Embed Size (px)
Citation preview

MINI-REVIEW
Lymphatic Transport of Proteins AfterSubcutaneous Administration
CHRISTOPHER J. H. PORTER, SUSAN A. CHARMAN*
Department of Pharmaceutics, Victorian College of Pharmacy Monash University, 381 Royal Parade,Parkville, Victoria, 3052, Australia
Received 2 September 1999; revised 15 November 1999; accepted 18 November 1999
ABSTRACT: This mini-review summarizes the relevant literature regarding the lym-phatic transport of proteins after subcutaneous administration. A review of the physi-ology of the lymphatics and inherent anatomical differences between blood and lymphcapillaries is presented followed by a brief overview of the general characteristics ofprotein absorption and bioavailability following S.C. injection. A description of factorsknown to directly affect the lymphatic uptake of macromolecules follows and is sup-ported by representative data from this laboratory. A brief perspective on the impor-tance of lymphatic uptake and transport in understanding the biopharmaceutical prop-erties of protein drugs and potentially targeting the lymphatics is presented. © 2000Wiley-Liss, Inc. and the American Pharmaceutical Association J Pharm Sci 89: 297–310, 2000
INTRODUCTION
Subcutaneous (S.C.) administration continues torepresent the primary route of delivery for pro-tein-based drugs despite significant efforts to de-velop non-parenteral delivery systems for theseagents. The reasons for this are many-fold andinclude the low and variable systemic bioavail-ability with many non-parenteral routes, the rela-tive ease and speed of development of parenteraldosage forms compared with more complicated,non-parenteral delivery systems (e.g., inhaledsystems), and stability considerations upon stor-age and administration. Even though S.C. deliv-ery has been utilized extensively for a number ofyears, very little is known about the processes
that govern the absorption of macromoleculesfrom the interstitial space and the resulting im-pact of these processes on bioavailability andpharmacokinetic profiles. Proteins larger thanabout 16–20 kDa are generally thought to betaken up primarily by the lymphatic system,1–7
but very few studies have experimentally inves-tigated this process. Furthermore, the effects ofvarious external factors, including the site andmethod of administration and even “simple” for-mulation variables (e.g., pH and ionic strength)on the lymphatic transport of subcutaneously-injected proteins are still largely undefined.
This mini-review summarizes the relevant lit-erature regarding the lymphatic transport of pro-teins after S.C. administration. A review of thephysiology of the lymphatics is presented, whichfocuses on the inherent anatomical differences be-tween blood and lymph capillaries which controltheir respective permeabilities. This is followed
*Correspondence to: S. A. Charman (E-mail: [email protected])Journal of Pharmaceutical Sciences, Vol. 89, 297–310 (2000)© 2000 Wiley-Liss, Inc. and the American Pharmaceutical Association
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 89, NO. 3, MARCH 2000 297

by a brief overview of the general characteristicsof protein absorption and bioavailability followingS.C. injection to provide a background of indirectevidence for potential transport via the lymphat-ics. Factors known to directly affect the lymphaticuptake of macromolecules from the injection sitewill then be discussed using recent data from thislaboratory to illustrate the role of lymphatic up-take and transport in the bioavailability of hu-man growth hormone (hGH) after S.C. adminis-tration. The final section will provide a brief per-spective on the importance of lymphatic transportfrom the standpoint of fully understanding thebiopharmaceutical properties of protein drugsand potentially targeting the lymphatics for thetreatment of various lymph-resident diseases andconditions. It is not within the scope of this com-munication to review the literature pertaining tolymphatic transport of particulates or micellar-and colloidal-based delivery systems for smallmolecular weight drugs. The reader is referred toother excellent reviews7–11 for further informa-tion on these topics.
OVERVIEW OF THE LYMPHATIC SYSTEM
Most of the constituents of plasma move freelythrough capillary walls to form interstitial fluid,however, more fluid leaves the blood capillariesthan is returned by absorption with the excessfluid (about 3 L/day) draining into the lymphaticsto form lymph. The lymphatics draining the in-terstitial spaces are responsible for the absorp-tion of excess fluid, protein, and cellular elementswhich are not reabsorbed by the blood capillaries.However, unlike the blood circulation, the flow oflymph is unidirectional, recovering fluid from theperiphery and returning it to the vasculature.12
The initial or terminal lymphatics collectlymph from the periphery and unite to formprenodal collecting vessels or afferent lymphaticswhich transport lymph to the regional lymphnodes. Postnodal (efferent) lymph vessels carrylymph between successive sets of nodes or tolarger lymphatic collecting vessels which thendrain the lymph from the final set of lymph nodesinto the principle lymph ducts. Lymph from theintestinal, hepatic, and lumbar areas finallydrains into the cisterna chyli, which acts as a col-lecting reservoir at the distal end of the thoraciclymph duct. The major lymphatic vessel, the tho-racic lymph duct, ascends from the cisterna chyli,receiving lymph from the mediastinum and even-
tually, from all parts of the body (except in somecases where the upper right quadrant is drainedby a “right” thoracic lymph duct), and then emp-ties directly into the venous blood at the junctionof the left internal jugular vein and the left sub-clavian vein.12
All lymph passes through at least one set oflymph nodes (and in many cases several sets ofnodes) on its passage from the periphery back tothe systemic circulation.13 Lymph enters thelymph nodes via one, or many, afferent lymphducts, flows through the medullary sinuses, andexits through the hilus into a single efferent lym-phatic. Exchange of various materials betweenthe blood and the lymph may occur in the lymphnodes, however, the mechanism of this exchangeis poorly understood. Large numbers of macro-phages line the medullary sinuses and are re-sponsible for the phagocytosis of cellular and par-ticulate material from the lymph. The lymphnodes are also a center for lymphocyte prolifera-tion with B-lymphocytes, T-lymphocytes, and B-lymphocyte-derived antibodies entering thelymph via the lymph nodes.14
Physiology of the Interstitial Space
The structural characteristics of the interstitialspace are similar in all tissues, consisting of afibrous collagen framework supporting a gelphase made up of glycosaminoglycans, salts, andplasma-derived proteins. The glycosaminoglycansare polyanionic polysaccharides that are fullycharged at physiological pH and which, with theexception of hyaluronan, are bound covalently toa protein backbone to form proteoglycans whichare immobilized in the interstitium. Hyaluronan,is not immobilized and may be removed from theinterstitium via the lymph in a flow-dependentmanner.15–17
The proteins present in the interstitial spaceare qualitatively the same as those in the plasma,although quantitatively, they are present in lowerconcentrations most likely due to restricted ex-travasation by transcapillary flux.12,18,19 One ofthe major functions of interstitial proteins is tomaintain extravascular colloid osmotic pressureand in this regard, protein concentrations in theinterstitium are approximately 50% of those inplasma resulting in the interstitial colloid osmoticpressure (COPI) being less than that in plasma.20
In comparison, the fluid interstitial hydrostaticpressure (Pi) is small and slightly negative.
Since the capillary endothelial barrier is rela-
298 PORTER AND CHARMAN
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 89, NO. 3, MARCH 2000

tively poorly permeable to large hydrophilic mac-romolecules, endogenous proteins are primarilycleared from the interstitium via the lymph and,at least in the initial lymphatics, the lymphaticprotein concentrations reflect those in the inter-stitial space.20 Endogenous protein removal fromthe interstitium has been estimated using albu-min to be approximately 2–2.5%/h and is sensi-tive to both physical and pathophysiologicalchanges, increasing 3–4-fold during muscle activ-ity or edema.21,22
Diffusion of macromolecules within the inter-stitium may be physically retarded by the fibrouscollagen network and the gel structure of the pro-teoglycans as well as by electrostatic interactionwith charged components of the interstitial archi-tecture. Although contradictory reports exist,23
the prevailing view is that the negative chargessupplied by hyaluronan and the proteoglycansseem likely to provide an overall net negativecharge in the interstitium.20,24 The interstitiumalso displays a high degree of structural hetero-geneity and it is thought that aqueous pores orchannels are present which provide a “free-fluid”phase in addition to the presence of a “colloid-rich” gel phase.25–29 Electron microscopic investi-gations suggest channel diameters of 50–100nm,28 whereas application of pore theory to thediffusivity of proteins across the interstitium sug-gests pore sizes some five times smaller (120–200Å).26 Other studies have suggested that the effec-tive interstitial distribution volumes are dictatednot only by the presence of a free-fluid phase anda gel phase, but also by the presence of endog-enous macromolecules within the gel phasethereby restricting “access” to the available vol-ume. This network is thought to effectively reducethe distribution volume such that the intersti-tium acts in a size exclusion manner, excludingvery large molecules and thereby promoting theirinterstitial transport.19,27,30–32
The process of macromolecular diffusion acrossthe interstitium is likely dictated by molecularsize, the presence of diffusional microdomains,and physical and electrostatic interactions withthe various components of the interstitium. Inthis regard, Bell and co-workers suggest thatsteric effects predominate,19 however, a clear pic-ture of these complex interactions is still elusive.The composition and structure of the interstitiumhas been extensively reviewed elsewhere,20,24,33
and the interested reader is directed to these re-views for further information.
Lymphatic Drainage of the Interstitial Space
The rate of filtration and reabsorption of fluidacross the vascular capillaries is high (20–40L/day) in comparison to the small quantities ofinterstitial fluid drained by the lymph (2–4L/day). Consequently, small molecules (<2,000molecular weight) which can access lymph andblood capillaries equally are predominantlycleared by the blood vessels, whereas particulatesand molecules of increasing molecular size appearto favor drainage into the more open capillaries ofthe lymph. Three different types of blood capillar-ies exist within the vasculature and may be clas-sified in terms of their endothelial structure aseither continuous, fenestrated or discontinuous.The blood capillaries supplying the subcutaneousspace are generally continuous in nature andcharacterized by tight interendothelial junctionsand an uninterrupted basement membrane.These blood capillaries are relatively permeableto the exchange of small, lipophilic molecules, andby virtue of capillary “pores” (probably a combi-nation of plasmalemmal vesicles, transendothe-lial channels, and endothelial junctions), somehydrophilic molecules such as water. In contrast,the endothelium of blood vessels constitutes a sig-nificant barrier to the transfer of large, hydro-philic molecules such as proteins.
The structure of the lymphatic capillaries dif-fers markedly from that of blood capillaries as itconsists of a single layer of overlapping endothe-lial cells with an incomplete basal lamina and anabsence of interendothelial tight junctions (Fig-ure 1). The lymphatic endothelium thus has amore “open” structure with larger intercellularjunctions than found in blood capillaries. Esti-mates of intercellular junctional distances varyfrom several microns34–36 to 15–20 nm.37,38 Thestructure of the lymphatic capillaries is main-tained by anchoring filaments which attach to thewall of the lymphatic capillary and to the collagenfibers of the interstitium.35,39 These anchoringfilaments, in association with the overlapping en-dothelial cells, provide an endothelial “flap,” orlymphatic endothelial microvalve, which allowsthe unidirectional flow of fluid into the initiallymphatics when interstitial fluid pressure israised. In the presence of an increase in intralu-minal pressure, the flap falls back against thelymph wall, preventing fluid flow back into theinterstitium.40 Transfer of various tracers such asferritin and horseradish peroxidase also occurs
MINI-REVIEW 299
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 89, NO. 3, MARCH 2000

across the lymphatic endothelium in associationwith cytoplasmic vesicles.38,41–43
The driving force for fluid transfer from theinterstitium into the initial lymphatics has beenthe subject of significant debate. Clearly, a poten-tial energy difference in the fluid phase betweenthe interstitium and the lymphatics is requiredand may take the form of a chemical gradient,with the associated osmotic or oncotic pressuregradients, or a hydrostatic pressure differential.Casley-Smith has suggested that initial lym-phatic filling is facilitated by an osmotic gradientset up in the initial lymphatics by the filtration ofprotein-poor fluid from the lymphatics into theinterstitium.44 However, other investigators haveshown that the colloid osmotic pressures in theinterstitium and the initial lymphatics are simi-lar at steady state.45 More recent studies suggestthat lymphatic filling is facilitated via periodicchanges in interstitial pressure and volume
which are transmitted via the anchoring fila-ments to the lymphatics causing them to expandand contract.46–51 The periodic tissue pressuresinherent in this explanation include mechanismsprevalent in “inactive” subjects such as arterialpressure pulsations, respiration, and contractionsof the heart,49,52 in addition to larger variationsstimulated by skeletal muscle contraction,51 skinrubbing,50,51 and external compression such asthat experienced during running or walking. Theadditional lymphatic filling pressures provided byphysical movement appear to explain the en-hanced ability of unanesthetized animals to com-bat edema via an increase in lymph flow.53–55
The initial lymphatics drain into larger collect-ing lymphatics which, unlike the initial lymphat-ics, contain a layer of smooth muscle makingthem capable of spontaneous contraction. This ac-tion propels lymph through the rest of the lym-phatic system and the lymph nodes through to thethoracic duct and into the systemic circulation.Even though the concentration of albuminchanges on passage through lymph nodes in re-sponse to alterations in venous pressure andlymph colloid osmotic pressure,56–58 there ap-pears to be almost complete recovery of albuminon passage through the lymphatics except atmarkedly increased lymphatic outflow pres-sures.59,60
ABSORPTION OF PROTEINS AFTERS.C. ADMINISTRATION
After S.C. administration, the absolute bioavail-ability of proteins is generally variable and in-complete relative to an I.V. dose with values rang-ing from about 20% up to 100% (Table I). Thebasis for the reduced S.C. bioavailability is notcurrently known, although degradation or me-tabolism at the site of injection has been proposedas a general mechanism.3,4,61,62 Subcutaneousdegradation has been specifically suggested forseveral proteins including hGH,63,64 erythropoie-tin (EPO),3,65 and insulin,66–68 however, direct ex-perimental evidence for this putative mechanismis limited. For example, whilst aprotinin, a serineprotease inhibitor, has been reported to enhancethe rate and extent of absorption of parathyroidhormone,69 calcitonin,69 and insulin,67,70,71 Lindeet al. have also demonstrated a concomitant in-crease in subcutaneous blood flow with aprotininwhich may account for the change in the absorp-tion kinetics.71
Figure 1. Electron micrographs illustrating the over-lapping endothelial cells of lymphatic capillaries. Theintercellular cleft regions are denoted by (*). Magnifi-cation (a) ×76,500, (b) ×21,250, (c) ×31,150, (d) ×23,800.(Reproduced from J. Cell Biol., 1971, 50, 300–323, bycopyright permission of The Rockefeller UniversityPress.)
300 PORTER AND CHARMAN
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 89, NO. 3, MARCH 2000

Rate of Protein Absorption AfterS.C. Administration
Subcutaneously administered proteins generallyexhibit a relatively slow rate of absorption as evi-denced by a prolonged terminal half-life in com-parison to that observed after I.V. administration.Maximum plasma concentrations after S.C. injec-tion occur from 2 to 20 h post-dosing (Table I)with the rate of absorption being dependent onvarious external factors including the site of in-jection, the subcutaneous blood flow, and the ap-plication of heat or massage.4
The influence of the site of injection on proteinabsorption has been demonstrated for insu-lin,70,72–74 hGH,75 and EPO.76 In these studies,the rate of absorption was increased with S.C.injection in the abdomen in comparison to moreperipheral extremities such as the thigh or theupper arm. While this effect is typically ascribedto differences in local blood flow, several authorshave also highlighted a possible link to regionalvariations in lymph flow.4,76 Although other ex-ternal factors such as exercise might be expected
to increase both blood and lymph flow, factorssuch as massage are also known to dramaticallyincrease lymph flow,20,49,50 without a measurableeffect on subcutaneous blood flow.77 Unfortu-nately, variations in blood and lymph flow at thedifferent anatomical sites utilized for S.C. injec-tions are not well defined.
The effect of blood flow on the rate of proteinabsorption from the interstitial space is fre-quently inferred; however, only a few studieshave simultaneously measured subcutaneousblood flow (SBF) and the rate of protein absorp-tion, and most of these studies have been con-ducted with insulin. Insulin absorption is typi-cally studied by monitoring the disappearance of125I-labeled material from the injection site withthe assumption that the resulting disappearancerate equals the rate of appearance in blood. In aseries of studies examining the disposition of in-sulin,78 an increased rate of absorption in re-sponse to alterations in injection site, skinfoldthickness, exercise, orthostatic changes, ambienttemperature, and other external factors were pri-
Table I. Representative Bioavailability Values and Times to Reach MaximumPlasma Concentrations Following S.C. Administration of Various Protein Drugs*
Protein
ApproximateMonomericMW (×103) Species
Absolute BA(%)
TMAX(h) Reference
Insulina 5.6 Humans 84 1–2 114–116IGF-1 7.6 Humans 100 7 117, 118IL-3 13.2 Monkeys 40 2–4 119IL-2 15.5 Humans 30–80 2–4 120, 121IL-10b 18.7 Humans 42 4–6 88IL-11 19 Humans 65 2–3 122TNF-a 17.4 Humans c 2 123, 124GM-CSFd 15.5–19.5 Humans 50 3 125G-CSFd 18–22 Monkeys 40–50 2–3 126hGH 22 Humans 50 5–6 127–129IFN-a 19.5 Humans >80 6–8 130, 131IFN-b 23 Rabbits 12 1 105IFN-gd 20–25 Humans 30–70 6–13 131, 132FSHb,d 36 Humans 66 0.5 133, 134EPOd 34–39 Humans 20–36 13–18 65, 135Factor IX 56 Dogs 63.5 19 136
* Abbreviations: insulin-like growth factor I (IGF-I), interleukin (IL), tumor necrosis factor(TNF), granulocyte macrophage-colony stimulating factor (GM-CSF), granulocyte-colony stimu-lating factor (G-CSF), human growth hormone (hGH), interferon (IFN), follicle stimulating factor(FSH), erythropoietin (EPO).
a Normally present as a hexamer.b Normally present as a dimer.c Too low to be assessed.d May be glycosylated.
MINI-REVIEW 301
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 89, NO. 3, MARCH 2000

marily attributed to increased SBF measured bydisappearance of 133Xe from the subcutaneous tis-sue. A curvilinear relationship between SBF andthe rate of disappearance of radiolabeled insulinwas found and as a result, factors other thanblood flow (i.e., depolymerization, interstitial dif-fusion, capillary permeability) were proposed asbeing rate limiting at high SBF. The authors wenton to describe the capillary diffusion capacity, de-fined as the amount of tracer passing the capil-lary membrane per 100 g of tissue per min, asbeing 5–10-fold lower for insulin than for inulin,which is of a similar monomeric molecular weightas insulin. On this basis, it was proposed thatinsulin must be transported within the intersti-tium in a polymeric form, yet lymphatic transportwas suggested to represent only a minor compo-nent of absorption. Further studies74,79–82 havealso shown an inverse relationship between therate of disappearance of radiolabeled insulin fromthe subcutaneous injection site and the averageeffective size of the insulin unit, although lym-phatic transport has not typically been thought tocontribute significantly to insulin absorption.Studies presented by Binder in 196983 supportthis hypothesis and suggest that lymphatic up-take does not play a significant role in the absorp-tion of porcine (hexameric) insulin, although morerecent results by Supersaxo et al.2 have shownthat lymphatic transport accounts for approxi-mately 20% of the absorption of subcutaneouslyadministered inulin, which is of a similar size tothe insulin monomer. Given the size of mono-meric insulin and of the insulin hexamer, it ispossible that multiple mechanisms control the ab-sorption and further studies are necessary tomore clearly define these processes.
Mathematical Models to CharacterizeProtein Absorption
Several mathematical models have been proposedto account for the slow absorption kinetics of pro-teins following S.C. administration. Initial phar-macokinetic models used to describe insulin ab-sorption assumed a split-pool model, whereby in-sulin absorption takes place from an undefinedpool secondary to the injection pool.84 More recentreports have utilized a combined diffusion–dissociation model to account for the absorptionkinetics and the differences in concentration andvolume effects for monomeric and hexameric in-sulin.85 While these models adequately describethe kinetic profiles for S.C. insulin and are in
agreement with clinical data,86 they do not pre-clude a potential lymphatic component for insulinabsorption, even though the contribution may beonly minor.
Other models have been proposed to describethe plasma pharmacokinetics of proteins afterS.C. administration assuming at least partial up-take via the lymphatics. Bocci et al.87 proposed athree-compartment model with parallel zero- andfirst-order input to describe the plasma concen-tration versus time profiles of interferon-a2 (IFN-a, MW 19,000) after S.C. administration in com-bination with albumin. The prolonged absorptionin the presence of albumin was attributed to en-hanced lymphatic transport due to an increase inthe colloid osmotic pressure of the interstitialfluid. Studies by Radwanski et al. published in199888 utilized a similar model to describe theplasma pharmacokinetics for subcutaneously ad-ministered interleukin-10 (IL-10, non-covalentdimer with monomeric MW 18,700). In thesestudies, the rapid appearance of the protein inplasma was attributed to direct delivery to theblood via a zero-order process, whereas the lagphase and the associated prolonged plasma con-centrations were ascribed to gradual uptake andtransport via the lymph as described by a first-order process presumed to be controlled primarilyby lymph flow rate. Based on the fitted absorptionparameters, the first-order lymphatic componentwas found to represent 95% of the overall absorp-tion process. These authors highlighted that thepresence of proteolytic enzymes in S.C. or lymphcompartments may partially account for the re-duced bioavailability (42% in the case of IL-10relative to an I.V. dose) with this delivery route.
It is apparent that the rate and extent of ab-sorption of proteins directly into the systemic cir-culation after S.C. administration is significantlylower than that commonly seen for small mol-ecules. Even though many studies have alluded tothe possibility of lymphatic transport of thesemolecules, confirmatory studies which define theextent of lymphatic transport and the contribu-tion of this pathway to the absorption kineticsand bioavailability are limited.
Factors Affecting Lymphatic Transport ofProteins after S.C. Administration
The lymphatic transport of exogenous macromol-ecules was first reported in the 1950s after intra-muscular and intrapleural administration of high
302 PORTER AND CHARMAN
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 89, NO. 3, MARCH 2000

molecular weight salts of antibiotic bases such asstreptomycin and neomycin.89 Transport of mono-clonal antibodies and radiolabeled macromol-ecules including dextran, albumin, and hydroxy-ethyl starch via the lymphatics has also been ex-tensively examined in relation to imaging agentsin lymphoscintigraphic studies, although the ab-solute extent of lymphatic transport has rarelybeen quantified.90–95 Muranishi and co-workers96
also utilized the lymph-directing qualities of dex-tran macromolecules by forming a dextran (MW500,000) prodrug of bleomycin (BLM) to enhancedelivery to the regional lymph nodes after injec-tion into the stomach wall of the rat. Takakuraand co-workers97–99 further confirmed the utilityof macromolecular prodrugs to enhance lym-phatic transport in studies using a series of dif-ferent sized (MW range of 10,000–500,000) posi-tively and negatively charged dextran prodrugs ofthe antitumor antibiotic, mitomycin C (MMC) af-ter intramuscular (I.M.) injection. In the latterstudies, macromolecules of increased size andpositive charge displayed lower rates of absorp-tion from the interstitial injection site, relativelyhigher affinity for local lymph nodes, and reducedappearance in the thoracic lymph, compared withsmaller, negatively charged prodrugs. Furtherevidence of the lymphotropic nature of macromo-lecular prodrugs was supplied by the studies ofMaeda and co-workers,100–102 who showed thataccumulation of a conjugate of the anti-tumoragent, neocarzinostatin (NCS) with a poly(maleicacid)/styrene oligomer in the regional lymphnodes was up to 10-fold higher after S.C. admin-istration than after I.V. administration.
Interest in the lymphatic disposition of thera-peutic proteins after S.C. or I.M. injection has in-creased relatively recently due primarily to theincreasing number of proteins in various stages ofdevelopment and the overwhelming prevalence ofparenteral administration for these drugs. In thisregard, Supersaxo and co-workers published a se-ries of seminal articles which quantified, for thefirst time, the extent of uptake of selected macro-molecules into the peripheral lymphatics after in-terstitial injection.2,103 Using a sheep model inwhich the efferent lymphatic duct of the popliteallymph node was cannulated, the studies demon-strated that the primary route of initial absorp-tion of recombinant interferon-a2a (IFN-a) afterintradermal or S.C. administration into the lowerhind leg was the regional lymphatics with ap-proximately 59% of the dose being recovered inthe popliteal lymph. Further studies examined
the lymphatic transfer of a series of compoundswith increasing molecular weights (5-fluoro-28-deoxyuridine, MW 246.2; inulin, MW 5,200; cyto-chrome c, MW 12,300; and IFN-a, MW 19,000)and showed a direct correlation between molecu-lar weight and the extent of recovery in the pop-liteal lymph (Figure 2).2 The correlation sug-gested that more than 50% of an administereddose would be absorbed by the regional lymphat-ics after S.C. administration for molecules withmolecular weights exceeding approximately16,000.
The lymphatic transport of IFN-a and glyco-sylated IFN-b into the central (thoracic) lymphhas also been widely studied.87,104–109 In contrastto the large extent of peripheral lymphatic trans-port of IFN-a reported by Supersaxo et al.,103 theamount of IFN-a recovered in the thoracic lymphof rabbits after a single S.C. injection was low(<0.1% of dose) but increased 4-fold when injectedat multiple sites. In the case of IFN-b, the extentof lymphatic transport was reported as the tho-racic lymph/plasma concentration ratio andranged from 1.2 after S.C. injection107 to 3.8107
and 1–2110 after I.M. injection. By way of com-parison, the lymph/plasma concentration ratiosestimated for thoracic lymph and IFN-a were ap-proximately 20–30,104 and the concentration ra-tios for IFN-a in peripheral lymph relative to sys-temic plasma were in the range of 2,000–8,000.103
Figure 2. Relationship between molecular weightand cumulative % dose recovered in popliteal lymphfollowing S.C. administration into the lower part of thehind leg of sheep (mean ± SD, n 4 3–4). Data fromSupersaxo et al. (●) and Charman et al. (s).
MINI-REVIEW 303
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 89, NO. 3, MARCH 2000
Subsequent studies examined the effect of al-bumin inclusion in the formulation, speculatingthat albumin would increase interstitial oncoticpressure thereby stimulating lymph flow. Bocci etal. showed a 2-fold increase in thoracic lymphatictransport of both IFN-a in the presence of 4% al-bumin104 and IFN-b in the presence of 13% albu-min107 after S.C. administration relative to albu-min-free formulations. Conversely, 13% albuminreduced the lymphatic transport of IFN-b afterI.M. injection, and other studies have shown thatintradermal administration of IFN-a with either0.5% or 13% albumin had no effect on the extentof IFN transport into the politeal (peripheral)lymph.103 Bocci et al. have also demonstrated in-creased lymphatic transport after inclusion of hy-aluronidase in formulations in an effort to stimu-late interstitial edema104 and increased lymphand blood transport with the inclusion of hista-mine or bradykinin as alternative edematogenicagents.109 Again, the extent of lymphatic trans-port in both cases was low in mass terms. Thetransport of human tumor necrosis factor (TNF,MW 20,000–40,000) into thoracic lymph afterS.C. injection to rats was also found to be ex-tremely low (0.02–0.03% of dose), although lym-phatic transport was considerably enhanced afterinjection into the stomach wall or gut wall.111
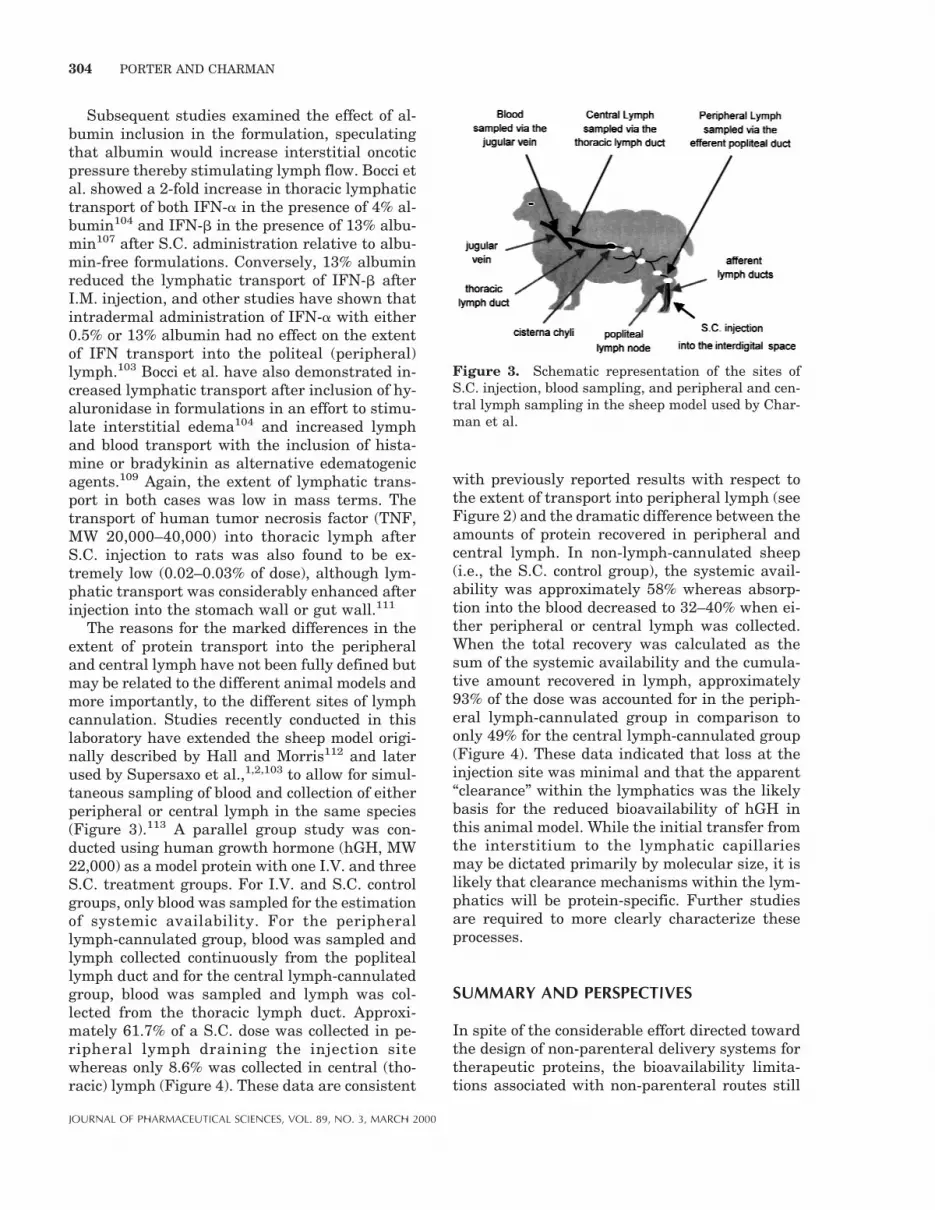
The reasons for the marked differences in theextent of protein transport into the peripheraland central lymph have not been fully defined butmay be related to the different animal models andmore importantly, to the different sites of lymphcannulation. Studies recently conducted in thislaboratory have extended the sheep model origi-nally described by Hall and Morris112 and laterused by Supersaxo et al.,1,2,103 to allow for simul-taneous sampling of blood and collection of eitherperipheral or central lymph in the same species(Figure 3).113 A parallel group study was con-ducted using human growth hormone (hGH, MW22,000) as a model protein with one I.V. and threeS.C. treatment groups. For I.V. and S.C. controlgroups, only blood was sampled for the estimationof systemic availability. For the peripherallymph-cannulated group, blood was sampled andlymph collected continuously from the popliteallymph duct and for the central lymph-cannulatedgroup, blood was sampled and lymph was col-lected from the thoracic lymph duct. Approxi-mately 61.7% of a S.C. dose was collected in pe-ripheral lymph draining the injection sitewhereas only 8.6% was collected in central (tho-racic) lymph (Figure 4). These data are consistent
with previously reported results with respect tothe extent of transport into peripheral lymph (seeFigure 2) and the dramatic difference between theamounts of protein recovered in peripheral andcentral lymph. In non-lymph-cannulated sheep(i.e., the S.C. control group), the systemic avail-ability was approximately 58% whereas absorp-tion into the blood decreased to 32–40% when ei-ther peripheral or central lymph was collected.When the total recovery was calculated as thesum of the systemic availability and the cumula-tive amount recovered in lymph, approximately93% of the dose was accounted for in the periph-eral lymph-cannulated group in comparison toonly 49% for the central lymph-cannulated group(Figure 4). These data indicated that loss at theinjection site was minimal and that the apparent“clearance” within the lymphatics was the likelybasis for the reduced bioavailability of hGH inthis animal model. While the initial transfer fromthe interstitium to the lymphatic capillariesmay be dictated primarily by molecular size, it islikely that clearance mechanisms within the lym-phatics will be protein-specific. Further studiesare required to more clearly characterize theseprocesses.
SUMMARY AND PERSPECTIVES
In spite of the considerable effort directed towardthe design of non-parenteral delivery systems fortherapeutic proteins, the bioavailability limita-tions associated with non-parenteral routes still
Figure 3. Schematic representation of the sites ofS.C. injection, blood sampling, and peripheral and cen-tral lymph sampling in the sheep model used by Char-man et al.
304 PORTER AND CHARMAN
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 89, NO. 3, MARCH 2000

dictate that the majority of proteins are currentlyadministered parenterally with the S.C. routepredominating. For the most part, the mecha-nisms underlying protein drainage from the injec-tion site and transport to the systemic circulationhave been only partially defined. It is apparentthat the lymphatic system plays a significant rolein the distribution of S.C. administered proteins,although the available data are complicated byvariations in the animals models used and thesites of lymphatic cannulation. Review of the lit-erature suggests that proteins drain from the in-jection site into both the peripheral lymph andthe blood capillaries and that uptake into the lym-phatics increases with molecular size in an ap-proximately linear manner. As such, greater than50% of a S.C. dose might be expected to drain intothe peripheral lymph for molecules with molecu-lar weights exceeding approximately 16,000. Fur-ther preliminary results from this laboratory sug-gest that protein “clearance” upon passagethrough the lymphatics may be significant lead-
ing to much lower concentrations in thoraciclymph than in peripheral lymph and possibly ac-counting, in part, for the reduced systemic avail-ability of these molecules.
A further understanding of the inherentlymph-directing properties of proteins after S.C.administration and the possibility of increasedresidence or uptake upon passage through thelymphatics has significant ramifications in termsof the activity and toxicity of these agents. Thelymphatics present an appealing target for im-munomodulatory agents, vaccines, and anti-metastatic compounds, and optimization of lym-phatic transport may prove beneficial for suchtherapeutic agents. Conversely, if lymphaticclearance leads to a reduction in systemic bio-availability, opportunities to reduce lymphatictransport may improve the availability and activ-ity of molecules for which the active site residesoutside of the lymphatics. Application of the para-digm which dictates that assessment of the “ex-posure” of patients to S.C. administered proteinsshould be via plasma or serum bioavailability es-timations may be inappropriate.
Realizing the importance of the potential roleof the lymphatics in the absorption and distribu-tion of therapeutic proteins after S.C. administra-tion, future studies might usefully address the po-tential effect of protein charge or protein modifi-cation on lymphatic uptake and/or clearance, aswell the importance of formulation variables suchas ionic strength, pH, and viscosity on the effec-tive size of proteins within the interstitium andthe resulting effect on lymphatic drainage.Greater insight into these and other factors mayindicate useful approaches to maximize the po-tential benefit of this route of absorption.
REFERENCES AND NOTES
1. Hein WR, Supersaxo A. 1988. Effect of interferonalpha-2a on the ouput of recirculating lympho-cytes from single lymph nodes. Immunology64:469–474.
2. Supersaxo A, Hein WR, Steffen H. 1990. Effect ofmolecular weight on the lymphatic absorption ofwater soluble compounds following subcutaneousadministration. Pharm Res 7:167–169.
3. Kompella UB, Lee VHL. 1991. Pharmacokineticsof peptide and protein drugs. In: Lee VHL, editor.Peptide and protein drug delivery. New York:Marcel Dekker, Inc. p 391–484.
4. Banerjee PS, Hosny EA, Robinson JR. 1991. Par-enteral delivery of peptide and protein drugs. In
Figure 4. Bar chart representing the cumulative pro-portion of a S.C. dose of hGH collected in peripheraland central lymph and the total percentage of the doserecovered (sum of systemic availability and cumulativeamount recovered in lymph) following S.C. administra-tion of 0.1 mg/kg. Hatched bars represent sheep withperipheral lymph cannulation, gray bars representsheep with central lymph cannulation, and the blackbar represents the non-lymph-cannulated controlsheep. Values represent the mean for n 4 4–6 animalsper treatment group, and error bars represent the stan-dard error of the means.
MINI-REVIEW 305
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 89, NO. 3, MARCH 2000

Lee VHL, editor. Peptide and protein drug deliv-ery. New York: Marcel Dekker, Inc. p 487–543.
5. Bocci V. 1992. Physicochemical and biologic prop-erties of interferons and their potential uses indrug delivery systems. Crit Rev Ther Drug Car-rier Syst 9:91–133.
6. Toon S. 1996. The relevance of pharmacokineticsin the development of biotechnology products. EurJ Drug Metab Pharmacokinet 21:93–103.
7. Porter CJH. 1997. Drug delivery to the lymphaticsystem. Crit Rev Ther Drug Carrier Syst 14:333.
8. Patel HM. 1988. Fate of liposomes in the lymphat-ics. In: Gregoriadis G, editor. Liposomes as drugcarriers. New York: Wiley. p 51–62.
9. O’Hagan DT, Christy NM, Davis SS. 1992. Par-ticulates and lymphatic delivery. In: CharmanWN, Stella VJ, editors. Lymphatic transport ofdrugs. London: CRC Press. p 279–315.
10. Kadir F, Zuidema J, Crommelin DJA. 1993. Lipo-somes as intramuscular and subcutaneous injec-tion drug delivery systems. In: Rolland A, editor.Pharmaceutical particulate carriers. New York:Marcel Dekker. p 165.
11. Hawley AE, Davis SS, Illum L. 1995. Targeting ofcolloids to lymph nodes: Influence of lymphaticphysiology and colloidal characteristics. Adv DrugDeliv Rev. 17:129–148.
12. Yoffey JM, Courtice FC. 1970. Lymphatics, lymphand the lymphomyeloid complex. London: Aca-demic Press.
13. O’Driscoll CM. 1992. Anatomy and physiology ofthe lymphatics. In: Charman WN, Stella VJ, edi-tors. Lymphatic transport of drugs. London: CRCPress. p 1–35.
14. Rhoades R, Pflanzer R. 1996. Body defense andthe immune response. In: Rhoades R, Pflanzer R,editors. Human physiology. Orlando: SaundersCollege Publishing. p 824–852.
15. Lebel L, Smith L, Risberg B, Gerdin B, LaurentTC. 1988. Effect of increased hydrostatic pressureon lymphatic elimination of hyaluronan fromsheep lung. J Appl Physiol 64:1327–1332.
16. Lebel L, Smith L, Risberg B, Laurent TC, GerdinB. 1989. Increased lymphatic elimination of inter-stitial hyaluronan during E. coli sepsis in sheep.Am J Physiol 256:1524–1531.
17. Pou NA, Roselli RJ, Parker RE, Clanton JC. 1993.Effects of air embolism on sheep lung fluid vol-umes. J Appl Physiol 75:986–993.
18. Bergstrom K, Werner B. 1966. Proteins in humanthoracic duct lymph. Studies on the distributionof some proteins between lymph and blood. ActaChir Scand 131:413–422.
19. Bell DR, Watson PD, Renkin EM. 1980. Exclusionof plasma proteins in interstitium of tissues fromthe dog hind paw. Am J Physiol 239:532–538.
20. Aukland K, Reed RK. 1993. Interetitial lymphatic
mechanisms in the control of extracellular fluidvolume. Physiol Rev 73:1–78.
21. Langgard H. 1963. The subcutaneous absorptionof albumin in edematous states. Acta Med Scand174:645–650.
22. Reed RK, Johansen S, Noddeland H. 1985. Turn-over rate of interstitial albumin in rat skin andskeletal muscle. Effects of limb movements andmotor activity. Acta Physiol Scand 125:711–718.
23. Gilanyi M, Kovach AG. 1991. Effect of local pH oninterstitial fluid pressure. Am J Physiol 261:627–631.
24. Comper WD, Laurent TC. 1978. Physiologicalfunction of connective tissue polysaccharides.Physiol Rev 58:255–315.
25. Gersh I, Catchpole HR. 1960. The nature ofground substance of connective tissue. PerspectBiol Med 3:282–319.
26. Granger HJ, Dhar J, Chen HI. 1976. Structureand function of the interstitium. In: Sgouris JT,Rene A, editors. Proceedings of the Workshop onAlbumin; Bethesda: NIH. p 114–125.
27. Watson PD, Grodins FS. 1978. An analysis of theeffects of the interstitial matrix on plasma-lymphtransport. Microvasc Res 16:19–41.
28. Casley-Smith JR, Vincent AH. 1978. The quanti-tative morphology of interstitial tissue channelsin some tissues of the rat and rabbit. Tissue Cell10:571–584.
29. Barber BJ, Nearing BD. 1990. Spatial distribu-tion of protein in interstitial matrix of rat mesen-teric tissue. Am J Physiol 258:556–564.
30. Watson PD, Bell DR, Renkin EM. 1980. Early ki-netics of large molecule transport betweenplasma and lymph in dogs. Am J Physiol239:525–531.
31. Bert JL, Mathieson JM, Pearce RH. 1982. Theexclusion of human serum albumin by humandermal collagenous fibres and within human der-mis. Biochemical J 201:395–403.
32. Wiig H, DeCarlo M, Sibley L, Renkin EM. 1992.Interstitial exclusion of albumin in rat tissuesmeasured by a continuous infusion method. Am JPhysiol 263:1222–1233.
33. Jackson RL, Busch SJ, Cardin AD. 1991. Gly-cosaminoglycans: Molecular properties, proteininteractions, and role in physiological processes.Physiol Rev 71:481–539.
34. Casley-Smith JR. 1980. The fine structure andfunctioning of tissue channels and lymphatics.Lymphology 13:177–183.
35. Casley-Smith JR. 1980. Are the initial lymphaticsnormally pulled open by the anchoring filaments?Lymphology 13:120–129.
36. Leak LV. 1980. Lymphatic removal of fluids andparticles in the mammalian lung. Environ HealthPerspect 35:55–76.
37. O’Morchoe PJ, Yang VV, O’Morchoe CC. 1980.
306 PORTER AND CHARMAN
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 89, NO. 3, MARCH 2000

Lymphatic transport pathways during volume ex-pansion. Microvasc Res 20:275–294.
38. Yang VV, O’Morchoe PJ, O’Morchoe CC. 1981.Transport of protein across lymphatic endothe-lium in the rat kidney. Microvasc Res 21:75–91.
39. Leak LV, Burke JF. 1968. Ultrastructural studieson the lymphatic anchoring filaments. J Cell Biol36:129–149.
40. Casley-Smith JR. 1972. The role of the endothe-lial intercellular junctions in the functioning ofthe initial lymphatics. Angiologica 9:106–131.
41. Dobbins WOd, Rollins EL. 1970. Intestinal muco-sal lymphatic permeability: An electron micro-scopic study of endothelial vesicles and cell junc-tions. J Ultrastruct Res 33:29–59.
42. Leak LV. 1971. Studies of the permeability oflymphatic capillaries. J Cell Biol 50:300–323.
43. O’Morchoe CC, Jones WRd, Jarosz HM, O’MorchoePJ, Fox LM. 1984. Temperature dependence ofprotein transport across lymphatic endotheliumin vitro. J Cell Biol 98:629–640.
44. Casley-Smith JR. 1982. Mechanisms in the for-mation of lymph. Int Rev Physiol 26:147–187.
45. Fadnes HO. 1981. Colloid osmotic pressure in in-terstitial fluid and lymph from rabbit subcutane-ous tissue. Microvasc Res 21:390–392.
46. Aukland K, Nicolaysen G. 1981. Interstitial fluidvolume: local regulatory mechanisms. PhysiolRev 61:556–643.
47. Reddy NP. 1986. Lymph circulation: physiology,pharmacology, and biomechanics. Crit RevBiomed Eng 14:45–91.
48. Mazzoni MC, Skalak TC, Schmid-Schonbein GW.1990. Effects of skeletal muscle fiber deformationon lymphatic volumes. Am J Physiol 259:1860–1868.
49. Schmid-Schonbein GW. 1990. Microlymphaticsand lymph flow. Physiol Rev 70:987–1028.
50. Ikomi F, Hunt J, Hanna G, Schmid-SchonbeinGW. 1996. Interstitial fluid, plasma protein, col-loid, and leukocyte uptake into initial lymphatics.J Appl Physiol 81:2060–2067.
51. Ikomi F, Schmid-Schonbein GW. 1996. Lymphpump mechanics in the rabbit hind leg. Am JPhysiol 271:173–183.
52. Skalak TC, Schmid-Schonbein GW, Zweifach BW.1984. New morphological evidence for a mecha-nism of lymph formation in skeletal muscle. Mi-crovasc Res 28:95–112.
53. Reed RK. 1981. Interstitial fluid volume, colloidosmotic and hydrostatic pressures in rat skeletalmuscle. Effect of venous stasis and muscle activ-ity. Acta Physiol Scand 112:7–17.
54. Dunbar BS, Elk JR, Drake RE, Laine GA. 1989.Intestinal lymphatic flow during portal venoushypertension. Am J Physiol 257:94–98.
55. Drake RE, Gabel JC. 1991. Effect of outflow pres-
sure on intestinal lymph flow in unanesthetizedsheep. Am J Physiol 260:668–671.
56. Adair TH, Moffatt DS, Paulsen AW, Guyton AC.1982. Quantitation of changes in lymph proteinconcentration during lymph node transit. Am JPhysiol 243:351–359.
57. Knox P, Pflug JJ. 1983. The effect of the caninepopliteal node on the composition of lymph. JPhysiol 345:1–14.
58. Adair TH, Guyton AC. 1983. Modification oflymph by lymph nodes. II. Effect of increasedlymph node venous blood pressure. Am J Physiol245:616–622.
59. Calnan JS, Rivero OR, Fillmore S, Mercurius-Taylor L. 1967. Permeability of normal lymphat-ics. Br J Surg 54:278–285.
60. Adair TH, Guyton AC. 1985. Modification oflymph by lymph nodes. III. Effect of increasedlymph hydrostatic pressure. Am J Physiol 249:777–782.
61. Lee VH. 1988. Enzymatic barriers to peptide andprotein absorption. Crit Rev Ther Drug CarrierSyst 5:69–97.
62. Ferraiolo BL, Mohler MA. 1992. Goals and ana-lytical methodologies for protein disposition stud-ies. In: Ferraiolo BL, Mohler MA, Gloff CA, edi-tors. Protein Pharmacokinetics and Metabolism.New York: Plenum Press. p 1–33.
63. Jorgensen JO, Flyvbjerg A, Lauritzen T, OrskovH, Christiansen JS. 1988. Subcutaneous degrada-tion of biosynthetic human growth hormone ingrowth hormone deficient patients. Acta Endocri-nol (Copenh) 118:154–158.
64. Laursen T, Moller J, Jorgensen JO, Orskov H,Christiansen JS. 1996. Bioavailability and bioac-tivity of intravenous vs subcutaneous infusion ofgrowth hormone in GH deficient patients. ClinEndocrinol 45:333–339.
65. Macdougall IC, Roberts DE, Coles GA, WilliamsJD. 1991. Clinical pharmacokinetics of epoetin(recombinant human erythropoietin). Clin Phar-macokinet 20:99–113.
66. Berger M, Halban PA, Girardier L, Seydoux J,Offord RE, Renold AE. 1979. Absorption kineticsof subcutaneously injected insulin. Evidence fordegradation at the infection site. Diabetologia17:97–99.
67. Berger M, Cuppers HJ, Halban PA, Offord RE.1980. The effect of aprotinin on the absorption ofsubcutaneously injected regular insulin in normalsubjects. Diabetes 29:81–83.
68. Ariza-Andraca CR, Altamirano-Bustamante E,Frati-Munari AC, Altamirano-Bustamante P,Graef-Sanchez A. 1991. Delayed insulin absorp-tion due to subcutaneous edema. Arch Invest Med22:229–233.
69. Parsons JA, Rafferty B, Stevenson RW, ZanelliJM. 1979. Evidence that protease inhibitors re-duce the degradation of parathyroid hormone and
MINI-REVIEW 307
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 89, NO. 3, MARCH 2000

calcitonin injected subcutaneously. Br J Pharma-col 66:25–32.
70. Berger M, Cuppers HJ, Hegner H, Jorgens V,Berchtold P. 1982. Absorption kinetics and bio-logic effects of subcutaneously injected insulinpreparations. Diabetes Care 5:77–91.
71. Linde B, Gunnarsson R. 1985. Influence of apro-tinin on insulin absorption and subcutaneousblood flow in type 1 (insulin-dependent) diabetes.Diabetologia 28:645–648.
72. Hildebrandt P, Sejrsen P, Nielsen SL, Birch K,Sestoft L. 1985. Diffusion and polymerization de-termines the insulin absorption from subcutane-ous tissue in diabetic patients. Scand J Clin LabInvest 45:685–690.
73. Vora JP, Burch A, Peters JR, Owens DR. 1992.Relationship between absorption of radiolabeledsoluble insulin, subcutaneous blood flow, and an-thropometry. Diabetes Care 15:1484–1493.
74. ter Braak EW, Woodworth JR, Bianchi R,Cerimele B, Erkelens DW, Thijssen JH, Kurtz D.1996. Injection site effects on the pharmacokinet-ics and glucodynamics of insulin lispro and regu-lar insulin. Diabetes Care 19:1437–1440.
75. Laursen T, Jorgensen JO, Christiansen JS. 1995.Pharmacokinetics and metabolic effects of growthhormone injected subcutaneously in growth hor-mone deficient patients: thigh versus abdomen[published erratum appears in Clin Endocrinol(Oxf). Clin Endocrinol 40:373–378 [Erratum]1994. Clin Endocrinol 42(1):109.
76. Jensen JD, Jensen LW, Madsen JK. 1994. Thepharmacokinetics of recombinant human erythro-poietin after subcutaneous injection at differentsites. Eur J Clin Pharmacol 46:333–337.
77. Linde B. 1986. Dissociation of insulin absorptionand blood flow during massage of a subcutaneousinjection site. Diabetes Care 9:570–574.
78. Hildebrandt P. 1991. Subcutaneous absorption ofinsulin in insulin dependent diabetic pateits. In-fluence of species, physico-chemical properties ofinsulin and physiological factors. Dan Med Bull38:337–346.
79. Vora JP, Owens DR, Dolben J, Atiea JA, Dean JD,Kang S, Burch A, Brange J. 1988. RecombinantDNA derived monomeric insulin analogue: com-parison with soluble human insulin in normalsubjects. Br Med J 297:1236–1239.
80. Brange J, Ribel U, Hansen JF, Dodson G, HansenMT, Havelund S, Melberg SG, Norris F, Norris K,Snel L, et al. 1988. Monomeric insulins obtainedby protein engineering and their medical implica-tions. Nature 333:679–682.
81. Brange J, Owens DR, Kang S, Volund A. 1990.Monomeric insulins and their experimental andclinical implications. Diabetes Care 13:923–954.
82. Kang S, Brange J, Burch A, Volund A, Owens DR.1991. Subcutaneous insulin absorption explained
by insulin’s physicochemical properties. Evidencefrom absorption studies of soluble human insulinand insulin analogues in humans. Diabetes Care14:942–948.
83. Binder C. 1969. Absorption of injected insulin. Aclinical-pharmacological study. Acta PharmacolToxicol (Copenh) 2:1–84.
84. Mosekilde E, Jensen KS, Binder C, Pramming S,Thorsteinsson B. 1989. Modeling absorption ki-netics of subcutaneous injected soluble insulin. JPharmacokinet Biopharmaceut 17:67–87.
85. Trajanoski Z, Wach P, Kotanko P, Ott A, SrkabaF. 1993. Pharmacokinetic model for the absorp-tion of subcutaneously injected soluble insulinand monomeric insulin analogues. Biomed Techn38:224–231.
86. Brange J, Volune A. 1999. Insulin analogs withimproved pharmacokinetic profiles. Adv Drug De-liv Rev 35:307–335.
87. Bocci V, Muscettola M, Naldini A, Bianchi E,Segre G. 1986. The lymphatic route. II. Pharma-cokinetics of human recombinant interferon-alpha 2 injected with albumin as a retarder inrabbits. Gen Pharmacol 17:93–96.
88. Radwanski E, Chakraborty A, Van Wart S, HuhnkRD, Cutler DL, Affrime MB, Jusko WJ. 1998.Pharmacokinetics and leukocyte responses of re-combinant human interleukin-10. Pharm Res15:1895–1901.
89. Malek P, Kolc J, Herold M, Hoffman J. 1958.Lymphotropic antibiotics: “Antibiolymphins.” In:Antibiotics Manual. New York: Medical Encyclo-pedia. p 546–551.
90. Steller MA, Parker RJ, Covell DG, Holton OD,Keenan AM, Sieber SM, Weinstein JN. 1986. Op-timization of monoclonal antibody delivery via thelymphatics: the dose dependence. Cancer Res46:1830–1834.
91. Wahl RL, Geatti O, Liebert M, Wilson B, ShreveP, Beers BA. 1987. Kinetics of interstitially ad-ministered monoclonal antibodies for purposes oflymphoscintigraphy. J Nucl Med 28:1736–1744.
92. Sadek S, Owunwanne A, Abdel-Dayem HM,Yacoub T. 1989. Preparation and evaluation of Tc-99m hydroxyethyl starch as a potential radio-pharmaceutical for lymphoscintigraphy: compari-son with Tc-99m human serum albumin, Tc-99mdextran, and Tc-99m sulfur microcolloid. Lym-phology 22:157–166.
93. Strand SE, Bergqvist L. 1989. Radiolabeled col-loids and macromolecules in the lymphatic sys-tem. Crit Rev Ther Drug Carrier Syst 6:211–238.
94. Weinstein JN. 1990. Antibody lymphoscintigra-phy. Cancer Treat Res 51:365–385.
95. Freedman DO, Bui T, De Almeida Filho PJ, BragaC, Maia e Silva MC, Maciel A, Furtado AF. 1995.Lymphoscintigraphic assessment of the effect of
308 PORTER AND CHARMAN
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 89, NO. 3, MARCH 2000

diethylcarbamazine treatment on lymphatic dam-age in human bancroftian filariasis. Am J TropMed Hyg 52:258–261.
96. Muranishi S, Takahashi Y, Hashida M, Sezaki H.1979. Effect of complexation with dextran sul-phate on the lymphatic delivery of bleomycin fol-lowing interstitial administration. J Pharmaco-bio-Dyn 2:383–390.
97. Takakura Y, Atsumi M, Hashida M, Sezaki H.1987. Development of a novel polymeric prodrugof mitomycin C-dextran conjugate with anioniccharge. II. Disposition and pharmacokinetics fol-lowing intravenous and intramuscular adminis-tration. Int J Pharm 37:145–154.
98. Takakura Y, Matsumoto S, Hashida M, Sezaki H.1984. Enhanced lymphatic delivery of mitomycinC conjugated with dextran. Cancer Res 44:2505–2510.
99. Takakura Y, Kitajima M, Matsumototo S, Ha-shida M, Sezaki H. 1987. Development of a novelpolymeric prodrug of mitomycin C-dextran conju-gate with anionic charge I. Physicochemical char-acteristics and in vivo and in vitro antitumouractivities. Int J Pharm 37:135–143.
100. Takeshita J, Maeda H, Kanamaru R. 1982. Invitro mode of action, pharmacokinetics, and organspecificity of poly (maleic acid-styrone)-conjugated neocarzinostatin, SMANCS. Gann73:278–284.
101. Maeda H, Takeshita J, Kanamaru R, Sato H,Khatoh J. 1979. Antimetastatic and antitumor ac-tivity of a derivative of neocarzinostatin: an or-ganic solvent- and water-soluble polymer-conjugated protein. Gann 70:601–606.
102. Maeda H, Takeshita J, Yamashita A. 1980. Lym-photropic accumulation of an antitumor antibioticprotein, neocarzinostatin. Eur J Cancer 16:723–731.
103. Supersaxo A, Hein W, Gallati H, Steffen H. 1988.Recombinant human interferon alpha-2a: deliv-ery to lymphoid tissue by selected modes of appli-cation. Pharm Res 5:472–476.
104. Bocci V, Muscettola M, Grasso G, Magyar Z,Naldini A, Szabo G. 1986. The lymphatic route. I.Albumin and hyaluronidase modify the normaldistribution of interferon in lymph and plasma.Experientia 42:432–433.
105. Bocci V, Muscettola M, Naldini A. 1986. The lym-phatic route. III. Pharmacokinetics of humannatural interferon-beta injected with albumin asa retarder in rabbits. Gen Pharmacol 17:445–448.
106. Bocci V, Pessina GP, Paulesu L, Nicoletti C. 1988.The lymphatic route. VI. Distribution of recombi-nant interferon-alpha 2 in rabbit and pig plasmaand lymph. J Biol Resp Mod 7:390–400.
107. Bocci V, Pessina GP, Paulesu L, Muscettola M,Valeri A. 1988. The lymphatic route. V. Distribu-
tion of human natural interferon-beta in rabbitplasma and lymph. J Interferon Res 8:633–640.
108. Bocci V, Muscettola M, Naldini A. 1986. The lym-phatic route. IV. Pharmacokinetics of human re-combinant interferon alpha 2 and natural inter-feron beta administered intradermally in rabbits.Int J Pharm 32:103–110.
109. Pessina GP, Bocci V, Carraro F, Naldini A,Paulesu L. 1993. The lymphatic route. IX. Distri-bution of recombinant interferon-alpha 2 admin-istered subcutaneously with oedematogenicdrugs. Physiol Res 42:243–250.
110. Yoshikawa H, Sutoh Y, Naruse N, Takada K,Muranishi S. 1985. Comparison of dissppearancefrom blood and lymphatic delivery of human fi-broblast interferon in rat by different routes. JPharmacobiodyn 8:206–210.
111. Kojima K, Takahashi T, Nakanishi Y. 1988. Lym-phatic transport of recombinant human tumor ne-crosis factor in rats. J Pharmacobiodyn 11:700–706.
112. Hall JG, Morris B. 1962. The output of cells inlymph from the Popliteal node of sheep. J ExpPhysiol 47:360–369.
113. Charman SA, Segrave AM, Edwards GA, PorterCJH. 2000. Systemic availability and lymphatictransport of human growth hormone adminis-tered by subcutaneous injection. J Pharm Sci89:168.
114. Kang S, Owens DR, Vora JP, Brange J. 1990.Comparison of insulin analogue B9AspB27Gluand soluble human insulin in insulin-treated dia-betes. Lancet 335:303–306.
115. Kang S, Brange J, Burch A, Volund A, Owens DR.1991. Absorption kinetics and action profiles ofsubcutaneously administered insulin analogues(AspB9GluB27, AspB10, AspB28) in healthy sub-jects. Diabetes Care 14:1057–1065.
116. Hoffman A, Ziv E. 1997. Pharmacokinetic consid-erations of new insulin formulations and routes ofadministration. Clin Pharmacokinet 33:285–301.
117. Wilton P, Sietnieks A, Gunnarsson R, Berger L,Grahnen A. 1991. Pharmacokinetic profile of re-combinant human insulin-like growth factor Igiven subcutaneously in normal subjects. ActaPaediatr Scand 377:111–114.
118. Grahnen A, Kastrup K, Heinrich U, GourmelenM, Preece MA, Vaccarello MA, Guevara-AguirreJ, Rosenfeld RG, Sietnieks A. 1993. Pharmacoki-netics of recombinant human insulin-like growthfactor I given subcutaneously to healthy volun-teers and to patients with growth hormone recep-tor deficiency. Acta Paediatr 82:9–13.
119. van Gils FC, Westerman Y, van den Bos C,Burger H, van Leen RW, Wagemaker G. 1993.Pharmacokinetic basis for optimal hemopoietic ef-fectiveness of homologous IL-3 administered torhesus monkeys. Leukemia 7:1602–1607.
120. Konrad MW, Hemstreet G, Hersh EM, Mansell
MINI-REVIEW 309
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 89, NO. 3, MARCH 2000
PW, Mertelsmann R, Kolitz JE, Bradley EC.1990.Pharmacokinetics of recombinant interleukin 2 inhumans. Cancer Res 50:2009–2017.
121. Gustavson LE, Nadeau RW, Oldfield NF. 1989.Pharmacokinetics of teceleukin (recombinant hu-man interleukin 2) after intravenous or subcuta-neous administration to patients with cancer. JBiol Resp Mod 8:440–449.
122. Aoyama K, Uchida T, Takanuki F, Usui T, Wa-tanabe T, Higuchi S, Toyoki T, Mizoguchi H.1997. Pharmacokinetics of recombinant humaninterleukin-11 (Rhil 11) in healthy male subjects.Br J Clin Pharmacol 43:571–578.
123. Saks S, Rosenblum M. 1992. Recombinant humanTNF-alpha: preclinical studies and results fromearly clinical trials. Immunol Ser 56:567–587.
124. Chapman PB, Lester TJ, Casper ES, GabriloveJL, Wong GY, Kempin SJ, Gold PJ, Welt S, War-ren RS, Starnes HF. 1987. Clinical pharmacologyof recombinant human tumor necrosis factor inpatients with advanced cancer. J Clin Oncol5:1942–1951.
125. Stute N, Furman WL, Schell M, Evans We. 1995.Pharmacokinetics of recombinant human granu-locyte macrophage colony-stimulating factor inchildren after intravenous and subcutaneous ad-ministration. J Pharm Sci 84:824–828.
126. Tanaka H, Tanaka Y, Shinagawa K, YamagishiY, Ohtaki K, Asano K. 1997. Three types of re-combinant human granulocyte colony stimulatingfactor have equivalent biological activities inmonkeys. Cytokine 9:360–369.
127. Zeisel HJ, Petrykowski Wv, Wais U. 1992. Phar-macokinetics and short-term metabolic effects ofmammalian cell-derived biosynthetic humangrowth hormone in man. Horm Res 37:5–13.
128. Laursen T, Susgaard S, Jensen FS, Jorgensen JO,Christiansen JS. 1994. Absorption kinetics of twohighly concentrated preparations of growth hor-mone: 12 IU/ml compared to 56 IU/ml. PharmacolToxicol 74:54–57.
129. Laursen T, Grandjean B, Jorgensen JOL, Chris-tiansen JS. 1996. Bioavailability and bioactivityof three different doses of nasal growth hormone(GH) administered to GH deficient patients. Com-parison with intravenous and subcutaneous ad-ministration. Eur J Endocrinol 135:309–315.
130. Wills RJ, Dennis S, Spiegel HE, Gibson DM,Nadler PI. 1984. Interferon kinetics and adversereactions after intravenous, intramuscular, andsubcutaneous injection. Clin Pharmacol Ther35:722–727.
131. Wills RJ. 1990. Clinical Pharmacokinetics of in-terferons. Clin Pharmacokinet 19:390–399.
132. Thompson JA, Cox WW, Lindgren CG, Collins C,Neraas KA, Bonnem EM, Fefer A. 1987. Subcuta-neous recombinant gamma interferon in cancerpatients: toxicity, pharmacokinetics, and im-munomodulatory effects. Cancer Immunol Immu-nother 25:47–53.
133. le Contonnec JY, Porchet HC, Beltrami V, KhanA, Toon S, Rowland M. 1994. Clinical pharmacol-ogy of recombinant human follicle-stimulatinghormone. II. Single doses and steady state phar-macokinetics. Fertil Steril 61:679–686.
134. Karlsson MO, Wade JR, Loumaye E, Munafo A.1998. The population pharmacokinetics of recom-binant- and urinary-human follicle-stimulatinghormone in women. Br J Clin Pharmacol45:13–20.
135. Salmonson T, Danielson BG, Wikstrom B. 1990.The pharmacokinetics of recombinant humanerythropoietin after intravenous and subcutane-ous administration to healthy subjects. Br J ClinPharmacol 29:709–713.
136. Liles D, Landen CN, Monroe DM, Lindley CM,Read MS, Roberts HR, Brinkhous KM. 1997. Ex-travascular administration of factor IX: potentialfor replacement therapy of canine and human he-mophilia B. Thromb Haemost 77:944–948.
310 PORTER AND CHARMAN
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 89, NO. 3, MARCH 2000





























