Embed Size (px)
Citation preview



FOREWORD
i
EDITORIAL ADVISORY BOARD MEMBERS
Robert EaglesDirector, Safety Operations & InfrastructureInternational Air Transport Association, Asia Pacific
Prof Henry FanProfessor, Centre for Infrastructure SystemsSchool of Civil and Environmental EngineeringNanyang Technological University, Singapore
Dr K RaguramanJoint Associate ProfessorDepartment of Geography and Civil EngineeringNational University of Singapore
Sivakant TiwariPrincipal, Senior State CounselAttorney-General’s Chambers, Singapore
Dr Jarnail SinghChairmanCivil Aviation Medical Board, Singapore
Cletus MJ PackiamChief, Airport Emergency ServiceCivil Aviation Authority of Singapore
Goh Chin EeDirector, Singapore Aviation AcademyCivil Aviation Authority of Singapore
EDITORIAL TEAM
Ms Chan Pin Pin
Ms Jasmin Ismail
Ms Addrienne Kang
Ms Eudora Tan
ii
CONTENTS
Aviation Safety
1 The Safety Reporting in Aviation: Safety Management
and Safety Culture in Interaction 1
Professor Patrick Hudson
Leiden University, The Netherlands
2 Aviation Safety Investigations – Cooperative, Independent,
No-blame and Accountable 13
Mr Alan Stray
Australian Transport Safety Bureau
3 Balancing Safety and Compliance in the Regulatory Environment 23
Mr William Voss
Flight Safety Foundation
Aviation Security
4 Benefits of Aviation Security Audits and Quality Control Systems 29
Mr Bernard Lim
Ministry of Transport, Singapore
Aircraft Accident Investigation
5 The Role of Safety Culture in Aircraft Accidents 37
Professor Graham Braithwaite
Cranfield University, UK
iii
Aviation Technology
6 State-of-the-Art Technology in Airport Pavement 47
Dr Satish K Agrawal
Federal Aviation Administration, US
Crisis Management
7 Evidence-based Medical Response to Mass Casualty Event at Airports 55
Dr Mark Leong
Singapore General Hospital
Airport Management
8 Opening of New Terminals – Changi Airport’s T3 experience 65
Mr Foo Sek Min
Civil Aviation Authority of Singapore
Sustainable Aviation
9 Towards Sustainable Aviation 73
Mr Michael Rossell
International Civil Aviation Organization
iv
ABSTRACT
Aviation Safety
ABSTRACT
This paper examines the necessity for safety reporting in terms of risk management, using the Bowtie model as a way of showing how reports of minor incidents can provide vital information about how well an organisation is managing the risks of the business. As the underlying causes of both major accidents and minor incidents are similar, reporting all types of incidents provides invaluable information that can be used to prevent accidents. In today’s commercial aviation industry, we cannot afford to learn these lessons from actual accidents, so there is no real choice if we are to avoid further major accidents.
The International Civil Aviation Organization has recognised this necessity in its definition of how Safety Management Systems (SMS) should operate. Nevertheless, there are many situations in which people are afraid to report, because of a blame culture, or do not feel it is worthwhile. This paper identifies three different types of blame culture, the Personal, the Professional and the Political and then examines how these might be countered, primarily by education and an understanding of how accidents are caused. The paper ends with a plea for all involved, from pilots and engineers to regulators, politicians and the media, to put aside natural tendencies to blame in favour of supporting full and open reporting in commercial aviation.
Safety Reporting in Aviation:
Safety Management and Safety Culture in Interaction
ABOUT THE AUTHOR ABOUT THE AUTHOR
Professor Patrick Hudson
Professor Patrick Hudson is with the Centre for Safety Research, Leiden University, Netherlands. He has been Project Leader of the Tripod Research Programme on Human Error for Shell International since 1988, cooperating closely with Prof. J. Reason of Manchester University, UK. He was involved in the early development of safety management systems as well as human factors programmes. He currently leads the Hearts and Minds research programme on the development of safety culture in the Oil and Gas industry.
Prof Hudson is a member of ICAO’s Human Factors Awareness Group and the Joint Aviation Authorities Human Factors Steering Group. His involvement with aviation includes working with companies such as Ansett Australia, Emirates, British Airways, Cathay Pacific, Shell Aircraft, KLM Helicopters and Swissair. He has over 180 publications in scientific journals, books and conference proceedings.
Safety Reporting in Aviation: Safety Management and Safety Culture in Interaction
1
Aviation Safety
Professor Patrick Hudson
Leiden University, The Netherlands
INTRODUCTION
Many incidents in aviation would go unknown unless
someone reports them. This is unfortunate, because learning
from minor incidents is the most cost-effective way of
making the aviation system safer. Accidents are obvious
and fortunately rare, but near misses and minor incidents
are much more common and can go undetected unless
someone is willing to tell what happened. The causes
of accidents and near misses are the same, especially at
the level of the underlying causes (Reason, 1997), which
is why they are commonly collected together under the
term incidents.
This paper will first discuss why it is so important to report
more than just the major incidents, placing reporting firmly
in the context of safety management, and then consider
why people find it so difficult to report, describing a
number of distinct organisational cultures. The paper then
considers the range of possible mechanisms for ensuring
reporting and concludes with a plea to put aside culturally
determined barriers in favour of encouraging a truly proactive
management of the risks of aviation.
WHY REPORT?
After a major incident, whether an actual accident or a very
public near miss, there will be a formal investigation to
discover what happened and, more importantly, why1. After
such an investigation, the results can be disseminated
throughout the industry and the expectation is that the
Safety Reporting in Aviation: Safety Management and Safety Culture in Interaction
1 ICAO Annex 13 is quite explicit in its requirement to uncover the reasons why an incident happened and to do this in a blame-free setting. This paper explores just why the blame-free element is so important, especially when incidents do not reach their full disastrous potential.

2
Safety Reporting in Aviation: Safety Management and Safety Culture in Interaction
safety of the system, as a whole, can be improved and possible accidents avoided. In the last
100 years of aviation, learning from accidents has been the main way in which the industry has
become safer; almost every line of the ICAO annexes can be traced back to an incident that now
need no longer be repeated.
Experience with major incidents in a great many different industries has shown that there are
almost always precursors that were, or could have been, identified in less serious incidents. In
many cases these minor incidents fall below the threshold that required them to be officially
reported and, subsequently, investigated (see Figure 1). These incidents will have breached one
or more barriers, “slices of cheese”, but will not have gone so far as to be classified as an actual
accident. Barriers are intended to prevent hazards from creating losses, such as an accident. Some
barriers may involve design and procedures, others may involve competence and vigilance. Poor
design or inappropriate procedures are latent conditions that are represented by ‘holes in the
cheese’, but an accident may be prevented by the competence and vigilance of an operator, such
as a pilot or air traffic controller. With the benefit of hindsight, such minor incidents have often
proven to be the harbingers of a future disaster. The immediate precursors that can be identified
from minor incidents will themselves have been caused by organisational failures or shortcomings,
such as lack of oversight, inappropriate procedures or a shortage of funding. These are all
factors that typically have an impact on a great many other possible defences that prevent
future accidents (Reason, 1997). It is this information that reporting of incidents can and should
provide. In an ideal world sufficient levels of proactive reporting of minor incidents, allowing
the identification of the underlying causes of potential incidents, should help drive down the
numbers of incidents where actual damage or injury occurs.
Figure 1: The Swiss Cheese model of accident causation (Courtesy J. Reason)
3
Journal Aviation Management 2008
REPORTING AND RISK MANAGEMENT
Reporting is one of the three major methods for acquiring information about how well
risks are being managed. This is the reason why incident reporting is stressed as one of the
major component of an SMS (ICAO, 2005). The other two are audits and, the most unforgiving,
accidents and major incidents where no one can deny that something went wrong. Reporting
enables us to identify systemic weaknesses as well as providing an important way of identifying
new hazards or threats that need to be managed to assure safety. To see reporting in context
it is necessary to understand how risk analysis is performed in other hazardous industries. Risk
analysis in general involves:
• Discovering how undesired consequences can occur and what hazards are involved (eg. terrain,
other aircraft, birds, Foreign Object Damage etc.);
• Uncovering both the superficial and the root or underlying causes of problems;
• Identifying how these causes can be managed effectively so that the problems do not arise.
Risk assessment goes further than analysis and involves quantifying the probabilities of such
consequences and identifying the frequency of underlying threats – how they may arise - and
assessing the effectiveness of preventative and mitigation barriers intended to prevent problems
from arising.
EXAMPLE – AIRSIDE COLLISIONS WITH NEW GENERATION COMPOSITE AIRCRAFT
There is a specific example which shows how reporting of apparently trivial incidents can no
longer be treated as a luxury. Future generations of aircraft will almost certainly increasingly
be constructed from composites, like the Boeing 787. One particular problem for such aircraft
lies exactly in their strength. Many components may fail to show, to simple visual inspection,
that they have been damaged to the point of threatening airworthiness as materials may
spring back after being hit. There are effective non-destructive techniques that are capable
of detecting such damage and allowing an assessment of whether repair is necessary or
not, but it is necessary first to know whether and where to look. Whether the damage is
caused by dropping tools in engineering or vehicle collisions on the ramp, the only way to
set a testing process in operation is to have someone report what happened and where; the
alternative of checking the whole of every such aircraft before every flight is unthinkable. At
the same time such reports also provide information about why such a collision occurred in
the first place; collecting such reports can show if there are trends, such as airside drivers
who may not have been given sufficient training to acquire the necessary competence to
drive heavy vehicles in the vicinity of composite aircraft.
In aviation, we are concerned with a wide range of possible consequences ranging from multiple
fatalities and aircraft loss, eg. Controlled Flight into Terrain (CFIT), to damage without injury and
reputation damage to airlines, airports, Air Traffic Mangement (ATM) providers and the sector as a

4
Safety Reporting in Aviation: Safety Management and Safety Culture in Interaction
whole. One of the lessons from other high-hazard industries is the need to manage the full
range of the problems that can cause such outcomes, not just by working backwards in the
hope of preventing specific outcomes like CFIT or runway incursions (Hudson, 2003a).
There are two basic approaches, viz reactive and proactive, to analysing the risks of an operation.
The reactive approach uses actual incidents and uncovers root causes by working backwards
from consequence to cause. A more proactive version of incident analysis imagines what possible
incidents could happen and again works backwards to ascertain how such an incident could
happen. An explicitly proactive approach, Failure Mode and Effect Analysis (FMEA), moves forward
from possible causes towards potential incidents, by systematically varying every element or
component in a system and seeing what failures can result. FMEA, while fully proactive, is labour
intensive and is usually only applied to engineering problems with a concentration on ‘hard’
component failures because of the difficulty in developing such a systematic approach with softer
human factors issues.
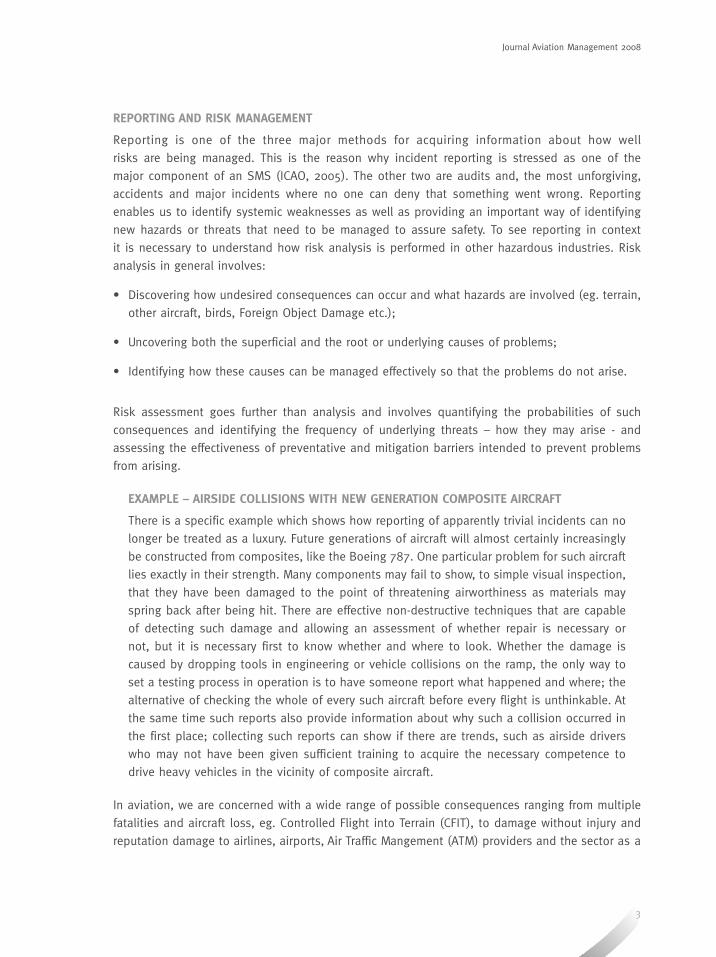
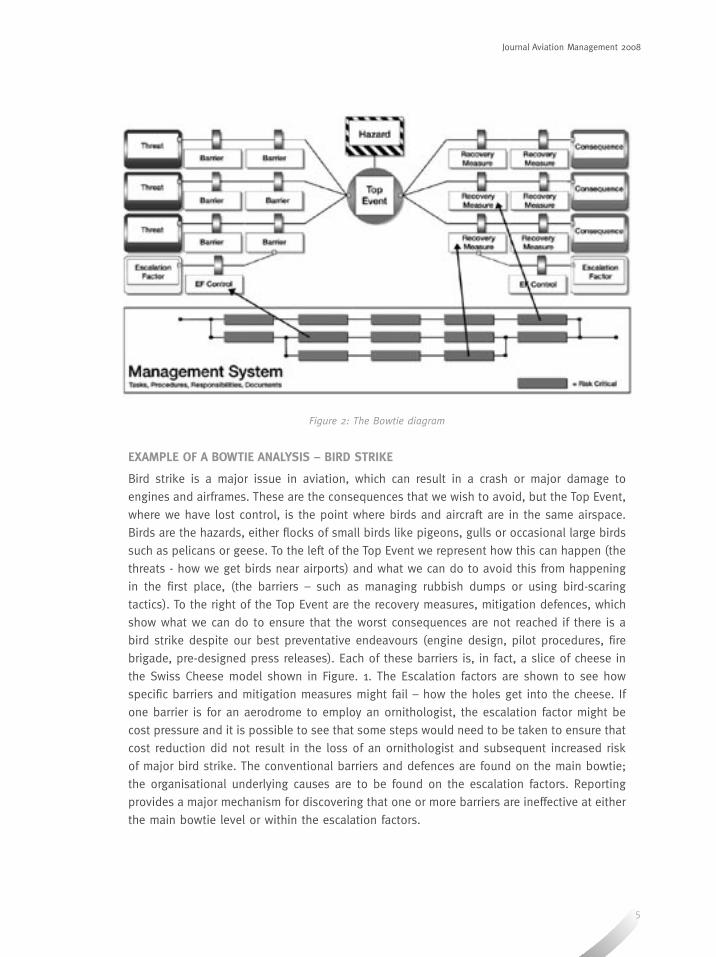
REPRESENTING RISKS - THE BOWTIE DIAGRAM
One way of understanding how accidents can be prevented involves using a risk analysis method
called the Bowtie, shown in Figure 2, which provides a way of combining these two approaches
while significantly reducing the complexity. Bowties are based around a top event, the point
at which no adverse consequences have yet occurred, but where control over the hazard has
been lost. There are a number of threats, ways in which the hazards can be released leading to
a top event and on to the undesirable consequences. To prevent hazards being released and
the consequences happening, we can place barriers on the threat pathway. These barriers may
depend on hard controls, such as designed hardware or softer controls such as procedures. The
barriers are explicit representations of the slices of cheese in the Swiss Cheese model. A full bowtie
represents a risk analysis, with all the threat pathways and barriers identified. If the frequencies of
threats and the effectiveness of the barriers are also quantified, then we have a risk assessment.
5
Journal Aviation Management 2008
Figure 2: The Bowtie diagram
EXAMPLE OF A BOWTIE ANALYSIS – BIRD STRIKE
Bird strike is a major issue in aviation, which can result in a crash or major damage to
engines and airframes. These are the consequences that we wish to avoid, but the Top Event,
where we have lost control, is the point where birds and aircraft are in the same airspace.
Birds are the hazards, either flocks of small birds like pigeons, gulls or occasional large birds
such as pelicans or geese. To the left of the Top Event we represent how this can happen (the
threats - how we get birds near airports) and what we can do to avoid this from happening
in the first place, (the barriers – such as managing rubbish dumps or using bird-scaring
tactics). To the right of the Top Event are the recovery measures, mitigation defences, which
show what we can do to ensure that the worst consequences are not reached if there is a
bird strike despite our best preventative endeavours (engine design, pilot procedures, fire
brigade, pre-designed press releases). Each of these barriers is, in fact, a slice of cheese in
the Swiss Cheese model shown in Figure. 1. The Escalation factors are shown to see how
specific barriers and mitigation measures might fail – how the holes get into the cheese. If
one barrier is for an aerodrome to employ an ornithologist, the escalation factor might be
cost pressure and it is possible to see that some steps would need to be taken to ensure that
cost reduction did not result in the loss of an ornithologist and subsequent increased risk
of major bird strike. The conventional barriers and defences are found on the main bowtie;
the organisational underlying causes are to be found on the escalation factors. Reporting
provides a major mechanism for discovering that one or more barriers are ineffective at either
the main bowtie level or within the escalation factors.
6
Safety Reporting in Aviation: Safety Management and Safety Culture in Interaction
Reports can be made about failures at any point on the trajectory from a hazard as well as about
novel hazards. At the level of consequences we will have had an actual accident, at the level of
the top event and where right-hand side barriers have failed, we will have had an incident that
can be easily recognised as a near miss. Prior to the top event, on the left-hand side, we could
have identified a failing preventative control. The bowtie diagram, in the case of any incident,
enables us to identify just which barriers failed and which barriers also worked to avoid the full
consequences. Accidents and public near-misses may suffice to set investigation in progress, but
there is already a cost, if only to reputation. The less obvious incidents, in contrast, can also be
analysed and can provide the same information at considerably less cost, at least in terms of
public exposure.
One thing is clear from this analysis of reporting as an integral part of the risk management
process. Reports have to be investigated to the point where they reveal information about
systemic shortcomings that could potentially impact operations and so cause more serious
incidents. Without such analysis, reporting is no more than a token exercise most likely to reflect
badly on the reporter. The problem is that professional investigation of incidents is often seen
as time-consuming and expensive, requiring extensive training if anything more than a superficial
re-description of the incident and some trivial trending is to be achieved. The bowtie, once in
place, provides an accessible and relatively rapid way of setting out the set of barriers available2,
allowing the investigator to identify which ones failed, which remained intact, and what if any
hazards and new threats can be identified.
WHY NOT REPORT?
If the case for reporting is so clear, why should people not report? The reality is that reporting in
many organisations and countries is sometimes infrequent; this despite the belief that there is
quite a lot happening, even in very safe operations, worthy of being reported, because individuals
fear being personally blamed for what went wrong, or more specifically, the consequences. Blame
cultures are those in which there is a strong desire to identify and punish those who have failed in
some way, typically those most closely identified with causing some bad outcome. They are found
in a wide variety of professions and in many national cultures.
Blame cultures can be understood in the light of two factors. One is a well-known and reliable
psychological phenomenon called the “Fundamental Attribution Error”. This refers to the disparity
in explanations of events between the individuals involved and observers; observers explain
individuals’ failures in terms of their poor internal psychological characteristics, while those same
individuals explain their actions with reference to the external environment. The term pilot error,
for instance, is used to blame the pilot, typically in terms of the individual pilot’s personal failings
while the pilot might point to the environmental factors3. The second factor is the belief that
people, unlike inanimate forces, have the power to control their own destiny. Taken in combination
with hindsight bias (Hudson, 2001; Fischhoff, 1975; Fischhoff & Beyth, 1975), where people believe
2 This is not necessarily to imply that the bowtie is the only possible methodology, but it sets a benchmark for quick and effective investigation of minor incidents that other methodologies will have to meet.3 In contrast people do tend to attribute their successes to their individual qualities, while outsiders may make reference to the
environment those individuals found themselves in.
7
Journal Aviation Management 2008
that “they knew it all along”, this leads to explanations of events in which a person can be
expected to have known what was happening and to have had the ability to prevent the bad
consequences from happening. The belief is that individuals, typically at the last moment, could
have and should have exercised sufficient control over their actions. The fact that they did not
makes them candidates for blame.
There appear to be three different types of blame culture, the Personal, the Professional and the
Political. In the Personal culture, there is a belief that people who immediately ‘cause’ an accident
should pay for it. Individuals are afraid of the consequences if they should report, especially when
it is their own actions, or inactions, that they are reporting. Even if they are not afraid of the
organisational consequences, such as punishment, they may still be keenly aware of the loss of
face reporting one’s own failures can incur. In many national cultures the fear of such outcomes
is enough to provide a significant impediment to reporting. These impediments to reporting can
be overcome if there is sufficient appreciation that front line operators, whose actions may have
been in error at the end of the whole incident trajectory, are equally the victims when there are
underlying causes over which they have little or no control (shown in Figure 1).
In the Professional culture, individuals may still feel ashamed of the fact that they have performed
below their own expectations and would rather not tell. Professional Cultures are those in which
the key individuals - pilots, engineers, and doctors form good examples – feel that they possess
exceptional characteristics and have been given special training so that any failure to exercise the
highest professional standards of performance must reflect upon them personally. In many ways
these groups may be seen to fall under a reversed attribution error; failure reflects on their failure
to exercise sufficient control whatever the circumstances, while success is only what would be
expected every day.
Finally, the Political culture covers the complex of public constituencies outside the organisation
that also seek to identify individuals to blame, from the law to the media. There may be
impediments to reporting from external agencies that mean that, even with an open culture
within the organisation with the understanding that everyone is fallible, reporting is still an open
invitation to some form of sanction, whether legal or in terms of reputation damage to either
individuals or the organisation as a whole. The law, almost by definition, institutionalises the
concept of blame and subscribes to the belief that identification and punishment of those who
fail, whether intentionally or not, is essential. Often there is a belief that punishment, especially
in public, will ensure that other people do not make the same errors – a belief that flies in the
face of 100 years of psychological study. The media is also served by providing easily understood
explanations of why things went wrong, especially after a public disaster – unfortunately accurate
explanations rapidly become too complex to capture in a sound bite or a headline, while pilot
error meets the bill easily. In commercial aviation the problem may be exacerbated by the public
perception that aviation is safe, therefore any failure of the system must be due to one or more
individuals who actively subverted that safe system.
8
Safety Reporting in Aviation: Safety Management and Safety Culture in Interaction
Some or all of these cultures may be in effect at the same time, they are different but not
incompatible because the same psychological mechanisms of blame underlie all three.
TYPES OF REPORTING SYSTEM
There are a variety of different ways to collect reports. A number of these systems are intended to
encourage reporting by avoiding some of the cultural pitfalls. This section describes the different
types of system available, the next section considers how they can be used to get people to
report. Barach & Small (2000) provide a comprehensive review of reporting systems.
• Anonymous reporting systems, while potentially capable of lowering the threshold to report,
suffer from a number of problems that make them effectively useless. One is that such systems
are open to abuse, allowing people to make reports that bring individuals into focus that may
be the result of malicious rather than well-intentioned intent. But more important is the fact
that it is hard, or impossible, to get the information that is really important; one is left with the
immediate description of what happened and little if any trustworthy information about why the
event happened. Yet I have argued above that this is the true value of reporting.
• Confidential reporting systems are intended to overcome the problems with anonymous
reporting, removing both malicious reporting and the inability to follow up reported incidents.
They should allow people who feel that they may be blamed to report anyway because their
names should never be released to those who will blame. The necessity of such systems reflects
on the overall culture of the organisation, as it is still felt necessary to protect reporters.
• Protected reporting systems are those that provide a degree of protection from prosecution.
The American ASRS provides immunity for those who report in a timely manner.
• Open reporting may be constrained, names are known but reports and their results are typically
published without references to persons, or totally open, as when access to all reports in the
system is available to everyone in the organisation, or limited to those with a need to know.
• Mandatory reporting is normally demanded by legal requirements. Such reports are invariably
specific about individuals, but may be confidential within the confines of the organisation
and the regulator, unless the legal authorities decide that they wish to intervene. ICAO
Annex 13 (Aircraft Accident & Incident Investigation) sets clear requirements for full and blame-
free investigation, implying the same for reporting on non-accident incidents, but the possibility
for prosecuting authorities to proceed has always remained, subject to the requirement that
they have to collect their own evidence4.
These different systems are intended to make reporting easier for reporters, except for mandatory
systems that simply require, with the clear threat of sanctions for non-reporting. It is clear that the
level of protection felt necessary to make people feel comfortable with reporting will be a function
of the overall safety culture of the organisation (Hudson 2003b), which primarily impacts on the
4 Most jurisdictions allow individuals to remain silent in the event that speaking would provide evidence of guilt in a criminal case. The requirement of Annex 13 is to ensure that the information needed to prevent future accidents becomes available, but the fact that something has been stated in the context of Annex 13 means that prosecutors would need to find other proof. The situation
in civil cases is, in my opinion, less clear.
9
Journal Aviation Management 2008
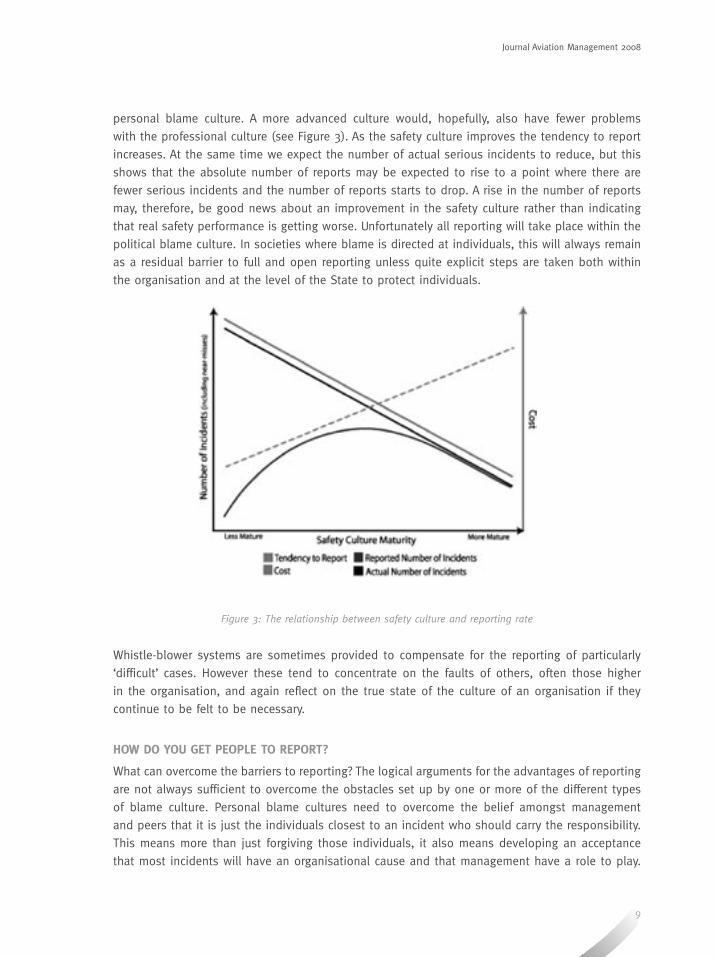
personal blame culture. A more advanced culture would, hopefully, also have fewer problems
with the professional culture (see Figure 3). As the safety culture improves the tendency to report
increases. At the same time we expect the number of actual serious incidents to reduce, but this
shows that the absolute number of reports may be expected to rise to a point where there are
fewer serious incidents and the number of reports starts to drop. A rise in the number of reports
may, therefore, be good news about an improvement in the safety culture rather than indicating
that real safety performance is getting worse. Unfortunately all reporting will take place within the
political blame culture. In societies where blame is directed at individuals, this will always remain
as a residual barrier to full and open reporting unless quite explicit steps are taken both within
the organisation and at the level of the State to protect individuals.
Figure 3: The relationship between safety culture and reporting rate
Whistle-blower systems are sometimes provided to compensate for the reporting of particularly
‘difficult’ cases. However these tend to concentrate on the faults of others, often those higher
in the organisation, and again reflect on the true state of the culture of an organisation if they
continue to be felt to be necessary.
HOW DO YOU GET PEOPLE TO REPORT?
What can overcome the barriers to reporting? The logical arguments for the advantages of reporting
are not always sufficient to overcome the obstacles set up by one or more of the different types
of blame culture. Personal blame cultures need to overcome the belief amongst management
and peers that it is just the individuals closest to an incident who should carry the responsibility.
This means more than just forgiving those individuals, it also means developing an acceptance
that most incidents will have an organisational cause and that management have a role to play.
10
Safety Reporting in Aviation: Safety Management and Safety Culture in Interaction
This is not such a burden as it might appear; incident reporting can uncover weaknesses in
the system, especially on the left-hand side of the bowtie, leading to improvements that are
typically cost-effective, benefiting the organisation as a whole, and where management can often
be happy that issues have been identified before anything wrong or blameworthy has happened.
Two major problems arise, one is the continuing belief of management in the reprehensibility of
individuals who could have prevented an incident at the last moment, the second is the belief
(and expectation) in such individuals that punishment will still be meted out, despite public
protestations to the opposite by senior staff.
Professional blame cultures are, if anything, more difficult to manage. Professionals like pilots
and surgeons have to learn the same lesson as management in the Personal culture, but now
applied to themselves. They need to understand that even though they may be put into impossible
situations, that it is worth reporting to uncover and remedy the reason for those problems.
Extending reporting requirements within an explicit framework of professional risk management
may help such people to realise that being professional involves discovering sources of error and
failure as well as combating them.
Political blame cultures are the hardest to circumvent. The historical and cultural background that
determines the attitudes of lawmakers and the media are outside the power of most organisations
to change. The one possibility that appears to work is supra-national regulation. ICAO, and
especially Annex 13, provides an example of how international regulation can be used to overcome
national tendencies. The European Union has also made a requirement for blame-free reporting
in directive 2003/42/EC. ICAO and the European Union have, unfortunately, little if any influence
on the media’s perception that when bad things have happened someone has to pay, and their
belief that retribution is what the public wants. Nevertheless even here a proactive approach to
the media, coupled with openness from senior management in the organisation, can result in a
change in opinion that the media can reflect. Figure 3 shows an interesting relationship between
the expected safety performance of an organisation and the number of reports, a message that
could be passed to those who immediately equate an increase in the number of reports with a
worsening situation5.
The lesson appears to be that education about how incidents actually happen, and how information
about failures can actually serve to make the system better rather than just provide evidence
that things are bad, can impact on blame cultures at all three levels. But there are two other
requirements that are essential. First, even with the development of the understanding of how
incidents can be illuminating rather than just symptomatic, it is essential that all parties can be
made to believe that reporting of all except the most egregious events should be blame-free (or
blame-light) and even rewarded (Hudson et al, 2008).
In order to do this a track record of reporting without negative consequences for the reporter
needs to be constructed, and this will take time. One way to develop such a track record
involves approaching individuals and essentially setting up a number of reports that ‘prime the
5 The question that can be asked in the aviation setting is, “Would you rather fly with an airline that reported, or one that didn’t?”

11
Journal Aviation Management 2008
pump’, together with publicity about the reports and the lessons learnt while clearly not naming
individuals (the message is that reporting makes things better and reporters do not receive bad
consequences). A later stage might then involve publishing the incident, the lessons learnt and
how the reporter was rewarded, thus bringing individuals out into the open in a positive way.
The second requirement interacts with the first, it is that reports should be handled in a timely
manner and that feedback be given to the reporter so that they feel that reporting is worthwhile.
Both of these are related to the development of trust; the first trust that reporters will not suffer
bad personal consequences, and may even be rewarded, the second that something useful will be
done with the information derived from the report.
CONCLUSION
Reporting, especially of apparently minor incidents, is of vital importance in all high hazard
industries, but particularly in commercial aviation where the numbers of victims in major accidents
can be considerable. Proactive reporting is one way to uncover underlying potential causes of
future accidents before they happen, along with considered risk analysis and thorough audits.
This paper has identified a number of reasons why people would not wish to report, some of
them are inherent to the industry, some are the result of failures of trust between reporters and
the management of their organisation, and some are the result of the behaviour, or expected
behaviour, of external bodies such as regulators or the media. There are a number of ways in
which reporting can be encouraged, ranging from making reports of certain types of incident
mandatory, providing ways of enduring freedom from prosecution, through confidential reporting
even to anonymous. The need for these different types of reporting system depends upon the
safety culture of the organisation, the regulatory bodies, the legal system and the media.
With recent developments in aviation, we can no longer afford the luxury of waiting to learn from
accidents, so there is really no alternative to having as full and open a reporting system as is
possible. The price we may have to pay to achieve a full and informative reporting system as
possible may be considerable. Pilots and engineers, for instance, must be willing to put aside their
feelings of professional pride for a greater good. Management of airlines must become convinced
that the benefits of reporting far outweigh their desire to punish individuals. Regulators and
other lawmakers must accept that heavy-handed intervention may well prove counterproductive
and smother reporting completely. Finally the media must learn to contain simplistic popular
interpretations, or at least accept responsibility for the long-term consequences of their actions.
Without such concessions from all parties we may remain doomed to continue learning from
accidents. In a world in which the consequences of accidents with aircraft like the A380 are almost
too considerable to be contemplated, for passengers, the airline and even the industry as a whole,
there is no alternative.

12
References
Barach, P. & Small, S.D. (2000) Reporting and preventing medical mishaps: Lessons from non-medical near miss
reporting systems. British Medical Journal, 320, 759-763
Fischoff, B. (1975) Hindsight /= foresight: The effect of outcome knowledge on judgement under uncertainty. Journal
of Experimental Psychology: Human Perception and Performance. 1, 288-299.
Fischhoff, B. & Beyth, R. (1975) “I knew it would happen”: Remembered probabilities of once-future things.
Organisational Behaviour and Human Performance. 13, 1-16.
Hudson, P.T.W. (2001) They didn’t see it coming: Hindsight and foresight on the road to disaster. In E.R. Mullaer &
C.J.J.M. Stolker (Eds.) Ramp en Recht: Beswchouwingen over rampen, verantwoordelijkheid en aansprakelijkheid.
Boom Juridische Uitgevers: Den Haag. Pp 91-102
Hudson, P.T.W. (2003a) Applying the lessons of high-risk industries to medicine. Quality and Safety in Health Care.
12, 7-12
Hudson, P.T.W. (2003b) Developing an aviation safety culture. Journal of Aviation Management. 4, 27-48.
Hudson, P.T.W., Vuijk, M., Bryden, R., Biela, D. & Cowley, C. (2008) Meeting Expectations: A new model for a just and
fair culture. In Proceedings of the 8th SPE International Conference of Health, Safety and Environment in Oil and Gas
Exploration and Production. Richardson, TX: Society of Petroleum Engineers. 6 pp. [CD-ROM]
ICAO (2005) ICAO Safety Management Manual. Doc 9859 AN/460 Montreal.
Reason, J.T. (1997) Managing the Risks of Organisational Accidents. Ashgate.
Safety Reporting in Aviation: Safety Management and Safety Culture in Interaction
ABSTRACT
Aviation Safety
ABSTRACT
The need for cooperation in investigations is a fundamental tenet and is now more important than ever. Cooperation is required to ensure the needs of the community are best served. Police, Coroners, Judicial and regulatory authorities in most States rely on effective cooperation with the aviation investigation authority to ensure they can also meet the needs of the community. However, in an era of low cost airlines and increasing globalisation, we are seeing airline ‘code sharing’ and ‘alliances’ resulting in more of the world’s population using air travel. People are using a broader cross section of airlines, from a range of flag States, than ever before.
Many States do not have, or do not dedicate, the resources to appropriately meet their ICAO Annex 13 obligations, thereby reducing the effectiveness of their safety oversight and investigation capabilities. This in turn reduces their ability to meet the needs of their citizens, and the citizens of many other countries when an aircraft is carrying passengers or crew of differing nationalities. This paper will briefly explore the need for broader cooperation in the conduct of independent, no-blame and accountable investigations not only within a State, but globally.
Aviation Safety Investigations – Cooperative, Independent, No-blame and Accountable
ABOUT THE AUTHOR ABOUT THE AUTHOR
Aviation Safety Investigations – Cooperative, Independent, No-blame and Accountable
Mr Alan Stray
Mr Alan Stray is Director International of the Australian Transport Safety Bureau (ATSB), with responsibility for international engagement/liaison with government and industry. He has been an aviation safety investigator since January 1987.
Mr Stray has been the Accredited Representative on a number of overseas major airline accidents, most recently the Garuda and AdamAir Boeing 737 tragedies in Indonesia. He has the lead in-country role in the ATSB’s cooperation with the Indonesian National Transportation Safety Committee, as part of the Australian Government’s Indonesia Transport Safety Assistance Programme. In January 2005 and 2008, he was awarded the Government’s Australia Day Council Achievement Medallion, for his contribution to aviation safety and support to the Indonesian Government in the Garuda 737 investigation respectively.
13
Aviation Safety
Mr Alan Stray
Australian Transport Safety Bureau
NEED FOR REGIONAL COOPERATION
International Civil Aviation Organization (ICAO) has
contemplated the need for Regional cooperation in
investigations and this was the subject of a working paper
that was discussed at the ICAO Accident Investigation
and Prevention (AIG) Divisional Meeting held in Montreal
in October 2008, the first such meeting since 1999.
In the working paper titled ‘Regional Cooperation in
Investigations’, the ICAO Secretariat states:
For the investigation of major accidents in States which do not have
the resources to carry out the investigation, other interested States
(e.g. the State of Design and Manufacture) may assist and provide
support to the State of Occurrence. However, many States also lack
the capability to investigate accidents other than the major ones,
and to investigate serious incidents. For many of those States, the
establishment of a regional accident investigation organisation, or
the creation of a regional pool of qualified investigators might be the
only options to enable the establishment of an effective accident and
incident investigation and prevention system.
ICAO has long been aware of the difficulties experienced by some
Contracting States in implementing Standards and Recommended
Practices (SARPs) and has tried to assist them accordingly. Safety
oversight audits conducted under the ICAO Universal Safety
Oversight Audit Programme (USOAP) have highlighted the extent
of deficiencies encountered by those States in meeting their safety
oversight obligations. In many cases, these deficiencies are the
result of insufficient resource allocation to the national civil aviation
body. Consequently, such States are unable to comply in full with
national and international requirements concerning the safety of civil
aircraft operations.
Aviation Safety Investigations – Cooperative, Independent, No-blame and Accountable
14
Aviation Safety Investigations – Cooperative, Independent, No-blame and Accountable
ICAO IDENTIFIES STATES’ SHORTFALLS
The ICAO Secretariat’s working paper on ‘Regional Cooperation in Investigations’ draws attention
to responsibilities of States in ensuring appropriate oversight and investigation, and highlights the
fact that many States are falling short of their responsibilities:
The Convention on International Civil Aviation (Chicago Convention) allocates responsibility for aviation safety to
individual States. Each State bears responsibility for the continuing airworthiness of aircraft; safe and efficient
aircraft operations; the licensing and/or certification of personnel; safe air traffic flow within its airspace, sufficient
airport infrastructure; and adequate investigations of aircraft accidents and incidents. At the November 1997
Conference of Directors-General of Civil Aviation, ICAO highlighted the findings of its safety oversight assessments,
which indicated that a significant number of Contracting States were experiencing problems in implementing SARPs,
recruiting qualified personnel and, in general, fulfilling their safety oversight obligations.
Safety oversight audits conducted under the ICAO Universal USOAP now include the audit of a
State’s capability with respect to compliance with Annex 13 SARPs. Since the inclusion of Annex 13
in the USOAP, the extent of deficiencies encountered by States in meeting their safety investigation
obligations has been highlighted. Some Contracting States have been found to have no Annex
13 enabling legislation or policies and procedures. Even in the States that have basic enabling
legislation, these deficiencies have been shown to result from insufficient resources, which
translates to a lack of qualified and experienced investigators; training opportunities; basic and
essential equipment; policies and procedures. Consequently, these States are unable to meet their
national and international aircraft accident and incident investigation obligations. The legal system
in a State itself may impact the relationship of the investigation legislation to other legislation.
ICAO GUIDANCE FOR REGIONAL OVERSIGHT
In 2006, ICAO published the Safety Oversight Manual and Part B — The Establishment and
Management of a Regional Safety Oversight System (Doc 9734–Part B). The manual provides
guidance on the establishment and management of a Regional Safety Oversight Organisation
(RSOO) and outlines the duties and responsibilities of ICAO Contracting States with respect to the
establishment and management of a regional safety oversight system. It is addressed to high-level
government decision-makers, as it highlights States’ obligations as signatories to the Chicago
Convention and provides information and guidance on the establishment and management of
an RSOO to assist Contracting States in fulfilling part or all of their safety oversight-related
obligations.
While Doc 9734–Part B does not specifically address aircraft accident and incident investigations,
it can be used as a reference for the establishment of regional accident investigation systems.
The manual provides guidance on how to establish and manage a regional system within a
particular region or sub-region. Consideration should be given to the need to ensure that the
establishment of a regional system for the investigation of accidents and incidents does not
affect the independence of the investigation process, which is not a matter covered in detail
in Doc 9734–Part B. The accident and incident investigation authority must be independent,
yet accountable.

15
Journal Aviation Management 2008
COOPERATION IS AN IMPORTANT ELEMENT
While the 1992 Accident Investigation and Prevention Divisional Meeting (AIG/92) discussed
the need to separate any judicial proceedings to apportion blame or liability from an accident
investigation, the meeting also discussed the necessity of good coordination between accident
investigation and judicial authorities during investigations. Following AIG/92, several provisions
covering those subjects were developed and introduced in Annex 13. ICAO has also developed
much guidance material to help States in implementing Annex 13 SARPs.
Many States do not have enabling legislation to ensure primacy, let alone protection of evidence,
for the agency conducting investigations in accordance with Annex 13 SARPs. For the investigation
of major accidents in States that do not have the resources to carry out investigations or have
extremely limited capability, other interested States (eg the State of Design and Manufacture) may
assist and provide support to the State of Occurrence. For many of those States, the establishment
of a regional accident investigation organisation, or the creation of a regional pool of qualified
investigators, might be the only options to enable the establishment of an effective accident and
incident investigation and prevention system.
One ICAO AIG working paper states:
In many areas of regional cooperation, States can produce economies of scale leading to increased efficiency due
to the possibility of sharing and pooling of human and financial resources. Participating States will also increase
their capacity to develop harmonised regulations adapted to their local environment and in compliance with SARPs.
In the international arena, the existence and effective operation of regional organisations is a demonstration of
regional solidarity and increases the involvement of individual States in aviation activities relating to the region or
sub-region.
COOPERATING WITH OTHER AUTHORITIES AND ORGANISATIONS
In recent years, some States have indicated that following an accident, the Judicial authorities have
control over the wreckage, which may delay or restrict the conduct of the Annex 13 investigation.
Many States do not have an independent investigation authority or appropriate procedures in
place for carrying out Annex 13 no-blame investigations. In this case, the investigation may be
done by the State’s regulator or the Judicial authority. These investigations are not Annex 13 no-
blame investigations, but nevertheless are necessary to ensure that the needs of the community
and the community’s expectation of natural justice are upheld. So when considering regional
cooperation to facilitate Annex 13 investigations for the conduct of no-blame safety investigations,
the needs of the community must be given very careful consideration.
WHAT IS INDEPENDENCE?
The principle of ‘independence’ is extremely important in aircraft accident and incident investigation.
Functional independence is required in order for the investigation to be conducted without ‘fear
or favour’ in the interest of seeking to fully determine all the causes or causal factors of the
accident or incident and report publicly, ensuring that appropriate safety action is taken. Functional
16
Aviation Safety Investigations – Cooperative, Independent, No-blame and Accountable
independence means that the roles and responsibilities of safety investigators need to be clearly
outlined in legislation, separate from judicial processes and not subject to direction in the conduct
of an investigation by third parties. Independence is not achieved where, for example, a division
of the regulator conducts the investigation of the accident or incident. Likewise, if a police aircraft
is involved in an accident, independence would not be achieved if a division of the police force
conducted the investigation. It is foreseeable that there may be systemic factors associated with
a regulatory or police agency that contributed to the accident. At the very least, if these agencies
commissioned the investigation, there is likely to be a community perception that all the factors
related to those agencies may not have been fully investigated and publicly reported on. Lack of
confidence in the investigation framework and processes will inevitably result.
HOW INDEPENDENT IS INDEPENDENT?
It is widely accepted that complete and totally unfettered independence is almost a myth. One
basic yet fundamental example is that the funding of investigation authorities in most States
is normally dependent on a government budgetary process. In many States, the investigation
authority may be responsible to a level of bureaucracy for public service administration. Therefore,
the term independence, in the context of aircraft accident and incident investigation, more typically
refers to functional or operational independence.
It is interesting to note that Article 6 of the European Union Directive, which covers aviation
investigation, states:
Investigating body or entity
1. Each member State shall ensure that technical investigations are conducted or supervised by a permanent civil
aviation body or entity. The body or entity concerned shall be functionally independent in particular of the national
aviation authorities responsible for airworthiness, certification, flight operation, maintenance, licensing, air traffic
control or airport operation and, in general, of any other party whose interests could conflict with the task entrusted
to the investigating body or entity.
2. Notwithstanding paragraph 1, the activities entrusted to this body or entity may be extended to the gathering and
analysis of air safety related data, in particular for prevention purposes, in so far as these activities do not affect its
independence and entail no responsibility in regulatory, administrative or standards matters.
There will always be a potential, perceived, or real conflict of interest where a person or organisation
involved in an accident or incident conducts the investigation.
INDEPENDENCE NOT JUST A MATTER FOR AVIATION INVESTIGATIONS
In the maritime world, there is also concern about independence. A proposed new Code for
Marine Casualty Investigations had been put forward for adoption at the International Maritime
Organisation’s Maritime Safety Committee meeting in May 2008. Chapter 11 of the Code which
would be mandatory will require that:
17
Journal Aviation Management 2008
Marine Safety Investigating State(s) must ensure that investigator(s) carrying out a Marine Safety Investigation
are impartial and objective. The Marine Safety Investigation must be able to report on the results of the Marine
Safety Investigation without direction or interference from any persons or organisations who may be affected by
its outcome.
ICAO GUIDELINES FOR FUNCTIONALLY INDEPENDENT INVESTIGATIONS
The following important information can be found in the Manual of Aircraft Accident and Incident Investigation and Part I — Organisation and Planning (Doc 9756):
2.1.1 In conformity with Article 26 of the Convention on International Civil Aviation, it is incumbent on the State
in which an aircraft accident occurs to institute an inquiry into the circumstances of the accident. This obligation
can only be met when appropriate legislation on aircraft accident investigation is in place. Such legislation
must establish an accident investigation authority (or commission, board or other body) for the investigation of
aircraft accidents.
2.1.2 The accident investigation authority must be strictly objective and totally impartial and must also be perceived
to be so. It should be established in such a way that it can withstand political or other interference or pressure.
Many States have achieved this objective by setting up their accident investigation authority as an independent
statutory body or by establishing an accident investigation organisation that is separate from the civil aviation
administration. In these States, the accident investigation authority reports direct to Congress, Parliament or a
ministerial level of government.
2.1.3 In many States it may not be practical to establish a permanent accident investigation authority. These States
generally appoint a separate accident investigation commission for each major accident to be investigated, the
members of which are often seconded from the civil aviation administration. It is essential that such a commission
report direct to a ministerial level of government so that the findings and safety recommendations of the investigation
are not diluted during passage through regular administrative channels.
COORDINATION WITH OTHER AUTHORITIES WHILE MAINTAINING NO-BLAME INVESTIGATIONS
The functional independence and primacy of investigations under Annex 13 are provided for in the ICAO Standards in paragraphs 5.4 and 5.6. However, cooperation and coordination with separate judicial or administrative inquiries are contemplated by Annex 13 and, if relevant, aviation security authorities (see paragraphs 5.10 and 5.11).
Coordination – Judicial authorities
5.10 The State conducting the investigation shall recognise the need for coordination between the investigator-in-
charge and the Judicial authorities. Particular attention shall be given to evidence which requires prompt recording
and analysis for the investigation to be successful, such as the examination and identification of victims and read-
outs of flight recorder recordings.
Note 1.— The responsibility of the State of Occurrence for such coordination is set out in 5.1.
Note 2.— Possible conflicts between investigating and Judicial authorities regarding the custody of flight recorders
and their recordings may be resolved by an official of the judicial authority carrying the recordings to the place of
read-out, thus maintaining custody.
18
Aviation Safety Investigations – Cooperative, Independent, No-blame and Accountable
Informing aviation security authorities
5.11 If, in the course of an investigation it becomes known, or it is suspected, that an act of unlawful interference was
involved, the investigator-in-charge shall immediately initiate action to ensure that the aviation security authorities
of the State(s) concerned are so informed.
This is reflected in Sections 7(2), 10 and 17 of Australia’s Transport Safety Investigation Act 2003,
which replaced Part 2A of the Air Navigation Act 1995. Such cooperation and coordination is
important and is achieved in the context of parallel inquiries.
These sections articulate the objectives of the Act to improve transport safety through reporting
safety matters, and the conduct of independent no-blame investigations. This is to be done through
cooperation between the investigation agency and other government agencies or any person who
has powers under another law to also investigate the matter. There is also a requirement to conduct
the investigation activities in a manner consistent with Australia’s international obligations.
The Australian Transport Safety Bureau (ATSB) seeks to ensure cooperation with other agencies
such as the aviation regulator, air traffic services provider, police and Coroner. Every effort is made
to facilitate these authorities being able to undertake parallel inquiries, short of them using ATSB
compelled witness statements and other sensitive documents. This also applies to Coroners and
officers assisting Coroners.
WHY DO INVESTIGATIONS NEED TO BE ‘NO-BLAME’
Annex 13 paragraph 3.1 states that “The sole objective of the investigation of an accident or
incident shall be the prevention of accidents and incidents. It is not the purpose of this activity to
apportion blame or liability”. However, in explaining what, why and how it happened, and seeking
to encourage safety actions to improve future safety, and trying to make sure an accident does not
happen again, aircraft accident investigation reports written in accordance with Annex 13 may be
read, particularly by the media, as implying blame.
ICAO Annex 13 Standard 5.12 requires non-disclosure of accident or incident records for purposes
other than accident or incident investigation unless a Judicial authority conducts a balancing
exercise and determines “that their disclosure outweighs the adverse domestic and international
impact such action may have on that or any future investigations”. The records covered by the
Standard include witness statements, operational communications, medical or private information,
cockpit voice recordings and transcripts, air traffic control recordings and transcripts, and opinions
expressed in the analysis of information including flight recorder information. Paragraph 5.12.1
states: “These records shall be included in the final report or its appendices only when pertinent
to the analysis of the accident or incident. Parts of the records not relevant to the analysis shall
not be disclosed,”. The Annex notes that:
19
Journal Aviation Management 2008
Information contained in the records listed above, which includes information given voluntarily by persons
interviewed during the investigation of an accident or incident, could be utilised inappropriately for subsequent
disciplinary, civil, administrative and criminal proceedings. If such information is distributed, it may, in the future,
no longer be openly disclosed to investigators. Lack of access to such information would impede the investigation
process and seriously affect flight safety.
Extensive legal guidance on the protection of safety information and data is provided in Attachment
E to Annex 13 which came into force on 23 November 2006. This guidance applies to all accident
investigation records.
The ‘no-blame’ principle is fundamental to encouraging the free flow of safety information to
an accident investigation. ICAO has done a tremendous job in encouraging States to implement
protection for accident investigation records as well as other safety information collected from
Safety Data Collection and Processing Systems. The promulgation of Attachment E to Annex 13
is an example of this. During the October 2008 AIG, the items that should be protected during
a no-blame investigation and included in Annex 13 Attachment E were discussed with the aim of
ensuring clearer guidance in facilitating the no-blame principle of safety investigation.
In addition to this ICAO material, in 2005 major aviation industry groups worked to develop a
‘Global Aviation Safety Roadmap’ (GASR) with key safety focus areas from 2006 to 2010 and
for several years beyond, which was presented to ICAO’s Air Navigation Commission on 25
January 2006. ICAO sought an implementation plan and the result in early 2007 was a detailed
document titled ‘Implementing the Global Aviation Safety Roadmap: A Strategic Action Plan for
Future Aviation Safety’ developed jointly by Airports Council International, Airbus, Boeing, Civil Air
Navigation Services Organisation, Flight Safety Foundation, International Air Transport Association
and International Federation of Air Line Pilots Associations for ICAO, States and the Industry (GASR
Implementation). Australia has supported the GASR and the GASR Implementation at meetings of
ICAO, Directors-General of Civil Aviation, and through training in our region (e.g. in Indonesia and
at the Singapore Aviation Academy).
The GASR Implementation emphasises that with the rapidly increasing aviation activity worldwide,
in order to prevent a rise in accidents, there is a need to share safety information and data more
freely and in better structured ways.
If a State is not able to establish a separate, functionally independent, no-blame accident and
incident investigation authority because of limited resources in its own State, the State should look
to the possibility of establishing such an authority in conjunction with other States in a regional
group. For many years the Interstate Aviation Committee based in Moscow has capably conducted
investigations on behalf of Russia and 11 other States. The Interstate Aviation Committee works
cooperatively with the 12 States and is a functionally independent, no-blame, accountable regional
investigation authority.

20
Aviation Safety Investigations – Cooperative, Independent, No-blame and Accountable
ACCOUNTABILITY
A separate, functionally independent accident and incident investigation authority needs to be able
to demonstrate accountability. The accident and incident investigation authority should be open
and transparent about its investigation processes. The precise means of achieving this openness
and transparency in order to provide accountability should be left to the individual States to
determine. However Annex 13 does provide a lead to investigation authorities into accountability
throughout the investigation process. Annex 13 Standard 6.3 instructs States to send the draft
Final Report to States with a material interest for a 60-day review and comment period; a period of
scrutiny. Accountability is further achieved through compliance with Annex 13 Standard 6.5, which
under the heading Release of the Final Report states:
6.5 In the interest of accident prevention, the State conducting the investigation of an accident or incident shall
release the Final Report as soon as possible.
This then leaves the report open to public scrutiny. A Coroner or an appropriate Judicial inquiry
may conduct an enquiry to determine the date, time, place, manner and cause of death. This will
normally include a detailed review of the Final Report. Further, as is the case in Australia, the ATSB
is subject to questioning from parliamentary committees about its investigations and processes.
HOW DOES THE ATSB ‘STACK UP’?
Australia, through the ATSB, has been conducting functionally independent, no-blame and
accountable investigations and has embarked on a significant programme of cooperation with its
regional neighbours for many years. More recently, under a structured program of cooperation with
the Republic of Indonesia titled the ‘Indonesian Transport Safety Assistance Program’ (ITSAP), the
ATSB has been working closely with the National Transportation Safety Committee team through
investigation and training cooperation in Jakarta, as well as in Canberra. Major activities in this
regional cooperation programme have been assistance in the Garuda and AdamAir Boeing 737
accidents that occurred in 2007. Working cooperatively led to the timely release of both Final
Reports and many safety actions being taken by the Indonesian regulator, air traffic services
provider and the airlines.
In an era of massive expansion of air services globally, cooperation with regional neighbouring
States is fundamentally important. This concept may lead to regional accident and incident
authorities being formed throughout the world to ensure the timely and effective use of resources
in the quest of transport safety enhancement. In many areas of regional cooperation, States can
produce economies of scale leading to increased efficiency due to the possibility of sharing and
pooling of human, technical and financial resources. Participating States will also increase their
capacity to develop harmonised regulations adapted to their local environment and in compliance
with SARPs.
The views and opinions expressed in this article reflect those of the author and not necessarily
those of the ASTB or the Australian Government.
21
Journal Aviation Management 2008
REFERENCES
ICAO (2008). ICAO AIG Working Papers, Used with permission of ICAO AIG Secretariat.
ICAO (2006). Safety Oversight Manual and Part B — The Establishment and Management of a Regional Safety
Oversight System (Doc 9734-part B).
ICAO (2001). Annex 13 Aircraft Accident and Incident Investigation, International Standards and Recommended
Practices, Amendment 11, 23 November 2006.
ICAO (2000). Manual of Aircraft Accident and Incident Investigation and Part I — Organisation and Planning (Doc 9756).
TSI Act (2003). Transport Safety Investigation Act (2003), Australian Government.
GASR Implementation Group (2005). Global Aviation Safety Roadmap (GASR).
GASR Implementation Group (2007). Implementing the Global Aviation Safety Roadmap: A Strategic action plan for
future aviation safety developed jointly by ACI, Airbus, Boeing, CANSO, FSF, IATA and IFALPA for ICAO States and
the Industry.

22
ABSTRACT
Aviation Safety
ABSTRACT
Safety management system (SMS) is a buzzword in the industry, and it is a system that will not work without voluntary disclosure of the evidence of risks in the system between operators and regulators. To continue this free disclosure, enforcement actions need to be carefully considered and sometimes waived if the risk factor is addressed promptly and appropriately. This novel concept is difficult for those outside the industry to understand, and political pressures have caused setbacks in the implementation of SMS. This paper discusses issues relating to balancing safety and compliance, and the importance of the operator-regulator relationship.
Balancing Safety and Compliance in the Regulatory Environment
ABOUT THE AUTHOR ABOUT THE AUTHOR
Balancing Safety and Compliance in the Regulatory Environment
Mr William Voss
Mr William Voss is President and CEO of the Flight Safety Foundation. Prior to that, he was Director of the Air Navigation Bureau at the International Civil Aviation Organization (ICAO), and was responsible for the development of major international safety initiatives. Before joining ICAO, Mr Voss spent 23 years at the Federal Aviation Administration (FAA), US, focusing on air traffic management and control. He was responsible for the development of global safety plans and led reform plans to expedite the process in which critical needs are identified and addressed. He is a certified air transport pilot, flight and ground instructor, airframe and power plant mechanic, and a qualified FAA control tower operator. He holds a Bachelor of Science degree in Aviation Maintenance and Management and a Master’s degree in Public Administration.
23
Aviation Safety
Mr William Voss
Flight Safety Foundation
INTRODUCTION
For decades, the aviation industry has been focusing on
the management of compliance. The thinking was simple
– find a problem, write a rule, comply with the rule, and
things will be safe. The idea is too simplistic and too
reactive. Now is an era of safety management that takes a
very different approach.
A lot has been done in the area of safety management
implementation. All over the world, airlines, airports,
regulators and air navigation service providers have
implemented new risk-based, proactive approaches.
However, this poses a problem as the public does not
understand these new emerging safety approaches; they
understood good old fashion simple compliance. They
want to understand why, as an industry, it was decided to
move past the simple concept of compliance, giving rise to
the need to explain these new actions.
THE LIMITS OF REGULATIONS
Without taking into account technical specifications and
recommendations set by the International Civil Aviation
Organization (ICAO), there are 13,000 Standards that
Governments are made to comply with. Adding to that
the technical requirements and recommended practices,
it amounts to approximately 30,000 ICAO Standards and
Recommended Practices (SARPs). The ICAO Council agreed
that it was time to start writing fewer rules. A new approach
had to be adopted.
It is important to remember that the States then have to
promulgate even more regulations and guidance materials
based on these SARPs. Companies that are subject to State
Balancing Safety and Compliance in the Regulatory Environment
24
regulations have to then develop internal regulations procedures that allow them to work within the regulatory environment. These would be things such as detailed procedures, operations manuals and technical guidelines. At the end of the day, the person actually trying to fly the airplane or run the airline is subjected to a dizzying array of thousands of regulations. The number of rules cannot simply increase with the expectations of things to happen. Rules are important but the potential of rules may have already been exhausted.
The first thousand standards were written in the 1940s and 1950s. These were probably very important standards. However, the next thousand standards would probably not be anywhere near as important as the first thousand. There is a point of diminishing returns which had been passed decades ago. For this reason, other approaches must be developed to ensure safety.
Out of necessity, a new approach i.e. safety management based on the management of risk rather than just the management of compliance, was developed for today. That leaves two approaches based on different philosophies, and these approaches have to be balanced.
The reality is that the balance that needs to be achieved is for the aviation professionals alone to decide. The reality is that much of what is done in the system is being driven by the public.
THE ROLES OF THE PUBLIC
The examples below discuss the big aviation changes in international aviation systems over the last five years.
The European Blacklist has certainly grabbed a lot of headlines. The establishment of the list came about when the public around the world saw numerous accidents happening in the summer of 2005. These made the public lose their trust in the aviation industry. It was particularly the case in Europe, where many had lost friends and family in foreign crashes. A tremendous amount of pressure was placed on the Director Generals and the Ministries to take action. The reality is that one of the biggest changes in the landscape of international aviation safety was not driven by the aviation professionals, but by the public.
Here is another example. After over 12 years of debate between the US National Transportation Board and Federal Aviation Administration (FAA), FAA announced its intention to issue a rule requiring the central fuel tanks in aircraft to be filled with inert gas in order to eliminate the chance of fuel tank explosions such as that which occurred in the Trans World Airline Flight 800. From the perspective of aviation safety risk management, it is hard to justify the high cost of that change.
Over the last 12 years, the FAA had issued countless directives that eliminated ignition sources and dramatically reduced the risks of that event occurring again. Comparing the price tag of the system and the resistible risk after the various procedure changes have been made, the FAA could say that they reduced the risk to nearly zero. However, this was not good enough for the public’s eye. There had to be reassurance and the risk had to be driven to zero no matter what the cost. This is an example of an expensive policy that is not based on data or analysis, but on the public’s need to feel reassured, which will affect aviation for years.
Balancing Safety and Compliance in the Regulatory Environment
25
Journal Aviation Management 2008
Another point would be the concept of collaboration. Collaboration between the industry and the government is central to the concept of system safety. It is clearly called out in ICAO documentation. In this regard, ICAO is not alone. The Global Aviation Safety Roadmap, Airport Council International, Airbus, Boeing, Civil Air Navigation Services Organisation, Flight Safety Foundation and the International Air Transport Association all clearly call out for renewed cooperation in safety between the government and the industry.
However, caution needs to be exercised. The concept of partnership, which the aviation system embraces broadly, can be viewed skeptically by the flying public. The public is very used to the notion that when the government and the industry collaborate, there is a tendency for the government and the industry to be corrupt. This leads to another problem – the industry was doing a lot of things right and lives were saved – but there is a need to reflect on how these actions are perceived and viewed by the outside world. If the power of the public is not considered, the ability to implement new safety changes and ultimately saving lives may be lost.
THE REALITY OF WHAT IS AT STAKE
To understand what is at stake, these new ideas including collaboration with industry and the proactive management of risk must be evaluated. These concepts started seeing broad implementation in the mid to late 1990s. While these practices were not adopted universally, they were clearly adopted by the airlines and regulators that transported the vast majority of the airline passengers. To put this in perspective, compare the accident rates internationally in 1996 when these ideas were new, and in 2006 when these ideas were well implemented. By taking the accident rates in 1996 and multiplying it by the number of flights in 2006, it worked out to about 30 potential major accidents. Yet, the actual number of accidents in 2006 was 11. That worked out to 19 airplanes full of people that did not crash.
The public thinks that governing bodies are going soft on the rules and that there is too much coziness between the government and the industry. The results however seem to suggest that this approach is saving lives. Try visualising the number of lives being saved. Imagine standing in a balcony overlooking a customs area and the customs shutting down while 19 planes arrive. Down in the crowded area, imagine baby strollers, businessmen and families on holiday. Imagine looking into that sea of people and seeing your own children’s faces looking back at you. This is what is at stake, and if this not communicated effectively to the public and politicians, there could be a terrible price to pay.
COMPLIANCE VERSUS SAFETY MANAGEMENT
This leads back to the balance that must be struck between the worlds of compliance and safety. Once this balance is struck, the public must understand it. The first step is to understand how different the philosophy of compliance is from the concept of safety management.
In the world of compliance, all rules are equal. In the world of safety management, some rules are vital, and some are nearly irrelevant. In safety management, the focus is on things that are most likely to cause risk whilst compliance focuses on complying to every rule even if they do not represent risk.
26
The other assumption in the world of compliance is that, if all rules are complied with, the risk of
an accident is zero. In safety management, it is known that the risk is never zero, but sometimes
it is acceptably low. This is where the public and politicians are lost. They want to be assured that
the possibility of an accident is zero, so they keep writing rules.
Another difference in the world of compliance is the notion that safety is supported by punishment.
The idea is to find the person who did not comply with the rule and punish him as an example.
Safety management philosophy is somewhat different. Safety is ensured when information flows
freely. Safety management acts on information on risks and incidents that would inform what the
next accident will be and how to prevent it. The safety management assumption is that people
will make mistakes even if punishment is mete out. The important thing is to anticipate the next
mistake that will be made.
Another assumption of the compliance model is that more inspections and more “cops on the
beat” will yield more safety. The logic is that more inspections equal more enforcement; more
enforcement equals more compliance; more compliance guarantees safety. In contrast, safety
management is not about more inspections, it is about making sure safety systems within an
airline work and making sure what is inspected is that which presents the most risk.
Looking at the philosophy underpinning the two approaches, it is easy to guess who understands
and supports which approach. The approach of compliance resonates with the public, politicians
and prosecutors. Compliance is easy to understand, provides reassurances, and resonates with
those who write laws and enforce them. On the other hand, only safety professionals understand
how safety management works and this notion has to change.
THE REALITY OF BALANCING THE TWO CONCEPTS
The good news is that compliance and safety management do not have to be at odds. They can
indeed complement each other. One such example is Canada.
Canada is a leader in safety management implementation. Everything they do in Canada is based
on risk. They deploy inspectors to the most serious problems. A number of years ago, the regulator
in Canada was having trouble with a low cost carrier. There were numerous incidents and reports
regarding this particular operator. This operator had not implemented safety management and was
barely dealing with the basics of operations. Fortunately, the regulator had implemented safety
management with many other carriers, including Air Canada. The regulator was able to look at
these mature airlines and determine that they could safely cut down on surveillance resources and
redirect these resources to the low cost carrier that was presenting more risk. The regulator took a
compliance-based approach to this problematic low cost carrier. Eventually this airline quietly went
into bankruptcy. The safety management approach that was appropriate for the more mature and
sophisticated airlines, actually freed up inspectors to deal with the more marginal carrier.
Balancing Safety and Compliance in the Regulatory Environment
27
Journal Aviation Management 2008
WHAT CAN GO WRONG
When the public and political world feel there is an imbalance between compliance and safety
management, things can go very wrong. The recent, very public hearing regarding the safety
oversight practices of the FAA is a very powerful example.
The US sets the highest record for safety in the history of aviation over the past five years. This
is remarkable when it is considered that all but two of the major airlines in the US were going
through bankruptcy at that time.
Yet, in recent hearings, this fact did not matter at all. The relationship between the FAA and the
industry was called into question. In spite of a remarkable safety record, politicians called into
question the appropriateness of the relationship between the government and the industry. They
also questioned the emphasis on risk management, and how some compliance issues could be
dismissed. This caused a backlash in the regulatory process and ultimately the travel of more that
300,000 passengers was disrupted while compliance issues were debated.
This type of intervention from the politicians and the public is not limited to the US. A similar
incident is taking place in Canada. The regulator in Canada is proposing safety management
legislation. It is being characterised by the press as “industry self-regulation”. As the newspaper
clips showed, the attacks on the regulator have been vicious. They call for vigorous enforcement
and compliance, and they dismiss collaboration and the exchange of safety information. Advocating
safety improvements without the understanding of the press, public and the politicians, is a
dangerous business.
Another area where things could go wrong with the debate between safety philosophies is the
courtroom. All over the world, it is seen that prosecutors are aggressively pursuing charges against
aviation personnel who had made mistakes. They are acting on the assumptions of a compliance
model, i.e. that punishment will prevent error. Recent events include the case of the Garuda crash,
the Concorde crash and the runway collision in Milan, Italy amongst many others.
The problem with this is that the philosophy of punishment runs against the philosophy of
information exchange that underlies safety management. The more cases are prosecuted, the
less likely the chances of voluntary disclosure of information that would allow the prediction and
prevention of accidents.
28
CONCLUSION
The aviation industry has to deal with two philosophies that can be conflicting if they are not
deliberately reconciled and balanced. It is not enough for the aviation industry to come to grips
with this. The audience is much bigger. Once the balance is struck, it must be communicated to
the politicians, media, public and prosecutors. If not, the balance will be rejected and focus will
swing back to old rule-based systems of compliance that we have all outgrown. That would take
the industry back in time with alarming accident rates. Everyone needs to reach a consensus in
the community on the right regulatory approach, then reach out to communicate it. It has to be
done – lives are at stake.
This paper was adapted from the lecture given by Mr William Voss, at the inaugural SAA Aviation
Insight Series on 31 July 2008
ABSTRACT
Aviation Security
Aviation security is a critical underpinning factor in the stability and growth of the global civil aviation industry. However, developing a set of aviation security standards and adopting various aviation security measures alone is insufficient to ensure that a sound security system is applied by airlines, airports, air cargo agents, and other relevant stakeholders. To ensure that aviation security standards are adhered to, reviewed and kept relevant, and that security measures are practical and effective, it is useful for stakeholders to establish and maintain an aviation security audit and compliance regime. An aviation security audit and compliance regime would help all stakeholders collaborate and coordinate with one another, as well as provide a reality check on the standards and measures in force to identify gaps, areas for improvements and areas that are adequately enforced.
It is also useful to consider the “six P’s” in an aviation security audit and compliance regime, namely (a) Patronage, (b) People, (c) Processes, (d) Preparation (e) Post-mortem and (f ) Perseverance. These guiding principles should help stakeholders to develop and sustain a meaningful and effective aviation security audit and compliance regime that would be adaptable to the changing global industry and security environment, and allow for better understanding and integration of efforts amongst all players responsible for effecting aviation security measures.
Benefits of Aviation Security Audits and Quality Control Systems
ABOUT THE AUTHOR
Mr Bernard Lim
Mr Bernard Lim is Director for International Relations and Security with the Ministry of Transport, Singapore. His key responsibilities include formulating and managing policy matters concerning international relations, transport security and transport emergency preparedness in Singapore. He is also the Vice-Chairman of the Asia-Pacific Economic Co-operation Aviation Security Experts Sub-Group, and member of the International Civil Aviation Organization Aviation Security Panel. Mr Lim holds a Master’s Degree in Public Administration from the University of Liverpool, UK, and was trained in crisis management at the Emergency Planning College in York, UK and in Leadership at the John. F. Kennedy School of Government, Harvard University. He was conferred the Airport Police Commander’s Award in 2000, the Singapore Armed Forces National Service Medal in 2001, the Ministry of Home Affairs’ Emergency Preparedness Commendation Award in 2002 and the Minister’s Innovation Distinguished Award in 2007.
Benefits of AviationSecurity Audits and Quality Control Systems
29
Aviation Security
Mr Bernard Lim
Ministry of Transport, Singapore
Benefits of Aviation Security Audits and Quality Control Systems
INTRODUCTION
The global civil aviation industry comprises a multitude of systems and sub-systems that involve regulations, processes, activities, infrastructure and facilities, which enable the carriage of people and goods across the world by air. Annually, some five billion passengers and close to 90 million metric tonnes of cargo move around the world by air.
The success and continued development of the global civil aviation industry rests on many players. These include regulators, airlines, airport operators, ground handling agents, suppliers, ground transport companies, air freight companies, catering companies and other stakeholders. Together, these stakeholders collaborate and coordinate with one another to ensure that air passengers and goods are moved safely, efficiently, and in a cost-effective and timely manner.
AVIATION SECURITY
There are many factors underpinning the stability and growth of the global civil aviation industry. A good level of aviation security is one of them. Aviation security encompasses a host of policies, legislation, national, airport and airline security frameworks and security programmes, as well as measures and procedures. Aviation security measures are needed to ensure that airport and airline operations are secure against the threats from unlawful interference that threaten to disrupt civil aviation operations and endanger lives of passengers and air crew. The terrorist attacks of 11 September 2001 where civilian aircraft were used as weapons of mass destruction further attest the need for effective aviation security measures across the entire civil aviation system.
30
AVIATION SECURITY AUDITS AND QUALITY CONTROL
To that extent, stakeholders have implemented various security measures across airline, airport
and airfreight operations. This is to achieve a level of security that is assessed to be reasonable
enough to protect their operations and minimise the threat from terrorist attacks. However,
implementing layers after layers of security measures is not necessarily the best way to achieve an
effective and practical level of security, be it for airline, airport, airfreight or other of civil aviation
operations. Rather, all stakeholders should periodically conduct audits to assess the effectiveness
of their existing aviation security plans, measures and procedures. As a basic approach, audit
checks are useful in helping stakeholders assess if their existing security measures comply with
the standards stakeholders have benchmarked to meet.
Aviation security audits and compliance regimes are not new. Regulators and the industry have
been undertaking audit checks for many years. Following the terrorist attacks in the US on 11
September 2001, the International Civil Aviation Organization (ICAO) established the ICAO Universal
Aviation Security Audit Programme (USAP). This programme involved the mandatory audit of all
190 ICAO Contracting States on their compliance with the aviation security standards under Annex
17 to the Chicago Convention. It also looked at measures taken by Contracting States to adopt or
achieve the objectives of the recommended practices for aviation security contained in Annex 17.
The first cycle of the ICAO USAP, which ran for five years from 2002 to 2007, has been completed.
ICAO continues to conduct follow-on audits for a number of Contracting States, while some others
have commenced their second cycle of ICAO USAP audits in 2008.
THE USEFULNESS OF AVIATION SECURITY AUDITS
Aviation security audits and compliance regimes are useful tools to help States and stakeholders
obtain an assessment of where they stand in relation to the standards that they are measured
against. Such audit exercises can also help regulators and stakeholders to identify gaps and areas
where security measures are lacking. These audit exercises further help to point out changes that
are needed in security measures and processes, and recognise those areas that are adequately
met. Audit checks provide a “health check” that would determine the overall prevailing level of
security in the State or for a specific civil aviation facility or organisation.
KEY FACTORS TO EFFECTIVE AVIATION SECURITY AUDITS
It can be argued that different stakeholders hold different perspectives and approaches towards
aviation security audits. Some may view aviation security audit exercises as constructive means
toward improving the level of security standards and measures in place. Others, on the other
hand, may view aviation security audits as an unnecessary hassle that consumes time and
resources. Nonetheless, at the end of each audit check, all stakeholders would like to hear that
their organisation has the necessary measures and that they had “passed” the audit checks with
flying colours.
Benefits of Aviation Security Audits and Quality Control Systems

31
Journal Aviation Management 2008
But the more important outcome of each aviation security audit exercise is not to simply know that an organisation had “done well”. Rather, the true value and desired outcome of aviation security audit exercises is to learn what needs to be done in order to implement the necessary aviation security measures effectively, close off any gaps, and engage in forward planning to deal with new security challenges that lie ahead. In order for any aviation security audit exercise to be meaningful, regulators and stakeholders could consider adopting the six “P’s” – Patronage, Processes, People, Preparation, Post-Mortem and Perseverance.
Patronage
In any organisation, the patronage of its top leaders is critical for any initiative to take off and to develop. With the patronage of the top management, there can be a strong assurance of commitment, effort and resources accorded to the whole aviation security audit effort. Periodic updates and reports to the top management on the audit preparations, outcome and follow-up actions will not only provide them with an accurate perspective of where the organisation stands in its compliance of aviation security standards, but also help identify areas that need to be addressed, including resources needed, so that decisions can be taken in directing the follow-on actions towards improving the aviation security measures.. Patronage is necessary at all levels, from the national level down to the individual stakeholder level. With strong commitment at all levels, all stakeholders will be able to work effectively towards achieving the best possible and practical outcomes to enhance the level of aviation security within the State.
Processes
As with any audit regime, it is necessary for regulators and stakeholders to establish a set of aviation security compliance regimes. Annex 17 to the Chicago Convention requires all Contracting States to establish a National Civil Aviation Security Quality Control Programme (NCASQCP) aimed at meeting the aviation security standards and recommended practices stipulated in Annex 17. At the minimum, each Contracting State should establish an NCASQCP. In addition, it is desirable that regulators and stakeholders establish other local aviation security audit programmes designed to meet the State’s national aviation security standards and requirements, as well as security requirements assessed as necessary for the individual organisation’s business and operations. For instance, the fuel providers at airports and the airline catering companies would have a set of common security objectives that would be in line with the State’s National Civil Aviation Security Programme and Airport Security Programme. In addition, these companies would have security requirements unique to their individual business considerations of providing fuel to airlines at the airport, and providing in-flight catering service.
Establishing clear and easily understandable aviation security compliance processes are useful. These processes should serve as guidance to regulators and stakeholders stipulating the objectives of the aviation security audit regimes, areas of focus, and recommended measures, processes and procedures which stakeholders can adopt to achieve the intended outcomes. These processes will also synchronise the work of the auditors and the actions by those audited. This would help minimise grey areas, ambiguities, and divergence in interpretations of the security objectives and intended outcomes. Follow-on actions after each audit exercise would also be much simpler with such a clear set of processes which stakeholders can refer to.

32
People
People are definitely the most important factor in successfully establishing and carrying out any aviation security audit programmes. The support of top managers and all personnel down to the rank and file is critical for any aviation security audit exercise to be meaningfully carried out. Aviation security regulators should have a team of auditors who are trained and knowledgeable in civil aviation operations, facilitation and procedures, and who possess the adequate expertise in aviation security requirements. Stakeholders (ie. those audited) should also have trained personnel who are familiar with the security objectives and standards, and a positive mindset and enthusiastic attitude in helping their organisation establish the necessary measures, initiatives and preparations to comply with the necessary aviation security requirements.
People are critical in many aspects. It is people that ensure that aviation security procedures are established and followed. It is people who maintain security equipment and infrastructure regularly and adequately to ensure that the equipment functions properly at all times. It is people who determine how open and agreeable stakeholders are to audit findings and recommendations, and give the support for follow-up actions to be taken. People can be argued as the start and end of the whole aviation security audit process, and the top management of all stakeholders must be willing to take the responsibility for the aviation security audit of their organisation and its
compliance with the aviation security standards as required.
Preparations
It is doubtful that any regulator or organisation can “breeze through” an aviation security audit exercise without adequate preparation. Preparation for audit exercises is necessary. Good preparation requires an investment in terms of time, commitment and resources. Preparation for aviation security audit exercises should start as early as possible. A dedicated core team of officers should be assigned the responsibility for all preparatory actions, and to help the organisation through the audit exercise. Preparation should involve all stakeholders concerned. They should be clearly informed of the purpose of the audit exercise, the security objectives to be assessed and met, and the desired outcomes to be achieved. A detailed audit preparatory programme should be developed mapping out the roles and responsibilities of all stakeholders concerned (eg. airport operator, security service providers, catering companies, fuel suppliers, immigration authority, airlines, ground handling agents, etc.). A preparatory committee comprising senior ranking officers from the relevant organisations should be established to oversee and monitor the preparation work for the audit exercise.
For national level audits, key milestones should be reported periodically to the National Civil Aviation Security Committee (NCASC) for policy guidance and decisions. For local or individual organisation audit preparations, key information and feedback should be given to senior management for their knowledge and for decision making. Pre-audit dry runs and rehearsals should be held with sufficient time to the actual audit exercise to allow organisations and individuals to iron out any grey areas, establish clear communication links and coordinate actions on the ground. A pre-audit exercise meeting should be held between the auditors and those who are audited so that clear ground rules and process steps are established to ensure smooth execution of the audit exercise.
Benefits of Aviation Security Audits and Quality Control Systems
33
Journal Aviation Management 2008
Post-Mortem
A post-mortem of each aviation security audit exercise is indeed useful. The purpose of post-
mortems should not be to witch hunt and pin blame on organisations or individuals for areas
that were found to be inadequate. On the other hand, post-mortems should also not be turned
into an exercise to heap praises and produce a glowing report of each stakeholder. Instead, clear
objectives and purpose of each post-mortem meeting should be established. Essentially, the aim
of such aviation security audit post-mortem meetings should be to objectively identify areas that
need to be improved on, be it in the area of aviation security plans, procedures, coordination or
equipment and infrastructure. These post-mortem discussions should also serve as a platform
for civil aviation stakeholders to work out corrective actions or plans to practically address the
security weaknesses identified. The approach should be forward moving towards improving the
level of security measures from the prevailing state.
Post-mortem exercises are also useful for regulators and stakeholders to review whether any
security standard in the National Civil Aviation Security Programme, Airport Security Programme,
Operator Security Programme, National Civil Aviation Security Training Programme, or any other
security regimes, are still relevant or require adjustment. As the civil aviation industry is a globally
dynamic industry where airline and airport operations are also constantly undergoing change
due to improvements in technology, new processes and improved facilitation needs, aviation
security standards should also be periodically reviewed to ensure relevance and effectiveness to
regulators, stakeholders and industry. Post-mortem meetings should be held at various levels,
including between auditor and those audited, amongst stakeholders who have been audited, and
within each individual organisation after the aviation security audit exercise. This is to understand
the strengths and weaknesses identified, map out the areas for improvements, and disseminate
the findings and recommended actions to all relevant personnel and to the management.
Perseverance
Finally, perseverance is an important factor for regulators and stakeholders to move on after each
aviation security audit exercise. It is important that organisations, from the top management down
to ground personnel, acknowledge the need to persevere on to address and overcome the security
gaps that had been identified, and to keep up those security measures and processes that were
found to be sound. Regulators and stakeholders should aim to avoid the trap of complacency,
where after each aviation security audit exercise, the findings are just noted with no concerted
effort to follow up to address the weaknesses that had been identified. Those security measures
found to be adequate should also not be taken for granted. Effort should continue to ensure that
the relevant personnel are trained, skills and knowledge updated, equipment maintained, and
procedures and processes periodically reviewed to check on their relevance and effectiveness over
time, especially if there are changes to factors like geography, technology and business operations.
Perseverance will also help sustain a positive mindset to plan for and pursue the acquisition of
needed resources and equipment to implement the desired aviation security measures that were
assessed through the audit exercise to be necessary, cost-effective and practical, especially in
situations where those resources are currently lacking.
34
SINGAPORE’S EXPERIENCE
Singapore was audited by ICAO under the ICAO USAP in November 2006. Singapore adopted
the six “P’s” amongst its approaches in preparing for and following up on the audit exercise.
To begin with, Singapore’s audit preparations were given top management and policy oversight
by the NCASC, chaired by the Deputy Secretary from the Singapore Ministry of Transport (MOT).
Periodic updates on the progress of the audit preparations were submitted to the Chairman of the
NCASC and key policy decisions were taken and approved, as relevant. The senior management
from the other Singapore Government agencies, such as the Civil Aviation Authority of Singapore
(CAAS), Singapore Police Force (SPF), Immigration and Checkpoints Authority (ICA), and industry
stakeholders (eg. the national carriers, ground handling agents, catering companies, security
service providers, concessionaires, etc.) were also kept informed of the audit preparations, roles
and involvement of the various agencies. Senior officials from the Singapore Government agencies
and airport community also participated actively throughout the audit exercise.
At the operational level, Singapore formed an aviation security audit task force led by the Airport
Police Division (APD) from the SPF, with members representing the various government organisations
and industry. The task force comprised a core team of personnel dedicated to overseeing the
preparatory work for the audit. Senior policy and operational staff from the various agencies were
also engaged in the discussions to ensure that the task force was adequately supported by people
with the relevant expertise and experience. Refresher training was given to officers as needed, and
training was provided to new officers who were involved in the audit exercise for the first time.
The aviation security audit task force ensured that all stakeholders were familiar with the aviation
security requirements as stipulated in the National Civil Aviation Security Programme, Airport
Security Programme, Operator Security Programme, and others as relevant. Agencies and individuals
also read through the procedures and processes for the ICAO USAP exercise to ensure that they
were familiar with how the audit exercise would be conducted and what was required from them.
This was useful in helping to optimise the time allocated for the audit exercise effectively.
The task force was formed at least one year ahead to prepare for the audit. Aside from establishing
the roles and responsibilities of agencies and individuals, the task force also reviewed the relevant
national civil aviation security programmes and Standard Operating Procedures (SOPs). Pre-
audit checks were carried out to ensure that procedures and measures were updated and clearly
understood by airport personnel responsible for executing these measures.
Following the end of the ICAO USAP audit of Singapore, the relevant Singapore agencies held in-
depth post-audit discussions on the findings and recommendations. These were followed up and
monitored by the APD and CAAS to ensure that the necessary corrective actions were undertaken.
In addition, the agencies took with them useful lessons from the audit exercise to conduct further
reviews of their own organisation SOPs and aviation security measures as they deemed relevant.
Benefits of Aviation Security Audits and Quality Control Systems

35
Journal Aviation Management 2008
Although the ICAO USAP audit of Singapore was held in 2006, the NCASC, MOT, SPF and CAAS continue
to monitor aviation security measures and procedures that could do with further improvement,
even if these measures were already in compliance with the standards and recommended practices
of Annex 17. In some cases, these could require investment in resources, equipment and training,
while in others, it could be a refinement to existing policies and procedures. Nonetheless, the
approach that has been adopted is one where, at both the national level and at the individual
organisation level, all parties would strive to enhance and improve their respective aviation security
measures in a practical and cost-effective manner that would meet the desired security objectives,
and balanced with the needs of facilitation, service and operations.
CONCLUSION
Aviation security audit exercises and compliance regimes are certainly useful in helping States
and industry players measure up to industry standards and practices to enhance the security
of their operations for the air travellers. In addition, aviation security audit exercises provide
all stakeholders with a unique opportunity to understand each other’s objectives, concerns and
business needs better. This would allow for better collaboration and coordination not only during
the audit exercise itself, but even thereafter on a day-to-day basis, where stakeholders can better
cooperate with each other to meet the common desired aviation security outcomes. Such aviation
security audit exercises also provide opportunities for networking and build closer people-to-
people relations amongst regulators and stakeholders. These relationships are certainly valuable
both within and outside the audit cycles.
Finally, aviation security audit exercises provide a very good reality check for all organisations
concerned. This will enable them to review and refine their aviation security approaches and more
often than not, lead them to adjust and adopt new and more cost-effective ways of carrying out
aviation security measures that best supports and enhances their business operations.
36
ABSTRACT
Aircraft Accident Investigation
In recent years, a great deal of emphasis has been placed on the role of safety culture in global aviation operations, particularly as part of an established safety management system. However, the way in which safety culture is both measured and managed is still the subject of much discussion. Furthermore, the investigation of safety culture following an accident adds further levels of complexity and potential bias to the task. This paper will discuss some of the issues and potential pitfalls surrounding the definition, measurement and investigation of safety culture and also examine the role of ‘Moments of Truth’ and the effect they have on both internal and external perceptions of safety culture.
The Role of Safety Culture in Aircraft Accidents
ABOUT THE AUTHOR ABOUT THE AUTHOR
Professor Graham Braithwaite
Professor Graham Braithwaite is Head of the Department of Air Transport and Director of the Safety and Accident Investigation Centre at Cranfield University, UK. A Fellow of the Royal Aeronautical Society and Member of the International Society of Air Safety Investigators, Prof Braithwaite has led the development and delivery of investigation, human factors and safety management courses for a range of external clients. He has also consulted extensively in safety and human factors matters. His research interests are in accident and incident investigation, human factors, safety management and the influence of culture on safety. Prof Braithwaite holds a Bachelor of Science (Hons) in Transport Management and Planning as well as a PhD in Aviation Safety Management from Loughborough University, UK.
The Role of Safety Culture in Aircraft Accidents
37
Aircraft Accident Investigation
Professor Graham Braithwaite
Cranfield University, UK
INTRODUCTION
With the publication of the Safety Management Manual in
2006, the International Civil Aviation Organization (ICAO)
signaled its intent that member States should require
operators to establish a formal safety management system
(SMS) by 1 January 2009. As the date approaches, a flurry
of activity is apparent across the industry. Whilst many of
the components that form an SMS are well established,
it is their interaction within a well designed system that
promises a tangible improvement in safety. Ultimately, the
facilitation of an SMS depends on the shared beliefs and
attitudes (culture) of the organisation if it is to go beyond
the theoretical framework.
Although much has been written about what safety culture
should look like, understanding its role in the causation
of incidents and accidents is harder to define. The biases
and traps that may affect investigators, analysts or other
interested parties can give a distorted view of the role of
safety culture and may be a factor in unwittingly shifting
blame from individuals to their managers. If safety culture
is to evolve positively, the industry needs to understand
not only where it is aiming, but how it reacts to apparent
failures of safety performance.
SAFETY CULTURE
The term safety culture first appeared after the catastrophic
reactor fire at Chernobyl nuclear power station located in
the Soviet Union near Pripyat, Ukraine in 1986. Since then,
the term has been widely discussed by the industry and
academia alike, although as Reason (1997) points out,
The Role of Safety Culture in Aircraft Accidents
38
The Role of Safety Culture in Aircraft Accidents
“few phrases are so widely used yet so hard to define as safety culture”. Whilst the term itself is
just over 20 years old, the role of an organisation’s way of doing things as a factor in accidents
has been known for rather longer.
The Royal Commission’s investigation into the 1979 Mount Erebus disaster provided a pivotal
role in changing the way accident investigation involving complex socio-technical systems was
conducted. Viewed in the context of modern safety thinking, the focus on organisational factors
is unremarkable. However, at the time, the Commissioner went far deeper than the technical
investigation did to examine the organisational and cultural factors within the operator and
regulator. The Commissioner experienced a strong political backlash when his findings were
released, not least because of the difficult conclusions he made about the honesty of the airline’s
senior management, summarising the evidence he had heard from them as “…an orchestrated
litany of lies” (Mahon, 1981).
Erebus was later cited in texts such as Beyond Aviation Human Factors (Maurino, Reason, Johnston
and Lee, 1995) and the ICAO Human Factors Digest No. 10 (ICAO, 1993) as an example of the way
in which actions taken close to the moment of occurrence had in many cases been seeded or
compounded by events, conditions or the way of working months or years before. With the work of
system safety specialists such as Perrow (1996), Rasmussen (1983 etc.) and Reason (1990, 1997b
etc.), the appreciation of organisational failings has grown considerably.
The fatal take-off accident at Dryden, Ontario, Canada in 1989 further highlighted the influence
of the wider safety system. The Commission of Inquiry examined factors from active failures on
the day through to deficiencies in the airline’s operation and the wider regulatory environment.
Concluding that the accident “...was a result of a failure in the air transport system”, Moshansky
(1992) highlighted systemic issues in a way that few technical investigations had been able to
do previously. A serious incident in the UK where the pilot of a BAC1-11 was nearly sucked out of
his aircraft after the windscreen failed allowed UK Air Accidents Investigation Branch (AAIB, 1992)
Inspectors to consider not just the errors of an individual (the shift supervisor who managed to fit
incorrectly-sized bolts to the aircraft), but also the processes and practices that should have been
in place to defend against the inevitability of human error.
These three accidents are well documented examples in which “the way of doing things”
compounded individual failures, errors and violations. However, as the enthusiasm for SMS gathers
pace, the question remains, how can we identify a failing safety culture prior to an accident, or
indeed diagnose the role of safety culture in an incident or accident?
MEASURING SAFETY CULTURE
Rod Eddington, former CEO of Ansett Australia and British Airways, often reminded his staff “…if
you can’t measure it, you can’t manage it”. In terms of safety culture, things are no different; the
transition from one level of safety culture to the next needs some sort of measurement. Hudson
(2001) builds on the work of Ron Westrum in describing the evolution of safety culture from
“pathological organisations” (who cares as long as we’re not caught?) to the ideal “generative
39
Journal Aviation Management 2008
culture” (safety is how we do business around here). Such stages of evolution are useful markers,
but identifying where an organisation finds itself on the scale is a little harder. The American
Institute of Chemical Engineers’ (2005) definition highlights why measurement is difficult: “Safety
culture is how the organisation behaves when no one is watching”. It is also conceivable that the
‘observer effect’ will modify the very thing being measured.
A number of researchers have investigated the measurement of safety culture with seminal work
published by both Zohar (1980) and Reason (1997b). The methods that were generally employed
included questionnaire-based techniques to score the organisation in a number of safety dimensions
according to the model being employed with Zohar correlating these dimensions against the
effectiveness of safety programmes within industrial organisations. However, questions exist as
to how well this industrial model relates to the aviation industry, although work has also been
carried out into specific safety culture surveys for aviation operations (Gibbons, von Thaden and
Wiegmann 2004).
The problem is compounded by a lack of data in the aviation industry and the, albeit desirable,
lack of accidents from which to obtain it. Recent investigation trends in the aviation industry have
seen the increased use of incidents as safety indicators and pre-emptors in an attempt to address
the lack of data and this has obvious parallels with Zohar’s later work (2003) to enhance both
modeling and measurement through the use of “micro accidents”.
One failure of the questionnaire-based approach is that it lacks any measure of observable
behaviours. Whilst some researchers highlight the relative accuracy of this approach and its ability
to capture change within an organisation, this presents a different challenge in accident or incident
investigations where pre-existing data may not be available and where the effect of the accident
on perceptions within the organisation may preclude any meaningful post-accident measurements.
The advantage of measuring observable behaviours is that awareness of the measurement criteria
will tend to improve those aspects; the disadvantage is that the same awareness will tend to
improve only those aspects.
When an incident or accident occurs, a questionnaire approach is unlikely to be appropriate, not
least because the event itself may have changed the perception of culture, or at least people’s
recollection of it prior to the event. This is part of what Reason refers to as outcome knowledge.
Just as all other aspects of investigation need multiple evidence sources and inductive reasoning
to corroborate any conclusions, so evidence of the effect of culture needs to be collected. One
way to achieve this is to test the organisation against established ideals for a safety culture (see
Reason, 1997b).
IDEALS FOR SAFETY CULTURE
An informed culture comprehends the hazards that it faces and the risk that each of them presents.
Yet, organisations cannot anticipate all of the hazards it is likely to face or accurately predict the
magnitude of all risks. Far from being a fatalistic attitude, this is an acknowledgement that the way
in which conditions and failures combine within a complex socio-technical system cannot easily

40
The Role of Safety Culture in Aircraft Accidents
be mapped, even in mature organisations. Aircraft accidents are rare events and there are many
examples where those with complex causality are the ones that slip through the safety net – the
so-called “impossible accidents” (Wagenaar and Groeneweg, 1987).
Where a no-blame approach was once advocated by many in the industry, there is now strong support
for just culture to be at the heart of an SMS. It remains appropriate for accident investigations
conducted through processes such as those found in the ICAO Annex (Aircraft Accident and Incident
Investigation) to be no-blame in order to preserve the integrity and independence of the process.
However, modern thinking on SMS highlights the need to make a clear distinction between what
is acceptable behaviour and what is not. Where resources and training support the employee to
make the right decision, a just culture will treat genuinely unintentional errors quite differently
from wilful violations. Indeed, when an incident or accident occurs, employees will look for fair
treatment of themselves and their colleagues, or behaviours will start to modify accordingly.
Misapplication of either no-blame or just culture will undermine the core value of a mature safety
culture – trust.
A reporting culture wants to know what is happening within the organisation – both good and
bad. Negative feedback is problematic, but a complete absence is arguably worse. In the airline
environment where serious incidents are rare, there can be a natural reluctance to be the bearer of
bad news. Following one incident, the accident investigation agency called the airline to say that
they thought it was unusual that their safety manager had not attended the site. For the safety
manager, this was the first news of an incident that had occurred two days previously that no one
had wanted to ‘trouble him’ with. When reviewing the role of reporting following an occurrence,
the investigator must consider whether the message was able to get through, whether it was
welcomed, or whether its presence was indicative that a problem had been identified, but not
dealt with.
A learning or proactive culture is one that recognises that incidents, near-misses and voluntary
reports can provide vital lessons before the onset of an accident. Indeed, there is a process in
place to collate and do something with the information. All too often, the collection of data has
become the focus and, with limited resources, there is little time to do anything with it other than
present trend data. Several options exist for safety promotion, ranging from publications and
presentations to training design and procedural changes. However, it should be borne in mind that
no safety improvements can exist in isolation from the financial health of an organisation. Budgets
are not limitless and choices need to be made in order to prioritise initiatives.
When an accident occurs, it is all too easy for digruntled employees, or perhaps those who
have been affected, to point to missed opportunities for the organisation to learn. However, it
is possible that the decision that was made at the time was the best one, based on available
evidence. A learning culture tries to understand the context of failures. In other words, as Dekker
(2002) remarks, “the point of an investigation is not to find where people went wrong. It is to
understand why their assessments and actions made sense at the time”.
41
Journal Aviation Management 2008
Finally, a flexible culture is adaptable to evolving threats and crises. It is this aspect that can often be overlooked when reactive investigations focus on what went wrong, rather than looking for things that reduced the potential consequences of an event. Whilst safety policies, processes and responsibilities need to be defined clearly as part of an SMS, the way in which an organisation responds to new situations is perhaps the greatest test of a safety culture. Encompassing all of the preceding elements, the ability to trap or mitigate against the impossible accident is the real test.
INTERPRETING SAFETY CULTURE
Mandating that organisations implement an SMS will not guarantee a sound safety culture. Regulators are faced with the unenviable task of attempting to measure and assess compliance using elements of a system that are not easy to measure, especially after an event. Although ICAO is clear that the intent of SMS is not something that can be achieved through a ‘tick in the box’ solution, the challenge of establishing what to measure and how to do it remains. ICAO (2006) acknowledges that “safety culture is… difficult to measure, especially when the principal criterion for measuring safety is the absence of accidents and incidents”. Does this mean that the occurrence of an accident suggests a poor safety culture?
Culture is easily misinterpreted, especially if it crosses organisational, professional or national boundaries. Spoken and body language, etiquette and customs are all examples of the variables that can be reflected across the culture of an organisation. Different combinations of cultural traits can be assembled to produce the same successful outcome – for example, a culture where questioning of authority does not come easily, can be balanced with strict adherence to standard operating procedures which include cross-checking.
The interpretation of data from certain elements of an SMS needs care to avoid false generalisations or false correlations. For example, an increase in incident reports may be symptomatic of either an increase in incidents or perhaps a greater willingness to report, or increased ease of reporting. Similarly, the operational requirements or conditions placed upon a certain group may yield results which can be misinterpreted. In the case of one major airline, the B737 fleet appeared to yield a higher proportion of unstable or rushed approaches than the other aircraft types. Was this symptomatic of the way the fleet was being managed or the crew trained? In fact, one of the influences was the type of flying that the B737 fleet was often being required to do, which involved short-notice replacement of aircraft types on sectors where the schedule needed making up – something that by definition was placing increased pressure on crews and even encouraging them to fly ‘enthusiastically’. A blame-oriented view was to see the managers as failing whereas a more enlightened view might be that business imperatives were creating risks that needed managing.
Identifying and quantifying the role of safety culture in an occurrence is not easy. Although certain accident investigation agencies (notably the Australian Transport Safety Bureau and the Transportation Safety Board of Canada) have prided themselves on their systemic approach to investigation and their willingness to examine organisational factors, this is far from the norm. Few, if any, accident investigation texts explain what to look for to establish whether safety culture deficiencies were a latent condition leading to an event. Is this something that is perhaps best diagnosed in terms of how well the organisation practises the ideals of safety culture?

42
The Role of Safety Culture in Aircraft Accidents
MOMENTS OF TRUTH
Former Scandanavian Airlines System (SAS) Group Chief Executive Office, Jan Carlzon (1989), spoke
of “Moments of Truth” when describing the 50 million times a year company employees came
into contact with the customer; their actions defining whether the company would succeed or fail.
Whilst Carlzon was writing from a business management perspective, such moments of truth are
equally valid when determining both the internal reality and external perception of safety culture.
For example, a recent event within a Maintenance, Repair and Overhaul (MRO) organisation tested
the commitment of senior management to its stated aim of developing a safety culture. The
MRO organisation was very busy and a customer’s aircraft was parked outside the hangar for
maintenance. The crew that was working on it went to start an air-powered jack which was placed
beneath the wing. Despite several attempts, the jack would not start and fitters were called to
repair it. After inspection and several attempts to fix it, it was concluded that a replacement
would be needed – something which would take an hour to arrange. At this point the maintainers
decided to take lunch early so that the jack would be available on their return and they could
keep to schedule. Unfortunately, whilst they were away, the jack (which had now dried out from
the water contamination that had caused it not to work) started to work and began to screw itself
up into the wing of the aircraft, causing considerable damage.
The initial reaction was to establish who was to blame. The maintainers agreed they had taken the
decision to go to lunch early as a group and as such they would take responsibility as a group.
The temptation for management was to start disciplinary action for the whole group – after all the
repair bill was potentially several million dollars. However, there was also recognition that the way
in which the event was dealt with would have aftershocks through the organisation. Although with
hindsight, a major error had been made in leaving the jack connected to the air supply, the intent
of the group in taking an early lunch was a positive one, related to their commitment to meet the
work schedule. Sacking the group would be an expensive mistake, not just in terms of the loss of
skills and capability, but also in sending a message to other staff that errors would be punished.
Even though the consequences carried high financial worth, the errors that led to it were no more
significant than for many other inconsequential near-misses.
Another moment of truth occurred as a result of a landing accident involving a B737 cargo aircraft at
Birmingham, UK in 2006. During landing approach at East Midlands airport, the pilot inadvertently
disconnected the autopilot leading to a high rate of descent. A go-around was called, but it was
too late to avoid contacting the ground, breaking off the right main landing gear. The aircraft
diverted to Birmingham where an emergency landing was subsequently made without injury.
The resulting Aircraft Accident Investigation Branch (AAIB) report (2008) highlighted a number of
causal and contributory factors, including inappropriate transmission of a company message at a
late stage (500 feet) of a Category III automatic approach, and ineffective training of the co-pilot
– the latter prompting a recommendation that the regulatory authority require the operator to
review their standard operating procedures. As a result of the accident, approximately one month
later, the operator sacked the pilot and was quoted (Mail Reporter, 2006) as saying, “Although the
AAIB investigation continues, it has been established that the automatic pilot was disengaged.

43
Journal Aviation Management 2008
That is down to human error. Although the pilots did manage to recover superbly and made a text
book emergency landing at Birmingham airport, they instigated the incident with a momentary
lapse and the company operates a zero accident tolerance level”.
The full facts are unlikely to be disclosed in the public domain, but if momentary lapses are to
be punished (or at least perceived to be punished) through a zero tolerance culture, the effect
on the safety culture is likely to be negative. Should the “superb recovery” and “text book
emergency landing” by the crew be taken into account in learning from the event or was the error
unforgivable?
In August 2007, an aircraft Captain allowed a Premiership footballer onto the flight deck of an
A320 private charter en route from Finland to Manchester, UK, contravening the stated policy of the
airline. The pilot later acknowledged that he had broken a rule but argued that he did “…interpret
the rule wasn’t quite as strict for a private charter, which this was. Everyone onboard knew each
other” (BBC, 2007). He was dismissed for gross misconduct with a spokesman for the operator
quoted as saying “We have a zero tolerance policy towards any actions which could endanger the
safety of our passengers and employees”.
In this case, the violation related to a security procedure; something which may be treated
differently to other flight safety issues in the current climate. However, the operator had the
added challenge of managing the dismissal of a ‘celebrity’ pilot and the involvement of a famous
footballer. In these circumstances, should the matter be treated any differently and were external
perceptions affected by those who were involved?
An alternative form of occurrence took place in January 2008 when the captain of a B777 performed
an unauthorised fly-by of the Boeing airfield during the delivery flight, reportedly passing within 28
feet of the ground with the undercarriage raised. The Captain was subsequently dismissed as he
had “…neither sought nor obtained the necessary company approval to undertake such a fly-by”
(Quinn 2008) and the co-pilot was subjected to disciplinary action.
The event was complicated by the presence of a large number of airline executives including
the Chairman, with the pilot allegedly even being pictured in the operator’s newsletter toasting
the maiden flight with airline executives who had been onboard. A senior pilot for the airline
was reported as saying “Maiden flights are treated as a bit of a jolly for executives with lots of
champagne flowing and these fly-bys used to be done for a wheeze in the old days. But they are
dangerous, because however good the pilot thinks he is, he isn’t trained for it and the planes
aren’t designed for it” (Batty, 2008).
Whilst the fly-by was a clear breach of current policy, it appears that a culture had existed where
this was an accepted practice and it is at least arguable that the presence and subsequent
“celebration” of the event by executives amounted to tacit cultural approval. The apparent inaction
of senior managers provides a strong case for the pilot to argue that he felt his actions to be
culturally acceptable. Indeed, as safety leadership starts at the top, were the senior managers not
equally culpable for the practice?

44
The Role of Safety Culture in Aircraft Accidents
It is interesting to reflect that these three cases arguably represent three levels of occurrence from
serious violation in the case of the fly-by, through procedural violation by the A320 captain to
momentary lapse in the case of the B737. Despite this, all three resulted in the same outcome of
dismissal of the pilot. However, it is difficult to imagine that all three affected the safety culture
of the organisation in the same way, or that effect on the internal and external perceptions were
the same.
BAD ACCIDENT: BAD SAFETY CULTURE?
Does the occurrence of an accident indicate the presence of a bad safety culture? Various
hindsight biases encourage observers to consider bad outcomes to be the result of bad people or
horrendous mistakes, something compounded by the instant news culture of looking for someone,
or something, to blame. Yet the reality is rarely so clear-cut – some of the most highly regarded
airlines have been involved in major accidents, often after long periods of accident-free operation.
For example, American Airlines had flown over nine million sectors without loss prior to a B757
colliding with terrain near Cali, Colombia in 1995. In other accidents such as those involving SAS
at Milan Linate, Italy in 2001 and DHL over Überlingen, Germany, in 2002, there was little more the
operator could have done to prevent them. However, such events have an effect on the culture of
the organisation and the perception of its customers.
CONCLUSION
The importance of safety culture has become widely accepted, but its measurement, particularly
following an occurrence, remains difficult. Whilst there is clear guidance as to where organisations
should aim to be, the response of an organisation to an event will provide a defining moment of
truth in establishing the future direction for its safety culture. Understanding how and why failures
occur is key to even a proactive approach and guidance on safety culture needs to be based on
an accurate understanding of how it contributes to accidents.
References
AAIB – Air Accidents Investigation Branch (2008) Report on the accident to Boeing 737-300, registration OO-TND at
Nottingham East Midlands Airport on 15 June 2006. UK Department for Transport, London.
AAIB – Air Accidents Investigation Branch (1992) Report on the accident on BAC 1-11, GBJRT over Didcot, Oxfordshire
on 10 June 1990. UK Department of Transport, London.
American Institute of Chemical Engineers (2005) Building Process Safety Culture: Tools to Enhance Process Safety
Performance. Center for Chemical Process Safety, New York.
Batty, D. (2008). Pilot sacked after fly-by prank ends up on internet [WWW]. http://www.guardian.co.uk/business/2008/
feb/25/theairlineindustry.usa
BBC (2007). Pilot sacked after Savage visit. [WWW]. http://news.bbc.co.uk/1/hi/england/coventry_warwickshire/7034412.
stm (28 May 2008)
45
Journal Aviation Management 2008
Carlzon, J. (1989) Moment of Truth. HarperPerennial, New York.
Dekker, S. W. A (2002) The Field Guide to Human Error Investigations. Ashgate, Aldershot.
Gibbons, A. M., von Thaden, T. L. and D. A. Wiegmann (2004). Exploration of the Correlation Structure of a Survey for
Evaluating Airline Safety Culture Technical Report AHFD-04-06/FAA-04-, Prepared for Federal Aviation Administration,
Atlantic City International Airport, NJ, USA.
Hendershot, D. (2007) Process Safety Culture. Journal of Chemical Health and Safety Volume 14, Issue 3, May-June
2007, Pages 39-40.
Hudson, P. (2001) Safety Culture: The Ultimate Goal. Flight Safety Australia September - October, CASA, Canberra.
ICAO (1993) Human Factors Digest No. 10: Human Factors, Management and Organization. Circular 247. International
Civil Aviation Organization, Montreal.
ICAO (2006) Safety Management Manual. Doc 9859 /460. International Civil Aviation Organization, Montreal.
Mahon, P. T. (1981) Report of the Royal Commission to inquire into the crash on Mount Erebus, Antarctica of a DC-10
aircraft operated by Air New Zealand Limited. Wellington.
Mail Reporter (2006) Crash Land Crew Axed [WWW] http://www.redorbit.com/news/
business/591262/crash_land_crew_axed__drama_pilot_error_behind_aircraft/index.html (28 May 2008)
Maurino, D. F., Reason, J., Johnston, N. and R. B. Lee (1995), Beyond Aviation Human Factors, Avebury Aviation,
Aldershot, UK.
Perrow, C. (1999) Normal Accidents, Princeton University Press.
Quinn, B. (2008). Jumbo jet pilot sacked for ‘fly-by’ at 28 feet [WWW]. http://www.timesonline.co.uk/tol/news/uk/
article3427696.ece (28 May 2008)
Rasmussen, J. (1983) Skills, Rules, and Knowledge: Signals, Signs, Symbols and Other Distinctions in Human
Performance Models. IEEE Transactions on Systems: Man and cybernetics, 13
Reason, J. (1990) Human Error. Cambridge University Press.
Reason, J. (1997) Corporate Culture and Safety. Paper presented at the National Transportation Safety Board Corporate
Culture and Transportation Safety Symposium. 24-25 April. Arlington, Virginia.
Reason, J. (1997b) Managing the Risks of Organizational Accidents. Ashgate, Aldershot.
Wagenaar, W. A. and Groeneweg, J. (1987) Accidents at Sea: Multiple Causes and Impossible Consequences,
International Journal of Man-Machine Studies 27, pp. 587–598.
46
The Role of Safety Culture in Aircraft Accidents
Zohar, D. (1980). Safety Climate in Industrial Organizations: Theoretical and Applied Implications. Journal of Applied
Psychology, 65, (1), pp. 96-102.
Zohar, D. (2000). A Group-Level Model of Safety Climate: Testing the Effect of Group Climate on Microaccidents in
Manufacturing Jobs. Journal of Applied Psychology, 85, (4), pp. 587-596.
ABSTRACT
Aviation Technology
Each new generation of aircraft has increased its capacity by becoming longer and wider while increasing the number of landing gear to support the extra weight. Pavement design procedures in existence before the introduction of these new aircraft were not adequate for analysing how these aircraft would affect the design life of existing pavements. Extrapolation of existing criteria indicated that the pavements would need to be strengthened at a cost of approximately US$1.7 billion over several years. The Federal Aviation Administration (FAA) undertook a 10-year comprehensive research and development (R&D) programme to resolve this dilemma. An essential element of the plan was a comprehensive test and verification programme performed on real pavements subjected to full-scale loading. The FAA’s National Airport Pavement Test Facility is capable of full-scale loading of up to 75,000 pounds per wheel on two landing gears with six wheels per gear. The 60-feet wide test sections provide two traffic lanes to compare the performance of six-wheel and four-wheel gears simultaneously. In operation since 1999, the facility is providing exciting new information in updating pavement design technologies around the world.
State-of-the-Art Technology in Airport Pavement
ABOUT THE AUTHOR
State-of-the-Art Technology in Airport Pavement
Dr Satish K Agrawal
Dr Satish K Agrawal is Manager of the Airport Technology Research and Development Team at the William J Hughes Technical Center in Atlantic City, New Jersey, US for the Federal Aviation Administration. He is responsible for formulating, directing, managing and conducting research in airport pavement technology, runway surface technology, airport visual guidance, runway incursions, wildlife hazards, airport planning and design technology, and post-crash aircraft rescue and fire-fighting. He earned his Master’s degree from the University of Iowa, US and his Doctorate from the Pennsylvania State University, US.
47
Aviation Technology
Dr Satish K Agrawal
Federal Aviation Administration, US
INTRODUCTION
In 1927, the Ford Motor Company built one of the world’s
first paved runways at Ford Airport in Dearborn, Michigan,
US. With no aviation experience and no airport pavement
design specifications, engineers built this and other early
runways using pavement thicknesses similar to those of
early highways. In fact, until World War II, airport engineers
based concrete pavement design on the anticipated loads
imposed by the trucks refueling the airplanes, rather than
the airplanes themselves.
For many years after the war, airport pavement research
and technology benefitted from advances in highway
research, as well as from the US Department of Defense
research supporting military aircraft and airfields. Added
complications in today’s design estimates, however, stem
from the fact that aircraft weigh far more than they did
when the basic relationships were established, and landing
gear layouts are far more complicated, with many more
wheels per gear and more gears per aircraft.
Runways, taxiways and aprons may be either “flexible” or
“rigid”, depending on the type of surface layer material.
Flexible pavements are constructed of asphalt, while rigid
pavements consist of concrete slabs. At larger airports,
both types of pavements generally include a stiffened,
or “stabilised”, base layer to provide additional support.
As aircraft get bigger and heavier, with new kinds of
landing gear, added stresses and strains are exerted on
airport pavements. Complex wheel load interactions within
pavement structures can contribute to premature failure of
the pavement structures, and must therefore be considered
in pavement design analyses. When traditional, empirically-
based pavement design methods are used to analyse loads
State-of-the-Art Technology in Airport Pavement

48
State-of-the-Art Technology in Airport Pavement
from the new generation of landing gear, they require pavements that seem unrealistically thick.
Hence, new heavy aircraft may require airports to overlay, reinforce, or even rebuild runways to
adapt to heavier loads.
PROBLEM STATEMENT
Moving ahead to 1995, the FAA was faced with the imminent introduction of a new generation of
heavy civil transport aircraft. These new aircraft included models that weighed up to 1.3 million
pounds and have complex, multiple-wheel, multiple truck landing gear systems. For example, the
Boeing 777 (B777) aircraft had two six-wheel main landing gears to support a gross weight of up
to 777,000 pounds. The six-wheel gear loads applied to airport pavements by this aircraft and
by the new aircraft from Airbus (i.e. the A380, weighing up to 1.3 million pounds) which are quite
different from the loads applied by the older generation of commercial airplanes.
Existing pavement thickness design procedures were inadequate for analysing the effect of these
new aircraft on the life of existing pavements. The question was whether the new aircraft would
cause more damage to existing runways than the existing aircraft in operation at that time. There
was no response or performance data, guidelines, or standards available anywhere in the world to
answer this question. Extrapolation of the existing criteria indicated that existing pavements would
need to be strengthened, costing approximately US$1.7 billion over several years.
Determining the compatibility of these new, heavier aircraft with the existing pavements was crucial
to the airlines and airport operators. If compatibility could not be established, there were two
options – operate the aircraft with reduced payload or pay increased landing fees to compensate
for the additional damage these aircraft would cause to the pavement. Neither of these options
were acceptable. The net effect would be a negative impact on the sale of aircraft to airline
operators or the unnecessary expenditure to strengthen airport pavements; the former effect
having a serious negative impact on the US economy and balance of trade.
THE RESEARCH & DEVELOPMENT PLAN
In response to this urgency, the FAA undertook a very comprehensive 10-year research and
development (R&D) programme aimed at upgrading and developing pavement design procedures
to accommodate these new aircraft. This programme was undertaken in response to these serious
contemporary issues facing airport pavement design. It utilises modern design and evaluation
procedures that concentrate on long-life pavements for existing as well as new and heavier
aircraft. It fulfills the US transportation needs by supporting the introduction of new aircraft,
protecting the multi-billion dollar investment in US airport pavements, and assuring continuing US
leadership in aviation technologies.

49
Journal Aviation Management 2008
The approach adapted by the FAA represents a return to fundamentals which will result in a
common pavement design methodology based on sound theoretical principles and full-scale
validation tests. It takes advantage of today’s enhanced computational abilities and provides the
flexibility to deal with new, complex landing gear configurations that were never visualised or
contemplated when the then current design procedures were developed. When completed, the
plan will reaffirm FAA’s leadership responsibilities as a key player of the aerospace industry.
THE NATIONAL AIRPORT PAVEMENT TEST FACILITY
An essential element in the development and implementation of new design procedures is a
comprehensive test and verification programme performed on real pavements subjected to full-
scale loading. The pavement test vehicle, with its ability to apply actual landing gear wheel loads
to test pavements, is the focal point of the National Airport Pavement Test Facility (NAPTF) (see
Figure 1). The NAPTF, located near Atlantic City, New Jersey, US, is where the FAA conducts full-scale
traffic tests on airport pavements.
The NAPTF was built to update pavement thickness design procedures for six-wheel airplane
landing gears, and to determine, through controlled tests, whether the existing procedures over
predict or under predict the load interaction effects from six wheels for the asphalt pavements. For
concrete pavements, the goals were similarly to get performance data to update outdated design
procedures, as well as to identify failure modes not adequately captured in the existing models.
In both cases, a fundamental approach to the problem requires conducting full-scale tests to total
pavement failure.
Figure 1: The National Airport Pavement Test Facility near Atlantic City, New Jersey, US
50
State-of-the-Art Technology in Airport Pavement
Facility Specifications
The test facility is capable of full-scale loading representing new generation, heavy civil transport
aircraft. This load may comprise up to 75,000 pounds per wheel on two landing gears with six
wheels per gear (total of 12 wheels). It will handle single, dual tandem, and tridem loading
configurations, and has the capability to change wheel spacing and gear spacing, with a maximum
tyre size at 56 inches (142 cm) overall diameter and 24 inches (61 cm) maximum width.
The test pavement is 900 feet (270 m) long and 60 feet (18 m) wide. The width of 60 feet is
necessary to investigate load interaction effects. It contains three subgrade materials (in the range
of three to 20 percent California Bearing Ratio or CBR) and asphalt and concrete surfaces, with a
total of nine test sections.
Tests are performed to the point of pavement structural failure, with the failure of one test
section to occur in one year or less. Speeds of the test vehicle represent worst case pavement
response, with the facility having the capability to conduct testing of up to a speed of 15 miles
per hour (24 km/h) while running tests in both directions. The facility is capable of accommodating
lateral wander patterns typical of airport runway operations. The test vehicle can be operated
continuously and automatically, with automatic tyre loading. Pavement response sensors measure
strain, deflection, pressure, moisture and temperature.
The 60-feet wide test pavement provides two traffic lanes so that two gear configurations can be
tested simultaneously. For example, it is possible to traffic a six-wheel B777 gear in one lane and a
four-wheel B747 gear in the other lane. The tests are run until all sections have completely failed.
Obviously we will have to define failure first. The test vehicle can be programmed to skip, or “fly
over”, a failed section or sections. This direct comparison of two different gears is particularly
important in finding a resolution for computing the aircraft classification number.
MAJOR ACCOMPLISHMENTS
The test facility became operational in 1999. A few major accomplishments from the 10-year R&D
plan are described below:
Development of the FAA Rigid and Flexible Iterative Elastic Layered Design – The New Pavement Thickness Design Procedure
To assess pavement requirements for heavier aircraft, and in an effort to create more cost-effective,
longer lasting airport pavements, FAA researchers have developed criteria and methods for design,
evaluation, performance and serviceability of airport pavements. In 2006, the FAA completed
a new consolidated, computerised design procedure called the FAA Rigid and Flexible Iterative
Elastic Layered Design (FAARFIELD). This procedure is contained in the FAA Advisory Circular
(AC) 150/5320-6E, ‘Airport Pavement Design and Evaluation’. A complete rewrite of this AC was
completed in March 2008 and is currently undergoing internal FAA review prior to public release.
51
Journal Aviation Management 2008
The design package, FAARFIELD, was developed after several intermediate efforts. Prior to the first flight of the B777 aircraft, the existing FAA design standard for airport pavements – the FAA AC 150/5320-6D, had been used for over 25 years. This standard, however, could not accurately assess damage to airport pavement as a result of the complex gear loads of the B777. To better predict wheel load interactions and to provide the airport community with a pavement design methodology addressing the needs of new, heavier aircraft, FAA researchers developed a design programme called the Layered Elastic Design (LED) FAA method, or LEDFAA.
As a result of this research effort, in 1995, the FAA issued a new Advisory Circular, AC 150/5320-16, implementing LEDFAA as a new standard for design of airport pavements intended to serve the B777 airplane. To ease the difficulties of implementing the LED procedure, and to empower design engineers with the required computational tools to perform the numerical computations, FAA’s researchers also developed the LEDFAA programme package with a user-friendly graphical interface. The programme minimises user input variables and the design thickness of the airport pavement is automatically computed. The next major revision came in 2004, when the FAA further modified the LEDFAA programme to accommodate the A380-800 aircraft. This effort was included in Change 3 to AC 150/5320-6. Change 3 specifies that LEDFAA can be used as an alternative FAA design standard for airport pavements handling all traffic mixes, not just those intended to serve the B777, and replaced AC 150/5320-16. The current revision to the design standard, AC 150/5320-6E, replaces both LEDFAA and the old design charts with the new programme, FAARFIELD.
From a user’s point-of-view, FAARFIELD is similar to LEDFAA. However, there are major internal changes. In this programme, a three-dimensional finite element model (3D-FEM) is used to describe the rigid pavement structure. The 3D-FEM method can handle greater detail and more complex characterisations of construction materials than the LED method. It is particularly useful for modelling rigid pavements, since the slab edges are often the critical components in rigid pavements. In addition, the 3D-FEM method can incorporate non-linear and non-elastic material models. Lastly, the 3D-FEM method is capable of more accurately simulating the structural response of airport pavements to complex loading configurations, including aircraft with six or more wheels per gear.
Aircraft Classification Number — an International Aircraft Compatibility Criteria
Another major accomplishment has been the resolution to the question of compatibility of the new heavy aircraft with airport runways around the world. In 1995, when the Boeing Company announced the introduction of B777 aircraft, the FAA did not have any data available to provide compatibility of this aircraft with existing runways in the US or anywhere else in the world. The compatibility of other large aircraft, such as B747, which were already operating, is determined by what is known as the Aircraft Classification Number (ACN). ACN is a measure of the amount of damage an aircraft causes to an airport pavement in relation to other airplanes operating on the pavement. For larger and heavier aircraft, the ACN is reduced by an “alpha factor” which is less than one. The International Civil Aviation Organization (ICAO) allowed the use of an interim “alpha factor” for the then new B777 aircraft. Selecting a suitable factor for permanent adoption was not possible because the B777 landing gear configuration had never been run in full-scale tests to pavement structural failure.
52
State-of-the-Art Technology in Airport Pavement
Between 2000 to 2002, comprehensive testing was conducted by the FAA covering most possible
variables and under the scrutiny of international researchers and ICAO. In 2006, ICAO proposed
that Alpha Factors at 100 coverages for four and six wheel gears be redefined for use in calculating
the ACN of airplanes operating on flexible pavements. The new Alpha Factor values are 0.800 and
0.720 for four and six wheel gears respectively, and are based on analysis of FAA NAPTF. With
these changes, Alpha Factors at other numbers of wheels, and over the full range of coverages for
design, required redefinition to maintain consistency in the CBR procedure for flexible pavement
thickness design, as required for ACN calculations.
Adoption of new Alpha Factors for computation of ACN was approved by ICAO on 19 June 2007,
and formally adopted on 16 October 2007 by a letter to the member States designating the new
Alpha Factors listed above as ‘Revised Alpha Factor Values’. The letter to the member States also
requested that the aircraft manufacturers revise the ACN values for their respective aircraft types
on various subgrade types, currently available as guidance material. The ICAO Pavement Design
Manual contains the new Alpha Factor values for one, two, four, six, eight, 12, 18, and 24 wheels;
it also contains information for computing Alpha Factors for other wheel combinations, and a
new methodology to allow calculation of Alpha Factor over the full range coverages. The new
methodology has been implemented in the computer programme COMFAA, which is available at
the FAA website.
Roughness Measurements
As pavements age and suffer damage from repeated loading or, more rarely, construction
deficiencies, their roughness increases and ride quality deteriorates. With increasing traffic and
airport utilisation rate, it is becoming evermore important to efficiently prioritise and schedule
maintenance. The need is increasing for airports to periodically survey their pavements and to
characterise the roughness using established methodologies. Improvements and availability of
equipment to accurately measure profiles and computer systems to do the analysis, together
with overall declining cost, are encouraging airports to include profile and roughness data in their
pavement management systems.
To address this new opportunity, the FAA is preparing a new AC intended to provide guidelines
for measuring and reporting airfield pavement roughness. Initially, the new Advisory Circular will
address the identification of isolated disturbances on pavements by the use of the Boeing Bump
criteria. When completed, the AC will address the problems of characterising the roughness of
a pavement over its full length and identifying numerical limits for triggering maintenance or
rehabilitation based on these alternative measures. Supporting the guidelines in the Circular is a
software package for analysing airfield pavement profiles called ProFAA. Figure 2 shows a vehicle
mounted profile measurement system.

53
Journal Aviation Management 2008
Figure 2: A portable profiler
8 AND 10 WHEEL LANDING GEAR
As the issues raised by the six-wheel gear are resolved, new questions are raised from the
operation of more complex wheel and gear design containing eight or more wheels per landing
gear. In order to remain a step ahead, we are adding new wheel modules to the NAPTF. The new
modules will allow us to test complex gear configurations. The capabilities of the test vehicle will
soon be expanded with the addition of two new load modules to supplement the existing three
load modules on each of its two movable carriages (see Figure 3). This enhancement will allow
researchers at the NAPTF to simulate eight and 10 in-line landing gear wheel loads.
Figure 3: Additional modules
While the existing configuration of the test vehicle was adequate to emulate almost all present
commercial airline landing gears, with the addition of the new load modules, the 10 in-line landing
gear wheel configuration of freighter aircraft manufactured by Antonov ASTC (see Figure 4) can
now be simulated. In addition, data derived from pavement testing using the new loading modules
will give commercial aircraft designers the ability to perform landing gear configuration studies for
future aircraft with more confidence than previously possible.
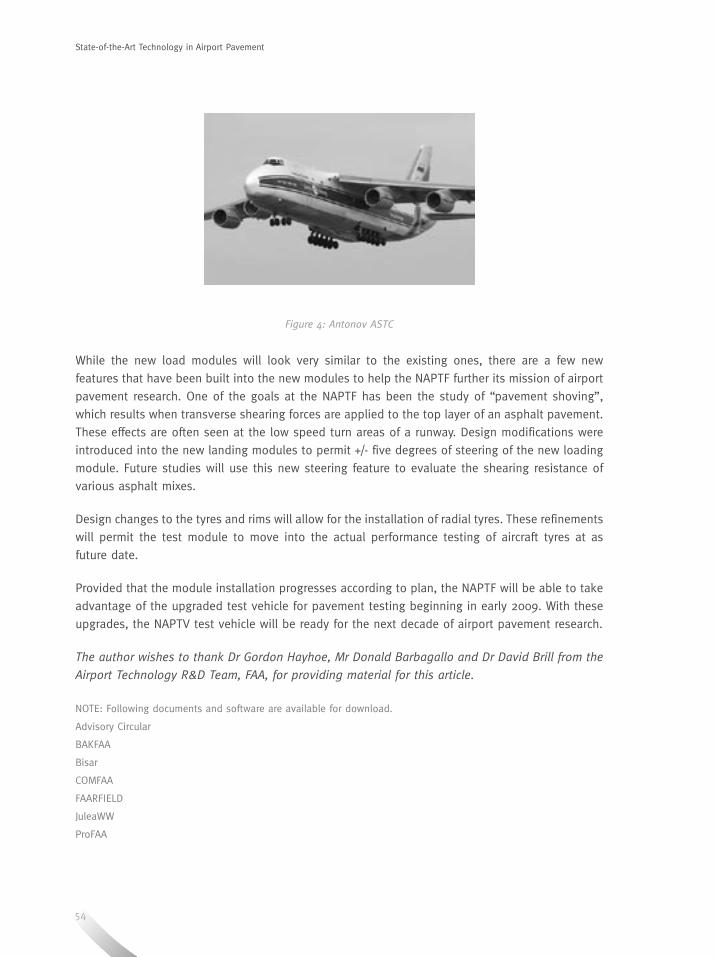
54
State-of-the-Art Technology in Airport Pavement
Figure 4: Antonov ASTC
While the new load modules will look very similar to the existing ones, there are a few new
features that have been built into the new modules to help the NAPTF further its mission of airport
pavement research. One of the goals at the NAPTF has been the study of “pavement shoving”,
which results when transverse shearing forces are applied to the top layer of an asphalt pavement.
These effects are often seen at the low speed turn areas of a runway. Design modifications were
introduced into the new landing modules to permit +/- five degrees of steering of the new loading
module. Future studies will use this new steering feature to evaluate the shearing resistance of
various asphalt mixes.
Design changes to the tyres and rims will allow for the installation of radial tyres. These refinements
will permit the test module to move into the actual performance testing of aircraft tyres at as
future date.
Provided that the module installation progresses according to plan, the NAPTF will be able to take
advantage of the upgraded test vehicle for pavement testing beginning in early 2009. With these
upgrades, the NAPTV test vehicle will be ready for the next decade of airport pavement research.
The author wishes to thank Dr Gordon Hayhoe, Mr Donald Barbagallo and Dr David Brill from the
Airport Technology R&D Team, FAA, for providing material for this article.
NOTE: Following documents and software are available for download.
Advisory Circular
BAKFAA
Bisar
COMFAA
FAARFIELD
JuleaWW
ProFAA
ABSTRACT
Crisis Management
Modern day emergency trauma care is based on the principles of the “golden hour”. Time from injury to definitive control of airway, and hemorrhage is vital if morbidity and mortality is to be minimised. To achieve this, urban communities in developed countries emphasise the importance of responsive and highly trained emergency medical services providing on scene trauma life support evaluation and interventions. Rapid transport to a recognised designated trauma centre has been shown to be of crucial importance.
Incidents involving airplanes often result in casualties with traumatic injuries just like in our day to day emergencies in the community. However, these incidents tend to produce more than one casualty and create additional challenges apart from providing the best care to a single casualty. This paper will explore the current evidence in trauma care that is of relevance to emergency planners involved in airport emergency planning. This will provide an opportunity for readers to re-visit and re-examine their own plans in relation to the current evidence.
Evidence-based Medical Response to Mass Casualty Event at Airports
ABOUT THE AUTHOR ABOUT THE AUTHOR
Dr Mark Leong
Dr Mark Leong is Senior Consultant and Deputy Head of Department of Emergency Medicine, Singapore General Hospital and Senior Consultant (Disaster Medicine) with Operation Readiness and Control Division, Ministry of Health.
He is actively involved in disaster and civil emergency planning and operations in Singapore and is currently the Field Medical Commander of Disaster Site Medical Command, Ministry of Health. His international and regional experience in natural disasters include leading and participating in humanitarian relief missions to India, Sri Lanka, Taiwan and Nias Indonesia.
Dr Leong holds a number of academic and teaching portfolios at the National University of Singapore and the Society of Emergency Medicine in Singapore and Ministry of Health. He is a fellow of the Royal College of Surgeons and Academy of Medicine Singapore.
Evidence-based Medical Response to Mass Casualty Event at Airports

55
Crisis Management
Dr Mark Leong
Singapore General Hospital
INTRODUCTION
The aviation industry is renowned for its quest towards
excellence in safety. However, with increasing air travel and
higher passenger carrying capacities of modern airplanes,
the potential exists for a major aircraft incident eg.
air crash causing traumatic mass casualties. Meanwhile,
responding agencies, eg. Fire and Rescue and Emergency
Medical Services (EMS) are facing increasing demands
from daily routine emergencies. Many services are facing
increasing response times, reduced capacity eg. hospital
beds, and longer waits. With emergency response agencies
and responders stretched, an added pressure of a major
aircraft incident at airports producing large numbers of
traumatic casualties will severely test the entire rescue
and medical chain. Communities that have to deal with
mass casualties on a more frequent basis, have come up
with strategies and recommendations to help others cope
with sudden surge in the need for medical services. This
paper examines the types of injuries that may arise from
an air crash, the principles of medical and mass casualty
management based on current available evidence, and the
current and future challenges confronting us.
INJURIES AFTER AN AIR CRASH
Are injuries sustained by passengers following an air crash
similar to those involved in a typical motor vehicle collision
on our roads? It is not difficult to imagine that being
in an aircraft is like being strapped in a motor vehicle
except that the passengers are being moved and hurled at
much higher speeds. Lillehei and Robinson (1994), in
their critical analysis of the fatal injuries resulting from
Continental flight 1713 disaster, found that the injuries
sustained were predominantly blunt injuries which were
Evidence-based Medical Response to Mass Casualty Event at Airports

56
remarkably similar to the deceleration injuries seen in motor vehicle collisions. Head and torso
injuries with associated spinal injuries were the most common cause of fatalities. For those who
survived the crash, burn injuries from resulting aircraft fires can be expected.
PRINCIPLES OF TRAUMA MANAGEMENT
The current widely accepted paradigm in managing a cardiac arrest victim is encapsulated in the
chain of survival starting from early access, cardiopulmonary resuscitation, cardiac defibrillation
and advanced cardiac life support. A chain of survival for the injured casualty should include the
following: bystander first aid, early access to EMS, on scene critical interventions, rapid evacuation,
hospital resuscitation, and access to advanced imaging, operating theatres and intensive care, and
rehabilitation services. The goal is to bring the casualty to a definitive medical facility with the
capability to arrest internal hemorrhage within one hour from the time of injury (ie. the “Golden
Hour”). The eventual outcome for the injured casualty is dependent on each and every element in
the chain. The strength of the chain is dependent on its weakest element. For medical responders
to mass casualties at airports, the emphasis is on pre-hospital elements of the chain.
1. Bystander first aid First aid is defined as assessments and interventions that can be performed by a bystander (or
by the victim) with minimal or no medical equipment. Following a major airport incident, it is
likely that the first responders will have more formal training than the lay public responding to
a road side motor vehicle collision. Responders eg. fire and rescue professionals should assess
imminent dangers and then begin rapid assessment of their casualties paying particular attention
to their airway, conscious level, breathing, and circulatory status while maintaining proper
cervical spine control in accordance to basic life support (BLS) guidelines. These knowledge
and skills are taught in courses such as International Trauma Life Support (ITLS, formerly Basic
Trauma Life Support) and Pre-Hospital Trauma Life Support (PHTLS). These courses provide
BLS training.
Many have also advocated paying particular attention in the first few minutes following injury.
The “Platinum Minutes” concept was developed to emphasise to pre-hospital care providers
the crucial first few minutes with relation to airway obstruction, undetected hypoxia, and
uncontrolled external hemorrhage. In response to this, many communities have promoted the
use of rapid access vehicles such as motorcycles to allow paramedics to deliver medical care in
the platinum minutes.
2. Early access to EMS With existing collaboration with other external agencies such as EMS, and Health, early
involvement of EMS is usually not a problem. However, if fire and rescue professionals are also
trained to provide BLS, life saving interventions with the platinum 10 minutes can be provided
much earlier.
Evidence-based Medical Response to Mass Casualty Event at Airports

57
Journal Aviation Management 2008
3. On scene critical interventions Casualties who are severely injured may require on scene critical interventions such as orotracheal
intubation, and chest decompression, skills which are not routinely taught to BLS providers.
Advanced life support (ALS) providers such as EMS/Medical/Health responders, often from other
agencies, are equipped with skills and equipment to perform these interventions. However, it is
important to note that despite the proven efficacy of these interventions performed in a hospital
setting, interventions have not been conclusively shown to be superior to just providing BLS to
injured casualties at the scene.
4. Rapid evacuation Current management of major trauma patients revolves around the concept of the “Golden
Hour”. Within an hour from the occurrence of an injury, the casualty should be in a definitive
medical facility with the capability of arresting any internal hemorrhage. This concept came
about following the work of Trunkey (1973, 1989) who first reported the trimodal distribution of
trauma deaths.
The first peak of death occurs minutes after the injury is a result of non survivable injuries such
as brain and major blood vessel injury. The second peak of death occurs over the next four
hours and is often attributed to uncorrected hypoxia from airway obstruction and respiratory
injuries, and hemorrhagic shock from uncontrolled external and internal hemorrhage. This
underpins the rationale of a “scoop and run” strategy from the scene to a medical facility where
definitive care can be provided. The debate and controversy of “scoop and run” versus “stay
and play” is still ongoing. The concept of “scoop and run” has been adopted by communities
who firmly believe that for severely injured casualties, rapid evacuation and timely access to a
major operating facility to stop ongoing internal hemorrhage is of paramount importance.
Other communities however emphasises the importance of providing initial resuscitation and
stabilisation on scene by highly trained paramedics and emergency physicians and transporting
them rapidly via land or air evacuation assets to the most appropriate hospital. The answer to
which system is best is a very complex and difficult one. In an urban environment with very
short transport times, it appears logical to employ a “scoop and run” strategy. However, in a
more rural environment with limited accessibility, greater travelling distances and transport
times, some form of initial stabilisation may be required for casualties to be delivered in a more
stable condition beyond the Golden Hour. The strategy to be used depends on many different
factors and the local operating environment.
58
5. Hospital management (Resuscitation, Major Operating Capabilities, Intensive Care and Rehabilitation)
From the pre-hospital perspective, the final delivery of the injured casualty to the nearest
medical facility within the “Golden Hour” appears to be the ultimate goal. However, with
global changes and rapid advancement in trauma management, delivering the casualty to the
nearest medical facility is no longer considered the standard of care. In the last four decades,
trauma care has evolved from rapid evacuation to the nearest facility to a designated trauma
centre which is part of a community based inclusive trauma care system. A recent study in the
US has shown that outcomes of injured patients were better when they were managed in a
trauma centre.
PRINCIPLES OF MASS CASUALTY MANAGEMENT
When a major airport incident occurs, a potential for mass casualties event eg. air crash exists.
The goals and challenges encountered in the delivery of trauma care to a single severely injured
casualty are now multiplied and magnified manifold placing severe stress on both the emergency
responders and their organisations. It is not unusual to find EMS and hospital services stretched
on a daily basis with an emphasis on prudence, productivity and efficiency. Unlike fire and rescue
agencies where the equipment and personnel are ready 24 hours a day to respond to any potential
incident, EMS and healthcare systems often function in an over capacity mode. This has resulted
in global problems such as emergency department overcrowding, high hospital bed occupancy
rates and increasing EMS response times. The coming together of these factors will invariably
produce an extremely challenging problem for health care providers, airport emergency planners and
policy regulators.
These challenges are not insurmountable. Communities who have experiences in dealing with
mass casualties on a more regular basis have developed strategies to cope. The fundamental
aims of a mass casualty event response are rapid evacuation from a hazardous incident scene
and reduce the mortality of critically injured casualties. Some important concepts in mass casualty
management for pre-hospital phase include:
• Disaster medical triage
• Appropriate intervention for appropriate casualty
• Multi-agency collaboration
• Incident command, control, communication and coordination
Disaster Medical Triage
In any mass casualty event, triage is perhaps the most crucial element that sets it apart
from single casualty incident. When demands on medical care exceed the capacity to provide
care, there is a need to conserve and prioritise care to those who most require it and benefit
from it. There is no place for futile care and “over-servicing” of casualties. In Fryberg’s (2002)
Evidence-based Medical Response to Mass Casualty Event at Airports

59
Journal Aviation Management 2008
study on mass casualty bombing events, it is shown that critical mortality of casualties
increase with an increase in over triage rates. In routine single casualty events, over triage
is the norm and a deliberate strategy to ensure no casualty slips through the safety net.
However, in mass casualty events, over triage over burdens the finite medical resources
– manpower, logistics and system, resulting in an increase in critical mortality. Conversely,
under triage (an underestimation of injury) can produce an equally bad outcome. Therefore
the act of segregating the casualties into several triage categories allows the limited number
of responders, equipment and supplies to focus on providing critical intervention and
expeditious evacuation of the critically injured, ensuring the lowest critical mortality rate.
There are many different disaster triage protocols in use. Regardless of the system used,
triage is performed by the most experienced responder with a good knowledge of the
medical system. This may initially be a senior experienced fire rescuer, a paramedic or senior
physician when more expertise becomes available.
Appropriate Intervention for Appropriate Casualty
During routine emergencies, emergency medical care at the scene is commonly provided
by first aiders (public) or EMS (EMTs, paramedics). However, in mass casualty events, ALS
medical teams from hospitals with physicians and nurses are often called upon to provide
care at the scene. As these ALS providers function in usually well equipped, environmentally
optimal infrastructure with the goal of delivering maximal care for the individual patient, they
may not be familiar with the constraints and limitations in performing critical interventions
on mass casualties. Experienced practitioners of mass casualty incidents advocate limiting
the critical interventions on scene of mass casualties to advanced airway maneuvers,
cervical spine stabilisation, chest decompression for tension pneumothorax and splinting
of fractures.
Multi-agency Collaboration
Very often agencies tend to be very focused on their own tasks and objectives. In mass
casualty events, all agencies have to come towards a common understanding and develop a
clear goal. From a health care perspective, the overriding goal is to ensure the best outcome
possible for all casualties ie. saving lives. It is imperative, regardless of primary responsibility
of all responding agencies, that the multiagency and multidisciplinary response is clearly
focused on producing such an outcome.
Incident Command, Control, Communications and Coordination
A clear chain of command is essential to bring order to an expected initial chaos with
multiple responding agencies, each with their own roles and responsibilities. Lessons from
recent mass casualty events continue to highlight communication and coordination as one of
the most challenging problems. Problems do not just lie with technology and its use, but can
often be due to poor human compliance and discipline. All agencies and incident command
systems must be able to continue with its response if all fails. An incident command system
and plan with minimal use of technology can be a good starting point with the availability
of modern digital and wireless communications a bonus.

60
AIRPORT EMERGENCY PLANNING
The International Civil Aviation Organization (ICAO) provides a model for emergency medical
response to a major aviation incident involving mass casualties within the airport. Casualties
are rescued, and moved to a casualty collecting area (CCA) where triage takes place and initial
emergency medical care can be provided. Casualties are then prioritised to be evacuated to the
most appropriate medical facility for definitive care.
In Singapore, the airport emergency plan (AEP) follows this recommendation. Casualties gathered
at the CCA usually within the vicinity of the crash but at a safe distance, are evacuated to a casualty
clearing station (CCS) where casualties can be triaged and given initial emergency medical care
by responding EMS units and field medical teams comprising of doctors and nurses from public
hospitals. After initial stabilisation, they are evacuated to hospitals under the direction of Ministry
of Health (MOH). Currently, the airport fire stations are designated as the CCS at Singapore Changi
Airport. It provides an easily recognisable, safe, environmentally stable and secured location for
initial casualty care by multi-agency and multi-disciplinary responders under mutual aid agreement
of the AEP.
CHALLENGES AND THE FUTURE
Does your AEP work? The short answer is it works when it works. Would a prior agreed upon
plan by all stakeholders that is regularly exercised gives us the assurance of a good outcome?
Lee et al, in their review of the emergency response after a B747 crashed on take off from Chiang
Kai Shek International Airport in 2000, showed that the anticipated benefits from having a mass
casualty plan with recent emergency preparedness and validation exercise were not achieved. The
main reasons cited for this failure is poor compliance by responders to a plan which has certain
structural problems. A major deviation from the plan was the absence of casualty triage and
initial management. This incident serves as a timely reminder to emergency planners and incident
managers the significant impact of how people and organisations are likely to act, rather than
expecting them to change their behavior to conform to the plan.
A proper and practically designed mass casualty incident (MCI) plan, good compliance of responders,
and a strong support system of responding agencies are the most important factors for successful
emergency response. An overly orchestrated exercise with less than realistic simulation to find out
whether a plan works is unlikely to produce the desired answers.
CONCLUSION
Major incidents in our airports are infrequent events which have the potential to generate a
complex event with mass casualties requiring a well prepared multi-agency response. Applying the
best evidence for trauma and mass casualty management, and learning from recent events will
result in the best possible outcome. Unrealistic planning and preparedness activities can result in
a false sense of assurance.
Evidence-based Medical Response to Mass Casualty Event at Airports
61
Journal Aviation Management 2008
References
Allgower M. Trauma care systems in Europe. Am J Surg. 1991; 161(2): 226-9
American Heart Association and American Red Cross (2005). Guidelines for First Aid. http://www.redcross.org/static/
file_cont4913_lang0_1727.pdf accessed 26 June 2008
Anantharaman V. Disaster - site medical support organization in a small country. PDM. 1991;6(1):43-6
Benson M, Koenig KL, Schultz CH. Disaster triage: START, then SAVE--a new method of dynamic triage for victims of
a catastrophic earthquake. Prehosp Disaster Med. 1996; 11(2):117-24
Campbell J E. International Trauma Life Support. ITLS for Prehospital Care Providers Manual 6th Edition ISBN 978-0-
13-237982-3
Cayten C, Murphy JG, Stahl W M. Basic Life Support versus Advanced Life Support for injured patients with an injury
severity score of 10 or more. J Trauma. 1993; 35(3):460-467.
Coats T J, Davis G. Prehospital care for road traffic casualties. BMJ 2002; 324 (11): 1135-1138
Cowley R A, Hudson F, Scanlan E, Gill W, Lally R J, Long W, Kuhn A O. An economical and proved helicopter program
for transporting the emergency critically ill and injured patient in Maryland. J Trauma. 1973; 13(12): 1029-38
Cummins RO, Ornato JP, Thies WH, et al. Improving survival from sudden cardiac arrest : the “chain of survival”
concept. Circulation 1991;83(5):1832-47.
Cummins RO. The “chain of survival” concept: how it can save lives. Heart Dis Stroke 1992;1(1):43-5.
Eckstein M, Chan L, Schneir A, Palmer R. Effect of Prehospital Advanced Life Support on Outcomes of Major Trauma
Patients. J Trauma. 2000; 48(4):643-648
Frykberg E R. Medical Management of Disasters and Mass Casualties from Terrorist Bombings: How can we cope? J
Trauma. 2002; 53(2): 201-212
Hirshberg A, Holcomb J, Mattox K L. Hospital Trauma Care in Multiple-Casualty Incidents: A Critical View. Ann Emerg
Med. 2001; 37(6): 647-652
Institute of Medicine. Hospital-Based Emergency Care: At the Breaking Point. 2006. National Academies Press. ISBN-
10: 0-309-10173-5.
International Civil Aviation Organization. 2005 ICAO Airport Services Manual Part 7. Airport Emergency Planning, Chp
9 – Triage and Medical Care.
Kennedy K, Aghababian R V, Gans L, Lewis C P. Triage: Techniques and Applications in Decisionmaking. Ann Emerg
Med. 1996; 28(2):136-144
62
Lee W H, Chiu T F, Ng C J, Chen J C. Emergency Medical Preparedness and Response to a Singapore Airliner Crash.
Acad Emerg Med. 2002, 9(3):194-198
Leong M K F, Briggs S. Classic Concepts in Disaster Medical Response – Chapter in “Humanitarian Crisis-The Medical
and Public Health Response”.1999, Harvard University Press
Liberman M, Mulder D. Sampalis J. Advanced or basic life support for trauma: meta-analysis and critical review of the
literature. J Trauma. 2000; 49:584–599
Liberman M, Mulder D, Lavoie A, Denis R, Sampalis J S. Multi Center Canadian study of prehospital trauma care. Ann
Surg. 2003; 237(2):153-160
Lillehei K O, Robinson M N. A Critical Analysis of the Fatal Injuries resulting from Continental flight 1713 airline
disaster: Evidence in favor of improved passenger restraint systems. J Trauma. 1994; 37(5):826-830
Lockey D J, MacKenzie R, Redhead J, Wise D, Harris T, Weaver A, Hines K, Davies G E. London bombings July 2005:
The immediate pre-hospital medical response.Resuscitation. 2005; 66: ix-xii
Mackenzie E J, Rivara F P, Jurkovich G J, Nathens A B, Frey K P, Egleston B L, Salkever D S, Scharfstein D O. A National
Evaluation of the effect of Trauma-Center care on mortality. NEJM. 2006; 354(4):366-378
Ministry of Health. Ministry of Health Emergency Response Plan, Operations Civil Emergency. 2005
Nathens A , Brunet F , Maier R. Development of trauma systems and effect on outcomes after injury. Lancet. 2004;
363:1794–801
National Association of Emergency Medical Technicians 2007. Pre Hospital Trauma Life Support Sixth Edition. Mosby
National Association of Emergency Medical Technicians. Pre-hospital trauma life support. St Louis: Mosby; 1994.
Oliveira M S, Egipto P, Costa I, Cunha-Ribeiro L M. Emergency Motorcycle: Has it a place in a medical emergency
system? AJEM. 2007; 25, 620–622
Potter D et al. A Controlled Trial of Prehospital Advanced Life Support in Trauma. Ann Emerg Med. 1988; 17(6):582-588
Quarantelli EL. Organizational behavior in disasters and implications for disaster planning, Report series 18. Newark,
DE: Disaster Research Center, University of Delaware; 1985
Rainer T H, Houlihan K P G, Robertson C E, Beard D, Henry J M, Gordon M W G. An evaluation of paramedic activities
in prehospital trauma care. Injury. 1997; 28:623-627
Redhead J, Ward P, Batrick N. .Prehospital and Hospital Care. NEJM. 2005; 353(6): 546-547
Sacco W J, Navin D M, Fiedler K E, Waddell R K , Long W B, Buckman R F Jr. Precise formulation and evidence-based
application of resource-constrained triage. Acad Emerg Med. 2005; 12(8):759-70
Evidence-based Medical Response to Mass Casualty Event at Airports
63
Journal Aviation Management 2008
Sampalis J S. Lavoie A, Williams J I, Mulder D, Kalina M. Impact of on-site, prehospital time, and level of in-hospital
care on survival in severely injured patients. J Trauma. 1993; 34(2):252-261
Sampalis J S, Denis R, Lavoie A, Frechette P, Boukas S, Nikolis A, Benoit D, Fleiszer D, Brown R, Churchill-Smith M,
Mulder D. Trauma Care Regionalization: A Process-Outcome Evaluation. J Trauma. 1999; 46(4):565-581
Super G, Groth S, Hook R. START: simple triage and rapid treatment plan. Newport Beach (CA): Hoag Memorial
Hospital Presbyterian; 1994
Stein M, Hirshberg A:Medical consequences of terrorism - the conventional weapon threat. Surg Clinics of North
America. 1999; 79(6):1537-1552
Trunkey DD. Trauma. Sci Am. 1983; 249(2):28-35
West J G, Trunkey D D, Lim R C. Systems of trauma care. A study of two counties. Arch Surg. 1979; 114(4): 455-60

64
ABSTRACT
Airport Management
The opening of new air passenger terminals at major airports has always attracted great attention, both from the local populace, as well as the mass media. This interest could be because air terminals are typically expensive investments with complex operations and have an infamous track record of newsworthy chaos or disruptions on opening day.
Singapore opened its new Terminal 3 (T3) on 9 January 2008, 27 years after Changi Airport started operations with its first terminal in 1981. This paper seeks to share the T3 experience in ensuring the smooth operations of the terminal on opening day and beyond.
Opening of New Terminals – Changi Airport’s T3 experience
ABOUT THE AUTHOR
Mr Foo Sek Min
Mr Foo Sek Min is currently Senior Director of the Airport Management Group at the Civil Aviation Authority of Singapore (CAAS) where he oversees the Airport Operations Division, Commercial Division and Aviation Security Unit. Mr Foo also serves on the Board of Crimson Logic Pte Limited, a leading Singapore-based IT service provider. Mr Foo has over 12 years of extensive experience in various aspects of passenger terminal and air cargo operations. He has been project lead for various infrastructural upgrading and expansion projects. These include the extension of the Terminal 2 finger piers, Terminal 2 upgrading, the construction and opening of Budget Terminal as well as the new Terminal 3.
Opening of New Terminals – Changi Airport’s T3 experience
65
Airport Management
Mr Foo Sek Min
Civil Aviation Authority of Singapore
INTRODUCTION
The opening of T3 is the fulfillment of the airport masterplan
envisioned in the 1970s. The seven-storey building with
three basements and four above-ground levels, occupies
380,000 square metres. T3 was built at a cost of S$1.75
billion and brings the total airport capacity to about 70
million passenger movements annually.
DESIGN CONCEPT
Clarity
Changi Airport planners recognised that a key stress point
for many travellers is wayfinding. T3 was hence designed to
allow travellers to find their passage through the terminal
with ease. This is possible as T3 adopts a see-through
layout concept, making it easier for travellers to orientate
themselves. Signage is upsized and multi-lingual to enhance
wayfinding. In current times, where air terminals tend to be
mega structures with high ceilings, it is important to ensure
that the font size of signage is not perceived to be small
relative to the huge expanse of space.
External Views
With a full glass facade, passengers have extensive visual
access to the external landscape that surround them.
This gives a sense of expansive space and openness,
besides giving travellers views of take-offs and landings
of airplanes.
Natural Lighting
T3 features a unique roof architecture which allows
soft natural light into the building while keeping the
tropical heat out. The first-of-its-kind roof design has 919
intelligent computer-controlled skylights with specially
Opening of New Terminals – Changi Airport’s T3 experience
66
designed butterfly-shaped reflectors which automatically adjust themselves according to the
outdoor sunlight intensity. This allows an optimal flow of soft and uniform daylight into the terminal
building during the day. Inside the terminal building, “louvers” spanning across the entire ceiling
deliberately diffuse the sunlight entering the building to create a warm and comfortable ambience.
At night, the skylights glow with artificial lighting delicately concealed below the reflector panels.
The overall effect is a soothing ambience at all times of the day.
Of course, for the airport operator, it is highly risky to create so many “holes” in the roof, especially
during the rainy season. A rigorous “wet” testing programme was carried out at each skylight and
a subsequent maintenance programme was put in place to ensure water-tightness. Recovery and
contingency plans were also developed to deal with leakage in the event it happens.
The introduction of abundance of natural light into the building in turn helped achieve two
objectives. Firstly, for about five hours a day, there is no need for artificial lighting. Together with
an air-conditioning system that emits cold air via binnacles rising from the ground, the result
was a substantial reduction in energy consumption and savings in energy bills. Secondly, lush
landscaping could be introduced into the building.
Going Back to Nature
Airport designs have evolved over the years, with newer airports and terminals developed with
striking architecture and each trying to carve out their own identities. For Changi Airport, T3 is a
reflection of Singapore’s Garden City image. Coming into T3, one will be awed by the five-storey
high vertical garden, called the “Green Wall”. Spanning 300 metres across the main building, it can
be admired from both the Departure and Arrival Halls. The “Green Wall” is a tapestry of climbing
plants, interspersed with four cascading waterfalls and a hand-carved sandstone art wall display.
At the transit mall, travellers can relax amongst fig trees, koi ponds or visit the World’s First
Butterfly Garden in an airport.
Comparison of Changi Airport’s Three Terminals
Terminal 1 Terminal 2 Terminal 3
Terminal floor area 280,020 m2 358,000 m2 380,000 m2
Handling capacity per annum
21 million 23 million 22 million
No. of aerobridge gates
29 35 28
No of A380 gates 5 5 6 8
Opening of New Terminals – Changi Airport’s T3 experience

67
Journal Aviation Management 2008
PREPARATIONS FOR OPERATIONS
Choosing an Operational Opening Date
Sufficient time of about six months should be given for the operational readiness programme,
which comprises integrated systems testing, operational testing and passenger-flight trials. This
often cannot be assessed until the building infrastructure is completed and individual stand-alone
systems installed, tested and commissioned. However, a firm date for operational opening is needed
for the airport operator to get stakeholders to ready themselves and for public communication
purposes to travellers.
From past experience, it is better to start operations during a quieter period than a period with
higher traffic, to allow the new terminal to open without excessive stress. Hence the opening
date should not coincide with peak periods of travel (such as school holidays, public holidays
or year-end travel season), when passenger traffic would be significantly heavier. In addition, it
is advisable to start operations on a quieter mid-week day (i.e. a Wednesday). This operational
opening date should also allow for a continuous ‘quiet’ period of at least three weeks for operations
to stabilise before the next peak travel event occurs. The operational opening date would also be
dependent on the expected date that the terminal building would receive its temporary occupation
permit (TOP).
To provide clarity for all the parties involved in T3 preparations, the opening date was communicated
internally to all airport agencies and stakeholders on 2 Nov 2006. This gave agencies a date to
focus on and also more than a year to prepare. The Minister for Transport, Mr Raymond Lim,
publicly announced the 9 January 2008 operational opening date during his visit to T3 on 29 May
2007. T3 received its TOP in two phases - 31 April 2007 and 19 July 2007.
ORGANISING OURSELVES
As airport operations is a multi-agency affair involving many complex and integrated systems, it
is necessary to organise efforts to track progress and resolve policy issues quickly and decisively.
A T3 Live Steering Committee, chaired by CAAS, comprising key members from top management
of airport organisations was formed in November 2006. Its aims were to jointly oversee the
operational readiness plan for T3 opening; set key policies and decisions related to T3; and to
align efforts and programmes of various agencies.
The Steering Committee was in turn supported by nine key subgroups and staffed by a secretariat
project team. Please see Figure 1.
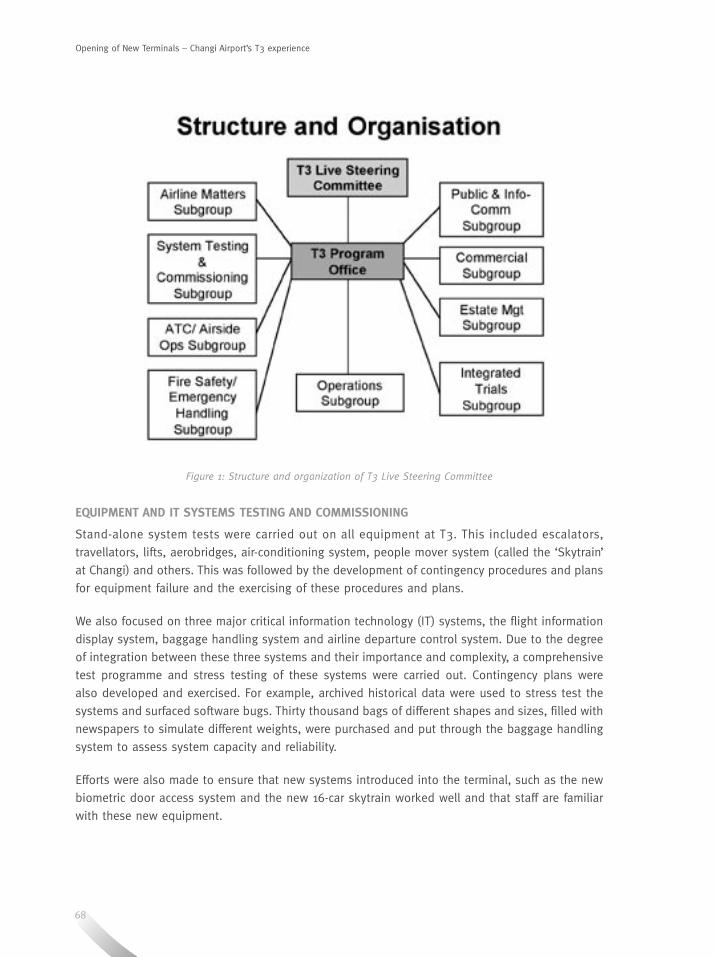
68
Figure 1: Structure and organization of T3 Live Steering Committee
EQUIPMENT AND IT SYSTEMS TESTING AND COMMISSIONING
Stand-alone system tests were carried out on all equipment at T3. This included escalators,
travellators, lifts, aerobridges, air-conditioning system, people mover system (called the ‘Skytrain’
at Changi) and others. This was followed by the development of contingency procedures and plans
for equipment failure and the exercising of these procedures and plans.
We also focused on three major critical information technology (IT) systems, the flight information
display system, baggage handling system and airline departure control system. Due to the degree
of integration between these three systems and their importance and complexity, a comprehensive
test programme and stress testing of these systems were carried out. Contingency plans were
also developed and exercised. For example, archived historical data were used to stress test the
systems and surfaced software bugs. Thirty thousand bags of different shapes and sizes, filled with
newspapers to simulate different weights, were purchased and put through the baggage handling
system to assess system capacity and reliability.
Efforts were also made to ensure that new systems introduced into the terminal, such as the new
biometric door access system and the new 16-car skytrain worked well and that staff are familiar
with these new equipment.
Opening of New Terminals – Changi Airport’s T3 experience

69
Journal Aviation Management 2008
STAFF FAMILIARITY AND TRAINING
Recognising that staff familiarity is crucial to the smooth operations of T3, all airport staff, both
new and existing, had to undergo site familiarisation and training before being issued with an
airport pass to work in T3. All airport employees were included, regardless of whether they were
operations staff, front-line staff or service staff. Even temporary employees such as airport guides
were also trained to ensure familiarity.
Existing staff who have to work in T3 were required to participate in the operational testing and
trials programme. As a guideline, all staff were required to operate the actual equipment at T3
onsite or to participate in trials at least twice.
Staff of third party service providers and maintenance contractors were also required to undergo
a similar familiarisation and training programme.
A T3 information kit was created and distributed to enhance staff’s knowledge of the workings,
layout, features and operations of the new T3. In the initial stages, bus shuttle services linking
T3 with other terminals were provided to facilitate staff to visit T3 on their own. Staff switched to
using the inter-terminal skytrain after it was ready for service.
A “Workshop on T3 Operations Readiness” was organised on 2-3 April 2007 as part of the airport-
wide preparation for T3 opening and to get the entire Changi community galvanised for the
terminal opening.
GROUND TRANSPORTATION
Besides focusing on airport staff who are directly employed onsite at the new Terminal, we also
engaged the various ground transport service providers to ensure that they are familiar with the
traffic patterns of the new Terminal. Taxi drivers were engaged via their company newsletters, car
decals and live taxi familiarisation exercises so that they would be familiar with the taxi holding
and taxi queue areas. Public buses and train companies were also engaged to start their services
at T3 earlier. Other transport service providers, such as ambulance drivers, limousine drivers and
tour coaches were also engaged to visit T3 to familiarise themselves with the traffic patterns.
RENOVATION AND MOVE-IN SCHEDULE
With over 100 shops and 40 food and beverage (F&B) outlets, we developed a three-stage move-
in schedule programme for all these tenants. These involved firstly working closely with the
Commercial division to ensure early award of tenders and allocation of office space. Secondly,
multiple parties were roped in to smoothen the approval process of shop designs and renovation
plans, followed by the actual renovation of the concession outlets and tenanted space. Lastly,
stocking-up and debris clearance plans were implemented.
70
INTEGRATED TRIALS AND LIVE FLIGHTS
A comprehensive trial programme was developed to integrate man, method and machine. The trials
started in June 2007 with volunteers from grassroots associations and students from local tertiary
education institutes acting as passengers. They were organised to simulate basic passenger arrival,
transit and departure flows and to test out wayfinding at the new terminal. Roadway and car park
trials were carried out by volunteers from car clubs to test out traffic flows and wayfinding and to
identify safety issues. Improvements were made following feedback from these basic trials.
The trials programme progressed to the next level of realism by operating live flights at T3.
Starting with chartered military flights from August 2007, actual travelling servicemen and their
meeters/greeters used T3 and tested the various systems and operational procedures.
Subsequently, chartered commercial flights with paying passengers were organised to use T3 in
September 2007.
By October 2007, T3 was ready for the first live commercial flight. In all, 43 departure and arrival
live commercial flights were conducted. The involvement of transfer passengers and baggage
increased the complexity of trials.
The integrated live flight trials culminated in a five-hour “live” cut-over exercise one week before
actual opening. This cutover exercise essentially replicated everything that would have occurred
on the actual opening day, down to the last detail. For example, the live commercial flights during
the exercise mirrored the flight schedule on opening day. All shop concessions were required to
operate as per opening day. All ground and service staff who are supposed to report to work on
Opening Day, did so for the cutover exercise.
PUBLIC OPEN HOUSE, INDUSTRY VISITS AND FEEDBACK
A public open house was organised over five weeks during the year end school holidays to give
the public a chance to visit the terminal before its actual opening. This would facilitate these future
customers who would be more familiar when they next use T3 for their flights. At the same time,
it would avoid having the public crowd the terminal unnecessarily during the operational opening
period. Lastly, opening the Terminal to the public would encourage the shop and restaurants to
complete their renovation on time in order to tap business from the visitors.
In addition, prior to the public open house, organised guided tours were held for groups ranging
from politicians, business partners, government agencies, travel trade industry, schools and
community centres. In all, about 16,000 visitors participated in these guided tours.
The T3 Public Open House event took place from 12 November to 9 December 2007 where more
than 240,000 members of the public explored the terminal on self-guided tours or join guided
tours of the transit area.
Opening of New Terminals – Changi Airport’s T3 experience
71
Journal Aviation Management 2008
PUBLICITY AND INFO-COMMUNICATIONS
A publicity and communication plan was developed to communicate two key messages, the actual
opening date and SIA’s expanded hub operations over two terminals.
With SIA operating from both T2 and T3, the challenge is to assist SIA to inform its departure
passengers on the correct terminal for their flights. At the same time, due to the need to optimise
SIA’s fleet utilisation, the arrival terminals are not fixed and arrival flight information would only
be available two hours prior to estimated arrival time.
To facilitate the communications on SIA’s expanded hub operations to travellers, measures were
put in place to remind passengers to check their flight information before they depart. Jointly
developed brochures were distributed onsite at the airport and up streamed to the travel trade
industry and overseas stations. Partners like transport operators, airport agencies, travel trade
and hospitality industry were also roped in to help disseminate the information and distribute
brochures to their customers/guests. Above-the-line campaigns were also launched, using online
and radio advertisements to communicate these messages to the general public.
ACTUAL OPENING – ORGANISATION
Various service recovery measures were anticipated beforehand and put in place in case passengers
ended up in the wrong terminal. Examples of such measures include free shuttle service between
T2 and T3, engagement of 100 temporary airport guides, additional signages and flight information
televisions.
The Civil Aviation Authority of Singapore had also set up a 24-hour Terminal Operations Command
Centre to monitor operations closely during the critical opening period. Daily co-ordination meetings
among the agencies were also convened to resolve operational issues and identify enhancements
to ground processes and airport facilities.
CONCLUSION
Precise planning and careful execution of all measures put in place is essential to ensure the
smooth opening of a new passenger terminal for all travelling passengers. T3 opened on 9 January
2008 with smooth flowing operations, marking yet another historical landmark in Singapore’s
aviation industry.

72
ABSTRACT
Sustainable Aviation
The ICAO States have risen to environmental challenges for aviation in the past: most notably on aircraft noise and on emissions which affect local air quality. The latest challenge is how the industry can develop a sustainable aviation sector which balances economic growth, social responsibility and environmental impact. In October 2007 the
36th ICAO Assembly agreed to the establishment of a senior level Group on International Aviation and Climate Change to develop a clear policy for international aviation. This will
be considered by the 15th Conference of the Parties to the United Nations Convention on Climate Change when it meets in Copenhagen at the end of 2009. This paper reviews previous ICAO measures on environmental matters and the present actions to address the development of a sustainable aviation industry.
Towards Sustainable Aviation
ABOUT THE AUTHOR ABOUT THE AUTHOR
Mr Michael Rossell
Michael Rossell is Representative of the United Kingdom on the Council of ICAO in September 2006. Mr Rossell headed up the international branch responsible for U.K. policy on aviation and the environment. He represented the UK in various working groups of the ICAO Committee on Aviation Environmental Protection (CAEP), and served as co-Rapporteur of a working group on market-based measures for reducing the environmental impact of aircraft engine emissions.
Towards Sustainable Aviation
73
Sustainable Aviation
INTRODUCTION
Growth of the aviation sector is likely to continue for as long
as increasing global wealth stimulates travel for business
and pleasure. But, aviation is a highly visible mode of
transport and its environmental impact is of growing
concern to the public and policy-makers. The International
Civil Aviation Organization (ICAO) has taken action over
the years to set standards for noise and emissions of
exhaust gases which affect local air quality, but there is a
pressing need for early action to limit or reduce emissions
of greenhouse gases. ICAO has made a start on this latest,
and most difficult challenge, through the agreement in
the 36th Assembly to establish the Group on International
Aviation and Climate Change (Resolution A36-22). Time is
pressing and ICAO must demonstrate leadership ahead
of the 15th Meeting of the Parties to the United Nations
Framework Convention on Climate Change (UNFCCC) at the
end of 2009.
SUSTAINABLE DEVELOPMENT
Sustainable development is not synonymous with
environmental protection. Sustainable development has
distinct, but closely linked, elements and in the UK are in
respect of five principles1. We should live within environmental
limits and achieve a just society, and do so by means of
sustainable economy, good governance and sound science.
Towards Sustainable AviationMr Michael Rossell
International Civil Aviation Organization
1 Internet, http://www.defra.gov.uk/sustainable/government/what/principles.htm (4 November 2008)
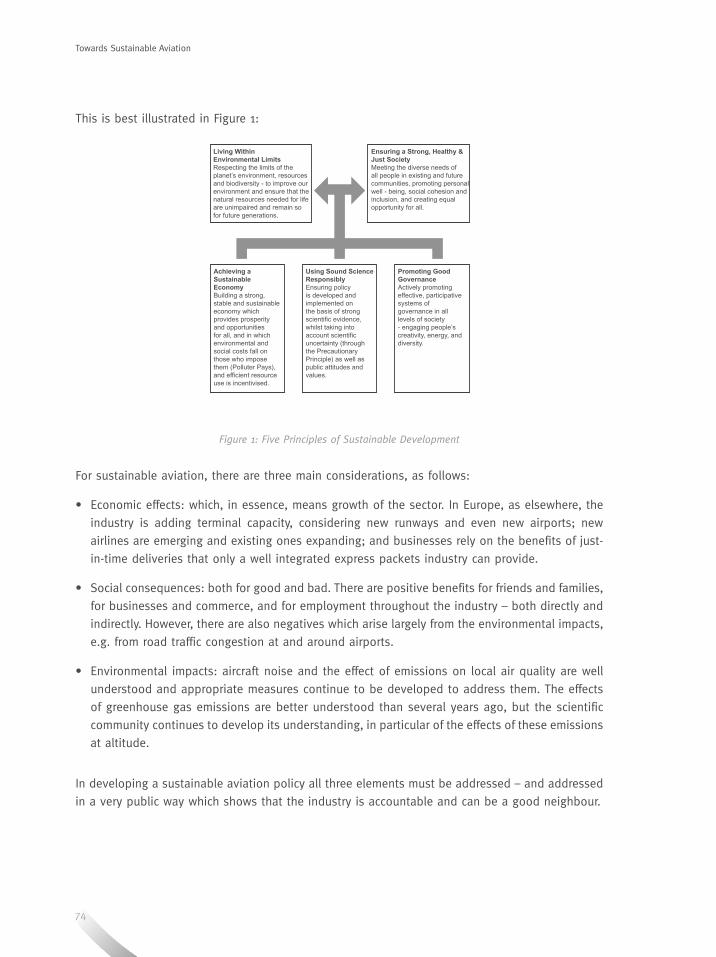
74
This is best illustrated in Figure 1:
Figure 1: Five Principles of Sustainable Development
For sustainable aviation, there are three main considerations, as follows:
• Economic effects: which, in essence, means growth of the sector. In Europe, as elsewhere, the
industry is adding terminal capacity, considering new runways and even new airports; new
airlines are emerging and existing ones expanding; and businesses rely on the benefits of just-
in-time deliveries that only a well integrated express packets industry can provide.
• Social consequences: both for good and bad. There are positive benefits for friends and families,
for businesses and commerce, and for employment throughout the industry – both directly and
indirectly. However, there are also negatives which arise largely from the environmental impacts,
e.g. from road traffic congestion at and around airports.
• Environmental impacts: aircraft noise and the effect of emissions on local air quality are well
understood and appropriate measures continue to be developed to address them. The effects
of greenhouse gas emissions are better understood than several years ago, but the scientific
community continues to develop its understanding, in particular of the effects of these emissions
at altitude.
In developing a sustainable aviation policy all three elements must be addressed – and addressed
in a very public way which shows that the industry is accountable and can be a good neighbour.
Towards Sustainable Aviation
Achieving a Sustainable EconomyBuilding a strong, stable and sustainable economy which provides prosperity and opportunities for all, and in which environmental and social costs fall on those who impose them (Polluter Pays), and efficient resource use is incentivised.
Using Sound Science ResponsiblyEnsuring policy is developed and implemented on the basis of strong scientific evidence, whilst taking into account scientific uncertainty (through the Precautionary Principle) as well as public attitudes and values.
Promoting Good GovernanceActively promoting effective, participative systems of governance in all levels of society - engaging people’s creativity, energy, and diversity.
Living Within Environmental LimitsRespecting the limits of the planet’s environment, resources and biodiversity - to improve our environment and ensure that the natural resources needed for life are unimpaired and remain so for future generations.
Ensuring a Strong, Healthy & Just SocietyMeeting the diverse needs of all people in existing and future communities, promoting personal well - being, social cohesion and inclusion, and creating equal opportunity for all.
75
Journal Aviation Management 2008
AIRCRAFT NOISE
Individually, newly designed and built aircraft are significantly quieter for their size, and often
in absolute terms, than aircraft of 20 years ago. The phase-out of the noisiest aircraft listed in
Chapter 2 at major airports around the world has meant that despite increased traffic, the number
of people living within a given noise footprint has reduced. However, the problem of aircraft noise
has not been solved. Increased traffic and sensitivity of people living near airports and under
flight paths – sometimes distant from airports – has meant that continuing efforts are necessary
to reduce the impact of aircraft further.
Developing standards and policies to deal with aircraft noise has been a major long term success
of co-operative work through ICAO. Over the years, successively stricter standards for aircraft
noise have been agreed upon. ICAO’s Committee on Aviation Environmental Protection (CAEP) has
worked in partnership with the industry to ensure that standards are environmentally effective,
technologically feasible and economically reasonable before recommending them to the ICAO
Council for adoption.
CAEP, Council and successive Assemblies have also developed Resolutions to promulgate policies
to get the best possible outcomes from the adoption of the new standards. Two important
Resolutions, still extant as A36-22, Appendix D and Appendix E (ICAO, 2007) deal respectively with:
the phasing out of the noisiest aircraft, starting with the developed countries and encouraging
others to do so as they are able; and, the adoption to the “balanced approach” to aircraft noise
management which encourages the application of land use planning measures and operational
measures before restricting the operation of certain aircraft types either at night (curfews) or at all
(e.g. by banning aircraft which do not meet specific certificated levels).
LOCAL AIR QUALITY
Smoke trailing behind departing aircraft prompted the first round of work within ICAO to develop
standards to reduce emissions which would have an impact on local air quality. This work
continues, consistent with the partnership approach with industry and the CAEP principles to
develop new standards for gaseous emissions including for nitrogen oxides (NOx) and to introduce
progressively stricter standards for new aircraft.
Emissions from aircraft are only part of those which have an impact on local air quality – they
are added to those which are in the ambient air for the region, from local industry, from road
transport and from airport-based vehicles. But, as measures are taken to reduce emissions from
other sources, and as the number and size of aircraft increases, the proportionate contribution
from aircraft will also increase unless corrective measures are taken.
Resolution A36-22, Appendix H (ICAO, 2007), recognises aviation’s impact on local air
quality and includes specific resolutions on the need to further develop understanding of the
processes, improve technological and operational practice, and to develop guidance on how the
76
impacts attributable to aviation might be ameliorated. There is also a specific Resolution which
requires the Council (advised by CAEP) “to continue its work to develop long-term technological
and operational goals with respect to aviation environmental issues, including nitrogen oxides
from aircraft.”
The manufacturing industry is acutely aware of the need to take action to reduce emissions of NOx
further, and in 2001 a report was published, which among its conclusions proposed an 80percent
cut in nitrogen oxide emissions from newly manufactured aircraft (Arguelles, P. et al, 2001). The
industry is investing heavily in new material development and technologies to achieve this. There
is also pressure on airports to reduce emissions from ground-based sources, such as tugs and
auxiliary power units, and also to increase the provision of public transport, so as to reduce the
number of private cars accessing airports.
GREENHOUSE GAS EMISSIONS
How aviation is to deal with its greenhouse gas emissions is currently its greatest challenge. How
ICAO responds to that challenge will mark its continued relevance in the field of aviation and the
environment.
The context in which emissions of greenhouse gases from aviation have to be considered is
established under the United Nations Framework Convention on Climate Change – UNFCCC (UNEP,
1999) and its Kyoto Protocol – KP (Climate Change Secretariat, 1998). Under Article 10 of the
UNFCCC, all Parties agree to work cooperatively, taking into account their common but differentiated
responsibilities and their specific national and regional development priorities, objectives and
circumstances but without introducing any new commitments for Parties not included in Annex I
(the developed countries).
In 1997, the Parties to the UNFCCC agreed in the KP to binding targets for the Annex 1 States. The
overall reduction would be 5.2percent in the period 2008 – 2012 compared to 1990. The KP also
established some flexible mechanisms by which emissions reductions could be achieved:
• Joint Implementation: projects between Annex 1 States,
• Clean Development Mechanism: projects where Annex 1 States could secure emissions reductions
in non-Annex 1 States, and
• Emissions Trading: which allowed States to use emissions reductions achieved in one area to
offset emissions somewhere else.
However, because of the complexities related to the allocation of emissions from international
aviation and shipping (bunker fuels), these emissions were not included in national totals under
the KP. Instead, Article 2.2 provided that Annex 1 Parties should pursue limitation or reduction of
them, working through the ICAO and the International Maritime Organization, respectively.
Towards Sustainable Aviation
77
Journal Aviation Management 2008
ICAO responded by initiating work with the Inter-governmental Panel on Climate Change (IPCC) to
assess the global impact of aviation on climate change. It produced a substantive peer-reviewed
report, the ‘IPCC Special Report on Aviation and Global Atmosphere’ in 1999. The report took
stock of what was known about the science of climate change and specifically aviation’s impact at
altitude, the available and projected technology, the anticipated trends in terms of growth of the
industry, and current and possible future measures which might be taken to mitigate the impacts
of aviation on the climate. Importantly, the report examined the known and possible impacts of
different gaseous emissions and developed quantified plausible scenarios for the future under
different policy choices. The document, which was finalised by government policy-makers in April
1999, was widely recognised as a step change in the understanding of aviation and climate change
and has established the basis for future work in this sphere.
This work has subsequently been updated by the IPCC 4th Assessment Report (IPCC, 2007),
which has estimated that aviation was responsible for around 2percent of global carbon dioxide
emissions. But these emissions are increasing as the industry grows and without further action
are expected to double within the next 20 years. In addition, emissions of NOx at high altitude,
through a complex chemical reaction with sunlight to produce ozone, increases the warming
effect of emissions from aviation. Furthermore, aircraft engines produce large quantities of water
vapour which create contrails and often persistent cirrus clouds – the warming potential of which
is thought to be significant but, as yet, difficult to quantify.
Some have asked the question “Is 2percent of CO2 emissions something we should worry about?”
To which the answer must be an emphatic yes. To put this amount in context, it is larger than most
countries’ individual emissions, and that is not taking into account the effects of NOx and water
vapour. Also, those Annex 1 States which are Parties to the KP have agreed to binding targets to
reduce their collective emissions by 5.2percent. Since international aviation emissions are outside
the national totals, any increase would erode that reduction.
Domestic aviation emissions fall within national totals and it is for States to make their own
policy decisions on how they address these in relation to emissions from other sources. Whether
they are treated in the same way or differently may depend in part on the relative quantity of
emissions from each source – consider for example the theoretical difference between the US with
its predominantly domestic market, and Singapore.
Since publication of the IPCC Special Report, CAEP and Council have continued to work on
improving their understanding and working on policy options, most notably in the development
of market-based measures. At the 33rd Assembly in 2001, the Assembly agreed Resolution
A33-7, Appendix I2 (ICAO, 2007), which for the first time recognised the need for a specific policy
on market-based measures regarding aircraft emissions. The Resolution specifically noted that
market-based measures were policy tools designed to achieve environmental goals at a lower cost
2 Superseded by A36-22
78
and in a more flexible manner than traditional regulatory measures, and the increasing recognition
of governments of their use in protecting the environment. The Resolution noted that work on
emissions trading was for the longer term whilst voluntary measures (under which industry and
governments agree on a target and/or to a set of actions to reduce emissions) could serve as a
first step.
RECENT DEVELOPMENTS
Although work continued in ICAO, it was developments outside which have set the pace. In
December 2006, the European Commission published a proposal to include emissions from
international aviation in its already operational emissions trading scheme (European Commission,
2006). The scheme had been established to deal with emissions from large point source emitters
such as power stations, cement works, smelters etc., but it could easily be adapted to include
other major emitters, provided it was possible to measure and account for their emissions. This
proposal has been refined through negotiation and the current position agreed with the European
Parliament is that the emissions trading scheme would apply to all services to and from the EU
from 2012. The cap for 2012 will be set at 97percent of the average annual emissions between
2004 and 2006; and the cap for 2013 at 95percent of those average annual emissions. 15percent
of the allocations would be auctioned.
There were also developments within the industry and at the International Air Transport Association
(IATA)’s AGM in 2007, Mr Giovanni Bisignani, Director General & CEO of IATA, challenged the
industry to adopt a bold vision of zero carbon aircraft by 20503 (Bisignani, G., 2007).
In September 2007, the 36th ICAO Assembly, fully cognisant of these developments, worked to
develop its own vision for the future. Under the chairmanship of the President of the Assembly, a
small group of “friends” worked to develop a draft Resolution to define this vision. While some
progress was made, a consensus was not possible. Instead, the President proposed, and the
Assembly agreed, to the establishment of a Group on International Aviation and Climate Change
(GIACC). The broad Terms of Reference for the group were established in Assembly Resolution A36-
22 Appendix K (ICAO, 2007). GIACC would be a small, senior level group of policy and decision-
makers – as distinct from CAEP’s technical experts – who would be charged with formulating a
coherent strategy for ICAO to address aviation’s impact on climate change.
GIACC met for the first time on 22-24 February 2008 in Montreal, Canada and took evidence from
senior representatives from the industry. It agreed on a way forward and specifically agreed that
Members should respond to a structured template of questions about States views on the role of
ICAO and its, and their own, response to greenhouse gas emissions from aviation.
The second meeting of GIACC was held on 14 - 16 July, again in Montreal, to review and debate
the collected responses to the templates. The initial discussions recognised that there were three
main clusters of policy to be addressed, these were:
3 This was adopted as IATA policy in April 2008.
Towards Sustainable Aviation
79
Journal Aviation Management 2008
• Goals for the short, medium and long term. Consistent with Appendix K the goals would be
aspirational and focus on improvements in fuel efficiency – but it was recognised that firmer
targets might be considered, in addition, for the medium and longer term.
• Measures to reduce greenhouse gas emissions. It was recognised that emissions reductions
would need to be achieved from a wide range of activities. These included design and
manufacture of more efficient aircraft; improved operations to reduce wastage from less than
optimal operational practice; improvements to management of airports to ensure maximum
efficiency of movements on the ground; optimisation of airspace design and control to permit
aircraft to fly the most direct routes and at the most efficient speed or on routes where they
could take advantage of jet-stream winds; and the use of market-based measures, both to
provide positive incentives for the foregoing, but also, through the KP flexible mechanisms to
enable the aviation industry to take advantage of emissions reductions in other areas at lower
cost than they could be achieved internally.
• Monitoring and reporting. This would be a key task to ensure that there was full information
collected on a consistent basis about fuel consumption, passenger/cargo miles flown etc. It
would be essential to have a transparent system so that participants have confidence that they
were operating in an equivalent environment with their competitors.
Although much work has already been done to examine these issues, GIACC agreed to establish
three Working Groups to develop this work in the context of a global strategy and to report back
to the Group as a whole in February 2009.
A degree of urgency had been injected into the process by the Secretariat of the UNFCCC who
explained that ICAO should prepare at least an interim response by mid-2009 if it was to be properly
considered by the 15th Conference of the Parties when it meets in Copenhagen at the end of 2009.
The UNFCCC had also been examining the issues surrounding emissions from international aviation
and shipping and had been considering options that would change the respective responsibilities
of ICAO and the Parties.
In addition, as explained above, in mid-2008 the European Parliament reached an agreement with
the Council of the European Union on the terms of aviation’s inclusion in the European Emissions
Trading Scheme.
At the time of writing, the Council of the EU had not formally agreed to the compromise but
was expected to do so later in the year, with just over three years before the provisions come
into effect.

80
NEXT STEPS
In setting up GIACC, the ICAO States recognised the important and complex interaction with the
UNFCCC process and in particular the need to establish a clear policy for international aviation for
the commitment period from 2013 to 2017, i.e. the successor to the KP. It therefore envisioned two
further meetings of GIACC – one in February 2009, and the other, fourth meeting later in the year.
Council would also need to determine when to hold a high level meeting with respect to the role
it wished to play in Copenhagen.
The Council would also need to prepare for the 37th ICAO Assembly scheduled for late 2010 in
which existing Resolutions would need to be reviewed and, if necessary, new ones agreed upon.
CONCLUSION
ICAO has a clear objective in Article 44(a) of the Chicago Convention to promote aviation. This means
promoting a sustainable industry which can continue to grow to deliver the many economic and
social benefits, that profit developed and developing countries alike. But, this must be consistent
with the third of ICAO’s Strategic Objectives, ie. it must be environmentally responsible.
ICAO has faced challenges on the environment in the past - on noise and on local air quality.
The Council and the Assembly have acted to produce consensus agreements. Climate change is
the biggest challenge yet and it will be essential that ICAO takes decisive action to address this
challenge. Without this action, ICAO will certainly lose its leadership role and the initiative will
pass to others – which will not have the interests of aviation foremost in their minds.
The GIACC has the opportunity to take bold steps, to set credible and demanding targets, to show
the way forward to achieving those targets, and to inject a leadership vision for international
aviation. For the sake of a sustainable future for aviation, the industry must fervently hope that
it succeeds.
REFERENCES
Arguelles, P. et al. (2001). European Aeronautics: A Vision for 2020, Meeting society’s needs and winning global
leadership. [WWW] http://www.acare4europe.com/docs/Vision%202020.pdf (15 July 2008).
Bisignani, G. (2007). Speech to the Annual General Meeting of the Arab Air Carriers’ Organisation. [WWW] http://www.
iata.org/pressroom/speeches/2007-24-10-01 (4 November 2008).
Climate Change Secretariat. (1998). United Nations Framework Convention on Climate Change, The Kyoto Protocol.
Germany. Climate Change Secretariat.
European Commission. (2006). Proposal for a Directive of the European Parliament and of the Council amending
Directive 2003/87/EC so as to include aviation activities in the scheme for greenhouse gas emission allowance trading
within the Community. [WWW] http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=COM:2006:0818:FIN:EN:PDF (4
November 2008).
Towards Sustainable Aviation
81
Journal Aviation Management 2008
ICAO. (1999). Aviation and the Global Atmosphere. Cambridge University Press.
ICAO. (2005). Annex 16 to the Convention on International Civil Aviation, Environmental Protection, Volume I Aircraft
Noise. Montreal.
ICAO. (2007). Assembly Resolutions in Force (as of 28 September 2007), Assembly Resolution A36- 22 Appendix D,
Doc 9902, Part I, p. 60. Montreal.
ICAO. (2007). Assembly Resolutions in Force (as of 28 September 2007), Assembly Resolution A36- 22 Appendix E,
Doc 9902, Part I, p. 61. Montreal.
ICAO. (2007). Assembly Resolutions in Force (as of 28 September 2007), Assembly Resolution A36- 22 Appendix H,
Doc 9902, Part I, p. 65. Montreal.
ICAO. (2007). Assembly Resolutions in Force (as of 28 September 2007), Assembly Resolution A36- 22 Appendix K,
Doc 9902, Part I, p. 68. Montreal.
ICAO. (2007). Assembly Resolutions in Force (as of 28 September 2007), Assembly Resolution A36- 22 Appendix L,
Doc 9902, Part I, p. 72. Montreal.
ICAO. (2008). Annex 16 to the Convention on International Civil Aviation, Environmental Protection, Volume II Aircraft
Engine Emissions. Montreal.
Inter-governmental Panel on Climate Change. (2007). IPCC 4th Assessment Report. [WWW] http://www.ipcc.ch/ (17
November 2007).
UNEP. (1999). United Nations Framework Convention on Climate Change, Convention on Climate Change, Article 10.
Switzerland. UNEP.

82
JOURNAL OF AVIATION MANAGEMENT 2009 CONTRIBUTOR GUIDELINES
The Journal of Aviation Management is an annual publication by the Singapore Aviation Academy,
the training arm of the Civil Aviation Authority of Singapore. It aims to provide an intellectual forum
for the sharing of views and experiences on new developments and topical management issues in
civil aviation amongst leading experts from Singapore and around the world.
It is distributed to a worldwide audience of experts and professionals in the field of civil aviation.
Journal papers are also posted on SAA’s Alumni website under ‘Article of the Month’. We welcome
contributions of papers and feedback from members of the aviation community.
CopyrightAuthors submitting papers for publication should warrant that the work is not an infringement
of any existing copyright (and will indemnify the publisher against any breach of such warranty).
Authors should indicate if their paper has been presented/published elsewhere. If he/she does not
do so, it will be assumed that the paper is an original contribution. Papers published will become
the legal copyright of the published, unless otherwise agreed.
Preparation of PaperLength: Preferred length is between 3,000 and 4,000 words.
Title: Should identify the subject matter as briefly and clearly as possible.
Abstract: Authors are requested to provide an abstract of about 150 words.
Figures and Tables: Should be typed separately from the text, and numbered and captioned
clearly.
Illustrations: Where possible, provide high resolution digital files. High quality black and white and
colour transparencies, slides or prints are also acceptable.
Footnotes: To be used as sparingly as possible. Footnotes should be numbered consecutively
(1,2,3) and appear on the page they are referred to.
ReferencingReferences to other works should be presented according to the APA Referencing Style as
follows:
• Reference to articles
Author (family name/last name followed by initials). Year of Publication in brackets. Title of article.
Name of the publication in which it appears, volume, issue (in brackets), page reference, date
of issue.
Example: Bells, W G. (1993). Guidelines for emergency management in fixed site installations.
Journal of Disaster Prevention and Management, 2, (4), pp. 6-16.
• References to books or preports
Author (surname followed by initials). Year of publication in brackets. Book title, including
subtitle (underlined). Edition (in brackets). Place of publication. Publisher.
Example: Wells, A T. (1996). Airport Planning and Management (3rd edn). New York. McGraw-Hill.
• References to websites or a WWW document
Author (surnamed followed by initials). Year of publication in brackets. Document title
(underlined). Format (WWW). URL including filename extension. Date accessed in brackets.
Example: Lee, J. (1999). Salvador Dali. (WWW)
http://dali.kores.ac.kr/SalvadorDali_biography.html (30 July 2001).
• Please list references chronologically in alphabetical order.
• Where necessary, in-text referencing should be included.
– When quoting, referencing should be reflected in brackets immediately after quote, as
(author’s surname, year, page reference)
Example: (Aust, 200,p75)
– When paraphrasing, referencing should be reflected as author’s surname (year, page
reference).
Example: Aust (2000,p.75) argued that….
Biography and Photograph
Authors are requested to submit a brief biography (50-100 words) outlining their current
title/appointment, qualifications and relevant career highlights, as well as a photograph of
themselves.
Submission of Paper
Authors are requested to submit a printed copy of the paper as well as a softcopy in cd or via
email, preferably in Microsoft Word format. Copy deadline for the 2009 issue is 31 March 2009.
Papers should be submitted to:
The Editor
Journal of Aviation Management
Singapore Aviation Academy
1 Aviation Drive
Singapore 499867
Fax: (65) 6542 9890/ 6543 2778
Email: [email protected]
JOURNAL OF AVIATION MANAGEMENT 2008
An annual publication since 2000, the Journal serves to provide an intellectual forum for sharing of views and experiences on critical issues affecting international civil aviation among leading experts from Singapore and around the world.
I wish to purchase copies of the Journal of Aviation Management at S$36* (inclusive of postage per copy. Please send them to:
Name: _____________________________________________________________________________________________
Designation: _______________________________________________________________________________________
Organisation: _______________________________________________________________________________________
Mailing Address:_____________________________________________________________________________________
___________________________________________________________________________________________________
Postal Code: _______________________________ Country: ________________________________________________
Tel No: ____________________________________________________________________________________________
Email Address: ______________________________________________________________________________________
No. of copies: ______________________________________________________________________________________
Total amount payable: S$ ____________________________________________________________________________
*Alumni members are entitled to a 10% discount.
Payment Details (Please tick where applicable)
Bank draft/ Money Order/ Cheque No.________________________________________________________________
Telegraphic transfer to Citibank, Main Office, Singapore Account No.:0-70203-25
Credit Card: Visa/ Mastercard/ Diners/ Amex Card No.: __________________________________________________
Expiry date: _____________________________________________________________________________________
Payment must be made in S$ to “Civil Aviation Authority of Singapore”. Cash-and-carry purchases are welcomed.
Journals will not be dispatched until payment has been received. Please submit completed Journal Order Forms with
payment to:
The Editor
Journal of Aviation Management
Singapore Aviation Academy
1 Aviation Drive, Singapore 499867
Fax: (65) 6542 9890/ 6543 2778
Orders for the Journal (including past issues) may also be made through the Singapore Aviation Academy website
at http://www.saa.com.sg.











![Download [ 11,06 MB ] - e-Gyanagar](https://img.pdfslide.net/doc/110x75/63201ead08dd9576940849a5/download-1106-mb-e-gyanagar.jpg)






![Download [ 5.27 MB ] - e-Gyanagar](https://img.pdfslide.net/doc/110x75/63352264b9085e0bf50959db/download-527-mb-e-gyanagar.jpg)







![Download [ 12.01 MB ]](https://img.pdfslide.net/doc/110x75/633748f1d63e7c790105b7e8/download-1201-mb-.jpg)
![Download [PDF, 4.32 MB] - ILO](https://img.pdfslide.net/doc/110x75/63125b6515106505030a96fd/download-pdf-432-mb-ilo.jpg)




