Embed Size (px)
Citation preview
The American Journal of Surgery (2013) 206 494-501
Clinical Science
Improving postoperative handover a prospectiveobservational study
Kamal Nagpal MS MRCS PhD May Abboudi BScChhavi Manchanda FRCA Amit Vats MRCS Nick Sevdalis PhDColin Bicknell MD FRCS Charles Vincent PhDKrishna Moorthy MS MD FRCS
Centre for Patient Safety and Service Quality Department
of Biosurgery and Surgical Technology Imperial CollegeLondon 10th floor QEQM St Maryrsquos Hospital South Wharf Road London W2 1NY UK
KEYWORDSPostoperativehandoverHandoverChecklistProforma
The authors declare no conflicts of in
This research was supported by the H
search Council (EPSRC)
Corresponding author Tel 100-4
E-mail address kamalnagpallahey
Manuscript received February 14 20
0002-9610$ - see front matter 2013
httpdxdoiorg101016jamjsurg20
AbstractBACKGROUND The information provided during the postoperative handover influences the delivery
of care of patients in the postoperative recovery unit through their care on the ward There is a need fora structured and systematic approach to postoperative handover The aim of this study was to improvepostoperative handover through the implementation of a new handover protocol which involved ahandover proforma and standardization of the handover process
METHODS This prospective pre-post intervention study demonstrated the improvement in post-operative handover through standardization There was a significant reduction in information omis-sions and task errors and improvement in communication and teamwork with the new handoverprotocol
RESULTS There was a significant reduction in overall information omissions from 9 to 3 (P 001)omissions per handover and task errors from 28 to 8 (P 001) with the new handover protocolTeamwork and nursesrsquo satisfaction score significantly improved from a median of 3 to 4 (P 001)and median of 4 to 5 (P 001) Duration of handover decreased from a median of 8 to 7 minutes(P 376)
CONCLUSIONS The study demonstrates that standardization of postoperative handover improvedcommunication and teamwork and reduced information omissions and task errors There was an im-provement in the quality of the handover after the introduction of the new handover protocol whichwas easy and simple to use 2013 Elsevier Inc All rights reserved
terest
ealth Foundation National Institute of Health Research (NIHR) and the UK Engineering and Physical Sciences Re-
4-207-886-7640 fax 100-44-207-886-6309
org
12 revised manuscript January 28 2013
Elsevier Inc All rights reserved
1303005
K Nagpal et al Improving postoperative handover 495
Handoverdthe transfer of professional responsibilityand accountability for some or all aspects of care for apatient or group of patients to another person orprofessional group on a temporary or permanent basis1
Good quality handover is central to the effective delivery ofhealth care2 The primary intention of any patient handover isthe accurate transfer of information about a patientrsquos state andcare plan to ensure the safety and continuity of patient care3 Itis an interactive communication allowing the opportunity forquestioning between the giver and receiver of patient informa-tionHandover is also one of themost frequent4 and influentialmoments of the patientrsquos journey through hospital as it plays acentral role in determining the future management plan of thepatient Missing or fragmented information may lead to delayin medical diagnosis wrong treatment life-threatening ad-verse events patient complaints increased health care expen-diture increased length of stay5 and potentially result inincreased morbidity and mortality1
From a review of sentinel events and root cause anal-yses handovers have been identified as the source ofsignificant medical error and adverse patient outcomesThey account for 20 of malpractice claims in the UnitedStates6 A joint commission reported lsquolsquocommunication fail-uresrsquorsquo to be the root cause in 70 of sentinel events7 ofwhich at least half were due to communication breakdownsduring handovers In a recent study of handovers from theoperating theater to the intensive care unit communicationerrors were present in 100 of handovers8 Although thelevel of detail of information exchanged during handoversvaries according to each individual case the lack of a sup-porting framework or predetermined format results in in-consistent and variable quality handovers9
The surgical patient is more vulnerable to handovererrors than patients in other clinical specialties because ofthe high number of transitions in care that occur throughoutthe preoperative intraoperative and postoperative phasesof care It is only logical to assume that the greater thenumber of transitions the greater the need for handoversduring the transitions and thus the greater the likelihood ofinformation being distorted or lost across the phases ofcare10 A standardized approach to handover would proba-bly help minimize errors
Postoperative handover is one such critical phase in thecare of surgical patients Fourteen percent of 419 adverseevents in the recovery room were reported to be due tocommunication failures during the handover process11
Another descriptive study highlighted that 14 of anesthe-tists failed to transfer essential verbal information duringthe handover In addition only one-third of anesthetists at-tained a maximum score for the quality of verbal informa-tion12 In a previous study we showed that postoperativehandover is characterized by a high number of informationomissions and that distractions during the handover com-promise the transfer of information13
Studies have been done to improve handover in theintensive care unit14 however no attempt has been made to
improve the quality of handover from the theater to thepostanesthesia care unit (PACU) The aim of this studywas to develop a simple easily trainable new handoverprotocol to improve the quality of handover of patients un-dergoing major general surgical operations
Methods
This was a prospective prendashpost intervention study withdirect observation of handover conducted in the PACU ofan acute teaching hospital in London A total of 90handovers were evaluated by a trained researcher 50 beforeand 40 after the introduction of a new handover protocolHandovers of patients who had undergone major vascular(n 5 41) and major gastrointestinal (n 5 49) surgicalprocedures were observed Operative patients included 55males and 35 females with a median age of 64 (inter-quartile range [IQR] 527 to 740)
Procedure
A trained researcher observed the handovers using anassessment tool to evaluate the quality of the handoverbefore and after the implementation of the new handoverprotocol The assessment tool has been described else-where15 Twenty percent of the handovers were observedby a 2nd observer to assess for interrater reliability
The outcome measures were as follows15
Information omissions Omissions were documentedwhen the information was not transferred verbally In-formation items were categorized as patient-specificinformation anesthesia information and surgicalinformation
Tasks errors Errors were classed when patient-specifictasks and equipment tasks were not completed appropri-ately For example ifmonitors and alarmswere not set upbefore the verbal handover this was classed as an error
Teamwork This was assessed using the behavioralpostoperative component of the Observational Team-work Assessment Tool for Surgery16 It consists of 5domains Leadership Communication CoordinationCooperation and Situational Awareness which wererated on a 7-point Likert scale (0 to 7)
Nurse satisfaction Recovery nurses rated their overall sat-isfactionwith thehandoverona5-pointLikert scale (1 to5)
Duration Measured from the time the patient and oper-ating theater team enters the PACU until theater staffleave the PACU
Development of a new handover protocol
The new handover protocol consisted of a postoperativehandover proforma and standardization of the handoverprocess
Figure 1 Information omissions per handover before and after the new handover protocol
496 The American Journal of Surgery Vol 206 No 4 October 2013
1 Proforma The development of the proforma has beendescribed elsewhere13 Appendix 1 demonstrates thenew postoperative handover proforma
2 Standardization of the handover process wasachieved by- Surgeon input The surgeon participated in thehandover in order to transfer the patientrsquos surgicalinformation
- Task sequence Equipment and patient-specific taskswere completed 1st followed by information transferfrom the anesthetist and then the surgeon
- Distractions No information was handed over untiltasks were completed Verbal handover of informa-tion occurred in a sterile environment with limitedinterruptions and distractions
Statistical analysis
Statistical methods included the Mann-Whitney Utest for continuous variables chi-squared test forcategorical variables and Spearman rank correlationto assess relationships using the Statistical Packagefor Social Sciences version 160 software (SPSSChicago IL)
Results
Interrater reliability
The interrater reliability calculated by Spearmancorrelation was found to be significant (r 5 964P 001)
Information omissions
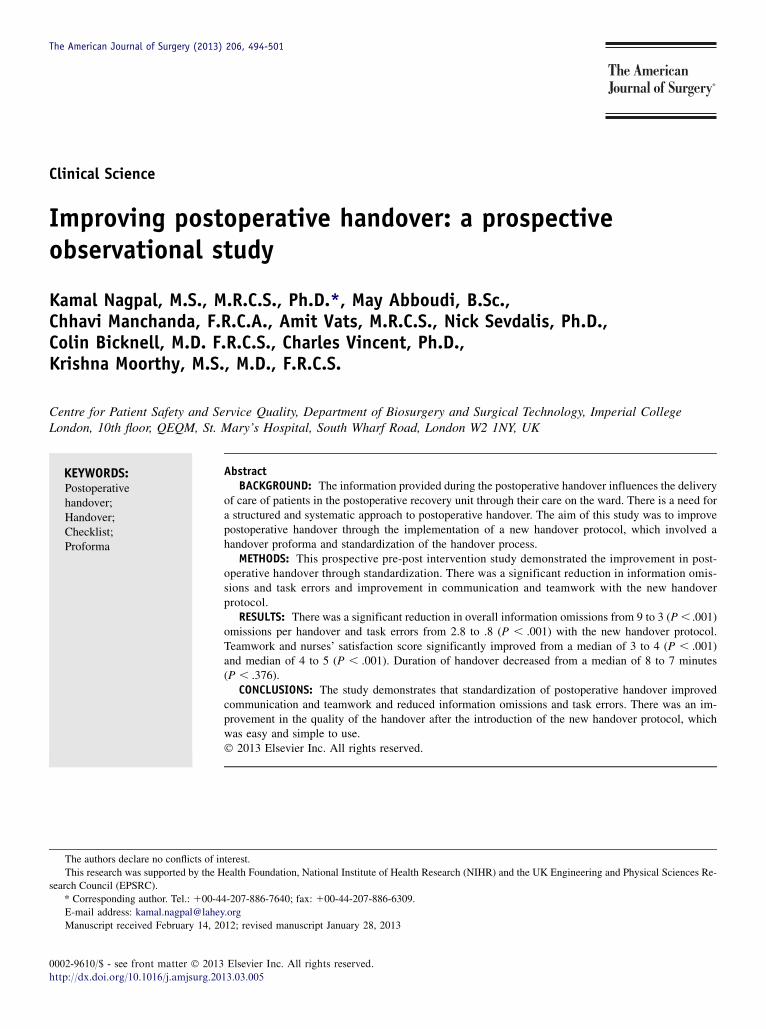
After the new handover protocol there was a signif-icant reduction in the number of information omissionsper handover from 9 to 3 (P 001) (Fig 1) Thelargest reduction in information omissions per handoverwas observed for surgical information which decreasedfrom 42 to 8 (P 001) Information omissions perhandover of both patient-specific information 26 to 13(P 001) and anesthetic information fell from 34 to15 (P 001)
Task errors
The overall number of task errors per handover reducedsignificantly from 28 to 8 task errors per handover (P 001)
Figure 2 Task errors before and after new handover protocol
Figure 3 Median teamwork score per handover before and afterthe new handover protocol
K Nagpal et al Improving postoperative handover 497
(Fig 2) The number of patient-specific task errors reducedsignificantly from 3 to 06 errors per handover (P 05)Finally there was a significant reduction in the number ofequipment task errors from 25 to 7 errors per handover(P 001)
Teamwork
Teamwork (all 5 components) improved significantlywith an overall improvement of median teamwork scorefrom 3 to 4 (P 001) (Fig 3)
Nurse satisfaction
The overall nursesrsquo satisfaction improved significantlyafter the new handover from a median of 4 to 5 (P 001Mann-Whitney test) After the new handover protocol 58of the handovers were awarded a score of 5 of 5 by the re-covery nurse compared with only 8 before the newprotocol
Duration
Duration of the postoperative handover reduced from amedian of 8 (IQR 5 to 12) to 7 (IQR 5 to 9) minutes afterthe new handover protocol however the reduction was notsignificant (P 5 376 Mann-Whitney)
Correlations
Spearman rank correlation identified a significant cor-relation between the number of information omissions andnumber of task errors per handover before and after the
498 The American Journal of Surgery Vol 206 No 4 October 2013
handover protocol (r 5 548 P 001) Thus informationomissions were more likely compounded by the task errors(ie information omissions is directly proportional to thetask errors) The communication component of the team-work score was negatively correlated with the number oftask errors (r 5 2625 P 001) demonstrating thatpoor communication during the handover is associatedwith more task errors
The 2-tailed Spearman rank correlation demonstrated anegative correlation between the number of informationomissions and teamwork score (r 5 2663 P 001)thereby highlighting the importance of teamwork as avital component in good quality handover informationtransfer
Comments
The new handover protocol produced a marked im-provement in the quality of handover Information omis-sions and task errors were significantly reduced and therewas considerable improvement in teamwork and nursesatisfaction scores In fact improvements were foundacross almost the entire process following its introductionThe structured approach to the transfer of information fromoperating theater staff to recovery staff and coordination oftasks performed contributed to the improved teamworkscore Although there was no significant reduction in theduration after the new protocol the nurses were moresatisfied with the overall handover
The protocol focused on the surgeonrsquos participation inthe handover process communication task sequence andleadership Most significant is the finding that team mem-bers working in a hectic and high-pressure clinical envi-ronment can successfully implement a change in theirhandover practice Several factors contributed to the suc-cess of the new handover protocol implementation in thestudy The surgical anesthetic and recovery team includeda consistent group of people who were supportive ofresearch The surgeonrsquos commitment was particularly crit-ical for the successful implementation which can be seenby the largest improvement in surgical information omis-sions Consistent with quality improvement initiatives thatinvolve health care professions we engaged in a continuousprocess with the participants receiving and providingcontinuous feedback The feedback of theater and recoverystaff both before and during the development of proformaprovided critical insight into the implementation processEngagement with the professionals may also have con-ferred a sense of ownership to participants which isessential to the success of quality improvement initiativesthat seek to change the behavior
Before the intervention the handover process wasnegatively affected by the lack of surgical informationprovided distractions during the handover and lack of aformalized structure The new protocol ensured the pres-ence of at least 1 member of the surgical team and adequate
transfer of all the information especially surgical informa-tion in a standardized format Furthermore the correlationbetween information omissions and teamwork emphasizedthe value of teamwork in achieving the lowest rate oferrors
Avoidance of any variability in the delivery of postop-erative handover through standardization of process im-plementation of postoperative handover proforma and tasksequence involvement of the lsquolsquocaptain of shiprsquorsquo (ie sur-geon) excellent teamwork and camaraderie performed inexactly the same manner every time were the key principlesof the successful outcome These led to changes in criticalclinical processes which eventually led to changes inoutcomes as discussed below We did not focus on out-comes therefore this parameter was not measured More-over adverse outcome measures were precluded by low ratesrequiring large sample sizes However we believe thatchanges in these clinical processes (ie information omis-sions task errors and teamwork) will impact the clinical andnonclinical outcomes
Our results echo the findings of poor quality handoverfrom theater to the PACU12 Our study also demonstratedthat 48 of anesthetic information was not transferred Inthe study conducted by Anwari12 nurses awarded the high-est marks to almost half the anesthetists however this fig-ure increased from 7 to 60 after the introduction of thenew protocol Very few studies have attempted to improvepostoperative handover A noteworthy exception is a studyby Catchpole et al14 which used Formula-1 concepts to im-prove the handover process in the pediatric intensive careunit They demonstrated a significant reduction in informa-tion omissions and technical errors after standardizing theirhandover process
As evident in other high-reliability industries standard-ization of the handover has been effective through team-work communication techniques flattening of hierarchymutual respect within and across disciplines and situationalawareness which are key components of a culture ofsafety17 Furthermore improving coordination of carethrough a structured communication process is particularlyimportant in environments in which interruptions and mul-titasking are common such as the PACU setting This coor-dination of care helps to create a lsquolsquoshared mental modelrsquorsquo ofa patientrsquos status and the expected clinical course18 As aresult any digression from the anticipated postoperativecourse is more promptly identified
There was evidence that clinically significant steps in theinformation transfer process were missed which at the veryleast eroded safety margins The potential of adverse eventsoccurring during the patientrsquos care became evident in thepreintervention phase Two patients did not receive deepvein thrombosis prophylaxis on their 1st postoperative daybecause of information omission during the handoverprocess Introduction of the proforma was effective inensuring that pertinent information was not overlookedduring the handover Additionally the proforma served as areminder to the surgeon to write instructions regarding deep
K Nagpal et al Improving postoperative handover 499
vein thrombosis prophylaxis on the drug chart on 4occasions which otherwise would not have been writtenand potentially not administered to the patient affecting thepatientrsquos safety Formalizing and producing a more stan-dardized handover was accomplished and the study can beseen as a step in meeting the joint commissionrsquos NationalPatient Safety Goals for a standardized approach to handoffcommunication19
There were several limitations to this study In anyobservational study the question of authenticity of data isof central concern In addition to mechanisms employed tominimize the observer or Hawthorne effect20 the observerrecorded evidence of this possible effect in the field notesFurthermore informal interviews with randomly selectedparticipants following each observation period contributedto our sense of the datarsquos representativeness Working groupmembers commented on whether data seemed representa-tive or not on no occasion did experts question thesedata Moreover the validity of data was also confirmedby significant interrater reliability Another limitation wasthe small sample size and the fact that the study was con-ducted on a single site each institution has its own barriersto changing culture therefore the results may not bebroadly generalized This study also suffers from the tradi-tional biases of a prendashpost test design specifically that wewere unable to control for all potential confounding influ-ences However a randomized controlled trial of this inter-vention within 1 institution would be impossible due to therisk of contamination between study groups and feasibilityissues Despite these limitations we believe that implemen-tation of the new handover protocol indeed standardizesand facilitates communication among health care providersin the PACU This study did not set out to determine if thisnew handover protocol improved patient outcomes Never-theless it is important that the likelihood of multiple errorswith individual patients was reduced as the avoidance ofcompounding errors is a fundamentally important compo-nent of safety21 and has been shown in other studies toaffect outcome22
A further limitation is that while the proforma iseffective to ensure that the necessary information is handedover it does not ensure that the information is understoodby the receiving nurse In this study the improved nursesrsquosatisfaction for the overall handover could indicate thattheir level of understanding of the information communi-cated during the handover improved
We also observed that the researcher had to facilitate theprocess by asking the anesthetist and a member of thesurgical team to use the proforma for the handover on 4occasions This and the high level of engagement with theclinical team during the study highlights the fact that thesuccessful implementation of the protocol was influencedto a large extent by the motivation of the clinical team andthat there was a certain amount of selection bias in thisstudy As the protocol is more widely implemented we willhave to be aware of the need for a strategy for engagement
with clinical teams This also raises the question ofsustainability of the protocol when someone is not presentto drive the use of the protocol
Conclusions
Despite any potential failings implementation of the newhandover protocol significantly improved the quality of thepostoperative handover through enhanced information trans-fer teamwork and reduced task errors In most health caresettings the handover in the PACU is the conduit to infor-mation downstream when patients are transferred to theirfinal recovery facility By improving postoperative handoverin the PACU we can ensure that information transferreddownstream is made more accurate comprehensive androbust This could potentially ensure a heightened state ofvigilance for postoperating complications improve postop-erative care by ensuring that key processes are undertakenand thus potentially improve postoperative outcomesWe arenow undertaking research to evaluate the impact of improvedhandover on postoperative care and outcomes
References
1 British Medical Association Safe handover safe patients Guid-
ance on clinical handover for clinicians and managers Vol 2009
2004
2 McCann L McHardy K Child S Passing the buck clinical handovers
at a tertiary hospital N Z Med J 2007120U2778
3 Sherlock C The patient handover a study of its form function and ef-
ficiency Nurs Stand 1995933ndash6
4 Whitt N Harvey R McLeod G et al How many health professionals
does a patient see during an average hospital stay N Z Med J 2007
120U2517
5 Australian Council for Safety andQuality in Health Care Clinical hand-
over and patient safety literature review report Vol 2009 2005
6 Singh H Thomas EJ Petersen LA et al Medical errors involving
trainees a study of closed malpractice claims from 5 insurers Arch
Intern Med 20071672030ndash6
7 Joint Commission on Accreditation of Healthcare Organizations Sen-
tinel event statistics Vol 2009 2005
8 Mistry K Landrigan C Goldmann D et al Communication during
post-operative patient handoff in the pediatric intensive care unit
Crit Care Med 200533A12
9 Hughes RG Clancy CM Improving the complex nature of care tran-
sitions J Nurs Care Qual 200722289ndash92
10 Williams RG Silverman R Schwind C et al Surgeon information
transfer and communication factors affecting quality and efficiency
of inpatient care Ann Surg 2007245159ndash69
11 Kluger MT Bullock MF Recovery room incidents a review of 419 re-
ports from the Anaesthetic Incident Monitoring Study (AIMS) Anaes-
thesia 2002571060ndash6
12 Anwari JS Quality of handover to the postanaesthesia care unit nurse
Anaesthesia 200257488ndash93
13 Nagpal K Arora S Abboudi M et al Postoperative handover prob-
lems pitfalls and prevention of error Ann Surg 2010252171ndash6
14 Catchpole KR de Leval MR McEwan A et al Patient handover
from surgery to intensive care using Formula 1 pit-stop and aviation
models to improve safety and quality Paediatr Anaesth 200717
470ndash8
500 The American Journal of Surgery Vol 206 No 4 October 2013
15 Nagpal K Abboudi M Fishler L et al Evaluation of postoperative
handover using a tool to assess information transfer and teamwork
Ann Surg 2011253831ndash7
16 Undre S Sevdalis N Healey AN et al Observational teamwork as-
sessment for surgery (OTAS) refinement and application in urological
surgery World J Surg 2007311373ndash81
17 Patterson ES Roth EM Woods DD et al Handoff strategies in set-
tings with high consequences for failure lessons for health care oper-
ations Int J Qual Health Care 200416125ndash32
18 McLeod J Chaffee S Interpersonal approaches to communication re-
search Am Behav Sci 197316469ndash99
19 Joint Commission National patient safety goals handbook 2008 Avail-
able at httpwwwpatientsafetygovTIPSDocsTIPS_JanFeb08pdf
Accessed June 23 2013
20 Franke R Kaul J The Hawthorne experiments first statistical interpre-
tation Am Sociol Rev 197843623ndash43
21 Catchpole KR Giddings AE de Leval MR et al Identification of sys-
tems failures in successful paediatric cardiac surgery Ergonomics
200649567ndash88
22 Hofer TP Hayward RA Are bad outcomes from questionable clinical
decisions preventable medical errors A case of cascade iatrogenesis
Ann Intern Med 2002137(Pt 1)327ndash33
K Nagpal et al Improving postoperative handover 501
Appendix 1
Postoperative handover proforma
Postoperative proforma
Patient specific Anesthetic Surgical
U Patient name amp ageU Medical historyU Allergy statusU Name of procedureU Current status
of patient
U Type of anesthesiaU Intraoperative course amp any complicationsU Anticipated postop problems bleeding
pain airwayU Monitoring amp range for physiological
parameters BP UOU Analgesia planU Plan for IV fluidsU Postop complicationsU Contact problems for any anesthetic problems
U Intraoperative surgicalcourse amp any complications
U Blood lossU Antibiotic planU Drugs to be restartedU DVT prophylaxis planU Plans for tubes amp drainsU NG tube amp feeding planU Postop investigationsU Contact number for any
surgical problems
BP 5 blood pressure DVT 5 deep vein thrombosis IV 5 intravenous NG 5 nasogastric UO 5 urinary output

K Nagpal et al Improving postoperative handover 495
Handoverdthe transfer of professional responsibilityand accountability for some or all aspects of care for apatient or group of patients to another person orprofessional group on a temporary or permanent basis1
Good quality handover is central to the effective delivery ofhealth care2 The primary intention of any patient handover isthe accurate transfer of information about a patientrsquos state andcare plan to ensure the safety and continuity of patient care3 Itis an interactive communication allowing the opportunity forquestioning between the giver and receiver of patient informa-tionHandover is also one of themost frequent4 and influentialmoments of the patientrsquos journey through hospital as it plays acentral role in determining the future management plan of thepatient Missing or fragmented information may lead to delayin medical diagnosis wrong treatment life-threatening ad-verse events patient complaints increased health care expen-diture increased length of stay5 and potentially result inincreased morbidity and mortality1
From a review of sentinel events and root cause anal-yses handovers have been identified as the source ofsignificant medical error and adverse patient outcomesThey account for 20 of malpractice claims in the UnitedStates6 A joint commission reported lsquolsquocommunication fail-uresrsquorsquo to be the root cause in 70 of sentinel events7 ofwhich at least half were due to communication breakdownsduring handovers In a recent study of handovers from theoperating theater to the intensive care unit communicationerrors were present in 100 of handovers8 Although thelevel of detail of information exchanged during handoversvaries according to each individual case the lack of a sup-porting framework or predetermined format results in in-consistent and variable quality handovers9
The surgical patient is more vulnerable to handovererrors than patients in other clinical specialties because ofthe high number of transitions in care that occur throughoutthe preoperative intraoperative and postoperative phasesof care It is only logical to assume that the greater thenumber of transitions the greater the need for handoversduring the transitions and thus the greater the likelihood ofinformation being distorted or lost across the phases ofcare10 A standardized approach to handover would proba-bly help minimize errors
Postoperative handover is one such critical phase in thecare of surgical patients Fourteen percent of 419 adverseevents in the recovery room were reported to be due tocommunication failures during the handover process11
Another descriptive study highlighted that 14 of anesthe-tists failed to transfer essential verbal information duringthe handover In addition only one-third of anesthetists at-tained a maximum score for the quality of verbal informa-tion12 In a previous study we showed that postoperativehandover is characterized by a high number of informationomissions and that distractions during the handover com-promise the transfer of information13
Studies have been done to improve handover in theintensive care unit14 however no attempt has been made to
improve the quality of handover from the theater to thepostanesthesia care unit (PACU) The aim of this studywas to develop a simple easily trainable new handoverprotocol to improve the quality of handover of patients un-dergoing major general surgical operations
Methods
This was a prospective prendashpost intervention study withdirect observation of handover conducted in the PACU ofan acute teaching hospital in London A total of 90handovers were evaluated by a trained researcher 50 beforeand 40 after the introduction of a new handover protocolHandovers of patients who had undergone major vascular(n 5 41) and major gastrointestinal (n 5 49) surgicalprocedures were observed Operative patients included 55males and 35 females with a median age of 64 (inter-quartile range [IQR] 527 to 740)
Procedure
A trained researcher observed the handovers using anassessment tool to evaluate the quality of the handoverbefore and after the implementation of the new handoverprotocol The assessment tool has been described else-where15 Twenty percent of the handovers were observedby a 2nd observer to assess for interrater reliability
The outcome measures were as follows15
Information omissions Omissions were documentedwhen the information was not transferred verbally In-formation items were categorized as patient-specificinformation anesthesia information and surgicalinformation
Tasks errors Errors were classed when patient-specifictasks and equipment tasks were not completed appropri-ately For example ifmonitors and alarmswere not set upbefore the verbal handover this was classed as an error
Teamwork This was assessed using the behavioralpostoperative component of the Observational Team-work Assessment Tool for Surgery16 It consists of 5domains Leadership Communication CoordinationCooperation and Situational Awareness which wererated on a 7-point Likert scale (0 to 7)
Nurse satisfaction Recovery nurses rated their overall sat-isfactionwith thehandoverona5-pointLikert scale (1 to5)
Duration Measured from the time the patient and oper-ating theater team enters the PACU until theater staffleave the PACU
Development of a new handover protocol
The new handover protocol consisted of a postoperativehandover proforma and standardization of the handoverprocess
Figure 1 Information omissions per handover before and after the new handover protocol
496 The American Journal of Surgery Vol 206 No 4 October 2013
1 Proforma The development of the proforma has beendescribed elsewhere13 Appendix 1 demonstrates thenew postoperative handover proforma
2 Standardization of the handover process wasachieved by- Surgeon input The surgeon participated in thehandover in order to transfer the patientrsquos surgicalinformation
- Task sequence Equipment and patient-specific taskswere completed 1st followed by information transferfrom the anesthetist and then the surgeon
- Distractions No information was handed over untiltasks were completed Verbal handover of informa-tion occurred in a sterile environment with limitedinterruptions and distractions
Statistical analysis
Statistical methods included the Mann-Whitney Utest for continuous variables chi-squared test forcategorical variables and Spearman rank correlationto assess relationships using the Statistical Packagefor Social Sciences version 160 software (SPSSChicago IL)
Results
Interrater reliability
The interrater reliability calculated by Spearmancorrelation was found to be significant (r 5 964P 001)
Information omissions
After the new handover protocol there was a signif-icant reduction in the number of information omissionsper handover from 9 to 3 (P 001) (Fig 1) Thelargest reduction in information omissions per handoverwas observed for surgical information which decreasedfrom 42 to 8 (P 001) Information omissions perhandover of both patient-specific information 26 to 13(P 001) and anesthetic information fell from 34 to15 (P 001)
Task errors
The overall number of task errors per handover reducedsignificantly from 28 to 8 task errors per handover (P 001)
Figure 2 Task errors before and after new handover protocol
Figure 3 Median teamwork score per handover before and afterthe new handover protocol
K Nagpal et al Improving postoperative handover 497
(Fig 2) The number of patient-specific task errors reducedsignificantly from 3 to 06 errors per handover (P 05)Finally there was a significant reduction in the number ofequipment task errors from 25 to 7 errors per handover(P 001)
Teamwork
Teamwork (all 5 components) improved significantlywith an overall improvement of median teamwork scorefrom 3 to 4 (P 001) (Fig 3)
Nurse satisfaction
The overall nursesrsquo satisfaction improved significantlyafter the new handover from a median of 4 to 5 (P 001Mann-Whitney test) After the new handover protocol 58of the handovers were awarded a score of 5 of 5 by the re-covery nurse compared with only 8 before the newprotocol
Duration
Duration of the postoperative handover reduced from amedian of 8 (IQR 5 to 12) to 7 (IQR 5 to 9) minutes afterthe new handover protocol however the reduction was notsignificant (P 5 376 Mann-Whitney)
Correlations
Spearman rank correlation identified a significant cor-relation between the number of information omissions andnumber of task errors per handover before and after the
498 The American Journal of Surgery Vol 206 No 4 October 2013
handover protocol (r 5 548 P 001) Thus informationomissions were more likely compounded by the task errors(ie information omissions is directly proportional to thetask errors) The communication component of the team-work score was negatively correlated with the number oftask errors (r 5 2625 P 001) demonstrating thatpoor communication during the handover is associatedwith more task errors
The 2-tailed Spearman rank correlation demonstrated anegative correlation between the number of informationomissions and teamwork score (r 5 2663 P 001)thereby highlighting the importance of teamwork as avital component in good quality handover informationtransfer
Comments
The new handover protocol produced a marked im-provement in the quality of handover Information omis-sions and task errors were significantly reduced and therewas considerable improvement in teamwork and nursesatisfaction scores In fact improvements were foundacross almost the entire process following its introductionThe structured approach to the transfer of information fromoperating theater staff to recovery staff and coordination oftasks performed contributed to the improved teamworkscore Although there was no significant reduction in theduration after the new protocol the nurses were moresatisfied with the overall handover
The protocol focused on the surgeonrsquos participation inthe handover process communication task sequence andleadership Most significant is the finding that team mem-bers working in a hectic and high-pressure clinical envi-ronment can successfully implement a change in theirhandover practice Several factors contributed to the suc-cess of the new handover protocol implementation in thestudy The surgical anesthetic and recovery team includeda consistent group of people who were supportive ofresearch The surgeonrsquos commitment was particularly crit-ical for the successful implementation which can be seenby the largest improvement in surgical information omis-sions Consistent with quality improvement initiatives thatinvolve health care professions we engaged in a continuousprocess with the participants receiving and providingcontinuous feedback The feedback of theater and recoverystaff both before and during the development of proformaprovided critical insight into the implementation processEngagement with the professionals may also have con-ferred a sense of ownership to participants which isessential to the success of quality improvement initiativesthat seek to change the behavior
Before the intervention the handover process wasnegatively affected by the lack of surgical informationprovided distractions during the handover and lack of aformalized structure The new protocol ensured the pres-ence of at least 1 member of the surgical team and adequate
transfer of all the information especially surgical informa-tion in a standardized format Furthermore the correlationbetween information omissions and teamwork emphasizedthe value of teamwork in achieving the lowest rate oferrors
Avoidance of any variability in the delivery of postop-erative handover through standardization of process im-plementation of postoperative handover proforma and tasksequence involvement of the lsquolsquocaptain of shiprsquorsquo (ie sur-geon) excellent teamwork and camaraderie performed inexactly the same manner every time were the key principlesof the successful outcome These led to changes in criticalclinical processes which eventually led to changes inoutcomes as discussed below We did not focus on out-comes therefore this parameter was not measured More-over adverse outcome measures were precluded by low ratesrequiring large sample sizes However we believe thatchanges in these clinical processes (ie information omis-sions task errors and teamwork) will impact the clinical andnonclinical outcomes
Our results echo the findings of poor quality handoverfrom theater to the PACU12 Our study also demonstratedthat 48 of anesthetic information was not transferred Inthe study conducted by Anwari12 nurses awarded the high-est marks to almost half the anesthetists however this fig-ure increased from 7 to 60 after the introduction of thenew protocol Very few studies have attempted to improvepostoperative handover A noteworthy exception is a studyby Catchpole et al14 which used Formula-1 concepts to im-prove the handover process in the pediatric intensive careunit They demonstrated a significant reduction in informa-tion omissions and technical errors after standardizing theirhandover process
As evident in other high-reliability industries standard-ization of the handover has been effective through team-work communication techniques flattening of hierarchymutual respect within and across disciplines and situationalawareness which are key components of a culture ofsafety17 Furthermore improving coordination of carethrough a structured communication process is particularlyimportant in environments in which interruptions and mul-titasking are common such as the PACU setting This coor-dination of care helps to create a lsquolsquoshared mental modelrsquorsquo ofa patientrsquos status and the expected clinical course18 As aresult any digression from the anticipated postoperativecourse is more promptly identified
There was evidence that clinically significant steps in theinformation transfer process were missed which at the veryleast eroded safety margins The potential of adverse eventsoccurring during the patientrsquos care became evident in thepreintervention phase Two patients did not receive deepvein thrombosis prophylaxis on their 1st postoperative daybecause of information omission during the handoverprocess Introduction of the proforma was effective inensuring that pertinent information was not overlookedduring the handover Additionally the proforma served as areminder to the surgeon to write instructions regarding deep
K Nagpal et al Improving postoperative handover 499
vein thrombosis prophylaxis on the drug chart on 4occasions which otherwise would not have been writtenand potentially not administered to the patient affecting thepatientrsquos safety Formalizing and producing a more stan-dardized handover was accomplished and the study can beseen as a step in meeting the joint commissionrsquos NationalPatient Safety Goals for a standardized approach to handoffcommunication19
There were several limitations to this study In anyobservational study the question of authenticity of data isof central concern In addition to mechanisms employed tominimize the observer or Hawthorne effect20 the observerrecorded evidence of this possible effect in the field notesFurthermore informal interviews with randomly selectedparticipants following each observation period contributedto our sense of the datarsquos representativeness Working groupmembers commented on whether data seemed representa-tive or not on no occasion did experts question thesedata Moreover the validity of data was also confirmedby significant interrater reliability Another limitation wasthe small sample size and the fact that the study was con-ducted on a single site each institution has its own barriersto changing culture therefore the results may not bebroadly generalized This study also suffers from the tradi-tional biases of a prendashpost test design specifically that wewere unable to control for all potential confounding influ-ences However a randomized controlled trial of this inter-vention within 1 institution would be impossible due to therisk of contamination between study groups and feasibilityissues Despite these limitations we believe that implemen-tation of the new handover protocol indeed standardizesand facilitates communication among health care providersin the PACU This study did not set out to determine if thisnew handover protocol improved patient outcomes Never-theless it is important that the likelihood of multiple errorswith individual patients was reduced as the avoidance ofcompounding errors is a fundamentally important compo-nent of safety21 and has been shown in other studies toaffect outcome22
A further limitation is that while the proforma iseffective to ensure that the necessary information is handedover it does not ensure that the information is understoodby the receiving nurse In this study the improved nursesrsquosatisfaction for the overall handover could indicate thattheir level of understanding of the information communi-cated during the handover improved
We also observed that the researcher had to facilitate theprocess by asking the anesthetist and a member of thesurgical team to use the proforma for the handover on 4occasions This and the high level of engagement with theclinical team during the study highlights the fact that thesuccessful implementation of the protocol was influencedto a large extent by the motivation of the clinical team andthat there was a certain amount of selection bias in thisstudy As the protocol is more widely implemented we willhave to be aware of the need for a strategy for engagement
with clinical teams This also raises the question ofsustainability of the protocol when someone is not presentto drive the use of the protocol
Conclusions
Despite any potential failings implementation of the newhandover protocol significantly improved the quality of thepostoperative handover through enhanced information trans-fer teamwork and reduced task errors In most health caresettings the handover in the PACU is the conduit to infor-mation downstream when patients are transferred to theirfinal recovery facility By improving postoperative handoverin the PACU we can ensure that information transferreddownstream is made more accurate comprehensive androbust This could potentially ensure a heightened state ofvigilance for postoperating complications improve postop-erative care by ensuring that key processes are undertakenand thus potentially improve postoperative outcomesWe arenow undertaking research to evaluate the impact of improvedhandover on postoperative care and outcomes
References
1 British Medical Association Safe handover safe patients Guid-
ance on clinical handover for clinicians and managers Vol 2009
2004
2 McCann L McHardy K Child S Passing the buck clinical handovers
at a tertiary hospital N Z Med J 2007120U2778
3 Sherlock C The patient handover a study of its form function and ef-
ficiency Nurs Stand 1995933ndash6
4 Whitt N Harvey R McLeod G et al How many health professionals
does a patient see during an average hospital stay N Z Med J 2007
120U2517
5 Australian Council for Safety andQuality in Health Care Clinical hand-
over and patient safety literature review report Vol 2009 2005
6 Singh H Thomas EJ Petersen LA et al Medical errors involving
trainees a study of closed malpractice claims from 5 insurers Arch
Intern Med 20071672030ndash6
7 Joint Commission on Accreditation of Healthcare Organizations Sen-
tinel event statistics Vol 2009 2005
8 Mistry K Landrigan C Goldmann D et al Communication during
post-operative patient handoff in the pediatric intensive care unit
Crit Care Med 200533A12
9 Hughes RG Clancy CM Improving the complex nature of care tran-
sitions J Nurs Care Qual 200722289ndash92
10 Williams RG Silverman R Schwind C et al Surgeon information
transfer and communication factors affecting quality and efficiency
of inpatient care Ann Surg 2007245159ndash69
11 Kluger MT Bullock MF Recovery room incidents a review of 419 re-
ports from the Anaesthetic Incident Monitoring Study (AIMS) Anaes-
thesia 2002571060ndash6
12 Anwari JS Quality of handover to the postanaesthesia care unit nurse
Anaesthesia 200257488ndash93
13 Nagpal K Arora S Abboudi M et al Postoperative handover prob-
lems pitfalls and prevention of error Ann Surg 2010252171ndash6
14 Catchpole KR de Leval MR McEwan A et al Patient handover
from surgery to intensive care using Formula 1 pit-stop and aviation
models to improve safety and quality Paediatr Anaesth 200717
470ndash8
500 The American Journal of Surgery Vol 206 No 4 October 2013
15 Nagpal K Abboudi M Fishler L et al Evaluation of postoperative
handover using a tool to assess information transfer and teamwork
Ann Surg 2011253831ndash7
16 Undre S Sevdalis N Healey AN et al Observational teamwork as-
sessment for surgery (OTAS) refinement and application in urological
surgery World J Surg 2007311373ndash81
17 Patterson ES Roth EM Woods DD et al Handoff strategies in set-
tings with high consequences for failure lessons for health care oper-
ations Int J Qual Health Care 200416125ndash32
18 McLeod J Chaffee S Interpersonal approaches to communication re-
search Am Behav Sci 197316469ndash99
19 Joint Commission National patient safety goals handbook 2008 Avail-
able at httpwwwpatientsafetygovTIPSDocsTIPS_JanFeb08pdf
Accessed June 23 2013
20 Franke R Kaul J The Hawthorne experiments first statistical interpre-
tation Am Sociol Rev 197843623ndash43
21 Catchpole KR Giddings AE de Leval MR et al Identification of sys-
tems failures in successful paediatric cardiac surgery Ergonomics
200649567ndash88
22 Hofer TP Hayward RA Are bad outcomes from questionable clinical
decisions preventable medical errors A case of cascade iatrogenesis
Ann Intern Med 2002137(Pt 1)327ndash33
K Nagpal et al Improving postoperative handover 501
Appendix 1
Postoperative handover proforma
Postoperative proforma
Patient specific Anesthetic Surgical
U Patient name amp ageU Medical historyU Allergy statusU Name of procedureU Current status
of patient
U Type of anesthesiaU Intraoperative course amp any complicationsU Anticipated postop problems bleeding
pain airwayU Monitoring amp range for physiological
parameters BP UOU Analgesia planU Plan for IV fluidsU Postop complicationsU Contact problems for any anesthetic problems
U Intraoperative surgicalcourse amp any complications
U Blood lossU Antibiotic planU Drugs to be restartedU DVT prophylaxis planU Plans for tubes amp drainsU NG tube amp feeding planU Postop investigationsU Contact number for any
surgical problems
BP 5 blood pressure DVT 5 deep vein thrombosis IV 5 intravenous NG 5 nasogastric UO 5 urinary output
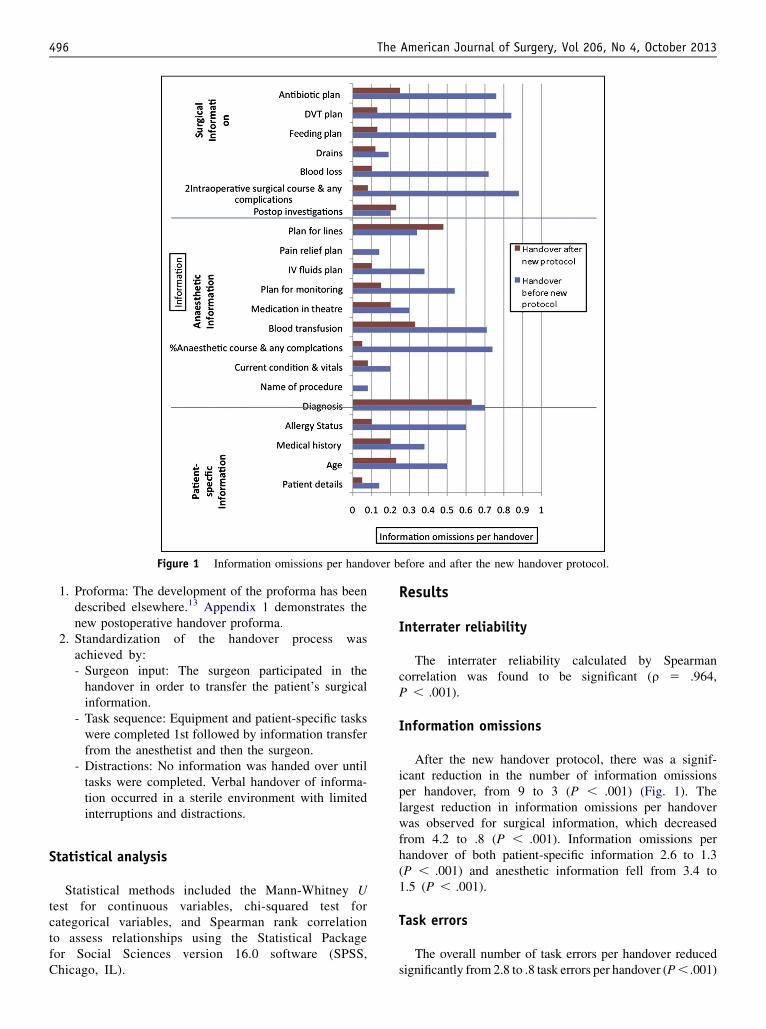
Figure 1 Information omissions per handover before and after the new handover protocol
496 The American Journal of Surgery Vol 206 No 4 October 2013
1 Proforma The development of the proforma has beendescribed elsewhere13 Appendix 1 demonstrates thenew postoperative handover proforma
2 Standardization of the handover process wasachieved by- Surgeon input The surgeon participated in thehandover in order to transfer the patientrsquos surgicalinformation
- Task sequence Equipment and patient-specific taskswere completed 1st followed by information transferfrom the anesthetist and then the surgeon
- Distractions No information was handed over untiltasks were completed Verbal handover of informa-tion occurred in a sterile environment with limitedinterruptions and distractions
Statistical analysis
Statistical methods included the Mann-Whitney Utest for continuous variables chi-squared test forcategorical variables and Spearman rank correlationto assess relationships using the Statistical Packagefor Social Sciences version 160 software (SPSSChicago IL)
Results
Interrater reliability
The interrater reliability calculated by Spearmancorrelation was found to be significant (r 5 964P 001)
Information omissions
After the new handover protocol there was a signif-icant reduction in the number of information omissionsper handover from 9 to 3 (P 001) (Fig 1) Thelargest reduction in information omissions per handoverwas observed for surgical information which decreasedfrom 42 to 8 (P 001) Information omissions perhandover of both patient-specific information 26 to 13(P 001) and anesthetic information fell from 34 to15 (P 001)
Task errors
The overall number of task errors per handover reducedsignificantly from 28 to 8 task errors per handover (P 001)
Figure 2 Task errors before and after new handover protocol
Figure 3 Median teamwork score per handover before and afterthe new handover protocol
K Nagpal et al Improving postoperative handover 497
(Fig 2) The number of patient-specific task errors reducedsignificantly from 3 to 06 errors per handover (P 05)Finally there was a significant reduction in the number ofequipment task errors from 25 to 7 errors per handover(P 001)
Teamwork
Teamwork (all 5 components) improved significantlywith an overall improvement of median teamwork scorefrom 3 to 4 (P 001) (Fig 3)
Nurse satisfaction
The overall nursesrsquo satisfaction improved significantlyafter the new handover from a median of 4 to 5 (P 001Mann-Whitney test) After the new handover protocol 58of the handovers were awarded a score of 5 of 5 by the re-covery nurse compared with only 8 before the newprotocol
Duration
Duration of the postoperative handover reduced from amedian of 8 (IQR 5 to 12) to 7 (IQR 5 to 9) minutes afterthe new handover protocol however the reduction was notsignificant (P 5 376 Mann-Whitney)
Correlations
Spearman rank correlation identified a significant cor-relation between the number of information omissions andnumber of task errors per handover before and after the
498 The American Journal of Surgery Vol 206 No 4 October 2013
handover protocol (r 5 548 P 001) Thus informationomissions were more likely compounded by the task errors(ie information omissions is directly proportional to thetask errors) The communication component of the team-work score was negatively correlated with the number oftask errors (r 5 2625 P 001) demonstrating thatpoor communication during the handover is associatedwith more task errors
The 2-tailed Spearman rank correlation demonstrated anegative correlation between the number of informationomissions and teamwork score (r 5 2663 P 001)thereby highlighting the importance of teamwork as avital component in good quality handover informationtransfer
Comments
The new handover protocol produced a marked im-provement in the quality of handover Information omis-sions and task errors were significantly reduced and therewas considerable improvement in teamwork and nursesatisfaction scores In fact improvements were foundacross almost the entire process following its introductionThe structured approach to the transfer of information fromoperating theater staff to recovery staff and coordination oftasks performed contributed to the improved teamworkscore Although there was no significant reduction in theduration after the new protocol the nurses were moresatisfied with the overall handover
The protocol focused on the surgeonrsquos participation inthe handover process communication task sequence andleadership Most significant is the finding that team mem-bers working in a hectic and high-pressure clinical envi-ronment can successfully implement a change in theirhandover practice Several factors contributed to the suc-cess of the new handover protocol implementation in thestudy The surgical anesthetic and recovery team includeda consistent group of people who were supportive ofresearch The surgeonrsquos commitment was particularly crit-ical for the successful implementation which can be seenby the largest improvement in surgical information omis-sions Consistent with quality improvement initiatives thatinvolve health care professions we engaged in a continuousprocess with the participants receiving and providingcontinuous feedback The feedback of theater and recoverystaff both before and during the development of proformaprovided critical insight into the implementation processEngagement with the professionals may also have con-ferred a sense of ownership to participants which isessential to the success of quality improvement initiativesthat seek to change the behavior
Before the intervention the handover process wasnegatively affected by the lack of surgical informationprovided distractions during the handover and lack of aformalized structure The new protocol ensured the pres-ence of at least 1 member of the surgical team and adequate
transfer of all the information especially surgical informa-tion in a standardized format Furthermore the correlationbetween information omissions and teamwork emphasizedthe value of teamwork in achieving the lowest rate oferrors
Avoidance of any variability in the delivery of postop-erative handover through standardization of process im-plementation of postoperative handover proforma and tasksequence involvement of the lsquolsquocaptain of shiprsquorsquo (ie sur-geon) excellent teamwork and camaraderie performed inexactly the same manner every time were the key principlesof the successful outcome These led to changes in criticalclinical processes which eventually led to changes inoutcomes as discussed below We did not focus on out-comes therefore this parameter was not measured More-over adverse outcome measures were precluded by low ratesrequiring large sample sizes However we believe thatchanges in these clinical processes (ie information omis-sions task errors and teamwork) will impact the clinical andnonclinical outcomes
Our results echo the findings of poor quality handoverfrom theater to the PACU12 Our study also demonstratedthat 48 of anesthetic information was not transferred Inthe study conducted by Anwari12 nurses awarded the high-est marks to almost half the anesthetists however this fig-ure increased from 7 to 60 after the introduction of thenew protocol Very few studies have attempted to improvepostoperative handover A noteworthy exception is a studyby Catchpole et al14 which used Formula-1 concepts to im-prove the handover process in the pediatric intensive careunit They demonstrated a significant reduction in informa-tion omissions and technical errors after standardizing theirhandover process
As evident in other high-reliability industries standard-ization of the handover has been effective through team-work communication techniques flattening of hierarchymutual respect within and across disciplines and situationalawareness which are key components of a culture ofsafety17 Furthermore improving coordination of carethrough a structured communication process is particularlyimportant in environments in which interruptions and mul-titasking are common such as the PACU setting This coor-dination of care helps to create a lsquolsquoshared mental modelrsquorsquo ofa patientrsquos status and the expected clinical course18 As aresult any digression from the anticipated postoperativecourse is more promptly identified
There was evidence that clinically significant steps in theinformation transfer process were missed which at the veryleast eroded safety margins The potential of adverse eventsoccurring during the patientrsquos care became evident in thepreintervention phase Two patients did not receive deepvein thrombosis prophylaxis on their 1st postoperative daybecause of information omission during the handoverprocess Introduction of the proforma was effective inensuring that pertinent information was not overlookedduring the handover Additionally the proforma served as areminder to the surgeon to write instructions regarding deep
K Nagpal et al Improving postoperative handover 499
vein thrombosis prophylaxis on the drug chart on 4occasions which otherwise would not have been writtenand potentially not administered to the patient affecting thepatientrsquos safety Formalizing and producing a more stan-dardized handover was accomplished and the study can beseen as a step in meeting the joint commissionrsquos NationalPatient Safety Goals for a standardized approach to handoffcommunication19
There were several limitations to this study In anyobservational study the question of authenticity of data isof central concern In addition to mechanisms employed tominimize the observer or Hawthorne effect20 the observerrecorded evidence of this possible effect in the field notesFurthermore informal interviews with randomly selectedparticipants following each observation period contributedto our sense of the datarsquos representativeness Working groupmembers commented on whether data seemed representa-tive or not on no occasion did experts question thesedata Moreover the validity of data was also confirmedby significant interrater reliability Another limitation wasthe small sample size and the fact that the study was con-ducted on a single site each institution has its own barriersto changing culture therefore the results may not bebroadly generalized This study also suffers from the tradi-tional biases of a prendashpost test design specifically that wewere unable to control for all potential confounding influ-ences However a randomized controlled trial of this inter-vention within 1 institution would be impossible due to therisk of contamination between study groups and feasibilityissues Despite these limitations we believe that implemen-tation of the new handover protocol indeed standardizesand facilitates communication among health care providersin the PACU This study did not set out to determine if thisnew handover protocol improved patient outcomes Never-theless it is important that the likelihood of multiple errorswith individual patients was reduced as the avoidance ofcompounding errors is a fundamentally important compo-nent of safety21 and has been shown in other studies toaffect outcome22
A further limitation is that while the proforma iseffective to ensure that the necessary information is handedover it does not ensure that the information is understoodby the receiving nurse In this study the improved nursesrsquosatisfaction for the overall handover could indicate thattheir level of understanding of the information communi-cated during the handover improved
We also observed that the researcher had to facilitate theprocess by asking the anesthetist and a member of thesurgical team to use the proforma for the handover on 4occasions This and the high level of engagement with theclinical team during the study highlights the fact that thesuccessful implementation of the protocol was influencedto a large extent by the motivation of the clinical team andthat there was a certain amount of selection bias in thisstudy As the protocol is more widely implemented we willhave to be aware of the need for a strategy for engagement
with clinical teams This also raises the question ofsustainability of the protocol when someone is not presentto drive the use of the protocol
Conclusions
Despite any potential failings implementation of the newhandover protocol significantly improved the quality of thepostoperative handover through enhanced information trans-fer teamwork and reduced task errors In most health caresettings the handover in the PACU is the conduit to infor-mation downstream when patients are transferred to theirfinal recovery facility By improving postoperative handoverin the PACU we can ensure that information transferreddownstream is made more accurate comprehensive androbust This could potentially ensure a heightened state ofvigilance for postoperating complications improve postop-erative care by ensuring that key processes are undertakenand thus potentially improve postoperative outcomesWe arenow undertaking research to evaluate the impact of improvedhandover on postoperative care and outcomes
References
1 British Medical Association Safe handover safe patients Guid-
ance on clinical handover for clinicians and managers Vol 2009
2004
2 McCann L McHardy K Child S Passing the buck clinical handovers
at a tertiary hospital N Z Med J 2007120U2778
3 Sherlock C The patient handover a study of its form function and ef-
ficiency Nurs Stand 1995933ndash6
4 Whitt N Harvey R McLeod G et al How many health professionals
does a patient see during an average hospital stay N Z Med J 2007
120U2517
5 Australian Council for Safety andQuality in Health Care Clinical hand-
over and patient safety literature review report Vol 2009 2005
6 Singh H Thomas EJ Petersen LA et al Medical errors involving
trainees a study of closed malpractice claims from 5 insurers Arch
Intern Med 20071672030ndash6
7 Joint Commission on Accreditation of Healthcare Organizations Sen-
tinel event statistics Vol 2009 2005
8 Mistry K Landrigan C Goldmann D et al Communication during
post-operative patient handoff in the pediatric intensive care unit
Crit Care Med 200533A12
9 Hughes RG Clancy CM Improving the complex nature of care tran-
sitions J Nurs Care Qual 200722289ndash92
10 Williams RG Silverman R Schwind C et al Surgeon information
transfer and communication factors affecting quality and efficiency
of inpatient care Ann Surg 2007245159ndash69
11 Kluger MT Bullock MF Recovery room incidents a review of 419 re-
ports from the Anaesthetic Incident Monitoring Study (AIMS) Anaes-
thesia 2002571060ndash6
12 Anwari JS Quality of handover to the postanaesthesia care unit nurse
Anaesthesia 200257488ndash93
13 Nagpal K Arora S Abboudi M et al Postoperative handover prob-
lems pitfalls and prevention of error Ann Surg 2010252171ndash6
14 Catchpole KR de Leval MR McEwan A et al Patient handover
from surgery to intensive care using Formula 1 pit-stop and aviation
models to improve safety and quality Paediatr Anaesth 200717
470ndash8
500 The American Journal of Surgery Vol 206 No 4 October 2013
15 Nagpal K Abboudi M Fishler L et al Evaluation of postoperative
handover using a tool to assess information transfer and teamwork
Ann Surg 2011253831ndash7
16 Undre S Sevdalis N Healey AN et al Observational teamwork as-
sessment for surgery (OTAS) refinement and application in urological
surgery World J Surg 2007311373ndash81
17 Patterson ES Roth EM Woods DD et al Handoff strategies in set-
tings with high consequences for failure lessons for health care oper-
ations Int J Qual Health Care 200416125ndash32
18 McLeod J Chaffee S Interpersonal approaches to communication re-
search Am Behav Sci 197316469ndash99
19 Joint Commission National patient safety goals handbook 2008 Avail-
able at httpwwwpatientsafetygovTIPSDocsTIPS_JanFeb08pdf
Accessed June 23 2013
20 Franke R Kaul J The Hawthorne experiments first statistical interpre-
tation Am Sociol Rev 197843623ndash43
21 Catchpole KR Giddings AE de Leval MR et al Identification of sys-
tems failures in successful paediatric cardiac surgery Ergonomics
200649567ndash88
22 Hofer TP Hayward RA Are bad outcomes from questionable clinical
decisions preventable medical errors A case of cascade iatrogenesis
Ann Intern Med 2002137(Pt 1)327ndash33
K Nagpal et al Improving postoperative handover 501
Appendix 1
Postoperative handover proforma
Postoperative proforma
Patient specific Anesthetic Surgical
U Patient name amp ageU Medical historyU Allergy statusU Name of procedureU Current status
of patient
U Type of anesthesiaU Intraoperative course amp any complicationsU Anticipated postop problems bleeding
pain airwayU Monitoring amp range for physiological
parameters BP UOU Analgesia planU Plan for IV fluidsU Postop complicationsU Contact problems for any anesthetic problems
U Intraoperative surgicalcourse amp any complications
U Blood lossU Antibiotic planU Drugs to be restartedU DVT prophylaxis planU Plans for tubes amp drainsU NG tube amp feeding planU Postop investigationsU Contact number for any
surgical problems
BP 5 blood pressure DVT 5 deep vein thrombosis IV 5 intravenous NG 5 nasogastric UO 5 urinary output
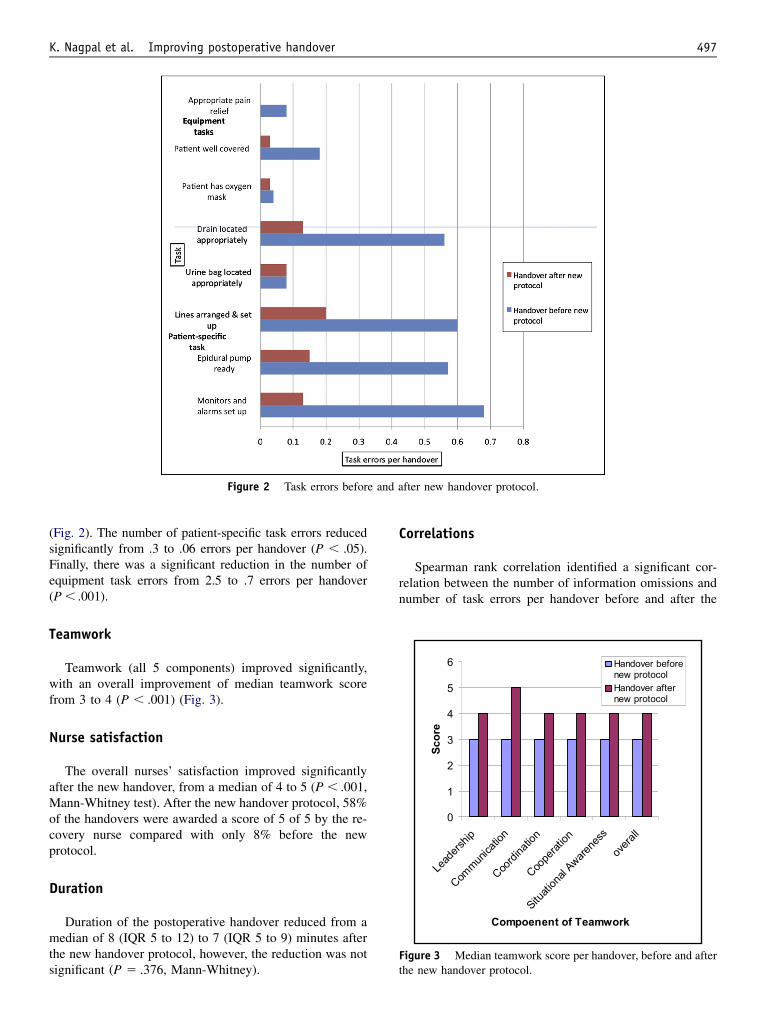
Figure 2 Task errors before and after new handover protocol
Figure 3 Median teamwork score per handover before and afterthe new handover protocol
K Nagpal et al Improving postoperative handover 497
(Fig 2) The number of patient-specific task errors reducedsignificantly from 3 to 06 errors per handover (P 05)Finally there was a significant reduction in the number ofequipment task errors from 25 to 7 errors per handover(P 001)
Teamwork
Teamwork (all 5 components) improved significantlywith an overall improvement of median teamwork scorefrom 3 to 4 (P 001) (Fig 3)
Nurse satisfaction
The overall nursesrsquo satisfaction improved significantlyafter the new handover from a median of 4 to 5 (P 001Mann-Whitney test) After the new handover protocol 58of the handovers were awarded a score of 5 of 5 by the re-covery nurse compared with only 8 before the newprotocol
Duration
Duration of the postoperative handover reduced from amedian of 8 (IQR 5 to 12) to 7 (IQR 5 to 9) minutes afterthe new handover protocol however the reduction was notsignificant (P 5 376 Mann-Whitney)
Correlations
Spearman rank correlation identified a significant cor-relation between the number of information omissions andnumber of task errors per handover before and after the
498 The American Journal of Surgery Vol 206 No 4 October 2013
handover protocol (r 5 548 P 001) Thus informationomissions were more likely compounded by the task errors(ie information omissions is directly proportional to thetask errors) The communication component of the team-work score was negatively correlated with the number oftask errors (r 5 2625 P 001) demonstrating thatpoor communication during the handover is associatedwith more task errors
The 2-tailed Spearman rank correlation demonstrated anegative correlation between the number of informationomissions and teamwork score (r 5 2663 P 001)thereby highlighting the importance of teamwork as avital component in good quality handover informationtransfer
Comments
The new handover protocol produced a marked im-provement in the quality of handover Information omis-sions and task errors were significantly reduced and therewas considerable improvement in teamwork and nursesatisfaction scores In fact improvements were foundacross almost the entire process following its introductionThe structured approach to the transfer of information fromoperating theater staff to recovery staff and coordination oftasks performed contributed to the improved teamworkscore Although there was no significant reduction in theduration after the new protocol the nurses were moresatisfied with the overall handover
The protocol focused on the surgeonrsquos participation inthe handover process communication task sequence andleadership Most significant is the finding that team mem-bers working in a hectic and high-pressure clinical envi-ronment can successfully implement a change in theirhandover practice Several factors contributed to the suc-cess of the new handover protocol implementation in thestudy The surgical anesthetic and recovery team includeda consistent group of people who were supportive ofresearch The surgeonrsquos commitment was particularly crit-ical for the successful implementation which can be seenby the largest improvement in surgical information omis-sions Consistent with quality improvement initiatives thatinvolve health care professions we engaged in a continuousprocess with the participants receiving and providingcontinuous feedback The feedback of theater and recoverystaff both before and during the development of proformaprovided critical insight into the implementation processEngagement with the professionals may also have con-ferred a sense of ownership to participants which isessential to the success of quality improvement initiativesthat seek to change the behavior
Before the intervention the handover process wasnegatively affected by the lack of surgical informationprovided distractions during the handover and lack of aformalized structure The new protocol ensured the pres-ence of at least 1 member of the surgical team and adequate
transfer of all the information especially surgical informa-tion in a standardized format Furthermore the correlationbetween information omissions and teamwork emphasizedthe value of teamwork in achieving the lowest rate oferrors
Avoidance of any variability in the delivery of postop-erative handover through standardization of process im-plementation of postoperative handover proforma and tasksequence involvement of the lsquolsquocaptain of shiprsquorsquo (ie sur-geon) excellent teamwork and camaraderie performed inexactly the same manner every time were the key principlesof the successful outcome These led to changes in criticalclinical processes which eventually led to changes inoutcomes as discussed below We did not focus on out-comes therefore this parameter was not measured More-over adverse outcome measures were precluded by low ratesrequiring large sample sizes However we believe thatchanges in these clinical processes (ie information omis-sions task errors and teamwork) will impact the clinical andnonclinical outcomes
Our results echo the findings of poor quality handoverfrom theater to the PACU12 Our study also demonstratedthat 48 of anesthetic information was not transferred Inthe study conducted by Anwari12 nurses awarded the high-est marks to almost half the anesthetists however this fig-ure increased from 7 to 60 after the introduction of thenew protocol Very few studies have attempted to improvepostoperative handover A noteworthy exception is a studyby Catchpole et al14 which used Formula-1 concepts to im-prove the handover process in the pediatric intensive careunit They demonstrated a significant reduction in informa-tion omissions and technical errors after standardizing theirhandover process
As evident in other high-reliability industries standard-ization of the handover has been effective through team-work communication techniques flattening of hierarchymutual respect within and across disciplines and situationalawareness which are key components of a culture ofsafety17 Furthermore improving coordination of carethrough a structured communication process is particularlyimportant in environments in which interruptions and mul-titasking are common such as the PACU setting This coor-dination of care helps to create a lsquolsquoshared mental modelrsquorsquo ofa patientrsquos status and the expected clinical course18 As aresult any digression from the anticipated postoperativecourse is more promptly identified
There was evidence that clinically significant steps in theinformation transfer process were missed which at the veryleast eroded safety margins The potential of adverse eventsoccurring during the patientrsquos care became evident in thepreintervention phase Two patients did not receive deepvein thrombosis prophylaxis on their 1st postoperative daybecause of information omission during the handoverprocess Introduction of the proforma was effective inensuring that pertinent information was not overlookedduring the handover Additionally the proforma served as areminder to the surgeon to write instructions regarding deep
K Nagpal et al Improving postoperative handover 499
vein thrombosis prophylaxis on the drug chart on 4occasions which otherwise would not have been writtenand potentially not administered to the patient affecting thepatientrsquos safety Formalizing and producing a more stan-dardized handover was accomplished and the study can beseen as a step in meeting the joint commissionrsquos NationalPatient Safety Goals for a standardized approach to handoffcommunication19
There were several limitations to this study In anyobservational study the question of authenticity of data isof central concern In addition to mechanisms employed tominimize the observer or Hawthorne effect20 the observerrecorded evidence of this possible effect in the field notesFurthermore informal interviews with randomly selectedparticipants following each observation period contributedto our sense of the datarsquos representativeness Working groupmembers commented on whether data seemed representa-tive or not on no occasion did experts question thesedata Moreover the validity of data was also confirmedby significant interrater reliability Another limitation wasthe small sample size and the fact that the study was con-ducted on a single site each institution has its own barriersto changing culture therefore the results may not bebroadly generalized This study also suffers from the tradi-tional biases of a prendashpost test design specifically that wewere unable to control for all potential confounding influ-ences However a randomized controlled trial of this inter-vention within 1 institution would be impossible due to therisk of contamination between study groups and feasibilityissues Despite these limitations we believe that implemen-tation of the new handover protocol indeed standardizesand facilitates communication among health care providersin the PACU This study did not set out to determine if thisnew handover protocol improved patient outcomes Never-theless it is important that the likelihood of multiple errorswith individual patients was reduced as the avoidance ofcompounding errors is a fundamentally important compo-nent of safety21 and has been shown in other studies toaffect outcome22
A further limitation is that while the proforma iseffective to ensure that the necessary information is handedover it does not ensure that the information is understoodby the receiving nurse In this study the improved nursesrsquosatisfaction for the overall handover could indicate thattheir level of understanding of the information communi-cated during the handover improved
We also observed that the researcher had to facilitate theprocess by asking the anesthetist and a member of thesurgical team to use the proforma for the handover on 4occasions This and the high level of engagement with theclinical team during the study highlights the fact that thesuccessful implementation of the protocol was influencedto a large extent by the motivation of the clinical team andthat there was a certain amount of selection bias in thisstudy As the protocol is more widely implemented we willhave to be aware of the need for a strategy for engagement
with clinical teams This also raises the question ofsustainability of the protocol when someone is not presentto drive the use of the protocol
Conclusions
Despite any potential failings implementation of the newhandover protocol significantly improved the quality of thepostoperative handover through enhanced information trans-fer teamwork and reduced task errors In most health caresettings the handover in the PACU is the conduit to infor-mation downstream when patients are transferred to theirfinal recovery facility By improving postoperative handoverin the PACU we can ensure that information transferreddownstream is made more accurate comprehensive androbust This could potentially ensure a heightened state ofvigilance for postoperating complications improve postop-erative care by ensuring that key processes are undertakenand thus potentially improve postoperative outcomesWe arenow undertaking research to evaluate the impact of improvedhandover on postoperative care and outcomes
References
1 British Medical Association Safe handover safe patients Guid-
ance on clinical handover for clinicians and managers Vol 2009
2004
2 McCann L McHardy K Child S Passing the buck clinical handovers
at a tertiary hospital N Z Med J 2007120U2778
3 Sherlock C The patient handover a study of its form function and ef-
ficiency Nurs Stand 1995933ndash6
4 Whitt N Harvey R McLeod G et al How many health professionals
does a patient see during an average hospital stay N Z Med J 2007
120U2517
5 Australian Council for Safety andQuality in Health Care Clinical hand-
over and patient safety literature review report Vol 2009 2005
6 Singh H Thomas EJ Petersen LA et al Medical errors involving
trainees a study of closed malpractice claims from 5 insurers Arch
Intern Med 20071672030ndash6
7 Joint Commission on Accreditation of Healthcare Organizations Sen-
tinel event statistics Vol 2009 2005
8 Mistry K Landrigan C Goldmann D et al Communication during
post-operative patient handoff in the pediatric intensive care unit
Crit Care Med 200533A12
9 Hughes RG Clancy CM Improving the complex nature of care tran-
sitions J Nurs Care Qual 200722289ndash92
10 Williams RG Silverman R Schwind C et al Surgeon information
transfer and communication factors affecting quality and efficiency
of inpatient care Ann Surg 2007245159ndash69
11 Kluger MT Bullock MF Recovery room incidents a review of 419 re-
ports from the Anaesthetic Incident Monitoring Study (AIMS) Anaes-
thesia 2002571060ndash6
12 Anwari JS Quality of handover to the postanaesthesia care unit nurse
Anaesthesia 200257488ndash93
13 Nagpal K Arora S Abboudi M et al Postoperative handover prob-
lems pitfalls and prevention of error Ann Surg 2010252171ndash6
14 Catchpole KR de Leval MR McEwan A et al Patient handover
from surgery to intensive care using Formula 1 pit-stop and aviation
models to improve safety and quality Paediatr Anaesth 200717
470ndash8
500 The American Journal of Surgery Vol 206 No 4 October 2013
15 Nagpal K Abboudi M Fishler L et al Evaluation of postoperative
handover using a tool to assess information transfer and teamwork
Ann Surg 2011253831ndash7
16 Undre S Sevdalis N Healey AN et al Observational teamwork as-
sessment for surgery (OTAS) refinement and application in urological
surgery World J Surg 2007311373ndash81
17 Patterson ES Roth EM Woods DD et al Handoff strategies in set-
tings with high consequences for failure lessons for health care oper-
ations Int J Qual Health Care 200416125ndash32
18 McLeod J Chaffee S Interpersonal approaches to communication re-
search Am Behav Sci 197316469ndash99
19 Joint Commission National patient safety goals handbook 2008 Avail-
able at httpwwwpatientsafetygovTIPSDocsTIPS_JanFeb08pdf
Accessed June 23 2013
20 Franke R Kaul J The Hawthorne experiments first statistical interpre-
tation Am Sociol Rev 197843623ndash43
21 Catchpole KR Giddings AE de Leval MR et al Identification of sys-
tems failures in successful paediatric cardiac surgery Ergonomics
200649567ndash88
22 Hofer TP Hayward RA Are bad outcomes from questionable clinical
decisions preventable medical errors A case of cascade iatrogenesis
Ann Intern Med 2002137(Pt 1)327ndash33
K Nagpal et al Improving postoperative handover 501
Appendix 1
Postoperative handover proforma
Postoperative proforma
Patient specific Anesthetic Surgical
U Patient name amp ageU Medical historyU Allergy statusU Name of procedureU Current status
of patient
U Type of anesthesiaU Intraoperative course amp any complicationsU Anticipated postop problems bleeding
pain airwayU Monitoring amp range for physiological
parameters BP UOU Analgesia planU Plan for IV fluidsU Postop complicationsU Contact problems for any anesthetic problems
U Intraoperative surgicalcourse amp any complications
U Blood lossU Antibiotic planU Drugs to be restartedU DVT prophylaxis planU Plans for tubes amp drainsU NG tube amp feeding planU Postop investigationsU Contact number for any
surgical problems
BP 5 blood pressure DVT 5 deep vein thrombosis IV 5 intravenous NG 5 nasogastric UO 5 urinary output

498 The American Journal of Surgery Vol 206 No 4 October 2013
handover protocol (r 5 548 P 001) Thus informationomissions were more likely compounded by the task errors(ie information omissions is directly proportional to thetask errors) The communication component of the team-work score was negatively correlated with the number oftask errors (r 5 2625 P 001) demonstrating thatpoor communication during the handover is associatedwith more task errors
The 2-tailed Spearman rank correlation demonstrated anegative correlation between the number of informationomissions and teamwork score (r 5 2663 P 001)thereby highlighting the importance of teamwork as avital component in good quality handover informationtransfer
Comments
The new handover protocol produced a marked im-provement in the quality of handover Information omis-sions and task errors were significantly reduced and therewas considerable improvement in teamwork and nursesatisfaction scores In fact improvements were foundacross almost the entire process following its introductionThe structured approach to the transfer of information fromoperating theater staff to recovery staff and coordination oftasks performed contributed to the improved teamworkscore Although there was no significant reduction in theduration after the new protocol the nurses were moresatisfied with the overall handover
The protocol focused on the surgeonrsquos participation inthe handover process communication task sequence andleadership Most significant is the finding that team mem-bers working in a hectic and high-pressure clinical envi-ronment can successfully implement a change in theirhandover practice Several factors contributed to the suc-cess of the new handover protocol implementation in thestudy The surgical anesthetic and recovery team includeda consistent group of people who were supportive ofresearch The surgeonrsquos commitment was particularly crit-ical for the successful implementation which can be seenby the largest improvement in surgical information omis-sions Consistent with quality improvement initiatives thatinvolve health care professions we engaged in a continuousprocess with the participants receiving and providingcontinuous feedback The feedback of theater and recoverystaff both before and during the development of proformaprovided critical insight into the implementation processEngagement with the professionals may also have con-ferred a sense of ownership to participants which isessential to the success of quality improvement initiativesthat seek to change the behavior
Before the intervention the handover process wasnegatively affected by the lack of surgical informationprovided distractions during the handover and lack of aformalized structure The new protocol ensured the pres-ence of at least 1 member of the surgical team and adequate
transfer of all the information especially surgical informa-tion in a standardized format Furthermore the correlationbetween information omissions and teamwork emphasizedthe value of teamwork in achieving the lowest rate oferrors
Avoidance of any variability in the delivery of postop-erative handover through standardization of process im-plementation of postoperative handover proforma and tasksequence involvement of the lsquolsquocaptain of shiprsquorsquo (ie sur-geon) excellent teamwork and camaraderie performed inexactly the same manner every time were the key principlesof the successful outcome These led to changes in criticalclinical processes which eventually led to changes inoutcomes as discussed below We did not focus on out-comes therefore this parameter was not measured More-over adverse outcome measures were precluded by low ratesrequiring large sample sizes However we believe thatchanges in these clinical processes (ie information omis-sions task errors and teamwork) will impact the clinical andnonclinical outcomes
Our results echo the findings of poor quality handoverfrom theater to the PACU12 Our study also demonstratedthat 48 of anesthetic information was not transferred Inthe study conducted by Anwari12 nurses awarded the high-est marks to almost half the anesthetists however this fig-ure increased from 7 to 60 after the introduction of thenew protocol Very few studies have attempted to improvepostoperative handover A noteworthy exception is a studyby Catchpole et al14 which used Formula-1 concepts to im-prove the handover process in the pediatric intensive careunit They demonstrated a significant reduction in informa-tion omissions and technical errors after standardizing theirhandover process
As evident in other high-reliability industries standard-ization of the handover has been effective through team-work communication techniques flattening of hierarchymutual respect within and across disciplines and situationalawareness which are key components of a culture ofsafety17 Furthermore improving coordination of carethrough a structured communication process is particularlyimportant in environments in which interruptions and mul-titasking are common such as the PACU setting This coor-dination of care helps to create a lsquolsquoshared mental modelrsquorsquo ofa patientrsquos status and the expected clinical course18 As aresult any digression from the anticipated postoperativecourse is more promptly identified
There was evidence that clinically significant steps in theinformation transfer process were missed which at the veryleast eroded safety margins The potential of adverse eventsoccurring during the patientrsquos care became evident in thepreintervention phase Two patients did not receive deepvein thrombosis prophylaxis on their 1st postoperative daybecause of information omission during the handoverprocess Introduction of the proforma was effective inensuring that pertinent information was not overlookedduring the handover Additionally the proforma served as areminder to the surgeon to write instructions regarding deep
K Nagpal et al Improving postoperative handover 499
vein thrombosis prophylaxis on the drug chart on 4occasions which otherwise would not have been writtenand potentially not administered to the patient affecting thepatientrsquos safety Formalizing and producing a more stan-dardized handover was accomplished and the study can beseen as a step in meeting the joint commissionrsquos NationalPatient Safety Goals for a standardized approach to handoffcommunication19
There were several limitations to this study In anyobservational study the question of authenticity of data isof central concern In addition to mechanisms employed tominimize the observer or Hawthorne effect20 the observerrecorded evidence of this possible effect in the field notesFurthermore informal interviews with randomly selectedparticipants following each observation period contributedto our sense of the datarsquos representativeness Working groupmembers commented on whether data seemed representa-tive or not on no occasion did experts question thesedata Moreover the validity of data was also confirmedby significant interrater reliability Another limitation wasthe small sample size and the fact that the study was con-ducted on a single site each institution has its own barriersto changing culture therefore the results may not bebroadly generalized This study also suffers from the tradi-tional biases of a prendashpost test design specifically that wewere unable to control for all potential confounding influ-ences However a randomized controlled trial of this inter-vention within 1 institution would be impossible due to therisk of contamination between study groups and feasibilityissues Despite these limitations we believe that implemen-tation of the new handover protocol indeed standardizesand facilitates communication among health care providersin the PACU This study did not set out to determine if thisnew handover protocol improved patient outcomes Never-theless it is important that the likelihood of multiple errorswith individual patients was reduced as the avoidance ofcompounding errors is a fundamentally important compo-nent of safety21 and has been shown in other studies toaffect outcome22
A further limitation is that while the proforma iseffective to ensure that the necessary information is handedover it does not ensure that the information is understoodby the receiving nurse In this study the improved nursesrsquosatisfaction for the overall handover could indicate thattheir level of understanding of the information communi-cated during the handover improved
We also observed that the researcher had to facilitate theprocess by asking the anesthetist and a member of thesurgical team to use the proforma for the handover on 4occasions This and the high level of engagement with theclinical team during the study highlights the fact that thesuccessful implementation of the protocol was influencedto a large extent by the motivation of the clinical team andthat there was a certain amount of selection bias in thisstudy As the protocol is more widely implemented we willhave to be aware of the need for a strategy for engagement
with clinical teams This also raises the question ofsustainability of the protocol when someone is not presentto drive the use of the protocol
Conclusions
Despite any potential failings implementation of the newhandover protocol significantly improved the quality of thepostoperative handover through enhanced information trans-fer teamwork and reduced task errors In most health caresettings the handover in the PACU is the conduit to infor-mation downstream when patients are transferred to theirfinal recovery facility By improving postoperative handoverin the PACU we can ensure that information transferreddownstream is made more accurate comprehensive androbust This could potentially ensure a heightened state ofvigilance for postoperating complications improve postop-erative care by ensuring that key processes are undertakenand thus potentially improve postoperative outcomesWe arenow undertaking research to evaluate the impact of improvedhandover on postoperative care and outcomes
References
1 British Medical Association Safe handover safe patients Guid-
ance on clinical handover for clinicians and managers Vol 2009
2004
2 McCann L McHardy K Child S Passing the buck clinical handovers
at a tertiary hospital N Z Med J 2007120U2778
3 Sherlock C The patient handover a study of its form function and ef-
ficiency Nurs Stand 1995933ndash6
4 Whitt N Harvey R McLeod G et al How many health professionals
does a patient see during an average hospital stay N Z Med J 2007
120U2517
5 Australian Council for Safety andQuality in Health Care Clinical hand-
over and patient safety literature review report Vol 2009 2005
6 Singh H Thomas EJ Petersen LA et al Medical errors involving
trainees a study of closed malpractice claims from 5 insurers Arch
Intern Med 20071672030ndash6
7 Joint Commission on Accreditation of Healthcare Organizations Sen-
tinel event statistics Vol 2009 2005
8 Mistry K Landrigan C Goldmann D et al Communication during
post-operative patient handoff in the pediatric intensive care unit
Crit Care Med 200533A12
9 Hughes RG Clancy CM Improving the complex nature of care tran-
sitions J Nurs Care Qual 200722289ndash92
10 Williams RG Silverman R Schwind C et al Surgeon information
transfer and communication factors affecting quality and efficiency
of inpatient care Ann Surg 2007245159ndash69
11 Kluger MT Bullock MF Recovery room incidents a review of 419 re-
ports from the Anaesthetic Incident Monitoring Study (AIMS) Anaes-
thesia 2002571060ndash6
12 Anwari JS Quality of handover to the postanaesthesia care unit nurse
Anaesthesia 200257488ndash93
13 Nagpal K Arora S Abboudi M et al Postoperative handover prob-
lems pitfalls and prevention of error Ann Surg 2010252171ndash6
14 Catchpole KR de Leval MR McEwan A et al Patient handover
from surgery to intensive care using Formula 1 pit-stop and aviation
models to improve safety and quality Paediatr Anaesth 200717
470ndash8
500 The American Journal of Surgery Vol 206 No 4 October 2013
15 Nagpal K Abboudi M Fishler L et al Evaluation of postoperative
handover using a tool to assess information transfer and teamwork
Ann Surg 2011253831ndash7
16 Undre S Sevdalis N Healey AN et al Observational teamwork as-
sessment for surgery (OTAS) refinement and application in urological
surgery World J Surg 2007311373ndash81
17 Patterson ES Roth EM Woods DD et al Handoff strategies in set-
tings with high consequences for failure lessons for health care oper-
ations Int J Qual Health Care 200416125ndash32
18 McLeod J Chaffee S Interpersonal approaches to communication re-
search Am Behav Sci 197316469ndash99
19 Joint Commission National patient safety goals handbook 2008 Avail-
able at httpwwwpatientsafetygovTIPSDocsTIPS_JanFeb08pdf
Accessed June 23 2013
20 Franke R Kaul J The Hawthorne experiments first statistical interpre-
tation Am Sociol Rev 197843623ndash43
21 Catchpole KR Giddings AE de Leval MR et al Identification of sys-
tems failures in successful paediatric cardiac surgery Ergonomics
200649567ndash88
22 Hofer TP Hayward RA Are bad outcomes from questionable clinical
decisions preventable medical errors A case of cascade iatrogenesis
Ann Intern Med 2002137(Pt 1)327ndash33
K Nagpal et al Improving postoperative handover 501
Appendix 1
Postoperative handover proforma
Postoperative proforma
Patient specific Anesthetic Surgical
U Patient name amp ageU Medical historyU Allergy statusU Name of procedureU Current status
of patient
U Type of anesthesiaU Intraoperative course amp any complicationsU Anticipated postop problems bleeding
pain airwayU Monitoring amp range for physiological
parameters BP UOU Analgesia planU Plan for IV fluidsU Postop complicationsU Contact problems for any anesthetic problems
U Intraoperative surgicalcourse amp any complications
U Blood lossU Antibiotic planU Drugs to be restartedU DVT prophylaxis planU Plans for tubes amp drainsU NG tube amp feeding planU Postop investigationsU Contact number for any
surgical problems
BP 5 blood pressure DVT 5 deep vein thrombosis IV 5 intravenous NG 5 nasogastric UO 5 urinary output

K Nagpal et al Improving postoperative handover 499
vein thrombosis prophylaxis on the drug chart on 4occasions which otherwise would not have been writtenand potentially not administered to the patient affecting thepatientrsquos safety Formalizing and producing a more stan-dardized handover was accomplished and the study can beseen as a step in meeting the joint commissionrsquos NationalPatient Safety Goals for a standardized approach to handoffcommunication19
There were several limitations to this study In anyobservational study the question of authenticity of data isof central concern In addition to mechanisms employed tominimize the observer or Hawthorne effect20 the observerrecorded evidence of this possible effect in the field notesFurthermore informal interviews with randomly selectedparticipants following each observation period contributedto our sense of the datarsquos representativeness Working groupmembers commented on whether data seemed representa-tive or not on no occasion did experts question thesedata Moreover the validity of data was also confirmedby significant interrater reliability Another limitation wasthe small sample size and the fact that the study was con-ducted on a single site each institution has its own barriersto changing culture therefore the results may not bebroadly generalized This study also suffers from the tradi-tional biases of a prendashpost test design specifically that wewere unable to control for all potential confounding influ-ences However a randomized controlled trial of this inter-vention within 1 institution would be impossible due to therisk of contamination between study groups and feasibilityissues Despite these limitations we believe that implemen-tation of the new handover protocol indeed standardizesand facilitates communication among health care providersin the PACU This study did not set out to determine if thisnew handover protocol improved patient outcomes Never-theless it is important that the likelihood of multiple errorswith individual patients was reduced as the avoidance ofcompounding errors is a fundamentally important compo-nent of safety21 and has been shown in other studies toaffect outcome22
A further limitation is that while the proforma iseffective to ensure that the necessary information is handedover it does not ensure that the information is understoodby the receiving nurse In this study the improved nursesrsquosatisfaction for the overall handover could indicate thattheir level of understanding of the information communi-cated during the handover improved
We also observed that the researcher had to facilitate theprocess by asking the anesthetist and a member of thesurgical team to use the proforma for the handover on 4occasions This and the high level of engagement with theclinical team during the study highlights the fact that thesuccessful implementation of the protocol was influencedto a large extent by the motivation of the clinical team andthat there was a certain amount of selection bias in thisstudy As the protocol is more widely implemented we willhave to be aware of the need for a strategy for engagement
with clinical teams This also raises the question ofsustainability of the protocol when someone is not presentto drive the use of the protocol
Conclusions
Despite any potential failings implementation of the newhandover protocol significantly improved the quality of thepostoperative handover through enhanced information trans-fer teamwork and reduced task errors In most health caresettings the handover in the PACU is the conduit to infor-mation downstream when patients are transferred to theirfinal recovery facility By improving postoperative handoverin the PACU we can ensure that information transferreddownstream is made more accurate comprehensive androbust This could potentially ensure a heightened state ofvigilance for postoperating complications improve postop-erative care by ensuring that key processes are undertakenand thus potentially improve postoperative outcomesWe arenow undertaking research to evaluate the impact of improvedhandover on postoperative care and outcomes
References
1 British Medical Association Safe handover safe patients Guid-
ance on clinical handover for clinicians and managers Vol 2009
2004
2 McCann L McHardy K Child S Passing the buck clinical handovers
at a tertiary hospital N Z Med J 2007120U2778
3 Sherlock C The patient handover a study of its form function and ef-
ficiency Nurs Stand 1995933ndash6
4 Whitt N Harvey R McLeod G et al How many health professionals
does a patient see during an average hospital stay N Z Med J 2007
120U2517
5 Australian Council for Safety andQuality in Health Care Clinical hand-
over and patient safety literature review report Vol 2009 2005
6 Singh H Thomas EJ Petersen LA et al Medical errors involving
trainees a study of closed malpractice claims from 5 insurers Arch
Intern Med 20071672030ndash6
7 Joint Commission on Accreditation of Healthcare Organizations Sen-
tinel event statistics Vol 2009 2005
8 Mistry K Landrigan C Goldmann D et al Communication during
post-operative patient handoff in the pediatric intensive care unit
Crit Care Med 200533A12
9 Hughes RG Clancy CM Improving the complex nature of care tran-
sitions J Nurs Care Qual 200722289ndash92
10 Williams RG Silverman R Schwind C et al Surgeon information
transfer and communication factors affecting quality and efficiency
of inpatient care Ann Surg 2007245159ndash69
11 Kluger MT Bullock MF Recovery room incidents a review of 419 re-
ports from the Anaesthetic Incident Monitoring Study (AIMS) Anaes-
thesia 2002571060ndash6
12 Anwari JS Quality of handover to the postanaesthesia care unit nurse
Anaesthesia 200257488ndash93
13 Nagpal K Arora S Abboudi M et al Postoperative handover prob-
lems pitfalls and prevention of error Ann Surg 2010252171ndash6
14 Catchpole KR de Leval MR McEwan A et al Patient handover
from surgery to intensive care using Formula 1 pit-stop and aviation
models to improve safety and quality Paediatr Anaesth 200717
470ndash8
500 The American Journal of Surgery Vol 206 No 4 October 2013
15 Nagpal K Abboudi M Fishler L et al Evaluation of postoperative
handover using a tool to assess information transfer and teamwork
Ann Surg 2011253831ndash7
16 Undre S Sevdalis N Healey AN et al Observational teamwork as-
sessment for surgery (OTAS) refinement and application in urological
surgery World J Surg 2007311373ndash81
17 Patterson ES Roth EM Woods DD et al Handoff strategies in set-
tings with high consequences for failure lessons for health care oper-
ations Int J Qual Health Care 200416125ndash32
18 McLeod J Chaffee S Interpersonal approaches to communication re-
search Am Behav Sci 197316469ndash99
19 Joint Commission National patient safety goals handbook 2008 Avail-
able at httpwwwpatientsafetygovTIPSDocsTIPS_JanFeb08pdf
Accessed June 23 2013
20 Franke R Kaul J The Hawthorne experiments first statistical interpre-
tation Am Sociol Rev 197843623ndash43
21 Catchpole KR Giddings AE de Leval MR et al Identification of sys-
tems failures in successful paediatric cardiac surgery Ergonomics
200649567ndash88
22 Hofer TP Hayward RA Are bad outcomes from questionable clinical
decisions preventable medical errors A case of cascade iatrogenesis
Ann Intern Med 2002137(Pt 1)327ndash33
K Nagpal et al Improving postoperative handover 501
Appendix 1
Postoperative handover proforma
Postoperative proforma
Patient specific Anesthetic Surgical
U Patient name amp ageU Medical historyU Allergy statusU Name of procedureU Current status
of patient
U Type of anesthesiaU Intraoperative course amp any complicationsU Anticipated postop problems bleeding
pain airwayU Monitoring amp range for physiological
parameters BP UOU Analgesia planU Plan for IV fluidsU Postop complicationsU Contact problems for any anesthetic problems
U Intraoperative surgicalcourse amp any complications
U Blood lossU Antibiotic planU Drugs to be restartedU DVT prophylaxis planU Plans for tubes amp drainsU NG tube amp feeding planU Postop investigationsU Contact number for any
surgical problems
BP 5 blood pressure DVT 5 deep vein thrombosis IV 5 intravenous NG 5 nasogastric UO 5 urinary output

500 The American Journal of Surgery Vol 206 No 4 October 2013
15 Nagpal K Abboudi M Fishler L et al Evaluation of postoperative
handover using a tool to assess information transfer and teamwork
Ann Surg 2011253831ndash7
16 Undre S Sevdalis N Healey AN et al Observational teamwork as-
sessment for surgery (OTAS) refinement and application in urological
surgery World J Surg 2007311373ndash81
17 Patterson ES Roth EM Woods DD et al Handoff strategies in set-
tings with high consequences for failure lessons for health care oper-
ations Int J Qual Health Care 200416125ndash32
18 McLeod J Chaffee S Interpersonal approaches to communication re-
search Am Behav Sci 197316469ndash99
19 Joint Commission National patient safety goals handbook 2008 Avail-
able at httpwwwpatientsafetygovTIPSDocsTIPS_JanFeb08pdf
Accessed June 23 2013
20 Franke R Kaul J The Hawthorne experiments first statistical interpre-
tation Am Sociol Rev 197843623ndash43
21 Catchpole KR Giddings AE de Leval MR et al Identification of sys-
tems failures in successful paediatric cardiac surgery Ergonomics
200649567ndash88
22 Hofer TP Hayward RA Are bad outcomes from questionable clinical
decisions preventable medical errors A case of cascade iatrogenesis
Ann Intern Med 2002137(Pt 1)327ndash33
K Nagpal et al Improving postoperative handover 501
Appendix 1
Postoperative handover proforma
Postoperative proforma
Patient specific Anesthetic Surgical
U Patient name amp ageU Medical historyU Allergy statusU Name of procedureU Current status
of patient
U Type of anesthesiaU Intraoperative course amp any complicationsU Anticipated postop problems bleeding
pain airwayU Monitoring amp range for physiological
parameters BP UOU Analgesia planU Plan for IV fluidsU Postop complicationsU Contact problems for any anesthetic problems
U Intraoperative surgicalcourse amp any complications
U Blood lossU Antibiotic planU Drugs to be restartedU DVT prophylaxis planU Plans for tubes amp drainsU NG tube amp feeding planU Postop investigationsU Contact number for any
surgical problems
BP 5 blood pressure DVT 5 deep vein thrombosis IV 5 intravenous NG 5 nasogastric UO 5 urinary output

K Nagpal et al Improving postoperative handover 501
Appendix 1
Postoperative handover proforma
Postoperative proforma
Patient specific Anesthetic Surgical
U Patient name amp ageU Medical historyU Allergy statusU Name of procedureU Current status
of patient
U Type of anesthesiaU Intraoperative course amp any complicationsU Anticipated postop problems bleeding
pain airwayU Monitoring amp range for physiological
parameters BP UOU Analgesia planU Plan for IV fluidsU Postop complicationsU Contact problems for any anesthetic problems
U Intraoperative surgicalcourse amp any complications
U Blood lossU Antibiotic planU Drugs to be restartedU DVT prophylaxis planU Plans for tubes amp drainsU NG tube amp feeding planU Postop investigationsU Contact number for any
surgical problems
BP 5 blood pressure DVT 5 deep vein thrombosis IV 5 intravenous NG 5 nasogastric UO 5 urinary output





























