Embed Size (px)
Citation preview
REVIEW
Minimally invasive oesophagectomy: current status and futuredirection
Nick Butler • Stuart Collins • Breda Memon •
Muhammed Ashraf Memon
Received: 24 February 2010 / Accepted: 26 July 2010
� Springer Science+Business Media, LLC 2011
Abstract
Background Oesophagectomy is one of the most chal-
lenging surgeries. Potential for morbidity and mortality is
high. Minimally invasive techniques have been introduced
in an attempt to reduce postoperative complications and
recovery times. Debate continues over whether these
techniques are beneficial to morbidity and whether onco-
logical resection is compromised. This review article will
analyse the different techniques employed in minimally
invasive oesophagectomy (MIO) and critically evaluate
commonly reported outcome measures from the available
literature.
Methods Medline, Embase, Science Citation Index,
Current Contents, and PubMed databases were used to
search English language articles published on MIO. Thirty-
one articles underwent thorough analysis and the data were
tabulated where appropriate. To date, only level III evi-
dence exists. Where appropriate, comparisons are made
with a meta-analysis on open oesophagectomy.
Results Positive aspects of MIO include at least compa-
rable postoperative recovery data and oncological resection
measures to open surgery. Intensive care unit requirements
are lower, as is duration of inpatient stay. Respiratory
morbidity varies. Negative aspects include increased
technical skill of the surgeon and increased equipment
requirements, increased operative time and limitation with
respect to local advancement of cancer. With increasing
individual experience, improvements in outcome measures
and the amenability of this approach to increasing neo-
plastic advancement has been shown.
Conclusion MIO has outcome measures at least as com-
parable to open oesophagectomy in the setting of benign
and nonlocally advanced cancer. Transthoracic oesophag-
ectomy provides superior exposure to the thoracic
oesophagus compared to the transhiatal approach and is
currently preferred. No multicentre randomised controlled
trials exist or are likely to come into fruition. As with all
surgery, careful patient selection is required for optimal
results from MIO.
Keywords Oesophagectomy � Laparoscopy �Oesophageal cancer � Retrospective studies � Prospective
studies � Comparative studies � Patient outcome �Intraoperative complications � Postoperative
complications � Hospitalisation � Human
Surgical resection and replacement of the neoplastic
oesophagus remains the definite therapeutic mode in order
to achieve cure. Other indications for operative interven-
tion include Barrett’s oesophagus with high-grade dyspla-
sia and benign disease refractory to medical or endoscopic
treatment. Irrespective of aetiology, oesophagectomy has
long been respected as one of the most challenging
N. Butler � S. Collins � B. Memon � M. A. Memon (&)
Department of Surgery, Ipswich Hospital, Chelmsford Avenue,
Ipswich, QLD, Australia
e-mail: [email protected]
M. A. Memon
Department of Surgery, University of Queensland, Brisbane,
QLD, Australia
M. A. Memon
Faculty of Health Sciences and Medicine, Bond University,
Gold Coast, QLD, Australia
M. A. Memon
Faculty of Health and Social Sciences, Bolton University,
Bolton, Lancashire, UK
123
Surg Endosc
DOI 10.1007/s00464-010-1511-2

surgeries, with the combination of oesophageal anatomy
and patient demographics giving a high potential for both
morbidity and mortality. Recently, larger centres have
introduced minimally invasive techniques in an attempt to
reduce postoperative complications and recovery times.
Since the advent of minimally invasive oesophagectomy
(MIO) over 15 years ago, debate has continued over
whether laparoscopic techniques are actually beneficial to
morbidity, and, further still, whether oncological resection
is compromised. This review article analyses the different
techniques employed in MIO and critically evaluates the
commonly reported outcome measures from available
literature.
Materials and methods
An electronic search for articles on the subject of laparo-
scopic oesophagectomy was performed through the Med-
line, Embase, Science Citation Index, Current Contents,
and PubMed databases. The search strategy involved
combining all of the available literature on the approach
(i.e., minimally invasive) with operation type (i.e., oeso-
phagectomy) for the disease process (i.e., oesophageal
cancer/neoplasm). Keywords used with respect to approach
were laparoscopy (MeSH terms, includes laparoscopic);
minimally AND invasive; minimally AND invasive AND
surgery (MeSH terms) OR operative OR procedures OR
operative procedures. Keywords used with respect to the
operation type were esophagectomy (MeSH term); oeso-
phagectomy (United Kingdom spelling). Keywords used
with respect to disease process were neoplasm (MeSH
terms); cancer. Further searches using keywords for oper-
ation subtypes (Ivor-Lewis; three-stage (o)esophagectomy;
transhiatal) did not reveal any further articles. Non-English
articles, articles pertaining only to benign processes, and
individual case reports were excluded. To date no ran-
domised controlled trials exist; the available literature is
limited to level III-2 evidence. All available case series and
reports on MIO for oesophageal cancer were included. The
minimally invasive techniques and reported data were
analysed, and from this a selection of commonly recogni-
sed outcome measures was generated. Following the defi-
nition of the important outcome measures, the studies were
separated into single-arm observational studies and com-
parative studies and also delineated by operative approach
and method of data collection (prospective versus retro-
spective). Data from case series with 15 or more patients
were included for data tabulation. Some overlap of data
was observed and was subsequently accounted for. Where
between-study homogeneity was clear, for example, mul-
tiple-case series reporting a purely minimally invasive
approach to both abdominal and thoracic components,
descriptive statistics were acquired using an electronic
statistics package (SPSS Statistics 17.0, SPSS Inc.). Using
the available data, we report the history of MIO, discuss
reported outcome measures, present thinking on current
best practice, and also postulate the future of oesophag-
ectomy. Where appropriate, comparisons were made with a
meta-analysis by Hulscher et al. [1] comparing open
transhiatal versus open transthoracic oesophagectomy.
Results
Thirty-one suitable articles [1], consisting of mainly pro-
spective and retrospective studies, were identified. Seven
series [25–31] directly compared open oesophagectomy
versus MIO; two of these [27, 28] were performed pro-
spectively. Review of 30 of the identified papers [2–31]
revealed three main groups of common outcome measures:
operative data, morbidity and mortality data, and onco-
logical resection data. Main operative outcome measures
were defined as total operative time, conversion rate, and
blood loss. Morbidity data was defined by early and late
complication rates, duration of intensive care requirement,
and total hospital stay. Complications of particular
importance were also recorded and comprised anastomotic
leaks, chylothorax, and specific respiratory morbidity.
Perioperative mortality was defined by death within
30 days from the procedure. Oncological outcome mea-
sures were pathological disease stage, margin involvement,
local recurrence, lymph node yield, and overall survival.
Neoadjuvant treatment numbers were included for each
study.
Twenty five case series containing 15 or more patients
were identified for data tabulation (Tables 1, 2, 3, 4, 5, 6, 7,
8). Operative time was recorded in 94% of the single-arm
observational studies and 86% of the comparative studies
(only one comparison study did not [27]). All 25 studies
included for data analysis reported important outcome
measures in percentages as follows: blood loss 81%, inci-
dence of anastomotic leak 68%, incidence of respiratory
morbidity 92%, incidence of chylothorax 96%, duration of
ICU stay 76%, duration of overall hospital stay 92%, 30-day
operative mortality 100%, extent of oncological resection
(positive margins/local recurrence and/or lymph node yield)
88%, survival at (variable) mean follow-up 72%.
Twelve case series [2–5, 8, 9, 13, 15, 25, 28, 29, 31]
directly reported results for completely minimally invasive
transthoracic oesophagectomy regardless of abdominal
component and anastomosis site. Selected results were as
follows (reported figures were weighted according to study
sample size, n is the number of studies included in the
calculation): mean operation time 312 min (range =
220–476 min) (n = 11); median blood loss 425 ml
Surg Endosc
123
(range = 65–700 ml) (n = 11); median incidence of
anastomotic leak 5.5% (range = 0–53.0%) (n = 9); med-
ian incidence of respiratory complications 31.7% (range =
0–223.5%) (n = 11); median incidence of chylothorax
5.2% (range = 2.2–26.7%) (n = 12); median duration of
ICU stay 1 day (range = 1–19 days) (n = 10); median
duration of hospital stay 13 days (range = 7–16 days)
(n = 12); median 30-day mortality 1.0% (range =
0–6.5%) (n = 12).
Nine case series [3, 5, 8, 13, 15, 25, 28, 29, 31] directly
reported results on a purely minimally invasive approach to
transthoracic oesophagectomy. Selected results from these
series were as follows: median operation time 330 min
(range = 220-413 min) (n = 9); median blood loss 279 ml
(range = 65–700 ml) (n = 9); median incidence of anas-
tomotic leak 5.6% (range = 0–40.0%) (n = 7); median
incidence of respiratory complications 7.8% (range =
3.1–60.0%) (n = 9); median incidence of chylothorax
3.0% (range = 1.0–4.0%) (n = 9); median duration of
ICU stay 1 day (range = 1–19 days) (n = 8); median dura-
tion of hospital stay 9 days (range = 7–14 days) (n = 9);
median 30-day mortality 1.0% (range = 0–3%) (n = 9).
Five case series [20–22, 24, 29] directly reported results
on a purely minimally invasive transhiatal technique.
Selected results from these series were as follows: mean
operation time 305 min (range = 200–415 min) (n = 5);
median blood loss 220 ml (range = 150–325 ml) (n = 4);
median incidence of anastomotic leak 8.0% (range =
7.7–29.2%) (n = 3); median incidence of respiratory
complications 9.0% (range = 8.3–25.0%) (n = 4); median
incidence of chylothorax 3.1% (range = 2.6–20.8%) (n =
5), median duration of ICU stay 1 day (range = 1–5 days)
(n = 3); median duration of hospital stay 12 days (ran-
ge = 7–17 days) (n = 5); median 30-day mortality 0%
(range = 0–4.6%) (n = 5).
Techniques of minimally invasive oesophagectomy
Two main techniques have been described for oesophageal
resection; transthoracic oesophagectomy and transhiatal
oesophagectomy. In total, three sites of exposure can be
utilised in oesophagectomy: the abdomen, the thorax, and
the neck. Transthoracic (Ivor-Lewis) resection involves
direct, and separate, abdominal and transthoracic access
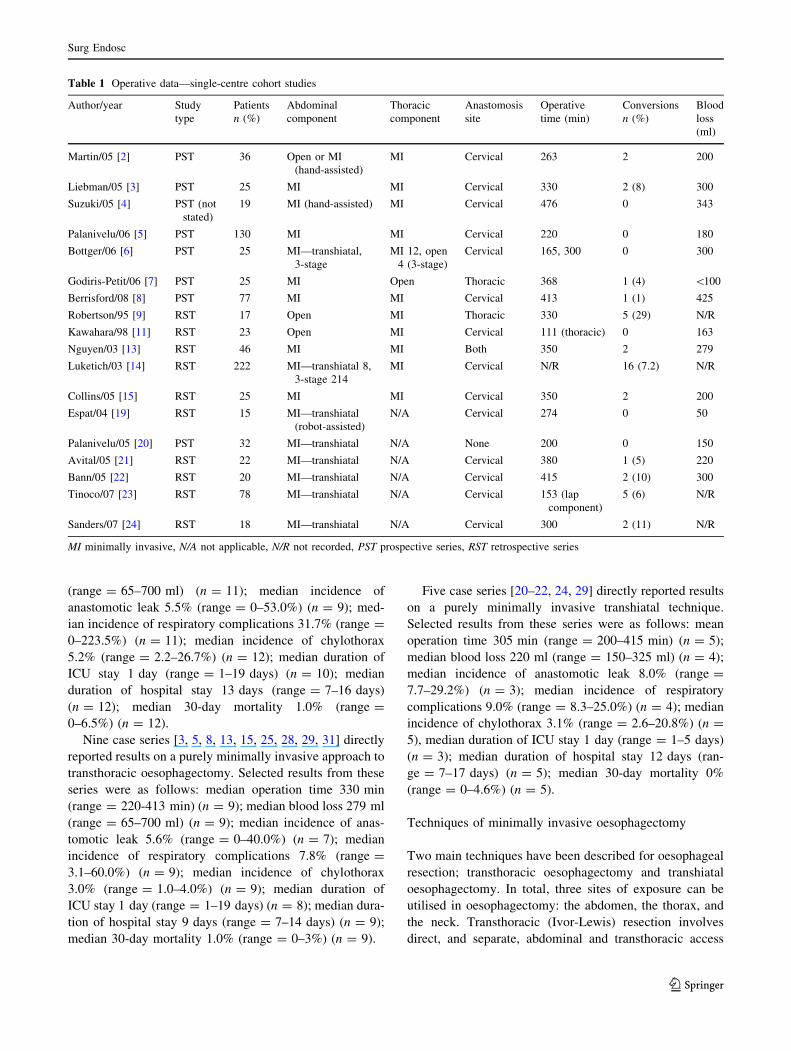
Table 1 Operative data—single-centre cohort studies
Author/year Study
type
Patients
n (%)
Abdominal
component
Thoracic
component
Anastomosis
site
Operative
time (min)
Conversions
n (%)
Blood
loss
(ml)
Martin/05 [2] PST 36 Open or MI
(hand-assisted)
MI Cervical 263 2 200
Liebman/05 [3] PST 25 MI MI Cervical 330 2 (8) 300
Suzuki/05 [4] PST (not
stated)
19 MI (hand-assisted) MI Cervical 476 0 343
Palanivelu/06 [5] PST 130 MI MI Cervical 220 0 180
Bottger/06 [6] PST 25 MI—transhiatal,
3-stage
MI 12, open
4 (3-stage)
Cervical 165, 300 0 300
Godiris-Petit/06 [7] PST 25 MI Open Thoracic 368 1 (4) \100
Berrisford/08 [8] PST 77 MI MI Cervical 413 1 (1) 425
Robertson/95 [9] RST 17 Open MI Thoracic 330 5 (29) N/R
Kawahara/98 [11] RST 23 Open MI Cervical 111 (thoracic) 0 163
Nguyen/03 [13] RST 46 MI MI Both 350 2 279
Luketich/03 [14] RST 222 MI—transhiatal 8,
3-stage 214
MI Cervical N/R 16 (7.2) N/R
Collins/05 [15] RST 25 MI MI Cervical 350 2 200
Espat/04 [19] RST 15 MI—transhiatal
(robot-assisted)
N/A Cervical 274 0 50
Palanivelu/05 [20] PST 32 MI—transhiatal N/A None 200 0 150
Avital/05 [21] RST 22 MI—transhiatal N/A Cervical 380 1 (5) 220
Bann/05 [22] RST 20 MI—transhiatal N/A Cervical 415 2 (10) 300
Tinoco/07 [23] RST 78 MI—transhiatal N/A Cervical 153 (lap
component)
5 (6) N/R
Sanders/07 [24] RST 18 MI—transhiatal N/A Cervical 300 2 (11) N/R
MI minimally invasive, N/A not applicable, N/R not recorded, PST prospective series, RST retrospective series
Surg Endosc
123
with or without dissection at the cervical oesophagus
depending on the site of anastomosis. Transhiatal oeso-
phagectomy negates direct access to the mediastinum
through the thoracic wall and also may require dissection
of the cervical oesophagus depending on anastomosis site.
The first described techniques for MIO were in transhiatal
procedures by DePaula et al. [32] in Brazil and by Swan-
strom et al. [10] in North America. Subsequent to these,
video assistance was employed for transthoracic oeso-
phagectomy. As skills and technology have developed,
laparoscopy has become increasingly successful for the
abdominal component of Ivor-Lewis oesophageal resec-
tion. Gastric preconditioning, whereby the stomach is
mobilised on the right gastric arterial pedicle to assess
conduit viability prior to the resection surgery, is not
mentioned by the proponents of MIO.
Transhiatal oesophagectomy
As described, minimally invasive transhiatal oesophagec-
tomy was developed first and negates the need for trans-
thoracic exposure in an attempt to reduce postoperative
pulmonary complications. Most proponents of this proce-
dure use 5-port laparoscopy with the patient in varying
degrees of anti-Trendelenburg position. Although tech-
niques continue to be refined, most proponents describe
operator positioning between the patient’s legs, with the
camera holder and instrument nurse to the patient’s left
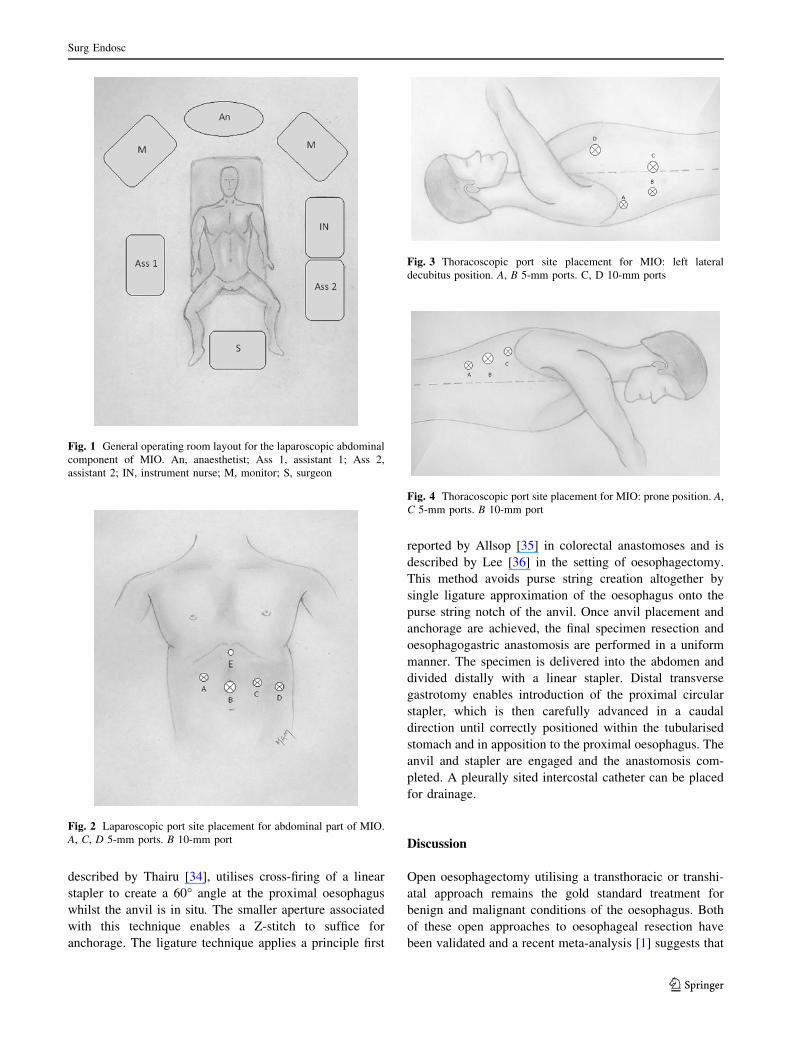
side and the second assistant to the right (Fig. 1). A con-
sensus on abdominal port placement is provided in Fig. 2.
All oncological oesophagectomies commence with a thor-
ough general inspection. The stomach may be mobilised
before or after oesophageal dissection. Irrespective of the
order, all lymph nodes and fatty tissue from the coeliac axis
and common hepatic and splenic arteries are cleared via an
incision through the lesser omentum; these are then swept
into the resection specimen. Oesophageal dissection begins
at the crura using harmonic shears with en bloc excision of
any locally involved tissue. The posterior mediastinum is
entered and adequate circumferential mobilisation of the
oesophagus is achieved by a combination of blunt and
sharp harmonic dissection. A tape may be passed around
the oesophagus to aid retraction, although some authors
[20] avoid this because of concern over tumour spill. A
proximal margin of at least 5 cm is the goal. The stomach
is mobilised in the usual fashion with preservation of the
right gastric artery and right gastroepiploic vascular arcade.
Although intrathoracic anastomosis has been described for
the transhiatal approach [29], this anastomosis site is
generally avoided with preference for a cervical anasto-
mosis following gastric pull-up. To achieve this, open
access and dissection are employed and the proximal
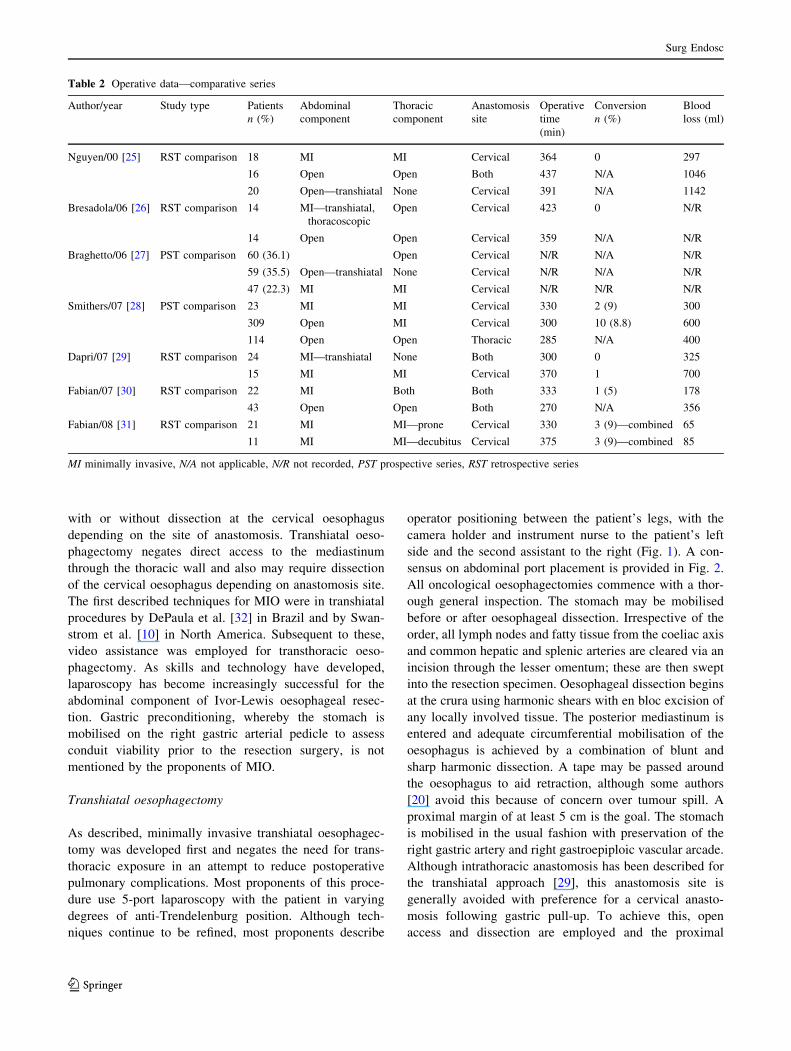
Table 2 Operative data—comparative series
Author/year Study type Patients
n (%)
Abdominal
component
Thoracic
component
Anastomosis
site
Operative
time
(min)
Conversion
n (%)
Blood
loss (ml)
Nguyen/00 [25] RST comparison 18 MI MI Cervical 364 0 297
16 Open Open Both 437 N/A 1046
20 Open—transhiatal None Cervical 391 N/A 1142
Bresadola/06 [26] RST comparison 14 MI—transhiatal,
thoracoscopic
Open Cervical 423 0 N/R
14 Open Open Cervical 359 N/A N/R
Braghetto/06 [27] PST comparison 60 (36.1) Open Cervical N/R N/A N/R
59 (35.5) Open—transhiatal None Cervical N/R N/A N/R
47 (22.3) MI MI Cervical N/R N/R N/R
Smithers/07 [28] PST comparison 23 MI MI Cervical 330 2 (9) 300
309 Open MI Cervical 300 10 (8.8) 600
114 Open Open Thoracic 285 N/A 400
Dapri/07 [29] RST comparison 24 MI—transhiatal None Both 300 0 325
15 MI MI Cervical 370 1 700
Fabian/07 [30] RST comparison 22 MI Both Both 333 1 (5) 178
43 Open Open Both 270 N/A 356
Fabian/08 [31] RST comparison 21 MI MI—prone Cervical 330 3 (9)—combined 65
11 MI MI—decubitus Cervical 375 3 (9)—combined 85
MI minimally invasive, N/A not applicable, N/R not recorded, PST prospective series, RST retrospective series
Surg Endosc
123
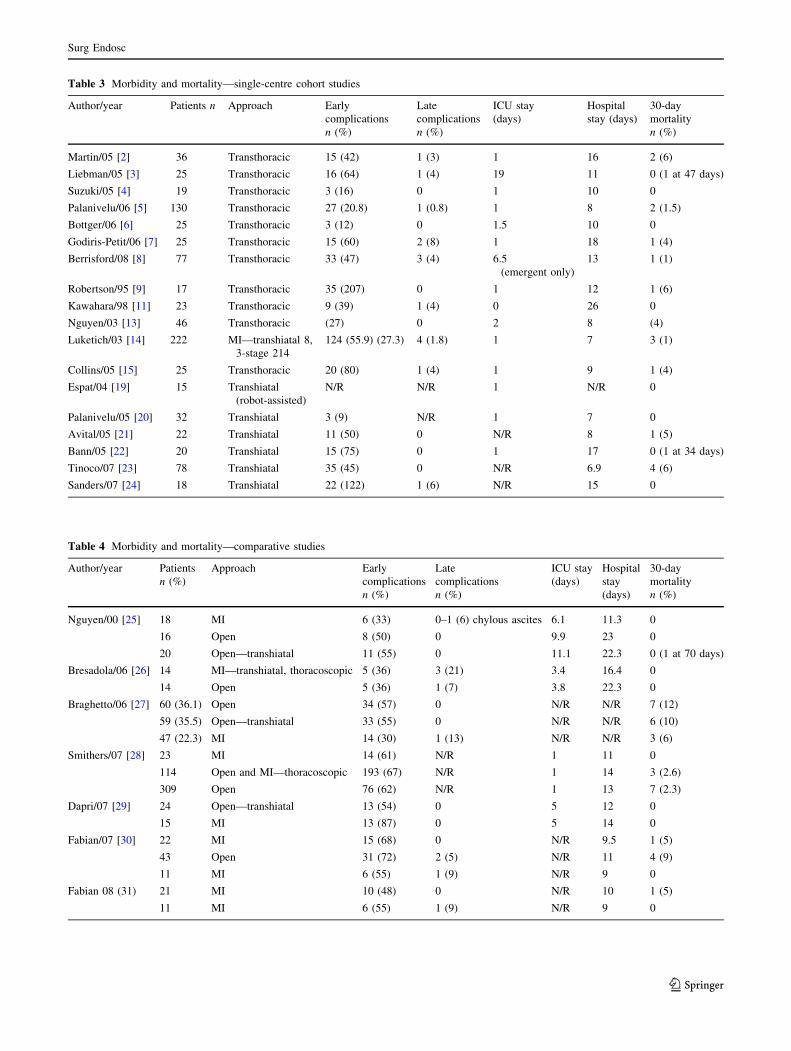
Table 3 Morbidity and mortality—single-centre cohort studies
Author/year Patients n Approach Early
complications
n (%)
Late
complications
n (%)
ICU stay
(days)
Hospital
stay (days)
30-day
mortality
n (%)
Martin/05 [2] 36 Transthoracic 15 (42) 1 (3) 1 16 2 (6)
Liebman/05 [3] 25 Transthoracic 16 (64) 1 (4) 19 11 0 (1 at 47 days)
Suzuki/05 [4] 19 Transthoracic 3 (16) 0 1 10 0
Palanivelu/06 [5] 130 Transthoracic 27 (20.8) 1 (0.8) 1 8 2 (1.5)
Bottger/06 [6] 25 Transthoracic 3 (12) 0 1.5 10 0
Godiris-Petit/06 [7] 25 Transthoracic 15 (60) 2 (8) 1 18 1 (4)
Berrisford/08 [8] 77 Transthoracic 33 (47) 3 (4) 6.5
(emergent only)
13 1 (1)
Robertson/95 [9] 17 Transthoracic 35 (207) 0 1 12 1 (6)
Kawahara/98 [11] 23 Transthoracic 9 (39) 1 (4) 0 26 0
Nguyen/03 [13] 46 Transthoracic (27) 0 2 8 (4)
Luketich/03 [14] 222 MI—transhiatal 8,
3-stage 214
124 (55.9) (27.3) 4 (1.8) 1 7 3 (1)
Collins/05 [15] 25 Transthoracic 20 (80) 1 (4) 1 9 1 (4)
Espat/04 [19] 15 Transhiatal
(robot-assisted)
N/R N/R 1 N/R 0
Palanivelu/05 [20] 32 Transhiatal 3 (9) N/R 1 7 0
Avital/05 [21] 22 Transhiatal 11 (50) 0 N/R 8 1 (5)
Bann/05 [22] 20 Transhiatal 15 (75) 0 1 17 0 (1 at 34 days)
Tinoco/07 [23] 78 Transhiatal 35 (45) 0 N/R 6.9 4 (6)
Sanders/07 [24] 18 Transhiatal 22 (122) 1 (6) N/R 15 0
Table 4 Morbidity and mortality—comparative studies
Author/year Patients
n (%)
Approach Early
complications
n (%)
Late
complications
n (%)
ICU stay
(days)
Hospital
stay
(days)
30-day
mortality
n (%)
Nguyen/00 [25] 18 MI 6 (33) 0–1 (6) chylous ascites 6.1 11.3 0
16 Open 8 (50) 0 9.9 23 0
20 Open—transhiatal 11 (55) 0 11.1 22.3 0 (1 at 70 days)
Bresadola/06 [26] 14 MI—transhiatal, thoracoscopic 5 (36) 3 (21) 3.4 16.4 0
14 Open 5 (36) 1 (7) 3.8 22.3 0
Braghetto/06 [27] 60 (36.1) Open 34 (57) 0 N/R N/R 7 (12)
59 (35.5) Open—transhiatal 33 (55) 0 N/R N/R 6 (10)
47 (22.3) MI 14 (30) 1 (13) N/R N/R 3 (6)
Smithers/07 [28] 23 MI 14 (61) N/R 1 11 0
114 Open and MI—thoracoscopic 193 (67) N/R 1 14 3 (2.6)
309 Open 76 (62) N/R 1 13 7 (2.3)
Dapri/07 [29] 24 Open—transhiatal 13 (54) 0 5 12 0
15 MI 13 (87) 0 5 14 0
Fabian/07 [30] 22 MI 15 (68) 0 N/R 9.5 1 (5)
43 Open 31 (72) 2 (5) N/R 11 4 (9)
11 MI 6 (55) 1 (9) N/R 9 0
Fabian 08 (31) 21 MI 10 (48) 0 N/R 10 1 (5)
11 MI 6 (55) 1 (9) N/R 9 0
Surg Endosc
123
oesophagus is divided using a linear stapler. After delivery
of the gastric conduit into the neck, cervical anastomosis is
achieved by either a hand-sewn interrupted technique or
stapler. In the event of any pleural breach, mediastinal
drains are placed, and prior to closure a feeding jejunos-
tomy is usually sited.
Transthoracic oesophagectomy
Minimally invasive transthoracic oesophagectomy involves
two or three stages depending on the site of oesophageal
anastomosis, and it has traditionally been felt that it offers
superior oncological resection when compared to the
transhiatal approach. Access to the abdomen and the cer-
vical area is generally achieved with the patient in the anti-
Trendelenburg position, whereas thoracoscopic access is
better with the lateral or prone position. Because of the
subsequent need for intraoperative repositioning, the order
by which the transthoracic technique is achieved tends to
depend on the site of anastomosis. For intrathoracic anas-
tomosis, it seems logical to fully complete the abdominal
component of the operation prior to repositioning for
thoracoscopic dissection and anastomosis, thus avoiding
the need for further unnecessary movement of the patient.
Likewise, in the situation of cervical anastomosis, com-
pleting the thoracoscopic dissection prior to the abdominal
and cervical components achieves the same economy of
movement.
Where cervical anastomosis is to be performed, the first
stage of the operation varies among authors; some prefer
initial dissection in the abdomen, whilst others prefer initial
oesophageal mobilisation in the thorax. As described
above, the latter approach reduces the required amount of
intraoperative repositioning. Irrespective of this, the
abdominal component of the procedure proceeds in a fairly
universal way. The anti-Trendelenburg position is acquired
and a 5-port laparoscopy is set up, not dissimilar in pattern
to that of the transhiatal procedure described above
(Figs. 1, 2); however, the operator usually stands on the
patient’s right side instead of between the legs. The pri-
mary assistant stands on the patient’s left with the monitor
placed at the patient’s head end. Stomach is most com-
monly used for conduit, but colon may be required in the
situation of distal tumour spread or previous gastrectomy.
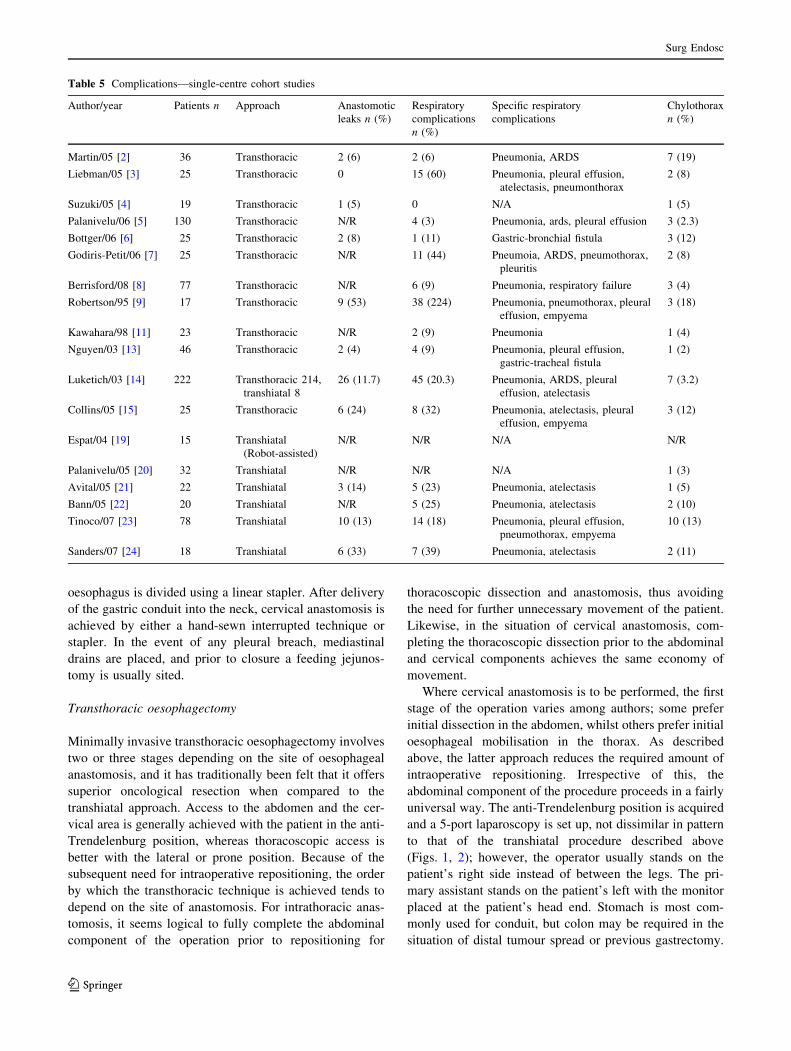
Table 5 Complications—single-centre cohort studies
Author/year Patients n Approach Anastomotic
leaks n (%)
Respiratory
complications
n (%)
Specific respiratory
complications
Chylothorax
n (%)
Martin/05 [2] 36 Transthoracic 2 (6) 2 (6) Pneumonia, ARDS 7 (19)
Liebman/05 [3] 25 Transthoracic 0 15 (60) Pneumonia, pleural effusion,
atelectasis, pneumonthorax
2 (8)
Suzuki/05 [4] 19 Transthoracic 1 (5) 0 N/A 1 (5)
Palanivelu/06 [5] 130 Transthoracic N/R 4 (3) Pneumonia, ards, pleural effusion 3 (2.3)
Bottger/06 [6] 25 Transthoracic 2 (8) 1 (11) Gastric-bronchial fistula 3 (12)
Godiris-Petit/06 [7] 25 Transthoracic N/R 11 (44) Pneumoia, ARDS, pneumothorax,
pleuritis
2 (8)
Berrisford/08 [8] 77 Transthoracic N/R 6 (9) Pneumonia, respiratory failure 3 (4)
Robertson/95 [9] 17 Transthoracic 9 (53) 38 (224) Pneumonia, pneumothorax, pleural
effusion, empyema
3 (18)
Kawahara/98 [11] 23 Transthoracic N/R 2 (9) Pneumonia 1 (4)
Nguyen/03 [13] 46 Transthoracic 2 (4) 4 (9) Pneumonia, pleural effusion,
gastric-tracheal fistula
1 (2)
Luketich/03 [14] 222 Transthoracic 214,
transhiatal 8
26 (11.7) 45 (20.3) Pneumonia, ARDS, pleural
effusion, atelectasis
7 (3.2)
Collins/05 [15] 25 Transthoracic 6 (24) 8 (32) Pneumonia, atelectasis, pleural
effusion, empyema
3 (12)
Espat/04 [19] 15 Transhiatal
(Robot-assisted)
N/R N/R N/A N/R
Palanivelu/05 [20] 32 Transhiatal N/R N/R N/A 1 (3)
Avital/05 [21] 22 Transhiatal 3 (14) 5 (23) Pneumonia, atelectasis 1 (5)
Bann/05 [22] 20 Transhiatal N/R 5 (25) Pneumonia, atelectasis 2 (10)
Tinoco/07 [23] 78 Transhiatal 10 (13) 14 (18) Pneumonia, pleural effusion,
pneumothorax, empyema
10 (13)
Sanders/07 [24] 18 Transhiatal 6 (33) 7 (39) Pneumonia, atelectasis 2 (11)
Surg Endosc
123
For gastric conduit, mobilisation of the stomach is per-
formed as per the transhiatal approach. Kocherisation of
the duodenum is required to mobilise the pylorus to the
oesophageal hiatus. Dissection of the lower oesophagus
can be achieved as far as the extent of direct vision. The
gastric conduit is created using multiple loads of a linear
cutting stapler, starting at the lesser curvature. Many
operators do not complete transection of the pathologic
specimen at this point as keeping this continuity later
facilitates retraction of the conduit into the chest.
The thoracic component is performed with the patient in
either a lateral or a prone position (Figs. 3, 4) to aid
exposure of the mediastinal oesophagus. The prone posi-
tion, in particular, places the oesophagus at the upper limit
in the thorax and enables the right lung to fall away under
gravity [12]. The clear disadvantages of the prone tech-
nique are the inherent practical issues of physically
achieving such a position and the associated difficulty with
airway management. There is little consensus on thoracic
port placements, which are dependent on patient position-
ing. Single-lung ventilation is required. Where patients
have not tolerated single-lung ventilation, low-pressure gas
insufflation has been successfully employed. Dissection is
achieved with ultrasonic shears, and manipulation of the
oesophagus is aided by looping tape around its circum-
ference from an early stage.
Following oesophageal mobilisation, the specimen can
be manipulated and transected in the thorax, abdomen, or
neck depending on disease site and surgeon’s preference.
Anastomosis sites and technique vary among authors.
When an intrathoracic anastomosis is required, technique is
particularly critical to reduce the risk of leak and its
associated morbidity. All minimally invasive techniques
for intrathoracic anastomosis describe use of a circular end-
to-end stapler. The detachable anvil may be introduced into
the proximal oesophagus via either abdomen or thorax, but
extension of thoracic port sites is avoided where possible.
Following ligature or clamp occlusion of the proximal
margin of the specimen, the anvil is introduced into the
proximal oesophagus via a transverse incision. Anvil
anchorage is now necessary and has been regarded as a
rate-limiting step. Two principal methods of anvil fixation
are subsequently described: purse string and ligature
techniques. The traditional method of purse string
placement is time consuming in MIO and has led to the
development of new instruments and techniques. The
Endo-Stitch device (US Surgical), described by Misawa
et al. [33], consists of a two-jawed endoscopic instrument
with each jaw capable of holding a double-ended straight
needle. Used on soft tissues, this instrument enables the
placement of running or interrupted sutures more effi-
ciently by one hand. The alternative Z-stitch technique,
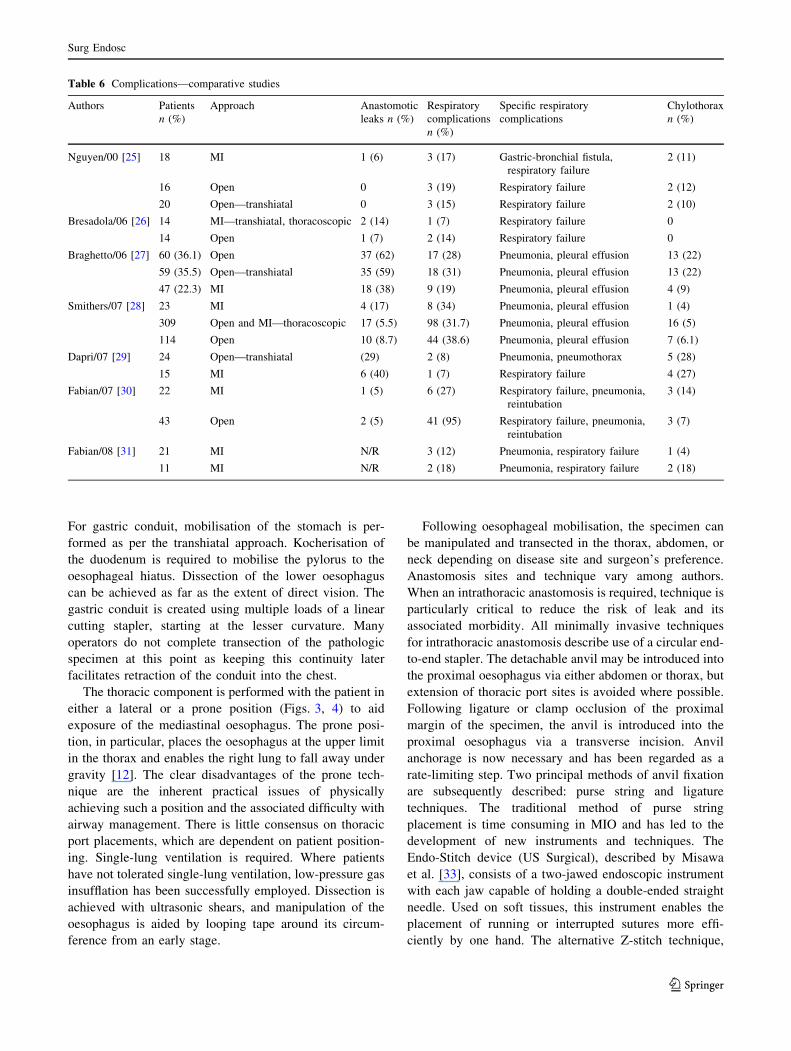
Table 6 Complications—comparative studies
Authors Patients
n (%)
Approach Anastomotic
leaks n (%)
Respiratory
complications
n (%)
Specific respiratory
complications
Chylothorax
n (%)
Nguyen/00 [25] 18 MI 1 (6) 3 (17) Gastric-bronchial fistula,
respiratory failure
2 (11)
16 Open 0 3 (19) Respiratory failure 2 (12)
20 Open—transhiatal 0 3 (15) Respiratory failure 2 (10)
Bresadola/06 [26] 14 MI—transhiatal, thoracoscopic 2 (14) 1 (7) Respiratory failure 0
14 Open 1 (7) 2 (14) Respiratory failure 0
Braghetto/06 [27] 60 (36.1) Open 37 (62) 17 (28) Pneumonia, pleural effusion 13 (22)
59 (35.5) Open—transhiatal 35 (59) 18 (31) Pneumonia, pleural effusion 13 (22)
47 (22.3) MI 18 (38) 9 (19) Pneumonia, pleural effusion 4 (9)
Smithers/07 [28] 23 MI 4 (17) 8 (34) Pneumonia, pleural effusion 1 (4)
309 Open and MI—thoracoscopic 17 (5.5) 98 (31.7) Pneumonia, pleural effusion 16 (5)
114 Open 10 (8.7) 44 (38.6) Pneumonia, pleural effusion 7 (6.1)
Dapri/07 [29] 24 Open—transhiatal (29) 2 (8) Pneumonia, pneumothorax 5 (28)
15 MI 6 (40) 1 (7) Respiratory failure 4 (27)
Fabian/07 [30] 22 MI 1 (5) 6 (27) Respiratory failure, pneumonia,
reintubation
3 (14)
43 Open 2 (5) 41 (95) Respiratory failure, pneumonia,
reintubation
3 (7)
Fabian/08 [31] 21 MI N/R 3 (12) Pneumonia, respiratory failure 1 (4)
11 MI N/R 2 (18) Pneumonia, respiratory failure 2 (18)
Surg Endosc
123
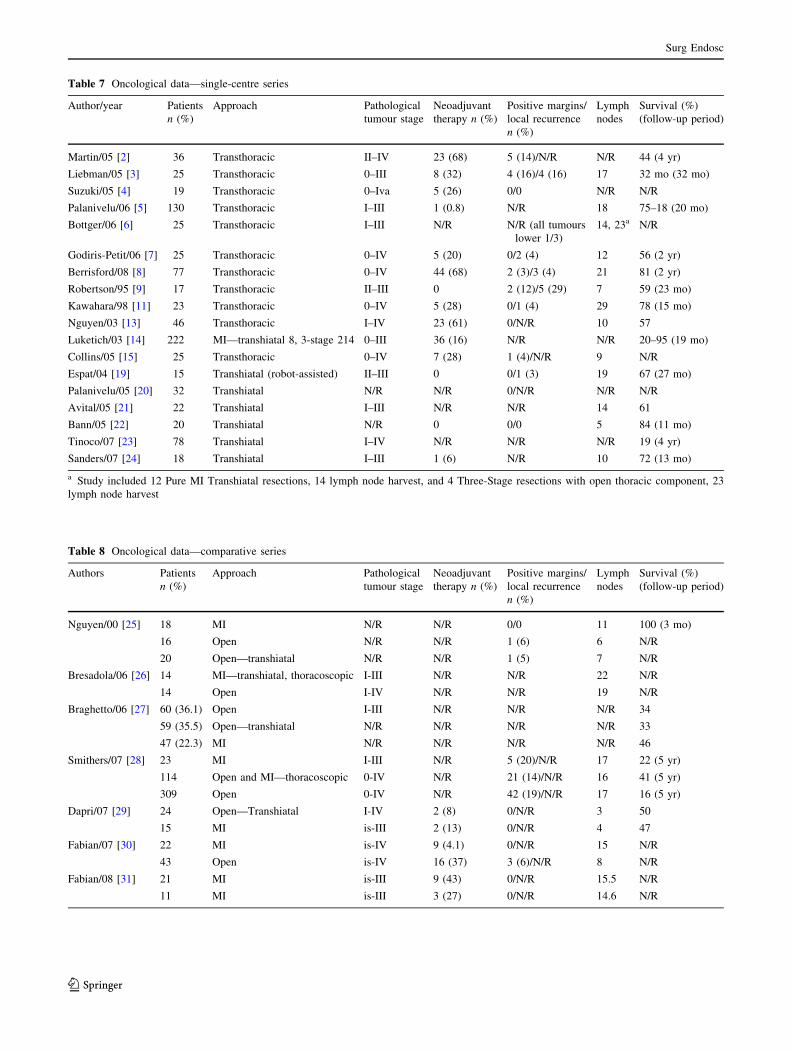
Table 7 Oncological data—single-centre series
Author/year Patients
n (%)
Approach Pathological
tumour stage
Neoadjuvant
therapy n (%)
Positive margins/
local recurrence
n (%)
Lymph
nodes
Survival (%)
(follow-up period)
Martin/05 [2] 36 Transthoracic II–IV 23 (68) 5 (14)/N/R N/R 44 (4 yr)
Liebman/05 [3] 25 Transthoracic 0–III 8 (32) 4 (16)/4 (16) 17 32 mo (32 mo)
Suzuki/05 [4] 19 Transthoracic 0–Iva 5 (26) 0/0 N/R N/R
Palanivelu/06 [5] 130 Transthoracic I–III 1 (0.8) N/R 18 75–18 (20 mo)
Bottger/06 [6] 25 Transthoracic I–III N/R N/R (all tumours
lower 1/3)
14, 23a N/R
Godiris-Petit/06 [7] 25 Transthoracic 0–IV 5 (20) 0/2 (4) 12 56 (2 yr)
Berrisford/08 [8] 77 Transthoracic 0–IV 44 (68) 2 (3)/3 (4) 21 81 (2 yr)
Robertson/95 [9] 17 Transthoracic II–III 0 2 (12)/5 (29) 7 59 (23 mo)
Kawahara/98 [11] 23 Transthoracic 0–IV 5 (28) 0/1 (4) 29 78 (15 mo)
Nguyen/03 [13] 46 Transthoracic I–IV 23 (61) 0/N/R 10 57
Luketich/03 [14] 222 MI—transhiatal 8, 3-stage 214 0–III 36 (16) N/R N/R 20–95 (19 mo)
Collins/05 [15] 25 Transthoracic 0–IV 7 (28) 1 (4)/N/R 9 N/R
Espat/04 [19] 15 Transhiatal (robot-assisted) II–III 0 0/1 (3) 19 67 (27 mo)
Palanivelu/05 [20] 32 Transhiatal N/R N/R 0/N/R N/R N/R
Avital/05 [21] 22 Transhiatal I–III N/R N/R 14 61
Bann/05 [22] 20 Transhiatal N/R 0 0/0 5 84 (11 mo)
Tinoco/07 [23] 78 Transhiatal I–IV N/R N/R N/R 19 (4 yr)
Sanders/07 [24] 18 Transhiatal I–III 1 (6) N/R 10 72 (13 mo)
a Study included 12 Pure MI Transhiatal resections, 14 lymph node harvest, and 4 Three-Stage resections with open thoracic component, 23
lymph node harvest
Table 8 Oncological data—comparative series
Authors Patients
n (%)
Approach Pathological
tumour stage
Neoadjuvant
therapy n (%)
Positive margins/
local recurrence
n (%)
Lymph
nodes
Survival (%)
(follow-up period)
Nguyen/00 [25] 18 MI N/R N/R 0/0 11 100 (3 mo)
16 Open N/R N/R 1 (6) 6 N/R
20 Open—transhiatal N/R N/R 1 (5) 7 N/R
Bresadola/06 [26] 14 MI—transhiatal, thoracoscopic I-III N/R N/R 22 N/R
14 Open I-IV N/R N/R 19 N/R
Braghetto/06 [27] 60 (36.1) Open I-III N/R N/R N/R 34
59 (35.5) Open—transhiatal N/R N/R N/R N/R 33
47 (22.3) MI N/R N/R N/R N/R 46
Smithers/07 [28] 23 MI I-III N/R 5 (20)/N/R 17 22 (5 yr)
114 Open and MI—thoracoscopic 0-IV N/R 21 (14)/N/R 16 41 (5 yr)
309 Open 0-IV N/R 42 (19)/N/R 17 16 (5 yr)
Dapri/07 [29] 24 Open—Transhiatal I-IV 2 (8) 0/N/R 3 50
15 MI is-III 2 (13) 0/N/R 4 47
Fabian/07 [30] 22 MI is-IV 9 (4.1) 0/N/R 15 N/R
43 Open is-IV 16 (37) 3 (6)/N/R 8 N/R
Fabian/08 [31] 21 MI is-III 9 (43) 0/N/R 15.5 N/R
11 MI is-III 3 (27) 0/N/R 14.6 N/R
Surg Endosc
123
described by Thairu [34], utilises cross-firing of a linear
stapler to create a 60� angle at the proximal oesophagus
whilst the anvil is in situ. The smaller aperture associated
with this technique enables a Z-stitch to suffice for
anchorage. The ligature technique applies a principle first
reported by Allsop [35] in colorectal anastomoses and is
described by Lee [36] in the setting of oesophagectomy.
This method avoids purse string creation altogether by
single ligature approximation of the oesophagus onto the
purse string notch of the anvil. Once anvil placement and
anchorage are achieved, the final specimen resection and
oesophagogastric anastomosis are performed in a uniform
manner. The specimen is delivered into the abdomen and
divided distally with a linear stapler. Distal transverse
gastrotomy enables introduction of the proximal circular
stapler, which is then carefully advanced in a caudal
direction until correctly positioned within the tubularised
stomach and in apposition to the proximal oesophagus. The
anvil and stapler are engaged and the anastomosis com-
pleted. A pleurally sited intercostal catheter can be placed
for drainage.
Discussion
Open oesophagectomy utilising a transthoracic or transhi-
atal approach remains the gold standard treatment for
benign and malignant conditions of the oesophagus. Both
of these open approaches to oesophageal resection have
been validated and a recent meta-analysis [1] suggests that
Fig. 1 General operating room layout for the laparoscopic abdominal
component of MIO. An, anaesthetist; Ass 1, assistant 1; Ass 2,
assistant 2; IN, instrument nurse; M, monitor; S, surgeon
Fig. 2 Laparoscopic port site placement for abdominal part of MIO.
A, C, D 5-mm ports. B 10-mm port
Fig. 3 Thoracoscopic port site placement for MIO: left lateral
decubitus position. A, B 5-mm ports. C, D 10-mm ports
Fig. 4 Thoracoscopic port site placement for MIO: prone position. A,
C 5-mm ports. B 10-mm port
Surg Endosc
123

they result in similar morbidity, mortality, and 5-year
survival rates. Theoretically, respiratory morbidity should
occur more frequently in the transthoracic approach but no
statistically significant difference has been shown.
No randomised controlled trials currently exist for MIO,
and it seems unlikely that any will be carried out given the
known limitations of the procedure for locally advanced
primary disease. This, in addition to the high dependence
of MIO on advanced technical skill, has resulted in a slow
acceptance of this technique as a valid or achievable
standard of care. The available comparative data do sug-
gest that MIO is as good as open oesophagectomy when
performed by an appropriately skilled and experienced
surgeon. Of particular note is the work of Luketich et al.
[14, 37], who have reported the largest series of MIO (222
patients), albeit noncomparatively. Morbidity rates are at
least comparable to open procedures in this series. Luke-
tich’s mortality rate of 1.3% is better than the mortality rate
of 5.7% for transhiatal oesophagectomy (THO) and 9.2%
for transthoracic oesophagectomy (TTO) reported in the
meta-analysis by Hulscher et al. [1] on open oesophagec-
tomy. It is generally accepted that outcome following open
oesophagectomy is better when performed in high numbers
by dedicated surgeons, and it is logical to extrapolate that
theory for MIO. Even so, MIO has been reported by
smaller centres with comparable outcome measures to open
oesophagectomy. For example, Bann et al. [22] reported on
a prospective series of 22 patients who underwent Ivor-
Lewis MIO at a district general hospital in the United
Kingdom with oncological resection and morbidity results
comparable to those of open oesophagectomy. Review of
the existing studies shows a number of commonly assessed
outcome measures for morbidity and oncological resection
which will now be addressed individually.
Operative data
Operative time
It is unanimously accepted that total operative time
(Tables 1, 2) is longer for MIO than for open surgery and
except for the limitation caused by local oncological stage,
this remains the major drawback in MIO. As with all
comparisons to open oesophagectomy, variability in study
size and subsequently induced statistical error need to be
considered, as does the inherent selection bias of patients
more likely to have less advanced and therefore more
easily resectable disease.
Blood loss
Blood loss is reported by most authors in this series, with
the range of averages between 50 and 700 ml (Tables 1, 2).
The study with the lowest blood loss was by Espat [19] in
2004, who used a robot-assisted transhiatal approach in 15
patients with no conversions. There are no other recorded
studies using this technology in the literature, which is not
surprising given that robot-assisted surgery still remains
very much in the avant-garde and is inaccessible to the vast
majority of institutions. Otherwise little solid comparative
data to open surgery exists, but there is certainly no
overwhelming evidence of any significant difference in
haemorrhage between MIO and open oesophagectomy.
Morbidity and mortality
Anastomotic leakage
Anastomotic leak is one of the most feared complications
in oesophagectomy surgery, with a historical mortality rate
of 50%. The definition of anastomotic leak varies between
authors although most in this series used radiographic
findings, whether carried out as a routine or because of
clinical suspicion. From our analysis, MIO leakage rate
ranged between 2.2 and 52.9% (Tables 5, 6), which is at
least comparable to the reported leakage rates for open
oesophagectomy [1], where rates vary from 3 to 50%. The
wide range of leakage rate reported following open oeso-
phagectomy was addressed by Hulscher et al. [1] in their
meta-analysis, and they concluded that this wide-ranging
result was more a reflection of the problem with definition
rather than true technical differences. There is no apparent
difference between leakage rates in thoracic or cervical
anastomosis following MIO. For open surgery, transhiatal
operations with cervical anastomoses seem to produce
almost twice the anastomotic leak compared to transtho-
racic operations, where a majority of anastomoses were
made through the chest (13.6 vs. 7.2%) [1]. From our
collated data this does not appear to be reflected in MIO.
Irrespective of absolute leakage rate, thoracic leakage tends
to result in higher morbidity than cervical leakage, and this
should be considered in addition to absolute numbers.
Respiratory morbidity
Major morbidity results from open transthoracic access.
The thoracotomy incision is painful and also exposes the
lungs to atmospheric pressure for extended periods,
increasing barotrauma risk. Open transhiatal techniques
were first developed in an attempt to avoid thoracotomy,
but the inherent element of blind resection in this technique
raised some concern over the adequacy of oncological
resection and led to the first minimally invasive thoraco-
scopic approaches. Analysis of respiratory complication
rate, however, shows fairly underwhelming results when
compared to open techniques. Analysis of the 12 case
Surg Endosc
123

series that report results on a transthoracic approach [2–5,
8, 9, 13, 15, 25, 28, 29, 31] provides a weighted median
respiratory complication rate of 31.7%, which is high
compared to the published data on open oesophagectomy;
the meta-analysis by Hulcher et al. [1] reports respiratory
complication rates of 18.7% for open transthoracic surgery
and 12.7% for open transhiatal oesophagectomy. This
alarming result is, however, probably more reflective of
variation in reporting than a true difference. The notable
extreme in respiratory complication rate was observed in
the retrospective review of 17 patients who underwent a
two-stage oesophagectomy performed by Robertson et al.
[9]. In this series radiographic evidence of atelectasis was
included in the complication rate irrespective of the clinical
picture and thus accounted for 76% of all patients alone.
Analysis of the available series that reported results of a
purely minimally invasive approach to both the abdominal
and the thoracic component reveals more promising
information, with a combined respiratory complication rate
of 7.8%. The largest available series by Luketich [14] was
not included in either of the above grouped case series
because 8 of 222 patients underwent transhiatal oeso-
phagectomy and could not be differentiated from the
remaining 214. This series reports a 12.6% combined
respiratory complication rate defined as pneumonia and/or
acute respiratory distress syndrome (ARDS). Meta-analysis
of the open technique by Hulscher et al. [1] grouped pul-
monary complications together, including pulmonary
embolus (PE) with pneumonia and ARDS. The addition of
PE to the Luketich et al. [14] data results in a morbidity
rate of 14% compared to 18.7% for open transthoracic and
12.7% for open transthoracic techniques. It should be noted
that Luketich et al. preferred the improved access of a
minimally invasive transthoracic approach and that their
morbidity result is at least comparable to that of the open
transhiatal technique but with the benefits of improved
mediastinal exposure.
Postoperative intensive care requirements
and hospital stay
Median duration of postoperative stay on the intensive care
unit (ICU) following MIO is 1 day in the majority of studies
(Tables 3, 4). Some postoperative care protocols following
MIO did not involve planned admission to ICU at all. In a
series of 77 patients who underwent minimally invasive
transthoracic oesophagectomy, Berrisford et al. [8] used
ward-based postoperative care with central venous moni-
toring. This approach resulted in a 14% emergency admis-
sion rate to the formal ICU, however, and median stay on the
ICU in these patients was longer at 6.5 days. It remains to be
proven whether the avoidance of routine admission to ICU
following MIO is a safe or cost-effective practice.
Mortality
Thirty-day mortality rates following MIO vary between 0
to 5.9% (Tables 3, 4), which compares to the open trans-
thoracic procedure mortality rate of 9.2% and open trans-
hiatal procedure mortality rate of 7.2% described by
Hulscher et al. [1] in their meta-analysis. Patient selection
for surgery may well bias these results, but most propo-
nents of MIO believe this technique to be superior to open
surgery in patients with early disease.
Oncological resection
Since the advent of MIO, the adequacy of oncological
resection compared to that of open surgery has been
questioned. Important and commonly reported outcome
measures are resection margins, lymph node numbers,
overall disease stage, and long-term survival.
All potentially curative oncological resections require
complete clearance of local disease and therefore clear
resection margins (i.e., R0) of the primary tumour are
subsequently of the utmost importance. During the initial
development of MIO, only benign or early-stage malignant
disease was considered, and for most proponents of MIO
this still remains the case. This practice is based on the
expert opinion of these surgeons that an open approach still
provides better oncological clearance for locally advanced
disease compared to MIO and that potential cure from this
outweighs the known difference in morbidity risk. The
range of final pathological stage following MIO for
malignant disease does range from 0 to IV (Tables 7, 8).
Where a pathological stage IV was reported, surgery was
usually completed on palliative grounds or when previ-
ously undiagnosed metastatic spread could be concomi-
tantly resected. It should also be remembered that stage
migration [38] can bias analysis of pathological stage. This
upstaging is based on the idea that a more extensive lym-
phatic dissection results in a higher probability of node
positive disease being diagnosed. Stage migration will also
result in a more favourable long-term outcome relative to
pathological stage.
Where reported, MIO results in clear resection margins
in the vast majority. Martin et al. [2] reported the highest
rate of resection margin involvement in a study of 36
patients who underwent hybrid three-stage transthoracic
oesophagectomy. The technique included thoracoscopic
mobilisation of the mediastinal oesophagus and hand-
assisted laparoscopy in 21 patients and open laparotomy in
the remaining 15. Of all resections, five had involved
margins. Two were found to have unresectable primary
disease irrespective of approach and three had positive
radial margins, none of whom had received neoadjuvant
therapy. On this note, at least one study [11] revealed an
Surg Endosc
123

excellent response of some tumours to neoadjuvant therapy
with significant pathological downstaging and subsequent
successful resection with minimally invasive techniques.
Even with open oesophagectomy, there is still debate as
to the best approach for optimal lymph node dissection.
Given this, we will not comment on comparative data
between transhiatal and transthoracic minimally invasive
techniques. Analysis of all articles that used minimally
invasive techniques on ten or more patients provides a
range of average lymph nodes sampled of between 5 and
29 (Tables 7, 8). Variations on the extent of lymphatic
dissection for any approach to oesophagectomy do exist
and will undoubtedly bias the quoted figures influencing
overall staging via stage migration.
Survival
Long-term survival following MIO varies. This is largely
due to the retrospective data collection in most of the
existing studies. If reliable 3- and 5-year survival follow-up
data were available, one would expect similar results
compared to stage-equivalent patients who underwent open
surgery where clear margins and ‘‘adequate’’ lymphatic
clearance were achieved, but this is speculative.
Learning curve/progression
The best example of progression in MIO comes from
Luketich et al. [14, 37], who have published serial data on
their experience. The initial approach was with laparo-
scopic transhiatal oesophagectomy, which changed to a
thoracoscopic transhiatal technique over time. The initial
description was of 77 patients who underwent MIO
between August 1996 and September 1999 [37]. This has
now been extended to include data for a total of 222
patients [14], the largest single series of any experience
with MIO. Median operative time for the first 20 cases was
450 min, which decreased to 270 min thereafter. Anasto-
motic leak rate from initial experience was 9%, which
increased slightly to 11.7% over all 222 patients. As
experience grew, the minor complication rate decreased
and the major complication rate increased. Overall mor-
tality rate for the 222 patients was 1.4%. Progressively
more advanced disease has become amenable to MIO
through this series and should be taken into account when
considering these data.
Conclusions
For benign disease and oesophageal cancer of stage III or
less, MIO appears to be at least as good as open techniques
when performed by experienced surgeons in large centres.
Trends show acceptable morbidity, improved postoperative
recovery time, and adequate oncological resection for early
malignant disease. The immediately obvious negative
aspects of MIO are the experience requirement, the need
for advanced minimally invasive skills and equipment, and
the increased operative time. Morbidity following tho-
racoscopic and transhiatal MIO techniques is similar.
Whilst the transhiatal approach requires less intraoperative
positioning, access to the mediastinum via the hiatus is
limited and may compromise the extent of oncological
resection. Thoracoscopy provides improved exposure to
the middle and upper oesophagus and thoracic lymph
nodes. Although the oncological outcome data following
transhiatal MIO is scarce and negates further objective
comparison to the thoracoscopic technique, achieving long-
term locoregional control is the primary goal in any cancer
surgery. For this reason, thoracoscopic mobilisation of the
oesophagus, with either an open or a laparoscopic
abdominal component, is the currently preferred technique
for most surgeons. It is still felt that locally advanced
disease is a strong contraindication to MIO, irrespective of
approach. There will always be an inherent conversion rate
for intraoperative complications, such as uncontrolled
haemorrhage, and patient factors, such as adhesions. Where
this occurs, morbidity arguably may be higher than with a
primary open procedure. There remains no level I evidence
on which to draw firmer conclusions and it is unlikely that
a multicentre randomised controlled trial will come to
fruition. In the eyes of proponents of MIO, this may be
irrelevant. When used for carefully selected patients with
benign disease or early cancer, data from the literature does
show that MIO can result in superior outcome measures
and is at least comparable to open resection in this group.
Disclosures Nick Butler, Stuart Collins, Breda Memon, and Mu-
hammed Ashraf Memon have no conflicts of interest or financial ties
to disclose.
References
1. Hulscher JB, Tijssen JG, Obertop H, van Lanschot JJ (2001)
Transthoracic versus transhiatal resection for carcinoma of the
esophagus: a meta-analysis. Ann Thorac Surg 72:306–313
2. Martin DJ, Bessell JR, Chew A, Watson DI (2005) Thoracoscopic
and laparoscopic esophagectomy: initial experience and out-
comes. Surg Endosc 19:1597–1601
3. Leibman S, Smithers BM, Gotley DC, Martin I, Thomas J (2006)
Minimally invasive esophagectomy: short- and long-term out-
comes. Surg Endosc 20:428–433
4. Suzuki Y, Urashima M, Ishibashi Y, Abo M, Omura N, Nakada
K, Kawasaki N, Eto K, Hanyu N, Yanaga K (2005) Hand-assisted
laparoscopic and thoracoscopic surgery (HALTS) in radical
esophagectomy with three-field lymphadenectomy for thoracic
esophageal cancer. Eur J Surg Oncol 31:1166–1174
5. Palanivelu C, Prakash A, Parthasarathi R, Senthilkumar R,
Senthilnathan PR, Rajapandian S (2007) Laparoscopic
Surg Endosc
123
esophagogastrectomy without thoracic or cervical access for
adenocarcinoma of the gastroesophageal junction: an Indian
experience from a tertiary center. Surg Endosc 21:16–20
6. Bottger T, Terzic A, Muller M, Rodehorst A (2007) Minimally
invasive transhiatal and transthoracic esophagectomy. Surg
Endosc 21:1695–1700
7. Godiris-Petit G, Munoz-Bongrand N, Honigman I, Cattan P,
Sarfati E (2006) Minimally invasive esophagectomy for cancer:
prospective evaluation of laparoscopic gastric mobilization.
World J Surg 30:1434–1440
8. Berrisford RG, Wajed SA, Sanders D, Rucklidge MW (2008)
Short-term outcomes following total minimally invasive oeso-
phagectomy. Br J Surg 95:602–610
9. Robertson GS, Lloyd DM, Wicks AC, Veitch PS (1996) No
obvious advantages for thoracoscopic two-stage oesophagecto-
my. Br J Surg 83:675–678
10. Swanstrom LL, Hansen P (1997) Laparoscopic total esophagec-
tomy. Arch Surg 132:943–947
11. Kawahara K, Maekawa T, Okabayashi K, Hideshima T, Shiraishi
T, Yoshinaga Y, Shirakusa T (1999) Video-assisted thoracoscopic
esophagectomy for esophageal cancer. Surg Endosc 13:218–223
12. Watson DI, Davies N, Jamieson GG (1999) Totally endoscopic
Ivor Lewis esophagectomy. Surg Endosc 13:293–297
13. Nguyen NT, Roberts P, Follette DM, Rivers R, Wolfe BM (2003)
Thoracoscopic and laparoscopic esophagectomy for benign and
malignant disease: lessons learned from 46 consecutive proce-
dures. J Am Coll Surg 197:902–913
14. Luketich JD, Alvelo-Rivera M, Buenaventura PO, Christie NA,
McCaughan JS, Litle VR, Schauer PR, Close JM, Fernando HC
(2003) Minimally invasive esophagectomy: outcomes in 222
patients. Ann Surg 238:486–494
15. Collins G, Johnson E, Kroshus T, Ganz R, Batts K, Seng J,
Nwaneri O, Dunn D (2006) Experience with minimally invasive
esophagectomy. Surg Endosc 20:298–301
16. Sutton CD, White SA, Marshall LJ, Berry DP, Veitch PS (2002)
Endoscopic-assisted intrathoracic oesophagogastrostomy without
thoracotomy for tumours of the lower oesophagus and cardia. Eur
J Surg Oncol 28:46–48
17. Wong SK, Chan AC, Lee DW, To EW, Ng EK, Chung SC (2003)
Minimal invasive approach of gastric and esophageal mobiliza-
tion in total pharyngolaryngoesophagectomy: total laparoscopic
and hand-assisted laparoscopic technique. Surg Endosc 17:
798–802
18. Costi R, Himpens J, Bruyns J, Cadiere GB (2004) Totally lapa-
roscopic transhiatal esophago-gastrectomy without thoracic or
cervical access. The least invasive surgery for adenocarcinoma of
the cardia? Surg Endosc 18:629–632
19. Espat NJ, Jacobsen G, Horgan S, Donahue P (2005) Minimally
invasive treatment of esophageal cancer: laparoscopic staging to
robotic esophagectomy. Cancer J 11:10–17
20. Palanivelu C, Prakash A, Senthilkumar R, Senthilnathan P, Par-
thasarathi R, Rajan PS, Venkatachlam S (2006) Minimally
invasive esophagectomy: thoracoscopic mobilization of the
esophagus and mediastinal lymphadenectomy in prone position–
experience of 130 patients. J Am Coll Surg 203:7–16
21. Avital S, Zundel N, Szomstein S, Rosenthal R (2005) Laparo-
scopic transhiatal esophagectomy for esophageal cancer. Am J
Surg 190:69–74
22. Bann S, Moorthy K, Shaul T, Foley R (2005) Laparoscopic
transhiatal surgery of the esophagus. JSLS 9:376–381
23. Tinoco R, El-Kadre L, Tinoco A, Rios R, Sueth D, Pena F (2007)
Laparoscopic transhiatal esophagectomy: outcomes. Surg Endosc
21:1284–1287
24. Sanders G, Borie F, Husson E, Blanc PM, Di Mauro G, Claus C,
Millat B (2007) Minimally invasive transhiatal esophagectomy:
lessons learned. Surg Endosc 21:1190–1193
25. Nguyen NT, Follette DM, Wolfe BM, Schneider PD, Roberts P,
Goodnight JE Jr (2000) Comparison of minimally invasive
esophagectomy with transthoracic and transhiatal esophagec-
tomy. Arch Surg 135:920–925
26. Bresadola V, Terrosu G, Cojutti A, Benzoni E, Baracchini E,
Bresadola F (2006) Laparoscopic versus open gastroplasty in
esophagectomy for esophageal cancer: a comparative study. Surg
Laparosc Endosc Percutan Tech 16:63–67
27. Braghetto I, Csendes A, Cardemil G, Burdiles P, Korn O, Val-
ladares H (2006) Open transthoracic or transhiatal esophagec-
tomy versus minimally invasive esophagectomy in terms of
morbidity, mortality and survival. Surg Endosc 20:1681–1686
28. Smithers BM, Gotley DC, Martin I, Thomas JM (2007) Com-
parison of the outcomes between open and minimally invasive
esophagectomy. Ann Surg 245:232–240
29. Dapri G, Himpens J, Cadiere GB (2008) Minimally invasive
esophagectomy for cancer: laparoscopic transhiatal procedure or
thoracoscopy in prone position followed by laparoscopy? Surg
Endosc 22:1060–1069
30. Fabian T, Martin JT, McKelvey AA, Federico JA (2008) Mini-
mally invasive esophagectomy: a teaching hospital’s first year
experience. Dis Esophagus 21:220–225
31. Fabian T, Martin J, Katigbak M, McKelvey AA, Federico JA
(2008) Thoracoscopic esophageal mobilization during minimally
invasive esophagectomy: a head-to-head comparison of prone
versus decubitus positions. Surg Endosc 22:2485–2491
32. DePaula AL, Hashiba K, Ferreira EAB (1996) Trans-hiatal
approach for esophagecotmy. In: Toouli J, Gossot D, Hunter JG
(eds) Endosurgery. Churchill Livingstone, New York, pp 293–299
33. Misawa K, Hachisuka T, Kuno Y, Mori T, Shinohara M,
Miyauchi M (2005) New procedure for purse-string suture in
thoracoscopic esophagectomy with intrathoracic anastomosis.
Surg Endosc 19:40–42
34. Thairu N, Biswas S, Abdulaal Y, Ali H (2007) A new method for
intrathoracic anastomosis in laparoscopic esophagectomy. Surg
Endosc 21:1887–1890
35. Allsop JR (1992) Ligature versus purse string for surgical stapled
anastomoses. Aust N Z J Surg 62:740–742
36. Lee KW, Leung KF, Wong KK, Lau KY, Lai KC, Leung SK,
Leung LC, Lau KW (1997) One-stage thoracoscopic oesophag-
ectomy: ligature intrathoracic stapled anastomosis. Aust N Z J
Surg 67:131–132
37. Luketich JD, Schauer PR, Christie NA, Weigel TL, Raja S,
Fernando HC, Keenan RJ, Nguyen NT (2000) Minimally inva-
sive esophagectomy. Ann Thorac Surg 70:906–911
38. Feinstein AR, Sosin DM, Wells CK (1985) The Will Rogers
phenomenon: stage migration and new diagnostic techniques as a
source of misleading statistics for survival in cancer. N Engl J
Med 312:1604–1608
Surg Endosc
123




























