Embed Size (px)
Citation preview

DOI: 10.1542/peds.2009-0357; originally published online December 21, 2009; 2010;125;e9Pediatrics
MarkestadAukland, Hallvard Reigstad, Terje Alsaker, Dag Moster, Rolv Terje Lie and Trond
Karen Rosendahl, Carol Dezateux, Kari Røine Fosse, Hildegunn Aase, Stein Magnusin Newborns
Immediate Treatment Versus Sonographic Surveillance for Mild Hip Dysplasia
http://pediatrics.aappublications.org/content/125/1/e9.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2010 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on May 29, 2013pediatrics.aappublications.orgDownloaded from
Immediate Treatment Versus SonographicSurveillance for Mild Hip Dysplasia in Newborns
WHAT’S KNOWN ON THIS SUBJECT: Recent observational andsmall randomized studies have indicated that active surveillancein stable but mildly dysplastic hips is appropriate in newborns;however, data have been lacking on accurate radiologicaloutcomes.
WHAT THIS STUDY ADDS: We report the long-term outcomes ofwatchful waiting for mild hip dysplasia.
abstractOBJECTIVE: We conducted a blinded, randomized, controlled trial toexamine whether mildly dysplastic but stable or instable hips wouldbenefit from early treatment, as compared with watchful waiting.
PATIENTS AND METHODS: A total of 128 newborns with mild hip dys-plasia (sonographic inclination angle [� angle] of 43°–49°) and stableor instable but not dislocatable hips were randomly assigned to re-ceive either 6 weeks of abduction treatment (immediate-treatmentgroup) or follow-up alone (active-sonographic-surveillance group). Themain outcome measurement was the acetabular inclination angle,measured by radiograph, at 1 year of age.
RESULTS: Both groups included 64 newborns, and there was no loss tofollow-up. With the exception of a small but statistically significantexcess of girls in the active-sonographic-surveillance group, therewere no statistically significant differences in baseline characteristicsbetween the 2 groups. The mean inclination angle at 12 months was24.2° for both groups (difference: 0.1 [95% confidence interval (CI):�0.8 to 0.9]), and all children had improved and were without treat-ment. The mean � angle was 59.7° in the treatment group and 57.1° inthe active-surveillance group for a difference of 2.6° evaluated after 1.5and 3months (95%CI: 1.8 to 3.4; P� .001). At 1.5months of age, the hipshad improved in all treated children but not in 5 children under activesurveillance (P � .06). Among the sonographic-surveillance group, 47%received treatment after the initial surveillance period of 1.5 months.
CONCLUSIONS: Active-sonographic-surveillance halved the number ofchildren requiring treatment, did not increase the duration of treat-ment, and yielded similar results at 1-year follow-up. Given a reportedprevalence of 1.3% for mildly dysplastic but stable hips, a strategy ofactive surveillance would reduce the overall treatment rate by 0.6%.Our results may have important implications for families as well as forhealth care costs. Pediatrics 2010;125:e9–e16
AUTHORS: Karen Rosendahl, MD, PhD,a,b Carol Dezateux,FMedSci,c Kari Røine Fosse, MD,d Hildegunn Aase, MD,d
Stein Magnus Aukland, MD,d Hallvard Reigstad, MD,e TerjeAlsaker, MD,e Dag Moster, MD, PhD,e Rolv Terje Lie, PhD,f
and Trond Markestad, MD, PhDe
aDiagnostic Radiology, Great Ormond Street Hospital forChildren, London, United Kingdom; bInstitute of SurgicalSciences and fDepartment of Public Health and Primary HealthCare, University of Bergen, Bergen, Norway; cMRC Centre ofEpidemiology for Child Health, UCL Institute of Child Health,London, United Kingdom; and Departments of dRadiology andePediatrics, Haukeland University Hospital, Bergen, Norway
KEY WORDSrandomized, controlled trial, hip dislocation, congenital, therapy
ABBREVIATIONSAI—acetabular indexAVN—avascular necrosisDDH—developmental dysplasia of the hip
This trial has been registered at www.clinicaltrials.gov(identifier NCT00843258).
www.pediatrics.org/cgi/doi/10.1542/peds.2009-0357
doi:10.1542/peds.2009-0357
Accepted for publication Jul 30, 2009
Address correspondence to Karen Rosendahl, MD, PhD, GreatOrmond Street Hospital for Children, Diagnostic Radiology, GreatOrmond Street, London WC1N 3JH, United Kingdom. E-mail:[email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2009 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
ARTICLES
PEDIATRICS Volume 125, Number 1, January 2010 e9 by guest on May 29, 2013pediatrics.aappublications.orgDownloaded from

Developmental dysplasia of the hip(DDH) is the most common musculo-skeletal disorder in infancy and variesin severity, ranging from neonatal hipinstability with or without associatedacetabular dysplasia to irreducibledislocation.1 In its severe form andeven with surgical treatment, DDH re-sults in shortening of the affected legand early osteoarthritis. Clinical testsfor DDH were described by Le Damanyand Saiget2 in 1910, Ortolani3 in 1937,Marx4 in 1938, Palmen5 in 1961, andBarlow6 in 1962. Although newbornscreening programs based on the Or-tolani3 and Barlow6 tests were intro-duced in the 1950s and 1960s withearly abduction splinting in 2% ofpatients who tested positive,7–9 theprevalence of late cases warrantingsurgery has remained stable, at ap-proximately 1 per 1000.10–12 Conse-quently, ultrasound has been intro-duced as an additional diagnostictest,13 and ultrasound screening is cur-rently offered to all newborns in Aus-tria and Germany14,15 and to newbornswith selected risk factors in theUnited Kingdom, Scandinavia, Italy,and France.16–22 These variations re-flect the uncertain evidence base forDDH screening policies, includingthat for treatment effectiveness, ashighlighted in 2 recent systematicreviews.23,24
These differences are important, be-cause 5% to 7% of all newborns aretreated after universal ultrasoundscreening, compared to 2% of new-borns treated with clinical screeningalone.15,25,26 This increase in abductionsplinting treatment is partly due to theinitiation of treatment of infants inwhom mild, stable hip dysplasia hasbeen identified. Furthermore, abduc-tion splinting is not without risk, withavascular necrosis (AVN) being re-ported in approximately 2% of thosepatients being referred before theage of 2 months.24,27,28 Although the
justification for such treatment hasbeen questioned, randomized trialsto inform clinical practice have beenlacking.23,24
We aimed to determine whether activesonographic surveillance would re-duce the likelihood of abduction splint-ing treatment without increasing therisk of persistent or more severe dys-plasia in later infancy.
PATIENTS AND METHODS
Participants
Participants recruited were healthyterm newborns born at the maternityunit at Haukeland University Hospital,Bergen, Norway, from February 1998 toApril 2003. Infants were eligible if mild
dysplasia in 1 or both hips was identi-fied on hip ultrasound. This ultrasoundis routinely undertaken at HaukelandUniversity Hospital after either the de-tection of clinical hip instability or theidentification of other risk factors forDDH (breech presentation at delivery,or first- or second-degree family his-tory of DDH) recognized at the new-born screening examination (Fig 1).The current practice is to review in-fants with mild dysplasia at 6 weeks ofage before initiating any treatment. In-fants with dislocated, dislocatable, orseverely dysplastic hips were excludedfrom this study because these infantswarrant immediate treatment. We alsoexcluded those who weighed �2.5 kg
FIGURE 1Routinemanagement of infants undergoing a neonatal hip screening at Haukeland University Hospitalduring the trial. a Family history in 1 or more first-degree relatives or 2 or more second-degreerelatives.
e10 ROSENDAHL et al by guest on May 29, 2013pediatrics.aappublications.orgDownloaded from

at birth or with major congenitalanomalies.
Newborn screening examinationswere undertaken at 1 to 3 days of ageby 1 of 8 physicians, who all had atleast 2 years’ pediatric experience.Each hip was classified as either sta-ble, instable (significant movement ofthe femoral head but not dislocatable),dislocatable (femoral head movescompletely out of the acetabulumduring the Barlow maneuver), ordislocated.
Ultrasound examinations were per-formed the following day at the mater-nity unit by 1 of 3 senior pediatric radi-ologists, who used a GE RT200machineand a linear 5-MHz transducer (Gen-eral Electric, Munchen, Germany). Hipmorphology and stability were as-sessed separately in each hip by usinga modified Graf technique to measurethe � angle (Fig 2).29,30 The � angle is ameasure of acetabular depth and wasused to classify each hip as either nor-mal (� �60°), immature (50° � � �60°), mildly dysplastic (43°� � � 50°),or severely dysplastic (� � 43°) (Fig3). Hip stability was assessed sono-graphically by performing a maneuversimilar to the Barlow test with the in-fant in a lateral position, and each hipwas classified as stable, instable, dis-locatable, or dislocated.
Mothers of eligible infants identified atultrasound in the maternity unit were
given written information about the trialby the same senior pediatric radiologist,and written informed consent was ob-tained according to our institutionalguidelines. The study was approved bythe Medical Research Ethics Committeeof the Western Region of Norway.
Once recruited, infants were referredto the pediatric outpatient depart-ment, where an experienced pediatricradiologist (Dr Rosendahl) performedanother ultrasound examination by us-ing a high-resolution ultrasound ma-chine (Acuson XP or ATL HDI 5000, lin-ear 5–10/12 MHz transducer) toconfirm sonographic mild dysplasia. Aclinical reexamination was under-taken by 1 of 4 senior pediatricians.
Interventions
Infants with persistent mild stable dys-plasia were then randomly assigned toreceive either immediate abductionsplinting treatment for at least 6weeks using a Frejka pillow splint withsonographic follow-up (immediate-
treatment group) or to receive activesonographic surveillance but no treat-ment before 6 weeks of age (active-sonographic-surveillance group). Astatistician (Dr Lie) performed the ran-domization as 1 single block by using acomputerized random-number genera-tor, and group assignments were put inopaque, sealed, and numbered enve-lopes. With the parent present but theradiologist absent, a senior nurseopened the envelopes in numerical se-quence for each infant at the outpatientclinic.
The treatment protocols included aspecific plan for discontinuing or initi-ating abduction treatment after 6weeks of age as appropriate in eachgroup. Thus, infants allocated to theimmediate-treatment group were fit-ted with a Frejka pillow splint, with re-view at 2 to 3 weeks of age for fittingand adjustment, and at 6 weeks and 3months for hip ultrasounds. Treatmentwas to be discontinued for those pa-
FIGURE 2Graf’s standard coronal section through the deepest part of the acetabulum illustrating key structures (A), the � angle (B), and the femoral headcoverage (C).
FIGURE 3Rosendahl’s modification of the Graf classification based on the standard coronal section: A, normal,� �60°; B, immature, 50°� � �60°; C, mild dysplasia 43°� � �50°; D, significant dysplasia, � �43°.
ARTICLES
PEDIATRICS Volume 125, Number 1, January 2010 e11 by guest on May 29, 2013pediatrics.aappublications.orgDownloaded from

tients with an � angle of �53° at 6weeks or �55° at 3 months. A studycoordinator was responsible for man-aging appointments and following upwith nonattendees.
Infants allocated to the active-sonographic-surveillance group werefirst reviewed at 6 weeks of age andagain at 3 months, with hip ultra-sounds performed on both occasions.Abduction splinting was not to bestarted before 6 weeks of age but wasto be initiated after 6 weeks for thosepatients with persistent dysplasia, asindicated by an � angle of �50° at 6weeks or�55° at 3 months.
The same pediatric radiologist per-formed the majority (80%) of follow-upultrasound examinations, and 2 otherpediatric radiologists performed the re-mainder. All treated infants had their ab-duction splinting device removed beforeentering the radiology department forimaging. In addition, parents were in-structed not to discuss their child’streatment with the radiologists to en-sure that the radiologists were blindedto the intervention assigned.
If treatment was to be continued be-yond 3 months in either group, theFrejka pillow splint was replaced witha simple, custom-fitted plastic cast thatprovided better support for the hips.Treatment was only discontinued whenthe � angle was normal (�60°), or theacetabular index (AI), assessed by stan-dardized anteroposterior pelvic radio-graphs at 6 months of age, was within2 SDs of the reference values for agepublished by Tonnis and Brunken31
(�35° at age 4.5 months [mean: 25°],�33° at age 5 to 6 months [mean 24°],and�30° at age 7 to 12months [mean:23°]) (Fig 4). Similar to the Frejka pil-low splint, the plastic cast was simpleto use, and could be removed easily tofacilitate diaper changes.
In this trial we tested the hypothesisthat acetabular depth at 1 year ofage would be greater in infants as-
signed to immediate treatment thanin those assigned to active sono-graphic surveillance.
Primary Outcome
The main aim of abduction splintingtreatment for DDH is to ensure that thehip is functionally unimpaired at skel-etal maturity, specifically through pro-moting normal acetabular develop-ment by ensuring hip stability andconcentric location of the femoralhead within the acetabulum. Becauseit was not feasible to specify outcomesat skeletal maturity for this trial andhip function at this age is not a reliableindicator of longer-term hip function,we selected the radiologic appearanceof the hip at the end of the first year oflife as a primary outcome. Specifically,we used the AI (Fig 4), assessed fromanteroposterior pelvic radiographsobtained with the child lying supine,with the thighs parallel and slightly el-evated to avoid hip adduction and apelvic tilt (in the sagittal plane).
All AI measurements were repeated bya fourth experienced radiologist (DrAase) who was blinded to the studygroup and previous findings and hadnot been involved in ultrasound as-sessments. On the basis of the AI, thehips were classified as normal (AIwithin 1 SD), acetabular ossificationdelay (1 SD� AI� 2 SD), or dysplasia
(AI � 2 SD), according to the classifi-cation system used by Tonnis andBrunken31(Fig 4).
Statistical Analysis
We assumed that a 3° difference in theAI between the 2 groups was clinicallyimportant at 1 year of age, which rep-resented approximately 1 normal SDat this age.10 A sample size of 128 pa-tients would have 80% power to detecta difference significant at the 5% level,and the size was increased to 140 par-ticipants in anticipation of a 10% lossto follow-up.
All analyses compared the immediate-treatment and active-sonographic-surveillance groups on an intention-to-treat basis. We used t tests tocompare continuous variables at base-line with �2 or exact tests when appro-priate. Both hips of each child weremeasured at several time points dur-ing the follow-up. In models estimatingthe difference in mean � angle duringthe follow-up period between theimmediate-treatment group and theactive-surveillance group, random ef-fects were used to account for corre-lations between the right and left hipsand between subsequent follow-up ob-servations of the same child. To lookfor consistency with the overall re-sults, we also performed analyses thatincluded only the initially worse hip
FIGURE 4On the basis of the AI, the hips were radiographically classified as normal (A), having delayed acetab-ular ossification (B), or dysplastic (C).
e12 ROSENDAHL et al by guest on May 29, 2013pediatrics.aappublications.orgDownloaded from

of each child and for each time pointduring follow-up. All analyses wereadjusted for gender. The statisticalanalyses were performed using the xt-mixed program in Stata 9 (Stata CorpLP, College Station, TX). All significancetests were 2 sided.
RESULTS
Patients
Figure 5 summarizes the flow of pa-tients through the trial.32,33 Therewas asmall but statistically significant ex-cess of girls in the active surveillancegroup, but with that exception no sta-tistically significant differences inbaseline characteristics between the 2groups (Table 1).
All infants in the immediate-treatmentgroup were treated according to theprotocol, and none were lost to follow-up. At 6 weeks of age, treatment wasdiscontinued in 24 infants and contin-
ued in 40 participants in whom the �angle was �53°. At 3 months of age,treatment was continued for an addi-tional 2 weeks for 5 infants in whomthe � angle was �55°. At 6 months,
treatment was restarted on 5 infantsfor whom splinting had been discon-tinued at 6 weeks because pelvic ra-diographs revealed the presence ofdysplasia as defined by an AI of �2SDs above the mean. All 5 infants haddiscontinued treatment by 1 year ofage.
All infants in the active-sonographic-surveillance group were treated ac-cording to the protocol. No infants inthis group received abduction splint-ing treatment before 6 weeks of age,and none were lost to follow-up. Withthe exception of 1 infant who was re-viewed at 8 weeks, all patients wereexamined at 6 weeks of age. Abductionsplinting was initiated for 12 infants inwhom the � angle was �50°, for anadditional 12 infants in whom the� an-gle was �55° at the 3-month review,and for 1 infant who was seen at 10weeks. At 6 months, treatment was ini-tiated for the first time in 5 infants inwhom the AI was �2 SDs above themean. All 5 infants had discontinuedtreatment by 1 year of age.
Themedian treatment duration was 12weeks (range: 6–24 weeks) in boththe immediate-treatment and active-sonographic-surveillance groups (Fig
FIGURE 5Flow of participants through the trial as shown in CONSORT (Consolidated Standards of ReportingTrials) format.
TABLE 1 Baseline Characteristics According to Treatment Allocation
Characteristic Immediate-TreatmentGroup (n� 64)
Active-SurveillanceGroup (n� 64)
Girls, n (%) 43 (67) 54 (84)a
Birth weight, mean (SD), g 3686 (465) 3758 (529)Family history of DDH, n (%)
�1 first- degree relative 23 (36) 23 (36)�2 second-degree relative 6 (9) 10 (16)
Breech presentation at delivery 8 (13) 6 (9)Findings on first clinical examination, n (%)At least 1 instable hip 18 (28) 14 (22)Bilateral instable hips 7 (10.9) 7 (10.9)Hip instability on clinical reexamination, n (%)At least 1 hip 14 (22) 13 (20)Both hips 7 (11.5) 9 (14.5)Sonographic hip instability, n (%)At least 1 hip 52 (81) 45 (70)Both hips 31 (48.4) 30 (46.9)Acetabular morphology
� angle worse hip, mean (SD), ° 47.0 (1.7) 47.0 (1.8)a P� .04.
ARTICLES
PEDIATRICS Volume 125, Number 1, January 2010 e13 by guest on May 29, 2013pediatrics.aappublications.orgDownloaded from
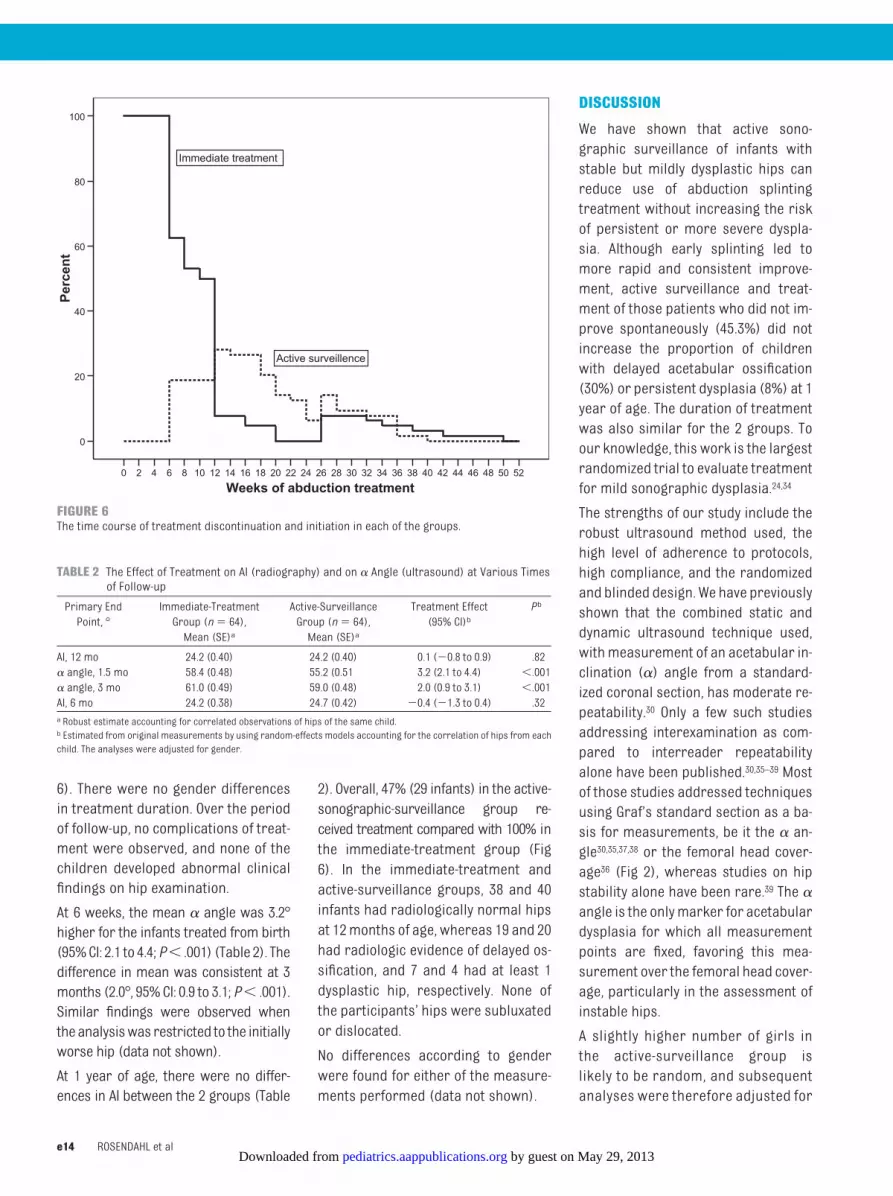
6). There were no gender differencesin treatment duration. Over the periodof follow-up, no complications of treat-ment were observed, and none of thechildren developed abnormal clinicalfindings on hip examination.
At 6 weeks, the mean � angle was 3.2°higher for the infants treated from birth(95%CI: 2.1 to 4.4;P� .001) (Table 2). Thedifference in mean was consistent at 3months (2.0°, 95%CI: 0.9 to 3.1;P� .001).Similar findings were observed whentheanalysiswas restricted to the initiallyworse hip (data not shown).
At 1 year of age, there were no differ-ences in AI between the 2 groups (Table
2). Overall, 47% (29 infants) in the active-sonographic-surveillance group re-ceived treatment compared with 100% inthe immediate-treatment group (Fig6). In the immediate-treatment andactive-surveillance groups, 38 and 40infants had radiologically normal hipsat 12months of age, whereas 19 and 20had radiologic evidence of delayed os-sification, and 7 and 4 had at least 1dysplastic hip, respectively. None ofthe participants’ hips were subluxatedor dislocated.
No differences according to genderwere found for either of the measure-ments performed (data not shown).
DISCUSSION
We have shown that active sono-graphic surveillance of infants withstable but mildly dysplastic hips canreduce use of abduction splintingtreatment without increasing the riskof persistent or more severe dyspla-sia. Although early splinting led tomore rapid and consistent improve-ment, active surveillance and treat-ment of those patients who did not im-prove spontaneously (45.3%) did notincrease the proportion of childrenwith delayed acetabular ossification(30%) or persistent dysplasia (8%) at 1year of age. The duration of treatmentwas also similar for the 2 groups. Toour knowledge, this work is the largestrandomized trial to evaluate treatmentfor mild sonographic dysplasia.24,34
The strengths of our study include therobust ultrasound method used, thehigh level of adherence to protocols,high compliance, and the randomizedand blinded design. We have previouslyshown that the combined static anddynamic ultrasound technique used,withmeasurement of an acetabular in-clination (�) angle from a standard-ized coronal section, has moderate re-peatability.30 Only a few such studiesaddressing interexamination as com-pared to interreader repeatabilityalone have been published.30,35–39 Mostof those studies addressed techniquesusing Graf’s standard section as a ba-sis for measurements, be it the � an-gle30,35,37,38 or the femoral head cover-age36 (Fig 2), whereas studies on hipstability alone have been rare.39 The �angle is the onlymarker for acetabulardysplasia for which all measurementpoints are fixed, favoring this mea-surement over the femoral head cover-age, particularly in the assessment ofinstable hips.
A slightly higher number of girls inthe active-surveillance group islikely to be random, and subsequentanalyses were therefore adjusted for
5250484644424038363432302826242220181614121086420
Weeks of abduction treatment
100
80
60
40
20
0
Perc
ent
Immediate treatment
Active surveillence
FIGURE 6The time course of treatment discontinuation and initiation in each of the groups.
TABLE 2 The Effect of Treatment on AI (radiography) and on � Angle (ultrasound) at Various Timesof Follow-up
Primary EndPoint, °
Immediate-TreatmentGroup (n� 64),Mean (SE)a
Active-SurveillanceGroup (n� 64),Mean (SE)a
Treatment Effect(95% CI)b
Pb
AI, 12 mo 24.2 (0.40) 24.2 (0.40) 0.1 (�0.8 to 0.9) .82� angle, 1.5 mo 58.4 (0.48) 55.2 (0.51 3.2 (2.1 to 4.4) �.001� angle, 3 mo 61.0 (0.49) 59.0 (0.48) 2.0 (0.9 to 3.1) �.001AI, 6 mo 24.2 (0.38) 24.7 (0.42) �0.4 (�1.3 to 0.4) .32a Robust estimate accounting for correlated observations of hips of the same child.b Estimated from original measurements by using random-effects models accounting for the correlation of hips from eachchild. The analyses were adjusted for gender.
e14 ROSENDAHL et al by guest on May 29, 2013pediatrics.aappublications.orgDownloaded from

gender, although no differences ineither AI or � angles were found be-tween genders at follow-up. Becausethe parents could not be blinded tothe intervention allocation, it is pos-sible that they could have disclosedthis information to the staff respon-sible for taking the outcome radio-graph; however, because the report-ing radiologist was blinded toallocation and had no direct contactwith families, we consider the out-come assessments to be unbiased.
Previous studies have shown thatmostimmature acetabular resolve physio-logically during the first weeks of life,and that the acetabular inclination asmeasured by the � angle reaches aplateau after 2 to 3 months of age.10,40
Our results are consistent with theseobservations and also demonstratethat acetabular maturation acceler-ates if treatment is given during thefirst 6 weeks of life. Although 5 infantsunder active surveillance in this studydeteriorated from birth to 6 weeks ofage, rapid improvement was seen af-ter the treatment was initiated. Inter-estingly, acetabular maturation wasnot different for the 2 groups by 12months of age. Residual immaturity asmeasured by the AI was, however,demonstrated in more than one thirdof the patients.31
Our results support observationsmade by Sampath et al41 in a study thatincluded 35 infants with stable, butmildly dysplastic hips. All but 2 in-
fants improved without treatmentand none required surgical interven-tion (follow-upwas not noted). Wood etal34 used a randomized design to exam-ine the effect of 6 weeks of early treat-ment in 44 infants (29 girls) with dys-plastic but stable hips who presentedat the age of 2 to 6 weeks. Although thefemoral head coverage as measuredby ultrasound increased from an aver-age of 32.8% to 54.3% in the splintedgroup during the first 3 months com-pared to 36.7% to 48.6% in the un-splinted group, there was no differ-ence in AI by 3 months and 2 years ofage. It is reasonable to believe that alow femoral head coverage of 32% instable hips corresponds to mild dys-plasia as assessed by an� angle of 43°to 50°.42 Neither of the 2 studies re-ported details of the final AIs; the re-searchers reported only that theywere within the “normal range” for thechildren’s age.
The threshold for initiating or continu-ing treatment at 6 weeks of age orlater was not clearly justified by anyestablished risks of later dysplasia ordislocation. This result reflected a lowthreshold for treatment that is gener-ally considered more acceptable inearly infancy despite the small risk ofAVN, which is typically reported in 2%of treated infants after early referral.28
Our study lacked power to comparecomplication rates between the 2groups. Furthermore, there has beenan insufficient duration of follow-up tocomment on the risk of AVN, which was
not seen in any infant. On the otherhand, treatment initiated after 2months of age is associated withhigher rates of AVN, up to 11% accord-ing to a recent meta-analysis.28 It isrecognized that abduction splintingimmobilizes the infant, impedes dailycare, and might, therefore, interferewith the relationship between infantsand their carers.43 Of interest is thefact that watchful waiting resulted inlater treatment as well as less treat-ment, potentially allowing motherstime to care for their infants and es-tablish breastfeeding. Conversely, de-laying treatment may limit an increas-ingly mobile child. We were unable toassess these more qualitative but im-portant outcomes in this trial. How-ever, the decision to treat should takeinto account the positive and negativeeffects of treatment from a variety ofperspectives.
CONCLUSIONS
Although universal treatment frombirth of infants with stable but mildlydysplastic hips may cause more rapidnormalization, surveillance and treat-ment reconsideration at the age of 6weeks did not result in more abnormalhips at 1 year of age. Given a reportedprevalence of 1.3% for mildly dysplas-tic but stable hips, a strategy of activesurveillance would reduce the overalltreatment rate by 0.6%. Our resultsmay have important implications forfamilies as well as for health carecosts.
REFERENCES
1. Aronsson DD, Goldberg MJ, Kling TF Jr, RoyDR. Developmental dysplasia of the hip. Pe-diatrics. 1994;94:201–208
2. Le Damany P. La luxation congenitalede la hanche. Etudes d’anatomie compareed’anthropogenienormaleet pathologique, de-ductions therapeutique. Alcan, Paris 1912
3. Ortolani M. Un segno noto e sua importanzaper la diagnosi precoce di prelussazionecongenita dell’anca. Pediatria (Napoli).1937;45:129–136
4. Marx VO. New observations in congenitaldislocation of the hip in the newborn.J Bone Joint Surg. 1938;20:1095
5. Palmen K. Preluxation of the hip joint. Diag-nosis and treatment in the newborn and thediagnosis of congenital dislocation of the hipjoint in Sweden during the years 1948–1960.Acta Paediatr Suppl. 1961;50:1–71
6. Barlow TG. Early diagnosis and treatment ofcongenital dislocation of the hip. Proc R SocMed. 1962;56:804–806
7. Barlow TG. Congenital dislocation of thehip. Nurs Mirror Midwives J. 1968;126(13):25
8. Catford JC, Bennet GC, Wilkinson JA. Con-genital hip dislocation: an increasing andstill uncontrolled disability? Br Med J. 1982;285(6354):1527–1530
9. Chan A, Cundy PJ, Foster BK, Keane RJ,Byron-Scott R. Late diagnosis of congenitaldislocation of the hip and presence of ascreening programme: South Australian
ARTICLES
PEDIATRICS Volume 125, Number 1, January 2010 e15 by guest on May 29, 2013pediatrics.aappublications.orgDownloaded from

population-based study. Lancet. 1999;354(9189):1514–1517
10. Burger BJ, Burger JD, Bos CF, ObermannWR, Rozing PM, Vandenbroucke JP. Neonatalscreening and staggered early treatmentfor congenital dislocation or dysplasia ofthe hip. Lancet. 1990;336:1549–1553
11. Mitchell GP. Problems in the early diagnosisand management of congenital dislocation ofthe hip. J Bone Joint Surg Br. 1972;54:4–12
12. Hiertonn T, James U. Congenital dislocationof the hip. Experiences of early diagnosisand treatment. J Bone Joint Surg Br. 1968;50:542–545
13. Graf R. The diagnosis of congenital hip-jointdislocation by the ultrasonic Comboundtreatment. Arch Orthop Trauma Surg. 1980;97:117–133
14. Grill F, Muller D. [Ergebnisse des Huftultra-schallscreenings in Osterreich.][in Ger-man]. Orthopade. 1997;26:25–32
15. von Kries R, Ihme N, Oberle D, et al. Effect ofultrasound screening on the rate of first op-erative procedures for developmental hipdysplasia in Germany. Lancet. 2003;362:1883–1887
16. Brown J, Dezateux C, Karnon J, Parnaby A,Arthur R. Efficiency of alternative policy op-tions for screening for developmental dys-plasia of the hip in the United Kingdom. ArchDis Child. 2003;88:760–766
17. Holen KJ, Tegnander A, Bredland T, et al. Uni-versal or selective screening of the neona-tal hip using ultrasound? A prospective,randomised trial of 15,529 newborn infants.J Bone Joint Surg Br. 2002;84:886–890
18. Rosendahl K, Markestad T, Lie RT. Ultra-sound screening for developmental dyspla-sia of the hip in the neonate: the effect ontreatment rate and prevalence of latecases. Pediatrics. 1994;94:47–52
19. Baronciani D, Atti G, Andiloro F, et al. Screen-ing for developmental dysplasia of the hip:from theory to practice. CollaborativeGroup DDH Project. Pediatrics. 1997;99:E5
20. Riboni G, Bellini A, Serantoni S, Rognoni E,Bisanti L. Ultrasound screening for develop-mental dysplasia of the hip. Pediatr Radiol.2003l;33:475–481
21. Ortore P, Fodor G, Silverio R, Milani C, Psen-ner K. [Ecografia dell’anca neonatale: stato
dell’arte e prospettive.]. Radiol Med(Torino). 1996;92:10–15
22. Rosendahl K, Toma P. Ultrasound in the di-agnosis of developmental dysplasia of thehip in newborns. The European approach. Areview ofmethods, accuracy and clinical va-lidity. Eur Radiol. 2007;17:1960–1967
23. Woolacott NF, Puhan MA, Steurer J, KleijnenJ. Ultrasonography in screening for devel-opmental dysplasia of the hip in newborns:systematic review. BMJ. 2005;330:1413
24. Shipman SA, Helfand M, Moyer VA, Yawn BP.Screening for developmental dysplasia ofthe hip: a systematic literature review forthe US Preventive Services Task Force. Pedi-atrics. 2006;117:e557–e576
25. Duppe H, Danielsson LG. Screening of neo-natal instability and of developmental dislo-cation of the hip. A survey of 132,601 livingnewborn infants between 1956 and 1999.J Bone Joint Surg Br. 2002;84:878–885
26. Altenhofen L, Allhoff PG, Niethard FU. [Hipultrasound screening within the scope ofU3–initial experiences][in German]. Z Or-thop Ihre Grenzgeb. 1998;136:501–507
27. Kalamchi A, MacEwen GD. Avascular necro-sis following treatment of congenital dislo-cation of the hip. J Bone Joint Surg Am.1980;62:876–888
28. Lehmann HP, Hinton R, Morello P, Santoli J.Developmental dysplasia of the hip practiceguideline: technical report. Committee onQuality Improvement, and Subcommittee onDevelopmental Dysplasia of the Hip. Pediat-rics. 2000;105:E57
29. Rosendahl K, Markestad T, Lie RT. Ultra-sound in the early diagnosis of congenitaldislocation of the hip: the significance of hipstability versus acetabular morphology. Pe-diatr Radiol. 1992;22:430–433
30. Rosendahl K, Aslaksen A, Lie RT, MarkestadT. Reliability of ultrasound in the early diag-nosis of developmental dysplasia of the hip.Pediatr Radiol. 1995;25:219–224
31. Tonnis D, Brunken D. [Differentiation of nor-mal and pathological acetabular roof anglein the diagnosis of hip dysplasia. Evaluationof 2294 acetabular roof angles of hip jointsin children]. Arch Orthop Unfallchir. 64:197–228, 1968
32. Moher D, Schulz KF, Altman DG. The CONSORTstatement: revised recommendations forimproving the quality of reports of parallel-
group randomised trials. Lancet. 2001;357:1191–1194
33. Altman DG, Schulz KF, Moher D, et al. Therevised CONSORT statement for reportingrandomized trials: explanation and elabora-tion. Ann Intern Med. 2001;134:663–694
34. Wood MK, Conboy V, Benson MK. Does earlytreatment by abduction splintage improvethe development of dysplastic but stableneonatal hips? J Pediatr Orthop. 2000;20:302–305
35. Bar-On E, Meyer S, Harari G, Porat S. Ultra-sonography of the hip in developmental hipdysplasia. J Bone Surg Br. 1998;80:321–324
36. Holen KJ, Terjesen T, Tegnander A, BredlandT, Saether OD, Eik-Nes SH. Ultrasoundscreening for hip dysplasia in newborns.J Pediatr Orthop. 1994;14:667–673
37. Roovers EA, Boere-BoonekampMM, GeertsmaTS, Zielhuis GA, Kerkhoff AH. Ultrasonographicscreening for developmental dysplasia of thehip in infants. Reproducibility of assessmentsmade by radiographers. J Bone Joint Surg Br.2003;85:726–730
38. Zieger M. Ultrasound of the infant hip. Part2. Validity of the method. Pediatr Radiol.1986;16:488–492
39. Andersson JE. Neonatal hip instability: nor-mal values for physiological movement ofthe femoral head determined by ananterior-dynamic ultrasound method. J Pe-diatr Orthop. 1995;15:736–740
40. Dunn PM, Evans RE, Thearle MJ, Griffiths HE,Witherow PJ. Congenital dislocation of thehip: early and late diagnosis and manage-ment compared. Arch Dis Child. 1985;60:407–414
41. Sampath JS, Deakin S, Paton RW. Splintagein development dysplasia of the hip: howlow can we go? J Pediatr Orthop. 2003;23:352–355
42. Falliner A, Schwinzer D, Hahne HJ, Hed-derich J, Hassenpflug J. Comparing ultra-sound measurements of neonatal hips us-ing the methods of Graf and Terjesen.J Bone Joint Surg Br. 2006;88:104–106
43. Gardner F, Dezateux C, Elbourne D, Gray A,King A, Quinn A. The hip trial: psychosocialconsequences for mothers of using ultra-sound to manage infants with developmen-tal hip dysplasia. Arch Dis Child Fetal Neo-natal Ed. 2005;90:F17–F24
e16 ROSENDAHL et al by guest on May 29, 2013pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2009-0357; originally published online December 21, 2009; 2010;125;e9Pediatrics
MarkestadAukland, Hallvard Reigstad, Terje Alsaker, Dag Moster, Rolv Terje Lie and Trond
Karen Rosendahl, Carol Dezateux, Kari Røine Fosse, Hildegunn Aase, Stein Magnusin Newborns
Immediate Treatment Versus Sonographic Surveillance for Mild Hip Dysplasia
ServicesUpdated Information &
lhttp://pediatrics.aappublications.org/content/125/1/e9.full.htmincluding high resolution figures, can be found at:
References
l#ref-list-1http://pediatrics.aappublications.org/content/125/1/e9.full.htmat:This article cites 42 articles, 8 of which can be accessed free
Citations
l#related-urlshttp://pediatrics.aappublications.org/content/125/1/e9.full.htmThis article has been cited by 6 HighWire-hosted articles:
Subspecialty Collections
eletal_systemhttp://pediatrics.aappublications.org/cgi/collection/musculoskMusculoskeletal Systemthe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
mlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhttables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2010 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on May 29, 2013pediatrics.aappublications.orgDownloaded from




























