Embed Size (px)
Citation preview

DOI: 10.1016/j.athoracsur.2007.03.091 2007;84:2120-2124 Ann Thorac Surg
Michael Stamos Ninh T. Nguyen, Marcelo Hinojosa, Christine Fayad, James Gray, Zuri Murrell and
InterpositionLaparoscopic and Thoracoscopic Ivor Lewis Esophagectomy With Colonic
http://ats.ctsnetjournals.org/cgi/content/full/84/6/2120located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2007 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on May 29, 2013 ats.ctsnetjournals.orgDownloaded from

LENJD
Mapeucs
StcvvtcwmtIohbbm
detSatLpgopwLfm
A
AB
©P
FEAT
UR
EA
RT
ICLES
HOW TO DO IT
aparoscopic and Thoracoscopic Ivor Lewissophagectomy With Colonic Interpositioninh T. Nguyen, MD, FACS, Marcelo Hinojosa, MD, Christine Fayad, BS,
ames Gray, BS, Zuri Murrell, MD, and Michael Stamos, MD
epartment of Surgery, University of California Irvine Medical Center, Orange, Californiagerr
inimally invasive esophagectomy is a feasible and safelternative to open esophagectomy. The stomach is thereferred conduit for gastrointestinal reconstruction aftersophagogastrectomy; however, if the stomach is notsable, the colon can be interposed as an alternativeonduit. We describe the technique of minimally inva-
ive Ivor Lewis esophagogastrectomy in a patient with aT
Aciiceecueal
opermaspc(gauc
AETssagll
ddress correspondence to Dr Nguyen, Department of Surgery, 333 Cityldg West, Suite 850, Orange, CA 92868; e-mail: [email protected].
2007 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
astric cardia cancer involving the gastric body and distalsophagus. Laparoscopic colonic interposition using theight colon based on the middle colic vessels was used toestore gastrointestinal continuity.
(Ann Thorac Surg 2007;84:2120–4)
© 2007 by The Society of Thoracic Surgeonsurgical treatment of the proximal stomach cancer iscomplex. The surgical options for treatment are
ailored according to the proximal and distal extent of theancer. Patients with gastric cardia cancer without in-olvement of the esophagus who have significant in-olvement of the gastric body may be a candidate forotal gastrectomy with Roux-en-Y esophageal-jejunal re-onstruction. Patients with isolated gastric cardia cancerithout involvement of the esophagus or the gastric bodyay be a candidate for an Ivor Lewis esophagogastrec-
omy with the use of a gastric tube for reconstruction [1].f feasible, the stomach is always the preferred conduit tobtain gastrointestinal continuity [2]. In patients whoave gastric cardia cancer with involvement of the gastricody and distal esophagus in which the stomach will note usable for restoring esophageal continuity, the colonay be used as an alternative conduit.Minimally invasive esophagectomy has been intro-
uced at selected institutions. At first, minimally invasivesophagectomy was done by a laparoscopic transhiatalechnique with construction of a cervical anastomosis.ubsequently the laparoscopic and thoracoscopic esoph-gectomy technique with construction of a cervical anas-omosis and the laparoscopic and thoracoscopic Ivorewis esophagogastrectomy were described [1, 3, 4]. Thereferred conduit in these series continues to be theastric tube. Colonic interposition poses a challengingperation, particularly if the esophagogastrectomy iserformed using laparoscopic techniques. In this report,e describe our technique of a minimally invasive Ivorewis esophagogastrectomy with colonic interposition
or the treatment of gastric cardia cancer with involve-ent of the distal esophagus.
ccepted for publication March 26, 2007.
echnique
43-year-old Hispanic male presented with dysphagiaaused by a malignancy extension from the gastric cardianto the esophagus approximately 39 cm from thencisors. The retroflex endoscopic view showed a largeircumferential mass involving the gastric cardia withxtension to the gastric fundus and gastric body. Anndoscopic biopsy showed poorly differentiated adeno-arcinoma. Work-up included an endoscopic esophagealltrasound, which showed a T3N1 lesion at the distalsophagus, and a computed tomography of the chest andbdomen showed a large gastric cardia mass withoutiver metastasis.
The need for an esophagogastrectomy for restorationf swallowing and possible cure was discussed with theatient. Because there is cancer involvement of the distalsophagus, a total gastrectomy with Roux-en-Y jejunaleconstruction will not be able to obtain a clear proximalargin without excessive tension on the reconstructed
nastomosis. We planned a laparoscopic and thoraco-copic Ivor Lewis esophagogastrectomy with colon inter-osition to establish esophageal continuity to ensurelear proximal and distal margins from the carcinomaFig 1). A preoperative colonoscopy and computed tomo-raphic angiogram were performed to evaluate the colonnd patency of the middle colic vessels. The patientnderwent a Nichols bowel preparation with anaerobicoverage the day prior to the operation.
bdominal Phase of Minimally Invasive Ivor Lewissophagogastrectomyhe patient was intubated with a double-lumen tube foringle lung ventilation. The procedure began laparo-copically with the patient in the supine position. Fivebdominal trocars were introduced (Fig 2). The hepato-astric ligament was divided and the left gastric vessels
eading to the gastric pouch were exposed. A celiac
ymphadenectomy was performed en bloc, and the gas-0003-4975/07/$32.00doi:10.1016/j.athoracsur.2007.03.091
by on May 29, 2013 als.org

ttstdtldrwo
lcmvswt
vsactapncbdmetsel
flrTg
F
Fd
2121Ann Thorac Surg HOW TO DO IT NGUYEN ET AL2007;84:2120–4 MINIMALLY INVASIVE IVOR LEWIS ESOPHAGOGASTRECTOMY
FEA
TU
RE
AR
TIC
LES
ric vessels were divided at their origin from the celiacrunk with a linear stapler. The greater curvature of thetomach was mobilized by dividing the gastrocolic omen-um. The mobilization continued toward the gastric fun-us by dividing the short gastric vessels and also toward
he first portion of the duodenum. The right gastroepip-oic vessels were divided and the stomach was dividedistally leaving a small gastric remnant above the pylo-us. An intraoperative frozen section of the distal marginas obtained and was clear of carcinoma. A partialmentectomy was also performed.The right colon was mobilized by dividing the white
ine of Tolt and the hepatic flexure. The entire transverseolon and splenic flexure were also mobilized. The ter-inal ileum was divided 4 cm proximal to the ileocecal
alve. The ileocolic vessels were divided with the lineartapler. The mesentery of the right colon was dividedith bipolar cautery. The blood supply for the right and
ig 1. Laparoscopic esophagogastric cancer with planned level ofistal resection and colonic interposition.
ransverse colon segment was based on the middle colic e
ats.ctsnetjournDownloaded from
essels. The transverse colon was divided proximal to theplenic flexure. The transected terminal ileum was re-nastomosed to the transverse colon proximal to theolonic splenic flexure. An enterotomy was made in bothhe transverse colon and terminal ileum. A side-to-sidenastomosis was performed using a 60-mm linear sta-ler. The remaining enterotomy was closed with a run-ing suture in two layers, and the mesenteric defect waslosed (Fig 3). Esophageal continuity was established firsty construction of a colonic gastric anastomosis. Theistal aspect of the transverse colon conduit was anasto-osed to the residual prepyloric gastric remnant. An
nterotomy was made in both the gastric remnant andhe colonic conduit. A side-to-side anastomosis was con-tructed using a 60-mm linear stapler. The remainingnterotomy was closed with a running suture in twoayers.
The distal esophagus was mobilized circumferentiallyor a segment of 6 cm into the mediastinum. Due to thearge size of the gastric mass, the tumor mass wasemoved transabdominally rather than transthoracically.he esophagus was divided at 4 cm proximal to theastroesophageal junction. The tip of the cecum was
ig 2. Laparoscopic port position for minimally invasive extended
sophagogastrectomy with colonic interposition.by on May 29, 2013 als.org

sccttgpTfcj
TETbrAtTddPaovrid
gc
pwt1tpoeaepiito(lBU
psir
Fc
Fc
2122 HOW TO DO IT NGUYEN ET AL Ann Thorac SurgMINIMALLY INVASIVE IVOR LEWIS ESOPHAGOGASTRECTOMY 2007;84:2120–4
FEAT
UR
EA
RT
ICLES
utured to the esophageal stump in preparation for aolonic pull-up (Fig 4). A Penrose drain was placedircumferentially around the distal esophagus and left inhe mediastinum for retrieval in the chest. The 12-mmrocar incision was extended to 4 cm to accommodate theastric mass. A plastic wound protector was placed torotect the wound from direct contact with the tumor.he large esophagogastric mass was removed and the
ascia layer was closed with interrupted sutures. A needleatheter jejunostomy tube was placed at the proximalejunum.
horacic Phase of Minimally Invasive Ivor Lewissophagogastrectomy With Colonic Interpositionhe patient was then repositioned in a left lateral decu-itus position. Under single-lung ventilation, four tho-acic trocars were introduced in the right thoracic cavity.
wound protector was placed at one of the thoracicrocars in preparation for introducing the circular stapler.he inferior pulmonary ligament was divided. The me-iastinal pleura overlying the distal esophagus wereivided until the Penrose drain was visualized. Theenrose drain around the distal esophagus was identifiednd used for esophageal retraction during mobilizationf the thoracic esophagus up to the level of the azygousein. The remaining distal esophagus and the attachedight colon were pulled through the esophageal hiatusnto the right chest. The esophagus was divided imme-
ig 3. Laparoscopic mobilization of right and transverse colon withonstruction of an ileocolic anastomosis.
iately below the level of the azygous vein. The esopha- c
ats.ctsnetjournDownloaded from
eal surgical specimen was separated from the coloniconduit and removed through the 2.5-cm trocar site.
A 25-mm anvil was inserted transthoracically andlaced into the esophageal stump. The anvil was securedith a pursestring suture. An enterotomy was created at
he terminal ileum. The ileocecal valve was dilated with a0-mm instrument. A 25-mm circular stapler was placedransthoracically through the 2.5-cm trocar incision andositioned through the terminal ileum into the side wallf the cecum in preparation for construction of thesophagocolonic anastomosis. The anvil from the esoph-geal stump was connected to the circular stapler and ansophagocolonic anastomosis was performed. The sta-led anastomosis was reinforced with a second layer of
nterrupted Lembert sutures. A nasogastric tube wasnserted into the colonic conduit. The enterotomy at theerminal ileum was closed with a linear stapler andversewn with a second layer of running Lembert sutureFig 5). An appendectomy was also performed using theinear staplers. A 28-French chest tube and a 10-Frenchlake drain (Johnson & Johnson Gateway, Livingston,K) were inserted for postoperative drainage.The operative time was 4 hours for the laparoscopic
ortion of the procedure and 2 hours for the thoraco-copic portion. The estimate blood loss was 100 mL. Nontraoperative or postoperative blood transfusion wasequired. Grossly, the esophagus has adenocarcinoma
ig 4. Laparoscopic construction of the gastrocolic anastomosis. Theecum is attached to the esophageal stump in preparation of thoracic
olonic pull-up.by on May 29, 2013 als.org
itcao
tacospswp
fgowcpa
C
WstcuctF
t
Fctmrc
Fca
2123Ann Thorac Surg HOW TO DO IT NGUYEN ET AL2007;84:2120–4 MINIMALLY INVASIVE IVOR LEWIS ESOPHAGOGASTRECTOMY
FEA
TU
RE
AR
TIC
LES
nvolvement to 3 cm above the gastroesophageal junc-ion. Histologic findings confirmed poorly differentiatedarcinoma with esophageal involvement. The proximalnd distal margins were negative for carcinoma. Sixteenf 18 lymph nodes had cancer involvement.
ig 6. Postoperative upper gastrointestinal contrast study showing
ig 5. Schematic diagram of the extended esophagogastrectomy witholonic interposition. There are three anastomoses: (1) ileocolic anas-omosis, (2) gastrocolic anastomosis, and (3) esophagocolic anasto-osis. An appendectomy was performed in the right chest. Inset rep-
esents construction of the esophagocolic anastomosis using aircular stapler.
uhe colonic interposition in the right chest cavity.
ats.ctsnetjournDownloaded from
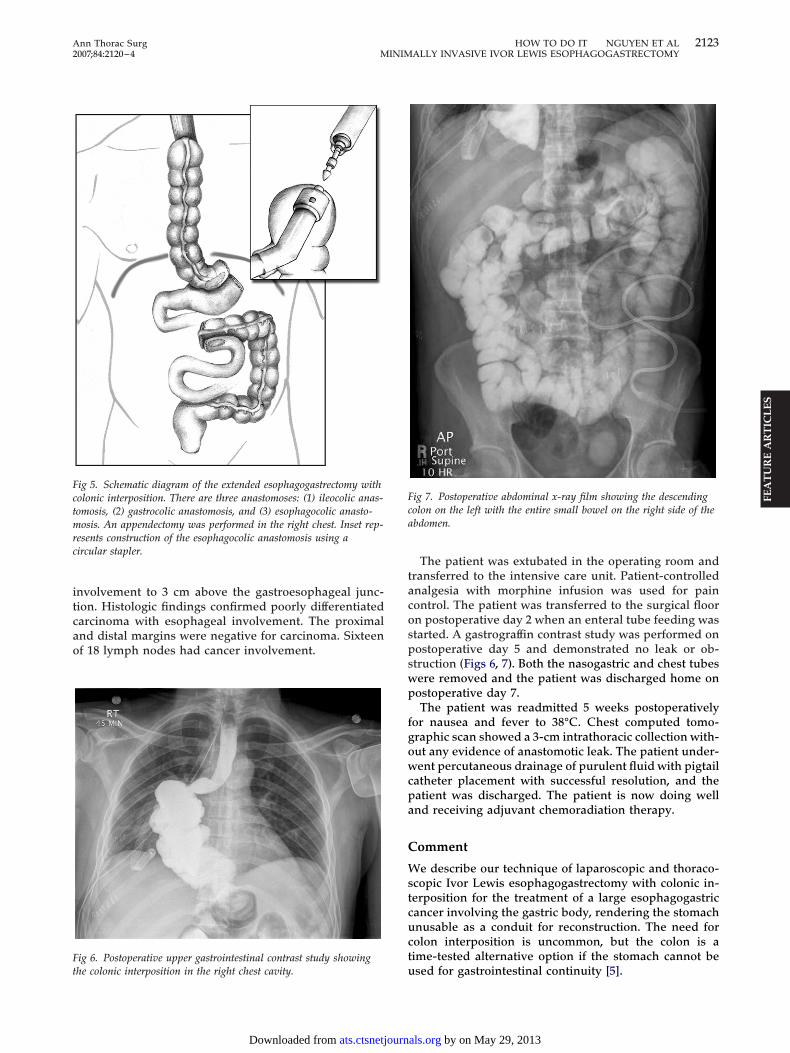
The patient was extubated in the operating room andransferred to the intensive care unit. Patient-controllednalgesia with morphine infusion was used for painontrol. The patient was transferred to the surgical floorn postoperative day 2 when an enteral tube feeding wastarted. A gastrograffin contrast study was performed onostoperative day 5 and demonstrated no leak or ob-truction (Figs 6, 7). Both the nasogastric and chest tubesere removed and the patient was discharged home onostoperative day 7.The patient was readmitted 5 weeks postoperatively
or nausea and fever to 38°C. Chest computed tomo-raphic scan showed a 3-cm intrathoracic collection with-ut any evidence of anastomotic leak. The patient under-ent percutaneous drainage of purulent fluid with pigtail
atheter placement with successful resolution, and theatient was discharged. The patient is now doing wellnd receiving adjuvant chemoradiation therapy.
omment
e describe our technique of laparoscopic and thoraco-copic Ivor Lewis esophagogastrectomy with colonic in-erposition for the treatment of a large esophagogastricancer involving the gastric body, rendering the stomachnusable as a conduit for reconstruction. The need forolon interposition is uncommon, but the colon is aime-tested alternative option if the stomach cannot be
ig 7. Postoperative abdominal x-ray film showing the descendingolon on the left with the entire small bowel on the right side of thebdomen.
sed for gastrointestinal continuity [5].
by on May 29, 2013 als.org

ctgdmsrirwcBedempaiodeicrdpfcdbmtbtcaa
erc
gseccnmcv
R
1
2
3
4
5
6
7
8
9
2124 HOW TO DO IT NGUYEN ET AL Ann Thorac SurgMINIMALLY INVASIVE IVOR LEWIS ESOPHAGOGASTRECTOMY 2007;84:2120–4
FEAT
UR
EA
RT
ICLES
Some of the advantages of a colonic interpositionompared with gastric pull-up are the lack of regurgita-ion and reflux esophagitis [6]. However, an esophago-astrectomy with colonic interposition is a technicallyemanding operation and can be associated with higherorbidity and mortality compared with the use of the
tomach as the conduit [7, 8]. Isolauri and colleagues [8]eported one of the largest experiences with open colonicnterposition with 248 patients in whom the mortalityate was 16% and the incidence of colon graft necrosisas 3%. We believe there has been no previous report of
olonic interposition performed by using a laparoscopy.uilding on our experience with minimally invasivesophagectomy and laparoscopic colon resection, weevised our technique of minimally invasive Ivor Lewissophagogastrectomy with colonic interposition. Mini-ally invasive esophagogastrectomy with colonic inter-
osition may reduce the morbidity and mortality associ-ted with this complex operation. In our patient, thenitial approach was the use of laparoscopy for evaluationf the gastric cardia cancer, particularly the proximal andistal extent of the cancer. Endoscopy was also intraop-ratively performed to localize the site of the tumor andts extension. Once we determined that the stomachould not be used as a conduit for reconstruction, a wideesection of the stomach was performed to obtain goodistal margins. In our case, the decision to keep theylorus was based on the fact that there is a lower risk
or anastomotic disruption with construction of a gastro-olic anastomosis compared with construction of a duo-enal-colic anastomosis. The right colon was chosen toe the conduit with the vascular supply based on theiddle colic vessels. One of the disadvantages of using
he right colon as the conduit is the size discrepancyetween the esophagus and cecum; however, an advan-
age of using the right colon is the long length of theonduit and dependable blood supply [8, 9]. A postoper-tive intrathoracic abscess that likely resulted from spill-
ge of colon contents during construction of theats.ctsnetjournDownloaded from
sophago-colic anastomosis developed in this patient. Inetrospect, copious antibiotic irrigation of the thoracicavity may have prevented this complication.
In summary, minimally invasive Ivor Lewis esophago-astrectomy with colonic interposition is technically fea-ible and safe. In this report we describe the technique ofxtended esophagogastrectomy with gastrointestinal re-onstruction using the right colon based on the middleolic vessels. This minimally invasive procedure is tech-ically demanding, requiring extensive experience ininimally invasive esophageal surgery and laparoscopic
olon surgery that can be obtained at centers with a higholume of esophageal and colon operations.
eferences
. Nguyen NT, Follette DM, Lemoine PH, et al. Minimallyinvasive Ivor Lewis esophagectomy. Ann Thorac Surg 2001;72:593–6.
. Cense HA, Visser MR, van Sandick JW, et al. Quality of lifeafter colon interposition by necessity for esophageal cancerreplacement. J Surg Oncol 2004;88:32–8.
. Luketich JD, Alvelo-Rivera M, Buenaventura PO, et al. Min-imally invasive esophagectomy: outcomes in 222 patients.Ann Thorac Surg 2003;238:486–95.
. Nguyen NT, Roberts P, Follette DM, et al. Thoracoscopic andlaparoscopic esophagectomy for benign and malignant dis-ease: lessons learned from 46 consecutive procedures. J AmColl Surg 2003;197:902–13.
. Renzulli P, Joeris A, Strobel O, et al. Colon interposition foresophageal replacement: a single-center experience. Langen-becks Arch Surg 2004;389:128–33.
. Yildirim S, Koksal H, Celayir F, et al. Colonic interposition vs.gastric pull-up after total esophagectomy. J Gastrointest Surg2004;8:675–8.
. Cerfolio RJ, Allen MS, Deschamps C, et al. Esophagealreplacement by colon interposition. Ann Thorac Surg 1995;59:1382–4.
. Isolauri J, Markkula H, Autio V. Colon interposition in thetreatment of carcinoma of the esophagus and gastric cardia.Ann Thorac Surg 1987;43:420–4.
. Furst H, Hartl WH, Lohe F, et al. Colon interposition foresophageal replacement: an alternative technique based on
the use of the right colon. Ann Surg 2000;231:173–8.by on May 29, 2013 als.org

DOI: 10.1016/j.athoracsur.2007.03.091 2007;84:2120-2124 Ann Thorac Surg
Michael Stamos Ninh T. Nguyen, Marcelo Hinojosa, Christine Fayad, James Gray, Zuri Murrell and
InterpositionLaparoscopic and Thoracoscopic Ivor Lewis Esophagectomy With Colonic
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/84/6/2120including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/84/6/2120#BIBL
This article cites 9 articles, 3 of which you can access for free at:
Subspecialty Collections
http://ats.ctsnetjournals.org/cgi/collection/esophagus_cancer Esophagus - cancer
following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on May 29, 2013 ats.ctsnetjournals.orgDownloaded from






















