Embed Size (px)
Citation preview

Imaging of neoplasms of the paranasal sinusesLaurie A. Loevner, MDa,*, Adina I. Sonners, BSb
aDepartment of Radiology, University of Pennsylvania Medical Center,
3400 Spruce Street, Philadelphia, PA 19104, USAbUniversity of Pennsylvania School of Medicine, University of Pennsylvania Medical Center,
3400 Spruce Street, Philadelphia, PA 19104, USA
Carcinomas of the sinonasal cavity constitute
3% to 4% of all head and neck neoplasms [1–4].
Squamous cell carcinoma accounts for approxi-
mately 80% of these cancers, whereas adenoid
cystic and adenocarcinomas account for 10%
[2,5]. In general, these carcinomas have a relatively
poor prognosis because many present at advanced
stages of disease. Reasons for delayed diagnosis
and presentation include a relative paucity of pain
associated with these neoplasms. Because there is
frequently coexistent inflammatory disease in the
paranasal sinuses that may elicit pain, a carcinoma
may initially be overlooked because the patient is
treated for presumed infection. Whereas pain in
the early stages of sinonasal malignancies is
uncommon, the presence of pain indicates ad-
vanced disease. Pain may indicate perineural
tumor spread, skull base extension, or spread to
the infratemporal fossa. Other clinical presenta-
tions include nasal congestion and epistaxis.
The assessment of sinonasal malignancies
requires a multidisciplinary team approach that
includes radiologists, head and neck surgeons,
neurosurgeons, oral prosthetics specialists, radia-
tion oncologists, and medical oncologists. Advan-
ces in pretherapeutic imaging have contributed
significantly to the management of sinonasal
tumors. CT and MR imaging play complementary
roles in the assessment and staging of these malig-
nancies [6–8].
The treatment of choice for sinonasal carci-
noma usually includes combined surgery and irra-
diation [9–13]. Overall survival rates for radiation
therapy prior to or following surgery are similar.
Orbital exenteration is performed for tumors
involving the periorbita, usually confirmed during
surgery by frozen section [14,15]. In the setting of
extension into the central skull base or the naso-
pharynx, curative surgery is usually not attempted.
The main cause of treatment failure is local recur-
rence [1,16].
Normal anatomy
To understand the clinical and radiologic
appearanceofneoplasmsoriginating fromthepara-
nasal sinuses, and the coexistant inflammatory
changes that usually occur with such tumors,
knowledge of the normal anatomy and the pat-
terns of pneumatization and drainage of sinus
secretions is necessary. An understanding of the
natural history of sinus carcinomas is also para-
mount in assessing patterns of tumor spread, in
determining surgical management, and in deter-
mining radiation portals.
There are paired maxillary, ethmoid, sphenoid,
and frontal sinuses, each named after the bones of
the skull in which they are localized. As each sinus
develops, pneumatization may extend into the
adjacent bones (ie, the frontal and maxillary
sinuses may extend into the zygomatic bones).
The maxillary sinuses are the first of the paranasal
sinuses to develop. The ethmoid air cells arise from
numerous evaginations from the nasal cavity,
beginning with the anterior air cells and progres-
sing to the posterior air cells. The ethmoid air cells
attain their adult proportions by puberty. The
sphenoid sinus usually develops by age 10. The
frontal sinuses are the only sinuses consistently
* Corresponding author.
E-mail address: [email protected] (L.A.
Loevner).
1064-9689/02/$ - see front matter � 2002, Elsevier Science (USA). All rights reserved.
PII: S 1 0 6 4 - 9 6 8 9 ( 0 2 ) 0 0 0 0 6 - 5
Magn Reson Imaging Clin N Am
10 (2002) 467–493

absent at birth. Their development is variable,
beginning during the first few years of life, and
completed in early adolescence.
The sinonasal cavity is lined by ciliated, pseu-
dostratified columnar epithelium, which contains
mucinous and serous glands. The common drain-
age pathway for the frontal sinuses, maxillary
sinuses, and anterior ethmoid air cells is through
the ostiomeatal complex, made up of the maxillary
sinus ostium, the infundibulum, the hiatus semilu-
naris, and the middle meatus (Fig. 1) [17]. Secre-
tions in the maxillary sinuses circulate to the
maxillary sinus ostium, propelled by cilia [18,19].
From the ostium, secretions circulate through the
infundibulum located lateral to the uncinate pro-
cess (an osseous extension of the lateral nasal
wall); through the hiatus semilunaris (an air-filled
channel anterior and inferior to the ethmoidal
bulla); and then pass into the middle meatus, the
nasal cavity, and the nasopharynx where they are
swallowed [18,19].
The frontal sinuses drain inferiorly via the fron-
tal recess/nasofrontal duct into the middle meatus,
also the common drainage site for the anterior eth-
moid air cells, which have ostia in contact with the
infundibulum of the ostiomeatal complex [17]. The
nasofrontal duct is between the inferomedial fron-
tal sinus and the anterior part of the middle meatus
[17]. The anterior-most ethmoid air cells are
located in front of the middle turbinates, which
are in turn located anterior, lateral, and inferior
to the frontal ethmoidal recess.
The posterior ethmoid air cells are located
behind the middle turbinate, and secretions drain
through the superior and supreme meati and other
tiny ostia under the superior turbinate into the
sphenoethmoidal recess, the nasal cavity, and
finally into the nasopharynx. Cilia are necessary
for the drainage of the spenoid sinus because the
ostia are located above the sinus floor.
There are paired superior, middle, and inferior
turbinates in the nasal cavity. Occasionally, there
Fig. 1. Anatomy of important landmarks in the sinonasal cavity shown on coronal CT imaging photographed for bone
detail. (A) Image obtained at the ventral sinonasal cavity. Frontal sinuses (F), cartilaginous nasal septum (C). (B) Image
at the level of the ostiomeatal unit. Medial orbital wall/laminae papyrecia (black arrows), uncinate process of the
ostiomeatal unit (short white arrow), cribriform plate (long white arrow), circulatory pathway of secretions (small white
squares), osseous nasal septum (N). (C) Coronal CT image at the level of the pterygoid bone shows the paired vidian
canals (arrows) and the foramen rotundum (r).
468 L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

may be a supreme turbinate located above the
superior turbinate. An aerated middle turbinate
(concha bullosa) is present in up to 50% of imaged
patients. Large, opacified concha bullosa may
obstruct the ostiomeatal complex. The nasal sep-
tum separates the right and left nasal turbinates,
dividing the nasal cavity in half. The anterior
and inferior nasal septum is made up of cartilage,
whereas the posterior portion is osseous. The
superoposterior osseous portion is the perpendicu-
lar plate of the ethmoid bone, whereas the infero-
posterior osseous portion is the vomer. The
septum within the nasal cavity is lined by squa-
mous epithelium.
There is normal cyclic passive congestion and
decongestion of each side of the nasal cavity and
ethmoid air cells that includes temporary unilat-
eral mucosal thickening of these structures. The
nasolacrimal duct courses from the lacrimal sac
at the medial canthus, runs along the anterior
and lateral nasal wall, and drains into the inferior
meatus.
Blood supply to the sinonasal structures comes
from the internal and external carotid arteries.
The arterial supply to the frontal sinuses is from
supraorbital and supratrochlear branches of
the ophthalmic artery, whereas venous drainage
is through the superior ophthalmic vein. The
Fig. 1 (continued )
469L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

ethmoid air cells and sphenoid sinus also receive
their blood supply from branches of the spheno-
palatine artery (arising from the external carotid)
and ethmoidal branches of the ophthalmic artery
(arising from the internal carotid). Venous drain-
age is via nasal veins into the nasal cavity, and/or
ethmoidal veins that drain into the opthalmic
veins, which then drain into the cavernous sinus.
The maxillary sinuses are predominantly sup-
plied by branches of the external carotid artery,
most notably the maxillary artery. These si-
nuses drain through facial and maxillary veins, the
latter communicating with the pterygoid venous
plexus.
Neoplasms
Squamous cell carcinoma
Squamous cell carcinoma accounts for 80% of
sinonasal malignancies [4]. Approximately 25%
to 60% of these carcinomas involve the maxillary
anthrum; however, the maxillary sinus is second-
arily involved by direct extension in 80% of
patients (Fig. 2). The nasal cavity is the site of
origin in approximately 30% of cases, and the
ethmoid air cells in 10% of cases. The sphenoid
and frontal sinuses account for less than 2% of
all sinonasal carcinomas [1]. These are typically
seen in patients who range in age from 60 to 70
years, more commonly in men [20]. Occupation
exposures include nickel, chromium pigment,
Bantusnuff,Thorotrast,mustardgas,polycyclichy-
drocarbons, and cigarettes [4,21]. People involved
in the production of wood furniture, isopropyl
alcohol, and radium also are at increased risk.
The average 5-year survival rate for squamous
carcinoma of the sinonasal cavity is approximately
25% to 30% [22]. More aggressive surgical man-
agement and improvements in administering ir-
radiation over the last decade may improve
survival rates. Local recurrences occur in approxi-
mately 25% to 35% of cases [1], and the most cases
present in the first year following diagnosis. Ten
percent of cases have distant metastases. Definitive
treatment for early lesions (T1 and T2) includes
surgery (maxillectomy) and/or radiation therapy.
Although the mainstay of therapy is surgery, some
small-scale studies have shown successful manage-
ment with irradiation alone. For advanced tumors
(T3 and T4), treatment requires surgery and irradi-
ation [10–13]. Adjuvant chemotherapy has
recently been added to the treatment regimen;
however, its impact remains to be determined.
Minor salivary gland malignancies
Approximately 10% of sinonasal tumors ori-
ginate in the glands [1]. There is a spectrum of
histologic types, including adenoid cystic, muco-
epidermoid,undifferentiated,andadenocarcinoma.
The adenocarcinomas may represent minor sali-
vary gland tumors or intestinal-type adenocarci-
nomas, and have a predilection for the ethmoid
sinuses [23,24]. These may be more common in
wood and leather workers [23]. They are fre-
quently advanced at presentation, with cribriform
plate erosion present in up to 50% of cases. Dural
invasion is not uncommon [24]. Treatment fre-
quently consists of craniofacial resection followed
by irradiation when tumors are close to or eroding
the cribriform plate, invading the dura, or in the
setting of positive surgical margins [24].
Most minor salivary gland tumors arise from
the palate and secondarily extend into the nasal
cavity and paranasal sinuses. Adenoid cystic carci-
nomas are most common, accounting for one third
of minor salivary gland neoplasms [25]. Up to one
half of these tumors arise in the maxillary sinus,
and one third arise in the nasal cavity. Less than
5% of tumors originate in the sphenoid and frontal
sinuses.
Adenoid cystic carcinomas have variable histo-
logic patterns (cribriform or tubular). They have a
relatively high incidence of perineural spread
(including skip lesions along nerves; Fig. 3), with
secondary extension into the orbit and intracranial
compartment. When feasible, surgical resection is
the treatment of choice. Adjuvant radiation ther-
apy allows for better local control. Local recur-
rence is seen in more than one half of patients at
1-year follow-up, and 75% of patients at 5 years
[1]. Tumors may progress from being well differ-
entiated (tubular), to moderately differentiated
(cribriform), to poorly differentiated [26]. Approxi-
mately one half of patients with adenoid cystic car-
cinoma have distant metastases, most commonly
to the lungs, brain, and bones [1]; therefore, CT
imaging of the chest, abdomen, and pelvis should
be included in the routine evaluation of these
patients.
Melanoma
Sinonasal melanomas may arise from melano-
cytes that have migrated during embryologic
development from the neural crest to the mucosa
of the sinonasal cavity [27]. Less than 4% of mela-
nomas arise in the sinonasal cavity, with most of
these originating in the nose [27,28]. Within the
470 L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

nasal cavity, the most common sites of melanomas
are the anterior nasal septum, lateral nasal wall,
and the inferior turbinates (Fig. 4) [29]. In the para-
nasal sinuses, the maxillary anthrum is the site of
origin in 80% of cases. Sinonasal melanomas may
be associated with melanosis, in which there is field
deposition of melanin along the mucosa in the
sinonasal cavity. This is best assessed on physical
Fig. 2. A 58-year-old man with squamous cell carcinoma of the maxillary sinus. (A) Axial fast-spin echo T2-weightedMR
image shows a large, poorly demarcated, hypointense mass (m) emanating from the right maxillary sinus, with frank
extension throughtheanterior sinuswall into the facial soft tissues/cheek. (B)Correspondingenhancedaxial fastmultiplanar
spoiled gradient echoMR image utilizing fat suppression shows extension outside the confines of the maxillary sinus.
471L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

examination. These tumors may also be multifocal
[29]. Most sinonasal melanomas are melanotic;
10% to 30% are amelanotic [30].
Wide local surgical resection with or without
postoperative radiation therapy is the standard
treatment. In general, sinonasal melanomas have
a poor prognosis, with a mean survival of approxi-
mately 2 years [31]. As many as 40% of patients
present with cervical nodal metastases. Up to
two thirds of patients have local recurrence or
Fig. 3. Perineural spread of adenoid cystic sinonasal carcinoma. Coronal CT image photographed for soft tissue detail
shows enlargement of the left vidian canal (v) and foramen rotundum (r), with soft tissue consistent with tumor in these
foramina.
Fig. 4. Nasal cavity melanoma. Axial T2-weighted MR image shows a hypointense mass (arrows) in the right nasal
cavity consistent with melanotic melanoma.
472 L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

metastases within the first year after treatment.
Hematogenous metastases affect the lungs, brain,
liver, and skin. Neurotrophic spread is not uncom-
mon (Fig. 5). Nasal melanomas have a better prog-
nosis than those originating in the paranasal
sinuses.
Olfactory neuroblastoma (esthesioneuroblastoma)
Esthesioneuroblastomas occur in the upper
nasal cavity/ethmoid vault, arising from the olfac-
tory nerves. They have a bimodal age distribution,
presenting in boys and middle-aged adults. They
have a marked propensity for crossing the cribri-
form plate and extending intracranially (Fig. 6)
[32,33]. When intracranial extension is present, a
craniofacial surgical approach and adjuvant radia-
tion therapy are necessary. Though uncommon,
subarachnoid seeding may occur. This spread
may be because of direct tumor extension or may
be a consequence of surgery.
Other neoplams
Other aggressive neoplasms involving the sino-
nasal cavity include ameloblastomas, sarcomas
(osteogenic sarcoma, chondosarcoma, fibroma/
fibrosarcoma), hemangiopericytomas (Fig. 7), and
lymphomas (Fig. 8); however, these constitute a
small fraction of all sinonasal malignancies.
Patterns of tumor spread
Sinonasal malignancies usually spread by direct
(see Figs. 6, 9) or perineural extension (see Figs. 3,
5) [6,8,34]; therefore, an understanding of the ana-
tomic boundaries of the individual paranasal
sinuses and their contiguous structures is impor-
tant in mapping the extent of disease and in deter-
mining the extent of surgical resection.
The superior and posterior boundaries of the
maxillary sinuses are important prognostically
and in designing the surgical management [15].
The maxillary sinuses are bounded superiorly by
the orbit and ethmoid air cells, and posteriorly
by the pterygoid plates and the pterygopalatine
fossa (PPF). Direct extension into the orbit, or
spread to the intracranial compartment via the
ethmoid air cells, makes obtaining tumor-free sur-
gical margins difficult. Extension posteriorly by
direct extension or perineural spread may result
in neoplastic invasion of the masticator space,
the orbit, and/or the intracranial compartment.
The other margins of the maxillary sinuses (medi-
ally the nasal cavity and inferiorly the alveolus)
are more readily resected en bloc and are less
problematic.
Important landmarks of the ethmoid air cells
include the fovea ethmoidalis and the cribriform
plate superiorly, which provide only a moderately
resilent barrier to intracranial spread [15]. Intra-
cranial spread usually necessitates a craniofacial
resection with the combined efforts of the head
and neck surgeons and neurosurgeons [9]. The lat-
eral wall of the ethmoid air cells—the lamina pap-
yracea—when violated, may result in intraorbital
spread that usually requires orbital exenteration
(see Fig. 9) [14,35–37]. Though rare, cancer arising
in the sphenoid sinus is difficult to resect because of
its central location in the skull base where it is sur-
rounded by numerous vital structures. The sphe-
noid sinus is bounded superiorly by the pituitary
sella and visual tracts; laterally by the carotid
arteries and cavernous sinuses; anteriorly by the
posterior ethmoid air cells; and inferiorly by the
vidian canal, the PPF, and the nasopharynx.
Metastases
Lymphatic drainage and nodal metastases
The lymph node drainage for sinonasal neo-
plasms is dependent on the origin of the neoplasm,
the stage of the neoplasm, and the histology.
Whereas the primary nodal drainage site for the
paranasal sinuses is the lateral retropharyngeal
nodes, these lymphatic channels may be incon-
stant. Therefore, the upper internal jugular and
submandibular nodes are the most common sites
for nodal metastases.
Regional lymph node metastases from sino-
nasal malignancies are relatively uncommon, but
when present are a poor prognostic sign and usu-
ally indicate tumor extension outside of the sino-
nasal cavity [38]. Cervical nodal metastases are
most common with tumors originating from the
maxillary anthrum, seen at presentation in up to
15% of cases. Nodal metastases are uncommon
with ethmoid cancers, and rare with sphenoid
and frontal sinus neoplasms.
Distant metastases
Less than 10% of all sinonasal carcinomas have
systemic metastases. Hematogenous spread to the
lungs is most common, with occasional bone meta-
stases. The presence of cervical nodal disease pla-
ces the patient at increased risk for distant
metastases [38]. Approximately one half of pa-
tients with adenoid cystic carcinomas have distant
473L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

Fig. 5. A 54-year-old woman with sinonasal melanoma. (A) Unenhanced axial T1-weighted MR image shows abnormal
soft tissue in the right pterygopalatine fossa (arrows) and extending into the skull base at the level of the vidian canal
(small white squares) and the clivus (c). (B) Corresponding enhanced fat-suppressed axial T1-weighted MR image shows
diffuse enhancement of the tissue consistent with tumor.
474 L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493
metastases, most commonly to the lungs, brain,
and bone. Hematogenous metastases are not
uncommon with melanoma and affect the brain,
liver, and skin. Although the incidence of meta-
static disease is relatively high with adenoid cystic
carcinoma and melanoma, it is important to recog-
nize that these tumors together account for less
than 8% of all sinonasal malignancies.
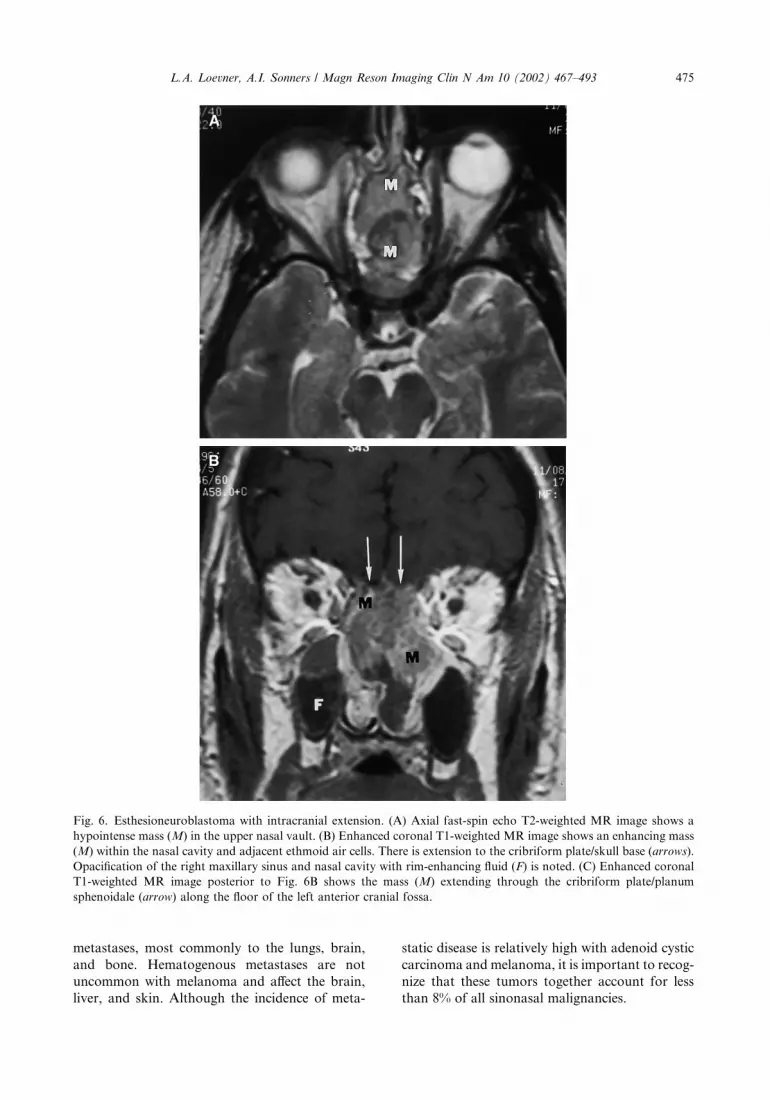
Fig. 6. Esthesioneuroblastoma with intracranial extension. (A) Axial fast-spin echo T2-weighted MR image shows a
hypointense mass (M) in the upper nasal vault. (B) Enhanced coronal T1-weighted MR image shows an enhancing mass
(M) within the nasal cavity and adjacent ethmoid air cells. There is extension to the cribriform plate/skull base (arrows).
Opacification of the right maxillary sinus and nasal cavity with rim-enhancing fluid (F) is noted. (C) Enhanced coronal
T1-weighted MR image posterior to Fig. 6B shows the mass (M) extending through the cribriform plate/planum
sphenoidale (arrow) along the floor of the left anterior cranial fossa.
475L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

Classification and staging
Staging systems are used to define the extent of
neoplastic disease, and to provide some basis to
determine prognosis. In the paranasal sinuses,
staging is usually discussed primarily in the
context of epithelial neoplasms because these
represent the vast majority of sinonasal tumors.
Carcinoma of the maxillary sinus is most common,
followed by ethmoid cancers. Malignancies of the
frontal and sphenoid sinsues are rare, and hence
are generally not included in staging.
T staging
Evaluation and staging of maxillary and eth-
moid sinus carcinomas is achieved through a com-
bination of clinical assessment and pretreatment
CT and MR imaging with close scrutiny of the
sinonasal cavity, orbits, nasopharynx, oral cavity,
and cranial nerves. Imaging is especially important
in assessing the skull base, intracranial compart-
ment, and in distinguishing tumor from coexistent
inflammatory changes.
The tumor, nodes, and metastases (TNM) sys-
tem of classification of maxillary sinus cancers is
based on Ohngren’s imaginary line drawn on a lat-
eral view extending from the medial canthus of the
eye to the angle of the mandible, separating the
maxillary anthrum into anteroinferior and supero-
posterior compartments. On a coronal view, the
maxillary anthrum may be divided into an infra-
structure, mesostructure, and suprastructure, with
the lines of division drawn through the anthral
floor of the maxillary sinus, and the anthral roof.
Tumors are usually resected by partial or total
maxillectomy; however, tumors extending into
the suprastructure also often require an orbital ex-
enteration. T1 tumors are confined to the mucosa,
T2 lesions are associated with osseous erosion or
destruction, and T3 and T4 tumors extend outside
the sinonasal cavity into the masticator space,
cheek (see Fig. 2), adjacent paranasal sinuses,
orbital apex, base of skull, nasopharynx, or intra-
cranially (Table 1) [39,40].
Ethmoid sinus carcinomas may be confined to
the ethmoid air cells (T1), or they may extend into
the nasal cavity (T2), the maxillary sinus and/or
anterior orbit (T3), the orbital apex, intracranial
compartment, skin, or frontal/sphenoid sinuses
(T4) (Table 2) [31].
N staging
In evaluating regional metastases, nodal size is
the major criterion by which N1 to N3 disease is
categorized (Table 3) [40]. To distinguish N1 from
N2 disease, 3 cm is used, whereas 6 cm distin-
guishes N2 from N3 disease [40].
Fig. 6 (continued )
476 L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

Imaging sinonasal neoplasms
It is often difficult for the radiologist to hone
down on a particular histologic diagnosis because
of the marked overlap of the imaging appearance
of different tumors on CT and MR images [41].
The major contribution by the radiologist is accu-
rate mapping of tumor extent and an understand-
ing of the anatomic sites that will influence or alter
surgical resection, treatment planning, and prog-
nosis. In the setting of sinonasal malignancies, a
combination of CT and MR imaging are usually
acquired [8,34,42]. When possible, these should
be completed prior to surgical intervention, includ-
ing biopsy. Preoperative imaging may allow opti-
mal localization for biopsy, and may be useful in
preparing and minimizing complications of sur-
gery, including blood loss in the setting of vascular
neoplasms. Tumors extending into the nasal cavity
may be amenable to transnasal biopsy.
CT andMR imaging play complementary roles
in the assessment of sinus neoplasms (see Fig. 9)
[2,4,8,34,43–45]. CT is more sensitive and accurate
in assessing the osseous margins of the sinonasal
cavity, the osseous floor of the anterior cranial
fossa, and the walls of the orbit [34,46,47]. CT
may detect early cortical skull base erosion [42,48].
Fig. 7. Hemangiopericytoma of the left maxillary sinus that grew during pregnancy in a 33-year-old woman who
presented with pain and numbness in the right cheek. (A) Enhanced axial CT shows an avidly enhancing mass (M) in the
right maxillary sinus. (B) CT image obtained at the level of the orbital floor shows extension of the tumor into the
infraorbital foramen (small squares), confirmed at biopsy.
477L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

Fig. 8. Sinonasal non-Hodgkin lymphoma in a 53-year-old patient following a lung transplant. (A) Unenhanced axial
CT image obtained at the skull base shows opacification of the pterygoid extension of the left sphenoid sinus with
osseous erosion (black arrows). There is also erosion of the posterior aspect of the ethmoid (white arrow). Note soft tissue
opacification of the left pterygopalatine fossa ( pf ). (B) Coronal T2-weighted MR image shows tumor (T) in the sphenoid
sinus, and replacing the pterygoid bone (P). Tumor is seen in the masticator space (curved arrows), with edema in the
temporalis muscle (t). (C) Unenhanced coronal T1-weighted MR image shows tumor in the sphenoid sinus with cortical
erosion of the roof of the sinus (thin arrows) and extension into the posterior aspect of the cavernous sinus (c). There is
tumor in foramen ovale on the left (thick arrows), with spread of disease into the left masticator space (M). (D) Enhanced
axial T1-weighted image shows extension of tumor through the lateral wall of the sphenoid sinus, and direct extension
along the dural margin (arrows) of the left middle cranial fossa. Note tumor (T) along the left temporalis muscle.
478 L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

MR imaging offers soft tissue resolution, con-
trast, and multiplanar capabilities. In most instan-
ces, excellent resolution may be acquired using a
standard head coil. On occasion, imaging of the
sinonasal cavity may be performed with a surface
coil positioned over the face [49]. MR imaging of
sinonasal tumors must include high-resolution
unenhanced and enhanced thin-section (3 mm)
images not only of the sinonasal cavity but also
of the orbit, skull base, and the adjacent intracra-
nial compartment [43,48,50,51]. Tumor extension
into these structures is frequently not evident on
clinical assessment and/or endoscopy. Images
should be acquired in both axial and coronal
planes. Contrast-enhanced imaging is essential to
assess the extent of local disease, and the presence
of perineural spread and intracranial extension.
Extension of neoplasm outside of the sinonasal
cavity into adjacent anatomic locations signi-
ficantly impacts on the following: the patient’s
Fig. 8 (continued )
479L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

operability, the type of resection that will occur,
the surgical approach, the necessity for radiation
therapy, the placement of radiation portals, and
the prognosis. Potential areas of tumor extension
that must be assessed in all patients with sinonasal
malignancies include intracranial spread (the ante-
rior and middle cranial fossa), the palate, the
orbits, the PPF, and the skull base [41,43,50,51].
The hallmark of malignancies involving the
sinonasal cavity is the presence of osseous destruc-
tion (see Figs. 2, 9) [41]. Bone involvement is seen
in approximately 80% of CT scans assessing sino-
nasal squamous cell carcinomas. Squamous and
adenocarcinomas, and the much less common
esthesioneuroblastoma, are usually intermediate
to hypointense on T2-weighted images compared
with gray matter (see Figs. 2, 6, 9), and most
enhance in a solid fashion [32]. Adenoid cystic car-
cinomas have variable signal intensity on MR
imaging, possibly reflecting the histologic pattern
(cribriform or tubular) and the presence of cystic
changes, tumor cellularity, and necrosis.
Tissue specificity is not possible withMR or CT
techniques except perhaps in some cases of mela-
noma. Inmostmelanomas, which containmelanin,
the neoplasms may be hyperintense to gray matter
on unenhanced T1-weighted images, with more
variable signal characteristics on corresponding
T2-weighted MR images [30,52]. Whereas the T1
hyperintensity of melanomas has been attributed
to the presence of blood products [53], T1 shorten-
ing in nonhemorrhagic, melanin-containing mela-
nomas is common because of the paramagnetic
effects of melanin [30,31,54]. Some investigators
believe that the T1 shortening is related to the pres-
ence of free radicals [54], whereas others speculate
Fig. 9. Sinonasal squamous cell carcinoma with orbital extension. (A) Coronal CT image photographed for bone detail
shows a mass in the right nasal cavity. There is destruction of the superolateral nasal wall and floor of the right frontal
sinus (black arrows) and marked thinning and bowing of the right medial orbital wall (white arrows). (B) Unenhanced
coronal T1-weighted MR image shows the mass in the right nasal cavity and adjacent ethmoid air cells (M). There
is extension through the floor of the right frontal sinus (white arrow), with hyperintense proteinaceous secretions (s)
filling the remainder of the right frontal sinus. There is nodularity at the interface between the tumor and the periorbita
(black arrows). At surgery, orbital invasion was confirmed. (C) Coronal T2-weighted MR image with fat sup-
pression acquired at the same level as Fig. 9B shows hypointense tumor, extension into the frontal sinus, and invasion of
the right periorbita. Inspissated secretions in the right frontal sinus are intermediate in signal intensity because of
protein.
480 L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

that the shortening effect is caused by paramag-
netic metal ions that may be bound tomelanin [55].
Differentiating secretions and inflammatory
changes from tumor
One of the advantages of MR imaging versus
CT is its ability to help discern complex sinonasal
secretions and inflammatory disease from malig-
nancy [32,47,56–58]. Secretions and mucosal
disease frequently have a high water content,
yielding high-signal intensity on T2-weighted
images with peripheral enhancement (Fig. 10). In
contrast, most histologic types of sinonasal tumors
are highly cellular, resulting in intermediate- to
low-signal intensity of these tumors on T2-
weighted images with a more solid pattern of
enhancement (see Figs. 2, 6) [57,59]. Benign masses
such as polyps, however, may also demonstrate
only peripheral enhancement (see Fig. 10).
A combination of T1- and T2-weighted images
is extremely useful in distinguishing secretions and
mucosal inflammation from neoplasm [58]. Both
pulse sequences are important because of the
marked variability in the signal intensity of sino-
nasal secretions, which is the result of variable pro-
tein concentrations, the presence and extent of
mobile water protons, and the viscosity that may
occur with inspissated secretions. The changes in
signal intensity associated with increasing protein
concentrations are likely caused by extensive
cross-linking of the glycoproteins present within
hyperproteinaceous secretions. As a result, the rel-
ative amount of mobile water protons decreases.
With low protein concentrations (\10%) and high
free-water content, secretions in the paranasal
sinuses are typically hypointense on T1-weighted
images and hyperintense on T2-weighted images
[60]. As the protein concentration increases, secre-
tions on T1-weighted images become more hyper-
intense. When concentrations approach 20% to
25%, secretions typically are hyperintense on both
T1-weighted and T2-weighted sequences. When
protein concentrations exceed 25%, they are
Fig. 9 (continued )
481L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

hyperintense on T1-weighted and hypointense on
T2-weighted images (see Figs. 9, 10). Finally, when
protein concentrations are extremely high (exceed-
ing 28%), they are hypointense on both T1- and
T2-weighted sequences and can mimic an aerated
sinus.
Bone destruction
Osseous erosion or destruction is most com-
monly seen with carcinomas (see Fig. 9) [41].
Though much less common, it may also be seen
with lymphomas, metastases, and sarcomas.
Sclerosis secondary to tumor is rare. The pres-
ence of sclerosis is normally related to coexistent
chronic inflammatory changes. Though uncom-
mon, osteomyelitis in the sinonasal cavities may
occur and is usually associated with rarefaction
and sclerosis of bone. Calcification of sinonasal
tumors is uncommon. Though prior literature
has suggested that the presence of calcification
with certain tumors is typical, it is more likely that,
in many cases, the findings interpreted as calcifica-
tions actually corresponded to fragmented bone.
Skull base invasion
Sinonasal masses that frequently erode the
skull base and spread intracranially include carci-
nomas (poorly or undifferentiated squamous cell),
esthesioneuroblastoma (see Fig. 6), lymphoma (see
Fig. 8), and sarcomas [42]. Benign lesions that may
erode the skull base include inverted papilloma,
polyps, and mucoceles. The pattern of osseous
destruction for benign and malignant lesions is
similar at the skull base, because osseous remodel-
ing in this location is unusual.
Whereas CT may detect cortical erosion of the
skull base [34], MR imaging is probably more sen-
sitive in assessing skull base invasion [61]. It is par-
ticularly well suited to study bone marrow because
it can differentiate fat from other tissues. The sig-
nal intensity is directly related to the relative
amounts of fat, water, and cells in the marrow.
Fig. 9 (continued )
482 L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493
In adults, the marrow in the normal skull base and
cranium is hyperintense on unenhanced T1-
weighted images because it contains predomi-
nantly fat [62–64]; therefore, skull base involve-
ment by tumor may be detected when the normal
hyperintense appearance caused by fat is replaced
with hypointense tissue (see Fig. 5) [65]. The pres-
ence of normal-appearing marrow at the skull base
is usually a good indicator of absence of skull base
invasion; however, fixation to the periosteum can-
not be excluded. The presence of hypointense tis-
sue, however, does not always mean the presence
of tumor. Hypointense tissue on unenhanced T1-
weighted images may also correspond to edema
or hematopoietic marrow [62,66,67]. In the pres-
ence of abnormal hypointense T1 signal, it is im-
portant to assess the corresponding T2-weighted
and enhanced images, which may help in differen-
tiating tumor from nonmalignant changes.
Perineural spread
An especially important anatomic location for
detection of tumor spread is the pterygopalatine
fossa (PPF; see Figs. 5, 8) [6,68]. When tumor from
the sinonasal cavity spreads to this location, exten-
sion into the adjacent orbit, infratemporal fossa,
skull base, and intracranial compartment may sub-
sequently occur [6,41,43]. Specifically, tumor may
spread from the PPF to the pterygomaxillary
fissure, allowing subsequent extension into the
masticator space. From the PPF, tumor may
extend to the inferior orbital fissure and the orbital
apex. Neoplasm may spread to the vidian canal,
and from there to the foramen lacerum and the
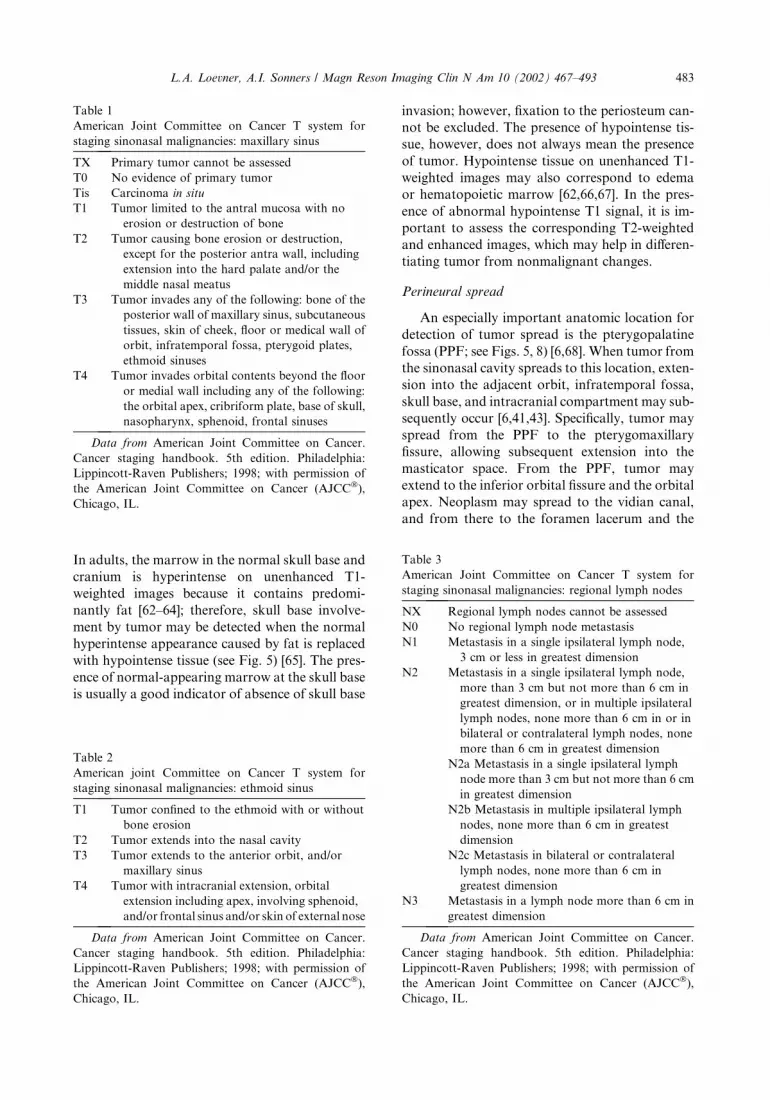
Table 1
American Joint Committee on Cancer T system for
staging sinonasal malignancies: maxillary sinus
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
Tis Carcinoma in situ
T1 Tumor limited to the antral mucosa with no
erosion or destruction of bone
T2 Tumor causing bone erosion or destruction,
except for the posterior antra wall, including
extension into the hard palate and/or the
middle nasal meatus
T3 Tumor invades any of the following: bone of the
posterior wall of maxillary sinus, subcutaneous
tissues, skin of cheek, floor or medical wall of
orbit, infratemporal fossa, pterygoid plates,
ethmoid sinuses
T4 Tumor invades orbital contents beyond the floor
or medial wall including any of the following:
the orbital apex, cribriform plate, base of skull,
nasopharynx, sphenoid, frontal sinuses
Data from American Joint Committee on Cancer.
Cancer staging handbook. 5th edition. Philadelphia:
Lippincott-Raven Publishers; 1998; with permission of
the American Joint Committee on Cancer (AJCC�),
Chicago, IL.
Table 2
American joint Committee on Cancer T system for
staging sinonasal malignancies: ethmoid sinus
T1 Tumor confined to the ethmoid with or without
bone erosion
T2 Tumor extends into the nasal cavity
T3 Tumor extends to the anterior orbit, and/or
maxillary sinus
T4 Tumor with intracranial extension, orbital
extension including apex, involving sphenoid,
and/or frontal sinus and/or skin of external nose
Data from American Joint Committee on Cancer.
Cancer staging handbook. 5th edition. Philadelphia:
Lippincott-Raven Publishers; 1998; with permission of
the American Joint Committee on Cancer (AJCC�),
Chicago, IL.
Table 3
American Joint Committee on Cancer T system for
staging sinonasal malignancies: regional lymph nodes
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node,
3 cm or less in greatest dimension
N2 Metastasis in a single ipsilateral lymph node,
more than 3 cm but not more than 6 cm in
greatest dimension, or in multiple ipsilateral
lymph nodes, none more than 6 cm in or in
bilateral or contralateral lymph nodes, none
more than 6 cm in greatest dimension
N2a Metastasis in a single ipsilateral lymph
node more than 3 cm but not more than 6 cm
in greatest dimension
N2b Metastasis in multiple ipsilateral lymph
nodes, none more than 6 cm in greatest
dimension
N2c Metastasis in bilateral or contralateral
lymph nodes, none more than 6 cm in
greatest dimension
N3 Metastasis in a lymph node more than 6 cm in
greatest dimension
Data from American Joint Committee on Cancer.
Cancer staging handbook. 5th edition. Philadelphia:
Lippincott-Raven Publishers; 1998; with permission of
the American Joint Committee on Cancer (AJCC�),
Chicago, IL.
483L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

Fig. 10. An 18-year-old man with a nasal choanal mass (M) protruding into the nasopharynx, and mucosal disease and
retained secretions in the left maxillary sinus. (A) Axial fast-spin echo T2-weighted MR image shows the mass (m) in the
right nasal cavity/nasopharynx. In the left maxillary sinus there is peripheral high signal intensity (small squares),
consistent with mucosal disease. The material in the central portion of the sinus is hypointense, consistent with
proteinaceous secretions (s). (B) Corresponding unenhanced axial T1-weighted MR image shows the peripheral mucosal
disease is hypointense and the central secretions (s) hyperintense, consistent with the presence of protein. (C) Enhanced
fat-suppressed axial T1-weighted MR image shows only minimal peripheral enhancement of the mucosal changes.
484 L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

intracranial compartment. In addition, tumor may
spread from the PPF to foramen rotundum, and in
such cases, patients may present with a fifth cranial
neuropathy (see Fig. 3). From the foramen rotun-
dum, perineural spread of tumor to the inferior
orbital fissure, the orbital apex, the superior orbi-
tal fissure, and subsequently the intracranial com-
partment may occur.
Orbital invasion
Tumor involvement of the orbit and nasolacri-
mal system impacts negatively on prognosis, and
significantly alters surgical planning [15]. The
absence of orbital symptoms is not a reliable indi-
cator of the absence of orbital invasion. The orbit
is a coned-shaped space contained within the fron-
tal bone, the greater and lesser wings of the sphe-
noid bone, the ethmoid bone, the lacrimal bone,
the zygoma, and the maxilla [69]. The periorbita
comprises the periosteum of these bones. It is con-
tinuous with the dura mater at the superior orbital
fissure and the optic foramen [69]. When tumor
penetrates through the periorbita (see Fig. 9),
exenteration is usually required if the patient is a
surgical candidate in order to obtain tumor-free
margins [14]. If the periorbita is intact, the eye
can be preserved and there is also a lower risk of
local recurrence [12,13,36,37,70]. Erosion of sino-
nasal malignancies through orbital bone without
invasion of the periorbita frequently may be man-
aged with orbital preservation [14,70]. In addition,
some investigators have suggested that when
tumor involves a limited amount of periorbita,
the eye might be preserved without increasing the
chance of local recurrence [14].
The preoperative imaging assessment of orbital
invasion has not been extensively studied. CT and
MR imaging are both important, each offering
their own advantages and pitfalls. Osseous
destruction with involvement of the orbital fat,
which manifests as soft tissue stranding in the
fat, has been one of the hallmarks used to suggest
orbital invasion (see Fig. 9); however, some inves-
tigators have found a significant number of false
negatives (low sensitivity: 40%, MR imaging;
60%, CT) for orbital fat involvement [50]. There-
fore, although the presence of orbital fat invasion
strongly indicates orbital invasion, the absence of
abnormality in the orbital fat cannot exclude inva-
sion. Other criteria evaluated include the follow-
ing: the relationship between the tumor and the
periorbita (abutting, displacing, or bowing the
periorbita), the presence of nodularity at the inter-
face between the tumor and the periorbita, assess-
ment of the extraocular muscles (enlargement,
displacement, and signal abnormalities), and
evaluation of the integrity of the osseous structures
comprising the orbital walls adjacent to tumor
[50]. None of these criteria is very accurate (each
�65%). Whereas tumor adjacent to the periorbita
was the most sensitive criterion, it suffered from
Fig. 10 (continued )
485L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

low specificity (29–44%). In this study, a compari-
son between the results of MR and CT findings for
orbital invasion showed CT to be more accurate
than MR imaging for most criteria [50]. The
strength of CT is its ability to evaluate both bone
and fat; however, it is difficult to distinguish tumor
that compresses versus invades the periorbita [35].
MR imaging tends to underestimate orbital inva-
sion, in part because it cannot distinguish perior-
bita from bone, because both are hypointense on
T1- and T2-weighted imaging. In cases in which
the imaging is ambiguous, intraoperative assess-
ment with histology on frozen section remains
the preferred method for determining invasion of
the periorbita.
Intracranial and dural invasion
Contrast-enhanced MR imaging allows better
identification of tumor extension intracranially,
including the optic canal, cavernous sinus, and
perineural spread at the skull base (see Figs. 5,
6, 8). MR imaging also provides more detailed
and accurate information than CT in assessing
for the presence of dural, pial, and parenchymal
brain invasion (Fig. 11) [43,51,71]. Smooth, con-
tinuous linear enhancement of the dura may be
present in the setting of malignant infiltration;
however, this appearance may also be seen in
benign reactive and/or fibrovascular changes and
therefore does not necessarily indicate dural tumor
[71]. MR imaging findings that favor the presence
of malignant involvement of the dura include the
presence of discontinuous dural enhancement
(multiple regions of enhancement with skip areas),
regions of thickening and/or nodularity greater
than 5 mm (see Fig. 8D), and the presence of T2
hyperintensity within the adjacent brain paren-
chyma [71]. Therefore, in addition to enhanced
fat-suppressed T1-weighted images, it is also
Fig. 11. A 21-year-old man with subarachnoid seeding of a poorly differentiated carcinoma of the ethmoid air cells. (A)
Enhanced axial T1-weighted MR image of the brain shows multiple areas of pathologic enhancement along the pia-
arachnoid/subarachnoid space (arrows) over the cerebral convexities. (B) Enhanced coronal T1-weighted MR image
shows tumor seeding the meninges of the cerebrum and cerebellum.
486 L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

important to acquire T2-weighted images to assess
for associated parenchymal abnormality. In the
setting of pial invasion (subarachnoid seeding),
multifocal areas of peripheral enhancement in
the subarachnoid spaces are present (see Fig. 11).
This spread may occur from direct extension of
the lesion or as a consequence of surgery.
Features of nodal metastases
In addition to size and location, other features
of pathologic nodes that should be assessed on
imaging include the presence of extracapsular
spread, carotid encasement, and nodal fixation,
all of which impact negatively on patient progno-
sis. Imaging findings that should be viewed as sus-
picious for the presence of extracapsular spread, in
addition to nodal size, are the presence of poorly
defined nodal margins and soft tissue stranding
of the fat and soft tissues in the adjacent neck.
The presence of carotid encasement is a relative
contraindication to surgery [72,73]. This complica-
tion of nodal metastases is relatively uncommon
in sinonasal malignancies; it is most prevalent
in patients with pharyngeal or laryngeal cancer
[74–76].
Functional imaging in the treated patient
New imaging techniques in addition to cross-
sectional imaging have focused on the physiologic
properties of tumors and tissue characterization,
rather than anatomic detail. Positron emission
tomography (PET) using 2-[F-18]fluoro-2-deoxy-
D-glucose (FDG) relies on the metabolic activity
of neoplasms relative to adjacent tissues (normal
neck soft tissues, scar, fibrosis, or inflammatory
changes) in positively identifying the presence of
tumor. In the setting of sinonasal cancers, PET
imaging may be useful in guiding endoscopic biop-
sies, in evaluating recurrent tumors [77,78], and in
distinguishing recurrent neoplasm from radiation
changes. One of the potential pitfalls of CT and
MR imaging is their inability to distinguish treat-
ment changes from recurrent tumor. Frequently,
the radiologist is asked to help aid in distinguish-
ing scar/fibrosis from neoplasm, and radiation
necrosis from tumor. In general, recurrent neo-
plasms show significant uptake of FDG compared
with fibrotic tissue and radiation-induced changes
[77–79]; however, occasionally, radiation necrosis
may demonstrate increased metabolic activity
resulting in significant uptake of FDG [80].
Fig. 11 (continued )
487L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

Furthermore, the timing of PET following irradia-
tion is important in the distinction of radiation
changes from tumor. PET performed shortly after
radiotherapymaynot accurately reflectdisease acti-
vity, whereas PET acquired several months after-
ward may more reliably identify recurrence [78,81].
Treatment decisions and planning
Sinonasal carcinoma is usually treatedwithboth
surgery and irradiation [10–13,15,82,83]. Although
the results in the literature differ, overall survival
rates for radiation therapy preoperatively or post-
operativelyare similar.Furthermore,postoperative
irradiation is associated with fewer complications
[1]. The main cause of treatment failure is local re-
currence [1]. Orbital exenteration is performed
for tumor involving the orbital periosteum, often
detected on imaging and documented during sur-
gery [14,35–37]. In the setting of extension into the
central skullbase, thePPF,and/or thenasopharynx,
curative surgery is usually not attempted.
Issues to consider when treating these patients
with surgery include preservation of social func-
tions (swallowing, phonation, speech), cosmetic
deformity, and limited surgical options regarding
complete resection because of the complexity of
the anatomy in and around the paranasal sinuses.
Surgical resection is usually done with the intent
to cure the patient. Tumors confined to the infra-
structure of the sinonasal cavity in which adequate
surgical margins may be achieved are managed
with primary surgical resection. In instances where
tumors extend superiorly or posteriorly, or where
tumors have vascular or neurotrophic spread, sur-
gery and radiation therapy are necessary. In
patients undergoing radiation therapy, and in those
with secondary sinusitis, an adequate drainage por-
tal for the sinonasal cavity must be created.
Palliative excisions may be performed in the
setting of intractable pain, to debulk massive
lesions prior to irradiation, to reduce cosmetic
deformity, or to allow for decompression of vital
structures (eg, the contents of the orbit/optic
chiasm). Criteria that may make a patient unre-
sectable include distant metastases, intracranial
extension, poor underlying general medical condi-
tion, and advanced age (Table 4).
Imaging following treatment
The follow-up of patients focuses predomi-
nantly on the early detection of recurrent tumor,
especially in the first 2 years after treatment. Clin-
ical assessment and cross-sectional imaging play
complementary roles. Issues include distinguishing
treatment changes from tumor recurrence, and
managing treatment-related complications, such
as cerebral radiation necrosis (Fig. 12) [84–86],
xerostomia related to changes in the salivary
glands included in the radiation field (associated
with prominent enhancement followed by atro-
phy), and cranial nerve palsies [87–95].
Tumor recurrence versus treatment changes
Tumor recurrence implies that the patient has
had a documented time interval following treat-
ment that was disease free, clinically and radiolog-
ically. Incomplete resolution of disease after
surgery and/or radiation therapy is completed rep-
resents residual (not recurrent) neoplasm.
One of the most significant challenges facing
the radiologist is distinguishing neoplasm from
scar. CT in this regard has limited utility because
these tissues frequently have overlapping densities,
making their distinction difficult. MR imaging can
be more sensitive in aiding in this distinction. Post-
operative granulation tissue, scar, and fibrosis are
dynamic tissues that may have a wide range of
intensity and enhancement characteristics. In the
paranasal sinuses, scar material may also have
overlapping imaging characteristics with mucosal
and inflammatory changes [49]. Early scar and
granulation tissue tend to be hyperintense on T2-
weighted images and enhance following the
administration of contrast material, which may
make distinction from tumor difficult. A baseline
post-treatment scan is useful, allowing the radiol-
ogist to assess on subsequent examinations for
increased mass effect in the surgical bed, suggesting
recurrent tumor and not contraction of tissue,
which favors scar but does not entirely exclude
tumor. A stable appearance or retraction of tissue
on serial examinations provides reassurance that
Table 4
Criteria for nonresectability of sinonasal malignancies
1. Distance metastases
2. Extensive cerebral involvement
3. Invasion of the optic chiasm
4. Bilateral cavernous sinus/carotid infiltration (it
should be noted that depending on the institution,
cavernous sinus and optic chiasm invasion are
relative contraindications for surgery)
5. Poor general medical condition–relative
6. Advanced age–relative
7. Patient refusal–relative
488 L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

the changes are related to treatment and not recur-
rent disease. Mature scar can usually be distin-
guished from tumor because it typically has little
or no mass effect, is hypointense on T2-weighted
images because of the presence of fibrosis, and
does not avidly contrast-enhance. In some instan-
ces, however, one is not able to exclude residual or
recurrent neoplasm, and in these cases, biopsy or
FDG-PET is necessary [77–79].
Complications of treatment
Radiation necrosis
Radiation necrosis is not an infrequent compli-
cation of nasopharyngeal, sinonasal, and skull
base neoplasms treated with irradiation [84–
86,96]. Because of the radiation portals and
the field covered, the temporal lobes are most
commonly affected (see Fig. 12), followed by the
frontal lobes. The total dose, duration, and frac-
tionation of radiation play an important role
in the development of radiation necrosis [86,96].
The incidence of radiation necrosis following the
treatment of head and neck cancer and skull base
neoplasms ranges from 3% to 10% [86,96,97].
Radiation necrosis is probably more common than
reported because many patients are asymptomatic
and therefore are not imaged, leading to underde-
tection. Irradiation can also result in radiation vas-
culitis, which affects the deep perforating arteries
leading to ischemic sequela in the basal ganglia,
thalami, brainstem, and the deep white matter
(Fig. 13). Symptoms of radiation arteritis are
dependent on the regions of the brain affected
and may include change in mental status, focal
neurologic deficits, and occasionally seizures.
Changes in the brain caused by radiation
necrosis may occur early (during therapy) or be
delayed. Delayed radiation changes can be further
divided into early (within 3 to 4 months of therapy)
and late (months to years following therapy). In
early and early-delayed injury, MRI typically
shows T2 hyperintensity representing edema and
demyelination, which is frequently reversible
[97,98]. Late-delayed injury is usually related to
vascular injury, demyelination, and inflammatory
infiltrates. This is characterized on MR imaging
by T2 hyperintensity, mass effect, and enhance-
ment that may be solid or ringlike (peripheral
enhancement around a necrotic cavity) [97,98]. In
burnt-out radiation necrosis, there is frequently
temporal lobe encephalomalacia. Whereas the
differential diagnosis of radiation necrosis includes
Fig. 12. A 55-year-old man previously treated with
irradiation for left ethmoid adenocarcinoma. The patient
was asymptomatic and presented for routine follow-up
at which time he was found to have cerebral radiation
necrosis. (A) Axial fluid attenuated inversion recovery
MR image obtained at the level of the cavernous sinus
shows abnormal signal intensity in the white matter of
the bilateral anteroinferior temporal lobes. (B) Corres-
ponding enhanced axial T1-weighted MR image shows
solid enhancement in the left temporal lobe (arrow).
489L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

metastatic disease, in the setting of primary head
and neck or skull base malignancies, cerebral
metastases are relatively uncommon. Intracranial
extension of these neoplasms usually presents with
extra-axial (extracerebral) masses, whereas the
changes of radiation necrosis are intracerebral.
Cranial neuropathies
The cranial nerves are relatively radioresistant.
The optic and hypoglossal nerves are most com-
monly affected [89,91,92,94]. Clinically, cranial
nerve XII nerve palsies may present with fascicula-
tions, weakness, and deviation of the tongue, and
problems with deglutitution [88,91]. On imaging,
ipsilateral edema in the early stages, followed later
by fatty replacement and atrophy, may be present
[91]. Optic neuritis caused by irradiation may
present with visual loss, enlargement and enhance-
ment of the involved optic tracts, or chiasm on
MR imaging [89,94]. Cranial nerves IV through
VII are less commonly affected and their involve-
ment may be related to primary changes in the
nerves themselves, or sequela of brainstem injury
from radiation vasculitis.
Radiation-induced neoplasms
Radiation-associated or radiation-induced
neoplasms typically occur in the radiated field. Cri-
teria in diagnosing a tumor induced by irradiation
include a histology different from the primary
tumor treated, and a latency period of at least 5
years. A wide spectrum of radiation-induced neo-
plasms have been reported, including meningio-
mas, sarcomas, schwannomas, squamous cell
carcinoma, and thyroid carcinoma [99–102].
Summary
The assessment of sinonasal malignancies
requires a multidisciplinary team approach.
Advances in pretherapeutic imaging have signifi-
cantly contributed to the management of sinonasal
tumors. CT and MR imaging play complementary
roles in the assessment and staging of these malig-
nancies by determining the presence or absence of
extension of disease into the skull base and its for-
amina, theorbit, and the intracranial compartment.
References
[1] Barnes L, Verbin RS, Gnepp DR. Diseases of the
nose, paranasal sinuses, and nasopharynx. In:
Barnes L, editor. Surgical pathology of the head
and neck. Vol 1. New York: Marcel Dekker; 1985.
p. 403–51.
Fig. 13. Radiation vasculitis in a 54-year-old man 1 year
following completion of radiation therapy for skull base
lymphoma, who presented with sensory deficits and
right-sided weakness. (A) Axial fluid attenuated in-
version recovery (FLAIR) MR image obtained at the
level of the upper pons shows multiple new foci of
increased signal intensity. (B) Axial FLAIR MR image
shows numerous foci of increased signal intensity in the
white matter of the corpus striatum and the deep gray
matter, consistent with radiation-induced vasculitis and
subsequent lacunar infarction.
490 L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

[2] Goldenberg D, Golz A, Fradis M, et al. Malignant
tumors of the nose and paranasal sinuses: a
retrospective review of 291 cases. Ear Nose Throat
J 2001;80:272–7.
[3] Muir C, Weiland L. Upper aerodigestive tract
cancers. Cancer 1995;75:147–53.
[4] Rao VM, el-Noueam KI. Sinonasal imaging.
Anatomy and pathology. Radiol Clin North Am
1998;36:921–39.
[5] Geopfert H, Luna MA, Lindberg RD, et al.
Malignant salivary tumors of the paranasal sinuses
and nasal cavity. Arch Otolaryngol 1983;109:
662–8.
[6] Curtin HD, Williams R, Johnson J. CT of
perineural tumor extension: pterygopalatine fossa.
AJNR Am J Neuroradiol 1984;5:731–7.
[7] Jeans WD, Gilani S, Bullimore J. The effect of CT
scanning on staging of tumors of the paranasal
sinuses. Clin Radiol 1982;33:173–9.
[8] Maroldi R, Farina D, Battaglia G, et al. MR of
malignant nasosinusal neoplasms. Frequently
asked questions. Eur J Radiol 1997;24:181–90.
[9] Osguthorpe JD, Patel S. Craniofacial approaches
to sinus malignancy. Otolaryngol Clin North Am
1995;28:1239–57.
[10] Sakai S, Hohki A, Fuchihata H, et al. Multi-
disciplinary treatment of maxillary sinus carci-
noma. Cancer 1983;52:1360–4.
[11] Shidnia H, Hornback NB, Saghafi N, et al. The
role of radiotherapy in treatment of malignant
tumors of the paranasal sinuses. Laryngoscope
1984;94:102–6.
[12] Sisson GA. Symposium III: treatment of malig-
nancies of paranasal sinuses. [discussion and
summary]. Laryngoscope 1970;80:945–53.
[13] Som ML. Surgical management of carcinoma of
the maxilla. Arch Otolaryngol 1974;99:270–3.
[14] McCary WS, Levine PA. Management of the eye
in the treatment of sinonasal cancers. Otolaryngol
Clin North Am 1995;28:1231–8.
[15] Van Tuyl R, Gissack GS. Prognostic factors
in craniofacial surgery. Laryngoscope 1991;101:
240–4.
[16] Alvarez I, Suarez C, Rodrigo JP, et al. Prognostic
factors in paranasal sinus cancer. Am J Otolaryn-
gol 1995;16:109–14.
[17] Zinreich SJ. Paranasal sinus imaging. Otolaryngol
Head Neck Surg 1990;103:863–8.
[18] Bangert BA. Imaging of paranasal sinus disease.
Pediatr Clin North Am 1997;44:681–99.
[19] Kennedy DW, Zinreich SJ, Rosenbaum AE, et al.
Functional endoscopic surgery: theory and diagno-
stic evaluation. Arch Otolaryngol 1985;111:576–82.
[20] Chaudhry AP, Gorlin RJ, Mosser DG. Carcinoma
of the antrum: a clinical and histopathologic study.
Oral Surg Oral Med Oral Pathol 1960;13:269–81.
[21] Keane WM, Atkins JP Jr, Wetmore R, et al.
Epidemiology of head and neck cancer. Laryngo-
scope 1981;91:2037–45.
[22] St. Pierre S, Baker SR. Squamous cell carcinoma
of the maxillary sinus: analysis of 66 cases. Head
Neck Surg 1983;5:508–13.
[23] Klintenberg C, Olofsson J, Hellquist H, et al.
Adenocarcinoma of the ethmoid sinuses: a review
of 38 cases with special reference to wood dust
exposure. Cancer 1984;54:482–8.
[24] Wax MK, Yun KJ, Wetmore SJ, et al. Adeno-
carcinoma of the ethmoid sinus. Head Neck
1995;17:303–11.
[25] Spiro RH, Koss LG, Hajdu SI, et al. Tumors of
minor salivary gland origin: a clinicopathologic
study of 492 cases. Cancer 1973;31:117–29.
[26] Yamamoto Y, Saka T, Makimoto K, et al.
Histological changes during progression of ade-
noid cystic carcinoma. J Laryngol Otol 1992;106:
1016–20.
[27] Lund VJ. Malignant melanoma of the nasal cavity
and paranasal sinuses. Ear Nose Throat J 1993;
72:285–90.
[28] Moore ES, Martin H. Melanoma of upper
respiratory tract and oral cavity. Cancer 1955;
8:1167–76.
[29] Barnes L, Peel RL. Head and neck pathology:
a text/atlas of differential diagnosis. New York:
Igaku-Shoin; 1990. 122–123.
[30] Yousem DM, Li C, Montone KT, et al. Primary
malignant melanoma of the sinonasal cavity: MR
evaluation. Radiographics 1996;16:1101–10.
[31] Matias C, Corde J, Soares J. Primary malignant
melanoma of the nasal cavity: a clinicopathologic
study of nine cases. J Surg Oncol 1988;39:29–32.
[32] Schuster JJ, Phillips CD, Levine PA. MR of
esthesioneuroblastoma (olfactory neuroblastoma)
and appearance after craniofacial resection. AJNR
Am J Neuroradiol 1994;15:1169–77.
[33] Som PM, Lidov M, Brandwein M, et al. Sinonasal
esthesioneuroblastoma with intracranial extension:
marginal tumor cysts as a diagnostic MR finding.
AJNR Am J Neuroradiol 1994;15:1259–62.
[34] Kraus DH, Lanzieri CF, Wanamaker JR, et al.
Complementary use of computed tomography and
magnetic resonance imaging in assessing skull base
lesions. Laryngoscope 1992;102:623–9.
[35] Graamans K, Slootweg PJ. Orbital exenteration in
surgery of malignant neoplasms of the paranasal
sinuses. Arch Otolaryngol Head Neck Surg 1989;
115:977–80.
[36] Perry C, Levine PA, Williamson BR, et al.
Preservation of the eye in paranasal sinus cancer
surgery. Arch Otolaryngol Head Neck Surg 1988;
114:632–4.
[37] Xuexi W, Pingxhang T, Yongfa Q. Management of
the orbital contents in radical surgery for squ-
amous cell carcinoma of the maxillary sinus. Chin
Med J 1995;108:123–5.
[38] Nishijima W, Takooda S, Tokita N, et al. Analysis
of distant metastases in squamous cell carcinoma
of the head and neck and lesions above the clavicle
491L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

at autopsy. Arch Otolaryngol Head Neck Surg
1993;119:65–8.
[39] Carinci F, Curioni C, Padula E, et al. Cancer of the
nasal cavity and paransal sinuses: a new staging
system. Int J Oral Maxillofac Surg 1996;25:34–9.
[40] Fleming I, Cooper J, Henson D, et al, editors.
AJCC cancer staging manual. 5th edition. Phila-
delphia: Lippincott-Raven; 1997.
[41] Phillips CD, Futterer SF, Lipper MH, et al.
Sinonasal undifferentiated carcinoma: CT and
MR imaging of an uncommon neoplasm of the
nasal cavity. Radiology 1997;202:477–80.
[42] Curtin HD, Hirsch WL. Base of the skull. In: Atlas
SW, editor. Magnetic resonance imaging of the
brain and spine. New York: Raven Press; 1991.
p. 668–706.
[43] Hermans R, De Vuysere S, Marchal G. Squamous
cell carcinoma of the sinonasal cavities. [review].
Semin Ultrasound CT MR 1999;20:150–61.
[44] Hudgins PA. Sinonasal imaging. Neuroimaging
Clin N Am 1996;6:319–31.
[45] Phillips CD. Current status and new developments
in techniques for imaging the nose and sinuses.
Otolaryngol Clin North Am 1997;30:371–87.
[46] Hahnel S, Ertl-Wagner B, Tasman AJ, et al.
Relative value of MR imaging as compared with
CT in the diagnosis of inflammatory paranasal
sinus disease. Radiology 1999;210:171–6.
[47] Rao VM, Sharma D, Madan A. Imaging of frontal
sinus disease: concepts, interpretation, and tech-
nology. Otolaryngol Clin North Am 2001;34:23–9.
[48] Lloyd G, Lund VJ, Howard D, et al. Optimum
imaging for sinonasal malignancy. J Laryngol Otol
2000;114:557–62.
[49] Loevner LA, Yousem DM, Lanza DC, et al. MR
evaluation of frontal osteoplastic flaps using
autogenous fat grafts to obliterate the sinus. AJNR
Am J Neuroradiol 1995;16:1721–6.
[50] Eisen MD, Yousem DM, Loevner LA, et al.
Preoperative imaging to predict orbital invasion by
tumor. Head Neck 2000;22:456–62.
[51] Eisen MD, Yousem DM, Montone KT, et al. Use
of preoperative MR to predict dural, perineural,
and venous sinus invasion of skull base tumors.
AJNR Am J Neuroradiol 1996;17:1937–45.
[52] Mafee MF, Carter BL. Nasal cavity and paranasal
sinuses. In: Valvassori GE, Mafee MF, Carter BL,
editors. Imaging of the head and neck. Stuttgart:
Thieme; 1995. p. 248–331.
[53] Hammersmith SM, Terk MR, Jeffrey PB, et al.
Magnetic resonance imaging of nasopharyngeal
and paranasal sinus melanoma. Magn Reson
Imaging 1990;8:245–53.
[54] Gomori JM, Grossman RI, Shields JA, et al.
Choroidal melanomas: correlation of NMR spec-
troscopy and MR imaging. Radiology 1986;
158:443–5.
[55] Enochs WS, Hyslop WB, Bennett HF, et al.
Sources of the increased longitudinal relaxation
rates observed in melanotic melanoma: an in vitro
study of synthetic melanins. Invest Radiol 1989;
24:794–804.
[56] Chong VF, Fan YF, Khoo JB. Computed tomo-
graphic and magnetic resonance imaging findings
in paranasal sinus involvement in nasopharyngeal
carcinoma. Ann Acad Med Singapore 1998;
27:800–4.
[57] Hasso AN, Lambert D. Magnetic resonance
imaging of the paranasal sinuses and nasal cavities.
Top Magn Reson Imaging 1994;6:209–23.
[58] Som PM, Shapiro MD, Biller HF, et al. Sinonasal
tumors and inflammatory tissues: differentiation
with MR imaging. Radiology 1988;167:803–8.
[59] Allbery SM, Chaljub G, Cho NL, et al. MR
imaging of nasal masses. Radiographics 1995;
15:1311–27.
[60] Som PM, Dillon WP, Fullerton GD, et al.
Chronically obstructed sinonasal secretions: obser-
vations on T1 and T2 shortening. Radiology
1989;172:515–20.
[61] Nishioka T, Shirato H, Kagei K, et al. Skull-base
invasion of nasopharyngeal carcinoma: magnetic
resonance imaging findings and therapeutic im-
plications. Int J Radiat Oncol Biol Phys 2000;47:
395–400.
[62] Kimura F, Kim KS, Friedman H, et al. MR
imaging of the normal and abnormal clivus. AJR
Am J Roentgenol 1990;155:1285–91.
[63] Okada Y, Aoki S, Barkovich AJ, et al. Cranial
bone marrow in children: assessment of normal
development with MR imaging. Radiology 1989;
171:161–4.
[64] Ricci C, Cova M, Kang YS, et al. Normal age-
related patterns of cellular and fatty bone marrow
distribution in the axial skeleton: MR imaging
study. Radiology 1990;177:83–8.
[65] Daffner RH, Lupetin AR, Dash N, et al. MRI in
the detection of malignant infiltration of bone
marrow. AJR Am J Roentgenol 1986;146:353–8.
[66] Poulton TB, Murphy WD, Duerk JL, et al. Bone
marrow reconversion in adults who are smokers:
MR imaging findings. AJR Am J Roentgenol
1993;161:1217–21.
[67] Shellock FG, Morris E, Deutsch AL, et al.
Hematopoietic bone marrow hyperplasia: high
prevalence on MR images of the knee in asympto-
matic marathon runners. AJR Am J Roentgenol
1992;158:335–8.
[68] Williams LS. Advanced concepts in the imaging of
perineural spread of tumor to the trigeminal nerve.
Top Magn Reson Imaging 1999;10:376–83.
[69] Weisman RA. Surgical anatomy of the orbit.
Otolaryngol Clin North Am 1988;21:1–12.
[70] McCary WS, Levine PA, Cantrell RW. Preserva-
tion of the eye in the treatment of sinonasal
malignant neoplasms with orbital involvement.
Arch Otolaryngol Head Neck Surg 1996;122:
657–9.
492 L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493

[71] Chong VFH, Fan YF, Khoo JBK. Nasopharyng-
eal carcinoma with intracranial spread: CT and
MRI characteristics. J Comput Assist Tomogr
1996;20:563–9.
[72] Brennan JA, Jafek BW. Elective carotid artery
resection for advanced squamous cell carcinoma of
the neck. Laryngoscope 1994;104:259–63.
[73] McCready RA, Miller SK, Hamaker RC, et al.
What is the role of carotid artery resection in the
management of advanced cervical cancer? J Vasc
Surg 1989;10:274–80.
[74] Kennedy JT, Krause CJ, Loevy S. The importance
of tumor attachment to the carotid artery. Arch
Otolaryngol 1977;103:70–3.
[75] Nieto CS, Solano JME, Martinez JB, et al.
Invasion of the carotid artery in tumors of the
head and neck. Clin Otolaryngol 1981;6:29–37.
[76] Yousem DM, Hatabu H, Hurst RW, et al. Carotid
artery invasion and neck masses: prediction with
MR imaging. Radiology 1995;195:715–20.
[77] Anzai Y, Carroll WR, Quint DJ. Recurrence of
head and neck cancer after surgery or irradiation:
prospective comparison of 2-deoxy-2-[F-18]-
fluoro-D-glucose PET and MR imaging diagnoses.
Radiology 1996;200:135–41.
[78] Greven KM, Williams DW III, Keyes JW Jr, et al.
Positron emission tomography of patients with
head and neck carcinoma before and after high
dose irradiation. Cancer 1994;74:1355–9.
[79] Mukherji SK, Drane WE, Mancuso AA, et al.
Occult primary tumors of the head and neck:
detection with 2-[F-18]fluoro-2-deoxy-D-glucose
SPECT. Radiology 1996;199:761–6.
[80] Fischman AJ, Thorton AF, Frosch MP, et al.
FDG hypermetabolism associated with inflamma-
tory necrotic changes following radiation of a
meningioma. J Nuc Med 1997;38:1027–9.
[81] Lapela M, Grenman R, Kurki T. Head and neck
cancer: detection of recurrence with PET and 2-
[F-18]fluoro-2-deoxy-D-glucose. Radiology 1995;
197:205–11.
[82] Janecka IP, Sen C, Sekhar L, et al. Treatment of
paranasal sinus cancer with cranial base surgery:
results. Laryngoscope 1994;104:553–5.
[83] Svane-Knudsen V, Jorgensen KE, Hansen O, et al.
Cancer of the nasal cavity and paranasal sinuses.
Rhinology 1998;36:12–4.
[84] Chong VE, Fan YF. Radiation-induced temporal
lobe necrosis [letter]. AJNR Am J Neuroradiol
1997;18:784–5.
[85] Chong VF, Rumpel H, Aw YS, et al. Temporal
lobe necrosis following radiation therapy for
nasopharyngeal carcinoma: 1H MR spectroscopic
findings. Int J Radiat Oncol Biol Phys 1999;
45:699–705.
[86] Lee AW, Foo W, Chappell R, et al. Effect of time,
dose, and fractionation on temporal lobe necrosis
following radiotherapy for nasopharyngeal carci-
noma. Int J Radiat Oncol Biol Phys 1998;40:
35–42.
[87] Bacskulin A, Guthoff R. Neuromyotonia of the
abducens nerve after hypophysectomy and radia-
tion. Strabismus 1999;7:37–40.
[88] Dejaeger E, Goethals P. Deglutition disorder as a
late sequel of radiotherapy for a pharyngeal tumor.
Am J Gastroenterol 1995;90:493–5.
[89] Ebner R, Slamovitis TL, Friedland S, et al. Visual
loss following treatment of spenoid sinus carci-
noma. Surv Ophthalmol 1995;40:62–8.
[90] Fu ER. Ocular neuromyotonia—an unusual ocu-
lar motility complication after radiation therapy
for nasopharyngeal cancer. Ann Acad Med Singa-
pore 1995;24:895–7.
[91] King AD, Ahuja A, Leung SF, et al. MR features
of the denervated tongue in radiation induced
neuropathy. Br J Radiol 1999;72:349–53.
[92] Leber KA, Bergloff J, Langmann G, et al.
Radiation sensitivity of visual and oculomotor
pathways. Stereotact Funct Neurosurg 1995;
64(Suppl):233–8.
[93] Marti-Fabregas J, Montero J, Lopez-Villegas D,
et al. Post-irradiation neuromyotonia in bilateral
facial and trigeminal nerve distribution. Neurology
1997;48:1107–9.
[94] Piquemal R, Cottier JP, Arsene S, et al. Radiation-
induced optic neuropathy 4 years after radiation:
report of a case followed up with MRI. Neuro-
radiology 1998;40:439–41.
[95] Yee RD, Purvin VA. Ocular neuromyotonia: three
case reports with eye movement recordings. J
Neuro-ophthalmol 1998;18:1–8.
[96] Lee AWN, Ng SH, Ho JHC, et al. Clinical
diagnosis of late temporal lobe necrosis following
radiation therapy for nasopharyngeal carcinoma.
Cancer 1988;61:1535–42.
[97] Rabin BM, Meyer JM, Berlin JW, et al. Radiation-
induced changes in the central nervous system and
head and neck. Radiographics 1996;16:1055–72.
[98] Hecht-Leavitt C, Grossman RI, Curran WJ Jr,
et al. MR of brain radiation injury: experimental
studies in cats. AJNR Am J Neuroradiol 1987;
8:427–30.
[99] Mark RJ, Bailet JW, Poen J, et al. Post-radiation
sarcoma of the head and neck. Cancer 1993;
72:887–93.
[100] Rubinstein AB, Reichenthal E, Borohov H.
Radiation-induced schwannomas. Neurosurgery
1989;24:929–32.
[101] Steeves RA, Bataini JP. Neoplasms induced by
megavoltage radiation in the head and neck region.
Cancer 1981;47:1770–4.
[102] Van der Laan BF, Baris G, Gregor RT, et al.
Radiation-induced tumors of the head and neck.
J Laryngol Otol 1995;109:346–9.
493L.A. Loevner, A.I. Sonners / Magn Reson Imaging Clin N Am 10 (2002) 467–493





















![[Paranasal sinus mycoses]](https://img.pdfslide.net/doc/110x75/6345ed21f474639c9b051166/paranasal-sinus-mycoses.jpg)







