Embed Size (px)
Citation preview

Long-term prognosis of bipolar I disorder
Turvey CL, Coryell WH, Solomon DA, Leon AC, Endicott J , Keller MR, Akiskal H. Long-term prognosis o f bipolar I disorder. Acta Psychiatr Scand 1999: 99: 1 10-1 19. ( Munksgaard 1999.
This study exaniincd the contribution of demographic. syndi-omal and longitudinal course variables t o the long-term prognosis of I65 bipolar patients prospectively observed over 10 years as part of the National Institute of Mental Health Collaborative Study o f Depression. Although most baseline clinical and demographic variables were not strong prognostic indicators, switching polarity within episodes was. Most episodes among the poor-prognosis patients were polyphasic, while most episodes among the comparison group with a better prognosis were monophasic. There was no evidence of shortening of cycle lengths over follow-up for either the poor- prognosis group o r the entire sample. The relevance of these findings to the ‘kindling’ model is discussed.
Introduction
The long-term course of bipolar disorder is difficult to predict, and can range from a course with few symptomatic periods to one with many episodes and marked disability (l), even among patients who are in treatment (2-12). Prior studies have found surprisingly few associations between prognosis and demographic variables such as age, sex and marital status (4, 7). In the absence of significant demographic and clinical predictors, investigators have turned to short-term course variables as possible indicators of long-term prognosis.
Perhaps the most widely investigated of these have been cycle length and frequency. Rapid cycling, the occurrence of four cycles within a 1- year period (13), has received considerable atten- tion because it is assumed by some to represent an end-stage form of bipolar illness. Post (14, 15) proposed that rapid cycling results from the gradual shortening of cycle lengths. According to Post’s theory, affective symptoms both within and between episodes are thought to have a ‘kindling’ or ‘sensitization’ effect with progressively lower thresholds for new episodes.
Studies investigating kindling must demonstrate that rapid cycling results from a gradual increase in the frequency of episodes, and that it is not simply characteristic of a subgroup of bipolar I patients who have a more severe condition and thereby have more frequent episodes. It is also possible that bipolar I patients characteristically display a
C. L.Turvey’, W. H. Coryel12, D. A. Solomon3, A. C. Leon4, J. Endicott5, M. B. Kelle?, H. Akiska16 ‘Department of Psychiatry and ’College of Medicine, Uriiversity of Iowa. luwa City. IA. ’School of Medicine, Brown University, Providence, RI, 4New York Hospital - Cornell Medical Center. N e w Yolk C~ty, NY, “New York State Psychiatric lristitutc. N e w York City, NY arid “College of Medicine, University of California -. San Diego, San Diego, CA USA
Key words bipolar disorder, mood disorders, prognosis. loiigitudirial stirdies
Carolyn L lurvey, Department of Psychiatry, University of Iowa. Psychiatry Research-MFB, Iowa City, IA 57742~1000, USA
Accepted for publication September 15, 1998
deteriorating course, yet this may not necessarily be due to sensitization. Several studies have described a shortening of cycle lengths over the course of the illness (16-22), but these studies have a number of methodological limitations.
Support for the kindling model is based on either retrospective or a combination of retrospective and prospective reports ( 16-22). Retrospective studies are subject to recall bias, which may contribute to thc apparent acceleration of episode frequency. Patients can often recall more recent episodes better than more distant ones, and this could give the overall impression of dccreasing interval length. For example, Angst et al. (21) report a shortening of cycle lengths in their sample, yet they also propose that there is a ‘self-limitation’ to the number of episodes, because the mean number of episodes was the same for patients undcr observa- tion for 40 years as for those under observation for 15 years. A limit on the total number of episodes, in and of itself, is inconsistent with the sensitization model, although it is possible that limitations in people’s ability to remember episodes underlie this finding.
Most studies cited as supportive of the kindling model have compared sequential interval lengths, not cycle lengths (17-20). This, however, does not adequately address the question of whether cycle lengths, which include both the duration of an episode and the following interval, shorten over
110

Long-term prognosis of bipolar 1 disorder
time. Studies investigating interval length cannot test for an increase in the frequency of switching within the same affective episode - the type of episode most often associated with rapid cycling.
In addition, longitudinal studies that compare change in interval lengths most often use group medians (1 7-20). This type of analysis is biased because patients who have longer cycle lengths will necessarily have fewer completed cycles within the observation period, and these cycle lengths will not be included in analyses comparing all completed cycles. A more appropriate analysis would examine whether each individual subject cxpericnced a shortening of cycle length, and would then test whether a significantly larger proportion of the sample showed a trend towards decreasing cyclc lengths.
In a reccnt study by Kcssing et al. (22), the rate of recurrence of successive episodes was examined in a unique case-register study using 20350 first- admission affectivc disorder paticnts. Aware o f thc potential for selection bias, these authors carefully analysed the data for the entire sample and then according to the total number of episodes observed during follow-up. They found evidence for both selection bias and a gradual deterioration in course. Patients with more episodes had a higher risk of recurrence from the first episode, yet there was also evidence that the risk of recurrence increased over the follow-up period. Since recurrence was based on documented hospital admissions, there is no potential for recall bias. However, the authors acknowledge that by limiting their definition of recurrence to hospitalization, they are eliminating episodes that were not severe enough to warrant admission. Moreover, if the patients were in fact hospitaliLed for every single episode, this may bias the sample towards more severe bipolar I patients, who may be more likely to show a deteriorating course.
Not all bipolar I patients show a deteriorating course. Roy-Byrne et al. (19) reported that 48% of a sample of bipolar patients treated at the National Institute of Mental Health (NIMH) have a random pattern to their episodes. Pretreatment era studies, such as the work of Lundquist (23), Bratfos & Haug (24) and Rennie (25 ) , also report a random or highly variable pattern to sequential interval lengths. Although Kraepelin is often cited in support of sensitization, his data is not entirely consistent with this model. He reports a decrease in interval, not cycle length. Moreover, he bases his comparisons on group medians and excludes cycle lengths of patients with infrequent episodes that occur outside the observation period. Kraepelin also discusses at length the unpredictability of episodes in bi'polar disorder, citing several case
examples that contradict his earlier conclusion about a pattern of decreasing interval lengths.
Two longitudinal studies show that the frequency of cycles does not appear to accelerate consistently over time. An analysis of data from thc Collabora- tive Depression Study round that only 25% of the original group of rapid cyclers continued to meet the frcquency criteria for rapid cycling in any one of follow-up years 2 to 5 (26). Similarly, Mai el al. (27) reported that only 18.9% of a sample o f 37 rapid cyclers continued to have four episodes ;i year throughout the 5-year follow-up period.
Howcvcr, several studies have documented that switching, rcgardless ot its frequency, is a sign of poor prognosis. Keller et al. (28) found that patients who switched polarity within one period of illness relapsed sooner after recovery than did those who had had monophasic episodes. Roy- Byrne et al. (19) and Maj ct al. (27) also reported associations between switching and higher relapse rates. Thcse findings suggest that polyphasic episodes are a common clinical presentation o f poor prognosis in bipolar I disorder.
This paper examines the contribution of demo- graphic, syndromal and longitudinal course vari- ablcs to the long-term prognosis of 165 bipolar 1 patients prospectively observed over I 0 years a s part of the NIMH Collaborative Study of Depres- sion. I t will first examine the association between demographic and baseline variables and long-term course. In addition, the association between prog- nosis and clinical factors found to be relevant in previous studies will be examined, such as the presence or absence of delusional symptoms, presence or absence of alcohol and drug abuse, and treatment intensity. It will then examine whether sequential cycle lengths decrease in duration over the course of follow-up. We propose that switching or polyphasic episodes will be associated with a poor prognosis, yet there will be no evidence of a shortening of cycle lengths over time.
Material and methods
Earlier reports describe the methods used in the National Institute of Mental Health Collaborative Program on the Psychobiology of Depression - Clinical Studies (29, 30) . Those methods that ark most relevant to the present analyses are as follows.
Patients with Research Diagnostic Criteria (RDC) (31) major deprcssivc disorder, bipolar or schizoaffective disorder were recruited at each of five tertiary care centres (Massachusetts General Hospital and Harvard Medical School in Boston, Rush-Presbyterian-St Luke's Medical Center in
111

Turvey et al.
Chicago, University of Iowa College of Medicine in Iowa City, New York State Psychiatric Institute and Columbia university in New York City, and Washington University School of Medicine in St Louis). Raters who were trained to a high level of reliability used the Schedule for Affective Dis- orders and Schi~ophrenia (SADS) (32) and RDC criteria to assign study diagnoses. Diagnoses were updated at years 5 and 10 based on follow-up information and medical records. Written informed consent was obtained from all participants.
The following analyses are limited to patients with a 10-year follow-up diagnosis of RDC bipolar I disorder or with schizoaffective mania, mainly affective type. Those with a full 10 years of follow- up ( n = 165) represent 71 % of the original sample of 231 bipolar I patients.
Raters interviewed the probands every 6 months for the first 5 years of follow-up and yearly for follow-up years 6 to 10. The Longitudinal Interview Follow-Up Evaluation (LIFE) and the Longitudi- nal Interview Follow-Up Evaluation-Version 11 (33) was used to assess the course of affective and comorbid syndromes. For each week of follow-up, raters quantified the symptom levels for each syndrome on a scale from 1 (no symptomatology) to 6 (severe symptomatology). Study participants were asked to recall the affective symptomatology that had occurred during the time period which had elapsed since the most recent interview. The weekly ratings are thus based on participants recall of affective symptoms for the 6 months prior to each follow-up interview in the first 5 years of the study, and for the entirc year before each follow-up interview for the last 5 years of the study. Interviewers also based these ratings on medical records. Comorbid syndromes such as alcohol dependence, drug abuse and delusional symptoms were also rated weekly on a scale of 1 to 3, where 3 indicated threshold symptomatology. The assess- ment of concurrent delusional symptoms did not begin until t he third year of follow-up.
Participation in the NIMH Collaborative Depression Study did not determine or influence treatment. However, the quality and quantity of treatment were systematically monitored as described elsewhere (34). The intensities of soma- totherapy, including ECT, were translated into scores on a 4-point scale to reflect the amount of treatment received in each week of follow-up. Treatment in this study was quantified as the total number of weeks in somatic treatment and the mean level of treatment, with larger numbers indicating higher levels of somatic therapy.
Psychosocial functioning was ascertained from 150 of the 165 subjects at the year 10 follow-up visit. Patients rated their overall level of satisfaction in
the month prior to the interview, and interviewers assessed the patients' global social adjustment using a scale ranging from 1 (very good) to 5 (very poor). The interviews also assessed the patients' functioning using the Global Assessment Scale (GAS) (35).
Baseline variables included age at onset, defined as the age at which the patient first fulfilled the criteria for major depressive disorder, mania or schizoaffectivc-manic disorder. The duration of illness was calculated by subtracting age of onset from age at intake. Raters used the Hollingshead and Rcdlich Scale (36) to assess socio-economic status and the Family History RDC (FH-RDC) (29) to assess family history. Two-thirds of the probands (n = 13 1 ) also participated in a family study in which raters who were blind to the proband diagnosis used the SADS-I, t o interview all consenting, adult first-degree relatives.
Definition of course variables
Affective episodes were defined according to RDC criteria based on weekly LIFE affective ratings. Recovery from an affective episode required 8 consecutive weeks with no more than one or two symptoms to no more than a mild degree. A new episode required full RDC symptom criteria and a duration of 1 week for mania and 2 weeks for depression.
All prospectively observed affective episodes in years 1 to 7 were charactcriyed as either mono- phasic, biphasic or polyphasic. Monophasic epi- sodes were exclusively manic or depressive, with no switching between polcs or mixed symptoms. Biphasic episodes consisted of one manic or hypomanic phase and one depressive phase, although not necessarily in that order. A polyphasic episode included at least two switches in polarity, although there were often more than two. Phases required the same duration as episodes, i.e. 1 week for mania or hypomania and 2 weeks for depres- sion. Mixed phases were relatively rare and mainly occurred in the context of a polyphasic episode. Each instance of a mixed phase was classified as a single polyphasic episode.
Cycle length is typically defined as the time period from the onset of one affective episode to the onset of the following episode. Unfortunately, studies vary in their definition of episodes, and some studies have failed to providc an exact definition. In previous papers, the Collaborative Study has defined episodes consistent with the RDC definition, which does not consider a switch- ing to the opposite affective pole as the onset of a
112

Long-term prognosis of bipolar I disorder
new episode. However, this switching is of parti- cular interest when examining rapid cycling.
DSM-IV (37) defines rapid cycling as 'at least four episodes of a mood disturbance in the previous 12 months ... . Episodes are demarcated by partial or full remission for at least 2 months or a switch to an episode of the opposite polarity' (p.391). In order to maintain consistency with prcvious Collaborative Study papers and the RDC, the definition of cpisodcs in this papcr will not include switching between affective poles. However, the definition of cycle length as the time between the onset of one episode and the onset of the next episode will be based on the DSM-IV demarcation of episodes provided above. This is in ordcr to capture switching between affective poles that occurs within an affective episode. However, it should be notcd that thc RDC definition of episodes, not the DSM-IV definition, is used in all of the analyses except those concerning cycle length.
Morbidity index
The prognosis was determined using a morbidity index originally described by Abou-Saleh & Coppen (38) for affective syndromes for follow- up years 8 to 10. Weekly affective ratings of 3 or above the syndromal level were summed for year 8, year 9 and year 10. For example, if a subject had a 7-week episode in one year, with 4 of the 7 weeks rated as 5 , and 3 of the 7 weeks rated as 3, his or her morbidity index for that year would be 29.
The poor-prognosis group consisted of those subjects in the highest quartile of the morbidity index for each of ycars 8, 9 and 10. Thus the poor- prognosis group not only had significant periods of affective dysfunction during the outcome period, but also had substantial dit'liculties in each of the three consecutive years. The remaining subjects who did not meet this criterion represented the comparison group. Therefore, the comparison group consisted of individuals who were quite well functioning as well as those who had more significant morbidity, yet not as much as that in the poor-prognosis group.
Data analysis
Differences between the poor-prognosis group and the comparison group on continuous variables assessed in follow-up years 1 to 7 were tested using the Wilcoxon rank-sum test with a Chi-square approximation. A logistic regression analysis was used to determine whether the association between phase charact6ristics of affective episodes and
prognosis could be attributed to other clinical variables shown to have prognostic importance in
the univariate analyses. In this model, prognostic grouping was the outcome variable. The number of polyphasic episodes, as wcll as the duration of illness, presence or absence of delusions, and presence or absencc of drug abuse were included as explanatory variables.
The trends with regard to changes in cycle length over the first 7 years of follow-up were examined by deriving a slope estimate from a linear regression model of sequential cycle lengths for each indivi- dual subject. An increase in cycle length over time would yield a positive slope, whereas shortening of cyclc lengths would yield a negative slope. A onc- sample Wilcoxon signed-rank statistic tested whether the slopes for the entire sample differed from Lero. A two-sample, Wilcoxon rank-sum statistic tested whether the poor-prognosis group was more likely than the comparison group to have decreasing cycle lengths. In total, 53 subjects ( 5 subjects from the poor prognosis group and 48 subjects from thc comparison group) did not have the two prospectively observed cycle lengths required to calculate a slope, and were therefore excluded from these analyses. Thcsc subjccts h a d fewer than two complete cycles over the course of the 7-year follow-up, so they could not show an increasing risk of recurrence. Spearman rank correlations were used to demonstrate associations between phase characteristics of episodes and psychosocial outcome variables. In order to adjust for multiple comparisons, the P-value threshold was set at P<O.Ol. All tests t'or significance were two-tailed.
Results
The poor-prognosis group
A total of 27 patients met the criteria for poor prognosis. Three of these patients had a 10-year RDC diagnosis of schizoaffective mania (mainly affective subtype), and the remaining subjects in both the poor-prognosis group and the comparison group had an RDC diagnosis of bipolar I disorder. Two of the 27 poor-prognosis patients had a period of remission during years 8, 9 and 10. However, 25 patients were in an affective episode for the entire years.
Of the 27 poor-prognosis patients, 16 subjects ( 5 9 % ) cycled between affective poles for the last 3 years of follow-up, yet only one fulfilled the criteria for rapid cycling. Three patients (11%) were in chronic manic monophasic episodes, and thrcc patients (1 1 %) were in chronic monophasic depressive episodes. The remaining five patients
113

Turvey et al.
Table 1 Cornparison between prognostic groups on demographic and baseline variables
Mean value (SD)
Comparison group
In= 138)
Poor-prognosis group
(n=27)
Wilcoxond
Xi ( d f = l ) P-value Variable
Age at intake (years)
Age of onset (years)
Duration of illness (years)
YQ Male
Socio-economic status
Family history positive for affective disorder'
Family history positive for mania'
35 I l l )
25 (101
10 (101
40% (49)
3 ( 1 ) 33% (17)
38 ( I l l
22 181
15 (81
31% 149)
4 (1)
31% (16)
169
169
10 03
0 01
1 1 9
0 21
a 1 9
0 19
0 002 0 18
0 27 0 65
6% (1 1 ) 4% (8) 0 53 0 47
" Statistic and Pvalue derived from Wilcoxon rank-sum test using a Chi-square approximation " 1 1 1 patients (80%) in the good-prognosis group and 22 patients (81%) in the poor-prognosis group consented to have family inembers interviewed for the farriily study Family
tiistory was modelled using the percentage of first-degree relatives affected
wcrc in cithcr chronic manic or depressive phases of polyphasic episodes that began before year 8.
prognosis group is not attributable to differences in
lcvel=3.23 (SD =0.83) vs. comparison group mean level = 3.1 1 (SD = 0.74); Wilcoxon x2 = 0.69, df = 1,
The grcatcr affective morbidity in the poor- P=0.44). - - treatment -intensity, since the two groups did not diffcr either in the total number of weeks in somatic Variables associated with poor prognosis
treatment in years 8 to 10 (poor prognosis Neither demographic variables nor family history mean = 132 weeks (SD =49) vs. comparison group were associated with prognostic grouping (Table 1). mean=112 weeks (SD=65); Wilcoxon x7=0.47, Females were not more likely to be in the poor- df = 1, P=0.49) or in the mean level of treatment prognosis group. The poor-outcome group and the for the weeks in treatment (poor-prognosis mean comparison group had similar ages at onset, but the
Table 2 Comparison between prognostic groups on course descriptors (n= 1651 ~ - -
Mean value (SO)
Comparisori
group ( / l = 138)
Poor-prognosis
group (n=27)
Wilcoxon '
XI
( d f = l ) Variable year 1-7 Pvalue
Cycles Number of cycles Cycle length
Weeks
Episodes Number of episodes Duration of episodes (weeks) Number of weeks manic Number of weeks depressed
4 1 (5 2) 131 (136)
7 6 (6 7) 66 (90)
8 10 6 96
0 004 0 008
5 (2) 28 (50) 32 (50) 47 (65)
3 (2) 83 (50) 80 (84)
191 (110)
8 80 31 3 10 14 33 26
0 003 0 0001 0 002 0 0001
Phase characteristics of episodesb Number of monophasic episodes Number of biphasic episodes Number of polyphasic episodes
68% (35) 8% (18)
24% (32)
38% (41) 4% (20)
58% (42)
6 48 186
18 19
0 01 0 17 0 0001
" Statistic and P-value derived from Wilcoxon rank-sum test using a Chi~square approximation ' Many patients did not have biphasic or polyphasic episodes, often making the mean number of monophasic, biphasic or polyphasic episodes less than 1 0 and difficult to
interpret For clarity, the mean values presented here are based on the proportion of the total number of episodes that were monophasic, biphasic or polyphasic However, in order to preserve the statistical independence of the three Wilcoxon rank-sum tests, the statistical analysis did not use the proportion of episodes. but simply the total number of each type of episode
114

Long-term prognosis of bipolar I disorder
Table 3 Coinparison between prognostic groups on clinical variables (n= 1651
Mean (SD)
Variable year 1 - I
Comparison Poor prognosis Wilcoxon’ group
(n- 138) x’
( d f = l l Pvalue
Concurrent syndromes Alcohol deperidence 1 % ) 15 77 Drug abuse 1 % ) 3 1 1 Delusions (%I 31 63
1 reatment Number of weeks on anti manic medication 238 (1351 288 11041 Meail intensity lpvel of 30310511 3 00 in 701
anti manic rncdicatioii
Number of weeks on all medication 259 (124) 272 1118) Mean intensity l rve l of 3 00 (0 581 7 88 (0 71)
dl l medication
0 80 3 72 9 81
0 27 1 4 1
0 22 0 007
0 37 0 054 o no2
0 60 0 22
0 64 0 93
’ Statistic and Pvalue derived from Wilcoxon rank-sum tcst using a Chi-square approxiination ‘’ Assessment of concurrent delusional symptoms did not begin uritil the second year of follow~uo
former group had significantly longer illness dura- tion at intake.
In contrast to demographic and baseline vari- ables, course variables were strong predictors of outcome (Table 2). Monophasic episodes were associated with lower subsequent morbidity, whereas polyphasic episodes were much more characteristic of the poor-prognosis group. Number of cycles and cycle length were associated with prognostic grouping. The comparison group actually had more episodes on average, but they were of significantly shorter duration. The poor- prognosis group had a higher total number of manic weeks and total number of depressed weeks. On average, the poor-prognosis group was depresscd for more than half of the 7-year follow-up.
Of the concurrent syndromes, presence of delusional symptoms was associated with poor prognosis (Table 3 ) . Presence of alcohol depen- dencc did not differ between thc two groups, but there was a trend for those in the poor-prognosis group to have abused drugs. The poor-prognosis patients did not have fewer weeks in treatment or less intensive treatment overall in follow-up years 1 to 7.
Cycle lengths
Over the 7-year follow-up period, there was no indication of a shortening of cycle length with each successive cycle in the sample of patients with at least two prospectively observed cycles (n = 1 12). In total, 54%0 of the sample showed an increase in cycle length and 46% showed a decrease in cycle
length. On average, the cycle lengths increased rather than dccrcased over the follow-up, with a mean increase of 8 weeks for each successive cycle (SD=S2) (Wilcoxon signed-rank tcst, P = O . l O ) . In total, 45% of the poor-prognosis group showed an increase in cycle length and 55% showed a decreasc. Likewise, the poor-prognosis group was no more likely than the comparison group to have a decreasing cycle length (Wilcoxon x2 = 0.04, df = 1 ,
It is possible that patients’ cycle lengths may have shortened before intake into the study. However, even patients who were in their first episode at intake (n = 17) showed a trend towards an increase rather than a decrease in cycle length, with a median increase of 7 weeks (SD=51.97; Wilcoxon signed-rank test, P= 0.15).
P=0.84).
Phase characteristics of episodes
Of the total sample, 33% had monophasic episodes exclusively, whereas 13% of the sample had polyphasic episodes exclusively. The remaining 54% had a heterogeneous course. The duration of phases in polyphasic episodes was actually
\ longer for the poor-prognosis group than for the comparison group (median phase length for poor- prognosis groups = 22 weeks (SD = 12.4) vs. com- parison group = 13 weeks (SD = 14); Wilcoxon x2=7.03, df= I , P=O.OI). Therefore, poor prog- nosis was characterized by extended polyphasic episodes rather than rapid cycling.
A multivariate analysis was performed to deter- mine whether the association between number of
115

Turvey et a].
Table 4 Spearman rank correlations between phase characteristics and measures of psychosocial functioning collected at year 10
Self-rated satisfaction in= 150)"
Interviewer's assessment of
patient's functioning (n= 152)''
Global Assessment
Scale in- 152f
Number of monophasic episodes Number of biphasic episodes Number of polyphasic episodes
0 005
0 77""" -0 07
-0 05 -0 10
0 30"""
-0 01 0 009 -0 21"""
* * P < O O l ~ * * * P < 0 0 0 1 Hated on a scale from 1 to 5 with higher numbers indicating poorer furictiunirig Hated on a scale from 0 to 100 with higher numbers indicating better functioning
polyphasic episodes and poor outcome remained after controlling for duration of illness and the two concomitant syndromes that were associated with poor prognosis, namely delusional symptoms and drug abuse. Number of polyphasic episodes was associated with prognostic grouping (x'= 6.6, df = 1, P=O.Ol) at a borderline level of significance. Presence of delusions (x2 = 9.6, df = 1, P = 0.002) and duration of illness in years (x2=6.9, d f = l , P = 0.009) predicted prognostic grouping, while the presence or absence of drug abuse did not (x2=3.8, d f = l , P=0.051).
Three ratings of psychosocial outcome were collected in year 10 of follow-up. The poor- prognosis group had lower scores on measures of satisfaction (x' = 21.47, df = 4, P = 0.001), overall functioning (x' = 41, df = 4, P = 0.004) and the GAS (Wilcoxon x2 = 35.8, df = 1, P < 0.0001). The median GAS rating for the poor-prognosis group was 40, indicating 'major impairment in several areas.' The comparison group's median rating was 70, indicat- ing 'some mild symptoms but generally functioning pretty well.' The phase characteristics of affective episodes predicted psychosocial outcomc much as they predicted the direct measures of morbidity (Table 4).
Stability of clinical presentation
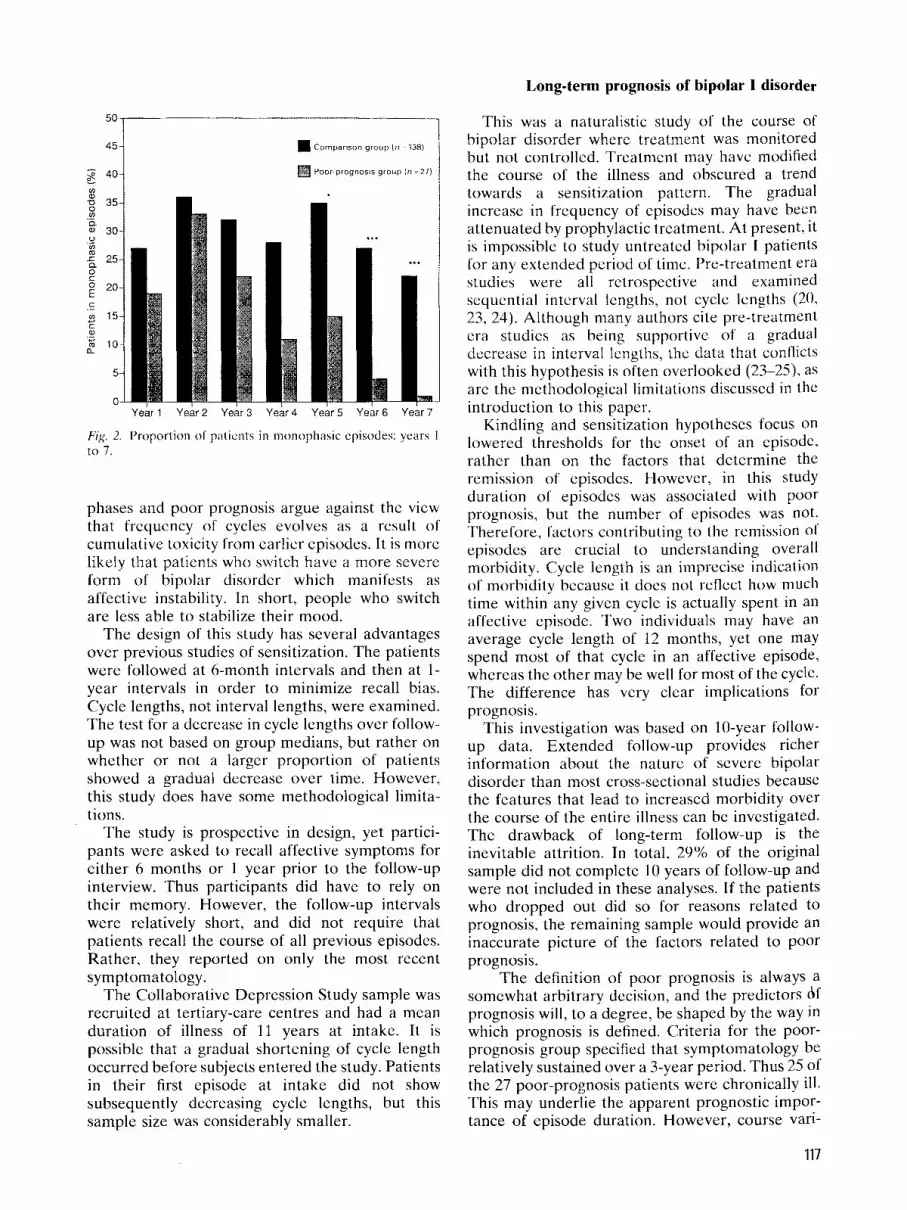
Patients in the poor-prognosis group were more likely to be in a polyphasic episode in each year of follow-up (Fig. 1). Similarly, a higher percen- tage of patients in the comparison group had monophasic episodes in each year of foollow-up, although this difference only reached the level of statistical significance in years 5 to 7 (Fig. 2). Some patients may have had both a polyphasic and a monophasic episode within the same calendar year, and were thus represented in both the monophasic and polyphasic episode estimates for that year. Since the episodes in the first year of follow-up often started before entry to the study, the phase characteristics of these
episodes could not be determined. Thcrefore, the percentage of patients in either monophasic or polyphasic episodes for year 1 underestimates the total number of subjects in affective episodes for that year.
Discussion
Consistent with earlier investigations of bipolar disorder, baseline and demographic variables had little bearing on long-term prognosis, whereas course indicators did. Longer episodes and a greater propensity to switching bctwccn poles both reflect impairment in affective regulation and may have a common genesis. Switching can be viewed as a failed attempt to stabilize mood in that the regulatory mechanism repeatedly over- shoots its mark when approaching euthymia. By comparison, monophasic episodes indicate a greater potential for restabilization. The lack of evidence for a clear progressive cycle length shortening and the association between longer
70
60 I
50- -0 v)
Q ._
.- 40- v)
r Q
-$ 30- Q C
w . _
; 20- ._ I
m a
10-
0-
.. .*.
Year 1 Year2 Year3 Year4 Year5 Year6 Year7
Fig I . Proportion of patients in polyphasic episodes: years I to 7.
116
Long-term prognosis of bipolar I disorder
50
45
40 !A
% 35 ._ 9 Q
U !A
a 30
25
.-
0 C ; 20 C .- !A 15
z l o
4- C W
5
.-
C
C
Fig. to 7.
Comparison group In 138)
Poor progi7osis group In 27)
Year1 Year2 Year3 Year4 Year5 Year6 Year7
I'roporlion o f patients in nionoptiasiic episodes: years I
phases and poor prognosis argue against the view that frequency of cycles evolves as a result o f cumulative toxicity from earlier episodes. It is more likely that patients who switch have a more severe lorm of bipolar disorder which manifests as affective instability. In short, people who switch are less able to stabilize their mood.
The design of this study has scveral advantages over previous studies of sensitization. The patients were followed at 6-month intervals and then at 1- year intervals in order to minimize recall bias. Cycle lengths, not interval lengths, were examined. The test for a decrease in cycle lcngths over follow- up was not based on group medians, but rather on whether or not a larger proportion o f patients showed a gradual decrease over time. However, this study does have some methodological limita- tions.
The study is prospective in design, yet partici- pants were asked to recall affective symptoms for either 6 months or 1 year prior to the follow-up interview. Thus participants did have to rely on their memory. However, the follow-up intervals were relatively short, and did not require that patients recall the course of all previous episodes. Rather, they reported on only the most recent symptomatology.
The Collaborative Depression Study sample was recruited at tertiary-care centres and had a mean duration of illness of 11 years at intake. It is possible that a gradual shortening of cycle length occurred before subjects entered the study. Patients in their first episode at intake did not show subsequently decreasing cycle lengths, but this sample size was considerably smaller.
This was a naturalistic study of the course of bipolar disorder where treatment was monitored but not conti-ollcd. Treatment may have modified the course of the illness and obscured a trend towards a sensitiLation pattern. The gradual increase in frequency o f episodes may have been attenuated by prophylactic treatment. At present, it is impossible to study untreated bipolar I patients lor any extended period of time. Pre-treatment era studies were all retrospective and examined sequential interval lengths, not cycle lengths (20, 23, 24). Although many authors cite pre-treatment era studies as being supportive of a gradual decrease in interval lengths, the data that conflicts with this hypothesis is often overlooked (23-25). as are the methodological limitations discussed in the introduction to this paper.
Kindling and sensitization hypotheses focus on lowered thresholds for the onset of an episode, rather than on the factors that determine the
i o n of episodes. Howcvcr, in this study n of episodes was associated with poor
prognosis, but the number of episodes was not. Therefore, factors contributing t o the remission of episodes are crucial to understanding overall morbidity. Cycle length is an imprccix indication of morbidity because it docs n o t reflect how much time within any given cycle is actually spent in an affective episodc. Two individuals may have an average cycle length of 12 months, yet one may spend most of that cycle in an affective episode, whereas the other may be well for most of the cycle. The difference has very clear implications for prognosis.
This investigation was based on 10-year follow- up data. Extended follow-up provides richer information about the nature o f severe bipolar disorder than most cross-sectional studies because the features that lead to increased morbidity over the course of the entire illness can be investigated. The drawback of long-term follow-up is the inevitable attrition. In total, 29% of the original sample did not complete 10 years of follow-up and were not included in these analyses. If the patients who dropped out did so for reasons rclated to prognosis, the remaining sample would provide an inaccurate picture of the factors related to poor prognosis.
The definition of poor prognosis is always a somewhat arbitrary decision, and the predictors bf prognosis will, to a degree, be shaped by the way in which prognosis is defined. Criteria for the poor- prognosis group specified that symptomatology be relatively sustained over a 3-year period. Thus 25 of the 27 poor-prognosis patients were chronically ill. This may underlie the apparent prognostic impor- tance of episode duration. However, course vari-
117

Turvey et al.
ables that predicted prognostic grouping also predicted poor functioning on psychosocial mea- sures. Furthermore, it was desirable to select a sample that had ongoing difficulties and to define the illness features that predispose bipolar patients to a inore compromised course with relatively few periods of relief from symptoms.
One aspect of poor prognosis that is consistently described in both pre-treatment and treatment era studies is polyphasic episodes (18-20, 23, 24, 27, 28). Rased on the findings of the prescnt study and several pre-treatment era studies, the poorest prognosis is associated with chronic polyphasic episodes and a lower frequency of switches in these episodes. The key prognostic feature of such episodes is not the frequency of switches, but rather the extended duration of the episode. Future investigations should study the biological process that allows bipolar I patients to stabilize their mood after a single phase rather than switch to a phase of thc opposite polarity.
References
1
2
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
GOOIIWIN FK, JAMISO\ KR. Manic depressive illness. New York: Oxford Ilniversity Press, 1090. GOLDHEKC; JF, HAKROW J, GKOSSMAN LS. Recurrent affective syndromes in bipolar and unipolar mood disorders at follow-up. Ur .I Psychiatry I995;166:382-385. GOLDBEKG JF, HARKOW J, GKOSSMAN LS. Course and outcome in bipolar affective disorder: a longitudinal kollow-up study. Am J Psychiatry 1995;152:379-384. GITIJN MJ. Swemsm J, HELLEK TL, HAMMEN C. Relapse and impairment in bipolar disorder. Am J Psychiatry 1995;152: lh35-- 1640. M A J M, P I K O ~ A R, M A G L I A N O L. Non-response to reinsti- tuted lithium prophylaxis in previously responsive bipolar patients: prevalence and predictors. Am .I Psychiatry I 995;152: 1 8 10-1 81 I , SOI.OMON DA, KFJTUEK GI, MILLER IW, SIIEA MT, KEI.I.ER MB. Course of illness and maintenance treatments for patients with bipolar disorder. J Clin Psychiatry 1995;56:5- 13. O’CONNFI.~. RA, MAYO JA. FLATLOW I,, CI;TITBT.KTSON B, O’iwAN BE. Outcome o f hipolar disorder on long- term treatment with lithium. Br J Psychiatry 1991;159: 123-1 29. Toiriih M, WAWKNALIX C M , TSUANG MT. Outcome in mania. Arch Gen Psychiatry 1990;47:1106-1111. HARROW M, GOI.DBFRG JF, GKOSSMAN LS. MELTZEK HY. Outcome in manic disorder. Arch Gen Psychiatry 1 990;47:665-671. TOHFN M, WATFKKAIIX CM, T S ~ I A N C ; MT, HI”. AT. Four- year follow-up o f twenty-four first-episode manic patients. Arch Gen Psychiatry 1990;19:79-86. AAGAAKD J, VFSTEKGAAKD P. Predictors of outcome in prophylactic lithium treatment: a 2-year prospective study. J Affect Disord 1990;18:259-266. MAJ M, PIKOZZI R, STAKACF F. Previous pattern of course of
IS a predictor of response to lithium prophylaxis in bipolar patients. J Affect Disord 1989;17:237-241. DUNNER DL. VIJAYALAKSHMY P, FIEVE RR. Rapid cycling
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
manic-depressive patients. Compr Psychiatry 1977;18:561- 566. Posr RE, RAI I ANGFK WP. The neurobiology o f mood disorder. New York: Plenum Press. 1990. POST R. Transduction of psychosocial stress into the neurobiology o f recurrent affective disorder. Am J Psychiatry 1992;149:909-10 10. CUTLER NR, Pus-r RM. Life course of illness in untreated manic-depressive patients. Compr Psychiatry I982:23:101- 1 IS. Zrs AP. GKOF P, WZHSIEK M. Gooowix FK. Prediction of relapse in recurrent affective disorder. Psychopharmacol Bull 1980;16:47-49, AK(jSI. J . Course of affective disorders. In: VANPRAAG HM. 1,Ar)I;t MH, RAFAFISFU OJ. SACHFK EJ. ed. Handbook of biological psychiatry. New York: Marcel Dekker. Inc.. 1981:225-242. ROY-BYKNF P, POST RM, UIIDE TW, PORCU T, DAVIS D. The longitudinal course of recurrent affcctive illness: life chart data from research patients at the NIMH. Acta Psychiatr Scand 1985:71:3-34. KKAI.IV.I I N E. Manic-depressivc insanity and paranoia. In: BAK(I.AY RM, trans. K U I ~ F K I S O K GM. ed. Edinburgh: E & S Livingstone, 1921. (Reprinted New York: Arno Press, 1976). AN(~SI .I. BAASIXI;P P, GKoI P, Hirwrrs H. POI I ) IN , I .K W, WEIS P. The course of monopolar depression and bipolar psychoses. Psychiatr Neurol Neurochir 1973;76:489-500. KI,SSIN(I LV. ANI)I:KSI:I\ PK, MOKII,USI:N PB, Hoi.wrc; TG. Recurrence in affective disorder. 1. Case-register study. Br J Psychiatry 1998:172:23-28. I A I N I ) O I I I S I ‘ G. Prognosis and course in manic-depressive psychoses: a follow-up study of 319 first admissions. Acta Psychiatr Scand 1945;2O(Suppl. 35):1-96. BKArros 0, H A ~ J ~ ; FO. The course of manic-depressive psychosis: follow-up investigation of 215 patients. Acta Psychiatr Scand 1968;44:89-112. RFNNIF T. Prognosis in manic-depressive psychoses. Am J Psychiatry 1942;98:801-818. CORYELL W, ENDICOTT J, KELLEK M. Rapidly cycling affective disorder. Arch Gen Psychiatry 1992;49:126-131. MAJ M, MAGLIANO L, PIKOZZI R, MAKASCO C, GUAKNERI M. Validity of rapid cycling as a course specifier for bipolar disorder. Am J Psychiatry 1994:151:1015-101 Y. KI:I.I.IX MB, I A V O K I PW, COKYEI .~ W et al. Differential outcome of pure manic, mixedkycling, and pure depressive episodes in patients with bipolar illness. J Am Med Assoc 1986;255:3138-3142. ANDREASEN NC, ENDICOTT J, SPITZER R, WINOKLIR G. The family history method using diagnostic criteria. Arch Gen Psychiatry 1 9 Y2;49: 126-1 3 1. ANDREASEN NC, GROVE WM, SHAPIRO RW, KELLER MB, HIKSCIIFEI.D RM, M~DOKALD-SCOTT P. Reliability of life- time diagnosis. Arch Gen Psychiatry IY77;34:1229-1235. SPITZER RL, ENDIVXT J, ROBINS E. Research diagnostic criteria: rationale and reliability. Arch Gen Psychiatry I978;35:773-782. ENDICOTT J, SWIZEK RL. A diagnostic interview: the Schedule for Affective Disorders and Schizophrenia. Arch Gen Psychiatry 1978;35:837-844. Km.i,ER MB, LAVOKI PW, FKIEIIMAN B et al. The longitudinal interval follow-up evaluation. Arch Gen Psychiatry 1979;36:555-559. K ~ L L E K MB, LAVUKI PW, KLEKMAK GL et al. Low levels and lack of predictors of somatotherapy and psychotherapy received by depressed patients. Arch Gen Psychiatry 1986;43:458466. ENDICOTT J, SPITZEK RL, FLEES JL. COHEN J. The Global

Long-term prognosis of bipolar I disorder
Assessment Scale: 21 procedurc [or measuring overall 17. American Psychiatric Association. I>ingnostic and statis- severity of psychiatric disturbance. Arch Gen Psychiatry tical manual of niental disorders, 4th edn. Washington, DC: 1976:33:766-77 I . American Psychiatric Press. 1994.
36. Mi1.1 I’K DC. The Hollingshead-Kedlicti scale. Handbook o f 38. ~ I W I - ~ A I PII MT. ( ‘ o i w s A . I’rcdictors o l long-term research design and social measurement, 4th edn. White outcome of mood disorder on prophylactic lithium. Plains. NY: Longnian, 1983. Lit hi um 1 99O:1:27--3S.
119






![[Bipolar disorder in children and adolescents: a difficult diagnosis]](https://img.pdfslide.net/doc/110x75/6329c6c056a016b67502a1c4/bipolar-disorder-in-children-and-adolescents-a-difficult-diagnosis.jpg)






















