Embed Size (px)
Citation preview

Expe
rim
enta
lPhy
siol
ogy
Exp Physiol 000.0 (2015) pp 1–11 1
Research PaperResearch Paper
Magnitude of muscle wasting early after on-pumpcoronary artery bypass graft surgery and explorationof aetiology
Dominique Hansen1,2, Loes Linsen1,3,4, Kenneth Verboven1, Marc Hendrikx1,5, Jean-Luc Rummens1,3,4,Monique van Erum1, Bert O. Eijnde1 and Paul Dendale1,2
1REVAL – Rehabilitation Research Center, BIOMED – Biomedical Research Center, Faculty of Medicine and Life Sciences, Hasselt University, Diepenbeek,Belgium2Heart Centre Hasselt, Jessa Hospital, Hasselt, Belgium3University Biobank Limburg, Hasselt, Belgium4Laboratory of Experimental Hematology, Jessa Hospital, Hasselt, Belgium5Department of Cardiothoracic Surgery, Jessa Hospital, Hasselt, Belgium
New Findings� What is the central question of this study?
It remains uncertain whether significant fat-free mass wasting occurs early after coronaryartery bypass graft surgery, and the aetiology of this wasting in these particular conditions isunexplored.
� What is the main finding and its importance?Significant fat-free mass wasting is present after coronary artery bypass graft surgery, and thiswasting effect is greater in younger patients and in patients with greater increments in bloodcortisol-to-testosterone ratios after surgery.
The magnitude and aetiology of muscle wasting early after coronary artery bypass graft (CABG)surgery remains unknown. In the present study, we assessed changes in fat-free mass early afterCABG surgery and explored the possible aetiology (relationships with postsurgical changesin blood hormones, insulin resistance, subject characteristics and inflammation) for thesechanges. Fat-free mass was assessed before and 23 (range: 25) days after CABG surgery in25 subjects. Blood testosterone, cortisol, insulin-like growth factor-1, growth hormone, sexhormone-binding globulin, glucose, insulin, C-peptide and C-reactive protein concentrationswere determined, and free androgen index, cortisol-to-testosterone ratio and HOMA-IR indexwere all calculated before surgery, during the first 3 days after surgery and at reassessment of bodycomposition. Relationships between changes in fat-free mass and changes in blood parametersafter surgery or subject characteristics were studied. After surgery, free androgen index and bloodsex hormone-binding globulin, testosterone and insulin-like growth factor-1 concentrationsdecreased significantly, while HOMA-IR index, cortisol-to-testosterone ratio, blood growthhormone, insulin and C-reactive protein concentrations increased significantly (P < 0.0025,observed α > 0.80). Whole-body fat-free mass decreased significantly [by −1.9 (range: 9.1) kg,P < 0.0025, observed α = 0.99] after surgery. According to regression analysis, greater absoluteloss of fat-free mass was observed after CABG surgery in subjects who were younger, whoexperienced a greater increase in blood cortisol-to-testosterone ratio after surgery and/or whounderwent earlier reassessment of body composition (P < 0.05). Significant decrements infat-free mass were observed early after CABG surgery, especially in younger subjects and/or
C© 2015 The Authors. Experimental Physiology C© 2015 The Physiological Society DOI: 10.1113/EP085053

2 Exp Physiol 000.0 (2015) pp 1–11D. Hansen and others
subjects with elevated blood cortisol-to-testosterone ratios after surgery. Interventions topreserve fat-free mass soon after CABG surgery are thus warranted.
(Received 6 January 2015; accepted after revision 8 May 2015; first published online 12 May 2015)Corresponding author D. Hansen: Hasselt University, Faculty of Medicine and Life Sciences, Agoralaan, Building A,3590 Diepenbeek, Belgium. Email: [email protected]
Introduction
More than 200,000 coronary artery bypass graft (CABG)surgical procedures are carried out each year in the USA(Weiss & Elixhauser, 2014). Coronary artery bypass graftsurgery is a procedure employed to restore or optimizemyocardial perfusion in coronary artery disease. In thissurgical intervention, a venous or arterial graft is usedto bypass the coronary occlusion or stenosis. Given thatcardioplegia (induction of temporary cardiac arrest) isoften executed, the patient’s circulation is coupled to acardiopulmonary bypass machine, and access to the heartis achieved by median sternotomy. After CABG surgery, a7–14 day hospital stay is generally required.
A likely consequence of CABG surgery is considerablemuscle wasting during the recovery period. This leads toa reduction in muscle strength, functional capacity andinsulin sensitivity, and elevated mortality, especially insubjects aged>50 years (Szulc et al. 2010). Mechanistically,the loss of fat-free mass during recovery has been linkedto a rapid decline in muscle protein synthesis rates (by�36%) in the first 4 h after CABG surgery (Caso et al.2008). Muscle wasting should thus be considered as asignificant adverse event after CABG surgery.
Nevertheless, whether muscle wasting genuinely occursafter CABG surgery remains a topic of debate. Miller et al.(2007) reported no significant changes in whole-bodyfat-free mass within 3 months after CABG surgery.Conversely, van Venrooij and colleagues (2012) reporteda modest (0.8 kg) but significant decrease in whole-bodyfat-free mass 2 months after CABG surgery. However, thesestudies were limited by the relatively late reassessment ofbody composition after surgery. It could be argued thatmuch of the reduction in fat-free mass was therefore notdetected and/or the patients had already participated inrehabilitation interventions or were engaged in regular(home-based) physical exercise, allowing some restorationof fat-free mass (Marzolini et al. 2008). At present itis recommended to initiate exercise-based rehabilitationinterventions (combination of endurance and resistanceexercises) early after CABG surgery (immediately afterhospital discharge; Piepoli et al. 2012), which we andothers routinely perform in clinical practice. Thus, it isnecessary to clarify the extent of fat-free mass loss duringrecovery from CABG surgery. This is important becauserecommendations on early tolerable muscle exercises arelikely to emerge in the event of acute fat-free mass wasting.
Moreover, the factors associated with fat-free masswasting after CABG surgery, if present, have not beenexplored in great detail. Previous studies have indicatedthat CABG surgery compromised endocrine function(alterations in the concentration of anabolic and catabolichormones in the blood), reduced insulin sensitivity andgenerated an inflammatory reaction (Lehot et al. 1992;Roth-Isigkeit et al. 1997, 2000; Henzen et al. 2003;Velissaris et al. 2004; Maggio et al. 2005). In addition,bed rest significantly reduced skeletal muscle proteinsynthesis rates, at least in healthy individuals (Kortebeinet al. 2007). Such endocrine and metabolic changes,together with inflammation, bed rest and/or insulinresistance, may ultimately lead to reductions in fat-freemass. Moreover, preoperative patient characteristics maydetermine changes in fat-free mass after CABG surgery. Adeeper understanding of the mechanisms and/or patientcharacteristics leading to fat-free mass wasting after CABGsurgery could lead to earlier preventive treatments and/orrehabilitation interventions.
In this study, the early impact of CABG surgeryon fat-free mass was examined, and the aetiology offat-free mass wasting after CABG surgery was explored.We hypothesized that significant fat-free mass wastingwas present early after CABG surgery, and that suchfat-free mass wasting was due to endocrine hormonedisturbances, insulin resistance, inflammation and/orsubject characteristics.
Methods
Ethical approval
This study was approved by the local medical ethicalcommittee (Jessa Hospital, Hasselt, Belgium); the studyconformed to the standards set by the latest revision of theDeclaration of Helsinki, and written informed consent wasobtained from all subjects.
Subjects
After inviting 119 eligible Dutch-speaking, Caucasiancandidates admitted to the hospital for elective CABGsurgery (from March 2011 to October 2013), 30subjects agreed to participate in this study (Fig. 1).The study sample size (n = 30) was based on
C© 2015 The Authors. Experimental Physiology C© 2015 The Physiological Society

Exp Physiol 000.0 (2015) pp 1–11 3Muscle wasting after coronary artery bypass graft surgery
previous studies assessing the impact of CABG surgeryon fat-free mass (Miller et al. 2007; van Venrooijet al. 2012). Owing to postoperative complications andprolonged hospitalization in five subjects, data from25 subjects were analysed. As a result, data from thepresent study reflected changes in blood parameters andbody composition after CABG surgery with a normalpostoperative course. Subjects were excluded prior tostudy when (mild) pulmonary, neurological, oncologicaland/or nephrological disease was present. Patients withmetal implants or previous CABG or valve surgerywere not included. Patients with previous percutaneouscoronary intervention and/or myocardial infarction, butwithout heart failure, were allowed to participate in thisstudy.
Design
This was a prospective observational study. The day beforeCABG surgery, body composition was assessed and afasting blood sample collected. On the first, second andthird day after CABG surgery, fasting blood samples werecollected [for measurement of blood testosterone, cortisol,
Subjects invited
(n = 119)
Subjects unwilling to participate (n = 89)
Subjects included
(n = 30)
Subjects experienced
complications and prolonged
hospitalization
(n = 5)
Subjects completed follow-up
(n = 25)
Figure 1. Study flowchartAfter inviting 119 eligible candidates admitted to the hospitalfor elective coronary artery bypass graft (CABG) surgery, 30subjects agreed to participate in this study. Owing topostoperative complications and prolonged hospitalization infive subjects, data from 25 subjects were analysed.
insulin-like growth factor-1 (IGF-1), growth hormone, sexhormone-binding globulin, C-reactive protein, glucose,insulin and C-peptide concentration, free androgenindex, cortisol-to-testosterone ratio and homeostatic modelassessment-insulin resistance (HOMA-IR) index]. At entryto rehabilitation [23 (range: 25) days after surgery], bodycomposition was reassessed and a fasting blood samplecollected.
Primary outcome measures
The primary outcome measure was whole-body fat-freemass.
Secondary outcome measures
Secondary outcomes measures were blood testosterone,cortisol, IGF-1, growth hormone, sex hormone-bindingglobulin, C-reactive protein, glucose, insulin andC-peptide concentrations, free androgen index, cortisol-to-testosterone ratio, HOMA-IR index, time to bodycomposition reassessment, duration of hospitalization,duration of surgery and duration of intubation.
Coronary artery bypass graft surgery
On-pump CABG surgery through median sternotomywas performed on all subjects by one surgeon withsimilar methodology. During this procedure, patients wereconnected to an open circuit extracorporeal circulation (orcardiopulmonary bypass), the aorta was cross-clampedand the heart was arrested by blood cardioplegia. Bodytemperature was lowered to 34°C. The average durationof the procedure (start of sternotomy incision untilend of closing sternotomy) was 227 (range: 248) min.During hospital stay [10 (range: 7) days], subjects receivedphysical therapy (daily breathing exercises for a durationof 15 min day−1 and endurance exercises (walking andcycling against resistance, arm cranking without appliedresistance) up to 30 min day−1 at a low intensity (exerciseheart rate <120 beats min−1).
Measurements
Body composition. After assessment of body weight andheight, segmental and whole-body adipose tissue mass andfat-free mass were determined in the fed condition usingwhole-body dual X-ray absorptiometry (DXA; LunarDPXL, WI, USA; Glickman et al. 2004). In four subjects,the composition of arm tissue could not be measuredbecause they did not fit under the scanner. In thesesubjects, whole-body fat-free and adipose tissue mass wascalculated by the sum of fat-free and adipose tissue massof the trunk and legs.
C© 2015 The Authors. Experimental Physiology C© 2015 The Physiological Society

4 Exp Physiol 000.0 (2015) pp 1–11D. Hansen and others
Blood parameters. Blood samples were collectedbetween 07.00 and 09.00 h after an overnight fast andwere processed and stored at the University BiobankLimburg (UBiLim). Analysis of blood parameters wasperformed by standard diagnostic tests at the clinicallaboratory of the Jessa Hospital. Blood glycosylatedhaemoglobin concentration was determined in wholeEDTA blood via a commercial HPLC-based method(Hi-Auto A1C Analyser; Menarini Diagnostics BeneluxS.A. Belgicastraat, Zaventem, Belgium). Serum tubeswere left to clot for 30 min and subsequently centrifugedfor 5 min at 2500g. These serum samples were used toasses blood hormones affecting skeletal muscle proteinsynthesis, such as total testosterone [by chemiluminescentenzyme-linked immunosorbent assay (ELISA) on anautomated ELISA device, Architect i2000SR; AbbottLaboratories, Illinois, USA], total cortisol (by directchemiluminescence sandwich ELISA on ADVIA CentaurXP analyser; Siemens Healthcare, The Netherlands),total IGF-1 [by immuneradiometric assay (IMRA)IGF-I kit; Beckman Coulter, ANALIS SA, Belgium] andtotal growth hormone (by hGH-IRMA kit; DIAsourceImmunoAssays SA, Louvain-la-Neuve - Belgium), aswell as for sex hormone-binding globulin (by two-stepChemiflex ImmunoAssay on automated ELISA deviceArchitect i2000SR; Abbott), insulin, C-peptide (both bydirect chemiluminescence sandwich ELISA on ADVIACentaur XP; Siemens) and blood glucose concentrations(by colorimetric hexokinase–glucose-6-phosphate dehy-drogenase method on a Beckman Coulter AU 2700chemical analyser; Beckman Coulter). Lithium heparinplasma was obtained by centrifuging blood samplesfor 5 min at 2500g. In these samples, the lipid profile(total cholesterol, triglycerides, low-density lipoproteincholesterol and high-density lipoprotein cholesterol) wasmeasured by enzymatic colorimetry, together with theinflammatory status based on blood C-reactive proteinconcentration by an antibody-based turbidimetricmethod, on a Beckman Coulter AU 2700 chemicalanalyser. The HOMA-IR index was calculated to estimatewhole-body insulin sensitivity, as follows: [insulin(in millunits per litre) × glucose (in millimoles perlitre)]/22.5 (Matthews et al. 1985). Free androgen indexwas calculated as follows: [blood total testosteroneconcentration (in nanomoles per litre) × 100]/blood sexhormone-binding globulin concentration (in nanomolesper litre) (Ho et al. 2006). Catabolic–anabolic hormonebalance was calculated as the blood total cortisolconcentration/blood total testosterone concentration.
Statistical analysis
Statistical analyses were executed using SPSS version22.0 (SPSS Inc., Chicago, IL, USA). Shapiro–Wilk tests
indicated that most data were not normally distributed.Therefore, data were expressed as the median (range),and non-parametric tests were applied. Changes inblood parameters during follow-up were analysed byrelated-sample Friedman variance of ranks tests, inwhich Bonferroni corrections for multiple comparisons(preoperative versus postoperative, n = 20) were applied(statistical significance was set at P < 0.0025). Changesin body composition were analysed by Wilcoxon signedranks tests, in which Bonferroni corrections for multiplecomparisons (preoperative versus postoperative, n = 20)were applied (statistical significance was set at P < 0.0025).Next, univariate Spearman correlations were calculated,and a forward stepwise multivariate regression model wasconstructed to examine relationships between changes inwhole-body fat-free mass and baseline parameters (bloodparameters, age, sex, baseline whole-body adipose andfat-free mass, intubation time, hospitalization duration,surgery duration and time to reassessment of bodycomposition) or changes in blood parameters after surgeryup to reassessment of body composition (area under thecurve minus preoperative value; Table 2). A multivariatelinear regression model was created, in which relationshipsbetween changes in whole-body fat-free mass and detectedsignificant independent predictors from the forwardstepwise multivariate regression model were examined. Inthese regression models, statistical significance was set atP < 0.05. Observed statistical power was calculated (byGPower v. 3.1, Heinrich-Heine-Universitat Dusseldorf,Germany).
Results
Subject characteristics
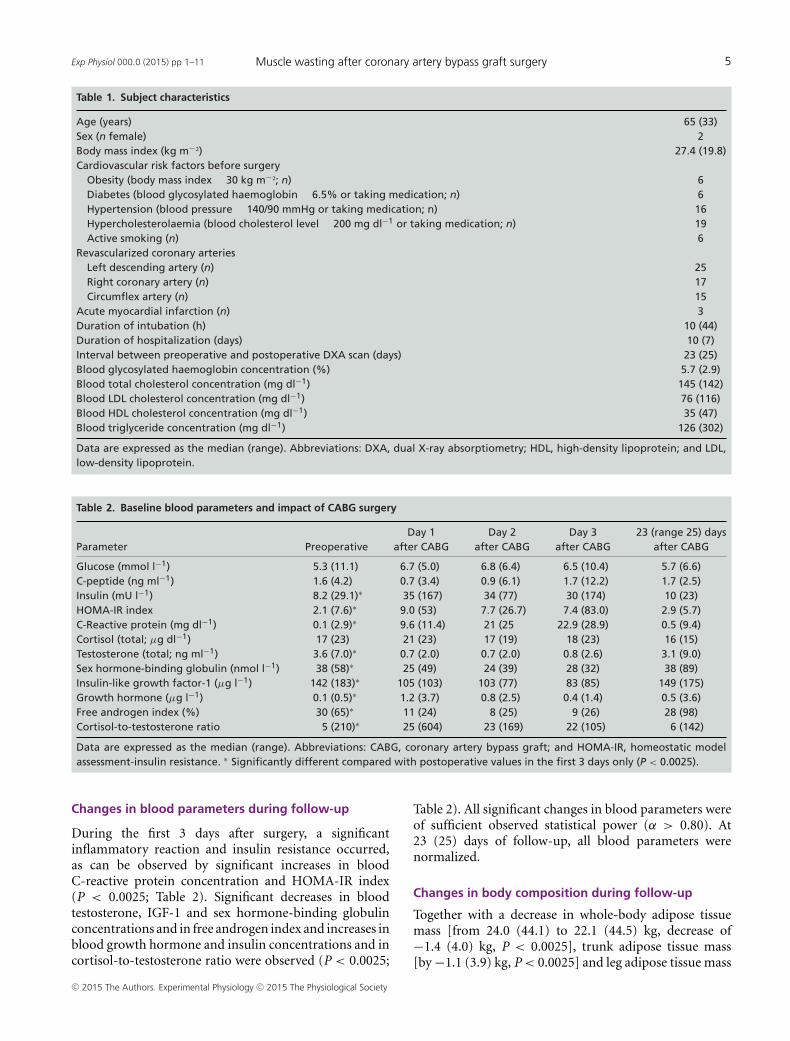
Twenty-five subjects were examined [two females;median age 65 (33) years; Table1]. Three subjects wererevascularized by CABG surgery after acute myocardialinfarction and others for stable angina with a positivestress test. Subjects were intubated for 10 (44) h afterCABG surgery and were hospitalized for 10 (7) days.The following medications were taken before surgery:anticoagulants (n = 23), nitrates (n = 11), β-blockers(n = 15), statins (n = 19), calcium antagonists (n = 3),metformin (n = 5), sulfonylurea (n = 2), insulin (n = 1),diuretics (n=3), angiotensin receptor blockers (n=1) andangiotensin-converting enzyme inhibitors (n = 9). Thefollowing medications were taken after surgery (on theday of body composition reassessment): anticoagulants(n = 24), nitrates (n = 4), β-blockers (n = 24),statins (n = 22), calcium antagonists (n = 7), metformin(n = 5), sulfonylurea (n = 2), insulin (n = 1), diuretics(n = 5), angiotensin receptor blockers (n = 1) andangiotensin-converting enzyme inhibitors (n = 5).
C© 2015 The Authors. Experimental Physiology C© 2015 The Physiological Society
Exp Physiol 000.0 (2015) pp 1–11 5Muscle wasting after coronary artery bypass graft surgery
Table 1. Subject characteristics
Age (years) 65 (33)Sex (n female) 2Body mass index (kg m−²) 27.4 (19.8)Cardiovascular risk factors before surgery
Obesity (body mass index � 30 kg m−²; n) 6Diabetes (blood glycosylated haemoglobin � 6.5% or taking medication; n) 6Hypertension (blood pressure � 140/90 mmHg or taking medication; n) 16Hypercholesterolaemia (blood cholesterol level � 200 mg dl−1 or taking medication; n) 19Active smoking (n) 6
Revascularized coronary arteriesLeft descending artery (n) 25Right coronary artery (n) 17Circumflex artery (n) 15
Acute myocardial infarction (n) 3Duration of intubation (h) 10 (44)Duration of hospitalization (days) 10 (7)Interval between preoperative and postoperative DXA scan (days) 23 (25)Blood glycosylated haemoglobin concentration (%) 5.7 (2.9)Blood total cholesterol concentration (mg dl−1) 145 (142)Blood LDL cholesterol concentration (mg dl−1) 76 (116)Blood HDL cholesterol concentration (mg dl−1) 35 (47)Blood triglyceride concentration (mg dl−1) 126 (302)
Data are expressed as the median (range). Abbreviations: DXA, dual X-ray absorptiometry; HDL, high-density lipoprotein; and LDL,low-density lipoprotein.
Table 2. Baseline blood parameters and impact of CABG surgery
Day 1 Day 2 Day 3 23 (range 25) daysParameter Preoperative after CABG after CABG after CABG after CABG
Glucose (mmol l−1) 5.3 (11.1) 6.7 (5.0) 6.8 (6.4) 6.5 (10.4) 5.7 (6.6)C-peptide (ng ml−1) 1.6 (4.2) 0.7 (3.4) 0.9 (6.1) 1.7 (12.2) 1.7 (2.5)Insulin (mU l−1) 8.2 (29.1)∗ 35 (167) 34 (77) 30 (174) 10 (23)HOMA-IR index 2.1 (7.6)∗ 9.0 (53) 7.7 (26.7) 7.4 (83.0) 2.9 (5.7)C-Reactive protein (mg dl−1) 0.1 (2.9)∗ 9.6 (11.4) 21 (25 22.9 (28.9) 0.5 (9.4)Cortisol (total; μg dl−1) 17 (23) 21 (23) 17 (19) 18 (23) 16 (15)Testosterone (total; ng ml−1) 3.6 (7.0)∗ 0.7 (2.0) 0.7 (2.0) 0.8 (2.6) 3.1 (9.0)Sex hormone-binding globulin (nmol l−1) 38 (58)∗ 25 (49) 24 (39) 28 (32) 38 (89)Insulin-like growth factor-1 (μg l−1) 142 (183)∗ 105 (103) 103 (77) 83 (85) 149 (175)Growth hormone (μg l−1) 0.1 (0.5)∗ 1.2 (3.7) 0.8 (2.5) 0.4 (1.4) 0.5 (3.6)Free androgen index (%) 30 (65)∗ 11 (24) 8 (25) 9 (26) 28 (98)Cortisol-to-testosterone ratio 5 (210)∗ 25 (604) 23 (169) 22 (105) 6 (142)
Data are expressed as the median (range). Abbreviations: CABG, coronary artery bypass graft; and HOMA-IR, homeostatic modelassessment-insulin resistance. ∗ Significantly different compared with postoperative values in the first 3 days only (P < 0.0025).
Changes in blood parameters during follow-up
During the first 3 days after surgery, a significantinflammatory reaction and insulin resistance occurred,as can be observed by significant increases in bloodC-reactive protein concentration and HOMA-IR index(P < 0.0025; Table 2). Significant decreases in bloodtestosterone, IGF-1 and sex hormone-binding globulinconcentrations and in free androgen index and increases inblood growth hormone and insulin concentrations and incortisol-to-testosterone ratio were observed (P < 0.0025;
Table 2). All significant changes in blood parameters wereof sufficient observed statistical power (α > 0.80). At23 (25) days of follow-up, all blood parameters werenormalized.
Changes in body composition during follow-up
Together with a decrease in whole-body adipose tissuemass [from 24.0 (44.1) to 22.1 (44.5) kg, decrease of−1.4 (4.0) kg, P < 0.0025], trunk adipose tissue mass[by −1.1 (3.9) kg, P < 0.0025] and leg adipose tissue mass
C© 2015 The Authors. Experimental Physiology C© 2015 The Physiological Society

6 Exp Physiol 000.0 (2015) pp 1–11D. Hansen and others
[by −0.2 (3.6) kg, P < 0.0025], whole-body fat-free massdecreased significantly [from 54.1 (24.8) to 52.7 (25.3) kg,decrease of −1.9 (9.1) kg, observed α = 0.99, P < 0.0025]after CABG surgery (Fig. 2). Furthermore, significant
60
*
*
*
*
*
Preoperative
Postoperative
*
50
40
30
20
10
Tis
sue m
ass (
kg)
0FM
total
FM
trunk
FM legs FM
arms
FFM
arms
FFM
total
FFM
trunk
FFM
legs
Figure 2. Changes in adipose tissue (FM) and fat-free mass(FFM) after CABG surgeryTogether with a decrease in whole-body adipose tissue mass,trunk adipose tissue mass and leg adipose tissue mass(P < 0.0025), whole-body fat-free mass decreased by−1.9 (9.1) kg (P < 0.0025) after CABG surgery. Significantdecreases in fat-free mass were observed in the arms [by−0.5 (0.8) kg, P < 0.0025] and legs [change of −0.5 (4.8) kg,P < 0.0025] after CABG surgery, but not in the trunk [changeof −0.7 (7.1) kg, P > 0.0025].
decreases in fat-free mass were observed in the arms[by −0.5 (0.8) kg, P < 0.0025] and legs [change of−0.5 (4.8) kg, P < 0.0025] after CABG surgery, but notin the trunk [change of −0.7 (7.1) kg, P > 0.0025]. Agreat heterogeneity in whole-body fat-free mass loss wasobserved (Fig. 3). Relative changes in fat-free mass inthe different body regions were as follows: whole-body[by −4.4 (15.3)%], trunk [by −2.8 (22.5)%], legs [by−2.8 (25.8)%] and arms [by −8.0 (8.2)%].
CorrelationsUnivariate correlations (P < 0.05) were found betweenthe magnitude of whole-body fat-free mass change aftersurgery and time to body composition reassessment(r = 0.43), age (r = 0.56), preoperative blood C-peptide(r = −0.53) and cortisol concentrations (r = 0.50),postoperative change in blood cortisol concentration(r = −0.50) and free androgen index (r = 0.47; Fig. 4).A correlation was found between age and changes inHOMA-IR (r = −0.45, P < 0.05) after CABG surgery,but not with changes in blood hormones or markers ofinflammation. Age was not correlated significantly withtime to reassessment of body composition (P > 0.05).Baseline fat-free mass was not correlated with changes infat-free mass after CABG surgery (P > 0.05).
Regression analysis
Greater increases in blood cortisol-to-testosterone ratioafter surgery (standardized coefficient β = 0.64,P < 0.001), younger age (standardized coefficient β= 0.68,
4
2
0
-2
-4
-6
-8
Subject
Change in fat-
free m
ass (
kg)
Figure 3. Changes in whole-body fat-free mass depicted for each individual separately (on x-axis)A great heterogeneity in whole-body fat-free mass loss was observed. Some subjects experienced severefat-free mass wasting (6.3 kg decrease in fat-free mass), while others did not (2.7 kg gain in fat-freemass).
C© 2015 The Authors. Experimental Physiology C© 2015 The Physiological Society

Exp Physiol 000.0 (2015) pp 1–11 7Muscle wasting after coronary artery bypass graft surgery
P < 0.001) and earlier reassessment of body composition(standardized coefficient β = 0.34, P = 0.028) wereindependently related to greater absolute whole-bodyfat-free mass loss after CABG surgery (model adjusted
r² = 0.75, P < 0.001). Also, a trend for a relationshipbetween the amount of fat-free mass loss and durationof surgery was found (standardized coefficient β = 0.28,P = 0.052).
A Relationship with time to reassessment of body composition (days)
D Relationship with preoperative blood cortisol concentration (μg dl-1)
E Relationship with change in blood cortisol concentration (μg dl−1) F Relationship with change in free androgen index (%)
C Relationship with preoperative blood C-peptide concentration (ng ml-1)
B Relationship with subject age (years)
45 90
80
70
60
50
40
30
20
10
0
40
35
30
25
20
15
10
5
-8 -6 -4 -2 -8 -6 -4 -20
-8 -6 -4 -2
60
40
20
0
0
-20
-40
-60
50
0
0
-50
-100
-150
-200
0
0 2 4
0
35
30
25
20
15
10
5
02 4
2 4
-8 -6 -4 -2
2 4-8 -6 -4 -2
2 4
-8 -6 -4 -2 2 4
0
6
5
4
3
2
1
0
Change in fat-free mass (kg)
Change in fat-free mass (kg)
Change in fat-free mass (kg)
Change in fat-free mass (kg)
Change in fat-free mass (kg)
Change in fat-free mass (kg)
Figure 4. Univariate correlations between changes in fat-free mass after CABG surgery and subjectcharacteristics/changes in blood parameters after CABG surgeryUnivariate correlations (P < 0.05) were found between the magnitude of whole-body fat-free masschange after surgery and time to body composition reassessment (r = 0.43), age (r = 0.56), preoperativeblood C-peptide (r = −0.53) and cortisol concentrations (r = 0.50), postoperative change in blood cortisolconcentration (r = −0.50) and free androgen index (r = 0.47).
C© 2015 The Authors. Experimental Physiology C© 2015 The Physiological Society

8 Exp Physiol 000.0 (2015) pp 1–11D. Hansen and others
Discussion
In the present study, we demonstrated that significantdecrements in fat-free mass occurred within the firstweeks after CABG surgery. Moreover, we also showedthat more severe absolute reductions in fat-free masswere experienced by younger subjects, subjects withgreater increases in blood cortisol-to-testosterone ratioafter surgery and/or subjects with earlier reassessment ofbody composition.
According to our data, CABG patients are likely toenter early rehabilitation programmes (within a few weeksafter surgery) with reduced fat-free mass. Especially inthe arms, a pronounced reduction in fat-free mass (by−8.1 ± 2.1%) was noticed. The reduction in fat-freemass could, however, have been mitigated by the earlyin-hospital rehabilitation programme after CABG surgery.Thus, it may be speculated that even greater fat-freemass decrements may be present after CABG surgerywhen such early rehabilitation intervention is absent. Areduction in body weight after CABG surgery shouldthus not be considered as a reduction in adipose tissuemass only. Given that fat-free mass wasting is associatedwith the development of insulin resistance, reducedmuscle strength and functional capacity and elevatedmortality (Szulc et al. 2010), attempts should be made tominimize such postoperative wasting in CABG patients.In this regard, exercise-based rehabilitation interventionsshould be implemented soon after CABG surgery.Such interventions should involve resistance exercises inpreference to endurance exercises because the former aremore strongly associated with hypertrophy and increasedstrength (Marzolini et al. 2008). In these interventions,the arm muscles must be targeted specifically. To optimizethe medical safety of resistance exercise training of theupper extremities early after CABG surgery, it is importantto avoid the Valsalva manoeuvre, to enssure that thesternum is stable and to execute only bilateral exerciseswith equal weights (Piepoli et al. 2012). It may alsobe speculated that nutritional support, such as proteinsupplementation (preferentially used in combination withresistance exercise) would augment fat-free mass regain inCABG patients (Cermak et al. 2012). Future studies shouldexplore whether such optimized early exercise trainingprogrammes could minimize or even prevent fat-free masswasting after CABG surgery.
In previous studies, only small changes in whole-bodyfat-free mass were observed after CABG surgery (Milleret al. 2007; van Venrooij et al. 2012). At first glance,this may seem to contradict our finding of considerablefat-free mass loss. However, in the present study, a smallerdecline in fat-free mass was observed in patients with alater re-examination of body composition after CABGsurgery. In agreement with this finding, Miller et al. (2007)did not observe changes in whole-body fat-free mass at
3 months after CABG surgery, while van Venrooij et al.(2012) found a small, significant decrease in whole-bodyfat-free mass at 2 months after CABG surgery. It couldbe hypothesized that a spontaneous regain in fat-freemass occurs after CABG surgery. Moreover, it could alsobe proposed that patients engaged in rehabilitation orhome-based physical activities within these 2–3 monthsafter CABG surgery in previous studies, resulting infat-free mass regain. In the present study, patients did notstart their ambulatory rehabilitation programme beforebody composition reassessment after surgery. However,we did not monitor home-based physical activity, soit remains uncertain whether spontaneous fat-free massregain occurs after CABG surgery or whether this regainis related to home-based physical activity.
Despite the significant fat-free mass wasting in the totalsubject cohort after CABG surgery, the severity of thiswasting was considerably different between individuals.Some subjects experienced severe fat-free mass wasting(6.3 kg decrease in fat-free mass), while others did not(2.7 kg gain in fat-free mass). Based on data fromthe present study, and in agreement with data fromprevious studies (Lehot et al. 1992; Roth-Isigkeit et al.1997, 2000; Henzen et al. 2003; Velissaris et al. 2004;Maggio et al. 2005), CABG surgery led to systemicinflammation and a decrease in blood anabolic hormoneconcentration (IGF-1 and testosterone), while bloodcatabolic hormone concentration (cortisol) remainedstable (suggesting a predominantly catabolic hormonalmilieu, based on cortisol-to-testosterone ratio). Moreover,subjects were intubated and subsequently hospitalizedfor 10 (7) days, which led to a reduced level ofphysical activity. In addition, subjects developed insulinresistance (six patients were diagnosed with diabetesbefore CABG surgery); patients were in need of exogenousinsulin administration (Actrapid R©) to prevent excessivehyperglycaemia (which explains, in part, the elevatedpostoperative blood insulin levels).
To explain the aetiology of the heterogeneity in fat-freemass wasting after CABG surgery, we therefore examinedwhich of those factors/changes and patient features wereindependently related to greater fat-free mass wastingafter CABG surgery. From this examination, it wasobserved that more severe fat-free mass wasting wasexperienced by subjects with greater increases in bloodcortisol-to-testosterone ratio after surgery and/or youngersubjects. Given that blood cortisol levels remained stableduring the first days after CABG surgery, but bloodtestosterone levels decreased significantly, a catabolichormonal environment developed. According to previousinvestigations, the relative predominance of blood cortisol(due to lowered blood testosterone concentration) couldlead to fat-free mass wasting by a combination oflowered protein synthesis (due to lowered transportof amino acids into the muscle, inhibition of insulin
C© 2015 The Authors. Experimental Physiology C© 2015 The Physiological Society

Exp Physiol 000.0 (2015) pp 1–11 9Muscle wasting after coronary artery bypass graft surgery
and IGF-1 action and/or inhibition of phosphorylationof eIF4E-binding protein-1 and ribosomal proteinS6 kinase-1) and increased protein breakdown [dueto activation of cellular proteolytic systems, such asthe ubiquitin–proteasome system, lysosomal system(cathepsins) and calcium-dependent system (calpains);Schakman et al. 2008]. In addition, lowered bloodtestosterone levels could also lead to fat-free mass wastingby an increase in muscle protein degradation due tolowered amino acid uptake into the cell, binding of thishormone to intracellular androgen receptors (causingless transcription of specific genes), decrease in IGF-1production and/or less inhibition of cortisol signalling(Vingren et al. 2010). Future studies are warranted toverify whether these physiological changes are indeedinstrumental to the fat-free mass wasting process afterCABG surgery. As a result of of the predominantlycatabolic hormonal environment after CABG surgeryand its relationship with fat-free mass wasting, otherlaboratories have already generated initial data concerningthe supplementation of testosterone after CABG surgeryto prevent fat-free mass wasting (Maggio et al. 2012).
Younger subjects experienced greater fat-free mass lossafter CABG surgery in the present study. The signallingpathways leading to muscle atrophy and the amount offat-free mass wasting seem to be significantly affected byage. For example, in young and old subjects, molecularsignalling pathways governing skeletal muscle proteinsynthesis decrease significantly as result of immobilization(Suetta et al. 2012). However, in older subjects higherAkt phosphorylation and early upregulation of IGF-1 Eaand mechano growth factor, in combination with loweratrogin-1 and muscle-specific muscle ring finger 1 mRNAexpression, has been observed during immobilization(Suetta et al. 2012). These adaptations collectively lead toless fat-free mass wasting as a result of immobilization inolder patients (Suetta et al. 2012). However, this hypothesisremains to be verified in CABG patients. As changes inblood hormones after surgery were not related to agein the present study, it is speculated that greater fat-freemass wasting in younger subjects is not due to differentchanges in blood hormones. It could be speculated thatyounger subjects had a greater preoperative fat-free mass,and thus greater reductions in fat-free mass can beanticipated in these subjects. However, in this study thepreoperative fat-free mass did not correlate (P > 0.05)with the magnitude of fat-free mass wasting after CABGsurgery.
It could be argued that fat-free mass wasting afterCABG surgery is mainly due to bed rest (whole-bodymuscle disuse). Indeed, previous studies have shown thata 7–14 day bed rest was associated with significant fat-freemass wasting (Ferrando et al. 1996; Drummond et al.2012) and that the anabolic response to amino acid intakewas significantly suppressed (Drummond et al. 2012).
The magnitude of fat-free mass wasting in the presentstudy seemed comparable to those previously publisheddata (Ferrando et al. 1996; Drummond et al. 2012).Considering the lack of a control subject who underwentbed rest only in this study, data from the present studyshould be evaluated in light of this shortcoming. However,subjects from the present study executed enduranceexercises on a daily basis under supervision of a physicaltherapist and were required to sit upright as often aspossible and to walk in a nearby corridor. Therefore, it islikely that substantially more physical activity was presentin our study as opposed to those previous studies (whererecruited healthy volunteers were not allowed to leavethe bed under carefully controlled laboratory conditions).Therefore, the observed fat-free mass wasting in thepresent study is probably not completely explained byphysical inactivity/bed rest alone. Unfortunately, physicalactivity was not monitored during hospitalization or athome in this study. Future studies should thus examine theimpact of postoperative physical activity level on fat-freemass after CABG surgery.
In the present study, CABG surgery led to somechanges in blood hormones that could be of interest forfurther study or are clinically relevant. However, it hasto be mentioned that the endocrine impact of CABGsurgery remains a topic of intense debate and is complex.After CABG surgery, hyperinsulinaemia occurred. TheCABG surgery provokes an inflammatory response(characterized by increased blood C-reactive proteinconcentration) and a reduction in blood testosteroneconcentration. Moreover, patients were sedated for severalhours, so skeletal muscle activity was significantlysuppressed. Although many more factors were involved,these changes would, at least in part, induce insulinresistance. To overcome this insulin resistance and avoidexcessive hyperglycaemia, exogenous insulin (Actrapid R©)was administered to the patients. This explains why a stateof hyperinsulinaemia was present after CABG surgery,while blood C-peptide levels (indicative of pancreaticactivity) remained stable after surgery. Moreover, inthe presence of an insulin-resistant state the proteinsynthesis-stimulating effect of insulin on muscle tissuecould have been suppressed (Bassil & Gougeon, 2013).In addition, CABG surgery, or any other major surgicalprocedure, is associated with rapid elevations in bloodgrowth hormone concentration (Wallin, 2007; Nakhjavaniet al. 2009). Although the aetiology for such postoperativegrowth hormone elevation remains speculative, ourfindings are in line with these observations. Moreover,patients who underwent CABG surgery seemed to developgrowth hormone resistance for currently unknownreasons (Wallin, 2007; Nakhjavani et al. 2009). Aconsequence of such growth hormone resistance is thelowering of blood IGF-1 levels (Wallin, 2007; Nakhjavaniet al. 2009), as was observed in the present study. A
C© 2015 The Authors. Experimental Physiology C© 2015 The Physiological Society

10 Exp Physiol 000.0 (2015) pp 1–11D. Hansen and others
reduction in circulatory IGF-1 levels in turn lowers insulinsensitivity (Wallin, 2007).
In the present study, significant decrements in adiposetissue mass were observed after CABG surgery. Thesefindings are in disagreement with the study of van Venrooijet al. (2012), where no changes in adipose tissue masswere observed after CABG surgery. The reason for thisdiscrepancy in outcomes between studies remains highlyspeculative. Data on the impact of CABG surgery onadipose tissue mass are, however, scarce but can beclinically relevant due to the relationship between (changesin) adipose tissue mass and clinical outcomes. It followsthat this topic should deserve greater attention in the nearfuture. In the present study, explaining the aetiology ofadipose tissue mass loss after CABG surgery is difficultbecause of a lack of detailed recordings of caloric andmacronutrient intakes during hospitalization.
This study may be limited by the small sample size.However, significant changes in body composition areobserved after CABG surgery (P < 0.0025), and changesin whole-body fat-free mass are of sufficient statisticalpower (α> 0.80). When using regression analyses to detectindependent predictors of fat-free mass wasting afterCABG surgery, findings are more robust when examininga large number of subjects. When using DXA scans, it isassumed that fat-free tissue hydration status is unalteredduring follow-up. This cannot be confirmed in the presentstudy. Subjects were predominantly male (92%). However,females were as frequently requested to participate in thisstudy as males.
As a result of CABG surgery, significant fat-freemass wasting is observed and more severe wasting isexperienced by subjects who are younger and/or witha greater increase in blood cortisol-to-testosterone ratioafter surgery. Interventions for preservation of fat-freemass should thus be implemented or studied early afterthe execution of CABG surgery.
References
Bassil MS & Gougeon R (2013). Muscle protein anabolism intype 2 diabetes. Curr Opin Clin Nutr Metab Care 16, 83–88.
Caso G, Vosswinkel JA, Garlick PJ, Barry MK, Bilfinger TV &McNurlan MA (2008). Altered protein metabolism followingcoronary artery bypass graft (CABG) surgery. Clin Sci 114,339–346.
Cermak N, Res PT, de Groot LC, Saris WH & van Loon LJ(2012). Protein supplementation augments the adaptiveresponse of skeletal muscle to resistance-type exercisetraining: a meta-analysis. Am J Clin Nutr 96, 1454–1464.
Drummond MJ, Dickinson JM, Fry CS, Walker DK,Gundermann DM, Reidy PT, Timmerman KL, MarkofskiMM, Paddon-Jones D, Rasmussen BB & Volpi E (2012). Bedrest impairs skeletal muscle amino acid transporterexpression, mTORC1 signaling, and protein synthesis inresponse to essential amino acids in older adults. Am JPhysiol Endocrinol Metab 302, E1113–E1122.
Ferrando AA, Lane HW, Stuart CA, Davis-Street J & Wolfe RR(1996). Prolonged bed rest decreases skeletal muscle andwhole body protein synthesis. Am J Physiol Endocrinol Metab270, E627–E633.
Glickman SG, Marn CS, Supiano MA & Dengel DR (2004).Validity and reliability of dual-energy X-ray absorptiometryfor the assessment of abdominal adiposity. J Appl Physiol 97,509–514.
Henzen C, Kobza R, Schwaller-Protzmann B, Stulz P & BrinerVA (2003). Adrenal function during coronary artery bypassgrafting. Eur J Endocrinol 148, 663–668.
Ho CKM, Stoddart M, Walton M, Anderson RA & Beckett GJ(2006). Calculated free testosterone in men: comparison offour equations and with free androgen index. Ann ClinBiochem 43, 389–397.
Kortebein P, Ferrando A, Lombeida J, Wolfe R & Evans WJ(2007). Effect of 10 days of bed rest on skeletal muscle inhealthy older adults. JAMA 297, 1772–1774.
Lehot JJ, Piriz H, Villard J, Cohen R & Guidollet J (1992).Glucose homeostasis: comparison between hypothermic andnormothermic cardiopulmonary bypass. Chest 102,106–111.
Maggio M, Ceda GP, De Cicco G, Cattadori E, Visioli S,Ablondi F, Beghi C, Gherli T, Basaria S, Ceresini G, ValentiG & Ferrucci L (2005). Acute changes in circulatinghormones in older patients with impaired ventricularfunction undergoing on-pump coronary artery bypassgrafting. J Endocrinol Invest 28, 711–719.
Maggio M, Nicolini F, Cattabiani C, Beghi C, Gherli T,Schwartz RS, Valenti G & Ceda GP (2012). Effects oftestosterone supplementation on clinical and rehabilitativeoutcomes in older men undergoing on-pump CABG.Contemp Clin Trials 33, 730–738.
Marzolini S, Oh PI, Thomas SG & Goodman JM (2008).Aerobic and resistance training in coronary disease: singleversus multiple sets. Med Sci Sports Exerc 40,1557–1564.
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, TreacherDF & Turner RC (1985). Homeostasis model assessment:insulin resistance and beta-cell function from fasting plasmaglucose and insulin concentrations in man. Diabetologia 28,412–419.
Miller LE, Pierson LM, Pierson ME, Kiebzak GM, Ramp WK,Herbert WG & Cook JW (2007). Changes in bone mineraland body composition following coronary artery bypassgrafting in men. Am J Cardiol 99, 585–587.
Nakhjavani M, Esteghamati A, Hamidi S, Esfahanian F, NabaviH, Abbasi M & Mirkhani SH (2009). Changes in growthhormone and insulin-like growth factor-I levels in the acutestage after open heart surgery and at the time of discharge.Exp Clin Endocrinol Diabetes 117, 413–416.
Piepoli MF, Corra U, Benzer W, Bjarnason-Wehrens B,Dendale P, Gaita D, McGee H, Mendes M, Niebauer J,Zwisler AD & Schmid JP; Cardiac Rehabilitation Section ofthe European Association of Cardiovascular Prevention andRehabilitation (2012). Secondary prevention throughcardiac rehabilitation: from knowledge to implementation.A position paper from the Cardiac Rehabilitation Section ofthe European Association of Cardiovascular Preventionand Rehabilitation. Eur J Cardiovasc Prev Rehabil 17,1–17.
C© 2015 The Authors. Experimental Physiology C© 2015 The Physiological Society

Exp Physiol 000.0 (2015) pp 1–11 11Muscle wasting after coronary artery bypass graft surgery
Roth-Isigkeit A, Dibbelt L, Schmucker P & Seyfarth M (2000).The immune–endocrine interaction varies with the durationof the inflammatory process in cardiac surgery patients.J Neuroendocrinol 12, 546–552.
Roth-Isigkeit AK & Schmucker P (1997). Postoperativedissociation of blood levels of cortisol andadrenocorticotropin after coronary artery bypass graftingsurgery. Steroids 62, 695–699.
Schakman O, Gilson H & Thissen JP. (2008). Mechanisms ofglucocorticoid-induced myopathy. J Endocrinol 197,1–10.
Suetta C, Frandsen U, Jensen L, Jensen MM, Jespersen JG, HvidLG, Bayer M, Petersson SJ, Shrøder HD, Andersen JL,Heinemeier KM, Aagaard P, Schjerling P & Kjaer M (2012).Aging affects the transcriptional regulation of humanskeletal muscle disuse atrophy. PLoS ONE 7, e51238.
Szulc P, Munoz F, Marchand F, Chapurlat R & Delmas PD(2010). Rapid loss of appendicular skeletal muscle mass isassociated with higher all-cause mortality in older men: theprospective MINOS study. Am J Clin Nutr 91,1227–1236.
van Venrooij LM, Verberne HJ, de Vos R, Borgmeijer-HoelenMM, van Leeuwen PA & de Mol BA (2012). Postoperativeloss of skeletal muscle mass, complications and quality oflife in patients undergoing cardiac surgery. Nutrition 28,40–45.
Velissaris T, Tang AT, Murray M, Mehta RL, Wood PJ, Hett DA& Ohri SK (2004). A prospective randomized study toevaluate stress response during beating-heart andconventional coronary revascularization. Ann Thorac Surg78, 506–512.
Vingren JL, Kraemer WJ, Ratamess NA, Anderson JM, Volek JS& Maresh CM (2010). Testosterone physiology in resistanceexercise and training: the up-stream regulatory elements.Sports Med 40, 1037–1053.
Wallin M (2007). The GH/IGF-1 system during surgery andcatabolism – focus on metabolism and heart function, pp.1–9. Doctoral thesis, Karolinska Institutet.
Weiss AJ & Elixhauser A (2014). Trends in operating roomprocedures in U.S. hospitals, 2001–2011. In: Healthcare Costand Utilization Project (HCUP) Statistical Briefs. Agency forHealth Care Policy and Research (USA), Rockville, MD,USA.
Additional information
Competing interests
None declared.
Author contributions
Conception and design of experiments: D.H., L.L., M.v.E., B.O.E.and P.D. Collection, analysis and interpretation of data: D.H.,L.L., K.V., J.-L.R., M.H. and P.D. Drafting the article or revisingit critically for important intellectual content: D.H., L.L., K.V.,M.H., M.v.E., B.O.E. and P.D. All authors approved the finalversion of the manuscript, all persons designated as authorsqualify for authorship, and all those who qualify for authorshipare listed.
Funding
This study was supported by an unrestricted research grant fromHartcentrum Hasselt vzw. L.L. is part of the ‘Limburg ClinicalResearch Program (LCRP) UHasselt-ZOL-Jessa’, supportedby the foundation Limburg Sterk Merk, province ofLimburg, Flemish government, Hasselt University, ZiekenhuisOost-Limburg and Jessa Hospital.
Acknowledgements
We are very thankful to Dr Benjamin Wall, PhD, from MaastrichtUniversity, The Netherlands, for a critical review of ourmanuscript.
C© 2015 The Authors. Experimental Physiology C© 2015 The Physiological Society





























