Embed Size (px)
Citation preview

UNIVERSIDADE CIDADE DE SÃO PAULO
MASTERS AND DOCTORAL PROGRAMS IN PHYSICAL THERAPY
CLINICAL RESEARCH:
METHODOLOGICAL QUALITY, REPORTING, SPIN AND
CONSISTENCY BETWEEN ABSTRACTS AND FULL TEXTS
Dafne Port Nascimento, PT
SÃO PAULO
2019

II
UNIVERSIDADE CIDADE DE SÃO PAULO
MASTERS AND DOCTORAL PROGRAMS IN PHYSICAL THERAPY
CLINICAL RESEARCH:
METHODOLOGICAL QUALITY, REPORTING, SPIN AND
CONSISTENCY BETWEEN ABSTRACTS AND FULL TEXTS
Dafne Port Nascimento, PT
SÃO PAULO
2019
Thesis presented to the Masters and Doctoral Programs in Physical Therapy at Universidade Cidade de São Paulo - UNICID, for the PhD degree, under the supervision of Prof. Leonardo Oliveira Pena Costa.

III
Sistema de Bibliotecas do Grupo Cruzeiro do Sul Educacional
N244c
Nascimento, Dafne Port. Clinical research: methodological quality, reporting, spin and consistency between abstracts and full texts. / Dafne Port Nascimento. São Paulo, 2019. 239 p. Includes bibliography Thesis (Doctoral) – Universidade Cidade de São Paulo - Supervision: Prof. Dr. Leonardo Oliveira Pena Costa. 1. Evidence-based practice. 2. Low back pain. 3. Randomized controlled trials as topic. 4. Methodology. 5. Systematic review. I. Costa, Leonardo Oliveira Pena, orient. II. Título.
CDD 615.8

IV
Examination board
Prof. Leonardo Oliveira Pena Costa
Universidade Cidade de São Paulo
Prof. Adriana Claudia Lunardi
Universidade Cidade de São Paulo
Prof. Bruno Tirotti Saragiotto
Universidade Cidade de São Paulo
Dr. Tiê Parma Yamato
University of Sydney
Prof. Luciana Patrícia Fernandes Abbade
Universidade Estadual Paulista

V
CONTENT
PAGE BIOGRAPHY VIII PUBLICATIONS AND PRESENTATIONS IX ACKNOWLEDGEMENTS XII PREFACE XV SUMMARY XVII RESUMO XXI CHAPTER 1 – Introduction 1 1.1. Evidence-based practice in healthcare 2 1.2. Literary sources for decision making of effectiveness of interventions 3
1.2.1. Methodological quality of randomized controlled trials 3 1.2.2. Methodological quality of systematic reviews 6
1.3. Common problems of abstracts 8
1.3.1. Reporting quality of abstracts 8 1.3.2. Consistency between abstracts and full texts 8
1.3.2.1. Spin of results and conclusions 8
1.4. Justification of the thesis 9
1.4.1. General objectives 10 1.4.2. Specific objectives 10
CHAPTER 2 – Randomized controlled trials in low back pain 17 2.1. Description of the randomized controlled trials 18
2.1.1. Description of low back pain clinical trials in physical therapy: a cross sectional study
19
2.2. Abstracts of the randomized controlled trials: reporting quality, spin and inconsistencies with the full text
39

VI
2.2.1. Abstracts of low back pain trials are poorly reported, contain spin of information and are inconsistent with the full text: an overview study
40
2.3. APPENDIXES: Common appendixes for Chapter 2 78
2.3.1. FIGURE 1. Flow chart of included randomized controlled trials. 79
2.3.2. APPENDIX A. Excluded trials. 81
2.3.3. APPENDIX B. Included trials. 89 CHAPTER 3 – Systematic reviews in low back pain 111
3.1. Description of the systematic reviews 112
3.1.1. Journals impact factor were associated with PRISMA endorsement, but not with the methodological quality of low back pain systematic reviews: a methodological review
113
3.2. Abstracts of the systematic reviews: reporting quality, spin and inconsistencies with the full text
131
3.2.1. Reporting of systematic review abstracts relevant to low back pain and inconsistencies with the full text: an overview study
132
3.2.2. Abstracts of low back pain systematic reviews presented spin and inconsistencies with the full text: an overview study
152
3.3. APPENDIXES: Common appendixes for Chapter 3 169
3.3.1. FIGURE 1. Flow chart of included reviews. 170
3.3.2. APPENDIX A. Excluded reviews. 172
3.3.3. APPENDIX B. Included reviews. 181
3.3.4. APPENDIX C. Number and percentage of individual items from the AMSTAR-2.
189
CHAPTER 4 – Abstracts in all healthcare areas 191 4.1. Abstracts of systematic reviews and randomized controlled trials: reporting quality, spin and inconsistencies with the full text
192
4.1.1. Abstracts of healthcare research need urgent action measures: A systematic review
193
CHAPTER 5 – Concluding remarks 223

VII
5.1. Visual abstracts 224 5.2. Abstracts influence in the media 226 5.3. Ethics and integrity in research 227 5.4. Actions to change journals` editorial policies 228
5.4.1. Clinical and research implications 229 5.4.2. Editorials 229

VIII
BIOGRAPHY
Dafne Port Nascimento obtained her Physical Therapy bachelor’s degree in 2007 at the
Universidade Cidade de Sao Paulo (UNICID) and initiated her scientific studies at the Faculdade
de Medicina da Universidade de Sao Paulo (FMUSP) in 2005. Since then, she has worked with
clinical research (at the University of Sydney and The George Institute for Global Health) and was
involved in research studies in the musculoskeletal field, mainly with low back pain. Parallel to
her research work, she has continuously worked and studied with Orthopedic, Postural and Sports
Physical Therapy in different clinical settings in Sydney (Australia; 2008-2011) and São Paulo
(Brazil; 2011-present). In 2015 she started her Master’s degree studies with methodology in
clinical research at UNICID, which has been converted into this thesis of direct PhD. Part of her
thesis was developed at the Vrije Universiteit (VU Amsterdam). Dafne main interest in research is
in methodology of clinical research, especially with transparency of reporting and interpretation of
research studies (avoiding bias and spin of information). Her main interest in the clinical field is to
continue learning and working in the field of Musculoskeletal, Postural and Sports Physical
Therapy.

IX
PUBLICATIONS AND PRESENTATIONS
Publications
• Nascimento DP, Gonzalez GZ, Costa LOP. Book title [published in Portuguese]:
Metodologia Científica aplicada à fisioterapia. Book Chapter 5: A base de dados em fisioterapia -
PEDro. Escola Bahiana de Medicina e Saúde Pública. Editora Sanar. 2018.
• Nascimento DP, Gonzalez GZ, Araujo AC, Costa LOP. Description of low back pain
clinical trials in physical therapy: a cross sectional study. Braz J Phys Ther. DOI:
10.1016/j.bjpt.2018.09.002 (Epub Ahead of Print). 2018.
• Nascimento DP, Costa LOP, Gonzalez GZ, Maher CG, Moseley AM. Abstracts of low
back pain trials are poorly reported, contain spin of information and are inconsistent with the full
text: an overview study. Arch Phys Med Rehabil. DOI: 10.1016/j.apmr.2019.03.024 (Epub Ahead
of Print). 2019.
• Nascimento DP, Gonzalez GZ, Araujo AC, Moseley AM, Maher CG,Costa LOP.
Abstracts of low back pain systematic reviews presented spin and inconsistencies with the full
text: an overview study. J Orthop Sports Phys Ther, accepted for publication. 2019.
• Gonzalez GZ, Moseley AM, Maher CG, Nascimento DP, Costa LDCM, Costa LOP.
Methodologic quality and statistical reporting of physical therapy randomized controlled trials
relevant to musculoskeletal conditions. Arch Phys Med Rehabil, 99(1): 129-136. 2018.
• Tomazoni SS, Costa LDCM, Guimarães LS, Araujo AC, Nascimento DP, Medeiros FC,
Avanzi MA, Costa LOP. Effects of photobiomodulation therapy in patients with chronic non-
specific low back pain: protocol for a randomized placebo-controlled trial. BMJ Open,
7(10):e017202. 2017.
• Araujo AC, Nascimento DP, Gonzalez GZ, Maher CG, Costa LOP. Impact of low back
pain clinical trials measured by the Altmetric score: cross sectional study. J Med Internet Res,
20(4):e86. 2018.
X
• Araujo AC, Nascimento DP, Gonzalez GZ, Costa LOP. How to increase the visibility of
scientific articles though social media? Braz J Phys Ther, 22(6):435-436. 2018.
Presentations
• Nascimento DP, Gonzalez GZ, Maher CG, Costa LOP. A qualidade e a veracidade de
resumos em fisioterapia para dor lombar. Poster presentation at the Congresso Internacional de
Fisioterapia em Coluna Vertebral (CONIFIC). Fortaleza – CE, Brazil. 2016.
• Nascimento DP, Costa LOP, Gonzalez GZ, Maher CG, Moseley AM. Abstracts of
randomized controlled trials relevant to low back pain are poorly reported and inaccurate: a cross
sectional study. Oral presentation (Speakers corner – Theme focused abstracts) at the International
Back and Neck Pain Research Forum 2017. Oslo, Norway. 2017.
• Nascimento DP, Costa LOP, Gonzalez GZ, Maher CG, Moseley AM. Abstracts of
randomized controlled trials relevant to low back pain are poorly reported and inaccurate: a cross
sectional study. Poster presentation at the World Confederation for Physical Therapy (WCPT)
Congress 2017. Cape Town, South Africa. 2017.
• Nascimento DP, Gonzalez GZ, Araujo AC, Moseley AM, Maher CG, Costa LOP. How
trustworthy are systematic reviews abstracts of interventions for low back pain? A methodological
review. Oral presentation at the Congresso Brasileiro de Fisioterapia (COBRAF). Belo Horizonte
– Minas Gerais, Brazil. 2018.
• Nascimento DP, Gonzalez GZ, Araujo AC, Moseley AM, Maher CG, Costa LOP.
Abstracts of low back pain systematic reviews are inaccurate with the full text: a cross sectional
study. Poster presentation at the Congresso Brasileiro de Fisioterapia (COBRAF). Belo Horizonte
– MG, Brazil. 2018.
• Araujo AC, Nascimento DP, Gonzalez GZ, Maher CG, Costa LOP. Impacto de ensaios
controlados aleatorizados em dor lombar por meio do Altmetric: estudo transversal. Oral
presentation at the Congresso Brasileiro de Fisioterapia (COBRAF). Belo Horizonte – Minas
Gerais, Brazil. 2018.

XI
• Nascimento DP, Gonzalez GZ, Araujo AC, Moseley AM, Maher CG, Costa LOP. Can we
trust what we read on reviews abstracts of interventions for low back pain? A methodological
review. Oral presentation at the Cochrane Colloquium Edinburgh. Edinburgh, Scotland. 2018.
• Araujo AC, Nascimento DP, Gonzalez GZ, Maher CG, Costa LOP. The impact of low
back pain clinical trials measured by the Altmetric score: a cross sectional study. Poster
presentation at the Cochrane Colloquium Edinburgh. Edinburgh, Scotland. 2018.
• Araujo AC, Nascimento DP, Gonzalez GZ, Maher CG, Costa LOP. The impact of low
back pain clinical trials measured by the Altmetric score: a cross sectional study. Oral presentation
at the 5AM Conference. London, United Kingdom. 2018.
• Nascimento DP, Costa LOP, Gonzalez GZ, Araujo AC, Vanin AA, Maher CG, Moseley
AM, van Tulder M, Ostelo R. Qualidade geral de resumos: podemos confiar na descrição e
interpretação dos autores?. Invited speaker at the Congresso Internacional de Fisioterapia em
Coluna Vertebral (CONIFIC). São Paulo – SP, Brazil. 2018.
• Nascimento DP, Gonzalez GZ, Araujo AC, Moseley AM, Maher CG, Costa LOP.
Abstracts of low back pain systematic reviews presented spin and poor completeness of reporting:
a cross sectional study. Oral presentation (Speakers corner – Theme focused abstracts) at the
International Back and Neck Pain Research Forum 2019. Quebec, Canada. 2019.

XII
ACKNOWLEDGEMENTS
I believe that great opportunities come to people who seek for them. I consider myself a
very blessed person, because I have been presented in life with so many great opportunities.
Certainly I owe the most to my parents, who built our amazing family, based on so much love,
believing and persistence. The person who has motivated me the most to always keep learning and
keep studying is my mum, and I am sure I will take this for life. Thank you mum, for this and for
so much more! You and dad are my best examples in life!
I met my supervisor Leonardo in Sydney. I was working as a research assistant at the
University of Sydney and he was finishing his PhD. At the time I decided to come back to Brazil,
Leo had recently been admitted at the UNICID as the head of the Masters and Doctoral Programs
of Physical Therapy. From then I knew I wanted to do my PhD with him. The last four years with
him as my supervisor were very enjoyable, I have learned a lot and have grown personally and
professionally. Thank you so much for these unforgettable years Leo!
Back in Sydney I also met Anne and Chris, who I admire and had the honour of working
with in Sydney, as well as in collaboration on some of my projects included here in this thesis.
Thank you greatly Anne and Chris!
A couple of years ago I met Maurits and Raymond in Amsterdam, when I was heading to
the International Back and Neck Pain Forum in Oslo. This year I had the pleasure of working with
them for a couple of months and it has been an amazing experience. Thank you Maurits and
Raymond for all your knowledge sharing and for receiving me with such a great attention and
caring!
During the past years I met many research colleagues, but some of them became my very
dear friends and I am so grateful for working with them and for their friendship. They made the
very difference for this PhD to become the most enjoyable. Thank you Amanda, Gabrielle, Flávia,
Adriane, Layana, Rafael and Leandro, you guys are the best! Thank you also all the other friends,
colleagues and professors who collaborated with work, laughs and learning!
Along those years I also would like to thank: my sister, brother and their families (and my
parents again of course), who gave me so much love to keep my balance between my personal and
professional lives; my childhood friends and their families, who are part of my family and are
always by my side; and my incredible man, who supported my decision of living overseas for a
while, understood me and helped me to keep my balance at all times. I love you all, thank you for
being part of my life!
Lastly, I would like to show my appreciation to São Paulo Research Foundation (grant#
XIII
2015/16953-2; grant# 2016/17853-4; grant# 2018/17932-7; Fundação de Amparo à Pesquisa do
Estado de São Paulo – FAPESP) for the financial support over those years, also allowing me to
participate in conferences in beautiful places over the world. Thank you FAPESP for the great
opportunities!

XIV
“We need less research, better research, and research done for the right reasons.”
Douglas Altman

XV
PREFACE
This PhD thesis contains five chapters discussing the importance of adequately reporting
and interpreting abstracts of clinical research. The main topics were: the overall quality of
abstracts of studies evaluating the effectiveness of interventions in physical therapy (CHAPTERS
2 and 3) and other healthcare related areas (CHAPTER 4). The Universidade Cidade de São
Paulo (UNICID) allows the inclusion of published papers during the PhD period in the thesis.
This PhD was initially funded for a short period in 2015 by a Masters scholarship from the
Coordination for the Improvement of Higher Education Personnel (CAPES). Still in 2015 the
studies in CHAPTER 2 were approved for a Masters scholarship from Sao Paulo Research
Foundation (FAPESP – grant# 2015/16953-2). Later on in 2016, the studies protocols described in
CHAPTERS 3 and 4 were added to the Masters protocol and were approved for a Direct
Doctorate (i.e. without a masters defense), also funded by FAPESP (grant# 2016/17853-4).
The studies here presented were conducted at the Masters and Doctoral Programs in
Physical Therapy of UNICID and at the Department of Health Sciences of the Vrije Universiteit
(VU) Amsterdam, The Netherlands, which was part of a fellowship program approved by FAPESP
(grant# 2018/17932-7). CHAPTERS 2 and 3 were conducted in collaboration with the Faculty of
Medicine and Health of The University of Sydney and the Institute of Musculoskeletal Health
from Sydney, Australia. CHAPTER 4 was conducted in collaboration with the Department of
Health Sciences of the VU Amsterdam and the Department of Epidemiology and Biostatistics of
the VU medical center from Amsterdam, The Netherlands.
CHAPTER 1 is an introduction of the common problems found in abstracts used for
decision making of effectiveness of interventions (randomized controlled trials and systematic
reviews) and the most common tools used to assess the methodological quality of those study
designs.
CHAPTER 2 is composed by two published papers related to randomized controlled trials
in physical therapy for low back pain and their abstracts reporting quality and consistency with the
full text. CHAPTER 3 is composed by three papers (one accepted for publication/ two under
review) related to systematic reviews in physical therapy for low back pain and their abstracts
reporting quality and consistency with the full text.

XVI
CHAPTER 4 is composed by one paper in the final stages of writing, which is related to
the reporting quality and consistency with the full text of abstracts of randomized controlled trials
and systematic reviews in all healthcare areas.
CHAPTER 5 is composed by the concluding remarks of this thesis, discussing important
topics related to abstracts used for clinical decision making, such as: novel use of visual abstracts;
ethics in publication; and actions to change journals` editorial policies with implications on
healthcare research.

XVII
SUMMARY
The use of the highest methodological quality and most recent evidence
available by healthcare professionals, together with their clinical experience and the
patients’ preferences and needs, compose the evidence-based practice in healthcare.
Essentially, healthcare practitioners should know how to critically appraise scientific
evidence in order to select high methodological quality studies, as well as they should
read the full text of an article. However many times the full version is not openly
accessible and the abstract poorly reported. Therefore, healthcare professionals may
take poor clinical decisions based on ineffective interventions. Abstracts of randomized
controlled trials and systematic reviews might present poor reporting quality,
inconsistencies between abstracts and full texts, and the presence of spin (interpretation
of study results that overemphasizes the beneficial effects of the intervention). These
issues related to abstracts have been investigated in psychiatry, general medicine,
oncology and cardiovascular fields for example. However, some other healthcare fields
still lack research on such concerns, as the abstracts of studies related to the
effectiveness of physical therapy interventions for low back pain. Furthermore, there is
no summarization of data discussing possible solutions and actions to be taken to
improve the overall quality of abstracts of studies related to treatment effects; or how
broad are those concerns related to abstracts; or how their improvement can affect the
daily lives of stakeholders and also influence their clinical and academic decision-
making. Given these reasons, the objectives of this thesis were to describe and analyze
the main characteristics of representative and recent samples of randomized controlled
trials and systematic reviews and their abstracts, in a specific population of studies
(physical therapy interventions for low back pain); and to describe and compare studies
that analyzed abstracts of randomized controlled trials and systematic reviews in all
healthcare areas. Our main goals were to increase awareness of the importance of a
well-written abstract in the academic and clinical healthcare fields, and also to call for
actions to change journal’s editorial policies in order to improve the quality of abstracts
in general.
Upon our analysis of 200 randomized controlled trials in physical therapy for
low back pain (2010-2015) retrieved from the Physiotherapy Evidence Database
(PEDro), their main characteristics were: published in journals with a mean Impact
Factor (IF) of 2.5, from which 55.5% endorsed the Consolidated Standards of Reporting
XVIII
Trials (CONSORT) recommendations; and moderate methodological quality (mean
score 5.8 on a scale of 0 to 10, the higher the better). Only a few journals publishing low
back pain trials had IF higher than 2.0, mean trial methodological quality higher than
6.0, endorsed CONSORT recommendations and offered papers as open access. In terms
of trials abstracts, we found that low back pain trials abstracts were incomplete, with
spin and inconsistent with the full text. Our conclusion was that a substantial number of
low back pain trials did not follow adequate reporting and methodological
recommendations. Also, we advise health care professionals to avoid making clinical
decisions based solely upon abstracts. Journal editors, reviewers and authors are jointly
responsible for improving abstracts, which could be guided by amended journals’
editorial policies.
The main characteristics of the 66 systematic reviews in low back pain retrieved
from PEDro (2015-2017) were: nearly 88.0% of journals presented a mean IF of 3.7 and
54.8% of journals endorsed the Preferred Reporting Items for Systematic reviews and
Meta-Analyses (PRISMA) recommendations. Methodological quality was classified as
critically low for 75.8% of reviews (mean IF 3.7), low for 10.6% (mean IF 1.9),
moderate for 6.1% and high for 7.7% (being all Cochrane reviews with an IF of 6.8).
Our results showed that the majority of reviews published in journals that endorsed the
PRISMA recommendations presented critically low methodological quality (36.4%). In
terms of abstracts, we found that low back pain systematic review abstracts were
incompletely reported, inconsistent with the full text (only Cochrane review abstracts
presented consistent interpretation with the full texts), and presented some form of spin
in 80.3% of abstracts. We concluded that most low back pain systematic reviews
presented critically low methodological quality, with exception to reviews published in
the Cochrane Database of Systematic Reviews. Based on these findings, it is very
important that clinicians know how to critically appraise the methodological quality of a
systematic review. Also, we advise readers to read the full text when using systematic
reviews to guide clinical practice. Journal editors and reviewers should follow and
check reporting checklists, and also ensure that abstracts are free of spin. Finally, we
suggest that authors write the abstract only when the manuscript is completed, paying
due attention to consistency and removal of spin.
In order to explore if the mentioned issues on abstracts can be generalized to all
healthcare areas, and also to call healthcare journal’s editorial boards for action, we
designed also a systematic review. The main objective was to descriptively analyze

XIX
overviews of randomized controlled trials and systematic reviews that summarized data
of healthcare abstracts on reporting of abstracts and consistency of abstracts with the
full text. We divided the results into two main groups: 1) Abstracts reporting quality: 27
overviews analyzing 5,194 randomized controlled trials and 866 systematic reviews
were retrieved. The standardized mean percentage score of fully reported items ranged
from 28.1% to 72.7% across healthcare areas; and 2) Abstracts consistency with the full
text: a total of 22 overviews analyzing 2,017 randomized controlled trials and 551
systematic reviews were included. The standardized mean percentage of inconsistent
abstracts ranged from 7.0% to 98.0% across healthcare areas, with abstracts results and
conclusions as the most inconsistent sections. Such results have shown that abstracts of
healthcare randomized controlled trials and systematic reviews have a large room for
improvement in reporting quality and consistency with the full texts. Abstracts are the
highest profile part of a research study and recommendations to authors, journal editors
and reviewers need to be put into action as highest priority.
Other than the usual research abstracts (with objectives, methods, results and
conclusion), the use of visual abstracts (through colored visual images of diagrams,
charts and figures) seems to be a great additional resource of spreading information of
research key results in social media. However, reading a visual abstract is not a
substitute for reading the actual research abstract, or even less for reading the full text,
reason why it should be consistent with the adequate reporting and interpretation of
healthcare abstracts and full texts. Clinicians should be careful on taking clinical
decisions based on abstracts, which are often misrepresented in press releases and news
coverage. Most of the spin detected is responsibility of the own authors, journal editors
and reviewers, as well as research disseminators that use social media.
The adequate reporting and interpretation of abstracts and full texts are part of
the research code of conduct and the principles of research integrity, which include
honesty, reliability, objectivity, impartiality, open communication, duty of care and
fairness. The communication between researchers, the overall public and the popular
media should be based on open access data and accurate references. Therefore, research
stakeholders have the obligation to follow the ethical principles on research (including
guidelines for ethical reporting), upon the conduct of a study, publication and
dissemination of results. That would avoid research misconduct leading to retracted
publications, which involves costs to funding sources and prejudice the researchers
careers. Reducing such research waste is needed and actions to change journals’

XX
editorial policies have been proposed, such as: investment by funding organizations on
training programs based on reporting guidelines and guidelines of ethics and integrity in
research (directed to journal editors, reviewers and authors); investment on the position
of a publications officer (who would manage those proper research trainings and also
provide guidance on submission of papers to journals); universities including mandatory
disciplines on training for graduate students in terms of study conduct, statistical
analysis, reporting and interpretation; guidance on how to follow the guidelines of
ethics and integrity in research as an integral part of doctoral programs; and online tools
and training module based on reporting guidelines for peer reviewers.
Clinical and research implications can be critically affected by the poor reporting
and misrepresentation of data, mainly to patients and policy makers. Initiatives on
recommendations given to funders, regulators, journals, academic institutions and
researches have been planned, in order to reduce waste and increase value in research.
Ultimately, clinical decision making based on high quality research must be an usual
practice in order to acquire better quality of life worldwide.
In order to take actions on improving the quality of abstracts once and for all, we
intend to develop some editorials directed to call attention of healthcare research
stakeholders. Our main goal is to share our findings with the International Committee of
Medical Journal Editors (ICMJE) and the International Society of Physiotherapy
Journal Editors (ISPJE) and call attention especially of healthcare journals editors and
reviewers. We hope that this thesis can be helpful on improving the awareness of
journal editors and reviewers, authors and readers in terms of transparency and integrity
of research healthcare abstracts and their dissemination to all stakeholders. We sincerely
hope that this awareness can stimulate publication of higher quality of healthcare
research.

XXI
RESUMO
A utilização da evidência disponível mais recente e de alta qualidade
metodológica, junto com a experiência clínica do profissional de saúde e as
preferências e necessidades dos pacientes, compõem a prática baseada em evidências
em saúde. Essencialmente, os profissionais de saúde devem saber avaliar criticamente
a evidência científica para selecionar estudos de alta qualidade metodológica, assim
como devem ler o texto completo do artigo. Porém muitas vezes a versão completa do
artigo não tem acesso aberto e o resumo é mal reportado, o que pode levar os
profissionais da saúde a tomar más decisões clínicas baseadas em intervenções
ineficazes. Resumos de ensaios controlados aleatorizados e revisões sistemáticas
podem apresentar má qualidade de descrição, inconsistência entre resumos e textos, e a
presença de ‘spin’ (interpretação dos resultados de um estudo que super enfatizam os
efeitos benéficos da intervenção). Essas questões relacionadas a resumos foram
investigadas por exemplo nas áreas de psiquiatria, clínica médica, oncologia e
cardiovascular. No entanto, algumas outras áreas da saúde ainda carecem de
pesquisas sobre tais questões, como resumos de estudos relacionados a efetividade de
intervenções em fisioterapia para dor lombar. Além disso, não existem estudos
sumarizando dados que discutam possíveis soluções e ações a serem tomadas para
melhorar a qualidade geral de resumos de estudos relacionados a efeitos do
tratamento; ou quão amplos são os problemas relacionados aos resumos; ou como sua
melhoria pode afetar o cotidiano das partes interessadas e também influenciar suas
tomadas de decisões clínicas e acadêmicas. Diante desses motivos, os objetivos dessa
tese foram descrever e analisar as principais características de amostras
representativas e recentes de ensaios controlados aleatorizados e revisões sistemáticas
e seus resumos em uma população específica de estudos (intervenções de fisioterapia
para dor lombar); e descrever e comparar estudos que analisaram resumos de ensaios
controlados aleatorizados e revisões sistemáticas em todas as áreas da saúde. Nossos
principais objetivos foram aumentar a conscientização da importância de um resumo
bem escrito nas áreas da saúde clínica e acadêmica, e também solicitar ações a serem
feitas para mudar as políticas editoriais de revistas, afim de melhorar a qualidade dos
resumos em geral.
Apos analisar 200 ensaios controlados aleatorizados em fisioterapia para dor
lombar (2010-2015) retirados do banco de dados PEDro (Physiotherapy Evidence

XXII
Database), suas características principais foram: publicados em revistas com media de
Fator de Impacto (FI) de 2.5, em que 55.5% endossaram as recomendações da
CONSORT (Consolidated Standards of Reporting Trials); e qualidade metodológica
moderada (pontuação media de 5.8 em uma escala de 0 a 10, quanto maior melhor).
Apenas algumas revistas que publicaram ensaios clínicos em dor lombar tiveram FI
maiores de 2.0, media de qualidade metodológica maior que 6.0, endossaram as
recomendações CONSORT e possuíam acesso aberto aos artigos. Em relação aos
resumos dos ensaios clínicos, encontramos que os resumos em dor lombar eram
incompletos, com ‘spin’ e inconsistentes com o texto completo. Nossa conclusão foi que
um numero substancial de ensaios controlados aleatorizados em dor lombar não
seguem as recomendações metodológicas e de escrita adequadas. Alem disso,
aconselhamos os profissionais de saúde a evitarem tomar decisões clínicas baseadas
apenas em resumos. Editores e revisores de revistas, assim como autores de artigos são
conjuntamente responsáveis por melhorar os resumos, que podem ser guiados por
alterações em políticas editorias de revistas.
As principais características das 66 revisões sistemáticas em dor lombar
retiradas da PEDro (2015-2017) foram: aproximadamente 88.0% das revistas
apresentaram media de FI de 3.7 e 54.8% das revistas endossavam as recomendações
PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses). A
qualidade metodológica foi classificada como criticamente baixa em 75.8% das
revisões (media de FI 3.7), baixa para 10.6% (media de FI 1.9), moderada para 6.1% e
alta para 7.7% (sendo estas revisões Cochrane com FI 6.8). Nossos resultados
mostraram que a maioria das revisões publicadas em revistas que endossavam as
recomendações PRISMA apresentaram qualidade metodológica criticamente baixa
(36.4%). Em relação aos resumos, nós encontramos que resumos de revisões
sistemáticas em dor lombar foram reportados inadequadamente, inconsistentes com o
texto completo (somente os resumos de revisões Cochrane apresentaram interpretação
consistente com os textos completos), e apresentaram alguma forma de ‘spin’ em 80.3%
dos resumos. Concluímos que a maioria das revisões sistemáticas em dor lombar
apresentou qualidade metodológica criticamente baixa, com exceção de revisões
publicadas na Cochrane Database of Systematic Reviews. Com base nesses resultados,
é extremamente importante que clínicos saibam avaliar criticamente a qualidade
metodológica de uma revisão sistemática. Alem disso, aconselhamos leitores de artigos
científicos a ler o texto completo quando utilizando revisões sistemáticas para guiar

XXIII
sua prática clínica. Editores e revisores de revistas devem seguir e checar checklists de
qualidade de descrição, e também assegurar que resumos não possuem ‘spin’.
Finalmente, nós sugerimos que autores escrevam resumos somente quando o artigo
está completo, com a devida atenção a consistência e remoção de ‘spin’.
Afim de explorar se estas questões sobre resumos podem ser generalizadas para
outras áreas da saúde, e também para solicitar ações de conselhos editorias de revistas
em saúde, nós projetamos uma revisão sistemática. O objetivo principal foi analisar
descritivamente estudos de visão geral que incluíram ensaios controlados aleatorizados
e revisões sistemáticas, sumarizando dados dos resumos em saúde em relação a
qualidade de descrição e consistência entre resumos e textos completos. Nós dividimos
os resultados em dois grupos principais: 1) Qualidade de descrição de resumos: 27
estudos de visão geral que analisaram 5,194 ensaios controlados aleatorizados e 866
revisões sistemáticas foram encontrados. A pontuação percentual media padronizada
de itens totalmente reportados variou de 28.1% a 72.7% nas áreas da saúde; e 2)
Consistência entre resumos e textos completos: um total de 22 estudos de visão geral
que analisaram 2,017 ensaios controlados aleatorizados e 551 revisões sistemáticas
foram incluídas. A porcentagem media padronizada de resumos inconsistentes variou
de 7.0% a 98.0% em todas as áreas da saúde, sendo as seções de resultados e
conclusões dos resumos as mais inconsistentes. Tais resultados mostraram que os
resumos de ensaios controlados aleatorizados e revisões sistemáticas em saúde tem um
grande espaço para melhora na qualidade de descrição e consistência com os textos
completos. Resumos são a parte mais importante de um estudo de pesquisa e
recomendações a autores, editores e revisores de revistas precisam ser colocadas em
prática como prioridade mais alta.
Alem dos resumos mais utilizados em pesquisa (com objetivos, métodos,
resultados e conclusão), o uso de resumos visuais (por meio de imagens visuais
coloridas de diagramas, gráficos e figuras) parece ser um ótimo recurso adicional para
disseminar informações de resultados-chave de pesquisa em mídias sociais. No entanto,
ler um resumo visual não substitui a leitura do resumo real do artigo, ou menos ainda a
leitura do texto completo, razão pela qual deve ser consistente em qualidade de
descrição e interpretação adequadas com os resumos e textos completos em saúde.
Clínicos devem ter cuidado ao tomar decisões clínicas baseadas em resumos, que são
muitas vezes distorcidos em comunicados de imprensa e coberturas de notícias. A
maioria do ‘spin’ detectado é de responsabilidade dos próprios autores, editores e

XXIV
revisores de revistas, assim como disseminadores de pesquisa que utilizam mídias
sociais.
A descrição e interpretação adequadas de resumos e textos completos fazem
parte do código de conduta e princípios de integridade em pesquisa, o que inclui
honestidade, confiabilidade, objetividade, imparcialidade, comunicação aberta, dever
de cuidado e justiça. A comunicação entre pesquisadores, o publico em geral e a mídia
popular deve ser baseada em acesso aberto aos dados e referencias precisas. Portanto,
as partes interessadas tem a obrigação de seguir os princípios de ética em pesquisa
(incluindo diretrizes de ética em descrição de dados), mediante a condução de um
estudo, publicação e disseminação de resultados. Isso evitaria a má conduta em
pesquisa que leva a retrações de publicações, o que envolve custos a fontes
financiadoras e prejudica as carreiras de pesquisadores. Reduzir tais desperdícios em
pesquisa é preciso e ações para mudar políticas editorias em saúde foram propostas,
como: investimento de organizações financiadoras em programas de treinamento
baseados em diretrizes de descrição e diretrizes de ética e integridade em pesquisa
(direcionados a autores, editores e revisores de revistas); investimento no cargo de
secretário de publicações (que gerenciaria devidamente estes programas de
treinamento e também forneceria orientação sobre a submissão de artigos a revistas);
universidades que incluam disciplinas obrigatórias de treinamento para estudantes de
graduação em termos de condução de um estudo, análise estatística, descrição e
interpretação; orientações em como seguir diretrizes de ética e integridade em pesquisa
como parte integral de programas de doutorado; e ferramentas online e módulos de
treinamento baseados em diretrizes de descrição para revisores por pares.
Implicações clínicas e em pesquisa podem ser criticamente afetadas pela má
descrição e distorção de dados, principalmente para pacientes e autoridades políticas.
Iniciativas sobre recomendações dadas a financiadores, reguladores, revistas,
instituições acadêmicas e pesquisas tem sido planejadas para reduzir o desperdício e
aumentar o valor da pesquisa. Enfim, a tomada de decisão clínica baseada em pesquisa
de alta qualidade deve ser uma prática comum, afim de adquirir melhor qualidade de
vida em todo o mundo.
Para que ações sejam tomadas para melhorar a qualidade de resumos de uma
vez por todas, pretendemos desenvolver alguns editorias direcionados a chamar a
atenção de todos aqueles interessados em pesquisa. Nosso objetivo principal é dividir
nossos resultados com o Comitê Internacional de Editores de Revistas Médicas

XXV
(International Committee of Medical Journal Editors – ICMJE) e com a Sociedade
Internacional de Editores de Revistas em Fisioterapia (International Society of
Physiotherapy Journal Editors – ISPJE) e chamar a atenção especialmente de editores
e revisores de revistas em saúde. Esperamos que essa tese possa ser útil para melhorar
a conscientização de editores e revisores de revistas, autores e leitores em termos de
transparência e integridade de resumos de pesquisa em saúde e suas disseminações por
todas as partes interessadas. Esperamos sinceramente que essa conscientização possa
estimular a publicação de pesquisa em saúde de maior qualidade.

CHAPTER 1
1
CHAPTER 1
Introduction

CHAPTER 1
2
1. Introduction
1.1. Evidence-based practice in healthcare
The idea of evidence-based practice using research articles to guide clinical
decision-making was firstly conceptualized by Archibald Cochrane from Scotland and
David Sackett from Canada1. Sackett et al have defined evidence-based practice as “the
conscientious, explicit and judicious use of current best evidence in making decisions
about the care of the individual patient. It means integrating individual clinical expertise
with the best available external clinical evidence from systematic research” [p. 712].
Over the past years, government organizations of several countries have
recognized the importance of evidence-based practice and have invested on the
integration of research findings into improving clinical care of patients3,4. Funders of
healthcare research encourage data sharing, registration of protocols and open access to
research information in order to avoid wasted data2 and to promote valuable research
uptake by policy-makers, researchers and healthcare practitioners5.
Not only the clinical experience of the healthcare professional composes the
clinical decision-making, but also the patients’ preferences and needs 6,7. However, the
responsibility of searching for the highest methodological quality and most recent
evidence available is given to the healthcare professionals6,7. In order to select high
methodological quality studies that compare the effectiveness of interventions, it is
essential that healthcare practitioners know how to critically appraise evidence6,7.
In physical therapy, the volume of randomized controlled trials is constantly
growing (doubles every 3.5 years), which improved the recognition and use of
evidence-based practice by physical therapists8-10. Despite those improvements, many
barriers to implement evidence-based physical therapy still remain11, such as lack of
time to search for evidence, lack of knowledge to understand statistical information or
the external validity of results, lack of support from employer or colleagues and even
lack of resources or interest. Other barriers that arise concern to healthcare literature are
related to difficulties in accessing the full manuscript12,13, questionable quality of
studies and conflicting results of studies analyzing the same topic10,14.

CHAPTER 1
3
1.2. Literary sources for decision making of effectiveness of interventions
In the hierarchy of evidence related to evaluation of treatment effects,
randomized controlled trials occupy the top of the pyramid15. Although one considers a
systematic review as a type of study design, it is in fact a way of summarizing evidence,
once it can summarize randomized controlled trials, cohort studies, case-control studies
and so on15. Nevertheless, it is unquestionable that systematic reviews of randomized
controlled trials do summarize the best evidence of interventions effectiveness.
Therefore, healthcare professionals should preferably read those types of study designs
(systematic reviews of randomized controlled trials and randomized controlled trials) to
make clinical decisions with regards to the effects of interventions6. However, evidence
has shown that randomized controlled trials not adequately conducted or reported can
result in biased estimates of treatment effects16,17. Also, poorly conducted and reported
systematic reviews can be wasteful18, as inadequate conduct can lead to misleading
results and poor reporting may bring difficulties in assessing the validity of methods
used.
1.2.1. Methodological quality of randomized controlled trials
The most used tools to evaluate the methodological quality of randomized
controlled trials are the Revised Cochrane risk of bias (RoB) tool19 and the
Physiotherapy Evidence Database scale (PEDro scale)20.
Differences between the Cochrane RoB tool and the PEDro scale21,22 have been
discussed with consideration on what approach to choose for clinical decision-making,
when evaluating the methodological quality of a randomized controlled trial. The tools
use different scoring systems for assessing the methodological quality of randomized
controlled trials. While the PEDro scale also offers individual scores for the eleven
items, it is more usual to use the generated summary score from zero to ten (the first
item is related to external validity and it is not included in the scoring system, whereas
the last two items of the scale are related to statistical reporting and are included in the
scoring system). The Revised Cochrane RoB tool analyzes each item individually,
which include six main criteria for judging risk of bias (selection bias, performance
bias, detection bias, attrition bias, reporting bias and other biases). The criteria from
Cochrane RoB tool include all items assessed in the PEDro scale, with exception to

CHAPTER 1
4
‘other biases’, which are directed to pre-specified questions mentioned in protocols.
TABLE 1 compared such tools, adding also the Cochrane Back and Neck RoB
guideline23, which included the broadest range of items.

CHAPTER 1
5
TABLE 1. Comparison of items related to assessment of methodological quality of randomized controlled trials in healthcare interventions. PEDro scale20 Revised Cochrane RoB tool19 Back and Neck RoB guideline23 Scoring system
Individual Items Yes/ No Yes/ Probably Yes/ Probably No/ No/ No information
Yes/ No/ Unclear
Judgment 0 to 10 (low to high methodological quality)
Low/ Unclear/ High risk of bias Low/ Unclear/ High risk of bias
Items Sequence allocation Item: 2 Item: Selection bias Item: Selection bias Allocation concealment Item: 3 Item: Selection bias Item: Selection bias Baseline comparability Item: 4 Not specified Item: Selection bias Blinding of subjects Item: 5 Item: Performance bias Item: Performance bias Blinding of healthcare professionals Item: 6 Item: Performance bias Item: Performance bias Blinding of outcome assessors Item: 7 Item: Detection bias Item: Detection bias Loss to follow-up Item: 8 Item: Attrition bias Item: Attrition bias Intention to treat analysis Item: 9 Not specified Item: Attrition bias Reporting of between group comparison Item: 10 Item: Attrition bias Item: Attrition bias Reporting of point estimates and variability Item: 11 Item: Attrition bias Item: Attrition bias Pre-specified questions mentioned in protocols Not specified Item: Other biases Item: Reporting bias Outcome measures not valid Not specified Not specified Item: Other biases Unclear reporting of conflict of interest Not specified Not specified Item: Other biases Co-interventions were avoided Not specified Not specified Item: Performance bias Compliance acceptable in all groups Not specified Not specified Item: Performance bias Timing of outcome assessment similar between groups Item: 10 Not specified Item: Detection bias Note: Acronyms: PEDro scale - Physiotherapy Evidence Database scale; RoB - Risk of bias.

CHAPTER 1
6
Despite the fact that the PEDro scale is mostly used to quantify the
methodological quality of physical therapy trials, it was originally judged by clinical
trials experts based on a Delphi list consensus of healthcare interventions, plus its items
are not directly related to physical therapy24. On the other hand, the Cochrane Back and
Neck RoB guideline23 is specific for the evaluation of healthcare interventions for spinal
conditions, even if it presented similar reliability and was strongly correlated with the
PEDro scale in pharmaceutical trials20. Therefore, researchers can use the PEDro scale
and the Revised Cochrane RoB tool for assessing trials that compare treatments in a
broad healthcare field. Another important point to be considered is the readiness of the
summary scores from the PEDro scale available for each randomized controlled trial
included in the PEDro website25, which can be more useful for physical therapists on
taking clinical decisions in a busy daily routine.
Interestingly, the latest version of the Cochrane Handbook for Systematic
Reviews of Interventions26 encourages the use of the term ‘risk of bias’ instead of
‘methodological quality’ because they consider that a study may present high
methodological quality and critical standards appraisal, yet still present some level of
risk of bias.
1.2.2. Methodological quality of systematic reviews
In order to assess the methodological quality of systematic reviews, the most
recently used tools are the AMSTAR-2 (A MeaSurement Tool to Assess systematic
Reviews – Version 2)27 and the Cochrane Collaboration tool to assess risk of bias in
systematic reviews (ROBIS)28.
Differences between the measurement properties of the older version of the
AMSTAR29, the AMSTAR-2 and the ROBIS are currently under investigation in the
fields of biomedicine and public health30. However, Banzi et al found that the older
AMSTAR and the ROBIS tools are similar in terms of reliability and positive
correlation between individual domains (moderate to substantial) and overall judgments
(fair)31. TABLE 2 compared the three tools: AMSTAR29, AMSTAR-227 and ROBIS28.

CHAPTER 1
7
TABLE 2. Comparison of items related to assessment of methodological quality of systematic reviews of healthcare interventions. AMSTAR29 AMSTAR-227 ROBIS28 Scoring system
Individual Items Yes/ No/ Not applicable/ Cannot answer
Yes/ Partial yes/ No/ No meta-analysis conducted
Yes/ Probably Yes/ Probably No/ No/ No information
Judgment Critically low/ Low/ Moderate/ High methodological quality
Critically low/ Low/ Moderate/ High methodological quality
Low/ Unclear/ High risk of bias
Adequate research question Not specified Item: 1 Items: 1.2 and 1.4 Prior statement of methods Item: 1 Item: 2 Item: 1.1 Study design explained Not specified Item: 3 Not specified Comprehensive literature search strategy Items: 3 and 4 Item: 4 Items: 1.3, 1.5, 2.1, 2.2, 2.3 and 2.4 Study selection in duplicate Item: 2 Item: 5 Item: 2.5 Data extraction in duplicate Item: 2 Item: 6 Item: 3.1 List of excluded studies with reasons Item: 5 Item: 7 Not specified Detailed description of included studies Items: 5 and 6 Item: 8 Items: 3.2 and 3.3 Adequate risk of bias assessment Item: 7 Item: 9 Item: 3.4 Sources of funding of studies reported Item: 11 Item: 10 Not specified Adequate statistical analyses Item: 9 Item: 11* Items: 4.1, 4.2 and 4.3 Potential impact of risk of bias on analyses Item: 8 Item: 12* Item: 3.5 Interpretation of data accounting for risk of bias Item: 8 Item: 13 Item: 4.6 Explanation for heterogeneity Not specified Item: 14 Item: 4.4 Adequate investigation of publication bias Item: 10 Item: 15* Item: 4.5 Conflict of interest reported Item: 11 Item: 16 Not specified Note: *Applicable only to studies performing meta-analysis. Acronyms: AMSTAR - A MeaSurement Tool to Assess systematic Reviews; AMSTAR-2 - A MeaSurement Tool to Assess systematic Reviews – Version 2; ROBIS - Cochrane Collaboration tool to assess risk of bias in systematic reviews.

CHAPTER 1
8
1.3. Common problems of abstracts
Reading the full text of an article is necessary to critically appraise evidence.
However, many times the full version is not openly accessible, or it can be accessed
only with an institutional account or under payment of a fee11,32. In addition, healthcare
professionals may read only the abstract of a study, due to lack of access to the full text
or lack of time for having a busy clinical schedule11,32,33. Abstracts bring the first
impression of the study and, therefore, abstracts must be clear, concise and reflect the
exact information stated in the full text34,35. If an abstract is poorly reported, healthcare
professionals may take poor clinical decisions based on ineffective interventions, which
shows even more the importance of a well-written abstract34,35.
1.3.1. Reporting quality of abstracts
Abstracts of randomized controlled trials and systematic reviews may present
poor reporting quality36-38, analyzed by the inclusion of items predefined in reporting
guidelines created by the Enhancing the Quality and Transparency of Health Research
(EQUATOR) Network39. The Consolidated Standards of Reporting Trials
(CONSORT)35 and the Preferred Reporting Items for Systematic Reviews and Meta-
Analysis (PRISMA)34 guidelines are specific for better guidance of reporting abstracts
for these type of studies.
1.3.2. Consistency between abstracts and full texts
Abstracts may present inconsistencies with their corresponding full text40. These
inconsistencies can be related to the information reported in the body of the full text
compared to the abstract, as well as to the interpretation of the results and conclusions
within the abstract, within the full text or also misinterpretation between abstract and
full text40.
1.3.2.1. Spin of results and conclusions
One way of checking for consistency between abstract and full text is through
the analysis of the interpretation of the study results and how consistent it is with the

CHAPTER 1
9
interpretation stated in the abstract. The misinterpretation of the study results may lead
to overstated conclusions either in the full text, the abstract, or both41-43. Such
misinterpretation has been denominated as ‘spin’, term defined by Boutron et al as: “a
misrepresentation of study results, regardless of motive (intentionally or
unintentionally) that overemphasizes the beneficial effects of the intervention and
overstates safety compared with that shown by the results” [p. 244]. Some examples of
common types of spin in abstracts are: omission of primary outcome or adverse events;
selective reporting of positive and negative primary outcomes; focus on positive
secondary outcomes; overstated interpretation of study results; recommendation of an
intervention without a clinically significant effect (different from statistically
significant); and recommendation of an intervention despite high risk of bias of the
outcomes analyzed41,43.
In the literature, the term ‘spin’ has been firstly mentioned in 1995 by Horton45
and later on discussed by Fletcher46 in 2007. However, the first study to evaluate the
presence of spin in clinical research was conducted by Boutron et al44 in 2010. The
authors of such study, together with the Cochrane Statistical Method Group, developed
a spin classification scheme based on discussions and agreement among authors44. The
discussions were over items that could lead to reporting biases related to non-significant
results for the primary outcomes, i.e. strategies of spin in each section of the abstract
and full texts of the articles analyzed44. Since then, other studies47-58 have analyzed spin
in clinical research, but no official list has been validated so far.
1.4. Justification of the thesis
As previously mentioned, the issues related to abstracts have been investigated
in studies of several healthcare related fields, as psychiatry37, general medicine38,
oncology41 and cardiovascular59 for example. However, some other healthcare fields
still lack research on such concerns, as the abstracts of studies related to the
effectiveness of physical therapy interventions for low back pain. Furthermore, there is
no summarization of data discussing possible solutions and actions to be taken to
improve the overall quality of abstracts of studies related to treatment effects
(randomized controlled trials and systematic reviews). Finally, there is no summary of
how broad are those concerns related to abstracts, how their improvement can affect the
daily lives of stakeholders (healthcare professionals, researchers, authors, peer

CHAPTER 1
10
reviewers, journal editors and publishers) and also influence their clinical and academic
decision-making. Given these reasons, we designed the objectives of this thesis.
1.4.1 General objectives
1) To describe and analyze the main characteristics of representative and recent
samples of randomized controlled trials and systematic reviews and their abstracts, in a
specific population of studies (physical therapy for low back pain). This objective will
be answered in CHAPTERS 2 and 3.
2) To describe and compare studies that analyzed abstracts of randomized
controlled trials and systematic reviews in all healthcare areas. This objective will be
answered in CHAPTER 4.
1.4.2 Specific objectives
Our main goals are to increase awareness of the importance of a well-written
abstract in the academic and clinical healthcare fields, and also to call for actions to
change journal’s editorial policies in order to improve the quality of abstracts in general.
This specific objective will be discussed in our concluding remarks in CHAPTER 5.
CHAPTER 1
11
REFERENCES
1. Claridge JA, Fabian TC. History and development of evidence-based medicine.
World J Surg. 2005;29(5):547-553.
2. Sackett DL, Rosenberg WMC, Gray MJA, Haynes BR, Richardson SW.
Evidence based medicine: what it is and what it isn't. BMJ. 1996;312:71-72.
3. Boon WM, Leves F. NHMRC initiatives to improve access to research outputs
and findings. Med J Aust. 2015;202(11):558.
4. Fauci AS, Collins FS. NIH research: think globally. Science.
2015;348(6231):159.
5. Conalogue DM, Kinn S, Mulligan JA, McNeil M. International consultation on
long-term global health research priorities, research capacity and research uptake in
developing countries. Health Res Policy Syst. 2017;15(1):24.
6. Herbert R, Jamtvedt G, Mead J, Hagen KB. Practical evidence-based
physiotherapy. 2nd Edition ed: Elsevier Butterworth-Heinemann; 2011.
7. Sackett D, Straus S, Richardson W, Rosenberg W, Haynes R. Evidence-based
medicine how to practice and teach EBM. 2a ed. Edinburgh: Churchill Livingstone;
2000.
8. PEDro. Statistics from Physiotherapy Evidence Database (PEDro)’ s website.
Sydney. 2019; https://www.pedro.org.au/english/downloads/pedro-statistics. Accessed
April 2nd 2019.
9. Kamper SJ, Moseley AM, Herbert RD, Maher CG, Elkins MR, Sherrington C.
15 years of tracking physiotherapy evidence on PEDro, where are we now? Br J Sports
Med. 2015;49(14):907-909.
10. Scurlock-Evans L, Upton P, Upton D. Evidence-based practice in physiotherapy:
a systematic review of barriers, enablers and interventions. Physiotherapy.
2014;100(3):208-219.
11. Silva TM, Costa LCM, Garcia AN, Costa LO. What do physical therapists think
about evidence-based practice? A systematic review. Man Ther. 2014;20(3):388-401.
12. Silva TM, Costa LCM, Costa LOP. Evidence-Based Practice: a survey about
behavior, knowledge, skills and resources, opinions and barriers faced by Brazilian
physical therapists from São Paulo state. Braz J Phys Ther. 2015;19(4).

CHAPTER 1
12
13. Wong G, Monatzerolghaem M, Gerzina T. Integrating Evidence-Based Practice
Into Oral Health Clinical Practice: Students' Perspectives. J Evid Based Dent Pract.
2019;19(1):79-85.
14. Spallek H, Song M, Polk DE, Bekhuis T, Frantsve-Hawley J, Aravamudhan K.
Barriers to implementing evidence-based clinical guidelines: a survey of early adopters.
J Evid Based Dent Pract. 2010;10(4):195-206.
15. Djulbegovic B, Guyatt GH. Progress in evidence-based medicine: a quarter
century on. Lancet. 2017;390(10092):415-423.
16. Nuesch E, Trelle S, Reichenbach S, et al. The effects of excluding patients from
the analysis in randomised controlled trials: meta-epidemiological study. BMJ.
2009;339:b3244.
17. Savovic J, Jones HE, Altman DG, et al. Influence of reported study design
characteristics on intervention effect estimates from randomized, controlled trials. Ann
Intern Med. 2012;157(6):429-438.
18. Page MJ, Shamseer L, Altman DG, et al. Epidemiology and Reporting
Characteristics of Systematic Reviews of Biomedical Research: A Cross-Sectional
Study. PLoS Med. 2016;13(5):e1002028.
19. Higgins JPT, Sterne JAC, Savović J, et al. A revised tool for assessing risk of
bias in randomized trials In: Chandler J, McKenzie J, Boutron I, Welch V (editors).
Cochrane Methods. Cochrane Database of Systematic Reviews. 2016(10 (Suppl 1)).
20. Yamato TP, Maher C, Koes B, Moseley A. The PEDro scale had acceptably
high convergent validity, construct validity, and interrater reliability in evaluating
methodological quality of pharmaceutical trials. J Clin Epidemiol. 2017;86:176-181.
21. Armijo-Olivo S, da Costa BR, Cummings GG, et al. PEDro or Cochrane to
Assess the Quality of Clinical Trials? A Meta-Epidemiological Study. PLoS One.
2015;10(7):e0132634.
22. Costa LO, Maher CG, Moseley AM, et al. da Costa and colleagues' criticism of
PEDro scores is not supported by the data. J Clin Epidemiol. 2013;66(10):1192-1193.
23. Furlan AD, Malmivaara A, Chou R, et al. 2015 Updated Method Guideline for
Systematic Reviews in the Cochrane Back and Neck Group. Spine (Phila Pa 1976).
2015;40(21):1660-1673.
24. Verhagen AP, de Vet HC, de Bie RA, et al. The Delphi list: a criteria list for
quality assessment of randomized clinical trials for conducting systematic reviews
developed by Delphi consensus. J Clin Epidemiol. 1998;51(12):1235-1241.

CHAPTER 1
13
25. PEDro website. Advanced search for clinical trials. Sydney: Physiotherapy
Evidence Database. 2019; https://search.pedro.org.au/advanced-
search/results?abstract_with_title=&therapy=0&problem=0&body_part=0&subdisciplin
e=0&topic=0&method=clinical+trial&authors_association=&title=&source=&year_of_
publication=&date_record_was_created=&nscore=&perpage=20&lop=and&find=&fin
d=Start+Search. Accessed April 17th 2019.
26. Higgins JPT, Altman DG, Sterne JACe. Chapter 8: Assessing risk of bias in
included studies. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS (editors),
Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated
June 2017), Cochrane. The Cochrane Collaboration; 2017. Available from
www.training.cochrane.org/handbook.
27. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for
systematic reviews that include randomised or non-randomised studies of healthcare
interventions, or both. BMJ. 2017;358:j4008.
28. Whiting P, Savovic J, Higgins JP, et al. ROBIS: A new tool to assess risk of bias
in systematic reviews was developed. J Clin Epidemiol. 2016;69:225-234.
29. Shea BJ, Grimshaw JM, Wells GA, et al. Development of AMSTAR: a
measurement tool to assess the methodological quality of systematic reviews. BMC Med
Res Methodol. 2007;7:10.
30. Gates A, Gates M, Duarte G, et al. Evaluation of the reliability, usability, and
applicability of AMSTAR, AMSTAR 2, and ROBIS: protocol for a descriptive analytic
study. Syst Rev. 2018;7(1):85.
31. Banzi R, Cinquini M, Gonzalez-Lorenzo M, Pecoraro V, Capobussi M, Minozzi
S. Quality assessment versus risk of bias in systematic reviews: AMSTAR and ROBIS
had similar reliability but differed in their construct and applicability. J Clin Epidemiol.
2018;99:24-32.
32. Maher CG, Sherrington C, Elkins M, Herbert RD, Moseley AM. Challenges for
evidence-based physical therapy: accessing and interpreting high-quality evidence on
therapy. Phys Ther. 2004;84(7):644-654.
33. Sriganesh K, Bharadwaj S, Wang M, et al. Quality of abstracts of randomized
control trials in five top pain journals: A systematic survey. Contemp Clin Trials
Commun. 2017;7:64-68.

CHAPTER 1
14
34. Beller EM, Glasziou PP, Altman DG, et al. PRISMA for Abstracts: reporting
systematic reviews in journal and conference abstracts. PLoS Med.
2013;10(4):e1001419.
35. Hopewell S, Clarke M, Moher D, et al. CONSORT for reporting randomised
trials in journal and conference abstracts. Lancet. 2008;371(9609):281-283.
36. Chhapola V, Tiwari S, Brar R, Kanwal SK. Reporting quality of trial abstracts-
improved yet suboptimal: A systematic review and meta-analysis. J Evid Based Med.
2018.
37. Song SY, Kim B, Kim I, et al. Assessing reporting quality of randomized
controlled trial abstracts in psychiatry: Adherence to CONSORT for abstracts: A
systematic review. PLoS One. 2017;12(11):e0187807.
38. Bigna JJ, Um LN, Nansseu JR. A comparison of quality of abstracts of
systematic reviews including meta-analysis of randomized controlled trials in high-
impact general medicine journals before and after the publication of PRISMA extension
for abstracts: a systematic review and meta-analysis. Syst Rev. 2016;5(1):174.
39. EQUATOR Network. Enhancing the QUAlity and Transparency Of health
Research. https://www.equator-network.org/reporting-guidelines/, 2019.
40. Li G, Abbade LPF, Nwosu I, et al. A scoping review of comparisons between
abstracts and full reports in primary biomedical research. BMC Med Res Methodol.
2017;17(1):181.
41. Boutron I, Altman DG, Hopewell S, Vera-Badillo F, Tannock I, Ravaud P.
Impact of spin in the abstracts of articles reporting results of randomized controlled
trials in the field of cancer: the SPIIN randomized controlled trial. J Clin Oncol.
2014;32(36):4120-4126.
42. Chiu K, Grundy Q, Bero L. 'Spin' in published biomedical literature: A
methodological systematic review. PLoS Biol. 2017;15(9):e2002173.
43. Yavchitz A, Ravaud P, Altman DG, et al. A new classification of spin in
systematic reviews and meta-analyses was developed and ranked according to the
severity. J Clin Epidemiol. 2016;75:56-65.
44. Boutron I, Dutton S, Ravaud P, Altman DG. Reporting and interpretation of
randomized controlled trials with statistically nonsignificant results for primary
outcomes. JAMA. 2010;303(20):2058-2064.
45. Horton R. The rhetoric of research. BMJ. 1995;310(6985):985-987.

CHAPTER 1
15
46. Fletcher RH, Black B. "Spin" in scientific writing: scientific mischief and legal
jeopardy. Med Law. 2007;26(3):511-525.
47. Arunachalam L, Hunter IA, Killeen S. Reporting of Randomized Controlled
Trials With Statistically Nonsignificant Primary Outcomes Published in High-impact
Surgical Journals. Ann Surg. 2017;265(6):1141-1145.
48. Assem Y, Adie S, Tang J, Harris IA. The over-representation of significant p
values in abstracts compared to corresponding full texts: A systematic review of
surgical randomized trials. Contemp Clin Trials Commun. 2017;7:194-199.
49. Austin J, Smith C, Natarajan K, Som M, Wayant C, Vassar M. Evaluation of
spin within abstracts in obesity randomized clinical trials: A cross-sectional review.
Clin Obes. 2019;9(2):e12292.
50. Chow JTY, Turkstra TP, Yim E, Jones PM. The degree of adherence to
CONSORT reporting guidelines for the abstracts of randomised clinical trials published
in anaesthesia journals: A cross-sectional study of reporting adherence in 2010 and
2016. Eur J Anaesthesiol. 2018:942-948.
51. Cooper CM, Gray HM, Ross AE, et al. Evaluation of spin in the abstracts of
otolaryngology randomized controlled trials. Laryngoscope. 2018.
52. Gewandter JS, McKeown A, McDermott MP, et al. Data interpretation in
analgesic clinical trials with statistically nonsignificant primary analyses: an ACTTION
systematic review. J Pain. 2015;16(1):3-10.
53. Hernandez AV, Pasupuleti V, Deshpande A, Thota P, Collins JA, Vidal JE.
Deficient reporting and interpretation of non-inferiority randomized clinical trials in
HIV patients: a systematic review. PLoS One. 2013;8(5):e63272.
54. Lieb K, von der Osten-Sacken J, Stoffers-Winterling J, Reiss N, Barth J.
Conflicts of interest and spin in reviews of psychological therapies: a systematic review.
BMJ Open. 2016;6(4):e010606.
55. Lockyer S, Hodgson R, Dumville JC, Cullum N. "Spin" in wound care research:
the reporting and interpretation of randomized controlled trials with statistically non-
significant primary outcome results or unspecified primary outcomes. Trials.
2013;14:371.
56. Patel SV, Chadi SA, Choi J, Colquhoun PH. The use of "spin" in laparoscopic
lower GI surgical trials with nonsignificant results: an assessment of reporting and
interpretation of the primary outcomes. Dis Colon Rectum. 2013;56(12):1388-1394.

CHAPTER 1
16
57. Roest AM, de Jonge P, Williams CD, de Vries YA, Schoevers RA, Turner EH.
Reporting Bias in Clinical Trials Investigating the Efficacy of Second-Generation
Antidepressants in the Treatment of Anxiety Disorders: A Report of 2 Meta-analyses.
JAMA Psychiatry. 2015;72(5):500-510.
58. Vera-Badillo FE, Shapiro R, Ocana A, Amir E, Tannock IF. Bias in reporting of
end points of efficacy and toxicity in randomized, clinical trials for women with breast
cancer. Ann Oncol. 2013;24(5):1238-1244.
59. Khan MS, Lateef N, Siddiqi TJ, et al. Level and Prevalence of Spin in Published
Cardiovascular Randomized Clinical Trial Reports With Statistically Nonsignificant
Primary Outcomes: A Systematic Review. JAMA Netw Open. 2019;2(5):e192622.

CHAPTER 2
17
CHAPTER 2
Randomized controlled trials in low back pain

CHAPTER 2
18
2.1. Description of the randomized controlled trials

CHAPTER 2
19
2.1.1. Description of low back pain clinical trials in physical therapy: a
cross sectional study
Published in: Brazilian Journal of Physical Therapy 2018 Sep 13
DOI: 10.1016/j.bjpt.2018.09.002 [Epub ahead of print]
CHAPTER 2
20
Description of low back pain clinical trials in physical therapy: a cross sectional
study
Dafne Port Nascimento1; Gabrielle Zoldan Gonzalez1; Amanda Costa Araujo1;
Leonardo Oliveira Pena Costa1 1Masters and Doctoral Programs in Physical Therapy, Universidade Cidade de São
Paulo, São Paulo, Brazil.
Corresponding author: Dafne Port Nascimento, Masters and Doctoral Programs in
Physical Therapy, Universidade Cidade de São Paulo. Rua Cesário Galeno 448,
Tatuapé, São Paulo, SP – Brazil, CEP 03071-000. Phone number: +55 11 994779119.
ORCID ID: https://orcid.org/0000-0002-8474-727X
Email address: [email protected]
Funding: This work was supported by a PhD scholarship from the Sao Paulo Research
Foundation (grant#2015/16953-2; Fundação de Amparo à Pesquisa do Estado de São
Paulo – FAPESP).
Declaration of interest: The authors declare no financial competing interest.
Furthermore, seven out of the 200 articles analyzed involved authors from our research
groups or collaborators.

CHAPTER 2
21
Description of low back pain clinical trials in physical therapy: a cross sectional
study
ABSTRACT
Purpose: To describe the main characteristics of low back pain randomized controlled
trials on the Physiotherapy Evidence Database (PEDro), and to rank the journals where
these trials were published according to their Impact Factor. Methods: This is a cross
sectional study based on a collection of randomized controlled trials. A random sample
of 200 low back pain trials published between 2010 and 2015 were selected from
PEDro in February 2016. We collected the following main characteristics of trials: 2015
journal Impact Factor; if the paper was published as open access; CONSORT
recommendations endorsement by the journal; methodological quality and statistical
reporting measured by the 0-10 items PEDro scale. Data was analyzed descriptively.
Results: Trials were published in journals with a mean Impact Factor of 2.5 (SD 2.5),
from which 55.5% endorsed the CONSORT recommendations. The methodological
quality was moderate with 5.8 points (SD 1.6). The top 3 journals according to Impact
Factor were: 1) British Medical Journal; 2) Annals of Internal Medicine; and 3) BMC
Medicine. Only 6 out of 97 journals publishing low back pain trials combined the
following factors: journal Impact Factor higher than 2.0, mean trial methodological
quality higher than 6.0 points, endorse CONSORT recommendations and offering
papers as open access. Conclusion: Clinicians interested in low back pain trials must
look for a wide variety of healthcare journals. A substantial number of low back pain
randomized controlled trials did not follow adequate reporting and methodological
recommendations.
Abbreviations: CONSORT - Consolidated Standards of Reporting Trials; PEDro -
Physiotherapy Evidence Database.

CHAPTER 2
22
INTRODUCTION
Low back pain is the leading cause of years lived with disability since 19901,
with a high prevalence and costs worldwide2-5. Low back pain affects not only high
income countries, but also high middle income and middle socio-demographic index
countries1. In order to measure treatment effectiveness for this condition, the best
evidence is provided by randomized controlled trials or systematic reviews of
randomized controlled trials6,7.
The usual treatment for low back pain patients is consisted of nonpharmacologic
therapies, education, reassurance and analgesic medication8. Nonpharmacologic
therapies have shown effectiveness on mind-body interventions, such as exercise,
psychological therapies, multidisciplinary rehabilitation, spinal manipulation, massage
and acupuncture9. Such interventions reinforce the essential role carried by physical
therapists in the long-term management of this condition10.
In order to implement treatments for low back pain, randomized controlled trials
should follow adequate reporting and methodological guidelines11. The methodological
quality of physical therapy randomized controlled trials varies across different
subdisciplines12. The methodological quality of trials in musculoskeletal physical
therapy has been associated with endorsement of reporting recommendations (i.e.
trials/journals that formally ask authors to report their trials using the Consolidated
Standards of Reporting Trials, CONSORT13), articles published recently and trials
published in English14. On the other hand, the methodological quality is not necessarily
associated with journal Impact Factor15.
The Physiotherapy Evidence Database (PEDro; www.pedro.org.au) is an open
access database that indexes clinical trials, systematic reviews and guidelines in
physical therapy16. PEDro is one of the four most comprehensive healthcare databases,
including CENTRAL, PubMed and EMBASE, but only PEDro is focused only in
physical therapy interventions17,18. Each clinical trial indexed on PEDro goes through a
methodological quality and statistical reporting assessment measured by the PEDro
scale19-22, which generates a score that ranges from 0 (low methodological quality) to 10
(high methodological quality). The items from the PEDro scale are: 1) Eligibility
criteria and source (not included on the total score); 2) Random allocation; 3) Concealed
allocation; 4) Baseline comparability; 5) Blinding of subjects; 6) Blinding of therapists;

CHAPTER 2
23
7) Blinding of assessors; 8) Adequate follow-up; 9) Intention-to-treat analysis; 10)
Between-group comparisons; 11) Point estimates and variability.
Clinicians treating low back pain patients should be aware about what would be
the core journals that publish randomized controlled trials in physical therapy for low
back pain. In addition, it is important to understand the strengths and weaknesses of
those trials11. Therefore, the primary objective of this study was to describe the main
characteristics of low back pain randomized controlled trials on PEDro, and to rank the
journals where these trials were published according to their Impact Factor. Our
secondary objective was to analyze the correlation between trials methodological
quality and journals Impact Factor.
METHODS
Study selection
We searched for all low back pain randomized controlled trials, published
between 2010 and 2015, and indexed on PEDro database on February 1st 2016. Then we
randomly selected a sample of approximately 40% of all eligible trials, using the
random number function in Excel. The eligibility criteria were: full-published articles;
written in English, Spanish or Portuguese; and published between 2010 and 2015. The
languages were restricted to English, Spanish and Portuguese, as they are languages
spoken by the authors of this manuscript and are within the most published languages
on PEDro14,23. Trials that were still in the recruitment stages, protocols, duplicates and
those involving any topic other than low back pain were excluded. We used the
advanced search strategy on PEDro, as follows: “clinical trial” for method; “lumbar
spine, sacroiliac joint or pelvis” for body part; “pain” for problem; and 2010 to 2015 for
year of publication.
Data extraction
One independent author extracted data in an Excel spreadsheet previously
formatted to describe the trials’ characteristics. Data extracted from the trials were: 1)
continent where trial was conducted; 2) language of publication, categorized into
English or non-English; 3) methodological quality, which was measured by total PEDro

CHAPTER 2
24
score and downloaded from PEDro database (0-10 points with higher values indicating
better methodological quality); 4) number of years since publication, calculated by
subtracting the year of publication from 2015; 5) number of citations normalized by the
number of years since publication (extracted from the Web of Science Clarivate
Analytics); 6) total sample size (i.e., number of participants randomized); 7) primary
outcomes, which were collected at most two outcomes. For articles that did not specify
the primary outcome, but had two outcomes mentioned only, we considered both as
primary. For articles that did not specify the primary outcome but had more than two
outcomes, we considered “pain” and “disability” as primary24. In the cases which the
article did not have any of these two outcomes, we collected the first two mentioned by
the authors. All primary outcomes were categorized into: pain, disability, function,
quality of life or other; 8) interventions, which included any type of physical therapy
intervention. Each intervention was categorized according to the intervention codes
used by PEDro25 (i.e., Acupuncture; Behavior modification; Education; Electrotherapy,
heat, cold; Fitness training; Health promotion; Hydrotherapy, balneotherapy;
Neurodevelopmental therapy, neurofacilitation; Ortheses, taping, splinting; Respiratory
therapy; Skill training; Strength training; Stretching, mobilization, manipulation,
massage; No appropriate value in this field); 9) comparators, which were categorized
into no-treatment control26, placebo27, addition of other treatment28, waiting list29,
minimal intervention28, usual care30 and/or other intervention31. We also classified the
trial in one of these groups if the authors of the trial classified the comparator group as
such.
Data extracted from journals were: 1) 2015 journal Impact Factor (from the Web
of Science, InCites Journal Citation Reports – Thomson Reuters’ website Clarivate
Analytics), and categorized in three strata (Journals without Impact Factor; Journals
with Impact Factor less than 2.0; Journals with Impact Factor more than 2.0); 2) if
journal was open access (yes or no), which was obtained from the Directory of Open
Access Journals, PubMed Central or the journal’s web-site; and 3) if journal endorses
the CONSORT recommendations32 (yes or no), which was extracted from the
“Instructions to authors” for each of the journals or from the CONSORT’s website13.

CHAPTER 2
25
Main outcome measures
The main outcome measures were: journal Impact Factor; if the paper was
published as open access; CONSORT recommendations endorsement by the journal;
and methodological quality measured by total PEDro score.
Data analysis
All trials characteristics were analyzed descriptively. Normality tests were
conducted and all data were normally distributed, except for the total sample size, which
was reported as median and interquartile range. The correlation between trials
methodological quality and journals Impact Factor was calculated using Pearson
correlation. We used SPSS software (Version 20.0) for all analyses.
RESULTS
The search strategy on PEDro database yielded 25.956 clinical trials. Using the
advanced search strategy 537 potentially eligible trials were retrieved. APPENDIX A
presents all excluded trials excluded (n=67) and reasons for these exclusions. From the
remaining 470 articles, we randomly selected a sample of 200 trials (APPENDIX B),
represented in the flow chart in FIGURE 1.
TABLE 1 presented the descriptive data of the 200 articles. Most of trials were
conducted in Europe and Asia, published in English, in open access journals and more
than half endorsed CONSORT recommendations.
TABLE 2 presented the frequency and percentage of the primary outcomes,
interventions and comparators. Most of trials evaluated pain and disability as primary
outcomes; strength training, stretching, mobilization, manipulation and/or massage as
interventions; and were mainly compared with other treatment or the addition of other
treatment.
The 200 trials were published in 97 different journals. We organized the journals
into: Impact Factor higher than 2.0 (30 journals with 81 articles); Impact Factor lower
than 2.0 (40 journals with 76 articles); and journals without Impact Factor (27 journals
with 43 articles) (TABLE 3). The top 3 journals were: 1) British Medical Journal; 2)
Annals of Internal Medicine; and 3) BMC Medicine. As our results showed, the higher

CHAPTER 2
26
the journal Impact Factor, the higher the methodological quality of the trials, and
apparently is also higher the likelihood of the journals to endorse CONSORT
recommendations and offer open access (Table 3). Combining those four characteristics
together (Impact Factor higher than 2.0, trial methodological quality higher than 6.0,
endorse CONSORT recommendations and open access journal), the top 3 journals
were: 1) BMC Medicine; 2) Annals of Family Medicine; and 3) Journal of Medical
Internet Research. Interestingly, only three other journals from our sample also
presented those four characteristics, which were the Journal of Physiotherapy, PLoS
ONE and BMC Pregnancy and Childbirth.
Trials methodological quality and statistical reporting measured by the PEDro
scale was weakly correlated with journals Impact Factor (r= 0.23; P=0.004).

CHAPTER 2
27
TABLE 1. Descriptive data of the total sample (n =200) with mean (standard deviation) and the frequency (percentage) of articles. Mean (SD) Number of Articles
(%) Continents - 200 (100.0)
Europe - 70 (35.0) Asia - 65 (32.5) North America - 33 (16.5) South America - 13 (6.5) Africa - 8 (4.0) Oceania - 11 (5.5)
Written in English - 198 (99.0) Portuguese and Spanish - 2 (1.0)
Open access articles - 115 (57.5) Trials published in journals that endorsed CONSORT recommendations
- 111 (55.5)
Total PEDro score/Methodological quality (0-10)+ 5.8 (1.6) 200 (100.0) Year of publication (years) *3.4 (1.7) 200 (100.0)
2010 - 28 (14.0) 2011 - 35 (17.5) 2012 - 36 (18.0) 2013 - 34 (17.0) 2014 - 29 (14.5) 2015 - 38 (19.0)
Journal InCites Journal Citation Reports Impact Factor 2015 2.5 (2.5) 157 (78.5) Articles in Journals without Impact Factor - 43 (21.5) Articles in Journals with Impact Factor lower than 2.0
1.4 (0.4) 76 (38)
Articles in Journals with Impact Factor higher than 2.0
3.7 (3.1) 81 (40.5)
Number of citations 2.6 (2.5) 144 (72.0) Not cited - 21 (10.5) Not indexed in Web of Knowledge - 35 (17.5)
Total sample size **73.5 (108.0)
200 (100.0)
+ The higher is the score, the better is the methodological/reporting quality. *Data presented as ‘number of years since publication’, which was calculated by subtracting the year of publication from 2015. **Data presented as median (Interquartile range).

CHAPTER 2
28
TABLE 2. Frequency (percentage) of the primary outcomes, interventions and comparators presented in the total sample (n =200). Number of Articles (%) Primary outcomes** 200 (100.0)
Pain 126 (63.0) Disability 93 (46.5) Function 18 (9.0) Quality of life 8 (4.0) Other 88 (44.0)
Interventions** 200 (100.0) Acupuncture 14 (7.0) Behavior modification 20 (10.0) Education 50 (25.0) Electrotherapy, heat, cold 25 (12.5) Fitness training 26 (13.0) Health promotion 7 (3.5) Hydrotherapy, balneotherapy 8 (4.0) Neurodevelopmental therapy, neurofacilitation 1 (0.5) Orthoses, taping, splinting 5 (2.5) Respiratory therapy 0 (0.0) Skill training 41 (20.5) Strength training 85 (42.5) Stretching, mobilization, manipulation, massage 88 (44.0) No appropriate value in this field 2 (1.0)
Comparators** 200 (100.0) No-treatment control 22 (11.0) Placebo 20 (10.0) Addition of other treatment 61 (30.5) Waiting list 4 (2.0) Minimal intervention 9 (4.5) Usual care 31 (15.5) Other treatment 82 (41.0)
**Some studies included more than one primary outcome, intervention or comparator.

CHAPTER 2
29
TABLE 3. Descriptive data of 200 trials published in 97 journals. Journals categorized into Impact Factor higher and lower than 2.0, and journals without Impact Factor. Ranking of journals is presented from higher to lower Impact factors (70 journals).
Name of Journal Number of articles (%)
Impact Factor 2015
Mean (SD) PEDro score 0-10
Open access journals
Journals endorsing CONSORT
30 Journals with Impact Factor higher than 2.0 *Mean (SD); **Number of journals (%) 81 (40.5) *3.7 (3.1) 6.3 (1.5) **16 (16.5) **21 (21.6) 1) British Medical Journal 1 (0.5) 19.7 8.0 (0.0) No Yes 2) Annals of Internal Medicine 2 (1.0) 16.4 6.5 (2.1) No Yes 3) BMC Medicine 3 (1.5) 8.0 7.0 (1.0) Yes Yes 4) British Journal of Sports Medicine 2 (1.0) 6.7 5.5 (0.7) No No 5) Pain 3 (1.5) 5.6 6.7 (1.2) No Yes 6) Annals of Family Medicine 1 (0.5) 5.1 9.0 (0.0) Yes Yes 7) Journal of Medical Internet Research 1 (0.5) 4.5 6.0 (0.0) Yes Yes 8) Health Technology Assessment 1 (0.5) 4.1 5.0 (0.0) Yes Yes 9) Medicine and Science in Sports and Exercise 1 (0.5) 4.0 7.0 (0.0) No No 10) Journal of Physiotherapy 2 (1.0) 4.0 8.0 (1.4) Yes Yes 11) Journal of Science and Medicine in Sport 1 (0.5) 3.8 8.0 (0.0) No No 12) International Journal of Nursing Studies 1 (0.5) 3.6 8.0 (0.0) No Yes 13) PLoS ONE 1 (0.5) 3.1 6.0 (0.0) Yes Yes 14) Archives of Physical Medicine and Rehabilitation 5 (2.5) 3.0 7.2 (0.8) No Yes 15) European Journal of Pain 2 (1.0) 2.9 7.0 (1.4) No Yes 16) Physical Therapy 8 (4.0) 2.8 7.0 (0.9) No Yes 17) The Clinical Journal of Pain 4 (2.0) 2.7 6.0 (0.0) No No 18) The Spine Journal 5 (2.5) 2.7 6.0 (1.2) No Yes 19) Lasers in Medical Science 2 (1.0) 2.5 7.0 (2.9) No No 20) Spine 16 (8.0) 2.4 5.6 (1.9) No Yes 21) Clinical Rehabilitation 5 (2.5) 2.4 6.6 (1.1) No No 22) Pain Medicine 1 (0.5) 2.3 6.0 (0.0) No No 23) Pain Practice 1 (0.5) 2.3 4.0 (0.0) No Yes 24) International Journal of Clinical Practice 1 (0.5) 2.2 4.0 (0.0) No Yes

CHAPTER 2
30
TABLE 3. Descriptive data of 200 trials published in 97 journals. Journals categorized into Impact Factor higher and lower than 2.0, and journals without Impact Factor. Ranking of journals is presented from higher to lower Impact factors (70 journals).
Name of Journal Number of articles (%)
Impact Factor 2015
Mean (SD) PEDro score 0-10
Open access journals
Journals endorsing CONSORT
25) BMC Pregnancy and Childbirth 1 (0.5) 2.2 6.0 (0.0) Yes Yes 26) European Spine Journal 3 (1.5) 2.1 6.3 (1.2) No No 27) American Journal of Physical Medicine & Rehabilitation 1 (0.5) 2.1 6.0 (0.0) No Yes 28) European Journal of Physical and Rehabilitation Medicine 5 (2.5) 2.1 4.5 (1.0) Yes Yes 29) Clinical Rheumatology 1 (0.5) 2.0 8.0 (0.0) No No 30) Family Practice 1 (0.5) 2.0 3.0 (0.0) No Yes 40 Journals with Impact Factor lower than 2.0 *Mean (SD); **Number of journals (%) 76 (38.0) *1.4 (0.4) 5.6 (1.4) **13 (13.4) **21 (21.6) 1) Evidence-Based Complementary and Alternative Medicine 1 (2.0) 1.9 6.5 (1.0) Yes No 2) Disability and Rehabilitation 1 (0.5) 1.9 8.0 (0.0) No No 3) Journal of Advanced Nursing 1 (0.5) 1.9 7.0 (0.0) No Yes 4) International Journal of Rheumatic Diseases 1 (0.5) 1.9 5.0 (0.0) No No 5) Manual Therapy 1 (2.0) 1.9 5.0 (0.8) No Yes 6) Physiotherapy 1 (0.5) 1.8 4.0 (0.0) No Yes 7) The American Journal of the Medical Sciences 1 (0.5) 1.8 3.0 (0.0) No No 8) Rheumatology International 1 (0.5) 1.7 5.0 (0.0) No Yes 9) BMC Musculoskeletal Disorders 1 (2.0) 1.7 6.5 (1.3) Yes Yes 10) International Journal of Gynaecology and Obstetrics 1 (0.5) 1.7 7.0 (0.0) No Yes 11) PM&R 2 (1.0) 1.7 5.0 (1.4) No Yes 12) Photomedicine and Laser Surgery 1 (0.5) 1.6 5.0 (0.0) No No 13) Journal of Sport Rehabilitation 1 (0.5) 1.6 6.0 (0.0) No No 14) Journal of Rehabilitation Medicine 5 (2.5) 1.6 6.6 (0.5) Yes Yes 15) Acupuncture in Medicine 2 (1.0) 1.6 8.0 (0.0) No Yes 16) Chinese Medicine 1 (0.5) 1.6 6.0 (0.0) Yes Yes 17) Swiss Medical Weekly 1 (0.5) 1.5 7.0 (0.0) Yes No 18) Ergonomics 1 (0.5) 1.4 5.0 (0.0) No No

CHAPTER 2
31
TABLE 3. Descriptive data of 200 trials published in 97 journals. Journals categorized into Impact Factor higher and lower than 2.0, and journals without Impact Factor. Ranking of journals is presented from higher to lower Impact factors (70 journals).
Name of Journal Number of articles (%)
Impact Factor 2015
Mean (SD) PEDro score 0-10
Open access journals
Journals endorsing CONSORT
19) The Journal of International Medical Research 2 (1.0) 1.4 6.5 (0.7) No Yes 20) Medical Science Monitor 2 (1.0) 1.4 4.5 (0.7) No No 21) Journal of Alternative & Complementary Medicine 2 (1.0) 1.4 7.5 (2.1) No Yes 22) Journal of Clinical Nursing 1 (0.5) 1.4 6.0 (0.0) No Yes 23) Psychology, Health & Medicine 1 (0.5) 1.3 4.0 (0.0) No No 24) Journal of Manipulative and Physiological Therapeutics 7 (3.5) 1.3 75 (1.3) No Yes 25) Clinics 1 (0.5) 1.3 7.0 (0.0) Yes No 26) Clinical Neurology and Neurosurgery 1 (0.5) 1.2 6.0 (0.0) No No 27) Indian Journal of Physiotherapy and Occupational Therapy 7 (3.5) 1.2 3.7 (1.1) No No 28) International Journal of Clinical and Experimental Medicine 1 (0.5) 1.1 5.0 (0.0) Yes No 29) Chung I Tsa Chih Ying Wen Pan [Journal of Traditional Chinese Medicine] 1 (0.5) 1.0 6.0 (0.0) Yes Yes 30) Military Medicine 1 (0.5) 1.0 6.0 (0.0) No Yes 31) Journal of Back and Musculoskeletal Rehabilitation 7 (3.5) 1.0 4.6 (0.8) No No 32) Revista Paulista de Medicina [Sao Paulo Medical Journal] 1 (0.5) 1.0 7.0 (0.0) Yes Yes 33) Southern Medical Journal 1 (0.5) 0.9 5.0 (0.0) No No 34) Neurosciences 1 (0.5) 0.5 7.0 (0.0) Yes Yes 35) Nigerian Journal of Clinical Practice 1 (0.5) 0.5 5.0 (0.0) Yes Yes 36) International Journal of Osteopathic Medicine 1 (0.5) 0.5 8.0 (0.0) Yes Yes 37) Turkish Neurosurgery 1 (0.5) 0.5 6.0 (0.0) Yes Yes 38) Revista de Investigacion Clinica 1 (0.5) 0.5 5.0 (0.0) No No 39) Acta Clinica Croatica 1 (0.5) 0.4 5.0 (0.0) No No 40) Isokinetics and Exercise Science 1 (0.5) 0.4 6.0 (0.0) No No 27 Journals without Impact Factor **Number (%) 43 (21.5) - 5.1 (1.7) **8 (8.2) **8 (8.2)

CHAPTER 2
32
DISCUSSION
Main characteristics of low back pain trials
Low back pain randomized controlled trials have been published in a variety of
healthcare journals, with Impact Factors ranging from 0.4 to 19.7, and even in some
journals that were not even indexed in the Web of Science. Most of these trials had
moderate methodological quality (with a PEDro mean score of 5.8 points out of 10.0)
and were published in open access journals that endorsed CONSORT recommendations.
Similar to a previous study in musculoskeletal physical therapy14, our results indicate a
positive, but weak correlation between methodological quality and Impact Factor. This
means that high quality low back pain trials are not necessarily published in journals
with high Impact Factor.
Low back pain trials characteristics and the literature
The sample size showed a median of 73.5 participants (IQR 109, minimum 10 –
maximum 4.325), which shows that some studies analyzed a small group of
participants, which probably did not reach the statistical power of detecting a clinical
important difference among the intervention and control groups33.
The primary outcomes most evaluated by the trials were pain and disability,
which agrees with the core outcome sets found in panel consensus for low back pain,
together with quality of life34. The instruments mostly recommended for physical
functioning are the Oswestry Disability Index and 24-item Roland-Morris Disability
Questionnaire, and the Numerical Pain Rating Scale 34. This shows that most of back
pain researchers are aligned with these recommendations.
The most frequent interventions analyzed in our sample were exercises (strength
training and stretching), manual therapy and education, which are the main
recommended interventions for low back pain according to the National Institute for
Health and Care Excellence (NICE) guidelines35, and also to a recent low back pain
series published by a panel of experts in the field 2-4. Maybe authors should investigate
further the effectiveness of interventions that were poorly or not investigated in these
trials for low back pain and which do not present much evidence according to

CHAPTER 2
33
previously published guidelines2-4,35, such as hydrotherapy and neurodevelopment
therapy, for example.
Strengths and limitations
A particular strength of our study is that we presented 30 possible options of
high Impact Factor journals that published low back pain trials, from which six journals
are highly recommended for reading and referred to when taking a clinical decision.
Also, we are confident that we have a representative sample of low back pain trials
published on PEDro in 2010 to 2015, once we selected 40% of the total ‘population’ of
eligible trials. However, our main limitation is that some journals might have been
missed and we could not generalize our results for all low back pain trials, including
trials involving surgery or drug trials.
Clinical and methodological implications
The analyzed trials comparing interventions for low back pain presented
moderate methodological quality. Readers should be very cautious on taking clinical
decisions based on poor methodological quality trials, which may increase the existing
gap between evidence and practice2-4. The research efforts and global initiatives to treat
this public health problem need also to focus on improving reporting and
methodological quality for future studies. Although 55.5% of journals already endorse
CONSORT recommendations, we suggest that the EQUATOR recommendations
(Enhancing the QUAlity and Transparency Of health Research; https://www.equator-
network.org/) become mandatory requirements for publication, as well as following the
items evaluated in methodological guidelines (e.g. Cochrane Risk of Bias tool or the
PEDro scale36). Journal editors and peer reviewers should strictly follow those
requirements in order to improve reporting and methodological quality of randomized
controlled trials. Therefore, actions of better reporting and conducting the studies
following adequate methodological guidelines will better address authors and journals
editors/reviewers to write and publish more trustworthy studies.

CHAPTER 2
34
CONCLUSION
Low back pain randomized controlled trials in the field of physical therapy
presented moderate methodological quality. Our findings also show that trial quality
was weakly correlated with Impact Factor. Clinicians interested in low back pain trials
may look for a wide variety of healthcare journals. A substantial number of low back
pain randomized controlled trials did not follow adequate reporting and methodological
recommendations.

CHAPTER 2
35
REFERENCES
1. Collaborators GDaIIaP. Global, regional, and national incidence, prevalence,
and years lived with disability for 328 diseases and injuries for 195 countries, 1990-
2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet.
2017;390(10100):1211-1259.
2. Buchbinder R, van Tulder M, Oberg B, et al. Low back pain: a call for action.
Viewpoint. Lancet. 2018.
3. Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why
we need to pay attention. Series. Low back pain 1. Lancet. 2018.
4. Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back
pain: evidence, challenges, and promising directions. Series. Low back pain 2. Lancet.
2018.
5. Asavasopon S. Chronification of low back pain: getting to the spine of the
problem. Braz J Phys Ther. 2018;22(1):1-6.
6. Herbert R, Jamtvedt G, Mead J, Hagen KB. Practical evidence-based
physiotherapy. 2nd Edition ed: Elsevier Butterworth-Heinemann; 2011.
7. Oliveira IS, Costa LOP, Garcia AN, Miyamoto GC, Cabral CMN, Costa L. Can
demographic and anthropometric characteristics predict clinical improvement in
patients with chronic non-specific low back pain? Braz J Phys Ther. 2018;22(4):328-
335.
8. Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet.
2017;389(10070):736-747.
9. Chou R, Deyo R, Friedly J, et al. Nonpharmacologic Therapies for Low Back
Pain: A Systematic Review for an American College of Physicians Clinical Practice
Guideline. Ann Intern Med. 2017;166(7):493-505.
10. Beattie PF, Silfies SP, Jordon M. The evolving role of physical therapists in the
long-term management of chronic low back pain: longitudinal care using assisted self-
management strategies. Braz J Phys Ther. 2016;20(6):580-591.
11. Hariohm K, Jeyanthi S, Kumar JS, Prakash V. Description of interventions is
under-reported in physical therapy clinical trials. Braz J Phys Ther. 2017;21(4):281-
286.
12. Moseley AM, Elkins MR, Janer-Duncan L, Hush JM. The Quality of Reports of
CHAPTER 2
36
Randomized Controlled Trials Varies between Subdisciplines of Physiotherapy.
Physiother Can. 2014;66(1):36-43.
13. PRISMA Endorsers. 2010; http://www.prisma-
statement.org/Endorsement/PRISMAEndorsers.aspx. Accessed September 2018.
14. Gonzalez GZ, Moseley AM, Maher CG, Nascimento DP, Costa L, Costa LO.
Methodologic Quality and Statistical Reporting of Physical Therapy Randomized
Controlled Trials Relevant to Musculoskeletal Conditions. Arch Phys Med Rehabil.
2018;99(1):129-136.
15. Costa LO, Moseley AM, Sherrington C, Maher CG, Herbert RD, Elkins MR.
Core journals that publish clinical trials of physical therapy interventions. Phys Ther.
2010;90(11):1631-1640.
16. Maher CG, Moseley AM, Sherrington C, Elkins MR, Herbert RD. A description
of the trials, reviews, and practice guidelines indexed in the PEDro database. Phys Ther.
2008;88(9):1068-1077.
17. Michaleff ZA, Costa LO, Moseley AM, et al. CENTRAL, PEDro, PubMed, and
EMBASE are the most comprehensive databases indexing randomized controlled trials
of physical therapy interventions. Phys Ther. 2011;91(2):190-197.
18. Moseley AM, Sherrington C, Elkins MR, Herbert RD, Maher CG. Indexing of
randomised controlled trials of physiotherapy interventions: a comparison of AMED,
CENTRAL, CINAHL, EMBASE, hooked on evidence, PEDro, PsycINFO and
PubMed. Physiotherapy. 2009;95(3):151-156.
19. de Morton NA. The PEDro scale is a valid measure of the methodological
quality of clinical trials: a demographic study. Aust J Physiother. 2009;55(2):129-133.
20. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of
the PEDro scale for rating quality of randomized controlled trials. Phys Ther.
2003;83(8):713-721.
21. Yamato TP, Maher C, Koes B, Moseley A. The PEDro scale had acceptably
high convergent validity, construct validity, and interrater reliability in evaluating
methodological quality of pharmaceutical trials. J Clin Epidemiol. 2017;86:176-181.
22. Shiwa SR, Costa LO, Costa Lda C, et al. Reproducibility of the Portuguese
version of the PEDro Scale. Cad Saude Publica. 2011;27(10):2063-2068.
23. 2018 SPED. Statistics from PEDro' s website. 2018;
https://www.pedro.org.au/english/downloads/pedro-statistics. Accessed July 2018.

CHAPTER 2
37
24. Chiarotto A, Deyo RA, Terwee CB, et al. Core outcome domains for clinical
trials in non-specific low back pain. Eur Spine J. 2015;24(6):1127-1142.
25. PEDro. Intervention codes from the Physiotherapy Evidence Database (PEDro).
2018; https://www.pedro.org.au/wp-content/uploads/PEDro_codes.pdf. Accessed July
2018.
26. Roussel NA, Kos D, Demeure I, et al. Effect of a multidisciplinary program for
the prevention of low back pain in hospital employees: a randomized controlled trial. J
Back Musculoskelet Rehabil. 2015;28(3):539-549.
27. Garcia AN, Costa Lda C, Hancock MJ, de Almeida MO, de Souza FS, Costa
LO. Efficacy of the McKenzie method in patients with chronic nonspecific low back
pain: a protocol of randomized placebo-controlled trial. Phys Ther. 2015;95(2):267-273.
28. Miyamoto GC, Costa LO, Galvanin T, Cabral CM. The efficacy of the addition
of the Pilates method over a minimal intervention in the treatment of chronic
nonspecific low back pain: a study protocol of a randomized controlled trial. J Chiropr
Med. 2011;10(4):248-254.
29. Hall AM, Maher CG, Lam P, Ferreira M, Latimer J. Tai chi exercise for
treatment of pain and disability in people with persistent low back pain: a randomized
controlled trial. Arthritis Care Res (Hoboken). 2011;63(11):1576-1583.
30. Lang E, Liebig K, Kastner S, Neundorfer B, Heuschmann P. Multidisciplinary
rehabilitation versus usual care for chronic low back pain in the community: effects on
quality of life. Spine J. 2003;3(4):270-276.
31. Macedo LG, Latimer J, Maher CG, et al. Effect of motor control exercises
versus graded activity in patients with chronic nonspecific low back pain: a randomized
controlled trial. Phys Ther. 2012;92(3):363-377.
32. Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 Explanation and
Elaboration: Updated guidelines for reporting parallel group randomised trials. J Clin
Epidemiol. 2010;63(8):e1-37.
33. Bernstein IA, Malik Q, Carville S, Ward S. Low back pain and sciatica:
summary of NICE guidance. BMJ. 2017;356:i6748.
34. Chiarotto A, Boers M, Deyo RA, et al. Core outcome measurement instruments
for clinical trials in nonspecific low back pain. Pain. 2018;159(3):481-495.
35. de Campos TF. Low back pain and sciatica in over 16s: assessment and
management NICE Guideline [NG59]. J Physiother. 2017;63(2):120.

CHAPTER 2
38
36. Armijo-Olivo S, da Costa BR, Cummings GG, et al. PEDro or Cochrane to
Assess the Quality of Clinical Trials? A Meta-Epidemiological Study. PLoS One.
2015;10(7):e0132634.

CHAPTER 2
39
2.2. Abstracts of the randomized controlled trials: reporting quality,
spin and inconsistencies with the full text

CHAPTER 2
40
2.2.1. Abstracts of low back pain trials are poorly reported, contain
spin of information and are inconsistent with the full text: an overview
study
Published in: Archives of Physical Medicine and Rehabilitation 2019 Jun 14
DOI: 10.1016/j.apmr.2019.03.024 [Epub ahead of print]

CHAPTER 2
41
Abstracts of low back pain trials are poorly reported, contain spin of information
and are inconsistent with the full text: An overview study
Dafne Port Nascimento1; Leonardo Oliveira Pena Costa1; Gabrielle Zoldan Gonzalez1;
Christopher G Maher2; Anne M Moseley2 1Masters and Doctoral Programs in Physical Therapy, Universidade Cidade de São
Paulo, São Paulo, Brazil. 2Musculoskeletal Health Sydney, School of Public Health, The University of Sydney,
Sydney, Australia.
Corresponding author: Dafne Port Nascimento, Masters and Doctoral Programs in
Physical Therapy, Universidade Cidade de São Paulo. Rua Cesário Galeno 448,
Tatuapé, São Paulo, SP – Brazil, CEP 03071-000. Phone number: +55 11 994779119.
ORCID ID: https://orcid.org/0000-0002-8474-727X
Email address: [email protected]
Funding: This work was supported by a PhD scholarship from the Sao Paulo Research
Foundation (grant#2015/16953-2; Fundação de Amparo à Pesquisa do Estado de São
Paulo – FAPESP).
Declaration of interest: The authors declare that, even though seven out of the 200
articles analyzed involved authors from our research groups, all articles were evaluated
with the same criteria and rigor.

CHAPTER 2
42
Abstracts of low back pain trials are poorly reported, contain spin of information
and are inconsistent with the full text: An overview study
ABSTRACT
Objective: To investigate trials abstracts evaluating treatments for low back pain with
regards to completeness of reporting, spin (i.e., interpretation of study results that
overemphasizes the beneficial effects of the intervention), and inconsistencies in data
with the full text. Data sources: The search was performed on Physiotherapy Evidence
Database (PEDro) in February 2016. Study Selection: This is an overview study of a
random sample of 200 low back pain trials published between 2010 and 2015. The
languages of publication were restricted to English, Spanish and Portuguese. Data
Extraction: Completeness of reporting was assessed using the CONSORT for
Abstracts checklist (CONSORT-A). Spin was assessed using a SPIN-checklist.
Consistency between abstract and full text were assessed by applying the assessment
tools to both the abstract and full text of each trial and calculating inconsistencies in the
summary score (paired t test) and agreement in the classification of each item (Kappa
statistics). Methodological quality was analyzed using the total PEDro score. Data
Synthesis: The mean number of fully reported items for abstracts using the CONSORT-
A was 5.1 (SD 2.4) out of 15 points and the mean number of items with spin was 4.9
(SD 2.6) out of 7 points. Abstract and full text scores were statistically inconsistent
(P=0.01). There was slight to moderate agreement between items of the CONSORT-A
in the abstracts and full text (mean Kappa 0.20 SD 0.13) and fair to moderate agreement
for items of the SPIN-checklist (mean Kappa 0.47 SD 0.09). Conclusions: The
abstracts were incomplete, with spin and inconsistent with the full text. We advise
health care professionals to avoid making clinical decisions based solely upon abstracts.
Journal editors, reviewers and authors are jointly responsible for improving abstracts,
which could be guided by amended editorial policies.
Abbreviations: CONSORT - Consolidated Standards of Reporting Trials; PEDro -
Physiotherapy Evidence Database.

CHAPTER 2
43
INTRODUCTION
Health care professionals use the results of randomized controlled trials to assist
their clinical decision making1. However, they should be mindful that trials that were
not adequately conducted and reported may tend to overestimate treatment effects2.
These exaggerated effects can be generated either due to bias in the conduct of the trials
or bias in the reporting of the trials3,4.
Reading the full report of trial results is necessary to critically appraise
evidence5,6. However, many health care professionals decide to read the full text of an
article only after reading the abstract and some may only have easy access to the
abstract6,7. Therefore the completeness of abstracts and consistency with full text is
important, also because trial abstracts are also widely used in the screening process of
systematic reviews8. Common problems with abstracts include incomplete and
inadequate reporting9,10 and inconsistencies between abstract and the full text11. Studies
that have examined completeness of trial abstracts12-17 using the CONSORT
(Consolidated Standards of Reporting Trials) for Abstracts checklist7 (CONSORT-A)
concluded that completeness of reporting of abstracts was poor. There appears to be an
association between completeness of reporting and the number of centers14, continent
where the trial was conducted18,19, abstract format14, and year of publication of a
trial18,19. Shiwa et at20 concluded that English trials were more likely to have better
methodological quality than trials written in other languages, therefore completeness of
reporting of abstracts might also be related to the language. Studies have also found
associations between better reporting quality and higher impact factor journals12,14,18,19,
journals endorsement of the CONSORT recommendations12,21, and abstracts with
higher word counts16. Studies that have compared abstracts and full texts in sports
injury prevention17, general medicine22, pharmacy23 and psychology24 found
inconsistencies in 13% to 80% of articles.
Spin of information25-27 is another factor that can influence the interpretation of
abstracts. In research, spin is defined as “a misrepresentation of study results, regardless
of motive (intentionally or unintentionally) that overemphasizes the beneficial effects of
the intervention and overstates safety compared with that shown by the results” [p. 228].
Spin may occur in a journal publication, academic press releases or media coverage of
research27,29-32. A study conducted in the oncology field33 evaluated the impact of spin
of results in trials abstracts using a 7-item SPIN-checklist and showed inconsistencies
CHAPTER 2
44
with the full text, such as selective reporting and overstated treatment effects. To the
best of our knowledge there is no study investigating association between abstracts
completeness of reporting and spin of information, or even associating spin in abstracts
with journal and trial characteristics.
The issues of abstracts completeness, spin and inconsistencies with the full text
have not been investigated in the low back pain field. This is an important gap to
address as low back pain is ranked the highest of all diseases for years lived with
disability and involves high costs worldwide34,35. A recent publication in one of the
world’s leading general medical journals stated that non-pharmacological interventions,
such as physiotherapy (including exercise, education, graded activity, manual therapy),
is the preferred first-line treatment option for low back pain36 and is congruent with
guideline recommendations37. Our primary questions were: (1) are abstracts of low back
pain randomized controlled trials incomplete as assessed with the CONSORT-A? (2) do
these abstracts contain spin as assessed with the SPIN-checklist? (3) are these abstracts
inconsistent with the full text in completeness and spin? Our secondary questions were:
(4) are these abstracts completeness associated with certain trial or journal
characteristics? and, (5) are abstracts spin associated with ‘negative results’ (i.e., lack of
statistical difference for primary outcomes reported, or no difference for primary
outcomes reported at all)?
METHODS
Eligibility criteria
This is an overview study of 200 trials reporting the results of randomized
controlled trials, both abstracts and full text. Firstly, we searched for all randomized
controlled trials coded as low back pain, and published between 2010 and 2015, that
were indexed on the Physiotherapy Evidence Database (PEDro; www.pedro.org.au).
We then selected a random sample of 40% from all potentially eligible trials for the
study. The selection was performed using the random number function in Excel. PEDro
was used because it is one of the most complete indexes of published reports of the
results of randomized controlled trials evaluating physiotherapy interventions, with no
restrictions on languages or journal of publication38. In addition, all trial reports indexed
on PEDro are rated for methodological quality using the PEDro scale39, which enabled

CHAPTER 2
45
us to include methodological quality as an independent variable in the analyses of trial
characteristics associated with abstract completeness. The eligibility criteria were: full-
published trial reporting the results of a randomized controlled trial evaluating at least
one physiotherapy intervention for low back pain; published in 2010 to 2015, inclusive;
and, written in English, Spanish or Portuguese. The search strategy performed on
PEDro was: “clinical trial” for method; “lumbar spine, sacroiliac joint or pelvis” for
body part; “pain” for problem; 2010 to 2015 for year of publication; and, English,
Spanish or Portuguese for language. This time period was selected as it was after the
release of the CONSORT-A in 20087, therefore we believe that authors would be prone
to use these recommendations. The language of publication was restricted to English,
Spanish and Portuguese, as these were the languages spoken by the authorship team of
this study and are among the most common languages of publication on PEDro40.
Data collection
Data extraction was divided into five, to answer our research questions: (1)
completeness of reporting of abstracts; (2) spin of information in abstracts; (3) abstracts
inconsistencies with the full text; and (4) association of abstract completeness and
abstract spin with trial and journal characteristics; (5) association of abstract spin with
negative results. These sections are described in detail below. Two independent authors
extracted data. Disagreements were resolved by discussion or arbitration by a third
author. Agreement of data extraction between raters before consensus was calculated
using Kappa statistics41. The agreement was calculated for each item of the CONSORT-
A and the SPIN-checklist for both abstract and full text.
1) Completeness of reporting of abstracts.
The 17-item CONSORT-A7 was used to evaluate completeness of reporting of
the abstracts of the included trials. However, we omitted two items in our data analyses
because they were not relevant to published articles of completed trials: “authors” (i.e.,
related to reporting of the contact details for the corresponding author in conference
proceedings) and “recruitment” (i.e., indicates phase of recruitment or ongoing). We
then modified the CONSORT-A to 15 items. Each item was classified as “fully reported”
(if reported all information specified in the item) and “not reported” (if partially

CHAPTER 2
46
reported the information specified in the item; or if no information specified in the item
were reported or when primary outcomes were not specified) for each trial. We also
generated a summary score (CONSORT-Abstract score) for each trial by counting the
number of items that were “fully reported”. The summary score could range from 0
(low level of completeness of reporting) to 15 (high level of completeness of reporting).
We considered primary outcomes to be those identified as ‘primary outcome’ or
‘main outcome’, or any synonyms of the word ‘outcome’ (e.g., endpoint). For trials that
presented one or two outcomes only, we considered them as primary.
2) Spin of information in abstracts.
We used a 7-item SPIN-checklist33 to evaluate spin of information in an abstract
by comparing the abstract conclusion to the abstract results. The list has been previously
used to measure spin in abstracts of randomized controlled trials in the field of
oncology33. Each item (items are listed in the results section) was classified as “yes”
(i.e., the spin was clearly present; or if the primary outcome results were not reported, or
omitted, which represented that the spin was also present) or “no” (i.e., the spin was not
present). For example, if the authors of the abstract gave a positive interpretation for a
non-significant result, we would classify Item 6 (over-enthusiastic interpretation of
outcomes) as “yes”. A summary score (SPIN-Abstract score) was calculated by
counting the items classified as “yes” (items classified as “no” were considered free of
spin of information). The summary score could range from 0 (low levels of spin) to 7
(high levels of spin). At this point, the abstract was assessed in isolation (not compared
to the full text). We did this because readers should be able to interpret the trial based
on the results section of the abstract.
The criterion for clinically important effects proposed by Ostelo et al42 was used
when scoring item 7 of the SPIN-checklist. These are: ≥15-point difference for the 0-
100 point Visual Analogue Scale, ≥2-point difference for the 0-10 point Numerical
Rating Scale, ≥5-point difference for the 0-24 point Roland Morris Disability
Questionnaire, ≥10-point difference for the 0-100 point Oswestry Disability Index, and
≥20-point difference for the 0-100 Quebec Back Pain Disability Scale.

CHAPTER 2
47
3) Abstracts inconsistencies with the full text.
Abstracts should reflect exactly what the full texts reported. Abstracts have been
compared to their corresponding full texts in terms of completeness of reporting of all
sections of a study and spin of information in the results and conclusion sections11,43.
We used the CONSORT-A and the SPIN-checklist to evaluate inconsistencies in
completeness of reporting and presence of spin between the abstract and the
corresponding full text, reason why we also applied the CONSORT-A and the SPIN-
checklist in the full texts. Summary scores were calculated for the full text (CONSORT-
Full text score and SPIN-Full text score) in order to be comparable to the abstract
(CONSORT-Abstract score and SPIN-Abstract score). It was not our intention to
analyze completeness of reporting of full texts themselves. In addition to that, for each
individual item from the CONSORT-A and the SPIN-checklist we calculated the
agreement of how the item was classified in the abstract with how it was classified in
the full text. Each full text was evaluated immediately after its abstract. If an item of the
full text was inconsistent with information reported in the abstract, we would re-score
such item in the abstract (e.g. using the CONSORT-A: if we had classified the results
for a primary outcome as “fully reported” in the abstract and in the full text we found
out there were two primary outcomes which were also “fully reported”, we would
downgrade the item in the abstract to “not reported”).
4) Description of trial and journal characteristics.
To investigate if trial and journal characteristics were associated with abstract
completeness and with abstract spin we defined two dependent variables and 10
independent variables. The dependent variables were the CONSORT-Abstract score and
the SPIN-Abstract score. The independent variables were: trial conducted in more than
one center, continent where trial was conducted, language of publication, 2015 journal
impact factor, if journal endorses the CONSORT recommendations, number of words in
abstract, structured abstract, total PEDro score, SPIN-Abstract score and number of
years since trial publication. The summary scores for the CONSORT-Abstract score and
SPIN-Abstract score are described in sections 1) and 2), respectively. For the
independent variables, we classified each trial as unicenter or multicenter (i.e, if the

CHAPTER 2
48
study had been conducted in one center or more). The country where the study was
conducted was extracted and categorized into continents (using dummy variables for
“Asia”, “Africa”, “Europe”, “North America”, “Oceania” and “South America”). The
language was classified as English or non-English. The journal impact factors from
2015 were downloaded from the InCites Journal Citation Reports (Thomson Reuters)’
website. Journal endorsement of the CONSORT recommendations44 was extracted from
the “Instructions to authors” for each of the journals or from the CONSORT
recommendations’ website45. The number of words in the abstract was counted using
the Microsoft Word “Word Count” function. The abstracts were classified as structured
or not structured46. The total PEDro score (0-10 points, higher values indicate better
methodological quality) was downloaded from PEDro. The number of years since trial
publication was calculated by subtracting the year of publication from 2015.
5) Description of negative results.
To investigate if trial negative results (i.e., statistically non-significant or not
reported between-group differences for the primary outcomes) were associated with
spin we defined seven independent variables (the individual items of the SPIN-
checklist) and one dependent variable (presence of statistically significant between-
group differences). The presence of statistical between-group differences was
determined for primary outcomes (two at most and preferably pain and disability) and
considering up to four intervention groups (the maximum number of groups from the
included trials), through confidence intervals or P values. If the statistical between-
group difference was in the opposite direction of the hypothesis for at least one primary
outcome, the trial was classified as “no” (or no statistical between-group difference). If
the between-group difference was not reported for at least one primary outcome, the
trial was classified as “not reported”. If all primary outcomes had statistical between-
group differences (in the direction of the hypothesis), the trial was classified as “yes”.
The trials classified as “no” and “not reported” were considered to have negative
results.
For descriptive analysis we also collected the maximum number of words
allowed in the abstract by the publishing journal. This was extracted from the
“Instructions to authors”. Trial abstracts were classified into four categories: those that
adhered to word limit (i.e., word count within 10 words of the word limit); those that

CHAPTER 2
49
used less words than the word limit; those that exceeded the word limit; and those
published in a journal without abstract word limits.
Data analysis
To investigate the completeness of reporting and spin of information in the
abstracts, the percentage of articles achieving each item of the CONSORT-A and the
SPIN-checklist were tabulated. The mean and standard deviation (SD) summary score
were calculated for each checklist (CONSORT-Abstract score and SPIN-Abstract
score). In order to investigate inconsistencies between abstract and full text we used
paired t tests between the CONSORT-Abstract scores with the CONSORT-Full text
scores and the SPIN-Abstract scores with the SPIN-Full text scores, with P<0.05.
Agreement between the abstract and full text for items 2-15 for the CONSORT-A (item
1 was excluded as it relates to the title) and all items from the SPIN-checklist were
calculated using Kappa coefficients41. Kappa values higher than 0.61 (i.e., “substantial”
to “almost perfect agreement”)41 was the criterion for “acceptable” agreement between
abstract and full text.
Linear regression models were built to evaluate the association between ten trial
and journal characteristics with the CONSORT-Abstract score and the SPIN-Abstract
score. We built both univariate and multivariate regression models. The independent
variables with P<0.20 in the univariate model were included in the final multivariate
model by using backward elimination method, until all independent variables achieved
P <0.05. Adjusted explained variance (adjusted R2), Beta coefficient (β) and its 95%
confidence intervals were reported for each variable with possible association. Linearity
was assessed by evaluation of linear relationship of the CONSORT-Abstract score with
each independent variable using simple scatter plots47. Multicollinearity was tested with
bivariate correlation analysis of the CONSORT-Abstract score with each independent
variable, and coefficients of independent variables with r ≥0.7 were not included in our
linear regression model48.
Chi-square tests were used to evaluate the association between trials with
negative results and the presence of spin in the abstract (i.e., classified as “yes”) for
each item of the SPIN-checklist. All seven items were evaluated to understand if
individual items could have different associations with negative results. SPSS software
(Version 20.0) was used for all analyses.

CHAPTER 2
50
RESULTS
The search strategy retrieved 537 potentially eligible trial reports from the
25,956 existing trials indexed in the PEDro database on February 1st 2016. Trials that
were still in the recruitment stage, protocols, duplicates and those involving not only
low back pain were excluded (n=67) and are detailed in APPENDIX A. From the
remaining 470 eligible trials, we randomly selected a sample of approximately 40%,
rounded up to 200 trials (APPENDIX B), as shown in the flow chart in Figure 1.
Journals and their impact factors are described in APPENDIX C. Descriptive data for
the 200 articles is presented in TABLE 1 and descriptive data of the 97 journals that
published the included trials are presented in APPENDIX C. Most trials were
conducted in Europe or Asia and published in English. Most journals had an impact
factor, more than half (51.5%) endorsed CONSORT recommendations, and 38.1% were
open access. The methodological quality of trials is presented in APPENDIX D.
The agreement of data extraction between raters for both abstract and full text
ranged from fair to almost perfect (see APPENDIX E). For the items of the
CONSORT-A the mean Kappa was 0.73 SD 0.18; and for the items of the SPIN-
checklist the mean Kappa was 0.67 (SD 0.11). We then resolved disagreements by
consensus.

CHAPTER 2
51
TABLE 1. Descriptive data for the included trials (n =200) with mean (standard deviation) plus the number and percentage (%) of articles.
Mean (SD) Number of
articles (%) Journal InCites Journal Citation Reports Impact Factor 2015 2.5 (2.5) 157 (78.5) Journals without Impact Factor 43 (21.5) Open access articles 115 (57.5) Written in English 198 (99.0) Written in Portuguese or Spanish 2 (1.0) Continents Europe 70 (35.0) Asia 65 (32.5) North America 33 (16.5) South America 13 (6.5) Africa 8 (4.0) Oceania 11 (5.5) Multicenter 17 (8.5) Unicenter 183 (91.5) Structured abstract 171 (85.5) Unstructured abstract 29 (14.5) Years since trial publication 3.4 (1.7)
2010 28 (14.0) 2011 35 (17.5) 2012 36 (18.0) 2013 34 (17.0) 2014 29 (14.5) 2015 38 (19.0)
Statistically significant between-group differences for the primary outcome(s)
70 (35.0)
No statistically significant between-group differences for the primary outcome(s)
96 (48.0)
Did not report between-group differences for the primary outcome(s)
34 (17.0)
Number of words in the abstract 258 (67.3) Articles published in journals with abstract word limits 178 (89.0) Abstracts that adhered to word limit 49 (24.5) Abstracts that used less words than the word limit 64 (32.0) Abstracts that exceeded the word limit 65 (32.5) Abstracts that published in a journal without abstract word limits 22 (11.0) Total PEDro score (/10) 5.8 (1.6)

CHAPTER 2
52
1) Completeness of reporting of abstracts.
The mean CONSORT-Abstract score was 5.1 (SD 2.4) out of 15 points. TABLE
2 presents the completeness of reporting for each item of the CONSORT-A. The items
with the highest completeness of reporting were specifying the objective (97.0%),
interventions (76.5%) and trial design (61.5%). The items with the lowest completeness
of reporting were specifying how participants were allocated to groups or randomization
(2.0%), blinding (2.5%) and a result for each group and the estimated effect size and its
precision for the primary outcomes (4.5%).
2) Spin of information in abstracts.
The mean (SD) SPIN-Abstract score was 4.9 (SD 2.6) out of 7 points, indicating
that most abstracts overstated the results. TABLE 3 presents the each item of the SPIN-
checklist. The most common problems were failing to mention adverse events (93.5%
of abstracts), selective reporting of outcomes (73.0% of abstracts) and recommendation
of a treatment (73.0% of abstracts). 98.0% of abstracts had at least one item of spin.

CHAPTER 2
53
TABLE 2. Percentage of included trials achieving each item of the CONSORT-A in the abstract and full text. Total sample n=200. ITEM DESCRIPTION Fully Reported (%) Abstract Full text 1. Title Identification of the study as randomized 58.5 2. Trial design Description of the trial design 61.5 63.0 Methods
3. Participants Eligibility criteria for participants and the settings where the data were collected 44.5 89.5 4. Interventions Interventions intended for each group 76.5 90.5 5. Objective Specific objective or hypothesis 97.0 95.5 6. Outcome Clearly defined primary outcome for this report 35.0 52.0 7. Randomization How participants were allocated to interventions 2.0 41.0
8. Blinding Whether or not participants, care givers, and those assessing the outcomes were blinded to group assignment 2.5 15.5
Results 9. Numbers randomized Number of participants randomized to each group 39.5 89.0 10. Numbers analyzed Number of participants analyzed in each group 10.5 88.0
11. Outcome For the primary outcome, a result for each group and the estimated effect size and its precision 4.5 32.5 12. Harms Important adverse events or side effects 7.0 29.5 13. Conclusions General interpretation of the results 24.0 34.5 14. Trial registration Registration number and name of trial register 20.0 32.5 15. Funding Source of funding 23.5 68.5

CHAPTER 2
54
TABLE 3. Percentage of included trials containing each item of the SPIN-checklist in the abstract and full text. Total Sample n=200.
Description of each item Yes (%) No (%)
Abstract Full text Abstract Full text
1. Omission of primary outcomes 56.0 40.5 44.0 59.5 2. Fail to mention adverse events of interventions 93.5 68.5 6.5 31.5 3. Selective reporting of positive results and omission of negative results of primary outcomes
73.0 53.5 27.0 46.5
4. Fail to report statistically non-significant primary outcomes 71.0 51.0 29.0 49.0 5. Focus on statistically significant outcomes other than the primary 62.5 49.0 37.5 51.0 6. Over-enthusiastic interpretation of statistically non-significant primary outcomes results as effective
61.5 47.5 38.5 52.5
7. Recommendation of a treatment without a clinically important effect on primary outcomes
73.0 60.5 27.0 39.5
Note: Abstracts and full texts free of spin are represented in column “no”; columns “yes” represent the percentage of abstracts and full-texts presenting spin of information.

CHAPTER 2
55
3) Abstracts inconsistencies with the full text.
Abstracts were reported less completely than the full text (P=0.01). The mean
CONSORT-Abstract score was 5.1 (SD 2.4) out of 15 compared to a mean CONSORT-
Full text score of 8.2 (SD 3.0), with a mean difference of -3.2 points (95% CI 2.8, 3.5).
Agreement between the abstract and full text for fourteen items from the CONSORT-A
ranged from slight to moderate agreement (mean Kappa 0.20 SD 0.14) (see APPENDIX
F). The percentage of trials achieving each individual item of the CONSORT-A for the
abstract and full text sections are presented in TABLE 2. No abstracts fully reported all
15 items (the highest number of items achieved was 13), while full reporting of full text
occurred for 3.0% of trials.
Abstracts presented more spin of information than the full text (P=0.01). The
mean SPIN-Abstract score was 4.9 (SD 2.6) out of 7 and mean SPIN-Full text score was
3.7 (SD 2.9), with a mean difference of 1.2 points (95% CI 0.9, 1.5). The ratings for the
seven items from the SPIN-checklist ranged from fair to moderate agreement (mean
Kappa 0.49 SD 0.11) between the abstract and full text (see APPENDIX F). Scoring for
the individual items of the SPIN-checklist for both the abstract and full text are
presented in TABLE 3. Only 2.0% abstracts and 17.0% full texts scored zero for the
SPIN-Abstract and SPIN-Full text scores, which means they were free of spin.
4) Association of abstract completeness and spin with trial and journal
characteristics.
All variables were included into the linear regression model exploring the
association between abstract completeness and spin with trial and journal
characteristics. Simple scatter plots confirmed the linearity assumption and bivariate
correlation coefficients were all less than 0.31 (i.e., multicollinearity assumption). The
final multivariate model explained 55% (adjusted R2=0.55) of the variance in
completeness of reporting of abstracts and 17% (adjusted R2=0.17) of the variance in
spin of information in abstracts (TABLE 4). Higher completeness of abstracts
(CONSORT-Abstract score) was associated with higher journal impact factor, journals
that endorse CONSORT recommendations, greater number of words in the abstract,
higher total PEDro score, and lower SPIN-Abstract score. Lower score of spin in

CHAPTER 2
56
abstracts (SPIN-Abstract score) was associated with multicenter trials, greater number
of words in the abstract and higher total PEDro score.
5) Association of abstract spin with negative results.
TABLE 5 presents the association between spin of information in the abstract
and the presence of negative results for each item of SPIN-checklist. We observed an
association (P<0.05) between negative results for three of the seven items: selectively
reported positive results and ignored negative results of primary outcomes; fail to report
primary outcomes statistically non-significant; and recommendation to use a treatment,
if it does not have an important minimal clinical change. In other words, the presence of
primary outcome negative results was associated with the presence of spin in the
abstract.

CHAPTER 2
57
TABLE 4. Final multivariate models of associations between trial and journal characteristics with the CONSORT-Abstract score and the SPIN-Abstract score.
Multivariate Regression Multivariate Regression Dependent variable: CONSORT-Abstract score Dependent variable: SPIN-Abstract score
Adjusted R2 = 0.55 Adjusted R2 = 0.17 Constant = 3.74 (95% CI 1.94, 5.54) Constant = 11.20 (95% CI 9.28, 13.11) Independent variables ß 95% CI P ß 95% CI P Number of centers 0.86 -1.58 -2.77, -0.39 **0.01 Continent 0.83 0.74 Language *0.23 *0.25 Journal impact factor 0.12 0.01, 0.23 **0.04 0.07 Journal endorses CONSORT recommendations 0.76 0.16, 1.36 **0.01 *0.26 Number of words in the abstract 0.01 0.00, 0.01 **0.01 -0.01 -0.01, -0.00 **0.01 Structured abstract 0.46 *0.58 Total PEDro score 0.23 0.04, 0.42 **0.02 -0.39 -0.60, -0.18 **0.01 SPIN-Abstract score -0.47 -0.58, -0.36 **0.01 N/A N/A N/A Years since trial publication *0.83 *0.29 Note: N/A: Not applicable; *eliminated in the univariate analysis, values with P <0.20 ; **values with P <0.05; CI: Confidence Interval.

CHAPTER 2
58
TABLE 5. Association of trials presenting negative results with percentage of abstracts indicating the presence of spin for each of the SPIN-checklist (n=200).
Description of each item Negative Results Chi-square values P
values 1. Omission of primary outcomes 37.0% 0.57 0.75 2. Fail to mention adverse events of interventions 60.5% 1.31 0.52 3. Selective reporting of positive results and omission of negative results of primary outcomes 50.0% 15.34 **0.01 4. Fail to report statistically non-significant primary outcomes 50.0% 15.40 **0.01 5. Focus on statistically significant outcomes other than the primary 41.0% 2.20 0.33 6. Over-enthusiastic interpretation of statistically non-significant primary outcomes results as effective 41.0% 3.88 0.15 7. Recommendation of a treatment without a clinically important effect on primary outcomes 47.0% 11.20 **0.01
Note: Negative results are the sum of percentage of articles with statistically non-significant between-group differences and those that did not report a statistically significant between-group difference. **values with P<0.05.

CHAPTER 2
59
DISCUSSION
Reporting of abstracts is incomplete in general medicine journals49, oncology14
and infectious diseases12 (mean CONSORT-Abstract scores= 12.1 measured on a 17-
point scale, 9.9 measured on a 18-point scale 0-18, and 7.7 measured on a 17-point
scale, respectively). Our analysis of trials evaluating physiotherapy interventions for
low back pain appears to have relatively lower completeness of reporting in the abstract
(mean CONSORT-Abstract score= 5.1). The description of items related to
randomization, blinding, results of primary outcomes, harms and trial registration were
particularly problematic.
The presence of spin of information in abstracts is evident in general medicine,
as one study reported 41% of abstracts with at least one type of spin27 whereas other
authors found that 68.1% had spin in at least one section of the abstract25. The abstracts
of trial reports in low back pain appear to contain more spin of information (98.0% of
abstracts have at least one item of spin) than in other areas of health care. Authors of
analyzed trial reports tended to either omit non-significant results for primary outcomes
or interpret them as beneficial, which can impact health care professionals interpretation
of abstracts results33.
Consistency between abstracts and the full text is far from perfect in the field of
pharmacy (61% classified as inconsistent with the full text)23, sports injury prevention
(80% had at least one major inconsistency with the full text)17, psychology (average of
13% inconsistent abstracts compared to the full text)24, and medicine (53% had data
inconsistencies compared to the full text)22. Using a differential approach, we have
determined that abstracts of trials evaluating physiotherapy interventions for low back
pain presented several inconsistencies with their full texts. Important to note that these
studies used different statistical approaches, therefore a direct comparison of our results
with the existing literature is not straightforward.
To simplify the evaluation of completeness of reporting and spin we generated
summary scores for the CONSORT-A and the SPIN-checklist, which quantified these
constructs as single dependent variables. Although this scale is not fully validated50, the
SPIN-checklist presented moderate to almost perfect agreement between raters. The use
of summary scores will facilitate future comparisons between different areas of health
care and evaluation of strategies to improve reporting and reduce spin.

CHAPTER 2
60
Spin of information can negatively impact health care as abstracts are commonly
used by health care professionals to inform treatment decisions33 and are widely
disseminated in the press and news27. Spin can happen for many reasons, including not
understanding scientific standards, young researchers copying previous bad practices,
unconscious bias, intentional attempts to influence the readers51, and academic press
releases to attract readers attention27,29-32. In addition, authors favoring or interpreting
results as effective, when those are not statistically significant, may induce journal
reviewers and editors to accept an article for publication52. Whatever the cause of spin,
this misinterpretation can potentially damage clinical practice and the integrity of
research53,54.
It seems that healthcare journals editors and reviewers are either unaware of the
importance of avoiding abstracts inconsistencies with the full text55 or not sufficiently
trained to detect methodological or reporting mistakes related to abstracts56.
Consequently, Moher and Altman57 described four actions to improve the completeness,
transparency, integrity, and value of abstracts and papers published: (1) employment of
a professional publication officer, (2) developing core competencies for editors and
reviewers, (3) training for authors to write complete and transparent papers, and (4)
training for peer reviewers. These training efforts could involve raising awareness of the
academic community to the available guidelines for reporting studies, ethics in
publication, integrity and responsibility in research, as well as highlighting the issue of
authors overstating their results25. Authors could also be encouraged to write the
abstract after the full text has been finalized. Programs with this type of content that
target authors, journal editors and reviewers could and should be implemented.
Our analysis of article characteristics associated with better abstract reporting
and avoiding spin in abstracts identified variables that predict better reporting and
interpretation. Higher completeness of reporting was associated with publication in
journals with higher impact factors and that endorse CONSORT recommendations,
greater number of words in the abstract, higher total PEDro score, and a lower SPIN-
Abstract score. Additionally, avoiding spin was also related to conducting the trial in
more than one center, which may be explained to the fact that different institutions are
involved in the writing process and consequently the manuscript is peer reviewed by a
broader group of researchers. Two possible strategies involve changing journal’s
editorial policies to increase the number of words permitted in the abstract to at least
350 words (500 words ideally) and endorsing (and using) the CONSORT

CHAPTER 2
61
recommendations, including the extension for abstracts. Recommendations on using
journal impact factor as reference for publication have been discussed since 2005 and
have been considered to be partially inappropriate58.
Study strengths and limitations
One of the strengths of this study is the representative sample of 42% of all trials
evaluating physiotherapy interventions for low back pain published in 2010 to 2015.
Additionally, we used the CONSORT-A7 to evaluate completeness of reporting. This
checklist has been used previously to compare conference abstracts with the abstract
subsequently used in the full publication of the trial17 and seems to be a good
measurement tool to compare the level of agreement between abstract and full text in
our study. Furthermore, the assessment of spin has been considered to be somewhat
subjective and difficult to evaluate50. To address this concern, we used a recent
developed SPIN-checklist33. In the attempt to limit subjectivity, we used two reviewers
to independently score the included trials, with disagreements resolved by consensus. A
limitation of this study was that abstracts not clearly defining the primary outcomes
were automatically classified as containing spin of information, as most of the items of
the SPIN-checklist relate to the primary outcomes. In order not to overestimate spin, if a
trial only reported one or two outcomes but did not explicitly state that the outcomes
were “primary”, we considered them to be the primary outcomes when applying the
SPIN-checklist. Another limitation relates to the evaluation of agreement between
raters, which did not take into account the interdependency of the items in the SPIN-
checklist.
CONCLUSIONS
Similar to other healthcare trials, the abstracts of randomized controlled trials
evaluating physiotherapy interventions for low back pain are incompletely reported,
contain spin of information and are inconsistent with the full text. Authors, reviewers
and journal editors need to improve the completeness of reporting and reduce spin of
results in abstracts. In order to do so, we encourage journal editors to consider changing
some editorial policies, such as increasing the number of words allowed in the abstract
and offering adequate training to improve peer reviewers attention to abstracts (in terms

CHAPTER 2
62
of reporting, interpretation of results and consistency of data between abstract and full
text). Journal editors and reviewers should jointly be responsible for improving research
integrity, transparency and ethics in the publication process. Finally, authors of trials
should carefully choose journals with strict methodological and reporting standards for
publication, as well as writing the abstract only when the full text has been finalized.
CHAPTER 2
63
REFERENCES
1. Herbert R, Jamtvedt G, Mead J, Hagen KB. Practical evidence-based
physiotherapy. 2nd Edition ed: Elsevier Butterworth-Heinemann; 2011.
2. Wood L, Egger M, Gluud LL, et al. Empirical evidence of bias in treatment
effect estimates in controlled trials with different interventions and outcomes: meta-
epidemiological study. BMJ. 2008;336(7644):601-605.
3. Costa LO, Maher CG, Lopes AD, de Noronha MA, Costa LC. Transparent
reporting of studies relevant to physical therapy practice. Rev Bras Fisioter.
2011;15(4):267-271.
4. Savovic J, Jones HE, Altman DG, et al. Influence of reported study design
characteristics on intervention effect estimates from randomized, controlled trials. Ann
Intern Med. 2012;157(6):429-438.
5. The PLoS Medicine Editors. The impact of open access upon public health.
PLoS Med. 2006;3(5):e252.
6. Gotzsche PC. Believability of relative risks and odds ratios in abstracts: cross
sectional study. BMJ. 2006;333(7561):231-234.
7. Hopewell S, Clarke M, Moher D, et al. CONSORT for reporting randomized
controlled trials in journal and conference abstracts: explanation and elaboration. PLoS
Med. 2008;5(1):201-209.
8. Dijkers MP. Searching the literature for information on traumatic spinal cord
injury: the usefulness of abstracts. Spinal Cord. 2003;41(2):76-84.
9. Chhapola V, Tiwari S, Brar R, Kanwal SK. Reporting quality of trial abstracts-
improved yet suboptimal: a systematic review and meta-analysis. J Evid Based Med.
2018.
10. Song SY, Kim B, Kim I, et al. Assessing reporting quality of randomized
controlled trial abstracts in psychiatry: Adherence to CONSORT for abstracts: A
systematic review. PLoS One. 2017;12(11):e0187807.
11. Li G, Abbade LPF, Nwosu I, et al. A scoping review of comparisons between
abstracts and full reports in primary biomedical research. BMC Med Res Methodol.
2017;17(1):181.
12. Bigna JJ, Noubiap JJ, Asangbeh SL, et al. Abstracts reporting of HIV/AIDS
randomized controlled trials in general medicine and infectious diseases journals:

CHAPTER 2
64
completeness to date and improvement in the quality since CONSORT extension for
abstracts. BMC Med Res Methodol. 2016;16(1):138.
13. Ghimire S, Kyung E, Kang W, Kim E. Assessment of adherence to the
CONSORT statement for quality of reports on randomized controlled trial abstracts
from four high-impact general medical journals. Trials. 2012;13:77.
14. Ghimire S, Kyung E, Lee H, Kim E. Oncology trial abstracts showed suboptimal
improvement in reporting: a comparative before-and-after evaluation using CONSORT
for Abstract guidelines. J Clin Epidemiol. 2014;67(6):658-666.
15. Guo JW, Iribarren SJ. Reporting quality for abstracts of randomized controlled
trials in cancer nursing research. Cancer Nurs. 2014;37(6):436-444.
16. Wang L, Li Y, Li J, et al. Quality of reporting of trial abstracts needs to be
improved: using the CONSORT for abstracts to assess the four leading Chinese medical
journals of traditional Chinese medicine. Trials. 2010;11:75.
17. Yoon U, Knobloch K. Assessment of reporting quality of conference abstracts in
sports injury prevention according to CONSORT and STROBE criteria and their
subsequent publication rate as full papers. BMC Med Res Methodol. 2012;12:47.
18. Lai R, Chu R, Fraumeni M, Thabane L. Quality of randomized controlled trials
reporting in the primary treatment of brain tumors. J Clin Oncol. 2006;24(7):1136-
1144.
19. Peron J, Pond GR, Gan HK, et al. Quality of reporting of modern randomized
controlled trials in medical oncology: a systematic review. J Natl Cancer Inst.
2012;104(13):982-989.
20. Shiwa SR, Moseley AM, Maher CG, Pena Costa LO. Language of publication
has a small influence on the quality of reports of controlled trials of physiotherapy
interventions. J Clin Epidemiol. 2013;66(1):78-84.
21. Turner L, Shamseer L, Altman DG, et al. Consolidated standards of reporting
trials (CONSORT) and the completeness of reporting of randomised controlled trials
(RCTs) published in medical journals. Cochrane Database Syst Rev.
2012;11:MR000030.
22. Fontelo P, Gavino A, Sarmiento RF. Comparing data accuracy between
structured abstracts and full-text journal articles: implications in their use for informing
clinical decisions. Evid Based Med. 2013;18(6):207-211.
23. Ward LG, Kendrach MG, Price SO. Accuracy of abstracts for original research
articles in pharmacy journals. Ann Pharmacother. 2004;38(7-8):1173-1177.

CHAPTER 2
65
24. Harris AH, Standard S, Brunning JL, et al. The accuracy of abstracts in
psychology journals. J Psychol. 2002;136(2):141-148.
25. Boutron I, Dutton S, Ravaud P, Altman DG. Reporting and interpretation of
randomized controlled trials with statistically nonsignificant results for primary
outcomes. JAMA. 2010;303(20):2058-2064.
26. Chiu K, Grundy Q, Bero L. 'Spin' in published biomedical literature: A
methodological systematic review. PLoS Biol. 2017;15(9):e2002173.
27. Yavchitz A, Boutron I, Bafeta A, et al. Misrepresentation of randomized
controlled trials in press releases and news coverage: a cohort study. PLoS Med.
2012;9(9):e1001308.
28. Haneef R, Yavchitz A, Ravaud P, et al. Interpretation of health news items
reported with or without spin: protocol for a prospective meta-analysis of 16
randomised controlled trials. BMJ Open. 2017;7(11):e017425.
29. The Lancet Editorial. Incomplete reporting of research in academic press
releases. Lancet. 2009;373(9679):1920.
30. Haneef R, Lazarus C, Ravaud P, Yavchitz A, Boutron I. Interpretation of results
of studies evaluating an intervention highlighted in Google Health News: a cross-
sectional study of news. PLoS One. 2015;10(10):e0140889.
31. Schwartz LM, Woloshin S, Andrews A, Stukel TA. Influence of medical journal
press releases on the quality of associated newspaper coverage: retrospective cohort
study. BMJ. 2012;344:d8164.
32. Woloshin S, Schwartz LM, Casella SL, Kennedy AT, Larson RJ. Press releases
by academic medical centers: not so academic? Ann Intern Med. 2009;150(9):613-618.
33. Boutron I, Altman DG, Hopewell S, Vera-Badillo F, Tannock I, Ravaud P.
Impact of spin in the abstracts of articles reporting results of randomized controlled
trials in the field of cancer: the SPIIN randomized controlled trial. J Clin Oncol.
2014;32(36):4120-4126.
34. Global Burden of Disease. Disability-adjusted life-years Hale Collaborators.
Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases
and injuries and healthy life expectancy (HALE), 1990-2015: a systematic analysis for
the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1603-1658.
35. Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why
we need to pay attention. Series. Low back pain 1. Lancet. 2018;391(10137):p2356‚Äö
Äì2367.

CHAPTER 2
66
36. Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back
pain: evidence, challenges, and promising directions. Series. Low back pain 2. Lancet.
2018;391(10137):p2368–2383.
37. Bernstein IA, Malik Q, Carville S, Ward S. Low back pain and sciatica:
summary of NICE guidance. BMJ. 2017;356:i6748.
38. Michaleff ZA, Costa LO, Moseley AM, et al. CENTRAL, PEDro, PubMed, and
EMBASE are the most comprehensive databases indexing randomized controlled trials
of physical therapy interventions. Phys Ther. 2011;91(2):190-197.
39. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of
the PEDro scale for rating quality of randomized controlled trials. Phys Ther.
2003;83(8):713-721.
40. Statistics from PEDro's website. Sydney: Physiotherapy Evidence Database.
2018; https://www.pedro.org.au/english/downloads/pedro-statistics.
41. Viera AJ, Garrett JM. Understanding interobserver agreement: the kappa
statistic. Fam Med. 2005;37(5):360-363.
42. Ostelo RW, Deyo RA, Stratford P, et al. Interpreting change scores for pain and
functional status in low back pain: towards international consensus regarding minimal
important change. Spine (Phila Pa 1976). 2008;33(1):90-94.
43. Assem Y, Adie S, Tang J, Harris IA. The over-representation of significant p
values in abstracts compared to corresponding full texts: a systematic review of surgical
randomized trials. Contemp Clin Trials Commun. 2017;7:194-199.
44. Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 Explanation and
Elaboration: Updated guidelines for reporting parallel group randomised trials. J Clin
Epidemiol. 2010;63(8):e1-37.
45. CONSORT Endorsers. 2010; http://www.consort-statement.org/about-
consort/endorsers. Accessed July 2018.
46. Nakayama T, Hirai N, Yamazaki S, Naito M. Adoption of structured abstracts
by general medical journals and format for a structured abstract. J Med Libr Assoc.
2005;93(2):237-242.
47. Zhou Z, Ku HC, Xing G, Xing C. Decomposing Pearson's chi(2) test: a linear
regression and its departure from linearity. Ann Hum Genet. 2018.
48. Prunier JG, Colyn M, Legendre X, Nimon KF, Flamand MC. Multicollinearity
in spatial genetics: separating the wheat from the chaff using commonality analyses.
Mol Ecol. 2015;24(2):263-283.

CHAPTER 2
67
49. Mbuagbaw L, Thabane M, Vanniyasingam T, et al. Improvement in the quality
of abstracts in major clinical journals since CONSORT extension for abstracts: a
systematic review. Contemp Clin Trials. 2014;38(2):245-250.
50. Horton R. The hidden research paper. JAMA. 2002;287(21):2775-2778.
51. Fletcher RH, Black B. "Spin" in scientific writing: scientific mischief and legal
jeopardy. Med Law. 2007;26(3):511-525.
52. Kien C, Nussbaumer B, Thaler KJ, et al. Barriers to and facilitators of
interventions to counter publication bias: thematic analysis of scholarly articles and
stakeholder interviews. BMC Health Serv Res. 2014;14:551.
53. Simera I, Altman DG. ACP Journal Club. Editorial: writing a research article
that is "fit for purpose": EQUATOR Network and reporting guidelines. Ann Intern Med.
2009;151(4):JC2-2, JC2-3.
54. Page MJ, McKenzie JE, Forbes A. Many scenarios exist for selective inclusion
and reporting of results in randomized trials and systematic reviews. J Clin Epidemiol.
2013;66(5):524-537.
55. Lazarus C, Haneef R, Ravaud P, Hopewell S, Altman DG, Boutron I. Peer
reviewers identified spin in manuscripts of nonrandomized studies assessing therapeutic
interventions, but their impact on spin in abstract conclusions was limited. J Clin
Epidemiol. 2016;77:44-51.
56. Hopewell S, Collins GS, Boutron I, et al. Impact of peer review on reports of
randomised trials published in open peer review journals: retrospective before and after
study. BMJ. 2014;349:g4145.
57. Moher D, Altman DG. Four proposals to help improve the medical research
literature. PLoS Med. 2015;12(9):e1001864.
58. Announcement: Nature journals support the San Francisco Declaration on
Research Assessment. Nature. 2017;544(7651):394.

CHAPTER 2
68
APPENDIX C. Percentage of trials per journal, 2015 impact factor, CONSORT recommendations endorsement and open access journals (n=200).
ITEM JOURNAL Percentage (%) Impact
factor 2015 Endorses CONSORT
recommendations Open access journals 1 Acta Anaesthesiologica Taiwanica 0.5 Not reported Yes Yes 2 Acta Clinica Croatica 0.5 0,412 No No 3 Acupuncture in Medicine 1.0 1,592 Yes No 4 American Journal of Physical Medicine & Rehabilitation 0.5 2,064 Yes No 5 An International Quarterly Journal of Research in Ayurveda 0.5 Not reported Yes Yes 6 Annals of Family Medicine 0.5 5,087 Yes Yes 7 Annals of Internal Medicine 1.0 16,440 Yes No 8 Annals of Rehabilitation Medicine 1.0 Not reported Yes Yes 9 Archives of Internal Medicine 0.5 Not reported Yes Yes
10 Archives of Physical Medicine and Rehabilitation 2.5 3,045 Yes No 11 BMC Medicine 1.5 8,005 Yes Yes 12 BMC Musculoskeletal Disorders 2.0 1,684 Yes Yes 13 BMC Pregnancy and Childbirth 0.5 2,180 Yes Yes 14 British Journal of Sports Medicine 1.0 6,724 No No 15 British Medical Journal 0.5 19,697 Yes No 16 Caspian Journal of Internal Medicine 0.5 Not reported No Yes 17 Chinese Medicine 0.5 1,580 Yes Yes 18 Chiropractic & Manual Therapies 0.5 Not reported Yes Yes 19 Chung I Tsa Chih Ying Wen Pan [Journal of Traditional Chinese Medicine] 0.5 1,023 Yes Yes 20 Clinical Neurology and Neurosurgery 0.5 1,198 No No 21 Clinical Rehabilitation 2.5 2,403 No No 22 Clinical Rheumatology 0.5 2,042 No No 23 Clinics 0.5 1,328 No Yes 24 Disability and Rehabilitation 0.5 1,919 No No 25 Ergonomics 0.5 1,449 No No 26 European Journal of Pain 1.0 2,900 Yes No 27 European Journal of Physical and Rehabilitation Medicine 2.0 2,063 Yes Yes 28 European Spine Journal 1.5 2,132 No No 29 Evidence-Based Complementary and Alternative Medicine 2.0 1,931 No Yes 30 Family Practice 0.5 2,022 Yes No 31 Fisioterapia em movimento 0.5 Not reported No No
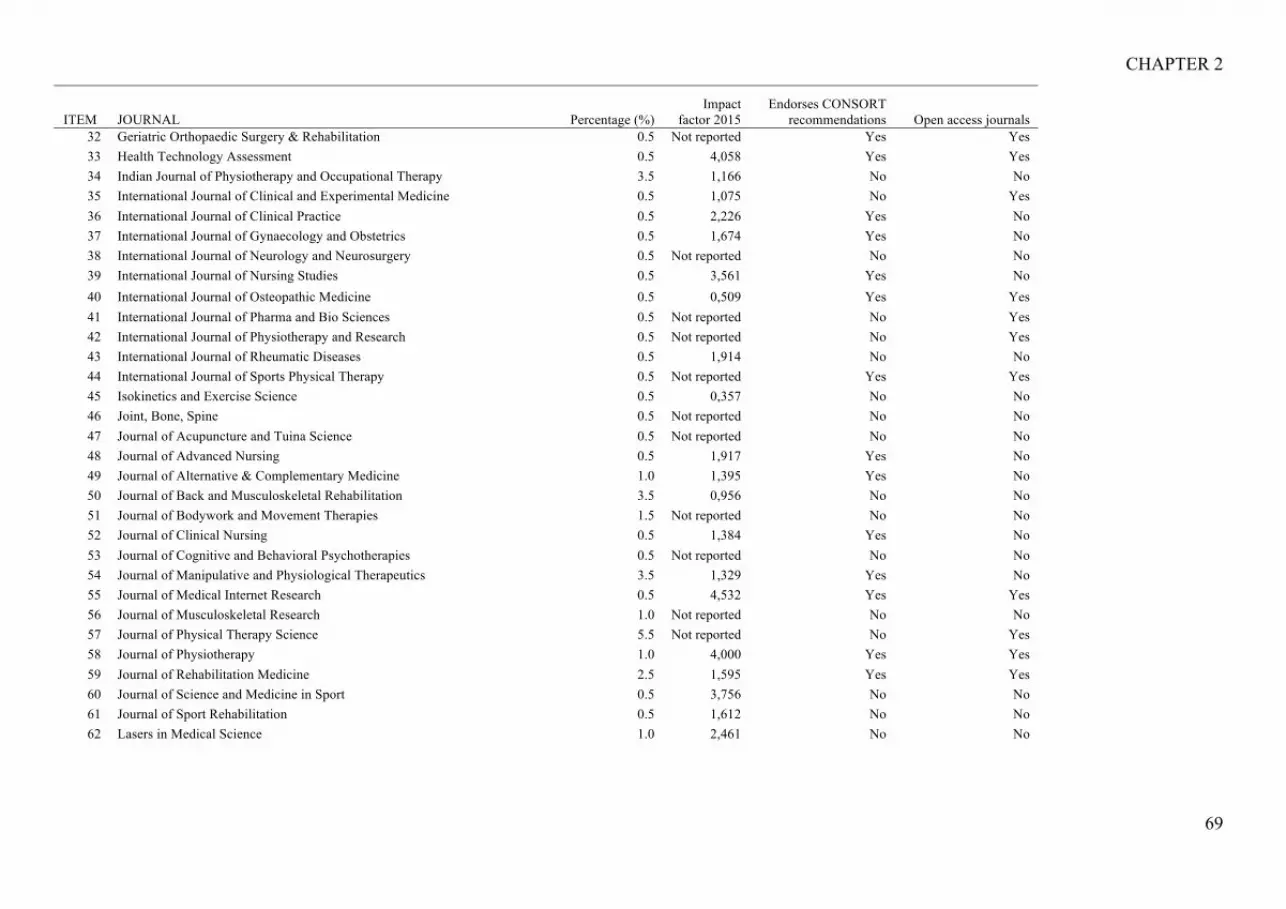
CHAPTER 2
69
ITEM JOURNAL Percentage (%) Impact
factor 2015 Endorses CONSORT
recommendations Open access journals 32 Geriatric Orthopaedic Surgery & Rehabilitation 0.5 Not reported Yes Yes 33 Health Technology Assessment 0.5 4,058 Yes Yes 34 Indian Journal of Physiotherapy and Occupational Therapy 3.5 1,166 No No 35 International Journal of Clinical and Experimental Medicine 0.5 1,075 No Yes 36 International Journal of Clinical Practice 0.5 2,226 Yes No 37 International Journal of Gynaecology and Obstetrics 0.5 1,674 Yes No 38 International Journal of Neurology and Neurosurgery 0.5 Not reported No No 39 International Journal of Nursing Studies 0.5 3,561 Yes No 40 International Journal of Osteopathic Medicine 0.5 0,509 Yes Yes 41 International Journal of Pharma and Bio Sciences 0.5 Not reported No Yes 42 International Journal of Physiotherapy and Research 0.5 Not reported No Yes 43 International Journal of Rheumatic Diseases 0.5 1,914 No No 44 International Journal of Sports Physical Therapy 0.5 Not reported Yes Yes 45 Isokinetics and Exercise Science 0.5 0,357 No No 46 Joint, Bone, Spine 0.5 Not reported No No 47 Journal of Acupuncture and Tuina Science 0.5 Not reported No No 48 Journal of Advanced Nursing 0.5 1,917 Yes No 49 Journal of Alternative & Complementary Medicine 1.0 1,395 Yes No 50 Journal of Back and Musculoskeletal Rehabilitation 3.5 0,956 No No 51 Journal of Bodywork and Movement Therapies 1.5 Not reported No No 52 Journal of Clinical Nursing 0.5 1,384 Yes No 53 Journal of Cognitive and Behavioral Psychotherapies 0.5 Not reported No No 54 Journal of Manipulative and Physiological Therapeutics 3.5 1,329 Yes No 55 Journal of Medical Internet Research 0.5 4,532 Yes Yes 56 Journal of Musculoskeletal Research 1.0 Not reported No No 57 Journal of Physical Therapy Science 5.5 Not reported No Yes 58 Journal of Physiotherapy 1.0 4,000 Yes Yes 59 Journal of Rehabilitation Medicine 2.5 1,595 Yes Yes 60 Journal of Science and Medicine in Sport 0.5 3,756 No No 61 Journal of Sport Rehabilitation 0.5 1,612 No No 62 Lasers in Medical Science 1.0 2,461 No No

CHAPTER 2
70
ITEM JOURNAL Percentage (%) Impact
factor 2015 Endorses CONSORT
recommendations Open access journals 63 Manual Therapy 2.0 1,869 Yes No 64 Medical Science Monitor 1.0 1,405 No No 65 Medicine and Science in Sports and Exercise 0.5 4,041 No No 66 Military Medicine 0.5 0,969 Yes No 67 Neurosciences 0.5 0,541 Yes Yes 68 New Zealand Journal of Physiotherapy 0.5 Not reported No No 69 Nigerian Journal of Clinical Practice 0.5 0,524 Yes Yes 70 Pain 1.5 5,557 Yes No 71 Pain Medicine 0.5 2,324 No No 72 Pain Practice 0.5 2,317 Yes No 73 Photomedicine and Laser Surgery 0.5 1,631 No No 74 Physical Therapy 4.0 2,779 Yes No 75 Physiotherapy 0.5 1,814 Yes No 76 PLoS ONE 0.5 3,057 Yes Yes 77 PM&R 1.0 1,655 Yes No 78 Psychology, Health & Medicine 0.5 1,347 No No 79 Rawal Medical Journal 0.5 Not reported No Yes 80 Revista de Investigacion Clinica 0.5 0,477 No No 81 Revista Paulista de Medicina [Sao Paulo Medical Journal] 0.5 0,955 Yes Yes 82 Rheumatology International 0.5 1,702 Yes No 83 South African Journal of Physiotherapy 1.0 Not reported No Yes 84 Southern Medical Journal 0.5 0,882 No No 85 Spine 8.0 2,439 Yes No 86 Swiss Medical Weekly 0.5 1,549 No Yes 87 The American Journal of the Medical Sciences 0.5 1,757 No No 88 The Clinical Journal of Pain 2.0 2,712 No No 89 The Journal of International Medical Research 1.0 1,431 Yes No 90 The Journal of Manual & Manipulative Therapy 0.5 Not reported No Yes 91 The Journal of the American Medical Association 0.5 Not reported Yes No 92 The Journal of the American Osteopathic Association 1.0 Not reported No No
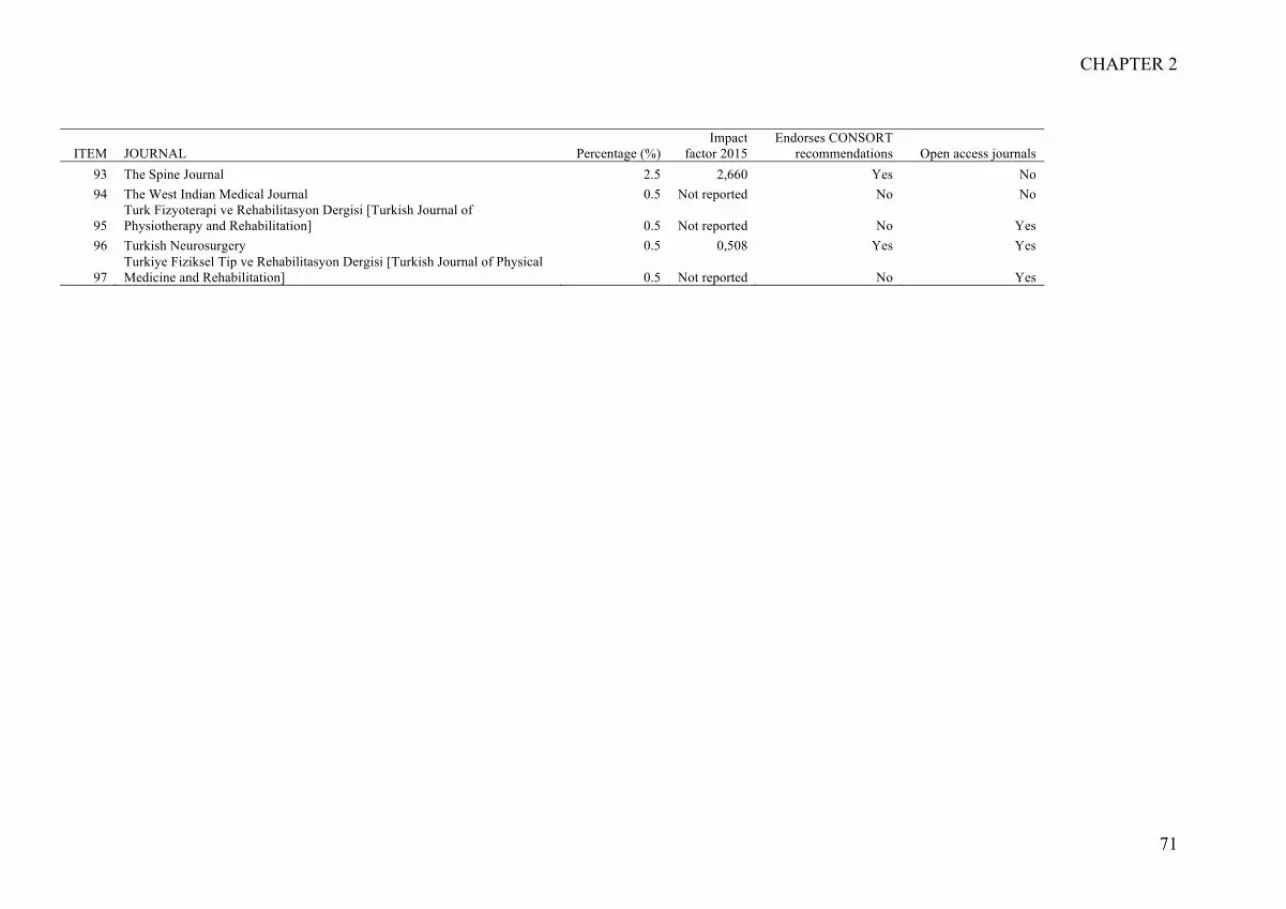
CHAPTER 2
71
ITEM JOURNAL Percentage (%) Impact
factor 2015 Endorses CONSORT
recommendations Open access journals 93 The Spine Journal 2.5 2,660 Yes No 94 The West Indian Medical Journal 0.5 Not reported No No
95 Turk Fizyoterapi ve Rehabilitasyon Dergisi [Turkish Journal of Physiotherapy and Rehabilitation] 0.5 Not reported No Yes
96 Turkish Neurosurgery 0.5 0,508 Yes Yes
97 Turkiye Fiziksel Tip ve Rehabilitasyon Dergisi [Turkish Journal of Physical Medicine and Rehabilitation] 0.5 Not reported No Yes

CHAPTER 2
72
APPENDIX D. Methodological quality of the 200 trials, measured by the PEDro scale [44, 45]. Data presented for the total PEDro score.
First author Year Journal Total PEDro score 0/10
Aboagye 2015 Journal of Rehabilitation Medicine 6 Alayat 2014 Lasers in Medical Science 5 Albaladejo 2010 Spine 7 Albert 2012 Spine 7 Aleksiev 2014 Spine 4 Alp 2014 Turkish Journal of Physical Medicine and Rehabilitation 6 Aluko 2013 Journal of Manipulative and Physiological Therapeutics 7 Apeldoorn 2012 European Spine Journal 7 Apeldoorn 2012 Spine 8 Bajaj 2010 Indian Journal of Physiotherapy and Occupational Therapy 5 Becker 2012 Spine 7 Bello 2010 Journal of Musculoskeletal Research 4 Bi 2013 The Journal of International Medical Research 7 Bronfort 2014 Annals of Internal Medicine 8 Bronfort 2011 The Spine Journal 8 Bruce-Low 2012 Ergonomics 5 Cambron 2014 Journal of Manipulative and Physiological Therapeutics 6 Campello 2012 Military Medicine 6 Cecchi 2012 European Journal of Physical and Rehabilitation Medicine 4 Chan 2011 Archives of Physical Medicine and Rehabilitation 7 Chen 2015 Clinical Neurology and Neurosurgery 6 Chen 2012 Acupuncture in Medicine 8 Chiauzzi 2010 Pain Medicine 6 Cho 2015 Journal of Physical Therapy Science 4 Christiansen 2010 Pain 6 Chuang 2012 Spine 5 Cramer 2013 Journal of Manipulative and Physiological Therapeutics 5 Cruz-Diaz 2015 Disability and Rehabilitation 8 Cuesta-Vargas 2012 Clinical Rheumatology 8 Cuesta-Vargas 2011 American Journal of Physical Medicine & Rehabilitation 6 de Oliveira 2013 Physical Therapy 8 del Pozo-Cruz 2013 Psychology, Health & Medicine 4 del Pozo-Cruz 2013 Clinical Rehabilitation 5 del Pozo-Cruz 2011 Journal of Rehabilitation Medicine 7 del Pozo-Cruz 2012 Journal of Rehabilitation Medicine 7 Demir 2014 European Journal of Physical and Rehabilitation Medicine 4 Dogan 2011 Southern Medical Journal 5 Dougherty 2014 Geriatric Orthopaedic Surgery & Rehabilitation 8 Eadie 2013 Archives of Physical Medicine and Rehabilitation 7 Ebadi 2012 BMC Musculoskeletal Disorders 8 Facci 2011 Sao Paulo Medical Journal 7 Fatemi 2015 Journal of Back and Musculoskeletal Rehabilitation 4 Ferrari 2015 Rheumatology International 5 Fiore 2011 European Journal of Physical and Rehabilitation Medicine 4 Flack 2015 BMC Pregnancy and Childbirth 6 Ford 2015 British Journal of Sports Medicine 6 Franca 2012 Journal of Manipulative and Physiological Therapeutics 4 Franca 2010 Clinics 7

CHAPTER 2
73
First author Year Journal Total PEDro score 0/10
Fritz 2015 The Journal of the American Medical Association 8 Froholdt 2011 The Spine Journal 6 Ganesh 2015 Journal of Back and Musculoskeletal Rehabilitation 5 Garcia 2013 Physical Therapy 6 Garcia 2015 Physical Therapy 6 George 2011 BMC Medicine 6 Grunnesjo 2011 Clinical Rehabilitation 7 Gunay 2014 Turkish Journal of Physiotherapy and Rehabilitation 7 Gupta 2012 Indian Journal of Physiotherapy and Occupational Therapy 2 Guthrie 2012 Journal of Sport Rehabilitation 6 Gutke 2010 Journal of Rehabilitation Medicine 6 Haakstad 2015 Journal of Rehabilitation Medicine 7 Haas 2014 The Spine Journal 5 Han 2011 Journal of Physical Therapy Science 4 Hartvigsen 2010 BMC Musculoskeletal Disorders 7 Hasegawa 2014 Acupuncture in Medicine 8 Hellum 2011 British Medical Journal 8 Henchoz 2010 Spine 6 Henchoz 2010 Swiss Medical Weekly 7 Henry 2014 The Spine Journal 6 Hidalgo 2015 Journal of Manipulative and Physiological Therapeutics 8 Hill 2015 Physical Therapy 6 Hoffman 2011 Manual Therapy 5 Homayouni 2015 Journal of Musculoskeletal Research 6 Hsieh 2014 Lasers in Medical Science 9 Huber 2011 Isokinetics and Exercise Science 6 Hugli 2015 Journal of Bodywork and Movement Therapies 7 Hurley 2015 Pain 6 Hwang 2013 Journal of Physical Therapy Science 4 Jacobson 2015 Evidence-Based Complementary and Alternative Medicine 7 Jain 2012 Indian Journal of Physiotherapy and Occupational Therapy 3 Jaromi 2012 Journal of Clinical Nursing 6 Javadian 2015 Caspian Journal of Internal Medicine 5 Javadian 2012 Journal of Back and Musculoskeletal Rehabilitation 4 Jensen 2012 BMC Musculoskeletal Disorders 5 Jensen 2015 Chiropractic & Manual Therapies 5 Jensen 2012 BMC Medicine 7 Johnsen 2014 Spine 5 Kamali 2012 Journal of Bodywork and Movement Therapies 6 Kawu 2011 Nigerian Journal of Clinical Practice 5 Kendall 2015 Journal of Science and Medicine in Sport 8 Khatri 2010 Indian Journal of Physiotherapy and Occupational Therapy 3 Kim 2015 International Journal of Osteopathic Medicine 8 Kluge 2011 International Journal of Gynaecology and Obstetrics 7 Kordi 2013 Journal of Back and Musculoskeletal Rehabilitation 5 Krammer 2015 New Zealand Journal of Physiotherapy 6 Kumar 2011 International Journal of Neurology and Neurosurgery 5 Lamb 2010 Health Technology Assessment 5 Lara-Palomo 2013 Clinical Rehabilitation 7 Lawand 2015 Joint, Bone, Spine 8 Learman 2013 Journal of Manipulative and Physiological Therapeutics 5

CHAPTER 2
74
First author Year Journal Total PEDro score 0/10
Lee 2015 Journal of Physical Therapy Science 5 Lee 2014 Journal of Physical Therapy Science 5 Lewis 2011 Journal of Physiotherapy 7 Licciardone 2013 The Journal of the American Osteopathic Association 7 Licciardone 2012 The Journal of the American Osteopathic Association 4 Licciardone 2013 Annals of Family Medicine 9 Lin 2015 PLoS ONE 6 Lomond 2014 Manual Therapy 5 Lu 2015 International Journal of Clinical and Experimental Medicine 5 Lurie 2014 Spine 5 Macedo 2010 Fisioterapia em movimento 5 Macedo 2012 Physical Therapy 8 Machado 2010 BMC Medicine 8 Mannion 2013 The Spine Journal 5 Masse-Alarie 2013 The Clinical Journal of Pain 6 Mattila 2011 European Spine Journal 7 McGregor 2012 Spine 1 McMorland 2010 Journal of Manipulative and Physiological Therapeutics 6 Meng 2011 The Clinical Journal of Pain 6 Miyamoto 2013 Physical Therapy 8 Monro 2015 Journal of Back and Musculoskeletal Rehabilitation 6 Monticone 2015 European Journal of Pain 8 Moon 2013 Annals of Rehabilitation Medicine 8 Moon 2015 Journal of Physical Therapy Science 4 Moore 2012 The American Journal of the Medical Sciences 3 Morone 2011 European Journal of Physical and Rehabilitation Medicine 6 Morris 2011 Spine 3 Naik 2010 Indian Journal of Physiotherapy and Occupational Therapy 4 Naqaish 2013 Rawal Medical Journal 4 Nassif 2011 Archives of Physical Medicine and Rehabilitation 8 Natour 2015 Clinical Rehabilitation 8 Nazzal 2013 Neurosciences 7 Nemcic 2013 Acta Clinica Croatica 5 Oestergaard 2012 Spine 6 Ohtsuki 2012 Journal of Physical Therapy Science 2 Okafor 2012 South African Journal of Physiotherapy 2 Oke 2013 The West Indian Medical Journal 4 Olmedo-Buenrostro 2010 Revista de Investigacion Clinica 5 Omar 2012 International Journal of Rheumatic Diseases 5 Onac 2012 Journal of Cognitive and Behavioral Psychotherapies 6 Ozdemir 2015 Journal of Advanced Nursing 7 Ozkara 2015 Turkish Neurosurgery 6 Pach 2013 Evidence-Based Complementary and Alternative Medicine 5 Park 2014 Journal of Physical Therapy Science 4 Parreira 2014 Journal of Physiotherapy 9 Petersen 2011 Spine 7 Prommanon 2015 Journal of Physical Therapy Science 7 Pushpika 2010 An International Quarterly Journal of Research in Ayurveda 3 Ratajczak 2011 Journal of Back and Musculoskeletal Rehabilitation 4 Rhee 2012 Medical Science Monitor 5 Riva 2014 Journal of Medical Internet Research 6

CHAPTER 2
75
First author Year Journal Total PEDro score 0/10
Rogerson 2010 Pain Practice 4 Sakulsriprasert 2010 Indian Journal of Physiotherapy and Occupational Therapy 4 Saliba 2010 International Journal of Sports Physical Therapy 7 Saper 2013 Evidence-Based Complementary and Alternative Medicine 7 Selhorst 2015 The Journal of Manual & Manipulative Therapy 7 Senna 2011 Spine 8 Sharma 2011 Indian Journal of Physiotherapy and Occupational Therapy 5 Sheeran 2013 Spine 6 Sherman 2011 Archives of Internal Medicine 7 Shin 2013 Pain 8 Siemonsma 2013 Physical Therapy 7 Simmerman 2011 PM&R 4 Sokunbi 2014 South African Journal of Physiotherapy 5 Son 2014 Journal of Physical Therapy Science 3 Sorensen 2010 BMC Musculoskeletal Disorders 6 Suni 2013 Spine 5 Szlezak 2011 Manual Therapy 4 Szulc 2015 Medical Science Monitor 4 Tavafian 2011 The Clinical Journal of Pain 6 Tellez-Garcia 2015 Journal of Bodywork and Movement Therapies 7 Tilbrook 2011 Annals of Internal Medicine 5 Tilbrook 2014 Physiotherapy 4 Unsgaard-Tondel 2010 Physical Therapy 7 Vallone 2014 Photomedicine and Laser Surgery 5 Vasseljen 2010 Manual Therapy 6 Verma 2013 International Journal of Physiotherapy and Research 5 Vibe 2013 European Journal of Pain 6 Vidal 2013 European Spine Journal 5 Vieira-Pellenz 2014 Archives of Physical Medicine and Rehabilitation 8 Vincent 2014 PM&R 6 Vong 2011 Archives of Physical Medicine and Rehabilitation 6 Wajswelner 2012 Medicine and Science in Sports and Exercise 7 Wand 2013 British Journal of Sports Medicine 5 Wand 2012 The Clinical Journal of Pain 6 Weis 2013 Journal of Alternative & Complementary Medicine 9 Xia 2011 Journal of Acupuncture and Tuina Science 3 Yardley 2010 Family Practice 3 Yeh 2010 Acta Anaesthesiologica Taiwanica 2 Yeh 2011 International Journal of Nursing Studies 8 Yildirim 2010 Journal of Back and Musculoskeletal Rehabilitation 4 Yoo 2014 International Journal of Clinical Practice 4 Yoon 2012 Annals of Rehabilitation Medicine 5 You 2014 Clinical Rehabilitation 6 You 2015 Journal of Physical Therapy Science 4 Yuan 2013 Evidence-Based Complementary and Alternative Medicine 7 Yun 2012 Journal of Alternative & Complementary Medicine 6 Zahari 2014 International Journal of Pharma and Bio Sciences 3 Zaringhalam 2010 Chinese Medicine 6 Zhang 2014 The Journal of International Medical Research 6 Zheng 2012 Journal of Traditional Chinese Medicine 6

CHAPTER 2
76
APPENDIX E. Agreement of data extraction between the two authors who collected the data. Kappa coefficient is presented for each item of the CONSORT-A and the SPIN-checklist for both abstract and full text (n=200).
Item Description Kappa coefficient 1. Title 0.96 2. Trial design 0.94 3. Participants 0.76 4. Interventions 0.47 5. Objective 0.52 6. Outcome 0.84 7. Randomization 0.75 8. Blinding 0.66 9. Numbers randomized 0.87 10. Numbers analyzed 0.72 11. Outcome results 0.35 12. Harms 0.81 13. Conclusions 0.53 14. Trial registration 0.94
CONSORT-A applied to the abstracts
15. Funding 0.87 1. Title 0.96 2. Trial design 0.91 3. Participants 0.69 4. Interventions 0.57 5. Objective 0.65 6. Outcome 0.90 7. Randomization 0.70 8. Blinding 0.54 9. Numbers randomized 0.58 10. Numbers analyzed 0.84 11. Outcome results 0.60 12. Harms 0.77 13. Conclusions 0.40 14. Trial registration 0.92 15. Funding 0.87
CONSORT-A applied to the full-text
Range from fair to almost perfect agreement Mean 0.73 (SD 0.18) 1. Omission of primary outcome 0.82 2. Fail to mention adverse events 0.80 3. Selective reporting of outcomes 0.53 4. Fail to report statistically non-significant outcomes 0.57 5. Focus on statistically significant outcomes 0.68 6. Over-enthusiastic interpretation of outcomes 0.66
SPIN-checklist applied to the abstracts
7. Recommendation of a treatment 0.49 1. Omission of primary outcome 0.81 2. Fail to mention adverse events 0.79 3. Selective reporting of outcomes 0.65 4. Fail to report statistically non-significant outcomes 0.71 5. Focus on statistically significant outcomes 0.63 6. Over-enthusiastic interpretation of outcomes 0.71 7. Recommendation of a treatment 0.53
SPIN-checklist applied to the full-text
Range from moderate to almost perfect agreement Mean 0.67 SD (0.11)

CHAPTER 2
77
APPENDIX F. Agreement between abstract and full text for the classifications of each item of the CONSORT-A and the SPIN-checklist (n=200). Calculated with Kappa coefficient. Item Description Kappa coefficient
1. Title *Not applicable 2. Trial design 0.33 3. Participants 0.12 4. Interventions 0.16 5. Objective 0.10 6. Outcome 0.45 7. Randomization 0.03 8. Blinding 0.19 9. Numbers randomized 0.10 10. Numbers analyzed 0.03 11. Outcome results 0.18 12. Harms 0.21 13. Conclusions 0.51 14. Trial registration 0.18
CONSORT-A classified as "fully reported" and "not reported". The checklist was applied to the abstract and to the full text.
15. Funding 0.25 Range from slight to moderate agreement Mean 0.20 (SD 0.14)
1. Omission of primary outcome 0.50 2. Fail to mention adverse events 0.26 3. Selective reporting of outcomes 0.49 4. Fail to report statistically non-significant outcomes 0.48 5. Focus on statistically significant outcomes 0.57 6. Over-enthusiastic interpretation of outcomes 0.53
SPIN-checklist classified as "yes” and “no”. The checklist was applied to the abstract and to the full text.
7. Recommendation of a treatment 0.57 Range from fair to moderate agreement Mean 0.49 (SD 0.11) *Note: The first item is ‘Not applicable’ because it is related to the title. Standard Deviation (SD).

CHAPTER 2
78
2.3. APPENDIXES: Common appendixes for Chapter 2

CHAPTER 2
79
2.3.1. FIGURE 1. Flow chart of included randomized controlled trials.

CHAPTER 2
80
FIGURE 1. Flow chart of included randomized controlled trials.
Records screened (n = 537)
Iden
tific
atio
n E
ligib
ility
In
clud
ed
Records identified through database searching
(n = 25.959)
Scre
enin
g
Records excluded, with reasons (n = 67)
Ongoing study (n = 1)
Protocol (n = 1)
Duplicate (n = 1)
Not only low back pain (n = 64) Full-text articles assessed
for eligibility (n = 470)
Studies included in qualitative synthesis
(n = 200)

CHAPTER 2
81
2.3.2. APPENDIX A. Excluded trials.
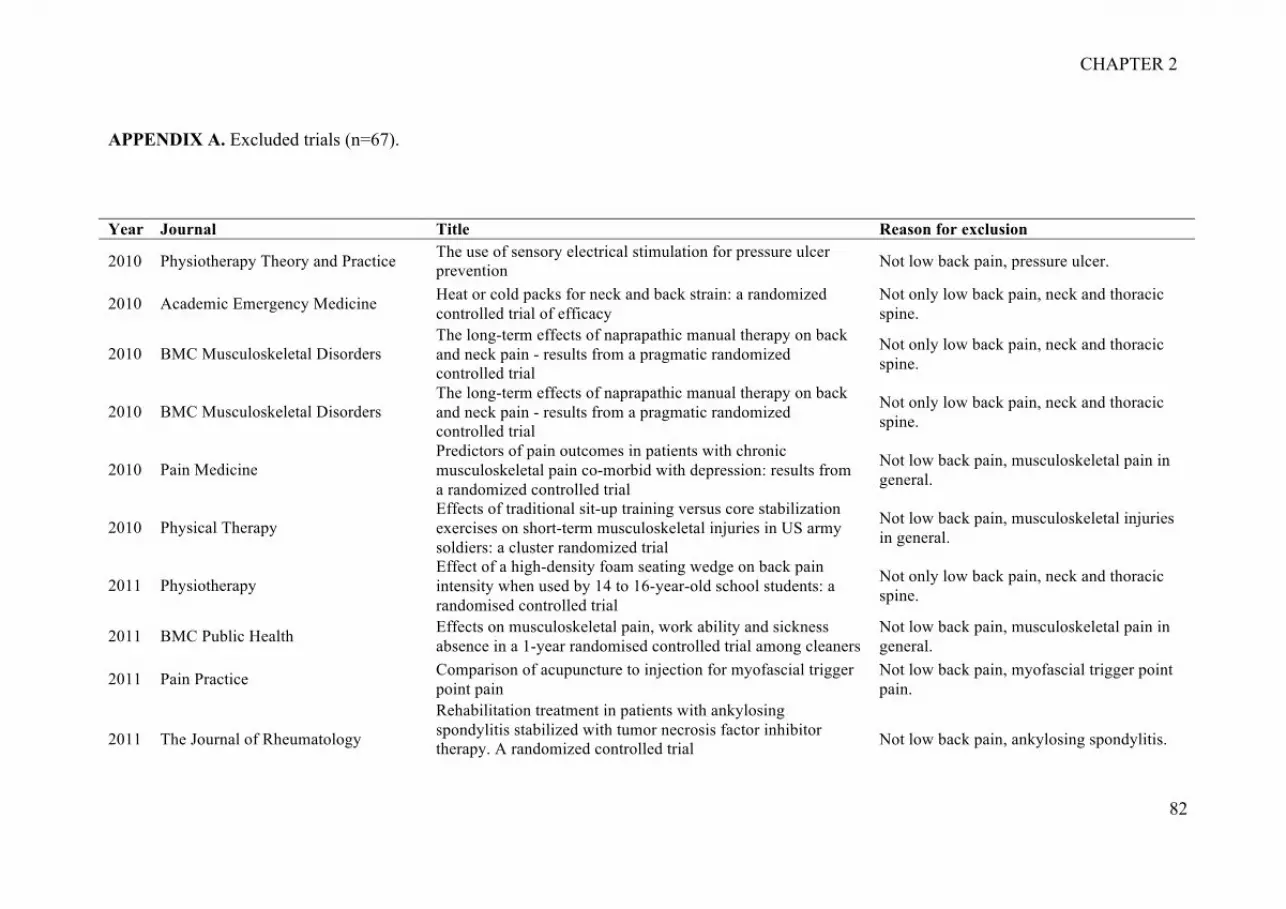
CHAPTER 2
82
APPENDIX A. Excluded trials (n=67).
Year Journal Title Reason for exclusion
2010 Physiotherapy Theory and Practice The use of sensory electrical stimulation for pressure ulcer prevention Not low back pain, pressure ulcer.
2010 Academic Emergency Medicine Heat or cold packs for neck and back strain: a randomized controlled trial of efficacy
Not only low back pain, neck and thoracic spine.
2010 BMC Musculoskeletal Disorders The long-term effects of naprapathic manual therapy on back and neck pain - results from a pragmatic randomized controlled trial
Not only low back pain, neck and thoracic spine.
2010 BMC Musculoskeletal Disorders The long-term effects of naprapathic manual therapy on back and neck pain - results from a pragmatic randomized controlled trial
Not only low back pain, neck and thoracic spine.
2010 Pain Medicine Predictors of pain outcomes in patients with chronic musculoskeletal pain co-morbid with depression: results from a randomized controlled trial
Not low back pain, musculoskeletal pain in general.
2010 Physical Therapy Effects of traditional sit-up training versus core stabilization exercises on short-term musculoskeletal injuries in US army soldiers: a cluster randomized trial
Not low back pain, musculoskeletal injuries in general.
2011 Physiotherapy Effect of a high-density foam seating wedge on back pain intensity when used by 14 to 16-year-old school students: a randomised controlled trial
Not only low back pain, neck and thoracic spine.
2011 BMC Public Health Effects on musculoskeletal pain, work ability and sickness absence in a 1-year randomised controlled trial among cleaners
Not low back pain, musculoskeletal pain in general.
2011 Pain Practice Comparison of acupuncture to injection for myofascial trigger point pain
Not low back pain, myofascial trigger point pain.
2011 The Journal of Rheumatology
Rehabilitation treatment in patients with ankylosing spondylitis stabilized with tumor necrosis factor inhibitor therapy. A randomized controlled trial
Not low back pain, ankylosing spondylitis.

CHAPTER 2
83
Year Journal Title Reason for exclusion
2011 Revista Brasileira de Fisioterapia [Brazilian Journal of Physical Therapy]
Effects of two physical therapy interventions in patients with chronic non-specific low back pain: feasibility of a randomized controlled trial
Partial analysis, study still ongoing.
2011 Pain Impact of biomedical and biopsychosocial training sessions on the attitudes, beliefs, and recommendations of health care providers about low back pain: a randomised clinical trial
Not low back pain, physiotherapists beliefs.
2011 Italian Journal of Physiotherapy Effect of a physiotherapy program in the management of musculoskeletal disorders in hairdressers: a randomized controlled trial
Not low back pain, musculoskeletal injuries in general.
2011 Journal of Bodywork and Movement Therapies
Fascial release effects on patients with non-specific cervical or lumbar pain
Not only low back pain, neck and thoracic spine.
2011 Turkish Journal of Rheumatology Long-term effects of comprehensive inpatient rehabilitation on function and disease activity in patients with chronic rheumatoid arthritis and ankylosing spondylitis
Not low back pain, chronic rheumatoid arthritis and ankylosing spondylitis.
2011 Scandinavian Journal of Work, Environment & Health
Kettlebell training for musculoskeletal and cardiovascular health: a randomized controlled trial
Not low back pain, musculoskeletal pain in general.
2011 Journal of Rehabilitation Medicine Efficacy of rehabilitation for patients with ankylosing spondylitis: comparison of a four-week rehabilitation programme in a Mediterranean and a Norwegian setting
Not low back pain, ankylosing spondylitis.
2011 Scandinavian Journal of Work, Environment & Health
The effectiveness of participatory ergonomics to prevent low-back and neck pain - results of a cluster randomized controlled trial
Not only low back pain, neck and thoracic spine.
2011 European Spine Journal Long-term effectiveness of a back education programme in elementary school children: an 8-year follow-up study
Not only low back pain, neck and thoracic spine.
2011 Journal of Bodywork and Movement Therapies
The immediate effects of traditional Thai massage on heart rate variability and stress-related parameters in patients with back pain associated with myofascial trigger points
Not only low back pain, neck and thoracic spine.
2011 Indian Journal of Physiotherapy and Occupational Therapy
Effectiveness of coccygeal manipulation in coccydynia: a randomized control trial
Duplicate.
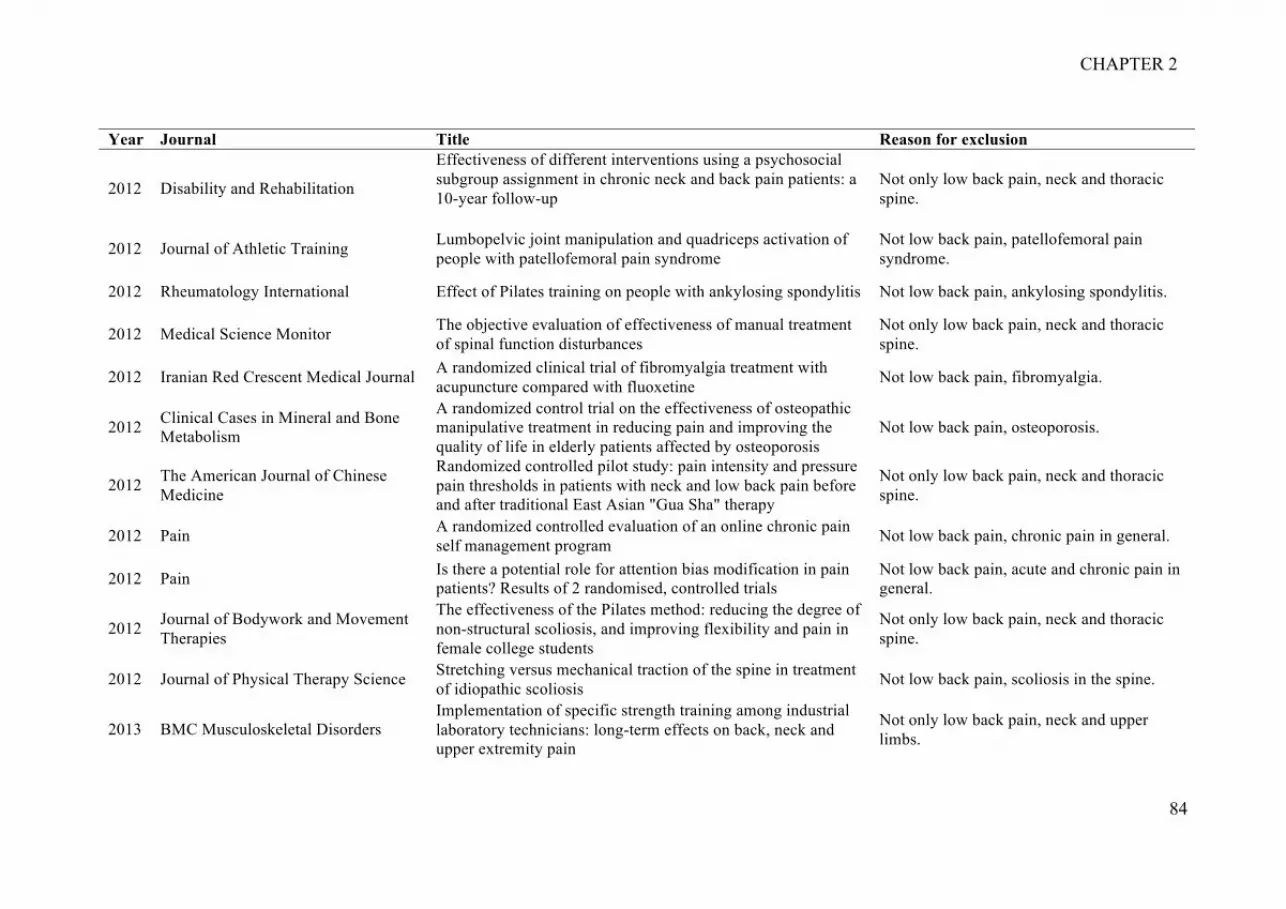
CHAPTER 2
84
Year Journal Title Reason for exclusion
2012 Disability and Rehabilitation
Effectiveness of different interventions using a psychosocial subgroup assignment in chronic neck and back pain patients: a 10-year follow-up
Not only low back pain, neck and thoracic spine.
2012 Journal of Athletic Training Lumbopelvic joint manipulation and quadriceps activation of people with patellofemoral pain syndrome
Not low back pain, patellofemoral pain syndrome.
2012 Rheumatology International Effect of Pilates training on people with ankylosing spondylitis Not low back pain, ankylosing spondylitis.
2012 Medical Science Monitor The objective evaluation of effectiveness of manual treatment of spinal function disturbances
Not only low back pain, neck and thoracic spine.
2012 Iranian Red Crescent Medical Journal A randomized clinical trial of fibromyalgia treatment with acupuncture compared with fluoxetine Not low back pain, fibromyalgia.
2012 Clinical Cases in Mineral and Bone Metabolism
A randomized control trial on the effectiveness of osteopathic manipulative treatment in reducing pain and improving the quality of life in elderly patients affected by osteoporosis
Not low back pain, osteoporosis.
2012 The American Journal of Chinese Medicine
Randomized controlled pilot study: pain intensity and pressure pain thresholds in patients with neck and low back pain before and after traditional East Asian "Gua Sha" therapy
Not only low back pain, neck and thoracic spine.
2012 Pain A randomized controlled evaluation of an online chronic pain self management program Not low back pain, chronic pain in general.
2012 Pain Is there a potential role for attention bias modification in pain patients? Results of 2 randomised, controlled trials
Not low back pain, acute and chronic pain in general.
2012 Journal of Bodywork and Movement Therapies
The effectiveness of the Pilates method: reducing the degree of non-structural scoliosis, and improving flexibility and pain in female college students
Not only low back pain, neck and thoracic spine.
2012 Journal of Physical Therapy Science Stretching versus mechanical traction of the spine in treatment of idiopathic scoliosis Not low back pain, scoliosis in the spine.
2013 BMC Musculoskeletal Disorders Implementation of specific strength training among industrial laboratory technicians: long-term effects on back, neck and upper extremity pain
Not only low back pain, neck and upper limbs.

CHAPTER 2
85
Year Journal Title Reason for exclusion
2013 Journal of Rehabilitation Medicine
A three-week multidisciplinary in-patient rehabilitation programme had positive long-term effects in patients with ankylosing spondylitis: randomized controlled trial
Not low back pain, ankylosing spondylitis.
2013 Journal of Strength & Conditioning Research
Effect of specific resistance training on musculoskeletal pain symptoms: dose-response relationship
Not low back pain, musculoskeletal pain in general.
2013 Turkish Journal of Rheumatology
A comparison of the efficacy of dry needling, lidocaine injection, and oral flurbiprofen treatments in patients with myofascial pain syndrome: a double-blind (for injection groups only), randomized clinical trial
Not low back pain, myofascial pain syndrome..
2013 Spine Short term usual chiropractic care for spinal pain: a randomised controlled trial
Not only low back pain, neck and thoracic spine.
2013 Applied Ergonomics Office ergonomics training and a sit-stand workstation: effects on musculoskeletal and visual symptoms and performance of office workers
Not low back pain, musculoskeletal pain in general.
2013 Clinical Rehabilitation Supervised training and home-based rehabilitation in patients with stabilized ankylosing spondylitis on TNF inhibitor treatment: a controlled clinical trial with a 12-month follow-up
Not low back pain, ankylosing spondylitis.
2013 Annals of Agricultural & Environmental Medicine
Physical therapy versus medical treatment of musculoskeletal disorders in dentistry - a randomised prospective study
Not low back pain, musculoskeletal pain in general.
2013 Arthritis Care & Research Effect of cardiovascular training on fitness and perceived disease activity in people with ankylosing spondylitis Not low back pain, ankylosing spondylitis.
2013 Spine Outcomes of Usual Chiropractic Harm (OUCH) randomised controlled trial of adverse events Protocol.
2013 Clinical and Experimental Rheumatology
Outcome of an education and home-based exercise programme for patients with ankylosing spondylitis: a nationwide randomized study
Not low back pain, ankylosing spondylitis.
2013 Swiss Medical Weekly
Culturally sensitive group therapy for Turkish patients suffering from chronic pain: a randomised controlled intervention trial
Not low back pain, chronic pain in general.

CHAPTER 2
86
Year Journal Title Reason for exclusion
2013 Rheumatology International The effects of combined spa therapy and rehabilitation on patients with ankylosing spondylitis being treated with TNF inhibitors
Not low back pain, ankylosing spondylitis.
2013 The Journal of Orthopaedic and Sports Physical Therapy
Efficacy of thrust and non-thrust manipulation and exercise with or without the addition of myofascial therapy for the management of acute post-inversion ankle sprain: a randomized clinical trial
Not low back pain, ankle sprain.
2013 Spine A randomized trial of balloon kyphoplasty and non-surgical management for treating acute vertebral compression fractures: vertebral body kyphosis correction and surgical parameters
Not low back pain, kyphosis correction.
2014 Rheumatology International
Effects of Pilates, McKenzie and Heckscher training on disease activity, spinal motility and pulmonary function in patients with ankylosing spondylitis: a randomized controlled trial
Not low back pain, ankylosing spondylitis.
2014 Journal of Physical Activity & Health Evaluation of Active Living Every Day in adults with arthritis Not low back pain, arthritis.
2014 Spine The effect of work-focused rehabilitation among patients with neck and back pain: a randomised controlled trial
Not only low back pain, neck and thoracic spine.
2014 Fisioterapia em Movimento [Physical Therapy in Movement]
Impact of dry needling and ischemic pressure in the myofascial syndrome: controlled clinical trial
Not low back pain, myofascial pain syndrome.
2014 The Clinical Journal of Pain Paraspinal stimulation combined with trigger point needling and needle rotation for the treatment of myofascial pain: a randomized sham-controlled clinical trial
Not low back pain, myofascial pain syndrome.
2014 Manual Therapy Manual therapy directed at the knee or lumbopelvic region does not influence quadriceps spinal reflex excitability Not low back pain, knee injury.
2014 BMC Musculoskeletal Disorders Adverse events after manual therapy among patients seeking care for neck and/or back pain: a randomized controlled trial
Not only low back pain, neck and thoracic spine.
2014 International Journal of Therapeutic Massage and Bodywork
Relief from back pain through postural adjustment: a controlled clinical trial of the immediate effects of muscular chains therapy (MCT)
Not only low back pain, musculoskeletal pain in the spine.

CHAPTER 2
87
Year Journal Title Reason for exclusion
2014 PLoS ONE Efficacy of high intensity exercise on disease activity and cardiovascular risk in active axial spondyloarthritis: a randomized controlled pilot study
Not low back pain, axial spondyloarthritis.
2014 Health Psychology Can we improve cognitive-behavioral therapy for chronic back pain treatment engagement and adherence? A controlled trial of tailored versus standard therapy
Not only low back pain, neck and thoracic spine.
2014 Rheumatology International Effect of aquatic exercise on ankylosing spondylitis: a randomized controlled trial Not low back pain, ankylosing spondylitis.
2014 Acupuncture in Medicine Efficacy and safety of auriculopressure for primary care patients with chronic non-specific spinal pain: a multicentre randomised controlled trial
Not only low back pain, neck and thoracic spine.
2015 Clinical Rehabilitation Inspiratory muscle training improves aerobic capacity and pulmonary function in patients with ankylosing spondylitis: a randomized controlled study
Not low back pain, ankylosing spondylitis.
2015 Occupational Therapy International Effect of an exercise programme for the prevention of back and neck pain in poultry slaughterhouse workers
Not only low back pain, neck and thoracic spine.
2015 European Journal of Physical and Rehabilitation Medicine
McKenzie training in patients with early stages of ankylosing spondylitis: results of a 24-week controlled study Not low back pain, ankylosing spondylitis.
2015 Medicina Clinica Efectos de un programa de ejercicio fisico y relajacion en el medio acuatico en pacientes con espondiloartritis: ensayo clinico aleatorizado
Not low back pain, spondyloarthritis.
2015 Scandinavian Journal of Work, Environment & Health
Effect of workplace- versus home-based physical exercise on musculoskeletal pain among healthcare workers: a cluster randomized controlled trial
Not low back pain, musculoskeletal pain in general.
2015 BMC Musculoskeletal Disorders Change in pain, disability and influence of fear-avoidance in a work-focused intervention on neck and back pain: a randomized controlled trial
Not only low back pain, neck and thoracic spine.
2015 Evidence-Based Complementary and Alternative Medicine
BEMER therapy combined with physiotherapy in patients with musculoskeletal diseases: a randomised, controlled double blind follow-up pilot study
Not low back pain, musculoskeletal injuries.

CHAPTER 2
88
Year Journal Title Reason for exclusion
2015 Scientific Reports Validation of placebo in a manual therapy randomized controlled trial Not low back pain, migraines.

CHAPTER 2
89
2.3.3. APPENDIX B. Included trials.

CHAPTER 2
90
APPENDIX B. Included trials (n=200).
1. Aboagye E, Karlsson ML, Hagberg J, Jensen I. Cost-effectiveness of early
interventions for non-specific low back pain: a randomized controlled study
investigating medical yoga, exercise therapy and self-care advice. J Rehabil Med. 2015
Feb;47(2):167-73.
2. Alayat MS, Atya AM, Ali MM, Shosha TM. Long-term effect of high-intensity
laser therapy in the treatment of patients with chronic low back pain: a randomized
blinded placebo-controlled trial. Lasers Med Sci. 2014 May;29(3):1065-73.
3. Albaladejo C, Kovacs FM, Royuela A, del Pino R, Zamora J, Spanish Back Pain
Research N. The efficacy of a short education program and a short physiotherapy
program for treating low back pain in primary care: a cluster randomized trial. Spine
(Phila Pa 1976). 2010 Mar 1;35(5):483-96.
4. Albert HB, Manniche C. The efficacy of systematic active conservative
treatment for patients with severe sciatica: a single-blind, randomized, clinical,
controlled trial. Spine (Phila Pa 1976). 2012 Apr 1;37(7):531-42.
5. Aleksiev AR. Ten-year follow-up of strengthening versus flexibility exercises
with or without abdominal bracing in recurrent low back pain. Spine (Phila Pa 1976).
2014 Jun 01;39(13):997-1003.
6. Alp A MG, Avsaroglu AH, Mert M, Sigirli D. Efficacy of core-stabilization
exercise and its comparison with home-based conventional exercise in low back pain
patients. Turkiye Fiziksel Tip ve Rehabilitasyon Dergisi [Turkish Journal of Physical
Medicine and Rehabilitation]. 2014;60(1):S36-S42.
7. Aluko A, DeSouza L, Peacock J. The effect of core stability exercises on
variations in acceleration of trunk movement, pain, and disability during an episode of
acute nonspecific low back pain: a pilot clinical trial. J Manipulative Physiol Ther. 2013
Oct;36(8):497-504 e1-3.
8. Apeldoorn AT, Bosmans JE, Ostelo RW, de Vet HC, van Tulder MW. Cost-
effectiveness of a classification-based system for sub-acute and chronic low back pain.
Eur Spine J. 2012 Jul;21(7):1290-300.
9. Apeldoorn AT, Ostelo RW, van Helvoirt H, Fritz JM, Knol DL, van Tulder
MW, et al. A randomized controlled trial on the effectiveness of a classification-based
system for subacute and chronic low back pain. Spine (Phila Pa 1976). 2012 Jul
15;37(16):1347-56.

CHAPTER 2
91
10. Bajaj S, Chitra K, Shallu S. Comparison of real-time ultrasound imaging and
pressure biofeedback training for performing abdominal drawing-in maneuver in low
back pain. Indian J Physiother Occup Ther. 2010;4(2):61-5.
11. Becker A, Held H, Redaelli M, Chenot JF, Leonhardt C, Keller S, et al.
Implementation of a guideline for low back pain management in primary care: a cost-
effectiveness analysis. Spine (Phila Pa 1976). 2012 Apr 15;37(8):701-10.
12. Bello AI, Kalu NH, Adegoke BOA, Agyepong-Badu S. Hydrotherapy versus
land-based exercises in the management of chronic low back pain: a comparative study.
J Musculoskelet Res. 2010;13(159).
13. Bi X, Zhao J, Zhao L, Liu Z, Zhang J, Sun D, et al. Pelvic floor muscle exercise
for chronic low back pain. J Int Med Res. 2013 Feb;41(1):146-52.
14. Bronfort G, Hondras MA, Schulz CA, Evans RL, Long CR, Grimm R. Spinal
manipulation and home exercise with advice for subacute and chronic back-related leg
pain: a trial with adaptive allocation. Ann Intern Med. 2014 Sep 16;161(6):381-91.
15. Bronfort G, Maiers MJ, Evans RL, Schulz CA, Bracha Y, Svendsen KH, et al.
Supervised exercise, spinal manipulation, and home exercise for chronic low back pain:
a randomized clinical trial. Spine J. 2011 Jul;11(7):585-98.
16. Bruce-Low S, Smith D, Burnet S, Fisher J, Bissell G, Webster L. One lumbar
extension training session per week is sufficient for strength gains and reductions in
pain in patients with chronic low back pain ergonomics. Ergonomics. 2012;55(4):500-7.
17. Cambron JA, Schneider M, Dexheimer JM, Iannelli G, Chang M, Terhorst L, et
al. A pilot randomized controlled trial of flexion-distraction dosage for chiropractic
treatment of lumbar spinal stenosis. J Manipulative Physiol Ther. 2014 Jul-
Aug;37(6):396-406.
18. Campello M, Ziemke G, Hiebert R, Weiser S, Brinkmeyer M, Fox B, et al.
Implementation of a multidisciplinary program for active duty personnel seeking care
for low back pain in a U.S. Navy Medical Center: a feasibility study. Mil Med. 2012
Sep;177(9):1075-80.
19. Cecchi F, Negrini S, Pasquini G, Paperini A, Conti AA, Chiti M, et al. Predictors
of functional outcome in patients with chronic low back pain undergoing back school,
individual physiotherapy or spinal manipulation. Eur J Phys Rehabil Med. 2012
Sep;48(3):371-8.

CHAPTER 2
92
20. Chan CW, Mok NW, Yeung EW. Aerobic exercise training in addition to
conventional physiotherapy for chronic low back pain: a randomized controlled trial.
Arch Phys Med Rehabil. 2011 Oct;92(10):1681-5.
21. Chen CY, Chang CW, Lee ST, Chen YC, Tang SF, Cheng CH, et al. Is
rehabilitation intervention during hospitalization enough for functional improvements in
patients undergoing lumbar decompression surgery? A prospective randomized
controlled study. Clin Neurol Neurosurg. 2015 Feb;129 Suppl 1:S41-6.
22. Chen M, Chen R, Xiong J, Chi Z, Sun J, Su T, et al. Evaluation of different
moxibustion doses for lumbar disc herniation: multicentre randomised controlled trial of
heat-sensitive moxibustion therapy. Acupunct Med. 2012 Dec;30(4):266-72.
23. Chiauzzi E, Pujol LA, Wood M, Bond K, Black R, Yiu E, et al. painACTION-
back pain: a self-management website for people with chronic back pain. Pain Med.
2010 Jul;11(7):1044-58.
24. Cho YK, Kim DY, Jung SY, Seong JH. Synergistic effect of a rehabilitation
program and treadmill exercise on pain and dysfunction in patients with chronic low
back pain. J Phys Ther Sci. 2015 Apr;27(4):1187-90.
25. Christiansen S, Oettingen G, Dahme B, Klinger R. A short goal-pursuit
intervention to improve physical capacity: a randomized clinical trial in chronic back
pain patients. Pain. 2010 Jun;149(3):444-52.
26. Chuang LH, Soares MO, Tilbrook H, Cox H, Hewitt CE, Aplin J, et al. A
pragmatic multicentered randomized controlled trial of yoga for chronic low back pain:
economic evaluation. Spine (Phila Pa 1976). 2012 Aug 15;37(18):1593-601.
27. Cramer GD, Cambron J, Cantu JA, Dexheimer JM, Pocius JD, Gregerson D, et
al. Magnetic resonance imaging zygapophyseal joint space changes (gapping) in low
back pain patients following spinal manipulation and side-posture positioning: a
randomized controlled mechanisms trial with blinding. J Manipulative Physiol Ther.
2013 May;36(4):203-17.
28. Cruz-Diaz D, Martinez-Amat A, Osuna-Perez MC, De la Torre-Cruz MJ, Hita-
Contreras F. Short- and long-term effects of a six-week clinical Pilates program in
addition to physical therapy on postmenopausal women with chronic low back pain: a
randomized controlled trial. Disabil Rehabil. 2016;38(13):1300-8.
29. CSG M, PC D, FM A. Efeito do isostretching na resistência muscular de
abdominais, glúteo máximo e extensores de tronco, incapacidade e dor em pacientes
com lombalgia (The Isostretching effect in the muscle strength of gluteus maximus,

CHAPTER 2
93
abdominal and the trunk extensor, incapacity and pain in patients with low back pain).
Fisioterapia em Movimento. 2010;23(1).
30. Cuesta-Vargas AI, Adams N, Salazar JA, Belles A, Hazanas S, Arroyo-Morales
M. Deep water running and general practice in primary care for non-specific low back
pain versus general practice alone: randomized controlled trial. Clin Rheumatol. 2012
Jul;31(7):1073-8.
31. Cuesta-Vargas AI, Garcia-Romero JC, Arroyo-Morales M, Diego-Acosta AM,
Daly DJ. Exercise, manual therapy, and education with or without high-intensity deep-
water running for nonspecific chronic low back pain: a pragmatic randomized
controlled trial. Am J Phys Med Rehabil. 2011 Jul;90(7):526-34; quiz 35-8.
32. de Oliveira RF, Liebano RE, Costa Lda C, Rissato LL, Costa LO. Immediate
effects of region-specific and non-region-specific spinal manipulative therapy in
patients with chronic low back pain: a randomized controlled trial. Phys Ther. 2013
Jun;93(6):748-56.
33. del Pozo-Cruz B, del Pozo-Cruz J, Adsuar JC, Parraca J, Gusi N. Reanalysis of a
tailored web-based exercise programme for office workers with sub-acute low back
pain: assessing the stage of change in behaviour. Psychol Health Med. 2013;18(6):687-
97.
34. del Pozo-Cruz B, Gusi N, del Pozo-Cruz J, Adsuar JC, Hernandez-Mocholi M,
Parraca JA. Clinical effects of a nine-month web-based intervention in subacute non-
specific low back pain patients: a randomized controlled trial. Clin Rehabil. 2013
Jan;27(1):28-39.
35. del Pozo-Cruz B, Hernandez Mocholi MA, Adsuar JC, Parraca JA, Muro I, Gusi
N. Effects of whole body vibration therapy on main outcome measures for chronic non-
specific low back pain: a single-blind randomized controlled trial. J Rehabil Med. 2011
Jul;43(8):689-94.
36. del Pozo-Cruz B, Parraca JA, del Pozo-Cruz J, Adsuar JC, Hill J, Gusi N. An
occupational, internet-based intervention to prevent chronicity in subacute lower back
pain: a randomised controlled trial. J Rehabil Med. 2012 Jun;44(7):581-7.
37. Demir S, Dulgeroglu D, Cakci A. Effects of dynamic lumbar stabilization
exercises following lumbar microdiscectomy on pain, mobility and return to work.
Randomized controlled trial. Eur J Phys Rehabil Med. 2014 Dec;50(6):627-40.
38. Dogan M, Sahin O, Elden H, Hayta E, Kaptanoglu E. Additional therapeutic
effect of balneotherapy in low back pain. South Med J. 2011 Aug;104(8):574-8.

CHAPTER 2
94
39. Dougherty PE, Karuza J, Dunn AS, Savino D, Katz P. Spinal Manipulative
Therapy for Chronic Lower Back Pain in Older Veterans: A Prospective, Randomized,
Placebo-Controlled Trial. Geriatr Orthop Surg Rehabil. 2014 Dec;5(4):154-64.
40. Eadie J, van de Water AT, Lonsdale C, Tully MA, van Mechelen W, Boreham
CA, et al. Physiotherapy for sleep disturbance in people with chronic low back pain:
results of a feasibility randomized controlled trial. Arch Phys Med Rehabil. 2013
Nov;94(11):2083-92.
41. Ebadi S, Ansari NN, Naghdi S, Jalaei S, Sadat M, Bagheri H, et al. The effect of
continuous ultrasound on chronic non-specific low back pain: a single blind placebo-
controlled randomized trial. BMC Musculoskelet Disord. 2012;13:192.
42. Facci LM, Nowotny JP, Tormem F, Trevisani VF. Effects of transcutaneous
electrical nerve stimulation (TENS) and interferential currents (IFC) in patients with
nonspecific chronic low back pain: randomized clinical trial. Sao Paulo Med J.
2011;129(4):206-16.
43. Fatemi R, Javid M, Najafabadi EM. Effects of William training on lumbosacral
muscles function, lumbar curve and pain. J Back Musculoskelet Rehabil.
2015;28(3):591-7.
44. Ferrari R. Effect of a pain diary use on recovery from acute low back (lumbar)
sprain. Rheumatol Int. 2015 Jan;35(1):55-9.
45. Fiore P, Panza F, Cassatella G, Russo A, Frisardi V, Solfrizzi V, et al. Short-
term effects of high-intensity laser therapy versus ultrasound therapy in the treatment of
low back pain: a randomized controlled trial. Eur J Phys Rehabil Med. 2011
Sep;47(3):367-73.
46. Flack NA, Hay-Smith EJ, Stringer MD, Gray AR, Woodley SJ. Adherence,
tolerance and effectiveness of two different pelvic support belts as a treatment for
pregnancy-related symphyseal pain - a pilot randomized trial. BMC Pregnancy
Childbirth. 2015 Feb 15;15:36.
47. Ford JJ, Hahne AJ, Surkitt LD, Chan AY, Richards MC, Slater SL, et al.
Individualised physiotherapy as an adjunct to guideline-based advice for low back
disorders in primary care: a randomised controlled trial. Br J Sports Med. 2016
Feb;50(4):237-45.
48. Franca FR, Burke TN, Caffaro RR, Ramos LA, Marques AP. Effects of
muscular stretching and segmental stabilization on functional disability and pain in

CHAPTER 2
95
patients with chronic low back pain: a randomized, controlled trial. J Manipulative
Physiol Ther. 2012 May;35(4):279-85.
49. Franca FR, Burke TN, Hanada ES, Marques AP. Segmental stabilization and
muscular strengthening in chronic low back pain: a comparative study. Clinics (Sao
Paulo). 2010;65(10):1013-7.
50. Fritz JM, Magel JS, McFadden M, Asche C, Thackeray A, Meier W, et al. Early
Physical Therapy vs Usual Care in Patients With Recent-Onset Low Back Pain: A
Randomized Clinical Trial. JAMA. 2015 Oct 13;314(14):1459-67.
51. Froholdt A, Holm I, Keller A, Gunderson RB, Reikeraas O, Brox JI. No
difference in long-term trunk muscle strength, cross-sectional area, and density in
patients with chronic low back pain 7 to 11 years after lumbar fusion versus cognitive
intervention and exercises. Spine J. 2011 Aug;11(8):718-25.
52. Ganesh GS, Chhabra D, Pattnaik M, Mohanty P, Patel R, Mrityunjay K. Effect
of trunk muscles training using a star excursion balance test grid on strength, endurance
and disability in persons with chronic low back pain. J Back Musculoskelet Rehabil.
2015;28(3):521-30.
53. Garcia AN, Costa Lda C, da Silva TM, Gondo FL, Cyrillo FN, Costa RA, et al.
Effectiveness of back school versus McKenzie exercises in patients with chronic
nonspecific low back pain: a randomized controlled trial. Phys Ther. 2013
Jun;93(6):729-47.
54. Garcia AN, Costa Lda C, Hancock M, Costa LO. Identifying Patients With
Chronic Low Back Pain Who Respond Best to Mechanical Diagnosis and Therapy:
Secondary Analysis of a Randomized Controlled Trial. Phys Ther. 2016
May;96(5):623-30.
55. George SZ, Childs JD, Teyhen DS, Wu SS, Wright AC, Dugan JL, et al. Brief
psychosocial education, not core stabilization, reduced incidence of low back pain:
results from the Prevention of Low Back Pain in the Military (POLM) cluster
randomized trial. BMC Med. 2011;9:128.
56. Grunnesjo MI, Bogefeldt JP, Blomberg SI, Strender LE, Svardsudd KF. A
randomized controlled trial of the effects of muscle stretching, manual therapy and
steroid injections in addition to 'stay active' care on health-related quality of life in acute
or subacute low back pain. Clin Rehabil. 2011 Nov;25(11):999-1010.

CHAPTER 2
96
57. Gunay S YY, Karadibak D. The effect of the muscle endurance training on the
chronic low back pain. Turk Fizyoterapi ve Rehabilitasyon Dergisi [Turkish Journal of
Physiotherapy and Rehabilitation] 2014;25(1):28-34.
58. Gupta M. Effectiveness of nerve mobilization in the management of sciatica.
Indian J Physiother Occup Ther. 2012;6(2):79-81.
59. Guthrie RJ, Grindstaff TL, Croy T, Ingersoll CD, Saliba SA. The effect of
traditional bridging or suspension-exercise bridging on lateral abdominal thickness in
individuals with low back pain. J Sport Rehabil. 2012 May;21(2):151-60.
60. Gutke A, Sjodahl J, Oberg B. Specific muscle stabilizing as home exercises for
persistent pelvic girdle pain after pregnancy: a randomized, controlled clinical trial. J
Rehabil Med. 2010 Nov;42(10):929-35.
61. Haakstad LA, Bo K. Effect of a regular exercise programme on pelvic girdle and
low back pain in previously inactive pregnant women: A randomized controlled trial. J
Rehabil Med. 2015 Mar;47(3):229-34.
62. Haas M, Vavrek D, Peterson D, Polissar N, Neradilek MB. Dose-response and
efficacy of spinal manipulation for care of chronic low back pain: a randomized
controlled trial. Spine J. 2014 Jul 01;14(7):1106-16.
63. Han G CM, Nam G, Moon T, Kim J, Kim S, Hong S, Cho B. The effects on
muscle strength and visual analog scale pain of aquatic therapy for individuals with low
back pain. Journal of Physical Therapy Science 2011;23(1):57-60.
64. Hartvigsen J, Morso L, Bendix T, Manniche C. Supervised and non-supervised
Nordic walking in the treatment of chronic low back pain: a single blind randomized
clinical trial. BMC Musculoskelet Disord. 2010;11:30.
65. Hasegawa TM, Baptista AS, de Souza MC, Yoshizumi AM, Natour J.
Acupuncture for acute non-specific low back pain: a randomised, controlled, double-
blind, placebo trial. Acupunct Med. 2014 Apr;32(2):109-15.
66. Hellum C, Johnsen LG, Storheim K, Nygaard OP, Brox JI, Rossvoll I, et al.
Surgery with disc prosthesis versus rehabilitation in patients with low back pain and
degenerative disc: two year follow-up of randomised study. BMJ. 2011 May
19;342:d2786.
67. Henchoz Y, de Goumoens P, Norberg M, Paillex R, So AK. Role of physical
exercise in low back pain rehabilitation: a randomized controlled trial of a three-month
exercise program in patients who have completed multidisciplinary rehabilitation. Spine
(Phila Pa 1976). 2010 May 20;35(12):1192-9.

CHAPTER 2
97
68. Henchoz Y, de Goumoens P, So AK, Paillex R. Functional multidisciplinary
rehabilitation versus outpatient physiotherapy for non specific low back pain:
randomized controlled trial. Swiss Med Wkly. 2010;140:w13133.
69. Henry SM, Van Dillen LR, Ouellette-Morton RH, Hitt JR, Lomond KV,
DeSarno MJ, et al. Outcomes are not different for patient-matched versus nonmatched
treatment in subjects with chronic recurrent low back pain: a randomized clinical trial.
Spine J. 2014 Dec 01;14(12):2799-810.
70. Hidalgo B, Pitance L, Hall T, Detrembleur C, Nielens H. Short-term effects of
Mulligan mobilization with movement on pain, disability, and kinematic spinal
movements in patients with nonspecific low back pain: a randomized placebo-
controlled trial. J Manipulative Physiol Ther. 2015 Jul-Aug;38(6):365-74.
71. Hill JJ, Keating JL. Daily exercises and education for preventing low back pain
in children: cluster randomized controlled trial. Phys Ther. 2015 Apr;95(4):507-16.
72. Hoffman SL, Johnson MB, Zou D, Harris-Hayes M, Van Dillen LR. Effect of
classification-specific treatment on lumbopelvic motion during hip rotation in people
with low back pain. Man Ther. 2011 Aug;16(4):344-50.
73. Homayouni K NM, Zaravar F, Zaravar L, Karimian H. Comparison of the effect
of aquatic physical therapy and conventional physical therapy in patients with lumbar
spinal stenosis (a randomized controlled trial). Journal of Musculoskeletal Research.
2015;18(1):1550002.
74. Hsieh RL, Lee WC. Short-term therapeutic effects of 890-nanometer light
therapy for chronic low back pain: a double-blind randomized placebo-controlled study.
Lasers Med Sci. 2014 Mar;29(2):671-9.
75. Huber J, Lisinski P, Samborski W, Wytrazek M. The effect of early isometric
exercises on clinical and neurophysiological parameters in patients with sciatica: an
interventional randomized single-blinded study. Isokinet and Exerc Sci.
2011;19(3):207-14.
76. Hugli AS, Ernst MJ, Kool J, Rast FM, Rausch-Osthoff AK, Mannig A, et al.
Adherence to home exercises in non-specific low back pain. A randomised controlled
pilot trial. J Bodyw Mov Ther. 2015 Jan;19(1):177-85.
77. Hurley DA, Tully MA, Lonsdale C, Boreham CA, van Mechelen W, Daly L, et
al. Supervised walking in comparison with fitness training for chronic back pain in
physiotherapy: results of the SWIFT single-blinded randomized controlled trial
(ISRCTN17592092). Pain. 2015 Jan;156(1):131-47.

CHAPTER 2
98
78. Hwang JA, Bae SH, Do Kim G, Kim KY. The effects of sensorimotor training
on anticipatory postural adjustment of the trunk in chronic low back pain patients. J
Phys Ther Sci. 2013 Sep;25(9):1189-92.
79. Jacobson EE, Meleger AL, Bonato P, Wayne PM, Langevin HM, Kaptchuk TJ,
et al. Structural integration as an adjunct to outpatient rehabilitation for chronic
nonspecific low back pain: a randomized pilot clinical trial. Evid Based Complement
Alternat Med. 2015;2015:813418.
80. Jain R, Hameed UA, Tuteja R. Effectiveness of slump stretching in comparison
to conventional physiotherapy in treatment of subacute non-radicular low back pain.
Indian J Physiother Occup Ther. 2012;6(1):123-6.
81. Jaromi M, Nemeth A, Kranicz J, Laczko T, Betlehem J. Treatment and
ergonomics training of work-related lower back pain and body posture problems for
nurses. J Clin Nurs. 2012 Jun;21(11-12):1776-84.
82. Javadian Y, Akbari M, Talebi G, Taghipour-Darzi M, Janmohammadi N.
Influence of core stability exercise on lumbar vertebral instability in patients presented
with chronic low back pain: A randomized clinical trial. Caspian J Intern Med. 2015
Spring;6(2):98-102.
83. Javadian Y, Behtash H, Akbari M, Taghipour-Darzi M, Zekavat H. The effects
of stabilizing exercises on pain and disability of patients with lumbar segmental
instability. J Back Musculoskelet Rehabil. 2012;25(3):149-55.
84. Jensen C, Jensen OK, Nielsen CV. Sustainability of return to work in sick-listed
employees with low-back pain. Two-year follow-up in a randomized clinical trial
comparing multidisciplinary and brief intervention. BMC Musculoskelet Disord.
2012;13:156.
85. Jensen RK, Kent P, Hancock M. Do MRI findings identify patients with chronic
low back pain and Modic changes who respond best to rest or exercise: a subgroup
analysis of a randomised controlled trial. Chiropr Man Therap. 2015;23:26.
86. Jensen RK, Leboeuf-Yde C, Wedderkopp N, Sorensen JS, Manniche C. Rest
versus exercise as treatment for patients with low back pain and Modic changes. A
randomized controlled clinical trial. BMC Med. 2012;10:22.
87. Johnsen LG, Hellum C, Storheim K, Nygaard OP, Brox JI, Rossvoll I, et al.
Cost-effectiveness of total disc replacement versus multidisciplinary rehabilitation in
patients with chronic low back pain: a Norwegian multicenter RCT. Spine (Phila Pa
1976). 2014 Jan 01;39(1):23-32.

CHAPTER 2
99
88. Kamali F, Shokri E. The effect of two manipulative therapy techniques and their
outcome in patients with sacroiliac joint syndrome. J Bodyw Mov Ther. 2012
Jan;16(1):29-35.
89. Kawu AA, Olawepo A, Salami AO. Facet joints infiltration: a viable alternative
treatment to physiotherapy in patients with low back pain due to facet joint arthropathy.
Niger J Clin Pract. 2011 Apr-Jun;14(2):219-22.
90. Kendall KD, Emery CA, Wiley JP, Ferber R. The effect of the addition of hip
strengthening exercises to a lumbopelvic exercise programme for the treatment of non-
specific low back pain: A randomized controlled trial. J Sci Med Sport. 2015
Nov;18(6):626-31.
91. Khatri SM JR, Nitsure P. Effectiveness of coccygeal manipulation in
coccydynia: a randomized control trial. Indian Journal of Physiotherapy and
Occupational Therapy 2010;4(4):93-5.
92. Kim BJ AJ, Cho H, Kim D, Kim T, Yoon B. Rehabilitation with osteopathic
manipulative treatment after lumbar disc surgery: a randomised, controlled pilot study.
International Journal of Osteopathic Medicine 2015;18(3):181–8.
93. Kluge J, Hall D, Louw Q, Theron G, Grove D. Specific exercises to treat
pregnancy-related low back pain in a South African population. Int J Gynaecol Obstet.
2011 Jun;113(3):187-91.
94. Kordi R, Abolhasani M, Rostami M, Hantoushzadeh S, Mansournia MA,
Vasheghani-Farahani F. Comparison between the effect of lumbopelvic belt and home
based pelvic stabilizing exercise on pregnant women with pelvic girdle pain; a
randomized controlled trial. J Back Musculoskelet Rehabil. 2013;26(2):133-9.
95. Krammer A HS, Tumilty S. Pulsed electromagnetic energy as an adjunct to
physiotherapy for the treatment of acute low back pain: a randomised controlled trial.
New Zealand Journal of Physiotherapy 2015;43(1):16-22.
96. Kumar SP, Cherian PJ. Efficacy of spinal mobilization in the treatment of
patients with lumbar radiculopathy due to disc herniation: a randomized clinical trial.
Int J Neurol. 2011;3(2):65-76.
97. Lamb SE, Lall R, Hansen Z, Castelnuovo E, Withers EJ, Nichols V, et al. A
multicentred randomised controlled trial of a primary care-based cognitive behavioural
programme for low back pain. The Back Skills Training (BeST) trial. Health Technol
Assess. 2010 Aug;14(41):1-253, iii-iv.

CHAPTER 2
100
98. Lara-Palomo IC, Aguilar-Ferrandiz ME, Mataran-Penarrocha GA, Saavedra-
Hernandez M, Granero-Molina J, Fernandez-Sola C, et al. Short-term effects of
interferential current electro-massage in adults with chronic non-specific low back pain:
a randomized controlled trial. Clin Rehabil. 2013 May;27(5):439-49.
99. Lawand P, Lombardi Junior I, Jones A, Sardim C, Ribeiro LH, Natour J. Effect
of a muscle stretching program using the global postural reeducation method for
patients with chronic low back pain: A randomized controlled trial. Joint Bone Spine.
2015 Jul;82(4):272-7.
100. Learman KE, Showalter C, O'Halloran B, Cook CE. Thrust and nonthrust
manipulation for older adults with low back pain: an evaluation of pain and disability. J
Manipulative Physiol Ther. 2013 Jun;36(5):284-91.
101. Lee SH, Kim TH, Lee BH. The effect of abdominal bracing in combination with
low extremity movements on changes in thickness of abdominal muscles and lumbar
strength for low back pain. J Phys Ther Sci. 2014 Jan;26(1):157-60.
102. Lee SW, Kim SY. Effects of hip exercises for chronic low-back pain patients
with lumbar instability. J Phys Ther Sci. 2015 Feb;27(2):345-8.
103. Lewis C, Souvlis T, Sterling M. Strain-Counterstrain therapy combined with
exercise is not more effective than exercise alone on pain and disability in people with
acute low back pain: a randomised trial. J Physiother. 2011;57(2):91-8.
104. Licciardone JC, Aryal S. Prevention of progressive back-specific dysfunction
during pregnancy: an assessment of osteopathic manual treatment based on Cochrane
Back Review Group criteria. J Am Osteopath Assoc. 2013 Oct;113(10):728-36.
105. Licciardone JC, Kearns CM, Hodge LM, Bergamini MV. Associations of
cytokine concentrations with key osteopathic lesions and clinical outcomes in patients
with nonspecific chronic low back pain: results from the OSTEOPATHIC Trial. J Am
Osteopath Assoc. 2012 Sep;112(9):596-605.
106. Licciardone JC, Minotti DE, Gatchel RJ, Kearns CM, Singh KP. Osteopathic
manual treatment and ultrasound therapy for chronic low back pain: a randomized
controlled trial. Ann Fam Med. 2013 Mar-Apr;11(2):122-9.
107. Lin SF, Chen YJ, Tu HP, Lee CL, Hsieh CL, Wu WL, et al. The Effects of
Extracorporeal Shock Wave Therapy in Patients with Coccydynia: A Randomized
Controlled Trial. PLoS One. 2015;10(11):e0142475.

CHAPTER 2
101
108. Lomond KV, Henry SM, Hitt JR, DeSarno MJ, Bunn JY. Altered postural
responses persist following physical therapy of general versus specific trunk exercises
in people with low back pain. Man Ther. 2014 Oct;19(5):425-32.
109. Lu T, Song QH, Xu RM, Zhang LY. Effect of Tai Chi exercise in combination
with auricular plaster on patients with lumbar muscle strain. Int J Clin Exp Med.
2015;8(2):2949-53.
110. Lurie JD, Tosteson TD, Tosteson AN, Zhao W, Morgan TS, Abdu WA, et al.
Surgical versus nonoperative treatment for lumbar disc herniation: eight-year results for
the spine patient outcomes research trial. Spine (Phila Pa 1976). 2014 Jan 01;39(1):3-
16.
111. Macedo LG, Latimer J, Maher CG, Hodges PW, McAuley JH, Nicholas MK, et
al. Effect of motor control exercises versus graded activity in patients with chronic
nonspecific low back pain: a randomized controlled trial. Phys Ther. 2012
Mar;92(3):363-77.
112. Machado LA, Maher CG, Herbert RD, Clare H, McAuley JH. The effectiveness
of the McKenzie method in addition to first-line care for acute low back pain: a
randomized controlled trial. BMC Med. 2010;8:10.
113. Mannion AF, Brox JI, Fairbank JC. Comparison of spinal fusion and
nonoperative treatment in patients with chronic low back pain: long-term follow-up of
three randomized controlled trials. Spine J. 2013 Nov;13(11):1438-48.
114. Masse-Alarie H, Flamand VH, Moffet H, Schneider C. Peripheral
neurostimulation and specific motor training of deep abdominal muscles improve
posturomotor control in chronic low back pain. Clin J Pain. 2013 Sep;29(9):814-23.
115. Mattila VM, Sillanpaa P, Salo T, Laine HJ, Maenpaa H, Pihlajamaki H. Orthotic
insoles do not prevent physical stress-induced low back pain. Eur Spine J. 2011
Jan;20(1):100-4.
116. McGregor AH, Henley A, Morris TP, Dore CJ, team F. An evaluation of a
postoperative rehabilitation program after spinal surgery and its impact on outcome.
Spine (Phila Pa 1976). 2012 Apr 1;37(7):E417-22.
117. McMorland G, Suter E, Casha S, du Plessis SJ, Hurlbert RJ. Manipulation or
microdiskectomy for sciatica? A prospective randomized clinical study. J Manipulative
Physiol Ther. 2010 Oct;33(8):576-84.
118. Meng K, Seekatz B, Roband H, Worringen U, Vogel H, Faller H. Intermediate
and long-term effects of a standardized back school for inpatient orthopedic

CHAPTER 2
102
rehabilitation on illness knowledge and self-management behaviors: a randomized
controlled trial. Clin J Pain. 2011 Mar-Apr;27(3):248-57.
119. Miyamoto GC, Costa LO, Galvanin T, Cabral CM. Efficacy of the addition of
modified Pilates exercises to a minimal intervention in patients with chronic low back
pain: a randomized controlled trial. Phys Ther. 2013 Mar;93(3):310-20.
120. Monro R, Bhardwaj AK, Gupta RK, Telles S, Allen B, Little P. Disc extrusions
and bulges in nonspecific low back pain and sciatica: Exploratory randomised
controlled trial comparing yoga therapy and normal medical treatment. J Back
Musculoskelet Rehabil. 2015;28(2):383-92.
121. Monticone M, Ambrosini E, Rocca B, Cazzaniga D, Liquori V, Foti C. Group-
based task-oriented exercises aimed at managing kinesiophobia improved disability in
chronic low back pain. Eur J Pain. 2016 Apr;20(4):541-51.
122. Moon HJ, Choi KH, Kim DH, Kim HJ, Cho YK, Lee KH, et al. Effect of lumbar
stabilization and dynamic lumbar strengthening exercises in patients with chronic low
back pain. Ann Rehabil Med. 2013 Feb;37(1):110-7.
123. Moon TY, Kim JH, Gwon HJ, Hwan BS, Kim GY, Smith N, et al. Effects of
exercise therapy on muscular strength in firefighters with back pain. J Phys Ther Sci.
2015 Mar;27(3):581-3.
124. Moore C, Holland J, Shaib F, Ceridan E, Schonard C, Marasa M. Prevention of
low back pain in sedentary healthy workers: a pilot study. Am J Med Sci. 2012
Aug;344(2):90-5.
125. Morone G, Paolucci T, Alcuri MR, Vulpiani MC, Matano A, Bureca I, et al.
Quality of life improved by multidisciplinary back school program in patients with
chronic non-specific low back pain: a single blind randomized controlled trial. Eur J
Phys Rehabil Med. 2011 Dec;47(4):533-41.
126. Morris S, Morris TP, McGregor AH, Dore CJ, Jamrozik K. Function after spinal
treatment, exercise, and rehabilitation: cost-effectiveness analysis based on a
randomized controlled trial. Spine (Phila Pa 1976). 2011 Oct 1;36(21):1807-14.
127. Naik PP, Heggannavar A, Khatri SM. Comparison of muscle energy technique
and positional release therapy in acute low back pain -- RCT. Indian J Physiother
Occup Ther. 2010;4(2):32-6.
128. Naqaish T RF, Ambreen S. Efficacy of Kegel exercises on lower back pain
control in patients of Cystocele. Rawal Medical Journal. 2013;38(3):275-8.

CHAPTER 2
103
129. Nassif H, Brosset N, Guillaume M, Delore-Milles E, Tafflet M, Buchholz F, et
al. Evaluation of a randomized controlled trial in the management of chronic lower back
pain in a French automotive industry: an observational study. Arch Phys Med Rehabil.
2011 Dec;92(12):1927-36 e4.
130. Natour J, Cazotti Lde A, Ribeiro LH, Baptista AS, Jones A. Pilates improves
pain, function and quality of life in patients with chronic low back pain: a randomized
controlled trial. Clin Rehabil. 2015 Jan;29(1):59-68.
131. Nazzal ME, Saadah MA, Saadah LM, Al-Omari MA, Al-Oudat ZA, Nazzal MS,
et al. Management options of chronic low back pain. A randomized blinded clinical
trial. Neurosciences (Riyadh). 2013 Apr;18(2):152-9.
132. Nemcic T, Budisin V, Vrabec-Matkovic D, Grazio S. Comparison of the effects
of land-based and water-based therapeutic exercises on the range of motion and
physical disability in patients with chronic low-back pain: single-blinded randomized
study. Acta Clin Croat. 2013 Sep;52(3):321-7.
133. Oestergaard LG, Nielsen CV, Bunger CE, Sogaard R, Fruensgaard S, Helmig P,
et al. The effect of early initiation of rehabilitation after lumbar spinal fusion: a
randomized clinical study. Spine (Phila Pa 1976). 2012 Oct 1;37(21):1803-9.
134. Ohtsuki K. The immediate changes in patients with acute exacerbation of
chronic lower-back pain elicited by direct stretching of the tensor fasciae latae, the
hamstrings and the adductor magnus. J Phys Ther Sci. 2012;24(8):707-9.
135. Okafor UA, Solanke TA, Akinbo SR, Odebiyi DO. Effect of aerobic dance on
pain, functional disability and quality of life on patients with chronic low back pain.
SAJPA. 2012;68(3):11-4.
136. Oke KI, Umebese PF. Evaluation of the efficacy of pulsed electromagnetic
therapy in the treatment of back pain: a randomized controlled trial in a tertiary hospital
in Nigeria. West Indian Med J. 2013 Mar;62(3):205-9.
137. Olmedo-Buenrostro BA, Trujillo-Hernandez B, Perez-Vargas FD, Diaz-Giner
VR, Delgado-Enciso I, Muniz-Murguia J, et al. [Comparison of three therapeutic
exercises protocols to lumbar hyperlordosis improvement in asyntomatic youths]. Rev
Invest Clin. 2010 Nov-Dec;62(6):568-76.
138. Omar AS, Awadalla MA, El-Latif MA. Evaluation of pulsed electromagnetic
field therapy in the management of patients with discogenic lumbar radiculopathy. Int J
Rheum Dis. 2012 Oct;15(5):e101-8.

CHAPTER 2
104
139. Onac IA MA, Onac I, Igna R, Pop L. Medication, physiotherapy and cognitive
behavior therapy for the treatment of chronic back pain: a clinical trial. Journal of
Cognitive and Behavioral Psychotherapies. 2012;12(1):23-37.
140. Ozdemir S, Bebis H, Ortabag T, Acikel C. Evaluation of the efficacy of an
exercise program for pregnant women with low back and pelvic pain: a prospective
randomized controlled trial. J Adv Nurs. 2015 Aug;71(8):1926-39.
141. Ozkara GO, Ozgen M, Ozkara E, Armagan O, Arslantas A, Atasoy MA.
Effectiveness of physical therapy and rehabilitation programs starting immediately after
lumbar disc surgery. Turk Neurosurg. 2015;25(3):372-9.
142. Pach D, Yang-Strobel X, Ludtke R, Roll S, Icke K, Brinkhaus B, et al.
Standardized versus Individualized Acupuncture for Chronic Low Back Pain: A
Randomized Controlled Trial. Evid Based Complement Alternat Med.
2013;2013:125937.
143. Park K, Seo K. The Effects on the Pain Index and Lumbar Flexibility of Obese
Patients with Low Back Pain after PNF Scapular and PNF Pelvic Patterns. J Phys Ther
Sci. 2014 Oct;26(10):1571-4.
144. Parreira Pdo C, Costa Lda C, Takahashi R, Hespanhol Junior LC, Luz Junior
MA, Silva TM, et al. Kinesio taping to generate skin convolutions is not better than
sham taping for people with chronic non-speci fi c low back pain: a randomised trial. J
Physiother. 2014 Jun;60(2):90-6.
145. Petersen T, Larsen K, Nordsteen J, Olsen S, Fournier G, Jacobsen S. The
McKenzie method compared with manipulation when used adjunctive to information
and advice in low back pain patients presenting with centralization or peripheralization:
a randomized controlled trial. Spine (Phila Pa 1976). 2011 Nov 15;36(24):1999-2010.
146. Prasert S, Roongtiwa V, Mantana V, Witchate P, Benjawan S. Effects of
physical therapy treatments with and without spinal mobilization in individuals with
acute nonspecific low back pain: A randomized trial. Indian J Physiother Occup Ther.
2010;4(4):107-11.
147. Prommanon B, Puntumetakul R, Puengsuwan P, Chatchawan U, Kamolrat T,
Rittitod T, et al. Effectiveness of a back care pillow as an adjuvant physical therapy for
chronic non-specific low back pain treatment: a randomized controlled trial. J Phys
Ther Sci. 2015 Jul;27(7):2035-8.

CHAPTER 2
105
148. Pushpika Attanayake AM, Somarathna KI, Vyas GH, Dash SC. Clinical
evaluation of selected Yogic procedures in individuals with low back pain. Ayu. 2010
Apr;31(2):245-50.
149. Ratajczak B, Hawrylak A, Demidas A, Kuciel-Lewandowska J, Boerner E.
Effectiveness of diadynamic currents and transcutaneous electrical nerve stimulation in
disc disease lumbar part of spine. J Back Musculoskelet Rehabil. 2011;24(3):155-9.
150. Rhee HS, Kim YH, Sung PS. A randomized controlled trial to determine the
effect of spinal stabilization exercise intervention based on pain level and standing
balance differences in patients with low back pain. Med Sci Monit. 2012
Mar;18(3):CR174-81.
151. Riva S, Camerini AL, Allam A, Schulz PJ. Interactive sections of an Internet-
based intervention increase empowerment of chronic back pain patients: randomized
controlled trial. J Med Internet Res. 2014 Aug 13;16(8):e180.
152. Rogerson MD, Gatchel RJ, Bierner SM. A cost utility analysis of
interdisciplinary early intervention versus treatment as usual for high-risk acute low
back pain patients. Pain Pract. 2010 Sep-Oct;10(5):382-95.
153. Saliba SA, Croy T, Guthrie R, Grooms D, Weltman A, Grindstaff TL.
Differences in transverse abdominis activation with stable and unstable bridging
exercises in individuals with low back pain. N Am J Sports Phys Ther. 2010
Jun;5(2):63-73.
154. Saper RB, Boah AR, Keosaian J, Cerrada C, Weinberg J, Sherman KJ.
Comparing Once- versus Twice-Weekly Yoga Classes for Chronic Low Back Pain in
Predominantly Low Income Minorities: A Randomized Dosing Trial. Evid Based
Complement Alternat Med. 2013;2013:658030.
155. Selhorst M, Selhorst B. Lumbar manipulation and exercise for the treatment of
acute low back pain in adolescents: a randomized controlled trial. J Man Manip Ther.
2015 Sep;23(4):226-33.
156. Senna MK, Machaly SA. Does maintained spinal manipulation therapy for
chronic nonspecific low back pain result in better long-term outcome? Spine (Phila Pa
1976). 2011 Aug 15;36(18):1427-37.
157. Sharma V, Sarkari E, Multani NK. Efficacy of neural mobilization in sciatica.
Indian J Physiother Occup Ther. 2011;5(1):125-7.
158. Sheeran L, van Deursen R, Caterson B, Sparkes V. Classification-guided versus
generalized postural intervention in subgroups of nonspecific chronic low back pain: a

CHAPTER 2
106
pragmatic randomized controlled study. Spine (Phila Pa 1976). 2013 Sep
1;38(19):1613-25.
159. Sherman KJ, Cherkin DC, Wellman RD, Cook AJ, Hawkes RJ, Delaney K, et al.
A randomized trial comparing yoga, stretching, and a self-care book for chronic low
back pain. Arch Intern Med. 2011 Dec 12;171(22):2019-26.
160. Shin JS, Ha IH, Lee J, Choi Y, Kim MR, Park BY, et al. Effects of motion style
acupuncture treatment in acute low back pain patients with severe disability: a
multicenter, randomized, controlled, comparative effectiveness trial. Pain. 2013
Jul;154(7):1030-7.
161. Siemonsma PC, Stuive I, Roorda LD, Vollebregt JA, Walker MF, Lankhorst GJ,
et al. Cognitive treatment of illness perceptions in patients with chronic low back pain: a
randomized controlled trial. Phys Ther. 2013 Apr;93(4):435-48.
162. Simmerman SM, Sizer PS, Dedrick GS, Apte GG, Brismee JM. Immediate
changes in spinal height and pain after aquatic vertical traction in patients with
persistent low back symptoms: a crossover clinical trial. PM R. 2011 May;3(5):447-57.
163. Sokunbi OG ML, Robinson P. A pilot study on using acupuncture and core
stability exercises to treat non-specific South African Journal of Physiotherapy.
2014;70(2):4-10.
164. Son JH, Park GD, Park HS. The effect of sacroiliac joint mobilization on pelvic
deformation and the static balance ability of female university students with si joint
dysfunction. J Phys Ther Sci. 2014 Jun;26(6):845-8.
165. Sorensen PH, Bendix T, Manniche C, Korsholm L, Lemvigh D, Indahl A. An
educational approach based on a non-injury model compared with individual symptom-
based physical training in chronic LBP. A pragmatic, randomised trial with a one-year
follow-up. BMC Musculoskelet Disord. 2010;11:212.
166. Suni JH, Taanila H, Mattila VM, Ohrankammen O, Vuorinen P, Pihlajamaki H,
et al. Neuromuscular exercise and counseling decrease absenteeism due to low back
pain in young conscripts: a randomized, population-based primary prevention study.
Spine (Phila Pa 1976). 2013 Mar 1;38(5):375-84.
167. Szlezak AM, Georgilopoulos P, Bullock-Saxton JE, Steele MC. The immediate
effect of unilateral lumbar Z-joint mobilisation on posterior chain neurodynamics: a
randomised controlled study. Man Ther. 2011 Dec;16(6):609-13.
168. Szulc P, Wendt M, Waszak M, Tomczak M, Cieslik K, Trzaska T. Impact of
McKenzie Method Therapy Enriched by Muscular Energy Techniques on Subjective

CHAPTER 2
107
and Objective Parameters Related to Spine Function in Patients with Chronic Low Back
Pain. Med Sci Monit. 2015 Sep 29;21:2918-32.
169. Tavafian SS, Jamshidi AR, Mohammad K. Treatment of chronic low back pain:
a randomized clinical trial comparing multidisciplinary group-based rehabilitation
program and oral drug treatment with oral drug treatment alone. Clin J Pain. 2011 Nov-
Dec;27(9):811-8.
170. Tellez-Garcia M, de-la-Llave-Rincon AI, Salom-Moreno J, Palacios-Cena M,
Ortega-Santiago R, Fernandez-de-Las-Penas C. Neuroscience education in addition to
trigger point dry needling for the management of patients with mechanical chronic low
back pain: A preliminary clinical trial. J Bodyw Mov Ther. 2015 Jul;19(3):464-72.
171. Tilbrook HE, Cox H, Hewitt CE, Kang'ombe AR, Chuang LH, Jayakody S, et al.
Yoga for chronic low back pain: a randomized trial. Ann Intern Med. 2011 Nov
1;155(9):569-78.
172. Tilbrook HE, Hewitt CE, Aplin JD, Semlyen A, Trewhela A, Watt I, et al.
Compliance effects in a randomised controlled trial of yoga for chronic low back pain: a
methodological study. Physiotherapy. 2014 Sep;100(3):256-62.
173. Unsgaard-Tondel M, Fladmark AM, Salvesen O, Vasseljen O. Motor control
exercises, sling exercises, and general exercises for patients with chronic low back pain:
a randomized controlled trial with 1-year follow-up. Phys Ther. 2010 Oct;90(10):1426-
40.
174. Vallone F, Benedicenti S, Sorrenti E, Schiavetti I, Angiero F. Effect of diode
laser in the treatment of patients with nonspecific chronic low back pain: a randomized
controlled trial. Photomed Laser Surg. 2014 Sep;32(9):490-4.
175. Vasseljen O, Fladmark AM. Abdominal muscle contraction thickness and
function after specific and general exercises: a randomized controlled trial in chronic
low back pain patients. Man Ther. 2010 Oct;15(5):482-9.
176. Verma Y GM, Narkeesh. Pain, range of motion and back strength in chronic
mechanical low back pain before and after lumbar mobilisation. International Journal
of Physiotherapy and Research. 2013(3):48-57.
177. Vibe Fersum K, O'Sullivan P, Skouen JS, Smith A, Kvale A. Efficacy of
classification-based cognitive functional therapy in patients with non-specific chronic
low back pain: a randomized controlled trial. Eur J Pain. 2013 Jul;17(6):916-28.

CHAPTER 2
108
178. Vidal J, Borras PA, Ponseti FJ, Cantallops J, Ortega FB, Palou P. Effects of a
postural education program on school backpack habits related to low back pain in
children. Eur Spine J. 2013 Apr;22(4):782-7.
179. Vieira-Pellenz F, Oliva-Pascual-Vaca A, Rodriguez-Blanco C, Heredia-Rizo
AM, Ricard F, Almazan-Campos G. Short-term effect of spinal manipulation on pain
perception, spinal mobility, and full height recovery in male subjects with degenerative
disk disease: a randomized controlled trial. Arch Phys Med Rehabil. 2014
Sep;95(9):1613-9.
180. Vincent HK, Vincent KR, Seay AN, Conrad BP, Hurley RW, George SZ. Back
strength predicts walking improvement in obese, older adults with chronic low back
pain. PM R. 2014 May;6(5):418-26.
181. Vong SK, Cheing GL, Chan F, So EM, Chan CC. Motivational enhancement
therapy in addition to physical therapy improves motivational factors and treatment
outcomes in people with low back pain: a randomized controlled trial. Arch Phys Med
Rehabil. 2011 Feb;92(2):176-83.
182. Wajswelner H, Metcalf B, Bennell K. Clinical pilates versus general exercise for
chronic low back pain: randomized trial. Med Sci Sports Exerc. 2012 Jul;44(7):1197-
205.
183. Wand BM, Abbaszadeh S, Smith AJ, Catley MJ, Moseley GL. Acupuncture
applied as a sensory discrimination training tool decreases movement-related pain in
patients with chronic low back pain more than acupuncture alone: a randomised cross-
over experiment. Br J Sports Med. 2013 Nov;47(17):1085-9.
184. Wand BM, Tulloch VM, George PJ, Smith AJ, Goucke R, O'Connell NE, et al.
Seeing it helps: movement-related back pain is reduced by visualization of the back
during movement. Clin J Pain. 2012 Sep;28(7):602-8.
185. Weiss J, Quante S, Xue F, Muche R, Reuss-Borst M. Effectiveness and
acceptance of acupuncture in patients with chronic low back pain: results of a
prospective, randomized, controlled trial. J Altern Complement Med. 2013
Dec;19(12):935-41.
186. Xia ZX YL, Zhang Y. Effect of auricular point sticking on pain due to lumbar
strain. Journal of Acupuncture and Tuina Science. 2011;9(6):384–7.
187. Yardley L, Dennison L, Coker R, Webley F, Middleton K, Barnett J, et al.
Patients' views of receiving lessons in the Alexander technique and an exercise

CHAPTER 2
109
prescription for managing back pain in the ATEAM trial. Fam Pract. 2010
Apr;27(2):198-204.
188. Yeh ML, Chung YC, Chen KM, Chen HH. Pain reduction of acupoint electrical
stimulation for patients with spinal surgery: a placebo-controlled study. Int J Nurs Stud.
2011 Jun;48(6):703-9.
189. Yeh ML, Tsou MY, Lee BY, Chen HH, Chung YC. Effects of auricular
acupressure on pain reduction in patient-controlled analgesia after lumbar spine surgery.
Acta Anaesthesiol Taiwan. 2010 Jun;48(2):80-6.
190. Yildirim Y, Soyunov S. Relationship between learning strategies of patients and
proper perception of the home exercise program with non-specific low back pain. J
Back Musculoskelet Rehabil. 2010;23(3):137-42.
191. Yoo JH, Kim SE, Lee MG, Jin JJ, Hong J, Choi YT, et al. The effect of horse
simulator riding on visual analogue scale, body composition and trunk strength in the
patients with chronic low back pain. Int J Clin Pract. 2014 Aug;68(8):941-9.
192. Yoon YS, Yu KP, Lee KJ, Kwak SH, Kim JY. Development and application of a
newly designed massage instrument for deep cross-friction massage in chronic non-
specific low back pain. Ann Rehabil Med. 2012 Feb;36(1):55-65.
193. You JH, Kim SY, Oh DW, Chon SC. The effect of a novel core stabilization
technique on managing patients with chronic low back pain: a randomized, controlled,
experimenter-blinded study. Clin Rehabil. 2014 May;28(5):460-9.
194. You YL, Su TK, Liaw LJ, Wu WL, Chu IH, Guo LY. The effect of six weeks of
sling exercise training on trunk muscular strength and endurance for clients with low
back pain. J Phys Ther Sci. 2015 Aug;27(8):2591-6.
195. Yuan WA, Huang SR, Guo K, Sun WQ, Xi XB, Zhang MC, et al. Integrative
TCM Conservative Therapy for Low Back Pain due to Lumbar Disc Herniation: A
Randomized Controlled Clinical Trial. Evid Based Complement Alternat Med.
2013;2013:309831.
196. Yun M, Shao Y, Zhang Y, He S, Xiong N, Zhang J, et al. Hegu acupuncture for
chronic low-back pain: a randomized controlled trial. J Altern Complement Med. 2012
Feb;18(2):130-6.
197. Zahari Z KK, Othman IR, Justine M. Effect of patient education combined with
physiotherapy treatment on fear-avoidance belief in low back pain sufferers.
International Journal of Pharma and Bio Sciences. 2014;5(2):B640-B8.

CHAPTER 2
110
198. Zaringhalam J, Manaheji H, Rastqar A, Zaringhalam M. Reduction of chronic
non-specific low back pain: a randomised controlled clinical trial on acupuncture and
baclofen. Chin Med. 2010;5:15.
199. Zhang Y, Wan L, Wang X. The effect of health education in patients with
chronic low back pain. J Int Med Res. 2014 Jun;42(3):815-20.
200. Zheng Z, Wang J, Gao Q, Hou J, Ma L, Jiang C, et al. Therapeutic evaluation of
lumbar tender point deep massage for chronic non-specific low back pain. J Tradit Chin
Med. 2012 Dec;32(4):534-7.

CHAPTER 3
111
CHAPTER 3
Systematic reviews in low back pain

CHAPTER 3
112
3.1. Description of the systematic reviews

CHAPTER 3
113
3.1.1. Journals impact factor were associated with PRISMA
endorsement, but not with the methodological quality of low back pain
systematic reviews: a methodological review
Under review in: Physiotherapy Journal 2019
Manuscript Number: PHYST-19-218

CHAPTER 3
114
Journals impact factor were associated with PRISMA endorsement, but not with
the methodological quality of low back pain systematic reviews: a methodological
review
Dafne Port Nascimento1, Gabrielle Zoldan Gonzalez1, Amanda Costa Araujo1,
Leonardo Oliveira Pena Costa1 1Masters and Doctoral Programs in Physical Therapy, Universidade Cidade de São
Paulo, São Paulo – SP, Brazil.
Corresponding author: Dafne Port Nascimento, Masters and Doctoral Programs in
Physical Therapy, Universidade Cidade de São Paulo. Rua Cesário Galeno 448,
Tatuapé, São Paulo, SP – Brazil, CEP 03071-000. Phone number: +55 11 994779119.
ORCID ID: https://orcid.org/0000-0002-8474-727X
Email address: [email protected]
Funding: This work was supported by a PhD scholarship from the Sao Paulo Research
Foundation (grant#2016/17853-4; Fundação de Amparo à Pesquisa do Estado de São
Paulo – FAPESP).
Declaration of interest: The authors declare that 15 out of the 66 reviews involved
authors from our research groups or collaborators (6 Cochrane and 8 non-Cochrane).
However, all reviews were evaluated with the same criteria and rigor.
CHAPTER 3
115
Journals impact factor were associated with PRISMA endorsement, but not with
the methodological quality of low back pain systematic reviews: a methodological
review
ABSTRACT
Background: There are inconsistent associations between some systematic review
characteristics and the journal impact factor the systematic review was published in.
Objective: To analyze the association of impact factor of the journals publishing low
back pain systematic reviews with whether these journals endorsed the PRISMA
recommendations and the reviews methodological quality. Data sources and eligibility
criteria: We searched the Physiotherapy Evidence Database on January 2018 for all
low back pain systematic reviews, published between 2015 and 2017. Synthesis
methods: Our primary outcomes were PRISMA recommendations endorsement by the
journal and 2017 journal impact factor. We assessed systematic review methodological
quality using the AMSTAR-2 (A MeaSurement Tool to Assess systematic Reviews) and
reported descriptive statistics. A multivariate linear regression model was built.
Results: We assessed 66 systematic reviews published in 42 journals. Thirty-seven
journals had an impact factor (mean 4.0, SD 4.8). 55% journals endorsed the PRISMA
recommendations. The methodological quality of 75.8% systematic reviews was
critically low. Journals with higher impact factor were associated with journals
endorsing the PRISMA recommendations (ß 3.7; 95% CI 1.2, 6.3), but were not
associated with the reviews methodological quality (ß -0.3; 95% CI -4.8, 4.3).
Conclusions: Three out of every four published low back pain systematic reviews had
critically low methodological quality. Journals with higher impact factor were
associated with journals endorsing the PRISMA recommendations. Clinicians must
know how to critically appraise reviews. Journals editorial policies should include the
assessment of study methodological quality and reporting in the review process of an
article.

CHAPTER 3
116
INTRODUCTION
Healthcare professionals prioritize information from systematic reviews when
contributing to clinical decisions1,2. The Preferred Reporting Items for Systematic
reviews and Meta-Analyses (PRISMA) checklist3 aimed to improve the reporting of
systematic reviews. Editorial organizations including the Cochrane Collaboration and
the International Society of Physiotherapy Journal Editors4, and 177 journals have
endorsed the PRISMA guidelines4,5. In addition to that, many healthcare professionals
assume that the quality of an article is highly associated with journal’s impact factor6.
Several studies in different healthcare areas have analyzed the association
between systematic reviews and journals characteristics7-11. Studies in the field of total
hip and knee arthroplasty11, psoriasis9 and depression7 found positive associations
between the methodological quality of such systematic reviews and the impact factor of
the journal they were published in. In health literacy and cancer screening systematic
reviews, there was a relationship between PRISMA recommendations endorsement and
journal impact factor.10 On the other hand, the methodological quality of pediatric
surgery systematic reviews were not associated with journal impact factor or with
PRISMA recommendations endorsement8. As such, it is unclear whether higher journal
impact factor is associated with journals endorsing reporting recommendations or either
with reviews methodological quality.
Low back pain is the leading cause of years lived with disability12, with high
prevalence and costs worldwide13-17. Therefore, we aimed to analyze systematic reviews
in the field of physiotherapy interventions for low back pain, which is one of the most
recommended treatment option for low back pain. Our objective was to analyze the
association of impact factor of the journals publishing low back pain systematic reviews
with whether these journals endorsed the PRISMA recommendations and the reviews
methodological quality.
METHODS
We searched the Physiotherapy Evidence Database (PEDro –
www.pedro.org.au) on January 10, 2018 for all indexed low back pain systematic
reviews that were published between January 2015 and December 2017. The eligibility
criteria for this cross sectional study were: full-published articles; and written in
CHAPTER 3
117
English, Spanish or Portuguese. We used the advanced search strategy on PEDro, as
follows: “systematic review” for method; “lumbar spine, sacroiliac joint or pelvis” for
body part; “pain” for problem; and 2015 to 2017 for year of publication.
Methodological quality assessment
Two assessors independently analyzed the methodological quality of the reviews
using the AMSTAR-218 (A MeaSurement Tool to Assess systematic Reviews).
Disagreements were resolved by discussion or arbitration by a third assessor. The
AMSTAR-2 is a reliable and validated tool19, with 16 items: 1) inclusion of the
components of PICO (Participants, Interventions, Comparisons and Outcomes) in the
research question; 2) review methods established prior to the conduct of the review; 3)
selection of study designs; 4) literature search strategy; 5) duplicate study selection; 6)
duplicate study data extraction; 7) list of excluded studies; 8) characteristics of included
studies; 9) risk of bias assessment; 10) report on funding sources for included studies;
11) methods to combine data; 12) impact of risk of bias in individual studies on meta-
analysis results; 13) impact of risk of bias in individual studies when interpreting the
results; 14) discussion about heterogeneity; 15) publication bias; and 16) conflicts of
interest and funding stated. Each item was classified as: “yes”, “partial yes”, “no” or
“not applicable”.
We judged the methodological quality of each review based on the number of
AMSTAR-2 items fulfilled: “high quality” (maximum of one non-critical weakness),
“moderate quality” (more than one non-critical weakness), “low quality” (one critical
flaw with or without non-critical weakness) or “critically low quality” (more than one
critical flaw with or without non-critical weakness)18. The non-critical weakness items
were: 1, 3, 5, 6, 8, 10, 12, 14 and 16. The critical flaws items were: 2, 4, 7, 9, 11, 13 and
15.
Data extraction
One independent author extracted data using an Excel spreadsheet previously
formatted to describe the reviews’ characteristics. Our primary outcomes were 2017
journal impact factor (IF) and PRISMA recommendations endorsement by the journal20.
The 2017 journals IF were downloaded from the Web of Science website (InCites

CHAPTER 3
118
Journal Citation Reports – Thomson Reuters). If the journal was not listed in this
website, it was considered as not having an IF. The PRISMA recommendations
endorsement20 was classified as yes or no. This information was extracted from the
“Instructions to authors” for each journal or from the PRISMA’s website5.
Descriptive data extracted from the reviews were: 1) continent where the review
was conducted, specified by the affiliation of the first author; 2) language of
publication; 3) time of difference between year the search was done in the systematic
review and the year the systematic review was published (in years); 4) primary
outcomes, classified into: pain; disability; function; and other; 5) interventions, which
included any type of physiotherapy intervention and were categorized according to the
codes used by PEDro21 (i.e., Acupuncture; Behavior modification; Education;
Electrotherapy, heat, cold; Fitness training; Health promotion; Hydrotherapy,
balneotherapy; Neurodevelopmental therapy, neurofacilitation; Orthoses, taping,
splinting; Respiratory therapy; Skill training; Strength training; Stretching,
mobilization, manipulation, massage; No appropriate value in this field); 6) duration of
low back pain, classified into: acute; chronic; acute or subacute; acute or chronic; acute,
subacute or chronic; and subacute or chronic; 7) classification of pain, classified into:
non-specific; disc herniation or prolapse; degenerative conditions; radiculopathy;
stenosis, spondylosis, spondylolisthesis; occupational; and other dysfunctions; 8)
number of meta-analyses in each review; 9) pooled sample of participants for each
systematic review; 10) article processing fees, classified into yes, no or not reported; 11)
mention to search period (yes or no); 12) presence of flow diagram (yes or no); 13)
presence of sensitivity analyses (yes or no); 14) registration of the review (yes or no);
15) primary outcome equivalent to registration/previously reported protocol,
categorized into yes, no, not applicable or not reported; 16) main searched databases
used by the included systematic reviews.
Data analysis
We built a multivariate linear regression model to explore the association
between journals 2017 impact factor with whether these journals endorsed the PRISMA
recommendations and the reviews methodological quality. The journal impact factor
was the dependent continuous variable. The independent variables were the journals
endorsing the PRISMA recommendations (categorized into dichotomous variables:

CHAPTER 3
119
“yes” or “no”) and the reviews methodological quality (categorized into dummy
variables named: “high”, “moderate”, “low” and “critically low”). We considered
association between variables if the independent variable reached P value < 0.05. We
used SPSS software (Version 20.0) for all analyses. We reported Beta coefficients (ß)
with 95% confidence intervals (CIs). The reviews characteristics were analyzed
descriptively. Normality tests were conducted before running the regression analysis
and data for the 2017 impact factors were normally distributed. We used SPSS software
(Version 20.0) for all analyses.
RESULTS
From our search strategy on January 10th 2018 in the PEDro database, 7,526
reviews were found, from which 126 fulfilled our search criteria (Figure 1). We
excluded 60 reviews. The main reasons for exclusion were: reviews with mixed
populations involving body segments other than the lower back (n=35) and the
participants not experiencing low back pain (n=19) (see APPENDIX A). The final
sample of reviews (n=66) can be found in APPENDIX B, from which 9 were Cochrane
reviews and 57 non-Cochrane reviews.
All outcomes analyzed were described in TABLE 1 by journal of publication.
Our sample of 66 reviews was published in 42 different journals, from which 10 were
specific for physiotherapy/rehabilitation, 6 for musculoskeletal conditions or spine
related and 3 for pain related journals. The top 3 journals by impact factor were: BMJ
(23.0), JAMA Internal Medicine (20.0) and Annals of Internal Medicine (19.4). One-
third of journals had an impact factor below 2.0. The majority of journals (88.1%)
presented IF, with a mean of 4.0 (SD 4.8), and 54.8% of journals endorsed the PRISMA
recommendations20. TABLE 2 described the reviews by classifications of
methodological quality, where the majority of reviews published in journals that
endorsed the PRISMA recommendations presented critically low methodological
quality (36.4%). Critically low methodological quality reviews were classified for most
reviews (75.8%, mean IF 3.7 SD 5.4), 10.6% for low (mean IF 1.9 SD 1.4), 6.1% for
moderate (n=4; all Cochrane reviews; with an IF of 6.8) and 7.7% for high
methodological quality (n=5; all Cochrane reviews; with an IF of 6.8). AMSTAR-2
individual items are described in APPENDIX C.

CHAPTER 3
120
TABLE 1. Number and percentage of presented journals organized according to higher impact factor. PRISMA endorsement and range of the methodological quality of 66 reviews are also described.
Item Journal of publication n (%) Impact factor
2017 PRISMA
endorsement Methodological quality (range)
1 BMJ 1 (1.5) 23.3 Yes Critically low 2 JAMA Internal Medicine 2 (3.0) 20.0 Yes Critically low 3 Annals of Internal Medicine 1 (1.5) 19.4 Yes Critically low 4 Cochrane Database of Systematic Reviews 9 (13.6) 6.8 Yes Moderate to high 5 Pain 1 (1.5) 5.5 Yes Critically low 6 Journal of Medical Internet Research 1 (1.5) 4.7 Yes Critically low 7 Archives of Physical Medicine and Rehabilitation 1 (1.5) 3.1 Yes Critically low 8 Physiotherapy 3 (4.5) 3.1 Yes Critically low 9 European Journal of Pain 1 (1.5) 3.0 Yes Low
10 Clinical Rehabilitation 2 (3.0) 2.9 Yes Critically low 11 Journal of Neurosurgery Spine 1 (1.5) 2.8 No Critically low 12 Pain Medicine 1 (1.5) 2.8 No Critically low 13 Spine 5 (7.6) 2.8 No Critically low to low 14 PLoS ONE 3 (4.5) 2.8 Yes Critically low to low 15 European Spine Journal 1 (1.5) 2.6 No Critically low 16 Acupuncture in Medicine 1 (1.5) 2.3 Yes Low 17 Clinical Rheumatology 1 (1.5) 2.1 No Critically low 18 Evidence-Based Complementary and Alternative Medicine 3 (4.5) 2.1 No Critically low 19 Journal of Evidence-Based Complementary & Alternative Medicine 1 (1.5) 2.1 Yes Critically low 20 BMC Musculoskeletal Disorders 1 (1.5) 2.0 No Critically low 21 Disability and Rehabilitation 1 (1.5) 2.0 No Critically low 22 Clinical Spine Surgery 1 (1.5) 2.0 Yes Critically low 23 Medicine 1 (1.5) 2.0 Yes Critically low 24 Physical Therapy in Sport 1 (1.5) 1.9 No Critically low 25 Applied Health Economics and Health Policy 1 (1.5) 1.9 Yes Critically low 26 PM&R 2 (3.0) 1.9 Yes Critically low 27 American Journal of Physical Medicine & Rehabilitation 2 (3.0) 1.8 Yes Critically low 28 Complementary Therapies in Clinical Practice 1 (1.5) 1.7 No Critically low 29 Occupational Medicine 1 (1.5) 1.5 Yes Critically low

CHAPTER 3
121
TABLE 1. Number and percentage of presented journals organized according to higher impact factor. PRISMA endorsement and range of the methodological quality of 66 reviews are also described.
Item Journal of publication n (%) Impact factor
2017 PRISMA
endorsement Methodological quality (range)
30 American Journal of Emergency Medicine 1 (1.5) 1.3 No Critically low 31 Journal of Back and Musculoskeletal Rehabilitation 2 (3.0) 1.0 No Critically low 32 Iranian Red Crescent Medical Journal 1 (1.5) 0.8 No Critically low 33 European Journal of Integrative Medicine 1 (1.5) 0.7 No Critically low 34 International Journal of Osteopathic Medicine 1 (1.5) 0.7 Yes Critically low 35 International Journal of Therapy and Rehabilitation 1 (1.5) 0.4 No Critically low 36 Journal of Physical Therapy Science 2 (3.0) 0.4 No Critically low 37 Journal of Bodywork and Movement Therapies 1 (1.5) 0.0 No Critically low 38 Nursing Research and Practice 1 (1.5) Not reported No Critically low 39 Scientifica 1 (1.5) Not reported No Critically low 40 Healthcare 1 (1.5) Not reported Yes Critically low 41 Journal of Chiropractic Medicine 1 (1.5) Not reported Yes Low 42 Physical Therapy Reviews 1 (1.5) Not reported Yes Low
TABLE 2. Comparison of the four classifications of reviews methodological quality with their mean journal impact factor, number (with percentage) of systematic reviews published in journals with and without impact factor, plus PRISMA endorsement. Total sample of 66 reviews.
Item
Journal impact factor
Mean (SD)
Reviews published in journals with impact factor
n (%)
Reviews published in journals without impact factor
n (%)
Reviews with PRISMA endorsement
n (%) Critically low methodological quality 3.7 (5.4) 47 (71.2) 3 (4.5) 24 (36.4) Low methodological quality 1.9 (1.4) 5 (7.6) 2 (3.0) 5 (7.6) Moderate methodological quality 6.8 (0.0) 4 (6.1) - 4 (6.1) High methodological quality 6.8 (0.0) 5 (7.6) - 5 (7.6)

CHAPTER 3
122
Journals with the highest IF were medical journals (BMJ, JAMA and Annals of
Internal Medicine), followed by the Cochrane Database of Systematic reviews.
Physiotherapy/rehabilitation, musculoskeletal/spine conditions or pain related journals
with the highest IF were Pain, Archives of Physical Medicine and Rehabilitation and
Physiotherapy.
Descriptive data are detailed in TABLE 3. In summary, all reviews were
published in English and most reviews were conducted in Europe, Oceania and North
America. Most reviews evaluated pain and disability as primary outcomes and analyzed
interventions classified into strength training, stretching, mobilization, manipulation and
massage. More than half of reviews classified the pain into non-specific low back pain,
whereas 19.7% did not classify the type of pain. More than half of reviews were
published in journals that did not charge article-processing fees. Less than half reviews
were registered, from which nearly 20% had primary outcomes equivalent to
registration or previously reported protocol. The most common databases the reviews
used for their search strategy were: MEDLINE, EMBASE, CINAHL, CENTRAL,
PubMed and PEDro.
We found that journals with higher impact factor were associated with journals
endorsing the PRISMA recommendations (ß 3.7; 95% CI 1.2, 6.3), but were not
associated with the reviews methodological quality (ß -0.3; 95% CI -4.8, 4.3) (see
TABLE 4). 24 systematic reviews (36.4% of 66) published in journals that endorsed the
PRISMA recommendations had critically low methodological quality (TABLE 2)

CHAPTER 3
123
TABLE 3. Descriptive data of the 66 systematic reviews of physiotherapy for low back pain indexed on PEDro between 2015 and 2017. Mean (SD) Articles n (%) Continents
Africa 3 (4.5) Asia 13 (19.7) Europe 19 (28.8) North America 14 (21.2) Oceania 16 (24.2) South America 1 (1.5)
Published in English 66 (100.0) Time of difference between year of search and year of publication 1.4 (1.0) 65 (98.5)
Year of search not reported 1 (1.5) Primary outcomes* 66 (100.0)
Pain 56 (84.8) Disability 36 (54.5) Function 13 (19.7) Other 16 (24.2)
Interventions* 66 (100.0) Acupuncture 7 (10.6) Behaviour modification 10 (15.2) Education 16 (24.2) Electrotherapy, heat, cold 5 (7.6) Fitness training 12 (18.2) Health promotion 2 (3.0) Hydrotherapy, balneotherapy 3 (4.5) Neurodevelopmental therapy, neurofacilitation 0 (0.0) Ortheses taping, splinting 2 (3.0) Respiratory therapy 1 (1.5) Skill training 25 (37.9) Strength training 36 (54.5) Stretching, mobilisation, manipulation, massage 26 (39.4) No appropriate value in this field 2 (3.0)
Duration of pain 66 (100.0) Acute 2 (3.0) Chronic 30 (45.5)

CHAPTER 3
124
TABLE 3. Descriptive data of the 66 systematic reviews of physiotherapy for low back pain indexed on PEDro between 2015 and 2017. Mean (SD) Articles n (%)
Acute or subacute 2 (3.0) Acute or chronic 1 (1.5) Acute, subacute or chronic 28 (42.4) Subacute or chronic 3 (4.5)
Classification of pain* 53 (80.3) Non-specific 39 (59.1) Disc herniation or prolapse 8 (12.1) Degenerative conditions 6 (9.1) Radiculopathy 6 (9.1) Stenosis, spondylosis, spondylolisthesis 3 (4.5) Occupational 1 (1.5) Other dysfunctions 4 (6.1) Not reported 13 (19.7)
Number of meta-analyses 5.0 (8.9) 66 (100.0) Pooled sample of participants #988.0 (74,964) 59 (90.8)
Not reported 7 (10.6) Article-processing fees (APF) 66 (100.0)
Yes 23 (34.8) No 41 (62.1) Not reported 2 (3.0)
Mention to search period 63 (95.5) Search period not reported 3 (4.5)
Flow diagram 54 (81.8) Sensitivity analyses 16 (24.2) Registration 29 (43.9)
Not registered 37 (56.1) Primary outcome equivalent to registration 13 (19.7)
Primary outcome not equivalent to registration/protocol 6 (9.1) Not applicable 41 (62.1) Not reported 6 (9.1)
Searched databases used by the included systematic reviews 66 (100.0) MEDLINE 54 (81.8) EMBASE 46 (69.7)

CHAPTER 3
125
TABLE 3. Descriptive data of the 66 systematic reviews of physiotherapy for low back pain indexed on PEDro between 2015 and 2017. Mean (SD) Articles n (%)
CINAHL 38 (57.6) CENTRAL 28 (42.4) PubMed 27 (40.9) PEDro 25 (37.9) ** Chinese Databases (CBM, CMCC, CNKI, VIP, Wanfang, other) 20 (30.3) Cochrane Library Database 19 (28.8) Allied and Complementary Medicine Database (AMED) 15 (22.7) PsyINFO 14 (21.2) Cochrane Back Review Group Trials Register 11 (16.7) SPORTDiscus 10 (15.2) Web of Science 8 (12.1) Scopus Elsevier 7 (10.6) ClinicalTrial.gov 7 (10.6) WHO international clinical trials registry platform 7 (10.6) Other 29 databases (Range of percentage) 59 (1.5 to 9.1)
Note: *Some studies included more than one primary outcome, intervention or classification of pain.**Usually these search databases were used in the same studies. #Median (Interquartile Range – IR)
TABLE 4. Linear regression model of associations between 2017 journal impact factor with whether these journals endorsed the PRISMA recommendations and the reviews methodological quality (n=66). Dependent variable 2017 journal impact factor Independent variable P value ß 95% CI PRISMA endorsement *0.01 3.7 1.2, 6.3 Reviews methodological quality
High 0.26 3.3 -2.5, 9.0 Moderate 0.29 1.6 -1.4, 4.7 Critically low 0.33 0.5 -0.6, 1.6 Low (excluded variable) Constant 0.91 -0.3 -4.8, 4.3
Note: ß = Beta coefficient; CI= Confidence Interval. *We considered association between variables if the independent variable reached P value < 0.05.

CHAPTER 3
126
DISCUSSION
We found that journals endorsing the PRISMA recommendations were
associated with higher impact factor journals. Furthermore, not always a high journal
impact factor means high methodological quality of a paper. We also found that 75.8%
of low back pain systematic reviews presented critically low methodological quality.
The Cochrane Database of Systematic Reviews was the only journal that published low
back pain systematic reviews with moderate to high methodological quality (IF 6.8).
The mean IF of journals that published 71.2% of the reviews with critically low
methodological quality was 3.7 (SD 5.4). 23 out of 42 journals (54.8%) endorsed
PRISMA recommendations, with 6 of these presenting better methodological quality
than the ones that did not endorse PRISMA. Additionally, most reviews evaluated pain
and disability as primary outcomes, which corroborate with the most recent core
outcome set in low back pain22. Despite less than half of low back pain reviews (43.9%)
were registered, such results were better than a survey of systematic reviews in
physiotherapy that showed 19% of reviews with registration23.
Systematic reviews and the literature
Our study described the main characteristics of systematic reviews in the field of
low back pain. Such characteristics have been analyzed in other healthcare fields and
most studies found association between methodological quality and journal IF7,9-11 or
with systematic reviews reporting quality24 25. However, systematic reviews in the field
of pediatric surgery found no associations between reviews methodological quality and
PRISMA recommendations endorsement, as well as better quality orthodontic reviews
published in the Cochrane Database of Systematic reviews8. Associations were found
between reporting quality and methodological quality of low back pain trials26, but were
associated with the reporting quality of abstracts only. Furthermore, republications of
Cochrane reviews in low back pain had lower methodological quality and presented
some form of overstated results (spin) in the abstracts, when compared to Cochrane
reviews27. Therefore, there are still many gaps in the conduct and reporting of
systematic reviews in many healthcare fields, including low back pain.

CHAPTER 3
127
Strengths and limitations
To our knowledge, this is the first study investigating the association between
journals impact factor with whether these journals endorsed the PRISMA
recommendations and the reviews methodological quality of systematic reviews in
physiotherapy for low back pain. Our main limitation is our sample limited to low back
pain systematic reviews of physiotherapy interventions from 2015 to 2017, and it cannot
be generalized to other study populations and interventions such as medical devices,
surgery and medication.
Clinical and methodological implications
Low back pain systematic reviews published in journals with lower IF not
always present lower methodological quality, and vice-versa. But more importantly,
authors of systematic reviews must follow reporting guidelines28,29, whether the journal
endorses PRISMA recommendations or not. Also clinicians must know how to critically
appraise the methodological quality of a systematic review, which corroborates with the
findings of a recent study on exercise therapy for low back pain30. Readers should not
always consider the journal IF to take their clinical decisions on low back pain
conditions31.
CONCLUSION
Our findings showed associations between journals with higher impact factor
and journals endorsing the PRISMA recommendations, but not with the reviews
methodological quality. Most low back pain systematic reviews presented critically low
methodological quality. Reviews published in the Cochrane Database of Systematic
Reviews were exception, presenting moderate to high methodological quality. Based on
these findings, it is very important that clinicians know how to critically appraise the a
systematic review, as well as journals editorial policies should include the assessment of
study methodological quality and reporting in the review process of an article. This is
necessary to ensure that clinical decisions on the management of low back pain are
based on the best available evidence.
CHAPTER 3
128
REFERENCES
1. Herbert R, Jamtvedt G, Mead J, Hagen KB. Practical evidence-based
physiotherapy. 2nd Edition ed: Elsevier Butterworth-Heinemann; 2011.
2. Oliveira IS, Costa LOP, Garcia AN, Miyamoto GC, Cabral CMN, Costa L. Can
demographic and anthropometric characteristics predict clinical improvement in
patients with chronic non-specific low back pain? Braz J Phys Ther. 2018;22(4):328-
335.
3. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items
for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg.
2010;8(5):336-341.
4. Costa LOP, Elkins MR. International Society of Physiotherapy Journal Editors.
Editorial. J Physiother. 2012;58.
5. PRISMA Endorsers. 2010; http://www.prisma-
statement.org/Endorsement/PRISMAEndorsers.aspx. Accessed September 2018.
6. Callaway E. Beat it, impact factor! Publishing elite turns against controversial
metric. Nature. 2016;535(7611):210-211.
7. Chung VCH, Wu XY, Feng Y, Ho RST, Wong SYS, Threapleton D.
Methodological quality of systematic reviews on treatments for depression: a cross-
sectional study. Epidemiol Psychiatr Sci. 2017:1-9.
8. Cullis PS, Gudlaugsdottir K, Andrews J. A systematic review of the quality of
conduct and reporting of systematic reviews and meta-analyses in paediatric surgery.
PLoS One. 2017;12(4):e0175213.
9. Gomez-Garcia F, Ruano J, Aguilar-Luque M, et al. Systematic reviews and
meta-analyses on psoriasis: role of funding sources, conflict of interest and bibliometric
indices as predictors of methodological quality. Br J Dermatol. 2017;176(6):1633-1644.
10. Sharma S, Oremus M. PRISMA and AMSTAR show systematic reviews on
health literacy and cancer screening are of good quality. J Clin Epidemiol. 2018;99:123-
131.
11. Wu X, Sun H, Zhou X, Wang J, Li J. Quality assessment of systematic reviews
on total hip or knee arthroplasty using mod-AMSTAR. BMC Med Res Methodol.
2018;18(1):30.
12. Collaborators GDaIIaP. Global, regional, and national incidence, prevalence,
and years lived with disability for 328 diseases and injuries for 195 countries, 1990-

CHAPTER 3
129
2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet.
2017;390(10100):1211-1259.
13. Ferreira G, Costa LM, Stein A, Hartvigsen J, Buchbinder R, Maher CG.
Tackling low back pain in Brazil: a wake-up call. Braz J Phys Ther. 2018.
14. Buchbinder R, van Tulder M, Oberg B, et al. Low back pain: a call for action.
Viewpoint. Lancet. 2018.
15. Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why
we need to pay attention. Series. Low back pain 1. Lancet. 2018.
16. Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back
pain: evidence, challenges, and promising directions. Series. Low back pain 2. Lancet.
2018.
17. Asavasopon S. Chronification of low back pain: getting to the spine of the
problem. Braz J Phys Ther. 2018;22(1):1-6.
18. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for
systematic reviews that include randomised or non-randomised studies of healthcare
interventions, or both. BMJ. 2017;358:j4008.
19. Shea BJ, Hamel C, Wells GA, et al. AMSTAR is a reliable and valid
measurement tool to assess the methodological quality of systematic reviews. J Clin
Epidemiol. 2009;62(10):1013-1020.
20. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting
systematic reviews and meta-analyses of studies that evaluate healthcare interventions:
explanation and elaboration. BMJ. 2009;339:b2700.
21. PEDro. Intervention codes from the Physiotherapy Evidence Database (PEDro).
2018; https://www.pedro.org.au/wp-content/uploads/PEDro_codes.pdf. Accessed July
2018.
22. Chiarotto A, Deyo RA, Terwee CB, et al. Core outcome domains for clinical
trials in non-specific low back pain. Eur Spine J. 2015;24(6):1127-1142.
23. Oliveira CB, Elkins MR, Lemes IR, et al. A low proportion of systematic
reviews in physical therapy are registered: a survey of 150 published systematic
reviews. Braz J Phys Ther. 2018;22(3):177-183.
24. Riado Minguez D, Kowalski M, Vallve Odena M, et al. Methodological and
Reporting Quality of Systematic Reviews Published in the Highest Ranking Journals in
the Field of Pain. Anesth Analg. 2017;125(4):1348-1354.

CHAPTER 3
130
25. Fleming PS, Seehra J, Polychronopoulou A, Fedorowicz Z, Pandis N. A
PRISMA assessment of the reporting quality of systematic reviews in orthodontics.
Angle Orthod. 2013;83(1):158-163.
26. Nascimento DP, Costa LOP, Gonzalez GZ, Maher CG, Moseley AM. Abstracts
of low back pain trials are poorly reported, contain spin of information and are
inconsistent with the full text: An overview study. Arch Phys Med Rehabil 2019.
27. Nascimento DP, Gonzalez GZ, Araujo AC, Moseley AM, Maher CG, Costa
LOP. Abstracts of low back pain systematic reviews presented spin and inconsistencies
with the full text: a cross sectional study. J Orthop Sports Phys Ther (under review).
2018.
28. Moher D, Tetzlaff J, Tricco AC, Sampson M, Altman DG. Epidemiology and
reporting characteristics of systematic reviews. PLoS Med. 2007;4(3):e78.
29. Page MJ, Shamseer L, Altman DG, et al. Epidemiology and Reporting
Characteristics of Systematic Reviews of Biomedical Research: A Cross-Sectional
Study. PLoS Med. 2016;13(5):e1002028.
30. Almeida MO, Yamato TP, Parreira P, Costa LOP, Kamper S, Saragiotto BT.
Overall confidence in the results of systematic reviews on exercise therapy for chronic
low back pain: a cross-sectional analysis using the Assessing the Methodological
Quality of Systematic Reviews (AMSTAR) 2 tool. Braz J Phys Ther. 2019.
31. Costa LO, Moseley AM, Sherrington C, Maher CG, Herbert RD, Elkins MR.
Core journals that publish clinical trials of physical therapy interventions. Phys Ther.
2010;90(11):1631-1640.

CHAPTER 3
131
3.2. Abstracts of the systematic reviews: reporting quality, spin and
inconsistencies with the full text

CHAPTER 3
132
3.2.1. Reporting of systematic review abstracts relevant to low back
pain and inconsistencies with the full text: an overview study
Under review in: Spine 2019
Manuscript Number: 158854

CHAPTER 3
133
Reporting of systematic review abstracts relevant to low back pain and
inconsistencies with the full-text: an overview study
Dafne Port Nascimento1; Gabrielle Zoldan Gonzalez1; Amanda Costa Araujo1; Anne M
Moseley2,3; Chris G Maher2,3; Leonardo Oliveira Pena Costa1 1Masters and Doctoral Programs in Physical Therapy, Universidade Cidade de São
Paulo, São Paulo – SP, Brazil. 2The University of Sydney, Sydney – NSW, Australia. 3Institute for Musculoskeletal Health, Sydney School of Public Health, Faculty of
Medicine and Health, Sydney – NSW, Australia.
Corresponding author: Dafne Port Nascimento, Masters and Doctoral Programs in
Physical Therapy, Universidade Cidade de São Paulo. Rua Cesário Galeno 448,
Tatuapé, São Paulo, SP – Brazil, CEP 03071-000. Phone number: +55 11 994779119.
ORCID ID: https://orcid.org/0000-0002-8474-727X
Email address: [email protected]
Funding: This work was supported by a PhD scholarship from the Sao Paulo Research
Foundation (grant#2016/17853-4; Fundação de Amparo à Pesquisa do Estado de São
Paulo – FAPESP).
Conflicts of Interest: The authors declare that 15 out of the 66 reviews involved
authors from our research groups or collaborators (6 Cochrane and 8 non-Cochrane).
However, all reviews were evaluated with the same criteria and rigor.
CHAPTER 3
134
Reporting of systematic review abstracts relevant to low back pain and
inconsistencies with the full-text: an overview study
ABSTRACT
Study Design: An overview study of systematic review abstracts. Summary of
Background Data: Inadequately reported abstracts of systematic reviews may be hard
to interpret. Objectives: 1. Are systematic reviews abstracts evaluating physiotherapy
interventions for low back pain fully reported? 2. Are these abstracts reporting
inconsistent with the full text? 3. Is abstract reporting associated with certain review or
journal characteristics? Methods: In 10th January 2018 we searched the Physiotherapy
Evidence Database (PEDro) for systematic reviews for low back pain published
between 2015 and 2017. Abstracts reporting was assessed with the Preferred Reporting
Items for Systematic Reviews and Meta-Analyses for abstracts checklist (PRISMA-A).
The differences between abstracts reporting with the full text were evaluated by
comparing scores for both abstract and full text, using also the PRISMA-A. Linear
regression analyses were also performed. A MeaSurement Tool to Assess systematic
Reviews (AMSTAR-2) was used to assess methodological quality of the reviews.
Results: 66 eligible systematic reviews were included, which were subdivided into
Cochrane (n=9) and non-Cochrane (n=57) reviews. Reviews presented ‘high’ to
‘critically low’ methodological quality. The mean (SD) PRISMA-abstract score (range
0-12 points for fully reported items) was 4.1 points (1.9) for non-Cochrane review
abstracts and 9.9 points (1.1) for Cochrane abstracts. Abstract and full text scores were
statistically inconsistent (P=0.01). Higher abstract reporting quality was associated with
higher abstract word count and less overstated results in abstracts conclusion.
Conclusions: Low back pain systematic review abstracts were incompletely reported
and inconsistent with the full text. Our recommendations target mainly journal editorial
policies and authors.
CHAPTER 3
135
INTRODUCTION
Abstracts of systematic reviews are frequently used to guide clinical decision-
making of health providers1. However, if the abstract is inadequately reported, the
review may be hard to interpret2. The Preferred Reporting Items for Systematic Reviews
and Meta-Analyses for abstracts checklist2 (PRISMA-A) was created to guide better
reporting of systematic review (SR) abstracts. Despite the publication of the PRISMA-
A, the reporting quality of SR abstracts in dentistry and general medicine remains
inadequate3-5. Worse than the abstract being poorly reported, is the abstract presenting
inconsistent information with the full-text, although either way readers are not able to
reliably assess abstracts findings.
The consistency of an abstract is related to the level of agreement between the
reporting and/or interpretation of results contained in the abstract and the corresponding
full-text6,7. One survey of biomedical reviews indicated further investigation and actions
to improve reporting inconsistencies between abstracts and full-texts7. Previous research
analyzed the presence of overstated results (‘spin’) in SR abstracts in low back pain8,
but no analyses on reporting quality has been reported so far for this field.
The adequacy of reporting of SR abstracts and consistency between abstract and
full-text in the field of low back pain (LBP) have not been investigated. Our focus was
on LBP as it is the most burdensome health condition globally in terms of disability9-12.
Additionally, we focused on physiotherapy interventions because they are the most
commonly used non-pharmacological and non-surgical treatment for LBP11,13-16.
Therefore, the primary research questions of this study were: 1. Are abstracts of SRs
evaluating physiotherapy interventions for LBP fully reported? 2. Are these abstracts
reporting inconsistent with the full-text? 3. Is abstract reporting associated with certain
review or journal characteristics?
METHODS
Data Sources and Searches
This overview study of SRs evaluating physiotherapy interventions for treating
LBP is a secondary analysis of previous research8. The search was performed in the
Physiotherapy Evidence Database (PEDro; www.pedro.org.au) on 10th of January 2018.

CHAPTER 3
136
Our search strategy was: “systematic review” for method; “lumbar spine, sacroiliac
joint or pelvis” for body part; “pain” for problem; 2015 to 2017 for year of publication.
The time period was selected because is two years after the publication of the PRISMA-
A2, therefore authors had a greater opportunity to adhere to these recommendations than
in older SRs. Eligibility criteria were: full journal publications (not abstract only);
evaluated one or more physiotherapy interventions for LBP; published between 2015
and 2017, and written in English, Spanish or Portuguese.
Data Extraction
Two independent authors evaluated the methodological quality, reporting quality
of abstracts and if abstract reporting was inconsistent with the full-text reporting for the
included reviews. They also extracted several review and journal characteristics from
the reviews. Disagreements were discussed by the two authors until consensus was
reached, if consensus could not be achieved there was arbitration by a third author.
Seven review features and three features of the publishing journals were
extracted for descriptive purposes. The review features were: (1) language of
publication; (2) year of publication to calculate the age (in years) of each review by
subtracting the year of publication from 2018; (3) open access on PubMed Central; (4)
number of collaborating centers based on the number of departments mentioned in the
author affiliations; (5) risk of bias tool used; (6) number of included studies and study
designs used; and, (7) the number of times the review had been cited, which was
downloaded from the Web of Knowledge (4th September 2018), and normalized by
dividing by the age of the review. The journal features were: (1) mention of the
PRISMA-A in the editorial policies and if implementation of the PRISMA for full-texts
checklist (PRISMA-FT) was compulsory; (2) the word limit for the abstract (extracted
from the “Instructions to authors”); and, (3) open access journal, obtained from the
Directory of Open Access Journals or the journal’s website.
Methodological Quality Assessment
The second edition of the 16-item A MeaSurement Tool to Assess systematic
Reviews (AMSTAR-2)17 checklist was used to evaluate the methodological quality of
CHAPTER 3
137
the included reviews. Each item was classified as: “no”, “yes”, “partial yes” or “not
applicable”.
The classification of the methodological quality for each review was based on
the AMSTAR-2 scores17, as follows: “high” (no or one non-critical weakness),
“moderate” (more than one non-critical weakness), “low” (one critical flaw with or
without non-critical weakness), or “critically low” (more than one critical flaw with or
without non-critical weakness). Non-critical weaknesses were related to items 1, 3, 5, 6,
8, 10, 12, 14 and 16; and critical flaws to items 2, 4, 7, 9, 11, 13 and 15.
Abstracts reporting
The 12-item PRISMA-A2 was used to evaluate the reporting quality of the
abstract of each included SR. Each item was classified as “fully reported” (contained all
information specified in the item), “partially reported” (contained some of the
information specified in the item) or “not reported” (contained none of the information
specified in the item). A summary score was generated for each review (called the
“PRISMA-abstract score”) by counting the number of items that were “fully reported”.
This score ranged from 0 (low reporting quality) to 12 (high reporting quality).
Abstracts reporting compared to the full-text
The abstracts reporting were evaluated by comparing the reporting of the
abstract to the full-text of the review. To achieve this, the full-text was evaluated also
with the PRISMA-A2 to produce a “PRISMA-full-text score”, but not to evaluate the
full-text itself. We then calculated if there was any difference between the PRISMA-
abstract scores and the PRISMA-full-text scores. Additionally, we also calculated
agreement of classification of each item from the PRISMA-A between abstract and full-
text (item 1 was omitted from this analysis as it relates to the title).
Associations between abstracts reporting and review and journal characteristics
To investigate if review and journal characteristics were associated with abstract
reporting we defined one dependent variable and seven independent variables that had
been previously identified in the literature4,18,19. The dependent variable was the total

CHAPTER 3
138
PRISMA-abstract score (range 0-12 points; described above, under ‘Abstracts
reporting’). Four independent variables were categorical: continent of the first author
(categorized as dummy variables for “Asia”, “Africa”, “Europe”, “North America”,
“Oceania” and “South America”); AMSTAR-2 methodological quality score (as
dummy variables for “high”, “moderate”, “low” or “critically low” – described above,
under ‘Quality Assessment’); PRISMA-FT20 endorsed by the publishing journal and
extracted from the “Instructions to authors” for each journal or from the PRISMA’s
website21(“yes” or “no”); and structured abstract required by the publishing journal22
(“yes” or “no”). Three independent variables were continuous: number of words in the
abstract (counted using the Microsoft Word “Word Count” function), SPIN-abstract
score (calculated with the SPIN 7-item checklist23; range 0-7 points; described below),
and 2017 journal Impact Factor (IF), downloaded from the InCites Journal Citation
Reports’ website (if a journal was not listed in this website, it was coded as not having
an IF).
The literature has defined spin as “a misrepresentation of study results,
regardless of motive (intentionally or unintentionally) that overemphasizes the
beneficial effects of the intervention and overstates safety compared with that shown by
the results” [p. 224]. We used a 7-item checklist23 to detect the presence of spin in an
abstract, by comparing the interpretation reported in the abstract conclusion and title to
the abstract results: 1) recommendations not supported by the findings; 2) title claims a
beneficial effect not supported by the findings; 3) selective reporting of outcomes or
analysis; 4) conclusion claims safety based on non-statistically significant results; 5)
conclusion claims beneficial effects despite high risk of bias; 6) selective reporting of
harm outcomes; and 7) the conclusion extrapolates the review’s findings to a different
intervention. Each item was classified as “yes” (i.e., spin was present), “no” (i.e., spin
was not present) or “not reported” (i.e., the item evaluated was not reported, or could
have been omitted, intentionally or not). We calculated the “SPIN-abstract score” for
each abstract by counting the items classified as “yes” and/or “not reported”. The score
could range from 0 (low levels of spin) to 7 (high levels of spin).
Data Analysis
Data were reported for all reviews and stratified into Cochrane and non-
Cochrane reviews. We separated the data for Cochrane and non-Cochrane reviews,
CHAPTER 3
139
because a previous research indicated that Cochrane reviews of physiotherapy
interventions have better reporting and methodological quality than non-Cochrane
reviews25. The methodological quality of reviews was reported in frequencies of “high”,
“moderate”, “low” and “critically low” scores (AMSTAR-2). We used SPSS software
for all analyses.
Abstracts reporting
We calculated the percentage of review abstracts achieving each item of the
PRISMA-A, as well as mean and standard deviation (SD) PRISMA-abstract score.
Abstracts reporting compared to the full-text
Differences of abstracts reporting with the full-texts were evaluated by
comparing the PRISMA-abstract score with the PRISMA-full-text score using paired t-
tests. Differences between abstract and full-text scores were considered with P<0.05.
Kappa coefficients26 were used to calculate agreement between the abstract and full-text
for items 2-12 for the PRISMA-A (item 1 was omitted as it relates to the title), using the
following criteria: <0 “less than chance”; 0.01-0.20 “slight”; 0.21-0.40 “fair”; 0.41-0.60
“moderate”; 0.61-0.80 “substantial”; and, 0.81-0.99 “almost perfect” agreement26. An
item was considered consistent if Kappa values were 0.61 or higher (i.e., “substantial”
to “almost perfect” agreement).
Associations between abstracts reporting and review and journal characteristics
We performed linear regression analyses to evaluate the association between
reporting of the abstract and seven independent variables. We built both univariable and
multivariable regression models. We included independent variables with univariable
model reaching P<0.20 in the final multivariable model. We used backward elimination
method until all independent variables achieved P<0.05. Adjusted explained variance
(adjusted R2), Beta coefficient (ß) and its 95% CIs were calculated for each possible
variable with association. Scatter plots of the PRISMA-abstract score (dependent
variable) with each independent variable were created to asses linear relationship
between variables in order to fit our model27. Coefficient values of r ≥0.7 analyzed by

CHAPTER 3
140
bivariate correlation (multicollinearity) were not included in our linear regression
model28. We also conducted similar analysis using data from the non-Cochrane reviews.
RESULTS
Our search retrieved 7,526 reviews from the PEDro database on 10 January
2018, of which 126 fulfilled our search criteria (FIGURE 1) and 60 reviews were
excluded because they did not fulfill our eligibility criteria (APPENDIX A). Our final
sample included 66 reviews (APPENDIX B). The AMSTAR-2 scores for
methodological quality were “critically low” for 50 (75.8%) reviews, “low” for 7
(10.6%), “high” for 5 (7.6%), and “moderate” for 4 (6.1%). Cochrane reviews had
higher methodological quality than non-Cochrane reviews. Methodological quality for
Cochrane reviews ranged from “moderate” to “high”, while methodological quality for
non-Cochrane reviews ranged from “critically low” to “low”. AMSTAR-2 individual
items scores are detailed in APPENDIX C.
The 66 reviews were published in 42 journals, the journal names along with the
IF, number of included reviews published in the journal, open access policy, and
endorsement of the PRISMA-FT are presented in APPENDIX D. All included reviews
were published in English, 59.1% were open access reviews (40.9% journals were open
access) and 89.2% had structured abstracts. Most reviews were written by a multicenter
collaboration (72.7%) and were conducted in Europe (28.8%), Oceania (24.2%) and
North America (21.2%). The mean number of included studies in the reviews was 14.4
(SD 15.9), of which 12.6 (SD 14.8) were randomized controlled trials and 1.7 (SD 4.0)
used other study designs. Descriptive data for the 66 included reviews, also separated
into non-Cochrane (n=9) and Cochrane (n=57), are shown in TABLE 1.

CHAPTER 3
141
TABLE 1. Characteristics of the included reviews, for the total sample (n=66) plus separately for non-Cochrane (n=57) and Cochrane (n=9) reviews. Variables Total sample (n=66) Non-Cochrane reviews (n=57) Cochrane reviews (n=9) Mean (SD) n (%) Mean (SD) n (%) Mean (SD) n (%) Age of review (years) 2.1 (0.7) 2.1 (0.7) 2.1 (0.8)
Published in 2015 21 (31.8) 18 (31.6) 3 (33.3) Published in 2016 30 (45.5) 26 (45.6) 4 (44.4) Published in 2017 15 (22.7) 13 (22.8) 2 (22.2)
Journal IF 2017 4.0 (4.8) 3.6 (5.1) 6.8 (0.0) Journals with an IF 61 (92.4) 52 (91.2) 9 (100.0) Journals without an IF 5 (7.6) 5 (8.8) 0 (0.0)
Number of citations normalized by age 4.7 (7.8) 4.6 (8.1) 5.3 (5.8) Reviews that had been cited 61 (92.4) 53 (93.0) 9 (100.0) Reviews that had not been cited 5 (7.6) 5 (8.8) 0 (0.0)
Number of words in the abstract #259.0 [909.0] #253.0 (716.0) #747.0 (514.0) Maximum words permitted in the abstract 279.9 (79.7) 259.3 (67 (6) 400.0 (0.0)
Reviews that had to meet a word limit 61 (92.4) 52 (91.2) 9 (100.0) Reviews that did not have to meet a word limit 5 (7.6) 5 (8.8) 0 (0.0)
Reviews published in journals with abstract word limits Reviews that adhered to word limit 25 (37.9) 24 (42.1) 0 (0.0) Reviews that used less words than the limit 19 (28.8) 19 (33.3) 0 (0.0) Reviews that exceeded the limit 18 (27.3) 9 (15.8) 9 (100.0) Reviews published in journals without abstract word limits 5 (7.6) 5 (8.8) 0 (0.0)
SPIN-abstract score (0-7) 2.3 (1.8) 2.5 (1.7) 0.3 (0.7) Risk of bias tool used
Cochrane risk of bias tool 41 (62.1) 32 (56.1) 9 (100.0) Physiotherapy Evidence Database scale 7 (10.6) 7 (12.3) 0 (0.0) Downs and Black Quality Index 2 (3.0) 2 (3.5) 0 (0.0) Jadad score 2 (3.0) 2 (3.5) 0 (0.0) Other 9 (13.5) 9 (15.8) 0 (0.0) Did not use a risk of bias tool 4 (6.2) 4 (7.0) 0 (0.0)
Note: Impact Factor (IF); #Median [interquartile range].

CHAPTER 3
142
Abstracts reporting
The mean (SD) PRISMA-abstract score was 4.9 (2.7) out of 12 for all reviews,
with 4.1 (2.0) for non-Cochrane reviews and 9.9 (1.1) for Cochrane reviews. The
number and percentage of full reporting for each item of the PRISMA-A is presented in
TABLE 2. For the total sample, the items with the best reporting were the title (87.7%),
objectives (74.2%), and information sources (51.15%). The items with the lowest
reporting were eligibility criteria (3.0%), registration (19.7%), and synthesis of results
(21.2%). With the exception of the risk of bias item, abstracts of Cochrane reviews had
a higher percentage achievement of all items compared to abstracts of non-Cochrane
reviews. The item with the largest absolute percentage difference between Cochrane
and non-Cochrane reviews was registration.
Abstracts reporting compared to the full-text
The mean (SD) PRISMA-full-text score was 8.6 (2.8) out of 12. Abstracts
reporting scores were inconsistent with the full-texts scores (P=0.01). Results were
similar for both Cochrane and non-Cochrane reviews (P<0.05). Only two items of the
PRISMA-A (objectives and registration) were classified as having “substantial” to
“almost perfect” agreement between the abstract and full-text (TABLE 3).
Additionally, four of the nine Cochrane reviews were republished in other journals29-32.
The republished version of the reviews had lower methodological quality and lower
PRISMA-abstract scores than the original Cochrane versions.

CHAPTER 3
143
TABLE 2. Number and percentage of fully reported items from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for abstracts checklist (PRISMA-A) for the abstract section of the included reviews for the total sample (n=66) plus separately for non-Cochrane (n=57) and Cochrane (n=9) reviews. Data are described in n (%).
ITEM DESCRIPTION Total Sample
(n=66) Non-Cochrane
(n=57) Cochrane
(n=9)
1. Title Identify the report as a systematic review, meta-analysis, or both 57 (87.7) 48 (84.2) 9 (100.0)
2. Objectives The research question including components such as participants, interventions, comparators, and outcomes 49 (74.2) 40 (70.2) 9 (100.0)
3. Eligibility criteria Study and report characteristics used as criteria for inclusion 2 (3.0) 0 (0.0) 2 (22.2) 4. Information sources Key databases searched and search dates 34 (51.5) 25 (43.9) 9 (100.0) 5. Risk of bias Methods of assessing risk of bias 22 (33.3) 19 (33.3) 3 (33.3) 6. Included studies Number and type of included studies and participants and relevant characteristics of studies 33 (50.0) 24 (42.1) 9 (100.0)
7. Synthesis of results Results for main outcomes (benefits and harms), preferably indicating the number of studies and participants for each. If meta-analysis was done, include summary measures and confidence intervals 14 (21.2) 6 (10.5) 8 (88.9)
8. Description of the effect
Direction of the effect (i.e., which group is favored) and size of the effect in terms meaningful to clinicians and patients 22 (33.3) 16 (28.1) 6 (66.7)
9. Strengths and Limitations of evidence
Brief summary of strengths and limitations of evidence (e.g., inconsistency, imprecision, indirectness, or risk of bias, other supporting or conflicting evidence) 33 (50.0) 24 (42.1) 9 (100.0)
10. Interpretation General interpretation of the results and important implications 19 (28.8) 12 (21.1) 7 (77.8) 11. Funding Primary source of funding for the review 25 (37.9) 16 (28.1) 9 (100.0) 12. Registration Registration number and registry name 13 (19.7) 4 (7.0) 9 (100.0)

CHAPTER 3
144
TABLE 3. Abstracts reporting quality scores compared to the full-text scores (Kappa coefficient) for each item of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for abstracts checklist (PRISMA-A). N=66. Item Kappa coefficient (95% CI) 1. Title *Not applicable 2. Objectives 0.69 (0.50, 0.87) 3. Eligibility criteria 0.05 (-0.02, 0.12) 4. Information sources 0.07 (-0.02, 0.16) 5. Risk of bias 0.15 (0.04, 0.25) 6. Included studies 0.13 (-0.01, 0.27) 7. Synthesis of results 0.48 (0.29, 0.66) 8. Description of the effect 0.32 (0.16, 0.47) 9. Strengths and Limitations of evidence 0.18 (0.04, 0.32) 10. Interpretation 0.27 (0.11, 0.42) 11. Funding 0.38 (0.22, 0.53) 12. Registration 0.61 (0.42, 0.80) Note: Item 1 in the PRISMA-A was considered as ‘Not applicable’ because it is related to the title. Items shaded in grey are classified as being “consistent” (Kappa value 0.61 or higher).
Associations between abstracts reporting and review and journal characteristics
The final multivariable model explained 73.0% of the variance in reporting of
abstracts (PRISMA-abstract score), presented in TABLE 4. Higher reporting quality of
abstracts was associated with greater number of words in the abstract (ß 0.01; 95% CI
0.00, 0.01) and lower levels of spin in the abstract (ß -0.57; 95% CI -0.80, -0.35).
The multivariable model using non-Cochrane reviews only explained 46.0% of
the variance in PRISMA-abstract score. Higher journal IF (ß 0.15; 95% CI 0.07, 0.23)
and lower levels of spin in the abstract (i.e., lower SPIN-abstract score; ß -0.57; 95% CI
-0.81, -0.33) were associated with higher reporting of non-Cochrane abstracts.

CHAPTER 3
145
TABLE 4. Univariable and multivariable model of associations between review characteristics and the PRISMA-abstract score (n=66). Univariable Regression Multivariable Regression Dependent variable Adjusted R2 = 0.73
Constant = 3.29 PRISMA-abstract score 95% CI = 2.20, 4.39 Independent variables Constant ß 95% CI P ß 95% CI P Continent 4.32 *0.01
Asia -0.85 -2.68, 0.97 Africa 0.01 -1.57, 1.58 North America 0.19 -0.26, 0.64 Oceania 0.50 0.16, 0.84 South America -0.22 -1.09, 0.65 0.93 Europe (excluded variable)
Journal endorsement of PRISMA for full-texts checklist 3.96 1.56 0.26, 2.89 *0.02 0.77 Structured abstract 3.00 2.16 0.16, 4.15 *0.04 0.12 2017 Journal Impact Factor 3.86 0.28 0.15, 0.41 *0.00 0.17 Number of words in the abstract 1.17 0.01 0.00, 0.01 *0.00 0.01 0.00, 0.01 *0.00 SPIN-abstract score 7.17 -1.02 -1.30, -0.73 *0.00 -0.57 -0.80, -0.35 *0.00 Methodological quality score (AMSTAR-2) 5.71 *0.00
High 4.09 1.98, 6.20 Moderate 2.14 1.01, 3.27 0.22 Critically low -0.46 -0.82, -0.10 Low (excluded variable)
Note: PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; Univariate Regression: *Values with P<0.20; Multivariate Regression: **Values with P <0.05; CI= Confidence Interval.

CHAPTER 3
146
DISCUSSION
Our sample of SRs evaluating physiotherapy interventions for LBP exhibited
low reporting quality of abstracts plus inconsistencies with the full-text. Higher
reporting quality of abstracts was associated with a larger word count in the abstract and
lower levels of spin in the abstract for all reviews. For non-Cochrane reviews, reporting
was associated with journal IF and spin. Abstracts of Cochrane reviews had higher
reporting quality and higher methodological quality compared to non-Cochrane
reviews.
Abstracts of SRs of physiotherapy interventions for LBP exhibited similar
reporting quality of other healthcare areas3-5, with reporting being particularly poor for
the treatment effects, harms, dates of search, assessment of risk of bias, and review
registration. Our comparison of the abstracts of Cochrane and non-Cochrane reviews
are also consistent with previous studies that indicated that Cochrane reviews have
higher methodological quality25 and better reporting quality33 compared to non-
Cochrane reviews. These differences may be due to the rigorous editorial processes and
higher word limits for abstracts used in Cochrane reviews33.
Reporting quality of abstracts could be improved by changing journal editorial
policies regarding the abstracts word count, use of the PRISMA-A plus by providing
training for editors, reviewers, and authors. We strongly encourage journal editors to
increase the abstracts word count7 (possibly to 400 words) and direct more attention to
abstracts during the peer review process. Journal editors could be more flexible with
authors exceeding abstract word count once all information needed is reported. The use
of the PRISMA-A (in addition to the PRISMA checklist for full-text) by journals in the
instructions for authors, along with editors and reviewers using these reporting
checklists during the review process, and completion of training programs about
reporting checklists for journal editorial board members, should be compulsory.
Additionally, awareness of the PRISMA-A could be enhanced by adding a reference to
the abstract section of the PRISMA-FT34,35, as occurs for the CONSORT for full-text
checklist36. Finally, we advise authors to write the abstracts only after completing the
full-text in order to ensure better consistency between abstracts and corresponding full-
text.

CHAPTER 3
147
Study limitations
The major strengths of our study were the tools used to evaluate reporting and
methodological quality, which have been created by well-known and highly respected
methodological research groups2,17. On the other hand, our findings may only apply to
SRs evaluating physiotherapy interventions for LBP and may not be generalized to
abstracts of SRs in general.
CONCLUSION
Abstracts of SRs evaluating physiotherapy interventions for LBP are
incompletely reported and inconsistent with the full-text. Our recommendations are
targeted to journal editorial policies (including increasing the word count in abstracts,
compulsory use of the PRISMA-A, and compulsory provision of training programs for
editors and reviewers). For authors we suggest writing the abstract after the full-text has
been completed, in order to ensure better reporting and consistency between abstracts
and corresponding full-texts.

CHAPTER 3
148
REFERENCES
1. Herbert R, Jamtvedt G, Mead J, Hagen KB. Practical evidence-based
physiotherapy. 2nd Edition ed: Elsevier Butterworth-Heinemann; 2011.
2. Beller EM, Glasziou PP, Altman DG, et al. PRISMA for abstracts: reporting
systematic reviews in journal and conference abstracts. PLoS Med.
2013;10(4):e1001419.
3. Hopewell S, Boutron I, Altman DG, Ravaud P. Deficiencies in the publication
and reporting of the results of systematic reviews presented at scientific medical
conferences. J Clin Epidemiol. 2015;68(12):1488-1495.
4. Kiriakou J, Pandis N, Fleming PS, Madianos P, Polychronopoulou A. Reporting
quality of systematic review abstracts in leading oral implantology journals. J Dent.
2013;41(12):1181-1187.
5. Seehra J, Fleming PS, Polychronopoulou A, Pandis N. Reporting completeness
of abstracts of systematic reviews published in leading dental specialty journals. Eur J
Oral Sci. 2013;121(2):57-62.
6. Assem Y, Adie S, Tang J, Harris IA. The over-representation of significant p
values in abstracts compared to corresponding full texts: a systematic review of surgical
randomized trials. Contemp Clin Trials Commun. 2017;7:194-199.
7. Li G, Abbade LPF, Nwosu I, et al. A scoping review of comparisons between
abstracts and full reports in primary biomedical research. BMC Med Res Methodol.
2017;17(1):181.
8. Nascimento DP, Gonzalez GZ, Araujo AC, Moseley AM, Maher CG, Costa
LOP. Abstracts of low back pain systematic reviews presented spin and inconsistencies
with the full text: a cross sectional study. J Orthop Sports Phys Ther (under review).
2018.
9. GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global,
regional, and national incidence, prevalence, and years lived with disability for 328
diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global
Burden of Disease Study 2016. Lancet. 2017;390(10100):1211-1259.
10. Ferreira G, Costa LM, Stein A, Hartvigsen J, Buchbinder R, Maher CG.
Tackling low back pain in Brazil: a wake-up call. Braz J Phys Ther. 2018.
11. Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why
we need to pay attention. Lancet. 2018;391(10137):2356-2367.
CHAPTER 3
149
12. Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet.
2017;389(10070):736-747.
13. Bardin LD, King P, Maher CG. Diagnostic triage for low back pain: a practical
approach for primary care. Med J Aust. 2017;206(6):268-273.
14. Beattie PF, Silfies SP, Jordon M. The evolving role of physical therapists in the
long-term management of chronic low back pain: longitudinal care using assisted self-
management strategies. Braz J Phys Ther. 2016;20(6):580-591.
15. Bernstein IA, Malik Q, Carville S, Ward S. Low back pain and sciatica:
summary of NICE guidance. BMJ. 2017;356:i6748.
16. Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back
pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368-
2383.
17. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for
systematic reviews that include randomised or non-randomised studies of healthcare
interventions, or both. BMJ. 2017;358:j4008.
18. Rice DB, Kloda LA, Shrier I, Thombs BD. Reporting quality in abstracts of
meta-analyses of depression screening tool accuracy: a review of systematic reviews
and meta-analyses. BMJ Open. 2016;6(11):e012867.
19. Song SY, Kim B, Kim I, et al. Assessing reporting quality of randomized
controlled trial abstracts in psychiatry: Adherence to CONSORT for abstracts: A
systematic review. PLoS One. 2017;12(11):e0187807.
20. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting
systematic reviews and meta-analyses of studies that evaluate healthcare interventions:
explanation and elaboration. BMJ. 2009;339:b2700.
21. PRISMA Endorsers. Preferred Reporting Items for Systematic Reviews and
Meta-Analyses. PRISMA Endorsers. 2015; http://www.prisma-
statement.org/Endorsement/PRISMAEndorsers.aspx. Accessed 5th November 2018.
22. Nakayama T, Hirai N, Yamazaki S, Naito M. Adoption of structured abstracts
by general medical journals and format for a structured abstract. J Med Libr Assoc.
2005;93(2):237-242.
23. Yavchitz A, Ravaud P, Altman DG, et al. A new classification of spin in
systematic reviews and meta-analyses was developed and ranked according to the
severity. J Clin Epidemiol. 2016;75:56-65.

CHAPTER 3
150
24. Haneef R, Yavchitz A, Ravaud P, et al. Interpretation of health news items
reported with or without spin: protocol for a prospective meta-analysis of 16
randomised controlled trials. BMJ Open. 2017;7(11):e017425.
25. Moseley AM, Elkins MR, Herbert RD, Maher CG, Sherrington C. Cochrane
reviews used more rigorous methods than non-Cochrane reviews: survey of systematic
reviews in physiotherapy. J Clin Epidemiol. 2009;62(10):1021-1030.
26. Viera AJ, Garrett JM. Understanding interobserver agreement: the Kappa
statistic. Fam Med. 2005;37(5):360-363.
27. Zhou Z, Ku HC, Xing G, Xing C. Decomposing Pearson's Chi2 test: a linear
regression and its departure from linearity. Ann Hum Genet. 2018.
28. Prunier JG, Colyn M, Legendre X, Nimon KF, Flamand MC. Multicollinearity
in spatial genetics: separating the wheat from the chaff using commonality analyses.
Mol Ecol. 2015;24(2):263-283.
29. Franke H, Fryer G, Ostelo RW, Kamper SJ. Muscle energy technique for non-
specific low-back pain. Cochrane Database Syst Rev. 2015(2):CD009852.
30. Saragiotto BT, Maher CG, Yamato TP, et al. Motor Control Exercise for
Nonspecific Low Back Pain: A Cochrane Review. Spine (Phila Pa 1976).
2016;41(16):1284-1295.
31. Yamato TP, Maher CG, Saragiotto BT, et al. Pilates for low back pain: complete
republication of a Cochrane review. Spine (Phila Pa 1976). 2016;41(12):1013-1021.
32. Zaina F, Tomkins-Lane C, Carragee E, Negrini S. Surgical Versus Nonsurgical
Treatment for Lumbar Spinal Stenosis. Spine (Phila Pa 1976). 2016;41(14):E857-868.
33. Page MJ, Shamseer L, Altman DG, et al. Epidemiology and Reporting
Characteristics of Systematic Reviews of Biomedical Research: A Cross-Sectional
Study. PLoS Med. 2016;13(5):e1002028.
34. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items
for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg.
2010;8(5):336-341.
35. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items
for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med.
2009;6(7):e1000097.
36. Schulz KF, Altman DG, Moher D, Group C. CONSORT 2010 statement:
updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332.

CHAPTER 3
151
APPENDIX D. Characteristics of the 42 journals publishing the included systematic reviews (n=66).
Journal Impact
factor 2017 n (%) Journal open
access PRISMA for
full-text PRISMA
for abstracts PRISMA
compulsory Acupuncture in Medicine 2.3 1 (1.5) No Yes No Yes American Journal of Emergency Medicine 1.3 1 (1.5) No No No No American Journal of Physical Medicine & Rehabilitation 1.8 2 (3.0) No Yes No Yes Annals of Internal Medicine 19.4 1 (1.5) No Yes No Yes Applied Health Economics and Health Policy 1.9 1 (1.5) No Yes No Yes Archives of Physical Medicine and Rehabilitation 3.1 1 (1.5) Yes Yes No Yes BMC Musculoskeletal Disorders 2.0 1 (1.5) Yes No No No BMJ 23.3 1 (1.5) No Yes Yes Yes Clinical Rehabilitation 2.9 2 (3.0) No Yes No Yes Clinical Rheumatology 2.1 1 (1.5) No No No No Clinical Spine Surgery 2.0 1 (1.5) No Yes No Yes Cochrane Database of Systematic Reviews 6.8 9 (13.6) Yes Yes Yes Yes Complementary Therapies in Clinical Practice 1.7 1 (1.5) No No No No Disability and Rehabilitation 2.0 1 (1.5) No No No No European Journal of Integrative Medicine 0.7 1 (1.5) No No No No European Journal of Pain 3.0 1 (1.5) Yes Yes No Yes European Spine Journal 2.6 1 (1.5) No No No No Evidence-Based Complementary and Alternative Medicine 2.1 3 (4.5) Yes No No No Healthcare Not reported 1 (1.5) Yes Yes No Yes International Journal of Osteopathic Medicine 0.7 1 (1.5) Yes Yes No Yes International Journal of Therapy and Rehabilitation 0.4 1 (1.5) No No No No Iranian Red Crescent Medical Journal 0.8 1 (1.5) Yes No No No JAMA Internal Medicine 20.0 2 (3.0) No Yes Yes Yes Journal of Back and Musculoskeletal Rehabilitation 1.0 2 (3.0) No No No No Journal of Bodywork and Movement Therapies 0.0 1 (1.5) No No No No Journal of Chiropractic Medicine Not reported 1 (1.5) Yes Yes Yes Yes Journal of Evidence-Based Complementary & Alternative Medicine 2.1 1 (1.5) Yes Yes No Yes Journal of Medical Internet Research 4.7 1 (1.5) No Yes No Yes Journal of Neurosurgery Spine 2.8 1 (1.5) No No No No Journal of Physical Therapy Science 0.4 2 (3.0) Yes No No No Medicine 2.0 1 (1.5) No Yes Yes Yes Nursing Research and Practice Not reported 1 (1.5) Yes No No No Occupational Medicine 1.5 1 (1.5) No Yes No Yes Pain 5.5 1 (1.5) No Yes No Yes Pain Medicine 2.8 1 (1.5) No No No No Physical Therapy in Sport 1.9 1 (1.5) No No No No Physical Therapy Reviews Not reported 1 (1.5) No Yes No Yes Physiotherapy 3.1 3 (4.5) No Yes Yes Yes PLoS ONE 2.8 3 (4.5) Yes Yes No Yes PM&R 1.9 2 (3.0) No Yes No Yes Scientifica Not reported 1 (1.5) Yes No No No Spine 2.8 5 (7.6) No No No No

CHAPTER 3
152
3.2.2. Abstracts of low back pain systematic reviews presented spin and
inconsistencies with the full text: an overview study
Accepted for publication in: Journal of Orthopaedic & Sports Physical Therapy 2019
Manuscript Number: 12-18-8962-LR.R2

CHAPTER 3
153
Abstracts of low back pain systematic reviews presented spin and inconsistencies
with the full text: an overview study
Dafne Port Nascimento1, Gabrielle Zoldan Gonzalez1, Amanda Costa Araujo1, Anne M
Moseley2,3, Chris G Maher2,3, Leonardo Oliveira Pena Costa1 1Masters and Doctoral Programs in Physical Therapy, Universidade Cidade de São
Paulo, São Paulo – SP, Brazil. 2Faculty of Medicine and Health, Sydney School of Public Health, The University of
Sydney, Sydney – NSW, Australia. 3Institute for Musculoskeletal Health, Sydney – NSW, Australia.
Corresponding author: Dafne Port Nascimento, Masters and Doctoral Programs in
Physical Therapy, Universidade Cidade de São Paulo. Rua Cesário Galeno 448,
Tatuapé, São Paulo, SP – Brazil, CEP 03071-000. Phone number: +55 11 994779119.
ORCID ID: https://orcid.org/0000-0002-8474-727X
Email address: [email protected]
Funding: This work was supported by a PhD scholarship from the Sao Paulo Research
Foundation (grant#2016/17853-4; Fundação de Amparo à Pesquisa do Estado de São
Paulo – FAPESP).
Conflicts of Interest: The authors declare that 15 out of the 66 reviews involved
authors from our research groups or collaborators (6 Cochrane and 8 non-Cochrane).
However, all reviews were evaluated with the same criteria and rigor.

CHAPTER 3
154
Abstracts of low back pain systematic reviews presented spin and inconsistencies
with the full text: an overview study
ABSTRACT
Study Design: Overview study. Background: Abstracts of systematic reviews have
presented ‘spin’ (i.e. overstated interpretation of study results) and inconsistency with
the full text. Objectives: 1. Do abstracts of low back pain reviews contain spin? 2. Do
these abstracts consistently represent the full text? 3. Is abstract spin associated with the
type of conclusion? Methods: Data was extracted from systematic reviews of
physiotherapy interventions for low back pain, published between 2015 and 2017. The
search was performed on the Physiotherapy Evidence Database (PEDro) in 10th January
2018. Spin was assessed using a SPIN 7-item spin checklist. Consistency was evaluated
by comparing information contained in the abstract and the full text using the SPIN 7-
item checklist with Kappa coefficient analysis. Logistic regression analysis was
performed to evaluate the association between spin in the abstract and type of
conclusion. The methodological quality of the reviews was evaluated using the
AMSTAR-2 (A MeaSurement Tool to Assess systematic Reviews). Results: We
included 66 eligible systematic reviews, subdivided into Cochrane (n=9) and non-
Cochrane (n=57) reviews. Some form of spin was observed in 80.3% of abstracts.
Abstracts of non-Cochrane reviews were not consistent with the full text (fair to
moderate agreement), while Cochrane review abstracts presented substantial to almost
perfect agreement with the full texts. Spin was not associated with the type of
conclusion (P < 0.05). The methodological quality ranged from ‘high’ to ‘critically
low’. Conclusions: The abstracts of systematic reviews evaluating physiotherapy
interventions for low back pain need some improvement. We advise readers to read the
full text when using systematic reviews to guide practice. Journal editors and reviewers
should follow and check reporting checklists, and also ensure that abstracts are free of
spin. We also suggest that authors write the abstract only when the manuscript is
completed, paying due attention to consistency and removal of spin.

CHAPTER 3
155
INTRODUCTION
Systematic reviews are widely read by healthcare professionals to guide clinical
decision-making1. However, if the systematic review abstract presents selective
reporting or ‘spin’ of results2, it can mislead the reader’s interpretation of the abstract
conclusions3-5. In addition to that, sometimes the abstract is the only available source of
information to readers, who cannot refer to the full text searching for detailed study
results6.
Spin is defined as “a misrepresentation of study results, regardless of motive
(intentionally or unintentionally) that overemphasizes the beneficial effects of the
intervention and overstates safety compared with that shown by the results” [p. 27].
Examples of spin of systematic reviews include8: the title, recommendations, or
conclusions claim a beneficial effect of the intervention that is not supported by the
findings; selective reporting of outcomes favoring the beneficial effect of the
intervention and downplaying of harms; and extrapolation of the review’s findings to a
different intervention. The consistency of an abstract can be measured by the percentage
of agreement or categorized rating (high/medium/low inconsistency) between the
reporting and/or interpretation of results contained in the abstract and the corresponding
full text6,9. A scoping review of biomedical reviews indicated that there was a low level
of consistency of reporting between the abstract and full text6 and further investigation
and action are urgently needed. Furthermore, to evaluate abstracts inconsistency with
the full text in terms of spin may be rather subjective, once spin could be happening
simultaneously in both the abstract and full text6.
There is a lack of summary showing spin in abstracts of systematic reviews10
and consistency with their respective full text6. We focused our work based on a sample
of low back pain (LBP) systematic reviews, as it is the most burdensome health
condition globally in terms of disability, major musculoskeletal condition and
enormously prevalence11-13. We focused on physiotherapy interventions because it is the
most commonly used non-pharmacological and non-surgical treatment for LBP13-17.
Therefore, the primary questions of this study were: 1. Do abstracts of low back pain
reviews contain spin? 2. Do these abstracts consistently represent the full text? 3. Is
abstract spin associated with the type of conclusion (positive, negative, neutral or
indeterminate)?

CHAPTER 3
156
METHODS
Data Sources and Searches
This is an overview study of abstracts of 66 systematic reviews. The eligibility
criteria for the reviews were: full publications (not abstract only); evaluate
physiotherapy interventions for the treatment of LBP; published in 2015 to 2017,
inclusive; and written in English, Spanish or Portuguese. The search for reviews was
performed on the Physiotherapy Evidence Database (PEDro; www.pedro.org.au) on 10th
of January 2018, using the following search strategy: “systematic review” for method;
“lumbar spine, sacroiliac joint or pelvis” for body part; “pain” for problem; 2015 to
2017 for year of publication. The time period was chosen because the PRISMA for
abstracts checklist5 had been published two years before, so authors had a greater
chance to better report their abstracts than in systematic reviews published before that
time period. The search was performed on PEDro because it is one of the most
comprehensive indexes of published systematic reviews in physiotherapy18.
Data Extraction and Quality Assessment
Two independent authors evaluated the methodological quality, spin of
information in the abstract, and consistency of the abstract compared to full text, plus
evaluated the type of conclusion for each of the included systematic reviews. Any
disagreements were resolved by a consensus discussion or, if necessary, arbitration by a
third author. Raters were both physiotherapists, with at least 8 years of experience in
research methods. In 2016 both authors completed a training program in appraising
articles19 and both attended lectures in advanced methodology in research at the
university during their masters and PhDs.
The second edition of the 16-item A MeaSurement Tool to Assess systematic
Reviews (AMSTAR-2)20 checklist was used, which has established validity and
reliability21. The 16 items are: 1) inclusion of the components of PICO (Participants,
Interventions, Comparisons and Outcomes) in the research question; 2) review methods
established prior to the conduct of the review; 3) selection of the study designs; 4)
literature search strategy; 5) duplicate study selection; 6) duplicate study data
extraction; 7) list of excluded studies; 8) characteristics of included studies; 9) risk of

CHAPTER 3
157
bias assessment; 10) report on the sources of funding for included studies; 11) methods
to combine data; 12) impact of risk of bias in individual studies on meta-analysis
results; 13) impact of risk of bias in individual studies when interpreting the results; 14)
discussion about the heterogeneity; 15) publication bias; and 16) conflicts of interest
and funding stated. Each item was classified as: “yes”, “partial yes”, “no” or “not
applicable”.
The methodological quality of each review was defined as: “high” (no
weaknesses or one non-critical weakness), “moderate” (more than one non-critical
weakness), “low” (one critical flaw with or without non-critical weakness), or “critically
low” (more than one critical flaw with or without non-critical weakness) based on the
AMSTAR-2 scores20. The non-critical weakness items are 1, 3, 5, 6, 8, 10, 12, 14 and
16. The critical flaws are related to items 2, 4, 7, 9, 11, 13 and 15.
Data Synthesis
1) Spin of information in the abstracts
We used a SPIN 7-item checklist. These seven items were selected by Yavchitz
et al8 using a consensus process of qualitative and quantitative methods among
members of the Cochrane Collaboration, as the most severe types of spin, out of 21
types that could happen in systematic review abstracts8. The SPIN 7-item checklist was
used in our study to evaluate the presence of spin of information in an abstract by
comparing the abstract results to the abstract conclusion. The abstract was assessed in
isolation because readers should be able to interpret the review based on the results
section of the abstract. The seven items are [p. 4, item 3.2.28]: “1) the conclusion
formulates recommendations for clinical practice not supported by the findings; 2) the
title claims or suggests a beneficial effect of the experimental intervention not supported
by the findings; 3) selective reporting of or overemphasis on efficacy outcomes or
analysis favoring the beneficial effect of the experimental intervention; 4) the
conclusion claims safety based on non-statistically significant results with a wide
confidence interval; 5) the conclusion claims a beneficial effect of the experimental
treatment despite high risk of bias in primary studies; 6) selective reporting of or
overemphasis on harm outcomes or analysis favoring the safety of the experimental
intervention; and 7) the conclusion extrapolates the review’s findings to a different
CHAPTER 3
158
intervention (i.e., claiming efficacy of one specific intervention although the review
covers a class of several interventions)”. Each item was classified as “yes” (i.e., spin
was clearly present or information was omitted or not reported) or “no” (i.e., spin was
not present). We calculated the percentage of each item presenting spin for all abstracts.
We measured the reliability between the two independent authors evaluating
spin of information in the abstracts and full texts, before consensus was performed.
2) Abstracts consistencies with the full text
The consistency of the abstract was evaluated by comparing the abstract to the
full text of the review, by evaluating differences between each individual item. The
abstract and full text were evaluated independently, using the SPIN 7-item checklist8.
Note that we also used the SPIN 7-item checklist to evaluate the presence of spin of
information in the full texts, however it was not our intention to analyze spin of
information in the full texts themselves. Each individual item of the SPIN 7-item
checklist was compared between abstract and full text in order to measure consistency
for each item individually. Item 2 of the SPIN 7-item checklist was omitted from this
analysis as it relates to the title.
3) Association of abstracts spin with the type of conclusion
To investigate if conclusions made were associated with the presence of spin, we
built logistic regression models using the presence of spin in the abstract (dichotomous
variable, categorized as yes or no) as the dependent variable and two independent
variables: type of conclusions in the abstract (categorized as dummy variables in
“positive”, “neutral”, “negative”, or “indeterminate”) and type of conclusion in the full
text (categorized in the same dummy variables that were used for the abstract). We
classified the type of conclusion for both the abstract and the full text. A “positive”
conclusion was defined when the author stated that there was evidence of effectiveness;
“neutral” when stated no evidence of effectiveness or reported no opinion; “negative”
when authors advised against the use of the intervention or it was not recommended; or
“indeterminate” when authors stated that there was insufficient evidence or that more
research is required22.

CHAPTER 3
159
Data Analysis
Frequencies of “high”, “moderate”, “low” and “critically low” scores were
reported for the AMSTAR-2. All data are reported for all reviews plus for Cochrane and
non-Cochrane reviews separately. SPSS software was used for all analyses.
Spin of information in the abstract and abstracts consistencies with the full text
The percentage of abstracts of included reviews achieving each item of the SPIN
7-item checklist (spin of information) was tabulated. In order to evaluate reliability
between the two independent authors, we used Kappa coefficients23,24. The following
criteria were used for interpreting the Kappa scores: <0 “less than chance”; 0.01-20
“slight”; 0.21-0.40 “fair”; 0.41-0.60 “moderate”; 0.61-0.80 “substantial”; and, 0.81-0.99
“almost perfect” agreement23,24.
In order to investigate abstract consistency, we used Kappa coefficients23,24 to
calculate the agreement between the abstract and full text for items 1 and 3-7 for the
SPIN 7-item checklist (item 2 is related to the title). We considered an item to be
consistent if the Kappa values were 0.61 or higher (i.e., “substantial” to “almost perfect”
agreement).
Association of spin of information with the type of conclusion
We built logistic regression models to evaluate the association between the
presence of spin in the abstract with the type of conclusion in the abstract and the full
text (two independent variables). We considered association between variables if the
independent variable reached P value < 0.05. We reported odds ratios (OR) with 95%
confidence intervals (CIs).
We also performed secondary analyses with data from the Cochrane and non-
Cochrane reviews separately, as non-Cochrane reviews are twice as likely to have
positive conclusions compared to Cochrane reviews22, plus Cochrane reviews of
physiotherapy have higher reporting and methodological quality25.

CHAPTER 3
160
RESULTS
From the 7,526 reviews indexed in the PEDro database on 10 January 2018, 126
fulfilled our search criteria. Sixty reviews were excluded (see APPENDIX A). Our
final sample of reviews (n=66) is listed in APPENDIX B.
The AMSTAR-2 quality rating was “critically low” for 50 (75.8%) reviews,
“low” for seven (10.6%), “high” for five (7.6%), and “moderate” for four (6.1%).
Cochrane reviews had higher quality ratings than non-Cochrane reviews. The quality
ratings for Cochrane reviews ranged from “moderate” to “high”, while the quality
ratings for non-Cochrane reviews ranged from “critically low” to “low”. Achievement
of AMSTAR-2 individual items are detailed in APPENDIX C.
All included reviews were published in English. The type of conclusion of the
66 reviews, collectively and separated into non-Cochrane (n=9) and Cochrane (n=57),
are shown in TABLE 1.
TABLE 1. Type of conclusion of the included reviews, for the total sample (n=66) plus separately for non-Cochrane (n=57) and Cochrane (n=9) reviews. Variables Total sample (n=66) Non-Cochrane
reviews (n=57) Cochrane
reviews (n=9) n (%) n (%) n (%) Conclusions in the abstract
Positive conclusions 25 (37.9) 24 (42.1) 1 (11.1) Neutral conclusions 4 (6.1) 4 (7.0) 0 (0.0) Negative conclusions 2 (3.0) 2 (3.5) 0 (0.0) Indeterminate conclusions 35 (53.0) 27 (47.4) 8 (88.9)
Conclusions in the full text Positive conclusions 21 (31.8) 20 (35.1) 1 (11.1) Neutral conclusions 4 (6.1) 4 (7.0) 0 (0.0) Negative conclusions 1 (1.5) 1 (1.8) 0 (0.0) Indeterminate conclusions 40 (60.6) 32 (56.1) 8 (88.9)
1) Spin of information in the abstracts
The number and percentage of reviews with each item of the SPIN 7-item
checklist for the abstract is presented in TABLE 2. Some form of spin was observed in
80.3% of abstracts. Selective reporting of harm outcomes of the experimental
intervention is the most common type of spin, presented in 72.7% of abstracts. 19.7% of
reviews had abstracts that were free of spin (6/57 non-Cochrane reviews and 7/9
Cochrane reviews). Our findings also suggest that the abstracts of Cochrane reviews
present less spin of information when compared to the abstracts of non-Cochrane

CHAPTER 3
161
reviews. Reliability between the two independent authors ranged from slight (Kappa =
0.09) to almost perfect agreement (Kappa = 1.0), with mean Kappa of 0.55 (detailed in
APPENDIX D).
TABLE 2. Number and percentages of reviews achieving each item of spin checklist in the abstract section for the total sample (n=66) plus separately for non-Cochrane (n=57) and Cochrane (n=9) reviews, data are n (%).
ITEM DESCRIPTION Total Sample (n=66)
Non-Cochrane (n=57)
Cochrane (n=9)
1. Recommendation Recommendation for clinical practice not supported by the findings
16 (24.2) 15 (26.3) 1 (11.1)
2. Title claims a beneficial effect not supported by the findings
The title claims a beneficial effect of the experimental treatment not supported by the findings
0 (0.0) 0 (0.0) 0 (0.0)
3. Selective reporting of outcomes
Selective reporting of outcomes favoring the beneficial effect of the experimental intervention
21 (31.8) 19 (33.3) 2 (22.2)
4. Safety based on non-statistically significant results
The conclusion claims safety based on non-statistically significant results
26 (39.4) 26 (45.6) 0 (0.0)
5. Beneficial effect despite high risk of bias
The conclusion claims the beneficial effect of the experimental treatment despite high risk of bias in primary studies
32 (48.5) 32 (56.2) 0 (0.0)
6. Selective reporting of harm outcomes
Selective reporting of harm outcomes of the experimental intervention
48 (72.7) 48 (84.3) 0 (0.0)
7. Conclusion extrapolates findings to a different intervention
The conclusion extrapolates the review’s findings to a different intervention
5 (7.6) 5 (8.8) 0 (0.0)
2) Abstracts consistencies with the full text
Only one item of the SPIN 7-item checklist (safety based on non-statistically
significant results) presented “substantial” to “almost perfect” agreement between the
abstract and full text for all the 66 abstracts, while all the other items presented fair to
moderate agreement. However, the consistency between abstracts and full texts of
Cochrane reviews were much better than non-Cochrane reviews (TABLE 3).
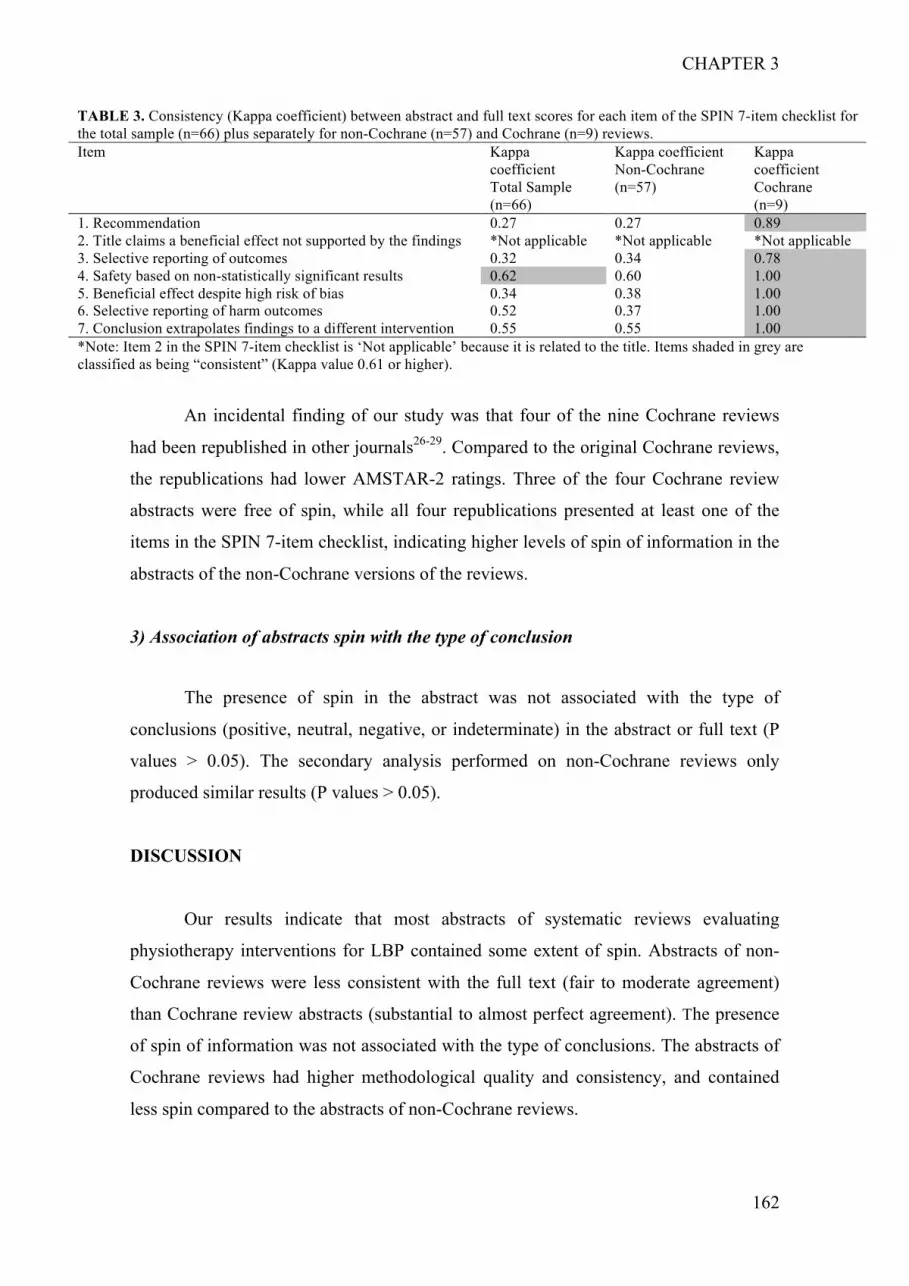
CHAPTER 3
162
TABLE 3. Consistency (Kappa coefficient) between abstract and full text scores for each item of the SPIN 7-item checklist for the total sample (n=66) plus separately for non-Cochrane (n=57) and Cochrane (n=9) reviews. Item Kappa
coefficient Total Sample (n=66)
Kappa coefficient Non-Cochrane (n=57)
Kappa coefficient Cochrane (n=9)
1. Recommendation 0.27 0.27 0.89 2. Title claims a beneficial effect not supported by the findings *Not applicable *Not applicable *Not applicable 3. Selective reporting of outcomes 0.32 0.34 0.78 4. Safety based on non-statistically significant results 0.62 0.60 1.00 5. Beneficial effect despite high risk of bias 0.34 0.38 1.00 6. Selective reporting of harm outcomes 0.52 0.37 1.00 7. Conclusion extrapolates findings to a different intervention 0.55 0.55 1.00 *Note: Item 2 in the SPIN 7-item checklist is ‘Not applicable’ because it is related to the title. Items shaded in grey are classified as being “consistent” (Kappa value 0.61 or higher).
An incidental finding of our study was that four of the nine Cochrane reviews
had been republished in other journals26-29. Compared to the original Cochrane reviews,
the republications had lower AMSTAR-2 ratings. Three of the four Cochrane review
abstracts were free of spin, while all four republications presented at least one of the
items in the SPIN 7-item checklist, indicating higher levels of spin of information in the
abstracts of the non-Cochrane versions of the reviews.
3) Association of abstracts spin with the type of conclusion
The presence of spin in the abstract was not associated with the type of
conclusions (positive, neutral, negative, or indeterminate) in the abstract or full text (P
values > 0.05). The secondary analysis performed on non-Cochrane reviews only
produced similar results (P values > 0.05).
DISCUSSION
Our results indicate that most abstracts of systematic reviews evaluating
physiotherapy interventions for LBP contained some extent of spin. Abstracts of non-
Cochrane reviews were less consistent with the full text (fair to moderate agreement)
than Cochrane review abstracts (substantial to almost perfect agreement). The presence
of spin of information was not associated with the type of conclusions. The abstracts of
Cochrane reviews had higher methodological quality and consistency, and contained
less spin compared to the abstracts of non-Cochrane reviews.
CHAPTER 3
163
The abstracts of systematic reviews of physiotherapy interventions for LBP
exhibit similar deficiencies to other areas of healthcare30-32. Our comparison of the
abstracts of Cochrane and non-Cochrane reviews are consistent with previous studies
that compared full reviews, indicating that Cochrane reviews have higher
methodological quality25 and contain less spin of information22,25. This difference might
be explained by the rigorous editorial processes, higher word limits for better reporting
of results, use of appendices, and inclusion of fewer study designs (randomized
controlled trials only in Cochrane reviews)33. Also two of the most frequent items found
in the present study are among the three least severe types of spin, in comparison to data
reported in the Yavchitz et al findings8. That might soften up the severity of spin
presented in the results of physiotherapy interventions for low back pain.
Editors and reviewers should emphasize the use of reporting checklists for
abstracts (such as the Preferred Reporting Items for Systematic Reviews and Meta-
Analyses – PRISMA – for abstracts checklist5), in order to guide the review process.
Authors could be encouraged to write the abstract after completing the review and to
ensure the results are consistent and free from spin of information. Future research
could test the impact of these suggestions comparing different editorial processes. Our
suggestions are in accordance with a recent scoping review6, which highly
recommended authors, reviewers and editorial staff to strictly inspect the consistency of
abstracts in the submission process, flexibility on word counts and guidance on the use
of checklists for abstracts.
To strengthen the quality of our study we used robust methods in our data
collection, including double data extraction using contemporary methodological
evaluation and exploring recent concerns in literature regarding spin of information2,8
and the consistency of abstracts6. Some limitations of our study are that, despite
similarities with other areas of healthcare2,6,8,9,30,31, the results may not be generalizable
to other systematic review abstracts other than physiotherapy interventions for low back
pain in recent years. Also, our findings are based upon seven items that aimed to
measure the most severe types of spin. Although these items have good face validity,
the instrument itself was not fully tested for its measurement properties. Therefore some
caution on our results is needed. Future research should investigate the validity and
reliability of instruments evaluating spin of results and conclusions, as our reliability
results add to previous research on the subjectivity of evaluating spin. Note that our
results add to the findings of Yavchitz et al8, where the seven items were ranked

CHAPTER 3
164
according to perceived severity, which makes more data available to support the validity
of the items. Our research group is currently addressing this limitation somehow, by
evaluating the concerns brought by literature regarding abstracts of both systematic
reviews and randomized controlled trial across a broad spectrum of healthcare areas34.
CONCLUSION
The abstracts of systematic reviews evaluating physiotherapy interventions for
LBP need some improvement. Most of abstracts presented spin of information and do
not consistently represent the full text, although spin was not associated with the type of
conclusion. We advise readers to read beyond the abstract when using systematic
reviews to guide practice. Some solutions proposed are relevant to journal editors and
reviewers, which includes following and checking both the full text and abstracts
reporting checklists, and also ensuring that abstracts are free of spin of information. We
suggest that authors write the abstract only when the manuscript is completed, paying
due attention to consistency and removal of spin. Finally, abstracts must be a reliable
summary of the systematic review for time-poor clinicians.

CHAPTER 3
165
REFERENCES
1. Herbert R, Jamtvedt G, Mead J, Hagen KB. Practical evidence-based
physiotherapy. 2nd Edition ed: Elsevier Butterworth-Heinemann; 2011.
2. Chiu K, Grundy Q, Bero L. 'Spin' in published biomedical literature: A
methodological systematic review. PLoS Biol. 2017;15(9):e2002173.
3. Costa LO, Maher CG, Lopes AD, de Noronha MA, Costa LC. Transparent
reporting of studies relevant to physical therapy practice. Rev Bras Fisioter.
2011;15(4):267-271.
4. Nascimento DP, Costa LOP, Gonzalez GZ, Maher CG, Moseley AM. Abstracts
of low back pain trials are poorly reported, inaccurate and contain spin of information:
A methodological review Arch Phys Med Rehabil (under review). 2018.
5. Beller EM, Glasziou PP, Altman DG, et al. PRISMA for Abstracts: reporting
systematic reviews in journal and conference abstracts. PLoS Med.
2013;10(4):e1001419.
6. Li G, Abbade LPF, Nwosu I, et al. A scoping review of comparisons between
abstracts and full reports in primary biomedical research. BMC Med Res Methodol.
2017;17(1):181.
7. Haneef R, Yavchitz A, Ravaud P, et al. Interpretation of health news items
reported with or without spin: protocol for a prospective meta-analysis of 16
randomised controlled trials. BMJ Open. 2017;7(11):e017425.
8. Yavchitz A, Ravaud P, Altman DG, et al. A new classification of spin in
systematic reviews and meta-analyses was developed and ranked according to the
severity. J Clin Epidemiol. 2016;75:56-65.
9. Assem Y, Adie S, Tang J, Harris IA. The over-representation of significant p
values in abstracts compared to corresponding full texts: a systematic review of surgical
randomized trials. Contemp Clin Trials Commun. 2017;7:194-199.
10. Boutron I, Dutton S, Ravaud P, Altman DG. Reporting and interpretation of
randomized controlled trials with statistically nonsignificant results for primary
outcomes. JAMA. 2010;303(20):2058-2064.
11. DALYs GBD, Collaborators H. Global, regional, and national disability-
adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy
(HALE), 1990-2015: a systematic analysis for the Global Burden of Disease Study
2015. Lancet. 2016;388(10053):1603-1658.

CHAPTER 3
166
12. Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet.
2017;389(10070):736-747.
13. Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why
we need to pay attention. Series. Low back pain 1. Lancet. 2018.
14. Bardin LD, King P, Maher CG. Diagnostic triage for low back pain: a practical
approach for primary care. Med J Aust. 2017;206(6):268-273.
15. Beattie PF, Silfies SP, Jordon M. The evolving role of physical therapists in the
long-term management of chronic low back pain: longitudinal care using assisted self-
management strategies. Braz J Phys Ther. 2016;20(6):580-591.
16. Bernstein IA, Malik Q, Carville S, Ward S. Low back pain and sciatica:
summary of NICE guidance. BMJ. 2017;356:i6748.
17. Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back
pain: evidence, challenges, and promising directions. Series. Low back pain 2. Lancet.
2018.
18. Michaleff ZA, Costa LO, Moseley AM, et al. CENTRAL, PEDro, PubMed, and
EMBASE are the most comprehensive databases indexing randomized controlled trials
of physical therapy interventions. Phys Ther. 2011;91(2):190-197.
19. PEDro scale training program. Sydney: The University of Sydney. 1999;
http://www.pedro.org.au/english/tutorial/pedro-scale-training-program/. Accessed 17 de
junho de 2015.
20. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for
systematic reviews that include randomised or non-randomised studies of healthcare
interventions, or both. BMJ. 2017;358:j4008.
21. Shea BJ, Hamel C, Wells GA, et al. AMSTAR is a reliable and valid
measurement tool to assess the methodological quality of systematic reviews. J Clin
Epidemiol. 2009;62(10):1013-1020.
22. Tricco AC, Tetzlaff J, Pham B, Brehaut J, Moher D. Non-Cochrane vs.
Cochrane reviews were twice as likely to have positive conclusion statements: cross-
sectional study. J Clin Epidemiol. 2009;62(4):380-386 e381.
23. Viera AJ, Garrett JM. Understanding interobserver agreement: the kappa
statistic. Fam Med. 2005;37(5):360-363.
24. Landis JR, Koch GG. The measurement of observer agreement for categorical
data. Biometrics. 1977;33(1):159-174.

CHAPTER 3
167
25. Moseley AM, Elkins MR, Herbert RD, Maher CG, Sherrington C. Cochrane
reviews used more rigorous methods than non-Cochrane reviews: survey of systematic
reviews in physiotherapy. J Clin Epidemiol. 2009;62(10):1021-1030.
26. Franke H, Fryer G, Ostelo RW, Kamper SJ. Muscle energy technique for non-
specific low-back pain. Cochrane Database Syst Rev. 2015(2):CD009852.
27. Saragiotto BT, Maher CG, Yamato TP, et al. Motor Control Exercise for
Nonspecific Low Back Pain: A Cochrane Review. Spine (Phila Pa 1976).
2016;41(16):1284-1295.
28. Yamato TP, Maher CG, Saragiotto BT, et al. Pilates for low back pain: complete
republication of a Cochrane review. Spine (Phila Pa 1976). 2016;41(12):1013-1021.
29. Zaina F, Tomkins-Lane C, Carragee E, Negrini S. Surgical Versus Nonsurgical
Treatment for Lumbar Spinal Stenosis. Spine (Phila Pa 1976). 2016;41(14):E857-868.
30. Hopewell S, Boutron I, Altman DG, Ravaud P. Deficiencies in the publication
and reporting of the results of systematic reviews presented at scientific medical
conferences. J Clin Epidemiol. 2015;68(12):1488-1495.
31. Kiriakou J, Pandis N, Fleming PS, Madianos P, Polychronopoulou A. Reporting
quality of systematic review abstracts in leading oral implantology journals. J Dent.
2013;41(12):1181-1187.
32. Seehra J, Fleming PS, Polychronopoulou A, Pandis N. Reporting completeness
of abstracts of systematic reviews published in leading dental specialty journals. Eur J
Oral Sci. 2013;121(2):57-62.
33. Page MJ, Shamseer L, Altman DG, et al. Epidemiology and Reporting
Characteristics of Systematic Reviews of Biomedical Research: A Cross-Sectional
Study. PLoS Med. 2016;13(5):e1002028.
34. Nascimento DP, Ostelo R, van Tulder M, et al. Reporting, interpretation and
consistency with the full text of healthcare research abstracts comparing interventions
effectiveness: a systematic review protocol JBI Database System Rev Implement Rep
(under review). 2018.

CHAPTER 3
168
APPENDIX D. Reliability of data extraction between the two authors who collected the data before consensus. Kappa coefficient is presented for each item of the SPIN 7-item checklist for abstracts and full texts (n=66).
Item Kappa coefficient 1. Recommendation 0.45 2. Title claims a beneficial effect not supported by the findings 1.00 3. Selective reporting of outcomes 0.48 4. Safety based on non-statistically significant results 0.42 5. Beneficial effect despite high risk of bias 0.64 6. Selective reporting of harm outcomes 0.67
SPIN 7-item checklist applied to the abstracts
7. Conclusion extrapolates findings to a different intervention 0.09 1. Recommendation 0.42 2. Title claims a beneficial effect not supported by the findings 1.00 3. Selective reporting of outcomes 0.49 4. Safety based on non-statistically significant results 0.54 5. Beneficial effect despite high risk of bias 0.54 6. Selective reporting of harm outcomes 0.67
SPIN 7-item checklist applied to the full-text
7. Conclusion extrapolates findings to a different intervention 0.25 Range from slight to almost perfect agreement Mean 0.55
CHAPTER 3
169
3.3. APPENDIXES: Common appendixes for Chapter 3

CHAPTER 3
170
3.3.1. FIGURE 1. Flow chart of included reviews.

CHAPTER 3
171
FIGURE 1. Flow chart of included reviews.
Incl
uded
E
ligib
ility
Sc
reen
ing
Iden
tific
atio
n Reviews indexed in PEDro (n = 7,526)
Reviews identified through database searching and
screened (n = 126)
Reviews excluded, with reasons (n = 60)
Published in 2013 (n = 1)
Other languages (n = 6)
Mixed populations (n = 34)
Not low back pain (n = 19) Full-text reviews assessed for eligibility
(n = 66)
Reviews included in quantitative synthesis
(n = 66)

CHAPTER 3
172
3.3.2. APPENDIX A. Excluded reviews.

CHAPTER 3
173
APPENDIX A. Excluded reviews (n=60).
Title. Journal. Year Reason for exclusion Interventions for preventing and treating low-back and pelvic pain during pregnancy. Cochrane Database of Systematic Reviews. 2015 Sep 30;(9):CD001139. doi: 10.1002/14651858.CD001139.pub4.
Not limited to low back pain, also pelvic pain.
Positioning and spinal bracing for pain relief in metastatic spinal cord compression in adults. Cochrane Database of Systematic Reviews. 2015 Sep 24;(9):CD007609. doi: 10.1002/14651858.CD007609.pub3.
Not limited to low back pain, also other areas of spine.
Comparative clinical effectiveness of management strategies for sciatica: systematic review and network meta-analyses. The Spine Journal. 2015 Jun 1;15(6):1461-77. doi: 10.1016/j.spinee.2013.08.049. Epub 2013 Oct 4. Published ahead of print in 2013.
Traditional Chinese medicine for neck pain and low back pain: a systematic review and meta-analysis. PLoS ONE. 2015 Feb 24;10(2):e0117146. doi: 10.1371/journal.pone.0117146. eCollection 2015.
Not limited to low back pain, also neck pain.
Acupuncture for acute postoperative pain after back surgery: a systematic review and meta-analysis of randomized controlled trials. Pain Practice. 2015 Mar;15(3):279-91. doi: 10.1111/papr.12208. Epub 2014 Apr 28.
Not limited to low back pain, also other areas of spine.
Walking exercise for chronic musculoskeletal pain: systematic review and meta-analysis. Archives of Physical Medicine and Rehabilitation. 2015 Apr;96(4):724-734.e3. doi: 10.1016/j.apmr.2014.12.003. Epub 2014 Dec 19.
Not limited to low back pain, also osteoarthritis and fibromyalgia.
The effectiveness of physiotherapist-delivered group education and exercise interventions to promote self-management for people with osteoarthritis and chronic low back pain: a rapid review part I. Manual Therapy. 2015 Apr;20(2):265-86. doi: 10.1016/j.math.2014.10.013. Epub 2014 Nov 1.
Not limited to low back pain, also osteoarthritis.
Tumour necrosis factor alpha inhibitor therapy and rehabilitation for the treatment of ankylosing spondylitis: a systematic review. Seminars in Arthritis and Rheumatism. 2015 Apr;44(5):542-550. doi: 10.1016/j.semarthrit.2014.09.012. Epub 2014 Sep 28.
Not limited to low back pain, ankylosing spondylitis.
Application of osteopathic manipulative technique in the treatment of back pain during pregnancy. Ginekologia Not limited to low back pain, also pelvic pain.

CHAPTER 3
174
Title. Journal. Year Reason for exclusion Polska [Polish Gynaecology]. 2015 Mar;86(3):224-8.
Cognitive-behavioural treatment for subacute and chronic neck pain (Cochrane review). Cochrane Database of Systematic Reviews. 2015 May 26;(5):CD010664. doi: 10.1002/14651858.CD010664.pub2. Not limited to low back pain, neck pain.
Auricular therapy for chronic pain management in adults: a synthesis of evidence. Complementary Therapies in Clinical Practice. 2015 May;21(2):68-78. doi: 10.1016/j.ctcp.2015.03.006. Epub 2015 Apr 4.
Not limited to low back pain, chronic pain in general.
The efficacy of conservative treatment of osteoporotic compression fractures on acute pain relief: a systematic review with meta-analysis. European Spine Journal. 2015 Apr;24(4):702-14. doi: 10.1007/s00586-015-3821-5. Epub 2015 Mar 1.
Not limited to low back pain, osteoporotic compression fractures.
(Effect of exercise therapy in an unstable surface on muscle activity pattern in patients with low back pain: a systematic review). [Persian]. Koomesh. 2015, 16(4): 495-504. In Persian language.
Physical activity in spondyloarthritis: a systematic review. Rheumatology International. 2015 Mar;35(3):393-404. doi: 10.1007/s00296-014-3141-9. Epub 2014 Oct 10.
Not limited to low back pain, spondyloarthritis.
Medical exercise therapy for treating musculoskeletal pain: a narrative review of results from randomized controlled trials with a theoretical perspective. Physiotherapy Research International. 2015 Sep;20(3):182-90. doi: 10.1002/pri.1632. Epub 2015 May 25.
Not limited to low back pain, musculoskeletal pain in general.
Effect of taping on spinal pain and disability: systematic review and meta-analysis of randomized trials. Physical Therapy. 2015 Apr;95(4):493-506. doi: 10.2522/ptj.20130619. Epub 2014 Nov 20.
Not limited to low back pain, also other areas of spine, myofascial pain syndrome and whiplash-associated disorders.
Local and distant acupuncture points stimulation for chronic musculoskeletal pain: a systematic review on the comparative effects. European Journal of Pain. 2015 Oct;19(9):1232-47. doi: 10.1002/ejp.671. Epub 2015 Feb 17.
Not limited to low back pain, chronic musculoskeletal pain in general.
Effects of home-based exercise intervention on health-related quality of life for patients with ankylosing spondylitis: a meta-analysis. Clinical Rheumatology. 2015 Oct;34(10):1737-44. doi: 10.1007/s10067-015-2913-
Not limited to low back pain, ankylosing spondylitis.

CHAPTER 3
175
Title. Journal. Year Reason for exclusion 2. Epub 2015 Mar 15.
Treatments for pregnancy-related lumbopelvic pain: a systematic review of physiotherapy modalities. Acta Obstetricia et Gynecologica Scandinavica. 2015 Nov;94(11):1156-67. doi: 10.1111/aogs.12681. Epub 2015 Jun 16.
Not limited to low back pain, also pelvic pain.
The efficacy of physiotherapy for the prevention and treatment of prenatal symptoms: a systematic review. International Urogynecology Journal. 2015 Nov;26(11):1575-86. doi: 10.1007/s00192-015-2684-y. Epub 2015 Mar 31.
Not limited to low back pain, any prenatal symptom.
Effect of birth ball on labor pain relief: a systematic review and meta-analysis. The Journal of Obstetrics and Gynaecology Research. 2015 Nov;41(11):1679-86. doi: 10.1111/jog.12802. Epub 2015 Sep 30.
Not limited to low back pain, labor pain relief.
A systematic review comparing the costs of chiropractic care to other interventions for spine pain in the United States. BMC Health Services Research. 2015 Oct 19;15:474. doi: 10.1186/s12913-015-1140-5.
Not limited to low back pain, also other areas of spine.
(Effects of exercise therapy on patients with low back pain: a meta-analysis). [Chinese]. Zhongguo Xunzheng Yixue Zazhi [Chinese Journal of Evidence-Based Medicine]. 2015;15(11):1317-1321. In Chinese language.
Concurrent intervention with exercises and stabilized tumor necrosis factor inhibitor therapy reduced the disease activity in patients with ankylosing spondylitis: a meta-analysis. Medicine. 2015 Dec;94(50):e2254. doi: 10.1097/MD.0000000000002254.
Not limited to low back pain, ankylosing spondylitis.
Effectiveness of trigger point dry needling for multiple body regions: a systematic review. The Journal of Manual & Manipulative Therapy. 2015 Dec;23(5):276-93. doi: 10.1179/2042618615Y.0000000014.
Not limited to low back pain, multiple body regions.
A systematic review of randomised controlled trials on the effectiveness of exercise programs on lumbo pelvic pain among postnatal women. BMC Pregnancy and Childbirth. 2015 Nov 26;15:316. doi: 10.1186/s12884-015-0736-4.
Not limited to low back pain, also pelvic pain.

CHAPTER 3
176
Title. Journal. Year Reason for exclusion Effektivitat von Kinesio-taping bei patienten mit ruckenschmerzen. [German] Krankengymnastik. 2015;67(3):30-38. In German language.
Physiotherapy commenced within the first four weeks post spinal surgery is safe and effective: a systematic review and meta-analysis. Archives of Physical Medicine and Rehabilitation. 2016 Feb;97(2):292-301. doi: 10.1016/j.apmr.2015.09.003. Epub 2015 Sep 25.
Not limited to low back pain, musculoskeletal pain in general.
Effect of education on non-specific neck and low back pain: a meta-analysis of randomized controlled trials. Manual Therapy. 2016 Jun;23:e3-4. doi: 10.1016/j.math.2016.03.005. Epub 2016 Mar 24.
Not limited to low back pain, also neck pain.
Timing of physical therapy initiation for nonsurgical management of musculoskeletal disorders and effects on patient outcomes: a systematic review. The Journal of Orthopaedic and Sports Physical Therapy. 2016 Feb;46(2):56-70. doi: 10.2519/jospt.2016.6138. Epub 2016 Jan 11.
Not limited to low back pain, also neck pain.
The effect of group training on pregnancy-induced lumbopelvic pain: systematic review and meta-analysis of randomized control trials. Journal of Exercise Rehabilitation. 2016 Feb 1;12(1):15-20. doi: 10.12965/jer.160277. eCollection 2016 Feb.
Not limited to low back pain, also pelvic pain.
Systematic review of acupuncture for chronic prostatitis/chronic pelvic pain syndrome. Medicine. 2016 Mar;95(11):e3095. doi: 10.1097/MD.0000000000003095.
Not limited to low back pain, chronic prostatitis/chronic pelvic pain syndrome.
Comparative effectiveness of conservative interventions for nonspecific chronic spinal pain: physical, behavioral/psychologically informed, or combined? A systematic review and meta-analysis. The Journal of Pain. 2016 Jul;17(7):755-74. doi: 10.1016/j.jpain.2016.01.473. Epub 2016 Feb 1.
Not limited to low back pain, also other areas of spine.
Effectiveness of Pilates exercise: a quality evaluation and summary of systematic reviews based on randomized controlled trials. Complementary Therapies in Medicine. 2016 Apr;25:1-19. doi: 10.1016/j.ctim.2015.12.018. Epub 2016 Jan 4.
Not limited to low back pain, musculoskeletal conditions in general.

CHAPTER 3
177
Title. Journal. Year Reason for exclusion Osteopathic manipulative treatment in gynecology and obstetrics: a systematic review. Complementary Therapies in Medicine. 2016 Jun;26:72-8. doi: 10.1016/j.ctim.2016.03.005. Epub 2016 Mar 7.
Not limited to low back pain, gynecology and obstetrics disorders.
Cost-effectiveness of physical therapy only and of usual care for various health conditions: systematic review. Physical Therapy. 2016 Jun;96(6):774-86. doi: 10.2522/ptj.20140333. Epub 2015 Dec 17.
Not limited to low back pain, various health conditions.
Effects of exercise on select biomarkers and associated outcomes in chronic pain conditions: systematic review. Biological Research for Nursing. 2016 Mar;18(2):147-59. doi: 10.1177/1099800415599252. Epub 2015 Aug 14.
Not limited to low back pain, any chronic pain condition.
Effectiveness of psychological interventions for chronic pain on health care use and work absence: systematic review and meta-analysis. Pain. 2016 Apr;157(4):777-85. doi: 10.1097/j.pain.0000000000000434.
Not limited to low back pain, any chronic pain condition.
Acupuncture for musculoskeletal pain: a meta-analysis and meta-regression of sham-controlled randomized clinical trials. Scientific Reports. 2016 Jul 29;6:30675. doi: 10.1038/srep30675.
Not limited to low back pain, also shoulder pain, osteoarthritis, myofascial pain and fibromyalgia.
(Effect of acupuncture therapy on patients with low back pain: a meta-analysis). [Chinese]. Zhongguo Gu Shang [China Journal of Orthopaedics and Traumatology]. 2016 May;29(5):449-455. In Chinese language.
The effectiveness of complementary manual therapies for pregnancy-related back and pelvic pain: a systematic review with meta-analysis. Medicine. 2016 Sep;95(38):e4723. doi: 10.1097/MD.0000000000004723.
Not limited to low back pain, also pelvic pain.
Programas de exercicio no domicilio e em grupo em doentes com espondilite anquilosante: revisao sistematica (Home based and group based exercise programs in patients with ankylosing spondylitis: systematic review). [Portuguese] Acta Reumatologica Portuguesa. 2016 Apr-Jun;41(2):104-111.
Not limited to low back pain, ankylosing spondylitis.
Comparison between specific exercises and physical therapy for managing patients with ankylosing spondylitis: a meta-analysis of randomized controlled trials. International Journal of Clinical and Experimental Medicine. 2016 Sep;9(9):17028-17039.
Not limited to low back pain, ankylosing spondylitis.

CHAPTER 3
178
Title. Journal. Year Reason for exclusion Effect of acupuncture on clinical symptoms and laboratory indicators for chronic prostatitis/chronic pelvic pain syndrome: a systematic review and meta-analysis. International Urology and Nephrology. 2016 Dec;48(12):1977-1991. Epub 2016 Sep 2.
Not limited to low back pain, chronic prostatitis/chronic pelvic pain syndrome.
Network meta-analysis of the efficacy of acupuncture, alpha-blockers and antibiotics on chronic prostatitis/chronic pelvic pain syndrome. Scientific Reports. 2016 Oct 19;6:35737. doi: 10.1038/srep35737.
Not limited to low back pain, chronic prostatitis/chronic pelvic pain syndrome.
Konservative therapie beim unspezifischen, chronischen kreuzschmerz: evidenz der wirksamkeit -- eine systematische literaturanalyse (Conservative treatment of nonspecific, chronic low back pain: evidence of the efficacy -- a systematic literature review). Der Orthopade. 2016 Jul;45(7):573-578.
In German language.
The effectiveness of specific exercise types on cardiopulmonary functions in patients with ankylosing spondylitis: a systematic review. Rheumatology International. 2017 Mar;37(3):409-421. doi: 10.1007/s00296-016-3603-3. Epub 2016 Nov 11.
Not limited to low back pain, ankylosing spondylitis.
Feldenkrais method on neck and low back pain to the type of exercises and outcome measurement tools: a systematic review. Polish Annals of Medicine. 2017 Feb;24(1):77-83.
Not limited to low back pain, also neck pain.
Effectiveness of global postural re-education for treatment of spinal disorders: a meta-analysis. American Journal of Physical Medicine & Rehabilitation. 2017 Feb;96(2):124-130. doi: 10.1097/PHM.0000000000000575.
Not limited to low back pain, also other areas of spine.
Crenotherapie (crenobalneotherapie) dans la lombalgie chronique: une revue critique (Spa therapy (crenobalneotherapy) in low back pain: a critical review). Revue du Rhumatisme Monographies. 2017 Feb;84(1):91-98.
In French language.
The efficacy of acupuncture in managing patients with chronic prostatitis/chronic pelvic pain syndrome: a systemic review and meta-analysis. Neurourology and Urodynamics. 2017 Feb;36(2):474-481. doi: 10.1002/nau.22958. Epub 2016 Jan 6.
Not limited to low back pain, chronic prostatitis/chronic pelvic pain syndrome.

CHAPTER 3
179
Title. Journal. Year Reason for exclusion Efficacy and safety of non-pharmacological and non-biological pharmacological treatment: a systematic literature review informing the 2016 update of the ASAS/EULAR recommendations for the management of axial spondyloarthritis. RMD Open. 2017 Jan 27;3(1):e000397. doi: 10.1136/rmdopen-2016-000397. eCollection 2017.
Not limited to low back pain, axial spondyloarthritis.
Interventions to increase adherence to therapeutic exercise in older adults with low back pain and/or hip/knee osteoarthritis: a systematic review and meta-analysis. British Journal of Sports Medicine. 2017 May;51(10):791-799. doi: 10.1136/bjsports-2016-096458. Epub 2017 Jan 13.
Not limited to low back pain, also hip/knee osteoarthritis.
Effect of acupuncture on pregnancy related low back pain and pelvic pain: a systematic review and meta-analysis. International Journal of Clinical and Experimental Medicine. 2017 Apr;10(4):5903-5912.
Not limited to low back pain, also pelvic pain.
Influence of exercise intervention on pain, quality of life and functional mobility in patients with osteoporotic vertebral fractures: a systematic review and meta-analysis. International Journal of Clinical and Experimental Medicine. 2017 Jul;10(7):9864-9870.
Not limited to low back pain, also other areas of spine.
Effectiveness of exercise programs in ankylosing spondylitis: a meta-analysis of randomized controlled trials. Archives of Physical Medicine and Rehabilitation. 2018 Feb;99(2):383-389.e1. doi: 10.1016/j.apmr.2017.07.015. Epub 2017 Aug 30.
Not limited to low back pain, ankylosing spondylitis.
The effectiveness of physiotherapy interventions for sacroiliac joint dysfunction: a systematic review. Journal of Physical Therapy Science. 2017 Sep;29(9):1689-1694. doi: 10.1589/jpts.29.1689. Epub 2017 Sep 15.
Not limited to low back pain, also pelvic girdle pain.
Exercise interventions for the prevention and treatment of groin pain and injury in athletes: a critical and systematic review. Sports Medicine. 2017 Oct;47(10):2011-2026. doi: 10.1007/s40279-017-0742-y.
Not limited to low back pain, groin pain and injury in athletes.
The role of land and aquatic exercise in ankylosing spondylitis: a systematic review. Rheumatology International. 2017 Dec;37(12):1979-1990. doi: 10.1007/s00296-017-3829-8. Epub 2017 Oct 5.
Not limited to low back pain, ankylosing spondylitis.

CHAPTER 3
180
Title. Journal. Year Reason for exclusion Osteopathic manipulative treatment for low back and pelvic girdle pain during and after pregnancy: a systematic review and meta-analysis. Journal of Bodywork and Movement Therapies. 2017 Oct;21(4):752-762. doi: 10.1016/j.jbmt.2017.05.014. Epub 2017 May 31.
Not limited to low back pain, also pelvic girdle pain.

CHAPTER 3
181
3.3.3. APPENDIX B. Included reviews.

CHAPTER 3
182
APPENDIX B. Included reviews (n=66).
1. Andronis L, Kinghorn P, Qiao S, Whitehurst DGT, Durrell S, McLeod H. Cost-
effectiveness of non-invasive and non-pharmacological interventions for low back pain:
a systematic literature review. Applied Health Economics and Health Policy 2017
Apr;15(2):173-201.
2. Blanchette MA, Stochkendahl MJ, Borges da Silva R, Boruff J, Harrison P,
Bussieres A. Effectiveness and economic evaluation of chiropractic care for the
treatment of low back pain: a systematic review of pragmatic studies. PLoS ONE 2016
Aug;11(8):e0160037.
3. Budhrani-Shani P, Berry DL, Arcari P, Langevin H, Wayne PM. Mind-body
exercises for nurses with chronic low back pain: an evidence-based review. Nursing
Research and Practice 2016 Jul 3;(9018036):Epub.
4. Chang WD, Lin HY, Lai PT. Core strength training for patients with chronic low
back pain. Journal of Physical Therapy Science 2015 Mar;27(3):619-622.
5. Chou R, Deyo R, Friedly J, Skelly A, Hashimoto R, Weimer M, et al.
Nonpharmacologic therapies for low back pain: a systematic review for an American
College of Physicians clinical practice guideline. Annals of Internal Medicine 2017 Apr
4;166(7):493-505.
6. Fernandez M, Hartvigsen J, Ferreira ML, Refshauge KM, Machado AF, Lemes
IR, et al. Advice to stay active or structured exercise in the management of sciatica: a
systematic review and meta-analysis. Spine 2015 Sep 15;40(18):1457-1466.
7. Franke H, Fryer G, Ostelo R, Kamper SJ. Muscle energy technique for non-
specific low-back pain (Cochrane review). Cochrane Database of Systematic Reviews
2015;Issue 2.
8. Franke H, Fryer G, Ostelo R, Kamper SJ. Muscle energy technique for non-
specific low-back pain. A Cochrane systematic review. International Journal of
Osteopathic Medicine 2016 Jun;20:41-52.
9. Furlan AD, Giraldo M, Baskwill A, Irvin E, Imamura M. Massage for low-back
pain (Cochrane review). Cochrane Database of Systematic Reviews 2005;Issue 9.
10. Gilmore SJ, McClelland JA, Davidson M. Physiotherapeutic interventions
before and after surgery for degenerative lumbar conditions: a systematic review.
Physiotherapy 2015 Jun;101(2):111-118.

CHAPTER 3
183
11. Glazov G, Yelland M, Emery J. Low-level laser therapy for chronic non-specific
low back pain: a meta-analysis of randomised controlled trials. Acupuncture in
Medicine 2016 Oct;34(5):328-341.
12. Gomes-Neto M, Lopes JM, Conceicao CS, Araujo A, Brasileiro A, Sousa C, et
al. Stabilization exercise compared to general exercises or manual therapy for the
management of low back pain: a systematic review and meta-analysis. Physical Therapy
in Sport 2017 Jan;23:136-142.
13. Gordon R, Bloxham S. A systematic review of the effects of exercise and
physical activity on non-specific chronic low back pain. Healthcare 2016 Apr
25;4(22):Epub.
14. Gurung T, Ellard DR, Mistry D, Patel S, Underwood M. Identifying potential
moderators for response to treatment in low back pain: a systematic review.
Physiotherapy 2015 Sep;101(3):243-251.
15. Hall A, Richmond H, Copsey B, Hansen Z, Williamson E, Jones G, et al.
Physiotherapist-delivered cognitive-behavioural interventions are effective for low back
pain, but can they be replicated in clinical practice? A systematic review. Disability and
Rehabilitation 2016 Nov 21:Epub ahead of print.
16. Hanney WJ, Masaracchio M, Liu X, Kolber MJ. The influence of physical
therapy guideline adherence on healthcare utilization and costs among patients with low
back pain: a systematic review of the literature. PLoS ONE 2016 Jun;11(6):e0156799.
17. Ishak NA, Zahari Z, Justine M. Effectiveness of strengthening exercises for the
elderly with low back pain to improve symptoms and functions: a systematic review.
Scientifica 2016;(3230427):Epub.
18. Ji M, Wang X, Chen M, Shen Y, Zhang X, Yang J. The efficacy of acupuncture
for the treatment of sciatica: a systematic review and meta-analysis. Evidence-Based
Complementary and Alternative Medicine 2015;(192808):Epub.
19. Kalin S, Rausch-Osthoff AK, Bauer CM. What is the effect of sensory
discrimination training on chronic low back pain? A systematic review. BMC
Musculoskeletal Disorders 2016 Apr 2;17(143):Epub.
20. Kamper SJ, Apeldoorn AT, Chiarotto A, Smeets R, Ostelo R, Guzman J, et al.
Multidisciplinary biopsychosocial rehabilitation for chronic low back pain: Cochrane
systematic review and meta-analysis. BMJ 2015 Feb 18;350:h444.

CHAPTER 3
184
21. Karagulle M, Karagulle MZ. Effectiveness of balneotherapy and spa therapy for
the treatment of chronic low back pain: a review on latest evidence. Clinical
Rheumatology 2015 Feb;34(2):207-214.
22. Kuss K, Becker A, Quint S, Leonhardt C. Activating therapy modalities in older
individuals with chronic non-specific low back pain: a systematic review. Physiotherapy
2015 Dec;101(4):310-318.
23. Lawford BJ, Walters J, Ferrar K. Does walking improve disability status,
function, or quality of life in adults with chronic low back pain? A systematic review.
Clinical Rehabilitation 2016 Jun;30(6):523-536.
24. Li X, Han Y, Cui J, Yuan P, Di Z, Li L. Efficacy of warm needle moxibustion
on lumbar disc herniation: a meta-analysis. Journal of Evidence-Based Complementary
& Alternative Medicine 2016 Oct;21(4):311-319.
25. Lin HT, Hung WC, Hung JL, Wu PS, Liaw LJ, Chang JH. Effects of Pilates on
patients with chronic non-specific low back pain: a systematic review. Journal of
Physical Therapy Science 2016 Oct;28(10):2961-2969..
26. Liu L, Huang QM, Liu QG, Thitham N, Li LH, Ma YT, et al. Evidence for Dry
Needling in the Management of Myofascial Trigger Points Associated With Low Back
Pain: A Systematic Review and Meta-Analysis. Arch Phys Med Rehabil.
2018;99(1):144-52 e2.
27. Lopez-de-Uralde-Villanueva I, Munoz-Garcia D, Gil-Martinez A, Pardo-
Montero J, Munoz-Plata R, Angulo-Diaz-Parreno S, et al. A systematic review and
meta-analysis on the effectiveness of graded activity and graded exposure for chronic
nonspecific low back pain. Pain Medicine 2016 Jan;17(1):172-188.
28. Macedo LG, Saragiotto BT, Yamato TP, Costa LOP, Menezes Costa LC, Ostelo
R, et al. Motor control exercise for acute non-specific low back pain (Cochrane review).
Cochrane Database of Systematic Reviews 2016;Issue 2.
29. Madera M, Brady J, Deily S, McGinty T, Moroz L, Singh D, et al. The role of
physical therapy and rehabilitation after lumbar fusion surgery for degenerative disease:
a systematic review. J Neurosurg Spine. 2017;26(6):694-704.
30. Matheve T, Brumagne S, Timmermans AAA. The effectiveness of technology-
supported exercise therapy for low back pain: a systematic review. American Journal of
Physical Medicine & Rehabilitation 2017 May;96(5):347-356.
31. McGregor A, Jones F, Mullane J, Hurley M. Rehabilitation following lumbar
fusion surgery: a systematic review and meta-analysis. Spine 2016 Jan;41(1):E28-E36.
CHAPTER 3
185
32. Meng XG, Yue SW. Efficacy of aerobic exercise for treatment of chronic low
back pain: a meta-analysis. American Journal of Physical Medicine & Rehabilitation
2015 May;94(5):358-365.
33. Nelson NL. Kinesio taping for chronic low back pain: a systematic review.
Journal of Bodywork and Movement Therapies 2016 Jul;20(3):672-681.
34. Nicholl BI, Sandal LF, Stochkendahl MJ, McCallum M, Suresh N, Vasseljen O,
et al. Digital Support Interventions for the Self-Management of Low Back Pain: A
Systematic Review. J Med Internet Res. 2017;19(5):e179.
35. Otoo SKW, Hendrick P, Ribeiro DC. The comparative effectiveness of
advice/education compared to active physiotherapy (manual therapy and exercise) in the
management of chronic non-specific low back pain. Physical Therapy Reviews 2015
Feb;20(1):16-26.
36. Parreira P, Heymans MW, van Tulder MW, Esmail R, Koes BW, Poquet N, et
al. Back Schools for chronic non-specific low back pain. Cochrane Database Syst Rev.
2017;8:CD011674.
37. Patti AB, Paoli A, Messina G, Montalto MA, Bellafiore M, Battaglia G, et al.
Effects of Pilates exercise programs in people with chronic low back pain: a systematic
review. Medicine 2015 Jan;94(4):e383.
38. Poon TH, Carus C. The effectiveness of laser therapy on the management of
chronic low back pain. International Journal of Therapy and Rehabilitation 2016
Sep;23(9):432-443.
39. Poquet N, Lin CWC, Heymans MW, van Tulder MW, Esmail R, Koes BW, et
al. Back schools for acute and subacute non-specific low-back pain (Cochrane review).
Cochrane Database of Systematic Reviews 2016;Issue 4.
40. Qin Z, Liu X, Wu J, Zhai Y, Liu Z. Effectiveness of acupuncture for treating
sciatica: a systematic review and meta-analysis. Evidence-Based Complementary and
Alternative Medicine 2015;(425108):Epub..
41. Richmond H, Hall AM, Copsey B, Hansen Z, Williamson E, Hoxey-Thomas N,
et al. The effectiveness of cognitive behavioural treatment for non-specific low back
pain: a systematic review and meta-analysis. PLoS ONE 2015 Aug;10(8):e0134192.
42. Rihn JA, Radcliff K, Norvell DC, Eastlack R, Phillips FM, Berland D, et al.
Comparative Effectiveness of Treatments for Chronic Low Back Pain: A Multiple
Treatment Comparison Analysis. Clin Spine Surg. 2017;30(5):204-25.

CHAPTER 3
186
43. Rothberg S, Friedman BW. Complementary therapies in addition to medication
for patients with nonchronic, nonradicular low back pain: a systematic review. The
American Journal of Emergency Medicine 2017 Jan;35(1):55-61..
44. Ruddock JK, Sallis H, Ness A, Perry RE. Spinal manipulation versus sham
manipulation for nonspecific low back pain: a systematic review and meta-analysis.
Journal of Chiropractic Medicine 2016 Sep;15(3):165-183.
45. Saragiotto BT, Maher CG, Yamato TP, Costa LOP, Costa LCM, Ostelo R, et al.
Motor control exercise for nonspecific low back pain: a Cochrane review. Spine 2016
Aug 15;41(16):1284-1295..
46. Saragiotto BT, Maher CG, Yamato TP, Costa LOP, Menezes Costa LC, Ostelo
R, et al. Motor control exercise for chronic non-specific low-back pain (Cochrane
review). Cochrane Database of Systematic Reviews 2016;Issue 1.
47. Searle A, Spink M, Ho A, Chuter V. Exercise interventions for the treatment of
chronic low back pain: a systematic review and meta-analysis of randomised controlled
trials. Clinical Rehabilitation 2015 Dec;29(12):1155-1167.
48. Shorthouse FM, Roffi V, Tack C. Effectiveness of educational materials to
prevent occupational low back pain. Occupational Medicine 2016 Nov;66(8):623-629.
49. Steele J, Bruce-Low S, Smith D. A review of the clinical value of isolated
lumbar extension resistance training for chronic low back pain. PM&R 2015
Feb;7(2):169-187.
50. Steffens D, Hancock MJ, Pereira LSM, Kent PM, Latimer J, Maher CG. Do
MRI findings identify patients with low back pain or sciatica who respond better to
particular interventions? A systematic review. European Spine Journal 2016
Apr;25(4):1170-1187.
51. Steffens D, Maher CG, Pereira LSM, Stevens ML, Oliveira VC, Chapple M, et
al. Prevention of low back pain: a systematic review and meta-analysis. JAMA Internal
Medicine 2016 Feb 1;176(2):199-208.
52. Straube S, Harden M, Schroder H, Arendacka B, Fan X, Moore RA, et al. Back
schools for the treatment of chronic low back pain: possibility of benefit but no
convincing evidence after 47 years of research -- systematic review and meta-analysis.
Pain 2016 Oct;157(10):2160-2172.
53. Traeger AC, Hubscher M, Henschke N, Moseley GL, Lee H, McAuley JH.
Effect of primary care-based education on reassurance in patients with acute low back

CHAPTER 3
187
pain: systematic review and meta-analysis. JAMA Internal Medicine 2015
May;175(5):733-743.
54. Wang L, Guo Q, Lu X, Ni B. Surgical versus nonsurgical treatment of chronic
low back pain: a meta-analysis based on current evidence. Journal of Back and
Musculoskeletal Rehabilitation 2016;29(3):393-401.
55. Wang X, Wanyan P, Tian JH, Hu L. Meta-analysis of randomized trials
comparing fusion surgery to non-surgical treatment for discogenic chronic low back
pain. Journal of Back and Musculoskeletal Rehabilitation 2015;28(4):621-627.
56. Wasser JG, Vasilopoulos T, Zdziarski LA, et al. Exercise Benefits for Chronic
Low Back Pain in Overweight and Obese Individuals. PM R 2017;9(2):181-92. doi:
10.1016/j.pmrj.2016.06.019
57. Wieland LS, Skoetz N, Pilkington K, Vempati R, d'Adamo CR, Berman BM.
Yoga treatment for chronic non-specific low back pain (Cochrane review). Cochrane
Database of Systematic Reviews 2017;Issue 1.
58. Wong JJ, Cote P, Sutton DA, Randhawa K, Yu H, Varatharajan S, et al. Clinical
practice guidelines for the noninvasive management of low back pain: a systematic
review by the Ontario Protocol for Traffic Injury Management (OPTIMa)
Collaboration. European Journal of Pain 2017 Feb;21(2):201-216.
59. Yamato TP, Maher CG, Saragiotto BT, Hancock MJ, Ostelo R, Cabral CMN, et
al. Pilates for low back pain: complete republication of a Cochrane review. Spine 2016
Jun;41(12):1013-1021..
60. Yamato TP, Maher CG, Saragiotto BT, Hancock MJ, Ostelo R, Cabral CMN, et
al. Pilates for low back pain (Cochrane review). Cochrane Database of Systematic
Reviews 2015;Issue 7.
61. Yang LH, Duan PB, Hou QM, Du SZ, Sun JF, Mei SJ, et al. Efficacy of
Auricular Acupressure for Chronic Low Back Pain: A Systematic Review and Meta-
Analysis of Randomized Controlled Trials. Evid Based Complement Alternat Med.
2017;2017:6383649.
62. Yeganeh M, Baradaran HR, Qorbani M, Moradi Y, Dastgiri S. The effectiveness
of acupuncture, acupressure and chiropractic interventions on treatment of chronic
nonspecific low back pain in Iran: A systematic review and meta-analysis. Complement
Ther Clin Pract. 2017;27:11-8.

CHAPTER 3
188
63. Zaina F, Tomkins-Lane C, Carragee E, Negrini S. Surgical versus non-surgical
treatment for lumbar spinal stenosis (Cochrane review). Cochrane Database of
Systematic Reviews 2016;Issue 1.
64. Zaina F, Tomkins-Lane C, Carragee E, Negrini S. Surgical versus nonsurgical
treatment for lumbar spinal stenosis. Spine 2016 Jul 15;41(14):E857-E868.
65. Zamiri S, Shaterzadeh Yazdi MJ, Maraghi E, Takamjani IE. The effectiveness of
classification-specific physical therapy for people with low back pain within dominant
movement-based schemes: a systematic review. Iranian Red Crescent Medical Journal
2016 Dec;18(12):e41959.
66. Zeng Y, Chung J-Y. Acupuncture for chronic nonspecific low back pain: an
overview of systematic reviews. European Journal of Integrative Medicine 2015
Apr;7(2):94-107.

CHAPTER 3
189
3.3.4. APPENDIX C. Number and percentage of individual items from
the AMSTAR-2.

CHAPTER 3
190
APPENDIX C. Number and percentage of individual items from the AMSTAR-2 (n=66).
AMSTAR-2 ITEM No Yes Partial
Yes n (%) n (%) n (%) 1. Did the research questions and inclusion criteria for the review include the components of PICO? 0 (0.0) 50 (75.8) 16 (24.2) 2. Did the report of the review contain an explicit statement that the review methods were established prior to the conduct of the review and did the report justify any significant deviations from the protocol? 43 (65.2) 22 (33.3) 1 (1.5) 3. Did the review authors explain their selection of the study designs for inclusion in the review? 54 (81.8) 7 (10.6) 5 (7.6) 4. Did the review authors use a comprehensive literature search strategy? 8 (12.1) 25 (37.9) 33 (50.0) 5. Did the review authors perform study selection in duplicate? 11 (16.7) 55 (83.3) 0 (0.0) 6. Did the review authors perform data extraction in duplicate? 12 (18.2) 49 (74.2) 5 (7.6) 7. Did the review authors provide a list of excluded studies and justify the exclusions? 36 (54.5) 16 (24.2) 14 (21.2) 8. Did the review authors describe the included studies in adequate detail? 3 (4.5) 21 (31.8) 42 (63.6) 9. Did the review authors use a satisfactory technique for assessing the risk of bias (RoB) in individual studies that were included in the review? 7 (10.6) 49 (74.2) 10 (15.2) 10. Did the review authors report on the sources of funding for the studies included in the review? 54 (81.8) 11 (16.7) 1 (1.5) 11. If meta-analysis was performed did the review authors use appropriate methods for statistical combination of results? 0 (0.0) *36 (54.5) 0 (0.0) 12. If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? 8 (12.1) *28 (42.4) 0 (0.0) 13. Did the review authors account for RoB in individual studies when interpreting/discussing the results of the review? 24 (36.4) 42 (63.6) 0 (0.0) 14. Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? 14 (21.2) 52 (78.8) 0 (0.0) 15. If they performed quantitative synthesis did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review? 4 (6.1) *32 (48.5) 0 (0.0) 16. Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? 9 (13.6) 57 (86.4) 0 (0.0) Note: *30 of articles (45.4%) did not perform meta-analyses.

CHAPTER 4
191
CHAPTER 4
Abstracts in all healthcare areas

CHAPTER 4
192
4.1. Abstracts of systematic reviews and randomized controlled trials:
reporting quality, spin and inconsistencies with the full text

CHAPTER 4
193
4.1.1. Abstracts of healthcare research need urgent action measures: A
systematic review
Will be submitted in: JAMA 2019

CHAPTER 4
194
Abstracts of healthcare research need urgent action measures: A systematic
review
Dafne Port Nascimento1; Raymond Ostelo2,3; Maurits Van Tulder2,4; Gabrielle Zoldan
Gonzalez1; Amanda Costa Araujo1; Adriane Aver Vanin1; Leonardo Oliveira Pena
Costa1 1Masters and Doctoral Programs in Physical Therapy, Universidade Cidade de São
Paulo, São Paulo – SP, Brazil 2Department of Health Sciences, Faculty of Science, Vrije Universiteit Amsterdam,
Amsterdam, The Netherlands 3Department of Epidemiology and Biostatistics, Amsterdam UMC, location VUmc
and the Amsterdam Movement Sciences Research Institute, Amsterdam, The
Netherlands 4Department of Physiotherapy & Occupational Therapy, Aarhus University Hospital,
Aarhus, Denmark
Corresponding author: Dafne Port Nascimento, Masters and Doctoral Programs in
Physical Therapy, Universidade Cidade de São Paulo. Rua Cesário Galeno 448,
Tatuapé, São Paulo, SP – Brazil, CEP 03071-000. Phone number: +55 11 994779119.
ORCID ID: https://orcid.org/0000-0002-8474-727X
Email address: [email protected]
Funding: This work was supported by a PhD scholarship from the Sao Paulo
Research Foundation (grant#2016/17853-4; grant# 2018/17932-7; Fundação de
Amparo à Pesquisa do Estado de São Paulo – FAPESP).
Conflict of interest: The authors declare no conflict of interest.

CHAPTER 4
195
Abstracts of healthcare research need urgent action measures: A systematic
review
ABSTRACT
Background: Clinicians often base their decision-making on the content of abstracts
of scientific studies. However, if the abstract is poorly reported or interpreted,
clinicians may choose ineffective interventions. Our primary objective was to
summarize the reporting quality of abstracts and inconsistencies between abstracts
and full texts in overviews of randomized controlled trials (RCTs) and systematic
reviews (SRs). Methods: This systematic review included overviews of RCTs and
SRs that summarized data of healthcare abstracts on reporting of abstracts and
consistency of abstracts with the full text. Searches were performed on PubMed,
Medline, Cochrane Central Register of Controlled Trials (CENTRAL), Cochrane
Library (records of Cochrane Reviews and Methods Studies) and EMBASE databases
from inception to February 2019. Two authors screened the overviews and extracted
the data. All analyses were made descriptively and divided into two main groups:
abstracts reporting quality; and abstracts consistency with the full text. Results: 27
overviews analyzing 5,194 RCTs and 866 SRs were retrieved for abstracts reporting
quality. The standardized mean percentage score of fully reported items ranged from
28.1% to 72.7% across healthcare areas. With regards to abstracts consistency with
the full text, a total of 22 overviews analyzing 2,017 RCTs and 551 SRs were
included. The standardized mean percentage of inconsistent abstracts ranged from
7.0% to 98.0% across healthcare areas, with abstracts results and conclusions as the
most inconsistent sections. Discussion: A strength of this systematic review is that it
described data of a large sample of healthcare interventions abstracts published in
peer-reviewed journals. A limitation was that it was not possible to evaluate the
methodological quality of the included overviews. Abstracts of healthcare RCTs and
SRs have shown a large room for improvement in reporting quality and consistency
with the full text. Abstracts are the highest profile part of a research study and
recommendations to authors, journal editors and reviewers need to be put into action
as highest priority.

CHAPTER 4
196
INTRODUCTION
Within the framework of evidence-based practice, healthcare professionals
should use evidence from randomized controlled trials (RCTs) and systematic reviews
(SRs) for clinical decisions on interventions1. Often the abstract of a scientific article
is the only available source of information for clinicians, due to lack of time and
access to the full text2-4. Therefore, if the abstract is poorly reported, clinicians may
choose ineffective or harmful interventions, as well as it may disseminate
misinterpreted research findings by academic press releases or media coverage of
research5,6.
Common problems found in abstracts of RCTs and SRs in healthcare research
are twofold: 1) Poor reporting quality7-9, which can be analyzed by the inclusion of all
relevant information reported in the study. The abstract should have enough details
and clarity that readers can assess study’s validity and applicability10,11; and 2)
Inconsistencies between the information contained in the full text and corresponding
abstract, which can be analyzed by comparing the reporting and interpretation of
sections of the abstract with the corresponding information in the full text12. Spin is
the term defined for the misinterpretation of study results, typically leading to
overstating the results in a more favorable way13-15. Examples of spin in abstracts are:
omission of primary outcome or adverse events; selective reporting of negative
primary outcomes; focus on positive secondary outcomes; overstated interpretation of
study results; recommendation of a treatment without a clinically important effect;
and also beneficial effect despite high risk of bias of outcomes analyzed13,15.
Researchers have been working on efforts to improve the quality, transparency,
integrity and value of abstracts and papers published, such as: stricter editorial
policies, stricter reporting guidelines endorsement and better guidance on abstracts
reporting guidelines8,12(Consolidated Standards of Reporting Trials for Abstracts
checklist10 [CONSORT-A] and Preferred Reporting Items for Systematic Reviews
and Meta-Analysis11 [PRISMA-A]); awareness of the prevalence of spin by journal
editors and reviewers14; and training programs for authors, journal editors and peer
reviewers16. Despite of these efforts, it seems that abstracts still present inadequate
reporting and inconsistencies with the full text7,12,14. It is also uncertain whether the
reporting quality and inconsistency of abstracts is specific for certain fields or can be
generalized to healthcare abstracts in general. Previous studies have suggested that

CHAPTER 4
197
more specific changes should be made in journals’ editorial policies, such as
increasing the word limits for abstracts12,17,18, however there is no consensus
summarized in literature on what measures should be taken.
In order to analyze how healthcare abstracts of RCTs have been reported, a SR
was performed7. However, this review included only comparisons for both the pre-
and post- CONSORT-A10 period7 and is now outdated, which might not give a
perspective of abstracts reporting quality in general after the CONSORT-A was
created19,20. Another scoping review recently published analyzed inconsistencies
between abstract and full text of primary studies, but included overviews analyzing
any study design and also conference abstracts12. Another concern in literature is
related to the terminology describing ‘inconsistencies’ (or inaccuracy, or
discrepancies) between abstracts and full texts, which seems to vary greatly between
studies12. Both systematic reviews mentioned above7,12 point to the need of efforts to
improve abstracts with poor reporting and inconsistencies with their full texts,
especially regarding stricter journal editorial policies. However, it seems that
recommendations have not been followed and it is unknown if such issues can be
generalized to all healthcare areas. In order to explore those gaps in literature and to
call healthcare journal’s editorial boards for action, we designed this systematic
review. Our primary objectives were: 1) summarize the reporting quality of RCTs and
SRs abstracts after the CONSORT-A10 and PRISMA-A11 release in all healthcare
areas; and 2) summarize the consistency between RCTs and SRs abstracts with their
corresponding full text in terms of reporting and spin of study results.
METHODS
This systematic review has not been suitable for registration at the
International Prospective Register Of Systematic Reviews (PROSPERO), because
they register only systematic reviews with direct link to human health.
Inclusion criteria
This systematic review included overviews of healthcare primary research
abstracts (RCTs and SRs only) that summarized data of abstracts reporting quality and
abstracts consistency with the full text. There were no language restrictions. Grey

CHAPTER 4
198
literature was not considered for our systematic review, however we checked the
reference lists for any other overview that could be included in our study, and
contacted authors when required.
1) Abstracts reporting quality:
• RCTs: the overviews had to have used the CONSORT-A to analyze the
abstracts. Such RCTs had to be published from 2008 onwards, as the CONSORT-A
was created in 200810;
• SRs: the overviews had to have used the PRISMA-A to analyze the abstracts.
Such SRs had to be published from 2013 onwards, as the PRISMA-A was created in
201311;
2) Abstracts consistency with the full text: Overviews assessing the consistency of
RCTs and SRs abstracts with the full text in terms of reporting and misinterpretation
of study results (spin), without restriction for time period.
Search Strategy
The search was performed on PubMed, Cochrane Central Register of
Controlled Trials (CENTRAL), Cochrane Library (records of Cochrane Reviews and
Methods Studies), Medline and EMBASE databases from inception to February 2019.
We narrowed our search to studies involving the analysis of abstracts and tried to
avoid retrieving conference abstracts. Therefore, our search strategy in each database
was limited to title and abstracts, with the following key-words: (abstracts not
conference* not congress* not meeting* not symposium not annual not convention*
not reunion* not workshop* not poster* not presentation* not forum* not
association*)[Title] and choosing the box “Abstracts” under “Limits” of the
Advanced Search.
Study selection
Two authors conducted the searches, identified potentially relevant studies and
removed duplicates. Titles and abstracts were screened for assessment against the
inclusion criteria and separated into two groups: Abstracts reporting quality; and

CHAPTER 4
199
Abstracts consistency with the full text. Eligible studies were retrieved in full
and assessed in detail. Reasons for exclusion of full text studies were recorded. Any
disagreements that arose between the reviewers at each stage of the study selection
process were resolved through discussion, or with a third reviewer.
Data extraction
Two authors extracted data independently. Disagreements were discussed in a
consensus meeting, and resolved by a third author if disagreements persisted. The
selected overviews and data extracted were stored in a Microsoft Excel spreadsheet.
The following data were extracted: first author; year of publication; healthcare field;
number of primary research abstracts; study design analyzed (RCTs or SRs); year
range of primary research abstracts; terminology used to describe consistency; aim of
the overview; methods used by the overviews to evaluate reporting and consistency of
the RCTs or SRs abstracts; and main findings of the overviews.
For each group we have detailed the main outcomes related to the main
findings of the overviews below:
1) Abstracts reporting quality of RCTs and SRs: the mean, median or percentage
overall score (with any measure of variability) of fully reported items from the
CONSORT-A10 (mean CONSORT-Abstract score) and PRISMA-A11 (mean
PRISMA-Abstract score); and percentage of abstracts reporting each item from the
checklists. We then calculated the standardized mean percentage of fully reported
items for each overview, by summing the percentage of each item, divided by the total
number of items. For overviews comparing the reporting quality of abstracts before-
and after-release of the abstracts checklists, we collected and analyzed information
regarding the after-period only;
2) Abstracts consistency with the full text: the percentage of abstracts presenting
inconsistencies with the full text (with any measure of variability). We calculated the
standardized percentage of inconsistent abstracts for each overview, including those
that reported only the odds ratio (OR). In this case, we divided the OR for one plus
the OR (percentage = OR / 1 + OR). When only the percentage of inconsistencies per
each item were reported, we calculated the standardized mean percentage of
inconsistent abstracts for each overview, by summing the percentage of each item,
divided by the total number of items.

CHAPTER 4
200
We also included the following information related to the main findings of the
overviews, if reported: the methodological quality of primary studies analyzed (the
overall judgment or overall score, range and scale used by the primary studies, e.g.
Cochrane risk of bias tool for RCTs21 and SRs22); information related to the number
of words in the primary research abstracts analyzed (mean word count or range
permitted in the journal of publication); associations found by the overviews between
the primary research abstracts (e.g. abstracts reporting quality) and journal or study
characteristics (e.g. journal impact factor); and recommendations given by the
overviews that were related to improvements of abstracts reporting quality and
consistency with the full text.
Data synthesis
All analyses were made descriptively for all studies and for subgroups of
different healthcare fields, by measurement of frequency and percentage of all
outcomes.
RESULTS
The searches were performed on 5th July 2018 and 5th March 2019. We found
in total 7,345 records indexed in all databases, with additional 12 identified
throughout the references of the analyzed studies. 122 overviews were assessed for
eligibility, from which 77 were excluded (APPENDIX A with reasons for exclusion
for each article). Our final sample of 45 overviews that were included in our
qualitative synthesis is listed in TABLE 1 for abstracts reporting quality of healthcare
RCTs and SRs (n=27); and TABLE 2 for abstracts consistency with the full text
(n=22). The flow chart of the included overviews is presented in a PRISMA flow
diagram23 (FIGURE 1). Four reviews were included in both groups24-27.

CHAPTER 4
201
Figure 1. Flow chart of the included overviews.
Records identified through database searching
(n = 7,333)
Scre
enin
g In
clud
ed
Elig
ibili
ty
Iden
tific
atio
n
Additional records identified through other sources
(n = 12)
Duplicates removed (n = 931)
Records screened (n = 6,414)
Records excluded (n =6,292)
Overviews assessed for eligibility (n = 122)
Full text overviews excluded, with reasons (n = 77) 29 not specific for RCTs or SRs 17 studies analyzed were published before the release of the abstracts reporting guidelines 9 analysis of other theme related to abstracts 7 did not evaluate all items of the EQUATOR abstracts reporting guidelines 6 comments/ letters 3 secondary analyses 2 protocols 2 systematic reviews of studies evaluating abstracts 1 pilot trials only 1 included conference abstracts
Overviews included in qualitative synthesis
(n = 45)
Abstracts reporting quality of healthcare RCTs
and SRs
(n = 27)
Abstracts consistency with
the full text of healthcare RCTs
and SRs (n = 22)

CHAPTER 4
202
1) Abstracts reporting quality
We included 27 overviews analyzing abstracts reporting quality of healthcare
RCTs and SRs8,9,24-48. Main characteristics are presented in TABLE 1. A total of
5,194 RCTs and 866 SRs were analyzed. The standardized mean percentage score of
fully reported items varied across healthcare areas, and ranged from 28.1% to 72.7%.
The healthcare fields with more than 50% mean percentage scores (standardized)
were: physical therapy, general medicine, dentistry, neurosurgical, pharmacy and
oncology. The healthcare fields with less than 50% of standardized mean percentage
scores were: psoriasis, psychiatry, infectious diseases, pain, anesthesia, low back pain,
dentistry, critical care and laser medicine. Twenty overviews8,9,24-28,31,34,35,37-40,42-47
investigated the relationship between journal and primary research characteristics
with abstracts reporting quality. Higher abstract reporting quality was associated with:
more recent publication date8,9,24,31,37,42,43,46,47, higher abstract word count8,9,25-27,44,
higher journal impact factor25,28,31,34,37, multicenter design8,39,42,45,47, higher number of
authors8,28,35, structured abstract8,9,31, reporting guidelines endorsement25,35,47, positive
outcomes statistical significance8,46, higher methodological quality25,35, less spin in the
abstracts25,26, European countries40 and academic funding source35. On the other hand,
some of the same variables have not been associated with abstracts reporting quality:
publication date25,38, abstract word count31,35,38,40, journal impact factor8,26,35,40,
number of centers25,34,37,38, number of authors9,31,34,37,38,40,45,49, abstract
format25,26,28,34,35,38,40, reporting guidelines endorsement8,9,26,28,40,46, outcomes
statistical significance34,38,39,42,45,47, methodological quality26, continent of first
author8,25,26,34,37-39,45 and funding source8,38,46,47. The most common items not
adequately reported (less than 50% of abstracts reporting) from the CONSORT-A
were: randomization, blinding, funding, numbers analyzed, harms, authors, trial
design, participants, primary outcomes results, registration, number randomized,
clearly defined primary outcomes, recruitment status, conclusions, interventions and
objectives; and for the PRISMA-A were: risk of bias, strengths and limitations of
evidence, funding, registration, information sources, and description of the effect.

CHAPTER 4
203
TABLE 1. Description of overviews analyzing abstracts reporting quality of healthcare RCTs and SRs. First author. Year of publication Aim of overview
Healthcare field Methods
Number of abstracts (year range) Main findings of abstracts reporting quality
Bigna. 20169 To assess abstracts reporting quality and to determine the factors associated with better reporting quality (before and after the release of the CONSORT-A).
Infectious diseases Data extracted using the original 17-item CONSORT-A: Mean CONSORT-Abstract score (scale 0-17; SD); Mean percentage score (95% CI); Percentage of abstracts reporting each item. Descriptive data to associate with abstracts reporting: journal IF; structured abstract; CONSORT endorser journal; intervention type (pharmacological or non-pharmacological); number of authors; publication on behalf of a research group; journal field (infectious diseases or general medicine).
153 RCTs (2014-2015) Mean CONSORT-Abstract score: 7.7 (SD 4.0); Mean percentage score: 58.6% (95% CI 57.6, 59.7); Range of abstracts reporting items: 12.0% (Blinding) to 93.0% (Interventions). Factors associated with better abstract reporting: non-pharmacological intervention type; higher number of authors; higher journal IF*.
Bigna. 201628 To assess abstracts reporting quality in journals with high IF and to determine the factors associated with better reporting quality (before and after the release of the PRISMA-A).
General medicine Data extracted using the 12-item PRISMA-A: Mean PRISMA-Abstract score (scale 0-12; SD); Percentage of abstracts reporting each item. Descriptive data to associate with abstracts reporting: publication date; abstract word count; PRISMA endorser journal; structured abstract; publication on behalf of a group; number of authors.
120 SRs (2014-2015) Mean PRISMA-Abstract score: 2014 6.8 (1.6); and 2015 7.5 (1.6); Range of abstracts reporting items (2015): 11.5% (Information sources) to 100.0% (Synthesis of results and Interpretation). Factors associated with better abstract reporting: more recent publication date; higher abstract word count (2014 and 2015); structured abstract (2014)*. <300 words: 22.5% abstracts; equal or >300 words: 77.5% words.
Blair. 201429 To assess abstracts reporting quality.
Pharmacy Data extracted using the modified 16-item CONSORT-A: Median CONSORT-Abstract score (scale 0-16; IQR); Median percentage score; Percentage of abstracts reporting each item.
63 RCTs (2009-2011) Median CONSORT-Abstract score: 9 (IQR 8 to 10); Median percentage score: 56.0% (IQR 50.0, 62.5); Range of abstracts reporting items: 0.0% (Registration and Funding) to 100.0% (Conclusions). Abstract word count range: 250-300.
Can. 201130 To assess abstracts reporting quality (before and after the release of the CONSORT-A).
Anesthesia Data extracted using the modified 16-item CONSORT-A: Mean percentage score (with 95% CI); Percentage of abstracts reporting each item.
252 RCTs (2008-2009) Mean percentage score: 29.0% (95% CI 27.2, 30.2%); Range of abstracts reporting items: 0.0% (Funding) to 90.1% (Objective). Journals abstract word limit range: 150-400.
Chen. 201831 To assess abstracts reporting quality and to determine the factors associated with better reporting quality (before and after the release of the CONSORT-A).
Dentistry Data extracted using the modified 16-item CONSORT-A: Mean CONSORT-Abstract score (scale 0-16; SD); Percentage of abstracts reporting each item. Descriptive data to associate with abstracts reporting: journal IF; number of authors; abstract word count; structured abstract; publication date.
87 RCTs (2010-2016) Mean CONSORT-Abstract score 6.1 (1.3). Range of abstracts reporting items: 0.0% (Randomization and Funding) to 100.0% (Interventions and Conclusions). Factors associated with better abstract reporting: higher journal IF; structured abstract; more recent publication date*. <200 words: 12.6% abstracts; 200-250 words: 40.2% abstracts; 250-300 words: 33.3% abstracts; >300 words: 13.8% abstracts. Journals abstract word limit range: 250-400.
Chow; 201824 To assess abstracts reporting quality and to determine whether there was an improvement over time.
Anesthesia Data extracted using the modified 16-item CONSORT-A: Median CONSORT-Abstract score (scale 0-16; IQR); Percentage of abstracts reporting each item. Descriptive data to associate with abstracts reporting: publication date.
395 RCTs (2010 and 2016) Median CONSORT-Abstract score for 2016 6.0 (5.0-8.0); Range of abstracts reporting item (2016): 0.0% (Funding) to 91.0% (Conclusions). Factors associated with better abstract reporting: more recent publication date. Journals abstract word limit range: 250-400.
Faggion. 201232 To assess abstracts reporting quality (before and after the release of the CONSORT-A).
Dentistry Data extracted using the modified 15-item CONSORT-A: Percentage of abstracts reporting each item.
209 RCTs (2009-2011) Range of abstracts reporting items: 0.0% (Funding) to 100.0% (Interventions and Conclusions).
Ghimire. 201233 To assess abstracts reporting quality in four journals with high IF.
General medicine Data extracted using the original 17-item CONSORT-A: Percentage of abstracts reporting each item.
271 RCTs (2010) Range of abstracts reporting items: 11.8% (Randomization) to 99.3% (Participants and Registration).

CHAPTER 4
204
TABLE 1. Description of overviews analyzing abstracts reporting quality of healthcare RCTs and SRs. First author. Year of publication Aim of overview
Healthcare field Methods
Number of abstracts (year range) Main findings of abstracts reporting quality
Ghimire. 201434 To assess abstracts reporting quality and to determine the factors associated with better reporting quality (before and after the release of the CONSORT-A).
Oncology Data extracted using the modified 18-item CONSORT-A: Mean CONSORT-Abstract score (scale 0-18; 95% CI); Mean percentage score (with 95% CI); Percentage of abstracts reporting each item. Descriptive data to associate with abstracts reporting: publication date; included journals (6 main journals and other); journal IF; continent of first author; number of authors; outcomes statistical significance (positive, negative or unclear); number of centers; structured abstract.
527 RCTs (2010-2012) Mean CONSORT-Abstract score: 9.9 (95% CI 9.7, 10.2); Mean percentage score: 55.2% (95% CI 53.8, 56.5); Range of abstracts reporting items: 6.8% (Randomization) to 100.0% (Interventions). Factors associated with better abstract reporting: trials published in the Lancet and Lancet Oncology; higher IF*.
Gómez-García. 201735 To assess abstracts reporting quality and to determine if the PRISMA-A indirectly captures the methodological quality and the risk of bias in the full texts.
Psoriasis Data extracted using the 12-item PRISMA-A: Median PRISMA-Abstract score (scale 0-12; range); Percentage of abstracts reporting each item. Descriptive data to associate with abstracts reporting: abstract word count; structured abstract; multiple affiliation and international collaboration (Cochrane or not); number of authors; funding source (academic, pharmaceutical or no funding); PRISMA endorser journal; journal IF; methodological quality.
139 SRs (2016-2017) Median PRISMA-Abstract score: 6.0 (2.0-11.0); Range of abstracts reporting items: 1.0% (Funding and Registration) to 95.0% (Objectives). Factors associated with better abstract reporting: higher number of authors; academic funding source; PRISMA endorser journal; higher methodological quality*. ≤300 words: 71.0% abstracts; >300 words: 29.0% abstracts.
Hays. 201636 To assess abstracts reporting quality in journals with high IF.
General medicine Data extracted using the modified 19-item CONSORT-A: Mean percentage score (with 95% CI); Percentage of abstracts reporting each item.
463 RCTs (2011-2014) Mean percentage score: 67.0% (95% CI 66.0, 68.0). Range of abstracts reporting items: 8.0% (Randomization) to 99.0% (Conclusions).
Hua. 201537 To assess abstracts reporting quality in journals with high IF and to determine the factors associated with better reporting quality (before and after the release of the CONSORT-A).
Dentistry Data extracted using the modified 16-item CONSORT-A: Mean CONSORT-Abstract score (scale 0-16; SD); Percentage of abstracts reporting each item. Descriptive data to associate with abstracts reporting: journal IF; continent of first author; publication date; number of authors; reported P value; number of centers.
159 RCTs (2010-2012) Mean CONSORT-Abstract score: 4.5 (SD 1.7). Range of abstracts reporting items: 0.6% (Randomization and Funding) to 98.1% (Objective and Conclusions). Factors associated with better abstract reporting: higher journal IF; more recent publication date*. <200 words: 25.8% abstracts; 200-250 words: 39.0% abstracts; 250-300 words: 28.9% abstracts; >300 words: 6.3% abstracts.
Janackovic. 201848 To assess abstracts reporting quality in seven journals with highest IF.
Anesthesia Data extracted using the 17-item CONSORT-A: Median percentage score (IQR); Percentage of abstracts reporting each item.
622 RCTs (2014-2016) Median percentage score 41.0% (IQR 35–53%); Range of abstracts reporting items: 0.2% (Funding) to 97.0% (Interventions). Journals abstract word limit range: 150-400.
Jin. 201638 To assess abstracts reporting quality in journals with high IF and to determine the factors associated with better reporting quality.
Laser medicine Data extracted using the modified 16-item CONSORT-A: Mean CONSORT-Abstract score (scale 0-16; SD); Percentage of abstracts reporting each item. Descriptive data to associate with abstracts reporting: 4 included journals; publication date; journal field (dentistry, dermatology, surgery or other); continent of first author; abstract word count; structured abstract; reported P value; outcomes statistical significance (positive or negative); number of centers; number of authors; sample size; funding source (yes or no); multiple affiliation and international collaboration.
129 RCTs (2014-2015) Mean CONSORT-Abstract score: 4.5 (SD 1.3). Range of abstracts reporting items: 0.0% (Recruitment, Primary outcomes results and Funding) to 98.4% (Objective). Factors associated with better abstract reporting: dermatology journal field*. <200 words: 5.4% abstracts; 200–250 words: 47.3% abstracts; 251–300 words: 31.8% abstracts; >300 words: 15.5% abstracts.
Kiriakou. 201439 To assess abstracts reporting quality and to determine the factors associated with better reporting quality.
Dentistry Data extracted using the modified 21-item CONSORT-A: Mean percentage score (with 95% CI); Percentage of abstracts reporting each item. Descriptive data to associate with abstracts reporting: 5 included journals; number of authors; continent of first author; outcomes statistical significance; number of centers.
163 RCTs (2008-2012) Mean percentage score: 58.6% (95% CI 57.6, 59.7); Range of abstracts reporting items: 0.0% (Registration) to 89.0% (Interventions). Factors associated with better abstract reporting: trials published in the European Journal of Oral Implantology; multicenter*.

CHAPTER 4
205
TABLE 1. Description of overviews analyzing abstracts reporting quality of healthcare RCTs and SRs. First author. Year of publication Aim of overview
Healthcare field Methods
Number of abstracts (year range) Main findings of abstracts reporting quality
Kumar. 201840 To assess abstracts reporting quality and to perform a bibliometric analysis.
Dentistry Data extracted using the modified 25-item CONSORT-A: Percentage of abstracts reporting each item. Descriptive data to associate with abstracts reporting: journal IF; abstract word count; number of authors; CONSORT endorser journal; continent of first author; structured abstract.
198 RCTs (2012) Range of abstracts reporting items: 0.0% (Funding) to 100.0% (Interventions). Factors associated with better abstract reporting: European countries of first author*. Abstract word count range: 48-569 (median 235, IQR: 205-269).
Kuriyama. 201741 To assess abstracts reporting quality (before and after the release of the CONSORT-A).
Critical care Data extracted using the modified 18-item CONSORT-A: Percentage of abstracts reporting each item.
166 RCTs (2011-2012) Range of abstracts reporting items: 1.8% (Randomization) to 97.0% (Conclusions). Journals abstract word limit range: 250-350.
Mbuagbaw. 201442 To assess abstracts reporting quality in journals with high IF (before and after the release of the CONSORT-A).
General medicine Data extracted using the original 17-item CONSORT-A: Mean CONSORT-Abstract score (scale 0–17; SD); Percentage of abstracts reporting each item. Descriptive data to associate with abstracts reporting: publication date; number of centers; intervention type (pharmaceutical or not); sample size; outcomes statistical significance (negative or positive).
100 RCTs (2012) Mean CONSORT-Abstract score: 12.1 (SD 2.2); Range of abstracts reporting items: 13.0% (Randomization) to 100.0% (Registration). Factors associated with better abstract reporting: post-CONSORT year of publication date; multicenter*.
Nascimento. 201925 To assess abstracts reporting quality and to determine the factors associated with better reporting quality.
Low back pain Data extracted using the modified 15-item CONSORT-A: Mean CONSORT-Abstract score (scale 0-15; SD); Percentage of abstracts reporting each item. Descriptive data to associate with abstracts reporting: number of centers; continent of first author; language (English or not); journal IF; CONSORT endorser journal; abstract word count; structured abstract; methodological quality; spin in the abstracts; date of publication.
200 RCTs (2010-2015) Mean CONSORT-Abstract score 5.1 (2.4). Range of abstracts reporting items: 2.0% (Randomization) to 97.0% (Objective). Factors associated with better abstract reporting: higher journal IF; CONSORT endorser journal; higher abstract word count; higher methodological quality; less spin in the abstracts*. Abstract mean word count: 258.0 (SD 67.3). Methodological quality (PEDro) mean score: 5.8 (SD 1.6; scale 0-10).
Nascimento. 201926 To assess abstracts reporting quality and to determine the factors associated with better reporting quality.
Low back pain Data extracted using the 12-item PRISMA-A: Mean PRISMA-Abstract score (scale 0-12; SD); Percentage of abstracts reporting each item. Descriptive data to associate with abstracts reporting: continent of first author; PRISMA endorser journal; structured abstract; journal IF; abstract word count; spin in the abstracts; methodological quality.
66 SRs (2015-2017) Mean PRISMA-Abstract score 4.9 (2.7); 4.1 (2.0) for non-Cochrane reviews and 9.9 (1.1) for Cochrane reviews. Range of abstracts reporting items: 3.0% (Eligibility criteria) to 87.7% (Title). Mean journals abstract word limit: Non-Cochrane 259.3 (SD 67.6); Cochrane 400.0. Methodological quality: 75.8% critically low; 10.6% low, 6.1% moderate (Cochrane only); 7.6% high (Cochrane only). Factors associated with better abstract reporting: higher abstract word count; less spin in the abstracts*. Median number of words: Non-Cochrane reviews 253.0 (IQR 716.0); Cochrane reviews 747.0 (IQR 514.0).
O’Donohoe. 201843 To assess abstracts reporting quality in 8 journals with highest IF.
Neurosurgical Data extracted using the modified 13-item PRISMA-A: Mean percentage score (95% CI). Descriptive data to associate with abstracts reporting: publication date.
257 SRs (2007-2017) Mean percentage score 56.5% (95% CI 47.8-60.9). Factors associated with better abstract reporting: post-PRISMA publication date.
Richter. 201644 To assess abstracts reporting quality.
Physical therapy Data extracted using the modified 20-item CONSORT-A: Percentage of abstracts reporting each item. Descriptive data to associate with abstracts reporting: word count.
150 RCTs (2009) Range of abstracts reporting items: 0.7% Randomization and Funding) to 100.0% (Trial design). Factors associated with better abstract reporting: higher word count.

CHAPTER 4
206
TABLE 1. Description of overviews analyzing abstracts reporting quality of healthcare RCTs and SRs. First author. Year of publication Aim of overview
Healthcare field Methods
Number of abstracts (year range) Main findings of abstracts reporting quality
Seehra. 201345 To assess abstracts reporting quality in seven journals with highest IF and to determine the factors associated with better reporting quality.
Dentistry Data extracted using the modified 21-item CONSORT-A: Mean percentage score (with 95% CI); Percentage of abstracts reporting each item. Descriptive data to associate with abstracts reporting: 7 included journals; continent of first author; number of authors; number of centers; outcomes statistical significance (positive or negative).
228 RCTs (2008-2011) Mean percentage score: 62.5% (95% CI 61.9, 63.0); Range of abstracts reporting items: 0.0% (Title) to 99.6% (Conclusions). Factors associated with better abstract reporting: multicenter*. Journals abstract word limit range: 200-250.
Sivendran. 201546 To assess abstracts reporting quality and to determine the factors associated with better reporting quality.
Oncology Data extracted using the modified 18-item CONSORT-A: Mean CONSORT-Abstract score (scale 0-18; SD); Percentage of abstracts reporting each item. Descriptive data to associate with abstracts reporting: CONSORT endorser journal; placebo controlled (yes or no); intervention type (chemotherapy, targeted or other); funding source (industry or other); intervention approved for another indication (yes or no); publication date; outcomes statistical significance (positive or negative); open access.
174 RCTs (2009-2011) Mean CONSORT-Abstract score: 9.2 (SD 2.7); Range of abstracts reporting items: 13.0% (Randomization) to 100.0% (Interventions). Factors associated with better abstract reporting: studies that had interventions approved for another indication; positive outcomes statistical significance; more recent publication date*.
Song. 20178 To assess abstracts reporting quality and to determine the factors associated with better reporting quality (before and after the release of the CONSORT-A).
Psychiatry Data extracted using the modified 18-item CONSORT-A: Mean CONSORT-Abstract score (scale 0-18; 95% CI); Mean percentage score (95% CI); Percentage of abstracts reporting each item. Descriptive data to associate with abstracts reporting: publication date; intervention type (pharmacological, psychological, both or others); journal field (general medicine or psychiatry journals; journal IF; number of authors; funding source (government, industry, both or none); continent of first author; number of centers; outcomes statistical significance (positive, negative or unclear); structured abstract; sample size; CONSORT endorser journal; abstract word count.
214 RCTs (2012-2014) Mean CONSORT-Abstract score: 8.2 (95% CI 7.8, 8.5); Mean percentage score: 45.4% (95% CI 43.5, 47.3); Range of abstracts reporting items: 2.0% (Randomization) to 99.0% (Conclusions). Factors associated with better abstract reporting: post-CONSORT publication date; pharmacological intervention type; general medicine journals; higher number of authors; multicenter; positive or negative outcomes statistical significance; structured abstract; higher abstract word count*. Abstract word count limit of 250, higher or no word limit: 88.8% abstracts.
Sriganesh. 201747 To assess abstracts reporting quality in five journals with high IF and to determine the factors associated with better reporting quality (before and after the release of the CONSORT-A).
Pain Data extracted using the original 17-item CONSORT-A: Mean CONSORT-Abstract score (scale 0–17; SD); Percentage of abstracts reporting each item. Descriptive data to associate with abstracts reporting: publication date; CONSORT endorser journal; number of centers; intervention type (non-pharmacological or pharmacological); sample size; outcomes statistical significance (positive or negative); funding source.
125 RCTs (2013-2015) Mean CONSORT-Abstract score: 7.1 (SD 1.9); Range of abstracts reporting items: 0.0% (Funding) to 99.2% (Interventions). Factors associated with better abstract reporting: post-CONSORT publication date; CONSORT endorser journal; multicenter; pharmacological intervention type*.
Tsou. 201627 To assess abstracts reporting quality.
General medicine Data extracted using the modified 15-item PRISMA-A: Mean PRISMA-Abstract score (scale 0-15; SD); Percentage of abstracts reporting each item. Descriptive data to associate with abstracts reporting: abstract word count.
200 SRs (2014) Mean PRISMA-Abstract score: 8.9 (SD 1.7). Range of abstracts reporting items: 1.0% (Funding) to 97.0% (Objectives). Factors associated with better abstract reporting: higher abstract word count. Mean abstract word count: 274.0 (SD 89.0).
Note: RCTs: Randomized Controlled Trials; SRs: Systematic Reviews; Mean CONSORT/PRISMA-Abstract score: mean number of items reported in all abstracts; Mean percentage score: mean percentage of items reported in all abstracts; CONSORT-A: Consolidated Standards of Reporting Trials for Abstracts checklist; PRISMA-A: Preferred Reporting Items for Systematic Reviews and Meta-Analysis for Abstracts checklist; CI: Confidence Interval; SD: Standard Deviation; IF: Impact Factor; IQR: Interquartile Range; PEDro scale: Physiotherapy Evidence Database scale. *There was no association between the remaining descriptive data.
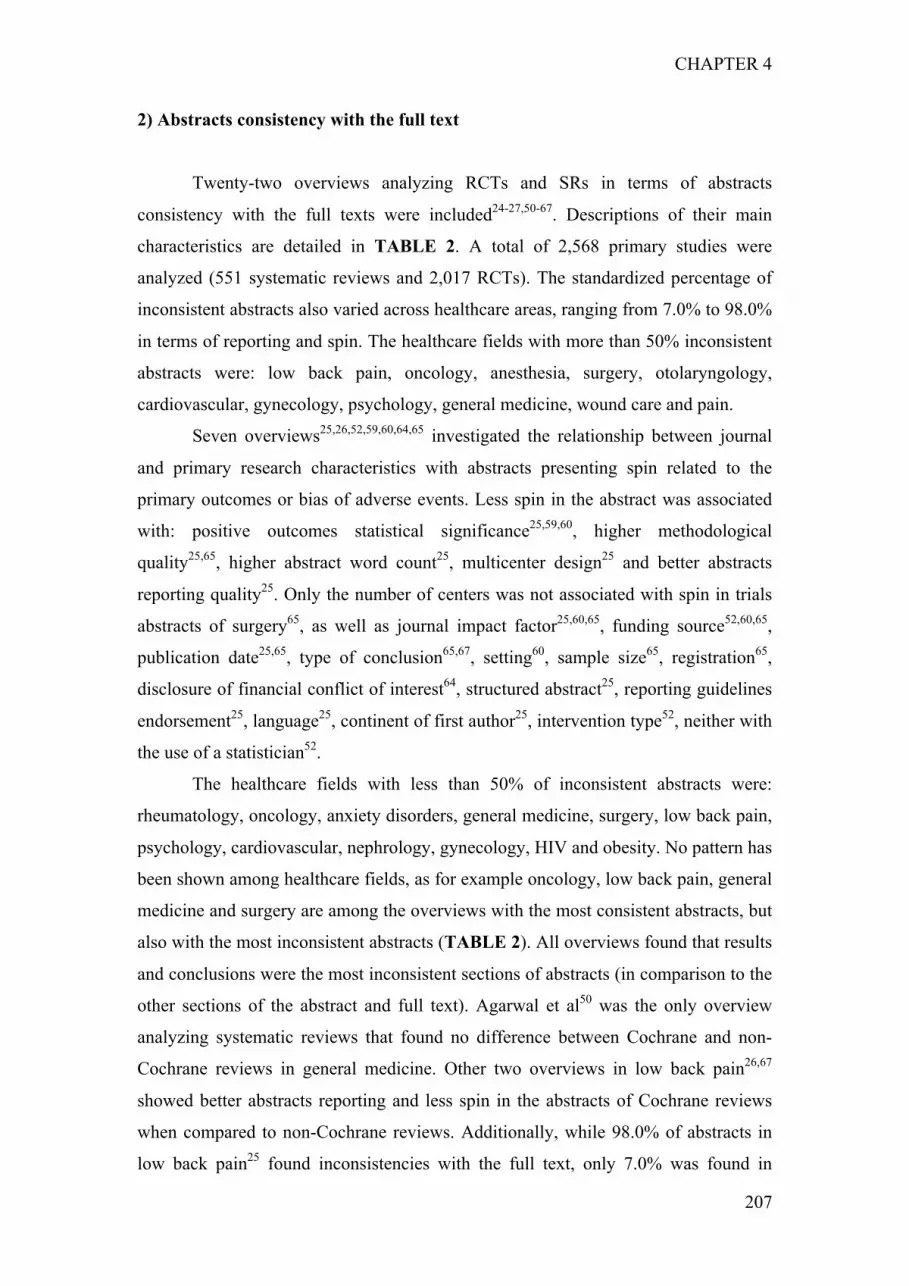
CHAPTER 4
207
2) Abstracts consistency with the full text
Twenty-two overviews analyzing RCTs and SRs in terms of abstracts
consistency with the full texts were included24-27,50-67. Descriptions of their main
characteristics are detailed in TABLE 2. A total of 2,568 primary studies were
analyzed (551 systematic reviews and 2,017 RCTs). The standardized percentage of
inconsistent abstracts also varied across healthcare areas, ranging from 7.0% to 98.0%
in terms of reporting and spin. The healthcare fields with more than 50% inconsistent
abstracts were: low back pain, oncology, anesthesia, surgery, otolaryngology,
cardiovascular, gynecology, psychology, general medicine, wound care and pain.
Seven overviews25,26,52,59,60,64,65 investigated the relationship between journal
and primary research characteristics with abstracts presenting spin related to the
primary outcomes or bias of adverse events. Less spin in the abstract was associated
with: positive outcomes statistical significance25,59,60, higher methodological
quality25,65, higher abstract word count25, multicenter design25 and better abstracts
reporting quality25. Only the number of centers was not associated with spin in trials
abstracts of surgery65, as well as journal impact factor25,60,65, funding source52,60,65,
publication date25,65, type of conclusion65,67, setting60, sample size65, registration65,
disclosure of financial conflict of interest64, structured abstract25, reporting guidelines
endorsement25, language25, continent of first author25, intervention type52, neither with
the use of a statistician52.
The healthcare fields with less than 50% of inconsistent abstracts were:
rheumatology, oncology, anxiety disorders, general medicine, surgery, low back pain,
psychology, cardiovascular, nephrology, gynecology, HIV and obesity. No pattern has
been shown among healthcare fields, as for example oncology, low back pain, general
medicine and surgery are among the overviews with the most consistent abstracts, but
also with the most inconsistent abstracts (TABLE 2). All overviews found that results
and conclusions were the most inconsistent sections of abstracts (in comparison to the
other sections of the abstract and full text). Agarwal et al50 was the only overview
analyzing systematic reviews that found no difference between Cochrane and non-
Cochrane reviews in general medicine. Other two overviews in low back pain26,67
showed better abstracts reporting and less spin in the abstracts of Cochrane reviews
when compared to non-Cochrane reviews. Additionally, while 98.0% of abstracts in
low back pain25 found inconsistencies with the full text, only 7.0% was found in

CHAPTER 4
208
abstracts of rheumatology59. Only a few overviews reported information regarding the
methodological quality of the studies, which were higher for Cochrane reviews in
comparison to non-Cochrane reviews26,67. Also just a few overviews25-27 reported the
mean (or median) abstract word count, which varied between 258 and 747, being the
higher number from Cochrane reviews abstracts. The most common terminology
presented in the overviews was: 77.0% for spin, 68.0% mislead, 64.0% bias, 59.0%
inconsistency/consistency, 45.0% for misrepresentation, and 41.0% for distortion,
inaccuracy/accuracy and reporting bias. Other terminology less frequent was:
misinterpretation, discrepancy, overemphasis, overestimate, deficiency, publication
bias, interpretation bias, comparison, discordance/concordance, overstate,
underestimate, wording, reporting mistakes, directional bias, over-representation and
restatement.
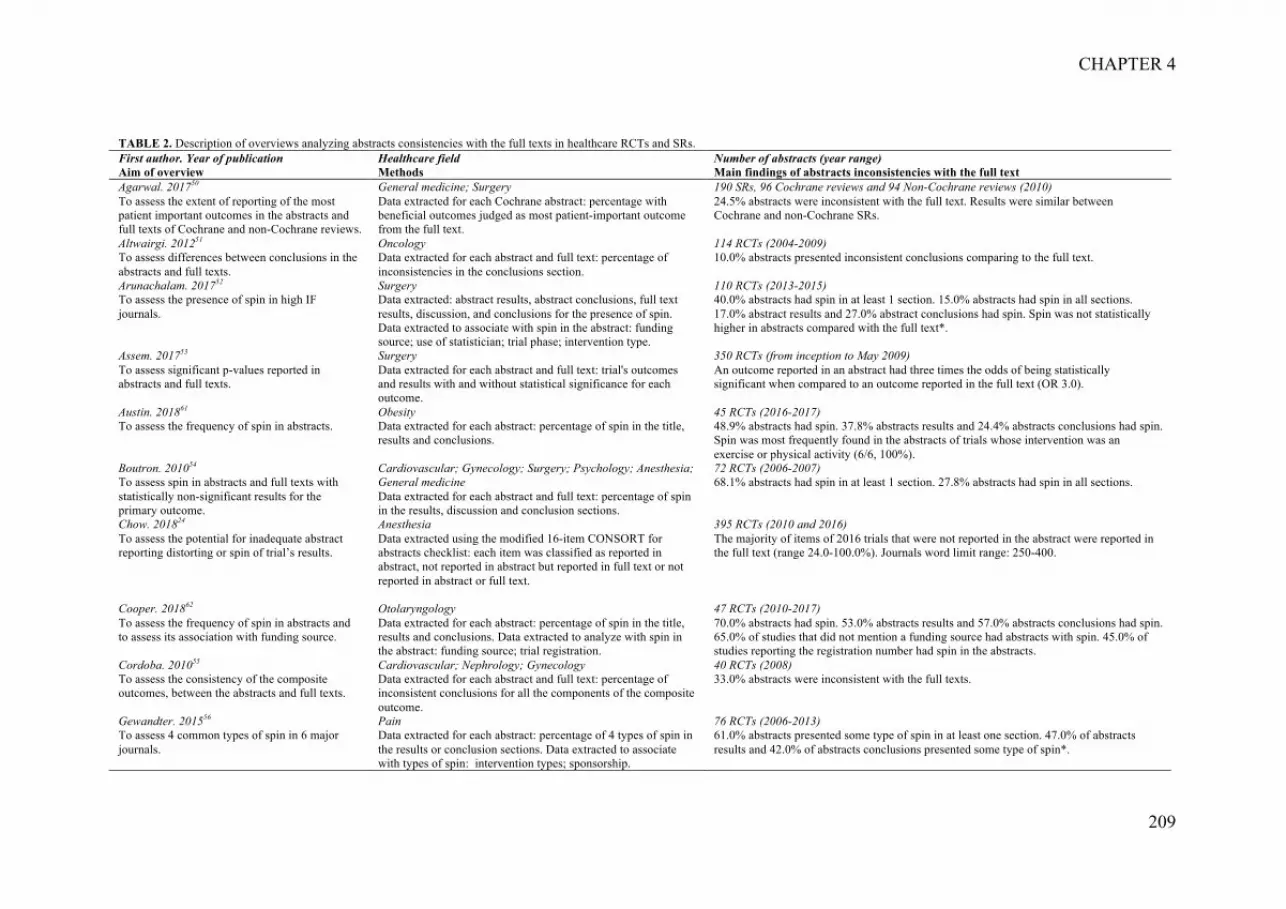
CHAPTER 4
209
TABLE 2. Description of overviews analyzing abstracts consistencies with the full texts in healthcare RCTs and SRs. First author. Year of publication Aim of overview
Healthcare field Methods
Number of abstracts (year range) Main findings of abstracts inconsistencies with the full text
Agarwal. 201750 To assess the extent of reporting of the most patient important outcomes in the abstracts and full texts of Cochrane and non-Cochrane reviews.
General medicine; Surgery Data extracted for each Cochrane abstract: percentage with beneficial outcomes judged as most patient-important outcome from the full text.
190 SRs, 96 Cochrane reviews and 94 Non-Cochrane reviews (2010) 24.5% abstracts were inconsistent with the full text. Results were similar between Cochrane and non-Cochrane SRs.
Altwairgi. 201251 To assess differences between conclusions in the abstracts and full texts.
Oncology Data extracted for each abstract and full text: percentage of inconsistencies in the conclusions section.
114 RCTs (2004-2009) 10.0% abstracts presented inconsistent conclusions comparing to the full text.
Arunachalam. 201752 To assess the presence of spin in high IF journals.
Surgery Data extracted: abstract results, abstract conclusions, full text results, discussion, and conclusions for the presence of spin. Data extracted to associate with spin in the abstract: funding source; use of statistician; trial phase; intervention type.
110 RCTs (2013-2015) 40.0% abstracts had spin in at least 1 section. 15.0% abstracts had spin in all sections. 17.0% abstract results and 27.0% abstract conclusions had spin. Spin was not statistically higher in abstracts compared with the full text*.
Assem. 201753 To assess significant p-values reported in abstracts and full texts.
Surgery Data extracted for each abstract and full text: trial's outcomes and results with and without statistical significance for each outcome.
350 RCTs (from inception to May 2009) An outcome reported in an abstract had three times the odds of being statistically significant when compared to an outcome reported in the full text (OR 3.0).
Austin. 201861 To assess the frequency of spin in abstracts.
Obesity Data extracted for each abstract: percentage of spin in the title, results and conclusions.
45 RCTs (2016-2017) 48.9% abstracts had spin. 37.8% abstracts results and 24.4% abstracts conclusions had spin. Spin was most frequently found in the abstracts of trials whose intervention was an exercise or physical activity (6/6, 100%).
Boutron. 201054 To assess spin in abstracts and full texts with statistically non-significant results for the primary outcome.
Cardiovascular; Gynecology; Surgery; Psychology; Anesthesia; General medicine Data extracted for each abstract and full text: percentage of spin in the results, discussion and conclusion sections.
72 RCTs (2006-2007) 68.1% abstracts had spin in at least 1 section. 27.8% abstracts had spin in all sections.
Chow. 201824 To assess the potential for inadequate abstract reporting distorting or spin of trial’s results.
Anesthesia Data extracted using the modified 16-item CONSORT for abstracts checklist: each item was classified as reported in abstract, not reported in abstract but reported in full text or not reported in abstract or full text.
395 RCTs (2010 and 2016) The majority of items of 2016 trials that were not reported in the abstract were reported in the full text (range 24.0-100.0%). Journals word limit range: 250-400.
Cooper. 201862 To assess the frequency of spin in abstracts and to assess its association with funding source.
Otolaryngology Data extracted for each abstract: percentage of spin in the title, results and conclusions. Data extracted to analyze with spin in the abstract: funding source; trial registration.
47 RCTs (2010-2017) 70.0% abstracts had spin. 53.0% abstracts results and 57.0% abstracts conclusions had spin. 65.0% of studies that did not mention a funding source had abstracts with spin. 45.0% of studies reporting the registration number had spin in the abstracts.
Cordoba. 201055 To assess the consistency of the composite outcomes, between the abstracts and full texts.
Cardiovascular; Nephrology; Gynecology Data extracted for each abstract and full text: percentage of inconsistent conclusions for all the components of the composite outcome.
40 RCTs (2008) 33.0% abstracts were inconsistent with the full texts.
Gewandter. 201556 To assess 4 common types of spin in 6 major journals.
Pain Data extracted for each abstract: percentage of 4 types of spin in the results or conclusion sections. Data extracted to associate with types of spin: intervention types; sponsorship.
76 RCTs (2006-2013) 61.0% abstracts presented some type of spin in at least one section. 47.0% of abstracts results and 42.0% of abstracts conclusions presented some type of spin*.

CHAPTER 4
210
TABLE 2. Description of overviews analyzing abstracts consistencies with the full texts in healthcare RCTs and SRs. First author. Year of publication Aim of overview
Healthcare field Methods
Number of abstracts (year range) Main findings of abstracts inconsistencies with the full text
Hernandez. 201363 To assess spin in trials in which non-inferiority was inconclusive or not established.
HIV Data extracted: spin in the abstracts results and conclusions; spin in the full text results, discussion and conclusions.
42 RCTs (1960-2011) 23/42 studies were evaluated for spin: 68.0% abstracts had spin in at least one section. 43.5% abstracts results and conclusions (or conclusions only) had spin. Poor overall quality by CONSORT extension.
Lehmen. 201457 To assess the prevalence of inconsistencies between abstracts and full texts.
Surgery Data extracted: percentage of items regarding inconsistencies or bias between the abstract and full text.
40 RCTs (2001-2010) 75.0% abstracts were inconsistent with the full texts and 10.0% abstracts conclusions were inconsistent with the full texts.
Lieb. 201664 To assess whether non-financial conflicts of interest increase the risk of spin in the conclusions of the reviews.
Psychology Data extracted: percentage of spin in the abstracts evaluated by consistency between the abstract conclusion with results in the full text. Data extracted to associate with spin in the abstract: journals with disclosure of financial conflicts of interest (financial, non-financial and personal).
95 SRs (2010-2013) 28.0% abstracts had spin. Reviews with inclusion of own primary studies showed more often spin than reviews without inclusion of own primary studies of the review authors (OR=2.08).*
Lockyer. 201358 To assess the frequency of statistically significant and non-significant outcomes in abstracts.
Wound care Data extracted for studies with statistically non-significant differences for the primary outcome: spin in the abstract results and conclusions, and full text results, discussion and conclusions.
71 RCTs (2004-2009) 63.0% abstracts and 59.0% abstract conclusions had spin. 89.0% of the industry-funded trials had spin in the abstract conclusions. 60.0% of not-for-profit funded trials had spin in the abstract.
Mathieu. 201259 To assess the prevalence of misleading conclusions in abstracts and to determine whether abstract conclusions are based on the primary outcome in the full text.
Rheumatology Data extracted: assessment of the results section of the full text, assessment of the abstract conclusions, and determining the existence of a misleading conclusion in the abstract. Data extracted to associate with misleading conclusions in the abstract: journal impact factor, sample size and outcome statistical significance (positive, negative and inaccurate).
144 RCTs (2006-2008) 22.9% abstracts conclusions were misleading and 7.0% were inconsistent with the full text. Negative trial results were associated with misleading abstract conclusions (OR 9.6)*.
Nascimento. 201925 To assess the frequency of spin in abstracts, consistency between abstracts and full text and association of spin with negative results.
Low back pain Data extracted: percentage of spin in each abstract and full text; consistency was calculated by evaluation of statistical difference between abstract and full text scores (for reporting and spin) and agreement for each item. Data extracted to associate with spin in the abstract: primary outcome statistical significance (positive or negative); abstracts reporting quality; number of centers; continent of first author; language (English or not); journal IF; CONSORT endorser journal; abstract word count; structured abstract; methodological quality; date of publication.
200 RCTs (2010-2015) 98.0% abstracts presented at least one item of spin. Abstracts reporting scores were inconsistent with the full texts and agreement for each item ranged from slight to moderate. Abstracts presented more spin than the full text and agreement for each item of spin ranged from fair to moderate between abstracts and full texts. Mean abstract word count: 258 (SD 67.3). Methodological quality (PEDro scale 0-10, the higher the better): 5.8 (SD 1.6). Less spin in the abstracts was associated with better abstracts reporting quality, positive primary outcome results, multicenter trials, higher abstract word count and higher methodological quality*.
Nascimento. 201967 To assess the frequency of spin in abstracts, consistency between abstracts and full text and association of spin with the type of conclusion.
Low back pain Data extracted: percentage of spin in each abstract and full text; consistency was calculated by agreement between each item of spin between abstract and full text. Data extracted to associate with spin in the abstract: types of conclusions (positive, negative, neutral or indeterminate).
66 SRs (2015-2017) 80.3% abstracts had some type of spin. Most items of spin had fair to moderate agreement between the abstract and full text (Cochrane reviews were better than non-Cochrane). 75.8% of reviews presented critically low methodological quality, 10.6% low, 7.6% high and 6.1% moderate. High and moderate quality were all Cochrane reviews.*

CHAPTER 4
211
TABLE 2. Description of overviews analyzing abstracts consistencies with the full texts in healthcare RCTs and SRs. First author. Year of publication Aim of overview
Healthcare field Methods
Number of abstracts (year range) Main findings of abstracts inconsistencies with the full text
Nascimento. 201926 To evaluate abstracts reporting consistencies with the full text.
Low back pain Data extracted using the 12-item PRISMA for abstracts checklist: consistency between abstract and full text scores by evaluation of statistical difference and agreement for each item.
66 SRs (2015-2017) Abstracts reporting scores were inconsistent with the full-texts scores, with similar results for both Cochrane and non-Cochrane reviews. Most items had slight to moderate agreement between the abstract and full text. Median number of words: Total sample 259.0 (IQR 909.0); Non-Cochrane reviews 253.0 (716.0); Cochrane reviews 747.0 (514.0). 75.8% of reviews presented critically low methodological quality, 10.6% low, 6.1% moderate and 7.6% high. Moderate and high were all Cochrane reviews.
Patel. 201365 To assess the prevalence of spin and possible associations with risk factors.
Surgery Data extracted: spin in the abstracts and the full texts conclusions. Data extracted to associate with spin in the abstract: date of publication (1992-2003 or 2004-2012); journal IF; disease types; sample size; trial registration; number of centers; authors’ conclusions; funding source (industry, nonindustry or not reported); items of methodological quality (adequate randomization, allocation concealment, blinding, intention-to-treat).
58 RCTs (1992-2012) 59.0% of abstracts had spin. Trials with adequate randomization were associated with an increased odds of spin (OR 0.3) and trials without an intention-to-treat analysis all had spin.*
Roest. 201566 To assess publication bias, outcome reporting bias and spin in trials abstracts.
Anxiety disorders Data extracted: publication bias, outcome reporting bias and spin (abstract conclusion not consistent with full text results on primary outcome).
49 RCTs (Inception-2012) 28.0% trials had publication bias, from those 19.0% had outcome reporting bias and spin in the abstract.
Tsou. 201627 To assess the clarity of abstracts conclusions.
General Medicine Data extracted for each abstract: assessment of the use of potentially misleading language in the conclusions, based on statistical significance of the primary outcome and vague or wishful wording.
200 SRs (2014) 62.0% abstracts conclusions made clear statements. 38.0% abstracts conclusions were unclear. The most common problem was simple restatement in 20.0% of abstracts. Mean abstract word count: 274 (SD 89).
Vera-Badillo. 201360 To assess reporting bias of the primary outcome and adverse events and to guide readers in judging the credibility of the conclusions.
Oncology Data extracted: prevalence of bias or spin for the primary outcome and adverse events in the abstracts conclusion comparing to the results of the full texts. Data extracted to associate with spin of primary outcomes and bias of adverse events in the abstract: funding source; journal IF; setting of the trial; outcome statistical significance.
164 RCTs (1995-2011) Trials with non-statistically significant results for the primary outcome were associated with spin in the conclusion section of the abstract (OR 5.2). Trials with statistically significant results for the primary outcome were associated with bias of adverse events (OR 2.0)*.
Note: RCTs: Randomized Controlled Trials; SRs: Systematic Reviews; OR: Odds Ratio; SD: Standard Deviation; PEDro scale: Physiotherapy Evidence Database scale; CONSORT: Consolidated Standards of Reporting Trials; IF: Impact Factor. *There was no association between the variables extracted.

CHAPTER 4
212
DISCUSSION
Abstracts reporting quality
The main finding is that even after the release of the CONSORT-A and
PRISMA-A, abstracts of RCTs and SRs reporting quality still remains suboptimal
with much room for improvement in all healthcare areas. There was no clear pattern
of abstracts reporting quality across healthcare areas, for example an overview that
analyzed dentistry RCTs presented 62.5% abstracts with fully reported items45, while
another overview analyzing also dentistry RCTs presented 28.1%37. Clear factors that
have been associated with higher abstracts reporting quality were: more recent
publication date8,9,24,31,37,42,43,46,47, higher abstract word count8,9,25-27,44, higher journal
impact factor25,28,31,34,37 and multicenter design8,39,42,45,47; as opposed to no association
with the following factors: abstract format25,26,28,34,35,38,40, number of
authors9,31,34,37,38,40,45,49, reporting guidelines endorsement8,9,26,28,40,46, outcomes
statistical significance34,38,39,42,45,47, continent of first author8,25,26,34,37-39,45 and funding
source8,38,46,47. Important considerations in terms of abstract word count are stated by
the CONSORT group68, in which 250 to 300 words are considered sufficient to
address all of the items in the CONSORT-A, while the PRISMA group has not
suggested any word limit11. Our results suggest that the number of words should be
higher than 300 words (400 or higher) for better abstracts reporting quality.
Adequately reporting abstracts help researchers and clinicians to properly interpret the
abstract with important decision-making on effectiveness of treatment for healthcare.
Most importantly, higher abstracts reporting quality has been associated with less spin
in the abstracts (with high percentages of explained variability25,26), as well as
systematic review abstracts with higher study methodological quality35 (Cochrane
reviews better than non-Cochrane26).
Abstracts consistency with the full text
All overviews analyzing consistency between abstracts and full texts stated
that the abstracts results and conclusion sections were the most inconsistent with their
corresponding full texts in terms of reporting and presence of spin. There was also no
pattern across healthcare areas for inconsistent abstracts, as an overview analyzing

CHAPTER 4
213
oncology RCTs presented 10.0% of inconsistent abstracts51 and another overview also
analyzing oncology RCTs presented 84.0%60. The terminology presented in the
overviews are in accordance with previous literature, which also found the terms
‘inconsistency/consistency’ and ‘inaccuracy/accuracy’ as two of the most frequent to
analyze differences between abstracts and full texts12. However, the most prevalent
terms we found were ‘mislead’, ‘spin’ and ‘bias’, all more related to interpretation
rather than reporting. The main factors associated with spin in abstracts seem to be
related to selective reporting of primary outcome statistical significance25,59,60, which
corroborate with the findings of Chiu et al14. In order to avoid spin in abstracts, better
checking of methodological and reporting guidelines, as well as more flexible
abstracts word count should be made. Abstracts with spin disseminated in press
releases and news coverage6,69-71 might look more attractive for readers, but it is most
likely to harm clinical decision-making13, which can bring serious consequences
affecting patients (e.g. oncology field)51.
Several recommendations have been given by all the included overviews,
which mainly directed to journal editors and reviewers for changing the quality of
future research. The most common recommendations to the journal editorial policies
were: explicit journal endorsement and stricter adherence to the abstracts reporting
checklist (highlighted as one of the 'instructions for authors')8,9,25-34,36-47,50-
56,59,60,62,63,67; better checking of abstracts consistency of reporting and interpretation
with the full text26,27,50,51,54-59,62,65-67, including consistency between the registration
protocol and the actual publication59,62,66; awareness of spin in the
abstracts25,46,47,50,52,58,60,61,63-66; critical appraisal skills training for all users of
research25,58,61,62,64,65, and revision of abstract word count26,27,67. Recommendations
were also directed to readers, so they do not rely solely on abstracts for decision-
making, when they should actually read and interpret the corresponding full texts25,51-
53,56-58,65.
It seems that healthcare journal editors and reviewers are either unaware of the
importance of avoiding inconsistencies between abstracts and full texts72 or not
sufficiently trained to detect interpretation or reporting mistakes in abstracts15,73-75.
We advise journal editors and reviewers to take aside the author’s conclusions of the
study being evaluated and to interpret the RCTs and SRs results by themselves, taking
into consideration items to evaluate spin across studies13-15. Other recommendations
in accordance with a SR on spin were to promote full access to open data to improve

CHAPTER 4
214
results interpretation among researchers, lessen the pressure to publish ‘positive’
results and be careful with dissemination of study results in the media14. Additionally,
this SR suggested further research on the development of a tool to assess spin of
results in abstracts and full texts14, which is a very challenging task due to the
subjectivity of terms to report the interpretation of study results (e.g. significant
results vs. statistically significant results vs. clinically important results).
Ultimately, research e-training programs should be implemented not only to
journal editors and reviewers, but also from the beginning of a researcher pathway as
a graduate student76. High quality and reliable abstracts are part of the research code
of conduct for research integrity77 and is also a matter of ethical principles on
research78. Abstracts of RCTs and SRs can be the only available source for healthcare
professionals2-4, can be harmful if poorly reported or mislead5,6. But an even more
important implication is to avoid dissemination of such abstracts among academic
press releases and media coverage of research5,6.
Strengths and limitations
Our systematic review has strengths in that we collected all overviews
analyzing a large sample of abstracts in all healthcare areas and we did not include
conference abstracts. Our main limitations are related to the possibility of duplicate
studies analyzed from the overviews and the fact that it was not possible to evaluate
the overviews methodological quality, as there is no guideline for assessing this type
of study design.
CONCLUSION
The results of the overviews are consistent in which abstracts of healthcare
RCTs and SRs have shown a great space for improvement in reporting quality and
consistency with the full text. Abstracts are the highest profile part of a research study
and recommendations to authors, journal editors and reviewers need to be put into
action as highest priority.

CHAPTER 4
215
REFERENCES
1. Herbert R, Jamtvedt G, Mead J, Hagen KB. Practical evidence-based
physiotherapy. 2nd Edition ed: Elsevier Butterworth-Heinemann; 2011.
2. Maher CG, Sherrington C, Elkins M, Herbert RD, Moseley AM. Challenges
for evidence-based physical therapy: accessing and interpreting high-quality evidence
on therapy. Phys Ther. 2004;84(7):644-654.
3. Bennett S, McKenna K, Hoffmann T, Tooth L, McCluskey A, Strong J. The
value of an evidence database for occupational therapists: an international online
survey. Int J Med Inform. 2007;76(7):507-513.
4. Silva TM, Costa LCM, Garcia AN, Costa LO. What do physical therapists
think about evidence-based practice? A systematic review. Man Ther.
2014;20(3):388-401.
5. Haneef R, Lazarus C, Ravaud P, Yavchitz A, Boutron I. Interpretation of
Results of Studies Evaluating an Intervention Highlighted in Google Health News: A
Cross-Sectional Study of News. PLoS One. 2015;10(10):e0140889.
6. Yavchitz A, Boutron I, Bafeta A, et al. Misrepresentation of randomized
controlled trials in press releases and news coverage: a cohort study. PLoS Med.
2012;9(9):e1001308.
7. Chhapola V, Tiwari S, Brar R, Kanwal SK. Reporting quality of trial
abstracts-improved yet suboptimal: A systematic review and meta-analysis. J Evid
Based Med. 2018.
8. Song SY, Kim B, Kim I, et al. Assessing reporting quality of randomized
controlled trial abstracts in psychiatry: Adherence to CONSORT for abstracts: A
systematic review. PLoS ONE. 2017;12(11):e0187807.
9. Bigna JJ, Um LN, Nansseu JR. A comparison of quality of abstracts of
systematic reviews including meta-analysis of randomized controlled trials in high-
impact general medicine journals before and after the publication of PRISMA
extension for abstracts: a systematic review and meta-analysis. Syst Rev.
2016;5(1):174.
10. Hopewel S, Clarke M, Moher D, et al. CONSORT for reporting randomized
controlled trials in journal and conference abstracts: explanation and elaboration.
PLoS Med. 2008;5(1):201-209.

CHAPTER 4
216
11. Beller EM, Glasziou PP, Altman DG, et al. PRISMA for Abstracts: reporting
systematic reviews in journal and conference abstracts. PLoS Med.
2013;10(4):e1001419.
12. Li G, Abbade LPF, Nwosu I, et al. A scoping review of comparisons between
abstracts and full reports in primary biomedical research. BMC Med Res Methodol.
2017;17(1):181.
13. Boutron I, Altman DG, Hopewell S, Vera-Badillo F, Tannock I, Ravaud P.
Impact of spin in the abstracts of articles reporting results of randomized controlled
trials in the field of cancer: the SPIIN randomized controlled trial. J Clin Oncol.
2014;32(36):4120-4126.
14. Chiu K, Grundy Q, Bero L. 'Spin' in published biomedical literature: A
methodological systematic review. PLoS Biol. 2017;15(9):e2002173.
15. Yavchitz A, Ravaud P, Altman DG, et al. A new classification of spin in
systematic reviews and meta-analyses was developed and ranked according to the
severity. J Clin Epidemiol. 2016;75:56-65.
16. Moher D, Altman DG. Four Proposals to Help Improve the Medical Research
Literature. PLoS Med. 2015;12(9):e1001864.
17. Page MJ, Shamseer L, Altman DG, et al. Epidemiology and Reporting
Characteristics of Systematic Reviews of Biomedical Research: A Cross-Sectional
Study. PLoS Med. 2016;13(5):e1002028.
18. Wang L, Li Y, Li J, et al. Quality of reporting of trial abstracts needs to be
improved: using the CONSORT for abstracts to assess the four leading Chinese
medical journals of traditional Chinese medicine. Trials. 2010;11:75.
19. Ghimire S, Kyung E, Kang W, Kim E. Assessment of adherence to the
CONSORT statement for quality of reports on randomized controlled trial abstracts
from four high-impact general medical journals. Trials. 2012;13:77.
20. Kiriakou J, Pandis N, Madianos P, Polychronopoulou A. Assessing the
reporting quality in abstracts of randomized controlled trials in leading journals of
oral implantology. J Evid Based Dent Pract. 2014;14(1):9-15.
21. Higgins JP, Altman DG, Gotzsche PC, et al. The Cochrane Collaboration's
tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928.
22. Whiting P, Savovic J, Higgins JP, et al. ROBIS: A new tool to assess risk of
bias in systematic reviews was developed. J Clin Epidemiol. 2016;69:225-234.
CHAPTER 4
217
23. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting
items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg.
2010;8(5):336-341.
24. Chow JTY, Turkstra TP, Yim E, Jones PM. The degree of adherence to
CONSORT reporting guidelines for the abstracts of randomised clinical trials
published in anaesthesia journals: A cross-sectional study of reporting adherence in
2010 and 2016. Eur J Anaesthesiol. 2018:942-948.
25. Nascimento DP, Costa LOP, Gonzalez GZ, Maher CG, Moseley AM.
Abstracts of low back pain trials are poorly reported and inconsistent with the full
text: An overview study. Arch Phys Med Rehabil (accepted for publication). 2019.
26. Nascimento DP, Gonzalez GZ, Araujo AC, Moseley AM, Maher CG, Costa
LOP. Reporting of systematic review abstracts relevant to low back pain and
inconsistencies with the full text: an overview study. Spine (under review). 2019.
27. Tsou AY, Treadwell JR. Quality and clarity in systematic review abstracts: an
empirical study. Res. 2016;7(4):447-458.
28. Bigna JJ, Noubiap JJ, Asangbeh SL, et al. Abstracts reporting of HIV/AIDS
randomized controlled trials in general medicine and infectious diseases journals:
completeness to date and improvement in the quality since CONSORT extension for
abstracts. BMC Med Res Methodol. 2016;16(1):138.
29. Blair DA, Hughes PJ, Woolley TW. Pharmacy journal abstracts published in
PubMed that abide by the CONsolidated Standards Of Reporting Trials (CONSORT)
guidelines. Journal of the Medical Library Association : JMLA. 2014;102(2):110-114.
30. Can OS, Yilmaz AA, Hasdogan M, et al. Has the quality of abstracts for
randomised controlled trials improved since the release of Consolidated Standards of
Reporting Trial guideline for abstract reporting? A survey of four high-profile
anaesthesia journals. Eur J Anaesthesiol. 2011;28(7):485-492.
31. Chen J, Li Z, Liu B, Gan X, Li C, Yu H. Quality improvement in randomized
controlled trial abstracts in prosthodontics since the publication of CONSORT
guideline for abstracts: a systematic review. J Dent. 2018:23-29.
32. Faggion CM, Jr., Giannakopoulos NN. Quality of reporting in abstracts of
randomized controlled trials published in leading journals of periodontology and
implant dentistry: a survey. J Periodontol. 2012;83(10):1251-1256.

CHAPTER 4
218
33. Ghimire S, Kyung E, Kang W, Kim E. Assessment of adherence to the
CONSORT statement for quality of reports on randomized controlled trial abstracts
from four high-impact general medical journals. Trials. 2012;13:77.
34. Ghimire S, Kyung E, Lee H, Kim E. Oncology trial abstracts showed
suboptimal improvement in reporting: A comparative before-and-after evaluation
using CONSORT for Abstract guidelines. J Clin Epidemiol. 2014;67(6):658-666.
35. Gomez-Garcia F, Ruano J, Aguilar-Luque M, et al. Abstract analysis method
facilitates filtering low-methodological quality and high-bias risk systematic reviews
on psoriasis interventions. BMC Med Res Methodol. 2017;17(1):180.
36. Hays M, Andrews M, Wilson R, Callender D, O'Malley PG, Douglas K.
Reporting quality of randomised controlled trial abstracts among high-impact general
medical journals: a review and analysis. BMJ Open. 2016;6(7):e011082.
37. Hua F, Deng L, Kau CH, Jiang H, He H, Walsh T. Reporting quality of
randomized controlled trial abstracts: survey of leading general dental journals.
Journal of the American Dental Association (1939). 2015;146(9):669-678.
38. Jin L, Hua F, Cao Q. Reporting quality of randomized controlled trial abstracts
published in leading laser medicine journals: an assessment using the CONSORT for
abstracts guidelines. Lasers Med Sci. 2016;31(8):1583-1590.
39. Kiriakou J, Pandis N, Madianos P, Polychronopoulou A. Assessing the
reporting quality in abstracts of randomized controlled trials in leading journals of
oral implantology. J. 2014;14(1):9-15.
40. Kumar S, Mohammad H, Vora H, Kar K. Reporting Quality of Randomized
Controlled Trials of Periodontal Diseases in Journal Abstracts-A Cross-sectional
Survey and Bibliometric Analysis. J Evid Based Dent Pract. 2018;18(2):130-141
e122.
41. Kuriyama A, Takahashi N, Nakayama T. Reporting of critical care trial
abstracts: a comparison before and after the announcement of CONSORT guideline
for abstracts. Trials. 2017;18(1):32.
42. Mbuagbaw L, Thabane M, Vanniyasingam T, et al. Improvement in the
quality of abstracts in major clinical journals since CONSORT extension for
abstracts: A systematic review. Contemp Clin Trials. 2014;38(2):245-250.
43. O'Donohoe TJ, Dhillon R, Bridson TL, Tee J. Reporting Quality of Systematic
Review Abstracts Published in Leading Neurosurgical Journals: A Research on
Research Study. Neurosurgery. 2019.

CHAPTER 4
219
44. Richter RR, Sebelski CA, Austin TM. The Quality of Reporting of Abstracts
in Physical Therapy Literature is Suboptimal: Cross-Sectional, Bibliographic Analysis.
Am J Phys Med Rehabil. 2016;95(9):673-684.
45. Seehra J, Wright NS, Polychronopoulou A, Cobourne MT, Pandis N.
Reporting quality of abstracts of randomized controlled trials published in dental
specialty journals. J. 2013;13(1):1-8.
46. Sivendran S, Newport K, Horst M, Albert A, Galsky MD. Reporting quality of
abstracts in phase III clinical trials of systemic therapy in metastatic solid
malignancies. Trials. 2015;16:341.
47. Sriganesh K, Bharadwaj S, Wang M, et al. Quality of abstracts of randomized
control trials in five top pain journals: A systematic survey. Contemporary Clinical
Trials Communications. 2017;7:64-68.
48. Janackovic K, Puljak L. Reporting quality of randomized controlled trial
abstracts in the seven highest-ranking anesthesiology journals. Trials. 2018;19(1):591.
49. Kiriakou J, Pandis N, Fleming PS, Madianos P, Polychronopoulou A.
Reporting quality of systematic review abstracts in leading oral implantology journals.
J Dent. 2013;41(12):1181-1187.
50. Agarwal A, Johnston BC, Vernooij RW, et al. Authors seldom report the most
patient-important outcomes and absolute effect measures in systematic review
abstracts. J Clin Epidemiol. 2017;81:3-12.
51. Altwairgi AK, Booth CM, Hopman WM, Baetz TD. Discordance between
conclusions stated in the abstract and conclusions in the article: analysis of published
randomized controlled trials of systemic therapy in lung cancer. J Clin Oncol.
2012;30(28):3552-3557.
52. Arunachalam L, Hunter IA, Killeen S. Reporting of Randomized Controlled
Trials With Statistically Nonsignificant Primary Outcomes Published in High-impact
Surgical Journals. Ann Surg. 2017;265(6):1141-1145.
53. Assem Y, Adie S, Tang J, Harris IA. The over-representation of significant p
values in abstracts compared to corresponding full texts: A systematic review of
surgical randomized trials. Contemporary Clinical Trials Communications.
2017;7:194-199.
54. Boutron I, Dutton S, Ravaud P, Altman DG. Reporting and interpretation of
randomized controlled trials with statistically nonsignificant results for primary
outcomes. Jama. 2010;303(20):2058-2064.

CHAPTER 4
220
55. Cordoba G, Schwartz L, Woloshin S, Bae H, Gotzsche PC. Definition,
reporting, and interpretation of composite outcomes in clinical trials: systematic
review. Bmj. 2010;341:c3920.
56. Gewandter JS, McKeown A, McDermott MP, et al. Data interpretation in
analgesic clinical trials with statistically nonsignificant primary analyses: an
ACTTION systematic review. J Pain. 2015;16(1):3-10.
57. Lehmen JA, Deering RM, Simpson AK, Carrier CS, Bono CM.
Inconsistencies between abstracts and manuscripts in published studies about lumbar
Spine surgery. Spine. 2014;39(10):841-845.
58. Lockyer S, Hodgson R, Dumville JC, Cullum N. "Spin" in wound care
research: the reporting and interpretation of randomized controlled trials with
statistically non-significant primary outcome results or unspecified primary outcomes.
Trials. 2013;14:371.
59. Mathieu S, Giraudeau B, Soubrier M, Ravaud P. Misleading abstract
conclusions in randomized controlled trials in rheumatology: comparison of the
abstract conclusions and the results section. Joint Bone Spine. 2012;79(3):262-267.
60. Vera-Badillo FE, Shapiro R, Ocana A, Amir E, Tannock IF. Bias in reporting
of end points of efficacy and toxicity in randomized, clinical trials for women with
breast cancer. Ann Oncol. 2013;24(5):1238-1244.
61. Austin J, Smith C, Natarajan K, Som M, Wayant C, Vassar M. Evaluation of
spin within abstracts in obesity randomized clinical trials: A cross-sectional review.
Clin Obes. 2019;9(2):e12292.
62. Cooper CM, Gray HM, Ross AE, et al. Evaluation of spin in the abstracts of
otolaryngology randomized controlled trials. Laryngoscope. 2018.
63. Hernandez AV, Pasupuleti V, Deshpande A, Thota P, Collins JA, Vidal JE.
Deficient reporting and interpretation of non-inferiority randomized clinical trials in
HIV patients: a systematic review. PLoS ONE. 2013;8(5):e63272.
64. Lieb K, von der Osten-Sacken J, Stoffers-Winterling J, Reiss N, Barth J.
Conflicts of interest and spin in reviews of psychological therapies: a systematic
review. BMJ Open. 2016;6(4):e010606.
65. Patel SV, Chadi SA, Choi J, Colquhoun PH. The use of "spin" in laparoscopic
lower GI surgical trials with nonsignificant results: an assessment of reporting and
interpretation of the primary outcomes. Dis Colon Rectum. 2013;56(12):1388-1394.

CHAPTER 4
221
66. Roest AM, de Jonge P, Williams CD, de Vries YA, Schoevers RA, Turner EH.
Reporting Bias in Clinical Trials Investigating the Efficacy of Second-Generation
Antidepressants in the Treatment of Anxiety Disorders: A Report of 2 Meta-analyses.
JAMA Psychiatry. 2015;72(5):500-510.
67. Nascimento DP, Gonzalez GZ, Araujo AC, Moseley AM, Maher CG, Costa
LOP. Abstracts of low back pain systematic reviews presented spin and
inconsistencies with the full text: an overview study. JOSPT (under review). 2019.
68. Hopewell S, Clarke M, Moher D, et al. CONSORT for reporting randomized
controlled trials in journal and conference abstracts: explanation and elaboration.
PLoS Med. 2008;5(1):e20.
69. Editorial. Incomplete reporting of research in academic press releases. Lancet.
2009;373(9679):1920.
70. Schwartz LM, Woloshin S, Andrews A, Stukel TA. Influence of medical
journal press releases on the quality of associated newspaper coverage: retrospective
cohort study. BMJ. 2012;344:d8164.
71. Sumner P, Vivian-Griffiths S, Boivin J, et al. The association between
exaggeration in health related science news and academic press releases: retrospective
observational study. BMJ. 2014;349:g7015.
72. Lazarus C, Haneef R, Ravaud P, Hopewell S, Altman DG, Boutron I. Peer
reviewers identified spin in manuscripts of nonrandomized studies assessing
therapeutic interventions, but their impact on spin in abstract conclusions was limited.
J Clin Epidemiol. 2016;77:44-51.
73. Hopewell S, Collins GS, Boutron I, et al. Impact of peer review on reports of
randomised trials published in open peer review journals: retrospective before and
after study. BMJ. 2014;349:g4145.
74. Dwan K, Gamble C, Williamson PR, Kirkham JJ, Reporting Bias G.
Systematic review of the empirical evidence of study publication bias and outcome
reporting bias - an updated review. PLoS One. 2013;8(7):e66844.
75. Wegwarth O, Schwartz LM, Woloshin S, Gaissmaier W, Gigerenzer G. Do
physicians understand cancer screening statistics? A national survey of primary care
physicians in the United States. Ann Intern Med. 2012;156(5):340-349.
76. Galipeau J, Barbour V, Baskin P, et al. A scoping review of competencies for
scientific editors of biomedical journals. BMC Med. 2016;14:16.

CHAPTER 4
222
77. European Science Foundation. Fostering Research Integrity in Europe. 2010;
http://archives.esf.org/fileadmin/Public_documents/Publications/ResearchIntegrity_re
port.pdf.
78. World Medical Association Declaration of Helsinki: ethical principles for
medical research involving human subjects. JAMA. 2013;310(20):2191-2194.

CHAPTER 4
223
APPENDIX A. Excluded reviews (n=77). First author Title Journal Year Reason for exclusion Alamri A corpus of potentially contradictory research claims from
cardiovascular research abstracts Journal of biomedical semantics 2016 Not specific for RCTs or SRs
Alasbali Discrepancy between results and abstract conclusions in industry- vs nonindustry-funded studies comparing topical prostaglandins
American Journal of Ophthalmology
2009 Not specific for RCTs or SRs
Assadi Evidence-based abstracts: what research summaries should contain to support evidence-based medicine
International journal of evidence-based healthcare
2012 Did not evaluete all items of the EQUATOR abstracts reporting guidelines
Baethge Tracing scientific reasoning in psychiatry: Reporting of statistical inference in abstracts of top journals 1975-2015
International Journal of Methods in Psychiatric Research
2018 Did not evaluete all items of the EQUATOR abstracts reporting guidelines
Baulig Reporting quality of randomised controlled trial abstracts on age-related macular degeneration health care: a cross-sectional quantification of the adherence to CONSORT abstract reporting recommendations
BMJ Open 2018 Studies analyzed were published before the release of the abstracts reporting guidelines
Baulig Reporting quality of randomised controlled trial abstracts on age-related macular degeneration health care: A cross-sectional quantification of the adherence to CONSORT abstract reporting recommendations
BMJ Open 2018 Studies analyzed were published before the release of the abstracts reporting guidelines
Berwanger The quality of reporting of trial abstracts is suboptimal: Survey of major general medical journals
Journal of Clinical Epidemiology 2009 Studies analyzed were published before the release of the abstracts reporting guidelines
Blake Beyond genes, proteins, and abstracts: Identifying scientific claims from full-text biomedical articles
Journal of Biomedical Informatics 2010 Not specific for RCTs or SRs
Boutron Impact of spin in the abstracts of articles reporting results of randomized controlled trials in the field of cancer: The SPIIN randomized controlled trial
Journal of Clinical Oncology 2014 Analysis of other theme related to abstracts
Buffel du Vaure
Reporting funding source or conflict of interest in abstracts of randomized controlled trials, no evidence of a large impact on general practitioners' confidence in conclusions, a three-arm randomized controlled trial
BMC Medicine 2014 Did not evaluete all items of the EQUATOR abstracts reporting guidelines
Cepeda Use of adjectives in abstracts when reporting results of randomized, controlled trials from industry and academia
Drugs in R & D 2015 Analysis of other theme related to abstracts
Chen Assessment of the quality of reporting in abstracts of randomized controlled trials published in five leading Chinese medical
PLoS One 2010 Studies analyzed were published before the release of the abstracts

CHAPTER 4
224
First author Title Journal Year Reason for exclusion journals reporting guidelines
Chhapola Reporting quality of trial abstracts-improved yet suboptimal: A systematic review and meta-analysis
Journal of Evidence Based Medicine
2018 Studies analyzed were published before the release of the abstracts reporting guidelines
Chhapola Reporting quality of trial abstracts-improved yet suboptimal: A systematic review and meta-analysis
Journal of Evidence-Based Medicine
2018 Systematic review of studies evaluating abstracts
Cohen The structural and content aspects of abstracts versus bodies of full text journal articles are different
BMC Bioinformatics 2010 Not specific for RCTs or SRs
Cui Does the CONSORT checklist for abstracts improve the quality of reports of randomized controlled trials on clinical pathways?
Journal of Evaluation in Clinical Practice
2014 Studies analyzed were published before the release of the abstracts reporting guidelines
Dijkers Searching the literature for information on traumatic spinal cord injury: the usefulness of abstracts
Spinal Cord 2003 Analysis of other theme related to abstracts
Faggion Assessment of the quality of reporting in abstracts of systematic reviews with meta-analyses in periodontology and implant dentistry
Journal of periodontal research 2014 Did not evaluete all items of the EQUATOR abstracts reporting guidelines
Fleming Reporting quality of abstracts of randomized controlled trials published in leading orthodontic journals from 2006 to 2011
American Journal of Orthodontics and Dentofacial Orthopedics
2012 Studies analyzed were published before the release of the abstracts reporting guidelines
Fontelo Comparing data accuracy between structured abstracts and full-text journal articles: Implications in their use for informing clinical decisions
Evidence-Based Medicine 2013 Not specific for RCTs or SRs
Froom Deficiencies in structured medical abstracts Journal of Clinical Epidemiology 1993 Not specific for RCTs or SRs Gazni Are the abstracts of high impact articles more readable?
Investigating the evidence from top research institutions in the world
Journal of Information Science 2011 Analysis of other theme related to abstracts
Germini Quality of reporting in abstracts of RCTs published in emergency medicine journals: A protocol for a systematic survey of the literature
BMJ Open 2017 Protocol
Ginsei The distribution of probability values in medical abstracts: an observational study
BMC Research Notes 2015 Not specific for RCTs or SRs
Gøtzsche Believability of relative risks and odds ratios in abstracts: Cross sectional study
British Medical Journal 2006 Not specific for RCTs or SRs
Gøtzsche Are relative risks and odds ratios in abstracts believable Ugeskr Laeger 2006 Secondary analysis

CHAPTER 4
225
First author Title Journal Year Reason for exclusion Graber Do abstracts of articles in major journals contain the same
information as the body of the paper? Am Fam Physician 2013 Comment
Guo Reporting quality for abstracts of randomized controlled trials in cancer nursing research
Cancer Nursing 2014 Studies analyzed were published before the release of the abstracts reporting guidelines
Harris The accuracy of abstracts in psychology journals The Journal of psychology 2002 Not specific for RCTs or SRs Hartley Clarifying the abstracts of systematic literature reviews Bulletin of the Medical Library
Association 2000 Did not evaluete all items of the
EQUATOR abstracts reporting guidelines
Hernandez Deficient Reporting and Interpretation of Non-Inferiority Randomized Clinical Trials in HIV Patients A Systematic Review
PLOS One 2013 Did not evaluete all items of the EQUATOR abstracts reporting guidelines
Hopewell Effect of editors' implementation of CONSORT guidelines on the reporting of abstracts in high impact medical journals: interrupted time series analysis
BMJ 2012 Studies analyzed were published before the release of the abstracts reporting guidelines
Isiguzo Quality of pilot trial abstracts in heart failure is suboptimal: a systematic survey
Pilot and Feasibility Studies 2018 Pilot trials only
Johansson Is qualitative research scientific, or merely relevant? Research-interested primary care and hospital physicians' appraisal of abstracts
Scandinavian Journal of Primary Health Care
2003 Not specific for RCTs or SRs
Kinder Presence of 'spin' in the abstracts and titles of anaesthesiology randomised controlled trials
British Journal of Anaesthesia 2018 Letter
Kiriakou Reporting quality of systematic review abstracts in leading oral implantology journals
Journal of dentistry 2013 Studies analyzed were published before the release of the abstracts reporting guidelines
Lazarus Classification and prevalence of spin in abstracts of non-randomized studies evaluating an intervention
BMC Medical Research Methodology
2015 Not specific for RCTs or SRs
Li A scoping review of comparisons between abstracts and full reports in primary biomedical research
BMC Med Res Methodol 2017 Systematic review of studies evaluating abstracts
Librero [Abstruse comparisons in abstracts of clinical trials in Spanish medical journals]. [Spanish]
Medicina Clinica 2001 Not specific for RCTs or SRs
Marcelo A comparison of the accuracy of clinical decisions based on full-text articles and on journal abstracts alone: A study among residents in a tertiary care hospital
Evidence-Based Medicine 2013 Not specific for RCTs or SRs

CHAPTER 4
226
First author Title Journal Year Reason for exclusion Maticic Assessment of reporting quality of abstracts of systematic reviews
with meta-analysis using PRISMA-A and discordance in assessments between raters without prior experience
BMC Medical Research Methodology
2019 Studies analyzed were published before the release of the abstracts reporting guidelines
McCoul Do abstracts in otolaryngology journals report study findings accurately?
Otolaryngology - Head and Neck Surgery
2010 Not specific for RCTs or SRs
Mills Professional medical writing support and the reporting quality of randomized controlled trial abstracts among high-impact general medical journals
F1000Research 2017 Secondary analysis
Nam Structuralizing biomedical abstracts with discriminative linguistic features
Computers in Biology and Medicine
2016 Analysis of other theme related to abstracts
Ngai A discourse analysis of the macro-structure, metadiscoursal and microdiscoursal features in the abstracts of research articles across multiple science disciplines
PLOS One 2018 Not specific for RCTs or SRs
Patel Spin in Minimally Invasive Transanal Total Mesorectal Excision Articles (TaTME) An assessment of the current literature
Colorectal Disease 2018 Not specific for RCTs or SRs
Petticrew Quality-assessed reviews of health care interventions and the Database of Abstracts of Reviews of Effectiveness (DARE)
International Journal of Technology Assessment in Health Care
1999 Not specific for RCTs or SRs
Pitkin Accuracy of data in abstracts of published research articles Journal of the American Medical Association
1999 Not specific for RCTs or SRs
Pitkin Can the accuracy of abstracts be improved by providing specific instructions? A randomized controlled trial
Jama 1998 Not specific for RCTs or SRs
Polychronopoulou
The reporting quality of meta-analysis results of systematic review abstracts in periodontology and implant dentistry is suboptimal
The journal of evidence-based dental practice
2014 Comment
Postma The quality of analytical information contained within abstracts and papers on new analytical methods
Analytica Chimica Acta 1992 Not specific for RCTs or SRs
Rice Reporting quality in abstracts of meta-analyses of depression screening tool accuracy: A review of systematic reviews and meta-analyses
BMJ Open 2016 Studies analyzed were published before the release of the abstracts reporting guidelines
Ries Comparing frequency of content-bearing words in abstracts and texts in articles from four medical journals: an exploratory study
Medinfo 2001 Not specific for RCTs or SRs

CHAPTER 4
227
First author Title Journal Year Reason for exclusion Rinchuse Scoping review of systematic review abstracts about
temporomandibular disorders: Comparison of search years 2004 and 2017
American Journal of Orthodontics and Dentofacial Orthopedics
2017 Analysis of other theme related to abstracts
Ruano Relationships between abstract features and methodological quality explained variations of social media activity derived from systematic reviews about psoriasis interventions
J Clin Epidemiol 2018 Studies analyzed were published before the release of the abstracts reporting guidelines
Scherer Full publication of results initially presented in abstracts Cochrane Database of Systematic Reviews
2018 Included conference abstracts
Schuemie Distribution of information in biomedical abstracts and full-text publications
Bioinformatics 2004 Not specific for RCTs or SRs
Seehra Reporting completeness of abstracts of systematic reviews published in leading dental specialty journals
European Journal of Oral Sciences 2013 Studies analyzed were published before the release of the abstracts reporting guidelines
Shin Is there any quality improvement in the randomized controlled trial abstracts in the Korean Journal of Anesthesiology after the publication of the CONSORT abstract guidelines in 2008?
Korean J Anesthesiol 2015 Letter
Siebers Data in abstracts of research articles. Are they consistent with those reported in the article?
British Journal of Biomedical Science
2002 Comment
Siebers Data inconsistencies in abstracts in the New Zealand Medical Journal
N Z Med J 2002 Letter
Siebers How accurate is data in abstracts of research articles? New Zealand Journal of Medical Laboratory Science
2000 Not specific for RCTs or SRs
Snedeker Completeness of reporting in abstracts from clinical trials of pre-harvest interventions against foodborne pathogens
Preventive Veterinary Medicine 2012 Studies analyzed were published before the release of the abstracts reporting guidelines
Sriganesh Reporting quality of abstracts of trials published in top five pain journals: A protocol for a systematic survey
BMJ Open 2016 Protocol
Stang Statistical inference in abstracts of major medical and epidemiology journals 1975-2014: a systematic review
European Journal of Epidemiology 2017 Not specific for RCTs or SRs
Taback A survey of abstracts of high-impact clinical journals indicated most statistical methods presented are summary statistics
Journal of Clinical Epidemiology 2008 Not specific for RCTs or SRs
Tfelt-Hansen CONSORT recommendations in abstracts of randomised, controlled trials on migraine and headache
Journal of Headache and Pain 2011 Did not evaluete all items of the EQUATOR abstracts reporting guidelines

CHAPTER 4
228
First author Title Journal Year Reason for exclusion Tsujimoto Physician characteristics associated with proper assessment of
overstated conclusions in research abstracts: A secondary analysis of a randomized controlled trial
PLOS One 2019 Secondary analysis
Vinkers Use of positive and negative words in scientific PubMed abstracts between 1974 and 2014: retrospective analysis
BMJ 2015 Not specific for RCTs or SRs
Wang The reporting quality of abstracts of stepped wedge randomized trials is suboptimal: A systematic survey of the literature
Contemporary Clinical Trials Communications
2017 Studies analyzed were published before the release of the abstracts reporting guidelines
Wang Quality of reporting of trial abstracts needs to be improved: using the CONSORT for abstracts to assess the four leading Chinese medical journals of Traditional Chinese Medicine
Trials 2010 Studies analyzed were published before the release of the abstracts reporting guidelines
Ward Accuracy of abstracts for original research articles in pharmacy journals
Annals of Pharmacotherapy 2004 Not specific for RCTs or SRs
Westergaard A comprehensive and quantitative comparison of text-mining in 15 million full-text articles versus their corresponding abstracts
PLoS Computational Biology 2018 Not specific for RCTs or SRs
Westergaard A comprehensive and quantitative comparison of text-mining in 15 million full-text articles versus their corresponding abstracts
PLOS Computational Biology 2018 Not specific for RCTs or SRs
Yavchitz A new classification of spin in systematic reviews and meta-analyses was developed and ranked according to the severity
Journal of Clinical Epidemiology 2016 Analysis of other theme related to abstracts
Yavchitz Impact of adding a limitations section to abstracts of systematic reviews on readers' interpretation: a randomized controlled trial
BMC Medical Research Methodology
2014 Analysis of other theme related to abstracts
Yoneoka Evaluating association between linguistic characteristics of abstracts and risk of bias: Case of Japanese randomized controlled trials
PLoS One 2017 Analysis of other theme related to abstracts

CHAPTER 5
229
CHAPTER 5
Concluding remarks

CHAPTER 5
230
5. Concluding remarks
5.1. Visual abstracts
Other than the usual research abstracts, the use of a summary of findings that
could be more understandable for lay audiences have been studied for almost 10 years1.
A recent and apparently successful alternative way of communicating research is using
the visual abstracts, also called infographics (word derived from ‘information
graphic’2), or graphical abstracts3,4. Such abstracts are graphically displayed, translating
and spreading information of research key results through colored visual images of
diagrams, charts and figures3,4. A recent published article5 has presented in visual
abstract format6 the frequency of injuries and illness by sports modality competing at
the 2016 Olympic Games.

CHAPTER 5
231
The use of visual abstracts seems to be a great additional resource of spreading
information, while it should not be considered for clinical decision making4. Reading a
visual abstract is not a substitute for reading the actual research abstract, or even less for
reading the full text4. Critical appraisal formats, such as the usual structured abstracts
(with objectives, methods, results and conclusion) have been considered clearer and
more understandable when compared to visual abstracts3, which were perceived as more
enjoyable for reading in the same comparison7. Both abstract formats were equally
effective in terms of translating research knowledge to the target readers7. Most
adequately, articles titles accompanied by visual abstracts have been compared to
mentioning only the title of the study on Twitter, which yielded a much higher number
of tweets and article visits for the articles tweeted with visual abstracts, rather than those
with the title only8.
The preferences and needs of the audience who is reading the research results
should be taken into consideration, as well as the purpose of reading such information.
Apparently, the overall public, patients and the media prefer visual abstracts, while
researchers and research funders prefer the usual structured abstracts3. Ultimately, once
a research manuscript has been accepted for publication, the visual abstract should be an

CHAPTER 5
232
additional form of disseminating its findings through social media, and should be
consistent with the adequate reporting and interpretation of healthcare abstracts and full
texts.
Several journals, organizations and institutions have adopted visual abstracts as a
strategy to spread the research results content into social media, including the BMJ
(British Medical Journal)9 and the JAMA Network10, among other leading healthcare
journals. Authors can also disseminate their visual abstracts in social media by using the
hashtag #VisualAbstract11, which has been widely spread out in the last couple of years.
Guides explaining the step by step process on how to create visual abstracts, as well as
useful tips on how to disseminate research findings into infographics can be found in
PDF documents available online4,12.
5.2. Abstracts influence in the media
Clinicians may take clinical decisions based on abstracts if the full text is not
freely available13,14. However, research abstracts findings are often misrepresented in
press releases and news coverage15-17, which most of times are associated with
overstated results (spin) favoring the experimental treatment18. Journalists might
enhance some results to make it more attractive to readers, but most of the spin detected
are responsibility of the own authors17. More importantly, journal editors and reviewers
are jointly responsible for the transparent reporting of research studies, as well as for
avoiding interpretation, reporting and publication biases16,18,19. Another important issue
to be risen is that the media should not generalize research studies taken on animals to
clinical benefits on humans, as the proper manner to generalize research findings is
performing adequate research in the specific population under study16.
Social media has become an essential way of research findings dissemination
through many platforms, such as Facebook, Twitter, LinkedIn, among others8.
Researchers and research disseminators that use social media to that end, should also
accurately report and interpret study results and be careful not to distort the information
posted11. In order to reach the challenging task of research communication with the
overall public, researchers could also adopt visual abstracts to disseminate their study
results11, always accompanied with the online reference to the full manuscript.
Additionally, some tips to increase the visibility of scientific articles through social
media are: submission of articles to high impact factor journals; use of provocative
CHAPTER 5
233
titles; and use of the Document Object Identifier (DOI) and/or the link to the article on
posting over social media20.
5.3. Ethics and integrity in research
The importance of adequate reporting and interpretation of abstracts and full
texts are highly mentioned in the research code of conduct for research integrity21.
Reporting should be complete, clearly defined and accurate, as well as interpretation
should not be misleading and must present data with honesty, transparency and
accuracy21,22. The communication between researchers, the overall public and the
popular media should be based on open access data and accurate references (unjustified
claims are forms of falsification)21,22. Some types of misconduct include making up
results and manipulation of data (changing or omitting information)21. Research
misconduct may happen intentionally and based on conflict of interests, and should be
distinguished from unintentional mistakes or inconsistent opinions21. The responsibility
to deal with misconduct is on the institutions that employ the researchers, which should
bring awareness to all stakeholders (researchers, authors, funders, journal editors and
reviewers) on the Good Research Practices to promote research integrity21,22. Evidence-
based practice are based on the code of conduct and the principles of research integrity,
which must include honesty, reliability, objectivity, impartiality, open communication,
duty of care and fairness21.
Research stakeholders do have the obligation to follow the ethical principles on
research (including guidelines for ethical reporting), upon the conduct of a study,
publication and dissemination of results22. Ethical reporting involves the reporting of
positive, negative and inconclusive results, as well as sources of funding, institutional
affiliations and conflicts of interest22.
Research misconduct my lead to retracted publications, involving costs to
funding sources and prejudice the researchers careers23. Reducing such research waste
has been a topic of discussion in recent years24-26. It is consensual that scientific editors
(Editorial Board, Associate Editor and Editor-in-Chief) are the responsible ones for
changing the journals content and policies24. Therefore, authors must follow the actions
proposed in the editorial policies in order to have their submitted articles accepted for
publication. The question that still remains is if the peer reviewers are adequately

CHAPTER 5
234
trained and if they consistently check reporting and methodological guidelines upon
evaluating the submitted articles.
5.4. Actions to change journals` editorial policies
Several research institutes are responsible for promoting research integrity, such
as national academies and foundations, universities, research organizations, funding
organizations and journals` editorial boards21. However, there is no international
standardized formal training for journal editors and reviewers, that could influence the
quality of the published studies and consequently the strength to obtain funding sources
and believability in such data24,25.
Funding organizations could and should invest on training programs based on
reporting guidelines and also guidelines of ethics and integrity in research, with such
trainings directed to journal editors, reviewers and authors24-27. Funders and universities
could employ the position of a publications officer, who would manage those proper
research trainings and also provide guidance on submission of papers to journals27.
Universities could include mandatory training for graduate students in terms of study
conduct, statistical analysis, reporting and interpretation24,27, which could be part of the
content of disciplines of methodology in clinical research and evidence based practice.
Additionally, guidance on how to follow the guidelines of ethics and integrity in
research were proposed to be an integral part of post graduation programs, and always
reminded in international conferences28.
A practical research protocol is currently being conducted to evaluate an online
tool for peer reviewers in biomedical publications, including an online tool and training
module based on reporting guidelines29. For journals editors, fourteen core
competencies have been developed under a consensus statement of experts30, which
comprises topics related to the editor qualities and skills, publication ethics and research
integrity, plus editorial principles and processes. Moreover, the utility of an institutional
publications officer over five research institutes has been assessed in a pilot study and
proved to improve publications knowledge and perceptions31, but it was limited to a
short period of time and a limited sample size.

CHAPTER 5
235
5.4.1. Clinical and research implications
Poor reporting and misrepresentation of data can bring critical consequences to
patients and policy makers32. For patients, believing this type of research disseminated
may bring false hope of recovering or healing from a disease, or even risk of worsening
a health condition32. For policy makers, unqualified research becoming base for new
laws or regulations may expose the population to unnecessary risks32. A solution
brought up into investigation was to train journalists to identify spin in research articles
developed by researchers15,32, but that would have to be way general and so perhaps
way complex for someone not familiar with the specific topic. Also the readers of
newspapers vary broadly in reading and interpretation levels17,32, which depend on their
education, culture, behavior and beliefs. What journalists could do is checking for
reporting consistency between the material presented in the news and the information
contained in the full text of the manuscript, and their ‘training’ could be that simple:
check the news with the research article.
Using properly press releases with adequate information has been proved to be
more efficient in terms of communication with the overall public15. Improper press
releases content are caused mainly within academic institutions17, which must focus on
improving the overall reporting and methodological quality of research. Other than that,
the financial costs in biomedical research would be much lower than the current
expenses26, which was estimated in a quarter of a trillion of dollars every year.
Initiatives on recommendations given to funders, regulators, journals, academic
institutions and researches have been planned26, in order to reduce waste and increase
value in research26,33,34. Ultimately, readers of healthcare research reproducibility based
on systematic reviews are not putting evidence into practice35. Clinical decision making
based on high quality research must be an usual practice in order to acquire better
quality of life worldwide.
5.4.2. Editorials
Upon the acceptance of publication of the manuscript detailed in Chapter 4,
some of the authors involved in this thesis will develop editorials directed to call
attention of healthcare research stakeholders to take actions on improving the quality of
abstracts once and for all. Our main goal is to share our findings with the International

CHAPTER 5
236
Committee of Medical Journal Editors (ICMJE) and the International Society of
Physiotherapy Journal Editors (ISPJE) and call attention especially of healthcare
journals editors and reviewers. We would like to propose actions to be taken by journal
editors and reviewers on:
1) Mandatory use of reporting guidelines, not only for full text but also
for abstracts, highlighted as one of the 'instructions for authors';
2) Proper checking if authors have followed the adequate reporting
guidelines for abstracts and full text, checking also for abstracts
consistency of reporting and interpretation with the full text;
3) Awareness of spin in the abstracts and full texts, with adequate
interpretation of results and conclusions of trials and reviews;
4) More flexibility with the abstract word count, with a minimum limit
of 400 words;
5) Critical appraisal skills training, including the previous items.
We hope that this thesis can be helpful on improving the awareness of journal
editors and reviewers, authors and readers in terms of transparency and integrity of
research healthcare abstracts and their dissemination to all stakeholders. We sincerely
hope that this awareness can stimulate publication of higher quality of healthcare
research.

CHAPTER 5
237
REFERENCES
1. Rosenbaum SE, Glenton C, Nylund HK, Oxman AD. User testing and
stakeholder feedback contributed to the development of understandable and useful
Summary of Findings tables for Cochrane reviews. J Clin Epidemiol. 2010;63(6):607-
619.
2. Lankow J, Ritchie J, Crooks R. Infographics: The power of visual storytelling.
2012.
3. Crick K, Hartling L. Preferences of Knowledge Users for Two Formats of
Summarizing Results from Systematic Reviews: Infographics and Critical Appraisals.
PLoS One. 2015;10(10):e0140029.
4. Ibrahim AM. Use of a VISUAL ABSTRACT to Disseminate Scientific
Research. 2018; https://www.surgeryredesign.com/s/VisualAbstract_Primer_v4_1.pdf.
5. Soligard T, Steffen K, Palmer D, et al. Sports injury and illness incidence in the
Rio de Janeiro 2016 Olympic Summer Games: A prospective study of 11274 athletes
from 207 countries. Br J Sports Med. 2017;51(17):1265-1271.
6. Soligard T, Steffen K, Palmer D, et al. Infographic: Injury and illness, the 2016
Olympic Games. Br J Sports Med. 2019;53(7):404-405.
7. Buljan I, Malicki M, Wager E, et al. No difference in knowledge obtained from
infographic or plain language summary of a Cochrane systematic review: three
randomized controlled trials. J Clin Epidemiol. 2018;97:86-94.
8. Ibrahim AM, Lillemoe KD, Klingensmith ME, Dimick JB. Visual Abstracts to
Disseminate Research on Social Media: A Prospective, Case-control Crossover Study.
Ann Surg. 2017;266(6):e46-e48.
9. BMJ. BMJ visual abstracts. British Medical Journal. 2018;
https://www.bmj.com/content/bmj-visual-abstracts.
10. Network J. Visual Abstract. For the Media. News releases & journal articles
from the JAMA Network. 2018; https://media.jamanetwork.com/news-item/visual-
abstract/.
11. Wray CM, Arora VM. #VisualAbstract: A Revolution in Communicating
Science? Ann Surg. 2017;266(6):e49-e50.
12. Stones C, Gent M. The 7 G.R.A.P.H.I.C. principles of public health infographic
design. 2015; https://visualisinghealth.files.wordpress.com/2014/12/guidelines.pdf.

CHAPTER 5
238
13. Maher CG, Sherrington C, Elkins M, Herbert RD, Moseley AM. Challenges for
evidence-based physical therapy: accessing and interpreting high-quality evidence on
therapy. Phys Ther. 2004;84(7):644-654.
14. Silva TM, Costa LCM, Garcia AN, Costa LO. What do physical therapists think
about evidence-based practice? A systematic review. Man Ther. 2014;20(3):388-401.
15. Schwartz LM, Woloshin S, Andrews A, Stukel TA. Influence of medical journal
press releases on the quality of associated newspaper coverage: retrospective cohort
study. BMJ. 2012;344:d8164.
16. Woloshin S, Schwartz LM, Casella SL, Kennedy AT, Larson RJ. Press releases
by academic medical centers: not so academic? Ann Intern Med. 2009;150(9):613-618.
17. Sumner P, Vivian-Griffiths S, Boivin J, et al. The association between
exaggeration in health related science news and academic press releases: retrospective
observational study. BMJ. 2014;349:g7015.
18. Yavchitz A, Boutron I, Bafeta A, et al. Misrepresentation of randomized
controlled trials in press releases and news coverage: a cohort study. PLoS Med.
2012;9(9):e1001308.
19. Incomplete reporting of research in academic press releases. Lancet.
2009;373(9679):1920.
20. Araujo AC, Nascimento DP, Gonzalez GZ, Costa LOP. How to increase the
visibility of scientific articles through social media? Braz J Phys Ther. 2018;22(6):435-
436.
21. European Science Foundation. Fostering Research Integrity in Europe. 2010;
http://archives.esf.org/fileadmin/Public_documents/Publications/ResearchIntegrity_repo
rt.pdf.
22. World Medical Association Declaration of Helsinki: ethical principles for
medical research involving human subjects. JAMA. 2013;310(20):2191-2194.
23. Stern AM, Casadevall A, Steen RG, Fang FC. Financial costs and personal
consequences of research misconduct resulting in retracted publications. Elife.
2014;3:e02956.
24. Galipeau J, Barbour V, Baskin P, et al. A scoping review of competencies for
scientific editors of biomedical journals. BMC Med. 2016;14:16.
25. Glasziou P, Altman DG, Bossuyt P, et al. Reducing waste from incomplete or
unusable reports of biomedical research. Lancet. 2014;383(9913):267-276.
CHAPTER 5
239
26. Moher D, Glasziou P, Chalmers I, et al. Increasing value and reducing waste in
biomedical research: who's listening? Lancet. 2016;387(10027):1573-1586.
27. Moher D, Altman DG. Four Proposals to Help Improve the Medical Research
Literature. PLoS Med. 2015;12(9):e1001864.
28. Kien C, Nussbaumer B, Thaler KJ, et al. Barriers to and facilitators of
interventions to counter publication bias: thematic analysis of scholarly articles and
stakeholder interviews. BMC Health Serv Res. 2014;14:551.
29. Chauvin A, Moher D, Altman D, et al. A protocol of a cross-sectional study
evaluating an online tool for early career peer reviewers assessing reports of randomised
controlled trials. BMJ Open. 2017;7(9):e017462.
30. Moher D, Galipeau J, Alam S, et al. Core competencies for scientific editors of
biomedical journals: consensus statement. BMC Med. 2017;15(1):167.
31. Cobey KD, Galipeau J, Shamseer L, Moher D. Assessing the utility of an
institutional publications officer: a pilot assessment. PeerJ. 2017;5:e3294.
32. Haneef R, Lazarus C, Ravaud P, Yavchitz A, Boutron I. Interpretation of Results
of Studies Evaluating an Intervention Highlighted in Google Health News: A Cross-
Sectional Study of News. PLoS One. 2015;10(10):e0140889.
33. Chalmers I, Glasziou P. Avoidable waste in the production and reporting of
research evidence. Lancet. 2009;374(9683):86-89.
34. Schnell-Inderst P, Hunger T, Conrads-Frank A, Arvandi M, Siebert U.
Recommendations for primary studies evaluating therapeutic medical devices were
identified and systematically reported through reviewing existing guidance. J Clin
Epidemiol. 2018;94:46-58.
35. Page MJ, Altman DG, Shamseer L, et al. Reproducible research practices are
underused in systematic reviews of biomedical interventions. J Clin Epidemiol.
2018;94:8-18.





























