Embed Size (px)
Citation preview
European Journal of Pharmacology 659 (2011) 213–223
Contents lists available at ScienceDirect
European Journal of Pharmacology
j ourna l homepage: www.e lsev ie r.com/ locate /e jphar
Cardiovascular Pharmacology
Investigation of the potential effects of metformin on atherothrombotic risk factors inhyperlipidemic rats
Somsuvra B. Ghatak a,⁎, Prakash S. Dhamecha b, Shraddha V. Bhadada a, Shital J. Panchal a
a Department of Pharmacology, Institute of Pharmacy, Nirma University, Sarkhej-Gandhinagar Highway, Ahmedabad-382 481, Gujarat, Indiab Torrent Pharmaceuticals Limited, Torrent Research Centre, Village Bhat, District – Gandhinagar – 382 428, Gujarat, India
⁎ Corresponding author. Tel.: +91 8141913478; fax:E-mail address: [email protected] (S.B. Ghat
0014-2999/$ – see front matter © 2011 Elsevier B.V. Aldoi:10.1016/j.ejphar.2011.03.029
a b s t r a c t
a r t i c l e i n f oArticle history:Received 3 October 2010Received in revised form 23 February 2011Accepted 21 March 2011Available online 2 April 2011
Keywords:MetforminHyperlipidemiaThrombosisOxidative stress
The increased mortality rate due to atherothrombotic events and related complications has necessitated thesearch for new pharmacological agents. Hyperlipidemia, thrombosis and oxidative stress are the primaryunderlying concerns in the pathogenesis of atherosclerosis. Metformin, although proved to be beneficial inmicro and macrovascular complications of diabetes mellitus, its effects on pure cardiovascular subjects arestill debatable. Hence, the aim of the present study was to investigate the effects of metformin onatherothrombotic risk factors in experimental hyperlipidemic rats. Hyperlipidemia was induced by an intra-peritoneal injection of criton X-100 (25 mg/kg). Assessment of the effects of metformin (300 mg/kg/day,400 mg/kg/day and 500 mg/kg/day) on lipid profile, coagulation time (activated partial thromboplastin timeand prothrombin time), fibrinogen level, thrombosis, lipid peroxidation, antioxidant enzymes level, plasmafluorescent oxidation products and aortic nitrite level revealed an overall improvement in the lipid profile atthe dose of 400 mg/kg along with a significant reduction in oxidative stress as compared to criton X-100treated control. Activated partial thromboplastin and prothrombin times were prolonged at all doses, whileplasma fibrinogen level remained unaffected. Metformin pre-treatment also reduced endothelial cell damagein ferrous chloride induced thrombosis in carotid arteries. Thus, the results indicate a potential protectiveeffect of metformin on atherothrombotic risk factors, as evident from an improvement in lipid profile,reduction in oxidative stress and thrombotic events.
+91 79 2717 241917.ak).
l rights reserved.
© 2011 Elsevier B.V. All rights reserved.
1. Introduction
Atherothrombosis, defined as atherosclerotic plaque disruptionwith superimposed thrombosis, is one of the leading causes ofmortality in the world. The atherosclerotic and thrombotic processesappear to be inter-dependent and could therefore be integrated underthe term “atherothrombosis”, including both atherosclerosis and itsthrombotic complications. Atherosclerosis is a diffuse process thatstarts early in the childhood and later, it is clinically manifested ascoronary artery disease, stroke, transient ischemic attack andperipheral arterial disease. From the clinical point of view, thisdisease should be envisioned as a single pathologic entity that affectsdifferent vascular territories (Juan et al., 2004). Many risk factors likediabetes, oxidative stress, dyslipoproteinemia, high level of lowdensity lipoprotein cholesterol (LDL-C), very low density lipoproteincholesterol (VLDL-C), cholesterol, low level of high density cholesterol(HDL-C), tobacco smoking, obesity, intake of trans-fat, homocysteine,elevated serum fibrinogen concentrations, serum C-reactive protein,chlamydia pneumoniae infection etc. contribute to the pathogenesis
of atherosclerosis and consequent atherothrombosis (Kumar et al.,2005). The morbidity and mortality due to atherothrombosis are stillunacceptably high although safe and efficient antihyperlipidemic andantithrombotic therapies are available. Recent evidence suggest thatimprovement in abnormal lipid profile, reduction in oxidative stress,inhibition of tissue factor or elements in the tissue factor pathway(i.e., factors VIIa and Xa, or thrombin) has the potential to furtherimprove the overall outcomes in atherothrombosis.
The current study is based on the concept of drug repurposing andinvolves a reverse step from relative clinical finding to pre-clinicalresearch.
Metformin, an insulin sensitizer belonging to the biguanide class,reduces hepatic glucose production and increases the sensitivity of liverand peripheral tissues to insulin. In the United Kingdom ProspectiveDiabetes Study (UKPDS), metformin monotherapy was found to beassociated with reduced macrovascular complications and all-causemortality in overweight patients with type 2 diabetes (Turner et al.,1998). Furthermore, administration of this drug has been shown to beassociatedwith decreased all-cause and cardiovascular risk of mortality(Johnson et al., 2002). In addition, a retrospective analysis, comprisingoftype 2 diabetes patients with heart failure, demonstrated reducedhospitalization and mortality with metformin as compared to sulpho-nylurea treatment (Eurich et al., 2005). This was corroborated in an
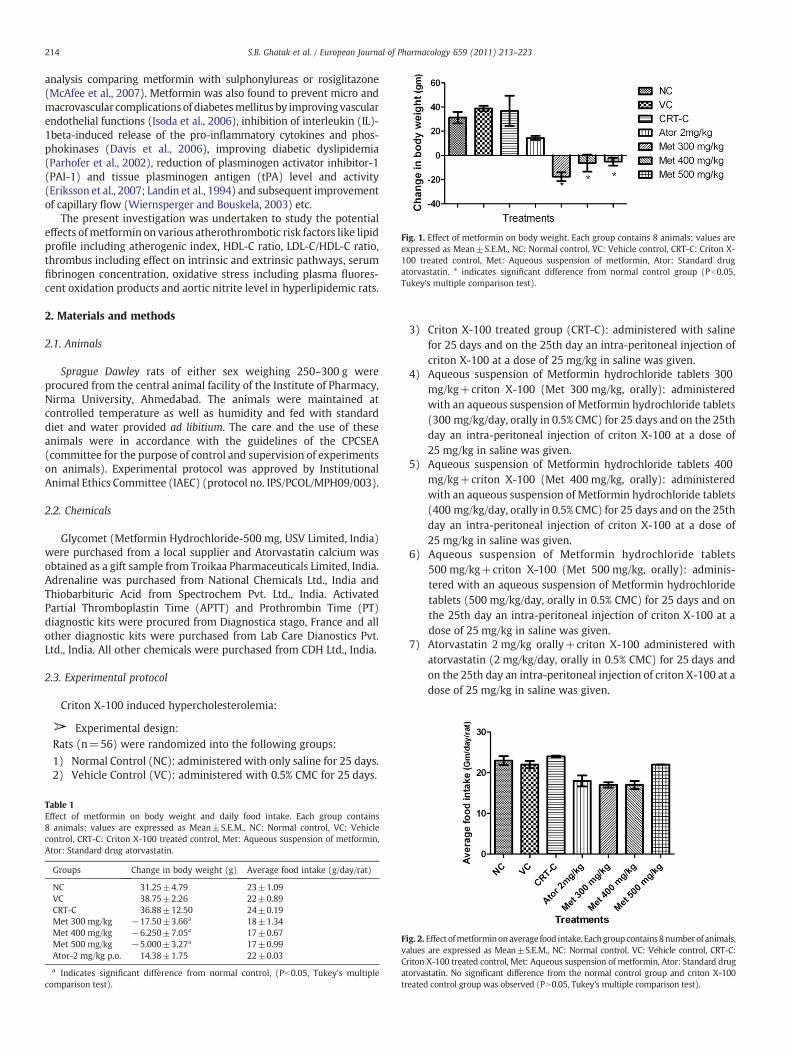
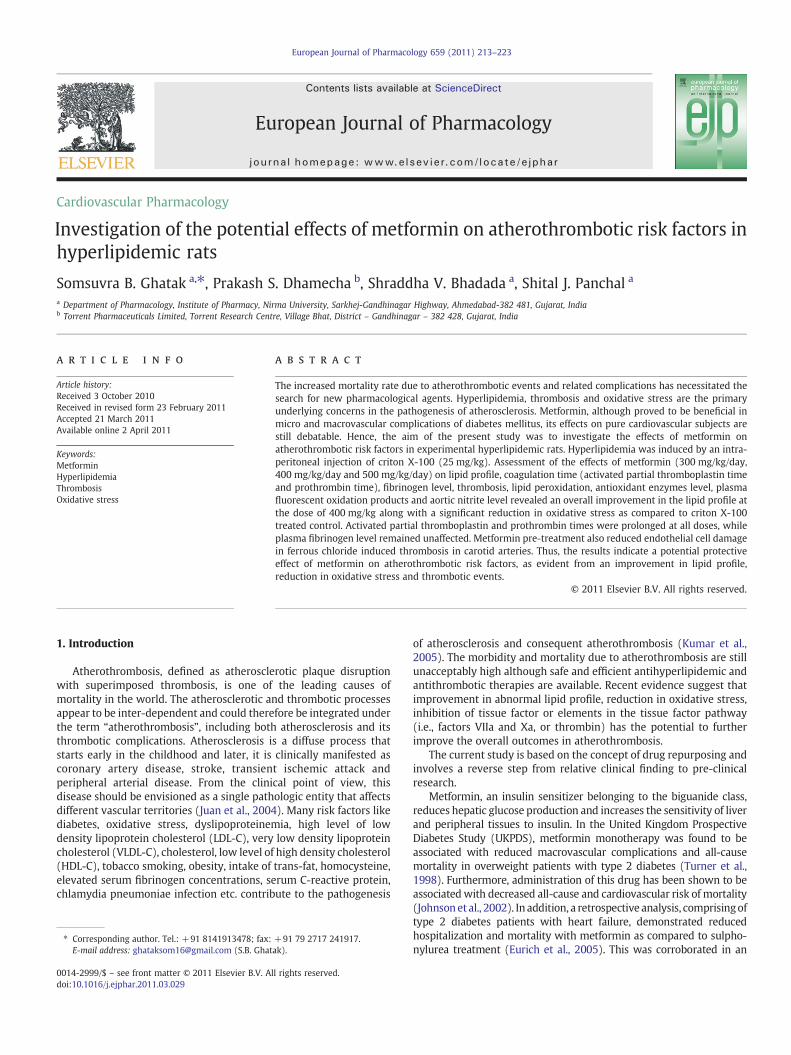
Fig. 1. Effect of metformin on body weight. Each group contains 8 animals; values areexpressed as Mean±S.E.M., NC: Normal control, VC: Vehicle control, CRT-C: Criton X-100 treated control, Met: Aqueous suspension of metformin, Ator: Standard drugatorvastatin. * indicates significant difference from normal control group (Pb0.05,Tukey's multiple comparison test).
214 S.B. Ghatak et al. / European Journal of Pharmacology 659 (2011) 213–223
analysis comparing metformin with sulphonylureas or rosiglitazone(McAfee et al., 2007). Metformin was also found to prevent micro andmacrovascular complications of diabetesmellitus by improvingvascularendothelial functions (Isoda et al., 2006), inhibition of interleukin (IL)-1beta-induced release of the pro-inflammatory cytokines and phos-phokinases (Davis et al., 2006), improving diabetic dyslipidemia(Parhofer et al., 2002), reduction of plasminogen activator inhibitor-1(PAI-1) and tissue plasminogen antigen (tPA) level and activity(Eriksson et al., 2007; Landin et al., 1994) and subsequent improvementof capillary flow (Wiernsperger and Bouskela, 2003) etc.
The present investigation was undertaken to study the potentialeffects ofmetformin on various atherothrombotic risk factors like lipidprofile including atherogenic index, HDL-C ratio, LDL-C/HDL-C ratio,thrombus including effect on intrinsic and extrinsic pathways, serumfibrinogen concentration, oxidative stress including plasma fluores-cent oxidation products and aortic nitrite level in hyperlipidemic rats.
2. Materials and methods
2.1. Animals
Sprague Dawley rats of either sex weighing 250–300 g wereprocured from the central animal facility of the Institute of Pharmacy,Nirma University, Ahmedabad. The animals were maintained atcontrolled temperature as well as humidity and fed with standarddiet and water provided ad libitium. The care and the use of theseanimals were in accordance with the guidelines of the CPCSEA(committee for the purpose of control and supervision of experimentson animals). Experimental protocol was approved by InstitutionalAnimal Ethics Committee (IAEC) (protocol no. IPS/PCOL/MPH09/003).
2.2. Chemicals
Glycomet (Metformin Hydrochloride-500 mg, USV Limited, India)were purchased from a local supplier and Atorvastatin calcium wasobtained as a gift sample from Troikaa Pharmaceuticals Limited, India.Adrenaline was purchased from National Chemicals Ltd., India andThiobarbituric Acid from Spectrochem Pvt. Ltd., India. ActivatedPartial Thromboplastin Time (APTT) and Prothrombin Time (PT)diagnostic kits were procured from Diagnostica stago, France and allother diagnostic kits were purchased from Lab Care Dianostics Pvt.Ltd., India. All other chemicals were purchased from CDH Ltd., India.
2.3. Experimental protocol
Criton X-100 induced hypercholesterolemia:
➢ Experimental design:Rats (n=56) were randomized into the following groups:
1) Normal Control (NC): administered with only saline for 25 days.2) Vehicle Control (VC): administered with 0.5% CMC for 25 days.
Table 1Effect of metformin on body weight and daily food intake. Each group contains8 animals; values are expressed as Mean±S.E.M., NC: Normal control, VC: Vehiclecontrol, CRT-C: Criton X-100 treated control, Met: Aqueous suspension of metformin,Ator: Standard drug atorvastatin.
Groups Change in body weight (g) Average food intake (g/day/rat)
NC 31.25±4.79 23±1.09VC 38.75±2.26 22±0.89CRT-C 36.88±12.50 24±0.19Met 300 mg/kg −17.50±3.66a 18±1.34Met 400 mg/kg −6.250±7.05a 17±0.67Met 500 mg/kg −5.000±3.27a 17±0.99Ator-2 mg/kg p.o. 14.38±1.75 22±0.03
a Indicates significant difference from normal control, (Pb0.05, Tukey's multiplecomparison test).
3) Criton X-100 treated group (CRT-C): administered with salinefor 25 days and on the 25th day an intra-peritoneal injection ofcriton X-100 at a dose of 25 mg/kg in saline was given.
4) Aqueous suspension of Metformin hydrochloride tablets 300mg/kg+criton X-100 (Met 300 mg/kg, orally): administeredwith an aqueous suspension of Metformin hydrochloride tablets(300 mg/kg/day, orally in 0.5% CMC) for 25 days and on the 25thday an intra-peritoneal injection of criton X-100 at a dose of25 mg/kg in saline was given.
5) Aqueous suspension of Metformin hydrochloride tablets 400mg/kg+criton X-100 (Met 400 mg/kg, orally): administeredwith an aqueous suspension of Metformin hydrochloride tablets(400 mg/kg/day, orally in 0.5% CMC) for 25 days and on the 25thday an intra-peritoneal injection of criton X-100 at a dose of25 mg/kg in saline was given.
6) Aqueous suspension of Metformin hydrochloride tablets500 mg/kg+criton X-100 (Met 500 mg/kg, orally): adminis-tered with an aqueous suspension of Metformin hydrochloridetablets (500 mg/kg/day, orally in 0.5% CMC) for 25 days and onthe 25th day an intra-peritoneal injection of criton X-100 at adose of 25 mg/kg in saline was given.
7) Atorvastatin 2 mg/kg orally+criton X-100 administered withatorvastatin (2 mg/kg/day, orally in 0.5% CMC) for 25 days andon the 25th day an intra-peritoneal injection of criton X-100 at adose of 25 mg/kg in saline was given.
Fig. 2. Effect ofmetforminonaverage food intake.Eachgroupcontains8numberof animals,values are expressed as Mean±S.E.M., NC: Normal control, VC: Vehicle control, CRT-C:Criton X-100 treated control, Met: Aqueous suspension of metformin, Ator: Standard drugatorvastatin. No significant difference from the normal control group and criton X-100treated control group was observed (PN0.05, Tukey's multiple comparison test).
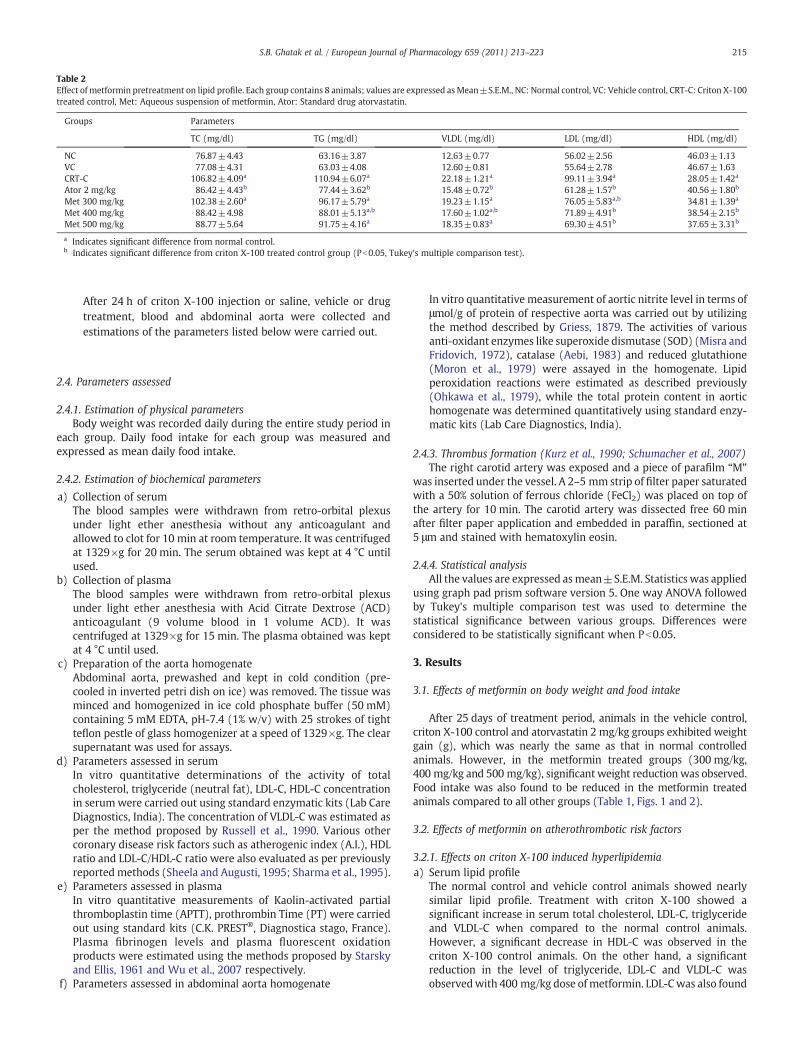
Table 2Effect of metformin pretreatment on lipid profile. Each group contains 8 animals; values are expressed asMean±S.E.M., NC: Normal control, VC: Vehicle control, CRT-C: Criton X-100treated control, Met: Aqueous suspension of metformin, Ator: Standard drug atorvastatin.
Groups Parameters
TC (mg/dl) TG (mg/dl) VLDL (mg/dl) LDL (mg/dl) HDL (mg/dl)
NC 76.87±4.43 63.16±3.87 12.63±0.77 56.02±2.56 46.03±1.13VC 77.08±4.31 63.03±4.08 12.60±0.81 55.64±2.78 46.67±1.63CRT-C 106.82±4.09a 110.94±6.07a 22.18±1.21a 99.11±3.94a 28.05±1.42a
Ator 2 mg/kg 86.42±4.43b 77.44±3.62b 15.48±0.72b 61.28±1.57b 40.56±1.80b
Met 300 mg/kg 102.38±2.60a 96.17±5.79a 19.23±1.15a 76.05±5.83a,b 34.81±1.39a
Met 400 mg/kg 88.42±4.98 88.01±5.13a,b 17.60±1.02a,b 71.89±4.91b 38.54±2.15b
Met 500 mg/kg 88.77±5.64 91.75±4.16a 18.35±0.83a 69.30±4.51b 37.65±3.31b
a Indicates significant difference from normal control.b Indicates significant difference from criton X-100 treated control group (Pb0.05, Tukey's multiple comparison test).
215S.B. Ghatak et al. / European Journal of Pharmacology 659 (2011) 213–223
After 24 h of criton X-100 injection or saline, vehicle or drugtreatment, blood and abdominal aorta were collected andestimations of the parameters listed below were carried out.
2.4. Parameters assessed
2.4.1. Estimation of physical parametersBody weight was recorded daily during the entire study period in
each group. Daily food intake for each group was measured andexpressed as mean daily food intake.
2.4.2. Estimation of biochemical parameters
a) Collection of serumThe blood samples were withdrawn from retro-orbital plexusunder light ether anesthesia without any anticoagulant andallowed to clot for 10 min at room temperature. It was centrifugedat 1329×g for 20 min. The serum obtained was kept at 4 °C untilused.
b) Collection of plasmaThe blood samples were withdrawn from retro-orbital plexusunder light ether anesthesia with Acid Citrate Dextrose (ACD)anticoagulant (9 volume blood in 1 volume ACD). It wascentrifuged at 1329×g for 15 min. The plasma obtained was keptat 4 °C until used.
c) Preparation of the aorta homogenateAbdominal aorta, prewashed and kept in cold condition (pre-cooled in inverted petri dish on ice) was removed. The tissue wasminced and homogenized in ice cold phosphate buffer (50 mM)containing 5 mM EDTA, pH-7.4 (1% w/v) with 25 strokes of tightteflon pestle of glass homogenizer at a speed of 1329×g. The clearsupernatant was used for assays.
d) Parameters assessed in serumIn vitro quantitative determinations of the activity of totalcholesterol, triglyceride (neutral fat), LDL-C, HDL-C concentrationin serumwere carried out using standard enzymatic kits (Lab CareDiagnostics, India). The concentration of VLDL-C was estimated asper the method proposed by Russell et al., 1990. Various othercoronary disease risk factors such as atherogenic index (A.I.), HDLratio and LDL-C/HDL-C ratio were also evaluated as per previouslyreported methods (Sheela and Augusti, 1995; Sharma et al., 1995).
e) Parameters assessed in plasmaIn vitro quantitative measurements of Kaolin-activated partialthromboplastin time (APTT), prothrombin Time (PT) were carriedout using standard kits (C.K. PREST®, Diagnostica stago, France).Plasma fibrinogen levels and plasma fluorescent oxidationproducts were estimated using the methods proposed by Starskyand Ellis, 1961 and Wu et al., 2007 respectively.
f) Parameters assessed in abdominal aorta homogenate
In vitro quantitative measurement of aortic nitrite level in terms ofμmol/g of protein of respective aorta was carried out by utilizingthe method described by Griess, 1879. The activities of variousanti-oxidant enzymes like superoxide dismutase (SOD) (Misra andFridovich, 1972), catalase (Aebi, 1983) and reduced glutathione(Moron et al., 1979) were assayed in the homogenate. Lipidperoxidation reactions were estimated as described previously(Ohkawa et al., 1979), while the total protein content in aortichomogenate was determined quantitatively using standard enzy-matic kits (Lab Care Diagnostics, India).
2.4.3. Thrombus formation (Kurz et al., 1990; Schumacher et al., 2007)The right carotid artery was exposed and a piece of parafilm “M”
was inserted under the vessel. A 2–5 mm strip of filter paper saturatedwith a 50% solution of ferrous chloride (FeCl2) was placed on top ofthe artery for 10 min. The carotid artery was dissected free 60 minafter filter paper application and embedded in paraffin, sectioned at5 μm and stained with hematoxylin eosin.
2.4.4. Statistical analysisAll the values are expressed asmean±S.E.M. Statistics was applied
using graph pad prism software version 5. One way ANOVA followedby Tukey's multiple comparison test was used to determine thestatistical significance between various groups. Differences wereconsidered to be statistically significant when Pb0.05.
3. Results
3.1. Effects of metformin on body weight and food intake
After 25 days of treatment period, animals in the vehicle control,criton X-100 control and atorvastatin 2 mg/kg groups exhibited weightgain (g), which was nearly the same as that in normal controlledanimals. However, in the metformin treated groups (300 mg/kg,400 mg/kg and 500 mg/kg), significant weight reduction was observed.Food intake was also found to be reduced in the metformin treatedanimals compared to all other groups (Table 1, Figs. 1 and 2).
3.2. Effects of metformin on atherothrombotic risk factors
3.2.1. Effects on criton X-100 induced hyperlipidemiaa) Serum lipid profile
The normal control and vehicle control animals showed nearlysimilar lipid profile. Treatment with criton X-100 showed asignificant increase in serum total cholesterol, LDL-C, triglycerideand VLDL-C when compared to the normal control animals.However, a significant decrease in HDL-C was observed in thecriton X-100 control animals. On the other hand, a significantreduction in the level of triglyceride, LDL-C and VLDL-C wasobservedwith 400 mg/kg dose of metformin. LDL-Cwas also found
Fig. 3. Effect of metformin pretreatment on lipid profile. A) Effects on total cholesterol, B) Effects on triglyceride, C) Effects on Very Low Density Cholesterol, D) Effects on LowDensityCholesterol and E) Effects on High Density Cholesterol. Each group contains 8 animals; values are expressed as Mean±S.E.M., NC: Normal control, VC: Vehicle control, CRT-C: CritonX-100 treated control, Met: Aqueous suspension of metformin, Ator: Standard drug atorvastatin. *Indicates significant difference from normal control, #Indicates significantdifference from criton X-100 treated control group (Pb0.05, Tukey's multiple comparison test).
216 S.B. Ghatak et al. / European Journal of Pharmacology 659 (2011) 213–223
to be reduced with metformin 500 mg/kg dose. Also, a remarkableincrease in HDL-C levels was seen in animals pretreated with400 mg/kg/day and 500 mg/kg/day of metformin. However, in ourstudy total cholesterol level was not significantly affected by anydose level of metformin pre-treatment (Table 2, Fig. 3) (all valuesfor serum lipid profile are expressed in mg/dl).
b) Atherogenic index, HDL-C ratio and LDL-C/HDL-C ratio (coronarydisease risk factors)Atherogenic index (A.I.), an indicator of the deposition of foamcells or plaque or fatty infiltration or lipids in aorta and liver, wasfound to be higher in the criton X-100 group as compared to thenormal and vehicle control group. Calculation of other coronary
disease risk predictor indices such as HDL ratio and LDL-C/HDL-Cin the criton X-100 group indicated that the values are atherogenicand undesirable. However, all these values returned to thedesirable ratio in the groups treated with metformin (Table 3).
3.3. Effects of metformin on oxidative stress
3.3.1. Effects on lipid peroxidation and antioxidant enzyme levelMalondialdehyde level was measured as an index of lipid
peroxidation in abdominal aorta homogenate. Criton X-100 controlledanimals showed a malondialdehyde (MDA) level (nmol/g protein)significantly higher than that observed in normal and vehicle control
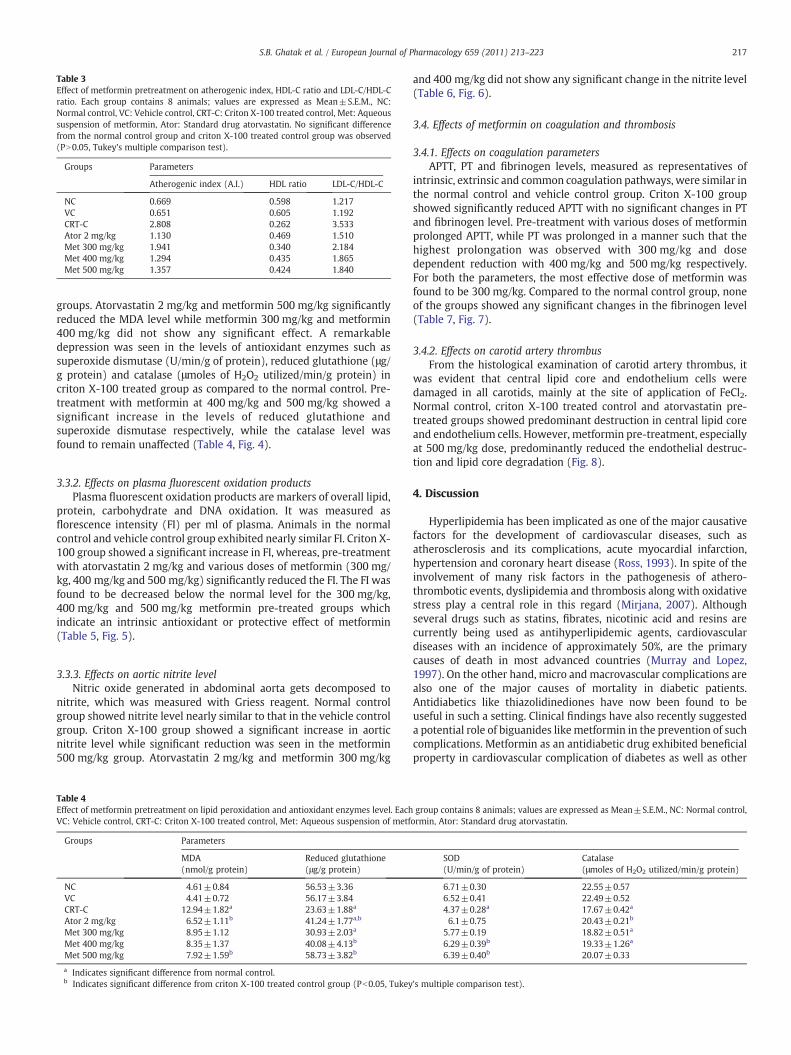
Table 3Effect of metformin pretreatment on atherogenic index, HDL-C ratio and LDL-C/HDL-Cratio. Each group contains 8 animals; values are expressed as Mean±S.E.M., NC:Normal control, VC: Vehicle control, CRT-C: Criton X-100 treated control, Met: Aqueoussuspension of metformin, Ator: Standard drug atorvastatin. No significant differencefrom the normal control group and criton X-100 treated control group was observed(PN0.05, Tukey's multiple comparison test).
Groups Parameters
Atherogenic index (A.I.) HDL ratio LDL-C/HDL-C
NC 0.669 0.598 1.217VC 0.651 0.605 1.192CRT-C 2.808 0.262 3.533Ator 2 mg/kg 1.130 0.469 1.510Met 300 mg/kg 1.941 0.340 2.184Met 400 mg/kg 1.294 0.435 1.865Met 500 mg/kg 1.357 0.424 1.840
217S.B. Ghatak et al. / European Journal of Pharmacology 659 (2011) 213–223
groups. Atorvastatin 2 mg/kg and metformin 500 mg/kg significantlyreduced the MDA level while metformin 300 mg/kg and metformin400 mg/kg did not show any significant effect. A remarkabledepression was seen in the levels of antioxidant enzymes such assuperoxide dismutase (U/min/g of protein), reduced glutathione (μg/g protein) and catalase (μmoles of H2O2 utilized/min/g protein) incriton X-100 treated group as compared to the normal control. Pre-treatment with metformin at 400 mg/kg and 500 mg/kg showed asignificant increase in the levels of reduced glutathione andsuperoxide dismutase respectively, while the catalase level wasfound to remain unaffected (Table 4, Fig. 4).
3.3.2. Effects on plasma fluorescent oxidation productsPlasma fluorescent oxidation products are markers of overall lipid,
protein, carbohydrate and DNA oxidation. It was measured asflorescence intensity (FI) per ml of plasma. Animals in the normalcontrol and vehicle control group exhibited nearly similar FI. Criton X-100 group showed a significant increase in FI, whereas, pre-treatmentwith atorvastatin 2 mg/kg and various doses of metformin (300 mg/kg, 400 mg/kg and 500 mg/kg) significantly reduced the FI. The FI wasfound to be decreased below the normal level for the 300 mg/kg,400 mg/kg and 500 mg/kg metformin pre-treated groups whichindicate an intrinsic antioxidant or protective effect of metformin(Table 5, Fig. 5).
3.3.3. Effects on aortic nitrite levelNitric oxide generated in abdominal aorta gets decomposed to
nitrite, which was measured with Griess reagent. Normal controlgroup showed nitrite level nearly similar to that in the vehicle controlgroup. Criton X-100 group showed a significant increase in aorticnitrite level while significant reduction was seen in the metformin500 mg/kg group. Atorvastatin 2 mg/kg and metformin 300 mg/kg
Table 4Effect of metformin pretreatment on lipid peroxidation and antioxidant enzymes level. EachVC: Vehicle control, CRT-C: Criton X-100 treated control, Met: Aqueous suspension of metf
Groups Parameters
MDA(nmol/g protein)
Reduced glutathione(μg/g protein)
NC 4.61±0.84 56.53±3.36VC 4.41±0.72 56.17±3.84CRT-C 12.94±1.82a 23.63±1.88a
Ator 2 mg/kg 6.52±1.11b 41.24±1.77a,b
Met 300 mg/kg 8.95±1.12 30.93±2.03a
Met 400 mg/kg 8.35±1.37 40.08±4.13b
Met 500 mg/kg 7.92±1.59b 58.73±3.82b
a Indicates significant difference from normal control.b Indicates significant difference from criton X-100 treated control group (Pb0.05, Tukey
and 400 mg/kg did not show any significant change in the nitrite level(Table 6, Fig. 6).
3.4. Effects of metformin on coagulation and thrombosis
3.4.1. Effects on coagulation parametersAPTT, PT and fibrinogen levels, measured as representatives of
intrinsic, extrinsic and common coagulation pathways, were similar inthe normal control and vehicle control group. Criton X-100 groupshowed significantly reduced APTT with no significant changes in PTand fibrinogen level. Pre-treatment with various doses of metforminprolonged APTT, while PT was prolonged in a manner such that thehighest prolongation was observed with 300 mg/kg and dosedependent reduction with 400 mg/kg and 500 mg/kg respectively.For both the parameters, the most effective dose of metformin wasfound to be 300 mg/kg. Compared to the normal control group, noneof the groups showed any significant changes in the fibrinogen level(Table 7, Fig. 7).
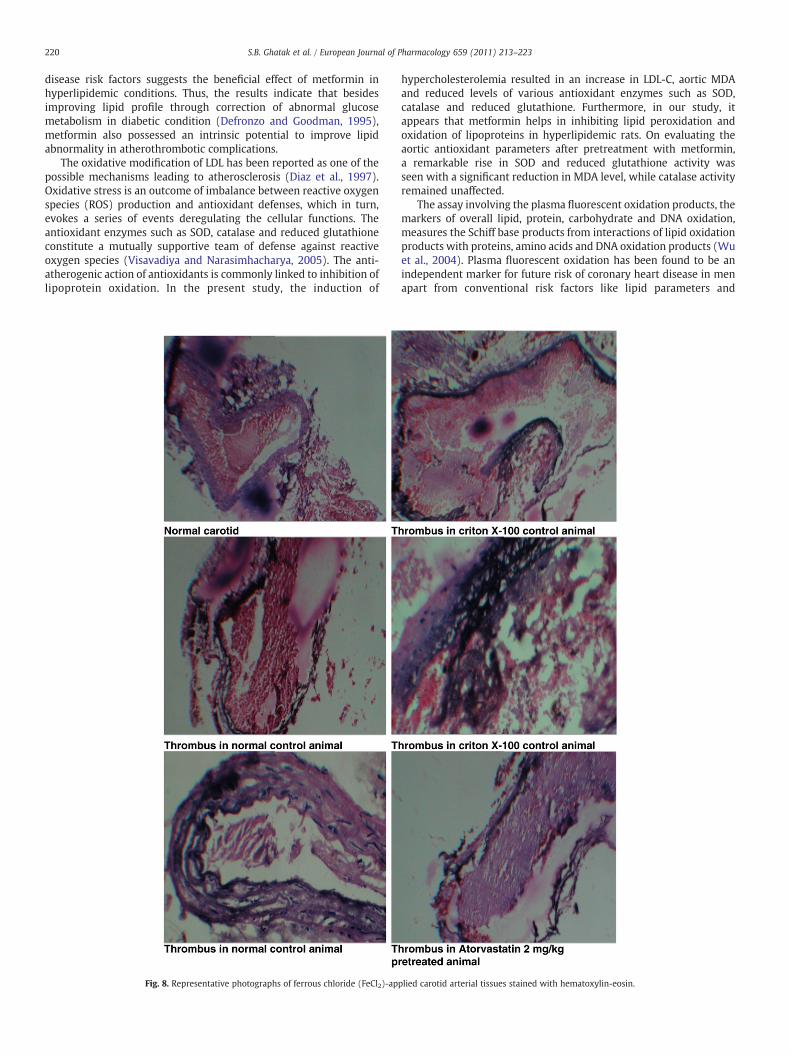
3.4.2. Effects on carotid artery thrombusFrom the histological examination of carotid artery thrombus, it
was evident that central lipid core and endothelium cells weredamaged in all carotids, mainly at the site of application of FeCl2.Normal control, criton X-100 treated control and atorvastatin pre-treated groups showed predominant destruction in central lipid coreand endothelium cells. However, metformin pre-treatment, especiallyat 500 mg/kg dose, predominantly reduced the endothelial destruc-tion and lipid core degradation (Fig. 8).
4. Discussion
Hyperlipidemia has been implicated as one of the major causativefactors for the development of cardiovascular diseases, such asatherosclerosis and its complications, acute myocardial infarction,hypertension and coronary heart disease (Ross, 1993). In spite of theinvolvement of many risk factors in the pathogenesis of athero-thrombotic events, dyslipidemia and thrombosis along with oxidativestress play a central role in this regard (Mirjana, 2007). Althoughseveral drugs such as statins, fibrates, nicotinic acid and resins arecurrently being used as antihyperlipidemic agents, cardiovasculardiseases with an incidence of approximately 50%, are the primarycauses of death in most advanced countries (Murray and Lopez,1997). On the other hand, micro and macrovascular complications arealso one of the major causes of mortality in diabetic patients.Antidiabetics like thiazolidinediones have now been found to beuseful in such a setting. Clinical findings have also recently suggesteda potential role of biguanides likemetformin in the prevention of suchcomplications. Metformin as an antidiabetic drug exhibited beneficialproperty in cardiovascular complication of diabetes as well as other
group contains 8 animals; values are expressed as Mean±S.E.M., NC: Normal control,ormin, Ator: Standard drug atorvastatin.
SOD(U/min/g of protein)
Catalase(μmoles of H2O2 utilized/min/g protein)
6.71±0.30 22.55±0.576.52±0.41 22.49±0.524.37±0.28a 17.67±0.42a
6.1±0.75 20.43±0.21b
5.77±0.19 18.82±0.51a
6.29±0.39b 19.33±1.26a
6.39±0.40b 20.07±0.33
's multiple comparison test).
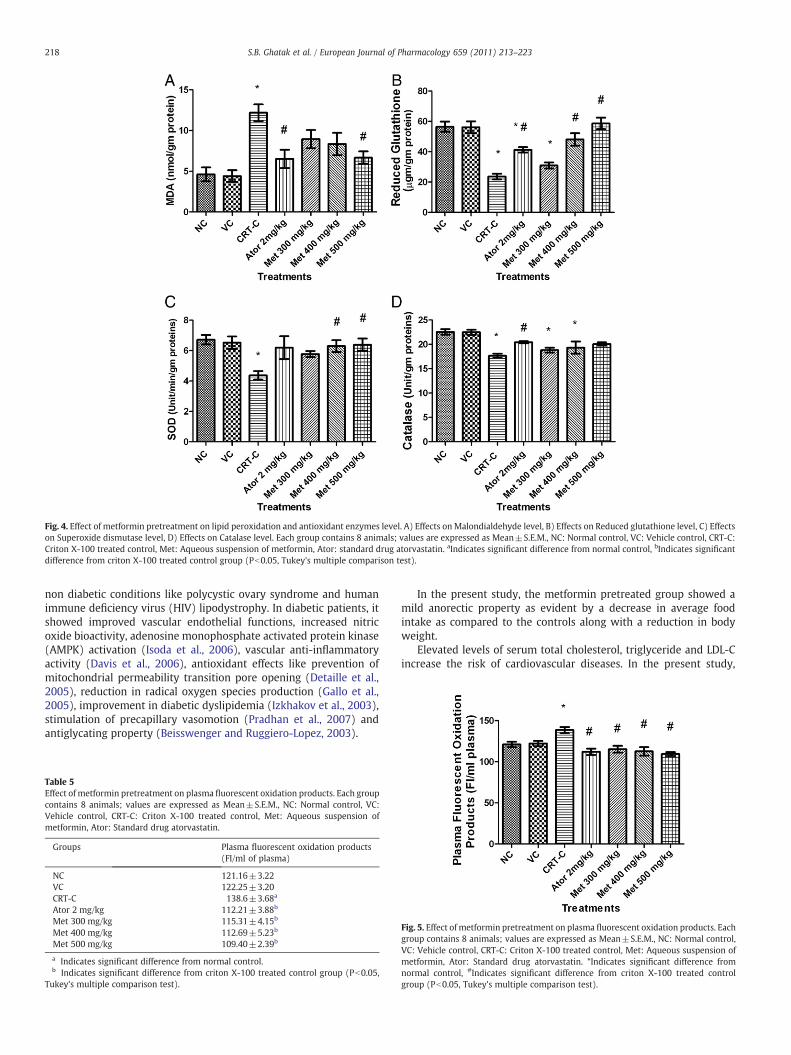
Fig. 4. Effect of metformin pretreatment on lipid peroxidation and antioxidant enzymes level. A) Effects onMalondialdehyde level, B) Effects on Reduced glutathione level, C) Effectson Superoxide dismutase level, D) Effects on Catalase level. Each group contains 8 animals; values are expressed as Mean±S.E.M., NC: Normal control, VC: Vehicle control, CRT-C:Criton X-100 treated control, Met: Aqueous suspension of metformin, Ator: standard drug atorvastatin. aIndicates significant difference from normal control, bIndicates significantdifference from criton X-100 treated control group (Pb0.05, Tukey's multiple comparison test).
218 S.B. Ghatak et al. / European Journal of Pharmacology 659 (2011) 213–223
non diabetic conditions like polycystic ovary syndrome and humanimmune deficiency virus (HIV) lipodystrophy. In diabetic patients, itshowed improved vascular endothelial functions, increased nitricoxide bioactivity, adenosine monophosphate activated protein kinase(AMPK) activation (Isoda et al., 2006), vascular anti-inflammatoryactivity (Davis et al., 2006), antioxidant effects like prevention ofmitochondrial permeability transition pore opening (Detaille et al.,2005), reduction in radical oxygen species production (Gallo et al.,2005), improvement in diabetic dyslipidemia (Izkhakov et al., 2003),stimulation of precapillary vasomotion (Pradhan et al., 2007) andantiglycating property (Beisswenger and Ruggiero-Lopez, 2003).
Table 5Effect of metformin pretreatment on plasma fluorescent oxidation products. Each groupcontains 8 animals; values are expressed as Mean±S.E.M., NC: Normal control, VC:Vehicle control, CRT-C: Criton X-100 treated control, Met: Aqueous suspension ofmetformin, Ator: Standard drug atorvastatin.
Groups Plasma fluorescent oxidation products(FI/ml of plasma)
NC 121.16±3.22VC 122.25±3.20CRT-C 138.6±3.68a
Ator 2 mg/kg 112.21±3.88b
Met 300 mg/kg 115.31±4.15b
Met 400 mg/kg 112.69±5.23b
Met 500 mg/kg 109.40±2.39b
a Indicates significant difference from normal control.b Indicates significant difference from criton X-100 treated control group (Pb0.05,
Tukey's multiple comparison test).
In the present study, the metformin pretreated group showed amild anorectic property as evident by a decrease in average foodintake as compared to the controls along with a reduction in bodyweight.
Elevated levels of serum total cholesterol, triglyceride and LDL-Cincrease the risk of cardiovascular diseases. In the present study,
Fig. 5. Effect of metformin pretreatment on plasma fluorescent oxidation products. Eachgroup contains 8 animals; values are expressed as Mean±S.E.M., NC: Normal control,VC: Vehicle control, CRT-C: Criton X-100 treated control, Met: Aqueous suspension ofmetformin, Ator: Standard drug atorvastatin. *Indicates significant difference fromnormal control, #Indicates significant difference from criton X-100 treated controlgroup (Pb0.05, Tukey's multiple comparison test).
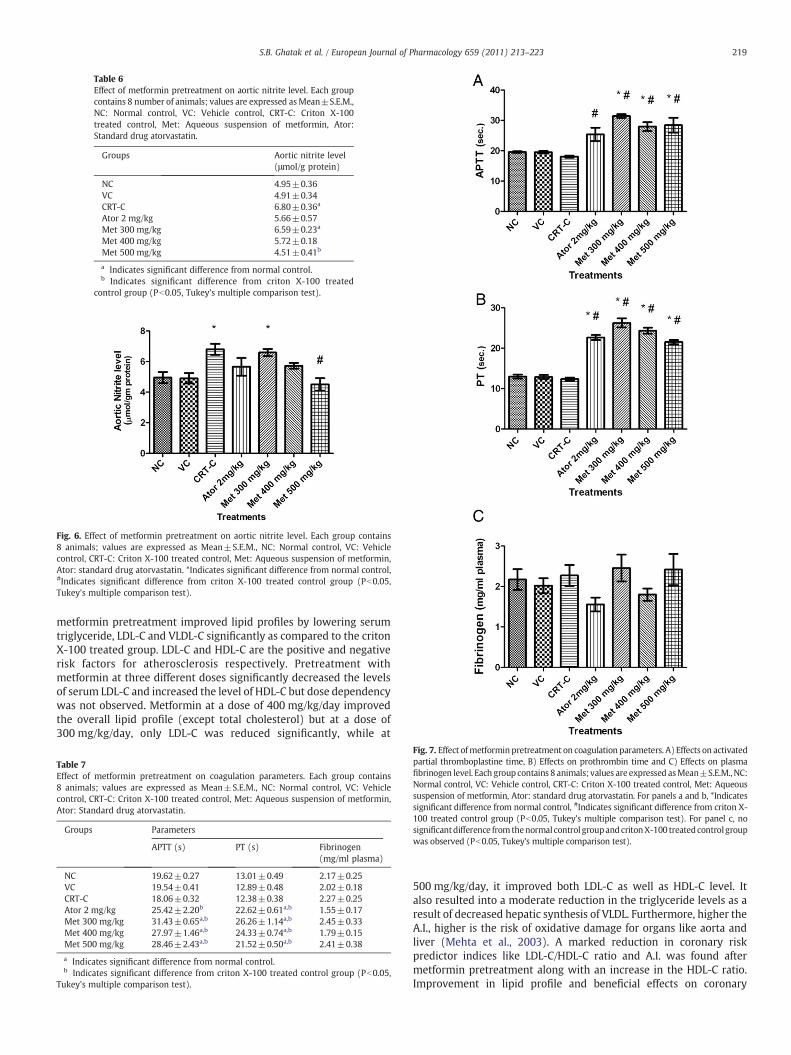
Table 6Effect of metformin pretreatment on aortic nitrite level. Each groupcontains 8 number of animals; values are expressed asMean±S.E.M.,NC: Normal control, VC: Vehicle control, CRT-C: Criton X-100treated control, Met: Aqueous suspension of metformin, Ator:Standard drug atorvastatin.
Groups Aortic nitrite level(μmol/g protein)
NC 4.95±0.36VC 4.91±0.34CRT-C 6.80±0.36a
Ator 2 mg/kg 5.66±0.57Met 300 mg/kg 6.59±0.23a
Met 400 mg/kg 5.72±0.18Met 500 mg/kg 4.51±0.41b
a Indicates significant difference from normal control.b Indicates significant difference from criton X-100 treated
control group (Pb0.05, Tukey's multiple comparison test).
Fig. 6. Effect of metformin pretreatment on aortic nitrite level. Each group contains8 animals; values are expressed as Mean±S.E.M., NC: Normal control, VC: Vehiclecontrol, CRT-C: Criton X-100 treated control, Met: Aqueous suspension of metformin,Ator: standard drug atorvastatin. *Indicates significant difference from normal control,#Indicates significant difference from criton X-100 treated control group (Pb0.05,Tukey's multiple comparison test).
219S.B. Ghatak et al. / European Journal of Pharmacology 659 (2011) 213–223
metformin pretreatment improved lipid profiles by lowering serumtriglyceride, LDL-C and VLDL-C significantly as compared to the critonX-100 treated group. LDL-C and HDL-C are the positive and negativerisk factors for atherosclerosis respectively. Pretreatment withmetformin at three different doses significantly decreased the levelsof serum LDL-C and increased the level of HDL-C but dose dependencywas not observed. Metformin at a dose of 400 mg/kg/day improvedthe overall lipid profile (except total cholesterol) but at a dose of300 mg/kg/day, only LDL-C was reduced significantly, while at
Table 7Effect of metformin pretreatment on coagulation parameters. Each group contains8 animals; values are expressed as Mean±S.E.M., NC: Normal control, VC: Vehiclecontrol, CRT-C: Criton X-100 treated control, Met: Aqueous suspension of metformin,Ator: Standard drug atorvastatin.
Groups Parameters
APTT (s) PT (s) Fibrinogen(mg/ml plasma)
NC 19.62±0.27 13.01±0.49 2.17±0.25VC 19.54±0.41 12.89±0.48 2.02±0.18CRT-C 18.06±0.32 12.38±0.38 2.27±0.25Ator 2 mg/kg 25.42±2.20b 22.62±0.61a,b 1.55±0.17Met 300 mg/kg 31.43±0.65a,b 26.26±1.14a,b 2.45±0.33Met 400 mg/kg 27.97±1.46a,b 24.33±0.74a,b 1.79±0.15Met 500 mg/kg 28.46±2.43a,b 21.52±0.50a,b 2.41±0.38
a Indicates significant difference from normal control.b Indicates significant difference from criton X-100 treated control group (Pb0.05,
Tukey's multiple comparison test).
Fig. 7. Effect ofmetforminpretreatment on coagulation parameters. A) Effects on activatedpartial thromboplastine time, B) Effects on prothrombin time and C) Effects on plasmafibrinogen level. Each group contains 8 animals; values are expressed asMean±S.E.M.,NC:Normal control, VC: Vehicle control, CRT-C: Criton X-100 treated control, Met: Aqueoussuspension of metformin, Ator: standard drug atorvastatin. For panels a and b, *Indicatessignificant difference from normal control, #Indicates significant difference from criton X-100 treated control group (Pb0.05, Tukey's multiple comparison test). For panel c, nosignificantdifference from thenormal control groupandcritonX-100 treatedcontrol groupwas observed (Pb0.05, Tukey's multiple comparison test).
500 mg/kg/day, it improved both LDL-C as well as HDL-C level. Italso resulted into a moderate reduction in the triglyceride levels as aresult of decreased hepatic synthesis of VLDL. Furthermore, higher theA.I., higher is the risk of oxidative damage for organs like aorta andliver (Mehta et al., 2003). A marked reduction in coronary riskpredictor indices like LDL-C/HDL-C ratio and A.I. was found aftermetformin pretreatment along with an increase in the HDL-C ratio.Improvement in lipid profile and beneficial effects on coronary
220 S.B. Ghatak et al. / European Journal of Pharmacology 659 (2011) 213–223
disease risk factors suggests the beneficial effect of metformin inhyperlipidemic conditions. Thus, the results indicate that besidesimproving lipid profile through correction of abnormal glucosemetabolism in diabetic condition (Defronzo and Goodman, 1995),metformin also possessed an intrinsic potential to improve lipidabnormality in atherothrombotic complications.
The oxidative modification of LDL has been reported as one of thepossible mechanisms leading to atherosclerosis (Diaz et al., 1997).Oxidative stress is an outcome of imbalance between reactive oxygenspecies (ROS) production and antioxidant defenses, which in turn,evokes a series of events deregulating the cellular functions. Theantioxidant enzymes such as SOD, catalase and reduced glutathioneconstitute a mutually supportive team of defense against reactiveoxygen species (Visavadiya and Narasimhacharya, 2005). The anti-atherogenic action of antioxidants is commonly linked to inhibition oflipoprotein oxidation. In the present study, the induction of
Fig. 8. Representative photographs of ferrous chloride (FeCl2)-ap
hypercholesterolemia resulted in an increase in LDL-C, aortic MDAand reduced levels of various antioxidant enzymes such as SOD,catalase and reduced glutathione. Furthermore, in our study, itappears that metformin helps in inhibiting lipid peroxidation andoxidation of lipoproteins in hyperlipidemic rats. On evaluating theaortic antioxidant parameters after pretreatment with metformin,a remarkable rise in SOD and reduced glutathione activity wasseen with a significant reduction in MDA level, while catalase activityremained unaffected.
The assay involving the plasma fluorescent oxidation products, themarkers of overall lipid, protein, carbohydrate and DNA oxidation,measures the Schiff base products from interactions of lipid oxidationproducts with proteins, amino acids and DNA oxidation products (Wuet al., 2004). Plasma fluorescent oxidation has been found to be anindependent marker for future risk of coronary heart disease in menapart from conventional risk factors like lipid parameters and
plied carotid arterial tissues stained with hematoxylin-eosin.
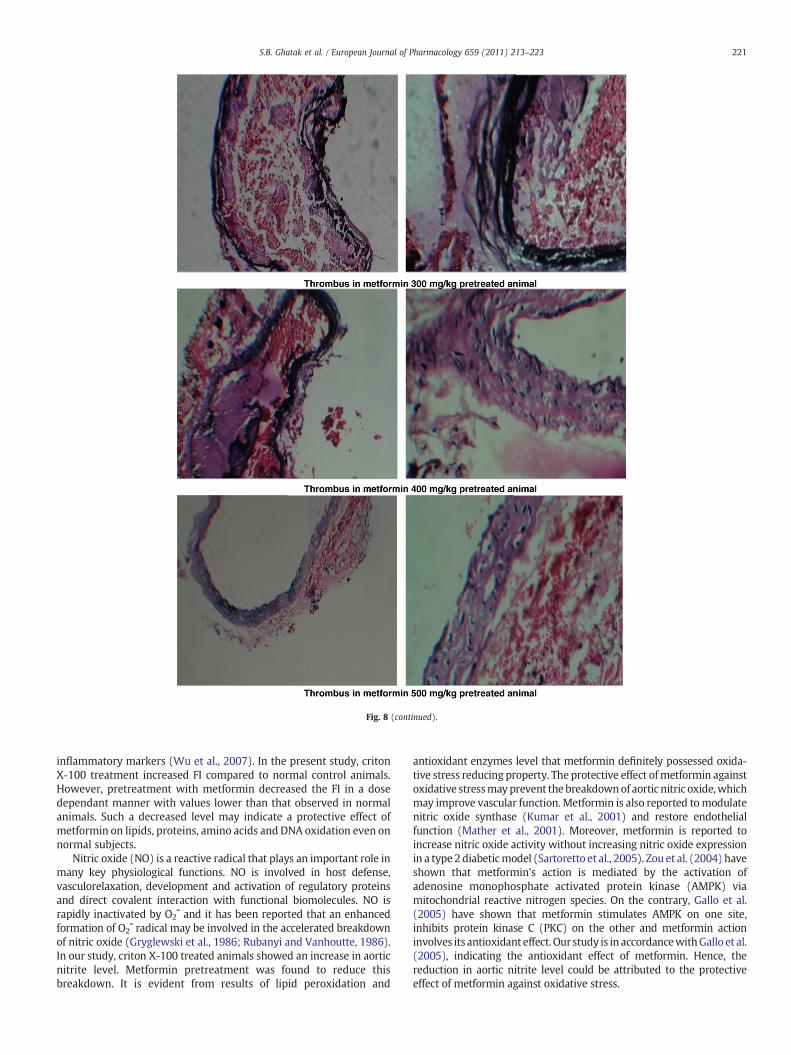
Fig. 8 (continued).
221S.B. Ghatak et al. / European Journal of Pharmacology 659 (2011) 213–223
inflammatory markers (Wu et al., 2007). In the present study, critonX-100 treatment increased FI compared to normal control animals.However, pretreatment with metformin decreased the FI in a dosedependant manner with values lower than that observed in normalanimals. Such a decreased level may indicate a protective effect ofmetformin on lipids, proteins, amino acids and DNA oxidation even onnormal subjects.
Nitric oxide (NO) is a reactive radical that plays an important role inmany key physiological functions. NO is involved in host defense,vasculorelaxation, development and activation of regulatory proteinsand direct covalent interaction with functional biomolecules. NO israpidly inactivated by O2¯ and it has been reported that an enhancedformation of O2¯ radical may be involved in the accelerated breakdownof nitric oxide (Gryglewski et al., 1986; Rubanyi and Vanhoutte, 1986).In our study, criton X-100 treated animals showed an increase in aorticnitrite level. Metformin pretreatment was found to reduce thisbreakdown. It is evident from results of lipid peroxidation and
antioxidant enzymes level that metformin definitely possessed oxida-tive stress reducing property. The protective effect ofmetformin againstoxidative stressmayprevent thebreakdownof aortic nitric oxide,whichmay improve vascular function.Metformin is also reported tomodulatenitric oxide synthase (Kumar et al., 2001) and restore endothelialfunction (Mather et al., 2001). Moreover, metformin is reported toincrease nitric oxide activity without increasing nitric oxide expressionin a type 2 diabeticmodel (Sartoretto et al., 2005). Zou et al. (2004) haveshown that metformin's action is mediated by the activation ofadenosine monophosphate activated protein kinase (AMPK) viamitochondrial reactive nitrogen species. On the contrary, Gallo et al.(2005) have shown that metformin stimulates AMPK on one site,inhibits protein kinase C (PKC) on the other and metformin actioninvolves its antioxidant effect. Our study is in accordancewithGallo et al.(2005), indicating the antioxidant effect of metformin. Hence, thereduction in aortic nitrite level could be attributed to the protectiveeffect of metformin against oxidative stress.

222 S.B. Ghatak et al. / European Journal of Pharmacology 659 (2011) 213–223
Preventionof lipidperoxidation, improvement in antioxidant enzymelevel (except catalase), reduction inplasmafluorescentoxidationproductand reduction in nitric oxide breakdown all accumulatively indicate aprotective effect of metformin against oxidative stress mediatedatherothrombotic complications.
Thrombotic mechanisms are thought to play a major role in thepathophysiology of acute coronary syndromes and other complicationsof atherosclerosis (Glass and Witztum, 2001). A variety of epidemio-logical studies have demonstrated an association between hypercho-lesterolemia and systemic markers of hypercoagulability (Maccallumet al., 2000, Griffin et al., 2001). Although the molecular mechanismsresponsible for this association are not understood completely, there areample evidence that the protein C anticoagulant pathway is altered inhyperlipidemia and the anticoagulant activity is enhanced by HDLcholesterol but not by LDL cholesterol (Griffin et al., 1999), whichsuggests a possiblemechanism for protection from thrombotic events inpatients with elevated HDL cholesterol. Other lipoproteins, includingtriglyceride-rich lipoproteins and oxidized LDL may accelerate pro-coagulant reactions (Moyer et al., 1998; Griffin et al., 1999). Theseobservations indicate that alterations in plasma lipoproteins duringatherosclerosis may influence both anticoagulant and pro-coagulantpathways. In the present study, APTT was reduced in criton X-100treated group while PT remained unaffected. Metformin pretreatmentat various doses prolonged both APTT and PT, which indicates theanticoagulant property of metformin. Prolongation of APTT and PTcompared to normal also suggests that metformin have effects on bothintrinsic as well as extrinsic coagulation pathways. In both the cases,coagulation time was more significantly prolonged in the metformin300 mg/kg/day treatment group. Further studies with decreasing dosesmay focus more light on this property. Fibrinogen level was found to beunaffected by any of the treatments. One of the possiblemechanisms forreduction of hypercoagulability and anticoagulant effect after pretreat-ment with metformin is its effect on intrinsic and extrinsic coagulationpathways. Further research is warranted to determine which factor(s)of these pathways are affected by metformin. Histological examinationof carotid artery also showed a reduction in endothelium and lipid coredamage with metformin pretreatment. Metformin was found tointerfere with factor XIII (FXIII) activation and fibrin polymerization(Standeven et al., 2002), suggesting that metformin may exert abeneficial effect against hypercoagulability and thrombotic eventsobserved in atherothrombotic complications.
5. Conclusion
The results of the current study indicate the beneficial effects ofmetformin on atherothrombotic risk factors, mainly by virtue of itspotential to improve the lipid profile and to reduce oxidative stressand thrombotic events, although more extensive studies are war-ranted to validate the same.
References
Aebi, H.E., 1983. Catalase, in methods of enzymatic analysis, In: Bergmeyer, H.U.,Bergmeyer, J., Grabl, M. (Eds.), third ed. Verlag Chemie, New York, pp. 273–286. 3.
Beisswenger, P., Ruggiero-Lopez, D., 2003. Metformin inhibition of glycation processes.Diabetes Metab. 29, 6S95-6S103.
Davis, B.J., Xie, Z., Viollet, B., Zou, M.H., 2006. Activation of the AMP-activated kinase byantidiabetes drug metformin stimulates nitric oxide synthesis in vivo by promotingthe association of heat shock protein 90 and endothelial nitric oxide synthase.Diabetes 55, 496–505.
Defronzo, R.A., Goodman, A.M., 1995. Efficacy of metformin in patient with non-insulindependent diabetes mellitus. N. Engl. J. Med. 333, 541–549.
Detaille, D., Guigas, B., Chauvin, C., 2005. Metformin prevents high-glucose-inducedendothelial cell death through a mitochondrial permeability transition-dependentprocess. Diabetes 54, 2179–2187.
Diaz, M.N., Frei, B., Vita, J.A., Keaney, J.F., 1997. Antioxidants and atherosclerotic heartdisease. N. Engl. J. Med. 337, 408–416.
Eriksson, A., Attval, S., Bonnier, M., Eriksson, J.W., Rosander, B., Kalrsson, F.A., 2007. Short-term effects of metformin in type 2 diabetes. Diabetes Obes. Metab. 9, 483–489.
Eurich, D.T., Majumdar, S.R., McAlister, F.A., Tsuyuki, R.T., Johnson, J.A., 2005. Improvedclinical outcomes associated with metformin in patients with diabetes and heartfailure. Diabetes Care 28, 2345–2351.
Gallo, A., Ceolotto, G., Pinton, P., Iori, E., Murphy, E., Rutter, G.A., 2005. Metforminprevents glucose-induced protein kinase C-beta2 activation in human umbilicalvein endothelial cells through an antioxidant mechanism. Diabetes 54,1123–1131.
Glass, C.K., Witztum, J.L., 2001. Atherosclerosis: the road ahead. Cell 104, 503–516.Griess, P., 1879. Bemerkungen zu der abhandlung der H.H. Weselsky und Benedikt
“Ueber einige azoverbindungen”. Chem. Ber. 12, 426–428.Griffin, J.H., Kojima, K., Banka, C.L., 1999. High-density lipoprotein enhancement of
anticoagulant activities of plasma protein S and activated protein C. J. Clin. Invest.103, 219–227.
Griffin, J.H., Fernandez, J.A., Deguchi, H., 2001. Plasma lipoproteins, hemostasis andthrombosis. Thromb. Haemost. 86, 386–394.
Gryglewski, R.J., Palmer, R.M.J., Moncada, S., 1986. Superoxide anion is involved in thebreakdown of endothelium-derived vascular relaxing factor. Nature 320, 454–456.
Isoda, K., Young, J.L., Zirlik, A., MacFarlane, L.A., Tsuboi, N., Gerdes, N., 2006. Metformininhibits proinflammatory responses and nuclear factor-kappaB in human vascularwall cells. Arterioscler. Thromb. Vasc. Biol. 26, 611–617.
Izkhakov, E., Meltzer, E., Rubinstein, A., 2003. Pathogenesis andmanagement of diabeticdyslipidemia. Treat. Endocrinol. 2, 231–245.
Johnson, J.A., Majumdar, S.R., Simpson, S.H., Toth, E.L., 2002. Decreased mortalityassociated with the use of metformin compared with sulfonylurea monotherapy intype 2 diabetes. Diabetes Care 25, 2244–2248.
Juan, F., Viles, G., Valentin, F., Juan, J.B., 2004. Atherothrombosis: a widespread diseasewith unpredictable and life-threatening consequences. Eur. Heart J. 25, 1197–1207.
Kumar, V.B., Bernardo, A.E., Vyas, K., Franko, M., Farr, S., Lakshmanan, L., Buddhiraju, C.,Morley, J.E., 2001. Effect of metformin on nitric oxide synthase in genetically obese(ob/ob) mice. Life Sci. 69, 2789–2799.
Kumar, V., Cotrans, R.S., Robbins, S.L., 2005. Robbins Basic Pathophysiology, seventh ed.Elsevier publication, Philadelphia, pp. 328–338.
Kurz, K.D., Main, B.W., Sandusky, G.E., 1990. Rat model of arterial thrombosis inducedby ferric chloride. Thromb. Res. 60, 269–280.
Landin, K., Tengborn, L., Smith, U., 1994. Effects of metformin and metoprolol CR onhormones and fibrinolytic variables during a hyperinsulinemic, euglycemic clampin man. Thromb. Haemost. 71, 783–787.
Maccallum, P.K., Cooper, J.A., Martin, J., 2000. Haemostatic and lipid determinants ofprothrombin fragment F1.2 and D-dimer in plasma. Thromb. Haemost. 83,421–426.
Mather, K.J., Verma, S., Anderson, T.J., 2001. Improved endothelial function withmetformin in type 2 diabetes mellitus. J. Am. Coll. Cardiol. 37, 1344–1350.
McAfee, A.T., Koro, C., landon, J., Ziyadeh, N., Walker, A.M., 2007. Coronary heart diseaseoutcomes in patients receiving antidiabetic agents. Pharmacoepidemiol. Drug Saf.16, 711–725.
Mehta, K., Balaraman, R., Amin, A.H., Bafna, P.A., Gulati, O.D., 2003. Effect of fruits ofMoringa oleifera on the lipid profile of normal and hypercholesterolaemic rabbits.J. Ethnopharmacol. 86, 191–195.
Mirjana, B., 2007. Pathogenetic aspects of atherosclerosis. Acta Med. Medianae 46,25–29.
Misra, H.P., Fridovich, I., 1972. The role of superoxide anion in the autoxidation ofepinephrine and a simple assay for superoxide dismutase. J. Biol. Chem. 247,3170–3179.
Moron, M.J., Diperre, J.W., Mannerv, K.B., 1979. Levels of glutathione, glutathionereductase and glutathione-S-transferase activities in rat lungs and liver. Biochem.Biophys. Acta 582, 67–71.
Moyer, M.P., Tracy, R.P., Tracy, P.B., 1998. Plasma lipoproteins support prothrombinaseand other procoagulant enzymatic complexes. Arterioscler. Thromb. Vasc. Biol. 18,458–465.
Murray, C.J., Lopez, A.D., 1997. Mortality by cause for eight regions of the world: globalburden of disease study. Lancet 349, 1269–1276.
Ohkawa, H., Ohishi, N., Yagik, S., 1979. Assay for lipid peroxides in animal tissues bythiobarbituric acid reaction. Anal. Biochem. 95, 351–358.
Parhofer, K.G., Laubach, E., Geiss, H.C., Otto, C., 2002. Effect of glucose control on lipidlevels in patients with type 2 diabetes. Dtsch. Med. Wochenschr. 127, 958–962.
Pradhan, R.K., Chakravarthy, V.S., Prabhakar, A., 2007. Effect of chaotic vasomotion inskeletal muscle on tissue oxygenation. Microvasc. Res. 74, 51–64.
Ross, R., 1993. The pathogenesis of atherosclerosis: a perspective for the 1990s. Nature362, 801–809.
Rubanyi, G.M., Vanhoutte, P.M., 1986. Superoxide anions and hyperoxia inactivateendothelium-derived relaxing factor. Am. J. Physiol. 250, H822–H827.
Russell, J.C., Koeslag, D.G., Dolphin, P.J., Amy, R.M., 1990. Prevention of myocardiallesions in JCR:LA-corpulent rat by nifedepine. Arteriosclerosis 10, 658–664.
Sartoretto, J.L., Melo, G.A., Carvalho, M.H., Nigro, D., Passaglia, R.T., Scavone, C., Cuman,R.K., Fortes, Z.B., 2005. Metformin treatment restores the altered microvascularreactivity in neonatal streptozotocin induced diabetic rats increasing NOS activity,but not NOS expression. Life Science 77, 2676–2689.
Schumacher, W.A., Bostwick, J.S., Ogletree, A.B., Hua, J., Rehfuss, R.P., 2007. Biomarkeroptimization to track the antithrombotic and hemostatic effects of clopidogrel inrats. J. Pharmacol. Exp. Ther. 322, 369–377.
Sharma, A., Mathur, R., Dixit, V.P., 1995. Prevention of hypercholesterolemia andatherosclerosis in rabbits after supplementation of Myristica fragrans seed extract.Indian J. Physiol. Pharmacol. 39, 407–410.
Sheela, C.G., Augusti, K.T., 1995. Antiperoxide effects of S-allyl cysteine sulfoxideisolated from Allium sativum Linn. and gugulipid in cholesterol fed rats. Indian J.Exp. Biol. 33, 337–341.

223S.B. Ghatak et al. / European Journal of Pharmacology 659 (2011) 213–223
Standeven, K.F., Ariens, R.A., Whitaker, P., Ashcroft, A.E., Weisel, J.W., Grant, P.J., 2002.The effect of dimethylbiguanide on thrombin activity, FXIII activation, fibrinpolymerization, and fibrin clot formation. Diabetes 51, 189–197.
Starsky, A., Ellis, B.C., 1961. A quick and accurate method for determination offibrinogen in plasma. J. Lab. Clin. Med. 59, 477–488.
Turner, R.C., Holman, R.R., Stratton, I.M., 1998. UK Prospective Diabetes Study (UKPDS)Group. Effect of intensive blood glucose control with metformin on complicationsin overweight patients with type 2 diabetes (UKPDS 34). Lancet 352, 854–865.
Visavadiya, N.P., Narasimhacharya, A.V., 2005. Hypolipidemic and antioxidant activitiesof Asparagus racemosus in hypercholesteremic rats. Indian J. Pharmacol. 37,376–380.
Wiernsperger, N.F., Bouskela, E., 2003. Microcirculation in insulin resistance anddiabetes: more than just a complication. Diabetes Metab. 29, 6S77-6S87.
Wu, T., Rifai, N., Roberts, L.J., Willett, W.C., Rimm, E.B., 2004. Stability of measurementsof biomarkers of oxidative stress in blood over 36 hours. Cancer Epidemiol.Biomarkers Prev. 13, 1399–1402.
Wu, T., Willett, W.C., Rifai, N., Rimm, E.B., 2007. Plasma fluorescent oxidation productsas potential markers of oxidative stress for epidemiologic studies. Am. J. Epidemiol.166, 552–560.
Zou, M.H., Kirkpatrick, S.S., Davis, B.J., Nelson, J.S., Wiles, W.G., Schlattner, U., Neumann,D., Brownlee, M., Freeman, M.B., Goldman, M.H., 2004. Activation of the AMP-activated protein kinase by the anti-diabetic drug metformin in vivo: role ofmitochondrial reactive nitrogen species. J. Biol. Chem. 279, 43940–43951.















![[Metformin increases serum concentration of high molecular weight (HMW-adiponectin) in nondiabetic obese subjects]](https://img.pdfslide.net/doc/110x75/634e61207c06afa1b60d99d0/metformin-increases-serum-concentration-of-high-molecular-weight-hmw-adiponectin.jpg)













