Embed Size (px)
Citation preview

Lung Scanning in the Diagnosis of Pulmonary Embolism: The Emperor Redressed
Jack E. Juni and Abass Alavi
Diagnosis and management of the patient wi th pulmo- nary embolism remains a vexing clinical problem. Emboli are often unsuspected clinically. Ventilation- perfusion (VQ) scintigraphy is known to miss some emboli found on pulmonary angiography. Some physi- cians recommend diagnostic approaches in which the lung scan plays a relatively minor role, and angiogra- phy is required for many patients. Major prospective studies recently have made available objective data for formulation and evaluation of diagnostic and thera- peutic strategies. These data suggest that the lung scan is a better predictor of patient outcome than has been previously appreciated. The goal of V / Q scanning is not detection of pulmonary emboli per se, but rather the identification of patients at a high or low risk for future embolic events if they are not anticoagulated.
Several studies have shown that some emboli found on angiography are clinically benign and, in the ab- sence of persistent thrombosis of the lower extremi- ties, do not require anticoagulation. Treatment trials and clinical fol low-up studies have shown that al- though the V / Q scan is not always predictive of angiogram results, i t is a reliable predictor of patient outcome. In the absence of deep vein thrombosis, the low.probabi l i ty scan identifies a patient population not requiring anticoagulation. When combined wi th objective studies of the venous system, the ventilation- perfusion lung scan provides a guide to management in the great majority of patients. Pulmonary angiogra- phy is required only occasionally. Copyright �9 1991 by W.B. Saunders Company
r I ~ H E DIAGNOSIS of pulmonary embolism 1 (PE) remains one of the most challenging of common problems in clinical medicine. Few diseases cut across so many specialties and present in such myriad ways. It has been esti- mated that there are approximately 630,000 cases of PE in the United States each year. Eleven percent of these individuals die within the first hour. Of those surviving, the diagnosis is missed in approximately 400,000 (71%). Ap- proximately 120,000 (30%) of these untreated individuals die. ~ In the 29% fortunate enough to receive anticoagulant therapy, mortality is re- duced to 10% to 16%. 2,3 Clearly, any therapy reducing mortality by two thirds should be made available to as many patients as possible. Antico- agulant therapy is not without its risks, however, and the diagnosis must be as firm as possible. 4 The ventilation-perfusion lung scan has become the launching pad of the diagnostic evaluation for PE. Is this appropriate? Is V/Q scanning accurate enough to eliminate the need for angiography? If so, how is the scan best per- formed, interpreted, and incorporated into diag- nostic and therapeutic planning?
HOW GOOD IS THE LUNG SCAN?
Almost since the beginning of modern ventila- tion-perfusion imaging, critics have proclaimed its lack of value. The lung scan has been humorously referred to as "an emperor with no clothes." More recently, others have been trou- bled by its apparent nonspecificity. 3'6-H Some
have advocated considering all scans with inter- pretations other than normal or high probability to be "nondiagnostic," and have suggested that the impact of the ventilation-perfusion scan is minimal in most patients. 3'6'n At this time, two large, well-designed, prospective clinical tri- als 7'8'12 have been reported. Although contro- versy still exists, the lung scan has proven to be of substantial clinical value. The diagnostic nihilism reflected in some recent reviews 8,H can now perhaps be tempered. The ventilation- perfusion lung scan, in combination with clini- cal examination and chest radiograph, is a powerful tool capable of guiding therapy in the majority of patients.
The Prospective Trials
In 1977, Biello et a113 proposed a system of scan interpretation that categorized scans into normal-, low-, intermediate-, or high-probabil- ity subgroups for PE. This work was based on a retrospective comparison of ventilation-perfu- sion scans to pulmonary angiograms, and has been modified and added to by many oth-
From the Nuclear Medicine Department, William Beaumont Hospital, Royal Oak, MI, and the Nuclear Medicine Depart- ment, Hospital of the University of Pennsylvania, Philadelphia, PA.
Address reprint requests to Jack E. Juni, MD, Nuclear Medicine Department, William Beaumont Hospital, 3601 W13 Mile Rd, Royal Oak, M148073-6769.
Copyright �9 1991 by W.B. Saunders Company 0001-2998/91/2104-0002505. 00/0
Seminars in Nuclear Medicine, Vol XXt, No 4 (October), 1991 : pp 281-296 281
282
e r s . 6'12A.18 The most comprehensive prospective studies to date are the Prospective Investigation of Pulmonary Embolism Diagnosis (PIOPED) 12 trial sponsored by the National Institutes of Health and the studies of Hull et al 7'1~ at McMaster University in Ontario. These studies are required reading for the practitioner of nuclear medicine.
The initial PIOPED study prospectively eval- uated a random sampling of 933 patients from a population of 1,493. Nine hundred and thirty- one of these patients underwent ventilation- perfusion scanning using technetium-99m (99~Tc) macroaggregated albumin (MAA) and xenon- 133 (133Xe). All patients with a scan interpreta- tion other than normal underwent pulmonary angiography (755 patients). Two hundred and fifty-one of these (33%) had embolism demon- strated on angiography. All patients were fol- lowed-up for 1 year. This follow-up was also extended to a large number of patients who either declined participation in the angiography arm of this study, were medically ineligible for pulmonary angiography, or were withdrawn by their physician. Scan interpretations were per- formed individually by two independent observ- ers blinded to patient history (other than that PE was considered a diagnostic possibility) and to the results of the angiography. A chest roentgenogram obtained within 24 hours of the scan was available for comparison. If the two interpretations were not similar, a consensus interpretation was obtained for comparison with clinical data and pulmonary angiography.
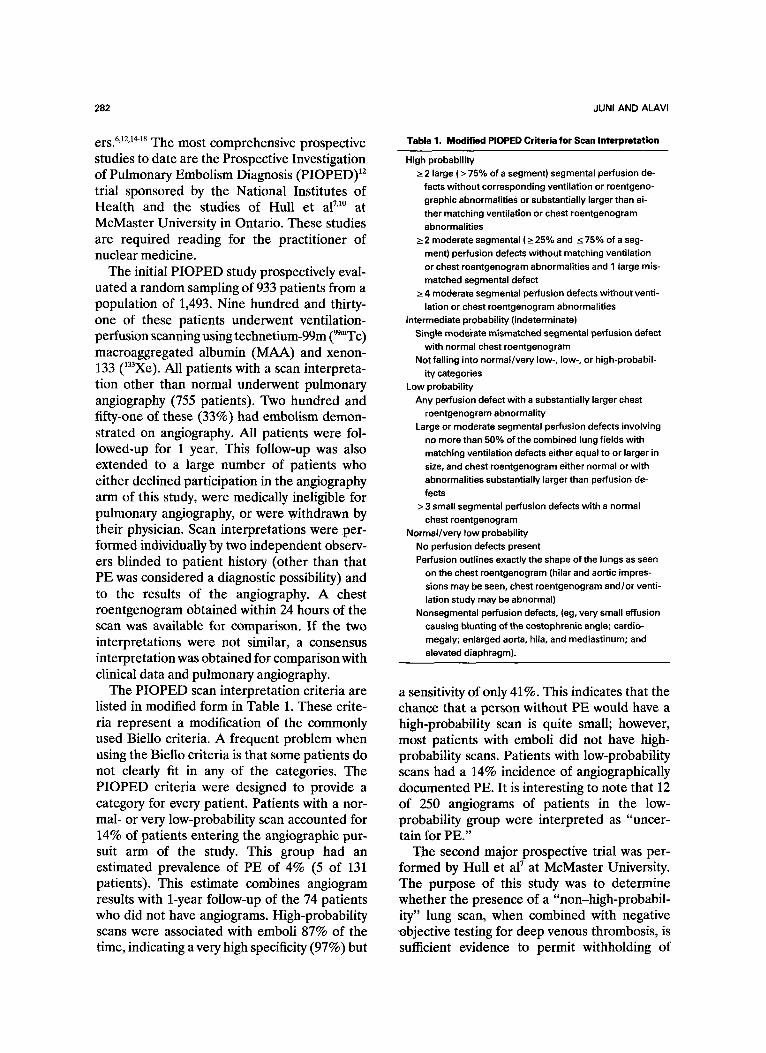
The PIOPED scan interpretation criteria are listed in modified form in Table 1. These crite- ria represent a modification of the commonly used Biello criteria. A frequent problem when using the BieUo criteria is that some patients do not clearly fit in any of the categories. The PIOPED criteria were designed to provide a category for every patient. Patients with a nor- mal- or very low-probability scan accounted for 14% of patients entering the angiographic pur- suit arm of the study. This group had an estimated prevalence of PE of 4% (5 of 131 patients). This estimate combines angiogram results with 1-year follow-up of the 74 patients who did not have angiograms. High-probability scans were associated with emboli 87% of the time, indicating a very high specificity (97%) but
JUNI AND ALAVI
Table 1. Modified PIOPED Criteria for Scan Interpretation
High probability _> 2 large ( > 75% of a segment) segmental perfusion de-
fects without corresponding ventilation or roentgeno- graphic abnormalities or substantially larger than ei- ther matching ventilation or chest roentgenogram abnormalities
___ 2 moderate segmental ( >_ 25% and ~ 75% of a seg- ment) perfusion defects without matching ventilation or chest roentgenogram abnormalities and 1 large mis- matched segmental defect
>_ 4 moderate segmental perfusion defects without venti- lation or chest roentgenogram abnormalities
intermediate probability (indeterminate) Single moderate mismatched segmental perfusion defect
with normal chest roentgenogram Not falling into normal/very low-, low-, or high-probabil-
ity categories Low probability
Any perfusion defect with a substantially larger chest roentgenogram abnormality
Large or moderate segmental perfusion defects involving no more than 50% of the combined lung fields with matching ventilation defects either equal to or larger in size, and chest roentgenogram either normal or with abnormalities substantially larger than perfusion de- fects
> 3 small segmental perfusion defects with a normal chest roentgenogram
Normal/very low probability No perfusion defects present Perfusion outlines exactly the shape of the lungs as seen
on the chest roentgenogram (hilar and aortic impres- sions may be seen, chest roentgenogram and/or venti- lation study may be abnormal)
Nonsegmental perfusion defects, (eg, very small effusion causing blunting of the costophrenic angle; cardio- megaly; enlarged aorta, hiM, and mediastinum; and elevated diaphragm).
a sensitivity of only 41%. This indicates that the chance that a person without PE would have a high-probability scan is quite small; however, most patients with emboli did not have high- probability scans. Patients with low-probability scans had a 14% incidence of angiographically documented PE. It is interesting to note that 12 of 250 angiograms of patients in the low- probability group were interpreted as "uncer- tain for PE."
The second major prospective trial was per- formed by Hull et a l 7 at McMaster University. The purpose of this study was to determine whether the presence of a "non-high-probabil- ity" lung scan, when combined with negative objective testing for deep venous thrombosis, is sufficient evidence to permit withholding of
LUNG SCANNING IN PULMONARY EMBOLISM 283
anticoagulant therapy. Ventilation-perfusion scans were grouped into three categories: nor- mal, high probability (defined as one or more large [ > 75%] segmental perfusion defects with normal ventilation), or non-high probability. Essentially all patients underwent impedance plethysmography (IPG) along with the scinti- graphic studies. IPG is a noninvasive electrical measure of the time course of blood drainage from the leg after release of an occluding cuff. It is both sensitive (86%) and specific (97%) for proximal vein thrombosis. 19 If IPG was negative, it was repeated every 2 to 3 days for 14 days. Anticoagulant therapy was withheld or with- drawn from all patients with no~-high-probabil- ity lung scans in whom serial IPG remained negative for 14 days.
A total of 874 patients with suspected PE was enrolled. Of these, 414 patients (47%) had lung scans that were not normal and not considered high probability. IPG was positive for proximal deep vein thrombosis in 1% of patients with normal lung scans, 19% of patients with high- probability scans, and only 8% of those with non-high-probability scans. Following the proto- col, 92% of those with nondiagnostic scans were not anticoagulated or had anticoagulants with- drawn. Patients were followed for 3 months to determine the number suffering from recurrent thromboembolism. During the follow-up, a re- currence was defined as either a documented PE or objectively documented deep venous thrombosis during th~ follow-up.
This course of treatment was remarkably successful. Only 1% of those patients with normal perfusion scans suffered a recurrence. Only 2.7% (10 of 371) of the group with non-high-probability scans and negative IPG had a recurrence despite withholding anticoagu- lant therapy. Of the group with high-probability scans, all of whom received anticoagulant ther- apy, 7% (5 of 66) had objectively documented symptomatic thromboembolism on follow,t~p. No untreated patient died during the study. The clear conclusion of this study was that patients with the combination of a non-high-probability V/Q scan and negative IPG for venous thrombo- sis could safely be managed without anticoagu- lant therapy. Interestingly, 7 of 9 of the positive IPG studies in this group were negative on the first exam. It is possible that some of these 7
patients benefited from being on anticoagulant therapy for several days to 2 weeks.
It should be noted that this study's criteria for high-probability scans were somewhat nonstand- ard. A V/Q scan was considered high probabil- ity if it demonstrated either segmental or greater mismatched defects (abnormal perfusion with normal ventilation) or large (greater than 75% of the segment) subsegmental defects with ven- tilation mismatch. This latter group is consid- eredintermediate probability by PIOPED crite- ria.
The reports of the M c M a s t e r group 7'1~ are outliers in several respects when compared with most other evaluations of ventilation-perfusion scanning. Not only are the criteria for high probability nonstandard, but also those for the normal and indeterminate (intermediate) scan categories. A substantially higher percentage of patients in the McMaster low-probability cate- gory had pulmonary embolus than in most other studies. The McMaster group also has a much higher percentage of low-probability interpreta- tions than most other groups--41% 2~ versus 14% in PIOPED. These differences, along with the referral bias caused by including only patients referred to a special thromboembolism unit (therefore selecting for somewhat sicker pa- tients), make the results of the McMaster group difficult to compare with those of PIOPED and other studies.
DIAGNOSTIC APPROACH TO PE
A large body of research over the last two decades has indicated that it is inappropriate to consider PE as a disease entity confined to the lungs. It is more appropriately considered as one serious complication of a broader disease entity: thromboembolismY Since virtually all pulmonary emboli are now felt to spring from venous thrombosis of the pelvis or lower extrem- ities, 21 treatment is directed towards preventing further thrombosis and embolization. There- fore, it is not always sufficient to exclude the diagnosis of PE and not consider deep venous thrombosis, which may well pose a similar overall risk to the patient. 22
Kelley et al 3 determined that lung scan inter- pretations of low- or intermediate-probability are not reliable enough to be clinically useful. They cite PIOPED data showing that interob-
284 JUNI AND ALAVI
server reproducibility for normal- and high- probability scans was 94% and 95%, respec- tively, but the intermediate- and low-probability categories had only 75% and 70% agreement between scan readers. Kelley et al note that 16% of PIOPED patients with low-probability scans had embolism on angiography while 32% of those with intermediate-probability scans had PE. They correctly argue that these percent- ages are too high to consider a low-probability scan alone as sufficient grounds for excluding the diagnosis of PE. H u l l 6 reports that 28 of 120 (23%) of patients with low-probability scans had pulmonary embolus. He argues that "the concept of a low-probability pattern is mislead- ing and, indeed, dangerous because of the frequency of this pattern among patients with pulmonary embolism. ''6 He suggests that lung scan findings be reported as either normal, high probability, or nondiagnostic. Bone 11 makes a similar argument, asserting that most patients with nonnormal lung scan patterns require an- giography.
Pulmonary angiography is the standard against which lung scans are traditionally compared. Before dismissing the lung scan for its imperfect correlation with the "gold standard," it be- hooves us to evaluate the standard itself.
Reliability of Pulmonary Angiography
In a 1986 review of diagnostic approaches to PE Sostman et a123 reported interobserver agree- ment on angiographic diagnosis ranging from 80% to 95%. In a 1987 study on the reliability of selective pulmonary arteriography in the diagno- sis of PE, three angiographers reviewed the arteriograms of a series of 60 patients. 24 The mean interobserver agreement was only 86%. All angiographers agreed on studies with PE graded as massive, lobar, or segmental, but agreed in only 2 of 15 cases in which the embolus was graded as subsegmental. In pa- tients with minor or more distal clots, both arteriography and V/Q scanning become more difficult to interpret. In Hull's 1~ prospective angiographic study, 51 of 283 patients were too ill for angiography; an additional 21 patients had contraindications to angiography (allergy, pregnancy, or primary cardiopulmonary dis- ease). Technical difficulties precluded angio- gram in 4 more patients. Angiography was
considered inadequate in 29 of 202 (14%) of patients eventually studied. In total, 37% of patients (105 of 283) had either nondiagnostic angiograrns or were unable to undergo the proce- dure.
In the PIOPED study, 12 the agreement among angiographers was 92% for positive scans and 83% for those read as negative for PE. In that study, however, three different interpretations of a technically adequate scan were permitted: positive for PE, negative for PE, and "uncer- tain." In actual medical practice, it is extremely rare for a pulmonary angiogram to be reported as uncertain or indeterminate. This is no doubt due to the perception of the angiogram as the ultimate diagnostic study that must give a defi- nite answer. The "uncertain" angiogram cate- gory was included in PIOPED because of the consensus among angiographers that there were, in fact, some angiograms in which a reliable diagnosis of the presence or absence of PE simply could not be made. Note that the "uncertain" category did not indicate inability of interpreters to come to agreement, but rather, an agreement between two blinded observers that the angiogram was not diagnostic. If the PIOPED patients in each of the three catego- ries of interpretations are added together, 650 of 755 (86%) of patients with a technically adequate angiogram had agreement between two observers (95% confidence interval, 83.6% to 88.6%). If both disagreements between ob- servers and uncertain angiograms are consid- ered as nondiagnostic, then only 83% of all angiograms in PIOPED were considered diag- nostic (95% confidence interval, 81.0% to 86.0%). Overall agreement in V/Q scan inter- pretation in all PIOPED patients was 730 of 931 (78%); 95% confidence interval, 75.8% to 81.1%). Thus, not only was the agreement rate of scan interpretation not significantly different from the agreement rate of angiogram interpre- tation in the statistical sense, the difference between 78% agreement in one test and 83% agreement in the other is unlikely to be a clinically significant difference.
Thus, in both large prospective studies and in a major retrospective study, the reliability of pulmonary arteriography as reflected in repro- ducibility of interpretation was 83% to 86%. Although data as to the rate of angiogram
LUNG SCANNING IN PULMONARY EMBOLISM 285
agreement in different scan probability catego- ries is not available from these studies, it is interesting to note that 21 of 24 (88%) of PIOPED angiograms read as uncertain oc- curred in patients whose lung scans were inter- preted as low or intermediate probability.
These studies indicate that V/Q scan and pulmonary angiography have quite similar reliabil- ity as assessed by agreement between two dif- ferent interpreters. It also appears that the patients with greatest disagreement between V/Q scan and pulmonary angiogram, those in the low- and intermediate-probability scan cate- gories, are also those in which there is least certainty in angiography. 24 It is reasonable to say that the angiogram and V/Q scan are likely to agree in a very high percentage of patients in whom the V/Q scan is interpreted as normal or high probability.
Prediction of Patient Outcome
If angiography is not the best indicator of the reliability of V/Q scanning, what measure can we use to assess its success at stratifying patients suspected of PE into various risk groups? The ultimate usefullness of all diagnostic procedures may be judged on how well they predict the patient's outcome or natural history. If an adverse course is predicted, appropriate treat- ment may be initiated. If the patient's untreated natural history is benign, no treatment is needed. The ultimate measure of the success or failure of ventilation-perfusion scanning is its ability to identify those patients who will do well or poorly if left untreated.
Dalen and Alpert a estimated that most pa- tients dying of acute PE die within the first hour. Of those that survive the first few hours but who are untreated, the cause of death is usually not the original embolus but a recurrent thromboem- bolic event. Treatment of PE patients not in acute cardiopulmonary distress is aimed at pre- venting a recurrent event, thereby altering the natural history of the disease. It is important to show not just how the scan correlates with angiograms, but rather to determine whether a given scan pattern is predictive of a patient's natural history. It is possible that some emboli detected by angiogram are clinically benign or inconsequential
The Normal Perfusion Scan
A V/Q scan interpreted as normal (Fig 1) reliably exludes the diagnosis of PE. Hull 7 found that only 1% of patients with a normal V/Q scan pattern had evidence of PE or deep vein thrombosis on 3-month follow-up despite with- holding anticoagulants. Kipper 5 found that none of 68 patients with normal scans had clinical evidence of pulmonary embolus on long-term follow-up. He concluded that if a normal scan misses any emboli, the emboli are unlikely to be of clinical significance. In another study, Hull 25 prospectively followed a large number of pa- tients with normal lung scans. On follow-up, only 0.6% had evidence of deep venous throm- bosis and 0.2% had PE. Only one death oc- curred during the follow-up that could be attrib- uted to deep vein thrombosis or PE. This was in a patient who had known deep vein thrombosis at the beginning of the study. This low incidence of thromboembolic events on follow-up is com- parable with that in patients with a normal pulmonary angiogram. In a study of 180 patients with negative arteriograms followed for at least 6 months each, 167 of whom received no treat- ment, there were no deaths attributable to thromboembolic disease and no patients had subsequent PE. 2 In the PIOPED study, 12 4% of patients with normal- or very low-probability scans had a positive angiogram. None of these had PE or other evidence of thromboembolism on follow-up. This percentage is higher than
Fig 1. Anterior view of a normal pulmonary perfusion study. The cardiac impression is clearly visible. Tracer uptake throughout the lungs is uniform,

286 JUNI AND ALAVI
most other studies and may represent a relative underrecruitment of true normal individuals. The PIOPED study group had a smaller propor- tion of patients with low-probability and near- normal or normal lung scans than did the population of patients who refused to enter the study. Thus, we can conclude that patients with a normal perfusion scan do not require angiography or anticoagulant therapy.
The High-Probability Scan
In PIOPED, ~2 the specificity of a high- probability lung scan is 97%; only 3% of pa- tients with normal angiograms will have a high- probability scan. In patients without a history of prior PE, 91% (89 of 97) with a high-probability scan will have positive angiograms. This positive predictive value drops to 74% in patients with history of prior PE due to the fact that many emboli do not resolve even after years. In patients without a prior history of PE, the certainty of diagnosis by high-probability lung scan is suffi- cient to begin anticoagulation without performing an angiogram in all but those with strong contrain- dications to anticoagulation.
The Low-Probability Scan
If high-probability scans and near-normal or normal scans are clinically reliable, what about low-probability scans? We have seen that a substantial number of patients with low-proba- bility scans will have positive angiograms. Does this mean that a low-probability scan is not useful in the patient with suspected PE?
One retrospective study involved a than 8-month follow-up of 183 patients with low- probability V/Q scans. 26 The incidence of clini- cally detectable recurrent PE was only 0.6% despite the absence of anticoagulant therapy. This extremely low incidence of clinical events on follow-up suggests that not all cases of small embolism detected by angiography are associ- ated with clinical consequences. It should be noted, however, that 34 patients with low- probability lung scans in this series were not included in the analysis due to death or perfor- mance of angiography soon after scintigraphy. They were excluded since they were felt t o represent a different patient population with a higher clinical suspicion of risk than the average low-probability patient. Excluding these pa-
tients would, however, tend to improve the results of a "hands-off" therapy trial.
Lee et a127 performed a similar study in which they reviewed the clinical records of 99 consecu- tive patients whose V/Q scans had been inter- preted as representing low probability of PE. No patients were treated for PE, but three were found to have venous thrombosis and were placed on anticoagulants. Two others had other indications for anticoagulants and were treated. The remaining 95 patients were untreated. No patient was felt to have clinical evidence of PE during a follow-up greater than 2 months (in most patients). None died of PE or other thromboembolic disease. More recently, Kahn et a128 retrospectively analyzed up to 1-year follow-up in 90 untreated patients in whom PE was suspected, but whose V/Q scans were interpreted as low probability. None of the 90 patients demonstrated clinical evidence of PE subsequent to the V/Q scan.
Although Hull and Raskob 6 recently found embolus on angiogram in 23% to 25% of pa- tients with low-probability scans, it is doubtful that many of these were clinically significant. Since untreated patients with PE have recur- rence rates of 26% to 50%, 1'26 it is difficult to imagine that such a high complication rate could have been missed by these long-term follow-up studies. 29 In fact, the incidence of embolism in the prospective trials may be artifi- cially increased because of (1) refusal of rela- tively healthy patients to join a study requiring angiography (PIOPED) and (2) the require-
men t for referral to a special team for treatment of thromboembolic disease (McMaster). In their prospective therapy trial, the McMaster group found that only 2.7% of untreated patients with low- or indeterminate-probability scans and negative IPG had recurrent thromboembolic events. We then can conclude that patients with a low-probability scan and no evidence of venous thrombosis may be safely left untreated.
Noninvasive Study of the Venous System
The important McMaster prospective trial withholding anticoagulant therapy from pa- tients with nondiagnostic scans has been dis- c u s s e d . 7 Unlike most centers, this group consid- ers all low- and intermediate-probability scans to be nondiagnostic, and lumps them together.
LUNG SCANNING IN PULMONARY EMBOLISM 287
Previous studies by this group have shown that proximal vein thrombosis may exist at the time of presentation in up to 50% of patients with PE. They used a "nondiagnostic" lung scan pattern to select patients with a low likelihood of PE. They then screened for simultaneous venous thrombosis by IPG. Patients with posi- tive IPG underwent venography and, if the diagnosis of thrombotic disease was confirmed, anticoagulant therapy. Since Hull's group has been the major proponent of IPG as an integral part of the initial diagnostic workup, it is impor- tant to note how often the results of venous studies are abnormal. Of 874 patients initially studied, 414 patients (47%) had non-high- probability scans. Of this group, only 34 (8%) had positive IPG on initial presentation, a surprisingly low rate. These patients were placed on anticoagulants. The remaining 380 patients underwent repeat testing with IPG at 2- to 3-day intervals for 14 days. An additional 9 patients (2% of the nondiagnostic scan cohort) had at least one positive IPG study on delayed serial testing. Therefore, a total of 43 (10%) of the non-~highprobability scan group had positive IPGs at some point within the first 2 weeks after presentation. On long-term follow-up of the 371 patients with non-high-probability scans and negative serial IPG results, only 10 patients (2.7%) developed objectively documented symp- tomatic thromboembolism (PE or deep vein thrombosis). Thus, this strategy of combining non-high-probability lung scans with IPG al- lowed identification of a large group of patients which, without anticoagulation, had only a 2.7% incidence of related complications on follow- up. Duplex ultrasound has accuracy comparable to IPG and is currently available in more institu- tions.30,31, 53
Is study of the venous system necessary in all patients? How do we account for the percent- age of patients receiving lung scans who had positive IPG in the two studies from McMaster (30% ~~ versus 7.4% [59 of 798]7)? The factors predisposing a patient to PE are the same factors that predispose to proximal vein throm- bosis. Similarly, those states predisposing to PE-surgery or significant trauma in the past 6 months: 9 malignancy, congestive heart failure, pregnancy, etc-also predispose to deep venous thrombosis. In the McMaster study, 34 of 414
(8%) of the patients with non-high-probability scans had evidence of proximal vein thrombosis on IPG. Although proximal vein thrombosis and PE are both components of the same disorder, the diagnostic workup for PE does not require IPG or Doppler ultrasound in all cases. Ninety percent of the non-high-probability scan group had at least one of the McMasters group's previously defined predisposing factors for prox- imal vein thrombosis (Table 2). Forty-seven percent had two or more predisposing factors. Clearly, those patients at high risk for venous thrombosis need objective evaluation because no more than 24% of patients with deep vein thrombosis can be expected to be symptomatic. 7 However, when low- and intermediate-probabil- ity patients are lumped together, only 10% will have positive IPG. The incidence of deep vein thrombosis in the low-probability group alone, although not separately analyzed by the McMas- ters group, would be expected to be much less than this.
If non-high-probability scans are such good discriminators in combination with IPG, how good would they be if used alone? Unfortu- nately, Hull et al do not break down their patient population into low- or intermediate- probability groups. This is doubtless due to their belief that these two groups cannot be sepa- rated. Nonetheless, the data from many retro- spective studies and the large PIOPED prospec- tive study indicate that, although there is interobserver variability, the group identified as intermediate probability has at least twice the incidence of PE as the group identified as low probability. In PIOPED, 32.5% of patients with interpretable angiograms and intermediate- probability scans had PE whereas only 16% of those with low-probability scans and interpret- able angiograms had PE. lz In spite of interob-
Table 2. Predisposing Factors for a Venous Thromboembolism
Age >_40yr History of deep vein thrombosis or PE, surgery, or trauma in
the past 6 months
Malignancy Congestive heart failure Leg paralysis Pregnancy Oral contraceptive use
Data from Hull. 7
288 JUNI AND ALAVI
server variability, it seems unwise to disregard any discriminator that indicates that some pa- tients will be at twice the risk of others.
How should we treat patients with intermedi- ate-probability scans? Must they all undergo angiography and/or venous studies? Could we withhold treatment in this group? Using the figures from Hull et al's 7 prospective series, if we were not to perform IPG, we would include in our untreated group 10% in whom IPG would have detected proximal vein thrombosis either on initial evaluation or on 14-day serial follow-up. Since PE is twice as common in the intermediate-probability scan group as in the low-probability group, then we would expect that about 3.3% of these patients with venous thrombosis would be included in our low- probability group and 6.6% in the intermediate- probability group. Thus, 97% of our low- probability scan group would belong in the original group of Hull et al with a vanishingly small incidence of complications if left un- treated. We can further stratify the 3.3% in whom proximal venous thrombosis would have been detected had 1PG been performed.
In Hull et al's 7 non-high-probability group, 67% (29 of 43) of positive IPGs occurred in patients with three or more predisposing factors for proximal vein thrombosis. Thus, if we were to refer patients with two or more risk factors for objective venous studies (IPG or duplex ultrasound), then of the 3% of our population at risk for proximal vein thrombosis, only one third of these would be expected to have a positive IPG if tested. Thus, by separating out patients with low- as opposed to intermediate- probability scans, and considering those with less than two predisposing factors for proximal vein thrombosis, we can identify a subset of patients in whom the risk of thromboembolism at the time of evaluation is approximately 1%. Even if this estimate is off by a factor of two, the risk of missing a patient with severe thromboem- bolic disease is extremely low.
Should we abandon IPG and duplex ultra- sound? Certainly not. Since they are noninva- sive, they should be performed, when available, in any patient with a high risk ie, several risk factors, of thromboembolic disease. If such testing is not immediately available, however, withdrawing anticoagulants in the patient with
less than two predisposing factors and a low- probability scan presents minimal risk.
Is the risk of proximal vein thrombosis at the time of presentation equal among all patients presenting for lung scans? The answer again is no. Compared with non-high-probability pa- tients, those with high-probability scans have more than twice the incidence on presentation of proximal venous thrombosis detectable by IPG, 19% versus 8%. 7
Even among these patients, we may make some rational assessments of the varying risk from patient to patient. Although many patients with proximal vein thrombosis will present with PE, not all patients in whom the diagnosis of PE is entertained are at the same risk for proximal vein thrombosis. In the patient who has recently undergone pelvic surgery or a prolonged period of immobility, the diagnosis of thromboembo- lism is strongly suggested and a low-probability lung scan should be followed by a noninvasive venous study such as IPG or duplex ultrasound. On the other hand, many patients presenting to nuclear medicine units for lung scanning have quite different histories. Some of these patients are at higher risk than the general population for proximal vein thrombosis, but many are not. The otherwise healthy patient with new onset of atrial fibrillation is suspected of having PE. If, however, a reasonable investigation (lung scan) indicates low probability, it makes little sense to pursue the diagnosis further in the absence of evidence pointing to proximal vein thrombosis. Likewise, consider the patient with shortness of breath due clinically to an exacerbation of pre-existing chronic obstructive pulmonary dis- ease. If a V/Q scan is low probability, the probability of detectable PE by angiography is low and, therefore, the patient is at an ex- tremely low risk of a thromboembolic complica- tions even without anticoagulant therapy. Since PE had a relatively low pretest (prescan) likeli- hood of causing the patient's symptoms, the chance that the patient also has an asymptom- atic proximal vein thrombosis is quite low.
The simple association of two phenomena, PE and venous thrombosis, does not mean the diagnostic workup for one should inevitably lead to an evaluation for the other. Nonethe- less, many conditions associated with symptoms of PE, eg, congestive heart failure, are associ-
LUNG S C A N N I N G IN P U L M O N A R Y E M B O L I S M 289
ated with increased risk of proximal vein throm- bosis, and these patients should be appropri- ately evaluated. But, if the clinical likelihood of PE and proximal vein thrombosis is felt to be low, this, in combination with a low-probability lung scan pattern, provides an appropriate level of certainty in allocating the patient to a low- risk group not requiring therapy. The long-term outcome of patients with non-high-probability scans and negative serial IPG results who were off anticoagulant therapy, has been found to be better than or at least equivalent to the outcome (7% thromboembolic events) in patients with high-probability lung scans who received antico- agulant therapy. 7 Likewise, the long-term out- come without treatment in patients with low- probability scans, even without performance of serial IPGs, is better than the outcome in treated patients with high probability scans. In view of the above data, we recommend that patients with multiple predisposing factors for venous thrombosis and low- or intermediate- probability scans should undergo noninvasive venous study of the legs before anticoagulants are withdrawn.
THE VALUE OF CLINICAL ASSESSMENT
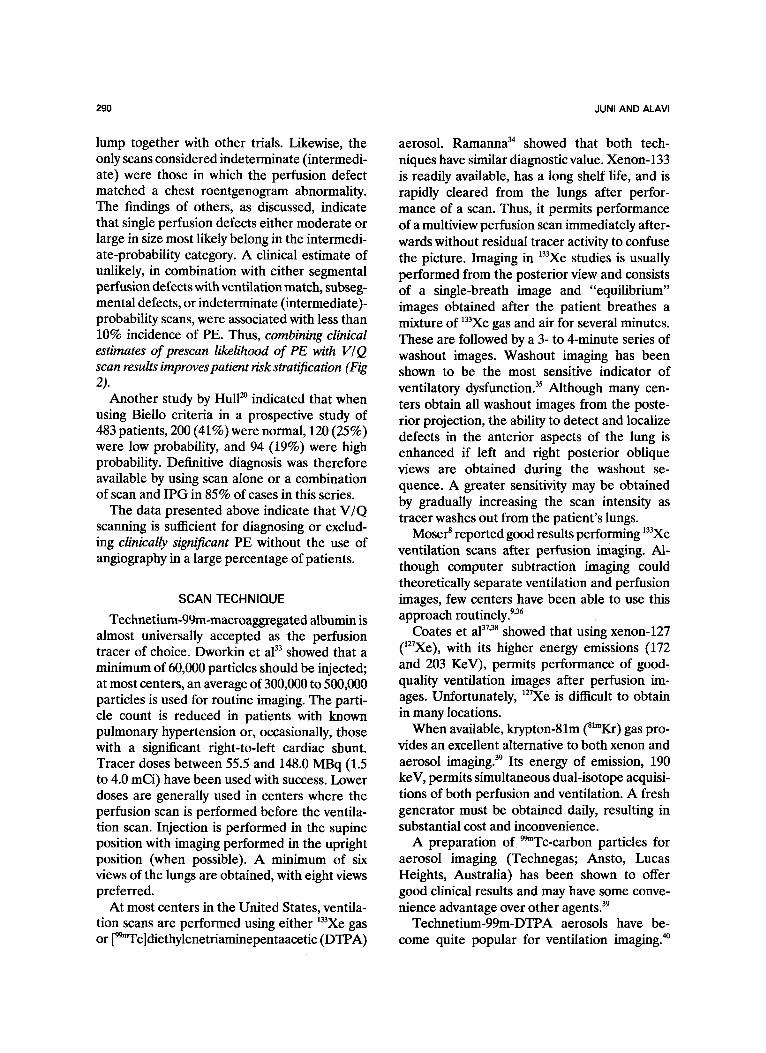
In the PIOPED study, clinical estimates of the likelihood of PE were determined for each patient before the scan was performed. These were based on clinical history, physical examina- tion, chest roentgenogram, and arterial blood gases. The clinical estimates reflected the exam- ining physician's personal assessment of disease likelihood and did not follow a predefined diagnostic algorithm or other set criteria for probability assessment. The number of physi- cians participating in this arm of the study was large and included staff from a number of separate institutions around the country. It is likely that, as a group, these judgements would be similar to those at other institutions. The clinical assessments were lumped into three broad categories, increasing the likelihood of consensus among observers: pulmonary embo- lus unlikely (estimated likelihood between 0% and 19%), likely (estimated likelihood of PE 80% to 100%), and uncertain (estimated likeli- hood between 20% and 79%). Combining the clinical assessments with the V/Q scan interpre- tations markedly improved the overall chance of
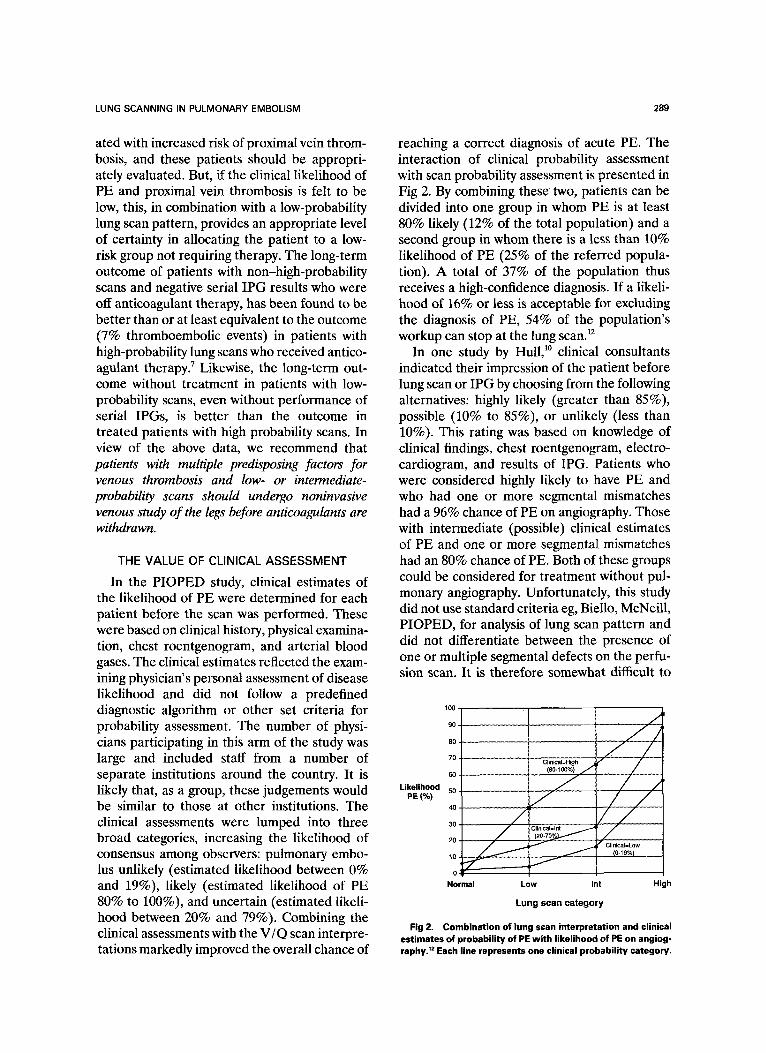
reaching a correct diagnosis of acute PE. The interaction of clinical probability assessment with scan probability assessment is presented in Fig 2. By combining these two, patients can be divided into one group in whom PE is at least 80% likely (12% of the total population) and a second group in whom there is a less than 10% likelihood of PE (25% of the referred popula- tion). A total of 37% of the population thus receives a high-confidence diagnosis. If a likeli- hood of 16% or less is acceptable for excluding the diagnosis of PE, 54% of the population's workup can stop at the lung scan. 12
In one study by Hull, 1~ clinical consultants indicated their impression of the patient before lung scan or IPG by choosing from the following alternatives: highly likely (greater than 85%), possible (10% to 85%), or unlikely (less than 10%). This rating was based on knowledge of clinical findings, chest roentgenogram, electro- cardiogram, and results of IPG. Patients who were considered highly likely to have PE and who had one or more segmental mismatches had a 96% chance of PE on angiography. Those with intermediate (possible) clinical estimates of PE and one or more segmental mismatches had an 80% chance of PE. Both of these groups could be considered for treatment without pul- monary angiography. Unfortunately, this study did not use standard criteria eg, Biello, McNeill, PIOPED, for analysis of lung scan pattern and did not differentiate between the presence of one or multiple segmental defects on the perfu- sion scan. It is therefore somewhat difficult to
Likelihood PE (%)
100
90 ,
/ 8O
70 Clinical~High ~"J
Normal Low Int High
Lung scan category
Fig 2. Combination of lung scan interpretation and clinical estimates of probability of PE with likelihood of PE on angiog- raphy. TM Each line represents one clinical probability category,
290 JUNI AND ALAVI
lump together with other trials. Likewise, the only scans considered indeterminate (intermedi- ate) were those in which the perfusion defect matched a chest roentgenogram abnormality. The findings of others, as discussed, indicate that single perfusion defects either moderate or large in size most likely belong in the intermedi- ate-probability category. A clinical estimate of unlikely, in combination with either segmental perfusion defects with ventilation match, subseg- mental defects, or indeterminate (intermediate)- probability scans, were associated with less than 10% incidence of PE. Thus, combining clinical estimates of prescan likelihood of PE with I/'/ Q scan results improves patient risk stratification (Fig 2).
Another study by Hull 2a indicated that when using Biello criteria in a prospective study of 483 patients, 200 (41%) were normal, 120 (25%) were low probability, and 94 (19%) were high probability. Definitive diagnosis was therefore available by using scan alone or a combination of scan and IPG in 85% of cases in this series.
The data presented above indicate that V/Q scanning is sufficient for diagnosing or exclud- ing clinically significant PE without the use of angiography in a large percentage of patients.
SCAN TECHNIQUE
Technetium-99m-macroaggregated albumin is almost universally accepted as the perfusion tracer of choice. Dworkin et a133 showed that a minimum of 60,000 particles should be injected; at most centers, an average of 300,000 to 500,000 particles is used for routine imaging. The parti- cle count is reduced in patients with known pulmonary hypertension or, occasionally, those with a significant right-to-left cardiac shunt. Tracer doses between 55.5 and 148.0 MBq (1.5 to 4.0 mCi) have been used with success. Lower doses are generally used in centers where the perfusion scan is performed before the ventila- tion scan. Injection is performed in the supine position with imaging performed in the upright position (when possible). A minimum of six views of the lungs are obtained, with eight views preferred.
At most centers in the United States, ventila- tion scans are performed using either 133Xe gas or [99~Tc]diethylenetriaminepentaacetic (DTPA)
aerosol. Ramanna 34 showed that both tech- niques have similar diagnostic value. Xenon-133 is readily available, has a long shelf life, and is rapidly cleared from the lungs after perfor- mance of a scan. Thus, it permits performance of a multiview perfusion scan immediately after- wards without residual tracer activity to confuse the picture. Imaging in 133Xe studies is usually performed from the posterior view and consists of a single-breath image and "equilibrium" images obtained after the patient breathes a mixture of 133Xe gas and air for several minutes. These are followed by a 3- to 4-minute series of washout images. Washout imaging has been shown to be the most sensitive indicator of ventilatory dysfunction. 35 Although many cen- ters obtain all washout images from the poste- rior projection, the ability to detect and localize defects in the anterior aspects of the lung is enhanced if left and right posterior oblique views are obtained during the washout se- quence. A greater sensitivity may be obtained by gradually increasing the scan intensity as tracer washes out from the patient's lungs.
Moser 8 reported good results performing 133Xe ventilation scans after perfusion imaging. Al- though computer subtraction imaging could theoretically separate ventilation and perfusion images, few centers have been able to use this approach routinely. 9'36
Coates et a137'38 showed that using xenon-127 (127Xe), with its higher energy emissions (172 and 203 KeV), permits performance of good- quality ventilation images after perfusion im- ages. Unfortunately, 127Xe is difficult to obtain in many locations.
When available, krypton-81m (81"Kr) gas pro- vides an excellent alternative to both xenon and aerosol imaging. 39 Its energy of emission, 190 keV, permits simultaneous dual-isotope acquisi- tions of both perfusion and ventilation. A fresh generator must be obtained daily, resulting in substantial cost and inconvenience.
A preparation of 99mTc-carbon particles for aerosol imaging (Technegas; Ansto, Lucas Heights, Australia) has been shown to offer good clinical results and may have some conve- nience advantage over other agents. 39
Technetium-99m-DTPA aerosols have be- come quite popular for ventilation imaging. 4~
LUNG SCANNING IN PULMONARY EMBOLISM 291
The tracer distribution in such a study is similar to that of the single-breath t33Xe scan. Aerosol imaging has the advantage of tracer remaining fixed in the lung for several minutes after inhalation. This permits ventilation images to be obtained from multiple views matching those of the perfusion scan. Performing a perfusion scan before the ventilation study permits the ventilation study to be obtained in the position most likely to demonstrate a defect. A disadvan- tage is the absence of washout images and the fact that both the ventilation and perfusion images are obtained using the same radionu- clide. Activity from whichever scan is performed first will "shine through" on the second scan. Delaying the second set of images until the first tracer has decayed is impractical in the clinical setting where an answer is needed fairly rapidly. So long as the injected dose of [~9~Tc]MAA is kept low, eg, 1.5 mCi (55.5 MBq), it is generally possible to obtain good-quality ventilation im- ages with [99~Tc]DTPA aerosol after perfusion imaging. A reasonable guideline is to adminis- ter enough aerosol that the count rate in the posterior view is three times that of the perfu- sion image alone. Schane et al 4~ showed that surface contamination in rooms in which radio- aerosol studies have been performed may be significant. Careful technique, with frequent wipe tests of imaging tables, equipment, and personnel (garments and skin), is essential when aerosol imaging is performed.
When the ventilation scan is routinely per- formed first, a substantial number of patients (those with normal perfusion) will undergo ventilation scans that are not helpful for diagno- sis. S o m e 9 have proposed that a perfusion study be performed first in patients in whom (1) the clinical suspicion of PE is low and (2) the chest roentgenogram is normal. Since most of these cases would be expected to have normal ventila- tion, only those cases in which the perfusion study is abnormal would require ventilation scans. In view of the many reports of successful performance of ventilation imaging after perfu- sion imaging, there seems to be little need for changing procedure from patient to patient. Performance of a perfusion image first will permit rapid identification of those patients needing no further diagnostic evaluation. If low
doses of [99~Tc]MAA are used as described above, ventilation imaging with 133Xe, techne- tium-DTPA aerosol, or 81mKr can be performed afterwards in those patients in whom it is needed. The advantage gained by being able to perform the ventilation scan from the projec- tion best showing perfusion defects is substan- tial.
CRITERIA FOR SCAN INTERPRETATION
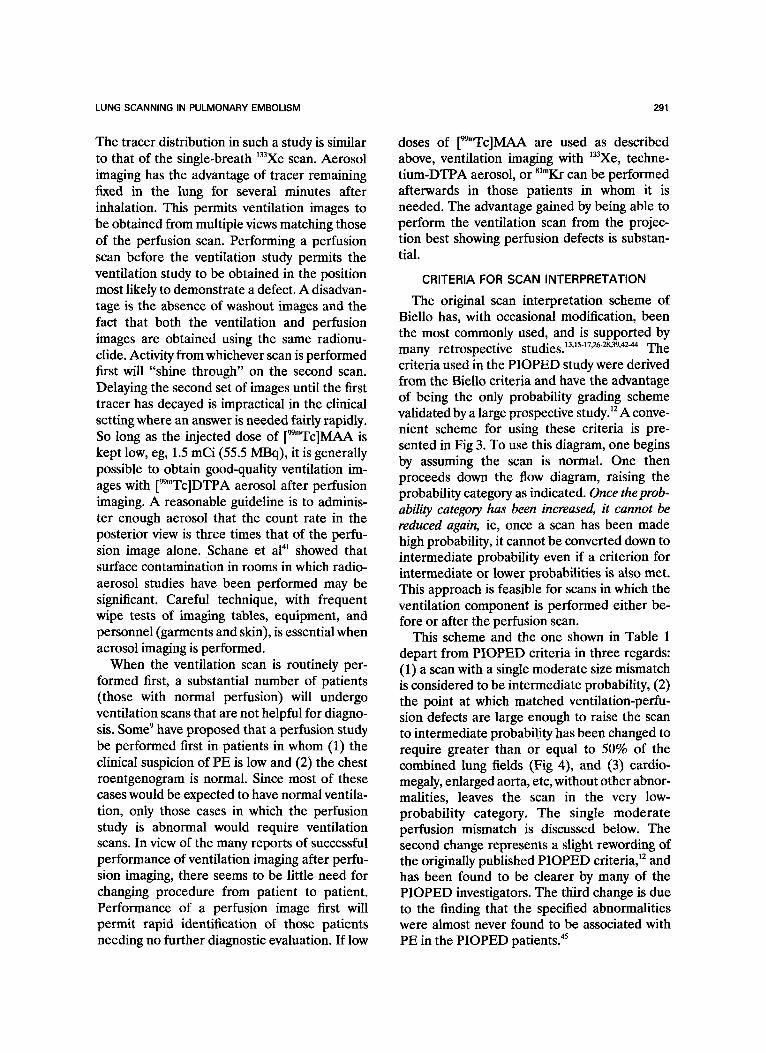
The original scan interpretation scheme of Biello has, with occasional modification, been the most commonly used, and is supported by many retrospective s t u d i e s . 13A5-17'2628'39'42-44 The criteria used in the PIOPED study were derived from the Biello criteria and have the advantage of being the only probability grading scheme validated by a large prospective study. ~2 A conve- nient scheme for using these criteria is pre- sented in Fig 3. To use this diagram, one begins by assuming the scan is normal. One then proceeds down the flow diagram, raising the probability category as indicated. Once the prob- ability category has been increased, it cannot be reduced again, ie, once a scan has been made high probability, it cannot be converted down to intermediate probability even if a criterion for intermediate or lower probabilities is also met. This approach is feasible for scans in which the ventilation component is performed either be- fore or after the perfusion scan.
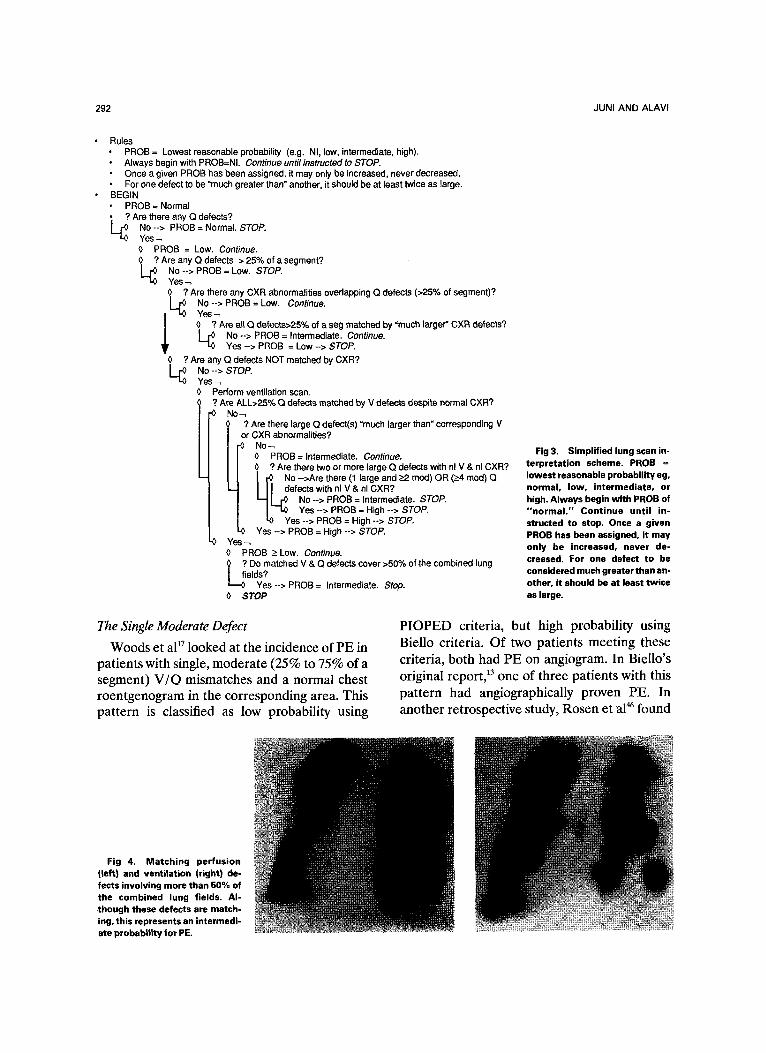
This scheme and the one shown in Table 1 depart from PIOPED criteria in three regards: (1) a scan with a single moderate size mismatch is considered to be intermediate probability, (2) the point at which matched ventilation-perfu- sion defects are large enough to raise the scan to intermediate probability has been changed to require greater than or equal to 50% of the combined lung fields (Fig 4), and (3) cardio- megaly, enlarged aorta, etc, without other abnor- malities, leaves the scan in the very low- probability category. The single moderate perfusion mismatch is discussed below. The second change represents a slight rewording of the originally published PIOPED criteria, 12 and has been found to be clearer by many of the PIOPED investigators. The third change is due to the finding that the specified abnormalities were almost never found to be associated with PE in the PIOPED patients. 45
292 JUNI AND ALAVI
Rules PROB = Lowest reasonable probability (e.g. NI, low, intermediate, high). Always begin with PROB=NI. Continue unti/ instructed to STOP. Once a given PROB has been assigned, it may only be increased, never decreased. For one defect to be "much greater than" another, it should be at least twice as large.
BEGIN PROB = Normal ? Are there any Q defects?
No --> PROB = Normal. STOP. Yes~ O PROB = Low. Continue. 0 ? Are any Q defects > 25% of a segment? L ~ No --> PROB = Low. STOP.
Yes 0 ? Are there any CXR abnormalities overlapping Q defects (>25% of segment)?
No --> PROB = Low, Continue.
0 ? Are all Q defects>25% of a seg matched by "much larger" CXR defects? No --> PROB = Intermediate. Continue. Yes --> PROB = Low --> STOP.
0 ? Are any Q defects NOT matched by CXR? L [~ No --> STOP.
Yes Perform ventilation scan.
Are ALL>25% Q defects matched by V defects despite normal CXR? -0 No~
? Are there large Q defect(s) =much larger than" corresponding V or CXR abnormalities?
No / [~ 0 PROB= Intermediate. Continue. / / 0 ? Are there two or more large Q defects with nl V & nl CXR? I I I t ~ No -->Are there (1 large and >_2 mod) OR (>_4 mod) Q I . ~ I I I defects with nl V & nl CXR? | =--~ ~ r ~ No --> PROB = Intermediate. STOP. l I 7-0 Yes --> PROB = High --> STOP. / t O Yes --> PROB = High --> STOP. L O Yes --> PROB = High --> STOP. Yes 0 PROB _> Low. Continue. ~of i ? Do matched V & Q defects cover >50% of the combined lung
elds? Yes--> PROB = Intermediate. Stop.
0 STOP
Fig 3. Simplified lung scan in- terpretation scheme. PROB = lowest reasonable probability eg, normal, low, intermediate, or high. Always begin with PROB of "normal ." Continue until in- structed to stop. Once a given PROB has been assigned, it may only be increased, never de- creased. For one defect to be considered much greater than an- other, it should be at least twice as large.
The Single Moderate Defect
Woods et a117 looked at the incidence of PE in patients with single, moderate (25% to 75% of a segment) V/Q mismatches and a normal chest roentgenogram in the corresponding area. This pattern is classified as low probability using
PIOPED criteria, but high probability using Biello criteria. Of two patients meeting these criteria, both had PE on angiogram. In Biello's original report, 13 one of three patients with this pattern had angiographically proven PE. In another retrospective study, Rosen et a146 found
Fig 4. Matching perfusion (left) and ventilation (right) de- fects involving more than 50% of the combined lung fields. Al- though these defects are match- ing, this represents an intermedi- ate probability for PE.
LUNG SCANNING IN PULMONARY EMBOLISM 293
that 5 of 11 patients (45%) with moderate subsegmental mismatches had PE. 44 This in- cluded 7 of their 16 patients with normal chest roentgenogram and three fourths of patients with V/Q mismatch and matching radiographic opacity. Catania and Caride 18 grouped moder- ate and large defects together. Fifty percent of all scans with single perfusion defects had PE. PE was found in 5 of 5 moderate and 9 of 13 large defects regardless of the ventilation scan or chest roentgenogram findings. In a review of the literature, they found that 40% of patients with single perfusion defects mismatch with ventilation scan had PE whereas 15% had PE if the ventilation matched the perfusion scan but chest roentgenogram was normal. Interestingly, if perfusion defects matched chest roentgeno- gram abnormalities in the presence of normal ventilation scans, 91% of patients had PE; 56% had PE if the perfusion scan, ventilation scan, and chest roentgenogram were all abnormal. Hull ~~ found that moderate V/Q mismatches were associated with PE in 57% of cases whereas a moderate ventilation-perfusion match accom- panied PE in 31% of cases. PIOPED publica- tions to date have not been analyzed regarding single perfusion defects, but Gottschalk 47 re- ports that in his analysis of the PIOPED data, one third of 30 patients with single moderate perfusion defects had PE.
Thus, although PIOPED criteria place a sin- gle moderate mismatch in low probability and a large mismatch in intermediate probability, the weight of evidence would indicate that both single moderate and large V/ Q mismatches should be classified as intermediate probability regardless
of chest roentgenogram findings. 4s A moderate ventilation-perfusion match could be classified as either low or intermediate probability.
Effects of Pleural Effusion
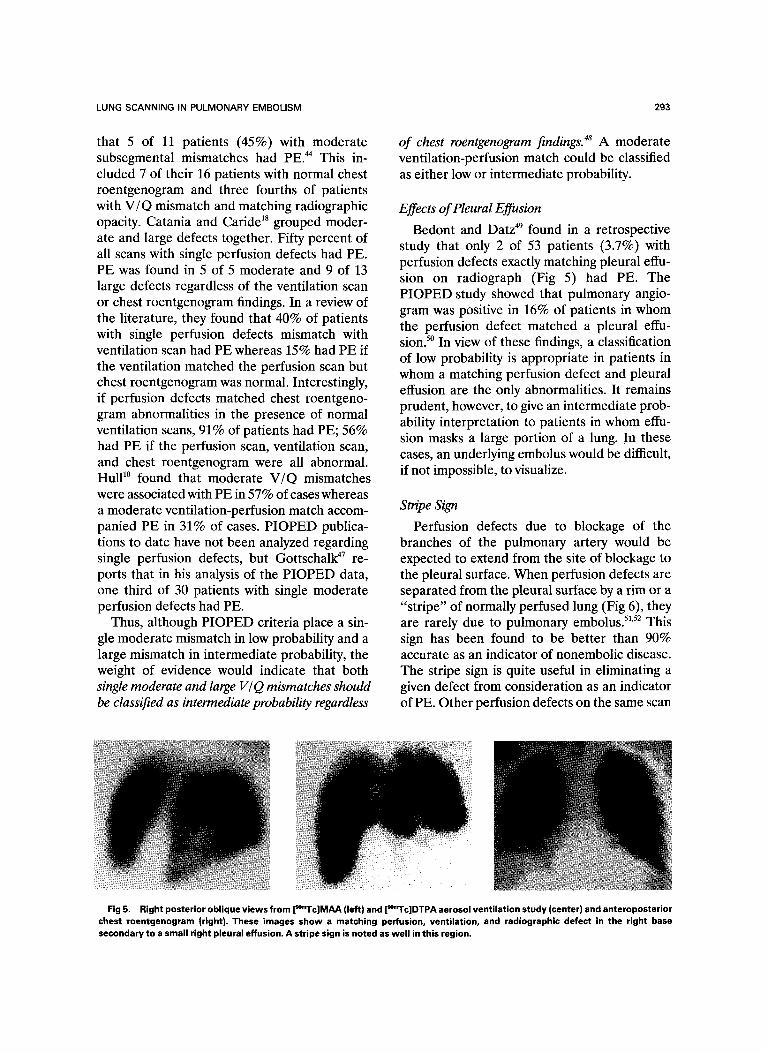
Bedont and Datz 49 found in a retrospective study that only 2 of 53 patients (3.7%) with perfusion defects exactly matching pleural effu- sion on radiograph (Fig 5) had PE. The PIOPED study showed that pulmonary angio- gram was positive in 16% of patients in whom the perfusion defect matched a pleural effu- sion. 5~ In view of these findings, a classification of low probability is appropriate in patients in whom a matching perfusion defect and pleural effusion are the only abnormalities. It remains prudent, however, to give an intermediate prob- ability interpretation to patients in whom effu- sion masks a large portion of a lung. In these cases, an underlying embolus would be difficult, if not impossible, to visualize.
Stripe Sign
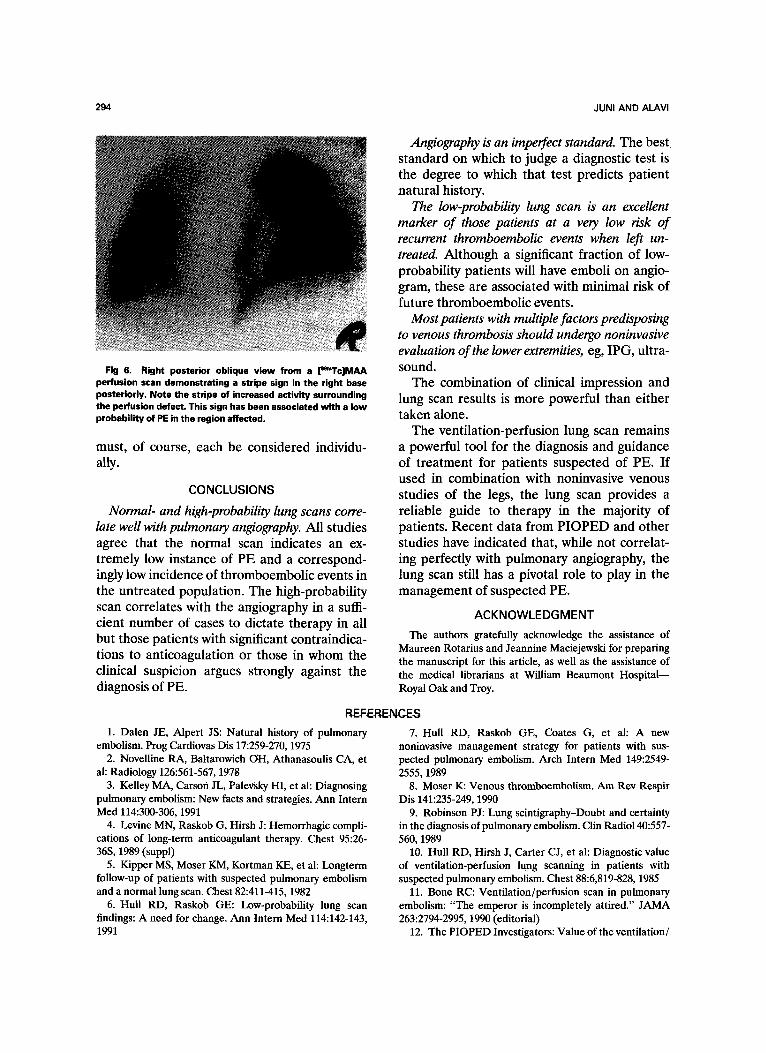
Perfusion defects due to blockage of the branches of the pulmonary artery would be expected to extend from the site of blockage to the pleural surface. When perfusion defects are separated from the pleural surface by a rim or a "stripe" of normally perfused lung (Fig 6), they are rarely due to pulmonary embolus. 51'52 This sign has been found to be better than 90% accurate as an indicator of nonembolic disease. The stripe sign is quite useful in eliminating a given defect from consideration as an indicator of PE. Other perfusion defects on the same scan
Fig 5. Right posterior oblique views from [~mTc]MAA (left) and ['gmTc]DTPA aerosol ventilation study (center) and anteroposterior chest roentgenogram {right). These images show a matching perfusion, ventilation, and radiographic defect in the right base secondary to a small right pleural effusion. A stripe sign is noted as well in this region.
294 JUNI AND ALAVI
Fig 6. Right posterior oblique view from a [m' rc ]MAA perfusion scan demonstrating a stripe sign in the right base posteriorly. Note the stripe of increased activity surrounding the perfusion defect. This sign has been associated with a low probability of PE in the region affected.
must, of course, each be considered individu- ally.
CONCLUSIONS
Normal- and high-probability lung scans corre- late well with pulmonary angiography. All studies agree that the normal scan indicates an ex- tremely low instance of PE and a correspond- ingly low incidence of thromboembolic events in the untreated population. The high-probability scan correlates with the angiography in a suffi- cient number of cases to dictate therapy in all but those patients with significant contraindica- tions to anticoagulation or those in whom the clinical suspicion argues strongly against the diagnosis of PE.
Angiography is an imperfect standard. The best standard on which to judge a diagnostic test is the degree to which that test predicts patient natural history.
The low-probability lung scan is an excellent marker of those patients at a very low risk of recurrent thromboembolic events when left un- treated. Although a significant fraction of low- probability patients will have emboli on angio- gram, these are associated with minimal risk of future thromboembolic events.
Most patients with multiple factors predisposing to venous thrombosis should undergo noninvasive evaluation of the lower extremities, eg, IPG, ultra- sound.
The combination of clinical impression and lung scan results is more powerful than either taken alone.
The ventilation-perfusion lung scan remains a powerful tool for the diagnosis and guidance of treatment for patients suspected of PE. If used in combination with noninvasive venous studies of the legs, the lung scan provides a reliable guide to therapy in the majority of patients. Recent data from PIOPED and other studies have indicated that, while not correlat- ing perfectly with pulmonary angiography, the lung scan still has a pivotal role to play in the management of suspected PE.
ACKNOWLEDGMENT
The authors gratefully acknowledge the assistance of Maureen Rotarius and Jeannine Maciejewski for preparing the manuscript for this article, as well as the assistance of the medical librarians at William Beaumont Hospital-- Royal Oak and Troy.
REFERENCES
1. Dalen JE, AlpeTt JS: Natural history of pulmonary embolism. Prog Cardiovas Dis 17:259-270, 1975
2. Novelline RA, Baltarowich OH, Athanasoulis CA, et al: Radiology 126:561-567, t978
3. Kelley MA, Carson JL, Palevsky HI, et al: Diagnosing pulmonary embolism: New facts and strategies. Ann Intern Med 114:300-306, 1991
4. Levine MN, Raskob G, Hirsh J: Hemorrhagic compli- cations of long-term anticoagulant therapy. Chest 95:26- 36S, 1989 (suppl)
5. Kipper MS, Moser KM, Kortman KE, et al: Longterm follow-up of patients with suspected pulmonary embolism and a normal lung scan. Chest 82:411-415, 1982
6. Hull RD, Raskob GE: Low-probability lung scan findings: A need for change. Ann Intern Med 114:142-143, 1991
7. Hull RD, Raskob GE, Coates G, et al: A new noninvasive management strategy for patients with sus- pected pulmonary embolism. Arch Intern Med 149:2549- 2555, 1989
8. Moser K: Venous thromboembolism. Am Rev Respir Dis 141:235-249, 1990
9. Robinson PJ: Lung scintigraphy-Doubt and certainty in the diagnosis of pulmonary embolism. Clin Radio140:557- 560, 1989
10. Hull RD, Hirsh J, Carter CJ, et al: Diagnostic value of ventilation-perfusion lung scanning in patients with suspected pulmonary embolism. Chest 88:6,819-828, 1985
11. Bone RC: Ventilation/perfusion scan in pulmonary embolism: "The emperor is incompletely attired." JAMA 263:2794-2995, 1990 (editorial)
12. The PIOPED Investigators: Value of the ventilation/
LUNG SCANNING IN PULMONARY EMBOLISM 295
perfusion scan in acute pulmonary embolism: Results of the Prospective Investigation of Pulmonary Embolism Diagno- sis (PIOPED). JAMA 263:2753-2759, 1990
13. BieUo DR, Mattar AG, McKnight RC, et al: Ventila- tion-perfusion studies in suspected pulmonary embolism. AJR 133:1033-1037, 1979
14. McNeil BJ, Holman L, Adelstein SJ: The scinti- graphic definition of pulmonary embolism. JAMA 227:753- 756, 1974
15. Alderson PO, Biello DR, Saehariah KG, et al: Scinti- graphic detection of pulmonary embolism in patients with obstructive pulmonary disease. Radiology 138:661-666, 1981
16. Webber MM, Gomes AS, Roe D, et al: Comparison of Biello, McNeil and PIOPED criteria for the diagnosis of pulmonary emboli on lung scans. AJR 154:975-981, 1990
17. Woods ER, Iles S, Jackson S: Comparison of scinti- graphic diagnostic criteria in suspected pulmonary embo- lism. J Can Assoc Radio140:194-197, 1989
18. Catania TA, Caride VJ: Single perfusion defect and pulmonary embolism: Angiographic correlation. J Nucl Med 31:296-310, 1990
19. Hull RD, Hirsh J, Carter CJ, et al: Pulmonary angiography, ventilation lung scanning, and venography for clinically suspected pulmonary embolism with abnormal perfusion lung scan. Ann Intern Med 98:891-899, 1983
20. Hull RD, Raskob GE: Low-probability lung scan findings: A need for change. Ann Intern Med 114:142-143, 1991
21. Moser KM, LeMoine JR: Is embolic risk conditioned by location of deep venous thrombosis? Ann Intern Med 94:439-444, 1981
22. Huisman MV, Buller HR, tenCate JW, et al: Unex- pected high prevalence of silent pulmonary embolism in pa- tients with deep venous thrombosis. Chest 95:498-502, 1989
23. Sostman HD, Rapoport S, Gottschalk A, et al: Imaging in pulmonary embolism. Invest Radiol 21:443-454, 1986
24. Quinn ME, Lundell CJ, Klotz TA, et al: Reliability of selective pulmonary arteriography in the diagnosis of pulmo- nary embolism. AIR 149:469-471, 1987
25. Hull RD, Raskob GE, Coates G, et al: Clinical validity of a normal perfusion lung scan in patients with suspected pulmonary embolism. Chest 97:23-26, 1990
26. Smith R, Maher JM, Miller RI, et al: Clinical out- comes of patients with suspected pulmonary embolism and low-probability aerosol-perfusion scintigrams. Radiology 164:731-733, 1987
27. Lee ME, Biello DR, Kumar B, et al: "Low-probability" ventilation-perfusion scintigrams: Clinical outcomes in 99 patients. Radiology 156:497-500, 1985
28. Kahn D, Bushnell DL, Dean R, et al: Clinical outcome of patients with a "low-probability" of pulmonary embolism on ventilation-perfusion lung scan. Arch Intern Med 149:377-379, 1989
29. Jacobs MP: "Low-probability" ventilation/perfusion scans. Ann Intern Med 114:604-605, 1991 (letter to the editor)
30. Huisman MV, Buller HR, TenCate JW, et ai: Serial impedance plethysmography for suspected deep venous thrombosis in outpatients. N Engl J Med 314:823-828, 1986
31. Hull RD, Hirsh J, Carter CJ, et al: Diagnostic efficacy of impedance plethysmography for clinically suspected deep- vein thrombosis. Ann Intern Med 102:21-28, 1985
32. Monreal M, Barroso C, Manzano JR, et al: Asymp- tomatic pulmonary embolism in patients with deep vein thrombosis. It is useful to take a lung scan to rule out this condition. J Cardiovasc Surg 30:104-107, 1989
33. Dworkin H J, Gutkowski RF, Porter W, et al: Effect of particle number on lung perfusion images: Concise commu- nication. J Nucl Med 18:260-262, 1977
34. Ramanna L, Alderson PO, Waxman AD, et al: Regional comparison of technetium-99m DTPA aerosol and radioactive gas ventilation (Xenon and Krypton) stud- ies in patients with suspected pulmonary embolism. J Nucl Med 27:1391-1396, 1986
35. Alderson PO, Biello DR, Khan AR, et al: Compari- son of 133Xe single-breath and washout imaging in the scintigraphic diagnosis of pulmonary embolism. Radiology 137:481-486, 1980
36. Kenny PA, Dowsett DJ, Vernon D, et al: A technique for digital image registration used prior to subtraction of lung images in nuclear medicine. Phys Med Bio135:679-685, 1990
37. Coates G, Garnett ES: The ventilation study: Before or after the perfusion lung scan. AJR 128:1037-1038, 1977 (letters to the editor)
38. Coates G, Nahmias C: Xenon-127, a comparison with Xenon-133 for ventilation studies. J Nucl Med 18:221-225, 1977
39. Peltier P, DeFaucal P, Chetanneau A, et al: Compar- ison of technetium-99m aerosol and krypton-81m in ventila- tion studies for the diagnosis of pulmonary embolism. Nucl Med Commun 11:631-638, 1990
40. Selby JB, Callcott F, Gordon L, et al: Utility of Tc-99m DTPA aerosol inhalation scans following perfusion lung scans in the diagnosis of pulmonary embolism. Clin Nucl Med 15:143-149, 1990
41. Schane EC, McGraw R, Culver C, et al: Room contamination following Tc99m-DTPA aerosol ventilation studies. J Nucl Med Technol 18:139, 1990
42. Carter WD, Brady TM, Keyes JW, et al: Relative accuracy of two diagnostic schemes for detection of pulmo- nary embolism by ventilation-perfusion scintigraphy. Radi- ology 145:447-451, 1982
43. Becker RC, Graor R, Hoiloway J: Pulmonary embo- lism: A review of 200 cases with emphasis on pathophysiol- ogy, diagnosis and treatment. Cleve Clin Q 51:519-529,1984
44. Selby JB Sr, Callcott F, Gordon L, et ai: Utility of Tc-99m DTPA aerosol inhalation scans following perfusion lung scans in the diagnosis of pulmonary embolism. Clin Nucl Med 15:143-149, 1990
45. Gottschalk A: PIOPED: Evaluation of criteria. Pre- sented at Spring 1991 Meeting of the Central Chapter of the Society of Nuclear Medicine, Milwaukee, WI, April 28,1991
46. Rosen JM, Palestro CJ, Markowitz D, et al: Signifi- cance of single ventilation/perfusion mismatches in Krypton- 81m/technetinm-99m lung scintigraphy. J Nucl Med 27:361- 365, 1986
47. Gottschalk A: Yearbook of Nuclear Medicine, St Louis, MO, Mosby, 1991, p 132

296 JUNI AND ALAVI
48. Gray HW: The single perfusion abnormality: "Quo vadis?" Nucl Med Commun 12:377-379, 1991
49. Bedont R.A, Datz FL: Lung scan perfusion defects limited to matching pleura] effusions: Low probability of pulmonary embolism. AIR 145:1155-1157, 1985
50. Gottschalk A, Stein PD: Lung scan perfusion defects limited to matching pleural effusions indicate a low probabil- ity of pulmonary embolism, but do not confidently exclude the diagnosis. (Abstract) J Nucl Med 32:951, 1991 (abstr)
51. Sostman HD, Gottschalk A: The stripe sign: A new sign for diagnosis of nonembolic defects on pulmonary perfusion scintigraphy. Radiology 142:737, 1982
52. Kotlyarov EV, Ruppel WF, Reba RC: Interpretation of perfusion lung scan based on presence and absence of "stripe sign," Invest Radiol 18:S15, 1983 (suppl)
53. White RH, McGahan JP, Daschbach MM, et al: Diagnosis of deep-vein thrombosis using duplex ultrasound. Ann Intern Med 111:297-304, 1989