Embed Size (px)
Citation preview

Intermittent loading improves resultsin mandibular alveolar distractionosteogenesis
Ugo ConsoloCarlo BertoldiDavide Zaffe
Authors’ affiliations:Ugo Consolo, Carlo Bertoldi, Department ofNeurosciences, Head–Neck, Rehabilitation, Sectionof Dentistry and Maxillofacial Surgery, Universityof Modena and Reggio Emilia, Modena, ItalyDavide Zaffe, Department of Anatomy andHistology, Section of Human Anatomy Universityof Modena and Reggio Emilia, Modena, Italy
Correspondence to:Prof. Davide ZaffeDipartimento di Anatomia e IstologiaSezione di Anatomia Umana NormaleVa Del Pozzo71- 41100 ModenaItalyTel.:þ þ39-0594224800Fax: þ þ 39-0594224861e-mail: [email protected]
Key words: alveolar distraction, bone structure, histology, osteogenesis
Abstract
Aim: To evaluate clinical and morphological effects on distractive callus after application of
an original protocol of bone stimulation.
Material and methods: Traditional or mechanically stimulated alveolar-distraction
osteogenesis was studied on 16 highly selected subjects subdivided into two groups.
Clinical, radiological, densitometric and histological (on biopsies) analyses were performed
6, 8 and 12 weeks after distraction was completed.
Results: In subjects undergoing stimulated alveolar-distraction osteogenesis, bone density
was higher and at histology, bone with ordered structure was observed after 6 weeks.
Moreover, bone trabeculae with oriented architecture and greater amounts of lamellar
bone were observed after 8 and 12 weeks in the same subjects.
Discussion and conclusions: In conclusion, although osteogenic processes were similar in
both groups, they were induced earlier and were better structured in subjects undergoing
stimulated alveolar-distraction osteogenesis. These encouraging results can only be
achieved and preserved by strict monitoring of distractive vectors.
Alveolar distraction osteogenesis (ADO) is
a process of new bone formation (Zaffe
et al. 2002) subjected to two fundamen-
tal biological principles (Ilizarov 1989a,
1989b, 1997): (1) tension/stress effects, in
which a force produces stress or strain and
induces growth of soft tissue and bone and
(2) load/morphology effects, in which load-
ing and blood supply influence the shape
and mass of skeletal segments. These prin-
ciples are defined as Ilizarov effects.
Ilizarov’s method has been successfully
applied in the oral and maxillo-facial field.
After initial animal studies (Snyder et al.
1973; Micheli & Miotti 1977), the method
was applied in humans starting in 1992
(McCarthy et al. 1992; Klein & Howaldt
1995; Molina & Monasterio 1995). The
vector in these distractive methods was
applied along the direction of the longitu-
dinal bone axis.
In relation to the longitudinal axis of the
bone, Block et al. (1996) on animals, and
subsequently Chin & Toth (1996) and
Chin (1999a, 1999b, 1999c) in humans,
studied a method of distraction with
transverse vectors. These studies were
fundamental to ADO development and
particularly suitable for corrections of eden-
tulous–alveolar–ridge defects. This pre-
prosthetic surgical method represented an
innovative approach for achieving newly
formed bone build-up in the short term at
a ‘moderate biological and surgical cost.’
The implementation of ADO for correct-
ing alveolar ridge defects is constrained by
general and local conditions. The lack of
these conditions can cause complicationsCopyright r Blackwell Munksgaard 2006
Date:Accepted 13 June 2005
To cite this article:Consolo U, Bertoldi C, Zaffe D. Intermittent loadingimproves results in mandibular alveolar distractionosteogenesis.Clin. Oral Impl. Res. 17, 2006; 179–187doi: 10.1111/j.1600-0501.2005.01213.x
179

such as dehiscence of soft tissues, fracture
and infection of the distracted bony seg-
ment, lesions to vessels or nerves, devia-
tion of the distraction vector, delayed
consolidation, unsatisfactory osteogenesis
and poor final therapeutic outcomes.
ADO is most effective when combined
with implant-based prostheses. This type of
prosthesis helps obviate the resorption of
new bony volumes and ensures a therapeu-
tic continuity by effectively reproducing
the type of loads propagated through teeth
to the surrounding bony tissue. Neverthe-
less, the combination of ADO and implant-
based prosthesis requires that implant alloca-
tion be meticulously planned temporally and
spatially to obtain a correct distribution of
masticatory loads in relation to implants and
through implants to the underlying bone.
At present, additional knowledge is re-
quired to achieve a more rational planning
of rehabilitation. An exhaustive under-
standing of callus stimulation procedures
suitable for achieving adequate bone induc-
tion (qualitatively and quantitatively struc-
tured and correlated to masticatory load)
would pave the road toward improvement.
The purpose of this work is to apply an
original system of bone stimulation to repro-
duce (after prosthetic rehabilitation) loading
of regenerated bony segment and to evaluate
its clinical and morphological effects.
Material and methods
Screening
Patients for the present study were selected
according to inclusion and exclusion cri-
teria, listed below, and typified according
to the classification of Lekholm & Zarb
(1985), supplemented by that of Cawood &
Howell (1988), considering the whole jaw
and intraforamina area, respectively, when
included in the defect.
Patients undergoing ADO accomplished
the following general indications: a medical
history of good health, particularly ruling
out bone disease; no medical history of
systemic therapy, e.g. chemotherapy, ra-
diation therapy, etc.; no respiratory, masti-
catory or swallowing disorders; no tobacco
and/or alcohol abuse; and suitable oral
hygiene and compliance. Oral hygiene
was estimated using the plaque index (PI)
(Silness & Loee 1964) and gingival index
(GI) (Loee & Silness 1963), when possible,
and in any case was considered as the
absence of signs of inflammation signs or
food traces.
Patients also showed the following spe-
cific indications: alveolar vertical atrophy
(greater than 3 mm) with more than 7 mm
of residual bone covering the lower alveolar
nerve; vertical thickness of the distractive
fragment greater than 4 mm; good bone
quality (by densitometry and clinically
confirmed at surgery); and no diseases
affecting the site metabolism; no spatial
obstacle to the use of the distractor. On the
contrary, patients were excluded from the
study if they fulfilled the following general
criteria: systemic conditions not allowing
distractive therapy; neurotic and psychotic
disorders; tetracycline or non-steroidal
anti-inflammatory drugs (NSAID) allergy;
pregnancy or lactation; and underage or
uncooperative. Patients were also excluded
if they fulfilled the following specific
criteria: poor oral hygiene; chronic or
pre-chronic infective diseases; chronic sto-
matitis in the surgical field; cancerous or
pre-cancerous lesions, treated within the
last 5 years; dental treatments unrelated to
the study; and parafunctions.
Sixteen patients matched for gender, age
and type of alveolar ridge defect were se-
lected; all subjects gave their informed
consent to the ADO procedure.
Control group (CG)
Ten patients, five males and five females,
aged 15–71 years (mean� SD¼ 42.8�19.9), were selected. Four (40%) were
completely edentulous and the rest were
partially edentulous. The alveolar bone
defect had a mesiodistal dimension of 27–
60 mm (mean� SD¼ 46.8� 12.2) and a
vertical dimension of 6.6–14 mm (mean
SD¼10.4� 3). According to Lekholm &
Zarb (1985), the degree of the defect was B/
2–3 in five patients and C/2–3 in the
remaining five. Cawood & Howell (1988)
degree 4 defects were present in two
patients and degree 5 in three patients.
According to clinical intraoperative and
densitometric criteria, the bone quality of
the patients was defined as degree 1–2
(Lekholm & Zarb 1985).
Loaded device group (LDG)
This group contained three males and
three females, aged 20–63 years (mean
SD¼38.7� 16.5). Two patients (33%)
were completely edentulous and the rest
were partially edentulous. The alveolar
bone defect had a mesiodistal dimension
of 30–60 mm (mean� SD¼ 49.5� 12.7)
and a vertical dimension of 6.6–14 mm
(mean� SD¼ 10.4� 3.3). According to
Lekholm & Zarb, the degree of the defect
was B/2–3 in three patients and C/2–3 in
the remaining three. Cawood & Howell
degree 4 defects were observed in one
patient and degree 5 in two patients. The
bone quality of the patients was degree 1–2.
Operative protocol
The same team carried out all clinical
evaluations during the pre-distractive, dis-
tractive and post-distractive phases. De-
scriptive criteria were used to classify the
initial appearance of tissue changes during
the ADO procedure and final results, since
indexes or classifications for alveolar dis-
tractive therapy are lacking.
Alveolar sites were examined by conven-
tional radioscopy (orthopantomography,
etc), Computer tomography (CT) with
transverse image digital reconstructions
(maximum slice¼1 mm) and densitome-
try. Densitometric evaluations (Kalander et
al. 1990), carried out by an auto-standar-
dizing apparatus (3-CTcytec, General Elec-
tric Healthcare Technologies, Waukesha,
WI, USA), were computed as Hounsfield
units (HU). A complete radiographic study
was performed before surgical inter-
ventions by the distractive protocol. The
radiologist, permitting reproducible, com-
parable and reliable evaluations, carefully
checked anatomical reference points for
each patient and apparatus collimation on
the basis of previous radiographs.
Pre-surgical phase
Chalk models of the dental arches, stan-
dard radiographies and CT with high-reso-
lution transverse reconstructions were
performed on patients to plan the therapy
of implant-based prosthesis.
Surgical phase
The surgical distraction protocol was per-
formed using the Hidding intra-oral extra-
alveolar distractor (Hidding et al. 1999;
Lazar et al. 1999) TRACK (Tissue Regen-
eration by Alveolar Callus distraction –
Koln) model (Martin, Tuttlingen, Ger-
many) under general anesthesia as pre-
viously described (Hidding et al. 1999;
Lazar et al. 1999; Consolo et al. 2000;
Consolo et al . Loading effect on distracted bone
180 | Clin. Oral Impl. Res. 17, 2006 / 179–187

Raghoebar et al. 2002; Zaffe et al. 2002).
To maintain the distractive vector constant
and to prevent lesions, a suitable TRACK
device was chosen depending on the degree
of correction of alveolar dismorphism. The
same surgical team performed surgery and
device application, according to the tar-
geted prosthetic outcomes.
Post-surgical phase
The protocol (traditional ADO – TADO)
recommended for the TRACK device was
followed for treating the CG (Table 1). A
protocol of stimulated ADO (SADO) de-
rived from our previous studies (Consolo
et al. 2000; Zaffe et al. 2002) was followed
for treating the LDG (Tables 1 and 2).
Moreover, the SADO protocol schedules
early implant insertion at removal of the
distraction device. Callus stimulation was
performed by cyclical distractive activa-
tions and deactivations for 8 weeks after
distraction was completed (Table 2).
In the two groups, clinical evaluations
were also repeated at the same time during
the latency, distractive and post-distractive
periods. An additional complete set of
radiographic examinations was performed
after distractor removal.
The postponed implant insertion of the
CG (TADO) calls for fewer radiographic
examinations. Nevertheless, radiographic
examinations were needed at implant in-
sertion in CG, 4 weeks after the end of
distraction. Simultaneous implant inser-
tion with distractor removal of the LDG
(SADO) required radiographic examina-
tions at 8 weeks but not at 12 weeks after
the end of distraction. Orthopantomogra-
phies and teleradiographies and plain radio-
graphic examinations were also performed
as required.
To mark newly formed bone during the
post-surgical phases, patients were given
tetracycline antibiotic (Bassado (doxycy-
cline) – 100 mg twice a day, for 3 days
starting 5 days prior to biopsy –Pharmacia
Upjhon, Nerviano, Italy).
Morphofunctional analysis of the tissues
was performed on cylindrical biopsies (two
biopsies for each patient) obtained by
means of a hollow mill (2 mm diameter),
operating at 600 rpm. under saline jet, at 8
and 12 weeks after the distraction proce-
dure. Biopsies were taken from the center
of the mesiodistal side of the callus, at a
right angle to the distractive membrane.
Due to causes unrelated to the study, four
patients (two for each group) were also
biopsied at 6 weeks after distraction was
completed. Unscheduled soft tissue surgi-
cal correction in 3 patients of the LDG
allowed an additional biopsy 12 weeks after
the end of distraction.
Statistics
Densitometric data were evaluated (Glantz
2003) with the Wilcoxon (matched pairs)
test, Mann–Whitney test (2 groups) or the
Kruskal–Wallis test (three groups). If P was
equal or inferior to 6% (P�0.06) groups
were considered statistically different and
then analyzed parametrically. Data were
evaluated by the paired Student’s t-test,
unpaired Student’s t-test (2 groups) or AN-
OVA test (three groups), both followed by
the Student–Newman–Keuls test when
the distribution was Gaussian. Groups
were considered statistically different if P
was equal or inferior to 5% (P�0.05).
Histology
Biopsies were fixed in 4% paraformalde-
hyde in 0.1 M phosphate buffer pH 7.2 for
1 h at room temperature and then dehy-
drated and embedded in methyl methacry-
late (PMMA) at 41C, as reported elsewhere
(Zaffe et al. 2002). Longitudinal thin
(5-mm-thick) and thick (200-mm-thick) sec-
tions were obtained from biopsies using an
Autocut 1150 bone microtome (Reichert-
Jung GmbH, Nussloch, Germany) and a
Leica 1600 diamond saw microtome (Leica
Microsystems, Wetzlar, Germany), respec-
tively (Zaffe et al. 2002). Thin sections
were stained with toluidine blue, tri-
chrome Gomori stain, total alkaline phos-
phatase (TAP) and tartrate-resistant acid
phosphatase (TRAP) methods, as reported
elsewhere (Zaffe et al. 2002). Thick sec-
tions were reduced to 100mm and X-ray
microradiographed (Zaffe et al. 2002).
Microradiographs and thin sections were
analyzed and photographed using an Axio-
phot Zeiss microscope (Carl Zeiss AG,
Oberkochen, Germany) under ordinary or
polarized light. New bone formation was
checked in thick sections using the micro-
scope under fluorescent light.
Trabecular bone volume (TBV, index of
bone tissue content – Parfitt et al. 1987)
and bone tissue structure (woven vs. la-
mellar bone) were evaluated by means of
a suitable image analyzer (VIDAS, Carl
Zeiss) on microradiographs and stained
sections, under polarized light, respective-
ly. Data were evaluated (Glantz 2003) with
the Mann–Whitney test (two groups).
Results
Clinical
The distraction procedure was successful
without serious complications in almost all
patients. No infection, dehiscence or neu-
rovascular injuries were observed. A satis-
factory post-surgical course was achieved
in all patients. Due to good vascularization,
soft tissues were trophic after suture
removal.
Pain was only reported in a few patients
of both groups during the activation phase.
The distraction procedure in these patients
Table 1. Distractive protocol
TADO ODP ! 1 week ! DS ! DE ! 8 weeks ! DR ! 4 weeks ! ISADO ODP ! 1 week ! DS ! DE ! 8 weeks ! DRI
TADO, traditional alveolar distraction osteogenesis; SADO, stimulated alveolar distraction osteogenesis; ODP, osteotomy and distractor positioning; DS,
distraction start; DE, distraction end; DR, distractor removal; DRI, distractor removal and implantology; I, implantology.
Table 2. SADO treatment schedule
Week Day
1 2 3 4 5 6 7
1 A D A D2 A D A3 D a d a4 d a d5 a d a d6 a d7 a d8 a d ###
A, 1 turn activation; D, 1 turn deactivation; a,
1/2 turn activation; d, 1/2 turn deactivation;
### , distractor removal and implant inser-
tion.
Consolo et al . Loading effect on distracted bone
181 | Clin. Oral Impl. Res. 17, 2006 / 179–187
was made more bearable by increasing the
frequency (4 daily activations to spread out
distraction) and, if needed, decreasing the
amount of activation (less than 1 mm per
day). Despite reduction of the treatment
scheduled by protocol (Table 2), some pa-
tients in the LDG reported pain during the
final activation–deactivation cycle.
Oral surgery was required 6 weeks after
the end of distraction in three patients (two
CG and one LDG). The latter LDG patient
and six other patients (four CG and two
LDG) underwent soft tissue treatment 12
weeks after the end of distraction to deepen
the oral vestibule and/or obtain keratinized
gingival buildup.
The planned angle of the distraction
vector was changed in four patients (two
CG and two LDG). In three of these pa-
tients (two CG and one LDG), the amount
of deviation was compatible with that
needed in implant-based prosthetic rehabi-
litation.
Unscheduled corrective surgery, required
due to the loss of anchorage of the distrac-
tion device and major deviation, was re-
quired 6 weeks after the end of distraction
in one patient (LDG). This clinical compli-
cation excluded the results obtained 6
weeks after distraction was completed in
this patient.
In all patients, the alveolar ridge was
suitable for the successive pre-prosthetic
surgical procedure at the end of the distrac-
tive protocol.
The distracted fragments ranged between
27 and 60 mm (mean� SD¼ 46.8� 12.2),
and bone buildup (verified at TC) ranged
from 6.6 to 14 mm (mean� SD¼ 10.4
� 3) in CG patients. The distracted frag-
ments (Fig. 1) ranged from 30 to 60 mm
(mean� SD¼ 49.5� 12.7), and the ach-
ieved bone buildup (CT verified) ranged
from 6.6 to 14 mm (mean� SD¼ 10.4
� 3.2) in patients of the LDG.
Due to the roughly triangular section of
the distracted bony segments, the actual
bone thickness could not be reliably and
exactly evaluated in either group; these
measurements were purposely omitted
since they would have produced arbitrary
results and were substantially of little clin-
ical importance. The longitudinal size
(P¼ 0.697) of the defect and consequently
of the distracted bone, and the height
(P¼ 0.956) of the defect and of the corre-
sponding correction were not statistically
different in the CG and LDG (Mann–
Whitney rank-sum test).
Radiograms clearly showed all skeletal
distracted segments and the hard tissue,
which originated from the cut edges. Quite
often radiograms did not show conspicuous
differences when the two groups were
compared at the same observation interval
(Fig. 1).
Densitometry
Bone densitometry (P¼ 0.871) was not
statistical by different at non-parametric
statistical analysis (Mann–Whitney rank-
sum test) between the LDG (n¼6, mean
SD¼792.5� 642.7 HU) and CG (n¼10,
mean� SD¼ 847.9� 527.5 HU) prior to
surgery (Fig. 2).
When the distraction device was re-
moved (8 weeks after distraction was com-
pleted), values in the LDG (mean� SD
¼1210� 547.5 HU) differed significantly
from those in the CG (mean� SD¼670.1
� 424.5 HU) (P¼0.044 – Student’s t-
test). In compensation, densitometric va-
lues (mean� SD¼ 755.1� 357.1 HU) in-
creased in the CG at implant insertion
(12 weeks after distraction was completed).
No statistical differences (P¼ 0.062 –
Student’s t-test) were found when compar-
ing the correspondent densitometric values
of the patients at implant insertion, i.e. the
values obtained 12 weeks after distraction
for CG vs. those obtained 8 weeks after
distraction for LDG.
Longitudinal comparisons (before sur-
gery vs device removal vs implant inser-
tion) of densitometric values of each group
did not reach statistical significance in CG,
at non-parametric statistical analysis
(Kruskal–Wallis test) (P¼ 0.532). On the
contrary, the correspondent values were
statistically significant in LDG, at non-
parametric statistical analysis (Wilcoxon
test) (Po0.032). These values were highly
significant in the LDG, at parametric sta-
tistical analysis (paired Student’s t-test)
(P¼0.001).
Histology
Six weeks after the end of distraction, the
regenerated tissue in subjects undergoing
TADO (CG) was almost exclusively com-
posed of fibrous tissue, in accord with our
previous study (Zaffe et al. 2002). How-
ever, several islands of high angiogenic
activity were found inside the soft callus.
A feeble osteogenetic activity was ob-
served, and a limited number of isolated
and small trabeculae surrounded by vessels
could be seen in the fibrous tissue. Osteo-
blasts were not laid down on the trabeculae
surface, since these small bony formations
were the result of a static osteogenetic
process (Ferretti et al. 2002). The bone
Fig. 1. Computed tomography with transverse im-
age digital reconstructions of subjects undergoing
traditional alveolar distraction osteogenesis (a) and
simulated alveolar distraction osteogenesis (b) at the
distractor removal step. Note the absence of large
radiographic differences between these subjects.
2000
1000
0CG LDG
before8 weeks
12 weeks
HU
Fig. 2. Graph showing the densitometric behavior in
all subjects of the two groups, before surgery, 8 and
12 weeks after the end of distraction. Note that 8
weeks after distraction was completed, values were
higher in loaded device group and lower in control
group than those before surgery.
Consolo et al . Loading effect on distracted bone
182 | Clin. Oral Impl. Res. 17, 2006 / 179–187
had a woven structure, containing charac-
teristic globe-shaped osteocytes.
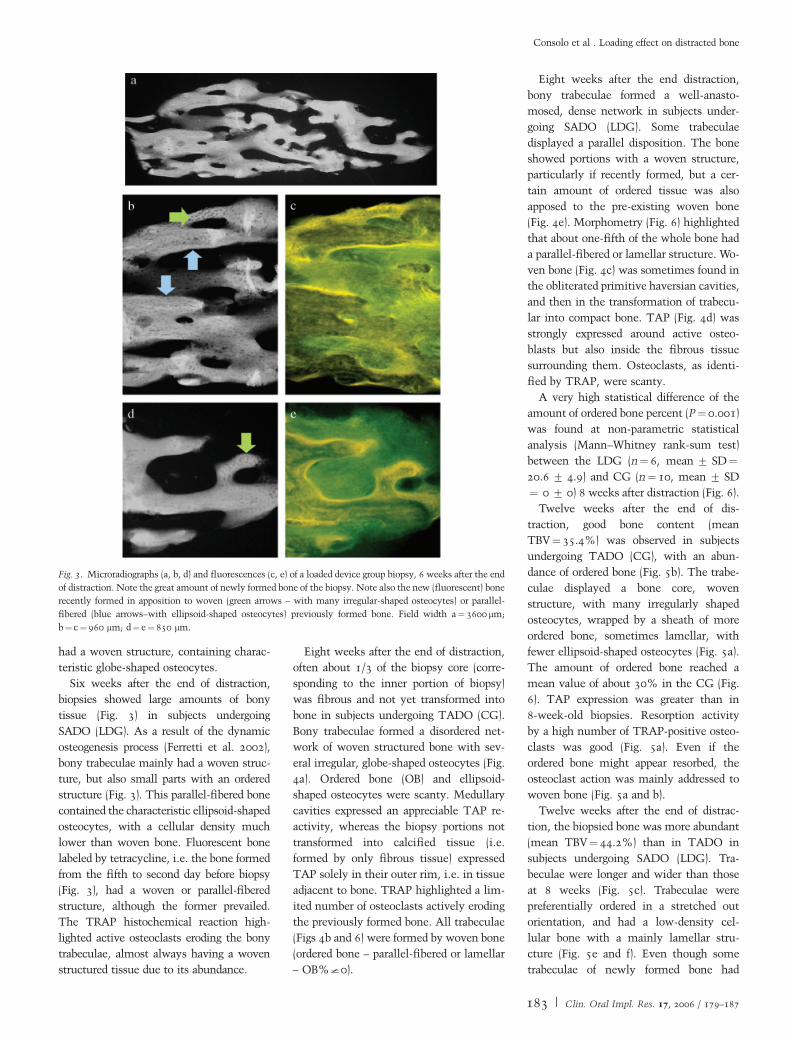
Six weeks after the end of distraction,
biopsies showed large amounts of bony
tissue (Fig. 3) in subjects undergoing
SADO (LDG). As a result of the dynamic
osteogenesis process (Ferretti et al. 2002),
bony trabeculae mainly had a woven struc-
ture, but also small parts with an ordered
structure (Fig. 3). This parallel-fibered bone
contained the characteristic ellipsoid-shaped
osteocytes, with a cellular density much
lower than woven bone. Fluorescent bone
labeled by tetracycline, i.e. the bone formed
from the fifth to second day before biopsy
(Fig. 3), had a woven or parallel-fibered
structure, although the former prevailed.
The TRAP histochemical reaction high-
lighted active osteoclasts eroding the bony
trabeculae, almost always having a woven
structured tissue due to its abundance.
Eight weeks after the end of distraction,
often about 1/3 of the biopsy core (corre-
sponding to the inner portion of biopsy)
was fibrous and not yet transformed into
bone in subjects undergoing TADO (CG).
Bony trabeculae formed a disordered net-
work of woven structured bone with sev-
eral irregular, globe-shaped osteocytes (Fig.
4a). Ordered bone (OB) and ellipsoid-
shaped osteocytes were scanty. Medullary
cavities expressed an appreciable TAP re-
activity, whereas the biopsy portions not
transformed into calcified tissue (i.e.
formed by only fibrous tissue) expressed
TAP solely in their outer rim, i.e. in tissue
adjacent to bone. TRAP highlighted a lim-
ited number of osteoclasts actively eroding
the previously formed bone. All trabeculae
(Figs 4b and 6) were formed by woven bone
(ordered bone – parallel-fibered or lamellar
– OB%I0).
Eight weeks after the end distraction,
bony trabeculae formed a well-anasto-
mosed, dense network in subjects under-
going SADO (LDG). Some trabeculae
displayed a parallel disposition. The bone
showed portions with a woven structure,
particularly if recently formed, but a cer-
tain amount of ordered tissue was also
apposed to the pre-existing woven bone
(Fig. 4e). Morphometry (Fig. 6) highlighted
that about one-fifth of the whole bone had
a parallel-fibered or lamellar structure. Wo-
ven bone (Fig. 4c) was sometimes found in
the obliterated primitive haversian cavities,
and then in the transformation of trabecu-
lar into compact bone. TAP (Fig. 4d) was
strongly expressed around active osteo-
blasts but also inside the fibrous tissue
surrounding them. Osteoclasts, as identi-
fied by TRAP, were scanty.
A very high statistical difference of the
amount of ordered bone percent (P¼ 0.001)
was found at non-parametric statistical
analysis (Mann–Whitney rank-sum test)
between the LDG (n¼ 6, mean� SD¼20.6� 4.9) and CG (n¼10, mean� SD
¼ 0� 0) 8 weeks after distraction (Fig. 6).
Twelve weeks after the end of dis-
traction, good bone content (mean
TBV¼35.4%) was observed in subjects
undergoing TADO (CG), with an abun-
dance of ordered bone (Fig. 5b). The trabe-
culae displayed a bone core, woven
structure, with many irregularly shaped
osteocytes, wrapped by a sheath of more
ordered bone, sometimes lamellar, with
fewer ellipsoid-shaped osteocytes (Fig. 5a).
The amount of ordered bone reached a
mean value of about 30% in the CG (Fig.
6). TAP expression was greater than in
8-week-old biopsies. Resorption activity
by a high number of TRAP-positive osteo-
clasts was good (Fig. 5a). Even if the
ordered bone might appear resorbed, the
osteoclast action was mainly addressed to
woven bone (Fig. 5a and b).
Twelve weeks after the end of distrac-
tion, the biopsied bone was more abundant
(mean TBV¼ 44.2%) than in TADO in
subjects undergoing SADO (LDG). Tra-
beculae were longer and wider than those
at 8 weeks (Fig. 5c). Trabeculae were
preferentially ordered in a stretched out
orientation, and had a low-density cel-
lular bone with a mainly lamellar stru-
cture (Fig. 5e and f). Even though some
trabeculae of newly formed bone had
Fig. 3. Microradiographs (a, b, d) and fluorescences (c, e) of a loaded device group biopsy, 6 weeks after the end
of distraction. Note the great amount of newly formed bone of the biopsy. Note also the new (fluorescent) bone
recently formed in apposition to woven (green arrows – with many irregular-shaped osteocytes) or parallel-
fibered (blue arrows–with ellipsoid-shaped osteocytes) previously formed bone. Field width a¼ 3600 mm;
b¼c¼960 mm; d¼e¼ 850 mm.
Consolo et al . Loading effect on distracted bone
183 | Clin. Oral Impl. Res. 17, 2006 / 179–187

a woven structure, woven bone gen-
erally formed the core of trabeculae
enwrapped in lamellar bone (Fig. 5F).
The amount of ordered bone was very
high in this group, reaching a mean value
of 51% (Fig. 6). TAP expression, i.e. os-
teogenesis marker, was reduced, although
consistently found around the few flat-
tened osteoblasts (Fig. 5d). On the con-
trary, TRAP-positive osteoclasts were
sometimes found to remove bone, gener-
ally woven structured.
On performing a non-parametric statis-
tical analysis (Mann–Whitney rank-sum
test), a statistical difference was found
in the percent amount of ordered bone
(P¼ 0.014) between the LDG (n¼ 3, mean
SD¼51.0� 10.5) and CG (n¼10, mean
SD¼28.9� 6.3) 12 weeks after dis-
traction (Fig. 6).
Discussion
Several authors (Widmark et al. 1998,
2001; Bahat & Fontanessi 2001) consider
regenerated bone as unreliable and ill-
suited, as compared with native bone, for
maintaining long-term stability for im-
plant-supported prosthetic rehabilitation.
Masticatory forces greatly affect native
oral bone during its formation. On the
contrary, regenerated alveolar bone is
formed without any mechanical load on
the distracted segment. The availability of
methods able to influence bone formation
positively might help transform the fea-
tures of regenerated bone into those of the
native ones.
Technical problems, arising when con-
siderable bony buildup is achieved by
distraction of segments, may underlie the
dearth of studies in this field. Several
variables affect the outcome of alveolar
distraction. We selected patients according
to strict criteria using few and well-defined
parameters that were amenable to statistic
evaluation in order to limit the number of
variables. Patients were split into groups,
matched for gender, age and type of
ridge defect to be corrected. However, the
small sample size forced us to apply non-
parametric methods. This analysis revealed
the absence of statistical significance
in the size of bony defects of the two
groups. Moreover, the clinical classifica-
tions of Lekholm & Zarb (1985) and
Cawood & Howell (1988), which are
still largely correlated to techniques for
correcting ridge deformities irrelevant to
our study, were not used to define clinical
outcome. These two classifications are
reliably inherent to a less narrow grate of
resolvable bony defects.
Clinical, radiological and cast pre-surgi-
cal evaluations were performed in order to
calculate the distractive vector suitable
for prosthetic needs. The bony defect
was vertically solved in all the patients.
On the contrary, four (sagittal and
horizontal) vectorial deviations in were
achieved. The recorded vectorial deviations
seem to be attributable to the two
respective sample sizes rather than the
different protocols applied in the two
groups.
Contrary to TADO, in SADO, activa-
tion (one turn) followed by deactivation
(one turn) were performed every 2 days
Fig. 4. Morphology (a, c, toluidine blue stain; b, e, under polarized light, trypan blue stain) and histochemistry
(d, total alkaline phosphatase) of the bone in control group (a, b) and loaded device group (c, d, e), 8 weeks after
distraction was completed. Note in b the woven structure of the trabeculae. The ordered bone (lamellar or
parallel fibered), in apposition to the previously formed woven bone, has been outlined by a light-blue broken
line in e, to point out the method used for bone morphometry. Field width a¼b¼c¼d¼ 306mm; e¼ 408 mm.
Consolo et al . Loading effect on distracted bone
184 | Clin. Oral Impl. Res. 17, 2006 / 179–187
for the first 2 weeks after distraction was
completed. The callus was adequately soft
to undergo these loading cycles without
stress reactions in the tissues, in particular,
bony tissue, surrounding the device fixing
screws. Activation and deactivation were
then reduced both in amplitude and fre-
quency over the following 6 weeks to avoid
stress reactions.
Clinical requirements leading to un-
scheduled surgical corrections over the
treatment period underscore the need to
harmonize the protocol for prosthetic reha-
bilitation. Obliteration of the oral vestibule
(displayed in four CG and three LDG
patients), and the consequent need for
surgical deepening, may be attributed to
the TRACK device used rather than to
reduced oral vestibule depth or to the
different (stimulation) protocol. These
‘first-generation’ devices have two metallic
guides that parallel the distractive screw,
and the guides may produce soft tissue
drag. This side effect along with a shallow
vestibule was common in patients who
required surgical deepening.
Algesthesia reported by some patients in
the final stages of stimulation was never so
intense as to require suspending the stimu-
lation or distractive procedure. Pain in the
LDG patient who dropped out of the study
due to high distractive vector deviation was
caused by buccal orthodontic traction dur-
ing vector correction. This finding and the
well-known problems related to internal
rigid fixation and soft tissue expansion
lead us to believe that ADO algesthesia is
probably related to an inappropriate effect
on the newly formed bony callus. The good
clinical results achieved must in part be
attributed to the psychological motivation
of the patients included in this study and to
the low rate of individual side effects,
despite the complex activities that the
patients were forced to perform.
The matched densitometric values
across the LDG and CG were a categorical
pre-operative condition for this study. A
decreasing densitometric trend was ob-
served in the CG (TADO). The small
number of patients in this group does not
allow a statistical significance to emerge
between protocol steps. On the contrary,
the lower variability of densitometric va-
lues leads to a statistically significant dif-
ference between protocol steps in the LDG
(SADO). Bone ridge densitometric values
have clinic and prognostic significance
(Schnitman el al. 1988; Hutton et al.
1995; Misch et al. 1998, 1999a, 1999b;
Misch 1999), and, if they exceed 800–
850 HU, they are an important factor for
implant insertion and success rate. In the
LDG, densitometries of the second step
essentially fulfill this densitometric re-
quirement and were statistically greater
than those of CG. The variability of the
distribution was probably the cause of the
statistical parity of densitometries of the
second step of the LDG as compared with
those of the third step of CG. This may
reflect a late acquisition of bone density in
the CG, whereas similar results are
achieved in a shorter time in the LDG.
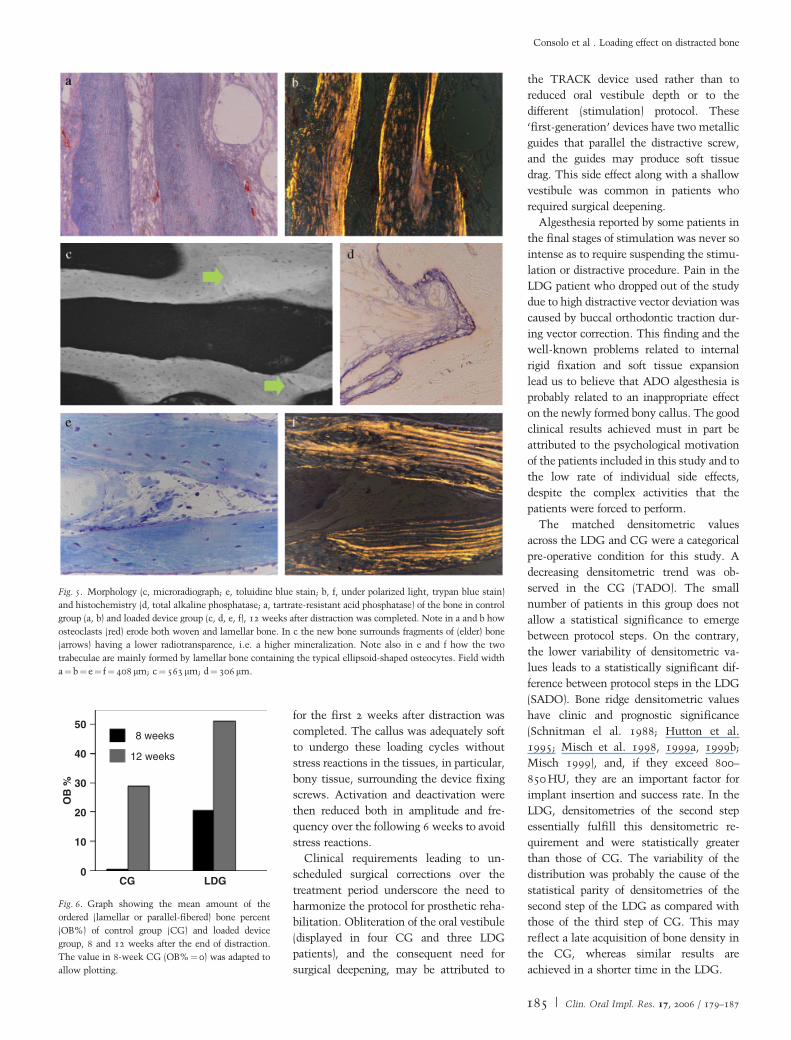
Fig. 5. Morphology (c, microradiograph; e, toluidine blue stain; b, f, under polarized light, trypan blue stain)
and histochemistry (d, total alkaline phosphatase; a, tartrate-resistant acid phosphatase) of the bone in control
group (a, b) and loaded device group (c, d, e, f), 12 weeks after distraction was completed. Note in a and b how
osteoclasts (red) erode both woven and lamellar bone. In c the new bone surrounds fragments of (elder) bone
(arrows) having a lower radiotransparence, i.e. a higher mineralization. Note also in e and f how the two
trabeculae are mainly formed by lamellar bone containing the typical ellipsoid-shaped osteocytes. Field width
a¼b¼e¼ f¼ 408 mm; c¼563 mm; d¼ 306 mm.
50
40
30
20
10
CG LDG
OB
%
8 weeks
12 weeks
0
Fig. 6. Graph showing the mean amount of the
ordered (lamellar or parallel-fibered) bone percent
(OB%) of control group (CG) and loaded device
group, 8 and 12 weeks after the end of distraction.
The value in 8-week CG (OB%¼ 0) was adapted to
allow plotting.
Consolo et al . Loading effect on distracted bone
185 | Clin. Oral Impl. Res. 17, 2006 / 179–187

Histology highlights relevant differences
between the LDG (SADO) and CG (TADO)
as early as 6 weeks after distraction was
completed. Despite good angiogenesis, new
bone formation is only occasionally found
in TADO, whereas new bone formation is
often found in SADO. In TADO, all bone
has a woven structure due to the static os-
teogenesis processes (Ferretti et al. 2002).
On the contrary, the more abundant newly
formed bone of SADO also had zones with a
more ordered structure (mainly parallel-fi-
bered structure). This bone is formed in app-
osition to the previously formed tissue
(therefore also woven ‘static’ bone) by dyna-
mic osteogenesis (Ferretti et al. 2002). As
showed at fluorescence microscopy, appreci-
able amounts of this type of bone were found
after only 6 weeks in SADO. At histology,
the process of bone formation is accelerated,
increasing after 6 weeks in SADO as com-
pared with conventional TADO.
Bone processes proved to be progressing
well in TADO 8 weeks after the end of
distraction. The bone was structured
mainly as woven tissue and showed a good
osteogenic index, in term of alkaline phos-
phatase expression, even if some (inner)
parts of the biopsies were still made up of
fibrous tissue. Alkaline phosphatase expres-
sion was higher and ordered bone was
greater in SADO 8 weeks after distraction
was completed. The bone shows small parts
with a woven structure and many parts
with a parallel-fibered or lamellar structure.
Unlike TADO, where deposition is archi-
tecturally disordered, bone trabeculae begin
to show preferential trajectories (probably
due to feeble loads) in SADO. Histology of
8-week-old biopsies seems to confirm the
previous results and points out both osteo-
genic processes, with structural and archi-
tectural bone improvement, in relation to
stimulated distraction as compared with
conventional TADO.
Even if bone with an ordered structure
was adequate, several parts of bone had a
woven structure in TADO 12 weeks after
the end of distraction. The trabeculae with a
fully woven structure are due to bone re-
sorption, which osteoclasts brought about
from the 8th to 12th week (Zaffe et al.
2002). To counterbalance resorbed tissue,
new bone with a woven structure is rapidly
formed (Consolo et al. 2000; Zaffe et al.
2002). The high osteogenic activity of
TADO produces new bone with an ordered
structure in apposition to previously formed
bone but also produces new bone with a
woven structured (new trabeculae). A re-
markable amount of bone with an ordered
(mostly lamellar) structure was found in
SADO 12 weeks after the end of the dis-
traction. Bone formation processes were
noticeably reduced: active osteoblasts were
scanty and bone surfaces were covered by
flattened osteoblasts or isolated cells (bone
lining cells). A small amount of bone resorp-
tion activities were detectable in SADO 12
weeks after the end of the distraction. The
results seem to highlight an advanced steady
state in SADO as compared with TADO.
The amount of ordered bone increases
in both groups 12 vs. 8 weeks after distrac-
tion. Morphometry reveals a statistical
significance and a consistently higher
amount of ordered bone in LDG vs. CG,
both 8 and 12 weeks after distraction.
Briefly, histological results highlight a
similar behavior in the two groups. All
morphostructural findings were anticipated
in subjects undergoing stimulated alveolar
distraction (SADO) and are tardily expressed
in subjects undergoing customary alveolar
distraction (TADO). From a qualitative
standpoint, the results of SADO biopsies
are fundamentally the same as those in
TADO biopsies. However, bone formation
and structure modification are realized be-
latedly and to a lower extent in conven-
tional distraction treatment (TADO).
Quantitative evaluations show that not
only are osteogenetic processes anticipated
in SADO but also bone formation time is
controlled. Osteogenetic processes (Ferretti
et al. 2002) begin with disordered layers of
osteoblasts that form woven bone in SADO
when angiogenic processes are not yet rea-
lized in TADO. Bone formation speed de-
celerates in both groups; ordered osteoblasts
layers form lamellar bone, but due to the
relatively shorter time, the slope of the
deceleration curve is steeper in TADO.
With a lower bone formation speed, great
ordered bone is formed.
The applied stimulative distraction
(SADO) protocol derives from the sugges-
tions of Prof. J. Hidding on the need to
stimulate the distractive callus properly to
prompt its evolution. We preferred to apply
a stimulation protocol, with extended and
mild cycles, from when distraction was
completed to avoid ‘overstimulation’ that
could modify the osteogenetic processes.
Even though we operated on selected pa-
tients with reduced loads, a moderate degree
of pain was recorded in some patients in the
terminal phases of stimulation. As early as
6 weeks after distraction, we clinically es-
tablished the tenacity of the stimulated
callus (SADO) during distractor removal in
the patient excluded from the study (LDG).
Callus stiffness was indirectly confirmed by
the ineffectiveness of the orthodontic trial,
in an attempt to correct vector deviation,
and the subsequent pain that followed.
In conclusion, our results provide firm
evidence for early formation, superior
structure quality and architectural displa-
cement of bone in patients undergoing
stimulated alveolar distraction osteogen-
esis. Bone displacement appears to be
more fitted to prosthetic implant-based
rehabilitation. Control of the distractive
vector, from which the congruence of al-
veolar stimulation and implant insertion
derives, and respect of the principles of
occlusal-based prosthetic rehabilitation ap-
pear to be particularly important. Since our
findings relate to a rather limited number
of patients, further studies will be neces-
sary to confirm our results.
Acknowledgements: We wish to
thank Dr John Pradelli, MD for assistance
in manuscript draft and revision. The
MIUR (Cofin 2003) Research Fund
supported this investigation.
Consolo et al . Loading effect on distracted bone
186 | Clin. Oral Impl. Res. 17, 2006 / 179–187

References
Bahat, O. & Fontanessi, R.V. (2001) Efficacy of
implant placement after bone grafting for three-
dimentional reconstruction of the posterior jaw.
International Journal of Periodontics and Re-
storative Dentistry 21: 220–231.
Block, M.S., Chang, A. & Crawford, C.H.
(1996) Mandibular alveolar ridge augmenta-
tion in the dog using distraction osteogenesis.
Journal of Oral and Maxillofacial Surgery 54:
309–314.
Cawood, J.I. & Howell, R.A. (1988) A classification
of edentulous jaws. International Journal of Oral
and Maxillofacial Surgery 17: 232–236.
Chin, M. (1999a) Alveolar distraction: endosseous,
self-retaining devices. In: Diner, P.A. &
Vazquez, M.P., eds. Proceedings of 2nd Interna-
tional Congress on Cranial and Facial Bone
Distraction Processes, 9–15. Paris: Monduzzi
Ed. S.p.A.
Chin, M. (1999b) Alveolar process reconstruction
using distraction osteogenesis. In: Diner, P.A. &
Vazquez, M.P., eds. Proceedings of 2nd Interna-
tional Congress on Cranial and Facial Bone
Distraction Processes, 51–54. Paris: Monduzzi
Ed. S.p.A.
Chin, M. (1999c) Reconstruction Alveolaire par
Distraction Osseuse Orthopedique. [Alveolar re-
generation by orthopedic bone distraction]. Jour-
nal de Parodontologie et d’Implantologie Orale
18: 199–210.
Chin, M. & Toth, B.A. (1996) Distraction osteogen-
esis in maxillofacial surgery using internal de-
vices: review of five cases. Journal of Oral and
Maxillofacial Surgery 54: 45–53.
Consolo, U., Bertoldi, C., Urbani, G. & Zaffe, D.
(2000) Valutazioni cliniche, analisi radiologiche ed
istologiche nelle procedure di distrazione alveolare
mandibolare. Studio preliminare. [Cinical evalua-
tions, radiologic and histologic analyses on
mandibular alveolar distraction procedures. A pre-
liminary report.]. Minerva Stomatologica 49:
475–484.
Ferretti, M., Palumbo, C., Contri, M. & Marotti G, .
(2002) Static and dinamic osteogenesis: two dif-
ferent types of bone formation. Anatomy and
Embryology 206: 21–29.
Glantz, S.A. (ed.) (2003) Statistica Per Discipline
Biomediche [Primer of Biostatistics]. Italian
Translation of 5th edition, 1–487. Milano, Italy:
Mc-Graw Hill Co, srl, Publ. Gr. Italia.
Hidding, J., Lazar, F. & Zoller, J.E. (1999)
Erste Ergebnisse bei der vertikalen Distraktion-
sosteogenese des atrophischen Alveolarkamms.
[Initial outcome of vertical distraction osteo-
genesis of the atrophic alveolar ridge.]. Mund-,
Kiefer und Gesichtschirurgie 3 (Suppl. 1):
S79–S83.
Hutton, J.E., Health, M.R., Chai, J.I., Harnett, J.,
Jemt, T., Johns, R.B., McKenna, S., McNamara,
D.C., van-Steenberghe, D., Taylor, R., Watson,
R.M. & Herrmann, I. (1995) Factors related to
success and failure rates at 3 years follow up in a
multicenter study of overdentures supported by
Branemark implants. International Journal of
Oral and Maxillofacial Implants 10: 33–42.
Ilizarov, G.A. (1989a) The tension-stress effect on
the genesis and growth of tissues: part I. The
influence of stability of fixation and soft-tissue
preservation. Clinical Orthopaedics and Related
Research 238: 249–281.
Ilizarov, G.A. (1989b) The tension-stress effect on
the genesis and growth of tissues: Part II. The
influence of the rate and frequency of distraction.
Clinical Orthopaedics and Related Research 239:
263–285.
Ilizarov, G.A. (1997) The principles of the Ilizarov
method. Bulletin Hospital for Joint Diseases New
York 56: 49–53.
Kalander, W.A., Seissler, W., Klotz, E. & Vock, P.
(1990) Spiral volumetric CT with single-breath-
hold technique, continuous transport, and contin-
uous scanner rotation. Radiology 176: 181–183.
Klein, C. & Howaldt, H.P. (1995) Lengthening of
the hypoplastic mandible by gradual distraction in
childhood: a preliminary report. Journal of
Craniomaxillofacial Surgery 23: 68–74.
Lazar, F., Hidding, J. & Zoller, J.E. (1999) Kno-
cherne Regeneration des Unterkieferalveolarfort-
satzes mit Hilfe der vertikalen Kallusdistraktion.
[Bone regeneration of mandibular alveolar pro-
cesses by vertical callus distraction.]. Deutsche
Zahnarztliche Zeitschrift 54: 51–54.
Lekholm, U. & Zarb, G.A. (1985) Patient selection
and preparation. In: Branemark, P.I., Zarb, G.A.
& Albrektsson, T., eds. Tissue-Integrated Pros-
theses, 199–209. Chicago: Quintessence Publish-
ing Co.
Loee, H. & Silness, J. (1963) Periodontal disease in
pregnancy. I. Prevalence and severity. Acta Odon-
tologica Scandinavica 21: 533–551.
McCarthy, J.G., Schreiber, J., Karp, N., Thorne,
C.H. & Grayson, B.H. (1992) Lengthening the
human mandible by gradual distraction. Plastic
and Reconstructive Surgery 89: 1–8.
Micheli, S. & Miotti, B. (1977) Lengthening of
mandibular body by gradual surgical orthodontic
distraction. Journal of Oral Surgery 35: 187–192.
Misch, C.E. (ed.) (1999) L’odontoiatria implantare
contemporanea [Contemporary Implant Dentis-
try]. Italian Translation of 2nd edition, 109–384.
Roma, Italy: Antonio Delfino Editore.
Misch, C.E., Dietsh-Misch, F., Hoar, J., Beck, G.,
Hazen, R. & Misch, C.M. (1999a) A bone quality-
based implant system: first year of prosthetic
loading. Journal of Oral Implantology 25:
185–197.
Misch, C.E., Hoar, J.B., Beck, G., Hazen, R. &
Misch, C.M. (1998) A bone quality based implant
system: a preliminary report of stage I and stage.
Implant Dentistry 7: 35–42.
Misch, C.E., Qu, Z. & Bidez, M.W. (1999b) Me-
chanical properties of trabecular bone in the hu-
man mandible: implications for dental implant
treatment planning and surgical placement.
Journal of Oral and Maxillofacial Surgery 57:
700–706.
Molina, F. & Monasterio, F.O. (1995) Mandibular
elongation and remodeling by distraction: a fare-
well to major osteotomies. Plastic and Recon-
structive Surgery 96: 841–842.
Parfitt, A.M., Drezner, M.K., Glorieux, F.H.,
Kanis, J.A., Malluche, H., Meunier, P.J., Ott,
S.M. & Beker, R.R. (1987) Bone histomorphome-
try: standardization of nomenclature, symbols and
units. Journal of Bone and Mineral Research 2:
595–610.
Raghoebar, G.M., Liem, R.S. & Vissink, A. (2002)
Vertical distraction of severely resorbed edentu-
lous mandible: a clinical, histological and electron
microscopic study of 10 treated cases. Clinical
Oral Implants Research 13: 558–565.
Schnitman, P.A., Rubenstein, J.E., Whorle, P.S.,
DaSilva, J.D. & Koch, G.G. (1988) Implants for
partial edentulism. Journal of Dental Education
52: 725–726.
Silness, J. & Loee, H. (1964) Periodontal disease in
pregnancy. II. Correlation between oral hygiene
and periodontal condiction. Acta Odontologica
Scandinavica 22: 121–135.
Snyder, C.C., Levine, G.A., Swanson, H.M. &
Browne, E.Z. (1973) Mandibular lengthening by
gradual distraction: a preliminary report. Plastic
and Reconstructive Surgery 51: 506–508.
Widmark, G., Andersson, B., Andrup, B., Carlsson,
G.E., Lindvall, A.M. & Ivanoff, C.J. (1998) Re-
habilitation of patients with severerly resorbed
maxillae by means of implants with or without
bone grafts. A 1 year follow-up study. Interna-
tional Journal of Oral and Maxillofacial Implants
13: 474–482.
Widmark, G., Andersson, B., Carlsson, G.E., Lind-
vall, A.M. & Ivanoff, C.J. (2001) Rehabilitation of
patients with severerly resorbed maxillae by
means of implants with or without bone grafts: a
3 to 5 year follow-up clinical report. International
Journal of Oral and Maxillofacial Implants 16:
73–79.
Zaffe, D., Bertoldi, C., Palumbo, C. & Consolo, U.
(2002) Morphofunctional and clinical study on
mandibular alveolar distraction osteogenesia.
Clinical Oral Implants Research 13: 550–557.
Consolo et al . Loading effect on distracted bone
187 | Clin. Oral Impl. Res. 17, 2006 / 179–187





























