Embed Size (px)
Citation preview

Managing patients with deliberate self harm who refuse treatmentin accident and emergency departments Education and debate p 905
Advice and procedure require correction
Editor—In their lesson of the week onmanaging patients with deliberate self harmwho refuse treatment in the accident andemergency department Hassan et al recom-mend that doctors must be fully conversantwith the law on assessing capacity to consentto treatment and its application.1 It is equallyimportant in these difficult cases to be famil-iar with the application of the Mental HealthAct 1983 or Mental Health (Scotland) Act1984, which Hassan et al seem not to be.They state: “If the overdose is considered tobe a consequence of a mental disorder thenthe patient can also be treated medically forthe overdose under the terms of the MentalHealth Act.” This statement is reiterated intheir proposed algorithm, recommendedfor use at accident and emergency depart-ments. This is simply not the case.
The Mental Health Act is for thetreatment of mental disorders. It does notauthorise the treatment of a physicaldisorder even if it arises as a consequence ofa mental disorder. Therefore the MentalHealth Act is of no help in the immediatemedical management of patients presenting
with deliberate self harm and refusing treat-ment, other than to permit detention in hos-pital if the patient is considered to besuicidal as a result of mental disorder.
Treatment for the overdose will remainunder common law based on assessment ofcompetency to refuse treatment and theneed to preserve life.
The Mental Health Act states thattreatment can be administered only if apatient is not capable of giving informedconsent, provided that it is in the patient’sbest interest, is urgently necessary, and is inaccordance with a practice accepted at thetime by a responsible body of medical opin-ion skilled in the particular form oftreatment in question.2 A study by theMacArthur group found that only aminority of psychiatric patients had signifi-cant impairment in ability to provide validinformed consent for treatment.3
The advice of Hassan et al and theiralgorithm require correction.Alastair Hull specialist registrar in [email protected]
Fabian Haut specialist registrar in psychiatryRoyal Dundee Liff Hospital, Dundee DD2 5NF
1 Hassan TB, MacNamara AF, Davy A, Bing A, Bodiwala GG.Managing patients with deliberate self harm who refusetreatment in the accident and emergency department. BMJ1999;319:107-9. (10 July.)
2 Bolam v Friern Hospital Management Committee [1957]1 W L R 582.
3 Grisso T, Appelbaum PS. The MacArthur treatment com-petence study. III. Abilities of patients to consent to psychi-atric and medical treatments. Law Hum Behav 1995;19:149-74.
No case law supports sectioning underthe Mental Health Act in thesecircumstances
Editor—In their lesson of the week onmanaging patients with deliberate self harmwho refuse treatment Hassan et al consultedneither psychiatrists nor the Mental HealthAct Commission, yet they make an unrefer-enced statement about the use of the MentalHealth Act which is misleading.1 Thisstatement is: “If the overdose is consideredto be a consequence of a mental disorder,then the patient can also be treatedmedically for the overdose under the termsof the Mental Health Act.”
Case law on this point derives from B vCroydon Health Authority,2 but the situationcovered in the case is not equivalent to thesituations about which the article advises. Bwas a psychiatric inpatient already under
section 3 of the Mental Health Act (atreatment order) when she stopped eating,and at issue was whether refeeding againsther stated wish could be instituted under theact. Enforced feeding is already recognisedas treatment for anorexia nervosa, andalthough B had a borderline personality dis-order, the Court of Appeal found that feed-ing was treatment for her mental disorder.
It is an unjustified extrapolation to saythat patients brought to hospital after an actof deliberate self harm may be placed undera section of the Mental Health Act in orderto be given medical treatment. There is nocase law in England and Wales to supportthis particular situation. The authors’ algo-rithm says that patients qualifying for thiscategory lack capacity; hence treatment forphysical illness may legitimately be given intheir best interests in circumstances ofnecessity under the common law. Waitingseveral hours for a patient to be placedunder a section of the Mental Health Act(requiring two medical recommendationsand an application by a social worker whomust interview the patient and a relative)wastes valuable time needed for urgentphysical treatment. Moreover, most patientswho deliberately harm themselves do notwarrant compulsory treatment orders forongoing psychiatric management.
Temporary mental incapacity also occursas a result of intoxication and in states of highemotional arousal. These factors are mostoften operating in uncooperative patientswho deliberately harm themselves.Eleanor Feldman Mental Health Act Adviser, RoyalCollege of Psychiatrists Liaison Psychiatry SectionDepartment of Psychological Medicine,John Radcliffe Hospital,Oxford OX3 [email protected]
1 Hassan TB, MacNamara AF, Davy A, Bing A, Bodiwala GG.Managing patients with deliberate self harm who refusetreatment in the accident and emergency department. BMJ1999;319:107-9. (10 July.)
2 B v Croydon Health Authority (1995) 1 All E R. 683.
Mental health professionals would bewary of detaining someone simply toimpose treatment for overdose
Editor—The lesson of the week by Hassanet al on the management of patients withdeliberate self harm who refuse treatment inan accident and emergency departmentaddresses a difficult and worrying issue formedical practitioners.1 The Mental HealthAct Commission is concerned, however, thatthe authors’ comments on the use of theMental Health Act 1983 are likely to causefurther confusion.
Hassan et al state under the headingHow should doctors proceed? that after a
Advice to authorsWe prefer to receive all responses electronically,sent either directly to our website or to theeditorial office as email or on a disk. Processingyour letter will be delayed unless it arrives in anelectronic form.
We are now posting all direct submissions toour website within 24 hours of receipt and ourintention is to post all other electronicsubmissions there as well. All responses will beeligible for publication in the paper journal.
Responses should be under 400 words andrelate to articles published in the precedingmonth. They should include <5 references, in theVancouver style, including one to the BMJ articleto which they relate. We welcome illustrations.
Please supply each author’s currentappointment and full address, and a phone orfax number or email address for thecorresponding author. We ask authors to declareany competing interest. Please send a stampedaddressed envelope if you would like to knowwhether your letter has been accepted or rejected.
Letters will be edited and may be shortened.
Letters
Website: www.bmj.comEmail: [email protected]
916 BMJ VOLUME 319 2 OCTOBER 1999 www.bmj.com
“psychiatric evaluation” the patient may be“detainable” under the act, adding: “If theoverdose is considered to be a consequenceof a mental disorder then the patient can betreated medically for the overdose under theterms of the Mental Health Act.”
Presumably, the use of the act is beingproposed to override the wishes of a patientwho has refused the treatment and has thecapacity to do so (if the person lacks capacitythe question whether treatment could begiven under common law would be consid-ered). However, the suggestion that a patientcan be detained under the act solely to receivetreatment for the overdose is misleading.
Although Hassan et al are correct insuggesting that a wide range of treatmentsmay be given under the act, such treatmentsmust be ancillary to the treatment for themental disorder. Furthermore, an essentialcondition for detention under the act is thatthe person has a mental disorder which war-rants assessment or treatment in hospital, orboth. In the recent case of R v Collins andOthers ex p S, which concerned thedetention of a woman who was refusingtreatment for her pregnancy, the Court ofAppeal found that the detention was unlaw-ful because there had been no intention toassess or treat her mental disorder.2 TheCourt of Appeal also made clear that “anapplication for an improper or collateralpurpose” would be susceptible to legal chal-lenge. For these reasons I suspect that men-tal health professionals would be extremelywary of detaining a person for the sole pur-pose of imposing treatment for an overdose.
A key function of the Mental Health ActCommission is to safeguard the rights ofdetained patients, and commissioners con-sidering a person’s detention under the actin these circumstances would wish to satisfythemselves that the criteria for detentionhad been met.William Bingley chief executiveMental Health Act Commission, Maid MarianHouse, Nottingham NG1 6BG
1 Hassan TB, MacNamara AF, Davy A, Bing A, Bodiwala GG.Managing patients with deliberate self harm who refusetreatment in the accident and emergency department. BMJ1999;319:107-9. (10 July.)
2 R v Collins and Others ex p S (No 2). The Times 1998Aug 3.
Authors’ reply
Editor—The concerns raised by corre-spondents about application of the MentalHealth Act to give medical treatment areunderstandable: this is a controversialsubject. Unfortunately (or fortunately) thereis at present no case law pertaining to thisparticular type of scenario in an accidentand emergency department. The algorithmwas, however, constructed after careful anddetailed discussion with medicolegal advis-ers from both medical defence organisa-tions. Doctors seeking urgent medicolegaladvice are likely to look to these bodies forsupport and be given similar advice.
A patient who refuses lifesaving medicaltreatment in the charged atmosphere of anaccident and emergency department poses asignificant challenge even to the most senior
clinicians in accident and emergency medi-cine. The duty of doctors is to do the best theycan for their patients, but how should theyproceed when the patient refuses offers oflifesaving treatment? Our study found thatdoctors in accident and emergency depart-ments lacked the appropriate knowledge tobe able to manage such patients correctly.They did not fully understand the term com-mon law and were unfamiliar with how to testcapacity. The algorithm sought to give someguidance on how best to manage thesepatients in a legal and pragmatic fashion.Many patients will respond to persuasionfrom doctors, nurses, or family. Others will bedeemed to lack capacity to make a valid deci-sion to refuse treatment and so could begiven essential medical treatment undercommon law. Unfortunately, much of thecorrespondence in the eBMJ1 and here hasdetracted from our central theme.
Feldman may believe that the extrapola-tion of B v Croydon Health Authority to ourcase is unjustified. However, Lord JusticeHoffman in the same case took a rather dif-ferent view: “It would seem to me strange if ahospital could without a patient’s consentgive him treatment directed to alleviating a. . . disorder showing itself in suicidal tenden-cies, but not without such consent be able totreat the consequences of a suicide attempt.”Presumably, his deliberations were takeninto account by the defence organisations,that in certain circumstances the MentalHealth Act might be used to detain a patientand treat him or her if the actions are theconsequences of a mental disorder. Obvi-ously, as pointed out by Feldman, this wouldbe only if time allowed and the correct pro-cedures were followed.
Doctors dealing with this group ofpatients need to follow a logical approachtaking into account the seriousness of themedical situation and the resulting level ofcapacity required. At all times they must con-tinue to try to gain the patient’s consent formedical treatment. Senior clinicians in acci-dent and emergency medicine and psychia-trists must become involved at an early stage.Taj Hassan consultant in accident and emergencymedicineLeeds General Infirmary, Leeds LS1 3EX
Aidan MacNamara consultant in accident andemergency medicineBirmingham Heartlands Hospital, BirminghamB9 5SS
Gautam Bodiwala headDepartment of Accident and Emergency Medicine,Leicester Royal Infirmary NHS Trust, LeicesterLE1 5WW
1 Electronic responses. Managing patients with deliberateself harm who refuse treatment in the accident and emer-gency department. eBMJ 1999;319 www.bmj.com/cgi/eletters/319/7202/107 (accessed 23 Sep 1999).
Relation between hostility andcoronary heart diseaseEvidence does not support link
Editor—The summary points of Heming-way and Marmot’s review of psychosocialrisk factors for coronary heart disease may
be misleading.1 The first of these states that“prospective cohort studies show a possibleaetiological role for type A/hostility.” How-ever, of the four prospective studies ofhostility, only two show any significantassociation between hostility and coronaryheart disease (one for women only). Six ofthe nine aetiological studies of type Abehaviour also show no association withcoronary heart disease. The other threestudies give no information on complete-ness of follow up or whether outcomes suchas angina were assessed in a blindedmanner. One of these studies had minimaladjustment for confounding. No studyshowed any prognostic role for type Abehaviour or hostility. Taken together, thesestudies do not represent robust evidencethat these psychological variables have animportant role in the development or prog-nosis of coronary heart disease.
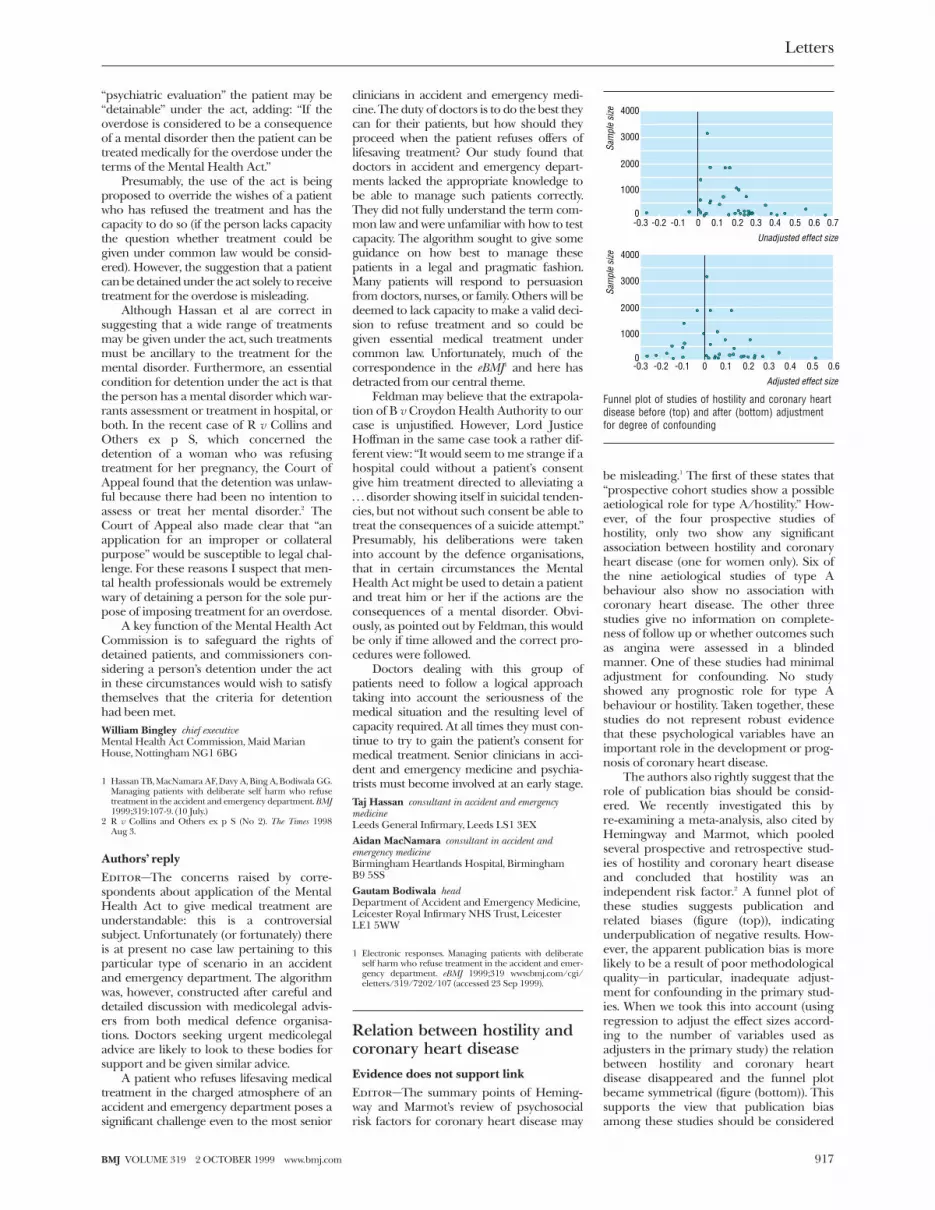
The authors also rightly suggest that therole of publication bias should be consid-ered. We recently investigated this byre-examining a meta-analysis, also cited byHemingway and Marmot, which pooledseveral prospective and retrospective stud-ies of hostility and coronary heart diseaseand concluded that hostility was anindependent risk factor.2 A funnel plot ofthese studies suggests publication andrelated biases (figure (top)), indicatingunderpublication of negative results. How-ever, the apparent publication bias is morelikely to be a result of poor methodologicalquality—in particular, inadequate adjust-ment for confounding in the primary stud-ies. When we took this into account (usingregression to adjust the effect sizes accord-ing to the number of variables used asadjusters in the primary study) the relationbetween hostility and coronary heartdisease disappeared and the funnel plotbecame symmetrical (figure (bottom)). Thissupports the view that publication biasamong these studies should be considered
4000
Sam
ple
size
3000
2000
1000
0-0.3 -0.2 -0.1 0 0.1 0.2 0.3 0.4 0.5 0.6 0.7
Unadjusted effect size
-0.3 -0.2 -0.1 0 0.1 0.2 0.3 0.4 0.5 0.6
Adjusted effect size
4000
Sam
ple
size
3000
2000
1000
0
Funnel plot of studies of hostility and coronary heartdisease before (top) and after (bottom) adjustmentfor degree of confounding
Letters
917BMJ VOLUME 319 2 OCTOBER 1999 www.bmj.com

only when other sources of bias, such asthe internal validity of the included studies,are taken into account, as suggested byEgger et al.3
Claims about the toxicity of type Abehaviour and hostility have led to thedevelopment of behavioural “treatments”for these putative risk factors. A recenteditorial also went as far as to suggest that, ashostility appeared to be a “toxic compo-nent,” we should all be nice to each other.4
Perhaps in the light of Hemingway andMarmot’s review, and the above comments,this advice should be reconsidered.Mark Petticrew associate directorMRC Social and Public Health Sciences Unit,University of Glasgow, Glasgow G12 8RZ
Simon Gilbody MRC health services researchtraining fellowNHS Centre for Reviews and Dissemination,University of York, York
Trevor A Sheldon professorYork Health Policy Group, University of York, York
1 Hemingway H, Marmot M. Psychosocial factors in the aeti-ology and prognosis of coronary heart disease: systematicreview of prospective cohort studies. BMJ 1999;318:1460-7. (29 May.)
2 Miller TQ, Smith TW, Turner CW, Guijarro ML, Hallet AL.A meta-analytic review of research on hostility and physi-cal health. Psych Bull 1996;19:322-48.
3 Egger M, Davey Smith G, Schneider M, Minder CE. Bias inmeta-analysis detected by a simple, graphical test. BMJ1997;315:629-34.
4 Whiteman MC, Fowkes FGR, Deary U. Hostility and theheart. BMJ 1997;315:379-80.
Authors’ reply
Editor—We welcome Petticrew et al’s appli-cation of methods more commonly used inthe context of clinical trials to our review ofobservational follow up studies. We agreewith their conclusion that these studies “donot provide robust evidence” of a relationbetween coronary heart disease and hostilityor type A behaviour. This is consistent withthe conclusion we reached, that the evidencefor hostility and type A behaviour was lessconsistent than that for depression andanxiety and social supports.
However, their attempt to take thesystematic review further raises some prob-lems. Firstly, Petticrew et al rightly raise theissue of completeness of follow up anddegree of blinding of outcomes such asangina. But they are wrong to say that thetwo studies incorporating these soft out-comes were unblinded. Furthermore, suchmethodological issues should be examinedsystematically across all studies, not just thepositive ones, since the direction of any biascannot be assumed.
Secondly, Petticrew et al reanalysed ahostility meta-analysis and showed an asym-metry in the plot of study size against effectsize. Such asymmetrical funnel plots may bedue to several potential biases. Petticrew et alpropose that inadequate adjustment forconfounding is likely to be most importantbecause their adjustment for the number ofconfounders used in the primary studiesmade the plot more symmetrical, althoughthe difference was not formally tested. Asdiscussed in our review, psychosocial factorsmay have effects on disease which are medi-ated by health related behaviours. Thus if
the causal chain involved hostile peoplebeing more likely to smoke,1 then adjustingfor smoking as a confounder would be mis-guided. Furthermore, the number of con-founders which were allowed for may itselfbe confounded. It is possible, for example,that studies which differ in respect to adjust-ment for confounding also differ in terms ofoverall methodological quality.
Empirical evidence of health benefitshould not be included among the groundsfor the ethical imperative “be nice to eachother.”Harry Hemingway senior [email protected]
Michael Marmot professorInternational Centre for Health and Society,Royal Free and University College London MedicalSchool, London WC1E 6BT
1 Siegler IC, Peterson BL, Barefoot JC, Williams RB. Hostil-ity during late adolescence predicts coronary risk factors atmid-life. Am J Epidemiol 1992;136:1-9.
Benzodiazepine use inpregnancy and majormalformations or oral clefts
Induced abortions should be included
Editor—Dolovich et al have reported theirmeta-analysis concerning use of benzo-diazepines during the first trimester of preg-nancy and the risk of oral clefts or majorcongenital malformations.1 In the cohortstudies no increased risk of congenitalmalformations was found, while case-control studies showed an increased risk ofboth oral clefts and major congenitalmalformations. The authors excluded stud-ies from the meta-analysis if only stillbirthsor abortions were included.
The paper missed important infor-mation about the criteria for inclusion in themeta-analysis. During the past 10-15 yearsprenatal diagnosis of congenital malforma-tions has increased significantly in manycountries and is often followed by termina-tion of pregnancy if severe malformationsare diagnosed.2 The Eurocat project is aEuropean epidemiological programme sur-veying congenital malformations. The Euro-cat registries are population based andbased on multiple sources of information;they include information about live births,deaths of fetuses with gestational age >20weeks, and induced abortions after prenataldiagnosis of malformations.
During 1990-4 there were 13 registriesfollowing strict Eurocat methodology andwhere induced abortion after prenatal diag-nosis of congenital malformations wasnoted. The 13 registries covered 1 284 599births. For this period the contribution ofinduced abortion in the registries rangedfrom 4.0-7.6 per 1000 births in the threeFrench registries to 0.7-3.1 per 1000 birthsin the other European countries.2 The tableshows the proportion of induced abortionamong cases of major congenital malforma-tions. If studies concerning risk factorsduring pregnancy include only information
from live births and stillbirths they will missthe large number of cases diagnosed pre-natally in which termination of pregnancy issubsequently carried out. This is notdiscussed in the paper.1
In studies from the 1970s and ’80s theproblem is of only minor importance. Forfuture studies of risk assessments duringpregnancy it is important also to includeterminations of pregnancies. These termina-tions often occur in the more severe cases,and prenatal diagnostic methods are moreoften performed in risk pregnancies, in anx-ious mothers taking benzodiazepines, and inmothers with epilepsy. If only live births arestudied the conclusions might be wrongbecause today live births occur in a selectedgroup of all pregnancies.Ester Game specialist in paediatricsEurocat, University of Southern Denmark, 5000Odense C, Denmark
Ulf Bergman visiting professorDepartment of Clinical Pharmacology, Universityof Southern Denmark
1 Dolovich L, Addis A, Vaillancourt JMR, Power JDB, KorenG, Einarson TR. Benzodiazepine use in pregnancy andmajor malformations or oral clefts: meta-analysis of cohortand case-control studies. BMJ 1998;317:839-43. (26September 1998.)
2 Eurocat Working Group. Eurocat report 7. Brussels:Scientific Institute of Public Health–Louis Pasteur, 1997.
Pooled results are sensitive to zerotransformation used
Editor—In 1994 Shapiro suggested thatmeta-analysis to combine the results ofobservational studies should be abandonedbecause the individual studies are open toparticular bias related to their study design.1
Dolovich et al have reported their meta-analysis of the use of benzodiazepinesduring the first trimester of pregnancy andthe risk of oral clefts or major congenitalmalformations.2 The differences they foundbetween the results of the cohort andcase-control studies suggest that it may bebias that is being pooled rather than trueeffects. The authors themselves expressreservations that most cases reported werederived from only three studies, so have thepatients with oral cleft been counted morethan once in the pooling process?
The statistical method used in this papercannot be relied on, as the pooled results aresensitive to the adjustment made for trials inwhich the number of malformations waszero. For example, the largest cohort study(that by Bergman et al, 1992) is calculated asshowing an odds ratio of 1.21, based on0/1354 exposed patients having oral cleft
Selected major congenital malformationsdetectable by prenatal ultrasound investigation(data from 13 Eurocat registries 1990-42)
No of cases
No (%) ofinduced
abortions
Anencephalus 447 375 (84)
Spina bifida 639 275 (43)
Hypoplastic left heart 316 80 (25)
Omphalocele 334 139 (42)
Bilateral renal agenesis 250 129 (52)
Letters
918 BMJ VOLUME 319 2 OCTOBER 1999 www.bmj.com

compared with 62/102 985 not exposed.This result suggests that the zeros have beenadjusted to 1 for the calculation (as odds ofzero cannot be turned into an odds ratio). Ifthe zero was counted as 0.5, however, theodds ratio for the study would fall to 0.61.
Even more bizarre is the study of epilepticpatients (that by Robert et al, 1986), in which0/4 compared with 1/144 is transformedinto an odds ratio of 10.63 on the basis of thezero transformation. Surely 0/4 is exactly theexpected finding if the odds ratio was 1 andthere was no difference between the exposedand non-exposed groups.
This paper seems to lend weight toShapiro’s suggestion that meta-analysisshould be confined to controlled clinicaltrials.Christopher Cates general practitionerBushey, Hertfordshire WD2 [email protected]
1 Shapiro S. Meta-analysis/Schmeta-analysis. Am J Epidemiol1994;140:771-7.
2 Dolovich L, Addis A, Vaillancourt JMR, Power JDB, KorenG, Einarson TR. Benzodiazepine use in pregnancy andmajor malformations or oral clefts: meta-analysis ofcohort and case-control studies. BMJ 1998;317:839-43.(26 September 1998.)
Quality of primary studies must influenceinferences made from meta-analyses
Editor—In a meta-analysis of cohort andcase-control studies on the association ofmalformations with use of benzodiazepinesin pregnancy, Dolovich et al recommend theuse of antenatal diagnostic tools for detectingmalformations in clinical practice.1 For futureresearch they say that further case-controlstudies are needed. They have disregardedthe importance of the quality of primarystudies in arriving at these conclusions.
In their analysis Dolovich et al stratifypooling of data according to the quality ofthe study. Higher quality studies (cohortstudies) showed lack of an association, whilepoor quality studies (case-control studies)showed an association. This is apparentfrom the graphic presentation of odds ratiosin the paper. To emphasise this point wehave performed logistic regression analysis,with fetal malformation (both major malfor-mation and oral cleft) as the binary depend-ent variable.
A logistic model was built to assess theimpact of the quality of the study on thestrength of the association between expo-sure to benzodiazepines and malformation.The value of the coefficient for theinteraction term between “study quality”(cohort v case-control) and “exposure”(exposure v non-exposure) provided an esti-mate of the bias in poor quality studies.2 Ouranalysis showed that the case-control studiesexaggerated the estimate of the odds ratiofor the association between malformationand exposure to benzodiazepines by 55%(95% confidence interval 28% to 72%,P = 0.0006) compared with cohort studies.
It has been well established that poorerquality literature tends to exaggerate theestimate of the strength of an association,and in this circumstance it is moreappropriate to base inferences on higher
quality evidence.3 Our conclusion on thebasis of meta-analysis of higher qualityevidence is that there is no associationbetween maternal exposure to benzo-diazepines and fetal malformation; furtherresearch should aim at generating highquality evidence in the form of cohortstudies rather than case-control studies.Khalid S Khan [email protected]
Catherine Wykes specialist registrarHarry Gee consultantDepartment of Obstetrics and Gynaecology,Birmingham Women’s Hospital, BirminghamB15 7TG
1 Dolovich LR, Addis A, Vaillancourt JMR, Power JDB,Koren G, Einarson TR. Benzodiazepine use in pregnancyand major malformation or oral cleft: meta-analysis ofcohort and case-control studies. BMJ 1998;317:839-43. (26September 1998.)
2 Khan KS, Daya S, Collins JA, Walter SD. Empiricalevidence of bias in infertility research: overestimation oftreatment effect in crossover trials using pregnancy as theoutcome measure. Fertil Steril 1996;65:939-45.
3 Khan KS, Daya S, Jadad AR. The importance of quality ofprimary studies in producing unbiased systematic reviews.Arch Intern Med 1996;156:661-6.
Vascular anomalies must beproperly classifiedEditor—Zameel Cader and Winer’s lessonof the week highlighted a common error ofterminology in describing vascular anoma-lies.1 The term cavernous haemangioma is aconfusing one and should ideally beavoided. The classification of vascularanomalies by Mulliken and Glowacki suc-cessfully categorised vascular anomalies in aconsistent and meaningful way according totheir endothelial cell characteristics.2 Theclassification distinguishes haemangiomasfrom vascular malformations.
A haemangioma is characterised histo-logically by high endothelial cell turnoverand in addition has a specific and character-istic clinical “life cycle”—strawberry naevus.3
All other lesions are vascular malforma-tions, which have normal endothelial cellturnover with abnormal gross vascularanatomy and are further subdivided intolow flow and high flow lesions. Low flowlesions include capillary, lymphatic, andvenous lesions or combinations of these,whereas high flow lesions include thearteriovenous malformations.
In the past the term cavernous haeman-gioma has been indiscriminately assigned toall categories of vascular anomalies.4 Thetable shows that each category not only hasa different clinical course but also has differ-ent treatment options.
Good classifications are important forcategorising information, recording it, yield-ing prognostic information, and ultimatelyguiding treatment plans.5 The Mulliken andGlowacki classification helps in this way andshould consequently be adhered to whenvascular anomalies are referred to. It is ourduty as clinicians to be consistent in our ter-minology in order to be able to communi-cate effectively, to promote research, and todevelop therapeutic strategies.Patrick Mallucci head and neck fellowRoyal Brisbane Hospital, Brisbane, [email protected]
1 Zameel Cader M, Winer JB. Cavernous haemangiomamimicking multiple sclerosis. BMJ 1999;318:1604-5. (12June.)
2 Mulliken JB, Glowacki J. Haemangiomas and vascular mal-formations in infants and children: a classification basedon endothelial characteristics. Plast Reconstr Surg1982;69:412.
3 Pasyk KA, Cherry GW, Grabb WC, Sasaki GH. Quantita-tive evaluation of mast cells in cellularly dynamic andadynamic vascular malformations. Plast Reconstr Surg1984;73:69-77.
4 Kane WJ, Morris S, Jackson IT, Woods JE. Significant hae-mangiomas and vascular malformations of the head andneck: clinical management and treatment outcomes. AnnPlast Surg 1995;35:133-43.
5 Kaban LB, Mulliken JB. Vascular anomalies of the maxillo-facial region. J Oral Maxillofac Surg 1986;44:203-13.
Choosing the right antibiotic
Right drug at right time in right dosesaves lives
Editor—Leibovici et al make a fundamentalpoint about the prescription of antimicro-bial drugs—the right antibiotic at the righttime saves lives1—and we should not forget it.Yet as the various commentators point out, itis not always easy to choose the right anti-microbial since we know that all drugs haveside effects, some are expensive, and someare more poisonous than others.
In intensive care, many patients presentwith septic shock, and we usually only get“one bite” at the cherry. I try to teach ourresidents a few of the “see-saw” principles ofantimicrobial prescribing that I have learntalong the way.
Classification distinguishing haemangiomas from vascular malformations
Haemangioma Vascular malformation
Histology High endothelial cell turnover Normal endothelial cell turnover
Presence at birth Usually absent Present (not always apparent clinically)
Clinical course Apparent by 6-8 weeks after birth, proliferativephase for 1-2 years, followed by spontaneousinvolution (majority)
Tends to grow in proportion with personthroughout life
Diagnosis Clinical history + appearance Vascular imagingMagnetic resonance angiography, Dopplerultrasonography, angiography
Treatmentoptions
Normally treated by observation onlyIf not involuted fully, minor surgical correctionIf very large or in anatomically sensitive area,systemic or intralesional steroids or interferongamma or surgical correction
Low flow lesions: Depending on site, size, symptoms,etc, from conservative only to laser for capillarymalformations, sclerotherapy with or withoutexcision, or surgery aloneHigh flow lesions: Depending on site, size, and stage,from conservative alone to embolisation plus surgeryor surgery alone
Letters
919BMJ VOLUME 319 2 OCTOBER 1999 www.bmj.com

Firstly, the right drug in the right dose(big) at the right time does save lives.Surprisingly to some, antibiotics do workand you need to get it right from the start.Secondly, there is not much point in savingyour “best” antibiotic for the postmortemroom. Next, we treat patients, not fevers,white cell counts, chest radiographs, orcultures. But on the other hand, just becausethe laboratory cannot grow something doesnot mean that there are no germs therecausing trouble. And it does not mean thatyou should not consult them. You should.Finally, try to avoid poisoning the patient butalways remember (and keep telling the man-agers) that saving lives costs money. There isnothing cheaper than a quick death.David Bihari associate professorIntensive Care Unit, St George Hospital, SydneyNSW [email protected]
1 Leibovici L, Shraga I, Andreassen S. How do you chooseantibiotic treatment? [with commentaries by Pauker SG,Rothberg M, Weinberg JR, Duerden BI, and DrickamerMA] BMJ 1999;318:1614-8 (12 June.)
Antibiotic choice may affect risk ofClostridium difficile infection
Editor—It is surprising that neither Leibo-vici et al nor the commentaries mention theissue of infection with Clostridium difficileinduced by antibiotics when discussing theappropriateness of antimicrobial treatmentof a severe urinary tract infection in a 83year old man.1 Despite evidence of under-reporting,2 notifications of C difficile con-tinue to increase in England and Wales.Over 17 000 predominantly hospitalacquired cases were reported to the Com-municable Disease Surveillance Centre in1998, 80% of which were in elderly people.
Cephalosporins such as cefuroxime andcefotaxime have been widely cited as pre-disposing to C difficile infection. Leibovici et alconsider cephalosporins but not fluoro-quinolones such as ciprofloxacin or ureido-penicillins for the empirical treatment ofsevere sepsis. Aminoglycosides, fluoro-quinolones, and ureidopenicillins have alower propensity to induce C difficile infec-tion.3 A prospective, crossover study in a geri-atric ward found that empirical treatmentwith piperacillin-tazobactam was seven timesless likely to induce C difficile infection thanwas treatment with cefotaxime.4
The proportion of British hospitalsreporting a change in antibiotic policies dueto C difficile infection increased from 5% to20% between 1993 and 1996.2 Elderlypatients with nosocomial C difficile infectionstay a median of three weeks longer in hos-pital, two weeks of which is spent in scarceisolation facilities, and a case-control studyfound an excess cost of over £4000 per case.5
Such costs dwarf those associated withbuying antibiotics and cannot be ignored incost effectiveness analyses of antimicrobialtreatment.
Care must be taken when extrapolatingaverage gains in studies to specific patients.Leibovici et al1 refer to data derived frompatients with a median age of 72 years andhospital or community acquired bacteraemia
or fungaemia. Outcome in an 82 year oldman with community acquired urinary tractinfection may well differ from these findings.The authors also give antibiotic susceptibilityrates for bacteraemic isolates, which includecommunity and hospital pathogens, thusbiasing towards resistant strains. Presumably,the figure of 77% susceptibility to gentamicinincludes Gram positive and Gram negativeisolates; community acquired Gram negativeisolates are likely to be more susceptible togentamicin. Once daily gentamicin may beassociated with lower nephrotoxicity and incombination with ampicillin would be apotential therapeutic choice.
The choice of antibiotic is complex.Workable antibiotic policies should aim toguide optimal treatment but will inevitablycontain compromises and assumptions, notleast because locally applicable and patientspecific data are rarely available. Although“appropriate” antimicrobial treatment is alaudable goal, side effects cannot berelegated to secondary considerations.Mark H Wilcox senior [email protected]
Jon Sandoe specialist registrarDepartment of Microbiology, General Infirmaryand University of Leeds, Leeds LS1 3EX
1 Leibovici L, Shraga I, Andreassen S. How do you chooseantibiotic treatment? [with commentaries by Pauker SG,Rothberg M, Weinberg JR, Duerden BI, and DrickamerMA] BMJ 1999;318:1614-8. (12 June).
2 Wilcox MH, Smyth ET. Incidence and impact ofClostridium difficile infection in the UK, 1993-1996. J HospInfect 1998;39:181-7.
3 Anand A, Bashey B, Mir T, Glatt AE. Epidemiology, clinicalmanifestations, and outcome of Clostridium difficilediarrhea. Am J Gastroenterol 1994;89:519-23.
4 Settle CD, Wilcox MH, Fawley WN, Corrado OJ, HawkeyPM. Prospective study of the risk of Clostridium difficilediarrhoea in elderly patients following treatment withcefotaxime or piperacillin-tazobactam. Alimentary Pharma-col Therapeutics 1998;12:1217-23.
5 Wilcox MH, Cunniffe JG, Trundle C, Redpath C. Financialburden of hospital-acquired Clostridium difficile infection.J Hosp Infect 1996;34:23-30.
Work of mental health reviewtribunals is increasing fasterthan detentionsEditor—Wall et al provide a helpful outlineof the significant increase in all psychiatricadmissions and in those admitted under theMental Health Act 1983.1 They mention, butdo not document, the effect of these trendson mental health review tribunals.
My study shows that the rate of appealsto, and hearings by, mental health review tri-bunals is increasing faster than increases inthe episodes of detention that warrant atribunal application. During 1991-3 thenumber of episodes of detention rose by4245 (15% of 1991 total), the number ofappeals to tribunals by 2032 (29%), and thenumber of hearings by 952 (26%). Theepisodes of detention include not only thoseadmitted to hospital under the act but alsothose inpatients who were converted fromanother status to an episode of detentionthat presented the opportunity for anappeal or further appeal—for example, aconversion from informal to section 2 or 3,or from section 2 to section 3. Thus not onlyhas the proportion of psychiatric inpatients
that are detained under the act risen but sohas the proportion of those detained whoappeal to and are heard by tribunals.
I also observed considerable differencesbetween NHS regions in the rate of detentionper unit of population. The figure shows therates of detention under section 2 and subse-quent appeals. Detentions under section 3showed a similar trend. Consequently, theburden of arranging and manning tribunalswill vary between regions.G E Langley medical member, mental health reviewtribunals, south and westHanningfields, Warborough Hill, Kenton, Exeter,Devon EX6 [email protected]
1 Wall S, Hotopf M, Wessely S, Churchill R. Trends in the useof the Mental Health Act 1984-96. BMJ 1999;318:1520-1.(5 June.)
Prophylaxis against earlyanaphylactic reactions to snakeantivenom
Stopping trials early may result ininsufficient evidence being accrued
Editor—Fan et al’s paper is the second inthe BMJ recently to investigate prophylaxisagainst adverse effects of snake antivenom.1
Earlier, Premawardhena et al in Sri Lankaconcluded that giving low dose subcutan-eous adrenaline before antivenom couldprevent acute adverse reactions.2 The Brazil-ian study (by Fan et al) showed no benefit inusing promethazine as pretreatment.1 Per-haps more interesting than the conclusions,however, is that both these clinical trials werestopped early because of interim analyses;they provide examples of the use and pitfallsof such analyses.
The Sri Lankan group stopped recruit-ment halfway through its study since theanalysis showed a significant reduction in allacute adverse effects when adrenaline wasused as pretreatment rather than placebo(P = 0.0002). Unfortunately, in subanalysis ofthe severity of adverse reactions in the twogroups the differences in incidence of mild,moderate, and severe reactions barelyreached significance due to the low power ofthe analysis (about 50%) and the small num-
Rate
per
100
0 po
pula
tion
North a
nd York
shire
Trent
South
Wester
n
Anglia
and O
xford
South
Tham
es
North T
hames
West M
idlan
ds
North W
est0
0.2
0.3
0.4
0.5
0.6
0.7
0.1
Appeals
Detentions
Rates of detention under section 2 of Mental HealthAct 1983 and appeals to mental health reviewtribunals per 1000 population of NHS regions,1994-95
Letters
920 BMJ VOLUME 319 2 OCTOBER 1999 www.bmj.com

bers. This is important since it is mainly themoderate and severe reactions that we wish toprevent. As it was, the trial was stoppedbecause of a supposed benefit, but we cannotadvise the use of subcutaneous adrenalinebecause of unconvincing evidence. In theBrazilian study the interim analysis was in theform of sequential analysis. The use of thismethod, and to some degree the negativeoutcome of the study, prevents arguments ofthe nature used above.
Interim analyses are often required onethical grounds, but final data analysis andclinical importance should be borne inmind when they are planned. Too often,emphasis is put on the ethics of continuing atrial in which some patients receive anapparently inferior treatment. Stopping thetrial may, however, result in the evidence forthe supposedly better treatment being insuf-ficient for policy changes to be recom-mended—this too is unethical.
Using and stating defined methodolo-gies, as in Fan et al’s study, can help, but wemust always bear in mind that statistics arean aid to reason, not a replacement for it.The dangers of stopping a trial too earlyhave been addressed recently by Pocock andWhite3 and need to be fully appreciated byclinical researchers.Douglas E Ball drug information pharmacist,department of pharmacyKlara Tisocki lecturer, department of clinicalpharmacologyUniversity of Zimbabwe, PO Box A178 Avondale,Harare, [email protected]
1 Fan HW, Marcopito LF, Cardoso JLC, França FOS,Malaque CMS, Ferrari RA, et al. Sequential randomisedand double blind trial of promethazine prophylaxisagainst early anaphylactic reactions to antivenom forbothrops snake bites. BMJ 1999;318:1451-2. (29 May.)
2 Premawardhena AP, de Silva CE, Fonseka MMD,Gunatilake SB, de Silva HJ. Low dose subcutaneousadrenaline to prevent acute adverse reactions toantivenom serum in people bitten by snakes: randomised,placebo controlled trial. BMJ 1999;318:1041-3. (17 April.)
3 Pocock S, White I. Trials stopped early: too good to betrue? Lancet 1999;353:943-4.
Author’s reply
Editor—Unfortunately, details on variablesand the formula for the calculation of thelimits of Wald’s graphic for the sequentialanalysis did not appear in the printed versionof our paper, but they are available on theBMJ ’s website (www.bmj.com).1 Ball andTisocki are invited to visit that site. On doingso, they may note that in Wald’s graphic therewas an initial trend in preferences for placebothat did not prevail. The trial was stoppedexactly when it was supposed to be stopped—that is, when one of the boundaries wasreached.
We share the authors’ concern aboutstatistics, but in this study the proportion ofreactions was virtually the same in bothgroups being compared (table 2 of theprinted version of our paper).Hui Wen Fan doctorHospital Vital Brazil, Instituto Butantan, 05503-900,Sao Paulo, [email protected]
1 Parameters and formula for calculation of limits of Wald’sgraphic. eBMJ 1999;318. www.bmj.com/cgi/content/full/318/7196/1451/DC1 (accessed 21 September 1999).
Naturalistic treatment study ofdepression in general practice
Clinical management is important intreatment of depression
Editor—The striking finding of Malt et al’sstudy in patients with depression is not thesuperiority of combined pharmacotherapyand psychotherapy but the 47% completeresponse rate to placebo and psychologicalsupport, which was present from about 12weeks onwards.1 Unfortunately, little infor-mation is given about the quantity and qual-ity of the psychological support provided,although reference is made to the clinicalmanagement protocol used in the NationalInstitute of Mental Health’s treatment ofdepression study, in which patients wereseen regularly for 20-30 minute sessions ofsupportive therapy.2 3 In that study, at 16weeks 42% of patients in the imipramine-clinical management group had recoveredcompared with 21% in the placebo-clinicalmanagement group.3
The difference between the studies isunlikely to be due to severity of illness as inboth studies the initial rating indicatedillnesses of moderate severity (Malt et al’sstudy, mean initial Montgomery Åsbergdepression rating scale = 26.7; NationalInstitute of Mental Health study, mean initialHamilton rating scale for depression = 19.5).However, the recovery criteria in Malt et al’sstudy were less stringent—namely, a 50%reduction in the score on the MontgomeryÅsberg depression rating scale and improve-ment to at least only mild illness remaining.To compare the results usefully with those ofother studies, data needed to be presentedon the proportion of patients achieving fullremission (a score < 6).
The authors state that the findings chal-lenge current guidelines that claim equalityof effect between drug and psychologicaltreatment in mild to moderate depression.These guidelines, however, have been basedon controlled trials of formal psychothera-pies rather than clinical management. In theNational Institute of Mental Health study,cognitive therapy and interpersonal therapywere both superior to placebo-clinical man-agement.3 What the findings do indirectlyconfirm is the crucial importance of goodclinical management in enhancing the effec-tiveness of drug treatment. This has beenshown in controlled trials showing the supe-riority of treatment based on guidelinescompared with usual treatment of depres-sion in primary care.4 5
Peter L Cornwall senior lecturer in communitypsychiatryUniversity Department of Psychiatry, Royal VictoriaInfirmary, Newcastle upon Tyne NE1 [email protected]
1 Malt UF, Robak OH, Madsu H-P, Bakke O, Loeb M. TheNorwegian naturalistic treatment study of depression ingeneral practice (NORDEP)–I: randomised double blindstudy. BMJ 1999;318:1180-4. (1 May.)
2 Fawcett J, Epstein P, Fiester SJ, Elkin I, Autry JH. Clinicalmanagement imipramine/placebo administration manual.Psychopharmacol Bull 1987;23:309-21.
3 Elkin I, Shea T, Watkins JT, Imber SD, Sotsky SM, Collins JF,et al. National Institute of Mental Health treatment of
depression collaborative research program. Arch GenPsychiatry 1989;46:971-82.
4 Katon W, Von Korff M, Lin E, Simon G, Walker E, Bush T,et al. Collaborative management to achieve treatmentguidelines. JAMA 1995;273:1026-32.
5 Schulberg HC, Block MR, Madonia MJ, Scott CP,Rodriguez E, Imber SD, et al. Treating major depression inprimary care practice. Eight month clinical outcomes. ArchGen Psychiatry 1996;53:913-9.
Antidepressants are overrated
Editor—The most interesting aspect of theresults of the trial by Malt et al is that the dif-ference between antidepressants and pla-cebo was not impressive and was of doubtfulclinical relevance.1 At most it consisted of adifference of 3 points on a scale with a maxi-mum of 60 points and a pretreatment aver-age value of 27. In most subjects whosedepression was classified as severe or majordepression the difference was smaller andnot significant.
At least part of this difference probablyrepresents the non-specific effects of takingan active drug as opposed to an inertplacebo. It has been found that bothresearchers and patients can distinguishantidepressants, including selective serot-onin reuptake inhibitors, from inert place-bos.2 3 This “unblinding” effect may beimportant, since trials comparing anti-depressants with active placebos havegenerally found smaller effects.4
Side effects are obviously an importantway in which the identity of a drug orplacebo is revealed. Unfortunately—especially since the doses of drugs used werehigher than those used routinely—Malt et alprovide no information on this outcomeexcept to say that side effects were “few andrather insignificant.” But patients may beable to identify that they are taking an activedrug without necessarily reporting sideeffects. The authors did not investigatewhether patients could identify which groupthey were in, but they do report that none ofthe general practitioners could identify thepatient-drug combination correctly. It is notclear, however, that this was assessed system-atically, since by chance some of the generalpractitioners would be expected to guesscorrectly.
These reservations about theimportance of Malt et al’s findings areconsistent with a recent meta-analysis whichfound that differences between antidepres-sants and placebo were less noticeable thanhas traditionally been assumed.5 Doctorsmust be cautious about recommending rou-tine drug treatment for mild and moderatedepression in general practice on ethical aswell as scientific grounds. It is clearly in theinterests of the pharmaceutical industry topromote the notion that drug treatment canresolve human unhappiness and the prob-lems of living. Professionals have a duty toconsider the wider implications of such ascenario.Joanna Moncrieff specialist registrar in psychiatryDepartment of Psychological Medicine, Chelseaand Westminster Hospital, London SW10 [email protected]
1 Malt U, Robak HO, Madsbu H-P, Bakke O, Loeb M. TheNorwegian naturalistic treatment study of depression in
Letters
921BMJ VOLUME 319 2 OCTOBER 1999 www.bmj.com

general practice (NORDEP)—1: randomised double blindstudy. BMJ 1999;318:1180-4. (1 May.)
2 White K, Kando J, Park T, Waternaux C, Brown WA. Sideeffects and the “blindability” of clinical drug trials. Am JPsychiatry 1992;149:1730-61.
3 Kranzler HR, Burleson JA, Korner P, del Boca FK, BohnMJ, Brown J, et al. Placebo controlled trial of fluoxetine asan adjunct to relapse prevention in alcoholics. Am JPsychiatry 1995;152:391-7.
4 Moncrieff JM, Wessely S, Hardy R. Meta-analysis of trialscomparing antidepressants with active placebos. Br JPsychiatry 1998;172:227-31.
5 Bollini P, Pampallona S, Tibaldi G, Kupelnick B, MunizzaC. Effectiveness of antidepressants. Meta-analysis ofdose-effect relationships in randomised clinical trials. Br JPsychiatry 1999;174:297-303.
Author’s reply
Editor—Cornwall asks for the proportionof patients achieving what he calls fullremission (score on the MontgomeryÅsberg depression rating scale < 7) in ourstudy to compare it with Elkin et al’s study.After 16 weeks 38/87 (44%) taking sertra-line (odds ratio 0.45; 95% confidenceinterval 0.23 to 0.89) and 31/84 (37%)taking mianserin (0.60; 0.30 to 1.20) had atotal score of < 7 compared with 23/89(26%) taking placebo.
Our results are comparable to those ofElkin et al’s study.1 Nevertheless, we thinkthat emphasising just a score of < 7 at agiven time addresses only part of thepicture. Because of the serious conse-quences of depression, differences in theproportion of subjects having final scores inthe range of 7-11 with a given treatment arealso clinically important. The difference inclinical disability between patients with ascore of, say, 8 or 18 may be that of beingable to work or not.
Moncrieff suggests that the additionalbenefit of drugs in our study is due tonon-specific effects of active treatment. Thisargument has less validity in primary care.The studies cited by Moncrieff et al are con-ducted with depressed outpatients, notprimary care attenders.2 In our experience,primary care attenders have strikingly fewerside effects than do psychiatric outpatients,whatever the drug given. In our study thegeneral practitioners were required toexplore possible side effects systematically.This method provides a higher prevalenceof side effects than just recording spontane-ously reported side effects. The meannumber of baseline-corrected side effectsduring the study was 7.11, 6.51, and 6.45after 8 weeks of treatment with sertraline,mianserin, or placebo respectively, and 3.16,3.09, and 3.02 after 24 weeks of treatment.
Unipolar and bipolar depressions arethe leading causes of the world’s totaldisability adjusted life years. When severalfeatures of this study (statistical power 0.95,70% completing 16 weeks of treatment, noexclusion of patients who responded to pla-cebo, measurement of serum drug concen-trations to control for compliance, reliableraters, psychological support as it is pro-vided in general practice) are considered,the superiority of combined drug-psychological treatment of depression inprimary care is remarkable. If this treatmentwas adopted worldwide a considerablereduction in disability adjusted life yearsshould be achieved.
We agree, however, that good clinicalmanagement is the key to therapeuticsuccess. The high response rate to goodclinical management and placebo is remark-able indeed. More research on identifyingpredictors of response to different treat-ments is obviously needed.Ulrik Fredrik Malt professor of psychiatryDepartment of Psychosomatic and BehaviouralMedicine, University of Oslo, N-0027 Oslo, [email protected]
1 Elkin I, Shea T, Watkins JT, Imber SD, Sotsky SM, CollingsJF, et al. National Institute of Mental Health treatment ofdepression collaborative resarch program. Arch GenPsychiatry 1989;46:971-82.
2 Moncrieff JM, Wessely S, Hardy R. Meta-analysis of trialscomparing antidepressants with active placebos. Br JPsychiatry 1998;172:227-31.
UK’s diagnostic criteria fordiabetes are different from US’sEditor—In the article on glycaemic controlin diabetes the American author states thatdiabetes is characterised by a fasting plasmaglucose concentration of >7.0 mmol/l or aplasma glucose concentration of >11.1mmol/l two hours after a 75 g oral glucoseload.1 Understandably, he has described theAmerican guidelines for diagnosingdiabetes,2 but these are not the same as thosein the United Kingdom.
Here, the World Health Organisation’scriteria are still used; these define the fastingplasma glucose cut off point as >7.8 mmol/l.3 The WHO may possibly adopt the Ameri-can guidelines in the future,4 but in themeantime we have to be wary of giving clini-cians conflicting advice which may lead todiagnostic difficulties with their patients.5
Eric S Kilpatrick consultant in chemical pathologyHull Royal Infirmary, Hull HU3 [email protected]
1 Herman WH. Clinical evidence: Glycaemic control indiabetes. BMJ 1999;319:104-6. (10 July.)
2 Expert Committee on the Diagnosis and Classification ofDiabetes Mellitus. Report of the expert committee on thediagnosis and classification of diabetes mellitus. DiabetesCare 1997;20:1183-97.
3 World Health Organisation. Diabetes mellitus: report of aWHO study group. WHO Tech Rep 1985;727.
4 WHO Consultation Group. Definition, diagnosis andclassification of diabetes mellitus and its complications.Part 1: diagnosis and classification of diabetes mellitus;provisional report of a WHO consultation. Diabetic Med1998;15:539-553.
5 DECODE Study Group. Will new diagnostic criteria fordiabetes mellitus change phenotype of patients withdiabetes? Reanalysis of European epidemiological data.BMJ 1998;317:371-5.
Money to modernise adultmental health services isinsufficientEditor—The government has great ambi-tions for adult mental health services andhas raised the public’s expectations thatcommunity care will be reformed. Unfortu-nately, the new funding available to mosthealth authorities for that purpose does notmatch the rhetoric or compensate for thedisinvestment in mental health services thatoccurred as the large psychiatric hospitalswere closed.1
With the publication of the new mentalhealth strategy the secretary of stateannounced £700m of new money formental health services from the modernisa-tion fund. It was stated that “the new invest-ment will provide extra beds of all kinds,better outreach services, better access to newanti-psychotic drugs, 24 hour crisis teams,more and better trained staff, regional com-missioning teams for secure services, anddevelopment teams.”2 This created theimpression that services for adults ofworking age would be the principal benefici-aries of the new funding and that allocationswould be sufficient to allow a major overhaulof local services. The true picture issomewhat different.
The £700m is to be allocated over threeyears. Altogether £46m of the first year’sallocation of £146m is for local authorities.Only £40m of the health authority alloca-tion is for adult mental health services, andjust £19m has actually been distributed tohealth authorities for one or more of threespecific purposes: to provide 24 hour staffedbeds, to develop assertive outreach teams,and to fund the prescription of more new“atypical” antipsychotic drugs. The remain-ing £21m is to establish new secure beds(£14m), to support a development fund toimplement the national service framework(£5m), and for a “beacon service challengefund” (£2m).
Decisions about the distribution of the£19m were based on three factors: servicegaps identified during the autumn review, ajudgment of need in each health authority,and evidence of greater need in London.The net result is that only two of the 100health authorities received more than £1madditional money for new developments inadult mental health for 1999-2000; 71received less than £100 000 and 53 receivedless than £50 000.
These are paltry sums when set againstsome of the incidental costs of modernmental health care borne by health authori-ties. A single placement in a private securehospital would cost about £100 000 a year;to provide a single acute psychiatric bedcosts £50 000-70 000 a year; and anindependent homicide inquiry would cost£0.5m-1.5m. The first year’s allocation of themodernisation fund also coincides with alarger than average staff pay award (onlypartially funded by the government) and therequirement for trusts to make the usualcost efficiency savings.Paul Lelliott directorRoyal College of Psychiatrists’ Research Unit,London SW1X 7EE
1 Lelliott P, Sims A, Wing J. Who pays for community care?The same old question. BMJ 1993;307:991-4.
2 Department of Health. Modernising mental health services:safe, sound and supportive. London: Department of Health,1998.
Letters
922 BMJ VOLUME 319 2 OCTOBER 1999 www.bmj.com





























