Embed Size (px)
Citation preview
JM Aranda, B Befeler, R Lazzara, A Embi and H Machadoand angiographic correlations
Mitral valve prolapse and coronary artery disease. Clinical, hemodynamic,
ISSN: 1524-4539 Copyright © 1975 American Heart Association. All rights reserved. Print ISSN: 0009-7322. Online
72514Circulation is published by the American Heart Association. 7272 Greenville Avenue, Dallas, TX
1975, 52:245-253Circulation
http://circ.ahajournals.org/content/52/2/245located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://www.lww.com/reprintsReprints: Information about reprints can be found online at [email protected]: 410-528-8550. E-mail: Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050. Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters http://circ.ahajournals.org//subscriptions/Subscriptions: Information about subscribing to Circulation is online at
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

Mitral Valve Prolapse and Coronary Artery Disease
Clinical, Hemodynamic, and Angiographic Correlations
By JUAN M. ARANDA, M. D., BENJAMIN BEFELER, M. D., RALPH LAZZARA, M.D.,
ABRAHAM EMBI, B.S., AND HUMBEBTO MACHADO, M.D.
SUMMARYAmong 95 patients with angina pectoris and angiographically documented coronary artery disease
(CAD), prolapse of the scallops of the posterior leaflet of the mitral valve (PLMV) was noted in 30 patients.Left ventriculograms in the right anterior oblique (RAO) projection revealed isolated prolapse of theposteromedial commissural scallop (PMCS) in 12 patients and the anterolateral commissural scallop (ALCS)in two patients. Seven patients had prolapse of both PMCS and ALCS, three had prolapse of the PMCS andmiddle scallop (MS), and six had prolapse of all three scallops of the PLMV.
Left ventricular dilatation with increased trabeculations was observed in 19 patients. Contractility deter-mined in a quantitative fashion by segmental motion analysis was markedly impaired in 29 patients. None ofthe patients had angiographic evidence of mitral insufficiency. Left ventricular dysfunction was
documented in 28 patients by either elevated left ventricular end-diastolic pressure (LVEDP), low cardiacindex (CI) or decreased ejection fraction (EF). In two patients in whom left ventricular contractility im-proved after aortocoronary bypass, previously prolapsed scallops could not be identified in the postoperativeventriculogram.
Prolapsed PLMV is a frequent angiographic finding in patients with angiographically observed CAD. Im-paired contractility of the ventricular myocardium and papillary muscles, left ventricular dilatation, andhypertrophy appear to play a significant role in the pathogenesis of this abnormality through distortion ofthe directional axis of the papillary muscles, asynergic contraction of the related free wall of the left ventri-cle, and changes in the normal spatial alignment necessary for mitral valve closure. The syndrome ofpapillary muscle dysfunction in patients with coronary artery disease represents a wider clinical spectrumthan previously described.
THE UNDERLYING CONDITIONS causingprolapse of the mitral valve leaflets are multiple
and include the Marfan syndrome, trauma, hyper-trophic obstructive cardiomyopathy, rheumatic en-
docarditis, congestive cardiomyopathy, atrial septaldefect and periarteritis nodosa.'` This syndrome in-cludes a spectrum of clinical findings which vary froma nonejection click without a systolic murmur to thepresence of mitral incompetence with a holosystolicmurmur and no click.6 7 Electrocardiographic findingscharacterized by ST and T wave changes in the in-ferior leads have been observed in some of the cases
reported.8 The findings are not specific, but may occur
in acquired mitral valve disease due to rheumaticfever or coronary atherosclerosis.9 10, 11 Since patientswith prolapsed mitral leaflets frequently develop
From the Cardiovascular Laboratory, Cardiology Section,Veterans Administration Hospital, and the Division of Cardiology,Department of Medicine, University of Miami School of Medicine,Mliami, Florida.
Supported in part by Institutional Research Funds.Address for reprints: Juan M. Aranda, M.D., Assistant Professor
of \Iedicine, Cardiology Section, Veterans Administration Hospital,University of Miami School of Medicine, 1201 N.W. 16th Street,Miami, Florida .33125.
Received November 25, 1974; revision accepted for publicationMarch 24, 197.5.
Circulation. Volume 52, August 1975
recurrent chest pain and ventricular arrhythmias, thepossibility that the electrocardiographic changes arecaused by coronary artery disease has beensuggested.9
Several recent reports in the literature have em-phasized angiographic-morphologic correlations'2 13and left ventricular abnormalities'4 in patients withthis syndrome. However, to date the frequency ofmitral valve prolapse in patients with coronary arterydisease has not been systematically studied. Thisreport describes the clinical, hemodynamic, andangiographic characteristics of patients with advancedcoronary artery disease who demonstrated prolapsedscallops of the posterior leaflet of the mitral valve.
Material and MethodsNinety-five patients, all males with angiographically
documented coronary artery disease referred to the Car-diovascular Laboratory for evaluation of chest pain,arrhythmias, or congestive heart failure, provided the datafor this report. An additional 12 patients studied because ofatypical chest pain, who had normal resting and exercisehemodynamics, coronary arteriograms, LV contractility,and no evidence of prolapsed mitral valve, cardiomyopathy,or valvular disease served as normal controls. All patientswere examined by at least two of the authors and all were ex-amined by one of us (BB).
After informed consent was obtained, right and left heart
245
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from
ARANDA ET AL.
catheterization and selective coronary cineangiography by amodification of the Sones technique"' was performed in thepostabsorptive state under mild sedation with diazepam andmeperidine. Angiographic images were recorded on 35 mmfilm at 60 frames per second. Pressure was registered on anElectronics for Medicine Multi-channel DR-16 recorder,utilizing Statham PD-23 transducers and fluid-filledcatheters. Cardiac output was determined in duplicate bythe dye dilution technique using indocyanine green.Isometric exercise was performed for 5 min using a hand-grip dynamometer. The maximal voluntary contraction wasdetermined before the procedure was started as the averageof three consecutive maximal attempts. Measurements weremade of the intracardiac pressures and cardiac output at restand at four minutes of sustained handgrip at 25% of max-imal voluntary contraction.
Left ventriculography was performed in all patients in theright anterior oblique projection at 300. Thirty-five to fiftyml of methylglucamine diatrizoate (Renografin-76) was in-jected into the left ventricle at a rate of 26 to 30 ml per sec-ond, using a Cordis II power injector.
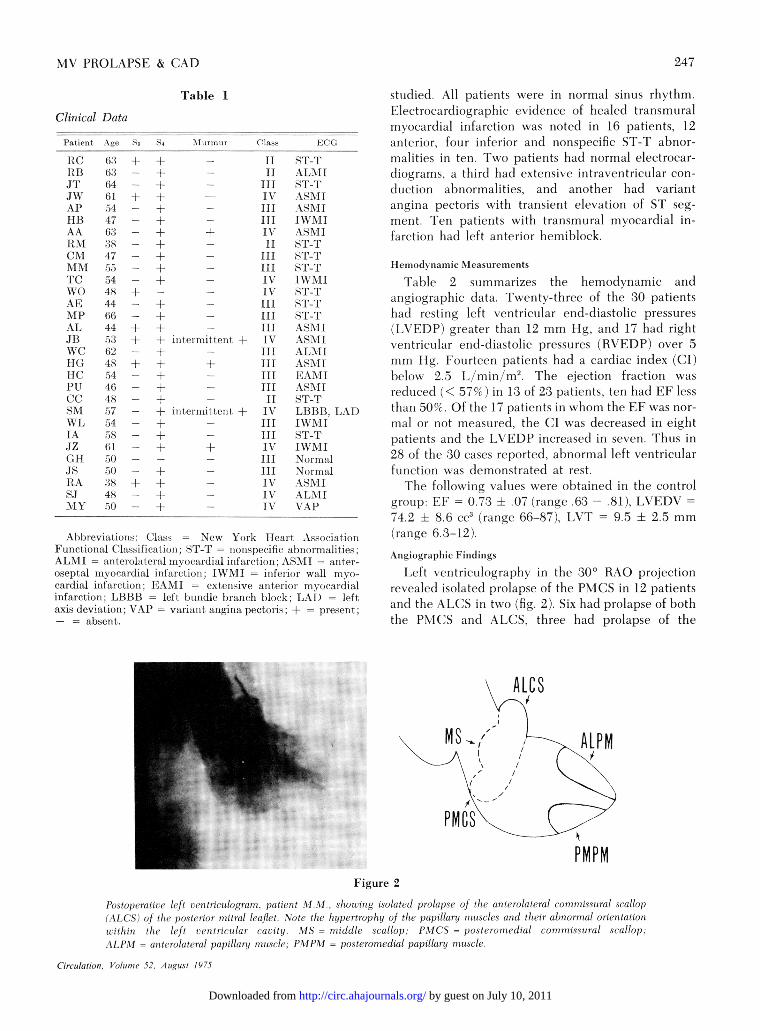
Individual systolic frames of the ventriculogram werecarefully studied. The mitral valve and the atrioventricularring at the base of the opacified left ventricle, as well as theposteromedial and anterolateral commissural areas, wereidentified. A distinct convex bulge in the area of theposteromedial or anterolateral commissure suggestedprolapse of the posteromedial (PMCS) or anterolateral com-missural scallop (ALCS), respectively. A distinct centralbulge was judged to be secondary to prolapse of the middlescallop (MS), as described by others.'6' 17
All angiograms were reviewed independently by at leasttwo observers who assessed the contractility of the left ven-tricle in a qualitative fashion. Regional wall segments wereclassified into one of four possible categories: normal,hypokinetic, akinetic, or dyskinetic. 1) normal - the seg-ment had synchronous and inward movement of goodamplitude during systole; 2) hypokinetic - a portion or allof a segment had inward movement judged qualitatively tobe diminished in amplitude; 3) akinetic- a portion or all ofthe segment had complete absence of wall motion; 4)dyskinetic - a portion or all of the segment had paradoxicalsystolic outward motion.
Quantitative angiographic methods were used to deter-mine volumes and ejection fractions (EF) using the area-length method of Dodge'8 modified for single planecalculations.'g The 35 mm cine film was viewed on a Tagar-no projector where a normal sinus beat was selected forvolume determination. The left ventricular end-systolic anddiastolic silhouettes were traced on paper and the areasmeasured by planimetry. The correction factor for volumedetermination was obtained by counting and planimeteringone centimeter squares in a grid that was filmed at the levelof the patient's left ventricle using the same fluoroscopicheight that was used during the ventriculogram. Thecounted area of the grid was then compared to itsplanimetered area recorded on cine film. Stroke volume ob-tained by this method correlated closely with the value ob-tained by dye dilution curves (r = 0.95).
Left ventricular hypertrophy was assessed cineangio-graphically in the RAO by the method ofGulotta.20 The leftventricular wall thickness (LVWT) in end-diastole wasmeasured anteriorly at a point midway between the apexand the aortic valve. The linear correction factor wasderived by comparing the projected longitudinal diameterof a grid to the known previously measured diameter (5cm).
PD
MD
AD
Figure 1
Schematic representation ofsuperimposed tracings of end-diastolic and end-systolicframes drawn directly from theprojected left ventriculogram.The long axis (L) of the left ven-tricle was quadrisected in-dependently at end-systole andend-diastole by three diametersdrawn perpendicular to it, (PD,MD, and AD). Shortening ofeach diameter was expressed aspercent shortening of its end-diastolic dimension.
The grid was filmed as previously described. Segmental mo-tion analysis was performed by superimposing tracings ofend-diastolic and systolic frames using the cardiac apex andmid-aortic valve as fixed points. The long axis of the left ven-tricle was determined from the midpoint of the aortic valveto the ventricular apex. It was quadrisected independentlyat end-systole and end-diastole by three diameters drawnperpendicular to it. These diameters were designated asproximal (PD), midventricular (MD), and apical (AP) seg-ment diameter.20 21 Shortening of each diameter was ex-pressed as a percent shortening of its end-diastolic dimen-sion (fig. 1).The head of the posteromedial papillary muscle was iden-
tified angiographically at end-systole and end-diastole in theRAO projection. Its orientation within the left ventricularcavity was determined as reported by Liedtke,2' by com-paring the ratio of the distances between the papillary mus-cle to the mitral valve ring and left ventricular apex to mitralvalve ring in end-systole and end-diastole.The same measurements were performed in the control
group. Left ventricular wall thickness between 12 and 15mm was considered as mild hypertrophy; 15-18 mm,moderate hypertrophy, and more than 18 mm, severe hyper-trophy. Left ventricular dilatation was considered to besignificant if the left ventricular end-diastolic volumemeasured by planimetry was more than two standarddeviations from the normal mean. The data was analyzed bymeans of the Student's t-test.
ResultsClinical and Electrocardiographic Features
Of the 95 patients studied, 30 had angiographicevidence of prolapse of the posterior mitral leaflet(table 1). Their average age was 54 years (range38-66). Twenty-six of the patients were significantlydisabled with Class III-IV symptoms of angina and/orcongestive heart failure (New York Heart Associationfunctional classification). A left ventricular lift waspalpable in 24 of 30 patients and in one it was diffuseand paradoxical, suggesting a ventricular aneurysm. Afourth heart sound was heard in 28 patients, a thirdheart sound in seven. Early or mid-systolic apical mur-murs (grade I-II) were detected in five patients andrecorded at the time of catheterization in threepatients. In two patients it was intermittently present.Systolic clicks were not heard in any of the cases
Circulation, Volume 52, August 1975
246
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from
MV PROLAPSE & (CAD
+
+
+
_+
_+
+
+ +
_+
_+
_+
iiite
i}tle
I iurimi r Class
-II
Il
'V
- III
_ Iv
TIII+ IxV-II_ 111
1 VIIv
-IIIIII
iniltttit +I IVIII
ITIlitIII
flltt(t +I IVsIIITI'
+ TVr
lII
- 'V
Iv
S'r-TALAMIST -T
ASM1ASXII
ASMI
ST-T
STl Tt
ST'-T
\SI\hIF
ALMI11AS-MIIKAXII.VASMI
LISBB, LAD
AXA,W;Xl :E
ST-TIWAI I
N.ormnalAISMIALlA[TVAP
Abbreviatilns: ('lass = New York Heart. Xtsso(c iailti1on1
Functional ClaTs-ifica nonspecificAILMI atelateral mxocardial inflection; ASIMlI - utater-oseptal mnyoeadial inflarction; IWMI = iniferiol wall myo-
cadlial infarction; EAXII = extensive anterior imyvocarldialinfarction; LIA3IB left bundle branch block; LAX) left
ax i . eili)l . &Vin ']atlgl. pectcaris; t= prMesenit;ais deviation YAP variant angi.,
=absent..
sttidiedl. All patients were in normal sintus rhythm.Electrocardiographic eviclence of healed transmuralmyvocardial infarctioni was noterd in 16 patients, 12anterior, four inferior an(l nonspecific ST-T abnor-mnalities in ten. Lxso patients had normal electrocar-dliograms, a third had extensive intraventricular con-riuction al)normalities, and another had variantanigina pectoris xvith transient elevation of ST seg-ment. Ten patients xith transmural myocardial in-farction had left anterior hemiblock.
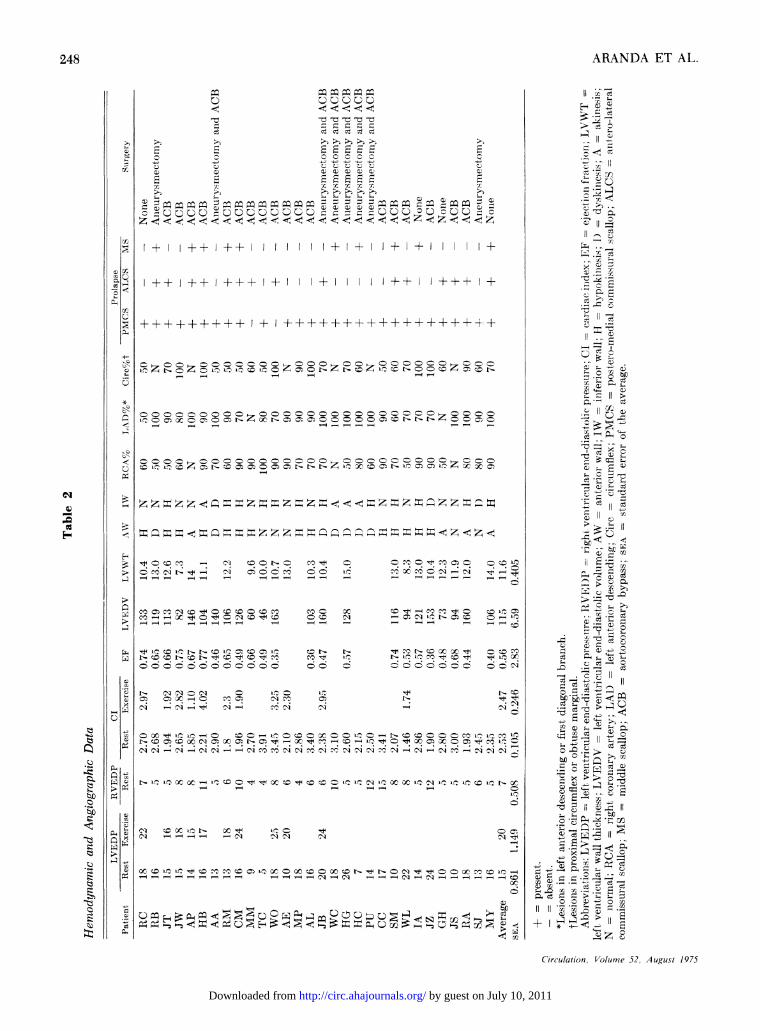
lIlcnodvnamiciNlcasuremnents
Table 2 suimmarizes the hemodlynamic andangiographic data. TFwenty-three of the 30 patieritshiad restinig left ventricular end-diastolic pressures(I VEDP) greater than 12 mm Jig, and 17 hadl rightvenitricular end-diastolic pressuires (RVEDP) over 5mm Hg. Fotirteen patients had a cardiac itidex (Cl)beloxw 2.5 L/min/m2. The ejection fraction wasreduced (< 57%e) in 13 of 23 patients, ten had EF lessthan .50%0. Of the 17 patients in whom the EF was nor-mal or not measuired, the C(l vas decreasedl in eightpatients and the 1VEDP increased in seven. Thuis in28 of the 30 cases reported, abnormal left ventricularfuinctioni was clemonstrated at rest.The following values were obtained in the control
group: FE 0.73 ± .07 (range .63 .81), INEDV =
74.2 ± 8.6 cc' (range 66-87), IAT 9.5 + 2.5mm(ranige 6.3-12).Angiographic Finidinigs
Left ventriculography in the 300 RAO projectionrevealed isolated prolapse of the PMCXS in 12 patientsand the ALICS in two (fig. 2). Six had prolapse of boththe PMCS and AUIPCS, three had prolapse of the
ALCS
ALPM
PMP
PMPMFigure 2
Poslopcratfice lft rentriculogram, patient M.M. shoeing isolated prolapse of tIle anriterolaterail comtmnissura/ scallopltps tt/ct h (>ie ltleitrolphti of the papillaril rnniscle,s and thleit abnormiial o tatti
ivithin il 1 laftuic MS = middle scallol); PMCS = posterormi dlial commzissural scallop1.
.I 1'X1 anterolateral papillary PIPMse/, = posteromnedial papillary mustcle.
Circulation, Col/unie 52 August 1975
Table 1
Clinical Data
llatient
NCN BJ rllriTJWx
AA
N:M(>1
TCW()Al,
ALJ1BWC
lfePIT(PC
IAJz(G111isRASiMY
Age
()46315447
63
47.5)a
.544844(6644
624%5;4648571545)615050)
48S1_,-)(4
48
51
247
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from
248 ARANDA ET AL.
ou | ° : 3 v ° ~~~~~~~~~~ C, C 1
I _ x Cs)5 c V- z VbzX- Uc, c,C;Cs V H;CC~ o- t- '-- c
t;¢ Ut ¢¢¢ ¢< <<¢ ¢¢ <¢¢ t; z;¢ <t c;~C1sl:CI~C 17C
xQ - m c c+Z+ I _
Q~ ~ ~~~c Tm 1 m I: m
> z t- t a Nbtm t :°tf. Al m -C (; L
* P^-e~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~c
cq Oq OOOOOOOOOO°OOOOOOOOOOCOOOOO......V1m b£ttb .....
Sooooooooocooco ......-
q I $ E m c ^ .^ cC z cc: c: ........... ~14
$ t o sn t-X so b o n+.ooOenosn j X.> o c: ca b tS : o c co c < n x 23 c c cq mP v o u; I PH s r-1 1 s E 4 1 w- w- I ~~~~~~~~~~CdXr l ¢ C5l > \ 1 dq < t s P ! Ct 1 t' tt-iCO5tC<;3;;. PS
W v [n. s ie b b s e s unsbb: Cqs tX m ro in o
X t- s D t- t >tsi t Q t X ? ! t [o. t_ L? Ln => t 4 t t Ln Ot C3 ; ; O_~~~bl
t.1°°D°°°°°° °° ° o o o o o o oc o o N s c:-e~~~~~~~~~~~~a
Circulation, Volumse 52, August 1975
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from
MV PROILAPSIE & (CAD2
PMCS
Figure 3
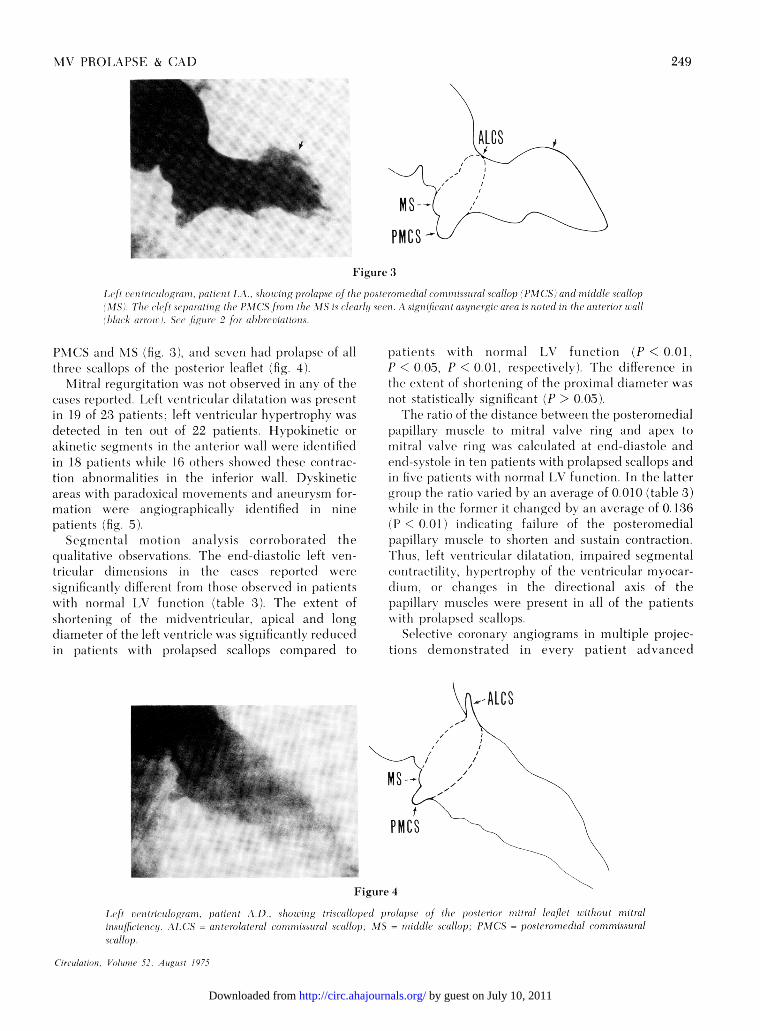
Ic1t/i -''tititri{lo'ugrai ati, ti(ut 1 X.A_ S/hJOlt ihig 1)trolaps,of { ) oste- roinedial co ii2 iss i ral saallo/) (PA CS nnrtaid(l lt sea(w/laop\1SS). /Th c'scIft s paratuuiuf te11c PXI 1(S fuo i/iIt XI. IS i sc/ealyrzx s en1i stpigJ ifia i t asel n rg{.cr ttrt a is riottt di1in hte anit i2ot uaala/rA anon. Se(o'io' 2 fo; tI/ubite ftutiuis.
1\ICS and \lS (fig. 3). an(l seveIn had prolapse of allthree scallops of the 1)osterior leaflet (fig. 4).
\litral regurgitation xxas not oIserve(l in any of thecases reported. Left ventricular clilatationi wxas presentin 19 of 23 patients, left x entrictular hvpertrophy xas(letected in ten out of 22 patients. Ilypokinetic orakinetic segmnents in the anterior wx all xxere idlentifiedin 18 patients xhile 16 others showeded these contrac-tioni abnormalities ini the inlferior xwall. Dx skineticareas wxith para(l\oical movex('erits a(ln aneurx sm fur-mation xx ere angiographically identified in ninepatients (fig. 5).Segmental miotion analysis corroborated the
qualitative ol)servations. The end-diastolic left vre-tr-icuilar dinevnsioins in the cases reported x iresigrnificantlx (different from those olserve(l irn patientswitlh narrnal IAV funiictionr (table 3). The extent ofshortening of the rnidxlventrictilar, apical aiid long(liameter of the left ventricle xwas significantly reduce(lin patienVts with prolapsed scallops compared to
patients xx iithiniorminal V\ futnictionri (P < 0.01,P < 0.05, P < 0.01, respectively). ihe difference inthe extent of shortening of the proximal (liameter wasriot statisticallv significant (P > 0.05).
Ich ratio of the clistance hetx een the posteromei(lialpapillary. mtuscle to miiitral valve ring aricl ape'x tomitral valve ringxwas calculated at endl-diastolle andend-sxstole in ten patients xw ith prolapsed scallops andini five patients x ithl niormal I-N futnction. In the lattergroll) thle ratit x aried hy ani average of 0 010 (table 3)while in the formeir it changed I)x an average of 0. 136(1) < 0.01 ) indlicatinig failurc of the posteromedialpapillary muscle to shlorten andl sustain contraction.Thus, left ventricular (lilatatiorn, impaired segmentalcontractilitx Ii ptertrophy of the veintricular rmv(car-tlimltri, tir chalnge s in the dlirectional axis of thepapillary imuscleles were present in all of the patientswx ith prolapse(l scallops.
Selective coronary atngiograms in multiple projec-titis dlelmonstratedl in everx patient acvanced
MS -
PMCS
Figure 4
I ft patient XI s/oiotg trist a/loped prolaps of the piosteri1ior uiittrall leafltt wiitliout miitralisuiff/itnttn. AV C S = antirtolateral oooiissuirl AstllpXIS = miuddll .sttallop; PXI(CS = }oterouJluiedil conuoitssuralsatllop.
Circulatuion, Vol/ant 52, At.guust /975
249
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from
ARANDA ET AL.
Figure 5
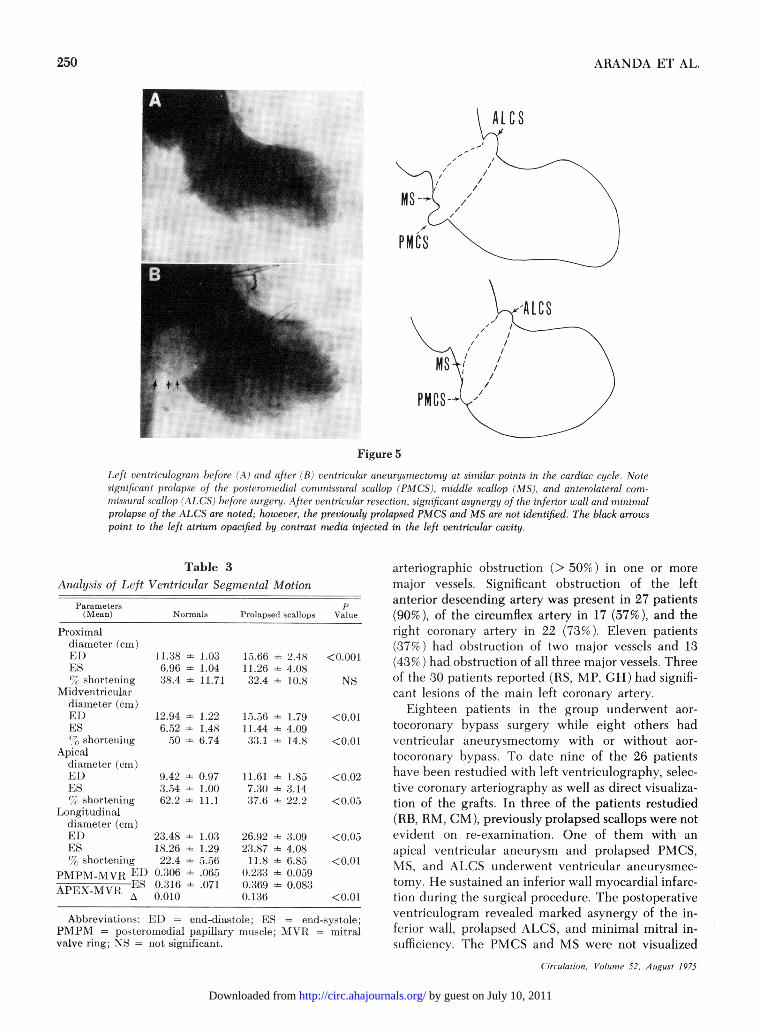
Left venitricuilogran l)efore (A) and after (B) ventricenlar anieurysmectorny at similar poiints in the cardiac cycle. Notesignlific,anit prolapse of the posterornedial comrynissntral scallop (PMCS), middle scallop (MS), and anterolateral corn-
niissural scallop (ALCS) before snrgery. Xfter ventricular resection, significant asyntergy of the inferior wall and mninimnal
prolapse of the ALCS are noted; however, the previously prolapsed PMCS and MS are not identified. The black arrows
point to the left atrium opacified by contrast media injected in the left ventricular cavity.
Table 3
Analysis of Left Ventrictular Segmental Motion
Parameters(Meaii)
Proximaldiameter (eni)E1)ES
, short,enllnlgMlidveint rlienlar
diameter ((en)El)
ESshorteniiig
Apicaldiametei (CIen)
El).ES
shlorteniniigLorngittudinal
diamet.er (ens)El)
ES
.short.ening
PMPM-MVI El)
APEX-MYI} A
p
Normals Prolapsel scallops Valuie
1I1 - 1.036.96 : 1.04
38.4 - 11.71
12.94 =E:
6.522
9.42 -3.54 ~
62.2 -
23.48 -18.26 -22.4
0.306 -0.316 -0.010
1.221.486.74
0.971.0011.1
1.031.295.56
.06,5
.071
15.66 =i- 2.48
11.26 - 4.0882.4 - 10.8
15.5- 6 - 1.7911.44 i 4.09.1 - 14.8
11.61 - 1.85
7.3) - 3.14
'37.6 - 22.2
26.9223.8711.8
0.2;330.3690.136
i 3.09= 4.08
= 6.85- 0.059
- 0.083
arteriographic obstruction (> 50%) in one or more
major vessels. Significant obstruction of the leftanterior descending artery was present in 27 patients(90%), of the circumflex artery in 17 (57%), and theright coronary artery in 22 (73%). Eleven patients(37%) had obstruction of two major vessels and 13(43%cr) had obstruction of all three major vessels. Threeof the 30 patients reported (RS, MP, GH) had signifi-cant lesions of the main left coronary artery.
Eighteen patients in the group underwent aor-
tocoronary bypass surgery while eight others hadventricular aneurysmectomy with or without aor-
tocoronary bypass. To date nine of the 26 patientshave been restudied with left ventriculography, selec-tive coronary arteriography as well as direct visualiza-tion of the grafts. In three of the patients restudied(RB, RM, CM), previously prolapsed scallops were notevident on re-examination. One of them with an
apical ventricular aneurysm and prolapsed PMCS,MS, and ALCS underwent ventricular aneurysmec-
tomy. He sustained an inferior wall myocardial infarc-tion during the surgical procedure. The postoperativeventriculogram revealed marked asynergy of the in-ferior wall, prolapsed ALCS, and minimal mitral in-sufficiency. The PMCS and MS were not visualized
Circulanon, Vo/unic 52, A ugunst 1975
Abbreviations: El) end-diastole; ES - enid-syst.ole;PMPM = posteiromedial papillary imousele; WM - mitralvalve ring; NS - Inot significanit.
250
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

MV PROLAPSE & CAD
(fig. 5). The two other patients underwent aor-tocoronary bypass surgery to the right posteriordescending and left anterior descending arteries. Inthe postoperative ventriculograms, the contractility ofthe inferior wall had improved, and the previouslyprolapsed ALCS were not identified in either patient.
DiscussionThe auscultatory findings of mitral valve prolapse
syndrome have been well documented in patientswith artherosclerotic heart disease.'0 22"26 However,there are no reports in the literature on clinical-an-giographic correlations of prolapsed mitral leaflets inpatients with advanced obstructive coronary arterydisease.The absence of clinical-angiographic correlations
may arise from the fact that there have been many dis-crepancies in the description of the mitral valve.There is still much controversy as to the definition ofthe commissural areas and arguments as to thenumber of leaflets of the mitral valve.27 28 Recently,Ranganathan et al.16 studied 50 normal mitral valvesfrom adults. Commissures identified by commissuralchordae tendineae divided the mitral valve intoanterior and posterior leaflets. They found that theposterior leaflet was further subdivided into scallopsby clefts or identations. In 92% of the hearts ex-amined, the posterior leaflet was constantly notchedand was divisible into three scallops. In 84% of thecases a large middle scallop was present with twosmaller scallops in either side; posteromedial andanterolateral commissural scallops. They suggestedthat prolapse of any part of the triscalloped structureof the posterior leaflet should be recognized in a leftventriculogram and that prolapse of commissuralscallops should be observed as bulges at either ex-tremity of the posterior leaflet area. In subsequentreports Ranganathan17 and Trent29 demonstrated theangiographic appearances of pathologic provenprolapses of the different scallops of the posteriormitral leaflet.The selection of patients in this study was based on
the angiographic observations of prolapsed scallops ofthe posterior leaflet of the mitral valve in patients withdocumented obstructive coronary artery disease. Ourseries differs from the series reported by Scampardoniset al.'4 and Gulotta et al.20 in that their patients wereselected because of the presence of nonejection clicks,late systolic murmurs, troublesome arrhythmias, ordisabling chest pains. Most of their cases had normalcoronary arteries and their series represented aheterogeneous clinical spectrum of patients with thissyndrome in which different etiological factors ac-counted for the abnormalities observed. Nonetheless,our observations are in agreement with these andCirculation, Volume 52, August 1975
other reports of asymmetric disordered patterns of leftventricular contraction in patients with systolic click,late systolic murmur, and prolapse of the posteriorleaflet of the mitral valve,4' 8, '3, 14, 20, 21, 30-33 but aredifferent from the observations made by Ranganathanet al.'6 '7 In their study prolapsed middle scallop wasmost frequently seen while isolated prolapse of a com-missural scallop occurred only once.The explanation for these observed differences is
not clear at the present time. However, the selectionof patients may account for some of these differences.In patients with coronary artery disease, infarction orfibrosis of papillary muscles, left ventricular abnor-malities, and normal mitral valves have beenreported.26 29 In patients with prolapsed mitral valveand normal coronary arteries, necropsy studies haveshown myxomatous degeneration of the valve, withelongated and thickened chordae but no intrinsicpathologic changes in the papillary muscles. '4, 17, 20This might be better understood if one considers theblood supply of the papillary muscles. The anteriorpapillary muscle receives its blood supply frombranches of the left anterior descending and cir-cumflex arteries, while the posterior muscle gets itsblood supply from branches of the right coronary andleft circumflex arteries in 70%, from the right coronaryartery alone in 20%, and the left circumflex artery in10% of the cases.34 36 The presence of severe obstruc-tive coronary artery disease in all of our cases appearsto be the most important contributing factor account-ing for the differences in the number of prolapsedscallops observed, since normal mitral valve functiondepends on a rather complex and finely coordinatedsystem of which the papillary muscle is one of theprincipal components.The high incidence of transmural myocardial in-
farction, ST-T wave abnormalities, hypokinesis, anddyskinesis of various segments of the left ventricularcavity found in our series agree with the recentclinical36 and experimental37 evidence that in-competence of the mitral valve depends not only onthe intrinsic dysfunction of the papillary muscles butalso upon distortion of the papillary muscle founda-tion by asynergic contraction of the related free wallof the left ventricle. Infarction of a portion of the leftventricular wall at the base of the papillary musclemay interfere with the proper functioning of the mus-cle by forming an aneurysm, thus changing the direc-tional axis of the papillary muscle.36 The paradoxicalexpansion of the wall of the aneurysm may carry thebase of the muscle away from its normal position, thuschanging the normal spatial three dimensional align-ment necessary for proper mitral valve closure. Therelatively high incidence of ventricular aneurysms inour patients agree with the above observations. In-
251
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from
ARANDA ET AL.
farction of the base of the papillary muscle or therelated free wall of the left ventricle may also interferewith its function by failure to provide adequateanchorage to the muscle and chordae tendineae dur-ing left ventricular systole.36
Considering the above mechanisms, we were notsurprised to find two patients who showed improvedleft ventricular contractility after aortocoronarybypass and whose previously prolapsed scallops were
absent in a postoperative ventriculogram. On theother hand, prolapse of the scallops of the posteriormitral leaflet might represent an intermediate stagebefore clinically apparent mitral insufficiency occurs.
As shown by the patient RB (fig. 5), infarction of thebase of the papillary muscle and its related free wall ofthe left ventricle interfered with proper closure of themitral valve by failure to provide anchorage to thepapillary muscle and chordae tendineae. As a result,the previously prolapsed leaflet became insufficient.The absence of mitral insufficiency in our group of
patients contrasts sharply with the previous angio-graphic documentation of mild to severe mitral insuffi-ciency in most patients with systolic click, late systolicmurmur, and prolapsed posterior leaflet.8 14, 17, 20 Inview of the findings of Ranganathan et al.17 it is in-teresting to speculate that since the middle scallop isusually the largest of the posterior leaflet, prolapse ofthis scallop might be accompanied more frequently bymild to moderate insuffciency than prolapse of thetwo smaller commissural scallops. In some of our cases
turbulence in the prolapsed scallop without regurgita-tion might have been responsible for the presence ofthe systolic murmur.8
The syndrome of papillary muscle dysfunction inpatients with coronary artery disease appears to repre-
sent a wider clinical spectrum than previouslydescribed. At one end of the spectrum are thosepatients with prolapsed scallops of the mitral valvewithout mitral insufficiency. In the middle of the spec-
trum are patients with systolic murmurs and/orsystolic clicks and compensated congestive heartfailure. At the other end of the spectrum are thosepatients with progressive cardiac decompensation andsevere mitral insufficiency.
In view of the recommendations regarding an-
tibiotic prophylaxis in patients with mitral valveprolapse syndrome2 38, 39 and considering the reportsof bacterial endocarditis complicating mitralregurgitation after an acute myocardial infarction,25the use of antibiotic prophylaxis should be consideredin patients with coronary artery disease and prolapsedscallops of the posterior leaflet of the mitral valve.
Although prolapse of the posterior mitral leaflethave heterogeneous origins, impaired contractility,left ventricular hypertrophy, and dilatation appear to
be the most significant contributing factors in patientswith coronary artery disease by causing distortion ofthe papillary muscle foundation during left ven-tricular contraction.
Acknowledgment
We acknowledge the secretarial help of Miss Diana Smith, MissBonnie Agnell and the medical artistry of Mr. Marcelino Obaya.
References
1. BARLOW JB, BOSMAN CK, POCOCK WA, MARCHAN P: Latesystolic murmurs and nonejection systolic clicks. An analysisof 90 patients. Br Heart J 30: 203, 1968
2. LINHATR JW, TAYLOR WJ: The late apical systolic murmur.Clinical, hemodynamic and angiographic observations. Am JCardiol 18: 164, 1966
3. MERCER EN, FRYE RL, GUJILIAN\I ER: Late systolic click innonobstructive cardiomyopathy. Br Heart J 32: 691, 1970
4. CRILEY JM, LEWIs KB, HUMPHRIES JO, Ross RS: Prolapse ofthe mitral valve: clinical and cine-angiocardiographic find-ings. Br Heart J 28: 488, 1966
a VICTORIC A BE, ELLIOT LP, GESSNER IH: Ostium secundumatrial septal defect associated with balloon mitral valve inchildren. Am J Cardiol 33: 668, 1974
6. BITTAR N, SOSA JA: The billowing mitral valve leaflet.Circulation 38: 763, 1968
7. GooCH AS, VICENCIO F, MARANHAO V, GOLDBERG H:Arrhythmias and left ventricular asynergy in the prolapsingmitral leaflet syndrome. Am J Cardiol 29: 611, 1972
8. LOBSTEIN HP, HORWVITz LD, CURRY G, MULLINS CB:Electrocardiographic abnormalities and coronary arterio-grams in the mitral click murmur syndrome. N Engl J Med289: 127, 1973
9. PoOCOK WA, BARLOW JB: Etiology and electrocardiographicfeatures of the billowing posterior mitral leaflet syndrome:Analysis of a further 130 patients with a late systolic murmuror nonejection click. Am J Med 51: 731, 1971
10. STEELMIAN RB, WHITE RS, HILL JC, NAGLE JB, CHEITLIN MD:Midsystolic clicks in arteriosclerotic heart disease: A newfacet in the clinical syndrome of papillary muscle dysfunc-tion. Circulation 44: 503, 1971
11. CHENG TO: Some new observations on the syndrome ofpapillarv muscle dysfunction. Am J Med 47: 924, 1969
12. JERESATY RM: Billowing of the mitral valve leaflets,angiographic study of 24 patients. Radiology 100: 45, 1971
13. STANNARD M, SLOMAN JG, HARE WS, GOBLES AJ: Prolapse ofthe posterior leaflet of the mitral valve: A clinical, familialand cineangiographic study. Br Med J 3: 71, 1967
14. SCANIPARDONIS G, YANCG SS, MARANHAO V, GOLDBERC. H, GOOCHAS: Left ventricular abnormalities in prolapsed mitral valveleaflet syndrome. Circulation 48: 287, 1973
15. WELLS D, BEFELER B, WIN-KLER J, MYERBURG RL, CASTELLANOSA, CASTILLO CA: A simplified method for left heartcatheterization including coronary arteriography. Chest 63:959, 1973
16. RANGANATHAN N, LANI JHC, WIGLE ED, SILVER MD:Morphology of the human mitral valve. II The valve leaflets.Circulation 41: 459, 1970
17. RANG-ANATHAN N, SILX ER MD, ROBINSON TI, KOSTUK WJ,FELDERHOF CH, PATT NL, WILSON JK, WIGLE ED:Angiographic-morphologic correlation in patients withsevere mitral regurgitation due to prolapse of the posteriormitral valve leaflet. Circulation 48: 514, 1973
Circulation, Volume 52, August 1975
252
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from
MV PROLAPSE & CAD
18. DODGE HT, SANDLER H, BALLEw FW, LORD JD: The use ofbiplane angiocardiography for measurement of left ven-tricular volume in man. Am Heart J 60: 762, 1960
19. KENNEDY JW, TRENHOLNME SE, KASSER IS: Left ventricularvolume and mass from single plane cineangiogram. A com-parison of antero-posterior and right anterior obliquemethods. Am Heart J 80: 343, 1970
20. GU-LOTTA SJ, GLLCO L, PADNIANAKHAN V, MILLER S: Thesyndrome of systolic click, murmur and mitral valve prolapse-A Cardiomyopathy. Circulation 49: 717, 1974
21. LIEDTKE AJ, GALLT JH, LEANIAN DM, BLUMENTHAL MS:Geometry of left ventricular contraction in the systolic clicksyndrome. Circulation 47: 27, 1973
22. BLRCH GE, DEPASQUALE NP, PHILLIPS JH: Clinicalmanifestations of papillary muscle dysfunction. Arch InternMed 112: 112, 1963
23. CHENG TO: Characterization of late systolic murmursassociated with coronary artery disease. Circulation 43(suppl II): 11-106, 1971
24. ORLANDO MD, WOOLEY CF, SCARPELLI D, RYAN JM: Mitralregurgitation caused by infarcted papillary muscle: report offifteen cases. Circulation 30 (suppl III): 111-136, 1964
25. BASHOLR FA: Mitral regurgitation following myocardialinfarction: the syndrome of papillary mitral regurgitation.Dis Chest 48: 113, 1965
26. HEIKKILA J: Mitral incompetence complicating acutemyocardial infarction. Br Heart J 29: 162, 1967
27. CHIECHI MA, LEES WM, THONIPSON R: Functional anatomy ofthe normal mitral valve. J Thorac Surg 32: 378, 1956
28. RLSTED IE, SCHEIFLEY CH, EDWARDS JE: Studies of the mitralvalve: I. Anatomic features of the normal mitral valve and
associated structures. Circulation 6: 825, 195229. TRENT JK, ADELMAN AG, WIGLE ED, SILVER MD: Morphology
of a prolapsed posterior mitral valve leaflet. Am Heart J 79:539, 1970
30. EHLERS KH, ENGLE MA, LEVIN AR, GROSSMAN H, FLEMING RJ:Left ventricular abnormality with late mitral insufficiencyand abnormal electrocardiogram. Am J Cardiol 26: 333, 1970
31. ENGLE MA: The syndrome of apical systolic click, late systolicmurmur and abnormal T waves. Circulation 39: 1, 1969
32. LEACHNIAN RD, DEFRANCHEsCHI A, ZAMALLOC 0: Late systolicmurmurs and clicks associated with abnormal mitral valvering. Am J Cardiol 23: 679, 1969
33. KARLINER JS, GAULT JH, ECKBERG D, MULLINS CB, Ross J:Mean velocity of fiber shortening. A simplified measure ofleft ventricular myocardial contractility. Circulation 44: 323,1971
34. ESTEs EH, ENTMIAN ML, DIXON HB, HACKEL DB: The vascularsupply of the left ventricular wall. Am Heart J 71: 58, 1966
35. JANIES TN: Anatomy of the coronary arteries in health anddisease. Circulation 32: 1020, 1965
36. SHELBURNE JC, RUBINSTEIN D, GORLIN R: A reappraisal ofpapillary muscle dysfunction. Am J Med 46: 862, 1969
37. TSAKIRIs AG, RASTELLI GC, ANIORIM D DE S, TITUS JL, WOODEH: Effects of experimental papillary muscle damage onmitral valve closure in intact anesthetized dogs. Proc MayoClin 45: 275, 1970
38. HANCOCK EW, CORN K: The syndrome associated with mid-systolic click and late systolic murmur. Am J Med 41: 183,1966
39. LEBAUER EJ, PERLOFF JK, DELIHER TF: The isolated systolicclick with bacterial endocarditis. Am Heart J 73: 534, 1967
Circulation, Volume 52, August 1975
253
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from





























