stay in ED at initial presentation § rate of re-‐presentation to ED within 14 days § rate of readmission within 14 days § rate of at least one re-‐siting of IV cannula during treatment § rates of complications, adverse events and allergic reactions § clinical features of cellulitis at initial presentation in the ED § microbiology results at baseline, 1 week and 3 months
in children treated with IV antibiotics at home (IV ceftriaxone) with children treated with IV antibiotics (IV flucloxacillin) in the hospital during the study period.
2. BACKGROUND/INTRODUCTION
2.1. STUDY DESIGN This study is a pragmatic, prospective, single-‐centre, open label non-‐inferiority randomised controlled trial (RCT) with economic analysis. This pragmatic trial aims to determine whether cellulitis treatment administered at home is non-‐inferior to (at least as good as) cellulitis treatment in the hospital, to inform decisions about practice. It will incorporate a two-‐arm, non-‐inferiority design with parallel groups and 1:1 allocation of children with moderate/severe cellulitis presenting to the RCH ED. A total of 188 children aged 6 months to <18 years will be recruited over 2 years from the Emergency Department (ED) at the Royal Children’s Hospital (RCH) and followed up for one year after initial ED presentation.
324
HREC34254E CHOICE Statistical Analysis Plan Page 6 of 15
(FORM-STAT-04A-01/Version 1.0)
2.2. TREATMENT GROUPS Types of treatment Patients who are randomised to the treatment in the Hospital-‐in-‐the-‐Home (HITH) group will be prescribed IV ceftriaxone (50 mg/kg once daily) and those randomised to the hospital ward will be prescribed IV flucloxacillin (50 mg/kg 6 hourly). The first dose of antibiotics will be administered in the Emergency Department (ED) before the child goes either home or to the ward. After randomisation, treatment decisions for the patient will be made by the appropriate treating physician, as per usual practice: if at home by the HITH paediatrician and if on the ward by the ward general paediatrician. Patients will be switched to oral antibiotics when there is clinical improvement of the cellulitis as judged by the treating clinician and discharged as per usual clinical practice. Oral antibiotics will be cephalexin 25 mg/kg 6 hourly (as per RCH guidelines), or the most appropriate antibiotic based on microbiology results (e.g. if methicillin-‐resistant Staphylococcus aureus is subsequently isolated). All participants will be followed up post-‐discharge as per the following schedule: - 7–14 days after starting antibiotics; - 3 months after starting antibiotics; - 1 year after starting antibiotics. At each time point, the following information will be collected regarding the interim period since the previous time point: overseas travel, primary care or hospital visits, hospital admissions, other antibiotic use, other infections, household member who has been admitted to hospital overseas. Randomisation process After a baseline assessment to ensure eligibility, the parent/guardian and/or child if adolescent will be given information about the study and have the opportunity to discuss the study with the researcher/clinician. After written consent is obtained, children will be randomised to either: - Hospital-‐in-‐the-‐Home (HITH) group, IV ceftriaxone (50 mg/kg once daily) - Hospital ward group, IV flucloxacillin (50 mg/kg 6 hourly)
with an allocation ratio of 1:1, using a web-‐based randomisation procedure. The randomisation schedule and web-‐based service will be provided by the Clinical Epidemiology and Biostatistics Unit (CEBU) at the Murdoch Children’s Research Institute. The randomisation will be in randomly permuted blocks of variable length, stratified by age (6 months to <9 years and 9 to <18 years) and periorbital cellulitis (absent and present). Web randomisation will be enabled through the REDCap (Research Electronic Data Capture) web-‐based application. Clinical management after randomisation is as per usual practice. Participants will be informed at the time of obtaining consent that they may withdraw from the study at any stage and that this will not affect the treatment or management of their medical condition or their relationship with RCH. Once consent is withdrawn, no more data or samples will be collected. Data, photos and samples collected prior to withdrawal of consent will be retained. Patients who withdraw will not be replaced.
325
HREC34254E CHOICE Statistical Analysis Plan Page 7 of 15
(FORM-STAT-04A-01/Version 1.0)
Patients who are determined after being randomised either not to have met inclusion criteria or to have met exclusion criteria will be replaced by further recruitment to maintain the required sample size. They will be clearly described.
2.3. STUDY POPULATION Inclusion Criteria • Children aged 6 months to <18 years. • Children presenting to RCH ED with moderate/severe cellulitis, that is, those assessed
as needing intravenous antibiotics. Currently, there is no validated scoring system on which to base the choice between intravenous or oral antibiotics, therefore clinician judgement is the current gold standard. Although reasons may differ between clinicians, this will be accounted for by randomisation. Reasons for starting intravenous antibiotics include:
A. Failed oral antibiotics (no improvement despite 24 h oral antibiotics). B. Rapidly spreading redness (patient/parent history). C. Significant swelling/redness/pain. D. Systemic symptoms/signs (eg, fever, lethargy). E. Difficult to treat areas (eg, face, ear, toe).
Exclusion Criteria Children will be excluded if they have: • Complicated cellulitis defined as follows: orbital cellulitis or unable to exclude orbital
cellulitis, penetrating injury/bites, suspected/confirmed foreign body, suspected fasciitis or myositis, varicella, undrained abscess including dental abscess.
• Toxicity: tachycardia when afebrile or hypotension (both as per the limits from the ‘Development of heart and respiratory rate percentile curves for hospitalised children’14), poor central perfusion (capillary refill >2 s).
• Underlying comorbidities: immunosuppression, liver disease. • Any concurrent infection necessitating different antibiotic treatment to intravenous
flucloxacillin or ceftriaxone monotherapy, for example, concurrent sinusitis or otitis media or lymphadenitis.
• Other medical diagnoses necessitating admission to hospital for observation or treatment relating to the known medical condition.
• Unable to obtain intravenous access. • Age <6 months old. • With mild cellulitis (ie, can be treated with oral antibiotics).
Non-‐English speakers will be included so long as at the time of obtaining consent, an interpreter is available. At our centre, an interpreter is available in person during normal working hours Monday to Friday and via telephone 24 h a day. An interpreter service will also be used for subsequent phone calls and clinic visits similar to routine clinical practice involving non-‐English speakers.
326
HREC34254E CHOICE Statistical Analysis Plan Page 8 of 15
(FORM-STAT-04A-01/Version 1.0)
2.4. SAMPLE SIZE Previous data from children at RCH with moderate/severe cellulitis showed a failure rate of treatment in hospital of approximately 5-‐7%. For patients treated out of the hospital and therefore less regularly reviewed we predicted a slightly increased failure rate of up to 10%. Based on the literature and discussion with clinicians, the maximum amount by which the failure rate in the HITH group could exceed the failure rate in the hospital treatment group before it would be considered to be inferior is 15%. Therefore, with a non-‐inferiority design, assuming the failure rate in the hospital ward group is 7% and the failure rate in the HITH group is 10%, if the maximum amount by which the failure rate in the HITH group could exceed that in the hospital group before it is considered to be inferior is 15%, 89 subjects in each treatment group gives a power to the study of approximately 81%. Thus, allowing for rates of 5% dropout and cross over between treatments, 94 participants are required in each treatment arm – 188 in total.
2.5. STUDY PROCEDURE
Assessment/ Procedure
ED presentatio
n Day 1
Day 2 Day 3 until
discharge
Day 7-‐14 after
discharge (after
finishing oral antibiotic or at resolution of cellulitis)
3 months after initial
ED presentatio
n
1 year after initial
ED presentatio
n
Informed Consent X Demographic Information X
Clinical assessment X X X Blood culture X Skin swab X Nasal swab (optional) X X X X Stool sample (optional) X X X X Photo on parent’s phone X X X
IV antibiotics X X X Anonymous questionnaire X X
Final review method option 1: RCH clinic (where parents willing) Optional stool for culture and sensitivity
X X
Final review method option 2: by telephone X
327
HREC34254E CHOICE Statistical Analysis Plan Page 9 of 15
(FORM-STAT-04A-01/Version 1.0)
(where parents unwilling to attend clinic) Parents to email photo of previously affected area if not seen in clinic
X
3. DEFINITION OF PROTOCOL VIOLATIONS, MISRANDOMISATIONS, AND STUDY POPULATIONS
3.1. MISRANDOMISATION
The following cases will be considered misrandomisations and will be excluded from all statistical analyses:
• A child found prior to commencing intravenous treatment to have met one of the predefined exclusion criteria
• Randomisation occurred after intravenous treatment commenced Participants who are found to be misrandomised will be excluded from the analysis and
replaced.
3.2. HANDLING OF STRATIFICATION ERROR Participants may have been stratified incorrectly at the point of initial data entry during randomisation process eg date of birth entered incorrectly, in this case the participant will be analysed as per the correct stratum.
3.3. PROTOCOL VIOLATIONS Major protocol violations include:
• Received treatment on the ward if randomised to the HITH arm • Received treatment under HITH at home if randomised to hospital arm • Did not receive any study treatment
Minor protocol violations include:
• Received oral flucloxacillin at discharge instead of oral cephalexin.
3.4. DEFINITIONS OF STUDY POPULATIONS AND ANALYSIS SETS Data analysis for the study will be performed by CEBU at MCRI. Statistical analysis will follow both intention to treat (ITT) and per-‐protocol (PP) approaches, which is a common standard method for non-‐inferiority randomised controlled trials. • The ITT population will include all randomised participants where outcome data are
available, regardless of treatment received. Misrandomised cases as defined in section 3.1 will be excluded from the intention to treat population and replaced.
• The PP population will include all individuals that received treatment as per randomised allocation and also did not encounter any major protocol violation as
328
HREC34254E CHOICE Statistical Analysis Plan Page 10 of 15
(FORM-STAT-04A-01/Version 1.0)
defined previously (subsection 3.3). Misrandomised cases as defined in section 3.1 will be excluded from the per protocol population and replaced.
4. OUTCOME VARIABLES
4.1. PRIMARY OUTCOME The primary outcome is treatment failure defined as lack of clinical improvement of cellulitis or an adverse event, resulting in a change of initial empiric antibiotics within 2 days (48 hours) of treatment from the start of the first antibiotic dose given in the ED. The features contributing to clinical improvement are assessed and recorded daily in the CRF by the treating clinician and include: reduction in fever (reduction in fever frequency or degree of temperature, if fever source is cellulitis and not concurrent illness), reduction in the cellulitis area (measured by largest diameter of erythema), reduction in the severity of swelling (judged as mild, moderate or severe) and a reduction in the intensity of erythema (judged on a scale of 0 to 5, 0=no erythema and 5=severe erythema).
4.2. SECONDARY OUTCOMES Rate of cessation of cellulitis spread at 24 h: Proportion of children whose cellulitis stopped spreading past the marked area within 24 hours from the start of the first dose in ED (Day 1). Rate of cessation of cellulitis spread at 48 h: Proportion of children whose cellulitis stopped spreading past the marked area within 48 hours from the start of the first dose in ED (Day 1). Duration of IV antibiotics: number of days (including fractions of days) elapsed from the start of the first dose in ED (Day 1) to the last dose.
Time to discharge: number of days (including fractions of days) elapsed from the time of presentation in ED to the time the patient is discharged from hospital or HITH care i.e. length of stay. (Discharge is defined as when patients admitted to hospital or HITH are deemed not to require any hospital or HITH funded care/intervention from a hospital or HITH based nurse/doctor. The time and date is registered on the electronic hospital database.) Length of stay in ED at initial presentation: from first presentation in ED to time the patient leaves ED to go either home under HITH or to hospital ward. Rate of re-‐presentation to ED: Proportion of children re-‐presenting to ED within 14 days of discharge and diagnosed to have incomplete resolution or recurrence of same cellulitis Rate of readmission: Proportion of children readmitted to hospital within 14 days of discharge date due to the same cellulitis
329
HREC34254E CHOICE Statistical Analysis Plan Page 11 of 15
(FORM-STAT-04A-01/Version 1.0)
Rate of at least one re-‐siting of IV cannula during treatment: Proportion of children who require at least one IV cannula to be re-‐sited to maintain IV access during IV treatment
4.3. OTHER SECONDARY PARAMETERS
DEMOGRAPHY AND BASELINE Age at baseline Sex Site of cellulitis Clinical assessment: - presence of systemic features - dimension of surface area affected (longest length axis multiply by the longest
perpendicular axis measured in cm2), - severity of swelling (judged by clinician as mild, moderate or severe) - intensity of erythema (judged by clinician on a scale of 0 to 5, 0=no erythema and
5=severe erythema) - tenderness of cellulitis area (judged by clinician from a scale of 0 to 5, 0=not tender
and 5=very tender) - impairment of function of affected area
SAFETY Complications of cellulitis: development of abscess requiring drainage after starting IV antibiotics, bacteremia. Adverse events: occurrences of anaphylaxis, allergic reaction (suspected or confirmed) necessitating change of empiric antibiotic, sepsis, death. MICROBIOLOGY (SHORT TERM) Microbiology, for participants who consented to samples: - Rate of ceftriaxone susceptibility in bacteria isolated from skin and/or nasal swabs.
Bacteria isolated by culture of a skin swab of the affected area and/or nasal swab will have susceptibility testing against ceftriaxone to document the rate of organism susceptibility to ceftriaxone
- Rate of Staphylococcus aureus (methicillin-‐sensitive and methicillin-‐resistant) nasal carriage collected within 48 hours, 7-‐14 days and 3 months of initial presentation to hospital
- Rate of resistant enteric bacteria present in stool sample collected within 48 hours, 7-‐14 days and 3 months of initial presentation to hospital
330
HREC34254E CHOICE Statistical Analysis Plan Page 12 of 15
(FORM-STAT-04A-01/Version 1.0)
4.4. LONGER-‐TERM PARAMETERS COST ANALYSIS Analysis of cost differences: Difference in average daily and total cost of treatment at home via HITH versus in hospital, incorporating direct (e.g. antibiotic cost, nursing visit) and indirect (e.g. computer use, overheads) costs QUALITY OF LIFE INDICATORS Quality of life (QOL) indicators: anonymous survey asking parents/patients how much admission to hospital or HITH disrupt their routine and including questions from a published quality of life (QOL) tool CLINICAL Infections with resistant bacteria: Rate of clinical infections with documented resistant bacteria within 1 year of initial presentation to ED; correlation with microbiology results MICROBIOLOGY (LONG TERM) Microbiology, for participants who consented to samples: - Rate of Staphylococcus aureus (methicillin-‐sensitive and methicillin-‐resistant) nasal
carriage collected 1 year after initial presentation to hospital - Rate of resistant enteric bacteria present in stool sample collected 1 year after initial
presentation to hospital - Differential effect of narrow spectrum (flucloxacillin) and broad spectrum
(ceftriaxone) antibiotic on the nasal and gastrointestinal microbiome from nasal swabs and stool samples collected within 48 hours, after 7-‐14 days, 3 months and 1 year after starting antibiotics
- Analysis of risk factors for acquisition of nasal or stool colonisation (e.g. travel overseas, other hospital admissions, household member a healthcare worker)
These longer-‐term parameters will be analysed later and published subsequently.
5. STATISTICAL METHODOLOGY
5.1. GENERAL METHODOLOGY
Baseline characteristics (such as patient demographics, underlying diagnosis, presence of systemic symptoms, site of cellulitis, characteristics of the cellulitis), safety and microbiology outcomes will be presented separately for participants in the two treatment groups using means and standard deviations (SD) for continuous data (or medians and inter-‐quartile ranges for non-‐normal data) and proportions for categorical data. HANDLING OF MISSING DATA The frequency and patterns of missing data will be examined. If the proportion of missing data on the primary outcome is greater than 5%, sensitivity analyses will be performed to
331
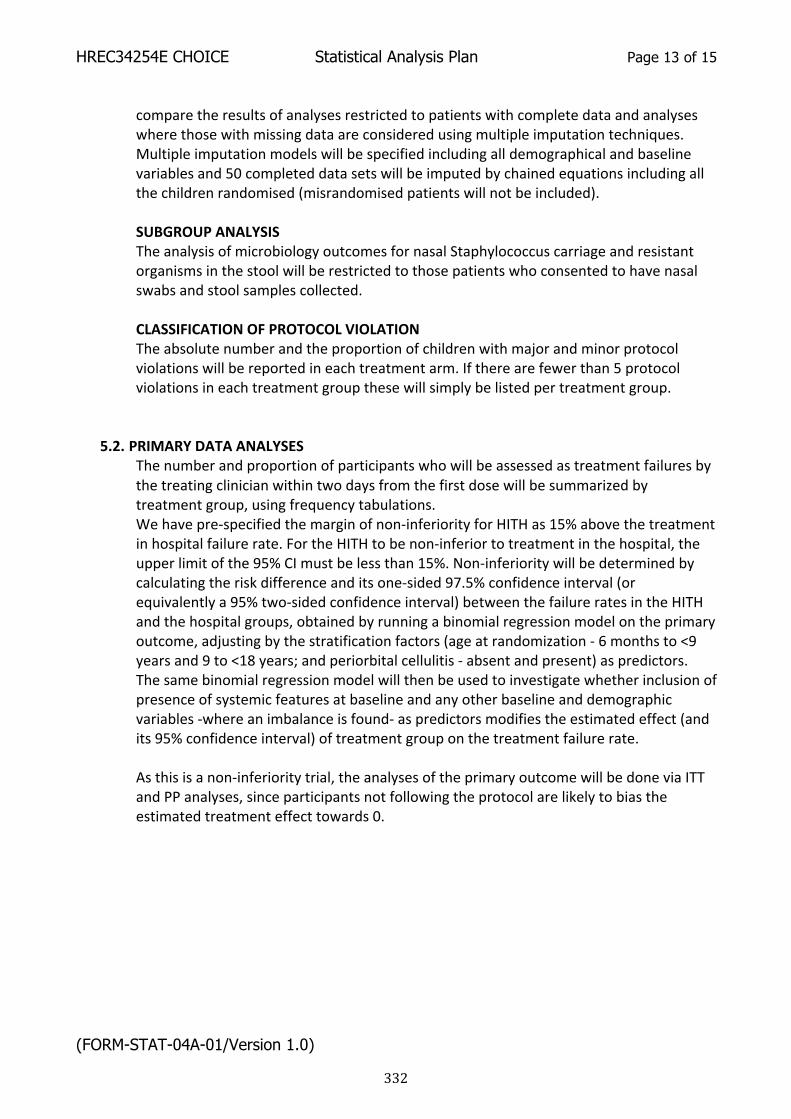
HREC34254E CHOICE Statistical Analysis Plan Page 13 of 15
(FORM-STAT-04A-01/Version 1.0)
compare the results of analyses restricted to patients with complete data and analyses where those with missing data are considered using multiple imputation techniques. Multiple imputation models will be specified including all demographical and baseline variables and 50 completed data sets will be imputed by chained equations including all the children randomised (misrandomised patients will not be included).
SUBGROUP ANALYSIS The analysis of microbiology outcomes for nasal Staphylococcus carriage and resistant organisms in the stool will be restricted to those patients who consented to have nasal swabs and stool samples collected. CLASSIFICATION OF PROTOCOL VIOLATION The absolute number and the proportion of children with major and minor protocol violations will be reported in each treatment arm. If there are fewer than 5 protocol violations in each treatment group these will simply be listed per treatment group.
5.2. PRIMARY DATA ANALYSES The number and proportion of participants who will be assessed as treatment failures by the treating clinician within two days from the first dose will be summarized by treatment group, using frequency tabulations. We have pre-‐specified the margin of non-‐inferiority for HITH as 15% above the treatment in hospital failure rate. For the HITH to be non-‐inferior to treatment in the hospital, the upper limit of the 95% CI must be less than 15%. Non-‐inferiority will be determined by calculating the risk difference and its one-‐sided 97.5% confidence interval (or equivalently a 95% two-‐sided confidence interval) between the failure rates in the HITH and the hospital groups, obtained by running a binomial regression model on the primary outcome, adjusting by the stratification factors (age at randomization -‐ 6 months to <9 years and 9 to <18 years; and periorbital cellulitis -‐ absent and present) as predictors. The same binomial regression model will then be used to investigate whether inclusion of presence of systemic features at baseline and any other baseline and demographic variables -‐where an imbalance is found-‐ as predictors modifies the estimated effect (and its 95% confidence interval) of treatment group on the treatment failure rate. As this is a non-‐inferiority trial, the analyses of the primary outcome will be done via ITT and PP analyses, since participants not following the protocol are likely to bias the estimated treatment effect towards 0.
332
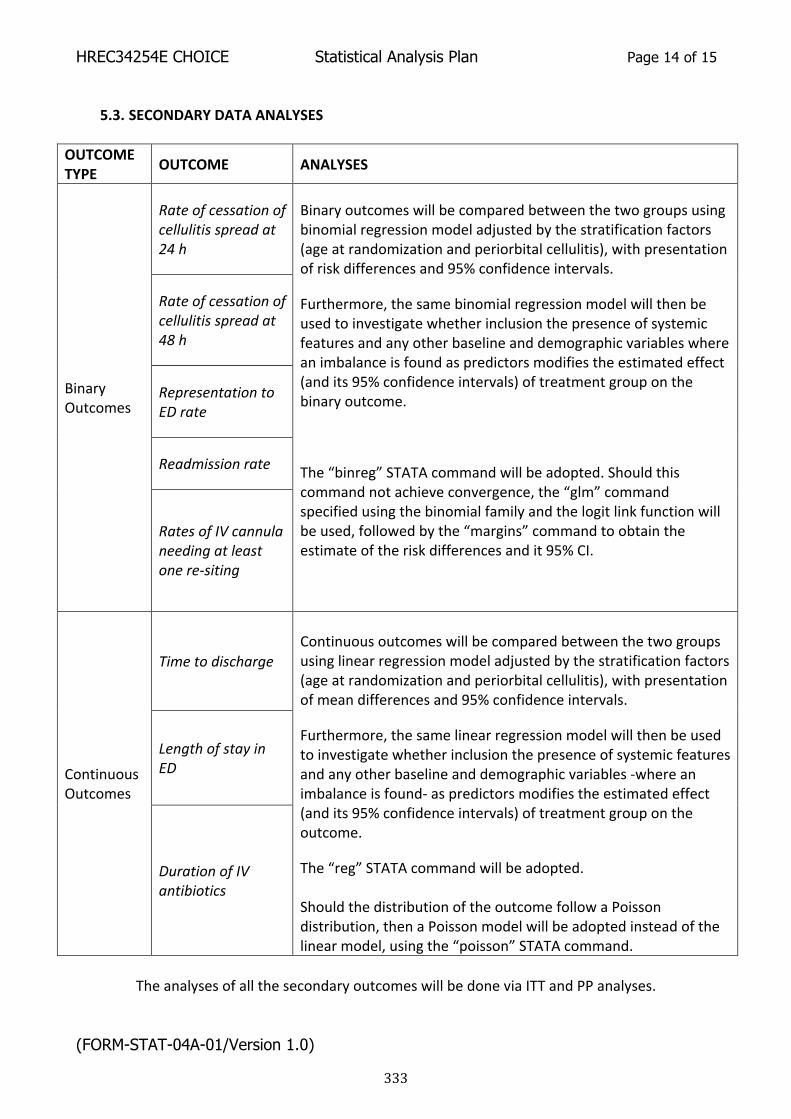
HREC34254E CHOICE Statistical Analysis Plan Page 14 of 15
(FORM-STAT-04A-01/Version 1.0)
5.3. SECONDARY DATA ANALYSES
OUTCOME TYPE OUTCOME ANALYSES
Binary Outcomes
Rate of cessation of cellulitis spread at 24 h
Binary outcomes will be compared between the two groups using binomial regression model adjusted by the stratification factors (age at randomization and periorbital cellulitis), with presentation of risk differences and 95% confidence intervals.
Furthermore, the same binomial regression model will then be used to investigate whether inclusion the presence of systemic features and any other baseline and demographic variables where an imbalance is found as predictors modifies the estimated effect (and its 95% confidence intervals) of treatment group on the binary outcome.
The “binreg” STATA command will be adopted. Should this command not achieve convergence, the “glm” command specified using the binomial family and the logit link function will be used, followed by the “margins” command to obtain the estimate of the risk differences and it 95% CI.
Rate of cessation of cellulitis spread at 48 h
Representation to ED rate
Readmission rate
Rates of IV cannula needing at least one re-‐siting
Continuous Outcomes
Time to discharge
Continuous outcomes will be compared between the two groups using linear regression model adjusted by the stratification factors (age at randomization and periorbital cellulitis), with presentation of mean differences and 95% confidence intervals.
Furthermore, the same linear regression model will then be used to investigate whether inclusion the presence of systemic features and any other baseline and demographic variables -‐where an imbalance is found-‐ as predictors modifies the estimated effect (and its 95% confidence intervals) of treatment group on the outcome.
The “reg” STATA command will be adopted. Should the distribution of the outcome follow a Poisson distribution, then a Poisson model will be adopted instead of the linear model, using the “poisson” STATA command.
Length of stay in ED
Duration of IV antibiotics
The analyses of all the secondary outcomes will be done via ITT and PP analyses.
333
HREC34254E CHOICE Statistical Analysis Plan Page 15 of 15
(FORM-STAT-04A-01/Version 1.0)
SIGNATURES PAGE Signature of Principal Investigator:
Date ___-___-_____
Print Name Laila Ibrahim
Signature of Trial Statistician:
Date 03-08-2017
Print Name Francesca Orsini
03 08 2017
334

335
Appendix 2 Blood Cultures in Cellulitis are not cost effective and should prompt investigation for an alternative focus

Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
118 | www.pidj.com The Pediatric Infectious Disease Journal • Volume 35, Number 1, January 2016
Aeromonas Associated With Swimming Pool
Folliculitis
Letters to the editor
To the Editors:
We read with interest the publicationby Trenchs et al1 ‘Blood Cultures
are not Useful in the Evaluation of Chil-dren with Uncomplicated Superficial Skin and Soft Tissue Infections’. This retrospective study showed that although 79% of patients had a blood culture, only 2 (0.6%) patients had a significant patho-gen isolated. The crucial information that is not clearly stated is whether these patients were clinically different from the other patients in the study. Without this, the question remains what risk phy-sicians are prepared to take by not tak-ing a blood culture. The authors also did not detail whether these positive culture results affected subsequent management such as other investigations or antibi-otic duration, which may be because of difficulties inherent in retrospective data collection.
We prospectively collected clinical and microbiological data on 162 patients with uncomplicated moderate/severe cel-lulitis (excluding complicated wounds, such as bites or containing foreign bod-ies, varicella and immunosuppression) receiving intravenous antibiotics. The majority—138 (85%) patients—had a blood culture. Only one (0.6%) patient had a positive culture, growing Staphylo-coccus aureus. He presented with 5 days of fever (38.5°C), lethargy and ano-rexia and 1 day of erythema and swell-ing over his left ankle. Difficulty with weight-bearing precipitated his hospital presentation. As data collection was pro-spective this culture result was deemed unusual. After 36 hours of antibiotics, he was afebrile with improving erythema, but the swelling remained. He therefore
Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.
ISSN: 0891-3668/16/3501-0118DOI: 10.1097/INF.0000000000000938
The Pediatric Infectious Disease Journal
35
1
Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.
0891-3668
PIDJ
PIDJ-215-688
Letters to the Editor
Letters to the Editor
2016
January
118
121
10.1097/INF.0000000000000938
2015
Priyamalini
Pediatr Infect Dis J
Lippincott Williams & Wilkins
Hagerstown, MD
XXX
The study is funded in part by grants from the RCH Foundation, the Murdoch Children’s Research Institute Infection and Immunity Theme and the Victorian Department of Health, Melbourne, Australia. The funding bodies do not have any authority in collection, management, analysis, and interpretation of data. The authors have no conflicts of interest to disclose.
Address for correspondence: Penelope A. Bryant, PhD; E-mail: [email protected]
Blood Cultures in Cellulitis are not Cost Effective and Should
Prompt Investigation for an Alternative Focus
had a bone scan that showed left f ibula osteomyelitis, which was treated with 3 weeks of antibiotics. He could have been differentiated at presentation from other patients with uncomplicated mod-erate/severe cellulitis by the prolonged history of fever. Although the positive blood culture prompted the diagnosis of osteomyelitis in this case, this would have otherwise been diagnosed based on incomplete clinical improvement. Two patients (1.2%) had blood culture contamination with coagulase-negative staphylococci, resulting in an unneces-sary additional day in hospital awaiting organism identification.
The Australian Medicare Benefits Schedule cost of blood cultures (incorpo-rating cost of consumables and scientist time for culture and sensitivities) at RCH is AU$30.75, so blood cultures in 85% of patients incurred AU$4244.2 The cost of the 2 contaminated blood cultures was 1 additional day in hospital and repeat blood culture for each patient: AU$2661, total-ing AU$7284 with no clear benefit. This is excluding additional costs of medical staff drawing the culture, transportation to the laboratory, etc.
On the basis of our additional data, we agree with Trenchs et al1 that blood cultures are unhelpful in celluli-tis in children and should not routinely be collected. In addition, as has previ-ously been found in adults, they are not cost effective.3 However, we suggest that if blood cultures are obtained, positive cultures with significant pathogens are sufficiently rare that they should prompt investigation for a metastatic focus or alternative diagnosis.
Penelope A. Bryant, PhDRCH@Home Department
Infectious Diseases UnitDepartment of General Medicine
Microbiology DepartmentMurdoch Children’s Research Institute
The Royal Children’s HospitalParkville, Australia
Franz E. Babl, MDEmergency Department
Murdoch Children’s Research InstituteThe Royal Children’s Hospital
Parkville, AustraliaDepartment of Paediatrics
University of MelbourneMelbourne, Australia
Andrew J. Daley, MBBSMicrobiology Department
The Royal Children’s HospitalParkville, Australia
Department of Paediatrics
University of MelbourneMelbourne, Australia
Sandy M. Hopper, MBBSEmergency Department
Murdoch Children’s Research InstituteThe Royal Children’s Hospital
Parkville, Australia
Laila F. Ibrahim, MB BCH, BAORCH@Home Department
Murdoch Children’s Research InstituteThe Royal Children’s Hospital
Parkville, AustraliaDepartment of Paediatrics
University of MelbourneMelbourne, Australia
REFERENCES1. Trenchs V, Hernandez-Bou S, Bianchi C, Arnan
M, Gene A, Luaces C. Blood cultures are not use-ful in the evaluation of children with uncomplicatedsuperficial skin and soft tissue infections. PediatrInfect Dis J. 2015;34:924–927.
2. Health AGDo. MBS Online. Medicare BenefitSchedule. Available from: http://www9.health.gov.au/mbs/fullDisplay.cfm?type=item&q=69354&qt=item&criteria=blood culture. Accessed July19, 2015.
3. Perl B, Gottehrer NP, Raveh D, et al. Cost-effectiveness of blood cultures for adult patientswith cellulitis. Clin Infect Dis. 1999;29:1483–1488.
The authors have no conflicts of interest to disclose.Address for correspondence: Veroniek Saegeman, MD,
PhD; E-mail: [email protected].
To the Editors:
In summer, it is common for childrento play in inflatable domestic swim-
ming pools. We report about a family with 4 children who developed moderate follic-ulitis after having played in their swimming pool. One day after the swimming pool was filled with fresh tap water without supple-mental chemical treatment of the water, the children did not show any signs of redness or folliculitis after their swim. The next day, the children swam in their swimming pool at noon. That evening all 4 children devel-oped small erythematous macules and pap-ules on the trunk and the back. The differ-ential diagnosis was sun burn and bacterial folliculitis. The morning afterwards, the folliculitis had extended to the cheeks in
Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.
ISSN: 0891-3668/16/3501-0118DOI: 10.1097/INF.0000000000000940
The Pediatric Infectious Disease Journal
0891-3668
INF
Letters to the Editor
Letters to the Editor
2016
January
2015
Pediatr Infect Dis J
Lippincott Williams & Wilkins
Hagerstown, MD
XXX
336

337
Appendix 3 Clinician survey questionnaire
31/12/2018 03:32 projectredcap.org
ConfidentialPage 1 of 8
Cellulitis at Home Or Inpatient in Children from ED(CHOICE) - Survey for Physicians
Thank you for taking part in this survey! By participating, you will increase our knowledgeabout doctors' perspectives on paediatric cellulitis management. Your responses will remainanonymous and confidential.
By completing all sections, you will also be in the draw to win one of three coffee and cakevouchers from Sandrock.
Please do not hesitate to contact the research team to address any questions and concerns. 1. In which department do you work? (Select all that EDapply) General Medicine
IDOther (Please specify)
__________________________________
2. Please state your current appointment (or most Consultantrecent if doing other e.g. Research) Fellow
RegistrarResidentIntern
338
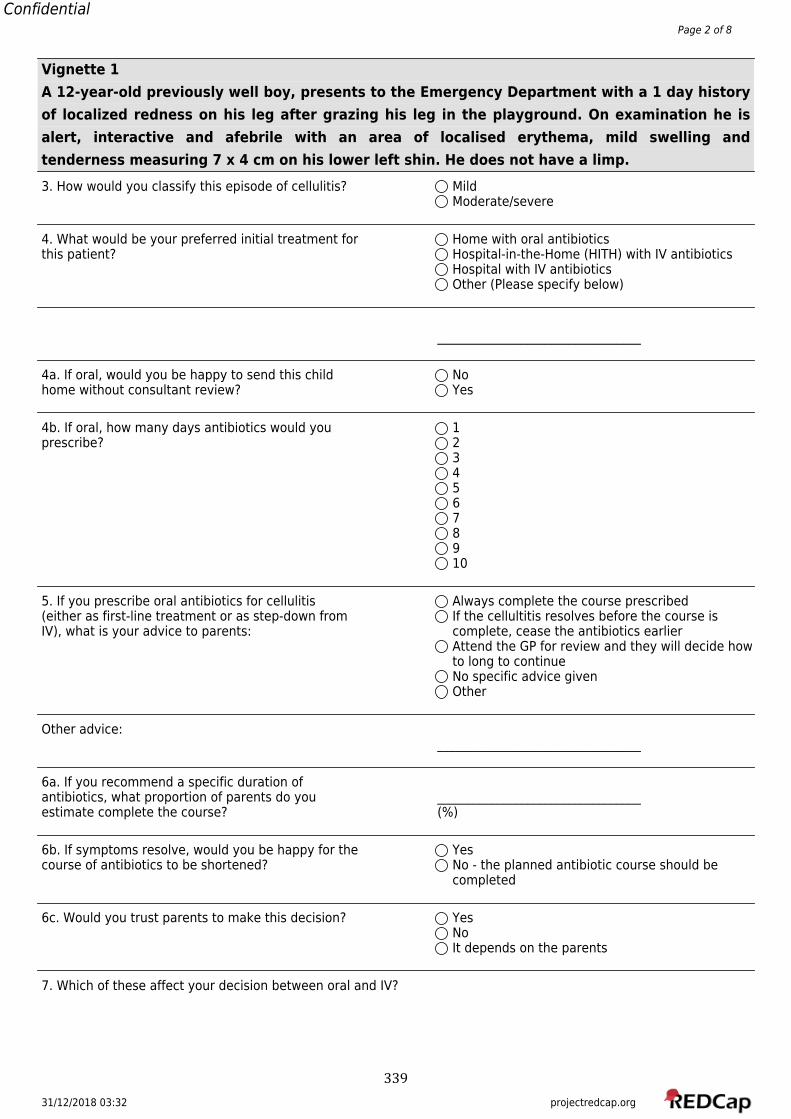
31/12/2018 03:32 projectredcap.org
ConfidentialPage 2 of 8
Vignette 1A 12-year-old previously well boy, presents to the Emergency Department with a 1 day historyof localized redness on his leg after grazing his leg in the playground. On examination he isalert, interactive and afebrile with an area of localised erythema, mild swelling andtenderness measuring 7 x 4 cm on his lower left shin. He does not have a limp.3. How would you classify this episode of cellulitis? Mild
Moderate/severe
4. What would be your preferred initial treatment for Home with oral antibioticsthis patient? Hospital-in-the-Home (HITH) with IV antibiotics
Hospital with IV antibioticsOther (Please specify below)
__________________________________
4a. If oral, would you be happy to send this child Nohome without consultant review? Yes
4b. If oral, how many days antibiotics would you 1prescribe? 2
345678910
5. If you prescribe oral antibiotics for cellulitis Always complete the course prescribed(either as first-line treatment or as step-down from If the cellultitis resolves before the course isIV), what is your advice to parents: complete, cease the antibiotics earlier
Attend the GP for review and they will decide howto long to continueNo specific advice givenOther
Other advice:__________________________________
6a. If you recommend a specific duration ofantibiotics, what proportion of parents do you __________________________________estimate complete the course? (%)
6b. If symptoms resolve, would you be happy for the Yescourse of antibiotics to be shortened? No - the planned antibiotic course should be
completed
6c. Would you trust parents to make this decision? YesNoIt depends on the parents
7. Which of these affect your decision between oral and IV?
339
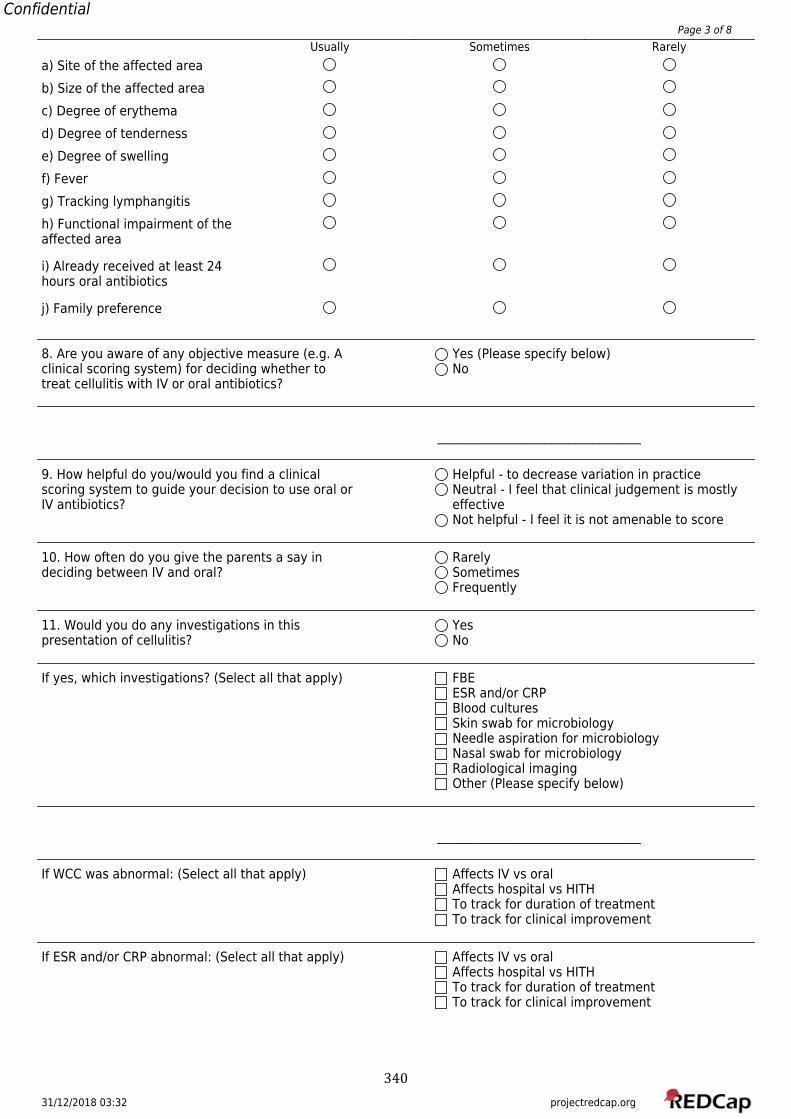
31/12/2018 03:32 projectredcap.org
ConfidentialPage 3 of 8
Usually Sometimes Rarelya) Site of the affected areab) Size of the affected areac) Degree of erythemad) Degree of tendernesse) Degree of swellingf) Feverg) Tracking lymphangitish) Functional impairment of theaffected area
i) Already received at least 24hours oral antibiotics
j) Family preference
8. Are you aware of any objective measure (e.g. A Yes (Please specify below)clinical scoring system) for deciding whether to Notreat cellulitis with IV or oral antibiotics?
__________________________________
9. How helpful do you/would you find a clinical Helpful - to decrease variation in practicescoring system to guide your decision to use oral or Neutral - I feel that clinical judgement is mostlyIV antibiotics? effective
Not helpful - I feel it is not amenable to score
10. How often do you give the parents a say in Rarelydeciding between IV and oral? Sometimes
Frequently
11. Would you do any investigations in this Yespresentation of cellulitis? No
If yes, which investigations? (Select all that apply) FBEESR and/or CRPBlood culturesSkin swab for microbiologyNeedle aspiration for microbiologyNasal swab for microbiologyRadiological imagingOther (Please specify below)
__________________________________
If WCC was abnormal: (Select all that apply) Affects IV vs oralAffects hospital vs HITHTo track for duration of treatmentTo track for clinical improvement
If ESR and/or CRP abnormal: (Select all that apply) Affects IV vs oralAffects hospital vs HITHTo track for duration of treatmentTo track for clinical improvement
340
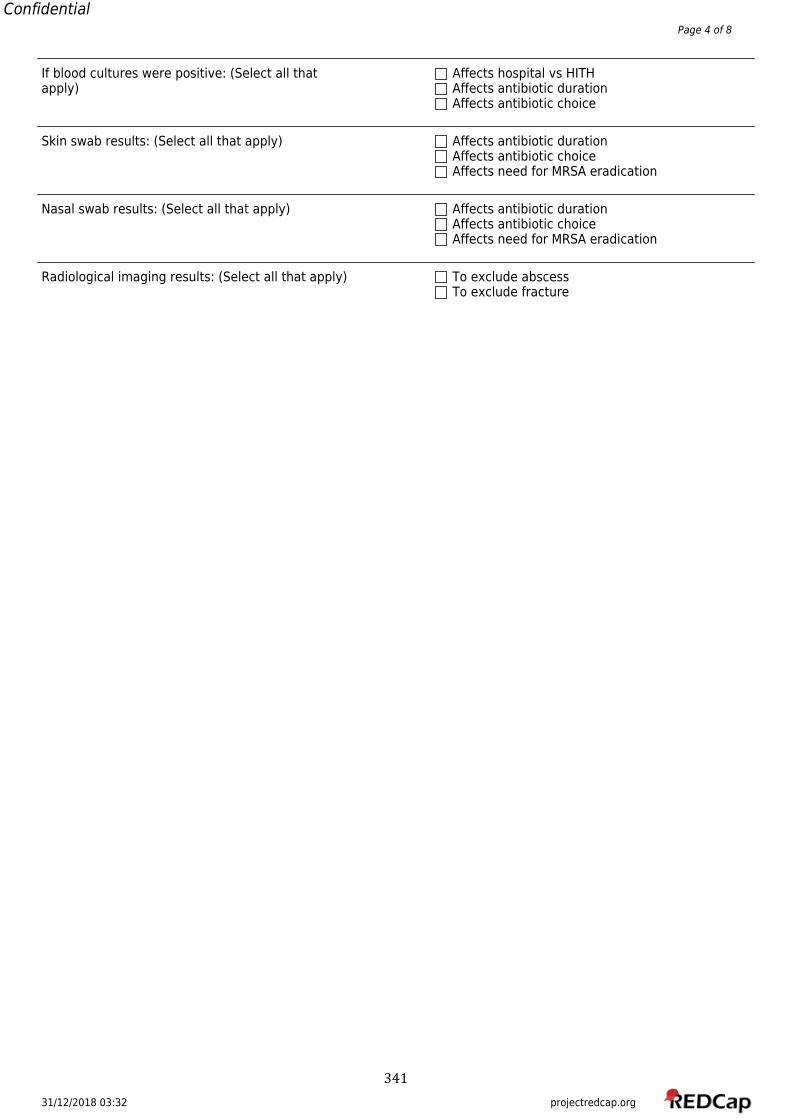
31/12/2018 03:32 projectredcap.org
ConfidentialPage 4 of 8
If blood cultures were positive: (Select all that Affects hospital vs HITHapply) Affects antibiotic duration
Affects antibiotic choice
Skin swab results: (Select all that apply) Affects antibiotic durationAffects antibiotic choiceAffects need for MRSA eradication
Nasal swab results: (Select all that apply) Affects antibiotic durationAffects antibiotic choiceAffects need for MRSA eradication
Radiological imaging results: (Select all that apply) To exclude abscessTo exclude fracture
341
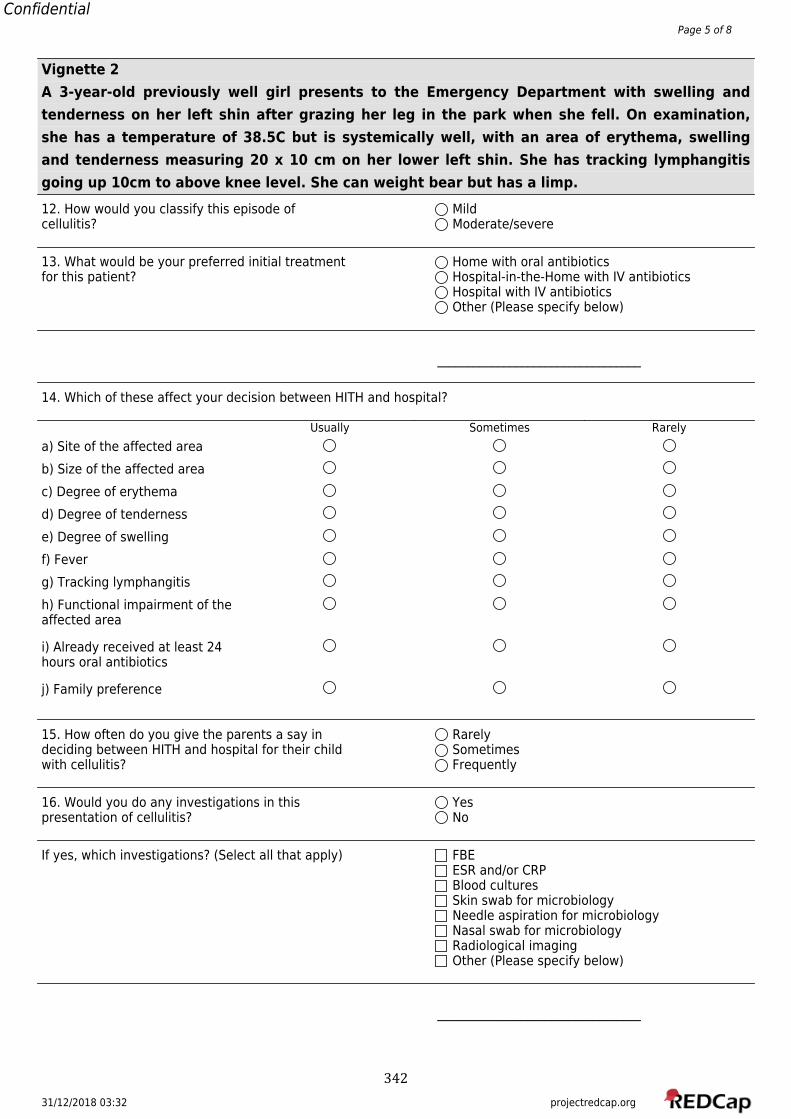
31/12/2018 03:32 projectredcap.org
ConfidentialPage 5 of 8
Vignette 2A 3-year-old previously well girl presents to the Emergency Department with swelling andtenderness on her left shin after grazing her leg in the park when she fell. On examination,she has a temperature of 38.5C but is systemically well, with an area of erythema, swellingand tenderness measuring 20 x 10 cm on her lower left shin. She has tracking lymphangitisgoing up 10cm to above knee level. She can weight bear but has a limp.12. How would you classify this episode of Mildcellulitis? Moderate/severe
13. What would be your preferred initial treatment Home with oral antibioticsfor this patient? Hospital-in-the-Home with IV antibiotics
Hospital with IV antibioticsOther (Please specify below)
__________________________________
14. Which of these affect your decision between HITH and hospital?
Usually Sometimes Rarelya) Site of the affected areab) Size of the affected areac) Degree of erythemad) Degree of tendernesse) Degree of swellingf) Feverg) Tracking lymphangitish) Functional impairment of theaffected area
i) Already received at least 24hours oral antibiotics
j) Family preference
15. How often do you give the parents a say in Rarelydeciding between HITH and hospital for their child Sometimeswith cellulitis? Frequently
16. Would you do any investigations in this Yespresentation of cellulitis? No
If yes, which investigations? (Select all that apply) FBEESR and/or CRPBlood culturesSkin swab for microbiologyNeedle aspiration for microbiologyNasal swab for microbiologyRadiological imagingOther (Please specify below)
__________________________________
342
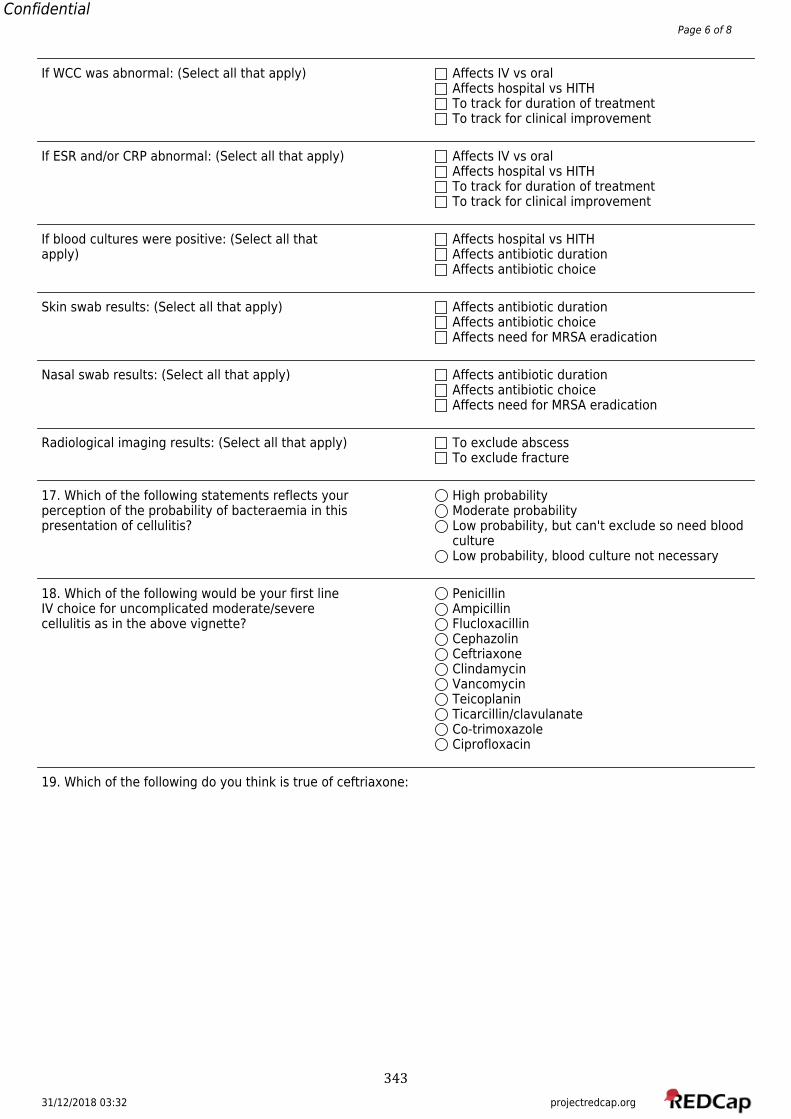
31/12/2018 03:32 projectredcap.org
ConfidentialPage 6 of 8
If WCC was abnormal: (Select all that apply) Affects IV vs oralAffects hospital vs HITHTo track for duration of treatmentTo track for clinical improvement
If ESR and/or CRP abnormal: (Select all that apply) Affects IV vs oralAffects hospital vs HITHTo track for duration of treatmentTo track for clinical improvement
If blood cultures were positive: (Select all that Affects hospital vs HITHapply) Affects antibiotic duration
Affects antibiotic choice
Skin swab results: (Select all that apply) Affects antibiotic durationAffects antibiotic choiceAffects need for MRSA eradication
Nasal swab results: (Select all that apply) Affects antibiotic durationAffects antibiotic choiceAffects need for MRSA eradication
Radiological imaging results: (Select all that apply) To exclude abscessTo exclude fracture
17. Which of the following statements reflects your High probabilityperception of the probability of bacteraemia in this Moderate probabilitypresentation of cellulitis? Low probability, but can't exclude so need blood
cultureLow probability, blood culture not necessary
18. Which of the following would be your first line PenicillinIV choice for uncomplicated moderate/severe Ampicillincellulitis as in the above vignette? Flucloxacillin
CephazolinCeftriaxoneClindamycinVancomycinTeicoplaninTicarcillin/clavulanateCo-trimoxazoleCiprofloxacin
19. Which of the following do you think is true of ceftriaxone:
343
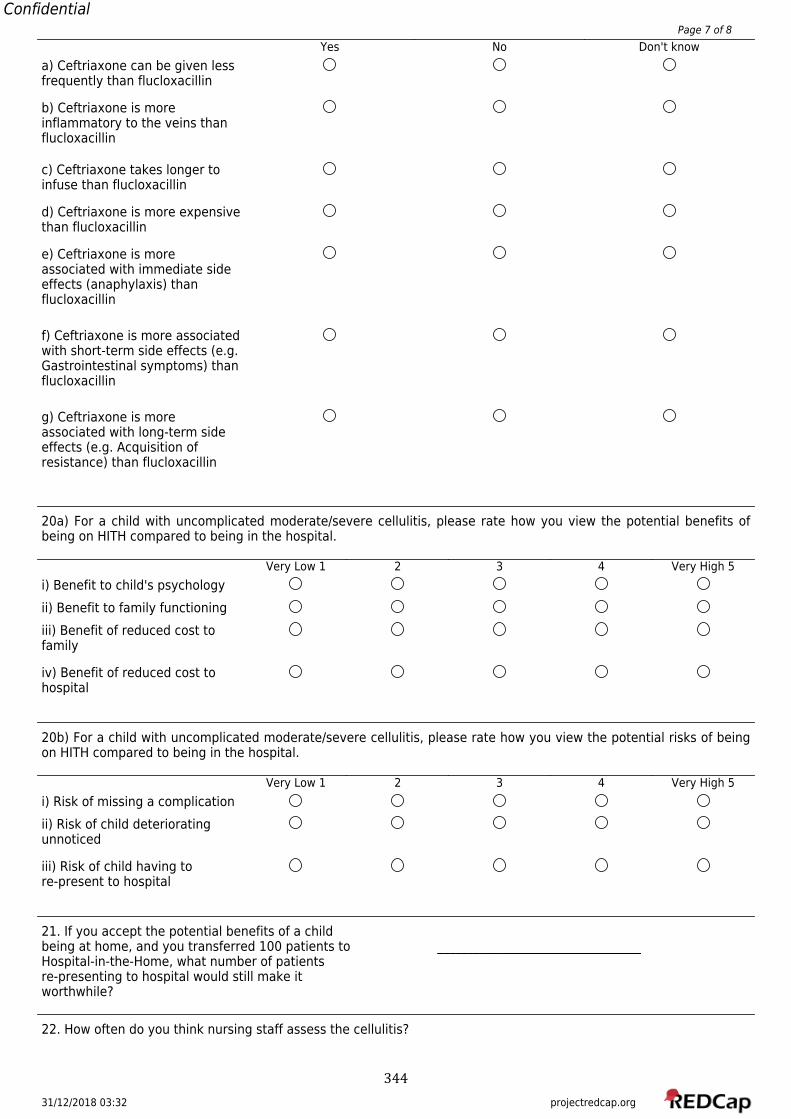
31/12/2018 03:32 projectredcap.org
ConfidentialPage 7 of 8
Yes No Don't knowa) Ceftriaxone can be given lessfrequently than flucloxacillin
b) Ceftriaxone is moreinflammatory to the veins thanflucloxacillin
c) Ceftriaxone takes longer toinfuse than flucloxacillin
d) Ceftriaxone is more expensivethan flucloxacillin
e) Ceftriaxone is moreassociated with immediate sideeffects (anaphylaxis) thanflucloxacillin
f) Ceftriaxone is more associatedwith short-term side effects (e.g.Gastrointestinal symptoms) thanflucloxacillin
g) Ceftriaxone is moreassociated with long-term sideeffects (e.g. Acquisition ofresistance) than flucloxacillin
20a) For a child with uncomplicated moderate/severe cellulitis, please rate how you view the potential benefits ofbeing on HITH compared to being in the hospital.
Very Low 1 2 3 4 Very High 5i) Benefit to child's psychologyii) Benefit to family functioningiii) Benefit of reduced cost tofamily
iv) Benefit of reduced cost tohospital
20b) For a child with uncomplicated moderate/severe cellulitis, please rate how you view the potential risks of beingon HITH compared to being in the hospital.
Very Low 1 2 3 4 Very High 5i) Risk of missing a complicationii) Risk of child deterioratingunnoticed
iii) Risk of child having tore-present to hospital
21. If you accept the potential benefits of a childbeing at home, and you transferred 100 patients to __________________________________Hospital-in-the-Home, what number of patientsre-presenting to hospital would still make itworthwhile?
22. How often do you think nursing staff assess the cellulitis?
344
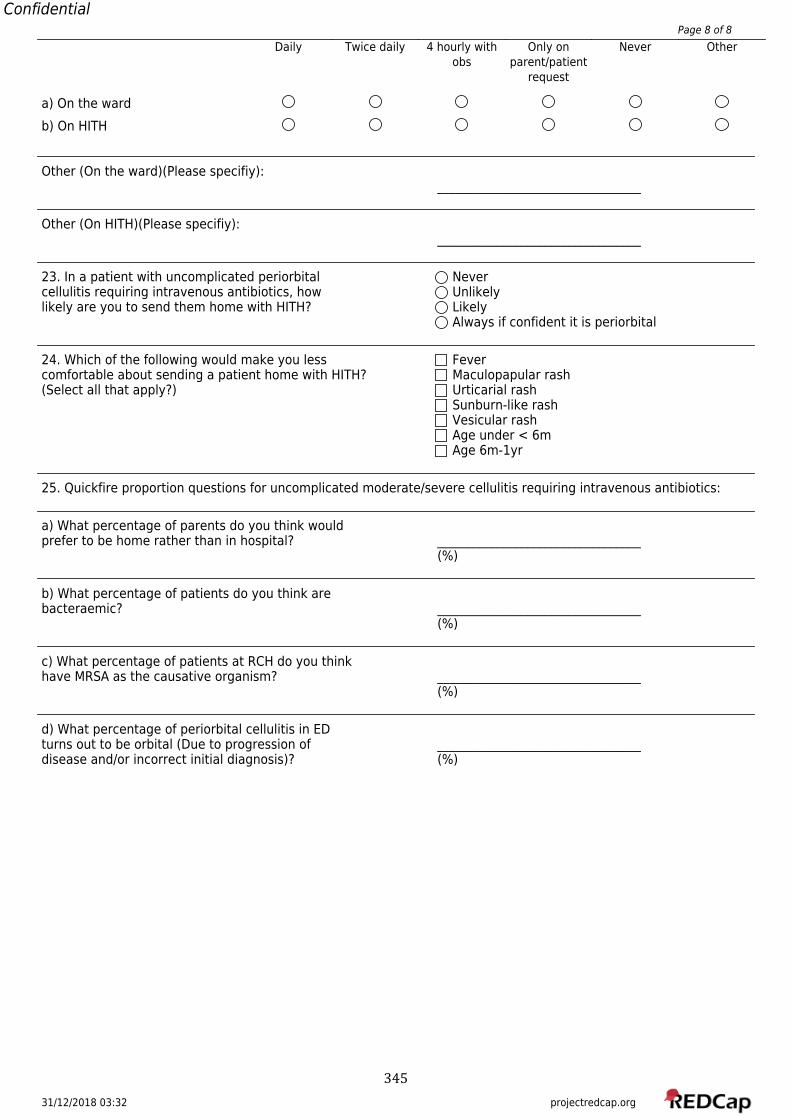
31/12/2018 03:32 projectredcap.org
ConfidentialPage 8 of 8
Daily Twice daily 4 hourly withobs
Only onparent/patient
request
Never Other
a) On the wardb) On HITH
Other (On the ward)(Please specifiy):__________________________________
Other (On HITH)(Please specifiy):__________________________________
23. In a patient with uncomplicated periorbital Nevercellulitis requiring intravenous antibiotics, how Unlikelylikely are you to send them home with HITH? Likely
Always if confident it is periorbital
24. Which of the following would make you less Fevercomfortable about sending a patient home with HITH? Maculopapular rash(Select all that apply?) Urticarial rash
Sunburn-like rashVesicular rashAge under < 6mAge 6m-1yr
25. Quickfire proportion questions for uncomplicated moderate/severe cellulitis requiring intravenous antibiotics:
a) What percentage of parents do you think wouldprefer to be home rather than in hospital? __________________________________
(%)
b) What percentage of patients do you think arebacteraemic? __________________________________
(%)
c) What percentage of patients at RCH do you thinkhave MRSA as the causative organism? __________________________________
(%)
d) What percentage of periorbital cellulitis in EDturns out to be orbital (Due to progression of __________________________________disease and/or incorrect initial diagnosis)? (%)
345

346
Minerva Access is the Institutional Repository of The University of Melbourne
Author/s:
Ibrahim, Laila Farah Binti
Title:
Home intravenous antibiotics in children: determining the population, efficacy, safety and
cost-effectiveness using cellulitis as a paradigm
Date:
2019
Persistent Link:
http://hdl.handle.net/11343/223034
File Description:
Complete thesis
Terms and Conditions:
Terms and Conditions: Copyright in works deposited in Minerva Access is retained by the
copyright owner. The work may not be altered without permission from the copyright owner.
Readers may only download, print and save electronic copies of whole works for their own
personal non-commercial use. Any use that exceeds these limits requires permission from
the copyright owner. Attribution is essential when quoting or paraphrasing from these works.





























