Embed Size (px)
Citation preview
Infant and Child DevelopmentInf. Child Dev. 15: 41–58 (2006)
Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/icd.428
Maternal Expectations about InfantDevelopment of Pre-term and Full-term Infants: A Cross-nationalComparison
Y. van Beeka,*, M.L. Gentab, A. Costabilec andA. Sansavinib
a Department of Developmental Psychology, Utrecht University, The Netherlandsb Department of Psychology, University of Bologna, Italyc Department of Educational and Psychological Sciences, University of Calabria,Italy
In three European regions (The Netherlands, Northern Italy andSouthern Italy) we investigated whether mothers of healthy pre-term infants (n=92) adjust their expectations for the timing ofdevelopmental milestones in the first years of life as compared tomothers of full-term infants (n=140). We examined whether theseadjustments could be seen as reflecting a pessimistic view, aswould be predicted from the ‘prematurity stereotype’ perspective.Partial corrections for prematurity were regularly made, but noindications were found for an overly pessimistic view. Moreover,the differences between the regions in the anticipated timing ofmastery of milestones were larger than the effects of prematur-ity. Copyright # 2006 John Wiley & Sons, Ltd.
Key words: maternal expectations; prematurity; developmental mile-stones
���������������������������
INTRODUCTION
It is widely assumed that parental beliefs concerning infant development andparenting are an important source of influence guiding children’s development(Harkness and Super, 1996; Miller and Goodnow, 1995). Parental beliefs aboutdevelopment contain expectations or goals about what their children can orshould achieve. Such goals may guide parental actions, and if such goals areunrealistic they may lead to disappointment and poor relationships (Goodnowand Collins, 1990). One group of infants for whom parental belief systems may be
Copyright # 2006 John Wiley & Sons, Ltd. Received March 2004Revised 27 April 2005Accepted 4 July 2005
*Correspondence to: Y. van Beek, Department of Developmental Psychology, UtrechtUniversity, PO 80.140, 3508 TC Utrecht, The Netherlands. E-mail: [email protected]
distorted are those born prematurely. Prematurity not only disrupts parentalbeliefs due to the unexpected timing of birth and the initial stressful hospitalexperiences, but also the process of forming expectations for their new infant andengaging in infant care (Goldberg and Di Vitto, 1995).
Prematurity may lead to a belief system in which increased vulnerability andless favourable outcomes are anticipated. This claim derives from a series ofstudies which showed that unfamiliar full-term infants labelled as prematurewere evaluated as being more vulnerable and feeble (Stern and Hildebrandt,1984, 1986; Stern and Hildebrandt Karraker, 1988, 1990). Moreover, during socialinteraction, they were touched less, were given more immature toys to play withand were perceived as more immature in appearance (i.e. smaller, finer-featuredand less cute). Such a ‘prematurity stereotype’ may serve as a self-fulfillingprophecy process, in which the parent’s behaviour toward the infant is guided bythese expectations. Over time, these biased expectations, behaviours andinterpretations will lead the adult to elicit the expected behaviour from theinfant, thereby resulting in a confirmation of the adult’s original expectancy.Consequently, Stern and colleagues (1986, 1990) held that the social and/orcognitive deficits which are manifested in children born prematurely mayactually be attributable to their social experiences rather than to medical factorsassociated with premature birth.
Although stereotyping has been found in both mothers of full-term and pre-term infants (Stern and Hildebrandt Karraker, 1988), the suggested effects ondevelopment have been criticized for several reasons. One is that even if mothersof pre-term infants stereotype an unfamiliar baby labelled as ‘premature’, thisdoes not necessarily mean that they do so with their own pre-term infant(Goldberg and Di Vitto, 1995). Furthermore, Ingleby and Tanke (1995) pointedout that, although they found similar indications of the prematurity stereotype ina Dutch sample, the normal effects of expectations on perception do notnecessarily constitute stereotyping. They argued that a stereotype can only besaid to exist when parents refuse to adjust their expectations in the face ofrepeated, clear-cut disconfirmation. Therefore it is important to examine mothersof low-risk pre-term infants, where negative outcomes are least expected. In high-risk pre-term infants it is very likely that the infants will indeed have the negativecharacteristics ascribed to them due to the effects of medical complications.Previous research in high-risk pre-term infants indicated that if they had beenvery ill early in life, parental concern remained long after the infant hadrecovered and ceased to show different behaviour as compared to the full-termgroup (Minde et al., 1983). However, this kind of ‘stereotype’ may be specific toinfants who have been very ill.
In a more recent study that addressed these questions (Stern et al., 2000), it wasshown that also mothers of healthy pre-term infants at the age of about 6 monthsresponded to the prematurity label in terms of more negative subjective ratingsand choosing less mature toys to play with. However, no differences in maternalbehaviours were detected between mothers of pre-term and full-term infantswhen interacting with the babies. Furthermore, the communicative behaviour ofmothers of pre-term infants was not affected by the prematurity label. Onlymothers of full-term infants touched infants labelled as ‘premature’ less. So,mothers of full-term infants seemed to exhibit more indications of prematuritystereotyping than mothers of pre-term infants, who had experience with theirown healthy pre-term infant.
Stern et al. (2000) further noted that the prematurity stereotype so far has onlybeen measured using relatively subjective rating-scales. An open question is
Y. van Beek et al.42
Copyright # 2006 John Wiley & Sons, Ltd. Inf. Child Dev. 15: 41–58 (2006)
whether the same kind of stereotyping can be found when using more objective,behaviourally anchored measures. Maternal expectations regarding theanticipated first age of appearance of well-known developmental milestonescould be such a measure. Parents usually have realistic expectations for thetiming of these milestones, and they have been used frequently in cross-culturalresearch on parental beliefs (Harkness and Super, 1996; Ninio, 1979). As such,these expectations can provide information about a possible negative bias in theexpectations and beliefs of mothers regarding their own infants instead of anunfamiliar baby labelled as premature. If less optimal developmental outcomesin pre-term infants are to be explained by different belief systems and subsequentdifferences in childrearing of their parents, as suggested by Stern and colleagues,parents of pre-term infants would be expected to have more negativeexpectations for the their infants’ development than mothers of healthy full-term infants.
The present study therefore examined whether more negative maternalexpectations exist in a relatively healthy pre-term sample as compared to anormal full-term group. In order to avoid possible influences from the initialstressful period in hospital, the expectations in the present study were sampledafter 40 weeks of gestational age so that parents of pre-term infants had had someexperience in child rearing (the selected pre-term children were born at least sixweeks early and discharged from hospital when the interview took place). Fewstudies have compared maternal expectations for developmental milestonesbetween full-term and pre-term groups before. The one study that we could find(Field, 1981), focussed more on the effects of teenage pregnancy (excluded fromthis study), and no selection was made for healthy pre-terms.
When can we speak of a negative bias in expectations? We should keep in mindthat if parents of premature babies are somewhat more pessimistic regarding thetiming of milestones, they are not necessarily unrealistic, even in low risk infants.There is much literature to show that the timing of most early developmentalmilestones should be at least partly corrected for prematurity, although differentcorrections may be necessary in different developmental domains (Allen, 1988,Belcher et al., 1987; Blasco, 1989; Kraemer et al., 1985; Lems et al., 1993; Palisano,1986). Motor development seems to be more determined by neurologicaldevelopment than experience and to require more correction for prematuritythan visuo-motor or mental development (Blasco, 1989; Palisano, 1986; Allen,1988; Lems et al., 1993). On the other hand, language development seems moreinfluenced by experience, for which no correction is favoured (Belcher et al.,1987). In general, research seems to show that in the first year some correction isusually necessary, but that full correction may already be over-correction, even inmotor development (Blasco, 1989). Of course, most parents are not familiar withthese specific research outcomes. Yet, in hospitals these days it is commonpractice to tell parents that development may be a bit slower due to thepremature birth, because not correcting for prematurity could be too optimistic,leading to disappointment when such expectations are not met (Goldberg and DiVitto, 1995). So when parents use less than full correction it cannot be concludedthat they are overly pessimistic.
Cultural Influences
The issue of possible effects of parental expectations on development is furthercomplicated by cultural values about child rearing (Harkness and Super, 1996).
Maternal Expectations about Pre-term Infants 43
Copyright # 2006 John Wiley & Sons, Ltd. Inf. Child Dev. 15: 41–58 (2006)
The general theoretical perspective proposes that timetables measure what adultsconsider as normal for child competencies to develop and subsequently serve asguidelines for adult behaviour, resulting in higher parental efforts to influence(e.g. by training, rewarding or punishing) those areas that are regarded asimportant. For example, one set of studies reported that a culturally constitutedsystem of physical training for infants acted as a mediating link betweenmaternal expectations about motor development and the subsequent ages ofattaining sitting and walking alone in a sample of Jamaican mothers and theirfull-term infants (Hopkins and Westra, 1988, 1989, 1990). Based on suchtheorizing, we not only asked for expectations regarding the timing ofmilestones, but also regarding the onset of parental didactical activities as wellas beliefs concerning the possibility to influence the timing of developmentalmilestones.
Furthermore, the present research included pre-term and full-term samplesfrom three different regions in Europe, namely The Netherlands, Northern Italyand Southern Italy. This was done for two reasons. Firstly, we wanted to comparethe effect of prematurity with another variable known to influence theseexpectations, which may give an indication of the importance of such an effect.Secondly, if mothers of pre-term infants show a negative bias in the expectationsfor their infants, this should be found irrespective of cultural background. It iswell known from the many follow-up studies that later behavioural and learningproblems in low-risk pre-term infants are found in many different countries,including The Netherlands and Italy (e.g. Verschoor et al., in press; Sansaviniet al., 1996). If the ‘vulnerable child’ perception of parents (and subsequentparenting) is held responsible for these findings, this negative bias should befound in all cultures.
The choice for these particular three European regions was pragmatic ratherthan theoretical (the same data were available for similar groups of infants due toan ongoing cooperation between the universities). There is no literature thatdirectly compares parental beliefs or strategies between these regions. Yet,studies on parental beliefs that include one of these regions do suggest thatdifferences may exist. It was found that Dutch mothers favour individualism(independence, assertiveness, self-development), speak about their children interms of their personal characteristics, and even young infants are expected toplay alone and take care of themselves early (Pels, 1991). Italian mothers howeverseemed not much concerned with academic success (patterns of infant careseemed to reflect a more explicit concern for the child’s physical well-being suchas growth, feeding, etc.), and infants were more enmeshed in a dense socialsetting (Bornstein, 1995; New and Richman, 1996). Bornstein et al. (1998), on thebasis such findings, summarized the ‘Italian way’ as: ‘In the traditional view,parenting per se is not thought to exert direct effects on child growth anddevelopment, mothers actively discourage early self-actualization skills, andmothers hold later expectations for children’s developmental accomplishments.’(p. 663). Although studies on differences between Southern and Northern Italy inthis respect are lacking, differences in family settings and values (e.g. largerfamilies, urban versus rural environment) and economical differences (Galati,1987; Galati and Sciaky, 1990) suggest that this traditional way of thinking may bemore clearly present in Southern Italy, and such differences do seem to affectparental behaviour (Camaioni et al., 1998).
As it is difficult to formulate specific hypotheses regarding the impact of thesecultural differences on parental beliefs regarding developmental timetables, thisresearch should be considered explorative in terms of the regional differences.
Y. van Beek et al.44
Copyright # 2006 John Wiley & Sons, Ltd. Inf. Child Dev. 15: 41–58 (2006)

The purpose, however, is not to find out where regional differences may comefrom, but rather to examine if such differences are important to consider whenstudying the effects of a pre-term birth on maternal expectations for develop-mental timetables.
Research Questions
In summary, the following research questions are addressed:Do mothers of healthy pre-term infants, as compared to those of full-term
infants, have more negative expectations regarding the timing of the onset ofdevelopmental milestones, the timing of parental didactical behaviours and/orbeliefs concerning their possibility to influence the timing of developmentalmilestones?
If so, are such differences found irrespective of possible regional differences inthese expectations?
METHODS
Participants
In total, 232 mothers of full-term (FT) and pre-term (PT) infants were interviewedwithin two weeks after term age (40 weeks gestational age). The participantswere recruited via hospitals and midwife-practices in The Netherlands(Amsterdam, Haarlem and Nijmegen), Northern Italy (Bologna, Ferrara andFiesole) and Southern Italy (Cosenza). The participants were interviewed at homeexcept for the majority of mothers from Northern Italy (Fiesole and Bologna),who were interviewed when visiting the hospital for a medical follow-up. Allparticipants were between 18 and 40 years of age.
The FT infants were healthy infants born after uncomplicated pregnancies witha gestational age between 38 and 42 weeks. The PT infants were born at least 6weeks prior to term age and had gestational ages between 27 and 34 weeks.Infants with serious medical complications (e.g. Grade III and IV haemorrhages,periventricular leucomalacia, postnatal asphyxia, neurological abnormalities)were excluded from the study (see van Beek et al., 1994a for a more detaileddescription of the exclusion criteria). All FT and PT infants were singletons.
Several variables reflecting SES were measured (occupation and educationallevel of both parents). As the variables were all highly correlated (r ranging from0.61 to 0.67) and data on maternal education were most complete, we onlyconsidered maternal education in our analyses. Maternal educational level wasdetermined on a 5-point scale ranging from university education to only primaryschool. However, because the majority of the participants had a medium tohigher educational level, it was reduced to a 3-point scale [1=university education,2=other extended professional education after high school, 3 ¼ no higher education(primary school to high school)]. The data on maternal educational level presentedin Table 1 do not always add up to the total number of participants due to somemissing data.
The number of firstborn infants was different between the three regions for theFT infants (w2 ¼ 18:6, df ¼ 2, p50.001), but not for the PT infants (w2 ¼ 3:8, df ¼ 2,p ¼ 0:15). In The Netherlands the number of firstborns was higher in the PT thanthe FT sample (w2 ¼ 7:4, df ¼ 1, p ¼50:01), whereas the reverse was the case inNorthern Italy (w2 ¼ 12:8, df ¼ 1, p ¼ 0:001).
Maternal Expectations about Pre-term Infants 45
Copyright # 2006 John Wiley & Sons, Ltd. Inf. Child Dev. 15: 41–58 (2006)
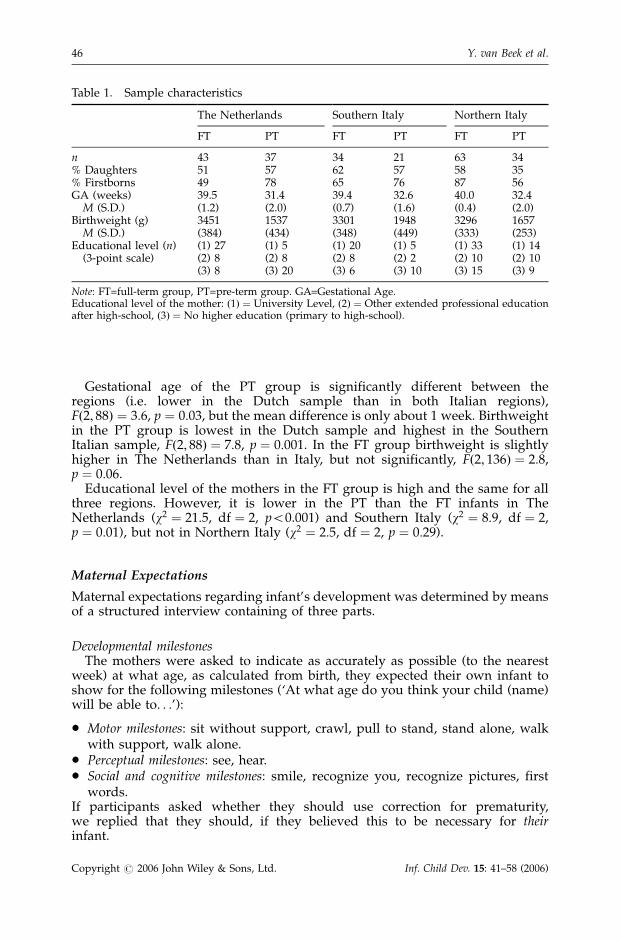
Gestational age of the PT group is significantly different between theregions (i.e. lower in the Dutch sample than in both Italian regions),Fð2; 88Þ ¼ 3:6, p ¼ 0:03, but the mean difference is only about 1 week. Birthweightin the PT group is lowest in the Dutch sample and highest in the SouthernItalian sample, Fð2; 88Þ ¼ 7:8, p ¼ 0:001. In the FT group birthweight is slightlyhigher in The Netherlands than in Italy, but not significantly, Fð2; 136Þ ¼ 2:8,p ¼ 0:06.
Educational level of the mothers in the FT group is high and the same for allthree regions. However, it is lower in the PT than the FT infants in TheNetherlands (w2 ¼ 21:5, df ¼ 2, p50.001) and Southern Italy (w2 ¼ 8:9, df ¼ 2,p ¼ 0:01), but not in Northern Italy (w2 ¼ 2:5, df ¼ 2, p ¼ 0:29).
Maternal Expectations
Maternal expectations regarding infant’s development was determined by meansof a structured interview containing of three parts.
Developmental milestonesThe mothers were asked to indicate as accurately as possible (to the nearest
week) at what age, as calculated from birth, they expected their own infant toshow for the following milestones (‘At what age do you think your child (name)will be able to. . .’):
* Motor milestones: sit without support, crawl, pull to stand, stand alone, walkwith support, walk alone.
* Perceptual milestones: see, hear.* Social and cognitive milestones: smile, recognize you, recognize pictures, first
words.If participants asked whether they should use correction for prematurity,we replied that they should, if they believed this to be necessary for theirinfant.
Table 1. Sample characteristics
The Netherlands Southern Italy Northern Italy
FT PT FT PT FT PT
n 43 37 34 21 63 34% Daughters 51 57 62 57 58 35% Firstborns 49 78 65 76 87 56GA (weeks) 39.5 31.4 39.4 32.6 40.0 32.4
M (S.D.) (1.2) (2.0) (0.7) (1.6) (0.4) (2.0)Birthweight (g) 3451 1537 3301 1948 3296 1657
M (S.D.) (384) (434) (348) (449) (333) (253)Educational level (n) (1) 27 (1) 5 (1) 20 (1) 5 (1) 33 (1) 14
(3-point scale) (2) 8 (2) 8 (2) 8 (2) 2 (2) 10 (2) 10(3) 8 (3) 20 (3) 6 (3) 10 (3) 15 (3) 9
Note: FT=full-term group, PT=pre-term group. GA=Gestational Age.Educational level of the mother: ð1Þ ¼ University Level, ð2Þ ¼ Other extended professional educationafter high-school, ð3Þ ¼ No higher education (primary to high-school).
Y. van Beek et al.46
Copyright # 2006 John Wiley & Sons, Ltd. Inf. Child Dev. 15: 41–58 (2006)
Onset of maternal teaching behavioursSimilarly, participants were asked to indicate at what age they would start:
* to teach their infant to drink from cup instead of bottle, toilet training, to teachtheir infant not to touch things that may break.
Expected influence on the timing of milestonesFor each of the motor, perceptual, social and cognitive milestones, mothers
were asked to indicate whether or not (yes/no) they believed they couldinfluence the timing of the first occurrence of this milestone.
Statistics and Preliminary Analyses
In all statistical tests an alpha of 0.05 was adopted. Although we are aware of theincreased risk of making type I errors because of the number of tests applied, wedid not to adapt the alpha accordingly. This choice was made because of thesmall group sizes, and we did not want to conclude too easily that there were nodifferences between the groups.
For the perceptual milestones and for the item ‘recognize you’ a largeproportion of the participants indicated that infants already showed this ability atbirth. Therefore, these data were dichotomized (at birth or later). Analyses ofthese items were done by means of log-linear analyses, using backwardelimination. Because such analyses can be regarded as the analyses of variancefor nominal data, results will be discussed in terms of ‘main’ and ‘interaction’effects while referring to the log-likelihood chi-square tests for the two-term[Milestone�Prematurity] or [Milestone�Region] and three-term [Milesto-ne�Prematurity�Region] interactions of log-linear analyses, respectively(testing the change in model fit when these terms are deleted from the model).
The other items were tested for normality. For those items for which the criteriawere upheld, a 2� 3 (Prematurity�Region) AN(C)OVA or MAN(C)OVA wasdone, with maternal education as covariate. For the motor items, six multivariateoutliers were removed on the basis of Mahanalobis distance values (they weremothers of firstborn FT infants from all three regions with deviations in thenormal order of expectancies, e.g. they expected walking before sitting), no otherdeviations from assumptions were noted. The distributions of ‘smile’, ‘teach todrink from cup’ and ‘teach not to touch things that may break’ showed such largedeviations from normality that we had to remove several outliers (12, 13 and 17,respectively, from full-term and pre-term groups and all regions) before analysesof variance (transformations could not solve the problem). To check the effects ofthese manipulations we also analysed the full data by means of Kruskal–Wallis orMann–Whitney-U tests. As these tests did not show any different results they willnot be reported here (but are available from the first author).
Because of the differences between the groups under study regarding thenumber of firstborn infants, educational level and birthweight of the PT infants,the possible confounding effects of these variables were examined where possibleand relevant. Maternal education was included as covariate in most analyses. Theeffects of ‘first- or later born’ were tested separately by including the variable inthe analyses (excluding the three-way interaction with region and prematurity toavoid small groups). At the end of the result section significant findings will bepresented and it will be discussed whether the effects of prematurity and/orregion could have been explained by differences in birth-status (full data are
Maternal Expectations about Pre-term Infants 47
Copyright # 2006 John Wiley & Sons, Ltd. Inf. Child Dev. 15: 41–58 (2006)
available from the first author). Birthweight of the PT group only correlated(negatively) with expectations in a few milestones (‘walk alone’, ‘first words’ and‘teach to drink from cup’). As there is no way to statistically control for theseeffects, we also did all analyses concerning these milestones after removal of sixDutch participants with the lowest birthweights (and GA) and three SouthernItalian participants with the highest birthweights, so that the significantdifferences in birthweight between the groups disappeared. As no differenceswere found from the findings for the full dataset we did not report these findingsin the results (available from the first author).
RESULTS
First the effects of premature birth and/or region on maternal expectations foreach of the developmental domains and beliefs regarding the timing ofdevelopmental milestones will be presented. Unlike maternal educational levelthe effects of birth-order could not be included as co-variate. Therefore, separateanalyses were done to examine the possible confounding effect of birth-order,which will be discussed in the last paragraph.
Maternal Expectations
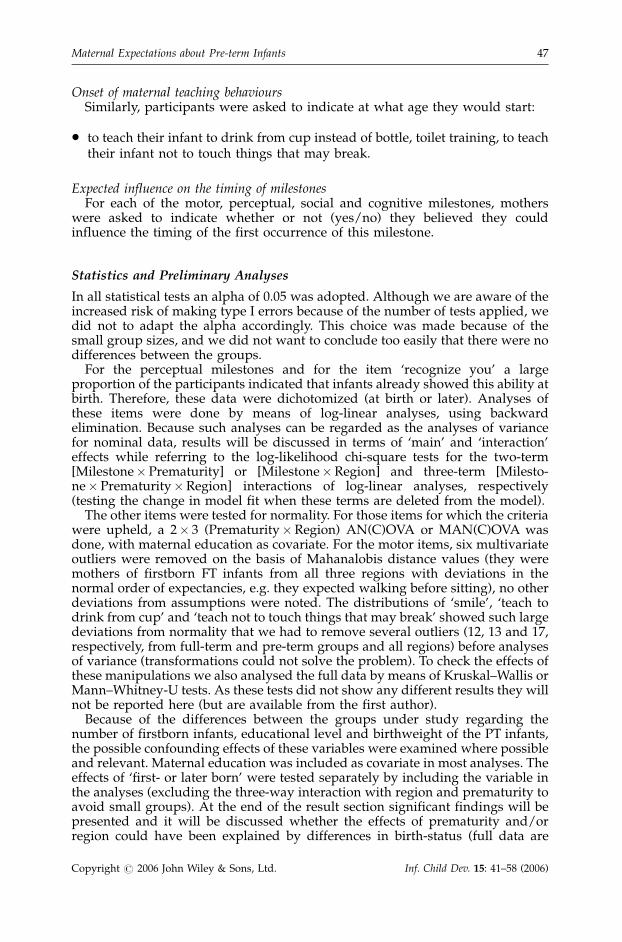
Motor milestonesIn Table 2 the means for each of the motor milestones are presented for the FT
and PT groups from all three regions.
Table 2. Mean expected ages (in weeks) for the motor milestones and results
The Netherlands Southern Italy Northern Italy Prem. Region Prem.�Reg.
Milestone FT PT FT PT FT PT df=1 df=2 df=2
Mean age in weeks (S.D.) F valuesSit 28.6 32.4 27.9 28.0 29.4 24.2 0.08 5.1** 4.2*
(7.6) (7.4) (10.1) (7.3) (8.7) (8.3)
Crawl 30.8 28.8 31.4 31.4 30.2 31.8 0.03 0.79 1.1(7.5) (8.7) (6.3) (6.4) (7.2) (7.2)
Pull to 41.2 38.7 32.8 35.8 37.1 32.7 0.12 7.6** 2.5stand (10.1) (8.2) (7.7) (9.8) (9.7) (10.3)
Stand alone 50.9 48.9 39.2 40.0 47.4 40.6 2.0 17.4*** 2.9(9.6) (7.9) (10.2) (8.4) (9.0) (10.6)
Walk with 49.8 52.4 42.4 46.0 44.8 44.8 4.2* 15.6*** 1.1support (8.8) (8.7) (6.4) (4.4) (8.3) (7.1)
Walk alone 57.4 61.1 47.4 48.0 53.2 50.0 0.07 36.2*** 3.9*(7.2) (9.5) (6.6) (6.6) (7.0) (7.3)
Note: PT ¼ pre-term group, FT ¼ full-term group, *p50.05, **p50.01, ***p50.001. Prem. (=prematur-ity) and Region refer to main effects and ‘Prem.�Reg.’ to the interaction effect between prematurityand region.
Y. van Beek et al.48
Copyright # 2006 John Wiley & Sons, Ltd. Inf. Child Dev. 15: 41–58 (2006)
A MANCOVA was done, with the expectations as dependent variables, region(The Netherlands, Southern Italy, Northern Italy) and prematurity (FT/PT) asindependent factors, and maternal educational level as co-variate. Multivariateanalyses (using Wilks lambda) indicated a main effect for region, Fð12; 384Þ ¼ 8:2,p50.001, with Dutch mothers expecting motor milestones to occur later thanItalian mothers. The main effect for prematurity was not significant, but therewas a significant prematurity� region interaction effect, Fð12; 384Þ ¼ 2:34,p ¼ 0:007. The interaction effect was largely caused by the surprising findingthat Northern Italian mothers expected motor-milestones to occur earlier in PTthan in FT infants. The covariate was not significant.
The subsequent analyses for the separate dependent variables (presented inTable 2) again showed no differences between mothers of FT and PT infants,except for ‘walk with support’, where mothers of PT infants expected themilestone a few weeks later. The main effects for region indicated that Dutchmothers expected all milestones except crawling to occur later than Italianmothers. In two items (sit, walk alone), significant interaction effects were foundbetween prematurity and region. Dutch mothers of PT infants expectedmilestones to occur 1–4 weeks later than their FT counterparts. So for thesemilestones they showed a partial correction for prematurity (full correctionwould be 7–8 weeks). The interaction effects were further caused by the fact thatNorthern Italian mothers expected motor-milestones to occur a few weeks earlierin PT than in FT infants.
In summary, the most evident finding is the effect for region, showing thatexpectations for most motor milestones were more moderate in The Netherlands.For only a few motor milestones were corrections for prematurity made. If therewas correction it was by no means full correction. On the contrary, in NorthernItaly the expectations for the PT group were often more optimistic than for the FTgroup.
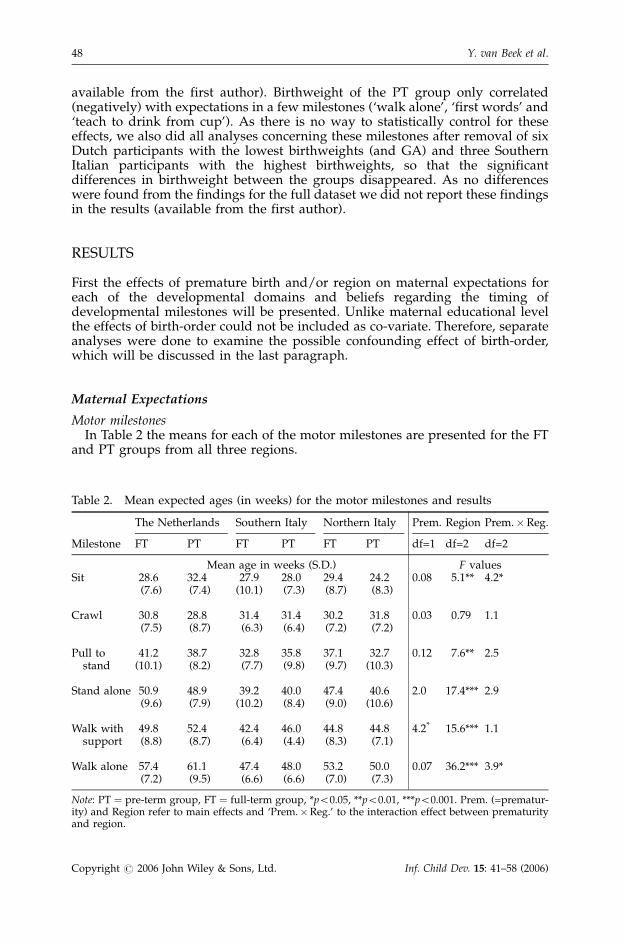
Perceptual milestonesTable 3 displays the proportion of mothers in each group who indicated that
their infants could see or hear at birth. Differences were tested by means of log-linear analyses, using backward elimination from a saturated model containingthe variables ‘see at birth’ or ‘hear at birth’ (yes/no), prematurity (PT/FT), andregion (The Netherlands/Southern Italy/Northern Italy).
Although there is an overall tendency for a larger proportion of FT mothers toindicate that their infants could already see at birth as compared to mothers of PTinfants, this difference was not significant, nor was the prematurity� regioninteraction effect. There was a significant main effect for region, showing that alarger proportion of the Dutch as compared to the Italian mothers assumed themilestone to be present at birth, LR w2 ¼ 14:9, df ¼ 2, p50.001.
Table 3. Proportion of mothers who believed the milestone to be present at birth
The Netherlands Southern Italy Northern Italy
Milestone FT (%) PT (%) FT (%) PT (%) FT (%) PT (%)
See 51.1 45.9 35.3 9.5 25.4 17.6Hear 76.2 71.4 67.6 38.1 68.3 50.0
Note: FT ¼ full-term group, PT ¼ pre-term group.
Maternal Expectations about Pre-term Infants 49
Copyright # 2006 John Wiley & Sons, Ltd. Inf. Child Dev. 15: 41–58 (2006)
For ‘hear at birth’ a larger proportion of mothers of FT infants indicated themilestone to be present at birth than of PT mothers, LR w2 ¼ 5:3, df ¼ 1, p ¼ 0:02.The prematurity� region interaction was not significant, nor was the tendencyfor a higher proportion in Dutch mothers.
As log-linear analyses do not allow co-variance analyses, we included thevariable ‘maternal education’ in the models for perceptual milestones. Only forhearing was an effect found. A higher proportion of the mothers with lowereducational levels believed ‘hearing’ not to be present at birth (47% of themothers with level 3, 40% of the mothers with level 2 and 25% of the motherswith level 1, w2 ¼ 9:0, df ¼ 2, p ¼ 0:01). However, with maternal education in themodel, the main effect of prematurity remained significant, LR w2 ¼ 7:0, df ¼ 2,p ¼ 0:008, indicating that both effects were independent.
In summary, more Dutch mothers believed that their infants could see at birththan Italian mothers and no effects were found for prematurity. For ‘hear atbirth’, however, fewer mothers of PT infants believed this ability to be present atbirth and no effects for region were found.
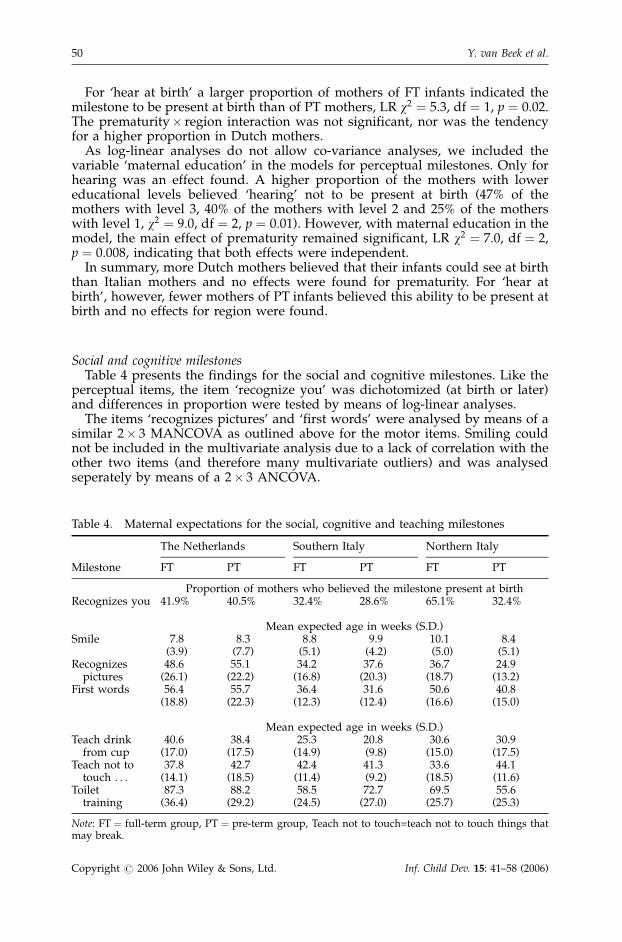
Social and cognitive milestonesTable 4 presents the findings for the social and cognitive milestones. Like the
perceptual items, the item ‘recognize you’ was dichotomized (at birth or later)and differences in proportion were tested by means of log-linear analyses.
The items ‘recognizes pictures’ and ‘first words’ were analysed by means of asimilar 2� 3 MANCOVA as outlined above for the motor items. Smiling couldnot be included in the multivariate analysis due to a lack of correlation with theother two items (and therefore many multivariate outliers) and was analysedseperately by means of a 2� 3 ANCOVA.
Table 4. Maternal expectations for the social, cognitive and teaching milestones
The Netherlands Southern Italy Northern Italy
Milestone FT PT FT PT FT PT
Proportion of mothers who believed the milestone present at birthRecognizes you 41.9% 40.5% 32.4% 28.6% 65.1% 32.4%
Mean expected age in weeks (S.D.)Smile 7.8 8.3 8.8 9.9 10.1 8.4
(3.9) (7.7) (5.1) (4.2) (5.0) (5.1)Recognizes 48.6 55.1 34.2 37.6 36.7 24.9
pictures (26.1) (22.2) (16.8) (20.3) (18.7) (13.2)First words 56.4 55.7 36.4 31.6 50.6 40.8
(18.8) (22.3) (12.3) (12.4) (16.6) (15.0)
Mean expected age in weeks (S.D.)Teach drink 40.6 38.4 25.3 20.8 30.6 30.9
from cup (17.0) (17.5) (14.9) (9.8) (15.0) (17.5)Teach not to 37.8 42.7 42.4 41.3 33.6 44.1
touch . . . (14.1) (18.5) (11.4) (9.2) (18.5) (11.6)Toilet 87.3 88.2 58.5 72.7 69.5 55.6
training (36.4) (29.2) (24.5) (27.0) (25.7) (25.3)
Note: FT ¼ full-term group, PT ¼ pre-term group, Teach not to touch=teach not to touch things thatmay break.
Y. van Beek et al.50
Copyright # 2006 John Wiley & Sons, Ltd. Inf. Child Dev. 15: 41–58 (2006)
For the milestone ‘recognize you’, there was a significant main effect forprematurity indicating that a lower proportion of mothers of PT than FT infantsassumed it to be present at birth (LR w2 ¼ 5:3, df ¼ 1, p ¼ 0:02). Also, a significantdifference was found between the regions (LR w2 ¼ 7:8, df ¼ 2, p ¼ 0:02), withhighest proportions in Northern Italy and lowest in Southern Italy. As can be seenin Table 4, the relatively high proportion of mothers in Northern Italy seemedmost responsible for these findings, yet the prematurity� region interaction onlyshowed a non-significant trend (LR w2 ¼ 4:8, df ¼ 2, p ¼ 0:09).
For the milestone ‘smile’ no significant differences between the mothers of FTand PT nor between mothers from different regions were found. The covariate‘maternal education’ was not significant either.
For ‘recognize pictures’ and ‘first words’ the multivariate results only indicateda significant effect for region, Fð4; 404Þ ¼ 18:6, p50.0001, particularly becauseDutch mothers expected the milestones to occur later. The covariate was notsignificant. The findings for the separate dependent variables again showedsignificant main effects for region, Fð2; 209Þ ¼ 22:8, p50.0001 and Fð2; 209Þ ¼ 21:1,p50.0001 for ‘first words’ and ‘recognizes pictures’, respectively. For ‘first words’a main effect for prematurity was also found Fð1; 209Þ ¼ 4; 1, p ¼ 0:04 in that themilestone was expected almost 4 weeks earlier in the PT group. Although thiseffect seems largest in the Northern Italian group, the interaction effect was notsignificant. For ‘recognizes pictures’ a significant prematurity� region interac-tion effect was found, Fð2; 209Þ ¼ 4:0, p ¼ 0:02. Dutch and Southern Italianmothers of PT infants expected the milestone to occur later than their FTcounterparts (6, respectively, 3 weeks), whereas the reverse was found inNorthern Italy (almost 12 weeks earlier).
In summary, only in some milestones were indications found that mothers ofPT infant corrected their expectations for prematurity. For ‘recognize you’ a lowerproportion of mothers of PT infants assumed the milestone present at birth. Onlyin the Dutch and Southern Italian mothers expectations were partially correctedfor the item ‘recognize pictures’. For ‘first words’ expectations seemed to beearlier for the PT than for the FT group, and not only in the Northern Italian groupas before. The effects of region were present in all milestones except ‘smile’,mostly indicating more moderate expectations in the Dutch group.
Onset of maternal teaching behavioursTable 4 also presents the findings for the expectations regarding maternal
teaching behaviours. The variables were not highly correlated and the number ofmultivariate outliers were very high. Therefore no multivariate analyses weredone and the results from separate ANCOVAs will be presented.
Table 4 shows that Italian mothers, and particularly those from the South,thought they would start teaching to drink from a cup earlier than Dutchmothers, Fð2; 195Þ ¼ 14:1, p50.0001. There were no differences between the FTand PT groups and the covariate for maternal education was not significant.
Mothers of PT infants expected to start ‘teaching not to touch things that maybreak’ 5–6 weeks later than mothers of FT infants, Fð1; 196Þ ¼ 5:5, p ¼ 0:02.Although this effect seemed largest in Northern Italy, the interaction effect wasnot significant, nor was there a main effect for region or maternal education.
‘Toilet training’ was expected to start later in The Netherlands than in Italy,Fð2; 219Þ ¼ 11:0, p50.001. No main effect was found for prematurity, but theinteraction effect, Fð2; 219Þ ¼ 4:6, p ¼ 0:01, meant that whereas Southern Italianmothers of PT infants expected to start toilet-training about 14 weeks later than
Maternal Expectations about Pre-term Infants 51
Copyright # 2006 John Wiley & Sons, Ltd. Inf. Child Dev. 15: 41–58 (2006)
those of FT infants, the reverse seemed the case in Northern Italy. The covariatewas significant in that mothers with the highest level of education expected tostart with toilet-training about 10 weeks later than mothers of lower education,Fð1; 206Þ ¼ 11:3, p ¼ 0:001.
In summary, (partial) corrections for prematurity were made for ‘teach not totouch things that may break’. More than partial correction was made for ‘toilettraining’, but only in the Southern Italian mothers, whereas the opposite was seenin Northern Italian mothers. Teaching to drink from a cup and toilet trainingwere expected later by the Dutch mothers.
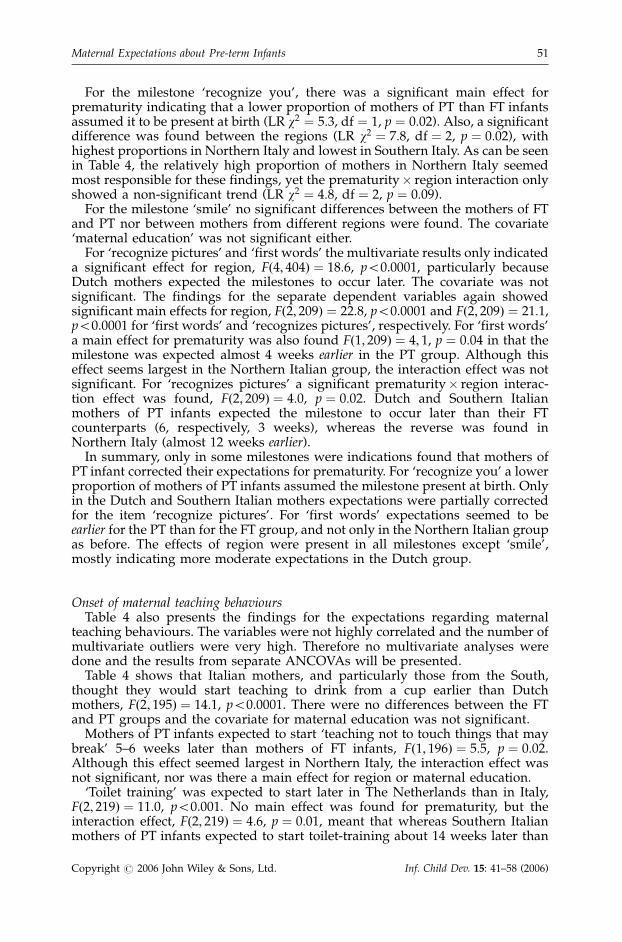
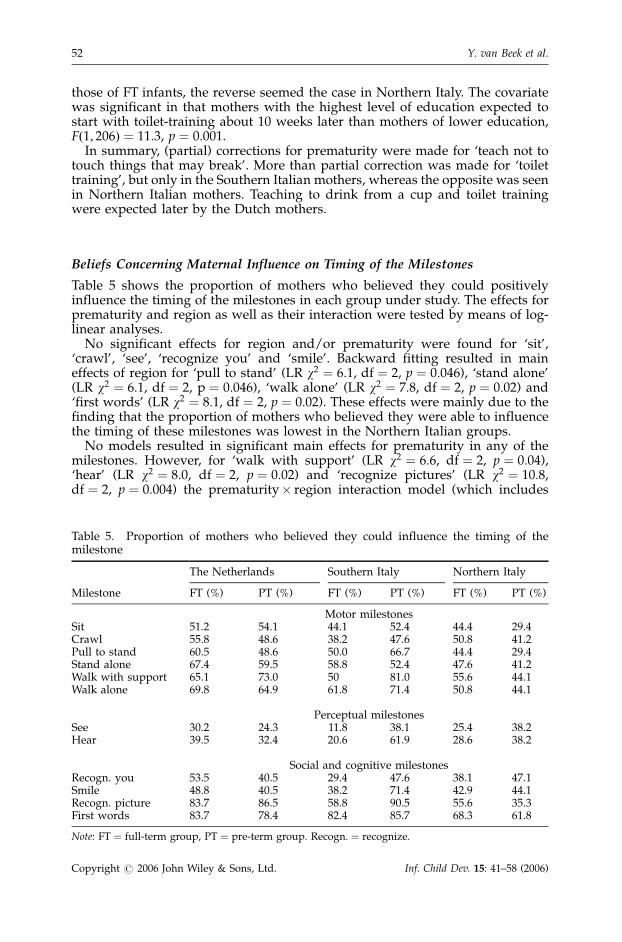
Beliefs Concerning Maternal Influence on Timing of the Milestones
Table 5 shows the proportion of mothers who believed they could positivelyinfluence the timing of the milestones in each group under study. The effects forprematurity and region as well as their interaction were tested by means of log-linear analyses.
No significant effects for region and/or prematurity were found for ‘sit’,‘crawl’, ‘see’, ‘recognize you’ and ‘smile’. Backward fitting resulted in maineffects of region for ‘pull to stand’ (LR w2 ¼ 6:1, df ¼ 2, p ¼ 0:046), ‘stand alone’(LR w2 ¼ 6:1, df ¼ 2, p ¼ 0:046), ‘walk alone’ (LR w2 ¼ 7:8, df ¼ 2, p ¼ 0:02) and‘first words’ (LR w2 ¼ 8:1, df ¼ 2, p ¼ 0:02). These effects were mainly due to thefinding that the proportion of mothers who believed they were able to influencethe timing of these milestones was lowest in the Northern Italian groups.
No models resulted in significant main effects for prematurity in any of themilestones. However, for ‘walk with support’ (LR w2 ¼ 6:6, df ¼ 2, p ¼ 0:04),‘hear’ (LR w2 ¼ 8:0, df ¼ 2, p ¼ 0:02) and ‘recognize pictures’ (LR w2 ¼ 10:8,df ¼ 2, p ¼ 0:004) the prematurity� region interaction model (which includes
Table 5. Proportion of mothers who believed they could influence the timing of themilestone
The Netherlands Southern Italy Northern Italy
Milestone FT (%) PT (%) FT (%) PT (%) FT (%) PT (%)
Motor milestonesSit 51.2 54.1 44.1 52.4 44.4 29.4Crawl 55.8 48.6 38.2 47.6 50.8 41.2Pull to stand 60.5 48.6 50.0 66.7 44.4 29.4Stand alone 67.4 59.5 58.8 52.4 47.6 41.2Walk with support 65.1 73.0 50 81.0 55.6 44.1Walk alone 69.8 64.9 61.8 71.4 50.8 44.1
Perceptual milestonesSee 30.2 24.3 11.8 38.1 25.4 38.2Hear 39.5 32.4 20.6 61.9 28.6 38.2
Social and cognitive milestonesRecogn. you 53.5 40.5 29.4 47.6 38.1 47.1Smile 48.8 40.5 38.2 71.4 42.9 44.1Recogn. picture 83.7 86.5 58.8 90.5 55.6 35.3First words 83.7 78.4 82.4 85.7 68.3 61.8
Note: FT ¼ full-term group, PT ¼ pre-term group. Recogn: ¼ recognize.
Y. van Beek et al.52
Copyright # 2006 John Wiley & Sons, Ltd. Inf. Child Dev. 15: 41–58 (2006)
main and interaction effects) fitted the data best. For ‘walk with support’ thisinteraction effect is mostly caused by the fact that in Northern Italy thepercentage was lower in the PT than the FT group, whereas the reverse wasfound in the other two regions. For ‘hear’ in Southern Italy a higher proportion ofmothers believed they could influence the timing of the milestone in the PTgroup (and a somewhat lower proportions was found in the FT group) than inthe other two regions. For ‘recognize pictures’ lower proportions were found inthe Italian FT groups. Moreover, in The Netherlands there was hardly anydifference between the FT and PT group, while in Northern Italy proportionswere lower in the PT group whereas the opposite was the case in Southern Italy.
In summary, for four milestones (three motor milestones and first words) alower percentage of mothers believed they were able to influence the timing ofmilestones in Italy, especially in the North. In three milestones (‘walk withsupport’, ‘hear’ and recognize pictures’) prematurity seemed to have a differenteffect on beliefs in the two Italian regions: in the South a much higher proportionof the mothers of PT than of FT infants believed to be able to influence the timingof these milestones, whereas the reverse was found in mothers from NorthernItaly (except for ‘hear’). In Holland, hardly any differences were found betweenmothers of FT and PT infants.
Possible Confounding Effects of Differences in Birth-order
In Table 1 it was shown that the number of firstborn infants was differentbetween the three regions for the FT infants, but not for the PT infants. Moreover,in The Netherlands the number of firstborns was higher in the PT than the FTsample, whereas the reverse was the case in Northern Italy. We thereforeexamined whether the above presented finding for region and prematurity couldhave been influenced by these differences in birth-order by including the variablein the analyses. Only for two milestones was an effect of birth-order onexpectations found.
For smiling, a significant interaction with prematurity was found,Fð1; 199Þ ¼ 5:36, p ¼ 0:02, i.e. in the PT group mothers of firstborn childrenexpected smiling 1.5 weeks later, whereas in the FT group they expected smiling1 week earlier. However, no effect for prematurity or region on expectations wasfound for this item and results remained the same if the variable was included.
Mothers of first-born children tended to expect the milestone ‘drink from cup’to occur earlier (mean difference about 7 weeks) than mothers of later bornchildren, Fð1; 194Þ ¼ 3:8, p ¼ 0:053, but particularly so in the FT group,Fð1; 194Þ ¼ 6:3, p ¼ 0:013. The effects of prematurity and/or region, however,were unaffected by the addition of this variable as independent factor in theanalyses.
In conclusion, birth-order influenced maternal expectations for only twomilestones and did not seem to have affected the findings for region orprematurity.
DISCUSSION
Prematurity and Maternal Expectations and Beliefs
For some of the developmental milestones the expectations of mothers of pre-term infants were a few weeks later, but usually no full correction for prematurity
Maternal Expectations about Pre-term Infants 53
Copyright # 2006 John Wiley & Sons, Ltd. Inf. Child Dev. 15: 41–58 (2006)
was made. For ‘hear’ and ‘recognize you’ fewer of the mothers in the pre-termgroup believed these abilities to be present at birth, but most of them believedthese milestones to be evident only a few weeks later. Here we should realize thatwe were not measuring expectations for future development, but rather mothersexpressed how they perceived this ability in the past (we asked their perceptionsaround term age, i.e. at least six weeks after birth).
An unexpected finding for many motor and some of the cognitive milestoneswas that mothers of Northern Italian pre-terms expected these milestones tooccur earlier than the mothers of the full-term group in the same region. This wasnot the case in The Netherlands and the South of Italy. Although seeming toindicate that this group has overly optimistic expectations, we should be careful.In all but two cases (sitting and recognize pictures), the mean expected age wascomparable with that of the full-term group in Southern Italy. Thus, it is difficultto say whether we should regard expectations for the pre-term group as toooptimistic or those for the full-term group as too pessimistic (these expectationswere often similar to those of Dutch mothers). The Northern Italian group of pre-term mothers also believed that they were less able to influence the timing ofsome milestones, and reported less sources of knowledge and support (notpresented in this paper) than the other groups. The overall impression of ourinterviewers was that these mothers seemed more upset and uncertain than theother pre-term groups. It remains unclear why this was the case. Perhaps the factthat the majority of mothers in this group were interviewed at the hospital mayhave contributed to this finding. But if so, it is unclear why a higher level ofdistress would result in more optimistic expectations regarding the timing ofmost milestones.
Also for maternal teaching behaviours correction for prematurity was rare and,if found, modest. More than full correction for prematurity was found for toilettraining, but only in Southern Italy, and for ‘teach not to touch things that maybreak’, but only in Northern Italy. Similar to the motor and cognitive milestones,earlier expectations in the Northern Italian pre-term group as compared to thefull-term group were found for toilet training.
Finally, effects were found of prematurity on beliefs concerning the possibilityto influence the timing of three developmental milestones, but only in the twoItalian sub-groups, and the effects in both groups were opposite in direction.
As we found only limited effects of prematurity overall, the type of expectation(objective/subjective, tailored to infant or parental behaviour) did not seem ofinfluence. There was also no indication for differentiation depending on thedevelopmental domain. However, one finding may be noteworthy. For ‘firstwords’ there was a general tendency to expect the milestone earlier in pre-termthan in full-term babies. Of all domains language development is indeedconsidered as less influenced by maturation and more by experience (Belcheret al., 1987). However, although the interaction effect was not significant, theNorthern Italian group contributed most to this finding, and this group showedthe same unexpected and unexplained optimistic expectations in many othermilestones.
In conclusion, it was shown that mothers of low-risk pre-term infants as agroup did not have very different beliefs from those with full-term offspring.Although small adjustments for prematurity were found regularly in two of theregions, there was no evidence for overly pessimistic expectations in the sensethat (more than) full correction was used. The adjustments made seem realistic,as literature indicates that at least partial correction is necessary, even in low-riskpre-term infants (e.g. Lems et al., 1993).
Y. van Beek et al.54
Copyright # 2006 John Wiley & Sons, Ltd. Inf. Child Dev. 15: 41–58 (2006)
Regional Differences
The most common regional finding is that Dutch mothers expected the motorand cognitive milestones to occur later than the Italian mothers. In the motordomain, they expected the milestones to occur 1–2 months later, and mostcognitive and language milestones as well as teaching behaviours were expected2–5 months later. Another regional effect was that more Dutch than Italianmothers correctly indicated that they believed that their infant was able to see atbirth. For ‘hear’ the same tendency existed, although the difference was notsignificant. A lack of knowledge regarding these perceptual abilities in parentshas been reported by others (Ninio, 1979; Crouchman, 1985). However, as thesemilestones occurred before the interview took place, and we therefore measuredperception rather than prediction, we cannot rule out the possibility that parentsdid not always have the same standard of mastery in mind, e.g. some may haveinterpreted ‘seeing’ as ‘seeing sharply’ and others as ‘seeing something’.Moreover, prematurity affected these beliefs more in the Italian than the Dutchgroups which also contributed to the regional effect.
With respect to the beliefs concerning parental influence on development, inseveral of the motor and cognitive milestones, a lower proportion of Italianmothers believed they were able to influence the timing of milestones,particularly in the full-term groups. This matches with the description of Italianbeliefs described by Bornstein et al. (1998). However, they proposed that Italianmothers would (therefore) have later expectations regarding the onset ofmilestones, whereas the reverse seemed to be the case in this study. Why Dutchmothers expect milestones later is yet unknown.
Most participants in this study came from urban societies and had relativelyhigh educational levels. As such, we do not know whether the regionaldifferences constitute differences in ‘cultural’ values that usually derive fromdifferences in religion, family background, rural versus urban societies, etc.Although the differences in educational level, number of first born infants andbirthweight of the pre-term groups did not seem to have large effects on ourfindings, and we feel quite confident that these factors were not responsible forthe regional effects reported, future studies could benefit from selecting groupsthat are more equal in this respect. More research is needed to understand wherethe regional differences came from.
General Discussion
If an effect of prematurity was found on expectations we wanted to compare itwith another factor in order to establish the importance of such an effect. Thefindings clearly showed that the effects for region were far larger and morecommon than those for prematurity. If we had adapted the alpha in order todecrease the likelihood of making type I errors, only the regional main effectswould have been significant. Moreover, the large regional differences indicatethat a criterion for ‘normal’ expectations is not easy to formulate. As regionaldifferences have such large impact on expectations, what criterion for‘pessimistic’ expectations should be used for pre-term infants? Full correctionfor prematurity (or more) as compared to the mean for mothers of full-terminfants of the same region (and with similar background characteristics) seemsreasonable, but what does such a bias mean in terms of effects on development ifregional differences in expectations are far larger? Moreover, if prematuritycauses a ‘vulnerable child’ perception it should be present in all regions, as
Maternal Expectations about Pre-term Infants 55
Copyright # 2006 John Wiley & Sons, Ltd. Inf. Child Dev. 15: 41–58 (2006)
similar developmental outcomes have been found in low-risk pre-terms in manydifferent countries and regions including the ones of the present study (e.g.Sansavini et al., 1996; Verschoor et al., in press). However, full correction or morewas very rare and, if found, only present in a specific region. Partial correctionwas more common, but only in the Dutch and/or Southern Italian groups.
What do these finding mean for the theory that a ‘prematurity-stereotype’ maycontribute, via parental beliefs and child-rearing, to less favourable outcomes inpre-term infants? Although research shows that also in mothers of low-risk pre-term infants the labelling experiment results in a prematurity stereotype (Sternet al., 2000), in this study hardly any indication was found that maternal beliefsand expectations were different from normal concerning their own low-risk pre-term infant. This may mean that the experience with their pre-term infantdiminished the ‘vulnerable child’ perception of mothers already at term age,similar to what Stern et al. (2000) showed regarding a lack of differences inmaternal interactive behaviour at the age of 6 months. However, inter-individualdifferences were considerable (although standard deviations were similar to thefull-term group), so there may have been mothers of pre-term infants who didnegatively adjust expectations. Moreover, further research is necessary to find outif negative beliefs may arise later in development, or for other characteristics ofthe infant (e.g. the quality of their skills rather that their first onset). Only if suchbeliefs exist and if they affect the way in which parents interact with their infant(correcting for differences in infant behaviour, see van Beek et al., 1994b for anexample) and such differences predict later outcome (correcting for otherpossible factors, e.g. indications for right-hemisphere damage, Verschoor et al., inpress) can we show that the ‘vulnerable child’ perception contributes to lessoptimal development in low-risk pre-term infants. The present study indicatesthat this line of research is further complicated by ‘cultural’ factors, as theyclearly influence beliefs and expectations regarding infant and maternalbehaviour.
ACKNOWLEDGEMENTS
We would like to thank Riccardo Stevens for his help with the data collection.
REFERENCES
Allen MC. 1988. Gross motor milestones in premature infants. Developmental Medicine andChild Neurology 30: 17.
van Beek Y, Hopkins B, Hoeksma JB. 1994a. Development of communicative behaviors inpreterm infants: the effects of birthweight and gestational age. Infant Behavior andDevelopment 17: 107–117.
van Beek Y, Hopkins B, Hoeksma JB, Samsom JF. 1994b. The development ofcommunication in pre-term infant-mother dyads. Behaviour 129: 35–61.
Belcher HME, Allen MC, Gittelsohn AM, Capute AJ. 1987. Longitudinal languageassessment of preterm infants: full versus partial correction for prematurity.Unpublished manuscript.
Blasco PA. 1989. Preterm birth: to correct or not to correct. Developmental Medicine and ChildNeurology 31: 816–826.
Bornstein MH. 1995. Parenting infants. In Handbook of Parenting, vol. 1: Children andParenting, Bornstein MH (ed.). Lea Mahwah: New Jersey; 3–41.
Y. van Beek et al.56
Copyright # 2006 John Wiley & Sons, Ltd. Inf. Child Dev. 15: 41–58 (2006)
Bornstein MH, Haynes OM, Azuma H, Galperin C, Maital S, Ogino M, Painter K, PascualL, Pecheux M-G, Rahn C, Toda S, Venuti P, Vyt A, Wright B. 1998. A cross-national studyof self-evaluations and attributions in parenting: Argentina, Belgium, France, Israel,Italy, Japan and the United States. Developmental Psychology 34: 662–676.
Camaioni L, Longobardi E, Venuti P, Bornstein MH. 1998. Maternal speech to 1-year-oldchildren in two Italian cultural contexts. Early Development and Parenting 7: 9–17.
Crouchman M. 1985. What mothers know about their newborns’ visual skills.Developmental Medicine and Child Neurology 27: 455–460.
Field TM. 1981. Early development of the preterm offspring of teenage mothers. In TeenageParents and Their Offspring, Scolt KG, Field TM, Robertson E (eds). Grune & Stralton:New York, 145–175.
Galati D. 1987. Il riconoscimento di antecedenti situazionali delle emozioni (Determiningthe situational background variables of emotions). Ikon 1: 143–158.
Galati D, Sciaky R. 1990. Antecedenti situazionali delle emozioni nel Nord en nel Sudd’Italia: un’ analisi testuale (Situational background variables of emotions in North andSouth Italy). Giornale Italiono di psicologia, XVII, 3: 461–485.
Goldberg S, Di Vitto B. 1995. Parenting children born preterm. In Handbook of Parenting: vol.1 Children and Parenting, Bornstein MH (ed.). Lea Mahwah: New Jersey; 209–233.
Goodnow JJ, Collins WA. 1990. Development According to Parents. The Nature, Sources, andConsequences of Parents’ Ideas. Lawrence Erlbaum Associates: Hove, UK.
Harkness S, Super C. 1996. Parents’ Cultural Belief Systems: Their Origins, Expressions andConsequences. Gilford Press: New York.
Hopkins B, Westra T. 1988. Maternal handling and motor development: an intraculturalstudy. Genetic, Social and General Psychology Monographs 114: 377–408.
Hopkins B, Westra T. 1989. Maternal expectations of their infants’ development: somecultural differences. Developmental Medicine and Child Neurology 31: 384–390.
Hopkins B, Westra T. 1990. Motor development, maternal expectations and the role ofhandling. Infant Behavior and Development 13: 117–122.
Ingleby JD, Tanke MJ. 1995. ‘Prematurity Stereotype’ in a sample of Dutch mothers: doresearcher suffer from a ‘prejudiced parent stereotype’? Infant Mental Health Journal 16:169–178.
Kraemer HC, Korner AF, Hurwitz S. 1985. A model for assessing the development ofpreterm infants as a function of gestational, conceptional or chronological age.Developmental Psychology 21: 806–812.
Lems W, Hopkins B, Samsom JF. 1993. Mental and motor development in preterm infants:the issue of corrected age. Early Human Development 34: 113–123.
Miller PJ, Goodnow JJ. 1995. Cultural practices: towards an integration of culture anddevelopment. In Cultural Practices as Context for Development, Goodnow JJ, Miller PJ,Kessel F (eds). Jossey-Bass: San Francisco; 5–17.
Minde K, Whitelaw A, Brown J, Fitzhardinge P. 1983. Effect of neonatal complications inpremature infants on parent–infant interactions. Developmental Medicine and ChildNeurology 24: 117–129.
New RS, Richman AL. 1996. Maternal believes and infant care practices in Italy and theUnited States. In Parents Cultural Belief Systems: Their Origins, Expressions, andConsequences, Harkness S, Super CM (eds). Guilford Press: New York; 385–404.
Ninio A. 1979. The naı̈ve theory of the infant and other maternal attitudes in twosubgroups in Israel. Child Development 50: 976–980.
Palisano RJ. 1986. Use of chronological and adjusted ages to compare motor developmentof healthy preterm and fullterm infants. Developmental Medicine and Child Neurology 28:180–187.
Pels T. 1991. Developmental expectations of Moroccan and Dutch parents. In ContemporaryIssues in Cross-cultural Psychology, Bleichrodt N, Drenth PJD (eds). Swets & Zeitlinger:Amsterdam; 64–71.
Sansavini A, Rizzardi M, Allessandroni R, Giovanelli G. 1996. The development of Italianlow and very-low birthweight infants from birth to 5 years: the role of biological andsocial risks. International Journal of Behavioral Development 19: 533–547.
Stern M, Hildebrandt KA. 1984. Prematurity stereotype: effects of labelling on adult’sperceptions of infants. Developmental Psychology 20: 360–362.
Stern M, Hildebrandt KA. 1986. Prematurity stereotyping: effects on mother-infantinteraction. Child Development 57: 308–315.
Maternal Expectations about Pre-term Infants 57
Copyright # 2006 John Wiley & Sons, Ltd. Inf. Child Dev. 15: 41–58 (2006)

Stern M, Hildebrandt Karrakker KA. 1988. Prematurity stereotyping by mothers ofpremature infants. Journal of Paediatric Psychology 13: 255–263.
Stern M, Hildebrandt Karrakker KA. 1990. The prematurity stereotype: empirical evidenceand implications for practice. Infant Mental Health Journal 11: 3–11.
Stern M, Hildebrandt Karraker K, Meldrum Sopko A, Norman S. 2000. The prematuritystereotype revisited: impact on mother’s interactions with premature and full-terminfants. Infant Mental Health Journal 21: 495–509.
Verschoor CA, Njiokiktjien C, Hopkins B, de Sonneville LMJ. in press. Neuropsychologicalprofiles after a low risk preterm birth. Follow-up at 18–30 months to 6 years.Developmental Neuropsychology.
Y. van Beek et al.58
Copyright # 2006 John Wiley & Sons, Ltd. Inf. Child Dev. 15: 41–58 (2006)































