Embed Size (px)
Citation preview

Intestinal microbiota and immune function in the pathogenesis of irritablebowel syndrome
Yehuda Ringel1 and Nitsan Maharshak1,2
1Division of Gastroenterology and Hepatology, University of North Carolina at Chapel Hill School of Medicine, Chapel Hill,North Carolina; and 2Department of Gastroenterology and Liver Diseases, Tel Aviv Sourasky Medical Center, Affiliated tothe Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
Submitted 16 May 2012; accepted in final form 17 July 2013
Ringel Y, Maharshak N. Intestinal microbiota and immune function in the pathogenesisof irritable bowel syndrome. Am J Physiol Gastrointest Liver Physiol 305: G529–G541,2013. First published July 25, 2013; doi:10.1152/ajpgi.00207.2012.—The pathophysiol-ogy of irritable bowel syndrome (IBS) is believed to involve alterations in thebrain-gut axis; however, the etiological triggers and mechanisms by which thesechanges lead to symptoms of IBS remain poorly understood. Although IBS is oftenconsidered a condition without an identified “organic” etiology, emerging evidencesuggests that alterations in the gastrointestinal microbiota and altered immunefunction may play a role in the pathogenesis of the disorder. These recent datasuggest a plausible model in which changes in the intestinal microbiota andactivation of the enteric immune system may impinge upon the brain-gut axis,causing the alterations in gastrointestinal function and the clinical symptomsobserved in patients with IBS. This review summarizes the current evidence foraltered intestinal microbiota and immune function in IBS. It discusses the potentialetiological role of these factors, suggests an updated conceptual model for thepathogenesis of the disorder, and identifies areas for future research.
inflammation; gastrointestinal; microbiota
IRRITABLE BOWEL SYNDROME (IBS) is the most common and beststudied condition of a larger group of functional gastrointesti-nal (GI) disorders. Functional GI disorders refer to the pres-ence of a variable combination of chronic or recurrent GIsymptoms not explained by structural or biochemical abnor-malities (130, 159). IBS is characterized by chronic or recur-ring abdominal pain or discomfort that is associated withaltered bowel habits (53, 99). The condition is often associatedwith other GI symptoms (e.g., bloating, distention, and gas),other functional GI disorders (e.g., functional dyspepsia), othernon-GI disorders (e.g., fibromyalgia, interstitial cystitis, mi-graine headache), and psychological disorders (e.g., depres-sion, anxiety, somatization) (96, 146, 167). Traditionally, IBShas been subtyped on the basis of the patient’s predominantsymptom/stool pattern (99). These subtypes include diarrheapredominant (IBS-D), constipation predominant (IBS-C), andmixed type (IBS-M), in which patients experience alternatingperiods of diarrhea and constipation. Unlike other conditionsthat can be associated with abdominal pain and abnormalbowel patterns such as inflammatory bowel diseases (IBD),IBS is not associated with any overt histopathology, structural,or biochemical abnormalities. IBS has been generally consid-ered to be caused by alterations in the brain-gut axis (thebidirectional communication network involving the entericnervous system, the autonomic nervous system, and the central
nervous system) (60, 108, 125), and the pathophysiologicalmechanisms behind this condition remain unclear. Tradition-ally, IBS is considered to be a multifactorial condition in whichmultiple environmental, genetic, physiological, and psychoso-cial factors contribute to the development of the disorderthrough direct or indirect effects on the brain-gut axis (65, 125,146). Bacterial infection, altered GI microbiota, dysregulatedimmune function, and low-grade inflammation are additionalfactors that have been gaining more interest as evidence sup-porting their contribution to the pathophysiology of IBS con-tinues to emerge. What remains unclear is how these factorsconverge to cause the observed abnormal GI function andfunctional GI symptoms reported in patients with IBS. Thisreview focuses on the potential roles of the intestinal microbi-ota and enteric immune function in the pathogenesis of IBS andwill discuss the evidence for how these factors may influencethe brain-gut axis, thus leading to the altered GI function andsymptoms of IBS.
THE INTESTINAL MICROBIOTA
Gastrointestinal bacteria play a critical role in the normalphysiological and immunological functions of the GI tract, andalterations in GI microbiota can lead to various GI and non-GIconditions (5, 145, 164). Specifically with regard to IBS,animal studies have shown that alterations in the GI microbiotacan lead to changes in GI functions, e.g., altered intestinalmotility and visceral hypersensitivity that are often observed inpatients with IBS and considered important factors in thepathophysiology of the disorder (12, 20, 25, 43, 80). Additionalevidence supporting the role of altered intestinal microbiota in
Address for reprint requests and other correspondence: Y. Ringel, Divisionof Gastroenterology and Hepatology, Univ. of North Carolina at Chapel HillSchool of Medicine, 4107 BioInformatics Bldg., CB# 7080, 130 Mason FarmRd., Chapel Hill, NC 27599-7080 (e-mail: [email protected]).
Am J Physiol Gastrointest Liver Physiol 305: G529–G541, 2013.First published July 25, 2013; doi:10.1152/ajpgi.00207.2012. Review
0193-1857/13 Copyright © 2013 the American Physiological Societyhttp://www.ajpgi.org G529

the pathogenesis of IBS has come from epidemiological ob-servations linking bacterial gastroenteritis and small intestinalbacterial overgrowth (SIBO) to IBS, microbiology studiesdescribing quantitative and qualitative alterations in the GImicrobiota in patients with IBS compared with healthy con-trols, and clinical studies demonstrating the efficacy of antimi-crobial and probiotic treatments in patients with IBS.
Postinfectious IBS
Postinfectious IBS (PI-IBS) refers to the development ofIBS following an episode of acute gastroenteritis. PI-IBSoccurs in �10% of patients with acute gastroenteritis, andacute gastroenteritis increases the odds of developing IBS six-to sevenfold (76, 157, 172). The extended duration of IBSsymptoms in these patients indicates that the condition persistslong after the initial infection has cleared. The precise mech-anisms by which IBS symptoms persist are not clear, althoughresearchers have speculated that genetic polymorphisms ingenes related to host immune response to microbial pathogens,ongoing altered immune function, or chronic low-grade in-flammation may be possible factors (26, 145, 170).
Small Intestinal Bacterial Overgrowth
The symptoms of SIBO and IBS overlap since SIBO canlead to similar symptoms and altered intestinal motility that areoften observed in patients with IBS (140). Detecting SIBO inpatients with IBS remains a challenge. Historically, SIBO hasbeen defined as �105 colony-forming units (cfu)/ml intestinalfluid (14). Using this definition, a study of bacterial cultures ofaspirates from patients with IBS compared with cultures fromhealthy volunteers showed no statistically significant differ-ences in the incidence of SIBO (141). However, when a lowercutoff concentration of �104 cfu/ml was used, significantdifferences were observed, suggesting increased numbers ofbacteria in the small intestine of patients with IBS.
Because of the limitations in obtaining intestinal cultures,SIBO is often diagnosed indirectly by hydrogen breath testing(HBT). A meta-analysis of studies using HBT reported apooled prevalence of SIBO in patients with IBS of 54–64%(61). However, the wide range of prevalence of SIBO reportedin individual studies [from 10% (186) to 84% (130)] reflectsthe lack of standardization of HBT and the possibility thatlactulose HBT results may reflect changes in small boweltransit time rather than the true presence of SIBO (194). Thesediagnostic limitations led to some controversies regarding thereal prevalence and the importance of SIBO in the pathogen-esis of IBS.
Nonetheless, the data from meta-analyses indicating in-creased prevalence of SIBO in IBS, the symptom overlapbetween the two conditions, and the improvement of symptomswith antibiotic treatment (47, 49, 59, 103, 131, 135, 136, 193)further support the hypothesis that alterations in the intestinalmicrobiota may have a role in the pathogenesis of IBS, at leastin some patients.
Alterations in Intestinal Microbiota
Several studies have investigated and compared the compo-sition of intestinal microbiota of patients with IBS with that ofhealthy individuals. Although early studies were relativelysmall with noticeable methodological limitations, their overall
findings suggested differences in the intestinal microbiota ofpatients with IBS and healthy controls (145, 153). These earlyfindings are further supported by recent studies using advancedmolecular biology techniques that are on the basis of thebacterial 16S ribosomal DNA (rDNA) gene. These includegenetic fingerprinting (e.g., denaturing gradient gel electropho-resis and terminal restriction fragment length polymorphism),16S rDNA high-throughput sequencing (e.g., 454-pyrose-quencing and Illumina), and phylogenetic microarray [e.g.,human intestinal tract chip (HITChip) and PhyloChip]. Thesetechniques enable detailed qualitative and quantitative infor-mation regarding the most abundant bacterial communities inthe intestinal microbiota (63). Recent studies using these ad-vanced molecular biology techniques have demonstrated quan-titative alterations of specific bacterial groups (33, 34, 81, 85,142, 154) and reduced diversity in gut microbial populations inpatients with IBS compared with healthy controls (33, 40).Limited data also suggest differences in mucosa-associatedmicrobiota (32, 33, 86, 129), reduced stability over time (106,107), rDNA, and differences between IBS subtypes (81, 104,129, 142). Overall, it appears that the composition of theintestinal microbiota and the relative abundance of specificbacterial species are altered in patients with IBS. Emergingdata demonstrate associations between altered intestinal micro-biota and abnormal intestinal functions that contribute to thepathophysiology of IBS as detailed below.
Altered Fermentation Processes
Poorly absorbed short-chain carbohydrates (e.g., fructoseand dietary starch) provide substrate for generation of short-chain fatty acids (SCFA) by colonic bacterial fermentation.Fecal SCFA have been shown to be increased in patients withIBS (175). In addition, a recent study reported higher counts ofacetic- and propionic-acid-producing bacteria (Veillonella andLactobacillus) in IBS patients and an association between thehigher levels of these SCFA and GI symptoms and quality oflife (171). From a mechanistic perspective, animal studiesdemonstrate that SCFA can initiate high-amplitude propagatedcolonic contractions (82) and increase intestinal transit andmotility via intestinal release of 5-hydroxytryptamine (66). Theassociation between certain dietary products and GI symptoms(e.g., abdominal bloating, distention, and pain) in patients withIBS (161) and the emerging data on the beneficial effects ofdietary manipulation, particularly elimination of highly fer-mentable short-chain carbohydrates (127), further support theimportance of altered fermentation processes by the intestinalmicrobiota in the pathogenesis of IBS.
Microbiota and the Intestinal Barrier
The gut microbiota have an important role in promoting thedevelopment, maintenance, and function of the intestinal bar-rier by increasing IgA production and mucin expression, pre-venting intestinal epithelial cell apoptosis, inhibiting coloniza-tion by enteric pathogens, and promoting physiological im-mune responses (113, 173, 178). Several in vivo studies inchildren and adults with IBS (56, 128, 162) and in vitro studiesof mucosal samples from IBS patients (132) demonstratedincreased intestinal permeability in IBS compared with healthycontrols. The mechanisms related to the increased permeabilityin IBS are not clear but alterations in intestinal microbiota and
Review
G530 MICROBIOTA AND IMMUNE FUNCTION IN IBS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00207.2012 • www.ajpgi.org

mucosal inflammation have been suggested (28). The increasedgut permeability of colonic biopsies from patients with IBSwas found to be associated with decreased expression of a tightjunction protein, zonula occludens-1 (ZO-1). When fecal su-pernatants from IBS patients were applied to colonic mucosafrom mice (67) or to Caco-2 cells (132), the expression ofZO-1 decreased and permeability increased. Furthermore, inpatients with D-IBS, this phenomenon was found to be asso-ciated with increased bacterial-related protease activity andtheir epithelial receptor PAR-2 (proteinase activated receptor2) (67). Additional support for the role of enteric bacteria inmaintaining normal barrier function is provided by data thatSCFA (e.g., butyrate and acetate) improve intestinal barrierfunction (64, 84). One small study found that administration ofbutyrate enemas in healthy volunteers resulted in decreased invisceral perception (180).
Microbiota and Enteric Sensorimotor Function
Intestinal microbiota may affect gut motility and pain per-ception. In mice, perturbation of the microbiota by exposure toantibiotics resulted in increased visceromotor responses tocolonic distension (182). Interestingly, in this model, treatmentof mice with Lactobacillus ameliorated inflammatory indexesin the gut wall and reduced the antibiotic-induced visceromotorresponse. Direct effects of bacterial products on gut sensori-motor functions have been shown in several in vitro studies.For example, stimulation of smooth muscle cells by superna-tants from Escherichia coli Nissle 1917 enhances coloniccontractility (9) and Lactobacillus rhamnosus and Bifidobac-terium lactis increases intestinal myoelectrical activity in rats(97). In addition, exposure of rats to L. reuteri (83) or L.acidophilus NCFM (151) reduce their pain response to balloondistension, through targeting ion channels in the enteric ner-vous system (83, 91) or increasing the expression of �-opioidand cannabinoid receptors in intestinal epithelial cells (151).
Several recent studies have demonstrated bile acid malab-sorption in a subset of patients with IBS (1, 29, 93, 192).Furthermore, reduced ileal absorption and excess of bile acid inthe colon can lead to acceleration of colonic transit by stimu-lating motility and secretion (8, 109). Since the intestinalmicrobiota are directly responsible for the transformation ofprimary into secondary bile acid it is tempting to hypothesizethat the intestinal dysbiosis observed in patients with IBS canaffect intestinal motility and lead to IBS symptoms through itseffect(s) on bile acid metabolism. Indeed, a recent small studyin patients with IBS demonstrated increase of primary bile acidin the feces of patients with IBS-D compared with healthysubjects (54). Interestingly, these differences correlated withstool consistency and frequency and were associated withdecreased levels of the Clostridium leptum group, which con-tains many of the bacteria that can transform primary intosecondary bile acid.
Emerging observations of perturbed composition of theintestinal microbiota and altered microbiota-related fermenta-tion, barrier, and sensorimotor functions in patients with IBSsupport the hypothesis that the intestinal microbiota contributeto the pathogenesis of the disorder. However, two key ques-tions remained unanswered. First, are the observed alterationsin the intestinal microbiota in IBS a cause or a consequence ofthe disorder? Relatedly, since the majority of the reported
studies were done at a single time point, it is not clear whetherand how the altered intestinal microbiota correlate with theclinical presentation and the IBS symptoms over time. Second,what are the relative contributions of the abnormal compositionvs. function of the intestinal microbiota and mechanisms bywhich these changes contribute to the pathogenesis of IBS?
Current advances in the area of microbiome research includ-ing advance in nucleic acid sequencing, metagenomics, andmetaproteomics allow investigation of structural and functionalaspects of the intestinal microbiome. Incorporating microbialresponse variables (e.g., taxonomy, microbial diversity, rich-ness, and stability) into future clinical studies in IBS is crucialto advance this field forward. However, controlling for all thevariables that influence the intestinal microbiota (e.g., diet andinterpatient variability) poses challenges to the design of clin-ical studies. Animal models may be useful by controlling forhost genotype, baseline microbiota, and diet. Furthermore,since the results from animal models cannot be generalized tohumans because of differences in the intestinal microbiota, it ispossible to improve mouse models of IBS by colonizinggerm-free animals with human-derived microbiota. The abilityof these systems to mimic human clinical conditions is unclearat present, but they can be useful to test hypotheses particularlyregarding causation.
In addition, the fact that genome sequence data for many ofthe bacterial species in the human gut microbiota are notavailable limits taxonomic assignments of the data with clini-cal, physiological, and metabolomic data. The anticipated ref-erence genome sequences generated by the Human Micro-biome Reference Genomes initiative, and the rapidly develop-ing analytic tools and bioinformatic technologies, are requiredto ensure progress.
THE INTESTINAL IMMUNE SYSTEM
Altered Intestinal Immune Function in IBS
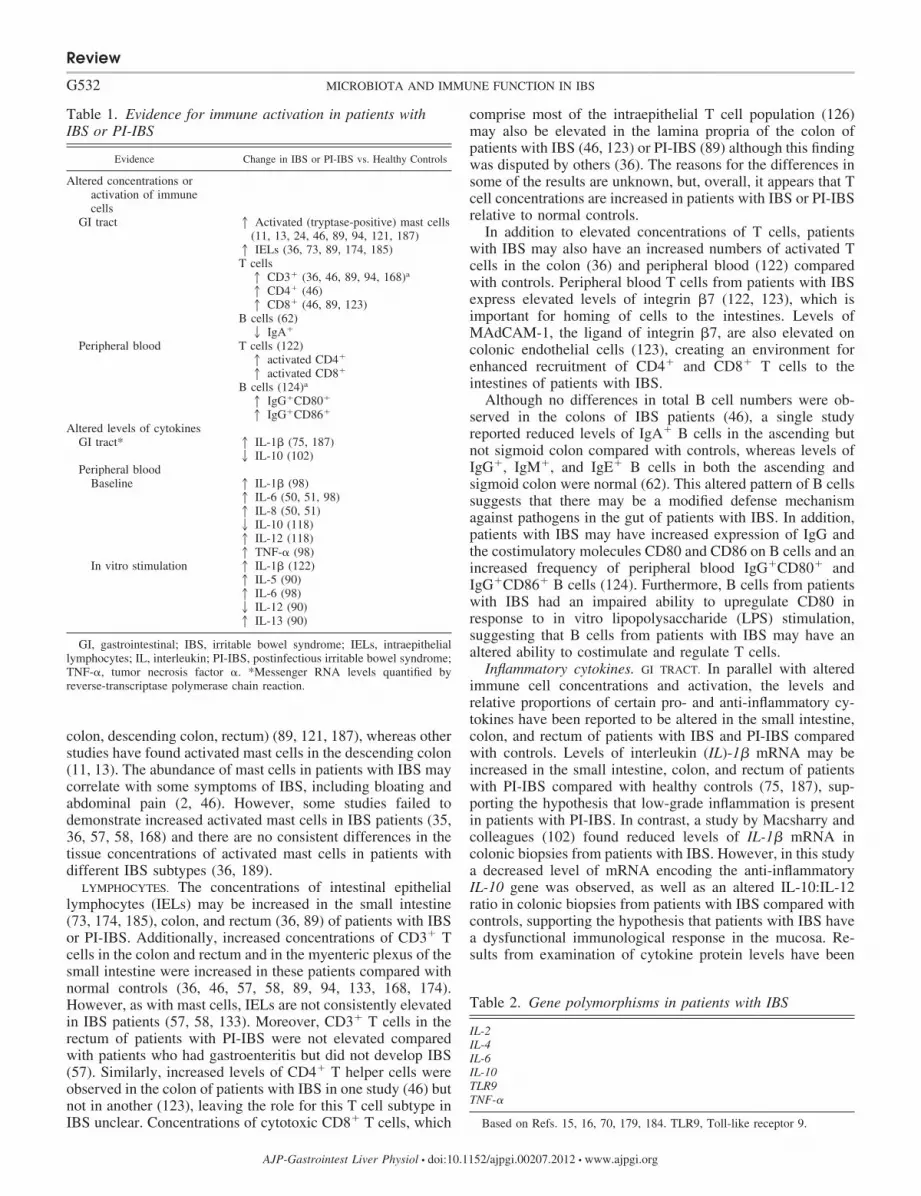
Although IBS is not generally considered an inflammatorydisease, there is growing appreciation for the hypothesis thatIBS may be a condition of low-grade inflammation and/orabnormal immune function, despite a lack of detectable inflam-mation on routine endoscopy or with conventional histology(48). Evidence supporting this hypothesis includes increasedconcentrations of inflammatory/immune cells in intestinal tis-sue from IBS patients, altered levels of pro- and anti-inflam-matory cytokines in the GI tract and peripheral blood ofpatients with IBS (Table 1) (11, 13, 24, 36, 46, 50, 51, 62, 73,75, 89, 90, 94, 98, 102, 118, 121–124, 168, 174, 185, 187), andIBS-associated polymorphisms in genes involved in immuneand inflammatory responses (Table 2) (15, 16, 70, 179, 184).This topic has been thoroughly reviewed recently (27).
Immune cells. MAST CELLS. Several studies have demon-strated increased concentrations of activated mast cells inpatients with IBS compared with controls (11, 13, 24, 46, 89,94, 121, 187). Interestingly, the activated mast cells were foundto be in close proximity to enteric nerves and correlated withabdominal pain/discomfort (11). Other studies have reportedelevated levels of histamine and tryptase release in patientswith IBS compared with controls (11, 13, 35, 73). Notably,some studies demonstrated an increase in activated mast cellsin biopsies from specific regions of the GI tract (i.e., cecum andterminal ileum) but not from other regions (e.g., ascending
Review
G531MICROBIOTA AND IMMUNE FUNCTION IN IBS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00207.2012 • www.ajpgi.org
colon, descending colon, rectum) (89, 121, 187), whereas otherstudies have found activated mast cells in the descending colon(11, 13). The abundance of mast cells in patients with IBS maycorrelate with some symptoms of IBS, including bloating andabdominal pain (2, 46). However, some studies failed todemonstrate increased activated mast cells in IBS patients (35,36, 57, 58, 168) and there are no consistent differences in thetissue concentrations of activated mast cells in patients withdifferent IBS subtypes (36, 189).
LYMPHOCYTES. The concentrations of intestinal epitheliallymphocytes (IELs) may be increased in the small intestine(73, 174, 185), colon, and rectum (36, 89) of patients with IBSor PI-IBS. Additionally, increased concentrations of CD3� Tcells in the colon and rectum and in the myenteric plexus of thesmall intestine were increased in these patients compared withnormal controls (36, 46, 57, 58, 89, 94, 133, 168, 174).However, as with mast cells, IELs are not consistently elevatedin IBS patients (57, 58, 133). Moreover, CD3� T cells in therectum of patients with PI-IBS were not elevated comparedwith patients who had gastroenteritis but did not develop IBS(57). Similarly, increased levels of CD4� T helper cells wereobserved in the colon of patients with IBS in one study (46) butnot in another (123), leaving the role for this T cell subtype inIBS unclear. Concentrations of cytotoxic CD8� T cells, which
comprise most of the intraepithelial T cell population (126)may also be elevated in the lamina propria of the colon ofpatients with IBS (46, 123) or PI-IBS (89) although this findingwas disputed by others (36). The reasons for the differences insome of the results are unknown, but, overall, it appears that Tcell concentrations are increased in patients with IBS or PI-IBSrelative to normal controls.
In addition to elevated concentrations of T cells, patientswith IBS may also have an increased numbers of activated Tcells in the colon (36) and peripheral blood (122) comparedwith controls. Peripheral blood T cells from patients with IBSexpress elevated levels of integrin �7 (122, 123), which isimportant for homing of cells to the intestines. Levels ofMAdCAM-1, the ligand of integrin �7, are also elevated oncolonic endothelial cells (123), creating an environment forenhanced recruitment of CD4� and CD8� T cells to theintestines of patients with IBS.
Although no differences in total B cell numbers were ob-served in the colons of IBS patients (46), a single studyreported reduced levels of IgA� B cells in the ascending butnot sigmoid colon compared with controls, whereas levels ofIgG�, IgM�, and IgE� B cells in both the ascending andsigmoid colon were normal (62). This altered pattern of B cellssuggests that there may be a modified defense mechanismagainst pathogens in the gut of patients with IBS. In addition,patients with IBS may have increased expression of IgG andthe costimulatory molecules CD80 and CD86 on B cells and anincreased frequency of peripheral blood IgG�CD80� andIgG�CD86� B cells (124). Furthermore, B cells from patientswith IBS had an impaired ability to upregulate CD80 inresponse to in vitro lipopolysaccharide (LPS) stimulation,suggesting that B cells from patients with IBS may have analtered ability to costimulate and regulate T cells.
Inflammatory cytokines. GI TRACT. In parallel with alteredimmune cell concentrations and activation, the levels andrelative proportions of certain pro- and anti-inflammatory cy-tokines have been reported to be altered in the small intestine,colon, and rectum of patients with IBS and PI-IBS comparedwith controls. Levels of interleukin (IL)-1� mRNA may beincreased in the small intestine, colon, and rectum of patientswith PI-IBS compared with healthy controls (75, 187), sup-porting the hypothesis that low-grade inflammation is presentin patients with PI-IBS. In contrast, a study by Macsharry andcolleagues (102) found reduced levels of IL-1� mRNA incolonic biopsies from patients with IBS. However, in this studya decreased level of mRNA encoding the anti-inflammatoryIL-10 gene was observed, as well as an altered IL-10:IL-12ratio in colonic biopsies from patients with IBS compared withcontrols, supporting the hypothesis that patients with IBS havea dysfunctional immunological response in the mucosa. Re-sults from examination of cytokine protein levels have been
Table 2. Gene polymorphisms in patients with IBS
IL-2IL-4IL-6IL-10TLR9TNF-�
Based on Refs. 15, 16, 70, 179, 184. TLR9, Toll-like receptor 9.
Table 1. Evidence for immune activation in patients withIBS or PI-IBS
Evidence Change in IBS or PI-IBS vs. Healthy Controls
Altered concentrations oractivation of immunecells
GI tract 1 Activated (tryptase-positive) mast cells(11, 13, 24, 46, 89, 94, 121, 187)1 IELs (36, 73, 89, 174, 185)T cells1 CD3� (36, 46, 89, 94, 168)a
1 CD4� (46)1 CD8� (46, 89, 123)
B cells (62)2 IgA�
Peripheral blood T cells (122)1 activated CD4�
1 activated CD8�
B cells (124)a
1 IgG�CD80�
1 IgG�CD86�
Altered levels of cytokinesGI tract* 1 IL-1� (75, 187)
2 IL-10 (102)Peripheral blood
Baseline 1 IL-1� (98)1 IL-6 (50, 51, 98)1 IL-8 (50, 51)2 IL-10 (118)1 IL-12 (118)1 TNF-� (98)
In vitro stimulation 1 IL-1� (122)1 IL-5 (90)1 IL-6 (98)2 IL-12 (90)1 IL-13 (90)
GI, gastrointestinal; IBS, irritable bowel syndrome; IELs, intraepitheliallymphocytes; IL, interleukin; PI-IBS, postinfectious irritable bowel syndrome;TNF-�, tumor necrosis factor �. *Messenger RNA levels quantified byreverse-transcriptase polymerase chain reaction.
Review
G532 MICROBIOTA AND IMMUNE FUNCTION IN IBS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00207.2012 • www.ajpgi.org

conflicting. In one study, levels of TNF-� were elevated, butlevels of IL-6 and interferon-� were decreased in mucosa ofpatients with IBS compared with controls (41). Ex vivo exam-ination of cytokine secretion by the colon failed to showelevation of proinflammatory cytokines or chemokines in pa-tients with IBS compared with controls (102).
PERIPHERAL BLOOD. A recent study demonstrated significantlyhigher levels of high-sensitivity C-reactive protein in patientswith IBS-D but not in patients with IBS-C or IBS-M comparedwith healthy controls (77). IL-6, which is a major regulator ofserum C-reactive protein levels, and IL-8 were also found to beincreased in the serum of patients with IBS compared withcontrols, supporting a proinflammatory profile in these patients(50, 51).
Additionally, IL-1�, IL-6, and TNF-� released from periph-eral blood mononuclear cells (PBMCs) were elevated in pa-tients with IBS-D but not in patients with IBS-C or IBS-M(98). Additionally, a decreased ratio of IL-10 to IL-12, indic-ative of a proinflammatory response, was demonstrated insupernatants of cultured PBMCs obtained from patients withIBS compared with controls (118). In this same study, normal-ization of the IL-10:IL-12 ratio in patients with IBS followingprobiotic treatment was paralleled by improvement in thesymptoms of IBS, thus supporting an association betweenchanges in the GI microbiota, the IL-10:IL-12 ratio, andsymptoms in patients with IBS. However, other studies did notobserve differences in IL-10 levels between IBS patients andcontrols (50, 51, 90), leaving the relevance of IL-10 levels inpatients with IBS unclear.
Cytokine secretion following in vitro stimulation of periph-eral blood lymphocytes/monocytes may also be altered inpatients with IBS (90, 98, 122). Increased secretion of TNF-�,IL-1�, and IL-6 by LPS-stimulated PBMCs was observed onlyin cells from patients with IBS-D but not in patients withIBS-C or IBS-M (98). In contrast, only IL-1� was secretedfollowing LPS stimulation of PBMCs obtained from IBS-Cpatients (98). Furthermore, increases in the secretion of TNF-�following LPS stimulation of PBMCs and of IL-1� followingT-cell anti-CD3/CD28 antibodies stimulation were signifi-cantly associated with anxiety (98) and bowel habit dissatis-faction and overall IBS symptoms (122), respectively. Overall,it seems that alterations in cytokine secretion by stimulatedperipheral blood cells appear to favor an activated immunestate (98, 122), and an altered immune response shifted towarda T-helper 2 phenotype(90) in IBS patients.
Immune-Related Genetic Alterations in IBS
Gene polymorphisms (188) in TNF-� (15, 179), IL-2 (16),IL-4 (16), IL-6 (15), and IL-10 (16, 70) have been associatedwith IBS or PI-IBS (Table 2). For example, IBS patients aremore likely to carry a combination of polymorphisms that leadto increased expression of TNF-� and decreased expression ofIL-10 compared with healthy controls (179). However, theprevalence of specific polymorphisms in the IL-10 gene inpatients with IBS are not consistent across studies and mayreflect the variety of ethnic groups in which these studies wereconducted (16). Genetic variation in promoter regions of theIL-6 and Toll-like receptor 9 (TLR9) genes were also identifiedas independent risk factors for the development of PI-IBS (26,184). Altered levels of IL-6, IL-10, and TNF-� in colon tissue
from IBS and PI-IBS patients suggest that the genetic poly-morphisms in immune genes may have functional conse-quences in patients with IBS. The presence of polymorphismsin the promoter of TLR9 suggests that patients with PI-IBS mayhave an inappropriate regulation of the immune response tomicrobial products.
Immune-Mediated Food Hypersensitivity in IBS
The majority of IBS patients believe that their IBS symp-toms are initiated or worsened by certain foods and many ofthem report intolerance (i.e., hypersensitivity) to a variety offoods (68). The mechanisms by which dietary factors lead toIBS symptoms are currently unknown. However, several stud-ies have documented IgG-mediated food hypersensitivity anddemonstrated that food-elimination diets based on IgG anti-bodies to specific food items improved IBS symptoms (4, 195,196), perhaps through amelioration of the immune response. Inaddition, few studies demonstrated increased peripheral bloodbasophil activation following stimulation with food antigens(30) and elevated levels of fecal tryptase and eosinophil cat-ionic protein (31) in patients with IBS and food hypersensitiv-ity, thus further suggesting possible inflammatory and alteredimmune etiology.
Although the mechanisms for food hypersensitivity in pa-tients with IBS are not clear, it can be postulated that dysregu-lated immune responses and possibly altered intestinal mucosalbarrier function may be involved.
Inflammation and Sensorimotor Function
The effects of inflammation on sensorimotor enteric functionhave been demonstrated in IBDs, where patients suffer fromabnormal intestinal motor function and enhanced sensory per-ception, even when inflammation is restricted to the mucosa(44, 143). In addition, human and animal studies have shownanatomical changes in the enteric nervous system (ENS)around inflammatory infiltrates in the gut wall (2, 11, 13).Functionally, intestinal inflammation is associated with in-creased expression of neuropeptides and mediators that are alsoinvolved with gut motility and sensation (e.g., VIP and sub-stance P) [for review, see Vasina et al. (181)]. Similar obser-vations have been made in IBS patients. One study thatsupports this association demonstrated a strong correlationbetween number of infiltrated colonic mast cells around nervesand the severity and frequency of abdominal pain in patientswith IBS (11).
MICROBIOTA, IMMUNE SYSTEM, AND THE BRAIN-GUT AXIS
The current understanding of IBS as a disorder of malfunc-tion in the bidirectional brain-gut communication suggests thatboth peripheral (GI) and central nervous system (CNS) factorsare involved in the pathophysiology of the disorder. Indeed, atthe gut level, the intestinal mucosal neuroimmune systemidentifies and responds to intestinal luminal food products,nutrients, bacteria, metabolites, and toxins. At the CNS level,the brain-gut axis connects environmental, cognitive, and emo-tional states with GI functions (191). For example, it has beenshown that physical and psychological stress (112), cognition(e.g., attention vs. distraction to aversive stimulus) (55), andearly life experience (e.g., sexual and physical abuse) (39, 149)can affect intestinal sensory perception. Furthermore, treat-
Review
G533MICROBIOTA AND IMMUNE FUNCTION IN IBS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00207.2012 • www.ajpgi.org

ments targeting the CNS, such as antidepressants and psycho-logical interventions, can reduce intestinal sensation/sensitivityand improve GI symptoms in patients with IBS (21, 111, 150,165).
The Intestinal Microbiota and Brain-Gut Axis
Recent data from animal and human studies have demon-strated that alterations in the intestinal microbiota have sub-stantial effects on the brain-gut axis at both the peripheral andcentral levels (Fig. 1). In the periphery, intestinal microbiotacan affect the ENS directly via release of bacterial substancesor metabolites, or indirectly by inducing the release of host-derived immune mediators that in turn impact the ENS (10,155). For example, production of the SCFA butyrate by bac-teria affects gene expression and the phenotype of entericneurons in a similar manner to that observed in the colons ofpatients treated with prokinetic agents (166, 169). Gastrointes-tinal microbiota may also contribute to the affective symptoms
associated with GI disorders by impacting the CNS via im-mune, hormonal, and neural mechanisms (17, 69, 155). Pre-liminary studies have demonstrated that alterations in the GImicrobiota can lead to long-term increased anxiety (69, 115,116) and altered exploratory behavior in mice (18, 19). Simi-larly, psychosocial stressors can change the composition of theintestinal microbiota and affect the brain-gut axis function (6,7, 119). For example, it has been shown that maternal separa-tion, a well-established rodent model of early life stress, canlead to significant alterations in the intestinal microbiota aswell as in brain-gut axis function, including increased plasmacorticosterone levels, systemic immune responses, and visceralsensation compared with a control group (119).
The Enteric Immune System and Brain-Gut Axis
The connection between altered intestinal immune functionand abnormal brain-gut axis in patients with IBS remainsunclear. However, some of the suggested mechanisms involve
Altered intestinalimmune system
• Mast cell activation
• Inflammatory cytokines
Altered intestinalmicrobiota
• Composition
• Function
CNS
HPAANS
ENS
Altered intestinal function
• Sensory-motor function
• Barrier function
Functional GI symptoms
Triggers and Predisposing Factors
Environmental factors
Central:
• Psychological stress
• Anxiety/Depression
Peripheral:
• Gastroenteritis
• Diet
• Medications
• Life habits
Host factors
• Genetics
• Disease conditions
Fig. 1. Interactions between the intestinal microbiota, immune system and brain-gut axis, and their effects on intestinal function and functional gastrointestinal(GI) symptoms. A number of factors and triggers, from both the environment and the host, combine to drive the complex interactions between the brain-gut axis,intestinal microbiota, and immune system toward altered intestinal functions and functional GI symptoms. Altered intestinal microbiota may affect the brain-gutaxis directly via effect on the mucosal barrier and intestinal neuroimmune system or indirectly via generation of bacterial-related metabolites. Immune activation(e.g., increased levels of proinflammatory cytokines) may affect the mucosal barrier, enteric nervous system (ENS) and peripheral nervous system [i.e., autonomicnervous system (ANS), hypothalamic-pituitary-adrenal (HPA) axis, central nervous system (CNS)]. The outcome of these complex interactions may alter theintestinal sensorimotor function and lead to functional GI symptoms.
Review
G534 MICROBIOTA AND IMMUNE FUNCTION IN IBS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00207.2012 • www.ajpgi.org

stress and psychological disturbances and disruption of muco-sal barrier function (120). For example, rats exposed to chronicstress exhibited activation of the hypothalamic-pituitary-adre-nal (HPA) axis, intestinal mucosal inflammation, increasedepithelial permeability, and colonic hyperalgesia (183). At theperipheral level, the close interaction between the immunesystem and the ENS in IBS is demonstrated by the increasedinfiltration of mast cells in the colonic mucosa in close prox-imity to enteric nerve fibers and by the increased number ofsensory nerve fibers surrounding the mast cells (2, 11, 13). Inaddition, several studies support the hypothesis that elevatedlevels of proinflammatory cytokines may affect the brain-gutaxis. For example, in rats elevated IL-1� and TNF-� secretionin response to the bacterial endotoxin LPS leads to visceralhyperalgesia via activation of sensory nerve pathways (42).Others showed that the proinflammatory cytokines IL-6, IL-1,and TNF-� affect the HPA axis through elevated release ofarginine vasopressin (AVP), corticotropin-releasing hormone(CRH), and adrenocorticotropic hormone (ACTH) (38, 176).AVP and CRH, by stimulating ACTH secretion, may affect theautonomic nervous system (38) and colonic sensorimotor func-tions (125, 152). Additionally, CRH may act directly onperipheral receptors of the ENS, independent of alterations inthe HPA axis, to impact sensorimotor functions in patients withIBS (152). Thus proinflammatory cytokines (e.g., IL-1�, IL-6,and TNF-�) may interact with the brain-gut axis at differentlevels, modulate its function, and lead to altered visceral andmotility function in patients with IBS (Fig. 1).
Interactions of the Intestinal Microbiota and ImmuneFunction in IBS
The effects of the intestinal microbiota on the development,function, and homeostasis of the enteric immune system arewell documented (5, 158). Enteric microbiota are crucial to thehost in numerous aspects including maturation of the systemicand enteric immune response, maintenance of the mucosalbarrier function, digestion of food, metabolism, and more (forreview, see Ref. 78). Although evidence is rapidly accumulat-ing that dysregulated immune responses to normal and “dys-biotic” enteric microbiota contribute to the pathogenesis ofIBD (105), there are limited data on the interactions betweenthe intestinal microbiota and the enteric immune system inIBS. However, some recent data suggest that IBS patients alsoexhibit dysregulated immune responses to commensal and/orpathogenic intestinal bacteria. For example, recognition ofbacterial components through Toll-like receptors (TLRs) isincreased in IBS patients. Expression of TLR4 (recognizesbacterial LPS) and TLR5 (recognizes flagellin, a commonbacterial antigen present in most motile bacteria in the gut) areincreased in colons of IBS patients compared with controls.TLRs have a central role in the mucosal innate immuneresponse and their increased expression is also associated withIBDs (23). In this regard, anti-flagellin antibodies were foundin almost 30% of IBS patients (mostly in PI-IBS) as opposedto only 7% of healthy controls (156). The importance of TLRsin IBS is further supported by a recent study in a mouse model,indicating that TLR4 stimulation by enteric microbiota can alsoaffect the enteric nervous system and intestinal motility (3).Moreover, the antimicrobial peptide �-defensin-2, which is aninnate immune molecule expressed by certain enteric epithelial
cells, is elevated in feces collected from IBS patients (similarlyto ulcerative colitis) compared with healthy controls (92).
The importance of the interaction between the intestinal micro-biota and immune system in IBS patients is demonstrated by a fewstudies in patients with PI-IBS, indicating activation of the GIimmune system following the acute GI infection (57, 58, 75, 89,94, 124, 168, 170, 187), and the recent animal studies showingthat stress-induced intestinal microbial changes are associatedwith altered immune response (6) and increased susceptibility toan enteric pathogen (183).
Clinical Implications
Manipulation of intestinal microbiota. The possible role ofthe altered intestinal microbiota, immune function, and theabnormal interaction between the two systems in the patho-genesis of IBS has led to the increased interest in targeting theintestinal microbiota and immune system in the treatment ofthis disorder. Early studies demonstrated symptom improve-ment in IBS patients whose SIBO was successfully treated withantibiotics, including neomycin, metronidazole, and the non-absorbable antibiotic rifaximin (47, 49, 59, 103, 131, 135, 136,193). Other studies have demonstrated beneficial effect ofantibiotics in patients with IBS regardless of either the diag-nosis of SIBO or the effect of antibiotics on HBT (95, 100,114, 134, 137–139, 160).
Several systematic reviews and meta-analyses suggest thatmodulation of intestinal microbiota with probiotics may im-prove some of the symptoms of IBS (22, 79, 110, 147, 148).The largest reported study was a randomized, double-blinded,placebo-controlled, multicenter study of 362 patients that dem-onstrated beneficial effects of Bifidobacterium infantis 35624over placebo on IBS composite score and individual symptomsof IBS (e.g., pain and bloating) (190). Although the effectswere modest, they were significant. Other smaller studiesreported some beneficial effects with other probiotic strainsincluding Bifidobacterium animalis DN-173 010 (74), Bifido-bacterium bifidum MIMBb75 (72), Lactobacillus plantarum299V (117), Saccharomyces boulardii (37), and combinationof Lactobacillus acidophilus NCFM and Bifidobacterium lactisBi-07 (144) and multispecies probiotic mixtures (71, 87, 88).Other approaches targeting the intestinal microbiota that haveshown benefit in the treatment of IBS include prebiotics (163)and dietary manipulation (127).
Currently, despite the demonstrated efficacy in subgroups ofpatients with IBS, antibiotics are not FDA-approved medica-tions for treatment of IBS, and there are no clear guidelines forthe use of probiotics, prebiotics, and diets in this disorder.Nevertheless, although the mechanisms of action are unclear,the available data suggest potential therapeutic benefit in tar-geting the intestinal microbiota in the treatment of IBS. Thedata underscore the need for further preclinical studies, includ-ing the use various animal model systems and well-designedhuman trials in this area. Future research should help directpatients and healthcare providers in making evidence-baseddecisions regarding the selection of patients, preferred productsand treatment regimens.
Anti-inflammatory treatment in IBS. An alternative, andperhaps complementary, therapeutic approach is to target thedysregulated immune response in IBS patients. Few studieshave investigated the use of anti-inflammatory medications in
Review
G535MICROBIOTA AND IMMUNE FUNCTION IN IBS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00207.2012 • www.ajpgi.org

IBS. A small, double-blind, randomized study of 20 IBSpatients showed that mesalamine 2.4 g/day for 8 wk failed toshow improvement in IBS symptoms despite a reduction in thenumber of total immune cells in colonic biopsies and improve-ment in general well-being (45, 177). Similarly, mesalamine3.2 g/day for 12 wk (168) and prednisolone 30 mg/day for 3 wk(52) were not effective in improving the GI symptoms inpatients with PI-IBS. A single small study suggests a possiblebenefit to targeting mast cells with sodium cromoglycate, amast cell stabilizer, in patients with IBS and food intolerance(101).
Taken together, the current available data do not support theclinical use of anti-inflammatory agents in the treatment ofIBS. However, the documented low-grade inflammation inIBS, the suggestive preliminary data from animal studies (52),and the noticeable paucity of clinical data in this area empha-size the need for further investigation to enable more solidconclusions regarding this treatment option in IBS. Under-standing the role of the immune system in IBS pathophysiol-ogy may further clarify the potential therapeutic role of target-ing the immune system in the treatment of IBS.
CONCLUSIONS
IBS has historically been considered a condition without anidentifiable organic etiology. However, accumulating observa-tions in animal models and in patients with IBS suggest aconceptual model in which environmental factors at both theperipheral (e.g., diet, GI infections, antibiotics) and central(e.g., psychological stress, anxiety, depression) levels can af-fect the intestinal microbiota and enteric immune system,which interact with each other and the brain-gut axis (Fig. 1).Alterations in these systems or in their interactions can affectGI function and lead to functional GI symptoms. Future re-search in this area may provide further insight into the rele-vance and relative importance of these interactions in thepathogenesis of IBS and improve our understanding of howmanipulating relevant environmental factors (e.g., diet andintestinal microbiota), and the immune and inflammatory pro-cesses may affect the brain-gut axis and improve patientoutcomes.
GRANTS
Y. Ringel is supported by National Institute of Diabetes and Digestive andKidney Diseases grants DK084294 and DK075621. N. Maharshak is supportedby the Crohn’s and Colitis Foundation of America Research Fellowship Awardand the American Physicians Fellowship for Medicine in Israel.
DISCLOSURES
Y. Ringel discloses Research Grant: Salix Pharmaceuticals, Danisco USA,Proctor & Gamble. Consultant: Salix Pharmaceuticals; Pfizer Inc.; Glaxo-SmithKline; Prometheus Laboratories; Schwabe North America. Travel grants:Nestlé; Institute of Health Sciences; Danone. Consultant: Proctor & Gamble,Ironwood Pharmaceuticals, Inc., Forest Laboratories, Inc. General Mills.Research grant: General Mills.
AUTHOR CONTRIBUTIONS
Y.R. conception and design of research; Y.R. and N.M. prepared figures;Y.R. and N.M. drafted manuscript; Y.R. and N.M. edited and revised manu-script; Y.R. and N.M. approved final version of manuscript.
REFERENCES
1. Abrahamsson H, Ostlund-Lindqvist AM, Nilsson R, Simren M,Gillberg PG. Altered bile acid metabolism in patients with constipation-
predominant irritable bowel syndrome and functional constipation. ScandJ Gastroenterol 43: 1483–1488, 2008.
2. Akbar A, Yiangou Y, Facer P, Walters JR, Anand P, Ghosh S.Increased capsaicin receptor TRPV1-expressing sensory fibres in irritablebowel syndrome and their correlation with abdominal pain. Gut 57:923–929, 2008.
3. Anitha M, Vijay-Kumar M, Sitaraman SV, Gewirtz AT, SrinivasanS. Gut microbial products regulate murine gastrointestinal motility viaToll-like receptor 4 signaling. Gastroenterology 143: 1006–1016.e4,2012.
4. Atkinson W, Sheldon TA, Shaath N, Whorwell PJ. Food eliminationbased on IgG antibodies in irritable bowel syndrome: a randomisedcontrolled trial. Gut 53: 1459–1464, 2004.
5. Bäckhed F, Fraser-Liggett C, Ringel Y, Sanders ME, Sartor RB,Sherman P, Versalovic J, Young V, Finlay BB. Defining a healthyhuman gut microbiome: current concepts, future directions, and clinicalapplications. Cell Host Microbe 12: 611–622, 2012.
6. Bailey MT, Dowd SE, Galley JD, Hufnagle AR, Allen RG, Lyte M.Exposure to a social stressor alters the structure of the intestinal micro-biota: implications for stressor-induced immunomodulation. Brain BehavImmun 25: 397–407, 2011.
7. Bailey MT, Dowd SE, Parry NM, Galley JD, Schauer DB, Lyte M.Stressor exposure disrupts commensal microbial populations in the in-testines and leads to increased colonization by Citrobacter rodentium.Infect Immun 78: 1509–1519, 2010.
8. Bampton PA, Dinning PG, Kennedy ML, Lubowski DZ, Cook IJ.The proximal colonic motor response to rectal mechanical and chemicalstimulation. Am J Physiol Gastrointest Liver Physiol 282: G443–G449,2002.
9. Bar F, Von Koschitzky H, Roblick U, Bruch HP, Schulze L, Sonnen-born U, Bottner M, Wedel T. Cell-free supernatants of Escherichia coliNissle 1917 modulate human colonic motility: evidence from an in vitroorgan bath study. Neurogastroenterol Motil 21: 559–566.e16–e17,2009.
10. Barbara G, Stanghellini V, Brandi G, Cremon C, Di Nardo G, DeGiorgio R, Corinaldesi R. Interactions between commensal bacteria andgut sensorimotor function in health and disease. Am J Gastroenterol 100:2560–2568, 2005.
11. Barbara G, Stanghellini V, De Giorgio R, Cremon C, Cottrell GS,Santini D, Pasquinelli G, Morselli-Labate AM, Grady EF, BunnettNW, Collins SM, Corinaldesi R. Activated mast cells in proximity tocolonic nerves correlate with abdominal pain in irritable bowel syn-drome. Gastroenterology 126: 693–702, 2004.
12. Barbara G, Vallance BA, Collins SM. Persistent intestinal neuromus-cular dysfunction after acute nematode infection in mice. Gastroenter-ology 113: 1224–1232, 1997.
13. Barbara G, Wang B, Stanghellini V, de Giorgio R, Cremon C, DiNardo G, Trevisani M, Campi B, Geppetti P, Tonini M, Bunnett NW,Grundy D, Corinaldesi R. Mast cell-dependent excitation of visceral-nociceptive sensory neurons in irritable bowel syndrome. Gastroenter-ology 132: 26–37, 2007.
14. Bardhan PK, Gyr K, Beglinger C, Vogtlin J, Frey R, Vischer W.Diagnosis of bacterial overgrowth after culturing proximal small-bowelaspirate obtained during routine upper gastrointestinal endoscopy. ScandJ Gastroenterol 27: 253–256, 1992.
15. Barkhordari E, Rezaei N, Ansaripour B, Larki P, Alighardashi M,Ahmadi-Ashtiani HR, Mahmoudi M, Keramati MR, Habibollahi P,Bashashati M, Ebrahimi-Daryani N, Amirzargar AA. Proinflamma-tory cytokine gene polymorphisms in irritable bowel syndrome. J ClinImmunol 30: 74–79, 2010.
16. Barkhordari E, Rezaei N, Mahmoudi M, Larki P, Ahmadi-AshtianiHR, Ansaripour B, Alighardashi M, Bashashati M, Amirzargar AA,Ebrahimi-Daryani N. T-helper 1, T-helper 2, and T-regulatory cyto-kines gene polymorphisms in irritable bowel syndrome. Inflammation 33:281–286, 2010.
17. Bércik P. The microbiota-gut-brain axis: learning from intestinal bacte-ria? Gut 60: 288–289, 2011.
18. Bercik P, Denou E, Collins J, Jackson W, Lu J, Jury J, Deng Y,Blennerhassett P, Macri J, McCoy KD, Verdu EF, Collins SM. Theintestinal microbiota affect central levels of brain-derived neurotropicfactor and behavior in mice. Gastroenterology 141: 599–609, 609.e1–e3,2011.
19. Bercik P, Verdu EF, Foster JA, Macri J, Potter M, Huang X,Malinowski P, Jackson W, Blennerhassett P, Neufeld KA, Lu J,
Review
G536 MICROBIOTA AND IMMUNE FUNCTION IN IBS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00207.2012 • www.ajpgi.org

Khan WI, Corthesy-Theulaz I, Cherbut C, Bergonzelli GE, CollinsSM. Chronic gastrointestinal inflammation induces anxiety-like behaviorand alters central nervous system biochemistry in mice. Gastroenterol-ogy 139: 2102–2112, 2010.
20. Bercík P, Wang L, Verdú EF, Mao YK, Blennerhassett P, Khan WI,Kean I, Tougas G, Collins SM. Visceral hyperalgesia and intestinaldysmotility in a mouse model of postinfective gut dysfunction. Gastro-enterology 127: 179–187, 2004.
21. Brandt LJ, Chey WD, Foxx-Orenstein AE, Quigley E, Schiller L,Schoenfeld P, Speigel B, Talley NJ, Moayyedi P. An evidence-basedsystematic review on the management of irritable bowel syndrome. Am JGastroenterol 104, Suppl 1: s8–s35, 2009.
22. Brenner DM, Moeller MJ, Chey WD, Schoenfeld PS. The utility ofprobiotics in the treatment of irritable bowel syndrome: a systematicreview. Am J Gastroenterol 104: 1033–1049, 2009.
23. Brint EK, MacSharry J, Fanning A, Shanahan F, Quigley EM.Differential expression of toll-like receptors in patients with irritablebowel syndrome. Am J Gastroenterol 106: 329–336, 2011.
24. Buhner S, Li Q, Vignali S, Barbara G, De Giorgio R, Stanghellini V,Cremon C, Zeller F, Langer R, Daniel H, Michel K, Schemann M.Activation of human enteric neurons by supernatants of colonic biopsyspecimens from patients with irritable bowel syndrome. Gastroenterol-ogy 137: 1425–1434, 2009.
25. Caenepeel P, Janssens J, Vantrappen G, Eyssen H, Coremans G.Interdigestive myoelectric complex in germ-free rats. Dig Dis Sci 34:1180–1184, 1989.
26. Camilleri M, Carlson P, McKinzie S, Zucchelli M, D’Amato M,Busciglio I, Burton D, Zinsmeister AR. Genetic susceptibility toinflammation and colonic transit in lower functional gastrointestinaldisorders: preliminary analysis. Neurogastroenterol Motil 23: 935–943.e398, 2011.
27. Camilleri M, Katzka DA. Irritable bowel syndrome: methods, mecha-nisms, and pathophysiology. Genetic epidemiology and pharmacogenet-ics in irritable bowel syndrome. Am J Physiol Gastrointest Liver Physiol302: G1075–G1084, 2012.
28. Camilleri M, Madsen K, Spiller R, Greenwood-Van Meerveld B,Verne GN. Intestinal barrier function in health and gastrointestinaldisease. Neurogastroenterol Motil 24: 503–512, 2012.
29. Camilleri M, Nadeau A, Tremaine WJ, Lamsam J, Burton D, OdunsiS, Sweetser S, Singh R. Measurement of serum 7alpha-hydroxy-4-cholesten-3-one (or 7alphaC4), a surrogate test for bile acid malabsorp-tion in health, ileal disease and irritable bowel syndrome using liquidchromatography-tandem mass spectrometry. Neurogastroenterol Motil21: 734–739.e43, 2009.
30. Carroccio A, Brusca I, Mansueto P, Pirrone G, Barrale M, Di PrimaL, Ambrosiano G, Iacono G, Lospalluti ML, La Chiusa SM, Di FedeG. A cytologic assay for diagnosis of food hypersensitivity in patientswith irritable bowel syndrome. Clin Gastroenterol Hepatol 8: 254–260,2010.
31. Carroccio A, Brusca I, Mansueto P, Soresi M, D’Alcamo A, Ambro-siano G, Pepe I, Iacono G, Lospalluti ML, La Chiusa SM, Di Fede G.Fecal assays detect hypersensitivity to cow’s milk protein and gluten inadults with irritable bowel syndrome. Clin Gastroenterol Hepatol 9:965–971.e3, 2011.
32. Carroll IM, Chang YH, Park J, Sartor RB, Ringel Y. Luminal andmucosal-associated intestinal microbiota in patients with diarrhea-pre-dominant irritable bowel syndrome. Gut Pathog 2: 19, 2010.
33. Carroll IM, Ringel-Kulka T, Keku TO, Chang YH, Packey CD,Sartor RB, Ringel Y. Molecular analysis of the luminal- and mucosal-associated intestinal microbiota in diarrhea-predominant irritable bowelsyndrome. Am J Physiol Gastrointest Liver Physiol 301: G799–G807,2011.
34. Carroll IM, Ringel-Kulka T, Siddle JP, Ringel Y. Alterations incomposition and diversity of the intestinal microbiota in patients withdiarrhea-predominant irritable bowel syndrome. Neurogastroenterol Mo-til 24: 521–530.e248, 2012.
35. Cenac N, Andrews CN, Holzhausen M, Chapman K, Cottrell G,Andrade-Gordon P, Steinhoff M, Barbara G, Beck P, Bunnett NW,Sharkey KA, Ferraz JG, Shaffer E, Vergnolle N. Role for proteaseactivity in visceral pain in irritable bowel syndrome. J Clin Invest 117:636–647, 2007.
36. Chadwick VS, Chen W, Shu D, Paulus B, Bethwaite P, Tie A, WilsonI. Activation of the mucosal immune system in irritable bowel syndrome.Gastroenterology 122: 1778–1783, 2002.
37. Choi CH, Jo SY, Park HJ, Chang SK, Byeon JS, Myung SJ. Arandomized, double-blind, placebo-controlled multicenter trial of saccha-romyces boulardii in irritable bowel syndrome: effect on quality of life.J Clin Gastroenterol 45: 679–683, 2011.
38. Chrousos GP. The hypothalamic-pituitary-adrenal axis and immune-mediated inflammation. N Engl J Med 332: 1351–1362, 1995.
39. Chung EK, Zhang X, Li Z, Zhang H, Xu H, Bian Z. Neonatal maternalseparation enhances central sensitivity to noxious colorectal distention inrat. Brain Res 1153: 68–77, 2007.
40. Codling C, O’Mahony L, Shanahan F, Quigley EM, Marchesi JR. Amolecular analysis of fecal and mucosal bacterial communities in irrita-ble bowel syndrome. Dig Dis Sci 55: 392–397, 2010.
41. Coeffier M, Gloro R, Boukhettala N, Aziz M, Lecleire S, Vandaele N,Antonietti M, Savoye G, Bole-Feysot C, Dechelotte P, Reimund JM,Ducrotte P. Increased proteasome-mediated degradation of occludin inirritable bowel syndrome. Am J Gastroenterol 105: 1181–1188, 2010.
42. Coelho AM, Fioramonti J, Buéno L. Systemic lipopolysaccharideinfluences rectal sensitivity in rats: role of mast cells, cytokines, andvagus nerve. Am J Physiol Gastrointest Liver Physiol 279: G781–G790,2000.
43. Collins S, Verdu E, Denou E, Bercik P. The role of pathogenicmicrobes and commensal bacteria in irritable bowel syndrome. Dig Dis27, Suppl 1: 85–89, 2009.
44. Collins SM. The immunomodulation of enteric neuromuscular function:implications for motility and inflammatory disorders. Gastroenterology111: 1683–1699, 1996.
45. Corinaldesi R, Stanghellini V, Cremon C, Gargano L, CogliandroRF, De Giorgio R, Bartesaghi G, Canovi B, Barbara G. Effect ofmesalazine on mucosal immune biomarkers in irritable bowel syndrome:a randomized controlled proof-of-concept study. Aliment PharmacolTher 30: 245–252, 2009.
46. Cremon C, Gargano L, Morselli-Labate AM, Santini D, CogliandroRF, De Giorgio R, Stanghellini V, Corinaldesi R, Barbara G. Muco-sal immune activation in irritable bowel syndrome: gender-dependenceand association with digestive symptoms. Am J Gastroenterol 104:392–400, 2009.
47. Cuoco L, Salvagnini M. Small intestine bacterial overgrowth in irritablebowel syndrome: a retrospective study with rifaximin. Minerva Gastro-enterol Dietol 52: 89–95, 2006.
48. De Giorgio R, Barbara G. Is irritable bowel syndrome an inflammatorydisorder? Curr Gastroenterol Rep 10: 385–390, 2008.
49. Dear KLE, Elia M, Hunter JO. Do interventions which reduce colonicbacterial fermentation improve symptoms of irritable bowel syndrome?Dig Dis Sci 50: 758–766, 2005.
50. Dinan TG, Clarke G, Quigley EMM, Scott LV, Shanahan F, CryanJ, Cooney J, Keeling PW. Enhanced cholinergic-mediated increase inthe proinflammatory cytokine IL-6 in irritable bowel syndrome: role ofmuscarinic receptors. Am J Gastroenterol 103: 2570–2576, 2008.
51. Dinan TG, Quigley EMM, Ahmed SMM, Scully P, O’Brien S,O’Mahony L, O’Mahony S, Shanahan F, Keeling PW. Hypothalamic-pituitary-gut axis dysregulation in irritable bowel syndrome: plasmacytokines as a potential biomarker? Gastroenterology 130: 304–311,2006.
52. Distrutti E, Sediari L, Mencarelli A, Renga B, Orlandi S, Russo G,Caliendo G, Santagada V, Cirino G, Wallace JL, Fiorucci S. 5-Ami-no-2-hydroxybenzoic acid 4-(5-thioxo-5H-[1,2]dithiol-3yl)-phenyl ester(ATB-429), a hydrogen sulfide-releasing derivative of mesalamine, ex-erts antinociceptive effects in a model of postinflammatory hypersensi-tivity. J Pharmacol Exp Ther 319: 447–458, 2006.
53. Drossman DA, Camilleri M, Mayer EA, Whitehead WE. AGAtechnical review on irritable bowel syndrome. Gastroenterology 123:2108–2131, 2002.
54. Duboc H, Rainteau D, Rajca S, Humbert L, Farabos D, Maubert M,Grondin V, Jouet P, Bouhassira D, Seksik P, Sokol H, Coffin B,Sabate JM. Increase in fecal primary bile acids and dysbiosis in patientswith diarrhea-predominant irritable bowel syndrome. NeurogastroenterolMotil 24: 513–520, e246–e247, 2012.
55. Dunckley P, Aziz Q, Wise RG, Brooks J, Tracey I, Chang L.Attentional modulation of visceral and somatic pain. NeurogastroenterolMotil 19: 569–577, 2007.
56. Dunlop SP, Hebden J, Campbell E, Naesdal J, Olbe L, Perkins AC,Spiller RC. Abnormal intestinal permeability in subgroups of diarrhea-predominant irritable bowel syndromes. Am J Gastroenterol 101: 1288–1294, 2006.
Review
G537MICROBIOTA AND IMMUNE FUNCTION IN IBS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00207.2012 • www.ajpgi.org

57. Dunlop SP, Jenkins D, Neal KR, Spiller RC. Relative importance ofenterochromaffin cell hyperplasia, anxiety, and depression in postinfec-tious IBS. Gastroenterology 125: 1651–1659, 2003.
58. Dunlop SP, Jenkins D, Spiller RC. Distinctive clinical, psychological,and histological features of postinfective irritable bowel syndrome. Am JGastroenterol 98: 1578–1583, 2003.
59. Esposito I, de Leone A, Di Gregorio G, Giaquinto S, de Magistris L,Ferrieri A, Riegler G. Breath test for differential diagnosis betweensmall intestinal bacterial overgrowth and irritable bowel disease: anobservation on non-absorbable antibiotics. World J Gastroenterol 13:6016–6021, 2007.
60. Feng B, La JH, Schwartz ES, Gebhart GF. Irritable Bowel Syndrome:Methods, Mechanisms, and Pathophysiology. Neural and neuro-immunemechanisms of visceral hypersensitivity in irritable bowel syndrome. AmJ Physiol Gastrointest Liver Physiol 302: (10) G1085–G1098, 2012.
61. Ford AC, Spiegel BMR, Talley NJ, Moayyedi P. Small intestinalbacterial overgrowth in irritable bowel syndrome: systematic review andmeta-analysis. Clin Gastroenterol Hepatol 7: 1279–1286, 2009.
62. Forshammar J, Isaksson S, Strid H, Stotzer PO, Sjovall H, SimrenM, Ohman L. A pilot study of colonic B cell pattern in irritable bowelsyndrome. Scand J Gastroenterol 43: 1461–1466, 2008.
63. Fraher MH, O’Toole PW, Quigley EM. Techniques used to character-ize the gut microbiota: a guide for the clinician. Nat Rev GastroenterolHepatol 9: 312–322, 2012.
64. Fukuda S, Toh H, Hase K, Oshima K, Nakanishi Y, Yoshimura K,Tobe T, Clarke JM, Topping DL, Suzuki T, Taylor TD, Itoh K,Kikuchi J, Morita H, Hattori M, Ohno H. Bifidobacteria can protectfrom enteropathogenic infection through production of acetate. Nature469: 543–547, 2011.
65. Fukudo S, Kanazawa M. Gene, environment, and brain-gut interactionsin irritable bowel syndrome. J Gastroenterol Hepatol 26, Suppl 3:110–115, 2011.
66. Fukumoto S, Tatewaki M, Yamada T, Fujimiya M, Mantyh C, VossM, Eubanks S, Harris M, Pappas TN, Takahashi T. Short-chain fattyacids stimulate colonic transit via intraluminal 5-HT release in rats. AmJ Physiol Regul Integr Comp Physiol 284: R1269–R1276, 2003.
67. Gecse K, Roka R, Ferrier L, Leveque M, Eutamene H, Cartier C,Ait-Belgnaoui A, Rosztoczy A, Izbeki F, Fioramonti J, Wittmann T,Bueno L. Increased faecal serine protease activity in diarrhoeic IBSpatients: a colonic lumenal factor impairing colonic permeability andsensitivity. Gut 57: 591–599, 2008.
68. Gibson PR. Food intolerance in functional bowel disorders. J Gastro-enterol Hepatol 26, Suppl 3: 128–131, 2011.
69. Goehler LE, Lyte M, Gaykema RPA. Infection-induced viscerosensorysignals from the gut enhance anxiety: implications for psychoneuroim-munology. Brain Behav Immun 21: 721–726, 2007.
70. Gonsalkorale WM, Perrey C, Pravica V, Whorwell PJ, HutchinsonIV. Interleukin 10 genotypes in irritable bowel syndrome: evidence foran inflammatory component? Gut 52: 91–93, 2003.
71. Guandalini S, Magazzù G, Chiaro A, La Balestra V, Di Nardo G,Gopalan S, Sibal A, Romano C, Canani RB, Lionetti P, Setty M.VSL#3 improves symptoms in children with irritable bowel syndrome: amulticenter, randomized, placebo-controlled, double-blind, crossoverstudy. J Pediatr Gastroenterol Nutr 51: 24–30, 2010.
72. Guglielmetti S, Mora D, Gschwender M, Popp K. Randomised clinicaltrial: Bifidobacterium bifidum MIMBb75 significantly alleviates irritablebowel syndrome and improves quality of life—a double-blind, placebo-controlled study. Aliment Pharmacol Ther 33: 1123–1132, 2011.
73. Guilarte M, Santos J, de Torres I, Alonso C, Vicario M, Ramos L,Martinez C, Casellas F, Saperas E, Malagelada JR. Diarrhoea-pre-dominant IBS patients show mast cell activation and hyperplasia in thejejunum. Gut 56: 203–209, 2007.
74. Guyonnet D, Chassany O, Ducrotte P, Picard C, Mouret M, MercierCH, Matuchansky C. Effect of a fermented milk containing Bifidobac-terium animalis DN-173 010 on the health-related quality of life andsymptoms in irritable bowel syndrome in adults in primary care: amulticentre, randomized, double-blind, controlled trial. Aliment Pharma-col Ther 26: 475–486, 2007.
75. Gwee KA, Collins SM, Read NW, Rajnakova A, Deng Y, GrahamJC, McKendrick MW, Moochhala SM. Increased rectal mucosal ex-pression of interleukin 1� in recently acquired post-infectious irritablebowel syndrome. Gut 52: 523–526, 2003.
76. Halvorson HA, Schlett CD, Riddle MS. Postinfectious irritable bowelsyndrome—a meta-analysis. Am J Gastroenterol 101: 1894–1899, 2006.
77. Hod K, Dickman R, Sperber A, Melamed S, Dekel R, Ron Y,Halpern Z, Berliner S, Maharshak N. Assessment of high-sensitivityCRP as a marker of micro-inflammation in irritable bowel syndrome.Neurogastroenterol Motil 23: 1105–1110, 2011.
78. Hooper LV, Littman DR, Macpherson AJ. Interactions between themicrobiota and the immune system. Science 336: 1268–1273, 2012.
79. Hoveyda N, Heneghan C, Mahtani KR, Perera R, Roberts N, Glas-ziou P. A systematic review and meta-analysis: probiotics in the treat-ment of irritable bowel syndrome. BMC Gastroenterol 9: 15, 2009.
80. Husebye E, Hellström PM, Sundler F, Chen J, Midtvedt T. Influenceof microbial species on small intestinal myoelectric activity and transit ingerm-free rats. Am J Physiol Gastrointest Liver Physiol 280: G368–G380, 2001.
81. Jeffery IB, O’Toole PW, Ohman L, Claesson MJ, Deane J, QuigleyEM, Simren M. An irritable bowel syndrome subtype defined byspecies-specific alterations in faecal microbiota. Gut 61: 997–1006, 2012.
82. Kamath PS, Hoepfner MT, Phillips SF. Short-chain fatty acids stim-ulate motility of the canine ileum. Am J Physiol Gastrointest LiverPhysiol 253: G427–G433, 1987.
83. Kamiya T, Wang L, Forsythe P, Goettsche G, Mao Y, Wang Y,Tougas G, Bienenstock J. Inhibitory effects of Lactobacillus reuteri onvisceral pain induced by colorectal distension in Sprague-Dawley rats.Gut 55: 191–196, 2006.
84. Kannampalli P, Shaker R, Sengupta JN. Colonic butyrate—algesic oranalgesic? Neurogastroenterol Motil 23: 975–979, 2011.
85. Kassinen A, Krogius-Kurikka L, Makivuokko H, Rinttila T, PaulinL, Corander J, Malinen E, Apajalahti J, Palva A. The fecal microbiotaof irritable bowel syndrome patients differs significantly from that ofhealthy subjects. Gastroenterology 133: 24–33, 2007.
86. Kerckhoffs APM, Samsom M, van der Rest ME, de Vogel J, Knol J,Ben-Amor K, Akkermans LM. Lower Bifidobacteria counts in bothduodenal mucosa-associated and fecal microbiota in irritable bowelsyndrome patients. World J Gastroenterol 15: 2887–2892, 2009.
87. Ki Cha B, Mun Jung S, Hwan Choi C, Song ID, Woong Lee H, JoonKim H, Hyuk J, Kyung Chang S, Kim K, Chung WS, Seo JG. Theeffect of a multispecies probiotic mixture on the symptoms and fecalmicrobiota in diarrhea-dominant irritable bowel syndrome: a random-ized, double-blind, placebo-controlled trial. J Clin Gastroenterol 46:220–227, 2012.
88. Kim HJ, Vazquez Roque MI, Camilleri M, Stephens D, Burton DD,Baxter K, Thomforde G, Zinsmeister AR. A randomized controlledtrial of a probiotic combination VSL# 3 and placebo in irritable bowelsyndrome with bloating. Neurogastroenterol Motil 17: 687–696, 2005.
89. Kim HS, Lim JH, Park H, Lee SI. Increased immunoendocrine cells inintestinal mucosa of postinfectious irritable bowel syndrome patients 3years after acute Shigella infection-an observation in a small case controlstudy. Yonsei Med J 51: 45–51, 2010.
90. Kindt S, Van Oudenhove L, Broekaert D, Kasran A, Ceuppens JL,Bossuyt X, Fischler B, Tack J. Immune dysfunction in patients withfunctional gastrointestinal disorders. Neurogastroenterol Motil 21: 389–398, 2009.
91. Kunze WA, Mao YK, Wang B, Huizinga JD, Ma X, Forsythe P,Bienenstock J. Lactobacillus reuteri enhances excitability of colonic AHneurons by inhibiting calcium-dependent potassium channel opening. JCell Mol Med 13: 2261–2270, 2009.
92. Langhorst J, Junge A, Rueffer A, Wehkamp J, Foell D, Michalsen A,Musial F, Dobos GJ. Elevated human beta-defensin-2 levels indicate anactivation of the innate immune system in patients with irritable bowelsyndrome. Am J Gastroenterol 104: 404–410, 2009.
93. Le Gall G, Noor SO, Ridgway K, Scovell L, Jamieson C, Johnson IT,Colquhoun IJ, Kemsley EK, Narbad A. Metabolomics of fecal extractsdetects altered metabolic activity of gut microbiota in ulcerative colitisand irritable bowel syndrome. J Proteome Res 10: 4208–4218, 2011.
94. Lee KJ, Kim YB, Kim JH, Kwon HC, Kim DK, Cho SW. Thealteration of enterochromaffin cell, mast cell, and lamina propria Tlymphocyte numbers in irritable bowel syndrome and its relationshipwith psychological factors. J Gastroenterol Hepatol 23: 1689–1694,2008.
95. Lembo A, Zakko SF, Ferreira NL, Ringel Y, Bortey E, Courtney K,Corse E, Forbes W, Pimentel M. Rifaximin for the treatment ofdiarrhea-associated irritable bowel syndrome: short term treatment lead-ing to long term sustained response [AGA abstract T1390]. Gastroen-terology 134, Suppl 1: A-545, 2008.
Review
G538 MICROBIOTA AND IMMUNE FUNCTION IN IBS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00207.2012 • www.ajpgi.org
96. Lembo T, Naliboff B, Munakata J, Fullerton S, Saba L, Tung S,Schmulson M, Mayer EA. Symptoms and visceral perception in patientswith pain-predominant irritable bowel syndrome. Am J Gastroenterol 94:1320–1326, 1999.
97. Lesniewska V, Rowland I, Laerke HN, Grant G, Naughton PJ.Relationship between dietary-induced changes in intestinal commensalmicroflora and duodenojejunal myoelectric activity monitored by radio-telemetry in the rat in vivo. Exp Physiol 91: 229–237, 2006.
98. Liebregts T, Adam B, Bredack C, Roth A, Heinzel S, Lester S,Downie-Doyle S, Smith E, Drew P, Talley NJ, Holtmann G. Immuneactivation in patients with irritable bowel syndrome. Gastroenterology132: 913–920, 2007.
99. Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F,Spiller RC. Functional bowel disorders. Gastroenterology 130: 1480–1491, 2006.
100. Low K, Hwang L, Hua J, Zhu A, Morales W, Pimentel M. Acombination of rifaximin and neomycin is most effective in treatingirritable bowel syndrome patients with methane on lactulose breath test.J Clin Gastroenterol 44: 547–550, 2010.
101. Lunardi C, Bambara LM, Biasi D, Cortina P, Peroli P, Nicolis F,Favari F, Pacor ML. Double-blind cross-over trial of oral sodiumcromoglycate in patients with irritable bowel syndrome due to foodintolerance. Clin Exp Allergy 21: 569–572, 1991.
102. Macsharry J, O’Mahony L, Fanning A, Bairead E, Sherlock G,Tiesman J, Fulmer A, Kiely B, Dinan TG, Shanahan F, Quigley EM.Mucosal cytokine imbalance in irritable bowel syndrome. Scand JGastroenterol 43: 1467–1476, 2008.
103. Majewski M, McCallum RW. Results of small intestinal bacterialovergrowth testing in irritable bowel syndrome patients: clinical profilesand effects of antibiotic trial. Adv Med Sci 52: 139–142, 2007.
104. Malinen E, Rinttilä T, Kajander K, Matto J, Kassinen A, Krogius L,Saarela M, Korpela R, Palva A. Analysis of the fecal microbiota ofirritable bowel syndrome patients and healthy controls with real-timePCR. Am J Gastroenterol 100: 373–382, 2005.
105. Manichanh C, Borruel N, Casellas F, Guarner F. The gut microbiotain IBD. Nat Rev Gastroenterol Hepatol 9: 599–608, 2012.
106. Mättö J, Maunuksela L, Kajander K, Palva A, Korpela R, KassinenA, Saarela M. Composition and temporal stability of gastrointestinalmicrobiota in irritable bowel syndrome—a longitudinal study in IBS andcontrol subjects. FEMS Immunol Med Microbiol 43: 213–222, 2005.
107. Maukonen J, Satokari R, Mättö J, Söderlund H, Mattila-SandholmT, Saarela M. Prevalence and temporal stability of selected clostridialgroups in irritable bowel syndrome in relation to predominant faecalbacteria. J Med Microbiol 55: 625–633, 2006.
108. Mayer EA, Tillisch K. The brain-gut axis in abdominal pain syndromes.Annu Rev Med 62: 381–396, 2011.
109. Mekjian HS, Phillips SF, Hofmann AF. Colonic secretion of water andelectrolytes induced by bile acids: perfusion studies in man. J Clin Invest50: 1569–1577, 1971.
110. Moayyedi P, Ford AC, Talley NJ, Cremonini F, Foxx-Orenstein A,Brandt L, Quigley E. The efficacy of probiotics in the treatment ofirritable bowel syndrome: a systematic review. Gut 59: 325–332, 2010.
111. Morgan V, Pickens D, Gautam S, Kessler R, Mertz H. Amitriptylinereduces rectal pain related activation of the anterior cingulate cortex inpatients with irritable bowel syndrome. Gut 54: 601–607, 2005.
112. Murray CDR, Flynn J, Ratcliffe L, Jacyna MR, Kamm MA, Em-manuel AV. Effect of acute physical and psychological stress on gutautonomic innervation in irritable bowel syndrome. Gastroenterology127: 1695–1703, 2004.
113. Natividad JM, Petit V, Huang X, de Palma G, Jury J, Sanz Y,Philpott D, Garcia Rodenas CL, McCoy KD, Verdu EF. Commensaland probiotic bacteria influence intestinal barrier function and suscepti-bility to colitis in Nod1�/�; Nod2�/� mice. Inflamm Bowel Dis 18:1434–1446, 2012.
114. Nayak AK, Karnad DR, Abraham P, Mistry FP. Metronidazolerelieves symptoms in irritable bowel syndrome: the confusion withso-called ‘chronic amebiasis.’ Indian J Gastroenterol 16: 137–139, 1997.
115. Neufeld KA, Kang N, Bienenstock J, Foster JA. Effects of intestinalmicrobiota on anxiety-like behavior. Commun Integr Biol 4: 492–494,2011.
116. Neufeld KM, Kang N, Bienenstock J, Foster JA. Reduced anxiety-likebehavior and central neurochemical change in germ-free mice. Neuro-gastroenterol Motil 23: 255–264, e119, 2011.
117. Niedzielin K, Kordecki H, Birkenfeld B. A controlled, double-blind,randomized study on the efficacy of Lactobacillus plantarum 299V inpatients with irritable bowel syndrome. Eur J Gastroenterol Hepatol 13:1143–1147, 2001.
118. O’Mahony L, McCarthy J, Kelly P, Hurley G, Luo F, Chen K,O’Sullivan GC, Kiely B, Collins JK, Shanahan F, Quigley EM.Lactobacillus and Bifidobacterium in irritable bowel syndrome: symptomresponses and relationship to cytokine profiles. Gastroenterology 128:541–551, 2005.
119. O’Mahony SM, Marchesi JR, Scully P, Codling C, Ceolho AM,Quigley EM, Cryan JF, Dinan TG. Early life stress alters behavior,immunity, and microbiota in rats: implications for irritable bowel syn-drome and psychiatric illnesses. Biol Psychiatry 65: 263–267, 2009.
120. O’Malley D, Quigley EM, Dinan TG, Cryan JF. Do interactionsbetween stress and immune responses lead to symptom exacerbations inirritable bowel syndrome? Brain Behav Immun 25: 1333–1341, 2011.
121. O’Sullivan M, Clayton N, Breslin NP, Harman I, Bountra C,McLaren A, O’Morain CA. Increased mast cells in the irritable bowelsyndrome. Neurogastroenterol Motil 12: 449–457, 2000.
122. Ohman L, Isaksson S, Lindmark AC, Posserud I, Stotzer PO, StridH, Sjovall H, Simren M. T-cell activation in patients with irritablebowel syndrome. Am J Gastroenterol 104: 1205–1212, 2009.
123. Ohman L, Isaksson S, Lundgren A, Simrén M, Sjovall H. A con-trolled study of colonic immune activity and �7� blood T lymphocytesin patients with irritable bowel syndrome. Clin Gastroenterol Hepatol 3:980–986, 2005.
124. Ohman L, Lindmark AC, Isaksson S, Posserud I, Strid H, Sjovall H,Simren M. B-cell activation in patients with irritable bowel syndrome(IBS). Neurogastroenterol Motil 21: 644–650, 2009.
125. Ohman L, Simrén M. New insights into the pathogenesis and patho-physiology of irritable bowel syndrome. Dig Liver Dis 39: 201–215,2007.
126. Ohman L, Simrén M. Pathogenesis of IBS: role of inflammation,immunity and neuroimmune interactions. Nat Rev Gastroenterol Hepatol7: 163–173, 2010.
127. Ong DK, Mitchell SB, Barrett JS, Shepherd SJ, Irving PM, Biesieki-erski JR, Smith S, Gibson PR, Muir JG. Manipulation of dietary shortchain carbohydrates alters the pattern of gas production and genesis ofsymptoms in irritable bowel syndrome. J Gastroenterol Hepatol 25:1366–1373, 2010.
128. Park DH, Kim MH, Chari ST. Recent advances in autoimmunepancreatitis. Gut 58: 1680–1689, 2009.
129. Parkes GC, Rayment NB, Hudspith BN, Petrovska L, Lomer MC,Brostoff J, Whelan K, Sanderson JD. Distinct microbial populationsexist in the mucosa-associated microbiota of sub-groups of irritablebowel syndrome. Neurogastroenterol Motil 24: 31–39, 2012.
130. Peery AF, Dellon ES, Lund J, Crockett SD, McGowan CE, Bulsie-wicz WJ, Gangarosa LM, Thiny MT, Stizenberg K, Morgan DR,Ringel Y, Kim HP, Dibonaventura MD, Carroll CF, Allen JK, CookSF, Sandler RS, Kappelman MD, Shaheen NJ. Burden of gastrointes-tinal disease in the United States: 2012 update. Gastroenterology 143:1179–1187.e1–e3, 2012.
131. Peralta S, Cottone C, Doveri T, Almasio PL, Craxi A. Small intestinebacterial overgrowth and irritable bowel syndrome-related symptoms:experience with rifaximin. World J Gastroenterol 15: 2628–2631, 2009.
132. Piche T, Barbara G, Aubert P, Bruley des Varannes S, Dainese R,Nano JL, Cremon C, Stanghellini V, De Giorgio R, Galmiche JP,Neunlist M. Impaired intestinal barrier integrity in the colon of patientswith irritable bowel syndrome: involvement of soluble mediators. Gut58: 196–201, 2009.
133. Piche T, Saint-Paul MC, Dainese R, Marine-Barjoan E, Iannelli A,Montoya ML, Peyron JF, Czerucka D, Cherikh F, Filippi J, Tran A,Hebuterne X. Mast cells and cellularity of the colonic mucosa correlatedwith fatigue and depression in irritable bowel syndrome. Gut 57: 468–473, 2008.
134. Pimentel M, Chatterjee S, Chow EJ, Park S, Kong Y. Neomycinimproves constipation-predominant irritable bowel syndrome in a fash-ion that is dependent on the presence of methane gas: subanalysis of adouble-blind randomized controlled study. Dig Dis Sci 51: 1297–1301,2006.
135. Pimentel M, Chow EJ, Lin HC. Eradication of small intestinal bacterialovergrowth reduces symptoms of irritable bowel syndrome. Am J Gas-troenterol 95: 3503–3506, 2000.
Review
G539MICROBIOTA AND IMMUNE FUNCTION IN IBS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00207.2012 • www.ajpgi.org

136. Pimentel M, Chow EJ, Lin HC. Normalization of lactulose breathtesting correlates with symptom improvement in irritable bowel syn-drome: a double-blind, randomized, placebo-controlled study. Am JGastroenterol 98: 412–419, 2003.
137. Pimentel M, Lembo A, Chey WD, Zakko S, Ringel Y, Yu J, MareyaSM, Shaw AL, Bortey E, Forbes WP. Rifaximin therapy for patientswith irritable bowel syndrome without constipation. N Engl J Med 364:22–32, 2011.
138. Pimentel M, Morales W, Chua K, Barlow G, Weitsman S, Kim G,Amichai MM, Pokkunuri V, Rook E, Mathur R, Marsh Z. Effects ofrifaximin treatment and retreatment in nonconstipated IBS subjects. DigDis Sci 56: 2067–2072, 2011.
139. Pimentel M, Park S, Mirocha J, Kane SV, Kong Y. The effect of anonabsorbed oral antibiotic (rifaximin) on the symptoms of the irritablebowel syndrome: a randomized trial. Ann Intern Med 145: 557–563,2006.
140. Pimentel M, Soffer EE, Chow EJ, Kong Y, Lin HC. Lower frequencyof MMC is found in IBS subjects with abnormal lactulose breath test,suggesting bacterial overgrowth. Dig Dis Sci 47: 2639–2643, 2002.
141. Posserud I, Stotzer PO, Björnsson ES, Abrahamsson H, Simrén M.Small intestinal bacterial overgrowth in patients with irritable bowelsyndrome. Gut 56: 802–808, 2007.
142. Rajilic-Stojanovic M, Biagi E, Heilig HGHJ, Kajander K, KekkonenRA, Tims S, de Vos WM. Global and deep molecular analysis ofmicrobiota signatures in fecal samples from patients with irritable bowelsyndrome. Gastroenterology 141: 1792–1801, 2011.
143. Rao SS, Read NW, Brown C, Bruce C, Holdsworth CD. Studies on themechanism of bowel disturbance in ulcerative colitis. Gastroenterology93: 934–940, 1987.
144. Ringel-Kulka T, Palsson OS, Maier D, Carroll I, Galanko JA, LeyerG, Ringel Y. Probiotic bacteria Lactobacillus acidophilus NCFM andBifidobacterium lactis Bi-07 versus placebo for the symptoms of bloatingin patients with functional bowel disorders: a double-blind study. J ClinGastroenterol 45: 518–525, 2011.
145. Ringel Y, Carroll IM. Alterations in the intestinal microbiota andfunctional bowel symptoms. Gastrointest Endosc Clin N Am 19: 141–150, 2009.
146. Ringel Y, Drossman DA. Irritable bowel syndrome. In: Netter’s Text-book of Internal Medicine (2nd ed.), edited by Runge MS, Greganti MA.Philadelphia, PA: Saunders Elsevier, 2009, p. 419–425.
147. Ringel Y, Quigley E, Lin HC. Probiotics and gastrointestinal disorders.Am J Gastroenterol Suppl 1: 34–40, 2012.
148. Ringel Y, Ringel-Kulka T. The rationale and clinical effectiveness ofprobiotics in irritable bowel syndrome. J Clin Gastroenterol 45 Suppl:S145–S148, 2011.
149. Ringel Y, Whitehead WE, Toner BB, Diamant NE, Hu Y, Jia H,Bangdiwala SI, Drossman DA. Sexual and physical abuse are notassociated with rectal hypersensitivity in patients with irritable bowelsyndrome. Gut 53: 838–842, 2004.
150. Roberts L, Wilson S, Singh S, Roalfe A, Greenfield S. Gut-directedhypnotherapy for irritable bowel syndrome: piloting a primary care-basedrandomised controlled trial. Br J Gen Pract 56: 115–121, 2006.
151. Rousseaux C, Thuru X, Gelot A, Barnich N, Neut C, Dubuquoy L,Dubuquoy C, Merour E, Geboes K, Chamaillard M, Ouwehand A,Leyer G, Carcano D, Colombel JF, Ardid D, Desreumaux P. Lacto-bacillus acidophilus modulates intestinal pain and induces opioid andcannabinoid receptors. Nat Med 13: 35–37, 2007.
152. Sagami Y, Shimada Y, Tayama J, Nomura T, Satake M, Endo Y,Shoji T, Karahashi K, Hongo M, Fukudo S. Effect of a corticotropinreleasing hormone receptor antagonist on colonic sensory and motorfunction in patients with irritable bowel syndrome. Gut 53: 958–964,2004.
153. Salonen A, de Vos WM, Palva A. Gastrointestinal microbiota inirritable bowel syndrome: present state and perspectives. Microbiology156: 3205–3215, 2010.
154. Saulnier DM, Riehle K, Mistretta TA, Diaz MA, Mandal D, Raza S,Weidler EM, Qin X, Coarfa C, Milosavljevic A, Petrosino JF,Highlander S, Gibbs R, Lynch SV, Shulman RJ, Versalovic J.Gastrointestinal microbiome signatures of pediatric patients with irritablebowel syndrome. Gastroenterology 141: 1782–1791, 2011.
155. Saulnier DM, Ringel Y, Heyman MB, Foster JA, Bercik P, ShulmanR, Versalovic J, Verdu E, Dinan TG, Hecht G, Guarner F. Theintestinal microbiome, probiotics, and prebiotics in neurogastroenterol-ogy. Gut Microbes 4: 17–27, 2013.
156. Schoepfer AM, Schaffer T, Seibold-Schmid B, Muller S, Seibold F.Antibodies to flagellin indicate reactivity to bacterial antigens in IBSpatients. Neurogastroenterol Motil 20: 1110–1118, 2008.
157. Schwille-Kiuntke J, Enck P, Zendler C, Krieg M, Polster AV,Klosterhalfen S, Autenrieth IB, Zipfel S, Frick JS. Postinfectiousirritable bowel syndrome: follow-up of a patient cohort of confirmedcases of bacterial infection with Salmonella or Campylobacter. Neuro-gastroenterol Motil 23: e479–e488, 2011.
158. Sekirov I, Russell SL, Antunes LCM, Finlay BB. Gut microbiota inhealth and disease. Physiol Rev 90: 859–904, 2010.
159. Shaheen NJ, Hansen RA, Morgan DR, Gangarosa LM, Ringel Y,Thiny MT, Russo MW, Sandler RS. The burden of gastrointestinal andliver diseases, 2006. Am J Gastroenterol 101: 2128–2138, 2006.
160. Sharara AI, Aoun E, Abdul-Baki H, Mounzer R, Sidani S, ElHajj I.A randomized double-blind placebo-controlled trial of rifaximin in pa-tients with abdominal bloating and flatulence. Am J Gastroenterol 101:326–333, 2006.
161. Shepherd SJ, Parker FC, Muir JG, Gibson PR. Dietary triggers ofabdominal symptoms in patients with irritable bowel syndrome: random-ized placebo-controlled evidence. Clin Gastroenterol Hepatol 6: 765–771, 2008.
162. Shulman RJ, Eakin MN, Czyzewski DI, Jarrett M, Ou CN. Increasedgastrointestinal permeability and gut inflammation in children with func-tional abdominal pain and irritable bowel syndrome. J Pediatr 153:646–650, 2008.
163. Silk DB, Davis A, Vulevic J, Tzortzis G, Gibson GR. Clinical trial: theeffects of a trans-galactooligosaccharide prebiotic on faecal microbiotaand symptoms in irritable bowel syndrome. Aliment Pharmacol Ther 29:508–518, 2009.
164. Simren M, Barbara G, Flint HJ, Spiegel BM, Spiller RC, Vanner S,Verdu EF, Whorwell PJ, Zoetendal EG. Intestinal microbiota infunctional bowel disorders: a Rome foundation report. Gut 62: 159–176,2013.
165. Simrén M, Ringström G, Björnsson ES, Abrahamsson H. Treatmentwith hypnotherapy reduces the sensory and motor component of thegastrocolonic response in irritable bowel syndrome. Psychosom Med 66:233–238, 2004.
166. Soret R, Chevalier J, De Coppet P, Poupeau G, Derkinderen P,Segain JP, Neunlist M. Short-chain fatty acids regulate the entericneurons and control gastrointestinal motility in rats. Gastroenterology138: 1772–1782, 2010.
167. Sperber AD, Dekel R. Irritable bowel syndrome and co-morbid gastro-intestinal and extra-gastrointestinal functional syndromes. J Neurogas-troenterol Motil 16: 113–119, 2010.
168. Spiller RC, Jenkins D, Thornley JP, Hebden JM, Wright T, SkinnerM, Neal KR. Increased rectal mucosal enteroendocrine cells, T lympho-cytes, and increased gut permeability following acute Campylobacterenteritis and in post-dysenteric irritable bowel syndrome. Gut 47: 804–811, 2000.
169. Suply E, de Vries P, Soret R, Cossais F, Neunlist M. Butyrate enemasenhance both cholinergic and nitrergic phenotype of myenteric neuronsand neuromuscular transmission in newborn rat colon. Am J PhysiolGastrointest Liver Physiol 302: G1373–G1380, 2012.
170. Swan C, Duroudier NP, Campbell E, Zaitoun A, Hastings M, DukesGE, Cox J, Kelly FM, Wilde J, Lennon MG, Neal KR, Whorwell PJ,Hall IP, Spiller RC. Identifying and testing candidate genetic polymor-phisms in the irritable bowel syndrome (IBS): association with TNFSF15and TNFalpha. Gut 62: 985–994, 2013.
171. Tana C, Umesaki Y, Imaoka A, Handa T, Kanazawa M, Fukudo S.Altered profiles of intestinal microbiota and organic acids may be theorigin of symptoms in irritable bowel syndrome. NeurogastroenterolMotil 22: 512–519, e114–e115, 2010.
172. Thabane M, Kottachchi DT, Marshall JK. Systematic review andmeta-analysis: the incidence and prognosis of post-infectious irritablebowel syndrome. Aliment Pharmacol Ther 26: 535–544, 2007.
173. Tlaskalova-Hogenova H, Stepankova R, Kozakova H, Hudcovic T,Vannucci L, Tuckova L, Rossmann P, Hrncir T, Kverka M, Zako-stelska Z, Klimesova K, Pribylova J, Bartova J, Sanchez D, FundovaP, Borovska D, Srutkova D, Zidek Z, Schwarzer M, Drastich P,Funda DP. The role of gut microbiota (commensal bacteria) and themucosal barrier in the pathogenesis of inflammatory and autoimmunediseases and cancer: contribution of germ-free and gnotobiotic animalmodels of human diseases. Cell Mol Immunol 8: 110–120, 2011.
Review
G540 MICROBIOTA AND IMMUNE FUNCTION IN IBS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00207.2012 • www.ajpgi.org

174. Törnblom H, Lindberg G, Nyberg B, Veress B. Full-thickness biopsyof the jejunum reveals inflammation and enteric neuropathy in irritablebowel syndrome. Gastroenterology 123: 1972–1979, 2002.
175. Treem WR, Ahsan N, Kastoff G, Hyams JS. Fecal short-chain fattyacids in patients with diarrhea-predominant irritable bowel syndrome: invitro studies of carbohydrate fermentation. J Pediatr Gastroenterol Nutr23: 280–286, 1996.
176. Turnbull AV, Rivier CL. Regulation of the hypothalamic-pituitary-adrenal axis by cytokines: actions and mechanisms of action. Physiol Rev79: 1–71, 1999.
177. Tuteja AK, Fang JC, Al-Suqi M, Stoddard GJ, Hale DC. Double-blind placebo-controlled study of mesalamine in post-infective irritablebowel syndrome — a pilot study. Scand J Gastroenterol 47: 1159–1164,2012.
178. Ulluwishewa D, Anderson RC, McNabb WC, Moughan PJ, WellsJM, Roy NC. Regulation of tight junction permeability by intestinalbacteria and dietary components. J Nutr 141: 769–776, 2011.
179. van der Veek PPJ, van den Berg M, de Kroon YE, Verspaget HW,Masclee AAM. Role of tumor necrosis factor-� and interleukin-10 genepolymorphisms in irritable bowel syndrome. Am J Gastroenterol 100:2510–2516, 2005.
180. Vanhoutvin SA, Troost FJ, Kilkens TO, Lindsey PJ, Hamer HM,Jonkers DM, Venema K, Brummer RJ. The effects of butyrate enemason visceral perception in healthy volunteers. Neurogastroenterol Motil21: 952–957.e76, 2009.
181. Vasina V, Barbara G, Talamonti L, Stanghellini V, Corinaldesi R,Tonini M, De Ponti F, De Giorgio R. Enteric neuroplasticity evoked byinflammation. Auton Neurosci 126–127: 264–272, 2006.
182. Verdu EF, Bercik P, Verma-Gandhu M, Huang XX, BlennerhassettP, Jackson W, Mao Y, Wang L, Rochat F, Collins SM. Specificprobiotic therapy attenuates antibiotic induced visceral hypersensitivityin mice. Gut 55: 182–190, 2006.
183. Vicario M, Alonso C, Guilarte M, Serra J, Martínez C, González-Castro AM, Lobo B, Antolín M, Andreu AL, García-Arumí E,Casellas M, Saperas E, Malagelada JR, Azpiroz F, Santos J. Chronicpsychosocial stress induces reversible mitochondrial damage and corti-cotropin-releasing factor receptor type-1 upregulation in the rat intestineand IBS-like gut dysfunction. Psychoneuroendocrinology 37: 65–77,2012.
184. Villani AC, Lemire M, Thabane M, Belisle A, Geneau G, Garg AX,Clark WF, Moayyedi P, Collins SM, Franchimont D, Marshall JK.Genetic risk factors for post-infectious irritable bowel syndrome follow-
ing a waterborne outbreak of gastroenteritis. Gastroenterology 138:1502–1513, 2010.
185. Walker MM, Talley NJ, Prabhakar M, Pennaneac’h CJ, Aro P,Ronkainen J, Storskrubb T, Harmsen WS, Zinsmeister AR, AgreusL. Duodenal mastocytosis, eosinophilia and intraepithelial lymphocyto-sis as possible disease markers in the irritable bowel syndrome andfunctional dyspepsia. Aliment Pharmacol Ther 29: 765–773, 2009.
186. Walters B, Vanner SJ. Detection of bacterial overgrowth in IBS usingthe lactulose H2 breath test: comparison with 14C-D-xylose and healthycontrols. Am J Gastroenterol 100: 1566–1570, 2005.
187. Wang LH, Fang XC, Pan GZ. Bacillary dysentery as a causative factorof irritable bowel syndrome and its pathogenesis. Gut 53: 1096–1101,2004.
188. Waterer GW, Wunderink RG. Science review: genetic variability inthe systemic inflammatory response. Crit Care 7: 308–314, 2003.
189. Weston AP, Biddle WL, Bhatia PS, Miner PB Jr. Terminal ilealmucosal mast cells in irritable bowel syndrome. Dig Dis Sci 38: 1590–1595, 1993.
190. Whorwell PJ, Altringer L, Morel J, Bond Y, Charbonneau D,O’Mahony L, Kiely B, Shanahan F, Quigley EM. Efficacy of anencapsulated probiotic Bifidobacterium infantis 35624 in women withirritable bowel syndrome. Am J Gastroenterol 101: 1581–1590, 2006.
191. Wilhelmsen I. Brain-gut axis as an example of the bio-psycho-socialmodel. Gut 47, Suppl IV: iv5–iv7, 2000.
192. Wong BS, Camilleri M, Busciglio I, Carlson P, Szarka LA, Burton D,Zinsmeister AR. Pharmacogenetic trial of a cannabinoid agonist showsreduced fasting colonic motility in patients with nonconstipated irritablebowel syndrome. Gastroenterology 141: 1638–1647.e31–e37, 2011.
193. Yang J, Lee HR, Low K, Chatterjee S, Pimentel M. Rifaximin versusother antibiotics in the primary treatment and retreatment of bacterialovergrowth in IBS. Dig Dis Sci 53: 169–174, 2008.
194. Yu D, Cheeseman F, Vanner S. Combined oro-caecal scintigraphy andlactulose hydrogen breath testing demonstrate that breath testing detectsoro-caecal transit, not small intestinal bacterial overgrowth in patientswith IBS. Gut 60: 334–340, 2011.
195. Zar S, Mincher L, Benson MJ, Kumar D. Food-specific IgG4 anti-body-guided exclusion diet improves symptoms and rectal compliance inirritable bowel syndrome. Scand J Gastroenterol 40: 800–807, 2005.
196. Zuo XL, Li YQ, Li WJ, Guo YT, Lu XF, Li JM, Desmond PV.Alterations of food antigen-specific serum immunoglobulins G and Eantibodies in patients with irritable bowel syndrome and functionaldyspepsia. Clin Exp Allergy 37: 823–830, 2007.
Review
G541MICROBIOTA AND IMMUNE FUNCTION IN IBS
AJP-Gastrointest Liver Physiol • doi:10.1152/ajpgi.00207.2012 • www.ajpgi.org





























