Embed Size (px)
Citation preview

Tcmdteotaigip[yf
Sappcugpgccrtt
eus
FPIMa
P
Im
©A
Metabolic Effects of Orally AdministeredAmino Acid Mixture in Elderly Subjects
with Poorly Controlled Type 2Diabetes Mellitus
Sebastiano B. Solerte, MD, Carmine Gazzaruso, MD, Nicola Schifino, MD,Eleonora Locatelli, MD, Tamara Destro, MD, Graziano Ceresini, MD, Ettore Ferrari, MD,
and Marisa Fioravanti, BS
wcsiOtbasdsacit
he reduction of muscle mass and increased proteinatabolism in aging can determine the occurrence ofetabolic alterations—such as hyperglycemia and re-uced insulin sensitivity—in elderly subjects with diabe-
es mellitus. Therefore, the aim of the study was tovaluate the effect of nutritional supplementation withral amino acid mixture (OAAM) in elderly subjects withype 2 diabetes. This approach was conducted in anttempt to antagonize muscle catabolism by means of
ncreased endogenous protein synthesis and to improvelucose metabolism and insulin sensitivity. A random-
zed, open-label, crossover study was conducted inoorly controlled (glycosylated hemoglobin levelHbA1c] >7%) elderly subjects (age range, 65 to 85ears) with type 2 diabetes. OAAM significantly reducedasting and postprandial blood glucose and HbA ,
1canis
ottheacostheth
y alu
icarepvebe
thseuliuch
pipgaitm
dpbmlctsdh
uaast
S
deo 2, Pavia, Italy. E-mail: [email protected].
2004 by Excerpta Medica, Inc.ll rights reserved.
hereas all parameters remained substantially un-hanged in the group treated with placebo. Fasting in-ulin levels and insulin resistance increased at baselinen all subjects with diabetes and decreased duringAAM supplementation. These results persisted also af-
er crossover from OAAM to placebo. No changes inlood lipid levels, creatinine, homocysteine, and urinarylbumin excretion rate were observed throughout thetudy, whereas a mild but significant increase of high-ensity lipoprotein cholesterol was found after OAAMupplementation. We suggest that increased amino acidvailability for skeletal muscle function and strengthould ameliorate metabolic control and insulin sensitivityn elderly patients with poorly controlled type 2 diabe-es. �2004 by Excerpta Medica, Inc.
Am J Cardiol 2004;93(suppl):23A–29A
inlyired
inontlyffort
net
en-hos-cend
insu-onn-acidn tod
val-oraltialin-n-
-
keletal muscle is the largest tissue in the bodycontains 50% of the body’s proteins. Muscle
mong the main targets of insulin action that promrotein anabolism; however, this occurs only inresence of either normal or high systemic aminooncentrations, thus regulating the rate of glucptake, storage, and utilization. In fact, 75% oflucose in a carbohydrate meal is taken up inostprandial state by muscle and stored mainllycogen. This tissue is therefore important for gose metabolism in normal and pathologic clinonditions (ie, obesity and diabetes mellitus) andesents an attractive therapeutic target for the preion of peripheral insulin resistance and type 2 diaes.1,2
The reduction of muscle mass and function inlderly could potentially result in impaired glucotilization and storage because of impaired insensitivity, a condition frequently observed in s
rom Department of Internal Medicine, Geriatric Clinic, University ofavia, Pavia, Italy (SBS, EL, TD, EF); Salvatore Maugeri Foundation,RCCS, Pavia, Pavia, Italy (CG); IIAARR Geriatric Hospital Santa
argherita, Pavia, Italy (NS); and Department of Internal Medicinend Medical Biosciences, University of Parma, Parma, Italy (GC).
The work was supported in part by a grant from the University ofavia, Pavia, Italy (project FAR, financial year 2002).
Address for reprints: Sebastiano B. Solerte, MD, Department ofnternal Medicine, Geriatric Clinic, University of Pavia, Piazza Borro-
d
e
ide
es
-l-n--
e
n
atients. It is well recognized that a reductionnsulin activity is often present in critically ill elderatients, as well as in elderly patients with impalucose tolerance and overt diabetes. Dietary amcid and protein requirements could be significa
ncreased in elderly patients with diabetes in an eo antagonize muscle catabolism and to stimulateuscle protein synthesis.3–7
Anabolic conditions that are able to enhanceogenous protein synthesis and adenosine triphate production by cells could potentially indueneficial effects in restoring muscle integrity aetabolic functions and, consequently, enhance
in activity and sensitivity of muscle. This situatiould be useful in elderly patients with poorly corolled diabetes and could be achieved by aminoupplementation; amino acids have been showecrease insulin resistance8 and reduce glycosylateemoglobin (HbA1c).9
The present investigation was undertaken to eate whether increased nutritional support with anmino acid mixture (OAAM) composed of essenmino acids could improve glycemic control andulin sensitivity in elderly patients with poorly corolled type 2 diabetes.
UBJECTS AND METHODSSubjects and study protocol: We conducted a ran
omized, open-label, crossover study of OAAM ver-
23A0002-9149/04/$ – see front matterdoi:10.1016/j.amjcard.2003.11.006

stfrltipd(waemt
sa�ftd
adha7soL
L
L
nT8
rfiowgaewt(gspa
(8ipHlhpl
iurfH3y
pam(HhDsiUaB�ptb
R
lTcsdidTawc1baa
be2tfCc(swpf(goat
2
us placebo in 34 consecutive elderly subjects withype 2 diabetes. All subjects gave their written in-ormed consent to participate in the study. The ageange of the subjects was 65 to 83 years, and theength of time since diabetes diagnosis ranged from 5o 15 years. Body weight (expressed as body massndex; range, 18 to 23) was within normal limits. Allatients had diabetes that was poorly controlled, asefined by metabolic control, with HbA1c �7%range, 7.2% to 10.5%). In all, 25 patients were treatedith oral hypoglycemic agents (9 with metformin
lone, 8 with the combination of metformin with glib-nclamide, 5 with the combination of repaglinide withetformin, 3 with glimepiride), and 9 patients were
reated with recombinant human insulin.Exclusion criteria for enrollment were as follows:
evere diabetic neuropathy and retinopathy, overt di-betic nephropathy (urinary albumin excretion rate200 �g/min), diabetic ketoacidosis, renal or hepatic
ailure, coronary and peripheral macroangiopathy, ar-erial hypertensive disease, and other systemiciseases.
OAAM (449 kcal/day) and placebo were ingesteds snacks at 10:00 AM and 6:00 PM, maintaining a totalaily caloric intake of 1,600 � 370 kcal (55% carbo-ydrates, 30% lipids, 15% proteins). Breakfast, lunch,nd dinner were scheduled at 7:00 AM, 12 noon, and:30 PM. The OAAM preparation (Big One; Profes-ional Dietetics SRL, Milan, Italy) contained 8 g/dayf amino acids, fractionated in the following manner:-leucine, 2.5 g; L-lysine, 1.3 g; L-isoleucine, 1.25 g;-valine, 1.25 g; L-threonine, 0.7 g; L-cysteine, 0.3 g;-histidine, 0.3 g; L-phenylalanine, 0.2 g; L-methio-ine, 0.1 g; L-tyrosine, 0.06 g; L-tryptophan, 0.04 g.otal lipids were 0.43 g, and carbohydrates were.15 g.
The randomized study consisted of 5 phases: (1) aun-in period and baseline examination 2 weeks be-ore OAAM or placebo administration; (2) random-zation into a 16-week treatment period with OAAMr placebo; (3) a washout period of 2 weeks (fromeek 16 to week 18); (4) crossover of the OAAMroup to placebo and the placebo group to OAAM;nd (5) a second period of 16 weeks of treatmentither on OAAM or on placebo. Of the 34 subjects, 18ere strictly assigned to group A (initial randomiza-
ion to OAAM) and 16 were assigned to group Binitial randomization to placebo). The crossover ofroup A to placebo and of group B to OAAM wascheduled after week 18 (end of the 2-week washouteriod). OAAM and placebo treatments were given inddition to conventional antidiabetic therapy.
The following measures were obtained at baseline2 weeks before the study and at the start) and after 4,, 12, 16, 18, 22, 26, 30, and 34 weeks: body massndex, arterial blood pressure, fasting blood glucose,ostprandial (1 hour and 2 hours) blood glucose,bA1c, total and high-density lipoprotein (HDL) cho-
esterol and triglycerides (TGs), fasting serum insulin,omocysteine, urinary albumin excretion rate (ex-ressed as micrograms per minute in a 24-hour col-
ection specimen), serum creatinine, and the degree of g4A THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 93 (8
nsulin resistance. Insulin resistance was estimatedsing the homeostasis model assessment for insulinesistance (HOMAIR): fasting insulin (�U/mL) �asting blood glucose (mmol/L)/22.5.10 The normalOMAIR value measured in our control population of50 healthy elderly subjects (age range, 67 to 81ears) was �2.4.
Laboratory procedures: Blood glucose (fasting andostprandial), creatinine, total and HDL cholesterol,nd TGs were determined by using a fully automatedethod following the single manufacturer’s protocols
Dasit-Ise Autoanalyzer; Dasit, Bareggio, Italy).bA1c and serum homocysteine were measured byigh-performance liquid chromatography (Bio-Radiagnostics Group, Hercules, CA). Fasting serum in-
ulin was determined by fluoroimmunoassay (Delfia-nsulin; PerkinElmer Life Sciences Inc., Boston, MA).rinary albumin excretion rate was measured by fully
utomated computerized immunonephelometry (Dadeehring, Milan, Italy).11 Data were expressed as mean
SD; 2-way analysis of variance with the Fisherrotected least-significant test and unpaired Student test were used for statistical analysis. A p value �0.05y the 2-tailed test was considered significant.
ESULTSNeither body weight nor arterial blood pressure
evels varied in group A or group B during the study.he results of the fasting and postprandial blood glu-ose levels are represented in Figures 1 through 3. Aignificant reduction in fasting blood glucose wasemonstrated in group A as soon as 8 weeks afternitiation of nutritional support with OAAM. The re-uction was more pronounced at 16 weeks (Figure 1).he effect was maintained during the washout periodnd after crossover from OAAM to placebo (fromeek 18 to week 34). Conversely, fasting blood glu-
ose was unchanged in group B from baseline through8 weeks; however, a significant decrease of fastinglood glucose was found when these patients weressigned to treatment with OAAM (after the crossovert week 18).
Similarly to what was found regarding fastinglood glucose, a significant but more consistent andarly decrease of postprandial blood glucose (at 1 andhours) was observed in group A (Figures 2 and 3);
his decrease was consistent throughout crossoverrom OAAM to placebo (from week 18 to week 34).onversely, postprandial blood glucose remained un-hanged in group B during treatment with placebofrom baseline to week 16), and only a borderlineignificant reduction of postprandial blood glucoseas observed at week 16. However, a significant andersistent decrease of postprandial blood glucose wasound when these patients were treated with OAAMie, after the crossover of week 18). Hence, in bothroups of elderly subjects with diabetes, the decreasef fasting and postprandial blood glucose was stronglyssociated with OAAM supplementation, parallelinghe period of treatment with OAAM and persisting in
roup A after crossover to placebo.A) APRIL 22, 2004

gpwraartfc
vs
cpdr8fsaonOi
Fo 0.0
Fs 0.0
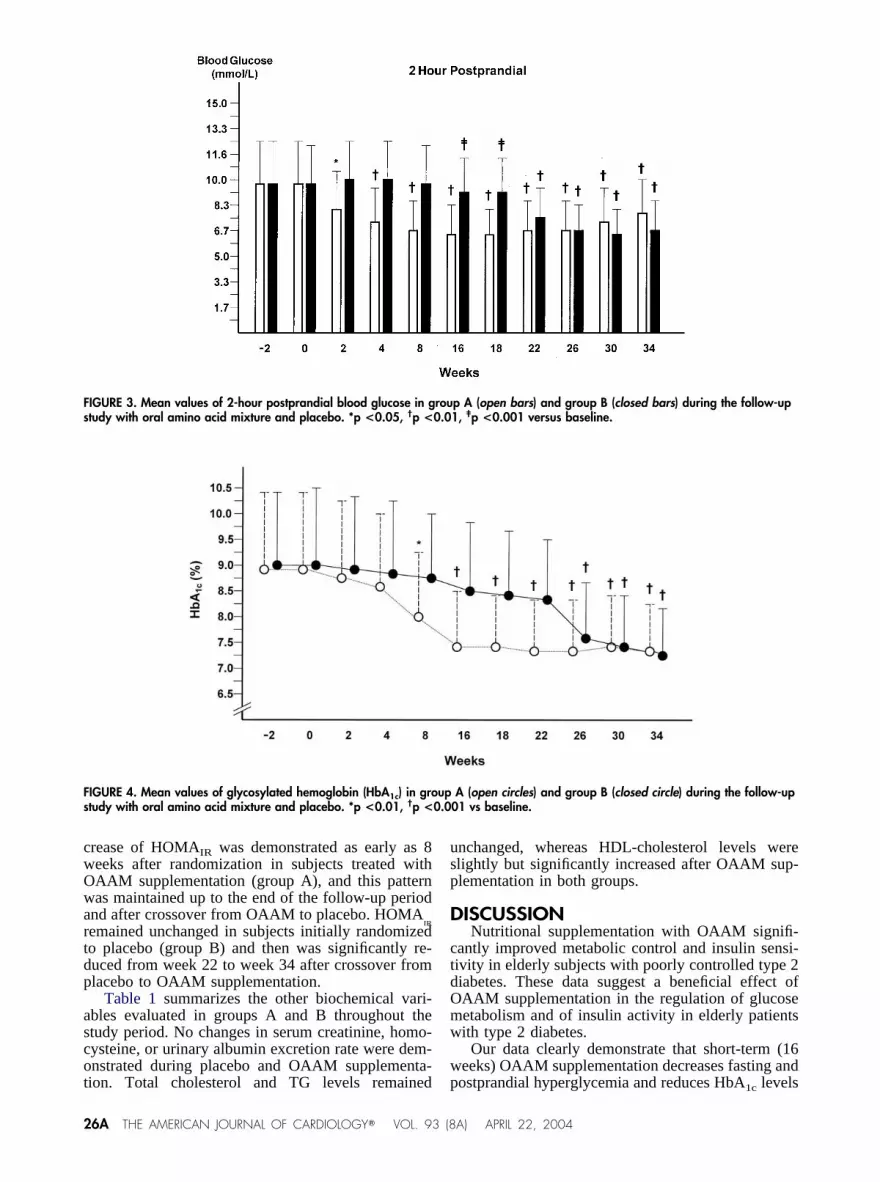
Figure 4 shows the mean variations of HbA1c inroups A and B throughout the 34-week follow-uperiod. A highly significant reduction of HbA1c levelsas demonstrated by 8 weeks in subjects initially
andomized to OAAM supplementation (group A),nd these findings were maintained in these subjectsfter the crossover from OAAM to placebo. HbA1cemained unchanged in subjects initially randomizedo placebo (group B), but it was significantly reducedrom week 26 to week 34, after crossover from pla-ebo to OAAM supplementation.
Figures 5 and 6 report serum insulin and HOMAIRariations in groups A and B during the study. Fasting
IGURE 1. Mean values of fasting blood glucose in group A (openral amino acid mixture and placebo. *p <0.05, †p <0.01, ‡p <
IGURE 2. Mean values of 1-hour postprandial blood glucose in gtudy with oral amino acid mixture and placebo. *p <0.05, †p <
erum insulin levels in groups A and B were signifi- d
A SYMPOSIUM: NUTR
antly higher than the insulin levels of the controlopulation of 350 healthy elderly subjects with noiabetes (10.6 � 2.2 �U/mL, p �0.001). A significanteduction in insulin concentration was observed afterweeks in subjects with diabetes initially randomized
or OAAM supplementation (group A), and these re-ults were consistent throughout OAAM treatmentnd after crossover to placebo. Similar to what wasbserved in group A, serum insulin levels were sig-ificantly reduced after crossover from placebo toAAM supplementation (from week 26 to week 34)
n group B.HOMAIR exhibited a similar pattern of decrease as
rs) and group B (closed bars) during the follow-up study with01 vs baseline.
p A (open bars) and group B (closed bars) during the follow-up01 vs baseline.
ba
rou
id serum insulin levels. In effect, a significant de-
ITIONAL SUPPLEMENTS IN CVD AND DIABETES MELLITUS 25A
cwOwartdp
ascot
usp
D
ctdOmw
w
Fs 0.0
Fs 0.0
2
rease of HOMAIR was demonstrated as early as 8eeks after randomization in subjects treated withAAM supplementation (group A), and this patternas maintained up to the end of the follow-up period
nd after crossover from OAAM to placebo. HOMAIR
emained unchanged in subjects initially randomizedo placebo (group B) and then was significantly re-uced from week 22 to week 34 after crossover fromlacebo to OAAM supplementation.
Table 1 summarizes the other biochemical vari-bles evaluated in groups A and B throughout thetudy period. No changes in serum creatinine, homo-ysteine, or urinary albumin excretion rate were dem-nstrated during placebo and OAAM supplementa-
IGURE 3. Mean values of 2-hour postprandial blood glucose in gtudy with oral amino acid mixture and placebo. *p <0.05, †p <
IGURE 4. Mean values of glycosylated hemoglobin (HbA1c) in grotudy with oral amino acid mixture and placebo. *p <0.01, †p <
ion. Total cholesterol and TG levels remained p
6A THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 93 (8
nchanged, whereas HDL-cholesterol levels werelightly but significantly increased after OAAM sup-lementation in both groups.
ISCUSSIONNutritional supplementation with OAAM signifi-
antly improved metabolic control and insulin sensi-ivity in elderly subjects with poorly controlled type 2iabetes. These data suggest a beneficial effect ofAAM supplementation in the regulation of glucoseetabolism and of insulin activity in elderly patientsith type 2 diabetes.
Our data clearly demonstrate that short-term (16eeks) OAAM supplementation decreases fasting and
p A (open bars) and group B (closed bars) during the follow-up1, ‡p <0.001 versus baseline.
A (open circles) and group B (closed circle) during the follow-up01 vs baseline.
rou
up
ostprandial hyperglycemia and reduces HbA1c levels
A) APRIL 22, 2004

wwe
mkipotatcmeni
lmss
otiiiItstfl
F( re a
Fo asel
ithin 8 weeks of treatment. These metabolic effectsere maintained during the crossover with placebo,
ven after the end of OAAM support.Several hypotheses can be proposed to explain the
echanisms involved in this phenomenon. It is wellnown that free amino acid plasma concentrations arencreased in long-term diabetes. This fact can be de-endent on increased protein turnover and catabolism,n increased gluconeogenesis, or on decreased syn-hesis of structural proteins.12 OAAM or parenteralmino acid supplementation may scavenge glucose,hereby decreasing hyperglycemia and glycemic ex-ursions and sparing the protein amino acids. OAAMay also positively affect protein anabolism by low-
ring amino acids in plasma13 and by stimulatinget muscle protein synthesis and glucose storage by
7,14
IGURE 6. Mean values of homeostasis model assessment for iclosed circles) during the follow-up study with oral amino acid mixtu
IGURE 5. Mean values of fasting serum insulin in group A (openral amino acid mixture and placebo. *p <0.01, †p <0.001 vs b
nsulin-sensitive tissues. This process is particu- a
A SYMPOSIUM: NUTR
arly evident in elderly subjects when OAAM supple-entation was introduced along with several other
trategies to counteract skeletal muscle loss andarcopenia.15
The capability of OAAM to increase protein anab-lism and muscle tissue synthesis is of definite impor-ance in restoring blood glucose levels and in improv-ng insulin sensitivity. Amino acids also upregulatensulin receptor synthesis and its autophosphorylationn animals and in individuals with type 2 diabetes.12,16
nsulin activity, in addition to insulin secretion, couldherefore be potentially enhanced during amino acidupplementation in subjects with diabetes, thus con-ributing to normalizing blood glucose levels. Thisact is demonstrated in our study. Fasting hyperinsu-inemia was significantly decreased during OAAM,
lin resistance (HOMAIR) in group A (open circles) and group Bnd placebo. *p <0.05, †p <0.01, ‡p <0.001 vs baseline.
les) and group B (closed circles) during the follow-up study withine.
nsu
circ
nd insulin sensitivity, which was evaluated by HO-
ITIONAL SUPPLEMENTS IN CVD AND DIABETES MELLITUS 27A

Msafmtctd
tccetticisculpsrciit
sc
wmwamfisiaa
apmoimsmrc
dottoarti
2
AIR, was also improved after the end of OAAMupplementation and after crossover to placebo. Themelioration of insulin sensitivity and the reduction ofasting hyperinsulinemia can be considered importantetabolic consequences of oral amino acid support in
hese elderly subjects with diabetes. These effectsould be dependent on recovery of insulin action onhe muscle target or could be due to an insulin-depen-ent increase of skeletal muscle anabolism and mass.
On the other hand, it has been well demonstratedhat oral supplementation with arginine, glycine, andysteine improves insulin sensitivity and muscle glu-ose metabolism; it has also been shown that leucinenhances protein synthesis in the skeletal musclehrough an insulin-dependent mechanism.17–21 All ofhese mechanisms could contribute to enhance thensulin-dependent action of glucose removal from cir-ulation and thereby enhance blood glucose reductionn postabsorptive conditions. The improvement of in-ulin sensitivity on skeletal muscle could permit in-reasing protein synthesis and glucose uptake andtilization within this tissue. In effect, adequate insu-in availability is necessary for the maintenance ofrotein synthesis and of normal glucose metabolism inkeletal muscle. The final metabolic effect may beepresented by increased consumption and use of glu-ose by muscle itself, thereby decreasing the circulat-ng glucose. These effects appear to be demonstratedn these elderly subjects during short-term supplemen-ation with OAAM.
The well-known substrate competition between in-ulin-mediated glucose disposal and amino acids
TABLE 1 Mean Variations � SD of Biochemical Variables in EldFollow-up Study with Oral Amino Acid Mixture and Placebo
GroupTiming(wk)
Creatinine(�mol/L)
UAER(�g/min)
H
A �2 138 � 18 65 � 28Baseline 145 � 20 71 � 20
2 143 � 23 68 � 234 140 � 16 65 � 308 145 � 21 73 � 28
16 137 � 24 70 � 2718 140 � 30 74 � 2522 146 � 28 67 � 2026 140 � 33 73 � 2530 135 � 41 70 � 2334 144 � 44 68 � 28
B �2 136 � 20 72 � 30Baseline 139 � 16 68 � 27
2 148 � 24 66 � 284 144 � 34 73 � 258 145 � 35 76 � 26
16 140 � 30 73 � 2418 144 � 28 71 � 2822 138 � 37 67 � 2626 147 � 40 65 � 2430 145 � 29 68 � 2634 149 � 18 70 � 23
HDL � high-density lipoprotein; UAER � urinary albumin excretion rate.*p �0.001 vs baseline.
ould contribute to hyperglycemia in elderly subjects r
8A THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 93 (8
ith type 2 diabetes, when protein catabolism anduscle degradation (conditions frequently associatedith aging) enhance the availability of circulating
mino acids. OAAM could powerfully antagonizeuscle catabolism, therefore reducing the amount of
ree amino acids in the circulation and increasing thensulin-mediated glucose disposal in peripheral tis-ues. On the other hand, OAAM supplementation usedn this study did not induce a consistent load of aminocids during exogenous infusion of different mixtures,s demonstrated by other studies.22,23
A possible effect of methionine content in themino acid mixture used in this study could be ex-ected to influence plasma homocysteine levels, aarker frequently associated with cardiovascular dis-
rders in diabetes and other diseases.24 Nevertheless,t is very important to observe that the content ofethionine in the composition of our mixture did not
ignificantly influence homocysteine levels, and ho-ocysteine remained unchanged throughout the pe-
iod of supplementation with OAAM and after therossover to placebo.
Based on the results of this pilot study and previousouble-blind pilot clinical trials, we hypothesize thatral amino acids may be promising antidiabetic agentshat may be useful as a nutritional supplement in thereatment of elderly patients with type 2 diabetes. Inrder to avoid the negative interaction between aminocids and carbohydrates when ingested together, theecommended timing of administration for OAAM ishe preprandial state. The absence of side effects dur-ng the study suggests a potentially useful long-term
Subjects with Type 2 Diabetes (Groups A and B) During the
cysteincol/L)
TotalCholesterol
(mg/dL)
HDLCholesterol
(mg/dL)Triglycerides
(mg/dL)
3 � 5 211 � 37 46 � 6 138 � 438 � 6 214 � 33 45 � 4 141 � 371 � 5 209 � 36 47 � 5 140 � 366 � 7 206 � 31 47 � 4 137 � 385 � 5 216 � 27 45 � 4 140 � 360 � 4 211 � 28 52 � 6* 135 � 403 � 5 217 � 27 54 � 6* 138 � 379 � 6 208 � 30 51 � 4* 141 � 367 � 6 209 � 32 49 � 5 144 � 412 � 5 214 � 34 48 � 4 141 � 404 � 4 219 � 37 47 � 5 139 � 399 � 6 207 � 28 44 � 7 142 � 393 � 5 213 � 30 45 � 6 140 � 355 � 4 206 � 31 43 � 5 137 � 378 � 6 214 � 33 42 � 6 141 � 346 � 5 211 � 30 44 � 5 144 � 362 � 4 207 � 27 46 � 4 137 � 381 � 6 205 � 32 45 � 5 139 � 407 � 6 209 � 36 44 � 6 135 � 344 � 5 206 � 31 49 � 5* 136 � 370 � 4 204 � 33 52 � 4* 140 � 365 � 5 209 � 28 54 � 6* 141 � 39
erly
omo(�m
18.18.19.18.18.19.19.18.18.19.19.17.18.18.18.18.19.19.18.19.19.18.
ole for OAAM supplementation in this population.
A) APRIL 22, 2004

Ns
1c2f23d3415J657a18d29ag1Rf41Fp11h1
1me1e11aN1gJ1g1Bic1KpD2Lw2i2d12Rd2pi
evertheless, well-planned, long-term clinical trialshould be conducted to confirm these results.
. DeFronzo RA. Lilly lecture 1987. The triumvirate: beta-cell, muscle, liver. Aollusion responsible for NIDDM. Diabetes 1988;37:667–687.. Shepherd PR, Kahn BB. Glucose transporters and insulin action: implicationsor insulin resistance and diabetes mellitus [review]. N Engl J Med 1999;341:48–257.. Barrett EJ, Schwartz RG, Young LH, Jacob R, Zaret BL. Effect of chroniciabetes on myocardial fuel metabolism and insulin sensitivity. Diabetes 1988;7:943–948.. Hoffer LJ. Protein consumption and diabetes mellitus: an overview. J Nutr998;128(suppl):321S–322S.. Hoffer LJ. Are dietary protein requirements altered in diabetes mellitus? CanPhysiol Pharmacol 1993;71:633–638.. Wolfe RR. Protein supplements and exercise. Am J Clin Nutr 2000;72(suppl):51S–557S.. Volpi E, Ferrando AA, Yeckel CW, Tipton KD, Wolfe RR. Exogenous aminocids stimulate net muscle protein synthesis in the elderly. J Clin Invest 1998;01:2000–2007.. Traxinger RR, Marshall S. Role of amino acids in modulating glucose-inducedesensitization of the glucose transport system. J Biol Chem 1989;264:20910–0916.. Sulochana KN, Punitham R, Ramakrishnan S. Beneficial effect of lysine andmino acids on cataractogenesis in experimental diabetes through possible anti-lycation of lens proteins. Exp Eye Res 1998;67:597–601.0. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, TurnerC. Homeostasis model assessment: insulin resistance and �-cell function from
asting plasma glucose and insulin concentrations in man. Diabetologia 1985;28:12–419.1. Solerte SB, Severgnini S, Locatelli M, Cerutti N, Rondanelli M, Netti MA,errari E, Fioravanti M. Nephelometry in the clinical assessment of glomerularroteinuria and tubular function in diabetic nephropathy. Clin Nephrol 1997;48:51–158.2. Allison TB, Bruhing SP, Crass MF 3rd, Eliot RS, Shipp JC. Reducedigh-energy phosphates in rat hearts. I. Effect of alloxan diabetes. Am J Physiol
976;230:1744–1750. 4A SYMPOSIUM: NUTR
3. Volpi E, Mittendorfer B, Wolfe SE, Wolfe RR. Oral amino acids stimulateuscle protein anabolism in the elderly despite higher first-pass splanchnic
xtraction. Am J Physiol 1999;277:E513–E520.4. Biolo G, Tipton KD, Klein S, Wolfe RR. An abundant supply of amino acidsnhances the metabolic effect of exercise on muscle protein. Am J Physiol997;273:E122–E129.5. Rasmussen BB, Wolfe RR, Volpi E. Oral and intravenously administeredmino acids produce similar effects on muscle protein synthesis in the elderly. Jutr Health Aging 2002;6:358–362.6. Iritani N, Sugimoto T, Fukuda H. Soybean protein increases insulin receptorene expression in fatty rats when dietary polyunsaturated fatty acid level is low.Nutr 1997;127:1077–1083.7. Gannon MC, Nuttall JA, Nuttall FQ. The metabolic response to ingestedlycine. Am J Clin Nutr 2002;76:1302–1307.8. Chevassus H, Renard E, Bertrand G, Mourand I, Puech R, Molinier N,ockaert J, Petit P, Bringer J. Effects of oral monosodium (L)-glutamate on
nsulin secretion and glucose tolerance in healthy volunteers. Br J Clin Pharma-ol 2002;53:641–643.9. Piatti PM, Monti LD, Valsecchi G, Magni F, Setola E, Marchesi F, Galli-ienle M, Pozza G, Alberti KG. Long-term oral L-arginine administration im-roves peripheral and hepatic insulin sensitivity in type 2 diabetic patients.iabetes Care 2001;24:875–880.0. Fulghesu AM, Ciampelli M, Muzj G, Belosi C, Selvaggi L, Ayala GF,anzone A. N-acetyl-cysteine treatment improves insulin sensitivity in womenith polycystic ovary syndrome. Fertil Steril 2002;77:1128–1135.1. Balon TW, Nadler JL. Evidence that nitric oxide increases glucose transport
n skeletal muscle. J Appl Physiol 1997;82:359–363.2. Ueland PM, Refsum H. Plasma homocysteine, a risk factor for vascularisease: plasma levels in health, diseases and drug therapy. J Lab Clin Med14:473–501.3. Natarajan Sulochana K, Lakshmi S, Punitham R, Arokiasamy T, Sukumar B,amakrishnan S. Effect of oral supplementation of free amino acids in type 2iabetic patients—a pilot clinical trial. Med Sci Monit 2002;8:131–137.4. Volpi E, Mittendorfer B, Rasmussen BB, Wolfe RR. The response of musclerotein anabolism to combined hyperaminoacidemia and glucose-induced hyper-nsulinemia is impaired in the elderly. J Clin Endocrinol Metab 2001;85:4481–
490.ITIONAL SUPPLEMENTS IN CVD AND DIABETES MELLITUS 29A





























