Embed Size (px)
Citation preview

MFUa
fuA
Pca
Lesser Metatarsal Phalangeal Joint Arthroscopy: AnatomicDescription and Comparative Dissection
Caio Nery, M.D., Michael J. Coughlin, M.D., Daniel Baumfeld, M.D.,Fernando C. Raduan, M.D., Fernanda Catena, M.D., Benjamim Dutra Macedo, M.D., and
Marco Antonio Percope de Andrade, M.D.
Purpose: The aim of this article is to describe the normal arthroscopic anatomy of the lesser metatarsophalangeal (MTP)joints and compare it with that seen in open dissection in cadaveric models. Methods: We performed arthroscopic ex-amination of 18 MTP joints of 6 normal fresh frozen feet. The second, third, and fourth MTP joints were studied because ofthe higher incidence of pathologic conditions found in these joints. During arthroscopy, each anatomic structure identifiedwas named and marked with different colored sutures using straight suture needles. After the arthroscopic procedure ofidentification and marking, each MTP joint was dissected, and all the anatomic structures were grossly identified. Withthese data, the correlation between the arthroscopic and the direct visualization of a normal MTP joint was established.Results: Considering the joint regions, we found that the examination accuracy of the medial gutter was 91%, whereasthe central joint accuracy reached 100% and the accuracy of the lateral gutter was 98%. The overall arthroscopic accuracyfor the lesser MTP joints was 96%. Conclusions: There is a high level of anatomic accuracy at the lesser MTP joint witharthroscopy. Clinical Relevance: The high overall level of anatomic accuracy of lesser MTP joint arthroscopy (96%)allows us to consider this resource as a valuable tool in the diagnosis and treatment of these joints, expanding the spectrumof indications using this method.
ith the improvement of technology and the
Wavailability of delicate instruments, arthroscopyfor small joints has become a promising tool, showing asignificant increase in its indications for minimal inva-sive surgery in the search for decreased surgicalcomplications.1,2Recently, several articles have presented experienceswith small joint arthroscopy of the foot, but its use isstill relatively limited.1,3 The majority of the techniquesused have been adapted from the experience with otherjoints, such as the ankle and subtalar and first meta-tarsophalangeal (MTP) joints.1
From UNIFESP-Federal University of São Paulo, Escola Paulista deedicina (C.N., F.C.R., F.C.), Escola Paulista de Medicina, São Paulo SP;elicio Rocho Hospital (D.B., B.D.M.), Belo Horizonte MG; and Federalniversity of Minas Gerais-UFMG (M.A.P.d.A.), Belo Horizonte MG, Brazil;nd St. Alphonsus Foot and Ankle Clinic (M.J.C.), Boise, Idaho, U.S.A.The authors report the following potential conflict of interest or source ofnding in relation to this article: C.N. and M.J.C. receive support fromrthrex.Received August 27, 2013; accepted March 20, 2014.Address correspondence to Caio Nery, M.D., Federal University of Sãoaulo, Escola Paulista de Medicina, 30380530, São Paulo SP, Brazil. E-mail:[email protected]� 2014 by the Arthroscopy Association of North America0749-8063/13622/$36.00http://dx.doi.org/10.1016/j.arthro.2014.03.018
Arthroscopy: The Journal of Arthroscopic and Related
First used by Watanabe4 in 1972 as a diagnostic tool,arthroscopy for the first MTP joint was implemented forthe treatment of cartilage lesions. Jaivin and Ferkel5
reported only a 4% rate of hallucal surgery when ac-counting for all foot and ankle procedures performedarthroscopically. In 1996, Maresca et al.6 reported thearthroscopic treatment of a patient with a secondmetatarsal Freiberg infraction. Hayashi et al.,7 in 2002,performed the same treatment for a bilateral Freiberginfraction of the second MTP joint. Later, in 2004, Carroet al.8 reported good results after the arthroscopicexcision of the second toe proximal phalangeal base forthe treatment of a final-stage case of Freiberg disease.Lui et al.,9,10 in 2007, reported an arthroscopicallyassisted technique for correction of the claw toedeformity associated with proximal plantar platetenodesis; good results with no major complicationswere reported.Although there has been a growing interest in these
procedures, to our knowledge until now there havebeen no publications regarding the normal arthroscopicanatomy of the lesser MTP joints, and there have beenno studies comparing arthroscopic versus open ap-proaches to these joints. Most reports detail the suc-cessful treatment of an osteochondral defect or thearthroscopically assisted part of a new technique
Surgery, Vol -, No - (Month), 2014: pp 1-9 1

Fig 1. (A) Positioning of the surgical team. (B) Surgeon isfacing the dorsum of the foot and both medial and lateraldorsal portals are in use to begin the process.
2 C. NERY ET AL.
without offering details on the methods of the proce-dure itself.6,8-11
The aim of this article is to describe the normal anat-omy of the lesser MTP joints identified by arthroscopyand compare it with that seen with open dissection incadaveric models. Our hypothesis is that there is a highcorrelation between arthroscopic visualization andidentification of anatomic structures and anatomic dis-section of the lesser toes.
MethodsWe performed arthroscopic examination of 18 MTP
joints in 6 normal fresh frozen feet. The second, third,and fourth MTP joints were studied because of thehigher incidence of pathologic conditions found inthese joints in clinical practice.12,13 Specimens with anytoe deformity or scars suggesting previous surgery ortrauma were excluded from the study.To standardize our arthroscopic findings, the exam-
iner was positioned facing the dorsal aspect of the footwith the specimen’s toes pointing up and the heellaying down on the surgical table surfacedthe sameposition suggested for performing an arthroscopic pro-cedure on the first MTP joint in a live patient. Thearthroscopic rack with the video screen and all theother electronic equipment and arthroscopic accessories
were positioned at the caudal extremity of the surgicaltable (Fig 1). Stabilization of the foot by an assistant wasnecessary to minimize motion of the cadaveric foot andto apply light manual traction on the tip of the toestudied, simulating regular surgical conditions.Two dorsal arthroscopic portals were used to access
the lesser MTP joints (the dorsal-medial and dorsal-lateral portals). Both of these portals were placed at orslightly distal to the MTP articular joint line, equidistant(4 to 5 mm) medially and laterally from the extensordigitorum longus tendon (Fig 2). Care must be takenwhen preparing the medial portal of the second MTPjoint because the dorsal digital branch of the deepperoneal nerve runs in the first intermetatarsal spacevery close to the medial border of the joint. For thisreason, the lateral portal was established first.With an 18-gauge needle, the adequate penetration
point was marked and 2 to 3 mL of saline solution wasinjected into the joint to confirm the proper placement.A No. 11 scalpel blade was used to incise the skin only,and a mosquito clamp was used to enter the joint,preventing injury to the neurovascular structures. Theclamp jaws were then opened to widen the approach inthe capsule. The ‘‘nick and spread’’ technique was usedto enter the capsule from both portals.A pump system was used to provide adequate intra-
articular saline flow and joint distention. Care mustbe taken to use the minimum effective pressure toachieve the desired surgical conditions. Because theliterature does not suggest parameters for the MTPjoints, we assumed the small joint arthroscopy levels of35 mm Hg and 100% flow rate as the initial marks inour study. Pressure and flow levels may be adjustedduring the procedure to ensure good visibility of theanatomic structures.Because of the small size of the lesser MTP joints,
small instruments are mandatory. We used a 2.7-mm30� arthroscope and light manual traction applied tothe toe to distract the joint space. A lightweight camerais preferred as well as small light cords. The light sourceis the same as for standard arthroscopic procedures. Asmall joint shaver system with 2.0-mm full-radiusblades is very important, as is a set of small surgicalinstruments such as probes, baskets, graspers, and cu-rettes. We consider it very important to also use anarthroscopic radiofrequency system and its miniwands
Fig 2. Arthroscopicportals to the second,third, and fourth metatarsophalangeal(MTP) joints.

Table 1. Suggested Equipment for Lesser MTP JointArthroscopy
TourniquetSterile toe trapShort 2.7 or 1.9 mm 30� arthroscopeSterile lightweight video cameraSmall joint shaving systemSmall joint probeNo. 2.0 full-radius shaving bladeNo. 2.0 basketNo. 2.0 buretteMinieradiofrequency wandsArthroscopic pump system
LESSER METATARSAL PHALANGEAL JOINT ARTHROSCOPY 3
to deal with hypertrophic synovial tissue, joint capsule,CLs, and the plantar plate itself (Table 1).With this arrangement, all intra-articular regions
could be visualized, inspected, and palpated. During thearthroscopic procedure, each anatomic structure iden-tified was named and marked with a different coloredsuture using straight suture needles (Fig 3). The correctidentification and marking was double-checked bychanging the arthroscope to the lateral portal andrepeating the articular inventory. Once this procedurewas finished, each foot was dissected through a dorsal
Fig 3. Arthroscopic identification of the anatomic structures ofneedles are being used to mark the structures with different-colorplantar plate. (B) The needle is pointing to the lateral insertion ofneedle is passing through the lateral portion of the plantar plate. (the plantar plate. (E) The salmon suture is passing through the lateto produce wide vision of the joint. (F) The needle is pointing to ththrough the medial collateral ligament (CL) while the orange suturThe same as in G, with the arthroscope positioned to produce wpointing to the medial wall of the MTP joint. (J) The salmon suturblue suture is passed through the medial CL, and the brown sutu(ACL).
incision, carefully removing the dorsal skin. The sub-cutaneous tissue and surrounding soft tissue wereremoved down to the level of the MTP joint, and at thispoint we could visualize the colored sutures at thedorsal part of the foot. We were careful to preserveintact the extensor tendons, the CLs, the plantar plate,and the capsule. At this moment, all anatomic struc-tures traversed by a colored suture were identified andthe relation of the suture color/structure name wasrecorded. After that, a dorsal capsular release was per-formed to expose the joint. With this exposure, wedissected all the structures with intra-articular andextra-articular visualization. The structures with intra-articular appearance were the metatarsal head, thearticular portion of the proximal phalanx, the lateraland medial accessory collateral ligaments (ACLs), thelateral and medial proper CLs, the medial and lateralbundles of the plantar plate, and the insertions on theproximal phalanx that form a central recess, which wasalso identified. At this point, the involved MTP jointwas inspected and the anatomic location of the coloredsutures was recorded (Fig 4). The relation of all extra-articular anatomic structures to the MTP joint was as-sessed, but this information was not used in the present
the second right metatarsophalangeal (MTP) joint. Note thated sutures. (A) The needle is pointing to the lateral half of thethe plantar plate at the base of the proximal phalanx. (C) TheD) The salmon suture is passing through the lateral portion ofral portion of the plantar plate; the arthroscope was positionede medial half of the plantar plate. (G) The blue suture is passinge is passed through the medial portion of the plantar plate. (H)ide vision of the medial gutter of the joint. (I) The needle ise is passed through the medial portion of the plantar plate, there is passed through the medial accessory collateral ligament
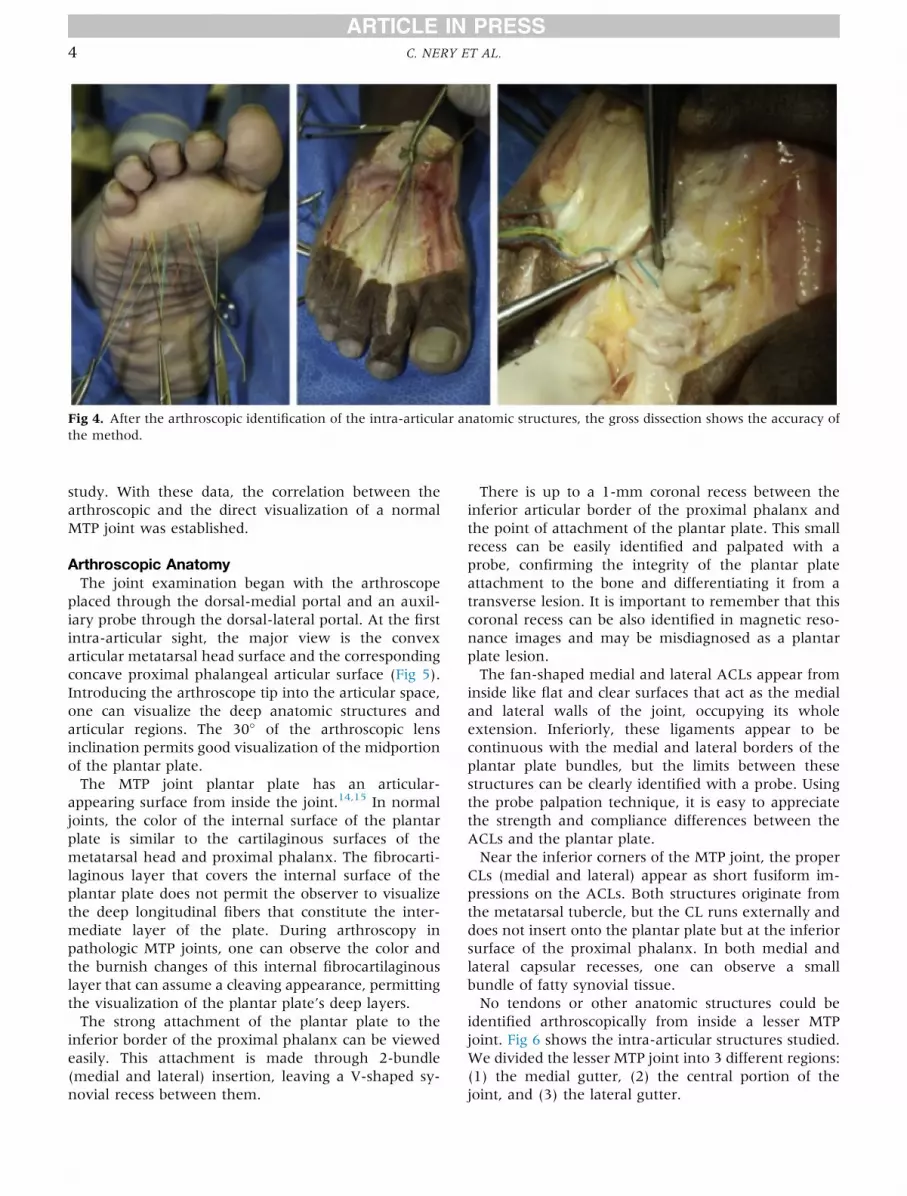
Fig 4. After the arthroscopic identification of the intra-articular anatomic structures, the gross dissection shows the accuracy ofthe method.
4 C. NERY ET AL.
study. With these data, the correlation between thearthroscopic and the direct visualization of a normalMTP joint was established.
Arthroscopic AnatomyThe joint examination began with the arthroscope
placed through the dorsal-medial portal and an auxil-iary probe through the dorsal-lateral portal. At the firstintra-articular sight, the major view is the convexarticular metatarsal head surface and the correspondingconcave proximal phalangeal articular surface (Fig 5).Introducing the arthroscope tip into the articular space,one can visualize the deep anatomic structures andarticular regions. The 30� of the arthroscopic lensinclination permits good visualization of the midportionof the plantar plate.The MTP joint plantar plate has an articular-
appearing surface from inside the joint.14,15 In normaljoints, the color of the internal surface of the plantarplate is similar to the cartilaginous surfaces of themetatarsal head and proximal phalanx. The fibrocarti-laginous layer that covers the internal surface of theplantar plate does not permit the observer to visualizethe deep longitudinal fibers that constitute the inter-mediate layer of the plate. During arthroscopy inpathologic MTP joints, one can observe the color andthe burnish changes of this internal fibrocartilaginouslayer that can assume a cleaving appearance, permittingthe visualization of the plantar plate’s deep layers.The strong attachment of the plantar plate to the
inferior border of the proximal phalanx can be viewedeasily. This attachment is made through 2-bundle(medial and lateral) insertion, leaving a V-shaped sy-novial recess between them.
There is up to a 1-mm coronal recess between theinferior articular border of the proximal phalanx andthe point of attachment of the plantar plate. This smallrecess can be easily identified and palpated with aprobe, confirming the integrity of the plantar plateattachment to the bone and differentiating it from atransverse lesion. It is important to remember that thiscoronal recess can be also identified in magnetic reso-nance images and may be misdiagnosed as a plantarplate lesion.The fan-shaped medial and lateral ACLs appear from
inside like flat and clear surfaces that act as the medialand lateral walls of the joint, occupying its wholeextension. Inferiorly, these ligaments appear to becontinuous with the medial and lateral borders of theplantar plate bundles, but the limits between thesestructures can be clearly identified with a probe. Usingthe probe palpation technique, it is easy to appreciatethe strength and compliance differences between theACLs and the plantar plate.Near the inferior corners of the MTP joint, the proper
CLs (medial and lateral) appear as short fusiform im-pressions on the ACLs. Both structures originate fromthe metatarsal tubercle, but the CL runs externally anddoes not insert onto the plantar plate but at the inferiorsurface of the proximal phalanx. In both medial andlateral capsular recesses, one can observe a smallbundle of fatty synovial tissue.No tendons or other anatomic structures could be
identified arthroscopically from inside a lesser MTPjoint. Fig 6 shows the intra-articular structures studied.We divided the lesser MTP joint into 3 different regions:(1) the medial gutter, (2) the central portion of thejoint, and (3) the lateral gutter.

Fig 5. Arthroscopic images of a normalright second metatarsophalangeal(MTP) joint. (A) View from the dorsal-lateral portal: inferior border of theproximal phalanx (1), MTP plantarplate (2), and metatarsal (MT) head (3).(B) View from the dorsal-lateral portal:lateral border of the MT head (3),accessory collateral ligament (ACL) (4),the lateral wall of the joint. (C) Viewfrom the dorsal-medial portal: inferiorcorner of the proximal phalanx (1), MThead (3), and ACL (4)dthe medial wallof the joint. (D) View from the dorsal-medial portal: proximal phalanx (1),MTP plantar plate (2), MT head (3), andproper CL impression (5). (E) Viewfrom the dorsal-lateral portal: proximalphalanx (1), MTP plantar plate (2), MThead (3), and central synovial recess(6). (F) View from the dorsal-lateralportal: proximal phalanx (1), lateralbundle of the plantar plate inserting atthe phalanx (2), and MT head (3).
Fig 6. Gross anatomy of a lesser metatarsophalangeal (MTP) joint: (1) proper collateral ligament; (2) accessory collateral liga-ment; (3) plantar plate; (4) fibrous flexor tendons sheath; (5) plantar fascia insertion to the plantar plate; (6) flexor tendons; (7)dorsal interossei tendon; (8) plantar interossei tendon; (9) lumbrical tendon; and (10) deep transversal intermetatarsal ligament.
LESSER METATARSAL PHALANGEAL JOINT ARTHROSCOPY 5

6 C. NERY ET AL.
In the medial gutter, we identified 5 anatomic struc-tures: the medial dome of the metatarsal head, theinferior medial corner of the proximal phalanx, themedial ACL, the proper medial CL, and the medialportion of the plantar plate. In the central portion of thejoint, we identified another 5 anatomic references: thecentral dome of the metatarsal head, the concavity ofthe proximal phalanx articular surface and its inferiorborder, the strong insertions of each half of the plantarplate at the base of the proximal phalanx (medial andlateral bundles), and a central synovial V-shapedrecess between them. In the lateral gutter, the samecorresponding medial anatomic structures were iden-tified: the lateral dome of the metatarsal head, theinferior lateral corner of the proximal phalanx, thelateral ACL, the proper lateral CL, and the lateralportion of the plantar plate.
Gross AnatomyThere is a fibrocartilage rectangular structure known
as the plantar plate, which acts as the firm and flexiblefloor and the most important and effective stabilizer ofthe lesser MTP joint. The portion that lies just beneaththe metatarsal head is broader and thicker than theother parts, but the central aspect is thinner than theborders. The length of the plantar plate ranges from 16to 23 mm, with an average of 19 mm, and the widthranges from 8 to 13 mm, with an average of 11 mmproximally and 9 mm distally16 (Fig 7).Its composition and anatomic relation correlate with
weight bearing and tension attenuating functions. Thestrongest insertion of the plantar plate is at the base ofthe proximal phalanx where the fibrous tissue of the
plate inserts into the bone through its 2 bundles thatderive directly from the 2 major bands of the plantarfascia. Between these 2 bundles, a synovial recess canbe found and cannot be misinterpreted as a lesion. Theproximal plantar plate insertion attaches to the plantaraspect of the metatarsal neck with a loose and fragilesynovial appearance and does not participate in thestabilization of the joint.From the medial and lateral metatarsal tubercles to
the plantar prominences of the proximal phalanx runsthe proper MTP CLs. These ligaments have little or noinsertions onto the plantar plate, but they can cause animpression on the most distal and plantar aspect of theMTP ACLs.As do the CLs, the MTP ACLs originate from the
metatarsal tubercle and insert directly onto the medialand lateral borders of the plantar plate. These fan-shaped ligaments are substantial structures that act asmain stabilizers of the plantar plates. The medial CLsand ACLs seem to be thinner and weaker than those onthe lateral side.17
The plantar plate also has connections on each sidewith the deep transverse intermetatarsal ligament(DTIL) and gives an insertion on the plantar side tothe fibrous flexor tendon sheath, the 2 longitudinalsepta of the plantar aponeurosis, the transverse headof the adductor halluces muscle, and vertical fibersextending to the superficial component of the plantaraponeurosis.18
The tendon of the lumbrical muscle runs plantar andmedial to the plantar plate just beneath the DTIL. Theinterossei tendons are dorsal to the DTIL and runadjacent to the plantar plate; the plantar interossei is
Fig 7. Stabilizers of the lesser MTPjoints include the proper collateral lig-ament (CL), accessory collateral liga-ment (ACL), plantar plate, fibrousflexor tendons sheath, plantar fasciainsertion to the plantar plate, flexortendons, dorsal interossei tendon,plantar interossei tendon, lumbricaltendon, and deep transversal inter-metatarsal ligament.

Table 2. Individual and Total Accuracy for the Anatomic Structures of Each MTP Joint and Its Regions
Articular Region/Anatomic Structure
Second MTP Joint Third MTP Joint Fourth MTP Joint Total
Proportion Accuracy Proportion Accuracy Proportion Accuracy Proportion Accuracy
Medial gutterMedial accessory collateral ligament 4 of 6 67% 6 of 6 100% 6 of 6 100% 16 of 18 89%Medial proper collateral ligament 5 of 6 83% 4 of 6 67% 6 of 6 100% 15 of 18 83%Medial plantar plate bundle 6 of 6 100% 6 of 6 100% 6 of 6 100% 18 of 18 100%
Accuracy medial gutter 15 of 18 83% 16 of 18 89% 18 of 18 100% 49 of 54 91%Central joint
Medial bundle of the plantar plate 6 of 6 100% 6 of 6 100% 6 of 6 100% 18 of 18 100%Lateral bundle of the plantar plate 6 of 6 100% 6 of 6 100% 6 of 6 100% 18 of 18 100%Central synovial recess 6 of 6 100% 6 of 6 100% 6 of 6 100% 18 of 18 100%
Accuracy central joint 18 of 18 100% 18 of 18 100% 18 of 18 100% 54 of 54 100%Lateral gutter
Lateral accessory collateral ligament 6 of 6 100% 6 of 6 100% 6 of 6 100% 18 of 18 100%Lateral proper collateral ligament 5 of 6 83% 6 of 6 100% 6 of 6 100% 17 of 18 94%Lateral plantar plate bundle 6 of 6 100% 6 of 6 100% 6 of 6 100% 18 of 18 100%
Accuracy lateral gutter 17 of 18 94% 18 of 18 100% 18 of 18 100% 53 of 54 98%Accuracy in all 3 articular regions 50 of 54 93% 52 of 54 96% 54 of 54 100% 156 of 162 96%
NOTE. Proportion refers to the number of true positive anatomic structure identifications in relation to the total of true positives þ falsepositives þ false negatives þ true negative identifications.MTP, metatarsophalangeal.
LESSER METATARSAL PHALANGEAL JOINT ARTHROSCOPY 7
medially located, whereas the dorsal interossei islaterally situated. All these tendons have subtle in-sertions onto the plantar plate through their course.The lateral plantar ligament is a small fibrous band
that originates on the lateral distal portion of theplantar plate that inserts onto a plantar phalangeal tu-bercle. The exact function of this structure remainsunclear.
Statistical AnalysisVariables analyzed in this study were summarized
according to the groups for descriptive statistics. Weused the accuracy assessment as a binomial test basedon the number of agreements (“true,” “success”) ordisagreement (“false,” “failure”) in this series.
ResultsDuring the systematic arthroscopic evaluation of the
18 lesser MTP cadaveric joints, as described previously,we attempted to identify the anatomic structuresmentioned. Each MTP joint was then dissected toestablish the correlation between the arthroscopic andgross anatomy.Table 2 shows the results of the correlation between
the arthroscopic and dissected specimens in the second,third, and fourth MTP joints in all the intra-articularregions, as well as the calculations of accuracy of themethod.At the second MTP joint, we found 67% accuracy for
the identification of the medial ACL and 83% accuracyfor the identification of the medial proper CL as well asthe lateral proper CL. For the second MTP joint, wefound 83% accuracy on identification of the structuresat the medial gutter, 100% accuracy at the central joint,and 94% accuracy at the lateral gutter. Considering
the second MTP joint, the accuracy for arthroscopicidentification of the anatomic intra-articular structureswas 93%.For the third MTP joint, the only problem was iden-
tifying the medial proper CL in 2 specimens (No. 1 andNo. 5), with 67% accuracy for this individual structure.For all other articular regions and anatomic structuresanalyzed we were 100% accurate. The accuracy for thisjoint was 89% in the medial gutter and 100% in thecentral joint and in the lateral gutter. Considering thethird MTP joint as a whole, the arthroscopic accuracywas 96%.We achieved 100% of accuracy in our sample for the
fourth MTP joint for all joint regions and all anatomicstructures studied.Considering the joint regions, we found that the ex-
amination accuracy of the medial gutter was 91%,whereas the central joint accuracy reached 100% andthe lateral gutter accuracy was 98%. The overallarthroscopic accuracy for the lesser MTP joints was 96%.Analyzing the lesser MTP intra-articular anatomic
structures, the most difficult to identify arthroscopicallyare the proper CLs (medial and lateral).
DiscussionUnderstanding the anatomy is important when
considering arthroscopic intervention. Recently, signif-icant progress has been made in the field of endoscopicfoot surgery, but small joint arthroscopy reports arelimited in the literature, and the techniques are stillbeing refined in comparison to those for the first MTPjoint.1,19
Regardless of the pathologic process, the surgeon musthave a firm understanding of the proper anatomic con-siderations, indications for use, predictable outcomes,

Fig 8. Arthroscopic images of right second metatarsophalangeal (MTP) joint in a patient with an osteochondral lesion of themetatarsal head. (A) The medial gutter of the joint was occupied by inflamed synovial tissue, where the round border of a freebody was easily seen. (B) Moving the arthroscope lightly backward, 2 cartilaginous free bodies were identified. (C) After the freebodies were removed, the lateral border of an osteochondral lesion of the metatarsal head was detected. (D) After debridement ofthe detached cartilaginous tissue, the osteochondral lesion can be inspected and measured. (E) A small set of ice pick instrumentswas used to produce microfractures at the bottom of the lesion. (F) While microfracturing the subchondral bone, little marrow fatdroplets could be seen floating inside the joint, indicating that the instrument reached adequate bone depth.
Fig 9. Arthroscopic images of lessermetatarsophalangeal (MTP) joints withplantar plate lesions (arrows). (A)Grade 1 lesion; (B) grade 2 lesion. (FDL,flexor digitorum longus; MT head,metatarsal head; Prox Pha, base of theproximal phalanx.)
8 C. NERY ET AL.

LESSER METATARSAL PHALANGEAL JOINT ARTHROSCOPY 9
and potential complications when deciding to proceedwith arthroscopic management of small joints. As weknow, arthroscopic techniques present less bleeding,infection rates, and scarring and allow faster rehabilita-tion and return to activities of daily living.2,3,20-22
Until now there have been only a few reports aboutlesser MTP joint arthroscopy, and most do not addressthe normal arthroscopic anatomy of these joints. Asshown by other authors,1,8,10 osteochondral defects ofthe lesser metatarsal head, resection of loose bodies,and synovectomy in patients with rheumatoid arthritiscan be adequately performed with this method (Fig 8).In recent publications, lesser toe arthroscopy was usedas a diagnostic method to confirm clinical assessmentand to plan the operative treatment for plantar platetears (Fig 9), but description of normal anatomy wasstill not reported.23-25
In our study, we show the efficacy of arthroscopy forthe lesser toes, with a direct and high correlation be-tween arthroscopic and anatomic dissection of thesejoints. The overall accuracy was 92% for the secondMTP joint, 96% for the third MTP joint, and 100% forthe fourth MTP joint. We believe that the second MTPjoint had the lowest accuracy because distraction in thisjoint is more difficult than in the others. This occursbecause of a normal long second metatarsal and a lessmobile metatarsal cuneiform joint.Although the gross anatomy of the forefoot and MTP
joints is complex, the arthroscopic anatomy of thesejoints is quite simple, with a few anatomic structuresrecognized during the endoscopic procedure. Becauseof this simplicity, we found very impressive levels ofaccuracy in all joint regions even in the smallest joints.
LimitationsAlthough we show a high level of accuracy between
arthroscopic and anatomic dissection of lesser MTPjoints, the limitations of our study are the small numberof joints analyzed.
ConclusionsThere is a high level of anatomic accuracy at the lesser
MTP joint arthroscopy.
References1. Derner R, Naldo J. Small joint arthroscopy of the foot. Clin
Podiatr Med Surg 2011;28:551-560.2. Myerson MS, Quill G. Ankle arthrodesis. A comparison of
an arthroscopic and an open method of treatment. ClinOrthop Relat Res 1991:84-95.
3. van Dijk CN, Veenstra KM, Nuesch BC. Arthroscopicsurgery of the metatarsophalangeal first joint. Arthroscopy1998;14:851-855.
4. Watanabe M. [Development of arthroscope] [Article inJapanese]. Ryumachi 1977;17:371-372.
5. Jaivin JS, Ferkel RD. Arthroscopy of the foot and ankle.Clin Sports Med 1994;13:761-783.
6. Maresca G, Adriani E, Falez F, Mariani PP. Arthroscopictreatment of bilateral Freiberg’s infraction. Arthroscopy1996;12:103-108.
7. Hayashi K, Ochi M, Uchio Y, Takao M, Kawasaki K,Yamagami N. A new surgical technique for treatingbilateral Freiberg disease. Arthroscopy 2002;18:660-664.
8. Carro LP, Golano P, Farinas O, Cerezal L, Abad J.Arthroscopic Keller technique for Freiberg disease.Arthroscopy 2004;20(suppl 2):60-63.
9. Lui TH. Arthroscopic-assisted correction of claw toe oroverriding toe deformity: Plantar plate tenodesis. ArchOrthop Trauma Surg 2007;127:823-826.
10. Lui TH. Arthroscopy and endoscopy of the foot and ankle:Indications for new techniques. Arthroscopy 2007;23:889-902.
11. Lui TH, Chan LK, Chan KB. Modified plantar platetenodesis for correction of claw toe deformity. Foot AnkleInt 2010;31:584-591.
12. Coughlin MJ. Lesser toe abnormalities. Instr Course Lect2003;52:421-444.
13. Smith BW, Coughlin MJ. Disorders of the lesser toes.Sports Med Arthrosc 2009;17:167-174.
14. Deland JT, Lee KT, Sobel M, DiCarlo EF. Anatomy of theplantar plate and its attachments in the lesser metatarsalphalangeal joint. Foot Ankle Int 1995;16:480-486.
15. Deland JT, Sung IH. The medial crosssover toe: A cadav-eric dissection. Foot Ankle Int 2000;21:375-378.
16. Johnston RB, Smith J, Daniels T. The plantar plate of thelesser toes: an anatomical study in human cadavers. FootAnkle Int 1994;15:276-282.
17. Suero EM, Meyers KN, Bohne WH. Stability of the met-atarsophalangeal joint of the lesser toes: A cadavericstudy. J Orthop Res 2012;30:1995-1998.
18. Armen K. Sarrafian’s anatomy of the foot and ankle: descrip-tive, topographic, functional, Ed 3. Philadelphia: LippincottWilliams & Wilkins, 2011.
19. Carreira DS. Arthroscopy of the hallux. Foot Ankle Clin2009;14:105-114.
20. Debnath UK, Hemmady MV, Hariharan K. Indications forand technique of first metatarsophalangeal joint arthros-copy. Foot Ankle Int 2006;27:1049-1054.
21. Shonka TE. Metatarsal phalangeal joint arthroscopy.J Foot Surg 1991;30:26-28.
22. Morgan CD, Casscells CD. Arthroscopic-assisted gleno-humeral arthrodesis. Arthroscopy 1992;8:262-266.
23. Coughlin MJ, Baumfeld DS, Nery C. Second MTP jointinstability: Grading of the deformity and description ofsurgical repair of capsular insufficiency. Phys Sportsmed2011;39:132-141.
24. Nery C, Coughlin MJ, Baumfeld D, Mann TS. Lessermetatarsophalangeal joint instability: Prospective evalua-tion and repair of plantar plate and capsular insufficiency.Foot Ankle Int 2012;33:301-311.
25. Nery C, Coughlin MJ, Baumfeld D, Mann TS, Yamada AF,Fernandes EA. MRI evaluation of the MTP plantar platescompared with arthroscopic findings: A prospective study.Foot Ankle Int 2013;34:315-322.





























