Embed Size (px)
Citation preview
Downloaded from UvA-DARE, the Institutional Repository of the University of Amsterdam (UvA)http://dare.uva.nl/document/107671
Description ThesisFile ID 107671Filename thesis.pdf
SOURCE, OR PART OF THE FOLLOWING SOURCE:Type DissertationTitle Advances in colorectal surgeryAuthor J. WindFaculty Faculty of MedicineYear 2008Pages 247
FULL BIBLIOGRAPHIC DETAILS: http://dare.uva.nl/record/274001
Copyrights It is not permitted to download or to forward/distribute the text or part of it without the consent of the copyright holder(usually the author), other then for strictly personal, individual use. UvA-DARE is a service provided by the Library of the University of Amsterdam (http://dare.uva.nl)

Advances in colorectal surgery
Wind (Chris).indb 1Wind (Chris).indb 1 28-05-2008 15:44:2028-05-2008 15:44:20

The printing of this thesis was financially supported by:
Nycomed B.V., Olympus Nederland B.V., W.L. Gore & Associates, Janssen-Cilag B.V., Nutricia
Nederland B.V., Novartis Oncology, Stichting tot bijstand Tergooiziekenhuizen, Covidien
Nederland B.V., Storz, MediRisk, Academic Medical Centre, Eurotec B.V., Smiths Medical
Nederland B.V., J.E. Jurriaanse Stichting, Bauerfeind Benelux B.V., B-Braun Medical B.V.,
Johnson & Johnson Medical B.V., KCI Medical B.V., Integraal Kankercentrum Amsterdam
(IKA) / Comprehensive Cancer Centre Amsterdam (CCCA)
The CCCA is one of the nine Comprehensive Cancer Centres (CCCs) in the Netherlands
Its area is the north-western part of the Netherlands and involves 2.800.000 inhabitants,
17 general hospitals, two university hospitals and the Netherlands Cancer Institute. The
CCCs in the Netherlands have been founded to provide comprehensive and high-quality
cancer care close to home for all cancer patients. The CCCA provides and coordinates
a collaboration of all health care professionals and institutions involved in cancer and
palliative care. The CCCA functions as a centre of knowledge and quality care that helps
to improve cancer treatment, patient care and clinical research as well as prevention of
cancer and decrease of cancer mortality.
Part of the studies in this thesis was financially supported by a grant from ZonMw.
Advances in colorectal surgery, Thesis, University of Amsterdam, the Netherlands
Copyright © 2008 Jan Wind, the Netherlands
No part of this thesis may be reproduced, stored or transmitted in any form or by any
means without prior permission of the author
Cover/ lay-out, printed by: Buijten and Schipperheijn, Amsterdam
ISBN- 978-90-9023243-0
Wind (Chris).indb 2Wind (Chris).indb 2 28-05-2008 15:44:2128-05-2008 15:44:21

Advances in colorectal surgery
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad van doctor
aan de Universiteit van Amsterdam
op gezag van de Rector Magnificus
prof. dr. D.C. van den Boom
ten overstaan van een door het college voor promoties ingestelde
commissie, in het openbaar te verdedigen in de Agnietenkapel
op vrijdag 27 juni 2008, te 14.00 uur
door
Jan Wind
geboren te Hilversum
Wind (Chris).indb 3Wind (Chris).indb 3 28-05-2008 15:44:2128-05-2008 15:44:21

PromotiecommissiePromotorProf. dr. W.A. Bemelman
Co-promotoresProf. dr. D.J. Gouma
Dr. J.F.M. Slors
Overige ledenProf. dr. M.A. Cuesta
Prof. dr. M.W. Hollmann
Prof. dr. F.J.W. ten Kate
Prof. dr. D.J. Richel
Dr. C.H.C. Dejong
Faculteit der Geneeskunde
Wind (Chris).indb 4Wind (Chris).indb 4 28-05-2008 15:44:2128-05-2008 15:44:21

“It is not the strongest of the species that survives,
nor the most intelligent that survives. It is the one
that is the most adaptable to change”
Charles Darwin (1809-1882)
Aan mijn ouders
Wind (Chris).indb 5Wind (Chris).indb 5 28-05-2008 15:44:2128-05-2008 15:44:21

Wind (Chris).indb 6Wind (Chris).indb 6 28-05-2008 15:44:2128-05-2008 15:44:21

7
Table of contents
General introduction and outline of the thesis 9
PART I Fast track colorectal surgery 23
Chapter 1 Fast track perioperative care programmes in colonic surgery 25
Chapter 2 Systematic review of enhanced recovery after surgery
(‘Fast Track’) programmes in colonic surgery 39
Chapter 3 Implementation of a fast track perioperative care programme:
what are the difficulties? 55
Chapter 4 Systematic review of laparoscopic versus open colonic resection
within a fast track perioperative care programme 71
Chapter 5 Perioperative strategy in colonic surgery; LAparoscopy and/or
FAst track multimodal management versus standard care
(LAFA trial). Design and rationale of a randomised controlled
multicentre trial 87
PART II Complications in colorectal surgery 99
Chapter 6 Installation of the pneumoperitoneum; technique and
complications 101
Chapter 7 Medical liability insurance claims on entry-related complications
in laparoscopy 117
Chapter 8 Laparoscopic reintervention for anastomotic leakage after
primary laparoscopic colorectal surgery; a comparative study 129
Chapter 9 S taple line failure using the Proximate® 100 mm linear cutter 139
Chapter 10 Temporary closure of the open abdomen; a systematic review
on delayed primary fascial closure in patients with an open
abdomen 147
Chapter 11 Single-stage closure of enterocutaneous fistula and stomas in
the presence of large abdominal wall defects using the
components separation technique 165
Wind (Chris).indb 7Wind (Chris).indb 7 28-05-2008 15:44:2228-05-2008 15:44:22

8
PART III Prognostication in colorectal cancer 177
Chapter 12 A systematic review on the significance of extracapsular
lymph node involvement in gastrointestinal malignancies 179
Chapter 13 The prognostic significance of extracapsular lymph node
involvement in node positive patients with colonic cancer 197
Chapter 14 Circulating tumour cells during laparoscopic and open surgery
for primary colonic cancer in portal and peripheral blood 211
Appendices Summary and conclusions 225
Nederlandse samenvatting 233
Dankwoord 241
Curriculum vitae 245
Wind (Chris).indb 8Wind (Chris).indb 8 28-05-2008 15:44:2228-05-2008 15:44:22

General introduction and outline of the thesis
Wind (Chris).indb 9Wind (Chris).indb 9 28-05-2008 15:44:2228-05-2008 15:44:22
10
General Introduction
Laparoscopy and fast track perioperative care programmesTwo major developments in colorectal surgery since the nineties have been the introduction
of laparoscopic surgery and the implementation of multimodal fast track perioperative
care programmes. Both focus on an enhanced recovery after surgery, reduced morbidity
and a shorter hospital stay as compared to open surgery in a traditional perioperative care
setting.
Laparoscopic segmental colectomy was first described in 1991.1 Ever since a great deal
of effort has been made to establish its feasibility and safety particularly in segmental
colectomy for cancer. Several randomised trials comparing laparoscopic with open
segmental colectomy have indicated that laparoscopic surgery can be applied safely for
both benign and malignant diseases.2-7 Furthermore, laparoscopic surgery, in a traditional
perioperative care setting, was associated with less morbidity, less postoperative pain, a
faster postoperative recovery and a shorter hospital stay.2;8;9 More recently, it has been
shown that short term cancer related outcomes such as cancer-free resection margins and
the number of harvested lymph nodes, as well as long term cancer related outcomes such
as disease free survival are comparable between laparoscopic and open surgery.2
At the same time, enthusiasm was raised for the so-called fast track perioperative care
programme, also referred to as Enhanced Recovery After Surgery (ERAS®). This essentially
is a modification of the programme initially developed by the Danish surgeon Henrik
Kehlet.10-12 The multimodal and multidisciplinary programme, involving optimization
of several aspects of the perioperative management of patients undergoing segmental
colectomy, enables patients to recover faster resulting in an earlier discharge as compared
to the traditional perioperative care setting. Lengths of postoperative hospital stay of
two to three days after open segmental colectomy have been reported. Furthermore,
postoperative morbidity might be reduced in a fast track perioperative care setting.13-18
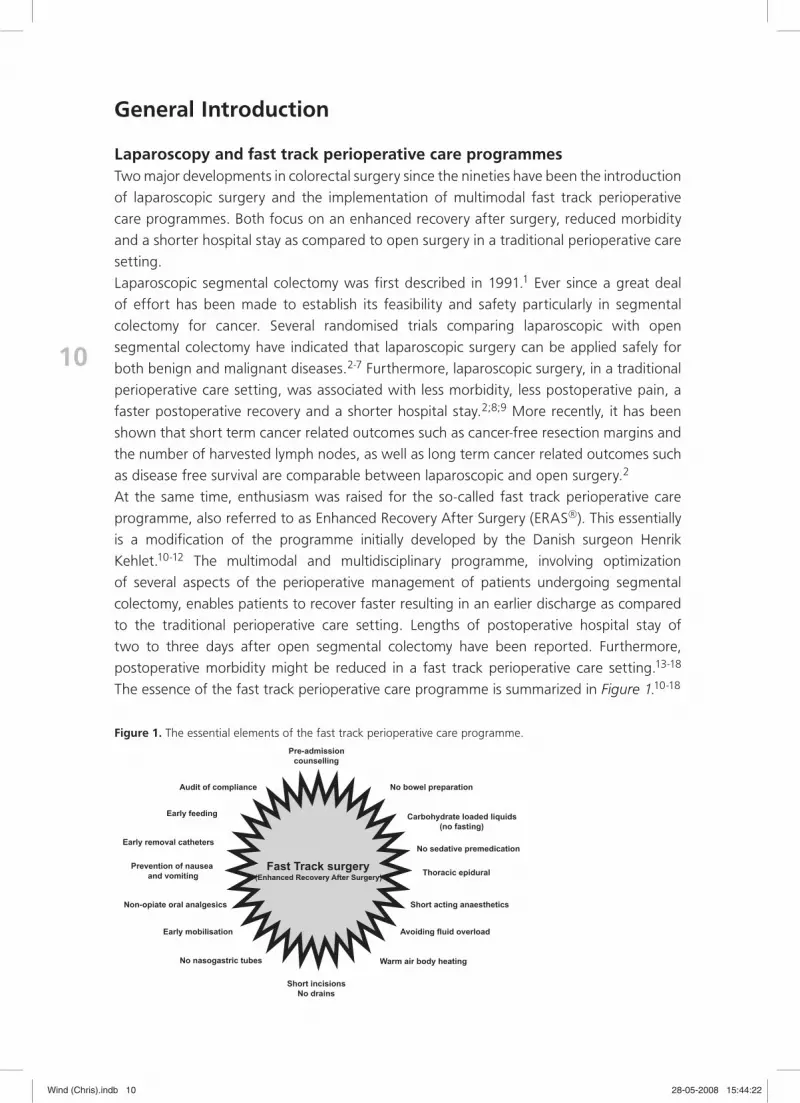
The essence of the fast track perioperative care programme is summarized in Figure 1.10-18
Fast Track surgery (Enhanced Recovery After Surgery)
Pre-admission counselling
No nasogastric tubes
No bowel preparation
Carbohydrate loaded liquids (no fasting)
No sedative premedication
Thoracic epidural
Short acting anaesthetics
Avoiding fluid overload
Short incisions No drains
Audit of compliance
Prevention of nausea and vomiting
Non-opiate oral analgesics
Early mobilisation
Warm air body heating
Early removal catheters
Early feeding
Figure 1. The essential elements of the fast track perioperative care programme.
Wind (Chris).indb 10Wind (Chris).indb 10 28-05-2008 15:44:2228-05-2008 15:44:22

11
Ch
apter 4
General intro
duction and outline of the thesis
During the early implementation, there were concerns regarding the number of
readmissions after fast track perioperative care programmes. Initial programmes of fast
track open colonic surgery had a planned two day postoperative hospital stay. This lead
to a high readmission rate (up to 20%).17 However, Andersen et al. reported that the
readmission rate declined when the planned postoperative hospital stay was increased
from two up to three days.19 Readmission rates decreased from 20% (period planned
hospital stay of two days) to 11% (period planned hospital stay of three days). The median
length of primary hospital stay was two days for the first group and three days for the
second, and median total hospital stay (including the readmissions) was three days in both
groups, respectively. Therefore, a reduction of hospital stay seems feasible with a lower
limit of postoperative day three. Several other studies have also reported no increase in
the number of readmissions after a primary hospital stay of three to four days.20;21
Nevertheless, despite the high level of evidence supporting the individual elements of the
fast track perioperative care programme, there seems to be no widespread implementation
of these elements. This is further demonstrated in a recent survey that investigated clinical
practice around colonic operations across 295 hospitals including several European
countries and the United States. Preoperative bowel clearance was still used in more than
85% of patients. A postoperative nasogastric tube was left in place in more than half
of the patients, to be removed about three days postoperatively. Furthermore, it took
three to four days until half of the patients first tolerated liquids and four to five days
until half of patients were eating and bowel movements were present.22 The delay in
integrating novel clinical management strategies within routine practice may be ascribed
to the time required to develop guidelines, the implementation process, the target group
of professionals, the patients, the cultural and social setting, and the organizational
and economic environment.23;24 Clearly, the issue of effective implementation and a
consequent high rate of compliance are essential in terms of problem solving, achieving
uniformity of patient management and finally postoperative recovery. Although fast track
perioperative care programmes have been evaluated in a variety of centres, little has
been published on the degree of compliance with such protocols when they have been
implemented. In a study by Maessen et al. the protocol compliance, regarding the individual
fast track elements, before and during the surgical procedure was high, but it was low in
the immediate postoperative phase.25 Also, there was a delay in the discharging of the
recovered patients. Patients fulfilled predetermined recovery criteria at a median of three
days after operation but were actually discharged at a median of five days after surgery.
Discharge delay and the development of major complications were the main reasons for
prolonged length of hospital stay. The phenomenon that the existence of a protocol is not
enough to enable discharge of patients on the day of functional recovery is also described
by others.26
In conclusion, despite the current enthusiasm regarding fast track perioperative care
programmes and laparoscopic surgery, there are only few data available that provide
evidence on the optimal combination (laparoscopic or open surgery and fast track or
traditional perioperative care) in terms of shorter lengths of hospital stay, number of
Wind (Chris).indb 11Wind (Chris).indb 11 28-05-2008 15:44:2228-05-2008 15:44:22

12
readmissions, reduced morbidity, quality of life and cost effectiveness.21;27-31 Furthermore,
the implementation of the evidence based individual fast track elements seems difficult.
The most effective way to implement the protocol is unclear. In addition to this, the effects
of protocol compliance on the outcome of fast track perioperative care programmes
remain unclear as well.
Laparoscopy-related complicationsAs mentioned before, laparoscopy has achieved broad acceptance nowadays and is a
fast expanding surgical discipline due to its short term advantages with respect to
open surgery.8;9;32 Although laparoscopy is favourable in terms of overall morbidity the
implementation of this new surgical discipline also implies the introduction of a new spectrum
of complications. These potential complications include those related to laparoscopy
itself and those related to the surgical procedure.33 Most of the laparoscopy-related
complications are associated with the entry into the peritoneal cavity, i.e. the creation of
the pneumoperitoneum and subsequently the introduction of the surgical instrumentation.
This remains a potentially dangerous first step, which is exclusively associated with the
laparoscopic approach. Several studies have demonstrated that 20 to 50% of all intra-
operative morbidity occurs during the creation of the pneumoperitoneum.34-36
Several techniques to establish the pneumoperitoneum have been described. Roughly,
entry techniques can be divided into two groups. The first group comprises entry
techniques performed without direct visual control, the so called blind-entry techniques.
The second group comprises of entry techniques performed under visual control. The
latter includes the open-entry technique and closed-entry techniques with optical
trocar devices. Concerning the prevention of entry related complications none of the
techniques is supported by solid evidence.37;38 Until today there is an ongoing debate
about the preferred technique, mainly between gynaecologists favouring the closed-entry
technique, and surgeons favouring the open-entry technique.36;39 Many general surgeons
suggest that the open-entry technique results in an equal amount of visceral lesions, but
significantly fewer vascular lesions compared to the closed-entry technique.35;39
Anastomotic leakageA feared complication after colorectal resection with anastomosis is anastomotic
insufficiency with subsequent leakage of intestinal contents into the abdominal cavity. The
frequency of anastomotic leakage following large bowel resection is quoted between 0.5
and 30%.40-44 Considerable variation is seen between surgeons but a realistic clinically
apparent leakage rate for experienced colorectal surgeons is likely to be between 3.4 and
6%.40-43 There seems to be no evident difference in the leak rate between laparoscopic
and open colorectal surgery. Furthermore, leak rates are broadly similar for all types of
bowel anastomosis proximal to the peritoneal reflection of the rectum, including small
bowel anastomosis.40;43;45 However, for anterior resection, clinically apparent leak rates
are higher, ranging between 2.9 and 15.3%.40;46;47 Moreover, a significant difference has
been demonstrated between leak rates following high and low anterior resection.40;48-50
Wind (Chris).indb 12Wind (Chris).indb 12 28-05-2008 15:44:2228-05-2008 15:44:22

13
Ch
apter 4
General intro
duction and outline of the thesis
Anastomotic insufficiency is a major cause of morbidity, including long intensive care
admittance, sepsis and several abdominal wall complications due to reinterventions and
wound infections. Apart from its immediate clinical consequences, anastomotic leakage
also has an independent negative association with survival after resections for colorectal
cancer.51;52 Postoperative mortality due to anastomotic leakage is considerable, ranging
between 6.0 and 39.3%.40 Moreover, the main cause of postoperative mortality after
elective segmental colorectal resections is anastomotic leakage.50;53-57
Several risk factors for anastomotic insufficiency have been identified, such as malnutrition,
weight-loss, long-course neo-adjuvant radiotherapy or neo-adjuvant chemo-radiotherapy,
preoperative steroid use, bowel obstruction, septic conditions, intra-operative blood loss
and intra-operative adverse events.56-58 Nevertheless, the most consistent factor to predict
leakage is low rectal anastomosis.40
In the traditional perioperative care setting it has been suggested that some elements
might reduce the leak rate. However, there is no evidence showing that preoperative
bowel preparation reduces the rate and consequences of leaks or any supporting the
use of drains when an anastomosis has been made outside the pelvis, though there is
evidence showing pelvic drainage may be important after anterior resection.59 The use
of covering stomas has not been shown to reduce leak rate but does mitigate the clinical
effects of leaks.40
Despite the identification of several potential risk factors the actual cause or contributing
factor(s) to anastomotic insufficiency is not always clear. With known risk factors aside,
surgical instruments used, in particular stapling and cutting devices, could also contribute
to anastomotic insufficiency if they malfunction or are used inappropriately.
Management of massive anastomotic leakage with peritonitis generally requires resuscitation
of the patient followed by prompt (re)laparotomy. However, with increasing numbers of
bowel resections being undertaken laparoscopically and the fact that over the past years
abdominal emergencies have been increasingly managed by laparoscopy, including those
patients with peritonitis the question arises whether postoperative complications in primary
laparoscopic operated patients should also be tackled laparoscopically.40;60-65 To date
reintervention for anastomotic leakage is generally performed by an open approach mainly
because of the fear of causing bowel injury due to distended bowel and lack of exposure for
cleaning the abdominal cavity. However, after primary laparoscopic surgery the previously
used trocar incisions can easily be re-used. Nevertheless, patients with an extensive ileus
and those with long standing peritonitis with pus pockets and inflammatory adhesions are
probably not amenable for laparoscopic treatment. Open-abdomen management might
be necessary because of abdominal compartment syndrome. Moreover, closure of the
abdominal wall after open reintervention might also be impossible due to extensive bowel
oedema after resuscitation. Therefore, in some cases full fascial closure is precluded by the
condition of the patient and open-abdomen treatment is started.
In general, there are three relatively frequent scenarios in which the operating surgeon
may decide to start open-abdomen treatment with temporary abdominal closure. These
are abdominal sepsis (peritonitis), intra-abdominal hypertension and following damage
Wind (Chris).indb 13Wind (Chris).indb 13 28-05-2008 15:44:2328-05-2008 15:44:23

14
control surgery.66-68 In these circumstances, the open abdomen needs to be closed
temporarily until the oedema has subsided and definitive closure can be attempted. Several
techniques and strategies for the temporary closure of the open abdomen are available.
These include the insertion of an (absorbable) mesh (with or without fluid suction system),
Bogota or intravenous bag, Velcro or zipper systems and in recent years, the abdominal
Vacuum Assisted Closure (VAC®) system was introduced.69-75
When the abdominal sepsis and visceral oedema has resolved and fascial closure of the
abdomen can be planned, the edges of the fascia have frequently retracted laterally due
to the continuous contraction of the oblique lateral abdominal musculature. This makes
full fascial closure of the abdomen difficult.66;67;76;77 When full fascial closure during
index admission is not possible, the fascial defect is left to heal by secondary intention
(granulation) or an absorbable mesh is used to close the abdomen without an attempt
to close the original fascia. Split thickness skin grafts are frequently used to cover the
wound and these planned ventral hernias can be corrected at a later stage.67;78 However,
due to the complicated course of these patients, the large defects are often associated
with enterocutaneous fistula and stomas.79 Closure of these fistula and stomas with
simultaneous closure of the large and contaminated abdominal wall defect requires
major surgery that includes extensive adhesiolysis, bowel resection with reanastomosing,
and closure of the abdominal wall. Ideally, a non-absorbable mesh is used to close the
abdominal wall.80 This technique ensures durable abdominal wall prosthesis. However,
application of a non-absorbable mesh is associated with an increased risk of infection,
especially if used in a contaminated surgical field.81;82 The use of an absorbable mesh
avoids infectious complications, but is only for temporary closure of the ventral hernia. The
most logical alternative for these large contaminated abdominal wall defects is the use of
autologous tissue repair,83 including the component separation technique, which was first
described by Ramirez et al.84 The separation of the muscle components of the abdominal
wall allows local advancement with complete continuity of the released muscle layers
over a greater distance compared to mobilisation of the entire abdominal wall as a block.
This enables closure of large abdominal wall defects under contaminated circumstances,
avoiding mesh infection.83
Prognostication after colorectal cancer resectionFor any individual patient, it is essential that their survival can be accurately predicted
and the likely sites of recurrence identified. The methods of prediction should be simple,
widely available, sensitive, specific and reproducible in any clinical setting. Mortality and
survival rates in colorectal cancer are highly influenced by the stage of the disease at
diagnosis, with the five-year survival rate dropping from 95% in Dukes A (T1-2N0M0) to
less than 10% in metastatic disease (Dukes D, T1-4N0-2M1).85 With respect to long-term
outcome haematogenous and lymphatic spread are the pathways of metastasis and are
therefore the most important factors associated with prognosis.86;87
Metastasis to regional lymph nodes, as determined by pathologic assessment, is one of
the factors that most strongly predict outcome following surgical resection, second only
Wind (Chris).indb 14Wind (Chris).indb 14 28-05-2008 15:44:2328-05-2008 15:44:23

15
Ch
apter 4
General intro
duction and outline of the thesis
to distant metastatic disease in importance.88-90 Besides the presence or absence of lymph
node metastasis per se, lymph node staging may be further refined by the identification
of different levels, the absolute number of lymph nodes with metastasis, the absolute
number of negative nodes, and the lymph node ratio (i.e. the number of involved nodes
over the total number of resected and identified nodes).91-94 Also, the presence of micro-
metastasis in lymph nodes has been identified as a prognostic factor.95;96
The prognostic value of extracapsular lymph node involvement has been studied for
several malignancies, including breast, oesophageal, prostate, vulva, bladder, lung, and
head and neck cancer.97-103 Extracapsular lymph node involvement is the extension
of cancer cells through the nodal capsule into the perinodal fatty tissue. Patients with
extracapsular lymph node involvement have a reduced overall and disease free survival in
these malignancies.97-104 However, in colonic cancer the prognostic value of extracapsular
lymph node involvement has not yet been established. Only two studies have been
published on extracapsular in both colonic and rectal cancer suggesting prognostic
significance of extracapsular lymph node involvement.105;106
As mentioned before, distant metastatic disease is the most important factor that predicts
outcome following surgical resection.88-90 However, the question whether circulating
tumour cells detected in peripheral blood of colorectal cancer patients represent metastatic
dissemination, or are merely cancer cells that have detached from the primary tumour
without metastatic potential, has been debated over half a century.107 In 1869, Ashworth
was the first to describe circulating tumour cells when he discovered cells in the blood
stream similar to those in the tumour at post-mortem studies.108 These circulating tumour
cells could be a potential cause of disease relapse particularly after surgery, therefore,
the presence or absence of circulating tumour cells has been considered by some to be
an important prognostic factor preoperatively and/or postoperatively, and an indicator
for the decision concerning adjuvant treatment and follow-up.109 However, this idea has
been questioned by others because the majority of circulating tumour cells shed from
solid tumours do not survive in the blood and only approximately 1% live long enough to
potentially form distant metastasis.86;110
Aim of the thesis
In this thesis, several aspects of colorectal surgery are highlighted. The aim of this thesis
is to critically appraise colorectal surgery and to evaluate potential improvements in
perioperative care (part I), complications (part II), and prognostication (part III).
Wind (Chris).indb 15Wind (Chris).indb 15 28-05-2008 15:44:2328-05-2008 15:44:23

16
Outline of the thesis
Part I: Fast track colorectal surgeryFast track perioperative care programmes have been successfully introduced in several
surgical procedures. In chapter 1 the application of fast track perioperative care in
colonic surgery is described. Furthermore, the individual elements of the programme are
reviewed. In chapter 2 the effect of the fast track perioperative care programme on the
outcome of, especially open colorectal surgery is systematically reviewed. In chapter 3
differences between open and laparoscopic surgery, both within a fast track perioperative
care programme are systematically reviewed. To investigate if the demonstrated benefits
of such a programme also apply to our own patient population, a pilot study was initiated,
which is described in chapter 4. Both the number of successfully applied pre-defined fast
track elements per patient (protocol compliance), as well as the combined effect of these
fast track perioperative care elements on postoperative recovery, are evaluated. The results
are compared to the results obtained in patients treated in a traditional perioperative care
setting. In chapter 5 a randomised controlled multi-centre trial is proposed to determine
whether laparoscopic surgery, fast track perioperative care, or a combination of both,
is to be preferred over open surgery with standard care in patients having segmental
colectomy for malignant disease.
Part II: Complications in colorectal surgeryThe creation of the pneumoperitoneum and subsequently the introduction of the surgical
instrumentation remains a potentially dangerous first step, which is exclusively associated
with the laparoscopic approach. In chapter 6 several techniques for the establishment
of the pneumoperitoneum are described including the equipment that is used and
the potential complications that can occur. In chapter 7 the number of entry related
complications that provoked medical liability insurance claims for laparoscopic surgery was
assessed at the largest medical liability mutual insurance company for institutions in health
care in the Netherlands. Furthermore, the used entry technique (i.e. open vs. closed),
distribution of injured organs, and predictive factors for litigation are described.
With the ongoing implementation of laparoscopy and the fact that over the past years
abdominal emergencies have been increasingly managed by laparoscopy, including those
patients with peritonitis, the question arises whether postoperative complications could be
tackled laparoscopically. The study described in chapter 8 evaluates whether a laparoscopic
reintervention for anastomotic leakage after primary laparoscopic surgery is technically
feasible and safe. Postoperative morbidity and recovery is assessed, and compared
with patients that had primary open surgery and subsequently open reintervention for
anastomotic leakage in the same period.
In chapter 9 potential usage concerns regarding linear cutters are described. An
incomplete linear staple line discovered during the stapling of an ileal pouch presented as
a case report in this chapter indicated that malfunctioning might occur when using linear
cutters.
Wind (Chris).indb 16Wind (Chris).indb 16 28-05-2008 15:44:2328-05-2008 15:44:23

17
Ch
apter 4
General intro
duction and outline of the thesis
Severe intra-abdominal sepsis may implicate repeated reinterventions and open-abdomen
management to control the sepsis. Moreover, closure of the abdominal wall might also
be impossible due to extensive bowel oedema after resuscitation. In chapter 10 different
strategies for open-abdomen treatment in terms of full fascial closure of the abdomen
are systematically reviewed. After open-abdomen management when full fascial closure
during index admission is not possible, the fascial defect can be left to heal by secondary
intention or an absorbable mesh can be used to close the abdomen. These planned
ventral hernias are often associated with enterocutaneous fistula and stomas. Closure of
enterocutaneous fistula and/or stomas in the presence of large abdominal wall defects
is a challenging problem. Simultaneous management of a large abdominal defect is an
accompanying problem making the combined procedure more difficult. In chapter 11 the
results of closure of enterocutaneous fistula and/or stomas and simultaneous abdominal
wall repair using the components separation technique are described.
Part III: Prognostication in colorectal cancerThe impact of extracapsular lymph node involvement has been studied for several
malignancies, including gastrointestinal malignancies. In chapter 12 the current evidence
on extracapsular lymph node involvement in gastrointestinal malignancies is systematically
reviewed in order to assess the incidence and extent of extracapsular lymph node
involvement. Furthermore, the relation between extracapsular lymph node involvement
and clinico-pathological factors, its prognostic value, its effect on the type of recurrence
and long term survival are evaluated. Since the prognostic significance of extracapsular
lymph node involvement is not yet established in colonic cancer, a retrospective study was
undertaken which is described in chapter 13.
Finally, in chapter 14 the presence and amount of circulating epithelial cells is assessed
focussing on differences in peripheral and portal blood. Furthermore, the role of
laparoscopy on the amount of circulating epithelial cells is also assessed.
Reference List
(1) Jacobs M, Verdeja JC, Goldstein HS. Minimally invasive colon resection (laparoscopic colectomy). Surg Laparosc Endosc 1991; 1(3):144-150.
(2) Reza MM, Blasco JA, Andradas E, Cantero R, Mayol J. Systematic review of laparoscopic versus open surgery for colorectal cancer. Br J Surg 2006; 93(8):921-928.
(3) Lacy AM, Garcia-Valdecasas JC, Delgado S, Castells A, Taura P, Pique JM et al. Laparoscopy-assisted colec-tomy versus open colectomy for treatment of non-metastatic colon cancer: a randomised trial. Lancet 2002; 359(9325):2224-2229.
(4) A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med 2004; 350(20):2050-2059.
(5) Leung KL, Kwok SP, Lam SC, Lee JF, Yiu RY, Ng SS et al. Laparoscopic resection of rectosigmoid carci-noma: prospective randomised trial. Lancet 2004; 363(9416):1187-1192.
Wind (Chris).indb 17Wind (Chris).indb 17 28-05-2008 15:44:2328-05-2008 15:44:23

18
(6) Maartense S, Dunker MS, Slors JF, Cuesta MA, Gouma DJ, van Deventer SJ et al. Hand-assisted laparo-scopic versus open restorative proctocolectomy with ileal pouch anal anastomosis: a randomized trial. Ann Surg 2004; 240(6):984-991.
(7) Tuynman JB, Bemelman WA, van Lanschot JJ. [Laparoscopic resection of colon carcinoma]. Ned Tijdschr Geneeskd 2004; 148(47):2315-2318.
(8) Abraham NS, Young JM, Solomon MJ. Meta-analysis of short-term outcomes after laparoscopic resection for colorectal cancer. Br J Surg 2004; 91(9):1111-1124.
(9) Schwenk W, Haase O, Neudecker J, Muller JM. Short term benefits for laparoscopic colorectal resection. Cochrane Database Syst Rev 2005;(3):CD003145.
(10) Fearon KC, Ljungqvist O, von Meyenfeldt M, Revhaug A, Dejong CH, Lassen K et al. Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr 2005; 24(3):466-477.
(11) Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg 2002; 183(6):630-641.
(12) Wilmore DW, Kehlet H. Management of patients in fast track surgery. BMJ 2001; 322(7284):473-476.
(13) Delaney CP, Zutshi M, Senagore AJ, Remzi FH, Hammel J, Fazio VW. Prospective, randomized, controlled trial between a pathway of controlled rehabilitation with early ambulation and diet and traditional postop-erative care after laparotomy and intestinal resection. Dis Colon Rectum 2003; 46(7):851-859.
(14) Zutshi M, Delaney CP, Senagore AJ, Mekhail N, Lewis B, Connor JT et al. Randomized controlled trial comparing the controlled rehabilitation with early ambulation and diet pathway versus the controlled rehabilitation with early ambulation and diet with preemptive epidural anesthesia/analgesia after laparo-tomy and intestinal resection. Am J Surg 2005; 189(3):268-272.
(15) Basse L, Madsen JL, Kehlet H. Normal gastrointestinal transit after colonic resection using epidural analge-sia, enforced oral nutrition and laxative. Br J Surg 2001; 88(11):1498-1500.
(16) Basse L, Raskov HH, Hjort JD, Sonne E, Billesbolle P, Hendel HW et al. Accelerated postoperative recovery programme after colonic resection improves physical performance, pulmonary function and body compo-sition. Br J Surg 2002; 89(4):446-453.
(17) Basse L, Thorbol JE, Lossl K, Kehlet H. Colonic surgery with accelerated rehabilitation or conventional care. Dis Colon Rectum 2004; 47(3):271-277.
(18) Hjort JD, Sonne E, Basse L, Bisgaard T, Kehlet H. Convalescence after colonic resection with fast-track versus conventional care. Scand J Surg 2004; 93(1):24-28.
(19) Andersen J, Hjort-Jakobsen D, Christiansen PS, Kehlet H. Readmission rates after a planned hospital stay of 2 versus 3 days in fast-track colonic surgery. Br J Surg 2007; 94(7):890-893.
(20) Anderson AD, McNaught CE, MacFie J, Tring I, Barker P, Mitchell CJ. Randomized clinical trial of multi-modal optimization and standard perioperative surgical care. Br J Surg 2003; 90(12):1497-1504.
(21) Raue W, Haase O, Junghans T, Scharfenberg M, Muller JM, Schwenk W. ‘Fast-track’ multimodal rehabilita-tion program improves outcome after laparoscopic sigmoidectomy: a controlled prospective evaluation. Surg Endosc 2004; 18(10):1463-1468.
(22) Kehlet H, Buchler MW, Beart RW, Jr., Billingham RP, Williamson R. Care after colonic operation--is it evidence-based? Results from a multinational survey in Europe and the United States. J Am Coll Surg 2006; 202(1):45-54.
(23) Schwenk W, Haase O, Raue W, Neudecker J, Muller JM. [Establishing “fast-track”-colonic surgery in the clinical routine]. Zentralbl Chir 2004; 129(6):502-509.
(24) Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patients’ care. Lancet 2003; 362(9391):1225-1230.
(25) Maessen J, Dejong CH, Hausel J, Nygren J, Lassen K, Andersen J et al. A protocol is not enough to imple-ment an enhanced recovery programme for colorectal resection. Br J Surg 2007; 94(2):224-231.
Wind (Chris).indb 18Wind (Chris).indb 18 28-05-2008 15:44:2328-05-2008 15:44:23

19
Ch
apter 4
General intro
duction and outline of the thesis
(26) Schwenk W, Gunther N, Wendling P, Schmid M, Probst W, Kipfmuller K et al. “Fast-track” rehabilitation for elective colonic surgery in Germany-prospective observational data from a multi-centre quality assur-ance programme. Int J Colorectal Dis 2007.
(27) Bosio RM, Smith BM, Aybar PS, Senagore AJ. Implementation of laparoscopic colectomy with fast-track care in an academic medical center: benefits of a fully ascended learning curve and specialty expertise. Am J Surg 2007; 193(3):413-415.
(28) Junghans T, Raue W, Haase O, Neudecker J, Schwenk W. [Value of laparoscopic surgery in elective colorectal surgery with “fast-track”-rehabilitation]. Zentralbl Chir 2006; 131(4):298-303.
(29) Mackay G, Ihedioha U, McConnachie A, Serpell M, Molloy RG, O’dwyer PJ. Laparoscopic colonic resection in fast-track patients does not enhance short-term recovery after elective surgery. Colorectal Dis 2007; 9(4):368-372.
(30) King PM, Blazeby JM, Ewings P, Franks PJ, Longman RJ, Kendrick AH et al. Randomized clinical trial comparing laparoscopic and open surgery for colorectal cancer within an enhanced recovery programme. Br J Surg 2006; 93(3):300-308.
(31) Basse L, Jakobsen DH, Bardram L, Billesbolle P, Lund C, Mogensen T et al. Functional recovery after open versus laparoscopic colonic resection: a randomized, blinded study. Ann Surg 2005; 241(3):416-423.
(32) Medeiros LR, Fachel JM, Garry R, Stein AT, Furness S. Laparoscopy versus laparotomy for benign ovarian tumours. Cochrane Database Syst Rev 2005;(3):CD004751.
(33) Wadlund DL. Laparoscopy: risks, benefits and complications. Nurs Clin North Am 2006; 41(2):219-29, vi.
(34) Harkki-Siren P, Kurki T. A nationwide analysis of laparoscopic complications. Obstet Gynecol 1997; 89(1):108-112.
(35) Hashizume M, Sugimachi K. Needle and trocar injury during laparoscopic surgery in Japan. Surg Endosc 1997; 11(12):1198-1201.
(36) Jansen FW, Kapiteyn K, Trimbos-Kemper T, Hermans J, Trimbos JB. Complications of laparoscopy: a prospective multicentre observational study. Br J Obstet Gynaecol 1997; 104(5):595-600.
(37) Neudecker J, Sauerland S, Lefering R, Neugebauer E. Closed versus open approach for laparoscopic surgery. (Protocol). Cochrane Database Syst Rev 2001;(3):CD003547. DOI: 10.1002/14651858.CD003547.
(38) Neudecker J, Sauerland S, Neugebauer E, Bergamaschi R, Bonjer HJ, Cuschieri A et al. The European Association for Endoscopic Surgery clinical practice guideline on the pneumoperitoneum for laparoscopic surgery. Surg Endosc 2002; 16(7):1121-1143.
(39) Jansen FW, Kolkman W, Bakkum EA, de Kroon CD, Trimbos-Kemper TC, Trimbos JB. Complications of laparoscopy: an inquiry about closed- versus open-entry technique. Am J Obstet Gynecol 2004; 190(3):634-638.
(40) Chambers WM, Mortensen NJ. Postoperative leakage and abscess formation after colorectal surgery. Best Pract Res Clin Gastroenterol 2004; 18(5):865-880.
(41) Alves A, Panis Y, Trancart D, Regimbeau JM, Pocard M, Valleur P. Factors associated with clinically signifi-cant anastomotic leakage after large bowel resection: multivariate analysis of 707 patients. World J Surg 2002; 26(4):499-502.
(42) Isbister WH. Anastomotic leak in colorectal surgery: a single surgeon’s experience. ANZ J Surg 2001; 71(9):516-520.
(43) Golub R, Golub RW, Cantu R, Jr., Stein HD. A multivariate analysis of factors contributing to leakage of intestinal anastomoses. J Am Coll Surg 1997; 184(4):364-372.
(44) Fielding LP, Stewart-Brown S, Blesovsky L, Kearney G. Anastomotic integrity after operations for large-bowel cancer: a multicentre study. Br Med J 1980; 281(6237):411-414.
(45) Bruce J, Krukowski ZH, Al-Khairy G, Russell EM, Park KG. Systematic review of the definition and measure-ment of anastomotic leak after gastrointestinal surgery. Br J Surg 2001; 88(9):1157-1168.
(46) Vignali A, Fazio VW, Lavery IC, Milsom JW, Church JM, Hull TL et al. Factors associated with the occurrence of leaks in stapled rectal anastomoses: a review of 1,014 patients. J Am Coll Surg 1997; 185(2):105-113.
Wind (Chris).indb 19Wind (Chris).indb 19 28-05-2008 15:44:2328-05-2008 15:44:23

20
(47) Tuson JR, Everett WG. A retrospective study of colostomies, leaks and strictures after colorectal anastomo-sis. Int J Colorectal Dis 1990; 5(1):44-48.
(48) Karanjia ND, Corder AP, Bearn P, Heald RJ. Leakage from stapled low anastomosis after total mesorectal excision for carcinoma of the rectum. Br J Surg 1994; 81(8):1224-1226.
(49) Law WI, Chu KW, Ho JW, Chan CW. Risk factors for anastomotic leakage after low anterior resection with total mesorectal excision. Am J Surg 2000; 179(2):92-96.
(50) Rullier E, Laurent C, Garrelon JL, Michel P, Saric J, Parneix M. Risk factors for anastomotic leakage after resection of rectal cancer. Br J Surg 1998; 85(3):355-358.
(51) Branagan G, Finnis D. Prognosis after anastomotic leakage in colorectal surgery. Dis Colon Rectum 2005; 48(5):1021-1026.
(52) Walker KG, Bell SW, Rickard MJ, Mehanna D, Dent OF, Chapuis PH et al. Anastomotic leakage is predic-tive of diminished survival after potentially curative resection for colorectal cancer. Ann Surg 2004; 240(2):255-259.
(53) Mealy K, Burke P, Hyland J. Anterior resection without a defunctioning colostomy: questions of safety. Br J Surg 1992; 79(4):305-307.
(54) Bozzetti F, Bertario L, Bombelli L, Fissi S, Bellomi M, Rossetti C et al. Double versus single stapling tech-nique in rectal anastomosis. Int J Colorectal Dis 1992; 7(1):31-34.
(55) Graf W, Glimelius B, Bergstrom R, Pahlman L. Complications after double and single stapling in rectal surgery. Eur J Surg 1991; 157(9):543-547.
(56) Soeters PB, de Zoete JP, Dejong CH, Williams NS, Baeten CG. Colorectal surgery and anastomotic leakage. Dig Surg 2002; 19(2):150-155.
(57) Alberts JC, Parvaiz A, Moran BJ. Predicting risk and diminishing the consequences of anastomotic dehis-cence following rectal resection. Colorectal Dis 2003; 5(5):478-482.
(58) Matthiessen P, Hallbook O, Andersson M, Rutegard J, Sjodahl R. Risk factors for anastomotic leakage after anterior resection of the rectum. Colorectal Dis 2004; 6(6):462-469.
(59) Guenaga KF, Matos D, Castro AA, Atallah AN, Wille-Jorgensen P. Mechanical bowel preparation for elec-tive colorectal surgery. Cochrane Database Syst Rev 2005;(1):CD001544.
(60) Sinha R, Sharma N, Joshi M. Laparoscopic repair of small bowel perforation. JSLS 2005; 9(4):399-402.
(61) Ramachandran CS, Agarwal S, Dip DG, Arora V. Laparoscopic surgical management of perforative perito-nitis in enteric fever: a preliminary study. Surg Laparosc Endosc Percutan Tech 2004; 14(3):122-124.
(62) Navez B, Tassetti V, Scohy JJ, Mutter D, Guiot P, Evrard S et al. Laparoscopic management of acute peri-tonitis. Br J Surg 1998; 85(1):32-36.
(63) Mutter D, Bouras G, Forgione A, Vix M, Leroy J, Marescaux J. Two-stage totally minimally invasive approach for acute complicated diverticulitis. Colorectal Dis 2006; 8(6):501-505.
(64) Sanabria AE, Morales CH, Villegas MI. Laparoscopic repair for perforated peptic ulcer disease. Cochrane Database Syst Rev 2005;(4):CD004778.
(65) Agresta F, De SP, Bedin N. The laparoscopic approach in abdominal emergencies: a single-center 10-year experience. JSLS 2004; 8(1):25-30.
(66) Bosscha K, Hulstaert PF, Visser MR, van Vroonhoven TJ, van der WC. Open management of the abdomen and planned reoperations in severe bacterial peritonitis. Eur J Surg 2000; 166(1):44-49.
(67) Jernigan TW, Fabian TC, Croce MA, Moore N, Pritchard FE, Minard G et al. Staged management of giant abdominal wall defects: acute and long-term results. Ann Surg 2003; 238(3):349-355.
(68) Miller RS, Morris JA, Jr., Diaz JJ, Jr., Herring MB, May AK. Complications after 344 damage-control open celiotomies. J Trauma 2005; 59(6):1365-1371.
(69) Stone PA, Hass SM, Flaherty SK, DeLuca JA, Lucente FC, Kusminsky RE. Vacuum-assisted fascial closure for patients with abdominal trauma. J Trauma 2004; 57(5):1082-1086.
Wind (Chris).indb 20Wind (Chris).indb 20 28-05-2008 15:44:2428-05-2008 15:44:24

21
Ch
apter 4
General intro
duction and outline of the thesis
(70) Miller PR, Meredith JW, Johnson JC, Chang MC. Prospective evaluation of vacuum-assisted fascial closure after open abdomen: planned ventral hernia rate is substantially reduced. Ann Surg 2004; 239(5):608-614.
(71) Tons C, Schachtrupp A, Rau M, Mumme T, Schumpelick V. [Abdominal compartment syndrome: preven-tion and treatment]. Chirurg 2000; 71(8):918-926.
(72) Ghimenton F, Thomson SR, Muckart DJ, Burrows R. Abdominal content containment: practicalities and outcome. Br J Surg 2000; 87(1):106-109.
(73) Garner GB, Ware DN, Cocanour CS, Duke JH, McKinley BA, Kozar RA et al. Vacuum-assisted wound closure provides early fascial reapproximation in trauma patients with open abdomens. Am J Surg 2001; 182(6):630-638.
(74) Zingales F, Moschino P, Carniato S, Fabris G, Vittadello F, Corsini A. Laparostomy in the treatment of severe peritonitis: a review of 60 cases. Chir Ital 2001; 53(6):821-826.
(75) Tsiotos GG, Luque-de LE, Soreide JA, Bannon MP, Zietlow SP, Baerga-Varela Y et al. Management of necrotizing pancreatitis by repeated operative necrosectomy using a zipper technique. Am J Surg 1998; 175(2):91-98.
(76) Cuesta MA, Doblas M, Castaneda L, Bengoechea E. Sequential abdominal reexploration with the zipper technique. World J Surg 1991; 15(1):74-80.
(77) Bose SM, Kalra M, Sandhu NP. Open management of septic abdomen by Marlex mesh zipper. Aust N Z J Surg 1991; 61(5):385-388.
(78) DeFranzo AJ, Argenta L. Vacuum-assisted closure for the treatment of abdominal wounds. Clin Plast Surg 2006; 33(2):213-24, vi.
(79) Schecter WP, Ivatury RR, Rotondo MF, Hirshberg A. Open abdomen after trauma and abdominal sepsis: a strategy for management. J Am Coll Surg 2006; 203(3):390-396.
(80) Luijendijk RW, Hop WC, van den Tol MP, de L, Braaksma MM, IJzermans JN et al. A comparison of suture repair with mesh repair for incisional hernia. N Engl J Med 2000; 343(6):392-398.
(81) White TJ, Santos MC, Thompson JS. Factors affecting wound complications in repair of ventral hernias. Am Surg 1998; 64(3):276-280.
(82) Morris-Stiff GJ, Hughes LE. The outcomes of nonabsorbable mesh placed within the abdominal cavity: literature review and clinical experience. J Am Coll Surg 1998; 186(3):352-367.
(83) de Vries Reilingh TS, Bodegom ME, van Goor H, Hartman EH, van der Wilt GJ, Bleichrodt RP. Autologous tissue repair of large abdominal wall defects. Br J Surg 2007; 94(7):791-803.
(84) Ramirez OM, Ruas E, Dellon AL. “Components separation” method for closure of abdominal-wall defects: an anatomic and clinical study. Plast Reconstr Surg 1990; 86(3):519-526.
(85) Yamaguchi K, Takagi Y, Aoki S, Futamura M, Saji S. Significant detection of circulating cancer cells in the blood by reverse transcriptase-polymerase chain reaction during colorectal cancer resection. Ann Surg 2000; 232(1):58-65.
(86) Khair G, Monson JR, Greenman J. Epithelial molecular markers in the peripheral blood of patients with colorectal cancer. Dis Colon Rectum 2007; 50(8):1188-1203.
(87) Liotta LA, Stetler-Stevenson WG. Tumor invasion and metastasis: an imbalance of positive and negative regulation. Cancer Res 1991; 51(18 Suppl):5054s-5059s.
(88) Cohen AM, Tremiterra S, Candela F, Thaler HT, Sigurdson ER. Prognosis of node-positive colon cancer. Cancer 1991; 67(7):1859-1861.
(89) Compton CC, Fielding LP, Burgart LJ, Conley B, Cooper HS, Hamilton SR et al. Prognostic factors in colorec-tal cancer. College of American Pathologists Consensus Statement 1999. Arch Pathol Lab Med 2000; 124(7):979-994.
(90) Wolmark N, Fisher B, Wieand HS. The prognostic value of the modifications of the Dukes’ C class of colorectal cancer. An analysis of the NSABP clinical trials. Ann Surg 1986; 203(2):115-122.
Wind (Chris).indb 21Wind (Chris).indb 21 28-05-2008 15:44:2428-05-2008 15:44:24

22
(91) Johnson PM, Porter GA, Ricciardi R, Baxter NN. Increasing negative lymph node count is independent-ly associated with improved long-term survival in stage IIIB and IIIC colon cancer. J Clin Oncol 2006; 24(22):3570-3575.
(92) Berger AC, Sigurdson ER, LeVoyer T, Hanlon A, Mayer RJ, Macdonald JS et al. Colon cancer survival is associated with decreasing ratio of metastatic to examined lymph nodes. J Clin Oncol 2005; 23(34):8706-8712.
(93) Wong JH, Severino R, Honnebier MB, Tom P, Namiki TS. Number of nodes examined and staging accuracy in colorectal carcinoma. J Clin Oncol 1999; 17(9):2896-2900.
(94) Tepper JE, O’Connell MJ, Niedzwiecki D, Hollis D, Compton C, Benson AB, III et al. Impact of number of nodes retrieved on outcome in patients with rectal cancer. J Clin Oncol 2001; 19(1):157-163.
(95) Liefers GJ, Cleton-Jansen AM, van d, V, Hermans J, van Krieken JH, Cornelisse CJ et al. Micrometastases and survival in stage II colorectal cancer. N Engl J Med 1998; 339(4):223-228.
(96) Yasuda K, Adachi Y, Shiraishi N, Yamaguchi K, Hirabayashi Y, Kitano S. Pattern of lymph node microme-tastasis and prognosis of patients with colorectal cancer. Ann Surg Oncol 2001; 8(4):300-304.
(97) Brasilino de CM. Quantitative analysis of the extent of extracapsular invasion and its prognostic signifi-cance: a prospective study of 170 cases of carcinoma of the larynx and hypopharynx. Head Neck 1998; 20(1):16-21.
(98) Fisher BJ, Perera FE, Cooke AL, Opeitum A, Dar AR, Venkatesan VM et al. Extracapsular axillary node extension in patients receiving adjuvant systemic therapy: an indication for radiotherapy? Int J Radiat Oncol Biol Phys 1997; 38(3):551-559.
(99) Fleischmann A, Thalmann GN, Markwalder R, Studer UE. Prognostic implications of extracapsular exten-sion of pelvic lymph node metastases in urothelial carcinoma of the bladder. Am J Surg Pathol 2005; 29(1):89-95.
(100) Griebling TL, Ozkutlu D, See WA, Cohen MB. Prognostic implications of extracapsular extension of lymph node metastases in prostate cancer. Mod Pathol 1997; 10(8):804-809.
(101) Myers JN, Greenberg JS, Mo V, Roberts D. Extracapsular spread. A significant predictor of treatment fail-ure in patients with squamous cell carcinoma of the tongue. Cancer 2001; 92(12):3030-3036.
(102) Ishida T, Tateishi M, Kaneko S, Sugimachi K. Surgical treatment of patients with nonsmall-cell lung cancer and mediastinal lymph node involvement. J Surg Oncol 1990; 43(3):161-166.
(103) van der Velden J, van Lindert AC, Lammes FB, ten Kate FJ, Sie-Go DM, Oosting H et al. Extracapsular growth of lymph node metastases in squamous cell carcinoma of the vulva. The impact on recurrence and survival. Cancer 1995; 75(12):2885-2890.
(104) Lagarde SM, ten Kate FJ, de Boer DJ, Busch OR, Obertop H, van Lanschot JJ. Extracapsular lymph node involvement in node-positive patients with adenocarcinoma of the distal esophagus or gastroesophageal junction. Am J Surg Pathol 2006; 30(2):171-176.
(105) Komuta K, Okudaira S, Haraguchi M, Furui J, Kanematsu T. Identification of extracapsular invasion of the metastatic lymph nodes as a useful prognostic sign in patients with resectable colorectal cancer. Dis Colon Rectum 2001; 44(12):1838-1844.
(106) Yano H, Saito Y, Kirihara Y, Takashima J. Tumor invasion of lymph node capsules in patients with Dukes C colorectal adenocarcinoma. Dis Colon Rectum 2006; 49(12):1867-1877.
(107) Tsavellas G, Patel H, len-Mersh TG. Detection and clinical significance of occult tumour cells in colorectal cancer. Br J Surg 2001; 88(10):1307-1320.
(108) Ghossein RA, Bhattacharya S. Molecular detection and characterisation of circulating tumour cells and micrometastases in solid tumours. Eur J Cancer 2000; 36(13 Spec No):1681-1694.
(109) Hardingham JE, Kotasek D, Sage RE, Eaton MC, Pascoe VH, Dobrovic A. Detection of circulating tumor cells in colorectal cancer by immunobead-PCR is a sensitive prognostic marker for relapse of disease. Mol Med 1995; 1(7):789-794.
(110) Fidler IJ. Metastasis: guantitative analysis of distribution and fate of tumor embolilabeled with 125 I-5-iodo-2’-deoxyuridine. J Natl Cancer Inst 1970; 45(4):773-782.
Wind (Chris).indb 22Wind (Chris).indb 22 28-05-2008 15:44:2428-05-2008 15:44:24

Part1Fast track colorectal surgery
Wind (Chris).indb 23Wind (Chris).indb 23 28-05-2008 15:44:2428-05-2008 15:44:24

Wind (Chris).indb 24Wind (Chris).indb 24 28-05-2008 15:44:2428-05-2008 15:44:24

1Chapter
Fast track perioperative care programmes in colonic surgery
J Wind
J Maessen
SW Polle
WA Bemelman
MF von Meyenfeldt
CHC Dejong
On behalf of the LAFA and ERAS study group
Nederlands Tijdschrift voor Geneeskunde 2006;150:299-304
Wind (Chris).indb 25Wind (Chris).indb 25 28-05-2008 15:44:2428-05-2008 15:44:24

26
Abstract
Fast track perioperative care programmes are intensive multimodal programmes, combining
a number of perioperative care elements with the goal to preserve normal preoperative
body composition, organ functions, and to actively enhance postoperative recovery. Fast
track perioperative care programmes have been introduced into the perioperative protocol
of several surgical procedures. This article reviews the use of fast track perioperative care
in colonic surgery.
The essence of fast track perioperative care in colonic surgery consists of extensive
preoperative counselling, no preoperative fasting but adequate nutrition, reducing surgical
trauma, abstaining routine use of drains and nasogastric tubes, tailored anaesthesiology
encompassing thoracic epidural, early and enhanced postoperative feeding and
mobilisation, and medicinal support with prokinetics and laxatives. A systematic review
demonstrates that fast track perioperative care programmes, in colonic surgery, enhance
recovery, and shorten primary and overall hospital stay.
26
Wind (Chris).indb 26Wind (Chris).indb 26 28-05-2008 15:44:2428-05-2008 15:44:24

27
Ch
apter 1
Fast track periop
erative care program
mes in colonic surg
ery
Introduction
In the previous decades, there has been a tendency to aim for a shorter hospital stay
following several surgical procedures, including colorectal surgery. There are many
reasons for this; firstly, increasing knowledge has improved the understanding of how the
postoperative convalescence of a patient can be accelerated. Secondly, the aim to reduce
hospital stay is based on economic efficiency. Furthermore, several technical developments
play an important role, including the introduction of minimally invasive (laparoscopic)
surgery, and the introduction of fast track perioperative care programmes also referred to
as Enhanced Recovery After Surgery (ERAS®). Fast track programmes combine a number
of perioperative elements (Figure 1), in order to preserve normal preoperative body
composition and organ functions, and to actively enhance postoperative recovery. This
results in a faster recovery, less morbidity and a shorter hospital stay.1-11
Kehlet et al. developed a multimodal fast track perioperative care programme specifically
for elective large bowel surgery. This programme is aimed to enhance postoperative
recovery and to avoid common reasons that interfere with early hospital discharge, such
as the need for parenteral analgesics or fluids, inadequate oral intake, delayed patient
mobilisation, complications, and lack of home care.1-6 The essence of Kehlet’s and other
fast track programmes in colonic surgery, comprises of extensive preoperative counselling,
adequate preoperative nutrition including no preoperative fasting but carbohydrate
loaded liquids until two hours prior to surgery, no bowel preparation, and no sedative
pre-medication. Furthermore, the fast track programme includes tailored anaesthesiology
Introduction
In the previous decades, there has been a tendency to aim for a shorter hospital stay
following several surgical procedures, including colorectal surgery. There are many
reasons for this; firstly, increasing knowledge has improved the understanding of how the
postoperative convalescence of a patient can be accelerated. Secondly, the aim to reduce
hospital stay is based on economic efficiency. Furthermore, several technical developments
play an important role, including the introduction of minimally invasive (laparoscopic)
surgery, and the introduction of fast track perioperative care programmes also referred to
as Enhanced Recovery After Surgery (ERAS®). Fast track programmes combine a number
of perioperative elements (Figure 1), in order to preserve normal preoperative body
composition and organ functions, and to actively enhance postoperative recovery. This
results in a faster recovery, less morbidity and a shorter hospital stay.1-11
Kehlet et al. developed a multimodal fast track perioperative care programme specifically
for elective large bowel surgery. This programme is aimed to enhance postoperative
recovery and to avoid common reasons that interfere with early hospital discharge, such
as the need for parenteral analgesics or fluids, inadequate oral intake, delayed patient
mobilisation, complications, and lack of home care.1-6 The essence of Kehlet’s and other
fast track programmes in colonic surgery, comprises of extensive preoperative counselling,
adequate preoperative nutrition including no preoperative fasting but carbohydrate
loaded liquids until two hours prior to surgery, no bowel preparation, and no sedative
pre-medication. Furthermore, the fast track programme includes tailored anaesthesiology
Figure 1. The essential elements of the fast track perioperative care programme.
Fast Track surgery (Enhanced Recovery After Surgery)
Pre-admission counselling
No nasogastric tubes
No bowel preparation
Carbohydrate loaded liquids (no fasting)
No sedative premedication
Thoracic epidural
Short acting anaesthetics
Avoiding fluid overload
Short incisions No drains
Audit of compliance
Prevention of nausea and vomiting
Non-opiate oral analgesics
Early mobilisation
Warm air body heating
Early removal catheters
Early feeding
Wind (Chris).indb 27Wind (Chris).indb 27 28-05-2008 15:44:2428-05-2008 15:44:24

28
encompassing thoracic epidural anaesthesia and short acting anaesthetics, non-opioid
pain management, avoiding perioperative fluid overload, minimal invasive surgery, no
routine use of drains and nasogastric tubes, early removal of bladder catheters, standard
laxatives and prokinetics, and early and enhanced postoperative feeding and mobilisation.
A reduction in hospital stay of up to two or three days after elective open segmental
colectomy has been reported, in a fast track care programme.1-6
Although many surgeons currently apply some of the fast track elements which are
not incorporated in a complete fast track perioperative care programme, such as the
omission of oral bowel preparation and drains, and early removal of the nasogastric
tube, considerable variation still exists throughout Europe in the degree into which these
elements are applied into daily practice.12-15
Apart from elective large bowel surgery, fast track programmes have been successfully
applied in several fields of elective surgery, e.g. for aortic aneurysm repair, pulmonary
lobectomy, and laparoscopic gastro-oesophageal reflux surgery.16-18
In this paper, the individual elements of fast track perioperative care will be discussed,
followed by a systematic review of prospective clinical controlled trials that have been
published on fast track perioperative care programmes used in elective segmental
colorectal resections.
Fast track perioperative care elements
Preoperative fast track care elementsIn fast track perioperative care, preoperative counselling is more extensive compared
to traditional care. Patients are informed on the important elements of fast track
perioperative care, such as the importance of early mobilisation and diet resumption to
reduce starvation and muscle loss, which is facilitated by tailored locoregional analgesia
and medicinal support. Furthermore, at this first meeting, the patient is informed on his/
her active role with specific tasks in the early postoperative period. These tasks include
targets for oral intake and mobilisation. It is also important to discuss when discharge can
be expected.19-22
Patients included in the fast track programme do not receive oral bowel preparation.
Patients only receive two enemas before surgery (evening before and preoperatively). In
recent meta-analyses on bowel preparation it has been shown that there are no advantages
of oral bowel preparation in colonic surgery.23-25 On the contrary, it is suggested that
after bowel preparation more anastomotic leaks might occur and there is also a trend
towards more wound infections, peritonitis and mortality. Other drawbacks of oral bowel
preparation include longer preoperative hospitalisation, induction of stress-response, and
disturbance of the physiological bowel motility and bacterial flora. Furthermore, bowel
preparation can result in dehydration and electrolyte abnormalities.
Besides the patients’ own medication, patients who are treated in a fast track perioperative
Wind (Chris).indb 28Wind (Chris).indb 28 28-05-2008 15:44:2528-05-2008 15:44:25

29
Ch
apter 1
Fast track periop
erative care program
mes in colonic surg
ery
care programme do not receive sedative pre-medication. Pre-medication, most often
consisting of benzodiazepines, might result in a somnolent/sedated patient both pre- and
postoperatively. As a consequence, provided information is not interpreted adequately
and active mobilisation is reduced.26 As the patient starts with oral intake and mobilisation
directly after surgery, sedation is undesirable.
The Dutch Anaesthesia Society states that intake of clear fluids up to 2-4 hours before
initiation of anaesthesia is safe. However, in daily practice this implies that a patient has
to fast from the evening before the operation. This is unnecessary because clear liquids or
carbohydrate loaded beverages are out of the stomach within 90 minutes and thereafter
there is no increased risk of aspiration.15;27-29 Another advantage of offering clear
carbohydrate loaded beverages two hours before surgery is that it reduces preoperative
thirst, hunger, anxiety, and glycogen depletion. Finally, postoperatively insulin resistance is
reduced with less risk of hyperglycaemia.15;29
Perioperative fast track care elementsAn important element of anaesthesiologic care in the fast track programme is thoracic
epidural analgesia which is commenced preoperatively and continued until two days
postoperatively. This thoracic epidural catheter provides optimal pain relief, with the
preservation of the patients’ normal capability of mobilisation (i.e. no motor function loss
of the legs). Furthermore, the use of epidural analgesia results in a reduction of systemic
opioid usage. Finally, afferent nerves from the surgical field are blocked (symphatic block)
resulting in a reduced stress-response, less gut paralysis, and a decreased risk of pulmonary
complications.15;30-32
General anaesthesia is accomplished by agents with short pharmaco-dynamic duration
resulting in a shorter stay in the recovery department. As a result pro-active recovery
is possible on the day of surgery. Postoperative nausea and vomiting are treated with a
combination of anti-emetic drugs.15;32;33
The surgical “access trauma” is reduced by using small incisions resulting in a reduction of
the inflammatory- and neuro-endocrine stressrespons.14;34-36 A further reduction might
be accomplished with a laparoscopic approach. In a meta-analysis on the safety and
effectiveness of elective laparoscopic segmental colorectal resections for malignancy it
has been demonstrated that laparoscopy, within a traditional care setting, is associated
with less morbidity, an enhanced recovery of gastro-intestinal motility, and a shorter
hospital stay.37 However, others have shown no differences between laparoscopic and
open surgery within a fast track perioperative care programme.38
Surgical incisions are infiltrated with a local anaesthetic agent which results in less wound
pain. Infiltration of the operative field prior to the incision, results in a better pain control
when compared to infiltration during wound closure.39;40
During (prolonged) operative procedures there is a risk of hypothermia. During re-warming
of the patient, catecholamines and cortisol are released which enhance the stress-response.
Prevention of hypothermia with upper-body forced-air heating covers (Bair Hugger®)
and infusion of warmed fluids, is important for the reduction of the stress-response,
Wind (Chris).indb 29Wind (Chris).indb 29 28-05-2008 15:44:2528-05-2008 15:44:25

30
complications, and organ dysfunction.14 It has been shown that active hypothermia
prevention reduces the risk of wound infection, blood loss, cardiac complications and
discomfort.41;42
Recent literature has demonstrated that restriction of perioperative i.v. fluids (1500-3000
ml) reduces postoperative morbidity and shortens postoperative ileus.32;43;44 Furthermore,
patients treated according to fast track perioperative care principles have a reduced need
for i.v. fluids because of the omission of oral bowel preparation and an increased oral
intake perioperatively. Patients with an epidural may experience vasodilatation leading to
hypotension. Judicious use of vasopressors in the treatment of this hypotension can avoid
excessive fluid administration.45
In two meta-analyses it has been demonstrated that routine nasogastric decompression
should be avoided after elective colorectal surgery.46;47 A nasogastric tube is very
unpleasant for the patient, hinders oral intake and prolongs (artificially) postoperative
ileus. Early removal of the nasogastric tube is not accompanied by an increased number of
complications. Moreover, the incidence of postoperative fever, atelectasis, and pneumonia
might be reduced. Therefore, in daily practice the nasogastric tube is removed during
extubation. If a patient develops nausea and vomiting postoperatively, treatment should be
started with a combination of anti-emetics and not directly by nasogastric tube insertion.
Postoperative fast track care elementsPostoperative bed rest results in an increased insulin resistance, muscle loss with decreased
strength, decreased pulmonary function and tissue oxygenation, and an increased risk of
thrombo-embolic complications.3;14;15
The presence of an abdominal drain represents a significant burden during early mobilisation.
It has never been demonstrated that the use of drains after colonic surgery beneficially
influences the occurrence of anastomotic leakage and morbidity.48;49 Therefore, the use
of abdominal drains should be minimized.
Also, urinary drainage holds patients back during mobilisation. For this reason, it
is recommended to use urinary bladder drainage only for the duration of epidural
analgesia.15
Since the day of surgery must be considered as the first day of recovery, patients are
mobilised directly after surgery. The aim is to have patients out of bed for two hours on
the day of surgery and at least six hours per day thereafter, until discharge. The early
mobilisation is facilitated by adequate pain relief with thoracic epidural analgesia and
encouragement to achieve the daily targets. The early mobilisation reduces the risk of
thrombo-embolic and pulmonary complications, decreases the amount of muscle loss and
increases muscle strength, and postoperative insulin resistance is also reduced.3;14;15
Early introduction of oral intake postoperatively is well tolerated by most patients. Early
feeding might increase bowel motility resulting in a shorter postoperative ileus and a
shorter hospital stay.50 A meta-analysis on early enteral or oral feeding versus “nil by
mouth” demonstrated that early feeding reduced both the risk of infectious complications
and hospital stay. Furthermore, there was a trend towards less anastomotic leakages.
Wind (Chris).indb 30Wind (Chris).indb 30 28-05-2008 15:44:2528-05-2008 15:44:25

31
Ch
apter 1
Fast track periop
erative care program
mes in colonic surg
ery
However, early feeding was associated with some gastro-intestinal symptoms, especially
vomiting.51
To further enhance oral intake, it is important to prevent postoperative gut dysfunction.
Postoperative ileus is partly caused by an inhibitory reflex from the surgical field. A thoracic
epidural, in contrast to a lumbar epidural, blocks this reflex and therefore might have a
positive effect on the prevention of paralytic ileus. Another important issue regarding
postoperative analgesia is opioid sparing and thereby avoiding opioid-related side
effects such as sedation and a negative effect on gut motility. For this reason, patients
additionally receive paracetamol and after discontinuation of the epidural a non steroidal
anti-inflammatory drug (NSAID) is started.14;15
Furthermore, it is important to avoid fluid overload (i.v. fluids) and medicinal support is
started such as oral magnesium oxide and pro-kinetic drugs.14;15;30;32
The implementation of the programme into daily practice
The relative contribution of each of the single elements in the fast track programme
remains uncertain. For some elements there is solid evidence that its implementation as
a single modality within a traditional care setting results in less morbidity and/or a faster
recovery, i.e. the omission of bowel preparation, removal of the nasogastric tube at the
time of extubation, and optimal pre- and postoperative nutritional care.23-28 For other
elements the evidence is less robust, and the implementation into the fast track programme
is in those cases either based on “common sense” or on consensus interpretation of
accumulating evidence.15
The effect of a fast track perioperative care programme might be, for an important part,
caused by working according to a clearly defined evidence-based protocol. Both patient
and care takers are well informed which targets have to be reached at a certain point in
the recovery of a patient.
In the fast track care programme it is important to discharge patients “under supervision”.
Once at home, patients are contacted by phone within 24-48 hours after discharge
to ensure that there are no questions or complications. Patients should be discharged
according to predefined discharge criteria. These discharge criteria include adequate pain
control with oral analgesics, absence of nausea, ability to take solid foods, passage of
flatus and/or stool, mobilisation and self support as compared to the preoperative level,
and finally acceptance of discharge by the patient.
When the postoperative course of a patient is uncomplicated, discharge can normally
be expected between the third and sixth postoperative day.2;7;8;52;53 Facilities should be
created to rapidly deal with complications that occur after discharge. Readmission in itself
does not always imply an overnight stay. Often patients can re-attend the hospital as an
out-patient, receive treatment (e.g. anti-emetics/fluids) and be discharged the same day.
Wind (Chris).indb 31Wind (Chris).indb 31 28-05-2008 15:44:2528-05-2008 15:44:25

32
Nevertheless, it is essential that there is a clear pathway for the prompt and safe readmission
of patients who experience major complications (e.g. anastomotic leakage).15
Most likely, fast track perioperative care programmes are not associated with an increased
workload of the first line home care takers (e.g. district nurse or general practitioner).
This is because patients are discharged in the same condition as formerly in a traditional
care setting. Moreover, the patient is instructed to contact the hospital if any questions or
complications may arise. First line home care takers should be involved earlier because the
discharge process has already started at the preadmission counselling session. Problems
regarding the patients’ social environment or special needs are addressed in this session
and if necessary first line care takers are contacted at this stage.15
There are no absolute contra-indications for fast track perioperative care itself. However,
there may be certain contra-indications for individual protocol elements. For example, in
patients with coagulation disorders the application of an epidural catheter is not possible.
In those circumstances only the contra-indicated elements are omitted, the other elements
are applied normally. It has been shown that fast track perioperative care is safe, feasible,
and associated with positive results in an older population or for patients with significant
co-morbidity.9;54 However, for this patient population it might be difficult to achieve
certain targets, such as the amount of postoperative mobilisation. In those cases targets
are set at the highest level possible.
It is important that the outcome is documented and evaluated during the introduction
of a fast track perioperative care programme. This not only ensures that morbidity and
mortality are optimal but also that feedback is provided on the protocol compliance to
the individual elements and to identify aspects of the programme that may need further
development of infrastructure and staff education.15
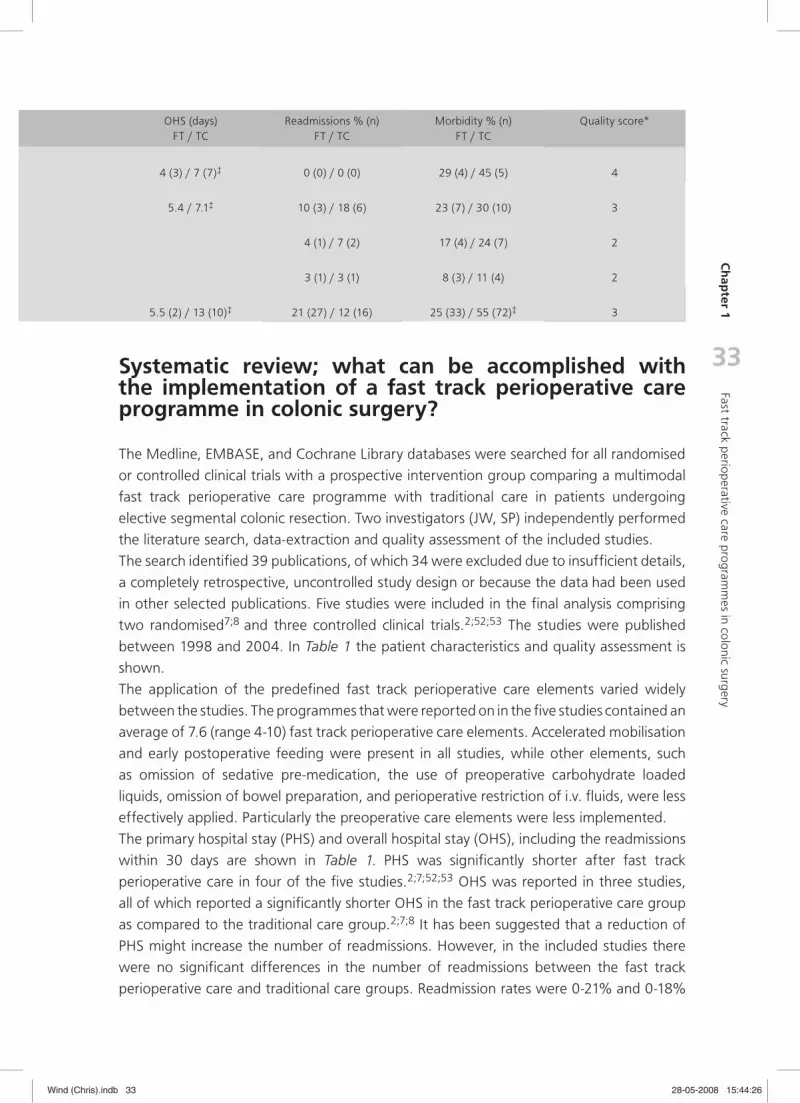
Study Design NFT / TC
Age (yr)FT / TC
% ASA I&IIFT / TC
PHS (days)FT / TC
Anderson et al.BJS 2003 RCT 14 / 11 64 / 68 93 / 91 4 (3) / 7 (7)‡
Delaney et al.DCR 2003 RCT 31 / 33 51 / 42‡ 61 / 79 5.2 / 5.8
Raue et al.Surg Endosc 2004 CCT 23 / 29 63 / 65 52 / 72 (4) / (7)‡
Bradshaw et al.J Am Coll Surg 1998 CCT 36 / 36 63 / 60 No ASA IV 4.9 / 6‡
Basse et al.DCR 2004 CCT 130 / 130† 72 / 74 60 / 77‡ 3.3 (2) / 10 (8)‡
Table 1. Patient characteristics, quality assessment, and results of the included studies
Continues data (age, PHS and OHS): mean (median); FT: Fast Track perioperative care; TC: Traditional Care; PHS: Primary Hospital Stay; OHS: Overall Hospital Stay (including readmissions within 30 days); RCT: Randomised Clinical Trial; CCT: Clinical Controlled Trial; ASA: American Society of Anaesthesiologists; ‡ p<0.05; †Traditional Care group retrospectively collected in another hospital; *Quality assessment: score ranging from 0 (worst)-5 (best) based on the cumulative score on the items randomisation, consecutivety, adequate follow-up (>30 days), independent collection of data and similarity of the groups.
Wind (Chris).indb 32Wind (Chris).indb 32 28-05-2008 15:44:2528-05-2008 15:44:25
33
Ch
apter 1
Fast track periop
erative care program
mes in colonic surg
ery
Systematic review; what can be accomplished with the implementation of a fast track perioperative care programme in colonic surgery?
The Medline, EMBASE, and Cochrane Library databases were searched for all randomised
or controlled clinical trials with a prospective intervention group comparing a multimodal
fast track perioperative care programme with traditional care in patients undergoing
elective segmental colonic resection. Two investigators (JW, SP) independently performed
the literature search, data-extraction and quality assessment of the included studies.
The search identified 39 publications, of which 34 were excluded due to insufficient details,
a completely retrospective, uncontrolled study design or because the data had been used
in other selected publications. Five studies were included in the final analysis comprising
two randomised7;8 and three controlled clinical trials.2;52;53 The studies were published
between 1998 and 2004. In Table 1 the patient characteristics and quality assessment is
shown.
The application of the predefined fast track perioperative care elements varied widely
between the studies. The programmes that were reported on in the five studies contained an
average of 7.6 (range 4-10) fast track perioperative care elements. Accelerated mobilisation
and early postoperative feeding were present in all studies, while other elements, such
as omission of sedative pre-medication, the use of preoperative carbohydrate loaded
liquids, omission of bowel preparation, and perioperative restriction of i.v. fluids, were less
effectively applied. Particularly the preoperative care elements were less implemented.
The primary hospital stay (PHS) and overall hospital stay (OHS), including the readmissions
within 30 days are shown in Table 1. PHS was significantly shorter after fast track
perioperative care in four of the five studies.2;7;52;53 OHS was reported in three studies,
all of which reported a significantly shorter OHS in the fast track perioperative care group
as compared to the traditional care group.2;7;8 It has been suggested that a reduction of
PHS might increase the number of readmissions. However, in the included studies there
were no significant differences in the number of readmissions between the fast track
perioperative care and traditional care groups. Readmission rates were 0-21% and 0-18%
OHS (days)FT / TC
Readmissions % (n)FT / TC
Morbidity % (n)FT / TC
Quality score*
4 (3) / 7 (7)‡ 0 (0) / 0 (0) 29 (4) / 45 (5) 4
5.4 / 7.1‡ 10 (3) / 18 (6) 23 (7) / 30 (10) 3
4 (1) / 7 (2) 17 (4) / 24 (7) 2
3 (1) / 3 (1) 8 (3) / 11 (4) 2
5.5 (2) / 13 (10)‡ 21 (27) / 12 (16) 25 (33) / 55 (72)‡ 3
Wind (Chris).indb 33Wind (Chris).indb 33 28-05-2008 15:44:2628-05-2008 15:44:26

34
respectively. The morbidity and mortality rates are shown in Table 1. With the exception
of one study that reported significant less morbidity in the fast track perioperative care
group, there were no further differences.2
Conclusion
Fast track perioperative care programmes are intensive multimodal and multidisciplinary
programmes with the goal to reduce loss of functional capacity and to enhance
postoperative recovery, resulting in a shorter hospital stay and an earlier return to normal
life.
Concerning cost-effectiveness, costs are reduced for the health care insurers and society on
the one hand. This is due to a reduction in hospital stay and an earlier resumption of work.
On the other hand, the costs for the hospital are increased because the hospital invests in
a multimodal and multidisciplinary programme which results in a shorter hospital stay and
correspondingly a smaller reimbursement by the health care insurer. To compensate for
this, an adjusted reimbursement should be introduced for procedures performed within a
fast track perioperative care programme.
When hospital stay is reduced, it is important to assure that patients are discharged in
the same condition as would have been the case in a traditional care situation: ‘an earlier
discharge is possible because the patient has recovered earlier’. This, in part, can be
achieved by applying strict discharge criteria. In addition to this, patients should be able to
easily contact the hospital for questions. Also, readmission procedures should be simplified
to assure that there is no delay in admission and to provide the necessary treatment.
Finally, the question remains how to implement such evidence based perioperative care
programmes on a broader basis in the Netherlands. Future studies should investigate
the added benefit of laparoscopic surgery within a fast track perioperative care
programme.12;55
Reference List
(1) Basse L, Jakobsen DH, Billesbølle P, Werner M, Kehlet H. A Clinical Pathway to Accelerate Recovery After Colonic Resection. Ann Surg 2000;232:51-57.
(2) Basse L, Thorbol JE, Lossl K, Kehlet H. Colonic surgery with accelerated rehabilitation or conventional care. Dis Colon Rectum 2004;47:271-278.
(3) Basse L, Raskov HH, Jakobsen H, Sonne E, Billesbolle P, Hendel HW, et al. Accelerated postoperative recovery programme after colonic resection improves physical performance, pulmonary function and body composition. Br J Surg 2002;89:446-453.
(4) Kehlet H, Dahl JB. Anaesthesia, surgery, and challenges in postoperative recovery. Lancet. 2003;362:921-1928.
Wind (Chris).indb 34Wind (Chris).indb 34 28-05-2008 15:44:2628-05-2008 15:44:26

35
Ch
apter 1
Fast track periop
erative care program
mes in colonic surg
ery
(5) Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg. 2002;183:630-641.
(6) Hjort Jakobsen D, Sonne E, Basse L, Bisgaard T, Kehlet H . Convalescence after colonic resection with fast-track versus conventional care. Scand J Surg. 2004;93:24-28
(7) Anderson AD, McNaught CE, MacFie J, Tring I, Barker P, Mitchell CJ. Randomized clinical trial of multi-modal optimization and standard perioperative surgical care. Br J Surg. 2003;90:1497-1504
(8) Delaney CP, Zutshi M, Senagore AJ, Remzi FH, Hammel J, Fazio VW. Prospective, randomized, controlled trial between a pathway of controlled rehabilitation with early ambulation and diet and traditional post-operative care after laparotomy and intestinal resection. Dis Colon Rectum. 2003;46:851-859.
(9) Delaney CP, Fazio VW, Senagore AJ, Robinson B, Halverson AL, Remzi FH. ‘Fast track’ postoperative management protocol for patients with high co-morbidity undergoing complex abdominal and pelvic colorectal surgery. Br J Surg. 2001;88:1533-1538
(10) Soop M, Carlson GL, Hopkinson J, Clarke S, Thorell A, Nygren J, et al. Randomized clinical trial of the effects of immediate enteral nutrition on metabolic responses to major colorectal surgery in an enhanced recovery protocol. Br J Surg. 2004;91:1138-1145.
(11) Fearon KC, Luff R. The nutritional management of surgical patients: enhanced recovery after surgery. Proc Nutr Soc. 2003;62:807-811.
(12) Nygren J, Hausel J, Kehlet H, Revhaug A, Lassen K, Dejong CH, et al. A comparison in five European Centres of case mix, clinical management and outcomes following either conventional or fast-track perioperative care in colorectal surgery. Clin Nutr. 2005;24:455-461.
(13) Lassen K, Hannemann P, Ljungqvist O, Fearon KC, Dejong CH, von Meyenfeldt MF, et al. Patterns in current perioperative practice: survey of colorectal surgeons in five northern European countries. BMJ. 2005;330:1420-1421.
(14) Wilmore DW, Kehlet H. Recent advances: management of patients in fast track surgery. BMJ 2001;322:473-476
(15) Fearon KC, Ljungqvist O, von Meyenfeldt M, Revhaug A, Dejong CH, Lassen K, et al. Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr. 2005;24:466-477
(16) Tovar EA, Roethe RA, Weissig MD, Lloyd RE, Patel GR. One-day admission for lung lobectomy: an inci-dental result of a clinical pathway. Ann Thorac Surg 1998:65;803-806
(17) Trondsen E, Mjaland O, Raeder J, Buanes T. Day-case laparoscopic fundoplication for gastro-oesopha-geal reflux disease. Br J Surg 2000;87:1708-1711
(18) Podore PC, Throop EB. Infrarenal aortic surgery with a 3-day hospital stay: a report on success with a clinical pathway. J Vasc Surg 1999;29:787-792.
(19) Egbert LD, Bant GE, Welch CE, Bartlett MK. Reduction of postoperative pain by encouragement and instruction of patients. N Engl J Med 1964;207:824-827
(20) Daltroy LH, Morlino CI, Eaton HM, Poss R, Liang MH. Preoperative education for total hip and knee replacement patients. Arthritis Care Res 1998;11:469-478
(21) Kiecolt-Glaser JK, Page GG, Marucha PT, MacCallum RC, Glaser R. Psychological influences on surgical recovery Perspectives from psychoneuroimmunology. Am Psychol 1998;53:1209-1218
(22) Disbrow EA, Bennett HL, Owings JT. Effect of preoperative suggestion on postoperative gastrointestinal motility. West J Med 1993;158:488-492
(23) Guenaga KF, Matos D, Castro AA, Atallah AN, Wille-Jorgensen P. Mechanical bowel preparation for elective colorectal surgery. Cochrane Database Syst Rev. 2005 25;(1):CD001544
(24) Bucher P, Mermillod B, Gervaz P, Morel P. Mechanical bowel preparation for elective colorectal surgery: a meta-analysis. Arch Surg. 2004;139:1359-1364
Wind (Chris).indb 35Wind (Chris).indb 35 28-05-2008 15:44:2628-05-2008 15:44:26

36
(25) Slim K, Vicaut E, Panis Y, Chipponi J. Meta-analysis of randomized clinical trials of colorectal surgery with or without mechanical bowel preparation. Br J Surg. 2004;91:1125-1130.
(26) Caumo W, Hidalgo MP, Schmidt AP, Iwamoto CW, Adamatti LC, Bergmann J, et al. Effect of pre-oper-ative anxiolysis on postoperative pain response in patients undergoing total abdominal hysterectomy. Anaesthesia. 2002;57:740-746.
(27) Ljungqvist O, Soreide E. Preoperative fasting. Br J Surg. 2003;90:400-406.
(28) Soop M, Nygren J, Myrenfors P, Thorell A, Ljungqvist O. Preoperative oral carbohydrate treatment atten-uates immediate postoperative insulin resistance. Am J Physiol Endocrinol Metab. 2001;280:E576-583.
(29) Nygren J, Thorell A, Jacobsson H, Larsson S, Schnell PO, Hylen L, et al. Preoperative gastric emptying. Effects of anxiety and oral carbohydrate administration. Ann Surg. 1995;222:728-734.
(30) Jorgensen H, Wetterslev J, Moiniche S, Dahl JB. Epidural local anaesthetics versus opioid-based anal-gesic regimens on postoperative gastrointestinal paralysis, PONV and pain after abdominal surgery. Cochrane Database Syst Rev. 2000;(4):CD001893.
(31) Rodgers A, Walker N, Schug S, McKee A, Kehlet H, van Zundert A, et al. Reduction of postoperative mortality and morbidity with epidural or spinal anaesthesia: results from overview of randomised trials. BMJ. 2000;321:1493.
(32) Schwenk W, Muller JM. Was ist fast track chirurgie? Dtsch Med Wochenschr. 2005;130:536-540.
(33) Apfel CC, Korttila K, Abdalla M, Kerger H, Turan A, Vedder I, et al. A factorial trial of six interventions for the prevention of postoperative nausea and vomiting. N Engl J Med. 2004;350:2441-2451.
(34) Kehlet H. Surgical stress response: does endoscopic surgery confer an advantage? World J Surg. 1999;23:801-807.
(35) Shea JA, Berlin JA, Bachwich DR, Staroscik RN, Malet PF, McGuckin M, et al. Indications for and outcomes of cholecystectomy: a comparison of the pre and postlaparoscopic eras. Ann Surg. 1998;227:343-350.
(36) Brown SR, Goodfellow PJ, Adam IJ, Shorthouse AJ. A randomised controlled trial of transverse skin crease vs. vertical midline incision for right hemicolectomy Tech Coloproctol. 2004;8:15-18.
(37) Abraham NS, Young JM, Solomon MJ. Meta-analysis of short-term outcomes after laparoscopic resec-tion for colorectal cancer. Br J Surg. 2004;91:1111-1124.
(38) Basse L, Jakobsen DH, Bardram L, Billesbolle P, Lund C, Mogensen T, et al. Functional recovery after open versus laparoscopic colonic resection: a randomized, blinded study. Ann Surg. 2005;241:416-423.
(39) Dath D, Park AE. Randomized, controlled trial of bupivacaine injection to decrease pain after laparo-scopic cholecystectomy. Can J Surg. 1999;42:284-288.
(40) Hannibal K, Galatius H, Hansen A, Obel E, Ejlersen E. Preoperative wound infiltration with bupivacaine reduces early and late opioid requirement after hysterectomy. Anesth Analg. 1996;83:376-381.
(41) Sessler DI. Complications and treatment of mild hypothermia. Anesthesiology. 2001;95:531-543.
(42) Sessler DI. Mild perioperative hypothermia. N Engl J Med. 1997;336:1730-1737.
(43) Lobo DN, Bostock KA, Neal KR, Perkins AC, Rowlands BJ, Allison SP. Effect of salt and water balance on recovery of gastrointestinal function after elective colonic resection: a randomised controlled trial. Lancet. 2002;359:1812-1818.
(44) Brandstrup B, Tonnesen H, Beier-Holgersen R, Hjortso E, Ording H, Lindorff-Larsen K, et al. Effects of intravenous fluid restriction on postoperative complications: comparison of two perioperative fluid regi-mens: a randomized assessor-blinded multicenter trial. Ann Surg. 2003;238:641-648.
(45) Holte K, Foss NB, Svensen C, Lund C, Madsen JL, Kehlet H. Epidural anesthesia, hypotension, and changes in intravascular volume. Anesthesiology. 2004;100:281-286.
(46) Nelson R, Edwards S, Tse B. Prophylactic nasogastric decompression after abdominal surgery. Cochrane Database Syst Rev. 2005 Jan 25;(1):CD004929
(47) Cheatham ML, Chapman WC, Key SP, Sawyers JL. A meta-analysis of selective versus routine nasogas-tric decompression after elective laparotomy. Ann Surg. 1995;221:469-476
Wind (Chris).indb 36Wind (Chris).indb 36 28-05-2008 15:44:2628-05-2008 15:44:26

37
Ch
apter 1
Fast track periop
erative care program
mes in colonic surg
ery
(48) Jesus EC, Karliczek A, Matos D, Castro AA, Atallah AN. Prophylactic anastomotic drainage for colorectal surgery. Cochrane Database Syst Rev. 2004 18;(4):CD002100.
(49) Petrowsky H, Demartines N, Rousson V, Clavien PA. Evidence-based value of prophylactic drainage in gastrointestinal surgery: a systematic review and meta-analyses. Ann Surg. 2004;240:1074-1084
(50) Stewart BT, Woods RJ, Collopy BT, Fink RJ, Mackay JR, Keck JO. Early feeding after elective open colorectal resections: a prospective randomized trial. Aust N Z J Surg. 1998;68:125-128.
(51) Lewis SJ, Egger M, Sylvester PA, Thomas S. Early enteral feeding versus “nil by mouth” after gastrointes-tinal surgery: systematic review and meta-analysis of controlled trials. BMJ. 2001;323:773-776.
(52) Raue W, Haase O, Junghans T, Scharfenberg M, Muller JM, Schwenk W. ‘Fast-track’ multimodal reha-bilitation program improves outcome after laparoscopic sigmoidectomy: a controlled prospective evalu-ation. Surg Endosc. 2004;18:1463-1468.
(53) Bradshaw BG, Liu SS, Thirlby RC. Standardized perioperative care protocols and reduced length of stay after colon surgery. J Am Coll Surg. 1998;186:501-506.
(54) DiFronzo LA, Yamin N, Patel K, O’Connell TX. Benefits of early feeding and early hospital discharge in elderly patients undergoing open colon resection. J Am Coll Surg. 2003;197:747-752
(55) Urbach DR, Baxter NN. Reducing variation in surgical care. BMJ. 2005;330:1401-1402.
Wind (Chris).indb 37Wind (Chris).indb 37 28-05-2008 15:44:2628-05-2008 15:44:26

Wind (Chris).indb 38Wind (Chris).indb 38 28-05-2008 15:44:2628-05-2008 15:44:26

2Chapter
Systematic review of enhanced recovery after surgery (‘Fast Track’) programmes in
colonic surgery
J Wind
SW Polle
PHP Fung Kon Jin
CHC Dejong
MF von Meyenfeldt
DT Ubbink
DJ Gouma
WA Bemelman
On behalf of the LAFA study and ERAS group
British Journal of Surgery 2006;93:800–809
Wind (Chris).indb 39Wind (Chris).indb 39 28-05-2008 15:44:2628-05-2008 15:44:26

40
Abstract
IntroductionFast track programmes optimise perioperative care in an attempt to accelerate recovery,
reduce morbidity and shorten hospital stay. Aim of this systematic review is to assess the
current evidence of fast track for elective segmental colonic resections.
MethodsA systematic review was performed of all randomised controlled trials (RCTs) and controlled
clinical trials (CCTs) on fast track colonic surgery. Main endpoints were number of applied
fast track elements, hospital stay, readmission rate, morbidity and mortality. Quality
assessment and data extraction were performed independently by three observers.
ResultsSix papers were eligible for analysis (3 RCTs and 3 CCTs), comprising 512 patients.
The fast track programmes contained an average of nine (range 4-12) of the 17 fast track
elements as defined in the literature. Primary hospital stay (weighted mean difference:
-1.56, 95%-confidence interval [CI]: -2.61 to -0.50) and morbidity (relative risk 0.54, 95%
CI: 0.42 to 0.69) were significantly lower in favour of fast track. Readmission rates were
not significantly different (relative risk 1.17, 95% CI: 0.73 to 1.86). No increase in mortality
was found.
ConclusionsBased on limited evidence, fast track appears safe and shortens hospital stay after
elective colorectal surgery. However, since the evidence is currently limited, a multi-centre
randomised trial seems justified.
40
Wind (Chris).indb 40Wind (Chris).indb 40 28-05-2008 15:44:2728-05-2008 15:44:27

41
Ch
apter 2
Systematic review
of fast track program
mes
Introduction
A recent development in elective large bowel surgery is the introduction and implementation
of fast track perioperative care, also referred to as Enhanced Recovery After Surgery
(ERAS®).1;2 Fast track perioperative care combines a number of perioperative elements
with the purpose to actively enhance recovery and to reduce the profound stress response
seen after surgery. This has been proposed to affect metabolic, neural, and other organ
functions beneficially, resulting in a reduction of morbidity, a faster recovery and a shorter
hospital stay.3-12
Kehlet et al. developed a multimodal fast track recovery programme for elective large
bowel surgery to enhance postoperative recovery and to avoid common reasons that
interfere with early hospital discharge, such as the need for parenteral analgesics or fluids,
delayed patient mobilisation, complications and the lack of home care.2-8 Main elements of
Kehlet’s, and similar fast track programmes, in colonic surgery are extensive preoperative
counselling, no bowel preparation, no pre-medication, the administration of synbiotics
preoperatively, no preoperative fasting but carbohydrate loaded liquids until two hours
prior to surgery, tailored anaesthesiology encompassing thoracic epidural anaesthesia
and short acting anaesthetics, perioperative high inspired O2 concentrations, avoiding
perioperative fluid overload, short incisions, non-opioid pain management, no routine use
of drains and nasogastric tubes, early removal of bladder catheters, standard laxatives and
prokinetics, and early and enhanced postoperative feeding and mobilisation.1-13
Apart from elective large bowel surgery, fast track programmes have been applied in
various other fields of elective surgery, e.g. for aortic aneurysm and lobectomy, reducing
hospital stay to three and two days respectively. Furthermore, laparoscopic gastro-
oesophageal reflux surgery has been reported to be successful in an ambulatory setting
using fast track programmes.7;14-16
The aim of this systematic review is to assess the current evidence on fast track perioperative
care in segmental colonic resections as compared with traditional care.
Methods
Data searchThe Medline database (from January 1966 to December 2005), EMBASE database
and the Cochrane Library (both from January 1980 to December 2005) were searched
using the following keywords; colon, colonic, colorectal, rectum, rectal, sigmoid, and
sigmoidal, in combination with fast, fast track, fast tract, enhanced, recovery, accelerated,
rehabilitation, convalescence, multimodal, rapid, perioperative care and ambulation. Three
investigators (JW, PFKJ, SP) independently performed the literature search. Electronic links
to related articles and references of selected articles were hand-searched as well. Leading
investigators in the field were contacted to inquire whether studies were missed or
Wind (Chris).indb 41Wind (Chris).indb 41 28-05-2008 15:44:2728-05-2008 15:44:27

42
publications were recently submitted. A hand search of relevant journals and conference
proceedings was not performed. The search was restricted to publications in the English,
Dutch or German language.
Study selection and data extractionFrom the potentially eligible studies randomised or controlled clinical trials with a prospective
intervention group comparing a multimodal fast track perioperative care programme with
traditional care in patients undergoing elective segmental colonic resection for malignant
and benign diseases were selected. In case of disagreement, full papers were obtained for
final judgement. Each of the selected trials was critically appraised by all three investigators,
using a critical review checklist for study validity as proposed by the Dutch Cochrane
Collaboration.17 Data were extracted from original articles only. Trials were selected if
they presented the following data: age, gender, ASA or POSSUM score, type of resection,
primary (PHS) and/or overall hospital stay (OHS), readmission rate, morbidity, mortality, and
at least four fast track elements were used in a fast track protocol. We identified 17 fast
track elements, 15 as proposed by Kehlet et al. and the Enhanced Recovery After Surgery
(ERAS®) study group with the addition of perioperative high inspired O2 concentrations,
and the administration of synbiotics preoperatively.1-13 The arbitrary number of four
fast track elements was chosen because of the fact that less elements might represent
“modern” traditional care. Duplicate publications and papers that reported on (parts of)
the same study population were excluded. In that situation only the largest or the most
recent publication was included. Final inclusion was done after consensus was reached. Discrepancies in judgement, if any, were resolved by discussion.
Analysis and presentation of dataHospital stay is expressed in days in hospital after surgery, where OHS represents PHS
including the hospitalisation period of patients readmitted within 30 days after surgery.
Table 1. Quality assessment and study design
Reference Study design N (FT vs TC) Consecutiveseries
Allocation concealment
Anderson et al.9 RCT 14 vs 11 Yes No
Delaney et al.10 RCT 31 vs 33 Unclear No
Gatt et al.13 RCT 19 vs 20 Yes No
Basse et al.4 CCT 130 vs 130 Yes No
prospective intervention group (hospital 1) vs. Retrospective control group (hospital 2)
Raue et al.19 CCT 23 vs 29 Yes No
Both groups prospective
Bradshaw et al.20 CCT 36 vs 36 Yes No
prospective intervention group vs. retrospective control group
FT: Fast Track; TC: Traditional Care; RCT: Randomised Controlled Trial; CCT: Controlled Clinical Trial
Wind (Chris).indb 42Wind (Chris).indb 42 28-05-2008 15:44:2728-05-2008 15:44:27

43
Ch
apter 2
Systematic review
of fast track program
mes
Blinding and data collection Similar groups Follow up Similar non-trial treatment
Not blinded Yes 30 days Yes
(Data collection by 2 individuals)
Not blinded Yes 30 days Yes
Not blinded Yes 30 days Yes
Not blinded Yes 30 days Yes
Institution bias
Not blinded Yes Unclear Yes
Operator bias
Not blinded Yes Unclear Not completely
Readmissions, morbidity and mortality are presented as a percentage of all included
patients. We defined morbidity as the reported morbidity in the included studies.
Quantitative data, if available were entered into Cochrane Review Manager 4.2 software
and analysed using RevMan Analyses 1.0.2 (The Cochrane Collaboration, Oxford, UK).
Summary estimates of treatment effects, including 95% confidence intervals (CI), were
calculated for each comparison. For continuous outcome data (hospital stay), means and
standard deviations were used to calculate a weighted mean difference (WMD) in the
meta-analysis. For dichotomous outcomes (readmissions, morbidity, mortality), the relative
risk (RR) was calculated.
Statistical heterogeneity was tested using Chi-square and I-square statistics. Data were
pooled using a fixed effect model if heterogeneity was limited; the random effect model
was used in case of moderate heterogeneity.
Results
Included studiesThe search identified 44 publications, of which 35 were excluded due to insufficient
details or a completely retrospective or uncontrolled study design. Furthermore, after
contacting the principal investigator, three studies were excluded because either part 18
or all of the data 5;8 had been used in other selected publications. Six studies were taken
into account in the final analysis comprising three randomised 9;10;13 and three controlled
clinical trials.4;19;20 These studies were published between 1998 and 2005 and reported
on a total of 512 patients, with a range of 25 to 260 patients per study. In Table 1 the
overall quality assessment and study designs are presented. Table 2 shows the patient
characteristics and results of the included studies.
Wind (Chris).indb 43Wind (Chris).indb 43 28-05-2008 15:44:2728-05-2008 15:44:27

44
The included studies had several limitations. It concerned single-centred, small studies,
and the studies were possibly insufficiently powered to detect important outcomes
such as quality of life and patient satisfaction. Only a few studies applied well-defined
discharge criteria, which is of major importance with hospital stay as one of the outcome
parameters. In the three randomised studies, randomisation was performed using sealed
envelopes. This may have threatened the concealment of allocation. In general, losses to
follow-up were not reported. Only Delaney et al. described an intention to treat principle.10
Blinding of the medical staff and patients was not possible owing to the nature of fast
track perioperative care. Data collection was not done by independent individuals. Only
Anderson et al. described data collection done by two separate individuals.9 In the study
by Basse et al. there was an institution bias because the intervention and control groups
were from two different hospitals.4 In the study by Bradshaw et al. and Basse et al. the
control group was retrospectively collected.4;20
Number of included fast track items The application of the 17 predefined fast track elements varied widely between the studies
(Table 3). The fast track programmes that were reported upon in the six studies contained
an average of nine (range 4-12) of the 17 fast track elements as defined in the literature.
Accelerated mobilisation and postoperative feeding were present in all studies, while
other elements, such as no use of premedication and active prevention of hypothermia
with warmed i.v. fluids and upper body air-warming were less frequently reported.
Primary and overall hospital stayAll six studies reported on PHS and this was significantly shorter after fast track
perioperative care in five of the six studies (Table 2). Only the study by Delaney et al.
showed no significant difference in PHS, although patients younger than 70 years
and patients treated by a surgeon experienced with the fast track programme had a
Table 2. Demographics, patient characteristics, and results of the included studies
Reference Age (years)FT / TC
% ASA I&IIFT / TC
Type of surgery
Anderson et al.9 64 / 68 93 / 91 LH, RH. All LT
Delaney et al.10 51 / 42* 61 / 79 Segmental intestinal resections. All LT
Gatt et al.13 67 / 67 Median ASA II in both groups RH, LH, SR, HM, AR, SC, PC, APR
Basse et al.4 72 / 74 60 / 77* Elective RH, LH, TR, SR, RS. All LT
Raue et al.19 63 / 65 52 / 72 Elective SR. All LS
Bradshaw et al.20 63 / 60 No ASA IV SR, RH, LH, SC, LA
FT: Fast Track; TC: Traditional Care; PHS: Primary Hospital Stay; OHS: Overall Hospital Stay; ASA: American Society of Anaesthesiologists; LH: Left Hemicolectomy; RH: Right Hemicolectomy; SC: Subtotal Colectomy; SR: Sigmoid Resection; RS: RectoSigmoid resection; LA: Low Anterior resection; TR: Transverse colon Resection; HM: Hartmann’s procedure; AR: Anterior Resection; PC: ProctoColectomy; APR: AbdominoPerineal Resection; LT: Laparotomy; LS: Laparoscopic; * p<0.05; NR: Not Reported; Continuous data: mean (median)
Wind (Chris).indb 44Wind (Chris).indb 44 28-05-2008 15:44:2728-05-2008 15:44:27

45
Ch
apter 2
Systematic review
of fast track program
mes
PHS (days)FT / TC
OHS (days)FT / TC
Readmissions % (n)FT / TC
Morbidity % (n)FT / TC
Mortality % (n)FT / TC
4 (3) / 7 (7)* 4 (3) / 7 (7)* 0 (0) / 0 (0) 29 (4) / 45 (5) 0 / 9 (1)
5.2 / 5.8 5.4 / 7.1* 10 (3) / 18 (6) 23 (7) / 30 (10) NR
6.6 (5) / 9.0 (7.5)* NR 5 (1) / 20 (4) 47 (9) / 75 (15) 5 (1) / 0
3.3 (2) / 10 (8)* 5.5 (2) / 13 (10)* 21 (27) / 12 (16) 25 (33) / 55 (72)* 5 (6) / 3 (4)
(4) / (7)* NR 4 (1) / 7 (2) 17 (4) / 24 (7) 0 / 0
4.9 / 6* NR 3 (1) / 3 (1) 8 (3) / 11 (4) NR
significantly shorter PHS. Also traditional care patients had a shorter PHS when they were
treated by a surgeon experienced with the fast track programme.10
After pooling available data, PHS in the fast track group was significantly lower than in the
group treated traditionally (WMD -1.56 days, 95% CI: -2.61 to -0.50 days, Figure 1).
OHS was reported in three studies, all of which reported a significantly shorter OHS in the
fast track group as compared to the traditional care group (Table 2).4;9;10 In the study by
Delaney et al., the significant shorter OHS was partly due to fewer readmissions in the fast
track group. Pooling could not be performed because only a few studies reported on this
outcome and because standard deviations were missing.
Readmission rateReadmission rates were reported in all studies and varied from 0 to 21% after fast track
care and from 0 to 20% after traditional care (Table 2). After pooling all available studies,
there was no significant difference in readmission rate between the fast track and
traditional care group (RR 1.17, 95% CI: 0.73 to 1.86, Figure 2). There was a trend to more
readmissions after fast track perioperative care in the non-RCTs due to the study of Basse
et al., the only study reporting more readmissions after fast track care.4 However, the
pooled data of the RCTs showed a trend to more readmissions after traditional care.
RCTs: Randomised Controlled TrialsNon-RCTs: Non Randomised Controlled Trials
Figure 1 Weighted mean difference (WMD) for primary hospital stay (PHS) in days
Wind (Chris).indb 45Wind (Chris).indb 45 28-05-2008 15:44:2828-05-2008 15:44:28

46
Table 3. Summary of outcomes and fast track items presented in the selected trials
Reference Type N
Anderson et al.9 RCT 25 √ √ √ √ √ √ √ √
Delaney et al.10 RCT 64 − √ √ √ √ √ √ − −
Gatt et al.13 RCT 39 √ √ √ √ − √ √ √ √
Basse et al.4 CCT 260 √ √ √ √ √ √ √ − −
Raue et al.19 CCT 52 √ √ √ √ − ∼ ∼ − −
Bradshaw et al.20 CCT 72 − √ √ √ − − √ − −
NG: Nasogastric; RCT: Randomised Controlled Trial; CCT: Controlled Clinical Trial; √: Adequately described/Present; -: Not Present/ Not studied; ~: Not adequately described/ partially present
Mo
rtal
ity
Mo
rbid
ity
Rea
dm
issi
on
s
Pri
mar
y H
osp
ital
Sta
y
Tota
l Ho
spit
al S
tay
Min
imu
m o
f 3
0 d
ays
follo
w-u
p
Pre
op
erat
ive
cou
nse
llin
g
Pre
op
erat
ive
feed
ing
Syn
bio
tics
RCTs: Randomised Controlled TrialsNon-RCTs: Non Randomised Controlled Trials
Figure 2 Relative Risk (RR) for readmission rates
Wind (Chris).indb 46Wind (Chris).indb 46 28-05-2008 15:44:2828-05-2008 15:44:28

47
Ch
apter 2
Systematic review
of fast track program
mes
Fast Track Items
√ − − √ − √ √ √ √ √ √ √ − −
− − − − − − − √ − √ √ − − −
√ − − √ − √ √ √ √ √ √ √ − −
− √ √ − − √ √ ∼ − √ √ √ √ √
− − √ − − √ √ √ − √ √ √ √ √
− − − − − √ − √ − √ √ ∼ − −
No
bo
wel
pre
par
atio
n
No
pre
med
icat
ion
Flu
id r
estr
icti
on
Per
iop
erat
ive
hig
h O
2 co
nce
ntr
atio
ns
Act
ive
pre
ven
tio
n o
f h
ypo
ther
mia
Epid
ura
l an
alg
esia
Min
imal
inva
sive
/ t
ran
sver
se in
cisi
on
s
No
ro
uti
ne
use
of
NG
tu
bes
No
use
of
dra
ins
Enfo
rced
po
sto
per
ativ
e m
ob
ilisa
tio
n
Enfo
rced
po
sto
per
ativ
e o
ral f
eed
ing
No
sys
tem
ic m
orp
hin
e u
se
Stan
dar
d l
axat
ives
Earl
y re
mo
val o
f b
lad
der
cat
het
er
Morbidity and mortalityMorbidity rates were reported in all included studies and ranged between 8% and 47%
in the fast track group and between 11% and 75% in the traditional care group (Table
2). Basse et al. reported significantly less morbidity in their fast track group, especially
cardiovascular and pulmonary (pneumonia) complications.4 Also the other studies reported
less morbidity in the fast track group, however not significantly different (Table 2).
The pooled data including all six studies showed significantly less morbidity in the fast
track group (RR 0.54, 95% CI: 0.42 to 0.69, Figure 3). The pooled data of the three RCTs,
showed only a trend towards reduced morbidity in the fast track group. The absolute
risk reduction of the pooled data was -0.15 (95% CI: -0.28 to -0.02). This means that the
number needed to treat is 6.7, i.e. for every seven patients receiving fast track perioperative
care, morbidity is avoided in one patient as compared with traditional care.
A feared complication after colonic surgery is anastomotic leakage. Only in the study by
Basse et al. were anastomotic leakages reported (3.8% in both groups).4 Four out of the
five patients with a leakage in the fast track group were readmitted with an anastomotic
leakage. The readmission was done promptly without mortality. Mortality was reported in
four of the included publications and ranged from 0 to 5% and from 0 to 9% in the fast
track and traditional care groups, respectively (Table 2).4; 9;13;19
Wind (Chris).indb 47Wind (Chris).indb 47 28-05-2008 15:44:2828-05-2008 15:44:28

48
Clinical outcome parameters
Gut function
Postoperative ileus, in terms of the necessity for reinsertion of a nasogastric decompression
tube, time until first defecation, or the number of days required postoperatively to attain
tolerance of solid food, was reduced in the fast track group (Table 4).
Pulmonary function
Raue et al. assessed pulmonary function by measuring forced vital capacity (FVC). FVC was
significantly better in the fast track group on the first postoperative day, but thereafter
no further differences were detected.19 In the studies by Anderson et al. and Gatt et al.
pulmonary function expressed as forced expiratory volume in one second (FEV1) was not
different at any time point between the two groups.9;13
Pain, fatigue, and quality of life.
In the study by Anderson et al. pain and fatigue, as measured using the visual analogue
scale (VAS-score), were a significantly more prominent feature in the traditional care
group.9 Delaney et al. found no difference in pain scores, measured using the VAS-score
and McGill pain score questionnaire (MGPQ), and quality of life, measured using the SF-36
and the Cleveland Clinic Global Quality of Life (CGQL) questionnaire, between traditional
care and fast track care groups.10 Raue et al. found no difference in pain scores, but
fatigue was increased in the traditional care group on the first two postoperative days. In
RCTs: Randomised Controlled TrialsNon-RCTs: Non Randomised Controlled Trials
Figure 3 Relative Risk (RR) for morbidity rates
Wind (Chris).indb 48Wind (Chris).indb 48 28-05-2008 15:44:2828-05-2008 15:44:28

49
Ch
apter 2
Systematic review
of fast track program
mes
this study both outcomes were measured using the VAS-score.19 Gatt et al. also used the
VAS-score to evaluate fatigue and pain and found no significant differences.13
Discussion
The results of this systematic review suggest that fast track multimodal perioperative
care programmes result in an enhanced recovery after surgery, reducing morbidity
rates, primary- and overall hospital stay. However, this systematic review demonstrates
that the evidence on fast track colonic surgery to date is scarce, and further research is
warranted.
Fast track programmes in colonic surgery have been introduced more than a decade ago
with favourable early results. Many elements of these fast track programmes are based
on solid evidence derived from randomised trials or meta-analyses. However, it is quite
surprising, that implementation in daily practice has so far stayed behind. This can partly,
be explained by the necessity to break with long-standing traditions, such as preoperative
fasting, slow postoperative advancement of oral feeding, and delayed mobilisation.
Nowadays, some of the fast track elements, such as omission of bowel preparation and
drains, early removal of nasogastric tubes, and early feeding and mobilisation have already
been incorporated in “modern” traditional care, although considerable variation still exists
throughout Europe.21;22 This modernisation of traditional care has been initiated, at least
to some extent, by the development of laparoscopic surgery.
The relative contribution of each of the single elements in the fast track programme
remains uncertain. For some elements there is solid evidence that its implementation
results in less morbidity and/or a faster recovery, i.e. removal of the nasogastric tube at
the time of extubation and no bowel preparation.23-28 For other elements the evidence is
less robust, and the implementation into the fast track programme is in those cases either
based on “common sense” or on consensus interpretation of accumulating evidence.2
However, in all cases this evidence is derived from traditional care settings. To distinguish
the critical elements in a fast track programme, further studies are needed that asses the
Table 4. Gut function in terms of the necessity for reinsertion of a nasogastric tube decompression, time until first defecation, and the number of days required postoperatively to attain tolerance of normal diet.
Reference % of reinserted NG tubes
FT / TC
First bowel movement
FT / TC
Tolerance of normal diet
FT / TC
Anderson et al.9 NR NR 2 / 3*
Delaney et al.10 6 / 9 NR NR
Gatt et al.13 NR NR 2 / 3.8*
Basse et al.4 2 / 15* 2 / 4.5* NR
Raue et al.19 13 / 21 2 / 3* 1 / 2*
Bradshaw et al.20 NR (2.5) / (3.7)* (1) / (2.9)*§
FT: Fast Track; TC: Traditional Care; *: p<0.05, Continuous data: median (mean); §: tolerance of fluid diet; NR: Not Reported; NG: Naso-Gastric
Wind (Chris).indb 49Wind (Chris).indb 49 28-05-2008 15:44:2928-05-2008 15:44:29

50
protocol compliance to each element. With this data the critical fast track elements might
be identified for example by using a regression model.
A drawback of the term fast track is the suggestion that the ultimate and main goal is
to discharge the patient earlier. This in fact is not the case; fast track programmes aim
at improving patient recovery postoperatively and reduce morbidity. In doing so, such
programmes enable the patient to go home earlier, if this is agreeable to the patient.
A fast track programme requires a dedicated and motivated team consisting of an
anaesthesiologist, surgeon, dietician, physiotherapist, social worker, and nursing team. This
is nicely illustrated in the paper by Basse et al., indicating that in the absence of the research
team (i.e. holidays), patients were not included in the fast track regimen.4 Experience with
the programme is another important factor for success. Delaney et al. reported that fast
track patients treated by an experienced fast track surgeon spent significantly less time
in the hospital compared with the fast track patients that were treated by a surgeon less
experienced with the programme. Also younger patients had more benefit of the fast track
programme compared with older patients.10 On the contrary in the study by Basse et al. the
ASA-classification of the fast track group was significantly higher.4 Others have confirmed
the safety, feasibility, and positive results of fast track in an older population or for patients
with significant co-morbidity.11;29 This is a confirmation of the view that particularly the old
and the frail patient will benefit from the application of fast track programmes.
One of the major concerns regarding fast track programmes is that reduction of the
PHS might result in an increased readmission rate. In this review there was no significant
difference in readmission rate. On the contrary, there was a trend to less readmissions
in the fast track group when only the randomised controlled studies are considered. The
trend to an increased readmission rate after fast track recovery, seen in the pooled result
of only the non-randomised studies is caused by the largest study by Basse et al., reporting
the largest reduction in PHS but also an increased readmission rate in the fast track group.
The other included studies reported a reduction in PHS also, albeit less pronounced, but
without an increased readmission rate. In other words there seemed to be a turning point
after which reducing the PHS further, the readmission rate would increase. This, in part,
can be prevented by applying strict discharge criteria. Only in this way, it is assured that
patients are discharged in the same condition as would have been the case in a traditional
care situation. This review shows that not all studies used such discharge criteria. In the
studies by Anderson et al., Delaney et al., and Gatt et al., discharge criteria had been
defined for both the fast track and traditional care patients. These discharge criteria
comprised the ability to tolerate solid food, full mobilisation, and pain medication limited
to oral analgesics.9;10;13 Delaney et al. defined additional discharge criteria concerning
passage of flatus or stool and agreement of the patient with the scheduled discharge.10
Bradshaw et al. used three discharge criteria for the fast track patients including normal
body temperature, return of gastrointestinal function and the tolerance of oral nutrition.20
In the other studies there were no properly defined or described discharge criteria.4;19
Secondly a higher readmission rate makes it necessary to simplify the readmission
procedure to assure that there is no delay in admission and treatment if necessary.
Wind (Chris).indb 50Wind (Chris).indb 50 28-05-2008 15:44:2928-05-2008 15:44:29

51
Ch
apter 2
Systematic review
of fast track program
mes
In this meta-analysis the PHS was reduced by 1.6 days. The study by Basse et al. was
excluded in the calculation of the weighted mean difference because a standard deviation
was not given. In this, relatively large, study the difference in mean PHS between fast
track and traditional care was 6.7 days in favour of fast track.4 If this study would be taken
into account, the difference would probably have been considerably greater than 1.6 days.
The reduction in PHS was partly facilitated by the prevention or reduction of postoperative
ileus and decreased morbidity, however, when only the randomised controlled studies
were considered in the morbidity analysis, the results were less pronounced, and no
longer significant. This may be explained by the remarkably great difference between the
fast track group and traditional care group in the large study by Basse et al.4 Furthermore,
this traditional care group was collected retrospectively from another institution.4 Gatt
et al. reported high morbidity rates in both the traditional care group and the fast track
group. This can partly be explained by the fact that minor morbidity such as vomiting and
diarrhoea were also taken into account.
This systematic review has many limitations; the overall quality of the included studies
was moderate with several sources of bias. Possibly, there also could be a publication bias
because all studies reported positive results in favour of fast track. The number of applied
fast track elements varied widely, in general only half of the pre-defined elements were
used. To partly deal with the heterogeneous nature of studies, a distinction was made
between the randomised and the non-randomised studies.
In conclusion, based on six comparative single centre studies, fast track programmes
were found to reduce the time spent in the hospital, and were found to be safe in major
abdominal surgery. Shortening hospital stay and morbidity reduction are attractive, since
both increase the availability of beds and might reduce the overall cost of hospital stay.
However, despite the current enthusiasm and implementation into daily practice this
systematic review shows that to date, there are few data available. The positive results, e.g.
shorter hospital stay, and reduced morbidity, should therefore encourage further studies on
fast track colonic surgery and not be used as a justification for broader implementation into
daily practice. Thus, multi-centre prospective randomised trials are needed to confirm the
broader applicability and favourable results of fast track programmes in colonic surgery.
Reference List
(1) Wilmore DW, Kehlet H. Recent advances: management of patients in fast track surgery. BMJ 2001;322:473-476.
(2) Fearon KC, Ljungqvist O, von Meyenfeldt M, Revhaug A, Dejong CH, Lassen K, et al. Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr. 2005;24:466-477
(3) Basse L, Jakobsen DH, Billesbølle P, Werner M, Kehlet H. A Clinical Pathway to Accelerate Recovery After Colonic Resection. Ann Surg 2000;232:51-57.
Wind (Chris).indb 51Wind (Chris).indb 51 28-05-2008 15:44:2928-05-2008 15:44:29

52
(4) Basse L, Thorbol JE, Lossl K, Kehlet H. Colonic sugery with accelerated rehabilitation or conventional care. Dis Colon Rectum 2004;47:271-278.
(5) Basse L, Raskov HH, Jakobsen H, Sonne E, Billesbolle P, Hendel HW et al. Accelerated postoperative recovery programme after colonic resection improves physical performance, pulmonary function and body composition. Br J Surg 2002;89:446-453.
(6) Kehlet H, Dahl JB. Anaesthesia, surgery, and challenges in postoperative recovery. Lancet 2003;362:1921-1928.
(7) Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg 2002;183:630-641.
(8) Hjort Jakobsen D, Sonne E, Basse L, Bisgaard T, Kehlet H . Convalescence after colonic resection with fast-track versus conventional care. Scand J Surg. 2004;93:24-28.
(9) Anderson AD, McNaught CE, MacFie J, Tring I, Barker P, Mitchell CJ. Randomized clinical trial of multi-modal optimization and standard perioperative surgical care. Br J Surg. 2003;90:1497-1504.
(10) Delaney CP, Zutshi M, Senagore AJ, Remzi FH, Hammel J, Fazio VW. Prospective, randomized, controlled trial between a pathway of controlled rehabilitation with early ambulation and diet and traditional post-operative care after laparotomy and intestinal resection. Dis Colon Rectum. 2003;46:851-859.
(11) Delaney CP, Fazio VW, Senagore AJ, Robinson B, Halverson AL, Remzi FH. ‘Fast track’ postoperative management protocol for patients with high co-morbidity undergoing complex abdominal and pelvic colorectal surgery. Br J Surg. 2001;88:1533-1538.
(12) Soop M, Carlson GL, Hopkinson J, Clarke S, Thorell A, Nygren J, et al. Randomized clinical trial of the effects of immediate enteral nutrition on metabolic responses to major colorectal surgery in an enhanced recovery protocol. Br J Surg. 2004;91:1138-1145.
(13) Gatt M, Anderson AD, Reddy BS, Hayward-Sampson P, Tring IC, MacFie J. Randomized clinical trial of multimodal optimization of surgical care in patients undergoing major colonic resection. Br J Surg. 2005;92:1354-1362.
(14) Podore PC, Throop EB. Infrarenal aortic surgery with a 3-day hospital stay: a report on success with a clinical pathway. J Vasc Surg 1999;29:787-792.
(15) Tovar EA, Roethe RA, Weissig MD, Lloyd RE, Patel GR. One-day admission for lung lobectomy: an inci-dental result of a clinical pathway. Ann Thorac Surg 1998:65;803-806.
(16) Trondsen E, Mjaland O, Raeder J, Buanes T. Day-case laparoscopic fundoplication for gastro-oesopha-geal reflux disease. Br J Surg 2000;87:1708-1711.
(17) Therapy checklist (Dutch extended version) of the Dutch Cochrane Centre.
(18) Nygren J, Hausel J, Kehlet H, Revhaug A, Lassen K, Dejong C, et al. A comparison in five European Centres of case mix, clinical management and outcomes following either conventional or fast-track perioperative care in colorectal surgery. Clin Nutr. 2005;24:455-561.
(19) Raue W, Haase O, Junghans T, Scharfenberg M, Muller JM, Schwenk W. ‘Fast-track’ multimodal reha-bilitation program improves outcome after laparoscopic sigmoidectomy: a controlled prospective evalu-ation. Surg Endosc. 2004;18:1463-1468.
(20) Bradshaw BG, Liu SS, Thirlby RC. Standardized perioperative care protocols and reduced length of stay after colon surgery. J Am Coll Surg. 1998;186:501-506.
(21) Lassen K, Hannemann P, Ljungqvist O, Fearon K, Dejong CH, von Meyenfeldt MF, et al. Patterns in current perioperative practice: survey of colorectal surgeons in five northern European countries. BMJ. 2005;330:1420-1421.
(22) Urbach DR, Baxter NN. Reducing variation in surgical care. BMJ. 2005;330:1401-1402.
(23) Slim K, Vicaut E, Panis Y, Chipponi J. Meta-analysis of randomized clinical trials of colorectal surgery with or without mechanical bowel preparation. Br J Surg. 2004;91:1125-1130.
(24) Guenaga KF, Matos D, Castro AA, Atallah AN, Wille-Jorgensen P. Mechanical bowel preparation for elective colorectal surgery. Cochrane Database Syst Rev. 2005; 25:CD001544.
Wind (Chris).indb 52Wind (Chris).indb 52 28-05-2008 15:44:2928-05-2008 15:44:29
53
Ch
apter 2
Systematic review
of fast track program
mes
(25) Bucher P, Mermillod B, Gervaz P, Morel P. Mechanical bowel preparation for elective colorectal surgery: a meta-analysis. Arch Surg. 2004;139:1359-1364.
(26) Cheatham ML, Chapman WC, Key SP, Sawyers JL. A meta-analysis of selective versus routine nasogas-tric decompression after elective laparotomy. Ann Surg. 1995;221:469-476.
(27) Nelson R, Edwards S, Tse B. Prophylactic nasogastric decompression after abdominal surgery. Cochrane Database Syst Rev. 2005;25:CD004929.
(28) Vermeulen H, Storm-Versloot MN, Busch OR, Ubbink DT. Nasogastric intubation after abdominal surgery: a meta-analysis of recent literature. Arch Surg. 2006 Mar;141(3):307-314.
(29) DiFronzo LA, Yamin N, Patel K, O’Connell TX.Benefits of early feeding and early hospital discharge in elderly patients undergoing open colon resection. J Am Coll Surg. 2003;197:747-752.
Wind (Chris).indb 53Wind (Chris).indb 53 28-05-2008 15:44:2928-05-2008 15:44:29

Wind (Chris).indb 54Wind (Chris).indb 54 28-05-2008 15:44:2928-05-2008 15:44:29
3Chapter
Implementation of a fast track perioperative care programme; what are
the difficulties?
SW Polle
J Wind
JW Fuhring
J Hofland
DJ Gouma
WA Bemelman
Digestive Surgery 2007;24:441-449
Wind (Chris).indb 55Wind (Chris).indb 55 28-05-2008 15:44:2928-05-2008 15:44:29

5656
Abstract
IntroductionThe aim of the present study was to evaluate the feasibility of a fast track programme and
its effect on postoperative recovery.
MethodsAll patients, scheduled for elective segmental colorectal resection were treated in a
fast track programme. Data were compared to a control-group operated for elective
colorectal resections and treated in a traditional care programme. Data from the fast track
group were collected prospectively, data from the traditional care group retrospectively.
Outcome-parameters included the number of successfully applied fast track modalities,
patient-satisfaction, morbidity rate, reoperation rate, primary (PHS) and total hospital stay
(THS), and readmission rate.
ResultsOne-hundred-and-seven patients were included (55 fast track group vs. 52 traditional care
group). The groups were comparable for patient-characteristics as age and cr-POSSUM-
score (p=0.22 and p=0.40). An average of 7.4 out of 13 predefined fast track modalities
were successfully achieved per patient. Patient-satisfaction was comparable (p=0.84).
Seven versus. five patients required a reoperation in the fast track and traditional care
group, respectively (p=0.52). Morbidity rate was comparable (n=16 vs. n=15, p=0.83).
Median PHS was 4.0 vs. 6.0 days and median THS was 4.0 vs. 6.5 days in the fast
track group and traditional care group (p<0.01 and p<0.03, respectively). Six versus
three patients were readmitted in the fast track and traditional care group, respectively
(p=0.49).
ConclusionImplementation of all fast track modalities was difficult since a rather low number
of pre-defined fast track modalities were effectively realized. Despite incomplete
implementation, PHS and THS were shorter in the fast track group without affecting
patient-satisfaction.
Wind (Chris).indb 56Wind (Chris).indb 56 28-05-2008 15:44:3028-05-2008 15:44:30

57
Ch
apter 3
Implem
entation of a fast track program
me
Introduction
Fast track programmes, also referred to as Enhanced Recovery After Surgery (ERAS®), are
supposed to reduce morbidity, accelerate recovery and consequently shorten hospital stay
of surgical patients.1;2 Kehlet and co-workers achieved a reduction in hospital stay from
10 to 3.3 days for patients undergoing segmental colonic resection.3 To a lesser degree,
others have also reported a reduction in hospital stay after the implementation of a fast
track programme.4-8 Although the number of studies reporting on advantages of fast
track care programmes are growing, the evidence is still rather limited; only three small
randomized controlled trials (RCTs), encompassing a total number of 64 patients treated
in a fast track perioperative care programme, have been published.9 Most of the available
non-randomised studies have a retrospective design or are case-series without adequate
control groups and without reporting on patient satisfaction with such a programme.10-13
Although the combination of laparoscopic surgery and fast track care might be the optimal
strategy, only two RCTs have compared laparoscopic to open surgery within a fast track
programme.14;15 The conflicting results of these reports justify further study.
While most authors have meticulously described the fast track modalities included in their
protocols (e.g. omission of bowel preparation and pre-medication, use of thoracic epidural
anesthesia for perioperative analgesia management, early post-operative mobilisation and
feeding), none of them actually described the degree of compliance with each of the single
fast track modalities as defined in their protocols. For this reason, the exact influence of
the number of and type of fast track modalities within a fast track programme remains
unknown. Moreover, most authors publishing on their results after introduction of a fast
track programme probably report on their results after an initial period of pilot testing
with such a programme. No data are available with respect to the encountered early
difficulties with the introduction of such a programme.
The objective of this study was therefore to describe our results from the start of
introduction of a fast track programme by evaluating both the number of successfully
applied pre-defined fast track modalities per patient as well as the combined effect of
these fast track modalities on postoperative recovery. These results were compared to
results of patients treated in a traditional care programme. The faced bottlenecks with the
introduction of the programme will be commented on.
Methods
In the Academic Medical Centre in Amsterdam two separate gastro-intestinal surgery
units are available. A fast track perioperative care programme was introduced in one of
the two gastrointestinal surgery units in August 2004. Patients scheduled for elective
abdominal segmental colorectal resection including ileo-colic (re-) resection in the period
August 2004 to July 2005, and admitted on the fast track unit, were treated according
Wind (Chris).indb 57Wind (Chris).indb 57 28-05-2008 15:44:3028-05-2008 15:44:30

58
to the fast track programme (fast track group). The allocation of patients to the unit
with fast track or the unit without fast track in this period, depended on the availability
of hospital beds on both units, the availability of a fast track nurse and the fast track
surgeon who initiated this project. A consecutive series of patients, scheduled for elective
segmental colorectal resection in the period June 2003 to January 2004 and admitted
on both gastrointestinal surgery units, was treated in a traditional care programme and
served as a control group (traditional care group). Only patients with American Society
of Anaesthesiologists (ASA) classification I or II were included in this study. In both study
groups, patients with prior segmental colorectal resections were included as were both
open and laparoscopic procedures. Patients requiring a palliative resection or an abdomino-
perineal resection (APR) for colorectal cancer were excluded. Outcome data of the fast
track group were recorded prospectively; outcome data of the traditional care group were
collected retrospectively from patients’ records. All data were analyzed according to an
intention-to-treat principle meaning that patients who were unable to fulfil (parts of) the
fast track programme were analyzed in the fast track group. Since each single modality
as applied in our fast track programme is an accepted form of treatment in daily care,
no ethics approval from our Ethic Committee was requested. Each patient was however
informed about the combination of these accepted and evidence based single modalities
applied in the fast track protocol.
Primary outcome parameters were the number of successfully applied fast track modalities
per patient and patient satisfaction. Secondary outcome parameters were overall morbidity
rate, reoperation rate, primary hospital stay, total hospital stay, readmission rate, and
mortality rate.
A total of 13 fast track modalities were identified (Table 1). For each patient each modality
was evaluated for successful implementation (e.g. if bowel preparation was omitted it was
scored as successful implementation, if it was not omitted it was considered unsuccessful).
Table 1. Evaluated fast track modalities
Omission of bowel preparation
Prevention of hypothermia
Pre-operative counselling by fast track nurse
Intake of 4 CHL drinks on day before surgery
Epidural anaesthesia
Prophylactic PONV medication
Intake of 2 CHL drinks 2 hours before surgery
Suprapubic catheter
Omission of evening medication
Omission of pre-medication
Intake of 2 CHL drinks on evening after surgery
Early extension of oral liquids
Early mobilisation
CHL: carbohydrate loaded drink (Nutridrink®)
Wind (Chris).indb 58Wind (Chris).indb 58 28-05-2008 15:44:3028-05-2008 15:44:30

59
Ch
apter 3
Implem
entation of a fast track program
me
In this manner all successfully applied items per patient were scored. Also the average
number of successfully applied items of all patients was calculated. Overall morbidity was
defined as any complication requiring an unplanned intervention within 30 days after the
operation. A major complication was considered any complication requiring a surgical
reintervention or resulting in permanent adverse sequel (such as myocardial infarction).
Total hospital stay was defined as primary hospital stay plus the hospitalisation period of
patients that were readmitted within 30 days after surgery.
Fast track vs. traditional care protocol Details of the fast track perioperative and traditional care protocols are summarized in Table
2. Discharge criteria were similar for both groups consisting of 1) adequate pain control
with oral medication, 2) absence of nausea, 3) passage of first flatus and/or stool, 4)
ability to tolerate solid food, 5) mobilisation and self support as preoperative and finally 6)
acceptance of discharge by the patient. Within 24 - 48 h after discharge, fast track patients
were contacted by telephone by a specially trained fast track senior nurse (JWF) to check
for complications. During this contact, patients were provided to ask questions about
Table 2. Differences between fast-track and traditional care protocol
Fast-track Care Traditional Care
Pre-operative phase
Outpatient department of Surgery
- Scheduling of operation- Information about FT- Informed consent
- Scheduling of operation
Outpatient department of anaesthesiology
- Pre-assessment for risk adjustment - Pre-assessment for risk adjustment
- Discussion focusing on placement of thoracic epidural catheter for management of perioperative analgesia
- Open discussion about different possibilities for management of perioperative analgesia (i.e. placement of epidural catheter on any level, patient controlled analgesia with morphine (PCA-morphine) or continuous IV morphine infusion
Pre-admission guided tour on surgical ward
- Yes - No tour
Day of admission
Pre-operative fasting - Last meal 6 h before operation- Last clear drink (CHL) 2h
before operation
- Last meal until midnight- No oral intake at the day of surgery
Pre-anaesthetic medication
- Lorazepam, 1 mg the evening before operation if necessary
- Lorazepam, 1 mg or temazepam 10 or 20 mg the evening before operation
- No sedative medication at the day of operation
- Lorazepam 1mg, temazepam 10 or 20 mg, or midazolam 7.5 mg at the day of operation
Wind (Chris).indb 59Wind (Chris).indb 59 28-05-2008 15:44:3028-05-2008 15:44:30

60
Day of Surgery
Anaesthetic management - Placement of thoracic epidural catheter (T6-T10, depending on the surgical resection); test-dose (bupivacaine 0.25% with adrenaline 1:200,000), top-up dose (bupivacaine 0.25% [±10 ml] with sufentanil 25 μg, followed by continuous infusion (bupivacaine 0.125% with fentanyl 2.5 μg.ml-1) until day 2 postoperative
- IV morphine loading (0.1 mg.kg-1) followed by continuous IV morphine infusion or PCA-morphine, OR placement of epidural catheter (T10-L1, test dose, top-up dose and continuous infusion in the same way as for fast track) when an open surgical procedure will be performed
- IV morphine loading (0.05-0.1 mg.kg-1) followed by PCA-morphine or continuous IV morphine infusion when a laparoscopic surgical procedure is performed
- Combined with balanced general anaesthesia
- Combined with balanced general anaesthesia
- Restricted per-operative fluid infusion regime (Ringers lactate 20 ml.kg-1 in the 1st h followed by RL 6 ml.kg-1.h-1)
- Standard per-operative fluid infusion regime (Ringers lactate 20 ml.kg-1 in the 1st h followed by RL 10-12 ml.kg-1.h-1)
- Use of vasopressor drugs as 1st choice for management of mean blood pressure drop > 20% of baseline
- Use of extra fluid challenge as 1st choice for management of mean blood pressure drop > 20% below baseline
- Forced body heating (Bair hugger system and warmed IV fluids)
- Forced body heating (Bair hugger system and warmed IV fluids)
- Removal of naso-gastric tube before extubation
- Naso-gastric tube remain until day 1 after surgery
- Prophylactic use of odansetron (4 mg) to prevent PONV
- Use of odansetron, dexamethason or droperidol for PONV management according to attending anaesthesiologist
Surgical Management - Minimal invasive incisions - Median laparotomy approach- Urine catheter according
to attending surgeon- No infiltration of surgical wounds
with local anaesthetic drugs
- Supra-pubic urine catheter
- Infiltration of surgical wounds with bupivacaine
Early post-operative management
- No standard use of abdominal drains - Standard use of abdominal drains
- Use of epidural catheter as mentioned before to which paracetamol 4 x 1 g.d-1 is added
- Continuous IV morphine infusion or PCA-morphine OR use of epidural catheter as mentioned before to which paracetamol 4 x 1 g.d-1 and/or diclofenac 3 x 50 mg.d-1 are added
- First oral drinks at 2 h post-surgery + IV infusion of RL 1.5 l.d-1
- Small amount of water orally + IV infusion of RL 2.5 l.d-1
- Mobilisation in the evening (>2 h out of bed)
- Bed rest
- First semi-solid food intake in the evening
Wind (Chris).indb 60Wind (Chris).indb 60 28-05-2008 15:44:3028-05-2008 15:44:30

61
Ch
apter 3
Implem
entation of a fast track program
me
Day 1 after Surgery - Oral intake > 2 l (including 4 units CHL drinks), offer solid food
- Diet increased on daily basis when normal bowel sounds are examined
- Stop IV fluid administration (leave canulla)
- IV fluid administration (2.5 l.d-1) is continued till adequate oral fluid intake
- Start laxative (MgO, 2 x 1g.d-1) - Start laxative (MgO, 2 x 1 g.d-1)
- Close supra-pubic urine catheter and remove when residue < 50 ml
- Expand mobilisation (> 6 h out of bed)
- Close supra-pubic urine catheter and remove when residue < 50 ml
Day 2 after surgery - Offer solid food- Expand mobilisation (> 8 hours)- Plan discharge
Continue as on day 1 until discharge criteria are fulfilled
Day 3 after surgery - Remove epidural catheter- Continue Paracetamol 4x 1000 mg- Add NSAID- Remove IV cannula- Expand mobilisation (> 8 hours)- Evaluating discharge criteria;
discharge if fulfilled
Continue as on day 1 until discharge criteria are fulfilled
Day 4 after surgery - Continue as on day 3 until discharge criteria are fulfilled
Continue as on day 1 until discharge criteria are fulfilled
FT: Fast-track; TC: Traditional care; CHL: carbohydrate loaded drink (Nutridrink®)
their recovery and reassured when necessary. All patients (both traditional care and fast
track) were seen at the outpatient department at a minimum of 30 days postoperatively.
Complications in the period after discharge, if any, were recorded.
Analysis of outcome parametersTo evaluate a possible learning effect with the implementation of the fast track protocol,
a comparison was made between the first and second half of patients treated since the
introduction of the fast track care programme (period I: 08-2004 to 12-2004 and period
II: 01-2005 to 07-2005).
To assess patient satisfaction with the hospitalisation, a self-report questionnaire consisting
of 16 modalities, was sent to all fast track patients within 30 days after discharge. This
questionnaire is routinely used in our hospital and includes questions concerning intake
on the surgical ward, degree of personal attention from the surgeon and nurse, transfer
of information of medical results, arrangement of discharge and questions concerning
aftercare. Patients were asked to rate their satisfaction with each single modality on a
Likert scale ranging from one (dissatisfied) to five (very satisfied). The scores of each
question are combined to form a total patient satisfaction score ranging from 16 (lowest
patient satisfaction) to 80 (highest patient satisfaction). The same questionnaire was used
previously to monitor patient satisfaction in the year 2003. Patient satisfaction of fast track
patients was compared to that of patients from the traditional care group.
Also a comparison was made between patients who underwent open resection with those
Wind (Chris).indb 61Wind (Chris).indb 61 28-05-2008 15:44:3028-05-2008 15:44:30

62
who underwent a laparoscopic resection, according to the type of perioperative care. So, a
subanalysis of four subgroups was performed: 1) open resection and fast track care (Open-
fast track group), 2) laparoscopic resection and fast track care (Lap-fast track group),
3) open resection and traditional care (Open-traditional care group) and 4) laparoscopic
resection and traditional care (Lap-traditional care group).
Statistical analysisData are presented as median values with ranges for continuous and discrete data,
unless otherwise specified. Categorical data are presented as frequencies or percentages.
Differences between groups were tested using Kruskal Wallis test or Mann-Whitney U
test for continuous data, depending on the number of groups compared. The Fisher’s
exact test or Chi-square test when appropriate were used to test for differences between
groups in case of categorical data. A p-value <0.05 was considered statistically significant
for all tests. Statistical analysis was done using the SPSS v.12.0 package (SPSS, Chicago,
Illinois, USA).
Results
A total of 107 patients were included in this study: 55 in the fast track group and 52 in the
traditional care group. None of the patients eligible for the fast track programme refused
participation in the study. Patient characteristics of the fast track and traditional care
patients are shown at Table 3. The fast track and traditional care group were comparable
for all patient characteristics although there were more open procedures and a trend to
more stomas in the traditional care compared to the fast track group. Within the fast track
group, patient characteristics of patients treated in the first and second fast track period
were comparable (data not shown). Patient characteristics of the four subgroups (data not
shown) were comparable except for a higher number of primary diverting stomas in the
open traditional care group compared to the laparoscopic fast track group (p<0.01).
Protocol complianceAn average of 7.4 out of a potential of 13 evaluated fast track modalities were successfully
applied per patient. Results of the degree of protocol compliance per fast track modality
are given at Table 4, ranging from 13% (intake of two CHL drinks the evening after surgery)
to 100% (prevention of hypothermia and omission of bowel preparation).
There were no differences in protocol compliance between the first and the second fast
track period in any of the evaluated variables, although a small improvement in the number
of patients receiving epidural analgesia in the second fast track period could be observed
(period II vs. period II: 58% vs. 81%, respectively; p=0.08).
Wind (Chris).indb 62Wind (Chris).indb 62 28-05-2008 15:44:3128-05-2008 15:44:31

63
Ch
apter 3
Implem
entation of a fast track program
me
Patient’s satisfaction
The response rate of the patient’s satisfaction questionnaire was 78% and 81% in the
fast track and traditional care group respectively. Total patients satisfaction score was
comparable in both groups (50.4 and 49.8 out of a potential 80 points in the fast track
and traditional care group respectively, p=0.84). The intake at the surgical ward was
evaluated more positively in the fast track group (mean score 3.8 and 3.3 in the fast track
and traditional care group respectively, P=0.02). Satisfaction between the two groups
with all of the other single modalities was comparable.
Outcome after fast track vs. traditional care (Table 5)Overall morbidity and number of major and minor complications of the fast track and
traditional care groups were comparable. However, it seemed that more patients in the fast
track group had an anastomotic leakage (n=6 (11%) vs. n=2 (4%), p=0.27). Reoperation
rate was comparable and median primary hospital stay was reduced by two days (p<0.01).
Despite an increase in the number of readmissions in the fast track group, total hospital
Table 3. Patient characteristics and type of resection according to care protocol
TCN=52
FTN=55
P†
Age (years)
-median (range) 47 (18-89) 49 (20-79) 0.224‡
ASA n (%) 0.402
-1 25.0 32.7
-2 75.0 67.3
Gender ratio (M:F) n 21:31 13:42 0.096
Body mass index (kg/m2)
-median (range) 24.0(15.2-37.7) 23.5(15.7-39.3) 0.803‡
CR-POSSUM operative severity score
-median (range) 7.0 (7-11) 7.0 (7-13) 0.395‡
Type of operation n (%) 0.804§
-ileocolic (re-) resection 15 (28.8) 19 (34.5)
-right hemicolectomy 10 (19.2) 6 (10.9)
-sigmoid resection 12 (23.1) 17 (30.9)
-rectal resection (anterior + low anterior) 10 (19.2) 10 (18.2)
-subtotal / total resection 3 (5.8) 2 (3.6)
-other partial colonic resection 2 (3.8) 1 (1.8)
Indication for resection n (%) 0.695
-malignant disease 21 (40.4) 20 (36.4)
-benign disease 31 (59.6) 35 (63.6)
Laparoscopic operation n (%) 17 (32.7) 29 (52.7) 0.051
Primary (temporary) stoma n (%) 13 (25.0) 7 (12.7) 0.138†Fisher´s exact test unless otherwise specified; ‡Mann Whitney U test; §Chi square test; TC: Traditional care; FT: Fast track care; CR-Possum: Colorectal Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity
Wind (Chris).indb 63Wind (Chris).indb 63 28-05-2008 15:44:3128-05-2008 15:44:31

64
Table 4. Degree of protocol compliance in fast track patients per evaluated modality
Evaluated modality Degree of compliance
Omission of bowel preparation n (%)
-yes 55 (100)
-no 0 (0)
Prevention of hypothermia n (%)
-yes 55 (100)
-no 0 (0)
Pre-operative counselling by FT nurse n (%)
-yes 48 (87.3)
-no 7 (12.7)
Intake of 4 CHL drinks on day before surgery n (%)
-yes 46 (83.6)
-no 8 (26.4)
Epidural anaesthesia n (%)
-yes 39 (70.9)
-T7-T10 level -22 (40.0)
-below T10 level -17 (30.9)
-no 16 (29.1)
Prophylactic PONV medication n (%)
-yes 37 (67.3)
-no 18 (32.7)
Intake of 2 CHL drinks 2 hours before surgery n (%)
-yes 37 (67.3)
-no 18 (32.7)
Suprapubic catheter n (%)
-yes 26 (47.3)
-no 29 (52.7)
Omission of evening medication n (%)
-yes 22 (40.0)
-no 33 (60.0)
Omission of pre-medication n (%)
-yes 17 (30.9)
-no 38 (69.1)
Intake of 2 CHL drinks on evening after surgery n (%)
-yes 7 (12.7)
-no 48 (87.3)
Total oral daily intake of fluids after operation (ml)
-POD 1 (first day after surgery) 944
-POD 2 1313
-POD 3 1622
Total duration of daily mobilisation after operation (min)
-POD 0 (day of surgery) 29
-POD 1 110
-POD 2 178
-POD 3 339
FT: Fast-track; POD0: day of surgery; POD1: first day after surgery; POD2: Second Day after surgery; POD3: Third day after surgery; CHL: carbohydrate loaded drink; PONV: post-operative nausea or vomiting prophylaxis
Wind (Chris).indb 64Wind (Chris).indb 64 28-05-2008 15:44:3128-05-2008 15:44:31

65
Ch
apter 3
Implem
entation of a fast track program
me
stay was reduced with 2.5 days (p=0.03). There was no mortality within 30 days after
surgery in either group.
Outcome after first fast track period compared to second fast track periodOverall morbidity rate seemed to decrease in the second compared to the first fast track
period (Period I: n=10 vs. Period II: n=5, p=0.07) as was the case for the number of major
complications (Period I: n=6 vs. Period II: n=2, p=0.07). Primary hospital stay was 4.0 days in
both periods and total hospital stay was 4.5 days in the first fast track period compared to
4.0 days in the second fast track period (p=0.43). All other evaluated outcome parameters
for both periods were comparable as well (data not shown).
Outcome differences of fast track vs. traditional care according to type of surgery (Table 6)Within the laparoscopic groups, there was no significant difference in primary and total
hospital stay (p=0.13 and p=0.44, respectively). There also was no difference in overall
morbidity (p=0.49). Major complications and reoperations occurred more frequent in the
fast track group (n=0 and n=5 for both major complication rate and reoperation rate in the
Table5. Postoperative results according to care protocol
TC N=52
FT N=55
P†
Overall morbidity <30 days n (%) 16 (30.8) 15 (27.3) 0.831
Major complications n (%) 8 (15.4) 8 (14.6) 1.000
- anastomotic leakage 2 6
- abdominal bleeding 2 0
- abdominal abscess 2 0
- myocardial ischemia 2 0
- persistent ileus requiring re-operation 0 1
- iatrogenic perforation requiring re-operation 0 1
Minor complications n (%) 8 (15.4) 7 (12.7) 0.784
- urinary tract infection 1 1
- wound infection 4 4
- supraventricular arrythmia 0 1
- NSAID gastritis 1 0
- high output stoma with dehydration 1 0
- persistent ileus treated conservatively 1 1
Re-operation n (%) 5 (9.6) 7 (12.7) 0.516
PHS (days)
-median (range) 6.0 (2-36) 4.0 (2-33) 0.002
THS (days)
-median (range) 6.5 (2-36) 4.0 (2-33) 0.027
Readmissions <30 days (%) 3 (5.8) 6 (10.9) 0.490
Mortality <30 days (n) 0 (0) 0 (0) -†TC vs. FT; PHS: primary hospital stay; THS: total hospital stay; TC: Traditional care; FT: Fast track care
Wind (Chris).indb 65Wind (Chris).indb 65 28-05-2008 15:44:3128-05-2008 15:44:31

66
Table 6. Subanalysis of postoperative results according to care protocol and type of surgery
Lap-TCN=17
Lap-FTN=29
Open-TCN=35
Open-FTN=26
P§
Overall morbidity <30 days n (%) 3 (17.6) 9 (31.0) 13 (37.2) 6 (23.1) 0.441
Major complications n (%) 0 (0.0) 5 (17.2) 8 (22.9) 3 (11.5) 0.167
Minor complications n (%) 3 (17.6) 4 (13.8) 5 (14.3) 3 (11.5) 0.907
Re-operation n (%) 0 (0.0) 5 (17.2) 5 (14.3) 2 (7.7) 0.243*
PHS (days)
-median (range) 5.0 (3-18) 4.0 (2-33) 8.0 (2-36) 4.5 (2-19) 0.000**
THS (days)
-median (range) 5.0 (3-18) 4.0 (2-33) 8.0 (2-36) 5.0 (2-23) 0.002***
Readmissions <30 days n (%) 0 (0.0) 3 (10.3) 3 (8.6) 3 (11.5) 0.566
Mortality <30 days n (%) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) -§Lap-TC vs. Lap-FT vs. Open TC vs. Open FT; PHS: primary hospital stay; THS: total hospital stay; TC: Traditional care; FT: Fast track care
P
* Re-operation rate: Lap TC vs Lap FT: 0.073
Lap FT vs Open TC: 0.557
Lap TC vs Open TC: 0.105
Lap FT vs Open FT: 0.232
Lap TC vs Open FT: 0.247
Open TC vs Open FT: 0.428
** PHS: Lap TC vs Lap FT: 0.131
Lap FT vs Open TC: 0.000
Lap TC vs Open TC: 0.003
Lap FT vs Open FT: 0.077
Lap TC vs Open FT: 0.762
Open TC vs Open FT: 0.017
***THS: Lap TC vs Lap FT: 0.437
Lap FT vs Open TC: 0.001
Lap TC vs Open TC: 0.001
Lap FT vs Open FT: 0.069
Lap TC vs Open FT: 0.314
Open TC vs Open FT: 0.083
FT: Fast-track group; TC: Traditional care group; Lap-TC: group of patients operated laparoscopically and treated in a traditional care programme; Lap-FT: group of patients operated laparoscopically and treated in a fast track programme; Open-TC: group of patients operated by an open approach and treated in a traditional care programme; Open-FT: group of patients operated by an open approach and treated in a fast track programme; PHS: Primary hospital stay; THS: Total hospital stay
Lap-traditional care and Lap-fast track group respectively; p=0.07).
Within the open groups there was a significant reduction in primary hospital stay in the
fast track compared to the traditional care group (8 vs. 4.5 days, p=0.02). Total hospital
Wind (Chris).indb 66Wind (Chris).indb 66 28-05-2008 15:44:3128-05-2008 15:44:31

67
Ch
apter 3
Implem
entation of a fast track program
me
stay was shorter as well, although not significantly (8 vs. 5 days, p=0.08). There were no
significant differences in overall morbidity, reoperation and major and minor complication
rates (Table 6).
Outcome differences of laparoscopic vs. open surgery according to type of perioperative care (Table 6)Within the fast track groups, both primary and total hospital stay seemed shorter in the
laparoscopic group (Table 6, reduction 0.5 and 1 day for primary hospital stay and total
hospital stay respectively, p=0.08 and p=0.07 respectively). There were no differences in
overall morbidity, and the number of major and minor complications between the open
and laparoscopic group (p=0.56, p=0.71, and p=0.70 respectively).
Within the traditional care groups, a reduction of three days of both primary and total
hospital stay was found in the laparoscopic compared to the open group (Table 4, p<0.01
and p<0.01, respectively). Overall morbidity rate and reoperation rate were higher in the
open group because of a significant higher rate of major complications in this group (Table
6, p=0.04).
Discussion
The present study showed that full implementation of a fast track care programme for
patients undergoing an elective segmental colorectal resection is troublesome, since overall
7.4 out of the predefined items were achieved. However despite a relatively low protocol
compliance, hospital stay is reduced without affecting overall morbidity and without
affecting patient satisfaction. It further indicates that the combination of laparoscopy and
fast track care might have an amplifying effect.
The implementation of a fast track care programme for colorectal surgery requires a
dedicated and motivated team of which the surgeon, anaesthesiologist and nursing team
are the mainsprings. The 180 degrees reversal in policy affecting current practice of three
different disciplines appeared difficult to apply in daily clinical practice. The change of
a delayed mobilisation into early mobilisation, the change of pre-operative fasting into
pre-operative feeding and the introduction of epidural analgesia in laparoscopic surgery
were important bottlenecks in the present study. The involved personnel need to be
trained, and probably the training must be repeated to maintain a high compliance. The
efforts to incorporate such an intensive and multidisciplinary programme in a hospital
should therefore not be underestimated.
Nonetheless, some of the fast track components are already implemented in a modern
traditional care programme; omission of bowel preparation, restrictive use of abdominal
drains and naso-gastric tubes, early mobilisation and advancement of oral diet, are
common practice in many hospitals. Those changes in daily practice are partly instigated
by the implementation of laparoscopic surgery.
Wind (Chris).indb 67Wind (Chris).indb 67 28-05-2008 15:44:3228-05-2008 15:44:32

68
Despite strenuous efforts of the study coordinators of the involved disciplines to comply
with all modalities of the fast track protocol, compliance with each of the single modalities
was relatively low; only a mean of 7.4 out of a potential 13 evaluated fast track modalities
per patient were achieved. In contrast to what could be expected, protocol compliance
did not improve significantly with increasing experience with the programme. Only, a
non-significant improvement in protocol compliance with the number of patients receiving
epidural analgesia in the second fast track period was observed. Possibly a much longer
period of training is necessary to break with the longstanding traditions in traditional care.
Still, despite the relatively low compliance, a significant reduction in primary and total
hospital stay was observed. This finding seems to suggest that it is rather the protocolised
way of perioperative treatment that enhances recovery, than it is the combined effect of
each of the single fast track modalities. Working according to the fast track protocol, there
is no argue about removal of i.v. drips, epidural catheters, urine catheters, advancement
of diet and mobilisation. Another important explanation could be the fact that by inviting
patients to participate in a “fast-track” programme, both the patient and the surgeon are
committed to work together striving for an enhanced recovery. The clear goals for the
patient to reach every day and possibly also the expectations that are being raised by the
term “fast” may have contributed to the reduced hospital stay as well.
In the present study, overall morbidity between the fast track and traditional care group
was comparable. This is in accordance with data from a meta-analysis comparing fast
track and traditional care in patients requiring segmental colonic resection.9 Although the
number of readmitted patients seemed higher in the fast track compared to the traditional
care group, total hospital stay was shorter in the fast track group. A feared complication of
fast track care programmes is an increased incidence of anastomotic leakages, supposed
to be caused by the early start of oral feeding. In the present study, more patients with an
anastomotic leakage were found in the fast track compared to the traditional care group.
This probably represents an unfortunate coincidence, since all leakages occurred in the
first fast track period and none occurred in the second fast track period. In literature there
is no association of anastomotic leakage with the absence of bowel preparation or early
feeding.9
Several randomised trials have demonstrated that a laparoscopic approach reduces
hospital stay after segmental colorectal resection for cancer16-19 and inflammatory bowel
disease20;21 in a traditional care programme. Theoretically, the combination of fast track
care with laparoscopy might be the most optimal combination. In this way the minimal
invasive incisions are combined with the advantages of the optimization package of the
fast track programme. Because the numbers of patients in each subgroup were too small,
no robust conclusions can be drawn from the comparison between the four subgroups in
which open and laparoscopic surgery as well as traditional care and fast track care were
compared. Nonetheless, a reduction in primary and total hospital stay in the open fast
track compared to the open traditional care group was found. This might be attributed
to the implementation of the fast track care programme. By combining laparoscopic
Wind (Chris).indb 68Wind (Chris).indb 68 28-05-2008 15:44:3228-05-2008 15:44:32
69
Ch
apter 3
Implem
entation of a fast track program
me
surgery and fast track care, a further decrease in primary and total hospital stay might be
achieved. Despite the relatively small number of patients in this pilot study, the findings
of the present study justify these findings to be tested in a randomised controlled trial.
At present such a study is being conducted in a multi-centre randomised setting.22 In this
trial the cost-effectiveness of the fast track programme compared to laparoscopy alone or
in combination with laparoscopy should be evaluated as well. ASA III patients, who were
not included in the present study are included in this multicentre trial as well. The reason
that only ASA I and ASA II patients were included in the present study was because it
was the authors expectation that ASA I and ASA II patients would optimally benefit from
the fast track protocol. Recent studies however have shown that ASA III patients may also
benefit from a fast track treatment protocol. This was unknown at the time the authors
started the study.
In conclusion, successful implementation of a fast track programme appeared difficult.
Despite a relatively low compliance, a reduction of 2.5 days of hospital stay was achieved,
indicating that it is rather the combination of the protocolised way of perioperative
treatment and patients expectations that enhances recovery. The role and necessity of
each single modality as well as the place of laparoscopy both within and compared to
such a programme remain to be determined.
Reference List
(1) Fearon KC, Ljungqvist O, von Meyenfeldt MF, Revhaug A, Dejong CH, Lassen K, et al. Enhanced recov-ery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr 2005;24:466-477.
(2) Wilmore DW, Kehlet H. Management of patients in fast track surgery. BMJ 2001;322:473-476.
(3) Basse L, Thorbol JE, Lossl K, Kehlet H. Colonic surgery with accelerated rehabilitation or conventional care. Dis Colon Rectum 2004;47:271-277.
(4) Anderson AD, McNaught CE, MacFie J, Tring I, Barker P, Mitchell CJ. Randomized clinical trial of multi-modal optimization and standard perioperative surgical care. Br J Surg 2003;90:1497-1504.
(5) Bradshaw BG, Liu SS, Thirlby RC. Standardized perioperative care protocols and reduced length of stay after colon surgery. J Am Coll Surg 1998;186:501-506.
(6) Delaney CP, Fazio VW, Senagore AJ, Robinson B, Halverson AL, Remzi FH. ‘Fast track’ postoperative management protocol for patients with high co-morbidity undergoing complex abdominal and pelvic colorectal surgery. Br J Surg 2001;88:1533-1538.
(7) Gatt M, Anderson AD, Reddy BS, Hayward-Sampson P, Tring IC, MacFie J. Randomized clinical trial of multimodal optimization of surgical care in patients undergoing major colonic resection. Br J Surg 2005;92:1354-1362.
(8) Raue W, Haase O, Junghans T, Scharfenberg M, Muller JM, Schwenk W. ‚Fast-track‘ multimodal reha-bilitation programme improves outcome after laparoscopic sigmoidectomy: a controlled prospective evaluation. Surg Endosc 2004;18:1463-1468.
Wind (Chris).indb 69Wind (Chris).indb 69 28-05-2008 15:44:3228-05-2008 15:44:32

70
(9) Wind J, Polle SW, Fung Kon Jin PH, Dejong CH, von Meyenfeldt MF, Ubbink DT, et al. Systematic review of enhanced recovery programmemes in colonic surgery. Br J Surg 2006;93:800-809.
(10) Bardram L, Funch-Jensen P, Kehlet H. Rapid rehabilitation in elderly patients after laparoscopic colonic resection. Br J Surg 2000;87:1540-1545.
(11) Basse L, Hjort JD, Billesbolle P, Werner M, Kehlet H. A clinical pathway to accelerate recovery after colonic resection. Ann Surg 2000;232:51-57.
(12) Kehlet H, Mogensen T. Hospital stay of 2 days after open sigmoidectomy with a multimodal rehabilita-tion programmeme. Br J Surg 1999;86:227-230.
(13) Zutshi M, Delaney CP, Senagore AJ, Fazio VW. Shorter hospital stay associated with fast track postop-erative care pathways and laparoscopic intestinal resection are not associated with increased physical activity. Colorectal Dis 2004;6:477-480.
(14) Basse L, Jakobsen DH, Bardram L, Billesbolle P, Lund C, Mogensen T, et al. Functional recovery after open versus laparoscopic colonic resection: a randomized, blinded study. Ann Surg 2005;241:416-423.
(15) King PM, Blazeby JM, Ewings P, Franks PJ, Longman RJ, Kendrick AH et al. Randomized clinical trial comparing laparoscopic and open surgery for colorectal cancer within an enhanced recovery programme. Br J Surg 2006;93:300-308.
(16) Abraham NS, Young JM, Solomon MJ. Meta-analysis of short-term outcomes after laparoscopic resec-tion for colorectal cancer. Br J Surg 2004;91:1111-1124.
(17) Curet MJ, Putrakul K, Pitcher DE, Josloff RK, Zucker KA. Laparoscopically assisted colon resection for colon carcinoma: perioperative results and long-term outcome. Surg Endosc 2000;14:1062-1066.
(18) Lacy AM, Garcia-Valdecasas JC, Delgado S, Castells A, Taura P, Pique JM et al. Laparoscopy-assisted colectomy versus open colectomy for treatment of non-metastatic colon cancer: a randomised trial. Lancet 2002;359:2224-2229.
(19) Schwenk W, Bohm B, Muller JM. Postoperative pain and fatigue after laparoscopic or conventional colorectal resections. A prospective randomized trial. Surg Endosc 1998;12:1131-1136.
(20) Maartense S, Dunker MS, Slors JF, Cuesta MA, Gouma DJ, van Deventer SJ et al. Laparoscopic-assisted versus open ileocolic resection for Crohn’s disease: a randomized trial. Ann Surg 2006;243:143-149.
(21) Milsom JW, Hammerhofer KA, Bohm B, Marcello P, Elson P, Fazio VW. Prospective, randomized trial comparing laparoscopic vs. conventional surgery for refractory ileocolic Crohn’s disease. Dis Colon Rectum 2001;44:1-8.
(22) Wind J, Hofland J, Preckel B, Hollmann MW, Bossuyt PM, Gouma DJ, et al. Perioperative strategy in colonic surgery; LAparoscopy and/or FAst track multimodal management versus standard care (LAFA trial).BMC Surg. 2006;6:16.
Wind (Chris).indb 70Wind (Chris).indb 70 28-05-2008 15:44:3228-05-2008 15:44:32

4Chapter
Systematic review of laparoscopic versus open colonic resection within a fast track
perioperative care programme
MS VlugJ Wind
DT UbbinkHA Cense
E van der ZaagWA Bemelman
Submitted
Wind (Chris).indb 71Wind (Chris).indb 71 28-05-2008 15:44:3228-05-2008 15:44:32

7272
Abstract
IntroductionFast track perioperative care programmes accelerate recovery, reduce morbidity and
shorten hospital stay. It is unclear what the effects are of laparoscopic and open surgery
within a fast track perioperative care programme. Aim of this systematic review was to
review the existing evidence.
MethodsA systematic review was performed of all randomised (RCTs) and controlled clinical trials
(CCTs) on laparoscopic and open surgery within a fast track perioperative care programme.
Main endpoints were primary and overall hospital stay, readmission rate, morbidity
and mortality. Study selection, quality assessment and data extraction were performed
independently by two observers.
ResultsOnly two RCTs and three CCTs were eligible for final analysis, which reported on 400
patients. Data could not be pooled because of clinical heterogeneity. Two studies stated a
shorter primary hospital stay in the laparoscopic group of two and three days. In one study
the readmission rate was lower in the laparoscopic group, the absolute risk reduction was
21.4% (95% confidence interval [CI]: 6% to 42.3%) and a “number needed to treat” (NNT)
of 4.7 patients. One study showed a 23 % difference in favour of the laparoscopic group
with regard to morbidity (95% CI: 6.3% to 39.1%), i.e. a NNT of 4.4 patients. There were
no significant differences in mortality rates.
ConclusionDue to the present lack of data, no robust conclusions can be made. A large randomised
controlled trial is required to compare laparoscopic with open surgery within a fast track
perioperative care setting.
Wind (Chris).indb 72Wind (Chris).indb 72 28-05-2008 15:44:3228-05-2008 15:44:32

73
Ch
apter 4
Systematic review
of laparoscopic versus open colonic resection
Introduction
A recent development in elective large bowel surgery is the introduction of enhanced
recovery programmes after surgery (ERAS®)1;2, also referred to as fast track perioperative
care. It combines a number of elements aiming at a faster recovery after surgery and
to reduce the surgical stress response.3-12 This multidisciplinary protocol is developed
by Kehlet et al. for all patients undergoing elective segmental colectomy enabling a
faster recovery resulting in an earlier discharge as compared to traditional care.4-6;9-11
Furthermore, postoperative morbidity might be reduced in a fast track perioperative
care setting.5-7;9;13;14 The essence of fast track perioperative care consists of extensive
preoperative counselling, no bowel preparation, no sedative premedication, carbohydrate
loaded liquids until two hours before surgery, thoracic epidural anaesthesia, short acting
anaesthetics, perioperative intravenous fluid restriction, small incisions, and no routine use
of drains and nasogastric tubes. Postoperative care includes non-opioid pain management,
early oral feeding, enforced mobilisation, early removal of bladder catheter and standard
laxative.1-12;15
Laparoscopic surgery was first described in 1991 and is still increasingly popular.16
Advantages of laparoscopic surgery are a reduced hospital stay of about four to eight
days17-22, less morbidity and less postoperative pain.17;21-26 After open colorectal surgery
postoperative hospital stay is about six to 11 days.17-22 It is unclear what the difference is
in hospital stay and clinical endpoints between laparoscopic and open surgery in a fast
track perioperative care programme. The aim of this systematic review was to appreciate
the existing high-level evidence on these differences.
Methods
Data searchMedline database (from January 1950 to August 2007), EMBASE and the Cochrane Library
(both from January 1980 to August 2007) were searched for randomised controlled trials
(RCTs) or controlled clinical trials (CCTs) with a prospective intervention group comparing
laparoscopic surgery with open surgery within an enhanced recovery programme,
using the following MeSH (Medical Subject Headings) terms and free text words; fast
track, enhanced recovery, ERAS, laparoscopy, laparoscopic, minimally invasive, surgery,
laparotomy, open, colon, colonic, colorectal or rectal.
Electronic links to related articles and references of selected articles were hand-searched
as well. Leading investigators in the field were contacted to inquire whether studies were
ongoing or publications were recently submitted. A hand-search of relevant journals and
conference proceedings was not performed. No language restriction was applied.
Wind (Chris).indb 73Wind (Chris).indb 73 28-05-2008 15:44:3328-05-2008 15:44:33

74
Study selection, quality assessment and data extractionFrom the potentially eligible studies, two investigators (JW, MSV) independently
selected suitable studies on the basis of their titles and abstracts. Studies were included
if they reported the following primary endpoints: age, gender, American Society of
Anaesthesiologists (ASA) classification, type of resection, primary (PHS) and/or overall
hospital stay (OHS), readmission rate, morbidity, mortality, and whether at least four fast
track elements were used in a standardised protocol. If an eligible study did not specify
at least one of these endpoints, it was excluded. The arbitrary number of four fast track
elements was chosen because fewer elements might represent ‘modern’ traditional care.
Secondary endpoints were: quality of life, gastrointestinal function, and the use of pain
medication.
In case of disagreement, full papers were obtained for final judgement. Discrepancies
were resolved by discussion. Final inclusion was done after consensus was reached. The
remaining trials were critically appraised using the standard checklist from the Dutch
Cochrane Collaboration.27 Subsequently, study data on the predefined endpoints were
extracted, again independently by the two investigators.
Data analysisPrimary hospital stay (PHS) is expressed as a median value and inter-quartile range (IQR) or
range for each surgical treatment group, calculated from the date of operation to the date
of discharge. Overall hospital stay (OHS) was defined as PHS including the hospitalisation
period of patients readmitted within 30 days of surgery. Readmission rate, morbidity
and mortality are presented as a percentage of the included patients in each surgical
treatment group. Morbidity was defined as the reported major and/or minor morbidity
rates within 30 days after surgery. The authors of the papers included, were asked to send
the median, inter-quartile range, and range of their PHS and OHS for proper statistical
analysis. For dichotomous outcomes (readmission, morbidity, and mortality) the Absolute
Risk Reduction (ARR), Number Needed to Treat (NNT) and 95% confidence intervals (CIs)
were calculated. In the absence of clinical heterogeneity a meta-analysis was attempted.
Results
Included studiesThe search identified 178 publications of which 171 were excluded, because those
studies did not match the criteria for inclusion. From the seven selected studies28-34 two
studies33;34 were excluded because all data was used in one of the other selected studies.
Of the three studies29;33;34 reporting on the same data, the study by Junghans et al.29
was included in the final analysis, because both other studies33;34 reported on smaller
sample sizes. Five studies28-32 remained for final analysis, comprising of two RCTs28;30 and
three CCTs.29;31;32 The selection process of the studies included is summarised in Figure 1.
Wind (Chris).indb 74Wind (Chris).indb 74 28-05-2008 15:44:3328-05-2008 15:44:33

75
Ch
apter 4
Systematic review
of laparoscopic versus open colonic resection
The included studies were published between 2004 and 2008 and reported on a total of
400 patients, ranging from 55 to 147 patients per study.
In Table 1 overall quality assessment is presented. Patient characteristics and results of the
included studies are shown in Table 2.
The individual data could not be pooled because of clinical heterogeneity among the
studies, for instance different inclusion criteria and different surgical procedures. Hence,
only individual study results are presented.
Methodological quality of the studiesTwo studies, by Basse et al.28 and King et al.30, were RCTs. The others by Mackay et al.31,
Junghans et al.29 and Polle et al.32 were CCTs. The five studies had several limitations.28-32 All
had relatively small sample sizes. One of the two RCTs did not describe how randomisation
was performed.28 Hence, allocation concealment was unclear. Only the study by Basse et
al. was double-blinded, i.e. for both patients and data assessors.28 The included patients
had an opaque dressing covering their whole abdomen, which was applied after surgery
and was not removed until the decision about discharge had been taken. In the other
studies the non-blinded study design and data collection may have caused observer bias,
which theoretically could have been in favour of the laparoscopic group. In the study
by Basse et al. the non-trial treatment differed between the groups.28 Patients in the
open group received an additional epidural dose of morphine. Only three studies applied
well-defined discharge criteria, which is of major importance as hospital stay is one of
Figure 1. Flow chart of study inclusion
Wind (Chris).indb 75Wind (Chris).indb 75 28-05-2008 15:44:3328-05-2008 15:44:33

76
the outcome parameters. The analysis of Polle et al.32 was a subgroup analysis. In this
study patients were included who underwent an elective open or laparoscopic segmental
colorectal resection within an enhanced recovery programme or traditional care setting.
The investigators mainly focused on the difficulties implementing fast track surgery.
Table 1. Quality assessment
Reference Year Study designConcealmentof allocation
Intention to treat
Blinding anddata collection
RCTs
Basse et al. 28 2005 RCT Unclear Yes Patient: yesPhysician: noObserver: yes
King et al.30 2005 RCT Yes Yes Not blinded
CCTs
MacKay et al.31 2006CCT
Both groups prospective
No Yes Not blinded
Junghans et al.29 2006CCT
Both groups prospective
No YesNot blinded
Polle et al. 322008
CCTBoth groups prospective
No YesNot blinded
Open: Open surgery; Lap: Laparoscopic surgery; RCT: Randomised Controlled Trial; CCT: Controlled Clinical Trial
Table 2. Demographics, patient characteristics, and results of the included studies
Reference N Lap / Open
Age (years)Lap / Open
% ASA I&IILap / Open
Type of surgery
RCTs
Basse et al.28 30 / 30 75.5 / 75 83 / 63 RH, SR
King et al.30 41 / 19 72.3 / 70.4(mean)
78 / 84 LH, RH, SR, AR, APR
CCTs
MacKay et al.31 21 / 57 72.0 / 73.2 77 / 74 LH, RH, AR, HC
Junghans et al.29 100 / 47 65 / 67 67 / 51.1 SR, RR
Polle et al.32 29 / 26 46.4 / 50.4 100 / 100 SC, IR
* p<0.05; NR: Not Reported; Continuous data: median (IQR or range); LH: Left Hemicolectomy; RH: Right Hemicolectomy;
SC: Subtotal Colectomy; SR: Sigmoid Resection; RR Rectal Resection; IR: Ileocolic Resection; AR: Anterior Resection;
APR: AbdominoPerineal Resection; HC: Hartmann Closure; ASA: American Society of Anaesthesiologists
Wind (Chris).indb 76Wind (Chris).indb 76 28-05-2008 15:44:3428-05-2008 15:44:34

77
Ch
apter 4
Systematic review
of laparoscopic versus open colonic resection
Comparability at baseline
Follow -upCompletefollow- up
Similar non-trial treatment
Yes 30 days 100 % NoIn open group additional dose of
epidural morphine
Yes 3 months 100 % Yes
Yes 3 months 88 % Yes
Yes 30 days 100 % Yes
Yes 30 days 100 % Yes
PHS (days)Lap / Open
OHS (days)Lap / Open
Readmissions % (n)Lap / Open
Morbidity % (n)Lap / Open
Mortality % (n)Lap / Open
2 (range 2-20) /2 (range 2-5)
2 (NR) /2 (NR)
20 (6) / 26.6 (8) 26.6 (8) / 20 (6) 0 / 10 (3)
5 (IQR 3-6) /8 (IQR 5-9.25)*
6 (IQR 3-11) / 8.5 (IQR 6-12.5)*
4.6 (2) / 26.3 (5)* 14.9 (6) / 26.3 (5) 2.4 (1) / 5.3 (1)
6 (IQR 5-9) /6 (IQR 5-10)
NR 0 / 3.4(2) 27.2 (6) / 22.4 (13) 4.5 (1) / 1.7 (1)
4 (range 3-123) /6 (range 3-79)*
NR NR 22 (22) / 44.7 (21)* 0 / 0
4 (IQR 3-5.5) / 4.5 (IQR 4-8.25)
4 (IQR 3-6.5) /5 (IQR 4-10.25)
10.3 (3) / 11.5 (3) 31.0 (9) / 23.1 (6) 0 / 0
Wind (Chris).indb 77Wind (Chris).indb 77 28-05-2008 15:44:3428-05-2008 15:44:34

78
Primary outcome parameters
Primary and overall hospital stay
All five studies reported on PHS.28-32 One RCT30 and one CCT29 reported a shorter PHS
after laparoscopy. The randomised trial of King et al. showed a significant difference in
PHS of three days. The PHS was five (IQR 3-6) days in the laparoscopic surgery group
versus eight (IQR 5-9.25) days in the open surgery group (Table 2).30 In the study by
Junghans et al. the authors reported a PHS of four (range 3-123) days in the laparoscopic
group versus six (range 3-79) days in the open group.29
Overall the PHS varied widely between the studies. The largest difference was seen
between the RCT of Basse et al.28 and the CCT of MacKay et al.31 Basse et al. reported
a PHS of two (range 2-20) days in the laparoscopic group and two (range 2-5) days in
the open group.28 MacKay et al. reported a PHS of six (IQR 5-9) days in the laparoscopic
group and six (IQR 5-10) days in the open group.31
Overall hospital stay was reported in three studies.28;30;32 Only the RCT of King et al.
showed a significant shorter OHS in the laparoscopic group; six (IQR 3-11) days versus 8.5
(IQR 6-12.5) days.30
Readmission rate
Readmission rates were reported in four studies.28;30-32 A large variation was observed in
readmission rates among the studies (Table 2). Concerning the laparoscopic surgery group,
the highest readmission rate of 20% was reported by Basse et al.28 and the lowest (0%)
was reported by MacKay et al.31 With respect to the open surgery group the same two
studies reported the highest (26.6%) and lowest (3.4%) readmission rates, respectively.
MacKay et al. who readmitted the lowest number of patients reported the longest PHS;
six days in both treatment groups.31
In the study by King et al. the readmission rate was significantly lower in the laparoscopic
group; ARR of 21% (95% CI: 0.6% to 42.3%), resulting in a NNT of 4.7 patients.30 The
other studies did not show a significant difference in readmission rates between the two
surgical techniques.
Morbidity and mortality
Morbidity rates were reported in all studies. Only in the study by Junghans et al. a 23%
difference in favour of the laparoscopic group was shown (95% CI: 6.3% to 39.1%), i.e.
a NNT of 4.4 patients.29 In the included studies, there were no significant differences
between the treatment groups with regard to mortality (Table 3).
Number of fast track items
The application of the 17 fast track perioperative care elements varied among the studies
(Table 4). The median number of fast track elements that was applied in the five studies was
13 (IQR 11.5-14.5). Preoperative counselling, fluid restriction, no routine use of nasogastric
tubes, enforced postoperative oral feeding/mobilisation, and early removal of the bladder
Wind (Chris).indb 78Wind (Chris).indb 78 28-05-2008 15:44:3428-05-2008 15:44:34

79
Ch
apter 4
Systematic review
of laparoscopic versus open colonic resection
catheter was required by protocol in all studies. Other fast track care elements, such as the
omission of bowel preparation and no premedication, were less frequently executed.
Table 3. Numbers needed to treat (NNT) and absolute reduced risk (ARR) with corresponding 95% confidence
intervals
Reference Readmissions Morbidity Mortality
RCTs
Basse et al.28 NNT 15.0ARR 0.067 (-0.147 - 0.280)
NNT -15.0ARR -0.067 (-0.280 - 0.147)
NNT 10ARR 0.100 (-0.007 - 0.207)
King et al.30 NNT 4.7ARR 0.214 (0.006 - 0.423)
NNT 8.5ARR 0.117 (-0.109 - 0.342)
NNT 35.5ARR 0.028 (-0.083 - 0.139)
CCTs
MacKay et al.31 NNT 28.5ARR 0.035 (-0.013 - 0.083)
NNT -17.3ARR -0.058 (-0.279 - 0.164)
NNT -33.2ARR -0.030 (-0.127 - 0.067)
Junghans et al.29 NR NNT 4.4ARR 0.227 (0.063 - 0.391)
NR
Polle et al. 32 NNT 84.0ARR 0.012 (-0.153 - 0.177)
NNT -12.5ARR -0.080 (-0.313 - 0.154)
NP
NP: not possible to calculate due to lack of data or zero in both groups; NR: not reported
Secondary outcome parameters
Quality of life
In the study by King et al.30 and MacKay et al.31 quality of life after surgery was evaluated.
Neither of these studies showed a statistical difference between the treatment groups.
King et al. did report that quality of life in both groups deteriorated two weeks after
surgery, but improved in both groups after six weeks. 30
Gastrointestinal function
Three studies reported on gastrointestinal function.28;29;31 Basse et al.28 and MacKay
et al.31 did not find any significant difference between the treatment groups regarding
nausea scores. Median time to first defecation was two days in both groups in the study
of Basse et al.28 In the study of Junghans et al. the median time to first defecation was
one (range 0-6) day postoperatively in the laparoscopic group versus two (range 0-6) days
in the open group.29 This difference was reported as significant. In the study by MacKay
et al. median times to first flatus and first defecation were similar between the treatment
groups.31
Wind (Chris).indb 79Wind (Chris).indb 79 28-05-2008 15:44:3428-05-2008 15:44:34

80
Table 4. Summary of outcomes and fast track items presented in the included trials
Reference N Mo
rtal
ity
Mo
rbid
ity
Rea
dm
issi
on
s
Pri
mar
y H
osp
ital
Sta
y
Tota
l Ho
spit
al S
tay
Min
imu
m o
f 3
0 d
ays
follo
w-u
p
Pre
op
erat
ive
cou
nse
llin
g
Pla
nn
ed d
isch
arg
e
Pre
op
erat
ive
feed
ing
No
bo
wel
pre
par
atio
n
No
pre
med
icat
ion
Flu
id r
estr
icti
on
Act
ive
pre
ven
tio
n o
f h
ypo
ther
mia
Epid
ura
l an
alg
esia
Min
imal
inva
sive
/ t
ran
sver
se in
cisi
on
s
No
ro
uti
ne
use
of
NG
tu
bes
RCTs
Basse et al.28 60 √ √ √ √ √ √ √ √ ∼ − √ √ √ √ ∼ √
King et al.30 62 √ √ √ √ √ √ √ √ √ − ∼ √ − √ √ √
CCTs
MacKay et al.31 78 √ √ √ √ − √ √ − √ √ − √ √ − − √
Junghans et al.29 147 √ √ − √ − √ √ √ ∼ − − √ √ √ √ √
Polle et al. 32 55 √ √ √ √ √ √ √ − √ √ √ √ √ √ √ √
√: Adequately described/Present; -: Not Present/ Not studied; ~: Not adequately described/ partially present
Pain medication
In the study by King et al. significantly more patients required additional opioid analgesics
in the open group; ARR of 52% (95% CI: 28.2% to 75.2%) and NNT of 1.9 patients.30
There were no significant differences reported in use of morphine, paracetamol and
tramadol between the groups in the study by MacKay et al.31
Discussion
This review might suggest a minimal superiority of laparoscopic surgery within a fast track
perioperative care setting with respect to hospital stay, readmission rates, and morbidity.
However, the available evidence is scarce due to a lack of good quality trials.
Of the two RCTs included in this review, only one showed a significantly lower primary
and overall postoperative hospital stay in the laparoscopic group.30 The differences
Wind (Chris).indb 80Wind (Chris).indb 80 28-05-2008 15:44:3528-05-2008 15:44:35

81
Ch
apter 4
Systematic review
of laparoscopic versus open colonic resection
between the two included RCTs in PHS and OHS were considerable.28;30 There are several
possible explanations. In the study of King et al. only patients with diagnosed colorectal
carcinoma were included.30 Basse et al. included patients with benign as well as malignant
conditions.28 The condition of the patients in the study of King et al.30 could therefore be
worse resulting in a longer postoperative recovery period. Furthermore, patients requiring
a rectal resection or not living independently were excluded in the study of Basse et
al.28, but were included by King et al.30 In the university hospital of Basse et al. fast track
surgery has been developed. Therefore, the results of their programme are likely to be
most favourable.28 Basse et al. demonstrated that a postoperative hospital stay of two
to three days after colonic surgery can be achieved both after laparoscopic and open
colectomy if performed in a fast track perioperative care setting. However, these results
were achieved at the expense of readmission rates up to 26.6%.28 Basse et al. showed a
remarkable high mortality rate in the open group of 10%. This can be explained by the
higher ASA scores in that group.28
The study of King et al. was not blinded.30 It is unclear how this affects hospital stay. On
the one hand an observer bias favouring the laparoscopic group, could have influenced the
No
use
of
dra
ins
Loca
l wo
un
d in
filt
rati
on
Enfo
rced
po
sto
per
ativ
e m
ob
ilisa
tio
n
Enfo
rced
po
sto
per
ativ
e o
ral f
eed
ing
No
sys
tem
ic m
orp
hin
e u
se
Stan
dar
d l
axat
ives
Earl
y re
mo
val o
f b
lad
der
cat
het
er
∼ √ √ √ √ √ √
√ √ √ √ − √ √
√ − √ √ − − √
√ − √ √ √ √ √
√ √ √ √ √ √ √
Wind (Chris).indb 81Wind (Chris).indb 81 28-05-2008 15:44:3528-05-2008 15:44:35

82
results of the study of King et al. reporting a significantly worse PHS, OHS, and readmission
rate in the open group.30 On the other hand, blinding with large bandages might give the
patient the impression they had open surgery hampering recovery and discharge.
In the three CCTs included in the present review,29;31;32 one study29 demonstrated a
significantly shorter PHS in the laparoscopic group. However, in this study almost half of
the patients in the open group had an ASA score of III or IV and more patients in this
group were operated because of a carcinoma.29 In the laparoscopic group, 33% of the
patients had an ASA score of III or IV and only 41% had a carcinoma. This might be an
explanation for the longer PHS and higher morbidity in the open group. In the study by
Polle et al. only patients with an ASA score of I and II were included.32
Morbidity was around 20 to 30% in four studies. Junghans et al. reported a 23% reduction
in morbidity in the laparoscopic group, but their morbidity of 44.7% in the open group is
very high.29 However, it was not clear whether patients with more than one complication
were counted twice resulting in this high morbidity rate. A readmission rate of 0% in the
laparoscopic group and 3.4% in the open group in the study by MacKay et al. suggests
that a longer hospital stay, reduces the number of readmissions.31 Recently, Kehlet’s
group confirmed this relation between hospital stay and readmissions. They achieved
lower readmission rates when hospital stay was prolonged with one day.35 The longer
hospital stay in the study of MacKay et al. may be caused by their use of patient-controlled
analgesia instead of epidural analgesia.31
Allocation bias could have influenced the results in favour of laparoscopic surgery in the
three CCTs by MacKay et al.31, Polle et al.32 and Junghans et al.29, because the surgeon
decided which patient would undergo laparoscopic or open surgery.
This systematic review was limited by a low number of studies. All studies had small
sample sizes and only one study used a proper sample size calculation. Overall quality
of the selected studies was found to be moderate. Of the five included studies, three
studies were CCTs, which increases the probability that bias occurs.29;31;32 Due to clinical
heterogeneity the data could not be pooled. Mean differences and 95% CIs could not be
calculated as data were not normally distributed.
Fast track perioperative care programmes in colonic surgery have been introduced more
then ten years ago. In the included studies the number of applied fast track elements in the
protocol were reported, but only one study, Polle et al.32 reported the number of elements
actually achieved. In this study 15 fast track elements were applied and 13 elements were
evaluated. An average of 7.4 of the elevated elements were successfully achieved per
patient. Nevertheless, despite this relatively low protocol compliance a significantly faster
recovery of the fast track group resulted in a shorter hospital stay. It is clear that a full
implementation of all fast track perioperative care elements encompassing the fast track
protocol requires a learning curve and a dedicated multidisciplinary functioning team.
Although there is evidence about most elements of the programme, it seems hard to
implement all different elements of fast track care as every discipline has to break with
long-standing traditions.
In conclusion, the presently available evidence does not allow a robust conclusion on
Wind (Chris).indb 82Wind (Chris).indb 82 28-05-2008 15:44:3528-05-2008 15:44:35

83
Ch
apter 4
Systematic review
of laparoscopic versus open colonic resection
the outcomes of laparoscopic versus open surgery within a fast track perioperative care
setting. Only five studies were available for analysis. So, the question remains whether
fast track or modern traditional care, laparoscopic or open surgery, or a combination of
both is the preferred strategy. This research question is the objective of the LAFA study,
compromising over 400 patients, that will hopefully provide the answer to this question
in the middle of 2009.36
Reference List
(1) Fearon KC, Ljungqvist O, Von Meyenfeldt MF, Revhaug A, Dejong CH, Lassen K, et al. Enhanced recov-ery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr 2005;24:466-477.
(2) Wilmore DW, Kehlet H. Management of patients in fast track surgery. BMJ 2001;322:473-476.
(3) Anderson AD, McNaught CE, MacFie J, Tring I, Barker P, Mitchell CJ. Randomized clinical trial of multi-modal optimization and standard perioperative surgical care. Br J Surg 2003;90:1497-1504.
(4) Basse L, Hjort JD, Billesbolle P, Werner M, Kehlet H. A clinical pathway to accelerate recovery after colonic resection. Ann Surg 2000;232:51-57.
(5) Basse L, Raskov HH, Hjort JD, Sonne E, Billesbolle P, Hendel HW, et al. Accelerated postoperative recov-ery programme after colonic resection improves physical performance, pulmonary function and body composition. Br J Surg 2002;89:446-453.
(6) Basse L, Thorbol JE, Lossl K, Kehlet H. Colonic surgery with accelerated rehabilitation or conventional care. Dis Colon Rectum 2004;47:271-277.
(7) Delaney CP, Fazio VW, Senagore AJ, Robinson B, Halverson AL, Remzi FH. ‘Fast track’ postoperative management protocol for patients with high co-morbidity undergoing complex abdominal and pelvic colorectal surgery. Br J Surg 2001; 88:1533-1538.
(8) Delaney CP, Zutshi M, Senagore AJ, Remzi FH, Hammel J, Fazio VW. Prospective, randomized, controlled trial between a pathway of controlled rehabilitation with early ambulation and diet and traditional post-operative care after laparotomy and intestinal resection. Dis Colon Rectum 2003;46:851-859.
(9) Hjort JD, Sonne E, Basse L, Bisgaard T, Kehlet H. Convalescence after colonic resection with fast-track versus conventional care. Scand J Surg 2004;93:24-28.
(10) Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg 2002;183:630-641.
(11) Kehlet H, Dahl JB. Anaesthesia, surgery, and challenges in postoperative recovery. Lancet 2003;362:1921-1928.
(12) Soop M, Carlson GL, Hopkinson J, Clarke S, Thorell A, Nygren J, et al. Randomized clinical trial of the effects of immediate enteral nutrition on metabolic responses to major colorectal surgery in an enhanced recovery protocol. Br J Surg 2004;91:1138-1145.
(13) Basse L, Madsen JL, Kehlet H. Normal gastrointestinal transit after colonic resection using epidural anal-gesia, enforced oral nutrition and laxative. Br J Surg 2001;88:1498-1500.
(14) Zutshi M, Delaney CP, Senagore AJ, Mekhail N, Lewis B, Connor JT, et al. Randomized controlled trial comparing the controlled rehabilitation with early ambulation and diet pathway versus the controlled rehabilitation with early ambulation and diet with preemptive epidural anesthesia/analgesia after lapa-rotomy and intestinal resection. Am J Surg 2005;189:268-272.
Wind (Chris).indb 83Wind (Chris).indb 83 28-05-2008 15:44:3528-05-2008 15:44:35

84
(15) Gatt M, Anderson AD, Reddy BS, Hayward-Sampson P, Tring IC, MacFie J. Randomized clinical trial of multimodal optimization of surgical care in patients undergoing major colonic resection. Br J Surg 2005;92:1354-1362.
(16) Jacobs M, Verdeja JC, Goldstein HS. Minimally invasive colon resection (laparoscopic colectomy). Surg Laparosc Endosc 1991;1:144-150.
(17) Laparoscopically assisted colectomy is as safe and effective as open colectomy in people with colon cancer Abstracted from: Nelson H, Sargent D, Wieand HS, et al; for the Clinical Outcomes of Surgical Therapy Study Group. A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med 2004;350: 2050-2059. Cancer Treat Rev 2004;30:707-709.
(18) Braga M, Vignali A, Gianotti L, Zuliani W, Radaelli G, Gruarin P, et al. Laparoscopic versus open colorec-tal surgery: a randomized trial on short-term outcome. Ann Surg 2002;236:759-766.
(19) Chapman AE, Levitt MD, Hewett P, Woods R, Sheiner H, Maddern GJ. Laparoscopic-assisted resection of colorectal malignancies: a systematic review. Ann Surg 2001;234:590-606.
(20) Janson M, Bjorholt I, Carlsson P, Haglind E, Henriksson M, Lindholm E, et al. Randomized clinical trial of the costs of open and laparoscopic surgery for colonic cancer. Br J Surg 2004;91:409-417.
(21) Lacy AM, Garcia-Valdecasas JC, Delgado S, Castells A, Taura P, Pique JM, et al. Laparoscopy-assisted colectomy versus open colectomy for treatment of non-metastatic colon cancer: a randomised trial. Lancet 2002;359:2224-2229.
(22) Leung KL, Kwok SP, Lam SC, Lee JF, Yiu RY, Ng SS, et al. Laparoscopic resection of rectosigmoid carci-noma: prospective randomised trial. Lancet 2004;363:1187-1192.
(23) Abraham NS, Byrne CM, Young JM, Solomon MJ. Meta-analysis of non-randomized compara-tive studies of the short-term outcomes of laparoscopic resection for colorectal cancer. ANZ J Surg 2007;77:508-516.
(24) Maartense S, Dunker MS, Slors JF, Cuesta MA, Gouma DJ, van Deventer SJ, et al. Hand-assisted laparo-scopic versus open restorative proctocolectomy with ileal pouch anal anastomosis: a randomized trial. Ann Surg 2004;240:984-991.
(25) Reza MM, Blasco JA, Andradas E, Cantero R, Mayol J. Systematic review of laparoscopic versus open surgery for colorectal cancer. Br J Surg 2006;93:921-928.
(26) Schwenk W, Haase O, Neudecker J, Muller JM. Short term benefits for laparoscopic colorectal resec-tion. Cochrane Database Syst Rev 2005;(3):CD003145.
(27) Dutch Cochrane Collaboration. http://www.cochrane.nl/index.html.
(28) Basse L, Jakobsen DH, Bardram L, Billesbolle P, Lund C, Mogensen T, et al. Functional recovery after open versus laparoscopic colonic resection: a randomized, blinded study. Ann Surg 2005;241:416-423.
(29) Junghans T, Raue W, Haase O, Neudecker J, Schwenk W. [Value of laparoscopic surgery in elective colorectal surgery with “fast-track”-rehabilitation]. Zentralbl Chir 2006;131:298-303.
(30) King PM, Blazeby JM, Ewings P, Franks PJ, Longman RJ, Kendrick AH, et al. Randomized clinical trial comparing laparoscopic and open surgery for colorectal cancer within an enhanced recovery programme. Br J Surg 2006;93:300-308.
(31) MacKay G, Ihedioha U, McConnachie A, Serpell M, Molloy RG, O’Dwyer PJ. Laparoscopic colonic resec-tion in fast-track patients does not enhance short-term recovery after elective surgery. Colorectal Dis 2007;9:368-372.
(32) Polle SW, Wind J, Fuhring JW, Hofland J, Gouma DJ, Bemelman WA. Implementation of a Fast-Track Perioperative Care Program: What Are the Difficulties? Dig Surg 2007;24:441-449.
(33) Proske JM, Raue W, Neudecker J, Muller JM, Schwenk W. [Fast track rehabilitation in colonic surgery: results of a prospective trial]. Ann Chir 2005;130:152-156.
(34) Schwenk W, Haase O, Raue W, Neudecker J, Muller JM. [Establishing “fast-track”-colonic surgery in the clinical routine]. Zentralbl Chir 2004;129:502-509.
Wind (Chris).indb 84Wind (Chris).indb 84 28-05-2008 15:44:3528-05-2008 15:44:35

85
Ch
apter 4
Systematic review
of laparoscopic versus open colonic resection
(35) Andersen J, Hjort-Jakobsen D, Christiansen PS, Kehlet H. Readmission rates after a planned hospital stay of 2 versus 3 days in fast-track colonic surgery. Br J Surg 2007;94:890-893.
(36) Wind J, Hofland J, Preckel B, Hollmann MW, Bossuyt PM, Gouma DJ, et al. Perioperative strategy in colonic surgery; LAparoscopy and/or FAst track multimodal management versus standard care (LAFA trial). BMC Surg 2006;6:16.
Wind (Chris).indb 85Wind (Chris).indb 85 28-05-2008 15:44:3628-05-2008 15:44:36

Wind (Chris).indb 86Wind (Chris).indb 86 28-05-2008 15:44:3628-05-2008 15:44:36

5Chapter
Perioperative strategy in colonic surgery; LAparoscopy and/or FAst track multimodal
management versus standard care (LAFA trial)
- design and rationale of a randomised controlled multicentre trial -
J Wind
WA Bemelman
On behalf of the LAFA study group
BMC Surgery 2006 29;6:16
Wind (Chris).indb 87Wind (Chris).indb 87 28-05-2008 15:44:3628-05-2008 15:44:36

8888
Abstract
Introduction Recent developments in large bowel surgery are the introduction of laparoscopic surgery
and the implementation of multimodal fast track recovery programmes. Both focus on a
faster recovery and shorter hospital stay. The randomised controlled multicentre LAFA-trial
(LAparoscopy and/or FAst track multimodal management versus standard care) was
conceived to determine whether laparoscopic surgery, fast track perioperative care or a
combination of both is to be preferred over open surgery with standard care in patients
having segmental colectomy for malignant disease.
MethodsThe LAFA-trial is a double blinded, multicentre trial with a two by two balanced factorial
design. Patients eligible for segmental colectomy for malignant colorectal disease i.e. right
and left colectomy and anterior resection will be randomised to either open or laparoscopic
colectomy, and to either standard care or the fast track perioperative care programme. This
factorial design produces four treatment groups; open colectomy with standard care (a),
open colectomy with the fast track programme (b), laparoscopic colectomy with standard
care (c), and laparoscopic surgery with the fast track programme (d). Primary outcome
parameter is postoperative hospital length of stay including readmission within 30 days.
Secondary outcome parameters are quality of life two and four weeks after surgery, overall
hospital costs, morbidity, patient satisfaction and readmission rate.
Based on a mean postoperative hospital stay of 9 +/- 2.5 days a group size of 400 patients
(100 each arm) can reliably detect a minimum difference of one day between the four arms
(alfa = 0.95, beta = 0.8). With 100 patients in each arm a difference of 10% in subscales of
the Short Form 36 (SF-36) questionnaire and social functioning can be detected.
ConclusionsThe LAFA-trial is a randomised controlled multicentre trial that will provide evidence on
the merits of fast track perioperative care and laparoscopic colorectal surgery in patients
having segmental colectomy for malignant disease (ISRCTN:79588422).
Wind (Chris).indb 88Wind (Chris).indb 88 28-05-2008 15:44:3628-05-2008 15:44:36

89
Ch
apter 5
Perioperative strateg
y in colonic surgery
Introduction
Recent developments in large bowel surgery are the introduction of laparoscopic surgery
and the implementation of multimodal fast track perioperative care programmes. Both
focus on enhanced recovery and shorter hospital stay as compared to open surgery and
traditional care. Laparoscopic colectomy was first described in 1991.1 Since then a lot
of effort has been made to establish its feasibility and safety particularly in laparoscopic
colectomy for cancer. Recently, several randomised trials comparing laparoscopic with
open colectomy indicated that laparoscopic surgery can be applied safely both for
malignant and benign diseases.2-7 Several systematic reviews that assessed the evidence
on the laparoscopic approach for colorectal cancer reported that laparoscopic surgery, in a
traditional perioperative care setting was associated with less morbidity, less postoperative
pain, earlier recovery and shorter hospital stay.2;8;9 Furthermore, short term cancer related
outcomes such as cancer free resection margins and the number of harvested lymph
nodes, as well as long term cancer related outcomes such as disease free survival were
comparable between laparoscopic and open surgery.2 These results stimulated many
surgeons in the Netherlands to set up a laparoscopic colorectal programme.
At the same time, enthusiasm was raised for the so-called fast track perioperative
care programme, also referred to as Enhanced Recovery After Surgery (ERAS®), which
essentially is a modification of the programme initially developed by the Danish surgeon
Henrik Kehlet.10-13 This multimodal programme, involving optimalisation of several
aspects of the perioperative management of patients undergoing colectomy, enables
patients to recover earlier and therefore go home as early as three days after open
colectomy. Furthermore, postoperative morbidity was reduced.14-19 The essence of a fast
track perioperative care programme consists of extensive preoperative counselling, no
bowel preparation, no sedative premedication, no preoperative fasting but carbohydrate
loaded liquids until two hours prior to surgery, tailored anaesthesiology encompassing
thoracic epidural anaesthesia and short acting anaesthetics, perioperative intravenous
fluid restriction, minimally invasive surgery (i.e. through small incisions or laparoscopy),
non-opioid pain management, no routine use of drains and nasogastric tubes, early
removal of bladder catheter, standard laxatives and prokinetics, and early and enhanced
postoperative feeding and mobilisation.10-19
As these new developments have been introduced in clinical practice, time has come
to evaluate their feasibility, safety, and cost-effectiveness in large bowel surgery in a
randomised controlled setting. It can be hypothesized that fast track and/or laparoscopy
are associated with less attenuation of the patient’s condition after surgery resulting in a
shorter postoperative hospital stay, a faster recovery to full activity at home, and a better
quality of life.
Since it has not been established which combination of perioperative management and
surgical approach i.e. standard care, fast track care, laparoscopic surgery or open surgery
is best in terms of postoperative hospital stay, quality of life, postoperative morbidity,
Wind (Chris).indb 89Wind (Chris).indb 89 28-05-2008 15:44:3628-05-2008 15:44:36

90
readmission rate, overall costs and patient satisfaction, this is the subject of the present
study proposal.
Methods
Study objectivesThe objective of this study is to determine whether laparoscopic surgery, fast track
perioperative care or a combination of both is to be preferred over open surgery with
standard care in patients undergoing segmental colectomy for malignant disease. The
objective is subdivided in three research questions; first, how laparoscopic surgery
compares to open surgery in terms of hospital stay, quality of life and costs? Second, how
fast track perioperative care compares to standard care in terms of hospital stay, quality
of life, and costs? Finally, what is the added benefit of the fast track perioperative care
programme in laparoscopic surgery in terms of hospital stay, quality of life and costs?
Study designThe LAFA-trial is a randomised multicentre trial, designed as a two by two balanced factorial
design. Patients are blinded for the type of intervention i.e. laparoscopic or open surgery.
Patients eligible for segmental colectomy, for malignant colorectal disease i.e. right and
left colectomy and anterior resection will be randomised to either open or laparoscopic
colectomy, and to either standard care or the fast track programme. This factorial design
results in four treatment groups; open colectomy with standard care (a), open colectomy
with fast track perioperative care (b), laparoscopic colectomy with standard care (c), and
laparoscopic surgery with fast track perioperative care (d) (see Figure 1).
Randomisation is performed by an Internet randomisation module. Block-randomisation is
used and the randomisation is stratified for the randomising centres.
Primary and secondary endpointsThe primary endpoint of the LAFA-study is total postoperative hospital stay in days,
including hospital stay of patients who are readmitted within 30 days after surgery.
Secondary endpoints are quality of life at two and four weeks after surgery. Quality of life
will be measured by two validated questionnaires; Short Form 36 (SF-36) and the Gastro-
Intestinal Quality of Life Index (GIQLI). Further secondary endpoints are; medical and non
medical costs, morbidity, and mortality within 30 days after surgery, patient satisfaction
measured by standardised questionnaires, and readmission rate.
Participating centresNine Dutch hospitals of the LAFA-study group, including three academic centres and four
non-academic centres, will enroll patients.
Wind (Chris).indb 90Wind (Chris).indb 90 28-05-2008 15:44:3628-05-2008 15:44:36

91
Ch
apter 5
Perioperative strateg
y in colonic surgery
Study populationThe study population consists of patients eligible for segmental colectomy for malignant
colorectal disease, i.e. right and left colectomy and anterior resection.
Inclusion criteria are; age between 40 and 80 years, colorectal cancer including colon and
recto-sigmoid cancers, ASA I-III, and informed consent.
Exclusion criteria are; prior midline laparotomy, ASA IV, laparoscopic surgeon not available,
emergency surgery and a planned stoma.
In Hospital: Patient characteristics, POSSUM score, surgical parameters, achieved discharge criteria, morbidity, length of stay, costs of material .
Out Hospital: Quality of life at two and four weeks (SF-36/GIQLI), medical and non-medical costs, readmissions, morbidity, sick leave, contact with general practitioner
Patients with colorectal cancer eligible for right/left colectomy and (recto)sigmoid resection
Check in- and exclusion criteria
R
Fast Track Laparoscopy
Fast track Open surgery
Standard care Open surgery
Standard care Laparoscopy
www.lafa-trial.nl
R: Randomisation; SF-36: Short Form 36; GIQLI: Gastro-Intestinal Quality of Life Index, POSSUM score: Physiological and Operative Severity Score for the enUmeration of Mortality and Morbidity
Figure 1. LAFA-study flowchart
Wind (Chris).indb 91Wind (Chris).indb 91 28-05-2008 15:44:3628-05-2008 15:44:36

92
EthicsThis study is conducted in accordance with the principles of the Declaration of Helsinki
and ‘good clinical practice’ guidelines. The independent medical ethics committees of the
participating hospitals have approved the study protocol. Prior to randomisation, written
informed consent will be obtained from all patients.
Study outlineInformed consent will be obtained at the outpatient department if the patient fulfils the
inclusion and exclusion criteria. Randomisation is performed instantly through the study
website.
The randomisation produces four treatment groups; open colectomy with standard care (a),
open colectomy with fast track perioperative care (b), laparoscopic colectomy with standard
care (c), and laparoscopic surgery with fast track perioperative care (d) (see Figure 1).
Patients that are randomised to fast track perioperative care will be informed by a
“fast track” trial nurse and by the anaesthesiologist about the essence of the fast track
programme. Appointments for these consultations will be made after consulting the
surgeon and randomisation has been done. All patients randomised to have a fast track
perioperative treatment will be admitted to a separate ”fast track” ward, where the nurses
and medical staff are trained in fast track perioperative management.
Patients who will receive standard treatment are not counselled by the fast track nurse
and will have a standard preassessment by the anaesthesiologist.
Patient and medical staff will be blinded for the surgical approach until the day of discharge
by applying a covering abdominal bandage.
SurgeryBoth open and laparoscopic surgery is done according to the technique applied by the
local surgeon. Antibiotic prophylaxis is done according to hospital protocol. All patients
will have two enemas before surgery (evening before and morning before). After surgery
the surgical wounds are covered with an abdominal dressing in order to blind the medical
staff for the type of approach. A requirement for the participating laparoscopic surgeons
to perform laparoscopic colectomy for cancer is a minimum of 20 laparoscopic colectomies
for benign disease as indicated by the proclamation of the American Society of the Colon
and Rectum Surgeons in 2004.20;21
Fast track and standard careComparison of the different strategies is only possible when a fast track programme
is running sufficiently and patients are nursed separately depending on the results of
randomisation either on a standard care or fast track ward in order to avoid a bias towards
fast track treatment by the nursing and medical staff. Patients that have standard care
cannot be nursed by nurses that have experience with fast track care. Fast track multimodal
management is done according to the protocol summarized in Table 1.
Wind (Chris).indb 92Wind (Chris).indb 92 28-05-2008 15:44:3728-05-2008 15:44:37

93
Ch
apter 5
Perioperative strateg
y in colonic surgery
Table 1. Differences between fast-track and traditional care protocol
Fast-track Care Traditional Care
Pre-operative phase
Outpatient department of Surgery
- Scheduling of operation- Information about FT- Informed consent
- Scheduling of operation
Outpatient department of anaesthesiology
- Pre-assessment for risk adjustment - Pre-assessment for risk adjustment
- Discussion focusing on placement of thoracic epidural catheter for management of perioperative analgesia
- Open discussion about different possibilities for management of perioperative analgesia (i.e. placement of epidural catheter on any level, patient controlled analgesia with morphine (PCA-morphine) or continuous IV morphine infusion
Pre-admission guided tour on surgical ward
- Yes - No tour
Day of admission
Pre-operative fasting - Last meal 6 h before operation- Last clear drink (CHL) 2h
before operation
- Last meal until midnight- No oral intake at the day of surgery
Pre-anaesthetic medication
- Lorazepam, 1 mg the evening before operation if necessary
- Lorazepam, 1 mg or temazepam 10 or 20 mg the evening before operation
- No sedative medication at the day of operation
- Lorazepam 1mg, temazepam 10 or 20 mg, or midazolam 7.5 mg at the day of operation
Day of Surgery
Anaesthetic management - Placement of thoracic epidural catheter (T6-T10, depending on the surgical resection); test-dose (bupivacaine 0.25% with adrenaline 1:200,000), top-up dose (bupivacaine 0.25% [±10 ml] with sufentanil 25 μg, followed by continuous infusion (bupivacaine 0.125% with fentanyl 2.5 μg.ml-1) until day 2 postoperative
- IV morphine loading (0.1 mg.kg-1) followed by continuous IV morphine infusion or PCA-morphine, OR placement of epidural catheter (T10-L1, test dose, top-up dose and continuous infusion in the same way as for fast track) when an open surgical procedure will be performed
- IV morphine loading (0.05-0.1 mg.kg-1) followed by PCA-morphine or continuous IV morphine infusion when a laparoscopic surgical procedure is performed
- Combined with balanced general anaesthesia
- Combined with balanced general anaesthesia
- Restricted per-operative fluid infusion regime (Ringers lactate 20 ml.kg-1 in the 1st h followed by RL 6 ml.kg-1.h-1)
- Standard per-operative fluid infusion regime (Ringers lactate 20 ml.kg-1 in the 1st h followed by RL 10-12 ml.kg-1.h-1)
- Use of vasopressor drugs as 1st choice for management of mean blood pressure drop > 20% of baseline
- Use of extra fluid challenge as 1st choice for management of mean blood pressure drop > 20% below baseline
Wind (Chris).indb 93Wind (Chris).indb 93 28-05-2008 15:44:3728-05-2008 15:44:37

94
- Forced body heating (Bair hugger system and warmed IV fluids)
- Forced body heating (Bair hugger system and warmed IV fluids)
- Removal of naso-gastric tube before extubation
- Naso-gastric tube remain until day 1 after surgery
- Prophylactic use of odansetron (4 mg) to prevent PONV
- Use of odansetron, dexamethason or droperidol for PONV management according to attending anaesthesiologist
Surgical Management - Minimal invasive incisions - Median laparotomy approach- Urine catheter according
to attending surgeon- No infiltration of surgical wounds
with local anaesthetic drugs
- Supra-pubic urine catheter
- Infiltration of surgical wounds with bupivacaine
Early post-operative management
- No standard use of abdominal drains - Standard use of abdominal drains
- Use of epidural catheter as mentioned before to which paracetamol 4 x 1 g.d-1 is added
- Continuous IV morphine infusion or PCA-morphine OR use of epidural catheter as mentioned before to which paracetamol 4 x 1 g.d-1 and/or diclofenac 3 x 50 mg.d-1 are added
- First oral drinks at 2 h post-surgery + IV infusion of RL 1.5 l.d-1
- Small amount of water orally + IV infusion of RL 2.5 l.d-1
- Mobilisation in the evening (>2 h out of bed)
- Bed rest
- First semi-solid food intake in the evening
Day 1 after Surgery - Oral intake > 2 l (including 4 units CHL drinks), offer solid food
- Diet increased on daily basis when normal bowel sounds are examined
- Stop IV fluid administration (leave canulla)
- IV fluid administration (2.5 l.d-1) is continued till adequate oral fluid intake
- Start laxative (MgO, 2 x 1g.d-1) - Start laxative (MgO, 2 x 1 g.d-1)
- Close supra-pubic urine catheter and remove when residue < 50 ml
- Expand mobilisation (> 6 h out of bed)
- Close supra-pubic urine catheter and remove when residue < 50 ml
Day 2 after surgery - Offer solid food- Expand mobilisation (> 8 hours)- Plan discharge
Continue as on day 1 until discharge criteria are fulfilled
Day 3 after surgery - Remove epidural catheter- Continue Paracetamol 4x 1000 mg- Add NSAID- Remove IV cannula- Expand mobilisation (> 8 hours)- Evaluating discharge criteria;
discharge if fulfilled
Continue as on day 1 until discharge criteria are fulfilled
Day 4 after surgery - Continue as on day 3 until discharge criteria are fulfilled
Continue as on day 1 until discharge criteria are fulfilled
FT: Fast-track; TC: Traditional care; CHL: carbohydrate loaded drink (Nutridrink®)
Wind (Chris).indb 94Wind (Chris).indb 94 28-05-2008 15:44:3728-05-2008 15:44:37

95
Ch
apter 5
Perioperative strateg
y in colonic surgery
Discharge criteria
Since hospital stay is a primary efficacy parameter, the discharge criteria are defined. Every
postoperative day will be noted whether the discharge criteria are met, and other reasons
of prolonged hospital stay e.g. social environment or patient inacceptance. The discharge
criteria include adequate pain control with oral analgesics, no nausea, ability to take solid
foods, passage of flatus and/or stool, mobilisation and self support as compared to the
preoperative level, and acceptance by the patient.
Statistical analysis
Intention to treat
The analysis will be performed in accordance with the intention to treat principle.
Sample size calculation
Since both, fast track care and laparoscopy focus on earlier recovery resulting in a
reduction of hospital stay, the latter is used as primary efficacy parameter. The mean
postoperative hospital stay for segmental bowel resection with standard care is nine days
with a standard deviation of 2.5 days in the Academic Medical Centre Amsterdam. Using
a 5% significance level, a total sample size of 400 would have a power of >95% to detect
a minimum reduction of one day in hospital stay between laparoscopic surgery and open
surgery, a one day reduction in hospital stay between fast track care and standard care,
and a power of 80% to detect the same difference between the combination of fast track
care with laparoscopic surgery and current treatment.
A much larger difference can be expected between the other treatment groups, for
instance open surgery and standard care compared to fast track perioperative care and
laparoscopic surgery. In order to obtain results with adequate precision we have calculated
group size using a difference of one day rather than the expected 2-4 days. With a group
size of one hundred patients per arm it is possible to find a significant difference (alfa=0.05,
beta=0.1) of at least 10% in subscales of the SF-36, a validated quality of life questionnaire,
at two weeks after surgery.22-24 Liem et al. demonstrated 20-30% differences in subscales
of the SF-36 between laparoscopic versus open hernia repair one week after surgery.24
Maartense et al. found a 10% difference in physical and social function two weeks after
surgery comparing laparoscopic versus open ileocolic resection in a randomised study
from our institution.25
Economic evaluation
The marginal direct medical, non-medical and time cost differences will be calculated for
the four treatment strategies. These will include the additional costs of laparoscopy, of
fast track care, as well as the differences due to complications and readmissions.
Wind (Chris).indb 95Wind (Chris).indb 95 28-05-2008 15:44:3728-05-2008 15:44:37

96
Data collection and monitoring
Data are collected via a secured internet module which is specially designed for the LAFA-
study. Data are collected daily until the day of discharge. Preoperatively, and at two and
four weeks postoperatively the questionnaires (SF-36 and GIQLI) are filled in by the patient.
One month postoperatively, the general practitioner is contacted to inform whether he/
she was contacted by the patient for problems related to the operation.
There will be regular contact between the study coordinators and the participating centres.
One research fellow will monitor the included data of every patient.
Discussion
Fast track programmes in colonic surgery have been introduced more than a decade ago
with favourable early results. Many elements of these fast track programmes are based
on solid evidence derived from randomised trials and systematic reviews. However, it
is quite surprising, that implementation in daily practice has so far stayed behind.26-28
This can partly be explained by the necessity to break with long-standing traditions, such
as preoperative fasting, slow postoperative advancement of oral feeding, and delayed
mobilisation. In a recent systematic review including six comparative single centre studies,
fast track programmes were found to reduce the time spent in the hospital and were found
to be safe in major abdominal surgery. However, this systematic review demonstrated that
the evidence on fast track colonic surgery was scarce.29
Both, laparoscopic surgery and fast track programmes are costly and require extensive
expertise. Laparoscopic surgery is costly due to expensive disposables and additional
operating time. Furthermore, a considerable learning curve must be mastered. Only 5-8%
of the colectomies are therefore done laparoscopically in the Netherlands. Fast track
multimodal perioperative care requires additional personnel trained in several aspects of
the fast track programme to make the programme work. It is clear that both, laparoscopic
surgery and fast track programmes enhance recovery and thereby reduce hospital
stay.2;8;29-32 Shortening hospital stay and reduction of morbidity are attractive, since
both increase the availability of beds and might reduce the overall cost of hospital stay.
However, despite the current enthusiasm and implementation into daily practice of fast
track care and laparoscopic surgery, there are few data available that provide evidence on
the optimal combination (laparoscopic or open surgery and fast track or standard care) in
terms of shorter hospital stay, reduced morbidity and cost effectiveness.
The largest reduction in hospital stay can probably be achieved by a combination of fast
track programmes and laparoscopic surgery. However, it is not known what the additional
costs of laparoscopic surgery or fast track programmes are compared to the reduction in
hospital stay that can be achieved with these programmes. Since the average postoperative
hospital stay after segmental colectomy is still considerable in the Netherlands as well
as throughout Europe, an enormous improvement can be expected applying fast track
Wind (Chris).indb 96Wind (Chris).indb 96 28-05-2008 15:44:3728-05-2008 15:44:37

97
Ch
apter 5
Perioperative strateg
y in colonic surgery
programmes and/or laparoscopy. The relative contribution to the reduction in hospital
stay of both methods is unknown. This must be assessed in a setting where patients are
blinded for the approach of surgery. The randomised controlled LAFA-trial was conceived
to determine whether laparoscopic surgery, fast track perioperative care or a combination
of both is to be preferred over open surgery with standard care in patients undergoing
segmental colectomy for malignant disease.
Reference List
(1) Jacobs M, Verdeja JC, Goldstein HS. Minimally invasive colon resection (laparoscopic colectomy). Surg Laparosc Endosc 1991;1:144-150.
(2) Reza MM, Blasco JA, Andradas E, Cantero R, Mayol J. Systematic review of laparoscopic versus open surgery for colorectal cancer. Br J Surg 2006;93:921-928.
(3) Lacy AM, Garcia-Valdecasas JC, Delgado S, Castells A, Taura P, Pique JM, et al. Laparoscopy-assisted colectomy versus open colectomy for treatment of non-metastatic colon cancer: a randomised trial. Lancet 2002;359:2224-2229.
(4) A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med 2004;350:2050-2059.
(5) Leung KL, Kwok SP, Lam SC, Lee JF, Yiu RY, Ng SS, et al. Laparoscopic resection of rectosigmoid carci-noma: prospective randomised trial. Lancet 2004; 363:1187-1192.
(6) Maartense S, Dunker MS, Slors JF, Cuesta MA, Gouma DJ, van Deventer SJ, et al. Hand-assisted laparo-scopic versus open restorative proctocolectomy with ileal pouch anal anastomosis: a randomized trial. Ann Surg 2004;240:984-991.
(7) Tuynman JB, Bemelman WA, van Lanschot JJ. [Laparoscopic resection of colon carcinoma]. Ned Tijdschr Geneeskd 2004;148:2315-2318.
(8) Abraham NS, Young JM, Solomon MJ. Meta-analysis of short-term outcomes after laparoscopic resec-tion for colorectal cancer. Br J Surg 2004;91:1111-1124.
(9) Schwenk W, Haase O, Neudecker J, Muller JM. Short term benefits for laparoscopic colorectal resec-tion. Cochrane Database Syst Rev 2005;(3):CD003145.
(10) Fearon KC, Ljungqvist O, von Meyenfeldt MF, Revhaug A, Dejong CH, Lassen K, et al. Enhanced recov-ery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr 2005;24:466-477.
(11) Wilmore DW, Kehlet H. Management of patients in fast track surgery. BMJ 2001;322:473-476.
(12) Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg 2002;183:630-641.
(13) Wind J, Maessen J, Polle SW, Bemelman WA, von Meyenfeldt MF, Dejong CH. [Elective colon surgery according to a ‘fast-track’ programmeme]. Ned Tijdschr Geneeskd 2006;150:299-304.
(14) Delaney CP, Zutshi M, Senagore AJ, Remzi FH, Hammel J, Fazio VW. Prospective, randomized, controlled trial between a pathway of controlled rehabilitation with early ambulation and diet and traditional post-operative care after laparotomy and intestinal resection. Dis Colon Rectum 2003;46:851-859.
(15) Zutshi M, Delaney CP, Senagore AJ, Mekhail N, Lewis B, Connor JT, et al. Randomised controlled trial comparing the controlled rehabilitation with early ambulation and diet pathway versus the controlled rehabilitation with early ambulation and diet with preemptive epidural anesthesia/analgesia after lapa-rotomy and intestinal resection. Am J Surg 2005;189:268-272.
Wind (Chris).indb 97Wind (Chris).indb 97 28-05-2008 15:44:3728-05-2008 15:44:37

98
(16) Basse L, Madsen JL, Kehlet H. Normal gastrointestinal transit after colonic resection using epidural anal-gesia, enforced oral nutrition and laxative. Br J Surg 2001;88:1498-1500.
(17) Basse L, Raskov HH, Hjort JD, Sonne E, Billesbolle P, Hendel HW, et al. Accelerated postoperative recov-ery programmeme after colonic resection improves physical performance, pulmonary function and body composition. Br J Surg 2002;89:446-453.
(18) Basse L, Thorbol JE, Lossl K, Kehlet H. Colonic surgery with accelerated rehabilitation or conventional care. Dis Colon Rectum 2004;47:271-277.
(19) Hjort JD, Sonne E, Basse L, Bisgaard T, Kehlet H. Convalescence after colonic resection with fast-track versus conventional care. Scand J Surg 2004;93:24-28.
(20) Otchy D, Hyman NH, Simmang C, Anthony T, Buie WD, Cataldo P, et al. Practice parameters for colon cancer. Dis Colon Rectum 2004;47:1269-1284.
(21) Tjandra JJ, Kilkenny JW, Buie WD, Hyman N, Simmang C, Anthony T, et al. Practice parameters for the management of rectal cancer (revised). Dis Colon Rectum 2005;48:411-423.
(22) Temple PC, Travis B, Sachs L, Strasser S, Choban P, Flancbaum L. Functioning and well-being of patients before and after elective surgical procedures. J Am Coll Surg 1995;181:17-25.
(23) Trus TL, Laycock WS, Waring JP, Branum GD, Hunter JG. Improvement in quality of life measures after laparoscopic antireflux surgery. Ann Surg 1999;229:331-336.
(24) Liem MS, Halsema JA, van der Graaf Y, Schrijvers AJ, van Vroonhoven TJ. Cost-effectiveness of extra-peritoneal laparoscopic inguinal hernia repair: a randomized comparison with conventional hernior-rhaphy. Coala trial group. Ann Surg 1997;226:668-675.
(25) Maartense S, Dunker MS, Slors JF, Cuesta MA, Pierik EG, Gouma DJ et al. Laparoscopic-assisted versus open ileocolic resection for Crohn’s disease: a randomized trial. Ann Surg 2006;243:143-149.
(26) Lassen K, Dejong CH, Ljungqvist O, Fearon K, Andersen J, Hannemann P et al. Nutritional support and oral intake after gastric resection in five northern European countries. Dig Surg 2005;22:346-352.
(27) Kehlet H, Buchler MW, Beart RW Jr., Billingham RP, Williamson R. Care after colonic operation--is it evidence-based? Results from a multinational survey in Europe and the United States. J Am Coll Surg 2006;202:45-54.
(28) Lassen K, Hannemann P, Ljungqvist O, Fearon K, Dejong CH, von Meyenfeldt MF, et al. Patterns in current perioperative practice: survey of colorectal surgeons in five northern European countries. BMJ 2005;330:1420-1421.
(29) Wind J, Polle SW, Fung Kon Jin PH, Dejong CH, von Meyenfeldt MF, Ubbink DT, et al. Systematic review of enhanced recovery programmemes in colonic surgery. Br J Surg 2006;93:800-809.
(30) Gatt M, Anderson AD, Reddy BS, Hayward-Sampson P, Tring IC, MacFie J. Randomized clinical trial of multimodal optimization of surgical care in patients undergoing major colonic resection. Br J Surg 2005;92:1354-1362.
(31) Raue W, Haase O, Junghans T, Scharfenberg M, Muller JM, Schwenk W. ‘Fast-track’ multimodal reha-bilitation programme improves outcome after laparoscopic sigmoidectomy: a controlled prospective evaluation. Surg Endosc 2004;18:1463-1468.
(32) Anderson AD, McNaught CE, MacFie J, Tring I, Barker P, Mitchell CJ. Randomized clinical trial of multi-modal optimization and standard perioperative surgical care. Br J Surg 2003;90:1497-1504.
Wind (Chris).indb 98Wind (Chris).indb 98 28-05-2008 15:44:3828-05-2008 15:44:38

Part2Complications in
colorectal surgery
Wind (Chris).indb 99Wind (Chris).indb 99 28-05-2008 15:44:3828-05-2008 15:44:38
Wind (Chris).indb 100Wind (Chris).indb 100 28-05-2008 15:44:3828-05-2008 15:44:38

6Chapter
Installation of the pneumoperitoneum; technique and complications
J Wind
WA Bemelman
Adapted from:
Handboek Endoscopische Chirurgie, Bohn Stafleu van Loghum, in press
Nederlands Tijdschrift voor Heelkunde 2007;16:429-432
Wind (Chris).indb 101Wind (Chris).indb 101 28-05-2008 15:44:3828-05-2008 15:44:38

102102
Abstract
A variety of techniques to establish a pneumoperitoneum have been described. Roughly,
techniques for the installation of the pneumoperitoneum can be divided in two groups.
The first group comprises of introductions performed without direct visual control, the
so-called blind-entry techniques. These blind-entries are performed by using a Veress
needle to establish the pneumoperitoneum followed by trocar insertion, or less frequently
used, direct trocar insertion without previously establishing a pneumoperitoneum. The
other group comprises of entry techniques performed with visual control, including the
open-entry technique and the closed-entry techniques with optical trocar devices.
For all the entry techniques there is a wide variety of reusable and disposable trocars, and
Veress needles designed and marketed with its individual advantages and disadvantages.
With respect to complications, approximately one half of all intra-operative laparoscopic
complications are caused during the establishment of the pneumoperitoneum and
introduction of the trocars. The reported incidence of vascular and bowel injuries varies
and is between 0.05 and 0.5 complication per 100 laparoscopic procedures. In literature,
it is suggested that the open-entry technique is the safest introduction technique because
an overshoot of the introduction, especially those resulting in retroperitoneal vascular
injury, can be avoided. However, an open-entry does not preclude bowel injury. In patients
who had no history of abdominal surgery the installation of the pneumoperitoneum by
using the reusable TrocDoc® trocar (“half open”) might be an effective and less expensive
alternative for the traditional open-entry technique according to Hasson. In obese patients
an open-entry technique can be technically difficult. For these patients the blind-entry
technique with the Veress needle remains a good alternative. Finally, the identification of
patients with an increased risk of an entry-related injury is essential for a safe installation
of the pneumoperitoneum to prevent injuries.
Wind (Chris).indb 102Wind (Chris).indb 102 28-05-2008 15:44:3828-05-2008 15:44:38

103
Ch
apter 6
Installation of the pneumop
eritoneum; technique and com
plications
Introduction
Several randomised controlled trials and meta-analyses have demonstrated that laparoscopic
surgery is superior to conventional open surgery in terms of morbidity, postoperative
recovery, and hospital stay.1-3 Due to these short term advantages, laparoscopic surgery
has achieved broad acceptance nowadays and is a fast expanding surgical discipline.
However, the initiation of laparoscopic surgery, i.e. the creation of a pneumoperitoneum
and subsequently the introduction of the surgical instrumentation, remains a potentially
dangerous first step, which is exclusively associated with the laparoscopic approach.
Several studies have demonstrated that 20% to 50% of all intra-operative morbidity during
laparoscopic surgery occurs during the installation of the pneumoperitoneum.4-6
Several techniques to establish the pneumoperitoneum have been described. Roughly,
entry techniques can be divided in two groups (Table 1). The first group comprises of
introductions performed without (direct) visual control, the so-called blind-entry techniques,
which are performed by using a Veress needle to establish the pneumoperitoneum
followed by primary trocar insertion or, less frequently used, direct trocar insertion
without previously establishing a pneumoperitoneum. The other group comprises of entry
techniques which are performed with visual control. This group includes the open-entry
technique and the closed-entry techniques with optical trocar devices. The open-entry
technique is performed through a small laparotomy. Successively, skin, rectus fascia, and
peritoneum are incised under direct vision, followed by blunt (Hasson’s) trocar insertion.
Subsequently, the pneumoperitoneum is created. This technique was firstly described by
the gynaecologist Harrith Hasson in 1971.7 Alternative techniques for the open placement
technique are closed-entry techniques with optical trocar devices. The transparent tip
of the optical trocar allows a controlled passage of the individual tissue layers of the
abdominal wall.8
Table 1. Overview of entry techniques
Visually controlled entry techniquesOpen-laparoscopy1.
Hasson’s technique- TrocDoc- ®
Closed-entry techniques2. Optiview- ® (Ethicon)Endotip- ® (Karl Storz)Visiport- ® (Auto-Suture)
Blind-entry techniquesDirect trocar insertion1. Veress needle 2.
normal pressure (12-15 mmHg)- high pressure (25-30 mmHg)- optical Veress needle-
Table 1. Overview of entry techniques
Wind (Chris).indb 103Wind (Chris).indb 103 28-05-2008 15:44:3828-05-2008 15:44:38

104
With respect to the prevention of entry-related injuries none of the above mentioned
techniques is supported by solid evidence and until today there is an ongoing debate,
mainly between gynaecologists favouring the closed-entry technique, and surgeons
favouring the open-entry technique, which technique is to be preferred.6;9 Many general
surgeons suggest that the open-entry technique results in an equal amount of visceral
lesions compared to the closed-entry technique, but significantly fewer (retroperitoneal)
vascular lesions.5;9
In this chapter several techniques for the establishment of the pneumoperitoneum are
described including the instrumentation that is used and the potential complications that
can occur.
Instrumentation
The Veress needleThe pneumonologist Janos Veress introduced a needle for the establishment of a
pneumoperitoneum in 1938. This so-called Veress needle has two working parts; an
outer needle with a sharp bevelled edge, and an inner, spring-loaded, retractable blunt
shaft that extends beyond the end of the needle point. During insertion, the blunt inner
part of the needle is pushed inwards resulting in a sharp tipped instrument. As soon as
the peritoneum is penetrated, the blunt shaft is propelled forward beyond the sharp tip
by the spring-loaded mechanism, thus making the instrument blunt. Theoretically, this
mechanism prevents that the sharp tip of the needle reaches the intra-abdominal organs
and blood vessels.
Standard lengths of the Veress needle are 10, 12, and 15 centimetres. Veress needles are
available in both disposable and reusable systems. Besides the standard Veress needle,
optical needles are also available. The outer shaft of the optical Veress needle has a
diameter of 2.1 millimetres and a length of 10.5 centimetres. After correct placement
of the needle a mini-laparoscope with a diameter of 1.2 millimetre is introduced though
the outer shaft. The optical Veress needle can be used in patients with an increased risk
of peri-umbilical adhesions. The optical system offers an intra-abdominal visual control
during the placement of the primary trocar. A panoramic view on the abdominal cavity
and subsequent visualisation of adhesions around the umbilical area can be established
after placement of the optical Veress needle at Palmer’s point (left upper quadrant). When
adhesions are absent the primary trocar can still be placed at the umbilicus.
Trocars Trocars are an essential part of the laparoscopic instrumentation. The word “trocar” is
originated from the French word “trois quarts”, which is the original name for a knife with
three cutting edges. All trocars share the common aim of allowing the passage of surgical
instruments into the peritoneal cavity, whilst simultaneously preventing gas leakage. The
latter is in general by means of a flapper-valve or rubber membrane mechanism. A wide
Wind (Chris).indb 104Wind (Chris).indb 104 28-05-2008 15:44:3828-05-2008 15:44:38
105
Ch
apter 6
Installation of the pneumop
eritoneum; technique and com
plications
variety of reusable and disposable trocars have been designed and marketed for the use
of laparoscopic surgery.
Disposable trocars are constructed predominantly of plastic materials. Many disposable
trocars have a built-in mechanism guarding their sharp tips, these are the so-called shielded
trocars. They usually rely on one of three basic designs; either a retractable external shield,
a retractable central blunt point, or an internal shield which protects the sharp outer
sleeve of the trocar. The shields are either retracted prior to placement of the trocar in
the wound or automatically retract during the placement. Once the sharp tip of the trocar
penetrates the abdominal wall and enters the abdominal cavity, the spring-loaded safety
shield automatically deploys, covering the cutting edges of the tip and locking in place.
Both the retractable spike and the internal shield may provide more effective protection
than the external shields, which can be retracted during the passage of the abdominal
wall by the surrounding tissues.10;11 Also, most reusable trocars do not have a guarded
design.
When assessing the costs per instrument used, disposables initially appear more expensive
due to the obvious higher purchase price. However, cleaning and sterilisation costs for
reusable trocars must also be taken into account.
In general, reusable trocars are less sharp compared to disposable trocars. Therefore,
during the insertion of a sharper disposable trocar less force is required. When performing
a blind-entry technique using the Veress needle, it might be advantageous to use a sharper
disposable trocar because “overshoot” of the introduction might be prevented due to the
fact that less force is required during insertion.
Besides threaded cannulas that do not require a trocar for entry and optical trocars,
trocars are created with a tip based on several designs including blunt, conical, round,
bladed, and pyramidal tipped trocars. Blunt trocars, such as the widely known Hasson
trocar, are used during the open-entry technique. Conical trocars, however, have a round
sharp tip and dilate the fascial and muscular tissue after a small opening is made. Each
side of pyramidal trocars forms a knife-like surface that slices open the tissue encountered.
Less force is used during the insertion of these pyramidal trocars as compared to conical
trocars.12
Optical trocar systems allow for placement of the laparoscope in the trocar during the
insertion, enabling the operating surgeon to continuously visualise the layers of the
abdominal wall throughout the insertion process.
Entry techniques
The patient is positioned supine on the table, without rotation or a head down or modified
Trendelenburg position. Because in these alternative positions, the relationships of the
great vessels and other gastro-intestinal structures to the abdominal landmarks such
as the umbilicus may be altered increasing the likelihood of injury.12 Verification of the
position of several important anatomical structures is vital. Localising the aortic bifurcation,
Wind (Chris).indb 105Wind (Chris).indb 105 28-05-2008 15:44:3828-05-2008 15:44:38

106
palpation of the promontorium and crista iliaca provide a contribution to the virtual image
of the abdominal cavity. Furthermore, organomegaly or intra-abdominal tumours should
be ruled out via palpation or percussion. An empty bladder is important to avoid bladder
injury and to provide more range of vision and working space. Bladder drainage can be
achieved by inserting a urine catheter or once-only catheterisation. A nasogastric tube
prevents gastric distension which reduces the risk of injury to the stomach and transverse
colon.13 Drainage of the bladder and stomach are especially important when performing
a blind-entry technique. Finally, the instrumentation to perform a laparotomy should be
close at hand in case of serious vascular injury caused by the introduction of the Veress
needle or trocar.
The open-entry technique During the open-entry technique according to Hasson, a small laparotomy is performed of
1-2.5 centimetres.7 Successively, skin, rectus fascia, and peritoneum are incised under direct
vision, followed by the insertion of a blunt trocar (Hasson trocar). During the incision of the
several layers, the abdominal wall should be lifted, for example with towel clips or clamps.
The introduction of the primary trocar is performed completely under direct visual control.
After the blunt trocar is inserted and its correct position is confirmed, the gas insufflation
can be initiated directly through the cannula with the obturator (inner removable part) still
in place. After the pneumoperitoneum has been established, the trocar is fixated with two
sutures. Modified Hasson trocars are manufactured with an inflatable balloon for a gas
tight fixation of the trocar. At the termination of the laparoscopic procedure the trocar
is removed with the laparoscope in it, followed by fascial closure. With the exception
of the blunt primary trocar and the instruments necessary for the mini-laparotomy, the
remaining instrumentation is identical to the other entry techniques. It is assumed that the
open-entry technique reduces retroperitoneal vascular injuries to a minimum. However,
the open-entry technique is less frequently used as compared to the blind-entry technique
with the Veress needle. Reasons for this are the assumed larger incision (scar) that has to
be made with the open-entry technique and the fact that more manipulations are needed
with the open-introduction technique. Furthermore, the occurrence of gas leakage at
the primary trocar site might be higher with the open-entry technique. Nevertheless,
several studies have demonstrated that the open-entry technique is faster and cheaper as
compared to entries with the Veress needle.
Besides the traditional Hasson trocar, several disposable and reusable blunt trocars have
been designed and marketed. One of these is the blunt TrocDoc® trocar which was derived
from a sharp tipped trocar. The tip of a 10/11-mm trocar was loosened from it shaft and
replaced by a longer blunt tip, which was 10 mm at the connection with the shaft tapering
to 5 mm at the tip. The peritoneal cavity is reached through an incision large enough to
facilitate the passage of the 5-mm blunt tip of the TrocDoc®. Due to the gradual increase
in diameter from 5 to 10 mm, the trocar can be pushed in gently by stretching the
abdominal fascia, providing a tight fit without gas leakage. This introduction technique
provides visual control and needs no fixating sutures as with the Hasson trocar.14;15
Wind (Chris).indb 106Wind (Chris).indb 106 28-05-2008 15:44:3828-05-2008 15:44:38

107
Ch
apter 6
Installation of the pneumop
eritoneum; technique and com
plications
Closed-entry techniques with optical trocar devicesOptical trocars (Optiview®, Visiport®) allow a visually controlled passage of the individual
tissue layers of the abdominal wall.8 The transparent trocar and the laparoscope are
inserted together. The layers of the abdominal wall can be visualised individually, at which
the peritoneal cavity depicts dark. In contrast, adhesive bowel and omentum depicts more
lighter. Furthermore, in the event of an injury it can be noticed directly.
Another instrument that allows a visually controlled insertion, is the so-called endoscopic
screw (Endotip®). The insertion of the endoscopic screw is performed without a prior
pneumoperitoneum. After a small incision is made in the fascia the endoscopic screw,
with the laparoscope in it, is ‘screwed’ in the fascia with a rotary motion. During the
insertion the tissue is pushed away instead of being devided.13;16 It must be stressed that
the recognition of the successive layers of the abdominal wall is not easy applying these
closed-entries using optical trocar devices.
Blind-entry technique with the Veress needleBefore using the Veress needle, the sharpness and the spring-loaded tip mechanism must
always be checked if it functions properly. Subsequently, after a small incision is made
and the abdominal wall is lifted, the needle is introduced at an angle to the abdominal
wall; normally this angle is approximately 30-45 degrees with respect to the vertical axis.
The slantwise introduction of the needle is because of the fact that the needle must be
introduced perpendicular with respect to the abdomen wall. When the abdomen wall is
lifted, an angle is then created with the horizontal axis. Lifting the abdominal wall is mainly
for fixation, otherwise the abdomen wall would be pushed inwards and the distance to
the retroperitoneal structures would be reduced. It should be noted that the distance
between the abdominal wall and the underlying structures is not increased during lifting
as long as there is no pneumoperitoneum because the intra-abdominal structures are
still situated against the abdomen wall (i.e. intra-abdominal vacuum). When the tip of
the needle reaches the abdominal cavity, a double click is heard or felt which is caused
by retraction of the blunt inner part of the needle after the penetration of the fascia and
peritoneum. Furthermore, a hissing sound caused by passing air into the peritoneal cavity
due to the negative intra-abdominal pressure can be heard. The correct position of the
Veress needle can be verified with several tests such as the “drip-test”. The test involves
of a drip of NaCl which is placed on top of the closed Veress needle. When the needle is
opened the drip of NaCl is sucked into the needle, especially when the abdominal wall is
lifted. Another test to confirm proper needle placement is Palmer’s aspiration test. Here,
a syringe filled with NaCl is connected to the Veress needle. Next, the NaCl is “injected”
intra-abdominally through the Veress needle. The NaCl should be inserted without any
resistance. Subsequently, with the same syringe an attempt is made to aspirate and during
this manoeuvre the aspiration of blood or bowel contents is abnormal. Other tests include
the disappearance of liver dullness during percussion, symmetrical distension of the
abdomen during insufflation, and confirmation of the negative intra-abdominal pressure
after connection with the insufflator during lifting of the abdominal wall.17 If the correct
Wind (Chris).indb 107Wind (Chris).indb 107 28-05-2008 15:44:3928-05-2008 15:44:39

108
position of the needle is verified, insufflation can be performed up to a pressure of 12-15
mmHg. Insufflation of CO2 gas with a flow of 2-3 l/min with a low counter pressure (< 5
mmHg) also indicates correct position of the needle.
Following the insertion of the needle and insufflation, the primary trocar is inserted at the
same place as the needle was positioned. Before the insertion of the primary trocar, it is
important to ensure that the skin incision is large enough. Resistance during the insertion
of the trocar is in general caused at skin level where the incision is not large enough and
not during the passage of the fascia. If the Veress needle can not be placed correctly,
another one or two attempts might be undertaken. Thereafter, an open-entry should be
performed.
The so-called radial distension trocar (Step®) is made up of a Veress needle with a
polymeric sleeve, both are inserted simultaneously. After the correct position of the
needle is checked and the abdomen is insufflated, the needle is retracted from the sleeve.
Subsequently, the sleeve is dilated with a blunt obturator.18 With this technique the
layers of the abdominal wall are pushed away instead of being perforated or incised. The
advantage of this technique is that the needle with the sleeve is the only sharp instrument
that is blindly inserted. Furthermore, stability of the trocar, less gas leakage, less tissue
damage, less postoperative pain, and a decreased risk of postoperative hernia are reported
as advantages as well.
With the hyperinsufflation technique, a higher abdominal pressure is applied during the
entry of the first trocar to prevent injury, especially injury of the large retroperitoneal
vessels. After the insertion of the Veress needle and confirmation of its correct position a
pneumoperitoneum is established with high pressures of 25-30 mmHg.13;19 Subsequently,
at the umbilical entry site, the primary trocar is inserted. After entrance of the abdominal
cavity with the trocar, the intra-abdominal pressure is decreased. The higher intra-abdominal
pressure increases the distance between the abdominal wall and the retroperitoneal
vessels. Furthermore, the high pressure gives more counter pressure during the insertion
of the trocar. The high pressure is maintained only for a short period, therefore the risk
of deep venous thrombosis, gas emboli, and subcutaneous emphysema is minimal. This
technique is applied mostly in young and healthy patients. In these patients the influence of
the high intra-abdominal pressure on the cardiovascular system and pulmonary functions
is limited. However, in the elderly and in patients with severe comorbidity the increased
intra-abdominal pressure might result in cardiovascular or pulmonary complications.
Therefore, this technique is only suitable in young and healthy patients.
Direct trocar insertionDirect insertion of the first trocar without previously establishing a pneumoperitoneum
can be applied in a selected group of patients with a mobile ventral abdominal wall and
without a history of abdominal surgery or infections.20;21 Sufficient muscle relaxation,
a skin incision large enough to facilitate the trocar without resistance, sharp trocars,
and knowledge of the position of important anatomical structures, such as the aortic
bifurcation, are essential when applying this technique. The advantage of this technique
Wind (Chris).indb 108Wind (Chris).indb 108 28-05-2008 15:44:3928-05-2008 15:44:39

109
Ch
apter 6
Installation of the pneumop
eritoneum; technique and com
plications
is that injuries caused by the introduction of the Veress needle are avoided. However, the
insertion of the primary trocar is still performed without any visual control and with the
risk of an overshoot of the introduction.
Secondary trocar placementInjury to the epigastric vessels during placement of secondary trocar(s) form a substantial
part of all vascular injuries.5 The secondary trocar should be placed in a well-controlled
manner and with direct visualisation to prevent injuries. The laparoscope is used to identify
the deep inferior epigastric vessels (typically located underneath the rectus muscles) and
transillumination is used to identify the superficial vessels.
Entry sitesThe usual site for the primary introduction is the lower border of the umbilicus, where the
abdominal wall is at its thinnest and the skin is in direct contact with the fascia despite the
presence of adiposity. It is important not to damage the intra-abdominal structures during
the incision of the skin and fascia since there are reports of severe vascular injuries made
with a scalpel during the skin incision. When there is a deformity of the umbilicus or when
the risk of intra-abdominal adhesions is increased, an introduction at the umbilicus might
be undesirable. Alternative introduction places include a point halfway the umbilicus and
the pubic symphysis, directly above the umbilicus, left or right at McBurney’s point or
between the seventh and eight costa in the midaxillairy line on the left side. Another
alternative, specially when adhesions at the umbilicus are expected or with bariatric
surgery, is Palmer’s point, which is located three centimetres caudal of the lowest costa in
the mid-clavicular line on the left.
Removal of the trocarsRemoval of the trocars should be performed under direct visual control. The last trocar is
removed with the laparoscope in the trocar. This allows identification of vascular injuries
which remained unnoticed because the bleeding was temporarily stopped due to the
pressure of the pneumoperitoneum or plugging by the trocar. Furthermore, bowel injury
and the occurrence of herniation can also be identified during the trocar removal.
Fascial defects created by 10-mm or larger trocars should be closed to prevent hernia
formation.22 All layers of the abdominal wall should be closed meticulously under direct
vision including the peritoneum.22-24 When active manipulation through a 5-mm port has
occurred during prolonged procedures or stretching the port side for retrieval, the fascia
should also be closed to prevent complications.22;25;26
Wind (Chris).indb 109Wind (Chris).indb 109 28-05-2008 15:44:3928-05-2008 15:44:39

110
Complications
It has been calculated that approximately one half of all intra-operative laparoscopic
complications is caused during the installation of the pneumoperitoneum and the
subsequent introduction of the trocars.4;6;27 Entry related injuries can be divided in two
different groups. The first group comprises of injuries to blood vessels and organs within
their normal anatomical position. The second group comprises of injuries to structures
which are located at an abnormal position, such as bowel or omentum which is adhesive to
the anterior abdominal wall. Besides direct injury to intra-abdominal structures during the
entry phase, the pneumoperitoneum itself influences the cardiovascular system due to the
increased intra-abdominal pressure. The cardiovascular effects of the pneumoperitoneum
occur mainly during its initiation. This should be considered when the intra-abdominal
pressure is initially increased for the introduction of access devices.27-30 In young and
healthy patients (ASA I and II) the hemodynamic and circulatory effects of a 15 mmHg
pneumoperitoneum are generally not clinically relevant. Care has too be taken when
establishing the pneumoperitoneum in the elderly and patients with severe co-morbidity
(ASA III and IV).27;29-31 Invasive measurement of blood pressure or circulating volume
should be considered. These patients should also receive adequate preoperative volume
loading and beta-blockers.27;32;33 If technically feasible, gasless or low pressure laparoscopy
might be an alternative for patients with limited cardiac function.27-29
IncidenceEntry-related injuries mostly involve bowel and blood vessel injuries. The reported incidence
of vascular and bowel injuries varies and is between 0.05 and 0.5 complications per 100
laparoscopic procedures.9;34-36 This is most likely an under-estimation as in the majority
of cases, most injuries are not reported. The result of major vascular and unrecognized
bowel injuries is serious, often leading to severe morbidity and even mortality. The overall
mortality rate is reported to be about 4%, increasing to 21% for unrecognized bowel
injury.34;36-40
The incidence of clinically relevant gas embolism is very rare (0.002-0.02%), but if it occurs
it can be a fatal complication.27;41 Gas embolism usually occurs during the installation
of the pneumoperitoneum using the Veress needle or less frequently a sharp trocar. The
usual cause of gas embolism is the accidental placement of a needle or trocar into a blood
vessel. Similarly, any injury to veins or parenchymal organs can result in direct gas inflow
into the systemic circulation, especially during liver surgery.27
The incidence of extraperitoneal insufflation is between approximately 0.4 and 3.5%.
Extensive preperitoneal insufflation can result in an altered outline of the abdominal cavity
which can severely hamper the exposure of the laparoscopic procedure. Furthermore,
extensive preperitoneal insufflation can result in serious complications such as a
pneumothorax, pneumomediastinum, or pneumopericardium.27
Wind (Chris).indb 110Wind (Chris).indb 110 28-05-2008 15:44:3928-05-2008 15:44:39

111
Ch
apter 6
Installation of the pneumop
eritoneum; technique and com
plications
Complications during open and blind-entriesHistorically, gynaecologists have been trained in the blind-entry technique with the
Veress needle. Although the technique of open-laparoscopy was first described by
the gynaecologist Hasson in 19717, only a few gynaecologists apply the open-entry
technique.9;42 Some have reported comparable or even higher complication rates when
applying the open-entry technique in gynaecological case series.9 However, in these studies
the participating gynaecologists did not frequently use the open-entry technique and if
used, this was mainly in selected patients who had prior abdominal surgery. Consequently,
these patients already were at a higher risk for entry related complications. This explains
why in a systematic review by Merlin et al. the risk of major complications initially appeared
to be higher for the open-entry technique. When only prospective series were taken into
account the opposite was shown; a relative risk of 0.30 (95% CI 0.09-1.03) was found in
favour of the open-entry technique. It was noted that retrospective studies compared a
high-risk with a low-risk patient population, while the prospective studies investigated an
unselected patient population.43
Recently, a review was performed concerning entry-related complications which included
all malpractice claims filed at the largest medical liability mutual insurance company for
hospitals in health care in the Netherlands.44 From January 1993 to December 2005,
229 laparoscopy-related claims were filed of which 41 (18%) claims were identified as
entry-related complications. Most were young (median age 35 years) female patients who
had routine, non-advanced laparoscopic procedures planned as short-stay or day-care
procedures. In these patients, a total of 51 structures were injured. There were 18
vascular structure injuries, mainly retroperitoneal arteries. Furthermore, there were 30
bowel injuries, in two patients the uterus was injured and one injury involved extensive
preperitoneal insufflation. An open-entry technique was used in only two (5%) of the
41 included patients. Both patients had a history of previous abdominal surgery and the
injured structure was bowel. In the remainder, a blind (Veress) entry technique had been
applied. Vascular injury was exclusively associated with the blind-entry technique. In only
19 (46%) patients the entry-related complication was diagnosed peroperatively. In the
remaining patients, the entry-related injury was diagnosed postoperatively, median on day
two (range 0-5).
In a recent survey of the U.S. Food and Drug Administration (FDA) by Fuller et al. reviewing
all reports in a period from January 1997 to June 2002, 31 fatal and 1353 nonfatal trocar
injuries were identified.39 Most fatalities involved vascular injuries. It was remarkable
that almost all the vascular injuries were caused with the Veress needle or trocar during
blind-entries. Bowel injury was reported in both the blind and open-entries. Furthermore,
many injuries were caused by disposable shielded trocars and optical trocars. Although,
the exact perspective concerning these FDA data is unclear because it is unknown how
many open and blind-entries are being performed and how many shielded and optical
trocars are used, it could carefully be concluded that neither shielded nor optical trocars
can guarantee a safe installation of the pneumoperitoneum. Furthermore, retroperitoneal
vascular injury seems to be associated with the blind-entry technique due to an “overshoot”
of the introduction of the Veress needle or trocar. This injury mechanism is not present
Wind (Chris).indb 111Wind (Chris).indb 111 28-05-2008 15:44:3928-05-2008 15:44:39

112
with the open-entry technique. However, an open-entry does not preclude bowel injury,
just as a formal laparotomy could be complicated by bowel injury.
Discussion
The European Association for Endoscopic Surgery (E.A.E.S; www.eaes-eur.org) practical
clinical guideline on the pneumoperitoneum does not state which of the entry techniques
is the preferred one.27 In literature, it is suggested that the open-entry technique is the
most safe entry technique because an overshoot of the introduction, especially those
resulting in retroperitoneal vascular injury, can be avoided. However, an open-entry does
not preclude bowel injury. Hashizume et al. reported in a retrospective study (1991-1995)
that during the study period 96.6% of the Japanese surgeons changed their method of
establishing a pneumoperitoneum from the closed technique to the open technique in
order to increase patient safety. The rate of complications related to needle and/or trocar
insertion subsequently decreased as the surgeon’s experience performing laparoscopic
surgery using the open-entry technique increased.5
In patients without abdominal surgery in their history, an entry with the reusable
TrocDoc® trocar (“half open”) might be an effective and less expensive alternative for
the open-introduction according to Hasson.14 With respect to obese patients the open-
entry technique can be technically difficult. For these patients, the blind-entry technique
with the Veress needle remains a good alternative. The presence of peritonitis is not an
absolute contra-indication for a laparoscopic approach. However, distended bowel poses
a risk for bowel injury during the installation of the pneumoperitoneum. Therefore, a well
controlled open-entry is in those circumstances the safest option.
In children and relatively thin adult patients the distance between the abdominal wall
and retroperitoneal structures is reduced. Therefore, in those patients the open-entry
technique might be the safest. Also, in pregnant females and in patients with ascites an
open-entry is preferred.27
Nevertheless, identification of patients who have an increased risk of an entry-related
injury is essential to prevent such injuries. Prior abdominal surgery, especially midline
laparotomy, is associated with a considerable increased risk of adhesions of bowel with
the anterior abdominal wall. After a Pfannenstiel incision in 31% of the patients adhesions
are present and in 10% of the patients these adhesions are extensive. After a midline
laparotomy, this is 51% and 30% respectively.45 Furthermore, a history of inflammatory
bowel disease, peritonitis, and radiotherapy is associated with intra-abdominal adhesions
and anatomical changes.
During physical examination it is important to search for abdominal wall herniations
to prevent that the installation of the pneumoperitoneum is performed at these sites.
Furthermore, the abdomen should be palpated to exclude organomegaly.
In conclusion, the installation of the pneumoperitoneum is exclusively associated with
the laparoscopic approach and remains a potentially dangerous first step. Moreover,
Wind (Chris).indb 112Wind (Chris).indb 112 28-05-2008 15:44:3928-05-2008 15:44:39

113
Ch
apter 6
Installation of the pneumop
eritoneum; technique and com
plications
approximately one half of all intra-operative laparoscopic complications are caused during
the establishment of the pneumoperitoneum and introduction of the trocars. Although
the incidence of entry-related injuries is very low for both the open and blind-entry
techniques, retroperitoneal vascular injury (“overshoot of the introduction”) might be
prevented by the open-entry technique. Based on available and reviewed literature, the
open-entry technique seems to be the most safe entry technique and is to be preferred in
most cases.
Reference List
(1) Abraham NS, Young JM, Solomon MJ. Meta-analysis of short-term outcomes after laparoscopic resec-tion for colorectal cancer. Br J Surg 2004;91:1111-1124.
(2) Medeiros LR, Fachel JM, Garry R, Stein AT, Furness S. Laparoscopy versus laparotomy for benign ovarian tumours. Cochrane Database Syst Rev 2005;(3):CD004751.
(3) Schwenk W, Haase O, Neudecker J, Muller JM. Short term benefits for laparoscopic colorectal resec-tion. Cochrane Database Syst Rev 2005;(3):CD003145.
(4) Harkki-Siren P, Kurki T. A nationwide analysis of laparoscopic complications. Obstet Gynecol 1997;89:108-112.
(5) Hashizume M, Sugimachi K. Needle and trocar injury during laparoscopic surgery in Japan. Surg Endosc 1997;11:1198-1201.
(6) Jansen FW, Kapiteyn K, Trimbos-Kemper T, Hermans J, Trimbos JB. Complications of laparoscopy: a prospective multicentre observational study. Br J Obstet Gynaecol 1997;104:595-600.
(7) Hasson HM. A modified instrument and method for laparoscopy. Am J Obstet Gynecol 1971;110:886-887.
(8) Mettler L, Schmidt EH, Frank V, Semm K. Optical trocar systems: laparoscopic entry and its complica-tions (a study of cases in Germany). Gynaecol Endosc 1999;8:383-389.
(9) Jansen FW, Kolkman W, Bakkum EA, de Kroon CD, Trimbos-Kemper TC, Trimbos JB. Complica-tions of laparoscopy: an inquiry about closed- versus open-entry technique. Am J Obstet Gynecol 2004;190:634-638.
(10) Dunn DC, Watson CJ. Disposable guarded trocar and cannula in laparoscopic surgery: a caveat. Br J Surg 1992;79:927.
(11) Watson DI. Disposable and reusable trocars. Endosc Surg Allied Technol 1995;3:140-142.
(12) Munro MG. Laparoscopic access: complications, technologies, and techniques. Curr Opin Obstet Gyne-col 2002;14:365-374.
(13) Admiraal JF. Laparoscopische insteektechnieken. Scoop 2002;7:2-5.
(14) Bemelman WA, de Wit LT, Busch OR, Den Boer KT, Klaase JF, Grimbergen CA, et al. Establishment of pneumoperitoneum with a modified blunt trocar. J Laparoendosc Adv Surg Tech A 2000;10:217-218.
(15) Bemelman WA, Dunker MS, Busch OR, Den Boer KT, de Wit LT, Gouma DJ. Efficacy of establishment of pneumoperitoneum with the Veress needle, Hasson trocar, and modified blunt trocar (TrocDoc): a randomized study. J Laparoendosc Adv Surg Tech A 2000;10:325-330.
(16) Ternamian AM. A second generation laparoscopic port system: EndoTIP. Gynaecol Endosc 1999;8:397-401.
(17) Semm K, Semm I. Safe insertion of trocars and the Veress needle using standard equipment and the 11 security steps. Gynaecol Endosc 1999;8:339-347.
Wind (Chris).indb 113Wind (Chris).indb 113 28-05-2008 15:44:3928-05-2008 15:44:39
114
(18) Turner D. Making the case for the radially expanding access system. Gynaecol Endosc 1999;8:391-395.
(19) Reich H, Ribeiro SC, Rasmussen C, Rosenberg J, Vidali A. High-pressure trocar insertion technique. JSLS 1999;3:45-48.
(20) Byron JW, Markenson G, Miyazawa K. A randomized comparison of Verres needle and direct trocar insertion for laparoscopy. Surg Gynecol Obstet 1993;177:259-262.
(21) Agresta F, De Simone P, Ciardo LF, Bedin N. Direct trocar insertion vs Veress needle in nonobese patients undergoing laparoscopic procedures: a randomized prospective single-center study. Surg Endosc 2004;18:1778-1781.
(22) Tonouchi H, Ohmori Y, Kobayashi M, Kusunoki M. Trocar site hernia. Arch Surg 2004;139:1248-1256.
(23) Callery MP, Strasberg SM, Soper NJ. Complications of laparoscopic general surgery. Gastrointest Endosc Clin N Am 1996;6:423-444.
(24) Velasco JM, Vallina VL, Bonomo SR, Hieken TJ. Postlaparoscopic small bowel obstruction. Rethinking its management. Surg Endosc 1998;12:1043-1045.
(25) Kopelman D, Schein M, Assalia A, Hashmonai M. Small bowel obstruction following laparoscop-ic cholecystectomy: diagnosis of incisional hernia by computed tomography. Surg Laparosc Endosc 1994;4:325-326.
(26) Nassar AH, Ashkar KA, Rashed AA, Abdulmoneum MG. Laparoscopic cholecystectomy and the umbili-cus. Br J Surg 1997;84:630-633.
(27) Neudecker J, Sauerland S, Neugebauer E, Bergamaschi R, Bonjer HJ, Cuschieri A, et al. The European Association for Endoscopic Surgery clinical practice guideline on the pneumoperitoneum for laparo-scopic surgery. Surg Endosc 2002;16:1121-1143.
(28) Stuttmann R, Vogt C, Eypasch E, Doehn M. Haemodynamic changes during laparoscopic cholecystec-tomy in the high-risk patient. Endosc Surg Allied Technol 1995;3:174-179.
(29) Nordentoft T, Bringstrup FA, Bremmelgaard A, Stage JG. Effect of laparoscopy on bacteremia in acute appendicitis: a randomized controlled study. Surg Laparosc Endosc Percutan Tech 2000;10:302-304.
(30) Koivusalo AM, Lindgren L. Respiratory mechanics during laparoscopic cholecystectomy. Anesth Analg 1999;89:800.
(31) Jackman SV, Weingart JD, Kinsman SL, Docimo SG. Laparoscopic surgery in patients with ventriculoperi-toneal shunts: safety and monitoring. J Urol 2000;164:1352-1354.
(32) Sungler P, Heinerman PM, Steiner H, Waclawiczek HW, Holzinger J, Mayer F, et al. Laparoscopic chole-cystectomy and interventional endoscopy for gallstone complications during pregnancy. Surg Endosc 2000;14:267-271.
(33) Feig BW, Berger DH, Dougherty TB, Dupuis JF, Hsi B, Hickey RC, et al. Pharmacologic intervention can reestablish baseline hemodynamic parameters during laparoscopy. Surgery 1994;116:733-739.
(34) Philips PA, Amaral JF. Abdominal access complications in laparoscopic surgery. J Am Coll Surg 2001;192:525-536.
(35) Bonjer HJ, Hazebroek EJ, Kazemier G, Giuffrida MC, Meijer WS, Lange JF. Open versus closed establish-ment of pneumoperitoneum in laparoscopic surgery. Br J Surg 1997;84:599-602.
(36) Bhoyrul S, Vierra MA, Nezhat CR, Krummel TM, Way LW. Trocar injuries in laparoscopic surgery. J Am Coll Surg 2001;192:677-683.
(37) van der Voort M, Heijnsdijk EA, Gouma DJ. Bowel injury as a complication of laparoscopy. Br J Surg 2004;91:1253-1258.
(38) Soderstrom RM. Bowel injury litigation after laparoscopy. J Am Assoc Gynecol Laparosc 1993;1:74-77.
(39) Fuller J, Ashar BS, Carey-Corrado J. Trocar-associated injuries and fatalities: an analysis of 1399 reports to the FDA. J Minim Invasive Gynecol 2005;12:302-307.
(40) Corson SL, Chandler JG, Way LW. Survey of laparoscopic entry injuries provoking litigation. J Am Assoc Gynecol Laparosc 2001;8:341-347.
Wind (Chris).indb 114Wind (Chris).indb 114 28-05-2008 15:44:3928-05-2008 15:44:39

115
Ch
apter 6
Installation of the pneumop
eritoneum; technique and com
plications
(41) Shulman D, Aronson HB. Capnography in the early diagnosis of carbon dioxide embolism during laparos-copy. Can Anaesth Soc J 1984;31:455-459.
(42) Levy BS, Hulka JF, Peterson HB, Phillips JM. Operative laparoscopy: American Association of Gynecologic Laparoscopists, 1993 membership survey. J Am Assoc Gynecol Laparosc 1994;1:301-305.
(43) Merlin TL, Hiller JE, Maddern GJ, Jamieson GG, Brown AR, Kolbe A. Systematic review of the safety and effectiveness of methods used to establish pneumoperitoneum in laparoscopic surgery. Br J Surg 2003;90:668-679.
(44) Wind J, Cremers JE, van Berge Henegouwen MI, Gouma DJ, Jansen FW, Bemelman WA. Medical liabil-ity insurance claims on entry-related complications in laparoscopy. Surg Endosc 2007;21:2094-2099
(45) Audebert AJ. The role of microlaparoscopy for safer wall entry: incidence of umbilical adhesions according to past surgical history. Gynaecol Endosc 1999;8:363-367.
Wind (Chris).indb 115Wind (Chris).indb 115 28-05-2008 15:44:4028-05-2008 15:44:40

Wind (Chris).indb 116Wind (Chris).indb 116 28-05-2008 15:44:4028-05-2008 15:44:40

7Chapter
Medical liability insurance claims on entry-related complications in laparoscopy
J Wind
JEL Cremers
MI van Berge Henegouwen
DJ Gouma
FW Jansen
WA Bemelman
Surgical Endoscopy 2007;21:2094-2099
Wind (Chris).indb 117Wind (Chris).indb 117 28-05-2008 15:44:4028-05-2008 15:44:40

118118
Abstract
IntroductionInstallation of the pneumoperitoneum is an essential part of laparoscopic surgery. Creation
can be performed by either the open or a closed technique. The aim of this study was to
assess the number of, and contributing factors to entry-related complications in medical
liability insurance claims in the Netherlands.
MethodsA retrospective chart review was performed including all malpractice claims filed at
MediRisk, which is presently the largest medical liability mutual insurance company for
institutions, mainly hospitals in health care in the Netherlands.
ResultsFrom January 1993 to December 2005, 41 claims were identified as entry-related
complications which comprised 18% of all laparoscopy-related complications leading
to claims. Most were young (median age 35 years) female patients who had routine,
non-advanced laparoscopic procedures planned as short-stay or day-care procedures. The
claims were equally divided between general surgery (n=20) and gynaecology (n=21). A
total of 51 structures were injured. There were 18 vascular structure injuries, 30 bowel
injuries and three other injuries. An open-entry technique was used in only two (5%)
patients. Vascular injury was exclusively associated with the closed-entry technique. In
only 19 (46%) patients the entry-related complication was diagnosed peroperatively,
consisting of 70% of the vascular and 25% of the bowel injuries. Twenty-six patients
(64%) were admitted to the Intensive Care Unit for a median of five days. There was no
mortality. Besides conversion, the majority of the patients filed a claim to compensate
for a longer hospital stay and related costs. A payment was made in 17 (57%) of the 30
settled claims.
ConclusionMedical liability claims concerning laparoscopic entry-related complications comprised
one fifth of all laparoscopy-related claims. Claims concerning entry-related complications
occurred in young patients who had routine, non-advanced procedures. In the investigated
cases most claims involved the closed-entry technique.
Wind (Chris).indb 118Wind (Chris).indb 118 28-05-2008 15:44:4028-05-2008 15:44:40

119
Ch
apter 7
Medical liability insurance claim
s on entry-related complications in laparoscopy
Introduction
Despite the ongoing technological advances in laparoscopic surgery, the creation of a
pneumoperitoneum and the additional introduction of surgical instruments remains a
potential dangerous first step that can result in serious injuries to the viscera and major
intra- and retroperitoneal vessels. The reported incidence of vascular and bowel injuries
varies and is between approximately 0.05–0.5 complications per 100 laparoscopic
procedures.1-4 Although the incidence of entry-related complications is rare, the result of
major vascular and unrecognized bowel injuries is serious, often leading to severe morbidity
and even mortality. The overall mortality rate is reported to be about 4% increasing to
21% for unrecognized bowel injury.5-7 In several reports the fatalities result from about
75% vascular injuries and the remaining 25% from unrecognized bowel injuries.4;5;8
Furthermore, it has been calculated that one half of all laparoscopic complications can be
blamed on the entry technique.9-11
In general, there are two techniques to establish the pneumoperitoneum and to enter
the abdominal cavity. The first is the closed (blind) entry, which is performed by using a
Veress needle to establish the pneumoperitoneum followed by trocar insertion or, less
frequently, direct trocar insertion without previously establishing a pneumoperitoneum.
The second method is the open technique, in which a small laparotomy is performed.
Successively, skin, rectus fascia, and peritoneum are incised under direct vision, followed
by blunt (Hasson’s) trocar insertion. Subsequently the pneumoperitoneum is created.1;12
With respect to the prevention of entry-related complications, neither of these two
techniques is supported by solid evidence and there is an ongoing debate, mainly
between gynaecologists who favour the closed-entry technique, and surgeons who favour
the open-entry technique, about which technique is better.1;10 Many general surgeons
suggest that the open-entry technique results in the same number of visceral lesions as
does the closed-entry technique, but significantly fewer vascular lesions.1;13 Furthermore,
it could be hypothesized that another advantage of the open-entry is that at least part of
the bowel injuries is immediately seen under direct vision. Because of the lack of evidence,
the European Association for Endoscopic Surgery (E.A.E.S.) practical clinical guideline on
the pneumoperitoneum could not state which of the entry techniques is preferred.9
To answer this questions with a high level of evidence a randomised comparison of the
open and closed access techniques with a sample size of over 200.000 patients would
be required to detect a reduction of major complications from one per 1000 to 0.5 per
1000.14 Therefore, it is important to continue to report on this topic because one has to
rely on accumulating evidence of a lower level. In this study medical liability data sources
were used to provide evidence on entry-related injuries.
The aim of this study was to assess the number of entry-related complications that
provoked medical liability insurance claims for laparoscopic surgery at the largest medical
liability mutual insurance company for institutions in health care in the Netherlands.
Furthermore, the used entry technique (i.e. open vs. closed), distribution of injured organs,
and predictive factors for litigation were assessed.
Wind (Chris).indb 119Wind (Chris).indb 119 28-05-2008 15:44:4028-05-2008 15:44:40

120
Methods
Data sourceA retrospective chart review was performed which included all malpractice claims filed at
MediRisk concerning entry-related complications in the period January 1993 to December
2005. MediRisk was founded in 1993 and is presently the largest medical liability mutual
insurance company for institutions, mainly hospitals in the healthcare industry in the
Netherlands. In 1993 MediRisk insured 21 hospitals. At the end of 2005 the number of
insured hospitals included 80 of the 101 Dutch hospitals (Figure 1). The insured institutes
are broadly representative of the Dutch teaching and non-teaching hospitals, with the
exception of all eight academic hospitals in the Netherlands, none of which are insured at
MediRisk.
Figure 1. The number of hospitals insured and the amount of claims that were filed between 1993 and 2005
Definitions and inclusion and exclusion criteriaAn entry-related complication was defined as a direct injury related to the insertion of
either the Veress needle or the first trocar, including preperitoneal insufflations and injuries
to epigastric vessels, intraperitoneal viscera and vessels, and retroperitoneal viscera and
vessels. Port-site hernias were excluded from this analysis.
Claims, in which the aetiology of the injury was not clear and other causes than insertion
(e.g. coagulation injury or other procedure-related complications) could not be ruled out,
based on operative reports and/or histological examination, were excluded. Furthermore,
injuries caused by second-trocar insertion were also excluded.
Claim characteristicsAll included claims were reviewed and the following data were extracted using a
preformatted sheet; age, gender, co-morbidity, prior abdominal surgery and/or
Wind (Chris).indb 120Wind (Chris).indb 120 28-05-2008 15:44:4028-05-2008 15:44:40

121
Ch
apter 7
Medical liability insurance claim
s on entry-related complications in laparoscopy
previous intra-abdominal infectious events, body mass index (BMI, kg/m2), specialty
(i.e. gynaecology or general surgery), urgency, experience (i.e. resident or consultant),
informed consent, indication for surgery, entry technique (i.e. open or closed), type of
entry-related complication, moment of diagnosis of the entry-related complication,
postoperative recovery including data such as reoperations, Intensive Care Unit (ICU)
admission, postoperative morbidity and mortality. The entry-related complications were
classified as ‘bowel’, ‘vascular’ or ‘other’. The gastrointestinal tract was divided into three
parts: stomach, small intestine and large intestine. Vascular injuries were divided into
retroperitoneal, intraperitoneal, and abdominal wall (epigastric vessels). Furthermore, the
vascular injuries were subdivided into arterial, venous, or vascular not specified.
StatisticsData were calculated as median values with ranges for continuous and discrete data,
unless otherwise specified. Categorical data are presented as frequencies or percentages.
Analysis was done using the SPSS v.12.0 package (SPSS, Chicago, Illinois, USA).
Results
Filed claims concerning laparoscopic procedures and entry-related complicationsIn the study period, a total of 10552 claims were filed at MediRisk (Figure 1) of which
229 (2%) involved gynaecological and surgical laparoscopic procedures. Of these 229
Figure 2. The relation between laparoscopy-related claims in total and entry-related injuries between 1993 and 2005
Wind (Chris).indb 121Wind (Chris).indb 121 28-05-2008 15:44:4128-05-2008 15:44:41

122
claims, 50 were identified as an entry-related complication. Subsequently, seven claims
were excluded because the aetiology of the injury was not clear and causes other than
Veress needle or trocar insertion could not be ruled out. Furthermore, two claims were
excluded because the injury was caused by insertion of the second-trocar. The final analysis
comprised 41 claims, which is 18% of all laparoscopy-related claims filed at MediRisk.
Figure 2 shows the relationship between all laparoscopy-related claims and the number
of entry-related complications. The yearly number of filed claims concerning entry-related
complications remained stable during the study period.
Characteristics of the entry-related complicationsThe median age of the 41 patients included in this study was 35 years (range 14-81).
Median BMI was 24.0 kg/m2 (range 18.6-55.9 kg/m2). Sixteen (39%) patients had a high
(> 25.0 kg/m2), and six (15%) had a low (< 20 kg/m2) BMI. Twenty-one patients (51%) had
a history of prior abdominal surgery (range 1-3 procedures). The ratio between general
surgery and gynaecology was 20:21. The surgical patients c onsisted of 17 (85%) females
and three (15%) males. Residents were involved in six (15%) claims. In both surgical and
gynaecological patients the planned procedures were routine and non-advanced and in
37 (90%) patients they were elective (Table 1).
Table 1. Planned operative procedures in the 41 patients with an entry-related complication
Planned procedure Number of patients (n=41)
Gynaecologysterilizationdiagnostic laparoscopy ovarian cystectomyadhesiolysisectopic pregnancyadnex extirpation
114221 1
Surgerycholecystectomydiagnostic laparoscopyappendectomyhernia repairgastric bandinggastric perforation
10‡
3 3 211
‡Including two open-entry techniques; in all other patients a closed-entry technique was used
A total of 51 structures were injured (Table 2). There were 18 vascular structure injuries
consisting mainly of retroperitoneal vessels (n=13, 72%) of arterial origin (n=10, 77%), 30
bowel injuries and three other injuries. Thirty-six patients had one injury, five (12%) patients
had a combination of entry-related complications (range 2-3). The injured retroperitoneal
arteries included the right iliac artery (n=2, 20%), the left iliac artery (n=2, 20%), and the
abdominal aorta (n=3, 30%); in the remaining three (30%) cases the injured artery was
not reported. The large bowel injuries comprised mainly the transverse (n=4, 40%) and
left sided colon (n=4, 40%). Two (5%) patients had an open entry-related complication.
Wind (Chris).indb 122Wind (Chris).indb 122 28-05-2008 15:44:4228-05-2008 15:44:42

123
Ch
apter 7
Medical liability insurance claim
s on entry-related complications in laparoscopy
Both patients had a history of a previous laparotomy. In one patient the exact type of
entry technique was not mentioned. A closed-entry technique was used in the remaining
38 (93%) patients. All vascular entry-related complications were seen after the closed-
entry technique. In 15 (39%) cases in which the closed-entry technique was used it could
not be determined whether the Veress needle or the primary trocar was responsible for
the injury. In the remaining closed-entry cases, the Veress needle was responsible in 12
(32%) and the first trocar in 11 (29%) cases. In only five of the latter cases the design of
the trocar was reported; four shielded trocars and one optical trocar.
Table 2. Type of entry-related complications (n=51) in the 41 patients included in this study
Type of entry-related complication
Gynaecology (n=21) Surgery (n=20)
Vascularepigastric vesselsretroperitoneal vesselsintraperitoneal vessels*
142
191
Bowelstomachsmall intestinelarge intestine
196
19‡
4‡
Otheruteruspreperitoneal insufflation
01
2†
0
*mesenterial artery or omental artery; †One patient was 22 weeks pregnant; ‡including one open-entry technique
Thirteen (32%) claims provided additional narrative comments by the surgeon on the
cause of the injury, citing various factors that contributed to the injury. These comments
included adhesions (n=4), “overshoot” with the trocar (n=2), distended intestine (n=2),
very thin patient (n=2), pregnancy (n=1), post partum (n=1), obesity (n=1), and device
problems during introduction (n=1).
Time of diagnosis and postoperative courseIn 19 (46%) cases the entry-related complication was diagnosed peroperatively resulting
in 16 conversions. In the remaining 22 (54%) cases the injury was diagnosed at median
postoperative day two (range 0-5), resulting in one or more reoperations and a complicated
postoperative course (Table 3). Eighty percent of the combined injuries and 70% of the
vascular injuries were diagnosed peroperatively, the remaining vascular and combined
injuries were diagnosed on the same day. Only 25% of the bowel injuries were diagnosed
peroperatively, the remainder were diagnosed at median postoperative day two. Twenty-
six patients (64%) were admitted to the ICU for a median of five days (range 1-60). Seventy
percent of the patients with a vascular injury were admitted to the ICU for a median of
two days (range 1-34). Fifty-eight percent of patients with a bowel injury were admitted
to the ICU for a median of eight days (range 1-60). There were no claims for fatal injuries.
Nine (22%) patients suffered permanent harm (> 1 year). The latter consisted of post
Wind (Chris).indb 123Wind (Chris).indb 123 28-05-2008 15:44:4228-05-2008 15:44:42

124
traumatic stress disorder (n=3), neuropathy (n=2), post ventilation lung damage (n=1),
premature childbirth due to uterus perforation (n=1), permanent enterocuteneous fistula
(n=1), and intermittent claudication (n=1).
Table 3. Time of diagnosis (no delay vs. delayed diagnosis) and postoperative course of the 41 patients included in this study
No delay(n=19)
Delayed diagnosis(n=22)
ICU stay- number of patients (%)- median days (range)
8 (42%)1 (1-18)
18 (82%)8 (1-60)
Patients with postoperative morbidity (%) 6 (32%) 17 (77%)
Permanent harm 5 (26%) 4 (18%)
ICU: Intensive Care Unit
From patient records only in 13 (32%) claims, informed consent was properly established,
i.e. documented and understood by the patient. In the remaining claims informed consent
was not documented or not given at all. In 48% of the claims complications such as
bowel injury or the chance of conversion to laparotomy were discussed preoperatively.
According to the records a postoperative meeting between surgeon and patient, in which
the complications that occurred were discussed, had taken place in only 16 (39%) cases.
The majority of the patients claimed financial compensation for the prolonged hospital stay,
related costs such as travelling expenses and domestic care and the midline laparotomy
scar. Thirty (73%) claims were settled at the end of the study period and a payment was
made in 17 (57%) of the settled claims.
Discussion
Several randomised controlled trials and meta-analyses have demonstrated that laparoscopic
surgery is superior to laparotomy in terms of morbidity, postoperative recovery, and length
of hospital stay.15;16 Having achieved broad acceptance, minimally invasive surgery is a fast-
expanding surgical discipline. Nevertheless, the initiation of laparoscopy, i.e. the creation
of a pneumoperitoneum followed by the introduction of the surgical instruments remains
a potentially dangerous first step, which is exclusively associated with the laparoscopic
approach.
The present study demonstrates that medical liability claims involving entry-related injuries
comprised about one fifth of all laparoscopic surgery-related claims filed at MediRisk. The
claims were equally distributed between general surgery and gynaecologic procedures.
However, this distribution does not implicate that the incidences of entry-related
complications are comparable because the number of laparoscopic procedures of both
specialities performed during the study period is not known.
In both the general surgery and gynaecology cases the planned procedure was generally a
routine one and elective in nature. Furthermore, these procedures involved mostly young
Wind (Chris).indb 124Wind (Chris).indb 124 28-05-2008 15:44:4228-05-2008 15:44:42

125
Ch
apter 7
Medical liability insurance claim
s on entry-related complications in laparoscopy
female patients who planned to be operated on in a day-care setting or in short stay
surgery. The consequences of an entry-related complication in these young patients who
underwent a routine procedure are striking, however. The entry-related complication
resulted in one or more laparotomies, stay in the ICU, and prolonged hospitalisation.
Furthermore, 22% of the patients suffered from permanent harm.
Since the first reports on entry-related complications many articles have been published
on this subject and trocars have been introduced with new design features, including
retractable shields and optical trocars to allow direct viewing during insertion.5;17
Furthermore, to avoid entry-related complications it is important to identify patients at
risk, e.g. those with adhesions from previous laparotomy and obese and very thin patients.
However, despite this identification entry-related complications still occur at a constant
rate.1;2;8 In a recent survey of the U.S. Food and Drug Administration (FDA) Fuller et al.,
who reviewed all reports from January 1997 to June 2002, identified 31 fatal and 1353
nonfatal trocar injuries. Most fatalities involved vascular injuries.5
In our study most claims were provoked by injuries caused by the closed-entry technique,
and vascular injury was exclusively caused by the closed-entry technique. However, this does
not mean that the incidence of entry-related complications for the closed-entry technique
is much higher compared with that of the open-entry technique because the numbers
of performed closed- and open-entry techniques are unclear. However, retroperitoneal
vascular injury is associated with “overshoot” of the introduction of the Veress needle
or the first trocar. Theoretically, this can be avoided by using an open introduction. It is
known that an open introduction might reduce the incidence of this serious complication.
On the other hand, bowel injuries are not fully avoided by the open-entry technique.
Historically, gynaecologists have been trained in the closed-entry technique. Although
the technique of open laparoscopy was first described by the gynaecologist Hasson
in 1971,12 only a few gynaecologists use the open-entry technique.1;18 Some have
reported comparable or even higher complication rates with the open-entry technique
in gynaecologic case series.1 However, in these studies gynaecologists did not use the
open-entry technique frequently; it was used mainly in selected patients who had prior
abdominal surgery. Consequently these patients already were at a higher risk for entry-
related complications. This explains why in a systematic review by Merlin et al. the risk
of major complications initially appeared to be higher for the open-entry technique.19
When only prospective series were taken into account the opposite was shown; a relative
risk of 0.30 (95% confidence interval 0.09-1.03) in favour of the open-entry technique.
It was noted that retrospective studies compared a high-risk with a low-risk patient
population, while the prospective studies investigated an unselected patient population.19
Furthermore, in a Japanese survey of laparoscopic surgeons, Hashizume et al. reported
that during the study period 96.6% of the surgeons changed their method of establishing
a pneumoperitoneum from the closed-entry technique to the open-entry technique to
increase patient safety. The rate of complications related to needle and/or trocar insertion
subsequently decreased as the surgeon’s experience performing laparoscopic surgery
using the open-entry technique increased.13
Wind (Chris).indb 125Wind (Chris).indb 125 28-05-2008 15:44:4228-05-2008 15:44:42
126
Our study also consists of a selected series of patients, because 51% percent of them
had a history of surgery, and only 46% of the patients had a normal BMI (20-25 kg/m2).
It is well recognized that the introduction of a pneumoperitoneum and trocars in obese
patients is difficult because of the lack of feeling the instruments penetrate the fascia or
the insertion is too deep. However, most patients at risk are lean. In these patients the
distance between the abdominal wall and the underlying structures is short so that a
Veress needle or trocar penetrating the abdominal fascia and peritoneum with a little too
much force puts these structures at risk. Furthermore, the risk of bowel injury is increased
in patients who had previous abdominal surgery because of adhesions of the small bowel
to the abdominal wall. Nevertheless, in the present series of patients a closed-entry
technique was used despite the increased risk of complications caused by an abnormal
BMI and the risk of adhesions after previous surgery.
It is remarkable that in only one third of the claims informed consent was properly given
and documented, and in only 48%, were complications discussed with the patient
preoperatively. An unexpected negative outcome, that is neither discussed preoperatively
nor explained postoperatively, is probably the most important trigger for litigation. A
properly informed patient is less likely to file a claim.20 This group of patients consisted
of young patients who underwent routine nonadvanced surgical procedures and both
surgeon and patient did not expect such a serious complication. Another factor that may
have provoked litigation is that more than half of the entry-related complications were
diagnosed with a delay and that several of these patients had already been discharged.
Therefore, it is important to discuss with the patient the risk of conversion to open surgery
and the risk of vascular and bowel injuries in general, and to point out that not all of these
injuries are diagnosed immediately. This conversation, including the informed consent of
the patient, must be documented and patients at risk (e.g. lean or obese patients or those
who had previous abdominal surgery) should be identified. Furthermore, it is important to
keep in mind that entry-related complications still occur at a constant rate, even in routine
procedures.
This study has several limitations. First, it probably represents only a part of all entry-
related complications that occur. Furthermore, the study consists of a small, retrospectively
collected, and selected population of patients, probably representing the most dramatic
cases. During the study period a (growing) fraction of the hospitals in the Netherlands
were insured at MediRisk. Because of insufficient record-keeping, we were unable to
clearly identify risk factors or specific trocar devices at risk. In general, this study does not
present any data on the total population who had a laparoscopic procedure by the same
surgeons responsible for the claims analysed. Therefore, the definite relationship between
several factors associated with entry-related injuries could no be established.
In conclusion, entry-related complications provoking litigation probably comprise one fifth
of all laparoscopy-related claims. Patients that filed a claim were mostly young females
with a history of abdominal surgery who were operated on in a day-care setting or had
short-stay surgery with severe consequences of the entry-related complication. Most
claims involved the closed-entry technique.
Wind (Chris).indb 126Wind (Chris).indb 126 28-05-2008 15:44:4228-05-2008 15:44:42

127
Ch
apter 7
Medical liability insurance claim
s on entry-related complications in laparoscopy
Reference List
(1) Jansen FW, Kolkman W, Bakkum EA, de Kroon CD, Trimbos-Kemper TC, Trimbos JB. Complications of laparoscopy: an inquiry about closed- versus open-entry technique. Am J Obstet Gynecol 2004; 190(3):634-638.
(2) Bonjer HJ, Hazebroek EJ, Kazemier G, Giuffrida MC, Meijer WS, Lange JF. Open versus closed establish-ment of pneumoperitoneum in laparoscopic surgery. Br J Surg 1997; 84(5):599-602.
(3) Philips PA, Amaral JF. Abdominal access complications in laparoscopic surgery. J Am Coll Surg 2001; 192(4):525-536.
(4) Bhoyrul S, Vierra MA, Nezhat CR, Krummel TM, Way LW. Trocar injuries in laparoscopic surgery. J Am Coll Surg 2001; 192(6):677-683.
(5) Fuller J, Ashar BS, Carey-Corrado J. Trocar-associated injuries and fatalities: an analysis of 1399 reports to the FDA. J Minim Invasive Gynecol 2005; 12(4):302-307.
(6) Soderstrom RM. Bowel injury litigation after laparoscopy. J Am Assoc Gynecol Laparosc 1993; 1(1):74-77.
(7) Corson SL, Chandler JG, Way LW. Survey of laparoscopic entry injuries provoking litigation. J Am Assoc Gynecol Laparosc 2001; 8(3):341-347.
(8) van der Voort M, Heijnsdijk EA, Gouma DJ. Bowel injury as a complication of laparoscopy. Br J Surg 2004; 91(10):1253-1258.
(9) Neudecker J, Sauerland S, Neugebauer E, Bergamaschi R, Bonjer HJ, Cuschieri A et al. The European Association for Endoscopic Surgery clinical practice guideline on the pneumoperitoneum for laparo-scopic surgery. Surg Endosc 2002; 16(7):1121-1143.
(10) Jansen FW, Kapiteyn K, Trimbos-Kemper T, Hermans J, Trimbos JB. Complications of laparoscopy: a prospective multicentre observational study. Br J Obstet Gynaecol 1997; 104(5):595-600.
(11) Harkki-Siren P, Kurki T. A nationwide analysis of laparoscopic complications. Obstet Gynecol 1997; 89(1):108-112.
(12) Hasson HM. A modified instrument and method for laparoscopy. Am J Obstet Gynecol 1971; 110(6):886-887.
(13) Hashizume M, Sugimachi K. Needle and trocar injury during laparoscopic surgery in Japan. Surg Endosc 1997; 11(12):1198-1201.
(14) Neudecker J, Sauerland S, Lefering R, Neugebauer E. Closed versus open approach for laparoscop-ic surgery. (Protocol). Cochrane Database Syst Rev 2001;(3):CD003547. DOI: 10.1002/14651858.CD003547.
(15) Medeiros LR, Fachel JM, Garry R, Stein AT, Furness S. Laparoscopy versus laparotomy for benign ovarian tumours. Cochrane Database Syst Rev 2005;(3):CD004751.
(16) Schwenk W, Haase O, Neudecker J, Muller JM. Short term benefits for laparoscopic colorectal resec-tion. Cochrane Database Syst Rev 2005;(3):CD003145.
(17) Levinson CJ. Laparoscopy is easy--except for the complications: a review with suggestions. J Reprod Med 1974; 13(5):187-194.
(18) Levy BS, Hulka JF, Peterson HB, Phillips JM. Operative laparoscopy: American Association of Gynecologic Laparoscopists, 1993 membership survey. J Am Assoc Gynecol Laparosc 1994; 1(4 Pt 1):301-305.
(19) Merlin TL, Hiller JE, Maddern GJ, Jamieson GG, Brown AR, Kolbe A. Systematic review of the safety and effectiveness of methods used to establish pneumoperitoneum in laparoscopic surgery. Br J Surg 2003; 90(6):668-679.
(20) Strasberg SM. Biliary injury in laparoscopic surgery: part 2. Changing the culture of cholecystectomy. J Am Coll Surg 2005; 201(4):604-611.
Wind (Chris).indb 127Wind (Chris).indb 127 28-05-2008 15:44:4228-05-2008 15:44:42
Wind (Chris).indb 128Wind (Chris).indb 128 28-05-2008 15:44:4328-05-2008 15:44:43

8Chapter
Laparoscopic reintervention for anastomotic leakage after primary laparoscopic colorectal surgery; a
comparative study
J Wind
AG Koopman
MI van Berge Henegouwen
JFM Slors
DJ Gouma
WA Bemelman
British Journal Surgery 2007;94:1562-1566
Wind (Chris).indb 129Wind (Chris).indb 129 28-05-2008 15:44:4328-05-2008 15:44:43

130130
Abstract
IntroductionAnastomotic leakage is associated with high morbidity and mortality. Aim of this study
was to assess potential benefits of a laparoscopic reintervention for anastomotic leakage
after primary laparoscopic surgery.
Methods
From January 2003 to January 2006, patients who underwent laparoscopic colorectal
resection and subsequently developed anastomotic leakage underwent a laparoscopic
reintervention (laparoscopic group, n=10). Relaparotomy was performed in patients who
had primary open surgery (open group, n=15).
Results Patient characteristics in both groups were comparable, including pre- and postoperative
APACHE II scores. Median length of time from first operation to reintervention was six days
in both groups. There were no conversions. Intensive Care Unit (ICU) stay was shorter in
the laparoscopic group (1 vs. 3 days; p=0.002). Resumption of a normal diet (3 vs. 6 days,
p=0.03) and first stoma output (2 vs. 3 days, p=0.04) occurred earlier in the laparoscopic
group. Postoperative 30-day morbidity was lower (40% vs. 80%, p=0.09), and hospital
stay shorter (9 vs. 13 days, p=0.06) in the laparoscopic group. The incidence of incisional
hernia was 0% in the laparoscopic group versus 33% in the open group (p=0.06).
Conclusions These data suggest that a laparoscopic reintervention for anastomotic leakage after primary
laparoscopic surgery is feasible and safe. It tends to be associated with less morbidity, a
faster recovery and fewer abdominal wall complications as compared to relaparotomy.
Wind (Chris).indb 130Wind (Chris).indb 130 28-05-2008 15:44:4328-05-2008 15:44:43

131
Ch
apter 8
Laparoscopic reintervention for anastomotic leakag
e
Introduction
Anastomotic leakage is the most important surgical complication following colorectal
resection with intestinal anastomosis. The reported clinical leakage rate after colorectal
resection depends on the site of anastomosis and ranges from 2 to 21 per cent.1-6
Anastomotic leakage after colorectal surgery is associated with high morbidity and even
mortality. Morbidity includes long Intensive Care Unit (ICU) admittance, sepsis and several
abdominal wall complications due to reinterventions and wound infections. Furthermore,
the risk of permanent stoma ranges from 10 to 100 per cent. In colorectal surgery, mortality
due to anastomotic leakage is considerable. Moreover, the main cause of postoperative
mortality are anastomotic complications.1-6
Elective laparoscopic colectomy was introduced in the early nineties.7 Since then several
randomised controlled trials have reported favourable results of laparoscopic colorectal
surgery as compared to open surgery. Laparoscopic surgery offers several advantages
including a faster postoperative recovery and a shorter hospital stay.8-10 Laparoscopic
colorectal surgery is associated with a similar anastomotic leak rate as compared to open
surgery.8
Massive anastomotic leakage and peritonitis generally requires prompt reintervention by
relaparotomy. Despite the short term benefits of laparoscopic colorectal resections and
the high implementation rate, reintervention for suspect anastomotic leakage is generally
done by an open approach. Most authors consider peritonitis to be a contraindication for
laparoscopic approach due to the risk of enhanced bacteraemia by pneumoperitoneum, risk
of bowel injury due to distended bowel, and presumed better visualization and irrigation
possibility of the abdomen by open surgery.10-13 In theory, laparoscopic reintervention
for anastomotic leakage after primary laparoscopic surgery might be beneficial when
considering abdominal wall complications and postoperative recovery. However,
laparoscopic reintervention in case of anastomotic leakage is not current practice yet, and
comparative data does not exist in the literature.
Therefore, the objective of this study was to evaluate whether a laparoscopic reintervention
for anastomotic leakage after primary laparoscopic surgery is technically feasible and safe.
Postoperative morbidity and recovery is assessed, and compared with patients that had
open surgery and open reintervention for anastomotic leakage in the same period.
Methods
The present study consists of a consecutive series of patients with anastomotic leakage
after open or laparoscopic colorectal resection operated on in the period January 2003 to
January 2006. Data were assessed in a retrospective manner. All patients who underwent
laparoscopic colorectal resection and subsequently developed anastomotic leakage were
reoperated laparoscopically (laparoscopic group). Relaparotomy was performed in patients
who had primarily open surgery (open group). One patient underwent a laparotomy
Wind (Chris).indb 131Wind (Chris).indb 131 28-05-2008 15:44:4328-05-2008 15:44:43

132
for anastomotic leakage after primary laparoscopic surgery, this patient was excluded.
Furthermore, all patients in which anatomotic leakage was managed by conservative
treatment were excluded. The decision to perform the initial operation laparoscopically
or open was based on referral to a surgeon capable of performing laparoscopic resection
and on patients’ and surgeons’ preference. Referral patterns for all surgeons were similar
throughout the whole study period.
Charts of the included patients were reviewed and the following data were extracted using
a preformatted sheet; age, gender, co-morbidity, previous midline laparotomy, Body Mass
Index (BMI, kg/m2) measured prior to primary surgery, ASA classification, indications for
the primary procedure, performed surgical procedure at the primary operation, time-span
between the primary intervention and the reintervention, “Acute Physiology and Chronic
Health Evaluation II” (APACHE II ) scores before and 24 hours after the reintervention,14
abdominal cavity cultures and postoperative recovery including ICU stay, resumption
of a normal diet, first stoma output, wound complications including incisional hernia,
postoperative mortality, and morbidity. Outcome and complications were noted during
clinical and out-patient clinic follow-up.
Operative proceduresIn all patients the suspicion of anastomotic leakage was established on clinical examination,
laboratory test and/or CT-scanning. Operative procedure consisted of inspection and
exploration, followed by culturing and rinsing of the abdominal cavity. Ileoanal, coloanal
and low colorectal anastomosis were diverted by creating a loop ileostomy and rinsing of
the rest colon. In case of major breakdown the afferent loop was exteriorized as an end
stoma. In case of anastomotic leakage after intra-abdominal resections, the anastomosis
was dismantled and an end colostomy was created in case of anatomotic leakage after
left-sided resections. An end ileostomy was created after right-sided resections.
During laparoscopic reintervention the prior trocar wounds were used for insertion of a
blunt TrocDoc® trocar establishing the pneumoperitoneum.15;16 The total reintervention
was performed laparoscopically and the mini-laparotomy, which was used for specimen
retrieval the first operation, was only opened when necessary. Wound closure and
postoperative wound care were at the discretion of the attending surgeon. All open
procedures were performed or supervised by one of the two colorectal surgeons. All
laparoscopic procedures and laparoscopic reinterventions were performed by a single
laparoscopic trained colorectal surgeon.
DefinitionsThe presence of anastomotic leakage was defined by clinical criteria and operative findings:
laboratory abnormalities and clinical deterioration with signs of peritonitis at physical
examination, with or without radiologically confirmed leakage. Operative finding had to
include a collection of pus or faecal material related to an insufficient anastomosis and
signs of (general) peritonitis. Furthermore, there had to be a positive culture indicating
intestinal bacteria. Morbidity was defined as all complications within 30 days after the
Wind (Chris).indb 132Wind (Chris).indb 132 28-05-2008 15:44:4328-05-2008 15:44:43

133
Ch
apter 8
Laparoscopic reintervention for anastomotic leakag
e
reintervention. Incisional herniation was assessed at long term follow up during a survey
in September 2006. ICU and hospital stay are given as the total number of days patients
stayed at the ICU or in the hospital respectively, after the reintervention.
StatisticsData are presented as median values with ranges for continuous data, unless otherwise
specified. Categorical data are presented as frequencies or percentages. Differences
between groups were tested using Mann-Whitney U test for continuous data. The Fisher’s
exact test was used to test for differences between groups in case of categorical data. A
p-value <0.05 was considered statistically significant for all tests. Statistical analysis was
done using the SPSS v.12.0 package (SPSS, Chicago, Illinois, USA).
Results
Patient characteristicsBetween January 2003 and January 2006, 398 consecutive patients underwent colorectal
resection with intestinal anastomosis and without diverting stoma. Two hundred fifty
one (63%) patients underwent open resection and 147 (37%) underwent a laparoscopic
resection. Subsequently, 26 (6.5%) patients were reoperated for anastomotic leakage.
In 11 (7.5%) patients the anastomotic leakage developed after a prior laparoscopic
colorectal resection. Ten patients were reoperated on laparoscopically and were included
in the laparoscopic group. The remaining patient was excluded from the analysis because
this patient underwent an open reintervention on postoperative day six after an initial
laparoscopic left colectomy. In this patient the anastomosis was dismantled and a
colostomy was constructed. Postoperatively, there was an episode of dyspnoea due to
cardiac decompensation. On postoperative day 14 the patient was discharged. No wound
or abdominal wall complications were observed. Relaparotomy for anastomotic leakage
was performed in 15 (6.0%) patients who had primary open surgery (open group).
Primary operations of the 25 included patients consisted of 16 segmental colonic
resections, five restorative proctocolectomies and four other procedures (Table 1). The
number of included open and laparoscopic procedures was comparable between the first
and second study period. Five patients participated in different randomised trials in which
patients were randomised between open and laparoscopic surgery.
Although, previous abdominal surgery was not an absolute contraindication there
was a non significant trend to more patients with a history of midline laparotomy in
the open group (p=0.09). Furthermore, patients in the laparaoscopic- and open group
were comparable for age, gender, ASA classification, surgical indication, type of initial
procedure, and preoperative APACHE II score (Table 1). Median length of time from the
primary operation to reintervention was six days in both groups.
Wind (Chris).indb 133Wind (Chris).indb 133 28-05-2008 15:44:4328-05-2008 15:44:43

134
Table 1. Patients characteristics of the 25 patients included in this study
laparoscopic group (n=10)
open group(n=15)
p-value
Age (years)† 45 (17-71) 45 (20-79) 0.78
Sex (male: female) 3:7 7:8 0.68
BMI (kg/m2)† 22.4 (16.6-28.1) 22.2 (16.8-32) 0.96
ASA I/II/III 5/5/0 6/8/1 0.67
Previous midline laparotomy* 1 (10%) 7 (47%) 0.09
Indication for surgery
- Inflammatory bowel disease
- Malignancy
- Diverticulitis
- Other
6
3
1
0
8
2
2
3
0.40
Initial procedure
- Right sided colonic resection
- Left sided colonic resection
- (Low) anterior resection
- Restorative proctocolectomy
- Other procedures
3
3
1
2
1
6
2
1
3
3
0.83
Length to reintervention (days)† 6 (3-9) 6 (2-11) 0.74
APACHE II score prior to reintervention† 10 (7-15) 10 (5-17) 0.89
†Median (range); *Absolute number (percentage); ASA: American Society of Anaesthesiologists; APACHE II: Acute Physiology and Chronic Health Evaluation II; BMI: Body mass index
ReinterventionThere were no conversions in the laparoscopic group. The minilaparotomy needed to be
opened in two (20%) patients, both after right sided resection in order to exteriorize the
afferent loop as an ileostomy and to exteriorize the efferent loop for closure or mucus
fistula creation.
In the laparoscopic group no intra-operative morbidity was reported. In the open group
there was one iatrogenic bowel perforation requiring an additional bowel resection.
Median operation time was not significantly different in the laparoscopic group as
compared to the open group (116 versus 105 minutes; p=0.52).
Four patients (27%) in the open group underwent a second reoperation compared to
none in the laparoscopic group (p=0.13). In two patients the reoperation was a planned
second look operation as part of a randomised trial comparing relaparotomy on demand
or planned laparotomy, one patient was reoperated for a blow out of the ascending colon,
and one patient was reoperated for a dehiscent fascia.
Short term outcomeMedian length of ICU admission was shorter in the laparoscopic group compared to
the open group. There was less postoperative morbidity within the first 30 days after
reintervention in the laparoscopic group, although this difference was not statistically
different (p=0.087). In the laparoscopic group four (40%) patients had one or more
complications. Complications in the laparoscopic group consisted of abscesses (n=3),
wound healing disorders (n=1), cardiovascular complications (n=1), psychiatric complications
Wind (Chris).indb 134Wind (Chris).indb 134 28-05-2008 15:44:4328-05-2008 15:44:43

135
Ch
apter 8
Laparoscopic reintervention for anastomotic leakag
e
(n=1), and prolonged postoperative ileus (n=1). In the open group 12 (80%) patients had
one or more complications. Complications in the open group consisted of abscesses
(n=5), wound healing disorders (n=3), (ongoing) sepsis (n=3), cardiovascular complications
(n=2), and respiratory complications (n=1). First stoma output and return to a normal
diet occurred significantly earlier in the laparoscopic group compared to the open group.
Median hospital stay in the laparoscopic group was nine (range 6-28) days compared to
13 (range 7-38) days in the open group (p=0.06). One patient (10%) in the laparoscopic
group and two (13%) patients in the open group were readmitted within 30 days (p=1.0).
Furthermore, in both the laparoscopic group and open group one patient was readmitted
after 30 days, respectively for abdominal abscesses and dehydration (see Table 2).
Table 2. Operative data of the reintervention and postoperative course of the 25 patients included in this study
laparoscopic group (n=10)
open group(n=15)
p-value
Operation duration (minutes)† 116 (59-181) 105 (59-328) 0.52
Procedure:
- end ileostomy
- diverting ileostomy
- end colostomy
- diverting colostomy
3
6
1
0
9
5
1
0
0.25
APACHE II score postoperatively† 14 (8-20) 13 (11-19) 0.70
ICU stay (days) † 1 (0-1) 3 (0-15) 0.002
Postoperative 30 day morbidity* 4 (40%) 12 (80%) 0.09
Resumption normal diet (days)† 3 (1-6) 6 (1-11) 0.03
First stoma output (days)† 2 (1-4) 3 (1-8) 0.04
Hospital stay (days)† 9 (6-28) 13 (7-38) 0.06
Readmissions within 30 days* 1 (10%) 2 (13%) 1.0
Incisional hernia* 0 5 (33%) 0.06
Stoma closure rate* 8 (80%) 9 (60%) 0.40
†Median (range); *Absolute number (percentage); APACHE II: Acute Physiology and Chronic Health Evaluation II; ICU: Intensive Care Unit
Long term outcomeThere were less patients with incisional hernias in the laparoscopic group; zero versus
five (33%), although this difference was not statistically significant (p=0.06). In eight
(80%) patients in the laparoscopic group the stoma had been closed. This was done
after a median of five (range 2-12) months. In nine (60%) patients in the open group the
stoma had been closed. This was done after a median six (range 3-16) months (p=0.40).
Two patients in the open group underwent an extensive abdominal wall reconstruction
during the same procedure the stoma was closed. In the laparoscopic group one patient
underwent a surgical correction of a post-stoma scar. There were no other abdominal wall
reconstructions in both groups during the study period. Median follow-up was 22 (range
12-28) months in the laparoscopic group and 22 (range 10-48) months in the open group
(p=0.72). None of the patients was lost to follow up.
Wind (Chris).indb 135Wind (Chris).indb 135 28-05-2008 15:44:4428-05-2008 15:44:44

136
Discussion
Laparoscopy has gained widespread acceptance in common surgical practice as a diagnostic
and therapeutic tool. Over the past years abdominal emergencies have been increasingly
managed by laparoscopy, including those patients with peritonitis.13;17-21 The present
study showed that a laparoscopic reintervention after primary laparoscopic surgery for
anastomotic leakage is feasible and may be safe in terms of conversions, intra-operative
morbidity, necessity of opening the minilaparotomy, and operating time. In addition,
laparoscopic reintervention may be associated with less postoperative morbidity, a faster
recovery and fewer abdominal wall complications as compared to open reintervention
after primary open surgery.
Reintervention for anastomotic leakage is generally done by an open approach mainly
because of the fear of causing bowel injury due to distended bowel and lack of exposure
for cleaning the abdominal cavity. After primary laparoscopic surgery the previously used
trocar incisions can easily be re-used. In this series of patients the pneumoperitoneum
was established through a prior trocar wound by an open entry technique using a blunt
trocar.22 This technique minimizes the risk of bowel injury, even in case of distended
bowel. A laparoscopic reintervention after open surgery might be appealing avoiding
wound problems and incisional hernia. However, installation of the pneumoperitoneum
is more difficult, because the trocars need to be inserted in open manner or blindly after
using the Veress needle.
The morbidity observed in our study is comparable with the percentage reported in
literature.5;6 However, in our series of patients no mortality was observed in both groups.
In part, this can be explained by the fact that in our series patients were relatively young,
since a great part of these patients were operated because of inflammatory bowel
diseases. Nonetheless, this observation is limited due to a small sample size. APACHE
II scores preoperatively and within 24 hours after surgery were moderately elevated,
indicating mild peritonitis and a non delayed diagnosis and reintervention for anatomotic
leakage in both the laparoscopic and the open group.
Laparoscopic reintervention after primary laparoscopic surgery can be initiated as an
early diagnostic tool to confirm the anastomotic leakage or to explore and identify other
causative pathology if patients do not improve as expected after laparoscopic surgery.
Recovery after laparoscopic surgery is generally fast.9;10 If the patient is not able to tolerate
a normal diet within a couple of days in combination with signs of infection, anastomotic
leakage must be suspected. For this reason, it could be hypothesized that patients after
laparoscopic surgery might have there reintervention earlier than after open surgery. This
earlier reintervention might prevent severe generalized peritonitis and systemic sepsis.
However, long standing peritonitis with pus pockets and inflammatory adhesions is
probably not amenable for laparoscopic treatment.
Following open surgery the systemic immunological function is depressed with adverse
alterations in cytokine levels and changes in the function of cellular components of the
systemic immune response. Furthermore, functions of the peritoneal macrophages are
Wind (Chris).indb 136Wind (Chris).indb 136 28-05-2008 15:44:4428-05-2008 15:44:44

137
Ch
apter 8
Laparoscopic reintervention for anastomotic leakag
e
better preserved when laparotomy is avoided. Others suggests that a laparoscopic approach
might be beneficial in the surgical management of intra-abdominal sepsis and results in
fewer postoperative septic complications.23;24 However, further research is warranted on
the effect of laparoscopy and the pneumoperitoneum on the intra-abdominal immune
system in the presence of peritonitis.
Another important advantage of laparoscopic reintervention might be a reduction in
wound complications such as early dehiscence and incisional herniation. However, the
results of the present study must be interpretated carefully because of several limitations.
First of all it comprises a small single centre retrospective study. Secondly, the surgical
indications and primary procedure were variable. Although patient characteristics were
comparable between both groups and considering the fact that the indication to perform
the initial procedure laparoscopically was mainly based on referral pattern, selection bias
could not be ruled out completely.
Furthermore, the included patients were not representative for the typical selection of
laparoscopic surgery. While the majority of laparoscopic resections are currently performed
for diverticular disease, adenoma and early stage cancer the majority of the laparoscopic
patients in the present study were operated on for inflammatory bowel disease.
The severity of the anastomotic leakage; i.e. the extent of peritonitis and severity of sepsis
were only assessed with the APACHE II scoring system and positive cultures. Although in
both groups patients had there reintervention at the same time after the first operation and
the APACHE II scores before and after the reintervention were the similar, we do not have
other objective data on the extent and severity of the peritonitis such as the Mannheim
peritonitis index or other scoring systems for severity of disease.25;26 Furthermore, all
laparoscopic procedures were performed by an experienced laparoscopic surgeon and
potentially this may have influenced the outcome.
Nonetheless, these preliminary data suggest that a laparoscopic reintervention for
anastomotic leakage after primarily laparoscopic surgery is probably feasible and might be
safe. While no conversions and intra-operative complications were observed. Furthermore,
a laparoscopic reintervention tends to be associated with less postoperative morbidity, a
faster recovery and fewer abdominal wall complications.
Ideally, a prospective trial should confirm these data. To evaluate the effect of laparoscopic
reintervention after primary laparoscopic surgery, it has to be part of a very large study
randomising patients for a laparoscopic or open initial procedure.
Reference List
(1) Mealy K, Burke P, Hyland J. Anterior resection without a defunctioning colostomy: questions of safety. Br J Surg 1992;79:305-307.
(2) Bozzetti F, Bertario L, Bombelli L, Fissi S, Bellomi M, Rossetti C et al. Double versus single stapling tech-nique in rectal anastomosis. Int J Colorectal Dis 1992;7:31-34.
Wind (Chris).indb 137Wind (Chris).indb 137 28-05-2008 15:44:4428-05-2008 15:44:44
138
(3) Graf W, Glimelius B, Bergstrom R, Pahlman L. Complications after double and single stapling in rectal surgery. Eur J Surg 1991;157:543-547.
(4) Rullier E, Laurent C, Garrelon JL, Michel P, Saric J, Parneix M. Risk factors for anastomotic leakage after resection of rectal cancer. Br J Surg 1998;85:355-358.
(5) Soeters PB, de Zoete JP, Dejong CH, Williams NS, Baeten CG. Colorectal surgery and anastomotic leak-age. Dig Surg 2002;19:150-155.
(6) Alberts JC, Parvaiz A, Moran BJ. Predicting risk and diminishing the consequences of anastomotic dehis-cence following rectal resection. Colorectal Dis 2003;5:478-482.
(7) Jacobs M, Verdeja JC, Goldstein HS. Minimally invasive colon resection (laparoscopic colectomy). Surg Laparosc Endosc 1991;1:144-150.
(8) Reza MM, Blasco JA, Andradas E, Cantero R, Mayol J. Systematic review of laparoscopic versus open surgery for colorectal cancer. Br J Surg 2006;93:921-928.
(9) Abraham NS, Young JM, Solomon MJ. Meta-analysis of short-term outcomes after laparoscopic resec-tion for colorectal cancer. Br J Surg 2004;91:1111-1124.
(10) Schwenk W, Haase O, Neudecker J, Muller JM. Short term benefits for laparoscopic colorectal resec-tion. Cochrane Database Syst Rev 2005;(3):CD003145.
(11) Sauerland S, Agresta F, Bergamaschi R, Borzellino G, Budzynski A, Champault G et al. Laparoscopy for abdominal emergencies: evidence-based guidelines of the European Association for Endoscopic Surgery. Surg Endosc 2006;20:14-29.
(12) Agresta F, De SP, Bedin N. The laparoscopic approach in abdominal emergencies: a single-center 10-year experience. JSLS 2004;8:25-30.
(13) Agresta F, Ciardo LF, Mazzarolo G, Michelet I, Orsi G, Trentin G et al. Peritonitis: laparoscopic approach. World J Emerg Surg 2006;1:9.
(14) Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med 1985;13:818-829.
(15) Bemelman WA, de Wit LT, Busch OR, Gouma DJ. Hand-assisted laparoscopic splenectomy. Surg Endosc 2000;14:997-998.
(16) Bemelman WA, de Wit LT, Busch OR, Den Boer KT, Klaase JF, Grimbergen CA et al. Establishment of pneumoperitoneum with a modified blunt trocar. J Laparoendosc Adv Surg Tech A 2000;10:217-218.
(17) Sinha R, Sharma N, Joshi M. Laparoscopic repair of small bowel perforation. JSLS 2005;9:399-402.
(18) Ramachandran CS, Agarwal S, Dip DG, Arora V. Laparoscopic surgical management of perforative peri-tonitis in enteric fever: a preliminary study. Surg Laparosc Endosc Percutan Tech 2004;14:122-124.
(19) Navez B, Tassetti V, Scohy JJ, Mutter D, Guiot P, Evrard S et al. Laparoscopic management of acute peritonitis. Br J Surg 1998;85:32-36.
(20) Mutter D, Bouras G, Forgione A, Vix M, Leroy J, Marescaux J. Two-stage totally minimally invasive approach for acute complicated diverticulitis. Colorectal Dis 2006; 8:501-505.
(21) Sanabria AE, Morales CH, Villegas MI. Laparoscopic repair for perforated peptic ulcer disease. Cochrane Database Syst Rev 2005;(4):CD004778.
(22) Hasson HM. A modified instrument and method for laparoscopy. Am J Obstet Gynecol 1971;110:886-887.
(23) Novitsky YW, Litwin DE, Callery MP. The net immunologic advantage of laparoscopic surgery. Surg Endosc 2004;18:1411-1419.
(24) Gupta A, Watson DI. Effect of laparoscopy on immune function. Br J Surg 2001; 88:1296-1306.
(25) Biondo S, Ramos E, Fraccalvieri D, Kreisler E, Rague JM, Jaurrieta E. Comparative study of left colonic Peritonitis Severity Score and Mannheim Peritonitis Index. Br J Surg 2006;93:616-622.
(26) Linder MM, Wacha H, Feldmann U, Wesch G, Streifensand RA, Gundlach E. [The Mannheim peritonitis index. An instrument for the intraoperative prognosis of peritonitis]. Chirurg 1987;58:84-92.
Wind (Chris).indb 138Wind (Chris).indb 138 28-05-2008 15:44:4428-05-2008 15:44:44

9Chapter
Staple line failure using the Proximate® 100 mm linear cutter
J Wind
F Safiruddin
MI van Berge Henegouwen
JFM Slors
WA Bemelman
Diseases of the Colon and Rectum, in press
Wind (Chris).indb 139Wind (Chris).indb 139 28-05-2008 15:44:4428-05-2008 15:44:44

140140
Abstract
IntroductionAn incomplete linear staple line that was discovered during the stapling of an ileal pouch
alerted us to evaluate potential usage concerns with linear cutters. This study was designed
to assess the integrity of the staple line of three different sizes of linear staplers.
MethodsIn an animal model three different lengths of linear cutters (Proximate®, Ethicon
Endo-Surgery) were used to cross-staple and transect the large bowel of one pig to check
for the integrity of the proximal end of the staple line.
ResultsCross-stapling and transecting across the pig’s large bowel demonstrated that if the
tissue is advanced up to the highest number on the scale of the 100 mm stapling device,
insufficient overlap between the proximal end of the staple line and the proximal end of
the cut line occur.
ConclusionAlthough a more than 100 mm staple line is delivered, the 100 mm cutter may not
produce a double-staggered row of staples at the most proximal end of the staple line
if the tissue is advanced past the 9.5 cm mark. Ethicon Endo-Surgery has agreed to add
indicator markers to the scale label on the instrument to provide the user with additional
guidance for tissue placement.
Wind (Chris).indb 140Wind (Chris).indb 140 28-05-2008 15:44:4428-05-2008 15:44:44

141
Ch
apter 9
Staple line failure using the Proximate
® 10
0 mm
linear cutter
Introduction
Several risk factors for anastomotic insufficiency have been identified.1-3 Despite the
identification of these risk factors, the actual cause or contributing factor(s) to anastomotic
insufficiency is not always clear. With known risk factors aside, surgical instruments used, in
particular stapling and cutting devices could contribute to anastomotic insufficiency if they
malfunction or are used inappropriately. Concerning surgical stapling devices the United
States Food and Drug Administration (FDA) received reports of 22,804 malfunctions, 2,180
injuries, and 112 deaths from 1992 up to July 1, 2001. These numbers include all types of
linear and circular stapling devices as well as clip appliers. Most of these reports comprised
device or user related errors of linear cutters and staplers. Furthermore, the majority of
operations reported were gastrointestinal. Failure of stapler devices to function or be
used properly, resulted in suture line separation or leak as the most commonly reported
problem.4 However, when interpreting these data it should be kept in mind that besides
the fact that staplers are used very frequently, the exact denominator is not known. This
subscribes the importance of understanding the correct usage of the device, as well as
the appropriate surgical techniques to inspect and verify staple lines and staple formation,
and the techniques to employ should issues occur.5 Nevertheless, despite correct usage
staple line failure might still occur.
The following case alerted us to evaluate the function of a linear cutter (Proximate® 100
mm-TLC10, Ethicon Endo Surgery).
CaseA patient with ulcerative colitis was referred for a laparoscopic restorative proctocolectomy
because of recurrent disease relapses despite extended medicinal therapy (no steroid use
preoperatively).
One firing of a 100 mm linear cutter (Proximate® TLC10, Ethicon Endo Surgery) was used
to construct the (relatively) small ileal pouch extracorporally. Subsequently, the anvil of the
circular stapler was placed in the base of the pouch to create a double-stapled ileoanal
anastomosis. The donuts were checked for their integrity and proved to be intact. During
the operation there was no significant blood loss and there were no intraoperative adverse
events.
The procedure was ended by the transanal insertion of a 24 Fr Foley catheter (outside
diameter 8 mm) in the pouch for temporary postoperative pouch decompression, because
there was no indication for a defunctioning ileostomy. During insertion it was noticed
that the drain could be pushed in much further than expected without resistance. This
unexpected observation urged reinstallation of the pneumoperitoneum. Inspection
showed that the drain emerged in between the mesentery of the pouch and the pouch
itself suggesting a failure of the posterior linear staple line. Subsequently, the drain was
pulled back and a defunctioning ileostomy was constructed. The defect in the pouch was
not repaired because of its difficult approachability.
Wind (Chris).indb 141Wind (Chris).indb 141 28-05-2008 15:44:4428-05-2008 15:44:44

142
The gap in the staple line was identified at the most proximal end of the linear cutter
staple line. After this incident, we investigated the proximal portion of the staple line of
three different sizes of linear cutters after cross-stapling of the large bowel of a pig.
Methods
To investigate whether insufficiency of the proximal staple line would occur if cross-stapling
of the bowel was performed according to the users’ manual three different lengths of
linear cutters from the same company (Proximate® 55 mm-TLC55, 75 mm-TLC75 and 100
mm-TLC10, Ethicon Endo-Surgery) were used to cross-staple the large bowel of one pig.
The pig (female, 10 weeks old, weight 30 kilograms) was sacrificed after a prior experiment
which was not related to the bowel. The large bowel of a pig was chosen because this
offered the same tissue characteristics as human tissue compared with artificial material
(e.g. PTFE). The complete experiment was approved by the institutional animal ethics
committee. Special attention was paid to the positioning of the bowel in the cutter; the
tissue was not advanced further than the end marks on the cutter.
After firing the cutter, the proximal area of the two double-staggered rows of staples was
photographed and visually evaluated for staple pattern and placement. Subsequently, in
the presence of a gap in the staple line, the gap was measured by using a pair of pickups.
The lab experiments were witnessed by representatives of the device manufacturer.
Results
Three different lengths of linear cutters (Proximate® 55 mm-TLC55, 75 mm-TLC75 and
100 mm-TLC10, Ethicon Endo Surgery) were used to cross-staple the large bowel of one
pig. Each cutter was fired three times.
The cross-stapling of the pigs large bowel demonstrated that the 100 mm cutter did not
produce a double-staggered row of staples at the most proximal end of the staple line if
the tissue was advanced up to the 10 mark on the stapling device. At the proximal end of
the staple line the bowel was cut but not stapled resulting in a gap ranging between three
and five mm (Figure 1). The 55 and 75 mm cutters produced visually adequate staple line
patterns, provided that the tissue was not squeezed or forced in beyond the five (TLC55)
and seven (TLC75) marks respectively during closure of the stapler. If tissue was squeezed
or forced proximal to these marks, cutting without stapling occurred. Inspection of the
three sizes of linear cutters demonstrated that the 100 mm cutter does not have a staple
overlap (double-staggered row) at the proximal end of the device. In Figure 2 it is shown
that the two double-staggered rows of staples stop at the 9.5 mark and only a single
staple is positioned proximally. Therefore, advancing the tissue to the 10 mark will cause
cutting without stapling resulting in a five mm gap. If the tissue is forced into the device
while closing, the gap is even longer.
Wind (Chris).indb 142Wind (Chris).indb 142 28-05-2008 15:44:4428-05-2008 15:44:44

143
Ch
apter 9
Staple line failure using the Proximate
® 10
0 mm
linear cutter
Figure 1. Large bowel of a pig after stapling close to the proximal end of the 100 mm Proximate® linear cutter (TLC10, Ethicon Endo Surgery). At the proximal end of the staple line, the bowel is cut but not stapled, leaving gap of 3 mm.
Figure 2. The proximal end of the 100 mm Proximate® linear cutter (TLC100, Ethicon Endo Surgery) in detail. The two double-staggered rows of staples stop already at 95 mm and a single staple is positioned proximal. Users should not position the tissue up to the 100 mm mark because the cutter divides the tissue beyond 100 mm, resulting in a small gap of several millimetres.
Wind (Chris).indb 143Wind (Chris).indb 143 28-05-2008 15:44:4528-05-2008 15:44:45

144
Discussion
Both the presented case and animal model demonstrated that when using the 100 mm
Proximate® linear cutter (TLC10, Ethicon Endo Surgery) care must be used when stapling
tissue close to the proximal end of the cutter. As shown in Figure 2 the row of staples
stops between the 10 and 9.5 indicators and only at the 9.5 mark a double-staggered row
is present. Beyond this point there is a possibility that the intestine is cut but not stapled,
leaving a gap of several millimetres.
Post market surveillance data by the manufacturer for the TLC10 device during a two-year
period showed no additional serious injury reports for leaking or incomplete staple lines,
which potentially could be related to the described staple pattern. The incidence of clinically
significant problems associated with this stapler is low, because it probably only occurs
when the 100 mm cutter is used for its full length, stapling large bowel and pouches.
Since the described incident occurred, we routinely inspect the pouch after linear stapling,
both anteriorly and posteriorly, by inversion of the pouch to check for insufficiency of
the proximal staple line. If an insufficiency is identified, it is most commonly located both
anteriorly and posteriorly, and the gap can usually accommodate at least one leg of a pair
of pickups (Figure 3). On the posterior site, the hole is oversewn and at the anterior site of
the pouch the hole is incorporated in the purse string of the anvil of the circular stapler.
In case of a side-to-end colonic anastomosis, the proximal end of the cross-stapling line is
routinely checked and oversewn if necessary.
Figure 3. Schematic drawing of the construction of a pouch using the 100 mm Proximate® linear cutter (TLC10, Ethicon Endo Surgery). A small gap of several millimetres arises when the cutter is used to its full length because of cutting without stapling (A, arrow). Both on the anterior and posterior site of the pouch, a small gap (*) is present because of cutting without stapling (B).
A
Wind (Chris).indb 144Wind (Chris).indb 144 28-05-2008 15:44:4528-05-2008 15:44:45
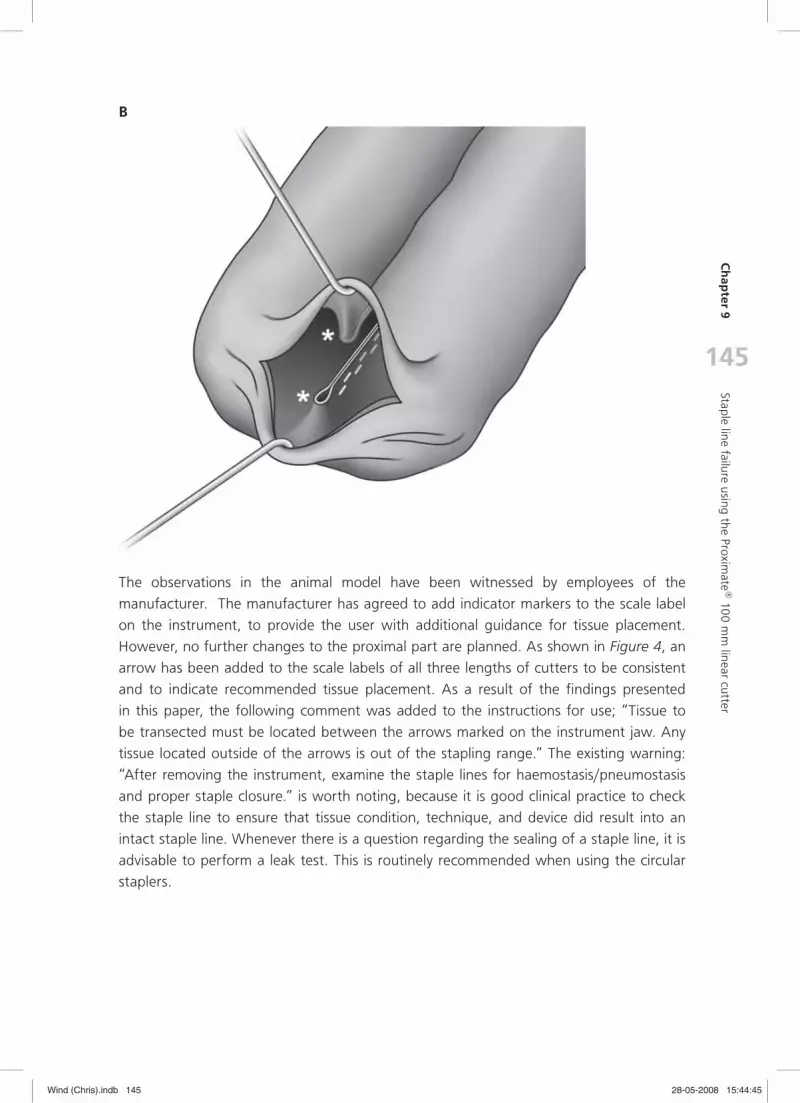
145
Ch
apter 9
Staple line failure using the Proximate
® 10
0 mm
linear cutter
B
The observations in the animal model have been witnessed by employees of the
manufacturer. The manufacturer has agreed to add indicator markers to the scale label
on the instrument, to provide the user with additional guidance for tissue placement.
However, no further changes to the proximal part are planned. As shown in Figure 4, an
arrow has been added to the scale labels of all three lengths of cutters to be consistent
and to indicate recommended tissue placement. As a result of the findings presented
in this paper, the following comment was added to the instructions for use; “Tissue to
be transected must be located between the arrows marked on the instrument jaw. Any
tissue located outside of the arrows is out of the stapling range.” The existing warning:
“After removing the instrument, examine the staple lines for haemostasis/pneumostasis
and proper staple closure.” is worth noting, because it is good clinical practice to check
the staple line to ensure that tissue condition, technique, and device did result into an
intact staple line. Whenever there is a question regarding the sealing of a staple line, it is
advisable to perform a leak test. This is routinely recommended when using the circular
staplers.
Wind (Chris).indb 145Wind (Chris).indb 145 28-05-2008 15:44:4528-05-2008 15:44:45

146
Figure 4. The anvils of the 100 mm, 75 mm, and 55 mm Proximate® linear cutters (Ethicon Endo Surgery), with the added arrows to indicate the tissue stapling range for the devices, to ensure presence of a double-staggered row of staples at the point of tissue placement.
Reference List
(1) Alberts JC, Parvaiz A, Moran BJ. Predicting risk and diminishing the consequences of anastomotic dehis-cence following rectal resection. Colorectal Dis 2003;5:478-482.
(2) Matthiessen P, Hallbook O, Andersson M, Rutegard J, Sjodahl R. Risk factors for anastomotic leakage after anterior resection of the rectum. Colorectal Dis 2004;6:462-469.
(3) Soeters PB, de Zoete JP, Dejong CH, Williams NS, Baeten CG. Colorectal surgery and anastomotic leak-age. Dig Surg 2002;19:150-155.
(4) Brown SL, Woo EK. Surgical stapler-associated fatalities and adverse events reported to the Food and Drug Administration. J Am Coll Surg 2004;199:374-381.
(5) Baker RS, Foote J, Kemmeter P, Brady R, Vroegop T, Serveld M. The science of stapling and leaks. Obes Surg 2004;14:1290-1298.
Wind (Chris).indb 146Wind (Chris).indb 146 28-05-2008 15:44:4628-05-2008 15:44:46

10Chapter
Temporary closure of the open abdomen; a systematic review on delayed primary
fascial closure in patients with an open abdomen
P Boele van Hensbroek
J Wind
MGW Dijkgraaf
ORC Busch
JC Goslings
Submitted
Wind (Chris).indb 147Wind (Chris).indb 147 28-05-2008 15:44:4628-05-2008 15:44:46

148148
Abstract
IntroductionIn some severe cases of peritonitis or abdominal trauma the abdomen cannot be closed
at the end of the laparotomy due to swelling of the abdominal contents or packing. This
so-called “open abdomen” must then be temporarily closed. The aim of the present study
was to systematically review the literature on temporary abdominal closure (TAC) of the
open abdomen and to assess which TAC technique, controlled for potential confounders
like age, sex, and the presence of fistulae or abscesses, is associated with the highest
delayed primary fascial closure (FC) rate.
MethodsThe Cochrane Register of Controlled Trials, MEDLINE and EMBASE databases were searched
until December 2007. References were checked for additional studies. Search criteria
included (synonyms of) “open abdomen”, “fascial closure”, “vacuum”, “re-approximation”
and “ventral hernia”. Open abdomen was defined as the inability to close the abdominal
fascia after laparotomy. Two reviewers independently extracted data from original articles
using a predefined checklist.
ResultsThe search identified 154 abstracts of which 96 were considered relevant. No comparative
studies were identified. After reading them, 51 articles, including 57 case series were
included. The techniques described were Vacuum Assisted Closure (VAC) (8 series),
Vacuum pack (15 series), Artificial burr (4 series), Mesh/sheet (16 series), Zipper (7 series),
Silo (3 series), Skin closure (2 series) Dynamic Retention Sutures (DRS), and Loose packing
(1 series each). The highest FC rates were seen in the Artificial burr (90%), DRS (85%),
and VAC (60%). The lowest mortality rates were seen in the Artificial burr (17%), VAC
(18%), and DRS (23%).
ConclusionsThese results suggest that the TAC techniques that keep permanent traction on the
fascial edges (e.g. VAC, DRS, and Artificial burr) show the highest FC rates and the lowest
mortality rates.
Wind (Chris).indb 148Wind (Chris).indb 148 28-05-2008 15:44:4628-05-2008 15:44:46

149
Ch
apter 10
Temporary closure of the op
en abdom
en
Introduction
At the end of most laparotomies, the abdominal fascia can be closed primarily at the end of
the operation. However, sometimes full fascial closure is precluded by the condition of the
patient or the bowel and open abdominal treatment is necessary. These patients are often
severely ill and the open abdomen is therefore associated with mortality rates over 50%.
In general, there are three relatively frequent scenarios in which the operating surgeon may
decide to start open abdomen treatment with temporary abdominal closure. These are
abdominal sepsis (peritonitis), Abdominal Compartment Syndrome (ACS) and abdominal
trauma (damage control surgery). Peritonitis is often caused by anastomotic leakage or bowel
perforation. The associated severe bowel oedema opposes fascial closure. Damage control
surgery in trauma patients consists of rapid assessment of the abdominal injuries and control
of bleeding by direct suture/ligation or packing with gauzes to stop the bleeding before
transport to the Intensive Care Unit (ICU) or angio-intervention for further resuscitation. The
bowel oedema due to massive resuscitation with intravenous fluids and/or the presence of
the packing gauzes may preclude full fascial closure in these patients.
ACS is characterized by an increased intra-abdominal pressure which compromises the
respiratory, renal, and cardiac function of a patient. This condition is commonly caused
by bowel oedema following intra-abdominal infection, abdominal trauma or massive fluid
resuscitation. A ‘decompressing laparotomy’ is often indicated to relieve the intra-abdominal
pressure. Due to the extended bowel and as part of the treatment, the abdomen is not
closed.
In open abdomen treatment, the need arises for temporary abdominal closure (TAC).
Several techniques for TAC have been described over the past years including mesh or
foil insertion, sterilised IV bag insertion, Velcro or zipper closure, and skin closure with
towel clips. Several articles have described the application of a fluid drainage system with
drains. In recent years, the application of the Vacuum Assisted Closure (VAC®) system has
been described and popularised for TAC of the open abdomen. All these techniques not
only vary in the way they cover the abdominal contents, but also the amount of traction
that is applied on the abdominal fascia to prevent lateral retraction, differs between the
techniques. Because, during open abdominal treatment, the fascial edges tend to retract
laterally due to continuous traction from the (oblique) lateral abdominal musculature which
might be prevented by traction to the fascial edges. The different techniques for TAC are
listed in Table 1.
Following open abdominal treatment, the abdominal fascia can be closed primarily, with a
mesh or granulation tissue covered by a split skin graft. Rationales for permanent coverage
of the open abdomen with a mesh or granulation tissue include persistent visceral
oedema, loss of domain due to trauma, infection, lateral retraction or delayed primary
fascial closure is simply not attempted at all. When delayed primary fascial closure is not
possible these patients develop a ventral hernia. The extent of these so-called ‘planned
ventral hernias’ varies from small and asymptomatic to very large. In case of physical or
cosmetic complaints, the ventral hernia needs to be surgically corrected once the patient
Wind (Chris).indb 149Wind (Chris).indb 149 28-05-2008 15:44:4628-05-2008 15:44:46

150
has recovered. However, recovery frequently takes several months in these patients and
a ventral hernia may cause a considerable burden. Furthermore, reconstructive surgery,
like every operative procedure, carries a risk of morbidity and mortality. These burdens
and risks associated with (planned) ventral hernias should be taken into account when
deciding on the strategy for TAC and whether or not to attempt fascial closure during the
index admission. Delayed primary fascial closure avoids ventral hernias and can therefore
be considered as the preferred outcome. However, no (randomised) comparative trials
have been conducted evaluating the effect of different strategies on the rate of delayed
primary fascial closure. Furthermore, it is unknown which other factors may influence the
fascial closure rate during index admission. Therefore, the aim of the present study was
Technique Description Re-approx*
Vacuum Assisted Closure (VAC®)
A perforated sheet is placed over the abdominal contents and under the fascial edges. A sponge is cut in the correct size and sutured to the facial edges. The entire wound is then covered by a drape which is opened in the middle to allow a suction drain pass through. The suction drain is connected to a pump and fluid collection system which keeps constant negative pressure on the wound.
Yes
Vacuum pack A perforated plastic sheet is laid over the abdominal contents and covered by damp surgical towels. A surgical drain is placed on top of the towels and the entire wound is covered by an airtight seal. The drain is then attached to two bulb suctions to keep negative pressure on the wound.
Yes
Artificial burr (Wittmann patch)
Two opposite Velcro sheets (hooks and loops, one on each side) are sutured to the fascial edges. This allows for easy access and stepwise re-approximation on the fascial edges.
Yes
Dynamic retention sutures
Horizontal sutures are placed through a large-diameter bolster and through the skin and fascia on both sides. The sutures may then be tightened to allow staged re-approximation of the fascial edges.
Yes
Plastic silo (Bogotá bag)
A sterile x-ray film cassette bag or sterile 3-Litre genitourinary irrigation bag is sutured between the fascial edges and opened in the middle. This allows for easy re-entry and can be taken in to approximate the fascial edges.
Yes
Mesh/sheet An absorbable or non-absorbable mesh or sheet is sutured between the fascial edges. The mesh or sheet can either be removed or left in place at the end of the open abdominal treatment. Examples are the Dexon mesh, Marlex mesh, and Vicryl mesh. Examples of Sheets are the Silastic or silicone sheets.
No
Loose packing The fascial defect is covered by dressing only. No
Skin approximation
The skin is closed over the fascial defect with either towel clips or a running suture.
No
Zipper A mesh or sheet with a sterilized zipper is sutured between the fascial edges. This only allows for easy re-entry.
No
Table 1. Temporary Abdominal Closure (TAC) techniques
* Re-approx: technique aimed at re-approximation of the edges of the abdominal fascia.
Wind (Chris).indb 150Wind (Chris).indb 150 28-05-2008 15:44:4628-05-2008 15:44:46

151
Ch
apter 10
Temporary closure of the op
en abdom
en
to systematically review the literature on temporary closure of the open abdomen and to
assess which TAC technique, controlled for potential confounders like age, sex, and the
presence of fistulae or abscesses, is associated with the highest delayed primary fascial
closure rates.
Methods
Literature searchThe Cochrane Database of systematic reviews, the Cochrane central register of controlled
trials, and MEDLINE databases were searched using keywords related to open abdominal
treatment (Table 2). The search period started in 1966 and extended until December
2007. Electronic links to related articles and references of selected articles were hand-
searched as well. A manual search of relevant journals and conference proceedings was
not performed. The search was not restricted to any language, however in the systematic
review only studies published in English, German or Dutch were taken into account.
Table 2. Search terms, as used in the systematic reviewSearch terms
MeSH: Free Text words:
Field: Limits:
Not used(open abdomen OR laparostomy OR open peritoneal cavity OR celiotomy OR open management abdomen OR abdominal wall defect OR open abdominal wound) AND (VAC OR V.A.C. OR vacuum OR closure OR re-approximation OR re-approximation OR fascial closure OR ventral hernia OR temporary abdominal closure OR bogota bag OR fascial dehiscence ) All FieldsNone
MeSH: medical subject headings
Study selection and data extractionFrom the potentially eligible publications only studies were included that reported on open
abdominal treatment and in which delayed primary fascial closure rates were reported.
Series of patients of less than five and studies with a non-consecutive inclusion period
were excluded. Furthermore, series that described patients with sub-costal incision, as well
as series that described the use of multiple TAC techniques in the same study population
were excluded. The definition of open abdominal treatment had to include the inability to
close the abdominal fascia after laparotomy. Two investigators (PBvH, JW) independently
extracted the following data, if reported, from the original studies using a preformatted
sheet; inclusion period, number of patients, type of patients (trauma, peritonitis, pancreatitis,
ACS), age, gender, Injury Severity Score (ISS), APACHE (Acute Physical And Chronic Health
Evaluation) II, type of open abdominal treatment (e.g. Vacuum pack, Vacuum Assisted
Closure (VAC) system, Bogota bag, Zipper, Mesh), mortality, complications (i.e. abscesses,
fistulae), number of surgical interventions until final closure, duration of open abdominal
Wind (Chris).indb 151Wind (Chris).indb 151 28-05-2008 15:44:4728-05-2008 15:44:47

152
treatment, percentage of full fascial closure, additional techniques for abdominal closure,
percentage of planned ventral hernias, ICU stay, length of hospital stay and length of
follow-up.
Each selected study was critically appraised by the two investigators, using a modified
form as proposed by the Dutch Cochrane Collaboration and assessing if a study was
randomised, consecutive, prospective or retrospective, and mentioned rates of full fascial
closure. In case of retrospective analysis of data collected prospectively, a study was defined
as prospective. Final inclusion was done after consensus was reached. Discrepancies in
judgment, if any, were resolved by discussion between the investigators. In case an article
described separate series with specific patient groups (either separate underlying causes or
TAC techniques) each series was assessed separately. In case of missing data the principal
investigators of those publications were contacted.
Analysis and presentation of dataThe characteristics of the included series were presented per technique. The delayed
primary fascial closure rate was calculated by dividing the number of patients with delayed
fascial closure by the total number of included patients. The mortality rate was calculated
by dividing the number of deceased patients by the total number of included patients.
The percentage of male patients, age, fistula rate, and abscess rate were described as the
median value (and range) of the concerning series.
The examined fascial closure rate (as a proportion) was derived from the series with
different TAC techniques. A random effect meta-regression approach was used to take
into account the differences in sample size between studies (putting more emphasis on
larger studies) and to account for remaining variability among studies beyond chance.
The logit-transformed fascial closure proportion was used as the outcome variable with
TAC technique as the main predictor of differences between studies, while adjusting for
other univariately significant predictors of fascial closure. A backward stepwise approach
was followed, starting with potential predictors with a p-value below 0.1 in the univariate
analyses. Final statistical significance was set at an alpha level of 0.05 or below. All analyses
were performed in SAS (Copyright © 2008 SAS Institute Inc., SAS Campus Drive, Cary,
North Carolina 27513, USA).
Results
Included studiesThe searches identified a total of 1493 manuscripts. Based on the title, 154 were selected.
The 1339 other titles were not considered relevant. After reading the abstracts, 58
manuscripts were excluded because they did not concern open abdominal treatment,
were case reports or reviews. Five of these abstracts were excluded because the articles
were written in Chinese, Norwegian, French (all once), or Russian (2 articles). Ninety six
abstracts were considered relevant and the complete articles were obtained. Of these, 45
Wind (Chris).indb 152Wind (Chris).indb 152 28-05-2008 15:44:4728-05-2008 15:44:47

153
Ch
apter 10
Temporary closure of the op
en abdom
en
articles did not meet the inclusion criteria and were therefore excluded. The remaining
51 articles were included in this review. These included articles were published between
1981 and 2007. There were no randomised controlled trials or other comparative studies.
The 51 articles included a total 57 case series describing various patient groups and TAC
techniques. The included case series described a total of 3169 patients. The inclusion
periods ranged from six to 168 months, with a median of 48 months.
Patient populationNineteen series described trauma patients only and an additional sixteen series described
a mixture of trauma, vascular surgery and general surgical patients. Twenty two series
described non-trauma patients of which eight with peritonitis patients only, and three with
vascular patients only. The remaining 11 series described a mixture of general surgical,
peritonitis, pancreatitis and vascular patients.
The gender distribution was described in 40 series (70%). The percentage of male patients
ranged from 62% in the one series with Dynamic Retention Sutures to 94% in the Artificial
burr series. In forty four series (77%) the mean age of the patients was reported. The
median age over these series was 40.1 years (range: 29.5 to 75). Median age was the
highest in the one Dynamic Retention Suture series (50 years), followed by the Zipper
series (46 years) and the Silo series (44 years). Twenty one series reported on the Injury
Severity Score (ISS). The median ISS ranged from 20.3 in the series that used Meshes or
sheets to 30.5 in the Artificial burr series. The APACHE II score was reported in 13 series
only and ranged from 17.8 in the Artificial burr series to 24.7 in the Mesh/sheet series.
Temporary closure techniques describedThe VAC technique was applied in eight series which were published since 2003 (Table
3a). The Vacuum pack has been described in 15 series published since 1995 (Table 3b). The
four series that described the application of the Artificial burr were published since 1990
(Table 3c). The VAC, Vacuum pack, and Artificial burr technique have all been published
until 2007.
The first series that described the use of Meshes or sheets was published in 1983. The
16 other series that used Meshes or sheets were before 2005 (Table 3d). The first of the
seven series that applied Zippers was published in 1991 and no series with Zippers have
been published since 2001 (Table 3e). The three series in which the Silo technique was
used were published between 2001 and 2007 and the two Skin only series were published
in 1992 and 2001. Loose packing and Dynamic Retention Sutures were each used in one
series published in 1981 and 2001 respectively (Table 3f).
Wind (Chris).indb 153Wind (Chris).indb 153 28-05-2008 15:44:4728-05-2008 15:44:47

154
Table 3a. The VAC series
Au
tho
r
Yea
r
Pro
spec
tive
/ r
etro
spec
tive
Gro
up
Pati
ents
(n
)
ISS
Tech
niq
ue
Du
rati
on
of
trea
tmen
t (m
ean
; day
s)
Re-
lap
aro
tom
ies
(mea
n)
Fist
ula
(%
)
Ab
sces
s (%
)
Mo
rtal
ity
(%)
Clo
sure
(%
)
Stonerock 2003 Retro Tr; Gs 15 17.6 VAC 12.0 0 7 7 67
Miller 2004 Prosp Tr 53 VAC 9.6 3.4 2 0 15 72
Stone 2004 Tr 48 25.0 VAC 4 10 33 54
Labler 2005 Tr; ACS; Pt 18 41.1 VAC 20.9 7.7 28 67
DeFranzo 2006 Retro Tr; Pt; CS; Gs; Om 30 VAC 0 10 33
Cothren 2006 Retro Tr; ACS 14 VAC 7.5 4.6 7 100
Oetting 2006 Pt; ACS; NF 36 VAC 13.0 11 0 22 72
Perez 2007 Prosp Pt; ACS 37 VAC 3.8 3 0 38 35
ACS: Abdominal Compartment Syndrome; GS: General Surgery; Gs: Gastroschisis; Om: Omphalocele; NF: Necrotising Fasciitis; Pt: Peritonitis; Tr: Trauma; Retro: retrospective inclusion; Prosp: prospective inclusion; Empty boxes indicate that these data were not reported.
Table 3b. The Vacuum pack series
Au
tho
r
Yea
r
Pro
spec
tive
/ r
etro
spec
tive
Gro
up
Pati
ents
(n
)
ISS
APA
CH
E II
(m
ean
)
Tech
niq
ue
Du
rati
on
of
trea
tmen
t (m
ean
; day
s)
Re-
lap
aro
tom
ies
(mea
n)
Fist
ula
(%
)
Ab
sces
s (%
)
Mo
rtal
ity
(%)
Clo
sure
(%
)Brock 1995 Retro Mi; RAAA; Pc 11 26.3 VP 36 36 18
Brock 1995 Retro Tr 17 19.0 VP 3.5 0 35 71
Smith 1997 Retro Pc; Mi; CD 38 VP 3.4 5 11 42 55
Sherck 1998 Retro Tr; Pt; Mi; Pc; Bl 50 27.0 VP 6 6 36 68
Barker 2000 Retro Tr 112 23.2 VP 4.7 1.9 4 4 26 55
Bosscha 2000 Retro Pt 67 13.0 VP 9.0 24 0 42 28
Foy 2003 Retro Tr; Pt; AAA 134 29.8 VP 6.5 2.3 5 4 38 47
Navsaria 2003 Retro Tr 55 35.0 VP 9.0 4.3 5 0 45 29
Chavarria-Aguilar 2004 Retro Tr 29 31.0 VP 1.9 0 21 10 76
Miller 2005 Retro Tr 344 19.0 VP 3.4 9 9 20 52
Barker 2007 Retro GS 120 VP 8.2 7 3 23 61
Barker 2007 Retro Va 22 VP 4.9 5 0 41 64
Barker 2007 Retro Tr 116 31.9 VP 3.5 3 4 26 58
van As 2007 Tr 60 27.5 VP 9.0 2.5 42 27
Wilde 2007 Prosp Pt; Mi; Bl 11 VP 3.9 1.7 0 91
(R)AAA: (Ruptured) Abdominal Aortic Aneurysm; Bl: Bleeding; CD: Crohns Disease; GS: General Surgery; Mi: Mesenterial ischemia; Pc: Pancreatitis; Pt: Peritonitis; Va: Vascular; Tr: Trauma; VP: Vacuum pack; Retro: retrospective inclusion; Prosp: prospective inclusion; Empty boxes indicate that these data were not reported.
Wind (Chris).indb 154Wind (Chris).indb 154 28-05-2008 15:44:4728-05-2008 15:44:47

155
Ch
apter 10
Temporary closure of the op
en abdom
en
Table 3c. The Artificial burr series
Au
tho
r
Yea
r
Pro
spec
tive
/ r
etro
spec
tive
Gro
up
Pati
ents
(n
)
ISS
APA
CH
E-II
(m
ean
)
Tech
niq
ue
Du
rati
on
of
trea
tmen
t (m
ean
; day
s)
Re-
lap
aro
tom
ies
(mea
n)
Fist
ula
(%
)
Ab
sces
s (%
)
Mo
rtal
ity
(%)
Clo
sure
(%
)
Aprahamian 1990 Prosp Tr 20 30.5 AB 3.6 0 15 20 75
Wittmann 2000 Pt 128 19.0 AB 6.8 2 19 93
Hadeed 2007 Retro Tr 26 AB 19.1 6.0 4 0 8 77
Keramati 2007 ACS 6 AB 9.0 67 33
ACS: Abdominal Compartment Syndrome; Pt: Peritonitis; Tr: Trauma; AB: Artificial burr; Retro: retrospective inclusion; Prosp: prospective inclusion; Empty boxes indicate that these data were not reported.
Table 3d. The Mesh or sheet series
Au
tho
r
Yea
r
Pro
spec
tive
/ r
etro
spec
tive
Gro
up
Pati
ents
(n
)
ISS
APA
CH
E-II
(m
ean
)
Tech
niq
ue
Du
rati
on
of
trea
tmen
t (m
ean
; day
s)
Re-
lap
aro
tom
ies
(mea
n)
Fist
ula
(%
)
Ab
sces
s (%
)
Mo
rtal
ity
(%)
Clo
sure
(%
)
Wouters 1983 Pt 20 M/S 5.0 0 20 20 75
Akers 1991 Va 6 M/S 12.5 50 67
Smith 1992 Tr 5 M/S 20 20
Cohn 1995 Retro Tr 14 M/S 3.2 29 64
Fansler 1995 Retro Tr; GS; Pc 26 19.0 M/S 7.0 2.1 42 42 12 15
Nagy 1996 Retro Tr 25 20.3 M/S 14 30 40
Yeh 1996 Retro Tr 36 M/S 0 0 28 22
Losanoff 1997 Pt 19 22.3 M/S 4.3 0 0 21 79
Sugrue 1998 Prosp Tr; Pt; GS; Va 49 31 M/S 2.6 6 43 33
Töns 2000 Tr; Pt, IL; Mi 377 M/S 21 18
Tremblay 2001 Retro Tr; Bl; Pc; Mi 12 23.6 M/S 33 8
Rasmussen 2002 Retro AAA 45 M/S 7 0 56 31
Schachtrupp 2002 Tr; Pt; Mi; ACS 40 M/S 4.4 20 58
Jernigan 2003 Tr 274 M/S 5 43 14
Howdieshell 2004 Tr 88 28.0 M/S 0 0 19 27
Mayberry 2004 Retro Tr 140 31.2 M/S 18.9 7 5 17 31
AAA: (Ruptured) Abdominal Aortic Aneurysm; ACS: Abdominal Compartment Syndrome; GS: General Surgery; Mi: Mesenterial ischemia; Pc: Pancreatitis; Pt: Peritonitis; Va: Vascular; Tr: Trauma; M/S: Mesh/Sheet; Retro: retrospective inclusion; Prosp: prospective inclusion; Empty boxes indicate that these data were not reported.
Wind (Chris).indb 155Wind (Chris).indb 155 28-05-2008 15:44:4828-05-2008 15:44:48

156
Table 3e. The zipper series
Au
tho
r
Yea
r
Pro
spec
tive
/ r
etro
spec
tive
Gro
up
Pati
ents
(n
)
APA
CH
E-II
(m
ean
)
Tech
niq
ue
Du
rati
on
of
trea
tmen
t (m
ean
; day
s)
Re-
lap
aro
tom
ies
(mea
n)
Fist
ula
(%
)
Ab
sces
s (%
)
Mo
rtal
ity
(%)
Clo
sure
(%
)
Cuesta 1991 Retro Pt 7 30.0 Zipper 5.0 29 0
Bose 1991 Retro Pt 5 Zipper 60 60 60 20
Hannon 1992 Pt; Mi 8 19.9 Zipper 12.6 5.1 0 100
Singh 1993 Pt 8 28.3 Zipper 10.5 4.6 38 25 38
Hubens 1994 Pt; NEC; Pc 23 20.3 Zipper 3.9 0 39 35
Goor, van 1997 Retro Pt; Mi 24 Zipper 14.0 6.6 17 4 29 54
Zingales 2001 Retro Pt; Pc; IC; Pi 60 19.7 Zipper 7.7 13 38 20
IC: Ischemic Colitis; Mi: Mesenterial ischemia; NEC: Necrotising Enteroclitis; Pc: Pancreatitis; Pi: Parietal Incompetence; Pt: Peritonitis; Tr: Trauma; Retro: retrospective inclusion; Prosp: prospective inclusion; Empty boxes indicate that these data were not reported.
Table 3f. The Silo, Skin, Loose packing, and Dynamic Retention Suture series
Au
tho
r
Yea
r
Pro
spec
tive
/ r
etro
spec
tive
Gro
up
Pati
ents
(n
)
ISS
(mea
n)
APA
CH
E-II
Tech
niq
ue
Du
rati
on
of
trea
tmen
t (m
ean
; day
s)
Re-
lap
aro
tom
ies
(mea
n)
Fist
ula
(%
)
Ab
sces
s (%
)
Mo
rtal
ity
(%)
Clo
sure
(%
)
Doyon 2001 Retro Pt 17 19.4 Silo 15.2 6.5 0 6 18 82
Tremblay 2001 Retro Tr; Bl; Pc; Mi 75 23.6 Silo 53 17
Kushimoto 2007 Retro Tr; NT 17 Silo 17.6 0 31 29
Smith 1992 Tr 8 Skin 25 75
Tremblay 2001 Retro Tr; Bl; Pc; Mi 93 23.6 Skin 40 40
Duff 1981 Retro Tr; Pt 18 LP 28 39 11
Koniaris 2001 Retro Tr; Pt; IL; AAA; CS; Pc 13 43.0 DRS 2.8 23 85
Bl: Bleeding; Mi: Mesenterial ischemia; NT: Non-Trauma; Pc: Pancreatitis; Pt: Peritonitis; Va: Vascular; Tr: Trauma; LP: Loose packing; Skin: Skin only closure; Silo: plastic silo closure; Retro: retrospective inclusion; Empty boxes indicate that these data were not reported.
Fascial closure As shown in Table 4, the highest pooled fascial closure rates corrected for study size
(1/variance) were achieved in the techniques that applied continuous traction on the
fascial edges to prevent lateral retraction. The series in which the Artificial burr was used
achieved the highest pooled closure rate (90%). The second highest pooled closure rate
was achieved by the one series that used the Dynamic Retention Sutures (85% closure),
followed, in third place, by the series that used the VAC technique (60% closure). The
Wind (Chris).indb 156Wind (Chris).indb 156 28-05-2008 15:44:4828-05-2008 15:44:48

157
Ch
apter 10
Temporary closure of the op
en abdom
en
closure rates in the other techniques ranged from 11% in the one series with Skin only
closure to 52% in the Vacuum pack series.
Fistulae and abscessesThe occurrence of fistulae as a complication of TAC was reported in 44 series (75%) and is
shown in Table 4. The highest pooled fistulae rate (1/variance) was observed in the series
that used Loose packing (28%). However, this was only one series with eighteen patients.
The second highest fistulae rate was observed in the Zipper (13.8%) series. The lowest
rates of fistulae were seen in the Silo series (0%), the Artificial burr series (2.0%), the VAC
series (2.9%), and the Vacuum pack series (5.7%).
The number of abscesses was reported in 29 series (49%) and the pooled rate varied per
technique (Table 4). The highest pooled abscesses rate (1/variance) was observed in the
Zipper series (5.8%). However, only two of the seven Zipper series reported the abscess
rate. The second highest median abscess rate (4.1%) was seen in the Artificial burr series.
The lowest pooled abscess rates were observed in the Mesh/sheet series (2.1%), the VAC
series (2.6%) and the Artificial burr series (3.0%).
MortalityThe pooled mortality rate (1/variance) over all techniques was 26% (95% CI: 24 – 27). The
highest overall mortality rates were seen in the Silo series (41%), and the Skin only series
(39%). The lowest overall mortality rates were observed in the Artificial burr series (17%)
and the VAC series (18%). The lowest mortality rates were observed in the four techniques
that showed the highest fascial closure rate (Table 4).
Meta-regression analysisBased on the results above, the authors identified a set of possible predictive factors
for delayed primary fascial closure (from the case series). These factors included intrinsic
pre-TAC factors; the TAC technique, nature of the underlying condition, gender, age, ISS,
and APACHE II. Intrinsic factors known during the TAC were duration of the treatment,
mortality, duration of hospital stay, duration of ICU stay, number of surgical reinterventions,
and percentage of fistulae and abscesses. Qualitative predictors which were known at
the start of the TAC were the year of inclusion and the country in which the study took
place.
Univariate logit-transformed meta-regression identified eight significant predictive factors.
Positive predictors were the Artificial burr and VAC technique. Negative predictors were series
with pancreatitis patients, the Mesh/sheet technique, number of surgical reinterventions,
duration of TAC, duration of ICU stay, and mortality. Multivariate logit-transformed meta-
regression analysis revealed that the Artificial burr is positively associated with delayed
primary fascial closure. The Mesh/sheet technique, duration of TAC, and mortality were
negative predictors for delayed primary fascial closure.
Wind (Chris).indb 157Wind (Chris).indb 157 28-05-2008 15:44:4828-05-2008 15:44:48
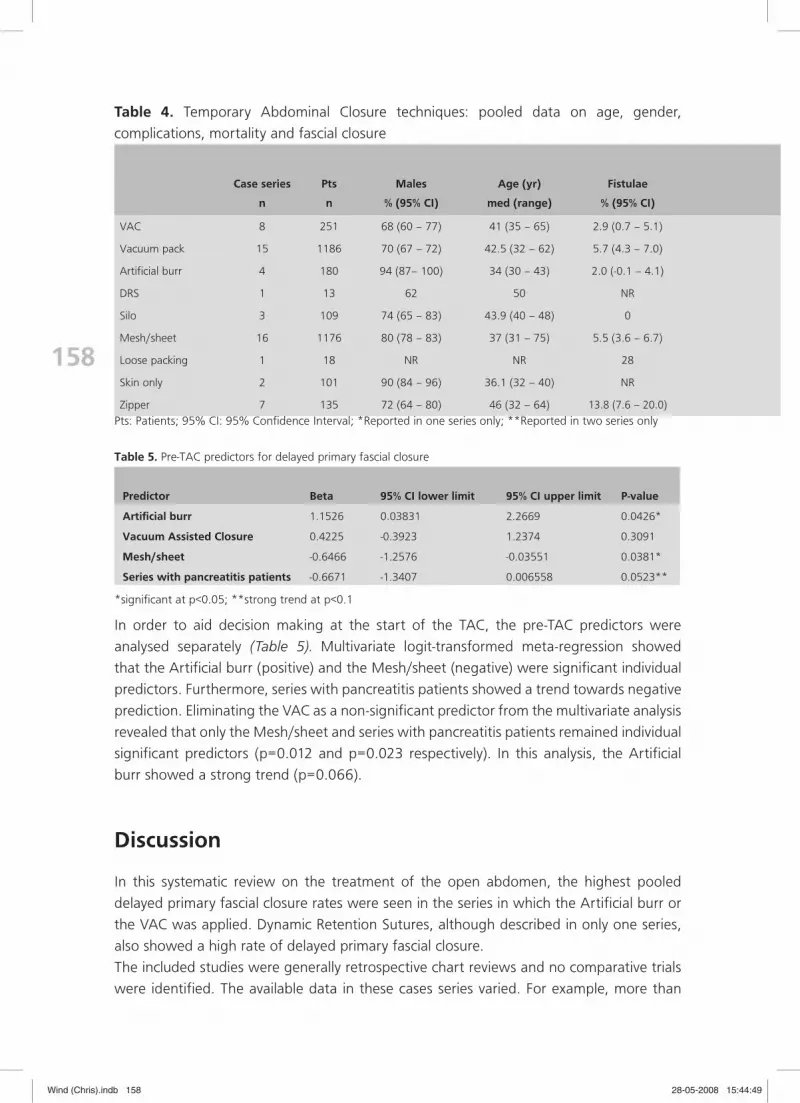
158
Table 4. Temporary Abdominal Closure techniques: pooled data on age, gender,
complications, mortality and fascial closure
Case series Pts Males Age (yr) Fistulae
n n % (95% CI) med (range) % (95% CI)
VAC 8 251 68 (60 – 77) 41 (35 – 65) 2.9 (0.7 – 5.1)
Vacuum pack 15 1186 70 (67 – 72) 42.5 (32 – 62) 5.7 (4.3 – 7.0)
Artificial burr 4 180 94 (87– 100) 34 (30 – 43) 2.0 (-0.1 – 4.1)
DRS 1 13 62 50 NR
Silo 3 109 74 (65 – 83) 43.9 (40 – 48) 0
Mesh/sheet 16 1176 80 (78 – 83) 37 (31 – 75) 5.5 (3.6 – 6.7)
Loose packing 1 18 NR NR 28
Skin only 2 101 90 (84 – 96) 36.1 (32 – 40) NR
Zipper 7 135 72 (64 – 80) 46 (32 – 64) 13.8 (7.6 – 20.0)
Pts: Patients; 95% CI: 95% Confidence Interval; *Reported in one series only; **Reported in two series only
Table 5. Pre-TAC predictors for delayed primary fascial closure
Predictor Beta 95% CI lower limit 95% CI upper limit P-value
Artificial burr 1.1526 0.03831 2.2669 0.0426*
Vacuum Assisted Closure 0.4225 -0.3923 1.2374 0.3091
Mesh/sheet -0.6466 -1.2576 -0.03551 0.0381*
Series with pancreatitis patients -0.6671 -1.3407 0.006558 0.0523**
*significant at p<0.05; **strong trend at p<0.1
In order to aid decision making at the start of the TAC, the pre-TAC predictors were
analysed separately (Table 5). Multivariate logit-transformed meta-regression showed
that the Artificial burr (positive) and the Mesh/sheet (negative) were significant individual
predictors. Furthermore, series with pancreatitis patients showed a trend towards negative
prediction. Eliminating the VAC as a non-significant predictor from the multivariate analysis
revealed that only the Mesh/sheet and series with pancreatitis patients remained individual
significant predictors (p=0.012 and p=0.023 respectively). In this analysis, the Artificial
burr showed a strong trend (p=0.066).
Discussion
In this systematic review on the treatment of the open abdomen, the highest pooled
delayed primary fascial closure rates were seen in the series in which the Artificial burr or
the VAC was applied. Dynamic Retention Sutures, although described in only one series,
also showed a high rate of delayed primary fascial closure.
The included studies were generally retrospective chart reviews and no comparative trials
were identified. The available data in these cases series varied. For example, more than
Wind (Chris).indb 158Wind (Chris).indb 158 28-05-2008 15:44:4928-05-2008 15:44:49

159
Ch
apter 10
Temporary closure of the op
en abdom
en
Abscesses Mortality Closure
% (95% CI) n % (95% CI) n % (95% CI)
2.6 (0.2 – 5.0) 56 18 (13 – 22) 149 60 (54 – 66)
4.1 (2.9 – 5.3) 340 27 (24 – 29) 611 52 (49 – 54)
3.0 (-1.9 – 7.9)** 34 17 (12 – 23) 156 90 (86 – 95)
NR 3 23 11 85
6 (*) 48 41 (32 – 51) 32 29 (20 – 37)
2.1 (0.7 – 3.6) 334 26 (23 – 28) 293 23 (20 – 25)
NR 7 39 2 11
NR 39 39 (29 – 48) 43 43 (34 – 53)
5.8 (-2.7 – 14.3)** 46 33 (25 – 41) 45 39 (31 – 47)
one third of the series did not report whether the patients were included prospectively
or retrospectively, or whether it concerned a consecutive series of patients. Furthermore,
the exact inclusion and exclusion criteria often were not reported. The decision to operate
a specific patient as well as the decision of TAC was usually left to the discretion of the
operating surgeon without an explanation of the rationale behind it. Scoring systems such
as the Acute Physiology and Chronic Health Evaluation II (APACHE II) and the Simplified
Acute Physiology II (SOFA II), both reflecting the severity of the disease, were reported
infrequently. The ISS in trauma patients was reported more frequently. However, differences
in severity of the patients’ conditions were still difficult to assess, because the ISS involves
all injuries to the body. These facts imply that the studies suffer from considerable bias in
both patient selection and treatment selection.
The fact that, over all series, three quarters of the patients were men could partly be explained
by the high percentage of male patients in the series with trauma patients. However, even
the series without trauma patients showed high percentages of male patients.
For the purpose of this study, the results were pooled per technique. However, no
standardised techniques were used in these series. By implication, even though series with
multiple techniques were excluded, an unknown amount of practice variation for each
technique remains.
Some techniques were used in only one series (Dynamic Retention Sutures and Loose
packing) with less than 20 patients per series. Other techniques were used in two (Skin)
or three series (Silo). These series, however, did include more than one hundred patients
each. Hence, the reliability of the pooled estimate of fascial closure per series differs.
In contrast to the other techniques, the VAC, Vacuum pack, and Mesh/sheet techniques
have been used in trauma series, mixed series as well as non-trauma patients. However,
subdivision of the results per patient group and technique, resulted in small numbers of
patients and heterogeneous rates of complications, mortality and fascial closure. Therefore
Wind (Chris).indb 159Wind (Chris).indb 159 28-05-2008 15:44:4928-05-2008 15:44:49

160
further subdivision of the results was omitted.
The availability and preference for the different techniques seems to have evolved over
the past 30 years. The first published studies on temporary closure of the open abdomen
concern mostly Mesh/sheet and Zipper techniques. Over the years, choice for temporary
abdominal closure technique seems to have shifted towards techniques that more actively
pursue abdominal drainage and fascial re-approximation. Furthermore, 85% of the studies
that were published since 1998 use a vacuum technique (Vacuum Assisted Closure or
Vacuum pack). Therefore, the surgeons preference seems to have shifted toward the
vacuum based techniques. The results show that this may be a good evolution because
these techniques show high closure rates and low complication rates. However, the
Artificial burr is better in terms of delayed primary fascial closure rate.
The best rates of delayed primary fascial closure were seen in the Artificial burr series and
the Dynamic Retention Suture series, although the latter concerned only one series. The
VAC and Vacuum pack also showed high closure rates which were comparable but in
favour of the VAC. The median closure rate in the Silo series is surprisingly low since this
technique allows for gradual re-approximation of the fascial edges. In other techniques,
this seems to result in higher fascial closure rates. After careful evaluation of these three
series, no clue was found for the reason of this low closure rate.
The results suggest that a more active approach towards fascial closure of the open
abdomen may result in higher fascial closure rates. The Artificial burr and the Dynamic
Retention Sutures, in which the fascial edges are actively pulled medially, showed the
highest closure rates.
As mentioned in the methods, the delayed primary fascial closure rate was calculated over
all included patients and not the survivors. This was done simply because the in-hospital
mortality often was not divided into pre-closure and post-closure mortality. However, it
is likely that most patients have died in the early stage of the open abdominal treatment
(i.e. before closure). Therefore, the delayed fascial closure rate of the survivors may indeed
have been even higher than the rates reported in this review. This applies to all TAC
techniques.
The Zipper series showed a surprisingly high median fistulae rate. Furthermore, although
reported in few series, the abscess rate was also high in the Zipper series. Surprisingly, the
Artificial burr series showed some of the lowest fistulae rates as well as the highest abscess
rate. In contrast, the VAC also showed one of the lowest fistulae rates, however, the VAC
series reported no abscesses. Of all possible complications of the open abdomen, fistulae
and abscesses were reported most consistently. However, the reported rates may be
underestimating the true number of fistulae and abscesses. This is because, in retrospective
chart reviews, complications may not have been reported and can be difficult to identify.
Especially the less grave complications which do not have therapeutic consequences may
be difficult to retrieve from the medical charts.
All included studies reported on mortality. Despite the high overall mortality, two series
reported a mortality rate of zero. This could partly be explained by the fact that these
two series concern few patients (8 and 11). Somewhat surprising is the fact that the three
Wind (Chris).indb 160Wind (Chris).indb 160 28-05-2008 15:44:4928-05-2008 15:44:49

161
Ch
apter 10
Temporary closure of the op
en abdom
en
techniques with the highest fascial closure rates, also showed the lowest mortality rates.
This may indicate that these techniques are indeed superior when it comes to fascial
closure and mortality. However, the fact that the general ICU treatment has improved
considerably over the years and that the VAC has only been used in recent years indicates
that there may be some confounding factors. However, contrary to this explanation, the
Artificial burr (which showed the highest closure rate as well as the lowest mortality rate)
was used over a large period of time.
Interestingly, the predictors from the univariate meta-regression analysis mainly concerned
TAC techniques and factors concerning hospital admission. The series with pancreatitis
patients was the only case in which the underlying condition predicted the outcome. This
partly contradicts the common surgeons’ phrase that delayed primary fascial closure is
easier in trauma patients because of the absent abdominal infection.
Four of the eight initial predictors for delayed primary fascial closure concerned factors
that are only fully known at the end of the TAC. These factors, although they predict the
outcome, are not suitable for clinical decision making pre-TAC. Therefore only the factors
that were known pre-TAC were further analysed.
The only two factors that remained significant were negative predictors. These results
suggest that, when using a Mesh or sheet, the probability of achieving delayed primary
facial closure is lower than for the other techniques described in this review. Furthermore,
the overall delayed primary fascial closure rate seems to be lower if the series contains
patients with pancreatitis. The former can be explained, because Meshes and sheets do
not keep appropriate tension on the fascial edges and therefore are in opposition to fascial
closure. It can be argued that the series with pancreatitis patients contain more severely ill
patients that may spend longer periods in the hospital and intensive care unit. However,
these factors, while significant in the univariate regression analysis, are not significant in
the multivariate analysis. Therefore, it is suggested that there may be unreported factors
that cause the decreased fascial closure in series with pancreatitis patients.
In conclusion, the results of this review suggest that temporary abdominal closure
techniques that keep traction on the fascial edges result in high rates of fascial closure.
Furthermore, techniques with high closure rates seem to result in low rates of fistulae,
abscesses, and mortality. The results of the meta-regression suggest that, of the reported
factors, Mesh/sheet use and series with pancreatitis patients negatively predict delayed
primary fascial closure. Randomised controlled trials are required to indicate more clearly
which technique produces higher delayed primary fascial closure rates.
Reference list
(1) Bose SM, Kalra M, Sandhu NP. Open management of septic abdomen by Marlex mesh zipper. Aust N Z J Surg. 1991;61:385-388.
(2) Keramati M, Srivastava A, Sakabu S, et al. The Wittmann Patchtrade mark as a temporary abdominal closure device after decompressive celiotomy for abdominal compartment syndrome following burn. Burns. 2007.
Wind (Chris).indb 161Wind (Chris).indb 161 28-05-2008 15:44:4928-05-2008 15:44:49

162
(3) Miller RS, Morris JA Jr., Diaz JJ Jr., Herring MB, May AK. Complications after 344 damage-control open celiotomies. J Trauma. 2005;59:1365-1371.
(4) Tons C, Schachtrupp A, Rau M, Mumme T, Schumpelick V. [Abdominal compartment syndrome: preven-tion and treatment]. Chirurg. 2000;71:918-926.
(5) Tremblay LN, Feliciano DV, Schmidt J, et al. Skin only or silo closure in the critically ill patient with an open abdomen. Am J Surg. 2001;182:670-675.
(6) Doyon A, Devroede G, Viens D, et al. A simple, inexpensive, life-saving way to perform iterative laparo-tomy in patients with severe intra-abdominal sepsis. Colorectal Dis. 2001;3:115-121.
(7) Wittmann DH. Staged Abdominal Repair: Development and Current Practice of an Advanced Operative Technique for Diffuse Suppurative Peritonitis. Acta Chir Austriaca. 2000;32:171-178.
(8) Cuesta MA, Doblas M, Castaneda L, Bengoechea E. Sequential abdominal reexploration with the zipper technique. World J Surg. 1991;15:74-80.
(9) Smith PC, Tweddell JS, Bessey PQ. Alternative approaches to abdominal wound closure in severely injured patients with massive visceral edema. J Trauma. 1992;32:16-20.
(10) Barker DE, Kaufman HJ, Smith LA, Ciraulo DL, Richart CL, Burns RP. Vacuum pack technique of tempo-rary abdominal closure: a 7-year experience with 112 patients. J Trauma. 2000;48:201-206.
(11) Suliburk JW, Ware DN, Balogh Z, et al. Vacuum-assisted wound closure achieves early fascial closure of open abdomens after severe trauma. J Trauma. 2003;55:1155-1160.
(12) Baker SP, O’Neill B, Haddon W Jr., Long WB. The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma. 1974;14:187-196.
(13) Ohmann C, Wittmann DH, Wacha H. Prospective evaluation of prognostic scoring systems in peritonitis. Peritonitis Study Group. Eur J Surg. 1993;159:267-274.
(14) Therapy checklist (Dutch extended version) of the Dutch Cochrane centre. www.cochrane.nl.
(15) Akers DL Jr., Fowl RJ, Kempczinski RF, Davis K, Hurst JM, Uhl S. Temporary closure of the abdominal wall by use of silicone rubber sheets after operative repair of ruptured abdominal aortic aneurysms. J Vasc Surg. 1991;14:48-52.
(16) Aprahamian C, Wittmann DH, Bergstein JM, Quebbeman EJ. Temporary abdominal closure (TAC) for planned relaparotomy (etappenlavage) in trauma. J Trauma. 1990;30:719-723.
(17) Barker DE, Green JM, Maxwell RA, et al. Experience with vacuum-pack temporary abdominal wound closure in 258 trauma and general and vascular surgical patients. J Am Coll Surg. 2007;204:784-792.
(18) Bosscha K, Hulstaert PF, Visser MR, van Vroonhoven TJ, van der Werken C. Open management of the abdomen and planned reoperations in severe bacterial peritonitis. Eur J Surg. 2000;166:44-49.
(19) Brock WB, Barker DE, Burns RP. Temporary closure of open abdominal wounds: the vacuum pack. Am Surg. 1995;61:30-35.
(20) Chavarria-Aguilar M, Cockerham WT, Barker DE, Ciraulo DL, Richart CM, Maxwell RA. Management of destructive bowel injury in the open abdomen. J Trauma. 2004;56:560-564.
(21) Cohn SM, Burns GA, Sawyer MD, Tolomeo C, Milner KA, Spector S. Esmarch closure of laparotomy inci-sions in unstable trauma patients. J Trauma. 1995;39:978-979.
(22) Cothren CC, Moore EE, Johnson JL, Moore JB, Burch JM. One hundred percent fascial approximation with sequential abdominal closure of the open abdomen. Am J Surg. 2006;192:238-242.
(23) DeFranzo AJ, Argenta L. Vacuum-assisted closure for the treatment of abdominal wounds. Clin Plast Surg. 2006;33:213-24, vi.
(24) Duff JH, Moffat J. Abdominal sepsis managed by leaving abdomen open. Surgery. 1981;90:774-778.
(25) Fansler RF, Taheri P, Cullinane C, Sabates B, Flint LM. Polypropylene mesh closure of the complicated abdominal wound. Am J Surg. 1995;170:15-18.
Wind (Chris).indb 162Wind (Chris).indb 162 28-05-2008 15:44:4928-05-2008 15:44:49

163
Ch
apter 10
Temporary closure of the op
en abdom
en
(26) Foy HM, Nathens AB, Maser B, Mathur S, Jurkovich GJ. Reinforced silicone elastomer sheeting, an improved method of temporary abdominal closure in damage control laparotomy. Am J Surg. 2003;185:498-501.
(27) Hadeed JG, Staman GW, Sariol HS, Kumar S, Ross SE. Delayed primary closure in damage control lapa-rotomy: the value of the Wittmann patch. Am Surg. 2007;73:10-12.
(28) Hannon RJ, Hood JM, Curry RC. Temporary abdominal closure: a new product. Br J Surg. 1992;79:820-821.
(29) Howdieshell TR, Proctor CD, Sternberg E, Cue JI, Mondy JS, Hawkins ML. Temporary abdomi-nal closure followed by definitive abdominal wall reconstruction of the open abdomen. Am J Surg. 2004;188:301-306.
(30) Hubens G, Lafaire C, De PM, et al. Staged peritoneal lavages with the aid of a Zipper system in the treat-ment of diffuse peritonitis. Acta Chir Belg. 1994;94:176-179.
(31) Jernigan TW, Fabian TC, Croce MA, et al. Staged management of giant abdominal wall defects: acute and long-term results. Ann Surg. 2003;238:349-355.
(32) Koniaris LG, Hendrickson RJ, Drugas G, Abt P, Schoeniger LO. Dynamic retention: a technique for closure of the complex abdomen in critically ill patients. Arch Surg. 2001;136:1359-1362.
(33) Kushimoto S, Yamamoto Y, Aiboshi J, et al. Usefulness of the bilateral anterior rectus abdominis sheath turnover flap method for early fascial closure in patients requiring open abdominal management. World J Surg. 2007;31:2-8.
(34) Labler L, Keel M, Trentz O. [New application of VAC (Vacuum Assisted Closure) in the Abdominal Cavity in Case of Open Abdomen Therapy]. Zentralbl Chir. 2004;129:S14-S19.
(35) Losanoff J, Kjossev K. Palisade dorsoventral lavage for neglected peritonitis. Am J Surg. 1997;173:134-135.
(36) Mayberry JC, Burgess EA, Goldman RK, Pearson TE, Brand D, Mullins RJ. Enterocutaneous fistula and ventral hernia after absorbable mesh prosthesis closure for trauma: the plain truth. J Trauma. 2004;57:157-162.
(37) Miller PR, Meredith JW, Johnson JC, Chang MC. Prospective evaluation of vacuum-assisted fascial closure after open abdomen: planned ventral hernia rate is substantially reduced. Ann Surg. 2004;239:608-614.
(38) Nagy KK, Fildes JJ, Mahr C, et al. Experience with three prosthetic materials in temporary abdominal wall closure. Am Surg. 1996;62:331-335.
(39) Navsaria PH, Bunting M, Omoshoro-Jones J, Nicol AJ, Kahn D. Temporary closure of open abdominal wounds by the modified sandwich-vacuum pack technique. Br J Surg. 2003;90:718-722.
(40) Oetting P, Rau B, Schlag PM. [Abdominal vacuum device with open abdomen]. Chirurg. 2006;77:586, 588-586, 593.
(41) Perez D, Wildi S, Demartines N, Bramkamp M, Koehler C, Clavien PA. Prospective evaluation of vacuum-assisted closure in abdominal compartment syndrome and severe abdominal sepsis. J Am Coll Surg. 2007;205:586-592.
(42) Rasmussen TE, Hallett JW Jr., Noel AA, et al. Early abdominal closure with mesh reduces multiple organ failure after ruptured abdominal aortic aneurysm repair: guidelines from a 10-year case-control study. J Vasc Surg. 2002;35:246-253.
(43) Schachtrupp A, Hoer J, Tons C, Klinge U, Reckord U, Schumpelick V. Intra-abdominal pressure: a reliable criterion for laparostomy closure? Hernia. 2002;6:102-107.
(44) Sherck J, Seiver A, Shatney C, Oakes D, Cobb L. Covering the “open abdomen”: a better technique. Am Surg. 1998;64:854-857.
(45) Singh K, Chhina RS. Role of zipper in the management of abdominal sepsis. Indian J Gastroenterol. 1993;12:1-4.
Wind (Chris).indb 163Wind (Chris).indb 163 28-05-2008 15:44:4928-05-2008 15:44:49
164
(46) Smith LA, Barker DE, Chase CW, Somberg LB, Brock WB, Burns RP. Vacuum pack technique of tempo-rary abdominal closure: a four-year experience. Am Surg. 1997;63:1102-1107.
(47) Stone PA, Hass SM, Flaherty SK, DeLuca JA, Lucente FC, Kusminsky RE. Vacuum-assisted fascial closure for patients with abdominal trauma. J Trauma. 2004;57:1082-1086.
(48) Stonerock CE, Bynoe RP, Yost MJ, Nottingham JM. Use of a vacuum-assisted device to facilitate abdomi-nal closure. Am Surg. 2003;69:1030-1034.
(49) Sugrue M, Jones F, Janjua KJ, Deane SA, Bristow P, Hillman K. Temporary abdominal closure: a prospec-tive evaluation of its effects on renal and respiratory physiology. J Trauma. 1998;45:914-921.
(50) van As AB, Navsaria P, Numanoglu A, McCulloch M. Modified sandwich vacuum pack technique for temporary closure of abdominal wounds: an African perspective. Acta Clin Belg Suppl. 2007;215-219.
(51) van Goor H, Hulsebos RG, Bleichrodt RP. Complications of planned relaparotomy in patients with severe general peritonitis. Eur J Surg. 1997;163:61-66.
(52) Wilde JM, Loudon MA. Modified Opsite sandwich for temporary abdominal closure: a non-traumatic experience. Ann R Coll Surg Engl. 2007;89:57-61.
(53) Wouters DB, Krom RA, Slooff MJ, Kootstra G, Kuijjer PJ. The use of Marlex mesh in patients with gener-alized peritonitis and multiple organ system failure. Surg Gynecol Obstet. 1983;156:609-614.
(54) Yeh KA, Saltz R, Howdieshell TR. Abdominal wall reconstruction after temporary abdominal wall closure in trauma patients. South Med J. 1996;89:497-502.
(55) Zingales F, Moschino P, Carniato S, Fabris G, Vittadello F, Corsini A. Laparostomy in the treatment of severe peritonitis: a review of 60 cases. Chir Ital. 2001;53:821-826.
Wind (Chris).indb 164Wind (Chris).indb 164 28-05-2008 15:44:4928-05-2008 15:44:49

11Chapter
Single-stage closure of enterocutaneous fistula and stomas in the presence of
large abdominal wall defects using the components separation technique
J Wind
PJ van Koperen
JFM Slors
WA Bemelman
American Journal of Surgery, in press
Wind (Chris).indb 165Wind (Chris).indb 165 28-05-2008 15:44:4928-05-2008 15:44:49

166166
Abstract
IntroductionClosure of an enterocutaneous fistula and/or stomas in the presence of large abdominal
wall defects is a challenging problem. In the present study the results of the components
separation technique are described.
MethodsAll patients with an enterocutaneous fistula and/or stomas in the presence of large
abdominal wall defects (i.e. laparostomy of ventral hernia) who underwent a single-stage
repair using the components separation technique in the period from January 2000 to July
2007 were reviewed retrospectively.
ResultsA total of 32 patients were included. Median operating time was 204 minutes (range
87-573). In 18 patients, additionally to the components separation, an absorbable mesh
was used. Postoperatively, in 16 patients 22 complications were reported. There were
nine patients with local wound problems. Median postoperative hospital stay was 12
days (range 5-74). Seven patients developed a ventral hernia. Four of them were small
asymptomatic recurrences. Four out of the 15 patients with an enterocuteneous fistula
developed a recurrent fistula. Median follow-up was 20 months (range 3-54).
ConclusionClosure of enterocutaneous fistula and/or stomas and simultaneous repair of large
abdominal wall defects is feasible using the components separation technique but
morbidity is considerable. Early recurrence of abdominal hernia and fistula is acceptable.
Wind (Chris).indb 166Wind (Chris).indb 166 28-05-2008 15:44:5028-05-2008 15:44:50

167
Ch
apter 11
Single-stage closure of entero
cutaneous fistula and stomas
Introduction
Patients surviving intra-abdominal catastrophes frequently have large abdominal wall
defects. These defects are generally the result of open abdomen management for severe
intra-abdominal sepsis, trauma, or other abdominal emergencies. These large defects are
often associated with enterocutaneous fistula and stomas.1
Closure of enterocuteneous fistula and/or stomas and simultaneous closure of the large
and contaminated abdominal wall defect requires major surgery that includes extensive
adhesiolysis, bowel resection with reanastomosing, and closure of the abdominal wall.
Morbidity and mortality rates are high in these often malnutritioned patients, particularly
those with high-output enterocuteneous fistula.2;3 The actual timing of the operation
requires thoughtful consideration. Planning the operation too soon may result in an
extremely difficult surgical procedure in an often fragile patient. Postponing the operation
for too long exposes the patient unnecessarily to the deleterious metabolic effects of the
fistula and catheter-related morbidity in case of parenteral nutrition.2;3
Ideally, a non-absorbable mesh is used to close the abdominal wall because primary fascial
closure is rarely possible in these patients.4 This technique ensures durable abdominal
wall prosthesis. However, the application of a non-absorbable mesh is associated with
an increased risk of infection, especially when used in a contaminated surgical field, for
instance in the presence of enterocutaneous fistula and stomas.5;6 Furthermore, the
implanted mesh might damage exposed bowel if the peritoneum or greater omentum are
not interposed between the mesh and the bowel. Therefore, many surgeons are reluctant
to use non-absorbable meshes in these complicated abdominal wall defects.5-7 The use of
an absorbable mesh avoids infectious complications, but is only for temporary closure of
the hernia.
The most logical alternative for these large and contaminated abdominal wall defects is the
use of autologous tissue repair including local tissue repair, autologous grafts and pedicled
or free vascularised flaps. In a recently published systematic review several techniques for
autologous repair of abdominal wall defects were reviewed.8 Despite the poor quality
of the included studies the components separation technique was the best documented
procedure. This technique, for the repair of large ventral hernias, was first described by
Ramirez et al.9 The separation of the muscle components of the abdominal wall allows
local advancement with complete continuity of the released muscle layers over a greater
distance compared to mobilisation of the entire abdominal wall as a block. This enables
closure of large abdominal wall defects under contaminated circumstances avoiding mesh
infection. Nevertheless, most of the studies included in the review concerned only clean or
clean-contaminated surgical fields.8
The aim of this study was to evaluate the results of closure of enterocutaneous fistula
and/or stomas and simultaneous abdominal wall repair using the components separation
technique.
Wind (Chris).indb 167Wind (Chris).indb 167 28-05-2008 15:44:5028-05-2008 15:44:50

168
Methods
The present study consists of a consecutive series of patients with enterocutaneous fistula
and/or stomas in the presence of a large abdominal wall defect (i.e. laparostomy or ventral
hernia). Patients had a single-stage closure of the enterocutaneous fistula and/or stomas
and simultaneous repair of the abdominal wall using the components separation technique
as described by Ramirez et al.9 All operations were performed electively in the period from
January 2000 to July 2007. Data were assessed in a retrospective manner. Patients under
18 years of age, large abdominal wall defects without the presence of enterocuteneous
fistula and/or stomas (i.e. surgical field contamination) and multi-staged procedures were
excluded from this study. Charts of the included patients were reviewed and the following
data were extracted using a preformatted sheet including age, gender, co-morbidity
and surgical history, Body Mass Index (BMI, kg/m2), signs of malnutrition defined as
a weight reduction of more than 10% in the previous six months and a low albumin
level (< 30 g/l)10, ASA classification, reasons for surgical field contamination, operating
time, concomitant surgical procedures, the use of mesh reinforcement, intra-operative
morbidity, 30-day morbidity and mortality, postoperative hospital stay, readmissions and
reoperations within 30 days. During long term follow-up recurrence of enterocutaneous
fistula or the development of ventral hernia was assessed. Outcome and complications
were noted during clinical and out-patient clinic follow-up.
Operative proceduresAll patients underwent general anesthesia and received preoperative parenteral antibiotic
prophylaxis (Ceforoxim 1500 mg/Clindamycine 600 mg, 30 minutes before surgery).
When the procedure lasted for more than four hours the same antibiotic prophylaxis was
repeated. Normal body temperature was maintained with standard bair hugger warming.
Perioperative glucose levels were not checked routinely. To avoid inadvertent bowel injury,
the abdomen was generally entered by dissecting the stomas when present. Otherwise
the laparotomy was started at the upper border of the incisional hernia or at the midline
above the laparostomy. A complete adhesiolysis was generally performed to get a clear
view on the anatomy and to free the bowel from the abdominal wall. If enterocutaneous
fistulas were present the segment(s) from which the fistula arose was identified and
isolated followed by a limited resection and reanastomosing of the two segments. If
stomas were present the bowel was reanastomosed and the fascia was closed using PDS
1 (Ethicon®) or the fascia was closed with a Vicryl mesh. Care was taken to reposition
the anastomosis or sutured small bowel lesions that occurred during adhesiolysis, as far
away from the abdominal wall as possible. The subsequent abdominal wall closure was
performed using the components separation technique (Figure 1 and 2). The skin and
subcutis were separated from the underlying abdominal musculature in lateral direction
up to the anterior axillary line. Next the aponeurosis of the external oblique muscle was
incised pararectally. Subsequently, the external oblique muscle was separated from the
underlying internal oblique muscle by blunt dissection in a relatively avascular plane.
Wind (Chris).indb 168Wind (Chris).indb 168 28-05-2008 15:44:5028-05-2008 15:44:50

169
Ch
apter 11
Single-stage closure of entero
cutaneous fistula and stomas
Figure 1. Cross-sectional view. Skin and subcutaneous tissue are separated from the underlying abdominal muscle in lateral direction up to the anterior axillary line. Next the aponeurosis of the external oblique muscle is incised pararectally and the external oblique muscle is separated from the underlying internal oblique muscle by blunt dissection (A and B). Additionally, the rectus muscle is separated from the posterior rectus sheath (C).
Wind (Chris).indb 169Wind (Chris).indb 169 28-05-2008 15:44:5028-05-2008 15:44:50

170
This was followed by the separation of the rectus muscle from the posterior rectus sheath.
The separation of the muscle components of the abdominal wall allowed mobilisation of
each unit over a greater distance with less tension. Subsequently the abdominal wall was
closed using PDS 1. Sometimes a temporary reinforcement consisting of an onlay Vicryl
mesh was sutured to the fascia. The skin was closed with running sutures. Two suction
drains were routinely used between the mobilised skin and abdominal wall musculature
to drain the death space. The skin was closed because leaving the skin open would not
guarantee adequate drainage (via the suction drains) of the large subcutaneous wound
surfaces. Therefore, skin closure combined with closed wound drainage (suction drains)
was preferred. Postoperatively, no abdominal binders were applied routinely. In case of a
wound infection the running sutures were (partly) removed for adequate drainage.
StatisticsData are presented as median values with ranges for continuous data, unless otherwise
specified. Categorical data are presented as number of patients and percentages. The
Chi-square or Fisher’s exact test was used to test for differences between groups. A
p-value <0.05 was considered statistically significant. Statistical analysis was done using
the SPSS v.12.0 package (SPSS, Chicago, Illinois, USA).
Figure 2. Frontal view. Additionally, parasagittal relaxing incisions can be made in the internal oblique muscle.
Wind (Chris).indb 170Wind (Chris).indb 170 28-05-2008 15:44:5028-05-2008 15:44:50

171
Ch
apter 11
Single-stage closure of entero
cutaneous fistula and stomas
Results
Demographics of the included patientsIn the study period a total of 32 patients were identified who underwent single-staged
closure of enterocutaneous fistula and/or stomas and simultaneous repair of the abdominal
wall using the components separation technique. There were 10 female and 22 male
patients with a median age of 43 years (range 19-78), median BMI of 21.7 kg/m2 (range
16-32) and a median ASA score of two (range 1-4). In nine (28%) patients there was
malnutrition (weight reduction of more than 10% in the previous six months and a low
albumin level) preoperatively. All patients were survivors of intra-abdominal catastrophes.
In 22 (69%) patients an intra-abdominal sepsis was managed with an open abdomen. In
the remaining patients a large incisional hernia was present expanding to at least half way
the upper and lower abdomen. In Table 1 the reasons for the surgical field contamination
are summarized. In four (13%) patients there was one source of contamination, in the
remaining patients there were several sources. There were 15 (47%) patients with an
enterocutaneous fistula of which nine were high output fistulas (>500 ml/24 hours). The
origin of the fistula was a small bowel segment in 12 patients and in three patients the
fistula arose from the large bowel. In 21 (66%) patients a stoma was closed comprising
of 15 ileostomies and six colostomies. Furthermore, 22 patients had large contaminated
granulating defects (i.e. laparostomy)
Table 1. Reasons for contamination of the surgical field
Reason for contamination Number of patients
Granulating defect (laparostomy)Osteomy closureEnterocuteneous fistula closureConcomitant bowel resection†
Abscess
222115 9 2
†Apart from resections of bowel segments from which the fistula arose in case of enterocuteneous fistula closure.
Operative dataMedian operating time was 204 minutes (range 87-573). In five patients complete fascial
approximation was not possible. In all these patients a Vicryl mesh was implanted.
Additionally, in 13 patients the components separation was reinforced with a Vicryl mesh.
This was done as an onlay procedure.
Concomitant bowel resections, apart from resections of bowel segments from which an
enterocuteneous fistula arose, were necessary in nine patients; one patient underwent
small and eight underwent large bowel resection(s). Furthermore, 21 patients underwent
stoma closure, 15 patients underwent closure of one or more enterocutaneous fistulas. In
three patients a stoma was constructed, two patients underwent a cholecystectomy, in two
patients an abscess was drained and in one patient an entero-vesico fistula was closed.
Wind (Chris).indb 171Wind (Chris).indb 171 28-05-2008 15:44:5128-05-2008 15:44:51

172
Short term outcomeThere was no postoperative mortality. Postoperatively, in 16 (50%) patients 22
complications were reported within the first 30 days. There were nine patients with
local wound problems; eight patients had a wound infection and one patient had a large
hematoma. One of these patients underwent a surgical debridement and drainage of the
wound. Furthermore, five patients had a cardiopulmonary complication, three patients had
a urine tract infection, two patients had a prolonged postoperative ileus, two patients had
intra-abdominal abscesses which were drained radiologically and one patient developed
an enterocutaneous fistula within the first 30 days. The local wound problems were not
correlated with the type of contamination (i.e. stoma or enterocutaneous fistula), with the
presence of an open abdomen or with the use of a Vicryl mesh.
Median postoperative hospital stay was 12 days (range 5-74). Three patients were
readmitted within the first 30 days. Reasons for these readmissions were; a recurrent
fistula, a wound infection, and dehydration due to nausea and vomiting.
Long term outcomeFour patients were lost to long term follow-up. No recurrent ventral hernia was found
during their median follow-up of 3.5 months (range 1-8). Median follow-up of the
remaining 28 patients was 20 months (range 3-54). Seven (25%) patients developed a
recurrent ventral hernia. Of the seven patients with a recurrence four had Vicryl mesh
reinforcement and in three patients the fascia could not be closed entirely during the
components separation. There was no correlation between recurrence and postoperative
wound infection. Two out of the eight patients with a wound infection had a recurrence
compared to five out of the 24 patients without a wound infection. Four recurrences
were small and asymptomatic which did not require repair. Three patients underwent
an uncomplicated mesh repair. However, two of these patients developed a second
recurrence and underwent a new mesh repair.
Four (27%) out of the 15 patients with an enterocutaneous fistula developed a recurrent
fistula after a median of four months (range 0-15). In one of the patients with a recurrence
after 15 months the fistula was due to activity of Crohn’s disease. Two patients had a
reoperation for their enterocutaneous fistula. In one patient a recurrent fistula was excised
without further recurrences. The second patient underwent three more operations due to
recurrent fistula (last operation August 2007). A Munchausen syndrome was suspected
in this patient.
Discussion
Closure of enterocutaneous fistula and/or stomas in the presence of large abdominal wall
defects is a challenging problem. The primary goal of surgery is to close the enterocutaneous
fistula or stoma. The presence and simultaneous management of a large abdominal
defect is an accompanying problem making the combined procedure more difficult. In
Wind (Chris).indb 172Wind (Chris).indb 172 28-05-2008 15:44:5128-05-2008 15:44:51
173
Ch
apter 11
Single-stage closure of entero
cutaneous fistula and stomas
the event that the abdominal reconstruction fails due to wound infection, burst abdomen
or infected prosthetic material, a laparostoma reoccurs with a high likelihood of intestinal
fistulisation. The results of the present study demonstrated that single-stage management
using the components separation technique is a feasible method avoiding early abdominal
wall dehiscence. Nevertheless, the incidence of postoperative morbidity was high mainly
due to wound infection. This is not surprising considering the contaminated condition and
the large wound surfaces.
Mesh repair is superior to suture repair without prosthetic material with respect to the
recurrence of hernia. After primary repair, rates of recurrences are reported up to 50 percent.
Repairs that include the use of a mesh have recurrence rates ranging between zero and
25 percent.4;11 The morbidity rate for mesh repair in these none contaminated incisional
hernias is approximately 20 percent including major complications as enterocuteneous
fistula and mesh infections.11;12
For the reconstruction of very large abdominal wall defects the lack of sufficient tissue
requires the insertion of prosthetic material or transposition of autologous material to
bridge the fascial gap. In a recently published interim analysis of a randomised study, 39
patients with large clean or clean-contaminated abdominal wall defects were randomised
between mesh repair (PTFE) and the components separation technique.13 Wound
complications were found in 53 percent after components separation and in 72 percent
after mesh repair. Reherniation occurred in 53 percent after components separation and
in 22 percent after mesh repair. However, in 39 percent of the patients having mesh
repair, the prosthesis had to be removed as a consequence of early or late infection.
The authors concluded that repair of large clean or clean-contaminated abdominal wall
hernias with the components separation technique compares favourably with prosthetic
repair. Although the reherniation rate after components separation was relatively high, the
trial was discontinued because the consequences of wound healing disturbances in the
presence of PTFE prosthesis were far-reaching, often resulting in loss of the prosthesis.13
The components separation technique provides midline advancement by sequential
incision and release of muscle layers. Bilateral partition and sequential relaxing incisions
provide approximately 10, 20, and 6 centimeters of advancement, in the upper, middle,
and lower thirds of the abdomen respectively.9;14
Data of large abdominal wall defects repair in contaminated surgical fields using the
components separation technique are rare. In a study by van Geffen et al. only patients
with severely contaminated abdominal wall defects were included.15 Twenty-six patients
were treated with the components separation technique. Morbidity was reported in 46
percent of the patients with wound infection as the most frequent complication. Only
eight percent of the patients developed a ventral hernia after a median follow-up of 27
months. Of the nine patients with an enterocutaneous fistula three developed a recurrent
fistula. Others have found comparable results with the components separation technique
in contaminated abdominal wall defects.14;16;17 In the present study 50 percent of the
patients developed one or more complications including 28 percent of the patients
Wind (Chris).indb 173Wind (Chris).indb 173 28-05-2008 15:44:5128-05-2008 15:44:51
174
with local wound problems. The recurrence rate was 22 percent. More than half of the
recurrences were small and asymptomatic. Others have also reported that the majority of
the recurrences after the components separation technique were small and asymptomatic
and needed no further treatment.13;15
The presence of local wound problems in several patients is not surprising as the skin and
subcutaneous tissue must be mobilised laterally over a large distance in order to reach
the aponeurosis of the external oblique muscle resulting in a large wound surface. The
extensive mobilisation endangers the blood supply, this may lead to skin necrosis and
an increased risk of infection. To reduce wound complications, modifications have been
described to preserve the blood supply of the skin and subcutaneous tissue by preserving
the musculocutaneous perforating arteries.18;19 Saulis et al. proposed that preserving the
periumbilical rectus abdominis perforators to the abdominal skin flaps will decrease the
prevalence of superficial wound complications. They maintain a cluster of vessels as a
broad stalk to the overlying skin at the level of the umbilicus. In a retrospective review
of 66 consecutive patients the authors described a decrease in superficial wound healing
complications when this technique is used (20% versus 2%, P<0.05).18
Jernigan et al. modified the components separation technique allowing more extensive
mobilisation and local advancement in order to achieve a higher rate of fascial closure in
very large defects and to reduce the amount of ventral hernias. The modification starts
with the standard separation of components; full-thickness skin flaps are dissected from
the fascia bilaterally to approximately the midaxillary line. Next, bilaterally the external
oblique component of the anterior rectus sheath is divided around one centimeter lateral
to the rectus muscle and continued longitudinally approximately six to eight centimeters
over the costal margin superiorly, and inferiorly to the pubis. After division of the external
oblique fascia, the posterior rectus fascia is separated from the rectus muscles bilaterally.
The last separation is the internal oblique component of the anterior rectus sheath. This
is divided superiorly from the costal margin and extending inferiorly to the arcuate line.
Reconstruction is completed by suturing the most medial portion of the posterior rectus
fascia to the lateral portion of the anterior rectus fascia, bilaterally. A five percent recurrent
hernia rate was reported with a follow-up interval of 24 months.20
Most surgeons are reluctant to use non-absorbable mesh in a contaminated operative
field.5-7 In the present series in some of the patients the components separation was
reinforced with an absorbable Vicryl mesh in case of closure under tension. The
presence of the Vicryl mesh did not correlate with local wound problems. Others have
reported favourable results using the components separation technique enforced with
non-absorbable meshes in the presence of contamination.15;17;21;22 The role of supporting
non-absorbable mesh has to be investigated in prospective studies.
The use of an acellular matrix (e.g. AlloDerm) which becomes vascularized and remodeled
into autologous tissue after implantation may represent an alternative with low infectious
morbidity. Patton et al. retrospectively analyzed 67 patients undergoing repair of
contaminated abdominal wall defects using an acellular dermal matrix.23 They reported
a complication rate of 35 percent and a recurrence rate of 18 percent after a limited
Wind (Chris).indb 174Wind (Chris).indb 174 28-05-2008 15:44:5128-05-2008 15:44:51

175
Ch
apter 11
Single-stage closure of entero
cutaneous fistula and stomas
mean follow-up of 11 months. Alaedeen et al. described a subset of eight patients in
whom a large contaminated abdominal wall defect was repaired with the components
separation technique with acellular matrix reinforcement.16 After a median follow-up
of 14 months they found no recurrences. The use of an acellular matrix appears to be
feasible in contaminated surgical fields. However, to date limited evidence is available on
the safety and long term outcome. Furthermore, these products are very expensive and
should therefore be validated in carefully controlled studies first.16;23;24
The results of the present study must be interpreted carefully because of several limitations.
First of all it comprises a small single centre retrospective study. Second, defect size was
not reported in many cases. All defects were described as large or huge defects while
exact measures were missing. Third, the follow-up period of 20 months is moderate. With
longer follow-up a higher rate of incisional hernia might be observed.
In conclusion, closure of enterocutaneous fistula or stomas in the presence of large
abdominal wall defects is feasible using the components separation technique. This
technique is one of the few options available to deal with this very difficult problem. Early
recurrence of abdominal hernia and fistula is acceptable but morbidity is considerable.
Suggested modifications to preserve the blood supply of the skin and subcutaneous tissue,
extended antibiotic therapy and changes in mesh repair might improve outcome.
Reference List
(1) Schecter WP, Ivatury RR, Rotondo MF, Hirshberg A. Open abdomen after trauma and abdominal sepsis: a strategy for management. J Am Coll Surg 2006;203:390-396.
(2) Sriussadaporn S, Sriussadaporn S, Kritayakirana K, Pak-art R. Operative management of small bowel fistulae associated with open abdomen. Asian J Surg 2006;29:1-7.
(3) Losanoff JE, Richman BW, Jones JW. Temporary abdominal coverage and reclosure of the open abdo-men: frequently asked questions. J Am Coll Surg 2002;195:105-115.
(4) Luijendijk RW, Hop WC, van den Tol MP, de Lange DC, Braaksma MM, IJzermans JN, et al. A compari-son of suture repair with mesh repair for incisional hernia. N Engl J Med 2000;343:392-398.
(5) White TJ, Santos MC, Thompson JS. Factors affecting wound complications in repair of ventral hernias. Am Surg 1998;64:276-280.
(6) Morris-Stiff GJ, Hughes LE. The outcomes of nonabsorbable mesh placed within the abdominal cavity: literature review and clinical experience. J Am Coll Surg 1998;186:352-367.
(7) Amid PK, Shulman AG, Lichtenstein IL, Hakakha M. Biomaterials for abdominal wall hernia surgery and principles of their applications. Langenbecks Arch Chir 1994;379:168-171.
(8) de Vries Reilingh TS, Bodegom ME, van Goor H, Hartman EH, van der Wilt GJ, Bleichrodt RP. Autolo-gous tissue repair of large abdominal wall defects. Br J Surg 2007;94:791-803.
(9) Ramirez OM, Ruas E, Dellon AL. “Components separation” method for closure of abdominal-wall defects: an anatomic and clinical study. Plast Reconstr Surg 1990;86:519-526.
(10) Lochs H, Allison SP, Meier R, Pirlich M, Kondrup J, Schneider S, et al. Introductory to the ESPEN Guideli-nes on Enteral Nutrition: Terminology, definitions and general topics. Clin Nutr 2006;25:180-186.
(11) Cassar K, Munro A. Surgical treatment of incisional hernia. Br J Surg 2002;89:534-545.
Wind (Chris).indb 175Wind (Chris).indb 175 28-05-2008 15:44:5128-05-2008 15:44:51
176
(12) Burger JW, Luijendijk RW, Hop WC, Halm JA, Verdaasdonk EG, Jeekel J. Long-term follow-up of a rando-mized controlled trial of suture versus mesh repair of incisional hernia. Ann Surg 2004;240:578-583.
(13) de Vries Reilingh TS, van Goor H, Charbon JA, Rosman C, Hesselink EJ, van der Wilt GJ, et al. Repair of giant midline abdominal wall hernias: “components separation technique” versus prosthetic repair : interim analysis of a randomized controlled trial. World J Surg 2007;31:756-763.
(14) Lowe JB III, Lowe JB, Baty JD, Garza JR. Risks associated with “components separation” for closure of complex abdominal wall defects. Plast Reconstr Surg 2003;111:1276-1283.
(15) van Geffen HJ, Simmermacher RK, van Vroonhoven TJ, van der Werken C. Surgical treatment of large contaminated abdominal wall defects. J Am Coll Surg 2005;201:206-212.
(16) Alaedeen DI, Lipman J, Medalie D, Rosen MJ. The single-staged approach to the surgical management of abdominal wall hernias in contaminated fields. Hernia 2007;11:41-45.
(17) Shestak KC, Edington HJ, Johnson RR. The separation of anatomic components technique for the recon-struction of massive midline abdominal wall defects: anatomy, surgical technique, applications, and limitations revisited. Plast Reconstr Surg 2000;105:731-738.
(18) Saulis AS, Dumanian GA. Periumbilical rectus abdominis perforator preservation significantly redu-ces superficial wound complications in “separation of parts” hernia repairs. Plast Reconstr Surg 2002;109:2275-2280.
(19) Maas SM, van Engeland M, Leeksma NG, Bleichrodt RP. A modification of the “components separation” technique for closure of abdominal wall defects in the presence of an enterostomy. J Am Coll Surg 1999;189:138-140.
(20) Jernigan TW, Fabian TC, Croce MA, Moore N, Pritchard FE, Minard G, et al. Staged management of giant abdominal wall defects: acute and long-term results. Ann Surg 2003;238:349-355.
(21) Geisler DJ, Reilly JC, Vaughan SG, Glennon EJ, Kondylis PD. Safety and outcome of use of nonab-sorbable mesh for repair of fascial defects in the presence of open bowel. Dis Colon Rectum 2003;46:1118-1123.
(22) Birolini C, Utiyama EM, Rodrigues AJ Jr., Birolini D. Elective colonic operation and prosthetic repair of incisional hernia: does contamination contraindicate abdominal wall prosthesis use? J Am Coll Surg 2000;191:366-372.
(23) Patton JH Jr., Berry S, Kralovich KA. Use of human acellular dermal matrix in complex and contaminated abdominal wall reconstructions. Am J Surg 2007;193:360-363.
(24) Schuster R, Singh J, Safadi BY, Wren SM. The use of acellular dermal matrix for contaminated abdomi-nal wall defects: wound status predicts success. Am J Surg 2006;192:594-597.
Wind (Chris).indb 176Wind (Chris).indb 176 28-05-2008 15:44:5128-05-2008 15:44:51

Part3Prognostication in
colorectal cancer
Wind (Chris).indb 177Wind (Chris).indb 177 28-05-2008 15:44:5128-05-2008 15:44:51

Wind (Chris).indb 178Wind (Chris).indb 178 28-05-2008 15:44:5128-05-2008 15:44:51

12Chapter
A systematic review on the significance of extracapsular lymph node involvement
in gastrointestinal malignancies
J Wind
SM Lagarde
FJW ten Kate
DT Ubbink
WA Bemelman
JJB van Lanschot
European Journal of Surgical Oncology 2007;33:401-408
Wind (Chris).indb 179Wind (Chris).indb 179 28-05-2008 15:44:5128-05-2008 15:44:51

180180
Abstract
IntroductionThe impact of extracapsular lymph node involvement has been studied for several
malignancies, including gastrointestinal malignancies. Aim of this study was to assess
the current evidence on extracapsular lymph node involvement as a prognostic factor for
recurrence in gastrointestinal malignancies.
MethodsThe Cochrane Database of systematic reviews, the Cochrane central register of controlled
trials, and MEDLINE databases were searched using a combination of keywords relating to
extracapsular lymph node involvement in gastrointestinal malignancies. Primary outcome
parameters were incidence of extracapsular lymph node involvement and overall five-year
survival rates.
ResultsFourteen manuscripts were included, concerning seven oesophageal, three gastric, one
colorectal, and three rectal cancer series with a total of 1528 node positive patients. The
pooled incidence of extracapsular lymph node involvement was 57% (95% confidence
interval [CI]: 53-61%) for oesophageal cancer, 41% (95% CI: 36-47%) for gastric cancer,
and 35% (95% CI: 31-40%) for rectal cancer. In nine of the 14 studies a multivariate analysis
was performed. In eight of these nine studies extracapsular lymph node involvement was
identified as an independent risk factor for recurrence.
ConclusionExtracapsular lymph node involvement is a common phenomenon in patients with
gastrointestinal malignancies. It identifies a subgroup of patients with a significantly
worse long-term survival. This systematic review highlights the importance of assessing
extracapsular lymph node involvement as a valuable prognostic factor. Pathologists and
clinicians should be aware of this important feature.
Wind (Chris).indb 180Wind (Chris).indb 180 28-05-2008 15:44:5128-05-2008 15:44:51

181
Ch
apter 12
Extracapsular lymph no
de involvement in gastrointestinal m
alignanies
Introduction
The presence and extent of lymphatic dissemination are among the most important
predictors for survival in gastrointestinal malignancies.1-4 Lymph node staging may be
further refined by the identification of different levels (i.e. proximate versus remote lymph
node stations), the absolute number of metastatic lymph nodes and/or the lymph node
ratio (i.e. the number of involved nodes over the total number of resected and identified
nodes).5-7 Furthermore, micro-metastasis defined as isolated tumour cells or small clusters
of cells, detected in lymph nodes, has also been identified as a prognostic factor.8
Extracapsular lymph node involvement is the extension of cancer cells through the nodal
capsule into the perinodal fatty tissue. The prognostic value of extracapsular lymph
node involvement has been studied for several malignancies, including breast, prostate,
vulva, bladder, lung, and head/neck cancer.9-15 Patients with extracapsular lymph node
involvement have a reduced overall and disease-free survival in these malignancies.9-15
However, in gastrointestinal malignancies, the prognostic value of extracapsular lymph
node involvement has not yet been completely established. The ability of cancer cells
not only to spread into a lymph node but also to invade through the lymph node capsule
in an immunologically hostile environment, probably reflects the invasiveness and thus
aggressiveness of the primary tumour.16;17
Only a limited number of small studies have been published on extracapsular lymph node
involvement, mainly concerning oesophageal, gastric, and rectal cancer.5;18-22 In the
majority of these studies extracapsular lymph node involvement was demonstrated to have
a negative effect on local control, disease-free and overall survival.5;18-22 Nonetheless, its
exact incidence is unclear. Moreover, it is as yet unknown if extracapsular lymph node
involvement is an early or late event in cancer progression. It has not been established
if extracapsular lymph node involvement is associated with local or haematogenous
recurrences.
Detection and quantification of extracapsular lymph node involvement in the surgical
resection specimen of gastrointestinal malignancies might be helpful not only for staging
purposes, but also for the stratification in future clinical trials and to individualize future
adjuvant strategies. Therefore, we performed a systematic review in order to assess
the incidence and extent of extracapsular lymph node involvement in gastrointestinal
malignancies. Furthermore, the relation between extracapsular lymph node involvement
and clinico-pathological factors, its prognostic value, its effect on the type of recurrence
and on long term survival were evaluated.
Wind (Chris).indb 181Wind (Chris).indb 181 28-05-2008 15:44:5228-05-2008 15:44:52

182
Methods
Literature searchThe Cochrane Database of systematic reviews, the Cochrane central register of controlled
trials, and MEDLINE databases were searched by using keywords related to extracapsular
lymph node involvement in gastrointestinal malignancies (Table 1) in order to identify
studies published up to May 2006. Two investigators (JW, SML) independently performed
the literature search. Electronic links to related articles and references of selected
articles were hand-searched as well. A hand search of relevant journals and conference
proceedings was not performed. The search was not restricted to any language, however
in the systematic review only studies published in English were taken into account.
Table 1. Search terms, as used in the systematic review
Search terms
MeSH: Not usedFree Text words: (extracapsular OR extranodal OR perilymphatic) AND (esophagus OR esophageal OR
oesophagus OR oesophageal OR stomach OR gastric OR junction OR liver OR pancreas OR pancreatic OR bile OR gallbladder OR peri ampullary OR Vater OR duodenum OR duodenal OR jejunum OR jejunal OR ileum OR ileal OR ileocolic OR papil OR bowel OR colon OR colonic OR rectum OR rectal OR colorectal)
Field: All Fields Limits: None
MeSH: medical subject headings
Study selection and data extractionFrom the potentially eligible publications only studies were included if they reported on
extracapsular lymph node involvement in gastrointestinal malignancies. Lympho-proliferative
disorders (e.g. Hodgkin disease, MALT lymphomas) and other rare malignancies located
in the gastrointestinal tract were excluded. Studies were included if they formulated a
clear definition of extracapsular lymph node involvement. The definition of extracapsular
lymph node involvement should include the extension of malignant cells through the
nodal capsule into the perinodal fatty tissue. Studies reporting exclusively on deposits of
metastatic cells without any recognizable lymph node structure were excluded.
The same two investigators independently extracted the following data, if reported, from
the original studies using a preformatted sheet; incidence of extracapsular lymph node
involvement, pTNM-stage, differentiation grade, radicality of resection, total number of
resected and identified lymph nodes, total number of positive lymph nodes, location
of positive nodes, lymphatic- and blood vessel invasion, perineural invasion, and finally
disease-free and/or overall survival rates. Furthermore, if possible the type of recurrence
was assessed in terms of loco-regional and/or distant (haematogenous) recurrence.
Duplicate publications and papers that reported on (parts of) the same study population
were excluded. In that situation only the largest or most recent publication was included.
Each of the selected studies was critically appraised by the two investigators, using a
modified form as proposed by the Dutch Cochrane Collaboration23 and assessed if a
Wind (Chris).indb 182Wind (Chris).indb 182 28-05-2008 15:44:5228-05-2008 15:44:52

183
Ch
apter 12
Extracapsular lymph no
de involvement in gastrointestinal m
alignanies
study was; randomised, consecutive, prospective or retrospective, had similar groups, and
if there was an adequate follow-up. In case of retrospective analysis of data collected
prospectively, a study was defined as prospective. Final inclusion was done after consensus
was reached. Discrepancies in judgment, if any, were resolved by discussion between the
authors.
Analysis and presentation of dataThe incidence of extracapsular lymph node involvement was calculated by the number
of patients with extracapsular lymph node involvement divided by the number of node
positive patients. Subsequently a weighted incidence with a 95% confidence interval (CI)
was calculated for each type of gastrointestinal malignancy. Survival rates were expressed
as overall- and disease-free five-year survival. The prognostic value of extracapsular lymph
node involvement in uni- and in multivariate analyses as reported in the original studies,
were expressed as a P-value and reported as a relative risk (RR), odds ratio (OR) or hazard
ratio (HR). Hazard or odds ratios and corresponding standard errors of the original
studies, corrected for other possible prognostic factors, were entered into Cochrane
Review Manager 4.2 software and analysed using RevMan Analyses 1.0.2 (The Cochrane
Collaboration, Oxford, UK). Summary estimates of prognostic significance, including 95%
CI, were calculated for the comparison of intracapsular lymph node involvement versus
extracapsular lymph node involvement. A weighted HR was calculated in the meta-analysis
using the inverse variance method. Statistical heterogeneity was tested using Chi-square
and I-square statistics.
Results
Included studiesThe searches identified 34 publications, of which 20 were excluded; six manuscripts were
excluded because they did not report on extracapsular lymph node involvement.24-29
Four were excluded because of an unclear definition of extracapsular lymph node
involvement30-33, seven because they reported on extranodal tumour deposits rather than
on extracapsular lymph node involvement.34-40 Subsequently, three manuscripts were
excluded because they were written in Japanese.41-43
In the final analysis 14 studies were included which have been published between 1963
and 2006, with a total of 1528 node positive patients, with a range of 28 to 251 node
positive patients per study.5;18-22;44-51 There were seven studies reporting on oesophageal
cancer20;22;44;45;47;49;51, three on gastric5;21;48, one on colorectal46, and three on rectal
cancer18;19;50 (Table 2).
The included studies had several limitations (Table 2). It concerned mostly retrospective
single-centre studies with generally small or moderate sample sizes. Only four studies had
a prospective study design.19;21;47;51 Furthermore, in half of the included studies it was not
clear if the patients were of a consecutive series.5;21;22;45;48;50;51
Wind (Chris).indb 183Wind (Chris).indb 183 28-05-2008 15:44:5228-05-2008 15:44:52

184
Table 2. Study designs of the 14 studies included in the systematic review
Study Year R/P Consecutive Inclusioncriteria
Oesophageal
Lagarde47 2006 P yes Curative surgery for adenocarcinoma of the distal oesophagus and GO-junction, node positive, including M1lym, transhiatal and transthoracic.
D’Journo51 2005 P - Transthoracic oesophagectomy for adenocarcinoma of the lower oesophagus (Siewert I/II).
Lerut49 2003 R yes Node positive T3 adenocarcinoma of the oesophagus or GO-junction.
Tachikawa20 1999 R yes Node positive oesophageal cancer with or without (neo) adjuvant therapy.
Nakano22 1999 R - Node positive carcinoma of the thoracic oesophagus.
Paraf45 1995 R - Adenocarcinoma arising in Barrett segment including patients with distant metastasis. None received radiotherapy.
Gatzinsky44 1985 R yes Surgically treated oesophageal cancer.
Gastric
Nakamura21 2005 P - Curative gastrectomy with D2 or D3 lymphadenectomy.
Di Giorgio51 1991 R - Elective total gastrectomy for node positive adenocarcinoma with curative intent.
Zacho48 1963 R - Gastric cancer, also palliative resection.
Rectal
Heide18 2004 R yes Stage II/III rectal, postoperative radiochemotherapy. Preoperative staging by ultrasonography/ CT scan and chest X-ray.
Lupatelli19 2001 P yes Stage II/III radically resected rectal adenocarcinoma ≤ 15 cm from the anal verge, capable to tolerate adjuvant therapy.
Ueno50 1998 R - Curative surgery for rectal adenocarcinoma.
Colorectal
Komuta46 2001 R yes Colorectal Dukes C carcinoma.
P: prospective; R: retrospective; CIS: carcinoma in situ; M1lym: distant lymph node metastasis; GO-junction: gastro-oesophageal junction; -: not reported or not clear.
Wind (Chris).indb 184Wind (Chris).indb 184 28-05-2008 15:44:5228-05-2008 15:44:52

185
Ch
apter 12
Extracapsular lymph no
de involvement in gastrointestinal m
alignanies
Exclusioncriteria
Follow-up(months)
Definition of extracapsular LNI
Direct postoperative deaths,residual disease. Other cancers than adenocarcinoma
> 12median 58
Extension through capsule into perinodal tissue. Deposits without a recognizable lymph node were considered as extracapsular LNI unless associated with perineural or vessel involvement.
- - Cells breaching the lymph node capsule.
Neo-adjuvant therapy, residual disease, organ metastasis, no lymphadenectomy.
Tumoural expansion that outgrows the node and extends beyond the capsule, not in afferent lymphatic vessels
- - Metastasis penetrating the capsule or accompanied by nodules such as extracapsular vessel invasion.
Residual disease, direct postoperative deaths.
18-166 Cancer cells in the perinodal soft tissue, lymphatic vessel invasion included.
Squamous cell carcinoma, CIS or dysplasia only.
> 24median 52
Invasion of the adipose tissue located beyond the nodal capsule.
- 24-144 Perinodular growth in metastatic lymph nodes.
Non curative resections, metastasis, specific types of gastric cancer.
> 21 Cancer cells beyond the capsule, excluding micro dissemination or vessel invasion in the adjacent tissues without spread through the capsule.
Stage T4 and M1. > 10 Infiltration of the capsule and extension beyond it by neoplastic tissue.
Multiple metastasis, anaplastic carcinoma.
- Penetration of the capsule and invasion of surrounding tissue.
- 14-104median 47
Extracapsular extension of lymph node metastasis.
Contraindications for adjuvant therapy, previous chemo- or radiotherapy, other malignancies, residual disease.
> 24median 57
Cells breaching the lymph node capsule.
Direct postoperative deaths,Follow-up less than 3 years
> 3 Cells breaching the capsule and spreading into the perinodal fatty tissue.
Neo-adjuvant therapy 36-108 Cancer cells invading the surrounding tissue of metastatic nodes, subdivided in less or more than five cells.
Wind (Chris).indb 185Wind (Chris).indb 185 28-05-2008 15:44:5228-05-2008 15:44:52

186
In only three studies the histological sections were screened for extracapsular lymph node
involvement by more than one researcher or pathologist.45;46;49 In general, the studies
applied variable in- and exclusion criteria with respect to the type and stage of tumours
and the use of (neo-) adjuvant therapies. Concerning oesophageal cancer, D’Journo et
al. applied neo-adjuvant therapy in half of the patients and Gatzinsky et al. in a few
patients44;51, while Tackikawa et al. applied both neo-adjuvant and adjuvant therapy in
most patients.20 Concerning rectal cancer, Heide et al. and Lupatelli et al. gave adjuvant
therapy to all patients.18;19
Furthermore, besides the extension of malignant cells through the capsule of a metastatic
lymph node, some studies included large deposits without a recognizable lymph node47,
or involvement of afferent lymphatic vessels adjacent to the lymph node20;22, while
others explicitly excluded lymphatic vessel invasion.21;47;49 Only Komuta et al. gave a
quantification of the extent of extracapsular lymph node involvement (i.e. more or less
than five cells invading the perinodal tissue; Table 2).46 Finally, only three studies provided
some detailed information on the prognostic value of the number of lymph nodes with
extracapsular lymph node involvement.20;47;49
Oesophageal cancerBoth squamous cell and adenocarcinomas of the oesophagus were included in the
present review. Four studies exclusively reported on adenocarcinomas45;47;49;51, one study
included both adenocarcinomas and squamous cell carcinomas44 and in two studies the
histological type was not stated.20;22 Six of the seven studies on oesophageal cancer
reported on the incidence of extracapsular lymph node involvement which ranged from
39% to 66% (Table 3).20;22;44;45;47;49 The pooled incidence for extracapsular lymph
node involvement in oesophageal cancer was 57% (95% CI: 53-61%).20;22;44;45;47;49 The
pooled incidence for extracapsular lymph node involvement in the studies that exclusively
reported on the extension of malignant cells through the capsule of a metastatic lymph
node and did not include vessel invasion and isolated deposits was comparable (61%; 95%
CI: 55-67%).44;45;49
Four of the seven studies related extracapsular lymph node involvement to various clinico-
pathological factors.20;44;45;47;49 Extracapsular lymph node involvement was significantly
related to transthoracic oesophagectomy47, T-stage20;44;47, N-stage20;47, number of positive
nodes20;47, lymph node ratio47, and degree of lymphatic20 and blood vessel invasion.45
Five of the seven studies reported on the five-year overall survival which ranged from 33%
to 53% for node positive patients with only intracapsular lymph node involvement and from
0% to 23% for patients with extracapsular lymph node involvement (Table 3).20;22;45;47;49
Lerut et al. and Lagarde et al. reported that patients with only one positive node identified
had a significantly worse five-year survival if extracapsular lymph node involvement was
present compared to patients in whom the tumour was confined within the lymph node
(33% vs. 86% and 20% vs. 60%, respectively).47;49 Furthermore, Lagarde et al. divided
patients with extracapsular lymph node involvement in three subgroups; patients with
only intracapsular lymph node involvement, patients with one node with extracapsular
Wind (Chris).indb 186Wind (Chris).indb 186 28-05-2008 15:44:5228-05-2008 15:44:52

187
Ch
apter 12
Extracapsular lymph no
de involvement in gastrointestinal m
alignanies
lymph node involvement and patients with two or more nodes with extracapsular lymph
node involvement. Compared to only intracapsular lymph node involvement, one node
and two or more nodes with extracapsular lymph node involvement were independent
prognostic factors with HR of 1.6 (95% CI: 1.1-2.4) and 3.7 (95% CI: 2.5-5.3), respectively
(personal communication). Patients who had two or more lymph nodes with extracapsular
lymph node involvement had a median survival of 12 months compared to 21 months in
patients who had only one lymph node with extracapsular lymph node involvement. Only
one of the 102 patients with two or more lymph nodes with extracapsular lymph node
involvement survived for more than five years.47 Finally, Tachikawa et al. found a better
survival, although not statistically significant, of patients with three or more positive lymph
nodes with only intracapsular lymph node involvement compared to those patients with
three or more positive nodes with extracapsular lymph node involvement.20
Nakano et al. found that 60% of the patients with extracapsular lymph node involvement
in the neck and/or upper mediastinum had a local recurrence in that region compared
to 21% of the patients without extracapsular lymph node involvement.22 Lagarde et
al. reported no difference in recurrence pattern between patients with and without
extracapsular lymph node involvement.47
In five studies a multivariate analysis was performed. In four of these studies, extracapsular
lymph node involvement was identified as an independent prognostic factor (Table
3).45;47;49;51 Pooling could not be performed because of different ways of reporting and
because standard deviations or 95% CIs were missing.
Gastric cancerBoth intestinal and diffuse type carcinomas of the stomach were included in the present
review. All three studies reported on the incidence of extracapsular lymph node involvement
which ranged from 29% to 58% (Table 3).5;21;48 The pooled incidence of extracapsular
lymph node involvement in gastric cancer was 41% (95% CI: 36-47%).5;21;48
In the study by Nakamura et al. extracapsular lymph node involvement was significantly
related to N-stage and serosal invasion of the tumour.21 In the study by Di Giorgio et al.
extracapsular lymph node involvement was significantly related to T-stage, N-stage, and
number of resected lymph nodes.5
The five-year overall survival ranged from 35% to 61% for node positive patients without
extracapsular lymph node involvement and from 5% to 23% for patients with extracapsular
lymph node involvement (Table 3).5;21;48
In two studies a multivariate analysis was performed, in both of which extracapsular
lymph node involvement was identified as an independent prognostic factor (Table 3).5;21
Nakamura et al. reported a RR of 6.9 (95% CI: 3.1-15.2) for the comparison of node
positive patients with or without extracapsular lymph node involvement.21 Pooling could
not be performed because only a few studies reported this outcome and if reported at
all they did this in different ways and with standard deviations or 95% CIs frequently
missing.
Wind (Chris).indb 187Wind (Chris).indb 187 28-05-2008 15:44:5328-05-2008 15:44:53

188
Table 3. Number of node positive patients, incidence of extracapsular lymph node involvement, and the prognostic significance of extracapsular lymph node involvement in uni- and multivariate analyses in the 14 included studies in the systematic review
Study Number of node positive patients
IncidenceELNI (%)
P-valueunivariate
Reported OR, RR or HR with 95%-CI
P-valuemultivariate
Oesophageal
Lagarde47 251 66 <0.001 HR 2.06 (1.45-2.93) <0.001
D’Journo51 28 - 0.02 OR 5.9 (1.0-32.0) 0.04
Lerut49 162 63 0.0001 HR 3.37 (1.75-6.49) 0.0003
Tachikawa20 46 39 <0.01 - -
Nakano22 159 41 0.012 - NS
Paraf45 34 65 <0.001 - sign
Gatzinsky44 43 51 - - -
Gastric
Nakamura21 135 29 <0.0001 RR 6.9 (3.1-15.2) <0.0001
Di Giorgio5 121 52 <0.05 - <0.01
Zacho48 47 58 - - -
Rectal
Heide18 96 33 0.041 RR 1.6 (1.01-2.7)† 0.044†
Lupatelli19 105 18 <0.0001 - <0.0001
Ueno50 217 45 - - -
Colorectal
Komuta46 84 55 <0.01 - -
ELNI: extracapsular lymph node involvement; OR: odds ratio; RR: relative risk; HR: hazard ratio; 95%-CI: 95% confidence interval †: for local control; -: not reported; sign: significant, no precise p-value given
(Colo)rectal cancerThe study of Komuta et al. was the only one reporting on extracapsular lymph node
involvement both in colon and in rectal cancer.46 The incidence of extracapsular lymph
node involvement in that study was 55%. They reported that extracapsular lymph node
involvement was seen more often in nodes that were occupied for more than 50% by cancer
cells compared to nodes with less than 50% occupation. Only nodes that were occupied
for more than 50% sometimes showed more than five cells invading the surrounding
tissue. Overall- and disease-free survival are indicated in Table 4. In patients without
extracapsular lymph node involvement, distant metastases were more frequent than local
recurrence (16% vs. 8%). For patients with extracapsular lymph node involvement, the risk
for local recurrence and distant metastases were comparable (35% vs. 43%).46
There were three studies reporting exclusively on rectal cancer with an incidence of
extracapsular lymph node involvement ranging from 18% to 45% (Table 3).18;19;50 The
pooled incidence of extracapsular lymph node involvement in rectal cancer was 35% (95%
CI: 31-40%).18;19;50
In the study by Heide et al. extracapsular lymph node involvement was significantly related
to a higher T- and N-stage, to the presence of lymphatic vessel involvement, and to a
lower differentiation grade.18 In the study by Ueno et al. the incidence of microscopic
Wind (Chris).indb 188Wind (Chris).indb 188 28-05-2008 15:44:5328-05-2008 15:44:53

189
Ch
apter 12
Extracapsular lymph no
de involvement in gastrointestinal m
alignanies
tumoural foci discontinuous with the primary lesion was significantly higher in patients
with extracapsular lymph node involvement.50
Five-year overall and disease-free survival are shown in Table 4. In two studies a multivariate
analysis was performed and in both studies extracapsular lymph node involvement was
identified as an independent prognostic factor.18;19 In the study by Heide et al. the
value of extracapsular lymph node involvement for the assessment of local failure risk
was confirmed in the Cox regression model, which revealed extracapsular lymph node
involvement as an independent prognostic factor (RR 1.6, 95% CI: 1.01–2.7). For distant
failure, however, extracapsular lymph node involvement did not independently predict
outcome.18 Pooling could not be performed because only a few studies reported this
outcome and if reported at all, they did this in different ways and with standard deviations
or 95% CIs frequently missing.
Table 4. The overall- and disease-free survival rates of node negative patients and node positive patients without and with extracapsular lymph node involvement as reported in the 14 included studies in the systematic review.
Study Node negative patientsoverall-/disease-free survival (5 years, %)
Node positive patients, no ELNI
overall-/disease-free survival (5 years, %)
Node positive patients with ELNI
overall-/disease-free survival (5 years, %)
Oesophageal
Lagarde47 - 44 / - 12 / -
D’Journo51 - - -
Lerut49 57 / - 40.9 / - 18 / -
Tachikawa20 - 53.3 / - 0 / -
Nakano22 - 39.4 / - 23.2 / -
Paraf45 56 / - 33 / - 0* / -
Gatzinsky44 - - -
Gastric
Nakamura21 91 / - 61 / - 23 / -
Di Giorgio5 - 44.8 / - 17.5 / -
Zacho48 38 / - 35 / - 5 / -
Rectal
Heide18 - / 83† - / 87† - / 58†
Lupatelli19 87 / 84 76.1 / 70.7 33.8 / 31.6
Ueno50 - 62 / - 44 / -
Colorectal
Komuta46 - 81 / 76 30-33‡ / 18-30‡
ELNI: extracapsular lymph node involvement; †: local control; *: no survivors at 2 years; -: not reported; ‡: more or less than five cells invading the surrounding tissue respectively
Wind (Chris).indb 189Wind (Chris).indb 189 28-05-2008 15:44:5328-05-2008 15:44:53

190
Discussion
The presence of extracapsular lymph node involvement harbours important prognostic
information. The present review emphasizes that extracapsular lymph node involvement is a
common phenomenon in patients with gastrointestinal malignancies. The pooled incidence
for oesophageal cancer was 57%, for gastric cancer 41%, and for rectal cancer 35%.
Furthermore, in all gastrointestinal malignancies, extracapsular lymph node involvement
identifies a subgroup of patients with a significantly worse long-term survival.
Extracapsular lymph node involvement probably is a late event in cancer progression
and reflects an advanced tumour stage. In several studies there was a higher chance
for extracapsular lymph node involvement with higher T-stage5;18;20;21;44;47, and with
higher N-stage.5;18;20;21;47 There was also a correlation between extracapsular lymph
node involvement and the number of positive nodes resected5;20;47 or lympho-vascular
invasion.18;20;45 However, in spite of this correlation with other well known prognostic
factors, extracapsular lymph node involvement was identified as an independent
prognosticator. In eight of the nine studies in which a multivariate analysis was performed
extracapsular lymph node involvement was a highly significant independent prognostic
factor.5;18;19;21;45;47;49;51
The prognostic significance is further highlighted by studies that reported comparable
survival in patients without lymph node involvement and patients with only intracapsular
lymph node involvement which is in contrast to the major decrease in survival observed
in patients with extracapsular lymph node involvement. This suggests that lymphatic
dissemination does not essentially deteriorate prognosis, provided that the lymph node
capsule remains intact.18;19;48;49 Furthermore, in patients with involvement of only one
single positive lymph node, extracapsular lymph node involvement was correlated with a
significantly worse prognosis.47;49
The results of this review supports the results of our earlier study on oesophageal
cancer also included in this review.47 However, the precise causative factor of this worse
prognosis is not yet clear. It could be hypothesized that extracapsular lymph node
involvement reflects the invasiveness and aggressiveness of the primary tumour, even in
an immunologically hostile environment. Another hypothesis could be that extracapsular
lymph node involvement reflects an extensive lymphatic spread which can lead to lymphatic
obstruction. It has been reported that lymphatic obstruction results in an aberrant flow
of lymph fluid leading to lymphaticovenous communication and thus to haematogenous
dissemination.52-54
This systematic review has several limitations. First, it comprises mostly single-centre
studies with generally small or moderate sample sizes, with mostly retrospective designs,
and in half of the included studies it was not clear if it concerned a consecutive series of
patients. In general, the studies applied different in- and exclusion criteria concerning type
and stage of tumours and the use of (neo-) adjuvant therapies. For oesophageal cancer
no correlation could be identified between extracapsular lymph node involvement and
histological type (i.e. squamous cell carcinoma versus adenocarcinoma). Also for gastric
Wind (Chris).indb 190Wind (Chris).indb 190 28-05-2008 15:44:5328-05-2008 15:44:53

191
Ch
apter 12
Extracapsular lymph no
de involvement in gastrointestinal m
alignanies
cancer such correlation could not be identified (i.e. intestinal type versus diffuse type).
Furthermore, only a few studies reported on the recurrence pattern.
A difficulty in assessing extracapsular lymph node involvement is the presence of
extranodal deposits which are discontinuous with the primary tumour. These deposits
have been identified in many gastrointestinal malignancies.36-40 It is unclear whether these
are lymph nodes that have been completely replaced by tumour tissue or manifestations
of multifocal metastatic disease.39 Tumour cells might be released from a primary lesion
and subsequently spread directly into the extranodal and extramural spaces. Alternatively,
extranodal deposits might occur subsequent to lymph node involvement as the ultimate
form of extracapsular lymph node involvement.40 In our systematic review the definition of
extracapsular lymph node involvement had to include the infiltration of cancer cells beyond
the capsule of the metastatic lymph node. However, besides that there was no uniform
definition; some studies included micro dissemination in adjacent tissues, while others
included deposits without a recognizable lymph node or involvement of afferent lymphatic
vessels adjacent to the lymph node. Nonetheless, no obvious differences were observed in
the incidence and prognostic significance between those studies that exclusively reported
on the extension of malignant cells through the capsule of a metastatic lymph node and
those studies that included vessel invasion and isolated deposits as well. However, the
number of studies was too small to be confirmative on this topic.
Furthermore, it is unclear if, and to which extent, there is an inter-observer variability
of the assessment of extracapsular lymph node involvement. In only three studies the
histological sections were screened for extracapsular lymph node involvement by more
than one researcher.45;46;49 In general, extracapsular lymph node involvement is often
associated with a desmoplastic reaction. Sometimes this reaction is so extensive that the
presence or absence of extracapsular lymph node involvement is difficult to interpret. In
cases of such difficulties an imaginary line that represents the pre-existing capsule can be
drawn to facilitate the interpretation.47
Detection and quantification of extracapsular lymph node involvement in the surgical
resection specimen of gastrointestinal malignancies might be helpful to individualize
postoperative therapeutic strategies in the adjuvant setting in patients in whom the
indication for adjuvant chemotherapy is not yet already been established based on
other pathological factors. To facilitate a tailored approach in the neo-adjuvant setting
it would be necessary to discriminate preoperatively between positive nodes with and
without extracapsular lymph node involvement. In this respect, the diagnostic accuracy of
endosonography, computer tomography and magnetic resonance imaging has only been
tested in small studies, without convincing results so far.49;55-57
However, the effect of (neo-) adjuvant therapy on the presence of extracapsular lymph
node involvement and its prognosis remains unclear because many studies did not include
patients who received such therapy.
In conclusion, based on the limited evidence available it can be concluded that extracapsular
lymph node involvement is a common phenomenon in patients with gastrointestinal
malignancies. It identifies a subgroup of patients with a significantly worse long-term
Wind (Chris).indb 191Wind (Chris).indb 191 28-05-2008 15:44:5328-05-2008 15:44:53

192
survival. This systematic review highlights the importance of assessing extracapsular
lymph node involvement as a valuable prognostic factor. Pathologists and clinicians
should be aware of this important feature. Further research is, however, warranted on
the correlation of extracapsular lymph node involvement with different histological types
(e.g. squamous cell carcinoma versus adenocarcinoma) and other important covariates,
such as the recurrence pattern and the effect of (neo-) adjuvant therapy. Possibly, in future
staging systems, not only the number of positive nodes and the lymph node ratio but also
the presence and number of lymph nodes with extracapsular lymph node involvement
should be considered.
Reference List
(1) de Manzoni G, Pedrazzani C, Verlato G, Roviello F, Pasini F, Pugliese R, et al. Comparison of old and new TNM systems for nodal staging in adenocarcinoma of the gastro-oesophageal junction. Br J Surg 2004;91:296-303.
(2) Eloubeidi MA, Desmond R, Arguedas MR, Reed CE, Wilcox CM. Prognostic factors for the survival of patients with esophageal carcinoma in the U.S.: the importance of tumor length and lymph node status. Cancer 2002;95:1434-1443.
(3) Korst RJ, Rusch VW, Venkatraman E, Bains MS, Burt ME, Downey RJ, et al. Proposed revision of the staging classification for esophageal cancer. J Thorac Cardiovasc Surg 1998;115:660-669.
(4) Nigro JJ, DeMeester SR, Hagen JA, DeMeester TR, Peters JH, Kiyabu M, et al. Node status in transmural esophageal adenocarcinoma and outcome after en bloc esophagectomy. J Thorac Cardiovasc Surg 1999;117:960-968.
(5) Giorgio DA, Botti C, Sammartino P, Mingazzini P, Flammia M, Stipa V. Extracapsular lymph node metas-tases in the staging and prognosis of gastric cancer. Int Surg 1991;76:218-221.
(6) Pocard M, Panis Y, Malassagne B, Nemeth J, Hautefeuille P, Valleur P. Assessing the effectiveness of mesorectal excision in rectal cancer: prognostic value of the number of lymph nodes found in resected specimens. Dis Colon Rectum 1998;41:839-845.
(7) Siewert JR, Bottcher K, Stein HJ, Roder JD. Relevant prognostic factors in gastric cancer: ten-year results of the German Gastric Cancer Study. Ann Surg 1998;228:449-461.
(8) Izbicki JR, Hosch SB, Pichlmeier U, Rehders A, Busch C, Niendorf A, et al. Prognostic value of immuno-histochemically identifiable tumor cells in lymph nodes of patients with completely resected esophageal cancer. N Engl J Med 1997;337:1188-1194.
(9) Brasilino de CM. Quantitative analysis of the extent of extracapsular invasion and its prognostic signif-icance: a prospective study of 170 cases of carcinoma of the larynx and hypopharynx. Head Neck 1998;20:16-21.
(10) Fisher BJ, Perera FE, Cooke AL, Opeitum A, Dar AR, Venkatesan VM, et al. Extracapsular axillary node extension in patients receiving adjuvant systemic therapy: an indication for radiotherapy? Int J Radiat Oncol Biol Phys 1997;38:551-559.
(11) Fleischmann A, Thalmann GN, Markwalder R, Studer UE. Prognostic implications of extracapsular extension of pelvic lymph node metastases in urothelial carcinoma of the bladder. Am J Surg Pathol 2005;29:89-95.
(12) Griebling TL, Ozkutlu D, See WA, Cohen MB. Prognostic implications of extracapsular extension of lymph node metastases in prostate cancer. Mod Pathol 1997;10:804-809.
Wind (Chris).indb 192Wind (Chris).indb 192 28-05-2008 15:44:5428-05-2008 15:44:54

193
Ch
apter 12
Extracapsular lymph no
de involvement in gastrointestinal m
alignanies
(13) Myers JN, Greenberg JS, Mo V, Roberts D. Extracapsular spread. A significant predictor of treatment failure in patients with squamous cell carcinoma of the tongue. Cancer 2001;92:3030-3036.
(14) Ishida T, Tateishi M, Kaneko S, Sugimachi K. Surgical treatment of patients with nonsmall-cell lung cancer and mediastinal lymph node involvement. J Surg Oncol 1990;43:161-166.
(15) van der Velden J, van Lindert AC, Lammes FB, ten Kate FJ, Sie-Go DM, Oosting H, et al. Extracapsular growth of lymph node metastases in squamous cell carcinoma of the vulva. The impact on recurrence and survival. Cancer 1995;75:2885-2890.
(16) Stitzenberg KB, Meyer AA, Stern SL, Cance WG, Calvo BF, Klauber-DeMore N, et al. Extracapsular exten-sion of the sentinel lymph node metastasis: a predictor of nonsentinel node tumor burden. Ann Surg 2003;237:607-612.
(17) Lyons AJ, Bateman AC, Spedding A, Primrose JN, Mandel U. Oncofetal fibronectin and oral squamous cell carcinoma. Br J Oral Maxillofac Surg 2001;39:471-477.
(18) Heide J, Krull A, Berger J. Extracapsular spread of nodal metastasis as a prognostic factor in rectal cancer. Int J Radiat Oncol Biol Phys 2004;58:773-778.
(19) Lupattelli M, Maranzano E, Bellavita R, Tarducci R, Latini R, Castagnoli P, et al. Adjuvant radiochemother-apy in high-risk rectal cancer results of a prospective non-randomized study. Tumori 2001;87:239-247.
(20) Tachikawa D, Inada S, Kotoh T, Futami K, Arima S, Iwashita A. An evaluation of malignancy and prognostic factors based on mode of lymph node metastasis in esophageal carcinoma. Surg Today 1999;29:1131-1135.
(21) Nakamura K, Ozaki N, Yamada T, Hata T, Sugimoto S, Hikino H, et al. Evaluation of prognostic significance in extracapsular spread of lymph node metastasis in patients with gastric cancer. Surgery 2005;137:511-517.
(22) Nakano S, Baba M, Shimada M, Shirao K, Noguchi Y, Kusano C, et al. How the lymph node metastases toward cervico-upper mediastinal region affect the outcome of patients with carcinoma of the thoracic esophagus. Jpn J Clin Oncol 1999;29:248-251.
(23) Therapy checklist (Dutch extended version) of the Dutch Cochrane centre. www.cochrane.nl. 2005. Internet Communication
(24) Matsuda J, Kitagawa Y, Fujii H, Mukai M, Dan K, Kubota T, et al. Significance of metastasis detected by molecular techniques in sentinel nodes of patients with gastrointestinal cancer. Ann Surg Oncol 2004;11(3 Suppl):250S-254S.
(25) Natsugoe S, Matsushita Y, Kijima F, Tokuda K, Shimada M, Shirao K, et al. Diffusely infiltrative squamous cell carcinoma of the esophagus. Surg Today 1998;28:129-134.
(26) Graham RA, Hohn DC. Management of inguinal lymph node metastases from adenocarcinoma of the rectum. Dis Colon Rectum 1990;33:212-216.
(27) Rugge M, Sonego F, Panozzo M, Baffa R, Rubio J Jr., Farinati F, et al. Pathology and ploidy in the prog-nosis of gastric cancer with no extranodal metastasis. Cancer 1994;73:1127-1133.
(28) Nagtegaal ID, Marijnen CA, Kranenbarg EK, van de Velde CJ, van Krieken JH. Circumferential margin involvement is still an important predictor of local recurrence in rectal carcinoma: not one millimeter but two millimeters is the limit. Am J Surg Pathol 2002;26:350-357.
(29) Ueno H, Mochizuki H, Hatsuse K, Hase K, Yamamoto T. Indicators for treatment strategies of colorectal liver metastases. Ann Surg 2000;231:59-66.
(30) Tanaka T, Kumagai K, Shimizu K, Masuo K, Yamagata K. Peritoneal metastasis in gastric cancer with particular reference to lymphatic advancement; extranodal invasion is a significant risk factor for perito-neal metastasis. J Surg Oncol 2000;75:165-171.
(31) Kumagai K, Tanaka T, Yamagata K, Yokoyama N, Shimizu K. Liver metastasis in gastric cancer with particular reference to lymphatic advancement. Gastric Cancer 2001;4:150-155.
(32) Natsugoe S, Mueller J, Kijima F, Aridome K, Shimada M, Shirao K, et al. Extranodal connective tissue invasion and the expression of desmosomal glycoprotein 1 in squamous cell carcinoma of the oesopha-gus. Br J Cancer 1997;75:892-897.
Wind (Chris).indb 193Wind (Chris).indb 193 28-05-2008 15:44:5428-05-2008 15:44:54

194
(33) Baba M, Aikou T, Natsugoe S, Kusano C, Shimada M, Kimura S, et al. Lymph node and perinodal tissue tumor involvement in patients with esophagectomy and three-field lymphadenectomy for carcinoma of the esophagus. J Surg Oncol 1997;64:12-16.
(34) Beresford M, Glynne-Jones R, Richman P, Makris A, Mawdsley S, Stott D, et al. The reliability of lymph-node staging in rectal cancer after preoperative chemoradiotherapy. Clin Oncol (R Coll Radiol ) 2005;17:448-455.
(35) Abad M, Ciudad J, Rincon MR, Silva I, Paz-Bouza JI, Lopez A, et al. DNA aneuploidy by flow cytometry is an independent prognostic factor in gastric cancer. Anal Cell Pathol 1998;16:223-231.
(36) Ueno H, Mochizuki H, Fujimoto H, Hase K, Ichikura T. Autonomic nerve plexus involvement and progno-sis in patients with rectal cancer. Br J Surg 2000;87:92-96.
(37) Ishikawa K, Hashiguchi Y, Mochizuki H, Ozeki Y, Ueno H. Extranodal cancer deposit at the primary tumor site and the number of pulmonary lesions are useful prognostic factors after surgery for colorec-tal lung metastases. Dis Colon Rectum 2003;46:629-636.
(38) Ueno H, Mochizuki H, Shinto E, Hashiguchi Y, Hase K, Talbot IC. Histologic indices in biopsy speci-mens for estimating the probability of extended local spread in patients with rectal carcinoma. Cancer 2002;94:2882-2891.
(39) Prabhudesai A, Arif S, Finlayson CJ, Kumar D. Impact of microscopic extranodal tumor deposits on the outcome of patients with rectal cancer. Dis Colon Rectum 2003;46:1531-1537.
(40) Etoh T, Sasako M, Ishikawa K, Katai H, Sano T, Shimoda T. Extranodal metastasis is an indicator of poor prognosis in patients with gastric carcinoma. Br J Surg 2006;93:369-373.
(41) Yoon T. Mode of metastasis of dukes C colorectal cancer in lymph nodes. Journal of japan society of colo-protology 1997;50:331-338.
(42) Yoshinaka H, Shimazu H, Natsugoe S, Haraguchi Y, Shimada M, Baba M, et al. [Histopathological features of the lymph node metastases in patients with thoracic esophageal cancer]. Nippon Geka Gakkai Zasshi 1992;93:1289-1296.
(43) Watanabe H, Kato H, Tachimori Y, Yamaguchi H, Itababashi M. [Characteristics of the spread pattern in esophageal carcinoma]. Kyobu Geka 1989;42(8 Suppl):682-689.
(44) Gatzinsky P, Berglin E, Dernevik L, Larsson I, William-Olsson G. Resectional operations and long-term results in carcinoma of the esophagus. J Thorac Cardiovasc Surg 1985;89:71-76.
(45) Paraf F, Flejou JF, Pignon JP, Fekete F, Potet F. Surgical pathology of adenocarcinoma arising in Barrett’s esophagus. Analysis of 67 cases. Am J Surg Pathol 1995;19:183-191.
(46) Komuta K, Okudaira S, Haraguchi M, Furui J, Kanematsu T. Identification of extracapsular invasion of the metastatic lymph nodes as a useful prognostic sign in patients with resectable colorectal cancer. Dis Colon Rectum 2001;44:1838-1844.
(47) Lagarde SM, ten Kate FJ, de Boer DJ, Busch OR, Obertop H, van Lanschot JJ. Extracapsular lymph node involvement in node-positive patients with adenocarcinoma of the distal esophagus or gastroesopha-geal junction. Am J Surg Pathol 2006;30:171-176.
(48) Zacho A, Fischermann K, Sorensen BL. Prognostic role of breach of lymph node capsule in nodal metastates from gastric carcinoma. Acta Chir Scand 1963;125:365-369.
(49) Lerut T, Coosemans W, Decker G, De LP, Ectors N, Fieuws S, et al. Extracapsular lymph node involve-ment is a negative prognostic factor in T3 adenocarcinoma of the distal esophagus and gastroesopha-geal junction. J Thorac Cardiovasc Surg 2003;126:1121-1128.
(50) Ueno H, Mochizuki H, Tamakuma S. Prognostic significance of extranodal microscopic foci discontinu-ous with primary lesion in rectal cancer. Dis Colon Rectum 1998;41:55-61.
(51) D’Journo XB, Doddoli C, Michelet P, Loundou A, Trousse D, Giudicelli R, et al. Transthoracic esophagec-tomy for adenocarcinoma of the oesophagus: standard versus extended two-field mediastinal lymph-adenectomy? Eur J Cardiothorac Surg 2005;27:697-704.
Wind (Chris).indb 194Wind (Chris).indb 194 28-05-2008 15:44:5428-05-2008 15:44:54

195
Ch
apter 12
Extracapsular lymph no
de involvement in gastrointestinal m
alignanies
(52) Yamagata K, Kumagai K. Experimental study of lymphogenous peritoneal cancer dissemination: migra-tion of fluorescent-labelled tumor cells in a rat model of mesenteric lymph vessel obstruction. J Exp Clin Cancer Res 2000;19:211-217.
(53) Burn JI. Obstructive lymphopathy. Ann R Coll Surg Engl 1968;42:93-113.
(54) Yamagata K, Kumagai K, Shimizu K, Masuo K, Nishida Y, Yasui A. Gastrointestinal cancer metastasis and lymphogenous spread: viewpoint of animal models of lymphatic obstruction. Jpn J Clin Oncol 1998;28:104-106.
(55) Steinkamp HJ, Beck A, Werk M, Rademaker J, Felix R. [Extracapsular spread of cervical lymph node metastases: diagnostic relevance of ultrasound examinations]. Ultraschall Med 2003;24:323-330.
(56) Steinkamp HJ, Beck A, Werk M, Felix R. [Extracapsular spread of cervical lymph node metastases: Diag-nostic value of magnetic resonance imaging]. Rofo Fortschr Rontg 2002;174:50-55.
(57) Steinkamp HJ, van der Hoeck E, Bock JC, Felix R. [The extracapsular spread of cervical lymph node metastases: the diagnostic value of computed tomography]. Rofo Fortschr Rontg 1999;170:457-462.
Wind (Chris).indb 195Wind (Chris).indb 195 28-05-2008 15:44:5428-05-2008 15:44:54

196
Wind (Chris).indb 196Wind (Chris).indb 196 28-05-2008 15:44:5428-05-2008 15:44:54

13Chapter
The prognostic significance of extracapsular lymph node involvement in node positive patients with colonic cancer
J Wind
FJW ten Kate
JJS Kiewiet
SM Lagarde
JFM Slors
JJB van Lanschot
WA Bemelman
European Journal of Surgical Oncology 2008;34:390-396
Wind (Chris).indb 197Wind (Chris).indb 197 28-05-2008 15:44:5428-05-2008 15:44:54

198198
Abstract
IntroductionIn colonic cancer the prognostic significance of extracapsular lymph node involvement is
not established and is therefore the objective of this study.
MethodsBetween January 1994 and May 2005, all patients who underwent resection for primary
colonic cancer with lymph node metastasis were reviewed. All resected lymph nodes were
re-examined to assess extracapsular lymph node involvement. In uni- and multivariate
analysis disease free survival (DFS) was correlated with various clinicopathologic factors.
ResultsOne hundred eleven patients were included. In 58 patients extracapsular lymph node
involvement was identified. Univariate analysis revealed that pN-stage (5-year DFS pN1
vs. pN2; 65% vs. 14%, p<0.001), extracapsular lymph node involvement (5-year DFS
intracapsular lymph node involvement vs. extracapsular lymph node involvement; 69%
vs. 41%, p=0.003), and lymph node ratio (5-year DFS < 0.176 vs. ≥ 0.176; 67% vs. 42%,
p=0.023) were significant prognostic indicators. Among these variables pN-stage (hazard
ratio 3.5, 95% confidence interval [CI]: 1.72 – 7.42) and extracapsular lymph node
involvement (hazard ratio 1.98, 95% CI: 1.00 – 3.91) were independent prognostic factors.
Among patients without extracapsular lymph node involvement, those receiving adjuvant
chemotherapy had a significantly better survival (p=0.010). In contrast, chemotherapy did
not improve DFS in patients with extracapsular lymph node involvement.
ConclusionTogether with pN2 stage, extracapsular lymph node involvement reflects a particularly
aggressive behaviour and has significant prognostic potential.
Wind (Chris).indb 198Wind (Chris).indb 198 28-05-2008 15:44:5428-05-2008 15:44:54
199
Ch
apter 13
Extracapsular lymph no
de involvement in colonic cancer
Introduction
The presence and extent of lymphatic dissemination are among the most important
predictors for survival in colonic cancer.1;2 For stage III colonic cancer, the 5-year survival
rate is approximately 50-60%.3-5 According to stages defined by the recently revised
American Joint Committee on Cancer (AJCC, sixth edition) 5-year stage specific survivals
were 83% for stage IIIa (T1-2N1), 64% for stage IIIb (T3-4N1), and 44% for stage IIIc
(T1-4N2).6 Adjuvant chemotherapy is standard in patients with stage III disease. Adjuvant
treatment with 5-fluorouracil and leucovorin reduces the risk of recurrence and death by
one third.4;7
Lymph node staging may be further refined by the identification of different levels, the
absolute number of lymph nodes with metastasis, the absolute number of negative nodes,
and/or the lymph node ratio (i.e. the number of involved nodes over the total number
of resected and identified nodes).8-10 Furthermore, the presence of micro-metastasis in
lymph nodes has also been identified as a prognostic factor.11;12
Extracapsular lymph node involvement is the extension of cancer cells through the nodal
capsule into the perinodal fatty tissue. The prognostic value of extracapsular lymph node
involvement has been studied for several malignancies, including breast, oesophageal,
prostate, vulva, bladder, lung, and head and neck cancer.13-19 Patients with extracapsular
lymph node involvement have a reduced overall and disease free survival (DFS) in these
malignancies.13-20 However, in colonic cancer the prognostic value of extracapsular lymph
node involvement has not yet been established. Only one study has been published on
extracapsular lymph node involvement in colonic cancer suggesting prognostic significance
of extracapsular lymph node involvement.21
Therefore, the aim of the present study was to assess the incidence and extent of
extracapsular lymph node involvement in patients with node positive colonic cancer.
Furthermore, its relation to other clinicopathologic factors was studied. Finally, its
prognostic significance in relation to the type of recurrence was analyzed.
Methods
Patient populationBetween January 1994 and May 2005, all patients who underwent segmental colonic
resection in the Academic Medical Centre in Amsterdam for primary colonic cancer
(rectal cancers and (sub-)total colectomies were excluded) were reviewed. All patients
with lymph node involvement (stage III) were included in the present study. Patients with
distant metastases (stage IV) diagnosed during preoperative staging, were excluded. Data
concerning patient characteristics and performed procedure were collected during chart
review using a preformatted sheet. Surgery was generally performed or supervised by a
colorectal surgeon. Operations were performed with curative intent, either via median
laparotomy or via laparoscopy.
Wind (Chris).indb 199Wind (Chris).indb 199 28-05-2008 15:44:5428-05-2008 15:44:54

200
Pathological processingRoutinely, after resection the pathologist who examined the operation specimen carefully
palpated the specimen and all palpable lymph nodes were collected and evaluated.
Routine H&E staining was performed using a standardized protocol. No additional
immunohistochemical staining techniques to detect micro-metastases were used. In
general all small nodes were completely embedded and serial sections were made. Larger
nodes were first laminated. Subsequently they were totally embedded and serial sections
were made. The findings of the pathologist were routinely discussed in a multidisciplinary
meeting to evaluate the indication for adjuvant therapy. During the whole study period
5-fluorouracil based adjuvant chemotherapy was offered to all patients with lymph node
involvement younger than 75 years old.
Data assessmentIn the summer of 2006 an experienced pathologist re-examined all available H&E slides
of both the primary tumour and all the collected lymph nodes to assess metastases
and extracapsular lymph node involvement. Furthermore, pT-stage, pN-stage (i.e. ≤ 3
positive nodes; pN1 vs. >3 positive nodes; pN2), differentiation grade of the tumour, the
presence or absence of lymphovascular invasion, total number of resected lymph nodes,
total number of positive lymph nodes, lymph node ratio and the presence or absence
of tumour deposits were recorded. The evaluation was done without knowledge of the
clinical outcome of the patients.
Extracapsular lymph node involvement was defined as metastatic adenocarcinoma
extending through the nodal capsule into the perinodal fatty tissue. Deposits of metastatic
adenocarcinoma without a recognizable lymph node were not considered as extracapsular
lymph node involvement but scored as separate tumour deposits and assessed as a
separate pathological factor. However, the size and contour of the deposits were not
taken into account in this study.
Extracapsular lymph node involvement is often associated with a desmoplastic stroma
reaction. Sometimes this reaction is so extensive that the presence or absence of
extracapsular lymph node involvement can be difficult to interpret. In that case, an
imaginary line representing the pre-existing capsule was drawn to facilitate proper
interpretation.20
Follow-upPatients’ hospital and outpatient clinic records were reviewed to assess recurrence. To
complete follow-up, a telephone survey contacting the patients’ general practitioner was
done in August 2006. Follow-up extended until August 2006, ensuring a minimal potential
follow-up of 15 months. Recurrence was classified as haematogenous recurrence, loco-
regional recurrence (including peritoneal recurrence) or both.
Wind (Chris).indb 200Wind (Chris).indb 200 28-05-2008 15:44:5428-05-2008 15:44:54

201
Ch
apter 13
Extracapsular lymph no
de involvement in colonic cancer
StatisticsStatistical calculations were performed using SPSS® version 12.0 (Statistical Package for
the Social Sciences, Chicago, IL, USA). Age, tumour diameter, total number of resected
lymph nodes (i.e. tumour positive and negative) and lymph node ratio were dichotomized
as less or more than the corresponding median value. To compare categorical data the
Chi-square or Fisher exact test was used when appropriate. The Mann-Whitney test was
used to compare continuous variables. Survival rates were calculated on an actuarial
basis with the Kaplan-Meier method, using the log-rank test for comparison. Multivariate
Cox regression analysis was carried out to identify independent prognostic factors. All
significant factors from a univariate analysis were entered in a multivariate analysis.
P-values < 0.05 (two-sided) were considered statistically significant.
Results
Included patientsIn the study period 398 patients underwent potentially curative segmental colonic
resection for primary colonic cancer. In 114 patients lymph node metastases were present
without other metastasis (stage III). Subsequently, three patients were excluded; two
patients died due to postoperative complications, in one patient a metastasis of an earlier
gastric carcinoma was diagnosed peroperatively.
In the final analysis 111 patients were included. There were 60 male and 51 female
patients. Median age was 66 (range 31-91) years. Sixteen patients were operated on in
an emergency setting, the remaining patients underwent elective surgery. There were
58 right sided colectomies, 15 left sided colectomies, and 38 sigmoid resections. In
the included patients, a total number of 1586 lymph nodes had been identified by the
pathologist who examined the resection specimen. A median of 12 (range 1-47) nodes
per patient had been identified in the specimen. In one patient only a single node was
identified. Metastases were detected in 332 lymph nodes. Tumour extension through the
lymph node capsule was identified in a total of 101 lymph nodes and in 58 of 111 lymph
node positive patients. Extracapsular lymph node involvement was confined to only one
lymph node in 35 of these patients.
Clinicopathologic characteristicsThe clinicopathologic characteristics of 53 patients with only intracapsular lymph node
involvement and 58 patients with extracapsular lymph node involvement are summarized
in Table 1. Extracapsular lymph node involvement was seen more often if the number of
positive nodes was higher, in patients with pN2 disease, with a higher lymph node ratio,
with poorer differentiated tumours and with invasion of lymphic or blood vessels.
Wind (Chris).indb 201Wind (Chris).indb 201 28-05-2008 15:44:5528-05-2008 15:44:55

202
Table 1. Clinicopathologic characteristics of 111 included patients with stage III colonic cancer. Patients are divided in groups with only intracapsular lymph node involvement (LNI) and patients with extracapsular LNI.
Only intracapsular LNI (n = 53) Extracapsular LNI (n = 58) P- value†
pT stage NS
T 1 1 0
T 2 1 1
T 3 50 56
T 4 1 1
Tumour diameter (cm)‡ 5.0 (1.3-12.0) 4.9 (2.0-12.0) NS
Resected nodes‡ 11 (1-47) 12 (4-39) NS
Positive nodes‡ 1 (1-8) 3 (1-21) <0.001
pN stage 0.002
N 1 48 38
N 2 5 20
Lymph node ratio‡ 0.11 (0.02-1.0) 0.24 (0.08-1.0) <0.001
Differentiation 0.001
good 3 2
moderate 48 38
poor 2 18
Lymphovascular invasion 0.031
no 38 30
yes 15 28
Extranodal deposits NS
no 40 41
yes 13 17
Adjuvant chemotherapy NS
no 17 26
yes 35 31
unknown 1 1
*Values are mean (SD); ‡Values are median (range); †Fisher’s exact test, Chi-square test, Mann-Whitney U test applied when appropriate; LNI: lymph node involvement; NS: not significant
Follow-up and survival analysis
The median potential follow-up period was 74 months (range 16-151). In the follow-
up period 45 patients developed recurrence; 26 patients developed haematogenous
recurrence, seven patients developed loco-regional recurrence and 11 patients had both
haematogenous and loco-regional recurrence. In one patient the type of recurrence was
unknown. The pattern of recurrence was comparable between patients with and without
extracapsular lymph node involvement (p=0.893).
Wind (Chris).indb 202Wind (Chris).indb 202 28-05-2008 15:44:5528-05-2008 15:44:55

203
Ch
apter 13
Extracapsular lymph no
de involvement in colonic cancer
Five-year DFS in patients with extracapsular lymph node involvement was 41% compared
to 69% for those who had only intracapsular lymph node involvement (p=0.003, Table
2, Figure 1). No difference in DFS was observed between patients (n=35) with only one
lymph node with extracapsular lymph node involvement as compared to patients (n=23)
with more than one lymph node with extracapsular lymph node involvement; 5-year DFS
was 41% vs. 40% (p=0.784) respectively.
Table 2. Univariate analysis of prognostic factors in patients with stage III colonic cancer
5 year disease free survival standard error P- value†
pT-stage NS
T1 -‡ -
T2 -‡ -
T3 54% 5%
T4 -‡ -
Tumour diameter (cm) NS
< 5 58% 7%
≥ 5 51% 7%
Number of resected nodes NS
< 12 50% 7%
≥ 12 59% 7%
pN stage <0.001
N 1 65% 6%
N 2 14% 8%
Lymph node ratio 0.023
< 0.176 67% 7%
≥ 0.176 42% 7%
Extracapsular LNI 0.003
no 69% 7%
yes 41% 7%
Differentiation NS
good 27% 23%
moderate 58% 6%
poor 45% 12%
Lymphovascular invasion NS
no 62% 6%
yes 43% 8%
Extra nodal deposits NS
no 58% 6%
yes 43% 10%
Adjuvant chemotherapy NS
no 43% 9%
yes 61% 6%
†Log-rank test; ‡too few patients and events; LNI: lymph node involvement
Wind (Chris).indb 203Wind (Chris).indb 203 28-05-2008 15:44:5528-05-2008 15:44:55

204
Figure 1. Recurrence in patients with lymph node positive (stage III) colonic cancer. Patients are divided in groups with only intracapsular lymph node involvement (LNI) and patients with extracapsular LNI (p= 0.003).
In 30 patients tumour deposits without any recognizable lymph node structure were
identified besides positive nodes. To assess whether the prognostic significance of
these tumour deposits was different from extracapsular lymph node involvement, the
study population was divided into three groups; intracapsular lymph node involvement
and tumour deposits, extracapsular lymph node involvement without deposits and
extracapsular lymph node involvement with tumour deposits. No difference in recurrence
was observed between the three groups; 5-year DFS was 49%, 44% and 38% respectively
(p=0.644).
Univariate analysis was performed to study the relation between the various factors and
DFS. Univariate analysis revealed that pN-stage (5-year DFS pN1 vs. pN2; 65% vs. 14%,
p<0.001), lymph node ratio (5-year DFS <0.176 vs. ≥ 0.176; 67% vs. 42%, p=0.023), and
extracapsular lymph node involvement (5-year DFS intracapsular lymph node involvement
vs. extracapsular lymph node involvement; 69% vs. 41%, p=0.003) were all significant
prognostic indicators for survival (Table 2). It was shown that the presence or absence of
tumour deposits was not a significant factor for recurrence in contrast to extracapsular
lymph node involvement.
Multivariate analysis demonstrated that among these variables pN-stage (hazard ratio 3.5,
95% confidence interval [CI]: 1.72 – 7.42) and extracapsular lymph node involvement
(hazard ratio 1.98, 95% CI: 1.00 – 3.91) were independent prognostic factors.
Adjuvant chemotherapySixty-six patients received adjuvant chemotherapy, 43 patients did not, and in two patients
it was unknown whether or not they had received adjuvant chemotherapy. Of the 77
patients younger than 75 years, 16 patients did not receive adjuvant chemotherapy due to
!
Wind (Chris).indb 204Wind (Chris).indb 204 28-05-2008 15:44:5528-05-2008 15:44:55
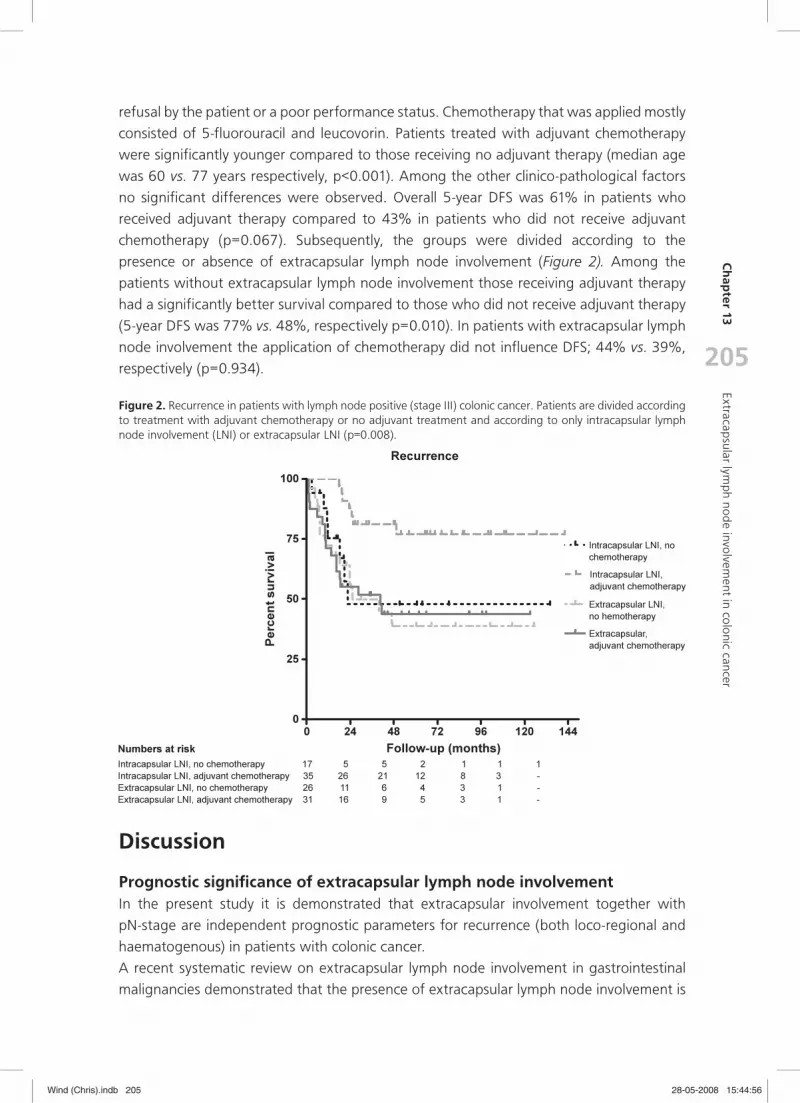
205
Ch
apter 13
Extracapsular lymph no
de involvement in colonic cancer
refusal by the patient or a poor performance status. Chemotherapy that was applied mostly
consisted of 5-fluorouracil and leucovorin. Patients treated with adjuvant chemotherapy
were significantly younger compared to those receiving no adjuvant therapy (median age
was 60 vs. 77 years respectively, p<0.001). Among the other clinico-pathological factors
no significant differences were observed. Overall 5-year DFS was 61% in patients who
received adjuvant therapy compared to 43% in patients who did not receive adjuvant
chemotherapy (p=0.067). Subsequently, the groups were divided according to the
presence or absence of extracapsular lymph node involvement (Figure 2). Among the
patients without extracapsular lymph node involvement those receiving adjuvant therapy
had a significantly better survival compared to those who did not receive adjuvant therapy
(5-year DFS was 77% vs. 48%, respectively p=0.010). In patients with extracapsular lymph
node involvement the application of chemotherapy did not influence DFS; 44% vs. 39%,
respectively (p=0.934).
Figure 2. Recurrence in patients with lymph node positive (stage III) colonic cancer. Patients are divided according to treatment with adjuvant chemotherapy or no adjuvant treatment and according to only intracapsular lymph node involvement (LNI) or extracapsular LNI (p=0.008).
Discussion
Prognostic significance of extracapsular lymph node involvement In the present study it is demonstrated that extracapsular involvement together with
pN-stage are independent prognostic parameters for recurrence (both loco-regional and
haematogenous) in patients with colonic cancer.
A recent systematic review on extracapsular lymph node involvement in gastrointestinal
malignancies demonstrated that the presence of extracapsular lymph node involvement is
Wind (Chris).indb 205Wind (Chris).indb 205 28-05-2008 15:44:5628-05-2008 15:44:56

206
a common phenomenon in patients with gastrointestinal malignancies. Furthermore, in all
these malignancies, extracapsular lymph node involvement identified a subgroup of patients
with a significantly worse long-term survival.22 However, for that review only one small
study concerning colorectal cancer was available,23 including a small subgroup of patients
with colonic cancer and showing that patients with extracapsular lymph node involvement
had significantly worse overall- and disease-free survival as compared to patients with only
intracapsular lymph node involvement. However, no multivariate analysis was performed.
More recently, a larger study was published showing an incidence of extracapsular lymph
node involvement of 49%. Extracapsular lymph node involvement was identified as the
only independent prognosticator for recurrence in multivariate analysis (hazard ratio 3.8,
95% CI: 1.6-8.9).21
The present study comprised of a consecutive series of lymph node positive patients with
colonic cancer. Extracapsular lymph node involvement was associated with a higher number
of positive nodes, pN2 stage, a higher lymph node ratio, poorly differentiated tumours,
and invasion of lymph- or blood vessels. The prognostic significance of extracapsular
lymph node involvement was confirmed in multivariate analysis demonstrating that it was
an independent prognostic factor (hazard ratio 1.98, 95% CI: 1.00 – 3.91). Five-year DFS
in patients with only intracapsular lymph node involvement was 69% compared to 41% in
patients with extracapsular lymph node involvement (p=0.003).
In some of the included patients lymph node staging was not adequate with less than
12 sampled nodes. However, in uni- and multivariate analysis including only patients in
whom 12 nodes or more were identified; the same variables were identified as significant
prognostic indicators (data not shown). Another limitation of the present study is the
retrospective study design. Since the resection specimen had been thrown away and only
the available slide could be assessed. However, all the available slides of both the primary
tumour and all the sampled nodes were re-assessed (prospectively).
The precise causative factor of the worse prognosis in patients with extracapsular lymph
node involvement is not yet clear. It could be hypothesized that the ability of cancer cells
to spread through the lymph node capsule, in an immunologically hostile environment,
probably reflects the invasive aggressiveness of the tumour.24;25 Another hypothesis could
be that extracapsular lymph node involvement reflects an extensive lymphatic spread
inducing lymphatic obstruction. It has been reported that lymphatic obstruction results
in an aberrant flow of lymph fluid leading to lympho-venous communication and thus
to haematogenous dissemination.26-28 However, in this study there was no correlation
between extracapsular lymph node involvement and recurrence pattern.
Adjuvant chemotherapyIn the present study no effect on survival of adjuvant chemotherapy was observed in
patients with extracapsular lymph node involvement. It can be hypothesized that the
extension through the barrier of the lymph node might reflect an aggressive behaviour
and/or a biological insensitivity for chemotherapy. It should be taken into account that
patients receiving no adjuvant therapy were significantly older, and therefore, part
of this observation could be biased. However, a pooled analysis of seven randomised
Wind (Chris).indb 206Wind (Chris).indb 206 28-05-2008 15:44:5728-05-2008 15:44:57

207
Ch
apter 13
Extracapsular lymph no
de involvement in colonic cancer
trials demonstrated no significant interaction between age and the efficacy of adjuvant
chemotherapy for resected colon cancer.29 The incidence of toxic effects was also not
increased among the elderly (age > 70 years). Furthermore, about 20% of the patients
younger than 75 years did not receive or refused adjuvant chemotherapy in the present
study. Finally, the study concerns a retrospectively collected series of patients in a large
period and the numbers in the subgroups were small introducing the risk of having a type-
II-error. Therefore, there is a need for unequivocal data from large prospective studies to
support this observation.
Extranodal tumour depositsThe proper assessment of extracapsular lymph node involvement can be difficult in the
presence of extranodal deposits which are discontinuous with the primary tumour. These
deposits have been identified in many gastrointestinal malignancies.30-34 It is unclear
whether these are lymph nodes that have been completely replaced by tumour tissue or
manifestations of multifocal metastatic disease.33 In the sixth edition of the TNM staging
system these tumour deposits are classified as regional lymph node metastasis if the
nodule has the shape and smooth contour of a lymph node. If the deposit has an irregular
contour, it is classified as pT3.35 However, if a deposit represents a completely overgrown
lymph node with extracapsular growth the contour will be irregular rather than a smooth
round contour. In earlier editions of the TNM staging system all deposits larger than
three millimetres in diameter were classified as regional lymph node metastasis. Tumour
deposits up to three millimetres in diameter were considered as discontinuous extension
and therefore classified as pT3.36 So the precise origin and prognostic implications of these
deposits remains unclear. Therefore, in the present study these deposits were assessed as
a separate factor. In the present study 27% of the patients showed these deposits. There
was no correlation between the presence of these deposits and extracapsular lymph node
involvement. Furthermore, these deposits had no significant effect on survival in univariate
analysis. On the other hand the survival of patients with only deposits and patients with
extracapsular lymph node involvement without deposits was comparable to survival of
patients with both deposits and extracapsular lymph node involvement. This suggests
that tumour deposits without a recognizable lymph node structure have a comparable
influence on survival as extracapsular lymph node involvement.
ConclusionIn conclusion, two independent study groups (ours and Yano’s) indicated that extracapsular
lymph node involvement in colonic cancer is an independent negative prognostic factor,
reflecting a particularly aggressive biological behaviour. It identifies a subgroup of patients
with a significantly worse DFS. Detection and quantification of extracapsular lymph
node involvement in the surgical resection specimen might be helpful in the future to
individualize postoperative therapeutic strategies in the adjuvant setting. Pathologists
should be aware of this clinically important feature and report its presence and extent
upon histological examination.
Wind (Chris).indb 207Wind (Chris).indb 207 28-05-2008 15:44:5728-05-2008 15:44:57

208
Reference List
(1) Cohen AM, Tremiterra S, Candela F, Thaler HT, Sigurdson ER. Prognosis of node-positive colon cancer. Cancer 1991; 67(7):1859-1861.
(2) Wolmark N, Fisher B, Wieand HS. The prognostic value of the modifications of the Dukes’ C class of colorectal cancer. An analysis of the NSABP clinical trials. Ann Surg 1986; 203(2):115-122.
(3) O’Connell MJ, Mailliard JA, Kahn MJ, Macdonald JS, Haller DG, Mayer RJ et al. Controlled trial of fluo-rouracil and low-dose leucovorin given for 6 months as postoperative adjuvant therapy for colon cancer. J Clin Oncol 1997; 15(1):246-250.
(4) Mamounas E, Wieand S, Wolmark N, Bear HD, Atkins JN, Song K et al. Comparative efficacy of adjuvant chemotherapy in patients with Dukes’ B versus Dukes’ C colon cancer: results from four National Surgi-cal Adjuvant Breast and Bowel Project adjuvant studies (C-01, C-02, C-03, and C-04). J Clin Oncol 1999; 17(5):1349-1355.
(5) Poplin EA, Benedetti JK, Estes NC, Haller DG, Mayer RJ, Goldberg RM et al. Phase III Southwest Oncol-ogy Group 9415/Intergroup 0153 randomized trial of fluorouracil, leucovorin, and levamisole versus fluorouracil continuous infusion and levamisole for adjuvant treatment of stage III and high-risk stage II colon cancer. J Clin Oncol 2005; 23(9):1819-1825.
(6) O’connell JB, Maggard MA, Ko CY. Colon cancer survival rates with the new American Joint Committee on Cancer sixth edition staging. J Natl Cancer Inst 2004; 96(19):1420-1425.
(7) O’Connell MJ, Laurie JA, Kahn M, Fitzgibbons RJ, Jr., Erlichman C, Shepherd L et al. Prospectively randomized trial of postoperative adjuvant chemotherapy in patients with high-risk colon cancer. J Clin Oncol 1998; 16(1):295-300.
(8) Berger AC, Sigurdson ER, LeVoyer T, Hanlon A, Mayer RJ, Macdonald JS et al. Colon cancer surviv-al is associated with decreasing ratio of metastatic to examined lymph nodes. J Clin Oncol 2005; 23(34):8706-8712.
(9) Johnson PM, Porter GA, Ricciardi R, Baxter NN. Increasing negative lymph node count is independently associated with improved long-term survival in stage IIIB and IIIC colon cancer. J Clin Oncol 2006; 24(22):3570-3575.
(10) Wong JH, Severino R, Honnebier MB, Tom P, Namiki TS. Number of nodes examined and staging accu-racy in colorectal carcinoma. J Clin Oncol 1999; 17(9):2896-2900.
(11) Liefers GJ, Cleton-Jansen AM, van de Velde CJ, V, Hermans J, van Krieken JH, Cornelisse CJ et al. Micro-metastases and survival in stage II colorectal cancer. N Engl J Med 1998; 339(4):223-228.
(12) Yasuda K, Adachi Y, Shiraishi N, Yamaguchi K, Hirabayashi Y, Kitano S. Pattern of lymph node microme-tastasis and prognosis of patients with colorectal cancer. Ann Surg Oncol 2001; 8(4):300-304.
(13) Brasilino de CM. Quantitative analysis of the extent of extracapsular invasion and its prognostic signifi-cance: a prospective study of 170 cases of carcinoma of the larynx and hypopharynx. Head Neck 1998; 20(1):16-21.
(14) Fisher BJ, Perera FE, Cooke AL, Opeitum A, Dar AR, Venkatesan VM et al. Extracapsular axillary node extension in patients receiving adjuvant systemic therapy: an indication for radiotherapy? Int J Radiat Oncol Biol Phys 1997; 38(3):551-559.
(15) Fleischmann A, Thalmann GN, Markwalder R, Studer UE. Prognostic implications of extracapsular exten-sion of pelvic lymph node metastases in urothelial carcinoma of the bladder. Am J Surg Pathol 2005; 29(1):89-95.
(16) Griebling TL, Ozkutlu D, See WA, Cohen MB. Prognostic implications of extracapsular extension of lymph node metastases in prostate cancer. Mod Pathol 1997; 10(8):804-809.
(17) Myers JN, Greenberg JS, Mo V, Roberts D. Extracapsular spread. A significant predictor of treatment failure in patients with squamous cell carcinoma of the tongue. Cancer 2001; 92(12):3030-3036.
(18) Ishida T, Tateishi M, Kaneko S, Sugimachi K. Surgical treatment of patients with nonsmall-cell lung cancer and mediastinal lymph node involvement. J Surg Oncol 1990; 43(3):161-166.
Wind (Chris).indb 208Wind (Chris).indb 208 28-05-2008 15:44:5728-05-2008 15:44:57

209
Ch
apter 13
Extracapsular lymph no
de involvement in colonic cancer
(19) van der Velden J, van Lindert AC, Lammes FB, ten Kate FJ, Sie-Go DM, Oosting H et al. Extracapsular growth of lymph node metastases in squamous cell carcinoma of the vulva. The impact on recurrence and survival. Cancer 1995; 75(12):2885-2890.
(20) Lagarde SM, ten Kate FJ, de Boer DJ, Busch OR, Obertop H, van Lanschot JJ. Extracapsular lymph node involvement in node-positive patients with adenocarcinoma of the distal esophagus or gastroesopha-geal junction. Am J Surg Pathol 2006; 30(2):171-176.
(21) Yano H, Saito Y, Kirihara Y, Takashima J. Tumor invasion of lymph node capsules in patients with Dukes C colorectal adenocarcinoma. Dis Colon Rectum 2006; 49(12):1867-1877.
(22) Wind J, Lagarde SM, ten Kate FJ, Ubbink DT, Bemelman WA, van Lanschot JJ. A systematic review on the significance of extracapsular lymph node involvement in gastrointestinal malignancies. Eur J Surg Oncol 2006.
(23) Komuta K, Okudaira S, Haraguchi M, Furui J, Kanematsu T. Identification of extracapsular invasion of the metastatic lymph nodes as a useful prognostic sign in patients with resectable colorectal cancer. Dis Colon Rectum 2001; 44(12):1838-1844.
(24) Stitzenberg KB, Meyer AA, Stern SL, Cance WG, Calvo BF, Klauber-DeMore N et al. Extracapsular exten-sion of the sentinel lymph node metastasis: a predictor of nonsentinel node tumor burden. Ann Surg 2003; 237(5):607-612.
(25) Lyons AJ, Bateman AC, Spedding A, Primrose JN, Mandel U. Oncofetal fibronectin and oral squamous cell carcinoma. Br J Oral Maxillofac Surg 2001; 39(6):471-477.
(26) Yamagata K, Kumagai K. Experimental study of lymphogenous peritoneal cancer dissemination: migra-tion of fluorescent-labelled tumor cells in a rat model of mesenteric lymph vessel obstruction. J Exp Clin Cancer Res 2000; 19(2):211-217.
(27) Burn JI. Obstructive lymphopathy. Ann R Coll Surg Engl 1968; 42(2):93-113.
(28) Yamagata K, Kumagai K, Shimizu K, Masuo K, Nishida Y, Yasui A. Gastrointestinal cancer metastasis and lymphogenous spread: viewpoint of animal models of lymphatic obstruction. Jpn J Clin Oncol 1998; 28(2):104-106.
(29) Sargent DJ, Goldberg RM, Jacobson SD, Macdonald JS, Labianca R, Haller DG et al. A pooled anal-ysis of adjuvant chemotherapy for resected colon cancer in elderly patients. N Engl J Med 2001; 345(15):1091-1097.
(30) Ueno H, Mochizuki H, Fujimoto H, Hase K, Ichikura T. Autonomic nerve plexus involvement and progno-sis in patients with rectal cancer. Br J Surg 2000; 87(1):92-96.
(31) Ishikawa K, Hashiguchi Y, Mochizuki H, Ozeki Y, Ueno H. Extranodal cancer deposit at the primary tumor site and the number of pulmonary lesions are useful prognostic factors after surgery for colorec-tal lung metastases. Dis Colon Rectum 2003; 46(5):629-636.
(32) Ueno H, Mochizuki H, Shinto E, Hashiguchi Y, Hase K, Talbot IC. Histologic indices in biopsy specimens for estimating the probability of extended local spread in patients with rectal carcinoma. Cancer 2002; 94(11):2882-2891.
(33) Prabhudesai A, Arif S, Finlayson CJ, Kumar D. Impact of microscopic extranodal tumor deposits on the outcome of patients with rectal cancer. Dis Colon Rectum 2003; 46(11):1531-1537.
(34) Etoh T, Sasako M, Ishikawa K, Katai H, Sano T, Shimoda T. Extranodal metastasis is an indicator of poor prognosis in patients with gastric carcinoma. Br J Surg 2006; 93(3):369-373.
(35) TNM Classification of Malignant Tumours. Sixth ed. New-York: Wiley-Liss; 2002.
(36) TNM Classiffication of Malignant Tumours. Fifth ed. New-York: Wiley; 1997.
Wind (Chris).indb 209Wind (Chris).indb 209 28-05-2008 15:44:5728-05-2008 15:44:57

Wind (Chris).indb 210Wind (Chris).indb 210 28-05-2008 15:44:5728-05-2008 15:44:57

14Chapter
Circulating tumour cells during laparoscopic and open surgery for
primary colonic cancer in portal and peripheral blood
J Wind
JB Tuynman
AGJ Tibbe
DJ Richel
MI van Berge Henegouwen
WA Bemelman
Submitted
Wind (Chris).indb 211Wind (Chris).indb 211 28-05-2008 15:44:5728-05-2008 15:44:57

212212
Abstract
IntroductionThe objective of this study was to detect and quantify circulating tumour cells (CTC) in
peripheral and portal blood of patients who had open or laparoscopic surgery for primary
colonic cancer.
MethodsPatients in the laparoscopic group were operated on in a medial to lateral approach
(“vessels first”), in the open group a lateral to medial approach was applied. The
enumeration of CTC was performed with the CellSearch System. Intra-operative samples
were taken paired-wise (from peripheral and portal circulation) directly after entering the
abdominal cavity (T1), after mobilisation of the tumour baring segment (T2), and after
tumour resection (T3). Ploidy of both the CTC and tissue of the primary tumour was
determined for chromosome 1, 7, 8 and 17.
ResultsThirty-one patients were included; 18 patients had open surgery, 13 patients were operated
on laparoscopically. The percentage of samples with CTC at T1 was 7% in peripheral blood
and 54% in portal blood (p=0.002). At T2, 4% and 31% respectively (p=0.031). And at T3,
4% and 26% respectively (p=0.125). The cumulative percentage of samples with CTC was
significantly higher during open surgery as compared to the laparoscopic approach. Both
the CTC and tissue of the primary tumour were diploid for chromosome 1, 7, 8 and 17.
ConclusionThe detection rate and quantity of CTC is significantly increased intra-operatively and is
significantly higher in portal blood compared to peripheral blood. Significantly less CTC
were detected during laparoscopic surgery probably as result of the medial to lateral
approach.
Wind (Chris).indb 212Wind (Chris).indb 212 28-05-2008 15:44:5728-05-2008 15:44:57

213
Ch
apter 14
Circulating tum
our cells during laparoscopic and open surg
ery
Introduction
It is of great importance that survival and the most likely sites of recurrence can be predicted
after surgery with curative intent. With respect to long-term outcome haematogenous and
lymphatic spread are the pathways of metastasis and are therefore the most important
factors associated with prognosis.1-5 Patients with unfavourable prognostic factors may
benefit from adjuvant chemotherapy. However, pathologic staging systems (TNM) fails to
adequately identify patients with stage II and III disease who will benefit from adjuvant
chemotherapy.2-5 Detection of circulating tumour cells (CTC) during and after resection
might be helpful to identify those patients who will benefit from adjuvant chemotherapy
and expand our knowledge about the biology of metastasis and potential role of surgery
in this process. CTC were first detected in patients with colorectal cancer more than 50
years ago.6;7
The introduction of the CellSearch™ system has provided a standardised method for the
enumeration and characterisation of CTC that permitted the evaluation of potential clinical
utilities of CTC through multi-centre prospective clinical trials.8 Prospective multi-centre
studies in metastatic breast, colorectal and prostate cancer showed that the presence of
CTC were associated with poor outcome and were an independent predictor of progression
free survival and overall survival.9-11 In primary colorectal cancer little is known about
the role of CTC although a relation with stage has been shown. The specificity of CTC
detection is lower at low frequencies making the data interpretation more difficult.12
In colorectal cancer surgery the principle of early lymphovascular ligation before manipulation
of the tumour has been termed the “no-touch isolation” technique.13;14 This technique was
proposed to reduce intra-operative dissemination.15 In laparoscopic colorectal surgery the
no-touch principles are represented in the so-called medial to lateral approach where the
supplying vessels are ligated early in the procedure. Several randomised trials comparing
laparoscopic with open segmental colectomy have indicated that laparoscopic surgery can
be applied safely for both benign and malignant diseases.16-21 Furthermore, it has been
shown that short term cancer related outcomes such as cancer free resection margins
and the number of harvested lymph nodes, as well as long term cancer related outcomes
such as disease-free survival are comparable between laparoscopic and open surgery.16
However, a potential oncological benefit of laparoscopic surgery in which a median to
lateral approach is applied is still debated.
The objective of this study was to determine whether CTC could be detected in peripheral
and portal blood during laparoscopic and open surgery for colonic cancer. Furthermore,
differences in the amount of CTC between peripheral and portal blood were assessed.
Finally, the effect of the surgical approach (i.e. open versus laparoscopic) on the presence
of CTC during surgery was assessed.
Wind (Chris).indb 213Wind (Chris).indb 213 28-05-2008 15:44:5828-05-2008 15:44:58

214
Methods
Study populationThe current study was performed on patients with primary colonic cancer (rectal cancers
were excluded) who underwent surgery with curative intent at the Academic Medical
Centre, Amsterdam between August 2005 and August 2007. All patients underwent
abdominal ultrasonography and chest radiography, to identify metastatic disease
preoperatively. Patients with distant metastases (stage IV) were excluded. Furthermore,
patients with prior abdominal surgery, emergency surgery, age over 85 years, and
American Society of Anaesthesiology (ASA) score above three were excluded. Surgery
was performed or supervised by a colorectal surgeon. Operations were performed with
curative intent, either via midline laparotomy or via laparoscopy. All laparoscopic operations
were performed according to the “no-touch isolation” technique, i.e. a medial to lateral
approach with early vessel ligation.14 A lateral to medial approach was performed during
open resections. In laparoscopic procedures pneumoperitoneum was established with
CO2 gas with an intra-abdominal pressure of 15 mmHg or less.
The majority of the patients (24/31) also participated in a randomised trial comparing
open and laparoscopic surgery (ISRCTN: 79588422).22 Tumour stage and grading were
classified according to the sixth edition of the TNM classification of the International Union
Against Cancer.23 Informed consent was obtained from all patients. The study protocol was
approved by the local medical ethics committee.
Blood collectionPeripheral whole blood samples were collected through an intravenous cannula. In
left sided colectomies, portal whole blood samples were collected by insertion of a 15
centimetres long 5.5 French catheter (Arrow-Howes™ Paediatric Multi-Lumen Central
Venous Line) into the inferior mesenteric vein which was advanced about 10-15 centimetres
to secure position at portal vein level. In laparoscopic procedures a 30 centimetres long
catheter was used which was positioned intra-abdominally through a large infusion needle.
Subsequently, a small hole was created in the inferior mesenteric vein with a pair of scissors
followed by insertion of the catheter laparoscopically. The catheter was advanced 10-15
centimetres to secure position at portal vein level and fixed with a purse-string suture. In
case of right sided colectomy a similar procedure was performed using a venous branch of
the right branch of the middle colonic vein to insert the catheter.
Blood samples were collected at four different time points which are shown in Figure 1.
The first sample was collected before surgery (only peripheral, T0). Subsequently samples
were taken paired-wise (peripheral and portal) after entry into the abdominal cavity and
before mobilisation of the tumour bearing segment (T1), after mobilisation of the tumour
bearing segment (T2), and after tumour resection (T3).
Wind (Chris).indb 214Wind (Chris).indb 214 28-05-2008 15:44:5828-05-2008 15:44:58

215
Ch
apter 14
Circulating tum
our cells during laparoscopic and open surg
ery
Enumeration of CTCBlood samples were drawn into 10 ml tubes which contained a cell preservative (CellSave
Preservative Tubes, Immunicon, Huntingdon Valley, USA). Samples were maintained
at room temperature and processed within 72 hours after collection. The CellSearch™
Circulating Tumour Cell Test (Veridex LLC, Warren, USA) was used for the isolation and
enumeration of circulating epithelial cells. The cell detection system consists of a sample
preparation and cell analysis platform that have been described elsewhere in detail.24
In brief, ferro-fluids coated with epithelial cell-specific EpCAM antibodies were used to
immuno-magnetically enrich epithelial cells from 7.5 ml of blood.25 The enriched samples
were stained with phycoerythrin conjugated antibodies directed against cytokeratins 8,
18, and 19, an allophycocyanin conjugated antibody to CD45 and the nuclear dye DAPI.
The isolated and stained CTC were transferred to a CellTracks® Cartridge and analysed
on the CellTracks® Analyser II, a four colour semi-automated fluorescence microscope
(Veridex). Image frames covering the entire surface of the cartridge for four different
fluorescence filter cubes were captured. From the captured images, a gallery of objects
meeting pre-determined criteria was automatically presented in a web-enabled browser
for interpretation by a trained operator who made the final selection of cells. The criteria
for an object to be defined as a CTC included round to oval morphology, a visible nucleus
(DAPI positive), positive staining for cytokeratin, and negative staining for CD45.24
Results of cell enumeration were expressed as the number of cells per 7.5 ml of blood.
The performance of the assay system is described in detail elsewhere.8 In this study the
presence of one or more CTC in the sample was considered CTC positive.12
Fluorescence in Situ Hybridization on CTC and primary tumour tissueTo determine cytogenetics changes of the CTC and as an additional identifier, Fluorescence
In Situ Hybridization (FISH) was applied to CTC containing cartridges. After the CTC were
isolated and identified as described in the previous section, the CTC were labelled with
fluorescent FISH probes against the centromeric region of chromosomes 1, 7, 8, and 17.26
The location of the previous identified tumour cells was maintained during FISH analysis
Figure 1. Time line which shows the different time points at which blood was collected. The first sample was collected before surgery (only peripheral, T0) and subsequently paired-wise (peripheral and portal) after entry into the abdominal cavity and before mobilisation of the tumour bearing segment (T1), after mobilisation of the tumour bearing segment (T2), and after tumour resection (T3).
Wind (Chris).indb 215Wind (Chris).indb 215 28-05-2008 15:44:5828-05-2008 15:44:58

216
which allows revisiting of the same cell. Fluorescence images of the FISH signals were
acquired and the number of FISH spots for each of the four chromosomes was determined
in each CTC. For the patients with the highest number of CTC the ploidy, on basis of
the number of copies of the chromosomes 1, 7, 8, and 17, of the CTC was compared
with the ploidy of the primary tumour tissue. Paraffin tissues of the primary tumour were
treated and hybridized and the number of FISH spots for chromosome 1, 7, 8, and 17 were
determined.
StatisticsStatistical calculations were performed using SPSS® version 12.0.2 (Statistical Package for
the Social Sciences, Chicago, IL, USA). To compare categorical data the Chi-square was
used. The Mann-Whitney test was used to compare continuous variables. The McNemar
and Wilcoxon tests were used to test for differences between the detection rate in
portal and peripheral blood with respect to the timing of blood collection. An unpaired
non-parametric test was used to assess the influence of open and laparoscopic surgery on
the detection rate of CTC.
Results
Study populationDuring the study period 38 patients were included. Subsequently, seven patients were
excluded; in five patients the cannulation of the inferior mesenteric vein was not successful
and a further two patients were excluded when histological evaluation of the resected
specimen revealed adenomas containing no invasive carcinoma. Thirty-one patients
remained for final analysis; 19 male and 12 female patients with a mean age of 67 (±12)
years. Eighteen patients had a laparotomy (open-group); the remaining 13 patients were
operated on laparoscopically (laparoscopic-group). There were 16 right-sided colectomies,
seven left-sided colectomies, seven (recto-) sigmoid resections, and one subtotal colectomy
(Table 1).
Wind (Chris).indb 216Wind (Chris).indb 216 28-05-2008 15:44:5828-05-2008 15:44:58

217
Ch
apter 14
Circulating tum
our cells during laparoscopic and open surg
ery
Table 1. Clinicopathologic characteristics of the included patients
Patients divided according to surgical approach
all patients open-group laparoscopic-group P-value†
(n=31) (n=18) (n=13)
Age* (yrs) 67 (12) 70 (10) 63 (13) 0.21
Male:female‡ 19 (61):12 (39) 1 (61):7 (39) 8 (62):5 (38) 0.98
Preoperative CEA level* 2.1 (2.5) 1.7 (1.8) 2.6 (3.4) 0.44
Operative procedure‡ 0.12
- right hemicolectomy 16 (51) 12 (67) 4 (31)
- left hemicolectomy 7 (23) 2 (11) 5 (38)
- (recto)sigmoidectomy 7 (23) 3 (17) 4 (31)
- subtotal colectomy 1 ( 3) 1 ( 5) 0
Operating time* (min) 178 (55) 153 (39) 224 (50) 0.001
pT stage‡ 0.06
- T 1
- T 2 5 (16) 1 ( 5) 4 (31)
- T 3 26 (84) 17 (95) 9 (69)
- T 4
Tumour diameter* (cm) 4.6 (2.0) 5.0 (2.3) 4.1 (1.4) 0.27
pN stage‡ 0.46
- N 0 21 (68) 12 (67) 9 (69)
- N 1 5 (16) 4 (22) 1 (8)
- N 2 5 (16) 2 (11) 3 (23)
Differentiation‡ 0.23
- good 1 (3) 1 ( 5) -
- moderate 24 (77) 12 (67) 12 (92)
- poor 6 (19) 5 (28) 1 (8)
Lymphovascular invasion‡ 0.09
- no 24 (77) 12 (67) 12 (92)
- yes 7 (23) 6 (33) 1 (8)
†Chi-square test, Mann-Whitney U test applied when appropriate; *Values are mean (SD); ‡Values are absolute numbers (%)
Clinicopathologic characteristicsThe clinicopathologic characteristics of the overall study population (n=31), the open-group
(n=18), and the laparoscopic-group (n=13) are summarised in Table 1. Operating times
were significantly longer in the laparoscopic-group compared to the open-group (153 vs.
224 minutes, p=0.001). Furthermore, there was a higher T-stage and more lymphovascular
invasion in the open-group as compared to the laparoscopic-group, although these
differences were not significant. In the laparoscopic group there was slightly more N2
disease. Finally, there were more right sided resections in the open group than in the
Wind (Chris).indb 217Wind (Chris).indb 217 28-05-2008 15:44:5828-05-2008 15:44:58

218
laparoscopic group, although this difference was not significant. Regarding the other
clinicopathologic characteristics the groups were comparable.
Enumeration of CTCIn Figure 2 the average number of CTC in patients who underwent laparoscopic or open
surgery at the subsequent time points is shown. Although the standard deviations were
large, the number of CTC detected in portal blood was higher at all subsequent time
points. In the samples taken at T1, CTC were identified in 7% of the peripheral samples
and in 45% of the portal samples (p=0.002). With respect to the samples taken at T2, CTC
were identified in 4% and in 31% respectively (p=0.031). Finally, at T3 the detection rate
was 4% and 26% respectively (p=0.125). Subsequently, to assess the overall difference
between peripheral and portal blood the dichotomous results on the three intra-operative
time points were summed, resulting in a score ranging from zero (all samples negative) to
three (all samples positive). The cumulative score was significantly higher in portal blood
compared to peripheral blood (p<0.001, Table 2)
Table 2. Cumulative result of the enumeration of CTC in peripheral and portal blood on the three intra-operative time points (p< 0.001)
peripheral blood portal blood
All samples negative 83% 28%
One sample positive 17% 45%
Two samples positive - 27%
All samples positive - 7%
The number of CTC in portal blood of patients who underwent open surgery was higher
compared to patients who underwent laparoscopic surgery. According to open vs.
laparoscopic surgery the percentage of samples with CTC at T1 was 0% vs. 18% (p=0.076)
in peripheral blood and 65% vs. 36% (p=0.142) in portal blood respectively. At T2, 0% vs.
8% (p=0.288) in peripheral blood and 44% vs. 9% (p=0.046) in portal blood respectively.
Finally, at T3, 8% vs. 0% (p=0.347) in peripheral blood and 29% vs. 20% (p=0.590) in
portal blood respectively. To assess the overall difference between open and laparoscopic
surgery the dichotomous results in portal blood (as this was more sensitive compared
to peripheral blood) on the three intra-operative time points were added up, resulting
in a score ranging from zero (all samples negative) to three (all samples positive). The
cumulative score was significantly higher in the open-group compared to the laparoscopic-
group (p=0.039, Table 3)
Table 3. Cumulative result of the enumeration of CTC in portal blood according open or laparoscopic surgery on the three intra-operative time points (p=0.039)
open-group laparoscopic-group
All samples negative 17% 45%
One sample positive 44% 45%
Two samples positive 28% 9%
All samples positive 11% -
Wind (Chris).indb 218Wind (Chris).indb 218 28-05-2008 15:44:5928-05-2008 15:44:59

219
Ch
apter 14
Circulating tum
our cells during laparoscopic and open surg
ery
Figure 2. Average number of CTC detected in the samples of patients who underwent laparoscopic or open surgery at the different time points.
CTC in relation to other clinicopathologic characteristicsTo assess potential associations between the presence or absence of CTC and certain
clinicopathologic characteristics all the available intra-operative samples, both peripheral
and portal, and the cumulative score (see above) of both peripheral and portal samples,
were tested in an univariate analysis. The following clinicopathologic characteristics were
analysed; age, gender, operative procedure, tumour diameter, tumour differentiation
grade, lymphovascular invasion, presence of lymph node metastasis per se, N-stage, and
T-stage (T1-T2 vs. T3-T4). Besides a non-significant trend towards a higher number of
samples with CTC during right-sided resections compared to left-sided resections (71% vs.
39%, p=0.085) there were no associations.
Morphology of the detected CTC The tumour cells detected in peripheral blood had a morphology that was similar to the
morphology in other carcinoma’s described elswhere.8;10 Different morphology was
observed for CTC detected in portal blood at T1 and T2. Cells present in these samples
looked frayed and appeared mostly as sheets and clumps of cellular material in which the
Wind (Chris).indb 219Wind (Chris).indb 219 28-05-2008 15:44:5928-05-2008 15:44:59

220
individual cells were difficult to discriminate. No difference in morphology between the
laparoscopic and open group was observed.
FISH As the morphology of the CTC in portal blood at T1 and T2 deviated, the ploidy of these
cells was determined as an additional tumour cell identifier, using chromosome 1, 7, 8
and 17. The CTC all contained two copies for each of the chromosomes. Subsequently,
the primary tumour tissue ploidy using chromosome 1, 7, 8 and 17, was compared to that
of the CTC. For each of the tested chromosomes the tumour tissue cells displayed also
two copies which was equal to the detected CTC. So, ploidy of the CTC and tissue of the
primary tumour did match, however both were diploid.
Discussion
The present study shows that the presence of CTC was significantly increased
intra-operatively and was significantly higher in portal blood (26-45%) as compared
to peripheral blood (4-7%). With respect to the surgical approach, the percentage of
CTC containing blood samples was significantly lower in the portal blood sample after
mobilisation of the tumour bearing segment during laparoscopic surgery compared to
open surgery (9% vs. 44%, p=0.046).
Others that assessed the presence of CTC intra-operatively, also found significant higher
detection rates in portal blood (50-65%) compared to peripheral blood (11-49%).27-30
Theoretically, tumour cells must pass through the liver, lungs and the microcirculation of
other tissues before they pass into the systemic venous circulation.15 Animal studies have
demonstrated that 80-100% of injected human colon carcinoma cells were trapped in the
capillary bed of the first organ encountered.31 Furthermore, a higher prevalence in portal
blood might be explained by the fact that there is some dilution in the larger blood volume
of the peripheral circulation.15 Yamaguchi et al. found a PCR-positive (CEA, cytokeratin 20)
detection rate of 31% in mesenteric blood and 15% in peripheral blood (p=0.033). The
presence of CEA and cytokeratin 20 mRNA in peripheral blood was not correlated with
survival. However, with respect to portal blood uni- and multivariate analysis indicated
that it was the only independent prognostic factor (hazard ratio 13.6, p=0.028).32
Various techniques have been described in the literature to study CTC and the large
differences in the reported results bring in question whether the same events are being
studied.1;33 We choose to use the CellSearch system for CTC evaluation as it has been
validated and used in prospective multi-centre trials.9-11;34 In this study the presence of
one or more CTC in the sample was considered a CTC positive sample. This low threshold
was chosen because of the significant relationship between the presence of one or more
CTC and poor outcome in patients with metastatic disease as shown by others.12 The
specificity of the CellSearch system is limited by the users ability to assign an event as a
tumour cell.12 We therefore tried to improve the specificity by investigating the ploidy of
Wind (Chris).indb 220Wind (Chris).indb 220 28-05-2008 15:45:0028-05-2008 15:45:00

221
Ch
apter 14
Circulating tum
our cells during laparoscopic and open surg
ery
the detected tumour cells. In the cases examined, however, both CTC and primary tumour
tissue were diploid for chromosome 1, 7, 8, and 17 thus not providing a definite answer
whether or not the detected CTC were true tumour cells or normal epithelial cells shed
into the portal blood through surgical trauma.
Since a considerable number of patients with resectable colorectal cancer subsequently
develop metastatic disease, dissemination is likely to be an early event that may happen pre-
or intra-operatively and is not detected by conventional staging techniques.35 In metastatic
breast, colorectal and prostate cancer the presence of CTC was associated with a short
progression free and overall survival and predicted treatment efficacy earlier and more
effectively than imaging in breast cancer and PSA in prostate cancer.9;11;34 Nevertheless,
the presence of CTC does not necessarily predict subsequent metastatic disease as this
process is very inefficient. Fidler reported that less than 0.1% of tumour cells placed into
the circulation survived to produce metastatic lesions in animals. However, activation
of blood coagulation and relative immune suppression due to the surgical stress might
enhance the metastatic potential of these intra-operatively spilled cells.35;36 So far, several
studies have demonstrated a negative effect of CTC on prognosis.27;37-39 Furthermore, in
some studies the presence of CTC was found as the only independent prognosticator.32;40
Nevertheless, others have found no association between CTC and survival.28;41 A major
difficulty in interpreting these results is the variety of detection methods, the small sample
sizes of the individual studies, and the relatively short follow-up.33
In the present study, less CTC were found in the laparoscopically operated patients.
Both the open-group and laparoscopic-group were comparable with respect to most
clinicopathologic characteristics, with the exception of a non-significant trend towards
more right-sided resections, a higher T-stage, and more lymphovascular invasion in the
open group, and longer operating times and more N2 disease in the laparoscopic-group.
Some have found an association between the presence of CTC and a higher T-stage, lymph
node involvement, poorer differentiated tumours, and lymph- and blood vessel invasion.
However, in these studies it was also demonstrated that in patients with early-staged
cancers the detection rates were also considerable.27;28;35 Moreover, in the present study it
was demonstrated that the only factor influencing the detection rate, besides the location
of sampling (i.e. peripheral vs. portal), was the surgical approach (i.e. laparoscopic or open
surgery) and that the other analysed factors were not associated with the presence or
absence of CTC.
It could be hypothesised that laparoscopic surgery with a medial to lateral approach with
early lymphovascular ligation is the ultimate form of no-touch surgery. In our open-group
a lateral to medial approach was applied, therefore this group could be considered as
‘conventional surgery’. The results obtained in the present study therefore support the
no-touch isolation technique rather than that the results suggest an oncological benefit
of laparoscopic surgery itself. In a recent review on the no-touch technique the overall
conversion rates (i.e. negative preoperatively, positive intra-operatively) for studies
employing the no-touch technique were 0–16%, compared to 0–80% for studies utilising
conventional surgery.15 Comparable to the present study, Bessa et al. assessed neoplastic
cell mobilisation in 50 patients who were randomly assigned to open or laparoscopic
Wind (Chris).indb 221Wind (Chris).indb 221 28-05-2008 15:45:0028-05-2008 15:45:00

222
surgery. In contrast to the present study, the no-touch isolation technique was applied
in both groups. In Bessa’s study, surgical neoplastic cell mobilisation was observed in
only four patients, with no difference with respect to the surgical approach.42 Therefore,
the detection rate of CTC might be unrelated to the surgical approach (i.e. laparoscopic
or open surgery) but related to the moment of lymphovascular ligation as these data
suggest that there is a trend towards reduced tumour cell dissemination for the no-touch
isolation method. The benefit of this in terms of improved patient survival remains to be
established.15
In conclusion, the detection rate and quantity of CTC is significantly increased
intra-operatively and is significantly higher in portal blood compared to peripheral blood.
Significantly less CTC were detected during laparoscopic surgery probably as result of the
medial to lateral approach.
AcknowledgementWe would like to thank dr. J.B. Reitsma from the department of Epidemiology and
Biostatistics for his statistical advise.
Reference List
(1) Khair G, Monson JR, Greenman J. Epithelial molecular markers in the peripheral blood of patients with colorectal cancer. Dis Colon Rectum 2007;50:1188-1203.
(2) Liotta LA, Stetler-Stevenson WG. Tumor invasion and metastasis: an imbalance of positive and negative regulation. Cancer Res 1991;51:5054s-5059s.
(3) Cohen AM, Tremiterra S, Candela F, Thaler HT, Sigurdson ER. Prognosis of node-positive colon cancer. Cancer 1991;67:1859-1861.
(4) Compton CC, Fielding LP, Burgart LJ, Conley B, Cooper HS, Hamilton SR, et al. Prognostic factors in colorectal cancer. College of American Pathologists Consensus Statement 1999. Arch Pathol Lab Med 2000;124:979-994.
(5) Wolmark N, Fisher B, Wieand HS. The prognostic value of the modifications of the Dukes’ C class of colorectal cancer. An analysis of the NSABP clinical trials. Ann Surg 1986;203:115-122.
(6) Engell HC. Cancer cells in the circulating blood; a clinical study on the occurrence of cancer cells in the peripheral blood and in venous blood draining the tumour area at operation. Acta Chir Scand Suppl 1955;201:1-70.
(7) Engell HC. [Cancer cells in the circulating blood; a clinical study on the occurrence of cancer cells in the peripheral blood and in venous blood draining the tumour area at operation.]. Ugeskr Laeger 1955;117:822-823.
(8) Allard WJ, Matera J, Miller MC, Repollet M, Connelly MC, Rao C, et al. Tumor cells circulate in the peripheral blood of all major carcinomas but not in healthy subjects or patients with nonmalignant diseases. Clin Cancer Res 2004;10:6897-6904.
(9) Moreno JG, Miller MC, Gross S, Allard WJ, Gomella LG, Terstappen LW. Circulating tumor cells predict survival in patients with metastatic prostate cancer. Urology 2005;65:713-718.
(10) Cohen SJ, Alpaugh RK, Gross S, O’Hara SM, Smirnov DA, Terstappen LW, et al. Isolation and charac-terization of circulating tumor cells in patients with metastatic colorectal cancer. Clin Colorectal Cancer 2006;6:125-132.
Wind (Chris).indb 222Wind (Chris).indb 222 28-05-2008 15:45:0028-05-2008 15:45:00

223
Ch
apter 14
Circulating tum
our cells during laparoscopic and open surg
ery
(11) Cristofanilli M, Budd GT, Ellis MJ, Stopeck A, Matera J, Miller MC, et al. Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N Engl J Med 2004;351:781-791.
(12) Tibbe AG, Miller MC, Terstappen LW. Statistical considerations for enumeration of circulating tumor cells. Cytometry A 2007;71:154-162.
(13) Barnes JP. Physiologic resection of the right colon. Surg Gynecol Obstet 1952;94:722-726.
(14) Turnbull RB Jr., Kyle K, Watson FR, Spratt J. Cancer of the colon: the influence of the no-touch isolation technic on survival rates. Ann Surg 1967;166:420-427.
(15) Atkin G, Chopada A, Mitchell I. Colorectal cancer metastasis: in the surgeon’s hands? Int Semin Surg Oncol 2005;2:5.
(16) Reza MM, Blasco JA, Andradas E, Cantero R, Mayol J. Systematic review of laparoscopic versus open surgery for colorectal cancer. Br J Surg 2006;93:921-928.
(17) Lacy AM, Garcia-Valdecasas JC, Delgado S, Castells A, Taura P, Pique JM, et al. Laparoscopy-assisted colectomy versus open colectomy for treatment of non-metastatic colon cancer: a randomised trial. Lancet 2002;359:2224-2229.
(18) A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med 2004;350:2050-2059.
(19) Leung KL, Kwok SP, Lam SC, Lee JF, Yiu RY, Ng SS, et al. Laparoscopic resection of rectosigmoid carci-noma: prospective randomised trial. Lancet 2004;363:1187-1192.
(20) Maartense S, Dunker MS, Slors JF, Cuesta MA, Gouma DJ, van Deventer SJ, et al. Hand-assisted laparo-scopic versus open restorative proctocolectomy with ileal pouch anal anastomosis: a randomized trial. Ann Surg 2004;240:984-991.
(21) Tuynman JB, Bemelman WA, van Lanschot JJ. [Laparoscopic resection of colon carcinoma]. Ned Tijdschr Geneeskd 2004;148:2315-2318.
(22) Wind J, Hofland J, Preckel B, Hollmann MW, Bossuyt PM, Gouma DJ, et al. Perioperative strategy in colonic surgery; LAparoscopy and/or FAst track multimodal management versus standard care (LAFA trial). BMC Surg 2006;6:16.
(23) TNM Classification of Malignant Tumours. Sixth ed. New-York: Wiley-Liss; 2002.
(24) Kagan M, Howard D, Bendele T, Mayes J, Silva J, Repollet M, et al. A sample preparation and analysis system for identification of circulating tumor cells. J Clin Ligand Assay 2002;25:104-110.
(25) Rao CG, Chianese D, Doyle GV, Miller MC, Russell T, Sanders RA Jr., et al. Expression of epithelial cell adhesion molecule in carcinoma cells present in blood and primary and metastatic tumors. Int J Oncol 2005;27:49-57.
(26) Tibbe AG, Swennenhuis JF, Terstappen LW. Detection of cytogenetic aberrations in circulating tumor cells. Proc Annu Meet Am Assoc Cancer Res 2006;74:-A3624.
(27) Taniguchi T, Makino M, Suzuki K, Kaibara N. Prognostic significance of reverse transcriptase-polymerase chain reaction measurement of carcinoembryonic antigen mRNA levels in tumor drainage blood and peripheral blood of patients with colorectal carcinoma. Cancer 2000;89:970-976.
(28) Sadahiro S, Suzuki T, Tokunaga N, Yurimoto S, Yasuda S, Tajima T, et al. Detection of tumor cells in the portal and peripheral blood of patients with colorectal carcinoma using competitive reverse transcriptase-polymerase chain reaction. Cancer 2001;92:1251-1258.
(29) Tien YW, Lee PH, Wang SM, Hsu SM, Chang KJ. Simultaneous detection of colonic epithelial cells in portal venous and peripheral blood during colorectal cancer surgery. Dis Colon Rectum 2002;45:23-29.
(30) Koch M, Weitz J, Kienle P, Benner A, Willeke F, Lehnert T, et al. Comparative analysis of tumor cell dissemination in mesenteric, central, and peripheral venous blood in patients with colorectal cancer. Arch Surg 2001;136:85-89.
(31) Mizuno N, Kato Y, Izumi Y, Irimura T, Sugiyama Y. Importance of hepatic first-pass removal in metasta-sis of colon carcinoma cells. J Hepatol 1998;28:865-877.
Wind (Chris).indb 223Wind (Chris).indb 223 28-05-2008 15:45:0028-05-2008 15:45:00

224
(32) Yamaguchi K, Takagi Y, Aoki S, Futamura M, Saji S. Significant detection of circulating cancer cells in the blood by reverse transcriptase-polymerase chain reaction during colorectal cancer resection. Ann Surg 2000;232:58-65.
(33) Tsavellas G, Patel H, len-Mersh TG. Detection and clinical significance of occult tumour cells in colorectal cancer. Br J Surg 2001;88:1307-1320.
(34) Cristofanilli M, Hayes DF, Budd GT, Ellis MJ, Stopeck A, Reuben JM, et al. Circulating tumor cells: a novel prognostic factor for newly diagnosed metastatic breast cancer. J Clin Oncol 2005;23:1420-1430.
(35) Weitz J, Kienle P, Lacroix J, Willeke F, Benner A, Lehnert T, et al. Dissemination of tumor cells in patients undergoing surgery for colorectal cancer. Clin Cancer Res 1998;4:343-348.
(36) Lundy J. Anesthesia and surgery: a double-edged sword for the cancer patient. J Surg Oncol 1980;14:61-65.
(37) Chen WS, Chung MY, Liu JH, Liu JM, Lin JK. Impact of circulating free tumor cells in the peripheral blood of colorectal cancer patients during laparoscopic surgery. World J Surg 2004;28:552-557.
(38) Patel H, Le MN, Wharton RQ, Khan ZA, Araia R, Glover C, et al. Clearance of circulating tumor cells after excision of primary colorectal cancer. Ann Surg 2002;235:226-231.
(39) len-Mersh TG, McCullough TK, Patel H, Wharton RQ, Glover C, Jonas SK. Role of circulating tumour cells in predicting recurrence after excision of primary colorectal carcinoma. Br J Surg 2007;94:96-105.
(40) Bosch B, Guller U, Schnider A, Maurer R, Harder F, Metzger U, et al. Perioperative detection of dissemi-nated tumour cells is an independent prognostic factor in patients with colorectal cancer. Br J Surg 2003;90:882-888.
(41) Bessa X, Pinol V, Castellvi-Bel S, Piazuelo E, Lacy AM, Elizalde JI, et al. Prognostic value of postoperative detection of blood circulating tumor cells in patients with colorectal cancer operated on for cure. Ann Surg 2003;237:368-375.
(42) Bessa X, Castells A, Lacy AM, Elizalde JI, Delgado S, Boix L, et al. Laparoscopic-assisted vs. open colec-tomy for colorectal cancer: influence on neoplastic cell mobilization. J Gastrointest Surg 2001;5:66-73.
Wind (Chris).indb 224Wind (Chris).indb 224 28-05-2008 15:45:0028-05-2008 15:45:00

Summary and conclusions
Wind (Chris).indb 225Wind (Chris).indb 225 28-05-2008 15:45:0028-05-2008 15:45:00

226
Summary and conclusions
In this thesis, several aspects of colorectal surgery are highlighted. The aim of this thesis
was to critically appraise colorectal surgery and to evaluate potential improvements in
perioperative care (part I), complications (part II), and prognostication (part III).
Part I: Fast track colorectal surgery
In chapter 1 the application of fast track perioperative care in colonic surgery is described.
Fast track perioperative care programmes have been introduced in several surgical
procedures. In colonic surgery fast track perioperative care is defined as an intensive
multimodal programme combining a number of perioperative elements with the purpose
to preserve preoperative body composition and organ functions and to actively enhance
postoperative recovery. The essence of fast track perioperative care consists of extensive
preoperative counselling, no preoperative fasting but adequate nutrition, omission of oral
bowel preparation, reducing the surgical trauma, no routine use of drains and nasogastric
tubes, tailored anaesthesiology encompassing thoracic epidural, early and enhanced
postoperative feeding and mobilisation and medicinal support with prokinetics and
laxatives. Furthermore, it is highlighted that for some elements there is solid evidence that
its implementation results in less morbidity and an enhanced postoperative recovery; e.g.
removal of the nasogastric tube at the time of extubation and the omision of oral bowel
preparation. For other elements the evidence is less robust, and the implementation into
a fast track perioperative care programme is in those cases either based on “common
sense” or on consensus interpretation of accumulating evidence. However, it should be
noted that concernig all the individual elements the available evidence is derived from
traditional perioperative care settings.
In chapter 2 a systematic review is performed of all randomised and clinical controlled
trials on fast track perioperative care in colonic surgery. The main endpoints were the
number of applied fast track perioperative care elements, postoperative hospital stay,
readmission rate, morbidity and mortality. After a systematically performed search in
several databases, six studies (three randomised and three clinical controlled trials) were
eligible for analysis, including 512 patients. The fast track perioperative care programmes
that were applied in the included studies contained an average of nine of the 17 fast
track elements as defined in the literature. The pooled analysis showed that fast track
perioperative care significantly reduced primary hospital stay (weighted mean difference:
-1.56, 95% confidence interval [CI]: -2.61 to -0.50) and morbidity (relative risk 0.54, 95%
CI: 0.42 to 0.69). Readmission rates were not significantly different and there was no
increase in mortality. Based on this limited evidence, fast track perioperative care appears
safe and enhances postoperative recovery after elective colorectal surgery. However, as
the evidence is limited, a multi-centre randomised trial seems justified.
To investigate whether the demonstrated benefits of fast track perioperative care
Wind (Chris).indb 226Wind (Chris).indb 226 28-05-2008 15:45:0028-05-2008 15:45:00

227
Sum
mary and conclusions
could also be applied on our own patient population, a pilot study was initiated at the
Academic Medical Centre. The results of this study are presented in chapter 3. All 55
patients, scheduled for elective segmental colorectal resection and treated in a fast track
perioperative care programme were compared to a control-group of 52 patients treated
in a traditional care setting. Successful implementation of the fast track care programme
demonstrated to be difficult, since only 7.4 out of 13 predefined and evaluated fast
track care elements were achieved per patient. Despite incomplete implementation and
a potentially higher incidence of readmissions, primary and overall hospital stay were
shorter after fast track perioperative care without affecting patient-satisfaction. Median
primary hospital stay was 4.0 vs. 6.0 days and median overall hospital stay was 4.0 vs.
6.5 days. No robust conclusions could be drawn from a subgroup analysis in which
open and laparoscopic surgery as well as traditional care and fast track perioperative
care were compared, because the numbers of patients were too small. Nonetheless, the
largest reduction in primary and overall hospital stay was observed in patients who had
laparoscopic surgery and fast track perioperative care.
To further assess the optimal combination, in chapter 4 a systematic review was
performed of all randomised and controlled clinical trials on laparoscopic and open surgery
both incorporated within a fast track perioperative care programme. Main endpoints
were primary and overall hospital stay, readmission rate, morbidity, and mortality. After
a systematically performed literature search only two randomised and three controlled
clinical trials were eligible for final analysis, which reported on a total of 400 patients.
The extracted data of the individual studies could not be pooled because of clinical
heterogeneity. Two studies of the five included studies reported a shorter primary hospital
stay in the laparoscopic group of two and three days. In one study the readmission rate
was lower after laparoscopic surgery (absolute risk reduction 21.4%, and a “numbers
needed to treat” of 4.7 patients). One study showed a 23% difference in favour of the
laparoscopic group with regard to morbidity, i.e. a “numbers needed to treat” of 4.4
patients. Concernig the main endpoints in the individual studies no further significant
differences between open and laparoscopic surgery within a fast track perioperative care
programme were found.
Despite some reported advantages of laparoscopic surgery, based on the lack of evidence,
no robust conclusions can be made. A large randomised controlled trial is required to
compare laparoscopic with open surgery within a fast track perioperative care setting.
In chapter 5 such a randomised controlled multi-centre trial is proposed. The LAFA-
trial (LAparoscopy and/or FAst track multimodal management versus standard care) is
conceived to determine whether laparoscopic surgery, fast track perioperative care
or a combination of both is to be preferred over open surgery with traditional care in
patients having segmental colectomy for malignant disease. The LAFA-trial is a double
blinded, multicentre trial with a two by two balanced factorial design. Patients eligible
for segmental colectomy for malignant colorectal disease i.e. right and left colectomy
and anterior resection are randomised to either open or laparoscopic colectomy, and
to either traditional care or fast track perioperative care. This factorial design produces
Wind (Chris).indb 227Wind (Chris).indb 227 28-05-2008 15:45:0028-05-2008 15:45:00

228
four treatment groups; open segmental colectomy with traditional care, open segmetal
colectomy with fast track perioperative care, laparoscopic segmental colectomy with
traditional care, and laparoscopic surgery with fast track perioperative care. The primary
outcome parameter is postoperative hospital stay including readmissions within 30 days.
Secondary outcome parameters are quality of life two and four weeks after surgery,
overall hospital costs, morbidity, patient satisfaction and readmission rate. The LAFA-trial
has started in 2005 and will be finished in the begining of 2009. Hopefully this trial will
answer the question which combination of perioperative care and type of surgery is the
most optimal combination.
Part II: Complications in colorectal surgery
In chapter 6 several techniques for the establishment of the pneumoperitoneum are
described including the equipment that is used and the potential complications that can
occur. Roughly entry techniques can be divided in two groups. The first group comprises
introductions performed without direct visual control, the so called blind entry techniques
(e.g. introductions with a Veress needle). The other group comprises of entry techniques
performed under visual control. The latter includes the open entry technique and
closed entry techniques with optical trocar devices. In this chapter it is demonstrated
that concerning entry-related complications approximately one half of all intra-operative
laparoscopic complications is caused during the establishment of the pneumoperitoneum
and introduction of the trocars. The reported incidence of vascular and bowel injuries
varies and is between approximately 0.05 and 0.5 complication per 100 laparoscopic
procedures. The reviewed literature in this chapter, suggests that the open-entry technique
is the safest introduction technique because an overshoot of the introduction, especially
those resulting in retroperitoneal vascular injury can be avoided. However, open-entry
techniques do not preclude bowel injury.
Chapter 7 describes a retrospective chart review including all malpractice claims concerning
entry-related injuries filed at MediRisk, which is presently the largest medical liability mutual
insurance company for institutions, mainly hospitals in health care in the Netherlands. From
January 1993 to December 2005, 229 laparoscopy-related claims were filed of which 41
(18%) claims were identified as entry-related complications. Therefore, medical liability claims
concerning laparoscopic entry-related complications comprise one fifth of all laparoscopy-
related claims. Patients that filed a claim were mostly young females with a history of
abdominal surgery who were operated on in a day-care setting or had short-stay surgery
with severe consequences of the entry-related complication. In the investigated cases most
claims involved the closed-entry technique. Vascular injury was exclusively associated with
the closed-entry technique. In more than half of the complications, the entry-related injury
was diagnosed with a delay. There was no mortality. Besides conversion, the majority of
the patients filed a claim to compensate for the longer hospital stay and related costs. A
payment was made in 17 (57%) of the 30 settled claims.
Wind (Chris).indb 228Wind (Chris).indb 228 28-05-2008 15:45:0128-05-2008 15:45:01

229
Sum
mary and conclusions
In chapter 8 the feasibility, safety, and potential benefits of a laparoscopic reintervention
for anastomotic leakage after primary laparoscopic surgery was assessed. From January
2003 to January 2006, ten consecutive patients who underwent laparoscopic colorectal
resection and subsequently developed anastomotic leakage, underwent a laparoscopic
reintervention. Relaparotomy was performed in fifteen consecutive patients who had
primary open surgery. In this chapter a laparoscopic reintervention after primary laparoscopic
surgery for anastomotic leakage appears feasible and safe in terms of conversions, intra-
operative morbidity, necessity of opening the minilaparotomy, and operating time. In
addition, laparoscopic reintervention was associated with less postoperative morbidity
(40% vs. 80%), shorter postoperative ileus (resumption of a normal diet; three vs. six
days), and a faster recovery (hospital stay; nine vs. 13 days). Furthermore, the incidence
of incisional hernia was zero percent in the laparoscopic group versus 33% in the open
group. Nonetheless, this are preliminary data and, ideally a prospective trial, should
confirm these data. To evaluate the effect of laparoscopic reintervention after primary
laparoscopic surgery, it has to be part of a very large study randomising patients for a
laparoscopic or open initial procedure.
In chapter 9 potential usage concerns regarding linear cutters are described. An
incomplete linear staple line discovered during the stapling of an ileal pouch presented
as a case report in this chapter indicated that malfunctioning might occur when using
linear cutters. Subsequently, in an animal model three different lengths of linear cutters
(Proximate®, Ethicon Endo-Surgery) were used to cross staple and transect the large bowel
of one pig to check for the integrity of the proximal end of the staple line. The experiment
demonstrated that when the tissue was advanced up to the highest number on the scale
of the 100 mm stapling device an insufficient overlap between the proximal end of the
staple line and the proximal end of the cut line occured. Although a more than 100 mm
staple line was delivered, the 100 mm cutter may not produce a double-staggered row of
staples at the most proximal end of the staple line when the tissue is advanced past the 9.5
centimeters mark. Ethicon Endo-Surgery has agreed to add indicator markers to the scale
label on the instrument to provide the user with additional guidance for tissue placement.
Nevertheless, it remains important to routinely inspect the pouch after linear stapling,
both anteriorly and posteriorly, by inversion of the pouch to check for insufficiency of the
proximal staple line. On the posterior site, the hole is oversewn and at the anterior site of
the pouch the hole is incorporated in the purse string of the anvil of the circular stapler.
In case of a side-to-end colonic anastomosis, the proximal end of the cross stapling line
should also be routinely checked and oversewn if necessary.
In chapter 10 literature regarding different strategies for open-abdomen treatment in
terms of full fascial closure of the abdomen is systematically reviewed. The aim of this
review was to investigate which temporary closure technique has the highest rate of
full fascial closure. The results of this review suggest that temporary abdominal closure
techniques that keep traction on the fascial edges, including Vacuum Assisted Closure
(VAC®) result in high rates of fascial closure. Furthermore, techniques with high closure
rates seemed to result in relatively low rates of fistula, abscesses, and mortality. After open-
Wind (Chris).indb 229Wind (Chris).indb 229 28-05-2008 15:45:0128-05-2008 15:45:01

230
abdomen management when full fascial closure during index admission is not possible,
the fascial defect can be left to heal by secondary intention or an absorbable mesh can
be used to close the abdomen. These planned ventral hernias are often associated with
enterocutaneous fistula and stomas. Closure of enterocutaneous fistula and/or stomas and
simultaneous management of a large abdominal defect is a difficult procedure. In chapter 11 the results of closure of enterocutaneous fistula and/or stomas and simultaneous
abdominal wall repair using the components separation technique were described. All
patients with enterocutaneous fistula and/or stomas in the presence of large abdominal
wall defects (i.e. laparostomy of ventral hernia) who underwent a single-stage repair using
the components separation technique in the period January 2000 to July 2007 were
reviewed retrospectively. The study demonstrated that closure of enterocutaneous fistula
or stomas in the presence of large abdominal wall defects is feasible using the components
separation technique. This technique is one of the few options available to deal with this
very difficult problem. Early recurrence of abdominal hernia (7/32) and fistula (4/15) was
acceptable but morbidity (16/32) was considerable. Suggested modifications to preserve
the blood supply of the skin and subcutaneous tissue, extended antibiotic therapy and
changes in mesh repair might improve outcome.
Part III: Prognostication in colorectal cancer
The impact of extracapsular lymph node involvement has been studied for several
malignancies, including gastrointestinal malignancies. In chapter 12 the literature on
extracapsular lymph node involvement in gastrointestinal malignancies is systematically
reviewed in order to assess the current evidence on extracapsular lymph node involvement
as a prognostic factor for recurrence in gastrointestinal malignancies. Based on the limited
evidence available it can be concluded that extracapsular lymph node involvement is a
common phenomenon in patients with gastrointestinal malignancies. The pooled incidence
of extracapsular lymph node involvement was 57% (95% CI: 53-61%) for oesophageal
cancer, 41% (95% CI: 36-47%) for gastric cancer, and 35% (95% CI: 31-40%) for rectal
cancer. Furthermore, extracapsular lymph node involvement identified a subgroup of
patients with a significantly worse long-term survival. This systematic review highlighted
the importance of assessing extracapsular lymph node involvement as a valuable
prognostic factor. Pathologists and clinicians should be aware of this important feature.
Further research is, however, warranted on the correlation of extracapsular lymph node
involvement with different histological types and other important covariates, such as the
recurrence pattern and the effect of (neo-) adjuvant therapy.
Since the prognostic significance of extracapsular lymph node involvement was not yet
established in colonic cancer as demonstrated in the above mentioned systematic review,
a retrospective study was undertaken which is described in chapter 13. Between January
1994 and May 2005, all patients who underwent resection for primary colonic cancer
with lymph node metastasis were reviewed. In a multivariate analysis, pN-stage (hazard
Wind (Chris).indb 230Wind (Chris).indb 230 28-05-2008 15:45:0128-05-2008 15:45:01

231
Sum
mary and conclusions
ratio 3.50, 95% CI: 1.72–7.42) and extracapsular lymph node involvement (hazard ratio
1.98, 95% CI: 1.00–3.91) were the only significant factors, indicating that extracapsular
lymph node involvement in colonic cancer is an independent negative prognostic factor,
reflecting a particularly aggressive biological behaviour. Interestingly, among patients
without extracapsular lymph node involvement, those receiving adjuvant chemotherapy
had a significantly better survival. In contrast, chemotherapy did not improve disease free
survival in patients with extracapsular lymph node involvement. Therefore, detection and
quantification of extracapsular lymph node involvement in the surgical resection specimen
might also be helpful in the future to individualize postoperative therapeutic strategies in
the adjuvant setting.
Finally, in chapter 14 the presence and amount of circulating tumour cells was assessed in
peripheral and portal blood of patients who had open or laparoscopic surgery for primary
colonic cancer. Patients in the laparoscopic group were operated on in a medial to lateral
approach (“vessels first”), in the open group a lateral to medial approach was applied. The
enumeration of circulating tumour cells was performed with immuno-magnetic isolation
and immuno-specific labelling. This technique not only counts complete cells instead of
cellular fragments as done by RNA identification by Polymerase Chain Reaction (PCR) but
also allows for evaluation of the morphology of the detected circulating tumour cells.
It was shown that the presence of circulating tumour cells was significantly increased
intra-operatively and was in general significantly higher in portal blood. Between 4-7%
of the pheripheral and 26-45% of the portal samples contained circulating tumour cells.
Significantly less circulating tumour cells were detected during laparoscopic surgery
possibly as result of the medial to lateral approach. Fluorescence In Situ Hybridization
(FISH) was applied as an additional tool to determine the true signature of these cells with
the different morphology. Both circulating tumour cells and primary tumour tissue were
diploid. Although the primary tumour tissue and circulating tumour cells showed the same
cytogenetic profile this does not provide a definite answer whether or not the detected
circulating tumour cells were true tumour cells or if these were normal epithelial cells that
were shed into the portal blood due to the surgical trauma.
Wind (Chris).indb 231Wind (Chris).indb 231 28-05-2008 15:45:0128-05-2008 15:45:01
Wind (Chris).indb 232Wind (Chris).indb 232 28-05-2008 15:45:0128-05-2008 15:45:01

Samenvatting en conclusies
Wind (Chris).indb 233Wind (Chris).indb 233 28-05-2008 15:45:0128-05-2008 15:45:01

234
Samenvatting en conclusies
In dit proefschrift worden verschillende aspecten van de colorectale chirurgie belicht met
als doel de colorectale chirurgie kritisch te beschouwen en potentiële verbeteringen te
evalueren. Dit zal gedaan worden in drie afzonderlijke onderdelen, waarbij de focus ligt op
de peri-operatieve zorg (deel I), complicaties (deel II) en het voorspellen van de overleving
van patiënten die wegens een colorectale maligniteit zijn geopereerd (deel III).
Deel I: Fast track colorectale chirurgie
In hoofdstuk 1 wordt fast track peri-operatieve zorg bij colon chirurgie beschreven. Fast
track peri-operatieve zorg is reeds geïntroduceerd bij verschillende chirurgische ingrepen.
Binnen de colon chirurgie kan fast track peri-operatieve zorg worden gedefinieerd als
een intensief multidisciplinair programma waarbij diverse peri-operatieve componenten
worden gecombineerd tot één protocol, met als doel het behoud van preoperatieve
lichaamssamenstelling en orgaanfuncties, en het actief stimuleren van het postoperatieve
herstel. In essentie komt fast track peri-operatieve zorg neer op uitgebreide preoperatieve
voorlichting, adequate voeding preoperatief met het vermijden van langdurig nuchter zijn,
het weglaten van orale darmvoorbereiding, minimaal invasieve chirurgie en anesthesie, het
vermijden van abdominale drains en maagsondes, adequate peri-operatieve pijnstilling met
behulp van ondermeer thoracale epiduraal anesthesie en analgesie, snelle mobilisatie en
snelle hervatting van voedselinname en medicamenteuze ondersteuning met pro-kinetica
en laxantia. Verder komt in dit hoofdstuk naar voren dat er voor een aantal componenten
in het fast track programma, zoals het weglaten van orale darmvoorbereiding en de
maagsonde postoperatief, gedegen wetenschappelijk bewijs bestaat waaruit blijkt dat de
implementatie van deze componenten morbiditeit reduceert en het herstel bespoedigt.
Voor andere componenten is er echter minder wetenschappelijk bewijs voorhanden. De
implementatie van deze componenten in het fast track programma berust op consensus
interpretatie van het bestaande bewijs of op basis van “common sense”. Belangrijk te
vermelden is dat voor alle afzonderlijke componenten van het fast track programma het
bestaande bewijs afkomstig is uit onderzoeken die zijn uitgevoerd in een traditionele zorg
setting.
In hoofdstuk 2 wordt een literatuur studie beschreven waarbij alle gerandomiseerde
en klinisch gecontroleerde studies naar de effecten van fast track peri-operatieve zorg
bij colorectale chirurgie zijn geïncludeerd. De voornaamste eindpunten die in dit review
werden beschouwd, zijn het aantal toegepaste fast track componenten, duur van het
postoperatief ziekenhuis verblijf, het aantal heropnames, morbiditeit en mortaliteit. Na
het systematisch doorzoeken van verschillende databestanden bleken er zes studies (drie
gerandomiseerde en drie klinisch gecontroleerde studies) geschikt, waarin 512 patiënten
waren geïncludeerd. De fast track programma’s die in de verschillende studies werden
toegepast bestonden gemiddeld slechts uit 9 van de 17 in de literatuur gedefinieerde
Wind (Chris).indb 234Wind (Chris).indb 234 28-05-2008 15:45:0128-05-2008 15:45:01

235
Sam
envatting en conclusies
fast track componenten. De gepoolde resultaten lieten zien dat fast track peri-operatieve
zorg de primaire opnameduur significant reduceerde (gemiddeld gewogen verschil:
-1.56, 95% betrouwbaarheidsinterval [BI]: -2.61 tot -0.50) en de morbiditeit significant
reduceerde (relatieve risico 0.54, 95% BI: 0.42 tot 0.69). Het aantal heropnames was
niet significant verschillend ten opzichte van traditionele zorg en er was geen toename
in mortaliteit. Gebaseerd op dit beperkte bewijs lijkt fast track peri-operatieve zorg bij
colorectale chirurgie veilig te zijn en bovendien het postoperatieve herstel te bespoedigen.
Omdat echter het aantal beschikbare relevante studies beperkt is, lijkt een multi-centrisch
gerandomiseerd onderzoek gerechtvaardigd.
Om te onderzoeken of een dergelijk fast track programma ook voordelen biedt binnen
onze eigen patiëntenpopulatie, werd een pilot-studie verricht in het Academisch Medisch
Centrum in Amsterdam. De resultaten van deze studie worden weergegeven in hoofdstuk 3. Vijfenvijftig consecutieve patiënten die electief een resectie ondergingen van de dikke
darm werden volgens fast track peri-operatieve zorg principes behandeld. Zij werden
vergeleken met 52 consecutieve patiënten die werden behandeld in een traditioneel
zorg programma. Succesvolle implementatie van het fast track programma bleek lastig;
slechts 7.4 van de 13 van tevoren gedefinieerde fast track componenten werden volledig
toegepast per patiënt. Echter, ondanks deze onvolledige implementatie en mogelijk
een hoger aantal heropnames, waren de primaire en de totale opnameduur korter in
de fast track peri-operatieve zorg groep zonder dat dit de patiënttevredenheid negatief
beïnvloedde. De mediane primaire opnameduur was 4.0 ten opzichte van 6.0 dagen en de
mediane totale opnameduur was 4.0 ten opzichte van 6.5 dagen. Aan de in dit hoofdstuk
uitgevoerde subgroep analyse, waarin zowel open en laparoscopische chirurgie als ook
fast track en traditionele zorg werden vergeleken, mogen geen harde conclusies worden
ontleend omdat de patiënt aantallen in de groepen klein waren. Desalniettemin werd de
grootste reductie van de primaire en totale opnameduur bereikt in de groep patiënten die
laparoscopisch werden geopereerd in een fast track programma.
Om meer inzicht te verkrijgen in de optimale combinatie van de manier van opereren en
peri-operatieve zorg, wordt er in hoofdstuk 4 een literatuur studie beschreven waarbij alle
gerandomiseerde en klinisch gecontroleerde studies naar open en laparoscopische chirurgie,
beiden in een fast track programma, werden geïncludeerd. De voornaamste eindpunten
die in dit review werden beschouwd zijn de primaire en totale opnameduur, het aantal
heropnames, morbiditeit en mortaliteit. Na het systematisch doorzoeken van verschillende
databestanden waren er slechts twee gerandomiseerde en drie klinisch gecontroleerde
studies beschikbaar waarin 400 patiënten waren geïncludeerd. De data uit de individuele
studies kon niet worden gepoold op basis van klinische heterogeniteit. In twee van de
vijf geïncludeerde studies werd een kortere primaire opnameduur gerapporteerd in de
laparoscopische groep van 2 en 3 dagen. In één studie was het percentage heropnames
significant lager na laparoscopische chirurgie (absolute risico reductie 21.4%, en “numbers
needed to treat” van 4.7 patiënten). Ten aanzien van morbiditeit rapporteerde één studie
een 23% verschil in het voordeel van laparoscopische chirurgie, neerkomend op een
“numbers needed to treat” van 4.4 patiënten. Verder werden in de geïncludeerde studies,
Wind (Chris).indb 235Wind (Chris).indb 235 28-05-2008 15:45:0128-05-2008 15:45:01
236
met betrekking tot de voornaamste eindpunten, geen significante verschillen beschreven
tussen de open en laparoscopische groep.
Ondanks enkele hierboven beschreven voordelen van laparoscopische chirurgie in een
fast track programma kunnen door een gebrek aan wetenschappelijk bewijs geen harde
conclusies worden getrokken. Een grote gerandomiseerde studie is daarom nodig om
laparoscopie met open chirurgie in een fast track programma te vergelijken.
In hoofdstuk 5 wordt een dergelijk gerandomiseerd multi-centrisch onderzoek voorgesteld.
Deze, zogehete LAFA-studie (LAparoscopie en/of FAst track peri-operatieve zorg versus
traditionele zorg), is ontworpen om te bepalen of laparoscopische chirurgie, fast track
peri-operatieve zorg of een combinatie van beide te prefereren is boven open chirurgie
met traditionele zorg bij patiënten die een segmentale colon resectie moeten ondergaan
wegens een maligniteit. De LAFA-studie is een dubbel blind gerandomiseerd multi-centrisch
onderzoek volgens een “2x2 balanced factorial design”. Patiënten die in aanmerking komen
voor een segmentale colon resectie wegens een maligniteit, dat wil zeggen een rechts- of
linkszijdige hemicolectomie en anterieure resecties, worden gerandomiseerd voor open of
laparoscopische chirurgie en voor traditionele zorg of voor fast track peri-operatieve zorg.
Door deze randomisatie ontstaan er vier behandelgroepen; open chirurgie met traditionele
zorg, open chirurgie met fast track peri-operatieve zorg, laparoscopische chirurgie met
traditionele zorg en laparoscopische chirurgie met fast track peri-operatieve zorg. Het
primaire eindpunt van deze studie is de duur van het ziekenhuisverblijf inclusief het aantal
heropnames binnen 30 dagen. Secundaire eindpunten zijn kwaliteit van leven twee en
vier weken postoperatief, totale ziekenhuiskosten, morbiditeit, patiënttevredenheid en het
aantal heropnames. De LAFA-studie is gestart in 2005 en zal in het begin van 2009 worden
afgerond. Hopelijk zal deze studie het antwoord geven op de vraag welke combinatie van
peri-operatieve zorg en manier van opereren het meest optimaal is.
Deel II: Complicaties in de colorectale chirurgie
In hoofdstuk 6 wordt een overzicht gegeven van de verschillende manieren om een
pneumoperitoneum aan te leggen, inclusief het daarbij benodigde instrumentarium en
potentiële complicaties die kunnen optreden. Grofweg zijn er twee groepen technieken
te onderscheiden voor het aanleggen van het pneumoperitoneum en de introductie van
de trocars. Allereerst zijn er introductie technieken die niet onder zicht plaatsvinden, de
zogenaamde blinde introducties, bijvoorbeeld met de Veress naald. Daarnaast zijn er
introductie technieken die plaatsvinden onder direct zicht. Tot deze laatste groep worden
de open introductie volgens Hasson en de gesloten introductie technieken met optische
trocar systemen gerekend. In dit hoofdstuk wordt beschreven dat ongeveer de helft van
alle intra-operatieve complicaties optreedt tijdens de introductiefase, nog voor er met
de daadwerkelijke ingreep is gestart. De incidentie van een darm- of vaatletsel varieert
in de literatuur tussen de 0.05-0.5 complicaties per 100 laparoscopische ingrepen. De
in dit hoofdstuk gerefereerde literatuur suggereert, dat de open introductie techniek
Wind (Chris).indb 236Wind (Chris).indb 236 28-05-2008 15:45:0128-05-2008 15:45:01

237
Sam
envatting en conclusies
de veiligste introductie biedt omdat “doorschiet” letsels, in het bijzonder letsels van de
grote retroperitoneale vaten kunnen worden vermeden. Echter, een open introductie sluit
darmletsel niet uit.
In hoofdstuk 7 wordt een retrospectieve analyse beschreven van alle medische
aansprakelijkheid claims betreffende aan de introductie gerelateerde complicaties die
werden ingediend bij de op dit moment grootste verzekeringsmaatschappij voor medische
aansprakelijkheid voor Nederlandse ziekenhuizen (MediRisk). Tussen januari 1993 en
december 2005 werden er 229 claims betreffende laparoscopische chirurgie ingediend
bij MediRisk. In 41 (18%) claims betrof het een introductie gerelateerde complicatie. Met
andere woorden, ongeveer een vijfde van alle laparoscopisch gerelateerde claims betreft
een introductie letsel. In deze studie betrof het voornamelijk jonge vrouwelijke patiënten
met in hun voorgeschiedenis één of meerdere buikoperaties, die werden geopereerd in
dagbehandeling of als korte opname, waarbij het introductie letsel ernstige gevolgen had.
In de onderzochte claims betrof het in bijna alle gevallen een blinde introductie techniek.
Alle vaatletsels werden veroorzaakt tijdens een blinde introductie. In meer dan de helft
van de introductie letsels werd de diagnose pas later gesteld. Er was in de geïncludeerde
claims geen sprake van mortaliteit. Naast het feit dat de laparoscopische procedure was
geconverteerd, diende de meerderheid van de patiënten een claim in ter compensatie
van een langere opnameduur en de daaruit voortvloeiende kosten. In 17 (57%) van de 30
afgehandelde claims werd er een uitbetaling gedaan.
In hoofdstuk 8 wordt de technische uitvoerbaarheid, veiligheid en het eventuele
voordeel van een laparoscopische reinterventie bij een verdenking op naadlekkage na
eerdere laparoscopische chirurgie geëvalueerd. In de periode januari 2003 tot januari
2006, ondergingen 10 consecutieve patiënten met een naadlekkage na een eerdere
laparoscopisch uitgevoerde colorectale resectie, een laparoscopische reinterventie.
Vijftien consecutieve patiënten die in dezelfde periode na een eerdere laparotomie een
naadlekkage ontwikkelden ondergingen een relaparotomie. De resultaten die in dit
hoofdstuk worden gepresenteerd suggereren dat een laparoscopische heroperatie wegens
naadlekkage technisch uitvoerbaar en veilig is wat betreft conversies, intra-operatieve
morbiditeit, de noodzaak om de mini-laparotomie te openen en operatietijd. Daarnaast
ging een laparoscopische reinterventie gepaard met minder postoperatieve morbiditeit
(40% versus 80%), een kortere postoperatieve ileus (tolereren van een normaal dieet; 3
versus 6 dagen) en een sneller herstel (opnameduur; 9 versus 13 dagen). Tot slot was de
incidentie van littekenbreuken 0% in de laparoscopische groep ten opzichte van 33% in de
open groep. Echter gezien het feit dat het om een kleine retrospectieve studie gaat moeten
deze data worden beschouwd als hypothesevormend. Idealiter moeten deze resultaten
worden bevestigd in een prospectieve studie. Om het effect van een laparoscopische
reinterventie na een eerdere laparoscopische ingreep te onderzoeken zou dit deel moeten
uitmaken van een zeer grote studie waarbij patiënten voor de eerste operatie al worden
gerandomiseerd voor een open of laparoscopische initiële procedure.
In hoofdstuk 9 wordt het potentieel niet goed functioneren van lineaire staplers
beschreven. Een defect in een gestapelde naad tijdens het aanleggen van een pouch
Wind (Chris).indb 237Wind (Chris).indb 237 28-05-2008 15:45:0128-05-2008 15:45:01

238
van het ileum na het gebruik van een lineaire stapler, gepresenteerd als een casus in dit
hoofdstuk, deed ons vermoeden dat er mogelijk een probleem zou kunnen bestaan met het
functioneren van de lineaire stapler. Om dit potentiële probleem verder te evalueren werd
in een dier experimenteel model het colon van een varken dwars gestapled gebruikmakend
van drie verschillende lengtes lineaire staplers (Proximate®, Ethicon Endo-Surgery). In het
experiment werd aangetoond dat wanneer het te stapelen weefsel wordt opgevoerd tot
het einde van de schaalaanduiding van de 100 mm stapler er een incomplete overlap
bestaat van de rij staples resulterend in een defect aan het proximale uiteinde. Hoewel de
staple rij een lengte heeft van meer dan 100 mm, kan het gebeuren dat er geen dubbele
rij staples wordt geplaatst ter plaatse van het proximale uiteinde wanneer het weefsel in
de stapler wordt opgevoerd voorbij het 9.5 centimeter markeringsteken. Ethicon Endo-
Surgery heeft op basis van deze bevindingen besloten om additionele markeringstekens
te plaatsen op de stapler om hiermee de gebruiker hulp te geven bij het juist plaatsen van
het weefsel in de stapler. Niettemin blijft het essentieel om routinematig het proximale
uiteinde van de pouch-naad te controleren, zowel aan de anterieure als aan de posterieure
zijde na het inverteren van de pouch. Aan de posterieure zijde wordt een eventueel
aanwezig defect overhecht, aan de anterieure zijde wordt het defect gereserceerd bij het
afvuren van de circulaire stapler. Ook bij het maken van een side-to-end colon anastomose
dient het proximale uiteinde van het dwars afgestapelde colon routinematig te worden
gecontroleerd en zonodig worden overhecht.
In hoofdstuk 10 wordt een systematische literatuur studie beschreven naar de verschillende
behandelstrategieën voor de open buik behandeling. Doel van dit review was te bepalen
welke techniek voor het tijdelijk sluiten van de open buik resulteert in het hoogste
percentage volledige fascie sluitingen tijdens de index opname. De resultaten die in dit
hoofdstuk worden gepresenteerd suggereren dat de technieken die tractie uitoefenen
op de fascie randen, zoals het Vacuum Assisted Closure (VAC®) systeem resulteren in de
hoogste percentages fascie sluiting. Daarnaast lijken deze technieken te zijn geassocieerd
met relatief weinig complicaties zoals fistels, abcessen en mortaliteit. Wanneer na een
open buik behandeling volledige fascie sluiting niet mogelijk is, kan het defect in de
fascie worden gesloten met een resorbeerbare mat of kan men het defect laten dicht
granuleren. Deze zogenaamde geplande ventrale hernia’s na een vaak gecompliceerd
beloop zijn echter vaak geassocieerd met enterocutane fistels en de aanwezigheid van
stoma’s. Het opheffen van deze stoma’s en enterocutane fistels met het gelijktijdig
corrigeren van het buikwanddefect is een moeilijke procedure. In hoofdstuk 11 worden
de resultaten van de Ramirez buikwandplastiek (“components separation”) beschreven
voor het opheffen van stoma’s en enterocutane fistels en het gelijktijdig stuiten van het
buikwanddefect. Een consecutieve serie patiënten met enterocutane fistels en/of stoma’s
in de aanwezigheid van een groot buikwanddefect (laparostoma of ventrale hernia) die
een correctie ondergingen in dezelfde procedure middels de Ramirez buikwandplastiek
werden retrospectief geanalyseerd. De studie periode betrof de periode januari 2000 tot
juli 2007. De resultaten toonden dat het opheffen van enterocutane fistels en stoma’s
Wind (Chris).indb 238Wind (Chris).indb 238 28-05-2008 15:45:0128-05-2008 15:45:01

239
Sam
envatting en conclusies
en het gelijktijdig corrigeren van een groot buikwanddefect haalbaar is met de Ramirez
buikwandplastiek. Deze techniek is een van de weinige opties voor de behandeling van
dit moeilijke probleem. Het aantal recidief ventrale hernia’s (7/32) en enterocutane fistels
(4/15) was acceptabel, de morbiditeit (16/32) was echter wel aanzienlijk. Mogelijk dat
technische aanpassingen aan de procedure om de bloedvoorziening van de huid en het
subcutane weefsels te behouden en uitgebreidere antibiotische behandeling de resultaten
verder kunnen verbeteren.
Deel III: Het voorspellen van de overleving bij het colorectaal carcinoom
De prognostische betekenis van extracapsulaire uitbreiding van een lymfklier metastase
is onderzocht bij diverse maligniteiten waaronder gastro-intestinale maligniteiten. In
hoofdstuk 12 wordt een systematische literatuur studie beschreven naar de prognostische
betekenis van extracapsulaire lymfklier uitbreiding bij gastro-intestinale maligniteiten.
Gebaseerd op beperkt wetenschappelijk bewijs kan worden geconcludeerd dat
extracapsulaire lymfklier uitbreiding een veel voorkomend fenomeen is bij gastro-intestinale
maligniteit. De gepoolde incidentie van extracapsulaire lymfklier uitbreiding was 57% (95%
BI: 53-61%) bij het slokdarmcarcinoom, 41% (95% BI: 36-47%) bij het maagcarcinoom en
35% (95% BI: 31-40%) bij het rectumcarcinoom. Extracapsulaire lymfklier uitbreiding was
sterk geassocieerd met een significant slechtere overleving. Dit hoofdstuk benadrukt het
belang van extracapsulaire lymfklier uitbreiding als een belangrijke prognostische factor.
Pathologen en clinici moeten zich hier dan ook van bewust zijn. Toekomstig onderzoek is
echter nodig naar de correlatie van extracapsulaire lymfklier uitbreiding en verschillende
histologische type tumoren en andere belangrijke factoren zoals het metastaseringspatroon
en het effect van (neo-) adjuvante behandeling.
Omdat de prognostische betekenis van extracapsulaire lymfklier uitbreiding nog niet
duidelijk is voor het coloncarcinoom, zoals duidelijk is geworden in het hierboven
genoemde review, wordt er in hoofdstuk 13 een retrospectieve studie beschreven die
als doel heeft dit te bestuderen. In de periode januari 1994 tot mei 2005 werden alle
patiënten die een resectie hadden ondergaan voor een primair coloncarcinoom waarbij
lymfklier metastasering was aangetoond retrospectief geanalyseerd. In een multivariate
analyse waren het pN-stadium (hazard ratio 3.50, 95% BI: 1.72–7.42) en extracapsulaire
lymfklier uitbereiding (hazard ratio 1.98, 95% BI: 1.00–3.91) de enige significante
variabelen. Dit betekent dat extracapsulaire lymfklier uitbereiding bij het coloncarcinoom
een onafhankelijke negatieve voorspeller is. Opmerkelijk was het feit dat patiënten met
lymfklier metastasering maar zonder extracapsulaire lymfklier uitbereiding een significant
betere overleving hadden na adjuvante chemotherapie terwijl chemotherapie de overleving
niet verbeterde bij patiënten die wel extracapsulaire lymfklier uitbereiding hadden. Daarom
zou het detecteren en kwantificeren van extracapsulaire lymfklier uitbereiding in het
Wind (Chris).indb 239Wind (Chris).indb 239 28-05-2008 15:45:0128-05-2008 15:45:01

240
resectie preparaat in de toekomst van waarde kunnen zijn bij de indicatiestelling omtrent
de keuze van adjuvante behandeling.
Tenslotte wordt er in hoofdstuk 14 een studie beschreven met als doel het detecteren
en kwantificeren van circulerende tumorcellen in perifeer en portaal bloed van patiënten
die een open of laparoscopische operatie ondergaan wegens een primair coloncarcinoom.
Patiënten in de laparoscopische groep werden geopereerd volgens een mediaal naar
laterale benadering (“no-touch” principe), in de open groep werd een lateraal naar
mediale benadering toegepast. Het detecteren en kwantificeren van de circulerende
tumorcellen werd gedaan middels immuno-magnetische isolatie en immuno-specifieke
labeling. Met deze techniek worden niet alleen complete cellen geïdentificeerd, maar ook
kan de morfologie van de gedetecteerde circulerende tumorcel worden geëvalueerd. Dit
in tegenstelling tot de cellulaire fragmenten welke gedetecteerd worden bij conventionele
bepaling van RNA middels Polymerase Chain Reaction (PCR). In deze studie kwam naar
voren dat de hoeveelheid circulerende tumorcellen significant was toegenomen intra-
operatief en significant hoger was in portaal bloed ten opzichte van perifeer bloed; tussen
de 4-7% van de perifere en 26-45% van de portale bloed afnamen waren positief voor de
aanwezigheid van circulerende tumorcellen. Significant minder circulerende tumorcellen
werden gevonden tijdens laparoscopische chirurgie. Dit kan mogelijk verklaard worden
door de gekozen benadering (mediaal naar lateraal). Fluorescentie in Situ Hybridisatie
(FISH) werd gebruikt als extra middel om de precieze herkomst van de geïdentificeerde
cellen te bepalen. Zowel de circulerende tumorcellen als de primaire tumor waren diploïd.
Alhoewel zowel de primaire tumor als de circulerende tumorcellen hetzelfde cytogenetische
profiel hebben, geeft dit geen definitief antwoord op de vraag of de geïdentificeerde
circulerende cellen daadwerkelijk tumorcellen zijn of dat het gaat om normale epitheliale
cellen die door het chirurgisch trauma in de bloedbaan zijn gekomen.
Wind (Chris).indb 240Wind (Chris).indb 240 28-05-2008 15:45:0128-05-2008 15:45:01

Dankwoord
Wind (Chris).indb 241Wind (Chris).indb 241 28-05-2008 15:45:0228-05-2008 15:45:02
242
Dankwoord
De totstandkoming van dit boekje was niet gelukt zonder de hulp en morele steun van
anderen. Ik wil iedereen die een bijdrage heeft geleverd aan dit proefschrift danken,
waarvan ik een aantal personen in het bijzonder wil noemen.
Mijn promotor, Prof. dr. Bemelman, beste Willem, ik beschouw het als een eer onderdeel
uitgemaakt te mogen hebben van jouw onderzoeksgroep. Ik heb door de jaren heen veel
bewondering gekregen voor jouw enthousiasme, energie en arbeidslust. Ik wil je danken
voor het vertrouwen en de vrijheid die je me hebt gegeven met uiteindelijk dit proefschrift
als resultaat. Ik hoop in de toekomst nog veel van je te mogen leren.
Mijn co-promotor, Prof. dr. Gouma, dank voor uw bijdrage aan dit proefschrift. Uw
kritische commentaar hebben zowel mijn manuscripten als mijn “wetenschappelijke blik”
scherper gemaakt.
Mijn andere co-promotor, Dr. Slors, beste Frederik, wat fijn waren jouw relativerende
opmerkingen. Dank dat je mijn co-promotor wilde zijn.
De overige leden van de promotiecommissie wil ik danken voor hun bereidheid het
proefschrift op zijn wetenschappelijke waarde te beoordelen. Dr. Dejong, beste Kees,
dank voor de inbreng bij alle fast track hoofdstukken. De NVGE en andere symposia
waren altijd gezellig ondanks het feit dat ik niet kan biljarten! Prof. dr. ten Kate, de vele
“kapseldoorbraak sessies” in de vroege morgen heb ik erg gewaardeerd, dank voor al uw
tijd. Prof. dr. Hollmann, beste Markus, erg efficiënt en prettig was de samenwerking met
de anesthesie. Ik hoop dat er mooie resultaten uit de “lidocaïne studie” komen. Prof. dr.
Cuesta, dank voor de korte lijntjes met de VU. Prof. dr. Richel, ik wil u danken voor uw
bereidheid zitting te nemen in de promotiecommissie.
Voor zover niet elders genoemd in dit dankwoord, wil ik alle co-auteurs van de hoofdstukken
danken voor hun bijdrage; Jan-Willem Fuhring, Jurriaan Tuynman, Prof. dr. van Lanschot,
Frank Willem Jansen, Jan Hofland, Jan Cremers, Prof. dr. von Meyenfeldt, Dr. Goslings,
Dr. Busch, Huib Cense, Edwin van der Zaag, Jordy Kiewiet, Arjan Tibbe, Dirk Ubbink, Jose
Maessen, Marcel Dijkgraaf en Roos Koopman.
Dr. van Berge Henegouwen, beste Mark, ik wil je danken voor je enthousiasme en je
bijdrage aan de manuscripten. Succes met de NOTES-onderzoekslijn!
De gehele LAFA-studiegroep en alle anderen die zich hebben ingespannen voor de
LAFA-studie, dank voor de goede samenwerking en de gastvrijheid in alle deelnemende
ziekenhuizen. Hopelijk dat er snel resultaten uit deze mooie studie komen!
Wind (Chris).indb 242Wind (Chris).indb 242 28-05-2008 15:45:0228-05-2008 15:45:02

243
D
ankwoord
De secretaresses van de afdeling Heelkunde, in het bijzonder Joke, Jaqueline, Trudi en
Carla, bedankt voor alles!
De G4 onderzoeksgroep. Ik wil jullie danken voor een onvergetelijke tijd; de Epstein bar,
NVGE, chirurgendagen, chirurgencup, de vele koffietjes maar ook de serieuze gesprekken,
ik zal ze missen! In willekeurige volgorde; Jikke, Sjoerd, Niels, Mark S, Emma, Mark van H,
Liselot, Philip, Oddeke, Ascelijn, Pieter, Teun, Eefje, Wytze, Robert, Ping, Steve, Marinke
en Koert.
Mijn opvolgster, Malaika, heel veel succes met de LAFA-studie en wat ziet mijn kamer er
opgeruimd uit!
Faiza, dank voor het corrigeren van hoofdstuk 1 en 6.
Alle onderzoekers van het chirurgisch lab, gelukkig een beetje geïntegreerd en dank voor
het opvangen van Paul!
Assistenten in het AMC, bedankt voor het geduld tijdens de operaties waarbij ik ontelbare
buisjes bloed nodig had.
Chirurgen en assistenten in Hilversum, wat geweldig is het om met jullie in de kliniek te
werken! Dank voor de tijd die ik nog aan dit boekje kon besteden.
Mijn vrienden en familie wil ik bedanken voor die heerlijke relativerende momenten, die er
eigenlijk veel te weinig waren, maar waar ik nu hopelijk weer meer tijd voor heb.
Mijn paranimfen en vrienden Bas en Paul. Wat hebben jullie mijn onderzoekstijd veel kleur
gegeven. Onze humor werd niet altijd door iedereen begrepen en gewaardeerd maar
dat maakte het alleen maar mooier. Het is me werkelijk een eer dat jullie naast me staan
tijdens de verdediging. Ik hoop nog veel met jullie te mogen samenwerken!
Rob, Carolien en Tessa, dank voor alle gezelligheid!
Lieve Oma, ik ben blij dat u erbij bent en ik ben trots dat u mijn oma bent!
Martin, dank voor de mooie en hachelijke avonturen op de “plassen”. Roeispanen zouden
ook steviger gemaakt moeten worden en één type benzine zou ook een uitkomst zijn. Ik
voel een mooi seizoen aankomen.
Marika, zusje, misschien heb ik dit proefschrift wel het meeste aan jou te danken. Immers
heb ik jouw weg gevolgd en ben ook geneeskunde gaan studeren. Anders was ik
waarschijnlijk toch brandweerman of timmerman geworden. Zus, ik ben trots op je!
Wind (Chris).indb 243Wind (Chris).indb 243 28-05-2008 15:45:0228-05-2008 15:45:02

244
Lieve pap en mam, dank voor al het vertrouwen, goede raad en bovenal liefde. Alles staat
of valt bij een goede fundering. Het boekje is daarom aan jullie opgedragen. Ik hoop nog
lang van jullie te mogen genieten!
Allerliefste Brenda (echtgenote!), jou ben ik het meest dankbaar van allemaal. Ik wil je
danken voor al je liefde, begrip en vooral je geduld. Jij was de grootste steun tijdens het
promoveren. Ik ga niet zeggen dat er een einde komt aan een hectische periode, want dit
is vast pas het begin. Maar met jou aan mijn zijde…kom maar op!!!
Wind (Chris).indb 244Wind (Chris).indb 244 28-05-2008 15:45:0228-05-2008 15:45:02

Curriculum Vitae
Wind (Chris).indb 245Wind (Chris).indb 245 28-05-2008 15:45:0228-05-2008 15:45:02

Wind (Chris).indb 246Wind (Chris).indb 246 28-05-2008 15:45:0228-05-2008 15:45:02
247
C
urriculum V
itae
Curriculum Vitae
On the sixth of May in 1979, a sunny Sunday morning, Jan Wind was born in Hilversum, the
Netherlands. He attended secondary school at the Comenius College in Hilversum, from
1991 until graduation in 1997. His medical study started in 1997 at the Free University
of Amsterdam. He passed his doctoral exam in 2001 and started the same year with his
internships. His medical degree was obtained in December 2003.
In January 2004 he started as a surgical resident at the Hilversum Hospital (currently
Tergooiziekenhuizen), where he worked until April 2005. In May 2005 he started
as a research fellow at the department of Surgery at the Academic Medical Centre in
Amsterdam (supervisor Prof. dr. W.A. Bemelman). The research performed during this
period resulted in the present thesis. In January 2008, he started his surgical training at
the Tergooiziekenhuizen in Hilversum (supervisor Dr. J.P. Eerenberg).
Wind (Chris).indb 247Wind (Chris).indb 247 28-05-2008 15:45:0228-05-2008 15:45:02

Wind (Chris).indb 248Wind (Chris).indb 248 28-05-2008 15:45:0228-05-2008 15:45:02





























