Embed Size (px)
Citation preview
MARKETIZATION, MANAGERS AND MORALSTRAIN: CHAIRMEN, DIRECTORS ANDPUBLIC SERVICE ETHOS IN THE NATIONALHEALTH SERVICE
ROD SHEAFF AND MICHAEL WEST
Survival of the public service ethos in Britain has been called into question followingintroduction of the ‘new public management’ and marketizing reforms in much ofthe public sector. This article examines how these developments have occurred inthe nhs, using survey data to analyse nhs board members’ substantive ethicalvalues. Unexpectedly the results suggest that nhs board members with a predomi-nantly nhs background appear less ethically conservative, more flexible and lessrisk-averse than those recruited from non-nhs backgrounds; and that as yet thenhs management ‘culture’ is not very homogenous in respect of ‘business ethics’.The nhs reforms also appear to accentuate the tensions between transparent publicaccountability in nhs management and incentives not to publicize certain types ofinformation. Recent codification of nhs ‘business ethics’ can be understood as anattempt to buttress the public service ethos against the increased moral strains ofa quasi-market.
SIGNS OF MORAL STRESS
As an alternative to the conventional privatization favoured elsewhere inthe public sector, nhs reform has focused on creating public-sectorcounterparts of the organizational forms, competition and contractingfound in conventional markets. Yet nhs bodies will mostly remain in thepublic sector and the nhs internal market is susceptible to being ‘managed’or ‘planned’ by the nhs Executive. Not only does the government havehealth policy reasons for wishing to retain a measure of control over thenhs but, on the experience of the last general election, the nhs reformsare a potential electoral liability (Guardian poll, 14 September 1992, table 4).A recent illustration of government sensitivity was the way in which minis-ters publicly distanced themselves from the Healthcare 2000 proposals forfurther marketization of the nhs (Guardian 19 and 20 September 1995;Healthcare 2000 1995). Governments thus confront a health policy dilemma:how to reconcile increasingly flexible nhs management, greater autonomy
Rod Sheaff is a Fellow in the Health Services Management Unit, Manchester University and MichaelWest is Professor in the mrc/esrc Social and Applied Psychology Unit, University of Sheffield.
Public Administration Vol. 75 Summer 1997 (189–206) Blackwell Publishers Ltd. 1997, 108 Cowley Road, Oxford OX4 1JF, UK and 350 Main Street,Malden, MA 02148, USA.
190 ROD SHEAFF AND MICHAEL WEST
for nhs purchasers and providers and competition with requirements formanageability of the nhs, for public accountability, and for political man-agement of an electorally visible part of the public sector.
The so-called ‘strategy of managerialism’ pursued since the first Griffiths‘report’ (Griffiths 1983) involved the attempt to create a new managerial‘culture’ in the nhs that would enable nhs activity to grow faster thannhs spending (cp. Flynn 1992, pp. 27–8) and shift the apparent source ofdecisions about resource ‘priorities’ (‘rationing’) from government (anddoctors) onto nhs managers. Since 1979 UK government has anywaytended to favour private sector management styles and culture (Flynn 1992,pp. 193–4), although public debates have often made crudely stereotypicalcontrasts between adaptable, dynamic, entrepreneurial private sector man-agement styles and bureaucratic, cautious, inflexible, rule-bound public sec-tor management. (Empirically nhs management behaviour is of coursemore complex: see Harrison et al. 1992; Dawson et al. 1995.)
A first attempt to recruit senior nhs managers from the private sectorduring implementation of the first Griffiths report (1983–5) largely failedbut a second opportunity came in recruiting the chairs, chief executives,executive directors and non-executive directors of nhs trusts and healthauthorities after 1989 (for short, chairmen, non-executive directors andexecutive directors are collectively referred to as ‘board members’ below).Besides overseeing the new internal market institutions the first (1991) gen-eration of board members had the tasks of continuing the implementationof the nhs reforms, cost improvement programmes and the ‘strategic shift’of resources from inpatient services toward ambulatory and communitycare. They therefore also faced the political difficulties and ethical dilemmasthat this transition entailed.
Meanwhile the term ‘sleaze’ entered British political vocabulary. Some‘sleaze’ was of a purely personal nature and some concerned private notpublic sector organizations, prompting the Cadbury report (Report of theCommittee on the Financial Aspects of Corporate Governance 1992). Othercases called the ethos of public administration into question: the Scottinquiry; payments for questions in the House of Commons; conflicts ofmps’ interests; and mismanagement of various quangos. Competitivetendering, outsourcing, the use of consultancies, privatizations and man-agement buyouts exposed public sector managers in general to greateropportunities for self-enrichment, fraud or corruption while increasingworkloads created new incentives and pressures for them to ‘cut corners’.Attempts to reduce the cost of public sector management allegedly weak-ened or removed ‘traditional’ mechanisms for ensuring integrity (Doig1995, pp. 197–9, 206). Government, its appointees and supporters in publicsector management also faced electoral and public relations incentives topublicize ‘successes’ and to gloss over any ‘failures’ of the marketizationpolicy. Performance-related pay, fixed-term contracts and individual per-
Blackwell Publishers Ltd. 1997
MARKETIZATION, MANAGERS AND MORAL STRAIN 191
formance review were giving many public sector managers financial andcareer incentives to do likewise.
In the nhs, Wessex rha’s waste of £20m on the risp information sys-tem became notorious (Guardian 25 July 1992). A district auditor’s reporton West Midlands rha concluded: ‘individually, many members wereaware to differing degrees of significant developments which: a) the Boardneither debated nor authorised b) were contrary to standing orders c) com-mitted the rha to spend over £10 million on projects which turned out tobe of little long term value’ (nhsme 1993b).
Also ‘standing orders were largely ignored. The orders themselves werebadly drafted and in need of revision’ (nhsme 1993b). National news-papers also scrutinized alleged relationships between Arthur AndersenConsulting (who had substantial nhs contracts) and leading ConservativeParty members (Guardian 20 December 1993) and ten health authoritiesreportedly made £813,000 of improper redundancy payments to staff dur-ing 1983 (Guardian 17 September 1994). During restructuring of the Londonnhs, Charing Cross Hospital reportedly drafted a business plan aimed at,among other things, ‘destabilizing’ one of its competitors (Evening Standard5 July 1994, p. 1). A long-standing controversy was re-ignited by researchsuggesting that in pursuit of private practice many nhs consultants wereroutinely neglecting their nhs duties (Yates 1995).
‘Economies with the truth’ about the effects of the nhs reforms alsoemerged. In the electorally sensitive matter of nhs waiting lists, data defi-nitions were changed (activity now being measured in ‘completed consult-ant episodes’ not ‘patient episodes’, yielding higher activity figures);patients waiting over two years for treatment by special health authorityhospitals were excluded from the totals; and waiting lists were ‘weeded’(Seng, Lessof and McKee 1993; Anon 1993). Some letters of public supportfor nhs trust applications in North London were in fact forged by man-agers (Guardian 2 November 1991). The Health Services Journal criticized thenhsme’s The nhs Reforms. The First Six Months (nhsme 1991), not onlyfor its content (mentioning only the successes and not mentioning that eventhese could be attributed to unusually generous funding in a pre-electionyear) but for its distribution. Advance copies were sent to pro-Conservativenewspapers such as the Daily Express and Daily Mail but not to the lesspartisan professional journals (Anon 1992). Cases of nhs managersattempting to silence ‘whistleblowers’ such as pathologist ChristopherChapman and nurse Graham Pink were also reported (Guardian 18 July1992 and 3 July 1992). A leaked nhs management internal discussion (notpolicy) document raised the question of how nhs managers should dealwith ‘“renegades, subversives and opposers of what is being attempted”’(Independent, 2 December 1991).
In response the nhsme (later renamed ‘nhs Executive’ (nhse)) estab-lished a ‘task force’ on corporate governance (House of Commons 1993;Department of Health 1993a) whose terms of reference were to review
Blackwell Publishers Ltd. 1997

192 ROD SHEAFF AND MICHAEL WEST
aspects of nhs corporate governance, in light of the Cadbury report andgood practice in other organizations. The internal nhsme announcementof this explained that ‘The independence of chairmen and non-executivedirectors from the chief executives and other non-executive directors willbe critical to any defence of accountability and the traditional standards ofconduct of public business in the post-reforms nhs’ (Department of Health1993b, §7). To inform the task force’s work, a survey of current attitudesto issues of probity was conducted among all chairmen, executives andnon-executives on rhas, dhas, fhsas and nhs trusts. It shed someunexpected light on present-day nhs managerial ‘culture’.
RESEARCH METHODS
The research method was a survey of all English nhs board members, i.e.the chairs, executive directors and non-executive directors of nhs healthauthorities (Regional, District, Special and Family Health Authorities) andtrusts. Among other topics the survey examined attitudes to: contractingwith suppliers; acceptance of gifts by nhs employees; hospitality; privatepersonal gain obtained in the course of nhs work; declaration of interests;commercial sponsorship; and conflicts of interest. These topics were allissues which had arisen in cases of alleged impropriety in public adminis-tration during the previous three years. In response to each of 53 items,board members were asked to indicate whether particular behaviours wereethically permissible on a five-point scale ranging through (1) ‘never per-missible’; (2) permissible ‘in exceptional circumstances only’; (3) ‘It dependsentirely on the situation’ whether permissible; (4) permissible ‘in most, butnot all circumstances’; and (5) ‘Always permissible’. Respondents also hadthe opportunity to indicate a ‘Don’t know’ category.
In a critical letter written after the research was concluded, a board mem-ber who had refused to respond pointed out that ‘Each of the statementswe were asked to rule on was capable of wide interpretation, and it wasnot possible to say many were “never permissible” as usually someinterpretation would allow it’ (Bedford 1994). This point about how to inter-pret the questionnaire results had also occurred to the researchers. So, thequestionnaire was followed up by a small amount of qualitative researchconducted by interview and intended to check the interpretation of the sur-vey results.
A letter explaining the purposes of the research, emphasizing confiden-tiality and anonymity, and encouraging a swift response was sent to allpotential respondents. Ten copies of each questionnaire and the explanatoryletter were sent to the chairs of every board in England, who were askedto distribute copies to all their executive and non-executive directors. Parti-cipants were asked to complete and return the questionnaires within threeweeks (so that answers could be processed within an nhsme deadline).Approximately 6,000 questionnaires were sent out and it is estimated that
Blackwell Publishers Ltd. 1997
MARKETIZATION, MANAGERS AND MORAL STRAIN 193
over 5,000 were received in time for board members to complete and returnthem. Some 2,600 completed questionnaires were received in time for analy-sis, representing a response rate of around 50 per cent. This is a highresponse rate for a mailed survey, especially in the short time availablefor responses.
Data were collected and held in ways which absolutely preserved respon-dents’ anonymity. No identifying information was collected and code num-bers were not used. Besides responding to the 53 questionnaire items,respondents were asked to indicate the most important and most difficultethical issues which they faced in their nhs work. Their responses weresubjected to category analysis.
The survey results described below pose several questions. Why didrespondents’ attitudes differ about what behaviour is ethically acceptablein certain circumstances? Why did some respondents take a comparativelypermissive view of the issues raised in the questionnaire? And why didattitudes differ between respondents with working backgrounds predomi-nantly outside and predominantly inside the nhs? To explore these ques-tions a file sample of 20 board members was selected for semi-structuredinterview, intended to provide a qualitative interpretation of some of therespondents’ survey answers. The structured element of the interview con-sisted of three scenarios with questions, the unstructured element beingfollow-up questions to check the interviewer’s understanding and toencourage respondents to amplify answers. The scenarios wereanonymized versions of real cases, selected to cover the issues on whichthe questionnaire results showed the widest divergence of opinion. Inter-viewees’ identities were obviously known to the interviewer but the resultswere collated in an aggregated, anonymous form.
RESULTS
The ‘Don’t know’ category in the questionnaire was rarely used, suggestingthat respondents had definite views about issues of probity. Figure 1 shows
Percentage average ofresponses
1. Honesty 22.82. Value for money 17.93. Conflicts of interest/personal gain 15.04. Fairness to patients 9.75. Financial honesty 6.06. High quality of care 5.27. Openness of decision-making/fairness to staff 4.48. Interactions with suppliers 2.99. Maintaining confidentiality 2.6
10. Other 8.9
FIGURE 1 Most important ethical issues that board members confront
Blackwell Publishers Ltd. 1997

194 ROD SHEAFF AND MICHAEL WEST
the categories of ethical issues which board members identified and thepercentage of responses falling within each. The most frequently used cate-gory was honesty. Responses referred to the need for board members tobe seen to be honest and publicly accountable for all decisions; for opennessand honesty in all contractual matters; for everything to be open to scrutiny;to be seen to follow correct procedures; to prevent corruption and financialfraud; and to maintain ethical integrity.
The second category board members most frequently used was value formoney. Board members were concerned about spending of scarce resourcesto ensure adequate provision of good care and treatment; spending in themost ethically correct and effective way; choices between spending on dif-ferent types of patient care; and maximizing good quality patient carewithin cash limits. Conflicts of interest over personal gain was the thirdcategory most frequently mentioned. It referred to pressure, influence and(financial and political) self-interest; to declaration of interests; to non-executives not using appointments to influence personal business; to con-flicts of interests between public and private interests; to personal use ofnhs facilities; and to collusion with suppliers. Fairness to patients was thenext most frequently cited category and this referred to protecting nhs
users’ rights; providing equality of treatment for all patients; fair allocationof resources; and awareness of needs of minority groups. Financial honestyaccounted for 6 per cent of responses and referred to the need to maintainprobity throughout the organization and ensure personal financial probity.
High quality of care was also mentioned by several board members. Thiscategory referred to maintenance of good medical practice and high qualityof service. Openness of decision-making, interactions with suppliers, main-taining confidentiality and fairness to staff were other issues raised byboard members. Board members were also asked to indicate what were themost difficult ethical issues they had to confront during their work. Higheston the list is conflict of interest over personal gain, accounting for 19.7 percent of responses (figure 2). This category referred to issues such as extra-organizational alliances affecting personal judgement; using knowledge ofcontracts outside the hospital in decision-making; or improper use of infor-
Percentage of responses
1. Conflicts of interest/personal gain 19.72. Determining treatment priorities 19.23. Disciplinary procedures 8.14. Flexibility interpreting rules 7.95. Public accountability/honesty 7.76. Fairness to all staff 6.17. Ensuring rules/decisions carried out 5.28. Conflict between private and public work in nhs 4.39. Rationalization 4.3
10. Other 17.4
FIGURE 2 Most difficult ethical issues that board members confront
Blackwell Publishers Ltd. 1997
MARKETIZATION, MANAGERS AND MORAL STRAIN 195
mation. The second most frequently cited category was determining treat-ment priorities. It covers cash control and decisions about which types oftreatment to fund and which not to; balancing financial restraints with pub-lic health needs; judgements about health gains; and determining prioritiesand choices between services.
Disciplinary procedures were also high on the list, including determiningconditions for disciplining or dismissing staff; assessing staff competence(especially that of medical staff) and taking appropriate action; dealing withmisconduct by doctors; professional competence of doctors and nurses; sev-erance payments in cases of incompetence or medical negligence; and ter-minations of employment for a cash settlement.
A number of board members referred to the need for flexibility in inter-preting rules to achieve the best for the nhs; and to avoid bureaucracy.Several respondents thought it desirable not to follow government direc-tions blindly but to consider what is good for the patient. Other categoriesthat board members considered difficult were being fair to everybodythroughout the organization, especially in relation to inequality of con-ditions and pay between senior and lower ranks. They were concernedabout satisfying and rewarding the aspirations of top executives whilstimposing pay restraints for employees lower down the hierarchy. Otherissues included: ensuring rules and decisions were implemented through-out the organization; rationalization of nhs services; and conflict betweenprivate and public work within the nhs. The latter is directly relevant tothe role of private medicine and the nature of nhs–private sector collabor-ation. One respondent referred to it as ‘running two agendas’.
Although some board members indicated cautiously conservative atti-tudes towards issues of probity or honesty, there was considerable variationin their responses to questionnaire items. On four of the 53 questionnaireitems there was more than 90 per cent agreement that particular practiceswere ethically ‘never permissible’. These items included ‘Allow a supplierin which one is a shareholder or director to tender for nhs work withoutdeclaring one’s interest’ (97 per cent agreement); ‘Omit to tell those appoint-ing an nhs director that a candidate is your near relative’ (91 per centagreement); ‘Use nhs money for entertaining nhs colleagues for non-nhs purposes’ (93 per cent agreement). However, the most striking aspectof the results is how very different the opinions of board members were.
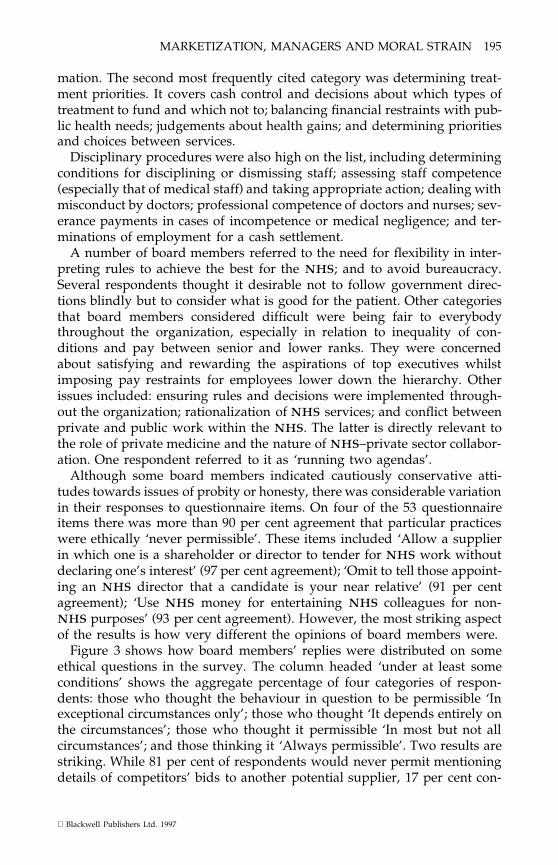
Figure 3 shows how board members’ replies were distributed on someethical questions in the survey. The column headed ‘under at least someconditions’ shows the aggregate percentage of four categories of respon-dents: those who thought the behaviour in question to be permissible ‘Inexceptional circumstances only’; those who thought ‘It depends entirely onthe circumstances’; those who thought it permissible ‘In most but not allcircumstances’; and those thinking it ‘Always permissible’. Two results arestriking. While 81 per cent of respondents would never permit mentioningdetails of competitors’ bids to another potential supplier, 17 per cent con-
Blackwell Publishers Ltd. 1997
196 ROD SHEAFF AND MICHAEL WEST
Behaviour Never Permissible underpermissible at least some
% conditions %
Sign contracts permitting expenditure first, and get 51 49authorization afterwards
Award severance or redundancy pay to directors or 53 43staff when they are known to be taking up anothernhs post immediately
Agree normal severance payments to a professional 43 56in your organization to avoid disciplinary proceduresfor professional incompetence/lack of probity/pursuitof personal gain
Turn a blind eye to infractions of rules or standing 53 46orders when these are in the nhs organization’sinterests
Undertake personal work (e.g. consultancy) for firms 43 55one has contact with through work with the nhs
Spend more than £5 per person on alcohol at a 38 59dinner/function at the expense of the nhs
Omit from the annual report serious problems with 60 38service quality which have been confronted in thepast year
Invite nhs staff to do work for oneself out of hours 36 62
Accept the gift of a study tour to a health care 65 34management conference abroad from a potentialsupplier
Discuss informally the possibility of privatizing parts 32 63of the organization before the arrangements anddecisions are finalized
Use nhs hospitality budgets to reward deserving 31 66members of staff in kind
Mention major gains of new business but not major 66 30losses of existing business in the annual report
Work as a consultant to a prospective purchaser of 70 29nhs assets
Become director to a supplier to the nhs whilst still 75 24an nhs director
Omit to declare every business connection (e.g. 81 17consultancies with a value less than £500) with nhs
organizations
Mention details of competitor’s bids in discussions 81 17with potential suppliers
Let business associates know informally of the 82 16organization’s intention to dispose of assets (e.g.land, housing) before tenders are published
Pay more than £50 per night hotel expenses for 9 88visits on nhs work
Use nhs resources for private work 44 50
FIGURE 3 Divergences in nhs board members’ ethical views (rounded percentages ofrespondents)
Blackwell Publishers Ltd. 1997
MARKETIZATION, MANAGERS AND MORAL STRAIN 197
sidered it to be permissible sometimes, despite hsg(93)5 of 18 January 1993expressly forbidding such disclosures. A substantial minority of respon-dents were also prepared to by-pass rules and regulations to achieve nhs
goals. Almost half (49 per cent) indicated that they would sign contractspermitting expenditure first and get authorization afterwards in some cir-cumstances. When that was in the nhs interest, 46 per cent would turn ablind eye to infractions of rules or standing orders. The separate last rowin figure 3 summarizes board members’ responses to seven questions aboutthe permissibility of using various nhs resources (secretarial time; infor-mation; software; copyright materials; and money) for one’s own privatework. Here too board members’ ethical views diverged: 92 per cent thoughtit was never permissible to use nhs hospitality budgets for non-nhs pur-poses but only 41 per cent thought this about making private use of nhs
information in articles or books.
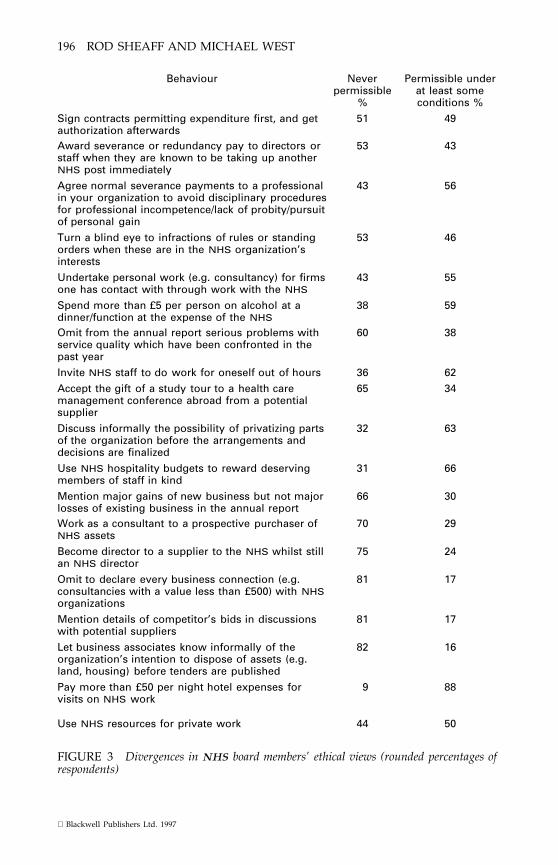
In order to compare chairs’, executives’ and non-executives’ responses soas to examine where the most marked differences lay, a total probity scorewas calculated by adding together responses to all the items on the ques-tionnaire. It was found that chairs had statistically significantly lower scoresthan non-executive board members (figure 4), who in turn had significantlylower scores than executive board members. In other words, chairs werethe most rigorous in their views and executives, the most permissive. Also,board members whose working experience had been predominantly in thenhs had significantly higher probity scores (i.e. were more permissive)than other board members.
A new feature of the 1991 reforms is the heterogeneous membership ofnhs boards. Many nhs executive directors have gained the majority oftheir previous work experience within the nhs and many non-executivesoutside the nhs. We therefore analysed the data according to respondents’
FIGURE 4 Total probity scores for chairmen, executive and non-executive directors*
*Lower scores indicate more ethically conservative attitudes(ANOVA: F = 90.06; df = 2,2523; p = ,0.001)
Blackwell Publishers Ltd. 1997
198 ROD SHEAFF AND MICHAEL WEST
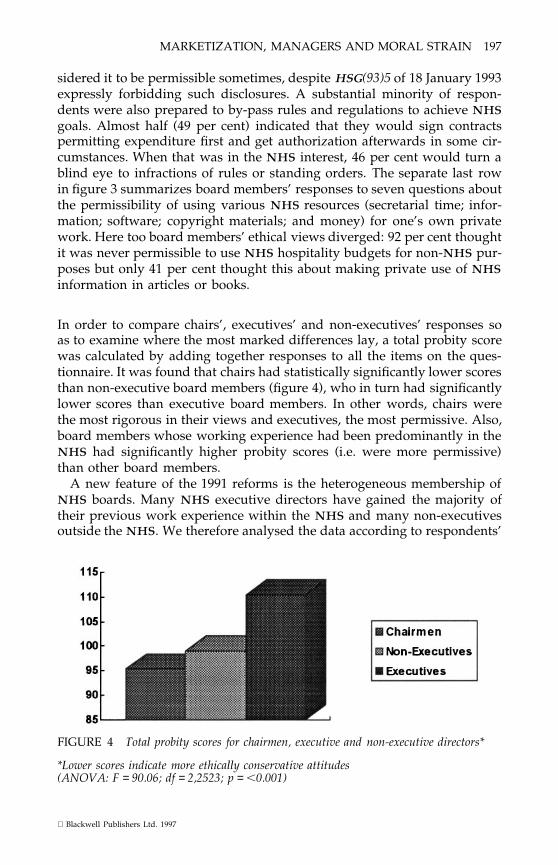
FIGURE 5 Total probity scores by previous work experience category*
*Lower scores indicate more ethically conservative attitudes.(ANOVA: F = 27.12; dF = 4,2427; p = ,0.001)
previous work experience (figure 5). Five principal groups were identifiedas those whose previous work had predominantly been in:
(1) The nhs (899 respondents)(2) Other UK public sector organizations (n = 371)(3) Private commercial organizations (n = 624)(4) Voluntary organizations (n = 210)(5) Self employment (n = 329)
Those whose previous experience had predominantly been in the nhs hadmore permissive attitudes than all other groups. Those whose experiencewas previously predominantly in the voluntary sector were less permissivethan all other groups. These findings were highly statistically significant.
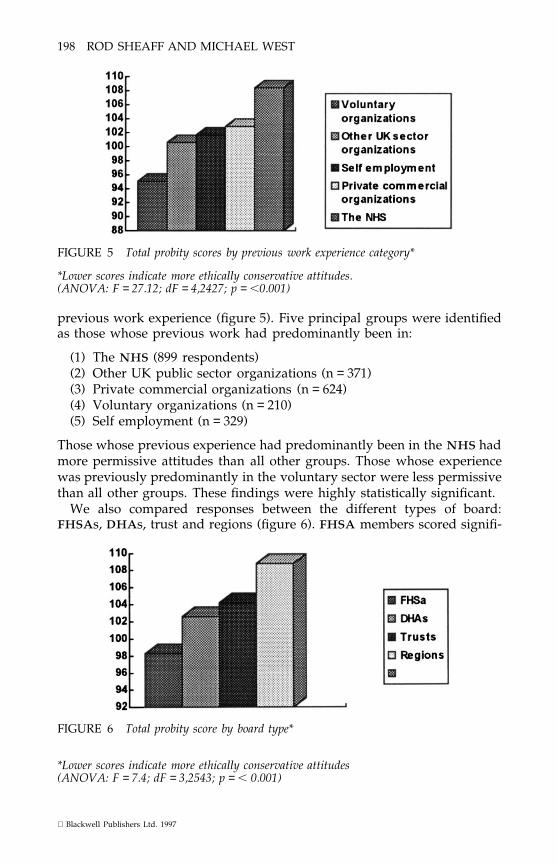
We also compared responses between the different types of board:fhsas, dhas, trust and regions (figure 6). fhsa members scored signifi-
FIGURE 6 Total probity score by board type*
*Lower scores indicate more ethically conservative attitudes(ANOVA: F = 7.4; dF = 3,2543; p = , 0.001)
Blackwell Publishers Ltd. 1997

MARKETIZATION, MANAGERS AND MORAL STRAIN 199
cantly lower than the other groups in terms of total probity indicating thatfhsa members were on average more ethically conservative in their atti-tudes. This finding may be partly explained by the fact that fhsas hadmore non-executive members than other boards did. (fhsas were mergedwith dhas in 1996.) Given our findings that non-executive members tendto be more ethically conservative than executive members, the differencein composition may account for some (but not all) of the variation foundhere. rhas were the least ethically conservative of nhs boards.
The interview findings gave some clues about the reasons for theseresults. Interviewees suggested what circumstances might excuse breachesof nhs rules or standing orders. Sometimes it is simply not practicable tofollow the rules strictly and literally; for instance if only one firm can supplya specific service or piece of equipment it becomes impossible to complywith rules that alternative suppliers should compete for contracts. Someinterviewees argued that board members sometimes have to manage prob-lems which were evidently not anticipated when rules or standing orderswere originally drafted. As examples they cited disciplinary problems andredundancies following the re-structuring of nhs trusts. Some inter-viewees also suggested that in some cases following the prescribed rulestoo scrupulously would cause avoidable harm, for instance by incurringlarge and unwarranted redundancy payments for the trust or authority.Several interviewees stipulated that one should first discuss with the trust’scheif executive or chairman whether the circumstances made it permissibleto breach or by-pass the rules. Some respondents argued that board mem-bers who break nhs rules or standing orders by mistake are less culpablethan those who do so out of self-interest or in order to cause deliberateharm to others.
Without exception the interviewees held that the same rules of probityshould apply to both public and private sectors; but if anything, there oughtto be greater accountability for the use of public money than for the use ofshareholders’ money. Interviewees expressed a feeling that nhs managersare more exposed to public scrutiny and criticism for unethical behaviourthan their private sector counterparts are. Several interviewees anticipateda potential dilemma in trying to guarantee probity without over-restrictingmanagerial freedoms or ‘entrepreneurship’ among nhs managers.
DISCUSSION AND CONCLUSIONS
Given the policy context, discussion of these results focuses on the statusof the results themselves; on how to interpret them; on their implicationsfor the availability and credibility of information about implementing thenhs reforms; and on further policy and research questions which theypose.
These results differ from earlier work on corporate governance (forexample, Ashburner et al. 1993; Ferlie et al. 1995) in focusing on the substan-
Blackwell Publishers Ltd. 1997
200 ROD SHEAFF AND MICHAEL WEST
tive ethical values of nhs board members. The results show greater caution(ethical conservatism) in attitudes than is truly the case, because peopletend to respond to this type of questionnaire in ways that they considersocially desirable. The Probity Score is also a fairly simple, ad hoc indicatorof ethical standpoint. Nevertheless the survey results can be taken as rep-resentative of the whole population of nhs board members.
nhs board members evidently see probity as concerning three maingroups of issues. By far the most important to the respondents was arequirement for transparency, accountability and avoiding illicit self-enrich-ment in taking decisions which are potentially open to improper influencefrom the personal interests of the decision-makers. Taken together theissues of ‘honesty’, ‘conflicts of interest/personal gain’, ‘financial honesty’and ‘interactions with suppliers’ account for 46.7 per cent of mentions(figure 1). Obtaining ‘value for [nhs] money’ came second (17.9 per cent).In third place issues about patients’ interests mustered only 14.9 per centof mentions, taking ‘fairness to patients’ together with ‘high quality of care’,rising to 17.5 per cent if one adds the issue of ‘maintaining confidentiality’.(However, board members are more likely to have taken the latter to meancommercial than medical confidentiality.) A similar picture emerges fromresponses about which ethical issues board members found most difficult(figure 2). Together the related issues ‘Conflicts of interest/personal gain’,‘flexibility interpreting rules’, ‘public accountability/honesty’ and ‘ensuringrules/decisions carried out’ accumulated 43.2 per cent of mentions. Ethicalissues more directly related to current health policy (‘determining treatmentpriorities’, ‘conflict between public and private work in the nhs’ and‘rationalization’) together accounted for only 27.8 per cent.
There are two possible interpretations of this. One is, that nhs boardmembers’ views as to which ethical issues are most ‘important’ and ‘diffi-cult’ simply differ from the priorities expressed in Working for Patients andsubsequent policy statements, which emphasize patients’ interests andvalue for money (in that order) as rationales for the nhs reforms(Department of Health 1989). By contrast nhs board members’ ethical con-cerns appear to focus more upon preventing illicit self-enrichment throughnhs transactions than upon the ethical implications of current health pol-icy. An alternative interpretation might be that respondents took the phrase‘most important ethical issue’ to mean ‘ethical issues which board membersmost often encounter in practice’ rather than ‘ethical issues with the mostweighty consequences’. In that case the issues of maintaining transparencyand preventing illicit self-enrichment in nhs transactions may haveseemed more difficult to deal with precisely because board membersencounter them more often than other ethical issues. Either way, the resultsare indirect evidence that in practice nhs board members’ ethical attentionis more oriented towards managerial decisions than towards the health pol-icy of the trust or authority.
Of all nhs board members it is the chair who is ultimately accountable
Blackwell Publishers Ltd. 1997
MARKETIZATION, MANAGERS AND MORAL STRAIN 201
for any lapses in probity which may explain why their probity scores arenoticeably less permissive than other board members (figure 4). Possiblythe difference also reflects different working backgrounds of chairs andother board members (figure 5). Of chairs 87.1 per cent reported previousworking experience predominantly outside the nhs, but only 52.3 per centof other board members.
Approximately a third of respondents saw no objection in principle toslanting their trust’s or authority’s annual report away from ‘bad news’about their organization’s performance. This finding suggests that a size-able minority of board members see the nhs annual reports more as apublic relations tool than as a means for public accountability or for a criti-cal overview of their organization’s work. (It also implies that futureresearchers should be cautious in using these reports as source material).
Three rather unexpected conclusions also emerge. Although somerespondents thought the survey unnecessary or that the answers to theethical questions were obvious, and few used the ‘don’t know’ category onthe questionnaires or in interview, the research indicates a considerablerange of opinion amongst nhs chairs, executive and non-executive direc-tors about what is the right way to act personally or in dealing with othersin the conduct of their nhs work. The extreme case was the question ofwhether it is legitimate to by-pass nhs rules or regulations if nhs interestswere thereby served. On this, respondents divided almost equally. How-ever a substantial minority of 20 per cent or more of the respondents dis-agreed with the majority view in respect of another 13 of the 53 issueswhich the survey covered. In ethical matters nhs managerial ‘culture’ isevidently not so homogeneous as the formal policy statements, codes andregulations – not to mention some nhs board members – might suggest.
Second, this research challenges the stereotype that directors and man-agers with a private sector background are more flexible, willing to bendrules and take risks to achieve quick results than directors and managerswith an nhs background are. Executive members, who mainly work fulltime for the nhs and are more likely than other board members to havespent the bulk of their working life in the nhs, had significantly higherProbity Scores (i.e. were more permissive) than non-executive members andchairs, who do not (figure 4). (Of executive directors, 82 per cent as against14 per cent of non-executives and only 7 per cent of chairs had spent thebulk of their working life in the nhs.) The difference was most markedon the questions of whether it is permissible to ‘Agree normal severancepayments for professional staff in your organization to avoid disciplinaryprocedures for professional incompetence/lack of probity/pursuit of per-sonal gain’ and whether it is permissible to use charitable trust funds topay for nhs facilities.
A third stereotype which our results challenge is the idea that recruitingboard members and managers with a non-nhs background can simply beequated with a relaxation of ethical standards (nhsme 1994, p. 8).
Blackwell Publishers Ltd. 1997
202 ROD SHEAFF AND MICHAEL WEST
How are these unexpected results to be explained? The research and theevents noted above suggest the following possible explanations which weoffer only provisionally, as hypotheses for further testing.
The diversity of nhs board members’ ethical views is more probably anindication of uncertainty than of moral laxity. It probably arises from thediversity of backgrounds and experience of those working on boards,apparently leading to a spectrum of views about what is ethically appropri-ate in the conduct of nhs business. But since a degree of diversity in theethical opinions of any group of new recruits to an occupation is probablyinevitable, this finding only raises the further question of why this diversitypersists among chairs and non-executive directors. Earlier research for thenhsme found that ‘the biggest discrepancy was between information[which new chairs and non-executive directors] received and that requiredon principles of corporate governance . . . almost none had received anysuch training prior to or since taking up their positions’ (Hardy and West1993, p. 10). Until the present research, little attention had been given todevising or promulgating ethical codes for nhs managers, although thisposition is changing. One might also hypothesize that the differences inresponse between those coming from outside the nhs and chairs and direc-tors whose working origins are inside the nhs, might partly reflect agreater sensitivity to public exposure and scrutiny on the part of those whohave worked outside the nhs for long periods; in contrast to a desensitiz-ation to it of those from within.
nhs managers have been expected since the first Griffiths report (1983)to work in increasingly entrepreneurial, flexible ways but within a frame-work of law, regulations and standing orders that still reflects an older,more rigid conception of public administration; and under increasinglybureaucratized and centralized managerial control (‘general management’,‘performance-related pay’, ‘individual performance review’). Neverthelessthe reformed nhs structures and managerial relations do increase man-agers’ discretion, creating new occasions for ethical uncertainty or even newopportunities for unethical behaviour. Conflicting pressures of these kindsmight be expected to produce ambivalence of attitudes and ethical views;and increase the tensions between rules or standing orders and the practicalexigencies of managing the nhs. There is also some evidence that policy-makers, media and management educators have promulgated unrealistic,ideologically coloured role models of private sector management to nhs
managers. For want of much contact with real private sector managers onemight conjecture that some nhs managers take these role models ratherliterally, ending up ‘more royalist than the king’.
In summary, there is considerable variation in attitudes towards issuesof probity amongst chairs, executive directors and non-executive directorsworking in rhas, dhas, fhsas and trusts. The research indicates thatthose whose previous work experience is largely outside the nhs, parti-cularly those from voluntary organizations, are likely to have more cau-
Blackwell Publishers Ltd. 1997
MARKETIZATION, MANAGERS AND MORAL STRAIN 203
tiously conservative attitudes towards issues of probity than those whoseprevious work experience has predominantly been within the nhs.Assuming that managers’ working practices correspond to their opinionsabout ‘business ethics’, it suggests that board members with a predomi-nantly nhs background are likely to be slightly less conservative, moreflexible and less risk-averse than those with a predominantly non-nhs
background. This casts doubt on the truth of the stereotypes of differentmanagerial styles which has tacitly underlain the ‘strategy of mana-gerialism’ for the nhs. It also suggests that as yet the nhs has no hom-ogenous management ‘culture’ in respect of ‘business ethics’.
AFTERMATH
After the task force reported (nhsme 1993d), nhs management startedto increase the provision of training for new board members (supported bysuch materials as Audit Commission 1995) and began more formal codifi-cation of nhs ‘business ethics’. The resulting codes of conduct and ofaccountability emphasize the general principles of probity, openness andaccountability (Department of Health 1994; nhsme 1993d, p. 10; nhsme
1994; nhse 1995a; nhse 1995b). The Institute of Health Services Manage-ment also published its Statement of Primary Values, fourteen somewhatanodyne points such as: ‘In making decisions and taking actions, managerswill respect the dignity of every individual’ or expecting managers to ‘useprocesses which are open’ and to ‘take personal responsibility’ (ihsm
1994). The new codes do address the issues which, according to the presentresearch, nhs board members find the most difficult and important, andother issues besides, but with one noteworthy exception.
New methods for appointing nhs chairmen and non-executive directorswere introduced in April 1995 (Department of Health and nhse 1995),using a national standard job description for non-executive directors and aperson specification. Board vacancies are now advertised. A sifting panelscreens the resulting applications and takes up references. Ministers makethe final decision on whom to appoint.
In respect of financial probity, one of the earliest pieces of post-reformguidance reiterated nhs employees’ legal duties: not to favour or disfavourpotential contractors for inducement or reward; not to use their nhs posi-tion for personal gain; to maintain commercial confidentiality; to refuse‘linked deals’ in which sponsorship is tacitly a reward for buying from thesponsor; and to declare any interests they have in potential contractors,especially private nursing homes or hostels (nhsme 1993a). They werealso reminded to declare any conflict of interests arising from employmentoutside the nhs. The noteworthy exception is private practice by (medical)consultants, which was expressly excused from this requirement. Privatemedical practice is still governed by an older policy document (dhss 1986)although that too is currently under revision (Department of Health 1995).
Blackwell Publishers Ltd. 1997

204 ROD SHEAFF AND MICHAEL WEST
Otherwise little has been done, apart from the publication of a tangentiallyrelevant report on pricing in private practice (by the Monopolies and Merg-ers Commission not the nhse (mmc 1994)) to review this conflict of inter-ests.
Subsequent nhs policy guidance has recognized the right and duty ofpotential ‘whistle-blowers’ to ‘raise matters of concern’ without fear of pen-alty. However: ‘Employees also have an implied duty of confidentiality andloyalty to their employer. Breach of this duty may result in disciplinaryaction, whether or not there is a clause in their contract of employmentexpressly addressing the question of confidentiality’ (nhsme 1993c, §9).Before informing the mass media about ‘matters of concern’, nhs
employees are first expected to exhaust an informal procedure, a formalprocedure and an appeal to a ‘designated officer’, all intended to deal withsuch issues internally not publicly (nhsme 1993c, para. 28). Ultimately,however, ‘An employee who has exhausted all the locally established pro-cedures . . . might also, as a last resort, contemplate the possibility of dis-closing his or her concern to the media. Such action, if entered into unjust-ifiably, could result in disciplinary action and might unreasonablyundermine public confidence in the Service’ (nhsme 1993c, §27). Sub-sequently an Audit Commission survey found that a third of the nhs staffit interviewed said they would take no action if they discovered an ‘impro-priety’ for fear of losing their job as a result (Audit Commission 1994). Asyet the task force’s recommendation for a ruling on whether to allow ‘gag-ging clauses’ in nhs contracts of employment has not been met (nhsme
1993d, p. 31). In June 1995 a Code of Practice on Openness in the nhs wasimplemented, listing seven main categories of information which trusts andhealth authorities must publish, and lists of types of information which‘may’ be published or ‘be available on request’ (el(95)42 4 April 1995;nhse 1995a; nhse 1995b). However it reserves the right to withhold‘management information, where disclosure would harm the proper andeffective operation of the nhs organization’ (nhse 1995a, p. 6). From1 April 1996 nhse regional offices replaced regional health authorities, thecode of practice on access to government information, not the nhs codeof practice, becoming their policy on open information.
Although the mere recruitment of managers and board members fromnon-nhs backgrounds does not in itself have that effect, and although theWessex and West Midlands cases predate the current nhs reforms (Ferlie,Ashburner and Fitzgerald 1995, p. 376), these responses implicitly acceptthat creating a quasi-market in healthcare increases nhs board members’and employees’ exposure to conflicts of interest, and opportunity for fraudand self-enrichment. They also tacitly recognize that the nhs reformsaccentuate the tensions between accountability and transparency in publicadministration (on the one hand) and political and commercial incentivesto conceal information (on the other). Codification of nhs business ethicscan therefore be understood as an attempt to buttress the public service
Blackwell Publishers Ltd. 1997

MARKETIZATION, MANAGERS AND MORAL STRAIN 205
ethos against the increased moral strains of a quasi-market. However,another policy response is possible. Recent health policy documents claimthat the nhs reforms are the latest in ‘a series of measures to improvethe way the nhs is managed’ (Department of Health 1989, p. 3) whilst‘maintaining the principles on which it was founded’ (Margaret Thatcher’sforeword to Department of Health 1989); and that government intend thenhs to remain a ‘managed’ or ‘planned’ quasi-market. In that case anothersolution would be to ‘manage’ or ‘plan’ (or redesign) the organization andstructure of the nhs internal market in new directions, neither bureaucraticnor commercial, so as to reduce these strains at source rather than tryingto buttress its public service ethos against commercializing forces whichexpose it to permanently increased strain.
ACKNOWLEDGEMENT
The survey element of the research described here was sponsored by thenhsme whose support we gratefully acknowledge. However the authorsemphasize that the narrative and conclusions expressed here are purely ourown; in no way should they be taken as representing an nhse standpoint,nor the standpoint of any other nhs body or the Department of Health.We are also grateful to David Golya and Jan Williams for checking ourstatistical calculations.
REFERENCES
Anonymous. 1992. ‘Editorial’. Health Services Journal 23 Jan.—. 1993. ‘Editorial’. The Health Summary x, 2, Feb.Ashburner, L., Fitzgerald, L. and Ferlie, E.B. 1993. Leadership by boards in health care. Bristol: nhstd.Audit Commission. 1994. Protecting the public purse 2, Ensuring probity in the nhs. London: hmso.—. 1995. Taken on board. Corporate governance in the nhs: developing the role of non-executive members. Lon-
don: hmso.Bedford, A. 1994. ‘Letter’. Health Services Journal 10 March, p. 20.Committee on the Financial Aspects of Corporate Governance. 1992. The financial aspects of corporate govern-
ance. London: Gee and Committee on the Financial Aspects of Corporate Governance (the Cadburyreport).
Committee on Standards in Public Life. 1995. First Report of the Committee on Standards in Public Life (theNolan report). London: hmso.
Dawson, S., Winstanley, D., Mole, V. and Sherval, J. 1995. Managing the nhs. A study of senior executives.London: hmso.
Department of Health. 1989. Working for patients. London: hmso.—. 1993a. Virginia Bottomley announces action to strengthen nhs corporate management. London: Department
of Health Press Release H93/865.—. 1993b. Corporate Governance Task Force: Addressing the task, unpublished paper cgtf/sg.2.—. 1994. Code of conduct. Code of accountability. Leeds: Department of Health.Department of Health and nhs Executive. 1995. The appointment of chairmen and non-executive directors to
nhs authorities and trusts. Guidance on appointment procedures. Leeds: nhse.Department of Health and Social Security. 1986. Management of private practice in health service hospitals in
England and Wales, under hc (86) 4, n.d. March 1986.
Blackwell Publishers Ltd. 1997
206 ROD SHEAFF AND MICHAEL WEST
Doig, A. 1995. ‘Mixed signals? Public sector change and the proper conduct of public business’, PublicAdministration 73, 2, 191–212.
Ferlie, A., Ashburner, L., and Fitzgerald, L. 1995. ‘Corporate governance and the public sector: some issuesand evidence from the nhs’, Public Administration 73, 3, 375–92.
Flynn, R. 1992. Structures of control in health management. London: Routledge.Griffiths, R. 1983. nhs Management enquiry. Letter of 6th October 1983, under HN 84 (13).Hardy, G. and West, M. 1993. Training and induction of chairmen and non-executives. Sheffield: mrc/esrc
Social and Applied Psychology Unit.Harrison, S., Marnoch, G. and Pollitt, C. 1992. Just managing. Power and culture in the National Health Service.
London: Macmillan.Harrison, S. and Goose, M. 1993. ‘Holding on while letting go’, Health Matters (autumn) xv, 6–7.Healthcare 2000. 1995. UK health and healthcare services. Challenges and policy options. London: Healthcare
2000 group.House of Commons. 1993. Written answer to Mr. Julian Brazier, Conservative mp for Canterbury, 12th July,
po 5904/1992/93.House of Commons Committee of Public Accounts. 1993. West Midlands Regional Health Authority: Regionally
managed services organisation; 57th report of the Committee of Public Accounts. London: hmso.Institute of Health Services Management. 1994. Statement of primary values. London: ihsm.Malin, H. 1992. ‘Allocating resources at different service levels’. Jachranka, Anglo–Polish Health Sym-
posium.Monopolies and Mergers Commission. 1994. Private medical services: A report on agreements and practices
relating to charges for the supply of private medical services by nhs consultants. London: mmc.nhs Executive. 1995a. Code of practice on openness in the NHS. Leeds: nhse.—. 1995b. Guidance on implementation of code of practice on openness in the nhs. Leeds: nhse.nhs Management Executive. 1991. The nhs reforms. The first six months. London: nhsme.—. 1993a. Standards of business conduct for nhs staff, under hsg(93)5, 18 Jan.—. 1993b. Chief Executive’s letter to nhs general managers and chief executives, 15 April.—. 1993c. Guidance for staff on relations with the public and the media, under EL(93)51, 8 June 1993.—. 1993d. Corporate governance in the nhs. Report of the Corporate Governance Task Force. Leeds: nhsme
(unpublished).—. 1994. Draft code of practice on openness in the nhs. Leeds: nhsme.—. 1995. Draft: A guide to the management of private practice in nhs hospitals in England and Wales. Leeds:
nhsme.National Steering Group in Costing. 1993. National costing manual. Leeds: nhsme.Seng, C., Lessof, L. and McKee, M. 1993. ‘Who’s on the fiddle’, Health Services Journal 7 Jan., 16–7.Yates, J. 1995. Private eye, heart and hip. Surgical consultants, the National Health Service and private medicine.
Edinburgh: Churchill Livingstone and ihsm.
Date received 13 November 1995. Date accepted 16 October 1996.
Blackwell Publishers Ltd. 1997


![Foretell[ing] Ruin': The Prophetic Ethos of Milton's 'Lycidas](https://img.pdfslide.net/doc/110x75/631c6b387051d371800f7797/foretelling-ruin-the-prophetic-ethos-of-miltons-lycidas.jpg)

























![Uncertainty and Scientific Ethos in the Silent Spring[s] of](https://img.pdfslide.net/doc/110x75/63219923887d24588e03dd24/uncertainty-and-scientific-ethos-in-the-silent-springs-of-.jpg)
