Embed Size (px)
Citation preview
CLINICAL IXISIUNOLOGY ASD IhlMUNOPATHOLOGY 1, 53-68 (1972)
Immunological Studies on Heroin Addiction
I. Methodology and Application of a Hemagglutination Inhibition
Test For Detection of Morphine1
FRANK L. ADLER, CHI-TAN LIU AND DON H. CATLIN
Hemagglutination-inhibitition techniques have been applied to measure mor- phine in sera and urines. A rapid screening test and a quantitative test, each capable of detecting 25 pg morphine, have been described. The former allows analysis of 50 specimens/hr, and both tests require only basic laboratory equipment. Methadone does not interfere; “false positive” reactions occur in urines from patients receiving codeine, meperidine, or dihydromorphinone. Dextromethorphan interferes slightly; diphenoxylate and dextropropoxyphene interfere slightly but not consistently. Ingestion of large amounts of poppy seeds results in positive urine tests. The appli- cability of hemagglutination-inhibition and other serological tests to the recognition of heroin abuse has been discussed. It is concluded that hemagglutination-inhibi- tion merits consideration for the screening of specimens, and for the quantitation of morphine. The extreme sensitivity of hemagglutination-inhibition and other sero- logical tests highly qualify these procedures for use as exclusion tests.
Recent success in the preparation of antisera reactive with morphine (1) has created new opportunities for the study of heroin addiction. Among these is the application of highly sensitive and specific serological methods to the problem of drug detection. A radioimmunoassay, capable of detecting pico- gram amounts of morphine, has been described and applied (2-4) and a test employing an electron spin resonance label has been developed (5). We have previously reported that a hemagglutination-inhibition test displays sensitiv- ity similar to these serological tests (6) and have called attention to the rapid- ity and simplicity of this procedure. It is the purpose of this paper to describe the application of a semiquantitative hemagglutination-inhibition test (QHI) to clinical specimens, to introduce a rapid screening test (RST) procedure, and to present some general considerations regarding the application of serological methods to the detection of drugs. In subsequent papers we shall deal with the significance of the sensitive detection techniques to problems of recognition and treatment of heroin addiction, and shall present data in which the several methods of morphine detection will be compared.
’ This work has been supported by Contract DADA17-72C-2052, Department of the Army, U. S. Army Medical Research and Development Command, Washington, D. C.
53 Copyright @ 1972 by Academic Press, Inc. All rights of reproduction in any form reserved.

54
MATERIALS AND METHODS
Hemagglutination-inhibition (HI) tests employ a constant, limiting amount of antibody specific for a soluble antigen, and red cells (indicator cells) to which this antigen has been bound. Agglutination of the indicator cells by the antibody can be inhibited by admixture or prior addition of the soluble an- tigen. The sensitivity of the test, i.e., the smallest amount of soluble antigen that can be detected by its ability to inhibit agglutination, is determined primarily by how much antibody is used over and above the minimal agglu- tinating amount. In general, the limiting amounts of antibody are in the order of lo-' to 10m" pg A’, and soluble antigens (or haptens) can usually be detected in the nanogram or picogram range. Haptens of low molecular weight that are firmly bound by their antibodies are readily detected and measured in amounts close to the lower limit of this range.
The technical details of the HI test have been previously described (6), and additional information is provided in sections of this paper which deal specifically with the RST, and the QHI. With regard to the preparation of suit- able anti-carboxymethylmorphine (antiCMM) sera it seems worthy of men- tion that in our experience with I2 rabbits, 2 1 sheep, and 50 mice immuniza- tion beyond two injections (6) only occasionally increased the “titers” of the sera and that most of the sera obtained 5-8 weeks after the first injection were satisfactory for the HI test.
The equipment required for the tests in their present form consists of a clinical centrifuge, assorted serological pipettes, flasks, graduates, and tubes, disposable Pasteur pipettes, and components of the microtiter (Cooke Engi- neering Co., Alexandria, Virginia) system, specifically hemagglutination trays with V-shaped wells, either of the permanent (Lucite), or disposable (polyeth- ylene) types, pipette droppers calibrated to deliver 0.025 or 0.05 ml amounts per drop, and, optionally, a device that allows multiple simultaneous serial dilutions to be made in the wells of the hemagglutination trays (“mul- timicrodiluter”).
The diluent used is that previously described, namely 0.25% heated (56”C/30 min) normal rabbit serum in a 1: 1 mixture of 0.15 M NaCl and 0. I5 M phosphate buffered at pH 7.6. The suspending medium for the indicator cells is 1% normal rabbit serum prepared in the same buffered saline solution.
One addition to the materials previously described (6) is the optional substi- tution of formalinized sheep red cells for the sheep erythrocytes stored in ci- trate solution. Formalinized erythrocytes are prepared as described by Czismas (7). After the removal of formalin by exhaustive washing, such cells are treated with tannic acid and then coated with the conjugate of rabbit serum albumin-carboxymethylmorphine (CMM-RSA) exactly as previously
2 In conducting the research described in this report. the in\ estigators adhered to the “Guidv for Laboratory Animal Facilities and Care,” as promulgated by the Committee on the Guide fol- Laboratory Animal Facilities and Care of the Institute of Laboratory Animal Resources, National Academy of Sciences-National Research Council.

SEROLOGICAL TESTS FOR MORPHINE 55
described. The cells are then suspended in 1% normal rabbit serum (in phosphate buffered saline, pH 7.6) to yield a 15% suspension. This suspen- sion is tubed in convenient amounts, subjected to quick freezing in a Dry Ice- alcohol bath and stored at -70°C. Just prior to use the cell suspension is thawed at 37°C and, after centrifugation, the supernatant is discarded and replaced by sufficient fresh 1% normal rabbit serum to yield the working sus- pension of indicator cells (0.75% suspension). Such formalinized and coated cells are slightly less sensitive indicator cells than those freshly prepared but offer the advantages of a reagent that can be stored for at least 3 months.
The working suspension of indicator cells, whether freshly prepared or preserved cells are used, should be kept cold during the day’s work. If merthiolate (1: 10,000) is added to the suspending medium, these prepara- tions are perfectly stable for at least 4-7 days at 4°C. However, it is necessary and essential that prior to subsequent use the cells be sedimented by centrifu- gation and the supematant be replaced with fresh suspending medium. This step is necessary because a small amount of antigen leaks from the cells and inhibits hemagglutination by interception of antibody. The antigen that remains bound to the cells is sufficient to maintain agglutinability at a con- stant level. Glutaraldehyde (8) has also been used by us but while it yielded stable and sensitive indicator cell suspensions it required much larger amounts of CMM-RSA than the methods outlined above.
In applying HI tests to the detection of morphine in sera or plasma, we have found it convenient to remove interference by subjecting the sera, after an ini- tial fivefold dilution in phosphate buffered saline (pH 7.6), to a 15-min incuba- tion in a boiling water bath. Coagulated protein is then removed by centrifu- gation (20,OOOg for 30 min) and the test is performed on the clear supernatant. This procedure destroys the activity of antibodies that might react with the in- dicator system and also reduces the protein content of the specimen to a level compatible with HI tests.
EXPERIMENTAL
The Rapid Screening Test (RST)
To meet the demand for a simple, sensitive, and rapid diagnostic test suit- able for mass screening and requiring only basic equipment, a semiquantita- tive test procedure has been developed. It allows one person to analyze about 50 specimens per hour; the results can be read in 90-120 min after addition of the last reagent.
As shown in Fig. lA, 8 of the 96 wells in a standard disposable hemagglu- tination tray are used for each specimen. Urine that is free of turbidity and, sediment, preferably the clear supematant of a specimen that has been stored overnight at 4”c, is diluted tenfold by adding two drops (0.06 ml) of urine from a disposable Pasteur pipette to 0.6 ml of diluent in a suitable test tube. Avoid- ance of particulate matter, and the dilution eliminate nonspecific agglutina- tion of the indicator cells by the urine specimen. Using the same pipette, 0.03 ml (one drop) of the diluted urine is then delivered to each of the eight wells.

56 ADLER, LIlI AND CAI’LIN
These are arranged in four pairs, allowing for duplicate tests at three levels of test sensitivity (pairs l-3), and for a duplicate control test (pair 4) in which 0.025 ml of diluent is added to the diluted urine instead of antiserum. This control assures that the diluted urine is free of agglutinating activity which, if present, could mask a positive test for morphine, i.e., could cause a false nega- tive reaction.
With the aid of a calibrated pipette dropper that delivers 0.025 ml per drop anti-CMM serum in three different dilutions is added to wells 1, 2, and 3, respectively. The dilutions are chosen so that their agglutinating activity against the indicator cells can be inhibited by 2.5, 0.25, and 0.025 ng mor- phine (in 0.025 ml), respectively. These amounts correspond to 100, 10, or 1 ng morphine/ml of diluted urine or ten times these amounts per milliliter of undiluted urine, respectively. Once serum or diluent has been added to all the wells in a tray, mixing of the reagents is insured by gentle tapping and ro- tation of the tray on the bench surface.
After an incubation period of at least 10 min at room temperature the in- dicator cells are added from a calibrated pipette dropper that delivers 0.05 ml/drop, and the trays are once again tapped and rotated to insure mixing. After 90-120 min of incubation at room temperature the patterns of agglutina- tion are read and recorded.
It will be noted in Fig. 1A that specimen E, urine that contained 10 ng morphine/ml prior to dilution, inhibited hemagglutination by the highest of the three dilutions of anti-CMM serum, but failed to inhibit agglutination by the other two dilutions of anti-CMM serum. For the sake of convenience, this pattern is scored as positive at the + level. By the same token, specimens con- taining sufficient morphine to extend hemagglutination inhibition to the next higher concentration of anti-CMM serum are scored as ++ (specimen D, con-
taining 100 ng morphine/ml before dilution). Those samples which inhibit hemagglutination by all three doses of anti-CMM serum are scored as +-tS- (specimens A, B, and C, containing lo”, 104, and 10:’ ng morphine/ml, respec- tively, prior to dilution). The ready distinction between agglutination and inhibition of agglutination, the agreement between duplicates, and the ab- sence of agglutination in the control wells are all evident.
Urines which after tenfold dilution contain 0.2-2.0 ng morphine/ml may cause partial inhibition of agglutination, or show inhibition of agglutination in one but not in the other of the duplicate wells to which the most dilute anti- CMM solution has been added. The significance of such borderline results, recorded as +-, will be discussed later. It should be noted, however, that many urines can be used in the test in dilutions of 1: 2 or 1: 4 (instead of the routine 1: 10 dilution) and that it is a simple matter to repeat the test with such speci- mens at higher urine concentration and thus made more sensitive.
Finally, it should be stressed that the three levels of sensitivity, namely IO, 100, and 1000 or more rig/ml undiluted urine, were selected in an arbitrary fashion. Experience with the test may well suggest that analysis at one or two levels of sensitivity may satisfy the needs of a diagnostic test. This, of course, would further simplify and expedite the procedure.

SEROLOGICAL TESTS FOR MORPHINE 57
FIG. 1A. The rapid screening test (RST). Morphine was added to normal urine specimens to result in the following concentrations (pglml). A: 100, B: 10, C: 1.0, D: 0.1, E: 0.01, F: none. After each sample had been diluted tenfold, 0.03 ml dilution was placed into each of the eight wells in each set. Wells in the fourth and eighth columns then received 0.025 ml diluent (control), wells in columns three and seven received 0.025 ml anti-CMM serum (181-1) 1: 1600; those in columns two and six anti-CMM 1:400, and those in columns one and five anti-CMM 1: 100. See text for further detail.
The Quuwtitatioe Hemugglutiraation-Illhibitiorl Test (QHZ)
The quantitative test requires slightly more time and effort than the RST but yields data which allow estimation of the morphine content of a specimen within a SO-200% range of the true value. The required serial twofold dilu- tion series of each specimen is either prepared in a series of tubes from which 0.025-ml amounts are then transferred to the wells of a hemagglutination tray, or dilutions are made in the wells with the aid of a simple piece of equipment (Cooke Engineering Co.) which allows simultaneous dilution of up to 12 spec- imens. The initial dilution of each specimen is best chosen after a preliminary RST has indicated its approximate morphine content. An anti-CMM serum, diluted to give the test the desired level of sensitivity, is then added in 0.025 ml amounts to all wells and the trays are gently tapped and rotated to insure
58 ADLER. LIU AND CATLIN
Y
100 25 6 1.5 0.4 0.1 DIL
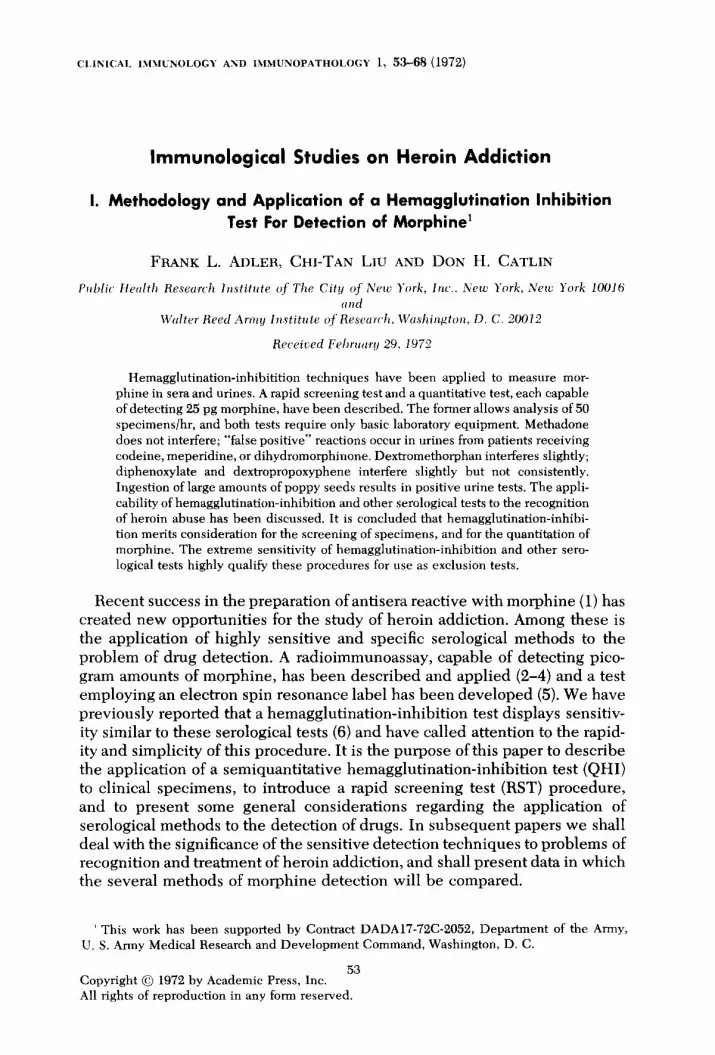
NANOGRAMS MORPHINE I ml FIG. 1B. The quantitative hemagglutination-inhibition test (QHI). The sensitivity ofthr test ah
a function of antibody concentration is demonstrated in this “checkerboard” titration. For details see text.
mixing of the reagents in the wells. The remainder of the procedure is exactly that described for the RST. The dilution of the anti-CMM serum to be used is determined by a preliminary titration such as that shown in Fig. 1B.
In this titration serial twofold dilutions of morphine, ranging from 100 to 0.1 rig/ml, were tested against a series of dilutions of an anti-CMM serum. It will be noted that the sensitivity of the test increased predictably as the anti-CMM serum was diluted. Serum diluted 1: 200 allowed the detection of morphine in solutions containing at least 3 ng morphine/ml. In contrast, hemagglutination by serum 1:SOO was effectively inhibited by a solution containing 0.4 ng of morphine/ml. At this level of test sensitivity the absolute amount of morphine detected in the 0.0025-ml sample was 0.01 ng or approximately 3.5 x lO-‘* moles of morphine. If, at this level of test sensitivity, the limiting dilution of an “unknown” specimen that inhibits HI is 1:20, it is concluded that the specimen contains 8 (4-16) ng morphine or morphine equivalents per milli- liter.
A typical application of the QHI test is depicted in Fig. 2. In this experi- ment the rate of disappearance of morphine from the serum of a rabbit that had been injected intracardially with 0.5 mg morphine/kg was measured. To compensate for the shortcomings of the serial twofold dilution method, each serum specimen obtained from the rabbit was titrated against three different dilutions of the anti-CMM serum chosen so that the end points (minimal amount of morphine inhibiting HA) were 6, 3, amd 0.8 ng morphine/ml. The plot of the data shows the triplicate experimental points and a straight line fitted to these points. The data indicate that during the period of 20-300 tin after injection morphine disappeared from the serum with an apparent half-life

SEROLOGICAL TESTS FOR MORPHINE 59
NANOGRAMS MORPHINE / ml SERUM
s:
0 2
8 8
g cl
i
FIG. 2. Clearance rate of morphine from serum. A I&kg rabbit received 1.0 mg morphine (alkaloid) in 10 ml saline intracardially at time 0.
of 47 min. This rate is quite comparable to that established for clearance of morphine from the serum of humans (3), rats (2), or dogs (9).
Acczcrucy of the Qzwntitntive Hemcl~~lutincltio72-Inlzibition Test (QHZ)
Since the QHI test applied to carefully prepared stock solutions of mor- phine serves as the standard both for the titration of anti-CMM sera and the examination of clinical specimens, a series of experiments was done to vali- date this procedure. In the experiment that yielded the data shown in Table 1, one anti-CMM serum, in two dilutions, was tested against four separately prepared stock solutions of morphine and also against two stock solutions of codeine. Independent duplicate twofold serial dilution series were made from the four morphine and two codeine replicate stock solutions.
The data presented in Table 1 show that differences between replicates and duplicates were within the expected limits of one dilution step. It will also be noted that with this particular anti-CMM serum, and within the range of dilu- tions in which it was used, a twofold decrease in antibody resulted in a four to eightfold decrease in the amount of hapten (morphine) that was required for inhibition of hemagglutination. Finally, it will be noted that with respect to this serum codeine was an approximately four times more effective inhibitor than morphine.
In yet other experiments some of the “strongest” of the addicts’ urines were used to estimate the error introduced when one and the same pipette is used to make all the twofold dilutions subsequent to the initial tenfold dilution. It was found that the apparent “titer” of such urines (some containing 300 pg morphine/ml) was at most one dilution higher when one pipette was em- ployed than when separate pipettes were used for each dilution.
Some of these urine specimens, together with stock solutions of morphine

60 ADLER. LIU AND CATLIN
Stock solution
Morphine Al A2 Bl B2 Cl c2 Dl D2
32” 1% 32 128
32-64 128-256 64 128-256
32-64 128-256 32-64 128-256 32-64 128
32 148-256
Codeine Al A2 Bl B2
64-128 512 64 512- 1024
64-128 512 128 512
” Reciprocal of highest dilution of stock solution that inhibited tlemagglutination. Use f&u stock solutions of morphine and two stock solutions of codeine were prepared independently Each contained 100 rig/ml. Each was serially diluted in duplicate.
in the usual diluent, were used as standards over a period of several months. They were stored at -20% and were subjected to repeated thawing and freezing. No indication of instability was observed. It should also be stressed that the presence of normal urine in morphine solutions does in no way inter- fere with the test, provided the urine has been cleared of particulate matter and its concentration is kept at 10% or less.
Reliability und Reproducibility of‘ the Rapid Scwening ?‘pst (RST)
Since the rapid screening test was specifically designed to serve as a prac- tical diagnostic procedure, and not as a research or precision tool, it appeared desirable to evaluate its performance under simulated field conditions. For this purpose a series of urines and sera from patients reporting to a metha- done clinic were coded by number. Some ofthese specimens were divided into two portions, each receiving a different number. All the specimens were then subjected but once to the RST procedure with emphasis on speed. Then, under more deliberate conditions and in duplicate assay, they were tested by QHI. Most of the specimens from this series were also examined by alternate serological and chemical tests for morphine, both in our laboratories and else- where. The results of these comparative studies will be published in a subsequent paper.
The results of RST and QHI tests on 197 specimens are shown in Fig. :3. It will be noted that those scored as +++ in the RST (putatively samples con- taining at least 1 pg morphine/ml) clustered around a mean of 5 ,ug/ml with a range of from 0.3 to 327 pg/ml. Specimens found to be ++ in the RST con-
SEROLOGICAL TESTS FOR MORPHINE 61
327660 -
61,920 -
20,400 -
- t St
RST
. URINE
o SERUM
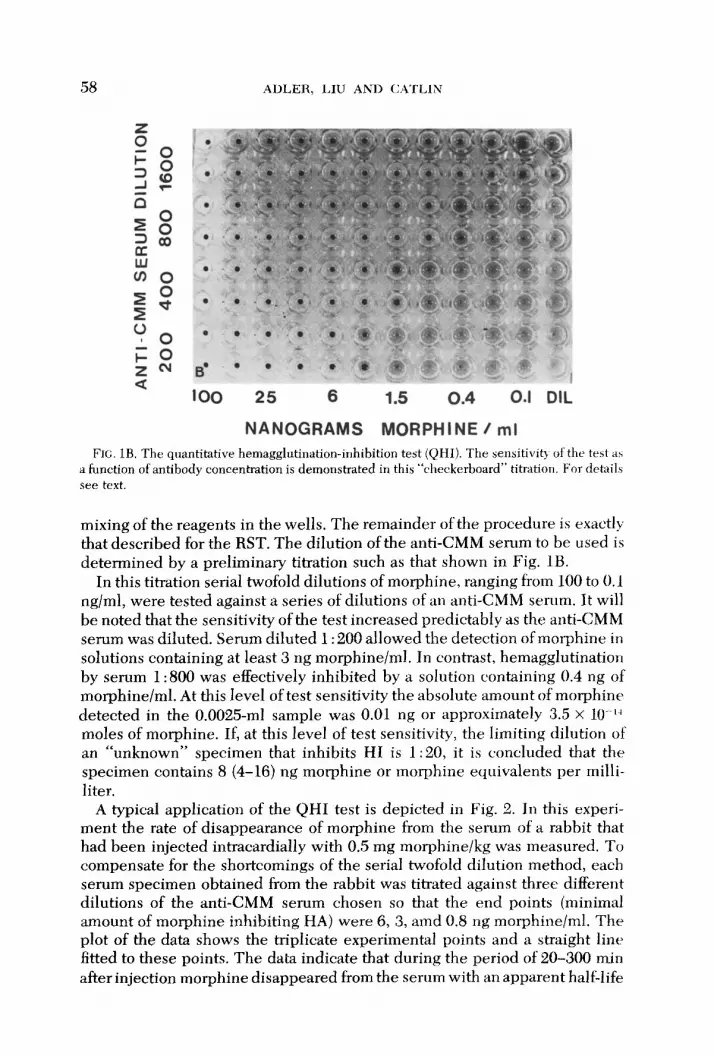
FIG. 3. Correlation between rapid screening test and quantitative hemagglutination-inhibition data. The results of tests on 59 sera and 138 urine specimens are plotted. The QHI titers are numerically identical with the estimated morphine concentration (nanograms) per milliliter of undiluted specimen.
tained 0.02-0.9 @g/ml with a mean of 0.16 pg/ml, and specimens scored as + in the RST were found to contain from <O.Ol to 0.3 pg/ml (mean of 0.02 pglml). It can also be seen that the presence of morphine, or its antigenic equivalents, was confirmed by the QHI test in all of the 93 specimens that had been scored as +++ or ++ in the RST, and also in 39 of the 46 specimens (85%) that had been classified +. The seven specimens (two sera and five urines) in the last group which, though + in the RST, could not be shown to contain at least 10 ng morphine/ml in the QHI, may be assumed to be samples with trace amounts of morphine only, or they may represent technical errors. We shall discuss the significance of + findings in the RST later, together with the meaning of the observation (Fig. 3) that 15 of the 58 specimens recorded as “-” in the RST (26%) were subsequently found to contain minimal amounts of morphine in the QHI tests, namely 0.01-0.03 kg/ml. It should be noted, however, with reference to this last group, that in compiling the data for Fig. 3 the + reactions from the RST were grouped with the “-” data.
The results of RST on split samples, involving 64 pairs of urine specimens, are shown in Fig. 4. These coded specimens had been tested at random as part of the general trial, and members of pairs were identified only after all the results had been recorded and the code had been broken. At that time one
62 ADLER, LIU AND CATLIN
I I - + +t ut
SPECIMEN A
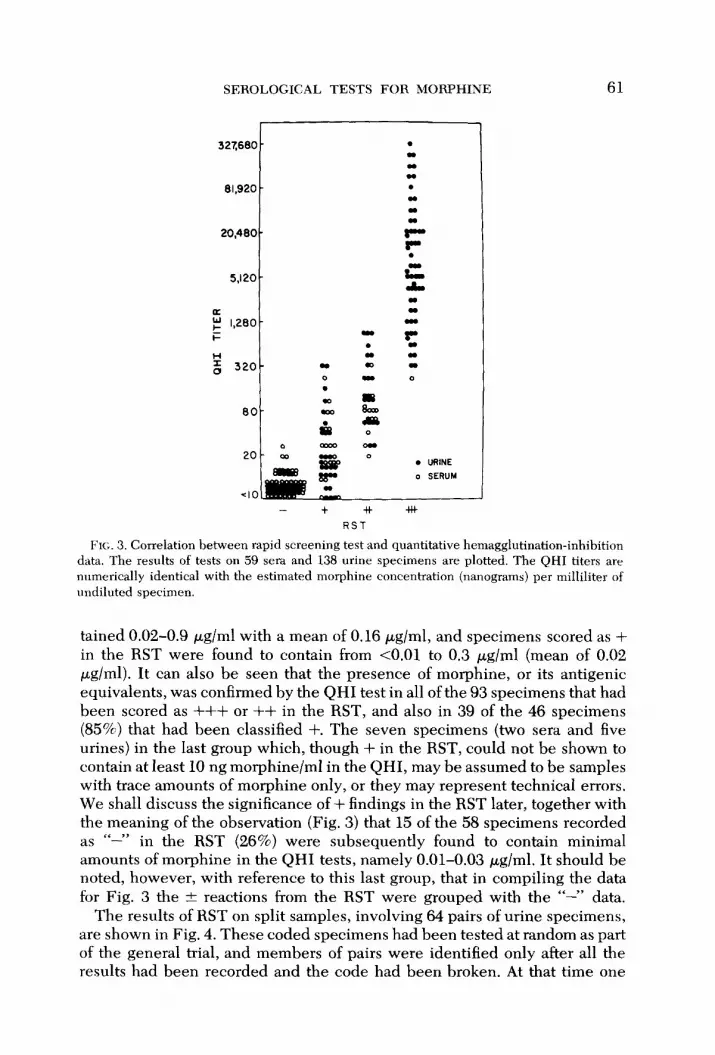
FIG. 4. Reproducibility of’ rapid screening test data. 64 pairs of “split samples” were a~~alyztxl.
sample of each pair was designated “A,” the other “B.” It can be seen that all of the +++ samples except one gave internally consistent results; in the one exception the “B” specimen was scored as ++. All the specimen scored I‘--” also yielded consistent results. Specimens scored + in the “A” series distrib- uted themselves between “--I’ and + in the “B” series, a result which is not surprising since subsequent QHI tests revealed that many of these contained only minimal amounts of morphine (lo-20 rig/ml). Disturbing, at face value, are the results obtained with those three pairs of samples which were nega- tive in the “B” series and -t+ in the “A” series. QHI tests confirmed the pres- ence of morphine in each of the three “A” specimens (320,60, and 60 nglml, respectively), and the absence of measurable amounts of morphine in the samples of the “B” series. It appears, therefore, that this discrepancy must have arisen from causes such as mislabeling or contamination of containers or pipettes.
Since one of the most frequent applications of diagnostic tests for morphine occurs in the supervision of patients in methadone maintenance programs, it appeared imperative that neither methadone taken orally in customary doses nor its metabolites give rise to false positive tests for morphine in urine or serum. We have reported previously that with the anti-CMM serum then in use, and after appropriate absorptions, the minimal inhibitory dose of metha- done was at least 3 x lo4 greater than the minimal inhibitory dose of morphine (6). Since then, Spector (2) has reported inhibition in the radioimmunoassay for morphine by methadone in doses 400 times greater than the required minimal dose of morphine. Examination of anti-CMM sera obtained from 12 rabbits and 1 sheep has shown that when assayed by QHI the majority of our sera resembled our original rabbit anti-CMM in that lo4 times or even more methadone was needed for inhibition than the minimal inhibitory dose of morphine, and that even in the worst of the sera this ratio was in excess of 1: 1000.
Most relevant to the immediate purpose on hand are the observations on sera and urines from patients who had taken prescribed oral doses of metha- done under supervision. Specimens were obtained 30 min to 48 hr after medi-

SEROLOGICAL TESTS FOR MORPHINE 63
cation and the presence of methadone in the specimens was ascertained in all but a few of the specimens. Doses of methadone taken ranged from lo-120 mg. Information on the last admitted use of heroin is included in the data.
It is apparent from the compilation of urine analyses in Table 2 that methadone taken in accepted doses by mouth does not give rise to false posi- tive RST or QHI tests for morphine provided a properly selected or appropri- ately absorbed anti-CMM serum is employed. Six plasma specimens from pa- tients given 50 to 120 mg methadone from 2-4 hr earlier also yielded uniformly negative tests for morphine.
The Effect of Other Drugs mad Dietary Supplements o11 RST und QHI Tests for Morphine
Knowledge of the immunochemistry of the morphine molecule is still too limited to allow predictions regarding the range of cross reactivities of anti- CMM antibodies. While appropriate studies are under way it was felt that with the practical application of the tests in mind an entirely empirical approach to the problem of cross reactivity would be useful. It also seemed more to the point to examine urines from patients taking drugs in preference
TABLE 2 URINE TESTS ON PATIENTS TAKING METHADONE"
Urine Methadone Heroin
Dose Time ___ Methadone Morphine
QHI specimen (ms) 04 Time TLC RST ndml
1 10 24 72 hr - (15 2 15 22 96 hr + Ik <15 3 15 24 72 hr N.T. - <15 4 20 20 22 hr + - <15 5 20 24 wk + - <15 6 25 24 96 hr + + 20 7 35 1 wk + - < 15 8 35 24 wk + - <15 9 40 24 wk + - <15
10 40 5 wk + - < 15 11 40 24 wk + - <15 12 50 24 (48 hr + - < 15 13 50 5.5 wk + - <15
14 60 0.5 wk + - < 15 15 60 32 wk + t <15 16 60 48 wk + - < 15 17 60 6 wk + * <15-15 18 75 2 wk + f <15 19 80 5 wk + - ‘c 15 20 80 24 wk + - < 15 21 85 23 wk + - <15 22 100 48 48 hr + * 15 23 100 3.5 wk + A < 15 - 15 24 100 24 <lwk N.T. - < 15 -
” Slethadone administration and urine collections were supervised. Time since last use of heroin was estimated by patient. QHI data expressed as nanograms of morphine (equivalents) per milliliter of urine.

64 ADLER, LILJ AND <:ATLIN
TABLE 3 RESUL~'S OF TESTS FOH MORPHINE ON Unri%s FHOW PATIEN'IX
TAKING ONE OH MORE OE‘ 'THE DRL’GS LISTEII
‘4rIfibiofic~s Ampicillin Oxacillin Cloxacillin Tetracycline Erythromycin Neomycin Nitrofurantoin Nalidixic acid Isoniazid Methenamine hippurate Methenamine mandelate
.~2tttitrr~u.s;t-c~s. cirlfi/~i.sf~ll,lill~(~.\.
trttd .u~/l~f~tntlrot,lirrlelic.a Diphenhydramine (Benadryl) Chlorpheniramine, phenyl-
propanolamine (Omade) Oxymetazoline (Afrin) Dextromethorphan’, glyceryi
guaiacolate (Robitussin DM) Chlorprophenpyridamine
(Chlor-Trimeton) Theophylline, ephedrine, phen~,-
barbital (Tedral) Theophylline, ethylenediamiue
l’ifamins
Folic acid Multi-vitamins Pyridoxine Vitamin B-complex
Sedatices, hypm~ticx. otd tmtlyrrilieers
Amobarbital Pentobarbital (Nembutal) Phenobarbital Secobarbital (Seconal) Chloral hydrate Meprobamate Methyprylon (Noludar) Chlordiazopoxide (Librium) Diazepam (Valium) Chlorpromazine (Thorazine) Prochlorperazine (Compazine) Thioridizine (Mellaril)
(Aminophylhne)
Cutllcrrticv trod Iumtic63
Diocytl Sodium Sulfosuccinate (Colace)
Cascara sagrada Castor oil
Narcotic, Awlgrsic,t Codeine” Meperidine” (Demerol) Dihydromorphinone* (Dilaudid) Morphine?’
Zfi.S~~~~/l~ltl~~~lf~~\ Digoxin Diphenylhydantoin (Dilantin) Methylphenidate (Ritalin) Benztropine mesylate (Cogentin) Trihexyphenidyl (Artane)
Tolbutamide (Orinase) Phenfonnin (DBI) Atropine Quinine Diphenoxylate” (Lomotil) Furosemide (Lasix) Amitriptyline (Elavil) Ferrous sulfate Ferrous gluconate
Notr-rwrcotic Anc~l~csics UIEC! clrdipyretics
Acetaminophen (Tylenol) Dextropropoxyphene5 (Darvon) Pentazocine (Talwin)
Insulin Stilbesterol Prednisone Dienestrol (Rentalon)
* False positive reaction for morphine. For each drug listed two to ten different specimens were tested.

SEROLOGICAL TESTS FOR MORPHINE 65
to doing tests on mixtures of drugs and normal urine since it appeared pos- sible that nonreacting drugs might be metabolized and excreted in a form reactive with anti-CMM antibodies.
Approximately 100 specimens from normal volunteers and about 250 speci- mens from hospitalized patients were examined. All of the latter were tested as coded unknowns and only after the results had been recorded were medi- cation charts consulted. Normal volunteers were requested to state what, if any, drugs they had taken within 48 hr. The results of this survey are listed in Table 3. Drugs that resulted in positive serological tests for morphine are iden- tified by asterisks.
Entirely expected were the strong positive reactions of urines from patients treated not only with morphine, but also from those given codeine, dihydro- morphinone (Dilaudid), and meperidine (Demerol) since these drugs have obviously close structural relatiopships to the immunizing antigen, carboxy- methylmorphine. Dextromethgrphan, an ingredient common to most cough syrups, consistently gave rise to false posit&e tests for morphine. Data presented in Table 4 indicate both the magnitude and the duration of this cross reaction.
Interference in the test by dextropropoxyphene (Darvon) or its excretion products was weak and inconsistent. For example, urine specimens collected from a volunteer who had taken twice 70 mg in 4 hr remained negative. This, of course, was only half of the recommended daily dose, and the interference may only be encountered if the total allowable dose has been taken. Individ- ual differences in drug excretion rates and possibily in type or amounts of the degradation products may also account for the inconsistent results. The posi- tive tests given by urine specimens from patients taking Lomotil were similarly weak and inconsistent. A single positive specimen from a patient who recalled only having taken phenobarbital can probably be discounted.
Interference in RST und QHZ by Food Products
In the survey of specimens from normal volunteers one, and only one indi- vidual repeatedly but inconsistently produced urine that gave weakly positive
TABLE 4 HEMAGGLUTINATION-INHIBITION BY URINE" AFTER INGESTION OF DEXTROMETHOFWHAN
Volume Hours (ml) RST QHI
0 - N.D. 2 110 + 0.03 5 120 + 0.03-0.06 9 150 + 0.03
13 loo * 0.008-0.015 27 - < 0.008
I‘ Volunteer ingested 5 ml of Robitussin-DM containing 3 mg dextromethorphan at 0 hr. QHI data are expressed as morphine equivalents (wg/ml urine).

66 ADLER, LIU AND C4TLIN
reactions for morphine. While it has not been possible, thus far, to identify the cause in this instance, this observation has led to an as yet preliminary survey of foods, primarily of vegetable origin. Volunteers were enlisted who agreed to furnish urine specimens before and from 2-12 hr after the ingestion of designated foods. The outstanding and, thus far, unique positive finding in this search is shown in the data of Table 5. It will be noted that 7/7 individuals who had eaten one to three helpings of pastry containing poppy seed filling developed strongly positive urine tests. Specimens obtained 4-5 hr after the meal contained 0.3-S kg morphine equivalents per milliliter of urine and all these specimens gave +++ reactions in the RST. It should be noted that the first two specimens (Table 5) were also examined by two additional sero- logical procedures (radioimmunoassay and electron spin resonance tests) and by two chemical methods (thin-layer chromatography and fluorometric assay). The serological procedures uniformly established the presence of “morphine” while the chemical methods yielded negative results.
It could also be shown that a saline extract of poppy seeds (5 gm seeds homogenized in 20 ml saline) contained in its aqueous phase the equivalent of about 1 Fug morphine/ml. Preliminary data from thin-layer chromatography suggest that while this extract contains some fast moving materials it is devoid of substances that resemble morphine in its Rf (10). The findings indicate, therefore, that poppy seeds contain material that is antigenically related to car- boxymethylmorphine. It must be kept in mind, of course, that this reactive material need not have any narcotic or other pharmacological activity,
Other plant or seed extracts that have been examined include black pepper (piperin), sesame, curry, and sunflower. All these yielded negative results but the presence of hemagglutinating activity in some seed extracts may well mask HI activity if it were present.
DISCUSSION
Some of the advantages of hemagglutination-inhibition techniques over other available or feasible serological tests for morphine are readily apparent.
TABLE 5 FALSE POSITIVE TEST FOH MOHPHINE AFTER IN~:LS~IOI\ ot POPW SEEDS
” Number of pieces of pastry containing poppy seed filling eaten. b Expressed as morphine equivalents (pgl m urine). Urine samples were collected immediate11 I
before and 4-5 hr after the meal.

SEROLOGICAL TESTS FOR MORPHINE 67
They include the lack of requirements for costly or potentially dangerous re- agents, and independence from expensive equipment. The minima1 amount of necessary handling of specimens tends to reduce the chances of errors. When quantitation is desired, the HI techniques provide the flexibility of “open end” tests because it is a simple matter to examine, in one operation, a broad range of dilutions of a given specimen. Quantitation by HI is, on the other hand, restricted in its accuracy by the error inherent in methods that employ serial twofold dilutions. Nevertheless, the data of Fig. 2 demonstrate that HI can be used for purposes such as the determination of clearance rates of morphine. If maximal precision is required, HI and radioimmunoassay can be advantageously used in tandem, the former to establish the approximate concentration, and the latter to attain ultimate precision. In data yet to be published, it will be shown that application of these two serological tech- niques to urine specimens yields results that are in very good agreement.
We have presented the detailed data concerning the occurrence of positive urine tests after the ingestion of poppy seeds (Table 5) in order to stress the need for proper interpretation of the HI or, for that matter, of any other serological test for morphine. The specificity of antibodies pertains to deter- minant groupings that may be shared by functionally unrelated substances. A positive serological test for morphine, no matter how strong, requires in- dependent confirmation by a nonserological procedure. The exquisite sensi- tivity of the HI test, in contrast, confers particular significance on negative results in properly controlled tests on urines or sera. If, for example, the an- tiserum employed in a test had been diluted to detect a minimum of 20 ng morphine/ml urine, a negative result clearly proves that the urine contains less than this amount of morphine. In another paper we shall present data on specimens from addicts in which urine and serum levels of morphine will be related to the time elapsed since the last admitted use of heroin. It is expected that analysis of these and of related data will provide guidelines to indicate what concentrations of morphine one might find in the urines of addicts who have abstained from heroin for 24,48, 72, or 96 hr. These data, in turn, will suggest the levels of sensitivity at which RST should be performed to meet the demands of a particular situation.
With regard to the requirement for independent confirmation of positive serological tests for morphine, strongly positive specimens containing 1000 rig/ml or more morphine per milliliter can readily be tested by thin-layer chromatography (lo), but at least 10 ml urine will be required to do so. Speci- mens containing morphine in low concentrations that are readily detected by serological methods, i.e., those containing nanogram amounts, present problems which, in some instances, could be resolved by appropriate extrac- tion and concentration procedures, and the application of highly sensitive and specific tests such as gas-liquid chromatography (11). In other instances it will undoubtedly be necessary to obtain additional specimens and, should none contain sufficient morphine for detection by nonserological tests, one may have to apply other criteria to determine whether drug abuse by the indi- vidual is indicated.

68 ADLER, LIU AND <:A?‘LIh
It seems fair to summarize these considerations by stating that the HI tests. and other serological procedures, are highly suitable for screening and for the purpose of excluding the possible abuse of opiates by an individual. The sim- plicity, rapidity, and sensitivity of the RST recommend its use in situations that require performance of a large number of tests. Whether applied to speci- mens from a general population or to those from patients in a methadone maintenance program, the elimination from further testing of all negative samples should reduce greatly the demands on laboratory space and effort.
The less than perfect reproducibility of RST data on urine specimens that contain less than 20 ng morphine/ml before, and thus less than 2 rig/ml after dilution (Figs. 3 and 4) results from the close approach to the lower limit of resolution of the test. As mentioned earlier, many urine specimens are suit- able for the RST when diluted two-or fourfold, rather than tenfold, Thus, samples that fall into the - to + range in the RST can be retested in higher concentrations to resolve uncertainties. Alternatively, one could sacrifict some of the test’s sensitivity and, by setting the lower limit of detectability to 30 rig/ml undiluted urine, avoid the entire problem.
Finally, even though our appropriate studies are still incomplete, prelimi- nary data strongly suggest that the HI tests detect glucuronide-bound as well as free morphine. Since substantial proportions of the excreted morphine are in the bound form, and because most currently used chemical screening tests avoid the hydrolysis step necessary to reveal bound morphine in these procedures, the detection of total morphine by HI would further increase the difference in sensitivity between HI and chemical tests.
ACKNOWLEDGMENTS
The authors gratefully acknowledge the cooperation of the Narcotics Treat- ment Administration, Washington, D. C, and the help and advice of Drs. S. .41- Askari, B. Davidow, V. Dole, W. Grace, and E. Mosbach. We are also indebted to Miss I. Kievman, Mrs. M. Stokes, and Mr. Wayne Hanson, and to Miss K. Kelly for their expert and dedicated technical and secretarial assistance, respectively. Credit is also due to Dr. U. Ahmed for her participation in some of the studies reported in this paper.
REFERENCES
1. SPECTOH, S. ANI) PARKEH, C. W. S’cim~ 168, 1347-1348, 1970.
2. SPECTOK, S. J. Phtrrfwcol fhy. T/xvx~~. 178, 253-258, 1971.
3. SPECTOH, S. 4ND &SELL, E. S. S’c,iorc,c, 174,421-422, 1971.
4. Ru~rv. J., P.4RKER. C. W., Ah’D WILLIAMS. R. C. Clirl. Hc.\. 19. 182. 1971.
5. ANONYMOUS. C&m. Etlg. ~~c~tc.s 49. 11-12. 1971.
6. ADLER, F. L. .AND Lru, C.-T. ,/. Immrlm/. 106, 1684-1685, 1971.
7. CZISMAS. L. PI-W. Sot. Esp. Bid. Med. 103, 157-160, 1960.
8. AVHAMEAS. S., TAL~DOU, B. ANI) CHUII.ON, S. Ir/ltl,cclrcjc,lrer,,i.vt,.!/ 6, 67-76, 1969. 9. ,IfULI$ S. J. AND WOoDS, L. A. J. Phtrmtrcd. E.v/,. Thvrrrj~. 136, 232-241, 1962.
LO. DAVIDOM’, B., PETRI, N. L. AND QUAME, B. ~\mer.,/. C/i/l. Ptrlhl. 50, 714-719, 1968.
11. WILKINSON, G. R. AND WAk, E. L. Rioc~/,cw. P/wrr,rtrc~~/. 18, 1435-1439, 1969.





























