Embed Size (px)
Citation preview
ISSN-2394-9465 (Print) ● ISSN-2395-180X (Electronic)
Volume 4 Number 2 July-December 2018
International Journal of Psychiatric NursingEDItor
Dr. r.K. SharmaFormerly, All-India Institute of Medical Sciences, New Delhi
Email: [email protected]
INtErNatIoNal EDItorIal BoarD 1. Dr. VidyaSeshan, (Assistant Dean), For Clinical And Community
Service, College of Nursing, Sultan Qaboos University, Muscat, Sultanate of Oman
2. Fatona, Emmanuel adedayo (Mr.), School of Nursing, Sacred Heart Hospital, Lantoro, Abeokuta, Ogun State, Nigeria
3. Dr. arnel Banaga Salgado, (Assistant Professor), (School Psychology, Education, Mental Health) RAK College of Dental Sciences (RAKCODS) & RAK College of Nursing, Ras Al Khaimah, United Arab Emirates
4. Erum akbar ali, (Working honorary), Department of Emergency Medicine, Aga Khan University Hospital, Karachi-Pakistan.
5. Sudhen Sumesh Kumar, (Lecturer), Haramaya University, Ethiopia
6. G. Nethaji, (Lecturer), Nobel Medical College, Biratnagar, Nepal
7. Dalal Shahin M, (Lecturer), Northern Border University- KSA
EDItorIal BoarD 1. Dr Chetan S. Patali, (Principal), A V School of Nursing, Behind
DurgaVihar, Station Road Bagalkot
2. andrea Pusey–Murray, Ministry of Health In-Service Education Unit, Evaluation of Post Basic Psychiatry Students In Clinical Area
3. lt Col M Jayalakshmi (retd), (Principal), Shri VinobaBhave College of Nursing, Silvassa, DNH (UT Administration) Government of India
4. Mrs. Kirupa P, (Associate Professor), Hod Departement of Psychiatric Nursing, K.Pandyaraja Ballal College of Nursing, Someswar Road, Ullal, Mangalore-20, Karnataka
6. Dr. Sripriya Gopalkrishnan, (Professor/Officiating Principal), Sadhu Vaswani College of Nursing, Pune
7. Dr. tessy treesa Jose, (Professor and Head) Department of Psychiatric/Mental Health Nursing, Manipal College of Nursing Manipal, Manipal University
8. Dr. G. radhakrishnan, Phd (N), (Principal), PD Bharatesh College of Nursing, Halaga, Belgaum, Karnataka, India
9. Josephine Jacquline Mary. N.I, (Professor Cum Principal) SI-MET College of Nursing,UdmaAyampara,Periya P.O, Kasargod, Dist. Kerala State
10. Pawan Kumar Sharma, (Associate Professor & Head of Department), Psychiatric Nursing, Institute of Nursing Education Guru Tegbahadur Sahib (C) Hospital, Ludhiana, Punjab
11. Manisha N. Pawar, (Professor Cum Vice Principal), Terna Nursing College, Nerul, Navimumbai
12. Manjeet Kaur Saggi, (Professor Cum Vice Principal), Mata Sahib Kaur College of Nursing
13. Bandana Bisht, (Vice Principal), Chitkara School of Health Sciences, Punjab
14. Dr. R. Sreevani, (Professor & HOD) Dept. Of Psychiatric Nursing, Dharwad Institute of Mental Health and Neurosciences (DIMHANS) Belgaum Road Dharwad
15. D. Elakkuvana Bhaskara raj, (Principal) Indira Gandhi School of Nursing, Amethi
16. Padmapriya S, (HOD & Professor), OBG Nursing DeptInVydehi Institute of Nursing Sciences and Research Center, Bangalore
17. Josephine Jacquline Mary, (Professor Cum Principal), SI –MET College of NursingUdma, Ayampara, Periya P.O. Kasaragod, Dist. Kerala State.
18. r. Jeyadeepa, (Vice Principal), Karuna College of Nursing, Palakkad, Kerala
19. Vijayaraddi B Vandali, (Asst. Prof), (Sumandeep Nursing College)Cum Officiating Nursing Superintendent (Dhiraj General Hospital), Sumandeep Vidyapeeth, Piperia, Waghodiya, Vadodara, Gujarat.
20. Dorothy Deena Theodore, (Principal & HOD), Psychiatric Nursing, Narayana Hrudayalaya College of Nursing
21. Ganapathy thilagavathy, (Professor, Principal & HOD), Obstetrics & Gynecological Nursing, NAAC COORDIATOR, IQAC-INTERNAL QUALITY ASSURENCE
22. Gururaj Udapi, (Assistant Professor Cum I/C HOD), KLE’S Institute of Nursing Sciences Belgaum
23. lekha Bist, (Associate Professor Cum Vice Principal), Nightingale Institute of Nursing, Noida NCR, (ChoudharyCharan Singh University) Meerut
24. Sasi V, (Professor & H.O.D.), Child Health Nursing,Vinayaka Mission’s College of Nursing, Puducherry
25. radha K, (Vice-Principal), Bhopal Nursing College, BMHRC, ICMR, UNDER MOH& FW, Govt of India, Bhopal.
26. Uma rani adhikari, (Professor Cum Vice Principal), Woodlands College of Nursing, Kolkata
27. D. S. Gayathry, (Asst. Professor Cum Principal), Shri USB College of Nursing
28. Mrs ashia Qureshi, (Dean Cum Principal), Prakash Institute Of Nursing, Physiotherapy And Rehabilitation & Allied Medical Sciences
29. Mrs. Nirmala Singh, (National Florence Nightingale Awardee by President of India), (Principal), College of Nursing, PGIMER & Dr. RML Hospital, New Delhi-01
30. ravindra HN. (Principal), Sumandeep Nursing College, Vadodara, Gujarat.
31. Mr. Sateesh Basanagouda Biradar, (Vice-principal), Maniba Bhula Nursing College, Uka Tarsadia University, Bardoli,Surat, Gujarat
32. Mrs. Grace Madonna Singh, (Asst. Professor, HOD), Himalayan College of Nursing, Swami Ram University, Jollygrant, Dehradun
SCIENtIFIC CoMMIttEE 1. Poonam Sharma, (Assistant Professor), I.N.E., Guru TegBahadur
Sahib (C) Hospital- Ludhiana, Punjab
2. asha Bose, (Assistant Professor), Santhi Institute of Medical Science And Research Centre, Calicut, Kerala, India
3. Bollineni Nirmala Jyothi, (Professor), NRI College of Nursing, Mangalagiri

International Journal of Psychiatric Nursing
Print- ISSN: 2394-9465, Electronic - ISSN: 2395-180XFrequency: Six Monthly
International Journal of Psychiatric Nursing is a double blind peer reviewed international journal. It deals with all aspects of Psychiatric Nursing.
Website: www.ijpn.co© All Rights reserved. The views and opinions expressed are of the authors and not of the Indian Journal of Physiotherapy and Occupational Therapy. The Indian Journal of Physiotherapy and Occupational Therapy does not guarantee directly or indirectly the quality or efficacy of any products or service featured in the advertisement in the journal, which are purely commercial.
EditorDr. r.K. Sharma
Institute of Medico-legal Publications501, Manisha Building, 75-76, Nehru Place,
New Delhi-110019 Printed, published and owned by
Dr. r.K. SharmaInstitute of Medico-legal Publications501, Manisha Building, 75-76, Nehru Place,
New Delhi-110019 Published at
Institute of Medico-legal Publications501, Manisha Building, 75-76, Nehru Place,
New Delhi-110019
4. Sreeja i, (Professor), College of Nursing, Ananthapuri Hospitals and Research Institute, Chackai, Trivandrum
5. Santhi S, (Professor), Dept. Psychiatric Nursing, SRU, Chennai
6. G. Vimala, (Assistant Professor), College of Nursing, PIMS (DU), Loni (Bk), Tal. Rahata, Dist. Ahmednagar.
7. ashok Kumar, (Assistant Professor), College of Nursing, All India Institute of Medical Sciences (AIIMS), Jodhpur, Rajasthan
8. V. Sathish, (Academic Officer), Allied Health Sciences, National Institute of Open Schooling,Ministry of Human Resource Development, Government of India
9. G. Neelakshi, (Professor), SRCON, SRU, Chennai
10. Sandhya Shrestha, (Lecturer, Assistant Professor & Class Coordinator), For 3rd Year (Community Health Nursing I& II, Behavioual Sciences, Psychiatric (Mental Health) Nursing, Nursing Education, Nursing Concept, Nutrition)
11. t. K. Sheshaadhiri, (Asst. Professor), Psychiatric Nursing, Teerthanker mahaveer college of nursing, Teerthanker mahaveer university, Moradabad.
12. Divya K Y, (Lecturer), Hiranandani College of Nursing, Powai, Mumbai
13. abin Varghese, (Nursing Tutor), Bhopal Nursing College, BMHRC, Bhopal, Madhyapradesh
14. M. Navaneetha, (Professor), PIMS College of Nursing, Pondicherry
15. S. Nilavansa Begum, (Associate Professor), S.G.L. Nursing College, Semi, Jalandhar
16. S. Sasikumar, (Professor), Vydehi Institute of Nursing Sciences & Research Centre, Bangalore
17. Jayesh N Patidar, Nootan College of Nursing, Visnagar, S.K. Campus, Nr. Kamana Crossing, Dist. Mehsana
18. Sophia lawrence, (Professor), in the Medical Surgical Area, College of Nursing , Christian Medical College, Vellore
19. ramandeep Kaur, (Assistant Professor), S.G.L. Nursing College, Jalandhar
20. Sheela Upendra, (Associate Professor), Symbiosis College of Nursing, Symbiosis International University, Pune
21. Shailza Sharma, (Assistant Professor), (16th Aug, 2011 To 12th March, 2014) At Institute of Nursing Education, Guru TegBhadur Sahib Charitable Hospital, Ludhiana, Punjab
22. Padmavathi Nagarajan, (Lecturer), College Of Nursing, JIPMER, Puducherry
23. rimple Sharma, (Lecturer), College of Nursing, AIIMS, New Delhi
24. Prabhuswami Hiremath, (Lecturer) (Dept of Mental Health Nursing) Krishna Institute of Nursing Sciences, Karad.
25. rakesh Joshi, (Asst. Lecturer), Trainee Hosp. Admin At GBH American Hospital, PGDHA (Hospital Admin.) Apollo Hyderabad, PGDMLS (Medico Legal) Symbiosis,Pune,
26. G. Neelakshi, (Professor), SRMC & RI (SRU)
27. MadhaviVerma, (Professor), Nursing, Amity University Gurgaon, Haryana
28. Bivin JB, (Sr Lecturer), in Psychiatric Nursing, Department of Psychiatric Mental Health, Mar Baselios College of Nursing, Kothamangalam, Keralam
29. Praveen S Pateel, (Assistant Professor), BVVS Sajjalashree Institute of Nursing Sciences Navanagar, Bagalkot
30. Dr. riaz K. M., (Assistant Professor), Department of Mental Health Nursing, Government College of Nursing Medical College Po -Thrissur, Kerala
31. Manjunathan C., (Lecturer and Clinical Instructor), Nursing (Medical-Surgical Nursing) Shri Anand Institute of Nursing
32. r. Krishnaveni, (Assistant Professor), Teerthanker Mahaveer College of Nursing,Teerthanker Mahaveer University
33. Sonia Sharma, (Working Assistant Professor), Obstetric AndGynecological Nursing, SGL Nursing College, Jalandhar
34. Syed Imran, (Assistant Professor), Yenepoya Nursing College, Yenepoya University, Deralakatte Mangalore
35. ramanpreet Kaur, (Lecturer), S.K.S.S., College of Nursing, Ludhiana.x
36. Jagjeet Kaur, (Assistant Professor), INE,GTBS(C)Hospital, Ludhiana
37. Sukhbir Kaur, (Assistant Professor), SGRD College of Nursing, Vallah, Sri Amritsar
38. N. Vijayanarayanan, (Prof. Owiasi College of Nursing), Owiasi Medical College And Hospital, Hyderabad
39. N. Gayathri, (Asst Professor), Rani Meyyammai College of Nursing, Annamalai University
40. Sheeba C, (Associate Professor), In Christian College of Nursing, Neyyoor, C.S.I. Kanyakumari Diocese
41. Janarthanan B, (Faculty of Psychiatric Nursing), College Of Nursing, Jawaharlal Institute Of Post Graduate Medical Education & Research (JIPMER), Puducherry “A Central Govt. Autonomous Institute, Govt. of India”
42. Sushil Kumar Maheshwari, (Associate Professor), (Psychiatric Nursing) University College of Nursing, BFUHS, Faridkot, Punjab
43. J. Jenifer, (Asst. Professor), Shri U S B College of Nursing, Abu Road ,Rajasthan.
44. Deepak K, (Assistant Professor), Manikaka Topawala Institute of Nursing, Charusat Campus, Changa, Petlad, Anand, Gujarat
II
International Journal of Psychiatric Nursing
www.ijpn.com
Volume 03 Number 02 July-December 2017
1. A Quasi-experimental Study to Assess the Effectiveness of Psycho Education on ........................................................... 01
Knowledge Regarding Psychological First Aid among Staff Nurses in Selected
Hospitals of Jalandhar, Punjab, 2017
Gagandeep Kaur, Rajratan Gupta, P Dhilip Kumar
2. Impact of Self Perceived Public Image of Nursing on Nurses Work Behavior .................................................................. 06
Kaur Pushpinder, Maheshwari S K, Rawat HC
3. Emotional Intelligence -Bring Into Play, Have an Impact! .................................................................................................... 12
Neha Peter Bhore
4. Prevalence, Awareness and Effects Of Nomophobia among Adolescents ......................................................................... 16
Preeti Maria Menezes, Shubhangi Pangam
5. A study to Assess the Knowledge Regarding Alzheimer's Disease ..................................................................................... 19
Among Students of Paramedical Courses in Selected Colleges of Vidarbha Region
Rashmi
6. A Study to Assess the Effectiveness of Laughter Therapy on Psychosocial Problems ..................................................... 24
among Institutionalized Elderly at Ernakulam District in Kerala
Soney M Varghese
7. A Study to Assess the Effectiveness of Video Assisted Teaching Programme on ............................................................. 31
Knowledge Regarding Mental Illness among General Public of Selected Area, Jalandhar (Punjab)
Gurleen Kaur, Rajratan Gupta
Contents
Content Final.pmd 9/27/2017, 11:29 AM1
International Journal of Psychiatric Nursingwww.ijpn.co
CONTENTS
Volume 4, Number 2 July-December 2018
1. EffectivenessofStructuredTeachingProgrammeRegardingtheKnowledgeofLifeSkillsTrainingProgramamongInmatesofaSelectedRehabilitationCenterofHyderabad 1Disney Sabatina, Anumol Joseph, Keerthi Samuel, Shiny P.T.
2.AwarenessandPracticesonToySafetyamongMothersofPreschoolChildren 6Hepsi Bai J, Sheela Rathi, Priyanka Lawrance, Angel Priya T
3.MaternalAwarenessandPerceptiononPhototherapyforNeonateswithHyperbilirubinemia 9Annie Mathew, Hepsi Bai J
4. EffectivenessofPelvicGirdleExerciseonPelvicGirdlePainandSpecificActivitiesamongPrimigravidaMothersAttendingAntenatalOPdatSelectedHospitals,Salem 12J Sathya, M. D. Santhi
5. StressandCopingbetweentheIntensiveCareUnitandGeneralWardNursesinSelectedHospital,Coimbatore 16S. Karthic, M. Baskaran, Esther Daisy Meerabai Joel
6. EffectivenessofVideoTeachingProgrammeonSelf-HelpTechniquesofOsteoarthritisamongElderlyinSelectedOldAgeHomes,Coimbatore 22M. D. Anuratha
7. EffectivenessofVideoTeachingProgrammeonNeonatalCareamongPrimigravidaMothersAdmittedinUrbanHealthMaternityCentres,Coimbatore 28M. D. Santhi
8.FactorsInfluencingClinicalLearningEnvironmentamongNursingStudents:ACrossSectionalStudy 33Manoj Kumar L, Libina Babu P. V.
9. HelpingArtofClinicalNursing:ApplicationofTheoryinEnhancingtheQualityofLifeofPatientswithPsoriasis 36Padmavathi Nagarajan
10. AStudytoAssesstheEffectivenessofStructuredTeachingProgrammeonKnowledgeRegardingPremenstrualSyndromeamongAdolescentGirlsStudyinginaSelectedEnglishMediumHighSchoolat
Bagalkot. 39Shivanagouda V Malagoudar, Praveen S. Pateel
11. FamilyFocusedNursingInterventionforFunctionalImprovementofBPAdClients-APilotStudyReport45

II
R R Kavitha, S Kamalam, Ravi Philip Rajkumar
12.Stress,AnxietyandcopingamongEngineeringStudentsatSelectedCollegeofPokhara,Kaski,Nepal 51Punam Pantha, Shrestha Sandhya
13. EffectivenessofStructuredTeachingProgrammeonLevelofKnowledgeRegardingSafeMotherhoodamongAntenatalMothersatMaternityCentre,Salem 57Santhi M. D., Kanaga Durga M., Manjula B., Sathya J.
14.AStudytoComparetheEffectsofMusicTherapyandLaughterTherapyonReducingLevelofdepressionamongOldAgePeopleOldAgeHomes 62Seema M. Boresa, Deepak Krishnamurthy
15.KnowledgeandAttitudeRegardingInclusiveEducationamongSchoolTeachers 67Sreeja i, Chinchu J
16.BurdenandFamilyFunctioningamongCaregiversofChronicSchizophrenia 73Sreeja I.
17. AssesstheLevelofSubjectivewellBeingandFindtheAssociationwithSocio-demographicVariablesofFarmersofSelectedVillagesofdharawadTaluka,Karnataka,India 78Shivananda Gejji, Sunanda G.T., R. Sreevani
18. EffectivenessofPsychoEducativeInterventiononBodyImageandAdjustmenttoCanceramongHeadandNeckCancerPatients 84T Sivabalan, Kavita Bhoknal
19.IssuesandChallengesinPsychiatricConsultation-LiaisonNurse(PCLN) 89Usha Marath
20.AReportondiabetesScreeningamongAdults 93W. Ashalata Devi, Manamaya Rana, A. L. Sharma
21. AStudytoAssessthedepressionamongElderlyResidinginOldAgeHomesofThiruvananthapuramdistrict,SouthKerala 96Athirarani M R, Aswany Sunil S, Anupama Paniker, Aparna S V, Ashifa A, Arya S, Arya S B
22.depressionamongOralCancerPatientsReceivingRadiationTherapyinSelectedCentre,Erode 100S. Manikandan, M. Baskaran, Prof. P. Subarani
23.LifeSkillsandNursing 104Buvaneswari R., Juliet Sylvia
24. AStudytoAssesstheKnowledgeandAttitudetowardsMentalIllnessamongAdultsatSelectedUrbanCommunityUdaipur,Rajasthan 108Digpal Singh Chundawat
25. AStudytoassesstheEffectivenessofSelectedNursingInterventiononActivitiesofdailyLiving,SelfEsteem,depressionandQualityofLifeamongElderlywithChronicIllnessatSelectedOldAgeHomesinBangalore,Karnataka 113D. Elakkuvana Bhaskara Raj, Kanniammal
26.UnderstandingWomenwithInfertility:Parse’sandSystem’sTheory 119
III
Porkodi Rabindran
27. AStudytoAssesstheEffectivenessofSelfInstructionalModuleRegardingReducingAcademicStressamongStudentsofB.scNursinginSelectedCollegesatJaipurCityRaj 123Manmohan Singh, Dinesh kumar Sharma, Rakesh Joshi
28. AStudytodeterminetheSources,EffectsandCausesforSubstanceUsedisordersandtodevelopanInformationalBookletonPreventionandManagementofSubstanceusedisordersinSelecteddrugde-
AddictionandRehabilitationCentersofNepal 127Rupshikha Mishra, Bindi Shauju, Veena Sharma
29.EffectofVideoAssistedTeaching(VAT)onImprovingPrimaryTeacher’sKnowledgeRegardingLearningdisabilities:AnIndianPerspective 133Amrinder Kaur, Betcy Mathew, Jithin Thomas Parel, Bince Varghese, Linsu Thomas
DOI Number: 10.5958/2395-180X.2018.00006.3
Effectiveness of Structured Teaching Programme Regarding the Knowledge of Life Skills Training Program among Inmates
of a Selected Rehabilitation Center of Hyderabad
Disney Sabatina1, Anumol Joseph2, Keerthi Samuel3, Shiny P.T.3
1MSc Nursing 2nd year student, 2Assistant Professor, 3Lecturer, Vijaymarie College of nursing, Hyderabad
AbSTRACT
Introduction:Skillsarethelearnedcapacitywhichhelpsustodoataskeffectively.Skillsareabilitiestouseknow-howtocompletetasks.
Aim: `Toassesstheknowledgeoflifeskillstrainingprogramamonginmatesofaselectedrehabilitationcenter.
Methodolody:Quantitativeapproachwasadoptedforthestudy.Theresearchdesignwaspreexperimentalonegrouppretestposttestdesign.ThirtyinmateswereselectedfromaRehabilitationCenterinHyderabad,Telangana throughconvenient sampling.Astructuredquestionnairewasadministered tocollect thedatafrom the subjects.The reliabilitywas computedby split halfmethodand found tobe1which indicatedperfectreliability.
Results: Itwas foundduringpre test that 36.6% inmateshadpoorknowledgeand63.3% inmateshadaverageknowledgeinpretest.However,afterlifeskillstraining(post-test)therewassignificantimprovementintheknowledgeas80%ofinmateshadgoodknowledgeandonly20%ofinmateshadaverageknowledgewhichindicatedthatstructuredteachingimprovedthelevelofknowledge.
Conclusion: Life skills training can promote interactive, decision-making, problem - solving, criticalthinkingandstressmanagementskillsandleadtomoresocialacceptability,whichinturnreducetheriskformentalillness.Itisrecommendedtoplanandperformconstantlifeskillstrainingworkshopsaseffectivetoolsfordevelopmentofpsychosocialskills.
Keywords: Life Skill Training; Inmates; Rehabilitation Center.
Corresponding Author:AnumolJosephAssistantProfessorVijaymarieCollegeofNursing,StreetNo.3,UmaNagarBegumpet,HyderabadMobile:9177101682Email:[email protected]
InTRoDuCTIon
Skillsarethelearnedcapacitywhichhelpsustodoa taskeffectively.Skills areabilities touseknowhowto complete tasks.They are acquired through practiceandpatience.Askilledpersonuseslesstime,energyandresourcestodoajobandproducesqualityresults.Skillsare gained through school/college, work experiences,
hobbies,books,elders,peersetc.Theycanbeimprovedifwecouldidentify,analyzeandpracticethem.(1)
World Health Organization estimates indicatea prevalence level of about 22% of the individualsdevelopingoneormorementalorbehavioraldisordersintheirlifetimeinIndia.Mentaldisordersafflict5croresoftheIndianpopulationandneedspecialcare.(2)
Initiatives to develop and implement life skillseducation in schools have been undertaken in manycountries around the world. The need for life skillseducation is highlighted, directly and indirectly in theConventionoftheRightsoftheChildandanumberofinternationalrecommendations.Lifeskillseducationisaimed at facilitating the development of psychosocialskills that are required to deal with the demands and
2 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
challengesofeveryday life. It includes theapplicationoflifeskillsinthecontextofspecificrisksituationsandinsituationswherechildrenandadolescentsandadultsneed to be empowered to promote and protect theirrights.(3)
“LifeSkillsareabilitiesforadaptiveandpositivebehaviorthatenableindividualstodealeffectivelywiththe demands and challenges of everyday life (WHO)Adaptivemeansthatapersonshouldhavetheflexibilityto adjust according to the situation. For positivebehavior,apersonneedstohavepositivethinkingandlookatopportunitiesevenindifficultsituations,inordertocopewiththesituation”.(4)
UNICEFdefinesLifeSkillsas“apositivebehaviororbehaviordevelopmentapproachdesignedtoaddressabalanceofthreeareas:knowledge,attitudeandskills”.Life Skills, are essentially those abilities that help topromotephysical,mentalandemotionalwell-beingandcompetence to face the realities of life.(5) Someof theimportant life skills identified throughdelphiMethodbyWHOare:(6)
z decisionmaking
z Problemsolving
z Creativethinking/lateralthinking
z Criticalthinking/perspicacity
z Effectivecommunication
z Interpersonalrelationships
z Self-awareness/mindfulness
z Assertiveness
z Empathy
z Equanimity
z Copingwithstress,traumaandloss
z Resilience
Life skills training is helpful to improve thinkingprocess.Itisbasedonthreeareasofchange.Firstareaisknowledge.Othertwoareaareattitudeandskills.Alifeskillenablestotransformknowledge,skill,attitudesandmoralsintoactualabilitiesthatiswhattodoandhowtodo thework,given thescopeandopportunity todoso.Presentstudyusedpower-pointpresentation to improvetheskillsoftheinmates.Wehavemanyonlinelifeskillstraining programmes available by which courses areprovidedwithevidencedbasedpracticeandtestimonies.(7)
METHoDoLogy
Quantitative approach was adopted for the study.Theresearchdesignwaspreexperimentalonegrouppretest post test design. 30 inmateswere selected from aRehabilitationCenterinHyderabad,Telanganathroughconvenient sampling. A structured questionnaire wasadministeredtocollect thedatafromthesubjects.Thereliabilitywascomputedbysplithalfmethodandfoundtobe1whichindicatedperfectreliability.datawasthenanalyzedusingdescriptiveandinferentialstatistics.
Table 1: Findings related to sample characteristics n = 30
S. no. Demographic Variables Frequency Percentage1. Age
YoungAdults(18-29yrs) 12 40%MiddleAge(30-49yrs) 16 53.3%
SeniorCitizens(50-65+Yrs) 02 6.6%2. gender
Male 13 43.3%Female 17 56.6%
3. Duration of Hospital Stay1month-3yrs 14 46.6%
4-6yrs 09 30%7-9yrs 05 16.6%
MoreThan10yrs 02 6.6%
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 3
Conted…
4. no. of HospitalizationOnce 13 43.3%
2-5Times 08 26.6%6-9Times 09 30%
MoreThan10Times 01 3.3%5. Diagnosis
Schizophrenia 15 50%BPAd 10 33.3%
Psychosis 02 6.6%Personalitydisorder 03 10%
The above table majority of the samples were ofmiddle aged that is 16(53.3%), males 13(43.3%) andfemaleswere17(56.6%)participatedinthestudy.Mostofthemwerehospitalizedforthedurationof1month-3yrs14(46.6%)andonly13(43.3%)wereonceadmittedforthementalillnessintherehabcenterwithmajorityofthemwerediagnosedwithSchizophrenia15(50%).
Table 2: Mean, mean difference, standard deviation effectiveness of structured teaching program (n = 30)
S. no. Tests Mean Mean Difference S D
1. Pretest 5.836.34
2.002. Posttest 12.17 1.60
Theabovetableshowsthatpretestandtheposttestscoresrevealedthatthemeanofpretestis5.83withSd2.00andPosttestscorerevealedmeanof12.17withSd1.60.
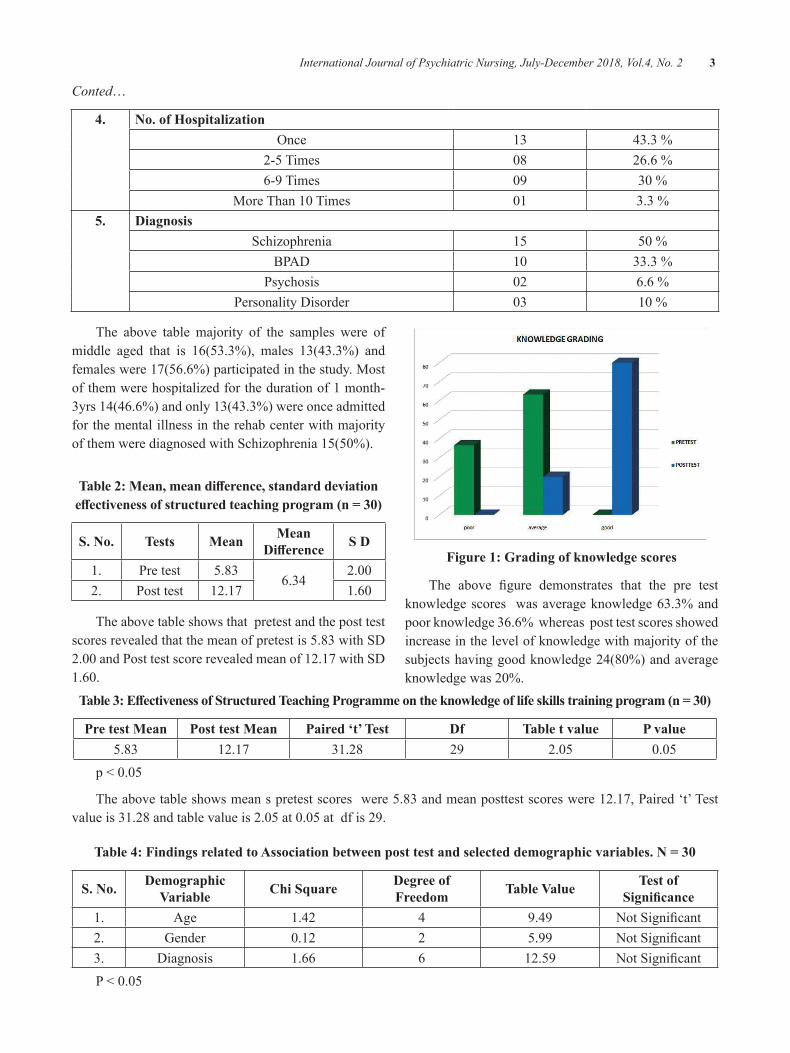
Figure 1: grading of knowledge scores
The above figure demonstrates that the pre testknowledgescores wasaverageknowledge63.3%andpoorknowledge36.6%whereasposttestscoresshowedincreaseinthelevelofknowledgewithmajorityofthesubjectshavinggoodknowledge24(80%)andaverageknowledgewas20%.
Table 3: Effectiveness of Structured Teaching Programme on the knowledge of life skills training program (n = 30)
Pre test Mean Post test Mean Paired ‘t’ Test Df Table t value P value5.83 12.17 31.28 29 2.05 0.05
p<0.05
Theabovetableshowsmeanspretestscoreswere5.83andmeanposttestscoreswere12.17,Paired‘t’Testvalueis31.28andtablevalueis2.05at0.05atdfis29.
Table 4: Findings related to Association between post test and selected demographic variables. n = 30
S. no. Demographic Variable Chi Square Degree of
Freedom Table Value Test of Significance
1. Age 1.42 4 9.49 NotSignificant2. Gender 0.12 2 5.99 NotSignificant3. diagnosis 1.66 6 12.59 NotSignificantP<0.05

4 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
Theabovetable:4showsthatthereisnosignificantassociationbetweenposttestandselecteddemographicvariableslikeAge,Genderanddiagnosis.
DISCuSSIon
Today, despite the deep cultural changes and thechangesinthewayoflife,manypeopledonothavethebasicandrequiredskillsindealingwithlife’problems,and that’swhy, they have been vulnerable in the faceoftheirproblemsandrequirementsoflife.Meanwhile,someprogramshavebeendesignedforpreventingandavoidingtheseproblems,whichoneofthemosteffectivekindofthemisthelifeskillseducationprogramthathasbeendesignedbyWorldHealthOrganization(WHO).
dr.Javad Khalatbari conducted a study onPsychological Explanation and Importance of lifeskillstrainingprogrammes,applicationsandchallengesfacing to it revealed that to determine the importanceof implementation and training of these skills throughpsychologicalorientation,andpaidabriefoverviewontheapplicationsand thechallengesfacing it in today’sworld. Life skills are simply a set of capabilities thatprovide field of adjustment and positive and helpfulbehavior.Numerousandextensiveresearchhaveshownthepositiveeffectoflifeskillsinreducingdrugabuse,preventingviolentbehaviors,strengtheningself-reliance,increasing skills to deal with pressures and stresses,establishingpositiveandeffectivesocialrelationships.(8) Thefindingsofthepresentstudyrevealedthatinpretest36.6%subjectshadpoorknowledgeand63.3%subjectshad average knowledge in pretest. After life skillstraining (post-test) there was significant improvementin theknowledgewith80%goodknowledgeand20%averageknowledge.
Tungpunkom et al., 2012 conducted a study oneffectivenessoflifeskillsonchronicmentalillnesseswithatotalof483participants.Allparticipantswerepeoplewithachronicmentalillness,mostlywithschizophreniaandschizophrenia-likedisorders.Thelifeskillsforthechronicmentally illpatientswaseffectiveandshowedgood results in both the genders.(10)The present studyis congruent with the study findings of Tungpunkomet al where the investigators would found significantimprovement in the knowledge scores.The findings ofthepresentstudyrevealedthatinpretest36.6%subjectshad poor knowledge and 63.3% subjects had average
knowledgeinpretest.Afterlifeskillstraining(post-test)there was significant improvement in the knowledgewith80%goodknowledgeand20%averageknowledge.
ConCLuSIon
Studieshaveshownthatifweprovideindividualsinthe rehabilitationcenterwith thenecessaryknowledgeandinformationandcreatesituationsinwhichtheycanpracticallyexperiencetheknowledgetheyhaveacquired,thisknowledgeaswellasthevalueandattitudewillbeturned into actualizedabilities.Life skills trainingcanpromoteinteractive,decision-making,problem-solving,criticalthinkingandstressmanagementskillsandleadtomore social acceptability, which in turn reduce therisk formental illness. It is recommended toplan andperformconstantLSTworkshopsaseffectivetoolsforinmatesinrehabilitationcenter.
Ethical Clearance:Permissionwasobtainedfromthecompetentauthorityoftherehabilitationcenter.
Source of Funding:Nofundingwasrequired
Conflict of Interest:Nil
REFEREnCES
1.Mary Townsend C. Psychiatric Mental HealthNursing. 8edt. India: Jaypee Brothers MedicalPublishers.
2.Partners in Life skills education- ConclusionsfromaUnitedNationsIntermeeting.departmentofMentalhealth,socialchangeandmentalhealthcluster. World Health Organization. Geneva1999:2-17 http://www.who.int/mental_health/media/en/30.
3.Sadock BJ, Sadock VA. Kaplan and Sadock’ssynopsis of psychiatry and behavioral sciences.8th ed. Philadelphia: Lippincott Williams andWilkins;2005:3183-98.
4.World Health Organization. (Translated byRobabeh Nouri Qasmabady and butterflyMohammadkhani).LifeSkillsTrainingProgram.Tehran:StateWelfareOrganization.CulturalandInternationalJournalofScientific&EngineeringResearch.August-2011:2(8)4:2229-5518

International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 5
5.University of West Indies. Strengthening thedelivery of Health and Family Life EducationinCaribbeandevelopmentcenter.July2013:15-21 available at https://www.open.uwi.edu/sites/default/files/HFLE%20final%20report%20revised%20-%20Aug%2019_2013.
6.EfCGLSEE team.GLSEE. (2012).GlobalLifeSkills Education Evaluation:draft Final Report(February).UNICEF
7.TenCore life skills byWHO.ReachOut India,portal foryouth.dec2015. Availableat:http://reachout.ind.in/whos-list-of-ten-core-life-skills/
8.dr.Javad Khalatbari, et al.A study to assess thePsychological explanation of importance oflife skills training programmes, applicationsand challenges facing to it. InternationalJournal of Scientific & Engineering Research.August-2011:4(8) 1. Available at: https://www.ijser.org/researchpaper/Psychological-explanation-of-the-importance-of-life-skills-training-programs-applications-and-challenges-facing-to-it.pdf
9.Tungpunkom P, Maayan N, Soares-WeiserK. Life skills programmes for chronicmental illnesses. Cochrane database ofSystematic Review(1)2012:Cd000381.doi:10.1002/14651858.Cd000381.pub3

Awareness and Practices on Toy Safety among Mothers of Preschool Children
Hepsi bai J1, Sheela Rathi2, Priyanka Lawrance2, Angel Priya T3
1Assistant Professor, Child Health Nursing Department, College of Nursing, AIIMS, Bhubaneswar; 2Clinical Instructor, Child Health Nursing Department, 3Principal, The Salvation Army Catherine Booth
College of Nursing
AbSTRACT
Poorparentalknowledgeandattitudesoftencontributetoinappropriatemanagementandpracticesofchildcare.Thisbaselinestudyaimedtoassesstheawarenessandpracticeofparentsofpreschoolchildrenregardingtoysafetyinaselectedchildren’shospitalatKanyakumaridistrict,TamilNadu.Usingadescriptiveresearchdesign, 60mothers of preschool childrenwere selected by convenience sampling technique. Structuredquestionnairewas distributed to assess the awareness and practice on toy safety. The finding showedthat93%ofmothershadinadequateawarenessand48%hadmoderatelyadequatepracticeontoysafety.Therewasastatisticallysignificantassociationbetweenlevelofawarenesswithmaternalage(p=0.0004),maternaloccupation(p=0.0001),fathersoccupation(p=0.0014)andmonthlyincome(p=0.0305).Thestudysuggests thatparentsneedtobetaughtontoysafetyguidelinesandpracticessothat toyrelatedinjuriescouldbeavoidedamongchildren.
Keywords: awareness, practice, toy safety, preschooler, mothers.
InTRoDuCTIon
Play is the key centre of a healthy child’s life.Playprovidestheopportunitiestobefree,creativeandexpressive. Toys aremeant to provide enjoyment andeducationforchildrenofallages,howevertheycanalsoprovideagreatdealofdanger.Toysafetyisthepracticeofensuringthattoys,especiallythosemadeforchildren,are safe, usually through the application of set safetystandards1. Parentsareconstantlylookingforwaysthattheycankeeptheirchildrensafewhentheyareplaying.Oneofthebestthingsthattheycandotomakesurethattheir children are safe is bymaking sure that the toysthattheypurchasefortheirchildrenaresafeoptionsforthemtoenjoy. Inordertochoosethebesttoys,parentsmusttakeintoconsiderationtheagethattheirchildrencurrentlyareandbuyaccordingly.Parentsalso shouldhavebetterawarenessandattitudeforbetterpracticeoftoysafetyinordertopreventtoysrelatedaccidents2.
bACKgRounD
Purchasing safe toys is something that all parentsshould focus onwhen they are buying a toy for theirchild.Thatisthebestwaytomakesurethattheirchild
willenjoy the toyandwillbeable tosafelyplaywithit. A survey done inUS (1999 -2010) on toy relatedinjuriesshowedthat3,278,073children<18yearsoldwere treated in emergencydepartments for toy-relatedinjuries. The number and rate of injuries peaked atage 2 years; 63.4%weremale children and 80.3% oftoyrelatedinjurieswereoccurredathome.Ridingtoysincluding non motorized scooters and small toy ballswereassociatedwithmostof thedeath.Mostof thesedeaths were associated with airway obstruction fromsmalltoys,drowningandmotorvehicleaccidentsduringplay.Most of the injuries were lacerations, contusionand abrasions, the head and faceswere the frequentlyaffected areas3. To prevent such incidents the patentsshouldhaveadequateawarenessontoysafetypractices.Comparing towestern literature very less informationwasfoundandwidegapwasidentifiedinIndiansetting,hencethepresentstudywasconducted.
METHoDoLogy
Using a descriptive research design, present wasconducted among60mothersof preschool children inaselectedchildren’shospitalatKanyakumaridistrict,
DOI Number: 10.5958/2395-180X.2018.00007.5
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 7
byconveniencesamplingtechnique.datawasobtainedafter getting approval from institutional researchcommittee, hospital authority and consent from themothers.Tomeetthestudyobjectivesthematerialusedwerestructuredquestionnaireonawareness,structuredpractice questionnaire on toy safety. descriptive(frequencyandpercentage)andinferentialstatistics(Chisquaretest)wasusedtoanalysisthecollecteddata.
RESuLTS
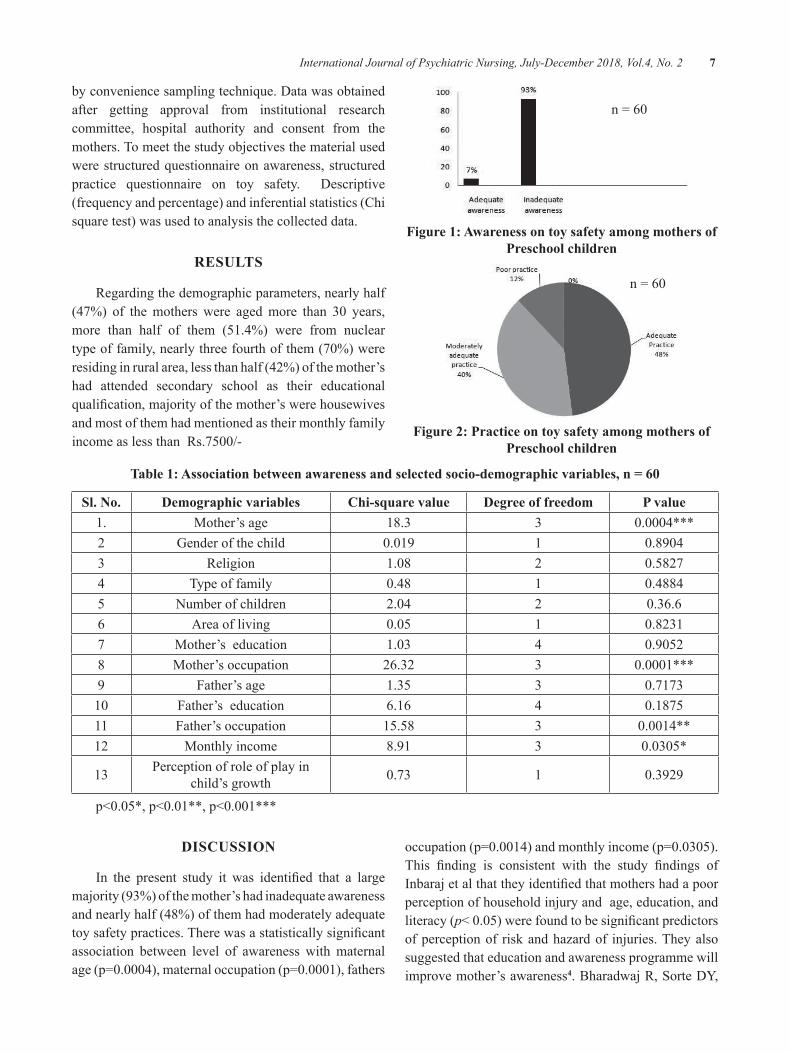
Regardingthedemographicparameters,nearlyhalf(47%) of themothers were agedmore than 30 years,more than half of them (51.4%) were from nucleartypeoffamily,nearlythreefourthofthem(70%)wereresidinginruralarea,lessthanhalf(42%)ofthemother’shad attended secondary school as their educationalqualification,majorityofthemother’swerehousewivesandmostofthemhadmentionedastheirmonthlyfamilyincomeaslessthanRs.7500/-
n=60
Figure 1: Awareness on toy safety among mothers of Preschool children
n=60
Figure 2: Practice on toy safety among mothers of Preschool children
Table 1: Association between awareness and selected socio-demographic variables, n = 60
Sl. no. Demographic variables Chi-square value Degree of freedom P value1. Mother’sage 18.3 3 0.0004***2 Genderofthechild 0.019 1 0.89043 Religion 1.08 2 0.58274 Typeoffamily 0.48 1 0.48845 Numberofchildren 2.04 2 0.36.66 Areaofliving 0.05 1 0.82317 Mother’seducation 1.03 4 0.90528 Mother’soccupation 26.32 3 0.0001***9 Father’sage 1.35 3 0.7173
10 Father’seducation 6.16 4 0.187511 Father’soccupation 15.58 3 0.0014**12 Monthlyincome 8.91 3 0.0305*
13 Perceptionofroleofplayinchild’sgrowth 0.73 1 0.3929
p<0.05*,p<0.01**,p<0.001***
DISCuSSIon
In the present study it was identified that a largemajority(93%)ofthemother’shadinadequateawarenessandnearlyhalf(48%)ofthemhadmoderatelyadequatetoysafetypractices.Therewasastatisticallysignificantassociation between level of awareness withmaternalage(p=0.0004),maternaloccupation(p=0.0001),fathers
occupation(p=0.0014)andmonthlyincome(p=0.0305).This finding is consistent with the study findings ofInbarajetalthattheyidentifiedthatmothershadapoorperceptionofhouseholdinjuryandage,education,andliteracy(p<0.05)werefoundtobesignificantpredictorsofperceptionof riskandhazardof injuries.Theyalsosuggestedthateducationandawarenessprogrammewillimprovemother’sawareness4.BharadwajR,SortedY,

8 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
GeorgeUalsofoundthatpretestknowledgescoreandpracticescores(14.37,28.00)waslessthanmeanposttestknowledge score and practice scores (20.74, 32.46)amongmothersofunderfivechildrenonmanagementofminorailmentswhichwasstatisticallysignificant(atp<0.05)5.
ConCLuSIon
Thestudyhasfoundthatthemothersofpreschoolchildren had inadequate awareness and moderatelyadequatetoysafetypractices.Thesefindingsemphasizethe importance of educating mothers on importanceof toy safety which helps to enhance the toy safetypracticessothattoyrelatedinjuriescouldbepreventedamong children. To protect the child from any injuryor hazard from toys, parents must follow toy safetyguidelines. Parents should avoid buying non-brandedtoys,plastictoys,toysoninternet,andbrightlycoloredtoysastheycontainhighercontentoflead.Also,parentsshouldcarefullyreadtheinstructionsgivenonthetoysoritsmanual;preferablybuytoysmadeupofclothsorwooden.
Ethical Clearance:Taken from “TheSalvationArmyCatherine Booth College of Nursing Ethical ResearchCommittee”
Source of Funding:Self
Conflict of Interest:Nil
REFEREnCES
1.Toxictoys:Overviewandhealthrisks.[internet]Available from: www.generationgreen.org/toys%20overview.htm
2.Kannan K. “Are toys safe?” Availablefrom: www.hindu.com/2004/04/02/stories/2004040206180400.htm [last accessedon2009Jul09]
3.Toy-Related Injuries Among Children Treatedin US Emergency departments, 1990-2011 | Request PDF. Available from: https://www.researchgate.net/publication/269178979_Toy-Related_Injuries_Among_Children_Treated_in_US_Emergency_departments_1990-2011 [accessedFeb282018].
4.Inbaraj LR, Rose A, George K, Bose A.Perception of unintentional childhood injuriesamong mothers in rural South India. Indian JPublicHealth[serialonline]2017[cited2018Feb28];61:211-4.Availablefrom:http://www.ijph.in/text.asp?2017/61/3/211/214812
5.BharadwajR,SortedY,GeorgeU.Effectivenessof Awareness Programme on Knowledge andPractice Regarding Management of MinorAilments among Care Givers of ChildrenUnder 5 Years. Pediatr Ther 7: 325. 2017 doi:10.4172/2161-0665.1000325

Maternal Awareness and Perception on Phototherapy for neonates with Hyperbilirubinemia
Annie Mathew1, Hepsi bai J2
1MSc (N) student, Sree Gokulam Nursing College, Trivandrum, Kerala; 2Assistant Professor, College of Nursing, AIIMS, Bhubaneswar
AbSTRACT
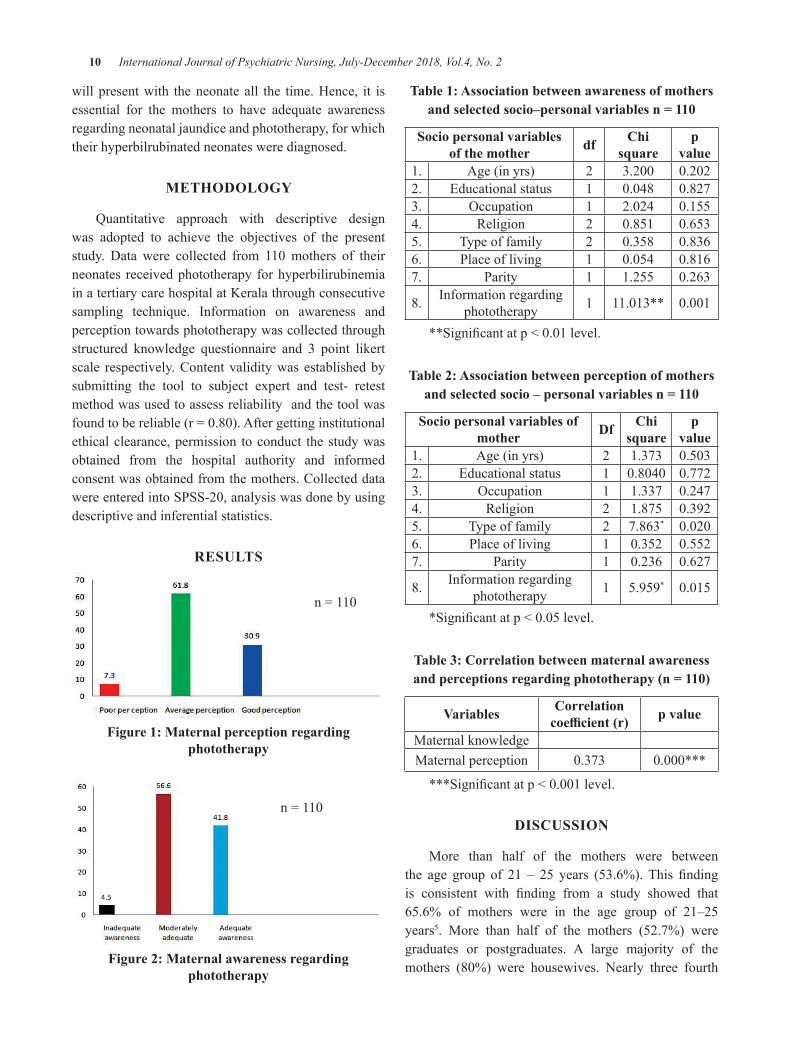
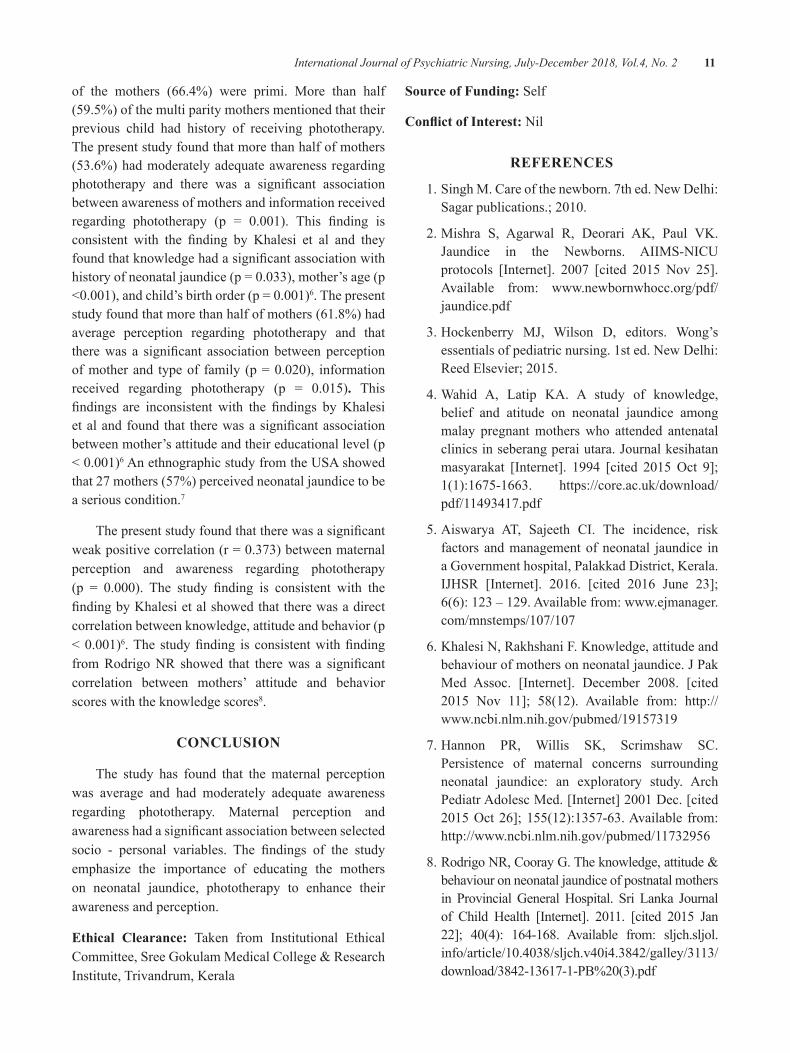
Phototherapy is the safest treatmentmodality for neonatal jaundice and it consists of the applicationoffluorescentlighttotheinfantsexposedskin.Thepresentstudywasaimedtoassessmaternalawarenessandperceptions regardingphototherapy among110mothersofneonates receivedphototherapy fromOBGwards.datawereobtainedby self reportmethod from themothersonperceptionandawareness. Theresultsshowedthatmorethanhalfofthemothers(61.8%)hadaverageperceptionand53.6%ofmothershadmoderatelyadequateawarenessregardingphototherapy.Therewasasignificantassociationbetweenmaternal perception on phototherapy and type of family (p = 0.020), information received regardingphototherapy(p=0.015).Therewasasignificantassociationbetweenawarenessofmotherandinformationreceivedregardingphototherapy(p=0.001).Therewasasignificantweakpositivecorrelation(r=0.373,p=0.000)betweenmaternalperceptionandawarenessregardingphototherapy.Thestudyemphasizestheimportanceofeducatingthemothersonneonatal jaundice,phototherapytoenhancetheirawarenessandperception.
Keywords: maternal perception; awareness; phototherapy; neonate
InTRoDuCTIon
Infants between birth and first 28 days of life arecalled newborns or neonates. Globally 130 millionbabiesareborneveryyear.Everyyearabout27millionbabies(20%ofglobalbirths)areborninIndia.Neonataljaundice is a common condition that pediatriciansencounterintheirpractice.Itisalsoasignificantcauseofneonatalmorbidityworld-wideandisestimatedtobepresent in 60% of term neonates and 80% of pretermbabies.Interventionstopreventprogressionofneonataljaundicesignificantlyreducethemorbidityandmortalityrate of neonate and one among the management isphototherapy1
bACKgRounD
Normally neonate’s body is able to maintain abalancebetweenthedestructionofRBCsandtheuseorexcretionofby-products.However,whendevelopmentallimitations or a pathologic process interferes with thisbalance,bilirubinaccumulates in the tissues toproducejaundice. If the bilirubin level is greatly elevated,symptoms may include yellowing of the skin and the
sclera, poor feeding and lethargy2 Managing neonataljaundice is by pharmacological (Phenobarbitone,Intravenous Immunoglobulins, Metalloporphyrins)and non pharmacological (phototherapy and exchangetransfusion)way.Phototherapyconsistsoftheapplicationoffluorescent light to theneonates exposed skin.Lightpromotes bilirubin excretion by photoisomerization,whichalters the structureofbilirubin toa soluble form(Lumirubin)foreasierexcretion.Studiesindicatethatbluefluorescentlightismoreeffectiveinreducingbilirubin.3
A cross-sectional studywas conducted to identifylevel of knowledge, belief and attitude on neonataljaundiceamong150MalaypregnantmotherswholiveinSeberangPeraiUtarastateandidentifiedthat,about50%oftherespondenthadinadequategeneralawarenesson neonatal jaundice, especially the knowledge oncomplicationsandidentifyingthebestmethodofjaundicedetection4 Since it is the mother who is wholly andsolelyresponsibleforcaringtheneonateitisnecessaryfor her to have adequate awareness on the treatmentorprocedurethebabyundergoes/receives.Inthefirstweekoflife,50%ofneonateshaveclinicallydetectablejaundiceandmothers are theprimarycaregiverswho
DOI Number: 10.5958/2395-180X.2018.00008.7
10 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
willpresentwith theneonateall the time.Hence, it isessential for the mothers to have adequate awarenessregardingneonataljaundiceandphototherapy,forwhichtheirhyperbilrubinatedneonateswerediagnosed.
METHoDoLogy
Quantitative approach with descriptive designwas adopted to achieve the objectives of the presentstudy. data were collected from 110mothers of theirneonates receivedphototherapy forhyperbilirubinemiainatertiarycarehospitalatKeralathroughconsecutivesampling technique. Information on awareness andperceptiontowardsphototherapywascollectedthroughstructured knowledge questionnaire and 3 point likertscale respectively.Contentvaliditywasestablishedbysubmitting the tool to subject expert and test- retestmethodwasusedtoassessreliabilityandthetoolwasfoundtobereliable(r=0.80).Aftergettinginstitutionalethicalclearance,permission toconduct thestudywasobtained from the hospital authority and informedconsentwasobtainedfromthemothers.CollecteddatawereenteredintoSPSS-20,analysiswasdonebyusingdescriptiveandinferentialstatistics.
RESuLTS
n=110
Figure 1: Maternal perception regarding phototherapy
n=110
Figure 2: Maternal awareness regarding phototherapy
Table 1: Association between awareness of mothers and selected socio–personal variables n = 110
Socio personal variables of the mother df Chi
squarep
value1. Age(inyrs) 2 3.200 0.2022. Educationalstatus 1 0.048 0.8273. Occupation 1 2.024 0.1554. Religion 2 0.851 0.6535. Typeoffamily 2 0.358 0.8366. Placeofliving 1 0.054 0.8167. Parity 1 1.255 0.263
8. Informationregardingphototherapy 1 11.013** 0.001
**Significantatp<0.01level.
Table 2: Association between perception of mothers and selected socio – personal variables n = 110
Socio personal variables of mother Df Chi
squarep
value1. Age(inyrs) 2 1.373 0.5032. Educationalstatus 1 0.8040 0.7723. Occupation 1 1.337 0.2474. Religion 2 1.875 0.3925. Typeoffamily 2 7.863* 0.0206. Placeofliving 1 0.352 0.5527. Parity 1 0.236 0.627
8. Informationregardingphototherapy 1 5.959* 0.015
*Significantatp<0.05level.
Table 3: Correlation between maternal awareness and perceptions regarding phototherapy (n = 110)
Variables Correlation coefficient (r) p value
MaternalknowledgeMaternalperception 0.373 0.000***
***Significantatp<0.001level.
DISCuSSIon
More than half of the mothers were betweenthe age group of 21 – 25 years (53.6%).This findingis consistent with finding from a study showed that65.6% of mothers were in the age group of 21–25years5. More than half of the mothers (52.7%) weregraduates or postgraduates. A large majority of themothers (80%) were housewives. Nearly three fourth
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 11
of the mothers (66.4%) were primi. More than half(59.5%)ofthemultiparitymothersmentionedthattheirprevious child had history of receiving phototherapy.Thepresentstudyfoundthatmorethanhalfofmothers(53.6%)hadmoderatelyadequateawarenessregardingphototherapy and there was a significant associationbetweenawarenessofmothersandinformationreceivedregarding phototherapy (p = 0.001). This finding isconsistent with the finding by Khalesi et al and theyfoundthatknowledgehadasignificantassociationwithhistoryofneonataljaundice(p=0.033),mother’sage(p<0.001),andchild’sbirthorder(p=0.001)6.Thepresentstudyfoundthatmorethanhalfofmothers(61.8%)hadaverage perception regarding phototherapy and thattherewas a significant association betweenperceptionofmotherand typeof family (p=0.020), informationreceived regarding phototherapy (p = 0.015). Thisfindings are inconsistent with the findings by Khalesietalandfoundthat therewasasignificantassociationbetweenmother’sattitudeandtheireducationallevel(p<0.001)6AnethnographicstudyfromtheUSAshowedthat27mothers(57%)perceivedneonataljaundicetobeaseriouscondition.7
Thepresentstudyfoundthattherewasasignificantweakpositivecorrelation(r=0.373)betweenmaternalperception and awareness regarding phototherapy(p = 0.000). The study finding is consistent with thefindingbyKhalesietalshowedthattherewasadirectcorrelationbetweenknowledge,attitudeandbehavior(p<0.001)6.The studyfinding is consistentwithfindingfromRodrigoNR showed that therewas a significantcorrelation between mothers’ attitude and behaviorscoreswiththeknowledgescores8.
ConCLuSIon
The study has found that thematernal perceptionwas average and had moderately adequate awarenessregarding phototherapy. Maternal perception andawarenesshadasignificantassociationbetweenselectedsocio - personal variables. The findings of the studyemphasize the importance of educating the motherson neonatal jaundice, phototherapy to enhance theirawarenessandperception.
Ethical Clearance: Taken from Institutional EthicalCommittee,SreeGokulamMedicalCollege&ResearchInstitute,Trivandrum,Kerala
Source of Funding:Self
Conflict of Interest:Nil
REFEREnCES
1.SinghM.Careofthenewborn.7thed.Newdelhi:Sagarpublications.;2010.
2.Mishra S, Agarwal R, deorari AK, Paul VK.Jaundice in the Newborns. AIIMS-NICUprotocols [Internet]. 2007 [cited 2015 Nov 25].Available from: www.newbornwhocc.org/pdf/jaundice.pdf
3.Hockenberry MJ, Wilson d, editors. Wong’sessentialsofpediatricnursing.1sted.Newdelhi:ReedElsevier;2015.
4.Wahid A, Latip KA. A study of knowledge,belief and atitude on neonatal jaundice amongmalay pregnantmotherswho attended antenatalclinicsinseberangperaiutara.Journalkesihatanmasyarakat [Internet]. 1994 [cited 2015Oct 9];1(1):1675-1663. https://core.ac.uk/download/pdf/11493417.pdf
5.Aiswarya AT, Sajeeth CI. The incidence, riskfactors andmanagementofneonatal jaundice inaGovernmenthospital,Palakkaddistrict,Kerala.IJHSR [Internet]. 2016. [cited 2016 June 23];6(6):123–129.Availablefrom:www.ejmanager.com/mnstemps/107/107
6.KhalesiN,RakhshaniF.Knowledge,attitudeandbehaviourofmothersonneonataljaundice.JPakMed Assoc. [Internet]. december 2008. [cited2015 Nov 11]; 58(12). Available from: http://www.ncbi.nlm.nih.gov/pubmed/19157319
7.Hannon PR, Willis SK, Scrimshaw SC.Persistence of maternal concerns surroundingneonatal jaundice: an exploratory study. ArchPediatrAdolescMed.[Internet]2001dec.[cited2015Oct26];155(12):1357-63.Available from:http://www.ncbi.nlm.nih.gov/pubmed/11732956
8.RodrigoNR,CoorayG.Theknowledge,attitude&behaviouronneonataljaundiceofpostnatalmothersin ProvincialGeneralHospital. Sri Lanka Journalof Child Health [Internet]. 2011. [cited 2015 Jan22]; 40(4): 164-168. Available from: sljch.sljol.info/article/10.4038/sljch.v40i4.3842/galley/3113/download/3842-13617-1-PB%20(3).pdf
Effectiveness of Pelvic girdle Exercise on Pelvic girdle Pain and Specific Activities among Primigravida Mothers Attending
Antenatal oPD at Selected Hospitals, Salem
J Sathya1, M. D. Santhi2
1Nursing Tutor, 2Professor cum HOD, Sri Gokulam College Of Nursing, Salem, TamilNadu
AbSTRACT
Introduction: Pregnancyisapreciousperiodandmemorablemomentforeverywomanwhofacesphysical,physiologicalandpsychologicalchangesresultingsomesortsofailment..OneamongthatisPelvicGirdlePain.Women with Pelvic Girdle Pain or symphysis pubis dysfunction during pregnancy has functionaldifficultiesthatsignificantlyaffectingqualityoflife.
objectives: AssesstheEffectivenessofPelvicGirdleExerciseonPelvicGirdlePainandSpecificActivitiesamongPrimigravidaMothers
Design: Quasiexperimentalresearchdesign(pre-testandpost-testcontrolgroupdesign)
Setting: SriGokulamHospital,SalemandSalemPolyClinicHospital.
Samples: 60primigravidamothers(30inexperimentalgroupand30incontrolgroup).
Measurements and Tools: ModifiedPelvicGirdleQuestionnaireandPatientSpecificFunctionalScale.descriptiveandInferentialstatisticswereused.
Findings: Inpre-testscoreinexperimentalgroup,66%ofmothershadmoderatepainwhereasinpost-testI&II(66%&97%)ofmothershadmildpainrespectively.Inpre-testtheexperimentalgroupmothershadmeanspecificactivitiesscoreof3.02±1.15whereasinpost-testI&IIthemeanscorewas4.36±0.90and6.30±0.78.Hence,itshowsthattherewasreductioninPelvicGirdlePainandimprovementinspecificactivities.Comparisonofposttestscoresand‘t’valueonPelvicGirdlePainandspecificactivitiesamongexperimentalandcontrolgroupshowsthatthemeanscorewas12.83±5.33,37.40±12.46and6.30±0.78,3.38±0.97respectively.TherewasnosignificantassociationwithdemographicvariablesandnegativecorrelationbetweenposttestscoresofPelvicGirdlePainandspecificactivitiesamongexperimentalgroupmothers.
Conclusion: PelvicgirdleexercisereducesPelvicGirdlePainandimprovesspecificactivitiesofthemother.Thisexerciseiseasytofollow,simpletodo,hasnoriskandeffectivetoreducePelvicGirdlePain.
Keywords: Pelvic girdle exercise, Pelvic girdle pain, Specific activities, Primigravida mothers
InTRoDuCTIon
AllovertheworldPelvicGirdlePainisasignificantproblem for pregnant women. Studies have revealedthatPregnancyrelatedPelvicGirdlePainisacommonsymptom among pregnant women in Europeanpopulation and in many studies the average reportedprevalence of Pregnancy related Low Back Pain andPelvicGirdlePainis45.3%.2
Majority (62.5%) of women having pelvic painget relieved within 1 month after delivery but 8.6%
continued to experience Pelvic Girdle Pain even twoyearsafterdeliveryindevelopingcountries.2
In 2005, theNational Centre for Health StatisticsreportedthattheprevalencerateofPGPis72%inIndia.5
A study conducted on ‘Prevalence of Pregnancyrelated Pelvic Girdle Pain in Indian primigravidamother’ at New delhi in India Concluded that 1 inevery 2 primigravida mothers suffered by Pregnancyrelated PelvicGirdle Pain and lumbo pelvic pain alsoshereportedthathighprevalenceofPelvicGirdlePainobservedat16and36weeksofgestation.1
DOI Number: 10.5958/2395-180X.2018.00009.9
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 13
PGPwasobserved74%infirstpregnancyitshowsthe frequency of pain increases as the pregnancyadvances, thatis12%inthefirst trimester,34%inthesecondtrimesterand52%inthethirdtrimester.3
Mostofthemothersnothavingadequateknowledgeregarding Pelvic Girdle Pain hence not seeking anytreatmentforit.SomanyresearcharticleshownthattheuntreatedPregnancyrelatedPelvicGirdlePainsustainsinpostpartumperiodandforsomewomenitcontinuesas a lifelong problem which is affecting their dailyactivities.6
Pelvic Girdle exercise is simple exercise able tofollowby themotherseasilyandhelps to improve thestability of pelvic and back thereby reduces pain andimproves specific activities. Comparativelywith othermodalities, Pelvic girdle exercise is simple, easy tofollowandeffectiveforPelvicGirdlePain.4
OBJECTIVES
1.ToidentifytheprimigravidamotherswithPelvicGirdle Pain of both experimental and controlgroup.
2.Toassess the levelofPelvicGirdlePainamongprimigravida mothers of both experimental andcontrolgroupbeforeandafterimplementationofPelvicgirdleexercise.
3.To assess the specific activities amongprimigravida mothers of both experimental andcontrolgroupbeforeandafterimplementationofpelvicgirdleexercise.
4.To associate thePelvicGirdlePain and specificactivities scores with selected demographicvariables among primigravida mothers of bothexperimentalandcontrolgroup.
5.To correlate post test scores of Pelvic GirdlePain and specific activities among primigravidamothersofbothexperimentalandcontrolgroup.
HyPoTHESES
1. H1:ThereisasignificantdifferencebetweenpreandposttestscoresonPelvicGirdlePainamongprimigravidamothersofExperimentalandcontrolgroupatp≤0.05level.
2. H2:Thereisasignificantdifferencebetweenpreandpost test scores of specific activities amongprimigravidamothersofExperimentalandcontrolgroupatp≤0.05level.
3. H3:Thereisasignificantdifferencebetweenpost-test score on Pelvic Girdle Pain and specificactivities among primi gravida mothers ofexperimentalandcontrolgroupatp≤0.05level.
4. H4: There is a significant association betweenpretestscoresofPelvicGirdlePainandspecificactivities with demographic variables amongprimigravida mothers of both experimental andcontrolgroupatp≤0.05level.
5. H5: There is a significant association betweenposttestscoresofPelvicGirdlePainandspecificactivities with demographic variables amongprimigravida mothers of both experimental andcontrolgroupatp≤0.05level.
6. H6: There is a significant correlation betweenposttestscoresofPelvicGirdlePainandspecificactivitiesofbothexperimentalandcontrolgroupmothersatp≤0.05level.
Theoritical Framework: Theoretical frameworkselected for this study was based on ModifiedWidenbach’s Prescriptive Theory-A helping art ofclinicalnursing.
MATERIALS AnD METHoD
AQuasiexperimentalresearchdesign(pre-testandpost-testcontrolgroupdesign)wasusedinthisstudy.Exp.Grouppretesttreatmentposttest1posttest2
Norandomization-----------------------------------------------------------------------
Con. Group pre test --------------- post test1posttest2
The study population includes the primigravidamothers at 36 weeks of gestation attending antenatalOPd. Written permission was obtained from theManagingdirectorofSriGokulamHospitalandSalemPolyclinic, Salem and written consent was obtainedfrom primigravida mothers. Modified Pelvic GirdleQuestionnairewasusedtoassessthelevelofPelvicGirdlePainandPatientSpecificFunctionalScalewasusedtoassess thespecificactivities forbothexperimentalandcontrolgroupmothers.Afterpretest,demonstratedthePelvicgirdle exercise for 3-5primigravidamothersofexperimentalgroupfor30minutes.Afterdemonstrationthemotherswereinstructedtoredemonstratetheexerciseand the investigator checked their performance, andalso insisted toperform this exerciseprogram2 timesdailyforaperiodof2weeksandalogbookwasgiven
14 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
torecordtheexercisewereperformedintheirhome.Attheendof1stand2ndweekoftheirantenatalvisittheposttestwasconductedbyusingsame tools.Thecollecteddata was organized, tabulated and analyzed by usingbothdescriptiveandinferentialstatistics.
FInDIngS
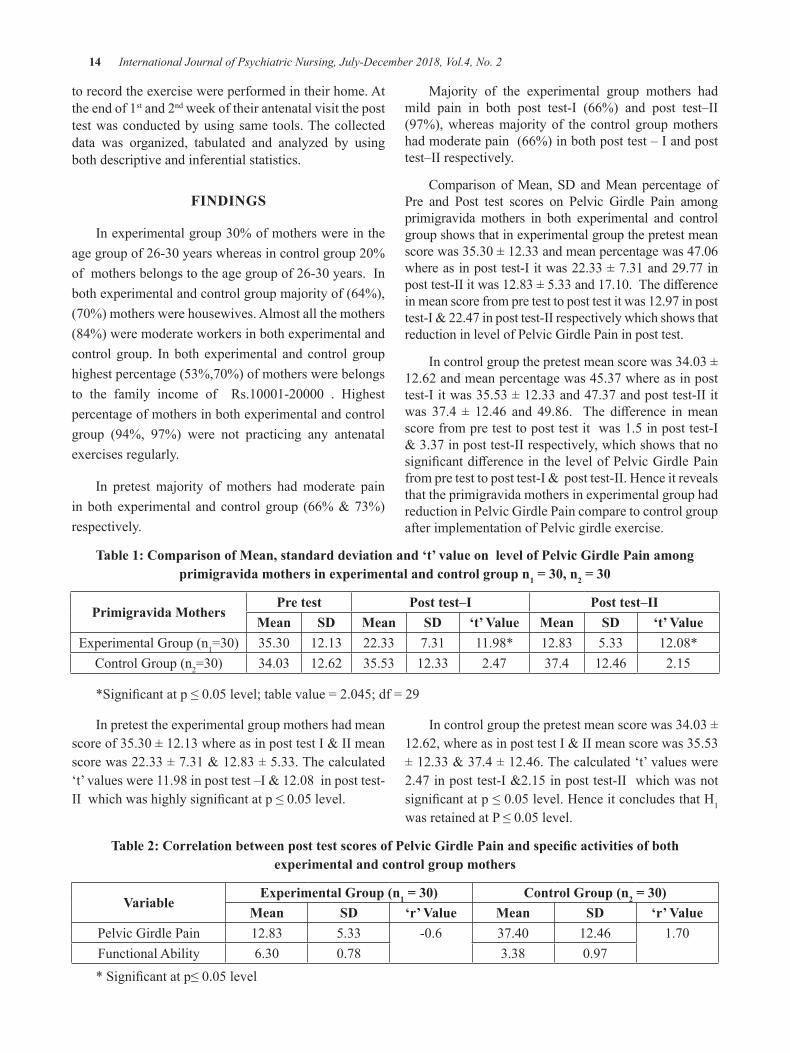
Inexperimentalgroup30%ofmotherswereintheagegroupof26-30yearswhereasincontrolgroup20%ofmothersbelongstotheagegroupof26-30years.Inbothexperimentalandcontrolgroupmajorityof(64%),(70%)motherswerehousewives.Almostallthemothers(84%)weremoderateworkersinbothexperimentalandcontrolgroup. Inbothexperimental andcontrolgrouphighestpercentage(53%,70%)ofmotherswerebelongsto the family income of Rs.10001-20000 . Highestpercentageofmothersinbothexperimentalandcontrolgroup (94%, 97%) were not practicing any antenatalexercisesregularly.
In pretest majority ofmothers hadmoderate paininbothexperimental andcontrolgroup (66%&73%)respectively.
Majority of the experimental group mothers hadmild pain in both post test-I (66%) and post test–II(97%),whereasmajorityof the controlgroupmothershadmoderatepain(66%)inbothposttest–Iandposttest–IIrespectively.
Comparison ofMean, Sd andMean percentage ofPre and Post test scores on Pelvic Girdle Pain amongprimigravidamothers in both experimental and controlgroupshowsthatinexperimentalgroupthepretestmeanscorewas35.30±12.33andmeanpercentagewas47.06whereasinposttest-Iitwas22.33±7.31and29.77inposttest-IIitwas12.83±5.33and17.10.Thedifferenceinmeanscorefrompretesttoposttestitwas12.97inposttest-I&22.47inposttest-IIrespectivelywhichshowsthatreductioninlevelofPelvicGirdlePaininposttest.
Incontrolgroupthepretestmeanscorewas34.03±12.62andmeanpercentagewas45.37whereasinposttest-Iitwas35.53±12.33and47.37andposttest-IIitwas 37.4 ± 12.46 and 49.86. The difference inmeanscorefrompretesttoposttestitwas1.5inposttest-I&3.37inposttest-IIrespectively,whichshowsthatnosignificantdifferenceinthelevelofPelvicGirdlePainfrompretesttoposttest-I&posttest-II.HenceitrevealsthattheprimigravidamothersinexperimentalgrouphadreductioninPelvicGirdlePaincomparetocontrolgroupafterimplementationofPelvicgirdleexercise.
Table 1: Comparison of Mean, standard deviation and ‘t’ value on level of Pelvic girdle Pain among primigravida mothers in experimental and control group n1 = 30, n2 = 30
Primigravida MothersPre test Post test–I Post test–II
Mean SD Mean SD ‘t’ Value Mean SD ‘t’ ValueExperimentalGroup(n1=30) 35.30 12.13 22.33 7.31 11.98* 12.83 5.33 12.08*
ControlGroup(n2=30) 34.03 12.62 35.53 12.33 2.47 37.4 12.46 2.15
*Significantatp≤0.05level;tablevalue=2.045;df=29
Inpretesttheexperimentalgroupmothershadmeanscoreof35.30±12.13whereasinposttestI&IImeanscorewas22.33±7.31&12.83±5.33.Thecalculated‘t’valueswere11.98inposttest–I&12.08inposttest-IIwhichwashighlysignificantatp≤0.05level.
Incontrolgroupthepretestmeanscorewas34.03±12.62,whereasinposttestI&IImeanscorewas35.53±12.33&37.4±12.46.Thecalculated‘t’valueswere2.47inposttest-I&2.15inposttest-IIwhichwasnotsignificantatp≤0.05level.HenceitconcludesthatH1
wasretainedatP≤0.05level.
Table 2: Correlation between post test scores of Pelvic girdle Pain and specific activities of both experimental and control group mothers
VariableExperimental group (n1 = 30) Control group (n2 = 30)
Mean SD ‘r’ Value Mean SD ‘r’ ValuePelvicGirdlePain 12.83 5.33 -0.6 37.40 12.46 1.70FunctionalAbility 6.30 0.78 3.38 0.97*Significantatp≤0.05level

International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 15
Therewasnegativecorrelationseeninexperimentalgroupandthecalculated‘r’valuewas-0.6whichwassignificantatp≤0.05level.Incontrolgrouptherewaspositive correlation and the calculated ‘r ‘ value was1.70whichwassignificantatp≤0.05 level. HenceH6
wasretained.
ConCLuSIon
Theresultofthisstudyshowedthat,thepre-testscorein experimental group, 66% ofmothers hadmoderatepainwhereasinpost-testI&II(66%&97%)ofmothershadmildpainrespectively.Inpre-testtheexperimentalgroupmothershadmeanspecificactivitiesscoreof3.02±1.15whereas inpost-test I&II themeanscorewas4.36± 0.90and6.30± 0.78.Hence,itshowsthattherewas reduction in PelvicGirdle Pain and improvementinspecificactivities.Comparisonofposttestscoresand‘t’ value on Pelvic Girdle Pain and specific activitiesamong experimental and control group shows that themeanscorewas12.83±5.33,37.40±12.46and6.30±0.78,3.38±0.97respectively.Hence,itshowsthattherewasreductioninPelvicGirdlePainandimprovementinspecific activities among experimental groupmothers.Pelvic girdle exercise reduces Pelvic Girdle Pain andimprovesspecificactivitiesofthemother.Thisexerciseiseasytofollow,simpletodo,hasnoriskand
IMPLICATIonS
nursing Education:
z EducationalprogrammeonPelvicGirdlePainandPelvic girdle exercise can be included in subjectcontent.
z Alternativepainreliefmanagementcanbeincludedinnursingcurriculum.
nursing practice:
z Pelvicgirdleexercisecouldbeadoptedinhospitalsandmaternitycentre.
z Staffdevelopmentprogrammecanbearrangedforstaffsworkinginthehospitalsandmaternitycentre.
Recommendations for further research:
z AcomparativestudycanbedonetodeterminetheeffectivenessofPelvicgirdleexerciseamongprimiandmultigravidamothers.
z Alongitudinalstudycanbedonetodeterminetheeffectivenessofpelvicgirdleexercise.
Conflict of Interest:Nil
Source of Funding:Self
Ethical Clearance:TakenfromtheInstitutionalEthicalCommittee.
REFEREnCES
1.Gupta Monika, Srivastava Shilpi, Khan SohrabA,(2014).Prevalenceofpregnancyrelatedpelvicgirdle pain in Indian primigravida: A Tertiarycare hospital. Indian Journal of Obstetrics and Gynecology Research, Vol.1,No.1,17-23.
2.HelenEldenetal.,(2004).Effectsofacupunctureand stabilizing exercises among women withpregnancy-relatedpelvicpain.American Journal of Obstetrics and Gynaecology, 330;761.doi:10.1136/bmj.38397.507014.
3.J. depledge, P. J. McNair, C. Keal-Smith, andM.Williams,(2005).Managementofsymphysispubisdysfunctionduringpregnancyusingexerciseandpelvic support belts.Physical Therapy, vol.85,no.12,
4.J.Klugeetal.,(2011),Specificexercisestotreatpregnancy-related low back pain in a SouthAfrican population. International Journal of Gynecology and Obstetrics ,113, 187–191.doi:10.1016/j.ijgo.2010.10.03.
5.Preetha Ramachandra, Arun G. Maiya, PratapKumar and Asha Kamath,(2015).Prevalenceof Musculoskeletal dysfunctions among IndianPresgnantWomen. Journal of pregnancy, Article ID 437105.
6.Stuge B , (2012). Pelvic girdle pain:examination, treatment, and the developmentand implementationof theEuropeanguidelines. Journal of the Association of Chartered Physiotherapists in Women’s Health, Autumn ,111,5–12.

Stress and Coping between the Intensive Care unit and general Ward nurses in Selected Hospital, Coimbatore
S. Karthic1, M. baskaran2, Esther Daisy Meerabai Joel3
1Senior Operations Manager, RPS Hospital, Chennai; 2Associate Professor, 3Professor and Former HOD, Department of Mental Health (Psychiatric) Nursing, PSG College of Nursing, Coimbatore, Tamil Nadu
AbSTRACT
Nursesstressisdefinedastheemotionaland physical reactions resultingfrom theinteractionsbetweenthenurseandher/hisworkenvironmentwherethedemandsofthejobexceedcapabilitiesandresources.Nursestressisoneofthecurrentproblemswhichaffectthenursesandthequalityofpatientcare.
objectives:
z TocomparethelevelofstressandcopingbetweenIntensiveCareUnitandGeneralWardnurses.
Material and Method: Theresearchdesignadoptedforthisstudywascomparativedescriptive.ThestudywasconductedinPSGHospital,Coimbatore.desiredsampleof150wereselectedaccordingtotheinclusionand exclusion criteria. demographic data and the stress of the nurses is assessed using a standardizedquestionnairedevelopedbyChaudhuryetal.,2004andcopingisassessedbyastandardizedratingscaledevelopedbyMcElfatricketal.,2000.Thedatawasanalyzedbyinferential&descriptivestatistics.
Results: ThestresslevelofintensivecareunitnursesissignificantlymorethanthegeneralwardnurseswhichhavebeenprovedbythevalueofZtest(10.98)whichisgreaterthanthetablevalue1.64.ThecopinglevelofintensivecareunitnursesissignificantlylessthanthegeneralwardnurseswhichhavebeenprovedbythevalueofZtest(15.22)whichisgreaterthanthetablevalue1.64.Thecorrelationcoefficient‘r’=0.425revealedthat,therewasamoderatelevelofsignificanceatp<0.01level.
Conclusion: This study shows that the intensive care unit nurses weremore stressed than the generalwardnursesandgeneralwardnurseshavemorecopingthantheintensivecareunitnurses.Itwasstronglyrecommendedthataregularassessmentofstressandstressreductionprogrammecanbearrangedtoreducethestressofintensivecareunitnurseswhichhelpstoimprovethequalityofcareforpatients.
Keywords: Stress, Coping, Intensive care unit, General ward, Nurses.
Corresponding Author:Mr.M.Baskaran,M.Sc(N),PhdScholarAssociateProfessordepartmentofMentalHealth(Psychiatric)Nursing.PSGCollegeofNursing,Coimbatore.TamilNaduEmail:[email protected]
InTRoDuCTIon
Nursingistheprofessionofcaringthesick.Nursestakecareofpatientandco-ordinatealltheservicesinthehealthcaresetting.Nursingcarethereforedemandscontinuous exercise of critical thinking, creativeimagination,independentjudgmentinproblemsolvinganddecisionmaking.
Nurse’s stress is defined as the emotional andphysical reactions resulting from the interactionsbetweenthenurseandhis/herworkenvironmentwherethe demands of the jobexceedcapabilitiesand.
need for the Study: A moderate level of stress or“Eustress” is an important motivating factor and isconsidered normal and necessary. If stress is intense,continuous, and repeated, it becomes a negativephenomenonor“distress,”whichcan lead tophysicalillness andpsychological disorders and thusmake lifeverymiserable.1
Stress experienced by workers at work is calledjobstress.Itmaybeduetoanumberoffactorssuchas
DOI Number: 10.5958/2395-180X.2018.00010.5

International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 17
poorworkingconditionexcessiveworkload,shiftwork,longhoursofwork,roleambiguity,roleconflicts,poorrelationshipswithboss, colleaguesor subordinates.2 A surveyconductedamongRegisterednursesofAmericashowedthat59%ofRegisterednursesreportedthattheirjobassostressfulandtheyfeltburnedout.3
REVIEW oF LITERATuRE
Research studies related to Stress and Coping Strategies Adopted by the Staff nurses: Adescriptivecomparativedesignwasconductedcomparethelevelofstress and coping strategies adopted by the staff nursesworking in various patient care settings. The 240 staffnurses were selected by stratified random sampling.data were collected by self-report method using sociodemographicperforma,PerceivedStressscaleandcopingscale. The result showed among staff nurses workingin generalwards, privatewards and ICU, severe stresswas experienced by ICU staff (42%) while majorityof the staff nurses in general wards and private wardswere experiencingmoderate level of stress. There wasno significant difference between the coping strategiesadoptedbystaffnursesworkingingeneralwards,privatewardsandICU.Thepresentstudyconcludesthatiftherewere effective management of stress among ICU andnovicenurses, theworkplaceerrorscanbeminimized;productivitycanbeincreasedtomaximumandultimatelycanenhancequalitypatientcare.4
Across-sectionalstudywasconductedtocomparestresslevelandjobstressorsoperatingintwodifferentunits,i.e.intensivecareunits(ICU)andgeneralwardsof a tertiary care hospital of North India. Convenientsample technique were used to selected 285 nurses(generalwards=176;ICU=109).ThestudyrevealedmoderatetohighstresslevelamonggeneralwardsandICU nurses with young female nurses experiencingmorestress.Further,workload,roleambiguityandlessersocial support accounted for significant amount stressamongnursesworkingonboththeunitswhileexternalfactors, such as physical environment and resourceshardlycontributed to stress. Itwasalso found that theICU nurses experienced stress more in the form ofexhaustion(11.9%);irritation(11.9%)andreducedself-confidence(0.9%)thatthoseworkingingeneralwards.However, the nurses on both the units use distraction,positivecoping,problem-solvingandreligiousstrategiestomanageandhandle their stress.Thefindingsof the
studygiveinsightintostressandstressorsrelatedtojobwhichcanbebufferedusingvariousstressmanagementstrategiesbythenursemanagers.5
A descriptive comparative design study wasconductedonperceivedstressamongnursesinJordan.310 were selected from various hospitals. NursesansweredtheArabicVersionofPerceivedStressScale10-Items Questionnaire (PSS10) and a CharacteristicChecklist.Thisstudyresultsshowedthatnursesworkinginpsychiatricdepartmentsperceived thehighest stresslevels followedbyoncologynurses (ONs), ICU/CCU,andERnursesrespectively.Medicalandsurgicalnursesreportedthelowestlevelofstress.Thisstudyconcludedthatpsychiatricnurseshavethehighestlevelsofstressamong all participated nurses. This might lead todissatisfactionwiththeworkandhighratesofburnoutandturnover.Allthesefactorscaneasilyaffectpatientscareandsafetyissue,especiallypsychiatricpatients.Itishighlyrecommendedthatnursemanagersandpolicymakers pay a particular attention to this phenomenonand looking for causes of such high level of stress isimportant.6
Statement of the Problem: A comparativestudytoassessthestressandcopingbetweenthe intensive care unit and general ward nurses inselectedhospital,Coimbatore
objectives:
z ToassessthestressandcopingbetweenIntensiveCareUnitandgeneralwardnurses.
z TocomparethelevelofstressandcopingbetweenIntensiveCareUnitandGeneralWardnurses.
z Tocorrelatethelevelof stressandcopingbetweenIntensiveCareUnitandGeneralWardnurses.
Assumptions:
z Thenursesworkinginintensivecareunitmayhavemore stress than the nurses working in generalward.
Hypothesis:
z There will be a difference in level of stress andcoping between nurses of intensive care unit andgeneralward.
z Therewillasignificantcorrelationbetweenlevelsof stress and coping strategies among nurses ofintensivecareunitandgeneralward.
18 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
operational Definitions:Stress:Stressisconsideredtoresult from an imbalance between the demands of theworkplaceandthenurse’sabilitytocope.
Coping Strategies: Coping strategies are the effortstaken by the nurses to manage the external and theinternaldemandsperceivedbythem.
Research Design: The research design selected forpresentstudyiscomparativedescriptivedesign.
Setting of the Study: Thestudywasconductedamongthe nurses who are working in PSG hospital criticalcare units and general ward. The PSG Hospital is amultispecialty910beddedhospitalandiswellequippedwithadequatefacilities.
Population:Thestudypopulationincludesnurseswhowere working in PSGHospital critical care units andgeneralward.
Samples: StaffNurses.
Sample Size:
Sample size of the study was 150 samples wereselected(intensivecareunit,n=75andgeneralwardn=75)totalsampleswere150.
Sampling Technique: Non-probability convenientsamplingtechnique
Instruments and Tools for Data Collection: A questionnaire for assessing the level of stress and aratingscalewasusedtoassessthecopinglevelamongthenurses.
Section I: Section I deals with the demographic dataof thesamples.Thedemographicprofile includedage,
sex,educationalqualification,familyprofile,individualincome, family income, place of domicile, distance toworkplace,modeoftravel,timeoftravel,experienceofnursesandhobbies.
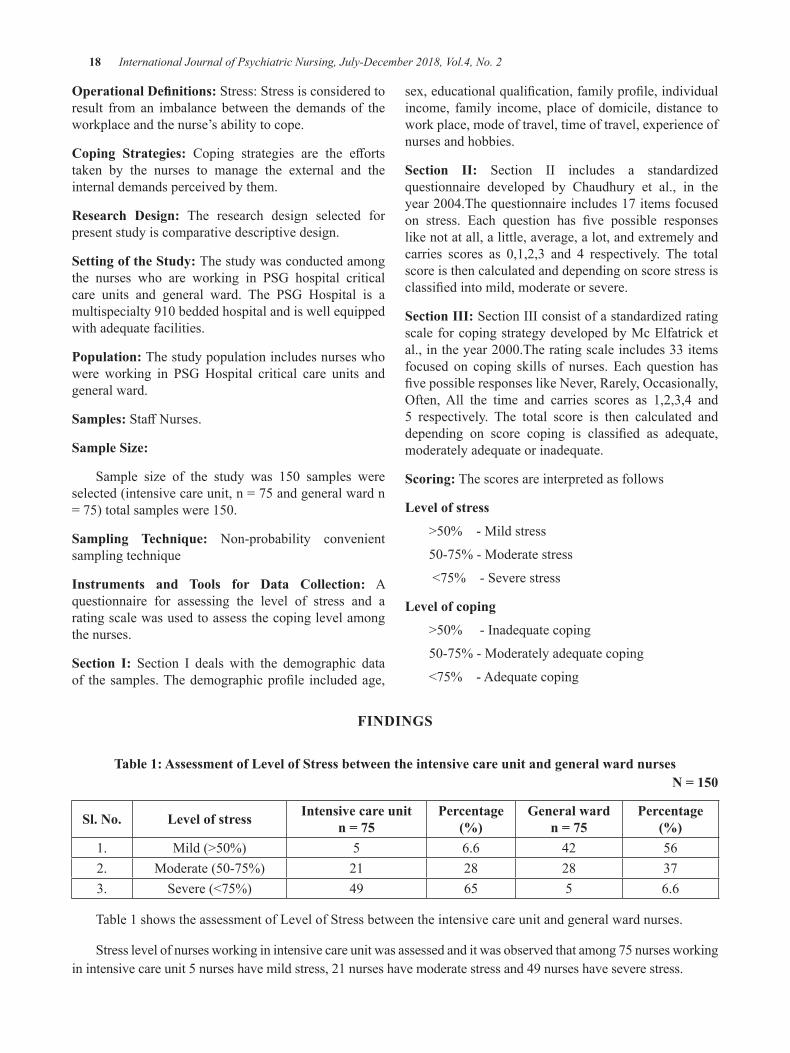
Section II: Section II includes a standardizedquestionnaire developed by Chaudhury et al., in theyear2004.Thequestionnaireincludes17itemsfocusedon stress. Each question has five possible responseslikenotatall,alittle,average,alot,andextremelyandcarries scores as 0,1,2,3 and 4 respectively. The totalscoreisthencalculatedanddependingonscorestressisclassifiedintomild,moderateorsevere.
Section III:SectionIIIconsistofastandardizedratingscaleforcopingstrategydevelopedbyMcElfatricketal.,intheyear2000.Theratingscaleincludes33itemsfocused on coping skills of nurses. Each question hasfivepossibleresponseslikeNever,Rarely,Occasionally,Often,All the time and carries scores as 1,2,3,4 and5 respectively. The total score is then calculated anddepending on score coping is classified as adequate,moderatelyadequateorinadequate.
Scoring:Thescoresareinterpretedasfollows
Level of stress
>50%-Mildstress
50-75%-Moderatestress
<75%-Severestress
Level of coping
>50%-Inadequatecoping
50-75%-Moderatelyadequatecoping
<75%-Adequatecoping
FInDIngS
Table 1: Assessment of Level of Stress between the intensive care unit and general ward nursesn = 150
Sl. no. Level of stress Intensive care unitn = 75
Percentage (%)
general wardn = 75
Percentage(%)
1. Mild(>50%) 5 6.6 42 562. Moderate(50-75%) 21 28 28 373. Severe(<75%) 49 65 5 6.6
Table1showstheassessmentofLevelofStressbetweentheintensivecareunitandgeneralwardnurses.
Stresslevelofnursesworkinginintensivecareunitwasassessedanditwasobservedthatamong75nursesworkinginintensivecareunit5nurseshavemildstress,21nurseshavemoderatestressand49nurseshaveseverestress.
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 19
Stresslevelofnursesworkingingeneralwardwasassessedanditwasobservedthatamong75nursesworkingingeneralward2nurseshavemildstress,28nurseshavemoderatestressand5nurseshaveseverestress.
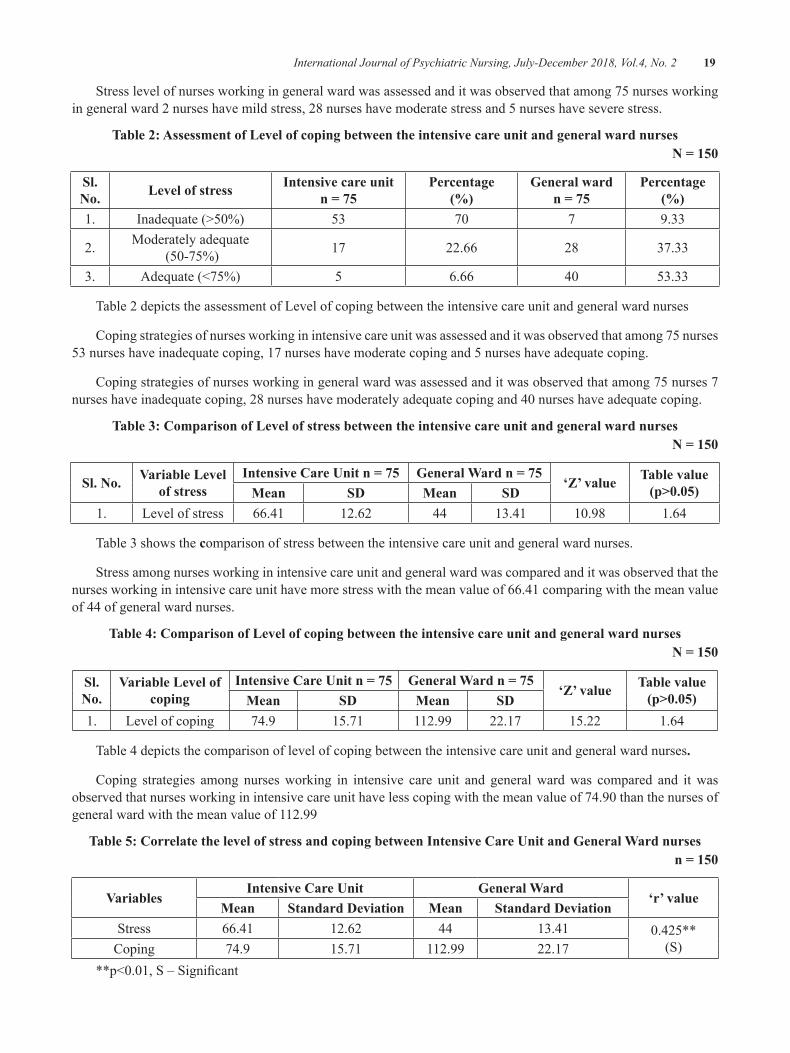
Table 2: Assessment of Level of coping between the intensive care unit and general ward nursesn = 150
Sl. no. Level of stress Intensive care unit
n = 75Percentage
(%)general ward
n = 75Percentage
(%)1. Inadequate(>50%) 53 70 7 9.33
2. Moderatelyadequate(50-75%) 17 22.66 28 37.33
3. Adequate(<75%) 5 6.66 40 53.33
Table2depictstheassessmentofLevelofcopingbetweentheintensivecareunitandgeneralwardnurses
Copingstrategiesofnursesworkinginintensivecareunitwasassessedanditwasobservedthatamong75nurses53nurseshaveinadequatecoping,17nurseshavemoderatecopingand5nurseshaveadequatecoping.
Copingstrategiesofnursesworkingingeneralwardwasassessedanditwasobservedthatamong75nurses7nurseshaveinadequatecoping,28nurseshavemoderatelyadequatecopingand40nurseshaveadequatecoping.
Table 3: Comparison of Level of stress between the intensive care unit and general ward nursesn = 150
Sl. no. Variable Level of stress
Intensive Care unit n = 75 general Ward n = 75‘Z’ value Table value
(p>0.05)Mean SD Mean SD1. Levelofstress 66.41 12.62 44 13.41 10.98 1.64
Table3showsthe comparisonof stressbetweentheintensivecareunitandgeneralwardnurses.
Stressamongnursesworkinginintensivecareunitandgeneralwardwascomparedanditwasobservedthatthenursesworkinginintensivecareunithavemorestresswiththemeanvalueof66.41comparingwiththemeanvalueof44ofgeneralwardnurses.
Table 4: Comparison of Level of coping between the intensive care unit and general ward nursesn = 150
Sl. no.
Variable Level of coping
Intensive Care unit n = 75 general Ward n = 75‘Z’ value Table value
(p>0.05)Mean SD Mean SD1. Levelofcoping 74.9 15.71 112.99 22.17 15.22 1.64
Table4depictsthecomparisonoflevelof copingbetweentheintensivecareunitandgeneralwardnurses.
Coping strategies among nursesworking in intensive care unit and generalwardwas compared and itwasobservedthatnursesworkinginintensivecareunithavelesscopingwiththemeanvalueof74.90thanthenursesofgeneralwardwiththemeanvalueof112.99
Table 5: Correlate the level of stress and coping between Intensive Care unit and general Ward nursesn = 150
VariablesIntensive Care unit general Ward
‘r’ valueMean Standard Deviation Mean Standard Deviation
Stress 66.41 12.62 44 13.41 0.425**(S)Coping 74.9 15.71 112.99 22.17
**p<0.01,S–Significant

20 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
Table 5 reveals the correlation the level of stressandcopingbetweenintensivecareunitandgeneralwardnurses.
Themeansscoreofintensivecareunitnurseslevelof stresswas66.41withthestandarddeviationof12.62and the mean score of GeneralWard nurses level of stresswas44withthestandarddeviationof33.41.Themeansscoreofintensivecareunitnurseslevelof copingwas74.9with the standarddeviationof15.71and themean score of General Ward nurses level of stresswas112.99with thestandarddeviationof22.17. Thecorrelation coefficient ‘r’ = 0.425 revealed that, therewasamoderatelevelofsignificanceatp<0.01level.
DISCuSSIon
AssessmentofStressofNursesWorkinginIntensiveCareUnit itwasobservedthatmajorityofnurses(49)among75nursesworkinginICUisexperiencingseverestressandonly5nursesreportedmildstress.Asimilarstudywhichhasbeenconductedtoidentifythestressofintensivecareunitnursesshowedthat50%ofthenurseshavesevereformofstressintheworkenvironment.7
AssessmentofStressofNursesWorkingInGeneralWarditwasobservedthatstresslevelwascomparativelyless.Among 75 nurses 42 nurses had mild stress, 28nurseshadmoderatestressand5nurseshadseverestress.Thisfindingwassupportedbyanotherstudyconductedamonggeneralwardnursessayingthat thestresslevelwillbelessfornursesworkingingeneralwards.8
Comparison of Stress among Nurses Working InIntensiveCareUnitandGeneralWarditwasobservedthatthenursesworkinginintensivecareunithavemorestresswiththemeanvalueof66.41comparingwiththegeneralwardnursesmeanstressvalueof44.AsimilarstudyhasbeenconductedtocomparethestresslevelofnursesworkinginICUandgeneralwardandithasbeenfound that the intensive care unit nurses experiencesmorestressthangeneralwardnurses.9
IMPLICATIonS
nursing practice: Thelevelofstressassessmentcanbedonefornursesandpropermanagementcanbegiven,whichcanimprovetheirpotencytoperformwell.
Recommendations: Periodic stress assessment shouldbe done for the nurses and necessary managementmeasureslikeregularrelaxationclassescanbearranged.
ConCLuSIon
Stressofnursesworkinginhospitalsisaworldwideproblem.Thisstudyhasbeendonetofindthestressandcopinglevelofthenursesinintensivecareunitandingeneralward,and itwasfoundthatmostof intensivecare unit nurses hasmore stress comparing to generalwardnursesandproperinterventionisneededtoreducethestresslevel.
Acknowledgement: The study was conducted in theintensive care unit, intensivemedical care unit, cardiaccareunit,neuro intensivecareunit,paediatric intensivecareunitandneonatalintensivecareunit,PSGhospitals,CoimbatoreaftergettingtheethicalclearanceandformalpermissionfromthedeanandtheNursingSuperintendentof PSG hospitals. PSG IMS&R Institutional HumanEthics Committee for their constant support andencouragement. This dissertation is submitted to TheTamilNadudr.M.G.R.MedicalUniversity,Chennai, inpartial fulfillment for the requirement of the degree ofMasterofScienceinNursing.
Conflict of Interest:Nil
Source of Funding:Selffunded.
REFEREnCES
1.Afecto PC. (2009). Evaluation of occupationalstressandburnoutinnursesofanintensivecareunit.Brazilianjournalofnursing,8(1)Pp76-85.
2.Mojoynola.J.K. (2008).Effect of job stress onhealth personal andwork behavior of nurses inpublichospital.Ethno–Med,2(2)Pp143–148.
3.Aone.(2002). Stress and burnout of nurses.Americanjournalofpsychology,53(3)Pp43-46.
4.GraceMariaJoseph.2016.ComparetheLevelofStressandCopingStrategiesAdoptedbytheStaffNursesWorkinginVariousPatientCareSettings.International Journal of Innovative Research &development.Vol5Issue7.
5.Ruchi Saini, Sukhpal Kaur, Karobi das.2016.Stress,StressReactions,JobStressorsandCopingamongNursesWorking in IntensiveCareUnitsandGeneralWards of aTertiaryCareHospital:A Comparative Study. Journal of PostgraduateMedicine, Education and Research, January-March2016;50(1):9-17

International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 21
6.Rami Masa’deh1. Perceived Stress in Nurses:AComparative Study.Global Journal ofHealthScience;Vol.9,No.6;2017
7.Saritha.,(2011).Astudytoassesstheoccupationalstress among nurses working in intensive careunitsatselectedhospitals,M.ScNursingThesis,royalcollegeofnursing,Bangalore,SubmittedtotheKarnatakaRajivGandhiuniversityandhealthsciences,Bangalore.
8.Jomonjoy.,(2008).Acomparativestudytoassessthestressandcopingstrategiesofnurseswhoareworking in general wards and in intensive care
unit in selected hospitals,M.ScNursingThesis,Akshaya college of nursing,Tumkur, Submittedto the Karnataka Rajiv Gandhi university andhealthsciences,Bangalore.
9.Jincy Antony., (2006). A study to assess theeffectiveness of self instructional module onknowledgeregardingburn-outanditspreventionamong staff nurses working in intensive careunitsatselectedhospitals,M.ScNursingThesis,Acharyacollegeofnursing,Bangalore,Submittedto the Karnataka Rajiv Gandhi university andhealthsciences,Bangalore.

Effectiveness of Video Teaching Programme on Self-Help Techniques of osteoarthritis among Elderly in Selected old
Age Homes, Coimbatore
M. D. Anuratha
Professor cum Nursing Superintendent, PSG Hospital, Coimbatore
AbSTRACT
Introduction:Osteoarthritisisadiseaseinwhichthecartilagewhichactsasacushioninbetweenbonesinjointsbeginstooverstress,resultinginswellingandpaininjointswhichaffectsnegatively.Itcouldbealsocalledasdegenerativearthritisordegenerativejointdisease.
objectives:AssesstheeffectivenessofvideoteachingprogrammeonSelf-HelptechniquesofOsteoarthritisamongElderlyforimprovingtheirknowledgeandpractice.
Design: Quasiexperimentaltimeseriesdesign
Setting:Oldagehomes,Coimbatore
Participants:272osteoarthritisclients.
Measurements and tools: Osteoarthritis identification tool, ModifiedWOMAC Index tool, structuredinterview schedule, observational checklist and video teaching programme on self-help techniques ofOsteoarthritis.BothdescriptiveandInferentialstatisticswereused.
Findings:distributionofosteoarthritisclientsaccordingtotheirseveritylevelofosteoarthritisshowsthat,inpre-test,97percentageofclientshadseverelevelofosteoarthritis,inposttest74percentageofclientsinmild level of severity through fully adaptation of self-help technique. Significant association formedbetweentheknowledgeandpracticeofOAclientswhencomparedtothedemographicvariables.differencebetweenthepreandpost-testknowledgeandpracticeofself-helptechniquesofosteoarthritisshowshighlysignificantdifference.KarlPearson’sco-relationco-efficientanalysisbetweenknowledgeandpracticescoreof thepost-test shows significantpositive relationship (r=0.882).Paired‘t’ testwascalculatedtoanalyzetheseverityofosteoarthritis,showsthatinpreandpost-testtherewasasignificantdifferenceinWOMACindex.difference inseverityofosteoarthritis inpreandpostassessmentbyusingonewayrepeatedmeasureANOVAshowstherewasasignificantimprovementintheobservationofreductioninseverityofosteoarthritis.
Conclusion:After implementationofvideo teachingprogrammeonself-help techniqueofosteoarthritisshowstheclientshadexcellentknowledgeandfullyadoptivepracticeofself-caremanagementaswellasreducedtheseverityofosteoarthritisgraduallyandsignificantly.
Keywords: Video teaching programme, Osteoarthritis, Elderly, Self-help techniques
InTRoDuCTIon
Osteoarthritisisacommondisorderoccurringinallpopulation,andoverallprevalenceisthesameinmenandwomen.Itisseenthatthereisamorerapidagerelatedincrease in theprevalenceofgeneralizedosteoarthritisinwomenmorethanmen.Bytheage40,90percentageof all persons can have such changes in their weight
bearing joints, thoughclinical symptomsaregenerallyabsent.Underageof45years,prevalencewasgreateramongmen,whereasaftertheageof55prevalencewasmoreinwomenthaninmen.Moderatetoseveregradesofosteoarthritiswas seen to a larger extent inwomencomparedtomen.Obesityhasacloseassociationwithdevelopmentofkneeosteoarthritis.1
DOI Number: 10.5958/2395-180X.2018.00011.7
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 23
InU.S.therearearound20millionofpeoplewitharthritis,whichmaygrowupto40millionby2020.2
Thereisaremarkableincreaseinthenumberoftheold age population. In India, 5.3 percentage of malesand4.8percentageoffemalewereagedwhoaremorethan65years.Theproportionatepercentageofoldagepeopleindevelopingcountriesislessbutindevelopedcountriestheabsolutenumberishigh.3
demographic changes in India estimated that thepopulationofpersonabove60yearswasaround76.62million in 2001, which can rise up to 179million by2031.dependencyratioin1991wasaround12.26anditmayriseupto14.12by2016andtherewerearound1,50,000centenariansinIndiain1991whichwillgrowtonearly2,00,000by2016.4
Themajorrelationshipbetweendietandarthritisisweight.Excessofbodyweightdoesnotholdgoodforjointhealth.Losingsomebodyweighthelpsinreducingthe strain of knees, hips, feet and lower back, thusimproving overall physical health andmobility.Manyresearchers have also shown that in combinationwithregularexercise,weight losshelps in reducingpain injointandstiffnessrelatedtoosteoarthritis.Otherseriousmedical conditions are commonly seen in peoplewhoareobese.So,reducingexcessweightnotonlyhelpstomanagebutpreventthisdiseaseconditions.5
Theosteoarthritisusuallyaffectstheknee,hipandhand. Osteoarthritis becomes more common with ageafter50yearsandwomenareaffectedmorethanmen.Alsosaidthattheageandsex-standardisedincidenceofosteoarthritisof thehand is100per1,00,000personsperyear,forthehipis88per1,00,000personsperyear,andthatofkneeis240per1,00,000personsperyear.6
OBJECTIVES
1.ToidentifytheclientsaffectedwithOsteoarthritisamongelderly.
2.To assess the self-care among elderly withOsteoarthritis.
3.ToimplementtheVideoTeachingProgrammetoclientswithosteoarthritisonSelf-HelpTechniquesofOsteoarthritis
4.To assess the effectiveness of Video TeachingProgramme on Self-Help Techniques ofOsteoarthritis.
5.Toassociatetheself-careknowledgeandpracticewith demographic variables of clients withosteoarthritis.
6.To compare the self-care practice in relation toknowledgeoftheclientswithosteoarthritis.
HyPoTHESIS
H1:There is a significant association betweenpre-testself-care knowledge anddemographic variables of theclientswithosteoarthritis.
H2:There is a significant association betweenpre-testself-care practice and demographic variables of theclientswithosteoarthritis.
H3:Thereisasignificantdifferencebetweenpreandpost-testself-careknowledgeofclientswithosteoarthritis.
H4: There is a significant difference between pre andpost-testself-carepracticeofclientswithosteoarthritis.
H5: There is a significant relation between the post-test self-care knowledge and practice of clients withosteoarthritis.
H6:ThereisasignificantdifferencebetweenthepreandpostassessmentonseverityofOsteoarthritis.
Theoritical Framework:Theoreticalframeworkchosenandmodifiedforthisstudy,wasGeneralSystem’stheorybyAlabwigVonBertanlanffy(2010).7
MATERIAL AnD METHoD
Quasiexperimentaltimeseriesdesignwasadoptedforthisstudy.
Experimental group:O1 X O2 X O3 X O4
The sample size was 272 osteoarthritis clientsfromold age homes,Coimbatore. Purposive samplingtechniquewasadoptedinthisstudy.Clientsmorethan50yearsofageandofboththesexeswereincludedforthestudy.Thetoolusedfordatacollectionwereosteoarthritisidentification tool, modified WOMAC Index tool toassesstheseverityofosteoarthritis,structuredinterviewschedule in tamil toassess theself-careknowledgeonosteoarthritis,observationalchecklisttoassesstheself-careabilitiesandvideoteachingprogrammeonself-helptechniquesofOsteoarthritis.
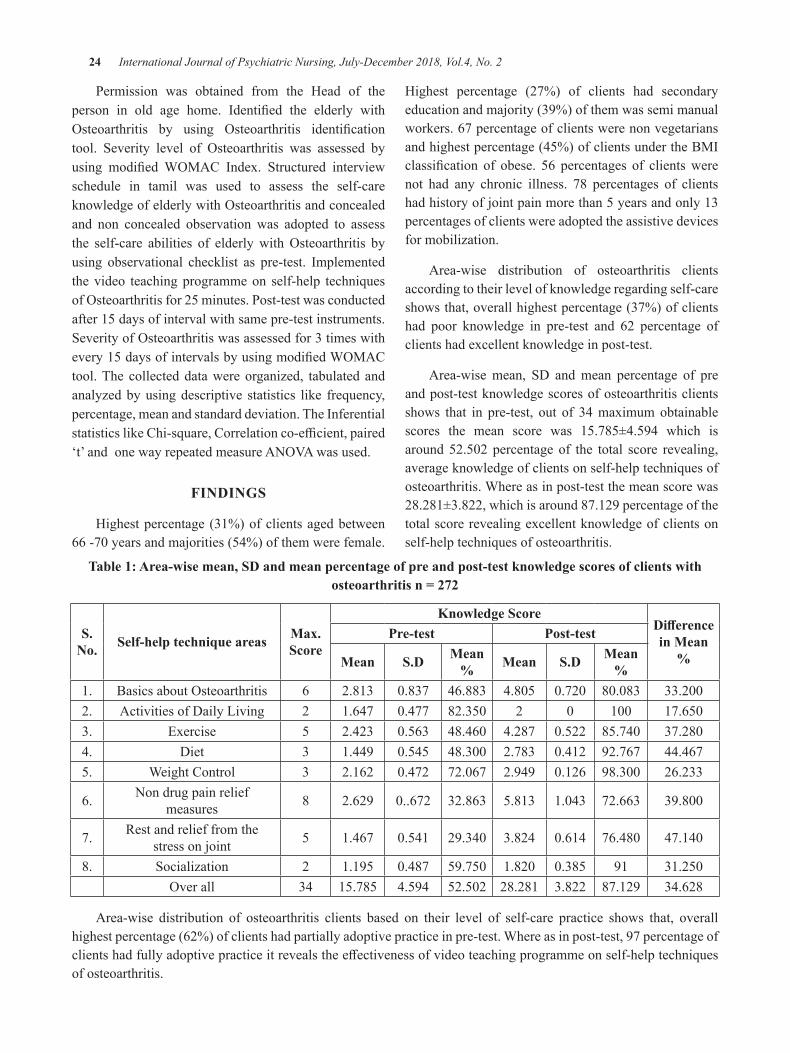
24 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
Permission was obtained from the Head of theperson in old age home. Identified the elderly withOsteoarthritis by using Osteoarthritis identificationtool. Severity level of Osteoarthritis was assessed byusing modifiedWOMAC Index. Structured interviewschedule in tamil was used to assess the self-careknowledgeofelderlywithOsteoarthritisandconcealedand non concealed observationwas adopted to assessthe self-care abilities of elderlywithOsteoarthritis byusing observational checklist as pre-test. Implementedthevideo teachingprogrammeon self-help techniquesofOsteoarthritisfor25minutes.Post-testwasconductedafter15daysofintervalwithsamepre-testinstruments.SeverityofOsteoarthritiswasassessedfor3timeswithevery15daysofintervalsbyusingmodifiedWOMACtool.Thecollecteddatawereorganized, tabulatedandanalyzedbyusingdescriptive statistics like frequency,percentage,meanandstandarddeviation.TheInferentialstatisticslikeChi-square,Correlationco-efficient,paired‘t’andonewayrepeatedmeasureANOVAwasused.
FInDIngS
Highestpercentage(31%)ofclientsagedbetween66-70yearsandmajorities(54%)ofthemwerefemale.
Highest percentage (27%) of clients had secondaryeducationandmajority(39%)ofthemwassemimanualworkers.67percentageofclientswerenonvegetariansandhighestpercentage(45%)ofclientsundertheBMIclassification of obese. 56 percentages of clientswerenot had any chronic illness. 78 percentages of clientshadhistoryofjointpainmorethan5yearsandonly13percentagesofclientswereadoptedtheassistivedevicesformobilization.
Area-wise distribution of osteoarthritis clientsaccordingtotheirlevelofknowledgeregardingself-careshowsthat,overallhighestpercentage(37%)ofclientshad poor knowledge in pre-test and 62 percentage ofclientshadexcellentknowledgeinpost-test.
Area-wisemean, Sd andmean percentage of preandpost-testknowledgescoresofosteoarthritisclientsshows that in pre-test, out of 34maximumobtainablescores the mean score was 15.785±4.594 which isaround52.502 percentage of the total score revealing,averageknowledgeofclientsonself-helptechniquesofosteoarthritis.Whereasinpost-testthemeanscorewas28.281±3.822,whichisaround87.129percentageofthetotalscorerevealingexcellentknowledgeofclientsonself-helptechniquesofosteoarthritis.
Table 1: Area-wise mean, SD and mean percentage of pre and post-test knowledge scores of clients with osteoarthritis n = 272
S. no. Self-help technique areas Max.
Score
Knowledge ScoreDifference in Mean
%
Pre-test Post-test
Mean S.D Mean % Mean S.D Mean
%1. BasicsaboutOsteoarthritis 6 2.813 0.837 46.883 4.805 0.720 80.083 33.2002. ActivitiesofdailyLiving 2 1.647 0.477 82.350 2 0 100 17.6503. Exercise 5 2.423 0.563 48.460 4.287 0.522 85.740 37.2804. diet 3 1.449 0.545 48.300 2.783 0.412 92.767 44.4675. WeightControl 3 2.162 0.472 72.067 2.949 0.126 98.300 26.233
6. Nondrugpainreliefmeasures 8 2.629 0..672 32.863 5.813 1.043 72.663 39.800
7. Restandrelieffromthestressonjoint 5 1.467 0.541 29.340 3.824 0.614 76.480 47.140
8. Socialization 2 1.195 0.487 59.750 1.820 0.385 91 31.250Overall 34 15.785 4.594 52.502 28.281 3.822 87.129 34.628
Area-wise distribution of osteoarthritis clients based on their level of self-care practice shows that, overallhighestpercentage(62%)ofclientshadpartiallyadoptivepracticeinpre-test.Whereasinpost-test,97percentageofclientshadfullyadoptivepracticeitrevealstheeffectivenessofvideoteachingprogrammeonself-helptechniquesofosteoarthritis.
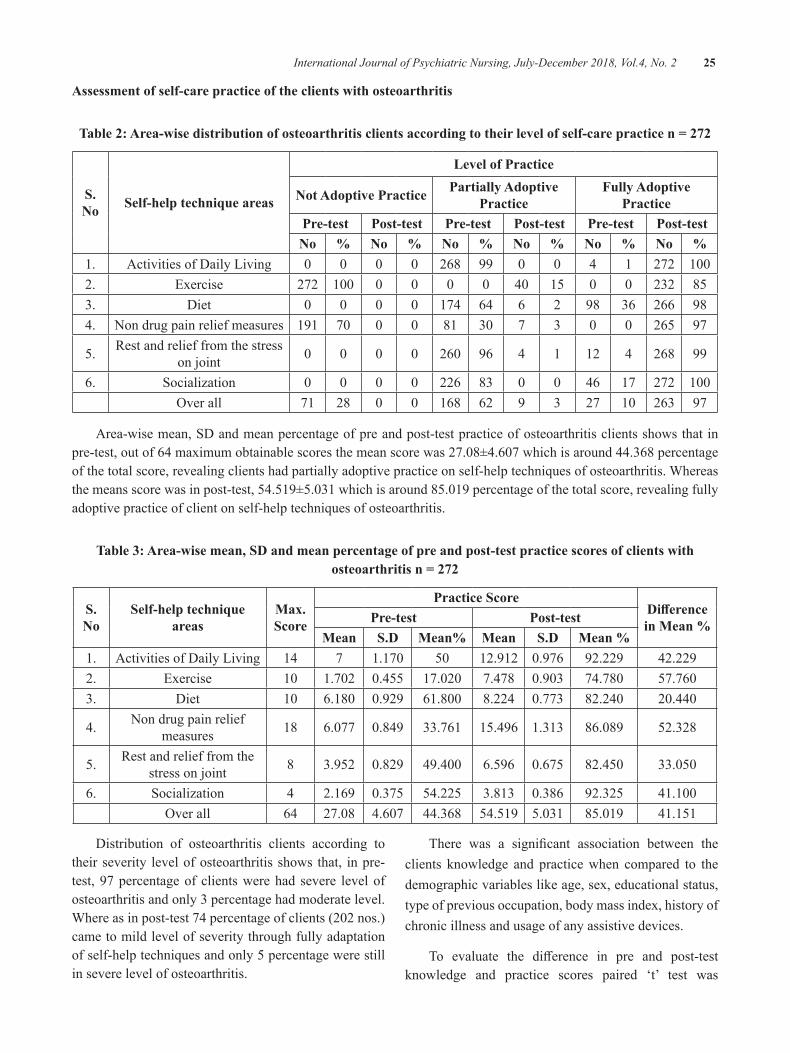
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 25
Assessment of self-care practice of the clients with osteoarthritis
Table 2: Area-wise distribution of osteoarthritis clients according to their level of self-care practice n = 272
S. No Self-help technique areas
Level of Practice
not Adoptive Practice Partially Adoptive Practice
Fully Adoptive Practice
Pre-test Post-test Pre-test Post-test Pre-test Post-testNo % No % No % No % No % No %
1. ActivitiesofdailyLiving 0 0 0 0 268 99 0 0 4 1 272 1002. Exercise 272 100 0 0 0 0 40 15 0 0 232 853. diet 0 0 0 0 174 64 6 2 98 36 266 984. Nondrugpainreliefmeasures 191 70 0 0 81 30 7 3 0 0 265 97
5. Restandrelieffromthestressonjoint 0 0 0 0 260 96 4 1 12 4 268 99
6. Socialization 0 0 0 0 226 83 0 0 46 17 272 100Overall 71 28 0 0 168 62 9 3 27 10 263 97
Area-wisemean,Sdandmeanpercentageofpreandpost-testpracticeofosteoarthritisclientsshowsthatinpre-test,outof64maximumobtainablescoresthemeanscorewas27.08±4.607whichisaround44.368percentageofthetotalscore,revealingclientshadpartiallyadoptivepracticeonself-helptechniquesofosteoarthritis.Whereasthemeansscorewasinpost-test,54.519±5.031whichisaround85.019percentageofthetotalscore,revealingfullyadoptivepracticeofclientonself-helptechniquesofosteoarthritis.
Table 3: Area-wise mean, SD and mean percentage of pre and post-test practice scores of clients with osteoarthritis n = 272
S. No
Self-help technique areas
Max. Score
Practice ScoreDifference in Mean %Pre-test Post-test
Mean S.D Mean% Mean S.D Mean %1. ActivitiesofdailyLiving 14 7 1.170 50 12.912 0.976 92.229 42.2292. Exercise 10 1.702 0.455 17.020 7.478 0.903 74.780 57.7603. diet 10 6.180 0.929 61.800 8.224 0.773 82.240 20.440
4. Nondrugpainreliefmeasures 18 6.077 0.849 33.761 15.496 1.313 86.089 52.328
5. Restandrelieffromthestressonjoint 8 3.952 0.829 49.400 6.596 0.675 82.450 33.050
6. Socialization 4 2.169 0.375 54.225 3.813 0.386 92.325 41.100Overall 64 27.08 4.607 44.368 54.519 5.031 85.019 41.151
distribution of osteoarthritis clients according totheirseverity levelofosteoarthritisshows that, inpre-test, 97percentageof clientswerehad severe levelofosteoarthritisandonly3percentagehadmoderatelevel.Whereasinpost-test74percentageofclients(202nos.)cametomildlevelofseveritythroughfullyadaptationofself-helptechniquesandonly5percentagewerestillinseverelevelofosteoarthritis.
There was a significant association between theclients knowledge and practicewhen compared to thedemographicvariableslikeage,sex,educationalstatus,typeofpreviousoccupation,bodymassindex,historyofchronicillnessandusageofanyassistivedevices.
To evaluate the difference in pre and post-testknowledge and practice scores paired ‘t’ test was
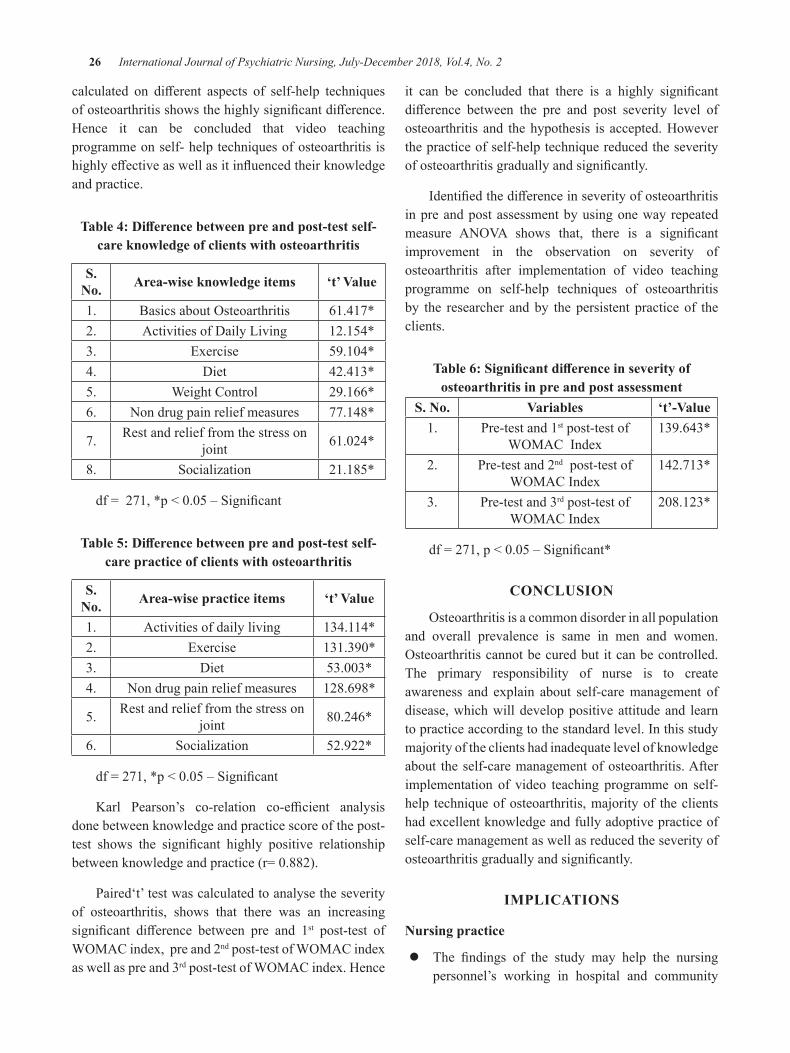
26 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
calculated on different aspects of self-help techniquesofosteoarthritisshowsthehighlysignificantdifference.Hence it can be concluded that video teachingprogrammeonself-helptechniquesofosteoarthritisishighlyeffectiveaswellasitinfluencedtheirknowledgeandpractice.
Table 4: Difference between pre and post-test self-care knowledge of clients with osteoarthritis
S. no. Area-wise knowledge items ‘t’ Value
1. BasicsaboutOsteoarthritis 61.417*2. ActivitiesofdailyLiving 12.154*3. Exercise 59.104*4. diet 42.413*5. WeightControl 29.166*6. Nondrugpainreliefmeasures 77.148*
7. Restandrelieffromthestressonjoint 61.024*
8. Socialization 21.185*
df=271,*p<0.05–Significant
Table 5: Difference between pre and post-test self-care practice of clients with osteoarthritis
S. no. Area-wise practice items ‘t’ Value
1. Activitiesofdailyliving 134.114*2. Exercise 131.390*3. diet 53.003*4. Nondrugpainreliefmeasures 128.698*
5. Restandrelieffromthestressonjoint 80.246*
6. Socialization 52.922*
df=271,*p<0.05–Significant
Karl Pearson’s co-relation co-efficient analysisdonebetweenknowledgeandpracticescoreofthepost-test shows the significant highly positive relationshipbetweenknowledgeandpractice(r=0.882).
Paired‘t’testwascalculatedtoanalysetheseverityof osteoarthritis, shows that there was an increasingsignificant difference between pre and 1st post-test ofWOMACindex,preand2ndpost-testofWOMACindexaswellaspreand3rdpost-testofWOMACindex.Hence
it can be concluded that there is a highly significantdifference between the pre and post severity level ofosteoarthritis and thehypothesis is accepted.Howeverthepracticeofself-helptechniquereducedtheseverityofosteoarthritisgraduallyandsignificantly.
Identifiedthedifferenceinseverityofosteoarthritisinpreandpostassessmentbyusingonewayrepeatedmeasure ANOVA shows that, there is a significantimprovement in the observation on severity ofosteoarthritis after implementation of video teachingprogramme on self-help techniques of osteoarthritisby the researcher andby the persistent practice of theclients.
Table 6: Significant difference in severity of osteoarthritis in pre and post assessment
S. no. Variables ‘t’-Value1. Pre-testand1stpost-testof
WOMACIndex139.643*
2. Pre-testand2ndpost-testofWOMACIndex
142.713*
3. Pre-testand3rdpost-testofWOMACIndex
208.123*
df=271,p<0.05–Significant*
ConCLuSIon
Osteoarthritisisacommondisorderinallpopulationand overall prevalence is same in men and women.Osteoarthritiscannotbecuredbutitcanbecontrolled.The primary responsibility of nurse is to createawareness and explain about self-caremanagement ofdisease,whichwilldeveloppositiveattitudeand learntopracticeaccordingtothestandardlevel.Inthisstudymajorityoftheclientshadinadequatelevelofknowledgeabout theself-caremanagementofosteoarthritis.Afterimplementation of video teaching programme on self-help techniqueofosteoarthritis,majorityof theclientshadexcellentknowledgeandfullyadoptivepracticeofself-caremanagementaswellasreducedtheseverityofosteoarthritisgraduallyandsignificantly.
IMPLICATIonS
nursing practice
z The findings of the study may help the nursingpersonnel’s working in hospital and community
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 27
knowing about the self-help techniques ofOsteoarthritis and helps in planning andimplementationofhealthteaching.
z Nursesneedtoupdatetheirknowledgeonvarioustreatmentoptionsavailableforosteoarthritistocaretheosteoarthritisclientseffectively.
z Nursesneedtofocusonthepreventionofobesitythroughweightcontrolespeciallythosewithkneeosteoarthritis could be benefitted from weightreduction.
nursing Research: Thisstudyhelpsthenurseresearcherstodevelopinsightintothedevelopmentofinterventionmodule for osteoarthritis clients towards promotionofquality of life and prevention of osteoarthritis relatedproblems.
Recommendations
z Acomparativestudyonpharmacologicalandnonpharmacologicalpainmanagementofosteoarthritiscanbestudied.
z Astudycanbeundertakeninhospitalsettings.
z Longitudinal study can be undertaken foridentifyingtheassociatefactorsofosteoarthritis.
z A comparative study can be conducted betweenclientswithosteoarthritisandrheumatoidarthritisabouttheeffectivenessofself-helptechnique.
Conflict of Interest:Nil
Source of Funding:SelfFunded
Ethical Clearance:EthicalclearancewasobtainedfromInstitutionalHumanEthicsCommitteeinPSGInstitute
of Medical Sciences and Research (PSG IMS&R),Coimbatore.
REFEREnCES
1.MdGolamNobi,AbulKalamAzad,BadrunnessaAhmed, Imamur Rashid, et.al., Effects ofActivitiesofdailyLiving(AdL)InstructionsonPatientwithOsteoarthritisoftheKnee.JournalofMedicine.2012;13(1).
2.ChristineGorman,AlicePark.TheageofArthritis.TheTIMEASIAJournal.2003,June,9;22:50.
3.Sharma.M.K,SwamiH.M,BhatiaV,VermaA,Bhatia SPS, Kaur G.An epidemiological studyof correlates of Osteo-Arthritis in GeriatricpopulationofUTChandigarh. Indian JounralofCommunity.2007,January-March;32(1):72-8.
4.Sundar Lal. Textbook pf CommunityMedicine,PreventiveandSocialMedicine.Noida.diamondAgencies,Pvt.Ltd.2ndedition.2010.pp.712-713
5.MohamedAhmed, NahidAli, Zia Ur Rahman,MisbahullahKhan.Astudyonprescribingpatternsinthemanagementofarthritisinthedepartmentoforthopaedics.derPharmaciaLettre. 2012;4(1):5-27.
6.JohannesWJBijlsma,FrancisBerenbaum,FlorisP J G Lafeber. Osteoarthritis: an update withrelevance for clinical practice. www.thelancet.com.2011,June18;377:2115–26
7.Karl Ludwig von Bertalanffy. General Systemtheory:Foundations,development,Applications,NewYork:GeorgeBraziller:1976.

Effectiveness of Video Teaching Programme on neonatal Care among Primigravida Mothers Admitted in urban Health
Maternity Centres, Coimbatore
M. D. Santhi
Professor cum HOD, Sri Gokulam College of Nursing, Salem
AbSTRACT
Introduction: Birthofahealthynewbornisoneofthefinestgiftsofnature.Theprocessofbirthtakesonlyafewhoursbutitisthemosthazardousperiodoflifesinceitisassociatedwithlargestnumberofdeathsascomparedtoanyotherphaseoflife.
objectives:assesstheeffectivenessofvideoteachingprogrammeonNeonatalcareamongPrimigravidamothersforimprovingknowledgeandpractice.
Design: Trueexperimentaldesignpreandpost-testcontrolgroupdesign
Setting:6urbanhealthmaternitycentres,Coimbatore.
Participants:266(147experimentalgroupand119controlgroup)primigravidamothersadoptedbySimplerandomsamplingtechnique.
Measurements and tools: Structured interview schedule, Observational checklist and video teachingprogrammeonneonatalcare.Bothdescriptiveandinferentialstatisticswereused.
Findings: Inexperimentalgroupthepre-testthemeanwas10.163±4.783,inpost-testitwas48.38±6.103,revealingexcellentknowledgeofmothersonthecomponentsofneonatalcare.Incontrolgrouppre-testmeanscorewas9.656±3.497whereasinpost-test,themeanscorewas9.656±3.825revealingverypoorknowledgeofprimigravidamothers. Inpracticeofneonatalcareshows that, inexperimentalgroup themeanscorewas56.412±3.272,revealingfullyadoptivepractice.Andincontrolgroup,themeanscorewas27.547±1.815,revealingmothershadpartiallyadoptivepractice.Therewashighlysignificantdifferenceinpost-testknowledgeandpracticescores.Positiverelationshipwasfoundbetweenknowledgeandpracticeofexperimentalgroupprimigravidamothers(r=0.79)andnosignificantrelationfoundbetweenknowledgeandpracticeofcontrolgroup(r=0.14).
Conclusion: Majorityoftheexperimentalandcontrolgroupmothershadinadequateknowledgeonneonatalcareinpre-test.Afterimplementationofvideoteachingprogrammeprimigravidamothersfromexperimentalgrouphadexcellentknowledgeandfullyadoptivepracticeofneonatalcare.
Keywords: Video teaching programme, Neonatal care, Primigravida mothers, Experimental and control group
InTRoDuCTIon
World’s one of the neglected health problem isneonatalmortality.Globally3.9millionneonataldeathsconstitute36percentageofunder-fivedeaths. In Indiaeveryyearnearly1.2millionneonataldeathsoccurred.Nearlyhalfoftheunderfivedeathsoccursinneonatalperiod. The World Health Organization guidelineson essential newborn care consists cleanliness,thermoregulation,earlysuctioning,earlybreastfeeding
initiationandexclusive,eyecare,immunization,minorillnessmanagement,andlowbirthweightneonatalcare.Andemphasizededucationtothemotherandherfamilyregardingpreparation,birthchoice,thermalcare,breastfeedingandpreparationofdangersigns.1
The under-5 child mortality rate in global showsdecreased continuously from 13.5 million in the year1980,to7.7to8.8millionin2008.Theneonataldeathsalsodecreasedfrom4.6millionintheyear1990to3.1
DOI Number: 10.5958/2395-180X.2018.00033.6
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 29
to3.6millionin2009.Whencomparingthesetwodatatheneonataldeathshaddeclinedonlyatalowerrate.2
Nearly1.2milliondieduringtheneonatalperiodoutof26millioninfants,beforecompleting4weeksoflife.Global under five including infantmortality rateswerereducedtopastfourdecades,whereasneonatalmortalityrateswasveryhighandremainsrelativelyunchanged.3
In 2008 Newborn Indicators Technical WorkingGroup (TWG)wasdevelopedby theSavingNewbornLives program at Save the Children to improve theindicators and arranging standard tools to measurethe newborn care interventions. The newborn careindicators likedrying,delayedbathing,umbilical cordcuttingwith sterile instruments, kangaroomother careandidentifyingtheevidencedbasedinterventions.4
In India among 26 million newborn babies, 1.2millionweredyingbeforecompletingtheirnewbornlifeeveryyear.ApproximatelyonefifthofIndianpopulationlives in slums,withhighermortality rate.According toSurvey Registration System 2009, India’s birth rate of22.22per1000populationandInfantmortalityratewas53per1000livebirths.Thehigherratesrecordedinslumand resettlement colonies. Therefore neonatal health tobeimposesamongpoorcommunities,whichisanationalpriority.Theinterventionsliketetanustoxoidvaccination,clean delivery, breast feeding, care of lowbirthweightbabiesandmanagingneonatalinfections.Thesemeasuresmayreducetheneonataldeathsupto72percentage.5
OBJECTIVES
1.To assess the level of knowledge on neonatalcare among experimental and control groupprimigravida mothers before implementation ofvideoteachingprogramme.
2.To implement the video teaching programmeon neonatal care among experimental groupprimigravidamothers.
3.To evaluate the effectiveness of video teachingprogrammeonneonatalcareamongprimigravidamothers.
4.To associate the post-test scores with selecteddemographicvariablesofbothexperimentalandcontrolgroupprimigravidamothers.
5.To correlate the post-test knowledge withpractice of both experimental and control groupprimigravidamothers.
HyPoTHESIS
H1:Thereisasignificantassociationbetweenpost-testknowledgeanddemographicvariablesofexperimentalandcontrolgroupprimigravidamothers
H2:Thereisasignificantassociationbetweenpost-testpracticeanddemographicvariablesofexperimentalandcontrolgroupprimigravidamothers.
H3: There is a significant difference between pre andpost-testknowledgeofexperimentalandcontrolgroupprimigravidamothersonneonatalcare.
H4: There is a significant difference between post-test knowledge of experimental and control groupprimigravidamothersonneonatalcare.
H5: There is a significant difference between post-test practiceof neonatal care amongexperimental andcontrolgroupprimigravidamothers.
H6: There is a significant relation between theknowledge and practice of experimental and controlgroupprimigravidamothersregardingneonatalcare.
Theoritical Framework:Theoreticalframeworkchosenandmodifiedforthisstudy,wasGeneralSystem’stheorybyAlabwigVonBertanlanffy(2010).6
MATERIAL AnD METHoD
Trueexperimentalpreandposttest-controlgroupresearchdesignwasadoptedforthisstudy.Random Exp group Pre-test Treatment Post-test
Assignment Cont group Pre-test Post-test
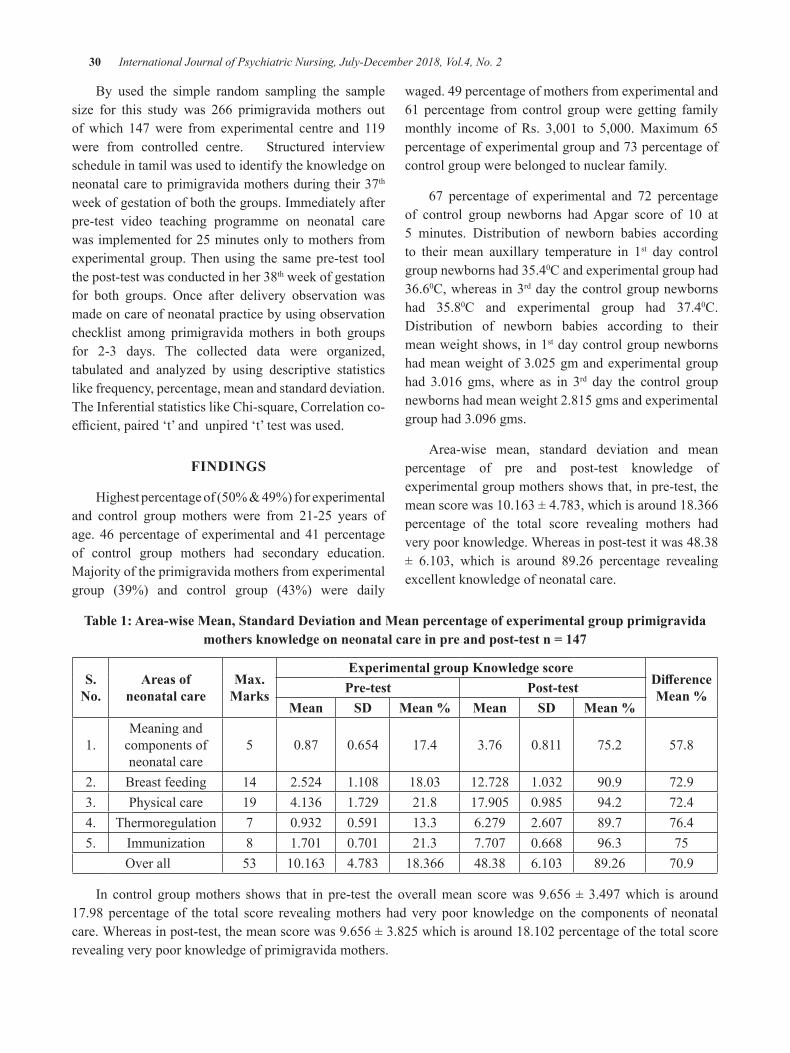
30 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
By used the simple random sampling the samplesize for this study was 266 primigravida mothers outofwhich 147were from experimental centre and 119were from controlled centre. Structured interviewscheduleintamilwasusedtoidentifytheknowledgeonneonatalcaretoprimigravidamothersduringtheir37th weekofgestationofboththegroups.Immediatelyafterpre-test video teaching programme on neonatal carewasimplementedfor25minutesonlytomothersfromexperimentalgroup.Thenusing the samepre-test toolthepost-testwasconductedinher38thweekofgestationfor both groups. Once after delivery observation wasmadeoncareofneonatalpracticebyusingobservationchecklist among primigravidamothers in both groupsfor 2-3 days. The collected data were organized,tabulated and analyzed by using descriptive statisticslikefrequency,percentage,meanandstandarddeviation.TheInferentialstatisticslikeChi-square,Correlationco-efficient,paired‘t’andunpired‘t’testwasused.
FInDIngS
Highestpercentageof(50%&49%)forexperimentaland control group mothers were from 21-25 years ofage. 46percentageof experimental and41percentageof control group mothers had secondary education.Majorityoftheprimigravidamothersfromexperimentalgroup (39%) and control group (43%) were daily
waged.49percentageofmothersfromexperimentaland61 percentage fromcontrol groupwere getting familymonthly income of Rs. 3,001 to 5,000.Maximum 65percentageofexperimentalgroupand73percentageofcontrolgroupwerebelongedtonuclearfamily.
67 percentage of experimental and 72 percentageof control group newborns hadApgar score of 10 at5 minutes. distribution of newborn babies accordingto their mean auxillary temperature in 1st day controlgroupnewbornshad35.40Candexperimentalgrouphad36.60C,whereasin3rddaythecontrolgroupnewbornshad 35.80C and experimental group had 37.40C.distribution of newborn babies according to theirmeanweightshows,in1stdaycontrolgroupnewbornshadmeanweightof3.025gmandexperimentalgrouphad 3.016 gms,where as in 3rd day the control groupnewbornshadmeanweight2.815gmsandexperimentalgrouphad3.096gms.
Area-wise mean, standard deviation and meanpercentage of pre and post-test knowledge ofexperimentalgroupmothersshowsthat,inpre-test,themeanscorewas10.163±4.783,whichisaround18.366percentage of the total score revealing mothers hadverypoorknowledge.Whereasinpost-testitwas48.38± 6.103, which is around 89.26 percentage revealingexcellentknowledgeofneonatalcare.
Table 1: Area-wise Mean, Standard Deviation and Mean percentage of experimental group primigravida mothers knowledge on neonatal care in pre and post-test n = 147
S. no.
Areas of neonatal care
Max. Marks
Experimental group Knowledge scoreDifference Mean %Pre-test Post-test
Mean SD Mean % Mean SD Mean %
1.Meaningandcomponentsofneonatalcare
5 0.87 0.654 17.4 3.76 0.811 75.2 57.8
2. Breastfeeding 14 2.524 1.108 18.03 12.728 1.032 90.9 72.93. Physicalcare 19 4.136 1.729 21.8 17.905 0.985 94.2 72.44. Thermoregulation 7 0.932 0.591 13.3 6.279 2.607 89.7 76.45. Immunization 8 1.701 0.701 21.3 7.707 0.668 96.3 75
Overall 53 10.163 4.783 18.366 48.38 6.103 89.26 70.9
In control groupmothers shows that in pre-test the overallmean scorewas 9.656±3.497which is around17.98 percentage of the total score revealingmothers had very poor knowledge on the components of neonatalcare.Whereasinpost-test,themeanscorewas9.656±3.825whichisaround18.102percentageofthetotalscorerevealingverypoorknowledgeofprimigravidamothers.
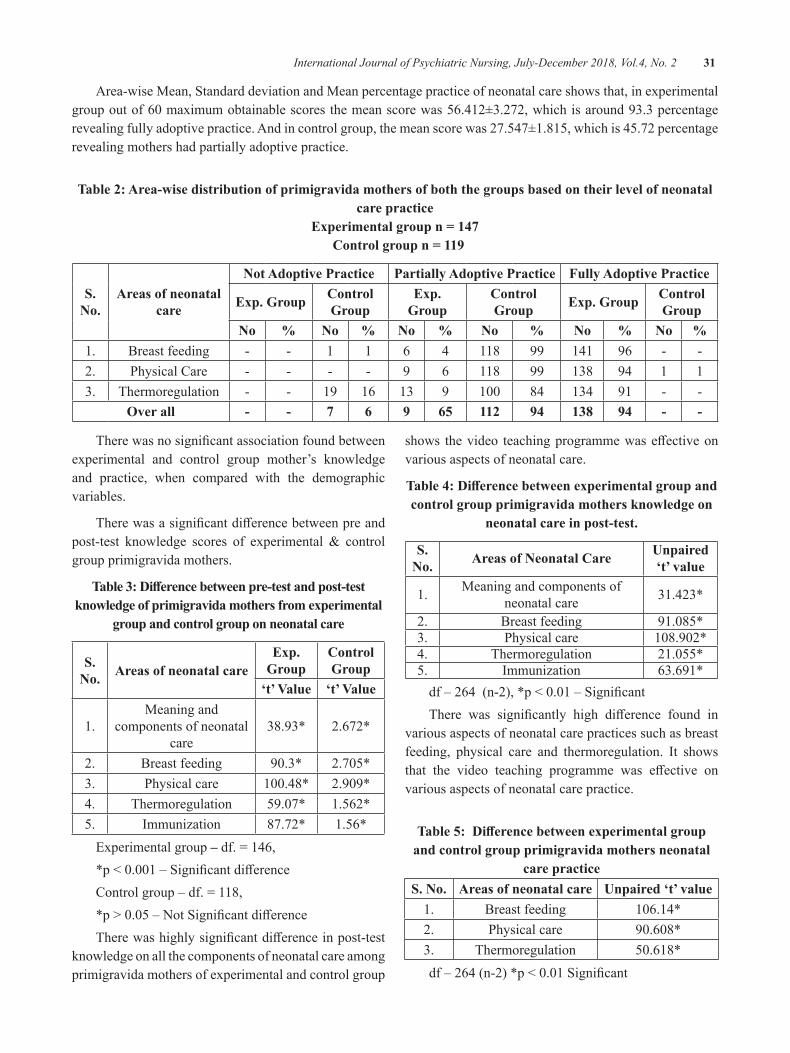
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 31
Area-wiseMean,StandarddeviationandMeanpercentagepracticeofneonatalcareshowsthat,inexperimentalgroupoutof60maximumobtainablescoresthemeanscorewas56.412±3.272,whichisaround93.3percentagerevealingfullyadoptivepractice.Andincontrolgroup,themeanscorewas27.547±1.815,whichis45.72percentagerevealingmothershadpartiallyadoptivepractice.
Table 2: Area-wise distribution of primigravida mothers of both the groups based on their level of neonatal care practice
Experimental group n = 147 Control group n = 119
S. no.
Areas of neonatal care
not Adoptive Practice Partially Adoptive Practice Fully Adoptive Practice
Exp. group Control group
Exp. group
Control group Exp. group Control
groupNo % No % No % No % No % No %
1. Breastfeeding - - 1 1 6 4 118 99 141 96 - -2. PhysicalCare - - - - 9 6 118 99 138 94 1 13. Thermoregulation - - 19 16 13 9 100 84 134 91 - -
over all - - 7 6 9 65 112 94 138 94 - -
Therewasnosignificantassociationfoundbetweenexperimental and control group mother’s knowledgeand practice, when compared with the demographicvariables.
Therewasasignificantdifferencebetweenpreandpost-test knowledge scores of experimental & controlgroupprimigravidamothers.
Table 3: Difference between pre-test and post-test knowledge of primigravida mothers from experimental
group and control group on neonatal care
S. no. Areas of neonatal care
Exp. group
Control group
‘t’ Value ‘t’ Value
1.Meaningand
componentsofneonatalcare
38.93* 2.672*
2. Breastfeeding 90.3* 2.705*3. Physicalcare 100.48* 2.909*4. Thermoregulation 59.07* 1.562*5. Immunization 87.72* 1.56*Experimentalgroup – df.=146,*p<0.001–SignificantdifferenceControlgroup–df.=118,*p>0.05–NotSignificantdifferenceTherewashighlysignificantdifferenceinpost-test
knowledgeonallthecomponentsofneonatalcareamongprimigravidamothersofexperimentalandcontrolgroup
shows thevideo teachingprogrammewaseffectiveonvariousaspectsofneonatalcare.
Table 4: Difference between experimental group and control group primigravida mothers knowledge on
neonatal care in post-test.
S. no. Areas of neonatal Care unpaired
‘t’ value
1. Meaningandcomponentsofneonatalcare 31.423*
2. Breastfeeding 91.085*3. Physicalcare 108.902*4. Thermoregulation 21.055*5. Immunization 63.691*df–264(n-2),*p<0.01–SignificantThere was significantly high difference found in
variousaspectsofneonatalcarepracticessuchasbreastfeeding, physical care and thermoregulation. It showsthat the video teaching programme was effective onvariousaspectsofneonatalcarepractice.
Table 5: Difference between experimental group and control group primigravida mothers neonatal
care practiceS. no. Areas of neonatal care unpaired ‘t’ value
1. Breastfeeding 106.14*2. Physicalcare 90.608*3. Thermoregulation 50.618*df–264(n-2)*p<0.01Significant
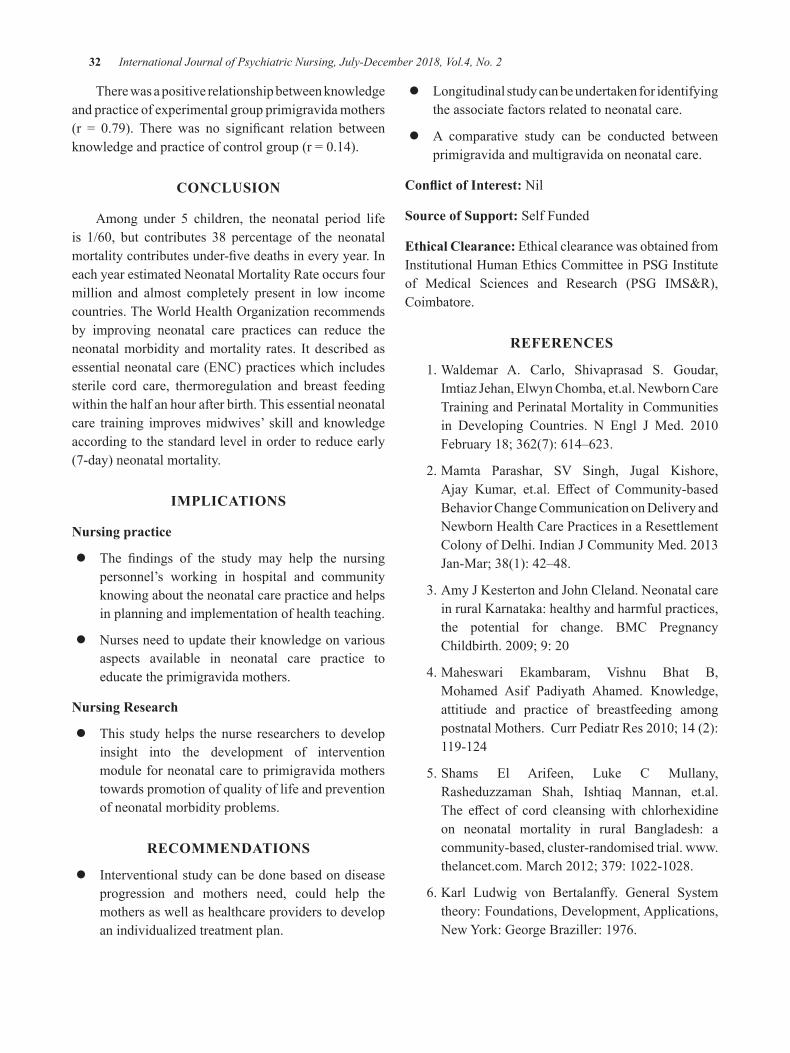
32 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
Therewasapositiverelationshipbetweenknowledgeandpracticeofexperimentalgroupprimigravidamothers(r = 0.79). There was no significant relation betweenknowledgeandpracticeofcontrolgroup(r=0.14).
ConCLuSIon
Among under 5 children, the neonatal period lifeis 1/60, but contributes 38 percentage of the neonatalmortalitycontributesunder-fivedeathsineveryyear.IneachyearestimatedNeonatalMortalityRateoccursfourmillion and almost completely present in low incomecountries.TheWorldHealthOrganizationrecommendsby improving neonatal care practices can reduce theneonatalmorbidity andmortality rates. It describedasessentialneonatalcare(ENC)practiceswhichincludessterile cord care, thermoregulation and breast feedingwithinthehalfanhourafterbirth.Thisessentialneonatalcare training improvesmidwives’ skill andknowledgeaccordingtothestandardlevelinordertoreduceearly(7-day)neonatalmortality.
IMPLICATIonS
nursing practice
z The findings of the study may help the nursingpersonnel’s working in hospital and communityknowingabouttheneonatalcarepracticeandhelpsinplanningandimplementationofhealthteaching.
z Nursesneedtoupdatetheirknowledgeonvariousaspects available in neonatal care practice toeducatetheprimigravidamothers.
nursing Research
z This studyhelps thenurse researchers todevelopinsight into the development of interventionmoduleforneonatalcare toprimigravidamotherstowardspromotionofqualityoflifeandpreventionofneonatalmorbidityproblems.
RECoMMEnDATIonS
z Interventionalstudycanbedonebasedondiseaseprogression and mothers need, could help themothersaswellashealthcareproviderstodevelopanindividualizedtreatmentplan.
z Longitudinalstudycanbeundertakenforidentifyingtheassociatefactorsrelatedtoneonatalcare.
z A comparative study can be conducted betweenprimigravidaandmultigravidaonneonatalcare.
Conflict of Interest:Nil
Source of Support:SelfFunded
Ethical Clearance:EthicalclearancewasobtainedfromInstitutionalHumanEthicsCommitteeinPSGInstituteof Medical Sciences and Research (PSG IMS&R),Coimbatore.
REFEREnCES
1.Waldemar A. Carlo, Shivaprasad S. Goudar,ImtiazJehan,ElwynChomba,et.al.NewbornCareTrainingandPerinatalMortalityinCommunitiesin developing Countries. N Engl J Med. 2010February18;362(7):614–623.
2.Mamta Parashar, SV Singh, Jugal Kishore,Ajay Kumar, et.al. Effect of Community-basedBehaviorChangeCommunicationondeliveryandNewbornHealthCarePracticesinaResettlementColonyofdelhi.IndianJCommunityMed.2013Jan-Mar;38(1):42–48.
3.AmyJKestertonandJohnCleland.NeonatalcareinruralKarnataka:healthyandharmfulpractices,the potential for change. BMC PregnancyChildbirth.2009;9:20
4.Maheswari Ekambaram, Vishnu Bhat B,Mohamed Asif Padiyath Ahamed. Knowledge,attitiude and practice of breastfeeding amongpostnatalMothers.CurrPediatrRes2010;14(2):119-124
5.Shams El Arifeen, Luke C Mullany,Rasheduzzaman Shah, Ishtiaq Mannan, et.al.The effect of cord cleansingwith chlorhexidineon neonatal mortality in rural Bangladesh: acommunity-based,cluster-randomisedtrial.www.thelancet.com.March2012;379:1022-1028.
6.Karl Ludwig von Bertalanffy. General Systemtheory:Foundations,development,Applications,NewYork:GeorgeBraziller:1976.

Factors Influencing Clinical Learning Environment among nursing Students: A Cross Sectional Study
Manoj Kumar L1, Libina babu P. V.1
1Assistant Professor, Department of Psychiatric Nursing, Sree Gokulam Nursing College, Trivandrum
AbSTRACT
Clinical learning is theessenceofnursingeducation.Manyfactorshavebeendemonstrated to influencestudents’developmentofclinicalcompetence.Anon-experimentaldescriptivestudywasconductedaimingtoassessthefactorsinfluencingclinical learningenvironment, toprioritizethosefactorsandtocomparewithdegreeanddiplomanursing.The studywasconductedamongstudentnurses ina selectednursingcollege inThiruvananthapuram district of Kerala. 100 student nurses including fifty B.Sc. nursing andfiftyGeneralnursingstudentswererecruitedusingstratifiedandsimplerandomsamplingtechniqueafterobtaininginstitutionalethicalcommitteeclearance.datawascollectedfromsamplesaftergettinginformedconsent; thetoolsusedwere:SectionA-PerformatocollectdemographiccharacteristicsofsubjectsandSectionB-AssessmentoffactorsinfluencingCLEwhichwasathreepointlikertscaleanditincludedfactorslike;Supervision-10items,Clinicalfacilities-5items,Organization-5items,Interpersonalrelationship-5itemsandStudentrelatedfactors-5items.descriptivestatisticalmeasuressuchasfrequency,percentageandmeanwereusedforanalyzedata.Thecollecteddatawasanalyzedusingstatisticalpackageforsocialsciences version 20.Themean score of distribution of factors affectingCLEwas found as supervision(24.59),clinicalfacilities(10.74),organization(10.60),IPR(11.68)andstudentrelatedfactors(11.33).Onprioritizing thefactorshighestmeanpercentagewasobtainedforsupervision(81.97)and the lowest fororganization(70.67).
Keywords: Clinical learning, nursing education, clinical competence
Corresponding Author:ManojKumarLAssistantProfessor,departmentofPsychiatricNursing,SreeGokulamNursingCollege,Trivandrum-695607Phone:9048595588Email:[email protected]
InTRoDuCTIon
Clinicalpracticeisavitalcomponentofthenursingcurriculumandhasbeenacknowledgedasbeingcentralto nursing education1. Based on this general premise,there is agreement that nursing curriculum should bedirectedtowardsimprovementofclinicalcompetenciesof nursing students2. during clinical learning, nursingstudentsfrequentlyfeelanxiousandevenvulnerableinthe clinical environment3. There have been numerousstudies4,5,6 examining the effects of clinical experienceonstudentlearningandtheproblemsstudentsencounter
atclinics.Thesestudiesalsoshownstressorsassociatedwithgoingoutintotheclinicalfieldforthefirsttime,thefearofmakingmistakes,anxietyoverpossiblecriticismsfrom peers, being able to communicate with healthpersonnelandpatients,providingcarefortheseriouslyill or terminal patients, having thenecessary technicalskillsforprocedures,attitudestowardsandexpectationsofstaffofstudents7,8,9
Inadditiontoabovementionedfactors,ithasbeenshown that the attitudes, experiences and knowledgeof mentors influence student learning. By contrast,an effective mentor who tries to enables students toput their knowledge into practice by creating learningopportunities helps students the best. Research alsoindicates that mentors should make use of supportivestrategiestofacilitatelearningintheclinicalsetting.Forexample,inastudy10foundthatstudentslearnedbetterby assuming responsibilities, having opportunities toimplement new interventions and receiving feedback
DOI Number: 10.5958/2395-180X.2018.00012.9
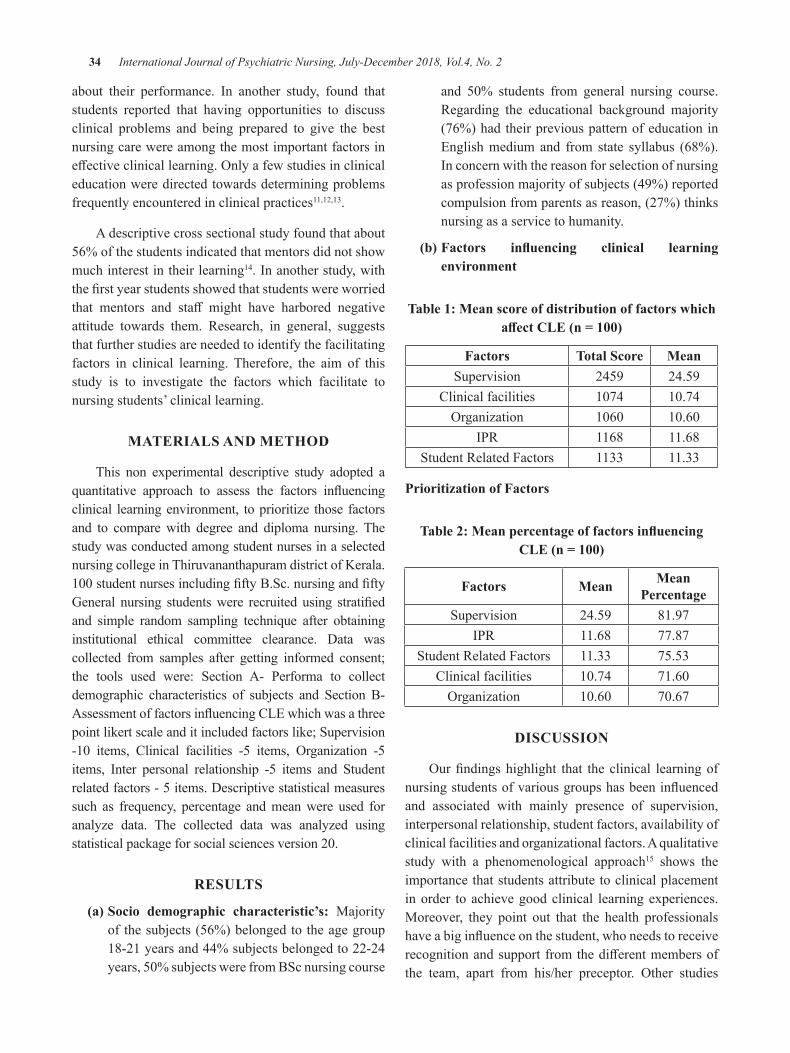
34 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
about their performance. In another study, found thatstudents reported that having opportunities to discussclinical problems and being prepared to give the bestnursingcarewereamongthemostimportantfactorsineffectiveclinicallearning.Onlyafewstudiesinclinicaleducationweredirectedtowardsdeterminingproblemsfrequentlyencounteredinclinicalpractices11,12,13.
Adescriptivecrosssectionalstudyfoundthatabout56%ofthestudentsindicatedthatmentorsdidnotshowmuchinterestintheirlearning14.Inanotherstudy,withthefirstyearstudentsshowedthatstudentswereworriedthat mentors and staff might have harbored negativeattitude towards them. Research, in general, suggeststhatfurtherstudiesareneededtoidentifythefacilitatingfactors in clinical learning. Therefore, the aim of thisstudy is to investigate the factors which facilitate tonursingstudents’clinicallearning.
MATERIALS AnD METHoD
This non experimental descriptive study adopted aquantitative approach to assess the factors influencingclinical learningenvironment, toprioritize those factorsand to comparewith degree and diploma nursing.ThestudywasconductedamongstudentnursesinaselectednursingcollegeinThiruvananthapuramdistrictofKerala.100studentnursesincludingfiftyB.Sc.nursingandfiftyGeneral nursing studentswere recruited using stratifiedand simple random sampling technique after obtaininginstitutional ethical committee clearance. data wascollected from samples after getting informed consent;the tools used were: Section A- Performa to collectdemographic characteristics of subjects and Section B-AssessmentoffactorsinfluencingCLEwhichwasathreepointlikertscaleanditincludedfactorslike;Supervision-10 items, Clinical facilities -5 items, Organization -5items, Inter personal relationship -5 items and Studentrelatedfactors-5items.descriptivestatisticalmeasuressuch as frequency, percentage andmeanwere used foranalyze data. The collected data was analyzed usingstatisticalpackageforsocialsciencesversion20.
RESuLTS
(a) Socio demographic characteristic’s: Majorityofthesubjects(56%)belongedtotheagegroup18-21years and44%subjectsbelongedto22-24years,50%subjectswerefromBScnursingcourse
and 50% students from general nursing course.Regarding the educational background majority(76%)hadtheirpreviouspatternofeducationinEnglishmediumand from state syllabus (68%).Inconcernwiththereasonforselectionofnursingasprofessionmajorityofsubjects(49%)reportedcompulsionfromparentsasreason,(27%)thinksnursingasaservicetohumanity.
(b) Factors influencing clinical learning environment
Table 1: Mean score of distribution of factors which affect CLE (n = 100)
Factors Total Score MeanSupervision 2459 24.59
Clinicalfacilities 1074 10.74Organization 1060 10.60
IPR 1168 11.68StudentRelatedFactors 1133 11.33
Prioritization of Factors
Table 2: Mean percentage of factors influencing CLE (n = 100)
Factors Mean Mean Percentage
Supervision 24.59 81.97IPR 11.68 77.87
StudentRelatedFactors 11.33 75.53Clinicalfacilities 10.74 71.60Organization 10.60 70.67
DISCuSSIon
Ourfindingshighlight that theclinical learningofnursingstudentsofvariousgroupshasbeeninfluencedand associated with mainly presence of supervision,interpersonalrelationship,studentfactors,availabilityofclinicalfacilitiesandorganizationalfactors.Aqualitativestudy with a phenomenological approach15 shows theimportancethatstudentsattributetoclinicalplacementinorder toachievegoodclinical learningexperiences.Moreover, they point out that the health professionalshaveabiginfluenceonthestudent,whoneedstoreceiverecognitionandsupportfromthedifferentmembersofthe team, apart from his/her preceptor. Other studies

International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 35
alsoconfirmthattherelationshipbetweenstudentsandclinicalnurseshasasignificantinfluenceonthelearningexperiences in clinical placement16. Other authors17 havenotedthatcommunicationandcooperationarethebasis of adequate supervisory relationships. Further,concluded that having meaningful learning situationswas a relevant aspect highlighted by students. Theseresultsareconsistentwiththoseobtainedinthepresentstudy, where the elements that were best perceivedby students focused on the good supervision andinterpersonalrelationshipeitherwiththeteamorwiththepreceptorandonthemotivationtolearn,hasbeenonthepositiveside18.
Conflict of Interest:Nil
Source of Funding:Self
REFEREnCES
1.dunn,S.V.,&Hansford,B.(1997).Undergraduatenursing students’ perception of their clinicallearning environment. Journal of AdvancedNursing,25(6),1299-1306.
2.Bradbury,Jones, C., Sambrook, S., & Irvine, F.(2007).Themeaningofempowermentfornursingstudents: a critical incident study. Journal ofAdvancedNursing,59(4),342–351.
3.Chow, F.L.W.,& Suen, L.K.P. (2001). Clinicalstaffasmentors inpre-registrationundergraduatenursing education: student’s perceptions ofthe mentor’s roles and responsibilities. NurseEducationToday,21(5),350-358.
4.Cimete, G. (1998). A qualitative study aboutstudent-teacher interaction. CumhuriyetÜniversitesi HemşirelikYüksekokuludergisi, 2(1),9-19
5.Cormack, d.F.S. (2006). The Research ProcessinNursing,(5thed.,pp.165.)Oxford:BlackwellPublishing.
6.Elcigil, A.,& Sarı, H.Y. (2007). determiningproblems experiencedby student nurses in theirwork with clinical educators in Turkey. NurseEducationToday,27(5),491-498.
7.Elo,S.&Kyngas.(2008).Thequalitativecontentanalysis process. Journal of Advanced nursing,62(1),107–115.
8.Ferguson, S. (1996). The lived experience ofclinicaleducators.JournalofAdvancedNursing,23(4),835–841.
9.Ip Wan Yim., & Chan, d.S.K. (2005). HongKongnursingstudents’perceptionoftheclinicalenvironment:aquestionnairesurvey.InternationalJournalofNursingStudies,42(6),665–672.
10.Kloster,T.,Hoie,M.,&Skar,R.(2007).Nursingstudents’careerpreferences:aNorwegianstudy.JournalofAdvancedNursing,59(2),155–162.
11.Lee, W.S., Cholowski, K., & Williams, A.K.(2002). Nursing student’ and clinical educatorsperceptions characteristics of effective clinicaleducators in anAustralian university school ofnursing. Journal of Advanced Nursing, 39(5),412-420
12.Mohan,R.,(2006).Emergingconceptsofnursingcare;Where does India stand. Indian Journal ofHolisticNursing.Volume1,Number4.
13.Binoy, S., (2009). Challenger towardsadvancement in clinical practice. Indian JournalofHolisticNursing.Volume1,Number4.
14.Latha, R., (2007). Promoting positive practiceenvironment fornurses- Issues andChallengers.KeralaNursesForum.Volume2,Number4.
15.PappI,MarkknenM,vonBonsdorffM.Clinicalenvironment as a learning environment: studentnurse perceptions concerning clinical learningexperiences. Nurse Educ Today. 2003;23:262–268.
16.AtackL,ComacuM.,KennyR,LabelleN,Millerd. Student and staff relationships in a clinicalpracticemodel:impactonlearning.JNursEduc.2000;39(9):387–395.]
17.daleB,LelandA,daleJG.WhatFactorsFacilitateGoodLearningExperiencesinClinicalStudiesinNursing: Bachelor Students’ Perceptions. ISRNNursing.2013;2013:1–7.
18.BisholtB,OhlssonU,EngströmAK,JohanssonAS,GustafssonM.Nursingstudents’assessmentof the learning environment in different clinicalsettings.NurseEducPract.2014;14(3):304–310.

Helping Art of Clinical nursing: Application of Theory in Enhancing the Quality of Life of Patients with Psoriasis
Padmavathi nagarajan
Assistant Professor, College of Nursing, JIPMER (Jawaharlal Institute of Post- Graduate Medical Education and Research), Pudhucherry
AbSTRACT
Psoriasis isachronicinflammatoryhyperproliferativediseaseoftheskinandaffectspeopleofallages.Inaddition to theskin and jointmanifestations,psoriasis impairsmanyaspectsof individualwell-being,includingemotional,physical,sexual, andfinancialstatus.Thecosmeticdisfigurementofpsoriasishasanegative impactonqualityof lifebycausingpsychologicalstress,disruptionofsocial relationshipsanddifficultiesindailylife.Helpingthepatientswithpsoriasistolearntolivewiththeirconditionisachallengingandimportantroleofnursesashealthprofessionals.Nursingpracticeshouldbetheorybasedanditenablestheresearchertolinkthefindingstonursing’sbodyofknowledge.Inthisarticle,theauthorexplainstheapplicationofWiedenbach’s“Helpingartofclinicalnursingtheory”indevelopingandadministeringaninterventiontoenhancethequalityoflifeofpatientswithpsoriasis.
Keywords: Nursing theory, Psoriasis, Quality of life
InTRoDuCTIon
Healthyskinisanessentialpartofpatientwellbeing.Skinproblemsarecommoninthegeneralpopulationandcompriseawidevarietyofdiagnosesrangingfrompurecosmetic conditions to tumors, genetic disturbances,autoimmunediseases and inflammatory skindiseases.1 Manyof thediseases seen indermatologyare chronicand life-long.due to thevisibleaspectofskin lesionsand their potentially high psychological impact, theevaluationofqualityoflifeinpsoriasisisaveryusefulcomplementtoclinicalstudies.
Magin et al 2 found that embarrassment, shame,impairedself-image,lowself-esteem,self-consciousnessandstigmatizationweremoreprominentamongpatientswith psoriasis.Many of the difficulties experienced bypatients with psoriasis make demands that outstrip thecoping measures of patient and their family or socialnetwork.Theyneedsufficienteducationandsupportfromhealthcareproviderstomanagetheirconditioneffectively.Today, dermatologic treatment of psoriasis has becomeincreasingly effective, can alleviate physical symptomsbut not cure the disease.A challenge to the patients isthereforetocopewithpsoriasisineverydaylife.
The World Health Organization (WHO) definesquality of life as “individual’s perception of their
position in life in the contextof the culture andvaluesystemsinwhichtheyliveandinrelationtotheirgoals,expectations, standards and concerns”. AccordingtoWHO, health-related quality of life (HRQoL) is abroad-rangingconceptaffectedinacomplexwaybyaperson’s physical health, psychological state, level ofindependence, social relationships, personal beliefs,and their relationship with salient features of theirenvironment(WHOQoLGroup,1995).3
Nurses are in unique position to address themultidimensional impactofpsoriasisonqualityof lifewith patients by allowing them to verbalize fears andconcerns, meeting with significant others, teachingpatientsaboutthediseaseprocessandassistingpatientstoparticipateintheiractivitiesofdailyliving.Hence,itisessentialtodevelopappropriatenursingstrategiestobringpositivepatientoutcomesonqualityoflife(QoL)amongpatientswithpsoriasis.
Generally, theories are used to explain the eventsthatoccurinpeople’slifeandintheirenvironment.Forexample,weconsiderstresstheoryastheexplanationforthetensedandimpatientbehavioursofthetrafficpolicemen because of their continued and uncomfortableworking situations. Similarly, nurses use theories toexplaintheiractivitiessignificancetonursing.Asound
DOI Number: 10.5958/2395-180X.2018.00013.0

International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 37
theoretical or conceptual framework strengthens thequalityofaresearchstudyandprovidesthefoundationonwhichtheresearchhasbeencarriedout.Oneofthemostcommon theory which has relevance and significanceto nursing practice is, Wiedenbach’s “HelpingArt ofClinicalNursingTheory”.4
ConCEPTS oF THE THEoRy
Wiedenbach proposes a prescriptive theory fornursing that directs action towards an explicit goal. Itconsists of three factors such as the central purpose,prescriptionandrealities.
(i)The central purpose refers to what the nurseresearcher wants to accomplish towards thepatient’sbenefitsorwellness.
(ii)The prescription refers to the plan of care forsubjectssufferingfrompsoriasis. It specifies thenatureofactionthatwillfulfillthenurse’scentralpurposeandtherationaleforthatactiontoachievethecentralpurpose.
(iii)Realities; It refers to the factors that come intoplayinasituationinvolvingnursingaction.Thefiverealitiesareagent,recipient,goal,meansandframework.
The nurse researcher as an agent interacts withpatientsdiagnosed tohavepsoriasis as recipientswithagoal to identify theneedforhelpanddevisesmeansto achieve the help within the framework of nursingpractice.4
Application of “Helping Art of Clinical nursing Theory”: According to this nursing theory, nursingpracticefocusesonidentifyingapatient’sneedforhelpwhohasbeendiagnosedwithpsoriasis,ministeringtheneededhelpandvalidatingthattheneededhelpwasmet.Theresearcheridentifiedapsoriasissufferer’sneedforhelpusingthepretestwhichassessedtheirknowledge,attitude and quality of life. The central purpose wasto reduce the negative effects of psoriasis on affectedpatientsandachievingabetterqualityoflife.
Basedonthecentralpurpose, thenurseresearcherprescribed theneededhelp i.e.administeredstructuredteachingprogrammeandprogressivemusclerelaxationalongwithdeepbreathingexercises.Thus,theresearcherhelped the patients with psoriasis to understand theirdiseaseprocess and reduced the stress associatedwithdailylifewhichpromotedabetterqualityoflife.
Afteradministering theprescription, the researchervalidatedwhetherthequalityoflifewasimprovedthroughapost test.When thequalityof lifewas improved, thepatientsexperiencedbettercontrolovertheirdiseaseandtheywereabletocopeupwithdailylife.Ifnot,theirneedforhelphadtobeidentifiedtotakefurtheractioninordertostrengthentheirabilitytocopeupwiththeirdiseasetilltheyachievedabetterqualityoflife.
Clients with psoriasis were assessed before theintroduction of nursing strategies regarding theirknowledge and attitude towards their disease. Further,the disability experienced in the day to day activitiesoftheirlifeandstressexperiencedbythembecauseoftheir illness were also studied. A structured teachingprogramme on psoriasis was taught to them with thehelp of video, pamphlets, charts and other necessarymedications and ointments for a period of threemonths alongwith simple relaxation techniques.Theywere assessed at different time intervals (at the endof one month, two months and three months afterthe interventions) to assess the changes that mighthave occurred during the study period. Based on theoutcomemeasures,theresearcherwasabletoassesstheeffectivenessofherstrategies.5-8
Thefindingshadshowedasignificantdifferenceinknowledge,attitudeandqualityoflifeafterthreemonthsofinterventionintheexperimentalgroupwhencomparedtothecontrolgroup.Thefindingsalsorevealedthattheimplementation of nursing strategieswere effective inimprovingthequalityoflifeofpatientswithpsoriasis.
ConCLuSIon
Psoriasis is a chronic skin disease which has animpact on health-related quality of life (QoL). It is adisease with profound impact on the psychologicaland social aspect of the patient, particularly becauseof its visibility. In thehealth team,nursesplay avitalrole in educating, training and providing variouspsychosocial therapies.Thenursesshouldbeawareofthestressassociatedwithpsoriasisamong theaffectedindividuals. By using various nursing strategies thatreduce the psychosocial burden and stress associatedwith the disease, nurses can help the patients to leadan independent and productive life. The theoreticalframeworkwhichwasbasedonWiedenbach’s“HelpingArt of Clinical Nursing” was useful to determine theeffectiveness of nursing strategies on quality of lifeamongpatientswithpsoriasis.
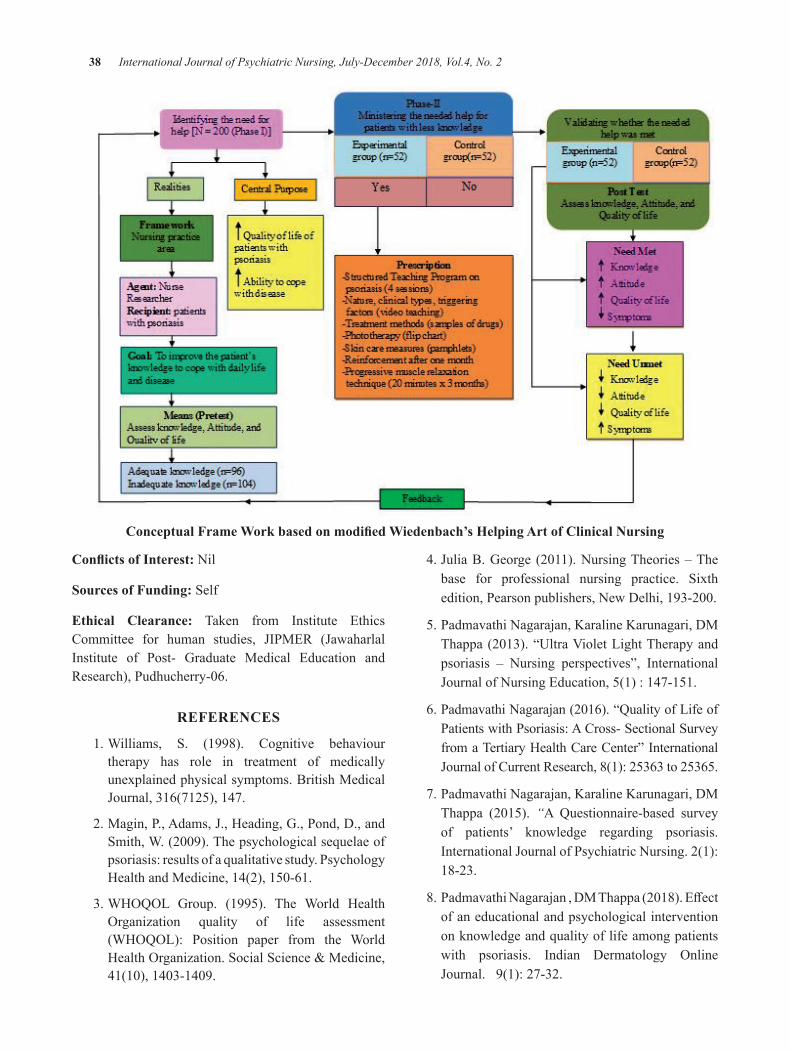
38 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
Conceptual Frame Work based on modified Wiedenbach’s Helping Art of Clinical nursing
Conflicts of Interest:Nil
Sources of Funding:Self
Ethical Clearance: Taken from Institute EthicsCommittee for human studies, JIPMER (JawaharlalInstitute of Post- Graduate Medical Education andResearch),Pudhucherry-06.
REFEREnCES
1.Williams, S. (1998). Cognitive behaviourtherapy has role in treatment of medicallyunexplainedphysicalsymptoms.BritishMedicalJournal,316(7125),147.
2.Magin,P.,Adams,J.,Heading,G.,Pond,d.,andSmith,W.(2009).Thepsychologicalsequelaeofpsoriasis:resultsofaqualitativestudy.PsychologyHealthandMedicine,14(2),150-61.
3.WHOQOL Group. (1995). The World HealthOrganization quality of life assessment(WHOQOL): Position paper from the WorldHealthOrganization.SocialScience&Medicine,41(10),1403-1409.
4.JuliaB.George (2011).NursingTheories–Thebase for professional nursing practice. Sixthedition,Pearsonpublishers,Newdelhi,193-200.
5.PadmavathiNagarajan,KaralineKarunagari,dMThappa(2013).“UltraVioletLightTherapyandpsoriasis – Nursing perspectives”, InternationalJournalofNursingEducation,5(1):147-151.
6.PadmavathiNagarajan(2016).“QualityofLifeofPatientswithPsoriasis:ACross-SectionalSurveyfromaTertiaryHealthCareCenter”InternationalJournalofCurrentResearch,8(1):25363to25365.
7.PadmavathiNagarajan,KaralineKarunagari,dMThappa (2015). “A Questionnaire-based surveyof patients’ knowledge regarding psoriasis.InternationalJournalofPsychiatricNursing.2(1):18-23.
8.PadmavathiNagarajan,dMThappa(2018).Effectofaneducationalandpsychologicalinterventiononknowledgeandqualityoflifeamongpatientswith psoriasis. Indian dermatology OnlineJournal.9(1):27-32.
A Study to Assess the Effectiveness of Structured Teaching Programme on Knowledge Regarding Premenstrual Syndrome
among Adolescent girls Studying in a Selected English Medium High School at bagalkot.
Shivanagouda V Malagoudar1, Praveen S. Pateel2
1Staff Nurse Gadag Institute of Medical Sciences, Gadag; 2Asso Professor and HOD of Nursing Foundation, B. V. V. Sangha’s Sajjalashree Institute of Nursing Sciences Navanagar, Bagalkot. Karnataka
AbSTRACT
Aonegrouppre-testpost-testexperimentaldesignhasbeenusedinthisstudy.Thesampleforthepresentstudycomposedof50adolescentgirlsattendingtheselectedEnglishmediumhighschoolofBagalkot.TheresultconcludedthatwithComparisonoflevelofknowledgeofAdolescentgirlsinpretestandposttestrevealsthatmajority66%ofadolescentgirlshadpoorknowledge,22%ofthemhadaverageknowledge,12%ofthemhadverypoorknowledgeandtherewerenoadolescentgirlshadgoodandexcellentknowledge.Whereasinposttest64%ofadolescentgirlshadexcellentKnowledgeand36%ofthemhadgoodknowledge.
Keywords: adolescent girls, knowledge, premenstrual syndrome STP.
Corresponding Author:Mr.PraveenS.PateelMScNursing(Phd)Asso.ProfessorandHOdofNursingFoundationB.V.V.Sangha’sSajjalashreeInstituteofNursingSciencesNavanagar,Bagalkot.KarnatakaCell:9743240191Email:[email protected]
InTRoDuCTIon
Adolescence is themost common time of life forpsychiatric illness toemerge. Thebehaviorsobservedduring adolescence represent a non-linear change thatcan be distinguished from childhood to adulthood, asevidencedbythenationalcenterforthehealthstatisticson adolescent behavior and mortality. Adolescencerepresents a period of intensive growth and changein nearly all aspects of the child’s physical, mental,social andemotional life. Adolescents areveryproneto emotional maladjustment. The most frequentlyobservedproblemduring thisperiodarepsychologicaldisorders like anxiety & depression, violent behavior,eatingdisorders, substanceabuse, sexually transmitteddiseases,premenstrualsyndrome1.
Premenstrualsyndromecanbedefinedasanymoodchange, physical or behavioral symptoms that appearinthelutealphaseofthemenstrualcycleanddisappearshortlyaftertheonsetofnextmenstruation.Menstruationisthesheddingoftheuterineliningthroughthevagina2.
Premenstrual syndrome (PMS) is a symptomcomplex recognized primarily by cyclical changesassociatedwithovulatorycycles.Itoccurs7–14daysprior tomenstruationand spontaneously resolves aftermenstruation.2 PMS is a common cause of sicknessabsenteeismfromschoolsandinterfereswiththedailyroutine activities of adolescent girls. It is a commonadolescent health problem with high prevalence andsuffering,leadingtolossofacademicachievements3.
Most common emotional PMS symptoms areIrritability, anger, depression, crying, over sensitivity,feeling nervous and anxious, alternating sadness andrage.Thesemood/emotionaldisturbancearethoughttobeconnectedtoriseandfallofhormonesspecificallyestrogen throughout the menstrual cycle. Estrogenlevel begins to rise slowly just after period ends andit peaks two weeks later. Then estrogen levels droplike a rock and begin rising slowly before droppingagain justbeforemenstruationstarts. Thesehormonal
DOI Number: 10.5958/2395-180X.2018.00014.2
40 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
peaks and valleys are thought to cause mood swingsand other menstrual symptoms. Stressful situationscannotcausePMSbut theycanmake itworse. Someresearch suggests that female hormones interact withthebrainchemicalsandeffectmoodinthosewithPMS.Reduced levels of estrogen during the luteal phaseof the cycle could possibly cause a drop in serotonin.Lowerserotonin levelsareassociatedwithdepression,irritabilityandcarbohydratecravings,allofwhichcanbePMSsymptoms4.
The Research problem statement:A study to assessthe effectivenessof structured teachingprogrammeonknowledge regarding premenstrual syndrome amongadolescentgirlsstudyinginaselectedEnglishmediumhighschoolatBagalkot
OBJECTIVES
z To assess the knowledge of adolescent girlsregardingpremenstrualsyndrome.
z ToassesstheeffectivenessofSTPamongadolescentgirlsregardingpremenstrualsyndrome.
z To associate the knowledge of adolescent girlsregarding premenstrual syndrome with theirselected demographic variables such as age,education.
Hypothesis
H1: There will be significant difference between pre-testandpost-testknowledgescoresofadolescentgirlsregardingpremenstrualsyndromeanditsmanagement.
H2:Therewillbesignificantassociationbetweenpre-test knowledge scores of Adolescent girls regardingpremenstrual syndromeand itsmanagementwith theirselectedsocio-demographicvariables.
Delimitations
1.Study is limited to adolescent girls in the agegroup(13-16)years.
2.Adolescent girls available during the period ofstudy.
3.Adolescent girls who are studying in selectedEnglishmediumhighschoolatBagalkot.
4.Study is limited to adolescent girls who haveattainedmenarche.
Conceptual Framework: The conceptual frameworkusedforthisthestudyisbasedonSystemsModel(VonLudwigBertalanffy).
METHoDoLogy
Research approach:Anevaluativeapproachusingpre-test(O1)andpost-test(O2)withoutacontrolgroupwasadoptedforthisstudy
Research design: A one group pre-test post-testexperimentaldesignhasbeenusedinthisstudy.
Experimental group Pre-test Intervention Post-test
R O1 X O2
Tableno1Aonegrouppre-testpost-testexperimentaldesignhasbeenusedinthisstudy
Setting of the Study: ThepresentstudywasconductedatStAnne’sLionsSchool,Bagalkot.
Population: The target population of the study isadolescentgirlsattendingselectedEnglishmediumhighschoolatBagalkot
Sample and Sample size: The sample for thepresentstudy composed of 50 adolescent girls attending theselectedEnglishmediumhighschoolofBagalkot.
Sampling Technique: Simple random samplingtechniquewasusedtoselecttheschoolandconveniencesampling techniquemethodwas adopted to select thesamplesforthepresentstudy
Development and Description of the Tool: The datacollectiontoolwasstructuredknowledgequestionnairefor knowledge assessment. Keeping this in mindstructuredquestionnairewasselectedanddevelopedonknowledge of adolescent girls regarding premenstrualsyndrome. The tool was prepared on the basis ofobjectives of the study. The following steps wereadoptedinthedevelopmentoftool.
z Theneedtoeducatetheadolescentgirlsregardingpremenstrualsyndrome.
z Relatedreviewofliterature.
z Consultationwithexpertsintherelevantfield.
z discussionandconsultationwiththestatistician.
z Thefinaltoolwaspreparedwiththeguidanceandsuggestionsoftheguide.
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 41
Description of the final Tool:Afterathoroughreviewof literature related to the topic and considering thesuggestions of experts a structured questionnaire wasdeveloped.
Thestructuredquestionnairecomprisedoftwoparts.
Part I:Consistsofitemsseekinginformationregardingsocio-demographic characteristics of adolescentgirls such as age, education, occupation of parents,type of family, monthly income in rupees, sources ofinformation.
Part II: Consists of 40 knowledge items related topremenstrualsyndrome.
Validity and Reliability: Theconstructedtoolwasgivento 3expertsof relatedfields forcontentvalidity.Theywere from the departments of Child Health Nursing,community health nursing, andmental health nursing.Thetoolwasmodifiedaccordingto thesuggestionsoftheexperts.
The reliability of the tool was established byusing splithalfmethod.4 subjectswere selected fromEnglishmediumhighschool,Bagalkot.KarlPearson’scoefficient correlation ‘r’ was computed for findingout thereliability.Theobtainedvalueof‘r’’was0.85,indicatingthatthetoolwashighlyreliableforknowledge.
RESuLTS
Part I: Description of socio-demographic characteristics of sample.
Out of 50 sample distribution of adolescent girlsaccordingtotheirageinyearsshowsthatMost64%oftheadolescentgirlswere15–17yearsold,and36%ofadolescentgirlswere13–15yearsold.majoradolescentgirlsaccording to theirReligionshows thatMajorityofadolescents90%werebelongingtoHindureligion,6%ofthemwereMuslimsand4%ofthemwerebelongingtoChristianreligion.Adolescentsgirlsmotherseducational
status reveals that Majority 46.00% of mothers haddegreeandabove,28.00percentofthemhadsecondaryeducation,14.00% them had PUC, 10.00% them hadprimary education, and remaining 2.00% mothers’ ofadolescentgirlswereilliterate.adolescentgirlsaccordingto theirageofattainedmenarcheshowsthatMost76%oftheadolescentgirlswere13–14yearsold,and22%ofadolescentgirlswere10–12yearsold,andremaining2percentofadolescentgirlswere15–16years.
Part II:
Section A: Assessment of pre-test knowledge of the adolescent girls regarding pre menstrual syndrome and its management.
Level of knowledge
Range of scores
number of respondents
Percentage (%)
Excellent 33-40 0 0Good 25-32 0 0Average 17–24 11 22Poor 9-16 33 66
Verypoor 0-8 6 12Total 40 50 100
Tableno2Assessmentofpre-testknowledgeoftheadolescentgirlsregardingpremenstrualsyndromeanditsmanagement
Section b: Area wise mean, SD and mean percentage of pre-test knowledge scores of Adolescent girls.
Knowledge Area Max. Score Mean SD Mean
%diseaseaspectofpremenstrual
syndrome23 7.6 2.041 33.04
Managementofpremenstrualsyndrome.
17 6.12 2.33 36
Total 40 13.72 3.31 34.3
Table 3: Comparison of level of knowledge of adolescent girls in pre-test and post-test. n = 50
Level of knowledge Pre–test Post Testno. of respondents Percentage no. of respondents Percentage
Excellent O 0.0 32 64.0Good 0 0.0 18 36.0Average 11 22.0 0 0.0Poor 33 66 0 0.0
Verypoor 6 12 0 0.0Total 50 100 50 100
42 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
Comparison of level of knowledge ofAdolescentgirls inpretestandposttest reveals thatmajority66%ofadolescentgirlshadpoorknowledge,22%ofthemhad average knowledge, 12% of them had very poorknowledgeandtherewerenoadolescentgirlshadgoodandexcellentknowledge.Whereasinposttest64%of
adolescentgirlshadexcellentKnowledgeand36%ofthemhadgoodknowledge.
Section b: Area- wise effectiveness of the STP on disease aspect of pre menstrual syndrome and its management.
Table 4: Area- wise effectiveness of the STP on disease aspect of pre menstrual syndrome and its management
Knowledge area Max. score
Pre-test (o1) Post-test (o2)Effectiveness
(o2-O1)Mean ± SD Mean % Mean ± SD Mean % Mean ± SD Mean %
diseaseaspectofpremenstrualsyndrome 23 7.6±2.04 33.04 18.88±1.34 82.09 11.28±2.2 49.04
Managementofpremenstrualsyndrome. 17 6.1±2.33 36 14.98±1.37 83.06 8.02±2.70 47.18
Total 40 13.72±3.31 34.3 33±2.02 82.5 19.28±3.9 48.2
Comparisonofmeanpercentageof theknowledgescoresof thepre-test andpost-test reveals an increaseof 48.2 percent in the mean knowledge score of theadolescent girls after STP. Comparison of area wisemean and Sd of the knowledge scores in the area of‘disease aspect of premenstrual syndrome’ shows thatthe pre-testmean percentage of knowledge scorewas33.04percentwithmeanandSd7.6±2.04whereaspost-testmeanpercentageofknowledge scorewas82.09%withmeanpercentwithmeanandSd18.88±1.34.Thisshowsanincreaseof49.04%inthemeanpercentageofknowledgescoresoftheadolescentgirls.
Section C: Testing of Hypothesis: Thecalculatedvaluesweremuchhigherthantablevalue(1.96).HencetheH1 stated is accepted. Findings reveal that the differencebetweenmeanpre-test(13.72±3.31)andpost-test(33±2.02)knowledgescoresofadolescentgirlsfoundtobestatisticallysignificantat0.05levelofsignificance[t=33.91,p<0.05].
Similarly the area wise difference between pre-test and post-test knowledge scores on premenstrualsyndromeanditsmanagementwerehighlysignificant.Meanofpost-testknowledgescoresinthearea‘diseaseaspect of premenstrual syndrome’ (18.88 ± 1.33) issignificantlyhigherthanthemeanofpre-testknowledgescores (6.12 ± 2.33) at 0.05 level of significance (t =35.17,p<0.05).SimilarlyMeanofpost-testknowledgescores in the area ‘management of premenstrualsyndrome’(14.98±1.37)issignificantlyhigherthanthemeanofpre-testknowledgescores(6.12±2.33)at0.05levelofsignificance(t=20.8,p<0.05).
Findingsrevealthatthereissignificantassociationbetween post-test knowledge scores of the adolescentgirlsandsociodemographicvariablessuchasmotherseducational status [x2 = 8.33, P, 0.05] and year ofstudy [x2 = 4.22, P < 0.05]. There is no significantassociation between post-test knowledge scores of theadolescentgirls and sociodemographicvariables suchasage,religion,typeoffamily,father’soccupation,andmothers’occupationmonthly incomeof family,ageofattained menarche and source of health information.Thus H2 state disaccepted for demographic variablessuchasmotherseducationalstatusandyearofstudyandrejectedfortheirothervariables.
Implications of the Study:The findings of the studycanbeusedinthefollowingareasofnursingprofession.
1. nursing Practice: Health education is animportanttoolofhealthcareagency.Itisoneofthemostcosteffectiveinterventions.It isconcernedwithpromotinghealthaswellasreducingstress.Theextendedandexpandedrolesofprofessionalnursehaveemphasizedmoreaboutthepreventiveandprimitiveaspectsofthehealth.
2. nursing Education: The curriculum isresponsibleforpreparingthefuturenurses.Thereitshouldemphasizeonpreventiveandpromotivehealth practices.The learning experience of thestudentsshouldgivemoreemphasisonteachingthe population who are at risk. Workshops,seminars and conferences can be conductedto educate the student nurses regarding pre
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 43
menstrualsyndromeand itsmanagementso thatthey could disseminate their knowledge to theadolescent girls. The student nurses should begiven opportunities during his/her training toplanandconducthealtheducationforadolescentsstudying indifferentcolleges regardingproblemsolvingtechniquesandcopingskills tomeet thechallengesofthetransitionalage.
3. nursing Administration: The nursingadministrator can take part in developingprotocols, standing orders related to designingthe health education programmes and strategiesfor school going adolescent girls regarding premenstrualsyndromeanditsmanagement.
Thenursingadministratorcanmobilizetheavailableresource personnel towards the health education ofschool going girls regarding pre menstrual syndromeanditsmanagement.
nursing Research: Thisstudyhelpsnurseresearcherstodevelopappropriatehealtheducationtoolsforeducatingtheschoolgoinggirlsregardingpremenstrualsyndromeaccording to their demographic, socio-economic andculturalcharacteristics.
Nurses should come forward to take up unsolvedquestions in the field of pre menstrual syndrome andits management to carryout studies and publish themfor the benefit of youth, public and nursing fraternity.Thepublicandprivateagenciesshouldalsoencourageresearchinthisfieldthroughmaterialsandfunds.
Limitations of the Study
z Thestudyislimitedtotheadolescentgirlsbetweentheagegroupof13-16years studying inEnglishmediumhighschoolatBagalkot.
z The study did not use a control group. Theinvestigatorhadnocontrolovertheeventsthattookplacebetweenpretestandposttest.
z Only a single domain that is knowledge isconsideredinthepresentstudy.
z The sample for the study was limited to 50adolescentgirls.Thiswasonlyasmallsampleforgeneralization.
z The researcher could not get a standardized toolto assess the knowledge of adolescent girls. Theresearcherhimselfdevelopedthetool.
z ThecontentofSTPwaslimitedtocoverwithin45minutes.
RECoMMEnDATIonS
Based on the findings of the study the followingrecommendationsarestated;
z A similar study can be undertaken with a largestratified sample including adolescent girls fromselectedEnglishmediumhighschooltogeneralizethefindings.
z Asimilar study canbeundertakenwith a controlgroupdesign.
z Astudycanbeconductedtofindouttheprevalenceofpremenstrualsyndromeamongadolescentgirls.
Suggestions
z Healthprofessionalscanconducthealtheducationprogramme on premenstrual syndrome and itsmanagementamongadolescentgirlsatschoolsandcolleges.
z Structured teachingprogrammecanbeconductedin a group including adolescent girls and theirparents, teachers, administrators and communitymembers.
ConCLuSIon
On the basis of the findings of the study, thefollowingconclusionsaredrawn:
z Assessment of the level of pre test knowledgeoftheadolescentgirlsrevealsthatmajority66%oftheadolescent girls had poor knowledge, 12 percentof themhadverypoorknowledgeandtherewereno adolescent girls who had good and excellentknowledgeregardingpremenstrualsyndrome.
z Asignificantdifferencewasfoundbetweenthepost-test and pre-test knowledge scores of adolescentgirls.The study showed that the STPwas highlyeffectiveinimprovingtheknowledgeofadolescentgirlsonpremenstrualsyndrome.
z There is significant association between post-testknowledgescoresoftheadolescentgirlsandsociodemographicvariablessuchasmothers’educationalstatus and year of study. There is no significant
44 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
association between post-test knowledge scoresof the adolescent girls andsocio demographicvariables such as age, religion, type of family,father’s occupation,mothers’ occupationmonthlyincome of family, age of attained menarche andsourceofhealthinformation.
Ethical Clearance: Taken from Shri B V V SSajjalashree Institute Of Nursing Sciences NavanagarEthicalclearance-committee
Source of Funding:Self
Conflict of Interest:Nil
REFEREnCES
1.Henshaw A. Premenstrual syndrome diagnosisetiology, assessment andmanagement.Article ofadvancesinpsychiatrictreatment.2007:13;139-146.
2.Mohammad Bakhshani, NowrooziMousavi,Khodabandeh. Prevalence and severity ofpremenstrual symptoms among Iranian femaleuniversity students.Journal of Pakistan medicalAssociation.2009;59:205.
3.Rusheed. P, Al-SowielemLS.Prevalence andPredictors of Premenstrual Syndrome among
College Aged Women in Saudi Arabia. (www.pubmed.com)
4.L A Heinemann, T d Minh, A Filonenko,Uhl-hochgraver. Explorative evaluation ofthe Williams.The importance of adolescence.Available from: URL: http:// www.google.com/theimportanceofadolescence.
5.Anandhalakshmi, S.priy m, Saravanan A.Prevalence of premenstrual syndrome anddysmenorrhoea among female medical studentsand its association with college absenteeism.International journal of Biological and medicalresearch .October 2011, Vol.2, Issue .4, 2(4);1011-1016.
6.dr.AminaMohamedRashid,HalaAhmadThabet,SamiaAboud .Effectsof aneducationalprogramonnursingstudentswithpremenstrualsyndrome.2002Sep;30(7):220-242.
7.Maine S, Shute R, Martin G. Effect of premenstrual syndrome educational programe onadolescentgirls.2005Sep;31(9):320-32.
8.Rapkin, Andrea Ja. Mikacich, Judith Aa. Knowledge of adolescents on pre menstrualsyndromeandpremenstrualdysphoricdisorderinUSA.2008Aug;8(11)400-416.

Family Focused nursing Intervention for Functional Improvement of bPAD Clients- A Pilot Study Report
R R Kavitha1, S Kamalam2, Ravi Philip Rajkumar3
1Tutor (PhD scholar), College of Nursing JIPMER, Puducherry, 2Principal, A G Padmavathi College of Nursing, Puducherry, 3Additional Professor, Department of Psychiatry, JIPMER, Puducherry
AbSTRACT
Introduction:Bipolaraffectivedisorderisachronic,episodicillnessthatcancreateproblemsanddisruptionsinsocial,occupational,andfamilyfunctioningofaclient.CurrentstudyaimedtoassessFamilyFocusedNursingInterventions(FFNI)onfunctionalimprovementonsampleofsymptomaticBipolardisorderclients.
Method: InviewofcheckingthefeasibilityofRandomizedcontrolledtrial involving208samples,asaPilottestingof46clientswithbipolaraffectivedisordershasbeenselectedforthisstudy.Studyhadequalnumberofcontrolandstudygroupparticipants23ineachgroup.Controlgroupreceivedroutinetreatment,studygroupreceivedFFNIin7sessions.Theprimaryoutcomeisfunctionallevelofclient,wasassessedusingFunctionalAssessmentShortTest -FASTScore.The collecteddatawas analysedusingSPSS20,Independentsamplet-test,ANOVAandPearsoncorrelationusedasdifferentstatisticalmethods.Pvaluelessthan.05wasconsideredasstatisticallysignificantresult.,
Results:At the end of pilot study 45 patients completed the treatment and follow-up. After the randomassignment to control and study group, the pre-test evaluation of functioning then repeated evaluation atdischarge,afteramonthandat2monthfollow-up.ResultsshowedthatbothgroupwerecomparableatbaselineandtherewasasignificantimprovementinthefunctionallevelafterFFNI.Studywasfeasibletoconduct.
Conclusion:Adjuvanttoroutinetreatmentfamilyfocusednurseledinterventionswillimprovethefunctionalabilityoftheclient.
Keywords: family focused, Bipolar illness, nursing intervention.
Corresponding Author:RRKavithaTutor(Phdscholar),CollegeofNursingJIPMER,PuducherryEmail:[email protected]
InTRoDuCTIon
Bipolarillnessestendtorecurandcausefunctionalimpairmentduringtherelapseandinremissionperiod.Bipolar illness is severe in nature and mood changesfromdepressiontomania.duringactiveillnessperiod,clients’functionalabilityisbecomingaggressivetonilactivity.Thisisaffectingpatients’social,occupational,recreational, relationship and family functioning. Thebipolar illness affects nearly 1% of world population.Bipolardisorder isassociatedwith impulsiveandself-destructive behavior1. Not surprisingly, families are
frequentlymost affectedby their bipolarmember, andthemselvesexperiencearangeofdeeplyfeltemotions,not the leastofwhich isa senseofhelplessness tofixbipolar symptoms. With appropriate drug treatment,about 40 percent of recovered patients will sufferrelapses(NIMH,2005).
Mood stabilizers, ECT and psychotherapy are thetreatmentmodalitiesforbipolardisorder.ThePrevalenceRateforbipolardisorder isapproximately1.1%of thepopulationovertheageof18or,inotherwords,atanyonetimeasmanyas51millionpeopleworldwidesufferfrombipolardisorder,8.7millionpeople inIndia.TheUnitedStateshadthehighestprevalencerateofbipolarspectrum(4.4percent),whileIndiahadthelowestrate(0.1 percent). More than half of those with bipolardisorder in adulthood note that their illness began intheiradolescentyears2.
DOI Number: 10.5958/2395-180X.2018.00015.4

46 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
Bipolar disorder has traditionally been associatedwith a better outcome than schizophrenia becauseof a presumed absence of cognitive impairment andseeminglynormalfunctioningbetweenepisodes3.Thus,generallylittleattentionhasbeengiventopsychosocialoutcomes in patientswith bipolar disorder4. However,in contrast to early studies3-4, recent studies point toa significant degree of psychosocial dysfunction evenwhenpatientsareeuthymic5,6.Functioningisacomplexconceptsinceitinvolvesthecapacitytowork,study,liveindependently and engage in recreation and romanticlife4. Functional recovery has been described as theability to achieve the level of functioning prior to themostrecentepisode5
Miklowitz and colleagues have pioneered family-focused8-12 psychoeducational treatments for bipolardisorder (2000, 2003and 2008). Their family-focusedtreatment involves all available immediate familymembers in 21 one-hour sessions delivered over 9months(12weekly,then6fortnightly,then3monthly).Itcomprisesthreeconsecutivemodules:
Psychoeducation focusing on the signs andsymptoms of bipolar disorder, the etiology of bipolarepisodes according to a stress-vulnerability modeland the development of strategies to prevent relapses;communication enhancement training sessions usingrole-playandbetween-session rehearsal to teach skillsforactivelistening,waystodeliverpositiveandnegativefeedback and constructiveways to request changes inbehaviour; Problem-solving skills training sessionsin which participants learn to identify specific familyproblems thatmight contribute to relapse anddevelopskillsforfindingacceptablesolutionstotheseproblems.The current study is expected to assess the functionalimpairment of bipolar affective disorder clients andthe effect of family-focused nursing intervention onfunctionalimprovementofclientswithbipolardisorder.Thisstudyisexpectedtodeterminetheeffectoffamily-focused nursing intervention and can be incorporatedtopracticeasawaytohelpthefamilyandclientswithbipolardisorder.
Tocheck thefeasibilityof themainstudywith46subjectspilotstudyhasbeenconducted.
METHoD AnD MATERIALS
Thisstudyaimed toa toassess the feasibilityandeffectoffamilyfocusednursingintervention(FFNI)on
functionalimprovementamongtheclientwithBdWiththeaboveobjectives,bipolarclientswhohaveadmittedtothepsychiatricwardatJIPMERwererecruitedwithfollowinginclusioncriteriasuchaspatienthasat leastoneprimarycaregiverabloodrelativeorapersonwhomclient stayswithmore than a year andwho iswillingto participate. A client who had ICd 10 diagnosisof the bipolar affective disorder has been included.Patients enrolled for any other psychological therapy,Primary caregiver withmental illness and Patient hasa co-morbidmajormental illness (alcoholdependence/another psychiatric diagnosis) were excluded fromthe study. The experimental group received routinepsychiatric treatment along with Family-FocusedNursing Intervention. Control group received routinepsychiatric treatment.Consecutive sampling techniquewas used to select the study participants. The clientswith Bipolar Affective disorders admitted in apsychiatricwardwhofulfilledtheinclusioncriteriawasselected alongwith their familymember afterwritteninformedconcern.ThisstudywasapprovedbyInstituteethicscommittee,JIPMERandregisteredunderCTRI.(CTRI/2017/09/009860)
Thecalculatedsamplesizewas208(n=101ineacharm)forthemainstudy.Butforfeasibilitycheckingonly46clients included.Blockrandomizationwithvaryingblock size used to randomize the clients into studyarms.Theblockrandomizationwithvaryingblockswasgeneratedusingacomputerprogram.
SociodemographicvariablessuchasAge,Gender,Maritalstatus,Religion,education,Occupation,monthlyFamily Income, type family: number of siblings,personalhabits,numberofhospitalization,durationofillnessinmonths,Totaldurationofillperiodinthelastyear in days, Level of functioning assessed by FAST(FunctionalAssessmentShortTest)AdrianeRRosaetal200718datawerecollectedfrompatientsadmittedtotheinpatientdepartmentofJIPMERhospitalwhosatisfytheinclusioncriteriaafterwritteninformedconsent.
Theyrandomlyassignedtocontrolgroupandstudygroup. Clients and primary caregiver interviewed forcollectingdemographicprofileandpre-testassessmentclientsfunctionusingFASTScale,thenFamily-focusednursing interventionwas given in 7 sessions to clientandfamilymembertheprimarycaregiverinaninpatientsetting.At discharge, after onemonth and at 2-monthassessmentdone to see the functional improvementofclientsatoutpatientsetting
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 47
Enr
ollm
ent
Allo
catio
nFo
llow
up
Ana
lysi
sAssessedforeligibility
(N=48)
Analyzed(n=22)Analyzed(n=23)
Randomized(n=46)
Excluded(n=2)Notmeetinginclusioncriteria
(n=1)Refusedtoparticipate
(n=1)
AllocatedtoFFNI(n=23)
Receivedallocatedintervention(n=23)
Losttofollowup(0,1and2ndmonth
followup)(n=0)
Losttofollowup(n=1)(AgainstMedicalAdvice)(0,1and2nd
monthfollowup)
AllocatedtoroutineRx(n=23)
Receivedallocatedintervention(n=23…)
Consort diagram: Family focused nursing intervention for functional improvement of bPAD
clients−A pilot study report
RESuLTS
Table 1: Demographic details of the client with bipolar disorders n = 45
Variable
Frequency (%)
Study group n = 23
Frequency (%)
Control groupn = 22
Sig*
SexMale 12(52.2) 13(59)
P=.644Female 11(47.8) 9(40.9)
Marital statusSingle 12(52.2) 11(50)
P=.887Married 11(47.8) 11(50)
ReligionHindu 19(82.6) 21(95.4)
P=.163Others 4(17.4) 1(4.5)
Conted…
Education Primary 4(17.4) 5(22.7)
P=.028Secondary 9(39.1) 6(27.3)Higher
secondary&Above
10(43.5) 11(50)
EmploymentEmployed 12(52.2) 13(59.1)
P=.029Unemployed 7(30.4) 5(22.7)
Student 4(17.4) 4(18.2)Income<2500 16(69.6) 16(72.7)
P=.0012501-10000 4(17.4) 5(22.7)
10001 -above 3(13) 1(4.5)
Family typeNuclear 19(82.6) 18(81.8)
P=.001Joint 4(17.4) 4(18.2)
Habits (Alcohol, smoking)Yes 6(26.1) 10(45.5)
P=.001No 17(73.9) 54.5)
*Chi-squaretestused
Table I shows that majority of the participantsdetailswere comparable.Meanageof theparticipantswere31.4±8.6.
Table 2: frequency and percentage distribution of Clinical factor of clients n = 45
Variable Study n = 23Frequency (%)
Control n = 22Frequency (%)
Family history
No 14(60.8) 14(63.6)
Yes 9(39.1) 8(36.4)Current episode
Mania 19(82.6) 20(90.9)Others 4(17.4) 2(9)Anti–
psychotics 22(95.7) 21(95.5)
Anti-manic 12(52.2) 12(54.5)Antianxiety 18(78.3) 16(72.6)
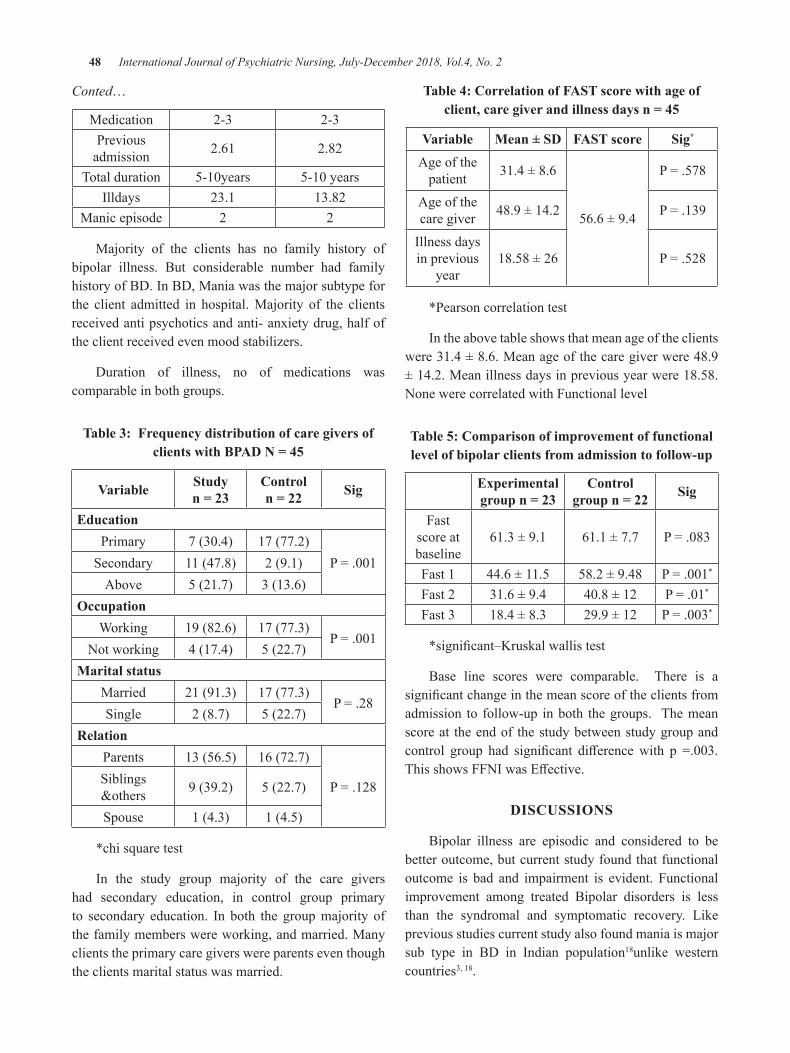
48 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
Conted…
Medication 2-3 2-3Previousadmission 2.61 2.82
Totalduration 5-10years 5-10yearsIlldays 23.1 13.82
Manicepisode 2 2
Majority of the clients has no family history ofbipolar illness. But considerable number had familyhistoryofBd.InBd,Maniawasthemajorsubtypeforthe client admitted in hospital.Majority of the clientsreceivedantipsychoticsandanti-anxietydrug,halfoftheclientreceivedevenmoodstabilizers.
duration of illness, no of medications wascomparableinbothgroups.
Table 3: Frequency distribution of care givers of clients with bPAD n = 45
Variable Studyn = 23
Controln = 22 Sig
EducationPrimary 7(30.4) 17(77.2)
P=.001Secondary 11(47.8) 2(9.1)Above 5(21.7) 3(13.6)
occupationWorking 19(82.6) 17(77.3)
P=.001Notworking 4(17.4) 5(22.7)
Marital statusMarried 21(91.3) 17(77.3)
P=.28Single 2(8.7) 5(22.7)
RelationParents 13(56.5) 16(72.7)
P=.128Siblings&others 9(39.2) 5(22.7)
Spouse 1(4.3) 1(4.5)
*chisquaretest
In the study group majority of the care givershad secondary education, in control group primaryto secondary education. In both the groupmajority ofthefamilymemberswereworking,andmarried.Manyclientstheprimarycaregiverswereparentseventhoughtheclientsmaritalstatuswasmarried.
Table 4: Correlation of FAST score with age of client, care giver and illness days n = 45
Variable Mean ± SD FAST score Sig*
Ageofthepatient 31.4±8.6
56.6±9.4
P=.578
Ageofthecaregiver 48.9±14.2 P=.139
Illnessdaysinprevious
year18.58±26 P=.528
*Pearsoncorrelationtest
Intheabovetableshowsthatmeanageoftheclientswere31.4±8.6.Meanageofthecaregiverwere48.9±14.2.Meanillnessdaysinpreviousyearwere18.58.NonewerecorrelatedwithFunctionallevel
Table 5: Comparison of improvement of functional level of bipolar clients from admission to follow-up
Experimental group n = 23
Control group n = 22 Sig
Fastscoreatbaseline
61.3±9.1 61.1±7.7 P=.083
Fast1 44.6±11.5 58.2±9.48 P=.001*
Fast2 31.6±9.4 40.8±12 P=.01*
Fast3 18.4±8.3 29.9±12 P=.003*
*significant–Kruskalwallistest
Base line scores were comparable. There is asignificantchangeinthemeanscoreoftheclientsfromadmission to follow-up inboth thegroups. Themeanscoreat theendof thestudybetweenstudygroupandcontrol group had significant differencewith p =.003.ThisshowsFFNIwasEffective.
DISCuSSIonS
Bipolar illness are episodic and considered to bebetteroutcome,butcurrentstudyfoundthatfunctionaloutcome is bad and impairment is evident. Functionalimprovement among treated Bipolar disorders is lessthan the syndromal and symptomatic recovery. Likepreviousstudiescurrentstudyalsofoundmaniaismajorsub type in Bd in Indian population18unlike westerncountries3,18.

International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 49
Mean FAST score level also was high whichexplainshigherdisabilityduringacuteperiod,similarfindings have been reported in south India as well asstudyconductedinAustralia18-20.
PooreroverallfunctionsinBdhavebeenreportedin the previous study conducted in Massachusetts 19 which supports current study findings. But studyconducted inChina had contrast findings than presentstudy that patients with schizophrenia have moresignificant deficits in everyday functioning skills thanhealthyindividualsand,insomedomains,patientswithaffective disorders20. Primary care givers weremostlyparent’seventhoughtheclienthadhisownfamily.
Main objective of the study was to check thefeasibility; it’s feasible toconduct the study.From thebase line functional impairment, client had improvedfunctionallevelsignificantlyattheendofthestudywhichwas statistically significant.The current findingsweresupportedbypreviousstudies,thatreportedIntensivepsychosocial treatment enhances relationshipfunctioningand life satisfaction amongpatientswithbipolardisorder16,17.
Limitations of the study was follow-up periodattritionwasunavoidable.2followuponlywaspossible.Since it’s a pilot study associations between variableswerenotestablished.
ConCLuSIon
Psychiatricnurseshouldassess thefunctionof theclientnotonlyduringadmissionevenduringremissionperiodandplanforrehabilitationservices.Sincefunctionisacomplexandtaxingtask.Butit’sveryimportanttobringbacktheclienttohisfullestpossibleleveltonormallifebyplanningeffectivepsychoeducationaboutillness,communication training and teaching problem solvingskills to client and family.Current study suggests thatfunctionalassessmentandnursinginterventioncanhelppatienttocomebacktonearnormalfunctionallevelnotonly during or inter episode euthymic period but alsoduringrelapseperiod.
Conflict of Interest:Nil
Ethical Clearance:InstituteEthicsCommitteeapproved
Source of Funding:Self
REFEREnCES
1.Rehm, LP,Wagner,AL, Ivens-Tyndal C.Mooddisorders:unpopularandbipolar.Comprehensivehandbook of psychopathology. New york: NY:PlenumPublisher;2001.
2.MerikangasKR,JinR,HeJ,KesslerRC,LeeS,SampsonNA,etal.Prevalenceandcorrelatesofbipolar spectrum disorder in the World MentalHealth Survey Initiative. Arch Gen Psychiatry.2011Mar;68(3):241-51.
3.Kraepelin E. Manic-depressive Insanity. NewYork:ArnoPress;1976.
4.Zarate CA Jr, TohenM, LandM, Cavanagh S.Functional impairment and cognition in bipolardisorder.PsychiatrQuaterly.2000;71(4):309–29.
5.TohenM,Hennen J, ZarateCA Jr,BaldessariniRJ,StrakowskiSM,StollA, et al.TheMclean-Harvard First Episode affective disorders withpsychotic features.Am J Psychiatry. 2000 Feb;157(2):220-28.
6.Sanchez-M J, Martinez-AA, Tabarés-SeisdedosR, Torrent C, Vieta E, Ayuso-Mateos J.L.Functioninganddisabilityinbipolardisorder:anextensive review. Psychother Psychosom .2009;78(3):285–97.
7.Tobiasd,danieleSK,LarsO,Schaerer,NaneC,Biedermannetal.InterpersonalandInstrumentalFunctioning of Patients With Bipolar disorderdepends on Remaining depressive Symptoms. GerJPsychiatry.2010;13:61-5.
8.MiklowitzdJ,BiuckiansA,RichardsJA.Early-onset bipolar disorder: A family treatmentperspective.devPsychopathol. 2006Fall;18(4):1247–65.
9.MiklowitzdJ,GeorgeEL,RichardsJA,SimoneauTL,SuddathRL.Arandomizedstudyoffamily-focused psychoeducation and pharmacotherapyintheoutpatientmanagementofbipolardisorder.ArchGenPsychiatry.2003Sep;60(9):904–12.
10.Miklowitz dJ, Otto MW, Frank E, Reilly-HarringtonNA,WisniewskiSR,KoganJN,etal.Psychosocial treatments for bipolar depression:A 1-year randomized trial from the SystematicTreatment Enhancement Program. Arch GenPsychiatry.2007Apr;64(4):419–27.
50 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
11.MiklowitzdJ,WisniewskiSR,MiyaharaS,OttoMW,SachsGS.Perceivedcriticismfromfamilymembers as a predictor of the 1-year course ofbipolardisorder.PsychiatryRes.2005Sep;136(2-3):101–11.
12.MiklowitzdJ,AxelsondA,George EL,TaylordO,SchneckCd,SullivanAE,etal.Expressedemotionmoderates theeffectsof family-focusedtreatment for bipolar adolescents. J Am AcadChildAdolescPsychiatry.2009;48:643–51.
13.Colom F Vieta E. Psychological interventionsin bipolar disorder: fromwishful thinking to anevidence-based approach.Acta Psychiatr ScandSuppl.2004;110(Suppl.422):34–8.
14.LamdH,WatkinsER,HaywardP,BrightJ,WrightK,KerrN,etal.Arandomizedcontrolledstudyofcognitivetherapyofrelapsepreventionforbipolaraffectivedisorder:outcomeofthefirstyear.ArchGenPsychiatry.2003Feb;60(2):145–52.
15.Lam d, Wright K, Sham P. Sense of hyper-positiveselfandresponsetocognitivetherapyinbipolardisorder.PsycholMed.2005;35:69–77.
16.Miklowitz dJ, Otto MW, Frank E, Reilly-HarringtonNA,WisniewskiSR,KoganJN,etal.Psychosocial treatments for bipolar depression:a 1-year randomized trial from the SystematicTreatment Enhancement Program. Arch GenPsychiatry.2007;64(4):419–26.
17.Miklowitz,dJ, OttoMW, Frank E, Reilly-Harrington NA, KoganJN., Sachs GS, et al
.Intensive Psychosocial Intervention EnhancesFunctioning inPatientsWithBipolardepression:ResultsFroma9-MonthRandomizedControlledTrial:AmJPsychiatry.2007Sep;164(9):1340–47.
18.Adriane RR, Jose S-M,AnabelM-A,Manel S,CarlaT,MariaR,etal.Validityandreliabilityofthe FunctioningAssessment Short Test (FAST)inbipolardisorder.ClinPract Epidemiol MentHealth2007,3:5d1-8.
19.Chopra MP, Kumar KV, Jain S, Murthy RS.Psycho-social outcomes for persons withbipolar-Idisorder:Eight-yearfollow-upofaruralcohortfromsouthIndia.AsianJPsychiatr.2010.Jun;3(2):55-9
20.HuaLL,WilensTE,MartelonM,WongP,WozniakJ, and Biederman J. Psychosocial functioning,familiality,andpsychiatriccomorbidityinbipolaryouthwith andwithout psychotic features. J ofClinPsychiatry.2011;vol.72:no.3,pp.397–405
21.McIntoshBJ,ZhangXY,KostenT,TanSP,XiuMH,HarveyPd.Performancebasedassessmentof functional skills in severe mental illness:Resultsofalarge-scalestudyinChina.Jofpsychresearch. 2011;45(8):1089-1094. doi:10.1016/j.jpsychires.2011.01.012.
22.duarte, W., Becerra, R., Cruise. K. TheRelationship Between NeurocognitiveFunctioning and Occupational Functioning inBipolardisorder:ALiteratureReview.Europe’sJofPsychology,2016;http://ejop.psychopen.eu/article/view/909

Stress, Anxiety and coping among Engineering Students at Selected College of Pokhara, Kaski, nepal
Punam Pantha1, Shrestha Sandhya2
1Staff Nurse, Norvic Hospital, Kathmandu, 2Assistant Professor, Manipal College of Medical Sciences (Nursing Program), Pokhara, Nepal
AbSTRACTbackground: Stresshasbeenidentifiedasa20thcenturydiseaseandhasbeenviewedasacomplexanddynamictransactionbetweenindividualandtheirenvironments.Stresscanberegardedasapsychologicalthreat,inwhichtheindividualperceivesasituationasapotentialthreat.
objectives: To assess the level of stress, anxiety and coping among engineering students at PokharaUniversity,Pokhara,Kaski,Nepalandtoassesstheassociationbetweendemographicvariableswithlevelofstressandlevelofanxietyrespectivelyandcorrelationbetweenlevelofstressandlevelofanxiety.
Methodology: ThedescriptivesurveyapproachwasadoptedforpresentstudyandconductedatPokharaUniversity,Pokhara,Kaski,Nepal.Purposivesamplingtechniquewasusedtoselectsamplesandsamplesizewas182.Thetoolconsistedofsociodemographicproforma,PerceivedStressScale,ZungSelfAnxietyRatingScaleandBriefCopeScale.datawascollectedbyselfadministeredquestionnaire.dataanalysisandinterpretationwasdoneusingSPSSforWindowsVersion16.0.
Results: Majorityofstudentshavemoderatelevelofstressandmostofstudentsexperiencedmildlevelanxiety.Mostofthestudentsuse“planning”categoryofcoping.Thereissignificantassociationbetweenlevelofstressandtypeoffamily,reasonforchoosingengineeringandnonsignificantassociationbetweenage,sex,levelofeducation,sourcesofincomeandresidenceandthereissignificanceassociationbetweenlevel of anxiety and reason for choosing engineering and non significant association between levelof anxiety andare, sex, levelof education, typeof family, sourcesof income, residence and reason forchoosingengineering.Thereispositivecorrelationbetweenlevelofstressandlevelofanxietyat0.05levelofsignificance(r=0.171).
Conclusion: Thepresent study concludes thatmajorityof students havemoderate level of stress .Mostof the students use “planning” category of coping. There is no significant association between sociodemographicvariablesandlevelofstressandthereissignificantassociationbetweenlevelofanxietyandsociodemographicvariables.There is significantcorrelationbetweenstressandanxietyat0.05 levelofsignificance(r=0.171).
Keywords: Stress, anxiety, coping, engineering students.
Corresponding Author:SandhyaShresthaAssistantProfessorManipalCollegeofMedicalsciences(NursingProgram),Pokhara,NepalEmail:[email protected]
InTRoDuCTIon
Stress is the “non-specific response of the bodytoanykindofdemandmadeuponit”.Stresshasbeenidentifiedasa20thcenturydiseaseandhasbeenviewedasacomplexanddynamictransactionbetweenindividuals
and their environments. Stress can be regarded as apsychological threat, inwhich the individualperceivesasituationasapotentialthreat.1
Epidemiological studies have shown more than50%ofcollegestudentssufferfromstressandanxietyworldwide and 70-80% of the diseases are related tostress. Studies show that more than 18% of collegestudents in US are experiencing stress and amongwhich30%ofthestressisduetotheacademicpressure.AccordingtoAmericanInstituteofstress8in10collegestudents say they frequently experience stress in theirdailybasis.13%ofthestudentsinUKareexperiencingstresseachyear.2
DOI Number: 10.5958/2395-180X.2018.00016.6
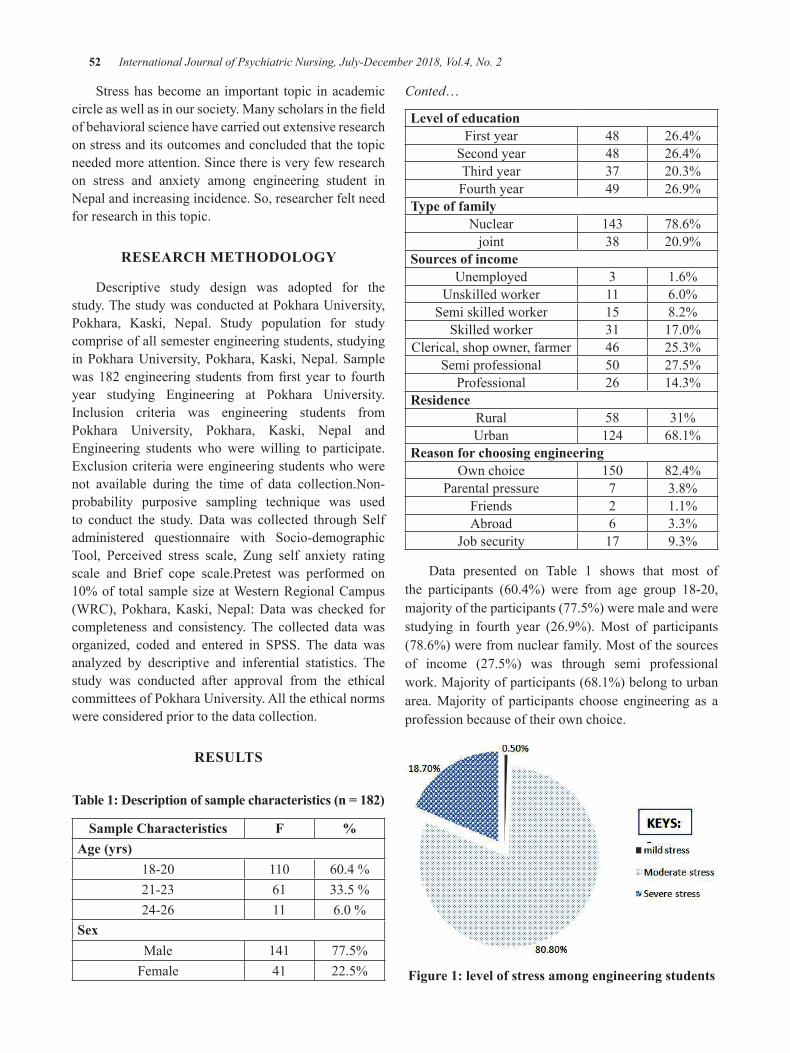
52 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
Stresshasbecomean important topic inacademiccircleaswellasinoursociety.Manyscholarsinthefieldofbehavioralsciencehavecarriedoutextensiveresearchonstressanditsoutcomesandconcludedthatthetopicneededmoreattention.Sincethereisveryfewresearchon stress and anxiety among engineering student inNepalandincreasingincidence.So,researcherfeltneedforresearchinthistopic.
RESEARCH METHoDoLogy
descriptive study design was adopted for thestudy.ThestudywasconductedatPokharaUniversity,Pokhara, Kaski, Nepal. Study population for studycompriseofallsemesterengineeringstudents,studyinginPokharaUniversity,Pokhara,Kaski,Nepal.Samplewas182engineering students fromfirstyear to fourthyear studying Engineering at Pokhara University.Inclusion criteria was engineering students fromPokhara University, Pokhara, Kaski, Nepal andEngineering students who were willing to participate.Exclusioncriteriawereengineeringstudentswhowerenot available during the time of data collection.Non-probability purposive sampling technique was usedto conduct the study.datawas collected through Selfadministered questionnaire with Socio-demographicTool, Perceived stress scale, Zung self anxiety ratingscale and Brief cope scale.Pretest was performed on10%of totalsamplesizeatWesternRegionalCampus(WRC),Pokhara,Kaski,Nepal:datawaschecked forcompleteness and consistency.The collected datawasorganized, coded and entered in SPSS. The data wasanalyzed by descriptive and inferential statistics. Thestudy was conducted after approval from the ethicalcommitteesofPokharaUniversity.Alltheethicalnormswereconsideredpriortothedatacollection.
RESuLTS
Table 1: Description of sample characteristics (n = 182)
Sample Characteristics F %Age (yrs)
18-20 110 60.4%21-23 61 33.5%24-26 11 6.0%
SexMale 141 77.5%Female 41 22.5%
Conted…
Level of educationFirstyear 48 26.4%Secondyear 48 26.4%Thirdyear 37 20.3%Fourthyear 49 26.9%
Type of familyNuclear 143 78.6%joint 38 20.9%
Sources of incomeUnemployed 3 1.6%
Unskilledworker 11 6.0%Semiskilledworker 15 8.2%Skilledworker 31 17.0%
Clerical,shopowner,farmer 46 25.3%Semiprofessional 50 27.5%Professional 26 14.3%
ResidenceRural 58 31%Urban 124 68.1%
Reason for choosing engineeringOwnchoice 150 82.4%
Parentalpressure 7 3.8%Friends 2 1.1%Abroad 6 3.3%
Jobsecurity 17 9.3%
data presented on Table 1 shows that most ofthe participants (60.4%) were from age group 18-20,majorityoftheparticipants(77.5%)weremaleandwerestudying in fourth year (26.9%).Most of participants(78.6%)werefromnuclearfamily.Mostofthesourcesof income (27.5%) was through semi professionalwork.Majorityofparticipants(68.1%)belongtourbanarea.Majority of participants choose engineering as aprofessionbecauseoftheirownchoice.
Figure 1: level of stress among engineering students
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 53
datarepresentedfromfig1indicatemajority(80.8%)ofengineeringstudentshadmoderatestress,18.7%haveseverestressandverylessi.e(0.5%)ofengineeringstudentshavemildstress.
KEyS
Figure 2: level of anxiety among engineering students
datarepresentedfromfig2indicatemajority(79.1%)ofengineeringstudentsneverexperienceanxiety,(20.3%)experiencemildlevelofanxiety,(0.5%)ofengineeringstudentsexperienceanxietyinmoderateamount.
Table 2: table showing frequency and percentage of Coping (n = 182)
Items never n (%)
Little bit n (%)
Moderate Amount n (%)
A lot n (%)
Self distractionturningtoworkorotheractivities 24(13.2) 62(34.1) 57(31.3) 39(21.4)
doingsomethingtothinkaboutitless. 11(6.0) 50(27.5) 73(40.1) 48(26.4)Active coping
concentratingmyeffortsondoingsomething 6(3.3) 47(25.8) 64(35.2) 65(35.7)takingactiontotrytomakethesituationbetter 8(4.4) 27(14.8) 68(37.4) 79(43.4)
Denialsayingtomyself“thisisn’treal.” 44(24.2) 70(38.5) 48(26.4) 20(11.0)
refusingtobelievethatithashappened. 47(25.8) 63(34.6) 51(28.0) 21(11.5)Substance abuse
usingalcoholorotherdrugstomakemyselffeelbetter. 119(65.4) 25(13.7) 18(9.9) 20(11.0)
usingalcoholorotherdrugstohelpmegetthroughit 112 (67.0) 28(15.4) 21(11.5) 11(6.0)
Emotional supportgettingemotionalsupportfromothers 27(14.8) 62(34.1) 47(25.8) 46(25.3)
gettingcomfortandunderstandingfromsomeone 20(11.0) 51(28.0) 66(36.3) 45(24.7)Instrumental support
gettinghelpandadvicefromotherpeople 17(9.3) 48(26.4) 64(35.2) 53(29.1)tryingtogetadviceorhelpfromotherpeopleaboutwhat
todo. 11(6.0) 52(28.6) 62(34.1) 57(31.3)
behavioral disengagementgivinguptryingtodealwithit. 66(36.3) 47(25.8) 45(24.7) 24(13.2)givinguptheattempttocope. 68(37.4) 49(26.9) 50(27.5) 15(8.2)
54 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
Conted…
Ventingsayingthingstoletmyunpleasantfeelingsescape 46(25.3) 71(39.0) 44(24.2) 21(11.5)
expressingmynegativefeelings. 59(32.4) 69(37.9) 35(19.2) 19(10.45)Positive reframingtryingtoseeitinadifferentlight,tomakeitseemmore
positive. 18(9.9) 40(22.0) 68(37.4) 56(30.8)
lookingforsomethinggoodinwhatishappening 4(2.25) 25(13.7) 69(37.95) 84(46.25)Planning
tryingtocomeupwithastrategyaboutwhattodo. 10(5.5) 35(19.25) 62(34.1) 74(40.7)thinkinghardaboutwhatstepstotake. 12(6.6) 29(15.9) 63(34.6) 78(42.9)
HumorI’vebeenmakingjokesaboutit. 51(28.0) 58(31.9) 35(19.2) 38(20.9)
I’vebeenmakingfunofthesituation. 41(22.5) 52(28.6) 43(23.6) 46(25.3)Acceptance
acceptingtherealityofthefactthatithashappened. 18(9.9) 30(16.5) 67(36.8) 67(36.8)learningtolivewithit. 10(5.5) 30(16.5) 73(40.1) 69(37.9)
datapresentedintable2showsthat40.1%ofparticipantsdosomethingtothinkaboutthestressless,suchasgoingtomovies,watchingTV,reading,daydreaming,sleepingorshoppinginmoderateamount.Majority43.4%oftheparticipantstakesanactiontotrytomakethesituationbetterasanactivecopingmethod.38.5%oftheparticipantssometimessaysthatthesituationisnotrealasadenialmethodofcoping.Majority67.0%oftheparticipantsneverusealcoholorotherdrugstohelpgetthroughthestressfulsituation.34.1%oftheparticipantsgetsemotionalsupportfromotherstocopeupwiththestressfulsituation.35.2%oftheparticipantsgethelpandadvicefromotherpeopletocopeandveryfew6.0%oftheparticipantsnevertrytogetadviceorhelpfromotherpeopleaboutwhattodo.37.4%oftheparticipantsnevergiveuptheattempttocopeandveryfew13.2%giveuptryingtodealwiththesituationmostofthetime.39.0%oftheparticipantsmostofthetimelooksforsomethinggoodinhappeningand9.9%nevertrytoseethethingsindifferentlighttomakeitseemmorepositive.42.9%oftheparticipantsdoplanningandthinkhardaboutfurtherstepstotakemostofthetimeand5.5%oftheparticipantsneverdoplanningupwithastrategyaboutwhattodo.31.9%oftheparticipantssometimeshavebeenmakingjokesaboutthesituationtocope.40.1%oftheparticipantsoftenacceptsthesituationandlearntolivewithitand9.9%oftheparticipantsneveraccepttherealityofthefactthathashappened.31.9%oftheparticipantsmostofthetimestrytofindcomfortintheirreligionorspiritualbeliefsand17.6%never try tofindcomfort in their religionor spiritualbeliefs.37.4%of theparticipantsnevercriticizethemselvesforthestressfulsituationand15.4%mostofthetimeblamethemselvesforthingsthathappened.
Table 3: Association between level of stress and selected socio demographic variables (n = 182)
Socio-demographic variables
Level of stress Chi-squaredf Significance Mild
stressModerate
StressSevere stress
Calculatedvalue
Tabulatedvalue
Type of familyNuclear 0 120 23 6.099 5.99 2 SJoint 1 27 10
Reason for choosing engineeringOwnchoice 0 124 26
15.705 15.51 8 SParentalpressure 0 4 3
Friends 0 1 1Abroad 0 6 0
Jobsecurity 1 12 4
Atp<0.05,NS=Nonsignificant,S=Significant
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 55
Table3revealsthatthereissignificantassociationbetweenlevelofstressandtypeoffamily,reasonforchoosingengineeringandnonsignificantassociationbetweenage,sex,levelofeducation,sourcesofincomeandresidence.
Table 4: Association between level of anxiety and selected socio demographic variables n = 182
Socio-demographic
variables
Level of anxiety Chi-square
df Significance normal Mild to
moderateModerate to Severe Extreme Calculated
valueTabulated
value
Reason of choosing engineeringOwnchoice 117 33 0 0
28.770 15.51 8 SParentalpressure 5 1 1 0
Friends 1 1 0 0Abroad 5 1 0 0
Jobsecurity 16 1 0 0
P<0.05,S=Significance,NS=Notsignificant
Table4revealsthatthereissignificanceassociationbetween level of anxiety and reason for choosingengineering and non significant association betweenlevel of anxiety and are, sex, level of education, typeoffamily,sourcesof income,residenceandreasonforchoosingengineering.
Table 5: Co-relation between level of stress and level of anxiety (n = 182)
Variables Correlation coefficient (r)
P value Significance
Levelofstress
0.171 0.021 SignificanceLevelofanxiety
Table5showsthatcorrelationbetweenlevelofstressandlevelofanxietywasfoundtobepositiveatsignificantlevelof0.05.Therefore, theresearcherrejects thenullhypothesisandacceptsthealternativehypothesiswhichcan be concluded that there is significant relationshipbetweenlevelofstressandlevelofanxiety.
DISCuSSIon
A comparative research study was conducted byKumar.S and Bhukar.j.p among engineering studentsinIndiashowedthatstresslevelwashighamonggirls3. Thisstudysupportsthepresentstudyas(22.20%)girlshadseverestressascomparedtoboys.
A descriptive study was conducted by LisaSchneideratCornellUniversityCollegeofengineeringshowedthatperceivedstresslevelvariedsignificantlybygender.4Thisstudysupportsthepresentstudyaslevelofperceivedstressdifferenceamongmaleandfemaleandseverestressishighamongfemale.
A Cross-sectional study was conducted byWaghachavare.V.B in Sangi district of westernMaharashtra Indiashowed that therewasnostatisticalsignificant between stress and environmental factors.5 Whichisconsistentwithpresentstudywherethereisnosignificantcorrelationbetweenstressandenvironmentalfactorssuchasresidence.
A Co relational study conducted by Aziah.A,Norzaidi.M, Choy Chong.S and et.all at Malaysia toexaminetherelationshipbetweenstressfactorsandthelevel of perceived stress at three different periods ofsemesterandtheirimpactontheacademicperformanceofdiplomaEngineeringstudents.Studyshowedthatinanoverallstudentsexpressedmoderatelevelofstress6.Thisstudysupportsthepresentstudywheremajorityofthestudentsexperiencesmoderatelevelofstress.
ConCLuSIon
The present study concludes that the majorityof students havemoderate level of stress andmost ofstudents experienced mild level of anxiety. Most ofthe students use “planning” category of coping.Thereis significant association between level of stress and

56 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
type of family, reason for choosing engineering andnon significant association between age, sex, level ofeducation, sources of income and residence and thereissignificanceassociationbetweenlevelofanxietyandreason for choosing engineering and non significantassociationbetweenlevelofanxietyandare,sex,levelofeducation,typeoffamily,sourcesofincome,residenceandreasonforchoosingengineering.There ispositivecorrelationbetweenlevelofstressandlevelofanxietyat0.05levelofsignificance(r=o.017,p=0.02).
Source of Funding:Self
Conflict of Interest:Nil
REFEREnCES
1. EswiAS, Radis andYoussri H. Stress/stressorsperceived by Baccalaureate Saudi Nursingstudents. Middle East Journal of scientificResearch.2013;14(2):193-202.
2.Stress,Anxietyanddepression.WashingtondC,Georgetown University, 2011. Available from
http://student health georgetown.edu/ health-issues/stressanxietydepression.
3.Kumar.S andBhukar.J.P. Stress level and copingstrategiesofcollegestudents.Journalofphysicaleducationandsportsmanagement2013;4(1):5-11.
4.Schneider.L.PerceivedStressamongEngineeringStudents 2002. Available from https://www.asee.org/documents/sections/st-lawrence/2007/Schneider-2007-Student-perceived-stress.pdf
5.Waghachavare.V.B, dhumale.G.B, Kadam.Y.RandGore.A.d.AStudyofStressamongStudentsof Professional Colleges from an urban areaIn India 2013; 13(3):429-436. Available from)http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3749028/
6.Rafidah.K. The impact of perceived stress andstress factors onAcademic performance of Pre-diploma Science Students:A Malaysian Study.International Journal of Scientific Research inEducation2009;2(1):13-26.

Effectiveness of Structured Teaching Programme on Level of Knowledge Regarding Safe Motherhood among Antenatal
Mothers at Maternity Centre, Salem
Santhi M. D.1, Kanaga Durga M.2, Manjula b.3, Sathya J.3
1Professor cum HOD, 2Asst. Professor, 3Lecturer, Sri Gokulam College of Nursing, Salem
AbSTRACT
Theworldhealthorganizationestimated that150millionpregnanciesoccurannually.pregnancy relatedcomplications die nearly 6, 00,000 each year; of these 99% of death occurs in developing countries.Quantitativeexperimentalresearchapproachwasadoptedforthisstudy.60sampleswereselected(n=60)atgestationalweeksof28-34weeksbasedoninclusioncriteriabyusingpurposivesamplingtechnique.Pre-testwasconductedwiththehelpofstructuredinterviewschedule.Structuredteachingprogrammeonsafemotherhoodwasgivenandposttestwasconductedafter15days.ThestudyfindingsshowedthatMajorityofthemothers(53%)werebetween33-34weeksofgestation.Inpretest88%ofmothershadinadequateknowledge,whereasinpost test68%ofmothershadmoderatelyadequateknowledge.Themeanpretestscorewas11.79±6.07whereasinposttestmeanscorewas32.66±6.47.Thecalculated‘t’valuewas26.14whichwashighlysignificantatp≤0.05level.Henceitwasprovedthatthestructuredteachingprogrammeonknowledgeregardingsafemotherhoodwaseffective. Therewasnosignificantassociationbetweenpreandposttestknowledgescoreswithdemographicvariables.
Keywords: Safe Motherhood, Pregnancy,Structured teaching programme
InTRoDuCTIon
The Safe Motherhood Initiative was launchedby the World Health Organization (WHO) and otherinternationalagencyincludesUNICEF,UNFPA,WorldBank, Population Council and IPPF in 1987 and wasimmediatelysupportedbyICM.Atthattimethenumberof women suffering maternal deaths worldwide wasestimated to be at least 600,000 each year with 99%ofdeathsoccurringinthedevelopingworld.Themostcommondirectcausesofsuchdeathsareknowntobesevere bleeding infection leading to sepsis the effectsofunsafeabortion,eclampsia,hypertension,obstructedlabour,anaemiaandmalnutrition.1
Almost 35% of women in developing countriesreceive no antenatal care during pregnancy; in somecountriesantenatalcoverageisaslowas26%.Millionsofwomendonothaveaccesstogoodqualityofhealthservices during pregnancy and childbirth, especially,womenwhoarepoor,uneducatedorwho live in ruralareas(UNFPA1996). 2
The goal of Safe Motherhood Initiative is to cutmaternal mortality by half by the year 2010, global
experience has shown that pregnancy related deathsare preventable and a significant body of research onstrategies for reducing maternal mortality has beengenerated.Itisaddressedtogovernments,policymakers,programmanagersandeachof therespectiveagenciespersonnelandisintendedtoguidetheirdecisionmakingtoensuresaferpregnancyandchildbirth.3
Theprimaryfocusofmodernobstetricalnursingisonpreventivecareofpregnantwomen.Themainaimofwhichistohelpthemotherstohaveasafeandnaturalchildbirth.Successfulantenatalcareandeducationcanbetterpreparewomenandfamiliestocareforthemselves.Asaresult,itreducestoonematernaldeathinavillageof1000populationandittakes9-10yearstoseeit.4
developments and trends of safe motherhoodinitiative since 1987, has identified, Essential stepsneeded to reduce maternal mortality, early diagnosedandnowemphasizesmaking skilledcareavailable foreachbirth.Countriesthatprovideskilledbirthattendantsand access to emergency obstetric care have cut theirmaternaldeaths.Tunisiareduceditsmaternalmortalityrate by 80% in 23 years with such a comprehensive
DOI Number: 10.5958/2395-180X.2018.00017.8
58 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
strategy and Sri Lanka reduced itsmaternalmortalityratefrommorethan1,500per100,000livebirthsinthe1960and30today. 5
Theworldhealthorganizationestimatedthat 150 million pregnancies occur annually.Among these women who die of pregnancyrelated complications, nearly 6,00,000 womendie each year; of these 99%of death occurs indevelopingcountries.6
India has a highmortality rate. In India, in every5 minutes 1 women dies from complications relatedto pregnancy and child birth. This adds upto total of1,21,000 women per year. Maternal mortality rate in1938was20per1000livebirthin1954.In1990maternalmortalityrateinIndiawasper1,00,000livebirth.Thetrendasnotchanged in last5years.Thismeansmorethan 1,00,000women die each year due to pregnancyrelatedtocauses.7
According to sample registration survey estimates1.1% of all deaths in the country in 1991 were dueto maternal causes. An estimate 82,93,770 deathsoccuredofwhich91,231wererelatedtopregnancyandchildbirth. Unless appropriate measures are taken itsmay reach its peak and endanger the life ofmother’s.Studies also indicate that it ismorewith the illiterateor for thosewhohave poor knowledge regarding safemotherhood.8
Statement of the Problem: A study to evaluate theEffectivenessofSTPon levelofknowledge regardingsafemotherhoodamongantenatalmothersatMaternityCentre,Salem.
OBJECTIVES
1.To assess the level of knowledge on safemotherhood among antenatal mothers beforeimplementationofstructuredteachingprogramme.
2.Toassesstheeffectivenessofstructuredteachingprogrammeonsafemotherhood.
3.To associate the pre and post test scores withselecteddemographicvariables amongantenatalmothers.
Hypotheses:
z H1: There is a significant difference between preandposttestknowledgescoresonsafemotherhoodamongantenatalmothersatp≤0.05level.
z H2: There is a significant association betweenpre and post test knowledge scoreswith selecteddemographicvariableamongantenatalmothersatp≤0.05level.
Conceptual Framework: The investigator adoptedModifiedWidenbach’s PrescriptiveTheory -A helpingart of Clinical Nursing(1964) theory as a basis ofconceptual framework, which is aimed to assess theeffectiveness of Structured Teaching Programme onSafemotherhoodamongantenatalmothers.
MATERIALS & METHoD
Quasiexperimentalonegrouppre-testandpost-testresearchdesignwasusedforthisstudy.ThestudywasconductedinAnnaMaternityCentre,Salem.PurposiveSampling technique was adopted and selected 60Antenatalmothersforthisstudy.TheinclusioncriteriawereMothersofbothprimiandmultigravidaandalsohave 28-34 weeks of gestation. Structured InterviewSchedule and structured Teaching Programme wereused to assess the pre test and post test knowledgescore. The researcher obtained permission from theMedicalOfficerofAnnaMaternityCentre.Pre-testwasconductedbystructuredinterviewschedule.Structuredteachingprogrammeonsafemotherhoodwasgivenandpost test was conducted after 15 days by using sameStructured Interview Schedule. descriptive statisticswere used to assess the level of knowledge regardingsafemotherhood. Inferentialstatisticssuchaspaired‘t’testwasused toassess thepreandpost test scoresonknowledge.Chi-squaretestwasusedtoassociatethepreandposttestscoreswiththeirdemographicvariables.
RESuLTS &DISCuSSIon
The highest percentage (63%) of mothers in theagegroupwere21-25years.Themaximumpercentage(35%)ofmotherswas completed secondaryeducationand Majority of the them (32%) were daily wages.Maximumhalfofthemothers(49%)belongstonuclearfamilyandhavethefamilyincomeoflessthanRs.3000(44%). Majority of the mothers (53%) were between33-34 weeks of gestation, and more or less similarpercentageofmotherswerebetween28-30weeks(27%)and 31-32 weeks of gestation (20%). The maximumpercentage(62%)ofmotherswereprimiand(38%)ofmothersweremultigravidamothers.Mostofthemothers(40%)receivedinformationregardingsafemotherhoodthroughtheirfamilymembersandmoreorlesssimilarpercentage of mothers obtained information throughRadioandTelevision(12%)andbooksandnewspaper(15%)respectively.
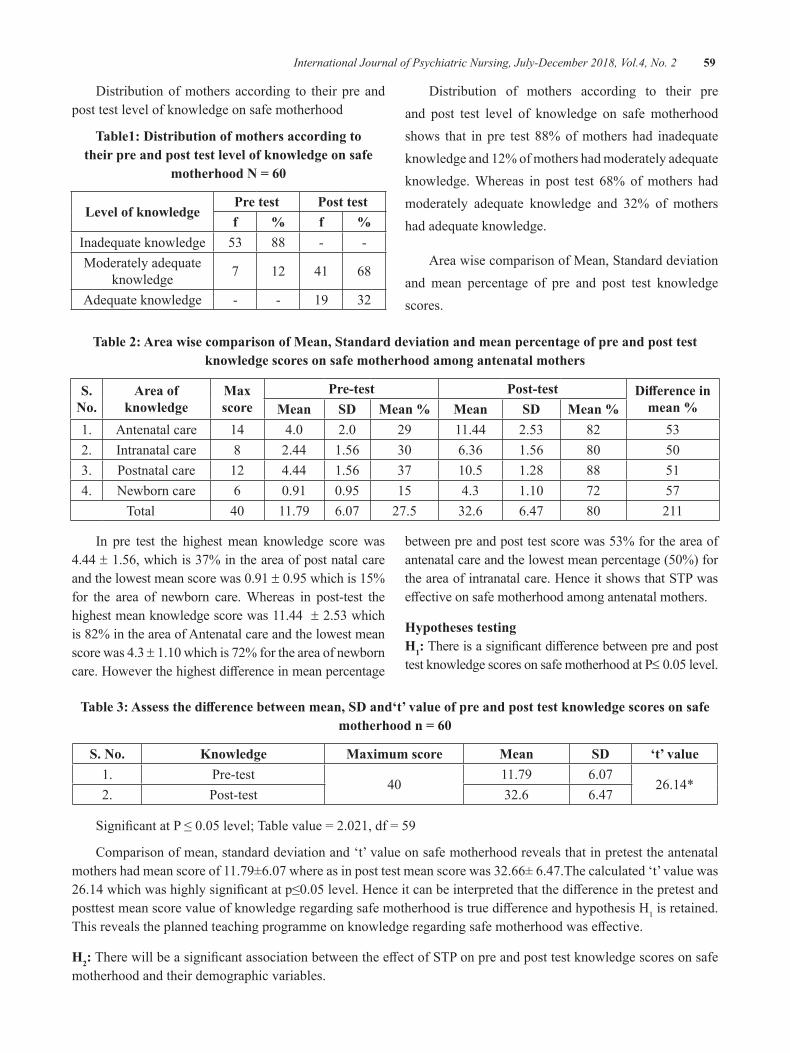
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 59
distributionofmothersaccording to theirpreandposttestlevelofknowledgeonsafemotherhood
Table1: Distribution of mothers according to their pre and post test level of knowledge on safe
motherhood n = 60
Level of knowledgePre test Post testf % f %
Inadequateknowledge 53 88 - -Moderatelyadequate
knowledge 7 12 41 68
Adequateknowledge - - 19 32
distribution of mothers according to their preand post test level of knowledge on safemotherhoodshows that inpre test 88%ofmothershad inadequateknowledgeand12%ofmothershadmoderatelyadequateknowledge.Whereas in post test 68% ofmothers hadmoderately adequate knowledge and 32% of mothershadadequateknowledge.
AreawisecomparisonofMean,Standarddeviationand mean percentage of pre and post test knowledgescores.
Table 2: Area wise comparison of Mean, Standard deviation and mean percentage of pre and post test knowledge scores on safe motherhood among antenatal mothers
S. no.
Area of knowledge
Max score
Pre-test Post-test Difference in mean %Mean SD Mean % Mean SD Mean %
1. Antenatalcare 14 4.0 2.0 29 11.44 2.53 82 532. Intranatalcare 8 2.44 1.56 30 6.36 1.56 80 503. Postnatalcare 12 4.44 1.56 37 10.5 1.28 88 514. Newborncare 6 0.91 0.95 15 4.3 1.10 72 57
Total 40 11.79 6.07 27.5 32.6 6.47 80 211
In pre test the highestmean knowledge score was4.44 ±1.56,whichis37%intheareaofpostnatalcareandthelowestmeanscorewas0.91± 0.95whichis15%for the area of newborn care.Whereas in post-test thehighestmeanknowledgescorewas11.44±2.53whichis82%intheareaofAntenatalcareandthelowestmeanscorewas4.3± 1.10whichis72%fortheareaofnewborncare.Howeverthehighestdifferenceinmeanpercentage
betweenpreandposttestscorewas53%fortheareaofantenatalcareandthelowestmeanpercentage(50%)fortheareaofintranatalcare.HenceitshowsthatSTPwaseffectiveonsafemotherhoodamongantenatalmothers.
Hypotheses testingH1:ThereisasignificantdifferencebetweenpreandposttestknowledgescoresonsafemotherhoodatP≤0.05level.
Table 3: Assess the difference between mean, SD and‘t’ value of pre and post test knowledge scores on safe motherhood n = 60
S. no. Knowledge Maximum score Mean SD ‘t’ value1. Pre-test
4011.79 6.07
26.14*2. Post-test 32.6 6.47
SignificantatP≤0.05level;Tablevalue=2.021,df=59
Comparisonofmean,standarddeviationand‘t’valueonsafemotherhoodrevealsthatinpretesttheantenatalmothershadmeanscoreof11.79±6.07whereasinposttestmeanscorewas32.66±6.47.Thecalculated‘t’valuewas26.14whichwashighlysignificantatp≤0.05level.HenceitcanbeinterpretedthatthedifferenceinthepretestandposttestmeanscorevalueofknowledgeregardingsafemotherhoodistruedifferenceandhypothesisH1isretained.Thisrevealstheplannedteachingprogrammeonknowledgeregardingsafemotherhoodwaseffective.
H2:TherewillbeasignificantassociationbetweentheeffectofSTPonpreandposttestknowledgescoresonsafemotherhoodandtheirdemographicvariables.
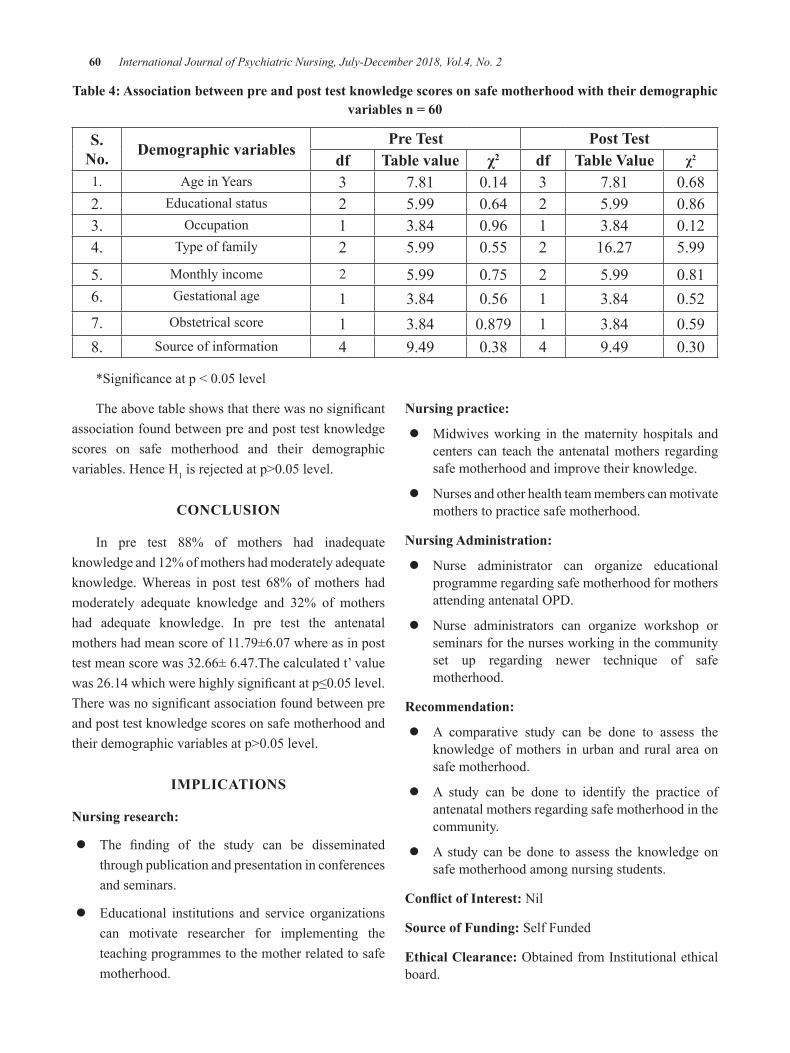
60 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
Table 4: Association between pre and post test knowledge scores on safe motherhood with their demographic variables n = 60
S. no. Demographic variables
Pre Test Post Testdf Table value χ2 df Table Value χ2
1. AgeinYears 3 7.81 0.14 3 7.81 0.682. Educationalstatus 2 5.99 0.64 2 5.99 0.863. Occupation 1 3.84 0.96 1 3.84 0.124. Typeoffamily 2 5.99 0.55 2 16.27 5.99
5. Monthlyincome 2 5.99 0.75 2 5.99 0.816. Gestationalage 1 3.84 0.56 1 3.84 0.527. Obstetricalscore 1 3.84 0.879 1 3.84 0.598. Sourceofinformation 4 9.49 0.38 4 9.49 0.30
*Significanceatp<0.05level
nursing practice:
z Midwivesworking in thematernity hospitals andcenters can teach the antenatalmothers regardingsafemotherhoodandimprovetheirknowledge.
z Nursesandotherhealthteammemberscanmotivatemotherstopracticesafemotherhood.
nursing Administration:
z Nurse administrator can organize educationalprogrammeregardingsafemotherhoodformothersattendingantenatalOPd.
z Nurse administrators can organize workshop orseminarsforthenursesworkinginthecommunityset up regarding newer technique of safemotherhood.
Recommendation:
z A comparative study can be done to assess theknowledgeofmothers inurbanand rural areaonsafemotherhood.
z A study can be done to identify the practice ofantenatalmothersregardingsafemotherhoodinthecommunity.
z A study can be done to assess the knowledge onsafemotherhoodamongnursingstudents.
Conflict of Interest:Nil
Source of Funding:SelfFunded
Ethical Clearance:ObtainedfromInstitutionalethicalboard.
Theabovetableshowsthattherewasnosignificantassociationfoundbetweenpreandposttestknowledgescores on safe motherhood and their demographicvariables.HenceH1isrejectedatp>0.05level.
ConCLuSIon
In pre test 88% of mothers had inadequateknowledgeand12%ofmothershadmoderatelyadequateknowledge.Whereas in post test 68% ofmothers hadmoderately adequate knowledge and 32% of mothershad adequate knowledge. In pre test the antenatalmothershadmeanscoreof11.79±6.07whereasinposttestmeanscorewas32.66±6.47.Thecalculatedt’valuewas26.14whichwerehighlysignificantatp≤0.05level.Therewasnosignificantassociationfoundbetweenpreandposttestknowledgescoresonsafemotherhoodandtheirdemographicvariablesatp>0.05level.
IMPLICATIonS
nursing research:
z The finding of the study can be disseminatedthroughpublicationandpresentationinconferencesandseminars.
z Educational institutions and service organizationscan motivate researcher for implementing theteachingprogrammestothemotherrelatedtosafemotherhood.
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 61
REFEREnCES
1.Susila C (2008) “level of self motivationamong primiparae mothers towards antenatalcare” Journal of clinical nursing, Education,Training and career development: Volume 3Number1,Januvary;p:7-9
2.AliYawarAlam,AkhalAliQuresi“comparatativestudyofknowledgeandpracticeamongantenatalcarefacilitiesutilizingandnon-utilisingwomen”perinatal(2007)december6:18059464
3.Nahala A Kishk “knowledge and practice ofwomen towards antenatal care rural urbancomparison”.Arch Gynecol/obstet 2009 sep2;19727783
4.Kathryn S Panaretlo “sustainable antenatalcare services in an urban community”MJA2007;187(18-22)
5.Hassan Ali “knowledge and practice amongAntenatalcare facilities”JPakmedAssociation2005Feb;55(2)p;53-56
6.Blondel B,Pusch d,Schmidit E “somecharacteristics of antenatal care in 13 EuropeanCountries”Br:J Obset Gynaecol,1985jan:92(6);565-568(pubmed)
7.Adil HIbnouf,Johannes AMaarse “utilizationof antenatal care services for women in theirreproductiveage”JournalofEgyptPublicHealthAssociation2002;77(5-6);479-98;17216974
8.Maternal health division department of familyWelfare Ministry of Health & Family WelfareGovernment of India “Guidelines forAntenatalcare”2005April(1_22)
A Study to Compare the Effects of Music Therapy and Laughter Therapy on Reducing Level of Depression among
old Age People old Age Homes
Seema M. boresa1, Deepak Krishnamurthy2
12nd year M.Sc. Nursing student, 2HOD of Mental Health Nursing, Manikaka Topawala Institute of Nursing–A constituent of Charotar University of science & Technology, Changa, Taluka : Petlad,
District: Anand, Gujarat, India
AbSTRACT
TheResearcheraims tocompare theeffectsofmusic therapyand laughter therapyon reducing levelofdepressionamongoldagepeopleinselectedoldagehomes.Reviewofliteratureshowsthatdepressionismostcommonpsychologicalproblemsamongoldagegroup.Musicandlaughtertherapyisaeffectivenonpharmacological,noninvasivetherapytoreducethelevelofdepressionamongelderlypeopleinoldagehomes.
Keywords: Music therapy, Laughter therapy, Level of depression, Old age people
Corresponding Author:Ms.SeemaMBoresa2ndyearM.Sc.Nursingstudent,ManikakaTopawalaInstituteofNursing–AconstituentofCharotarUniversityofscience&Technology,Changa,Taluka:Petlad,district:Anand-388421,Gujarat,IndiaEmail:[email protected]
InTRoDuCTIon
The world’s population is rapidly aging anddeveloping countries are more involved with suchissue. According to the United Nations’ estimates,elderlypopulationispredictedtoincreasefromalmost10.5%ofthetotalpopulationin2007to28.8%by2050.[1]Aging is a worldwide issue in our society, Elderlypeoplelivinginoldagehomesmaysufferfromsadness,painandisolation.NumerousstudieshavedocumentedahighprevalenceofdepressedmoodandotherdepressivesymptomsinelderlyPersonslivinginthecommunity.[2]
TheNationalInstituteofMentalHealth’sepidemiologiccatchmentArea (ECA)program found that one of themostcommonmentaldisordersofelderlyaredepressivedisorders.[3] Music therapy minimizes the pain andenhances sleep. Music therapy has been recognized
as an effectivemethod in helping the elderly improveboththeirphysicalandmentalhealth.[4]Laughtertherapyhasbeenalsousedtoreducedepressionamongelderlypeople.Laughtertherapyisauniqueconceptwhichuseslaughterasagroupexercise,asitisaphysicallyorientedtechnique.Laughter therapy is theonly technique thatallows adults to achieve sustained laughter withoutinvolvingincognitivethought.[5]
MATERIAL METHoDS AnD FInDIngS
Thestudyistocomparetheeffectsofmusictherapyandlaughtertherapyonlevelofdepressionamongoldagepeopleinoldagehomes.
REVIEW oF LITERATuRE
1.Haejinko and Changho youn conducted studyto investigate the effects of laughter therapy ondepression, cognitive function, quality of life,andsleepoftheelderlyinacommunity.BetweenJulyandSeptember2007,thetotalstudysampleconsistedof109subjectsagedover65dividedintotwo groups; 48 subjects in the laughter therapygroupand61 subjects in thecontrolgroup.Thesubjectsinthelaughtertherapygroupunderwentlaughtertherapyfourtimesover1month.Study
DOI Number: 10.5958/2395-180X.2018.00018.X
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 63
compared Geriatric depression Scale (GdS),Mini-MentalStateExamination(MMSE),Short-Form Health Survey-36 (SF-36), InsomniaSeverityIndex(ISI)andPittsburghSleepQualityIndex(PSQI)betweenthetwogroupsbeforeandafter laughter therapy.Therewerenosignificantdifferences in baseline characteristics betweenthe twogroups. Laughter therapy is consideredto be useful, cost-effective and easily-accessibleinterventionthathaspositiveeffectsondepression,insomnia,andsleepqualityintheelderly.[6]
2.ArandomisedcontrolledstudywasconductedbyMoon Fai Chan, ZiYangWong,HideakiOnishiand Naidu Vellasamy Thayala, from July 2009–June 2010 at participants’ home in Singapore.In total, 50 older adults (24using music and 26control)completedthestudyafterbeingrecruited.Participantslistenedtotheirchoiceofmusicfor30minutes per week for eight weeks. depressionscoreswerecollectedonceaweekforeightweeks.depression levels reduced weekly in the musicgroup, indicating a cumulativedose effect, and astatistically significant reduction in depressionlevels was found over time in the music groupcompared with non-music group. So Listeningto music can help older people to reduce theirdepression level.Music isanon-invasive,simpleandinexpensivetherapeuticmethodofimprovinglifequalityincommunity-dwellingolderpeople.[7]
3. J korean conducted study to investigate theeffects of visiting laughter therapy on depressionand insomnia in the vulnerable elderly.A quasi-experimental non equivalent control group pretests-posttestdesignwasusedforthisstudy.Theparticipantswere 87 elderlywhowere registeredin the Tailored Visiting Health Program ofpublic health centers. data were collected fromSeptember to November 2010.The experimentalgroup received 10~15 min of laughter therapyonceaweekfor8weeks.TheinstrumentsincludedGeriatricdepressionScaleandInsomniaSeverityIndex tomeasure depression and sleep problemsbefore and after the laughter therapy.The resultsshowedthatvisitinglaughtertherapywaseffectivein decreasing depression and insomnia amongthe vulnerable elderly. These findings indicatethat laughter therapymaybeaneffectivenursinginterventiontoimprovedepressionandinsomnia.[8]
4.JaakkoErkkila¨,Marko Punkanen, Jo¨rgFachner,EsaAla-Ruona,IngaPo¨ntio¨,MariTervaniemi,MaunoVanhalaandChristianGoldetal,conductedstudytodeterminetheefficacyofmusictherapyadded to standard care compared with standardcare only in the treatment of depression amongworking-agepeoplein2011.Participants(n=79)with an ICd–10 diagnosis of depression wererandomised to receive individual music therapyplus standard care (20 bi-weekly sessions) orstandard careonly, and followedup at baseline,at3months(afterintervention)andat6months.Theresponseratewassignificantlyhigherforthemusictherapyplusstandardcaregroupthanforthestandardcareonlygroup(oddsratio2.96,95%CI1.01to9.02).Individualmusictherapycombinedwith standard care is effective for depressionamongworking-agepeoplewithdepression.[9]
5.Jinliangwang, Haizhenwang, and dajunzhangconductedstudytoexamine theeffectsofgroupmusic therapy on depression and mental healthamong college students in 2011. The balancegrouppre-test andpost-test experimental designwas used. The college students with the scoreof self-rating depression scale, greater than 40and score of depression factors of SCL-90, thesymptomchecklist,greaterthan2.18areselectedastheparticipants.80studentsparticipatedinthisstudy,with40assignedtocontrolgroupandother40 assigned to experimental group. The resultsshowed that after the group music therapy, forthe experimental group, the depression scoreshavereducedsignificantlyandthementalhealthscores have improved, while for the controlgroup,nosignificantdifferencewasobtainedonthe depression and mental health scores. Thisindicatesthatgroupmusictherapycaneffectivelyreducedepressionandimprovementalhealth.[10]
6.Ravikumar conducted study to aseess theeffectiveness of music therapy on level ofdepression among elderly people residing inselected old age home in Pune in 2012.QuasiExperimental study with pre-test and post-testdesign was used. 60 samples (30 experimentaland30controls)wereselectedaspertheinclusioncriteria using Non-Probability PurposiveSampling. In pre -test 76.7%of elderly peopleof experimental Group were having moderate
64 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
depression score (11-15). In pre -test 73.3% ofelderly people of control Group were havingmoderate depression score (11-15). In post test,intheexperimentalgroup,50%ofthepeoplehadmilddepressionscore(6-10). Inpost-test, in thecontrol group, 80%of the people hadmoderatedepression score (11-15), which indicates thatthe music therapy is effective in reducing thedepression of the elderly people residing in oldagehome.[11]
7.JayaraniGeorgeandVineethaJacobconductedstudy to assess the effectiveness of laughtertherapy on depression among elderly people inselected old age homes at Mangalore in 2014.The study design was two group pre-test post-test design. Purposive sampling technique wasused for selecting 60 samples above the ageof 60 years. The tool used for the study weredemographic proforma and modified Geriatricdepression Scale. There was a significantdifferencebetweenpre-testdepressionscoreandthe post-test depression scores (t = 37.696, p <0.05).The findings of the study shows that theinterventionprogrammewaseffectiveinreducingthedepressionamongelderlypeople.[12]
8.TheexperimentalstudywasconductedbyElhamMohamadEsmailandTaiebeAhromiBoshehritocomparetheeffectsoflaughtertherapyandplaytherapy on reduction of depression symptomsin primary school girls. 36 sample of Tehran’sprimary schoolgirlswere selectedbypurposivesamplingandrandomlyassignedinthreegroupsPlaytherapy,laughtertherapyandthecontrolgroupintheacademicyear2014/15.ResearchtoolwasCSI-4questionnaire.Eighttherapysessionswereconsidered for every experimental group. Thenthepost-testwasadministered.Theresultsofone-wayANOVAindicatedlaughtertherapyandplaytherapyreduceddepressivesymptoms.Accordingto findings, laughter therapy and play therapytechniques, recommended topsychotherapists inorder to reduce the symptoms of depression inchildren.[13]
9.The pre experimental study was conducted byShineGeorgeJosephandRiazK.M.toassessingthe effect of laughter therapy on depressionamong30elderlybetweentheagegroupof60-80yearsresidinginselectedoldagehomesofkerala
in2015.Semistructuredinterviewschedulewasusedtocollectsociodemographicdata;ModifiedBeck depression Inventory was used to assessthe level of depression of elderly. The laughtertherapy given to elderly residing in an old agehome has significantly reduced their level ofdepression (P0.05).The study reveals that therewas no significant association between level ofdepression and selected demographic variables(P>0.05).Laughtertherapymaybeaninnovativeoption to promote a healthy environment forindividuals in family and in other communitysettings.[5]
10.Pre-experimental one group pre-test post teststudywas conducted bySrinivasan to evaluatethe effectiveness ofmusic therapyonquality oflife with 40 elderly inmates in Old age home(InbaIllam),PasumalaiatMadurai in2015.Totalenumerativesamplingwasusedandthedatawascollected by WHO QOL old BREF scale withinterviewtechniquebeforeandaftermusictherapy.StudysubjectsweregivenwithMusictherapyinopenmodetechniquetoallsamplesdailyfor30minutes for the period of 24 days.Therewas asignificantdifferenceinthemeanscoreofqualityoflifebeforeandaftermusictherapyanditwasstatisticallysignificantat0.05level.Furthertherewas a significant association between the levelqualityoflifeandeducationat0.05level.Thus,study finding concludes thatmusic therapywassignificantly effective to improve quality of lifeamongelderly.[4]
11.Padmapriya,Prabavathy,andRenukhaconductedstudy to assess the effectiveness of MusicTherapyonlevelofdepressionamongelderlyinVolontariatHome,Oupalam,Puducherryin2015.A Quantitative Quasi Experimental study (Pre-experimental-onegrouppreandposttestdesign)done among40elderlypeoplewithdepression.datawere collected usingHamiltondepressionScale.dataanalysiswasdoneusinginferentialanddescriptivestatistics.MajorityofthesampleshadNormalandMildlevelofdepression.Themeanpretestvaluesofdepressionscorehadsignificantdifferenceduringposttestmeasurementofmeandepression score which proved that there wassignificant reduction in the level of depressionamongElderlyduetoMusictherapy.Thisstudy
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 65
it was proven that Music therapy reduces thelevelofdepressionamongElderlysufferingfromdepression.[14]
12.The pre–experimental study was conducted byGangadghar Rao Kalapala to investigate theeffectiveofmusic therapyondepressionamongelderly people staying in the old age home inHyderabad IN 2017.The study employs thepre-test and post–test for assessing the level ofdepressionamong theelderlypersons in theoldagehomes,andwithrespecttothedemographicvariableswhichareusedforassessingthelevelsofdepressionamongbothmalesandfemalesfromthestudy.Findingsclearlyshowedthattherewasmild level of depression among elderly peoplebeforetheinterventionandthelevelofdepressionwas decrease after the intervention. Overall63.3% of samples 38 havemild depression and20% of the samples 12 have severe depressionandremainingarenormalinpre-test.Themusictherapyplaysacrucialroleinreducingdepressionamongtheelderlypersonswhoareresidingattheoldagehomes.[2]
ConCLuSIon
ResearcherfeltthatMusicandlaughtertherapycanbeeffectivenonpharmacological,non invasive therapy.Sothatthepresentstudytocomparetheeffectivenessoftherapytoreducethelevelofdepressionamongelderlypeopleinoldagehomesisplannedtoassessmoreeffectivemeanstoreducedepressionamongoldagepeople.
Conflict of Interest:None
Source of Funding:Noseparatefundingwasreceivedforthisstudy.
Ethical Clearance:Theethicalclearanceobtainedfromourinstitute.
REFEREnCES
1.Fariba Ghodsbin, Zahra Sharif Ahmadi, IranJahanbin, Farkhondeh Sharif. Int J CommunityBased Nurs Midwifery. 2015 Jan; 3(1): 31–38 ( Cited on 7 June2017). Available from :https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4280555/
2.Gangadhar Rao Kalapana. Int J innovativeknowledgeconcepts.2017March;3(1);Issue3( Cited on 6 June 2017)Available from :http://www.ijikc.co.in/sites/ijikc/index.php/ijikc/article/view/338
3.Anuraj Mathew. Rajiv Gandhi universityof health science Bangalore Karnataka. 26June 2010 (Cited on 5 June 2017). Availablefrom:http://webcache.googleusercontent.com/search?q=cache:a5JbK0-xCy0J:www.rguhs.ac.in/cdc/onlinecdc/uploads/05_N161_27648.doc+&cd=1&hl=en&ct=clnk&gl=in
4.Srinivasan. Int. J of Applied Research 2015;1(13):432-434(citedon5June2017).Availablefrom:http:/ /www.allresearchjournal.com/archives/2015/vol1issue13/PartG/1-13-119.pdf
5.Shine George Joseph, Riaz. Int. J innovativeResearch&development;September2015;V(4);issue10 (citedon4 June2017).Available from:http://www.ijird.com/index.php/ijird/article/view/80071
6.Hie jin ko, Changho youn. Geriatrics &GerontologyInternational11(3):267-74·July2011(citedon5 June2017 ).Available from :https://www.researchgate.net/publication/49761638_Effects_of_laughter_therapy_on_depression_cognition_and_sleep_among_the_community-dwelling_elderly
7.MoonFaiChan,ZiYangWong,HideakiOnishiandNaiduVellasamyThayala.JournalofclinicalNursing; 2011: 21:776-786 (Cited on 6Jne2017). Availablefrom:http://www.academia.edu/6711868/Effects_of_music_on_depression_in_older_people_a_randomised_controlled_trial
8.EunokPark. JKoreanAcadCommunityHealthNurs. 2013 Jun;24(2):205-213(Cited on 5June 2017). Available from: https://jkachn.org/search.php?where=aview&id=10.12799/jkachn.2013.24.2.205&code=0200JKACHN&vmode=PUBREAdER#!po=10.0000
9.Jaakko Erkkila , Marko Punkanen et al. TheBritish JournalofPsychiatry; (2011):199,132–139(Citedon6June2017).Availablefrom:http://bjp.rcpsych.org/content/bjprcpsych/199/2/132.full.pdf

66 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
10.JinliangWang1, HaizhenWang2, dajun Zhang.Impactofgroupmusictherapyonthedepressionmood of college students; 28 February 2011:3(3): 151-155(Cited on 3 June 2017).Availablefrom: https://file. scirp.org/ pdf/ Health20110300005_56316734.pdf
11.RaviPimple.SinhgadCollegeofNursing.Pune.2012(Citedon8June2017).Availablefrom:http://www.sinhgad.edu/sinhgadnursingcollege-ejournal/Vol_II_Issue_II/Author_6.pdf
12.JayaRaniGeorge,VineethaJacob.Int.JofNursingEducation;June2014;6(1):152-154(Citedon7June2017).Availablefrom:http://www.i-scholar.in/index.php/ijne/article/view/52446
13.ElhamMohamadEsmail,TaiebeAhromiBoshehri.JournalofAppliedEnvironmentalandBiologicalSciences;2015:5(10):155-158 (Citedon3 June2017). Available from: https://www.textroad.com/pdf/JAEBS/J.%20Appl.%20Environ.%20Biol.%20Sci.,%205(10)155-158,%202015.pdf
14.Padmapriya, Prabavathy ,Renukha. Journal ofNursingandHealthScience;Sep.-Oct.2015:V(4), Issue 5 : 31-33 ( Cited on 6 June 2017).Available from:http://www.iosrjournals.org/iosr-jnhs/papers/vol4-issue5/Version-3/F04533133.pdf

Knowledge and Attitude Regarding Inclusive Education among School Teachers
Sreeja i1, Chinchu J2
1Professor, 22nd year M.Sc Nursing Student, College of Nursing, Ananthapuri Hospitals and Research Institute, Trivandrum, Kerala
AbSTRACT
Inclusiveeducationmeanstheprocessofplacingstudentswithdisabilitiesorspecialneedsinclassroomswith childrenwhodonothave suchdisabilitiesorneeds.Thepresent studyaimed to assess the schoolteacher’sknowledgeandattituderegardinginclusiveeducation.Themainobjectiveofthestudywastoassesstheknowledgeandattituderegardinginclusiveeducationamongschoolteachers.Theresearchapproachwasquantitativeanddescriptivedesignwasusedforthestudy.ThesettingofthestudywasselectedschoolsinVenganoorPanchayathTrivandrum.Sampleconsistedof50 teachers selectedbymultistagesamplingtechnique.Inthefirststage,2schools(1fromGovernmentand1fromprivate)inVenganoorpanchayathwereselected.Inthesecondstage,25teachersworkingineachschoolwereselectedrandomlybylotterymethod.Structuredself-administeredquestionnairewasusedtoassesstheknowledgeandratingscalewasused toassess theattitude regarding inclusiveeducationamongschool teachers.datawerecollectedbyself-reportmethodaftergettinginformedconsentfromthestudyparticipants.Resultsrevealedthatmajorityoftheteachers66%werehavingaverageknowledgeregardinginclusiveeducation,10%werehavinglowknowledge and 24%were having high knowledge.Themean score for overall knowledgewas 6.4 andstandarddeviationwas1.54.Outofthe50subjects,80%hadpositiveattitudetowardsinclusiveeducationand18%hadaneutralattitude.Themeanscoreforoverallattitudewas58.4andstandarddeviationwas6.53.Therewassignificantassociationbetweenknowledgeof teachersandeducationalstatus.Selectedsocio-demographicvariablesuchasgenderandeducationalqualificationwasfoundtohavesignificantassociationwithattitude.Itcanbeconcludedthatschoolteacherslackappropriateknowledgeeventhoughtheyhadpositiveattituderegardinginclusiveeducation.Thereisaneedforschoolstoprovidemorespecialeducationalneedstraining,forimplementingthespecialeducationalneeds(SEN)strategiesintheclassroomsaswellasofferingteachersnewstrategiesonimprovingtheirknowledgeandattitudetowardsinclusiveeducation.
Keywords: Knowledge, Attitude, Inclusive education, School teachers
Corresponding Author:dr.SreejaI.Professor,CollegeofNursing,AnanthapuriHospitalsandResearchInstituteChackai,Trivandrum-695024,KeralaEmail:[email protected]
InTRoDuCTIon
Education is the most powerful and effectiveinstrumentforincludingradicalchangesinthebehaviorofstudents.It isreportedthattenpercentofourschoolaged children show evidences of specific learningdisabilitiesandtheycanbeconsideredaschildrenwith
special needs. Children with special needs are thosewhodeviatementally,socially,educationally,physicallyorculturallyfromnormalchildren.Suchchildrenneedspecial educational care and their learning problemsare tobe tackled in a specialmanner.Educating thesedifferentlyabledchildrenisachallengingtaskinhumanresourcedevelopment.Untilthelate18thandearly19thcenturiesnoattemptsweremadetotreatdisadvantagedindividualsinahumanfashion.1
UNICEF’sReportontheStatusofdisabilityinIndia2000statesthattherearearound30millionchildreninIndiasufferingfromsomeformofdisability.TheSixthAll-India Educational Survey (NCERT, 1998) reportsthatof India’s200million school-agedchildren (6–14
DOI Number: 10.5958/2395-180X.2018.00019.1
68 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
years),20millionrequirespecialneedseducation.Whilethe national average for gross enrolment in school isover90percent,lessthanfivepercentofchildrenwithdisabilitiesareinschool.2
Inclusionineducationisanapproachtoeducatingstudents withspecial educational needs. Children withspecial needs have always been segregated from theirpeers.Parentsofthosechildrenwerediscriminatedandhumiliated.1The plan of action to improve educationsystem created by the EducationCommission (1964 -66) suggested that people with disabilities should beincludedinmainstreamandattemptsshouldbemadetobringinasmanychildreninintegratedprograms.Theconceptofincludingchildrenwithdisabilitiesinregulareducationenvironmentshasbeenidentifiedusingmanylabelsmainstreaming, integration,andmostcurrently,inclusion. Inclusion seeks to educate children withdisabilities in regulareducationclassroomsrather thanin segregated settings.2A successful inclusive learningcommunityfosterscollaboration,problemsolving,selfdirectedandcriticaldiscourse,italsoallows(a)studentswith extra rate (b) studentswho progress slower thantheaveragetomoveat thebestof theirabilityand(c)students with specific learning challenges to receivecreativeandeffectivesupporttomaximizethesuccess.
The movement towards inclusive education hasvarious potential advantages not only for the childwith special educational needs, but also for the childwithoutanydisability. In thecaseof thechildwithoutadisability,thiscanleadtopositivechangesinattitudetowardsdisability.Inaddition,growingopportunitiesforsocialcontactwithfellowlearnerswhoarenotdisabledcan create tolerance towards diversity and facilitatefriendships.2
The government has recently launched theSarvaShikshaAbhiyan (SSA). This proposes toimplement ‘universalization of elementary education’(UEE) in a mission mode with a focus on providingqualityelementaryeducation toall children in theagegroup 6–14 years. Inclusive education is an integralcomponent of SSA, and promises tomake ‘educationforall’arealityby2010.2
Survey of various studies conducted on inclusiveeducationinIndiaandabroadhelpstounderstandmoreabout inclusion and its importance today. It clearlyemphasizeshowimportanttheroleofschoolandteacheris, indealingwithinclusion,andmakingitsuccessful.Methodsand techniquesaredeveloped togiveSpecial
educationforspecificdisabilitiesinspecialschoolsbutfor inclusive education few efforts about program &curriculacanbelistedoutespeciallyinIndia.Providingaccesstoeducationisonlythefirststageinovercomingexclusionordiscrimination.Thereisaneedforashiftinperspectivesandvaluessothatdiversityisappreciatedand even welcomed, while teachers are given skillsto provide all children, including those with differentlearningneeds,withqualityeducation.
Nayak(2008)focusedontheattitudeofparentsandteacherstowardsinclusiveeducation.Findingsindicatedsignificantdifferencebetweentheopinionsofparentsofdifferentiallyabledchildren,parentsofnormalchildrenandteachersofnormalchildren.3
Inthepresentscenario, it isseenthattheprevioussystemofeducation-generalschoolsandspecialschoolsisnowchangingasinclusiveschools.Inthisrespectitbecomesessentialtoassesstheattitudeandknowledgelevel of teachers. Attitude of the teachers towardsinclusionisofmuchimportance.
Teacherrequiresrighttypeofawarenessandattitudeon various aspects of diverse abilities, causes andcharacteristics, identification and assessment, teachingand trainingmethods and guidance and counseling tothe children with diverse abilities, their parents andcommunity.4Suchanawarenessandattitudewillleadtobettercompetenciesinteachers.Ateacherwithrighttypeofawareness,attitudeandcompetenciesisanassettoanyinstitutionofferingprogrammesforthedifferentlyabled.Byconsideringallthesefactors,investigatorsdecidedtofindouttheknowledgeandattitudeofteacherstowardsinclusiveeducation.
METHoDoLogy
The present study was conducted to assess theknowledge and attitude regarding inclusive education.A prior permission was obtained from the concernedauthority of the schools of Venganoor Panchayath,Thiruvananthapuram for conducting the study. Ethicalclearance was obtained from the institutional ethicscommittee. Informed consent was obtained fromthe participants and data collection was done overone week among 50 teachers who met the inclusioncriteria.SubjectswereselectedbyMultistagesamplingtechnique. Questionnaire was distributed amongparticipantsandinformationwascollectedbyselfreportmethod. The subjects took about 20 – 30 minutes toanswerthequestions.
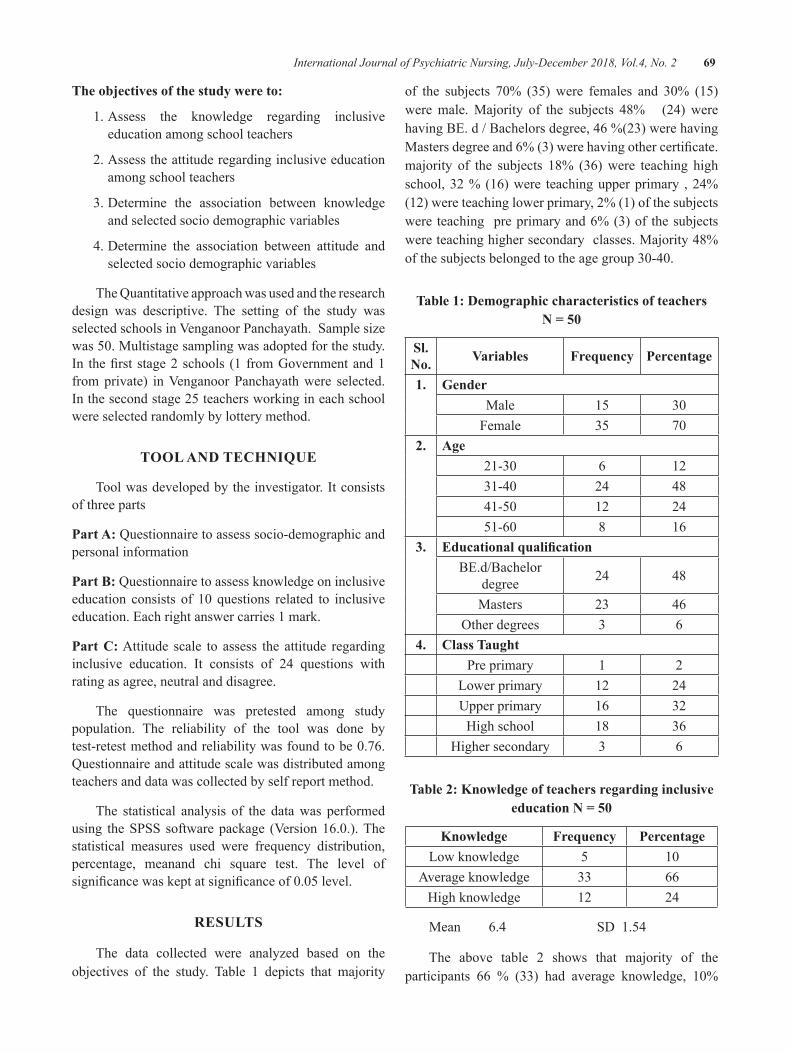
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 69
The objectives of the study were to:
1.Assess the knowledge regarding inclusiveeducationamongschoolteachers
2.Assesstheattituderegardinginclusiveeducationamongschoolteachers
3.determine the association between knowledgeandselectedsociodemographicvariables
4.determine the association between attitude andselectedsociodemographicvariables
TheQuantitativeapproachwasusedandtheresearchdesign was descriptive. The setting of the study wasselectedschoolsinVenganoorPanchayath.Samplesizewas50.Multistagesamplingwasadoptedforthestudy.In thefirst stage2schools (1 fromGovernmentand1fromprivate) inVenganoorPanchayathwere selected.Inthesecondstage25teachersworkingineachschoolwereselectedrandomlybylotterymethod.
TooL AnD TECHnIQuE
Toolwasdevelopedbytheinvestigator.Itconsistsofthreeparts
Part A:Questionnairetoassesssocio-demographicandpersonalinformation
Part b:Questionnairetoassessknowledgeoninclusiveeducation consists of 10 questions related to inclusiveeducation.Eachrightanswercarries1mark.
Part C:Attitude scale to assess the attitude regardinginclusive education. It consists of 24 questions withratingasagree,neutralanddisagree.
The questionnaire was pretested among studypopulation. The reliability of the tool was done bytest-retestmethodandreliabilitywasfoundtobe0.76.Questionnaireandattitudescalewasdistributedamongteachersanddatawascollectedbyselfreportmethod.
The statistical analysis of the datawas performedusing theSPSS softwarepackage (Version16.0.).Thestatistical measures used were frequency distribution,percentage, meanand chi square test. The level ofsignificancewaskeptatsignificanceof0.05level.
RESuLTS
The data collected were analyzed based on theobjectives of the study. Table 1 depicts that majority
of the subjects 70% (35)were females and 30% (15)weremale.Majority of the subjects 48% (24) werehavingBE.d/Bachelorsdegree,46%(23)werehavingMastersdegreeand6%(3)werehavingothercertificate.majority of the subjects 18% (36)were teaching highschool,32%(16)were teachingupperprimary ,24%(12)wereteachinglowerprimary,2%(1)ofthesubjectswere teaching preprimaryand6%(3)of thesubjectswereteachinghighersecondaryclasses.Majority48%ofthesubjectsbelongedtotheagegroup30-40.
Table 1: Demographic characteristics of teachers n = 50
Sl. no. Variables Frequency Percentage
1. genderMale 15 30Female 35 70
2. Age21-30 6 1231-40 24 4841-50 12 2451-60 8 16
3. Educational qualificationBE.d/Bachelor
degree 24 48
Masters 23 46Otherdegrees 3 6
4. Class TaughtPreprimary 1 2
Lowerprimary 12 24Upperprimary 16 32Highschool 18 36
Highersecondary 3 6
Table 2: Knowledge of teachers regarding inclusive education n = 50
Knowledge Frequency PercentageLowknowledge 5 10
Averageknowledge 33 66Highknowledge 12 24
Mean6.4Sd1.54
The above table 2 shows that majority of theparticipants 66 % (33) had average knowledge, 10%
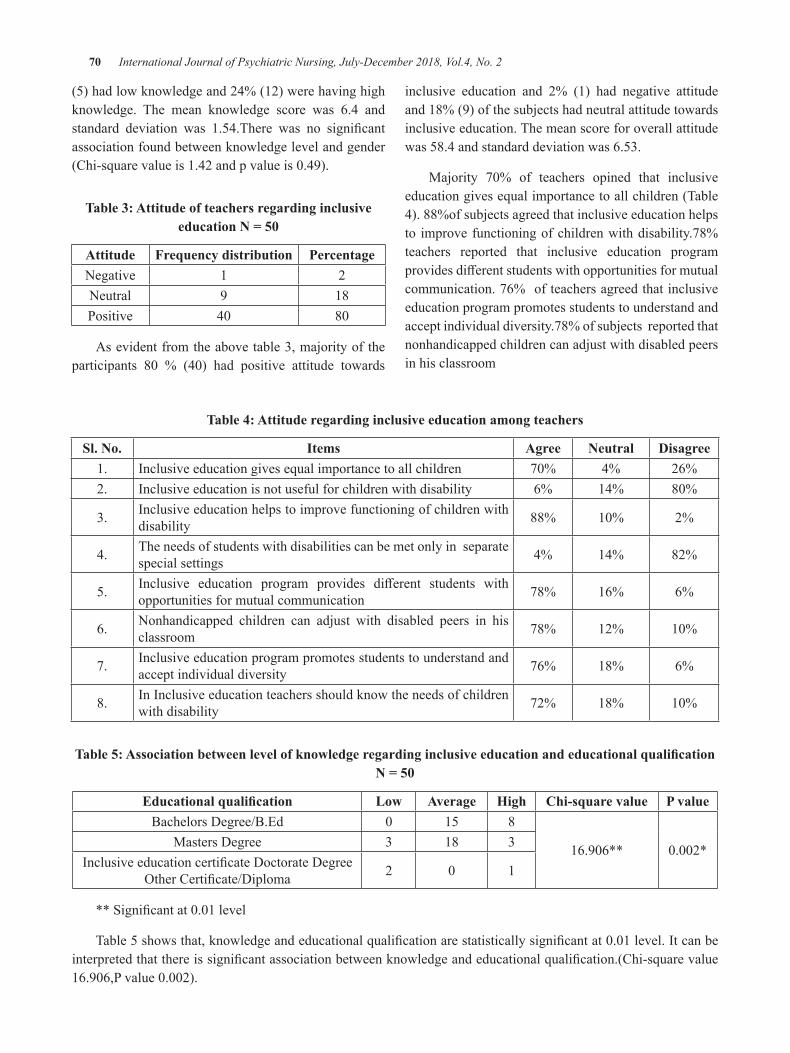
70 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
(5)hadlowknowledgeand24%(12)werehavinghighknowledge. The mean knowledge score was 6.4 andstandard deviation was 1.54.There was no significantassociationfoundbetweenknowledgelevelandgender(Chi-squarevalueis1.42andpvalueis0.49).
Table 3: Attitude of teachers regarding inclusive education n = 50
Attitude Frequency distribution PercentageNegative 1 2Neutral 9 18Positive 40 80
Asevidentfromtheabovetable3,majorityoftheparticipants 80 % (40) had positive attitude towards
inclusive education and 2% (1) had negative attitudeand18%(9)ofthesubjectshadneutralattitudetowardsinclusiveeducation.Themeanscoreforoverallattitudewas58.4andstandarddeviationwas6.53.
Majority 70% of teachers opined that inclusiveeducationgivesequalimportancetoallchildren(Table4).88%ofsubjectsagreedthatinclusiveeducationhelpsto improvefunctioningofchildrenwithdisability.78%teachers reported that inclusive education programprovidesdifferentstudentswithopportunitiesformutualcommunication.76%ofteachersagreedthatinclusiveeducationprogrampromotesstudentstounderstandandacceptindividualdiversity.78%ofsubjectsreportedthatnonhandicappedchildrencanadjustwithdisabledpeersinhisclassroom
Table 4: Attitude regarding inclusive education among teachers
Sl. no. Items Agree neutral Disagree1. Inclusiveeducationgivesequalimportancetoallchildren 70% 4% 26%2. Inclusiveeducationisnotusefulforchildrenwithdisability 6% 14% 80%
3. Inclusiveeducationhelpstoimprovefunctioningofchildrenwithdisability 88% 10% 2%
4. Theneedsofstudentswithdisabilitiescanbemetonlyinseparatespecialsettings 4% 14% 82%
5. Inclusive education program provides different students withopportunitiesformutualcommunication 78% 16% 6%
6. Nonhandicapped children can adjust with disabled peers in hisclassroom 78% 12% 10%
7. Inclusiveeducationprogrampromotesstudentstounderstandandacceptindividualdiversity 76% 18% 6%
8. InInclusiveeducationteachersshouldknowtheneedsofchildrenwithdisability 72% 18% 10%
Table 5: Association between level of knowledge regarding inclusive education and educational qualification n = 50
Educational qualification Low Average High Chi-square value P valueBachelorsdegree/B.Ed 0 15 8
16.906** 0.002*Mastersdegree 3 18 3Inclusiveeducationcertificatedoctoratedegree
OtherCertificate/diploma 2 0 1
**Significantat0.01level
Table5showsthat,knowledgeandeducationalqualificationarestatisticallysignificantat0.01level.Itcanbeinterpretedthatthereissignificantassociationbetweenknowledgeandeducationalqualification.(Chi-squarevalue16.906,Pvalue0.002).
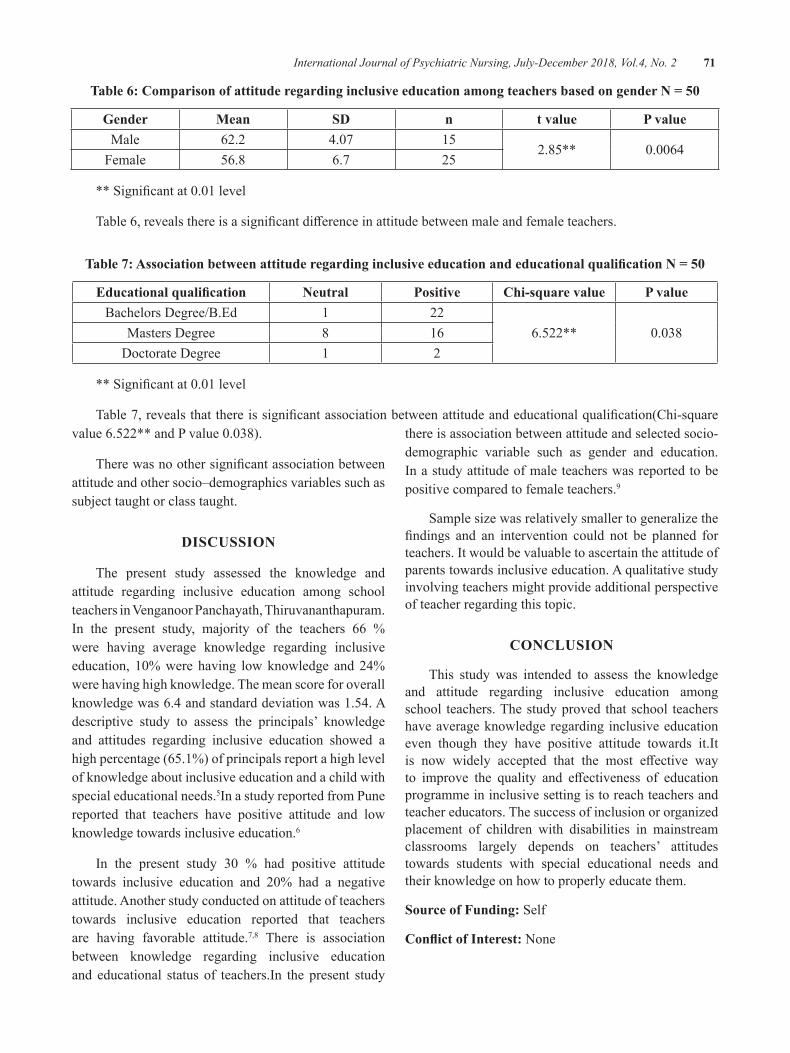
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 71
Table 6: Comparison of attitude regarding inclusive education among teachers based on gender n = 50
gender Mean SD n t value P valueMale 62.2 4.07 15
2.85** 0.0064Female 56.8 6.7 25
**Significantat0.01level
Table6,revealsthereisasignificantdifferenceinattitudebetweenmaleandfemaleteachers.
Table 7: Association between attitude regarding inclusive education and educational qualification n = 50
Educational qualification neutral Positive Chi-square value P valueBachelorsdegree/B.Ed 1 22
6.522** 0.038Mastersdegree 8 16doctoratedegree 1 2
**Significantat0.01level
Table7,revealsthatthereissignificantassociationbetweenattitudeandeducationalqualification(Chi-squarevalue6.522**andPvalue0.038).
Therewasnoothersignificantassociationbetweenattitudeandothersocio–demographicsvariablessuchassubjecttaughtorclasstaught.
DISCuSSIon
The present study assessed the knowledge andattitude regarding inclusive education among schoolteachersinVenganoorPanchayath,Thiruvananthapuram.In the present study, majority of the teachers 66 %were having average knowledge regarding inclusiveeducation, 10%werehaving lowknowledge and24%werehavinghighknowledge.Themeanscoreforoverallknowledgewas6.4andstandarddeviationwas1.54.Adescriptive study to assess the principals’ knowledgeand attitudes regarding inclusive education showed ahighpercentage(65.1%)ofprincipalsreportahighlevelofknowledgeaboutinclusiveeducationandachildwithspecialeducationalneeds.5InastudyreportedfromPunereported that teachers have positive attitude and lowknowledgetowardsinclusiveeducation.6
In the present study 30 % had positive attitudetowards inclusive education and 20% had a negativeattitude.Anotherstudyconductedonattitudeofteacherstowards inclusive education reported that teachersare having favorable attitude.7,8 There is associationbetween knowledge regarding inclusive educationand educational status of teachers.In thepresent study
thereisassociationbetweenattitudeandselectedsocio-demographic variable such as gender and education.Inastudyattitudeofmaleteacherswasreportedtobepositivecomparedtofemaleteachers.9
Samplesizewasrelativelysmallertogeneralizethefindings and an intervention could not be planned forteachers.Itwouldbevaluabletoascertaintheattitudeofparentstowardsinclusiveeducation.Aqualitativestudyinvolvingteachersmightprovideadditionalperspectiveofteacherregardingthistopic.
ConCLuSIon
This study was intended to assess the knowledgeand attitude regarding inclusive education amongschool teachers.Thestudyprovedthatschool teachershaveaverageknowledgeregardinginclusiveeducationeven though they have positive attitude towards it.Itis now widely accepted that the most effective wayto improve the quality and effectiveness of educationprogrammeininclusivesettingistoreachteachersandteachereducators.Thesuccessofinclusionororganizedplacement of children with disabilities in mainstreamclassrooms largely depends on teachers’ attitudestowards students with special educational needs andtheirknowledgeonhowtoproperlyeducatethem.
Source of Funding:Self
Conflict of Interest:None

72 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
REFEREnCES
1.GuruJournalofBehavioralandSocialSciences... Volume2Issue1(Jan–Mar, 2014).ISSN:2320-9038www.gjbss.org. G.J. B. S. S.Volume2. Issue 1.2014.Editor.Jayan,C.ManikandanK.
2.UNICEF (2003). Examples of inclusiveeducation in India.https://www.unicef.org/rosa/InclusiveInd.pdf
3.Nayak, Jyotirmayee (2008).Attitude of Parentsand Teachers towards Inclusive educationEdUTRACKS-AMonthlyScannerofTrendsinEducation,7(6),20-23
4.NaeemMohsin, Abdul Ghafar, Tahir MuhmoodTabsum.AttitudeofParentsandTeacherstowardsInclusiveEducation.SecondaryEducationJournal2(1)19-33
5.MthethwaGS.Principals’knowledgeandattitudesregarding inclusive education: implications forcurriculumandassessment(doctoraldissertation).
6.Kern, Evangeline. Survey of Teacher AttitudeRegarding Inclusive Educationwithin anUrbanSchool district. 2006. PCOM psychologydissertations70
7. dapudong Richel C. teachers’ knowledge andattitude towards inclusive education: basis foranenhancedprofessionaldevelopmentprogram.Internationaljournaloflearninganddevelopment.Internationaljournaloflearninganddevelopment.4(4);2014. doi:10.5296/ijld.v4i4.6116 URL:http://dx.doi.org/10.5296/ijld.v4i4.6116
8.Anita M. Belapurkar. Knowledge and attitudeabout Inclusive Education of school teachers:A study scholarly research journal forinterdidciplinarystudies
9.Sonam Bansal. A study of attitude of primaryschool teachers towards inclusive education.InternationalJournalofEducationIssueOctober2013,Vol.1

burden and Family Functioning among Caregivers of Chronic Schizophrenia
Sreeja I.
Professor, College of Nursing, Ananthapuri Hospitals and Research Institute, Trivandrum
AbSTRACT
Introduction:Schizophrenia isachronicmajorpsychoticdisordermanifestedbydistorted thinkingandpooremotionalresponse.Familiesofpatientswithschizophreniafacemanychallengessuchascareburden,fearandembarrassmentaboutillness,signsandsymptoms,uncertaintyaboutcourseofthedisease,lackofsocialsupport,andstigma.
objective:1.Assesstheperceivedburdenofcaregiversofpatientshavingchronicschizophrenia.2.Assessfamily functioning of caregivers of patients having chronic schizophrenia.3.determine the relationshipbetweenburdenandfamilyfunctioning.
Methods:Adescriptivedesignandconsecutivesamplingwasadoptedforthestudy.ThepopulationunderstudywascaregiversofpatientshavingchronicschizophreniainThiruvananthapuramdistrict.Onehundredandseventyseven(177)constitutedstudysample.Burdenassessmentscheduleandfamilyfunctioningscalewasusedtoassessburdenandfamilyfunctioning.datawascollectedbyselfreport.
Results: Healthy familiesperceived significantly (t175=3.4,p<0.01)moreburdencompared tounhealthyfamilies.Burdensubscalesoffamilyrelations,physicalandmentalhealthweresignificantlyhighinhealthyfamilies.
Conclusion:Thisstudydemonstratedthattheperceptionofburdenisdifferentforhealthyandunhealthyfamilies.FamilyinterventioncanbeincludedasatreatmentmodalityforpatientswithSchizophrenia.
Keywords: family functioning, caregiver burden
InTRoDuCTIon
Schizophrenia causes significant social andwork problems to the sufferer.1With the advent ofdeinstitutionalization, the focus of care has shiftedfromhospitaltocommunity.InacountrylikeIndia,thetermcommunitycaremeanspatientsremainingoutsidehospitals with family members. Families of patientswith schizophrenia facemany challenges such as careburden,fearandembarrassmentaboutillness,signsandsymptoms,uncertaintyaboutcourseofthedisease,lackofsocialsupport,andstigma.2
Familiescaringforamemberwithachronicseveremental illness have to cope with a lot of burden anddistress. The concept of family burden illustrates theimpactofmental illnessonfamilies.Objectiveburdenincludes the practical, day-to-day problems and issuesrelatedtohavingafamilymemberwithamentalillness,such as loss of income and disruption of household
routines.Subjectiveburden includes thepsychologicaland emotional impact of mental illness on familymembers, including feelings of grief and worry. Thestress of illness exacerbations coupled with limitedsocial and coping capabilities contribute to subjectiveburden.1,3
Familyisabasicunitthatisresponsibleinpreservingtheintegrityofindividuals,whoformtheunit.Familiesextendemotional,social,andeconomicsupporttotheirmembers. Having a relation with schizophrenia alsoaffectstherolesandinteractionswithinthefamily.Thelifetime emotional, social, and financial consequencesexperienced by individuals with schizophrenia havesignificant effects on their families. Findings indicatethatfamilypsychologicaldistressandpatientbehavioralproblems are important factors in family functioning.A high functioning family helps in maintaining thedimensionsofcommunication,emotionalandbehavioral
DOI Number: 10.5958/2395-180X.2018.00020.8
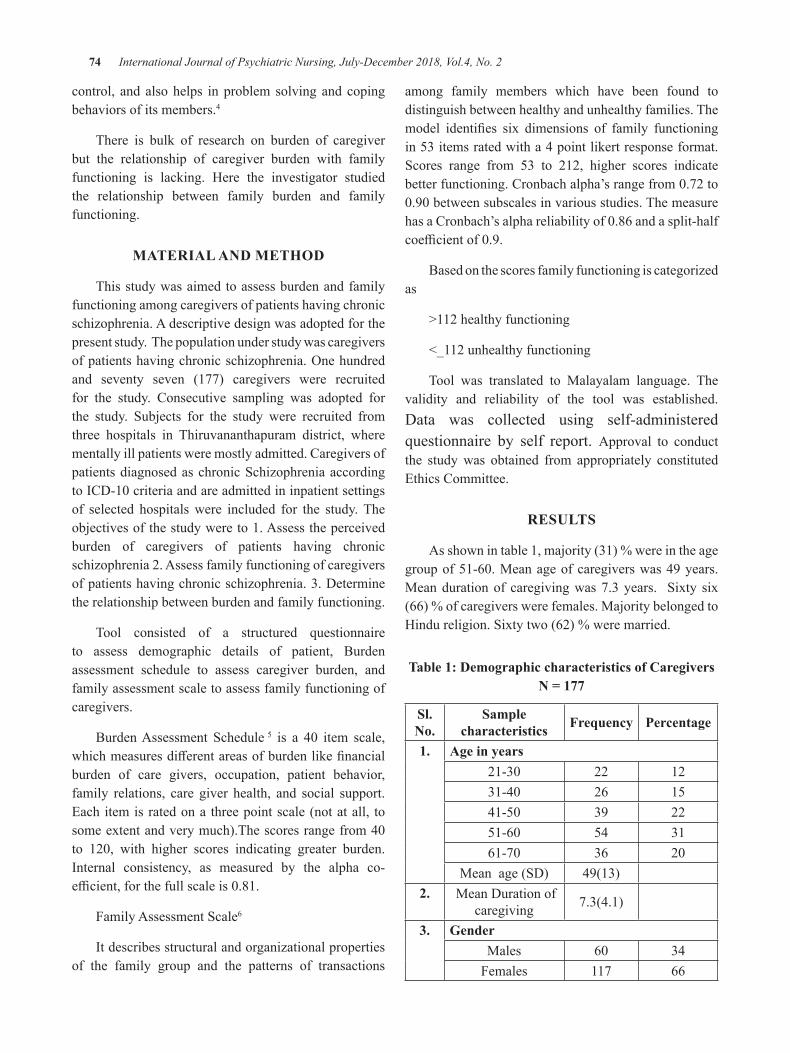
74 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
control, andalsohelps inproblemsolvingandcopingbehaviorsofitsmembers.4
There is bulk of research on burden of caregiverbut the relationship of caregiver burden with familyfunctioning is lacking. Here the investigator studiedthe relationship between family burden and familyfunctioning.
MATERIAL AnD METHoD
Thisstudywasaimedtoassessburdenandfamilyfunctioningamongcaregiversofpatientshavingchronicschizophrenia.Adescriptivedesignwasadoptedforthepresentstudy.Thepopulationunderstudywascaregiversofpatientshavingchronicschizophrenia.Onehundredand seventy seven (177) caregivers were recruitedfor the study. Consecutive sampling was adopted forthe study. Subjects for the study were recruited fromthree hospitals in Thiruvananthapuram district, wherementallyillpatientsweremostlyadmitted.CaregiversofpatientsdiagnosedaschronicSchizophreniaaccordingtoICd-10criteriaandareadmittedininpatientsettingsof selected hospitalswere included for the study.Theobjectivesofthestudywereto1.Assesstheperceivedburden of caregivers of patients having chronicschizophrenia2.Assessfamilyfunctioningofcaregiversofpatientshavingchronicschizophrenia.3.determinetherelationshipbetweenburdenandfamilyfunctioning.
Tool consisted of a structured questionnaireto assess demographic details of patient, Burdenassessment schedule to assess caregiver burden, andfamilyassessmentscaletoassessfamilyfunctioningofcaregivers.
BurdenAssessment Schedule 5 is a 40 item scale,whichmeasuresdifferentareasofburdenlikefinancialburden of care givers, occupation, patient behavior,family relations, care giver health, and social support.Eachitemisratedona threepointscale(notatall, tosomeextentandverymuch).Thescoresrangefrom40to 120, with higher scores indicating greater burden.Internal consistency, as measured by the alpha co-efficient,forthefullscaleis0.81.
FamilyAssessmentScale6
Itdescribesstructuralandorganizationalpropertiesof the family group and the patterns of transactions
among family members which have been found todistinguishbetweenhealthyandunhealthyfamilies.Themodel identifies six dimensions of family functioningin53itemsratedwitha4pointlikertresponseformat.Scores range from 53 to 212, higher scores indicatebetterfunctioning.Cronbachalpha’srangefrom0.72to0.90betweensubscalesinvariousstudies.ThemeasurehasaCronbach’salphareliabilityof0.86andasplit-halfcoefficientof0.9.
Basedonthescoresfamilyfunctioningiscategorizedas
>112healthyfunctioning
<_112unhealthyfunctioning
Tool was translated to Malayalam language. Thevalidity and reliability of the tool was established.data was collected using self-administeredquestionnaire by self report. Approval to conductthe studywas obtained from appropriately constitutedEthicsCommittee.
RESuLTS
Asshownintable1,majority(31)%wereintheagegroupof51-60.Meanageofcaregiverswas49years.Meandurationof caregivingwas7.3years. Sixty six(66)%ofcaregiverswerefemales.MajoritybelongedtoHindureligion.Sixtytwo(62)%weremarried.
Table 1: Demographic characteristics of Caregivers n = 177
Sl. no.
Sample characteristics Frequency Percentage
1. Age in years21-30 22 1231-40 26 1541-50 39 2251-60 54 3161-70 36 20
Meanage(Sd) 49(13)2. Meandurationof
caregiving 7.3(4.1)
3. genderMales 60 34Females 117 66
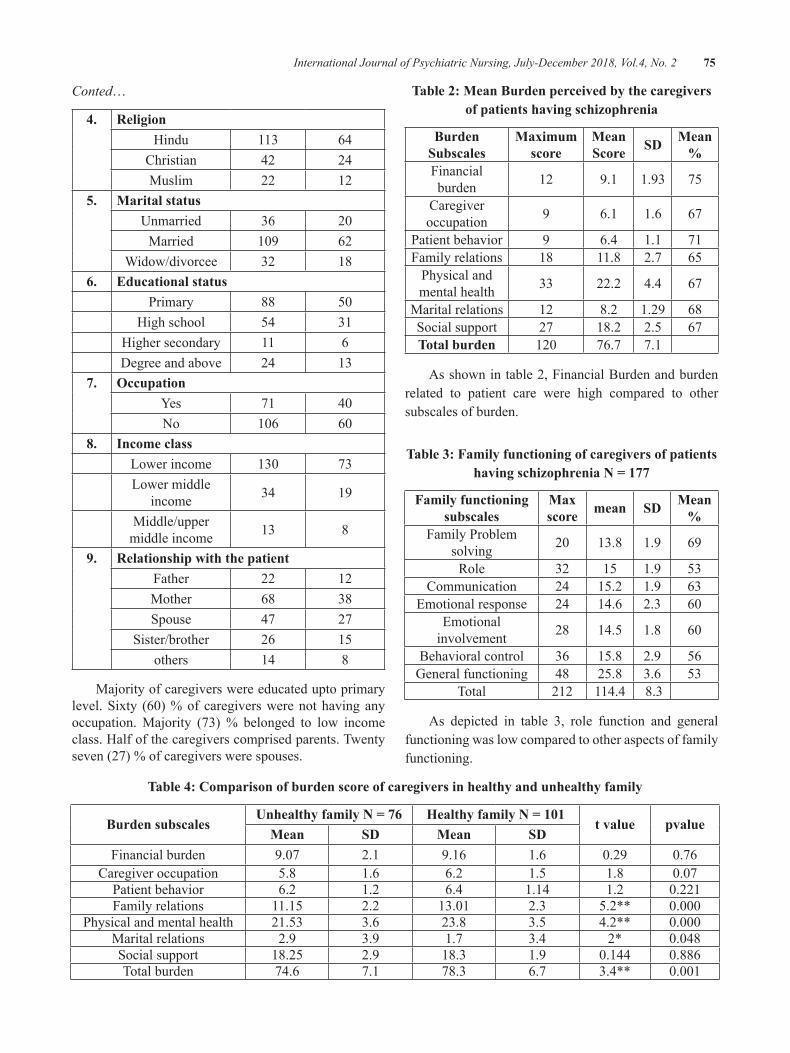
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 75
Conted…
4. ReligionHindu 113 64
Christian 42 24Muslim 22 12
5. Marital statusUnmarried 36 20Married 109 62
Widow/divorcee 32 186. Educational status
Primary 88 50Highschool 54 31
Highersecondary 11 6degreeandabove 24 13
7. occupationYes 71 40No 106 60
8. Income classLowerincome 130 73Lowermiddle
income 34 19
Middle/uppermiddleincome 13 8
9. Relationship with the patientFather 22 12Mother 68 38Spouse 47 27
Sister/brother 26 15others 14 8
Majorityofcaregiverswereeducateduptoprimarylevel.Sixty (60)%of caregiverswerenothavinganyoccupation.Majority (73)% belonged to low incomeclass.Halfofthecaregiverscomprisedparents.Twentyseven(27)%ofcaregiverswerespouses.
Table 2: Mean burden perceived by the caregivers of patients having schizophrenia
burden Subscales
Maximum score
Mean Score SD Mean
%Financialburden 12 9.1 1.93 75
Caregiveroccupation 9 6.1 1.6 67
Patientbehavior 9 6.4 1.1 71Familyrelations 18 11.8 2.7 65Physicalandmentalhealth 33 22.2 4.4 67
Maritalrelations 12 8.2 1.29 68Socialsupport 27 18.2 2.5 67Total burden 120 76.7 7.1
Asshownintable2,FinancialBurdenandburdenrelated to patient care were high compared to othersubscalesofburden.
Table 3: Family functioning of caregivers of patients having schizophrenia n = 177
Family functioning subscales
Max score mean SD Mean
%FamilyProblem
solving 20 13.8 1.9 69
Role 32 15 1.9 53Communication 24 15.2 1.9 63
Emotionalresponse 24 14.6 2.3 60Emotionalinvolvement 28 14.5 1.8 60
Behavioralcontrol 36 15.8 2.9 56Generalfunctioning 48 25.8 3.6 53
Total 212 114.4 8.3
As depicted in table 3, role function and generalfunctioningwaslowcomparedtootheraspectsoffamilyfunctioning.
Table 4: Comparison of burden score of caregivers in healthy and unhealthy family
burden subscalesunhealthy family n = 76 Healthy family n = 101
t value pvalueMean SD Mean SD
Financialburden 9.07 2.1 9.16 1.6 0.29 0.76Caregiveroccupation 5.8 1.6 6.2 1.5 1.8 0.07Patientbehavior 6.2 1.2 6.4 1.14 1.2 0.221Familyrelations 11.15 2.2 13.01 2.3 5.2** 0.000
Physicalandmentalhealth 21.53 3.6 23.8 3.5 4.2** 0.000Maritalrelations 2.9 3.9 1.7 3.4 2* 0.048Socialsupport 18.25 2.9 18.3 1.9 0.144 0.886Totalburden 74.6 7.1 78.3 6.7 3.4** 0.001
76 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
As shown in table 4, healthy families perceivedsignificantly(t175=3.4,p<0.01)moreburdencomparedto unhealthy families. Burden subscales of familyrelations,physicalandmentalhealthweresignificantlyhigh in healthy families. It can be interpreted thatthe perception of burden is different for healthy andunhealthyfamilies.
DISCuSSIon
Sixty (60)%ofcaregivers in thepresentstudydidnothaveoccupation.Caregiversareforcedtocutdowntheirworkhourstoprovidecarefortheirpatient.AnotherstudycarriedoutbyAwadandVoruganti7reportedthosefamilymemberswholeavetheirjobstoprovidecarefortheir ill relativewith schizophrenia ranged from1.2%forthefirstepisodeand2.5%forlong-termpatients.Thepresent studyfindingsareconsistentwith thepreviousstudy.Thefearofleavingaschizophrenicpatientalonemakesthecaregiversresideathomemostofthetimeandconsequentlyisolatethemselvesfromthesocialcontactortheoutsideworld.Majority(65%)belongedtourbanarea.Urbansiteshadsignificantlyhigherincidenceratesofschizophreniathanruralsites.8
In thepresent study, family role functionwas lowcomparedtootherdomainsoffamilyfunctioning.Neenareported that dimensions of the family functioningis correlated to the social support perceived from thefamilyintheschizophrenicpatients.
The result highlight that there is a need forpsychoeducation/intervention for family members ofpatients with schizophrenia. disturbed behavior is agreaterdeterminantofseverityofburdenthanpsychiatricdiagnosis;henceappropriatetreatmentisthefirststepinreducingcaregiverburden.9
Caregivers of schizophrenia experience enormousburdenandareatriskformentaldisorders.Theseverityoftheburdenisrelatedtothelevelofpsychopathologyandmedicaladherence.
The relationship between caregiver-burden andfamilyrelationshipappearstobeacomplexone.Moremethodologically sound investigations are required tounderstandthisintricatearea,withthehopethatabetterunderstandingwillhelp thecauseofbothpatientsandtheir caregivers. Sixty six (66) % of caregivers werefemale caregivers, out ofwhich 38%mainlymothers.
Asmanyotherstudiesreportedintheliterature,femalesarepredominantlyinvolvedincaregivingtask.3
Caregivers reported financial burden and patientbehaviormore compared to other domains of burden.Thesefindingsareinaccordancewiththestudyfindingsof Kareem and Aarthi Jaganathan.10In developingcountries, quality of life is affected by the caregivers’economic burden.9 decreased quality of life may beassociated with the caregivers’ burden, lack of socialsupport,thecourseofthediseaseandfamilyrelationshipproblems.
z There may be discrepancy in the perception ofburden among family members. A similar studyincludingallfamilymemberscanbeconducted.
z Thereshouldbemorepostcreationofcommunitymentalhealthnurseswhoshouldactivelyworkforthewelfareoffamilyofpatients.
ConCLuSIon
ItcanbeconcludedfromthestudyFamilycaregiversofpatientshavingschizophreniaperceivehighburden.Family members’ functioning are disturbed due to illmemberinthefamily.
Source of Funding:Self
Acknowledgement:Studyparticipants
Conflict of Interest:Nil
Ethical Clearance: Ethical clearance was obtainedfromappropriatelyconstitutedethicscommittee.Aletterexplainingthepurposeof thestudywashandedout tosubjects.Consentformsweresignedbeforeparticipatinginthestudy.
REFEREnCES
1.Thara R, Padmavati R, Aynkran JR, John S.Community mental health in India: a rethink.International Journal of mental health system2008;2:11
2.Awad AG, Voruganti LN. The burden ofschizophrenia on caregivers: a review.Pharmacoeconomics2008;26(2):149-62
3.Lasebikan VO, Ayinde OO. Family burdenin caregivers of schizophrenia patients:
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 77
Prevalence and socio-demographic correlates.Indian J Psychol Med [internet]2013[cited2014May5];35:60-6.Availablefrom: http://www.ijpm.info/text.asp?2013/35/1/60/112205
4.NeenaSSawant,KamalSJethwani.Understandingfamily functioning and social support inunremitting schizophrenia: a study in India.IndianJPsychiatry2010April-June;52(2):145-9
5.Thara R, Padmavati R, Kumar S, SrinivasanL. BurdenAssessment Schedule: Instrument toassessburdenoncaregiversof chronicmentallyill.IndianJournalofPsychiatry1998;40:21-29.
6.Endicott J, Spitzer RL, Fleiss JL, CohenJ: “The Global Assessment Scale: AProcedure for Measuring Overall Severity ofPsychiatric disturbance. Archives of GeneralPsychiatry33:766-771,1976.
7.Avasthi A. Preserve and strengthen familyto promote mental health. Indian journal ofpsychiatry2010;52:113-26
8.OliverMI,AartiJagannathan,JagadishaThirthalli,Ameer HamzaHR, NagendraBN, Gangadhar.Predictors Of Family Caregiver Burden InSchizophrenia: Study From An In-PatientTertiary Care Hospital In India.Asian Journalof Psychiatry2014; 8:94-98. dOI:10.1016/j.ajp.2013.12.018
9.Pearson N, Gunnell d. Help-seeking behaviorin men and women with common mentalhealth problems: cross sectional study. Br JPsychiatry2005;186:297-301.
10.Joseph Peuskens, Vibeke Porsdal, JanPecenak, Peter Handest, Yulia d’yachkova, Radim Brousil, Walter deberd. Schizophreniasymptoms and functioning in patients receivinglong-term treatment with olanzapine long-acting injection formulation: a pooled analysis.BMC Psychiatry 2012, 12:130 availableat: http://www.biomedcentral.com/1471-244X/12/130doi:10.1186/1471-244X-12-130
Assess the Level of Subjective well being and Find the Association with Socio-Demographic Variables of Farmers of
Selected Villages of Dharawad Taluka, Karnataka, India
Shivananda gejji1, Sunanda g.T.2, R. Sreevani3
1Lecturer, Govt. College of Nursing, BIMS, Belagavi; 2Assistant Professor, 3Professor & HOD, Department of Psychiatric Nursing, Dharwad Institute of Mental Health and Neurosciences,
Belagavi Road, Dharwad, India
AbSTRACT
background: Farmingisassociatedwithuniquesetofstressorthatincludeunpredictableenvironmental,financialandsocialimpactarefeltseriousreductioninincomeforfarmerandsubjectivewell-beingisanalternatemeasureofpovertyanddeprivation amongfarmers.
Aim: Toassessthelevelofsubjectivewell-beingoffarmers,
Method:The studyusedconvenient sampling techniqueandcollecteddata from100 farmers,byusinginterviewingmethod.Thetoolsusedwere(i)Socio-demographicdatasheet(ii)Subjectivewellbeingscale.Thedatawasanalyzedbyusingdescriptiveandinferentialstatistics.
Results:Thefindingsshowsthat,65%ofthefarmershadmediumlevelofsubjectivewellbeing,22%ofthemhadlowlevelofsubjectivewellbeingand13%farmershadhigherlevelofsubjectivewellbeingwiththeoverallmedianscoreof51.50.andthereisastatisticallysignificantassociationfoundbetweenthelevelofsubjectivewellbeingandsociodemographicvariablesuchasamountofdebt’sandcropfailureatthelevelofp<0.05.
Conclusion: Thestudyresultsrecommendedthatpoliciesinthefutureaimedataddressingdeprivationoflowsubjectivewell-beingoffarmerswhodependontheagriculturallabourasalivelihoodstrategy.
Keywords: Subjective well-being, farmers, agriculture.
Corresponding Author:dr.SunandaG.T.M.Sc(N),Phd,RN,AssistantProfessordepartmentofPsychiatricNursingdharwadInstituteofMentalHealthandNeurosciencesBelagaviRoad,dharwad-580008,IndiaPhone:9611814496Email:[email protected]
InTRoDuCTIon
Indiaisalandofvillagesandmostofthepopulationsresiding in villages are farmers. Agriculture employsmore thanhalfof the Indianpopulation.Todayalmost70%oftheIndianpopulationwaslivingonagriculturalincome.ThemajoroccupationamongruralresidentsofKarnatakaisagriculture.
In India more than two decades suicides amongfarmersare increased.Economicproblems,psychiatricillness,andstressfullifeeventswerefoundtobeimportantcontributors to farmers’ suicides. Important economicrisk factorswereprocurementofdebt,especially frommultiple sources and for nonagricultural reasons andleasingoutfarms.Cropfailure,interpersonalproblems,medicalillness,andmarriageoffemalefamilymemberweresignificantstressfullifeevents.1
Wellbeingisafundamentalissue.Materialwealthand fulfillment of one’s desires, human relationships,development of one’s potentialities and one’spsychologicalstate,faithinareligionandspiritualityareconsideredasrelevantandsignificantinthiscontextintheconceptualizationofsubjectivewellbeing.2
DOI Number: 10.5958/2395-180X.2018.00021.X

International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 79
A person’s wellbeing is influenced by theirenvironment anddisposition, their safety and security,theirphysicalandmentalhealth,theirrelationshipsandsocial networks, their access to goods and services.Farmersarenodifferenttootherpeopleinthisregard,and these factors will affect their overall wellbeing.However, understanding the wellbeing of farmers isespecially complex as, in addition to the usual factorsthat influence wellbeing, farming is associated with anumberofoccupationspecificfactorsthatcanchallengewellbeing. Climatic variability such as the experienceof drought, pest and disease outbreaks, rising inputcosts,complexgovernmentbureaucracyandgeographicisolationwithassociatedlackofaccesstoservices,andsocialisolationforfarmers.3
Farmersworklonghours,havephysicallydemandingwork,areoftenisolatedsociallyandgeographicallyfromservices,arelesslikelytotakevacationsandlesslikelyto retire thanpeople inotheroccupations, In addition,farming has suffered recent pressures in the form of;globalization,economicrationalization,pestanddiseaseoutbreaks, diminishing rural populations, drought, andclimatechange.Thereforefarmerscouldbeconsideredto be a vulnerable population and the associationbetween work and health is particularly pertinent fortheirlivelihoodandwellbeing.4
Farmer’s suicides have been receiving a lot ofsocial and public policy attention. Suicides weremainlyconcentratedinKarnataka,AndhraPradeshandMaharashtra. These incidents raised serious questionsofeconomichardshipsfacedbyfarmers.Theresearcherhad comeacrossmany farmers in hospital setting andaswellatcommunitysetting,observeddistressrelatedmanifestations among farmerswhichwere associationwith their social status.And also the suicides amongfarmingpopulationhavedrasticallyincreasedasperthereportsbyvariousstudiesconductedandnewspapers.By observing all these factors the researcher felt theneedtodeterminetheassociationbetweenthesubjectivewellbeingandsociodemographicvariableoffarmers.
MATERIALS & METHoD
Research design: descriptive research design wasadoptedinthisstudy.
Setting of the study: The study was conducted inselected villages of dharawad Taluka, dharwad.Karnataka.India.
Population: Targetpopulationforthepresentstudywere100 farmers’ who were actively involved in farmingselectedfromvillagesofdharawadTaluka.dharwad.
Sampling: Convenient sampling technique was usedinthepresentstudy.InclusioncriteriaareFarmersagedbetween18 to60years,whoare available at the timeofdatacollection,andwhoarewillingtoparticipateinthe study.Farmerswhoare sufferingwith any typeofchronicmedicalorpsychiatric illnesseswereexcludedfromthestudy.
Tools:
Sections i: It includes‘18’items related to the sociodemographicvariablescomprisethreeparts,
(a) Socio demographic characteristics
(b) Socio agro economic characteristic.
(c) Socio psychological characteristics
Sections ii: Subjective wellbeing scale: SubjectiveWell-BeingInventoryisaselfreportquestionnaireconsistingof40itemsdesignedtomeasureanindividual‘smentalstatusregardingoverallfeelingaboutlife.5
Procedure for data collection: Priortothestudyformalpermissionwasobtained from the subjects.Structuredinterviewschedulewasadoptedfor thedatacollectionandwas carried outwithin given period of 12weeks.Before interviewing the subjects,purposeof the studywas explained with self-introduction. Privacy wasmaintained during the interview. Subjects were madetobecomfortableandrelaxduringinterview.Thedatacollection process for each individual took 40 - 50minutes,5-6subjectswereinterviewedperday.
DATA AnALySIS
Aftercompletionofthedatacollection,thedatawascodedandwasanalyzedintermsoftheobjectivesofthestudyusingdescriptiveandinferentialstatistics.
RESuLTS
A. Distribution of based on frequency and percentage of socio-demographic characteristics.
(a) Socio demographic characteristics: The description of socio-demographiccharacteristics of farmers. Regarding agegroupthemajorityoffarmers(34%)belongsto
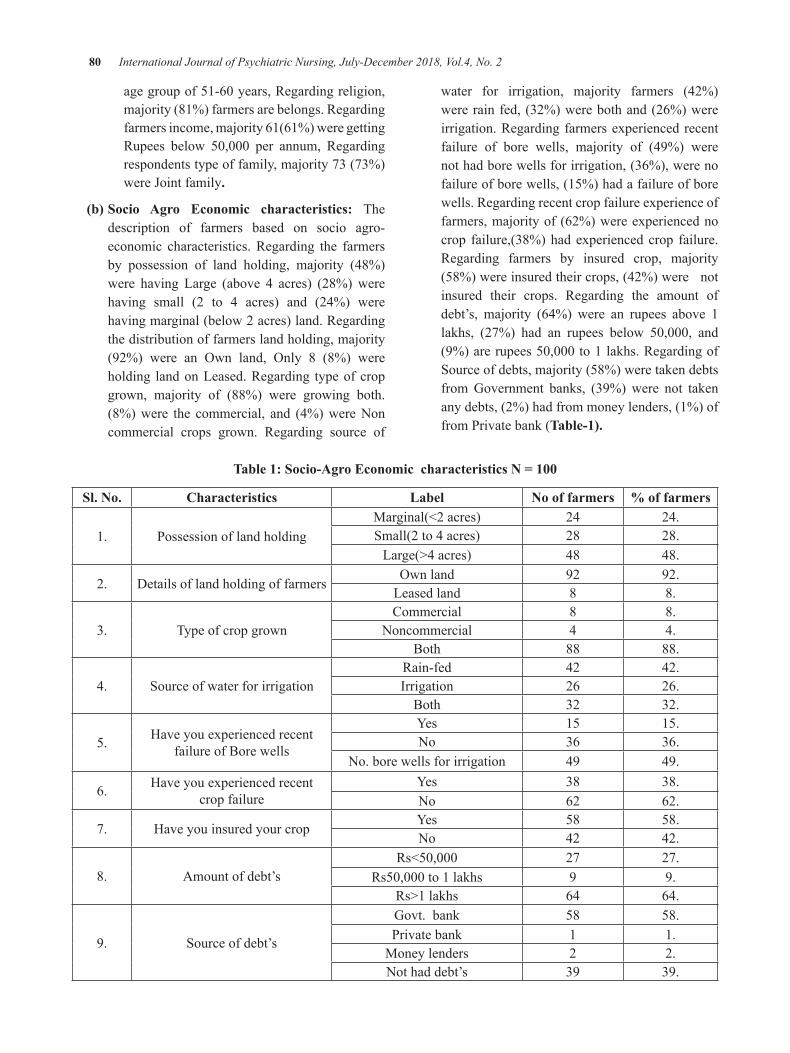
80 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
agegroupof51-60years,Regardingreligion,majority(81%)farmersarebelongs.Regardingfarmersincome,majority61(61%)weregettingRupees below 50,000 per annum, Regardingrespondentstypeoffamily,majority73(73%)wereJointfamily.
(b) Socio Agro Economic characteristics: Thedescription of farmers based on socio agro-economic characteristics.Regarding the farmersby possession of land holding, majority (48%)were having Large (above 4 acres) (28%)werehaving small (2 to 4 acres) and (24%) werehavingmarginal(below2acres)land.Regardingthedistributionoffarmerslandholding,majority(92%) were an Own land, Only 8 (8%) wereholding landonLeased.Regarding typeofcropgrown, majority of (88%) were growing both.(8%)were the commercial, and (4%)wereNoncommercial crops grown. Regarding source of
water for irrigation, majority farmers (42%)wererainfed,(32%)werebothand(26%)wereirrigation.Regardingfarmersexperiencedrecentfailure of bore wells, majority of (49%) werenothadborewellsforirrigation,(36%),werenofailureofborewells,(15%)hadafailureofborewells.Regardingrecentcropfailureexperienceoffarmers,majorityof(62%)wereexperiencednocrop failure,(38%)hadexperiencedcrop failure.Regarding farmers by insured crop, majority(58%)wereinsuredtheircrops,(42%)werenotinsured their crops. Regarding the amount ofdebt’s, majority (64%) were an rupees above 1lakhs, (27%) had an rupees below 50,000, and(9%)arerupees50,000to1lakhs.RegardingofSourceofdebts,majority(58%)weretakendebtsfromGovernment banks, (39%)were not takenanydebts,(2%)hadfrommoneylenders,(1%)offromPrivatebank(Table-1).
Table 1: Socio-Agro Economic characteristics n = 100
Sl. no. Characteristics Label no of farmers % of farmers
1. PossessionoflandholdingMarginal(<2acres) 24 24.Small(2to4acres) 28 28.Large(>4acres) 48 48.
2. detailsoflandholdingoffarmersOwnland 92 92.Leasedland 8 8.
3. TypeofcropgrownCommercial 8 8.
Noncommercial 4 4.Both 88 88.
4. SourceofwaterforirrigationRain-fed 42 42.Irrigation 26 26.Both 32 32.
5. HaveyouexperiencedrecentfailureofBorewells
Yes 15 15.No 36 36.
No.borewellsforirrigation 49 49.
6. Haveyouexperiencedrecentcropfailure
Yes 38 38.No 62 62.
7. HaveyouinsuredyourcropYes 58 58.No 42 42.
8. Amountofdebt’sRs<50,000 27 27.
Rs50,000to1lakhs 9 9.Rs>1lakhs 64 64.
9. Sourceofdebt’s
Govt.bank 58 58.Privatebank 1 1.Moneylenders 2 2.Nothaddebt’s 39 39.
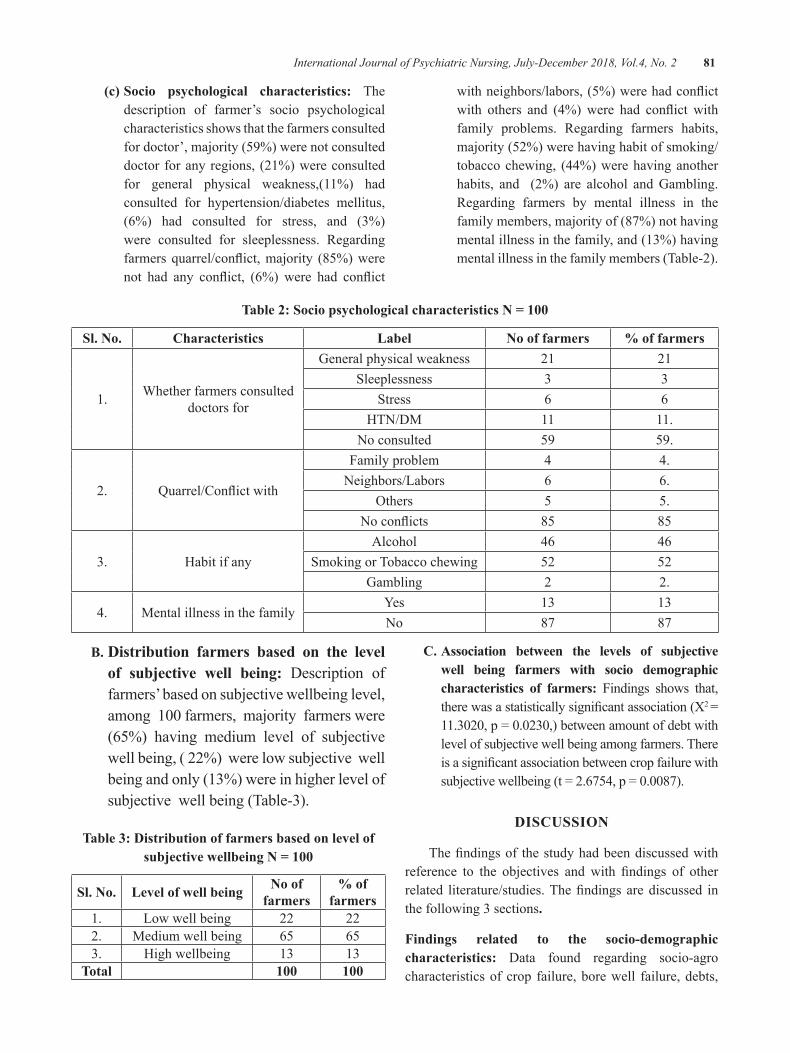
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 81
(c) Socio psychological characteristics: Thedescription of farmer’s socio psychologicalcharacteristicsshowsthatthefarmersconsultedfordoctor’,majority(59%)werenotconsulteddoctorforanyregions, (21%)wereconsultedfor general physical weakness,(11%) hadconsulted for hypertension/diabetes mellitus,(6%) had consulted for stress, and (3%)were consulted for sleeplessness. Regardingfarmersquarrel/conflict,majority (85%)werenot had any conflict, (6%) were had conflict
withneighbors/labors,(5%)werehadconflictwith others and (4%)were had conflict withfamily problems. Regarding farmers habits,majority(52%)werehavinghabitofsmoking/tobaccochewing, (44%)werehavinganotherhabits, and (2%) are alcohol andGambling.Regarding farmers by mental illness in thefamilymembers,majorityof(87%)nothavingmentalillnessinthefamily,and(13%)havingmentalillnessinthefamilymembers(Table-2).
Table 2: Socio psychological characteristics n = 100
Sl. no. Characteristics Label no of farmers % of farmers
1. Whetherfarmersconsulteddoctorsfor
Generalphysicalweakness 21 21Sleeplessness 3 3
Stress 6 6HTN/dM 11 11.
Noconsulted 59 59.
2. Quarrel/Conflictwith
Familyproblem 4 4.Neighbors/Labors 6 6.
Others 5 5.Noconflicts 85 85
3. HabitifanyAlcohol 46 46
SmokingorTobaccochewing 52 52Gambling 2 2.
4. MentalillnessinthefamilyYes 13 13No 87 87
b. Distribution farmers based on the level of subjective well being: description offarmers’basedonsubjectivewellbeinglevel,among100farmers,majorityfarmerswere(65%) having medium level of subjectivewellbeing,(22%)werelowsubjectivewellbeingandonly(13%)wereinhigherlevelofsubjectivewellbeing(Table-3).
Table 3: Distribution of farmers based on level of subjective wellbeing n = 100
Sl. no. Level of well being no of farmers
% of farmers
1. Lowwellbeing 22 222. Mediumwellbeing 65 653. Highwellbeing 13 13
Total 100 100
C. Association between the levels of subjective well being farmers with socio demographic characteristics of farmers: Findings shows that,therewasastatisticallysignificantassociation(X2 =11.3020,p=0.0230,)betweenamountofdebtwithlevelofsubjectivewellbeingamongfarmers.Thereisasignificantassociationbetweencropfailurewithsubjectivewellbeing(t=2.6754,p=0.0087).
DISCuSSIon
Thefindingsof thestudyhadbeendiscussedwithreference to the objectives and with findings of otherrelated literature/studies.Thefindingsarediscussed inthefollowing3sections.
Findings related to the socio-demographic characteristics: data found regarding socio-agrocharacteristicsofcrop failure,borewell failure,debts,

82 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
andhabitsliketobaccoandalcoholareshownmajority.It indicates that majority farmers were experiencedcropfailure,borewellfailure,havingdebts,theselosesmay be provoking the farmers to cultivate un-healthyhabitslikeusingtobaccoandconsumingalcohol.So,itisawarningsignalthatfarmersmentalhealthgoingtobe affects and risk formental illnesses likedepressivedisorders, alcohol dependence syndrome, and othersubstanceabusedisordersandalsoincreasetheriskforfarmerssuicide.Manyresearchstudiessupportsforthesame results. Farmer’s suicides have been receiving alotofsocialandpublicpolicyattention.SuicidesweremainlyconcentratedinKarnataka,AndhraPradeshandMaharashtra.AlargenumberofsuicideswerereportedinKarnatakainthefirstthreeyearsofthedecadestarting2000-01,whileAndhraPradeshhadmaximumin2004-05. In 2006, therewas virtually a suicide epidemic inMaharashtra. These incidents raised serious questionsofthestateoftheagrarianeconomyandtheeconomichardshipsfacedbyfarmers.6
TheearlierstudyreportstheresultsofpresentstudyconductedcountyinIowa.Participantsaged18orolderwere asked about suicidal ideation in the past year aswellasmood,alcoholuse,socialsupport,andstressfullifeevents.About8.2%ofthesamplereportedsuicidalideation.depressivesymptoms,problemsresultingfromalcoholuse,infrequentsocialcontactandfinanciallosscharacterizedthesuicidalgroup.depressivesymptomswere thestrongestcorrelateofsuicidal ideation in thisrural sample. This suggests that change in financialstatus rather than chronic poverty poses a risk forsuicidalideation.7
Level of subjective wellbeing among farmers: Thelevel of subjective wellbeing among farmers wasassessedbystructured interviewtheresultsshows thatsubjectivewellbeingwith the overallmedian score of51.50.Thefindingsshowsthatthemajorityoffarmersexperiencing the moderate or low level of subjectivewellbeing. The results of the present study supportedbythestudyconductedin1981toidentifydeterminantsof subjective wellbeing among farmers. The studyconcludedthatthesubjectivewellbeingamongfarmersvaryandisconsiderablylesserthanthatofotherworkers.Thesalientfindingsrevealedthatnearaboutcentpercent(98.58%)selectedfarmerswerehavinghighcompositeindexofagrariandistress.8
Association between the levels of subjective well-being with socio- demographic variables: There isastatistically significant association found between thelevel of subjective well being and socio demographicvariables such asAmount of debt’s at the level ofp<0.05.Theresultsofthepresentstudyareinconsistentwiththestudycarriedoutandreportedwiththepurposeof determining the effects of off-farm employment onperceptionsofqualityoflife.9
Theearlierstudyresultssupportsthepresentstudyreports reveal that exploring the relationship betweensubjective wellbeing and groundwater attitudes andpracticesoffarmersinRuralIndia.Theresultssuggestasingular relianceon initiatives to improvehouseholdincome is unlikely tomanifest as improved individualsubjective wellbeing for the dharta and Meghrajwatersheds.Correlatesweretabulatedintoasystematicdecisionframeworktoassistthedesignofparticipatoryprocesses at the village level, by targeting specificfactors likely to jointly improve aquifer sustainabilityandhouseholdwellbeing.10
Nursing personnel especially mental health andcommunity health nurses can contribute much forprevention and management of ill well being amongfarmersandnursesplayanimportantroleinpreventionofseriousconsequenceslikementalhealthproblemsandevensuicidesamongfarmersthroughearlyidentificationandpromptintervention.
ConCLuSIon
The changing values of society, globalization,urbanization,industrializationandclimaticallychangingetcarecausinggeneralwellbeingnegativeandpositiveeffectinfarmer’slife.Henceitisnecessarytoaddressthefarmers’needofstressmanagement.Itisanticipatedthat this research may help mental health nurses andcommunitymentalhealthpersonalstoidentifythementalhealthstatuswithviewingtheirsubjectivewellbeingandtoplaneffectivementalhealthneedsoffarmerssothatfurtherdamageorconsequencesofdistressof farmerscanbepreventedbytimelyintervention.
Ethical Clearance:ObtainedfromdIMHANSEthicalcommittee, dharwad Institute of Mental Health &Neurosciences,dharwad,Karnataka,India.
Source of Funding:Selffunding.

International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 83
Conflict of Interest: No conflict of interest has beendeclaredbytheauthor(s)
REFEREnCES
1.BhiseMC,BeherePB.RiskFactorsforFarmers’Suicides in Central Rural India:MatchedCase-control Psychological Autopsy Study. Indian JPsycholMed.2016Nov-dec;38(6):560-566.
2.KirankumarSK.AnIndianconceptionofwellbeing.BritishPsychologicalSociety.2003;2(1):2-10.
3.Berry,H.L.,Hogan,A.,Owen,J.,Rickwood,d.,Fragar, L., (2011).Climate change and farmers’mental health: risksandresponses.Asia-PacificJournalofPublicHealth,23(2),119S–132S.
4.Brewetal.ThehealthandwellbeingofAustralianfarmers:Alongitudinalcohortstudy.BMCPublicHealth2016;16:988.
5.Nagpal & Helmut Sell. The Subjective Well-BeingInventory(SUBI) InternationalJournalofMentalHealthVol.23,No.3.pp.89-102.
6.Bhende M. J. and Thippaiah P. An EvaluationStudyofPrimeMinister’s.RehabilitationPackageforFarmers inSuicide-Pronedistricts,Ministryof Agriculture, Government of India, ISECBangalore.2010.Pp-17-57.ISSN-2250-1991
7.KearneyGd,RaffertyAP,LaurenR,HendricksLR,AllendL,RobinTM.OriginalarticleACross-Sectional Study of StressorsAmong Farmers inEasternNorthCarolina.NCMedJ.2014;75(6):384-92.
8.Pateletal.Theinterplaybetweenhouseholdfoodsecurityandwellbeingamongsmall-scalefarmersin thecontextof rapidagrarianchange in India.AgriandFoodSecur.Research-2015;4:16
9.Thekiso MS. Psychological well-being, healthand the quality of life of farm workers. Well-beingresearchinSouthAfrica,2013;123:61-72.
10.Melinda McCoy, Glen Filson, Working off thefarm:Impactsonqualityoflife,SocialIndicatorsResearch,February1996,Volume37,Issue2,pp149–163.

Effectiveness of Psycho Educative Intervention on body Image and Adjustment to Cancer among Head and neck Cancer Patients
T Sivabalan1, Kavita bhoknal2
1Dean, Faculty of Nursing, 2Asst. Professor, Pravara Institute of Medical Sciences (Deemed to be University), College of Nursing, Loni (Bk), Tal. Rahata, Dist. Ahmednagar, Maharashtra
AbSTRACT
background: CancerisoneofthemajorpublichealthproblemsinIndia.despitethesignificantadvancementincancermanagement,it’sstillamostdreadfuldiseasethathastremendousburdenonindividual,familyandsociety.Headandneckcancerpatientsexperienceconsiderablestress,poorqualityoflifeandimpairmentof adjustment to cancer. The aim of present studywas to determine effectiveness of psycho educativeinterventiononbodyimageandadjustmenttocanceramongheadandneckcancerpatients.
Material and Method: Anexperimentalstudy,preandposttestdesignwasundertakenamongheadandneckcancerpatientsofPravaraRuralHospital,Loni(Bk).Atotalof60cancerpatientswereselectedbysystematicrandomsamplingtechniquewhofulfillstheinclusioncriteria’s.Pretestedstructuredquestionnaire[a)BodyImageScaleandb)MentalAdjustmenttoCancerScale]wasusedtocollectdata.StudywasapprovedbyIEC/IRCandinformedconsentwasobtainedfromalltheparticipants.Afterpretestingpsychoeducativeinterventionwasimplementedindividuallyandposttestwasconductedaftersixsessionsofintervention.Thedescriptiveandinferentialstatisticswereappliedwhereverwasrequired.
Results: Majorityofpatientshadpartiallyadoptivenesstocancerdiseaseaftertheintervention,andfoundstatisticallysignificantatp<0.05level.Itwasearlierfoundtobenotadoptiveduringpretestassessment.Inrelationtobodyimage,patientsdidnothavesignificantchangeinbodyimageafterthepsychoeducation.Itwasnotedthatbodyimagehadsignificantassociationwithdemographicvariableslikeage(x2 =4.29),gender(x2 =3.58)andsiteofcancer(x2 =7.04);similarlyadjustmenttocancerhadassociationwithage(x2
=3.92)anddurationofillness(x2 =6.81)p<0.05level.
Conclusion: Studyoutcomerevealedthatpsychoeducativeinterventionwasfoundeffective,andplayedsignificantroleforadjustmenttocancer.Theplannedpsychoeducationalprogramhelpspatientsandtheirfamiliestocopewithcancerdiseaseaswellasenablestoenhancequalityoflife.
Keywords: effectiveness, psycho educative intervention, body image and adjustment to cancer
Corresponding Author:dr.T.Sivabalan,Phd(N)dean,FacultyofNursing,PravaraInstituteofMedicalSciences(dU)CollegeofNursing,Loni(Bk),Tal.Rahatadist.Ahmednagar,MS–413736Mobile:+919960783747Email:[email protected]
InTRoDuCTIon
Cancerisoneof themajorpublichealthproblemsin India, and despite the significant advancement in
cancer treatment, it’s still a most dreadful diseasethat has tremendous burden on individual and family.Headandneckcanceristhefifthmostcommoncancerworldwide, and males are predominantly affected. InIndia the prevalence rate of head and neck cancer is23%.Cancer patients including head and neck cancerpatientsexperienceconsiderablestress,poorqualityoflifeandimpairmentofadjustmenttocancer.1
Cancerpatientshasnumerousandintensesymptomswhichleadstopoorqualityoflifeanddeteriorationinhealth status.The life of patientswith advanced headand neck cancer gets involved in abundant physical,emotional and psychological symptoms. Scholarly
DOI Number: 10.5958/2395-180X.2018.00022.1

International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 85
studieshavefoundthecommonhealthproblemswhicharepain(>85%),dysphagia(>60%),airwayobstruction,fungatingwound,andmucosaldrynessarethealarmingproblemsinpatientswithheadandneckcancers2,3.
Headandneckcancersarethecommonestcancersamongmales in Indiaandaroundmore than two thirdpresents in advanced stage with significant burden ofvarietyofsymptoms.Majorityofthemhavepoorqualityoflifeandemotionalwellbeingaswellasactivitiesofdaily living.The top four common symptomsof headand neck cancer patients are pain, insomnia, loss ofappetiteandfatigue4.
Cancer and its treatment strategies usually resultsinmajoralterationsofbodyimageduetolossofbodypart,disfigurement,scarsorskinchanges.Radiotherapycause tissue damagewith insidious changes formanyyears, the effects of surgery are immediate and oftenpermanent,whereastransient,reversiblechangesresultsfrom chemotherapy. Thus, large numbers of patientsacrossmanydiseasegroupsandtreatmenttypescanbeaffected.5
ScholarlyarticleonQOLincancerpatientsrevealedthatmajority (81%)hadapoorqualityof lifewherein(59%)hadpoorQOLbecauseofphysicalpainandmorethanhalf(58%)wereverydissatisfiedwiththeirhealthcondition.Aconsiderableproportionhaddissatisfactionwith themselves, dissatisfaction with their sexual life(65%)and(62%)respectively.Onethird(35%)ofthemhad increased frequency of having negative feelingssuchasbluemood,despair,anxiety,depression.6
Psycho education is an effective psychosocialapproach of specialized education that consists ofeducational and psychosocial endeavors with an aimtocreateterminalbehaviorchangeinpatientsandtheirfamilies. Planned psycho educational programs assistpatientsandtheirfamiliestocopewithandadapttothedifficulties associatedwith thedisease, enable them todevelop theirproblemsolvingskillsand increase theirqualityoflife.7
The women participating in psycho educationalprogramhad increased levels of adjustment to cancer;theinterventiongrouphadhigherlevelsoffightingspirit,lower levelsofhelplessnessandhopelessness,anxiouspreoccupationandfatalismincomparisontothecontrolgroup.Itwasevidentthatthepsychoeducationledtoa
changeinlevelsofadjustmentincancerpatients.8Thusthepresentcommunicationwasundertakentoexaminethe effectiveness of psycho educative intervention onbody image, adjustment to cancer and correlate withclinicalcharacteristicsofheadandneckcancerpatients.
MATERIAL AnD METHoD
Aquantitative research, experimental studywherepreandposttestdesignwasundertakenamongheadandneckcancerpatientsadmittedatPravaraRuralHospital,Loni (Bk),Maharashtra.A total of 60 head and neckcancerpatientsabove18yearsofageofbothgender,andwillingtoparticipatewereselectedbysystematicrandomsamplingtechnique.ThesamplesizewascalculatedwithOpenepi,version2,opensourcecalculator–SSP.Cancerpatientswho are acutely ill, has comorbid conditionsandsecondarymetastasiswasexcludedfromthestudy.Pretestedandvalidatedstructuredquestionnairesuchasa)Body ImageScale (BIS)andb)MentalAdjustmenttoCancerScale (MAC)was used to collect data.TheresponsesforallitemsofBISaregradedonfourpointscale(3=Verymuch,2=Quiteabit,1=Alittleand0 =Not at all), and the responses forMAC scale aregradedona fourpoint scale (1–4, one fordefinitelydoes not applies tome and 4 for definitely applies tome). The study was approved by Institutional EthicsCommittee/Institutional Research Committee (IEC /IRC)andwritten informedconsentwasobtained fromallparticipants.
The psycho educative intervention comprised ofa) basic information about head and neck cancer b)importanceofnutritionc)healthproblemsofheadandneckcancerd)measurestoadjust/copewithcancerande) sources of social support and financial support. Itwasimplementedafterpretestingindividuallythroughdidactic lecture and discussion (in Marathi language)for six sessions with 45 minutes of duration at eachfollow up visit of patients. Along with education aninformative pamphlets and leaflets are supplementedfor enhancement and reinforcement of awareness andcomplianceoftreatment,andtheposttestwasconductedaftersixsessionsofpostintervention.Thecollecteddatawascoded,tabulatedandanalyzedbyusingdescriptive(mean,Sd) and inferential statistics (t test, chi squaretest)whereverrequired,andp<0.05wasconsideredasstatisticallysignificant.
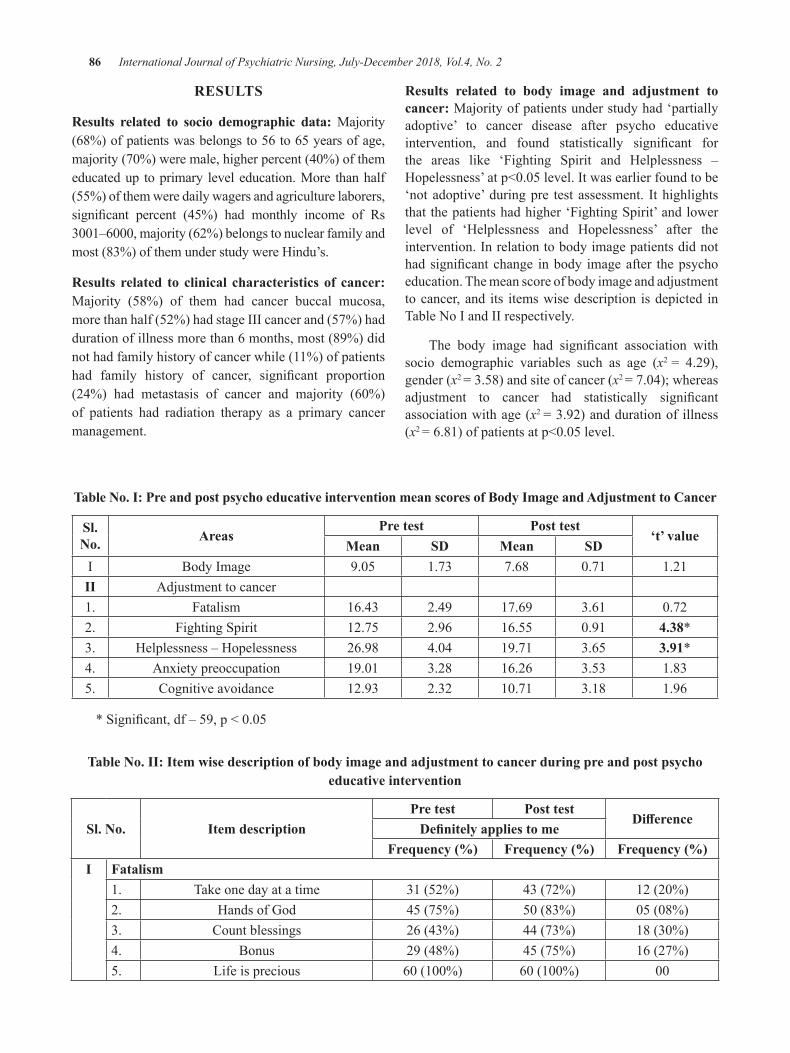
86 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
RESuLTS
Results related to socio demographic data:Majority(68%)ofpatientswasbelongsto56to65yearsofage,majority(70%)weremale,higherpercent(40%)ofthemeducatedup toprimary leveleducation.More thanhalf(55%)ofthemweredailywagersandagriculturelaborers,significant percent (45%) had monthly income of Rs3001–6000,majority(62%)belongstonuclearfamilyandmost(83%)ofthemunderstudywereHindu’s.
Results related to clinical characteristics of cancer: Majority (58%) of them had cancer buccal mucosa,morethanhalf(52%)hadstageIIIcancerand(57%)haddurationofillnessmorethan6months,most(89%)didnothadfamilyhistoryofcancerwhile(11%)ofpatientshad family history of cancer, significant proportion(24%) had metastasis of cancer and majority (60%)of patients had radiation therapy as a primary cancermanagement.
Results related to body image and adjustment to cancer: Majorityofpatientsunderstudyhad‘partiallyadoptive’ to cancer disease after psycho educativeintervention, and found statistically significant forthe areas like ‘Fighting Spirit and Helplessness –Hopelessness’atp<0.05level.Itwasearlierfoundtobe‘notadoptive’duringpre test assessment. Ithighlightsthatthepatientshadhigher‘FightingSpirit’andlowerlevel of ‘Helplessness and Hopelessness’ after theintervention.Inrelationtobodyimagepatientsdidnothadsignificantchange inbody imageafter thepsychoeducation.Themeanscoreofbodyimageandadjustmenttocancer,and its itemswisedescription isdepicted inTableNoIandIIrespectively.
The body image had significant association withsocio demographic variables such as age (x2 = 4.29),gender(x2 =3.58)andsiteofcancer(x2 =7.04);whereasadjustment to cancer had statistically significantassociationwithage(x2 =3.92)anddurationof illness(x2 =6.81)ofpatientsatp<0.05level.
Table no. I: Pre and post psycho educative intervention mean scores of body Image and Adjustment to Cancer
Sl. no. Areas
Pre test Post test‘t’ value
Mean SD Mean SDI BodyImage 9.05 1.73 7.68 0.71 1.21II Adjustmenttocancer1. Fatalism 16.43 2.49 17.69 3.61 0.722. FightingSpirit 12.75 2.96 16.55 0.91 4.38*3. Helplessness–Hopelessness 26.98 4.04 19.71 3.65 3.91*4. Anxietypreoccupation 19.01 3.28 16.26 3.53 1.835. Cognitiveavoidance 12.93 2.32 10.71 3.18 1.96
*Significant,df–59,p<0.05
Table no. II: Item wise description of body image and adjustment to cancer during pre and post psycho educative intervention
Sl. no. Item descriptionPre test Post test
DifferenceDefinitely applies to me
Frequency (%) Frequency (%) Frequency (%)I Fatalism
1. Takeonedayatatime 31(52%) 43(72%) 12(20%)2. HandsofGod 45(75%) 50(83%) 05(08%)3. Countblessings 26(43%) 44(73%) 18(30%)4. Bonus 29(48%) 45(75%) 16(27%)5. Lifeisprecious 60(100%) 60(100%) 00
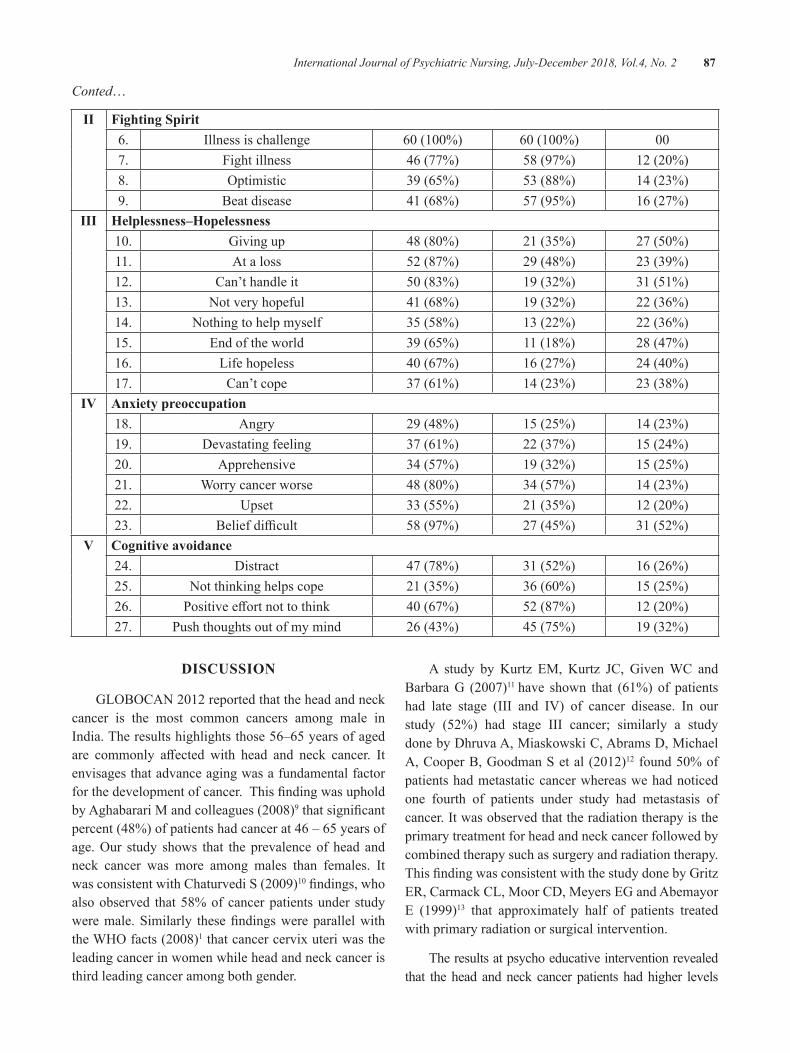
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 87
Conted…
II Fighting Spirit6. Illnessischallenge 60(100%) 60(100%) 007. Fightillness 46(77%) 58(97%) 12(20%)8. Optimistic 39(65%) 53(88%) 14(23%)9. Beatdisease 41(68%) 57(95%) 16(27%)
III Helplessness–Hopelessness10. Givingup 48(80%) 21(35%) 27(50%)11. Ataloss 52(87%) 29(48%) 23(39%)12. Can’thandleit 50(83%) 19(32%) 31(51%)13. Notveryhopeful 41(68%) 19(32%) 22(36%)14. Nothingtohelpmyself 35(58%) 13(22%) 22(36%)15. Endoftheworld 39(65%) 11(18%) 28(47%)16. Lifehopeless 40(67%) 16(27%) 24(40%)17. Can’tcope 37(61%) 14(23%) 23(38%)
IV Anxiety preoccupation18. Angry 29(48%) 15(25%) 14(23%)19. devastatingfeeling 37(61%) 22(37%) 15(24%)20. Apprehensive 34(57%) 19(32%) 15(25%)21. Worrycancerworse 48(80%) 34(57%) 14(23%)22. Upset 33(55%) 21(35%) 12(20%)23. Beliefdifficult 58(97%) 27(45%) 31(52%)
V Cognitive avoidance24. distract 47(78%) 31(52%) 16(26%)25. Notthinkinghelpscope 21(35%) 36(60%) 15(25%)26. Positiveeffortnottothink 40(67%) 52(87%) 12(20%)27. Pushthoughtsoutofmymind 26(43%) 45(75%) 19(32%)
DISCuSSIon
GLOBOCAN2012reportedthattheheadandneckcancer is the most common cancers among male inIndia.Theresultshighlightsthose56–65yearsofagedare commonly affected with head and neck cancer. Itenvisagesthatadvanceagingwasafundamentalfactorforthedevelopmentofcancer.ThisfindingwasupholdbyAghabarariMandcolleagues(2008)9thatsignificantpercent(48%)ofpatientshadcancerat46–65yearsofage.Our study shows that theprevalenceofhead andneck cancer was more among males than females. ItwasconsistentwithChaturvediS(2009)10findings,whoalsoobserved that58%ofcancerpatientsunder studyweremale.Similarly thesefindingswereparallelwiththeWHOfacts(2008)1thatcancercervixuteriwastheleadingcancerinwomenwhileheadandneckcanceristhirdleadingcanceramongbothgender.
A study by Kurtz EM, Kurtz JC, GivenWC andBarbaraG (2007)11 have shown that (61%)of patientshad late stage (III and IV) of cancer disease. In ourstudy (52%) had stage III cancer; similarly a studydonebydhruvaA,MiaskowskiC,Abramsd,MichaelA,CooperB,GoodmanSetal(2012)12 found50%ofpatientshadmetastaticcancerwhereaswehadnoticedone fourth of patients under study had metastasis ofcancer.Itwasobservedthattheradiationtherapyistheprimarytreatmentforheadandneckcancerfollowedbycombinedtherapysuchassurgeryandradiationtherapy.ThisfindingwasconsistentwiththestudydonebyGritzER,CarmackCL,MoorCd,MeyersEGandAbemayorE (1999)13 that approximately half of patients treatedwithprimaryradiationorsurgicalintervention.
Theresultsatpsychoeducativeinterventionrevealedthat thehead andneck cancerpatients hadhigher levels
88 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
of ‘fightingspirit’, and lower levelsof ‘helplessnessandhopelessness’, ‘anxious preoccupation’ and ‘cognitiveavoidance’ related to adjustment to cancer while therewasnosignificantchangeinbodyimagebeforeandafterintervention.Thisfindingwere incongruencewithstudycarried out bydastanNB,BuzluS (2013)14 that psychoeducationinterventionwaseffectivetoimproveadjustmenttocanceramongfirst–secondstagecancerpatients.
ConCLuSIon
The results highlight that psycho educativeinterventionwaseffectiveandplayedsignificantroleforadjustmenttocancerofheadandneckcancerpatients.Thoughitdidnothavesignificantimpactonbodyimagechanges, certainly the intervention helps patients andfamilies to cope or adjustment to cancer disease, andenablestoenhancethewellbeingandqualityoflife.Inconclusion,Regular thepsychoeducation–Better thesenseofcontrolandadjustment tocancerdisease;and‘Never give up, life isworth living, there is life evenafterhavingcancer’.
Source of Funding:Self
Conflict of Interest:Nil
Ethical Clearence: The study was approved byInstitutional Research Committee and InstitutionalEthics Committee (IRC/IEC) of Pravara Institute ofMedicalSciences–deemedtobeUniversity,Loni(Bk),Maharashtra. The ethical guidelines for biomedicalresearchonhumanparticipantswerestrictlyfollowed.
REFEREnCES
1.WorldHealthOrganization(WHO).CancerStats,2008. International Agency for Research onCancer(IARC)SectionofCancerInformation
2.Teunissen SC, Wesker W, Kruitwagen C, HaesHC,VoestEE,GraeffA.Symptomprevalence inpatientswithincurablecancer:Asystematicreview.JPainSymptomManage,2007;34:94–104.
3.Whitmer KM, Pruemer JM, Nahleh ZA, JaziehAR. Symptom management needs of oncologyoutpatients.JPalliatMed,2006;9:628–30.
4.Gandhi AK, Roy S, Thakar A and Sharma A.SymptomburdenandQOLinadvancedheadandneckcancerpatients.IndianJournalofPalliativeCare,2014;20(3):189–193
5.HopwoodP,FletcherI,LeeAandGhazalAI.Abody image scale for use with cancer patients.EuropeanJournalofCancer,2001;37:189–197
6.Arunachalam d, Thirumoorthy A, devi S andThennarasu. Quality of Life in cancer patientswithdisfigurementduetocanceranditstreatment.IndianJPalliatCare2011;17:184–90
7.Reid J, Lloyd C, de Groot L. The psychoeducationneedsofparentswhohaveanadultsonor daughter with a mental illness. Australian JAdvMentalHealth,2005;4:1–13
8.dastan NB, Buzlu S. Psycho educationIntervention to Improve Adjustment to CanceramongTurkishStageI–IIBreastCancerPatients:ARandomizedControlledTrial.Asian Pacific JCancerPrev,2012;13(10):5313–5318
9.Aghabarari M, Ahmadi F, AghaAlinejad H,Mohammadi E and Hajizadeh E. Effect ofdesignedExerciseProgramonFatigueinWomenwith Breast Cancer Receiving Chemotherapy.IranianJPublHealth,2008;37(1):92–98.
10.ChaturvediS.What’simportantforqualityoflifetoIndians:inrelationtocancer?IndianJournalofPalliativeCare,2009;9(2):62–70.
11.Kurtz EM, Kurtz JC, Given WC and Barbara.Symptom clusters among cancer patients andeffects of an educational symptom controlintervention.CancerTherapy,2007;5:105–112.
12.dhruvaA, Miaskowski C, Abrams d, MichaelA,CooperB,GoodmanS andHechtFM.Yogabreathing for cancer chemotherapy-associatedsymptoms and quality of life: results of a pilotrandomizedcontrolledtrial.JAlternComplementMed.2012;18(5):473–79.
13.Gritz ER, Carmack CL,Moor Cd,Meyers EGandAbemayorE.Firstyearafterheadandneckcancer: Quality of Life. J Clin Oncol, 1999;17:352–360
14.dastan NB, Buzlu S. Psycho educationintervention to improve adjustment to canceramongTurkishstageI–IIbreastcancerpatients:ARandomizedControlledTrial.Asian Pacific JCancerPrev,2013;13(10):5313–18

Issues and Challenges in Psychiatric Consultation- Liaison nurse (PCLn)
usha Marath
Professor cum Principal, Lisie College of Nursing, Ernakulam. Kerala
AbSTRACT
Mentalhealthproblemsarenotcurrentlygiventhesameimportanceasphysicalhealth.Nurses,particularlythoseworkinginnon-psychiatricsettings,reportthattheydonotfeeladequatelypreparedtomeetthementalhealthneedsofpatients.Thepsychiatricconsultation-liaisonnursingrolehasariseninpart,asaresponsetothesedifficultiesandaimstofacilitateaccesstomentalhealthnursingexpertiseforgeneralhospitalpatientsandstaff.
Keywords: Psychiatric-liaison nurse, consultation-liaison nurse.
Corresponding Author:dr.UshaMarath,ProfessorcumPrincipal,LisieCollegeofNursing,LisieHospital,Ernakulam-682018,KeralaEmail:[email protected]
InTRoDuCTIonThe mind and the body are more than married, for they are most intimately united; and when
one suffers, the other sympathizes. —Lord Chesterfield
Consultation-Liaison Psychiatry is a serviceprovided to patients who are admitted to a generalhospital for a non-psychiatric condition, but whomay exhibit symptoms of a psychiatric condition andwhosecasemaybeenhancedbytheexpertiseofhealthworkerswithmental health care training.This serviceis provided either throughdirect consultationwith thepatient, or indirectly, through support, education andadvicetootherhealthprofessionalsresponsibleforthecareand treatmentof thepatient.Evidenceshows that25%ofallpatientsadmittedtohospitalwithaphysicalillnessalsohaveamentalhealthcondition,andinmostcasesthisisnottreatedwhilstthepatientisinhospital.In termsof long-termconditions,25–33%ofpatientswith a long-term physical health problem also havea concurrent mental illness that increases the risk of
physical health complications and increases the costsof treating thephysical illness.1There isnowgrowingevidence for the impact of liaisonpsychiatry services.descriptiveevidenceshowsalistofbenefits includingdecreased length of stay, reduction in psychologicaldistress, improved service user experience, improveddementia care and enhanced knowledge and skill ofgeneralhospitalclinicians.2
InIndia,althoughtheGeneralHospitalPsychiatricunits were established in 1930s, C-L Psychiatry hasnever been the main focus of training and research.3 Theintroductionofanursingpositionofaconsultation-liaison psychiatric nurse is yet to take its birth in theIndian health care system, even though there is agrowingbodyofevidencetosuggestthatnursesworkingin general hospital settings do not generally considerthemselvesadequatelyprepared,skilledorexperiencedtocareforpatientswithmentalhealthproblems.4-6Thusthe Psychiatric Consultation-Liaison Nurse (PCLN) rolearisesasaresponsetothesedifficultiesandaimstofacilitate access tomental health nursing expertise forgeneralhospitalpatientsandstaff.
ISSuES AnD CHALLEngESThe challenges associatedwith caring for patients
whoexperienceamentalillnessinacutesecondarycaresettings in particular are often linked with the notionthathealthprofessionalsarenot immune to theeffectsof stigma attached to mental illness; despite formal
DOI Number: 10.5958/2395-180X.2018.00023.3

90 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
educationinpsychiatry.7Mentalhealthproblemsarenotcurrentlygiventhesameimportanceasphysicalhealthproblems.Insimpletermsitmeansgivingmentalhealthequalvaluetophysicalhealth,forexamplethroughequalaccess to effective care, and equal efforts to improvethequalityofcare.Thus there isaneedtofill thegaparoundthementalhealthneedsofpeoplewithphysicalhealthproblems.“Thestatusof liaisonpsychiatry thusshouldchange.Itneedstoberecognizedasanessentialingredient of modern health care and not an optionalextrawhichismerelynicetohave.”2Thiscallsfortheneedtosensitizethestakeholders,policymakersforthegrowthandsustenanceofPCLN.Agoodliaisonservicefunctionsbestasadiscrete,specialized,fullyintegratedteam comprising multi-professional health care staff,undersingleleadershipandmanagement.
Various models of psychiatric consultation aredescribed in literature depending on the focus ofconsultation, function and focus ofwork.Themodelsbased on the focus of consultation include patientorientedapproach, crisisorientedapproach, consultee-oriented approach, situation oriented approach andexpanded psychiatric consultation.8 depending on thefunction, the models of consultation-liaison includeconsultationmodel,liaisonmodel,bridgemodel,hybridmodelandautonomouspsychiatricmodel.9dependingonthefocusofworkthedifferentmodelsincludecriticalcaremodel,biologicalmodel,Milieumodelandintegralmodel.10Thus themodelof serviceneed tobecreatedwhichisamenabletolocalflexibilityandcloseworkingrelationshipsbetweenallkeystakeholders.
Theallianceorliaisonrelationshipiscentraltotheclinical practice of a PCLN.11The liaison relationshipbetweenthePCLNandthestaff,unitsandtheorganizationasawholeunderpinsboththeclinicalandorganizationalconsultationprocesses.Sheferetal12showedthatadultnursesbelievetheyhavetodefertotheMHLteam,andnotedthatwhiletheliaisonteam’spresencewas‘usefulin many ways, it can have adverse consequences, inparticular increatinga reduced senseof responsibilityofemergencystaffforpatientstheyseeasbelongingtoanotherteam’.Thisillustratesthegulfthatcharacterizesmuchoftheinteractionbetweenmentalhealthspecialistsand their colleagues. Clear communication process isakey to success. Properdescriptionof their rolewillhelptopreventoverlapwithotherhealthprofessionals.11 Hence, it is important that the PCLN role within theCLteamisclearlyarticulated togeneralhospitalstaff.
The development of skilled multidisciplinary teamsemphasizing close collaborations between psychiatricand non-psychiatric personnel is essential elementfor the functioningof theCL team.Until recently, thegeneral health and psychiatric sectors of the publichealthsystemhasbeenquiteseparate.Culturebrokeringisofparticularimportanceinbridgingthegapbetweenthese artificially disparate areas of nursing. Culturebrokering ‘... is definedas the actofbridging, linkingor mediating between groups or persons of differingcultural backgrounds for the purpose of reducingconflictorproducingchange.’13Theskillsofmediation,negotiation and innovation are important if greatercommunicationandagreaterunderstandingbetweenthegeneralandpsychiatricculturesistobeachieved.
Muchattentionisgiventooutcomesofhealthcare,but structure and process must also receive attentionas they underpin the outcome. If the structure of, andprocesses within a service are not well defined andarticulated, then it is likely that the outcomemay notbe as desirable. Under ‘structure’, consideration ofcomponents such as the PCLN position description(responsibilities, specifications, remunerationand linesofaccountability),physicalstructure(office,equipment,teaching aids, communication devices) and resource/budgetissuescanbearticulated.Animportantchallengeisthephysicalenvironmentinthegeneralwardcontextof a hospital when caring for patients who have co-morbid mental illness. Patients experiencing mentaldisorders often require a therapeutic milieu to aidrecovery,andwhenpatientsareconsideredasnotfittingintothepurposeoftheenvironment,healthprofessionals’attitudescanalter,frustrationsincreaseandfearsbecomeapparentwithstigmatizingandstereotypingbehaviors.14 Under ‘process’, the model of service deliveryincluding the choice of theory underpinning practice,clinical supervision arrangements, policies, standards,mechanisms for documentation and evaluation needto be considered. The ‘outcome’ of PCLNwork mayinclude whether or not the interventions improve thepsychosocial care of general hospital patients, thelevel of satisfaction that consultees have with theservice, or whether changes in the nurses’ knowledgeofpsychosocialnursingandintheirattitudestopeoplewith mental illness has occurred. Assessment ofoutcomemayprove to be themost challenging as theoutcomemeasures andkeyperformance indicators forC-LPsychiatryarenotwell-developed.15&16

International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 91
The issue of the educational preparation of thePCLN has only been given cursory attention.17 It isstrongly suggested in the literature that the PCLN isconsidered an advanced psychiatric nurse practitionerwithanumberofyearsexperienceinclinicalpsychiatricnursing practice. Robinson18 indicates that it is anexpectationthatadvancedpracticeasaPCLNrequiresa Masters-prepared psychiatric nurse who has alsocompleted post-graduate studies in C-L psychiatryand received supervision of his/her practice by anexperienced qualified preceptor. Hence this calls forjudiciouscurriculumreframingandtrainingtomeetthespecificcompetenciesrequiredforaPCLN.
Liaisonpsychiatryprovisionisoftenpatchy,despiteitscoreroleinriskmanagementandinfacilitatinggoodphysical health care. Existing liaison services tendtypicallytobeforadultswithmentalhealthneeds,andnot for children, young people and older adults. Animportantdevelopmentwouldbetocommissionliaisonservicesthatareage-inclusive. “Thewayaheadforthelong-termdevelopmentofliaisonpsychiatryislikelytolieprimarilyintheexpandedprovisionofcommunity-facingservices.”2
ConCLuSIon
The role of the Psychiatric Consultation-LiaisonNurse (PCLN) not only provides potential for thedevelopmentofaNursePractitionerrole,butitalsoofferspsychiatricnursesanopportunitytoimprovethequality-of-care for the psychological and psychiatric needs ofpatientswithin the general hospital setting.19A robustpsychiatric-liaison service to be implemented requirestheabovementionedissuestobeconsideredwhichwillthen cater to the health care needs of individuals andcommunityholistically.20
The primary aim of this paper was to commencedebateanddiscussionregardingtheroleof thePCLN.To this end, issues and challenges related to thePCLNessential forpracticeand the levelofeducationwhich should be mandatory for the PCLN have beenconsidered.Itisintendedthatthisisthebeginningofamuchdeeperexploration,and that furtherexaminationofthemodelforpracticeanditsapplicabilitytovariouspracticesettingsneedstooccur.
Conflict of Interest:Nil
Ethical Clearance:Notapplicable
Source of Funding:Notapplicable
REFEREnCES
1.Naylor,C., Parsonage,M.,Mcdaid,d.,Knapp,M.,Fossey,M.&Galea,A.(2012).Long-termconditions and mental health: the cost of co-morbidities.London:TheKing’sFundandCentreforMentalHealth.
2.ParsonageM,FosseyM,TuttyC.(2012).LiaisonPsychiatry in theModernNHS.London:CentreforMentalHealth.
3.Grover S. (2011). State of consultation liaisonpsychiatryinIndia:Currentstatusandvisionforfuture.IndianJPsychiatry,53:202-13.
4.Sharrock,J.L.(2000).Strivingforcompetenceinprovidingmentalhealthcare:Agroundedtheoryanalysis of nurses’ experiences. UnpublishedMaster of Health Science (Psychiatric Nursing)Thesis.RMITUniversity,Bundoora,Victoria.
5.Bailey,S.R.(1998).Anexplorationofcriticalcarenurses’anddoctors’attitudestowardspsychiatricpatients.AustralianJournalofAdvancedNursing,15:8–14.
6.Gillette, J.,Bucknell,M.&Meegan,E. (1996).Evaluation of Psychiatric Nurse ClinicalConsultancyinEmergencydepartmentsProject. Bundoora,Victoria:FacultyofNursing BundooraRMIT.
7.ThornicroftG(2008).Stigmaanddiscriminationlimit access to mental health care. EpidemiolPsichiatrSoc.17:14-19.
8.Meyer E, Mendelson M.(1961). Psychiatricconsultations with patients on medical andsurgical wards: Patterns and processes.Psychiatry,24:197-220.
9.StrainJJ.(1996).LiaisonPsychiatry.In:RundellJR,WiseMG,editors.TextbookofConsultation-Liaison Psychiatry. Washington dC: AmericanPsychiatricPress;37-51.
10.Leigh H. (2008). Evolution of Consultation-LiaisonPsychiatryandPsychosomaticMedicine.In: Leigh H, Streltzer J, editors. Handbook ofConsultation-LiaisonPsychiatry.Springer;3-11.
92 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
11.Joint Commissioning Panel for Mental Health(2012). Guidance for commissioners of liaisonmentalhealthservicestoacutehospitals.Availableatwww.jcpmh.info
12.Shefer G, Cross S, Howard L et al (2015).Improving the diagnosis of physical illnessin patients with mental illness who present inemergencydepartments:consensusstudy.JournalofPsychosomaticResearch,78(4):346-351.
13.Jezewski,M.A. (1993). Culture brokering as amodel for advocacy. Nursing and Health Care,14:78–85.
14.Zolnierek Cd and Clingerman EM (2012). Amedical-surgical nurse’s perceptions of caringfor a person with severe mental illness. J AmPsychiatr Nurses Assoc. 18 : 226-35. doi:10.1177/1078390312446223.
15.Wilson, L. & Goldsmidt, P. (1995). Qualitymanagementinhealthcare.Roseville:McGraw-Hill.
16.Greenhill MH. (1977). The development ofliaisonprograms.In:UsdinG,editor.PsychiatricMedicine.NewYork:BrunnerMazel;115-91.
17.Anderson, G. & Hicks, S. (1986). The clinicalnurse specialist-role overview and futureprospects.AustralianNursesJournal,15:36–53.
18.Robinson, L. (1991). Psychiatric consultation–liaisonnursing. InF.K. Judd&G.d.Burrows(Eds),Handbook of Studies on general hospitalpsychiatry.Amsterdam: Elsevier SciencePublishers.
19.Tunmore,R. (1990b).Liaisonpsychiatry settingthepace.NursingTimes,86:29–32.
20.Sharrock J and Happell B . The psychiatricconsultation-liaison nurse: Towards articulatingamodelforpractice (PdFdownloadAvailable).Available from: https://www.researchgate.net/publication/12062113 The psychiatricconsultation-liaisonnurseTowardsarticulatingamodelforpractice[accessedMar052018].

A Report on Diabetes Screening among Adults
W. Ashalata Devi1, Manamaya Rana2, A. L. Sharma3
1Assistant Professor, 2Lecturer, Manipal College of Medical Sciences (Nursing Programme), 3Professor, Manipal College of Medical Sciences
AbSTRACT
Ascreeningprogrammewasconductedfrom5-7thApril2016ontheoccasionofWorldHealthdaythemeon“HalttheRiseBeatdiabetes”,atManipalTeachingHospital.Theobjectivesofthescreeningprogrammeweretoassesstheprevalencerate,riskfactorsfordevelopingdiabetesandtogiveawarenessondiabetes.The totalparticipantswere325adultsagegroupof20andaboveyears.ThescreeningprogrammewasconductedwithpriorpermissionfromthedeanManipalCollegeofMedicalSciences.Theresultof thescreening programme showed that 56% of the participants had no history of both HTN and diabetes,30.8%hadfamilyhistoryofdiabetes,and10.2%alreadyhadHTN.Outofthetotalparticipants,47.4%oftheparticipantshadoverweight,32%hadnormal,19.1%hadobese,and1.5%hadbelownormallevel.RegardingGRBS,77.8%oftheparticipantshadnormal,11.4%hadpre-diabetes,5.5%hadthechancetohavediabetesand5.2%hadbelownormalrange.
Keywords: Adults, Diabetes, Screening
Corresponding Author:W.AshalatadeviAssistantProfessorManipalCollegeofMedicalSciences(NursingProgramme)
InTRoDuCTIon
diabetesisachronicdiseasethatoccurseitherwhenthepancreasdoesnotproduceenoughinsulinorwhenthebodycannoteffectivelyusetheinsulinitproduces.Insulin,ahormonethatregulatesbloodsugar,givesustheenergythatweneedtolive.Ifitcannotgetintothecellstobeburnedasenergy,sugarbuildsuptoharmfullevels in the blood. Over time, high blood sugar canseriously compromise every major organ system inthebody,causingheartattacks,strokes,nervedamage,kidneyfailure,blindness,impotenceandinfectionsthatcanleadtoamputations1.
bACKgRounD
WHOestimatesthattherewillbe1328000casesofdiabetesinNepalby2030.Accordingtothe2011–2012annualreportofthedepartmentofhealthservices,84%ofthetotalnumberofoutpatientvisitsand90%ofthetotal number of inpatients discharged in Nepal wereattributedtoNCds.2
diabetes is one of the major causes of prematuredeaths and disability, and people with diabetes are atincreased risk of dying from cardiovascular disease.Exposure to diabetes-related risk factors, and limitedaccess to early diagnosis andmanagement of diabetes,is not only associated with micro- and macrovascularcomplications but also leads to catastrophic healthexpenditure.Asdiabetesisprevalentinadultsofworkingage,itthreatenstofurtherimpoverishindividuals,familiesandthecommunityasawhole,inacountrywhereout-of-pocketexpenditureforhealthremainshigh.3
People with diabetes need access to appropriatemedicinesandawiderangeofhealth-careservicesinthecourseoftheirdisease.Earlydiagnosisandmanagementare key to prevention and control of diabetes. Therearewide variations in the availability of diabetes careservices, and their availability and utilization acrossdifferent socioeconomic and geographical populationgroups, indicating the challenge of access and equity.diabetesservicesaremainlycenteredinurbanareasandareinaccessibletomanyNepalesepeople.Therearenogovernmenthealth-financingschemesfordiabetescareandnoneoftheservicesarefundedorsubsidizedbythegovernment.All services such asdiagnosis, treatment,medicationsandlaboratorytestsarefundedbyindividualsand households out of pocket.There is also a lack ofawareness of diabetes and its complications amongthe general population.There is no nationwide robust
DOI Number: 10.5958/2395-180X.2018.00024.5
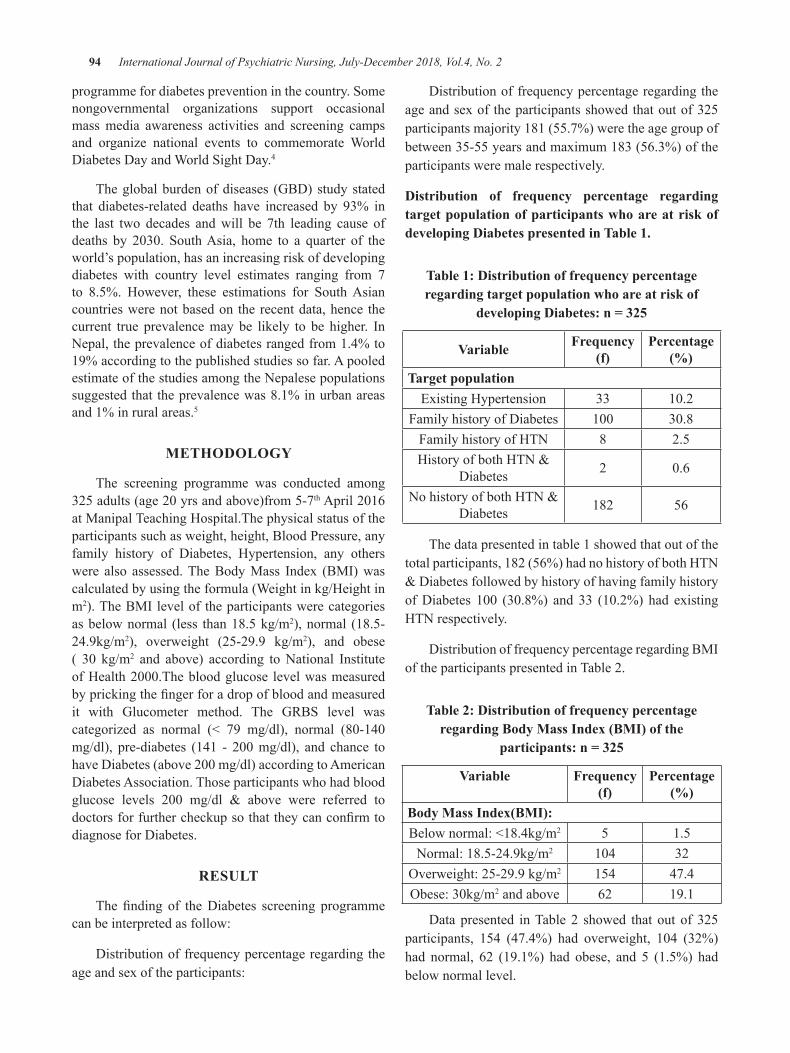
94 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
programmefordiabetespreventioninthecountry.Somenongovernmental organizations support occasionalmassmedia awareness activities and screening campsand organize national events to commemorate WorlddiabetesdayandWorldSightday.4
Theglobalburdenofdiseases (GBd)studystatedthat diabetes-related deaths have increased by 93% inthe last two decades andwill be 7th leading cause ofdeaths by 2030. SouthAsia, home to a quarter of theworld’spopulation,hasanincreasingriskofdevelopingdiabetes with country level estimates ranging from 7to 8.5%. However, these estimations for SouthAsiancountrieswerenotbasedon therecentdata,hence thecurrent true prevalencemay be likely to be higher. InNepal,theprevalenceofdiabetesrangedfrom1.4%to19%accordingtothepublishedstudiessofar.ApooledestimateofthestudiesamongtheNepalesepopulationssuggestedthattheprevalencewas8.1%inurbanareasand1%inruralareas.5
METHoDoLogy
The screening programme was conducted among325adults(age20yrsandabove)from5-7thApril2016atManipalTeachingHospital.Thephysicalstatusoftheparticipantssuchasweight,height,BloodPressure,anyfamily history of diabetes, Hypertension, any otherswere also assessed.TheBodyMass Index (BMI)wascalculatedbyusingtheformula(Weightinkg/Heightinm2).TheBMIleveloftheparticipantswerecategoriesasbelownormal (less than18.5kg/m2),normal (18.5-24.9kg/m2), overweight (25-29.9 kg/m2), and obese( 30 kg/m2 and above) according toNational InstituteofHealth2000.Thebloodglucose levelwasmeasuredbyprickingthefingerforadropofbloodandmeasuredit with Glucometer method. The GRBS level wascategorized as normal (< 79 mg/dl), normal (80-140mg/dl), pre-diabetes (141 - 200mg/dl), and chance tohavediabetes(above200mg/dl)accordingtoAmericandiabetesAssociation.Thoseparticipantswhohadbloodglucose levels 200 mg/dl & above were referred todoctorsforfurthercheckupsothattheycanconfirmtodiagnosefordiabetes.
RESuLT
Thefinding of thediabetes screening programmecanbeinterpretedasfollow:
distributionoffrequencypercentageregardingtheageandsexoftheparticipants:
distributionoffrequencypercentageregardingtheageandsexoftheparticipantsshowedthatoutof325participantsmajority181(55.7%)weretheagegroupofbetween35-55yearsandmaximum183(56.3%)oftheparticipantsweremalerespectively.
Distribution of frequency percentage regarding target population of participants who are at risk of developing Diabetes presented in Table 1.
Table 1: Distribution of frequency percentage regarding target population who are at risk of
developing Diabetes: n = 325
Variable Frequency (f)
Percentage (%)
Target populationExistingHypertension 33 10.2
Familyhistoryofdiabetes 100 30.8FamilyhistoryofHTN 8 2.5HistoryofbothHTN&
diabetes 2 0.6
NohistoryofbothHTN&diabetes 182 56
Thedatapresentedintable1showedthatoutofthetotalparticipants,182(56%)hadnohistoryofbothHTN&diabetesfollowedbyhistoryofhavingfamilyhistoryofdiabetes 100 (30.8%) and 33 (10.2%) had existingHTNrespectively.
distributionoffrequencypercentageregardingBMIoftheparticipantspresentedinTable2.
Table 2: Distribution of frequency percentage regarding body Mass Index (bMI) of the
participants: n = 325
Variable Frequency (f)
Percentage (%)
body Mass Index(bMI):Belownormal:<18.4kg/m2 5 1.5Normal:18.5-24.9kg/m2 104 32
Overweight:25-29.9kg/m2 154 47.4Obese:30kg/m2andabove 62 19.1
datapresented inTable2 showed that out of 325participants, 154 (47.4%) had overweight, 104 (32%)had normal, 62 (19.1%) had obese, and 5 (1.5%) hadbelownormallevel.
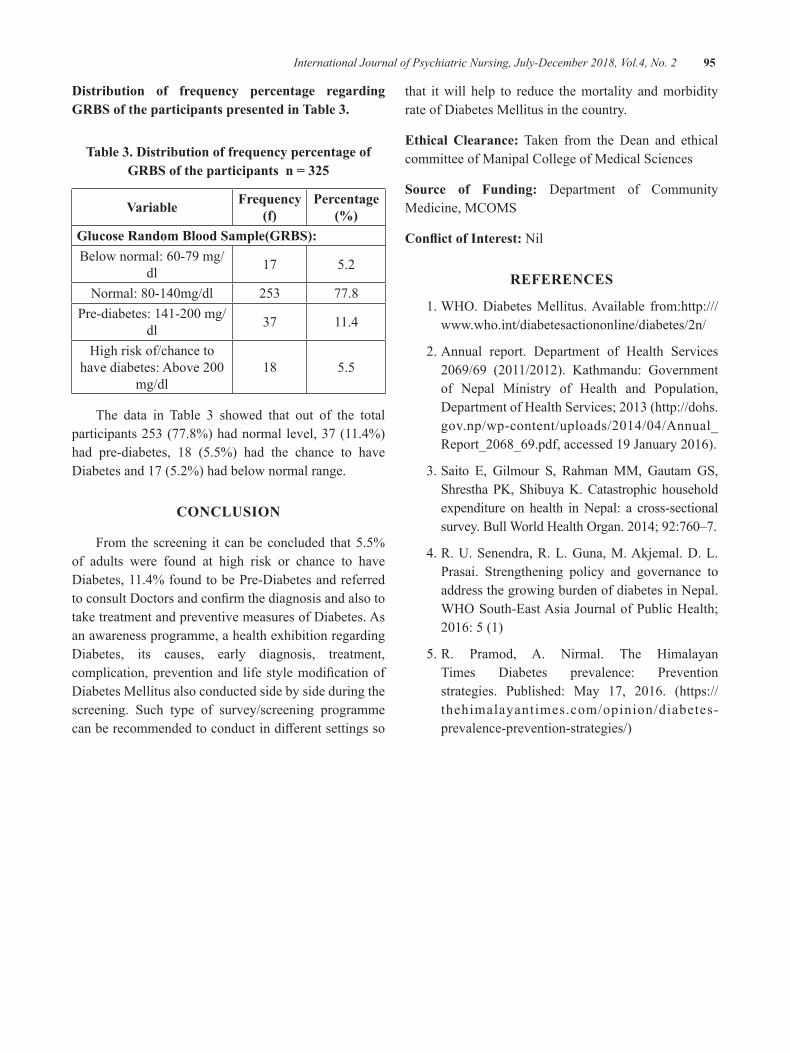
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 95
Distribution of frequency percentage regarding gRbS of the participants presented in Table 3.
Table 3. Distribution of frequency percentage of gRbS of the participants n = 325
Variable Frequency (f)
Percentage (%)
glucose Random blood Sample(gRbS):Belownormal:60-79mg/
dl 17 5.2
Normal:80-140mg/dl 253 77.8Pre-diabetes:141-200mg/
dl 37 11.4
Highriskof/chancetohavediabetes:Above200
mg/dl18 5.5
The data in Table 3 showed that out of the totalparticipants253(77.8%)hadnormallevel,37(11.4%)had pre-diabetes, 18 (5.5%) had the chance to havediabetesand17(5.2%)hadbelownormalrange.
ConCLuSIon
From the screening it canbeconcluded that5.5%of adults were found at high risk or chance to havediabetes,11.4%foundtobePre-diabetesandreferredtoconsultdoctorsandconfirmthediagnosisandalsototaketreatmentandpreventivemeasuresofdiabetes.Asanawarenessprogramme,ahealthexhibitionregardingdiabetes, its causes, early diagnosis, treatment,complication,preventionand lifestylemodificationofdiabetesMellitusalsoconductedsidebysideduringthescreening. Such type of survey/screening programmecanberecommendedtoconductindifferentsettingsso
that itwill help to reduce themortality andmorbidityrateofdiabetesMellitusinthecountry.
Ethical Clearance: Taken from the dean and ethicalcommitteeofManipalCollegeofMedicalSciences
Source of Funding: department of CommunityMedicine,MCOMS
Conflict of Interest:Nil
REFEREnCES
1.WHO.diabetesMellitus.Available from:http:///www.who.int/diabetesactiononline/diabetes/2n/
2.Annual report. department of Health Services2069/69 (2011/2012). Kathmandu: Governmentof Nepal Ministry of Health and Population,departmentofHealthServices;2013(http://dohs.gov.np/wp-content/uploads/2014/04/Annual_Report_2068_69.pdf,accessed19January2016).
3.Saito E, Gilmour S, RahmanMM, Gautam GS,ShresthaPK,ShibuyaK.Catastrophichouseholdexpenditure on health inNepal: a cross-sectionalsurvey.BullWorldHealthOrgan.2014;92:760–7.
4.R.U.Senendra,R.L.Guna,M.Akjemal.d.L.Prasai. Strengthening policy and governance toaddressthegrowingburdenofdiabetesinNepal.WHOSouth-EastAsiaJournalofPublicHealth;2016:5(1)
5.R. Pramod, A. Nirmal. The HimalayanTimes diabetes prevalence: Preventionstrategies. Published: May 17, 2016. (https://thehimalayantimes.com/opinion/diabetes-prevalence-prevention-strategies/)

A Study to Assess the Depression among Elderly Residing in old Age Homes of Thiruvananthapuram District,
South Kerala
Athirarani M R1, Aswany Sunil S2, Anupama Paniker2, Aparna S V2, Ashifa A2, Arya S2, Arya S b2
1Assistant Professor, Govt. College of Nursing, Alappuzha
AbSTRACT
Introduction: Population ageing is ultimate consequence of demographic transition. due to increasedindustrializationandmodernizationandduetotheshrinkageofjointfamilyintonuclearfamilymanyofelderlyfindtheirwaytooldagehomes.Studiesindicatedthatolderadultsarecommonlysubjectedtodepression.Oldageconsistofagesnearingorsurpassingtheaveragelifespanofhumanbeingsandthustheendofhumanlifecycle.
objective: AssessthedepressionamongelderlyresidinginoldagehomesofThiruvananthapuramdistrict.
Methodology: OurpresentstudyistoassessthedepressionamongelderlyresidinginoldagehomesofThiruvananthapuramdistrict.Thepopulationconsistedofelderlypeoplelivinginteholdagehomes.Thestudyisdescriptiveinnatureandusingsemi-structuredquestionnaireandgeriatricdepressionratingscaleweassessedthedepressionamong100elderly.
Results: Thefindingsofourstudyshowedthat13%ofourstudyparticipantshavenodepression,37%havemilddepression50%haveseveredepression.
Keywords: Depression, Elderly, Old age home
Corresponding Author:dr.AthiraraniMRAssistantProfessorGovt.CollegeofNursingAlappuzha
InTRoDuCTIon
Ageing is an inevitable change largelycharacterised by a decline in functional ability anddecreased capability. It is time related change thatoccurs throughout life.Ageing involves all aspects oforganism.Asan individualadvances from infancyoldage he accumulates a wealth of impression skills andknowledgeanddevelopshisownlife1.defineageinginterms of the biology referring to “the regular changesthatoccurinmaturegeneticallyrepresentativeorganismliving under reprehensive environmental conditions astheyadvance in chronologicalorder”2.Asmangrows,his reduced activities, income and consequent declineinthepositioninthefamilyandsocietymakeshislife
morevulnerable3.Anoldpersonbeginstofeelthatevenhis children don’t look upon him with that degree ofrespect,whichheusedtogetsomeyearsearlier.Theoldpersonfeelsneglectedandhumiliated.Thismayleadtopsychologicalshunningthecompanyofothers.Geriatricdepression is a major health hazard with devastatingoutcomes.depressioninoldageismuchcomplexanddifficult to diagnose due tomedical illnesses. I createmanyproblemsintheactivitiesofdailyliving.Inotherwords there is increased dependency on others andhealthcaresystems.
bACKgRounD
Old age is a process of unfavourable progressivechanges usually correlated to the passage of time,becoming apparent after maturity and terminatinginvariably in death of individual4 . Rapid growth ofindustryandmodernisationinIndia,ithasalsoaffectedthepeopleinmanyways.Thetraditionofjointfamilyisdisappearingslowly,whichwasbasedonlove,affectionandtradition.Ithasalsotransformedthelifeoffamily,
DOI Number: 10.5958/2395-180X.2018.00025.7

International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 97
affectedtheemotionofthepeople.duetothesereasonsnumber of old age homes have been increasing 4,5. Thoughthebeliefpersistthatdepressionissynonymouswith ageing and that depression in fact inevitable,there has been recent researches which dispels theirpsychologicalproblem.Studieshave found that age isnot always significantly related to level of depression,and that the oldest of folds may even have bettercopingskillstodealwithdepressionmakingdepressivesymptomsmorecommonbutnotsevereas inyoungerage6.India,world’spopulouscountrybloomtheshareof India’s population ages 50 and older relativelyincrease tremendously.All else being equal, an olderpopulationhasgreaterneedsforhealthcare8.Oldagemeansreducedphysicalability,decliningmentalability,thegradualgivingupofroleplayinginsocioeconomicactivities, anda shift in economic statusmoving fromeconomicindependencetoeconomicdependenceuponothers for support9. Family is themain source of caregiving to all its members. In a globalisingworld, themeaning of old age is changing across cultures andwithincountriesandfamilies10.Itisimportantthatthestate,civilsocietyandcommunityrecognises therightneedsoftheelderlywomenandmakesuitablepolicieshealthandsecurityschemefortheelderlywhichalreadyexists. There should be laws which ensure adequatesocial,physicalandmentalprotectionfortheelderly11.
nEED AnD SIgnIFICAnCE
The last centuryhaswitnesseda rapid increase inpopulation in elderly people.This phenomenon is notrestrictedtowesterncountriesonly,butmanycountriessuchasoursarenowfacingtheimpactofthistransaction.India ranks 4th in place of absolute size of elderlypopulation. Thecountry isnoadequatelyequipped tolookafter theirspecialhealthneeds and thechangingtraditionalvaluesystem12.Thetraditionalsenseofdutyandobligationof theyounger generation towards theoldergenerationisbeingeroded.Theoldergenerationiscaughtbetweenthedeclineinmentalandphysicalhealthinonehandandtheabsenceofadequatesocialsupportin eachother13. Old age homes are a needof today’slifestyle changes fast and diminishing acceptance offamily responsibilities towards one’s elders. Otherpeopleareinneedofvitalsupporttheiroverallqualityoflife.Weshouldthoroughlyunderstandtheconceptofold agehomes and theproblemsof elderly inold agehomes14.According toWHO report 1999, ageing can
becomemanifestnotonlyphysicallybutalsomentallyat almost any period of life. The care of the elderlypeople needs special emphasis because of their frailtyandvulnerability.InIndiawedonothavespecialareasorsettingstotakecareofold.duetorapidurbanisationandgrowingnumberofnuclearfamiliesmoreagedfeelneglected in their families.Need foe old age home isincreasingas theyouthof todaydoesn’thave time tospendwitholdpeople15.Theelderlycitizenareinneedofurgentattention.Theynoneedourpity,butunderstandingloveandcareof thefellowbeing.It isourdutytoseethattheydonotspendthetwilightyearsoftheirlifeinisolation,painandmisery.Olderpersonsareinneedofvitalsupportthatwillkeeptheirimportantaspectsofthelifestyleintactwhileimprovingtheiroverallqualityoflife16.Alongwiththephysicalillnessesmentalillnessalsoincreasedinelderpopulationduetolonelinessfromthenearanddear 17. Ageingisnotasin.Butitseemsfromanglesthattheagedsufferalotduetodenialbythenearones.Somewillinglywhileotherfindtheirwaytooldagehomes.Astheelderlypopulationisshootinginthesedecadesthenumberofoldagehomesarealsoincreasing.But they areonlymerehomes from therethey are not getting life satisfaction which leads tovarious health andmental problems.This lead to thepurposeofourstudyorletwaytoourstudy.
Statement of the Problem: A study to assess thedepressionamongelderlyresidinginoldagehomesofThiruvananthapuramdistrict,Kerala.
OBJECTIVE
AssessthedepressionamongelderlyresidinginoldagehomesofThiruvananthapuramdistrict.
oPERATIonAL DEFInITIon
Depression: It is defined as a feeling of sadness asmanifestedbyhopelessness,helplessness,worthlessness.
old age homes: It refers to an organization whereelderlyareresidingtomeettherebasicneedsofphysicalpsychologicalandsocialcomfort.
METHoDoLogy
Research Approach:Quantitativeapproach.
Design:descriptivedesign-Crosssectionalsurvey
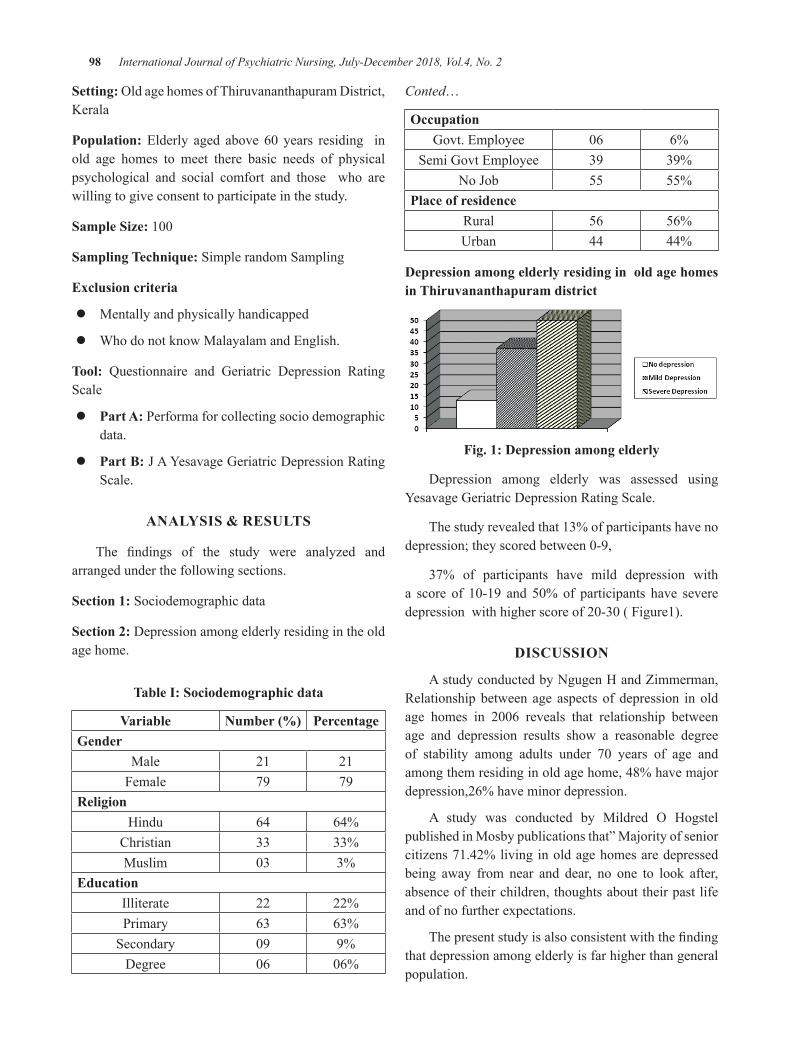
98 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
Setting:OldagehomesofThiruvananthapuramdistrict,Kerala
Population: Elderly aged above 60 years residing inold age homes to meet there basic needs of physicalpsychological and social comfort and those who arewillingtogiveconsenttoparticipateinthestudy.
Sample Size: 100
Sampling Technique:SimplerandomSampling
Exclusion criteria
z Mentallyandphysicallyhandicapped
z WhodonotknowMalayalamandEnglish.
Tool: Questionnaire and Geriatric depression RatingScale
z Part A:Performaforcollectingsociodemographicdata.
z Part b:JAYesavageGeriatricdepressionRatingScale.
AnALySIS & RESuLTS
The findings of the study were analyzed andarrangedunderthefollowingsections.
Section 1:Sociodemographicdata
Section 2:depressionamongelderlyresidingintheoldagehome.
Table I: Sociodemographic data
Variable number (%) Percentagegender
Male 21 21Female 79 79
ReligionHindu 64 64%
Christian 33 33%Muslim 03 3%
EducationIlliterate 22 22%Primary 63 63%Secondary 09 9%degree 06 06%
Conted…
occupationGovt.Employee 06 6%
SemiGovtEmployee 39 39%NoJob 55 55%
Place of residenceRural 56 56%Urban 44 44%
Depression among elderly residing in old age homes in Thiruvananthapuram district
Fig. 1: Depression among elderly
depression among elderly was assessed using YesavageGeriatricdepressionRatingScale.
Thestudyrevealedthat13%ofparticipantshavenodepression;theyscoredbetween0-9,
37% of participants have mild depression witha score of 10-19 and 50%of participants have severedepressionwithhigherscoreof20-30(Figure1).
DISCuSSIon
AstudyconductedbyNgugenHandZimmerman,Relationshipbetweenage aspectsof depression inoldage homes in 2006 reveals that relationship betweenage and depression results show a reasonable degreeof stability among adults under 70 years of age andamongthemresidinginoldagehome,48%havemajordepression,26%haveminordepression.
A study was conducted by Mildred O HogstelpublishedinMosbypublicationsthat”Majorityofseniorcitizens71.42%livinginoldagehomesaredepressedbeing away from near and dear, no one to look after,absenceoftheirchildren,thoughtsabouttheirpastlifeandofnofurtherexpectations.
Thepresentstudyisalsoconsistentwiththefindingthatdepressionamongelderlyisfarhigherthangeneralpopulation.

International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 99
ConCLuSIon
Inoursociety,duetotheincreasedindustrialization,modernizationandbytheshrinkageofjointfamilymostoftheelderlyarethrowntooldagehomesortheyfindtheirwaytooldagehomes.Geriatricdepressionisamajorhealthhazardwithdevastatingoutcomes.depressioninoldageismuchcomplexanddifficulttodiagnoseduetomedical illnesses. It createsmanyproblems inactivityofdailyliving.ThisstudywasconductedtoassessthedepressionamongelderlyresidinginoldagehomesofThiruvananthapuramdistrict.
Conflict of Interest:Nil
Source of Funding:Self
Ethical Clearance:TheethicalclearancewastakenfromcommitteeandSchoolauthoritiesbeforeconductingthestudy
REFEREnCES
1.LissyFJarvice(1998),Ageinginto21stcentuary,pageno-231
2.SaranjithUppalandSisiraSarma(2007),”AgeingHealth,TheCaseof India”WorldHealthandPopulation,9no:4:79-97.
3.dhara R.d and Yogsun Y.A(2013), depressionandPsychologicalwellbeinginoldage3:117:vol-3,issue-3.
4.Lansing (1984) In search of the agents for selfcare,JournalofGerontology;11(7):(10-16)
5.Sharma K. L(2007) Studies of Gerontology ,RawatPublications,Newdelhi,132
6.JarvikL.F(2006)Ageinganddepression,someunanswered questions, Journal of Gerontology,31,(324-326).
7.Today’sResearchonAgeing,ProgramandPolicyImplications,PopulationReferenceBureau(2015),(2):(1)
8.Smith J. Borchelt , Joppd. (2000), Health andWellbeinginyoung andoldestold,JournalofSocialissues,58(4):733
9.GouriG.B(2003),Attitudetowardsoldageandageing as shown by humour, Gerontologist,17(2);220-22638
10.BergeronL.R(2001),Anelderlyabusecasestudy;JornalofGerontologistsocialwork,34(3);47-63
11.Bhat K (20010, Ageing in India; driftingInternationalrelations,challengesandoptions,CambridgeJournalOnline,21:621-640
12.ArunadubeyandSeemaBasin(2011),Astudyofelderlylivinginoldagehomeandwithinfamilysetup,5(2);(93-98)
13.GormalK(2003),AgedinIndia,TissPublishers,9(2);52-69
14.MohanthN,Begum.F.A(2011),Geriatricdepressionand Psychological wellbeing. Indian Journal ofPsychologicalandmentalhealth5:(53-61)
15.WorldHealthMagazineofWHO(1998):177
16.dantekar K (1993), The elderly in India , Newdelhi,Sagepublishers17(2);241-250
17.ElderlypopulationandfutureprojectionsinIndia,UnitedNationPopulationdivision(2008)39

Depression among oral Cancer Patients Receiving Radiation Therapy in Selected Centre, Erode
S. Manikandan1, M. baskaran2, Prof. P. Subarani3
1Clinical Nurse Specialist, Psychiatric Department, PSG Hospital; 2Associate Professor, Mental Health (Psychiatric) Nursing, PSG College of Nursing, Coimbatore; 3Professor and HOD, Department of Mental
Health (Psychiatric) Nursing, Saveetha College of Nursing, Saveetha University, Chennai Tamil Nadu
AbSTRACT
Canceristheleadingcauseofdiseaseworldwide.Anestimated12.7millionnewcancercasesoccurredin2008.Cancerofthelipandoralcavityaccountedfor2%ofcancercasesworldwide.1
objectives: Theobjectivesofthestudywereto
z Assessthelevelofdepressionamongoralcancerpatient.
z Associatethelevelofdepressionwiththeselecteddemographicvariables.
Methodology: descriptiveresearchdesignwasadopted.Convenientsamplingtechniquewasusedand60patientswereselectedatErodeCancerCentre,Erode.Thedatawascollected,organizedandanalyzedintermsofbothdescriptiveandinferentialstatistics.
Result: Thestudyresultsshowedthatavastmajorityofthemie.135(50%)hadmoderatelevelofdepressionfollowedby9(6%)ofthemwhohadmilddepression,4(2.7%)whohadseverlevelofdepressionandmean37.34andstandarddeviation18.18.Chisquaretestrevealedtherewasasignificantassociationinthelevelofdepressionoforalcancerpatientreceivingradiationtherapywiththeselecteddemographicvariablessuchasage,gender,maritalstatus, availabilitythefamilysupport,&educationalstatusatp<0.05level.
Conclusion: Thisfindingwouldbeusefulandbeneficial tohealthcareserviceswhichmight improve inmanagementandinterventiononpsychologicalofpatientundergoingradiationtherapy.Otherfactorsthatcontributedtodepressionamongcancerpatientalsoneedtobeinvestigated.
Keywords: Depression, Oral, Cancer, Patients, Radiation Therapy
Corresponding Author:Mr.M.BaskaranAssociateProfessordepartmentofMentalHealth(Psychiatric)Nursing.PSGCollegeofNursing,Coimbatore.TamilNaduEmail:[email protected]
InTRoDuCTIon
Cancer is the second leading cause of deathglobally,andwasresponsiblefor8.8milliondeaths in2015.Globally, nearly 1 in 6 deaths is due to cancer.Approximately 70% of deaths from cancer occur inlow-andmiddle-incomecountries.Aroundonethirdofdeathsfromcancerareduetothe5leadingbehavioralanddietaryrisks:highbodymass index, lowfruitand
vegetableintake,lackofphysicalactivity,tobaccouse,andalcoholuse.Tobaccouseisthemostimportantriskfactor for cancer and is responsible for approximately22%ofcancerdeaths.2
nEED FoR THE STuDy
Cancer is the leadingcauseofdiseaseworldwide.Anestimated12.7millionnewcancercasesoccurredin2008.Cancerofthelipandoralcavityaccountedfor2%ofcancercasesworldwide.1
Oral mucositis can have potential seriousconsequences for patients. Painful lesions cancompromise the patient’s nutritional status and oralhygiene,andcanresult inlocalorsystemicinfections.
DOI Number: 10.5958/2395-180X.2018.00026.9
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 101
This can have a profound and debilitating effect onthe patient’s quality of life. The patient may sufferfrom malnutrition, dehydration, weight loss and havedifficultywithcommunication.Patientswithadamagedoralmucosalareatahigherriskofdevelopinginfections.
Radiotherapy is an important treatment modalityforpatientswithcancer,butitisnotwithoutitsphysicalandpsychologicalsideeffects.Nurseshaveanimportantrole is the supportive care of patients undergoingradiotherapy, whether it is radiotherapy alone or incombination with other treatment modalities such aschemotherapy.Many past supportive care practices inradiotherapyhavebeenanecdotalandbasedonhistoricalpractices.This is improving; however, research of theimpactofradiationtreatmentonanincreasinglyageingpopulationisminimal.Asweprogressourpracticeintothefuture,thiscareneedstobebasedongoodevidence.Thisopensupmanyavenuesfornursesinthisspecialitytoengagewithresearchtoprovidethisevidence.3
REVIEW oF LITERATuRE
Section–a: Studies related to depression among oral cancer patients receiving radiation therapy: A cross-sectional descriptive studywas conducted at theradiation therapy day Care Centre of North BengalMedical College and Hospital.A total of 174 cancerpatientswereselectedandinterviewed.BriefEdinburghdepressionScalewasusedtofindout.Theresultsdepictsout of 174 cancer patients, 97 (55.7%)were found tobedepressed.depressionwascomparativelyhigher inpatients≥50years;inmales;thosebelongingtoreligionotherthanHindus;whoreceivedhighereducation;hadmonthlyfamilyincome≥5000rupeesandwereinvolvedin moderate or heavy work. Nearly 70.6% of bloodcancerpatients;64.3%ofthosewhohadbeenreceivingchemotherapyfor≥6monthsand56.9%ofthoseintheir4th or less cycleof radiation therapywere found tobedepressed.Thestudyrevealeddepressionissubstantiallyhighamongcancerpatientsundergoingradiationtherapyinthisarea.diagnosisandtreatmentofcancerpatientsneedtobecomplementedbypsychologicalsupportforthecancerpatients.4
Across-sectionalandcorrelationaldesignwasusedtocollectdataforthisstudyconductedinnorthernTaiwan.Asetofquestionnaireswasusedtomeasuredepression,symptomdistress,performancestatus,socialsupport,anddemographic and disease-related information. Logistic
regressionwasconductedtodetermineimportantfactorspredictingdepression.Theresultsshowsthatatotalof132 oral cancer patients participated in this study. Ofthese, 18.2%were identified as depression cases.Thepatient average performance status score was 90 orhigher. Patients reported mild-to-moderate levels ofsymptom distress.Themajority of social supportwasfrom families. Religious belief, alcohol use, symptomdistress, and social support from family were foundto be important factors predicting depression. Patientswith religious beliefwith alcohol use reported greatersymptomdistress,andthosewithlowerlevelsofsocialsupport from families were significantly more likelyto develop depression. Conclusions of the studywereclinicians should assess patient emotional status andmanagesymptomsinatimelymannertoenhancecopingabilities.Supportivecareprovidesassuranceduringtheacutesurvivorphase.5
Statement of the Problem: AStudytoAssesstheLevelof depression among Oral Cancer Patients ReceivingRadiationTherapyinselectedCentre,erode.
OBJECTIVES
z Toassessthelevelofdepressionamongoralcancerpatientsreceivingradiationtherapy.
z Toassociate the levelofdepressionwithselectedthedemographicvariables.
Hypothesis
H1: Thereissignificantlevelofdepressionamongoralcancerpatient receiving radiation therapyasmeasuredbybeckdepressioninventory
oPERATIonAL DEFInITIonS
Assess: Itistheestimationoflevelofdepressionamongoralcancerpatientsreceivingradiationtherapy.
Depression: In this study it refers to a group ofsymptoms, feeling of sadness, loneliness, despair, lowselfesteem,withdrawalfrominterpersonalcontactandPhysiologicalsymptomsof insomnia,anorexia,weightloss,andlossofhairexperiencedbycancerpatients.
Cancer: In this study it refers to the diagnosis ofcancerwhichisconfirmedbyadiagnosticcriteriaanditincludesthedurationofillness,siteofcancerandstagesofcancer.
102 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
Radiation Therapy: The patient selected as they arereceivingradiationtherapy.
Assumptions: The hospitalized cancer patients havemaydepressioninvariouslevelsofdepression.
Research Design: The research design selected forpresentstudyiscomparativedescriptivedesign.
Setting of the Study:Thestudywasconductedamongthe nurses who are working in PSG hospital criticalcare units and general ward. The PSG Hospital is amultispecialty910beddedhospitalandiswellequippedwithadequatefacilities.
Population: The study population includes bothmaleand female oral cancer patient receiving radiationtherapy.
Samples:Oralcancerpatient.
Sample Size: The sample sizewas60 cancerpatientswithreceivingradiationtherapy
Sampling Technique: Non-probability convenientsamplingtechnique
Description of the tool: Thetoolconsistsoftwoparts.
Part–I: It deals with demographic variable consistsof, Age .Gender, duration of illness, Marital status,Availabilityoffamilysupport,Educationalstatus.
Part–II: Beckdepressionscaleisthemostappropriateinstrumenttoassessthepresenceandlevelofdepressionsymptomswhichwas developed byAaron beck. Thisquestionnaireconsistsof21ofstatements.Thepatienthastoreadandthenonestatementineachsamplethatbestdescribesthewayhe/shehaswithinthepast2weeksincludingthedayofinventorytotalscoreis63anditisclassifiedasfollows.
Score Interpretation:Milddepression-<50%Moderatedepression-50–75%Severedepression-(>75%
FInDIngS
Table 1: Distribution of level of depression among oral cancer patient receiving radiation therapy
(n = 60)
Sl. no.
Level of Depression Frequency Percentage
1. Mild(<50%) 20 33.3
2. Moderate (50–75%) 30 50
3. Severe(>75%) 10 16.6
Table 1 shows regarding the higher percentageof oral cancer patient receiving radiation therapy hadmoderatelevelofdepression30(50%).
Table 2: Mean and standard deviation of level of depression among oral cancer patient receiving
radiation therapy(n = 60)
Sl. no.
Level of Depression MEAN Standard
Deviation1. depression 37.34 18.18
Table 2 depicts the mean 37.34 and standarddeviation18.18oflevelofdepressionamongoralcancerpatientreceivingradiationtherapy.
Table 3: Association of demographic variables with level of depression among oral cancer patient with receiving radiation therapy
(n = 60)
Sl. no.
Demographic Variables
Mild Depression Moderate Depression Severe Depressionc2 value
no. % no. % no. %1. Age
18-30yrs 3 5 1 1.6 - -46.16d.f=6(S)*
31-40yrs 15 25 8 13.3 - -41-50yrs 2 3.3 18 30 2 3.3
Above50yrs 0 0 3 5 8 13.32. gender
Male 12 20 22 36.6 9 15 6.38d.f=2(N.S)Female 8 13.3 8 13.3 1 1.6
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 103
Conted…
3. Duration of illness>6month 10 16.6 7 11.6 1 1.6 21.3
d.f=4(N.S)
7-12months 10 16.6 18 30 3 513-24months - - 5 8.3 6 10
4. Marital statusMarried 20 33.3 30 50 10 16.6 44.1
d.f=2(S)*Unmarried - - - - - -5. Availability the family support
Yes 20 33.3 30 50 10 16.6 44.1(S)*No - - - - - -
6. Educational statusNoformaleducation 17 28.3 10 16.6 - - 32.51
d.f=4(S)*Primaryeducation 3 5 16 26.6 4 6.6
Highschool - - 4 6.6 6 10
*(S-Significant),(N.S-Notsignificant)
Table 3 reveals that thereshowed that therewasasignificant association in the levelofdepressionoforalcancerpatientreceivingradiationtherapywiththeselected demographic variables such as age, gender,marital status, availability the family support, &educationalstatusatp<0.05level.
ConCLuSIon
This finding would be useful and beneficial tohealthcareserviceswhichmightimproveinmanagementandinterventiononpsychologicalofpatientundergoingradiation therapy. Other factors that contributed todepression among cancer patient also need to beinvestigated.
Acknowledgement: Thestudywasconducted inErodeCancerCentre,Erodeafterobtainingformalpermissionfrom the InstitutionalReviewBoard, ScientificReviewBoard and Ethical Committee of Saveetha Universityand Ethical Board of Erode Cancer, Erode. ThisdissertationissubmittedtoTheTamilNadudr.M.G.R.MedicalUniversity,Chennai,inpartialfulfillmentfortherequirementofthedegreeofMasterofScienceinNursing.
Conflict of Interest:Nil
Source of Funding:Selffunded
REFEREnCES
1.FerlayJ,ShinHR,BrayF,Formand,MathersCd,Parkind.GLOBOCAN2008,Cancer Incidence
and Mortality Worldwide: IARC CancerBaseNo. 10. Lyon, France: InternationalAgency forResearch on Cancer; Year. Available at: http://globocan.iarc.fr.2010.Lastaccessed8/17/2010.
2.GBd 2015 Risk Factors Collaborators. Global,regional, and national comparative riskassessmentof79behavioural,environmentalandoccupational, andmetabolic risks or clusters ofrisks, 1990-2015: a systematic analysis for theGlobal Burden of disease Study 2015. Lancet.2016Oct;388(10053):1659-1724.
3.WellsM,donnanPT,SharpL,AcklandC,FletcherJ, dewar JA.2008. A study to evaluate nurse-led on-treatment review for patients undergoingradiotherapy for head and neck cancer. J ClinNurs.Jun;17(11):1428-39.Epub2007dec18.
4.SutanayBhattacharyya,SharmisthaBhattacherjee,Tanuka Mandal, dilip Kumar das(2017).depressionincancerpatientsundergoingradiationtherapyinatertiarycarehospitalofNorthBengal,India. Indian Journal of Public Health. Volume61.Issue1.January-March
5.Shu-Ching Chen, Bing-Shen Huang, Chien-YuLin(2013).depressionandPredictorsinTaiwaneseSurvivorswithOralCancer.AsianPacificJournalofCancerPrevention,Vol14,2013
Life Skills and nursing
buvaneswari R.1, Juliet Sylvia2
1Ph.D. Scholar and Lecturer, College of Nursing, JIPMER (Jawaharlal Institute of Post Graduate Medical Education and Research); 2Professor cum Vice Principal, Sacred Heart Nursing College, Madurai.
AbSTRACT
Life skills are a category of soft skills that are needed to successfully navigate the challenges of dailylife, both personal and professional.They include the ability to set and achieve goals,make decisions,solveproblems,andeffectivelymanageone’stime.Lifeskillsarethosesoftskillsthatlargelyrestintheindividual.Oncemastered,lifeskillshelpapersonineveryaspectofhislife.Acomprehensiveliteraturesearchwasperformedusingspecifickeywords.Mainfocusoftheliteraturesearchwasaboutlifeskillsandits relationwithnursing.Literature shows that life skills training causes significant improvement in thenurses’physicalfunctioning,bodilypain,generalhealth,vitality,socialfunctioning,mentalhealth,physicalhealthandultimatelyqualityoflife.Alsoitincreasesnurse’shappiness.
Keywords: life skills; nursing; self awareness.
Corresponding Author:Mrs.R.BuvaneswariEmail:[email protected]
InTRoDuCTIonIfamanishungry,don’tgivehimfish toeat,butteachhimtocatchfish.
Chineseadage
Lifeskillisthepositivebehaviorandabilitytoadjustefficiently with the needs and challenges of everydaylife.Theextenttowhichapersonexposestothedesiredskills and practice, determines the level of his overalldevelopment. It also helps to solve the physiological,psychologicalandsocialproblems.1
Life skills are used everymoment of our lives in
various situations. Life skills are the building blocksofone’sbehavior andneed tobe learntwell to leadahealthy,meaningfulandproductivelife.2
Definition:
WHo has defined life skills as, “the abilities foradaptive and positive behavior that enable individualstodealeffectivelywiththedemandsandchallengesofeverydaylife”.3
unICEF defineslifeskillsas“abehaviorchangeorbehavior development approach designed to address abalanceofthreeareas:knowledge,attitudeandskills”.4
Life skills fall into three basic categories, which complement and reinforce each other:
Social skills Cognitive skills Emotional coping skillsCommunicationNegotiation/refusalskillsAssertivenessskillsInterpersonalskillsCooperationskillsEmpathy
decisionmaking/problemsolvingskillsUnderstandingtheconsequencesofactions.determiningalternativesolutiontoproblemsCriticalthinkingskillsAnalyzingpeerandmediainfluencesAnalyzing one’s perceptions of social norms &benefitsSelfevaluationandvalueclarification
ManagingstressManaging feelings, includingangerSkills for increasing internallocus of control (selfmanagement,selfmonitoring)
Core Life Skills:TheTencoreLifeSkillsaslaiddownbyWHOare:
1. Self Awareness: Selfawarenessistheawarenessabout oneself (self consciousness). It includes
DOI Number: 10.5958/2395-180X.2018.00027.0
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 105
one’srecognitionofthem,one’scharacter,one’sstrengths and weaknesses, desires and dislikes.This helps the individual to understand his/herselfworth and builds his/her confidence to facelifeboldly.
2. Empathy: Empathyisone’sabilitytounderstandandacceptdifferentkindsofpeoplearoundthemwhoaredifferentinmanyrespects.Empathyalsohelps to encourage nurturing behavior towardspeopleinneedofcareandassistanceortolerance.
3. Effective communication: EffectiveCommunication is an efficient tool for theestablishment and maintenance of good socialandworkingrelationshipswithpeople.Itenablesanindividualtoexpresshisopinions,desiresandfearsclearlybyusingbothverbalcommunicationandnon-verbalexpressions.
4. Inter Personal Relationship: Inter PersonalRelations are known as survival skills which isveryimperativeforestablishingandmaintainingsocial relationships. Interpersonal skill is toinitiate and maintain positive relationship withother individuals and de-link unconstructiverelationship,withminimumdisturbancestoboth.Itteachesanindividualtorelatetootherpeopleinapositivemanner.
5. Creative thinking: Creativity is the ability togenerate innovative ideas and manifest themfromthoughtintoreality.Ithelpstorespondinaflexiblemannertovariouschallengesoflife.Thisskillhelpsinbothproblemsolvinganddecision-making.
6. Critical Thinking: Critical thinking is definedaslogicalthinkingandreasoningincludingskillssuch as comparison and classification. It alsohelpstorecognizefactorslikefamilyvalues,peerandmediapressures that influence attitudes andbehavior.
7. Decision-making: decision Making is theability to choose the best amongst the variousalternativesoroptionsinmanylifesituations.Theskill toanalysisandweigh theprosandconsofalternatives and accepting responsibility for theconsequencesofthedecisionwithconfidence.
8. Problem solving: Problemsolving skills enableustodealconstructivelywithproblemthatarises
in our live. It enables the person to get out oftheuncomfortablesituationandaccomplishone’sneed without using anger, coercion, defiance,aggressivebehaviororforce.
9. Coping with emotions: Coping with emotionshelps the individual to understand feelings ofthemandothers.Thisskillhelps toknowthat itisnormaltohavestrongfeelingsandthatfeelingsareneitherpositivenornegative.Lifeskillsenablethe individual to learnhealthy,positiveandsafewaystoexpressthesefeelings.
10. Coping with Stress: Copingwith stress enabletheindividual torecognizethesourcesofstress,understanding its effects and relax withoutmaking the situation worse. This skill providesthestrengthtofacepositiveornegativestressfulsituations.
LIFE SKILLS AnD nuRSIng
In the last few years, reforms in public healthbrought significant changes to nursing. The sphere oftheir independent activities is expanding. The WorldMedicalAssemblydefinesthemaintaskofthenursingpersonnel as “maintaining health, preventing diseases,determiningthepatient’sneedsandtakingactionsaimedatsolvingtheseissuestogetherwiththepatient”.5
NotEveryoneCanBeANurse Acareerinnursingencompassesskillsthatcanonlybefoundincertaintypesofpeople.Whetheryou’re alreadyanurse, training tobecomeanurse,orsimplyconsideringnursingasafuturecareeroption,it’scrucialthatyoucultivatethespecificlife-skillslikestressmanagement,communicationskill,patience,compassionandselflessness,problemsolvingandendurance.6
A high priority needs to be placed on preparingnursesandmidwivestomeetthecomplexityofcurrentandfuturenursing/midwiferypractice.7
Nursesandmidwivesdailywitnesspeople’smournsand pains in clinical environment. Nurses’ specialhospitalsituationssuchaspatients’sighandtheircriticalconditionanddeath,nurses’insomnia,lackofassurance,anddisturbancesintheirinterpersonalcommunicationsinall levelsenhancenurses’andmidwives’stress,andworsentheviciouscycleofanxiety,whichleadstotheirphysicalproblemsultimately influencing theoutputofhealthsystemandthemannerandqualityoftheircare.8
106 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
IMPoRTAnCE oF LIFE SKILLS In nuRSIng
z Nursesworkinavarietyofenvironmentssotherearealwaysavarietyofchallengesandpossibilities.Ifnurseshavetheskillsandtheyarewillingtoinvestthe time and effort into a lifelong career, nursingcould provide them with a fulfilling challengingprofession.
z Lifeskillsofferthenurseanopportunitytoacquireselfknowledge,totakeapositiveapproachtoselfand to develop personal growth and enrichment.Personal growth and enrichmentwill support thenurseinpursuitofprofessionalgrowth.
z Life skills enable the nurse to act effectively inrelationtootherpeopleandtorenderholisticnursingcare by applying life skills while supporting thepatientinthepursuitandmaintenanceofphysical,mental,andspiritualhealth.
z Life skills empower the nurse to develop andenhanceacaringattitudeinthenursingofpatients.They enable the nurse to listen to beyond whatthepatient is saying, and tobeassertive,manageconflictandmakecarefullyconsidereddecisions.
z Life skills develop emotional maturity, whichincludes honesty, openness, loyalty to people,kindness,keepingofpromisesandconfidence.9
z Lifeskillstrainingcausessignificantimprovementinthenurses’physicalfunctioning,bodilypain,generalhealth, vitality, social functioning, mental health,physicalhealthandultimatelyqualityoflife.10
z Research study indicates that life skills educationcouldsignificantlyincreasethehappinessofnurses.11
Importance of Life skills for nursing students
z NursingstudentsneedAnalyticalabilities,Psycho-Social-Behavioral Abilities, Physical Abilities,SensoryAbilities,andEmotionalIntelligence.
z Increasethelevelsofemotionalintelligenceofthestudents
z Academicsuccess
z Increasedstresstolerance
z Improveselfefficacy
z Reducesubstanceabuse
ConCLuSIon
Life skills are abilities helping to behaveappropriately and wisely in different situations andadaptively communicate with one’s self and others.These skills assist in solving the problems with noaggression and feeling happy in life while beingsuccessful.Learningtheseabilitiesyieldsmentalhealthpromotion, human relations enrichment, and increasedhealthybehaviors.
Conflict of Interest:Nil
Ethical Clearance: Obtained from institute ethicalcommittee
Source of Funding:Self
REFEREnCES
1.RajasenanNairV.Lifeskillsforpersonalityandleadership. Sriperumbathur: department of lifeskillseducationRajivGandhinationalinstituteofYouthdevelopment;2010.
2.Srikala Bharath, Kishore kumar, Vranda MN.Activity manual for the teachers on healthpromotionusinglifeskillsapproach,departmentofPsychiatryNIMHANS;2002.
3.WorldHealthOrganization,Partnersinlifeskillseducation.Geneva:1998.Available from:www.who.int/mental_health/media/en/30.pdf
4.Subhasree R, Radhakrishnana Nair A. TheLife Skills Assessment Scale: the constructionand validation of a new comprehensivescaleformeasuringLifeSkills. IOSRJournalofHumanities And Social Science (IOSR-JHSS)[Internet].2014[cited2014Sep30];19(1):50-8.Availablefrom:www.iosrjournals.org.
5.Richard IVES. Manual on Life skills training inschools.CouncilofEurope,PompidouGroup,2005.
6.MackenzieThompson.6skillsrequiredforyoursuccessful nursing career. National healthcareprovider solutions (NGO). Apr 12, 2015.https://nhcps.com/six-skills-required-for-your-successful-nursing-career/
7.World Health Organization. Adolescent HealthanddevelopmentinNursingandMidwiferyLifeEducation.Geneva2004.

International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 107
8.Mohammad Sahebalzamani, HojjatollahFarahani,, Fariba Feizi, Efficacy of life skillstrainingongeneralhealthinstudents.IranJNursMidwiferyRes.2012Nov-dec;17(7):553-5.
9.Juta’sManualofnursing.2nded.Lansdowne:Juta&Co.Ltd;2009.
10.Javadi M, Sepahvand M J, Mahmudi H. TheEffectofLifeSkillsTrainingonQualityofLifein
NursesofKhorramabadHospitals.SciJHamadanNursMidwiferyFac.2013;21(1):32-42.
11. Farahnaz Farnia, Fateme Rahighee Yazdi1,Maryam Salehzadeh Abarghouei. Effect of lifeskillseducationonnurses’happiness.AmJExpClinRes2016;3(2):157-160.

A Study to Assess the Knowledge and Attitude towards Mental Illness among Adults at Selected urban Community udaipur,
Rajasthan
Digpal Singh Chundawat
Principal, Tirupati College of Nursing, Pacific Medical University Campus, Bhilo-Ka-Bedla, Udaipur, Rajasthan
AbSTRACT
background of the Study: As a worldwide phenomenon, no one is immune- mental illnesses affectpeopleofallages,cultures,educationalandincomelevels.Thestudiesconductedindevelopingcountrieshave revealed that during their life time;more than25%of individualsdeveloponeormoremental orbehavioraldisorders.AccordingtoWHOreport-about450millionpeoplewereestimatedtobesufferingfromneuropsychiatryconditions.
Therehavebeentremendousadvancesinourunderstandingofthecausesandtreatmentofmentalillnessmostofthesetreatmentscanbeprovidedeffectivelybyageneralorcommunityhealthworkerbyhavinggoodknowledgeandfavorableattitudetowardsmentalillness.
Method: AdescriptivestudywasconductedtoassesstheknowledgeandAttitudetowardsmentalillnessamonganadultatselectedurbancommunity,Udaipurdistrict,Rajasthan.ConvenientorPurposiveSamplingtechniquewasusedtocollectdataamong40adultsbetween18-40yearsofage.Thedatawerecollectedusingselfadministeredstructuredknowledgeandattitudequestionnairetoolscomprisingof:demographicPerforma,knowledgeassessmentquestionnaireandfivepointattitudescale.Thedatawasanalyzedusingdescriptiveandinferentialstatistics.
Results: The study findings shows that majority of an adult had good knowledge (47.5%), excellentknowledge(42.5%),andnoonehadpoorknowledgeregardingmentalillness.
92.5%ofadultshadfavorableattitudetowardsmentalillness.Thestudyrevealedapositivescorrelationbetweenknowledgeandattitudescores.Noassociationwasfoundbetweenadultsknowledgeandselecteddemographicvariables.
Conclusion: Thestudysuggests thatnursescanplayavital role ineducating thepeoples in relation tomentalhealthandmentalillnessanditsprevention.
Keywords: Knowledge, Attitude, Mental illness, Adults.
InTRoDuCTIon“ThesecretofNationalHealthliesinthepeoplewithSoundMentalHealth”
MentalHealthconcernseveryone.Itaffectsourabilitytocopewithandmanagechange,lifeeventsandtransition.The definition of ‘Health’ according toWHO- “State ofphysical, mental, social and Spiritual well being of anindividual,notmerelyabsenceofanydisease”.Itcanbeevidentbyabovedefinitionthatphysicalaspectscomprisesany25%of totalhealthconceptwhileotherentities like
Mental, Social and Spiritual have greater relevance andsignificanceinthefieldofPsychiatryNursing.
There is more good health than just a physicallyhealthbody;apersonshouldalsohaveahealthymind.Apersonwith a healthymind shouldbe able to thinkclearly,solve thevariousproblemsfaced in life,enjoygood relations with friends, colleagues at work andfamilyandbringhappinesstoothersinthecommunity.It is these aspects of health that can be considered asmentalhealth.Eventhoughwetalkaboutthemindand
DOI Number: 10.5958/2395-180X.2018.00028.2

International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 109
bodyasiftheywereseparate,inrealityareliketwosidesofthesamecoin.Theyshareagreatdealwitheachother,butpresentadifferencefacetotheworldaroundus.ifoneofthetwoisaffectedinanywaythentheotherwillalmostcertainlyalsobeaffected.Justbecausewethinkaboutthemindandbodyseparately.Itdoesnotmeanthattheyareindependentofeachother.Justasthephysicalbodycanfallill,sotoocanthemind.ThiscanbecalledMentalIllness.Mentalillnessis“Anyillnessexperiencedby a personwhich affects their emotions, thoughts orbehavior, which is out of keeping with their culture,beliefs and personality, and is producing a negativeeffectontheirlivesorthelivesoftheirfamilies”.Therehavebeentremendousadvancesinourunderstandingofthecausesandtreatmentofmentalillness.Mostofthesetreatments canbeprovidedeffectivelybyageneralorcommunity health worker(1).Mental illness includes abroadrangeofhealthproblems.Formostpeoplementalillnessisathoughtofasanillnessassociatedwithseverebehavioral disturbances such as violence, agitationand being sexually inappropriate. Such disturbancesare usually associated with severe mental disorders.However,thevastmajorityofthosewithamentalillnessbehavesandlooksnodifferentfromanyoneelse.Thesecommon mental health problems include depression,anxiety, sexual In the past and in the present also, inthefieldofhealth,ourmindhasbeenpreoccupiedwithcommunicable disease because they are the biggestcauseofdeathinthepopulation(2).
We have been looking at health in terms ofphysical health, while neglecting mental health. Overtheyears,mentalillnesshasincreasedmanifold.WHOreport-2017:7.5%Indianssufferfrommentaldisorders.Not only do 56million Indians -- or 4.5% of India’spopulation -- suffer from depression at this moment,another38millionIndianssufferfromanxietydisorders.Thus,accordingtothelatestWorldHealthOrganizationreport on depression released, almost 7.5%of Indianssuffer from major or minor mental disorders thatrequire expert intervention(3). Referred to the findingsofthevariousstudies:“Indianeedstotalkaboutmentalillness;” Every sixth Indian needsmental health help.8%ofpeopleinKarnatakahavementalillness,Mentalproblems more in 30–49 age group or over 60; lowincome linked to occurrence of mental disorders andurbanareas tobemostaffected.TheNMHS(NationalMentalHealthSurvey)isamilestoneinunderstandingthe epidemiology of mental disorders in the country.
Psychiatric epidemiology has been an area of greatinterest among all the leading psychiatrists.The othersimilarareaofinterestisthepsychiatricclassifications.In both these fields, there are more “failures” thansuccesses in the past 60 years(4). Barriers to effectivecareincludelackofresources,dearthoftrainedhealth-care providers, and social stigma associated withmentaldisorders.India,forinstance,haslessthan4,000psychiatriststotreatitsmentallyillpeople(5).
Although there has been a demographical study,psychiatristestimatesthatabouttwopercentofIndianssuffers from mental illness, a staggering 20 millionoutofapopulationof100million.Arecent surveyof500 working women in delhi by Hamara Parivar, afamilywelfareprogramme,hasfoundthat78%ofthemsufferfromdepressionduetosociologicalpressureandbreakdownofpersonalrelationships(6).EpidemiologicalsurveysdoneinIndiaaswellasinmanyotherpartsoftheworldhaveamplyconfirmedthatatanygiventimeonetotwopercentofthepopulationsuffersfromseriousmental illness.While10 to15percent suffers fromsocalledmentaldisorderslikeanxiety,depression,somaticsymptomsdue to tension, alcohol and drug abuse etc.womenseemtobemorepronetoanxietyanddepressionwhilementoalcoholanddrugsmoreoften.OnetotwopercentofIndianssufferfrommanic-depressiveillnessalone.NinemillionspeoplehaveschizophreniainIndia(Oneoutof1000)(7).
obJECTIVES oF THE STuDy
1.To determine the level of knowledge of adultstowardsmentalillness.
2.To assess the attitude of adults towards mentalillness.
3.To find out the co-relation between knowledgescoreandattitudescoreofadults.
4.To find out the association between knowledgescore adults toward mental illness and selecteddemographicvariables.
HyPoTHESIS
H1: There will be significant co-relation between theknowledge score and attitude score of adults towardmentalillness.
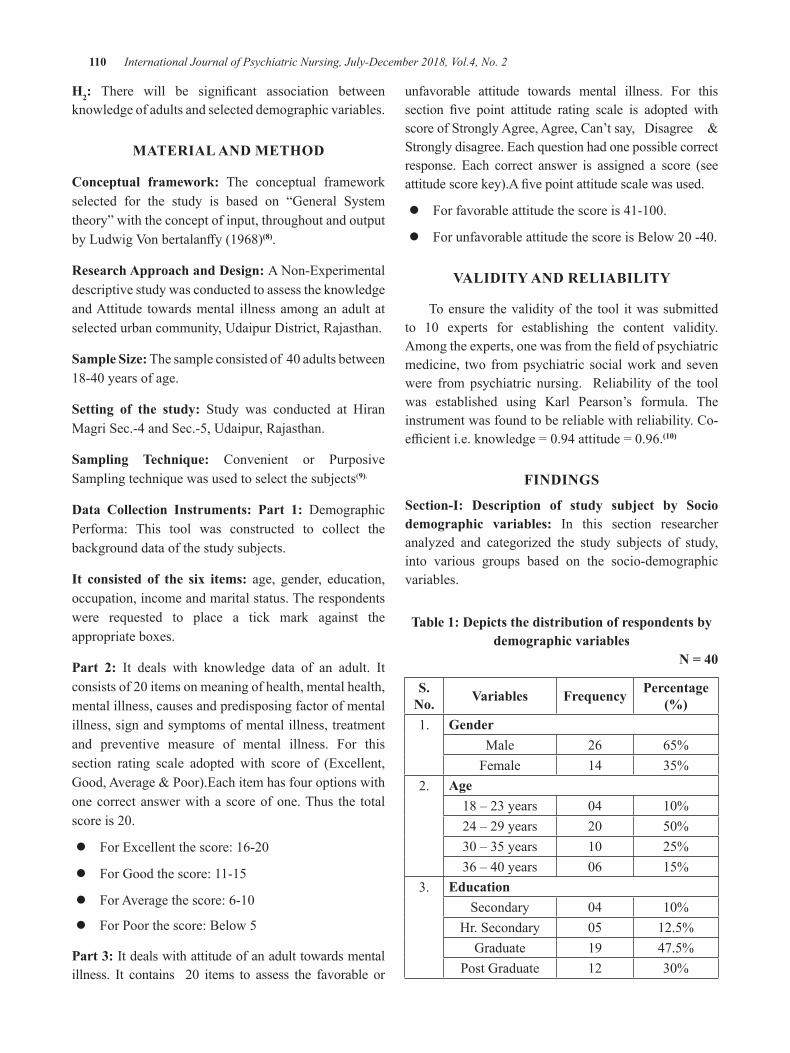
110 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
H2: There will be significant association betweenknowledgeofadultsandselecteddemographicvariables.
MATERIAL AnD METHoD
Conceptual framework: The conceptual frameworkselected for the study is based on “General Systemtheory”withtheconceptofinput,throughoutandoutputbyLudwigVonbertalanffy(1968)(8).
Research Approach and Design: ANon-ExperimentaldescriptivestudywasconductedtoassesstheknowledgeandAttitude towardsmental illness amonganadult atselectedurbancommunity,Udaipurdistrict,Rajasthan.
Sample Size: Thesampleconsistedof40adultsbetween18-40yearsofage.
Setting of the study: Study was conducted at HiranMagriSec.-4andSec.-5,Udaipur,Rajasthan.
Sampling Technique: Convenient or PurposiveSamplingtechniquewasusedtoselectthesubjects(9).
Data Collection Instruments: Part 1: demographicPerforma: This tool was constructed to collect thebackgrounddataofthestudysubjects.
It consisted of the six items: age, gender, education,occupation,incomeandmaritalstatus.Therespondentswere requested to place a tick mark against theappropriateboxes.
Part 2: It deals with knowledge data of an adult. Itconsistsof20itemsonmeaningofhealth,mentalhealth,mentalillness,causesandpredisposingfactorofmentalillness,signandsymptomsofmentalillness,treatmentand preventive measure of mental illness. For thissection rating scale adopted with score of (Excellent,Good,Average&Poor).Eachitemhasfouroptionswithonecorrectanswerwithascoreofone.Thus the totalscoreis20.
z ForExcellentthescore:16-20
z ForGoodthescore:11-15
z ForAveragethescore:6-10
z ForPoorthescore:Below5
Part 3:Itdealswithattitudeofanadulttowardsmentalillness. It contains 20 items to assess the favorable or
unfavorable attitude towards mental illness. For thissection five point attitude rating scale is adopted withscoreofStronglyAgree,Agree,Can’tsay, disagree &Stronglydisagree.Eachquestionhadonepossiblecorrectresponse. Each correct answer is assigned a score (seeattitudescorekey).Afivepointattitudescalewasused.
z Forfavorableattitudethescoreis41-100.
z ForunfavorableattitudethescoreisBelow20-40.
VALIDITy AnD RELIAbILITy
Toensure thevalidityof the tool itwassubmittedto 10 experts for establishing the content validity.Amongtheexperts,onewasfromthefieldofpsychiatricmedicine, two frompsychiatric socialworkand sevenwere frompsychiatric nursing. Reliability of the toolwas established using Karl Pearson’s formula. Theinstrumentwasfoundtobereliablewithreliability.Co-efficienti.e.knowledge=0.94attitude=0.96.(10)
FInDIngS
Section-I: Description of study subject by Socio demographic variables: In this section researcheranalyzed and categorized the study subjects of study,into various groups based on the socio-demographicvariables.
Table 1: Depicts the distribution of respondents by demographic variables
n = 40
S. no. Variables Frequency Percentage
(%)1. gender
Male 26 65%Female 14 35%
2. Age18–23years 04 10%24–29years 20 50%30–35years 10 25%36–40years 06 15%
3. EducationSecondary 04 10%
Hr.Secondary 05 12.5%Graduate 19 47.5%
PostGraduate 12 30%
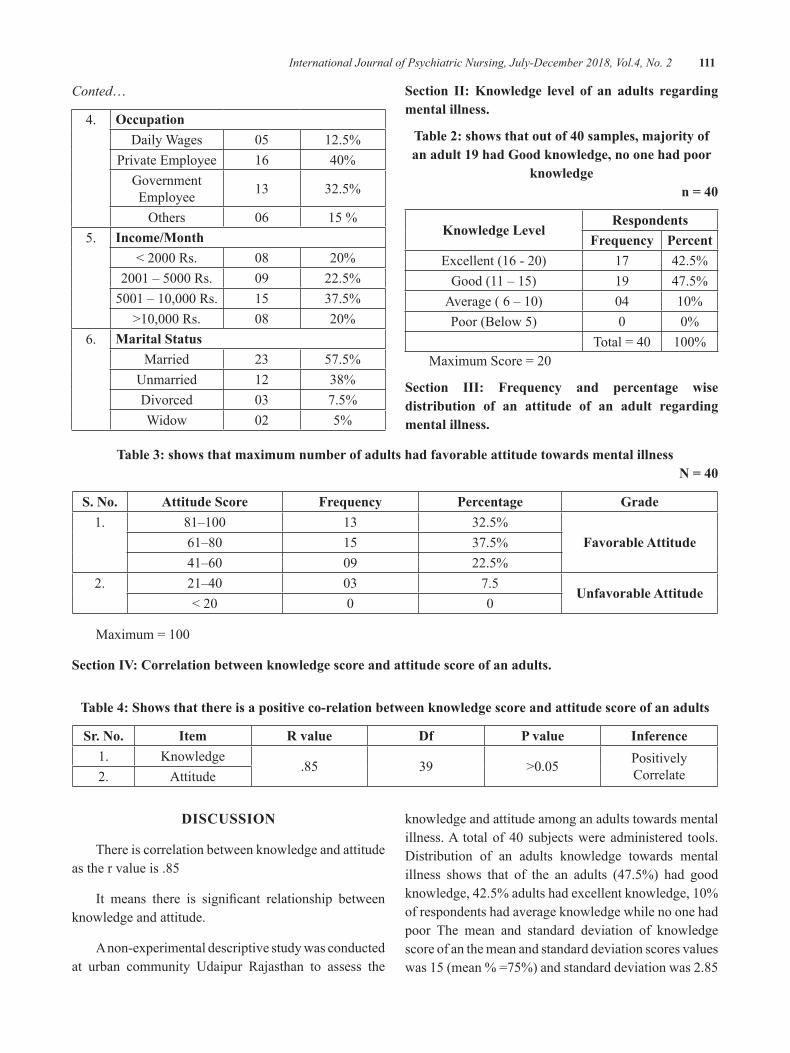
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 111
Conted…
4. occupationdailyWages 05 12.5%
PrivateEmployee 16 40%GovernmentEmployee 13 32.5%
Others 06 15%5. Income/Month
<2000Rs. 08 20%2001–5000Rs. 09 22.5%5001–10,000Rs. 15 37.5%
>10,000Rs. 08 20%6. Marital Status
Married 23 57.5%Unmarried 12 38%divorced 03 7.5%Widow 02 5%
Section II: Knowledge level of an adults regarding mental illness.
Table 2: shows that out of 40 samples, majority of an adult 19 had good knowledge, no one had poor
knowledgen = 40
Knowledge LevelRespondents
Frequency PercentExcellent(16-20) 17 42.5%Good(11–15) 19 47.5%Average(6–10) 04 10%Poor(Below5) 0 0%
Total=40 100%MaximumScore=20
Section III: Frequency and percentage wise distribution of an attitude of an adult regarding mental illness.
Table 3: shows that maximum number of adults had favorable attitude towards mental illnessn = 40
S. no. Attitude Score Frequency Percentage grade1. 81–100 13 32.5%
Favorable Attitude61–80 15 37.5%41–60 09 22.5%
2. 21–40 03 7.5unfavorable Attitude
<20 0 0
Maximum=100
Section IV: Correlation between knowledge score and attitude score of an adults.
Table 4: Shows that there is a positive co-relation between knowledge score and attitude score of an adults
Sr. no. Item R value Df P value Inference1. Knowledge
.85 39 >0.05 PositivelyCorrelate2. Attitude
DISCuSSIon
Thereiscorrelationbetweenknowledgeandattitudeasthervalueis.85
It means there is significant relationship betweenknowledgeandattitude.
Anon-experimentaldescriptivestudywasconductedat urban community Udaipur Rajasthan to assess the
knowledgeandattitudeamonganadultstowardsmentalillness.A totalof40subjectswereadministered tools. distribution of an adults knowledge towards mentalillness shows that of the an adults (47.5%) had goodknowledge,42.5%adultshadexcellentknowledge,10%ofrespondentshadaverageknowledgewhilenoonehadpoor The mean and standard deviation of knowledgescoreofanthemeanandstandarddeviationscoresvalueswas15(mean%=75%)andstandarddeviationwas2.85
112 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
(14.3%). It seems that an adults had good knowledgetowardsmentalillness.distributionofanadultsattitudetowardsmentalillnessshowsthatmajorityoftheadults(92.5%)hadfavourableattitudetowardsmentalillness.Mean attitude score was 70 (70%) standard deviationwas 8.9%. Positive correlation was found (+0.85)betweenknowledgescoreandattitudescoreofanadulttowardsmentalillness.Onthebasisofanalysistherewasno associationbetweenknowledge score and selected,becausethecalculatedvaluesislessthatvalueofX2=3.34,atthe0.05levelofsignificance.
RECoMMEnDATIonS
z Similarstudycanbeundertaken inruralareaandonalongersample
z sizetogeneralizethefindings.
z Acomparativestudycanbeconductedonruralandurbanadults.
z Astudymaybeconductedasexperimentalstudy.
z A study may be undertaken to evaluate theeffectivenessofselfinstructionalmodulepreparedonthetopic.
ConCLuSIon
The conclusionweredrawnon thebasis ofmajorfindingsofthestudywereasfollows.
z An adults had higher knowledge score in role of47.5% and no one had poor knowledge towardsmentalillness.
z An adults had higher attitude score in role of anadults 92.5% (favorable) and 7.5% unfavorableattitudetowardsmentalillness.
z The correlation coefficient (R) = +0.85 obtainedbetween knowledge and attitude towards mentalillness found to be positive indicating higher theknowledgebetteristheattitude.
z There was no significant association observedbetween adults knowledge with demographicvariables.
Conflict of Interest:Therewasnoconflictofinterest.
Ethical Clearance:PermissionhasobtainedfromCMO,Govt. SatelliteHospital,HiranMagri, Sec.5,Udaipur,Rajasthanandconsentweretakenfromsubjects.
Source of Funding:Self
REFEREnCES
1.M.S. Bhatia(1999), Essential of psychiatry,SecondEdition,P:6–38.
2.dr.LalithaK.(2001),“Independent livingskillsfor psychiatrics patients”, “Nurse of India”, amonthlypublicationofIndia.Com,Vol-3,P:7-8.
3.Timesof India,MalathyIyer. (2017),16:38ISThttps://timesofindia.indiatimes.com/india/7-5-indians-suffer-from-mental-disorders-who-report/articleshow/57344807.cms
4.MurthyR.S.(2017),Nationalmentalhealthsurveyofindia,2015-2016.IndianJPsychiatry;59:12-6.
5.B. S. Chauhan, (2006), ECT: “Knowledge andtheir attitude amongpatient and their relatives”,“IndianJournalofPsychiatry”,48;1:34–38.
6.Jugal Kishore et al: (2009) “Belief andattitudes towards mental health among medicalprofessionals in delhi” Vol-32 No.3 (2007 –2009).
7.HeatherStuart.(2005).OpenthedoorsTrainingManual:Worldpsychiatricassociationprogrammeto reduce stigma and discrimination because ofschizophrenia.http://www.opendoors.com.
8.Polit dF and Hungler BP,(1999). NursingResearch Principles andMethods, Philadelphia,J.BLippincott,P:134-143.
9.BT. Basavanthappa,(2007) “Nursing Research;Sampling and Sampling techniques” 2nd Edi.Jappy. Brother’s medical publishers (p) Ltd.,P:188–195.
10.Suresh K. Sharma(2015),Nursing Research &Statistics,2ndEd.,Elsevier,NewdelhiP.:43
A Study to assess the Effectiveness of Selected nursing Intervention on Activities of Daily Living, Self Esteem,
Depression and Quality of Life among Elderly with Chronic Illness at Selected old Age Homes in bangalore, Karnataka
D. Elakkuvana bhaskara Raj1, Kanniammal2
1Principal, Indira Gandhi School & College of Nursing, Amethi; 2Dean, SRM College of Nursing, Chennai
AbSTRACT
Introduction: Elderly are themost rapidlygrowing segmentof population. In India there are about77millionelderlypopulationswhereasinKarnatakaoutofapopulationof5.5crores,8percentareelderly1.
objectives: 1.TTo compare thepre andpost test activities of daily living, self esteem,depression andqualityoflifeamongelderlywithchronicillnessbetweenexperimentalandcontrolgroup.2.Tocorrelatebetweenactivitiesofdailyliving,selfesteem,depressionandqualityof lifeamongelderlywithchronicillnessinexperimentalandcontrolgroup.
Methodology:Trueexperimentaltwogrouppre–posttestcontrolgroupdesignusedtoconductthestudy.Simplerandomsampletechniqueusedtocollect40elderlyfromselectedoldagehome.
Results: Therewasstatisticalsignificantatp<0.01inAdL,Selfesteem,depressionandQoLamongelderlywithchronicillnessbetweenexperimentalandcontrolgroup.ItshowspositivecorrelationbetweenAdL,SelfesteemandQOLamongelderlywithchronicillness.ItshowsnegativecorrelationbetweendepressionwithAdL, Self esteem and QOL among elderly with chronic illness. This indicates statistically highcorrelationbetweenactivitiesofdailyliving,selfesteem,depressionandqualityoflifeamongelderlywithchronicillnessinexperimentalGroup.
Keywords: chronic ill, elderly, old age home
InTRoDuCTIon
The elderly population (aged 60 years or above)accountfor7.4%oftotalpopulationin2001.Formalesitwasmarginallylowerat7.1%,whileforfemalesitwas7.8%.Both the shareand sizeofelderlypopulation isincreasingovertime.From5.6%in1961itisprojectedtoriseto12.4%ofpopulationbytheyear20261.
Thelossofphysicalabilitiesisacommonproblemfortheelderlyinoldagehomes.
Physical illness can result in excess disabilitybecauseof inactivity. Inactivityduringphysical illnesscan lead to a decline in skeletal muscle strength andaerobic capacity. These effects of inactivity result inexcessdisability5.
Physical illness such as cardiovascular diseases,stroke, respiratory diseases, and musculoskeletal
diseasesmayleadtoadeclineinskeletalmusclestrengthandaerobiccapacityduetoinactivity6.
Consequences of excess disability
Theyare:1) increasedmorbidityandmortality,2)increased “true” disability, 3) increased cost, and 4)decreasedqualityoflife2.
About64perthousandelderlypersonsinruralareasand55per thousand inurbanareassuffer fromoneormore disabilities. Most common disability among theagedpersonswas locomotordisabilityas3%of themsufferfromit.
According to theCenters fordiseaseControl andPrevention(CdC),chronicdiseasesareamongthemostcommon,costly,andpreventableofallhealthproblems.More than 2.5 – 3.0 million people die of a chronicdiseaseeachyear.
DOI Number: 10.5958/2395-180X.2018.00029.4
114 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
Additionally, approximately 80% of older adultshaveatleastonechronicillness,andatleast50%haveatleasttwo.Unfortunately,chronicconditionsmayleadtopainanddisability,whichmayresultinalowerqualityoflife1.
In thepopulationover70yearsofage,more than50% suffer fromone ormore chronic conditions.Thechronicillnessesusuallyincludehypertension,coronaryheartdisease,andcancer.
According to Government of India statistics(2011), cardiovascular disorders account for one-thirdof elderlymortality. Respiratory disorders account for10%mortality while infections including tuberculosisaccountforanother10%7.
objectives of the study
1.Toassessthepreandposttestlevelofactivitiesofdailyliving,selfesteem,depressionandqualityof life among elderly with chronic illness inexperimentalandcontrolgroup.
2.To compare the pre and post test activities ofdaily living, self esteem, depression and qualityoflifeamongelderlywithchronicillnessbetweenexperimentalandcontrolgroup.
3.To correlate between activities of daily living,selfesteem,depressionandqualityoflifeamongelderlywith chronic illness in experimental andcontrolgroup.
RESEARCH HyPoTHESES
H1: There is significant difference between the meanscorepre-testandposttestactivitiesofdailyliving,selfesteem, depression and quality of life among elderlywith chronic illness between experimental group andcontrolgroup.
H2: Thereisasignificantrelationshipbetweenactivitiesofdailyliving,selfesteem,depressionandqualityoflifeamongelderlywithchronicillnessinexperimentalandcontrolgroup.
RESEARCH METHoDoLogy
Research Design: The researcher was adopted trueexperimental,twogroup-pretest-posttestcontrolgroupdesigntofulfiltheobjectivesofthestudy.Subjectsinthe
experimental group received a Self-Care Self-EfficacyEnhancementProgram.Simultaneously,subjectsinthecontrolgroupreceivedsocialvisits3.
Variables
z Independent variable: In this study independentvariable was selected nursing intervention(SCSEEP).
z Dependent variables:Thedependentvariablesareactivities of daily living, self esteem, depressionand quality of life among elderly with chronicillness.
z Demographic variables: It includes age, sex,religion, educational status, previous occupation,numberofchildren,historyofchronic illnessanddurationofillness.
Setting of the study: ThestudywasconductedinAshaSevaoldagehomesatsouthBangalore.
Sample size:Samplesizewas40(20experimentaland20control)
Sample technique: Random allocation of subjects by simple random samplingusinglotterymethod
Criteria for selecting sample:
Inclusion criteria
z Oldagehomeelderlyrangedfrom60to80years.
z Those are not cognitively impaired. Cognitivelyintactasmeasuredbyascoreof23orgreaterontheMini-MentalStateExamination(MMSE)
Exclusion criteria
z Thosearebedridden
Tools & Techniques: Researcherwas used structuredinterviewscheduleafterdetailedreviewofliteratureanddiscussionwithexperts.
Section A:Itincludesbaselineinformationofelderly
Section b: ToassessActivitiesofdailyLivingbyKatzIndexofindependenceinactivitiesofdailyliving(AdL)forelderlywithchronicillness.
Section C: Rosenberg Self esteem scale was used toassessselfesteem
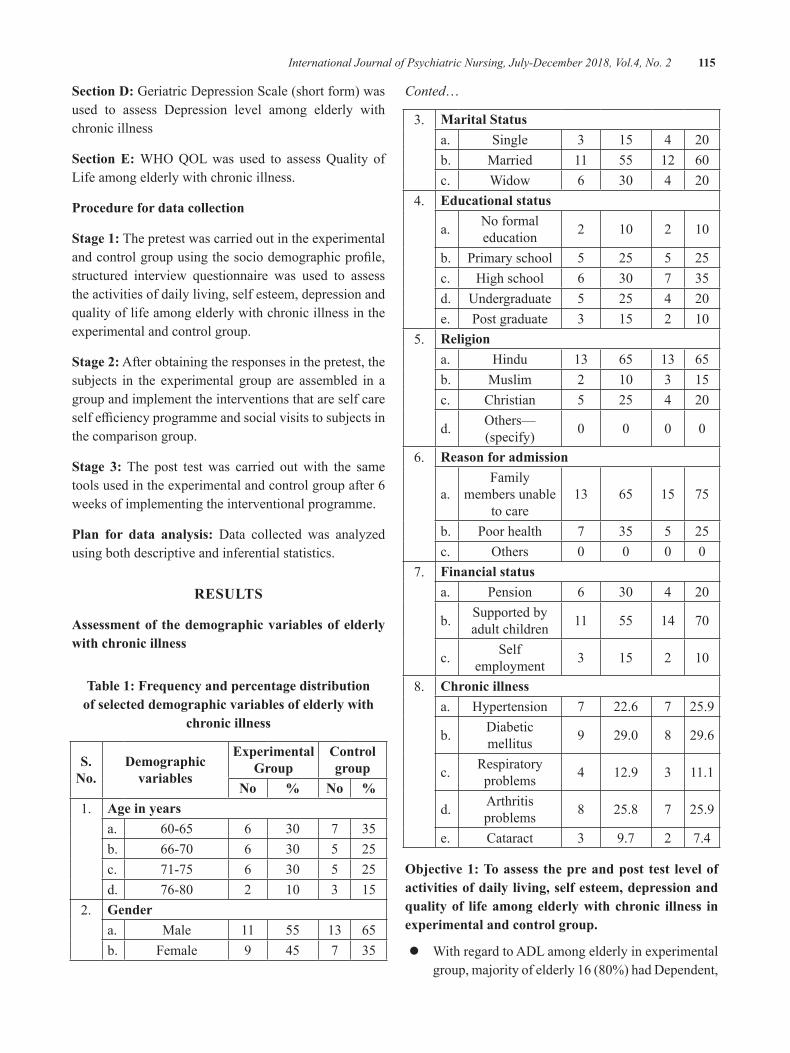
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 115
Section D:GeriatricdepressionScale(shortform)wasused to assess depression level among elderly withchronicillness
Section E: WHOQOLwas used to assessQuality ofLifeamongelderlywithchronicillness.
Procedure for data collection
Stage 1:Thepretestwascarriedoutintheexperimentalandcontrolgroupusingthesociodemographicprofile,structured interview questionnaire was used to assesstheactivitiesofdailyliving,selfesteem,depressionandqualityoflifeamongelderlywithchronicillnessintheexperimentalandcontrolgroup.
Stage 2:Afterobtainingtheresponsesinthepretest,thesubjects in the experimental group are assembled in agroupandimplementtheinterventionsthatareselfcareselfefficiencyprogrammeandsocialvisitstosubjectsinthecomparisongroup.
Stage 3: The post testwas carried outwith the sametoolsusedintheexperimentalandcontrolgroupafter6weeksofimplementingtheinterventionalprogramme.
Plan for data analysis: data collected was analyzedusingbothdescriptiveandinferentialstatistics.
RESuLTS
Assessment of the demographic variables of elderly with chronic illness
Table 1: Frequency and percentage distribution of selected demographic variables of elderly with
chronic illness
S. no.
Demographic variables
Experimental group
Control group
No % No %1. Age in years
a. 60-65 6 30 7 35b. 66-70 6 30 5 25c. 71-75 6 30 5 25d. 76-80 2 10 3 15
2. gender a. Male 11 55 13 65b. Female 9 45 7 35
Conted…
3. Marital Statusa. Single 3 15 4 20b. Married 11 55 12 60c. Widow 6 30 4 20
4. Educational status
a. Noformaleducation 2 10 2 10
b. Primaryschool 5 25 5 25c. Highschool 6 30 7 35d. Undergraduate 5 25 4 20e. Postgraduate 3 15 2 10
5. Religiona. Hindu 13 65 13 65b. Muslim 2 10 3 15c. Christian 5 25 4 20
d. Others—(specify) 0 0 0 0
6. Reason for admission
a.Family
membersunabletocare
13 65 15 75
b. Poorhealth 7 35 5 25c. Others 0 0 0 0
7. Financial statusa. Pension 6 30 4 20
b. Supportedbyadultchildren 11 55 14 70
c. Selfemployment 3 15 2 10
8. Chronic illnessa. Hypertension 7 22.6 7 25.9
b. diabeticmellitus 9 29.0 8 29.6
c. Respiratoryproblems 4 12.9 3 11.1
d. Arthritisproblems 8 25.8 7 25.9
e. Cataract 3 9.7 2 7.4
objective 1: To assess the pre and post test level of activities of daily living, self esteem, depression and quality of life among elderly with chronic illness in experimental and control group.
z WithregardtoAdLamongelderlyinexperimentalgroup,majorityofelderly16(80%)haddependent,
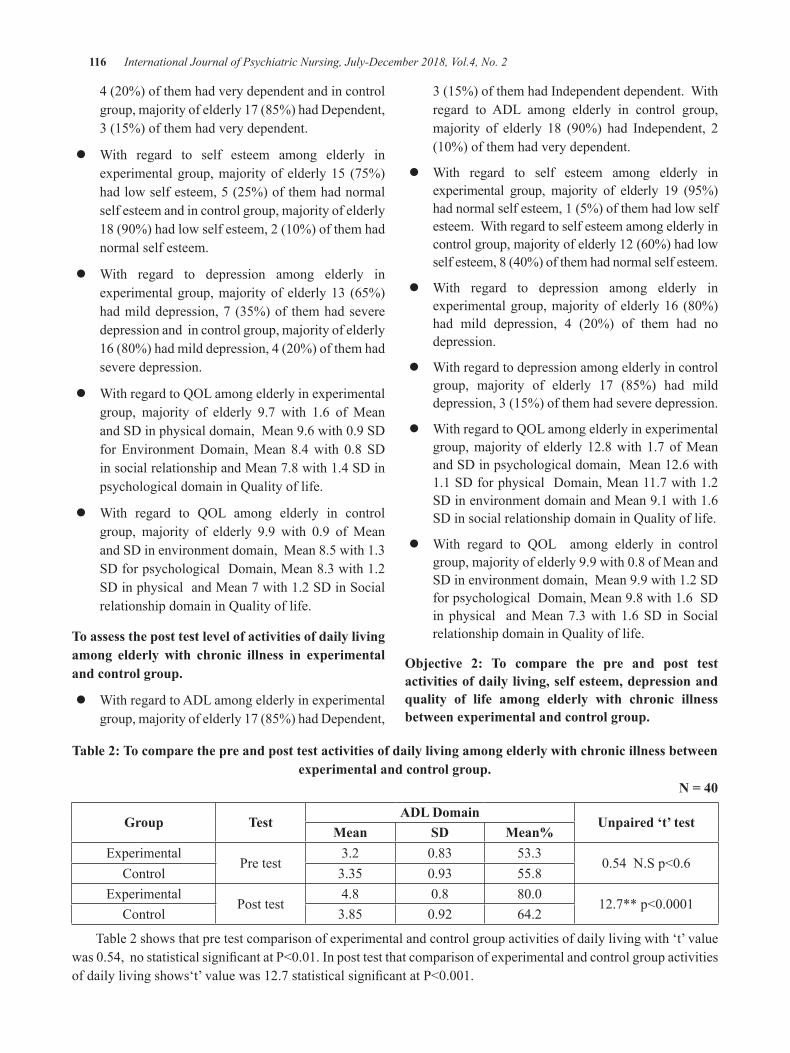
116 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
4(20%)ofthemhadverydependentandincontrolgroup,majorityofelderly17(85%)haddependent,3(15%)ofthemhadverydependent.
z With regard to self esteem among elderly inexperimentalgroup,majorityofelderly15 (75%)hadlowselfesteem,5(25%)ofthemhadnormalselfesteemandincontrolgroup,majorityofelderly18(90%)hadlowselfesteem,2(10%)ofthemhadnormalselfesteem.
z With regard to depression among elderly inexperimentalgroup,majorityofelderly13 (65%)hadmilddepression,7 (35%)of themhadseveredepressionandincontrolgroup,majorityofelderly16(80%)hadmilddepression,4(20%)ofthemhadseveredepression.
z WithregardtoQOLamongelderlyinexperimentalgroup, majority of elderly 9.7 with 1.6 of MeanandSdinphysicaldomain,Mean9.6with0.9Sdfor Environmentdomain,Mean 8.4with 0.8 SdinsocialrelationshipandMean7.8with1.4SdinpsychologicaldomaininQualityoflife.
z With regard to QOL among elderly in controlgroup, majority of elderly 9.9 with 0.9 of MeanandSdinenvironmentdomain,Mean8.5with1.3Sdforpsychologicaldomain,Mean8.3with1.2SdinphysicalandMean7with1.2SdinSocialrelationshipdomaininQualityoflife.
To assess the post test level of activities of daily living among elderly with chronic illness in experimental and control group.
z WithregardtoAdLamongelderlyinexperimentalgroup,majorityofelderly17(85%)haddependent,
3(15%)ofthemhadIndependentdependent.Withregard to AdL among elderly in control group,majority of elderly 18 (90%) had Independent, 2(10%)ofthemhadverydependent.
z With regard to self esteem among elderly inexperimental group, majority of elderly 19 (95%)hadnormalselfesteem,1(5%)ofthemhadlowselfesteem.Withregardtoselfesteemamongelderlyincontrolgroup,majorityofelderly12(60%)hadlowselfesteem,8(40%)ofthemhadnormalselfesteem.
z With regard to depression among elderly inexperimentalgroup,majorityofelderly16 (80%)had mild depression, 4 (20%) of them had nodepression.
z Withregardtodepressionamongelderlyincontrolgroup, majority of elderly 17 (85%) had milddepression,3(15%)ofthemhadseveredepression.
z WithregardtoQOLamongelderlyinexperimentalgroup,majorityof elderly12.8with1.7ofMeanandSdinpsychologicaldomain,Mean12.6with1.1Sdforphysicaldomain,Mean11.7with1.2SdinenvironmentdomainandMean9.1with1.6SdinsocialrelationshipdomaininQualityoflife.
z With regard to QOL among elderly in controlgroup,majorityofelderly9.9with0.8ofMeanandSdinenvironmentdomain,Mean9.9with1.2Sdforpsychologicaldomain,Mean9.8with1.6Sdin physical andMean7.3with 1.6Sd inSocialrelationshipdomaininQualityoflife.
objective 2: To compare the pre and post test activities of daily living, self esteem, depression and quality of life among elderly with chronic illness between experimental and control group.
Table 2: To compare the pre and post test activities of daily living among elderly with chronic illness between experimental and control group.
n = 40
group TestADL Domain
unpaired ‘t’ testMean SD Mean%
ExperimentalPretest
3.2 0.83 53.30.54N.Sp<0.6
Control 3.35 0.93 55.8Experimental
Posttest4.8 0.8 80.0
12.7**p<0.0001Control 3.85 0.92 64.2
Table2showsthatpretestcomparisonofexperimentalandcontrolgroupactivitiesofdailylivingwith‘t’valuewas0.54,nostatisticalsignificantatP<0.01.Inposttestthatcomparisonofexperimentalandcontrolgroupactivitiesofdailylivingshows‘t’valuewas12.7statisticalsignificantatP<0.001.
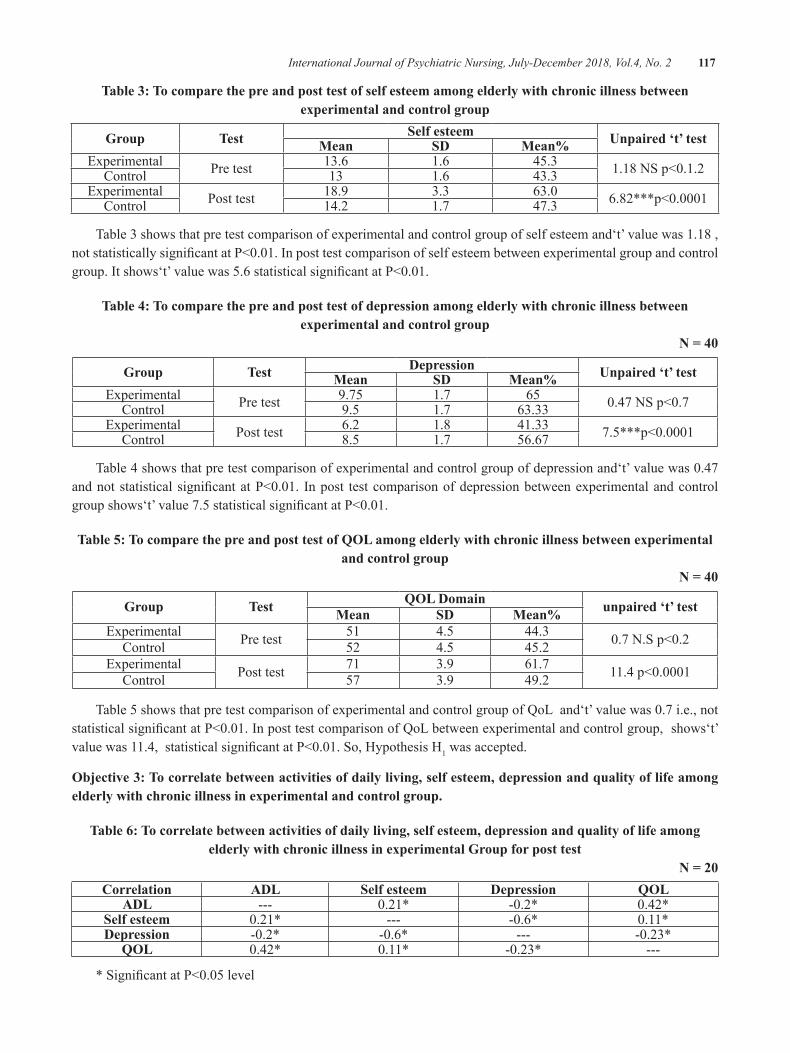
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 117
Table 3: To compare the pre and post test of self esteem among elderly with chronic illness between experimental and control group
group Test Self esteem unpaired ‘t’ testMean SD Mean%Experimental Pretest 13.6 1.6 45.3 1.18NSp<0.1.2Control 13 1.6 43.3Experimental Posttest 18.9 3.3 63.0 6.82***p<0.0001Control 14.2 1.7 47.3
Table3showsthatpretestcomparisonofexperimentalandcontrolgroupofselfesteemand‘t’valuewas1.18,notstatisticallysignificantatP<0.01.Inposttestcomparisonofselfesteembetweenexperimentalgroupandcontrolgroup.Itshows‘t’valuewas5.6statisticalsignificantatP<0.01.
Table 4: To compare the pre and post test of depression among elderly with chronic illness between experimental and control group
n = 40
group Test Depression unpaired ‘t’ testMean SD Mean%Experimental Pretest 9.75 1.7 65 0.47NSp<0.7Control 9.5 1.7 63.33Experimental Posttest 6.2 1.8 41.33 7.5***p<0.0001Control 8.5 1.7 56.67
Table4showsthatpretestcomparisonofexperimentalandcontrolgroupofdepressionand‘t’valuewas0.47andnotstatisticalsignificantatP<0.01. Inpost testcomparisonofdepressionbetweenexperimentalandcontrolgroupshows‘t’value7.5statisticalsignificantatP<0.01.
Table 5: To compare the pre and post test of QoL among elderly with chronic illness between experimental and control group
n = 40
group Test QoL Domain unpaired ‘t’ testMean SD Mean%Experimental Pretest 51 4.5 44.3 0.7N.Sp<0.2Control 52 4.5 45.2Experimental Posttest 71 3.9 61.7 11.4p<0.0001Control 57 3.9 49.2
Table5showsthatpretestcomparisonofexperimentalandcontrolgroupofQoLand‘t’valuewas0.7i.e.,notstatisticalsignificantatP<0.01.InposttestcomparisonofQoLbetweenexperimentalandcontrolgroup,shows‘t’valuewas11.4,statisticalsignificantatP<0.01.So,HypothesisH1wasaccepted.
objective 3: To correlate between activities of daily living, self esteem, depression and quality of life among elderly with chronic illness in experimental and control group.
Table 6: To correlate between activities of daily living, self esteem, depression and quality of life among elderly with chronic illness in experimental group for post test
n = 20Correlation ADL Self esteem Depression QoL
ADL --- 0.21* -0.2* 0.42*Self esteem 0.21* --- -0.6* 0.11*Depression -0.2* -0.6* --- -0.23*
QoL 0.42* 0.11* -0.23* ---
*SignificantatP<0.05level
118 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
Table 6 shows that positive correlation betweenAdL,SelfesteemandQOLamongelderlywithchronicillness.ItshowsnegativecorrelationbetweendepressionwithAdL, Self esteem andQOL among elderly withchronicillness.So,HypothesisH2wasaccepted.
ConCLuSIon
Thedatawascollectedfrom40elderlywithchronicillness (20 experimental and 20 control group) fromselectedoldagehome settingbystructured interviewschedule.
Therewas statistical significant at p<0.01inAdL,Self esteem, depression and QoL among elderly withchronicillnessbetweenexperimentalandcontrolgroup.
It shows positive correlation between AdL, SelfesteemandQOLamongelderlywithchronicillness.Itshows negative correlation between depression withAdL,SelfesteemandQOLamongelderlywithchronicillness. This indicates statistically high correlationbetweenactivitiesofdailyliving,selfesteem,depressionandqualityoflifeamongelderlywithchronicillnessinexperimentalGroup.
Conflict of Interest:Nil
Source of Funding:Self
Ethical Clearance: 1.Thestudywasapprovedbytheresearchcommitteeandaformalpermissionwasobtainfromheadoftheinstitution.
2.Writtenconsentofeachofthesubjectswasobtainbeforestartingdatacollection.
3.The subjects was assured confidentiality havemaintainofinformation.
4.Thesubjectsareinformedthattheirparticipationisvoluntary,hadthefreedomtowithdrawfromthestudy.
5.Sameinterventionwasgivenforthecontrolgroupafterthecompletionofdatacollection.
REFEREnCES
1.UnitedNationsPopulationFund(UNFPA).IndiaAgeing Report 2017. Newdelhi; UNPF; 2017.Available from; india.unfpa.org/.../India%20Ageing%20Report%20-%202017%
2.Aberg, A. C, Sidenvall, B., Hepworth, M.,O’Reilly, K., & Lithell, H. On loss of activityand independence, adaptation improves lifesatisfaction in old age. Qual Life Res. 2005 May;14(4):1111-25.
3.Adams,d.L.Analysisofalifesatisfactionindex.JournalofGerontology.1969;24(1):470-474.
4.Allison, M. J., & Keller, C. Self-efficacyintervention effect on physical activity in olderadults. Western Journal of Nursing Research.2004Feb;26(1):31-46.
5.Chen, Y. C. Chinese values, health and nursing.JournalofAdvancedNursing.2001;36(2):270-273.
6.Kalinowaski, J., Guntualli, V. K., Stuart, A.,& Saltuklaroglu, T.. Self- reported efficacyof an ear-level prosthetic device that deliversalteredauditoryfeedbackforthemanagementofstuttering.InternationalJournalofRehabilitationResearch.2004;27(2).167-170.
7.department of Health, Executive Yuan, Taiwan,RepublicofChina.(n.d.).RetrievedAugust12,2004,fromhttp://www.doh.gov.tw/statistic/index.htm

understanding Women with Infertility: Parse’s and System’s Theory
Porkodi Rabindran
Tutor, College of Nursing, JIPMER, Puducherry
AbSTRACT
Nursingdevelopsitsknowledgebasefromnetworkoffacts,conceptsandapproachestoinquiryofhumanexperiences. Health comprises biological, psychological, social and spiritual components that follow aprocessofchangingvaluepriorities.Thedynamicstateofhealthrequiresbody-mind-spiritperspectivetohelpsmanfixprioritiesinlife.Manchooseswaysoflivingbyexploringoptions,hispersonalrealitiesandpossibleoutcomes.Childbearingandraisingchildrenareextremelyimportanteventsinhumanlifeandarestronglyassociatedwith theultimategoalsofcompleteness,happinessandfamily integration. Infertilityoftenpushesthewomenwithinfertilityintocauldronofemotionaldisturbance.Nurseshouldprovidecarekeeping inmind the interplayofherpersonalcharacteristics, familyand thesocietyat large.ThispaperattemptstointegrateParse’sHumanBecomingtheoryandBowen’sFamilysystemtheorytounderstandthenumerousissuesofwomenwithinfertility.
Keywords: Infertility, Human Becoming, Family system
InTRoDuCTIon
Themostbasicnecessityofhumanraceisprocreationand inability to bear a child leads to devastatingemotionalandpsychologicaldistress.Thesocialstigmaof infertility is gender biased and impacts heavily onwomen. Inadditiontotheinfertilitystatus, thehigh-techreproductive technologiesavailablebringsalongmanyassociated psychological and ethical issues that thewomenwithinfertilityinevitablyendure.Therefore,itisimportantforthehealthcareprofessionalstounderstandtheinterplayofnumerousissuessurroundinginfertilityanditstreatment.
Family plays an important role in the experiencesof an individual.Across cultures of theworldwomenaresubjectedtovariedtraditionalmethodsandreligiouspractices, including visits to temples, abstaining fromvisitingaplacewhereawomanhasdelivereda child,observingtantricrites,wearingcharms,participatinginritualsandvisitingastrologers.2ThestressesassociatedwithinfertilityandIVFtreatmenthadanegativeimpacton women’s psychological health status and maritalquality.3Thesefindingsemphasize theneed to includepsychological and socio-cultural considerations withanymedicalinterventionsforinfertility4.
THEoRETICAL APPRoACH
The complexity of humanbehavior is a challengeto decipher. When it is compounded with conditionsthat pose a severe psychosocial impact the task isoverwhelming.Nursetheoristshaveprovidedtheoreticalframeworks tohelpus in theprocessofunderstandingandcaringforourclients.
An individual should be considered within thecontext of their life situations and relationships tounderstandtheirbehavioursanddecisions.Thedomainsofhealth thatare important toan individualshouldbeassessedtoprovidemultidimensionaltreatment.5Nursetheorist Rosemarie Rizzo Parse iterates this view inherwords, “medicalmodelwas limitedas aguide fornursing practice. Why do people not follow healthteachingandlikesomepeoplewhodo,donotgetwell?Thereisaneedfornewperspectivethanthetraditionalview of nursing.” The importance of the individual’sperspectivewhich is shaped by their lived experience(phenomenology) is the philosophical underpinningof her theory. This philosophical approach led to thedevelopment of “human becoming theory”. The livedexperiencesarearesultofinteractionwiththepeopleinaparticulartimeframeandplace.
DOI Number: 10.5958/2395-180X.2018.00034.8
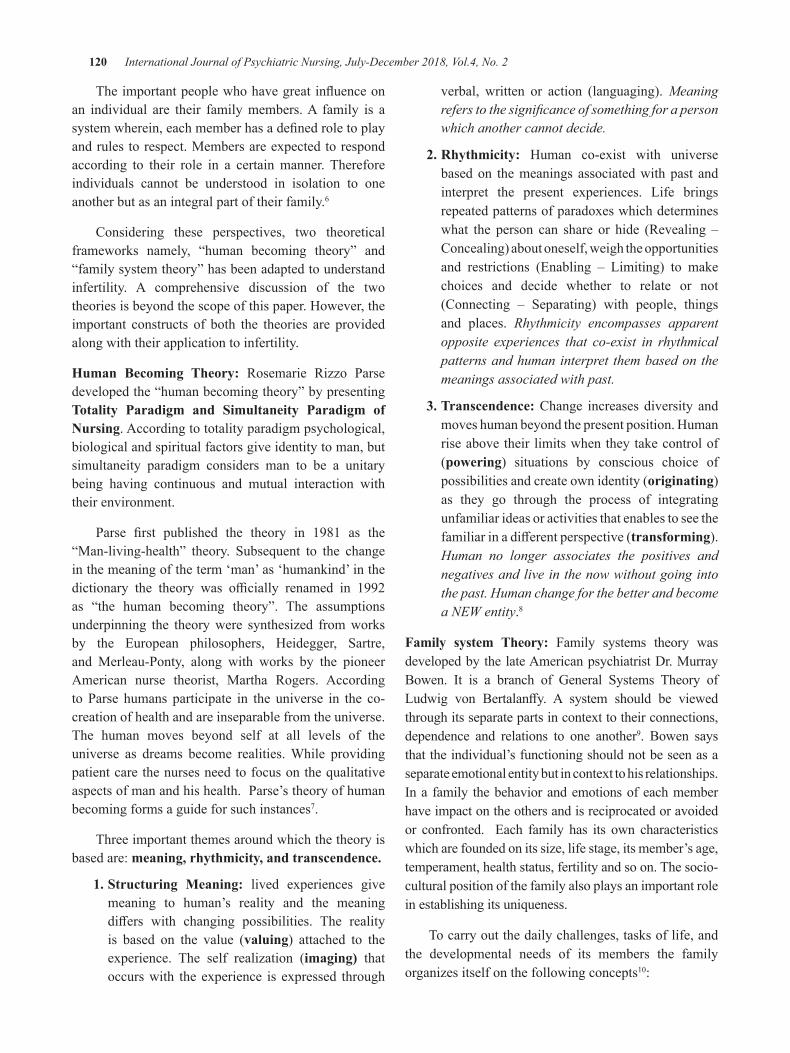
120 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
Theimportantpeoplewhohavegreatinfluenceonan individual are their familymembers.A family is asystemwherein,eachmemberhasadefinedroletoplayandrulestorespect.Membersareexpectedtorespondaccording to their role in a certainmanner. Thereforeindividuals cannot be understood in isolation to oneanotherbutasanintegralpartoftheirfamily.6
Considering these perspectives, two theoreticalframeworks namely, “human becoming theory” and“familysystemtheory”hasbeenadaptedtounderstandinfertility. A comprehensive discussion of the twotheoriesisbeyondthescopeofthispaper.However,theimportant constructs of both the theories are providedalongwiththeirapplicationtoinfertility.
Human becoming Theory: Rosemarie Rizzo Parsedevelopedthe“humanbecomingtheory”bypresentingTotality Paradigm and Simultaneity Paradigm of nursing.Accordingtototalityparadigmpsychological,biologicalandspiritualfactorsgiveidentitytoman,butsimultaneity paradigm considers man to be a unitarybeing having continuous and mutual interaction withtheirenvironment.
Parse first published the theory in 1981 as the“Man-living-health” theory. Subsequent to the changeinthemeaningoftheterm‘man’as‘humankind’inthedictionary the theory was officially renamed in 1992as “the human becoming theory”. The assumptionsunderpinning the theorywere synthesized fromworksby the European philosophers, Heidegger, Sartre,and Merleau-Ponty, along with works by the pioneerAmerican nurse theorist, Martha Rogers. Accordingto Parse humans participate in the universe in the co-creationofhealthandareinseparablefromtheuniverse.The human moves beyond self at all levels of theuniverse as dreams become realities.While providingpatientcarethenursesneedtofocusonthequalitativeaspectsofmanandhishealth.Parse’stheoryofhumanbecomingformsaguideforsuchinstances7.
Threeimportantthemesaroundwhichthetheoryisbasedare:meaning, rhythmicity, and transcendence.
1. Structuring Meaning: lived experiences givemeaning to human’s reality and the meaningdiffers with changing possibilities. The realityis based on the value (valuing) attached to theexperience. The self realization (imaging) thatoccurswith theexperience is expressed through
verbal, written or action (languaging).Meaning refers to the significance of something for a person which another cannot decide.
2. Rhythmicity: Human co-exist with universebasedon themeanings associatedwithpast andinterpret the present experiences. Life bringsrepeatedpatternsofparadoxeswhichdetermineswhat the person can share or hide (Revealing –Concealing)aboutoneself,weightheopportunitiesand restrictions (Enabling – Limiting) to makechoices and decide whether to relate or not(Connecting – Separating) with people, thingsand places. Rhythmicity encompasses apparent opposite experiences that co-exist in rhythmical patterns and human interpret them based on the meanings associated with past.
3. Transcendence:Change increasesdiversity andmoveshumanbeyondthepresentposition.Humanriseabovetheir limitswhentheytakecontrolof(powering) situations by conscious choice ofpossibilitiesandcreateownidentity(originating) as they go through the process of integratingunfamiliarideasoractivitiesthatenablestoseethefamiliarinadifferentperspective(transforming). Human no longer associates the positives and negatives and live in the now without going into the past. Human change for the better and become a NEW entity.8
Family system Theory: Family systems theory wasdevelopedbythelateAmericanpsychiatristdr.MurrayBowen. It is a branch of General Systems Theory ofLudwig von Bertalanffy. A system should be viewedthroughitsseparatepartsincontexttotheirconnections,dependence and relations to one another9. Bowen saysthattheindividual’sfunctioningshouldnotbeseenasaseparateemotionalentitybutincontexttohisrelationships.Ina family thebehaviorandemotionsofeachmemberhaveimpactontheothersandisreciprocatedoravoidedor confronted. Each family has its own characteristicswhicharefoundedonitssize,lifestage,itsmember’sage,temperament,healthstatus,fertilityandsoon.Thesocio-culturalpositionofthefamilyalsoplaysanimportantroleinestablishingitsuniqueness.
Tocarryoutthedailychallenges,tasksoflife,andthe developmental needs of its members the familyorganizesitselfonthefollowingconcepts10:
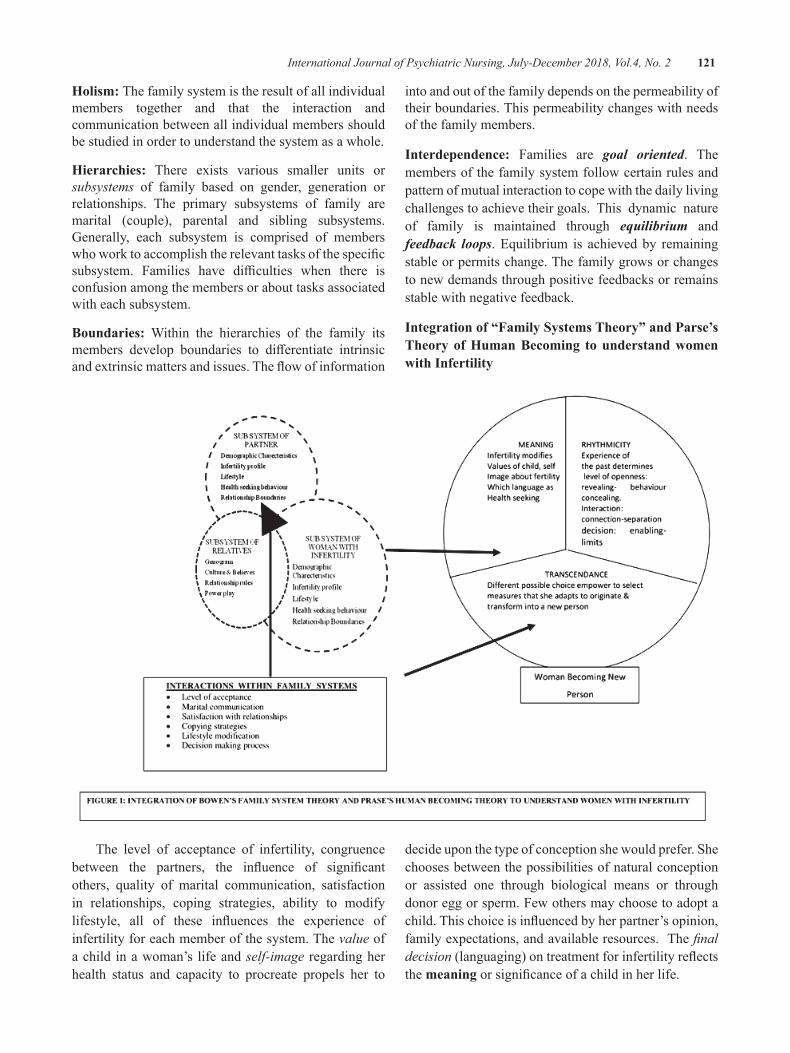
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 121
Holism: Thefamilysystemistheresultofallindividualmembers together and that the interaction andcommunicationbetweenallindividualmembersshouldbestudiedinordertounderstandthesystemasawhole.
Hierarchies: There exists various smaller units orsubsystems of family based on gender, generation orrelationships. The primary subsystems of family aremarital (couple), parental and sibling subsystems.Generally, each subsystem is comprised of memberswhoworktoaccomplishtherelevanttasksofthespecificsubsystem. Families have difficulties when there isconfusionamongthemembersorabouttasksassociatedwitheachsubsystem.
boundaries: Within the hierarchies of the family itsmembers develop boundaries to differentiate intrinsicandextrinsicmattersandissues.Theflowofinformation
intoandoutofthefamilydependsonthepermeabilityoftheirboundaries.Thispermeabilitychangeswithneedsofthefamilymembers.
Interdependence: Families are goal oriented. Themembersofthefamilysystemfollowcertainrulesandpatternofmutualinteractiontocopewiththedailylivingchallengestoachievetheirgoals. This dynamic natureof family is maintained through equilibrium andfeedback loops.Equilibrium is achievedby remainingstableorpermitschange.Thefamilygrowsorchangestonewdemandsthroughpositivefeedbacksorremainsstablewithnegativefeedback.
Integration of “Family Systems Theory” and Parse’s Theory of Human becoming to understand women with Infertility
The level of acceptance of infertility, congruencebetween the partners, the influence of significantothers, quality of marital communication, satisfactionin relationships, coping strategies, ability to modifylifestyle, all of these influences the experience ofinfertilityforeachmemberofthesystem.Thevalueofachild inawoman’s lifeandself-image regardingherhealth status and capacity to procreate propels her to
decideuponthetypeofconceptionshewouldprefer.Shechoosesbetweenthepossibilitiesofnaturalconceptionor assisted one through biological means or throughdonoreggorsperm.Fewothersmaychoosetoadoptachild.Thischoiceisinfluencedbyherpartner’sopinion,familyexpectations,andavailableresources.Thefinal decision(languaging)ontreatmentforinfertilityreflectsthemeaningorsignificanceofachildinherlife.

122 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
Oncethedecisionismadesheexpressesdifficultiesandfeasibilitiesintermsofoneself,familyandsocietalconstraintstothelevel she deems appropriate(revealing-concealing)soastoparticipateintheinfertilitytreatmentprocess.Theinteractionswiththehealthcarepersonnelwillhelphertorealize factors that will help or hinder (enabling-limiting) her in the process.This realizationenables (connecting-separating) her to connect to the supporting factors like interacting with other womenwithasimilarproblemorthosewhoarecompassionateandunderstandingandembracinglifestylemodification.At the same time, she also distances herself from the stressful factorslikesituationsandpersonswhoquestionortauntherself-worthandpracticesthataredetrimentaltoconception.Thelevelofappropriateness,factorsthathelporhinderandwhatissupportiveorstressfultothewomanmayfollowarepetitivefashionorrhythmicity. Theseexperiencesfinallyhelpthe womantounderstandherstatusinlightofherdecisionabouthertreatment.
This realization empowers (powering) her tocollaboratewithhersignificantotherstomakeappropriatedecisions on treatment modalities that will fit her individuality(originating).Thussheisnowanew person (transforming) who is able to accept the situation andmoveforwardwiththenecessarychanges.Therealizationofselfasbeingdifferentandunderstandingtheimportanceofembracingthediversitiesofinfertilitytreatmentisthetranscendenceseeninwomenwithinfertility.
ConCLuSIon
Thehumanbehaviorbeingcomplexandinterwovenwithintheirrelationshipsnecessitatesnursestorecognizethe client’s needs in the context of their families andsocietyat large inacomprehensivemanner toprovideholistic nursing care.This effort of integratingParse’shuman becoming theory and Bowen’s family systemstheorywassuchanattempttounderstandthenumerousfacetsofwomenseekinginfertilitytreatment.
Conflict of Interest:Theauthordeclaresnoconflictofinterest.
Source of Support:Self
Ethical Clearance:TakenfromJIPMERInstituteEthicsCommittee.
REFEREnCES
1.Widge.A &C leland.J. The public sector’s rolein infertilitymanagement in India.Retrievedon28/01//13fromhttp://heapol.oxfordjournals.org
2.Tripathi N. Infertility among Indian Women:EmergingevidenceandneedforPolicyMeasures. paa2011.princeton.edu/papers/110609
3.ReidK,AlfredA.Qualityoflife,copingstrategiesand support needs ofwomen seekingTraditionalChinese Medicine for infertility and viablepregnancyinAustralia:amixedmethodsapproach.BMCWomensHealth.2013Apr;9:13-7.
4.WangK,Li J, Zhang JX,ZhangL,Yu J, JiangP.Psychological characteristics and maritalqualityofinfertilewomenregisteredforinvitrofertilization-intracytoplasmic sperm injection inChina.FertilityandSterility.2007Apr;87(4):792-8.Epub2007Jan12
5.Shane J Mc Inerney S J Mc. Introducing theBiopsychosocial Model for good medicine andgooddoctors.BMJ2015;324:1533
6.ParkerME.NursingTheoriesandNursingPractice.2nded.Philadelphia,F.A.davisCompany,2005.
7.KarenL.Melnechenko.Parse’sTheoryofHumanBecoming:AnAlternativeGuidetoNursingPracticeforPediatricOncologyNurses.JournalofPediatricOncologyNursing.1995;Vol.12,No.3,122-7
8.Fawcett J. The Nurse Theorist: 21st centuryupdates - Rosemarie Rizzo Parse. Scholarlydialogue.NursSciQ.2001Apr;14(2):126-31.
9.Family Systems Theory–Basic concepts/propositions[Internet]2017Availablefrom:http://family.jrank.org/pages/597/Family-Systems-Theory-Basic-Concepts-Propositions.html
10.Kerr,MichaelE.“OneFamily’sStory:APrimeronBowenTheory.”TheBowenCenterfortheStudyoftheFamily.2000.http://www.thebowencenter.org.
A Study to Assess the Effectiveness of Self Instructional Module Regarding Reducing Academic Stress among Students
of b.sc nursing in Selected Colleges at Jaipur City Raj
Manmohan Singh1, Dinesh kumar Sharma2, Rakesh Joshi3
1Nursing Lecturer USB College of Nursing Abu Road, Dist. Sirohi; 2Nursing Tutor,College of Nursing Aiims Rishikesh; 3Deputy Registrar Geetanjali University Udaipur
AbSTRACT
Thetermstressmeanspressureandinhumanlifeitrepresentsanuneasyexperience.It isanunpleasantpsychological and physiological state caused due to some internal or external demands that go beyondourcapacity. It refers to theconsequenceof thefailureofanorganismtorespondadequately tomental,emotionalorphysicaldemands,eitheractualorimagined. objectives: Theobjectives of the studywere 1)To assess the level of academic stress among studentsofB.Sc.Nursing .2)Toassess the effectivenessof self-instructionalmodule in reducingacademic stressamongB.Sc.NursingStudents.3Tofindouttheassociationbetweenpost-teststressscoresandselecteddemographicvariables.
Methodology:Theresearchapproachadoptedforthestudywaspre-experimentalresearchapproach.Theresearchdesignadoptedforthestudywaspre-experimentalresearchdesign.Thedatawascollectedthroughthetoolwhichispreparedbytheinvestigator.Thesampleconsistsofthe50students.Thetoolusedforthedatacollectionwasstructuredstressknowledgequestionnaire,whichhastwosections:Section A: Itemsonsocio-demographicvariables Section b: Itemsonstressquestionnaresregarding,stressrelatedtoacademiccondition,stressrelatedtosocialcondition,stressrelatedtofamily/environmentalcondition.
Results:showsthatthemaximummeanpercentageobtainedbythestudentsisfoundintheaspectofstressrelatedtosocialcondition(52.52%)followedbystressrelatedtogeneral/personalcondition(52.24%),stressrelated to family/environmental condition(49.66%) and leastmean percentage obtained in the aspect ofstressrelatedtoacademiccondition(49.60%).TheoverallMean±Sdofpost-testlevelofacademicstresswas46.13±2.42andmeanpercentageof46.13%.
Conclusion:Theoverallfindingsofthestudyrevealedthattherewasoverallmeanknowledgescoreobtainedbythestudentswas46.13andwithstandarddeviation2.42andthemeanpercentagewas51.25%,Sothisindicatesthatlevelofacademicstressisreducedamongstudents
Keywords: Assess, self instructional module,stress,academic stress,Effectiveness.
InTRoDuCTIonEducation make a people easy to lead butdifficulttodrive,easytogovernbutimpossibletoenslave
−Peterbrougham
Psychiatricnursingisaspecializedareaofnursingpractice,whichemploystheoriesofhumanbehaviour.Ithelpstheindividualfortheuseofselfinunderstandingthediagnosisandtreatmentofhumanresponsestoactualorpotentialmentalhealthproblems.1
The termstressmeanspressure and inhuman lifeit represents an uneasy experience. It is an unpleasantpsychological and physiological state caused due tosome internalorexternaldemands thatgobeyondourcapacity2.Stressistheterminpsychologyandbiologyborrowedfromphysicsandengineeringandfirstusedinthebiologicalcontextin1930`s,whichhasinmorerecentdecadesbecomecommonlyusedinpopulationbalance.Itreferstotheconsequenceofthefailureofanorganismtorespondadequatelytomental,emotionalorphysicaldemands,eitheractualorimagined.3academicstressisa
DOI Number: 10.5958/2395-180X.2018.00030.0

124 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
veryimportanttypeaffectingeachandeverystudentinthisfastpacedliferunningonthebasisofperformancein academy. Academic period is never easy, it is atime of uncertainty, insecurity and sometimes feelingof inadequacy. Life events are many like transitionperiod from childhood to adolescence, academicstress, marital stress, occupational stress, retirementstress.4 The reasons are separation from parents, poorinfrastructure, inexperience and inadequate teachers,academic overload, new and vast subjects, languageproblem, presentation problem and lack of practicalskills5. They may have difficulty adjusting to morerigorousacademicexpectationsandtheneedtolearntodealwith individuals of differing cultures and beliefs.Thus, stress may result from being separated fromhome for the first time, the transition from a personalto an impersonal academic environment, and the verystructure of the academic experience at the collegelevel6.Significantchangesinlivingconditions,thenoveldemandsofthecollegeacademicenvironment,andthelargechangeinsocialsurroundingsarejustafewofthepotentialsourcesofstressforacollegestudent7.Collegestudents experience high stress at predictable timeseachsemesterduetoacademiccommitments,financialpressures, and lack of timemanagement skills. Stressresults from the interaction between stressors and theindividual’s perception and reaction to those stressors.Other potential sources of stress for college studentsinclude excessive homework, unclear assignments,anduncomfortableclassrooms.Inadditiontoacademicrequirements, relationswithfacultymembersand timepressuresmayalsobesourcesofstress8.
nEED FoR THE STuDy
According to Mental HealthAmerica’s estimates,20% of teens are clinically depressed, and the realtragedy lies with how their parents and teachersapproach the subject. Because so many dismiss thesymptomsofdepressionasmereadolescentadjustments,a disconcerting number of these teens go without thetreatment they need to enjoy a healthy, happy life.Obviously, depression stems from numerous factorsbeyond just heightened academic pressures. But theycertainly render alreadypainful situations evenworse,regardlessofwhetherornottheyexistastherootcause.
Mypurposeforconductingthisstudywastoexploretheundergraduatestudents’perceptionofmajorsourcesof academic stress. I wanted to know how studentsperceiveacademicstressandhowtheycopewithiton
dailybasis,astheyarestrugglingtoreduceandcontrolthenegativeeffectson theirhealthand theiracademicperformance. In my opinion, it is very important forundergraduate students to learn how to manage theacademic stress, even if it cannot be eliminated. Inthe mtvAssociated Press survey for 2009, more thanhalf of students (60%) reported that severe stressinterferedwiththeirabilitytocompletetheirschoolworkmoreoften thanonce,and that thisstatistic reflectsanincrease from2008.All India figures show that 8,046students ended their lives last year.Maharashtra,with1,191, reported the highest number of students takingtheextremestep.KarnatakacamefifthwhileNagalandreportedthelowest,withnumberofvictimsrunninginsingledigitsforthepastthreeyears
The Spring 2013 edition of the National CollegeHealth Assessment, where the average age of thosesurveywas21years,reportedthatalmosthalf(46.3%)of all undergraduate students surveyed felt trauma oroverwhelmedinregardtotheiracademicresponsibilities.Almost half of students surveyed reported they havemorethanaverageorextremestress.
Problem statement: “Astudytoassesstheeffectivenessof Self Instructional Module regarding reducingacademic stress among students ofB.SC Nursing inselectedcollegesatJaipurcity”.
objectives of the study
1.To assess the level of academic stress amongstudentsofB.Sc.Nursing.
2.To assess the effectiveness of self-instructionalmoduleinreducingacademicstressamongB.Sc.NursingStudents.
3.Tofindouttheassociationbetweenpost-teststressscoresandselecteddemographicvariables
Hypothesis
H1: There will be a difference between pre-test andpost-teststressscoresofstudents.
H2:Therewillbeanassociationbetweenpost-teststressscoreofBachelorofScience inNursingstudentswiththeselecteddemographicvariables.
Assumptions: Thestudyassumesthat
1.All the fresher students will have some sort ofacademicstress.
2.TheknowledgeofacademicstresswillbedifferentamongstudentsofB.Sc.(N)1styearaccordingtoselecteddemographicvariables.
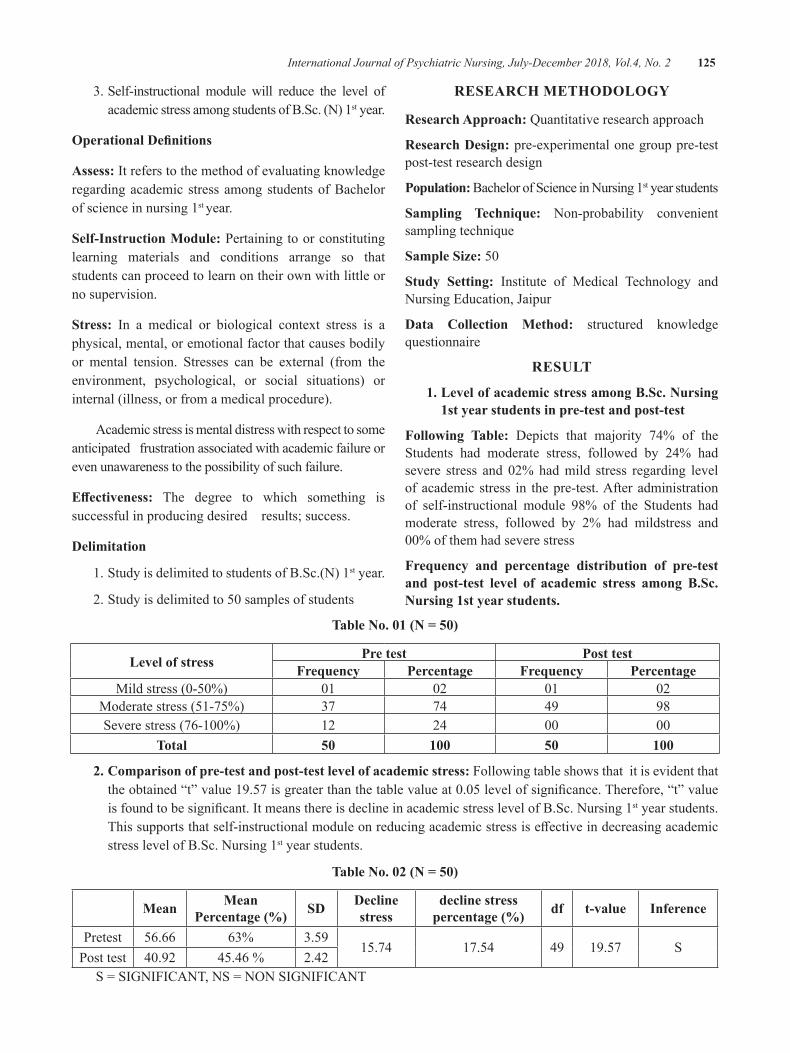
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 125
3.Self-instructional module will reduce the level ofacademicstressamongstudentsofB.Sc.(N)1styear.
operational Definitions
Assess:ItreferstothemethodofevaluatingknowledgeregardingacademicstressamongstudentsofBachelorofscienceinnursing1styear.
Self-Instruction Module:Pertainingtoorconstitutinglearning materials and conditions arrange so thatstudentscanproceedtolearnontheirownwithlittleornosupervision.
Stress: In a medical or biological context stress is aphysical,mental,oremotionalfactorthatcausesbodilyor mental tension. Stresses can be external (from theenvironment, psychological, or social situations) orinternal(illness,orfromamedicalprocedure).
Academicstressismentaldistresswithrespecttosomeanticipatedfrustrationassociatedwithacademicfailureorevenunawarenesstothepossibilityofsuchfailure.
Effectiveness: The degree to which something issuccessfulinproducingdesiredresults;success.
Delimitation
1.StudyisdelimitedtostudentsofB.Sc.(N)1styear.
2.Studyisdelimitedto50samplesofstudents
RESEARCH METHoDoLogy
Research Approach: Quantitativeresearchapproach
Research Design: pre-experimentalonegrouppre-testpost-testresearchdesign
Population: BachelorofScienceinNursing1styearstudents
Sampling Technique: Non-probability convenientsamplingtechnique
Sample Size: 50
Study Setting: Institute of Medical Technology andNursingEducation,Jaipur
Data Collection Method: structured knowledgequestionnaire
RESuLT
1. Level of academic stress among b.Sc. nursing 1st year students in pre-test and post-test
Following Table: depicts that majority 74% of theStudents had moderate stress, followed by 24% hadsevere stress and 02%hadmild stress regarding levelofacademicstress in thepre-test.Afteradministrationof self-instructional module 98% of the Students hadmoderate stress, followed by 2% had mildstress and00%ofthemhadseverestress
Frequency and percentage distribution of pre-test and post-test level of academic stress among b.Sc. nursing 1st year students.
Table no. 01 (n = 50)
Level of stress Pre test Post testFrequency Percentage Frequency Percentage
Mildstress(0-50%) 01 02 01 02Moderatestress(51-75%) 37 74 49 98Severestress(76-100%) 12 24 00 00
Total 50 100 50 100
2. Comparison of pre-test and post-test level of academic stress: Followingtableshowsthatitisevidentthattheobtained“t”value19.57isgreaterthanthetablevalueat0.05levelofsignificance.Therefore,“t”valueisfoundtobesignificant.ItmeansthereisdeclineinacademicstresslevelofB.Sc.Nursing1styearstudents.Thissupportsthatself-instructionalmoduleonreducingacademicstressiseffectiveindecreasingacademicstresslevelofB.Sc.Nursing1styearstudents.
Table no. 02 (n = 50)
Mean Mean Percentage (%) SD Decline
stressdecline stress
percentage (%) df t-value Inference
Pretest 56.66 63% 3.5915.74 17.54 49 19.57 S
Posttest 40.92 45.46% 2.42S=SIGNIFICANT,NS=NONSIGNIFICANT
126 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
DISCuSSIon
1. Demographic characteristics of students. z Inthestudymajority92%ofthestudentswereagedbetween17-20years&06%ofthemagedbetween21-24years,02%ofthemwereagedabove25-29yearsand0%ofthemaged29andabove.
z Inthestudymajority92%oftheStudentsaremales,08%arefemales.
z Themajority42%ofthestudentsbelongstoruralarea and32%of thembelongs to urban area andremaining26%belongstosemi-urbanarea.
z Themajority56%ofthestudentsarefromnuclearfamily, 40% from joint family & 04% fromextendedfamily.
z Themajority92%ofthestudentsbelongstomiddleclassand06%belongstopoorclassand02%fromupperclass.
2. Level of academic stress among b.Sc. nursing 1st year students in pre-test and post-test: Themajority74%oftheStudentshadmoderatestress,followedby24%hadseverestressand02%hadmildstressregardinglevelofacademicstressinthepre-test.Afteradministrationofself-instructionalmodule98%oftheStudentshadmoderatestress,followedby2%hadmildstressand00%ofthemhadseverestress.
3. Comparison of pre-test and post-test level of academic stress: The obtained “t” value 19.57is greater than the table value at 0.05 level ofsignificance. Therefore, “t” value is found to besignificant. Itmeans there isdecline in academicstresslevelofB.Sc.Nursing1styearstudents.Thissupportsthatself-instructionalmoduleonreducingacademicstressiseffectiveindecreasingacademicstresslevelofBscNursing1styearstudents.
4. Association of post-test stress scores of b.Sc. nursing students with selected demographic variables:χ2valuecomputedbetween the levelof academic stress and selected demographicvariables.Variables such as age, area of living,type of family, income group of family, familyincome,educationoffather,educationofmotherwere significant at 0.05 level.Variables such asgenderwerenotsignificantat0.05levelThereforethehypothesisstatedtherewillbeanassociationbetween pre-test stress score of Bachelor ofScience in Nursing students with the selecteddemographicvariablesisaccepted.
RECoMMEnDATIonSOnthebasisoffinding,thestudyrecommendations
areasfollows
z ASimilarstudycanbereplicatedonlargesampleinordertogeneralizethefindings.
z An experimental study can be conducted withcontrol group for the effective comparison of theresults.
z Astudycanbeconductedtoevaluatetheefficiencyof teaching strategy like lesson plan shows onreducingacademicstressamongstudents.
ConCLuSIon
Theoverallfindingsofthestudyrevealedthattherewas overall mean knowledge score obtained by thestudentswas46.13andwithstandarddeviation2.42andthemeanpercentagewas51.25%,Sothisindicatesthatlevelofacademicstressisreducedamongstudents.
Source of Funding:SelfFunding
Conflict of Interest:NIL
Ethical Clearance: Ethical ClearanceAlready TakenFromMTINCONJaipur.
REFEREnCES 1.R.Sreevani.A guide to Mental Health and
Psychiatric Nursing.2nd edition. Jaypee BrotherMedicalpublishers;2008.
2.I. clement. Text book on communication andeducational technology. 1st edition EMMESSmedicalpublishers2008.
3.Articles related to mental disorders, the freeencyclopedia.Available from: URL:http://www.en.wikipedia.org
4.BhatiaMS.AConcisedTextbookonPsychiatricNursing. First Edition. CBS Publishers. Newdelhi;1997.
5.Ahuja.N.AShortTextBookofPsychiatry.Thirdedition. Jaypee Brothers. Medical publishers.Newdelhi;1999.
6.Shields N: Stress, active coping, and academicperformanceamongpersistingandnonpersistingstudents. Journal of Applied BiobehavioralResearch2001,6(2):65-81.
7.Tamina Toray: Coping in Women CollegeStudents:TheInfluenceofExperience.JournalofCollegeStudentdevelopment;1998.
8.MisraR,McKeanM:Collegestudents’academicstress and its relation to their anxiety, timemanagement, and leisure satisfaction.AmericanJournalofHealthStudies2000,16(1):41-51.
A Study to Determine the Sources, Effects and Causes for Substance use Disorders and to Develop an Informational booklet
on Prevention and Management of Substance use Disorders in Selected Drug De-Addiction and Rehabilitation Centers of nepal
Rupshikha Mishra1, bindi Shauju2, Veena Sharma3
1Lecturer, Kathmandu Medical College, Kathmandu, Nepal; 2Assistant Professor, 3Associate Professor, Rufaida College of Nursing, Jamia Hamdard, New Delhi
AbSTRACT
Themainobjectivesofthestudyweretodeterminesources,causesandeffectsofsubstanceusedisorders,todevelopanddisseminateaninformationalbookletonpreventionandmanagementofsubstanceusedisordersforthepatientsandtoseekrelationshipbetweeneffectsofsubstanceusedisordersandselecteddemographicvariables,suchas,age,maritalstatus,familyincome,occupation,educationalqualification.
AconceptualmodelofsubstanceabusebyClarkHWwasusedastheconceptualframework.Adescriptivesurvey approach with cross-sectional design was used to achieve the objectives of the study.A semistructuredquestionnaire,toassessthesources,causesandeffectsofsubstanceusedisorderwasdeveloped.ThetoolwasvalidatedbytheexpertsfromthefieldofPsychiatricNursing,PsychologyandPsychiatry.ThereliabilityofthetoolwasestablishedbyusingCronbach’sAlphaandthereliabilitycoefficientwas0.87.ThestudywasconductedatTheRichmondFellowship,Chobar,Kathmandu,Nepal.Purposivesamplingtechniquewasemployedtoselect60patientsattendingdrugde-addictionandrehabilitationcentres.
data gathered was analyzed and interpreted using both descriptive and inferential statistics. The studyshowedthatmostofthestudysubjectswereintheagegroupof15-25yearsandunmarried,mostofthestudysubjectsconsumedalcoholasaddictivesubstance,mostofthepatientsprocuredsubstancesfromfriendsandusedtoconsumeattheirhome.Mostofthestudysubjectsconsumedsubstancesforpleasureandalsoastheyfeltlonely.Aspertheseverity,75%ofthestudysubjectshadmoreharmfuleffectsofthesubstanceusedisorders.Amongthecausesofsubstanceusedisorders,psychologicalcausesrankedthehighest.Therewasnosignificantrelationshipbetweentheeffectofsubstanceusedisordersandtheselectedvariables.
Keywords: Substance abuse, effectiveness, sources, effect, causes, prevention, management.
InTRoDuCTIonThecauseofworldwideconsumptionofHasis,Opium,WineandTobaccoliesnotinthetastenor in anypleasure, recreationormirth.Theyafford but simply inman’s need to hide fromhimselfthedemandsofconscience”
−Tolstoy
People abuse substances suchas alcohol, tobacco,and other drugs for varied and complicated reasons,but it is clear that our society pays a significant cost.Thetollforthisabusecanbeseeninourhospitalsandemergencydepartmentsboth throughdirectdamage to
healthbysubstanceabuseanditslinktophysicaltrauma.Jailstallydailythestrongconnectionbetweencrimeanddrugdependenceandabuse.Althoughuseofsomedrugssuchascocainehasdeclinedinrecentyears,useofotherdrugssuchasheroinand«clubdrugs”hasincreased.1
Substance use is very rampant in developingcountrieslikeNepal.GovernmentofNepalhasincludedcontrol of “substance abuse including alcohol andtobacco”,asoneofthemaininterventionsinEssentialHealthCareServices(EHCS).2
According to World Health Organization (WHO)and theAmerican PsychiatricAssociation (APA), drug
DOI Number: 10.5958/2395-180X.2018.00031.2
128 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
abuseistheillicitconsumptionofnaturallyoccurringorpharmaceuticalsubstancesforthepurposeofchangingtheway,inwhichapersonfeels,thinksorbehaves,withoutunderstandingortakingintoconsiderationthedamaging,physicalandmentalsideeffectsthatarecaused.3
background of the Study:InNepal,thedrinkingcultureprobablyfitsintothesecondmodelwhereabstinenceandpermissivenesstowardsdrinkingco-exists.AlcoholuseiscloselyrelatedwiththecastesystemofNepal.Manypeople foster theuseofalcoholbeverageaccording totheirsocial,religiousandculturaltraditions.Thepeopleof Mangoloid origin used alcohol for the purpose ofritualsandonreligiousoccasions,aswellasforsocialdrinkingduringfestivalsandspecialoccasionslikebirthanddeath.Ontheotherhand,theHindusociety,basedonthecodeofManu,prohibitedalcoholuseamongthehighercasteofBrahminandChhetri.4
Nepalisamulti-ethnic,multicultural,multireligiousand multi-linguistic society with a rich repertoire ofcustomsandtraditions.Itisalsoageographicallydiversecountryandacasteboundsociety.Inthemiddleperiod,Newars adoptedand followed theTrantrism-a sectofHindusim which emphasized Matsya (fish), Mamsha(meat) and Madira (alcohol) among food items evenduringtherituals.TheNewarsmadevarietyofalcoholicbeveragesfromrice,fruitsandmillets.4
need for the Study: InNepal,drugdelinquencyarisesduetoparentrelatedcauses,theabstenceofappropriatecontrol reactive patterns ofmisbehavior and a lack ofinterpersonalrelationshipandcommunication.Inordertoavoidpsychological terror inafamily,effectiveandcontinuous guidance care and counseling should beprovidedtothefamilyandpeopleeffectedbytheproblemofdrugabuse.Especially,youngNepaleseaddictscomefromdifferentstrataofsociety.Researchfindingsshowthey come from upper income group. They are moreseriouslyinvolvedindrugaddiction.Thereareprimaryfour ways of drug control: controlling consumption,production,processingandtrafficking.Psychologicallytheissueofdrugcontrolisverycomplex.Itcanbesolvedbyamultipleapproachwiththeeffortofgovernmentalorganization, NGOs and individuals. On the whole,researchhas shown that anykindofdrug treatment iseffectivewhentheyareavailabletodrugusersatatimewhenheorshevoluntarilyseekshelp.5
METHoDoLogy
The purpose of the present study conducted atselecteddrugde-addictionandrehabilitationcentresofNepal,wastoaccomplishresearchobjectivesthatwere:
1.To determine sources, causes and effects ofsubstanceusedisorders.
2.To develop and disseminate an informationalbooklet on prevention and management ofsubstanceusedisordersforthepatients.
3.Toseekrelationshipbetweeneffectofsubstanceusedisorderandselecteddemographicvariables,such as, age, marital status, family income,occupation,educationalqualification.
Research Approach: Asthepresentstudyisaimedtotheeffectsofsubstanceusedisordersamongthepatientsattending de-addiction and rehabilitation centres aquantitative(descriptivesurvey)approachwasfoundtobeappropriateforthestudy.
Setting of the Study: Permissionwasobtainedfromtheadministrative authority to conduct a pilot study fromde-addiction center of Govindapuri, New-delhi, andfinal study from drug de-addiction and rehabilitationcentres ofTheRichmondFellowshipNepal,Chobhar,Kathmandu,Nepal.
Criteria for Selecting Sample
The criteria for selecting sample were:
z Patients at the selected de-addiction andrehabilitation centres who were willing andavailabletoparticipateinthestudy.
z Patients who are able to understand English orNepali.
z Patientswhowerepolydrugusers,namelyalcohol,narcoticsandcannabis.
Exclusion criteria:
z Newly admitted patients at the selected drug de-addiction and rehabilitation centers of RichmondFellowship,Chobhar,Kathmandu,Nepal.
DATA CoLLECTIon TooLS AnD TECHnIQuES
Basedontheconceptualframeworkandobjectivesof the study, the following tool was developed togeneratedata:
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 129
Semi-structuredquestionnairetoexplorethesource,causesandeffectsofsubstanceusedisorders.
Development of Tool: In order to develop the semi-structured questionnaire to assess sources, causes andeffectsofsubstanceusedisorders,followingstepsweretaken:
z Extensivereviewofliteraturetodeveloptheneeditemsandscoringtechniqueforthetool.
z Formulationoftheitems.
z Categorizationoftheitemsunderdifferentsection(personal data, sources, causes and effects ofsubstanceusedisorders)
Preparation of the blue print of differentquestionnaires,scoringandinterpretationofthescores.
Description of the Tool: The toolwas divided into 4sections.
Section 1:Consistedofquestionsrelatedtodemographicdata such as age, gender, marital status, religion,education, father’s occupation, mother’s occupation,educationalstatusoffather,educationalstatusofmother,monthlyincomeofthefamilyandtheoccupation.
Section 2: Consistedoffivequestionsrelatedtosourcesofsubstanceusedisorders.
Section 3: Consistedofonequestionrelated tocausesof substance use disorders in various aspects such asbiological,psychological,social,culturalandreligious.
Section 4: Consistedofthirtyfourquestionsrelatedtotheeffectsofthesubstanceusedisordersinthevariousaspects such as biological, social, psychological,spiritualandfinancial.
Development of Information booklet: Informationalbooklet was prepared on prevention and managementof substance use disorders through review of researchandnon-researchliterature,discussionwithpeergroupand experts opinion. Certain aspects were consideredwhilepreparingthebookletlikesimplicityoflanguage,illustration,handy,self-pacingandindependentlearning.ThematerialwasdevelopedinsimpleEnglishlanguagewith help of language experts in order to facilitateindependent/selflearning.ThebookletwastranslatedinHindiforpilotstudyandinNepaliforthemainstudy.
The Steps Taken in Developing the Information booklet:
z developmentofCriteriaRatingScale.
z PreparationofInformationBooklet.
z ContentvalidityofInformationBooklet
z PreparationoffinaldraftofInformationBooklet
Plan For Data Analysis: Plan for data analysis waschalked out by employing descriptive and inferentialstatistics.Thefollowingplansofanalysisweredevelopedwithexperts’opinions:-
z Computation of frequency and percentagedistributiontodescribethesamplecharacteristics.
z Frequency and percentage distribution of thesubjects by the sources, causes and effects ofsubstanceusedisorders.
z Mean,median,mode, standard deviation, possiblerangeofscoresandrangeofobtainedscoresofeffectofthesubstanceuseonthestudysubjectsattendingdrugde-addictionandrehabilitationcentres.
z FrequencyandPercentageofstudysubjectsbasedon severity of the Effects of the Substance Usedisorders.
z Areawiseanalysisofeffectsofthesubstanceuseinstudysubjects,meanmodifiedmeanandrankorderofdifferentareasofeffectsofsubstanceuse.
z ComputationofFisher testvalues toestablish therelationship between selected factors and effectscoresofsubstanceusedisorders.
AnALySIS AnD InTERPRETATIon
Section 1:Consistedofquestionsrelatedtodemographicdata such as age, gender, marital status, religion,education, father’s occupation, mother’s occupation,educationalstatusoffather,educationalstatusofmother,monthlyincomeofthefamilyandtheoccupation.
Table no. 1: Frequency and Percentage Distribution of the Study Subjects Attending Drug De-addiction and Rehabilitation Centres by their Demographic
Characteristics (Age, Sex and Marital Status)n = 60
S. no.
Demographic Characteristics Frequency Percentage
(%)1. Age
15–25years 25 41.726–35years 20 33.336–45years 9 15
Morethan46years 6 10
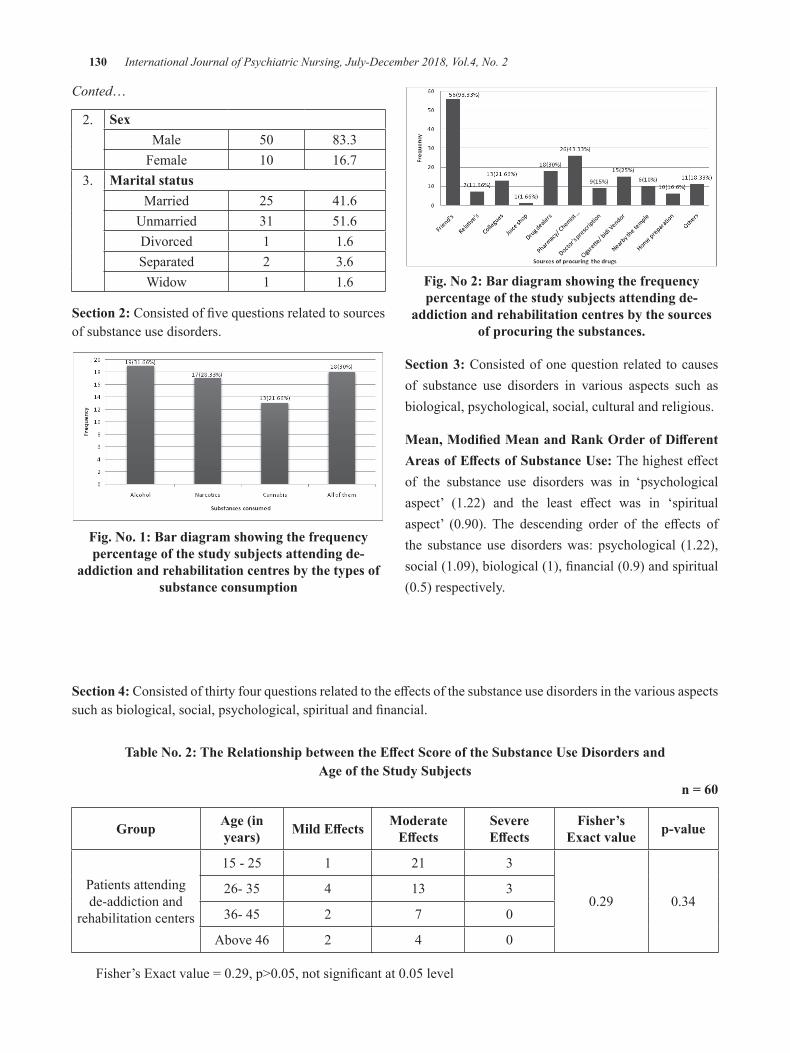
130 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
Conted…
2. SexMale 50 83.3Female 10 16.7
3. Marital statusMarried 25 41.6Unmarried 31 51.6divorced 1 1.6Separated 2 3.6Widow 1 1.6
Section 2:Consistedoffivequestionsrelatedtosourcesofsubstanceusedisorders.
Fig. no. 1: bar diagram showing the frequency percentage of the study subjects attending de-
addiction and rehabilitation centres by the types of substance consumption
Fig. no 2: bar diagram showing the frequency percentage of the study subjects attending de-
addiction and rehabilitation centres by the sources of procuring the substances.
Section 3: Consistedofonequestionrelated tocausesof substance use disorders in various aspects such asbiological,psychological,social,culturalandreligious.
Mean, Modified Mean and Rank order of Different Areas of Effects of Substance use: Thehighesteffectof the substance use disorders was in ‘psychologicalaspect’ (1.22) and the least effect was in ‘spiritualaspect’ (0.90). The descending order of the effects ofthe substance use disorderswas: psychological (1.22),social(1.09),biological(1),financial(0.9)andspiritual(0.5)respectively.
Section 4: Consistedofthirtyfourquestionsrelatedtotheeffectsofthesubstanceusedisordersinthevariousaspectssuchasbiological,social,psychological,spiritualandfinancial.
Table no. 2: The Relationship between the Effect Score of the Substance use Disorders and Age of the Study Subjects
n = 60
group Age (in years) Mild Effects Moderate
EffectsSevere Effects
Fisher’s Exact value p-value
Patientsattendingde-addictionand
rehabilitationcenters
15-25 1 21 3
0.29 0.3426-35 4 13 3
36-45 2 7 0
Above46 2 4 0
Fisher’sExactvalue=0.29,p>0.05,notsignificantat0.05level
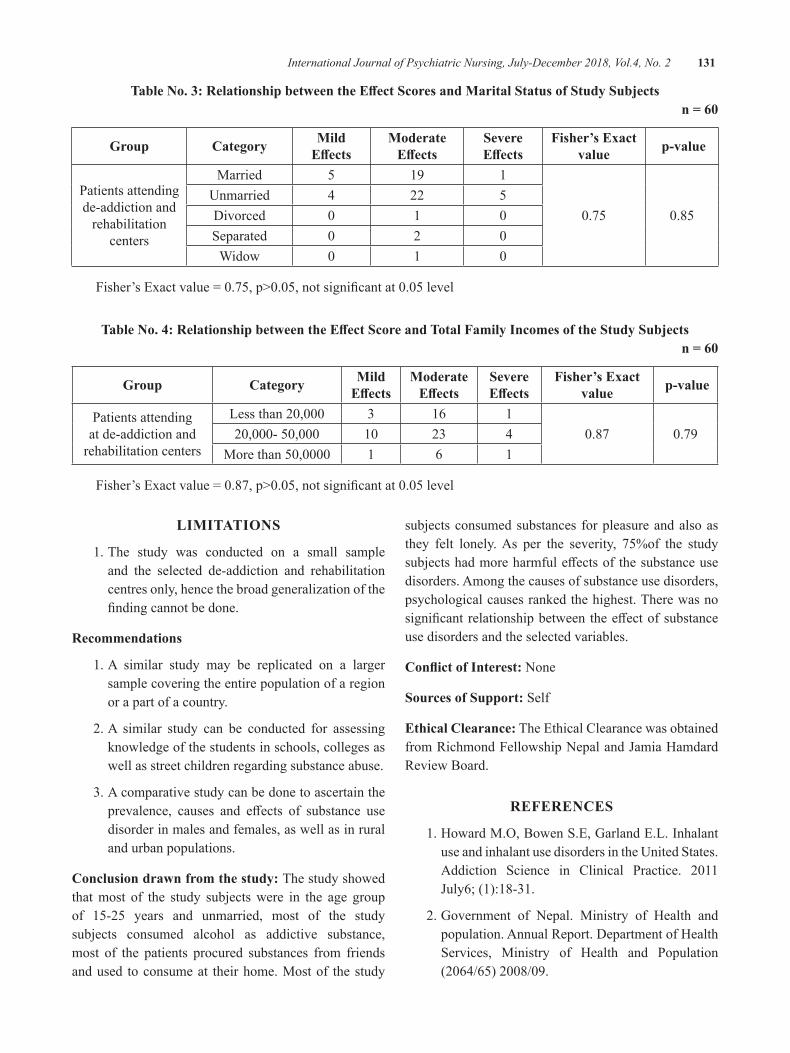
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 131
Table no. 3: Relationship between the Effect Scores and Marital Status of Study Subjectsn = 60
group Category Mild Effects
Moderate Effects
Severe Effects
Fisher’s Exact value p-value
Patientsattendingde-addictionandrehabilitation
centers
Married 5 19 1
0.75 0.85Unmarried 4 22 5divorced 0 1 0Separated 0 2 0Widow 0 1 0
Fisher’sExactvalue=0.75,p>0.05,notsignificantat0.05level
Table no. 4: Relationship between the Effect Score and Total Family Incomes of the Study Subjectsn = 60
group Category Mild Effects
Moderate Effects
Severe Effects
Fisher’s Exact value p-value
Patientsattendingatde-addictionandrehabilitationcenters
Lessthan20,000 3 16 10.87 0.7920,000-50,000 10 23 4
Morethan50,0000 1 6 1
Fisher’sExactvalue=0.87,p>0.05,notsignificantat0.05level
LIMITATIonS
1.The study was conducted on a small sampleand the selected de-addiction and rehabilitationcentresonly,hencethebroadgeneralizationofthefindingcannotbedone.
Recommendations
1.A similar study may be replicated on a largersamplecoveringtheentirepopulationofaregionorapartofacountry.
2.A similar study can be conducted for assessingknowledgeofthestudentsinschools,collegesaswellasstreetchildrenregardingsubstanceabuse.
3.Acomparativestudycanbedonetoascertaintheprevalence, causes and effects of substance usedisorderinmalesandfemales,aswellasinruralandurbanpopulations.
Conclusion drawn from the study: Thestudyshowedthatmost of the study subjectswere in the age groupof 15-25 years and unmarried, most of the studysubjects consumed alcohol as addictive substance,most of the patients procured substances from friendsandused toconsumeat theirhome.Mostof thestudy
subjectsconsumedsubstances forpleasureandalsoasthey felt lonely.As per the severity, 75%of the studysubjectshadmoreharmfuleffectsofthesubstanceusedisorders.Amongthecausesofsubstanceusedisorders,psychologicalcausesrankedthehighest.Therewasnosignificantrelationshipbetweentheeffectofsubstanceusedisordersandtheselectedvariables.
Conflict of Interest:None
Sources of Support:Self
Ethical Clearance:TheEthicalClearancewasobtainedfromRichmondFellowshipNepalandJamiaHamdardReviewBoard.
REFEREnCES
1.HowardM.O,BowenS.E,GarlandE.L.InhalantuseandinhalantusedisordersintheUnitedStates.Addiction Science in Clinical Practice. 2011July6;(1):18-31.
2.Government of Nepal. Ministry of Health andpopulation.AnnualReport.departmentofHealthServices, Ministry of Health and Population(2064/65)2008/09.

132 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
3.ChakrabortyN.Effectivenessofcontinuingnursingeducation programme on substance use disorder.[M.Sc.Nursing].Mangalore.2001Feb;56.
4.dhital R, Subedi G, Gurung YB, Hamal P.Alcohol and drug use in Nepal with reference
to children.Nepal:CWIN (ChildrenWorkers inNepalConcernedCentre.2001.
5.dr. Upadhyay Prasad N. drug Abuse AmongyoungstersinNepal.TheKathmanduPost.2000Nov2:Health:13.
Effect of Video Assisted Teaching (VAT) on Improving Primary Teacher’s Knowledge Regarding Learning
Disabilities: An Indian Perspective
Amrinder Kaur1, betcy Mathew2, Jithin Thomas Parel3, bince Varghese4, Linsu Thomas5
1M.Sc. Nursing, 2Professor & HOD, Department of Psychiatric Nursing, Adesh University, Bathinda, Punjab; 3HOD & Assistant Professor, Department of Psychiatric Nursing, JIET College of Nursing, Jodhpur, Rajasthan; 4Lecturer, Hind College of Nursing, Lucknow, Uttar Pradesh; 5Nursing Officer,
All India Institute of Medical sciences (AIIMS), Jodhpur, Rajasthan, India
AbSTRACT
objectives:Formallearninginclassroomisapartandparcelofcurrenteducationalsystem.Teachersareinauniquepositiontoidentifythechildren’slacunaesinthedevelopmentallearningprocesses.CurrentStudywasdonetoassessthepreinterventionalknowledgeofprimaryschoolteachersregardingselectedlearningdisabilitiesamongprimaryschoolchildren,evaluatetheeffectofVideoAssistedTeaching(VAT)andtofindtheassociationbetweenknowledgescoresandselectedsocio-demographicvariables.
Method:Pre-experimentalonegroupPretest-posttestdesignwasusedamong60primaryschoolteachersselected through convenient sampling. Researcher developed structured questionnairewas administeredafterobtaininginformedconsent.Reliabilityandvaliditywereestablished.Onehourgroupsession-Videoassisted teaching(VAT)wasadministeredfor7daysconsecutivedays.Theoreticalandpracticalaspectsofselected learningdisabilitiesand itsmanagementmeasureswerediscussed.datawereassessedusingdescriptiveandinferentialstatistics.
Results:Majority33(55%)ofprimaryschool teachershadaverageknowledgefollowedby22(36.6%)hadpoorknowledgeand5(8.3%)hadgoodlevelofknowledgescore.Therewasastatisticallysignificantdifferenceintheknowledgescorebeforeandaftertheinterventionatp<0.01.
Conclusion: Teachers play a paramount role in identifying and managing learning disabilities.A wellinformedteachercantransformthesedisabilitiesintopossibilities,whichcanbringoutthebestinthechild.
Keywords: Learning disabilities; Knowledge; Primary school teachers; Video assisted teaching.
InTRoDuCTIon
“Learningdisability” is a generic term that refersto a heterogeneous group of disorders manifested bysignificant difficulties in the acquisition and use oflistening, speaking, reading, writing, reasoning ormathematical abilities.These disorders are intrinsic totheindividualandpresumedtobeduetoCentralNervousSystemdysfunction.Eventhoughalearningdisabilitymay occur concomitantly with other handicappingconditions(e.g.sensoryimpairment,mentalretardation,social and emotional disturbance) or environmentalinfluences (e.g. cultural differences, insufficiency orinappropriateinstruction,psychogenicfactors)anditisnotthedirectresultofthoseconditionsorinfluences.1
The term Learning disability was first coined bySamuel Kirk on 1963 to describe children who haveserious learning problems in schools but do not fallunder other categories of handicap.The term referredto a discrepancy between a child’s apparent capacityto learnandhisorher levelofachievement.Learningdisorderisalsotermedas‘specificlearningdisorder’or‘specificacademicskilldisorder’.2
Identification of disorder prior to school age isdifficult due to the instability of results obtained fromformaltestingprocedures.Teachersarethefirstpersonto notice that the child is not learning as expected.Shaw andMac (2005) stated that for students with alearning disorder, “Planning, monitoring, regulating
DOI Number: 10.5958/2395-180X.2018.00032.4

134 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
and scheduling” are difficult. These students requirecontinuous help to adapt learning situations. Selvin(2004)inananalysisofchallengingbehavioursamongpeople with learning disorder suggests that thesechildrenareamajorchallengeforteachersandmembersofcaringfamilies.3
Learning disability is usually identified amongpreschoolandprimaryschoolchildrenalthoughittendstoprogressintoadulthood.Often,thesechildrenmaytryvery hard to follow instructions, concentrate, and “begood” at homeand in school. Yet, despite this effort,heorsheisnotmasteringschooltasksandfallsbehind.4
APrevalencerateof20-33%ofpsychiatricdisordersinschoolchildrenhasbeenreportedinIndia.7%ofthemare developmental disorders. Among them, learningdisorder constitute 1 in 10 children. In India, ever7sectionof the school is likely to have around15-25%ofstudents,whoarenotabletomaintainasatisfactoryscholasticperformanceinschool.5
Similarlyastudywasconducteddalwaietal.(2010)assessed the awareness and sensitivity amongparents,teachers,schoolmanagementandcounsellorsregardinglearning disability in 35 Schools of Mumbai. Aboutthe conceptual understanding of learning disabilities.Amongthem,52%teachershadnoawareness,37%hadminimal awareness and 11% had adequate awareness.About aetiology 72% had no awareness, 14% hadminimal awareness and 14%had adequate awareness.Aboutthetypesoflearningdisabilities75%ofteacherswerenotaware.6
A quasi-experimental study was conducted bydaniel LT, Gupta S, Sagar R (2013) at NIMHANSBangalore, to assess the effectiveness of structuredteachingprogrammeonthelevelofknowledgeofteachertraineestowardslearningdisabilities.Thesampleswere32 teacher trainees where, pre-test knowledge meanscore was 17.75, which was improved to a post-testknowledge mean score of 28.78 significant at 0.001.The findings supports the administration of teachingprogrammes in improving knowledge of teachers onlearningdisabilities.7
The Indian educational perspective students areacclimatized to a rigid structured curriculum. Theyare owe to a plethora of academic assignments andexamination. due to inadequate knowledge and
awareness,theteachersseldomgiveindividualattentionfor children with disabilities. Where the existing oremerging learning difficulties are not identifyingpromptly, and the less academic performances furtherdemotivatesthechild.Misunderstandingofthedisabilityand negative reinforcement from teachers and parentscaneventuallyleadtopooracademicoutputsandschooldropouts.Inthiscontext,astructuredteachingmodulecan endorse the insight of teachers regarding learningdisabilities especially in primary level. In the currentresearch,avideoassisted teachingmoduleonselectedlearning disabilities was developed to evaluate theeffectivenessamongprimaryschoolteachers.
Thestudyaimsto assesstheknowledgeofprimaryschool teachers regarding selected learningdisabilitiesamong primary school children by conducting pre-test, to assess the effectiveness of structured teachingprogramme on knowledge of primary school teachersregarding selected learningdisabilities amongprimaryschool children by conducting post-test and to findthe association between knowledge scores of primaryschool teachers regarding selected learningdisabilitiesamongprimaryschoolchildrenwiththeirselectedsocio-demographicvariables.
METHoD
The researchwas conducted inonegrouppre-testandpost-testdesignamong60primaryschoolteachersfrom selected Primary schools of Punjab, India usingconvenientsamplingtechnique.Astructuredknowledgequestionnairewas developed by the researcher,wherethecontentvalidityof the toolwasevaluatedby the5experts. reliabilitywasevaluatedbysplithalfmethodby using Karl Pearson correlation coefficient and thescoreobtainedwas0.83.PilotstudywasconductedinaselectedSchoolinPunjab.Thestudywasapprovedbythe Institutional Ethical Committee. Informed consentwasobtainedand theconfidentialityandanonymityofthesubjectsweremaintained.
Pre-testwasfollowedbytheadministrationofvideoassistedteachingsessions(1hourperday)forthenext7consecutivedays.After7daysapost-testwasconductedby using the same questionnaire, data collected wastabulatedandanalysedwiththehelpofdescriptiveandinferentialstatistics.
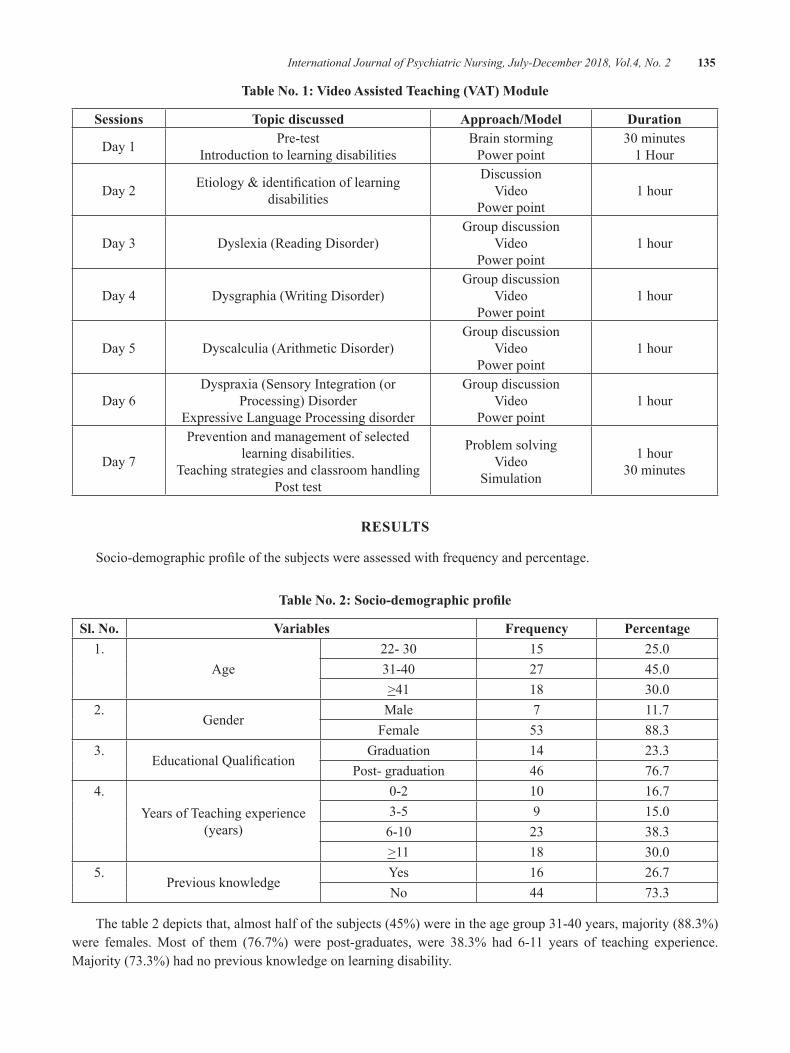
International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 135
Table no. 1: Video Assisted Teaching (VAT) Module
Sessions Topic discussed Approach/Model Duration
day1 Pre-testIntroductiontolearningdisabilities
BrainstormingPowerpoint
30minutes1Hour
day2 Etiology&identificationoflearningdisabilities
discussionVideo
Powerpoint1hour
day3 dyslexia(Readingdisorder)Groupdiscussion
VideoPowerpoint
1hour
day4 dysgraphia(Writingdisorder)Groupdiscussion
VideoPowerpoint
1hour
day5 dyscalculia(Arithmeticdisorder)Groupdiscussion
VideoPowerpoint
1hour
day6dyspraxia(SensoryIntegration(or
Processing)disorderExpressiveLanguageProcessingdisorder
GroupdiscussionVideo
Powerpoint1hour
day7
Preventionandmanagementofselectedlearningdisabilities.
TeachingstrategiesandclassroomhandlingPosttest
ProblemsolvingVideo
Simulation
1hour30minutes
RESuLTS
Socio-demographicprofileofthesubjectswereassessedwithfrequencyandpercentage.
Table no. 2: Socio-demographic profile
Sl. no. Variables Frequency Percentage1.
Age22-30 15 25.031-40 27 45.0>41 18 30.0
2.Gender
Male 7 11.7Female 53 88.3
3.EducationalQualification
Graduation 14 23.3Post-graduation 46 76.7
4.YearsofTeachingexperience
(years)
0-2 10 16.73-5 9 15.06-10 23 38.3>11 18 30.0
5.Previousknowledge
Yes 16 26.7No 44 73.3
Thetable2depictsthat,almosthalfofthesubjects(45%)wereintheagegroup31-40years,majority(88.3%)were females.Most of them (76.7%)were post-graduates, were 38.3% had 6-11 years of teaching experience.Majority(73.3%)hadnopreviousknowledgeonlearningdisability.
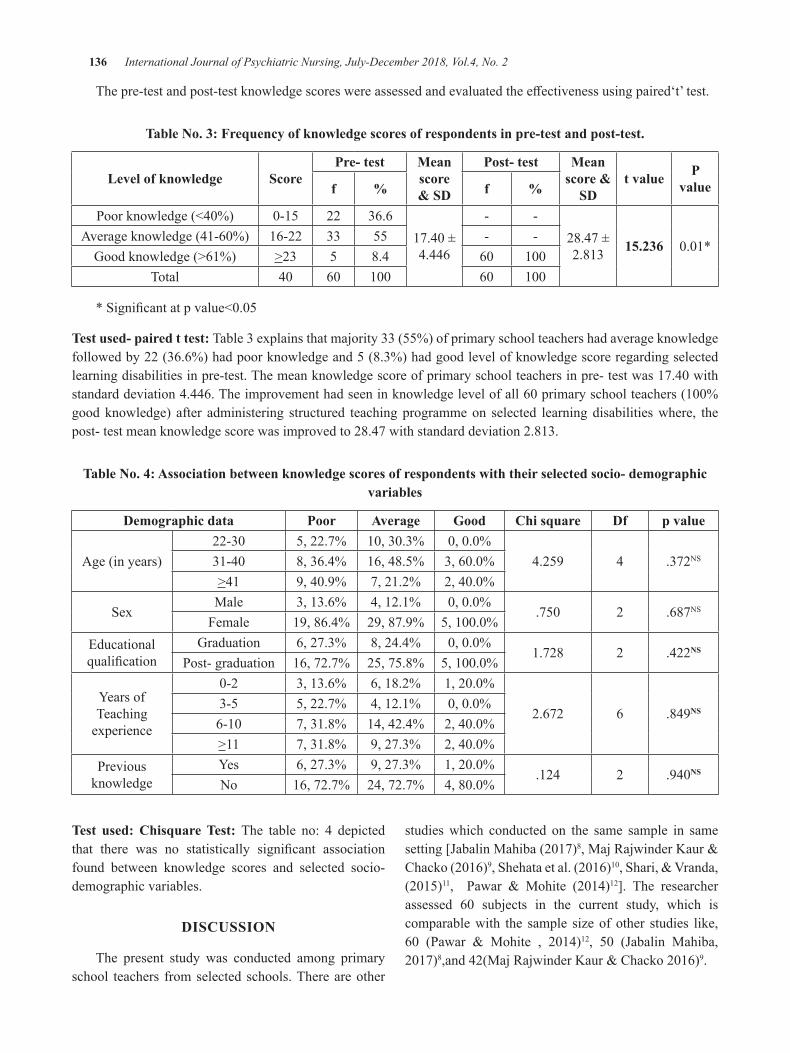
136 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
Thepre-testandpost-testknowledgescoreswereassessedandevaluatedtheeffectivenessusingpaired‘t’test.
Table no. 3: Frequency of knowledge scores of respondents in pre-test and post-test.
Level of knowledge ScorePre- test Mean
score & SD
Post- test Mean score &
SDt value P
valuef % f %
Poorknowledge(<40%) 0-15 22 36.617.40±4.446
- -28.47±2.813 15.236 0.01*
Averageknowledge(41-60%) 16-22 33 55 - -Goodknowledge(>61%) >23 5 8.4 60 100
Total 40 60 100 60 100
*Significantatpvalue<0.05
Test used- paired t test: Table3explainsthatmajority33(55%)ofprimaryschoolteachershadaverageknowledgefollowedby22(36.6%)hadpoorknowledgeand5(8.3%)hadgoodlevelofknowledgescoreregardingselectedlearningdisabilitiesinpre-test.Themeanknowledgescoreofprimaryschoolteachersinpre-testwas17.40withstandarddeviation4.446.Theimprovementhadseeninknowledgelevelofall60primaryschoolteachers(100%goodknowledge) after administering structured teachingprogrammeon selected learningdisabilitieswhere, thepost-testmeanknowledgescorewasimprovedto28.47withstandarddeviation2.813.
Table no. 4: Association between knowledge scores of respondents with their selected socio- demographic variables
Demographic data Poor Average good Chi square Df p value
Age(inyears)22-30 5,22.7% 10,30.3% 0,0.0%
4.259 4 .372NS31-40 8,36.4% 16,48.5% 3,60.0%>41 9,40.9% 7,21.2% 2,40.0%
SexMale 3,13.6% 4,12.1% 0,0.0%
.750 2 .687NSFemale 19,86.4% 29,87.9% 5,100.0%
Educationalqualification
Graduation 6,27.3% 8,24.4% 0,0.0%1.728 2 .422NS
Post-graduation 16,72.7% 25,75.8% 5,100.0%
YearsofTeachingexperience
0-2 3,13.6% 6,18.2% 1,20.0%
2.672 6 .849NS3-5 5,22.7% 4,12.1% 0,0.0%6-10 7,31.8% 14,42.4% 2,40.0%>11 7,31.8% 9,27.3% 2,40.0%
Previousknowledge
Yes 6,27.3% 9,27.3% 1,20.0%.124 2 .940NS
No 16,72.7% 24,72.7% 4,80.0%
Test used: Chisquare Test: The table no: 4 depictedthat there was no statistically significant associationfound between knowledge scores and selected socio-demographicvariables.
DISCuSSIon
The present study was conducted among primaryschool teachers fromselected schools.Thereareother
studieswhich conducted on the same sample in samesetting[JabalinMahiba(2017)8,MajRajwinderKaur&Chacko(2016)9,Shehataetal.(2016)10,Shari,&Vranda,(2015)11, Pawar & Mohite (2014)12]. The researcherassessed 60 subjects in the current study, which iscomparablewith the sample sizeofother studies like,60 (Pawar & Mohite , 2014)12, 50 (Jabalin Mahiba,2017)8,and42(MajRajwinderKaur&Chacko2016)9.

International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2 137
Theresearcherusedvideoassisted teachingas theintervention, where the other studies used differentinterventionalmodules like, self- instructionalmodule(Pawar&Mohite2014),structuredteachingprogramme[JabalinMahiba,(2017)8,MajRajwinderKaur&Chacko(2016)9,Shehataetal.(2016)0,AmitKadu,(2016)13].
Inpresentstudyduringthecomparisonofpre-testand post- test knowledge of primary school teachersregarding selected learning disabilities it was foundthatmeanknowledgescoreofpre- testwas17.40withstandarddeviation4.446andpost-testmeanknowledgescore28.47withstandarddeviation2.813.ThefindingsfromstudyconductedbyPawar&Mohite(2014)[Meanpre-test knowledge score 13.48.& posttest knowledge21.13]12supportedtheresults.Inmajorityofthestudiesteachersreportedwithlessoraveragepretestknowledge[Pawar & Mohite, (2014)12, Jabalin Mahiba, (2017)8,AmitKadu,(2016)13].
Inthecurrentstudy,thedifferencebetweenthepre-testandpost-testmeanknowledgescorewasstatisticallysignificantatp<0.001level,whichwaswellsupportedby,danielLT,GuptaS,SagarR(2013)atNIMHANS,Bangalore,theyfoundpre-testknowledgemeanscoreas17.75,andthepost-testknowledgemeanscoreas28.78,.The paired difference between the pre-test knowledgeandpost-testknowledgeshowedtheknowledgegainandthevaluewas11.3and‘p’valuewassignificantat0.001.This indicated that study was effective in improvingknowledgeofteachersonlearningdisabilities”.7
There was no significant association foundbetweenthepretestknowledgeandsocio-demographicvariables,whichwas contradictory to the study resultsbyAmitKadu,(2016)whofoundsignificantassociationfound between the knowledge and demographicvariables like age, educational qualification, andyearsofteachingexperiences.13
Implications of practice: Primary teachers are to bewell versed in identifying and screening childrenwithlearning disability. In service education and academictraining would be conducted for the primary schoolteachers to develop a favourable attitude, adequateknowledge and child handling skills in concern tolearning disability. Classroom management techniqueto handle these students coupled with easy learningtechniquesshouldbeprovidedtothechildren.
RECoMMEnDATIonS
Largescalestudycanbeconductedtoimprovethegeneralizability. The same study can be donewith anexperimentalresearchapproachwithacontrolgroup.Acomparativestudycanbeconductedonspecialeducationteachers&generaleducationteachers.Followuppost-testsassessmentcanbeplannedinfrequentintervalsinordertochecktheretentionofteacher’sknowledgeandapplicationofthestrategiesinclassrooms.
LIMITATIonS
Convenientsampletechniqueandsmallsamplesizeadoptedinthecurrentstudyreducedthegeneralizabilityof the findings. Extraneous variables like informationgivenbyotherhealthprofessional,massmedia,werenotunderthecontroloftheinvestigator.
ConCLuSIon
Teachershadinadequateknowledgebeforethevideoassisted teaching which was significantly improvedafter the intervention. This would definitely enhancethe competency of the teachers to screen andmanagethe studentwith learning disability.The added role ofprimary teachers to identify and manage the learningdisabilityisun-doubtfullyaccepted.
Source of Funding:Self
Conflict of Interest:Nil
REFEREnCES
1.The National Joint Committee for Learningdisabilities (NJCLd).Learning disabilitydefinition,(online),2017,Availablefrom:URL:http://www.ldonline.org/about/partners/njcld
2.dr.PanditRP.Factorsaffectinglearningdisabilityin Mathematics: A study of central region ofNepal. [Online]. 2006(Cited 2010); AvailablefromURL:http://www.nepjd.info
3.Sinesd,SelvinE.Theroleofcommunitynursesforpeoplewithlearningdisabilities:workingwithpeople who challenge. International Journal ofNursingStudies.2005
4.2012AmericanAcademyofChildandAdolescentPsychiatry Children with Learning disorders,
138 International Journal of Psychiatric Nursing, July-December 2018, Vol.4, No. 2
“FactsforFamilies,”No.16(08/13).Washington,d.C:APA;2000.
5.Shelton d. Child Mental Health Policy ofPeadiatric Nursing. 5th ed. Jaypee publications.Newdelhi2000.
6.dalwai S, Kanade d, Sane M, Chatterjee S.Awarenessandsensitivity-TheAlphaandOmegaoflearningdisability.2010Aug6
7.daniel LT, Gupta S, Sagar R. Effect ofeducational module on knowledge of primaryschool teachers regarding early symptoms ofchildhoodpsychiatricdisorders.IndianJPsycholMed. 2013 Oct; 35(4):368-72. Available from:http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3868088/
8.P. Jabalin Mahiba, effectiveness of structuredteaching programme among primary schoolteachers regarding learning disorder ofchildren,JournalofAdvancedNursingPractice.2017;4(1):1-3.
9.Maj Rajwinder Kaur, Lt ColMeena Chacko,AStudy toAssess the Effectiveness of StructuredTeaching Programme on Knowledge of SchoolTeachers Regarding Learning disordersAmongChildren in Selected Schools, InternationalJournalOfScientificResearch,Volume:5|Issue:11|November2016•ISSNNo2277–8179
10.AmalShehata,EnasMahrousAbdElAziz,EnamAbd El latif Farrag, Zeinab, Hassan Hassan,Effectiveness of StructuredTeaching Program onKnowledge,Attitude and Management StrategiesAmong Teachers of Primary School towardChildren with Attention deficit Hyperactivitydisorders,JournalofNursingandHealthScience(IOSR-JNHS),e-ISSN:2320–1959.p-ISSN:2320–1940Volume5,Issue6Ver.VII(Nov.-dec.2016),PP29-37,availablefrom:www.iosrjournals.org
11.ShariM1,MysoreNarasimhaVranda,Knowledgeof Primary School Teachers in IdentifyingChildrenwithLearningdisabilities, disability-CBR- Inclusive journal, (online)Vol. 26, No.3,2015;available from: http://dcidj.org/article/view/443
12.ShivajiH.Pawar,VaishaliR.Mohite,Effectivenessof Self Instructional Module on Knowledge ofPrimary School Teachers Regarding LearningdisordersAmongChildreninSelectedSchoolsatKaradCity, InternationalJournalofScienceandResearch,Volume3Issue7,July2014
13.Amit Kadu,A Study to assess the Effectivenessof Structured Teaching Program on KnowledgeregardingLearningdisabilityamongthePrimarySchool Teachers of Ahmednagar, Maharashtra,InternationalJournalofEducationandResearchinHealthSciences,July-September2016;2(3):34-35
64 International Journal of Psychiatric Nursing. January-June 2017. Vol. 3, No. 1
Call for Papers/ Article Submission
Article submission fee
• Please note that we charge manuscript handling charges for all publications.Charges can be enquired by sending mail.
• In cases of urgent publication required by author, he /she should write to editor for discretion.
• Fast tracking charges are applicable in urgent publication
• Please note that we charge only after article has been accepted for publication, not at the time of submission.
• Authors have right to withdraw article if they do not wish to pay the charges.
Article Submission Guidelines
Please submit paper in following format as far as applicable
1. Title.
2. Names of authors.
3. Your Affiliation (designations with college address).
4. Corresponding author- name, designations, address, E-mail id.
5. Abstract with key words.
6. Introduction or back ground.
7. Material and Methods.
8. Findings.
9. Discussion / Conclusion.
10. Conflict of Interest.
11. Source of Support.
12. References in Vancouver style.
13. Word limit 2500-3000 words, MSWORD Format, single file.
14. Please quote references in text by superscripting.
Our Contact Info:Institute of Medico-legal Publications
501, Manisha Building, 75-76, Nehru Place New Delhi -110019
www.imlp.inTel No 91-9971888542
CALL FOR SUBSCRIPTIONS
ABOUT THE JOURNAL International Journal of Psychiatric Nursing is a double blind peer reviewed international journal which has commencedits publication from January 2015. The journal is half yearly in frequency. The journal covers all aspects of Psychiatric Nursing. The journal has been assigned ISSN 2394-9465 (Print Version) & 2395 180X (Electronic Version).
Journal TitlePricing of Journals
Indian Foreign
International Journal of
Psychiatric Nursing
OnlyPrint+Online
Online
Only
OnlyPrint+Online
Online
Only
INR
5000
INR
7000
INR
3000
USD
250
USD
400
USD
200
NOTE FOR SUBSCRIBERS• Advance payment required by cheque/demand draft in the name of
“ Institute of Medico-Legal Publications“ payable at New Delhi.
• Cancellation not allowed except for duplicate payment.
• Claim must be made within six months from issue date.
• A free copy can be forwarded on request.
International Journal of Psychiatric NursingInstitute of Medico-legal Publications
501, Manisha Building, 75-76, Nehru Place New Delhi -110019
www.imlp.inTel No 91-9971888542
Send all payment to:
Institute of Medico-legal Publications 501, Manisha Building,
75-76, Nehru Place New Delhi -110019
www.imlp.inTel No 91-9971888542




![Kamau, C. (2014). Effects of shadowing and supervised on-the-job inductions on mental health nurses. Journal of Psychiatric and Mental Health Nursing, 21, 379–382. [FULL TEXT]](https://img.pdfslide.net/doc/110x75/63199472d4191f2f9307abaf/kamau-c-2014-effects-of-shadowing-and-supervised-on-the-job-inductions-on-mental.jpg)

























