Embed Size (px)
Citation preview

Deanna St. Germain, D.O.Family Medicine
Children's Medical Resource Network107 McKinley St.Anna, IL 62906
Assistant Professor of Clinical PediatricsDepartment of Pediatrics
Southern Illinois University School of MedicineSpringfield, IL
Clinical Assistant ProfessorFamily and Community Medicine
Southern Illinois University School of MedicineCarbondale, IL
Last revision August 2008.
Special thanks to:
Kay Saving, M.D. and Linda Simkins, LCSW, Pediatric Resource Center, University of Illinois, Peoria, IL Michele Lorand, M.D., Department of Pediatrics, Stroger Hospital, Chicago, ILCheryl Peterson, PhD, Children’s Justice Task Force, Department of Children and Family Services, Springfield, IL.Jill Harley, PA-C, Kid’s Center, Bend, OR.
1

This publication has been developed under a grant from the Illinois Department of Children and Family Services
2

TABLE OF CONTENTS
TABLE OF CONTENTS 2
DEFINITION 3
TYPES 3
RISK FACTORS 3
PURPOSE OF EXAM 5
TIMING OF EXAMS 6
INTERVIEW/HISTORY 7
PHYSICAL EXAM 9
LABORATORY 15
TREATMENT 17
DOCUMENTATION 20
DIAGNOSIS 21
COMMON DEFENSE MYTHS 27
CONDITIONS THAT MAY BE CONFUSED
WITH SEXUAL ABUSE 28
TESTIFYING 29
Bibliography 32
3

DEFINITIONThe American Academy of Pediatrics defines child sexual abuse as
follows:
Sexual abuse occurs when a child is engaged in sexual activities that the child cannot comprehend for which the child is developmentally unprepared, and cannot give consent, and/or violate the law or social taboos of society. 1-p507
Medical providers should be aware of state laws pertaining to sexual abuse and sexual assault in the state where they practice.
TYPESSexual activities that constitute abuse and assault may include, but
are not limited to the following:
1. Sexual penetration: genital, anal or oral.
2. Sexual contact: inappropriate touching of the genitalia and/or breasts or forcing a child to touch one’s genitalia.
3. Sexual conduct and sexual exploitation: exhibitionism, use of objects on a child, forcing sex between a child and another individual for the sexual gratification of watching, forcing a child into prostitution, taking nude photographs for sexual gratification or for pornographic reasons, forcing a child to view pornography or sexual nudity.
RISK FACTORSSexual abuse of children crosses ALL socioeconomic, racial,
religious, and ethnic boundaries. Twelve to 25% of female and 8 to 10% of male children are believed to be abused. 2 The difference between females and males may be due to a lower reporting of abuse among male victims. As with all forms of abuse, children at higher risk may live in family environments that can be categorized as chaotic and disorganized or isolated and tightly structured.
Risk factors must be considered in combination with assessments of children’s behavior and other aspects of the complete investigation. Clinicians should be cautious when considering risk factors since children can be abused in homes that demonstrate no risk
4

factors. Some of the following factors may be associated with a higher risk for sexual abuse:
For the abuser in general: being under-educated, unemployed, blue collar, as well as scoring high on emotional and sexual need scales, and being previously abused.³
For fathers who abuse: scoring high on distress, loneliness, rigidity and unhappiness scales.³
For mothers of sexually abused children: scoring high on tension, depression, anger and confusion scales; being more psychologically distressed and symptomatic and/or with a greater number of stressful life events.³
For the family: residing in dangerous communities and one parent families, those who live in poverty, mothers in a second marriage, parents less satisfied as parents, experiencing an unsatisfactory marital relationship, domestic violence, as well as mothers perceiving a low level of emotional support, mothers who neglect their children, and/or families who experience poor mother/daughter relationships.³
Other reported risk factors include: children with multiple caretakers, drug and alcohol abuse by caretakers, social isolation of the family, and children with poor self esteem. Also at risk are: children living without their mother at some time in their life, having a sexually repressive mother; children without physical affection from father and children with two or fewer friends in childhood.
BEHAVIORAL CHANGESIn conjunction with history and environmental risk factors,
behavioral changes in children may corroborate abuse. However, one third to one half of sexually abused children will have no symptomatology.²,³
Recognized potential behavior changes include: sexualized behaviors, symptoms of post-traumatic stress disorder, anxiety, irritability, nightmares, bed-wetting, not wanting to sleep alone, fear, new onset mental illness, aggression, school problems, eating disorders, hyperactivity, regression, withdrawal, self-injurious behavior, psychosomatic complaints and substance abuse.3,6
5

Again, these behaviors in conjunction with a history of sexual abuse may be considered corroborative but they are not diagnostic. There has been discussion in the literature regarding the usefulness of child sexual behavior scales., “To date, the literature does not identify any constellation of behaviors as a reliable indicator of sexual abuse.”²-
p213
Appendix A provides a well recognized Child Sexual Behavior Inventory with items at the top of the list being the most rare (“puts mouth on sex parts”) and those at the bottom the most common (“touches sex parts at home”).9 Certainly, behaviors in the rare and aggressive range are very worrisome and deserve a full investigation and work up. These behaviors in a child with a clear and consistent history of sexual abuse would be supportive of that disclosure and supportive of a diagnosis of sexual abuse.
Problematic sexual behaviors are more worrisome when: the behavior continues after the child has been told to stop10 or told to do it in private; also concerning is when the child focuses on these activities excluding other more age appropriate interests; when the child’s behavior upsets other children, or the child uses force, coercion or manipulation to engage in sexual behavior with other children; and/or if the sexualized behavior produces feelings of shame or embarrassment.2
So many factors affect a child’s behavior including stress from any source that each child’s behavior should be evaluated on a case by case basis.
PURPOSE OF EXAMDr. Astrid Heger writes “The true value of the medical examination
for possible sexual abuse is for the protection, the treatment and the reassurance of the child.”6p-8 Purposes of the thorough examination of a child suspected to have been sexually abused include:
1. To identify the signs and symptoms of child sexual abuse.11
2. To address the concerns of the child.11
3. To assess the physical well-being of the child and administer appropriate medical treatment. This includes looking for signs and symptoms of sexually transmitted diseases, physical abuse and/or neglect.12
6

4. To assess the emotional and psychological well-being of the child.12
5. To intervene on the child’s behalf to protect them from further harm. 12
6. To document a complete and accurate medical evaluation and, when appropriate, to collect potential evidence. 12
7. To report to appropriate authorities in accordance with state law. 12*
8. To support exam findings with documentation and court testimony (if indicated) to protect children from further abuse. 12
9. To attempt to get appropriate intervention and examinations for other children in the household. 12
10. To obtain a history. 12
11. To explore alternative explanations for concerns. 12
12. To assess the child’s developmental level. 12
* Remember, as mandated reporters, there need only be “a reasonable suspicion of abuse”. The investigation and litigation will be completed by others.
TIMING OF EXAMS
Unfortunately, a large percentage of children fail to report their abuse at the time of the incident. This fact largely contributes to the lack of physical findings upon examination. It is extremely important that children disclosing their assaults acutely be examined as soon as possible, preferably within the first 24 hours.
1. Acute: children with a history of assault within 72 hours or a serious presenting complaint, such as serious physical assault, genital pain, bleeding or discharge, severe emotional lability, suicidal ideation, or possibility of pregnancy should be examined immediately.13 Under most circumstances, a sexual assault evidence kit should be completed according to the detailed
7

instructions contained within the kit. Most law enforcement officers carry these kits and most Emergency Departments keep them on hand.
Injuries to the mucous membranes, such as those sustained during a sexual assault, heal very quickly, many within 24-72 hours ( notice the next time you accidentally bite the inside of your cheek, which is a mucous membrane, then notice when you can no longer feel any changes associated with the injury).
More serious injuries heal within 30 days most by 16 days.14
In young children, most forensic evidence is lost after 24 hours.15
In the prepubescent child, unless you have reason to believe that the child is presenting with an acute assault and DNA evidence is likely to exist, it may not be prudent to proceed with a sexual abuse exam on an emergency basis, but to refer the child to the most skilled clinician in your community for an urgent exam; a clinician with special training in the interpretation of the non-acute physical findings associated with blunt, penetrating trauma to the genitals.
a. Very rarely are examinations under anesthesia needed. Examples would include: severe trauma requiring sutures and/or exploration of the injuries, foreign bodies that cannot be easily and comfortably removed during the exam, and the extremely uncooperative child. Exams under anesthesia or sedation should be used only when there is likelihood of serious injury requiring repair, or a strong possibility of forensic evidence that will be lost if the exam is postponed and if the benefits outweigh the risks.12 If none of these situations exist, then the appointment should be rescheduled in an attempt to accomplish the necessary examination without the use of sedatives or anesthetics.
b. Children older than approximately 18-24 months of age should not be held down or coerced into submitting to the examination, unless there are deemed to be small costs with large benefits and parental permission.
c. Remember to perform photo-documentation both before and after any surgical repair.
2. Sub-acute: children with a history of assault within the past week or with less severe presenting complaints such as genital itching, discharge or signs and symptoms of sexually transmitted disease should be examined as soon as possible.
8

3. Non-acute: children with a history of assault weeks, months or years ago without significant physical or psychological concerns can be examined at the next available appointment time.
The child should be evaluated by the clinician in your community who is most skilled in the examination of sexually abused children. In fact, it is advised that a child with a history of sexual abuse who presents to an unskilled clinician, be examined appropriately (i.e. thoroughly enough) to rule out any acute trauma or infection or other condition that needs immediate treatment. The child should then be referred to the medical provider in the community who is the most skilled to perform the complete examination for child sexual abuse. A notation should be made in the chart to reflect that a detailed examination was not undertaken or that the child is being referred for “further medical evaluation”. A 2002 study by Makoroff et al showed children examined by pediatric emergency room physicians were more likely to have their exams interpreted as abnormal, whereas, a physician with training in child sexual abuse exams found their exams normal or nonspecific.16
CONSENTClinicians should be knowledgeable regarding the laws of their
state defining consent. In Illinois, Senate Bill 1618 provides that: “any minor who is a sexual assault survivor who seeks emergency hospital services and forensic services or follow-up healthcare under this Act shall be provided such services without the consent of the parent, guardian or custodian of the minor.” In addition, the release of the sexual assault evidence collection kit can be consented to by any child of 13 years or older, children under the age of 13 can have their evidence collection kits released “at the written request of the parent, guardian, investigating law enforcement officer, or Department of Children and Family Services”.17
Most medical providers will not perform a sexual abuse evaluation on a child who refuses to consent verbally no matter what their age (once they are past an age or developmental level that allows them to understand the proceedings) despite the wishes of their guardian. If, as mentioned above, the potential benefit of an examination outweighs the potential risks to sedation or anesthesia, an older child can be examined without having to be restrained but this is very, very rarely undertaken.
9

INTERVIEW/HISTORYThe interview with the child should, ideally, be conducted in a
private, quiet, reassuring atmosphere. Having a child friendly space without distractions is optimal but not always possible. In all aspects of interaction, allow the child as much freedom and choice over the situation as possible. Talk to the child alone, without parents or other caretakers present.
Given the small percentage of definitive physical findings in cases of prepubescent children who have been sexually abused, the medical history is an extremely important part of the sexual abuse evaluation.
Behavioral indicators and physical findings, the other two components of the evaluation, support the history given by the child.18
Before talking with a child, it is important to ascertain if the child has had a victim sensitive interview conducted by child welfare, law enforcement or a Children’s Advocacy Center (CAC) in regard to a specific disclosure or allegation of abuse. If a child has already been questioned thoroughly, the investigative agency should share essential information from the previous interview with the clinician. The medical interview with the child can then be brief and more specifically focused.
An in-depth interview should be conducted by the professional in your community with the most experience and training in the victim sensitive interviewing of young children.
1. Why we obtain a medical history/interview:
a. To document the alleged abusive incident.
b. To direct the physical examination.
c. To develop rapport with the child.
d. To evaluate the emotional/psychological manifestations of the abuse.
e. To document physical symptoms and medical history.
2. Techniques:
a. Take an appropriate history from the accompanying caretaker, including what they know about this incident and the child’s medical history. Do not do this in front of the child.
10

b. Speak to the child separately from parents or caretakers.
c. Sit at eye level, and speak in an age appropriate manner.
d. Inform the child that they can say “I don’t know” or “I don’t remember” and that they can correct you if you are wrong.
e. Begin by asking general questions about the child’s age, school, pets, interests, etc.
f. Learn the child’s names for appropriate body parts.
g. Ask about the basics of what happened and who did it, physical symptoms such as pain, bleeding, pain with defecation and urination, discharge and physical symptoms. Ask these questions in an open-ended manner: what, who, when, where. Leading questions include “Did Uncle Joe put his private in your pee pee?” Open ended questions include “tell me more…” and “what happened next?” Do not associate a specific act with a specific person in the same sentence unless the child has done so previously.
h. Keep your reactions to yourself. Be relaxed and non-threatening and non-authoritative.
i. Thank the child for their effort during the interview.
j. Use this time to lead into the physical exam, explain what the exam will involve, familiarize the child with the equipment that will be used.
k. Document what the child told you with his/her precise words using quotation marks. Do not use the word “alleged”.
l. Ask if the child has any questions or concerns that can be addressed now or during the physical examination.
More complete guidelines for an investigative interview (including many mentioned above) can be found in the American Professional Society on the Abuse of Children’s (APSAC) 2002 practice guidelines.19
11

PHYSICAL EXAMSome medical providers allow the child to choose a support person
who accompanies them through the medical examination and some states may have a Victim Bill of Rights that allows them to have a support person present.19 Others prefer only the child and medical personnel be present. In that case, medical personnel can include a support person for the child who is a neutral party such as nurse, child advocate or social worker. A clinician should always have another responsible party in the room when he or she completes a child sexual abuse examination.
Do not disrobe the child until just before you are ready to start the exam. Have child-sized exam gowns. Allow the child as much control as possible. Reading or other activities help to distract young children from the genital exam but you should constantly explain each step of the exam before you touch the child.
If the unwashed clothing, worn at the time of the assault, is available, have the child undress on a clean, white sheet. Fold soiled spots inward, and place clothing in a plain, PAPER bag; do the same with the sheet. Note the condition of the clothing. If the child is not wearing the clothing, collect only the clothing that was in direct contact with the genital areas of either the child or the perpetrator (or their excretions). Encourage law enforcement to collect all objects, furniture or linens that may have been soiled from the scene in the same manner. Dried semen can be detected on unwashed clothing and bed linens up to several months after the event, but as a rule, most forensic evidence is lost after one week.20 In fact, the majority of forensic evidence secured in the examination of prepubescent children is found on clothing or linens. 15
Know your normal genital anatomy. The best way to become familiar with normal prepubescent genitalia is to include a genital exam in well child exams or exams for other complaints that are appropriate, such as urinary tract infections, discharge or itching. Once familiar with the usual prepubescent genital appearance, the abnormal becomes more obvious.
12

Posterior commisure (in prepubertal children the labia minora are not completely formed and do not connect posteriorly; in the adolescent female this areais referred to as the posterior fourchette)21
Fossa navicularis (3 dimensional space from the posterior edge of the posterior hymenal rim to the posterior commissure)
Posterior hymenal rim
Hymenal orifice (vagina can sometimes be seen beyond here)
Anterior hymen(not seen with crescentic hymens) Anterior vaginal wall
(can sometimes be seen)
Urethral orifice
Clitoris
Labia minora
Urethralorifice
Anteriorvaginalwall
Labia minora
Anteriorhymenalrim
Hymenalorifice
Fossa navicularis Posterior hymenal rim
Posterior commissure
Figure 1: Simplified prepubescent female anatomy Figure 2: Colposcopic photo with labeled anatomy, prepubescent female
Urethra
Shaft of penis
Corona
Glans
ScrotumMedianraphe
Figure 3: Simplified prepubescent male anatomy Figure 4: Prepubescent male anatomy
13

Internal anal sphincter closed
Pectinate line with anal papilla is sometimes visible
External anal sphincter relaxed
Anal verge
Anal verge
Prominent rugae
External anal sphincter slightly relaxed
Internal anal sphincter closed
Figure 5: Simplified anal anatomy Figure 6: Colposcopic photo with anal anatomy labeled
DO A COMPLETE HEAD TO TOE PHYSICAL EXAMINATION OF THE CHILD VISUALIZING ALL BODY PARTS.
Hymenal variations include: annular (concentric), crescentic, septate with or without duplication of vagina, fimbriated, imperforate, cribiform (multiple openings) and redundant (see Appendix B).
Inspect the skin, look for and descriptively document (with both narrative and body chart) any contusions, hematomas, abrasions, lacerations, erythema, edema, petechiae, scars, contractures, friability, injection or increased vascularity, skin tags, alopecia, bite marks, burns, induration or discharges, tenderness, stains, suspected seminal products, ligature marks, or any other abnormalities or asymmetry.
14

In addition to providing a routine physical exam, you should be concerned about all other forms of abuse and extra-genital trauma including fractures, abdominal trauma, retinal hemorrhages, head injury, nutritional neglect, skin lesions and developmental delays. Any concerns should be worked up with appropriate X-ray, laboratory and/or other diagnostic means necessary.
Consider documenting hygiene status. Think about a drug screen if appropriate; some of the current “date rape” drugs do not appear on routine drug screens but be aware that the most commonly abused “drug” used to facilitate sexual assault is alcohol.22
With regard to the examination of the external genitalia:
A PREPUBESENT FEMALE SHOULD NOT UNDERGO A SPECULUM OR VAGINAL MANUAL EXAMINATION WITHOUT GENERAL ANESTHESIA.12
If the injuries necessitate a speculum exam they should be extensive enough to warrant an exam under anesthesia.
Small children do best in the “frog leg” position while supine on the exam table; adolescents can use the stirrups. Prepubescent children can also be examined being held by the caretaker who is on the table with them. The knee chest position often provides a better view of the posterior hymenal rim in prepubertal girls and the anterior hymen in pubertal females. This position should be included as part of the exam for this reason, and is highly recommended if an abnormality of the posterior rim is noted. In the supine position, labial traction allows the pelvic floor to relax and allows the best view of the hymen and vestibule. Separation of the labia and the buttocks are also useful techniques in either supine or knee chest position.23
Figure 7: Supine “frog leg” position Figure 8: Prone “knee chest” position
15

If any child has trouble with the knee chest position because it is the position the abuse occurred in, a reasonable alternative is the lateral recumbent position.13
If there is difficulty observing the hymenal edges, they can often be “floated” by applying a few drops of warm saline or using a moistened cotton-tipped swab. In the case of an estrogenized hymen, a balloon catheter can be inserted through the hymenal orifice, the balloon inflated and then slowly and gently pulled forward to expose the edges of the hymen.12 It should be noted that the prepubescent hymen is very sensitive and even gentle touching with a cotton-tipped swab is often perceived as painful, the estrogenized hymen is less sensitive and often tolerates manipulation.
A colposcope is often used to observe and document the genital exam, either by photo or video. A Medscope™ and other digital video devices can also be used to document genital injuries for use in departments that cannot afford a colposcope. Even a hand held otoscope is a good alternative when used with careful documentation and drawings. A competent photographer may use a 35mm camera to document genital injuries as an alternative to the colposcope and should also document any other external injuries. All extra-genital injuries should be photographed in color, using a coin or a ruler to illustrate the size of an injury. Make sure all photographs of this type include a ruler for sizing and are documented with a patient identifier, date and time the photo was taken, location of injury if not obvious, and the name of the person who took the photograph.
16
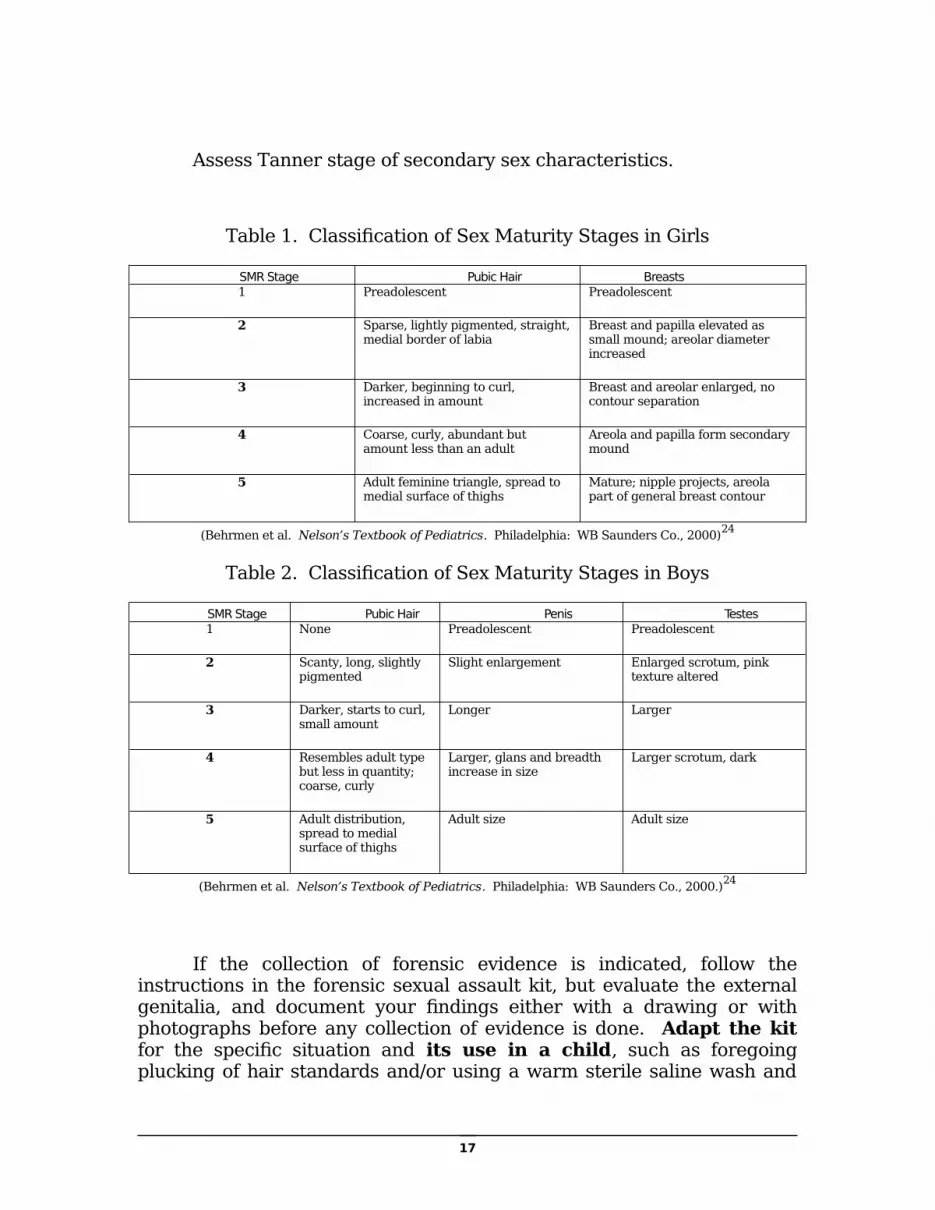
Assess Tanner stage of secondary sex characteristics.
Table 1. Classification of Sex Maturity Stages in Girls
SMR Stage Pubic Hair Breasts1 Preadolescent Preadolescent
2 Sparse, lightly pigmented, straight, medial border of labia
Breast and papilla elevated as small mound; areolar diameter increased
3 Darker, beginning to curl, increased in amount
Breast and areolar enlarged, no contour separation
4 Coarse, curly, abundant but amount less than an adult
Areola and papilla form secondary mound
5 Adult feminine triangle, spread to medial surface of thighs
Mature; nipple projects, areola part of general breast contour
(Behrmen et al. Nelson’s Textbook of Pediatrics. Philadelphia: WB Saunders Co., 2000)24
Table 2. Classification of Sex Maturity Stages in Boys
SMR Stage Pubic Hair Penis Testes1 None Preadolescent Preadolescent
2 Scanty, long, slightly pigmented
Slight enlargement Enlarged scrotum, pink texture altered
3 Darker, starts to curl, small amount
Longer Larger
4 Resembles adult type but less in quantity; coarse, curly
Larger, glans and breadth increase in size
Larger scrotum, dark
5 Adult distribution, spread to medial surface of thighs
Adult size Adult size
(Behrmen et al. Nelson’s Textbook of Pediatrics. Philadelphia: WB Saunders Co., 2000.)24
If the collection of forensic evidence is indicated, follow the instructions in the forensic sexual assault kit, but evaluate the external genitalia, and document your findings either with a drawing or with photographs before any collection of evidence is done. Adapt the kit for the specific situation and its use in a child, such as foregoing plucking of hair standards and/or using a warm sterile saline wash and
17

foley catheter to obtain evidence from the vagina without performing a speculum exam. Save any painful procedures for the end of the exam such as cultures or blood draws. Viscous lidocaine can be used topically to decrease the discomfort of genital culture collection.
These kits standardize the collection of evidence that may remain on the victim but belong to the perpetrator such as DNA from various sources (blood, semen, skin, saliva), hair, blood type, semen, p30 (human seminal protein) and semen acid phosphatase.25 Remember that one person must stay with the sexual assault kit at all times to establish the chain of custody. DNA evidence from sloughed skin cells may be detected by newer evidentiary techniques.26
Despite previous recommendations, a Wood’s lamp is inadequate for fluorescing semen on the skin. If done at all, a Blue Max 500 alternative light source (or equivalent) should be used, and suspicious areas swabbed per instructions in the evidence kit.27
Be aware that children do not always disclose or are not aware of the extent of the assault. Christian et al found that the disclosure and the forensic evidence did not correlate well in prepubescent children so the decision to collect forensic evidence is best made using the time from assault (less than 24 hours) rather than the child’s description of the assault.15
Toluidine blue dye can be applied to accentuate superficial abrasions of the mucosa,20 but the red-free filter on the colposcope will provide similar information without the mess of the dye. This dye will adhere to any denuded area without regard to cause and should therefore, be used appropriately and interpreted with caution.28 Again, do not do this until you have documentation without foreign substances.
Note the appearance of the breasts, medial thighs, external genitalia, and anus. As stated above, no speculum or vaginal exams are necessary in prepubescent females. If the trauma is severe enough to require an internal examination, the child should be examined under anesthesia. An internal rectal exam is not necessary to evaluate the rectum, unless a severe traumatic injury is suspected. If the child is being seen acutely after an anal assault, consider anoscopy (usually under sedation or anesthesia), to document internal lacerations or injuries.28 The decision whether to do this under anesthesia would have to be made on a case by case basis considering risks and benefits, always erring on the side of being humane to the child who is disclosing anal assault.
The most important contribution an unskilled examiner can make to the physical examination of a prepubescent child, done on an acute
18

basis, is a detailed description and diagram of the genitalia. No knowledge or interpretation is necessary to describe what the hymen, penis, scrotum, anus and their surrounding tissue look like.
Specifically, note the appearance of the clitoris, the labia minora and majora, the urethra, hymen, fossa navicularis, posterior commissure, perineum, glans and shaft of the penis, scrotum, testicles, and anus. Describe the type of hymen, thickness and configuration of the edges, any bumps, tags, notches, or intravaginal ridges. Describe findings by using the face of a clock, and note whether the child is in supine or knee-chest position when naming the position of injuries. Note whether the male child is circumcised, and note the urethral opening in both sexes. Describe the anus’ configuration and any fissures, mounds, tags, venous congestion, or relaxation.
Abnormal findings could include: erythema, labial adhesions, hematomas, mucosal abrasions, submucosal hemorrhages, petechiae, blood blisters, scarring, friability of the posterior commissure, edema, swelling, injection, lacerations or hymenal transections, anal lacerations, anal dilation of 2 cm. or greater without stool in the ampulla and occurring within 30 seconds, marked irregularity of the anal orifice, and evidence of STI’s or pregnancy. After fellatio, there can be injury to the frenulum of either the lips or the tongue and petecchiae on the palate.28
Note that not all of these findings are specific for abuse and consideration should be given to whether the examination is acute or non-acute when weighing certain physical findings. Please refer to the section on diagnosis and see appendix B for photo plates of genital findings.
Beware midline abnormalities. Although many transections of the hymen occur in the midline so do congenital anomalies. If there is a question about injury vs. congenital anomaly, have the child return in a few weeks for a recheck. The congenital defect will be unchanged, whereas the injury will change as it heals. If an injury has already reached maximum healing, this approach won’t help. If symmetrical, smooth, and unchanging on serial exams, consider that this might be a congenital anomaly or normal variant. Describe it in detail, make a diagram, obtain pictures and consult with a clinician skilled in the medical evaluation of prepubescent children who have been sexually abused.
Myhre et al and Emans suggest “floating” the posterior rim of the hymen with saline when there is concern about thinning of the hymen to less than 1 mm since the hymen can fold over on itself, and when this happens it may appear smaller than it actually is.29,13
19

Make certain to document everything you do with written words and drawings.
Remember the importance of assessing the emotional, behavioral, developmental and mental health of the child and document that assessment.
LABORATORYSexually transmitted infection (STI) cultures are not necessary in
every case of child sexual abuse involving prepubescent children since the incidence is reported to be less than or equal to 5%. Commonly used adult rapid tests for Chlamydia trachomatis and Gonorrhea are not reliable in this age group. Actual culture media should be used both to insure accuracy and legal admissibility. Any positive results for STI’s should have confirmatory tests done by a different method to avoid false positives, particularly HIV, syphilis, and Gonorrhea/Chlamydia by nucleic acid amplification tests.30
Culture children who:
1. Have signs or symptoms of an STI or a genital infection contracted sexually.31
2. Were assaulted by an alleged offender who is known to harbor or be at high risk for harboring an STI.31
3. Give a history of, or have physical findings consistent with, penetration or ejaculation.31
4. Are consensually sexually active. 31
5. Live in communities with high rates of STI’s.31
6. Have siblings or household contacts with STI’s.31
7. The patient or parent requests testing or are anxious about STI’s.31
8. Are adolescent.31
9. Were assaulted by multiple perpetrators.32
10. Have a last date of contact with the perpetrator that is proximate to the time of the examination. For example, children who have no signs or symptoms of infection and
20

whose last exposure to the perpetrator was a year ago need not undergo testing.31
11. Are likely to be lost to follow up.
STI cultures and pregnancy tests (in females) should be considered in all adolescents. Remember that the swabs obtained for the forensic evidence kit will not be used to test for STI’s. Separate STI swabs must be obtained and processed in the local lab.
The AAP Red Book® 2006 recommends the following to be decided on a case by case basis as outlined above: rectal, throat, male urethral and vaginal cultures for Gonorrhea; rectal, male urethral and vaginal cultures for Chlamydia; as well as serology for HIV, Hepatitis B and syphilis. Sexual transmission of Hepatitis C is uncommon and routine screening in child sexual abuse victims is not currently recommended.31
Consider obtaining a wet prep for microscopic exam from the vagina (look for WBCs, clue cells, trichomonas, moniliasis and for semen if proximate to the assault) as well as Trichomonas vaginalis cultures.31
You may want to do routine pathogen culture and sensitivity in children with a history of a discharge, not just those cultures associated with STI’s.
Ulcerated areas can be cultured for HSV and growths suggestive of HPV can be biopsied though that is not routinely recommended, the diagnosis should be made clinically. Bacterial vaginosis can be diagnosed using wet prep, pH and potassium hydroxide testing. Pediculosis pubis can be diagnosed with the naked eye or magnifying glass.31
A note about human papilloma virus is appropriate here. When a new diagnosis of venereal warts occurs in children, a report to DCFS should be made but due to the marked presence of HPV in adult females, the presence of that infection alone in children under approximately 6 years of age should not be the basis of a diagnosis of child sexual abuse.33
The AAP (American Academy of Pediatrics) Committee on Pediatric HIV for 2002-2003 outlines the risk and recommendations for transmission of HIV in sexual abuse victims.34 Consulting that periodical is highly recommended. In summary, the risk of HIV transmission in children who have been sexually abused appears to be low, though it has occurred. The decision to use post-exposure prophylaxis (PEP) in prepubescent sexually abused children needs to be made on a case by case basis taking into account the amount of time since the exposure, the
21

perpetrator(s), a discussion with the parents/guardians and consultation with a pediatric infectious disease physician with experience treating HIV/AIDS. If you decide to treat, treatment with two or three antiretroviral drugs should be instituted as soon as possible, no later than 72 hours post exposure and continued for 28 days under close supervision as these drugs can be associated with toxicity and must be taken as prescribed. The risk for transmission is highest with unprotected anal receptive intercourse (0.5%-3.2%); is intermediate for receptive vaginal intercourse (0.05%-0.15%) and lowest for insertive vaginal intercourse (0.03%-0.9%); the risk from oral sex is unknown. The perpetrator’s HIV risk must be assessed and PEP is recommended for unprotected, anal, receptive intercourse with an HIV positive perpetrator, it should be considered for other levels of risk unless there is no risk from the assault (i.e. fondling) or the perpetrator’s HIV status is known to be negative.34
TREATMENTTreat all injuries noted and any medical conditions such as urinary
tract infection or coincidental pharyngitis, otitis or cellulitis. Address any neglect or developmental concerns. Consider tetanus and hepatitis B immunizations, pregnancy prophylaxis, and begin treatment for STI’s per guidelines provided in the AAP Red Book® or this text.
The prophylactic treatment of asymptomatic prepubescent children is not recommended unless the child is likely to be lost to follow up or there is a known STI or high risk for an STI in the perpetrator. Table 3 contains the recommendations for prophylactic treatment of a prepubescent. Consider follow up exams for STI’s or recommend the child be examined by the primary care provider in 2 weeks, 6 weeks, 3 months, 6 months, and an optional 12 months if there is a high likelihood of STI’s.31
If a child develops signs and symptoms of an STI (the provider should instruct parents/caretakers about usual signs and symptoms), he or she should be seen immediately, and treated, if necessary, with appropriate follow up. When an STI is identified, unless noted below, a test for cure is recommended. If a child has any STI’s, testing should be completed for all STI’s.
Any child with gonorrhea (beyond the neonatal period) should be treated concomitantly for Chlamydia infection. Test of cure is not necessary if treated with ceftriaxone unless they remain in a high risk
22

environment. The same is true for Chlamydia.31 Table 4 contains treatment recommendations for children with STI’s.
In children sexually exposed to individuals with known (or high risk for) Hepatitis A or B, prophylactic treatment should be considered. Most children receive the recommended Hepatitis B immunizations, if their post immunization status is unknown, they should receive one booster immunization. If their vaccination status is unknown, they should receive Hepatitis B immune globulin and start the immunization series as soon as possible, preferably less than or equal to 24 hours post exposure. They should receive subsequent Hepatitis B immunizations as routinely recommended. 31
Child victims of perpetrators with Hepatitis A should receive immune globulin as soon as possible after the assault, up to two weeks post exposure. They can also receive the first Hepatitis A vaccine at that time and follow with the series as routinely recommended. 31
Hepatitis C is not efficiently transmitted sexually and there is no post-exposure prophylaxis at this time. 31
Clinicians should remember to report appropriate infections to their local public health departments as required by the state in which they practice.
Table 3
STI prophylaxis of prepubertal children31
Weight <100 pounds STI Weight >100 pounds
Ceftriaxone 125mg IM X 1
Gonorrhea Ceftriaxone 125mg IM X 1
OR
Cefixime 400 mg PO X 1
PLUS
Azithromycin 20mg/kg to max of 1 g, PO X 1
OR
Chlamydia PLUS
Azithromycin 1 g PO X 1
OR
Doxycycline 100mg BID X 7 days (at least 8 yrs old)
23

Erythromycin base or ethylsuccinate 50mg/kg/day PO in 4 doses X 14 days
PLUS
Begin or complete hepatitis B virus immunization if not already immunized
Hepatitis B PLUS
Begin or complete hepatitis B virus immunization if not already immunized
PLUS
Metronidazole 15mg/kg/day PO in 3 doses X 7 days
Trichomonas or bacterial vaginosis
PLUS
Metronidazole 2 g PO X 1
24
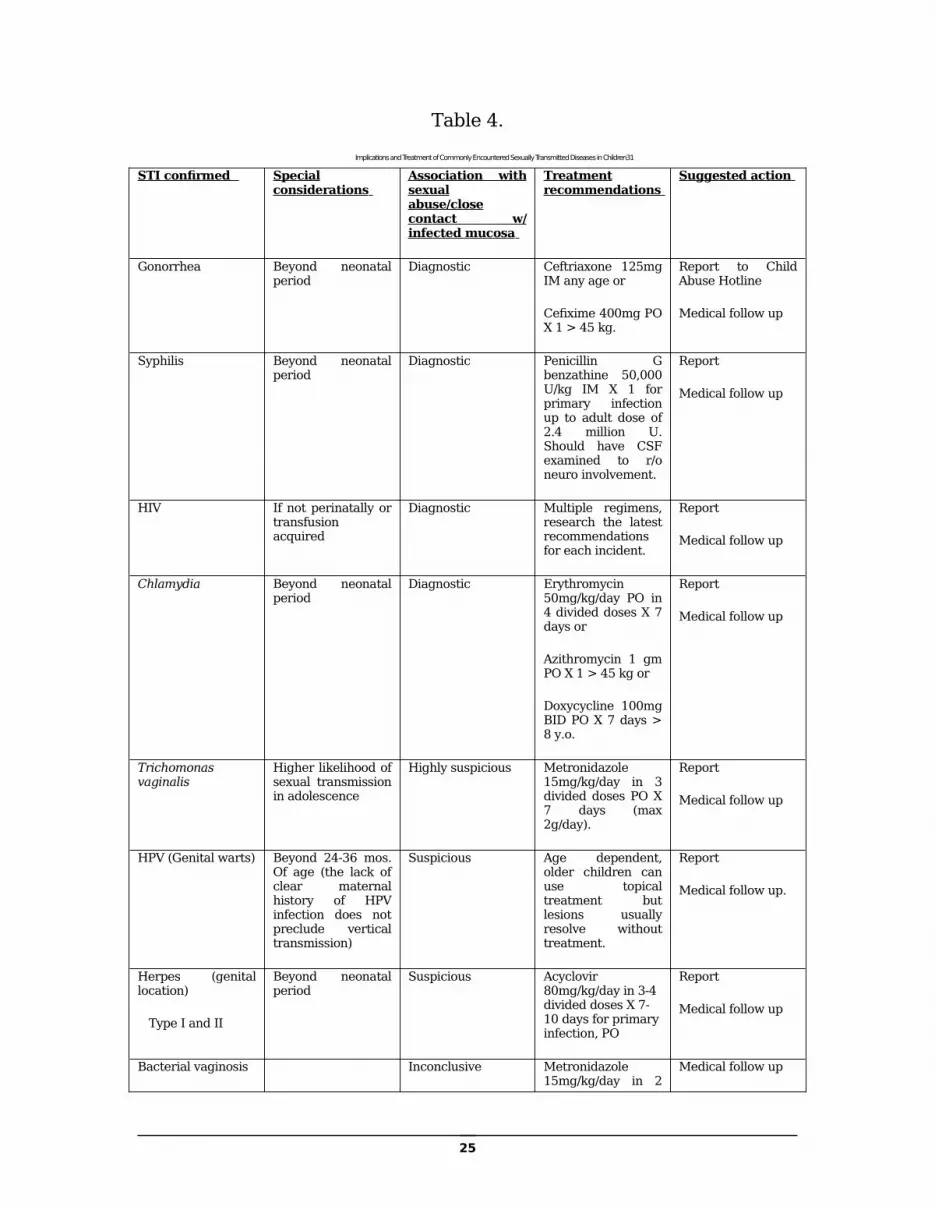
Table 4.
Implications and Treatment of Commonly Encountered Sexually Transmitted Diseases in Children31
STI confirmed Special considerations
Association with sexual abuse/close contact w/ infected mucosa
Treatment recommendations
Suggested action
Gonorrhea Beyond neonatal period
Diagnostic Ceftriaxone 125mg IM any age or
Cefixime 400mg PO X 1 > 45 kg.
Report to Child Abuse Hotline
Medical follow up
Syphilis Beyond neonatal period
Diagnostic Penicillin G benzathine 50,000 U/kg IM X 1 for primary infection up to adult dose of 2.4 million U. Should have CSF examined to r/o neuro involvement.
Report
Medical follow up
HIV If not perinatally or transfusion acquired
Diagnostic Multiple regimens, research the latest recommendations for each incident.
Report
Medical follow up
Chlamydia Beyond neonatal period
Diagnostic Erythromycin 50mg/kg/day PO in 4 divided doses X 7 days or
Azithromycin 1 gm PO X 1 > 45 kg or
Doxycycline 100mg BID PO X 7 days > 8 y.o.
Report
Medical follow up
Trichomonas vaginalis
Higher likelihood of sexual transmission in adolescence
Highly suspicious Metronidazole 15mg/kg/day in 3 divided doses PO X 7 days (max 2g/day).
Report
Medical follow up
HPV (Genital warts) Beyond 24-36 mos. Of age (the lack of clear maternal history of HPV infection does not preclude vertical transmission)
Suspicious Age dependent, older children can use topical treatment but lesions usually resolve without treatment.
Report
Medical follow up.
Herpes (genital location)
Type I and II
Beyond neonatal period
Suspicious Acyclovir 80mg/kg/day in 3-4 divided doses X 7-10 days for primary infection, PO
Report
Medical follow up
Bacterial vaginosis Inconclusive Metronidazole 15mg/kg/day in 2
Medical follow up
25

divided doses PO X 7 days with max of 500mg per dose.
Molluscum contagiosum
Inconclusive Not usually required
Medical follow up
Alternate regimens are available for adolescents.
Labial adhesions can be treated with estrogen cream applied to the area daily for two to six weeks until the edges separate then treated with triple antibiotic cream.35 Prolonged use of estrogen cream may cause estrogenization of the external genitalia. Do not attempt to manually separate adhesions without the child under anesthesia.
You should insure that the child and siblings are discharged to a safe environment. In some states medical providers have the right to take a child into protective custody if they feel that the child is in imminent danger. As always, the physician should make every effort to keep the caretakers informed, explain the mandatory reporting law, and the requirement of safety for the child. One should have law enforcement or security in place before advising the caretakers that you do not intend to let them leave with the child. Law enforcement officers can legally prevent the caretaker from leaving the facility with the child. Most people respect law enforcement and avoid confrontations; if an altercation ensues, the officers are trained to deal with it.
Next, a Child Abuse Hotline report should be made to notify child protection services that you are taking protective custody of the child. Usually, a child protection worker will be immediately dispatched and a safe environment will be provided for the child. If law enforcement and/or child protection are not available, the child can be admitted to the hospital for observation in order to assure safety. Hospital security should be alerted to keep the caretakers from removing the child. Any child with severe injuries which warrant hospitalization should be admitted and protected in a similar manner.
DOCUMENTATIONThe forms provided in Appendix C are suggested as examples of
documentation in child sexual abuse (and most child physical abuse cases), they can be amended to meet your facility’s needs. Give narrative descriptions including all the components of the examination detailed in these guidelines, as well as lab and X-ray data, treatment
26

given, disposition and your opinion. Always make a line drawing of the genital findings immediately after the exam, so you do not have to rely on photographs alone.
In order to protect a child, it is not necessary to obtain a release of information from the legal guardian when supplying information to law enforcement or investigators from the Department of Children and Family Services. However, it is best practice to do so whenever possible. For release of information to all other parties, including the parents themselves, a signed release should be on file. There may be exceptions to this policy such as subpoenas or court orders.
Remember not to use the word “alleged” when documenting what the child told you about the incident. Instead, use phrases like “the child reports” and quotation marks using the child’s own words.
Remember, the history is the single most important part of the diagnostic procedure.
DIAGNOSISIn the setting of an acute assault when the examination is more
likely to yield physical findings of trauma such as contusions, abrasions, petechiae, and lacerations the diagnosis is significantly enhanced by the acute findings. Most clinicians have difficulty in making a diagnosis when the disclosure is remote from the event and no acute findings exist.
Reassure parents and child that the child is physically “okay,” if that is true. Otherwise, describe the injuries in terms they understand, explain that any injuries sustained have been or will be treated, and assure them, whenever consistent with the case, that the injuries described will not be obvious to anyone else, even an intimate partner.
The colposcopic and Medscope™ pictures in Appendix B depict normal and non-specific genital findings (or congenital variations) as well as acute anal findings, non-acute hymenal and anal findings. Even if you cannot interpret the physical findings, it is important to document them descriptively in a detailed manner so that physicians reviewing the document can interpret them at a later date.
The following are the recommendations of the American Academy of Pediatrics1 regarding the decision making process for sexual abuse. This is helpful regarding the decision to report abuse to the proper authorities, but it is not helpful regarding the diagnosis since it
27

presupposes the interpretation of the physical findings as either nonspecific or specific.
Table 5
Remember, you DO NOT have to do an investigation and prove abuse before reporting it to the authorities (either law enforcement or DCFS Hotline). Report abuse if you have any suspicions. In most states, physicians and health care workers are mandated reporters of child abuse and can be sanctioned for not reporting suspected child abuse. Physicians and health care workers are protected from prosecution or litigation when reporting in good faith.
As you have learned, the specialized medical exam for the prepubescent child is not traumatic, it is similar to a yearly physical with more attention paid to the genitals but children are usually easily distracted from that part of the exam and take the entire process in stride. Child welfare investigations exist to protect the child and investigators work hard to decrease the impact of their investigations on the children. Clinicians should report abuse when they suspect it in the circumstance of objective, reasoned concerns.
28

The following is a copy of Joyce Adams’ Classification System. These guidelines clearly define the current consensus in the profession regarding the interpretation and significance of physical findings noted during the child sexual abuse evaluation in a prepubescent child.12
29

30
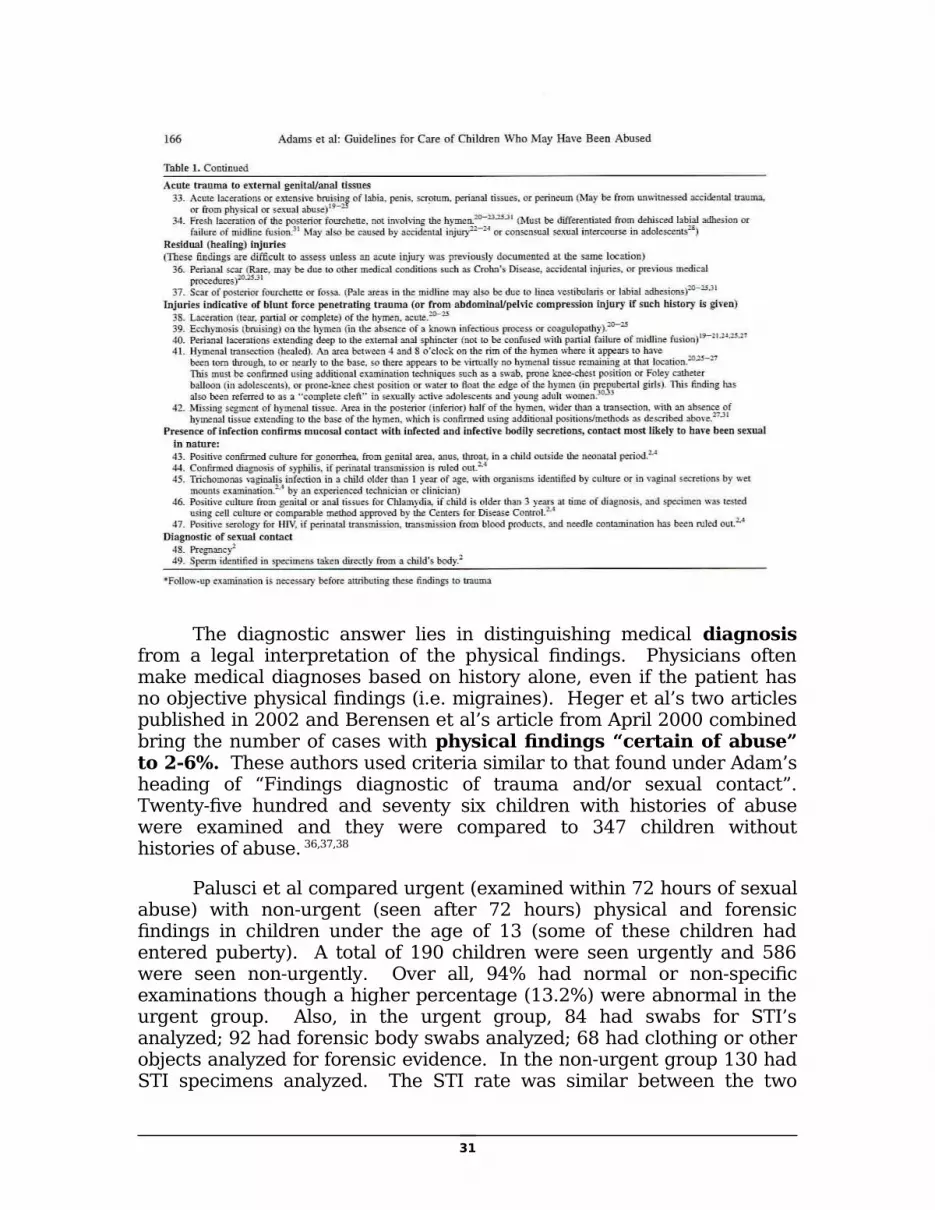
The diagnostic answer lies in distinguishing medical diagnosis from a legal interpretation of the physical findings. Physicians often make medical diagnoses based on history alone, even if the patient has no objective physical findings (i.e. migraines). Heger et al’s two articles published in 2002 and Berensen et al’s article from April 2000 combined bring the number of cases with physical findings “certain of abuse” to 2-6%. These authors used criteria similar to that found under Adam’s heading of “Findings diagnostic of trauma and/or sexual contact”. Twenty-five hundred and seventy six children with histories of abuse were examined and they were compared to 347 children without histories of abuse. 36,37,38
Palusci et al compared urgent (examined within 72 hours of sexual abuse) with non-urgent (seen after 72 hours) physical and forensic findings in children under the age of 13 (some of these children had entered puberty). A total of 190 children were seen urgently and 586 were seen non-urgently. Over all, 94% had normal or non-specific examinations though a higher percentage (13.2%) were abnormal in the urgent group. Also, in the urgent group, 84 had swabs for STI’s analyzed; 92 had forensic body swabs analyzed; 68 had clothing or other objects analyzed for forensic evidence. In the non-urgent group 130 had STI specimens analyzed. The STI rate was similar between the two
31
groups at 5% and 4%. Of the 93 children seen urgently who had one or more forensic test analyzed, 17 had one or more positive result for an 18.3% rate (9% if you use the total of 190 seen acutely rather than the number with tests analyzed). No child younger than 10 years of age had positive forensic findings if examined after 24 hours. Pubertal females were more likely to have positive exam findings.39
In John McCann et al’s 2007 article “Healing of Hymenal Injuries in Prepubertal and Adolescent Girls: A Descriptive Study”, the researchers followed children with acute anogenital injuries until they healed. Only the deepest, most severe lacerations left any sign of previous trauma,14 therefore, the history is the single most important consideration in making the diagnosis of child sexual abuse, particularly in the non-acute setting; the behavioral and physical findings support the history. Heppenstall-Heger et al’s 2003 article reports similar findings of complete healing after acute trauma.40
This same McCann article added some useful information with regard to timing acute injuries. Only petechiae correlated with the amount of time since injury. When noted, petechiae always resolved within 72 hours but the number of research subjects was 73, so more research is necessary before using this data to firmly interpret physical findings. Finding petechiae would be supportive of the child’s history of assault within 72 hours. The only physical finding that persisted past 16 days was blood blisters, all other injuries, including surgical repair of deep lacerations were healed by day 16.14
Dr. Boos et al, report a series of four children run over at a slow pace by motor vehicles with resultant anogenital injuries similar to those seen in child sexual abuse.41
Herrmann and Crawford report two cases of young females injured while using in-line skates. The injuries were perineal and did not create any hymenal lacerations.42
There are anecdotal reports of girls experiencing vaginal lacerations from water being forced into their vaginas while water-skiing, playing with hoses or the water jets of tubs or pools. 43
The significance of the child’s history cannot be made any more apparent than it is in Kellogg, et al’s 2004 article, “Normal Genital Anatomy in Pregnant Adolescents: normal does not mean nothing happened”. In this study, only two of thirty-six pregnant teens had definitive findings of penetrating injury. And it should be noted that 56% of these pregnancies were reported to have resulted from sexual abuse. 44
32

Boys rarely exhibit healed residua from trauma to the penis or scrotum during sexual abuse. Boys and girls do experience anal penetration during sexual abuse, this can result in healed residua. 11
Heppenstall-Heger et al reported only 2 out of 31 acute anal injuries showed persistent scarring after healing and those two required surgical repair. 40
Obtaining a history of dysuria immediately following the reported abusive incident is considered corroborative. 11
In some circumstances, medical providers will be asked if they have made a diagnosis and if that diagnosis was made with “a reasonable degree of medical certainty”. This is generally accepted to be the level of certainty used every day to make a diagnosis and treat a patient. 45
The legal system usually concerns itself with the physical findings. The legal system would like a definitive statement correlating physical findings with the allegations, such as “the only possible explanation of these physical findings is an inflicted penetrating injury”. Some legal systems seem to believe physical findings are needed to “prove” the history from the child, not merely support it. It does seem counter-intuitive that young children can be penetrated and heal without observable, objective signs of trauma. The following are suggested reasons for normal genital findings in so many children with detailed histories of sexual penetration:
a. Elasticity of the hymenal tissue. 12
b. Rapid healing of injuries that do occur. 12
c. Fondling or oral-genital contact only. 12
a. Nothing happened. 12
b. Prolonged interval between the incident and the disclosure (and therefore, examination).
c. Vulvar and intra-gluteal coitus. Vulvar coitus is the penetration of the penis between the labia, but not through the hymenal opening. Intra-gluteal coitus is achieved by rubbing the penis in the gluteal cleft between the buttocks and over, but not through, the anal verge. 11
d. The routine passage of large stools through the anal sphincter without injury.
33

e. The use of lubricants was employed.
f. The gentle nature of the violation; some perpetrators want to be able to have continued access to the child and take care to avoid painful experiences for the child.
g. The genital changes that accompany puberty may cover injuries from earlier abuse.
Different clinicians use different styles when reporting their findings. Some use a classification system to report their findings in that manner. Some use words like “suspicious” and “highly suspicious” in their diagnosis.
Dr. M. Finkel suggests a narrative approach with regard to diagnosis, such as “the history/behavior is descriptive of inappropriate sexual contact; however, no diagnostic residual is evident;” or “the history/behavior is descriptive, and diagnostic findings are present, which are reflective of the contact (i.e. trauma, STIs and/or seminal products)”; or “the history is diagnostic of inappropriate sexual contact without healed residua;” or “the history/observations are limited, and although the behaviors observed by the parent have raised concern, there are insufficient historical or behavioral details to support a concern of inappropriate sexual contact.” 11
With regard to physical findings and the legal system, one study found that in one 12-month period 76% of felony cases resulted in conviction of the perpetrator on felony charges. Physical evidence was present in just 23% of those cases. The conviction rate was 79% in cases without physical evidence and 67% of those with. The conclusion was that physical evidence was not necessary for successful prosecution. The quality of the verbal evidence and the child’s testimony were more predictive of success. 46
One should remember, when making decisions about the physical findings, that the medical findings do not identify the perpetrator. Only the child’s testimony and the forensic evidence can do that. The medical findings merely support the child’s history. Therefore, physicians should not be swayed to over interpret physical evidence. They should remain balanced and objective. Conversely, clinicians should not be so afraid of making a positive statement and/or appearing in court that they never “see” the physical findings of abuse.
Remember, the majority of sexually abused children have no specific physical findings and the lack of physical findings does not mean they were not abused. The documentation in the medical
34

record should reflect this fact. Most positive findings are discovered when the child presents immediately after the assault, (for prepubertal girls, the percentage of acute injuries can climb as high as 40% when they present acutely47) yet most children are examined after some appreciable length of time has elapsed.
MEDICAL PROVIDERS Adams et al, 2007 clearly states the recommended guidelines
regarding the qualification of medical providers who perform child sexual abuse examinations on prepubertal children:
The Child sexual abuse medical provider who is responsible for the interpretation of findings, diagnosis and treatment of alleged sexual abuse should have relevant training and clinical experience…12p-169
Clinicians should consult that document in deciding if they meet the criteria set forth for training, experience, peer review, adequate familiarity with the most recent research in the medical literature, proficiency, understanding of physical findings that can be mistaken for sexual abuse, ongoing educational activities, collaboration with a multidisciplinary team, comfort and competence in court testimony as well as community activity. 12
COMMON DEFENSE MYTHSMedical providers need to be aware of facts that can be used to counter common defenses of offenders with regard to genital injuries:
1. Congenitally absent hymen; there have been no documented cases of children born without hymens who have otherwise normal appearing genitalia.11,48
2. Hymenal injuries caused by masturbation or tampon use; masturbation and atraumatic tampon use do not result in specific findings of penetrating injuries.43,49
3. Hymenal injuries caused through normal play; children with straddle injuries are injured as the soft tissue hits the pubic bone. The injuries are high and/or lateral and the hymen is not torn unless there is a penetrating object involved in the trauma.40
35

CONDITIONS THAT MAY BE CONFUSED WITH SEXUAL ABUSE
Conditions that may be confused with sexual abuse in children:
1. Lichen sclerosis
2. Nonspecific vulvovaginitis and proctitis
3. Congenital midline defects
4. Vertical transmission of STI’s
5. Urethral prolapse
6. Varicella presenting in mucous membranes of genital area before other parts of the body
7. Accidental straddle or impaling injury.
8. Group B Streptococcus vaginitis or proctitis
9. Shigella vaginitis
10. Diaper dermatitis
11. Foreign bodies
12. Paralysis of the lower extremities.
13. Chronic gastrointestinal diseases, such as, Crohn’s disease
14. Hirschprung’s disease
15. Vitiligo
16. Vulvar pemphigoid
17. Behcet’s disease
18. Rhabdomyosarcoma
19. Hemangioma
20. Estrogen producing ovarian tumors
21. Sarcoma botryoides
36
22. Imperforate hymen with cystic appearance
23. Anal fissures from constipation, or other irritation. 11,43,51,52
Girls younger than six years old with vaginal bleeding or concerning discharge is addressed in Striegel et al. The study looked at 24 girls with vaginal bleeding or concerning discharge using non-invasive imaging, pelvic exam under anesthesia as well as vaginoscopy and cystoscopy. The non-invasive imaging identified 5 of 7 foreign bodies but only 2 of 6 malignancies and 0 of 2 benign papillomas. The malignancies were rhabdomyosarcomas and endodermal sinus tumors. None of the procedures added to the available information used to make a diagnosis of sexual abuse. Therefore, girls in this age group without an obvious source of bleeding (i.e. vulvar, hymenal or anal trauma or pathology) should be referred for a more extensive work up. 53
This protocol defines best practice suggestions. The clinician should always exercise his or her best judgment when considering all aspects of an individual case or circumstance and proceed accordingly.
TESTIFYINGA medical expert should be unbiased, neutral, knowledgeable,
make sound opinions, and be willing to explain those opinions.
A physician, nurse practitioner or physician’s assistant may be established as an “expert” by testifying to his/her special knowledge, skill, experience, training, or education. The other possibility is for a medical provider to testify as a treating physician or a “fact” witness regarding the condition of the patient they examined without being an expert.
Strategies for court testimony:
1. Do not testify without receiving a subpoena, and be sure it is accompanied by a properly signed release allowing you to disclose personal medical information45 and/or, follow the laws of your state regarding the disclosure of protected, confidential medical information.
2. Encourage and participate in pre-trial meetings with the examining attorney. 54
37

a. Establish the purpose of your testimony (treating physician vs. expert witness or fact vs. opinion). 54
Establish your qualifications54 as well as the key medical issues.
b. Discuss how the testimony will best be presented. 54
You can review specific facts and opinions as well as the sequence for presentation. 55 Familiarize yourself with the legal jargon and courtroom decorum.
i. Identify and alleviate problem areas where possible.54
ii. Plan exhibits and demonstrations. 55
iii. Consider possible cross-examination questions and what kind of opposing opinion can be expected. 55
iv. To decrease waiting time, discuss exactly what time you will be needed54 or agree to be on call for a certain time period and respond promptly.
3. Check that equipment to be used in court is working properly just before your appearance. 55
4. In general, don’t run scared. Do your homework and be prepared by thoroughly reviewing relevant medical records54, memorize the most substantive facts (not your testimony) and put your ideas in order.
5. Put your nervousness to work for you. Some degree of stress helps to raise our competence levels. 55
6. Be very careful of your dress54 and demeanor in and around the courtroom (including the parking lot). 55 Find out where to wait until you are needed in the courtroom, do not enter the courtroom without instruction. Do not discuss the case with anyone at the courthouse.
7. Sit up straight in the witness chair with your feet flat on the floor leaning forward slightly. 55
8. Keep good records and documentation. Do not alter records without documenting time and date and signing
38

the additional comments. 54 Never enter comments into the record that you wouldn’t want to read in open court.
9. Use language a lay person can easily understand or explain medical terms after you use them without talking down to the jury. 54
10. As a general rule, look at the person asking the question when answering. 54 If you are informing the jury then look at the jury directly; think of them as a patient to whom you are explaining a medical problem. 55
11. Prepare for a deposition as though it was court and review it carefully before going to court although participation in a deposition may negate the need to testify. 54
12. Be confident, not conceited. You are not expected to know everything so if you don’t know, say so. You may be able to explain why. 54
13. Review the relevant medical literature and make the examining attorney aware of the literature. 54
14. Be aware of some common cross-examination techniques; it is best to:
a. Remember, when asked about fees, you are being reimbursed for your time, not your answers on the witness stand. 55
b. Listen to the entire question before answering. 54
Think before you start to speak and speak with a normal pace. 55
c. Answer questions that make assumptions with a statement to be clear about the facts or your opinion. If you cannot answer a question with a yes or no reply, then do not do so54 and state why you cannot (you may need to ask the judge’s permission to do so).
d. Ask for clarification54, rewording, or repetition of the question if a question becomes confusing, vague, has too many parts to it or is leading; or again, you may need to answer the question with a statement rather than a yes or no response.
39

e. Make sure hypothetical questions are based on the facts of the case being presented.
f. Avoid providing information without being asked directly about it. 54
g. Avoid being lulled into thinking the cross-examining attorney is taking a benign approach. Do not allow yourself to become angry on the stand. Calmly correct an attorney if they misstate prior testimony. 54
12. Regarding the opposing attorney:
a. In most situations, the decision to speak with opposing counsel prior to testimony is up to you. You do not have to talk with them before you see them in the courtroom.
b. If you do talk to them, everything you say in that meeting can, and will be compared to how you testify in the courtroom.
c. If you do talk to them, you should be polite and succinct and answer only the questions asked. Keep careful notes, a tape recording of the interview or ask that a court reporter be provided to create a transcript so that you can review the information before court.
d. If you do not talk to them prior to testimony, expect to field a question related to that upon cross–examination. “Did you meet with the prosecuting attorney in this case? (Usually the answer will be yes) Did you refuse to meet with me, the defense attorney in this case? Why is that doctor?”
e. You do not have to take articles or textbooks from opposing counsel to read just before testifying. If you didn’t use it to form your opinion, you cannot be questioned on it. Be sure you know an article or text in depth before you testify about it; avoid agreeing that any author is the absolute last word on any subject.
40

“The more experience one has in the cross-examination of the medical witness, and particularly the expert medical witness, the more one must come to the conclusion that the cross-examination of a truthful, honest, efficient, and capable expert medical witness who isn’t given to exaggeration is not only dangerous but usually harmful to the trial lawyer.” Irving Goldstein, J.D. quoted in Testifying in Court . 55p-9
_________________________________
1. Kellogg N, Block R, Hibbard R, Jenny C, Spivack B, Stirling J; for the American Academy of Pediatrics’ Committee on Child Abuse and Neglect. Clinical Report: The evaluation of sexual abuse in children. Pediatrics. August 2005;116(2)506-512.
2. Ricci L, Wientzen J. Sexual abuse overview. In: Giardino A, Alexander R. Child Maltreatment: A Clinical Guide and Reference. 3rd ed. St. Louis, MO: G.W. Medical Publishing, Inc.;2005:209-221.
3. Black D, Heyman R, Smith Slep A. Risk factors for child sexual abuse. Aggression and Violent Behavior. 2001;6:203-229.
4. Botash A. Pediatrics, child sexual abuse (monograph online). eMedicine. April 6, 2006. http://www.emedicine.com/emerg/topic369.htm. Accessed June 6, 2008.
5. Koverola C, Friedrich W. Psychological effects of child sexual abuse. In: Heger A, Emans S J, Muram D. Evaluation of the Sexually Abused Child. New York, NY: Oxford University Press; 2000:21-37.
6. Heger A. Making the diagnosis of sexual abuse: Ten years later. In: Heger A, Emans S J, Muram D. Evaluation of the Sexually Abused Child. New York, NY: Oxford University Press; 2000:1-9.
7. Friedrich W, Trane S, Gully K. Letter to the Editor: Re: It is a mistake to conclude that sexual abuse and sexualized behavior are not related: a reply to Drach, Wientzen, and Ricci (2001). Child Abuse & Neglect. 2005;29:297-302.
41

8. Ricci L, Drach K, Wientzen J. Letter to the Editor: Further comment on the lack of utility of sexual behavior problems as measured by the child sexual behavior inventory in diagnosing sexual abuse: A reply to Friedrich, Gully, and Trane (2004). Child Abuse & Neglect. 2005;29:303-306.
9. Friedrich W, Fisher J, Broughton D, Houston M, Shafran C. Normative sexual behavior in children: A contemporary sample. Pediatrics [serial online]. April 1998;101(4)e9. http://www.pediatrics.org/cgi/content/full/101/4/e9. Accessed June 9, 2001.
10. Sapp M, Vandeven A. Update on childhood sexual abuse. Curr Opin Pediatr. April 2005, 17(2):258-264.
11. Finkel M. Sexual abuse: The medical examination. In: Giardino A, Alexander R. Child Maltreatment: A Clinical Guide and Reference. 3rd ed. St. Louis, MO: G.W. Medical Publishing, Inc.;2005:253-284.
12. Adams J, Kaplan R, Starling S, et al. Guidelines for medical care of children who may have been abused. J Pediatr Adolesc Gynecol. 2007;20:163-172.
13. Emans SJ. Physical examination of the child and adolescent. In: Heger A, Emans S J, Muram D. Evaluation of the Sexually Abused Child. New York, NY: Oxford University Press; 2000:57-76.
14. McCann J, Miyamoto S, Boyle C, Rogers K. Healing of hymenal injuries in prepubertal and adolescent girls: a descriptive study. Pediatrics. May 2007;119(5):e1094-106. http://www.pediatrics.org/cgi/content/full/119/5/e1094. Accessed November 7, 2007.
15. Christian C, Lavelle J, DeJong A, Loiselle J, Brenner L, Joffe M. Forensic evidence findings in prepubertal victims of sexual assault. Pediatrics. July 2000;106:100-104. http://www.pediatrics.org/cgi/content/full/106/1/100. Accessed August 12, 2008.
16. Makoroff K, Brauley J, Brandner A, Myers P, Shapiro R. Genital examinations for alleged sexual abuse of prepubertal girls: findings by pediatric emergency medicine physicians compared with child abuse trained physicians. Child Abuse and Neglect. December 2002;26(12):1235-1242.
42

17. Illinois State Senate Bill 1618. http://www.ilga.gov/legislation/publicacts/fulltext.asp?Name=095-0432 . Accessed March 22, 2007.
18. Monteleone J. Personal communication. Cardinal Glennon Children’s Hospital. St. Louis, MO;July 1987.
19. Pence D, Everson M, Wilson C; for APSAC Task Force on Investigative Interviews in Cases of Alleged Child Abuse. APSAC Practice Guidelines: Investigative Interviewing in Cases of Alleged Child Abuse. American Professional Society on the Abuse of Children (APSAC). 2002.
20. Jenny C. Forensic examination: The role of the physician as “medical detective”. In: Heger A, Emans S J, Muram D. Evaluation of the Sexually Abused Child. New York, NY: Oxford University Press; 2000:79-90.
21. McCann J; for APSAC Interpretation of physical findings in child sexual abuse subcommittee. Glossary of terms and the interpretations of findings for child sexual abuse evidentiary examinations. APSAC. 1998.
22. Hall J, Moore C. Drug facilitated sexual assault. J Forensic Leg Med. July 2008;15:291-297.
23. Boyle C, McCann J, Miyamoto S, Rogers K. Comparison of examination methods used in the evaluation of prepubertal and pubertal female genitalia: a descriptive study. Child Abuse & Neglect. February, 2008;32(2):229-243.
24. Needlman R. Adolescence. In: Behrman R, Kliegman R, Jenson H, eds. Nelson’s Textbook of Pediatrics. 16th ed. Philadelphia, PA: W. B. Saunders Company;2000:54.
25. Kuriger J. Collection and testing of forensic evidence in child sexual assault cases. Hennepin County Medical Center Education (online). October 4, 2006.. http://www.hcmc.org/education/cme/documents/childsexassault_000.ppt#2. Accessed on July 30, 2008.
26. Bell K, Archambault J, O’Donnell P. DNA evidence. In: Giardino A, Alexander R. Child Maltreatment: A Clinical Guide and Reference. 3rd ed. St. Louis, MO: G.W. Medical Publishing, Inc.;2005:861-914.
43

27. Nelson D, Santucci K. An alternate light source to detect semen. Acad Emerg Med. October 2002;9(10):45-48.
28. Finkel M, DeJong A. Medical findings in child sexual abuse. In: Reece R, Ludwig S, eds. Child Abuse Medical Diagnosis and Management. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins;2001:207-279.
29. Myhre A, Berntzen K, Bratlid D. Genital anatomy in non-abused preschool girls. Acta Paediatr. 2003; 92:1453-1462.
30. Workowski K, Berman S; for U. S. Department of Health and Human Services Centers for Disease Control. Sexually transmitted diseases treatment guidelines, 2oo6. Morbidity and Mortality Weekly Report. August 4, 2006;55(RR-11):1-94.
31. Pickering L, ed. Red Book: 2006 Report of the Committee on Infections Diseases. 27th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2006:169-177.
32. Sirotnak A. Sexually transmitted diseases. In: Giardino A, Alexander R. Child Maltreatment: A Clinical Guide and Reference. 3rd ed. St. Louis, MO: G.W. Medical Publishing, Inc.;2005:289-310.
33. Adams J. Genital warts and HPV in children: What do they mean and what do we do about them. In: The 21st Annual San Diego International Conference on Child and Family Maltreatment. January 22-26, 2007; San Diego, CA.
34. Haven P; for American Academy of Pediatrics Committee on Pediatric AIDS 2002-2003. Clinical Report: Postexposure prophylaxis in children and adolescents for nonoccupational exposure to human immunodeficiency virus. Pediatrics. June 2003;111(6):1475-1489.
35. Alagiri M. Labial adhesions (monograph online). eMedicine. March 30, 2006. http://www.emedicine.com/ped/topic1267.htm . Accessed June 12, 2008.
36. Heger A, Ticson L, Velasquez O, Bernier R.. Children referred for possible sexual abuse: medical findings in 2384 children. Child Abuse Negl. June 2002;26(6-7)645-659.
37. Heger A, Ticson L, Guerra L, et al. Appearance of the genitalia in girls selected for nonabuse: review of hymenal morphology and nonspecific findings. J Pediatr Adolesc Gynecol. 2002;15:27-35.
44
38. Berenson A, Chacko M, Wiemann C, Mishaw C, Friedrich W, Grady J. A case controlled study of anatomic changes resulting from sexual abuse. Am J Obstet Gynecol. April 2000;182(4)820-31.
39. Palusci V, Cox E, Shatz E, Schultze J. Urgent medical assessment after child sexual abuse. Child Abuse & Neglect. 2006;30: 367-380.
40. Heppenstall-Hegar A, McConnell G, Ticson L, Guerra L, Lister J, Zaragoza T. Healing patterns in anogenital injuries: a longitudinal study of injuries associated with sexual abuse, accidental injuries, or genital surgery in the preadolescent child. Pediatrics. Oct 2003;112(4):829-837.
41. Boos S, Rosas A, Boyle C, McCann J. Anogenital injuries in child pedestrians run over by low-speed motor vehicles: four cases with findings that mimic child sexual abuse. Pediatrics. July 2003;112(1):e77-84. http://pediatrics.aappublications.org/cgi/reprint/112/1/e77. Accessed October 24, 2003.
42. Herrmann B, Crawford J. Genital injuries in prepubertal girls from inline skating accidents. Pediatrics. August 2002;110(2)e16. http://www.pediatrics.org/cgi/content/full/110/2/e16. Accessed June 7, 2005.
43. Adams J. Medical evaluation of suspected child sexual abuse. J Pediatr Adolesc Gynecol. June 2004;17(3):191-197..
44. Kellogg N, Menard S, Santos A. Genital anatomy in pregnant adolescents: “normal” does not mean “nothing happened”. Pediatrics. January 2004; 113(1):e67-69. http://www.pediatrics.org/cgi/content/full/113/1/e67. Accessed March 11, 2008.
45. Ricci L. Preparing to give expert testimony. In: Giardino A, Alexander R. Child Maltreatment: A Clinical Guide and Reference. 3rd ed. St. Louis, MO: G.W. Medical Publishing, Inc.;2005:761-771.
46. DeJong A, Rose M. Legal proof of child sexual abuse in the absence of physical evidence. Pediatrics. September 1991;88(3):506-511.
47. McCann J. Healing of genital injuries. In: 17th Annual San Diego Conference on Child and Family Maltreatment. February 3-7, 2003; San Diego, CA.
45

48. Berenson A, Heger A, Andrews S. Appearance of the hymen in newborns. Pediatrics. April 1991;87(4):458-465.
49. Adams J, Botash A, Kellogg N. Difference in hymenal morphology between adolescent girls with and without a history of consensual sexual intercourse. Arch Pediatr Adolesc Med. March 2004; 158:280-285.
50. Emans S J, Woods E, Allred E, Grace E. Hymenal findings in adolescent women: impact of tampon use and consensual sexual activity. The Journal of Pediatrics. July 1994; 125(1)153-160.
51. Heger A. Photographic atlas. In: Heger A, Emans S J, Muram D. Evaluation of the Sexually Abused Child. New York, NY: Oxford University Press; 2000:115-122.
52. Bays J. Conditions mistaken for sexual abuse. In: Reece R, Ludwig S, eds. Child Abuse Medical Diagnosis and Management. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins;2001:287-303.
53. Striegel A, Myers J, Sorensen M, Furness P, Koyle M. Vaginal dishcharge and bleeding in girls younger than 6 years. J Urol. December 2006;176(6 pt 1):2632-2635.
54. Hanes M, McAuliff T. Preparation for child abuse litigation: Perspectives of the prosecutor and the pediatrician. Pediatric Annals. May 1997;26(5)288-295.
55. Horsley, J. Testifying in Court, 4th ed. Los Angeles, CA: Practice Management Information Corporation, 1992.
56. The American Heritage Dictionary, 4th ed. Boston, MA: Houghton Mifflin Company, 2001.
57. Dorland’s Illustrated Medical Dictionary, 31st ed. Philiadelphia, PA: Saunders Elsevier, 2007.
Glossary
AAP- American Academy of Pediatrics. Abrasion- an injury to the surface of skin or mucous membrane caused by a
mechanical process. 21
Adhesion- abnormal fusion of adjacent surfaces. 57
Alleged- stated but without proof. 56
Alopecia- absence of hair where it is normally present. 57
Ampulla- dilation of a tubular structure, as at the end of the colon in the rectum. 57
46

Anal receptive intercourse- anus receiving the penetrating penis. Anomaly- deviation from the norm, i.e. as a result of congenital defect. 57
Anoscopy- examination of the anus through a speculum. 57
Anus- the lower opening of the digestive tract found between the buttocks. 57
Annular hymen- hymenal membrane covers the vaginal orifice circumferentially. 21
APSAC- American Professional Society on the Abuse of Children. 21
Areolar- circular area of pigmentation around the nipple on the breast.57
Asymmetry- a lack of balance in corresponding parts. 57
Bacterial vaginosis- change in the normal balance of the bacterial content of the vagina causing discharge and inflammation. 21
Behcet’s Disease- recurrent ulcerative disease of the mucous membranes and other body systems. 57
Blood blister- vesicle containing blood. 57
CAC- Children’s Advocacy Center, a national movement to create regionally accessible centers to support child victims by decreasing the number of interviews, creating multidisciplinary teams investigating child abuse and providing child friendly environments.
Candidal fungal infections- yeast infection. 21 Chlamydia trachomatis- sexually transmitted organism causing infection
and inflammation of the genital tract. 21
Clarification- to make clearer. 56
Cleft- a “V” shaped indentation along the edge of the hymen. 21
Clitoris- the erectile body of the female genitalia. 57
Clue cells- epithelial cells from the vagina with collections of bacteria on the surface. 57
Coagulopathy- disorder of blood coagulation (clotting). 57
Coercion- compelling by force. 56
Coitus- sexual intercourse between a male and female. 57
Collaboration- working together. 56
Colposcope- a magnifying instrument used to examine tissue57, often has a still or video camera attached.
Concentric hymen- another word for annular hymen. 21
Concomitantly- accompanying; along with. 56
Condyloma accuminata- venereal warts caused by human papilloma virus. 21
Congenital- born with; existing at birth. 57
Consensually- by agreement; with consent. 56 Contracture- shortening of a tissue due to resistance to stretch. 57
Contusions- a bruise. 57
Corona of the glans penis- rounded border of the glans and the shaft of the penis. 21
Corroborative- supportive. 56
Cresentic hymen- hymen does not circumferentially cover the vaginal orifice but attaches on either side giving a “half moon” appearance to the hymen. 21
Cribiform hymen- hymen with multiple openings. 21
Culture media- substance used to cultivate living cells, such as bacteria.
57
Cystoscopy- placement of a small scope to visualize the bladder. 57
Denuded- layed bare. 57 Dermatitis- inflammation of the skin. 57
Diastasis ani- congenital variation due to the absence of the muscles around the anus causing loss of normal folds, seen at 6 and 12 o’clock. 21
47

Didactic- instructive. 56
Dilation- to become wider or larger. 57
DNA- deoxyribonucleic acid, the basic chromosomal material of living cells. 57
Dysuria- painful urination. 57
Ecchymosis- bleeding into the skin or mucous membrane. 57
Edema- swelling due to increased fluids. 57
Ejaculation- expulsion of semen from the male urethra. 57
Elasticity- flexibility; able to return to normal after being stretched. 57
Endodermal sinus tumor- a malignant germ cell tumor of children. 57
Erythema- observed redness of the tissue due to dilation of small blood vessels (capillaries). 57
Estrogenized- affected by estrogen, the female sex hormone (which causes thickening of the hymen during puberty).
Evidentiary- bearing on or establishing the point in question in a court of law. 56
Examination positionsa. lateral recumbent- patient lying on their side with the opposite
knee drawn towards the chest. 21 b. prone knee-chest- patient on their knees, face down, with upper
chest against exam table and buttocks in the air so that the back is swayed. 21
c. supine “frog leg”- patient lying supine (on their back) with knees bent and hips rotated outward so that the bottom of the feet touch. 21
Excretions- normal waste material from the body. 57
Exploitation- to make unethical use of for one’s own profit. 56 Fellatio- penis penetrates the mouth for oral stimulation. 21 Fimbriated hymen- hymen with multiple indentations along the edge. 21
Fissure- superficial break in the surface of a tissue. 21
Foley catheter- flexible tube passed into a cavity57, typically through the urethra to the bladder with a inflated tip to hold it in place in order to drain urine from the bladder.
Fondling- touching sex organs with the hand. 56
Forensic- pertaining to legal matters. 56
Fossa navicularis- three dimensional concavity from the posterior aspect of the hymen to the posterior commissure. 21
Frenulum- small amount of mucous membrane that attaches one structure to another such as the tongue to the floor of the mouth or the lips to the gums to limit movement. 57
Friability- tissue bleeding easily when manipulated. 57
Gardnerella vaginalis- bacteria found in sexually active females associated with bacterial vaginosis. 21
Glans (of penis)- head of the penis, is covered by the foreskin in the uncircumcised male. 21
Gonorrhea- sexually transmitted infection with the bacteria Neisseria gonorrhoeae. 21
Gynecology- specialty of medicine dealing with the diseases of the genital tract in women. 57
Hemangioma- benign tumor composed of newly formed blood vessels. 57
Hematoma- localized collection of blood. Hepatitis B- viral infection which can be sexually transmitted and can
cause liver disease. 57
Hepatitis C- viral infection which can be sexually transmitted and can cause liver disease. 57
48

Hirschprung’s Disease- abnormally large colon, may be congenital or acquired. 57
HIV- human immunodeficiency virus, which may be sexually transmitted causing a breakdown in the normal immune function. 34
HPV- human papilloma virus which may be sexually transmitted causing venereal warts. 21
HSV- herpes simplex virus (1 and 2), an ulcerative sexually transmitted disease. 21
Hymen- membrane partially covering the opening to the vagina. 21
Hypopigmented- loss of usual pigment or color. 57
Hypothetical- based on an unproved theory. 56
Ideation- a plan or scheme. 56
Imperforate hymen- hymenal membrane completely covers the opening of the vagina therefore menstrual blood cannot flow, requires surgery to alleviate. 21
Induration- the quality of being hard. 57
Injection- liquid forced into the vascular tree. 57
Insertive vaginal intercourse- penis penetrating a vagina. 21
Intra-gluteal coitus- penis rubbed between the buttocks in the intra-gluteal cleft. 21
Intravaginal ridges- raised tissue on the vaginal wall that may attach to the inner aspect of the hymen. 21
Labia majora- outer lips, folds of skin forming the outer boundary of the vulva. 21
Labia minora- inner lips, folds of skin within the labia majora. 21
Labial separation- pulling the labia apart, down and laterally. 21
Labial traction- pulling the labia towards the examiner. 21
Laceration- a cut through tissue such as skin, mucous membrane or other structures. 57
Lability- instability. 56
Lichen sclerosis et atrophicus- a skin disease causing hypopigmented and erythematous areas seen around the genitals and perianal area. 57
Ligature- a tie or bind. 57
Linea vestibularis- vertical, hypopigmented line in the fossa navicularis or at the posterior commissure. 21
Litigation- contesting in a lawsuit. 56
Masturbation- manual stimulation of the genitals. 56
Median raphe- line at the union of the two halves of the perineum. 21 Medscope™- video instrument with magnification used to document
trauma. Microperforate hymen- hymen with a much smaller than usual opening. 21
Millimeter- one thousandth of a meter; slightly less than 4 one-hundredths of an inch (there are 25.4 mm in an inch). 57
Molluscum contagiosum- viral infection of the skin and other tissue which is benign and common in children but may be sexually transmitted.
21
Mound- distinct, rounded area of tissue on the hymenal edge. 21
Mucousal- pertaining to mucous membrane, the lining of various canals and cavities in the human body. 57
Multidisciplinary team- collaborative effort by individuals representing appropriate disciplines56 such as child welfare, law enforcement, psychology, medical, and prosecution, toward a common goal.
Neonatal- pertaining to an infant’s first four weeks of life. 57
Notch- indentation, see cleft. 21
49

Nucleic acid amplification test- laboratory test utilizing replication of the basic cellular building blocks of a bacteria or virus allowing for identification of an existing infection.
Nurse practitioner- an advanced degree nurse having completed the equivalent of a Master’s Degree in Nursing.
Orifice- the opening of a structure. 57
Palate- roof of the mouth. 57
Papilla (breast)- small projection or elevation. 57
Pathology- the branch of medicine studying the nature of disease; pertaining to the manifestation of disease. 57
PEP- postexposure prophylaxis. 34
Pectinate line- also called dentate line, anal structures with saw-tooth appearance seen with anal dilation. 21
Pediculosis pubis- pubic hair infested with lice. 57
Penis- male sex organ with erectile tissue and urethral orifice. 21
Perianal- around the anus. 21
Perineum- the pelvic floor and associated structures usually used to identify the area between the vulva and the anus or the scrotum and the anus. 57
Periurethral bands- supporting structures around the urethra. 21
Petechiae- tiny red lesions caused by blood leaking out of capillaries (small blood vessels). 57
pH- the degree to which a substance is acidic or alkaline. 57
Physician assistant- a licensed medical professional, qualified to render medical care for routine diagnoses under the supervision of a physician.
Pigmented- having color. 57
Posterior commissure- the union of the labia posteriorly (toward the anus) in the prepubescent female. 21
Posterior fourchette- the union of the labia minora posteriorly (toward the anus) in the postpubertal female. 21
Post-exposure prophylaxis- medication given to prevent infection after exposure to a potentially infected person. 34
Potassium hydroxide- solution used to test for bacterial vaginosis. 21
Pregnancy prophylaxis- medication intended to prevent implantation of a fertilized egg.
Prepubescent- prior to puberty. 57
Proctitis- inflammation of the rectum (the end of the digestive tract). 57 Prone- face down. 57
Prosecution- conducting legal action against. 56
Proximate- near to. 56
Psychosomatic- physical complaints made worse by one’s emotional or psychological state. 57
Pubertal- maturing of the secondary sex characteristics with the capacity for sexual reproduction. 57
Pubic bone- anterior portion of the pelvis. 57
Rapport- harmony. 56
Receptive vaginal intercourse- vagina being penetrated by a penis.
Redundant hymen- hymenal edges that are overlapping or folded over on themselves. 21
Regression- backward movement. 56
Relaxation- becoming less tense. 56
Repressive- holding back; subdued. 56
Residua- left behind. 57
Rhabdomyosarcoma- cancer of the muscle. 57
50

Sarcoma botryoides- a type of rhabdomyosarcoma from submucosal tissue. 57
Scrotum- pouch below the penis which holds the testicles. 21 Seminal products- pertaining to semen, ejaculate. Septal remnant- small tag attached to the edge of the hymen. 21
Septate (hymen or vagina)- band(s) of tissue that creates two openings (of the hymen) or two vaginas. 21
Serologic- pertaining to antigen-antibody reactions. 57
Shaft (of penis)- long, slender part. 21
Sloughed- a layer cast off. 57
Speculum- an instrument used to open a body orifice to allow visual inspection. 57
Semen acid phosphatase- substance present in semen. 25
Sphincter- a ring-like muscle. 57
STI- sexually transmitted infection. Submucousal- just below a mucous membrane. 57
Subpoena- a written legal order to appear in court to testify. 56
Superficial- on the surface. 56
Supine- face up. 57
Symmetrical- a balance to corresponding parts. 56
Syphilis- infection caused by the Treponema pallidum spirochete usually sexually transmitted. 21
Tag- a projection of tissue from the hymen or the anus. 21
Testicles- the male sex organ that produces sperm and testosterone (male hormone) encased in the scrotum. 21
Toluidine blue dye- a blue dye that adheres to denuded areas of mucous membranes. 57
Transection (hymenal)- cutting or tearing across, strict definition implies a complete tear. 21
Trichomonas vaginalis- infection with a single celled protozoan, usually sexually transmitted. 21
Ulcer- a defect usually caused by sloughing of tissue. 57
Urethra- the canal that carries urine from the bladder to the exterior of the body. 57
Urethral prolapse- protrusion of the inner lining of the urethra to the outside of the body. 57
Vagina- the canal in the female between the vulva and the cervix that receives the penis during coitus. 21
Vaginitis- inflammation of the vagina. 57
Vaginoscopy- placement of a small scope with a camera attached into the vagina for inspection. 57
Varicella- viral infection that causes ulcers of the mucous membranes. 57
Vascularity- dilation of blood vessels near the surface of skin or mucous membrane. 57
Venereal warts- viral tumor caused by the human papilloma virus which can be transmitted sexually. 57
Venous congestion- superficial collection of blood in the veins causing a purplish discoloration to the tissues. 57
Vertical transmission- transmitted to the fetus prior to or at the time of birth. 57
Vesicle- a small, membrane bound sac. 57
Vestibule- the cavity within the vulva containing the vagina, urethra and ducts of glands. 21
Vestibular bands- supporting bands of the vestibule. 21
51

Victim Sensitive Interview- a child friendly, non-leading, legally sound interview of a child who has experienced trauma.
Viscous lidocaine- local anesthetic. Vitiligo- a skin condition causing destruction of the pigment cells causing
patches of pale or white skin. 57
Vulva- the external genitalia of the female. 21
Vulvar coitus- rubbing the penis between the labia without penetrating the vagina. 21
Vulvar pemphigoid- skin condition affecting the mucous membranes. 57
Vulvovaginitis- inflammation of the vulva and vagina. 57
WBC- white blood cell, associated with inflammation. 57 Wet prep- laboratory test using saline and vaginal secretions looking for
WBC’s, clue cells, spermatozoa and yeast.
52





























