Embed Size (px)
Citation preview
Maxillary Major Connectors
Six basic types of maxillary major connectors are
considered:
1. Single palatal strap
2. Combination anterior and posterior palatal strap- type
connector
3. Palatal plate-type connector
4. U-shaped palatal connector
5. Single palatal bar
6. Anterior-posterior palatal bars
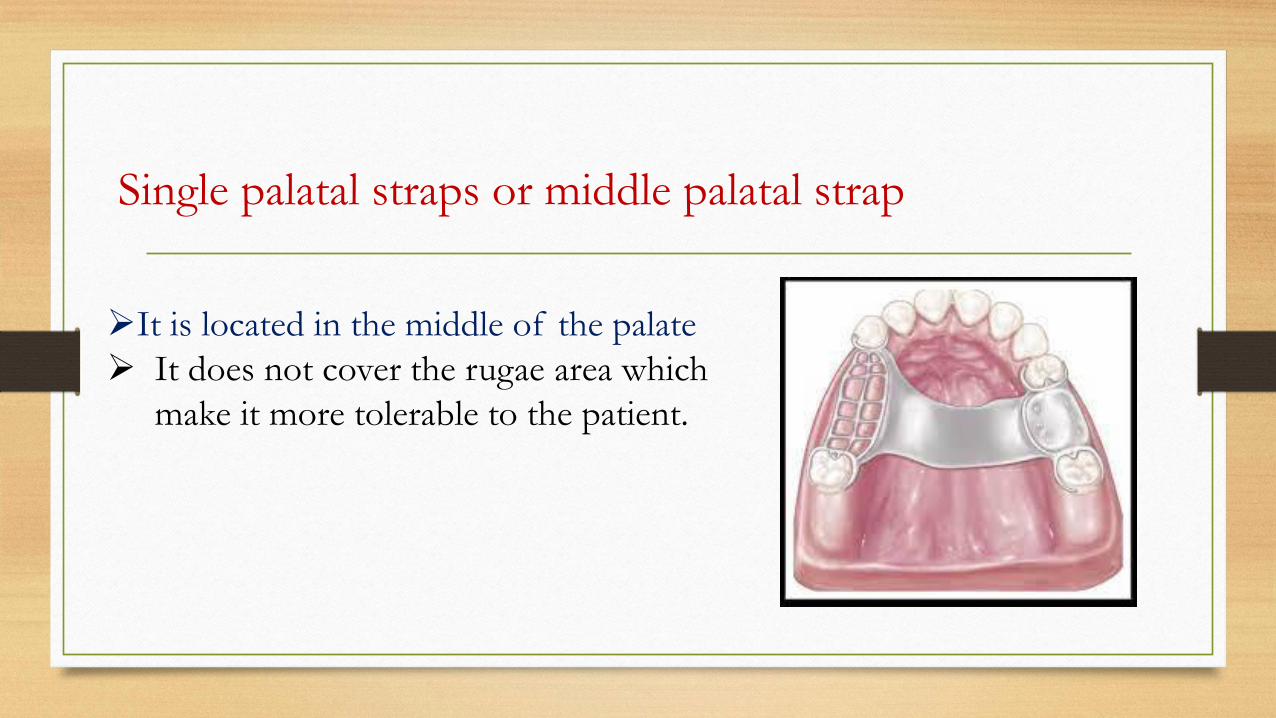
➢It is located in the middle of the palate
➢ It does not cover the rugae area which
make it more tolerable to the patient.
Single palatal straps or middle palatal strap
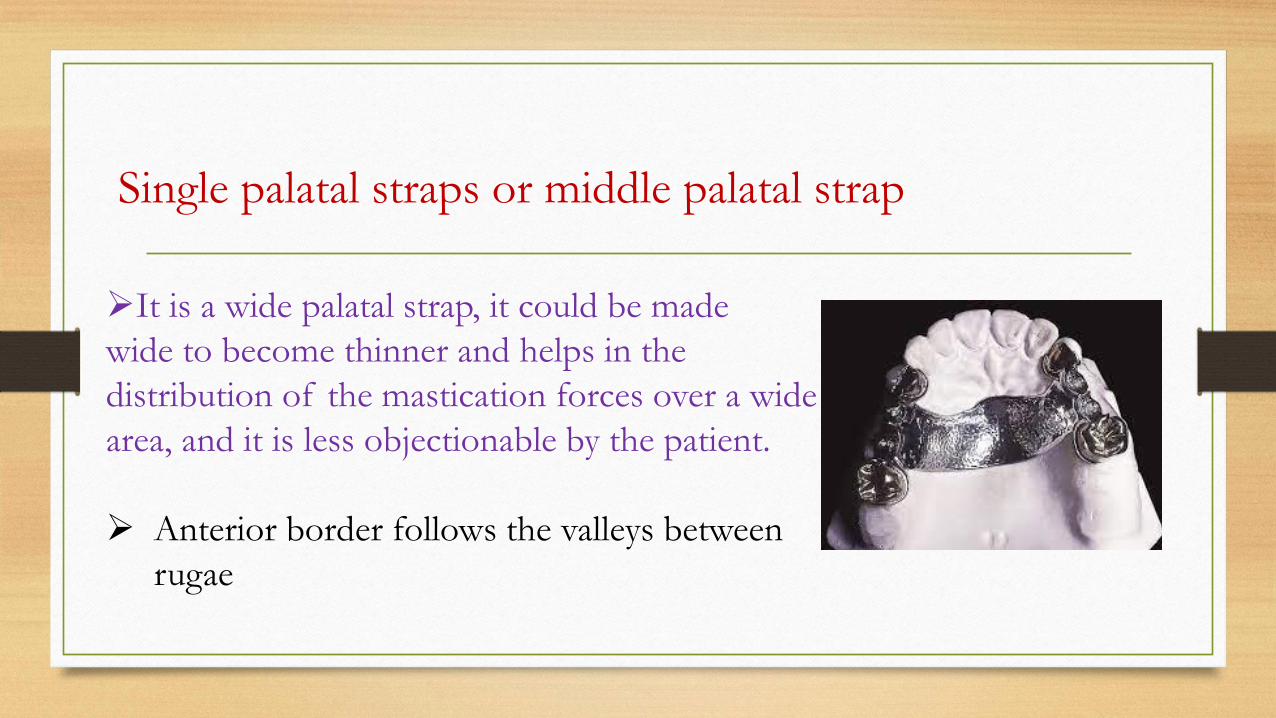
➢It is a wide palatal strap, it could be made
wide to become thinner and helps in the
distribution of the mastication forces over a wide
area, and it is less objectionable by the patient.
➢ Anterior border follows the valleys between
rugae
Single palatal straps or middle palatal strap
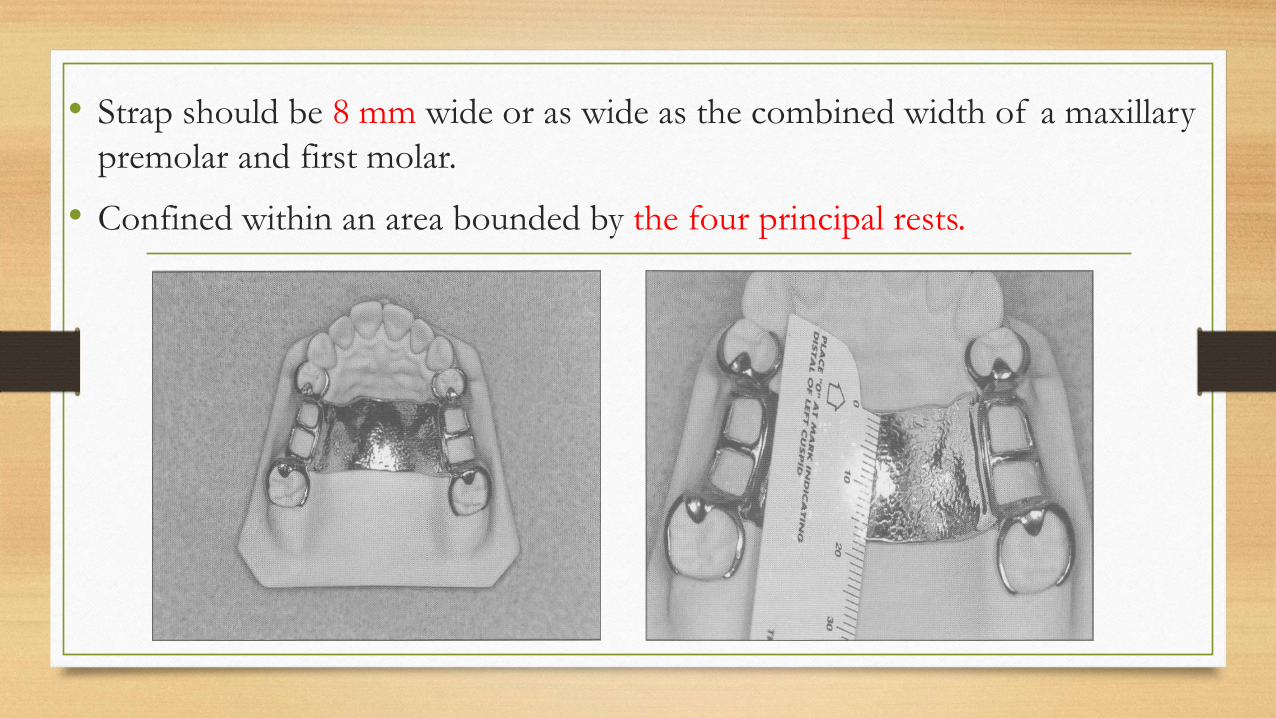
• Strap should be 8 mm wide or as wide as the combined width of a maxillary
premolar and first molar.
• Confined within an area bounded by the four principal rests.
Indications:
Bilateral and unilateral edentulous spaces of short span in a tooth-
supported
restoration (CL III & CLIII mod 1).
Contraindications:1. Tooth- tissue supported removable partial denture (RPD).
2. Palatal torus.
3. Extremely long tooth supported edentulous space.
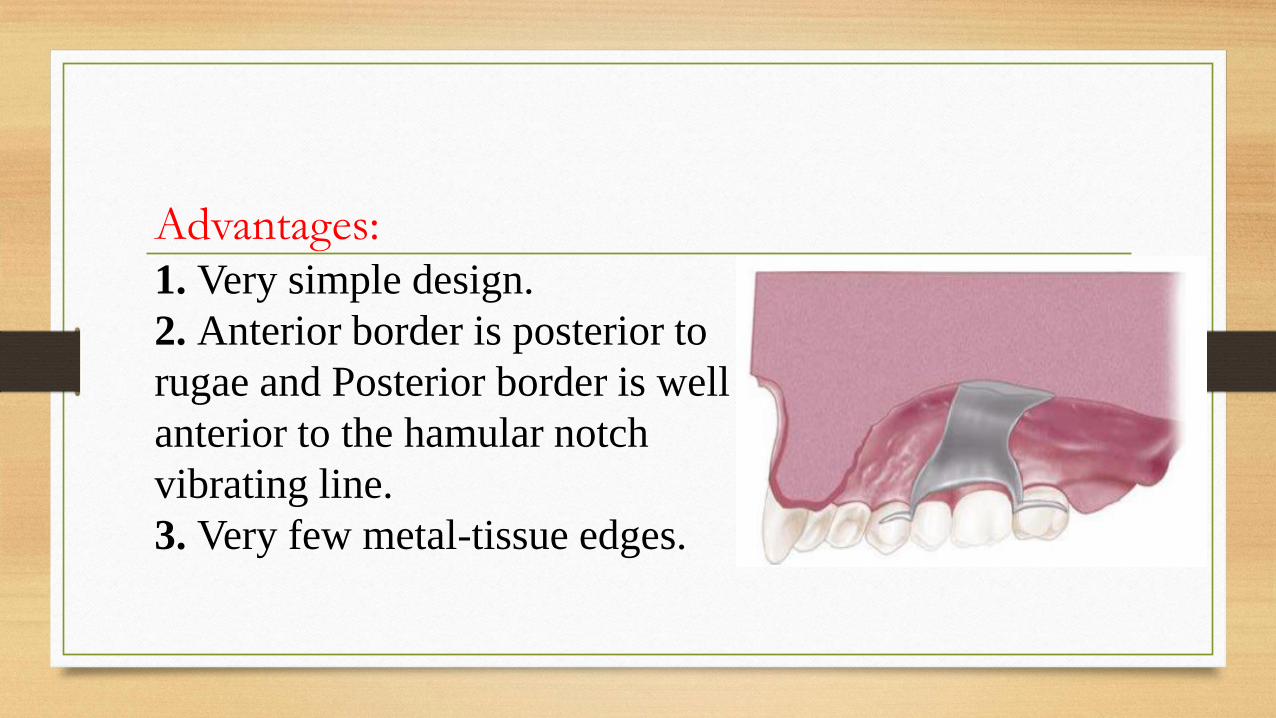
Advantages:1. Very simple design.
2. Anterior border is posterior to
rugae and Posterior border is well
anterior to the hamular notch
vibrating line.
3. Very few metal-tissue edges.
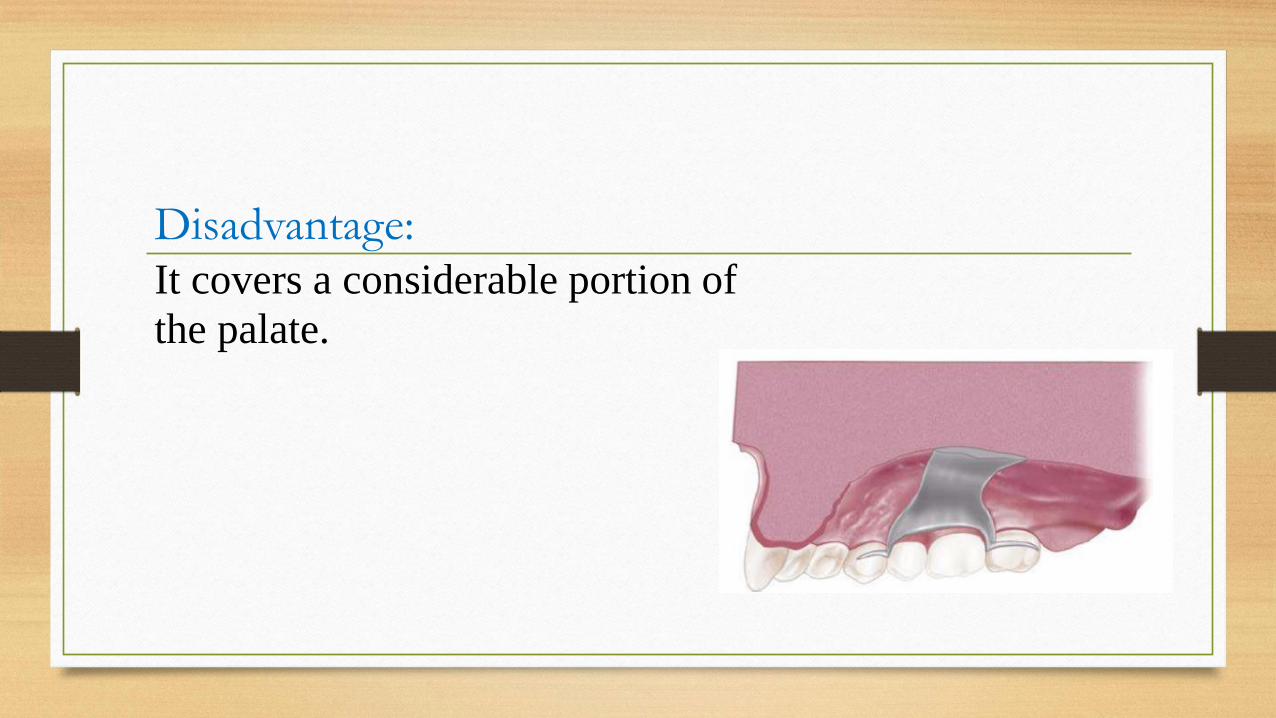
Disadvantage:It covers a considerable portion of
the palate.
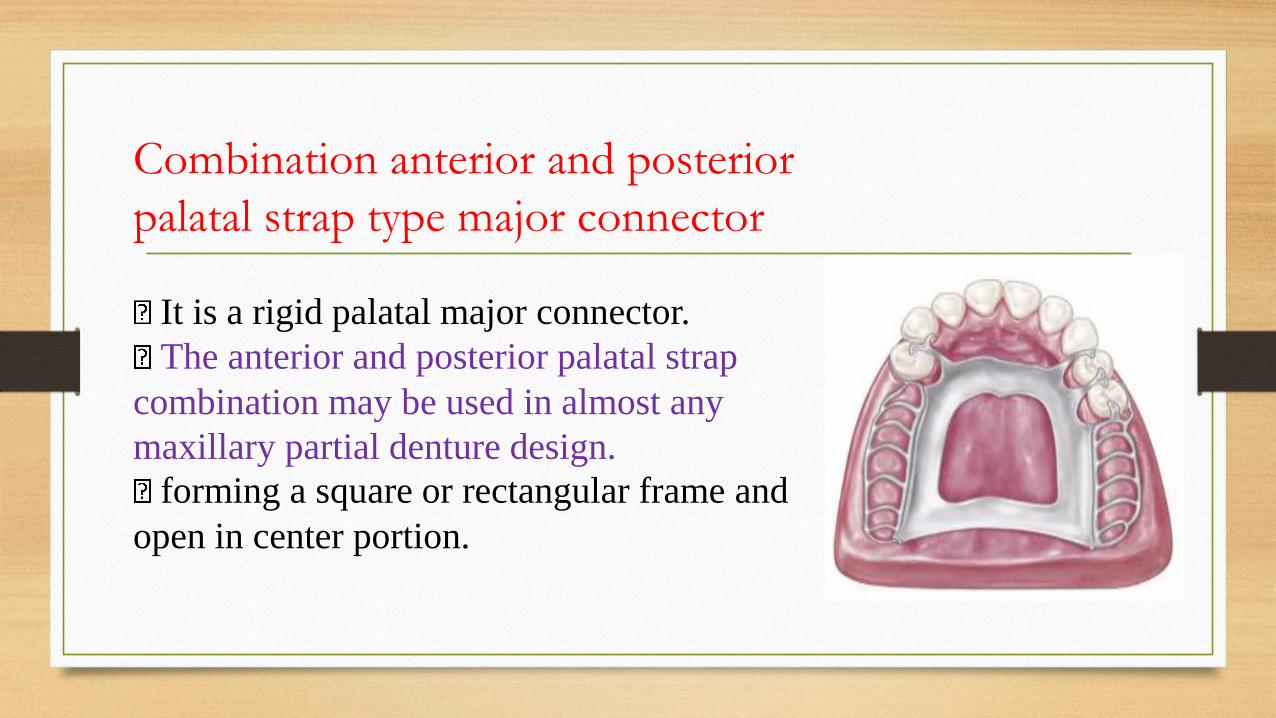
Combination anterior and posterior
palatal strap type major connector
It is a rigid palatal major connector.
The anterior and posterior palatal strap
combination may be used in almost any
maxillary partial denture design.
forming a square or rectangular frame and
open in center portion.
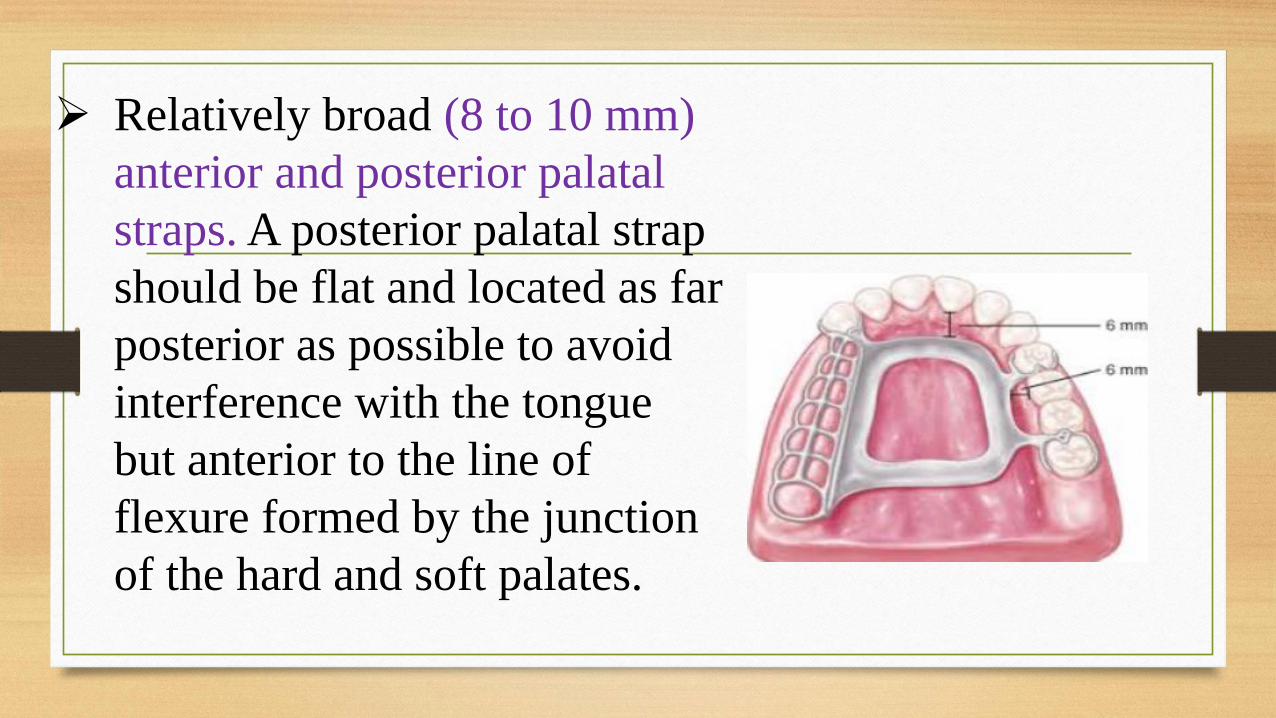
➢ Relatively broad (8 to 10 mm)
anterior and posterior palatal
straps. A posterior palatal strap
should be flat and located as far
posterior as possible to avoid
interference with the tongue
but anterior to the line of
flexure formed by the junction
of the hard and soft palates.
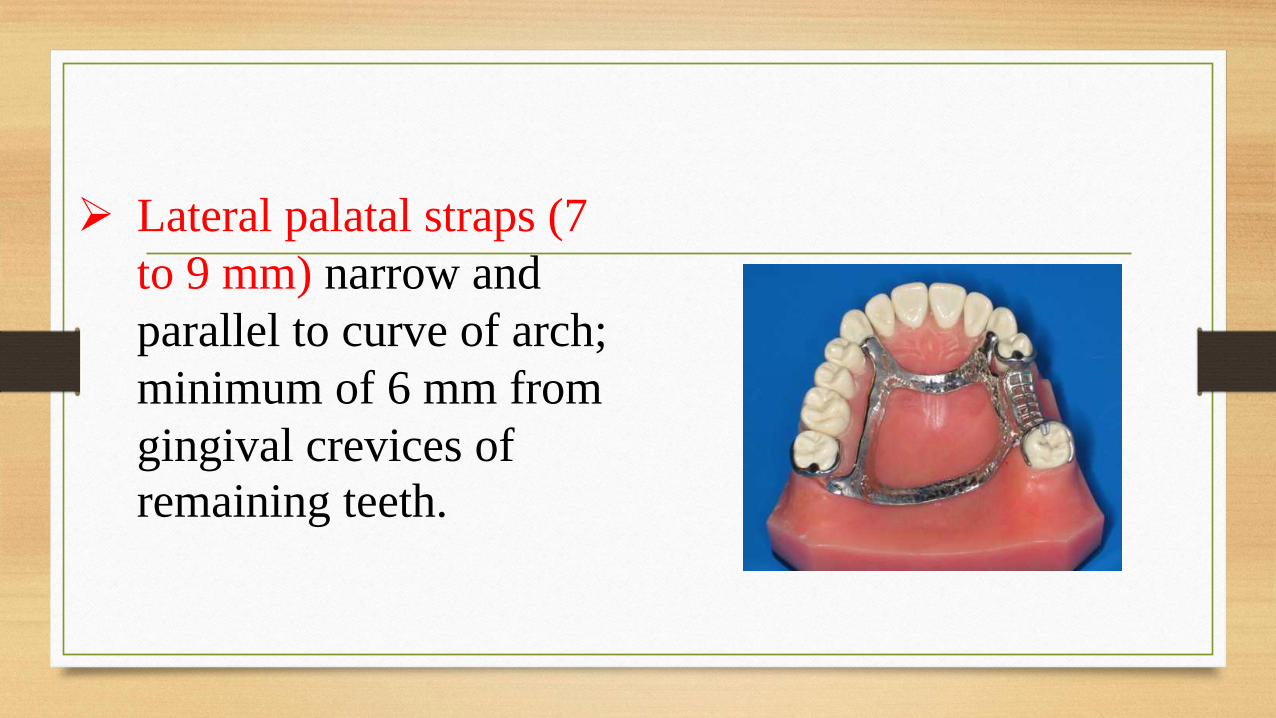
➢ Lateral palatal straps (7
to 9 mm) narrow and
parallel to curve of arch;
minimum of 6 mm from
gingival crevices of
remaining teeth.
Indications:
1. In Class I and II arches in which excellent
abutment and residual ridge support exists, and direct
retention can be made adequate without the need for
indirect retention from palate (palatal plate).
2. Long edentulous spans in Class II mod. 1 arches.
Indications:
3. In Class IV arches in which anterior teeth must be
replaced with a removable partial denture.
4. Inoperable palatal tori that do not extend
posteriorly to the junction of the hard and soft
palates.
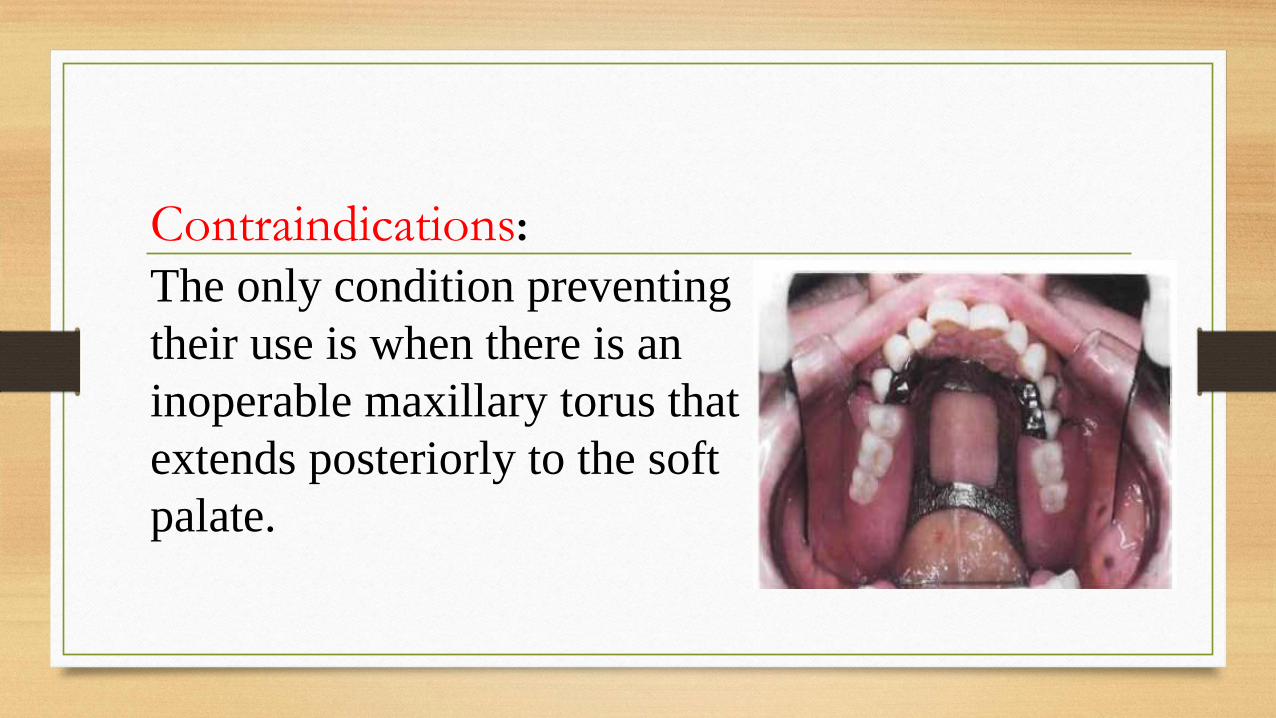
Contraindications:
The only condition preventing
their use is when there is an
inoperable maxillary torus that
extends posteriorly to the soft
palate.
Advantages:
It covers a minimum of palatal tissues.
Disadvantages:
1. Very complex design.
2. A lot of metal-tissue edges.
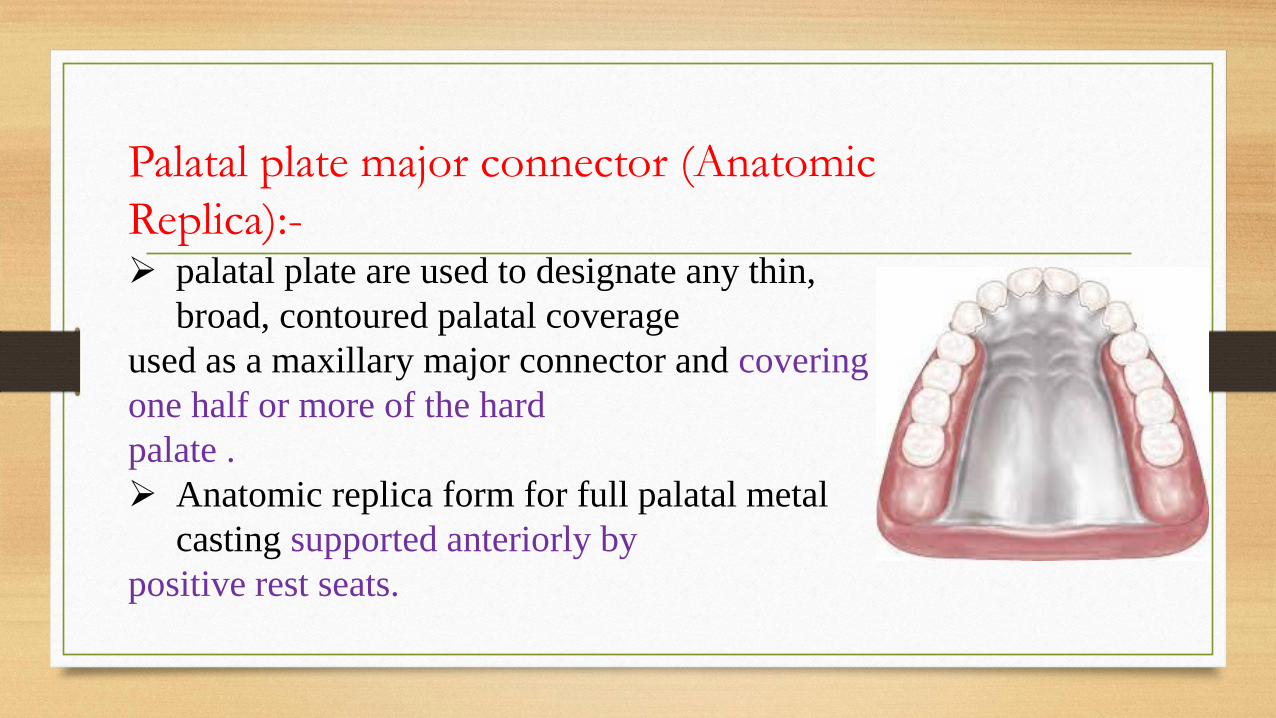
Palatal plate major connector (Anatomic
Replica):-➢ palatal plate are used to designate any thin,
broad, contoured palatal coverage
used as a maxillary major connector and covering
one half or more of the hard
palate .
➢ Anatomic replica form for full palatal metal
casting supported anteriorly by
positive rest seats.
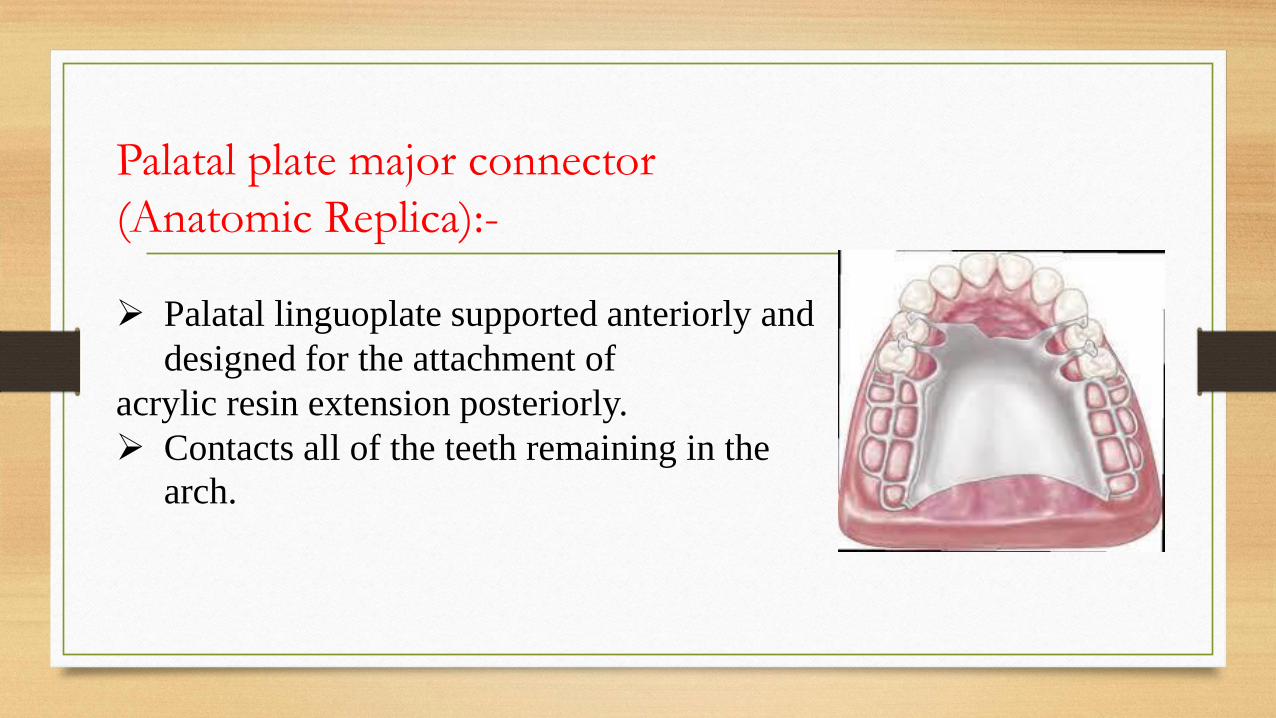
Palatal plate major connector
(Anatomic Replica):-
➢ Palatal linguoplate supported anteriorly and
designed for the attachment of
acrylic resin extension posteriorly.
➢ Contacts all of the teeth remaining in the
arch.
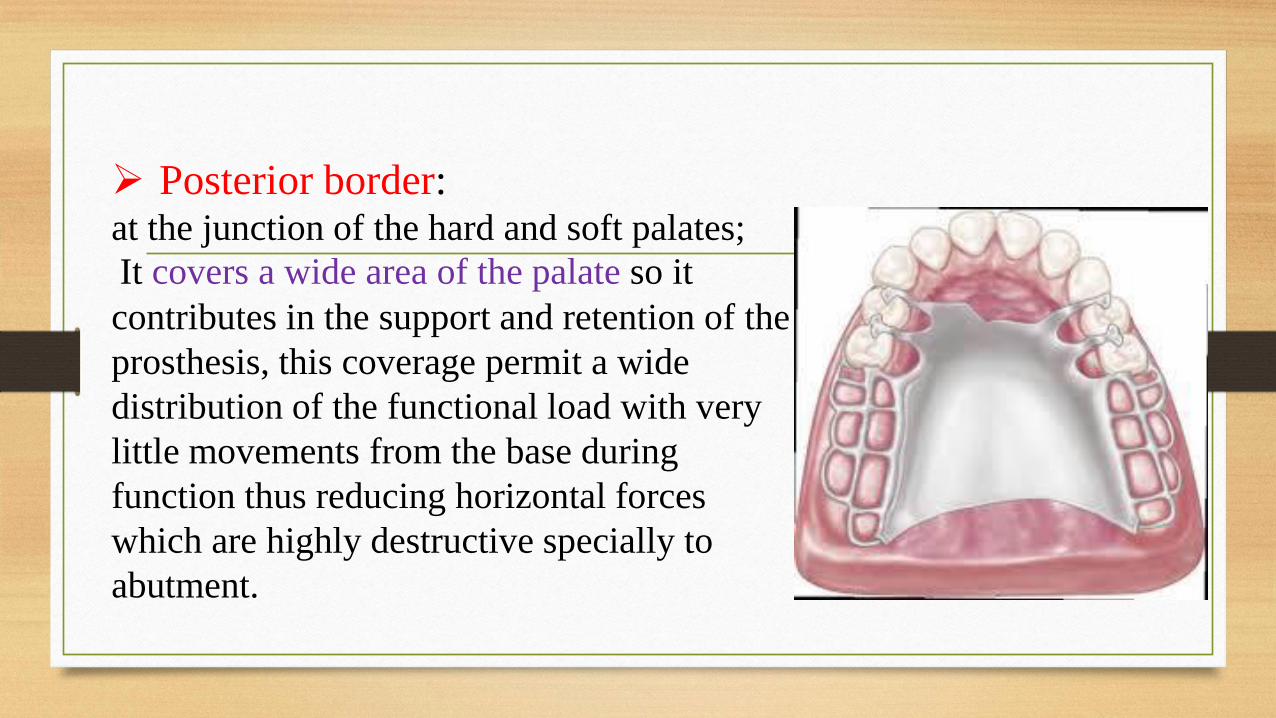
➢ Posterior border: at the junction of the hard and soft palates;
It covers a wide area of the palate so it
contributes in the support and retention of the
prosthesis, this coverage permit a wide
distribution of the functional load with very
little movements from the base during
function thus reducing horizontal forces
which are highly destructive specially to
abutment.
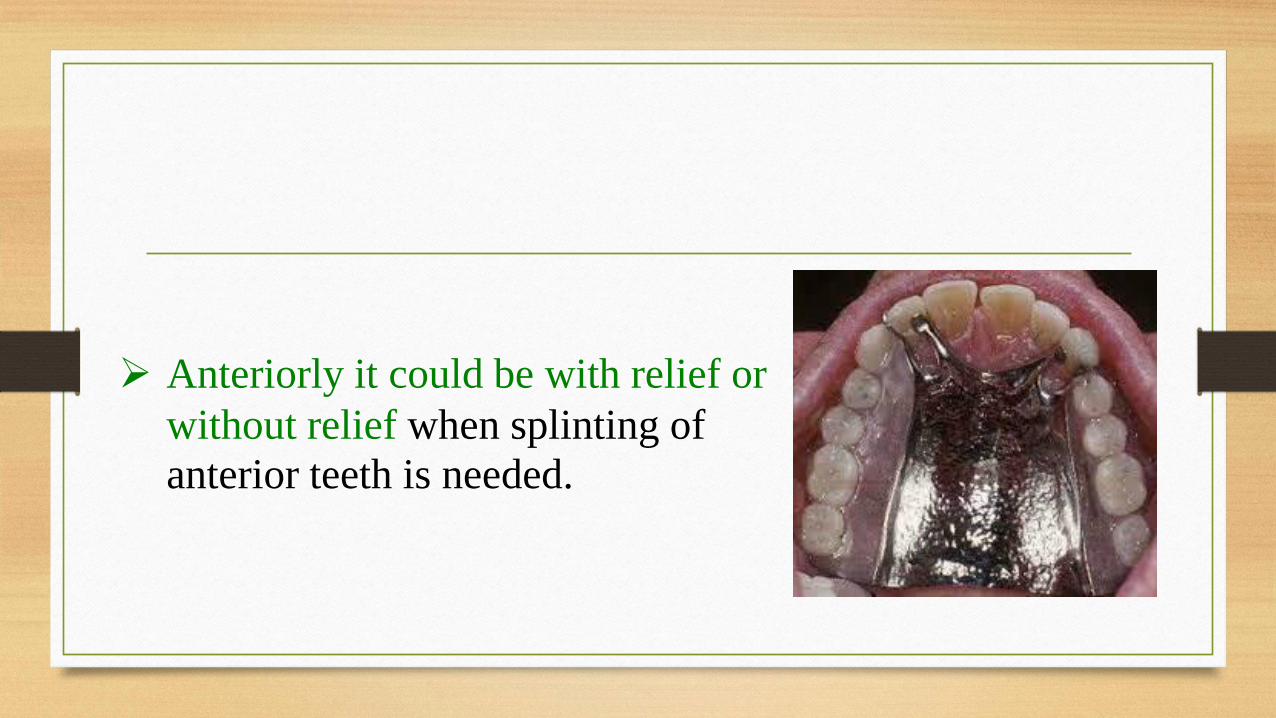
➢ Anteriorly it could be with relief or
without relief when splinting of
anterior teeth is needed.
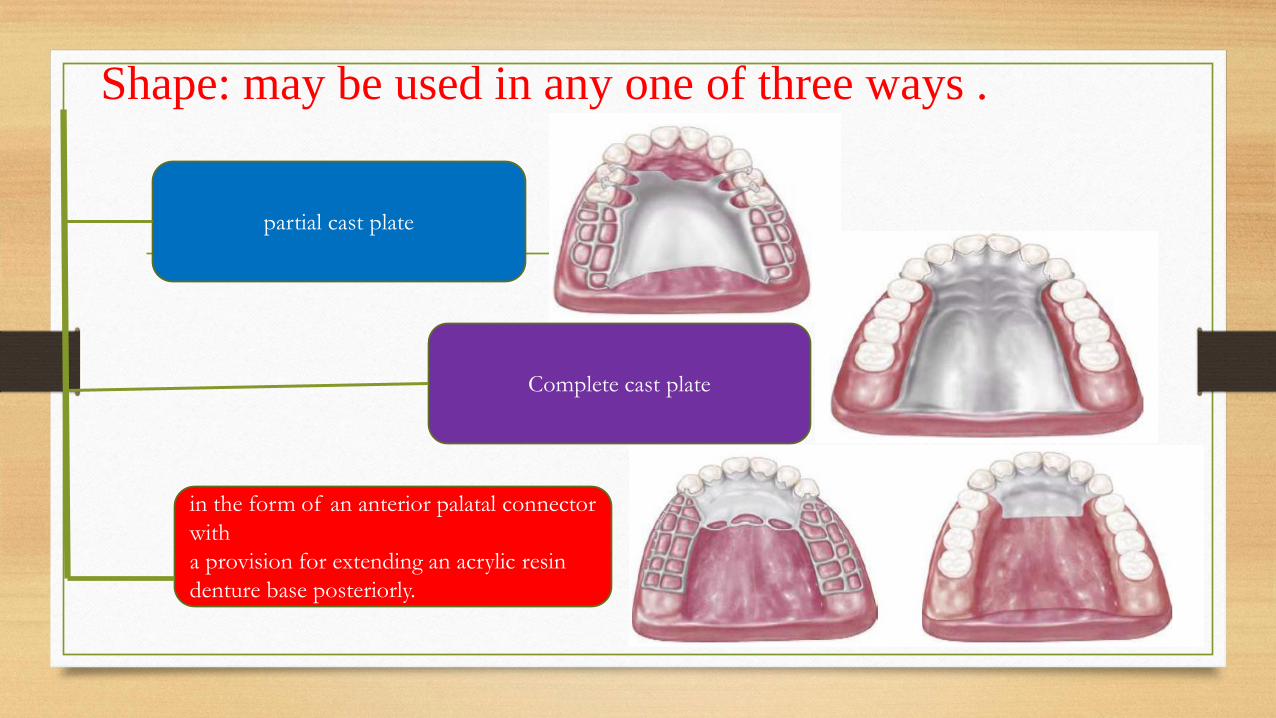
Shape: may be used in any one of three ways .
partial cast plate
Complete cast plate
in the form of an anterior palatal connector
with
a provision for extending an acrylic resin
denture base posteriorly.
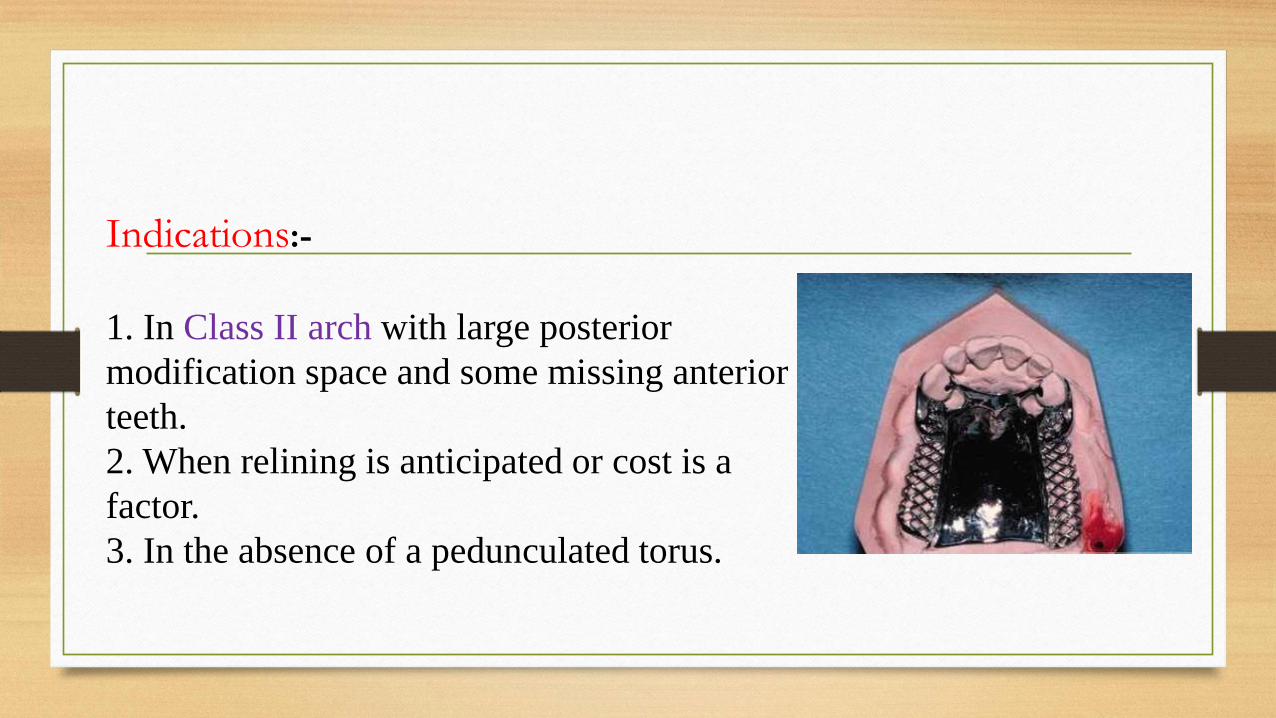
Indications:-
1. In Class II arch with large posterior
modification space and some missing anterior
teeth.
2. When relining is anticipated or cost is a
factor.
3. In the absence of a pedunculated torus.
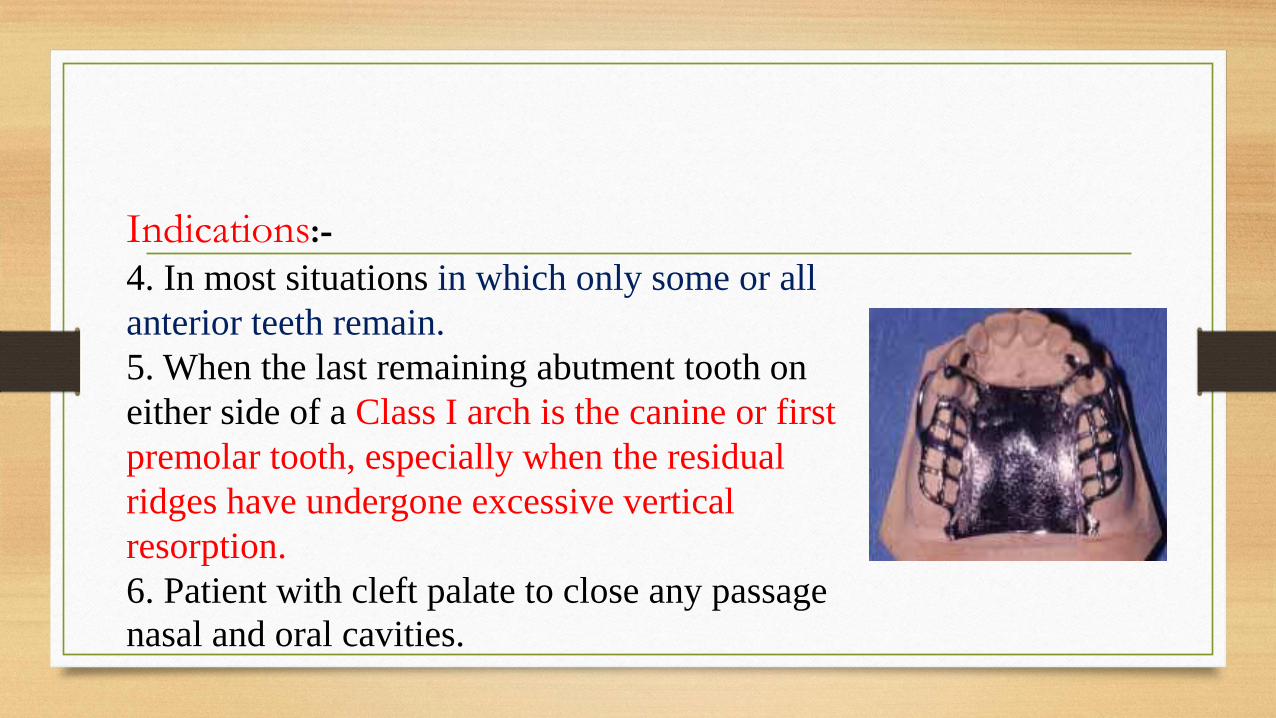
Indications:-
4. In most situations in which only some or all
anterior teeth remain.
5. When the last remaining abutment tooth on
either side of a Class I arch is the canine or first
premolar tooth, especially when the residual
ridges have undergone excessive vertical
resorption.
6. Patient with cleft palate to close any passage
nasal and oral cavities.
Contraindications:
When less than complete palatal coverage is necessary and there are
sufficient remaining natural teeth to use a palatal plate major connector.
Advantages:
1. It permits the making of a uniformly thin metal plate that reproduces
faithfully
the anatomic contours of the patient’s own palate. Its uniform thinness and
the thermal conductivity of the metal are designed to make the palatal
plate more readily acceptable to the tongue and underlying tissue.
Advantages:
2. The corrugation in the anatomic replica adds strength to
the casting; thus a thinner casting with adequate rigidity can
be made.
3. Surface irregularities are intentional rather than accidental;
therefore electrolytic polishing is all that is needed, the
original uniform thickness of the plastic pattern is thus
maintained.
Advantages:
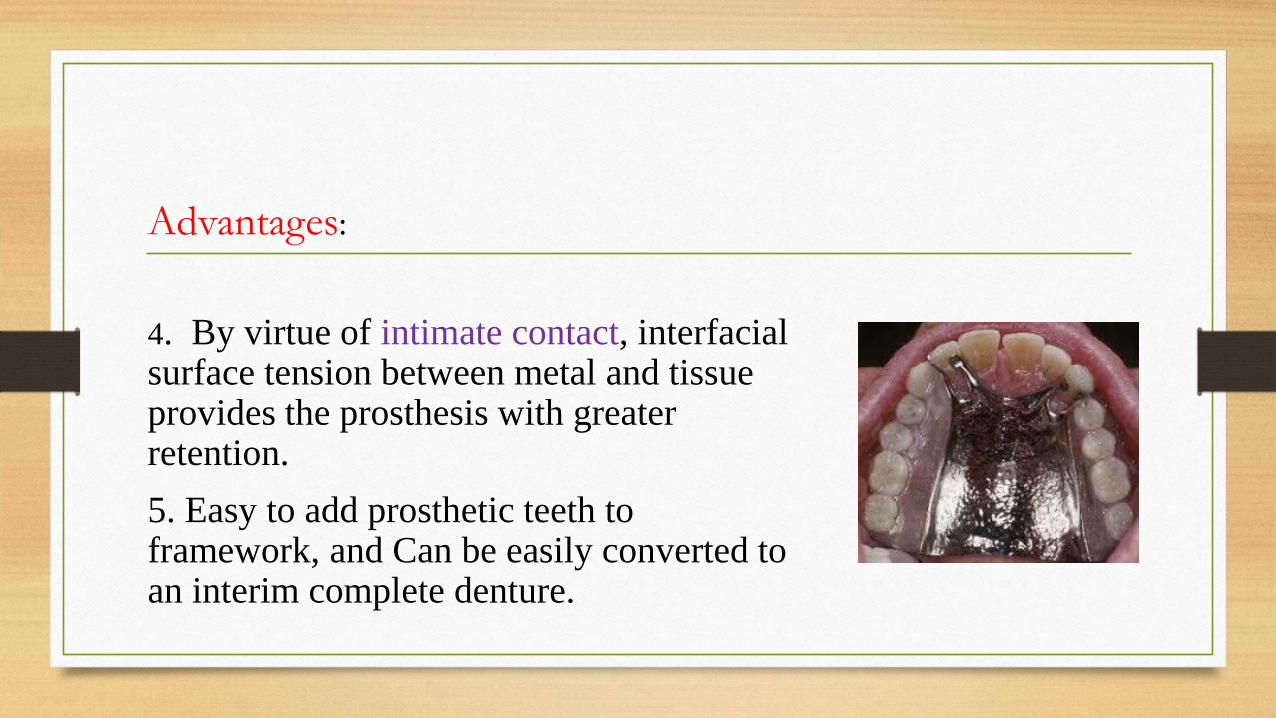
4. By virtue of intimate contact, interfacial surface tension between metal and tissue provides the prosthesis with greater retention.
5. Easy to add prosthetic teeth to framework, and Can be easily converted to an interim complete denture.
Disadvantages:1. Covers more tooth and tissue surface than any other major connector.
2. Design difficulties:
a) The hamular notch vibrating line area must be located on the master cast.
b) Difficult to adjust the metal-tissue contact.
c) Difficult to reline the metal portion of the palatal contact.
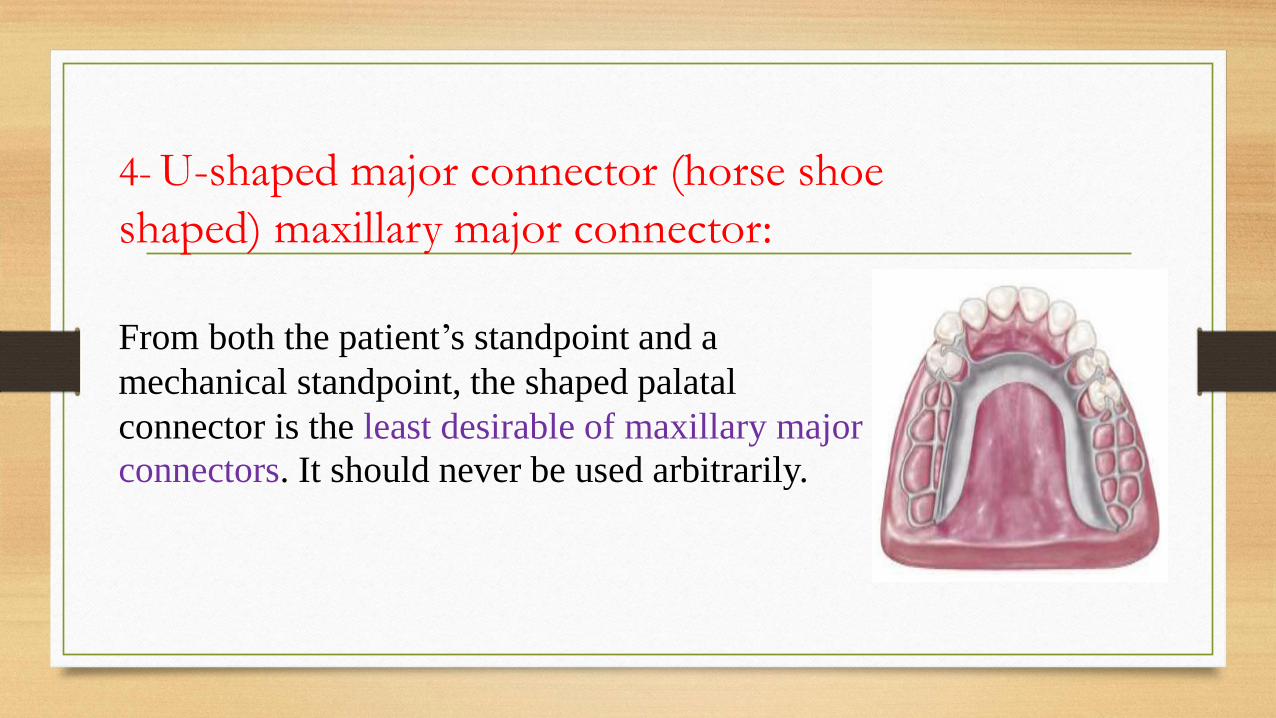
4- U-shaped major connector (horse shoe
shaped) maxillary major connector:
From both the patient’s standpoint and a
mechanical standpoint, the shaped palatal
connector is the least desirable of maxillary major
connectors. It should never be used arbitrarily.
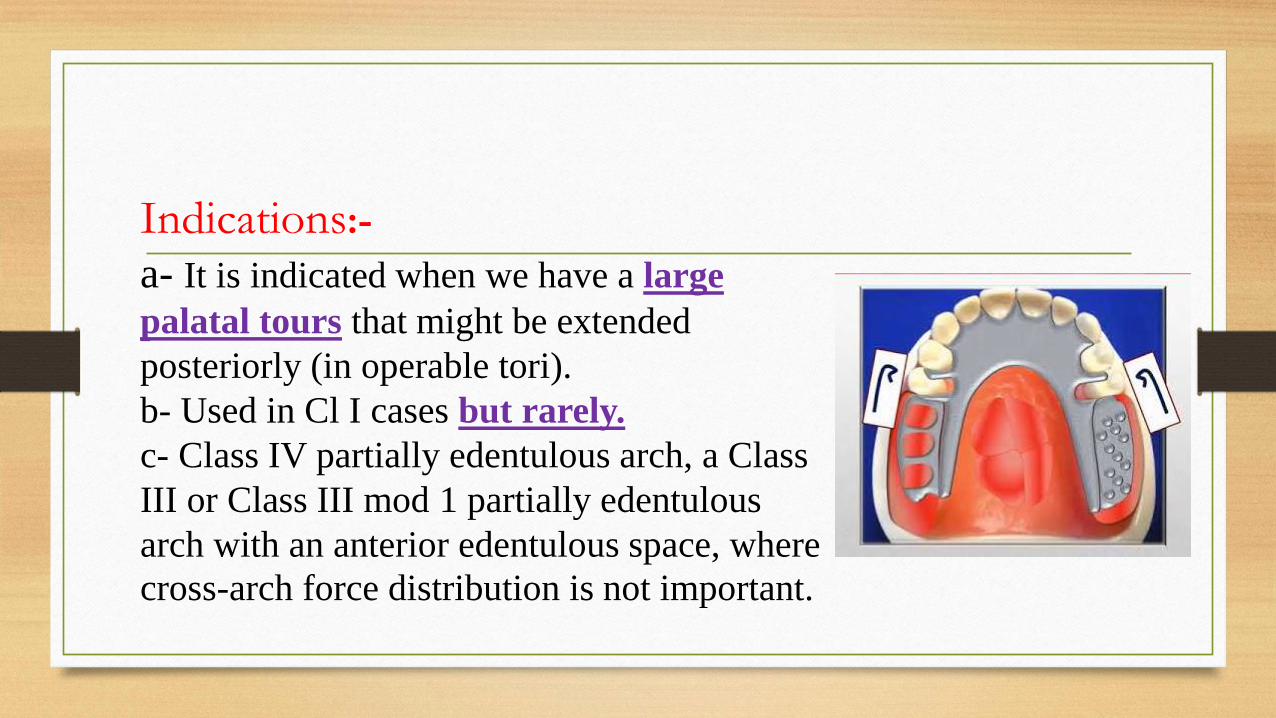
Indications:-
a- It is indicated when we have a large
palatal tours that might be extended
posteriorly (in operable tori).
b- Used in Cl I cases but rarely.
c- Class IV partially edentulous arch, a Class
III or Class III mod 1 partially edentulous
arch with an anterior edentulous space, where
cross-arch force distribution is not important.
Contraindications:
1. Where support, retention, bracing, and direct- indirect retention
from the palate is necessary
2. Where cross-arch force distribution is necessary.
Advantages:
1. Minimal coverage of the palate and fewer metal-tooth or tissue
edges than the AP design
2. Fairly simple design.
The disadvantages of this type:
1. It is flexible and not rigid (allows lateral flexure under occlusal
forces, which may induce torque or direct lateral force to abutment
teeth).
2. It has the disadvantages of being bulky for the tongue and thus
interferes with the phonetics causing this comfort to the patient, so it
is objectionable from both, the patients and mechanical stand point.
The disadvantages of this type:
3. Also (gingival irritation) the design may permit impingement
of tissues underline, its palatal border when subjected to occlusal
loads (fails to provide good support).
4. Movement may occur at the open ends.
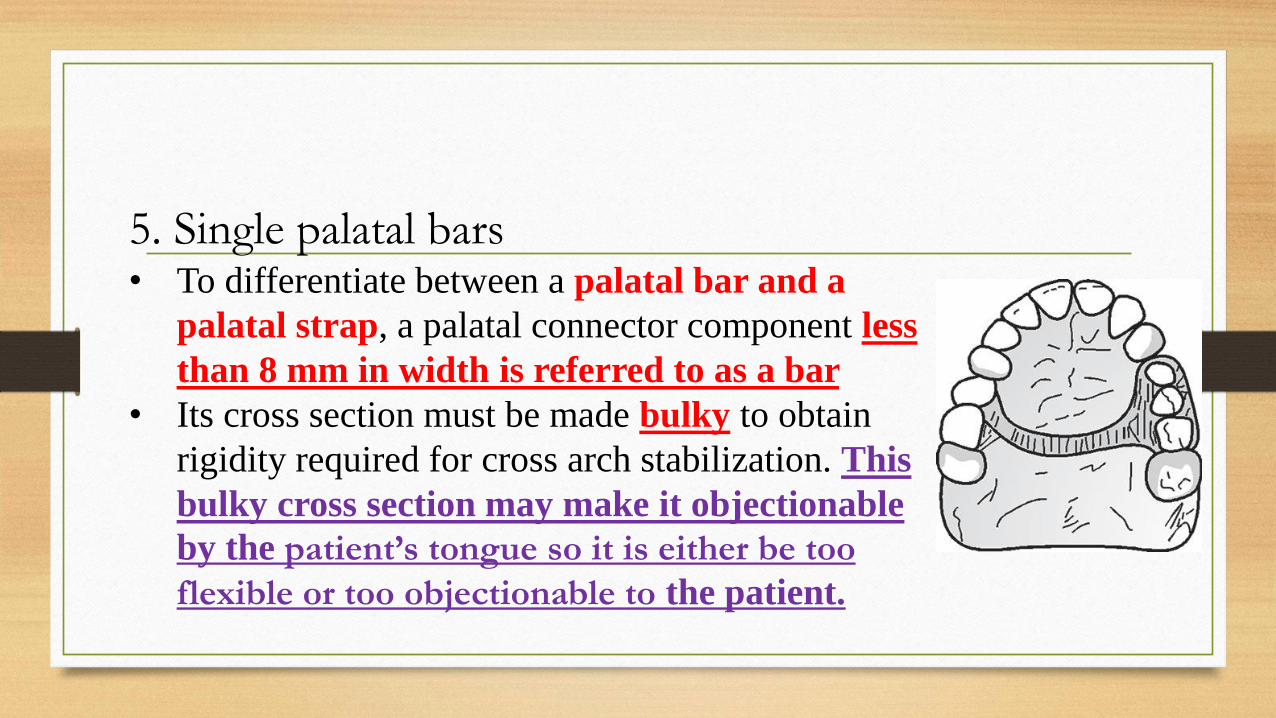
5. Single palatal bars• To differentiate between a palatal bar and a
palatal strap, a palatal connector component less
than 8 mm in width is referred to as a bar
• Its cross section must be made bulky to obtain
rigidity required for cross arch stabilization. This
bulky cross section may make it objectionable
by the patient’s tongue so it is either be too
flexible or too objectionable to the patient.
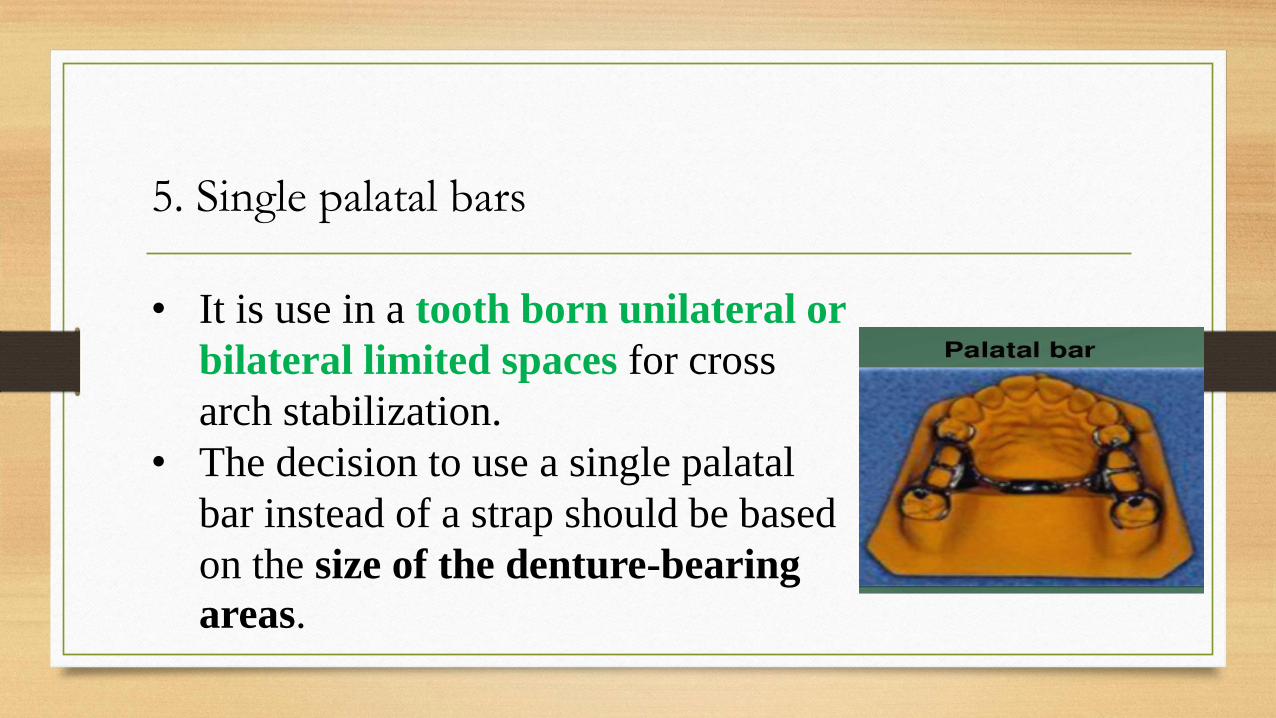
5. Single palatal bars
• It is use in a tooth born unilateral or
bilateral limited spaces for cross
arch stabilization.
• The decision to use a single palatal
bar instead of a strap should be based
on the size of the denture-bearing
areas.
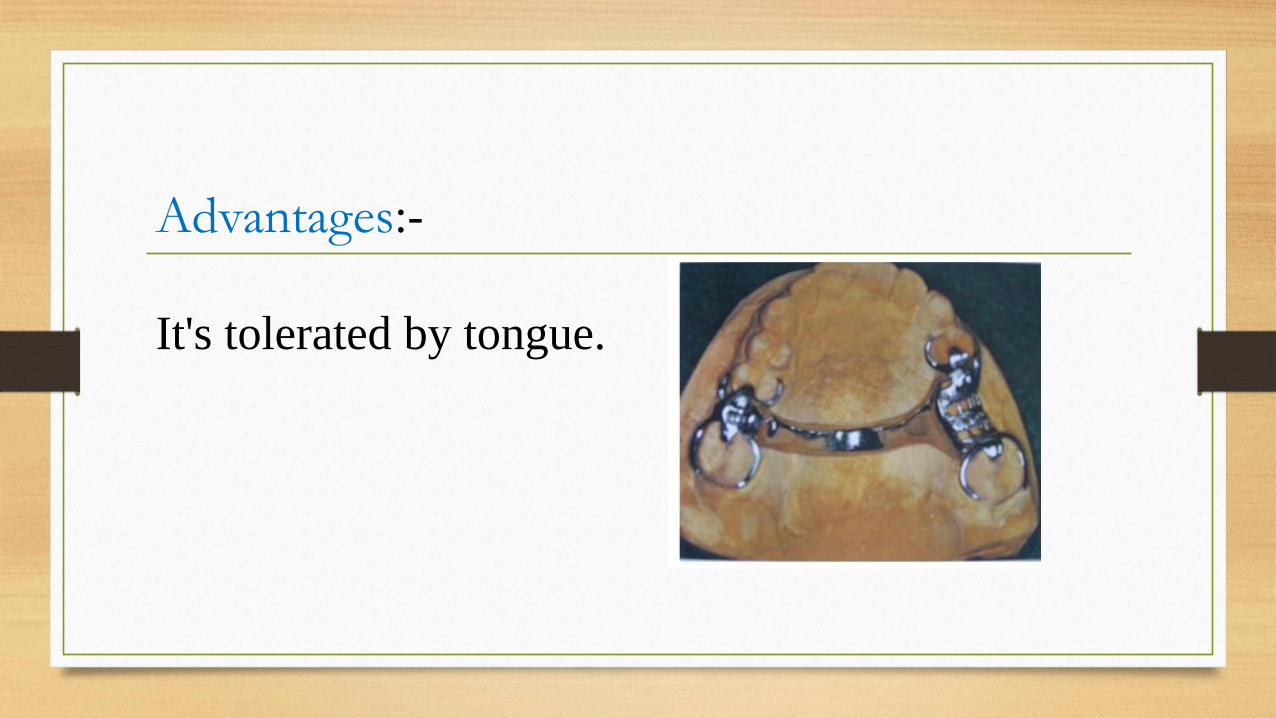
Advantages:-
It's tolerated by tongue.
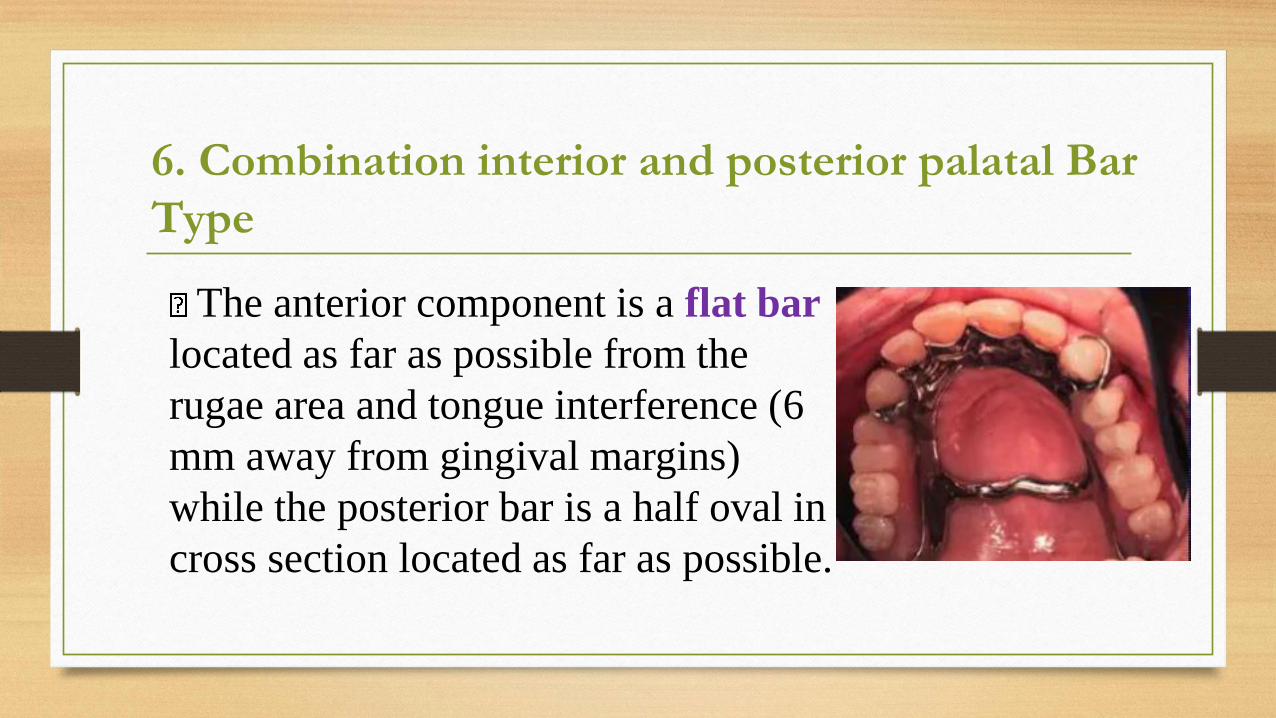
The anterior component is a flat bar
located as far as possible from the
rugae area and tongue interference (6
mm away from gingival margins)
while the posterior bar is a half oval in
cross section located as far as possible.
6. Combination interior and posterior palatal Bar
Type
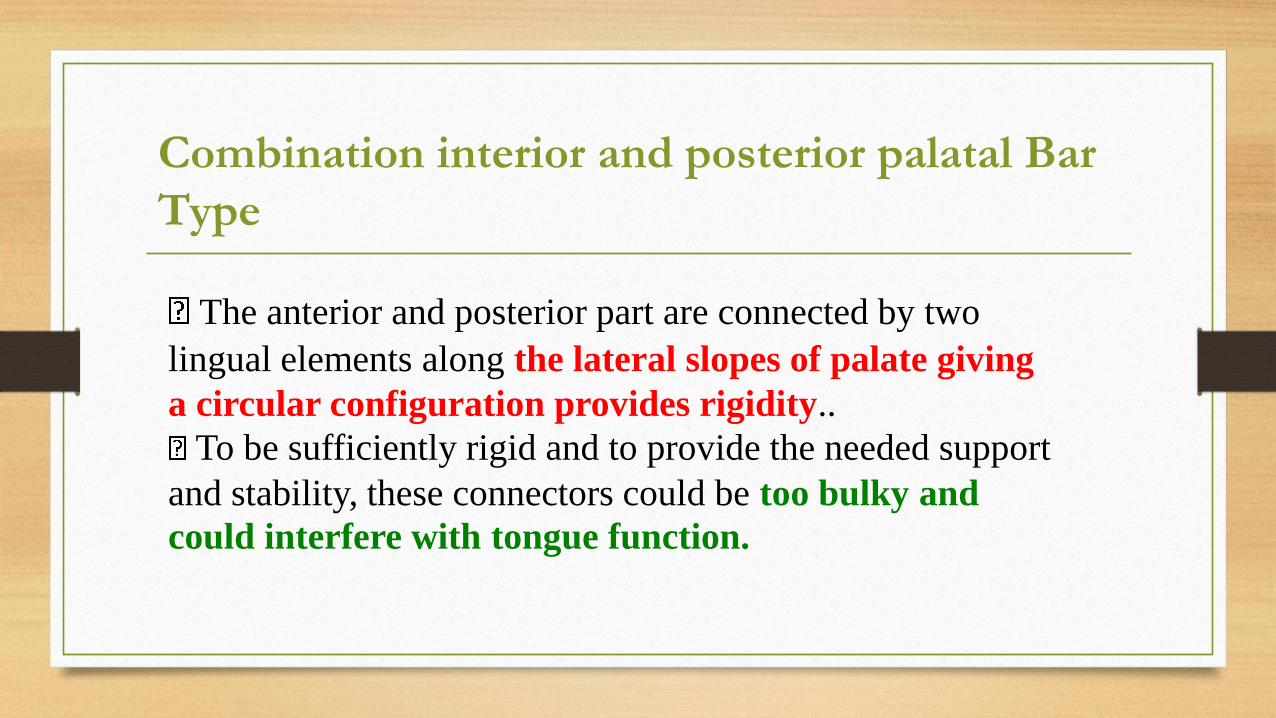
The anterior and posterior part are connected by two
lingual elements along the lateral slopes of palate giving
a circular configuration provides rigidity..
To be sufficiently rigid and to provide the needed support
and stability, these connectors could be too bulky and
could interfere with tongue function.
Combination interior and posterior palatal Bar
Type

Advantages:
Strong.
Limited soft tissue coverage.
Disadvantages:
Limited support from the palate.
Uncomfortable as it has multiple
borders.
Selection of the type of connector(s) is based on four
factors:
1. mouth comfort
2. rigidity
3. location of denture bases
4. indirect retention.
❖ Connectors should be of minimum bulk and
should be positioned so that interference with the
tongue during speech and mastication is not
encountered.
❖ Connectors must have a maximum of rigidity to
distribute stress bilaterally.
Quiz
Major Connector must be Rigid or
Flexible, and why?
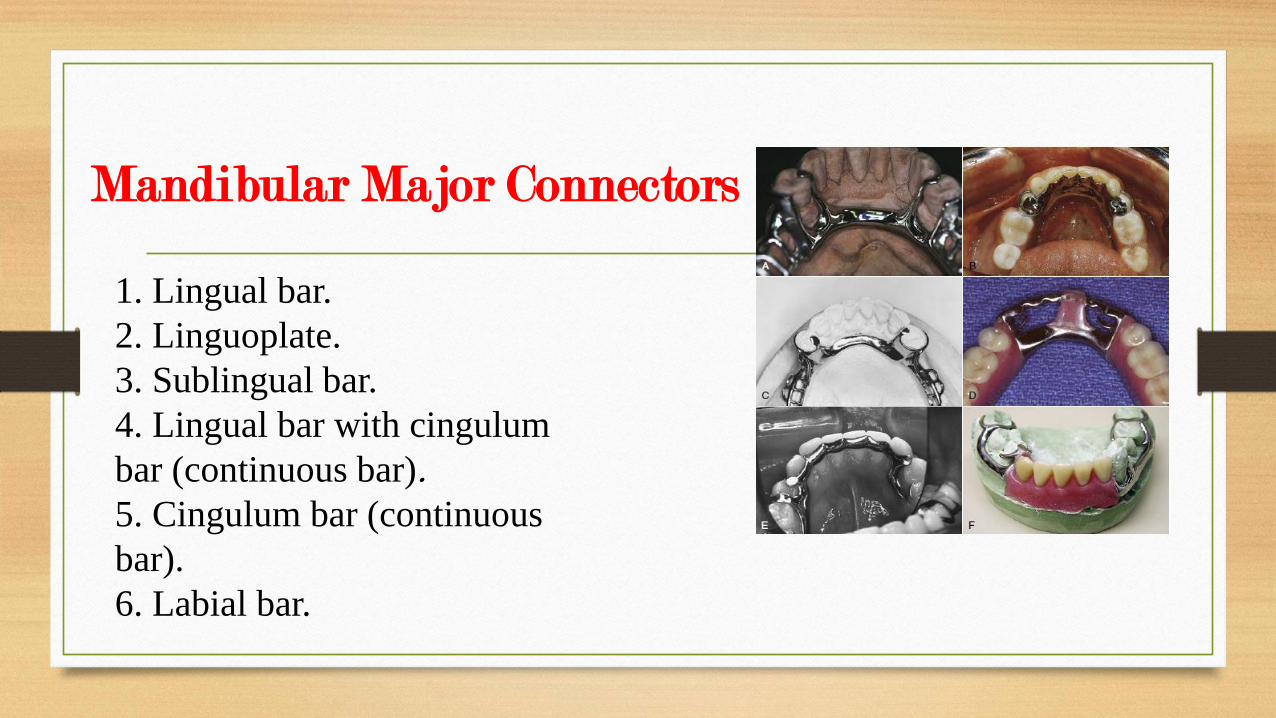
Mandibular Major Connectors
1. Lingual bar.
2. Linguoplate.
3. Sublingual bar.
4. Lingual bar with cingulum
bar (continuous bar).
5. Cingulum bar (continuous
bar).
6. Labial bar.
Note
• The lingual bar and the linguoplate are by far the most common
major connectors used in mandibular removable partial
dentures.
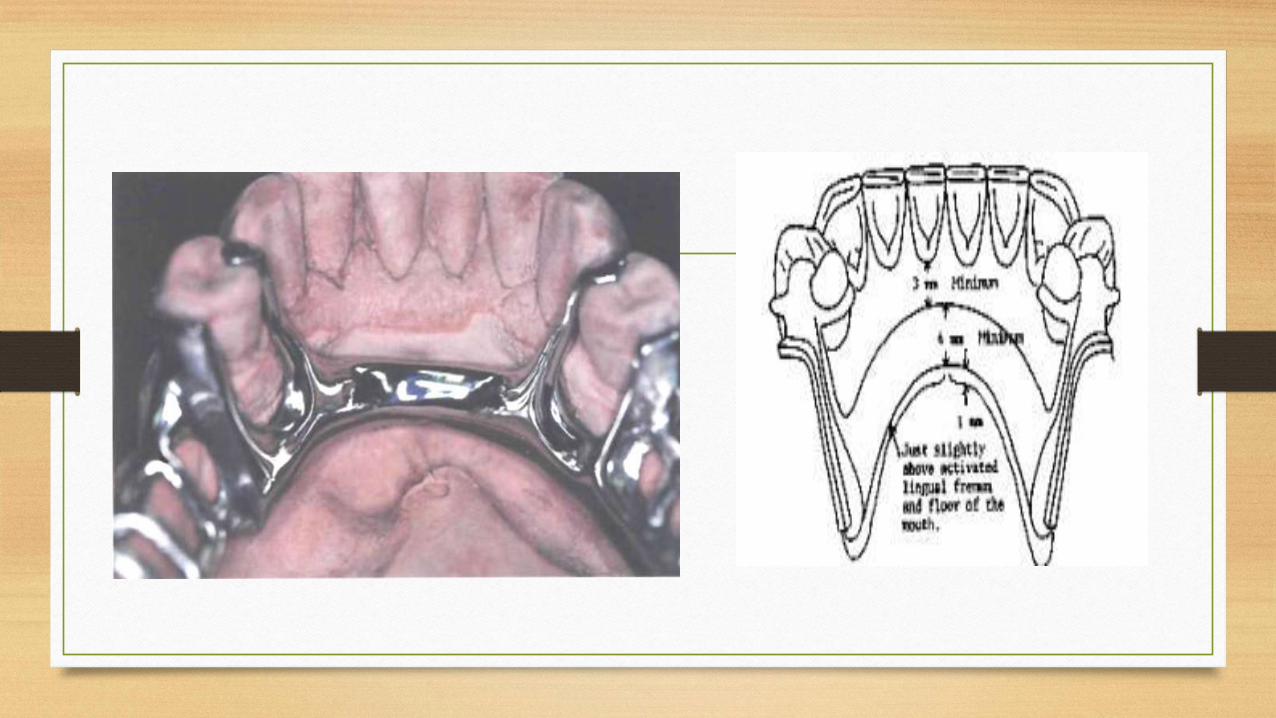
1. Lingual Bar
• Characteristics and location:-
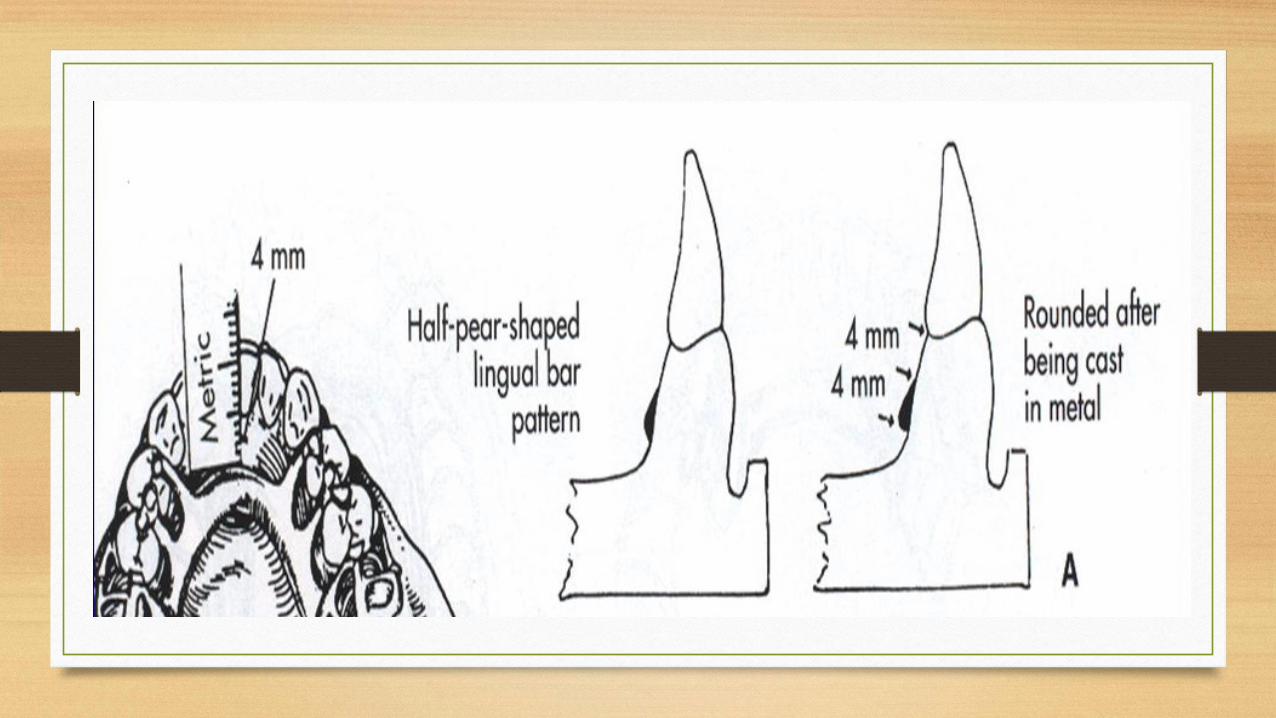
Half-pear shaped with bulkiest portion inferiorly located.
The superior border of a lingual bar connector should be tapered toward the gingival tissue superiorly with its greatest bulk at the inferior border.
The superior border should be at located 3-4mm away from the gingival margin & more if possible to prevent blood constriction.
1. Lingual Bar
Characteristics and location:-
Half-pear shaped with bulkiest portion inferiorly located. The inferior border of
the lingual bar should be slightly rounded. A rounded border will not impinge on
the lingual tissue when the denture bases rotate inferiorly under occlusal loads.
Inferior border located at the ascertained height of the alveolar lingual sulcus
when the patient's tongue is slightly elevated.
Frequently, additional bulk is necessary to provide rigidity, particularly when the
bar is long or when a less rigid alloy is used.
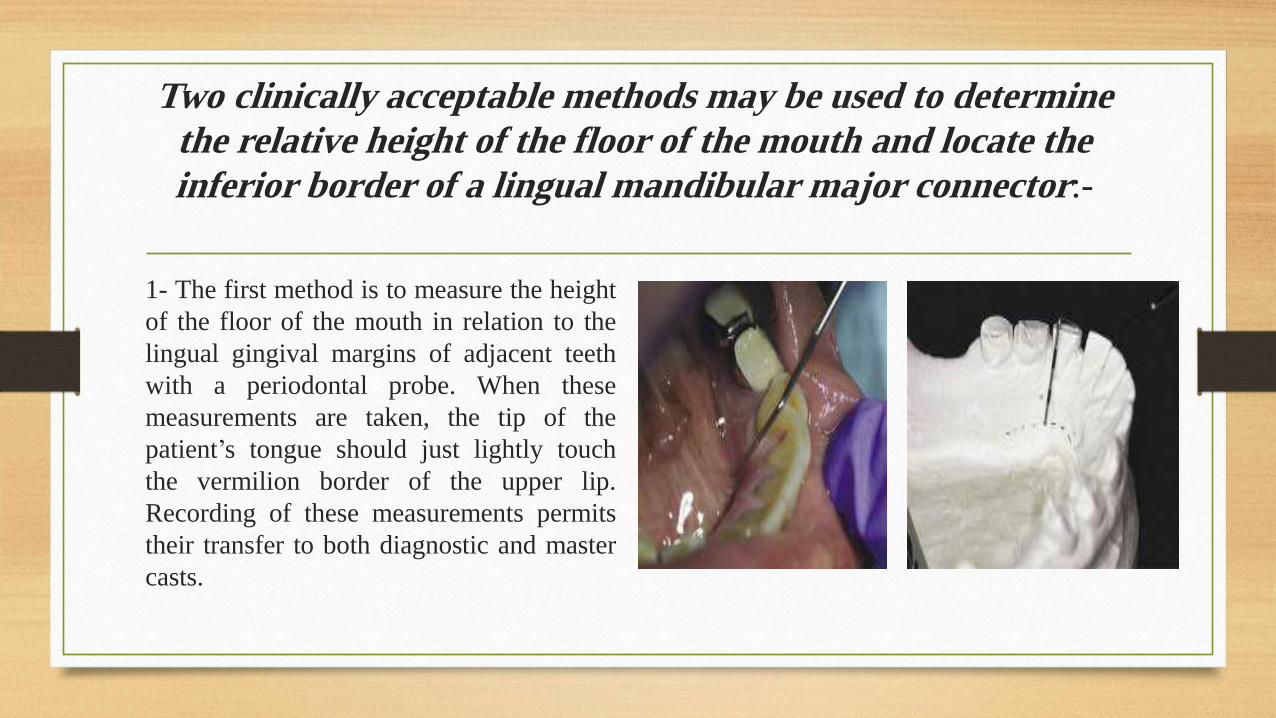
Two clinically acceptable methods may be used to determine
the relative height of the floor of the mouth and locate the
inferior border of a lingual mandibular major connector:-
1- The first method is to measure the height
of the floor of the mouth in relation to the
lingual gingival margins of adjacent teeth
with a periodontal probe. When these
measurements are taken, the tip of the
patient’s tongue should just lightly touch
the vermilion border of the upper lip.
Recording of these measurements permits
their transfer to both diagnostic and master
casts.
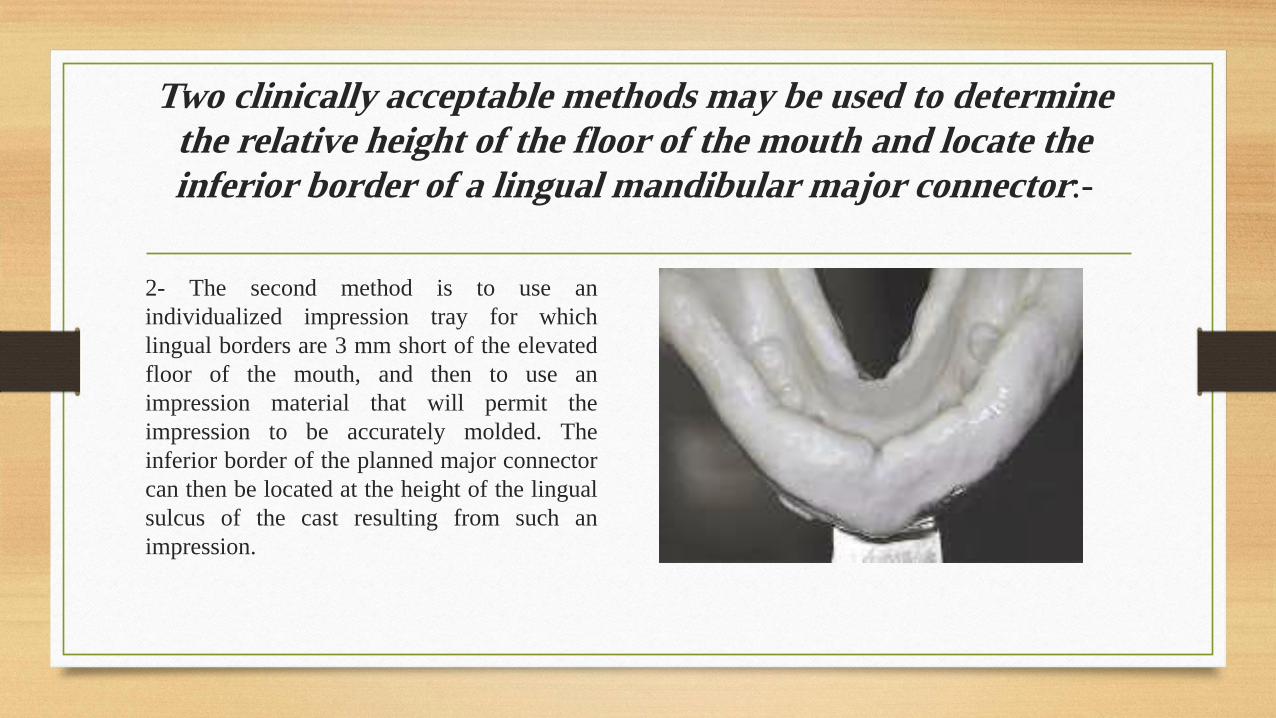
Two clinically acceptable methods may be used to determine
the relative height of the floor of the mouth and locate the
inferior border of a lingual mandibular major connector:-
2- The second method is to use an
individualized impression tray for which
lingual borders are 3 mm short of the elevated
floor of the mouth, and then to use an
impression material that will permit the
impression to be accurately molded. The
inferior border of the planned major connector
can then be located at the height of the lingual
sulcus of the cast resulting from such an
impression.
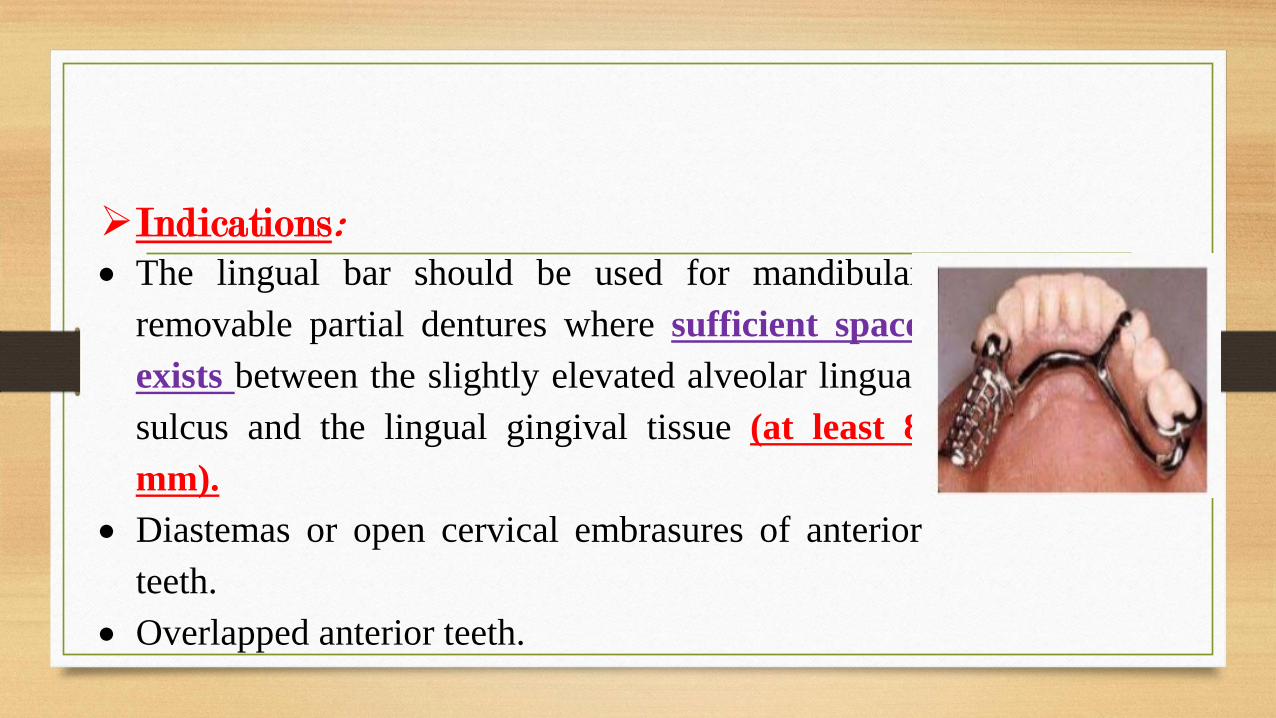
➢Indications:
• The lingual bar should be used for mandibular
removable partial dentures where sufficient space
exists between the slightly elevated alveolar lingual
sulcus and the lingual gingival tissue (at least 8
mm).
• Diastemas or open cervical embrasures of anterior
teeth.
• Overlapped anterior teeth.
➢Contraindications:
• Less than 8mm between the marginal gingival & the activated
lingual frenum & floor of the mouth.
• Only few remaining anterior teeth which must be contacted to
provide a reference for fitting the framework & indirect retention.
And when the future replacement of one or more incisor teeth
➢Contraindications:
• Lingually inclined teeth.
• An undercut lingual alveolar ridge which would result in an
excessive space between the bar & the mucosa.
➢Advantages:
• Covers a minimum of surface area of teeth & tissue therefore
the potential for caries, periodontal & mucositis caused by plaque
being held in contact with teeth & tissues is minimal.
• Esthetic.
➢Disadvantages:
• Less rigidity compared with other types.
• Difficult to add additional prosthetic teeth to framework.
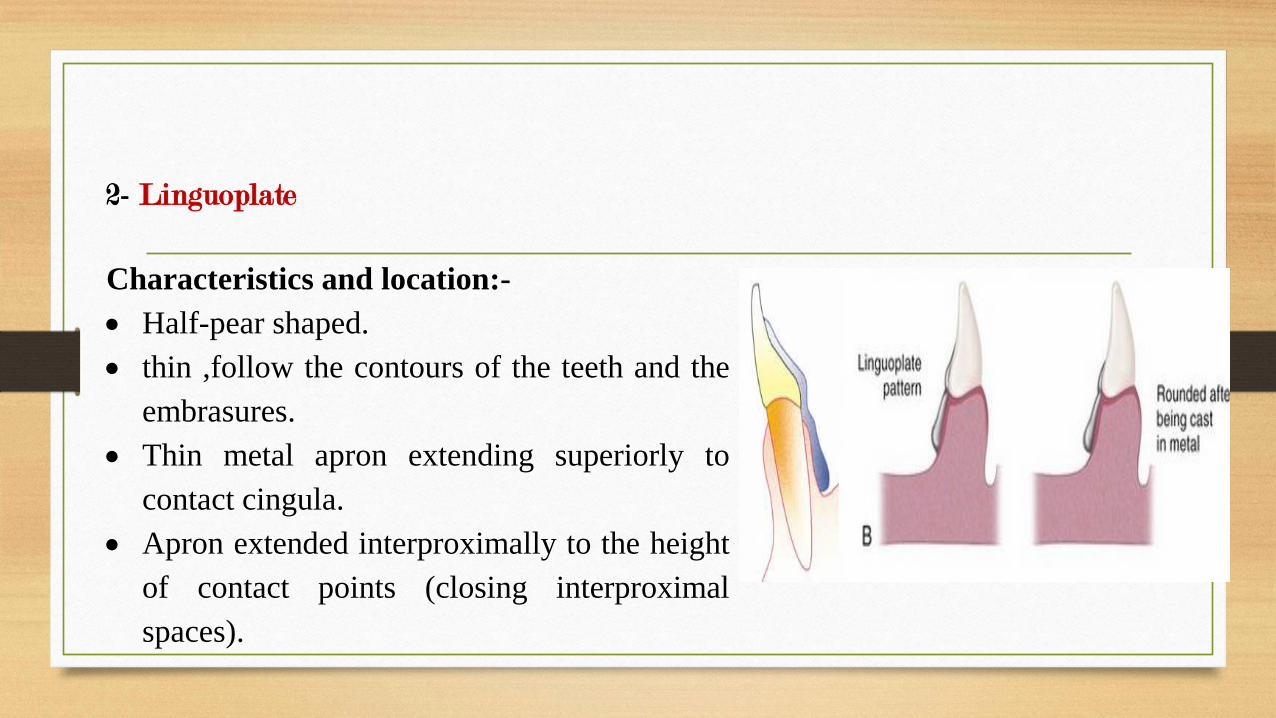
2- Linguoplate
Characteristics and location:-
• Half-pear shaped.
• thin ,follow the contours of the teeth and the
embrasures.
• Thin metal apron extending superiorly to
contact cingula.
• Apron extended interproximally to the height
of contact points (closing interproximal
spaces).
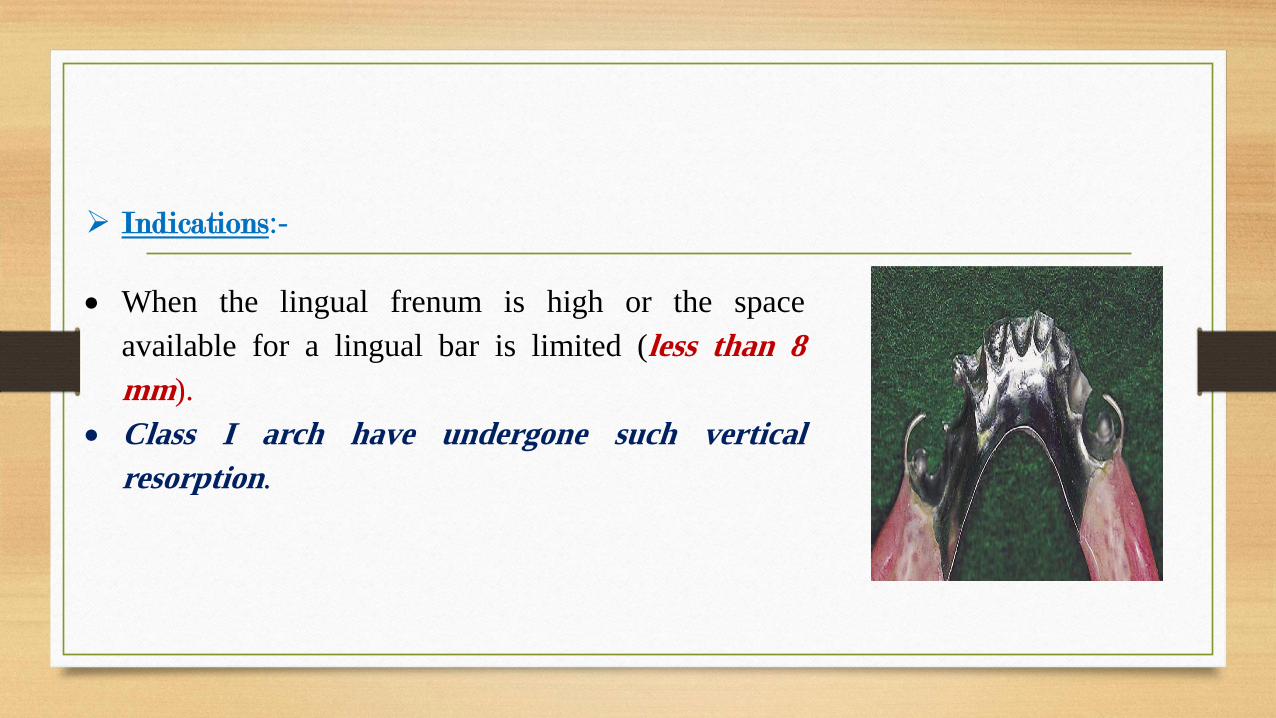
➢ Indications:-
• When the lingual frenum is high or the space
available for a lingual bar is limited (less than 8
mm).
• Class I arch have undergone such vertical
resorption.
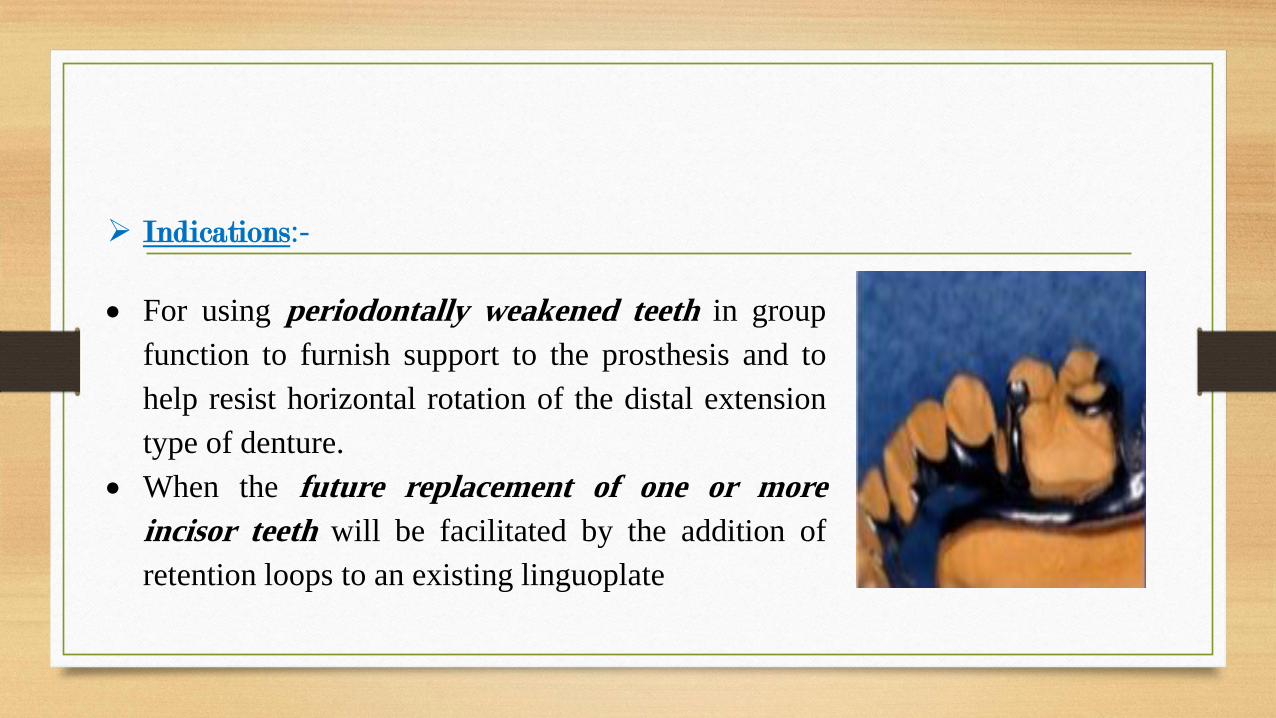
➢ Indications:-
• For using periodontally weakened teeth in group
function to furnish support to the prosthesis and to
help resist horizontal rotation of the distal extension
type of denture.
• When the future replacement of one or more
incisor teeth will be facilitated by the addition of
retention loops to an existing linguoplate
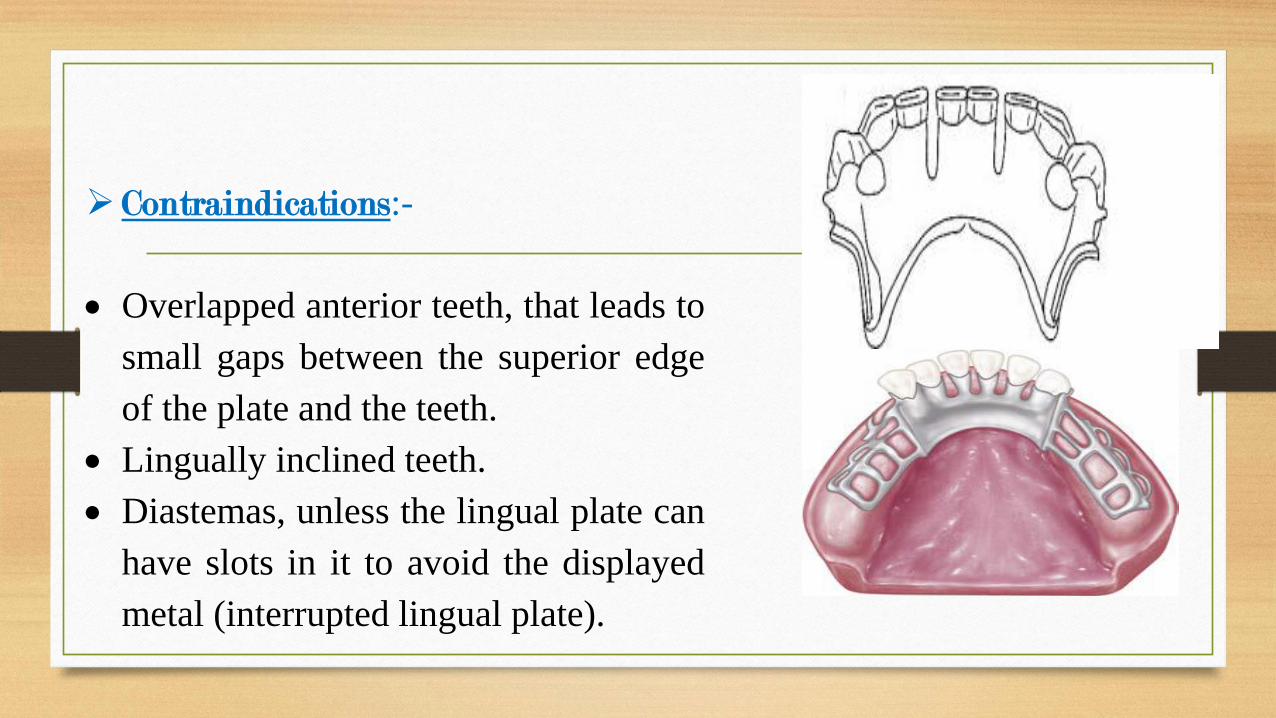
➢ Contraindications:-
• Overlapped anterior teeth, that leads to
small gaps between the superior edge
of the plate and the teeth.
• Lingually inclined teeth.
• Diastemas, unless the lingual plate can
have slots in it to avoid the displayed
metal (interrupted lingual plate).
➢Advantages:
• Structurally simple & rigidity more than a lingual
bar.
• Easy to add additional prosthetic teeth to
framework.
➢Disadvantages:• Covers more tissue surface & teeth than lingual bar.
• May be more noticeable to patient than lingual bar.
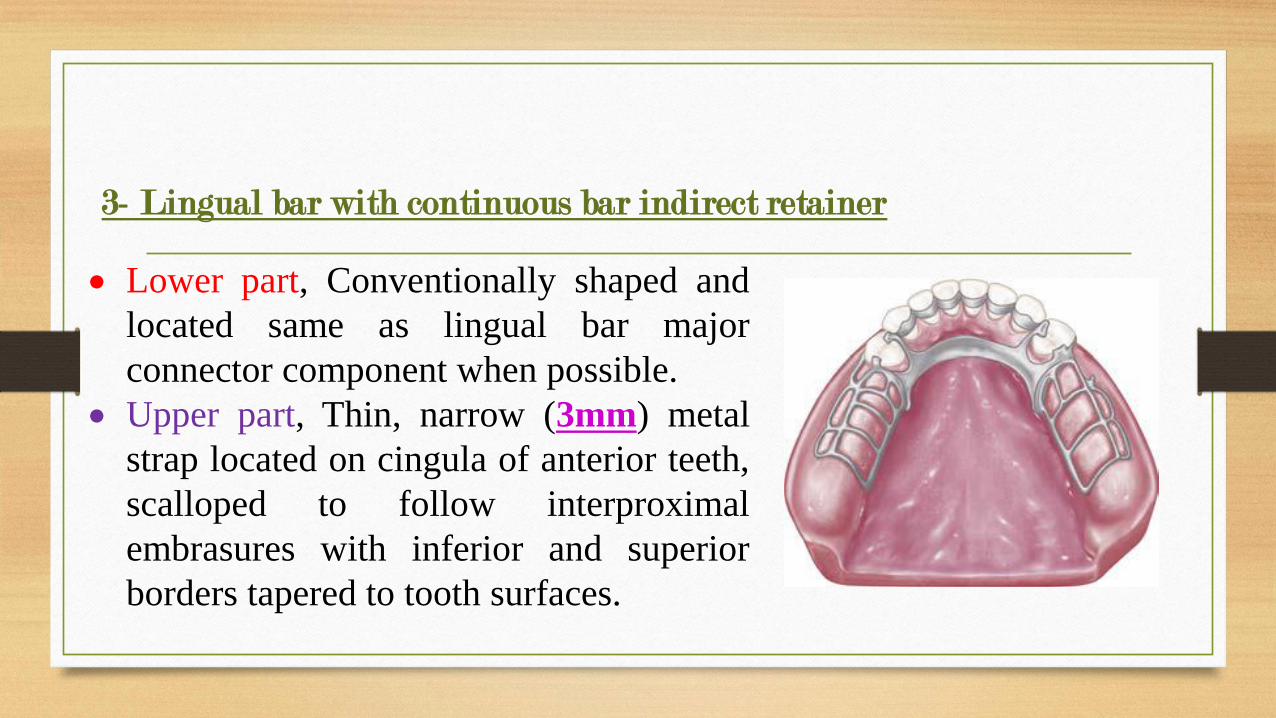
3- Lingual bar with continuous bar indirect retainer
• Lower part, Conventionally shaped and
located same as lingual bar major
connector component when possible.
• Upper part, Thin, narrow (3mm) metal
strap located on cingula of anterior teeth,
scalloped to follow interproximal
embrasures with inferior and superior
borders tapered to tooth surfaces.
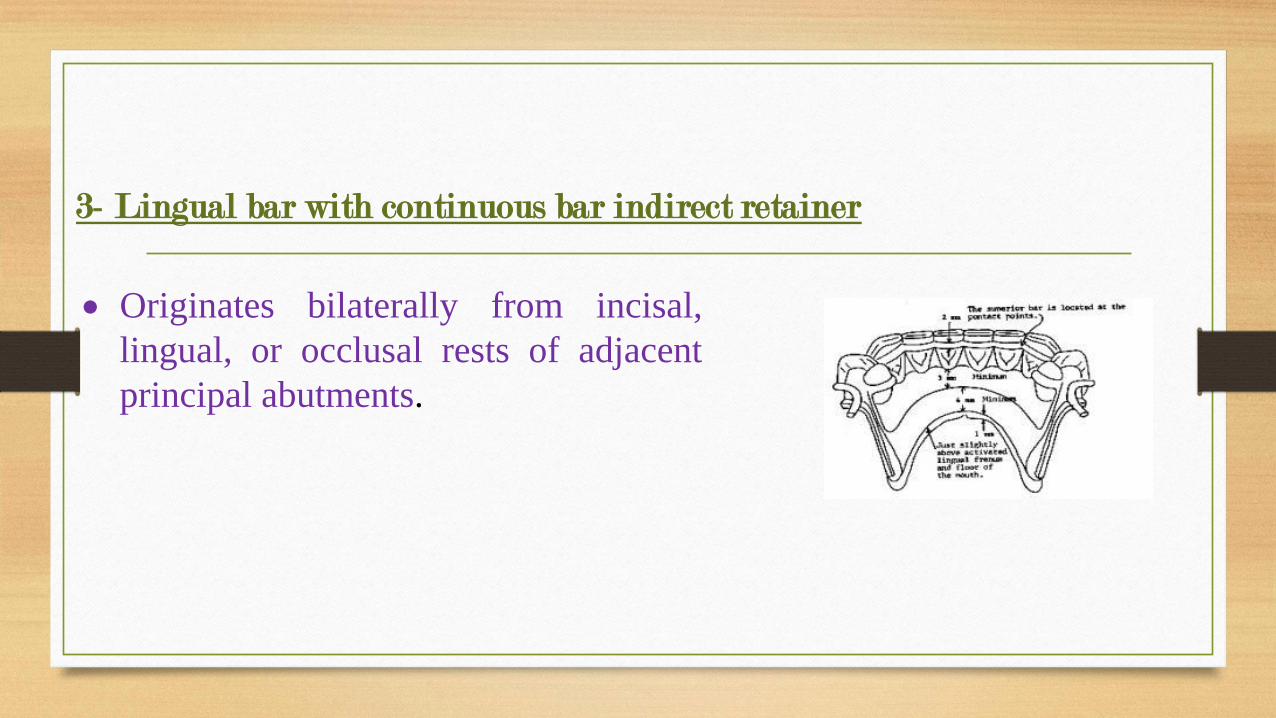
3- Lingual bar with continuous bar indirect retainer
• Originates bilaterally from incisal,
lingual, or occlusal rests of adjacent
principal abutments.
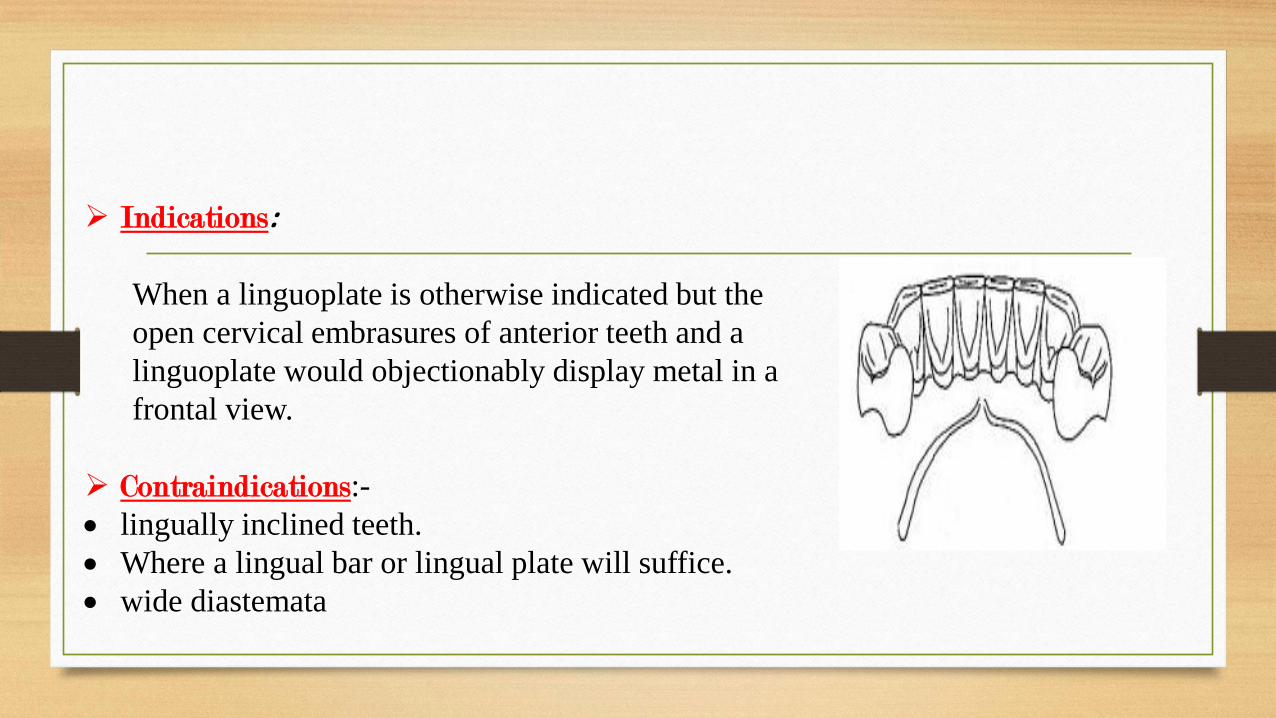
➢ Indications:
When a linguoplate is otherwise indicated but the
open cervical embrasures of anterior teeth and a
linguoplate would objectionably display metal in a
frontal view.
➢ Contraindications:-
• lingually inclined teeth.
• Where a lingual bar or lingual plate will suffice.
• wide diastemata
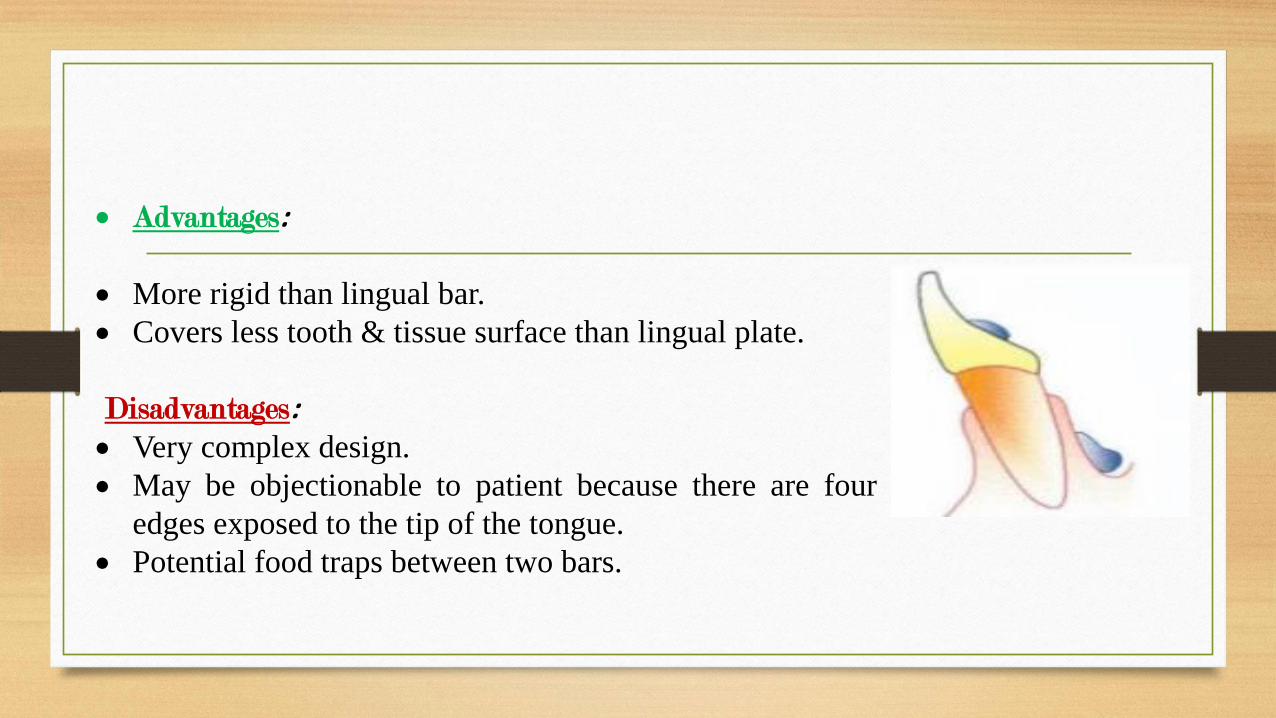
• Advantages:
• More rigid than lingual bar.
• Covers less tooth & tissue surface than lingual plate.
Disadvantages:• Very complex design.
• May be objectionable to patient because there are four
edges exposed to the tip of the tongue.
• Potential food traps between two bars.
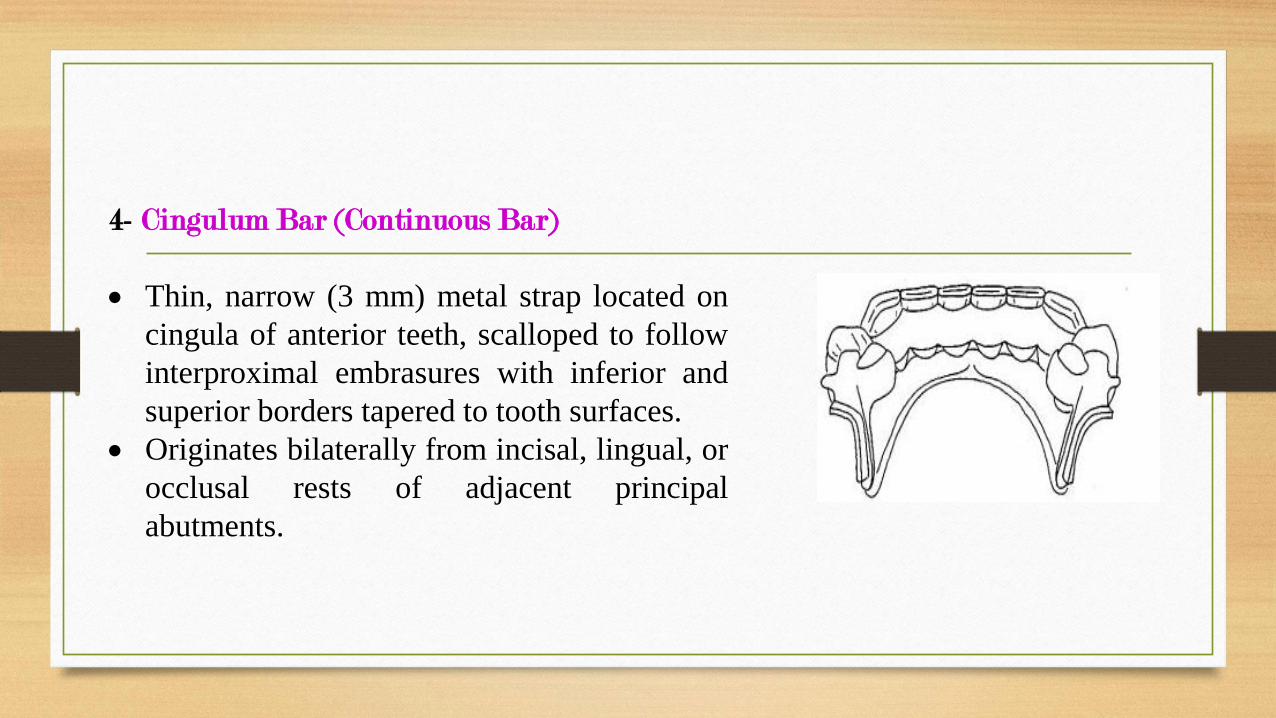
4- Cingulum Bar (Continuous Bar)
• Thin, narrow (3 mm) metal strap located on
cingula of anterior teeth, scalloped to follow
interproximal embrasures with inferior and
superior borders tapered to tooth surfaces.
• Originates bilaterally from incisal, lingual, or
occlusal rests of adjacent principal
abutments.
➢ Indications:-
• When a linguoplate is the major
connector of choice, but the axial
alignment of the anterior teeth is such
that excessive block out of
interproximal undercuts must be
made, a cingulum bar may be
considered.
• .
➢ Indications:-
• Height of activated lingual frenum and
floor of the mouth at the same level as
marginal gingiva.
• Inoperable tori or exostosis at the same
level as the marginal gingiva.
• Severely undercut lingual alveolus.
5- Sublingual Bar
modification of the lingual bar that has
been demonstrated to be useful when the
height of the floor of the mouth does not
allow placement of the superior border of
the bar at least 4 mm below the free
gingival margin.
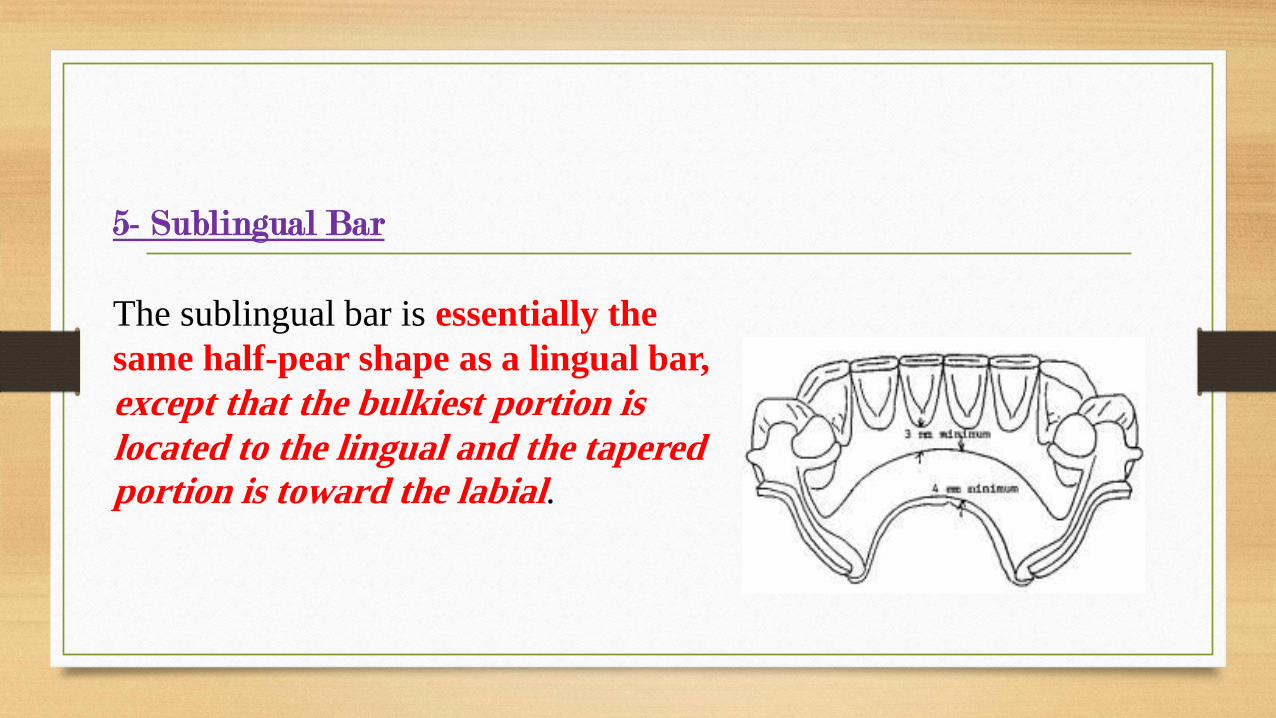
5- Sublingual Bar
The sublingual bar is essentially the
same half-pear shape as a lingual bar,
except that the bulkiest portion is
located to the lingual and the tapered portion is toward the labial.
➢Indications:
• The sublingual bar should be used for mandibular removable
partial dentures when the height of the floor of the mouth in
relation to the free gingival margins will be less than 6 mm.
➢Contraindications:
1. Interfering with lingual tori.
2. High attachment of lingual frenum.
3. Interference with elevation of the floor of the mouth during
functional movements.
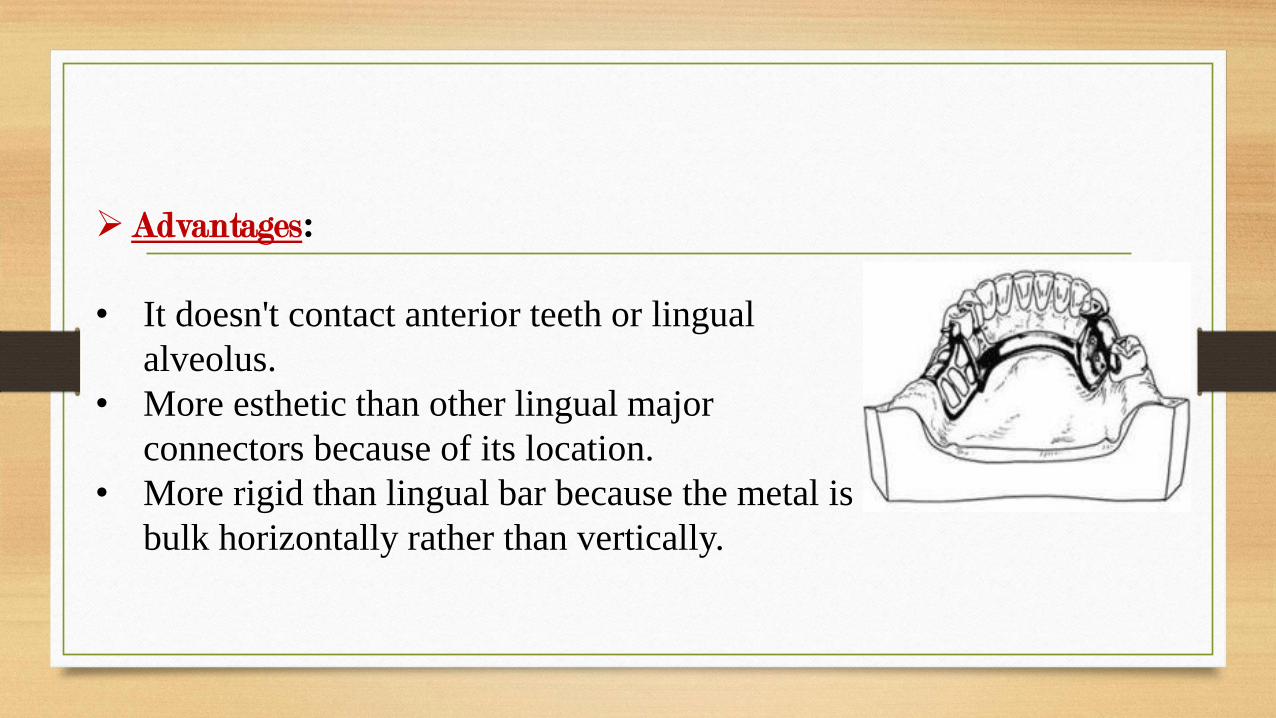
➢Advantages:
• It doesn't contact anterior teeth or lingual
alveolus.
• More esthetic than other lingual major
connectors because of its location.
• More rigid than lingual bar because the metal is
bulk horizontally rather than vertically.
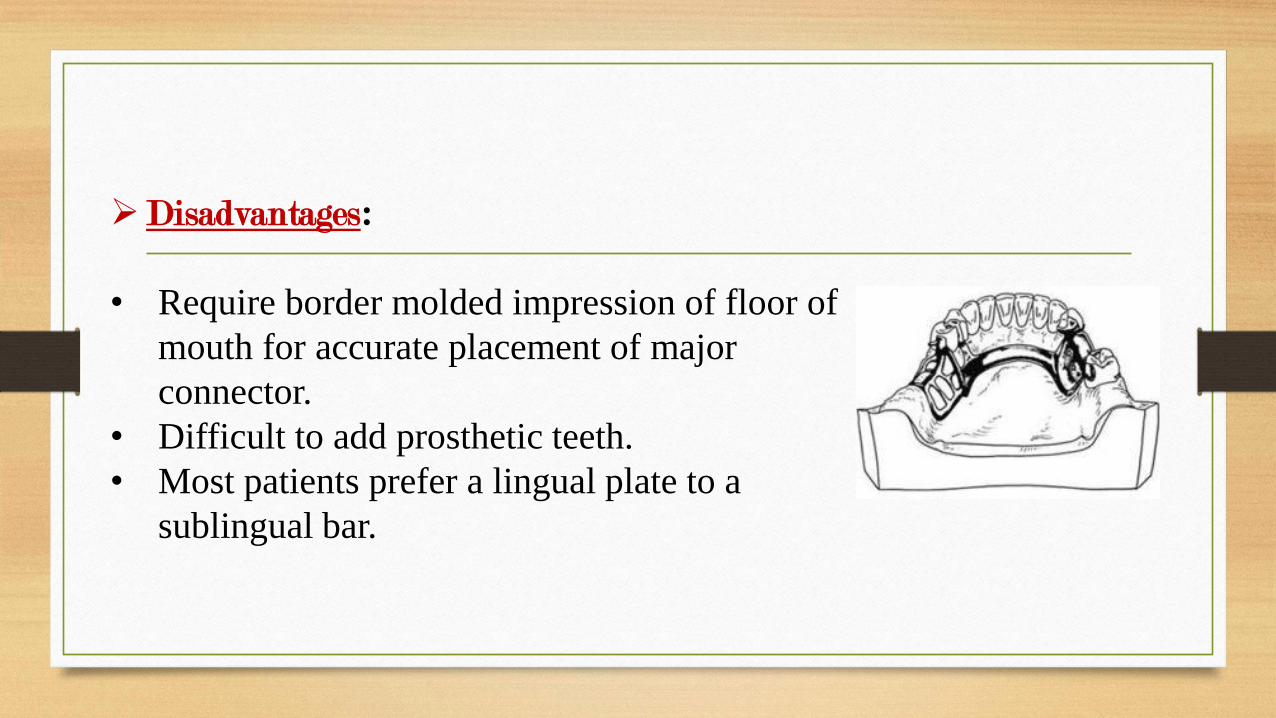
➢Disadvantages:
• Require border molded impression of floor of
mouth for accurate placement of major
connector.
• Difficult to add prosthetic teeth.
• Most patients prefer a lingual plate to a
sublingual bar.
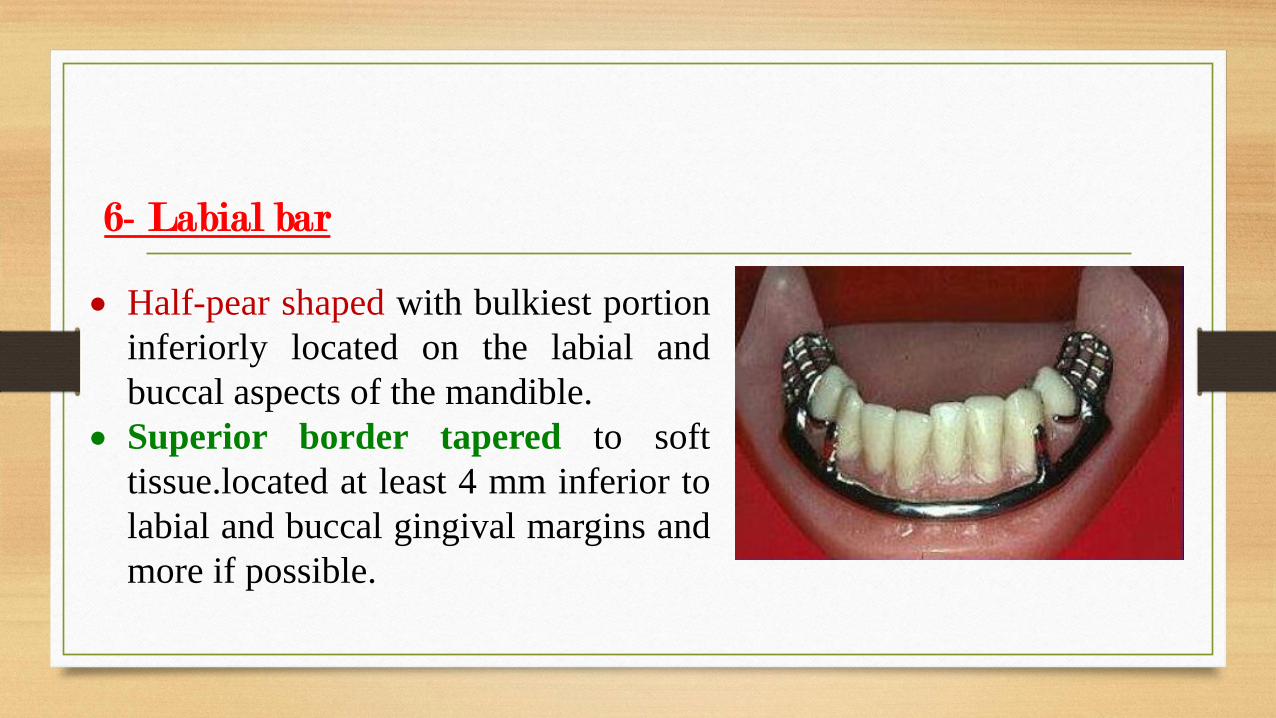
6- Labial bar
• Half-pear shaped with bulkiest portion
inferiorly located on the labial and
buccal aspects of the mandible.
• Superior border tapered to soft
tissue.located at least 4 mm inferior to
labial and buccal gingival margins and
more if possible.
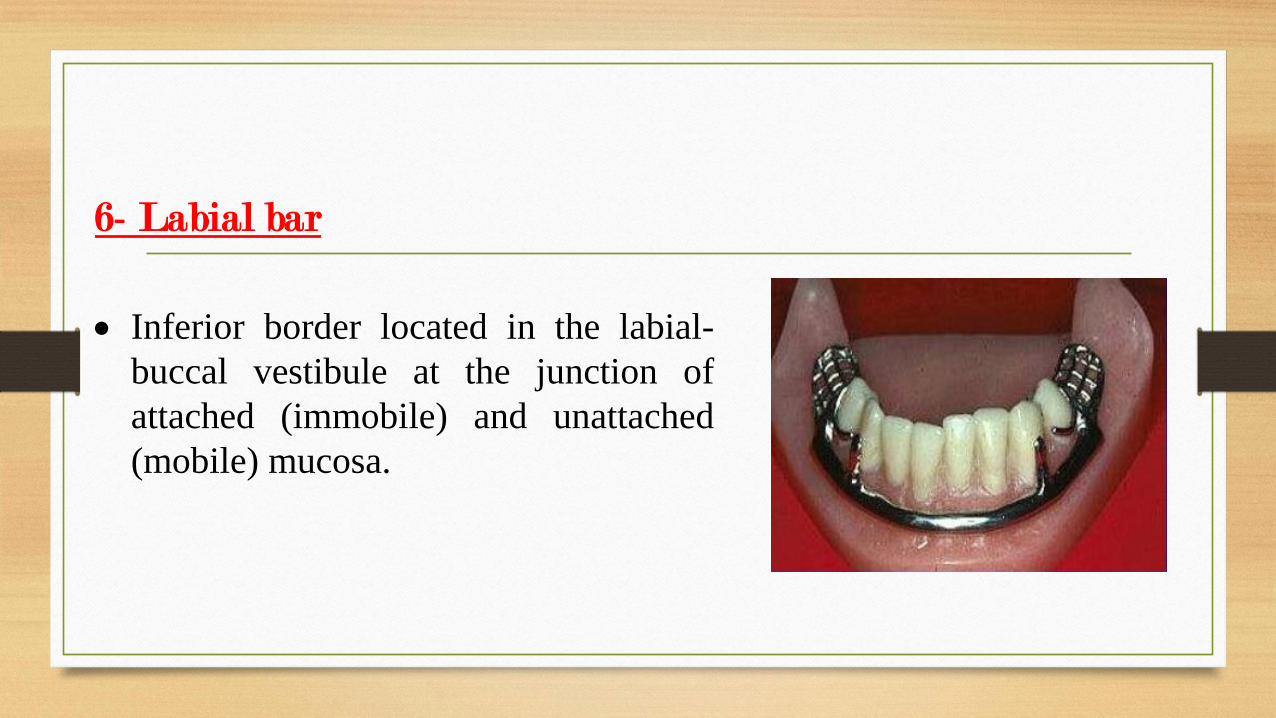
6- Labial bar
• Inferior border located in the labial-
buccal vestibule at the junction of
attached (immobile) and unattached
(mobile) mucosa.
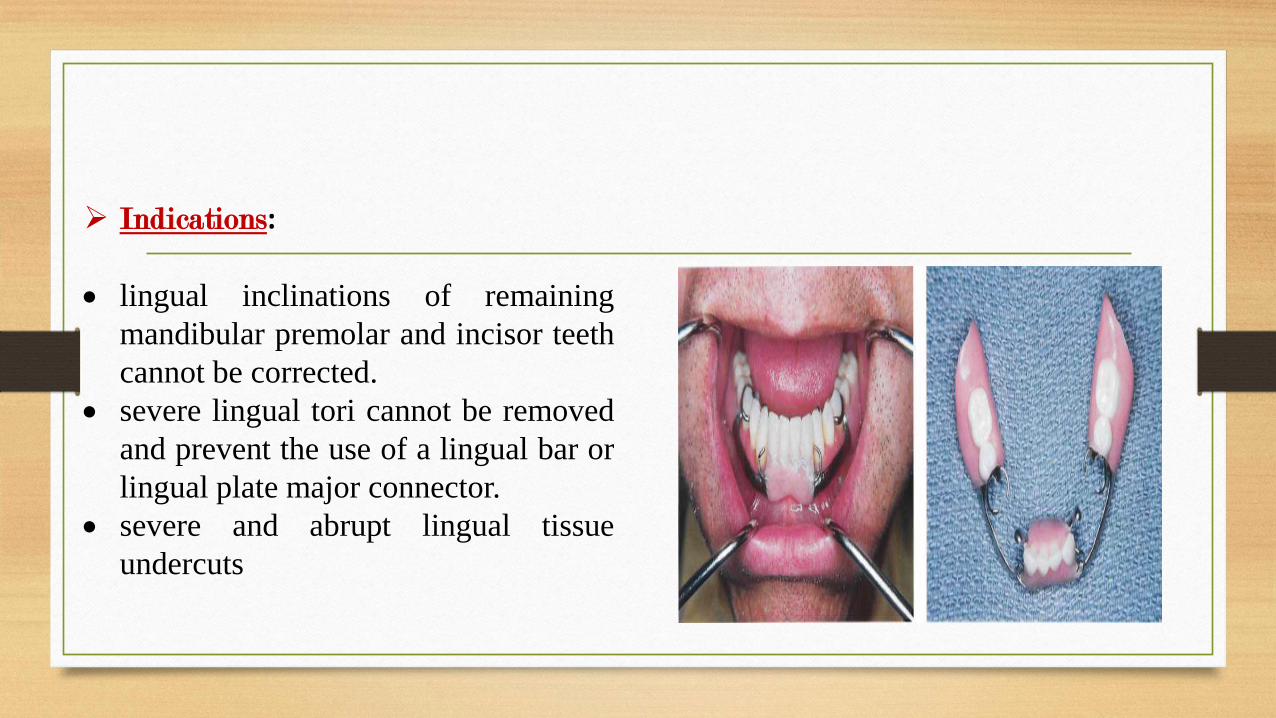
➢ Indications:
• lingual inclinations of remaining
mandibular premolar and incisor teeth
cannot be corrected.
• severe lingual tori cannot be removed
and prevent the use of a lingual bar or
lingual plate major connector.
• severe and abrupt lingual tissue
undercuts
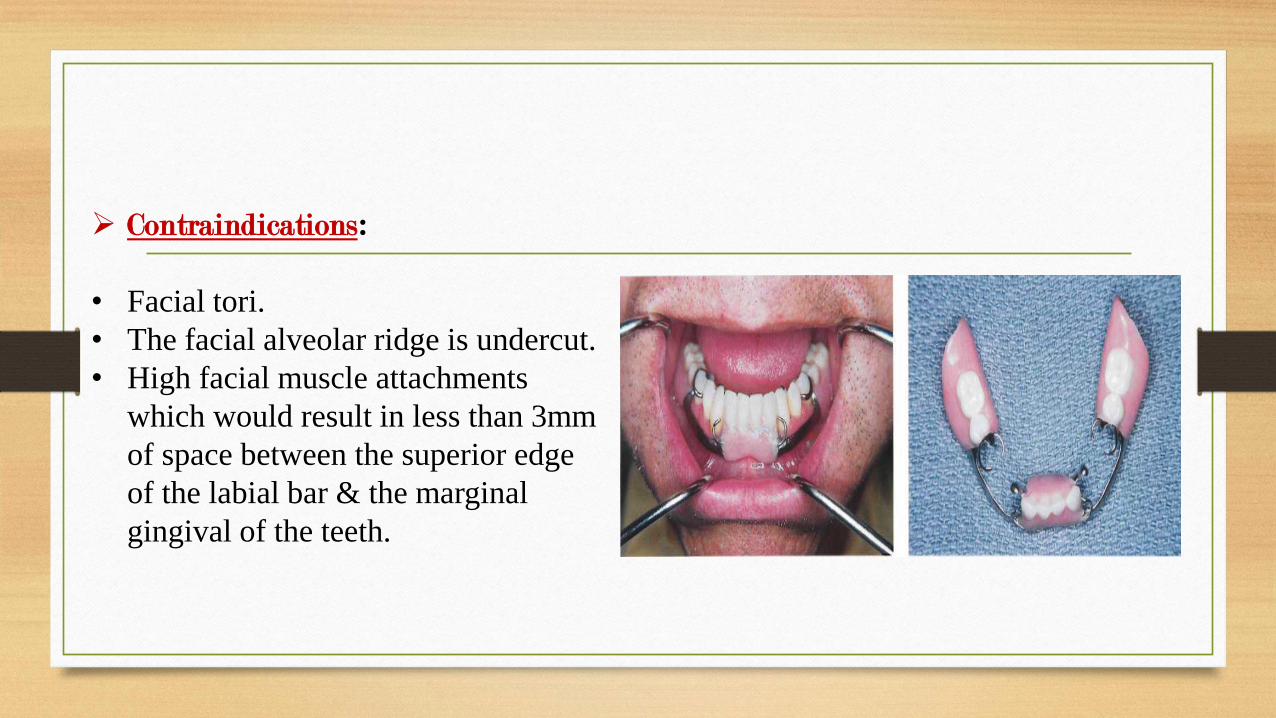
➢ Contraindications:
• Facial tori.
• The facial alveolar ridge is undercut.
• High facial muscle attachments
which would result in less than 3mm
of space between the superior edge
of the labial bar & the marginal
gingival of the teeth.
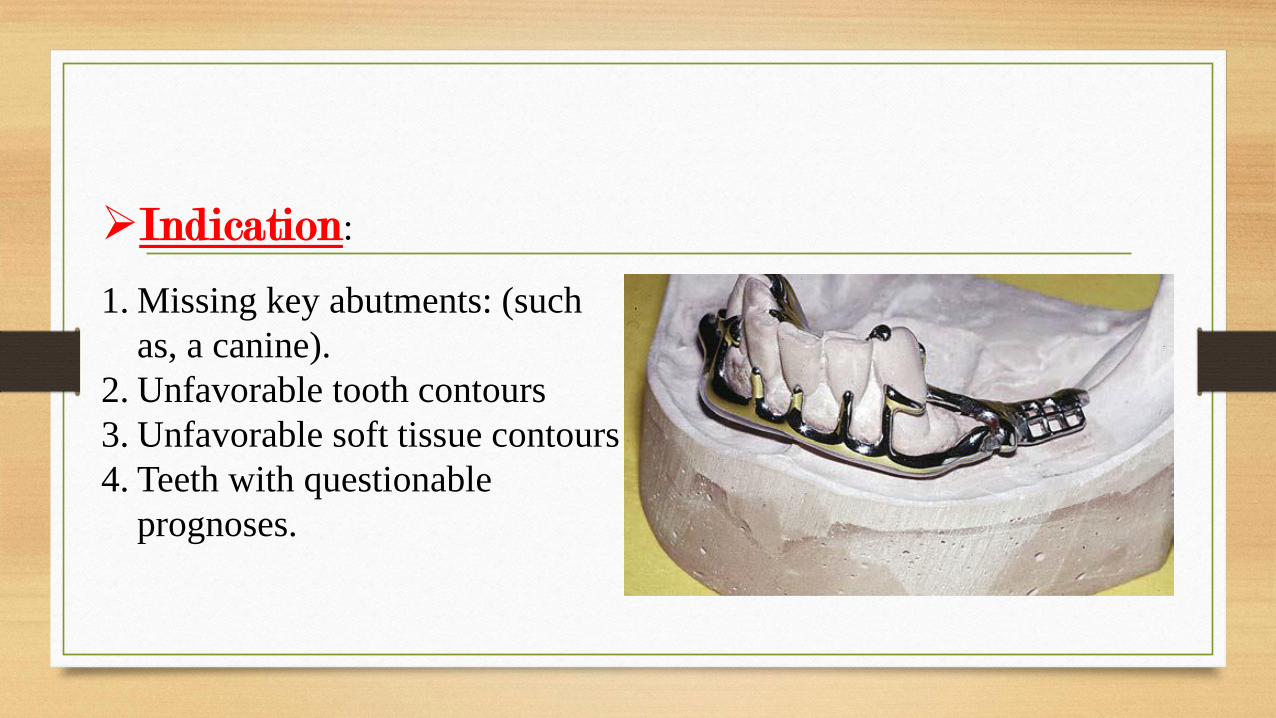
➢Indication:
1. Missing key abutments: (such
as, a canine).
2. Unfavorable tooth contours
3. Unfavorable soft tissue contours
4. Teeth with questionable
prognoses.
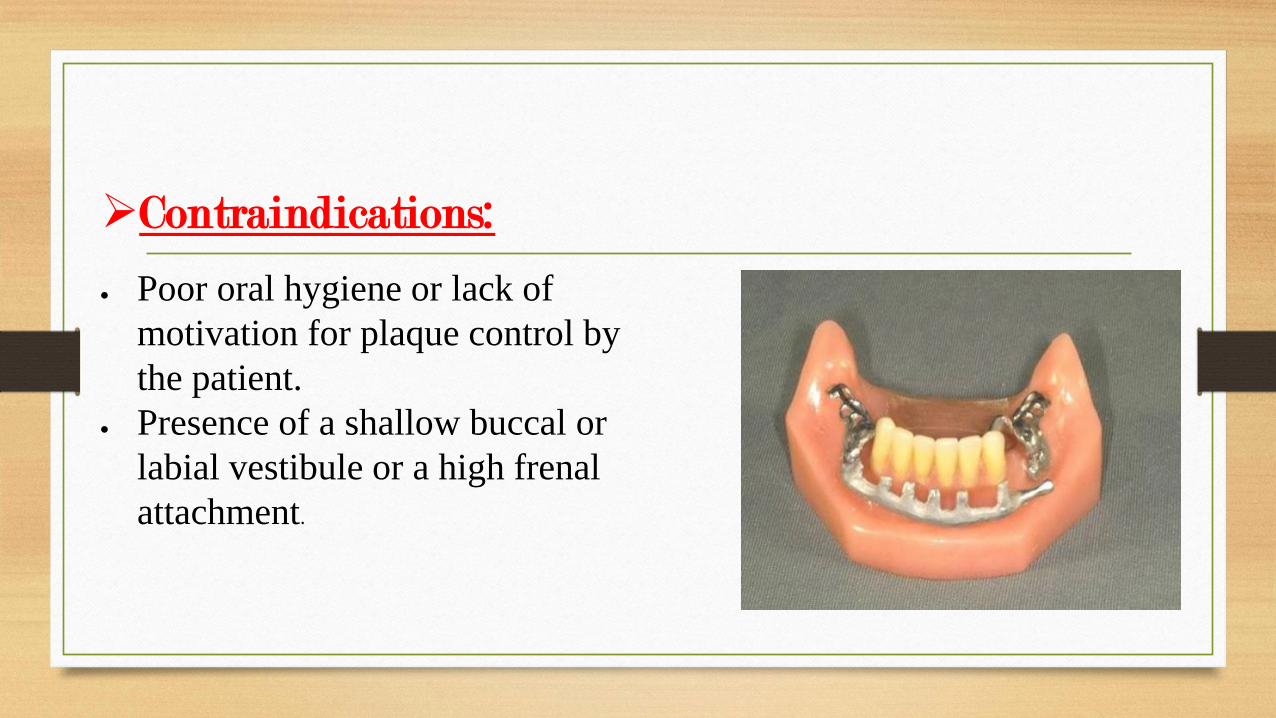
➢Contraindications:
• Poor oral hygiene or lack of
motivation for plaque control by
the patient.
• Presence of a shallow buccal or
labial vestibule or a high frenal
attachment.






























