Embed Size (px)
Citation preview

Available online at www.sciencedirect.com
www.elsevier.com/locate/ymgme
Molecular Genetics and Metabolism 93 (2008) 275–281
Commentary
Methods for a prompt and reliable laboratory diagnosisof Pompe disease: Report from an international consensus meeting
The Pompe Disease Diagnostic Working GroupB. Winchester a,*, D. Bali b, O.A. Bodamer c, C. Caillaud d, E. Christensen e, A. Cooper f,
E. Cupler g, M. Deschauer h, K. Fumic i, M. Jackson j, P. Kishnani b, L. Lacerda k,J. Ledvinova l, A. Lugowska m, Z. Lukacs n, I. Maire o, H. Mandel p, E. Mengel q,
W. Muller-Felber r, M. Piraud o, A. Reuser s, T. Rupar t, I. Sinigerska u, M. Szlago v,F. Verheijen s, O.P. van Diggelen s, B. Wuyts w, E. Zakharova x, J. Keutzer y
a Biochemistry Research Group, UCL Institute of Child Health, Great Ormond Street Hospital, University College London,
30 Guilford Street, London WC1N 1EH, UKb Division of Medical Genetics, Department of Pediatrics, Duke University Medical Center, Durham, NC, USA
c Division of Biochemical and Pediatric Genetics, University Children’s Hospital Vienna, Vienna, Austriad Laboratoire de Biochimie et Genetique Moleculaire, Hopital Cochin, Paris, France
e Department of Clinical Genetics, Rigshospitalet, Copenhagen, Denmarkf Willink Biochemical Genetics Unit, Royal Manchester Children’s Hospital, Manchester, UK
g Neuromuscular Diseases Center, Oregon Health and Science University, Portland, OR, USAh Department of Neurology, University of Halle-Wittenberg, Halle/Saale, Germany
i Clinical Institute of Laboratory Diagnosis, Zagreb University School of Medicine and Clinical Hospital Center, Zagreb, Croatiaj The Enzyme Laboratory, Department of Chemical Pathology, Great Ormond Street Hospital, London, UK
k Unidade de Enzimologia, Instituto de Genetica Medica Jacinto Magalhaes, Porto, Portugall Institute of Inherited Metabolic Disorders, First Faculty of Medicine, Charles University, Prague, Czech Republic
m Department of Genetics, Institute of Psychiatry and Neurology, Warsaw, Polandn Department of Pediatrics, Metabolic Laboratory Hamburg University Medical Center, Hamburg, Germany
o Centre d’Etude des Maladies Hereditaires du Metabolisme, Hopital Debrousse, Lyon, Francep Metabolic Unit, Rambam Medical Center, Haifa, Israelq Pediatric Clinic, University of Mainz, Mainz, Germany
r Haunersche Kinderklinik, Children’s Hospital, Ludwig-Maximilians-University, Munich, Germanys Department of Clinical Genetics, Erasmus MC, Rotterdam, The Netherlands
t Child & Parent Resource Institute, Department of Biochemistry and Pediatrics, University of Western Ontario, London, Ont., Canadau National Genetic Laboratory, University Hospital of Obstetrics and Gynecology, Sofia, Bulgaria
v Laboratorio de Neuroquımica ‘‘Dr. N. A. Chamoles’’, FESEN, Buenos Aires, Argentinaw Department of Clinical Chemistry, Laboratory of Metabolic Disorders, University Hospital Ghent, Gent, Belgium
x Research Centre for Medical Genetics, Moscow, Russiay Genzyme, Cambridge, MA, USA
Received 11 September 2007; accepted 11 September 2007Available online 19 December 2007
Abstract
Pompe disease is an autosomal recessive disorder of glycogen metabolism caused by a deficiency of the lysosomal enzyme acid a-glu-cosidase (GAA). It presents at any age, with variable rates of progression ranging from a rapidly progressive course, often fatal by one-year of age, to a more slowly, but nevertheless relentlessly progressive course, resulting in significant morbidity and premature mortality.
1096-7192/$ - see front matter � 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.ymgme.2007.09.006
* Corresponding author. Fax: +44 207 404 6191.E-mail address: [email protected] (B. Winchester).

276 B. Winchester et al. / Molecular Genetics and Metabolism 93 (2008) 275–281
In infants, early initiation of enzyme replacement therapy is needed to gain the maximum therapeutic benefit, underscoring the need forearly diagnosis. Several new methods for measuring GAA activity have been developed. The Pompe Disease Diagnostic Working Groupmet to review data generated using the new methods, and to establish a consensus regarding the application of the methods for the lab-oratory diagnosis of Pompe disease. Skin fibroblasts and muscle biopsy have traditionally been the samples of choice for measuring GAAactivity. However, new methods using blood samples are rapidly becoming adopted because of their speed and convenience. MeasuringGAA activity in blood samples should be performed under acidic conditions (pH 3.8–4.0), using up to 2 mM of the synthetic substrate4-methylumbelliferyl-a-D-glucoside or glycogen (50mg/mL), in the presence of acarbose (3–9 lM) to inhibit the isoenzyme maltase–glucoamylase. The activity of a reference enzyme should also be measured to confirm the quality of the sample. A second test shouldbe done to support the diagnosis of Pompe disease until a program for external quality assurance and proficiency testing of the enzymaticdiagnosis in blood is established.� 2007 Elsevier Inc. All rights reserved.
Keywords: Pompe disease; Glycogen storage disease type II; Acid maltase deficiency; Diagnosis; Lysosomal acid a-glucosidase; Enzyme assay, Acarbose
Introduction
Pompe disease, which is also called glycogen storagedisease type II and acid maltase deficiency, is an autoso-mal recessive disorder of glycogen metabolism with anestimated incidence of one in 40,000 births [1–3]. It iscaused by a deficiency of the lysosomal enzyme acid a-glucosidase (GAA). As in other inborn errors of metabo-lism, Pompe disease is associated with a range of clinicalphenotypes with varying organ involvement, age of onset,and severity. The most rapidly progressive form of thedisease, with onset of symptoms in the first year of life,is characterized by cardiomegaly, hypotonia, and deathdue to cardiorespiratory failure often before the age ofone-year [4,5]. In older children and adults, where the dis-ease involves primarily skeletal and respiratory muscles,clinical manifestations and rate of progression are muchmore variable, and the patients can typically die of respi-ratory failure.
Prior to 2006, treatment for patients with Pompe diseasewas primarily palliative [6,7]. The development of alglucos-idase alfa enzyme replacement therapy (Myozyme�; Gen-zyme Corporation, Cambridge, MA, USA), representsthe first effective, disease-specific treatment for patientswith Pompe disease [8,9]. In infants, the early initiationof enzyme replacement therapy is essential in order to gainthe maximum therapeutic benefit, underscoring the needfor early diagnosis [8,10]. Early diagnosis requires bothincreased awareness among clinicians regarding the clinicalcharacteristics of Pompe disease, [1,10–12], and fast andreliable GAA activity assays to confirm the GAA defi-ciency. Several clinical diagnostic algorithms for Pompedisease have been proposed [2,11,13], but no standardizedprotocol exists for the laboratory diagnosis. Muscle biop-sies can be used to measure GAA activity, but are not incommon usage as the primary tissue to measure enzymeactivity. Measurement of GAA activity in skin fibroblastsis often used to confirm the diagnosis of Pompe disease,in patients that present with symptoms consistent withPompe disease. However, growing fibroblasts to confluencefrom a skin biopsy takes several weeks, which delays diag-nosis and treatment initiation. The measurement of GAA
in mixed leukocytes and whole blood is complicated bythe presence of maltase glucoamylase (MGA), another a-glucosidase, which is active at an acid pH and masks thedeficiency of GAA. Recently, assays that exploit inhibitionof MGA to measure GAA activity in blood samples havebeen developed.
The Pompe Disease Diagnostic Working Group assem-bled to establish a consensus regarding the application ofthese new assays for the laboratory diagnosis of Pompedisease. The Working Group consists of scientists, genet-icists, and clinicians working in the field of Pompe dis-ease. The group met in December 2006 in London, UK,and formed a consensus on several points, as well as iden-tifying areas for further research. This article summarizesthe key outcomes from the meeting (Table 1). Implica-tions for population screening were only briefly discussed;therefore, the consensus statements found in this articlerefer to the diagnosis of patients with clinical symptomssuggestive of Pompe disease, and do not pertain to new-born screening.
Laboratory diagnosis of Pompe disease
The diagnosis of Pompe disease in a patient who haspresented with clinical symptoms requires the demonstra-tion of a deficiency of GAA activity. In general, infantswith Pompe disease have GAA activities in muscle tissueand skin fibroblasts that are less than 1% of the meanactivity in normal controls [1,7]. In older children andadults, GAA activity is reduced, but generally higherthan that seen in infants [11,14,15]. Assays that use bloodto diagnose Pompe disease were developed because theavailable methods were considered slow and invasive.The Working Group agreed that the new blood sampleGAA activity assays can be used to diagnose Pompe dis-ease, and a second test should be performed to confirmthe diagnosis (Fig. 1). When a patient older than one-year presents with a general myopathy without clearsymptoms of Pompe disease, the recommendation is toperform a GAA activity assay in a blood sample, evenif a muscle biopsy has been taken for histologicalexamination.
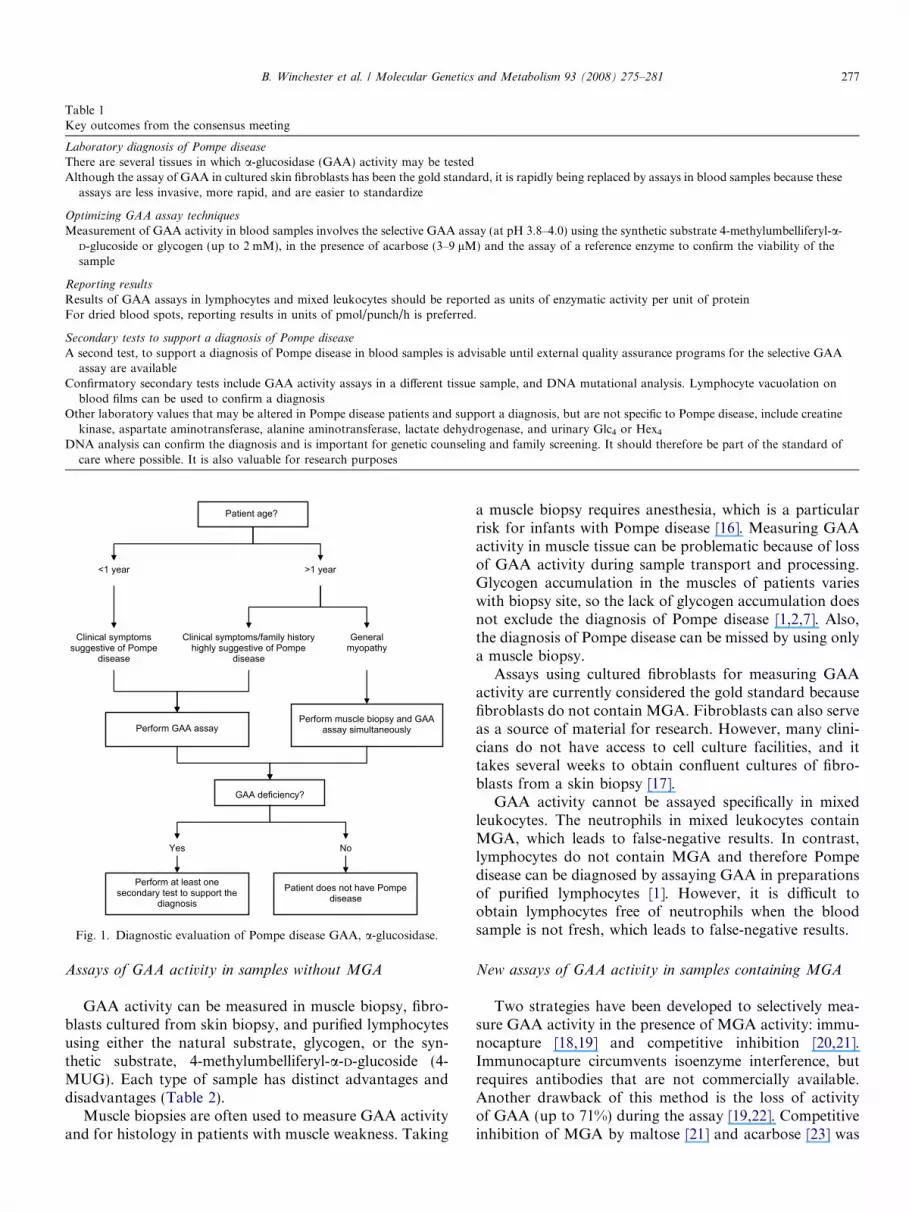
Table 1Key outcomes from the consensus meeting
Laboratory diagnosis of Pompe disease
There are several tissues in which a-glucosidase (GAA) activity may be testedAlthough the assay of GAA in cultured skin fibroblasts has been the gold standard, it is rapidly being replaced by assays in blood samples because these
assays are less invasive, more rapid, and are easier to standardize
Optimizing GAA assay techniques
Measurement of GAA activity in blood samples involves the selective GAA assay (at pH 3.8–4.0) using the synthetic substrate 4-methylumbelliferyl-a-D-glucoside or glycogen (up to 2 mM), in the presence of acarbose (3–9 lM) and the assay of a reference enzyme to confirm the viability of thesample
Reporting results
Results of GAA assays in lymphocytes and mixed leukocytes should be reported as units of enzymatic activity per unit of proteinFor dried blood spots, reporting results in units of pmol/punch/h is preferred.
Secondary tests to support a diagnosis of Pompe disease
A second test, to support a diagnosis of Pompe disease in blood samples is advisable until external quality assurance programs for the selective GAAassay are available
Confirmatory secondary tests include GAA activity assays in a different tissue sample, and DNA mutational analysis. Lymphocyte vacuolation onblood films can be used to confirm a diagnosis
Other laboratory values that may be altered in Pompe disease patients and support a diagnosis, but are not specific to Pompe disease, include creatinekinase, aspartate aminotransferase, alanine aminotransferase, lactate dehydrogenase, and urinary Glc4 or Hex4
DNA analysis can confirm the diagnosis and is important for genetic counseling and family screening. It should therefore be part of the standard ofcare where possible. It is also valuable for research purposes
Patient age?
<1 year >1 year
Clinical symptoms/family history highly suggestive of Pompe
disease
General myopathy
Perform muscle biopsy and GAA assay simultaneously
Clinical symptoms suggestive of Pompe
disease
Perform GAA assay
Perform at least one secondary test to support the
diagnosis Patient does not have Pompe
disease
GAA deficiency?
Yes No
Fig. 1. Diagnostic evaluation of Pompe disease GAA, a-glucosidase.
B. Winchester et al. / Molecular Genetics and Metabolism 93 (2008) 275–281 277
Assays of GAA activity in samples without MGA
GAA activity can be measured in muscle biopsy, fibro-blasts cultured from skin biopsy, and purified lymphocytesusing either the natural substrate, glycogen, or the syn-thetic substrate, 4-methylumbelliferyl-a-D-glucoside (4-MUG). Each type of sample has distinct advantages anddisadvantages (Table 2).
Muscle biopsies are often used to measure GAA activityand for histology in patients with muscle weakness. Taking
a muscle biopsy requires anesthesia, which is a particularrisk for infants with Pompe disease [16]. Measuring GAAactivity in muscle tissue can be problematic because of lossof GAA activity during sample transport and processing.Glycogen accumulation in the muscles of patients varieswith biopsy site, so the lack of glycogen accumulation doesnot exclude the diagnosis of Pompe disease [1,2,7]. Also,the diagnosis of Pompe disease can be missed by using onlya muscle biopsy.
Assays using cultured fibroblasts for measuring GAAactivity are currently considered the gold standard becausefibroblasts do not contain MGA. Fibroblasts can also serveas a source of material for research. However, many clini-cians do not have access to cell culture facilities, and ittakes several weeks to obtain confluent cultures of fibro-blasts from a skin biopsy [17].
GAA activity cannot be assayed specifically in mixedleukocytes. The neutrophils in mixed leukocytes containMGA, which leads to false-negative results. In contrast,lymphocytes do not contain MGA and therefore Pompedisease can be diagnosed by assaying GAA in preparationsof purified lymphocytes [1]. However, it is difficult toobtain lymphocytes free of neutrophils when the bloodsample is not fresh, which leads to false-negative results.
New assays of GAA activity in samples containing MGA
Two strategies have been developed to selectively mea-sure GAA activity in the presence of MGA activity: immu-nocapture [18,19] and competitive inhibition [20,21].Immunocapture circumvents isoenzyme interference, butrequires antibodies that are not commercially available.Another drawback of this method is the loss of activityof GAA (up to 71%) during the assay [19,22]. Competitiveinhibition of MGA by maltose [21] and acarbose [23] was

Table 2Tissue samples in which a-glucosidase activity can be measured
Specimen Advantages Disadvantages Comments
Dried blood spot (DBS) Minimally invasive, relatively easy to collect andtransport, small sample volume required,provides rapid results; may be applied tonewborn screening
Most laboratories/hospitals areunfamiliar with DBS sample collectionand assay
Uses acarbose to eliminate the interference bymaltase glucoamylase (MGA)
Mixed leukocytes Minimally invasive, whole blood samples easilycollected; fewer preparation steps, comparedwith purified lymphocyte assay
Shipment for more than 2 daysreduces enzyme activity
Uses acarbose to eliminate the interference byMGA
Purified lymphocytes Minimally invasive, whole blood samples easilycollected
Purification requires additionalpreparation, compared with mixedleukocyte assay
Inclusion of acarbose isrecommended to eliminate theinterference by MGA whenneutrophils are present
Fibroblasts Establishes a patient-specific cell line for furtherresearch and genotyping. Provides a reliableassay of a-glucosidase activity with 4-methylumbelliferyl-a-D-glucoside substrate inabsence of acarbose, and may discriminatebetween clinical subtypes
Time-consuming: results take 4–6weeks
The culture conditions affectenzyme activity
Requires cell culture facilitiesMore invasive skin biopsy
Muscle biopsy Biopsy allows for both enzyme assay andhistological evaluation. The latter is useful in thedifferential diagnosis of Pompe disease andother muscle disorders
Invasive; requires anesthesia Lack of glycogen accumulationdoes not rule out Pompe diseaseSite of biopsy can affect morphologic
results; areas with muscle weakness aremore likely to have large glycogendepositsNeed liquid nitrogen and shipping indry ice
278 B. Winchester et al. / Molecular Genetics and Metabolism 93 (2008) 275–281
demonstrated in GAA assays in dried blood spots (DBS).Acarbose performed better when the two inhibitors werecompared [15,24]. DBS are relatively easy to obtain, mak-ing them useful for rapid diagnosis in newborns and chil-dren. DBS are stable during shipping, which permits easytransport to specialized laboratories for diagnosis. GAAactivity can be assayed selectively in mixed leukocytes byinhibiting neutrophil MGA by acarbose [25]. The additionof acarbose to assays using purified lymphocytes preventsfalse-negative results from contaminating neutrophils [26].
Based on these observations and personal experiences,the Working Group agreed that GAA assays using bloodsamples can now be considered the method of choice forthe enzymatic diagnosis of Pompe disease because theyare reliable, less invasive, more convenient, and faster.
Optimizing GAA assay techniques
Assessment of GAA activity requires at least two assays:the selective GAA assay, and the assay of a referenceenzyme to confirm the quality of the sample. The selectiveGAA assay is performed under acidic conditions (pH3.8–4.0) using up to 2 mM of 4-MUG or glycogen(50 mg/mL), in the presence of acarbose (3–9 lM). TheWorking Group concluded that acarbose is preferred overmaltose for MGA inhibition. At concentrations of 3–9 lM,
acarbose completely inhibits MGA activity at acidic pHwithout affecting GAA activity at substrate (4-MUG) con-centrations, up to 2 mM, in mixed leukocytes [25], lympho-cytes [26], and DBS [24]. Higher concentrations ofacarbose, for example 80 lM, inhibit GAA [24,25]. Vary-ing the concentration of 4-MUG can affect the resultsand the required concentration of acarbose. Although theassay with the synthetic substrate 4-MUG, is easier thanthe one with glycogen, better discrimination between nor-mal controls and patients in the mixed leukocyte assay isachieved with the natural substrate glycogen [25]. How-ever, the assay with the natural substrate does not distin-guish individuals homozygous for the commonpseudodeficiency allele from patients [25]. The pH usedvaries among laboratories, but most assays are carriedout within the range of pH 3.8–4.0.
The Working Group felt that it was very important toemphasize the necessity of including a reference enzymetest. Other lysosomal enzymes, for example b-galactosidaseor b-hexosaminidase, should be assayed as a referenceactivity to confirm sample quality. A sample of poor qual-ity often has low GAA activity, which could lead to a false-positive diagnosis of Pompe disease. Low activity of thereference lysosomal enzyme will reveal a poor sample. Evenin a poor sample, the ratio of the GAA activity to the ref-erence enzyme activity may still indicate a provisional diag-

Table 3Secondary tests to support a diagnosis of Pompe disease based on a-glucosidase assay in blood samples
Confirmatory
a-Glucosidase (GAA) assay in culture of skin fibroblasts or musclebiopsy (will also provide histological information)
Detection of disease-causing mutations in GAA gene by DNA analysisDetection of vacuolation of lymphocytes in blood film, only if carried
out in experienced laboratory
Supportive non-specific laboratory parameters
Abnormal values forCreatine kinaseAspartate aminotransferaseAlanine aminotransferaseLactate dehydrogenaseHex4 in urine and plasmaGlc4 in urine and plasma
B. Winchester et al. / Molecular Genetics and Metabolism 93 (2008) 275–281 279
nosis, necessitating a request for a fresh sample and confir-mation by a repeated enzymatic test.
Sample collection and enzyme assays should be per-formed in accordance with standard laboratory guidelines.It is inevitable that protocols will vary to some degreeamong laboratories, which may complicate direct compar-isons of results. However, the priority for laboratoriesshould be to establish a working protocol that includesboth positive and negative internal control samples, anda reference enzyme. In the future, efforts may be taken todevelop a single protocol that can be implemented globally.
Reporting results
Currently, there is no standard approach to reportingthe results of GAA assays. However, the Working Groupfelt that standardization is important because it will allowfor better comparisons among laboratories. The ratio ofGAA activity to the control enzyme’s activity may be cal-culated although, in most cases, the benefit of thisapproach is not required. The results should be expressedas units of enzyme activity per unit of protein for lympho-cytes and mixed leukocytes, and as units of pmol/punch/hfor DBS.
Secondary tests to support the diagnosis of Pompe disease
Clinicians often prefer to perform a second test to sup-port a diagnosis of Pompe disease based on GAA assays(Fig. 1), not only because of the lifelong implications forpatients and their families, but also to support treatmentwith enzyme replacement therapy. The selective GAAassay using 4-MUG and acarbose is relatively new. Sys-tems for the external quality assurance and proficiency test-ing of the assay are in development [27], but have not beenimplemented widely. The Working Group recognized that,during this transitional period, a second test is needed tosafeguard against errors in diagnosis. However, the needfor a second test should be reviewed once the quality assur-ance systems are available.
Several tests are available to support a preliminary diag-nosis of Pompe disease based on measurement of GAAactivity in a blood sample (Table 3). Some tests are defini-tive confirmatory tests, such as the demonstration of a defi-ciency of GAA in another tissue, or the detection ofdisease-causing mutation(s) in the GAA gene. Some labora-tories have used lymphocyte vacuolation on blood films toconfirm a diagnosis of Pompe disease [28]. Other tests onlysupport the enzymatic diagnosis.
A non-specific marker of Pompe disease in most patientsis elevation of the urinary and plasma concentrations of thetetrasaccharides Hex4 and Glc4 [29–32]. This test is non-invasive [11] and the concentrations of Glc4 and Hex4 havebeen shown to correlate with the treatment effects ofenzyme replacement therapy. The concentrations are gen-erally reduced in patients who have clinical improvementfollowing treatment initiation [32,33]. Other laboratory
parameters that may be abnormal in Pompe diseasepatients include creatine kinase, aspartate aminotransfer-ase, alanine aminotransferase, and lactate dehydrogenase[34,35]. These parameters, however, are not specific toPompe disease and can be normal in patients with Pompedisease. If clinical suspicion is strong, but these non-specifictests are negative, a confirmatory test should be carriedout. In contrast, if a confirmatory secondary test is nega-tive, for example normal GAA activity in muscle or fibro-blasts, or absence of a mutation in the GAA gene, a fullclinical and biochemical investigation needs to be repeated.The choice of secondary test is left to the individual labo-ratory, and typically depends on available resources andexpertise.
The identification of disease-causing mutation(s) in thegene encoding GAA by DNA analysis is not essential forthe diagnosis of Pompe disease, but provides valuableinformation for family screening and genetic counseling.In the rare situation where the diagnosis is not clear byenzyme activity analysis, mutation analysis may be helpfulin confirming the diagnosis. The identification of a muta-tion(s) in a patient, and genotyping of the parents shouldbe considered part of the management of patients withPompe disease. As with other lysosomal storage disorders,carriers cannot be detected reliably using enzyme activityassay, but can be detected through genotyping. DNA anal-ysis is extremely useful for investigating genotype/pheno-type relationships.
Summary and future directions
Pompe disease is a progressive, debilitating and oftenfatal neuromuscular disorder that manifests as a contin-uum of clinical phenotypes that vary with respect to organinvolvement, age of onset, and severity. Recently, a dis-ease-specific treatment option (alglucosidase alfa; Myo-zyme�; Genzyme Corporation, Cambridge, MA, USA)for patients with Pompe disease has become available.Early initiation of alglucosidase alfa therapy can be life

280 B. Winchester et al. / Molecular Genetics and Metabolism 93 (2008) 275–281
saving and could prevent irreversible muscle damage,emphasizing the need for early diagnosis. For patients withclinical symptoms suggestive of Pompe disease, diagnosis isbased on the demonstration of deficient GAA activity.Table 1 summarizes the key outcomes from the consensusmeeting by the Pompe Disease Diagnostic Working Group.Blood GAA assays have rapidly become a reliable test fordiagnosing Pompe disease as they are quick, easy, and non-invasive. Regardless of the type of blood enzyme assay, theaddition of acarbose is necessary and has indeed becomecommon practice.
Laboratory protocols for the diagnosis of Pompe dis-ease are expected to continue to evolve, as current tech-niques are refined. Further efforts are needed tostandardize sample collection and improve regional accessto laboratories able to perform the necessary diagnosticassays.
Disclosure of Conflict of Interest
The authors received editorial/writing support in thepreparation of this manuscript, funded by GenzymeCorporation. The authors were fully responsible for contentsand editorial decisions for this manuscript. The content ofthis manuscript is based on a meeting of the Pompe DiseaseDiagnostic Working Group (London, December 2006),which was sponsored by Genzyme Corporation.
Dr. Winchester has received fees for lectures and consul-tation and support for research from Genzyme Corpora-tion and Shire. Dr. Kishnani and Dr. Bali have receivedresearch/grant support from Genzyme Corporation.Dr. Kishnani is a member of the Pompe Disease AdvisoryBoard for Genzyme Corporation. Dr. Cupler is a memberof the Genzyme Speaker Bureau and is a consultant forGenzyme. Dr. Ledvinova has received research supportfrom Genzyme for the diagnosis of all lysosomal storagedisorders. Dr. Lukacs has received research support fromGenzyme. Dr. Maire and Dr. Piraud have received lecturefees from Shire, and support for research from Genzyme.Dr. Mandel has received fees for lectures and support forresearch from Genzyme Corporation. Dr. Zakharova hasreceived research support from Genzyme. Dr. Muller-Felberis a member of the Advisory Board for the Pompe Registry.Dr. van Diggelen, Dr. Mengel, Dr. Cooper, Dr. Deschauerand Dr. Rupar have received lecture fees from Genzyme.The following authors have no conflict of interest:Dr. Bodamer, Dr. Caillaud, Dr. Christensen, Dr. Fumic,Dr. Jackson, Dr. Lacerda, Dr. Lugowska, Dr. Reuser,Dr. Sinigerska, Dr. Szlago, Dr. Verheijen, and Dr. Wuyts.Dr. Keutzer is an employee of Genzyme Corporation.
The clinical trials with rhGAA mentioned in this manu-script have been supported by a grant from Genzyme Cor-poration at the various sites that patients were treated.rhGAA, in the form of Genzyme’s product, Myozyme�,has now been approved by the US FDA and the EuropeanUnion as therapy for Pompe disease. Duke University andinventors for the method of treatment and predecessors of
the cell lines used to generate the enzyme (rhGAA) used inclinical trials may benefit financially pursuant to theUniversity’s Policy on Inventions, Patents and TechnologyTransfer, even if those cell lines are not used in the com-mercialized therapy. Dr. Kishnani and Dr. Bali are affili-ated to Duke University.
The clinical trials with rhGAA at the Rambam MedicalCenter, Haifa, Israel, have been supported by a grant fromGenzyme Corporation. Dr. Mandel is affiliated to RambamMedical Center. Genzyme’s product, Myozyme�, has nowbeen approved by the Israeli medical authorities as the onlytreatment of Pompe disease.
References
[1] R. Hirschhorn, A.J. Reuser, Glycogen storage disease type II: acid a-glucosidase (acid maltase) deficiency, in: C.R. Scriver, A.L. Be audet,W.S. Sly, D. Valle, B. Vogelstein, B. Childs (Eds.), The Metabolicand Molecular Bases of Inherited Disease, eighth ed., McGraw-HillPublishing Co., New York, 2001, pp. 3389–3420.
[2] M.G. Ausems, J. Verbiest, M.M. Hermans, M.A. Kroos, F.A.Beemer, J.H. Wokke, L.A. Sandkuijl, A.J. Reuser, A.T. van derPloeg, Frequency of glycogen storage disease type II in TheNetherlands: implications for diagnosis and genetic counselling,Eur. J. Hum. Genet. 7 (1999) 713–716.
[3] F. Martiniuk, A. Chen, A. Mack, E. Arvanitopoulos, Y. Chen, W.N.Rom, W.J. Codd, B. Hanna, P. Alcabes, N. Raben, P. Plotz, Carrierfrequency for glycogen storage disease type II in New York andestimates of affected individuals born with the disease, Am. J. Med.Genet. 79 (1998) 69–72.
[4] H.M. van den Hout, W. Hop, O.P. van Diggelen, J.A. Smeitink, G.P.Smit, B.T. Poll-The, H.D. Bakker, M.C. Loonen, J.B. de Klerk, A.J.Reuser, A.T. van der Ploeg, The natural course of infantile Pompe’sdisease: 20 original cases compared with 133 cases from the literature,Pediatrics 112 (2003) 332–340.
[5] P.S. Kishnani, W.L. Hwu, H. Mandel, M. Nicolino, F. Yong, D.Corzo, Infantile-Onset Pompe Disease Natural History Study Group,a retrospective, multinational, multicenter study on the naturalhistory of infantile-onset Pompe disease, J. Pediatr. 148 (2006) 671–676.
[6] D.D. Koeberl, P.S. Kishnani, Y.T. Chen, Glycogen storage diseasetypes I and II: treatment updates, J. Inherit. Metab. Dis. 30 (2007)159–164.
[7] P.S. Kishnani, R.R. Howell, Pompe disease in infants and children, J.Pediatr. 144 (Suppl. 5) (2004) S35–S43.
[8] P.S. Kishnani, D. Corzo, M. Nicolino, B. Byrne, H. Mandel, W.L.Hwu, N. Leslie, J. Levine, C. Spencer, M. McDonald, J. Li, J.Dumontier, M. Halberthal, Y.H. Chien, R. Hopkin, S. Vijayaragh-avan, D. Gruskin, D. Bartholomew, A. van der Ploeg, J.P. Clancy, R.Parini, G. Morin, M. Beck, G.S. De la Gastine, M. Jokic, B.Thurberg, S. Richards, D. Bali, M. Davison, M.A. Worden, Y.T.Chen, J.E. Wraith, Recombinant human acid [alpha]-glucosidase:major clinical benefits in infantile-onset Pompe disease, Neurology 68(2007) 99–109.
[9] J.M. Van den Hout, J.H. Kamphoven, L.P. Winkel, W.F. Arts,J.B. De Klerk, M.C. Loonen, A.G. Vulto, A. Cromme-Dijkhuis,N. Weisglas-Kuperus, W. Hop, H. Van Hirtum, O.P. VanDiggelen, M. Boer, M.A. Kroos, P.A. Van Doorn, E. Van derVoort, B. Sibbles, E.J. Van Corven, J.P. Brakenhoff, J. Van Hove,J.A. Smeitink, G. de Jong, A.J. Reuser, A.T. Van der Ploeg,Long-term intravenous treatment of Pompe disease with recombi-nant human alpha-glucosidase from milk, Pediatrics 113 (2004)e448–e457.
[10] R.R. Howell, B. Byrne, B.T. Darras, P. Kishnani, M. Nicolino, A.van der Ploeg, Diagnostic challenges for Pompe disease: an under-

B. Winchester et al. / Molecular Genetics and Metabolism 93 (2008) 275–281 281
recognized cause of floppy baby syndrome, Genet. Med. 8 (2006) 289–296.
[11] P.S. Kishnani, R.D. Steiner, D. Bali, K. Berger, B.J. Byrne, L.E.Case, J.F. Crowley, S. Downs, R.R. Howell, R.M. Kravitz, J.Mackey, D. Marsden, A.M. Martins, D.S. Millington, M. Nicolino,G. O’Grady, M.C. Patterson, D.M. Rapoport, A. Slonim, C.T.Spencer, C.J. Tifft, M.S. Watson, Pompe disease diagnosis andmanagement guideline, Genet. Med. 8 (2006) 267–288.
[12] L.P. Winkel, M.L. Hagemans, P.A. van Doorn, M.C. Loonen, W.J.Hop, A.J. Reuser, A.T. van der Ploeg, The natural course of non-classic Pompe’s disease; a review of 225 published cases, J. Neurol.252 (2005) 875–884.
[13] P.J. Meikle, E. Ranieri, H. Simonsen, T. Rozaklis, S.L. Ramsay, P.D.Whitfield, M. Fuller, E. Christensen, F. Skovby, J.J. Hopwood,Newborn screening for lysosomal storage disorders: clinical evalua-tion of a two-tier strategy, Pediatrics 114 (2004) 909–916.
[14] A.J. Reuser, M.A. Kroos, M.M. Hermans, A.G. Bijvoet, M.P.Verbeet, O.P. Van Diggelen, W.J. Kleijer, A.T. Van der Ploeg,Glycogenosis type II (acid maltase deficiency), Muscle Nerve 3 (1995)S61–S69.
[15] H. Kallwass, C. Carr, J. Gerrein, M. Titlow, R. Pomponio, D. Bali, J.Dai, P. Kishnani, A. Skrinar, D. Corzo, J. Keutzer, Rapid diagnosisof late-onset Pompe disease by fluorometric assay of alpha-glucosi-dase activities in dried blood spots, Mol. Genet. Metab. 90 (2007)449–452.
[16] L.Y. Wang, A.K. Ross, J.S. Li, S.M. Dearmey, J.F. Mackey, M.Worden, D. Corzo, C. Morgan, P.S. Kishnani, Cardiac arrhythmiasfollowing anesthesia induction in infantile-onset Pompe disease: acase series, Paediatr. Anaesth. 17 (2007) 738–748.
[17] M.J. Heukels-Dully, M.F. Niermeijer, Variation in lysosomal enzymeactivity during growth in culture of human fibroblasts and amnioticfluid cells, Exp. Cell Res. 97 (1976) 304–312.
[18] J.F. Koster, R.G. Slee, W.C. Hulsmann, The use of leukocytes as anaid in the diagnosis of glycogen storage disease type II (Pompe’sdisease), Clin. Chim. Acta 51 (1974) 319–325.
[19] K. Umapathysivam, J.J. Hopwood, P.J. Meikle, Determination ofalpha-glucosidase activity in blood spots as a diagnostic test forPompe disease, Clin. Chem. 47 (2001) 1378–1383.
[20] D.M. Broadhead, J. Butterworth, Pompe’s disease: diagnosis inkidney and leucocytes using 4-methylumbelliferyl-alpha-D-glucopy-ranoside, Clin. Genet. 13 (1978) 504–510.
[21] N.A. Chamoles, G. Niizawa, M. Blanco, D. Gaggioli, C. Casentini,Glycogen storage disease type II: enzymatic screening in dried bloodspots on filter paper, Clin. Chim. Acta 347 (2004) 97–102.
[22] K. Umapathysivam, A.M. Whittle, E. Ranieri, C. Bindloss, E.M.Ravenscroft, O.P. van Diggelen, J.J. Hopwood, P.J. Meikle, Deter-mination of acid alpha-glucosidase protein: evaluation as a screeningmarker for Pompe disease and other lysosomal storage disorders,Clin. Chem. 46 (2000) 1318–1325.
[23] Y. Li, C.R. Scott, N.A. Chamoles, A. Ghavami, B.M. Pinto, F.Turecek, M.H. Gelb, Direct multiplex assay of lysosomal enzymes in
dried blood spots for newborn screening, Clin. Chem. 50 (2004) 1785–1796.
[24] H. Zhang, H. Kallwass, S.P. Young, C. Carr, J. Dai, P.S. Kishnani,D.S. Millington, J. Keutzer, Y.T. Chen, D. Bali, Comparison ofmaltose and acarbose as inhibitors of maltase–glucoamylase activityin assaying acid alpha-glucosidase activity in dried blood spots for thediagnosis of infantile Pompe disease, Genet. Med. 8 (2006) 302–306.
[25] T. Okumiya, J.L. Keulemans, M.A. Kroos, N.M. Van der Beek, M.A.Boer, H. Takeuchi, O.P. Van Diggelen, A.J. Reuser, A new diagnosticassay for glycogen storage disease type II in mixed leucocytes, Mol.Genet. Metab. 88 (2006) 22–28.
[26] R.M. Jack, C. Gordon, C.R. Scott, P.S. Kishnani, D. Bali, The use ofacarbose inhibition in the measurement of acid alpha-glucosidaseactivity in blood lymphocytes for the diagnosis of Pompe disease,Genet. Med. 8 (2006) 307–312.
[27] G.J. Ruijter, M. Boer, C.W. Weykamp, R. de Vries, I. van den Berg,J. Janssens-Puister, K. Niezen-Koning, R.A. Wevers, B.J. Poorthuis,O.P. van Diggelen, External quality assurance programme forenzymatic analysis of lysosomal storage diseases: a pilot study, J.Inherit. Metab. Dis. 28 (2005) 979–990.
[28] G. Anderson, V.V. Smith, M. Malone, N.J. Sebire, Blood filmexamination for vacuolated lymphocytes in the diagnosis of metabolicdisorders; retrospective experience of more than 2,500 cases from asingle centre, J. Clin. Pathol. 58 (2005) 1305–1310.
[29] Y. An, S.P. Young, S.L. Hillman, J.L. Van Hove, Y.T. Chen, D.S.Millington, Liquid chromatographic assay for a glucose tetrasaccha-ride, a putative biomarker for the diagnosis of Pompe disease, Anal.Biochem. 287 (2000) 136–143.
[30] S.P. Young, R.D. Stevens, Y. An, Y.T. Chen, D.S. Millington,Analysis of a glucose tetrasaccharide elevated in Pompe disease bystable isotope dilution-electrospray ionization tandem mass spec-trometry, Anal. Biochem. 316 (2003) 175–180.
[31] M.A. Chester, A. Lundblad, A. Hager, S. Sjoblad, C. Loonen, J.M.Tager, D. Zopf, Increased urinary excretion of a glycogen-derivedtetrasaccharide in heterozygotes with glycogen storage diseases type IIand III, Lancet 1 (1983) 994–995.
[32] S.P. Young, D. Corzo, P. Kishnani, D.D. Koeberl, D. Bali, D.Peterson, Y.T. Chen, D.S. Millington, Diagnostic value of urinaryand plasma glucose tetrasaccharides in infantile and late onsetglycogen storage disease type II, Mol. Genet. Metab. 84 (2005) 241–242.
[33] Y. An, S.P. Young, P.S. Kishnani, D.S. Millington, A. Amalfitano,D. Corzo, Y.T. Chen, Glucose tetrasaccharide as a biomarker formonitoring the therapeutic response to enzyme replacement therapyfor Pompe disease, Mol. Genet. Metab. 85 (2005) 247–254.
[34] M.G. Ausems, P. Lochman, O.P. van Diggelen, H.K. Ploos vanAmstel, A.J. Reuser, J.H. Wokke, A diagnostic protocol for adult-onset glycogen storage disease type II, Neurology 52 (1999) 851–853.
[35] M.T. Di Fiore, R. Manfredi, L. Marri, A. Zucchini, L. Azzaroli, G.Manfredi, Elevation of transaminases as an early sign of late-onsetglycogenosis type II, Eur. J. Pediatr. 152 (1993) 784.





























