Embed Size (px)
Citation preview

lable at ScienceDirect
Annals of Epidemiology xxx (2014) 1e8
Contents lists avai
Annals of Epidemiology
journal homepage: www.annalsofepidemiology.org
Original article
Hypercholesterolemia and its associated risk factorsdKingdomof Saudi Arabia, 2013
Mohammed Basulaiman MDa, Charbel El Bcheraoui PhD, MSc b, Marwa Tuffaha MDb,Margaret Robinson BSc b, Farah Daoud BSc b, Sara Jaber MDb, Sarah Mikhitarian BSc b, Shelley Wilson BAb,Ziad A. Memish MD a, Mohammed Al Saeedi MDb, Mohammad A. AlMazroa MD a, Ali H. Mokdad PhD b,*
aMinistry of Health of the Kingdom of Saudi Arabia, Riyadh, Saudi Arabiab Institute for Health Metrics and Evaluation, University of Washington, Seattle
a r t i c l e i n f o
Article history:Received 1 July 2014Accepted 14 August 2014
Keywords:HypercholesterolemiaSaudi ArabiaNoncommunicable diseases
Conflicts of interest: The salaries of the authorsMetrics and Evaluation were fully or partially paid thistry of Health (MOH) of the Kingdom of Saudi Arabiacollection for this study.* Corresponding author. Department of Global Healt
and Evaluation, University of Washington, 2301 5th A98121. Tel.: þ1 206 897 2849; fax: þ1 206 897 2899.
E-mail address: [email protected] (A.H. Mokdad).
1047-2797/$ e see front matter � 2014 Elsevier Inc. Ahttp://dx.doi.org/10.1016/j.annepidem.2014.08.001
Please cite this article in press as: BasulaimaAnnals of Epidemiology (2014), http://dx.do
a b s t r a c t
Purpose: To assess the prevalence of hypercholesterolemia and its associated factors in the Kingdom ofSaudi Arabia.Methods: A national multistage representative sample of Saudis aged 15 years or older was surveyedthrough face-to-face interviews. Data on sociodemographics, risk factors, and health information werecollected, and blood sample analysis was performed. Data were analyzed using SAS 9.3 to account for thesample weights and complex survey design.Results: Between April and June 2013, a total of 10,735 participants completed the survey. Overall, 8.5% ofSaudis had hypercholesterolemia. Another 19.6% had borderline hypercholesterolemia. Among hyper-cholesterolemic Saudis, 65.1% were undiagnosed, 2.3% were treated uncontrolled, 28.3% were treatedcontrolled, and 4.3% were untreated. The risk of being hypercholesterolemic increased with age andamong individuals who reported consuming margarine, obese individuals, and those who have beenpreviously diagnosed with hypertension or diabetes.Conclusions: More than a million Saudis have hypercholesterolemia, and 700,000 of them are unaware oftheir condition which can be controlled through early detection campaigns and lifestyle change andmedication. An urgent awareness and screening campaign is needed in Kingdom of Saudi Arabia toprevent and avoid disease progression toward more serious stages.
� 2014 Elsevier Inc. All rights reserved.
Introduction
Cholesterol is essential for the body, specifically for hormonesynthesis, fat digestion, and formation of cell membranes [1].However, large amounts of cholesterol in the bloodstream lead tomyocardial infarction, stroke, ischemic injury, and organ failure [2].Hypercholesterolemia can be prevented, and measures such as di-etary changes and clinical follow-up must be taken for high-riskindividuals to reduce adverse events [3e7].
The Global Burden of Disease 2010 study estimated that highcholesterol is a leading risk factor for death from cardiovasculardiseases in the Kingdom of Saudi Arabia (KSA). It accounted for
from the Institute for Healthrough a grant from the Min-. The MOH managed the data
h, Institute for Health Metricsvenue, Suite 600, Seattle, WA
ll rights reserved.
n M, et al., Hypercholesteroli.org/10.1016/j.annepidem.20
about 5.14% of total deaths, 3.96% of years of life lost, and 1.99% ofdisability-adjusted life years. From 1990 to 2010, the burden ofhypercholesterolemia remained very high in KSA as it rankedeighth among the risk factors for total deaths [8].
Previous studies reportedonprevalence of hypercholesterolemiain KSA. In the early 80s, prevalence of hypercholesterolemia was 7%for males and 8% for females and increased with age and body massindex (BMI) [9,10]. Since the late 90s, data on hypercholesterolemiaare limited [11]. However, prevalence of hypercholesterolemia wasreported as 18.6% for males and 19.7% for females in 2005 [12].
To assess the current status of hypercholesterolemia in KSA, weanalyzed the 2013 Saudi Health Interview Survey (SHIS) to describethe magnitude of hypercholesterolemia in KSA by different socio-demographic groups and risk factors.
Materials and methods
SHIS is a nationalmultistage survey of individuals aged15 years orolder. Households were randomly selected from a national sampling
emia and its associated risk factorsdKingdom of Saudi Arabia, 2013,14.08.001

M. Basulaiman et al. / Annals of Epidemiology xxx (2014) 1e82
frame maintained and updated by the Census Bureau. KSA wasdivided into 13 regions. Each regionwas divided into subregions andblocks. All regions were included, and a probability proportional tosize was used to randomly select subregions and blocks. Householdswere randomly selected from each block. A roster of householdmembers was collected, and an adult aged 15 years or older wasrandomlyselected tobe surveyed.Weight, height, andbloodpressureweremeasured at the household bya trainedprofessional. AnOmronHN286 scale (SN: 201207-03163F) and Omron M6 Comfort monitor(HEM-7223-E) were used to measure weight and blood pressure.
The survey included questions on sociodemographic character-istics, including age, sex, education, and marital status, tobaccoconsumption, diet, physical activity, health care utilization, differenthealth-related behaviors, and self-reported chronic conditions.
We usedmeasured weight and height to calculate BMI as weight(kilogram)/height2 (square meter). Participants were classified intofour groups: (1) underweight, BMI less than18.5; (2) normal weight,BMI 18.5 to 24.9; (3) overweight, BMI 25.0 to 29.9; or (4) obese, BMIgreater than or equal to 30.0. Respondents were considered to becurrent smokers if they reported ever smoking any tobacco productsand still currently smoking tobacco, and were considered pastsmokers if they reported smoking in the past but not anymore. Weassessed the type of fat most consumed by asking respondents:“What type of oil or fat is most often used for meal preparation inyour household?” Respondents could choose between vegetableoils, olive oil, butter or ghee, margarine, or none in particular.Vegetable and olive oil were combined into one category of vege-table oil, and butter and ghee were considered animal fat.
We computed the servings of fruits and vegetables and redmeats and chicken consumed per day from the detailed dietaryquestionnaire as the sum of the average daily consumption of fruits,fruit juices, and vegetables, and redmeats and chicken.We used theInternational Physical Activity questionnaire [13] to classify re-spondents into four groups of physical activity: (1) met vigorousphysical activity level, (2) met moderate physical activity level, (3)insufficient physical activity to meet vigorous or moderate levels,and (4) no physical activity.
To calculate the time spent on watching television, respondentswere asked: “In a typicalweek,howmuch timedoyouusually spend infront of the television or on the computer?” Time was recorded inminutes orhours and then computed to create four categories inhours.
To assess diagnosed hypertension, prediabetes, diabetes, andhypercholesterolemia status, respondents were asked four separatequestions: “Have you ever been told by a doctor, nurse, or other
Table 1Sociodemographic characteristics of Saudis aged 15 years or older, 2013
Sociodemographic and risk factors Categories
Sex MalesFemales
Age (y) 15e2425e3435e4445e5455e6465þ
Marital status Currently marriedNever marriedSeparated, divorced, or widowed
Education Primary school* or lessElementaryy or high school completedCollege degree or higher education
SE ¼ Standard error.* Six years of schooling after kindergarten.y Three years of schooling after primary school.
health professional that you had: (1) high blood pressure, other-wise known as hypertension; (2) prediabetes mellitus, otherwiseknown as prediabetes, borderline diabetes, impaired fastingglucose, impaired glucose tolerance, or impaired sugar tolerance;(3) diabetes mellitus, otherwise known as diabetes, sugar diabetes,high blood glucose, or high blood sugar; (4) hypercholesterolemia,otherwise known as high or abnormal blood cholesterol?” Womendiagnosed with diabetes or hypertension only during pregnancywere counted as not having these conditions. Those who werediagnosedwith either of these conditions were further asked if theyare currently receiving any treatment for their condition. Similarly,the same types of questions were used to determine previousdiagnosis of stroke, myocardial infarction, atrial fibrillation, cardiacarrest, congestive heart failure, chronic obstructive pulmonarydisease, asthma, renal failure, and cancer. We considered a personto be diagnosed with a chronic condition if they reported beingdiagnosed with any of the conditions cited earlier.
Respondents who reported being diagnosed with hypercholes-terolemia were asked: “During the past 30 days, or since yourdiagnosis, have you ever taken medication for this condition?”Those who reported being on treatment were asked to provide thename of the drugs they are using.
Respondents who completed the questionnaire were invited tolocal primary health care clinics to provide a blood sample for labo-ratory analysis. A Roche Hitachi COBAS 8000 system was used tomeasure cholesterol. Respondents were considered to be hypercho-lesterolemic if they met any of the following criteria: (1) measuredcholesterol equal to or exceeding 6.2 mmol/L or (2) measuredcholesterol not exceeding 6.2 mmol/L, but the respondent reportedtaking medications for hypercholesterolemia. Respondents wereconsidered tohaveborderlinehypercholesterolemia if (1) theydidnotreport taking drugs for hypercholesterolemia and (2) their measuredblood cholesterol level was between 5.18 and 6.2 mmol/L. Re-spondents under treatment for hypercholesterolemia were consid-ered controlled if their measured cholesterol levels were below6.2 mmol/L.
Levels of high-density lipoproteins (HDL), low-density lipopro-teins (LDL), and triglycerides were alsomeasured. Respondents wereconsidered to have low HDL if their measured HDL was below1.0 mmol/L or 1.3 mol/L for males and females, respectively. Re-spondents were considered to have high LDL if their measured LDLwas greater or equal to 4.13 mmol/L. They were considered to havehypertriglyceridemia if theirmeasured triglycerides levelwasgreateror equal to 2.3 mmol/L.
Complete sample Clinical examination sample
N Weighted % SE N Weighted % SE
5253 50.64 0.69 2576 52.86 1.085482 49.36 0.69 3014 47.14 1.082382 40.31 0.73 1163 42.32 1.142757 21.50 0.52 1299 22.05 0.842339 15.18 0.41 1241 14.35 0.581520 12.38 0.40 860 11.51 0.55862 6.47 0.29 485 6.03 0.40875 4.17 0.20 542 3.74 0.24
3286 26.32 0.58 2024 28.39 0.914872 52.83 0.68 2325 51.92 1.072557 20.85 0.53 1236 19.69 0.826976 49.35 0.69 3657 46.52 1.052829 45.87 0.71 1423 49.74 1.08897 4.78 0.23 492 3.75 0.27
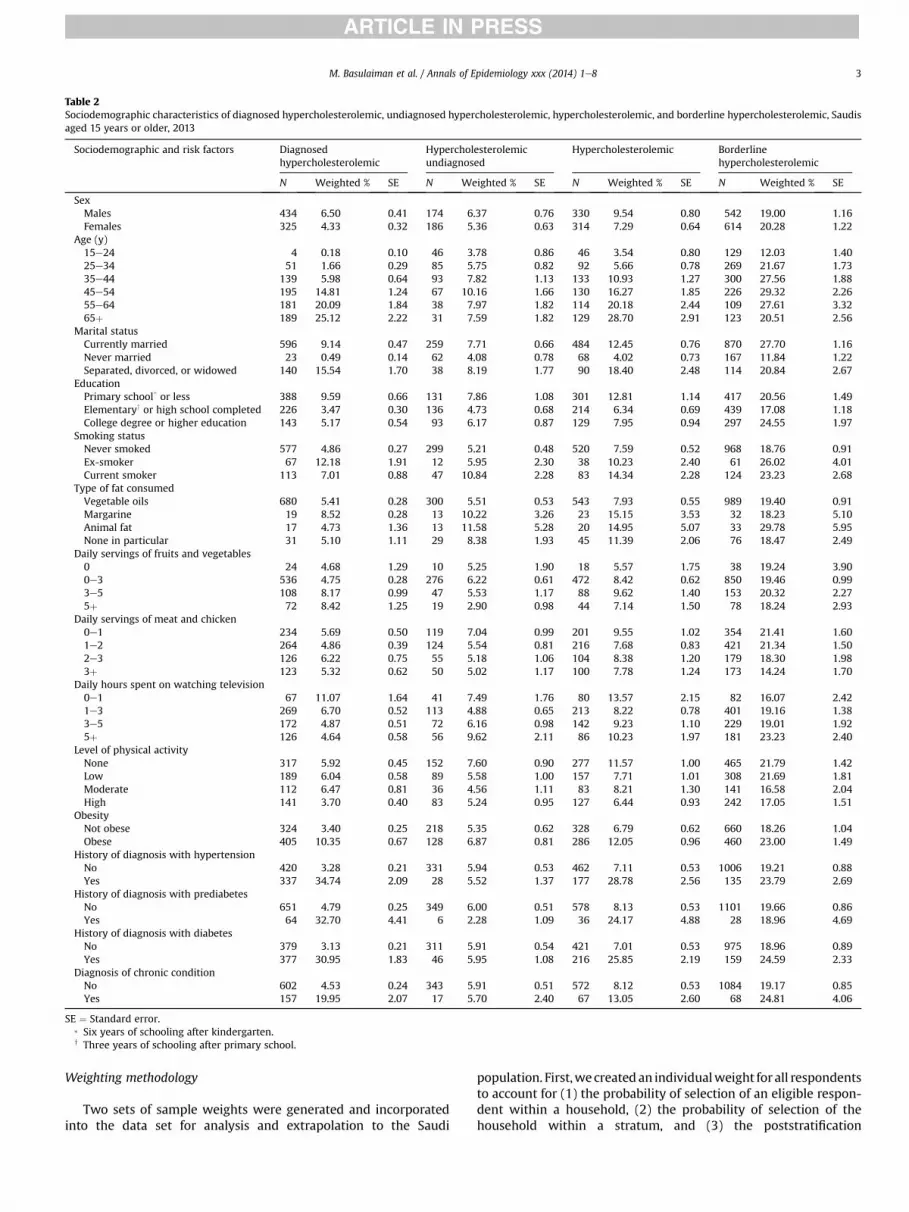
Table 2Sociodemographic characteristics of diagnosed hypercholesterolemic, undiagnosed hypercholesterolemic, hypercholesterolemic, and borderline hypercholesterolemic, Saudisaged 15 years or older, 2013
Sociodemographic and risk factors Diagnosedhypercholesterolemic
Hypercholesterolemicundiagnosed
Hypercholesterolemic Borderlinehypercholesterolemic
N Weighted % SE N Weighted % SE N Weighted % SE N Weighted % SE
SexMales 434 6.50 0.41 174 6.37 0.76 330 9.54 0.80 542 19.00 1.16Females 325 4.33 0.32 186 5.36 0.63 314 7.29 0.64 614 20.28 1.22
Age (y)15e24 4 0.18 0.10 46 3.78 0.86 46 3.54 0.80 129 12.03 1.4025e34 51 1.66 0.29 85 5.75 0.82 92 5.66 0.78 269 21.67 1.7335e44 139 5.98 0.64 93 7.82 1.13 133 10.93 1.27 300 27.56 1.8845e54 195 14.81 1.24 67 10.16 1.66 130 16.27 1.85 226 29.32 2.2655e64 181 20.09 1.84 38 7.97 1.82 114 20.18 2.44 109 27.61 3.3265þ 189 25.12 2.22 31 7.59 1.82 129 28.70 2.91 123 20.51 2.56
Marital statusCurrently married 596 9.14 0.47 259 7.71 0.66 484 12.45 0.76 870 27.70 1.16Never married 23 0.49 0.14 62 4.08 0.78 68 4.02 0.73 167 11.84 1.22Separated, divorced, or widowed 140 15.54 1.70 38 8.19 1.77 90 18.40 2.48 114 20.84 2.67
EducationPrimary school* or less 388 9.59 0.66 131 7.86 1.08 301 12.81 1.14 417 20.56 1.49Elementaryy or high school completed 226 3.47 0.30 136 4.73 0.68 214 6.34 0.69 439 17.08 1.18College degree or higher education 143 5.17 0.54 93 6.17 0.87 129 7.95 0.94 297 24.55 1.97
Smoking statusNever smoked 577 4.86 0.27 299 5.21 0.48 520 7.59 0.52 968 18.76 0.91Ex-smoker 67 12.18 1.91 12 5.95 2.30 38 10.23 2.40 61 26.02 4.01Current smoker 113 7.01 0.88 47 10.84 2.28 83 14.34 2.28 124 23.23 2.68
Type of fat consumedVegetable oils 680 5.41 0.28 300 5.51 0.53 543 7.93 0.55 989 19.40 0.91Margarine 19 8.52 0.28 13 10.22 3.26 23 15.15 3.53 32 18.23 5.10Animal fat 17 4.73 1.36 13 11.58 5.28 20 14.95 5.07 33 29.78 5.95None in particular 31 5.10 1.11 29 8.38 1.93 45 11.39 2.06 76 18.47 2.49
Daily servings of fruits and vegetables0 24 4.68 1.29 10 5.25 1.90 18 5.57 1.75 38 19.24 3.900e3 536 4.75 0.28 276 6.22 0.61 472 8.42 0.62 850 19.46 0.993e5 108 8.17 0.99 47 5.53 1.17 88 9.62 1.40 153 20.32 2.275þ 72 8.42 1.25 19 2.90 0.98 44 7.14 1.50 78 18.24 2.93
Daily servings of meat and chicken0e1 234 5.69 0.50 119 7.04 0.99 201 9.55 1.02 354 21.41 1.601e2 264 4.86 0.39 124 5.54 0.81 216 7.68 0.83 421 21.34 1.502e3 126 6.22 0.75 55 5.18 1.06 104 8.38 1.20 179 18.30 1.983þ 123 5.32 0.62 50 5.02 1.17 100 7.78 1.24 173 14.24 1.70
Daily hours spent on watching television0e1 67 11.07 1.64 41 7.49 1.76 80 13.57 2.15 82 16.07 2.421e3 269 6.70 0.52 113 4.88 0.65 213 8.22 0.78 401 19.16 1.383e5 172 4.87 0.51 72 6.16 0.98 142 9.23 1.10 229 19.01 1.925þ 126 4.64 0.58 56 9.62 2.11 86 10.23 1.97 181 23.23 2.40
Level of physical activityNone 317 5.92 0.45 152 7.60 0.90 277 11.57 1.00 465 21.79 1.42Low 189 6.04 0.58 89 5.58 1.00 157 7.71 1.01 308 21.69 1.81Moderate 112 6.47 0.81 36 4.56 1.11 83 8.21 1.30 141 16.58 2.04High 141 3.70 0.40 83 5.24 0.95 127 6.44 0.93 242 17.05 1.51
ObesityNot obese 324 3.40 0.25 218 5.35 0.62 328 6.79 0.62 660 18.26 1.04Obese 405 10.35 0.67 128 6.87 0.81 286 12.05 0.96 460 23.00 1.49
History of diagnosis with hypertensionNo 420 3.28 0.21 331 5.94 0.53 462 7.11 0.53 1006 19.21 0.88Yes 337 34.74 2.09 28 5.52 1.37 177 28.78 2.56 135 23.79 2.69
History of diagnosis with prediabetesNo 651 4.79 0.25 349 6.00 0.51 578 8.13 0.53 1101 19.66 0.86Yes 64 32.70 4.41 6 2.28 1.09 36 24.17 4.88 28 18.96 4.69
History of diagnosis with diabetesNo 379 3.13 0.21 311 5.91 0.54 421 7.01 0.53 975 18.96 0.89Yes 377 30.95 1.83 46 5.95 1.08 216 25.85 2.19 159 24.59 2.33
Diagnosis of chronic conditionNo 602 4.53 0.24 343 5.91 0.51 572 8.12 0.53 1084 19.17 0.85Yes 157 19.95 2.07 17 5.70 2.40 67 13.05 2.60 68 24.81 4.06
SE ¼ Standard error.* Six years of schooling after kindergarten.y Three years of schooling after primary school.
M. Basulaiman et al. / Annals of Epidemiology xxx (2014) 1e8 3
Weighting methodology
Two sets of sample weights were generated and incorporatedinto the data set for analysis and extrapolation to the Saudi
population. First,wecreated an individualweight for all respondentsto account for (1) the probability of selection of an eligible respon-dent within a household, (2) the probability of selection of thehousehold within a stratum, and (3) the poststratification

Fig. 1. Percent distribution of diagnosis and treatment status among hypercholester-olemic, Saudis aged 15 years older, 2013.
M. Basulaiman et al. / Annals of Epidemiology xxx (2014) 1e84
differences in age and sex distribution between the sample and theSaudi population.
For individuals who completed the laboratory-based bloodanalysis, we computed an additional weight used in analyzing datafrom clinic visits to account for (1) the individual weight describedpreviously, (2) the probability of visiting a clinic, (3) sociodemo-graphic, behavioral, and health differences between respondentswho visited the clinic and those who did not, and (4) the post-stratification differences in age and sex distribution between therespondentswhovisited the clinic and the general Saudi population.
Statistical analysis
We used a multivariate logistic regression model to measureassociation between outcome variables and sociodemographicfactors first. Then, we used a backward elimination multivariatelogistic regression model to measure the association betweenoutcome variables and all associated factors. All factors were firstincluded in the models. Then variables were eliminated based on aWald c2 test for the analysis of effect. Variables were removed oneby one based on the significance level of their effect on the model,starting with the variable with the highest P > .5, till all variableskept had a P � .5 in the analysis of effect. We used SAS 9.2 (SASInstitute Inc., Cary, NC) for the analyses and to account for weightsand the complex sampling design.
Results
Between April and June 2013, a total of 10,735 participantscompleted the SHISdresponse rate of 89.4%dand were invited tothe local health clinics. The remaining 1265 participants completedpart of the household enumeration, or all of it, but the selectedadult did not complete the survey. A total of 5590 individuals wentto the local clinics and provided blood samples for analysesdaresponse rate of 52.1%. The characteristics of respondents whocompleted the questionnaire and the laboratory examination arepresented in Table 1.
Overall, an estimated 693,106 Saudis (5.4%) reported beingdiagnosed with hypercholesterolemia. However, an estimated1,107,296 Saudis (8.5%) aged 15 years or older had hypercholester-olemia as measured by our laboratory tests with blood cholesterollevel greater or equal to 6.2 mmol/L or reported currently takingcholesterol medication. Of these, 65.1% were undiagnosed or un-aware of their condition. Moreover, 19.6% of Saudis, an estimated2,397,211 participants, had borderline hypercholesterolemia withmeasured blood cholesterol levels between 5.18 and 6.2 mmol/Land not currently taking blood cholesterol lowering medication.Characteristics of respondents with undiagnosed hypercholester-olemia, hypercholesterolemia, and borderline hypercholesterole-mia are presented in Table 2.
Among participants diagnosed with hypercholesterolemia,92.9% reported taking medication for their condition. More than95% of those being treated were taking statins for their condition.The vast majority of hypercholesterolemic patients (92.6%) whowere on medication had their blood cholesterol level controlled.Among those who were hypercholesterolemic, 65.1% were undi-agnosed, 2.3% were treated uncontrolled, 28.3% were treatedcontrolled, and 4.3% were untreated (Fig. 1).
A high percent of Saudis (48.7%) have low HDL, 7.4% have highLDL, and 8.5% have hypertriglyceridemia. Distributions of thesethree conditions by sociodemographic and risk factors are pre-sented in Table 3.
Age, type of fat mostly consumed, obesity, and diagnosis historyof hypertension and diabetes were associated with hypercholes-terolemia (Table 4). The risk of being hypercholesterolemic
increased with age (adjusted odds ratios [AOR] ¼ 1.03; 95% confi-dence intervals [CI], 1.01e1.04), among individuals who reportedconsuming margarine (AOR ¼ 2.17; 95% CI, 1.17e4.00), obese in-dividuals (AOR¼ 1.40; 95% CI, 1.03e1.89), and those who have beenpreviously diagnosed with hypertension (AOR ¼ 1.82; 95% CI,1.31e2.53) and diabetes (AOR ¼ 1.85; 95% CI, 1.28e2.69). On theother hand, sex, marital status, education, smoking status, timespent onwatching television, and level of physical activity were notassociated with the risk of hypercholesterolemia (Table 4). The riskof borderline hypercholesterolemia increased with age and timespent on watching television (Table 5).
The risk of being undiagnosed when one is hypercholesterol-emic was associated only with age (Table 6). Older individuals weremore likely to be undiagnosed while hypercholesterolemic(AOR ¼ 1.02; 95% CI, 1.01e1.03).
Discussion
To our knowledge, this is the first national study to report oncholesterol levels in KSA. We found high rates of undiagnosedcholesterol and borderline levels in a country where chronic dis-eases are the major health burden. Our findings call for awarenesscampaigns to educate the public about the danger of high choles-terol levels and the importance of early diagnosis. Indeed, becauseSaudis have free medical care, receive free medication whenneeded, and our data show high control levels of cholesterol onceon medication, our recommendation will reduce the burden ofcholesterol-related outcomes in KSA. Moreover, if these campaignsinclude messages on changing health behaviors such as diet andphysical activity, they will have a larger impact on health.
Our findings about lack of diagnosis and treatment of hyper-cholesterolemia in KSA have been previously reported; themajorityof hypercholesterolemic Saudi individuals are unaware of theircondition, and hypercholesterolemia remains undertreated [14]. InKSA, ischemic heart disease is the leading cause of death [8] as isthe case for the whole Arab world, geographically comprised 22countries known as the Arab league [15], and it has been reportedthat hypercholesterolemia is a major risk factor for this disease,both in KSA and worldwide [16,17]. Hypercholesterolemia has beenreported as the eighth risk factor for death in the Arab World inGlobal Burden of Disease 2010 study. In our study, type of fatconsumed, obesity, and sedentary activities were associated withhypercholesterolemia and borderline hypercholesterolemia. Hence,health authorities in KSA should develop public health campaignsthat promote healthier lifestyles, encourage people to exercise, andmake informed decisions around their eating habits.

Table 3Distribution of HDL, LDL, and triglycerides by sociodemographic and risk factors
Sociodemographicand risk factors
HDL LDL Hypertriglyceridemia
Not diagnosed ortreated
Diagnosed and treated Not diagnosed ortreated
Diagnosed andtreated
Not diagnosed ortreated
Diagnosed andtreated
N Weighted % SE N Weighted % SE N Weighted % SE N Weighted % SE N Weighted % SE N Weighted % SE
SexMales 947 38.89 1.57 59 39.84 5.94 194 8.29 0.87 6 4.74 2.42 249 9.93 0.91 23 12.85 4.08Females 1717 59.77 1.56 72 63.77 6.31 171 6.67 0.84 5 5.44 3.20 185 6.52 0.72 14 13.60 3.87
Age (y)15e24 558 45.33 2.04 0 0 0 41 3.69 0.88 0 0 0 43 4.14 0.86 0 0 025e34 617 47.91 2.11 2 63.98 29.86 79 7.52 1.17 0 0 0 81 7.13 1.08 1 12.84 13.7835e44 641 53.42 2.09 11 45.03 14.22 95 11.62 1.62 4 9.06 5.99 121 13.48 1.56 3 8.40 5.1345e54 428 54.74 2.57 31 48.37 10.30 68 13.85 2.10 3 6.84 4.58 93 15.07 2.01 7 11.44 5.9855e64 214 56.31 3.79 38 53.99 8.37 47 13.32 2.73 0 0 0 53 18.78 3.21 8 14.81 7.1465þ 206 50.04 3.66 49 43.94 7.05 35 13.53 3.07 4 5.07 3.35 43 12.54 2.49 18 15.05 4.06
Marital statusCurrently married 1741 53.16 1.26 95 43.54 5.22 263 11.01 0.93 7 4.84 2.25 348 12.99 0.92 30 12.40 3.36Never married 665 44.39 1.86 1 44.10 31.99 60 4.31 0.82 0 0 0 57 4.27 0.78 0 0 0Separated, divorced,or widowed
250 58.43 4.15 35 75.36 7.93 41 11.89 2.54 4 6.84 4.31 28 9.34 2.24 7 19.66 7.48
EducationPrimary school* or less 997 55.29 1.92 85 44.51 5.89 136 10.37 1.36 5 3.26 1.97 161 9.87 1.11 24 12.58 2.90Elementaryy or highschoolcompleted
1068 46.10 1.66 31 58.42 8.90 144 5.88 0.78 5 7.46 4.39 168 6.61 0.79 9 16.65 7.88
College degree or highereducation
597 47.34 2.37 15 39.78 10.18 85 8.15 1.23 1 6.02 5.87 104 10.65 1.44 4 7.35 4.47
Smoking statusNever smoked 2359 49.47 1.22 102 46.52 5.29 300 6.75 0.61 8 4.96 2.24 341 6.94 0.56 26 11.72 2.80Ex-smoker 82 39.92 5.29 12 40.31 14.77 16 8.94 2.87 0 0 0 26 13.73 3.97 6 12.22 6.53Current smoker 221 47.29 3.48 17 60.60 12.61 47 12.37 2.50 3 7.84 6.46 65 16.91 2.69 5 21.32 12.77
Type of fat consumedVegetable oils 2297 48.83 1.23 117 49.06 5.17 303 7.11 0.64 11 6.21 2.47 373 8.39 0.65 35 15.07 3.51Margarine 81 53.28 5.95 4 35.31 18.16 16 11.88 3.64 0 0 0 14 6.24 2.28 0 0 0Animal fat 75 54.50 6.52 4 73.39 18.94 10 12.67 6.03 0 0 0 6 5.58 3.00 0 0 0None in particular 172 46.79 3.80 3 31.54 19.29 29 10.78 2.51 0 0 0 32 9.49 1.97 1 7.01 7.05
Daily servings of fruitsand vegetables0 71 49.90 5.96 4 35.54 26.00 8 4.78 1.92 0 0 0 10 6.71 2.42 0 0 00e3 2057 49.05 1.30 98 49.72 5.67 283 7.74 0.72 10 6.95 2.83 332 8.49 0.71 28 12.41 3.013e5 322 46.31 3.16 17 39.73 10.72 49 8.07 1.74 0 0 0 54 8.01 1.42 5 8.68 4.255þ 178 48.56 4.29 7 47.67 15.72 21 5.77 1.59 1 1.52 1.57 30 7.51 1.82 4 30.16 16.53
Daily servings of meatand chicken0e1 789 49.40 2.05 40 42.97 8.63 119 8.61 1.03 2 6.21 4.39 123 7.57 0.96 8 12.16 6.071e2 974 49.48 1.88 41 49.47 8.00 134 7.79 1.13 4 3.74 2.94 159 8.95 1.05 15 13.38 4.082e3 415 46.92 2.88 29 56.79 11.18 65 7.18 1.34 2 5.48 4.32 76 9.51 1.61 5 13.43 8.923þ 458 47.83 2.68 19 46.86 10.90 43 5.48 1.34 3 4.24 2.83 70 7.34 1.36 9 14.92 5.59
Daily hours spent onwatchingtelevision0e1 186 53.74 4.77 15 35.00 10.12 36 8.72 2.09 3 12.27 7.89 29 6.48 1.63 4 12.89 6.481e3 915 48.64 1.93 48 58.57 7.67 122 7.07 0.99 1 0.45 0.46 150 8.41 0.99 16 16.65 6.093e5 543 45.28 2.46 40 40.63 8.08 82 8.62 1.34 2 4.42 3.69 96 7.99 1.23 9 12.52 5.565þ 399 48.43 2.88 8 24.60 10.04 59 10.77 2.20 2 17.04 13.52 57 8.43 1.70 4 19.89 10.00
Level of physical activityNone 1091 58.45 1.78 53 48.67 7.71 141 9.58 1.26 5 3.98 2.60 158 8.47 0.91 12 12.76 5.04Low 674 50.70 2.20 37 51.93 8.21 102 7.81 1.23 3 8.66 5.39 114 8.48 1.25 9 10.49 3.69Moderate 316 43.46 3.05 20 32.64 9.08 37 5.79 1.30 1 3.78 3.77 54 6.87 1.31 10 16.54 7.96High 583 40.98 2.12 21 59.90 11.77 85 6.30 0.99 2 2.65 1.93 108 8.67 1.16 6 14.27 6.65
ObesityNot obese 1575 45.81 1.41 48 41.04 7.03 207 6.41 0.70 7 7.05 3.55 244 6.73 0.66 11 6.20 2.27obese 1005 56.58 1.87 79 55.01 6.18 147 9.81 1.14 4 3.64 2.32 183 12.46 1.27 24 19.18 5.09
History of diagnosis withhypertensionNo 2432 48.54 1.17 59 43.08 7.50 328 7.42 0.63 6 5.75 3.10 389 8.09 0.61 10 5.37 2.02Yes 220 56.74 3.72 72 51.96 5.80 35 10.12 2.30 5 4.44 2.53 45 15.53 2.49 27 18.71 4.64
History of diagnosis withprediabetesNo 2563 48.63 1.15 111 47.97 5.26 351 7.64 0.62 10 5.01 2.13 410 8.12 0.60 30 13.96 3.48Yes 54 59.44 7.27 16 61.82 11.03 8 3.68 1.55 0 0 0 13 18.82 5.98 5 7.10 3.87
History of diagnosis withdiabetesNo 2356 48.62 1.19 47 51.98 7.51 317 7.35 0.64 2 0.89 0.66 341 7.51 0.61 10 10.13 4.10Yes 289 55.54 2.98 84 45.39 5.82 43 10.24 1.90 9 8.34 3.50 92 21.38 2.48 27 15.34 4.18
(continued on next page)
M. Basulaiman et al. / Annals of Epidemiology xxx (2014) 1e8 5

Table 3 (continued )
Sociodemographicand risk factors
HDL LDL Hypertriglyceridemia
Not diagnosed ortreated
Diagnosed and treated Not diagnosed ortreated
Diagnosed andtreated
Not diagnosed ortreated
Diagnosed andtreated
N Weighted % SE N Weighted % SE N Weighted % SE N Weighted % SE N Weighted % SE N Weighted % SE
Diagnosis of chronic conditionNo 2526 48.93 1.16 102 46.79 5.19 347 7.53 0.62 10 5.60 2.38 406 8.18 0.60 24 10.03 2.64Yes 138 47.08 4.65 29 53.62 11.01 18 7.56 2.90 1 2.48 2.48 28 10.42 2.85 13 25.87 10.08
SE ¼ Standard error.* Six years of schooling following kindergarten.y Three years of schooling following primary school.
M. Basulaiman et al. / Annals of Epidemiology xxx (2014) 1e86
Our findings showed that older individuals should be targetedfor early detection and encouraged to change their lifestyle orseek treatment, especially because health care and medications inKSA is free and readily available to citizens. As seen in our data,most Saudis treated for hypercholesterolemia are prescribedstatins, and the fact that 92% of treated subjects are able tocontrol their cholesterol blood level is an encouraging finding inour study. Moreover, the risk of hypercholesterolemia increasedamong diabetic and hypertensive patients. Screening for hyper-cholesterolemia should be prioritized among these patients ascomorbid individuals who are at higher risk of serious healthcomplications.
The last reported study of hypercholesterolemia rates in KSAwas in 2005 and revealed a 19.1% prevalence of hyper-cholesterolemiadcutoff point of 5.2 mmol/Ldamong Saudis aged15 to 64 years [12]. When restricted to the same age groups andusing the same cutoff point, our data revealed a prevalence of 25.3%.However, in our survey, we applied poststratification weights to
Table 4Multivariate logistic regression for sociodemographic characteristics, risk factors, and hy
Sociodemographic and risk factors Categories
Sex MalesFemales
Age (y)Marital status Currently married
Never marriedSeparated, divorced, or widowed
Education Primary school* or lessElementaryy or high school compCollege degree or higher educatio
Smoking status Never smokedEx-smokerCurrent smoker
Type of fat consumed Vegetable oilsMargarineAnimal fatNone in particular
Daily hours spent on watching television 0e11e33e55þ
Level of physical activity NoneLowModerateHigh
Obesity Not obeseObese
History of diagnosis with hypertension NoYes
History of diagnosis with diabetes NoYes
AOR ¼ Adjusted odds ratio; CI ¼ Confidence interval.* Six years of schooling after kindergarten.y Three years of schooling after primary school.
reflect the Saudi population and adjusted for the increased proba-bility of sick individuals to agree to visit the health facility forphysical and blood samples. This was not done for the previoussurvey. Indeed, when we did not apply adjustments based onpoststratification and the predicted probability of completing theclinic visit; our hypercholesterolemia estimates were 30.1% (95% CI,29.0e32.4). Clearly, this indicates a rise in the prevalence ofcholesterol in KSA and calls for programs to prevent and controlcholesterol levels given its role as a major risk factor for ischemicheart disease, the leading cause of death in KSA [8].
Our study has some limitations. First, our data are from a cross-sectional study; hence, we cannot assess causality. Second, many ofour behavioral data, such as diet and physical activity, are self-reported and subject to recall and social desirability biases. Onthe other hand, our study is based on a large sample size and used astandardized methodology for all its measures. Third, only 52% ofrespondents completed the visit to the health clinics and had theirblood drawn for analysis. However, our weighting methodology
percholesterolemia, Saudis aged 15 years or older, 2013
Sociodemographic model Full model
AOR 95% CI AOR 95% CI
d d d d
0.73 0.56e0.95 0.72 0.50e1.031.04 1.03e1.05 1.03 1.01e1.04d d d d
0.71 0.47e1.06 0.79 0.49e1.271.23 0.83e1.82 1.49 0.96e2.33d d d d
leted 0.97 0.65e1.44 d d
n 1.00 0.66e1.50 d d
d d d d
d d 0.62 0.28e1.34d d 1.70 0.98e2.94d d d d
d d 2.17 1.17e4.04d d 1.00 0.34e2.95d d 1.25 0.72e2.19d d d d
d d 0.82 0.52e1.27d d 1.14 0.70e1.87d d 1.19 0.68e2.06d d d d
d d 0.73 0.48e1.12d d 0.83 0.52e1.33d d 0.68 0.43e1.09d d d d
d d 1.40 1.03e1.89d d d d
d d 1.85 1.28e2.69d d d d
d d 1.88 1.31e2.70

Table 5Multivariate logistic regression for sociodemographic characteristics, risk factors, and borderline hypercholesterolemia, Saudis aged 15 years or older, 2013
Sociodemographic and risk factors Categories Sociodemographic model Full model
AOR 95% CI AOR 95% CI
Sex Males d d d d
Females 1.09 0.86e1.37 1.02 0.76e1.35Age (y) 1.02 1.01e1.03 1.02 1.00e1.03Marital status Currently married d d d d
Never married 0.43 0.31e0.60 0.43 0.29e0.64Separated, divorced, or widowed 0.67 0.46e0.98 0.69 0.44e1.10
Education Primary* school or less d d d d
Elementaryy or high school completed 1.32 0.98e1.78 1.19 0.84e1.69College degree or higher education 1.63 1.17e2.26 1.29 0.88e1.91
Type of fat consumed Vegetable oils d d d d
Margarine d d 1.25 0.54e2.87Animal fat d d 1.96 0.99e3.87None in particular d d 1.09 0.69e1.73
Daily servings of meat and chicken 0e1 d d d d
1e2 d d 1.00 0.73e1.382e3 d d 0.76 0.51e1.123þ d d 0.74 0.49e1.11
Daily hours spent on watching television 0e1 d d d d
1e3 d d 1.44 0.96e2.173e5 d d 1.66 1.05e2.635þ d d 2.00 1.25e3.20
Level of physical activity None d d d d
Low d d 1.00 0.72e1.39Moderate d d 0.73 0.47e1.12High d d 0.81 0.57e1.14
History of diagnosis with prediabetes No d d d d
Yes d d 0.54 0.27e1.08History of diagnosis with diabetes No d d d d
Yes d d 1.19 0.80e1.75Diagnosis of chronic condition No d d d d
Yes d d 1.31 0.65e2.62
AOR ¼ Adjusted odds ratio; CI ¼ Confidence interval.* Six years of schooling after kindergarten.y Three years of schooling after primary school.
M. Basulaiman et al. / Annals of Epidemiology xxx (2014) 1e8 7
accounted for this bias by applying a poststratification adjustmentusing sociodemographic characteristics, health behavior, previouslydiagnosed noncommunicable diseases, and anthropometric mea-surements of respondents from the household survey.
The prevalence of hypercholesterolemia in KSA is not as highas in many developing countries but is a shared risk factor fordeath with the remaining Arab World [15]. For instance, inSwitzerland, 17.4% of adults aged 15 years or older were self-reportedly hypercholesterolemic in 2007 [18], double the preva-lence of KSA. In the United States in 2005 to 2008, 23% of adultsaged 20 to 64 years had hypercholesterolemia, defined similarly
Table 6Multivariate logistic regression for sociodemographic characteristics, risk factors, and un
Sociodemographic and risk factors Categories
Sex MalesFemales
Age (y)Marital status Currently married
Never marriedSeparated, divorced, or widowed
Education Primary school or lessElementary or high school completCollege degree or higher education
History of diagnosis with prediabetes NoYes
History of diagnosis with diabetes NoYes
History of diagnosis with hypertension NoYes
AOR ¼ Adjusted odds ratio; CI ¼ Confidence interval.
to our study [19]. In KSA, only 6.7% of adults of the same agegroup were affected in 2013. On the other hand, the prevalence inKSA is similar to its neighboring countries. For example, inKuwait, about 7% of individuals aged 20 to 69 years had bloodcholesterol levels at or above 6.2 mmol/L in 2009 [20].
We found a large prevalence of undiagnosed hypercholesterole-mia, amajor risk factor for ischemicheartdisease, the leadingcauseofdeath in KSA [8]. Despite its relatively low prevalence, the issue ofhypercholesterolemia should be addressed to reduce the risk ofischemic heart disease and death, especially because Saudi patientshave been successful in lowering their blood cholesterol levels.
diagnosis of hypercholesterolemia, Saudis aged 15 years or older, 2013
Sociodemographic model Full model
AOR 95% CI AOR 95% CI
d d d d
0.75 0.54e1.04 0.78 0.54e1.131.01 1.00e1.03 1.02 1.01e1.03d d d d
0.64 0.41e1.01 0.68 0.43e1.071.04 0.61e1.78 1.07 0.62e1.84d d d d
ed 0.74 0.45e1.21 d d
0.85 0.52e1.38 d d
d d d d
d d 0.27 0.09e0.79d d d d
d d 0.80 0.49e1.31d d d d
d d 0.68 0.37e1.27

M. Basulaiman et al. / Annals of Epidemiology xxx (2014) 1e88
Indeed, concerned Saudi health professionals are already calling forsteps, such as food labeling, to prevent cardiovascular diseases [21].
Conclusions
Our findings call for urgent measures by the Saudi Ministry ofHealth to reduce the burden of hypercholesterolemia in KSA. Tar-geted blood cholesterol screening campaigns are required to detectindividuals with hypercholesterolemia and refer them for medicalfollow-up. Moreover, the early detection campaigns should offerthose with borderline hypercholesterolemia means to control theircholesterol levels through behavioral changes or medication if theyhave other risk factors. In addition, these early detection campaignsshould include screening for blood pressure or diabetes tomaximizetheir benefits. Finally, educational campaigns are needed topromotehealthier lifestyles through physical activity and healthy eatinghabits. Indeed, changing health behaviors among Saudis will have atremendous impact on the burden of disease in KSA.
Acknowledgment
This study was financially supported by a grant from the Min-istry of Health (MOH) of the Kingdom of Saudi Arabia. The authorswould like to acknowledge Adrienne Chew at the Institute forHealth Metrics and Evaluation, Seattle, WA for editing this paper.
References
[1] Widmaier E, Raff H, Strang K. Vander’s Human physiology: the mechanisms ofbody function. 13th ed. New York: McGraw-Hill Science/Engineering/Math;2013.
[2] Kashyap ML. Cholesterol and atherosclerosis: a contemporary perspective.Ann Acad Med Singapore 1997;26:517e23.
[3] Ziegler O, Got I, Jan P, Drouin P. [Diet therapy of hypercholesterolemia. Fromtheory to practice]. Ann Cardiol Angéiol 1989;38:249e53.
[4] Darnton-Hill I, Nishida C, James WPT. A life course approach to diet, nutritionand the prevention of chronic diseases. Public Health Nutr 2004;7:101e21.
[5] Diet, nutrition and the prevention of chronic diseases. World Health OrganTech Rep Ser 2003;916:ieviii. 1e149, backcover.
[6] Griffin BA. Nonpharmacological approaches for reducing serum low-densitylipoprotein cholesterol. Curr Opin Cardiol 2014.
[7] McNamara DJ, Howell WH. Epidemiologic data linking diet to hyperlipidemiaand arteriosclerosis. Semin Liver Dis 1992;12:347e55.
[8] GBD Compare. IHME n.d.[9] Al-Nuaim AR, Al-Rubeaan K, Al-Mazrou Y, Al-Attas O, Al-Daghari N. Prevalence
of hypercholesterolemia in Saudi Arabia, epidemiological study. Int J Cardiol1996;54:41e9.
[10] Al-Nuaim AR. Serum total and fractionated cholesterol distribution andprevalence of hypercholesterolemia in urban and rural communities in SaudiArabia. Int J Cardiol 1997;58:141e9.
[11] Abalkhail BA, Shawky S, Ghabrah TM, Milaat WA. Hypercholesterolemia and5-year risk of development of coronary heart disease among university andschool workers in Jeddah, Saudi Arabia. Prev Med 2000;31:390e5.
[12] WHO j STEPwise approach to chronic disease risk factor surveillance. WHO n.d.[13] Downloadablequestionnaires - InternationalPhysicalActivityQuestionnairen.d.[14] Arafah MR, Mahmeed AAW. The undertreatment of hypercholesterolemia in
Saudi Arabia and the Gulf states: results of the CEPHEUS study. J Saudi HeartAssoc 2012;24:276e7.
[15] Mokdad AH, Jaber S, Aziz MIA, AlBuhairan F, AlGhaithi A, AlHamad NM, et al.The state of health in the Arab world, 1990-2010: an analysis of the burden ofdiseases, injuries, and risk factors. Lancet 2014;383:309e20.
[16] Al-Nozha MM, Arafah MR, Al-Mazrou YY, Al-Maatouq MA, Khan NB, Khalil MZ,et al. Coronary artery disease in Saudi Arabia. Saudi Med J 2004;25:1165e71.
[17] Wilson PWF, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB.Prediction of coronary heart disease using risk factor categories. Circulation1998;97:1837e47.
[18] Estoppey D, Paccaud F, Vollenweider P, Marques-Vidal P. Trends in self-reported prevalence and management of hypertension, hypercholesterole-mia and diabetes in Swiss adults, 1997-2007. BMC Public Health 2011;11:114.
[19] Products - Data briefs - number 57-January 2011 n.d.[20] Ahmed F, Waslien C, Al-Sumaie M, Prakash P. Trends and risk factors of hy-
percholesterolemia among Kuwaiti adults: National Nutrition SurveillanceData from 1998 to 2009. Nutrition 2012;28:917e23.
[21] Mandatory food labeling urged to warn consumers of risks to health. YahooMaktoob News n.d.





























