Embed Size (px)
Citation preview
iCAN Self-Management Technology
Helping Patients Adhere to Medical Appointments
June 20, 2014
Maen Mahfoud - MPH
Agenda1. The Problem
3. The Intervention - iCAN
4. Implementation & Evaluation
2. Causes & Rationale
5. Challenges
‘Missing appointments cost the NHS above £600 million per year, enough to run two medium-size hospitals.’ BBC 2009
Rate of non-attendance in the UK is 12%. Cost: disrupt the flow, interfere with the continuity of healthcare
Directly: through underutilization of administrative resources
Indirectly: through increasing hospital readmission rate.
The Problem
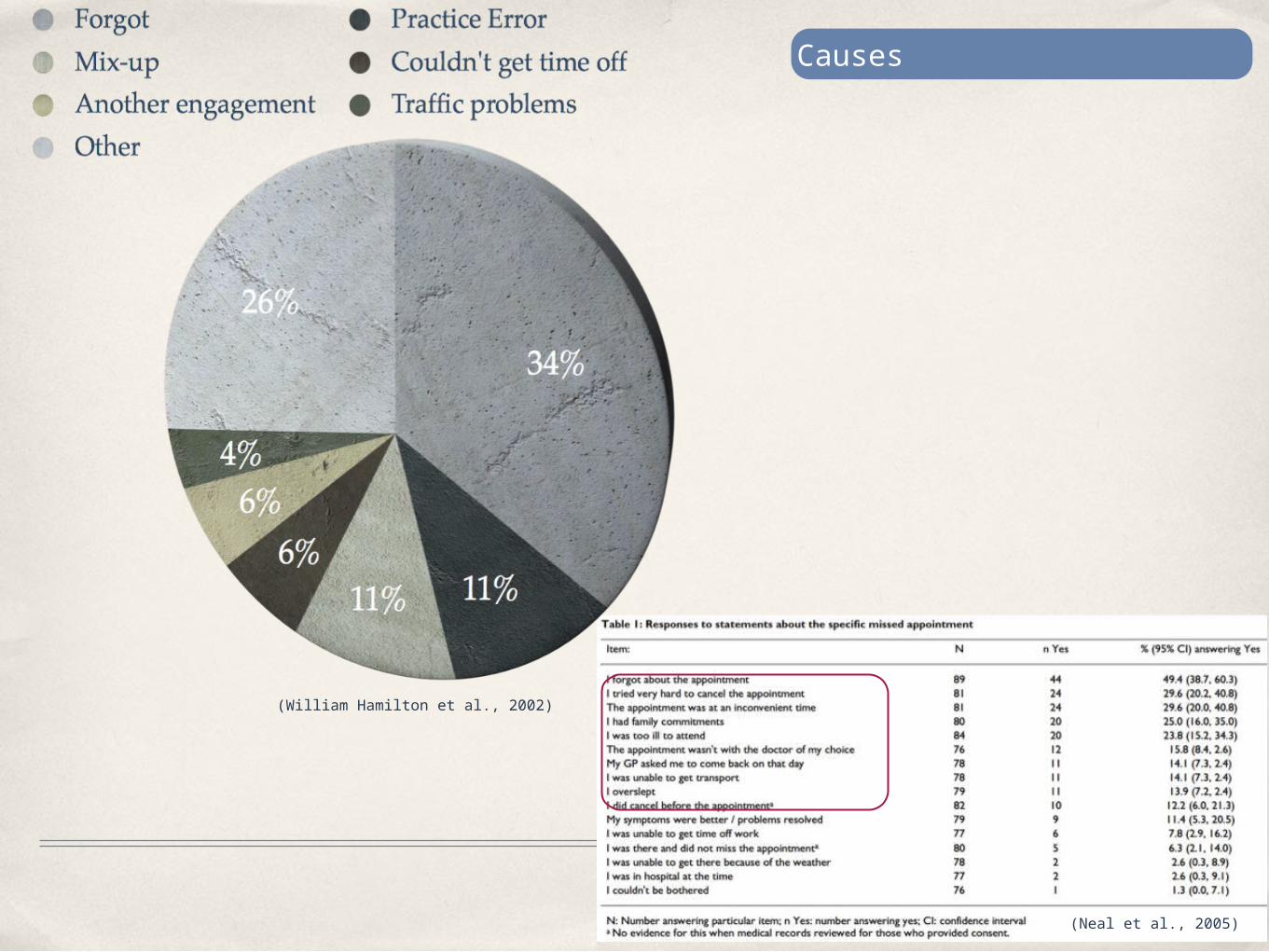
(William Hamilton et al., 2002)
(Neal et al., 2005)
Causes
Patient Disengagement
Current Interventions
Incentives / Fines Overbooking
Phone Reminders SMS Reminders
Postal Reminders Online Consultation
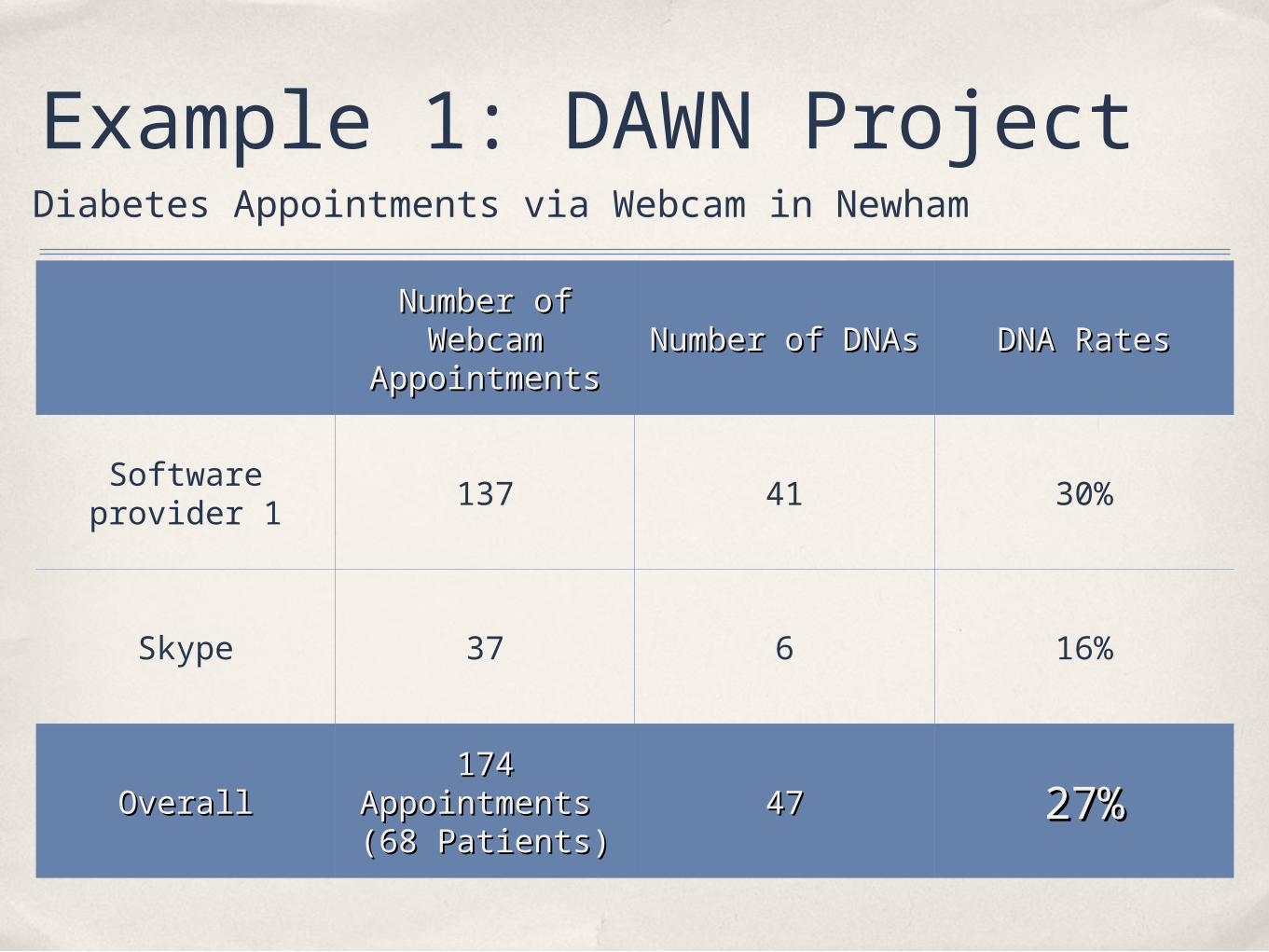
Example 1: DAWN Project
Number of Number of Webcam Webcam
AppointmentsAppointmentsNumber of DNAsNumber of DNAs DNA RatesDNA Rates
Software provider 1 137 41 30%
Skype 37 6 16%
OverallOverall174 174
Appointments Appointments (68 Patients)(68 Patients)
4747 27%27%
Diabetes Appointments via Webcam in Newham
Design a Patient-Centered environment
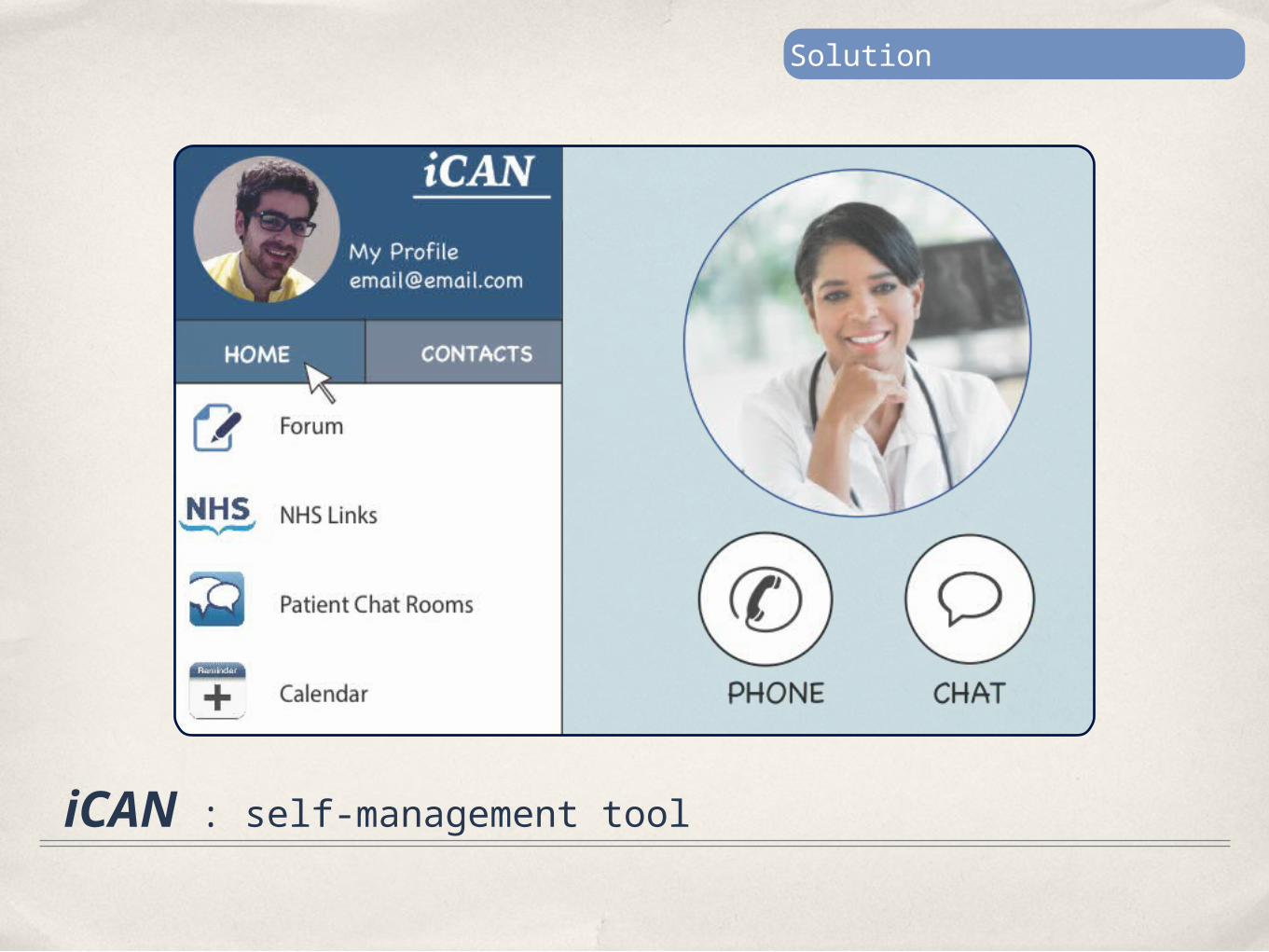
iCAN : self-management tool
Solution
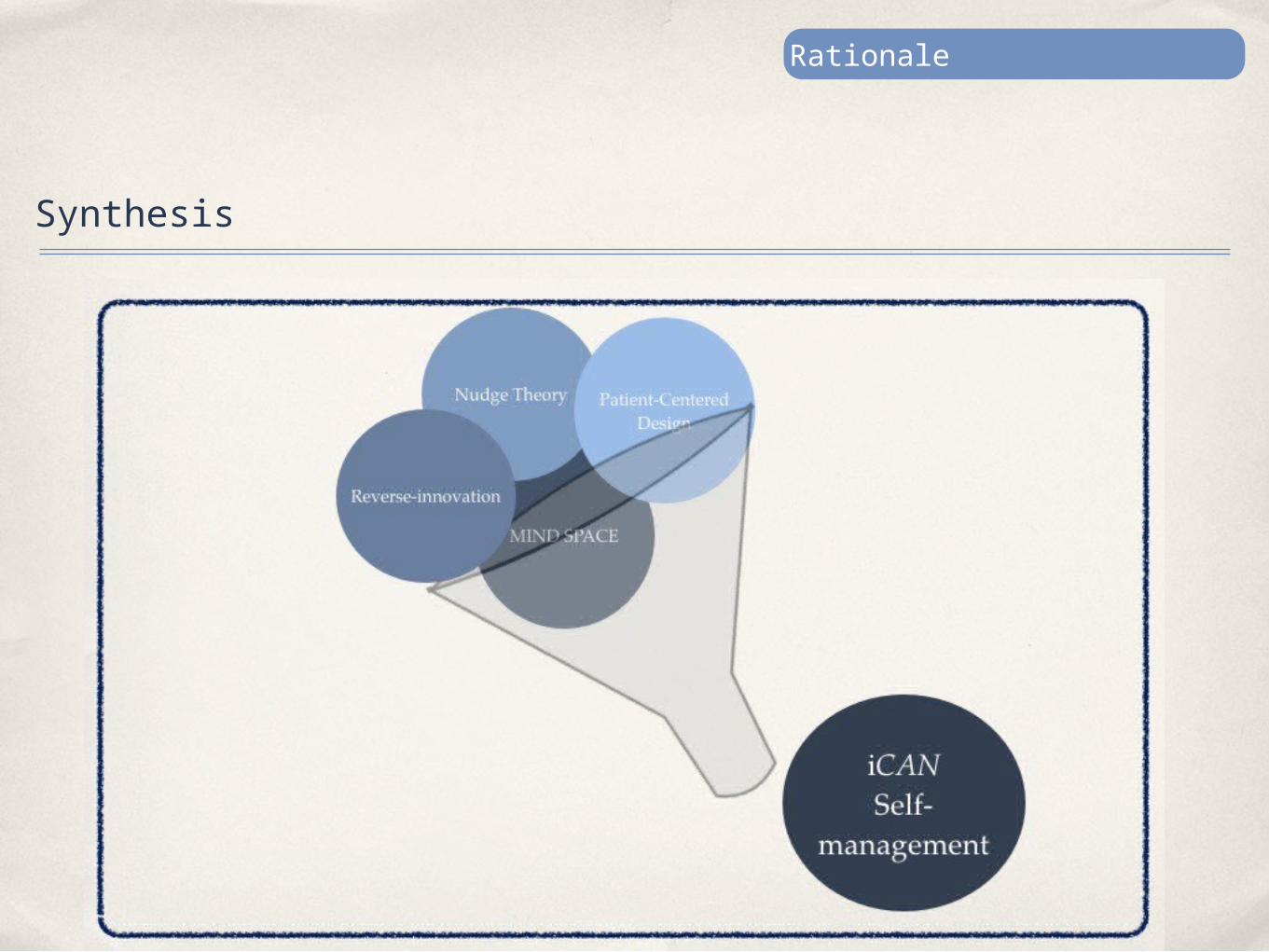
iCAN takes insight from:
1. Disruptive innovation
2. Nudge Theory
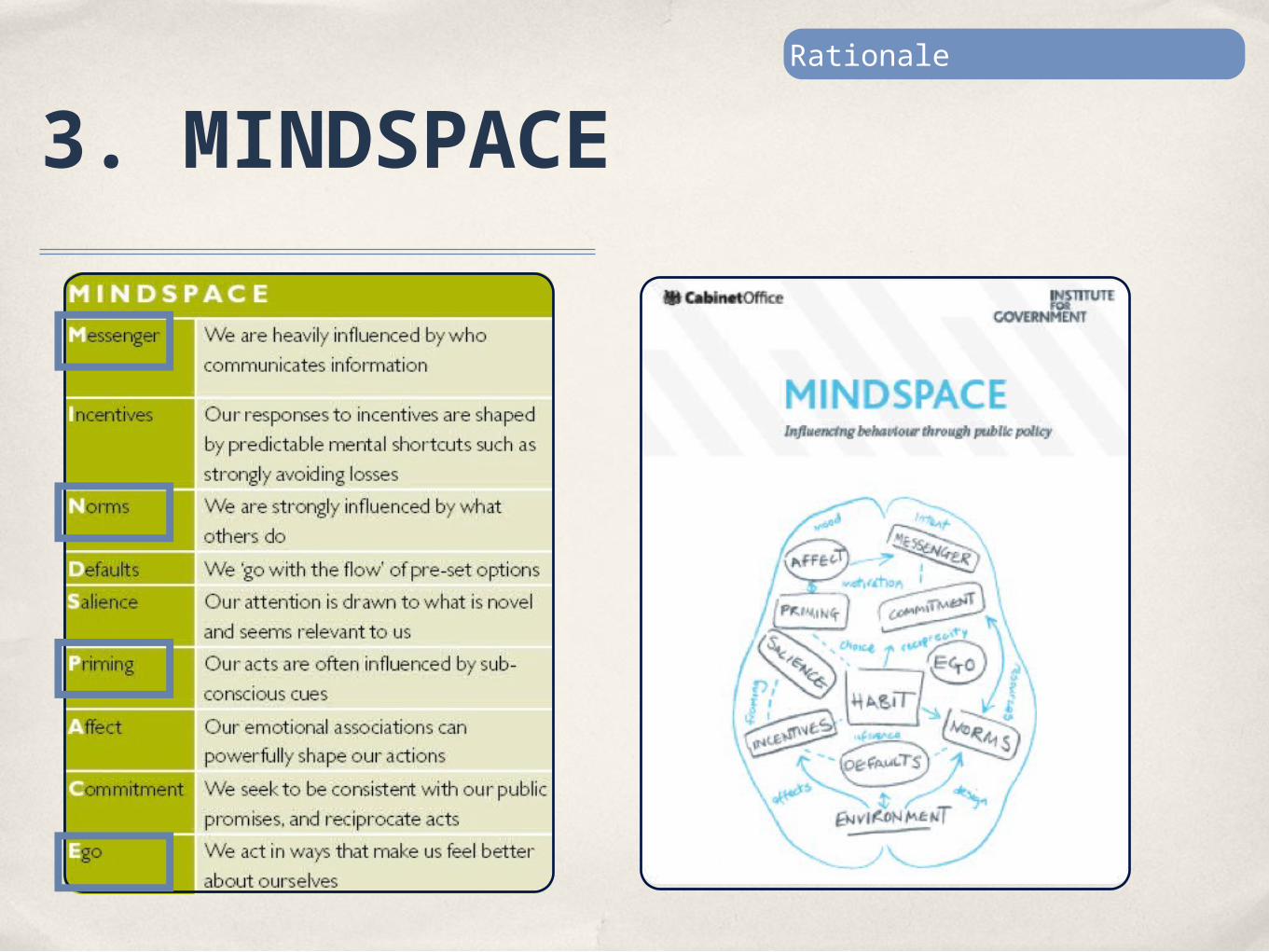
3. MIND SPACE
4. Patient-centered design
Rationale
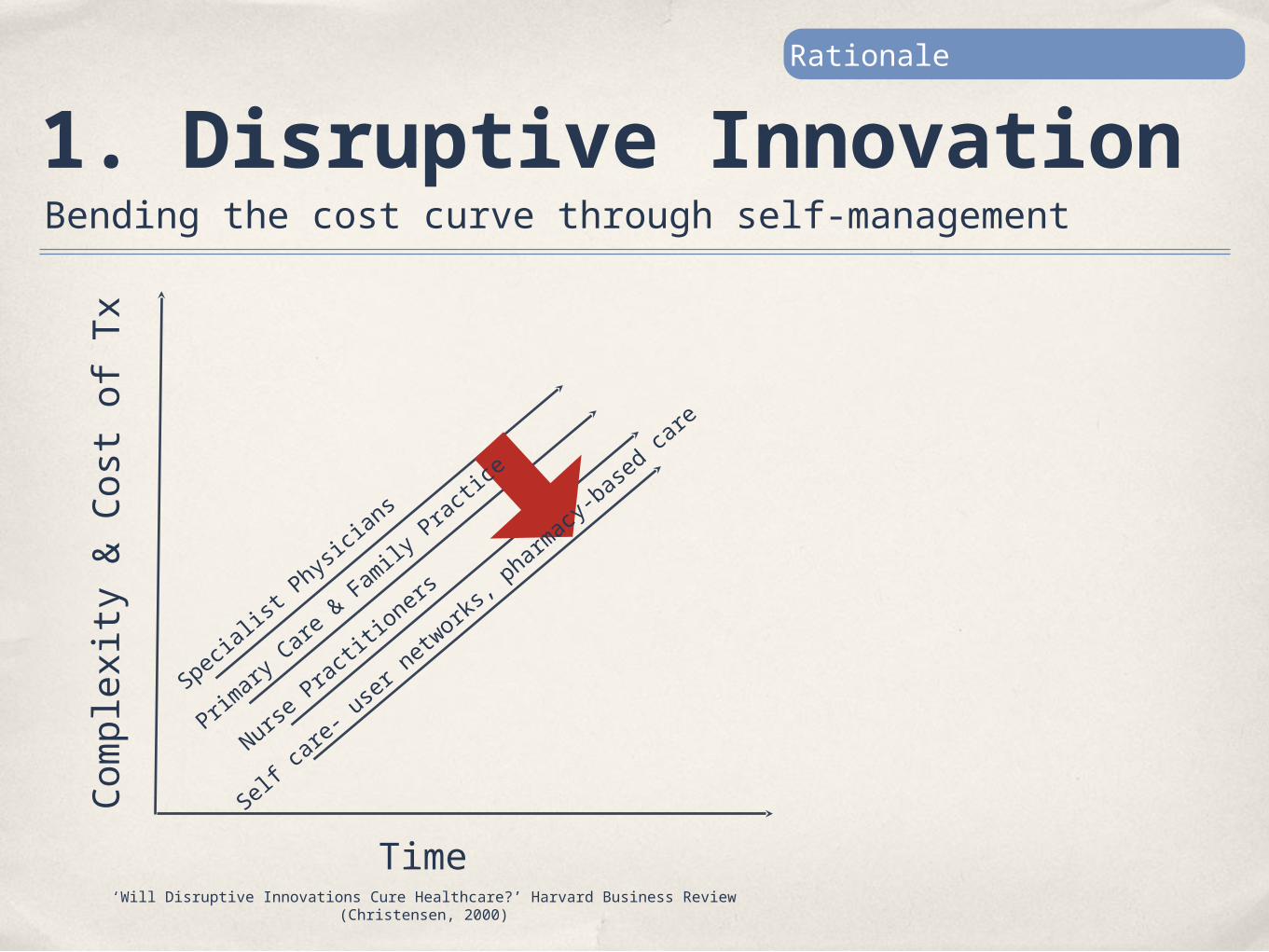
1. Disruptive Innovation
Time
Comp
lexi
ty &
Cos
t of
Tx
Specia
list P
hysici
ans
Primar
y Care
& Fam
ily Pr
actice
Nurse
Practi
tioner
s
Self c
are- u
ser ne
tworks
, phar
macy-b
ased c
are
‘Will Disruptive Innovations Cure Healthcare?’ Harvard Business Review (Christensen, 2000)
Bending the cost curve through self-management
Rationale
2. Nudge Theory Rationale
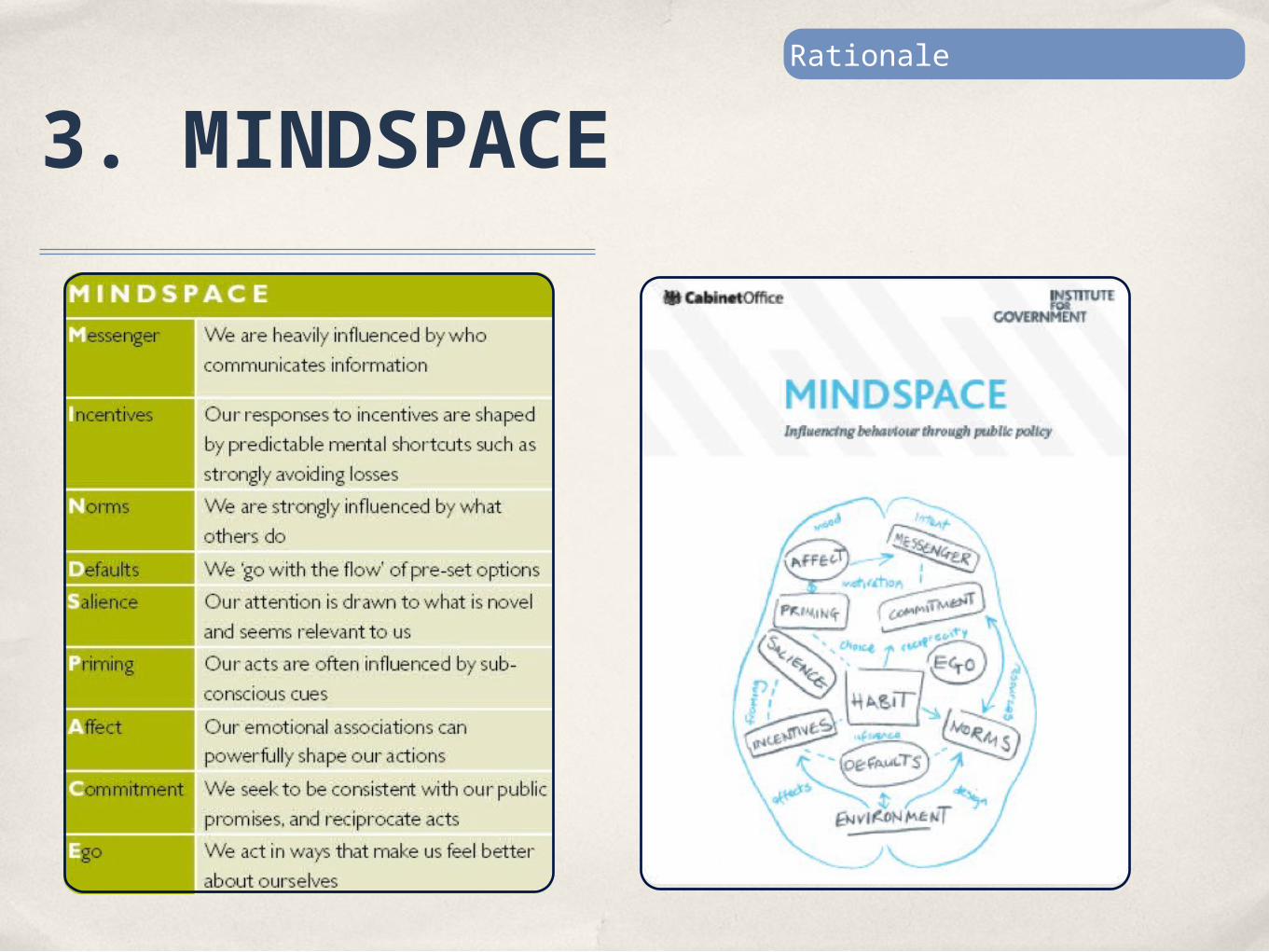
3. MINDSPACE Rationale
3. MINDSPACE Rationale
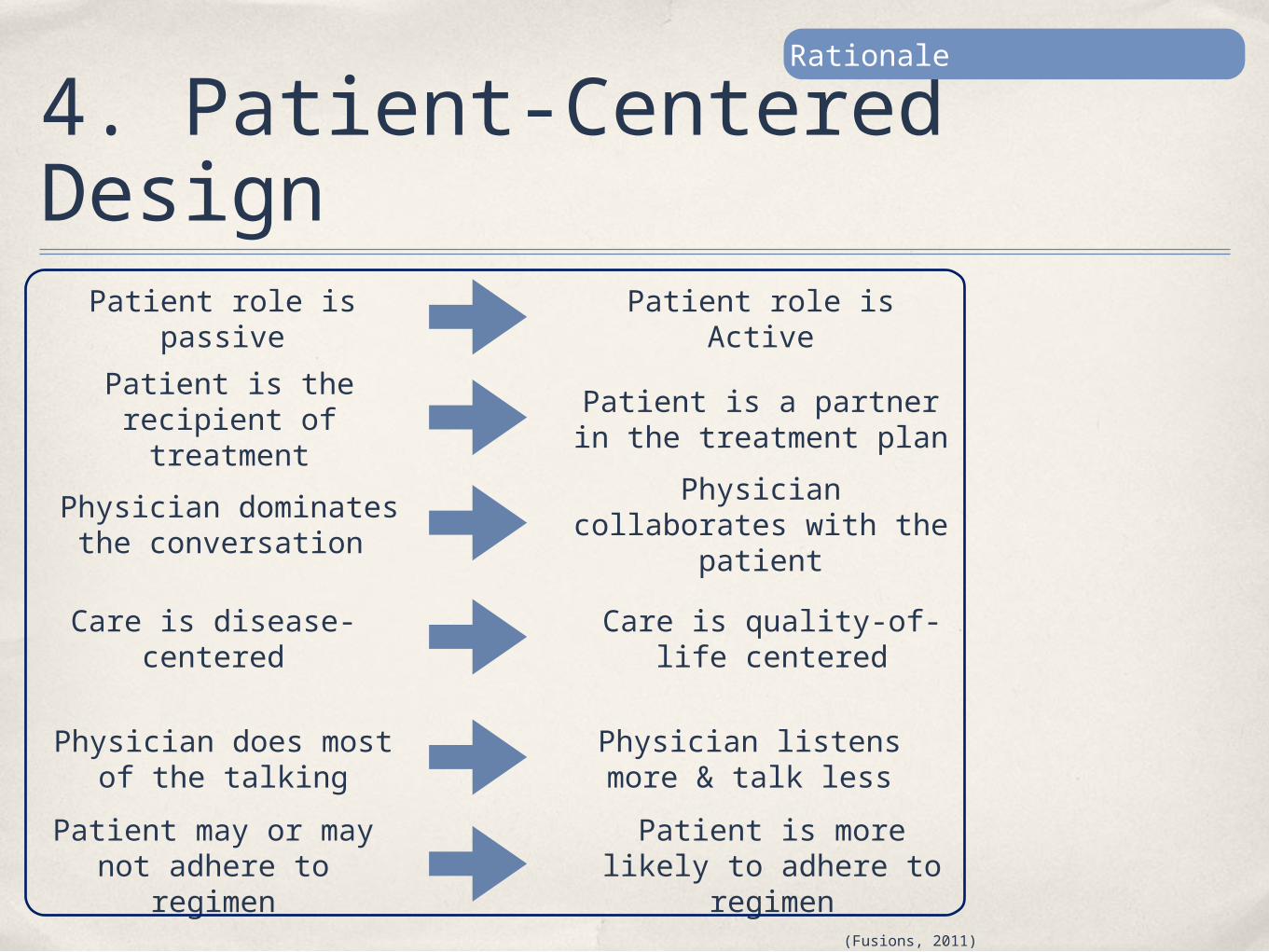
4. Patient-Centered Design
Patient role is passive
Patient is the recipient of treatment
Physician dominates the conversation
Care is disease-centered
Physician does most of the talking
Patient may or may not adhere to
regimen
Patient role is Active
Patient is a partner in the treatment plan
Physician collaborates with the
patient
Care is quality-of-life centered
Physician listens more & talk lessPatient is more
likely to adhere to regimen
(Fusions, 2011)
Rationale
Rationale
Synthesis
The Intervention
iCAN is an electronic self-management tool aimed to provide an engaging environment for diabetic outpatients to gain control over their health, and ultimately adhere to their medical appointments.
iCAN Framework
IMMERSEPatients will be immersed in their health by using iCAN technology
CONTROLPatients will gain control of their environment
ADHEREPatients will adhere and commit to showing up and take medication
NETWORKPatients will be able to share their concerns via iCAN forum & Chat rooms

iCAN User Interface Design & Delivery
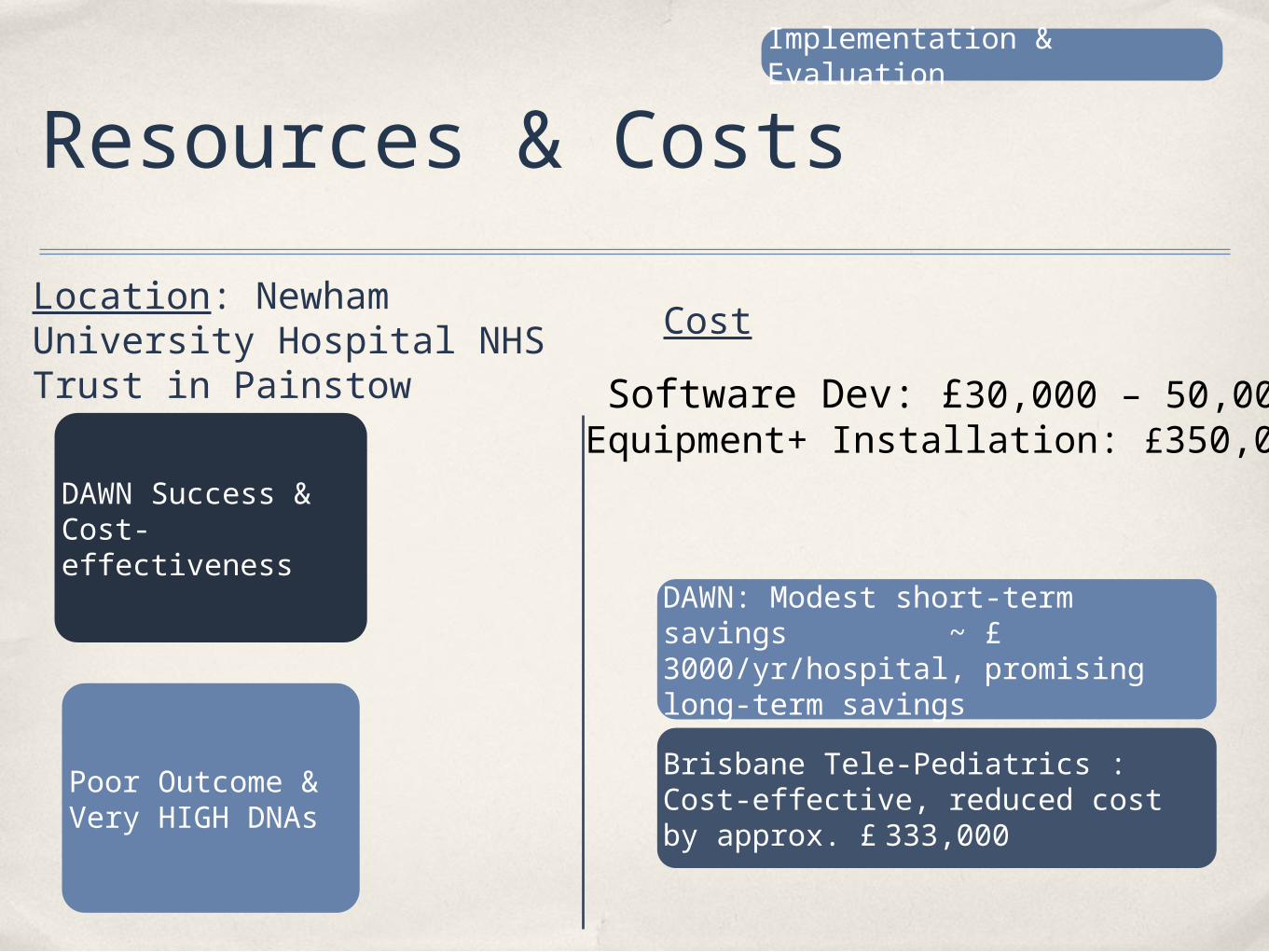
Resources & CostsLocation: Newham University Hospital NHS Trust in Painstow
DAWN Success & Cost-effectiveness
Poor Outcome & Very HIGH DNAs
Cost
DAWN: Modest short-term savings ~ £ 3000/yr/hospital, promising long-term savingsBrisbane Tele-Pediatrics : Cost-effective, reduced cost by approx. £ 333,000
Implementation & Evaluation
Software Dev: £30,000 – 50,000Equipment+ Installation: £350,000
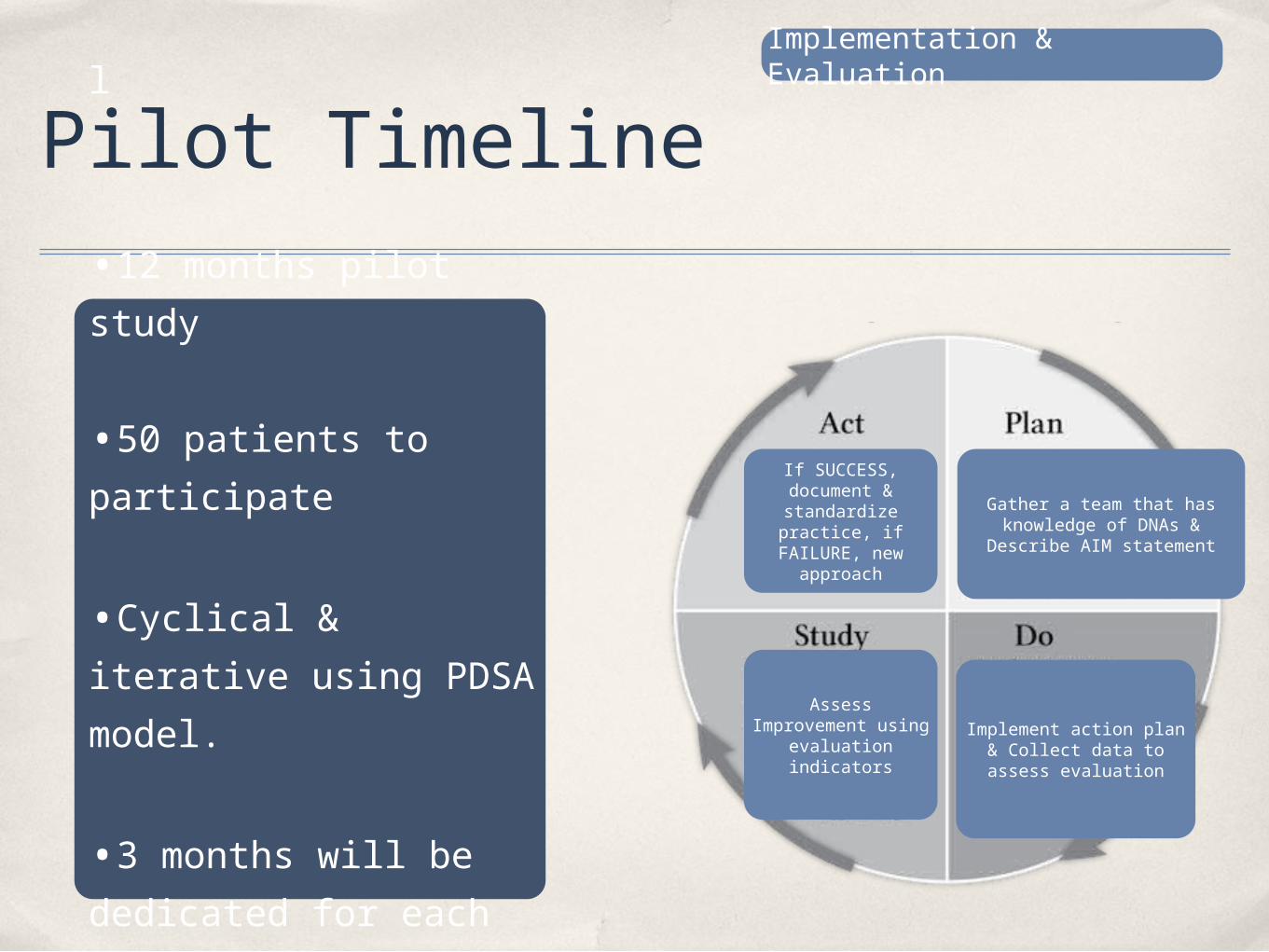
Pilot Timeline
If SUCCESS, document & standardize practice, if FAILURE, new
approach
Gather a team that has knowledge of DNAs &
Describe AIM statement
Assess Improvement using
evaluation indicators
Implement action plan & Collect data to assess evaluation
l
•12 months pilot study
•50 patients to participate
•Cyclical & iterative using PDSA model.
•3 months will be dedicated for each of the 4 stages.
Implementation & Evaluation
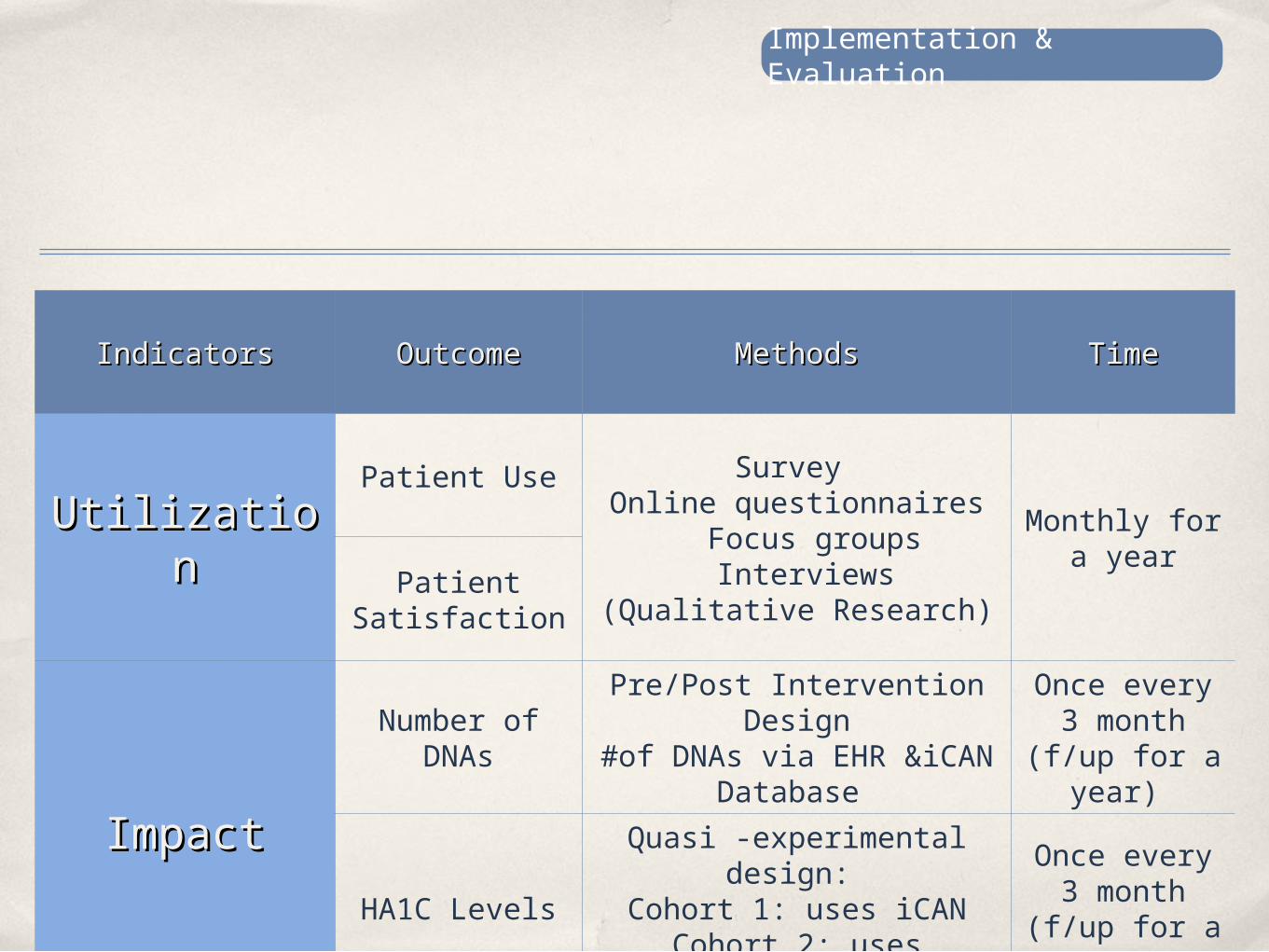
IndicatorsIndicators OutcomeOutcome MethodsMethods TimeTime
UtilizatioUtilizationn
Patient Use Survey Online questionnaires
Focus groups Interviews
(Qualitative Research)
Monthly for a year
Patient Satisfaction
ImpactImpact
Number of DNAs
Pre/Post Intervention Design
#of DNAs via EHR &iCAN Database
Once every 3 month
(f/up for a year)
HA1C Levels
Quasi -experimental design:
Cohort 1: uses iCANCohort 2: uses traditional
Once every 3 month
(f/up for a year)
Implementation & Evaluation
Limitations & Discussion
Recommendation: Invest inSimple, scalable, cheap & frugal technologies
Availability
Accessibility
Acceptability
Challenges
‘ A surge in digital health investing reflects how rapidly confidence in this space is growing. We can clearly see a future where a doctor’s prescription sends you to an immersive online experience as often as it does to a pharmacy.’
Sean Duffy, CEO and Co-Founder, Omada Health
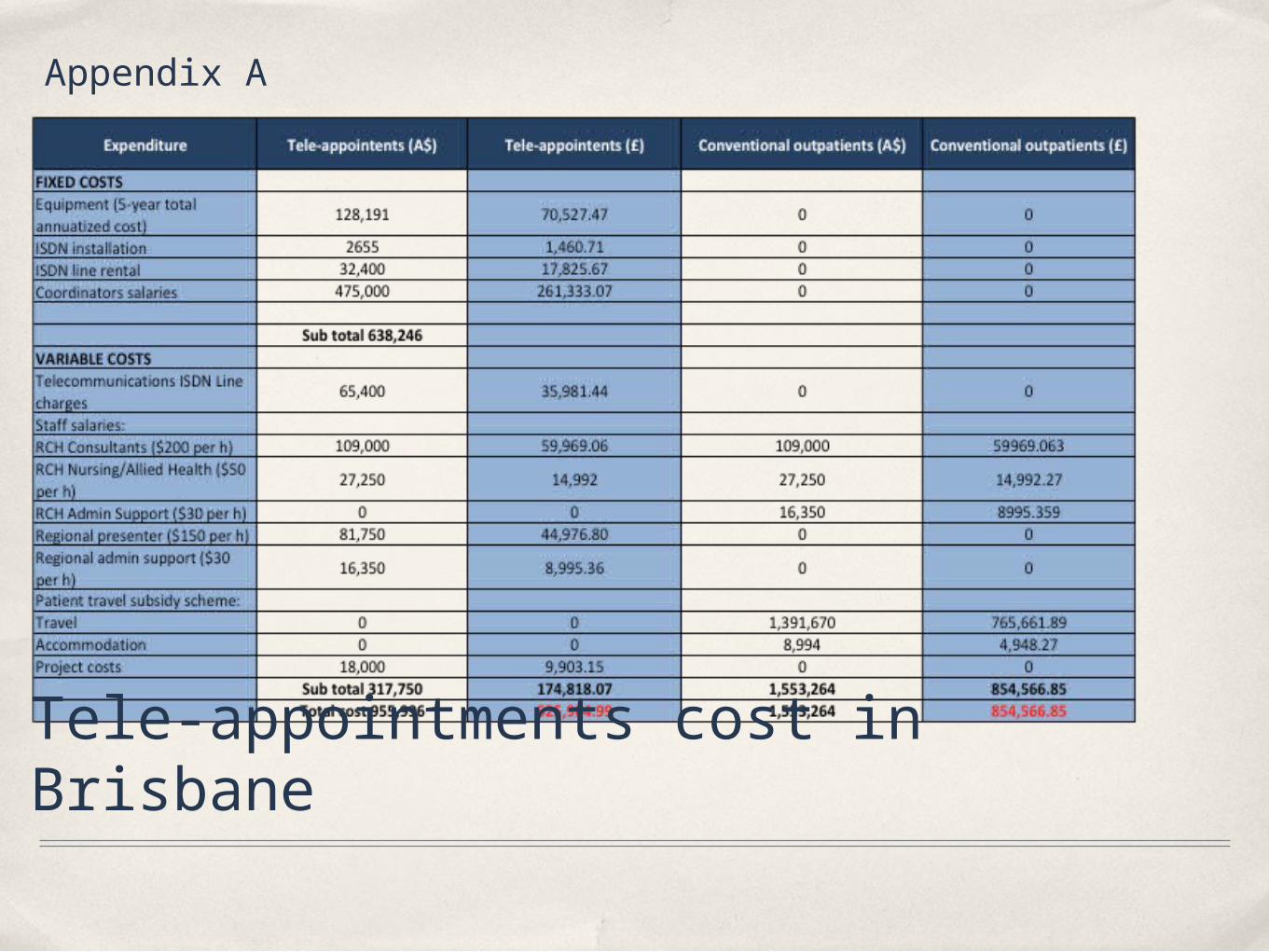
Tele-appointments cost in Brisbane
Appendix A
IMMERSEPatients will be immersed in their health when using this
application. By signing in to this software, the program will: •Send patients reminders about their appointments;•Enforce positive behaviour changes through other users success stories;•Empower patients by educating them about their condition;•Encourage exercise through community forums; •Engage with providers through accessible promotion links;•Inform patients about appointments through calendar alerts;•Eliminate fear associated with medicine through shared experiences in chat rooms;•Provide a user-friendly calendar to encourage people to set schedules and improve their efficiency. CONTROL
Patients will gain control of their environment; the platform will allow them to:
•Avoid waiting times in hospitals;•Feel in control by meeting from their homes or offices;•Avoid negative emotions about hospitals, GPs, and clinics;•Choose a time that does not interfere with their commitments;•Choose their preferred physician, hence increasing responsiveness; •Have clear expectations about their provider’s role in their health
ADHEREiCAN will use the following techniques to improve
adherence among diabetics: •Show the risks of not controlling glucose appropriately through the educational links provided;•Make patients sign a contract to show commitment to attend appointments;•Prime participants with motivational pictures (athletes, alerts, medication) to encourage adherence;•Show success stories of patients who are leading healthy lives. NETWORK
The software will foster networking by enabling patients to:•Communicate with other patients and share concerns;•Learn new methods to cope with appointments and medication;•Organize socials events and perhaps exercise with each other;•Network and exchange useful links and articles;•Motivate each other to take challenges
References BBC. 2009. 'No shows' cost the NHS millions BBC News, 19/4/2014.CHRISTENSEN, C. 2000. Will Disruptive Innovations Cure
Healthcare? [Online]. Harvard Business Review. Available: http://hbr.org/web/extras/insight-center/health-care/will-disruptive-innovations-cure-health-care-sb2 [Accessed 1/5/2014.
CHRISTENSEN, C. 2000. Will Disruptive Innovations Cure Healthcare? [Online]. Harvard Business Review. Available: http://hbr.org/web/extras/insight-center/health-care/will-disruptive-innovations-cure-health-care-sb2 [Accessed 1/5/2014.
DOLAN, P., HALLSWORTH, M., HALPERN, D., KING, D. & VLAEV, I. 2009. MIND SPACE: Influencing behaviour through public policy. UK: Institute For Government.
DUFFY, S. 2014. What If Doctors Could Finally Prescribe Behavior Change? [Online]. Forbes. Available: http://www.forbes.com/sites/sciencebiz/2014/04/17/what-if-doctors-could-finally-prescribe-behavior-change/ [Accessed 2/5/2014.
SHINE. 2011. Newham University Hospital NHS Trust: Web based outpatient consultations in diabetes [Online]. The Health Foundation: Inspiring Improvement Available: http://www.health.org.uk/areas-of-work/programmes/shine-eleven/related-projects/newham-university-hospital/ [Accessed 1/5/2014.
SMITH, A. C., SCUFFHAM, P. & WOOTTON, R. 2007. The costs and potential savings of a novel telepaediatric service in Queensland. BMC Health Serv Res, 7, 35.
WILLIAM HAMILTON, BARNFIELD HILL SURGERY, MANJO LUTHRA, SMITH, T. & EVANS, A. P. 2002. Non-attendance in general practice: a questionnaire survey. Primary Health Care Research and Development, 3.
WM, B. 1980. Failed appointments. Who misses them, why they are missed, and what can be done. Prime Care, 4.





























