Embed Size (px)
Citation preview
Models of ambulance service delivery for rural Victoria
Full Name and Degrees of Candidate:
Peter Francis O’Meara Student No. 8401608 Admitted to the Degree of Bachelor of Health Administration The University of New South Wales 22 May 1992 Admitted to the Degree of Master of Public Policy Deakin University 8 May 1998
Full Title:
Models of ambulance service delivery for rural Victoria.
Institution:
The University of New South Wales School of Public Health and Community Medicine
Submission Date:
1 June 2002.
© Peter O’Meara 2002.

Models of ambulance service delivery for rural Victoria
Abstract
The primary aim of the research project was to develop conceptual models of rural ambulance service delivery based on different worldviews or philosophical positions, and then to compare and contrast these new and emerging models with existing organisational policy and practice. Four research aims were explored: community expectations of pre-hospital care, the existing organization of rural ambulance services, the measurement of ambulance service performance, and the comparative suitability of different pre-hospital models of service delivery.
A unique feature was the use of soft systems methodology to develop the models of service delivery. It is one of the major non-traditional systems approaches to organisational research and lends itself to problem solving in the real world. The classic literature-hypothesis-experiment-results-conclusion model of research was not followed. Instead, policy and political analysis techniques were used as counter-points to the systems approach.
The program of research employed a triangulation technique to adduce evidence from various sources in order to analyse ambulance services in rural Victoria. In particular, information from questionnaires, a focus group, interviews and performance data from the ambulance services themselves were used. These formed a rich dataset that provided new insight into rural ambulance services.
Five service delivery models based on different worldviews were developed, each with its own characteristics, transformation processes and performance criteria. The models developed are titled: competitive; sufficing; community; expert; and practitioner. These conceptual models are presented as metaphors and in the form of holons and rich pictures, and then transformed into patient pathways for operational implementation.
All five conceptual models meet the criteria for systemic desirability and were assessed for their political and cultural feasibility in a range of different rural communities. They provide a solid foundation for future discourse, debate and discussion about possible changes to the way pre-hospital services are delivered in rural Victoria.
Keywords Ambulance Rural Australia Pre-hospital Model Soft Systems Policy Problem-solving
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy i
Table of Contents
SECTION 1 INTRODUCTION...........................................................................1
1.0 Overview of Study............................................................................................................................ 1 1.1 Rationale for the study ................................................................................................................... 1 1.2 Aims and objectives....................................................................................................................... 4 1.3 Research methods used.................................................................................................................. 5
1.4 Main findings 7
1.5 Future directions .......................................................................................................................... 10
SECTION 2 THEORY AND METHODS .........................................................11
2.0 Theoretical Framework and Empirical Foundations ................................................................ 11 2.1 Introduction .................................................................................................................................. 12 2.2 Systems theory ............................................................................................................................. 14 2.3 Socio-political context ................................................................................................................. 27 2.4 Health policy context ................................................................................................................... 36 2.5 Ambulance context ...................................................................................................................... 46 2.6 Aims and objectives..................................................................................................................... 72
3.0 Methods ........................................................................................................................................... 74 3.1 Introduction .................................................................................................................................. 75 3.2 The communities and ambulance stations................................................................................... 79 3.3 Determining expectations of rural ambulance services .............................................................. 85 3.4 Structure and culture of ambulance services in rural Victoria.................................................... 90 3.5 Measuring performance of ambulance services .......................................................................... 98 3.6 Formulating models of service delivery .................................................................................... 104 3.7 Integration of findings................................................................................................................ 112
SECTION 3 FINDINGS AND DISCUSSION.................................................119
4.0 Rural Communities and Respondents to Study ....................................................................... 119 4.1 Introduction ................................................................................................................................ 120 4.2 Sample rural communities ......................................................................................................... 121 4.3 Respondents to study ................................................................................................................. 129 4.4 Discussion .................................................................................................................................. 133
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy ii
5.0 Expectations of Rural Communities .......................................................................................... 136 5.1 Introduction ................................................................................................................................ 137 5.2 Expectations of health professionals and community members ............................................... 138 5.3 Suggested changes to rural ambulance services........................................................................ 144 5.4 Discussion .................................................................................................................................. 166
6.0 Structure and Culture of Rural Ambulance Services.............................................................. 172 6.1 Introduction ................................................................................................................................ 173 6.2 Rural ambulance structure in Victoria....................................................................................... 177 6.3 Cultural landscape of Rural Ambulance Victoria ..................................................................... 193 6.4 Discussion .................................................................................................................................. 217
7.0 Performance of Rural Ambulance Services.............................................................................. 223 7.1 Introduction ................................................................................................................................ 224 7.2 Satisfaction with services........................................................................................................... 230 7.3 Operational performance ........................................................................................................... 235 7.4 Performance framework............................................................................................................. 244
8.0 Models of Service Delivery.......................................................................................................... 256 8.1 Introduction ................................................................................................................................ 257 8.2 Competitive model..................................................................................................................... 269 8.2 Sufficing model.......................................................................................................................... 278 8.4 Community model...................................................................................................................... 289 8.4 Expert model .............................................................................................................................. 299 8.6 Practitioner model ...................................................................................................................... 308 8.7 Using the models to make changes............................................................................................ 321
SECTION 4 CONCLUSION ..........................................................................325
9.0 Policy Implications of the Models .............................................................................................. 325 9.1 Summary of thesis...................................................................................................................... 326 9.2 Future directions ........................................................................................................................ 328
BIBLIOGRAPHY .............................................................................................332
APPENDICES..................................................................................................357
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy iii
List of Tables
Table 1 Morgan’s Paradigms and Metaphors
Table 2 Problem Categories
Table 3 Structure of Rural, Remote & Metropolitan Areas (RRMA) Classification
Table 4 Beaulieu and Berry’s EMS Models
Table 5 Studies Examining Utilization Rates
Table 6 EMS System Attributes
Table 7 Core Elements of Successful Rural EMS Systems
Table 8 Spaite’s EMS System Types
Table 9 Overview of Data Management
Table 10 Sample Towns – population and rurality classification
Table 11 RRMA Categorization and ARIA Ranges
Table 12 Rurality Classification of Ambulance Stations in Sample
Table 13 Potential Informants for Study
Table 14 Data Request to Rural Ambulance Services for 1996/97 Fiscal Year
Table 15 Seven Stages of Soft Systems Methodology
Table 16 CATWOE mnemonic
Table 17 Profile of Former Rural Ambulance Services, 1996/97
Table 18 Sample Stations in Study
Table 19 Population Profile of the Sample Ambulance Stations
Table 20 Sample Population by Rurality Classification
Table 21 Hospital Services by Rurality
Table 22 General Practitioner Numbers by Rurality
Table 23 Emergency Service Availability
Table 24 Questionnaire Responses
Table 25 Responses by Perceived and Actual Rurality Bands
Table 26 Responses by Modified Rurality Band
Table 27 Gender of Respondents
Table 28 Experience of Self or Family as a Patient
Table 29 Frequency of Contact with Ambulance Service
Table 30 Expectations of Survey Participants
Table 31 Expectations by Survey Respondent
Table 32 Expectations by Locality
Table 33 Expectations by Respondent Gender
Table 34 Expectations by Self or Family Experience
Table 35 Expectations by Respondent Contact Frequency
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy iv
Table 36 Rural Ambulance Victoria at a Glance
Table 37 Management Changes at Selected Sample Stations
Table 38 University Affiliated Institutions Offering Ambulance Courses
Table 39 Telemedicine and Ambulance Service Delivery
Table 40 Boundary Permeability of Rural Ambulance Victoria
Table 41 Perceived Performance
Table 42 Perceived Community Capacity by Ambulance Performance
Table 43 Performance by Perceived Rurality (RRMA)
Table 44 Performance by Rurality (modified RRMA)
Table 45 Performance by Personal Experience
Table 46 Performance by Contact Frequency
Table 47 Performance by Respondent
Table 48 Summary of Utilization and Performance
Table 49 Age and Gender Ratio of Patients
Table 50 Percentage of Population using Ambulance Services by Age
Table 51 Utilization Rates of Total Study Sample
Table 52 Ambulance Response Rate Ranges by Rurality
Table 53 Response Times to Incident (hours/minutes) by Rurality
Table 54 Scene Times by Rurality
Table 55 Time from Scene to Destination by Rurality
Table 56 Average Trip Distances by Rurality
Table 57 National Health Performance Committee Performance Framework
Table 58 Definition of Outcome Categories
Table 59 SAAS Success Measurements and Key Performance Indicators
Table 60 Performance Framework for Rural Ambulance Services
Table 61 Relative Strengths and Weaknesses of Abstract Ambulance Models
Table 62 Root Definition of Competitive Model
Table 63 Competitive Model – Transformation Process
Table 64 Root Definition of Sufficing Model
Table 65 Sufficing Model – Transformation Process
Table 66 Root Definition of Community Model
Table 67 Community Model – Transformation Process
Table 68 Root Definition of Expert Model
Table 69 Expert Model – Transformation Process
Table 70 Root Definition of Practitioner Model
Table 71 Practitioner Model – Transformation Process
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy v
List of Figures
Figure 1 Navigation Map of Thesis
Figure 2 Navigation Map of Thesis
Figure 3 System Elements
Figure 4 State of Victoria in Australia
Figure 5 Systems Frame of Reference
Figure 6 Navigation Map of Thesis
Figure 7 Types and Sources of Data
Figure 8 Sample Towns and Stations
Figure 9 Drivers for Rural Ambulance Service Delivery Systems
Figure 10 Research Methodology Outline
Figure 11 Process of Logical Analysis
Figure 12 Analysis Process of Thesis
Figure 13 Role Description
Figure 14 Overview of ‘system’ Social System
Figure 15 Web of Interests
Figure 16 Navigation Map of Thesis
Figure 17 Age Structure by Rurality
Figure 18 Navigation Map of Thesis
Figure 19 Strength of Respondent Change Agenda
Figure 20 Strength of Change Agenda according to Rurality
Figure 21 Change Themes for Rural Ambulance Services
Figure 22 Navigation Map of Thesis
Figure 23 Structure of Victoria’s Ambulance Services
Figure 24 Rural Ambulance Victoria Organizational Structure
Figure 25 Typical Area Organizational Structure in RAV
Figure 26 Rural Urgent Care Context
Figure 27 Large Rural Centres Profile
Figure 28 Small Rural Centres Profile
Figure 29 Small Towns Profile
Figure 30 Little Townships Profile
Figure 31 Remote Areas Profile
Figure 32 Navigation Map of Thesis
Figure 33 Emergency Management Performance Framework
Figure 34 Ambulance Utilization and Age for Total Study Population
Figure 35 Utilization Rates by Rurality
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy vi
Figure 36 Time to Destination by Rurality
Figure 37 Navigation Map of Thesis
Figure 38 Modern Soft Systems Methodology Cycle
Figure 39 Basic Model Structure
Figure 40 Systems Hierarchy
Figure 41 Picture of the Competitive Model
Figure 42 Rich Picture of Competitive Model
Figure 43 Patient Pathway for Competitive Model
Figure 44 Picture of Sufficing Model
Figure 45 Rich Picture of Sufficing Model
Figure 46 Patient Pathway for Sufficing Model
Figure 47 Picture of Community Model
Figure 48 Rich Picture of Community Model
Figure 49 Patient Pathway for Community Model
Figure 50 Picture of Expert Model
Figure 51 Rich Picture of Expert Model
Figure 52 Patient Pathway for Expert Model
Figure 53 Nesting of the Chain of Survival within the Practitioner Model
Figure 54 Picture of Practitioner Model
Figure 55 Rich Picture of Practitioner Model
Figure 56 Patient Pathway for Practitioner Model
Figure 57 Interplay of Rural Context and Service Delivery Models
Figure 58 Simple Planetary Relationship of an Ambulance System and Models
Figure 59 Navigation Map of Thesis
Figure 60 Integrating Rural Pre-hospital Models into Policy and Practice
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy vii
Abbreviations
ABS Australian Bureau of Statistics
ACAP Australian College of Ambulance Professionals
ACEP American College of Emergency Physicians
AIHW Australian Institute of Health and Welfare
ALP Australian Labor Party
ALS Advanced Life Support
AMPDS Advanced Medical Priority Dispatch System
AOTC Ambulance Officers’ Training Centre
ARIA Accessibility/Remoteness Index of Australia
ASA Ambulance Services Association – United Kingdom
ASNSW Ambulance Service of New South Wales
ASV Ambulance Service Victoria
BLS Basic Life Support
BN Bush Nurse
CAO Community Ambulance Officer
CERT Community Emergency Response Team
CFA Country Fire Authority
CMIS CSIRO Mathematical and Information Sciences
CPR Cardio Pulmonary Resuscitation
CSU Charles Sturt University
DHSV Department of Human Services Victoria
DHHST Department of Health and Human Services, Tasmania
Displan State Disaster Plan, including Medical Displan
ED Emergency Department
EMS Emergency Medical Service
EMSOP Emergency Medical Services Outcomes Project
GIS Geographic Information Systems
GISCA Geographic Information Systems Co-operative of Adelaide
GP General Practitioner
HHSC Hospitals and Health Services Commission (UK)
JRCALC Joint Royal Colleges Ambulance Liaison Committee (UK)
KPIs Key Performance Indicators
MAS Metropolitan Ambulance Service (Melbourne)
MICA Mobile Intensive Care Ambulance
MODP Multiple-Option Decision Point
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy viii
MTS Major Trauma Service
MUCAPS Monash University Centre for Ambulance and Paramedic Studies
NHMBWG National Health Ministers’ Benchmarking Working Group
NHPC National Health Performance Committee
NHS National Health Service (United Kingdom)
NHTSA National Highway Traffic Administrator – United States
NP Nurse Practitioner
NRHA National Rural Health Alliance (Australia)
NRHA - US National Rural Health Association (United States)
OPALS Ontario Prehospital Advanced Life Support (OPALS) Study
ORCON Operational Research Consultancy (UK)
PBRC Public Bodies Review Committee
PCR Patient Care Record
PEC Practitioner in Emergency Care
PIIC Performance Indicators Implementation Committee of ASV
QAS Queensland Ambulance Service
RAF Resource Allocation Formula
RAR Road Accident Rescue
RAV Rural Ambulance Victoria
RCCECC Regional Critical Care and Emergency Consultative Committee
RCCAEP Rural Committee of Canadian Association of Emergency Physicians
RDAV Rural Doctors Association of Victoria
RN Registered Nurse
RRMA Rural Remote and Metropolitan Areas
RTS Regional Trauma Service
RWAV Rural Workforce Agency, Victoria
SAAS South Australian Ambulance Service
SCRCSSP Steering Committee for the Review of Commonwealth/State Service Provision
SES State Emergency Service
SSM Soft Systems Methodology
TAFE Technical and Further Education
UWA University of Western Australia
VASA Victorian Ambulance Services’ Association
VICPOL Victoria Police
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy ix
Key Terms in Soft Systems Methodology
Real world The unfolding and interacting flux of events and ideas experienced as everyday life.
Systems-thinking world
The world in which conscious reflection on the real world takes place, making use of systems ideas.
Problem situation A real-world situation in which there is a sense of unease, a feeling that things could be better than they are, or some perceived problem requiring attention.
Analysis One Analysis in terms of roles: client (caused the study to take place), problem solver (undertakes the enquiry), and problem owner (roles from which the problem can be viewed).
Analysis Two Analysis of social and cultural aspects of the problem situation by considering roles, norms, and values.
Analysis Three Analysis of the political (power-related) aspects of the problem situation, by considering the commodities of power.
Rich pictures Diagrammatic representations of the structures (entities), processes, relationships, and issues.
Root definitions Concise verbal description of activity systems that are relevant to exploring the problem situation. Usually written in the form 'Do X by Y in order to achieve Z'.
CATWOE Elements considered when formulating root definitions. Standing for C (customers, who can be victims or beneficiaries), A (actors, carrying out the activities), T (transformation of some entity), W (Weltanschauung, world-view or perspective), O (owner, who controls the system), and E (environmental constraints, taken as given).
The five Es Criteria by which a transformation can be judged. Comprising efficacy, efficiency, effectiveness, ethicality, and elegance.
Conceptual model The set of activities necessary to carry out the root definition. Consists of an operational subsystem and a control subsystem.
Comparison Comparing the conceptual models and the perceived real world, in order to generate debate and possible changes to improve the problem situation.
Desirable and feasible changes
Possible changes that are systemically desirable and culturally feasible for the people in the system at this time.
Action Real-world action to improve the problem situation as a result of the learning cycle of SSM.
Sources: Hindle & Braithwaite 2001; Checkland & Scholes 1990.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy x
Statement of Original Authorship The University of New South Wales
Doctor of Philosophy
I hereby declare that this submission is my own work and that, to the best of my
knowledge it contains no material previously published or written by another person,
nor material which to a substantial extent has been accepted for the award of any other
degree or diploma at UNSW or any other educational institution, except where due
acknowledgement is made in the thesis. Any contribution made to the research by
others, with whom I have worked at UNSW or elsewhere, is explicitly acknowledged in
the thesis.
I also declare that the intellectual content of the thesis is the product of my own work,
except to the extent that assistance from others in the project’s design and conception or
in style, presentation and linguistic expression is acknowledged.
Name: Peter Francis O’Meara
Signed: ................................................................................................................
Date: 1 June 2002.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy xi
Acknowledgements
Rural Ambulance Victoria (RAV) and the five former regional ambulance services in rural Victoria are acknowledged for their cooperation while I undertook the research for this thesis. Both current and past ambulance service personnel who supplied data and other information, completed questionnaires and participated in interviews and the focus group are specifically thanked.
I also thank those general practitioners, nurses, ambulance officers and members of the public who completed questionnaires for the study. Many of these respondents and their colleagues discussed the preliminary findings with me from time-to-time and generally maintained my enthusiasm for the research. It is acknowledged that many ideas and insights about rural ambulance systems and models were discussed with others throughout the course of the research process. However, the inferences and interpretation of the data are my responsibility.
Completion of the thesis would have been more difficult without the support and encouragement of my colleagues at the Monash University School for Rural Health. Apart from these intangibles that are so important, they also provided their time and patience to discuss theoretical concepts, style of presentation and technical matters. Their contribution strengthened the input of my supervisors at the University of New South Wales School of Public Health and Community Medicine. Associate Professor Jeffrey Braithwaite managed to keep in touch and sustain my motivation for the duration of the research despite being located in Sydney over 1,000 kilometres distant. Associate Professor Johanna Westbrook, as co-supervisor later in the process strengthened the methods and findings chapters through constructive criticism and suggestions for improvement in the structure of the thesis.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy xii
Publications and presentations of the author arising from or contributing to this thesis
O’Meara, P. (1995) Resource Allocation for Gippsland Ambulance. Ambulance Service Victoria - South Eastern Region. Ref Type: Unpublished Work
Kelly, H. O’Meara, P. and Burley, M. (1999) Urgent care in Victorian rural towns: Final Report. Monash University, Traralgon.
O’Meara, P. and Somers, G. (1999) ‘Ambulance Service Delivery in Emerald: a pilot study’, Health Services Research Conference, Sydney, 8-11 August 1999.
O’Meara, P. (2000) ‘Ambulance Service Delivery in Emerald: a pilot study’, 5th Biennial Australian Rural and Remote Health Scientific Conference, Toowoomba, 24-26 February 2000.
O’Meara, P. (2000) ‘Assisting rural communities meet their urgent care needs’, 1st Conference on the Future of Australia's Country Towns, Bendigo, 28-30 June 2000.
O’Meara, P. and Burley, M. (2000) Immediate Care Service Model for Lakes Entrance: a co-ordinated approach to urgent care services for Lakes Entrance. Monash University Centre for Rural Health. Traralgon.
O’Meara, P. Strasser, R. Marrow, A. and Le Leivre, P. (2001) ‘An integrated approach to the role of the Ambulance Medical Officer in rural Australia’, Pre-hospital Immediate Care. 5(1): 24-26.
O’Meara, P. (2001) ‘Professional and community expectations of rural ambulance services in Australia’, Pre-hospital Immediate Care. 5(1): 27-30.
O’Meara, P. and Burley, M. (2001) Feasibility of extending and improving urgent care in Lakes Entrance. Monash University School of Rural Health. Traralgon.
O’Meara, P. and Boyle, M. (2001) ‘From Roadside to Hospital: An investigation of the factors influencing the time taken to deliver trauma patients to a regional hospital’. Monash Rural Health Bulletin. 8(1). www.med.monash.edu.au/mrh/education/cpe/v8n1-bulletin.html [accessed 7/01/02].
O’Meara, P. (2001) ‘Using Soft Systems Methodology to develop rural ambulance models’. Health Services Research and Policy Conference, Wellington, New Zealand, 2-4 December 2001.
O’Meara, P. (2001) Moe After Hours Medical Service Evaluation, Final Report. Monash University School of Rural Health, Traralgon.
O’Meara, P. and Strasser, R. (2002) ‘Moe After Hours Medical Service: ‘pillars’ of success’. Australian Health Review. 25(2): 107-117.
O’Meara, P. Burley, M. and Kelly, H. (2002) ‘Rural urgent care models: what are they made of?’ Australian Journal of Rural Health. 10: 45-51.
O’Meara, P. Burley, M. Pendergast, C. and Kirkbright, S. (2002) Transforming Rural Health Systems. Monash University, School of Rural Health, Traralgon.
O’Meara, P. (2002) Featured Conference Speaker at the 6th Annual Canadian EMS Chiefs and Directors Conference, Vancouver, British Columbia, Canada, 18-20 September 2002.
O’Meara. (2002) ‘Would a pre-hospital practitioner model improve patient care in rural Australia?’ Emergency Medicine Journal. [submitted for publication April 2002]
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
1
SECTION 1 INTRODUCTION
1.0 Overview of Study
1.1 Rationale for the study
This is the only known comprehensive, empirical study of rural ambulance service
systems and models of service delivery that has been undertaken in Australia or other
developed countries. It is the sole one using soft systems methodology. In common with
at least one other study in the United Kingdom, this study set out to stimulate
discussion, dialogue and debate about the future shape of ambulance services (Nicholl
et al 2001). The main emphasis is on the formulation of alternative models of service
delivery that meet the needs and expectations of rural Victoria, and how they may
impact on future policy and practice within the pre-hospital sphere.
The planning, operation and assessment of ambulance services in Australia has been in
a state of flux for at least the last 20 years (PBRC 1984; Capp 1992; ASNSW 1992a;
Baragwanath 1997a & 1997b; DHSV 1998a; Allen Consulting 1999; Audit Office NSW
2001). Reflecting this state of confusion, ambulance services have tended to have
organizational structures and cultures that are more akin to emergency services than as
providers of emergency health services (NHTSA 1996; Audit Office NSW 2001).
Contacts between ambulance paramedics and other rural health professionals were
limited until the 1980s. Even now there is only limited collaboration or evidence of
organized interdisciplinary training, education or research with other members of the
health care team (O’Meara et al 2001).
In common with other ambulance services in Australia, the planning and management
of Victorian rural ambulance service was reactive, with industrial disputation and other
external factors driving their agenda until their amalgamation in 1999. It was best
described as a crisis management culture (Baragwanath 1997a and 1997b; DHSV
1998a; Allen Consulting 1999). An almost complete dearth of empirical evidence, either
quantitative or qualitative, allowed this culture of reactive management to thrive.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
2
Despite the existence of these organizational problems throughout the country, there
have been few attempts to study Australian ambulance services in any systematic way
(Jacobs 2000). There is little Australian research specifically addressing the challenges
of delivering rural ambulance services. The studies undertaken have tended to be
snapshots that have made promising beginnings without really addressing the recurring
issues and problems of rural ambulance services (Gilligan et al 1999; O’Meara 2000).
Urban research has been drawn on to address rural issues surrounding the delivery of
pre-hospital care. In the absence of other evidence, this approach is better than the
alternative of relying on myth and tradition to formulate and deliver rural pre-hospital
care. However, the means of delivering this service in rural areas may need to be
modified substantially to account for distance, terrain or lack of resources. The
assumption that if a model works in urban areas, it will therefore be suitable for rural
areas may not always be true.
This study was uniquely concerned with the whole service delivery model as an
operational system within the rural social, economic and political context, rather than as
a set of individual components in isolation from each other, the community, and the
health delivery system. It also breaks new ground in its examination of community
expectations and consideration of a coherent performance framework for rural
ambulance services as part of the model development process.
Rural ambulance services in the Australian State of Victoria were used as the focus of
the study, to take advantage of the profound organizational changes taking place at the
time of the study in the late 1990s. These changes resulted in the formation in early
1999 of Rural Ambulance Victoria (RAV) a specialized rural ambulance service
providing for the emergency ambulance needs of all but a small area of rural Victoria.
This organizational structure is unique in Australia, with other States opting for single
state-wide ambulance services.
This rural setting provided a unique opportunity to view rural ambulance services as a
distinct discipline or area of study, in which rural issues and concerns are not subsumed
into an urban-orientated view of the world. This rural-orientated management of
ambulance services also stands in contrast to the locally based management of
ambulance in much of the rural United States of America, where most of the ambulance
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
3
or Emergency Medical Services research literature is derived. It can also be
distinguished from ambulance service arrangements in the United Kingdom, where the
factors of time and distance from emergency medical facilities are less acute.
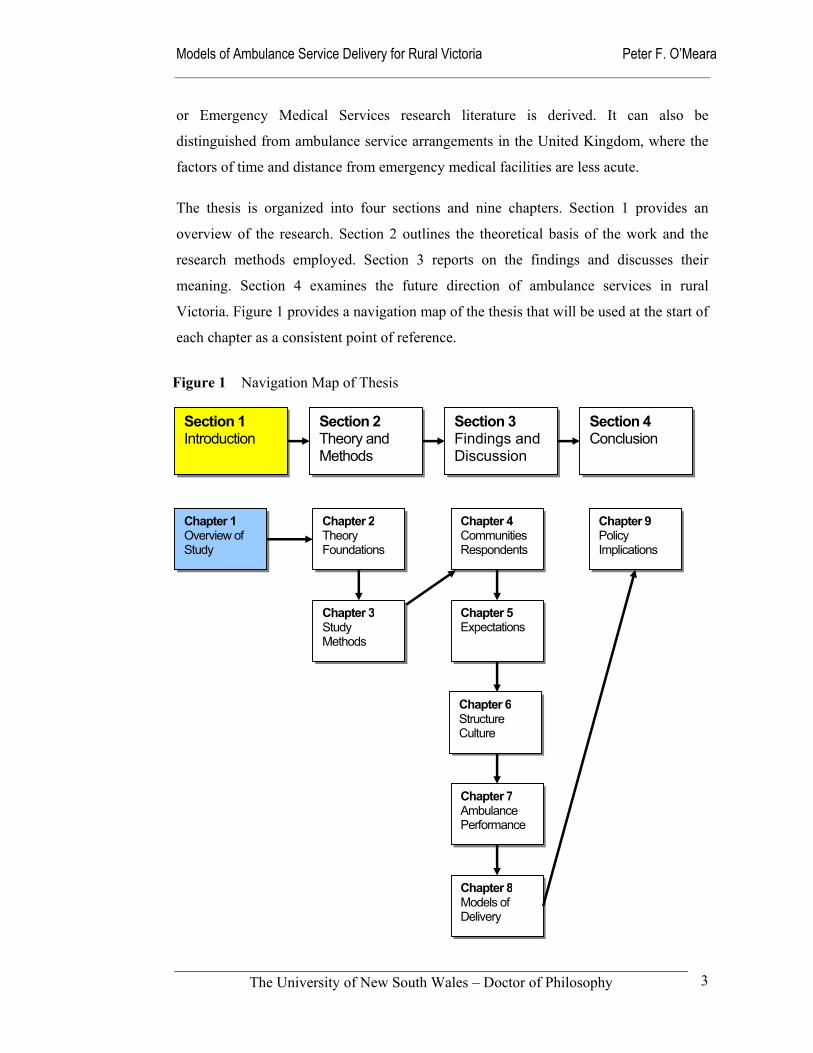
The thesis is organized into four sections and nine chapters. Section 1 provides an
overview of the research. Section 2 outlines the theoretical basis of the work and the
research methods employed. Section 3 reports on the findings and discusses their
meaning. Section 4 examines the future direction of ambulance services in rural
Victoria. Figure 1 provides a navigation map of the thesis that will be used at the start of
each chapter as a consistent point of reference.
Section 1 Introduction
Section 2 Theory and Methods
Section 3 Findings and Discussion
Section 4 Conclusion
Chapter 1 Overview of Study
Chapter 2Theory Foundations
Chapter 4Communities Respondents
Chapter 5Expectations
Chapter 6Structure Culture
Chapter 7Ambulance Performance
Chapter 8Models of Delivery
Chapter 9 Policy Implications
Chapter 3Study Methods
Figure 1 Navigation Map of Thesis
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
4
1.2 Aims and objectives
The primary aim of the study was to develop conceptual models to stimulate discussion
and debate about models of ambulance service delivery and to provide a foundation for
determining the most suitable models for rural Victoria. Analysis of the formulated
models of service delivery will assist in addressing the current significant gap in
knowledge and understanding of rural ambulance systems. Four research questions were
addressed through this research to reach this point in a positive and innovative manner.
The specific research aims were to:
1. Identify the professional and community expectations of rural ambulance
services in Victoria, and to suggest improvements in how they operate;
2. Describe the structure and culture of rural ambulance services within their socio-
political climate, along with the educational and technological changes that
continue to shape their evolution;
3. Compare the perceived and actual performance of rural ambulance services in
different geographical areas in terms of utilization rates and time intervals with a
view to developing a useful performance framework for rural ambulance
services; and
4. Develop models of ambulance service delivery from different philosophical
perspectives to stimulate debate about models that may be most suitable for rural
Victoria.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
5
1.3 Research methods used
A systems approach was used to conceptualise the issues and to structure the research
activities. This allowed the policy and empirical components to be brought together into
a manageable whole. Using specific ‘systems’ tools – in particular, soft systems
methodology (Checkland & Scholes 1990; Checkland 1999) – provided the
management tools for the conduct of the research, then the integration and analysis of
the findings. It allowed for the cultural environment to be contrasted with the logic-
driven approach often employed to manage and direct large organizations. It added
‘richness’ to the analysis and conclusions that would otherwise have been missing. Soft
systems methodology was combined with basic epidemiological techniques and the use
of metaphor to describe the formulated models, in order to provide some clarity of
thought during the modelling process.
As a precursor to the formulation of the models, the preliminary research audited and
described the ambulance services operating in rural Victoria using data obtained
through the cooperation of the rural ambulance services from their operational data and
strategic planning documents. Questionnaires seeking information about local
ambulance resources, the local environment, and other health and emergency services,
were also distributed to the officers in charge of sample stations, supplemented with
documents from Rural Ambulance Victoria, interviews with industry experts and a
focus group of ambulance managers.
Observation of the overt decision-making processes (such as any public consultation)
and planning processes that have shaped the evolution of the current service delivery
models, resulted in a more political perspective of the recent organizational changes in
rural Victoria. The broader impact of these changes, were examined through an analysis
of responses to questionnaires sent to ambulance staff, other health professionals and
members of the public in 40 sample communities of over 400,000 people throughout the
State. At the time of the research there were 117 ambulance stations in rural Victoria.
For the purposes of analysis, the sample stations were categorised into five distinct
groups on the basis of town population and the degree of isolation from major services.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
6
For the quantitative phase of the research, Victorian rural ambulance services made
available electronic data from the 1996/97 fiscal year on the number and urgency of
ambulance cases, the time intervals for case responses, age and gender of patients, trip
distance, and patient pick-up and destination points by postcode. Of critical importance
was the collation of demographic data describing the catchment population for each
community studied. These were obtained through a combination of questionnaires to the
ambulance services, examination of maps, and data from the Australian Bureau of
Statistics 1996 Census.
Questionnaires were distributed to ambulance officers (paramedics and volunteers),
general practitioners, registered nurses and members of the public in the sample towns
and regional centres. Respondents were asked to express their expectations of their local
ambulance services, their level of satisfaction and any suggestions they may have for
improvement. This is the only known study to include these professional groups and
members of the public in the one study.
Systems thinking, with its emphasis on looking at the service delivery as a whole
system was used to formulate five models. As a matter of process, the models could not
be definitively determined at the onset – they were formed, constantly reviewed and
modified throughout the research process. Action research of this nature is iterative; it
does not follow the classic literature-hypothesis-experiment-results-conclusion model.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
7
1.4 Main findings
Following an overview of the sample rural communities in terms of demography, health
system and an emergency services profile, the four substantive chapters in Section 4
respond to the research aims of:
1 Determining community expectations of rural ambulance services;
2 Reporting on the structure and culture of rural ambulance services;
3 Looking at performance measures; and
4 Developing models of service delivery.
Expectations – satisfaction – improvement ideas
Respondents to the study indicated that their main expectations of rural ambulance
services were:
Service availability;
Speed of response;
Competent and skilled staff;
Communication and teamwork with health and emergency services; and
Professional and ethical behaviour from staff.
All these can be considered generic qualities that should be expected in all ambulance
services irrespective of location or the service delivery model being used. While
generally satisfied with their rural ambulance services, respondents suggested that
improvements needed to be made in the areas of:
Staff numbers, skills and support;
Local management autonomy, with the place of centralized dispatch centres
coming under sustained criticism; and
The need to clarify the future role of the ambulance services within the health
system.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
8
Structural and cultural dimensions
Ambulance services in Australia, rural and urban, are changing from hierarchal systems
to knowledge-driven models, with greater interaction occurring with other health
professionals through opportunities for shared education, collaborative research, and
improvements in teamwork. Culturally, the two major driving forces on rural ambulance
services are education and technology. Together, they open up the possibility of an
ever-expanding range of education programs, and clinical assessment and intervention
possibilities in the pre-hospital environment.
The formation of Rural Ambulance Victoria has enabled rural ambulance services to
speak with one voice, and as a result develop wider stakeholder relationships than was
previously possible as a disparate group of autonomous regions that were informally
aligned through common interests. Despite claims that its ‘flat’ organizational structure
makes it less hierarchical than its predecessors, Rural Ambulance Victoria as an
organization has high levels of complexity, formalization and centralization. The
emerging challenges for rural ambulance services, as they integrate more closely with
other components of the health system, will be their ability to accommodate a more
independent ambulance paramedic profession and to develop a greater ability to form
and maintain key partnerships.
Measuring performance
Performance measures used in rural ambulance services have been adhoc and often fail
the test of being specific, measurable, action-orientated, relevant, and timely. There has
been a concentration on easily collectable time intervals of dubious accuracy, while
there is little accessible information on clinical matters. Drawing from a now
inappropriate emergency services model, response times have tended to be used as a
proxy for effective ambulance service performance.
A performance framework has been constructed for rural ambulance services, which
incorporates the National Health Performance Committee’s structural dimensions of
effectiveness, appropriateness, safety, capability, continuity, accessibility and equity,
acceptability, and efficiency.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
9
Models of service delivery
Five potentially overlapping service delivery models were formulated on the basis of
five distinct worldviews, or ‘Weltanschauung’ using soft systems terminology. The
description of these models of service delivery has the capacity to open up dialogue and
debate about the strategic choices that need to be made if these or other new models are
to be implemented, the cultural and social aspects of these choices, and the political
forces that both promote and hinder policy initiatives. The models and their implicit
worldviews are briefly described below:
competitive model
This is a market model, based on a view that competitive environments result in a more
efficient delivery of ambulance services. It tends to avoid the problem of the service
being ‘captured’ by unions and other pressure groups.
sufficing model
Views the delivery of ambulance services as a public good, with all citizens entitled to a
minimum level of service irrespective of income, geographic location, gender or race. It
is often characterised by internal conflict and resource allocation distortions.
community model
Community self-reliance and control is highly valued, with the model concentrating on
satisfying the expectations of the local community. However, it can become unstable
because of its isolation from professional support mechanisms.
expert model
Based on the notion that there is information asymmetry and the ‘professionals’,
through their training and experience, are best able to determine the needs of the
community. Letting communities have a direct say would distort priorities and result in
less than ‘best practice’ standards.
practitioner model
This is based on a view that health care is best integrated, with professional staff sharing
roles that effectively utilize their skills and knowledge within a unified health system. It
is an aspirational model, which would need to overcome major professional barriers
before it could be widely implemented.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
10
1.5 Future directions
Three of the five models formulated in this study, ‘sufficing’, ‘community’ and ‘expert’,
are recognisable within the Australian context. The ‘competitive’ model is largely
confined to the United States, although the Metropolitan Ambulance Service in
Melbourne had a brief flirtation with it in the 1990s. The ‘practitioner’ model is more
speculative and builds on dialogue taking place in the United States of America, the
United Kingdom and in South Australia about expanding the scope of ambulance
paramedic practice. The principles that underlie the practitioner model are consistent
with discussions in rural Australia exploring the development of generalist roles for
allied health professionals and the implementation of generalist health science degrees
for rural health professionals.
While aspects of all the models are familiar, they are nonetheless abstract systems and
do not exist. In the real world, service delivery models are messy and imperfect, with
service delivery models more likely to be amalgams of different models in response to
their local contexts, and confused and contradictory policy imperatives. Because the
five models formulated are based on an understanding that pre-hospital care is part of
the health system, each is compatible with an ambulance system that is integrated within
the health system.
These potentially overlapping models provide useful points of reference for debate and
discussion about the future policy, practice and research directions of rural ambulance
services. Immediate policy concerns identified in this study are: how rural ambulance
services will manage their further integration with the health system; adapt to a more
professionalised workforce; foster the involvement of rural communities; and maintain
the level of resources necessary for the provision of a first-class service to rural
communities.
Rural ambulance services will also share with other health and emergency services, the
challenge of meeting the rising expectations within the context of continual social and
technological change.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
11
SECTION 2 THEORY AND METHODS
2.0 Theoretical Framework and Empirical Foundations
Section 1 Introduction
Section 2 Theory and Methods
Section 3 Findings and Discussion
Section 4 Conclusion
Chapter 1 Overview of Study
Chapter 2Theory Foundations
Chapter 4Communities Respondents
Chapter 5Expectations
Chapter 6Structure Culture
Chapter 7Ambulance Performance
Chapter 8Models of Delivery
Chapter 9Policy Implications
Chapter 3Study Methods
Figure 2 Navigation Map of Thesis
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
12
2.1 Introduction
The general approach taken in the thesis was to use a systems approach to conceptualise
the theoretical and empirical work relevant to the research aims. Using a systems
approach allowed this body of work to be combined together into a manageable whole.
In particular, soft systems methodology – provided valuable tools for the conduct of the
research, integration and analysis of the findings.
Simeon’s ‘funnel of causality’ was utilized as a conceptual device to assemble and
organize the theoretical and empirical work of others for the thesis. Through this device
a metaphorical window was formed and the impact of ideology, power and conflict on
the development of rural ambulance service delivery models was examined (Simeon
1976). Through this it was possible to look at the ways in which policy-makers interact
during the highly political processes of planning and change. These processes include
both the overt and covert exercises of power that influence the final decisions on the
shape and character of the ambulance service delivery models adopted in rural areas.
To come to an understanding of the context in which the rural ambulance services
operate, it was necessary to:
understand who the participants are, what interests they represent, and the resources they can marshal, mobilize and command for the exercise of power;
look at the policy-makers’ values and ideologies to determine why they act the way they do; and
appreciate how institutions are constrained and the opportunities that may exist.
(Simeon 1976: 121).
Focusing on the decision-making processes allowed the modus operandi and the
strategies and tactics of the participants to be observed through the socio-economic
environment, the political and structural variables. From this conceptualisation, it
became clear that the official and unofficial policy-makers interact through the
environmental, political and institutional variables before any decision is finally arrived
at (Simeon 1976: 121).

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
13
To take advantage of this conceptual framework for the thesis, the review of the
theoretical and empirical literature was segmented into four broad categories:
1. systems theory; (Chapter 2.2)
2. socio-political context; (Chapter 2.3)
3. health policy context; (Chapter 2.4) and
4. ambulance context. (Chapter 2.5)
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
14
2.2 Systems theory
The reason for embracing systems theory was the recognition that ambulance service or
pre-hospital research needed to move on from component research toward a more
integrated approach. That is, the study sought to move from reductionist to systematic
thinking. It was through this research device that I aimed to produce an informed and
multi-model response to the principal research aim to develop models of ambulance
service delivery from different philosophical perspectives to stimulate debate about
models that may be most suitable for rural Victoria.
2.2.1 General Systems Theory
Kauffman (1980), Lilienfeld (1978) and others provide descriptions of the genesis of
systems thinking from the 1920s, when researchers sought to find a means of dealing
with ‘messy problems’ through the development of a consistent frame of reference.
Drawing largely from the biological sciences, von Bertalanffy, Pepper, Henderson, and
Cannon are considered to have been the forerunners of more sophisticated systems
thinkers (Lilienfeld 1978: 7-32). The use of general systems theory had a major impact
on many scientific fields, including the development of computerization and
automation. Central to this was the idea that a system is a collection of parts that interact
with each other to function as a whole (Kauffman 1980: 1).
Flood and Jackson (1991) provide an excellent description of the concept of a ‘system’
and chart the development of modern systems theory and how the concept allows
researchers and managers to draw on other organizational theories. Describing the
evolution of systems thinking from the mechanistic or closed concept to open systems,
they describe the difference between the two concepts:
In mechanistic thinking a “system” is an aggregate of parts in which the whole is equal to the sum of the parts. In systems thinking, a “system” is a complex and highly interlinked network of parts exhibiting synergistic properties – the whole is greater than the sum of its parts.
(Flood & Jackson 1991: 4)
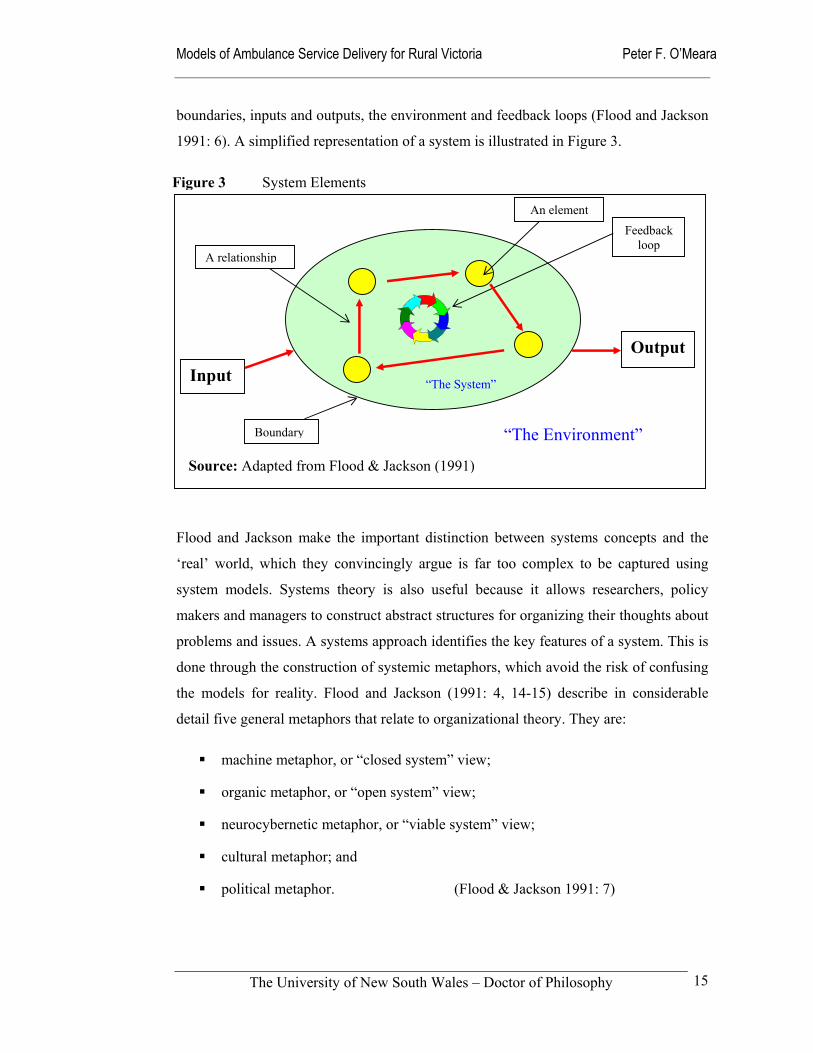
Flood and Jackson’s (1991: 5-6) description of a system provides a useful heuristic tool.
They describe a system in terms of elements (actors and resources), relationships,
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
15
boundaries, inputs and outputs, the environment and feedback loops (Flood and Jackson
1991: 6). A simplified representation of a system is illustrated in Figure 3.
Flood and Jackson make the important distinction between systems concepts and the
‘real’ world, which they convincingly argue is far too complex to be captured using
system models. Systems theory is also useful because it allows researchers, policy
makers and managers to construct abstract structures for organizing their thoughts about
problems and issues. A systems approach identifies the key features of a system. This is
done through the construction of systemic metaphors, which avoid the risk of confusing
the models for reality. Flood and Jackson (1991: 4, 14-15) describe in considerable
detail five general metaphors that relate to organizational theory. They are:
machine metaphor, or “closed system” view;
organic metaphor, or “open system” view;
neurocybernetic metaphor, or “viable system” view;
cultural metaphor; and
political metaphor. (Flood & Jackson 1991: 7)
“The Environment”
An element
OutputInput “The System”
A relationship
Feedback loop
Figure 3 System Elements
Source: Adapted from Flood & Jackson (1991)
Boundary
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
16
Of these models, the machine and open metaphors were promising approaches to the
analysis of the current emergency ambulance services provided to rural and remote
Australians. Their cybernetic metaphor also fits the ‘modern’ computer aided dispatch
systems used by most emergency services in Australia, where staff are expected to
follow established protocols and directives in order to deliver short response times and
standardized treatment protocols. The problem with this cybernetic system view of the
world is that it tends to assume a mindless contribution from staff who are in practice
required to make highly autonomous clinical decisions (Mahony 2001). The organic or
open metaphor provides a useful approach when considering the degree of change –
both organizational and technological – that rural ambulance services are facing as they
enter the third millennium. Senge (1998) argues that the age of the machine
organization is over, with the ‘living system’ a more promising approach to organizing
institutions and corporations. A related approach is that of Clegg et al (1996) who
describe how environmentalists have argued for an ecological systems approach to
problem solving and organizing.
The political metaphor was the most useful theoretical perspective for the thesis at the
analytical level. It provided three descriptions of the political environment – labelled
unitary, pluralist and coercive – based on issues of interests, conflict and power (Flood
& Jackson 1991). The strength of the political metaphor is its ability to balance the
rather naïve perspective of the open systems approach that emphasizes functionality and
order. It recognizes the strains and tensions that characterize the observed behaviour of
ambulance services in Australia. However, concentrating on this political facet of the
question at the expense of the functional would have run the risk of neglecting other
factors, such as organizational structure and the development of clear goals, which are
essential to the success of any model of service delivery.
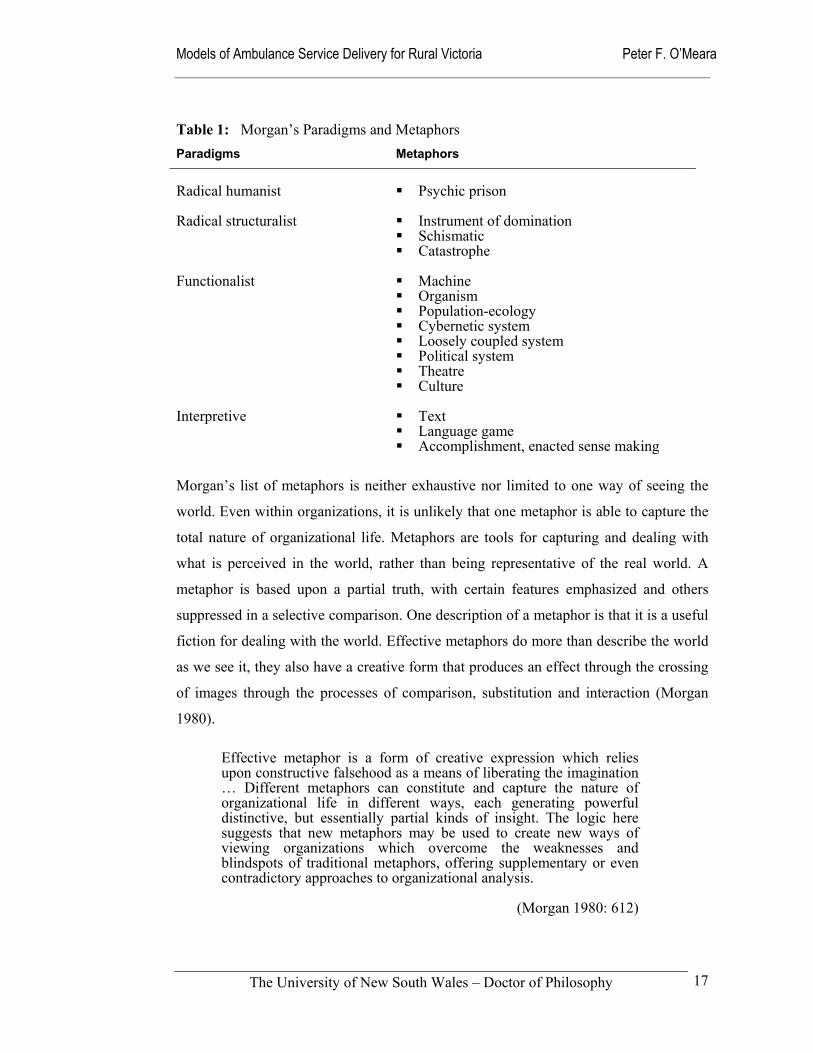
Morgan (1980) argues that this open-closed dichotomy and related metaphors are
imprisoned within the functionalist paradigm or world-view. He identifies three other
distinct world-views and a total of fifteen metaphors or schools of thought. From these
metaphors are spawned puzzle-solving activities that may be described as models.
Morgan’s metaphors are summarized in Table 1.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
17
Table 1: Morgan’s Paradigms and Metaphors
Paradigms Metaphors
Radical humanist Psychic prison
Radical structuralist Instrument of domination
Schismatic Catastrophe
Functionalist Machine
Organism Population-ecology Cybernetic system Loosely coupled system Political system Theatre Culture
Interpretive Text
Language game Accomplishment, enacted sense making
Morgan’s list of metaphors is neither exhaustive nor limited to one way of seeing the
world. Even within organizations, it is unlikely that one metaphor is able to capture the
total nature of organizational life. Metaphors are tools for capturing and dealing with
what is perceived in the world, rather than being representative of the real world. A
metaphor is based upon a partial truth, with certain features emphasized and others
suppressed in a selective comparison. One description of a metaphor is that it is a useful
fiction for dealing with the world. Effective metaphors do more than describe the world
as we see it, they also have a creative form that produces an effect through the crossing
of images through the processes of comparison, substitution and interaction (Morgan
1980).
Effective metaphor is a form of creative expression which relies upon constructive falsehood as a means of liberating the imagination … Different metaphors can constitute and capture the nature of organizational life in different ways, each generating powerful distinctive, but essentially partial kinds of insight. The logic here suggests that new metaphors may be used to create new ways of viewing organizations which overcome the weaknesses and blindspots of traditional metaphors, offering supplementary or even contradictory approaches to organizational analysis.
(Morgan 1980: 612)
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
18
In later work Morgan (1997) describes eight images of organizations, within which he
uses a number of metaphors to expand on alternate views of organizations. Amongst the
more helpful are those shedding further light on the political system and those that seek
to explain change and the transformation of organizations. The latter draws on the idea
that the universe is in a constant state of flux: He explores four ‘logics of change’ to
explain this position. These are the theory of autopoiesis, chaos and complexity theory,
that change is embedded within circular relations, and the idea that change is the
product of tensions within opposites (Morgan 1997: 252). However, he cautions that
metaphor can provide only partial insight.
As has been shown, metaphors create insight. But they also distort. They have strengths. But they also have limitations. In creating ways of seeing they tend to create ways of not seeing.
(Morgan 1997: 348)
From a management perspective, Forrester (1980) provides an excellent description of
complex systems and how all larger organizations share these characteristics to varying
degrees. His work also provides an excellent discussion of the characteristics, uses and
limitations of model building to describe the structure and interrelationships of a system
(Forrester 1969: 112-114). Forrester’s work is structuralist, emphasizing his belief in
avoiding the mere collection of observations, practices and conflicting incidents.
However, his faith in the centrality of structure is rather inflexible and largely avoids the
importance of cultural and political processes in the operation of systems and
organizations. Lilienfeld (1978) is very critical of Forrester’s and others’ ambitious
claims for systems theory; in addition to doubting the universal utility of systems
thinking, Lilienfeld characterizes the theories as ideological imperialism that tends to
exclude other management approaches.
Other writers, such as Alderfer and Cooper (1980) added useful insights to systems
thinking, dividing systems into underbounded and overbounded components. This
theory is based on the premise that system boundaries, both physical and psychological,
are the defining characteristic of systems and that permeability is the crucial property of
system boundaries.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
19
‘Overbounded’ systems show less boundary permeability than is optimal for the system’s relationship to its environment, and ‘underbounded’ systems show more boundary permeability than is optimal for the system’s relationship to its environment. The primary threat to overbounded systems is that they become closed off to their environments and lose the capacity to respond adaptively to environmental changes and to reverse the build-up of entropy. The primary threat to underbounded systems is that they will become totally caught up in their environmental turbulence and lose a consistent sense of their own identity and coherence. Thus, being extremely underbounded is a greater threat to a system’s survival, especially in the short run, than being overbounded.
(Alderfer & Cooper 1980: 269)
This theoretical perspective provides a valuable framework to judge the ability of rural
ambulance services to interact with the wider health system, other health professionals
and the community at large. Alderfer and Cooper (1980: 269-277) have identified
eleven interdependent variables to differentiate between underbounded and
overbounded systems. This set of variables is considered during the research process in
order to explore the organizational health of the rural ambulance services. These
variables are:
Goals Affect distribution
Authority relations Intergroup dynamics
Economic relations Unconscious basic assumptions
Role definitions Time-span
Communication patterns Cognitive work
Human energy
General management literature also picks up the concepts of systems thinking. Dunham
and Pierce (1989) relate systems theory to the relationship between organizations and
their environment. They describe Burns and Stalker’s studies relating the organic and
mechanistic system organizational responses to environmental change. They argue
strongly that organizations need to create different management systems to deal with the
characteristics of the task environment and the uncertainty of their environment.
‘Organic management systems appear appropriate for high levels of environmental
change and segmentation, mechanistic systems for more stable environments and lower
levels of uncertainty’ (Dunham & Pierce 1989: 56). They also describe the perspective
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
20
of organizations in relation to their external environment in terms of whether the system
is open or closed (Dunham & Pierce 1989: 56-58).
Senge (in Adams 1986: 134-157) explores the relationship between systems theory and
leadership, in which he argues the development of systemic thinking is important if
leaders are to understand their own organization. He sees a systemic viewpoint being of
most value through its ability to distinguish between high and low-leverage changes.
His feedback structures appear a little like the cogs and chain-wheels on a bicycle,
where different combinations produce different outcomes. In The Fifth Discipline,
Senge links systems thinking to the concept of change in his description of it as a:
… conceptual framework, a body of knowledge and tools that has been developed over the past fifty years, to make the full patterns clearer, and to help us see how to change them effectively.
(Senge 1990: 7)
An important characteristic of systems thinking is its distinction from reductionalism
where the use of ‘snapshots’ provides simple, and largely simplistic, solutions to
complex problems (Senge 1990). Senge’s colleagues, Roberts and Kleiner, define
systems by their elements having a common purpose, and behaving in common ways
because they are interrelated toward that purpose (in Senge 1999: 137). They go on to
describe four forms of systems thinking relevant to organizational change:
Open Systems: Seeing the world through flows and constraints;
Social Systems: Seeing the world through human interaction;
Process Systems: Seeing the world through information flow; and
Living Systems: Seeing the world through the interaction of its self-creating entities.
(Roberts & Kleiner in Senge 1999: 137-145)
Shortell and Kaluzny (1994: 14) describe health service organizations as complex social
systems, with a constant tension between the need for predictability, order, and
efficiency on the one hand and openness, adaptability and innovation on the other. The
former is consistent with a closed system view of an organization, while the latter is
consistent with an open system view. They make the point that both approaches are

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
21
needed; something that should not be lost on rural ambulance services as they strive to
maintain control of a geographically diverse organization and maintain meaningful
dialogue with the wider health system and rural communities. More recently, others
(Plsek & Greenhalgh 2001; Plsek & Wilson 2001) have supported the value of using the
idea of health care as part of a complex adaptive system, and have criticised traditional
reductionist thinking based on command and control.
Robbins and Barnwell (1994: 10-15, 52-55) describe the systems perspective in relation
to the workings of an organization. They critique the often quoted open-closed
dichotomy of organizational systems, arguing that this should more accurately be
considered as a range rather than two separate classifications. Open systems share the
characteristics of having inputs, transformation processes and outputs. Gardner (1992)
uses these same characteristics to describe how the health system operates. A criticism
of these descriptions is their neglect of the transformation processes, which appear to
produce outputs through some ‘magical’ process that is not shared with the reader.
Robbins and Barnwell (1994: 15) note the value of systems theory as a framework for
students and managers to conceptualise organizations and to enable them to see the
organization as a whole. They also draw attention to the limitations of a systems
framework; the most telling of which is its abstractness. On the other hand, as Flood and
Jackson (1991) argue, it is this characteristic of systems theory that is its strength. It is
the confusion between models and abstractions with the political and cultural
dimensions of the organization that potentially causes problems for researchers and
managers alike.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
22
2.2.2 Soft Systems Methodology
Flood and Jackson (1991: 31-43) examine a range of different systems thinking
approaches, each of which is based on different metaphorical understandings and
different views of reality. They list the following systems approaches:
Operational research Socio-technical systems thinking
Systems analysis Social systems design
Systems engineering Strategic assumption surfacing and testing
System dynamics Interactive planning
Viable system diagnosis Soft systems methodology
General systems theory Critical systems heuristics
Contingency theory
Rather than attempting to use a great number of these approaches to address a particular
problem, researchers need to decide which approach to adopt. Otherwise the paradigm
proliferation will defeat them. Flood and Jackson (1991: 32-43) address this problem
through the grouping of problem contexts according to the dimensions of systems and
participants.
The systems dimension refers to relative complexity in terms of the “system” or “systems” that make up the problem situation, and within which other difficult pluralist or coercive issues of concern may be located.
The participants dimension refers to the relationship (of agreement or disagreement) between individuals or parties who stand to gain (or lose) from a systems intervention. It thus allows us to build pluralistic and coercive appreciations of problem situations into any understanding of complexity that is promoted through the systems dimension.
(Flood & Jackson 1991: 33)
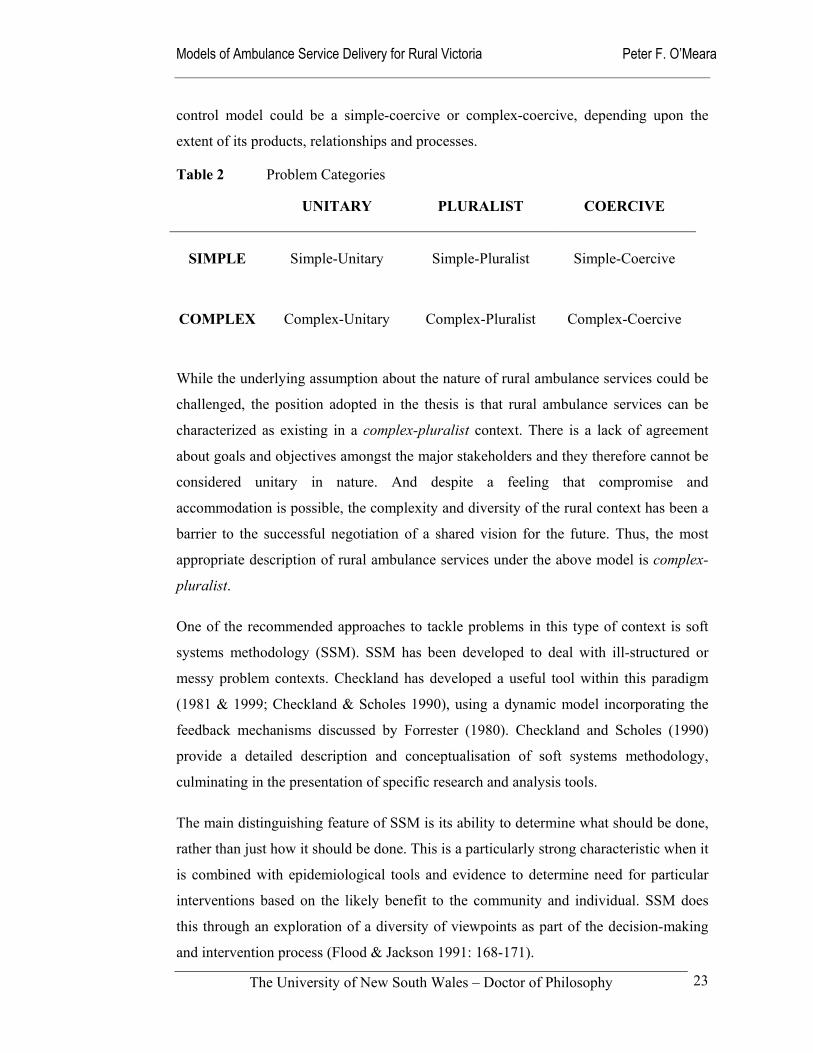
Their combination of relative complexity and the political metaphor provides six ideal-
type problem categories illustrated in Table 2, into which a given situation can be
placed (Flood & Jackson 1991: 35). For instance, a garbage collection service is likely
to be classified in the simple-unitary category. A university department is more likely to
be categorized as complex-pluralist, and a factory if it is operated on a command and
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
23
control model could be a simple-coercive or complex-coercive, depending upon the
extent of its products, relationships and processes.
Table 2 Problem Categories
UNITARY
PLURALIST COERCIVE
SIMPLE
Simple-Unitary
Simple-Pluralist
Simple-Coercive
COMPLEX
Complex-Unitary
Complex-Pluralist
Complex-Coercive
While the underlying assumption about the nature of rural ambulance services could be
challenged, the position adopted in the thesis is that rural ambulance services can be
characterized as existing in a complex-pluralist context. There is a lack of agreement
about goals and objectives amongst the major stakeholders and they therefore cannot be
considered unitary in nature. And despite a feeling that compromise and
accommodation is possible, the complexity and diversity of the rural context has been a
barrier to the successful negotiation of a shared vision for the future. Thus, the most
appropriate description of rural ambulance services under the above model is complex-
pluralist.
One of the recommended approaches to tackle problems in this type of context is soft
systems methodology (SSM). SSM has been developed to deal with ill-structured or
messy problem contexts. Checkland has developed a useful tool within this paradigm
(1981 & 1999; Checkland & Scholes 1990), using a dynamic model incorporating the
feedback mechanisms discussed by Forrester (1980). Checkland and Scholes (1990)
provide a detailed description and conceptualisation of soft systems methodology,
culminating in the presentation of specific research and analysis tools.
The main distinguishing feature of SSM is its ability to determine what should be done,
rather than just how it should be done. This is a particularly strong characteristic when it
is combined with epidemiological tools and evidence to determine need for particular
interventions based on the likely benefit to the community and individual. SSM does
this through an exploration of a diversity of viewpoints as part of the decision-making
and intervention process (Flood & Jackson 1991: 168-171).
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
24
Flood and Jackson provide the following clear description of soft systems methodology
stages:
start with an unstructured problem situation;
work towards a problem situation expressed and name some relevant human activity systems;
formulate root definitions of relevant human activity systems;
undertake comparison of conceptual models of the system named in the root definitions;
undertake comparison of conceptual models with the expression of the problem situation;
discuss culturally feasible and systematically desirable changes;
take action to improve the problem situation.
(Flood & Jackson 1991: 39)
While not discarding the approach, which they believe is extremely adept at providing
creative solutions to problems depending on the environment and circumstances
practitioners may find themselves, Flood and Jackson recommend that SSM be used in
contexts in which there is a lack of agreement about goals and objectives among
participants, but where some genuine compromise is achievable. Complex-pluralist
contexts satisfy this requirement.
The principal criticisms of SSM by Flood and Jackson (1991:186-190) are couched in
terms of theory, methodology, ideology and utility. A significant criticism of SSM they
argue is its inability to conceptualise that individuals and groups can have real
differences that cannot be resolved within the existing political and economic structures.
Because the methodology fails to provide clear ground rules for participation it runs the
risk of supporting those in already powerful decision making positions. This criticism is
reminiscent of the one Lilienfeld (1978) directed at earlier systems theorists.
The methodological criticism of SSM is the dominance of the cultural metaphor over
the organismic metaphor. Again, the issue of how power is distributed within and
between organizations is discussed; in particular, SSM’s neglect of how the dominant
culture will decide the real feasibility and acceptability of a change. Flood and Jackson
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
25
(1991: 186-190) find the approach to be fundamentally idealist, with its emphasis on
autonomous ideas rather than recognizing the force of material and economic interests.
These views are probably a little harsh, given the general dominance of logic-driven
analysis in the decision-making processes of organizational management and the
feedback mechanisms inherent in SSM. Checkland’s achievement was to break away
from the hard systems approach of earlier theorists who regarded problems as real and
solvable, with their means-end approach.
Watson and Smith’s (1988) report on eighteen applications of SSM in Australia,
including two in the health sector, support the suitability of SSM for researching an
ambulance system in rural Australia. The first evaluated the operation of the
Community Health Program within the Australian Capital Territory and the second was
used to plan an integrated hospital management information system for the Health
Department of Western Australia. More recently, Hindle and Braithwaite (2001) have
written a manual on the use of soft systems methodology for Australian health care
professionals. They refine SSM to the four activities of finding out about the problem,
formulating activity models, using the models to debate the situation, and taking action
to improve the situation (Hindle & Braithwaite 2001: 24-25).
Davies and Ledington (1981) describe the use of the SSM within the setting of the
British Army. Davies tells the story of how she used SSM to describe the army’s system
of effectively training then losing highly skilled staff. This use of negative modelling
resulted in her exclusion from army property and restrictions being placed on contact
with army personnel. In a sense, it is a description of how not to deal with a client.
While Victoria’s ambulance services are uniformed and hierarchical in nature, it is
doubtful that the management personnel are equally sensitive to criticism. On the other
hand, some of the cultural characteristics of Australian ambulance services are derived
from military influences (Willis and McCarthy 1986; Audit Office NSW 2001).
Patching (1990: 106-113) provides a guide to building models using SSM. Of particular
relevance is his explanation of how to move from high-level models to a situation where
these simple representations of activities, resources, information and communications
links can be expanded to the point where all the activities that are desirable can be listed
and described. This in turn leads to identification of resource needs, measures of

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
26
performance, feedback and control mechanisms. While Patching warns that this
approach is tortuous, he argues that its strength is its ability to produce a list of factors
that are relevant to the organization examined. Through its ability to add flesh to the
theoretical situation, Patching’s approach effectively bridges the gap between systems
thinking and the real situation.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
27
2.3 Socio-political context
One way of getting a little closer to the research questions was to focus on the
underlying ideological and cultural forces at work in the State of Victoria (Figure 4).
While doing this, it was important to bear in mind that the concepts of ideology and the
underlying culture of a community are extremely difficult to separate and may be
legitimately treated as one. A useful definition of ideology comes from Sargent:
... a value or belief system that is accepted as fact or truth by some group. It is composed of sets of attitudes towards various institutions and processes of society. It provides a believer with a picture of the world both as it is and as it should be, and, in doing so, it organizes the tremendous complexity of the world into something fairly simple and understandable.
(Sargent 1972: 1)
Figure 4 State of Victoria in Australia
In the mid to late-1990s the driving force in government administration in the State of
Victoria was a mixture of economic rationalism and an entrepreneurial business style.
These ingredients formed the essence of the Liberal/National Party Government led by
Premier Jeffrey Kennett, which Hodge (2000) has described as the “ … fastest privatiser
on earth”. He saw the privatisation policies of the Kennett Government as part of a
bigger culture of domination and control prevalent at that time. To understand the
operation of the Victorian Liberal/National Party Government of the 1990s, I chose to
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
28
use two filters; the competitive imperative and the political dimension. Each provides a
means of understanding the pressures and constraints that have been placed on the
delivery of ambulance services in rural Victoria.
2.3.1 The Competitive Imperative
The dominant forces in the State of Victoria during the late 1990s were the orthodoxy of
economic-rationalism and the ascendancy of the Kennett Liberal/National Party
government (Hancock 1999: 1). In relation to the former, the most important tenet has
been the adoption of the National Competition Policy as espoused in the Hilmer Report
presented to the Council of Australian Governments in August 1993. The reform agenda
recommended by the Hilmer Committee was based on six principles:
1. Limiting anti-competitive conduct.
2. Reforming regulation which unjustifiably restricts competition.
3. Reforming the structure of public monopolies to facilitate competition.
4. Providing third party access to facilities that are essential to competition.
5. Restraining monopoly pricing behaviour. 6. Fostering ‘competitive neutrality’ between government and private business when
they compete. (Hilmer 1993)
The dominance of this economic-rationalist agenda is highlighted in the discussion
paper of the Department of Human Services, reviewing the Ambulance Services Act
1986 (DHSV 1998: 10). The Review itself was charged with the responsibility of
considering three key issues:
the contestability of ambulance services;
broad structural alternatives; and
the regulatory and purchasing framework. (DHSV 1998: 10).
Hancock (1999: v-viii) considers this market approach of running health care as a
business a ‘transient fashion’, with health policy now passing into a ‘post-market era’
characterized by a greater emphasis on public health, collaborative partnerships and
public involvement. Her view is debatable, given the strengthening of the private health
sector as a result of strong Federal Government support for private health insurance at
the expense of the public health system (Palmer & Short 2000: 67). Hancock concedes
that there have been useful outcomes from the market approach to health care. These
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
29
include a clearer specification of service goals, better planning and performance
indicators, and the design of services that respond to the needs of users. The negatives
have been the higher transaction costs of real or quasi markets, the loss of citizenship
and the damage to service ethos and morale.
In spite of its underlying ideological premise, the Department’s discussion paper
provides a good overview of the ambulance services in Victoria at that time, along with
a basic contextual description in regard to the National Competition Policy and the
wider health sector. It is also a valuable reference as it discusses the significant
differences between metropolitan and rural ambulance services; it highlights the
challenges rural services face and some of the opportunities for innovative solutions.
An important theme is the acknowledgement of differences between rural and metropolitan markets for ambulance (and other) services in terms of demographics, economies of scale and scope, utilisation rates and social issues. The key question appears to be the extent to which there are opportunities for the closer integration of, and greater cooperation with, other emergency and human services in rural areas.
(DHSV 1998: 11)
In describing the components of the Ambulance Services Act 1986, the paper also
proposes six alternate models of service delivery from a ‘competition’ perspective:
Single Statutory Authority; Statutory Authority with Ring-Fenced Business Unit;
Purchaser and Provider; Funder, Purchaser and Provider; Multiple Geographic
Franchises and Unbundled Service Contracts (DHSV 1999: 38-39).
i) Single Statutory Authority
This has been the traditional model for the provision of ambulance services in Australia.
Victoria has been the only Australian State to resist the concept of a ‘single-service’
structure for its ambulance service. A statutory authority pursues a charter to provide
services, balancing regulatory, purchaser and business objectives. From a ‘competition’
perspective, this model creates a problem when there are also private providers who are
subject to the statutory body’s regulatory regime. It may be an attractive structure where
increased contestability is not thought to provide significant net public benefit.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
30
ii) `Statutory Authority with Ring-Fenced Business Unit
Under this structure, the provider function is operated as a separate internal business
unit with a degree of management autonomy. In the early 1990s a variation of this
approach was attempted within the Metropolitan Ambulance Service in Melbourne – it
was later abandoned for a more integrated management system. It is considered a more
acceptable ‘competition’ structure than the traditional model as it internally separates
the purchaser and provider functions.
iii) Purchaser and Provider
Under this alternative, there is a clear split between the purchaser/regulatory role and
the provider role. The government takes the purchaser/regulatory role and the provision
of services is undertaken by a separate entity – usually a Government Business
Enterprise. A service contract exists between the purchaser and the provider. This model
implies that a monopoly license would be granted. This alternative is suitable when
there are strong synergies and economies of scale and scope in the provider’s operation
that may be lost under more aggregated models.
iv) Funder, Purchaser and Provider
Under this arrangement, the government as funder enters into a high-level purchasing
agreement with the purchaser, who enters into more detailed contracts or agreements
with the provider. An example of this model is the relationship between the
government, a regional health care authority and a hospital. A criticism is the high
transaction costs that characterize this structure, particularly when smaller contracts are
involved.
v) Multiple Geographic Franchises
Individual providers are given the exclusive rights to operate within a defined
operational area. While there are opportunities to benchmark services, there are
problems when the operational zones overlap. In Victoria before the 1987
regionalization of the previous 16 services into six regions, these ‘territorial’ issues
characterized and in some cases dominated the relationships between at least some of
the District Services providing services in ‘exclusive’ geographic zones.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
31
vi) Unbundled Service Contracts
Under this model the ambulance service is unbundled into a number of elements, which
may be operational capabilities or support services. The purchaser assumes strong
central coordination. A variation of this approach is seen in the Melbourne Metropolitan
Ambulance Service which has unbundled routine transport services, dispatch systems
and fleet management to the private sector, while maintaining overall control of the total
ambulance system.
While the Department’s discussion paper acknowledges some shortcomings of
competitive markets in the health sector, each of the alternate models adopt the
principles of the National Competition Policy that have underpinned the general thrust
of the health reforms in Victoria. These reforms have seen a shift towards
purchaser/provider splits, increasing focus on output-based service contracts, and
greater involvement of the private sector through capital investment and the provision of
services (DHSV 1998: 19).
Apart from the ideological flavour of these alternatives, the discussion paper also
identifies three important issues that cut across these and other alternate models of
service delivery. These are:
Synergies and integration – are there potential synergies from greater integration with other emergency services or the health sector?
Community involvement – are there ways to retain the benefits of community involvement within a competitive framework?
Transitional issues – if there is to be change, how can it be managed to minimize key risks?
(DHSV 1998: 12)
These three issues are addressed in the thesis as important components of alternate
models of service delivery in rural Victoria. The first is critical to the effective
performance of the whole emergency health system response to acute injury and illness.
However, opportunities for ambulance services to develop synergies with health and
emergency services through integration are scarce in rural towns without hospitals.
While other emergency services, which are often voluntary, offer only restricted
opportunities for professional interaction in most rural towns (Allen Consulting 1999:
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
32
77). The second is crucial when considering the long-term viability of the different
models of service delivery. It is known that the level of community involvement and
acceptance of service delivery models is vital to the sustainability of rural health
services (Reich 1991; Harvey et al 1995; NRHA 1998; Humphreys & Mathews-Cowey
1999; Bryant & Strasser 1999). The third issue acknowledges the social and cultural
problems associated with implementing changes to service delivery models.
Even those advocating the adoption of market mechanisms for the provision of
emergency ambulance services have acknowledged the distinction between urban and
rural environments (Allen Consulting 1999: 38-39).
Larger and more concentrated populations in metropolitan areas provide for economies of scale in service delivery compared to smaller, more dispersed populations in rural areas. This is particularly important where there are large increments of supply and/or fixed costs relatively large compared to the size of the market.
(Allen Consulting 1999: 38)
2.3.2 The Political Dimension
The second major force impacting on rural ambulance services in Victoria has been the
radical State government led by Premier Kennett. This Government dominated the
ideological and cultural agenda in Victoria from its first election victory in 1992 until its
demise in 1999, with its emphasis on what it saw as service efficiency and value for the
tax-payer. This economic rationalist approach to government arguably allowed the
dominant elite to marginalise concerns about equity, fairness and a sense of community.
The ideological and cultural position of the Kennett Government, along with the
prevailing confidence in managerialism would have had little practical impact on social
policy without the government possessing real power. Between its initial election in
1992 and its fall from power in 1999 the Kennett government had a disproportionate
share of formal power at its disposal; having a large parliamentary majority in both
Houses of Parliament made it unusual amongst Australian State governments, which
generally face hostile upper houses. Queensland is the exception, with its unicameral
parliament. This concentration of power weakened the pluralist nature of the decision-
making environment, with it tending more towards an elitist system. The major source
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
33
of power was seen to be personality – Kennett had a crash through approach – self-
confidence, and self-righteousness. Kennett has often been compared with former
British Prime Minister Margaret Thatcher in terms of ideology, outlook and style.
Amongst the Government’s aims was the desire to reduce the power of public sector
unions in Victoria, including the Ambulance Employees Association (Forbes 1999;
Hodge 2000). However, this political-industrial agenda needs to be placed in
perspective. For no matter how strongly the Ambulance Employees Association may
have felt persecuted, the foundations of the Kennett government’s ‘Contract State’
rested on a substantial ideological foundation unrelated to the existence or activities of
one small union representing ambulance service employees. It is unlikely that there was
any special Government pre-occupation with the Ambulance Employees Association
amongst the many public sector unions that opposed the Government’s ideological
position.
The Kennett reform efforts of the public sector in Victoria were more about a
redistribution of power than about economics. For the critics of the reforms, a key
lesson in Victoria was “ … that when government ideology takes over from sensible
organisation and business operations, government itself becomes dumbed down and
hollowed out” (Hodge 2000).
Alford and O’Neill (1994) describe these ideological foundations of the Kennett
Government, linking them to the managerialist model of government instituted during
the Cain Labor government of the 1980’s and more particularly to Osborne and
Gaebler’s, Reinventing Government (1993). This approach to government inspired the
Victorian Commission of Audit (1993) to adopt ‘three principles’ for structuring
government. Firstly, that each government Department would be responsible for setting
policy, regulating and ultimately contracting for the provision of goods and services.
Under this principle the Department contracting for the provision of services would be
clearly separated from the organizations providing the goods and services. This is
described as separating the ‘steering’ from the ‘rowing’. The second principle is the
emphasis on outcomes or outputs rather than funding inputs such as wages and salaries.
And finally, the government should foster competition between organizations supplying
or providing goods and services (Alford & O’Neill 1994: 5).
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
34
From the Audit Report, the Victorian Kennett Government developed a Management
Improvement Initiative (Alford & O’Neill 1994: 4-5), which elaborated five policy
principles for public sector reform:
1. Focus on clear responsibility and accountability for results;
2. Empowering consumers;
3. Minimizing government bureaucracy;
4. Preference for market mechanisms; and
5. Professional and business-like management of public agencies.
According to Osborne and Gaebler (1993: 32), the benefits to government of the
separation of policy decisions from service provision are considerable. For example,
alleged benefits include allowing policy makers to concentrate on overall direction,
without being caught up in operational management matters or coming under undue
influence from sectional interests such as unions and consumer groups. This
marginalisation of the consumer seems to be at odds with the second of the
Management Improvement Initiative policy principles of empowering consumers.
Osborne and Gaebler also suggest that competition between providers can be used to
overcome resistance to change in the public sector and the public service.
The implementation of the Commission of Audit principles produced a loss of
government services in many parts of rural Victoria, where communities saw the
closure of hospitals, schools and other community services throughout the term of the
Kennett Government. Similar policies at the National level added to this deleterious
impact on rural infrastructure.
While the community ‘backlash’ against the Government and other unpopular large
institutions, such as banks, had been noisy until the 1999 Victorian State Election, it
was generally insufficient to reverse the direction of the Government’s reform program.
In 1996 the first of two rural independent members of Parliament was elected, closely
followed by the second at a by-election. At the 1999 election these two rural
independents were re-elected and joined by a third. As a result of this ‘community
anger’ in rural Victoria being converted into a more general swing away from the

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
35
Liberal and National Parties, the Kennett Government fell. The outcome of the election
was a minority Labor Government, reliant on the support of the three rural
independents. A major plank of this alliance between the Labor Party and the
independents is the “Charter for Good Governance” (Hodge 2000); it includes specific
reference to the administration of the Metropolitan Ambulance Service contracts for
outsourcing their dispatching system. One of the first decisions of the new Labor
administration was to establish a Royal Commission into outsourcing in the
Metropolitan Ambulance Service. It subsequently had its terms of reference diluted and
changed before it reported.
The operations of rural ambulance services were disrupted and destabilized either
directly or indirectly as the result of the former Government’s actions – manifested
mainly through industrial action. However, the changes to the ambulance services were
largely restricted to the centralization of dispatch systems, changes of management and
pressure on support services. In fact the changes have been more substantial since the
change of government with the amalgamation of the previous regional services into
Rural Ambulance Victoria and an increase in government expenditure (DHSV 2000).
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
36
2.4 Health policy context
2.4.1 Health or Public Safety Paradigm?
Australia’s ambulance service delivery systems operate within the broad contexts of
both the health system and the public safety system. An example of the former is the
role of the ambulance service as a component of the emergency trauma system in each
State. Another way of describing the ambulance service, to borrow the term from
Baume (1995), is as a provider of ‘salvage medicine’ dealing with the downstream
consequences of disease and illness. While not what many would like to hear, it is in
some sense an accurate description of a service established to react to others’ crises.
These larger health systems are all encompassing and are not confined to rural areas.
The National Rural Health Alliance (1999: 21) has recognized the futility of rural and
remote Australia addressing its health needs in isolation from the broad health system.
There is however, a need for metropolitan-based health services and professionals to
improve their understanding of rural health issues and directions.
Unlike in many comparable countries, the Australian ambulance system is deeply
embedded in the wider health and medical system, rather than the public safety system,
with its emphasis on law enforcement and fire fighting. Because of this relatively strong
connection with the health system, Australian ambulance services have been largely
spared the fragmentation that has beset American pre-hospital systems. They may be
operated through fire departments, hospitals or the private sector and have as a result
been described as lacking “… a strong, cohesive identity” (Erich 2001). One
manifestation of this Australian ambulance connection with the health system, is
demonstrated in the education of ambulance officers and in a common occupational
culture that is shared to some extent with both medicine and nursing. This close
connection with the health sector has both advantages and disadvantages from a
planning and management standpoint. From a research perspective, comparisons with
ambulance systems in other countries need to be treated with caution; in particular,
when considering their organizational and cultural characteristics.
In the United Kingdom, Nicholl et al (2001:4) have recommended that ambulance
services need to integrate even more with other health care providers and to extend their
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
37
clinical role in caring for patients. This includes the implementation of the idea of
Practitioners in Emergency Care who cross the boundary between paramedics and
nurses. They report that:
There is widespread agreement within Ambulance Service [sic] that the Ambulance Service should become the emergency arm of the health care services rather than the health care arm of the emergency services.
(Nicholl et al 2001: 11)
In Australia, Field (1994), Wellard (1995) and Butson (1999) identify the tension
between the health and public safety paradigms. They all identify the future place of
ambulance within the health system. Like most other components of the health sector,
the Ambulance Service is based on the ‘medical model’ of service delivery, with a
strong reliance on the use of technology and the associated technical skills. Daniel’s
study of how medical dominance developed and has been maintained in the health
sector is of importance when considering the emergence of both a strong industry union
and the emergence of a ‘professional’ culture in the Victorian Ambulance Service
(Daniel 1993). For example, the ambulance union appears to have borrowed the
Australian Medical Association’s tactics of using the media to achieve its industrial and
political ends.
At the professional end of the spectrum, the Australian College of Ambulance
Professionals has adopted a Code of Ethics not dissimilar to medical and nursing
professional bodies. Willis and McCarthy (1986) provide a sociological account of the
development of ambulance providers as health professionals from their blue-collar
origins. Mayski (1999) has attempted an examination of the culture influences on the
members of the Melbourne Metropolitan Ambulance Service using the variables of
mission, consistency, involvement and adaptability.
These steps toward professionalisation within the ambulance sector follow the lead of
other professionals. Like ambulance paramedics, these professionals have historically
asserted their autonomy through the establishment of ‘self-regulation’ and control of
their work (Friedson 1970). Hancock reports on the shifting of the power base within
the health system with the emergence of other health professions such as nurse
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
38
practitioners and a general erosion of the status of professionals generally amongst a
more educated and informed public (Hancock 1999: 42-47).
The distinction between the health system and the public safety system is important, as
interpretation of the ambulance system is partially dependent on where the provision of
ambulance services is placed. Is it a health service, or an emergency service? Palmer
and Short help locate the ambulance service in the health system when they distinguish
health policy from general public policy on the basis of:
the dominant role of the medical profession in shaping and constraining health policy;
the complexity of health care provision, which makes the application of competitive models without substantial modifications fraught with difficulty when consumers suffer from information asymmetry;
the nature of decision-making in health matters, where life and death may be involved, leads the community to see health care and its providers in a different light to other goods and services.
(Palmer & Short 1994: 26)
These three criteria are met within the ambulance service system of service delivery.
The medical profession does constrain the policies of the ambulance system through the
control of training standards and the restriction of treatment protocols, there are clearly
problems with competition models (particularly in rural areas), and life and death is an
issue for the providers and the community. The restraining role of the medical
profession is addressed in Chapter 2.5.1.
Palmer and Short (1994: 29-32) describe the nature of decision-making, introducing the
concept of a systems model of decision-making. Like Simeon (1976), they acknowledge
the influence of the wider social, economic and technological contexts in which the
health system operates. In particular, they note the ability of powerful interest groups to
shape the agenda (Palmer & Short 1994: 35). Daniel raises the importance of history to
inform research and the centrality of culture when carrying out health research (Daniel
1993: 10-11). This latter point is very relevant when researching an organization as
traditionally based as the ambulance service, with its hierarchical structure and culture
of rugged independence (Willis & McCarthy 1996; Bird 1999; Audit Office NSW
2001).
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
39
2.4.2 Rural Health Environment
In order to better understand the operation and planning of rural ambulance services, it
was essential to contextualise their operation. Like all rural health services, the
geographic, economic and political context in which they operate is a major influence
on their performance. Beaulieu and Berry (1994) describe the common problems that
health services face in the rural areas of the United States. While the various regions and
areas in rural Australia may differ in the specifics, they share many of the difficulties in
the United States, such as:
low population densities;
long distances;
poor roads and/or rough terrain;
lower levels of health care;
older population;
lower income and insurance cover;
hazardous occupations; and
undersupply of health professionals & facilities.
(Bealieu & Berry 1994: 136)
The Australian Institute of Health and Welfare (AIHW) provide a quantitative picture of
the health and welfare of rural Australians. Using socio-demographic, hospital and
Medicare data they describe rural and remote communities with markedly different
health status and needs from those in metropolitan areas (Strong et al 1998). From an
ambulance perspective, the most significant findings are the significantly higher injury
and motor vehicle accident rates in rural Australia. Despite these findings, the AIHW
made no attempt to analyse the need for, or use of, ambulance services in rural
Australia. This same omission is apparent in the National Rural Health Alliance Healthy
Horizons paper, even after noting the difficult task of retaining safe emergency and
urgent care services for Australians living in rural, regional and remote Australia
(NRHA 1999: 1).
The AIHW uses a comparison of Australian Bureau of Statistics’ mortality and
morbidity statistics across Rural, Remote and Metropolitan Areas (RRMA) to highlight
the verifiable disadvantage suffered outside the metropolitan areas of Australia. Table 3
provides a summary of its structure. While the classifications themselves, which were
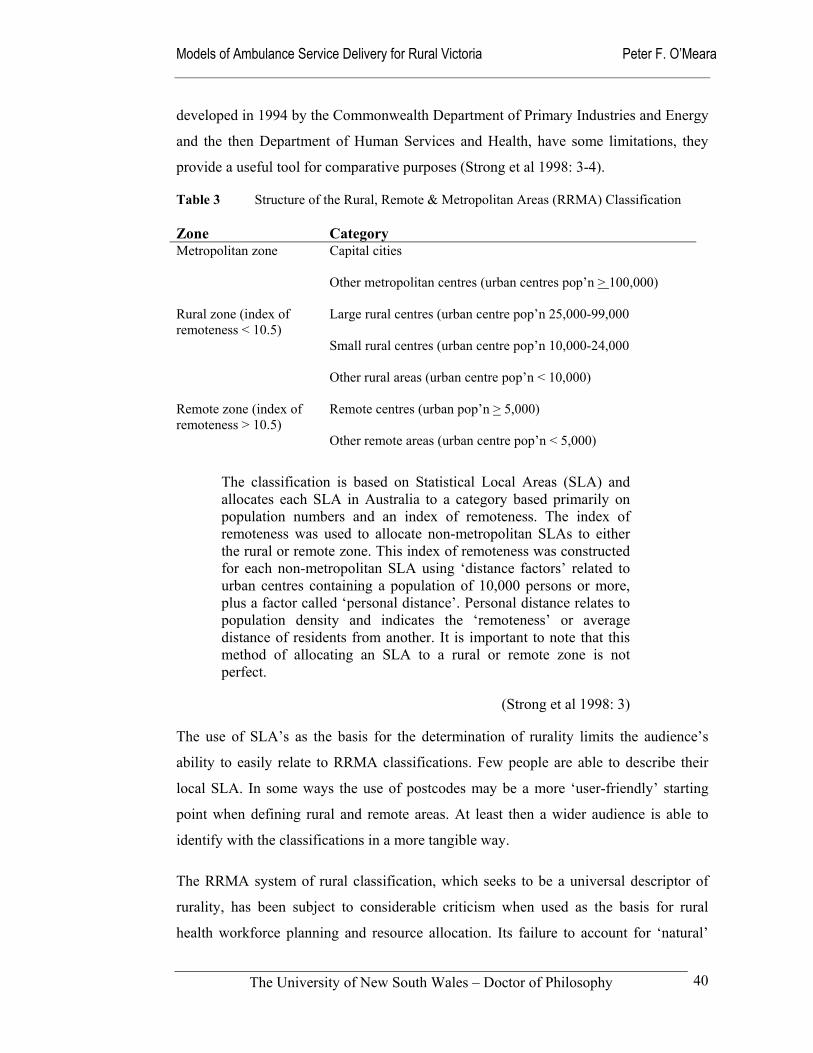
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
40
developed in 1994 by the Commonwealth Department of Primary Industries and Energy
and the then Department of Human Services and Health, have some limitations, they
provide a useful tool for comparative purposes (Strong et al 1998: 3-4).
Table 3 Structure of the Rural, Remote & Metropolitan Areas (RRMA) Classification Zone Category Metropolitan zone Capital cities
Other metropolitan centres (urban centres pop’n > 100,000)
Rural zone (index of remoteness < 10.5)
Large rural centres (urban centre pop’n 25,000-99,000
Small rural centres (urban centre pop’n 10,000-24,000
Other rural areas (urban centre pop’n < 10,000)
Remote zone (index of remoteness > 10.5)
Remote centres (urban pop’n > 5,000)
Other remote areas (urban centre pop’n < 5,000)
The classification is based on Statistical Local Areas (SLA) and allocates each SLA in Australia to a category based primarily on population numbers and an index of remoteness. The index of remoteness was used to allocate non-metropolitan SLAs to either the rural or remote zone. This index of remoteness was constructed for each non-metropolitan SLA using ‘distance factors’ related to urban centres containing a population of 10,000 persons or more, plus a factor called ‘personal distance’. Personal distance relates to population density and indicates the ‘remoteness’ or average distance of residents from another. It is important to note that this method of allocating an SLA to a rural or remote zone is not perfect.
(Strong et al 1998: 3)
The use of SLA’s as the basis for the determination of rurality limits the audience’s
ability to easily relate to RRMA classifications. Few people are able to describe their
local SLA. In some ways the use of postcodes may be a more ‘user-friendly’ starting
point when defining rural and remote areas. At least then a wider audience is able to
identify with the classifications in a more tangible way.
The RRMA system of rural classification, which seeks to be a universal descriptor of
rurality, has been subject to considerable criticism when used as the basis for rural
health workforce planning and resource allocation. Its failure to account for ‘natural’

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
41
boundaries, liveability or environmental attractiveness of rural areas is considered a
weakness (Humphreys & Mathews-Cowey 1999).
Having noted some of the limitations and difficulties with the RRMA classification,
there are no other entirely satisfactory substitutes available at this time. Faulkner and
French in 1983 made an attempt to develop an index of remoteness based on population
and distances to urban centres. Griffith proposed a system using Census Collection
Districts as its basic unit, rather than the heavily criticised SLA’s. Fragar (1997) has
developed another classification system based on industry or commodity type
predominant in an area.
The University of Adelaide, National Key Centre for Social Applications in Geographic
Information Systems, has developed a new classification system which will allow the
investigation of population, industry, and geographical characteristics in a flexible way
and not be reliant on fixed boundaries (NRHA 1999: 1; Hugo 1999). The
Accessibility/Remoteness Index of Australia (ARIA) model was developed on the basis
of a geographical approach, which defines remoteness in terms of environmental
parameters influencing access on a scale of zero to twelve (GISCA 1999: 6). Its
proponents claim that ARIA “… was designed to be comprehensive, sufficiently
detailed, as simple as possible, transparent, defensible, and stable over time; and makes
sense ‘on the ground’…” (GISCA 1999: 2). It is proposed that ARIA replace the well-
established RRMA classification system as the accepted rurality framework for health
service planning (Best 1999).
In the United States, Ricketts et al (1998) describe the two major definitions of rurality
from the Office of Management and Budget, and from the US Bureau of Census. In
common with the Australian experience:
Neither of these two principal, nationally-applicable definitions completely and adequately captures the essence of what is rural nor provides a universally-applicable methods that precisely separates urban from rural populations or places.
(Ricketts et al 1998: 1)
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
42
A Canadian, Rourke (1997) makes the point that when defining ‘rural’ we are faced
with the challenge of perspective, which is dependent on person, place and context. He
describes three factors, community and lifestyle, nature of rural practice, and
professional isolation and support. These factors are derived from rurality indices and
models from Canada, New Zealand and Australia. While the concepts are designed for
general practice, they are useful for the analysis of rurality in ambulance services when
considering the issues of recruitment and retention of the workforce.
However, it is equally important that the rural environment and the health system
environment be studied within its socio-economic, political and demographic contexts.
Throughout the 1990’s John Humphreys and his co-writers (Humphreys & Rolley 1991;
Humphreys & Weinand 1991; Humphreys et al 1992; Humphreys 1993; Humphreys et
al 1996; Humphreys 1998; Humphreys & Mathews-Cowey 1999) have provided the
broadest descriptive and analytical accounts of the rural context in which health services
operate.
Rural health researchers in Australia have been informed by a five-yearly census
providing statistics relating to the differences between urban, rural and remote
population characteristics. They have also followed up these data with qualitative
research examining rural perceptions of their health and health service needs through
the eyes of both health professionals and rural residents. Humphreys and Weinand
(1991: 734) found that the most valued health services in country towns are doctors and
hospital services, with pharmacy and ambulance services rating at equal importance just
below the first choices. Dentists, social workers and community nurses are rated as
relatively unimportant. Reid and Solomon (1992) reported similar findings.
In 1988 Kelleher summarized the health problems of rural areas and the deficiencies in
health service provision – in particular in rural towns of less than 10,000 people. He
highlighted the primacy of politics and economics when trying to understand rural
health (Kelleher 1988).
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
43
The public health problems of rural Australia so often mask political and economic problems of a national kind. Rural Australia as a region, has been in economic decline since the mid to late sixties. Some argue that the process began even earlier than this. The health problems in the country reflect this process of marginalisation. The service provision problems, however, have additional underlying reasons for their inadequacy. Problems in service provision so often mask ideological and political bias of interest groups which are urban based and who favour interventionist and technology orientated programmes. Rural dwellers and those health and welfare professionals who represent them are up against lobby groups with greater resources and influence than they.
(Kelleher 1988: 6)
As a result of these and other studies, political pressure and the continuing health deficit
in rural and remote Australia, Governments have come to recognize that metropolitan
solutions and rigid guidelines cannot always be successfully applied in rural, regional
and remote communities. Health providers and communities must be able to develop
solutions and service models that reflect their needs and circumstances (NRHA 1999:
14). The National Rural Health Alliance suggest that guidelines for the provision of
quality health services in rural areas should include:
Clinical standards;
Service benchmarks;
Performance indicators; and
Accreditation standards. (NRHA 1999: 15)
Dunne et al (1994) provide an example set in Tasmania of a needs analysis of health
service provision in rural and remote areas. It is a benchmark study that employs socio-
economic and demographic research tools to study the quantitative data and qualitative
data derived from questionnaires and interviews with general practitioners, other health
providers and community representatives. As they express it:
Our findings provide a model for further studies of the health needs of rural and remote communities, using the perceptions of local GPs and other health providers together with available secondary data.
(Dunne et al 1994)
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
44
It is within this broad policy context that the ambulance services operate in the rural
environment. Significant characteristics of this rural context in the late twentieth/early
twenty-first century include declining rural economic activity, decaying infrastructure,
ageing demographics and a growing sense of isolation (Harrison 1997).
The National Rural Health Association in the United States (NRHA-US 1998) and a
range of Australian writers (Harvey et al 1995; Humphreys & Mathews-Cowey 1999;
Bryant & Strasser 1999) emphasise the importance of this economic and social vitality
to the health and effectiveness of the rural health system. Reich (1991) links the same
issues to the sustainability of small rural ambulance services in the United States. It is
the strength of rural communities themselves as the organizing and sponsoring entities
that are so important in rural areas. Humphreys and Mathews-Cowey (1999: ix & xv)
identified eight critical components associated with the provision of appropriate and
effective delivery of health care. This included the involvement of the community in
each stage of the planning approach, with customers involved in the determination of
their needs and the selection of the model that may work best for them. The National
Rural Health Association in the United States provides a set of principles that correlate
with community success in sustaining rural health systems that can be used as a guide
for community providers to compare their efforts, choices and decisions. These
sustainability principles are:
Broad community-wide support for and participation in the work to sustain local health services.
Local control of the elements of the delivery system - both institutions, such as hospitals and long-term care facilities, and provider practices.
A bold vision of both the desired local services and the degree of local control, as well as assertive advocacy on behalf of this vision.
Effective local health care leadership, especially from physicians and other providers.
High level of teamwork, respect and collaboration among community providers.
A willingness to take risks on behalf of their vision - in contrast to risk aversion behaviours that paralyze efficient and timely community decision-making.
Willingness, in the current environment, to be open to partnerships and affiliations with other regional providers and with value-compatible urban providers.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
45
Access to relevant, practical information and successful rural models.
Successful coordination and control of local health care dollars, both through expanding the range of services and the market share, and by assuming appropriate levels of financial control and financial risk.
Well informed community providers and residents about state and federal policies that impact rural health services.
(NRHA-US 1998)
Hancock (1999: 7-10) covers similar ground to the American NRHA when suggesting
ten criteria for evaluating health policy generally. These evaluation criteria are useful
analytical signposts and are re-visited in Chapter 7.
These observations about health services generally and rural health services in
particular, need to be considered when examining rural ambulance services in terms of
their context, activities, and the available research on current performance and future
developments. On the other hand, a more aggressive approach can be taken on the
variations in the provision of health services. In a recent investigation into ambulance
services in the United Kingdom Nicholl et al (2001) do not explicitly consider rural and
remote ambulance service provision; however they make the strong point that:
‘Post-code prescribing’, by which is meant geographic variations in health care policy and practice, is no longer politically or socially acceptable. It is expected that the same services and treatments will be available to all NHS patients wherever they live.
(Nicholl et al 2001: 24)
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
46
2.5 Ambulance context
Prima facie, the literature relating to the management and operation of ambulance
services and emergency medical services are the most important source of insight into
the topic of determining service delivery models in rural ambulance services. If the
disciplines of pre-hospital or ambulance research were more mature, this preliminary
observation may have a greater degree of validity.
A number of writers in Australia, the United States and the United Kingdom lament the
lack of pre-hospital research and discuss the barriers to ambulance managers and
paramedics undertaking research. The main reasons given are the lack of a developed
research culture and the dearth of research skills amongst ambulance professionals
(Johnson 1991; Callaham 1997; Cooke & Wilson 1999; Woollard et al 2000; Jacobs
2000; Brice et al 2000). Australian accounts of ambulance practice tend to concentrate
on the education and training of ambulance professionals (Wellard 1995; Bailey 1996;
Lord 1998; Field & Lord 1999; Field et al 1999).
Apart from these education and training-focused accounts, the Australian research
literature related to ambulance service delivery consists of little more than a number of
weighty official reports. These have been produced as a result of government reviews
and inquiries (ASNSW 1992a; Capp 1992; Diagnosis 1992; Health Solutions 1992;
PIIC 1992; Baragwanath 1997a & 1997b; DHSV 1998a; Allen Consulting 1999; Audit
Office NSW 2001). These official reports are largely descriptive in nature. While of
considerable value as historical records, they generally suffer from a lack of strong
direction and clarity of thought. They tend to be atheoretical and instrumental in nature.
Like many official reports, they tend to provide the answers the government of the day
wants.
Moving beyond these descriptive reports and articles, the remaining literature can be
categorized according to the epidemiological, bio-medical and systems paradigms and
the literature that looks toward future developments in service delivery models. While
the epidemiological and bio-medical factors are important and are called upon to
support and strengthen the thesis findings and conclusions, as noted above the
concentration here is on the systems paradigm which has the role of bringing the
epidemiological and bio-medical together.
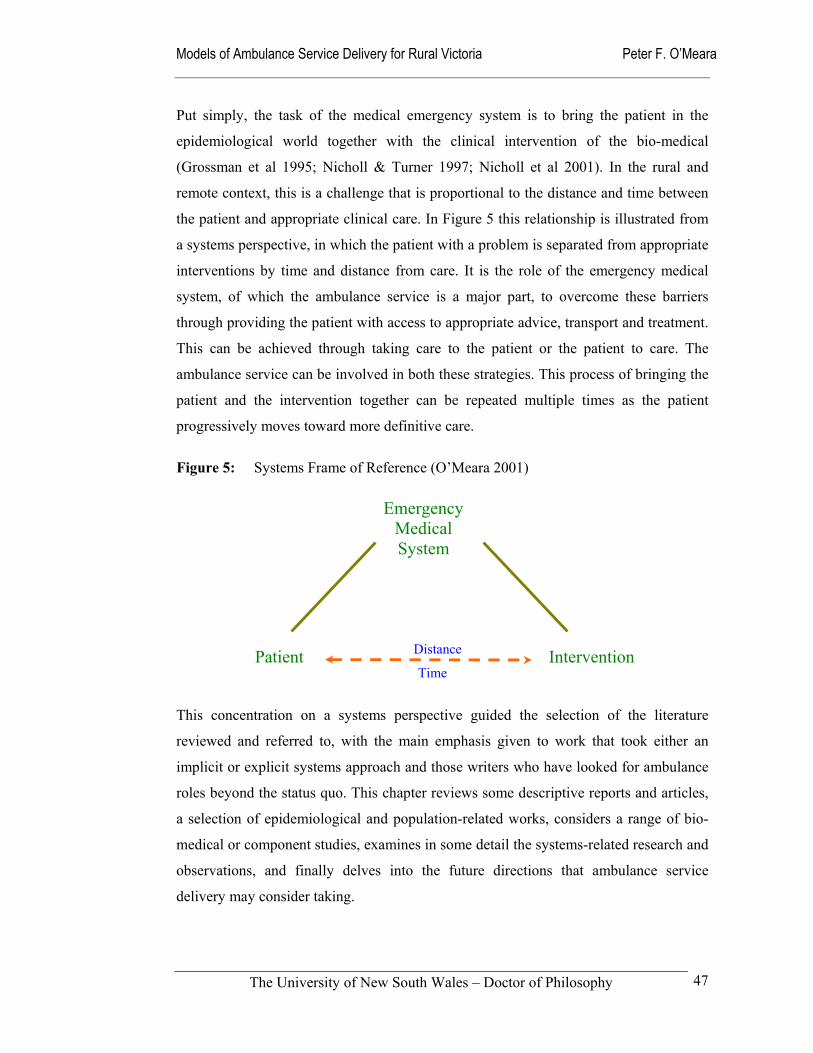
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
47
Put simply, the task of the medical emergency system is to bring the patient in the
epidemiological world together with the clinical intervention of the bio-medical
(Grossman et al 1995; Nicholl & Turner 1997; Nicholl et al 2001). In the rural and
remote context, this is a challenge that is proportional to the distance and time between
the patient and appropriate clinical care. In Figure 5 this relationship is illustrated from
a systems perspective, in which the patient with a problem is separated from appropriate
interventions by time and distance from care. It is the role of the emergency medical
system, of which the ambulance service is a major part, to overcome these barriers
through providing the patient with access to appropriate advice, transport and treatment.
This can be achieved through taking care to the patient or the patient to care. The
ambulance service can be involved in both these strategies. This process of bringing the
patient and the intervention together can be repeated multiple times as the patient
progressively moves toward more definitive care.
This concentration on a systems perspective guided the selection of the literature
reviewed and referred to, with the main emphasis given to work that took either an
implicit or explicit systems approach and those writers who have looked for ambulance
roles beyond the status quo. This chapter reviews some descriptive reports and articles,
a selection of epidemiological and population-related works, considers a range of bio-
medical or component studies, examines in some detail the systems-related research and
observations, and finally delves into the future directions that ambulance service
delivery may consider taking.
Figure 5: Systems Frame of Reference (O’Meara 2001)
Distance
Time
Emergency Medical System
Intervention Patient
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
48
2.5.1 Descriptive Reports
In the Victorian context, a number of the reviews and reports that have been
commissioned in recent years – for instance, those commissioned by the Victorian
Ambulance Services’ Association (VASA) – remain closed to researchers for reasons of
‘commercial confidentiality’. This is unfortunate, as the VASA reports, even with their
narrow focus on efficiency, constitute one of the few specific research efforts into rural
ambulance services in Australia. This culture of ‘secrecy’ in the State of Victoria, has
been commented on by the former Victorian Auditor General, who criticized the former
Government’s interests for overwhelming the public interest (Baragwanath 1997a &
1997b). The change to the Brack’s Labor Government in 1999, has tended to unravel
this shroud of secrecy over time.
With the exception of Government and Parliamentary inquiries, such as those conducted
by the Victorian Auditor General, there have been few reviews of Ambulance Services
as systems. The last public review of the Ambulance Services in Victoria was in 1992.
This recommended that Victoria’s Ambulance Services be amalgamated into one state-
wide service, consistent with that operating in other Australian States (Capp 1992).
Australia’s largest State, New South Wales, also experienced a major government
initiated inquiry into the delivery of ambulance services in the same year (ASNSW
1992a). Since then there have been two confidential reports (KPMG 1997, Coopers &
Lybrand 1997) into Victoria’s rural Ambulance Services recommending the
amalgamation into one rural Ambulance Service. The result of these inquiries was the
formation on 1 March 1999 of Rural Ambulance Victoria, an amalgamated rural
ambulance service. The Victorian Auditor General has also inquired into Victoria’s
metropolitan and rural ambulance services (Baragwanath 1997a & 1997b). Other
Australian States have also seen official inquiries carried out since the 1980s, with the
most recent being in New South Wales (Audit Office NSW 2001).
Beaulieu and Berry (1994) describe rural emergency services in the United States,
including both pre-hospital and in-hospital systems. After describing the elements of an
Emergency Medical System (EMS), they explain the trends in rural America including
the growing need of hospitals and ambulance services to coordinate their efforts and
develop a ‘peaceful co-existence’ through co-operation (Beaulieu & Berry 1994: 153).

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
49
They outline four different conceptual models (Table 4) based on the two variables of
organizational choice and environmental determinism.
Table 4 Beaulieu and Berry’s EMS Models
Model Description
Natural selection Achieved through market forces without government regulation or attempts to view health care as justifying certain exceptions to market assumptions.
Differentiation Exists in a ‘competitive’ environment with considerable regulation defining the ‘rules of the game’.
Strategic choice Characterized by a maximum of choice and is more prevalent in high population areas with a minimum of competition, where change is affected by design in a benign environment.
Undifferentiated choice Characteristic of health services in remote areas, where the services offered may fail to meet the needs of the community because of limited resources.
(Adapted from Beaulieu & Berry 1994: 146-150)
Narad (2000) approaches the emergency medicine organizational structures from the
same market-oriented approach when describing emerging structures in the United
States. He cites emerging models such as consolidated ambulance services and
networks, demand management programs and public-private joint ventures. Using a
more historical approach, Eisenberg et al (1996) describe the evolution of pre-hospital
cardiac care in the United Kingdom and the United States. The radical break from the
then existing practices was the establishment in 1966 of a pre-hospital cardiac care
system in Belfast to resuscitate sudden cardiac arrest victims. While the concept was
widely adopted in the United States and elsewhere, the Belfast physician-staffed model
was not widely imitated. In common with the current Australian situation, paramedic-
staffed programs were implemented in the United States in cities like Seattle where the
concept of the ‘tiered response’ was developed. Unlike the situation in Australia, most
of these early American paramedic programs were based in fire departments.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
50
While the American models of service delivery have a strong influence on Australian
practices and systems, this is not necessarily the case in many other countries. In
Europe, physicians and nurses continue to play a major role in pre-hospital services.
France for instance operates a two-tier system, with basic life support (BLS)
ambulances run by the fire department and advanced life support (ALS) ambulances run
by hospitals. Aggressive physician-operated triage results in only 65 percent of requests
for service resulting in the dispatch of an ambulance. Apart from this significant
difference from the North American system and the Australian service delivery models,
the major distinguishing factor of the French system is its staffing of the ALS
ambulances, namely a driver, plus a physician on a 24-hour basis (Nikkanen et al 1998).
This physician dominated system is unlikely to change in the near future as ... sentiment among physicians still runs against releasing control of what they consider the exclusive purview of physicians.
(Nikkanen et al 1998)
Wright et al (2000) describe a similarly physician-dominated system in the Ukraine, in
which doctors and nurses staff ambulances. Ukrainian doctors complete 18 months of
additional training for the role. Van Olden et al (1994) compare the ambulance system
in the Netherlands with the United States. They note the superior training of ambulance
attendants and dispatchers in the United States, and the greater use of protocols for
dispatch of ambulances. A significant difference between the two systems is the
extensive use of nurses to staff ambulances in the Netherlands.
In the Republic of Ireland, poor response times in rural areas have been heavily
criticised. The Association of Ambulance Personnel has suggested that up to 700
persons die each year as a result of poor response times and the limited range of
protocols available to ambulance technicians (Payne 2000). Their claim that in the
previous seven years 5,000 people had died who could have been saved if a 24-hour
service had been put in place is similar to the rhetoric of Australian ambulance staff
associations when campaigning for salary and staff increases. Breen et al (2000) use
empirical research into Irish response times to put the same case in a more rational way.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
51
In Jordan the pre-hospital emergency care has developed in its own unique way, where
it is the responsibility of the Civil Defence Directorate, which provides medics who
provide first aid at the scene and transportation to hospital. Civil Defence Directorate
fire fighters are trained as first responders. The Jordanian air force provides helicopters
for medical evacuations (Abbadi et al 1997).
In Africa the geography and population density dictate the delivery systems for pre-
hospital and emergency care that is provided. In Namibia a state-run ambulance service
provides basic patient transport to state-run hospitals. While there is no ‘000’ or ‘911’
system in place, the system does provide a full range of services with modern
equipment and vehicles (Tintinalli 1998). The South African pre-hospital system is
evolving with the development of a new integrated health care system with equal access
for all citizens (Clarke 1998). Doherty and Price (1998) provide an outline of the
improvements taking place in the delivery of ambulance services in rural South Africa.
The Australian ambulance system shares many of the characteristics of ambulance
services operating in the United Kingdom, where ambulance services are medically
based, government controlled systems with mainly full-time professional staff providing
services to the public. British ambulance services face the problems of rising demand,
tight budgets, and increasing patient expectations (Cooke & Wilson 1999; Victor et al
1999; Nicholl et al 2001). As in Australia, there is considerable debate about the clinical
value of employing highly trained paramedics rather than more basically trained
ambulance technicians (Weston & McCabe 1992; Rainer et al 1997; Nguyen-Van-Tam
et al 1997; Nicholl et al 1998). The National Health Service (NHS) has set performance
targets for rural ambulance services, however there is little research into the rural
dimension of providing emergency ambulance services. While a number of American
studies address this issue at a systems level (Cayten et al 1993; Auble et al 1995), they
fail to consider the political and industrial relations factors that appear more prominent
in the Australian context.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
52
2.5.2 Population-based Research
A number of researchers have approached ambulance and pre-hospital research from a
population-based perspective. One of the more recent is a retrospective cohort study of
out-of-hospital cardiac deaths in Scotland (Capewell et al 2001). The population-based
ambulance research in Australia has taken place within Victoria, New South Wales and
Queensland, with the Queensland work being published in peer-reviewed journals
(Clark et al 1998; Clark & Fitzgerald 1999). Most of these population-based studies
relate to determining utilization rates and the factors that influence ambulance usage.
These studies date from the early 1970s to the beginning of the twenty-first century.
Table 5 summarises the most relevant studies from throughout the world for this study
in chronological order.
Table 5 Studies Examining Utilization Rates
Author Description of Study or Report
Aldrich et al 1971
This old American study attempted to develop a model to explain variations in utilization and predict ambulance emergency rates in an urban area. They concluded that demand was highly predictable using economic variables, quality of services variables, and land use variables.
Sosnin et al 1989
A clinical study of emergency ambulance utilization in the northern suburbs of Melbourne. They found that most calls were associated with cardio-respiratory episodes, loss of consciousness, and trauma. In 13 percent of cases MICA were used. Twenty-three percent of calls did not result in a patient transport to hospital because of patient refusal or the absence of any medical need. They identified the need for further studies on patterns of utilization of ambulance services.
Cadigan & Bugarin 1989
An American study that developed a formula to predict utilization in rural communities in communities of between 2,535 and 65,113 persons. They developed two rules of thumb that predicted 3.5 transports per 100 persons or one transport per 10,000 population per day. A number of definitions for demand were provided and they examined the impact of demographic and economic factors on utilization rates.
Wears 1989 A critique of Cadigan and Bugarin, raising the problems of: poor data; unmet need; problems of matching demand with resources in small communities; and a lack of consideration of other factors that influence system design. He criticized Cadigan and Bugarin’s report as ‘flawed and incomplete at best’, because of the difficulty they had with inconsistent data and un-measurable differences between communities.
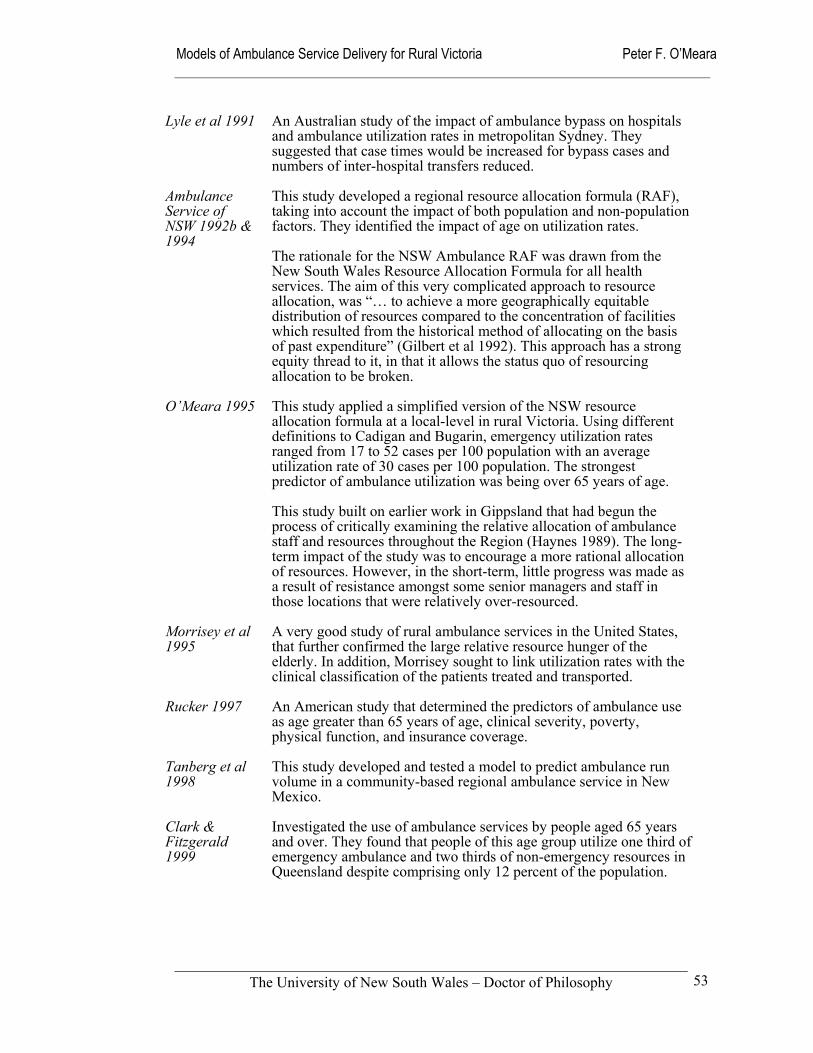
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
53
Lyle et al 1991 An Australian study of the impact of ambulance bypass on hospitals and ambulance utilization rates in metropolitan Sydney. They suggested that case times would be increased for bypass cases and numbers of inter-hospital transfers reduced.
Ambulance Service of NSW 1992b & 1994
This study developed a regional resource allocation formula (RAF), taking into account the impact of both population and non-population factors. They identified the impact of age on utilization rates.
The rationale for the NSW Ambulance RAF was drawn from the New South Wales Resource Allocation Formula for all health services. The aim of this very complicated approach to resource allocation, was “… to achieve a more geographically equitable distribution of resources compared to the concentration of facilities which resulted from the historical method of allocating on the basis of past expenditure” (Gilbert et al 1992). This approach has a strong equity thread to it, in that it allows the status quo of resourcing allocation to be broken.
O’Meara 1995 This study applied a simplified version of the NSW resource allocation formula at a local-level in rural Victoria. Using different definitions to Cadigan and Bugarin, emergency utilization rates ranged from 17 to 52 cases per 100 population with an average utilization rate of 30 cases per 100 population. The strongest predictor of ambulance utilization was being over 65 years of age.
This study built on earlier work in Gippsland that had begun the process of critically examining the relative allocation of ambulance staff and resources throughout the Region (Haynes 1989). The long-term impact of the study was to encourage a more rational allocation of resources. However, in the short-term, little progress was made as a result of resistance amongst some senior managers and staff in those locations that were relatively over-resourced.
Morrisey et al 1995
A very good study of rural ambulance services in the United States, that further confirmed the large relative resource hunger of the elderly. In addition, Morrisey sought to link utilization rates with the clinical classification of the patients treated and transported.
Rucker 1997 An American study that determined the predictors of ambulance use as age greater than 65 years of age, clinical severity, poverty, physical function, and insurance coverage.
Tanberg et al 1998
This study developed and tested a model to predict ambulance run volume in a community-based regional ambulance service in New Mexico.
Clark & Fitzgerald 1999
Investigated the use of ambulance services by people aged 65 years and over. They found that people of this age group utilize one third of emergency ambulance and two thirds of non-emergency resources in Queensland despite comprising only 12 percent of the population.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
54
Victor et al 1999
A study of the growing demands made of the London Ambulance Service 999 system. It found that persons over 65 years of age constituted one third of callers and that the most common reasons for calling were accidents and medical conditions such as respiratory, cardiac and obstetric conditions.
Clark et al 2000
This Queensland study set out to establish the demographic, health status and insurance determinants of pre-hospital ambulance non-usage for patients with emergency medical needs. Age and trauma were found to be the highest predictors of ambulance usage, while non-English speaking background was predictive of non-usage.
In the United Kingdom there has been sufficient concern about the high emergency
demand on ambulance service for the National Health Service to commission research
on alternatives, such as nurse-led telephone triage services, to reduce service demand
(George 1998). It is alleged that ‘misuse’ is the major reason for the growing demand of
emergency ambulance services in the United Kingdom – 28 percent increase in demand
in the three years to 1996-7 in the Westcountry Ambulance Service and a 30 percent
increase in the London Ambulance Service in the five years to 1996-7. However,
investigations have been unable to find any satisfactory explanation (Mann & Guly
1998; Snooks et al 1998; Victor et al 1999). Further research has been called for to
determine why people call the emergency ambulance number for non-emergencies. It is
more likely to be related to other components of the health system, such as the
availability of after-hours medical services, than any characteristics of the ambulance
system.
2.5.3 ‘Bio-medical’ Research
Publications and discussion of ambulance services or Emergency Medical Systems
(EMS) research are prolific in the United States and Canada. However, the quality of
the North American research reported has been questioned on the grounds of its lack of
rigor and the absence of randomised clinical trials (Callaham 1997; Marcum &
Callaham 1998). In the United Kingdom, the same observation about the lack of
randomised trials is raised. However, a different conclusion is reached, with Brazier
(1999) for instance recommending that as evidence based policy-making cannot depend
on randomised controlled trials, alternate information sources must be used.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
55
Not unexpectedly, a major emphasis of this North American work has been on ‘bio-
medical’ research. There is no shortage of studies and reports of specific clinical and
procedural interventions in North America; that is, whether a specific clinical
intervention – procedural or pharmacological – is effective for a specific cohort of
patients. Growing from this are a number of studies comparing the patient outcomes in
different types of ambulance systems. Most of these have concentrated on survival from
ventricular fibrillation after pre-hospital defibrillation.
While there is a growing literature on ambulance topics from other parts of the world,
the majority of the available research literature on ambulance services still comes from
North America (Cooke & Wilson 1999). Specific clinical interventions such as
intubation (Spaite 1998, Sayre et al 1998), intravenous fluids (Kaweski et al 1990) and
defibrillation (Auble et al 1995; White et al 1996) are well represented. Canadian
writers McCallum and Rubes (1996) have examined a number of emergency pre-
hospital care interventions.
In the United Kingdom there has been a review of cardiac arrest outcomes in the West
Midlands Ambulance Service (Robinson et al 1998). As in the United States the general
consensus in the United Kingdom is that “ … there is a dearth of good research
evidence to justify some of the therapeutic interventions used in pre-hospital care.”
(Nicholl et al 2001)
In Canada, Steil and the Ontario Prehospital Advanced Life Support (OPALS) study
team have embarked on what is claimed to be the largest pre-hospital study yet
conducted (Steil et al 1996; Steil et al 1998; Steil et al 1999a; Steil et al 1999b). The
OPALS study will involve more than 25,000 cardiac arrest, trauma, and critically ill
patients over an eight-year period. The study aims to evaluate the incremental benefit of
rapid defibrillation and pre-hospital Advanced Cardiac Life Support measures for
cardiac arrest survival and the benefit of Advanced Life Support for patients with
traumatic injuries and other critically ill pre-hospital patients. While the study is limited
to the period from 1994 to 2002, it offers valuable preliminary results and
methodological information, including clearly defined definitions of key events and
outcomes in the pre-hospital system.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
56
In Western Australia, Jacobs and Oxer (1990) compared ventricular fibrillation
survivors who were treated by paramedics and those treated by ambulance officers with
a defibrillation-only protocol. They found that the key determinant in survival from
ventricular fibrillation occurring outside hospital is how rapidly defibrillation can be
initiated. Callaham and Madsen (1996) reported similar findings in the United States,
where they used neurologic quality as the outcome measure. These studies conceptually
articulate with the systems research being undertaken in the thesis.
Spaite et al (1995) critiques component research and recommends the use of system
research methodology as a tool for examining EMS systems. The rationale for this is
that it is of little benefit to the community if the very best staff, equipment and protocols
are inaccessible to those in need if the system used to deploy them is ineffective. This
rationale is at the crux of this thesis, in its exploration of models of ambulance service
delivery for rural Victoria.
2.5.4 Ambulance Systems Research
While much has been written about specific clinical interventions in ambulance or EMS
care, in comparison, relatively little has been published about the nature and operation
of ambulance service delivery systems. Research related to EMS systems such as the
‘chain of survival’ (Steill et al 1993; Stratton & Niemann 1998; Jacobs et al 2001),
Priority Dispatching (Stout 1984) and time and motion studies (Cone et al 1998) have
been completed. Their main emphasis has rested on cardiac related emergencies where
early access, early cardio-pulmonary resuscitation, early defibrillation and early
advanced care have become the underlying concept for the treatment of out-of-hospital
cardiac arrest (Jacobs et al 2001).
Other writers have identified the elements that form successful ambulance or EMS
systems in both urban and rural areas (Oranto et al 1984; Reich 1991; Vukor et al 1988;
Gallehr & Vukor 1993; Moore 1999; O’Meara et al 2002). Internationally, the challenge
of researching rural EMS models and systems is taken up by a limited number of
authors (Anderson: 1992; Smith et al 1997; Williams et al 2001). Linwood (1999),
McCoy (1996) and McCoy et al (1997) describe the introduction of ‘quality systems’
into Australian ambulance services. These Australian articles are positive, ‘feel-good’
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
57
descriptions of fashionable developments in the Queensland and Victorian ambulance
services.
White links aspects of component research with systems research when studying the
processes and discharge survival rates after rapid defibrillation (White et al 1996), in
particular the impact of police and paramedic response systems (White et al 1994;
White et al 1998). Auble et al (1995) has carried out a meta-analysis of defibrillation by
Basic Life Support (BLS) providers on cardiac arrest mortality. Jacobs et al (2001),
summarizes 20 journal articles to determine rates of survival to discharge using
neurologic function as the outcome measure. Specifically relevant to the thesis is the
work of Gallehr and Vukov (1993) who attempted to define the benefits of emergency
medical technician-defibrillation in rural communities through comparison of outcomes
in communities of greater than or less than 15,000. Their conclusions were that:
Small rural communities cannot expect statistics for prearrest neurologic survival after cardiac arrest to be similar to those from large rural communities. Many emergency medical system factors, such as delay to system access, lack of first-responder CPR, and absence of full-time EMTs, may prevent EMT-D programs in small rural communities from experiencing comparable cardiac arrest survival.
(Gallehr & Vukov 1993)
That study built on Vokov’s earlier work that identified early CPR and short
defibrillation times as essential prerequisites to a successful rural defibrillation program
(Vukov et al 1988). Even earlier than this, Ornato had identified that the major problem
with EMT defibrillation in rural areas was maintenance of skills and continuing
education (Ornato et al 1984). Anderson (1992) has explicitly examined rural EMS
system development in the context of technological advance, while Johnson (1991) has
looked at response time and staffing benchmarks for EMS systems in urban, rural and
suburban environments.
Until recently, a comparatively small number of published studies had been reported in
the United Kingdom. This now appears likely to change, with the National Health
Service (NHS) having commissioned a number of studies. These relate to the efficacy of
dispatch systems, the use of paramedics, emergency response times, first responder
systems, and the extension of ambulance practice (Nicholl 1996; Knapp 1996; Duck &
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
58
Ord 1999). These systems studies are of particular relevance when determining the
feasibility and acceptability of rural models of ambulance service delivery. Nicholl has
been commissioned to evaluate the prioritised dispatch for ambulance services and the
impact of new ambulance service response time standards in the United Kingdom
(Nicholl 1996). Duck and Ord (1999) have examined the introduction of community
first responder programs that have been proposed as a strategy for reducing response
times. The most comprehensive outcome of this research activity has been the report of
the Strategic Review of Options for the Future of Ambulance Services carried out on
behalf of the Ambulance Service Association (Nicholl et al 2001). Their report positions
the ambulance service as a core part of the health system with a focus on health care
rather than emergencies. They propose a Health Care Service Model, which links
ambulance services to the other components of the health system that is most likely to
meet the strategic aspirations of the Ambulance Service in the United Kingdom (Nicholl
et al 2001: 12). In doing so, their report also considers the drivers of change such as
rising expectations and technological developments, the means of delivering services,
and the measurement of performance in meaningful and useful ways.
It was this body of systems research that was of most relevance to the thesis. However,
as already outlined the quality of the clinical EMS research in the United States has
been heavily criticized for its lack rigor. Spaite, for example, is very critical of
ambulance systems that lack any evidence of their success or otherwise.
Personnel in these systems probably “think” they save people from sudden death. However, very few have attempted the rigorous evaluation necessary to prove what they believe.
(Spaite et al 1997)
The ‘chain-of-survival’ concept is an example of research that has incorporated a
systems-analysis to understand and alter current practice (Strattan & Niemann 1998;
Martinez 1998; Jacobs et al 2001). However, the lack of out-of-hospital care systems
research aside from that related to cardiac arrest is a research gap. One international
exception is Joó (2000), who describes the German ‘chain of rescue’ system for road
accident response that forms the basis of that country’s emergency medical services.
The four links of first aid, emergency call, emergency medical service and hospital
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
59
constitute the German ‘chain of rescue’. While there has been research conducted into
trauma, Spaite argues that:
... approaches that have been used to develop the current pre-hospital trauma literature do not permit the development of a consensus on the impact of each system component on patient outcome. In fact, most pre-hospital trauma research has emphasized the wrong issues, asked the wrong questions, and used the wrong methods.
(Spaite et al 1995)
In Victoria the Ministerial Taskforce on Trauma and Emergency Services (1999),
through its review of the State’s trauma and emergency services, has addressed these
shortcomings to some degree. Other studies have supplemented this report (McDermont
et al 1996; Danne et al 1998; Cooper et al 1998). The purpose of the Ministerial Review
was to advise the State Government on an appropriate system-wide structure,
arrangements for ongoing monitoring of the accessibility and responsiveness of
emergency and trauma services, and education and training issues. Its report identified a
number of system-wide deficiencies adversely impacting on the outcomes for severely
injured patients.
Examples of the deficiencies in the Victorian trauma system identified are:
Inadequate availability of prehospital and emergency department advanced life support skills.
Prolonged times at the scene of accidents.
Inadequate reception in emergency departments by junior staff and delayed investigation and surgical consultation.
Triage of patients to hospitals without optimal skills or resources to manage time-critical major trauma patients.
Delays in, and inadequate medical escort for, rural and metropolitan interhospital transfer of major trauma patients.
(Ministerial Taskforce on Trauma 1999: 4)
The taskforce’s ‘solution’ to the problems was to bypass local hospitals and transport
patients to Major Trauma Centres. Somers’ analysis of the same data is that improved
care in rural areas rather than routine ‘bypass’ is the key to improved patient outcomes.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
60
He advocates the teaming together of ambulance officers and appropriately trained rural
general practitioners to provide early definitive care, appropriate ‘aggressive’
resuscitation and appropriate triage (Somers 1999).
The politically powerful Victorian Health Association (VHA) has also expressed a
number of concerns about the 1999 proposals to change the structure of trauma and
critical care services in Victoria. Its major concern relates to the centralized structure of
two adult and one paediatric Major Trauma Centres, resulting in the by-passing of
Metropolitan and Regional Trauma Services and a consequent detrimental impact on
their clinical viability as a result of reduced case load and de-skilling of key staff.
Insofar as ambulance services are concerned, VHA was concerned that the additional
out-of-area travel will reduce availability of ambulances and increase the cost of
operating ambulance services (VHA 1999).
One of the objectives of the trauma system for which the ambulance service has major
responsibility is getting the right patient to the right hospital at the right time (Grossman
et al 1995; Nicholl & Turner 1997). The extant pre-hospital trauma literature has been
criticized for its inability to permit the development of a consensus on the impact of this
and other system components on patient outcomes (Spaite et al 1995).
As already mentioned, the Victorian Ministerial Taskforce on Trauma and Emergency
Services (1999) addressed these shortcomings through its identification of a number of
system-wide deficiencies that adversely impact on the outcomes for severely injured
patients. One of these deficiencies is the prolonged times at the scene of accidents of
more than 20 minutes for un-trapped patients. Aside from airway management
deficiencies, delays at the scene were identified as the most significant pre-hospital care
problem. Danne et al (1998) recommended further research into the reasons for pre-
hospital deficiencies in the care of trauma patients. It was recognized that in the rural
context, significant distances and scattered medical resources are often responsible for
delays in getting patients to appropriate hospitals for definitive care, and that solutions
will vary in different geographical regions. In Australia, a study is being undertaken to
examine the environmental and system factors that influence extended scene time for
patients being received at one Victorian regional hospital (O’Meara & Boyle 2001).
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
61
Extended scene times are also of concern in other developed countries. In the United
Kingdom, Cooke (1999) extends the argument beyond ‘scoop and run’ and ‘stay and
play’. He discusses the organisational structure of ambulance services and the training
and education of ambulance paramedics. His suggestion is that more highly trained staff
with improved patient assessment capabilities will make informed decisions about what
is appropriate at the scene. Lendrum et al (2000) has raised the need to match the
training of ambulance staff to the workload mix if an extended role is to be considered.
In Denmark, Birk et al (2000) studied the relationship between the number of basic pre-
hospital interventions used and at scene time. In this unpublished study it is noted that
there is little evidence of a positive effect on outcome from most pre-hospital
interventions and that a shorter pre-hospital time may be an important factor in survival
for trauma patients. In Mexico, Arreola-Risa et al (2000) report improvements in pre-
hospital outcomes associated with improved response times and the introduction of a
pre-hospital trauma life support course. The improved pre-hospital treatment did not
increase the mean scene time in this six-month study.
The North American literature brings a rural and remote perspective on pre-hospital
care in trauma systems. Grossman et al (1995) conducted a study to examine the role of
rural hospitals and pre-hospital agencies in the care of motor vehicle accidents prior to
the regionalization of trauma care. The study provides an excellent guide on data
linkages between pre-hospital agencies, receiving hospitals and coroner reports. As part
of the study, they examined pre-hospital time intervals, with ambulance median scene
time of 15 minutes and scene to emergency department arrival of 36 minutes. In another
study Grossman et al (1997) compared the time intervals of advanced paramedics to
trauma incidents in rural and urban locations in the state of Washington. Mean scene
times in rural areas were slightly longer than in urban areas, while mean response and
transport times were significantly greater. Longer response times in rural areas were
associated with higher mortality rates. The study was unable to find any association
between the severity of injuries and the length of pre-hospital time intervals. A longer
scene time for more severely injured patients was expected if more severely injured
patients require a higher number of advanced life support procedures. Their study did
not have information regarding the use of procedures and therefore was unable to assess
whether more severely injured patients actually received more procedures. Other

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
62
American studies to examine rural pre-hospital scene times include Morrissey et al
(1996) in Georgia, Stripe and Susman (1991) in Nebraska, and Esposito et al (1995)
comparing urban and rural outcomes.
The Tasmanian Department of Health and Human Service (1999) Medical Emergency
Services Plan for Rural and Remote Areas addresses the issue of providing timely and
effective responses to medical emergencies in rural areas. The report documents the
strategies to achieve this based on four key elements. These are: prevention wherever
possible of medical emergencies; preparedness of the community for medical
emergencies; effective response to each medical emergency; and recovery of the
individuals and community affected by a medical emergency (DHHST 1999: 6).
Four key issues were identified during the Department’s consultation process: firstly,
the characteristics of services providers; secondly, clinical standards and training;
thirdly, medical equipment and drugs; and fourthly, communication systems. Drawing
on these findings and work previously carried out in Queensland, the Tasmanian
authorities recognized the pivotal role of ordinary rural community members. As a
result they adopted an, ‘All Agencies’ approach, which requires a partnership between:
community members;
voluntary and community organizations;
local general practitioners;
others with medical emergency response training;
all levels of government; and
statutory authorities.
(DHHST 1999).
In the United States, to a much greater degree than in Australia, the EMS system has
developed at the intersection of the public safety and medical care systems (Martinez
1998). The community therefore has the dual expectation of a rapid response and
competent medical care in the pre-hospital environment. There is also an evolving set of
expectations that concentrate on the capacity of the EMS systems to provide acute-care
triage, enhanced integration with primary care, increased participation in public health
and prevention activities, and limiting transportation to medical emergencies (NRHA-
US 1997). The American National Rural Health Association has produced an issues
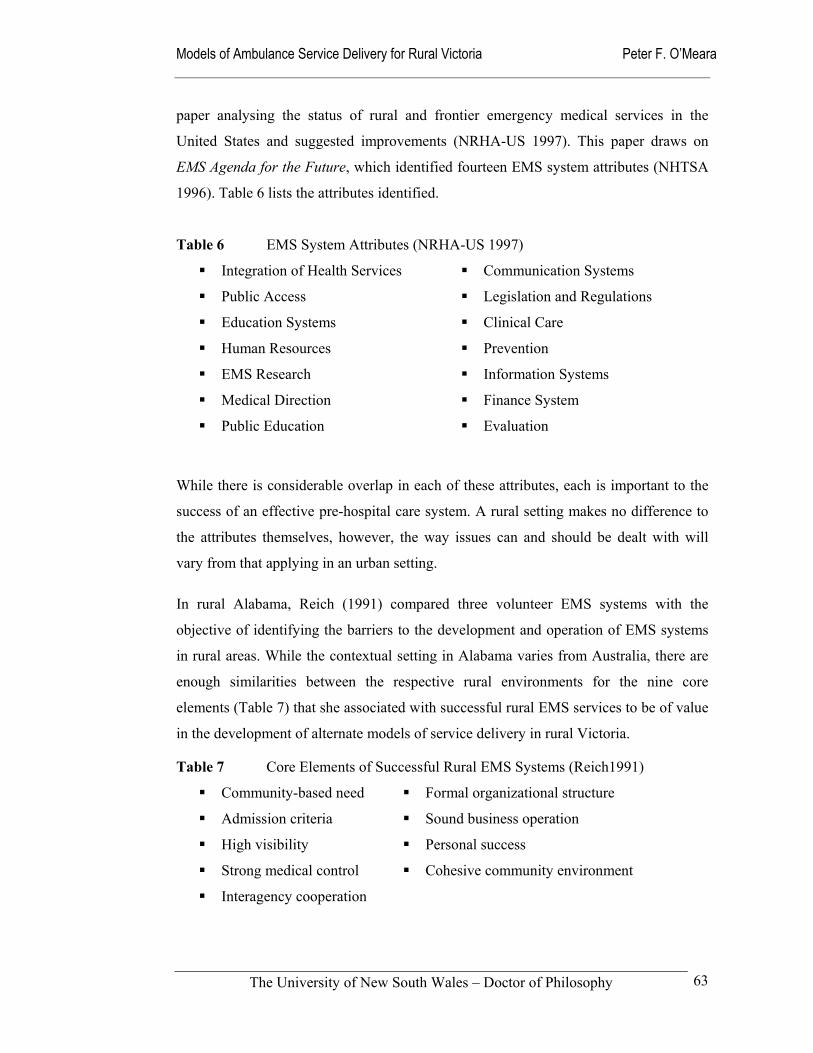
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
63
paper analysing the status of rural and frontier emergency medical services in the
United States and suggested improvements (NRHA-US 1997). This paper draws on
EMS Agenda for the Future, which identified fourteen EMS system attributes (NHTSA
1996). Table 6 lists the attributes identified.
Table 6 EMS System Attributes (NRHA-US 1997)
Integration of Health Services Communication Systems
Public Access Legislation and Regulations
Education Systems Clinical Care
Human Resources Prevention
EMS Research Information Systems
Medical Direction Finance System
Public Education Evaluation
While there is considerable overlap in each of these attributes, each is important to the
success of an effective pre-hospital care system. A rural setting makes no difference to
the attributes themselves, however, the way issues can and should be dealt with will
vary from that applying in an urban setting.
In rural Alabama, Reich (1991) compared three volunteer EMS systems with the
objective of identifying the barriers to the development and operation of EMS systems
in rural areas. While the contextual setting in Alabama varies from Australia, there are
enough similarities between the respective rural environments for the nine core
elements (Table 7) that she associated with successful rural EMS services to be of value
in the development of alternate models of service delivery in rural Victoria.
Table 7 Core Elements of Successful Rural EMS Systems (Reich1991)
Community-based need Formal organizational structure
Admission criteria Sound business operation
High visibility Personal success
Strong medical control Cohesive community environment
Interagency cooperation
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
64
Her framework of attributes or elements is particularly relevant to the development,
management and monitoring of volunteer or community-based ambulance services that
are prevalent in the more remote and sparsely populated areas of Victoria. With the
exception of the work completed in Tasmania, little research has been undertaken into
volunteer ambulance systems in Australia. However, it is possible to draw on the work
completed that examined the state of volunteer fire services in country Victoria
(Reinholtd 1999; Aitken 2000).
Narad (1998) is critical of this emphasis on elements, as it neglects the relationships
between the different components of an EMS system. He suggests a ‘multicratic
organizational’ system for managing the multiple autonomous organizations that make
up the typical EMS system. Narad also describes five potential EMS management
approaches for communities. They are:
laissez-faire, where even voluntary co-ordination efforts are not tried;
voluntary co-operation efforts, such as co-ordinating councils;
external planning agencies, without regulatory control;
framework organizations, with regulatory control over system participants; and
bureaucratization, placing system participants within a single organizational hierarchy.
Amongst the few contributions to the development of effective ambulance systems is
the work of Morrisey et al (1995) who carried out research in rural Georgia in the
United States. That study reported on the services provided, the volume of use and the
mix of patients in a population of 195,161. This is comparable in size to the aggregate
size of the sample towns examined in this thesis. It therefore provides a useful
benchmark for this study of Victoria’s rural ambulance services.
A useful contribution comes from Anderson (1992), who describes in some detail the
characteristics of the EMS systems in the rural areas of the United States. Of particular
note is his lament that the resources allocated to rural areas are inadequate in relation to
the demonstrated needs. Williams et al (2001), reiterate this when they argue that the
practice of emergency medicine in rural areas is different than practice models
commonly found in urban areas of the country.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
65
The delivery of high-quality emergency care in a rural setting requires a conceptual framework quite different from that required in urban and surburban environments, given that available resources are limited in a rural setting.
(Williams et al 2001: 323)
The findings of both the Australian Institute of Health and Welfare (Strong et al 1999)
and the Ministerial Taskforce on Trauma and Emergency Services (1999) appear to
support this notion that available resources fail to meet the needs of rural communities.
In the United States, rural EMS has also been examined within the context of the Rural
Hospital Flexibility Program. Schoenman et al (1999) identify EMS as a critical element
in the rural health care delivery system. This project team visited twelve sites in five
States to track EMS developments funded through the Rural Hospital Flexibility
Program. Initiatives included development of training programs, scholarships, creation
of multi-county EMS systems, strengthening of medical direction, development of
dispatch systems, examination of possible expansions to the scope of practice for rural
EMS providers, and development of EMS quality assessment tools.
2.5.5 Future Directions for Ambulance
From a methodological perspective, Callaham (1997) is very critical of the dearth of
strong scientific evidence to support many of the pre-hospital clinical interventions
practiced in the United States. His paper mirrors the historical tendency in Australia of
making decisions about the introduction of specific clinical interventions before
significant and verifiable evidence of their effectiveness has been produced. Nor is
controlled evaluation always planned before the introduction of new practices. While
Callaham’s research only examines urban EMS, he has a point when he argues that
many clinical interventions rest on the flimsy notion:
... that there are large numbers of prehospital patients who will materially benefit from only 15 to 20 minutes of treatment, in an environment more difficult than any hospital or medical office, by individuals with less formal training and direct supervision than nurses or nurse practitioners or physicians, with essentially no verifiable medical history or records about the patient, treating an almost unlimited variety of ailments, and unsupported by extensive diagnostic tools that so greatly improve the accuracy and safety of treatment in a hospital environment.
(Callaham 1997)
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
66
Callaham’s challenge to pre-hospital researchers and providers alike, is to re-examine
the basis on which the service delivery system is based, and to monitor and report
clinical outcomes at the same standard as hospitals. Of particular relevance is the need
to ensure that harm from current interventions is measured and then minimized. He
makes an appeal to those who promote EMS as ‘saving lives’; this he posits is
unrealistic, as relatively few patients benefit from aggressive interventions. For most
patients, reassurance and transport is the only intervention EMS can provide. Shapiro
(2000) also expresses concern about the lack of evidence to support the view that pre-
hospital care saves lives.
In North America, the Emergency Medical Services Outcomes Project (EMSOP) is
taking up Callaham’s challenge (Maio et al 1998; Spaite et al 2001). This project aims
to develop a methodologically acceptable outcomes model for emergency medical
services using the ‘Episode of Care Model’ and its sub-unit the ‘Out-of-Hospital Unit of
Service Model’.
At the level of the individual ambulance paramedic, these arguments about the dearth of
evidence are unlikely to be highly valued in an environment where the community
expects ambulance paramedics, doctors and nurses to take action in emergency
situations. Health professionals are often driven toward action in their efforts to help
individual patients and they are not concerned about research and evaluation studies
when they believe they can help their patient. However, Callahan’s and Shapiro’s
concerns are similar to Johnson’s earlier work (1991); he also lamented the lack of
evidence to support pre-hospital interventions. His argument is that planning for EMS
systems must strive to maximize access to proven interventions. On this basis the goals
of an EMS system should be:
1. Basic life support within four minutes;
2. Advanced life support within eight minutes; and
3. Arrival at a definitive trauma facility within an hour, preferably one-half hour, of the original injury.
Unlike the targets for the United Kingdom’s National Health Service or the Department
of Human Services - Victoria, these targets are not quantified in terms of percentiles.
The achievement of these targets in all cases is not possible in the context of limited
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
67
resources and dispersed populations. Johnson is also concerned about uncritical
application of interventions in both urban and non-urban environments, asking:
In selecting interventions, inadequate consideration has been given to the differences in emergency medical services personnel training, frequencies of their exposure to patients, frequencies of skill use, and available of effective continuing education programs in the urban and nonurban environments.
(Johnson 1991)
He found that the cornerstones of a rural EMS system are: its ability to get help to the
patient in a timely fashion, initiation of sound airway management, CPR, defibrillation,
and control of bleeding. Other measures require consideration, based on the available
evidence. Given the diversity of rural settings, it is unlikely that implementation of a
one-system model will be effective. It is this point that runs through this study and is
also expressed, for example, in the Tasmanian Medical Emergency Services Plan for
Rural and Remote Areas (DHHST 1999).
More recently in the United States, the future of EMS has been canvassed. Delbridge et
al (1998) used the fourteen attributes already mentioned from EMS Agenda for the
Future to develop a vision for the future. Their vision is of a community-based
undertaking that is fully integrated with the overall health system; this vision would
include EMS personnel taking roles in health promotion and monitoring. Potentially,
this model has considerable merit in the Victorian rural context where ambulance
officers and paramedics experience an estimated 50 percent of their time as ‘down
time’.
Spaite et al (1997) advocates a carefully designed expanded-scope EMS system that
incorporates evaluation frameworks to determine the impact of system changes. These
suggestions for expanded-scope services, like Delbridge et al (1998), place an emphasis
on contributions to public health activities in prevention, public education and public
safety. The American College of Emergency Physicians has offered cautious support to
the concept of an expanded scope of practice for EMS, provided some basic principles
related to system design and medical oversight are observed (ACEP 1997).
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
68
At the Sand Key Conference in 1994, programs and proposals to expand or transform
EMS were presented (Garza 1994). The key points that resulted from the conference
included the importance of: determining local needs and resources; customizing
programs to meet local requirements; working together with other health care providers;
and sharing ideas and information as EMS evolves.
The Joint Royal Colleges Ambulance Committee in the United Kingdom has examined
the future role and education of paramedics. Their paper offers an overview of the
merging concepts in relation to paramedic education and training for ambulance
services of the future. They provide a strong multidisciplinary flavour to the discussion,
with suggestions that ambulance paramedics should be educated more broadly in
universities and evolve into a new professional category titled ‘Practitioner in
Emergency Care’ who could be employed in a wider range of settings (JCALC 2000).
Edwards (1998) provides an overview of the Bachelor of Medical Science degree that is
being offered at the University of Sheffield for ambulance paramedics.
In Australia, a number of accounts have been published regarding the transfer of
ambulance education and training from industry-based apprenticeship-type systems to
university-style courses in Faculties of Medicine and Health Sciences (Field 1994;
Wellard 1995; DeWitt 1997; Lord 1998; Field & Lord 1999; Field et al 1999). A total of
six Australian universities currently offer ambulance and paramedic courses at the
undergraduate level.
In the United Kingdom, Nicholl supports the implementation of the “… idea of
Practitioners in Emergency Care who cross the boundary between paramedics and
nurses, and lead to a wider clinical role for ambulance services and better care for
patients.” (Nicholl et al 2001: 4). Roberts (1998) makes the then rhetorical suggestion
that rather than becoming a new profession, pre-hospital care could become a sub-
specialty of nursing with practitioners moving between the pre-hospital environment,
hospitals and primary care. For Spaite, three main issues in relation to expanded-scope
EMS systems need to be considered: cost-effectiveness, lack of standardized systems
models, and the overall lack of good EMS research for comparison. Spaite et al (1997)
is critical of existing evaluation practices.
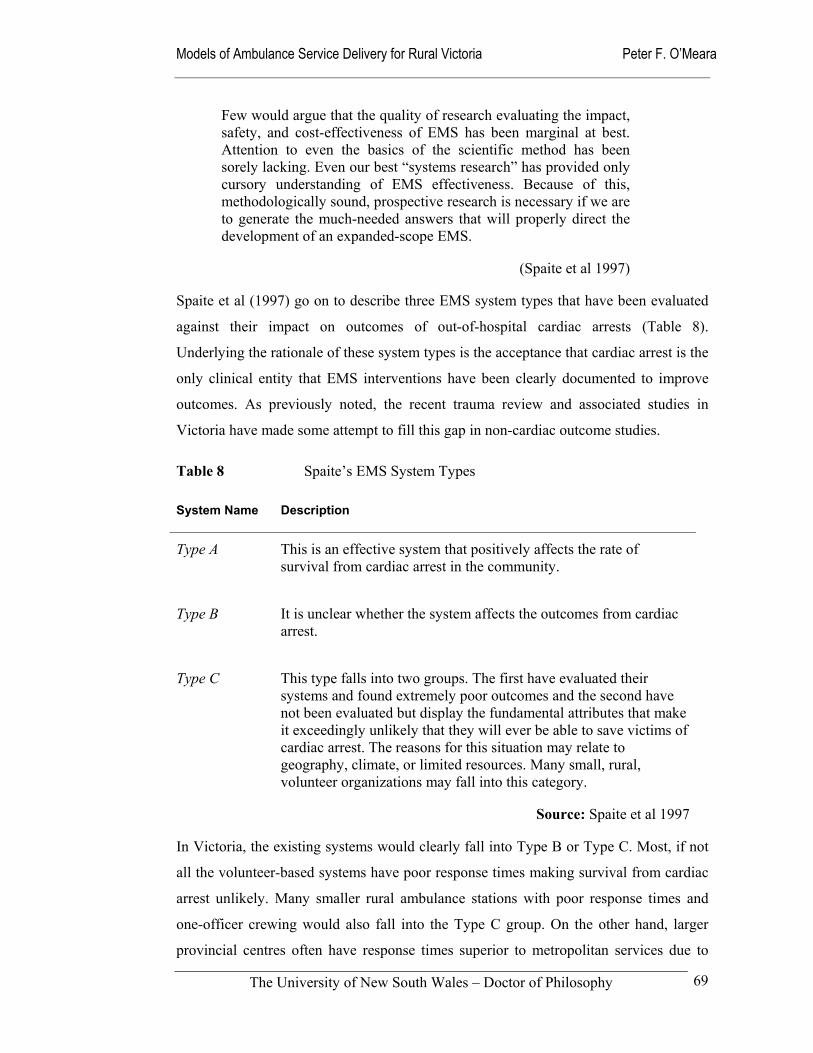
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
69
Few would argue that the quality of research evaluating the impact, safety, and cost-effectiveness of EMS has been marginal at best. Attention to even the basics of the scientific method has been sorely lacking. Even our best “systems research” has provided only cursory understanding of EMS effectiveness. Because of this, methodologically sound, prospective research is necessary if we are to generate the much-needed answers that will properly direct the development of an expanded-scope EMS.
(Spaite et al 1997)
Spaite et al (1997) go on to describe three EMS system types that have been evaluated
against their impact on outcomes of out-of-hospital cardiac arrests (Table 8).
Underlying the rationale of these system types is the acceptance that cardiac arrest is the
only clinical entity that EMS interventions have been clearly documented to improve
outcomes. As previously noted, the recent trauma review and associated studies in
Victoria have made some attempt to fill this gap in non-cardiac outcome studies.
Table 8 Spaite’s EMS System Types
System Name Description
Type A
This is an effective system that positively affects the rate of survival from cardiac arrest in the community.
Type B
It is unclear whether the system affects the outcomes from cardiac arrest.
Type C
This type falls into two groups. The first have evaluated their systems and found extremely poor outcomes and the second have not been evaluated but display the fundamental attributes that make it exceedingly unlikely that they will ever be able to save victims of cardiac arrest. The reasons for this situation may relate to geography, climate, or limited resources. Many small, rural, volunteer organizations may fall into this category.
Source: Spaite et al 1997
In Victoria, the existing systems would clearly fall into Type B or Type C. Most, if not
all the volunteer-based systems have poor response times making survival from cardiac
arrest unlikely. Many smaller rural ambulance stations with poor response times and
one-officer crewing would also fall into the Type C group. On the other hand, larger
provincial centres often have response times superior to metropolitan services due to
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
70
close proximity and easy access to patients. They may fit the criteria for Type B
systems. What is clear however is that few systems have collected and analysed
sufficient evidence to validly claim to belong to the elite Type A system. As in many
parts of the world, response times tend to be used as a proxy for effective performance.
This lack of more appropriate outcome measures is addressed in Chapter 7 drawing on
the Emergency Medical Services Outcomes Project (EMSOP) in the United States and
other generic performance frameworks for emergency management and health systems
(Aday 1998; NHMBWG 1998; Duckett 1999; Hancock 1999; Humphreys & Mathews-
Cowey 1999; NHPC 2000; SCRCSSP 2000: 859).
Spaite’s earlier work suggests the use of a ‘systems-analysis’ framework for future
research. He says that incorporation “... of this multidiscipline approach into EMS
research is essential if there is to be any hope of finding answers to many of the
important questions that remain in the arena of out-of-hospital health care.” (Spaite et al
1995)
Out-of-hospital emergency care was designed around the concept of a system of interrelated events that combine to offer a patient the best possible care outside the hospital. However, in contrast to the actual operations of the emergency medical service (EMS) systems, research has not typically used systems-based models as the method for evaluation.
(Spaite et al 1995)
Neely argues that the same forces that are transforming the wider health care delivery
system are also reshaping EMS systems (Neely et al 1997). While the legislative and
financial structures are different in the United States than in Australia, the demands
made on Australian ambulance services are similar. Australian State Governments, like
American health maintenance organizations, are demanding predictable costs and
appropriate utilization of services.
Neely’s vision is a multi-option decision point (MODP) model, based on clinically
based pathways to guide patient movement from point to point (Neely et al 1997).
Under this system, multiple options would be offered at each of the decision points - at
dispatch, on-scene, and upon transport - rather than the current American single-option
system. Under this system, the dispatchers may distinguish between callers who require
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
71
urgent attention and those who could be served by non-emergency care. They may also
refer the patient to a telephone triage system to be managed at home (Neely et al 1997).
To implement such a system, well-constructed and validated decision rules are required.
Studies in Portland, Oregon are seeking to do this through the development of new
triage guidelines for on-scene paramedics, which stratify patients into four categories:
1. Requires ambulance transport to an emergency department;
2. Needs emergency department evaluation, but may safety go by alternate means;
3. Referred to his or her primary care provider; or
4. Requires field treatment only.
The primary goal of any EMS system is to provide emergency services to those in needs. That mission must remain intact. EMS systems of the future will have an additional mission: to get the right patient to the right place at the right time.
(Neely et al 1997)
In the British NHS, ambulance crews currently have no option other than transporting
the patient to a hospital accident and emergency department (JRCALC 2000; Nicholl et
al 2001). The London Ambulance Service is developing new protocols to assist crews to
assess patient needs and, as appropriate, offer treatment or direct referral to other
agencies (Snooks 1998).
In terms of field practice, the rural Australian scene often incorporates these elements,
albeit without a clear rationale linking the components of the system together; it has
tended to evolve in a haphazard manner with little research to guide implementation.
Priority dispatching systems have operated in Victoria’s rural ambulance services for
many years. The major variation in Neely’s model is the authorization for paramedics to
provide or instruct patients to use other means of available transportation to an
emergency department or other care provider. In Australia there continues to be
reluctance to overturn the ultimate decision-making power of the medical practitioner.
However, it has been recently reported that in New South Wales, some forty percent of
ambulance calls do not result in transportation to hospital. The concern in the medical
community is whether ambulance officers have the capacity to make these alternate
referrals (Hill 2001: 5 & 13).

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
72
2.6 Aims and objectives
This extensive literature review of systems theory, the socio-political context, health
policy, and the state of pre-hospital research firmly locates Australian rural ambulance
services within the health care system. They provide a service that rural health
professionals and communities value and support. While public expectations of a
prompt emergency service can be satisfied through the public safety system, the
expected skills and clinical judgement can only be developed, nurtured and monitored
as part of an integrated health system (Nicholl & Munro 2000). The specific ambulance
roles will vary according to the local ambulance service’s capacity and the range of
other services available in that community.
The most persistent and important variable influencing the long-term development and
performance of rural ambulance services is the rural environment in which they operate.
This contextual factor influences the type and scope of services that are necessary and
possible; limitations are placed on the ambulance service characteristics through the
level and availability of basic infrastructure and staff in individual locations. Crucial
issues for rural ambulance service delivery are local leadership, education and training,
skills maintenance, and the maintenance of local community support.
These fundamental characteristics of the rural environment suggest that a range of
different ambulance service delivery models need to be developed and implemented to
meet local needs. Important environmental factors which affect the long-term
expectations and performance of rural ambulance services throughout Australia include
the population drift to larger centres, an ageing population, economic stagnation, some
degree of isolation from other health services, and the withdrawal of complementary
medical and health services from many country areas. Despite the withdrawal of many
health services from rural and remote areas, ambulance service links to general
practitioners, community nurses and hospitals have been maintained and continue to be
important. Some rural areas without the necessary infrastructure, such as hospitals and
medical practitioners, also have to cope with seasonal influxes of additional visitors,
either for seasonal work or for recreation.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
73
A potential weakness in the organization and delivery of rural ambulance services is the
lack of organizational models designed to match the needs of local communities. From
the medium to longer-term perspective, the most critical issues for rural ambulance
services that require attention are the:
need for acknowledgement that ambulance services constitute an important element of the emergency medical system;
equitable allocation of resources based on contemporary need, rather than historic patterns;
development and implementation of agreed performance standards (operational, clinical, financial); and
changing nature of ambulance officers, their education, career aspirations and professional practice.
The failure to develop coherent service delivery models or to adequately address these
issues, are associated with the high levels of conflict and industrial disputation seen in
Victoria’s rural ambulance services. This industrial disruption has resulted in reduced
effectiveness, equity and efficiency, to say nothing of the damage to the reputation of
the rural ambulance services. In isolation, it is unlikely that the amalgamation of
Victoria’s rural ambulance services will improve outcomes unless these challenges are
addressed in a constructive and creative way.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
74
3.0 Methods
Section 1 Introduction
Section 2 Theory and Methods
Section 3 Findings and Discussion
Section 4 Conclusion
Chapter 1 Overview of Study
Chapter 2Theory Foundations
Chapter 4Communities Respondents
Chapter 5Expectations
Chapter 6Structure Culture
Chapter 7Ambulance Performance
Chapter 8Models of Delivery
Chapter 9 Policy Implications
Chapter 3Study Methods
Figure 6 Navigation Map of Thesis
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
75
3.1 Introduction
The research methods were designed to answer four principal research aims. These were
to:
1. Identify the professional and community expectations of rural ambulance services in
Victoria, and to suggest improvements in how they operate;
2. Describe the structure and culture of rural ambulance services within their socio-
political climate, including the educational and technological changes that continue
to shape their evolution;
3. Compare the perceived and actual performance of rural ambulance services in
different geographical areas in terms of utilization rates and time intervals with a
view to developing a useful performance framework for rural ambulance services;
and
4. Develop models of ambulance service delivery from different philosophical
perspectives to stimulate debate about models that may be most suitable for rural
Victoria.
Ethics Committee approval for the research project was obtained from the institutional
Ethics Committee at the University of New South Wales on 16 February 1999
(Approval Number 98202). Participants in the study were all provided with explanatory
statements and asked to complete a consent form before completing questionnaires,
being interviewed, or participating in the focus group.
The data and findings are reported on a collective basis, with the opinions or
performance of individual informants and towns remaining anonymous. Where
practicable, the analytical results were reported on the basis of rurality and informant
category. This acknowledged the sensitivity of critical comments and findings, along
with a need to use robust data based on adequate sample sizes.
Reporting the insights of the ambulance staff presented some challenges. To obtain
frank and honest answers, the confidentiality of their individual responses was
guaranteed. The purpose of any questionnaires or other interactions with individuals
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
76
was always made clear to participants. Despite this, there was some initial reluctance to
be open during a time of considerable organizational upheaval and consequent
uncertainty. Another factor contributing to this reticence to participate may have been
the lack of any strong research culture within the ambulance service at the time of the
study compared to the other health professions (Jacobs 2000; Woollard et al 2000).
All data used were obtained through a transparent process of direct inquiry to the
relevant authorities, such as the Department of Human Services, the former Victorian
Ambulance Services’ Association, and the then six existing rural Ambulance Services.
Following the reorganization of the rural ambulance services, inquiries were directed
through Rural Ambulance Victoria and the Alexandra and District Ambulance Service.
Unfortunately, the Alexander and District Ambulance Service chose not to fully
participate. Other information used was obtained from publicly available documents or
through direct approaches to the relevant authorities.
The first step in this process of inquiry was the selection of sample rural communities of
different sizes, determination of respondents, and observation of the setting. Chapter 3.2
describes these community and respondent samples in detail. The research aims called
for both qualitative and qualitative data to draw a picture of the current state of rural
ambulance services, and to evaluate models of service delivery that were subsequently
formulated.
Figure 7 summarizes the type and sources of data that were examined during the study.
These data enabled the four research aims to be answered with a degree of confidence
that the findings and conclusions drawn had solid empirical foundations.
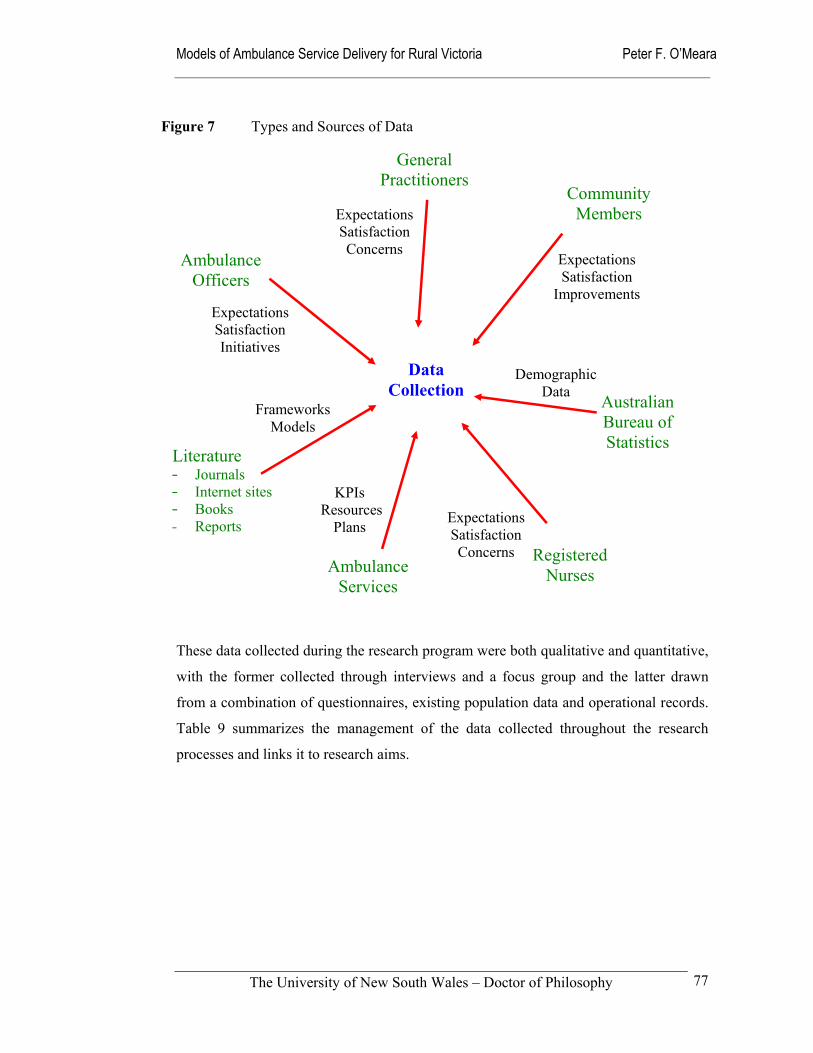
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
77
These data collected during the research program were both qualitative and quantitative,
with the former collected through interviews and a focus group and the latter drawn
from a combination of questionnaires, existing population data and operational records.
Table 9 summarizes the management of the data collected throughout the research
processes and links it to research aims.
Figure 7 Types and Sources of Data
Community Members
Ambulance Officers
Registered Nurses
Data Collection
General Practitioners
Ambulance Services
Expectations Satisfaction Concerns
Expectations Satisfaction Initiatives
KPIs Resources
Plans Expectations Satisfaction Concerns
Australian Bureau of Statistics
Demographic Data
Expectations Satisfaction
Improvements
Literature — Journals — Internet sites — Books — Reports
Frameworks Models
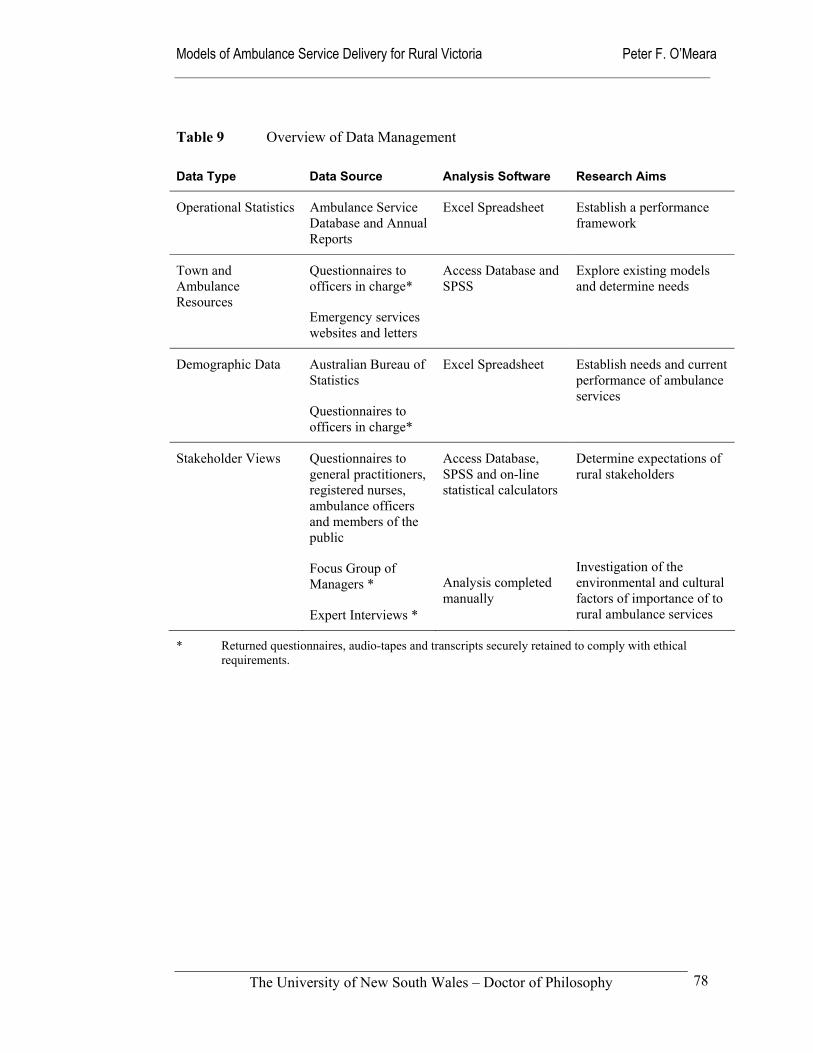
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
78
Table 9 Overview of Data Management
Data Type Data Source Analysis Software Research Aims
Operational Statistics Ambulance Service Database and Annual Reports
Excel Spreadsheet Establish a performance framework
Town and Ambulance Resources
Questionnaires to officers in charge*
Emergency services websites and letters
Access Database and SPSS
Explore existing models and determine needs
Demographic Data Australian Bureau of Statistics
Questionnaires to officers in charge*
Excel Spreadsheet Establish needs and current performance of ambulance services
Stakeholder Views Questionnaires to general practitioners, registered nurses, ambulance officers and members of the public
Focus Group of Managers *
Expert Interviews *
Access Database, SPSS and on-line statistical calculators
Analysis completed manually
Determine expectations of rural stakeholders
Investigation of the environmental and cultural factors of importance of to rural ambulance services
* Returned questionnaires, audio-tapes and transcripts securely retained to comply with ethical requirements.
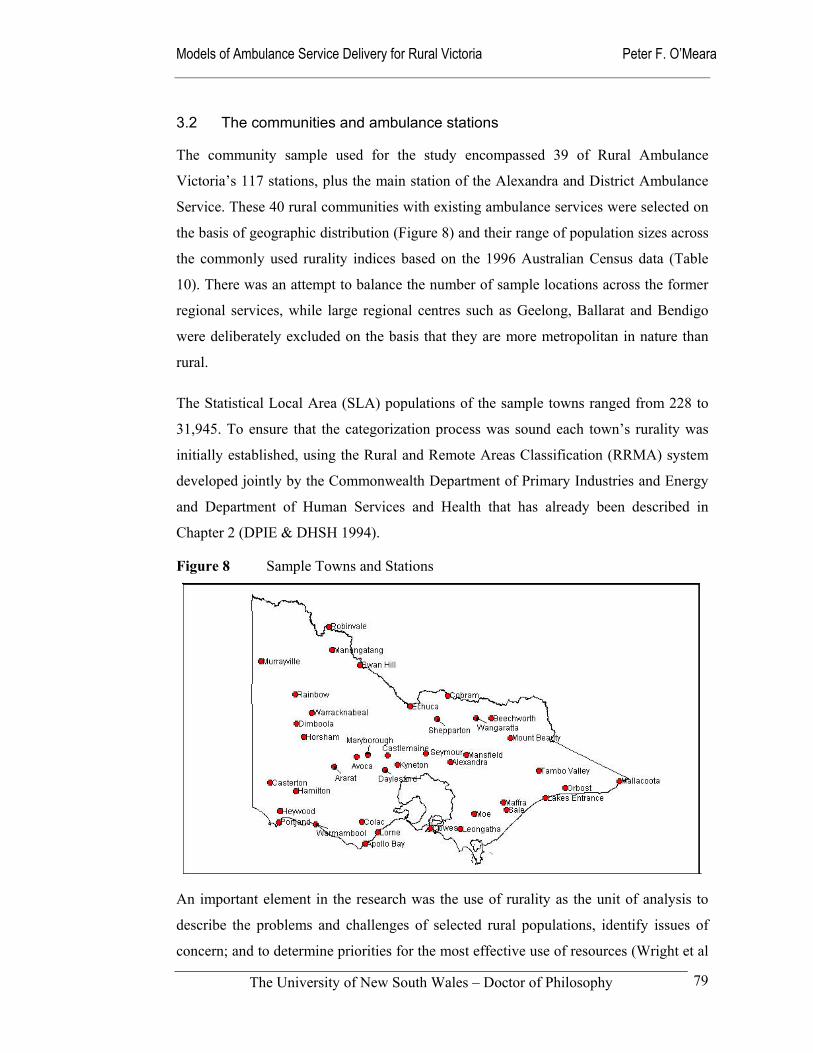
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
79
3.2 The communities and ambulance stations
The community sample used for the study encompassed 39 of Rural Ambulance
Victoria’s 117 stations, plus the main station of the Alexandra and District Ambulance
Service. These 40 rural communities with existing ambulance services were selected on
the basis of geographic distribution (Figure 8) and their range of population sizes across
the commonly used rurality indices based on the 1996 Australian Census data (Table
10). There was an attempt to balance the number of sample locations across the former
regional services, while large regional centres such as Geelong, Ballarat and Bendigo
were deliberately excluded on the basis that they are more metropolitan in nature than
rural.
The Statistical Local Area (SLA) populations of the sample towns ranged from 228 to
31,945. To ensure that the categorization process was sound each town’s rurality was
initially established, using the Rural and Remote Areas Classification (RRMA) system
developed jointly by the Commonwealth Department of Primary Industries and Energy
and Department of Human Services and Health that has already been described in
Chapter 2 (DPIE & DHSH 1994).
Figure 8 Sample Towns and Stations
An important element in the research was the use of rurality as the unit of analysis to
describe the problems and challenges of selected rural populations, identify issues of
concern; and to determine priorities for the most effective use of resources (Wright et al
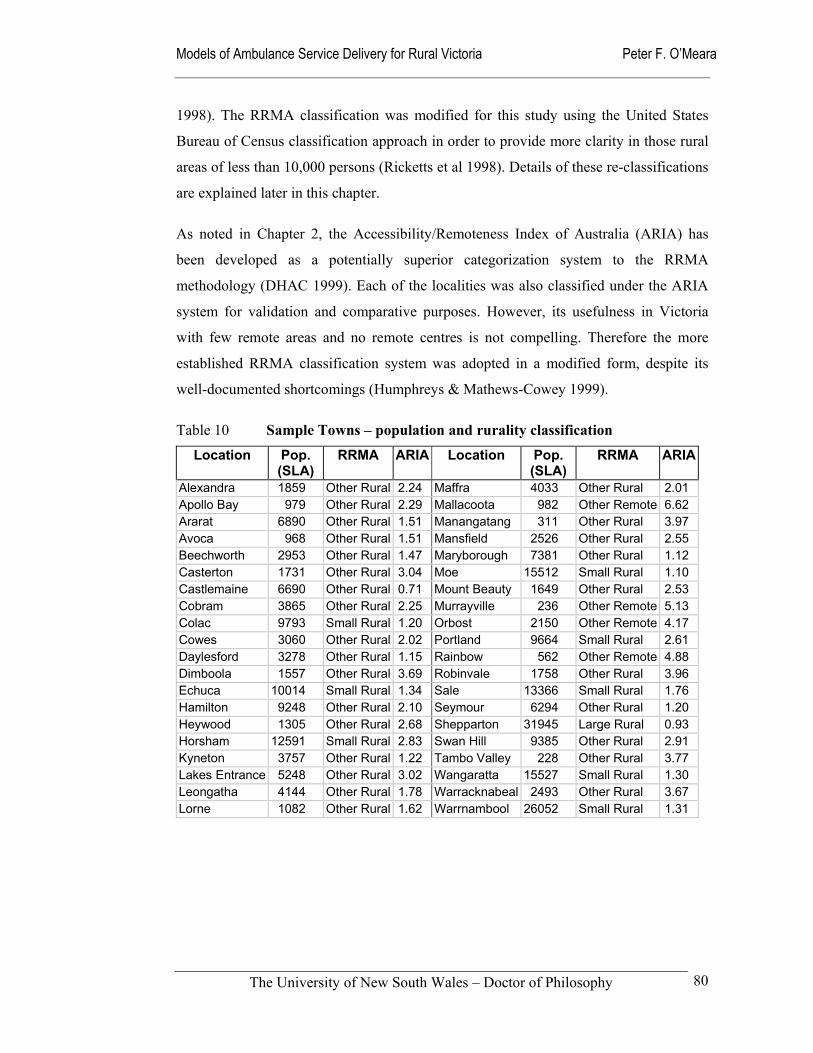
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
80
1998). The RRMA classification was modified for this study using the United States
Bureau of Census classification approach in order to provide more clarity in those rural
areas of less than 10,000 persons (Ricketts et al 1998). Details of these re-classifications
are explained later in this chapter.
As noted in Chapter 2, the Accessibility/Remoteness Index of Australia (ARIA) has
been developed as a potentially superior categorization system to the RRMA
methodology (DHAC 1999). Each of the localities was also classified under the ARIA
system for validation and comparative purposes. However, its usefulness in Victoria
with few remote areas and no remote centres is not compelling. Therefore the more
established RRMA classification system was adopted in a modified form, despite its
well-documented shortcomings (Humphreys & Mathews-Cowey 1999).
Table 10 Sample Towns – population and rurality classification
Location Pop. (SLA)
RRMA ARIA Location Pop. (SLA)
RRMA ARIA
Alexandra 1859 Other Rural 2.24 Maffra 4033 Other Rural 2.01 Apollo Bay 979 Other Rural 2.29 Mallacoota 982 Other Remote 6.62 Ararat 6890 Other Rural 1.51 Manangatang 311 Other Rural 3.97 Avoca 968 Other Rural 1.51 Mansfield 2526 Other Rural 2.55 Beechworth 2953 Other Rural 1.47 Maryborough 7381 Other Rural 1.12 Casterton 1731 Other Rural 3.04 Moe 15512 Small Rural 1.10 Castlemaine 6690 Other Rural 0.71 Mount Beauty 1649 Other Rural 2.53 Cobram 3865 Other Rural 2.25 Murrayville 236 Other Remote 5.13 Colac 9793 Small Rural 1.20 Orbost 2150 Other Remote 4.17 Cowes 3060 Other Rural 2.02 Portland 9664 Small Rural 2.61 Daylesford 3278 Other Rural 1.15 Rainbow 562 Other Remote 4.88 Dimboola 1557 Other Rural 3.69 Robinvale 1758 Other Rural 3.96 Echuca 10014 Small Rural 1.34 Sale 13366 Small Rural 1.76 Hamilton 9248 Other Rural 2.10 Seymour 6294 Other Rural 1.20 Heywood 1305 Other Rural 2.68 Shepparton 31945 Large Rural 0.93 Horsham 12591 Small Rural 2.83 Swan Hill 9385 Other Rural 2.91 Kyneton 3757 Other Rural 1.22 Tambo Valley 228 Other Rural 3.77 Lakes Entrance 5248 Other Rural 3.02 Wangaratta 15527 Small Rural 1.30 Leongatha 4144 Other Rural 1.78 Warracknabeal 2493 Other Rural 3.67 Lorne 1082 Other Rural 1.62 Warrnambool 26052 Small Rural 1.31
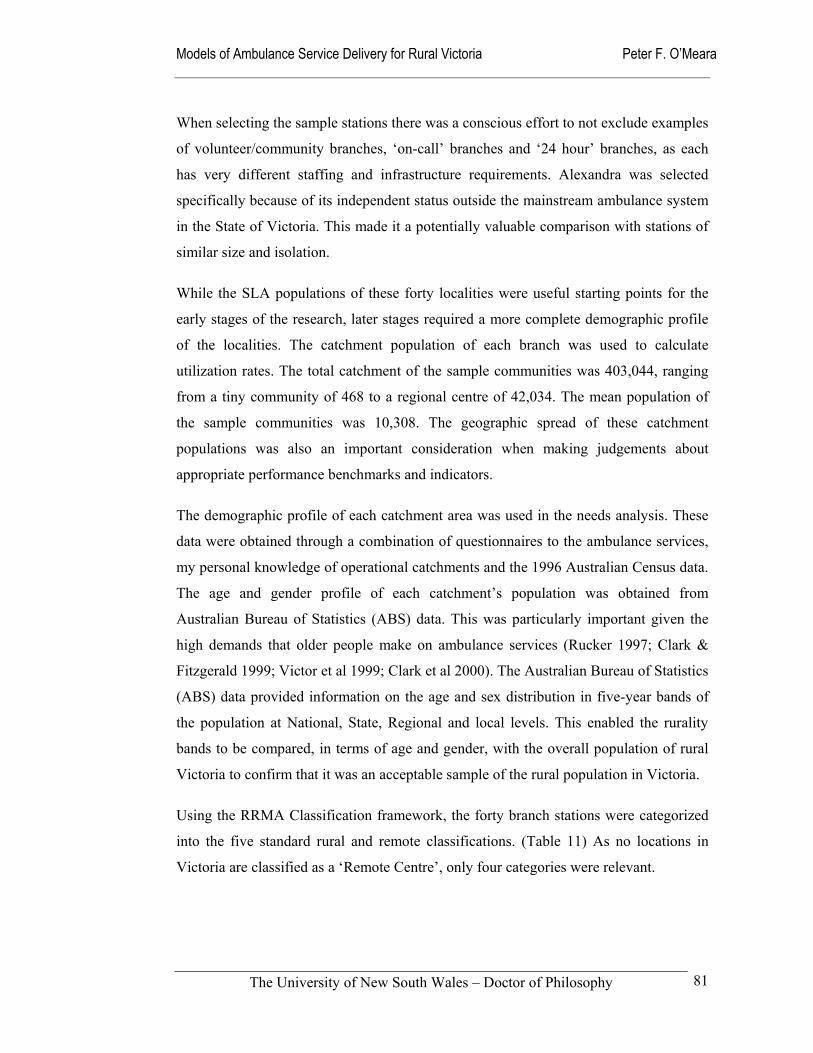
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
81
When selecting the sample stations there was a conscious effort to not exclude examples
of volunteer/community branches, ‘on-call’ branches and ‘24 hour’ branches, as each
has very different staffing and infrastructure requirements. Alexandra was selected
specifically because of its independent status outside the mainstream ambulance system
in the State of Victoria. This made it a potentially valuable comparison with stations of
similar size and isolation.
While the SLA populations of these forty localities were useful starting points for the
early stages of the research, later stages required a more complete demographic profile
of the localities. The catchment population of each branch was used to calculate
utilization rates. The total catchment of the sample communities was 403,044, ranging
from a tiny community of 468 to a regional centre of 42,034. The mean population of
the sample communities was 10,308. The geographic spread of these catchment
populations was also an important consideration when making judgements about
appropriate performance benchmarks and indicators.
The demographic profile of each catchment area was used in the needs analysis. These
data were obtained through a combination of questionnaires to the ambulance services,
my personal knowledge of operational catchments and the 1996 Australian Census data.
The age and gender profile of each catchment’s population was obtained from
Australian Bureau of Statistics (ABS) data. This was particularly important given the
high demands that older people make on ambulance services (Rucker 1997; Clark &
Fitzgerald 1999; Victor et al 1999; Clark et al 2000). The Australian Bureau of Statistics
(ABS) data provided information on the age and sex distribution in five-year bands of
the population at National, State, Regional and local levels. This enabled the rurality
bands to be compared, in terms of age and gender, with the overall population of rural
Victoria to confirm that it was an acceptable sample of the rural population in Victoria.
Using the RRMA Classification framework, the forty branch stations were categorized
into the five standard rural and remote classifications. (Table 11) As no locations in
Victoria are classified as a ‘Remote Centre’, only four categories were relevant.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
82
Table 11 RRMA Categorization and ARIA Ranges
RRMA Classification Frequency of Localities ARIA Range
Large Rural Centres (including Warrnambool #)
2 0.93 to 1.31
Small Rural Centres 7 1.10 to 2.61
Other Rural Areas 27 0.71 to 3.97
Remote Centres 0 Not applicable
Other Remote Areas 4 4.17 to 6.62
# Under the RRMA system Warrnambool is classified as a Small Rural Centre, but meets the criteria for Large Rural Centre. The latter was used for the purposes of this study.
The apparent anomalies in the classifications and population figures are a characteristic
of the RRMA system that attempts to combine both population size and isolation in the
one classification system. This weakness is also apparent when catchment populations
are used to capture the operational range of each ambulance station in the sample.
While there is overlap in both the RRMA and ARIA
classification systems, the major concern was the vast
range within the Other Rural Areas under RRMA. The
localities range from the very small populations
encompassing less than 1,000 persons to district centres
of close to 10,000 persons. To further differentiate
stations within the other rural areas categories, they were
sub-divided further using the United States Bureau of
Census definitions. Firstly, they were split into those
centres with a raw population of less than 2,500, referred
to in the thesis as Little Townships, and secondly, into
those with a population between 2,500 and 10,000,
referred to here as Small Towns (Ricketts et al 1998).
Table 12 categorizes all the sample localities on this
modified basis.
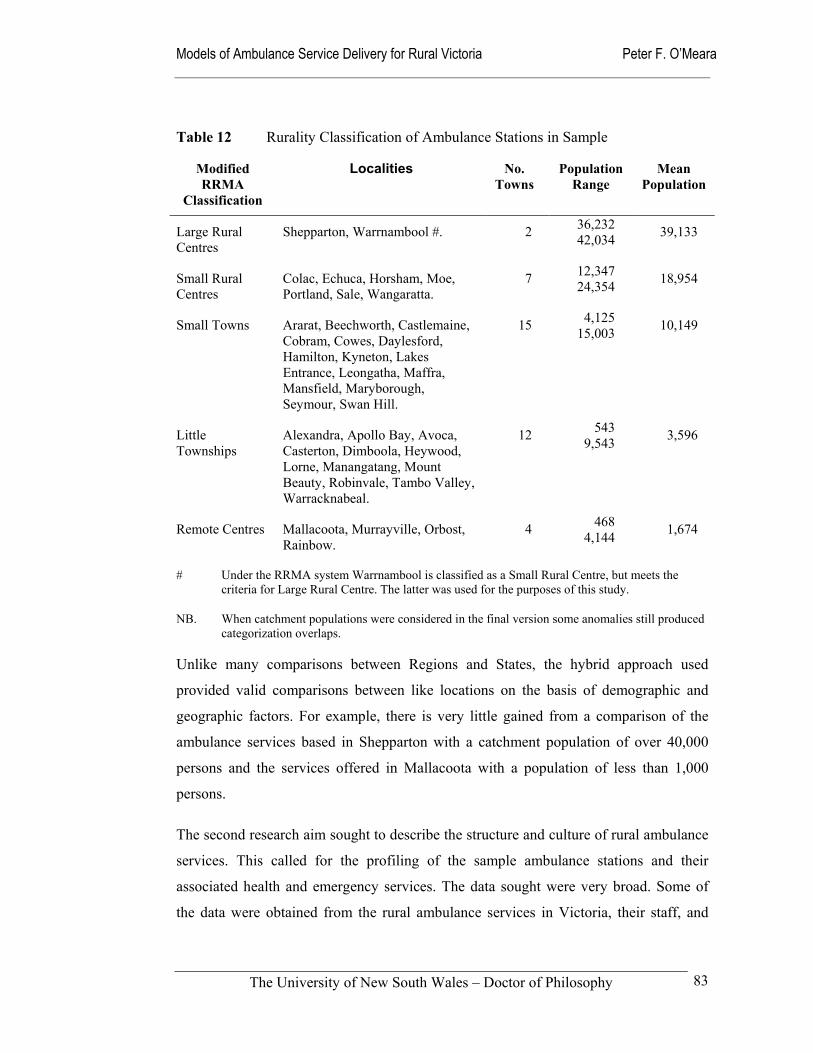
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
83
Table 12 Rurality Classification of Ambulance Stations in Sample
Modified RRMA
Classification
Localities
No. Towns
Population Range
Mean Population
Large Rural Centres
Shepparton, Warrnambool #. 2 36,232 42,034 39,133
Small Rural Centres
Colac, Echuca, Horsham, Moe, Portland, Sale, Wangaratta.
7 12,347 24,354 18,954
Small Towns Ararat, Beechworth, Castlemaine, Cobram, Cowes, Daylesford, Hamilton, Kyneton, Lakes Entrance, Leongatha, Maffra, Mansfield, Maryborough, Seymour, Swan Hill.
15 4,125 15,003 10,149
Little Townships
Alexandra, Apollo Bay, Avoca, Casterton, Dimboola, Heywood, Lorne, Manangatang, Mount Beauty, Robinvale, Tambo Valley, Warracknabeal.
12 543 9,543 3,596
Remote Centres Mallacoota, Murrayville, Orbost, Rainbow.
4 468 4,144 1,674
# Under the RRMA system Warrnambool is classified as a Small Rural Centre, but meets the criteria for Large Rural Centre. The latter was used for the purposes of this study.
NB. When catchment populations were considered in the final version some anomalies still produced categorization overlaps.
Unlike many comparisons between Regions and States, the hybrid approach used
provided valid comparisons between like locations on the basis of demographic and
geographic factors. For example, there is very little gained from a comparison of the
ambulance services based in Shepparton with a catchment population of over 40,000
persons and the services offered in Mallacoota with a population of less than 1,000
persons.
The second research aim sought to describe the structure and culture of rural ambulance
services. This called for the profiling of the sample ambulance stations and their
associated health and emergency services. The data sought were very broad. Some of
the data were obtained from the rural ambulance services in Victoria, their staff, and
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
84
other significant stakeholders through questionnaires (see Appendix), annual reports,
and in some instances direct approaches to key staff.
The balance of the data was found in published documents, officially commissioned
reports, and information available from sources such as municipal councils, other
emergency services and the Australian Bureau of Statistics. The main sources of data
for this purpose were:
Ambulance Service Annual Reports from 1996/97.
Rural Ambulance Victoria Annual Report 2000.
Reports from the Victorian Auditor General in 1997.
Other Government-commissioned Reports, such as the Victorian Ministerial Taskforce on Trauma and Emergency Services Report (1999).
Websites of the SES, CFA and Victoria Police supplemented by direct requests via email.
This approach had the advantage of accessing a large volume of descriptive data about
rural ambulance services, health and emergency services in each individual town.
Descriptive statistics in the form of tables were mainly used to present and summarize
the discrete and continuous data derived from these data sources. This produced
relatively distinct profiles of catchment areas using five rurality bands as a variable.
These profiles incorporated ambulance resource levels, and other health and emergency
infrastructure.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
85
3.3 Determining expectations of rural ambulance services
A cornerstone of the research was an examination of the professional and community
expectations of rural ambulance services through the eyes of ambulance officers,
general practitioners, registered nurses, and members of the public in selected Victorian
rural communities. These questions and related issues are linked to the sustainability
principles of community support, local control of the delivery system, local leadership
and provider teamwork and collaboration that have been described in Chapter 2. The
first of the research aims addressed in the thesis was to:
Identify the professional and community expectations of rural ambulance services in Victoria, and to suggest improvements in how
they operate.
The aim of this component of the research was to establish key respondents’
expectations and perceptions of their local ambulance services. These articulated
expectations are related to the overlapping concepts of need, demand and supply that
Wright et al (1998) have described in the following ways:
Need in health care is commonly defined as the capacity to benefit. If health needs are to be identified then an effective intervention should be available to meet these needs and improve health. There will be no benefit from an intervention that is not effective or if there are no resources available.
Demand is what patients ask for; ... Demand from patients for a service can depend on the characteristics of the patient or on the media’s interest in the service. Demand can be induced by supply: ...
Supply is the health care provided. This will depend on the interests of health professionals, the priorities of politicians, and the amount of money available.
(Wright et al 1998)
Sample
The key respondent groups who participated in the study – ambulance officers, general
practitioners, registered nurses and community members – were sought for their overall
level of knowledge about ambulance services from their own perspectives. They were
preferred from a larger potential group on the basis of their expertise, range of
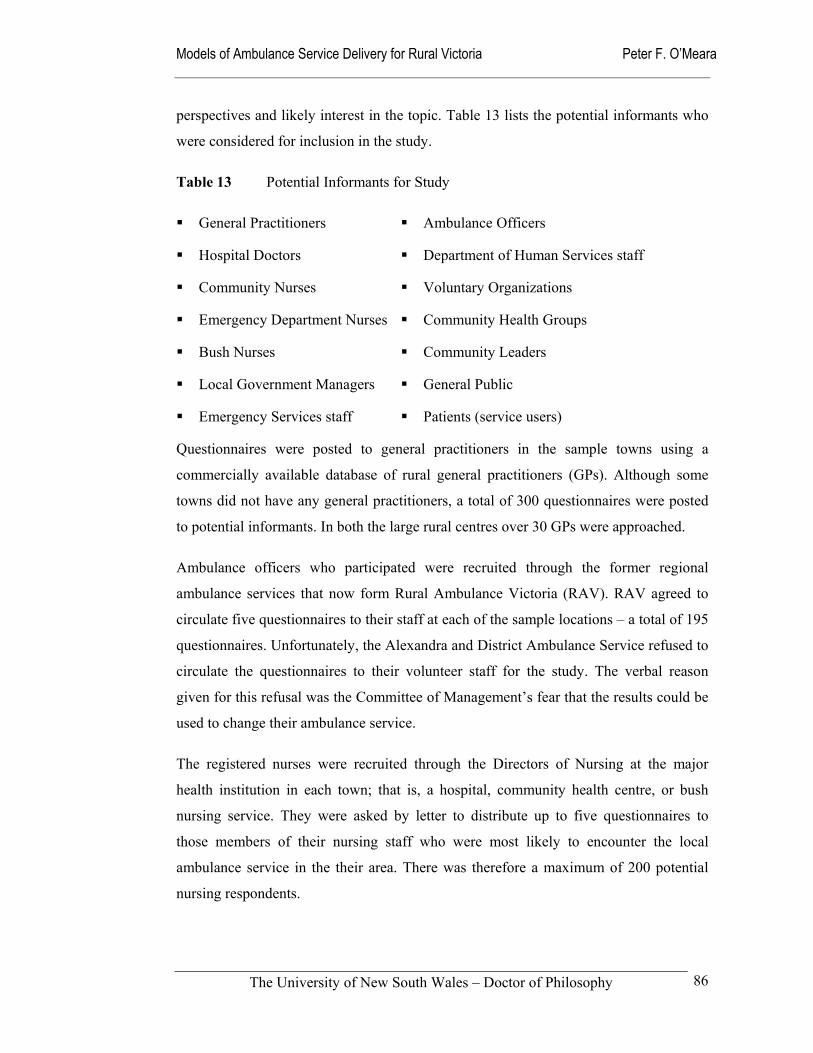
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
86
perspectives and likely interest in the topic. Table 13 lists the potential informants who
were considered for inclusion in the study.
Table 13 Potential Informants for Study
General Practitioners
Hospital Doctors
Community Nurses
Emergency Department Nurses
Bush Nurses
Local Government Managers
Emergency Services staff
Ambulance Officers
Department of Human Services staff
Voluntary Organizations
Community Health Groups
Community Leaders
General Public
Patients (service users)
Questionnaires were posted to general practitioners in the sample towns using a
commercially available database of rural general practitioners (GPs). Although some
towns did not have any general practitioners, a total of 300 questionnaires were posted
to potential informants. In both the large rural centres over 30 GPs were approached.
Ambulance officers who participated were recruited through the former regional
ambulance services that now form Rural Ambulance Victoria (RAV). RAV agreed to
circulate five questionnaires to their staff at each of the sample locations – a total of 195
questionnaires. Unfortunately, the Alexandra and District Ambulance Service refused to
circulate the questionnaires to their volunteer staff for the study. The verbal reason
given for this refusal was the Committee of Management’s fear that the results could be
used to change their ambulance service.
The registered nurses were recruited through the Directors of Nursing at the major
health institution in each town; that is, a hospital, community health centre, or bush
nursing service. They were asked by letter to distribute up to five questionnaires to
those members of their nursing staff who were most likely to encounter the local
ambulance service in the their area. There was therefore a maximum of 200 potential
nursing respondents.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
87
Members of the public were recruited through 29 local municipal councils. They were
requested via letters to distribute the questionnaires to members of the community who
they judged had an interest in ambulance services. Again five questionnaires were
targeted for each catchment area, irrespective of size.
In some cases the potential numbers of informants was much lower than the number of
questionnaires nominally distributed. For instance, a number of the very small locations
do not have general practitioners and the number of registered nurses is small. In some
branches the number of ambulance officers is very small or is confined to volunteer
staff. Based on another similar study, the expected response rate was twenty-five to
thirty percent (Kelly et al 1999).
Data collection
An eleven-question open-ended survey was designed to elicit the information required
to answer those research questions that relied on opinions from stakeholders. The
questionnaire (see Appendix) sought information about the respondents such as locality,
which of the respondent groups they belonged to, age and gender, and their previous
contact with their local ambulance service. Specific questions asked participants about
their expectations of their ambulance service, level of satisfaction and suggestions for
improvement. They were also asked to judge their community’s overall capacity to
respond to medical emergencies on a five-point scale from excellent to very poor.
The questionnaires were purposefully worded to focus on each respondent’s local
ambulance service, rather than the more distant abstract entities of statutory authorities
or regional services, which may have become convenient targets of criticism. It was
estimated that the questionnaires would take 10 minutes for each respondent to
complete.
Pilot testing of the questionnaire was an essential element of the research program.
Emerald, a rural area on the edge of the Melbourne Metropolitan area was chosen as a
pilot site for the research project based on its exclusion from the rural ambulance
services, its rural nature, and the ability to access key informants through existing
contacts. This pilot study, which commenced in November 1998, provided an important
exploratory device, as it allowed the identification of issues relevant to the research
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
88
questions. The pilot was limited to surveying a total of five ambulance officers and five
general practitioners following a field visit to the town. Minor changes to the
questionnaire were made to correct questions that were ambiguous or confusing
(O'Meara 2000).
The amended questionnaires were then distributed to the sample respondents, along
with an explanatory statement and consent form (see Appendix), to the potential
respondents with a request that the completed questionnaire be returned in the addressed
return envelope. Postage was not supplied for reasons of cost.
Data management procedures
Following the return of the questionnaires, the responses were entered into an Microsoft
Access database for secure storage. Question 1 asked where the respondent lived and
the responses were assigned to one of the 40 catchment areas as discrete data.
Responses to questions 2 to 8 and 11 were discrete variables that were entered directly
into the database. Answers to questions 9, 11 and 12 were in the form of short-sentences
and were entered in full with minimal changes such as obvious spelling errors.
In this form, each response could be categorized and analysed according to the variables
of:
gender of respondent;
respondent occupational category;
rurality bands according to RRMA and the modified rurality classifications used for the study;
frequency of contact with ambulance services;
direct contact with ambulance services; and
levels of satisfaction with the services offered.
The dataset was then downloaded into SPSS software for analysis. The answers to
questions 10 and 11 were categorized according to respondent category and rurality
within Microsoft Access. Textual analysis was then manually undertaken to determine
common threads and themes. Open-ended short question answers were analysed and
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
89
categories of themes and issues of interest were identified. The statistical package SPSS
was used to analyse these data, with the findings being presented in terms of rurality and
respondent categories. The returned questionnaires were securely retained to comply
with ethical requirements.
Analysis of stakeholder responses
Respondents’ expectations were manually aggregated into groups of expectations
according to common words and phrases. For example, all those responses that
mentioned time and speed were placed together into one category, while those related to
skills, education and clinical judgement were grouped together. Ten groups of responses
were initially identified, which were then reduced to five. After these five groups were
coded they were cross-tabulated against the variables of rurality and respondent using
SPSS. A Chi-squared test for statistical significance was applied using a Web Chi
Square Calculator (Georgetown 1996).
The cross-tabulation of expectations with the characteristics of the study participants
and the size of the communities enabled the question of expectations in different sized
communities and amongst different participants to be tested for common themes and
differences of emphasis. These analysed findings acted as catalysts for the later focus
group with RAV managers that explored the structural and cultural characteristics of
Rural Ambulance Victoria (reported in Chapter 6). These expectations were also drawn
on in Chapter 8 where models of service delivery were developed.
The questions seeking suggestions for changes and other comments were used to further
explore expectations of local services, and to provide the means of identifying any
suggestions for change that that may be desirable. The expert status of the three
professional groups – ambulance officers, general practitioners and registered nurses –
provided some assurance that the views expressed would be well-informed. The results
were compared to the existing literature on pre-hospital care and emergency medicine to
validate the results from a clinical perspective.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
90
3.4 Structure and culture of ambulance services in rural Victoria
The second aim of the research was to describe the existing ambulance service delivery
models in terms of their overall structure (governance, staff numbers, clinical
qualifications and roster configurations) and culture (management style, professional
ethos and linkages with other health and emergency services). This was completed
through examination of the sample stations and reference to Rural Ambulance Victoria,
the organization now predominately responsible for the delivery of ambulance services
to rural Victoria.
The contextual environment of rural ambulance services was explored through the
determination of RAV’s philosophical basis, its objectives and corporate strategies. The
educational and technological forces impacting upon rural ambulance services were also
identified and described. The second aim of the thesis thus set out to:
Describe the structure and culture of rural ambulance services within their socio-political climate, along with the educational and
technological changes that continue to shape their evolution.
A corporate approach, relying on official sources of data, was used to collect
organizational and community data for the study. While this ran the risk of blurring the
distinction between need and demand and between science and vested interests, the
intimate, detailed knowledge approach was essential if the findings of the study were to
be sensitive to local circumstances. The approach allowed measurement of the special
circumstances facing rural ambulance services in rural Victoria in the late-1990s and
early 21st century.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
91
Sample ambulance stations
Forty selected ambulance branch stations were compared with each other in terms of
clinical ambulance services offered, staffing levels, and rostering arrangements. This
information was initially gathered through a survey to the officers-in-charge of each
station in 1999, information from the 1996/97 annual reports of the former regional
services, my personal and professional knowledge, and government-commissioned
reports.
Data collection
The respective officers-in-charge were requested to complete an eleven question survey
(see Appendix) relating to the situation in 1996. Other data sources, such as road maps,
were used to fill in the gaps this approach left when some officers-in-charge failed to
respond or fill in all details. The questionnaire sought information about catchment
areas, perceptions of rurality, and resourcing and staffing details. Internally
commissioned reports from the former Victorian Ambulance Services’ Association
were unsuccessfully sought as supplementary material.
Rural Ambulance Victoria’s Annual Report of 2000 covering its first full year of
operation was used as source document to elicit RAV’s organisational vision, mission
and objectives. A commissioned operational plan for RAV was unavailable due to the
Department of Human Services delaying approval of its contents for financial and
political reasons. Bringing the survey data and the Annual Report information together
was a focus group with five middle-level managers in June 2001. Participants in the
focus group were middle-level managers who volunteered to participate after being
approached through one of their peers. Their comments were used to both supplement
and validate the findings from other research methods (Baume 1998: 160).
This approach provided a more contemporary picture of rural ambulance services in
Victoria following the establishment and consolidation of a single rural ambulance
service, for all but the small area of the State under the control of the Alexandra and
District Ambulance Service in the central highlands.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
92
Focus group participants were asked to reflect on the characteristics of Rural
Ambulance Victoria in terms of its activities, elements and relationships – in soft
systems methodology (SSM) terms, they were describing the transformation processes
of the organization. Other questions to the group related to the remaining SSM
components described in the CATWOE mnemonic. This mnemonic encompasses the
elements considered when formulating root definitions. The letters stand for C
(customers, who can be victims or beneficiaries), A (actors, carrying out the activities),
T (transformation of some entity), W (Weltanschauung, world-view or perspective), O
(owner, who controls the system), and E (environmental constraints, taken as given)
(Hindle & Braithwaite 2001).
Focus group participants were encouraged to describe RAV in terms of its:
Philosophical basis (Worldview)
Customers/clients (Customers)
Location of power (Owners)
Providers of service (Actors)
Rural environment (Environment)
The focus group participants were asked to describe RAV’s achievements to date and
the challenges of the future. Specific topics raised included the issues of ambulance
service resourcing, local community autonomy, and the role of the ambulance service in
the future. In some cases, the issues raised were further researched by using media
archives and the Hansard record of the Victorian Parliament.
In addition to the focus group, an assessment was made of the technological and
educational developments influencing ambulance service delivery through review of the
relevant literature and interviews with experts in the field. The most coherent work
addressing technological and educational developments in pre-hospital systems was the
strategic review of ambulance services in the United Kingdom (Nicholl et al 2001).
Although it was useful, the North American literature lacked overall coherence and
seemed less culturally and organizationally relevant in comparison with the British
material.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
93
Two interviews were conducted with established experts in the fields of pre-hospital
technology and pre-hospital education from Deakin University and Rural Ambulance
Victoria respectively. The technology expert was an established British researcher in the
pre-hospital field who was visiting Australia on a Fellowship, with a special interest and
expertise in the use of communications technology in combination with clinical
decision-making. That is, the use of telemedicine systems. He had been undertaking
telemedicine research in western Victoria in collaboration with RAV.
Educational developments were researched through reference to the literature in
Australia, the United States and the United Kingdom where degree level courses for
ambulance paramedics have either been established or under consideration. A senior
paramedic educator from RAV was interviewed to discuss the impact these education
and training changes are having on rural ambulance paramedics and the way in which
they practice.
Procedure
During 1999 the survey forms were forwarded to the officers-in-charge of the RAV
sample branches through rural ambulance Victoria. Following earlier telephone contact
with the officer-in-charge, the survey form for the Alexandra station was posted in early
1999. Further telephone contact was made some time later in an unsuccessful effort to
convince that small independent service to participate in the study. An offer was made
to make a presentation to the Committee of Management to allay their fears, however
this was declined.
The survey forms were sent to each station, together with a covering letter, the
ambulance officer questionnaires, explanatory statements and consent forms. Self-
addressed return envelopes were enclosed with each form.
The request for RAV managers to participate in a focus group was made through a letter
to the Chief Executive Officer explaining the issues that would be discussed and the
general approach being taken. This was followed up with a delegated member of the
management group via email and telephone. Arrangements for the focus group took
approximately six months to finalize because of the difficulty in finding a day on which
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
94
the selected managers were available. RAV selected the participants, the location, date
and time of the focus group.
The one-hour focus group was conducted in mid-June 2001 at the RAV Head Office in
Ballarat. Five middle-level managers based in Ballarat participated in the focus group.
Three were very well acquainted with me, having either past or current professional
relationships, while two had not met me before. Their respective responsibilities were
service planning, business development, clinical management and education, and
operational management. All were male.
On arrival, the participants were provided with an explanatory statement and consent
form to read and sign. They were asked whether they understood the purpose of the
focus group and whether they had any objection to the interview being taped for further
analysis. No objection was raised to this procedure.
Following completion of the consent forms, the focus group was initiated with
participants being asked to describe the structure and culture of Rural Ambulance
Victoria in terms of its activities, elements and relationships. They were asked to tell me
about the activities of RAV, the physical resources it uses and the key relationships that
it sustains. Following considerable discussion, participants were then asked about the
philosophical basis on which RAV rests; that is, its organizational values. This question
drew responses that covered other planned questions about RAV’s customers, who
provided services to them, and the impact of the rural environment on the services
provided.
Following this period of the participants speaking for themselves, a more confronting
question asking about where power rested within RAV was put to them. It sought to
have the focus group participants identify:
who the decision-makers are in rural ambulance circles;
who controls the agenda; and
who implements strategic objectives.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
95
The focus group ended with a positive question, asking participants about the
achievements of RAV to date and the future challenges it faces in the immediate to
medium-term future. Their responses concentrated on the important issues of the
organizational identity of RAV. The technological and educational determinants or
drivers of service delivery systems were barely addressed.
These unanswered questions were explored in the interviews with the pre-hospital
experts in technology and education. The pre-hospital technology expert participated in
a telephone interview in late-July 2001, following informal discussions and the
furnishing of possible questions. The 30-minute interview was taped to allow
confirmation of notes taken and for the further analysis that is incorporated into the
findings in Chapter 6.
In November 2001, a senior ambulance paramedic educator was interviewed in person.
He was asked to reflect on the impact of the changes in ambulance education over the
last decade. The most important changes explored were the transfer of ambulance
education to the university sector and the introduction of advanced clinical training to
rural areas in the guise of Advanced Life Support (ALS) and the extension of MICA
Paramedic training to rural areas. The interviewee was encouraged to explore the impact
this had made on ambulance paramedics’ views of their place in the health and
emergency response teams and how their relationships with the community and other
health professionals had changed.
Analysis
The data collected through questionnaires to the officer-in-charge of each of the stations
were used to define the sample stations’ catchment areas and develop profiles of each
sample community’s health and emergency services relevant to ambulance service
delivery. A second round of requests directly through Rural Ambulance Victoria failed
to improve the response rate. Other sources of information (maps, annual reports and
other organizations’ data) and my personal knowledge were used to construct the branch
profiles in those areas that failed to respond. After being entered into an MS Access
database, the data were analysed in SPPS using rurality as the variable. The results are
presented descriptively in tables in Chapter 5.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
96
The nature of the data gained from the focus group and the interviews allowed them to
be analysed for their textual content and character. Due to the comparatively small
volume of data, this was carried out manually. The focus group took one hour to
complete and ran to over eleven thousand words of transcript. Participants were asked a
few broad questions, such as:
Describe RAV to me?
What is the philosophical basis of RAV?
Where does the power rest in RAV? Who makes the decisions? Who controls
the agenda?
Can you tell me about the achievements of RAV in terms of resourcing?
What do you see as the future challenges for RAV?
The responses to these questions were reported as the story of the formation of RAV
and the resultant structural, cultural and political changes that have taken place. Key
issues were then identified and considered in the Chapter 6 discussion using a
combination of SSM and policy analysis techniques.
The interviews with the pre-hospital technological and educational experts concentrated
on identifying the technological and educational changes that may impact on future
ambulance service delivery. The findings were compared with the existing literature
relating to these areas of interest. The thesis sought to bridge the gap between the
reporting of new technologies, procedures and educational processes, with the impact
they may have on community expectations, interactions with other health professionals
and the deployment and management of rural ambulance services in the future.
The influences identified during the research process are described as the drivers of
rural ambulance systems and classified into eight groups of inter-related influences.
They are illustrated in Figure 9. For the purposes of reporting and discussion of the
findings, these influences are grouped into three main categories that looked at the
structure of Rural Ambulance Victoria, its cultural shape, and the political landscape in
which it is located. From these themes, the most pressing ongoing issues for rural
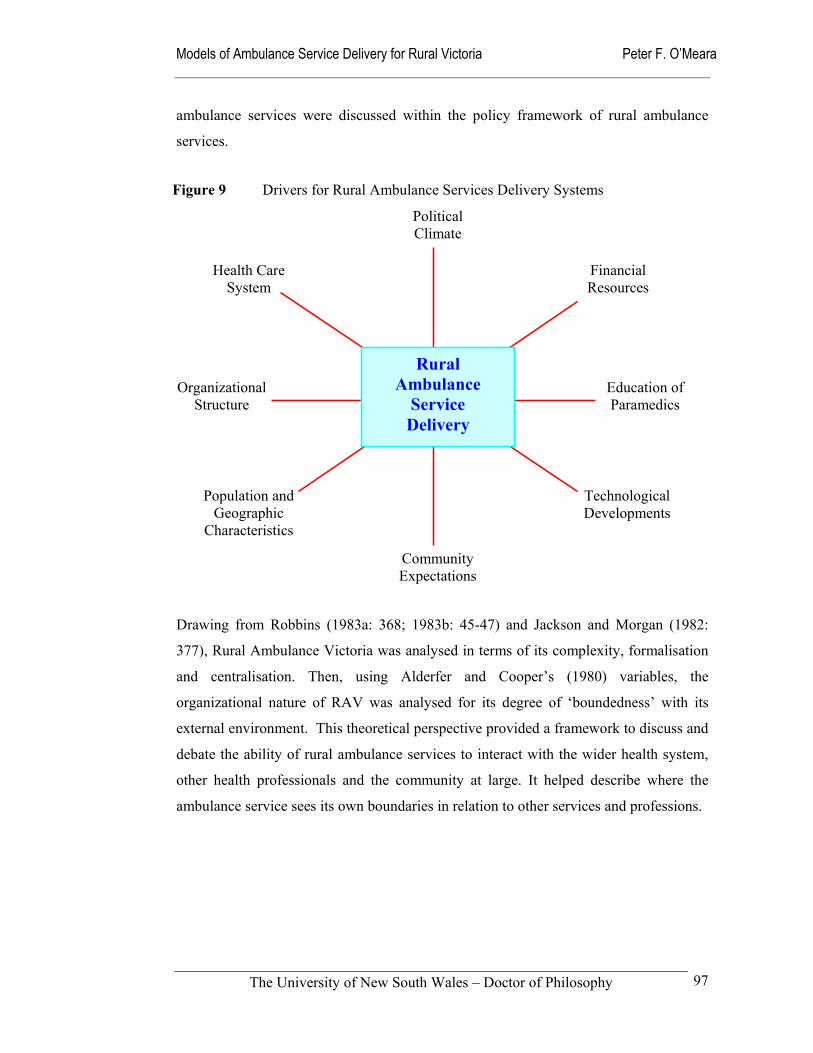
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
97
ambulance services were discussed within the policy framework of rural ambulance
services.
Drawing from Robbins (1983a: 368; 1983b: 45-47) and Jackson and Morgan (1982:
377), Rural Ambulance Victoria was analysed in terms of its complexity, formalisation
and centralisation. Then, using Alderfer and Cooper’s (1980) variables, the
organizational nature of RAV was analysed for its degree of ‘boundedness’ with its
external environment. This theoretical perspective provided a framework to discuss and
debate the ability of rural ambulance services to interact with the wider health system,
other health professionals and the community at large. It helped describe where the
ambulance service sees its own boundaries in relation to other services and professions.
Health Care System
Community Expectations
Population and Geographic
Characteristics
Political Climate
Education of Paramedics
Technological Developments
Organizational Structure
Financial Resources
Rural Ambulance
Service Delivery
Figure 9 Drivers for Rural Ambulance Services Delivery Systems
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
98
3.5 Measuring performance of ambulance services
Despite the time and resources channelled into the collection of operational data in
ambulance services, there is a lack of accepted performance benchmarks in Australian
rural ambulance services (Baragwanath 1997b). This shortfall in accepted measures of
performance highlights the need for a performance framework for rural ambulance
services. In order to make progress toward this outcome, the standard operational data
from rural ambulance services are reported on in the thesis, along with measures of
satisfaction from the surveys of respondents according to rurality. The existing
performance framework literature was then used to reflect on these data and used to:
Compare the perceived and actual performance of rural ambulance services in different geographical areas in terms of utilization rates and time intervals with a view to developing a useful performance framework for rural ambulance services.
Sample
As in the earlier questions, key respondents (ambulance officers, general practitioners,
nurses and members of the public) from 40 stations were surveyed. In this case, they
were asked to rate the performance of their local ambulance service and the capacity of
their community to respond to emergencies.
In order to directly measure performance, the former five major regional ambulance
services and Alexandra and District Ambulance Service were requested to provide
operational data including patient profiles, reaction and response times for 1996/97
covering the 40 sample branch stations. The specific operational information requested
from the rural Ambulance Services is detailed in Table 14. The operational performance
measures requested were selected because of their anticipated availability and
widespread use, rather than their confirmed value as measures of performance.
Additional information about clinical conditions that are theoretically coded on each
patient care record (PCR) were not sought as the data set was known to be incomplete
as a result of the turbulent industrial relations environment within the Victorian
ambulance services at that time.
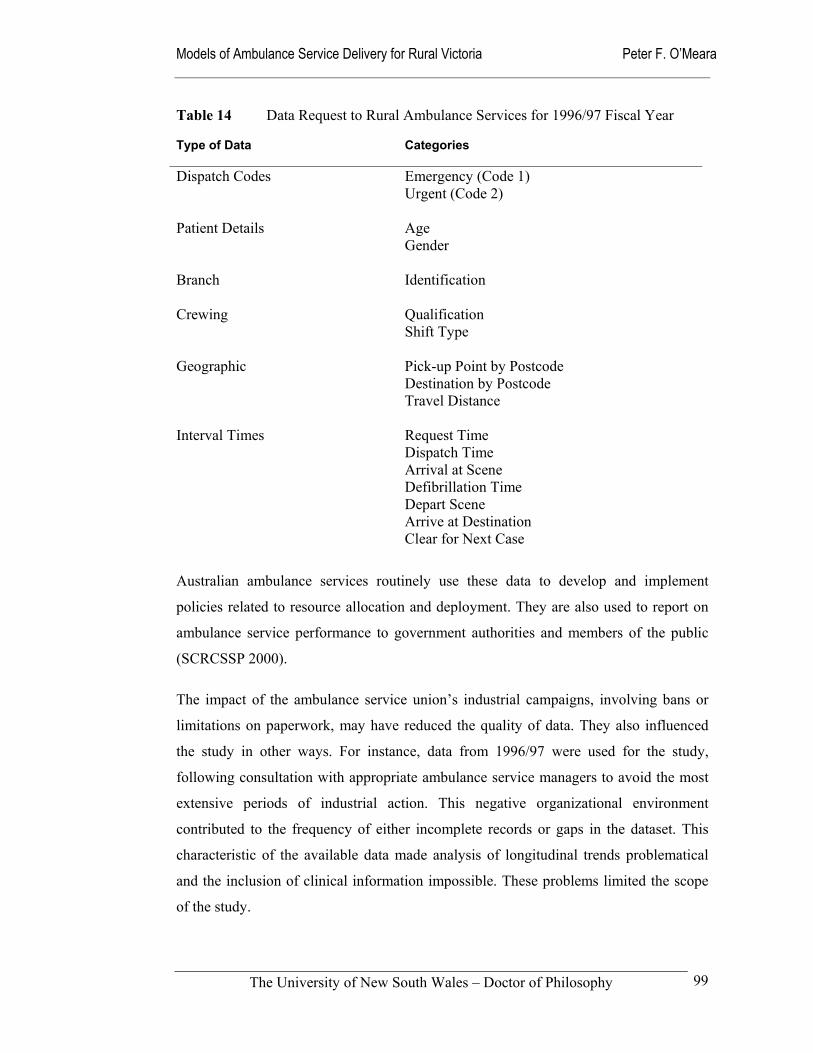
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
99
Table 14 Data Request to Rural Ambulance Services for 1996/97 Fiscal Year Type of Data
Categories
Dispatch Codes Emergency (Code 1) Urgent (Code 2) Patient Details Age Gender Branch Identification
Crewing Qualification Shift Type
Geographic Pick-up Point by Postcode Destination by Postcode Travel Distance
Interval Times Request Time Dispatch Time Arrival at Scene Defibrillation Time Depart Scene Arrive at Destination Clear for Next Case
Australian ambulance services routinely use these data to develop and implement
policies related to resource allocation and deployment. They are also used to report on
ambulance service performance to government authorities and members of the public
(SCRCSSP 2000).
The impact of the ambulance service union’s industrial campaigns, involving bans or
limitations on paperwork, may have reduced the quality of data. They also influenced
the study in other ways. For instance, data from 1996/97 were used for the study,
following consultation with appropriate ambulance service managers to avoid the most
extensive periods of industrial action. This negative organizational environment
contributed to the frequency of either incomplete records or gaps in the dataset. This
characteristic of the available data made analysis of longitudinal trends problematical
and the inclusion of clinical information impossible. These problems limited the scope
of the study.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
100
Data collection
The survey data were collected as part of the process used to answer the earlier research
aims. Stakeholder respondents were asked to rate their satisfaction levels with their
local ambulance service and the community’s overall capacity to cope with medical
emergencies on a five-point scale (see Appendix). They also had the opportunity to
make other comments in two other questions asking for their suggestions for
improvement and any other comments they may have. These latter questions were also
drawn on to answer questions about stakeholder expectations of rural ambulance
services.
In the first instance, the operational data, less patient and staff identifiers, were
requested in electronic form from the Department of Human Services, Victoria in late
1998. The Department advised that the data were available from the individual
ambulance services directly, subject to Ethics Committee approval. By this time, the
major rural ambulance services in Victoria were in the process of amalgamating into
one entity. Letters were written and direct telephone contact made to request the
required data and other assistance from the new organization, Rural Ambulance
Victoria, and the continuing Alexandra and District Ambulance Service in early 1999.
The 1996/97 operational data for the five former regional ambulance services were
supplied some months later in the form of five separate data sets stored in Microsoft
Excel. Operational data from Alexandra and District Ambulance Service were not made
available, apart from utilization rates that were obtained through the Department of
Human Services. It was therefore not included in the analysis of performance.
Using these data allowed the option of investigating whether the performance of the
ambulance service in individual locations differed markedly from that provided
elsewhere. Although the results required sensitive interpretation, comparative analysis,
process and outcome indicators helped identify differences in the provision of services
(Stevens & Gilliam 1998). Earlier work developing a resource allocation formula for
Gippsland in Victoria indicated that there was some value to be gained from this
comparative approach (O’Meara 1995).
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
101
Procedure
The survey results were entered into an Microsoft Access database for ease of entry,
before being transferred to SPPS for analysis. The completed questionnaires were then
categorized according to respondent groups and stored securely.
The operational data were supplied in five separate Microsoft Excel databases, with two
different formats. These were combined into one database of almost 20,000 records.
They were then analyzed according to the rurality classifications of the stations. At
each stage, the quality of the data was of concern and data that were obviously incorrect
were excluded. While the large number of records hindered the extent of the
corrections, it also provided the opportunity to use statistical methods that reduced the
impact of outliner results and overcame most of these data quality problems. Despite
audit of the data, the interpretation and application of the ambulance service operational
statistics needs to be tempered by the known weaknesses in both data recording and data
entry. These problems with the ambulance service data were constant.
The genesis of the problem lies in the data collection processes. For instance, the
recorded age of patients transported saw both the very young and very old over-
represented in the records. Adjustments were made to counter the skewing that resulted
from inaccurate data collection. One possibility was that the problems stem from the
information being collected in five separate dispatch centres. In all but one of these
centres, the time interval data were recorded onto the patient care records after patients
were safely deposited at their destination, rather than directly onto an electronic
database. Understandably, ambulance staff tend to be more concerned about the clinical
care of the patient than accurately recording interval times on patient care records. One
demonstration of this data collection flaw was the inordinately high number of
ambulance cases with a ‘zero’ response time. It is not credible that such a high number
of cases could be received, dispatched to and arrive at the scene in less than one minute,
including some from one postcode area to another. Independent and more recent data
from Rural Ambulance Victoria verifies this observation; its suggests that two to three
minutes should be added to the response time data to account for this inherent problem.
In other cases the time at scene times reported were more than twelve hours – these
were judged to be typographical errors during the data entry process.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
102
Analysis
To some degree, the information collected fits into Donabedian’s evaluation framework
of structure, process and outcome (Donabedian 1980). In other ways it fits into Aday’s
(1998) framework of effectiveness, efficiency and equity. Checkland and Scholes
(1990: 39) suggest that comparisons of any system or model should be made on the
basis of efficacy, efficiency or effectiveness. Efficacy means whether the intervention
undertaken actually works to achieve the desired output. Efficiency is an economic
indicator related to the use of resources. While effectiveness, examines the longer-term
outcomes of an activity in relation to its aims. For example, defibrillation does work for
many patients in ventricular fibrillation, it can be delivered economically under some
models of service delivery, but it may not necessarily improve the long-term objective
of improving patient discharges from hospital.
In common with the earlier analysis, respondents’ satisfaction levels were cross-
tabulated against rurality, occupational group, gender, and contact with ambulance
services. A Chi-squared test for statistical significance was applied where appropriate
using a Web Chi Square Calculator (Georgetown 1996). Their comments in the open
questions were also considered as part of the overall picture of how the respondents saw
the performance of the ambulance service.
Australian Bureau of Statistics demographic data for each catchment with the
Ambulance Services’ operational data were combined with the operational data to
calculate the utilization rates across the whole sample, each individual station and
according to rurality band. This provided a measure of the need for ambulance services
in rural Victoria. Despite some difficulties with these data, age and gender comparisons
were also made between the general rural population and patients transported within the
sample.
The time interval data were used to calculate individual response times, time at scene,
and time to destination; it was not possible to determine reaction times due to
incomplete data. These time intervals were then analysed to determine the percentile
response times according to the rurality of the stations. This procedure fits in with the
widely accepted ORCON (Operational Research Consultancy) standards used in the
United Kingdom (DHSS 1990; Barrett & Guly 1999a). Using the mean response times

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
103
would have run the risk of skewing the results in those locations with only a small
number of cases. The misuse of mean response times as a performance indicator is a
good example of how the performance data routinely collected have not been designed
to fit into any particular performance framework. The reality is that the performance
measures traditionally used in Australian ambulance services are often a collection of
those that can be collected, and those that government departments and the public have
demanded because they provide a simple one-figure snapshot. On the whole, they are
based on the emergency service model, rather than the health service model.
The concept of developing a performance framework for rural ambulance services is
developed in light of this observation. This effort drew on the work of Asplin (1997),
Carrington (1997), Moore (1999), Maio et al (1999) and Spaite et al (2001) in
ambulance services evaluation, and Duckett (1999), Aday (1998), Sheldon (1998) and
Hancock (1999) in health services management more generally. Of particular value was
the proposed national performance framework developed by the National Health
Ministers’ Benchmarking Working Group (2000), who had drawn heavily from
developmental work in both the United Kingdom and Canada. The work undertaken in
the South Australian Ambulance Service provided a clinical perspective on ambulance
service performance in contrast to the more traditional emergency service perspective
that is common elsewhere.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
104
3.6 Formulating models of service delivery
Addressing each of the first three research aims provided information and understanding
of the issues required to answer the fourth aim that sought to:
Develop models of ambulance service delivery from different philosophical perspectives to stimulate debate about models that may
be most suitable for rural Victoria.
The challenge was to develop models of service delivery that would bring about
changes in service delivery that are beneficial to the health of the rural population
(Stevens & Gilliam 1998). The socio-political environment in which rural ambulance
services operate in Australia dictates that changes to service delivery will take place
incrementally through a reallocation of existing resources and often amidst resistance
from stakeholders. This is not to diminish the value of good strategic planning; only to
acknowledge the nature of the rural ambulance service policy environment.
In this study both quantitative and qualitative research methods were called on to
untangle a number of the different ambulance service delivery models already operating
in rural Victoria. Other options that are not seen locally were also investigated and
assessed for their potential to improve service delivery. The research identified relevant
issues and problem situations, and explored each models’ activities, elements and
relationships.
Checkland’s soft systems methodology (SSM) was used to develop and critically
appraise five models of service delivery (Checkland 1981; Checkland & Scholes 1990;
Checkland 1999). As one of the major-non-traditional systems analysis/management
science approaches to organisational research, SSM was used for this research because
it:
is well established in the literature of management sciences;
is distinctly non-traditional in philosophy and operation;
has a recognisable degree of formal structure (Ledington & Donaldson 1997);
has not been used extensively in health sector analysis (Hindle & Braithwaite 2001); and
has not been used at all in ambulance service research.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
105
Soft System Methodology
The process of determining potential service delivery models for Victoria’s rural
ambulance services was not something that could be finalised at the onset of the
research. It was constantly reviewed and modified throughout the research process. The
process was iterative. SSM was used to build and analyse a range of different service
delivery models through the provision of:
an analytical framework for the findings related to the first three research aims (Chapters 5 to 7);
the creative development of useful models of ambulance service delivery in rural Victoria (Chapter 8); and
an integration framework used in the conclusion to bring together the sometimes conflicting empirical data (Chapter 9).
Checkland and Scholes quote von Bulow to explain the nature of these iterative and
reflective qualities of SSM.
The learning takes place through the iterative process of using systems concepts to reflect upon and debate perceptions of the real world, taking action in the real world, and again reflecting on the happenings using systems concepts. The reflection and debate is structured by a number of systemic models. These are conceived as holistic ideal types of certain aspects of the problem situation rather than as accounts of it. It is taken as given that no objective and complete account of a problem situation can be provided.
(von Bulow 1989, quoted in Checkland & Scholes 1990: 28)
The significant difference between this systems approach and the classical management
approaches is that it takes account of both the logic and the broader cultural context of
the situation. It is this consideration of the cultural feasibility that is the peculiar and key
feature that distinguishes SSM.
The idea of culture powerfully guides the SSM user, stating categorically that there are organisational and/or social constraints in the “real world” which potential changes, recommended by intervention, must meet. This clearly reflects the philosophical base of SSM, particularly the idea of the cohesiveness of social rules and practices.
(Flood & Jackson 1991: 171)
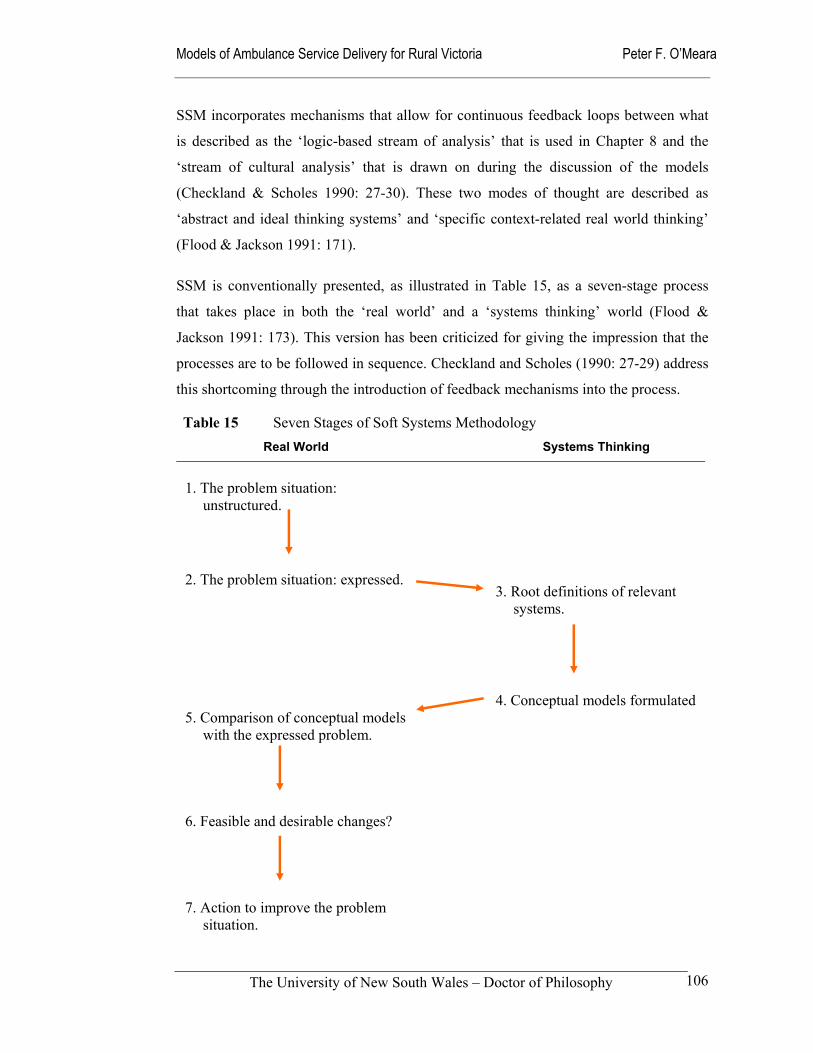
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
106
SSM incorporates mechanisms that allow for continuous feedback loops between what
is described as the ‘logic-based stream of analysis’ that is used in Chapter 8 and the
‘stream of cultural analysis’ that is drawn on during the discussion of the models
(Checkland & Scholes 1990: 27-30). These two modes of thought are described as
‘abstract and ideal thinking systems’ and ‘specific context-related real world thinking’
(Flood & Jackson 1991: 171).
SSM is conventionally presented, as illustrated in Table 15, as a seven-stage process
that takes place in both the ‘real world’ and a ‘systems thinking’ world (Flood &
Jackson 1991: 173). This version has been criticized for giving the impression that the
processes are to be followed in sequence. Checkland and Scholes (1990: 27-29) address
this shortcoming through the introduction of feedback mechanisms into the process.
Table 15 Seven Stages of Soft Systems Methodology Real World Systems Thinking
1. The problem situation:
unstructured.
2. The problem situation: expressed. 5. Comparison of conceptual models
with the expressed problem. 6. Feasible and desirable changes? 7. Action to improve the problem
situation.
3. Root definitions of relevant
systems.
4. Conceptual models formulated
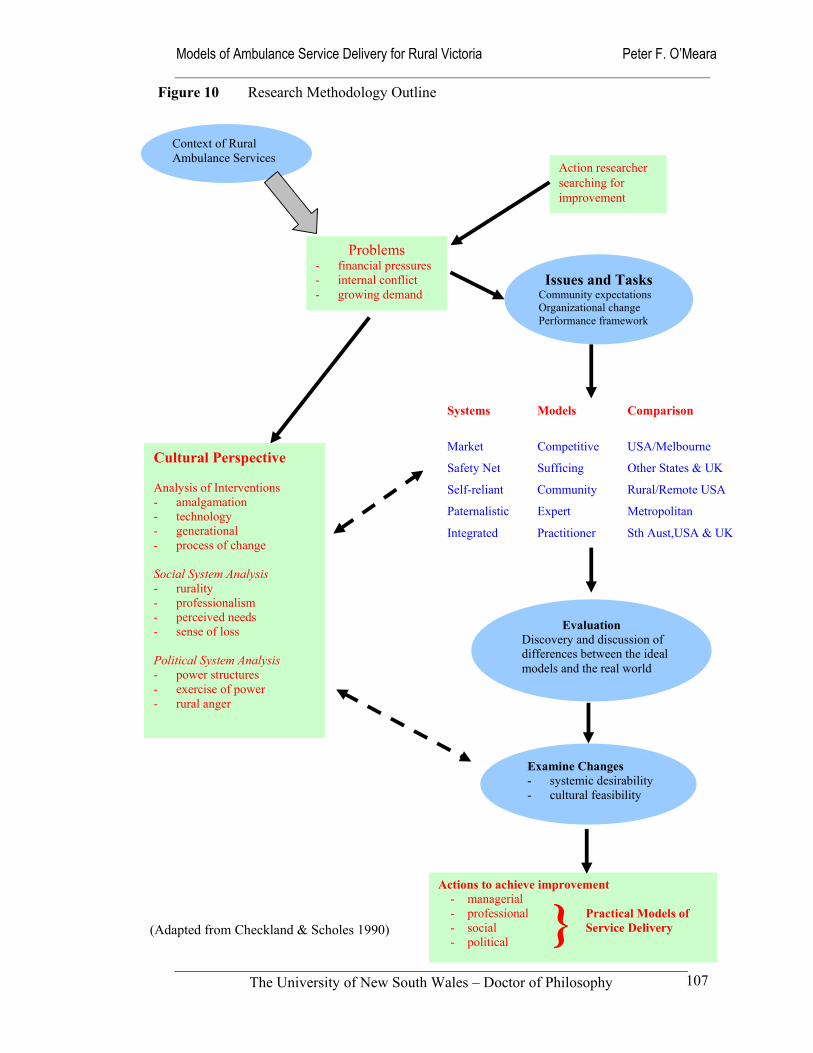
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
107
(Adapted from Checkland & Scholes 1990)
Context of Rural Ambulance Services
Action researcher searching for improvement
Issues and Tasks Community expectations Organizational change Performance framework
Problems - financial pressures - internal conflict - growing demand
Cultural Perspective Analysis of Interventions - amalgamation - technology - generational - process of change Social System Analysis - rurality - professionalism - perceived needs - sense of loss Political System Analysis - power structures - exercise of power - rural anger
Systems Models Comparison
Market Competitive USA/Melbourne
Safety Net Sufficing Other States & UK
Self-reliant Community Rural/Remote USA
Paternalistic Expert Metropolitan
Integrated Practitioner Sth Aust,USA & UK
Examine Changes - systemic desirability - cultural feasibility
Evaluation Discovery and discussion of differences between the ideal models and the real world
Actions to achieve improvement - managerial - professional - social - political }
Practical Models of Service Delivery
Figure 10 Research Methodology Outline
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
108
The overall methodological approach to the question of formulating service delivery
models is summarized in Figure 10. It moves the research process from the
identification of problems, through the identification of the issues and tasks while
answering aims one, two and three of the thesis, through to the process of identifying
abstract models of service delivery. In the thesis, five models – competitive; sufficing;
community; expert; and practitioner - were tested against the ‘real world’ for the
systemic desirability. Parallel to this process a cultural analysis examined the models’
feasibility from a socio-political perspective.
The outcomes of this two-pronged approach are suggestions for the future introduction
of innovative models of service delivery or the strengthening of older models that have
been re-visited. SSM’s strength throughout the research process was its ability to draw
on the answers to the first three research aims and then to inform the fourth aim of
developing models that stimulate debate about which models of ambulance service
delivery may be of value to rural communities.
Logic-based Stream of Analysis
The logic-based stream of analysis was used as a fulcrum to move through the
identification of expectations (Chapter 5), description of the existing organizational
context, structure and culture (Chapter 6), and the development of a performance
framework (Chapter 7), to the development of service delivery models (Chapter 8). This
stream of analysis, illustrated in Figure 11, consists of four main components; the
selection of relevant systems; the naming or describing of them; their modelling; and
then their comparison with real-world situations.
While it is important to recall that the systems are essentially abstractions, there are
essentially two types of systems that can be selected. At one end of the continuum are
those that focus on the primary task and at the other end those concentrating on the
issues (Checkland & Scholes 1990: 32). Much of the research was to conceptualise a
range of service delivery systems for Victoria’s rural ambulance services, develop
models and where possible find examples of communities where they operate, and
compare them to the actual situation as it occurs elsewhere in rural areas.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
109
Figure 11 Process of Logical Analysis
i) Choosing relevant systems
This first step in the logical process required an open mind to identify a range of
systems that may have been relevant. As mentioned above, this process offers two
approaches. The first approach focuses on the primary-task system that will provide the
specified service, for example the provision of an emergency response to medical
emergencies. The second, an issue-based system, is more concerned with determining
what the service ought to be, and is therefore more challenging; it can be used to
address the issues of resource allocation and the provision of equitable services. As
Checkland and Scholes explain, the reality is not as clear-cut as this description may
imply.
The distinction between primary task and issue-based relevant systems is not sharp or absolute, rather these are ends of a spectrum. At the extremes, primary task systems map on to institutionalized arrangements; issue-based systems, on the other hand, are relevant to mental processes which are not embodied in formalized real-world arrangements.
(Checkland & Scholes 1990: 32)
Reality Testing
Observation Informal discussions Interviews and focus groupSocio-political analysis
Modelling relevant systems Inputs-Processes-Outputs Activities-Elements-RelationshipsPerformance framework
Naming relevant systems ‘CATWOE’
Choosing relevant systems Primary-task systems Issue-based systems
(Adapted from Checkland & Scholes 1990)
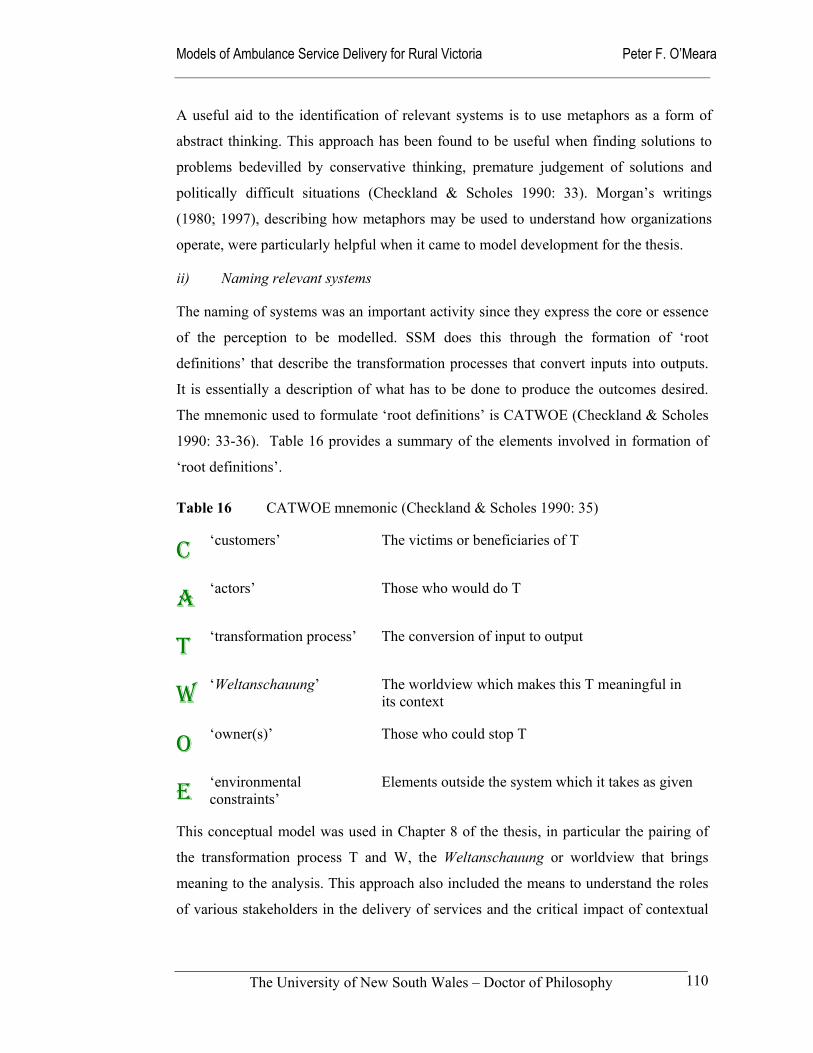
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
110
A useful aid to the identification of relevant systems is to use metaphors as a form of
abstract thinking. This approach has been found to be useful when finding solutions to
problems bedevilled by conservative thinking, premature judgement of solutions and
politically difficult situations (Checkland & Scholes 1990: 33). Morgan’s writings
(1980; 1997), describing how metaphors may be used to understand how organizations
operate, were particularly helpful when it came to model development for the thesis.
ii) Naming relevant systems
The naming of systems was an important activity since they express the core or essence
of the perception to be modelled. SSM does this through the formation of ‘root
definitions’ that describe the transformation processes that convert inputs into outputs.
It is essentially a description of what has to be done to produce the outcomes desired.
The mnemonic used to formulate ‘root definitions’ is CATWOE (Checkland & Scholes
1990: 33-36). Table 16 provides a summary of the elements involved in formation of
‘root definitions’.
Table 16 CATWOE mnemonic (Checkland & Scholes 1990: 35)
C ‘customers’ The victims or beneficiaries of T
A ‘actors’ Those who would do T
T ‘transformation process’ The conversion of input to output
W ‘Weltanschauung’ The worldview which makes this T meaningful in its context
O ‘owner(s)’ Those who could stop T
E ‘environmental constraints’
Elements outside the system which it takes as given
This conceptual model was used in Chapter 8 of the thesis, in particular the pairing of
the transformation process T and W, the Weltanschauung or worldview that brings
meaning to the analysis. This approach also included the means to understand the roles
of various stakeholders in the delivery of services and the critical impact of contextual
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
111
factors such as technological advances, and the prevailing economic and social
conditions.
iii) Modelling relevant systems
The modelling process consisted of assembling and structuring the minimum necessary
activities to carry out the tasks that are necessary. For instance, the provision of
adequate clinical care to trauma victims requires a range of activities such as the
training of personnel, supply of relevant equipment and transport, coordination with
other health services and effective communications. The resulting models describe the
transformation of inputs into outputs. Flowcharts, in the form of patient pathways, were
also used to further describe each models decision processes from the perspectives of
the community setting, pre-hospital system, and health system domains.
An important part of building models is to determine performance criteria for each
dimension of the systems modelled (Checkland & Scholes 1990: 39). While evaluation
may be in the form of the generic performance measures of efficacy, effectiveness and
effectiveness, a stronger alternative is through the means of a purpose-designed
performance framework. This latter approach was taken in Chapter 7, with the
exploration of a performance framework for rural ambulance services.
iv) Comparing models with reality
There were a variety of methods employed to carry out comparisons of the abstract
models with reality. These included informal discussions with interested and informed
people, the use of formal questioning techniques that were used in this study, and the
observation of similar models operating in the real world.
Patching (1990: 106-109) provided a simplified conceptual framework that bridged the
gap between high-level systems thinking and the real world of activities, resources,
information and communication links during this comparative stage. One of his useful
approaches is question generation, which links activities and performance indicators.
This device was used to generate questions for the expert interviews and the focus group
with RAV managers. It was also used as a critical device when reviewing RAV
corporate plans throughout the discussions in Chapter 5 to 9.
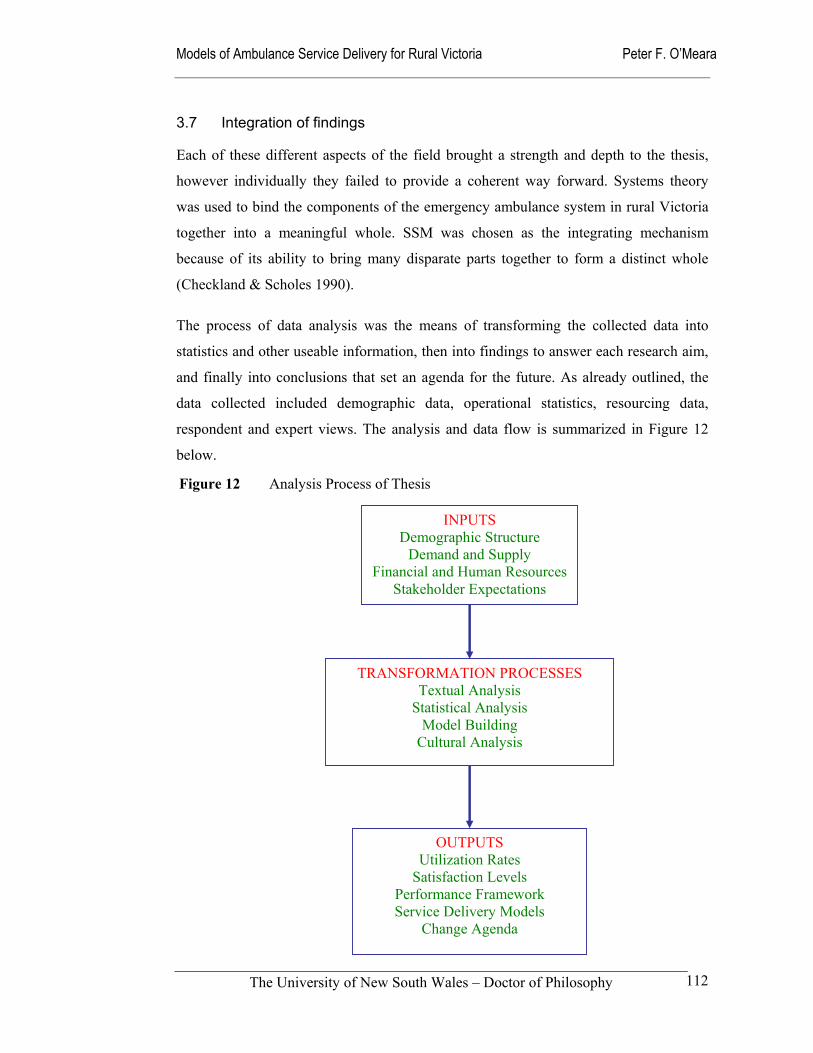
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
112
3.7 Integration of findings
Each of these different aspects of the field brought a strength and depth to the thesis,
however individually they failed to provide a coherent way forward. Systems theory
was used to bind the components of the emergency ambulance system in rural Victoria
together into a meaningful whole. SSM was chosen as the integrating mechanism
because of its ability to bring many disparate parts together to form a distinct whole
(Checkland & Scholes 1990).
The process of data analysis was the means of transforming the collected data into
statistics and other useable information, then into findings to answer each research aim,
and finally into conclusions that set an agenda for the future. As already outlined, the
data collected included demographic data, operational statistics, resourcing data,
respondent and expert views. The analysis and data flow is summarized in Figure 12
below.
Figure 12 Analysis Process of Thesis
INPUTS Demographic Structure
Demand and Supply Financial and Human Resources
Stakeholder Expectations
OUTPUTS Utilization Rates
Satisfaction Levels Performance Framework Service Delivery Models
Change Agenda
TRANSFORMATION PROCESSES Textual Analysis
Statistical Analysis Model Building
Cultural Analysis
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
113
The outputs that flowed directly from the analysis of these data included, branch
catchment populations, utilization rates, time intervals, staffing profiles and satisfaction
levels. These outputs were further developed in Chapter 8 through the application of
SSM to produce ideal system types and abstract models. The data analysis phase formed
the intermediate step (transformation) between the collection of the data (inputs) and the
findings (outputs).
The findings from the four research aims were integrated into an agenda for debate and
discussion in Chapter 9 using the SSM cultural stream of analysis. Debate about the
future directions for rural ambulance services was structured using a modified version
of Patching’s extended analysis tool. This device generated detailed ideas about the
transformation activities, the required resources and communication links. One
omission from Patching’s approach was any direct consideration of the key
relationships that bind the activities and resources of an organization or system together
in order to successfully complete tasks. The modification used in the thesis, which has
been used in another study of rural urgent care services, produces a triad of activities-
element-relationships as a decomposing tool (O’Meara & Burley 2001). The extended
use of metaphors to describe the essence of the findings also assisted in this process of
binding the findings together into manageable whole that is coherent and
understandable to policy makers.
Having compared the systems and models with the reality of the Victorian rural
environment to determine the systematic changes that may be desirable, the next step
taken was to come to a determination about the cultural feasibility of the suggested
changes or modifications. It was at this concluding stage that the stream of cultural
analysis became central to the analysis process.
The use of a stream of cultural analysis to carry out this research was as important as the
use of logic-driven thinking already described. Its use allowed the introduction of
feedback loops, which facilitated reality checks for the research findings and the
conclusions being drawn. It also avoided the fate that befell one researcher who used
SSM to examine the British Army. Because she misunderstood who held power over
her project, she was barred from further contact with army personnel before the research
was complete (Davies & Ledington 1991). This unfortunate experience was a timely
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
114
warning to all researchers dealing with traditional, hierarchical organizations such as
ambulance services.
The stream of cultural analysis allowed a structured acknowledgement of the contextual,
social and political forces that both drive and hold back changes in rural ambulance
services. It is this ‘culture’ that is ultimately crucial to the success of any organizational
and system changes that may be suggested.
... although facts and logic have a part to play in human affairs, the feel of them, their felt texture, derives equally (or more) from the myths and meanings which human beings attribute to their professional (and personal) entanglements with their fellow beings.
(Checkland & Scholes 1990: 44)
In many ways the political variables are the most important in relation to rural
ambulance services. They act on the socio-economic environment and can be broadly
categorized under the headings of power, ideology and culture. Each of these has
considerable influence on the determination of Government policy in regard to
ambulance services; the eventual policy emerging from the play of economic, social and
political forces and manifested in and through institutions and processes (Simeon 1976:
100).
One way of representing the cultural forces impacting on the rural ambulance services is
to record relationships and connections through pictures - described as ‘holons’ and
‘rich pictures’ (Checkland & Scholes 1990: 36-45). This technique was used throughout
the study to describe the ownership of the problems, their social and professional
relationships, and the political forces at work. Chapter 8 makes extensive use of the
technique. Using SSM allowed examination of the cultural perspective through three
inter-related filters that analyse the intervention, the social system and the political
system respectively (Checkland & Scholes 1990: 44-52):
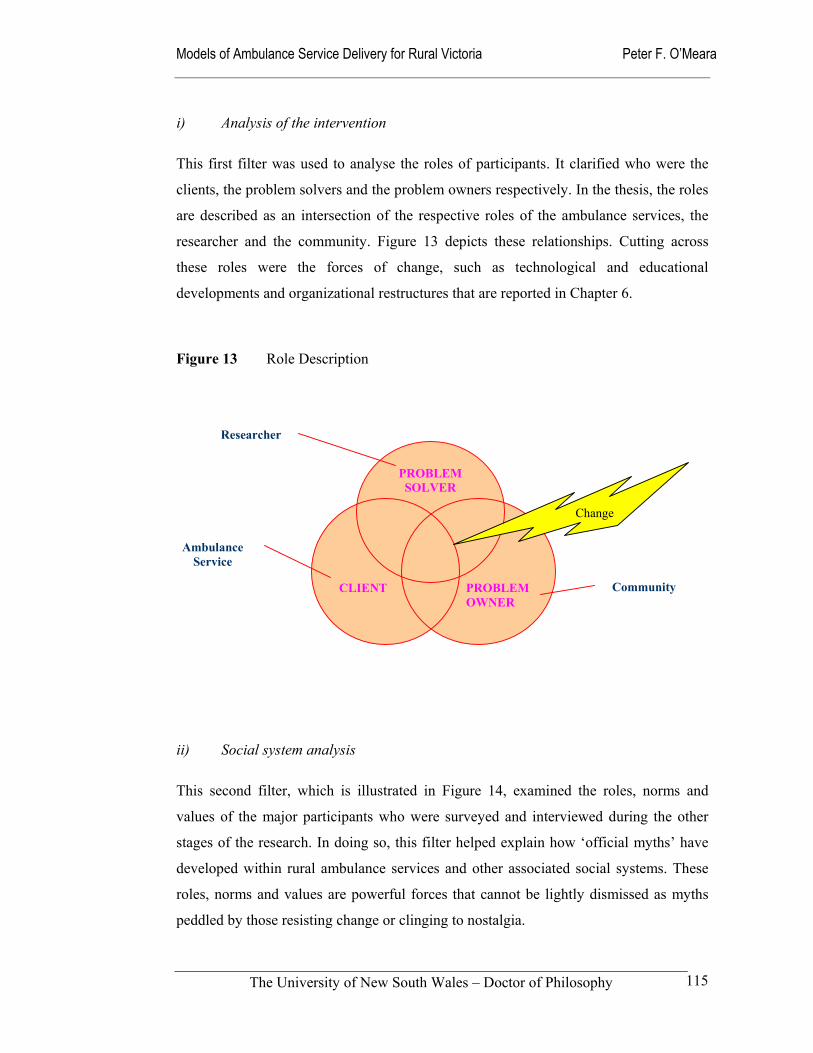
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
115
i) Analysis of the intervention
This first filter was used to analyse the roles of participants. It clarified who were the
clients, the problem solvers and the problem owners respectively. In the thesis, the roles
are described as an intersection of the respective roles of the ambulance services, the
researcher and the community. Figure 13 depicts these relationships. Cutting across
these roles were the forces of change, such as technological and educational
developments and organizational restructures that are reported in Chapter 6.
Figure 13 Role Description
ii) Social system analysis
This second filter, which is illustrated in Figure 14, examined the roles, norms and
values of the major participants who were surveyed and interviewed during the other
stages of the research. In doing so, this filter helped explain how ‘official myths’ have
developed within rural ambulance services and other associated social systems. These
roles, norms and values are powerful forces that cannot be lightly dismissed as myths
peddled by those resisting change or clinging to nostalgia.
CLIENT
PROBLEM SOLVER
PROBLEMOWNER
Community
Ambulance Service
Researcher
Change
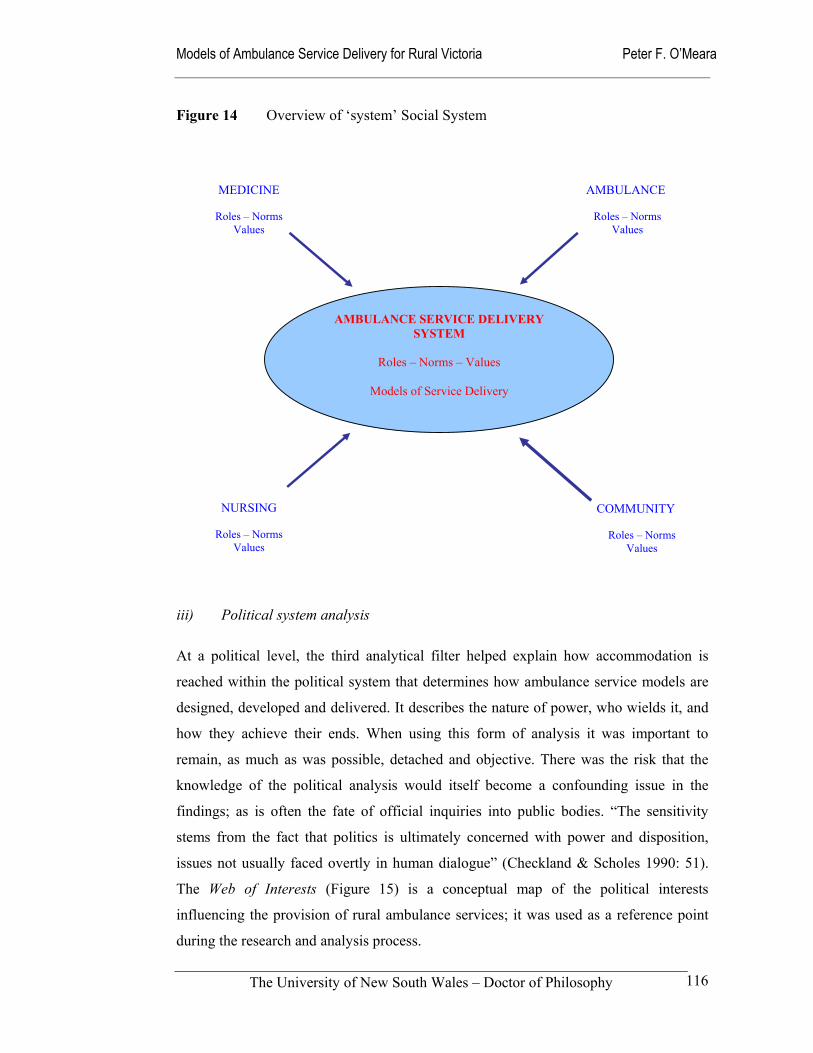
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
116
Figure 14 Overview of ‘system’ Social System
iii) Political system analysis
At a political level, the third analytical filter helped explain how accommodation is
reached within the political system that determines how ambulance service models are
designed, developed and delivered. It describes the nature of power, who wields it, and
how they achieve their ends. When using this form of analysis it was important to
remain, as much as was possible, detached and objective. There was the risk that the
knowledge of the political analysis would itself become a confounding issue in the
findings; as is often the fate of official inquiries into public bodies. “The sensitivity
stems from the fact that politics is ultimately concerned with power and disposition,
issues not usually faced overtly in human dialogue” (Checkland & Scholes 1990: 51).
The Web of Interests (Figure 15) is a conceptual map of the political interests
influencing the provision of rural ambulance services; it was used as a reference point
during the research and analysis process.
MEDICINE
Roles – Norms
Values
AMBULANCE
Roles – Norms
Values
COMMUNITY
Roles – Norms
Values
NURSING
Roles – Norms
Values
AMBULANCE SERVICE DELIVERY SYSTEM
Roles – Norms – Values
Models of Service Delivery
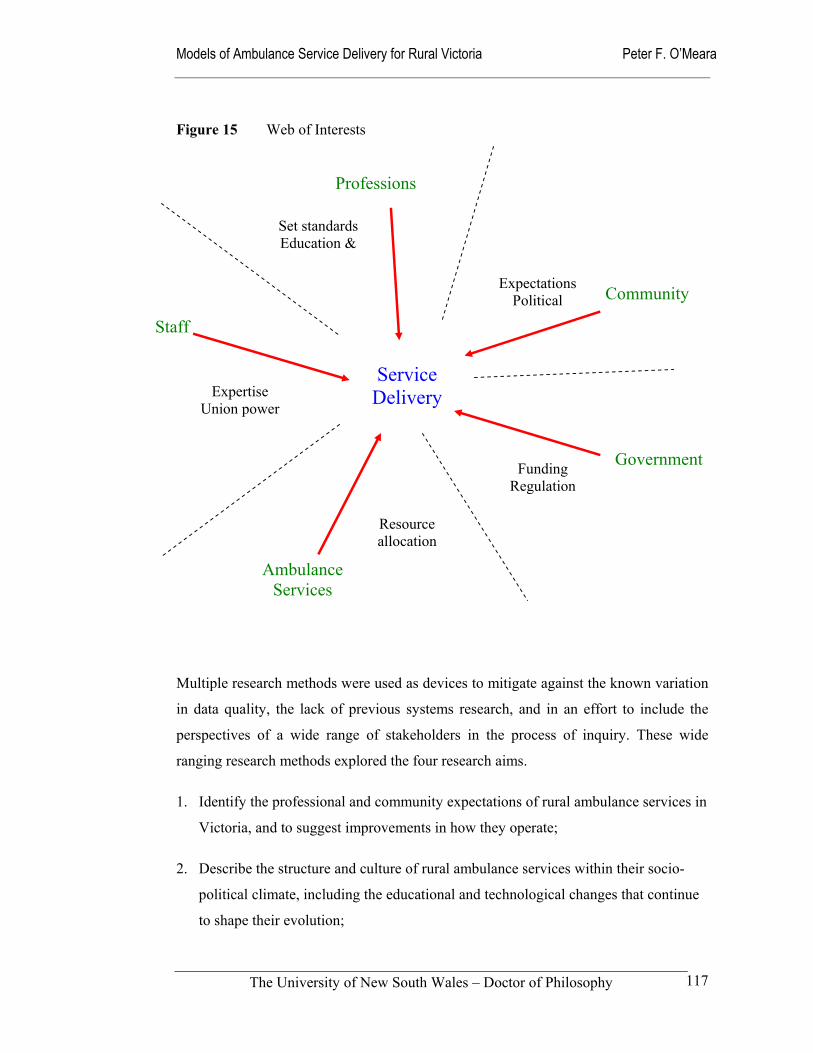
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
117
Figure 15 Web of Interests
Multiple research methods were used as devices to mitigate against the known variation
in data quality, the lack of previous systems research, and in an effort to include the
perspectives of a wide range of stakeholders in the process of inquiry. These wide
ranging research methods explored the four research aims.
1. Identify the professional and community expectations of rural ambulance services in
Victoria, and to suggest improvements in how they operate;
2. Describe the structure and culture of rural ambulance services within their socio-
political climate, including the educational and technological changes that continue
to shape their evolution;
Community
Staff
Government
Service Delivery
Professions
Ambulance Services
Set standards Education &
Expertise Union power
Expectations Political
Resource allocation
Funding Regulation
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
118
3. Compare the perceived and actual performance of rural ambulance services in
different geographical areas in terms of utilization rates and time intervals with a
view to developing a useful performance framework for rural ambulance services;
and
4. Develop models of ambulance service delivery from different philosophical
perspectives to stimulate debate about models that may be most suitable for rural
Victoria.
The following findings chapters report on the study setting and sample (Chapter 4),
expectations of rural ambulance services (Chapter 5), the structure and culture of rural
ambulance services in Victoria (Chapter 6), performance frameworks (Chapter 7) and
five models of service delivery (Chapter 8). The implications for future policy and
practice are addressed in the conclusion to the thesis (Chapter 9).
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
119
SECTION 3 FINDINGS AND DISCUSSION 4.0 Rural Communities and Respondents to Study
Section 1 Introduction
Section 2 Theory and Methods
Section 3 Findings and Discussion
Section 4 Conclusion
Chapter 1 Overview of Study
Chapter 2Theory Foundations
Chapter 4Communities Respondents
Chapter 5Expectations
Chapter 6Structure Culture
Chapter 7Ambulance Performance
Chapter 8Models of Delivery
Chapter 9 Policy Implications
Chapter 3Study Methods
Figure 16 Navigation Map of Thesis
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
120
4.1 Introduction
This first findings chapter describes the demographics of the sample communities
included in the study and the respondents who completed and returned questionnaires. It
sets the parameters of the analytical variables used throughout the thesis. These are the
occupational groupings – ambulance officers, general practitioners, registered nurses
and members of the public – and the modified rurality bands - Large Rural Centres,
Small Rural Centres, Small Towns, Little Townships and Remote Areas.
The collective community
profiles and descriptions of the
respondents provide a frame of
reference for the findings
reported in subsequent
chapters. For example, the
occupational groupings and the
rurality bands are used
extensively as analytical
variables when discussing the expectations and performance of rural ambulance services
in Chapters 5 and 7 respectively. The descriptions of the different-sized rural
communities are used as points of reference when different models of service delivery
are developed and analysed in Chapter 8.
In Chapter 4.2 the 40 communities studied are collectively described in terms of their
catchment populations, health and emergency services (excluding ambulance
infrastructure), and their relative rurality. Chapter 4.3 reports on the respondents to the
study, categorizing their response rates according to four occupational groups and five
rurality bands. Their responses are also described according to gender, and their past
and current interactions with rural ambulance services. Chapter 4.4 concludes with a
discussion of these findings and how they relate to the remainder of the thesis.
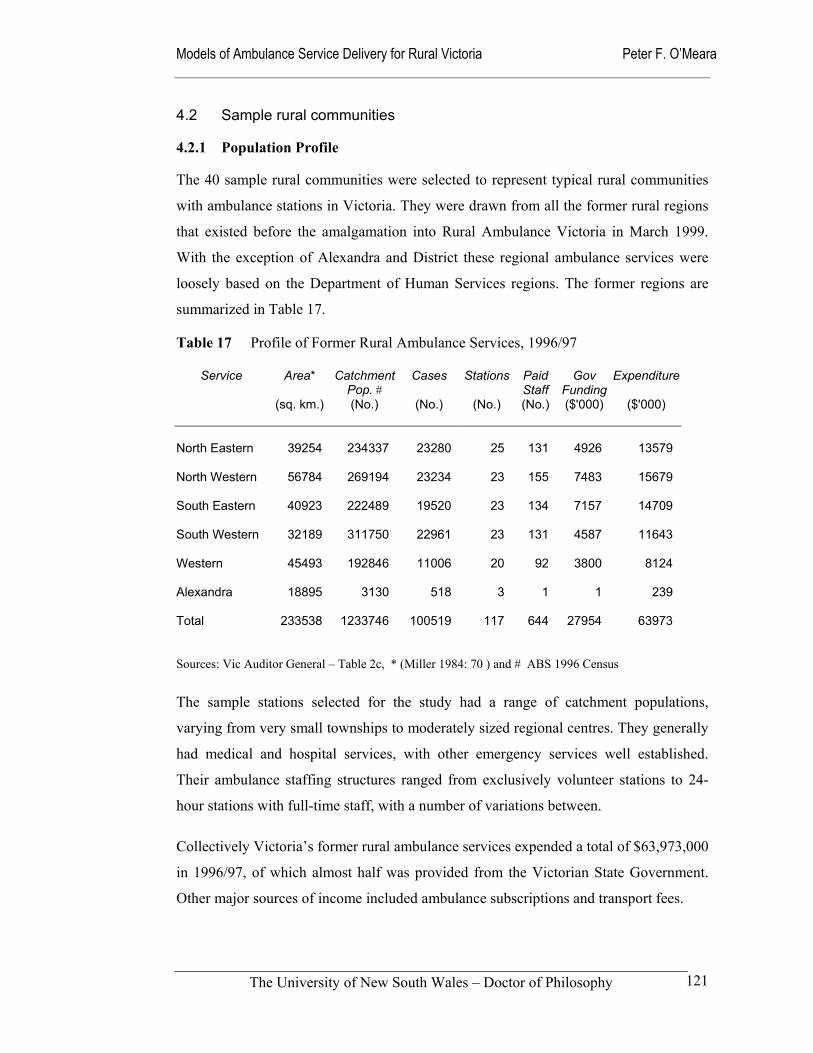
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
121
4.2 Sample rural communities
4.2.1 Population Profile
The 40 sample rural communities were selected to represent typical rural communities
with ambulance stations in Victoria. They were drawn from all the former rural regions
that existed before the amalgamation into Rural Ambulance Victoria in March 1999.
With the exception of Alexandra and District these regional ambulance services were
loosely based on the Department of Human Services regions. The former regions are
summarized in Table 17.
Table 17 Profile of Former Rural Ambulance Services, 1996/97
Service Area* Catchment Pop. #
Cases Stations Paid Staff
Gov Funding
Expenditure
(sq. km.) (No.) (No.) (No.) (No.) ($'000) ($'000)
North Eastern
39254
234337
23280
25
131
4926
13579
North Western 56784 269194 23234 23 155 7483 15679
South Eastern 40923 222489 19520 23 134 7157 14709
South Western 32189 311750 22961 23 131 4587 11643
Western 45493 192846 11006 20 92 3800 8124
Alexandra 18895 3130 518 3 1 1 239
Total 233538 1233746 100519 117 644 27954 63973
Sources: Vic Auditor General – Table 2c, * (Miller 1984: 70 ) and # ABS 1996 Census
The sample stations selected for the study had a range of catchment populations,
varying from very small townships to moderately sized regional centres. They generally
had medical and hospital services, with other emergency services well established.
Their ambulance staffing structures ranged from exclusively volunteer stations to 24-
hour stations with full-time staff, with a number of variations between.
Collectively Victoria’s former rural ambulance services expended a total of $63,973,000
in 1996/97, of which almost half was provided from the Victorian State Government.
Other major sources of income included ambulance subscriptions and transport fees.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
122
With the formation of RAV in 1999, the size and complexity of the new organization
now rivals that of the Melbourne Metropolitan Ambulance Service. The total estimated
budget for RAV in 2000/2001 is now approaching $80 million. It remains highly
dependent on direct government funding for its operation.
Major provincial centres such as Geelong, Bendigo and Ballarat were deliberately
excluded from this study, as they are more likely to share the organizational
characteristics of a metropolitan ambulance service. It is doubtful that they have any
special rural flavour. Two relatively large centres, Shepparton and Warrnambool, were
included in the sample to potentially act as a comparison group. The stations selected
for the study are listed in Table 18. In Chapter 3, the rationale for the selections, their
geographic locations, catchment populations and rurality classifications were explained
in detail.
Table 18 Sample Stations in Study Alexandra Daylesford Maffra Rainbow
Apollo Bay Dimboola Mallacoota Robinvale
Ararat Echuca Manangatang Sale
Avoca Hamilton Mansfield Seymour
Beechworth Heywood Maryborough Shepparton
Casterton Horsham Moe Swan Hill
Castlemaine Kyneton Mount Beauty Tambo Valley
Cobram Lakes Entrance Murrayville Wangaratta
Colac Leongatha Orbost Warracknabeal
Cowes Lorne Portland Warrnambool
While acknowledging that the concept of ‘community’ is one of the more contested in
the social sciences, the sample communities are considered to be representative of rural
Victoria (Jewkes & Murcott 1996). Over the last decade rural Victorian communities
have experienced the reorganization of hospital services, had constant difficulties
recruiting medical practitioners, and are have experienced growing concerns about the
continued willingness of citizens to actively support volunteer organizations. These
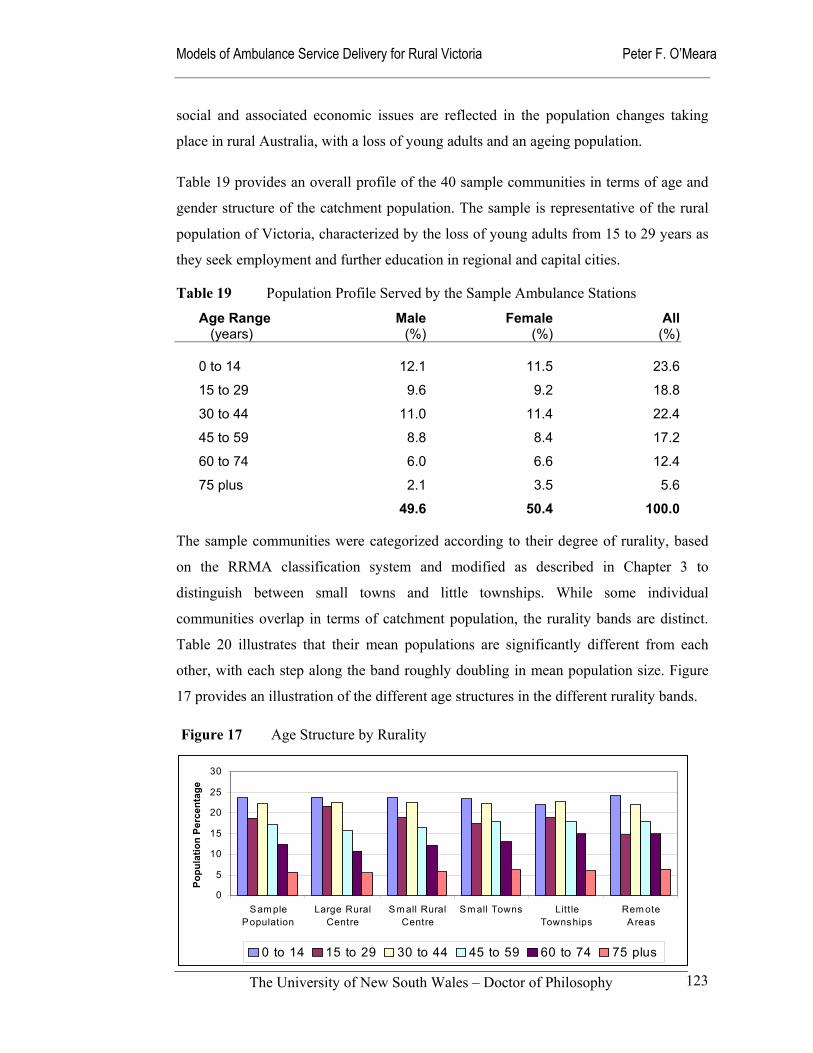
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
123
social and associated economic issues are reflected in the population changes taking
place in rural Australia, with a loss of young adults and an ageing population.
Table 19 provides an overall profile of the 40 sample communities in terms of age and
gender structure of the catchment population. The sample is representative of the rural
population of Victoria, characterized by the loss of young adults from 15 to 29 years as
they seek employment and further education in regional and capital cities.
Table 19 Population Profile Served by the Sample Ambulance Stations
Age Range (years)
Male(%)
Female(%)
All(%)
0 to 14 12.1 11.5 23.6
15 to 29 9.6 9.2 18.8
30 to 44 11.0 11.4 22.4
45 to 59 8.8 8.4 17.2
60 to 74 6.0 6.6 12.4
75 plus 2.1 3.5 5.6
49.6 50.4 100.0
The sample communities were categorized according to their degree of rurality, based
on the RRMA classification system and modified as described in Chapter 3 to
distinguish between small towns and little townships. While some individual
communities overlap in terms of catchment population, the rurality bands are distinct.
Table 20 illustrates that their mean populations are significantly different from each
other, with each step along the band roughly doubling in mean population size. Figure
17 provides an illustration of the different age structures in the different rurality bands.
Figure 17 Age Structure by Rurality
0
5
10
15
20
25
30
Sam plePopulation
Large RuralCentre
Sm all RuralCentre
Sm all Towns Litt leTownships
Rem oteAreas
Popu
latio
n Pe
rcen
tage
0 to 14 15 to 29 30 to 44 45 to 59 60 to 74 75 plus
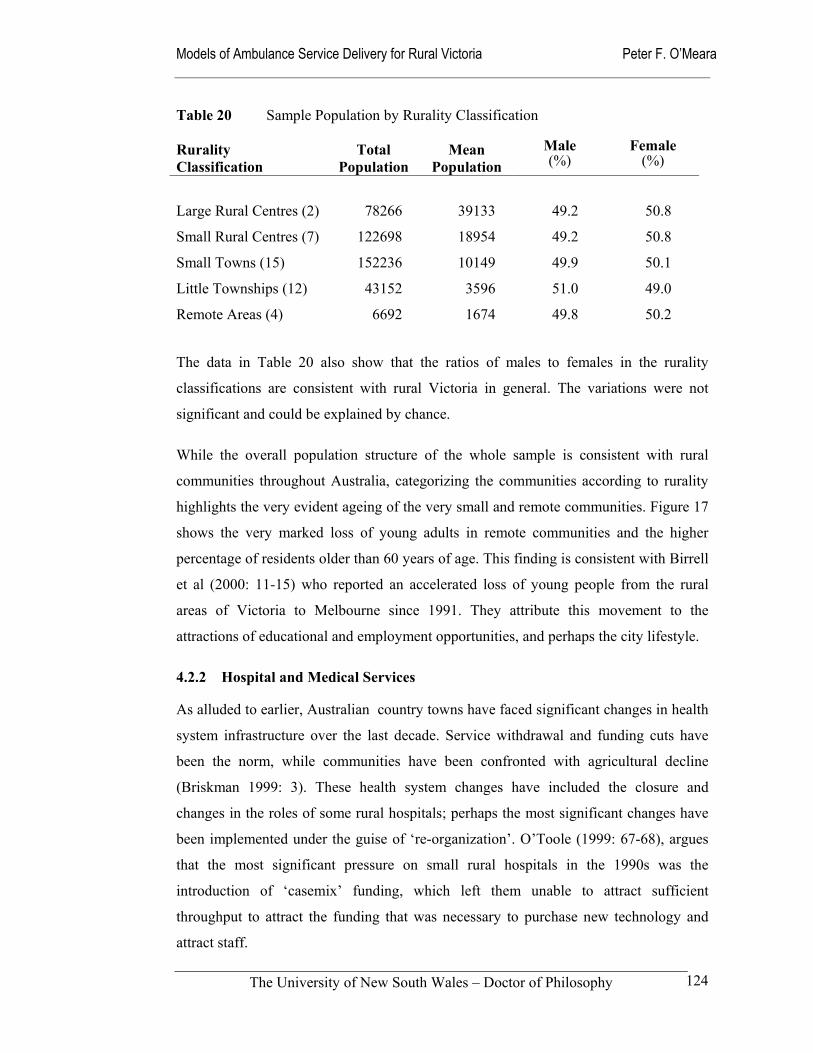
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
124
Table 20 Sample Population by Rurality Classification Rurality Classification
Total
Population
Mean
Population
Male (%)
Female
(%)
Large Rural Centres (2) 78266 39133 49.2 50.8
Small Rural Centres (7) 122698 18954 49.2 50.8
Small Towns (15) 152236 10149 49.9 50.1
Little Townships (12) 43152 3596 51.0 49.0
Remote Areas (4) 6692 1674 49.8 50.2
The data in Table 20 also show that the ratios of males to females in the rurality
classifications are consistent with rural Victoria in general. The variations were not
significant and could be explained by chance.
While the overall population structure of the whole sample is consistent with rural
communities throughout Australia, categorizing the communities according to rurality
highlights the very evident ageing of the very small and remote communities. Figure 17
shows the very marked loss of young adults in remote communities and the higher
percentage of residents older than 60 years of age. This finding is consistent with Birrell
et al (2000: 11-15) who reported an accelerated loss of young people from the rural
areas of Victoria to Melbourne since 1991. They attribute this movement to the
attractions of educational and employment opportunities, and perhaps the city lifestyle.
4.2.2 Hospital and Medical Services
As alluded to earlier, Australian country towns have faced significant changes in health
system infrastructure over the last decade. Service withdrawal and funding cuts have
been the norm, while communities have been confronted with agricultural decline
(Briskman 1999: 3). These health system changes have included the closure and
changes in the roles of some rural hospitals; perhaps the most significant changes have
been implemented under the guise of ‘re-organization’. O’Toole (1999: 67-68), argues
that the most significant pressure on small rural hospitals in the 1990s was the
introduction of ‘casemix’ funding, which left them unable to attract sufficient
throughput to attract the funding that was necessary to purchase new technology and
attract staff.
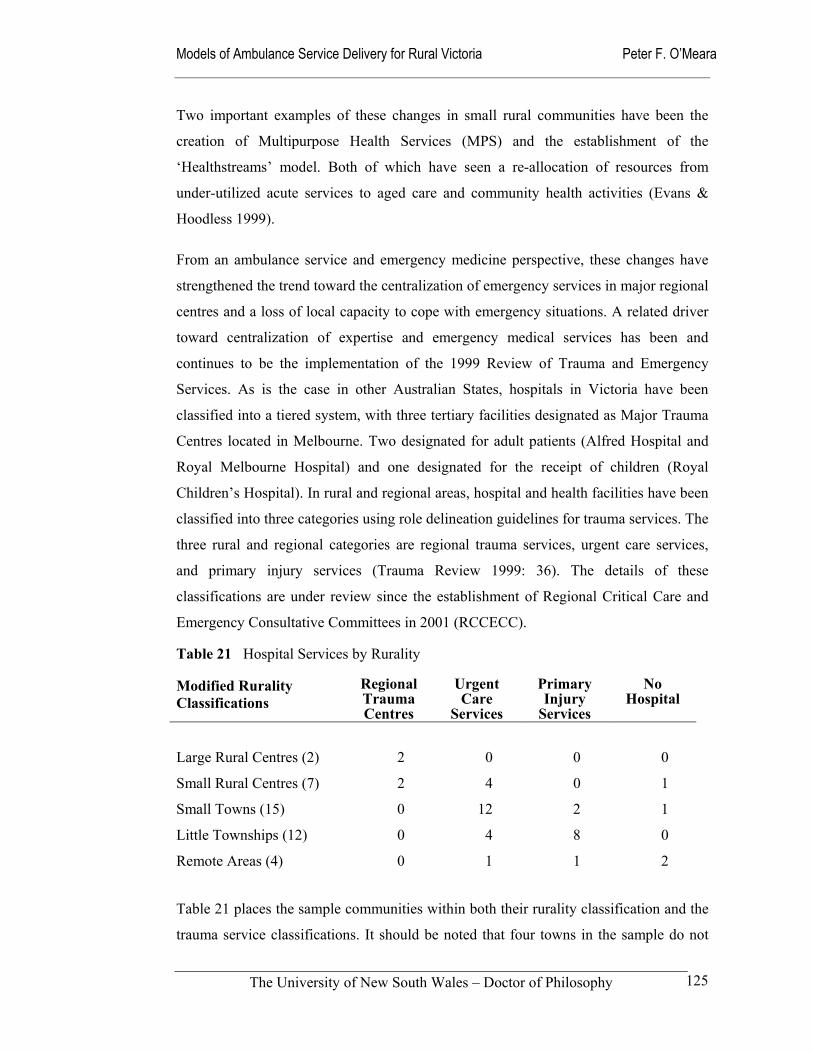
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
125
Two important examples of these changes in small rural communities have been the
creation of Multipurpose Health Services (MPS) and the establishment of the
‘Healthstreams’ model. Both of which have seen a re-allocation of resources from
under-utilized acute services to aged care and community health activities (Evans &
Hoodless 1999).
From an ambulance service and emergency medicine perspective, these changes have
strengthened the trend toward the centralization of emergency services in major regional
centres and a loss of local capacity to cope with emergency situations. A related driver
toward centralization of expertise and emergency medical services has been and
continues to be the implementation of the 1999 Review of Trauma and Emergency
Services. As is the case in other Australian States, hospitals in Victoria have been
classified into a tiered system, with three tertiary facilities designated as Major Trauma
Centres located in Melbourne. Two designated for adult patients (Alfred Hospital and
Royal Melbourne Hospital) and one designated for the receipt of children (Royal
Children’s Hospital). In rural and regional areas, hospital and health facilities have been
classified into three categories using role delineation guidelines for trauma services. The
three rural and regional categories are regional trauma services, urgent care services,
and primary injury services (Trauma Review 1999: 36). The details of these
classifications are under review since the establishment of Regional Critical Care and
Emergency Consultative Committees in 2001 (RCCECC).
Table 21 Hospital Services by Rurality Modified Rurality Classifications
Regional Trauma Centres
Urgent Care
Services
Primary Injury
Services
No Hospital
Large Rural Centres (2)
2
0
0
0
Small Rural Centres (7) 2 4 0 1
Small Towns (15) 0 12 2 1
Little Townships (12) 0 4 8 0
Remote Areas (4) 0 1 1 2
Table 21 places the sample communities within both their rurality classification and the
trauma service classifications. It should be noted that four towns in the sample do not

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
126
have hospital services; two have had hospitals closed and the other two have never had
a hospital.
Regional trauma services tend to be located in major regional centres and provide a
regional focus in trauma management receiving appropriate trauma referral from the
surrounding catchment areas. A number of them have regional retrieval services and
helipads available for the arrival of seriously injured or ill patients. Urgent care services
operate in smaller rural communities where higher levels of trauma care are not
accessible and they provide initial resuscitation and limited stabilization prior to early
transfer. In some cases these hospitals were formerly described as Base Hospitals and
have the capacity to cope with the seriously ill or injured, while others currently have
very basic capabilities. It is expected that the level of services operated will become
more consistent as the Trauma Review recommendations are implemented. Primary
injury services include hospitals that provide limited stabilization only, as well as a
number of hospitals designated for bypass of all major trauma cases.
The key characteristics of the Victorian State Trauma System being implemented are
threefold. Firstly, providers of trauma care will be integrated into a coordinated state-
wide trauma care system with comprehensive and inclusive representation from
metropolitan and rural providers. Secondly, hospitals will be designated to levels within
a tiered trauma system structure providing different complexities of care. And finally,
trauma patients will be treated by a service that is appropriate to the level of care
needed.
Under this system the optimal clinical outcomes for major trauma patients are said, to
be associated with:
minimization of time to definitive treatment;
triage to a specialist trauma hospital that is best able to provide definitive care, rather than to the nearest hospital, within logistic and safety parameters; and
concentration of expertise. (Trauma Report 1999: 37)
Associated with the closure and re-organization of hospital services in rural Victoria, is
the relative loss of general practitioners in rural towns (Evans & Hoodless 1999). While
the number of general practitioners (GPs) varies across the sample, Table 22 indicates
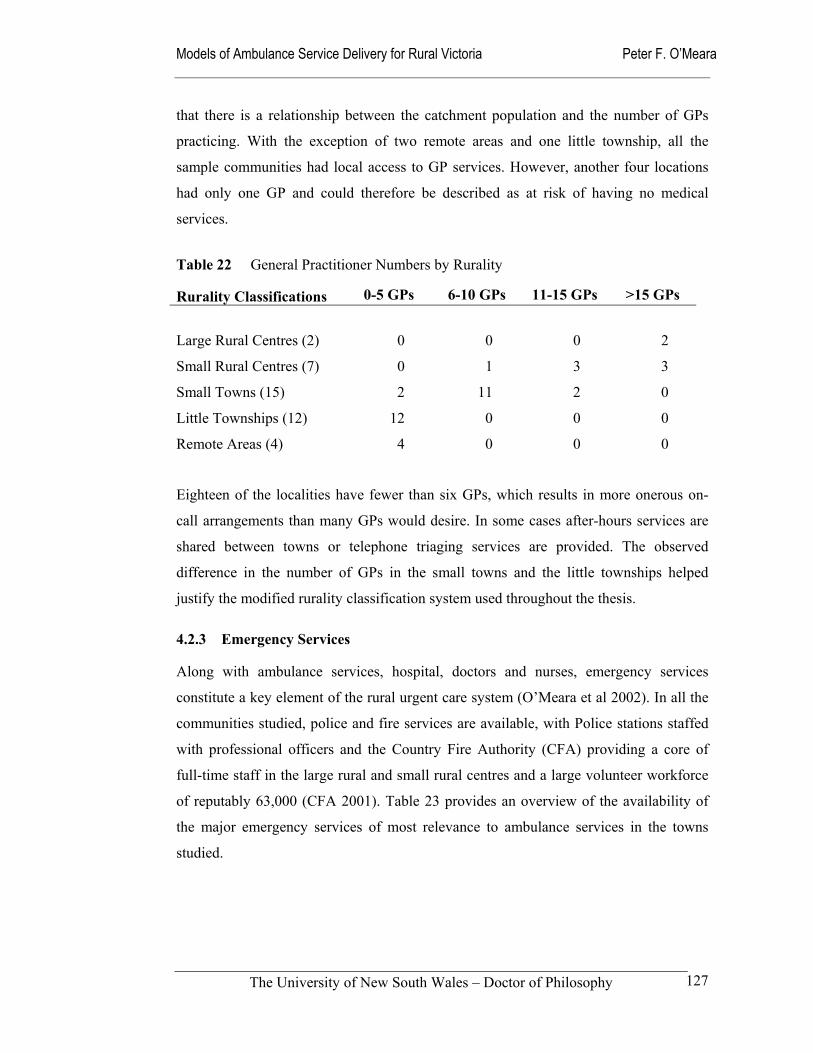
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
127
that there is a relationship between the catchment population and the number of GPs
practicing. With the exception of two remote areas and one little township, all the
sample communities had local access to GP services. However, another four locations
had only one GP and could therefore be described as at risk of having no medical
services.
Table 22 General Practitioner Numbers by Rurality Rurality Classifications 0-5 GPs 6-10 GPs 11-15 GPs >15 GPs
Large Rural Centres (2)
0
0
0
2
Small Rural Centres (7) 0 1 3 3
Small Towns (15) 2 11 2 0
Little Townships (12) 12 0 0 0
Remote Areas (4) 4 0 0 0
Eighteen of the localities have fewer than six GPs, which results in more onerous on-
call arrangements than many GPs would desire. In some cases after-hours services are
shared between towns or telephone triaging services are provided. The observed
difference in the number of GPs in the small towns and the little townships helped
justify the modified rurality classification system used throughout the thesis.
4.2.3 Emergency Services
Along with ambulance services, hospital, doctors and nurses, emergency services
constitute a key element of the rural urgent care system (O’Meara et al 2002). In all the
communities studied, police and fire services are available, with Police stations staffed
with professional officers and the Country Fire Authority (CFA) providing a core of
full-time staff in the large rural and small rural centres and a large volunteer workforce
of reputably 63,000 (CFA 2001). Table 23 provides an overview of the availability of
the major emergency services of most relevance to ambulance services in the towns
studied.
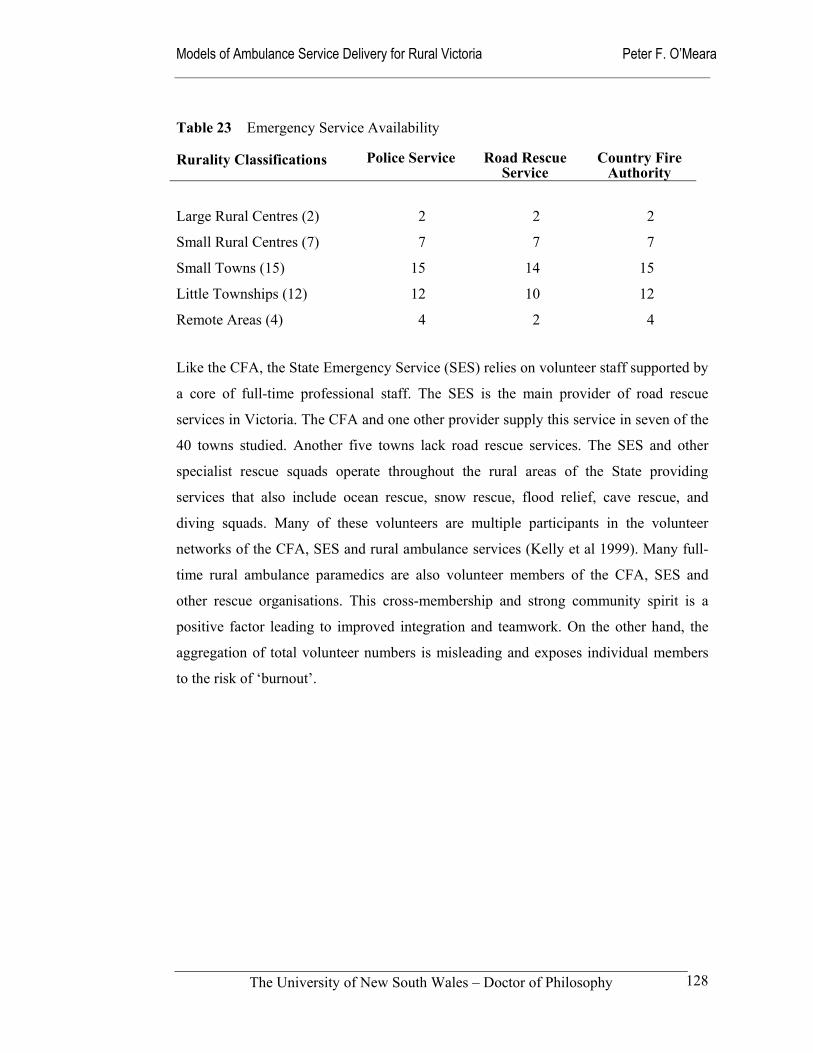
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
128
Table 23 Emergency Service Availability Rurality Classifications Police Service Road Rescue
Service Country Fire
Authority
Large Rural Centres (2)
2
2
2
Small Rural Centres (7) 7 7 7
Small Towns (15) 15 14 15
Little Townships (12) 12 10 12
Remote Areas (4) 4 2 4
Like the CFA, the State Emergency Service (SES) relies on volunteer staff supported by
a core of full-time professional staff. The SES is the main provider of road rescue
services in Victoria. The CFA and one other provider supply this service in seven of the
40 towns studied. Another five towns lack road rescue services. The SES and other
specialist rescue squads operate throughout the rural areas of the State providing
services that also include ocean rescue, snow rescue, flood relief, cave rescue, and
diving squads. Many of these volunteers are multiple participants in the volunteer
networks of the CFA, SES and rural ambulance services (Kelly et al 1999). Many full-
time rural ambulance paramedics are also volunteer members of the CFA, SES and
other rescue organisations. This cross-membership and strong community spirit is a
positive factor leading to improved integration and teamwork. On the other hand, the
aggregation of total volunteer numbers is misleading and exposes individual members
to the risk of ‘burnout’.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
129
4.3 Respondents to study
As already described in Chapter 3, potential respondents were asked to participate
through the completion and return of a twelve-question survey. The overall response
rate of 32 percent from participants as summarized in Table 24 was consistent with a
study involving a similar group of participants in rural Victoria (Kelly et al 1999). As
illustrated in Tables 25 to 27, the responses came from all the target groups across all
five rurality bands. Respondents from 37 communities returned questionnaires, with
three small towns failing to produce any returned questionnaires.
Table 24 Questionnaire Responses
Target Group
Questionnaires Distributed
Returned Questionnaires
Ambulance Paramedics
200
44 (22 %)
General Practitioners 300 93 (31 %)
Registered Nurses (Div 1) 200 86 (43 %)
Members of the Public 200 62 (31 %)
TOTAL 900 285 (32 %)
The response rate from ambulance service staff was reasonable under the circumstances
existing at the time of the survey. Up to half the stations had volunteer staff or less than
five paid staff, while a number of the Officers-in-Charge failed to pass on the
questionnaires. The one independent Ambulance Service in rural Victoria chose not to
participate in the study. These factors effectively reduced the number of potential
replies from ambulance paramedics to as few as 100. Another complicating factor was
the instability of the rural ambulance services at the time when the questionnaires were
being distributed. It coincided with the period when Rural Ambulance Victoria was
being formed from the former five rural regions.
In the case of registered nurses, the response rate was good, given that small hospitals
and bush nursing centres often have fewer than five nursing staff. In the case of general
practitioners and members of the public, the response rates were comparable to other
similar studies (Kelly et al 1999).
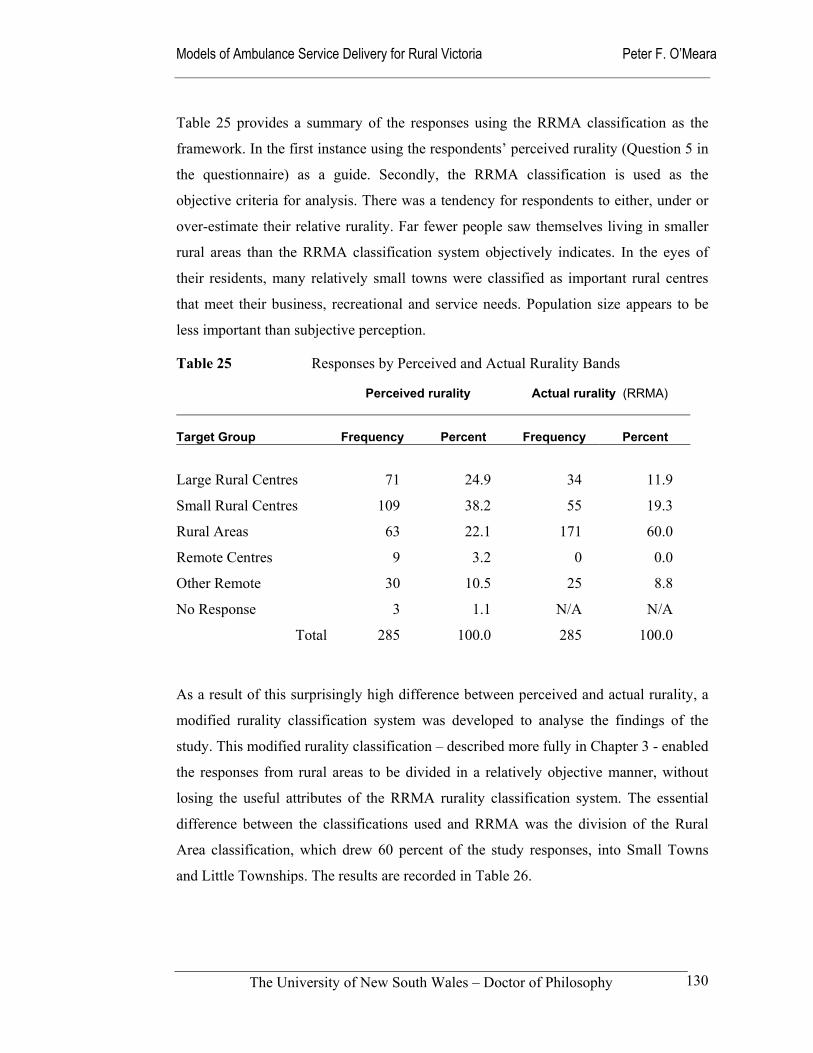
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
130
Table 25 provides a summary of the responses using the RRMA classification as the
framework. In the first instance using the respondents’ perceived rurality (Question 5 in
the questionnaire) as a guide. Secondly, the RRMA classification is used as the
objective criteria for analysis. There was a tendency for respondents to either, under or
over-estimate their relative rurality. Far fewer people saw themselves living in smaller
rural areas than the RRMA classification system objectively indicates. In the eyes of
their residents, many relatively small towns were classified as important rural centres
that meet their business, recreational and service needs. Population size appears to be
less important than subjective perception.
Table 25 Responses by Perceived and Actual Rurality Bands
Perceived rurality Actual rurality (RRMA)
Target Group
Frequency
Percent
Frequency
Percent
Large Rural Centres
71
24.9
34
11.9
Small Rural Centres 109 38.2 55 19.3
Rural Areas 63 22.1 171 60.0
Remote Centres 9 3.2 0 0.0
Other Remote 30 10.5 25 8.8
No Response 3 1.1 N/A N/A
Total 285 100.0 285 100.0
As a result of this surprisingly high difference between perceived and actual rurality, a
modified rurality classification system was developed to analyse the findings of the
study. This modified rurality classification – described more fully in Chapter 3 - enabled
the responses from rural areas to be divided in a relatively objective manner, without
losing the useful attributes of the RRMA rurality classification system. The essential
difference between the classifications used and RRMA was the division of the Rural
Area classification, which drew 60 percent of the study responses, into Small Towns
and Little Townships. The results are recorded in Table 26.
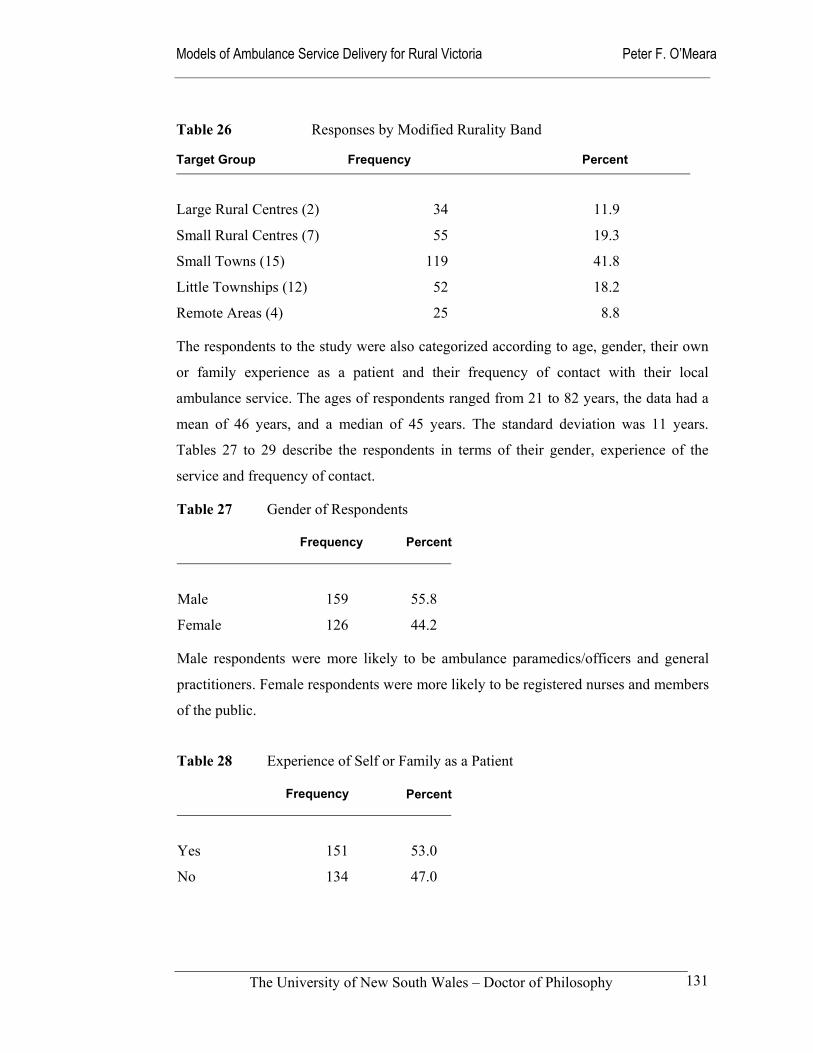
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
131
Table 26 Responses by Modified Rurality Band Target Group
Frequency
Percent
Large Rural Centres (2)
34
11.9
Small Rural Centres (7) 55 19.3
Small Towns (15) 119 41.8
Little Townships (12) 52 18.2
Remote Areas (4) 25 8.8
The respondents to the study were also categorized according to age, gender, their own
or family experience as a patient and their frequency of contact with their local
ambulance service. The ages of respondents ranged from 21 to 82 years, the data had a
mean of 46 years, and a median of 45 years. The standard deviation was 11 years.
Tables 27 to 29 describe the respondents in terms of their gender, experience of the
service and frequency of contact.
Table 27 Gender of Respondents
Frequency Percent
Male
159
55.8
Female 126 44.2
Male respondents were more likely to be ambulance paramedics/officers and general
practitioners. Female respondents were more likely to be registered nurses and members
of the public.
Table 28 Experience of Self or Family as a Patient
Frequency Percent
Yes
151
53.0
No 134 47.0
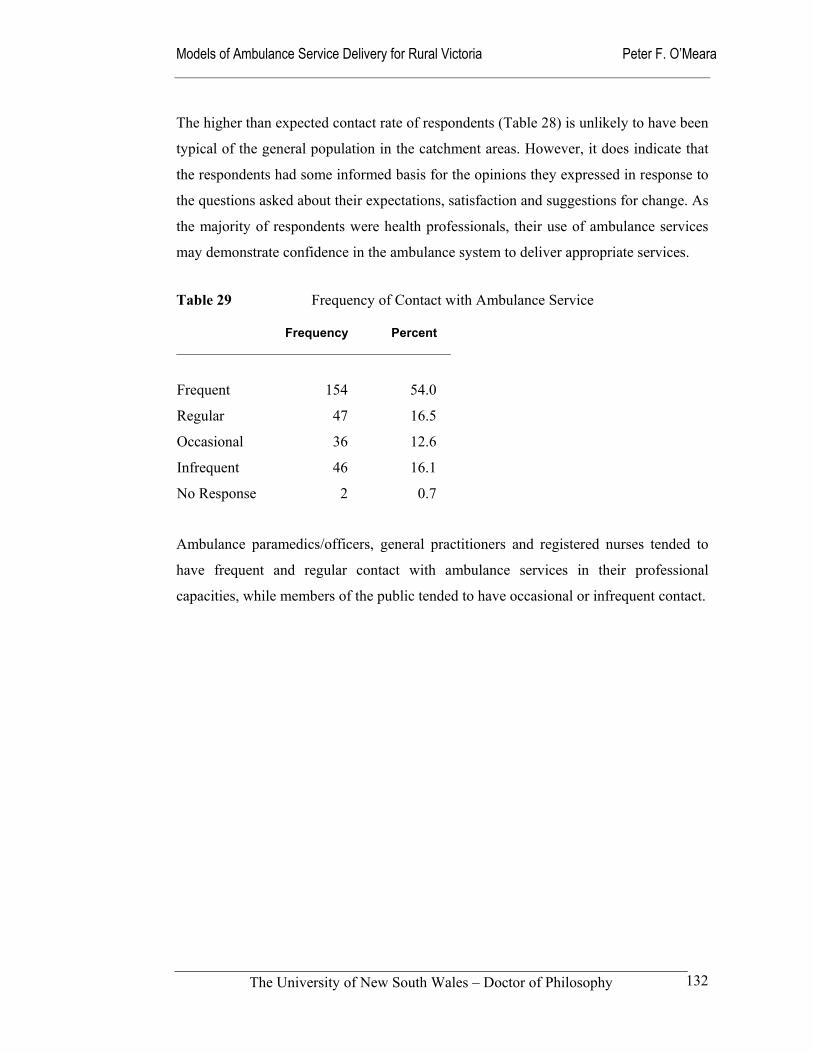
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
132
The higher than expected contact rate of respondents (Table 28) is unlikely to have been
typical of the general population in the catchment areas. However, it does indicate that
the respondents had some informed basis for the opinions they expressed in response to
the questions asked about their expectations, satisfaction and suggestions for change. As
the majority of respondents were health professionals, their use of ambulance services
may demonstrate confidence in the ambulance system to deliver appropriate services.
Table 29 Frequency of Contact with Ambulance Service
Frequency Percent
Frequent
154
54.0
Regular 47 16.5
Occasional 36 12.6
Infrequent 46 16.1
No Response 2 0.7
Ambulance paramedics/officers, general practitioners and registered nurses tended to
have frequent and regular contact with ambulance services in their professional
capacities, while members of the public tended to have occasional or infrequent contact.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
133
4.4 Discussion
This chapter has briefly described the rural communities studied within their assigned
classifications and profiled the respondents to the study. With only a third of the
questionnaires to the Officers-in-Charge being returned, the information about
catchment areas and the local infrastructure was largely collected through other health
services and emergency services. Many of the ambulance service first-line supervisors
passed up the opportunity to have direct input into the study. This was disappointing
when contrasted with the quality of the input of those who did participate. This
reluctance may have been the result of general apathy at a time of organizational
dislocation or may be linked to the general lack of a ‘research culture’ in ambulance
services.
The study refrained from the temptation to debate the meaning of community or concept
of rurality from a philosophical perspective. This could be the focus of a separate study.
Community was defined geographically as the primary catchment area of each
ambulance station. The RRMA rurality classification system was used as the basis for
the categorization of each community into rurality bands for the purposes of analysis.
The community profiles highlight the changing demographic structure of rural
communities, especially the smaller townships and more remote areas that are
progressively ageing with the movement of young people to larger regional centres and
Melbourne. This demographic change is likely to progressively place considerable
stress on small towns as current volunteers age. Volunteer emergency services have
traditionally recruited young people into voluntary organizations such as the fire
brigade, rescue services and ambulance services through junior programs like those that
the CFA runs, with the expectation that they will stay in the area and graduate to senior
ranks.
Associated with this population shift has been a change in health service needs, such as
more demand for aged care facilities. Along with the economic and financial pressures,
these changing needs have resulted in changes in hospital roles, some hospital closures
and centralization of specialist hospital services.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
134
An example of these system changes is the establishment of a state-wide trauma system
that sees ambulance services triaging patients directly to major trauma centres in
Melbourne, where the specialist emergency medicine expertise is concentrated, rather
than to the nearest hospital. The resulting tensions that these clinical assumptions cause
between rural ambulance services and general practitioners, hospitals and nurses are
reported in Chapter 5. Table 21 illustrated that regional trauma centres, which are
capable of effectively managing most trauma cases and medical emergencies that
ambulance services are often called to, are concentrated in those towns classified as
large rural centres and small rural centres.
Four localities in the study have no hospital services. The one in the small rural centres
category no longer has any hospital services following the former hospital’s closure.
Emergency cases are now taken to a new hospital 20 kilometres distant. Since the
closure of the previous hospital campus, ambulance service staffing has been
progressively increased from five staff to eleven, with plans for the station to become a
24-hour roster station.
The locality in the small towns
category without a hospital, has never
had a hospital for historical reasons
and patients attend a hospital 30
kilometres away. As in the small rural
centre above, there are plans to
increase ambulance staffing at this
station from three full-time staff
supported by volunteer Community
Ambulance Officers (CAO) to seven
full-time staff with continued support
from CAOs. The Ambulance Employees Association opposes the continued
involvement of COA at this station despite support from local staff and the community.
Clearly, having no hospital is an important factor in the deployment of ambulance
resources. It is something that policy makers and funders should take into account when
considering changes to rural hospital services. They need to take a ‘whole-of-system’

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
135
approach and therefore avoid the financial and structural gains in one part of the system
being lost in another part of the local health sector, be that in ambulance service staffing
or in the loss of general practitioners to the community.
While only two of the remote localities have no hospital services, small townships and
remote areas often have rudimentary hospital-type services in the form of Primary
Injury Services. These small and remote ambulance stations are the most likely to rely
on volunteer staff and have few, if any, medical staff (Table 22). While the numbers of
volunteers in emergency services looks healthy, Kelly et al (1999) found that the
membership of the SES, CFA and volunteer ambulance workers is often shared with
individuals undertaking multiple roles within their communities. This is taking place in
an environment where volunteerism is declining within falling and ageing rural
populations (Reinholtd & Smith 1998; Townsend et al 1999).
It was from these diverse rural communities that the participants in the qualitative
component of the study were recruited. In retrospect, more members of the public could
have been invited to participate to reduce the bias toward health professionals in the
sample. Perhaps it is always the case that more research can be done, or a larger sample
used. That said, the co-operation of the municipal councils in sending the questionnaires
to potential respondents was outstanding and seeking more respondents may simply
have meant the law of diminishing returns would have been encountered. All
respondents provided a wealth of information on their expectations, suggestions for
change and satisfaction levels that are reported in Chapters 5 and 7. The data were also
useful when examining the structure and culture of Rural Ambulance Victoria in
Chapter 6 and were considered during the modelling processes undertaken in Chapter 8.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
136
5.0 Expectations of Rural Communities
Section 1 Introduction
Section 2 Theory and Methods
Section 3 Findings and Discussion
Section 4 Conclusion
Chapter 1 Overview of Study
Chapter 2Theory Foundations
Chapter 4Communities Respondents
Chapter 5Expectations
Chapter 6Structure Culture
Chapter 7Ambulance Performance
Chapter 8Models of Delivery
Chapter 9Policy Implications
Chapter 3Study Methods
Figure 18 Navigation Map of Thesis
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
137
5.1 Introduction
This is the second of the five findings chapters. It reports on the first research aim that
sought to:
Identify the professional and community expectations of rural ambulance services in Victoria, and to suggest improvements in
how they operate.
These expectations and desired changes are described, then categorized according to the
major variables of respondent occupation and rurality classification. The findings are
consistent with the pre-hospital literature. They indicate that rural communities expect
their ambulance services to deliver five core elements of service. These expectations
are:
Service availability;
Speedy response;
Competent and skillful staff;
Communication and teamwork with health and emergency services; and
Professional and ethical behaviour from staff.
Also reported are the changes that respondents to the study said they would like to see.
These have been grouped into the themes of improving staff resources, improving local
management autonomy, and changes to the role of ambulance services and ambulance
paramedics. In Chapter 8 of the thesis, these themes are linked to five conceptual
models of service delivery that have been formulated.
In the discussion of this chapter the implications of these expectations and hopes for the
future are pursued further. They are linked to their rural context; be that the socio-
political, health policy, or the specifically ambulance contexts. The discussion
highlights the importance of understanding how rural communities see their ambulance
services. This information has the potential to influence the development of
organizational structures and processes (Chapter 6), help develop key performance
indicators (Chapter 7), and facilitate the building of service delivery models that meet
the aspirations of rural communities (Chapter 8).
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
138
5.2 Expectations of health professionals and community members
A total of 279 respondents identified 1,049 expectations of their local ambulance
services. A grounded approach to the analysis of these text data was taken. Using key
words and phrases the responses were initially grouped into ten categories, plus a small
number (n = 5) of other responses that defied categorization. The initial ten categories
were:
Timely and prompt; Transport;
Clinically competent and skilled; Local knowledge;
Communication and teamwork; Caring and compassionate;
Professional and ethical; Efficient; and
Accessible and available; Adequate resources
Two primary categories emerged from this analysis – ‘timely and prompt’ (n = 243) and
‘clinically competent and skilled’ (n = 255). This left 551 responses distributed across
the other eight categories. To make the categories clearer and the analysis more
statistically robust, the original ten expectation categories were reduced to five areas,
with the remainder classified as other expectations. The latter included a range of
responses that individually were small in number, such as transport, and local
knowledge of staff. The final five categories to emerge from the data were:
1. Service availability; incorporating adequate resourcing, efficient management and
accessibility. This category included staffing issues, vehicles, equipment and general
infrastructure.
2. Speed of response; included both the time to reach emergency incidents and
promptness of services when transferring patients to higher levels of care. There was
no mention of ‘time at scene’ despite this having been identified in the trauma
literature as an important indicator for the management of trauma patients (Danne et
al 1998).
3. Competence and skills of staff; covering clinical skills of staff, driving skills, level
of formal training and decision-making ability.
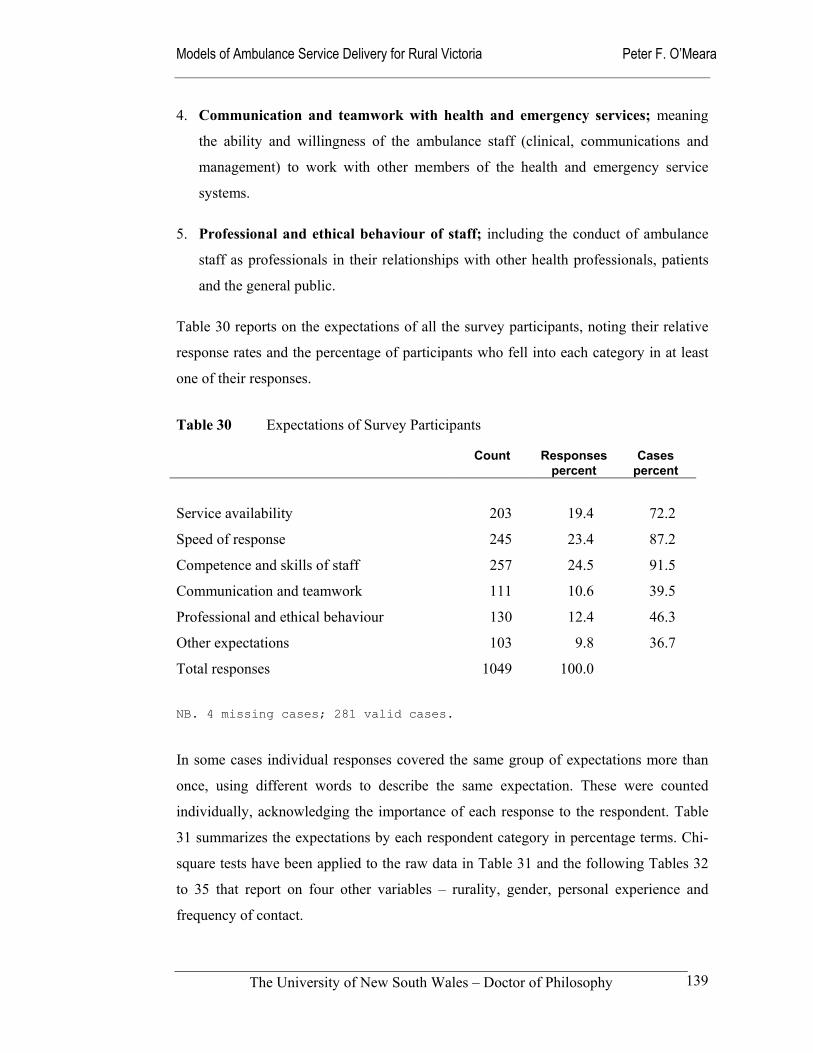
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
139
4. Communication and teamwork with health and emergency services; meaning
the ability and willingness of the ambulance staff (clinical, communications and
management) to work with other members of the health and emergency service
systems.
5. Professional and ethical behaviour of staff; including the conduct of ambulance
staff as professionals in their relationships with other health professionals, patients
and the general public.
Table 30 reports on the expectations of all the survey participants, noting their relative
response rates and the percentage of participants who fell into each category in at least
one of their responses.
Table 30 Expectations of Survey Participants
Count Responses percent
Cases percent
Service availability
203
19.4
72.2
Speed of response 245 23.4 87.2
Competence and skills of staff 257 24.5 91.5
Communication and teamwork 111 10.6 39.5
Professional and ethical behaviour 130 12.4 46.3
Other expectations 103 9.8 36.7
Total responses 1049 100.0
NB. 4 missing cases; 281 valid cases.
In some cases individual responses covered the same group of expectations more than
once, using different words to describe the same expectation. These were counted
individually, acknowledging the importance of each response to the respondent. Table
31 summarizes the expectations by each respondent category in percentage terms. Chi-
square tests have been applied to the raw data in Table 31 and the following Tables 32
to 35 that report on four other variables – rurality, gender, personal experience and
frequency of contact.
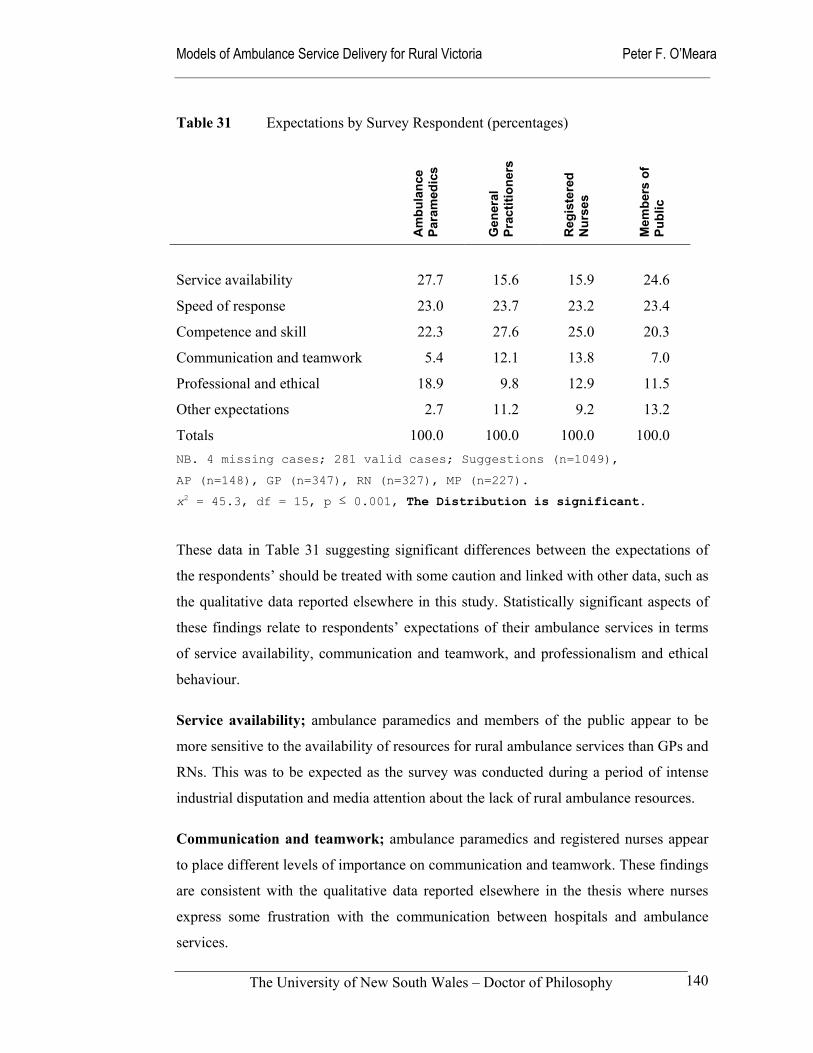
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
140
Table 31 Expectations by Survey Respondent (percentages)
Am
bula
nce
Para
med
ics
Gen
eral
Pr
actit
ione
rs
Reg
iste
red
N
urse
s
Mem
bers
of
Publ
ic
Service availability
27.7
15.6
15.9
24.6
Speed of response 23.0 23.7 23.2 23.4
Competence and skill 22.3 27.6 25.0 20.3
Communication and teamwork 5.4 12.1 13.8 7.0
Professional and ethical 18.9 9.8 12.9 11.5
Other expectations 2.7 11.2 9.2 13.2
Totals 100.0 100.0 100.0 100.0 NB. 4 missing cases; 281 valid cases; Suggestions (n=1049),
AP (n=148), GP (n=347), RN (n=327), MP (n=227).
x2 = 45.3, df = 15, p ≤ 0.001, The Distribution is significant.
These data in Table 31 suggesting significant differences between the expectations of
the respondents’ should be treated with some caution and linked with other data, such as
the qualitative data reported elsewhere in this study. Statistically significant aspects of
these findings relate to respondents’ expectations of their ambulance services in terms
of service availability, communication and teamwork, and professionalism and ethical
behaviour.
Service availability; ambulance paramedics and members of the public appear to be
more sensitive to the availability of resources for rural ambulance services than GPs and
RNs. This was to be expected as the survey was conducted during a period of intense
industrial disputation and media attention about the lack of rural ambulance resources.
Communication and teamwork; ambulance paramedics and registered nurses appear
to place different levels of importance on communication and teamwork. These findings
are consistent with the qualitative data reported elsewhere in the thesis where nurses
express some frustration with the communication between hospitals and ambulance
services.
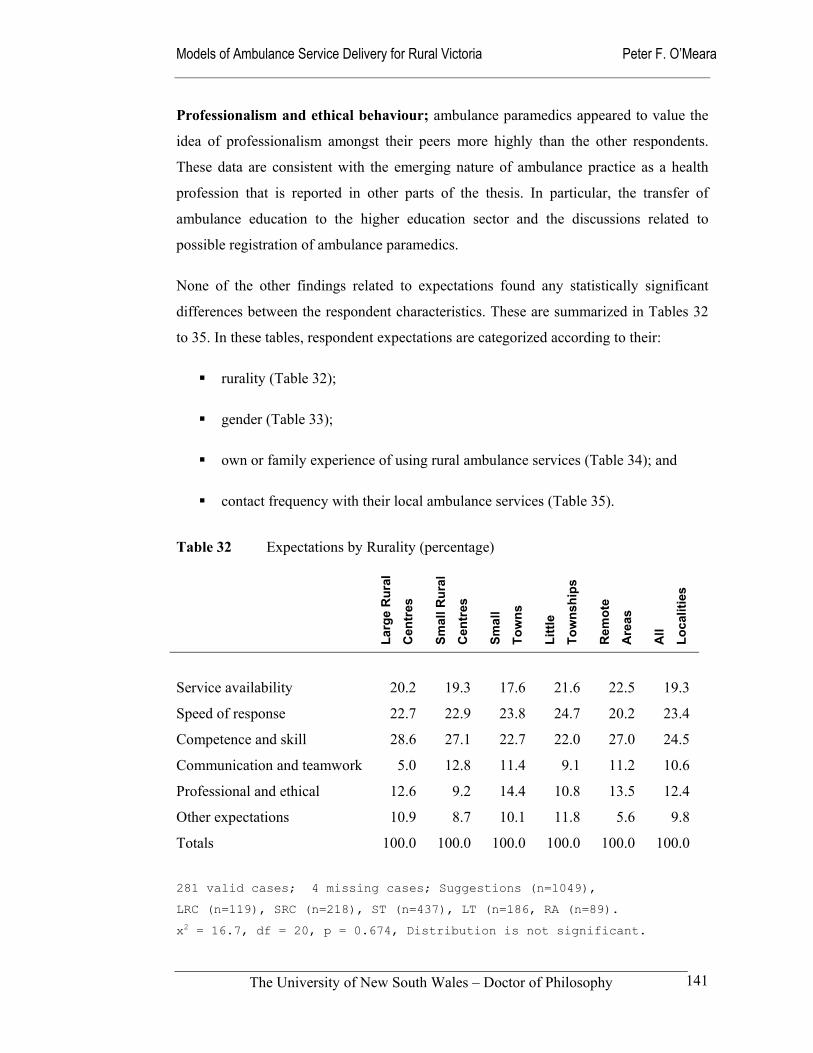
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
141
Professionalism and ethical behaviour; ambulance paramedics appeared to value the
idea of professionalism amongst their peers more highly than the other respondents.
These data are consistent with the emerging nature of ambulance practice as a health
profession that is reported in other parts of the thesis. In particular, the transfer of
ambulance education to the higher education sector and the discussions related to
possible registration of ambulance paramedics.
None of the other findings related to expectations found any statistically significant
differences between the respondent characteristics. These are summarized in Tables 32
to 35. In these tables, respondent expectations are categorized according to their:
rurality (Table 32);
gender (Table 33);
own or family experience of using rural ambulance services (Table 34); and
contact frequency with their local ambulance services (Table 35).
Table 32 Expectations by Rurality (percentage)
Larg
e R
ural
Cen
tres
Smal
l Rur
al
Cen
tres
Smal
l
Tow
ns
Littl
e
Tow
nshi
ps
Rem
ote
Are
as
All
Loca
litie
s
Service availability 20.2 19.3 17.6 21.6 22.5 19.3
Speed of response 22.7 22.9 23.8 24.7 20.2 23.4
Competence and skill 28.6 27.1 22.7 22.0 27.0 24.5
Communication and teamwork 5.0 12.8 11.4 9.1 11.2 10.6
Professional and ethical 12.6 9.2 14.4 10.8 13.5 12.4
Other expectations 10.9 8.7 10.1 11.8 5.6 9.8
Totals 100.0 100.0 100.0 100.0 100.0 100.0
281 valid cases; 4 missing cases; Suggestions (n=1049),
LRC (n=119), SRC (n=218), ST (n=437), LT (n=186, RA (n=89).
x2 = 16.7, df = 20, p = 0.674, Distribution is not significant.
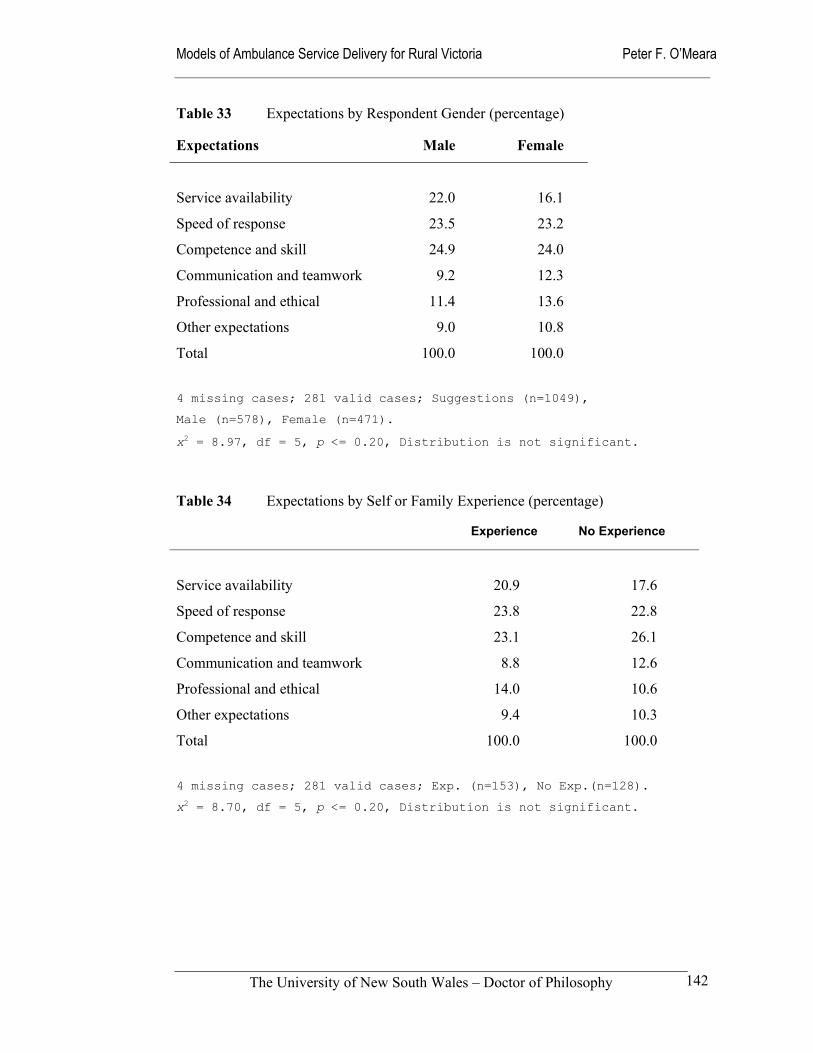
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
142
Table 33 Expectations by Respondent Gender (percentage) Expectations Male Female
Service availability 22.0 16.1
Speed of response 23.5 23.2
Competence and skill 24.9 24.0
Communication and teamwork 9.2 12.3
Professional and ethical 11.4 13.6
Other expectations 9.0 10.8
Total 100.0 100.0
4 missing cases; 281 valid cases; Suggestions (n=1049),
Male (n=578), Female (n=471).
x2 = 8.97, df = 5, p <= 0.20, Distribution is not significant. Table 34 Expectations by Self or Family Experience (percentage) Experience No Experience
Service availability
20.9
17.6
Speed of response 23.8 22.8
Competence and skill 23.1 26.1
Communication and teamwork 8.8 12.6
Professional and ethical 14.0 10.6
Other expectations 9.4 10.3
Total 100.0 100.0
4 missing cases; 281 valid cases; Exp. (n=153), No Exp.(n=128).
x2 = 8.70, df = 5, p <= 0.20, Distribution is not significant.
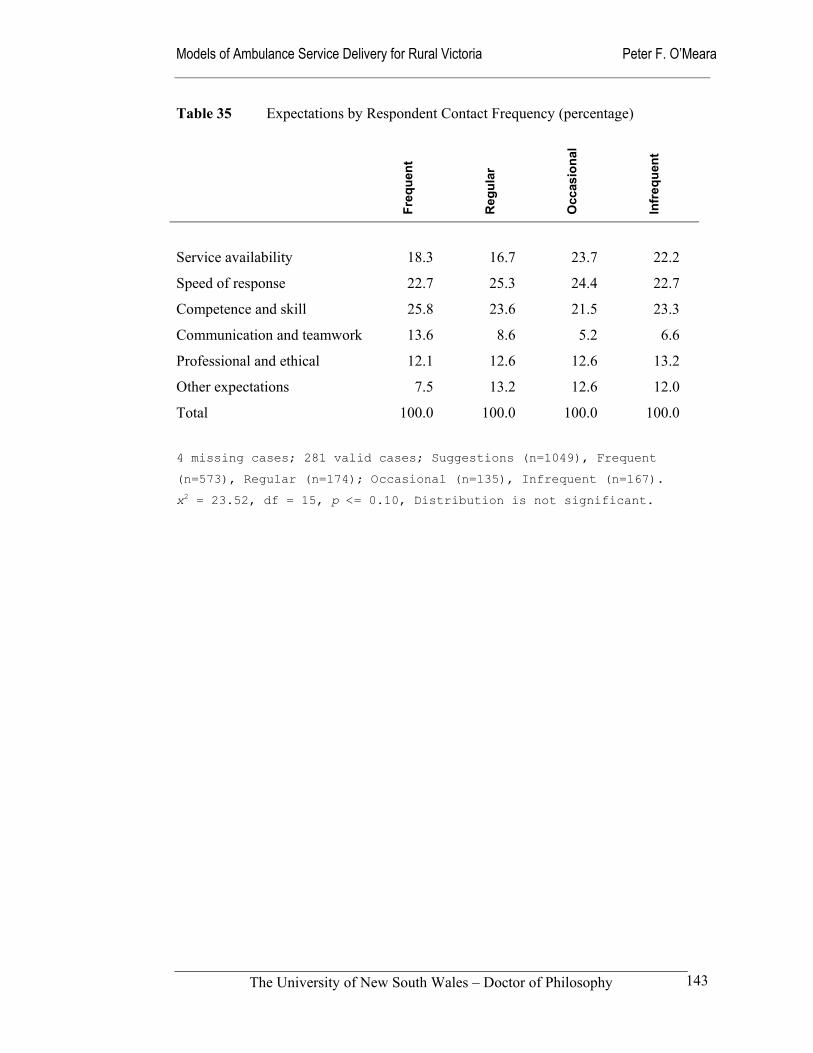
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
143
Table 35 Expectations by Respondent Contact Frequency (percentage)
Freq
uent
Reg
ular
Occ
asio
nal
Infr
eque
nt
Service availability 18.3 16.7 23.7 22.2
Speed of response 22.7 25.3 24.4 22.7
Competence and skill 25.8 23.6 21.5 23.3
Communication and teamwork 13.6 8.6 5.2 6.6
Professional and ethical 12.1 12.6 12.6 13.2
Other expectations 7.5 13.2 12.6 12.0
Total 100.0 100.0 100.0 100.0
4 missing cases; 281 valid cases; Suggestions (n=1049), Frequent
(n=573), Regular (n=174); Occasional (n=135), Infrequent (n=167).
x2 = 23.52, df = 15, p <= 0.10, Distribution is not significant.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
144
5.3 Suggested changes to rural ambulance services
Following the compilation of the responses to questions 11 and 12 in the respondent
questionnaire, common themes were identified and analysed according to respondent
and the rurality classifications. The two questions sought unstructured, short responses
at the end of the questionnaire (see Appendix). The two questions were:
Question 11.
Would you like to change anything about your local ambulance service?
Question 12.
Do you have any other comments about other aspects of your local ambulance
service?
Question 11 received a very good response rate, with 94 percent (268 of 285) of
respondents completing the question. Of these 17 percent (46 of 285) indicated that they
did not want to change anything about their local service. A number of respondents
made positive comments about the service provided. In total 78 percent (222 of 285)
had suggestions for improvement. These ranged from the blunt ‘Yes!!’ to narratives of
50 to 100 words. In this question, a ‘no response’ or ‘no’ was taken as an indication that
the respondent was satisfied with the current services being offered.
Question 12 produced a smaller response with 52 percent (148 of 285) responding apart
from those indicating that they had no comment to make. Many of these responses were
additions to those in Question 11, while others were positive comments about their local
services and staff.
This chapter provides a narrative summary of these responses, using respondent and
rurality classifications as the variables. While each variable is reported separately, three
themes were identified in the responses - staff resources; local autonomy; and
ambulance role. They are placed in the wider context in the discussion at the end of this
chapter.
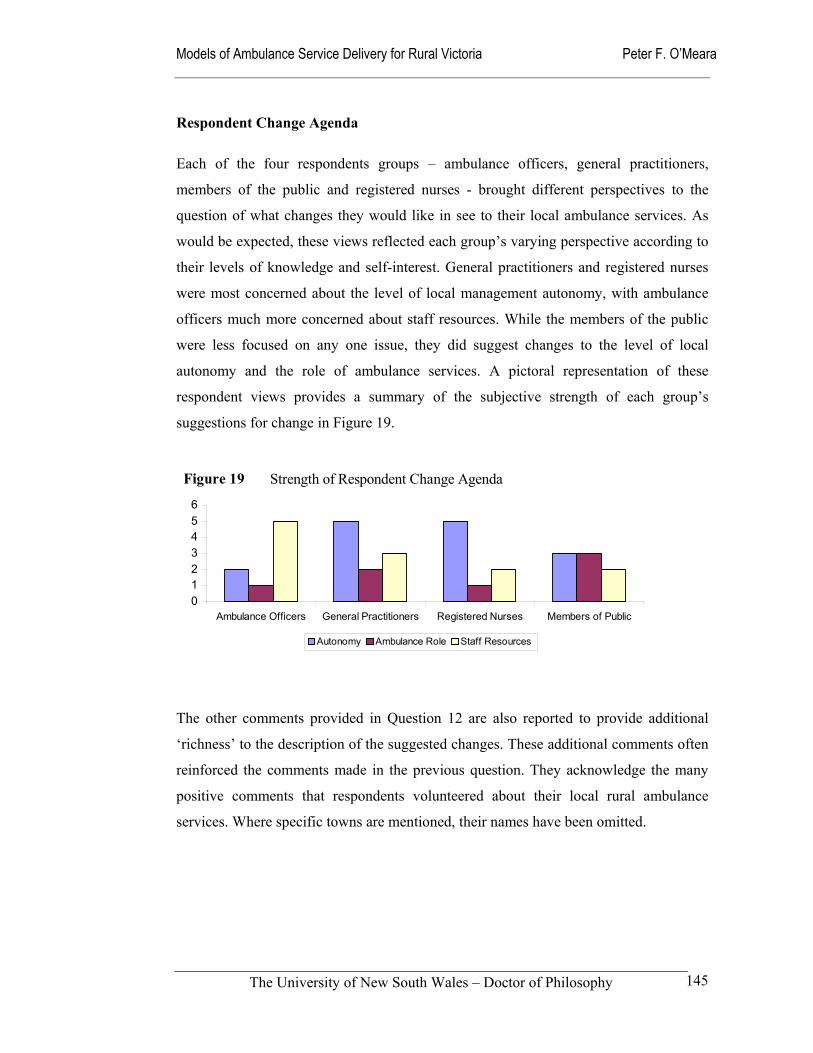
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
145
Respondent Change Agenda
Each of the four respondents groups – ambulance officers, general practitioners,
members of the public and registered nurses - brought different perspectives to the
question of what changes they would like in see to their local ambulance services. As
would be expected, these views reflected each group’s varying perspective according to
their levels of knowledge and self-interest. General practitioners and registered nurses
were most concerned about the level of local management autonomy, with ambulance
officers much more concerned about staff resources. While the members of the public
were less focused on any one issue, they did suggest changes to the level of local
autonomy and the role of ambulance services. A pictoral representation of these
respondent views provides a summary of the subjective strength of each group’s
suggestions for change in Figure 19.
The other comments provided in Question 12 are also reported to provide additional
‘richness’ to the description of the suggested changes. These additional comments often
reinforced the comments made in the previous question. They acknowledge the many
positive comments that respondents volunteered about their local rural ambulance
services. Where specific towns are mentioned, their names have been omitted.
Figure 19 Strength of Respondent Change Agenda
0123456
Ambulance Officers General Practitioners Registered Nurses Members of Public
Autonomy Ambulance Role Staff Resources
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
146
Ambulance Officers’ Change Agenda
The biggest issue for the 37 ambulance officers who responded to Question 11 was the
need for more staffing resources. They had a very strong desire for guaranteed two-
officer crewing as is the case in metropolitan areas. A number of the ambulance officer
respondents linked the levels of staffing to their preference for 24-hour shifts over the
use of on-call rosters. This is consistent with the on-going industrial disputation that
afflicted Victorian ambulance services during the 2000/2001 negotiation of a renewed
enterprise agreement with the Ambulance Employees’ Association.
Another related suggestion was that resources be provided to increase the number of
MICA-trained staff who could be available either locally or within a reasonable distance
and time. One respondent recognized that ‘younger staff would be required to meet this
recommendation’. The opportunity for existing staff to gain more advanced paramedic
qualifications and then be authorized to practice was a major point of contention.
Another ambulance officer made the point that:
The service needs to recognize the remote areas covered and the time lag involved in patient retrieval and therefore provide better patient outcomes by allowing officers to practice those advanced skills obtained in their own time and at their own expense.
A secondary issue for ambulance officers was the local control of resources. Some
wanted ‘more input and direction on a local level’, others expressed doubt that
centralization of dispatch procedures had been of advantage to the public. Underlying
this concern was the latent concern about the then pending amalgamation of the regional
services into one unified rural service.
In Question 12, ambulance officers made another 25 comments about their local
ambulance service. Their comments were generally positive, saying that their model
was working well within the available resources. One ambulance officer noted that the
Service ‘would fall into a heap without community support’. Another said that, ‘we have
a local Auxiliary, thus people have pride in our service’. Others suggested that ‘more
work needs to be done within the community to boost understanding of ambulance’ and
‘the service needs to promote themselves and their abilities to the general public’.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
147
Other ambulance officer concerns related to the service ‘becoming more remote and
isolated as more centralization takes place’, and the competitive environment that was
prevalent at the time of the questionnaire distribution. That is, prior to the change of
State Government in Victoria in late 1999.
General Practitioners’ Change Agenda
A total of 70 rural general practitioners provided responses to the question asking them
to describe the changes they desired in their rural ambulance services. In common with
ambulance officers, they were concerned about staffing configurations and the
availability of MICA-trained staff. One GP raised the issue of members of the public
being required to drive the ambulance when the single-officer crew treated the patient.
A number felt that having two-officer crews available locally would also improve
response times for urgent transfers from small rural hospitals to regional hospitals.
Cases of having to wait for crews from regional centres for over one hour were cited as
cause for concern. Others suggested increases in the numbers of vehicles in their towns,
and in some cases argued for the establishment of new branch stations in some small
towns.
Many of the GPs suggested an ‘increased
availability of paramedic (MICA) trained
ambulance officers’. They suggested that all
ambulance officers be brought up to and
maintain the same standard of training so that
they can cope with most emergencies.
Coming from an alternative perspective, one
GP reported ‘a slightly gung-ho approach
with inappropriate resuscitation’ and a
tendency of ambulance officers to go beyond
their training and skills when dealing with
elderly patients. According to this GP, they
unilaterally decide that the patient does not
GP Concerns Co-locate service to Accident and Emergency of local hospital. Time and funding to attend workshops with GPs and nurses. It should be based at the local emergency centre, rather than separated from it. This could better integrate ambulance services to the rest of the community health services. More involved in local hospital activities. eg. be based at local hospital.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
148
need to go to hospital without consulting with the patient’s medical officer. Despite
these concerns, GPs generally saw potential for ambulance stations and ambulance
officers to be more closely integrated into local health and emergency services.
By far the most strongly expressed concern amongst GPs was the issue of local
management autonomy, with considerable concern expressed about the transfer of
dispatching to distant communication centres in recent years. A large number of the GP
respondents wanted a ‘return to locally-based telephone answering and directing
service’. It did not matter if the control centre was 40, 75 or 300 kilometres distant the
sentiment was the same. The centralized communications centres were described as
‘remote’.
The central ambulance base is in [name omitted] – I’m frequently stuck on the phone trying to describe where the ambulance needs to come to, with someone with NO knowledge of the local area. The base should have stayed in [name omitted]. Spending 5-10 minutes on the phone during an emergency is laughable.
In addition to a perceived lack of local knowledge in
centralized communications centres, some GPs indicated
a lack of tangible connection with a service that was
remote and sometimes at an ‘undisclosed location’.
Some said they were denied the opportunity to contact
the local service.
Forty-five of the general practitioners offered other
comments in response to Question 12. Many of them
took the opportunity comment further on problems with
centralized control of the service to remote locations.
One made the point that, ‘I am not convinced that the
delays are minimized since central control moved away
from our region – they seem worse’. Another GP, who is
an Area Medical Co-ordinator with Medical Displan, felt
that he was no longer noticed after the centralization of
dispatch and control.
GP Criticisms
“Diplomacy” training for MICA ambulance officers from other areas. Problems with transfer of ventilated patients when MICA ambulance staff think they know more than the anesthetists who have resuscitated the patients. Inefficient use of resources because of a lack of A & E centre in the town, and poor co-operation with medical practitioners.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
149
One GP was so impressed with
the local volunteer ambulance
service, that he said, ‘please we
do not want paid officers’.
Others were pleased to see more
highly qualified staff being
appointed and reported that it
had improved services. One
described their local full-time
staff as ‘Very competent staff.
Service more effective than city
service.’
Views about the current and
future role of ambulance officers
ranged across a spectrum of
positions from criticism of
performance, to praise of current
performance and suggested
enhancements.
GP Compliments Those who do it provide an invaluable and life saving service - vital to preserve and enhance. Professional and competent officers. Their involvement is commendable. [referring to volunteers] Ambulance officers overall excellent and pleasant to work with. The GPs and ambulance officers have a good working relationship and cooperate well. Ambulance officers generally handle patients and emergencies well. Very high quality service. Very good support for GPs. They are a great asset and undervalued by the press and the public.
GP enhancement suggestions Could they become more community health orientated. Talk to schools etc. Their role facilitating healthy participation is (understandably) underdone. There is a need for it to work closer with GPs, via Medical Displan and Divisions of GP.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
150
Members of Public Change Agenda
The responses from the 42 members of the public who made suggestions for change
were the most prosaic of all the respondents. This possibly reflected their ‘lay’
qualifications and their lack of self-interest, as those with nursing, ambulance or
medical qualifications were deliberately excluded from this category. A further twelve
members of the public clearly indicated that they wanted no changes to be made to their
local ambulance service.
While a few members of the public said they wanted more staff and improved training,
there were far more comments related to the use of volunteer staff in their local area
than from other respondents. The role and performance of volunteer staff was generally
supported. However, respondents indicated that the appointment of full-time,
professionally qualified staff would be welcomed in small remote stations that currently
rely on voluntary staff. It was argued that some locations need permanent and qualified
staff because of their remoteness. There was also concern about single-officer crewing
in some areas. A comment that captured the feeling was:
It is of concern that nearly always only one officer is available to attend. This means that the patient being transported can only receive attention en-route if the ambulance stops or if a bystander is conscripted to drive the ambulance.
In common with GPs, the members of the public wanted to ‘be able to ring a local
number answered by local people’. They lacked confidence in remote communications
centres. A typical comment was ‘ calls are directed to [name omitted] who do not
always have adequate knowledge to direct calls to the right place’.
Members of the public were of the view that the role of ambulance staff could be
extended and be more integrated with other health services. This included suggestions
that ‘staff should perform other duties while awaiting calls’, and that co-location be
considered. One interesting suggestion was that ‘recognition needs to be given to the
community safety role they play’.
The 36 members of the public who provided other comments in response to Question 12
reiterated their regret that the service was no longer locally managed. A large number of
their remaining comments highlighted the important role of voluntary staff in small and

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
151
remote communities. One positive comment made was, ‘We have a very dedicated
available volunteer staff who are well trained and very professional.’
On the other hand another respondent felt that the task was ‘Too complex for local
volunteers to fully embrace.’
Registered Nurses’ Change Agenda
Some 69 nurses made suggestions for change, while twelve indicated that they wanted
no changes to be made. Their suggestions ranged from the very basic – ‘lots’ – to
lengthy answers that indicated a strong interest in the issues. As a group, nurses were
the most articulate respondents to the study. The need for additional staff and vehicles
was a continuing thread throughout the nursing responses, with concerns about the
impact one-officer crewing has on inter-hospital transfers. Related to this was a concern
about the ‘privatization of inter-hospital transports and the lack of ability of the
ambulance service to compete with them [referring to private ambulance services]’.
Community Views of Volunteers
Local service is provided by community-minded professionals with involvement in other emergency services (SES and CFA) and available to perform first aid classes. To continue the excellent work they currently perform. Totally comprised of "Community Ambulance Officers" (casual). The [name omitted] community has caring reliable ambulance officers who also have full-time or part-time jobs. Nothing other than to commend the volunteers - they waited at the hospital to see that I was okay! Volunteer service very good, but could be resourced and supported better. We are very lucky to have committed people who regularly give up time to operate their on call time at the centre.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
152
Nurses recognized the financial difficulty of having full-time professional staff in very
small towns, while hoping that the numbers could be increased as a means of improving
the service provided. One nurse made the suggestion to ‘have an ambulance officer on
hand who is actually trained by the service. That is, a fully-fledged ambulance officer’.
Nurses’ concerns about centralized
communications centres took a slightly
different form to that of the other
respondents. While a number preferred a
local response over a central response,
nurses as a group were much more
concerned about strategies for improving
communication between hospitals and
communication centres. This included,
booking procedures, prior notification of
emergency departments of patient arrivals,
and arranging inter-hospital transfers. There
was a large number of concerns and
constructive suggestions about the reliability
of ambulance notification to emergency
departments.
Even though they were complimentary of local ambulance officers’ skills and attitudes,
nurses made no specific comments about any changes in ambulance officer roles in
response to Question 11.
Fifty-seven nurses provided additional comments about their local ambulance service in
Question 12. They cited examples of where tensions between themselves and
centralized control centres have been manifested. One of the most direct said, ‘Local
ambulance officers pleasant and get on well with staff. Resentment of staff when
controllers “call the tune”, as when things will be transferred or if they can wait until
the following day! In other words, over-riding medical decisions due to lack of
resources.’
Communication with Emergency Departments System of notification to Accident and Emergency department prior to arrival of patient needs to improve. In my opinion it is important to notify rural hospitals of the impending transfer of a patient from the community to the hospital. This at present has been changed and is causing major confusion. Using [name omitted] as a phone base is ridiculous – often mix up address. Don’t always notify us of impending arrivals. Direct notification from officers rather than third-hand through Control 100 kilometres away.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
153
A topic that nurses raised in additional comments was that of volunteer ambulance
officers or, as they are now described in Victoria, Community Ambulance Officers. One
positive comment came from a nurse where CAO’s had been re-introduced to
complement full-time ambulance paramedics, who said ‘Addition of Community
Ambulance Officers has made a great deal of improvement and service to the
community.’ Another noted that ‘Mostly one officer and one volunteer do a great job.’
Unlike the majority of comments
from GPs and members of the
public, nurses were not always
complimentary about clinical
standards or the level of support
afforded the volunteers. While
making positive comments such
as, ‘The commitment of local
volunteers is to be commended
and should be recognized’,
‘Compliment to the volunteer
ambulance officers on their
commitment’, ‘The volunteers do
a terrific job’, nurses also made
less positive comments about
volunteer standards (see Box).
Tensions with Communications Centres
I have had a couple of occasions where I have found control not enthusiastic in helping arrange transport to meet appointment times in Melbourne of a patient being transported. Sometimes the distance of the control room leads to inadequate directions to locations for local crew – better maps or satellite guidance or other method for improvement? Why does a call for an ambulance have to go to Melbourne, then be referred back? This is very distressing to the client, particularly older persons trying to make contact.
Nurses’ Views of Volunteer Performance
Volunteer service is inadequate. As it is the only voluntary ambulance in Victoria, it is probably more difficult to obtain excellence from members. Would be better off with a regular ambulance service??? Sometimes a lack of confidentiality in a small town. Mostly a very good service. Our service is staffed by volunteers from the community. Considering their limited training, lack of experience (practical) and paucity of numbers, they do a great job. Often only one officer on duty and a volunteer has to be collected to help. More liaison (? with education) between our facility and volunteer ambulance.
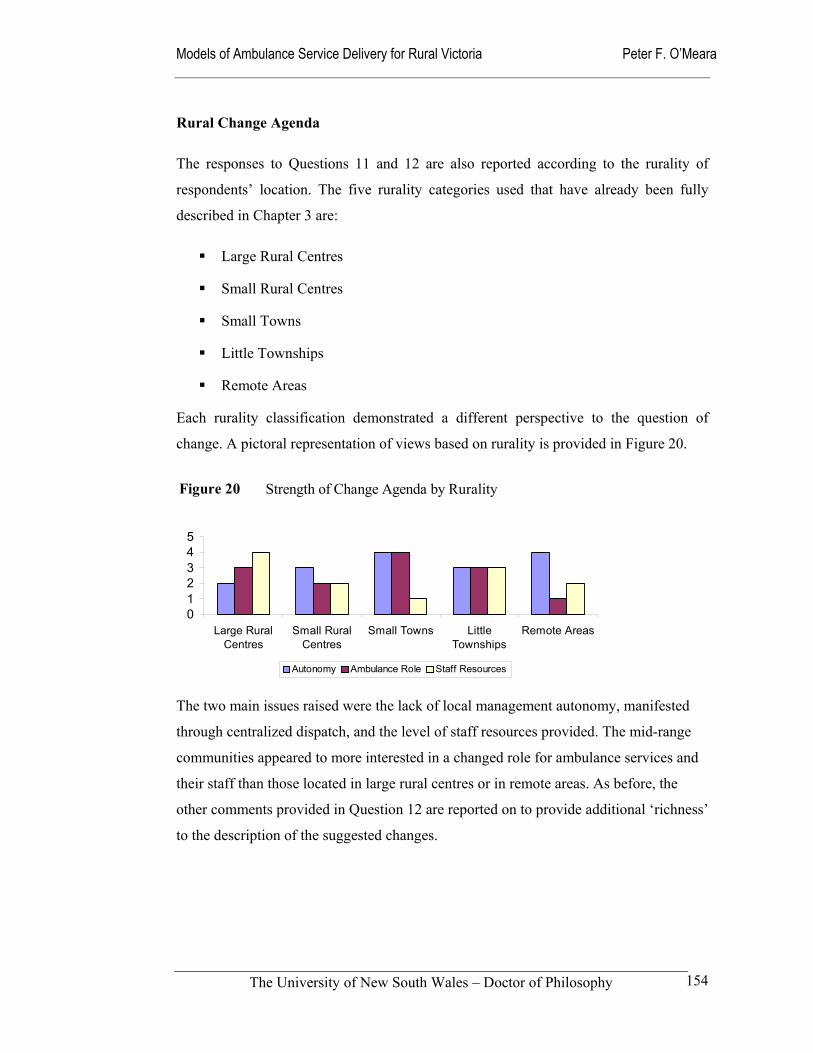
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
154
Rural Change Agenda
The responses to Questions 11 and 12 are also reported according to the rurality of
respondents’ location. The five rurality categories used that have already been fully
described in Chapter 3 are:
Large Rural Centres
Small Rural Centres
Small Towns
Little Townships
Remote Areas
Each rurality classification demonstrated a different perspective to the question of
change. A pictoral representation of views based on rurality is provided in Figure 20.
The two main issues raised were the lack of local management autonomy, manifested
through centralized dispatch, and the level of staff resources provided. The mid-range
communities appeared to more interested in a changed role for ambulance services and
their staff than those located in large rural centres or in remote areas. As before, the
other comments provided in Question 12 are reported on to provide additional ‘richness’
to the description of the suggested changes.
Figure 20 Strength of Change Agenda by Rurality
012345
Large RuralCentres
Small RuralCentres
Small Towns LittleTownships
Remote Areas
Autonomy Ambulance Role Staff Resources
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
155
Large Rural Centres Change Agenda
The 29 respondents from large rural centres had two main suggestions for change:
1. Increases in staff and other resources.
2. A return to local management autonomy.
Both the large rural centres in the study have had two-officer crewing for many years,
so the staffing issues raised concentrated on ‘maintenance of adequate crewing’
throughout the whole week and ‘more after-hours availability’. A number of
respondents were concerned about the facilities offered to staff. Some also suggested
the establishment of new stations in towns close to these large rural centres – so-called
satellite stations.
The issue of local management
autonomy was very acute in
these large rural centres that
had in the past been regional
headquarters with their own
communications centres. They
were suffering a very real
sense of loss at the removal of
their local management and
decision-making power. There
was particularly strong
criticism of one
communications centre that
had taken over the dispatch
functions from the ‘old’
regional headquarters.
Large Rural Centres and Dispatch Centres Operators with local knowledge would make initial contact easier. Local rather than Regional control. Direct contact instead of going through to [name omitted] and Melbourne. Cannot contact local service itself. Management of the agency from outside the area. Cost! Using [name omitted] as a phone base is ridiculous - often mix up re; address. Don't always notify us of impending arrivals. Have a telephone contact for service in [name omitted] rather than [name omitted]/Melbourne. Have the emergency call person centred here as opposed to the central remote location. Phone operators are distant … so don't know local area. Phone operators have little medical knowledge and no sense of urgency.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
156
The eighteen additional comments provided in the large rural centres were mainly
complimentary of ambulance staff and the services provided. There were suggestions
for ‘improved training curriculum for treating psychiatric patients’.
Small Rural Centre Change Agenda
Respondents from the small rural centres provided 42 suggestions for change that
encompassed the three themes of local autonomy, staff resourcing and the role of
ambulance officers. One respondent challenged the whole concept of a local ambulance
service with the comment that, ‘we do not have a local ambulance service, it is a state-
wide service’. Others doubted the effectiveness of centralized control (see Box below).
The twin staffing issue of
providing two-officer crews and
the availability of MICA-trained
staff was an area in which changes
were desired. Respondents had a
clear expectation that ambulances
should be fully-staffed with a
minimum of two officers to avoid
the situation where ‘the patient
being transported can only receive
attention en-route if the ambulance
stops or if a bystander is
conscripted to drive the
ambulance.’ Locally based MICA-
trained officers were wanted so
that the station would not be
Positive Comments from Large Regional Centres Professional and competent officers. Very competent staff. Service more effective than city service.
Centralized Control in Small Rural Centres System of notification Accident and Emergency department prior to arrival of patient needs to improve. Yes - immediate telephone access to our local ambulance officers - rather than through a remote (75 kms away) communications centre. LOCAL control for dispatching ambulances, not from [name omitted] (3 hours and 300 kms away). Ability to use own ambulance for immediate transfer of urgent cases!! Calls are directed to [name omitted] who do not always have adequate knowledge to direct calls to the right place. Local dispatch would lead to more efficient service delivery (Vs. [name omitted] dispatch).
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
157
reliant on crews from other areas. One respondent suggested ‘more trained MICA staff
so that there are sufficient to meet emergencies’. The issues of the long-term
recruitment and retention of
ambulance paramedics to regional
areas was also raised as an area of
future concern.
A number of respondents recognized
the desirability of ambulance staff
using their operational downtime
more productively through closer
liaison with local hospitals where
their skills could be utilized. These
suggestions included, team training,
integration within health agencies,
and the performance of other duties
between calls.
Thirty respondents in small rural centres
offered additional comments in response
to Question 12. Most continued to
comment about the loss of jobs and local
control since the regionalization of
communications centres in the 1990s.
Other comments related to the provision
of service delivery, with particular
concern about the long waiting times for
transfer of patients to regional and
metropolitan hospitals. Again, the concern
seemed to be with one specific
communications centre.
Some Additional Comments from Small Regional Centres Most people I have talked to would prefer to be able to contact their local ambulance directly, as local people have local knowledge. It is no longer local. Regional controllers are sometimes rude. It is disappointing the administration has been consolidated with the loss of local jobs. Sometimes the distance of the control room leads to inadequate directions to locations for local crews - better maps or satellite guidance or other method for improvement?
Problems with Patient Transfers The transfer of patients to a larger medical facility is too cumbersome and takes too long to get a two-man car from [name omitted]. Transfer of ill patients to other facilities can take far too long. Eg. Subarachnoid haemorrhage patient from [name omitted] to Melbourne - two hours to get ambulance from [name omitted] to pick up patient in [name omitted], then four to five hours to get to Melbourne. No air services available. This type of thing occurs often. Arrangements have to be done through HQ in [name omitted]!
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
158
There was one concern expressed about the clinical scope of ambulance paramedics
during inter-hospital transfers, with one respondent relating problems with the ‘transfer
of ventilated patients when MICA ambulance staff think they know more than the
anaesthetists who have resuscitated the patients.’
The ambulance service was described as ‘an essential community service and should not
be privatized’. Another noted rather optimistically that ‘there needs to be a more cost-
efficient service balanced with highly trained and experienced officers’.
Many respondents noted that ambulance officers were pleasant to work with and had
excellent communication and liaison with emergency departments. Others suggested,
that the role of ambulance officers could be enhanced by becoming more community
orientated. One nurse said that, ‘they don't receive the recognition they deserve from
medical officers’.
Small Towns Change Agenda
The dominant theme of the 88 responses to
Question 11 received from small towns respondents
was the inadequacy of staff resources for rural
ambulance services. In particular, staffing levels
and on-call requirements, crew deployment and
configuration, and improved skill levels of
paramedics were consistently alluded to in
responses. Although the comments often overlap,
the responses related to staffing issues have been
categorized into these three main areas of concern.
In Chapter 6, the responses of Rural Ambulance
Victoria to these concerns are outlined.
The need for more ambulance resources in small
towns was very strong, with a split between those
respondents who felt it would be good to have more
resources, and those who positively demanded
more staff and ambulances.
Demands for More Resources in Small Towns
Nothing other than staff increase.
More ambulance officers.
More staff officers covering stations / excessive overtime equals burnout.
More ambulances.
Increased manning.
More members and cars for area.
Increase staff and vehicles.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
159
In terms of staffing the small town
respondents were most concerned
about the provision of two-officer
crews, with one respondent saying
that, “… having one ambulance
officer on duty at a time is
ridiculous.” Others were concerned
about the well being of the
ambulance officers.
Calls to Increase Resources for Small Towns
Ideally would like two man car available in [name omitted] (often have to wait for car from [name omitted]).
An increase in numbers of officers as they are on call for long hours.
Often some delays due to ambulance being on another call. Perhaps another crew and ambulance.
Another Paramedic would be helpful.
Need more staffing for safety of rural area.
Have more ambulance vehicles based at rural towns so that they can arrive at destination within minutes.
Possibly more full time personnel available in local area.
More available staff and ambulances.
Increased availability and personnel.
Two-Officer Crewing
Change to two-man ambulance service.
Two staff to attend all call outs.
To have two officers on call.
More two-officer cars.
Two-person rather than one-person crews.
Easier to access to two-man car.
Recommend two-man crews for all rural calls. Two-man car could be available more often without such long delay (> 1 hr).
Dealing with Tourism in Small Towns
Sufficient staff on call during tourist season. Perhaps additional vehicle during above.
Increase staffing levels - currently no recognition of tourism throughout the year.
During winter months extra staff and vehicles.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
160
In addition to these staff resourcing issues, respondents
in small towns made positive suggestions for greater
integration with other health and emergency services,
the co-location of ambulance stations and the
desirability of inter-disciplinary training. One
respondent suggested, ‘More regular training. Cross
training with Police, CFA, doctors, hospital and
nurses.’ Probably because of its high visibility in the
public domain, the suggested introduction or expansion
of MICA units in small towns was a common
suggestion. Others just wanted an improvement in skill
levels locally, or access to units with those skills within
a reasonable timeframe.
Support for Improved Skill Levels in Small Towns
I would like a local two-man crew on standby in town. Improve nursing skills.
Two officer crewing on all vehicles. Availability of advanced life support skills/MICA within an adequate timeframe.
A pressing need for two officer crewing for emergency responses (at least). Upgrade skills to advanced life support for all officers.
More than one qualified officer on duty.
Ensure situations where member of public has to drive (because officer tending patient) do not occur - it is not satisfactory.
Abolish single officer crewing. Increase ALS skills.
MICA in Small Towns
Two-man at all times. MICA availability.
2 X 2 officer/MICA cars 24 hour per day.
Yes, another MICA unit.
Improve opportunity for officers to gain MICA paramedic qualifications.
Around the clock MICA coverage.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
161
The other major issue or theme that comes from the small towns category was
respondents’ desire to have more direct contact with, and greater local control of, their
ambulance service. It was evident that the technical advantages of a centralized
communication and dispatch system had not been adequately communicated to the local
community.
A total of 63 other comments in response to Question 12 were received from the small
towns category. While these responses were generally complimentary of their local staff
and service, they canvassed a wide range of topics and opinions. These included
comments that the ambulance service ‘are a great asset and undervalued by the press
and the public’, that the ‘staff perform well under the current political climate within
ambulance’. An example of the high regard for the local ambulance staff was at one
station where ‘[name omitted] has had remarkable continuity of ambulance officers -
two Station Officers in over 42 years. Their dedication has been exemplary and may not
be typical of all towns.’
Local Contact with Ambulance – improvement suggestions
Be able to ring local number answered by local people.
Have it controlled from the local area.
Communication with Control Service is usually good but has occasionally led to nonsense. Eg. Local crew nearby and crew sent from elsewhere.
Their communications in remote areas.
Co-ordinate service through local ambulance rather than through ambulance 40 kms away.
Return to locally-based telephone answering and directing service.
Increased co-operation with local medical practitioners. More efficient use of resources.
Direct notification from officers rather than third-hand through Control 100 kms away.
Some recent changes to dispatch procedures have not been to the advantage of the public.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
162
Once again, many comments were made about the problems of centralized
communications centres, with one cutting comment being ‘Excellent performance,
except for the clerks at end of telephone!!’
Little Townships Change Agenda
Question 11 elicited 40 responses from these much
smaller locations. Like the small towns, the main changes
suggested were related to additional staff resources. With
greater reliance on volunteers, respondents from the little
townships were less concerned with having officers with
advanced skills and more focused on having enough
ambulance officers. Some respondents had a preference
for paid staff over volunteer staff, while others wanted
more and better supported volunteers.
Other suggestions related to the provision of ‘better and
more frequent training’, particularly for older staff
members in the use of new equipment. One respondent
said, their volunteer staff needed a ‘more professional
attitude and better skills’, which they rated ‘from poor to
excellent’.
Communications Centre Gripes I am not convinced that the delays are minimized since central control moved away from our Region - they seem worse. Generally easy to work with locally - problems more at Regional level. We must have this service retained locally. Triage person needs to be polite and conscientious. Problems with control being remote from this area. Local Ambo's pleasant and get on well with staff. Resentment of staff when controllers “call the tune” .
Volunteer Woes in Little Townships Make it a paid position, rather than rely on volunteers. Although it may not warrant it, a fully qualified ambulance person would be a huge bonus. Local officers require more support in training. Additional staff. Need permanent staff. Staff. Presently only manned by volunteer ambulance officers creating time delay for more critical cases.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
163
Others suggested more and better trained staff who could provide two-officer crewing
and more advanced skills, such as the ‘ability to utilize intravenous injections in
emergencies’ and higher level skills, ‘able to administer intravenous fluids, adrenaline’.
More problems with centralized control surfaced, including a lack of input and direction
at a local level and a failure to notify rural hospitals of pending patient arrivals. One
respondent wanted ‘emergency calls to local controller, rather than central controller’.
As one respondent expressed it:
Improve communication with local hospital both in cases of emergency and booked transfers. I perceive some problems with centralized call centre.
When respondents were presented
with the opportunity to make other
comments about their local
ambulance service, 37 offered their
opinions. A small number suggested
that, ‘the ambulance service be co-
located at the health service complex,
so that “down time” could be more
appropriately utilized.’ Others
commented on the poor radio
communication in remote areas.
However, most of the additional
comments related to the pros and
cons of volunteer staff. One GP had
strong views on volunteers, saying:
Currently semi-independent service covering [towns X, Y and Z], ambulance covering each town. 100% volunteer service (no paid officers) with over 40 volunteers. Please, we do not want paid officers.
On the other hand, another respondent from the same town commented that:
As it is the only voluntary ambulance in Victoria, it is probably more difficult to obtain excellence from members. Would be better off with a regular ambulance service???
More Comments on Volunteers
The volunteers do a terrific job.
More liaison (? with education) between our facility and volunteer ambulance.
Our service is staffed by volunteers from the community. Considering their limited training, lack of experience (practical) and paucity of numbers, they do a great job.
We are very lucky to have committed people who regularly give up time to operate their on call time at the centre.
Volunteer service very good, but could be resourced and supported better.
No, except to say, we need to keep ambulance service here.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
164
Remote Areas Agenda
The seventeen suggestions for change from respondents in remote areas concentrated on
staffing issues. While they recognized the work of volunteers and the scarcity of
financial resources, remote respondents indicated a desire to have full-time and fully-
trained staff appointed in recognition of their remoteness from other health services.
One person suggested that remote areas should, ‘have an ambulance officer on hand
who is actually trained by the service. That is, is a fully fledge ambulance officer - not
just the holiday period.’
Calls for Full-time Staff in Remote Areas They [volunteer staff] are very good. In an environment of scarce financial resources, small population and remoteness it would be unreasonable to expect more. Perhaps appointment of a full-time ambulance officer. Better qualified ambulance officers because of remoteness. Too complex for local volunteers to fully embrace. A MICA trained officer (in remote areas like ours) would be beneficial to the area. Permanent full-time officer, Higher level training of officers (volunteers).

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
165
Remote respondents raised the issue of local control a couple of times, while the issue
of changing ambulance roles was not raised. Their other comments in response to
Question 12 followed up their concentration on volunteer ambulance officers, with
largely positive comments being made about their dedication and performance.
Appreciation of Volunteers We have a very dedicated available volunteer staff who are well trained and very professional. The commitment of local volunteers is to be commended and should be recognized – ‘rewarded’. Nothing other than to commend the volunteers - they waited at the hospital to see that I was okay! It is extremely difficult to get interested and conscientious people from the community interested to maintain a service.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
166
5.4 Discussion
Provision of emergency ambulance services to rural communities in Australia has been
based on historic resource allocations, metropolitan norms and the financial constraints
of ambulance services. At times, these factors are in conflict with each other and lead to
tensions that are often manifested through organizational conflict. The experience in
Australia has been that once resources are allocated to specific communities attempts to
adjust resource allocations or models of service delivery in response to changes in
circumstances are met with either apathy or hostility from stakeholders.
There is little evidence in the ambulance or emergency medical service (EMS) literature
of any systematic determination of the emergency ambulance expectations of rural
communities. A ‘top-down’ approach is more typical of the approaches taken to the
determination of needs. For example, Callaham (1997) argues that future planning for
EMS systems must strive to maximize access to proven interventions. On this basis the
goals of an EMS system should be:
1. Basic life support within four minutes;
2. Advanced life support within eight minutes; and
3. Arrival at a definitive trauma facility within an hour, preferably one-half hour, of the original injury.
These goals for emergency medical systems are laudable and based on well-founded
research. However, it has not been tested whether rural communities share these
expectations or whether professional providers are imposing their views on
communities. There is also the question of whether, the expectations of rural
communities are related to their size and isolation (rurality), and whether the key
stakeholders in a rural emergency medical system have different expectations of
ambulance services to each other?
These findings have described the expectations of rural ambulance paramedics, general
practitioners, registered nurses, and members of the public in 37 communities in rural
Victoria. The three most important expectations of rural ambulance services identified
were: service availability; speed of response; and competence and skills of staff. Other
expectations rated highly were: communication and teamwork; and the professional and
ethical behaviour of ambulance paramedics.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
167
These results highlight a number of important issues for policy makers, the providers of
ambulance services, and for those charged with responsibility of educating and training
ambulance professionals and volunteers. Ambulance paramedics themselves also need
to examine their own practices in light of these data.
The identified expectations are all important in their own right. Few people would argue
with the primacy of service availability, speed of response, and the competence and
skills of staff. These issues are addressed in the objectives of Rural Ambulance Victoria
and in the EMS literature. The findings on communication and teamwork are instructive
for those who place the provision of emergency ambulance services within the wider
health or emergency response system. Ambulance paramedics appear to place less
emphasis on inter-disciplinary teamwork than some other health professionals.
Alternately, differing perceptions of teamwork and how it relates to control may be a
factor. Professional and ethical behaviour is important in an organization with a
workforce consisting of both highly trained paramedics and community volunteers.
If ambulance paramedics are going to
work effectively with other health
professionals, they need to be better
trained in communication and
teamwork. There appears to be a case
for nurses and ambulance paramedics
to train and work together in order to
develop improved communication
and teamwork. A number of
respondents made suggestions along
these lines.
Allied to the problem of poor communication and teamwork is the need for an
understanding of the ethical and professional issues that relate to the role of ambulance
paramedics. For instance, the issue of patient confidentiality was highlighted in those
areas using CAO s.
These results highlight the importance of adequately educating and training ambulance
paramedics, including volunteer staff, in the clinical and decision-making skills that
Teamwork
I would like the ambulance service to be part of the health service complex; with ambulance officers ‘down-time’ utilized in the acute wards. – a nurse.
I would like to see the ambulance service co-located at the health service complex, so that ‘down time’ could be more appropriately utilized – a nurse.
There is a need for it to work closer with GPs, via Medical Displan and Divisions of GP. – a general practitioner.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
168
equip them to provide safe and effective care. How to provide and maintain this
standard of training in small communities with small caseloads presents many
challenges that need to be met if the expectations of rural communities are to be
satisfied.
In this study, the expectations of people living and working in small or isolated
communities were not fundamentally different to those in larger regional centres. When
the expressed expectations were analyzed through cross-tabulation with participant
descriptions and location, the results showed no significant difference between the
expectations of those residing in different-sized communities. Expectations of local
ambulance services were independent of the respondents’ level of rurality, they all
expect adequately resourced ambulance services that are able to respond quickly to their
needs with well-trained staff who behave in a professional manner.
These results provide an argument to policy makers and ambulance service boards that
they need to provide sufficient resources to ensure the rapid response of appropriately
trained ambulance personnel on an equitable basis. These expectations may include
access to services locally and more advanced services provided through specialized
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
169
response units or rotary-winged aircraft. In rural Australia, this will require a major
review of how resources are allocated if equitable outcomes are to be achieved. The
argument that people in small or isolated communities expect less than their peers in
larger centres is without foundation. The real question is how can this be achieved, not
if it is expected.
An overall summary of respondents suggested changes is presented here in the form of a
concept map (Figure 21). It identifies and links the three main themes that respondents
raised – staff resources, management autonomy, and the role of the ambulance service,
and identifies some of the contemporary issues that rural ambulance services are facing.
It also makes some tenuous links between them and the five models under consideration
in Chapter 8 of the thesis. The suggestion is that these issues and the types of service
delivery model adopted are intimately linked within a systems paradigm.
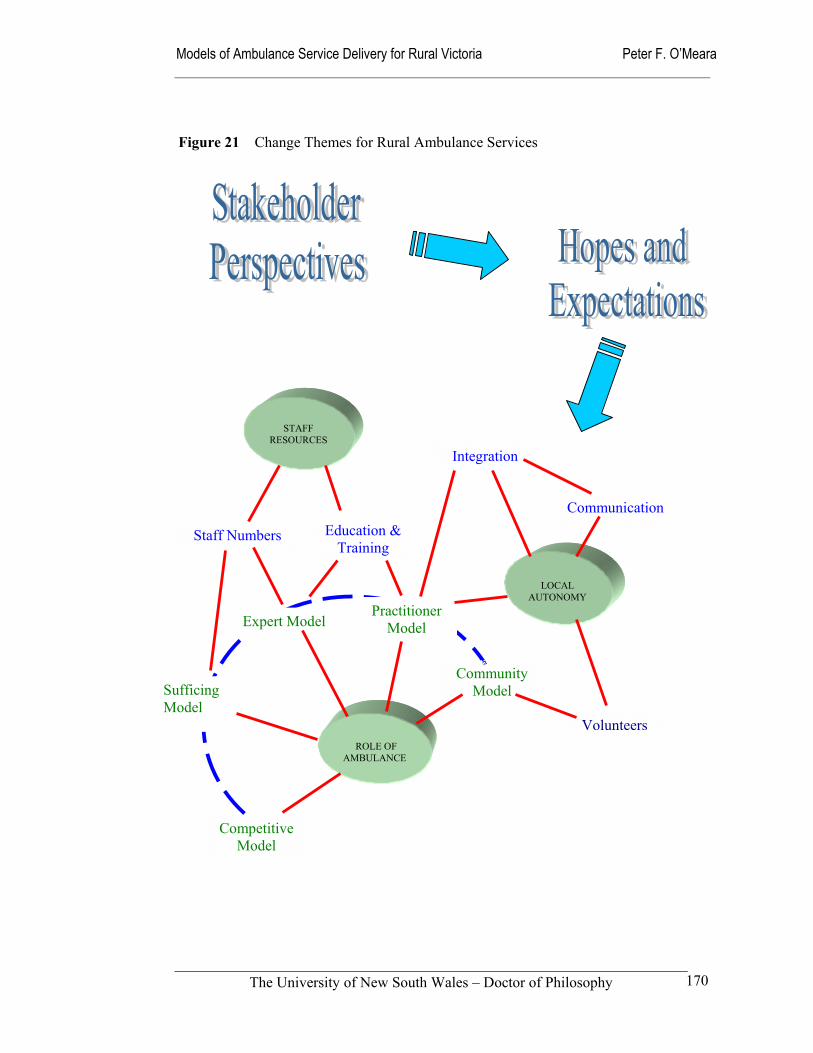
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
170
Figure 21 Change Themes for Rural Ambulance Services
ROLE OF
AMBULANCE
STAFF
RESOURCES
LOCAL
AUTONOMY
Staff Numbers
Integration
Communication
Volunteers
Education & Training
Community Model
Practitioner Model Expert Model
Sufficing Model
Competitive Model
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
171
Related to the concepts of expectation and change agendas are the concepts of demand
and need. Throughout the developed world there is the growing demand for after hours
medical services and emergency ambulance services (Pegram 2000). Rural ambulance
services in Australia are not immune to these demand pressures, and like ambulance
services elsewhere are seeking explanations for this growth in demand and planning
responses to these pressures. Chapter 6 examines the demand for emergency ambulance
services in rural Victoria, and notes some of the policy and operational responses to
these challenges. Suggested reasons for this observed growth in demand include:
greater awareness and raised expectations of ambulance services through media images of a more professional group of providers;
ageing of the population, which results in more need of ambulance services;
improved service availability as a result of improved resourcing;
improved quality of service following the impact of technological change and
more advanced training of personnel;
loss of other medical and health services such as country hospitals, including the de-institutionalization of psychiatric care.
Within the rural context, policy makers, ambulance services, funders and educators have
responded to community expectations, operational performance, public satisfaction
levels and hopes for the future with changes in funding arrangements and organizational
re-structures. Sometimes these responses have been planned while in other cases they
have been the products of external forces such as political and social changes, or
technological advances in communications systems or emergency medicine
interventions. Critics could say that, the planning and implementation processes have
often followed the contours of the land, rather than ploughing the furrows in ways that
would improve service delivery.
In rural Victoria some of the improvement initiatives taken have been widely supported,
while others have been contested. Clearly, the major stakeholders have pursued their
own interests according to their own worldviews. In Chapter 6, the responses of rural
ambulance services and educational providers are reported within the cultural, social
and political context of rural Victoria.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
172
6.0 Structure and Culture of Rural Ambulance Services
Section 1 Introduction
Section 2 Theory and Methods
Section 3 Findings and Discussion
Section 4 Conclusion
Chapter 1 Overview of Study
Chapter 2Theory Foundations
Chapter 4Communities Respondents
Chapter 5Expectations
Chapter 6Structure Culture
Chapter 7Ambulance Performance
Chapter 8Models of Delivery
Chapter 9 Policy Implications
Chapter 3Study Methods
Figure 22 Navigation Map of Thesis
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
173
6.1 Introduction
This third chapter of Section 3 (Findings and Discussion) addresses the second aim of
the thesis. It seeks to:
Describe the structure and culture of rural ambulance services within their socio-political climate, along with the educational and
technological changes that continue to shape their evolution.
The interaction between the structural and cultural aspects of rural ambulance services
with their socio-political environment, are fundamentally important determinants of
how services are delivered. The melding of these two aspects and their internal
consistency impact on the character of the transformation processes which constitute the
core of rural ambulance service delivery models. The structure of Rural Ambulance
Victoria has been used to illustrate how the cultural, social and political environment
influences the development of ambulance services in rural Australia.
This chapter describes the changes that have taken place leading up to and following the
1999 amalgamation of the five major regional ambulance services in rural Victoria
(Figure 23). In the first instance, the official story of the amalgamation is told through a
description of the structural changes that have taken place, the new organization’s
articulated vision, mission, values and objectives. These changes in organizational
arrangements are then placed within their cultural and political contexts. The
technological and educational developments that are impacting on Australian pre-
hospital systems are examined for their contribution to the service delivery systems of
rural ambulance services within these frames of reference. In the discussion, some of
the issues that rural ambulance services need to address now and in the future are
examined through these structural and cultural filters.
Rural ambulance services in Victoria have shared with other rural health services the
challenge of adjusting to a sometimes less than benign political and economic climate
over the last two decades. Since the mid-1980s ambulance services have faced the
corporatisation tide and greater ‘contestability’ within a competitive paradigm. This
‘mindset’ was encouraged on a bipartisan basis through the National Competition
Policy. A Victorian example of this was when in August 1993, the Kennett government
deregulated the ambulance transport fees for non-emergency patients. This
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
174
encouragement of private operators was a major destabilizing factor for the established
ambulance services. The continued existence and apparent profitability of private
ambulance transport services is testament to the long-term impact of this policy change.
Victorian rural ambulance services experienced varying degrees of difficulty responding
to this move toward a competitive market. Their organizational structures had been
designed to provide emergency services, not compete in the marketplace with private
providers. Those regional ambulance services with larger, relatively concentrated and
affluent populations were initially able to overcome the apparent inflexibility of their
organizational and cost structures. Compared to the smaller regions, they had the
advantage of relative economies of scale, a strong subscriber base, and for some time
sizable cash reserves.
In addition to these ‘competitive’ pressures, the rural ambulance services were
experiencing difficulties with largely union-imposed restrictive work practices. Unlike
the Melbourne Metropolitan Ambulance Service, the rural services because of their
smaller caseload and larger geographic areas did not realistically have the option of
splitting service delivery into emergency and non-emergency categories (Baragwanath
1997b). A further blow to their ability to compete occurred in July 1997 when the
Victorian Government introduced the Principles of Competitive Neutrality to the
ambulance services, which stripped services of any competitive advantages they may
have enjoyed as Government enterprises. At the same time, the ambulance services
were still trying to grapple with both a hostile industrial relations climate and budget
restraints.
The outcome of this environmental pressure was that in March 1999, the five major
rural ambulance regions were amalgamated into Rural Ambulance Victoria. Its
corporate headquarters was established in the provincial city of Ballarat, 100 kilometres
west of the State capital Melbourne. Figure 23 provides a picture of the pre-1999 and
current structure of publicly funded ambulance services in Victoria. This organizational
re-structure was another step in the rationalization of the sixteen ambulance services
originally formed in the mid-1950s and reduced to six in 1987 as a result of the 1984
Public Bodies Review Committee inquiry (PBRC 1984).
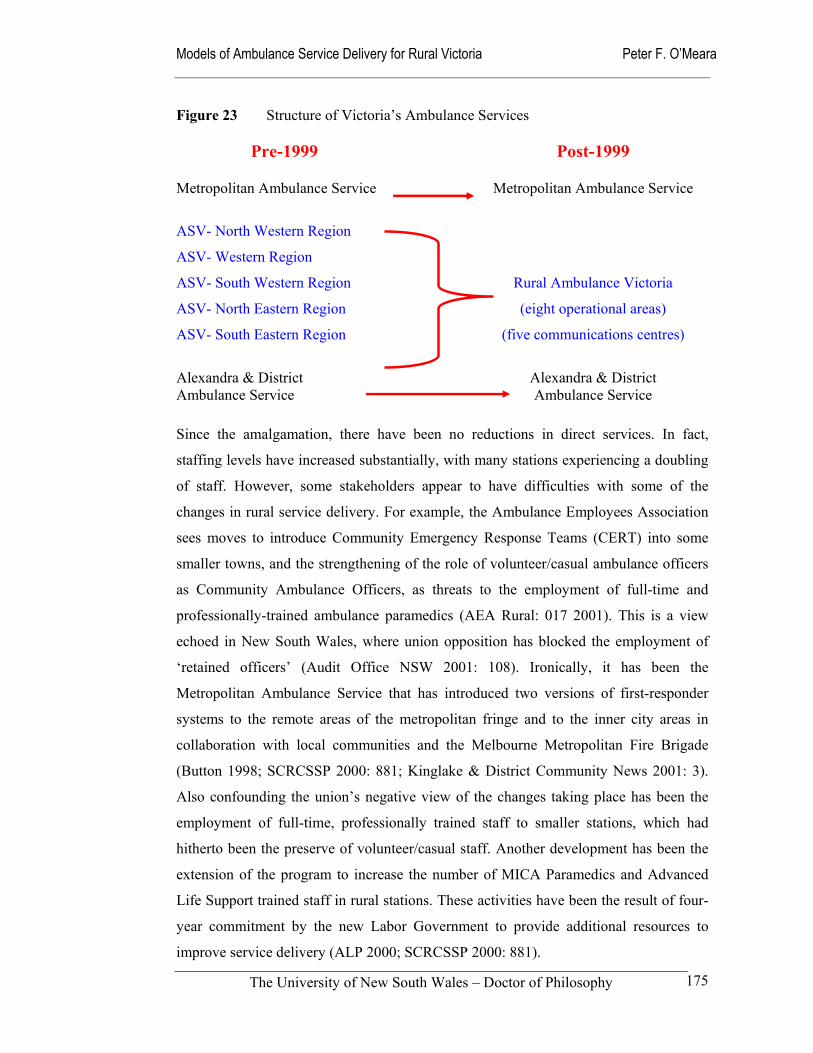
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
175
Figure 23 Structure of Victoria’s Ambulance Services Pre-1999
Post-1999
Metropolitan Ambulance Service Metropolitan Ambulance Service
ASV- North Western Region
ASV- Western Region
ASV- South Western Region Rural Ambulance Victoria
ASV- North Eastern Region (eight operational areas)
ASV- South Eastern Region (five communications centres)
Alexandra & District Ambulance Service
Alexandra & District Ambulance Service
Since the amalgamation, there have been no reductions in direct services. In fact,
staffing levels have increased substantially, with many stations experiencing a doubling
of staff. However, some stakeholders appear to have difficulties with some of the
changes in rural service delivery. For example, the Ambulance Employees Association
sees moves to introduce Community Emergency Response Teams (CERT) into some
smaller towns, and the strengthening of the role of volunteer/casual ambulance officers
as Community Ambulance Officers, as threats to the employment of full-time and
professionally-trained ambulance paramedics (AEA Rural: 017 2001). This is a view
echoed in New South Wales, where union opposition has blocked the employment of
‘retained officers’ (Audit Office NSW 2001: 108). Ironically, it has been the
Metropolitan Ambulance Service that has introduced two versions of first-responder
systems to the remote areas of the metropolitan fringe and to the inner city areas in
collaboration with local communities and the Melbourne Metropolitan Fire Brigade
(Button 1998; SCRCSSP 2000: 881; Kinglake & District Community News 2001: 3).
Also confounding the union’s negative view of the changes taking place has been the
employment of full-time, professionally trained staff to smaller stations, which had
hitherto been the preserve of volunteer/casual staff. Another development has been the
extension of the program to increase the number of MICA Paramedics and Advanced
Life Support trained staff in rural stations. These activities have been the result of four-
year commitment by the new Labor Government to provide additional resources to
improve service delivery (ALP 2000; SCRCSSP 2000: 881).
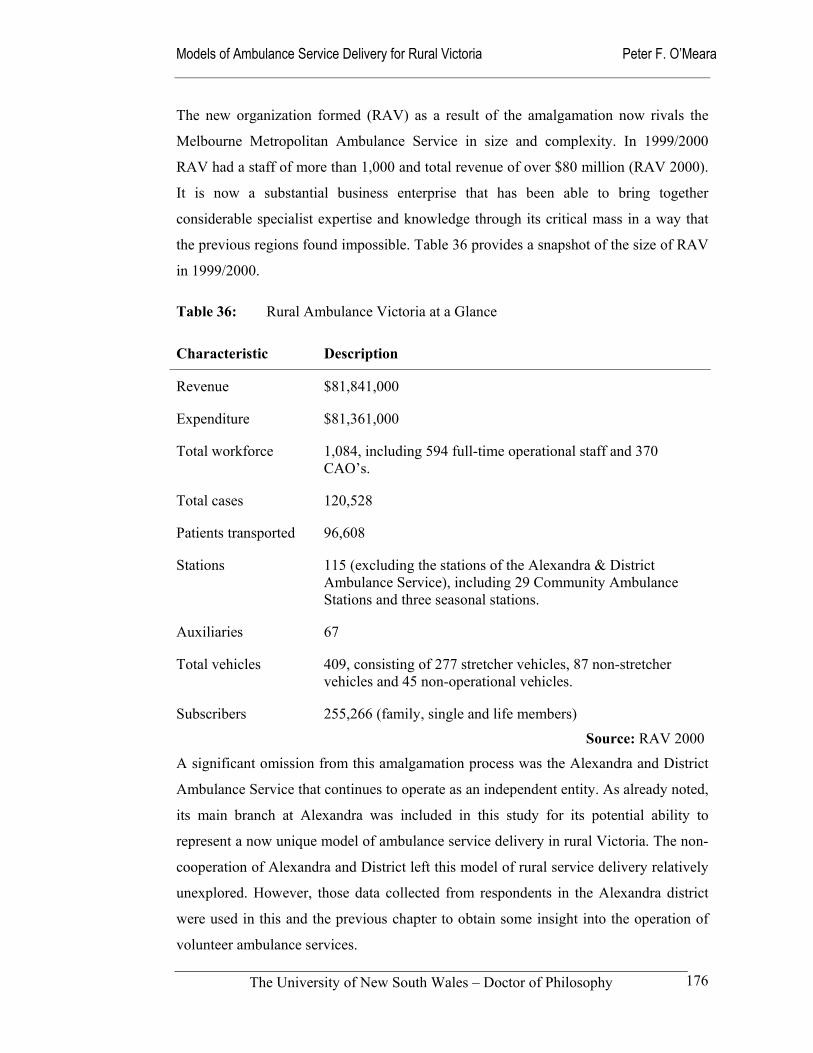
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
176
The new organization formed (RAV) as a result of the amalgamation now rivals the
Melbourne Metropolitan Ambulance Service in size and complexity. In 1999/2000
RAV had a staff of more than 1,000 and total revenue of over $80 million (RAV 2000).
It is now a substantial business enterprise that has been able to bring together
considerable specialist expertise and knowledge through its critical mass in a way that
the previous regions found impossible. Table 36 provides a snapshot of the size of RAV
in 1999/2000.
Table 36: Rural Ambulance Victoria at a Glance
Characteristic Description
Revenue $81,841,000
Expenditure $81,361,000
Total workforce 1,084, including 594 full-time operational staff and 370 CAO’s.
Total cases 120,528
Patients transported 96,608
Stations 115 (excluding the stations of the Alexandra & District Ambulance Service), including 29 Community Ambulance Stations and three seasonal stations.
Auxiliaries 67
Total vehicles 409, consisting of 277 stretcher vehicles, 87 non-stretcher vehicles and 45 non-operational vehicles.
Subscribers 255,266 (family, single and life members)
Source: RAV 2000
A significant omission from this amalgamation process was the Alexandra and District
Ambulance Service that continues to operate as an independent entity. As already noted,
its main branch at Alexandra was included in this study for its potential ability to
represent a now unique model of ambulance service delivery in rural Victoria. The non-
cooperation of Alexandra and District left this model of rural service delivery relatively
unexplored. However, those data collected from respondents in the Alexandra district
were used in this and the previous chapter to obtain some insight into the operation of
volunteer ambulance services.
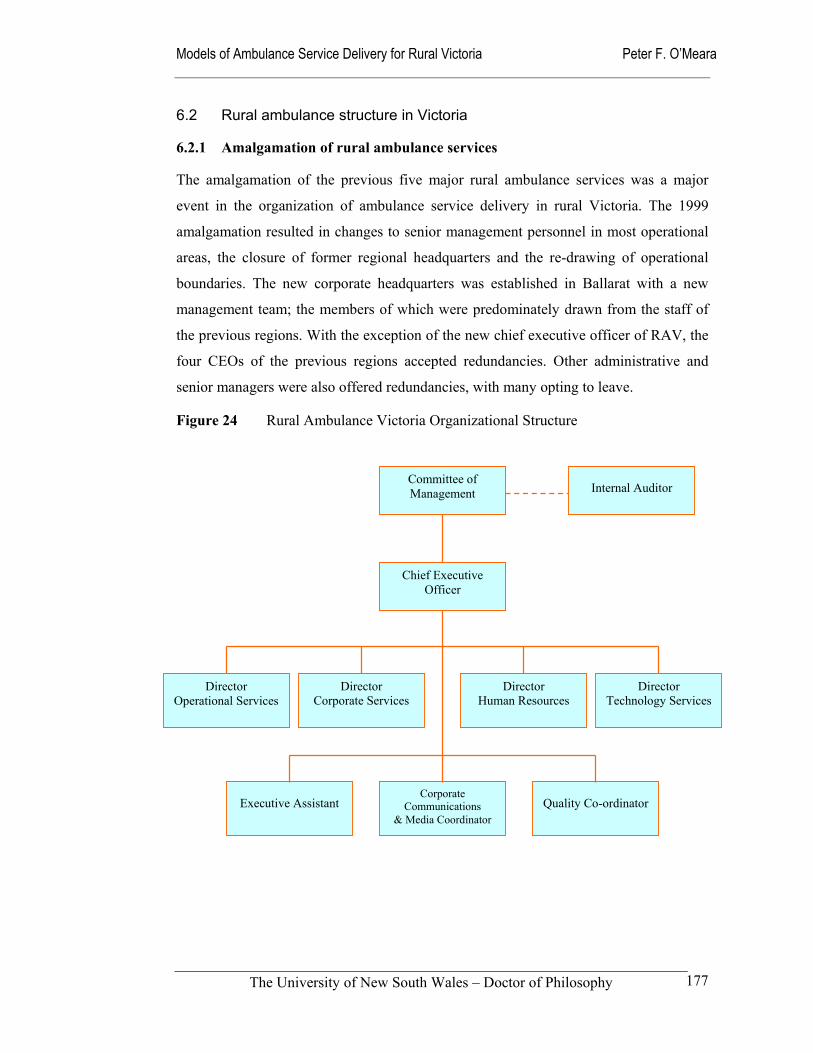
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
177
6.2 Rural ambulance structure in Victoria
6.2.1 Amalgamation of rural ambulance services
The amalgamation of the previous five major rural ambulance services was a major
event in the organization of ambulance service delivery in rural Victoria. The 1999
amalgamation resulted in changes to senior management personnel in most operational
areas, the closure of former regional headquarters and the re-drawing of operational
boundaries. The new corporate headquarters was established in Ballarat with a new
management team; the members of which were predominately drawn from the staff of
the previous regions. With the exception of the new chief executive officer of RAV, the
four CEOs of the previous regions accepted redundancies. Other administrative and
senior managers were also offered redundancies, with many opting to leave.
Figure 24 Rural Ambulance Victoria Organizational Structure
Director Technology Services
Director Human Resources
Director Corporate Services
Director Operational Services
Committee of Management
Chief Executive Officer
Internal Auditor
Corporate Communications
& Media Coordinator
Executive Assistant
Quality Co-ordinator
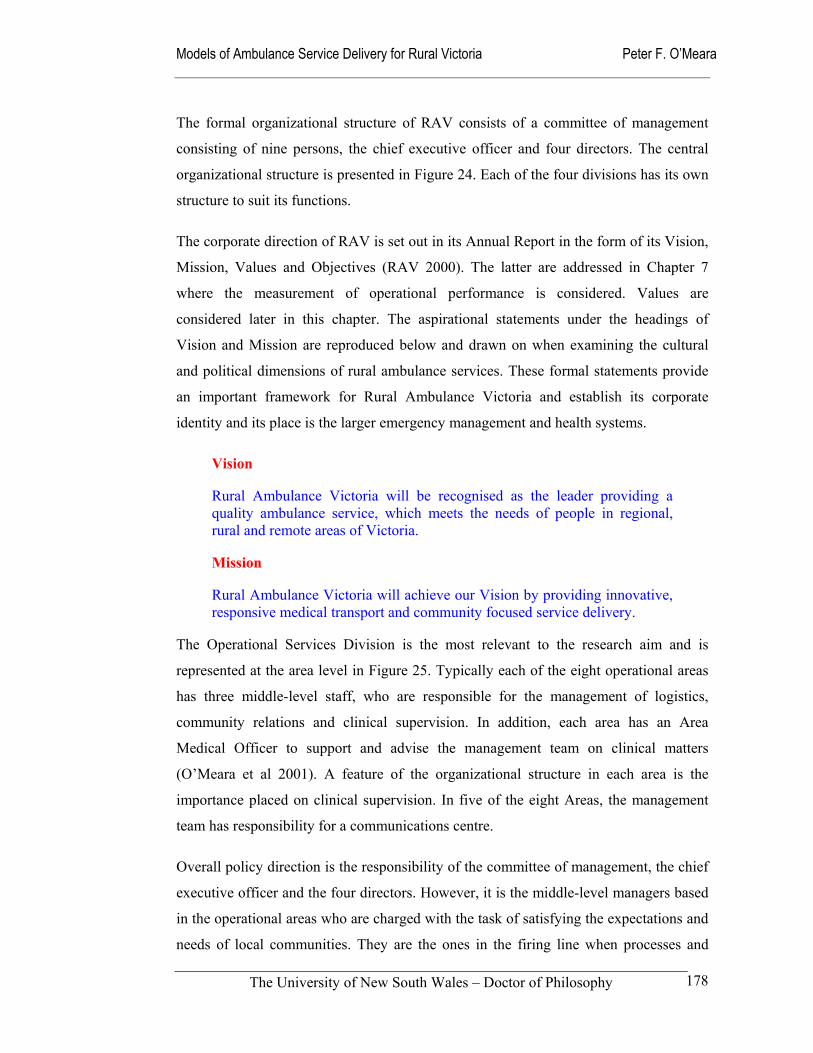
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
178
The formal organizational structure of RAV consists of a committee of management
consisting of nine persons, the chief executive officer and four directors. The central
organizational structure is presented in Figure 24. Each of the four divisions has its own
structure to suit its functions.
The corporate direction of RAV is set out in its Annual Report in the form of its Vision,
Mission, Values and Objectives (RAV 2000). The latter are addressed in Chapter 7
where the measurement of operational performance is considered. Values are
considered later in this chapter. The aspirational statements under the headings of
Vision and Mission are reproduced below and drawn on when examining the cultural
and political dimensions of rural ambulance services. These formal statements provide
an important framework for Rural Ambulance Victoria and establish its corporate
identity and its place is the larger emergency management and health systems.
Vision
Rural Ambulance Victoria will be recognised as the leader providing a quality ambulance service, which meets the needs of people in regional, rural and remote areas of Victoria.
Mission
Rural Ambulance Victoria will achieve our Vision by providing innovative, responsive medical transport and community focused service delivery.
The Operational Services Division is the most relevant to the research aim and is
represented at the area level in Figure 25. Typically each of the eight operational areas
has three middle-level staff, who are responsible for the management of logistics,
community relations and clinical supervision. In addition, each area has an Area
Medical Officer to support and advise the management team on clinical matters
(O’Meara et al 2001). A feature of the organizational structure in each area is the
importance placed on clinical supervision. In five of the eight Areas, the management
team has responsibility for a communications centre.
Overall policy direction is the responsibility of the committee of management, the chief
executive officer and the four directors. However, it is the middle-level managers based
in the operational areas who are charged with the task of satisfying the expectations and
needs of local communities. They are the ones in the firing line when processes and
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
179
outcomes cause concern amongst stakeholders. For instance, the local managers are
responsible for ensuring the community receives prompt and competent ambulance
services within the structural, cultural and financial constraints that are largely imposed
from the external environment. They are the ones who are expected to deal with the
issues described in Chapter 5: these may be angry general practitioners and nurses who
want a return to ‘local’ dispatching, or the challenge of providing consistent clinical
standards when their workforce is divided between full-time, professionally-trained staff
and remote volunteers with Basic Life Support training.
Figure 25 Typical Area Organizational Structure in RAV
Senior Operations Officer - Logistic
Area Manager
Station Officers
Area Medical Officer
Radio Technician
Communications &
Dispatch Centre Clinical Specialists
Clinical Educators
Senior Operations Officer - Clinical
Clinical Instructors
MICA Paramedics – Ambulance Paramedics – Community Ambulance Officers
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
180
6.2.2 Components of rural ambulance services
While the management structure of RAV is largely based on its geography and its own
needs to provide direction and ensure accountability, the principal components of its
operations are common to most ambulance services. They are call-taking and dispatch,
emergency medical response, pre-hospital care, non-emergency transport, and major
incident and disaster preparedness (DHSV 1998: 21). It is hard to see any model of
ambulance service delivery omitting any of these components as their core
transformation processes. These components of service delivery may be delivered
within the ambulance service or contracted to other providers as some of the
competition models suggest. Each component is described below as a reference point
for when models are developed in Chapter 7. These components can be organized into
the well-known ‘chain of survival’ model or into what has been termed the ‘interfaces
of care’ model that has been designed for universal implementation in both developed
and developing countries (Turner et al 2000).
Call-taking and dispatch
This is the communications and scheduling function, that is a vital part of the system
that ensures rapid and effective responses. It often relies on computer and
communications technology, skilled staff and appropriate protocols. RAV has five
communications centres across its eight operational areas. The communication centres’
geographic areas of responsibility continue to follow the previous regional boundaries.
Logically, this arrangement must cause some level of
confusion amongst staff, other health and emergency
services. It is not clear whether there are plans to align these
conflicting arrangements in the future. Alternately, at the risk
of industrial disputation and public concern, current
technology makes it possible to amalgamate them into one communications centre for
whole of rural Victoria. This option would run the risk of causing even more hostility
amongst stakeholders than that already reported in Chapter 5. The lack of research
related to rural communications centres makes such a course of action even harder to
defend to a sceptical audience. One suggestion has been to rationalize the number of
centres to two, with each one acting as a back-up for the other (Interview Respondent).

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
181
Emergency medical response
Emergency medical response is the rapid activation and response of specially equipped
ambulances and trained staff to time-sensitive medical emergencies, including
emergency responses where lights and sirens are required. It also encompasses urgent
responses that do not require lights and sirens. Through recent and planned increases in
staff numbers, establishment of more fully staffed stations, and continued support for
Community Ambulance Officers RAV has improved its logistical ability to respond to
calls for assistance.
Many of the stations included in this study have seen
substantial increases in staff during the last five years.
For example, the Lakes Entrance station had a full-
time staff complement of three ambulance paramedics
and supporting casual staff in 1996 and is projected to
have eleven full-time staff working a 24-hour roster in
2002. Likewise, the Moe station had five staff in 1996 and now has eleven working a
24-hour roster. It has also been announced that Cowes will double its staff numbers in
the near future.
Pre-hospital care
Pre-hospital care is described as the early and effective medical intervention by
ambulance paramedics at the scene of an incident or en route to hospital. This phase is
claimed to be often critical in both saving lives and in reducing the impact on the patient
and cost of further treatment in the medical system. The rapid extension of the MICA
Paramedic system to rural Victoria and the widespread introduction of Advanced Life
Support trained staff have greatly improved the quality of pre-hospital care provided to
patients. On the other hand, there has been considerable criticism of paramedics
undertaking excessive procedures on scene and thereby delaying arrival at hospitals
(Danne et al 1998). Based on the responses of the focus group of managers, it is
reasonable to say that RAV prides itself on having a clinical focus to its operations and
management, with most of its senior management staff having clinical backgrounds.
The clinical structure illustrated previously in Figure 25 supports this assertion.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
182
Non-emergency medical transport
This component of the system consists of inter-hospital transfers, stretcher and clinic
transport car transport of medical cases that are less time sensitive. While RAV still
offers this service, private operators increasingly undertake this work on behalf of third
parties such as hospitals and insurers. In some cases, private operators are sub-
contracted to either MAS or RAV. Many of the business owners and ambulance
attendants are former staff of the old regional services and the Metropolitan Ambulance
Service. Ambulant patients are encouraged to use community transport options or make
private arrangements for transport to medical consultations and treatment. This is a
major concern in rural areas that often lack the public transport infrastructure that is
taken for granted in metropolitan areas (Kelly et al 1999). The relatively poor socio-
economic profile of rural communities further exacerbates this problem. In some rural
areas, hospitals have initiated volunteer driver systems to alleviate the lack of public
transport infrastructure.
Major incident / disaster preparedness
Major incident and disaster planning is carried out in concert with other emergency
service organizations and agencies at local, regional and state levels. It is a traditional
emergency management activity. Since the formation of RAV, the role and influence of
rural ambulance services in the planning for major incidents and disasters have
substantially increased. The managers in the focus group reported that because of the
increased size and unity of one rural ambulance service, they now have more influence
within the emergency services sector. An important aspect of this is their ability to
specifically raise rural issues that may be less apparent to metropolitan-based
emergency services personnel.
6.2.3 Organizational Change in Rural Ambulance Services
The formation of RAV and the earlier regionalization of services in 1987 have impacted
on all ambulance stations in rural Victoria. Amongst these changes are the level of
resources available and their management arrangements. As already indicated, some of
the stations in the sample have benefited from large staff increases and an extension of
advanced skills training. Other stations have had to cope with a change in their
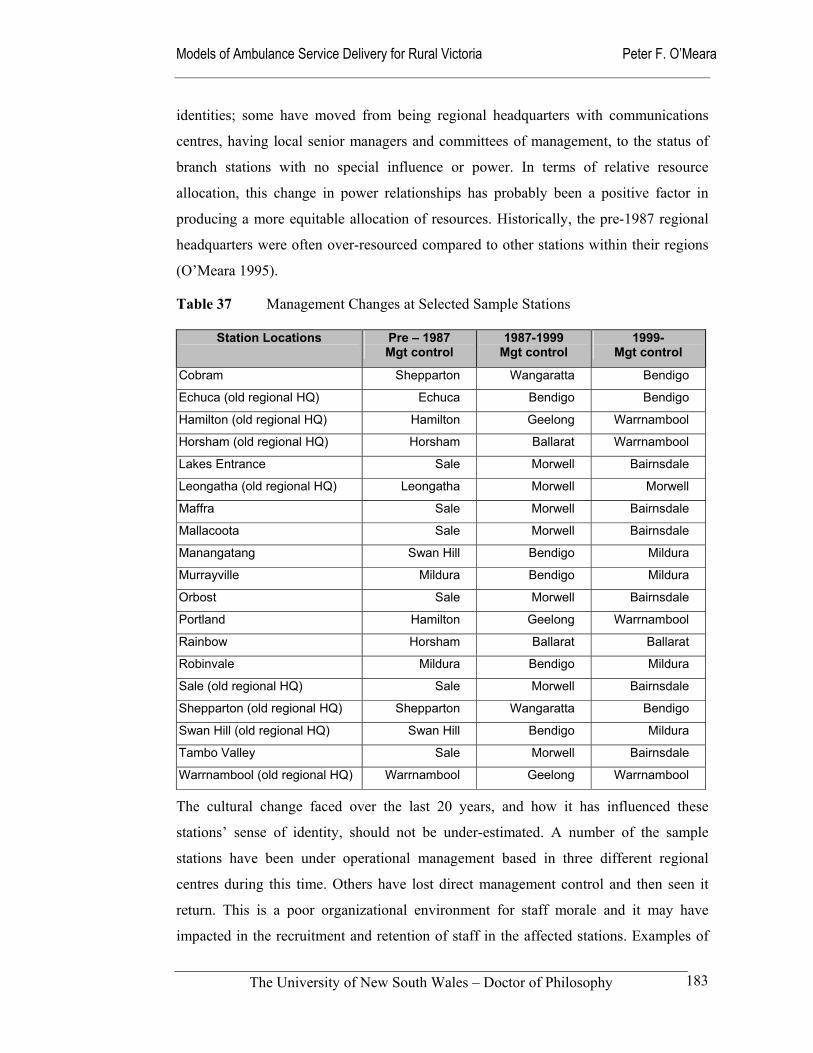
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
183
identities; some have moved from being regional headquarters with communications
centres, having local senior managers and committees of management, to the status of
branch stations with no special influence or power. In terms of relative resource
allocation, this change in power relationships has probably been a positive factor in
producing a more equitable allocation of resources. Historically, the pre-1987 regional
headquarters were often over-resourced compared to other stations within their regions
(O’Meara 1995).
Table 37 Management Changes at Selected Sample Stations
Station Locations Pre – 1987 Mgt control
1987-1999 Mgt control
1999- Mgt control
Cobram Shepparton Wangaratta Bendigo
Echuca (old regional HQ) Echuca Bendigo Bendigo
Hamilton (old regional HQ) Hamilton Geelong Warrnambool
Horsham (old regional HQ) Horsham Ballarat Warrnambool
Lakes Entrance Sale Morwell Bairnsdale
Leongatha (old regional HQ) Leongatha Morwell Morwell
Maffra Sale Morwell Bairnsdale
Mallacoota Sale Morwell Bairnsdale
Manangatang Swan Hill Bendigo Mildura
Murrayville Mildura Bendigo Mildura
Orbost Sale Morwell Bairnsdale
Portland Hamilton Geelong Warrnambool
Rainbow Horsham Ballarat Ballarat
Robinvale Mildura Bendigo Mildura
Sale (old regional HQ) Sale Morwell Bairnsdale
Shepparton (old regional HQ) Shepparton Wangaratta Bendigo
Swan Hill (old regional HQ) Swan Hill Bendigo Mildura
Tambo Valley Sale Morwell Bairnsdale
Warrnambool (old regional HQ) Warrnambool Geelong Warrnambool
The cultural change faced over the last 20 years, and how it has influenced these
stations’ sense of identity, should not be under-estimated. A number of the sample
stations have been under operational management based in three different regional
centres during this time. Others have lost direct management control and then seen it
return. This is a poor organizational environment for staff morale and it may have
impacted in the recruitment and retention of staff in the affected stations. Examples of

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
184
this phenomenon of ‘management ping-pong’ are illustrated in Table 37 for 19 of the 40
sample stations.
6.2.4 Rural pre-hospital infrastructure of the sample stations
Part of the rationale for grouping the sample stations in rurality bands was to break
away from the entrenched views of the individual stations’ status. The reason some
stations have relatively high staff numbers and 24-hour rosters have been their pre-1987
history as a ‘regional’ headquarters, rather than any analysis of objective need. Other
stations with larger populations and seemingly more need have historically been
expected to cope with inadequate resources as a result of their lack of internal political
power.
In order to obtain a clearer picture of the existing infrastructure, the officers-in-charge
of each station were requested to provide descriptions of their stations ambulance
resources, along with other emergency services and health infrastructure. Additional
data were gathered from other organizations, including local councils, professional
organizations and other emergency services. Much of the information was directly
accessible through the Internet. Since the data were collected in 1998, RAV has been
formed and major increases in resources have been implemented at many individual
stations. In some ways this vindicates the use of rurality bands, unrelated to
organizational structures, as one of the variables for the study. The resource increases
have removed some of the anomalies that were initially identified indicating that some
of the sample stations were under-resourced compared to their needs. Earlier plans to
compare relative resource allocation amongst the sample stations were abandoned,
when it became apparent that policy changes had overtaken the probable findings.
The five modified rurality categories are reported on in terms of staffing profile and the
types of staff rosters being operated at the time of the survey. They are indicative
profiles, rather than absolute descriptions that are subject to variation as priorities and
resource availability respond to the political and economic climate. Reflecting the
diversity of the rural context, the remote areas and little townships categories had
individual anomalies, however, each category was consistent enough to be of analytical
value. A point of departure in most categories was the use of volunteers, or as they are
now termed in Victoria, Community Ambulance Officers. Their deployment was not
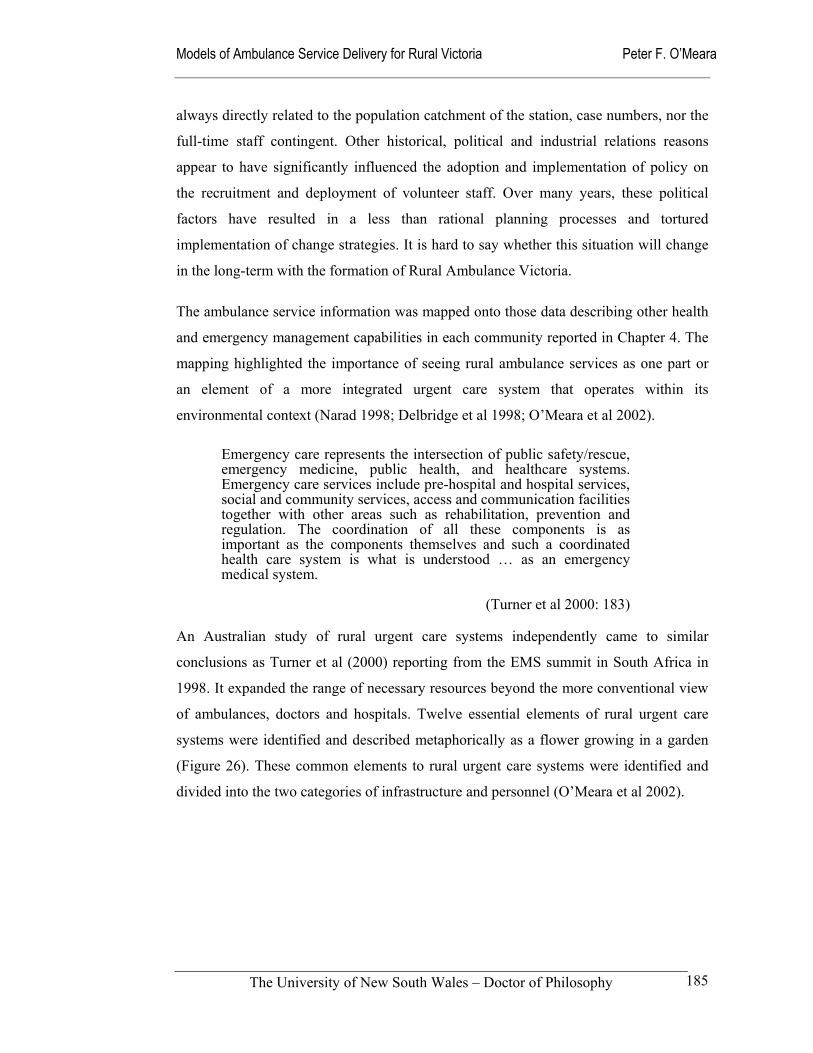
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
185
always directly related to the population catchment of the station, case numbers, nor the
full-time staff contingent. Other historical, political and industrial relations reasons
appear to have significantly influenced the adoption and implementation of policy on
the recruitment and deployment of volunteer staff. Over many years, these political
factors have resulted in a less than rational planning processes and tortured
implementation of change strategies. It is hard to say whether this situation will change
in the long-term with the formation of Rural Ambulance Victoria.
The ambulance service information was mapped onto those data describing other health
and emergency management capabilities in each community reported in Chapter 4. The
mapping highlighted the importance of seeing rural ambulance services as one part or
an element of a more integrated urgent care system that operates within its
environmental context (Narad 1998; Delbridge et al 1998; O’Meara et al 2002).
Emergency care represents the intersection of public safety/rescue, emergency medicine, public health, and healthcare systems. Emergency care services include pre-hospital and hospital services, social and community services, access and communication facilities together with other areas such as rehabilitation, prevention and regulation. The coordination of all these components is as important as the components themselves and such a coordinated health care system is what is understood … as an emergency medical system.
(Turner et al 2000: 183)
An Australian study of rural urgent care systems independently came to similar
conclusions as Turner et al (2000) reporting from the EMS summit in South Africa in
1998. It expanded the range of necessary resources beyond the more conventional view
of ambulances, doctors and hospitals. Twelve essential elements of rural urgent care
systems were identified and described metaphorically as a flower growing in a garden
(Figure 26). These common elements to rural urgent care systems were identified and
divided into the two categories of infrastructure and personnel (O’Meara et al 2002).
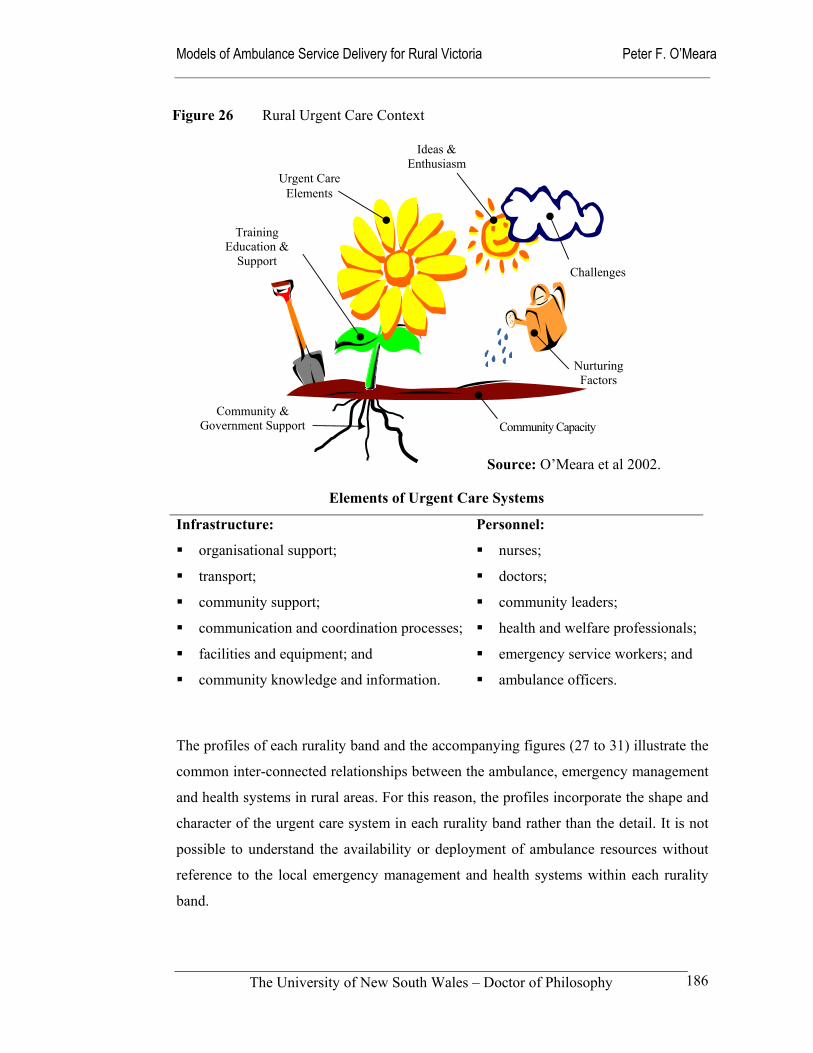
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
186
Elements of Urgent Care Systems
Infrastructure: Personnel:
organisational support; nurses;
transport; doctors;
community support; community leaders;
communication and coordination processes; health and welfare professionals;
facilities and equipment; and emergency service workers; and
community knowledge and information. ambulance officers.
The profiles of each rurality band and the accompanying figures (27 to 31) illustrate the
common inter-connected relationships between the ambulance, emergency management
and health systems in rural areas. For this reason, the profiles incorporate the shape and
character of the urgent care system in each rurality band rather than the detail. It is not
possible to understand the availability or deployment of ambulance resources without
reference to the local emergency management and health systems within each rurality
band.
Figure 26 Rural Urgent Care Context
Urgent Care Elements
Ideas & Enthusiasm
Challenges
Nurturing Factors
Community & Government Support
Training Education &
Support
Community Capacity
Source: O’Meara et al 2002.
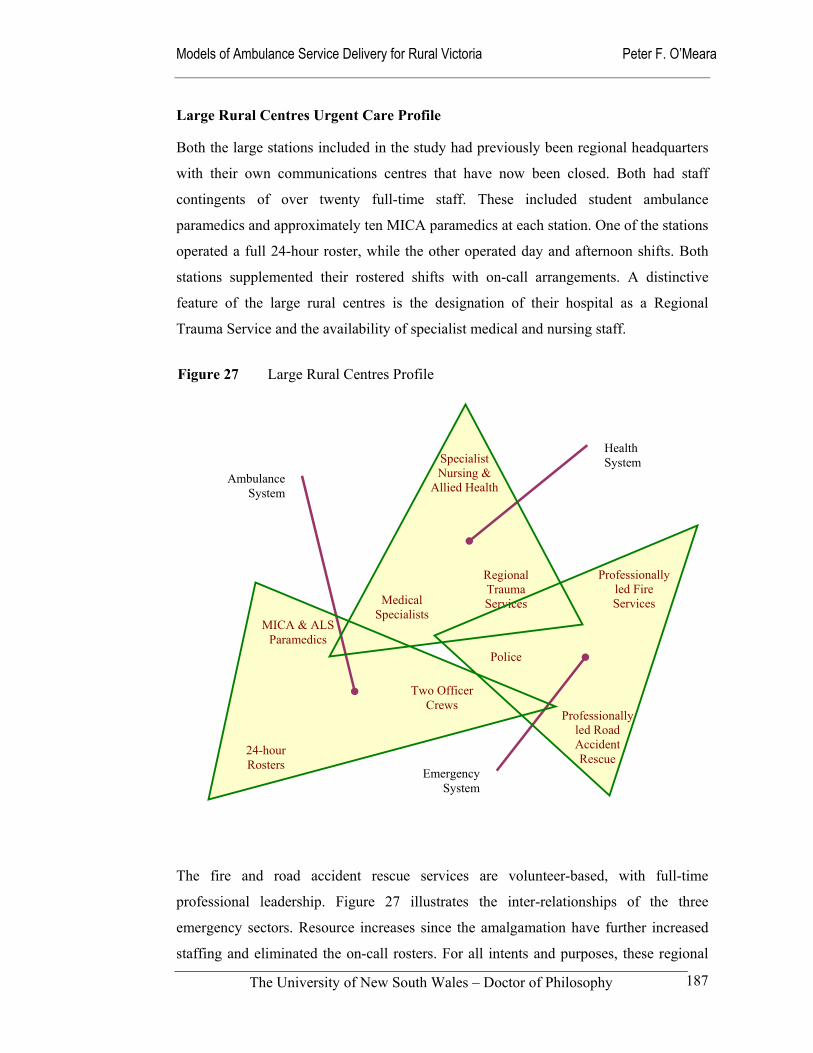
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
187
Large Rural Centres Urgent Care Profile
Both the large stations included in the study had previously been regional headquarters
with their own communications centres that have now been closed. Both had staff
contingents of over twenty full-time staff. These included student ambulance
paramedics and approximately ten MICA paramedics at each station. One of the stations
operated a full 24-hour roster, while the other operated day and afternoon shifts. Both
stations supplemented their rostered shifts with on-call arrangements. A distinctive
feature of the large rural centres is the designation of their hospital as a Regional
Trauma Service and the availability of specialist medical and nursing staff.
The fire and road accident rescue services are volunteer-based, with full-time
professional leadership. Figure 27 illustrates the inter-relationships of the three
emergency sectors. Resource increases since the amalgamation have further increased
staffing and eliminated the on-call rosters. For all intents and purposes, these regional
Two Officer Crews
MICA & ALS Paramedics
24-hour Rosters
Professionally led Fire Services
Professionally led Road Accident Rescue
Police
Medical Specialists
Specialist Nursing &
Allied Health
Regional Trauma Services
Health System
Ambulance System
Emergency System
Figure 27 Large Rural Centres Profile
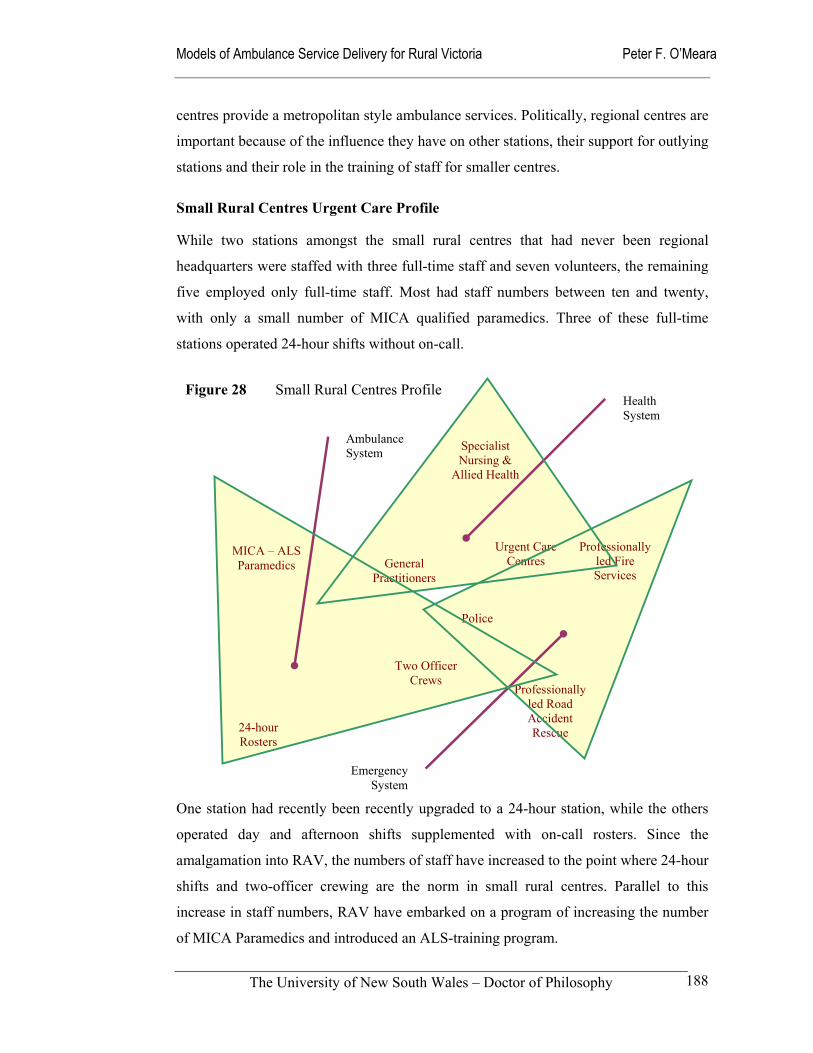
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
188
centres provide a metropolitan style ambulance services. Politically, regional centres are
important because of the influence they have on other stations, their support for outlying
stations and their role in the training of staff for smaller centres.
Small Rural Centres Urgent Care Profile
While two stations amongst the small rural centres that had never been regional
headquarters were staffed with three full-time staff and seven volunteers, the remaining
five employed only full-time staff. Most had staff numbers between ten and twenty,
with only a small number of MICA qualified paramedics. Three of these full-time
stations operated 24-hour shifts without on-call.
One station had recently been recently upgraded to a 24-hour station, while the others
operated day and afternoon shifts supplemented with on-call rosters. Since the
amalgamation into RAV, the numbers of staff have increased to the point where 24-hour
shifts and two-officer crewing are the norm in small rural centres. Parallel to this
increase in staff numbers, RAV have embarked on a program of increasing the number
of MICA Paramedics and introduced an ALS-training program.
Two Officer Crews
MICA – ALS Paramedics
24-hour Rosters
Professionally led Fire Services
Professionally led Road Accident Rescue
Police
General Practitioners
Specialist Nursing &
Allied Health
Urgent Care Centres
Figure 28 Small Rural Centres Profile Health System
Ambulance System
Emergency System
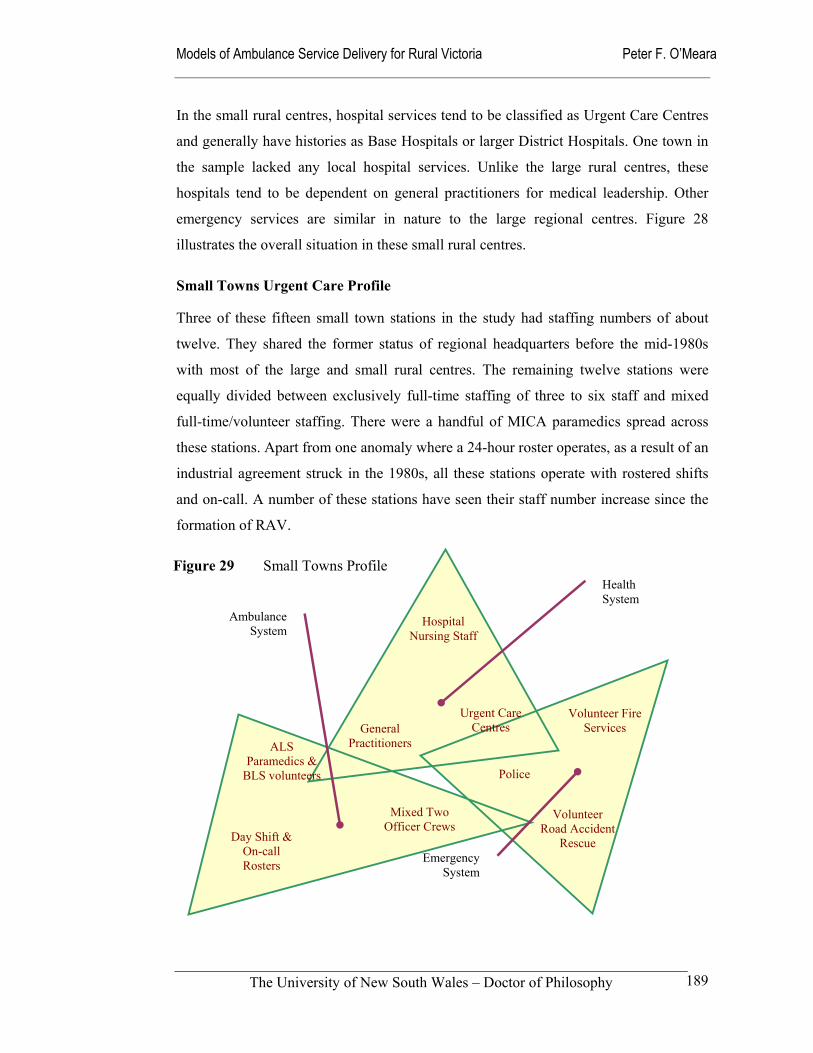
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
189
In the small rural centres, hospital services tend to be classified as Urgent Care Centres
and generally have histories as Base Hospitals or larger District Hospitals. One town in
the sample lacked any local hospital services. Unlike the large rural centres, these
hospitals tend to be dependent on general practitioners for medical leadership. Other
emergency services are similar in nature to the large regional centres. Figure 28
illustrates the overall situation in these small rural centres.
Small Towns Urgent Care Profile
Three of these fifteen small town stations in the study had staffing numbers of about
twelve. They shared the former status of regional headquarters before the mid-1980s
with most of the large and small rural centres. The remaining twelve stations were
equally divided between exclusively full-time staffing of three to six staff and mixed
full-time/volunteer staffing. There were a handful of MICA paramedics spread across
these stations. Apart from one anomaly where a 24-hour roster operates, as a result of an
industrial agreement struck in the 1980s, all these stations operate with rostered shifts
and on-call. A number of these stations have seen their staff number increase since the
formation of RAV.
Figure 29 Small Towns Profile
Mixed Two Officer Crews
Day Shift & On-call Rosters
Volunteer Fire Services
Volunteer Road Accident
Rescue
Police
General Practitioners
Hospital Nursing Staff
Urgent Care Centres
ALS Paramedics &
BLS volunteers
Ambulance System
Health System
Emergency System
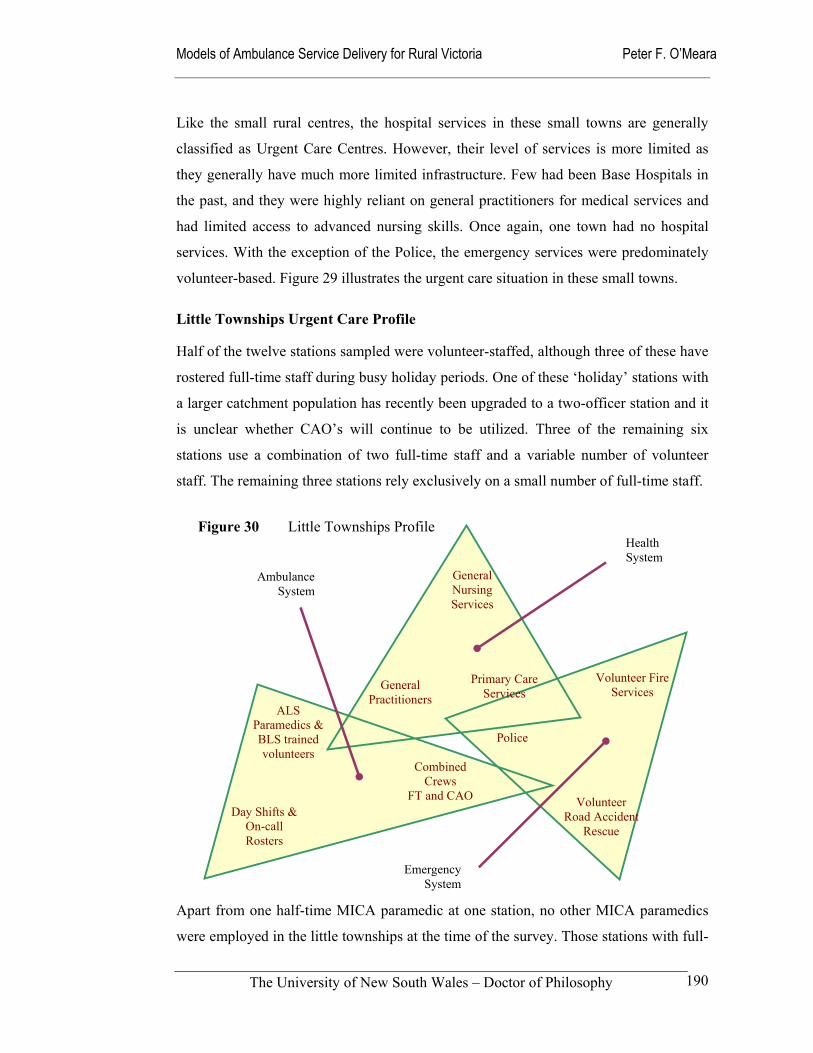
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
190
Like the small rural centres, the hospital services in these small towns are generally
classified as Urgent Care Centres. However, their level of services is more limited as
they generally have much more limited infrastructure. Few had been Base Hospitals in
the past, and they were highly reliant on general practitioners for medical services and
had limited access to advanced nursing skills. Once again, one town had no hospital
services. With the exception of the Police, the emergency services were predominately
volunteer-based. Figure 29 illustrates the urgent care situation in these small towns.
Little Townships Urgent Care Profile
Half of the twelve stations sampled were volunteer-staffed, although three of these have
rostered full-time staff during busy holiday periods. One of these ‘holiday’ stations with
a larger catchment population has recently been upgraded to a two-officer station and it
is unclear whether CAO’s will continue to be utilized. Three of the remaining six
stations use a combination of two full-time staff and a variable number of volunteer
staff. The remaining three stations rely exclusively on a small number of full-time staff.
Apart from one half-time MICA paramedic at one station, no other MICA paramedics
were employed in the little townships at the time of the survey. Those stations with full-
Combined Crews
FT and CAO
ALS Paramedics & BLS trained volunteers
Day Shifts & On-call Rosters
Volunteer Fire Services
Volunteer Road Accident
Rescue
Police
General Practitioners
General Nursing Services
Primary Care Services
Figure 30 Little Townships Profile Health System
Ambulance System
Emergency System
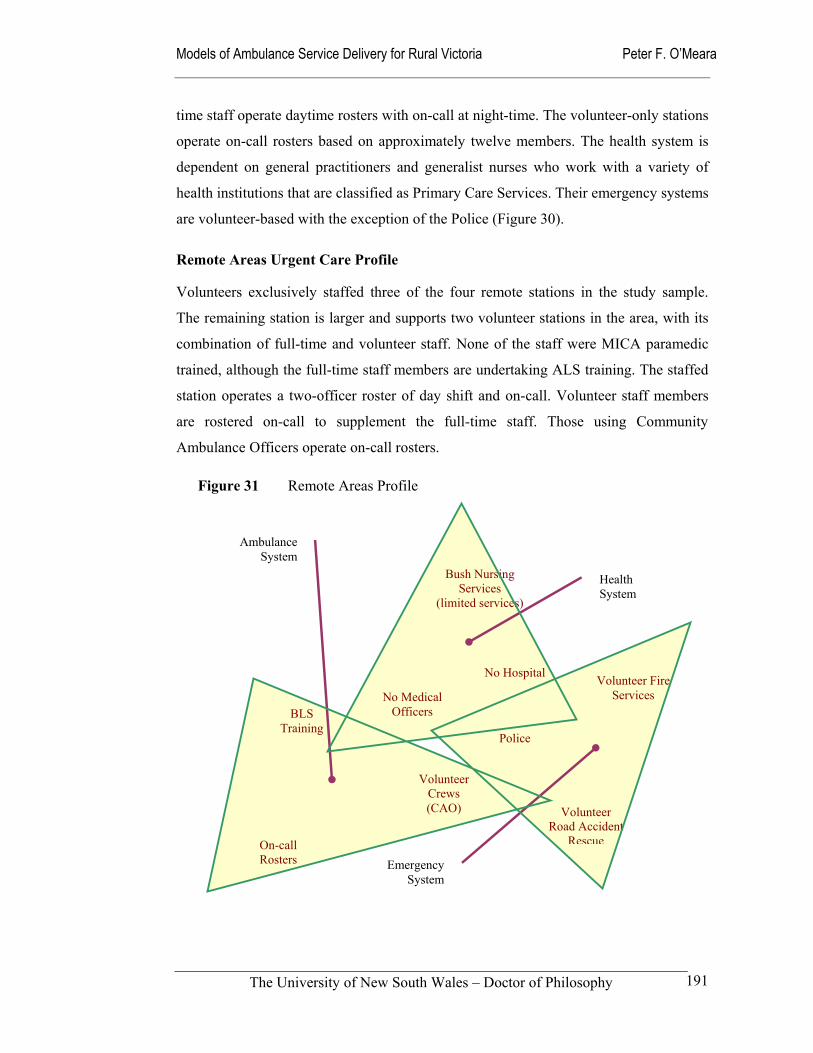
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
191
time staff operate daytime rosters with on-call at night-time. The volunteer-only stations
operate on-call rosters based on approximately twelve members. The health system is
dependent on general practitioners and generalist nurses who work with a variety of
health institutions that are classified as Primary Care Services. Their emergency systems
are volunteer-based with the exception of the Police (Figure 30).
Remote Areas Urgent Care Profile
Volunteers exclusively staffed three of the four remote stations in the study sample.
The remaining station is larger and supports two volunteer stations in the area, with its
combination of full-time and volunteer staff. None of the staff were MICA paramedic
trained, although the full-time staff members are undertaking ALS training. The staffed
station operates a two-officer roster of day shift and on-call. Volunteer staff members
are rostered on-call to supplement the full-time staff. Those using Community
Ambulance Officers operate on-call rosters.
Volunteer Crews (CAO)
BLS Training
On-call Rosters
Volunteer Fire Services
Volunteer Road Accident
Rescue
Police
No Medical Officers
Bush Nursing Services
(limited services)
No Hospital
Figure 31 Remote Areas Profile
Health System
Ambulance System
Emergency System
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
192
While the larger centre in the sample has both a hospital (UCS) and general practitioner
services, in general these Remote Area urgent care systems lack hospital services and
their general practitioner services may be limited to visiting services. In practice, they
are often highly reliant on bush nursing services for professionally trained emergency
health professionals. Like the Little Townships, the Remote Areas are highly dependent
on volunteer fire and road accident rescue services, with a small Police presence
supporting them (Figure 31).
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
193
6.3 Cultural landscape of Rural Ambulance Victoria
6.3.1 Contextual background
The changes in Victoria’s rural ambulance services reflect and often parallel the
fundamental changes taking place in Victoria’s rural health services. And like these
broader circumstances it is important that for their policies and programs “... to be
effective in bringing about improved health outcomes it is imperative that they be based
on a sound understanding of the rural health issues and an appreciation of the wider
rural scene” (Humphreys 1998: 3). Because of the ambulance service’s traditionally
insular nature, it is important that these wider forces are understood and appreciated
before a more contemporary sense of identity is fashioned out of the collective history
of rural ambulance services.
Apart from providing an opportunity to determine whether the development of uniquely
rural models of service delivery models for ambulance service delivery is justified, the
formation of a single rural ambulance service in Victoria provides a timely opportunity
to study organizational change within a system undergoing something of a revolution.
Contributing to this process of change are the technological and educational advances in
emergency medical care that are occurring throughout the developed world. The scope
of pre-hospital care has been broadened through the enhancement of communications
systems, the development of mobile diagnostic equipment and other clinical tools, and
the transfer of the education and training of ambulance paramedics to universities.
This research sought to study these issues at what was an opportune time in the history
of rural ambulance services in Victoria. The amalgamation of the rural regions into one
rural ambulance service for Victoria is an Australian first, if not a world first. Other
Australian states have opted for state-wide services to address the problems of
disjointed regional or district ambulance services. However, both the New South Wales
and South Australian Ambulance Services now have separate rural and metropolitan
operational divisions (Audit Office NSW 2001: 57). These organizational problems
were identified as far back as 1976 in a report to the Federal Minister of Health (HHSC
1976a).
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
194
Other developed countries have often opted for more geographically focused systems
that have their own inherent sets of problems (Erich 2001). In addition, the role of the
private sector in other systems is also of comparative relevance to the study of
ambulance service delivery models in rural Victoria.
The culture of rural ambulance services has not been explicitly studied in Australia.
However, a handful of efforts have been made to describe the cultural influences within
the Melbourne Metropolitan Ambulance Service and its predecessors (Willis &
McCarthy 1986; Mayski 1999).
The complex historical process, the current phase of which is medical dominance, has seen many Ambulance Officers emerge from their working class, low status, poorly trained ‘meat wagon’ driving origins, through a process of collective social mobility to an established paramedical location of which MICA Officers are the ‘cutting edge’.
(Willis & McCarthy 1986)
The relationship of ambulance to medicine has been described as adjunct, partially
separate and therefore not particularly threatening. In metropolitan areas, the process of
re-defining ambulance roles in relation to the medical profession has taken place in a
linear fashion. These, like other accounts exploring the education of ambulance officers,
note the emotional attachment of ambulance personnel to para-military symbols and
rituals (Field 1994; Wellard 1995; Mahony 2001). Even recently, the New South Wales
Ambulance Service has been unfavourably compared to its interstate counterparts for its
continued attachment to para-military structures (Audit Office NSW 2001: 66). Butson
(1999) has also noted the administrative movement of responsibility for ambulance
services in the Australian Capital Territory from the health portfolio, to urban services
and finally to the Department of the Attorney-General as an agency of the ACT
Emergency Services Bureau.
The shift of departments demonstrates the multiple perceptions governments have of the Ambulance Service with regard to its classification.
Is the Ambulance Service a health provider? An emergency service? A body of autonomous providers of pre-hospital care, or simply, in this case, an exploitable commodity able to be shuffled to suit economic figures?
(Butson 1999)
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
195
While there is little in the literature concerning the cultural fabric of rural ambulance
service, the services themselves have attempted to articulate their values. For instance,
Rural Ambulance Victoria has articulated their values in Annual Reports and other
planning documents with the following statement:
Values
In Rural Ambulance Victoria we value:
Competence, professionalism and the development of our people;
Integrity and honesty in the way we operate;
Equity in access to the delivery of our services;
Accountability and consistency in everything we do: and
Community participation and contribution.
During the research, the management focus group highlighted the positive impact these
issue-orientated value statements are having on RAV, particularly when combined with
the task-orientated operational objectives that are also being pursued. These values are
the elements that are helping form RAV’s preferred sense of identity and provide its
committee of management, its staff and community supporters’ with pride and a sense
of belonging to a worthwhile enterprise. It is less clear whether this enthusiasm for the
new organization is shared amongst those stakeholders outside the ‘inner-circle’
associated with the corporate headquarters. Anecdotally, some staff members express
considerable frustration with the ‘top-down’ style of management that has been adopted
in the corporate headquarters. This frustration at the ‘coal-face’, amongst on-road
ambulance officers, has been reported in a study of another Australian ambulance
service (Mahony 2001). Many members of the RAV workforce feel that the values in
the statement are being imposed from above and are not reflective of their extant values.
Thus the publishing of the values statement encounters the same type of problems as
many other large organizations face. There has certainly been little relief from industrial
disputation in Victoria between MAS and RAV, and the Ambulance Employees
Association during the negotiation of the latest enterprise agreement. This culture of
hostility has persisted despite massive additional resources being made available to
increase staff resources, fund pay rises and facilitate additional training opportunities.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
196
The organizational situation in Victoria since the formation of RAV was described
earlier from a structuralist perspective. At an individual station level, the re-organization
has had a diverse impact. As indicated earlier in Table 37, some stations have
experienced little change, others have returned to something resembling their pre-1987
regionalization operational boundaries, while other have faced a third change of
management control since 1987. While in some cases, the most recent changes may
have had the affect of re-establishing some of the bonds that were lost over the last
decade, others may be at risk of losing their identity and sense of connection with those
who lead and manage the new organization.
The comments from the focus group participants, who are beneficiaries of the
organizational changes, fail to make it clear whether the management group appreciates
the sense of dislocation that may have been experienced at the ‘far-flung’ edges of the
organization. It was observed during the study that a number of the focus group
participants had very little power and influence in the former Regions, and this is
perhaps reflected in the following comment describing the opportunities that the new
organization offers them.
… the ability to go off and negotiate things to put up ideas and to make change and influence change within that context is very rewarding, its one of the opportunities this job gives you to be able to influence things occurring and to make change are incredible which never occurred at the previous Regions.
(Focus Group Participant)
Perhaps their relatively new roles within RAV, contributed toward the focus group
participants’ enthusiasm and excitement about the direction of the new organizational
entity. From a senior management perspective, these qualities amongst middle managers
would be a heartening and positive outcome of their efforts to develop a new sense of
organizational identity. This process was started before the formation of RAV, with
many middle-level and senior staff of the former regions embarking on quality
improvement activities and taking courses such as ‘Investment in Excellence’ from The
Pacific Institute. These organizational activities stressed the central place of the
customer or client in the ‘transformed organization’. One focus group participant had
certainly picked up the rhetoric when asked about where power lies within RAV.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
197
I suggest its the community itself that actually holds the majority of power through their lobbying. They change what occurs and in this kind of political environment. The community has significant power because they are listened to and we are encouraged and mandated to be reactive and responsive to the community because at the end of the day we are their ambulance service.
(Focus Group Participant)
From a critical perspective, the ‘cultural change’ program being undertaken in RAV is a
strategy “… to replace the obvious and much maligned top-down bureaucratic control
with the less obvious but just as centralising cultural control” (Mahony 2000: 195). This
process has seen the attitudes, beliefs and management skills of the ‘old guard’
demonised because they were required to be ‘generalist managers’ rather than
specialists. This has had the effect of labelling the operational, economic and financial
problems they faced as a cultural problem (Mahony 2000: 188, 189). Fortuitously for
RAV and its new management team, the change of State government resulted in a large
increase in capital and recurrent funding to redress the macro-economic problems that
were largely created as a result of cost cutting in the 1990s.
Despite the shared values and beliefs that were expressed amongst the focus group
participants, one person also identified signs of organizational change fatigue when
asked about the future challenges of RAV. He said:
The only ones [problems] that stand out is that beware of the very flat organization. There is not one Area Manager in this organization who would work less than sixty hours per week and as a result it is going to take its toll at some point. So if the organization recognises that its looking at building its support structures, the strength of the organization being flat is that we can achieve change and achieve it relatively easily. The down side of that is that at some point its going to burn out the people that work in it and that’s probably the biggest challenge we’re facing at the moment.
(Focus Group Participant)
This concern is consistent with Mahony’s concerns about flatter organizational
structures (Mahony 2000; Mahony 2001). In particular, the expectation of the advocates
of cultural integration that employees are expected to work long unpaid hours to
demonstrate their loyalty and commitment (Mahony 2000: 191). Continuing to expect
such high levels of commitment from management staff could prove counterproductive
in the longer term.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
198
6.3.2 Education and technology influences
Amongst the major influences on the evolution pre-hospital systems are advances in
pre-hospital education and the adoption of emerging technological innovations. When
these influences have been combined impressive advances have been made in
emergency responses, clinical care in the pre-hospital environment and communication
with hospital-based emergency medical services. The importance of education and skill
development amongst ambulance staff has been long recognized as central to the rate
and nature of change in ambulance services (HHSC 1976a: 31, 32). More recently, the
New South Wales Ambulance Service has recognised the continued importance of
technology and education:
… world wide, ambulance services are addressing industry changes driven by technology, rising skills as ambulance officers emerge as health professionals and an increasing emphasis on accountability, quality and efficiency of services.
(Audit Office NSW 2001: 9)
For this study, the pre-hospital literature and the Internet were searched for evidence of
past, current and future educational and technological developments. These data
provided background material prior to interviews with two pre-hospital experts. The
first interviewee was an expert in pre-hospital education and training, who has worked
in two Australian States. He is currently employed in rural Victoria as a clinical
educator and supervisor. The second interviewee was an international expert in pre-
hospital technology who was visiting Australia from the United Kingdom as a Research
Fellow at Deakin University. He is undertaking research activities in conjunction with
Rural Ambulance Victoria related to the linking of expert clinicians - medical and
ambulance - to those delivering pre-hospital care in the field through the use of
information technology and advanced diagnostic tools.
Educational Influences on Pre-hospital Systems
Australia’s ambulance services are in the process of seeing the transfer of ambulance
officer/paramedic training from industry-based institutions to university-based
education at diploma and degree levels. Generally, ambulance services or government
departments provide core funding for the conduct of the courses offered. Monash
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
199
University Centre for Ambulance and Paramedic Studies is the major provider of
undergraduate education of ambulance paramedics in Victoria. Although not initially
recognized within the industry and therefore forced to offer only fee-paying courses,
pre-employment and post-graduate courses are also being offered by Victoria University
(DHSV 1998: 34). It also offers courses to overseas students from south-east Asian
countries on a fee-paying basis. Although entry to most of the university courses is
dependent on employment with an ambulance service, Flinders University in South
Australia and Charles Sturt University in New South Wales have offered a small
number of direct-entry places for anyone seeking a career as an ambulance officer,
including school leavers. Based on the Flinders University experience, where a Tertiary
Entrance Rank (matriculation score) of 89.40 out of a possible 100 was required in
2001, future demand for places in undergraduate ambulance courses will be very
competitive (Flinders University 2001).
Historically, the training of ambulance officers in Australia was the sole responsibility
of State health authorities. These courses varied in content and were generally not
recognized across State boundaries and for many years lacked any link with the
education system (HHSC 1976a: 32). In Victoria, the training of ambulance
officers/paramedics was undertaken through the Ambulance Officers’ Training Centre
that was originally established under the auspices of the Hospitals and Charities
Commission in 1965. Initially established at the Geelong Hospital, the site of the
Victorian training centre was then located at three separate sites in Metropolitan
Melbourne. While initially an entirely ‘in-house’ Certificate course with no formal links
with the broader education systems (the Hospitals & Charities Commission issued the
certificates), ambulance qualifications gradually evolved into recognized educational
qualification through the Technical and Further Education (TAFE) system. The move to
a university-based system was partly in response to the need to extend this recognition
to the more advanced paramedic course (MICA) that despite its high status in the health
and medical system, offered no formal educational accreditation (DHCS 1994: 15).
Contrary to the views of some internal critics, Australian ambulance paramedics have
made rapid progress in the quest for improved education and training since the early
1960s when formal in-house training was first introduced. Ambulance training is now
offered through six Australian universities; courses are offered at Certificate, Diploma
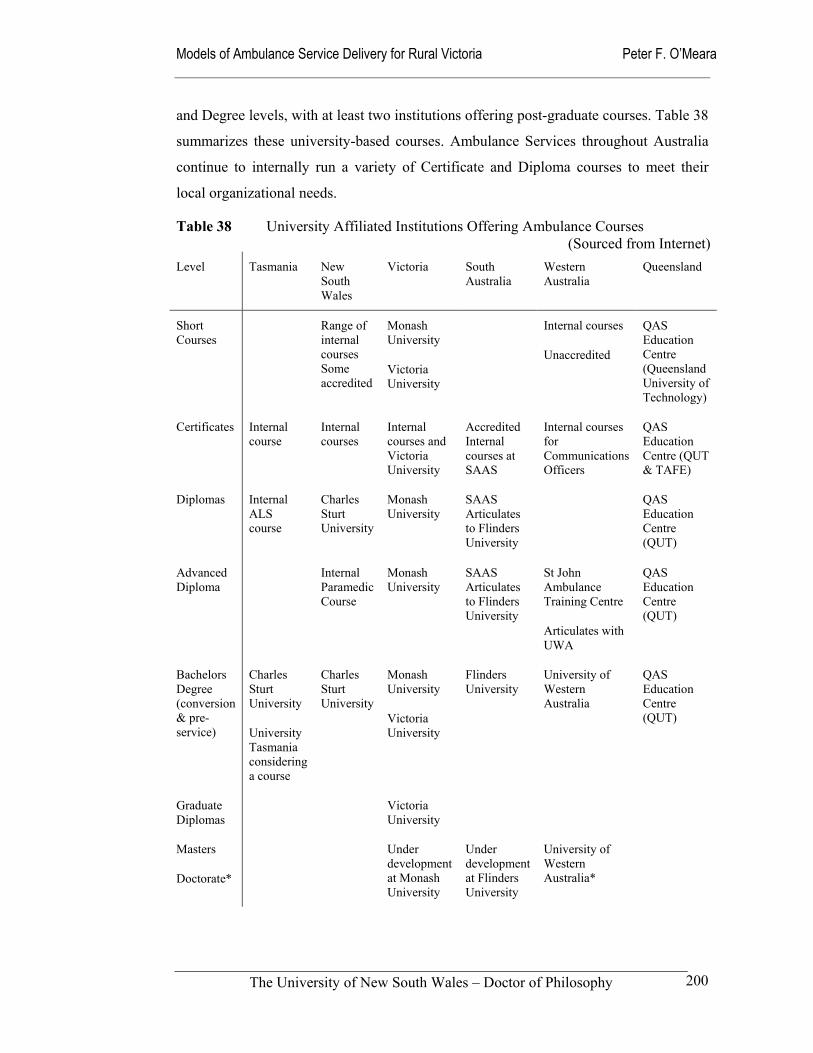
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
200
and Degree levels, with at least two institutions offering post-graduate courses. Table 38
summarizes these university-based courses. Ambulance Services throughout Australia
continue to internally run a variety of Certificate and Diploma courses to meet their
local organizational needs.
Table 38 University Affiliated Institutions Offering Ambulance Courses (Sourced from Internet)
Level Tasmania New South Wales
Victoria South Australia
Western Australia
Queensland
Short Courses
Range of internal courses Some accredited
Monash University
Victoria University
Internal courses
Unaccredited
QAS Education Centre (Queensland University of Technology)
Certificates Internal course
Internal courses
Internal courses and Victoria University
Accredited Internal courses at SAAS
Internal courses for Communications Officers
QAS Education Centre (QUT & TAFE)
Diplomas Internal ALS course
Charles Sturt University
Monash University
SAAS Articulates to Flinders University
QAS Education Centre (QUT)
Advanced Diploma
Internal Paramedic Course
Monash University
SAAS Articulates to Flinders University
St John Ambulance Training Centre
Articulates with UWA
QAS Education Centre (QUT)
Bachelors Degree (conversion & pre-service)
Charles Sturt University
University Tasmania considering a course
Charles Sturt University
Monash University
Victoria University
Flinders University
University of Western Australia
QAS Education Centre (QUT)
Graduate Diplomas
Victoria University
Masters
Doctorate*
Under development at Monash University
Under development at Flinders University
University of Western Australia*
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
201
A number of contradictory forces are at work in the transfer of ambulance officer
training to the university sector. On the one hand, the supply of qualified staff will be
improved through a more open training system, similar in style to that operating for
other health professionals. However, the greater recognition of ambulance paramedics
as professionals may tend to push wages up and open further career options to
individuals who may become more mobile across State borders and disciplines. This is a
potential problem for rural ambulance services. If the experience of medicine, nursing
and allied health are any guide, the recruitment and retention situation could deteriorate
to the point where incentives may become necessary to recruit and retain ambulance
staff in some rural areas. It is therefore understandable that ambulance authorities have
supported the move to professionally recognized education and training with some
misgivings.
While the motivation for advocating this higher level of ‘professionalism’ doubtless
varies between different players, the view that it is desirable is widely held in the
ambulance unions, professional organizations such as the Australian College of
Ambulance Professionals (ACAP), and amongst the officers and paramedics
themselves. Ambulance professionals are no different to other emerging or established
health workers in that they:
... have a broad interest in defining situations as requiring health work, and defining themselves as the only appropriate group which should be authorised to do the work.
(Hay et al 1993: 22)
One impact of training ambulance paramedics at Monash University in the Faculty of
Medicine (recently re-structured into the Faculty of Medicine, Nursing and Health
Sciences) will be an increase in the degree of medical control over ambulance models of
service delivery. This is in contrast to the competing emergency services model, which
continues to exert a strong influence on the planning and operational processes of
ambulance services throughout the world. In New South Wales and Tasmania, the main
university provider is Charles Sturt University, which lacks a Faculty of Medicine. In
contrast to the views of the ‘mainstream’ ambulance educators and managers who
supported the move to Monash University, the dominant ambulance union in Victoria
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
202
(the Ambulance Employees Association) supports the courses offered at Victoria
University, which has no medical school.
In addition to these academic-style courses, universities continue to offer advanced
clinical courses that allow ambulance paramedics to practice at advanced levels. In
Victoria, there are now two advanced clinical courses – the recently introduced
Advanced Life Support (ALS) and the more established MICA Paramedic course.
While the availability of the MICA Paramedic course since the early 1990s had a
significant impact on ambulance services in large regional centres, it was largely
irrelevant in other parts of rural Victoria. Widespread access to ALS in rural areas
promises to be a revolutionary development in the training and skills enhancement of
ambulance paramedics.
The relatively recent introduction of the Rural MICA Paramedic program has gone some way to addressing the pre-hospital health needs of rural Victorian, however it has proven logistically difficult to expand and sustain the full MICA program in remote areas.
(Monash University 2001)
When asked to describe the achievements of RAV to date, the participants in the
management focus group identified the standardization of training as a major
achievement of RAV. This achievement included the introduction of ALS training
across rural Victoria and the development of a recognized qualification for Community
Ambulance Officers under the Australian Qualifications Framework. The focus group
participants told the story of how RAV was formed from the previous regional services
and that this resulted in a “… central body [that] provides a focus, which gives
consistent direction in terms of the things that get done and the way in which they get
done” (Focus Group Participant). An example cited of where consistency was now more
apparent was in the implementation of advanced life support (ALS) systems.
… we had this thing called ALS and it was one thing in Ballarat, another thing in Wodonga, meant nothing in Morwell … and I think now we’ve actually, its all been brought back to a stream where there’s consistent control and its not about someone siting somewhere and saying “this is what we do”, its actually thought through.
(Focus Group Participant)
The ALS course is an industry-funded subject on behalf of the State Government and is
conducted in short block teaching modules to those students selected by RAV or MAS.
At Monash University, the ALS subject involves 40 hours of classroom and scenario

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
203
based training, supported by flexible delivery strategies to total of 156 hours of student
work. It articulates with both the Advanced Diploma of MICA Paramedic Studies and
gives students a six-point credit towards the Bachelor of Paramedic Studies (Monash
2001).
Many ambulance paramedics
expected that the transfer of
ambulance education would be little
more than a transfer of existing
programs from the Ambulance
Officers’ Training Centre to Monash
University’s Frankston campus. My
education interviewee remarked that,
“… in fact there has been quite a bit
of buying in by Monash itself as to
what AOTC now does … it is
highlighted in the way courses have
been changed …” (Education
Interviewee).
As already alluded to, one of the
unique characteristics of the
ambulance education and training in
Victoria compared to other Australian
States is that there are two major
providers. Victoria University offers
fee-paying courses to both the
Victorian and international markets, and it is estimated that forty percent of ALS
training is conducted through Victoria University (Education Interviewee). In the future,
contracts to supply the bulk of the education and training services to MAS and RAV
will be open to competition from the two Victorian universities, along with others from
interstate.
Summary of ALS Subject at Monash University This subject develops in the student the necessary knowledge, understanding, skills and attitudes to be able to provide ALS Ambulance Paramedic care in the circumstances of selected trauma and medical emergencies. The subject is underpinned by an ALS Ambulance paramedic clinical approach, clinical problem solving and clinical decision making model. The subject will describe and explain the ALS Ambulance Paramedic Clinical Practice Guidelines related to the management of cardiac arrest, analgesia and trauma. Advanced airway care and ventilation techniques using the laryngeal mask and intravenous adrenaline in the management of patients in cardiac arrest will be developed. Trauma care is approached from the contextual perspective of trauma systems, time critical guidelines and in-field triage criteria. Consideration of the shock process and the patient with hypovolaemia will be combined with skill development in perfusion status assessment and fluid resuscitation. The management of tension pneumothorax will be discussed and related skills developed. The use of parenteral analgesia in the management of patients with pain of cardiac and/or traumatic origin will be included. In addition to clinically related topics, this subject will also develop in the student appropriate skills in: communication; teamwork; and managing critical incident stress. As a final consideration, the student will develop and understanding of legal and occupational health and safety issues. (Monash University 2001)
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
204
This raises the issue of whether ambulance education, training and research activities
are better conducted in a University Faculty with a major medical presence or through a
more generic Health Sciences Faculty. In Australia, the status of the Faculties offering
ambulance education varies. Flinders University, Monash University and the University
of Western Australia have strong medical faculties, while the other providers – Victoria
University, Charles Sturt University and Queensland University of Technology – have
located their ambulance/pre-hospital courses in faculties of health sciences without a
major medical presence. When asked about the relative importance of the location of
ambulance training, the education interviewee expressed no great concern, being more
concerned about the quality of the educational program being offered.
I would suggest that the one with the Medical School [Monash University] have the cultural support for what they are trying to achieve … the universities without Medical Faculties such as Victoria University are putting together very, very sound educational programs that are being tested currently and found to be doing the job.
(Education Interviewee)
Moving to a situation where the education of ambulance paramedics is separated from
the major employers provides an opportunity to move from the Artisan Model to that of
Professional Practitioners. In other countries, the trend toward university-based
education and training has been linked to the changing role of pre-hospital systems and
the registration of ambulance paramedics (Sweet 1997; Edwards 1998). The possible
role changes have been described in Chapter 2; they are further development in Chapter
8 in the context of developing alternate service delivery models. Suffice to say here that,
the adoption of extended roles such as ‘community paramedics’ or ‘practitioners in
emergency care’ will require an extension to current paramedic education programs
(JRCALC 2000; Wood 2000: 132-135). In the British context, Woollard and Ellis
(1999) make the pitch for a broader ambulance education.
Undertaking such a role would, however, require an extension to the current paramedic education programme in order to provide staff with the underpinning knowledge necessary to effectively fulfil this task.
(Woollard & Ellis 1999:104)
There are now a number of paramedic degree courses being implemented throughout
the United Kingdom that have the potential to fill this knowledge gap. One of these is a
full-time Bachelor of Medical Science at the University of Sheffield that is based on the
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
205
medical degree course and offered through its medical school. Interest in the course has
been huge, with an application to placement ratio of greater than sixteen to one
(Edwards 1998: 224-226).
One of the cited strengths of the Sheffield
University course has been its location
within the Department of Surgery and
Anaesthetic Sciences. Here, access can be
gained to all the necessary medical
specialties within the university’s hospital
network, teaching by consultant medical
staff and exposure to a wide variety of
different medical areas (Edwards 1998:
224). Other British universities that offer
bachelor degree programs in collaboration
with their local ambulance services include
the University of Hertfordshire and the
University of Staffordshire. In Northumbria
the ambulance service has taken a different
approach, collaborating with Charles Sturt
University in Australia through the
establishment of a College of Paramedical
Studies in Northumberland (Battersby
1999: 114). Running parallel to proposed
role changes and the enhancement of education and training have been calls to register
ambulance paramedics (Allen Consulting 1999).
[Registration] … implies a code of professional practice, a broad range of knowledge and skills, an understanding of the role in the context of the wider community, self regulation [my emphasis] and a collective concern for improvement through education and research.
(Wellard 1995: 43)
Members of the Australian College of Ambulance Professionals (ACAP), formerly
known as the Institute of Ambulance Officers, have been lobbying in favour of
AUSTRALIAN COLLEGE OF AMBULANCE PROFESSIONALS
CODE OF ETHICS
As a member of the Australian College of Ambulance Professionals I shall uphold:
The Principle that ambulance service is part of
the whole health care of people;
That the best health care be available to all without consideration of race, creed or
religion;
That I, equally with others devoted to health care, will observe the traditions of honesty, integrity, confidentiality and whole-hearted
effort to save life and lesson suffering;
That due respect is owed to those with greater knowledge and skill in the arts of caring for the
sick and that I shall ever be ready to give proper consideration to their advice and
counsel;
That I shall share, without seeking gain, my knowledge and shall teach my skill to any
other person with responsibility for health care;
That I shall support at all times the aims of the Australian College of Ambulance
Professionals.
(ACAP 2001b)
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
206
registration for a number of years without any great progress. The official policy of the
ACAP is that registration should be introduced on a voluntary basis, with statutory
registration to ultimately follow (ACAP 2001a). These efforts have been meet with
tepid responses from ambulance authorities who have historically held the power of
approval to practice through their near monopoly as employers. Registration would
result in ambulance services having to share their power with an independent profession
and allow a greater degree of employment mobility than has generally been the case.
Ambulance services may not be ready to do this in Australia, where there remains a
strong culture of institutional control and regulation.
The move toward occupational professionalism perhaps brings the issues of meeting
expectations, managing demand, and measuring performances together. This emerging
professionalism within the planning and delivery of pre-hospital care brings together the
strands of community ownership, professional practice and the provision of resources.
Like other emerging health professionals, ambulance paramedics have been establishing
their own occupational territory, in particular negotiating space between medicine and
nursing. Ambulance paramedics have been described as having no clear occupational
territory, with no statutory registration. The previous Victorian state government
recognised this during their 1999 review of the Ambulance Services Act. The
consultants who conducted the review saw a need for some form of registration to
protect the public within a competitive industry structure (Allen Consulting 1999: xiii,
87). Their blueprint for an Ambulance Officers Registration Board was that it would
have the following roles:
Independent, self-funding Board appointed by government to administer occupational registration of ambulance officers for the purposes of protection of consumers.
Protects the use of certain titles (eg ‘Registered Ambulance Officer’) at a number of appropriate levels to those with appropriate qualifications and experience.
Provides for disciplinary and complaints handling provisions.
Purchasers of ambulance services may require operators to use employees with appropriate registration as a condition of a contract.
(Allen Consulting 1999: 82)
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
207
While the implementation of ambulance paramedic registration has advanced little in
Australia, progress in the United Kingdom has been more rapid; paramedics there have
been recognised by the Council for Professions Supplementary to Medicine. It is
anticipated that professional registration will shortly be a prerequisite for practising as a
paramedic in the United Kingdom (Nicholl et al 2001: 18).
In the rural context, the possible introduction of professional registration will need to be
reconciled with the continuing reliance on the employment of Community Ambulance
Officers in some areas. A challenge for all concerned will be the need to maintain a
culture of teamwork and co-operation amongst these community volunteers and
registered paramedics. While the hostile attitude of fully qualified paramedics to
volunteers is understandable in the context of an emerging health profession that is
continuing to negotiate its place in the hierarchy of health professionals, it is an issue
that will need to be confronted. Otherwise the outcome of this aggressive ‘staking out’
of territory will have the effect of alienating members of the local community and
diminishing access to services. This is closely related to the challenge ambulance
paramedics are facing in their efforts to work more effectively with other health
professionals as already discussed in Chapter 5. Registration of itself is no substitute for
behaving in a professional and ethical manner.
Technological Influences on Pre-hospital Systems
In terms of technological influences on pre-hospital care, my main interest was in
looking at the new and emerging technology to see how it might influence the way
ambulance services are delivered in rural areas. The intention was to move beyond
seeing telemedicine as video-conferencing. Two particular areas of interest were, the
improvement in support to first responders and CAOs, and the possibility of de-skilling
ambulance paramedics.
The pre-hospital technological changes are a world-wide phenomenon, with technical
advances being made in the design and capability of pre-hospital equipment, along with
related developments in telemedicine and information technology, making the delivery
of some clinical interventions more feasible than in the past. These telemedicine
developments do this through the transfer of information rather than patients and the
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
208
subsequent ability to deliver the right care by the right person at the right place at the
right time (Navein & Driscoll 2000).
The importance to pre-hospital care of technological developments lies in two important
areas. Firstly, the rapid development of mobile medical equipment has extended the
range of clinical interventions in the pre-hospital environment. For example, the
introduction of portable defibrillators has seen the care of cardiac arrest patients
extended from the hospital domain to that of first responders and volunteer staff trained
in basic life support. This is has provided the opportunity to redesign models of service
delivery in new and exciting ways. On the other hand, these opportunities have
threatened an emerging profession that is only starting to emerge from medical
dominance and its image of being drivers and rescuers.
Secondly, technological advances have seen a massive improvement in
communications. Almost all ‘first-world’ ambulance services, in both urban and rural
areas, are now able to operate modern computer-aided dispatch systems, incorporating
call-line identification, decision-support tools, and geographic information systems.
Despite the technical advantages of these improved communications systems, they are
yet to win the hearts and minds of many rural communities that continue to value their
personal contact with local ambulance staff. Improvements in communications systems
now allow ambulance paramedics to obtain consultant physician-level medical advice
while en route to hospitals.
The gurus of telemedicine can tend to be overly optimistic about the ability of the
technology to overcome problems and maybe a little naïve about the acceptability of the
technology in the field. Certainly, rural areas do not appear to be any more likely to
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
209
embrace telemedicine technology than any other areas (Navein & Driscoll 2000;
Neergaard 2001). The technological expert I interviewed certainly expressed an
optimistic view of the future of pre-hospital care and telemedicine.
… telemedicine will become very, very common, very widespread and so long as the paramedic is able to interact with a specialist at a significant level, adequate level, I think that this is what will happen. There will be a whole lot more pre-hospital stuff done not talking so much about first-responders but really the advanced paramedic.
(Technology Interviewee)
My interviewee went on to describe the value of telemedicine in remote settings,
including isolated areas, large oil-rigs and mines. He saw few insurmountable technical
problems for pre-hospital systems, saying that, “… even if it is some sort of science
fiction at this point, it is very likely to become a reality down the track.” The bigger
challenges are philosophical, with fear of the unknown and a lack of vision
predominating. For instance, he noted the potential that the new mobile telephone
technology offered for expanding the role of ambulance paramedics in newer health
services such as ‘Hospital-in-the-Home’.
A by-product of these technological developments has been the tendency of ambulance
crews to bypass local hospitals and general practitioners, and instead transport patients
directly to major hospitals under the authority of city-based senior medical consultants.
The challenge for smaller rural hospitals and medical practitioners is to convince the
major referral hospitals that there is value in their intervention before the transfer of
patients to tertiary hospitals (Somers 1999). One outcome of this trend toward hospital
bypass has been a straining of relations between the ambulance service, and local
general practitioners and nurses who feel that their skills are being ignored. Likewise,
the centralization of communications and dispatch, made possible through technological
innovation, do not always meet with universal approval in rural areas (see Chapter 5).
The lack of evidence on the effectiveness and efficacy or otherwise of centralized
dispatch systems does not help the argument for centralization of dispatch and is a gap
in Australian pre-hospital research.
For these reasons, the ability of modern telecommunication to support centralized
dispatching systems and decision-support systems are relevant to the results of this

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
210
study. Local and district communications systems had a key role in the management and
coordination of ambulance resources until the mid-1990s when economic pressures
alone forced the amalgamation of existing district communications centres into larger
regional centres. There were no accompanying technological improvements designed to
improve performance (personal recollection as a senior manager at the time). As
indicated in the results described in Chapter 5, the introduction of prioritised
dispatching processes has not meet with universal approval; nurses and general
practitioners in particular, complain about the loss of local contact and operational
control.
Paradoxically, it is the ambulance services capability to combine the clinical skills of its
paramedics with its expertise in information and communications technology that offers
it the opportunity to contribute more fully to health care provision (Woollard & Ellis
1999). Logically, the combination
of expanded practice and
technology may reduce the
frequency of local ‘by-pass’ in rural
areas. It is not in the financial and
operational interests of rural
ambulance services to have vehicles
and crews out of their operational
areas for extended periods.
… if the many patients who do not require the resources of a fully equipped A&E department could be treated locally, this would keep ambulances closer to their normal area of operations and result in shorter journey times. It would also free up these expensive resources more quickly to respond to the next call.
(Woollard & Ellis 1999)
The recent development of integrated decision-support tools for pre-hospital care as part
of a computerised patient care record (pictured above) may help overcome the dearth of
accurate data for both clinical audit and research purposes. The educational expert
interviewed was very excited about the potential this technology has in rural Victoria
where it is being trialed.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
211
Victoria will be the first place to actually have it [an electronic PCR] in use daily on the ground. … What is interesting about it is the clinical data is so extensive you will be able to say what age groups suffered asthma, what period of time. All those things and when we go back looking for data in relation to a subject from the introduction of this sheet we will be able to find it.
(Educational Interviewee)
While the system is being promoted within RAV as a world-first, it is in fact very
similar to a system that is operating in Uppsala, Sweden (Karlsten & Sjöqvist 2000).
Both systems are essentially information management systems that are used for data
communication, documentation, triaging and the presentation of checklists. The
introduction of this technology provides an excellent case study of how the combination
of enhanced education and technological developments may improve patient outcomes.
The technology is neither designed for nor capable of compensating for inadequate
education and training of pre-hospital providers. For small rural and remote areas, one
interesting design feature of the system is the ability to print a patient care record (PCR)
from a personal computer located in the hospital or medical clinic. Alternately, it is
possible to print the PCR in the ambulance. Table 39 summarises the predicted
advantages of the computerised PCR, decision support tools and other telemedicine
technologies for pre-hospital service delivery.
While Karlsten and Sjöqvist (2000) stress the importance of documenting medical
evaluations and advanced treatments in the pre-hospital setting, they also note the
importance of simplifying the documentation process so that it can be completed while
the patient in under the care of the paramedic.
In this way the paramedic can use the case-sheet as a medical protocol with built-in triage and advice. Depending on the patient’s chief complaint, different computer-based forms can be chosen: if the complaint is altered level of consciousness then a specific form for that condition is used. In this way the computer helps the paramedic in the examination and evaluation of the patient by pointing out important issues for that specific condition.
(Karlsten & Sjöqvist 2000)
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
212
Table 39 Telemedicine and Ambulance Service Delivery
Intervention Stage
Advantages of ambulance telemedicine
Access Locates appropriate resources according to location and clinical capability using a Global Positioning System.
Diagnosis Uses integrated diagnostic aids, including remote telemetry to alert hospitals of the clinical condition of impending arrivals.
Treatment Allows consultation with medical experts and the use of checklists to improve timeliness and quality of clinical interventions.
Transport Improves triage of patients to appropriate medical facilities consistent with their clinical condition and the capabilities of receiving medical facilities.
Hospital handover
Provides more accurate clinical data to hospitals and medical staff. When transport time is longer than ideal, the handover can be commenced before arrival at the hospital.
Clinical audit Integrates ambulance records with hospital medical records, enabling better evaluation of clinical outcomes. Each clinical intervention will be recorded digitally in real time providing a ‘water tight audit trail’ (Navein & Driscoll 2000).
Research and learning
Collects consistent operational and clinical data in an accessible form that will facilitate more pre-hospital research.
The impact of technological change on the pre-hospital field is a specialized topic
outside the scope of this work. The adoption of advanced technology has had many
positive aspects from the provision of safe and effective defibrillators, improved
education and training opportunities for remote staff, and improved communications.
It has even greater potential for the future development of
rural ambulance services, which lack the physical
infrastructure to otherwise support extended care training
and development programs. When allied with a
commitment to the provision of improved services the
combination of education and technology are very
powerful tools. However, a strong commitment will need to be more than rhetoric;
moving forward in the rural environment will require considerable management support
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
213
and financial resources. The challenges of maximising the advantages of advanced pre-
hospital technology in rural areas include the:
Influence of time and distance in rural settings, and the associated deficits in the quality of telecommunications in remote areas;
Limited caseloads of small and remote ambulance stations, which rely on staff with limited knowledge, skills and support; and
Communities with poor health and emergency service infrastructures.
6.3.3 Strength in unity
The strongest message from the focus group with the RAV managers was their
articulated sense of unity and purpose. They saw the major advantage of forming RAV
as the opportunity, as a larger business enterprise, to employ and develop specialist
managers in contrast with the former regions where management staff operated as
generalists who were sometimes in competition in the pursuit of resources and staff.
The change in organizational size and focus has provided management staff with the
opportunity to develop their knowledge and skills in specialist areas. This view echoes
the hopes expressed in New South Wales during the amalgamation of regional
ambulance services during the 1980s; unfortunately, little appears to have changed
(Audit Office NSW 2001: 54-55). The formation of RAV has also enabled rural
ambulance to speak with one voice, and as a result develop wider stakeholder
relationships than was possible as five separate regions. One example cited was how the
relationship with the Department of Human Services has changed.
… we’ve gotten to a size now where people consider its worth talking to us … So if there is going to be a re-development of a hospital site, someone actually comes and asks whether we’re thinking about re-developing an ambulance station there as well and whether we ought to piggy back onto this project. That was something we could never get out of the Department [of Human Services] years ago.
(Focus Group Participant)
The formation of RAV has changed the relationship with the Melbourne Metropolitan
Ambulance Service, which many other stakeholders had hitherto considered the de facto
State Ambulance Service. RAV is now considered a key player in health and emergency
service planning and policy development. Another significant development has been the
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
214
establishment of a rural ambulance service Medical Standards Committee with
representatives of rural stakeholders such as rural doctors through direct representation
of the Rural Doctors Association of Victoria and Monash University School of Rural
Health. One manager made the point that the formation of the RAV Medical Standards
Committee has “… given us the opportunity to partner and develop more strategic
relationships than we were ever able to do before.”
Strategic relationships have been formed and strengthened at a state-level with the
Victorian Farmers Federation, the Country Fire Authority, the State Emergency Service,
the Department of Justice, the Department of Human Services and Monash University
School of Rural Health. The inexperience of some members of the focus group
participants in senior management positions before the amalgamation of the former
Regions should temper the interpretation of their comments about the previous
management culture and practices that operated in a far more difficult financial and
political environment. Despite the expressed views of this group, my own professional
recollection is that the senior management staff of the old Regions had good links with
emergency services and the Department of Human Services.
This greater emphasis on connecting with rural stakeholders is a reflection of RAV’s
understanding that they aspire to having a uniquely rural focus in their approach to
delivering ambulance services. When specifically asked to describe the philosophical
basis of RAV, one participant replied with:
Core value is we’re a rural ambulance service, first and foremost and we are about working strategically with rural communities and the rural health care [system], we cannot do it alone and we need to do it in partnership with … communities.
(Focus Group Participant)
With the formation of RAV there was a fear that the new organization would lose touch
with the community. To address this potential problem, RAV has formed a Community
Reference Group to “… ensure that the communication between rural ambulance and
the rural people actually continues” (Focus Group Participant). Membership of the
group is drawn from across rural Victoria and its members meet regularly with the chief
executive officer and the directors. Their role is to act as a conduit between RAV and
the community. In addition to this strategy, the RAV committee of management is
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
215
conducting quarterly meetings with rural communities across the State. One focus group
participant described the management philosophy with the neat phrase:
Community and the Ambulance, the Ambulance and the Community.
In reality, the phrase appears to be a variation of one of RAV’s themes: “Community in
Ambulance; Ambulance in the Community” (Audit Office NSW 2001: 93). While the
focus group participants expressed a commitment to provide one standard of service to
all rural people, they acknowledged that there is more than one way of delivering the
service in rural and remote areas. For example, RAV are considering the utilization of
first responders, CAOs, and the use of other organizations to respond and deliver care in
some rural and remote locations as service delivery options.
RAV management sees the voluntary system as making a significant contribution to delivering ambulance services in rural and remote locations in Victoria that do not have sufficient demand to support the allocation of full time ambulance officers.
(Audit Office NSW 2001: 93)
Similar developments are taking place in the United Kingdom (Nicholl et al 2001: 22).
This sharing of responsibility is a large cultural shift for an organization that has
traditionally claimed exclusive responsibility to organize and deliver all ambulance care
and transport. Incorporation of other providers into the system of pre-hospital care
raises the issue of how best to manage those services. Should they be organised
centrally through large ambulance services or through smaller services? In the United
Kingdom, opinions are divided about the virtues of amalgamations and mergers when
the future role of ambulance services is discussed.
Although larger Ambulance Services may be more operationally effective. There was widespread unease about the process of mergers, which need to be justified on the grounds of improving care.
(Nicholl et al 2001: 4)
The Ambulance Service Association sponsored review of ambulance services in the
United Kingdom favoured the adoption of a Health Care Service ambulance model in
which there would be a greater focus on health care than on emergencies than is
inherent in the traditional public safety or emergency service model. Adoption of this
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
216
clinically broader, but more locally managed out-of-hospital model health care network
model, raises questions about the appropriateness of large regional ambulance services
for the provision of operationally effective units (Nicholl et al 2001: 11, 15, 26).
While RAV falls short of being a state-wide ambulance service, it is nonetheless of a
size that it potentially has the management problems of any large organization. These
may include:
the occurrence of large transaction costs;
ignoring of local conditions;
unwieldy decision-making and implementation processes; and
the stifling of innovation and creativity.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
217
6.4 Discussion
At the onset, the aims of this chapter were largely descriptive with limited analytical
ambitions. In the end, the findings illuminated the organizational, socio-political,
educational and technological issues and tensions that exist within rural ambulance
services. The resulting description can be viewed through the structural concepts of
complexity, formalization and centralization (Robbins 1983b: 45).
The formation of Rural Ambulance Victoria from the former regional ambulance
services was designed to replace a complex and disunited group of organizations that
were battling to achieve their goals in a difficult financial and political environment.
Both their critics and supporters argued that these medium-sized regional ambulance
services lacked the human and financial resources to cope with the expectations and
demands made of them. The creation of Rural Ambulance Victoria has resulted in an
organization with high levels of complexity, formalization and centralization that are
not necessarily in accord with each other. These tensions are important pointers or
indicators for those managing, studying or interacting with RAV.
An assessment based on these three concepts provides only a partial picture of RAV
based on structural variables. Another approach is needed to look more deeply into the
character or culture of RAV and rural ambulance services more generally. The approach
used here is to examine the nature of its relationship with its environment and ask how
RAV manages its relationship with the external environment? Alderfer and Cooper
offer a means of describing this through the concept of ‘boundary permeability’. It
describes organizational systems on a continuum from the one extreme of
underbounded systems that can lose a sense of their own identity and overbounded
systems that lack the ability to adapt to environmental change (Alderfer & Cooper 1980:
269). They use eleven variables as markers for the degree of boundary permeability. For
the purposes of this study, I rated each variable on the basis of my ambulance service
management expertise as exhibiting high, medium and low levels of boundary
permeability.
One of the observed characteristics of the newly established of RAV is its high level of
complexity. Complexity can be defined as “… the level of knowledge and expertise in
an organisation …” (Jackson & Morgan 1982: 377). Robbins (1983a: 368-370: 1983b:

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
218
45-47) describes complexity, formalization and centralization as the three key
components of organizational structure. He breaks complexity into three inter-related
parts. Horizontal differentiation refers to the degree of differentiation between units
based on the orientation of members, the nature of the tasks they perform, and their
education and training. Vertical differentiation refers to the depth of the organizational
hierarchy that is necessary to coordinate tasks and to bring them into a coordinated
whole. Spatial differentiation encompasses the degree to which the location of an
organization’s facilities and personal are geographically dispersed.
The findings reported in this chapter indicate a growth in the complexity of rural
ambulance services in Victoria associated with increasing size, technological advances
and organizational change. The spatial differentiation is clear for all to see, with little
chance of RAV escaping its geography. None of this came as a great surprise. However,
the articulated responses of the focus group participants appeared to be inconsistent with
this theoretical position. The respondents clearly identified the increasing horizontal
differentiation through greater role specialization, more comprehensive education and
training, and a trend toward independent clinical practice. It was very interesting that
they did not identify the increasing vertical differentiation that has taken place through
the introduction of a stronger and more centrally-controlled clinical career structure that
has been gradually replacing the older formal career structures that dominated the
previous regional ambulance services.
Formalization refers to the degree to which jobs within the organization are
standardized through the adoption of firm policies and procedures. This may be through
explicit job descriptions, many rules and clearly defined procedures that give staff little
scope for discretionary behaviour. Formalization is a measure of standardization
(Robbins 1983b: 61). RAV has greatly increased the level of formalization through
strategies such as accreditation through the ISO quality framework, tightly written
clinical practice guidelines and the implementation of standardized continuing
education programs for all staff. The planned introduction of a decision support tool as
part of the electronic patient care record will only add to the level of formalization.
These trends have many advantages for the consistent delivery of clinical care.
However, they are a potential point of tension with the emerging profession of pre-
hospital care, which has ambitions of becoming an autonomous health profession.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
219
Centralization is considered the most problematic of the three components of structure.
Generally speaking it refers to the degree to which decision-making is concentrated at a
single point in the organization (Robbins 1983b: 76-78). The degree of centralization
within RAV appears to be related an individual’s location within its structure and power
centres. The focus group participants perceived RAV as more decentralized in terms of
decision-making than the previous regional services; their evidence for this was the
‘flatter’ organizational structure of RAV.
On the other hand, informal discussions with staff outside the central management
group provided an altogether different perspective. They expressed the view that they
were as alienated from RAV as they ever were with the former regions. The levels of
discretion in relation to decision-making regarding major expenditure, the sharing of
information with the media and staff, and variations in clinical practice supports this
relatively sceptical perspective. Clinical practice is an example where behaviour will be
even more closely monitored in the future with the electronic patient care record. This
finding is consistent with observations in the United Kingdom, where one ambulance
service is reported to have combined a flat management structure with centralised
control and authority more indicative of a classic bureaucracy. In many ways, the
organizational outcome was little different to the comparative Australian ambulance
service in the same study, with its paramilitary and centralised line of command with
many hierarchical levels (Mahony 2001).
So what sort of structure and identity is being formed through the creation of one large
rural ambulance service? For this analysis, Alderfer and Cooper’s concept of
underbounded and overbounded systems is mobilised. As already described in Chapter
2, this theory is based on the premise that system boundaries, both physical and
psychological, are the defining characteristic of systems and that permeability is the
crucial property of system boundaries. Alderfer and Cooper (1980: 269-277) have
identified eleven interdependent variables to differentiate between underbounded and
overbounded systems. In Table 40, observations are recorded and judgements made
about these variables in terms of their level of boundary permeability within Rural
Ambulance Victoria.
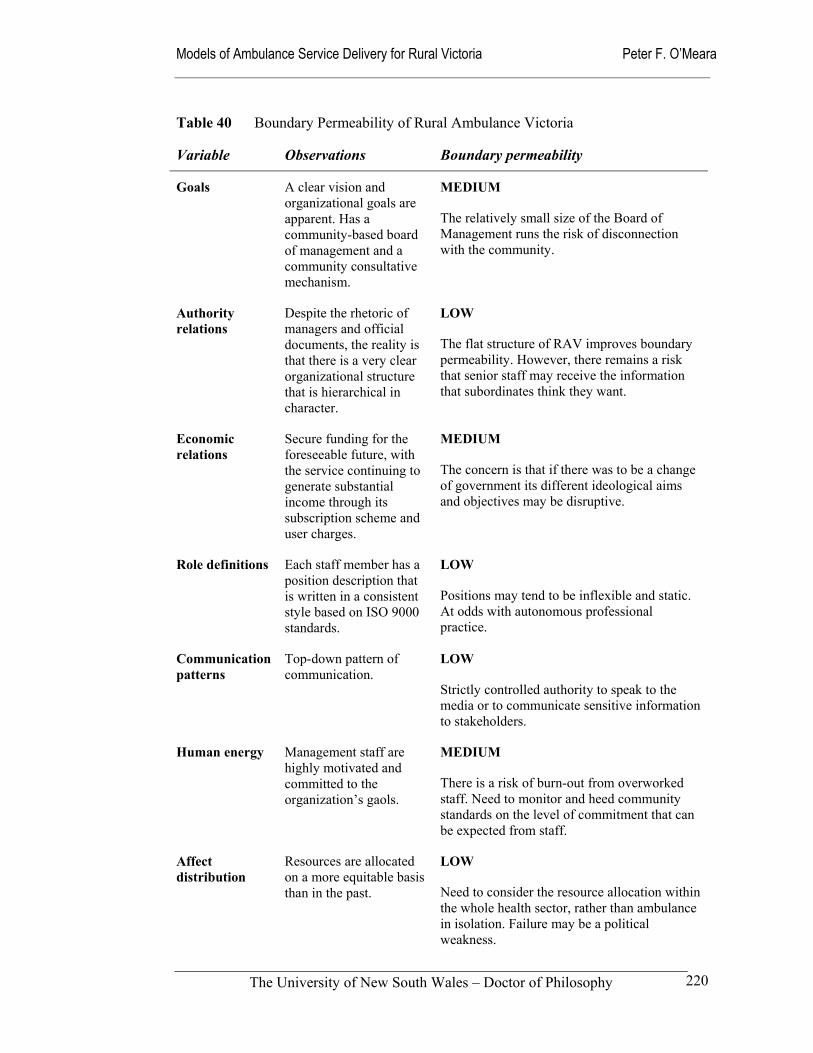
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
220
Table 40 Boundary Permeability of Rural Ambulance Victoria
Variable Observations Boundary permeability
Goals A clear vision and organizational goals are apparent. Has a community-based board of management and a community consultative mechanism.
MEDIUM
The relatively small size of the Board of Management runs the risk of disconnection with the community.
Authority relations
Despite the rhetoric of managers and official documents, the reality is that there is a very clear organizational structure that is hierarchical in character.
LOW
The flat structure of RAV improves boundary permeability. However, there remains a risk that senior staff may receive the information that subordinates think they want.
Economic relations
Secure funding for the foreseeable future, with the service continuing to generate substantial income through its subscription scheme and user charges.
MEDIUM
The concern is that if there was to be a change of government its different ideological aims and objectives may be disruptive.
Role definitions Each staff member has a position description that is written in a consistent style based on ISO 9000 standards.
LOW
Positions may tend to be inflexible and static. At odds with autonomous professional practice.
Communication patterns
Top-down pattern of communication.
LOW
Strictly controlled authority to speak to the media or to communicate sensitive information to stakeholders.
Human energy Management staff are highly motivated and committed to the organization’s gaols.
MEDIUM
There is a risk of burn-out from overworked staff. Need to monitor and heed community standards on the level of commitment that can be expected from staff.
Affect distribution
Resources are allocated on a more equitable basis than in the past.
LOW
Need to consider the resource allocation within the whole health sector, rather than ambulance in isolation. Failure may be a political weakness.
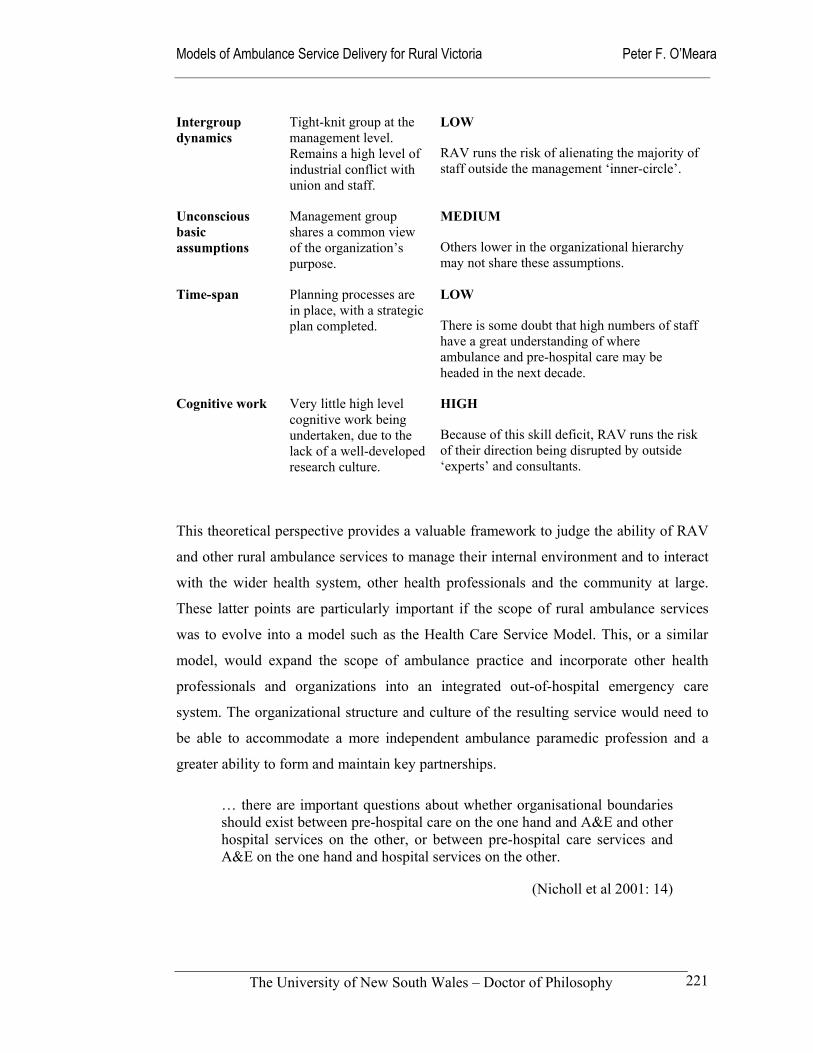
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
221
Intergroup dynamics
Tight-knit group at the management level. Remains a high level of industrial conflict with union and staff.
LOW
RAV runs the risk of alienating the majority of staff outside the management ‘inner-circle’.
Unconscious basic assumptions
Management group shares a common view of the organization’s purpose.
MEDIUM
Others lower in the organizational hierarchy may not share these assumptions.
Time-span Planning processes are in place, with a strategic plan completed.
LOW
There is some doubt that high numbers of staff have a great understanding of where ambulance and pre-hospital care may be headed in the next decade.
Cognitive work Very little high level cognitive work being undertaken, due to the lack of a well-developed research culture.
HIGH
Because of this skill deficit, RAV runs the risk of their direction being disrupted by outside ‘experts’ and consultants.
This theoretical perspective provides a valuable framework to judge the ability of RAV
and other rural ambulance services to manage their internal environment and to interact
with the wider health system, other health professionals and the community at large.
These latter points are particularly important if the scope of rural ambulance services
was to evolve into a model such as the Health Care Service Model. This, or a similar
model, would expand the scope of ambulance practice and incorporate other health
professionals and organizations into an integrated out-of-hospital emergency care
system. The organizational structure and culture of the resulting service would need to
be able to accommodate a more independent ambulance paramedic profession and a
greater ability to form and maintain key partnerships.
… there are important questions about whether organisational boundaries should exist between pre-hospital care on the one hand and A&E and other hospital services on the other, or between pre-hospital care services and A&E on the one hand and hospital services on the other.
(Nicholl et al 2001: 14)

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
222
This idea of full integration into the health system is unlikely to happen in the near
future. However, discussion and debate of the concept does encourage consideration of
how ambulance services see themselves both now and in the future. In summary, the
newly established Rural Ambulance Service has, on balance, a level of boundary
permeability that is appropriate to this stage of its development. The maturing process
should ensure that many of these concerns with the culture and structure are addressed.
Mahony (2001), when talking about occupational stressors in ambulance services, very
neatly sums up the challenge for ambulance services:
The situation in terms of work autonomy in both services [one in the UK and another in Australia] was quite paradoxical. Although all participants reported having a high level of clinical autonomy at the scene of an emergency, the way that their work was organised meant that they had little autonomy in deciding their workload, hours or recuperative periods after stressful assignments. Officers were expected to use their initiative and to make judgements concerning diagnosis and treatment in life and death situations yet management via Co-ordination (the centre where the emergency telephone calls are received and crews deployed) could send them anywhere at any time.
(Mahony 2001: 139)
This evolutionary process of organisational development will involve the development
of an independent ambulance profession and the adoption of relevant professional
standards and measurable performance targets. Chapter 7 addresses the matter of
performance frameworks for rural ambulance services.
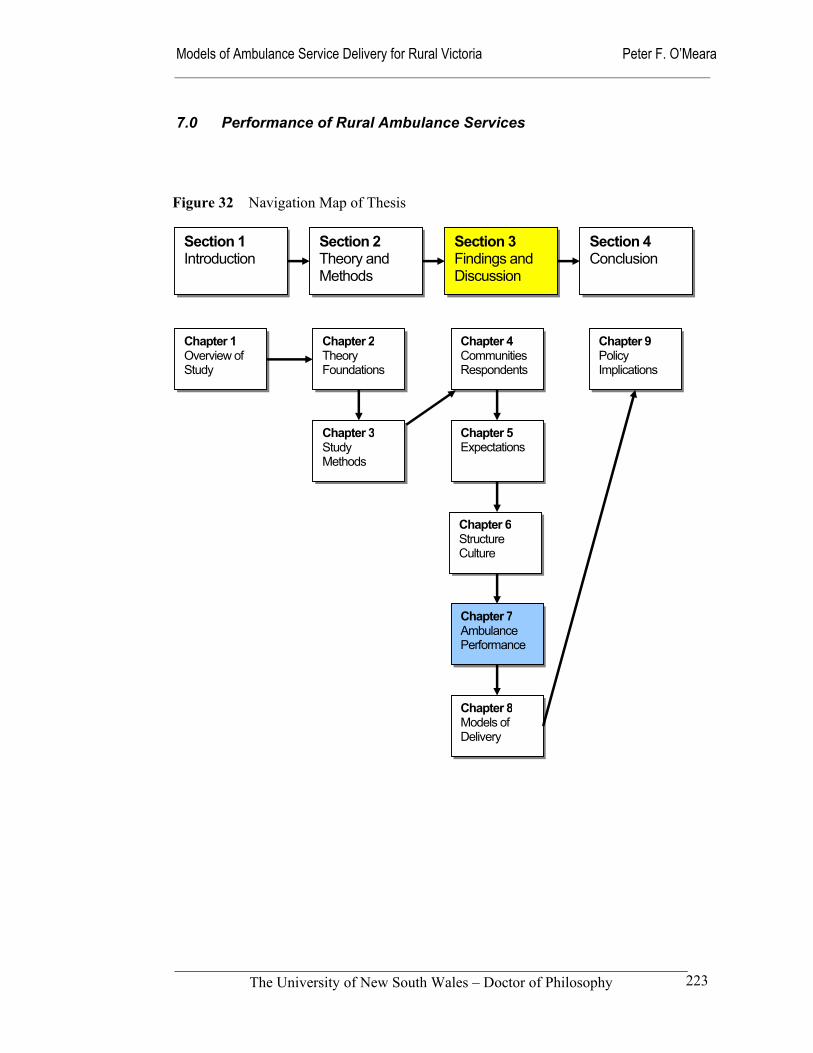
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
223
7.0 Performance of Rural Ambulance Services
Section 1 Introduction
Section 2 Theory and Methods
Section 3 Findings and Discussion
Section 4 Conclusion
Chapter 1 Overview of Study
Chapter 2Theory Foundations
Chapter 4Communities Respondents
Chapter 5Expectations
Chapter 6Structure Culture
Chapter 7Ambulance Performance
Chapter 8Models of Delivery
Chapter 9 Policy Implications
Chapter 3Study Methods
Figure 32 Navigation Map of Thesis
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
224
7.1 Introduction
Ambulance services throughout the world make efforts to measure and improve their
performance. Depending on their needs and technical capacity, they do this at the
strategic, managerial and operational levels. However, despite the resources expended
collecting data and the importance attached to the measurement of performance there is
a continuing dearth of agreed performance frameworks that are suitable for rural
ambulance services. As a result, staff and members of the community do not always
trust the data or its interpretation when it is used for planning and resource allocation
purposes (Hickey 2001b).
The publicly reported performance measures of Rural Ambulance Victoria are limited,
being restricted to financial performance, numbers of cases and basic response time data
(RAV 2000b). The empirical data from operational records of rural ambulance services
in Victoria (1996/97 year) and responses from a survey of stakeholders in this study
provided an opportunity to examine the state of play for rural ambulance services in
Victoria and ambulance services elsewhere. These data and an emerging literature were
combined to:
Compare the perceived and actual performance of rural ambulance services in different geographical areas in terms of utilization rates and
time intervals with a view to developing a useful performance framework for rural ambulance services.
This chapter briefly describes some of the performance frameworks that are in place for
ambulance services, reports on the analysed data collected during the course of this
research (Chapter 7.2 & 7.3), and then discusses the future directions that ambulance
services may take in response to the need to report on their performance (Chapter 7.4).
Performance reporting will become increasingly important as ambulance services
position themselves strategically within the community, and in relation to the
emergency management and health systems. The development of performance measures
is a key activity that must complement the formulation and implementation of different
models of service delivery. It is the means of providing meaningful data to guide
decision makers in policy development and implementation.
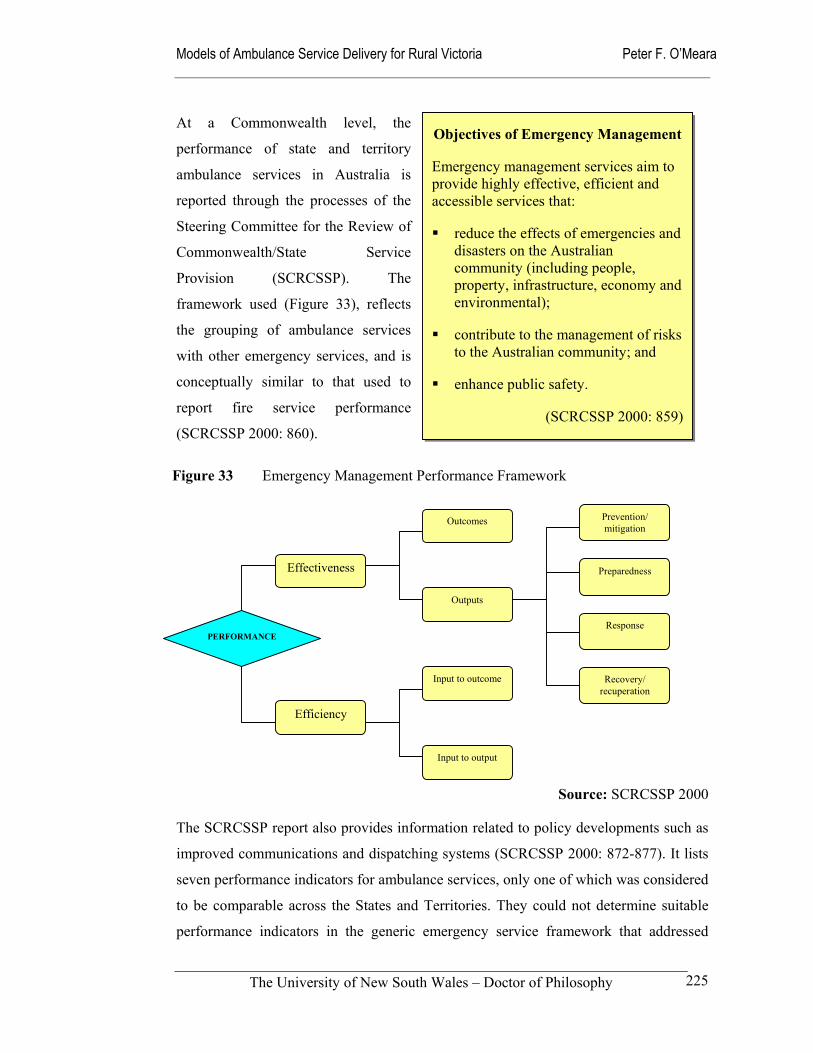
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
225
At a Commonwealth level, the
performance of state and territory
ambulance services in Australia is
reported through the processes of the
Steering Committee for the Review of
Commonwealth/State Service
Provision (SCRCSSP). The
framework used (Figure 33), reflects
the grouping of ambulance services
with other emergency services, and is
conceptually similar to that used to
report fire service performance
(SCRCSSP 2000: 860).
Source: SCRCSSP 2000
The SCRCSSP report also provides information related to policy developments such as
improved communications and dispatching systems (SCRCSSP 2000: 872-877). It lists
seven performance indicators for ambulance services, only one of which was considered
to be comparable across the States and Territories. They could not determine suitable
performance indicators in the generic emergency service framework that addressed
Figure 33 Emergency Management Performance Framework
Effectiveness
Efficiency
Outcomes
Outputs
Input to outcome
Input to output
Prevention/ mitigation
Preparedness
Response
Recovery/ recuperation
PERFORMANCE
Objectives of Emergency Management
Emergency management services aim to provide highly effective, efficient and accessible services that:
reduce the effects of emergencies and disasters on the Australian community (including people, property, infrastructure, economy and environmental);
contribute to the management of risks to the Australian community; and
enhance public safety.
(SCRCSSP 2000: 859)
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
226
‘prevention/mitigation’ and ‘recovery’. Those indicators that have been agreed at
Commonwealth level are: (SCRCSSP 2000: 872)
Survival rate from out-of-hospital cardiac arrest.
Proportion of emergency cases which receive a paramedic level of response.
50th percentile and 90th percentile response times.
Level of patient satisfaction (considered to be comparable).
Unit cost.
Expenditure per urgent and non-urgent response.
Expenditure per person.
This performance framework continues to make the assumption that ambulance services
are the health arm of the emergency services, rather than the emergency arm of the
health system; a notion that has already been challenged in the thesis. Outside the
straight-jacket of Commonwealth/State relationships, researchers and ambulance
services are exploring more appropriate performance indicators that better reflect the
needs of the community, health service planners, and patients entering the health system
through the pre-hospital system. Researchers have concentrated on studies of utilization
characteristics (Cadigan & Bugarin 1989; Jacobs & Oxer 1990; Morrisey et al 1995;
Clark et al 2000), time intervals (Morrissey et al 1996; Nicholl 1996; Cone et al 1998;
Guppy & Woollard 2000), and outcomes (Steil et al 1996; Robinson et al 1998; Maio et
al 1998; Spaite et al 2001). The Commonwealth framework for health services would
seem to be a more appropriate approach to the measurement of ambulance service
performance; it uses outcomes, access and equity, appropriateness, quality, and inputs
per output unit as its performance criteria (SCRCSSP 2000: 9).
Ambulance authorities have become interested in the development of these performance
measures, to measure their financial performance and to ensure that public monies are
used efficiently and effectively. The Australian Convention of Ambulance Authorities
has established a working group to improve the standardisation of definitions and to
develop a common set of core indicators to enable more meaningful comparative
analysis of ambulance service performance to be undertaken (Audit Office NSW 2001:
101). In New South Wales, the ambulance service has established a Performance
Information Unit to expand upon and improve the analysis and utility of its key
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
227
performance indicators (Audit Office NSW 2001: 6). Other States have instigated
similar processes to improve data collection and the reporting of performance.
As already indicated, time intervals of one sort or another are widely used to report on
the performance of ambulance services. This out-of-hospital time interval that has been
previously validated, variously incorporates activation time, call processing, allocation
of resources, mobilisation, travel to the scene, time at scene, travel to hospital, and time
spent at the hospital (Spaite et al 1993; Guppy & Woollard 2000; Spaite et al 2001).
The most widely cited performance framework for ambulance services are the ORCON
standards that the Organisational Research Consultancy developed in the United
Kingdom. The original ORCON report was issued in 1974 and recommended measures
and standards of service for emergency and urgent calls (DHSC 1974). These
recommendations specified that:
95 per cent of activation times should lie within 3 minutes;
in Metropolitan Services 50 per cent of calls should receive response times within 7 minutes and 95 percent within 14 minutes;
in Non-Metropolitan Services 50 per cent of calls should receive response times within 8 minutes and 95 per cent within 20 minutes.
Since that time, the ORCON standards have been reviewed and revised on numerous
occasions that take into account changing expectations, technology, and the challenge of
meeting metropolitan standards in rural and sparsely populated areas (DHSS 1990). The
shortcomings of relying exclusively on response times as a performance measure is well
recognised in the United Kingdom with performance targets now tiered and targeted
toward ensuring the fastest response times for those patients with life-threatening
conditions. Unlike the earlier standards, the newer standards are more patient-focused
and clinically meaningful (Nicholl et al 2001: 8-9, 15-16). Perhaps a little off-handedly,
the Ambulance Service of New South Wales disposed of the United Kingdom’s
standards with the following comment:
It should also be noted that the “ORCON standards” initially developed in 1976 [sic] are no longer considered relevant as a method of measuring modern ambulance performance.
(Audit Office NSW 2001: 101)

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
228
In North America, one of the most outstanding efforts to develop clinically relevant
performance measures is the Emergency Medical Services Outcomes Project (EMSOP).
It is a five-year project with the purpose of developing a foundation and a framework
for out-of-hospital outcomes research (Maio et al 1998; Spaite et al 2001). While
acknowledging that this is an enormous task, proponents say that “… the development,
dissemination and use of meaningful methods for EMS outcomes research is a key to
the future of EMS system development and maintenance” (Spaite et al 2001). At this
time they have used two models to inform their research: the Episode of Care Model;
and the Out-of-Hospital Unit of Service Model. The potential value of their conceptual
models is discussed later.
In common with all publicly funded or subsidised public services, rural ambulance
services in Australia are under pressure from stakeholders to develop performance
management and improvement processes. These stakeholders include government
funders and regulators, health and emergency systems managers, the community who
are reliant on the services provided, and others with an interest in their performance. On
the other hand, those within ambulance services have sometimes seen the development
and management of performance frameworks as a low priority; one that absorbs
valuable resources that could otherwise be used to provide services. More recently,
Australian ambulance authorities have recognised the importance of developing
performance indicators that demonstrate the clinical outcomes of ambulance service
activities and the extent to which ambulance paramedics make a contribution to the
condition and welfare of their patients. A number of Australian ambulance services,
including Rural Ambulance Victoria, are developing clinical information systems to
improve the timeliness and quality of data collection and analysis (Audit Office NSW
2001: 32; Kurowski 2002).
This tension between an external need for performance indicators and an internal culture
of scepticism, makes it essential that any performance management strategy should
answer the questions of why the information is needed, what activity or outcome is
sufficiently important that it should be measured, how the data are to be collected and
analysed, and who is to receive the information? The advocates of complexity theory
take the argument one step further and argue:

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
229
… that effective organisation and delivery of health care does not need detailed targets and specifications, nor should it focus primarily on “controlling the process” or “overcoming resistance.” Rather, those who seek to change an organisation should harness the natural creativity and organising ability of its staff and stakeholders through such principles as generative relationships, minimum specification, the positive attractors of change, and a constructive approach to variations in areas of practice where there is only moderate certainty and agreement.
(Plsek & Wilson 2001)
The next two sections of this chapter use indicative data to examine the performance of
rural ambulance services in Victoria. The data were collected in the period prior to and
shortly after the formation of Rural Ambulance Victoria. While it is clearly recognised
that many policies and processes have changed as a result of this major organisational
change, using the data to analyse perceived and actual performance remained a valuable
exercise in light of the continuing difficulty ambulance authorities and researchers have
with existing data collection methods and performance measurement. The final part of
this chapter explores the development of a performance framework for rural ambulance
services.
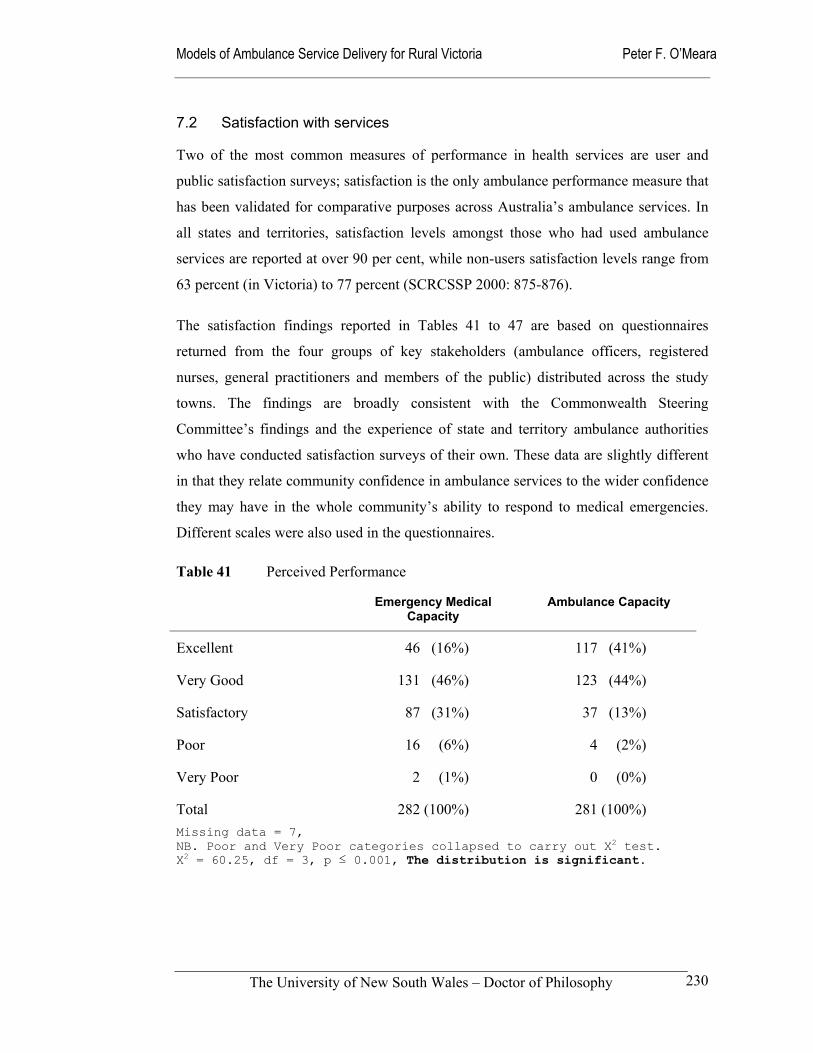
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
230
7.2 Satisfaction with services
Two of the most common measures of performance in health services are user and
public satisfaction surveys; satisfaction is the only ambulance performance measure that
has been validated for comparative purposes across Australia’s ambulance services. In
all states and territories, satisfaction levels amongst those who had used ambulance
services are reported at over 90 per cent, while non-users satisfaction levels range from
63 percent (in Victoria) to 77 percent (SCRCSSP 2000: 875-876).
The satisfaction findings reported in Tables 41 to 47 are based on questionnaires
returned from the four groups of key stakeholders (ambulance officers, registered
nurses, general practitioners and members of the public) distributed across the study
towns. The findings are broadly consistent with the Commonwealth Steering
Committee’s findings and the experience of state and territory ambulance authorities
who have conducted satisfaction surveys of their own. These data are slightly different
in that they relate community confidence in ambulance services to the wider confidence
they may have in the whole community’s ability to respond to medical emergencies.
Different scales were also used in the questionnaires.
Table 41 Perceived Performance
Emergency Medical Capacity
Ambulance Capacity
Excellent 46 (16%) 117 (41%)
Very Good 131 (46%) 123 (44%)
Satisfactory 87 (31%) 37 (13%)
Poor 16 (6%) 4 (2%)
Very Poor 2 (1%) 0 (0%)
Total 282 (100%) 281 (100%) Missing data = 7, NB. Poor and Very Poor categories collapsed to carry out X2 test. X2 = 60.25, df = 3, p ≤ 0.001, The distribution is significant.
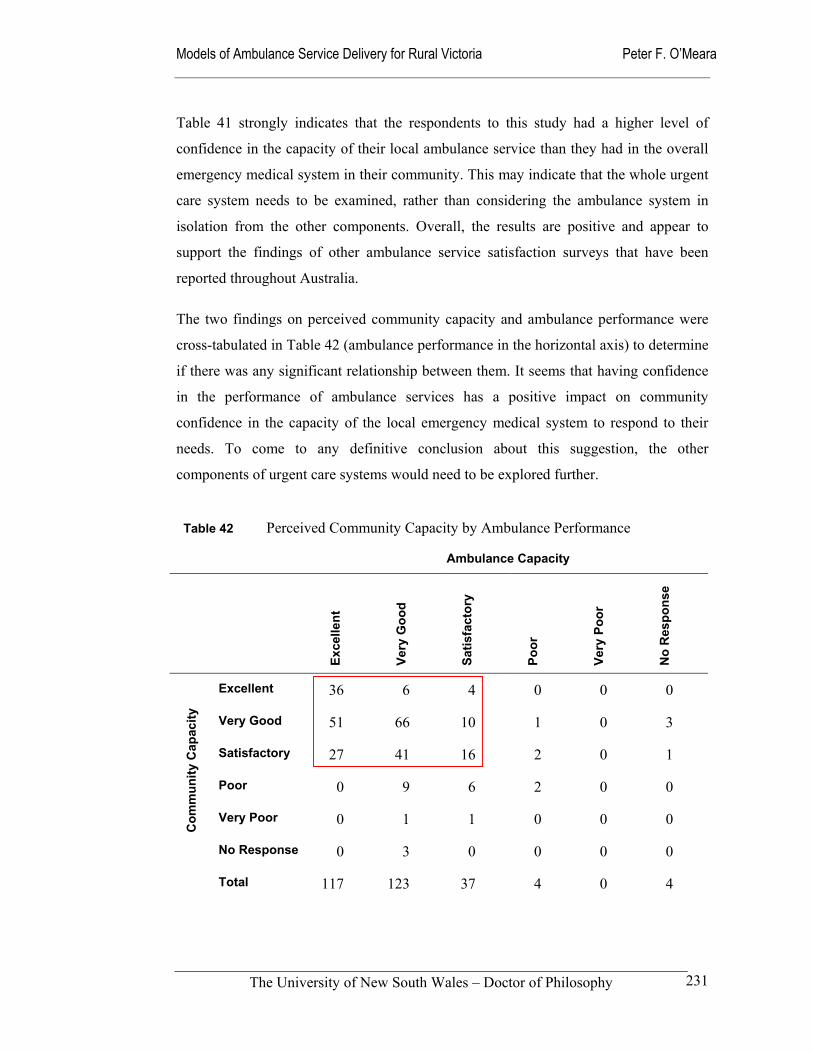
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
231
Table 41 strongly indicates that the respondents to this study had a higher level of
confidence in the capacity of their local ambulance service than they had in the overall
emergency medical system in their community. This may indicate that the whole urgent
care system needs to be examined, rather than considering the ambulance system in
isolation from the other components. Overall, the results are positive and appear to
support the findings of other ambulance service satisfaction surveys that have been
reported throughout Australia.
The two findings on perceived community capacity and ambulance performance were
cross-tabulated in Table 42 (ambulance performance in the horizontal axis) to determine
if there was any significant relationship between them. It seems that having confidence
in the performance of ambulance services has a positive impact on community
confidence in the capacity of the local emergency medical system to respond to their
needs. To come to any definitive conclusion about this suggestion, the other
components of urgent care systems would need to be explored further.
Table 42 Perceived Community Capacity by Ambulance Performance
Ambulance Capacity
Exce
llent
Very
Goo
d
Satis
fact
ory
Poor
Very
Poo
r
No
Res
pons
e
Excellent 36 6 4 0 0 0
Very Good 51 66 10 1 0 3
Satisfactory 27 41 16 2 0 1
Poor 0 9 6 2 0 0
Very Poor 0 1 1 0 0 0 Com
mun
ity C
apac
ity
No Response 0 3 0 0 0 0
Total 117 123 37 4 0 4
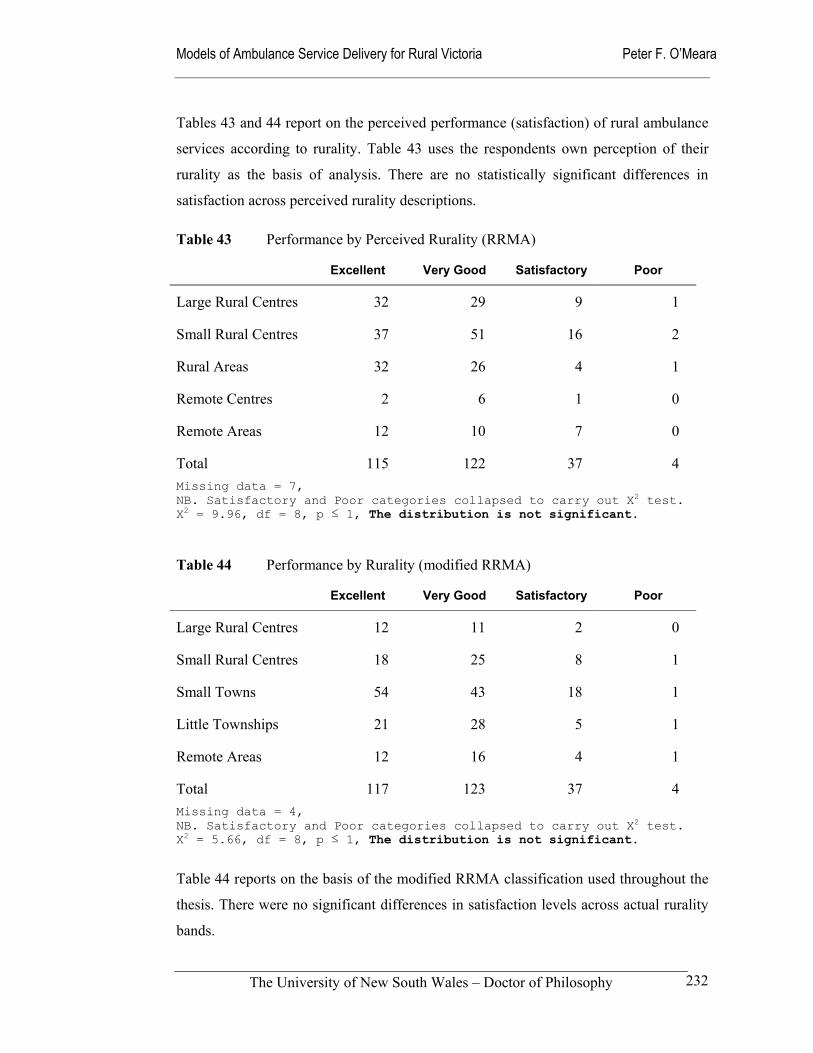
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
232
Tables 43 and 44 report on the perceived performance (satisfaction) of rural ambulance
services according to rurality. Table 43 uses the respondents own perception of their
rurality as the basis of analysis. There are no statistically significant differences in
satisfaction across perceived rurality descriptions.
Table 43 Performance by Perceived Rurality (RRMA)
Excellent Very Good Satisfactory Poor
Large Rural Centres 32 29 9 1
Small Rural Centres 37 51 16 2
Rural Areas 32 26 4 1
Remote Centres 2 6 1 0
Remote Areas 12 10 7 0
Total 115 122 37 4 Missing data = 7, NB. Satisfactory and Poor categories collapsed to carry out X2 test. X2 = 9.96, df = 8, p ≤ 1, The distribution is not significant.
Table 44 Performance by Rurality (modified RRMA)
Excellent Very Good Satisfactory Poor
Large Rural Centres 12 11 2 0
Small Rural Centres 18 25 8 1
Small Towns 54 43 18 1
Little Townships 21 28 5 1
Remote Areas 12 16 4 1
Total 117 123 37 4 Missing data = 4, NB. Satisfactory and Poor categories collapsed to carry out X2 test. X2 = 5.66, df = 8, p ≤ 1, The distribution is not significant.
Table 44 reports on the basis of the modified RRMA classification used throughout the
thesis. There were no significant differences in satisfaction levels across actual rurality
bands.
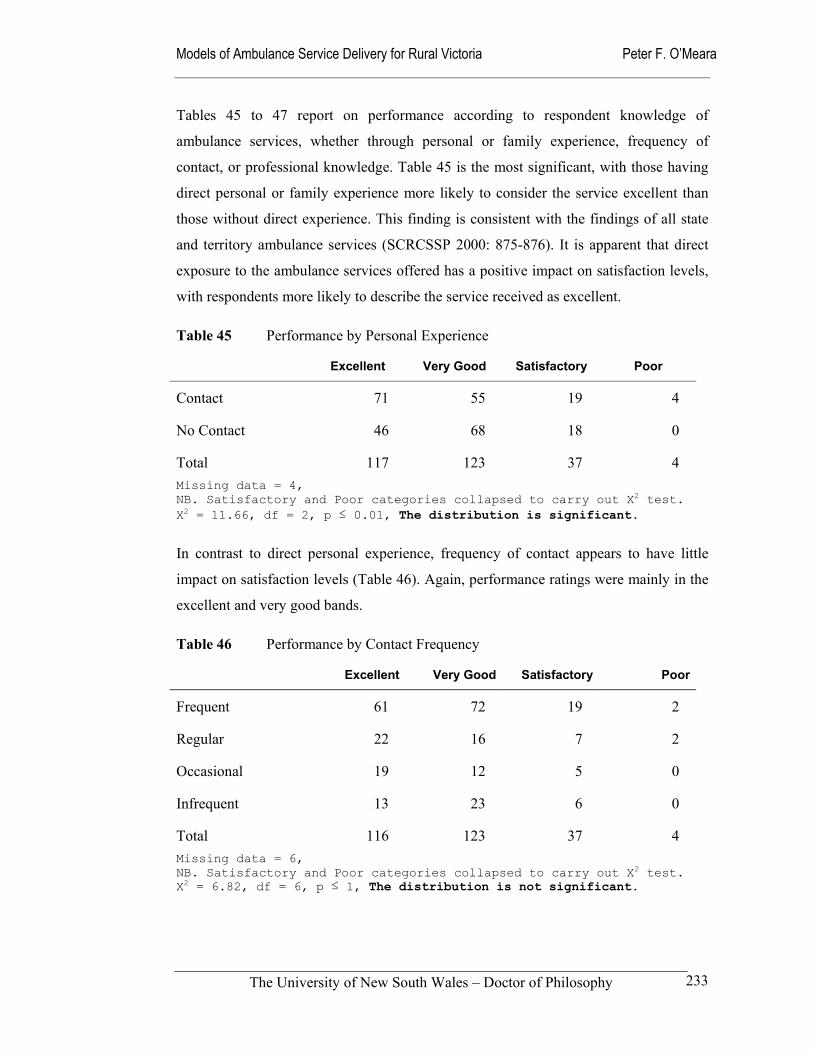
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
233
Tables 45 to 47 report on performance according to respondent knowledge of
ambulance services, whether through personal or family experience, frequency of
contact, or professional knowledge. Table 45 is the most significant, with those having
direct personal or family experience more likely to consider the service excellent than
those without direct experience. This finding is consistent with the findings of all state
and territory ambulance services (SCRCSSP 2000: 875-876). It is apparent that direct
exposure to the ambulance services offered has a positive impact on satisfaction levels,
with respondents more likely to describe the service received as excellent.
Table 45 Performance by Personal Experience
Excellent Very Good Satisfactory Poor
Contact 71 55 19 4
No Contact 46 68 18 0
Total 117 123 37 4 Missing data = 4, NB. Satisfactory and Poor categories collapsed to carry out X2 test. X2 = 11.66, df = 2, p ≤ 0.01, The distribution is significant.
In contrast to direct personal experience, frequency of contact appears to have little
impact on satisfaction levels (Table 46). Again, performance ratings were mainly in the
excellent and very good bands.
Table 46 Performance by Contact Frequency
Excellent Very Good Satisfactory Poor
Frequent 61 72 19 2
Regular 22 16 7 2
Occasional 19 12 5 0
Infrequent 13 23 6 0
Total 116 123 37 4 Missing data = 6, NB. Satisfactory and Poor categories collapsed to carry out X2 test. X2 = 6.82, df = 6, p ≤ 1, The distribution is not significant.
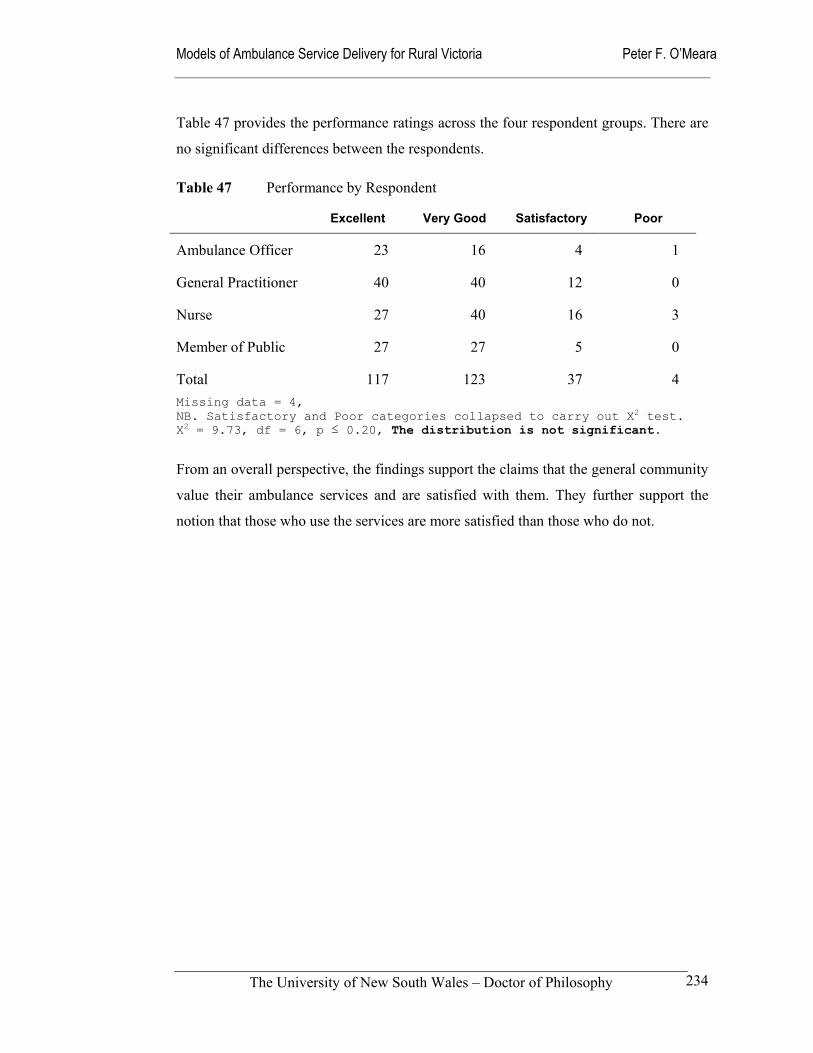
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
234
Table 47 provides the performance ratings across the four respondent groups. There are
no significant differences between the respondents.
Table 47 Performance by Respondent
Excellent Very Good Satisfactory Poor
Ambulance Officer 23 16 4 1
General Practitioner 40 40 12 0
Nurse 27 40 16 3
Member of Public 27 27 5 0
Total 117 123 37 4 Missing data = 4, NB. Satisfactory and Poor categories collapsed to carry out X2 test. X2 = 9.73, df = 6, p ≤ 0.20, The distribution is not significant.
From an overall perspective, the findings support the claims that the general community
value their ambulance services and are satisfied with them. They further support the
notion that those who use the services are more satisfied than those who do not.
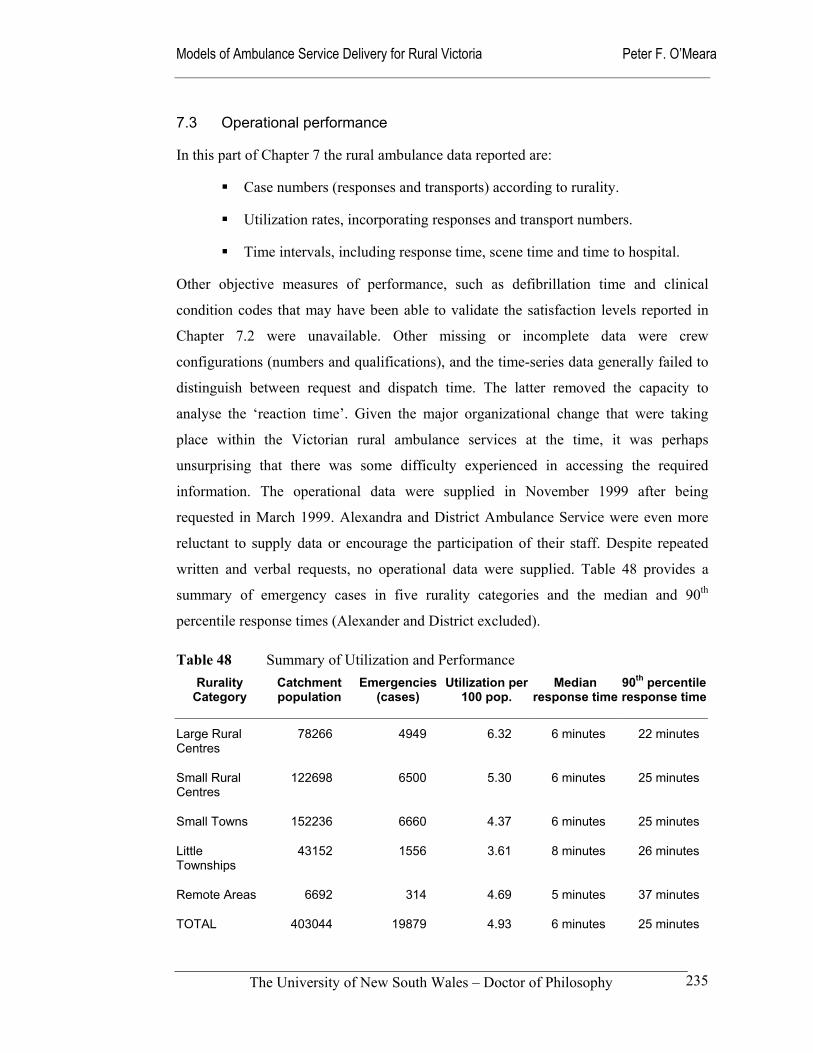
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
235
7.3 Operational performance
In this part of Chapter 7 the rural ambulance data reported are:
Case numbers (responses and transports) according to rurality.
Utilization rates, incorporating responses and transport numbers.
Time intervals, including response time, scene time and time to hospital.
Other objective measures of performance, such as defibrillation time and clinical
condition codes that may have been able to validate the satisfaction levels reported in
Chapter 7.2 were unavailable. Other missing or incomplete data were crew
configurations (numbers and qualifications), and the time-series data generally failed to
distinguish between request and dispatch time. The latter removed the capacity to
analyse the ‘reaction time’. Given the major organizational change that were taking
place within the Victorian rural ambulance services at the time, it was perhaps
unsurprising that there was some difficulty experienced in accessing the required
information. The operational data were supplied in November 1999 after being
requested in March 1999. Alexandra and District Ambulance Service were even more
reluctant to supply data or encourage the participation of their staff. Despite repeated
written and verbal requests, no operational data were supplied. Table 48 provides a
summary of emergency cases in five rurality categories and the median and 90th
percentile response times (Alexander and District excluded).
Table 48 Summary of Utilization and Performance Rurality
Category
Catchment population
Emergencies(cases)
Utilization per 100 pop.
Median response time
90th percentileresponse time
Large Rural Centres
78266 4949 6.32 6 minutes 22 minutes
Small Rural Centres
122698 6500 5.30 6 minutes 25 minutes
Small Towns 152236 6660 4.37 6 minutes 25 minutes
Little Townships
43152 1556 3.61 8 minutes 26 minutes
Remote Areas 6692 314 4.69 5 minutes 37 minutes
TOTAL 403044 19879 4.93 6 minutes 25 minutes
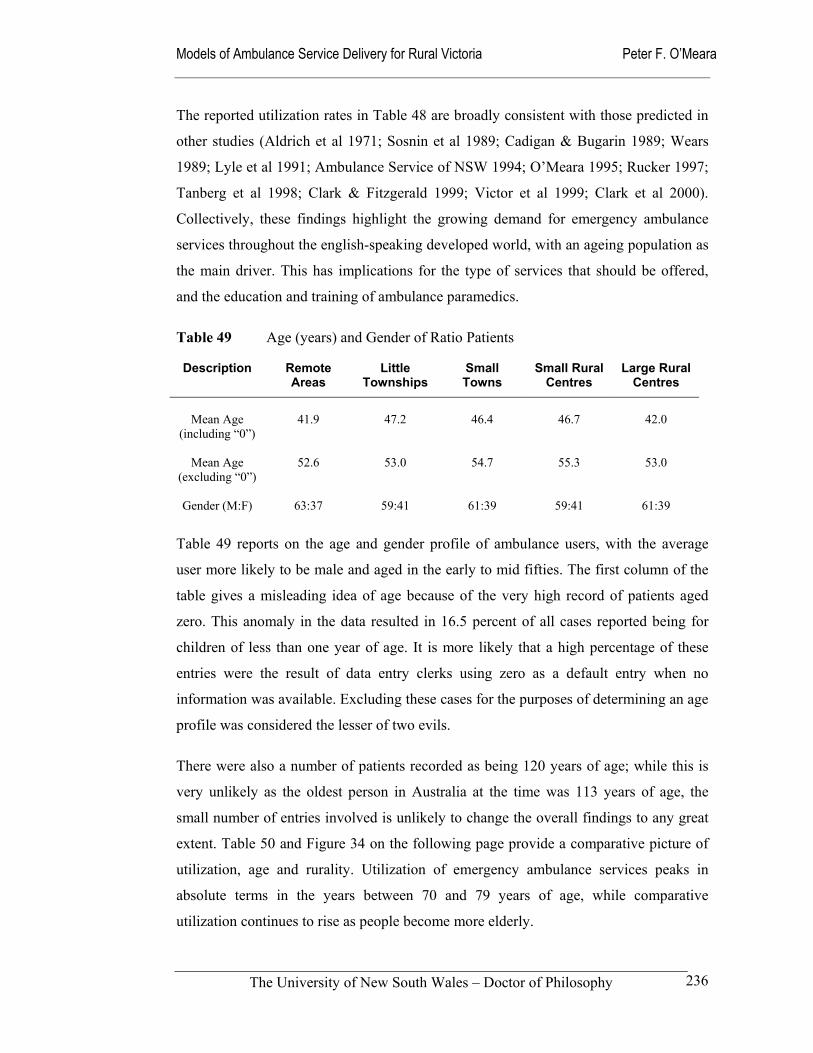
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
236
The reported utilization rates in Table 48 are broadly consistent with those predicted in
other studies (Aldrich et al 1971; Sosnin et al 1989; Cadigan & Bugarin 1989; Wears
1989; Lyle et al 1991; Ambulance Service of NSW 1994; O’Meara 1995; Rucker 1997;
Tanberg et al 1998; Clark & Fitzgerald 1999; Victor et al 1999; Clark et al 2000).
Collectively, these findings highlight the growing demand for emergency ambulance
services throughout the english-speaking developed world, with an ageing population as
the main driver. This has implications for the type of services that should be offered,
and the education and training of ambulance paramedics.
Table 49 Age (years) and Gender of Ratio Patients
Description Remote Areas
Little Townships
Small Towns
Small Rural Centres
Large Rural Centres
Mean Age
(including “0”)
41.9
47.2
46.4
46.7
42.0
Mean Age
(excluding “0”)
52.6
53.0
54.7
55.3
53.0
Gender (M:F)
63:37
59:41
61:39
59:41
61:39
Table 49 reports on the age and gender profile of ambulance users, with the average
user more likely to be male and aged in the early to mid fifties. The first column of the
table gives a misleading idea of age because of the very high record of patients aged
zero. This anomaly in the data resulted in 16.5 percent of all cases reported being for
children of less than one year of age. It is more likely that a high percentage of these
entries were the result of data entry clerks using zero as a default entry when no
information was available. Excluding these cases for the purposes of determining an age
profile was considered the lesser of two evils.
There were also a number of patients recorded as being 120 years of age; while this is
very unlikely as the oldest person in Australia at the time was 113 years of age, the
small number of entries involved is unlikely to change the overall findings to any great
extent. Table 50 and Figure 34 on the following page provide a comparative picture of
utilization, age and rurality. Utilization of emergency ambulance services peaks in
absolute terms in the years between 70 and 79 years of age, while comparative
utilization continues to rise as people become more elderly.
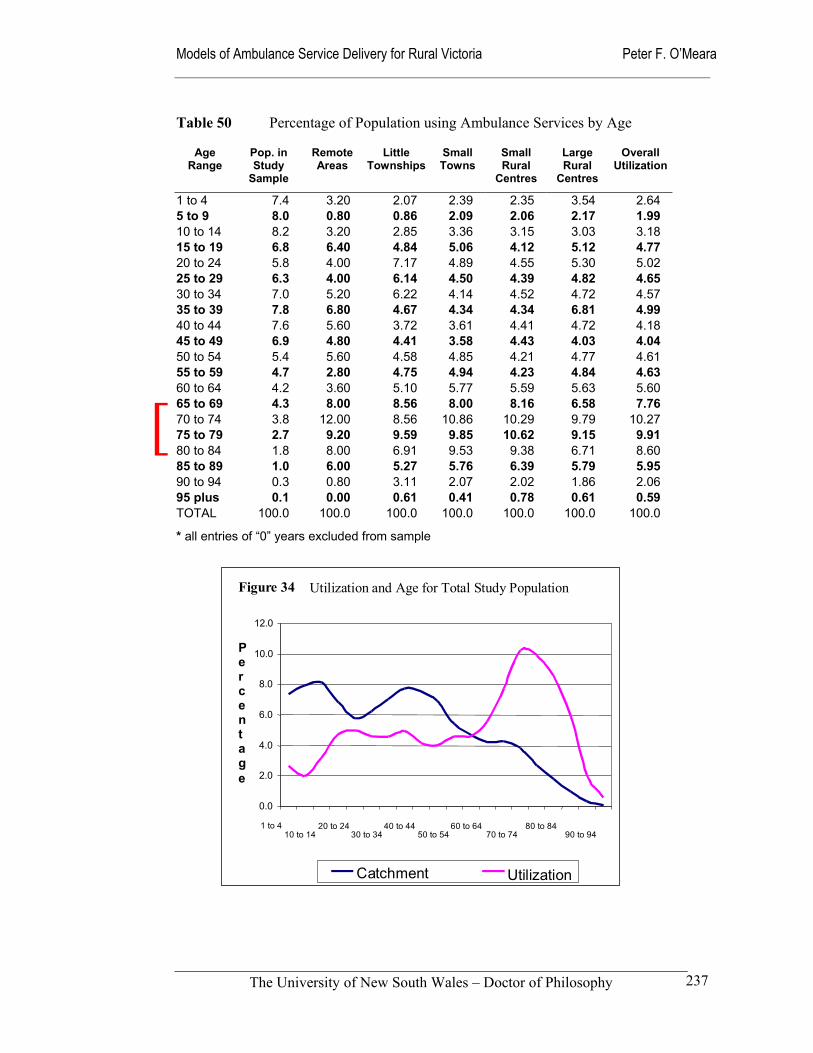
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
237
Table 50 Percentage of Population using Ambulance Services by Age
Age Range
Pop. in Study
Sample
Remote Areas
Little Townships
Small Towns
Small Rural
Centres
Large Rural
Centres
Overall Utilization
1 to 4 7.4 3.20 2.07 2.39 2.35 3.54 2.64 5 to 9 8.0 0.80 0.86 2.09 2.06 2.17 1.99 10 to 14 8.2 3.20 2.85 3.36 3.15 3.03 3.18 15 to 19 6.8 6.40 4.84 5.06 4.12 5.12 4.77 20 to 24 5.8 4.00 7.17 4.89 4.55 5.30 5.02 25 to 29 6.3 4.00 6.14 4.50 4.39 4.82 4.65 30 to 34 7.0 5.20 6.22 4.14 4.52 4.72 4.57 35 to 39 7.8 6.80 4.67 4.34 4.34 6.81 4.99 40 to 44 7.6 5.60 3.72 3.61 4.41 4.72 4.18 45 to 49 6.9 4.80 4.41 3.58 4.43 4.03 4.04 50 to 54 5.4 5.60 4.58 4.85 4.21 4.77 4.61 55 to 59 4.7 2.80 4.75 4.94 4.23 4.84 4.63 60 to 64 4.2 3.60 5.10 5.77 5.59 5.63 5.60 65 to 69 4.3 8.00 8.56 8.00 8.16 6.58 7.76 70 to 74 3.8 12.00 8.56 10.86 10.29 9.79 10.27 75 to 79 2.7 9.20 9.59 9.85 10.62 9.15 9.91 80 to 84 1.8 8.00 6.91 9.53 9.38 6.71 8.60 85 to 89 1.0 6.00 5.27 5.76 6.39 5.79 5.95 90 to 94 0.3 0.80 3.11 2.07 2.02 1.86 2.06 95 plus 0.1 0.00 0.61 0.41 0.78 0.61 0.59 TOTAL 100.0 100.0 100.0 100.0 100.0 100.0 100.0
* all entries of “0” years excluded from sample
Figure 34 Utilization and Age for Total Study Population
0.0
2.0
4.0
6.0
8.0
10.0
12.0
1 to 4 10 to 14
20 to 24 30 to 34
40 to 44 50 to 54
60 to 64 70 to 74
80 to 84 90 to 94
Percent age
Catchment Utilization
[
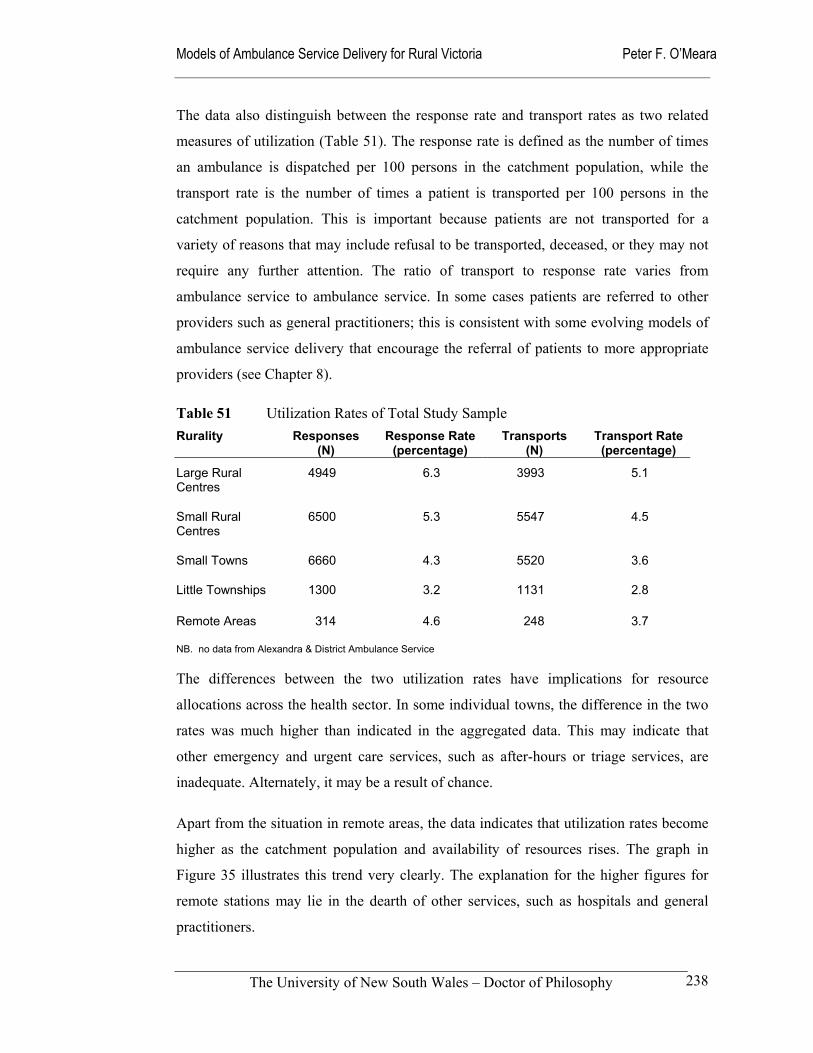
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
238
The data also distinguish between the response rate and transport rates as two related
measures of utilization (Table 51). The response rate is defined as the number of times
an ambulance is dispatched per 100 persons in the catchment population, while the
transport rate is the number of times a patient is transported per 100 persons in the
catchment population. This is important because patients are not transported for a
variety of reasons that may include refusal to be transported, deceased, or they may not
require any further attention. The ratio of transport to response rate varies from
ambulance service to ambulance service. In some cases patients are referred to other
providers such as general practitioners; this is consistent with some evolving models of
ambulance service delivery that encourage the referral of patients to more appropriate
providers (see Chapter 8).
Table 51 Utilization Rates of Total Study Sample Rurality Responses
(N) Response Rate
(percentage) Transports
(N) Transport Rate (percentage)
Large Rural Centres
4949 6.3 3993 5.1
Small Rural Centres
6500 5.3 5547 4.5
Small Towns 6660 4.3 5520 3.6
Little Townships 1300 3.2 1131 2.8
Remote Areas 314 4.6 248 3.7
NB. no data from Alexandra & District Ambulance Service
The differences between the two utilization rates have implications for resource
allocations across the health sector. In some individual towns, the difference in the two
rates was much higher than indicated in the aggregated data. This may indicate that
other emergency and urgent care services, such as after-hours or triage services, are
inadequate. Alternately, it may be a result of chance.
Apart from the situation in remote areas, the data indicates that utilization rates become
higher as the catchment population and availability of resources rises. The graph in
Figure 35 illustrates this trend very clearly. The explanation for the higher figures for
remote stations may lie in the dearth of other services, such as hospitals and general
practitioners.
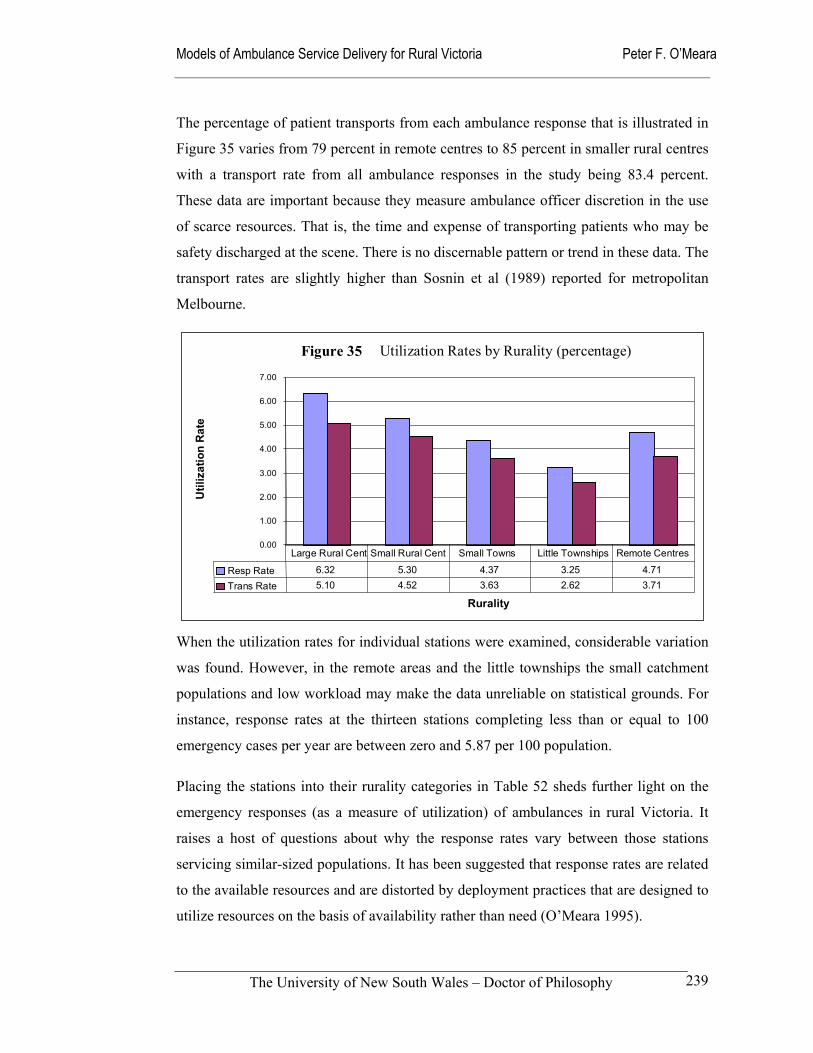
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
239
The percentage of patient transports from each ambulance response that is illustrated in
Figure 35 varies from 79 percent in remote centres to 85 percent in smaller rural centres
with a transport rate from all ambulance responses in the study being 83.4 percent.
These data are important because they measure ambulance officer discretion in the use
of scarce resources. That is, the time and expense of transporting patients who may be
safety discharged at the scene. There is no discernable pattern or trend in these data. The
transport rates are slightly higher than Sosnin et al (1989) reported for metropolitan
Melbourne.
When the utilization rates for individual stations were examined, considerable variation
was found. However, in the remote areas and the little townships the small catchment
populations and low workload may make the data unreliable on statistical grounds. For
instance, response rates at the thirteen stations completing less than or equal to 100
emergency cases per year are between zero and 5.87 per 100 population.
Placing the stations into their rurality categories in Table 52 sheds further light on the
emergency responses (as a measure of utilization) of ambulances in rural Victoria. It
raises a host of questions about why the response rates vary between those stations
servicing similar-sized populations. It has been suggested that response rates are related
to the available resources and are distorted by deployment practices that are designed to
utilize resources on the basis of availability rather than need (O’Meara 1995).
Figure 35 Utilization Rates by Rurality (percentage)
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
Rurality
Util
izat
ion
Rat
e
Resp Rate 6.32 5.30 4.37 3.25 4.71Trans Rate 5.10 4.52 3.63 2.62 3.71
Large Rural Cent Small Rural Cent Small Towns Little Townships Remote Centres
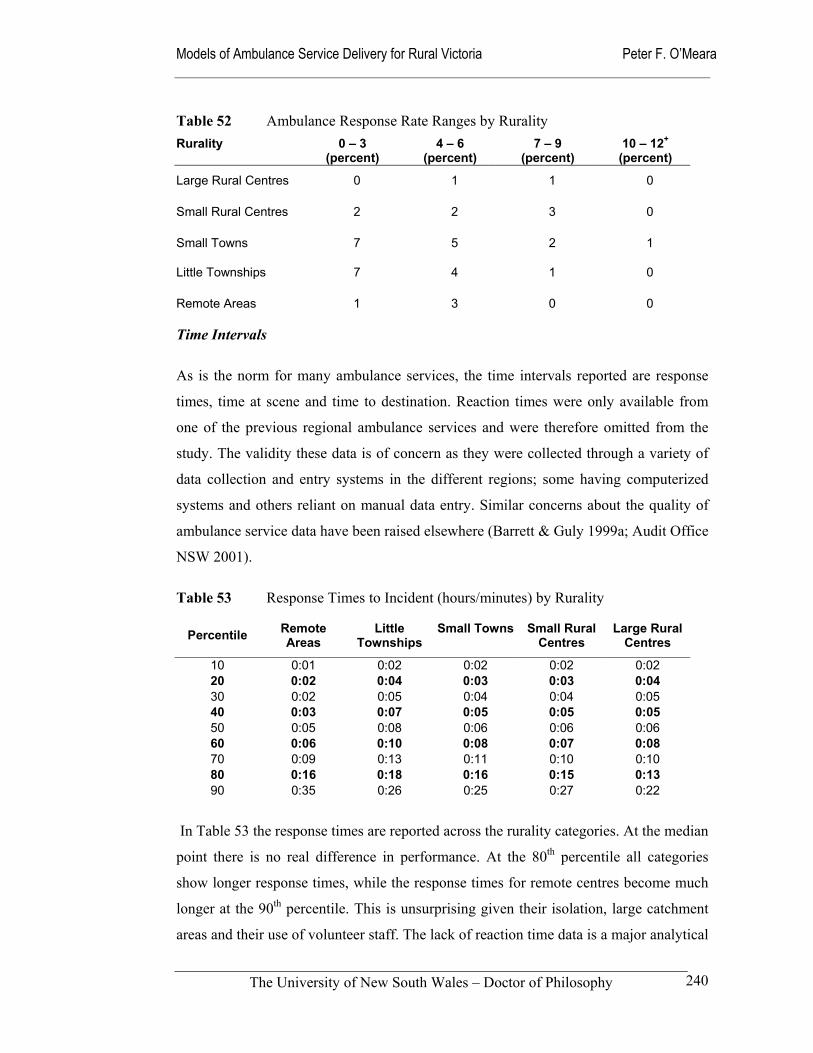
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
240
Table 52 Ambulance Response Rate Ranges by Rurality Rurality 0 – 3
(percent) 4 – 6
(percent) 7 – 9
(percent) 10 – 12+
(percent)
Large Rural Centres 0 1 1 0
Small Rural Centres 2 2 3 0
Small Towns 7 5 2 1
Little Townships 7 4 1 0
Remote Areas 1 3 0 0
Time Intervals
As is the norm for many ambulance services, the time intervals reported are response
times, time at scene and time to destination. Reaction times were only available from
one of the previous regional ambulance services and were therefore omitted from the
study. The validity these data is of concern as they were collected through a variety of
data collection and entry systems in the different regions; some having computerized
systems and others reliant on manual data entry. Similar concerns about the quality of
ambulance service data have been raised elsewhere (Barrett & Guly 1999a; Audit Office
NSW 2001).
Table 53 Response Times to Incident (hours/minutes) by Rurality
Percentile Remote
Areas Little
Townships Small Towns Small Rural
Centres Large Rural
Centres
10 0:01 0:02 0:02 0:02 0:02 20 0:02 0:04 0:03 0:03 0:04 30 0:02 0:05 0:04 0:04 0:05 40 0:03 0:07 0:05 0:05 0:05 50 0:05 0:08 0:06 0:06 0:06 60 0:06 0:10 0:08 0:07 0:08 70 0:09 0:13 0:11 0:10 0:10 80 0:16 0:18 0:16 0:15 0:13 90 0:35 0:26 0:25 0:27 0:22
In Table 53 the response times are reported across the rurality categories. At the median
point there is no real difference in performance. At the 80th percentile all categories
show longer response times, while the response times for remote centres become much
longer at the 90th percentile. This is unsurprising given their isolation, large catchment
areas and their use of volunteer staff. The lack of reaction time data is a major analytical
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
241
problem in the smaller areas and remote areas, as it disguises any potential problems of
on-call and volunteer crew activation. More complete data from fully computerized
dispatch systems may shed light on this question in the future.
Grouping the median response times according to rurality classifications produced no
meaningful insights. For instance, the eleven stations with median response times of
over eight minutes were found in four of the five categories. Small rural centres were
the exception. The lower performing stations had volunteer staff in some cases, in
others full-time staff and 24-hour shifts. The response rates of these poorly performing
stations ranged from 0.89 to 12.65 cases per 100 population. If reaction time data had
been available, they may have provided some useful findings.
Comparatively speaking, the median response times reported earlier in Table 48
compare well with other Australian ambulance services that range from six minutes in
the Australian Capital Territory to ten minutes in New South Wales and Tasmania. The
90th percentile response times rated poorly compared to response times of eleven to
twenty-two minutes reported elsewhere (SCRCSSP 2000: 875). RAV and NSW
ambulance service data supplied to the NSW Audit Office confirm that there is a
comparative problem with the 90th percentile response times in rural areas (Audit Office
NSW: 23).
The time at scene is particularly important in the case of trauma cases, with Danne et al
(1998) suggesting that scene times for trauma cases should be no more than 20 minutes
unless unforeseen events such as entrapment intervene. While Danne and McDermont et
al (1996) have examined road traffic fatalities in relation to at scene delays, little is
known about overall scene times. The Monash University School of Rural Health is
currently undertaking research to determine this information in a rural Victorian setting
(O’Meara and Boyle 2001). The already mentioned lack of clinical coding in the RAV
data made it impossible to distinguish between trauma and non-trauma cases in this
study. Table 54 shows that scene time for all emergency cases according to rurality are
not significantly different despite the large rural centres and small rural centres having
large numbers of MICA paramedics who would be expected to undertake a greater
number of invasive interventions than staff in the small towns and remote areas. As the
number of MICA paramedics rises even more in these larger stations, this situation may
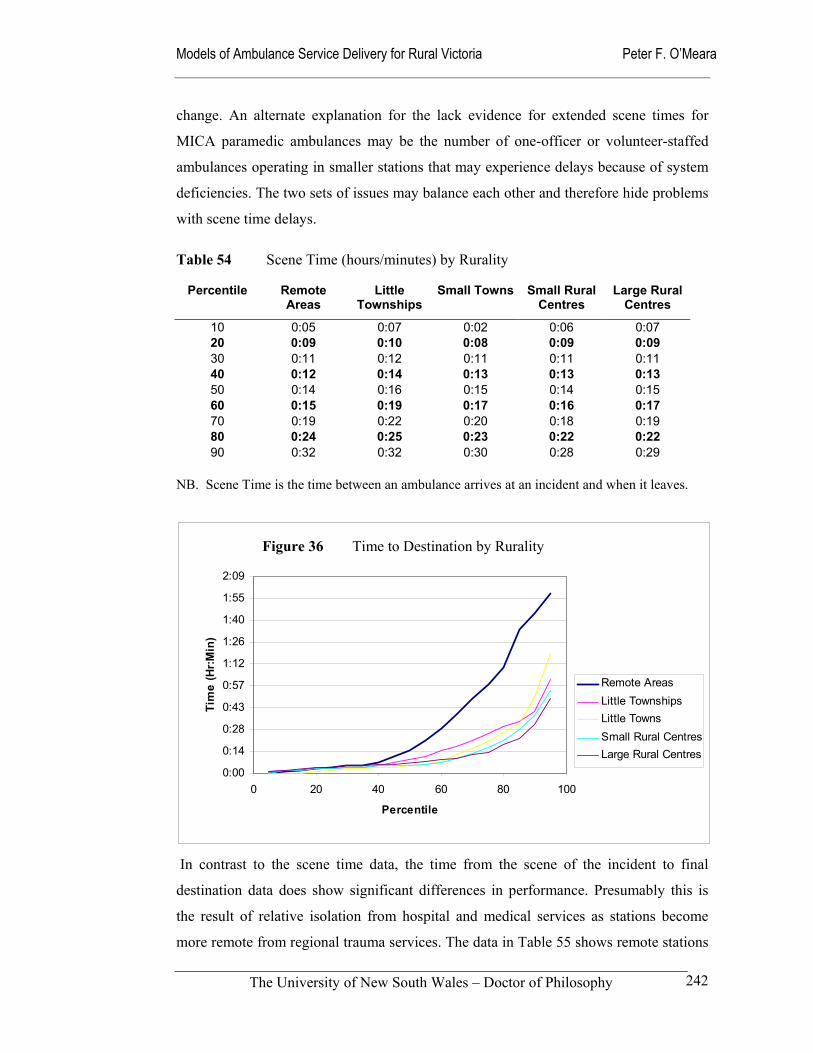
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
242
change. An alternate explanation for the lack evidence for extended scene times for
MICA paramedic ambulances may be the number of one-officer or volunteer-staffed
ambulances operating in smaller stations that may experience delays because of system
deficiencies. The two sets of issues may balance each other and therefore hide problems
with scene time delays.
Table 54 Scene Time (hours/minutes) by Rurality
Percentile Remote Areas
Little Townships
Small Towns Small Rural Centres
Large Rural Centres
10 0:05 0:07 0:02 0:06 0:07 20 0:09 0:10 0:08 0:09 0:09 30 0:11 0:12 0:11 0:11 0:11 40 0:12 0:14 0:13 0:13 0:13 50 0:14 0:16 0:15 0:14 0:15 60 0:15 0:19 0:17 0:16 0:17 70 0:19 0:22 0:20 0:18 0:19 80 0:24 0:25 0:23 0:22 0:22 90 0:32 0:32 0:30 0:28 0:29
NB. Scene Time is the time between an ambulance arrives at an incident and when it leaves.
In contrast to the scene time data, the time from the scene of the incident to final
destination data does show significant differences in performance. Presumably this is
the result of relative isolation from hospital and medical services as stations become
more remote from regional trauma services. The data in Table 55 shows remote stations
Figure 37 To Destination - Rurality
0:00
0:14
0:28
0:43
0:57
1:12
1:26
1:40
1:55
2:09
0 20 40 60 80 100
Percentile
Tim
e (H
r:Min
)
Remote AreasLittle TownshipsLittle TownsSmall Rural CentresLarge Rural Centres
Figure 36 Time to Destination by Rurality
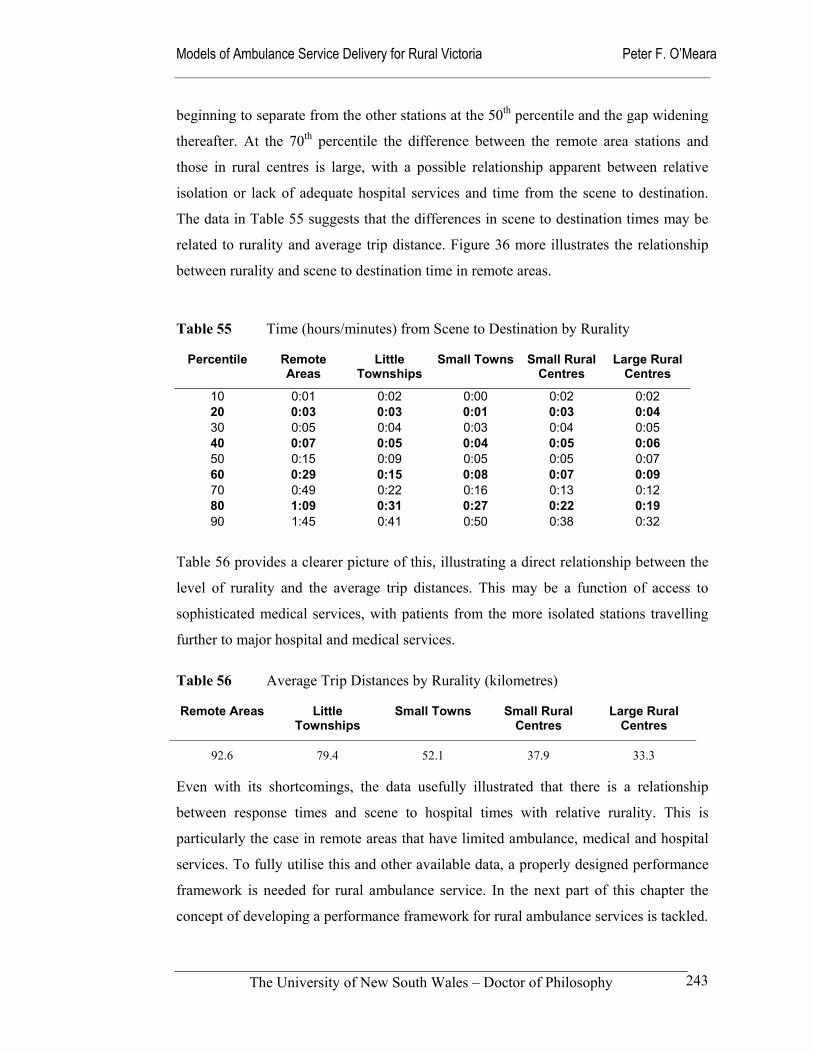
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
243
beginning to separate from the other stations at the 50th percentile and the gap widening
thereafter. At the 70th percentile the difference between the remote area stations and
those in rural centres is large, with a possible relationship apparent between relative
isolation or lack of adequate hospital services and time from the scene to destination.
The data in Table 55 suggests that the differences in scene to destination times may be
related to rurality and average trip distance. Figure 36 more illustrates the relationship
between rurality and scene to destination time in remote areas.
Table 55 Time (hours/minutes) from Scene to Destination by Rurality
Percentile Remote Areas
Little Townships
Small Towns Small Rural Centres
Large Rural Centres
10 0:01 0:02 0:00 0:02 0:02 20 0:03 0:03 0:01 0:03 0:04 30 0:05 0:04 0:03 0:04 0:05 40 0:07 0:05 0:04 0:05 0:06 50 0:15 0:09 0:05 0:05 0:07 60 0:29 0:15 0:08 0:07 0:09 70 0:49 0:22 0:16 0:13 0:12 80 1:09 0:31 0:27 0:22 0:19 90 1:45 0:41 0:50 0:38 0:32
Table 56 provides a clearer picture of this, illustrating a direct relationship between the
level of rurality and the average trip distances. This may be a function of access to
sophisticated medical services, with patients from the more isolated stations travelling
further to major hospital and medical services.
Table 56 Average Trip Distances by Rurality (kilometres)
Remote Areas Little Townships
Small Towns Small Rural Centres
Large Rural Centres
92.6 79.4 52.1 37.9 33.3
Even with its shortcomings, the data usefully illustrated that there is a relationship
between response times and scene to hospital times with relative rurality. This is
particularly the case in remote areas that have limited ambulance, medical and hospital
services. To fully utilise this and other available data, a properly designed performance
framework is needed for rural ambulance service. In the next part of this chapter the
concept of developing a performance framework for rural ambulance services is tackled.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
244
7.4 Performance framework
The terms ‘performance indicator’, performance measurement’, benchmark’ and benchmarking’ are often used interchangeably even though they deal with different but related concepts.
(NHMBWG 1998: 7)
Performance measurement can be defined as the process of collecting and collating
individual indicators. According to the National Health Ministers’ Benchmarking
Working Group, there are two types of health service performance indicators: health
resource indicators, such as those measuring labour force and expenditure; and health
service use or utilization (NHMBWG 1998: 14). Healthcare professionals and
researchers are likely to also consider other broad indicators such as effectiveness and
equity of importance (Duckett 1999; Hancock 1999; Humphreys & Matthews-Cowey
1999). In the United States, Aday (1998) suggests three main performance criteria:
equity, efficiency and effectiveness.
Performance reporting systems need to be directly aligned with organizational strategic
goals and focus on encouraging action by measuring the things that matter to
consumers, service providers, health care organizations and funders. For example, in
South Africa an attempt has been made to evaluate the operation of rural ambulance
services in regard to staff motivation and the allocation of resources (Doherty & Price
1998). Other important factors worthy of measurement may include the expectations of
stakeholders, described in Chapter 5 as:
Service availability;
Speed of response;
Competence and skills of staff;
Communication and teamwork with health and emergency services; and
Professional and ethical behaviour of staff.
Whatever the performance measure or benchmark is, performance indictors need to be
reliable, cost effective to collect, and easily understood (NHPC 2000). One of the
failings of ambulance performance measurement throughout the world is that it
generally draws upon a narrow band of performance indicators that are based on
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
245
availability rather than any coherent framework. It is for example, unlikely that any
single indicator such as the commonly used response times will adequately reflect the
overall performance of an ambulance service. While response times and other time
intervals are valuable in many ways, they fail to describe clinical processes or
outcomes. There is also the risk that over reliance on response times as a performance
indicator will distort management practices and the deployment of resources (Mahony
2001).
Specific performance indicators and benchmarks need to be examined in the context of
their economic, social and cultural environment. Understanding the reasons for
variations is an important part of the improvement process. “Used alone, indicators may
be ambiguous, and hide important differentials within populations and population
subgroups.” (NHMBWG 1998: 14) Another concern expressed, is that some pre-
hospital interventions may be ineffective and in some cases harmful, while current
performance indicators and associated research often provide little evidence either way
(Shapiro 2000; Pepe 2000; Guppy & Woollard 2000; Jacobs 2000).
The earlier findings in this chapter showed that that there are sometimes variations
between individual ambulance stations that cannot be explained without access to a
wider range of data and considerable analysis. These anomalies include structural,
process and outcome variations, such as in staffing levels, operational time intervals and
utilization rates. From these observations, some patterns are discernable. For example,
some of the variations appear to be related to the population-age profile of the
communities, their size and the availability of resources. To some degree, these factors
are all related to the rurality of communities.
Unfortunately, as in other Australian states, the regular banning of documentation as an
industrial relations weapon has also contributed toward shortcomings in performance
measurement (Audit Office NSW 2001: 26). Also contributing to the poor quality and
availability of data may be the lack of evaluation and research activities that regularly
use this information (Jacobs 2000; Woollard et al 2000). In short, there seems to be a
lack of a research culture within ambulance services. Staff may see little point in
conscientiously documenting information that is rarely used for anything other than the
preparation of transport accounts.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
246
Ambulance service managers, funders and regulators, and users require performance
measures that lead to improved outcomes. They want a performance management
system that assures availability, responsiveness, and quality patient care through the
effective and efficient use of resources. Development of a coherent performance
framework would capture the structural elements, service delivery processes, and
outcomes of the service delivery system. The desirability of having a structured and
considered approach to the measurement of performance in ambulance services is
consistent with a broader interest in measuring performance across the health system.
Driving this interest are concerns about expenditure constraints, demands for the
adoption of new technologies and rising consumer expectations (NHPC 2000).
Consumers and funding agencies have driven this trend for greater accountability from
providers of health and emergency services (Moore 1999). They want to be able to
assess performance against their expectations, policy goals and objectives.
Rural ambulance services, in common with their urban counterparts, have been
encouraged to develop performance measures that satisfy the need for improved
accountability and more effective and efficient operational management (Baragwanath
1997a; Baragwanath 1997b; Audit Office NSW 2001). In addition, quality improvement
strategies have demanded a means of identifying areas in which the quality and
responsiveness of service delivery can be improved through system changes (Sheldon
1998; McCoy 1997). These demands have placed ambulance services under pressure to
develop performance management and improvement processes. Unfortunately, there are
few validated indicators of effectiveness and quality in ambulance systems, and
therefore few universally accepted methods of measurement (Guppy 2000; Shapiro
2000). Considerable effort has been wasted developing, collecting and analysing
performance indicators that are irrelevant to system design, quality or effectiveness
(PIIC 1992). Alternately, performance indicators may not be readily measurable
because these data may be un-collectable or inaccurate. An example of the latter is the
skewed age distribution of patients found in this study as result of the large number of
patients recorded as being aged less than one year.
Within the ambulance sector various attempts have been made to grapple with the
challenge of providing emergency care in terms of access, quality and cost as a triad;
Asplin (1997) has suggested that achieving all three may be impossible. Managing the

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
247
balance between these elements of an ambulance system is a challenge that ambulance
services face in rural Australia. While Aday’s three objectives of equity, efficiency and
effectiveness can be complementary, the conflict between them is particularly acute in
rural ambulance services where the combination of sparse populations, long distances to
definitive care and workforce limitations exacerbate any system problems. Reflecting
Asplin’s dilemma, a key question for decision-makers is the degree to which each can
be traded off or sacrificed to achieve the other (Aday 1998). Unless they are measured
in some way, these decisions are made without any valid rationale.
The measurement of performance in rural ambulance services has been adhoc, and has
often failed the test of being specific, measurable, action-orientated, relevant, and timely
(Moore 1999). There has been a concentration on easily collectable time intervals of
dubious accuracy, while there is little accessible information on clinical matters. The
associated questioning of the value of many pre-hospital interventions has stimulated
interest in developing measurable outcomes that go beyond mortality measures (Maio
1999).
Potential performance frameworks
In the general Australian health services literature, Duckett (1999) provides a
performance framework for the Australian health care system based on the criteria of
equity, efficiency and acceptability. Duckett includes effectiveness as part and parcel of
efficiency. The National Report on Health Sector Performance Indicators adopts
effectiveness and efficiency as its basic building blocks, it defines effectiveness as
quality, appropriateness and accessibility and equity (NHMBWG 1998: 8).
An American, Morrissey (1997) describes the general requisites for effective provision
of health services as accessibility, flexibility and integration. The concept of
accessibility should see an acceptable and affordable service based on population needs.
Flexibility refers to the service delivery models ability to address specific service needs,
while integration is concerned with a service model’s place within a coordinated
framework of service. Back in Australia, Hancock (1999) suggests evaluation criteria
for health services that have analytical signposts that highlight the ten areas of:
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
248
Access and affordability Quality of care
Social equity and social justice Public interest accountability
Democratic participation and openness of decision-making
Effective healthcare treatment and care
Longer-term sustainability Respect for patient autonomy
Economic efficiency A rights-based framework for decision-making
In the rural context, Humphreys and Mathews-Cowey (1999) provide an alternative way
of evaluating the effectiveness and sustainability of health services in rural Australia.
They propose that service delivery models be evaluated with respect to seven key
considerations:
Level of service that can be realistically provided
Availability and accessibility when required
Appropriateness of services
Role delineation of health workers
Educational & training needs of health workers
Needs for co-ordination between health workers
Need for collaboration among services providing services
(Humphreys & Mathews-Cowey 1999)
Probably the most comprehensive work in Australia on performance frameworks is that
of the National Health Performance Committee, which has developed a comprehensive
four-part national performance framework that looks at: health outcomes; determinants
of health; health system performance; and health system infrastructure and community
capacity (NHPC 2000).
Its eight-point performance framework for the health system, summarized in Table 57,
has been largely derived from the Canadian Health Indicators Framework and the work
undertaken in the National health Service (NHS) in the United Kingdom where a three
part strategy to improve performance has been put into place. As part of this process in
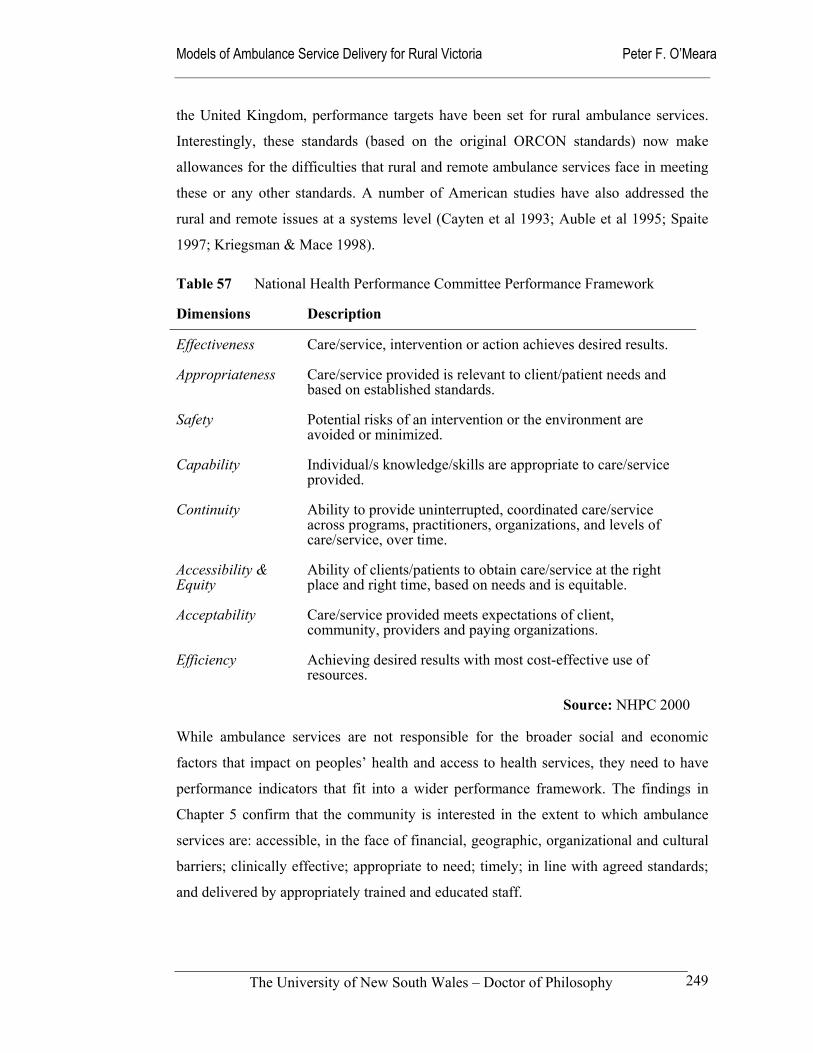
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
249
the United Kingdom, performance targets have been set for rural ambulance services.
Interestingly, these standards (based on the original ORCON standards) now make
allowances for the difficulties that rural and remote ambulance services face in meeting
these or any other standards. A number of American studies have also addressed the
rural and remote issues at a systems level (Cayten et al 1993; Auble et al 1995; Spaite
1997; Kriegsman & Mace 1998).
Table 57 National Health Performance Committee Performance Framework
Dimensions Description
Effectiveness Care/service, intervention or action achieves desired results.
Appropriateness Care/service provided is relevant to client/patient needs and based on established standards.
Safety Potential risks of an intervention or the environment are avoided or minimized.
Capability Individual/s knowledge/skills are appropriate to care/service provided.
Continuity Ability to provide uninterrupted, coordinated care/service across programs, practitioners, organizations, and levels of care/service, over time.
Accessibility & Equity
Ability of clients/patients to obtain care/service at the right place and right time, based on needs and is equitable.
Acceptability Care/service provided meets expectations of client, community, providers and paying organizations.
Efficiency Achieving desired results with most cost-effective use of resources.
Source: NHPC 2000
While ambulance services are not responsible for the broader social and economic
factors that impact on peoples’ health and access to health services, they need to have
performance indicators that fit into a wider performance framework. The findings in
Chapter 5 confirm that the community is interested in the extent to which ambulance
services are: accessible, in the face of financial, geographic, organizational and cultural
barriers; clinically effective; appropriate to need; timely; in line with agreed standards;
and delivered by appropriately trained and educated staff.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
250
A way forward
Drawing from a now inappropriate emergency services model, response times have
tended to be used as a proxy for effective ambulance service performance (Harvey
1999; Narad & Driesbock 1999; SCRCSSP 2000). Aside from the importance of
responding quickly to cardiac arrests and similar time critical incidents, the centrality of
response times as a performance indicator is rather fragile with little empirical evidence
supporting their relevance to a wider range of incidents. The clinical, cultural and
political reality is that there are other important performance criteria that are valued in
local ambulance services, even if they are not so easily quantified.
To better reflect this situation, ambulance services need a coherent performance
framework in which their evaluation and research activities can be placed. This level of
evaluation, which moves beyond response times and other similar time intervals, has not
been apparent in Victoria’s ambulance services. While the traditional quantitative
measures of performance will always remain important, it is time to move toward both
outcome orientated measures of performance and a range of more holistic performance
measures that account for factors such as integration with other health services and
community engagement. Moore (1999) has suggested ten useful criteria for EMS
system performance measures:
Should be structure-, process-, and outcome-orientated
Designed for ease in data collection
Able to measure quality and effectiveness of various system components
Adjustable for system demographics
Practical and relevant Continuously evaluated for relevance
Based on scientific evidence when possible
Accompanied by explicit instructions for consistency in use and interpretation
Subject to ongoing review Reproducible, precisely defined, and specific to ensure uniform application
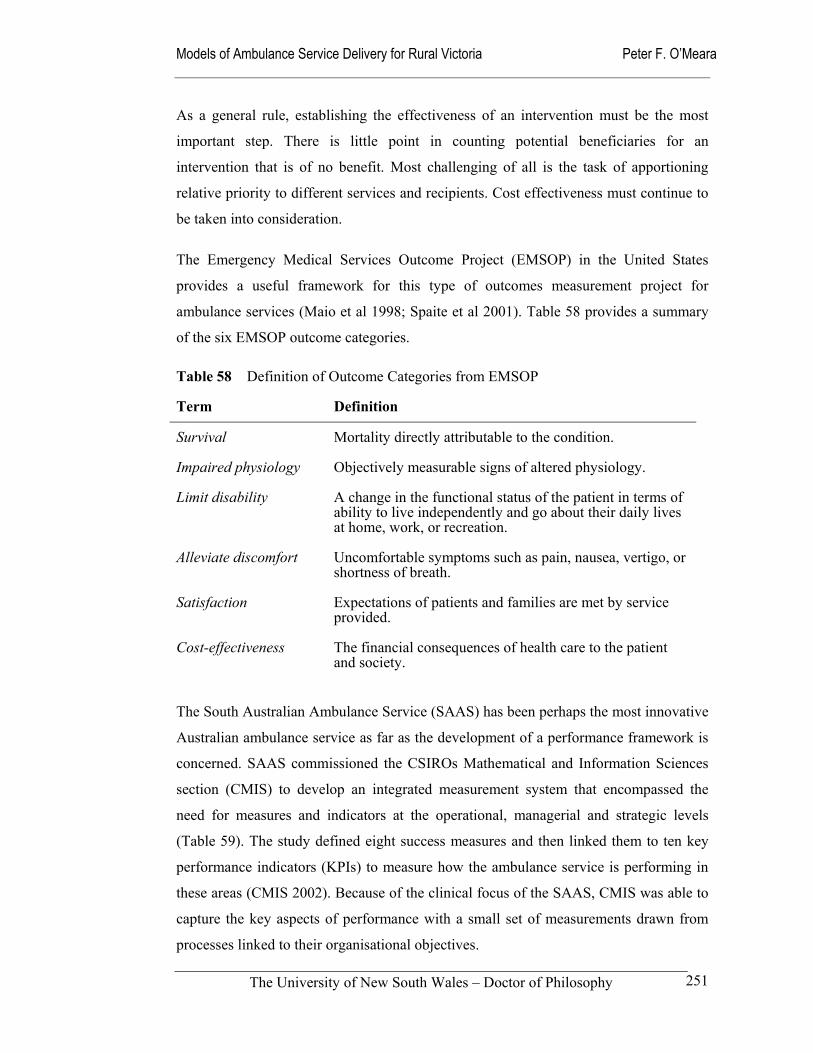
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
251
As a general rule, establishing the effectiveness of an intervention must be the most
important step. There is little point in counting potential beneficiaries for an
intervention that is of no benefit. Most challenging of all is the task of apportioning
relative priority to different services and recipients. Cost effectiveness must continue to
be taken into consideration.
The Emergency Medical Services Outcome Project (EMSOP) in the United States
provides a useful framework for this type of outcomes measurement project for
ambulance services (Maio et al 1998; Spaite et al 2001). Table 58 provides a summary
of the six EMSOP outcome categories.
Table 58 Definition of Outcome Categories from EMSOP
Term Definition
Survival Mortality directly attributable to the condition.
Impaired physiology Objectively measurable signs of altered physiology.
Limit disability A change in the functional status of the patient in terms of ability to live independently and go about their daily lives at home, work, or recreation.
Alleviate discomfort Uncomfortable symptoms such as pain, nausea, vertigo, or shortness of breath.
Satisfaction Expectations of patients and families are met by service provided.
Cost-effectiveness The financial consequences of health care to the patient and society.
The South Australian Ambulance Service (SAAS) has been perhaps the most innovative
Australian ambulance service as far as the development of a performance framework is
concerned. SAAS commissioned the CSIROs Mathematical and Information Sciences
section (CMIS) to develop an integrated measurement system that encompassed the
need for measures and indicators at the operational, managerial and strategic levels
(Table 59). The study defined eight success measures and then linked them to ten key
performance indicators (KPIs) to measure how the ambulance service is performing in
these areas (CMIS 2002). Because of the clinical focus of the SAAS, CMIS was able to
capture the key aspects of performance with a small set of measurements drawn from
processes linked to their organisational objectives.
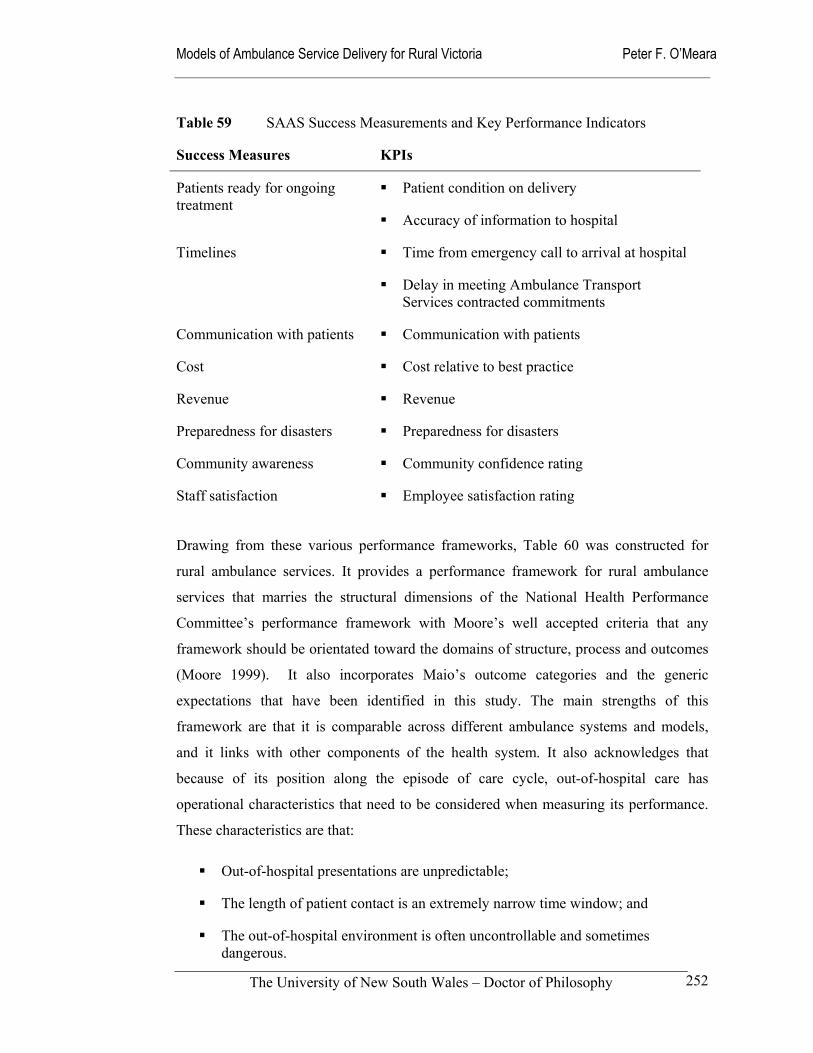
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
252
Table 59 SAAS Success Measurements and Key Performance Indicators
Success Measures KPIs
Patients ready for ongoing treatment
Patient condition on delivery
Accuracy of information to hospital
Timelines Time from emergency call to arrival at hospital
Delay in meeting Ambulance Transport Services contracted commitments
Communication with patients Communication with patients
Cost Cost relative to best practice
Revenue Revenue
Preparedness for disasters Preparedness for disasters
Community awareness Community confidence rating
Staff satisfaction Employee satisfaction rating
Drawing from these various performance frameworks, Table 60 was constructed for
rural ambulance services. It provides a performance framework for rural ambulance
services that marries the structural dimensions of the National Health Performance
Committee’s performance framework with Moore’s well accepted criteria that any
framework should be orientated toward the domains of structure, process and outcomes
(Moore 1999). It also incorporates Maio’s outcome categories and the generic
expectations that have been identified in this study. The main strengths of this
framework are that it is comparable across different ambulance systems and models,
and it links with other components of the health system. It also acknowledges that
because of its position along the episode of care cycle, out-of-hospital care has
operational characteristics that need to be considered when measuring its performance.
These characteristics are that:
Out-of-hospital presentations are unpredictable;
The length of patient contact is an extremely narrow time window; and
The out-of-hospital environment is often uncontrollable and sometimes dangerous.
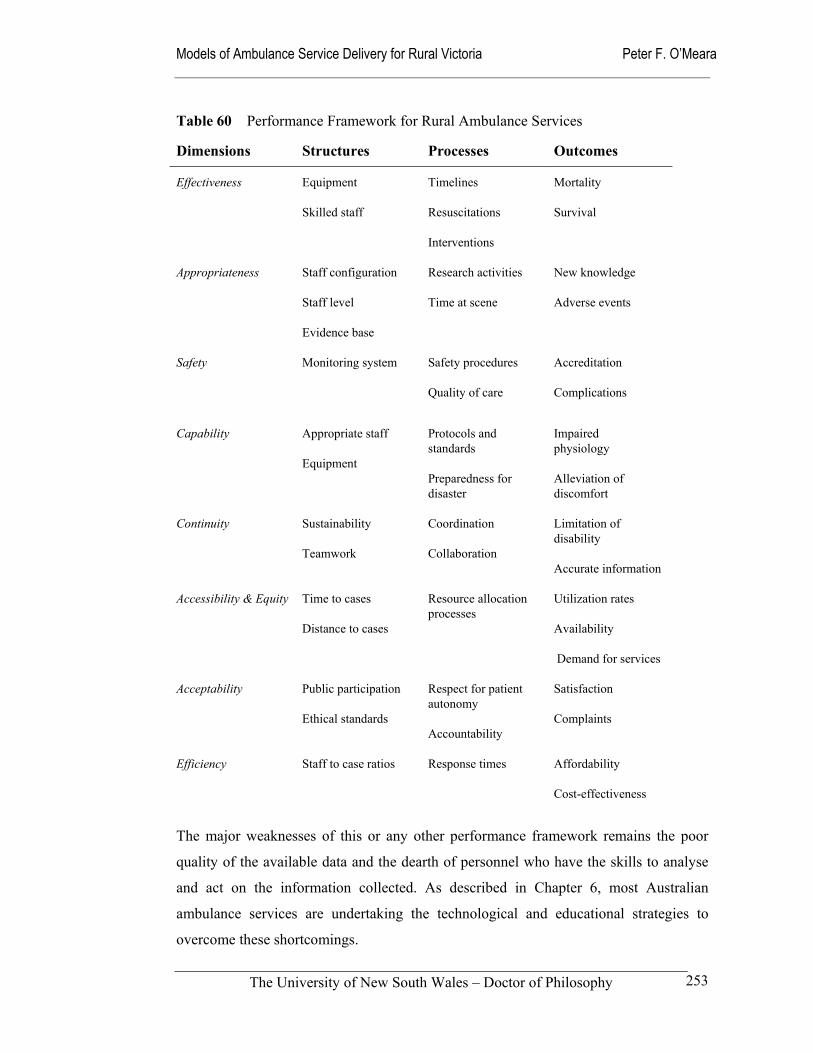
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
253
Table 60 Performance Framework for Rural Ambulance Services
Dimensions Structures Processes Outcomes
Effectiveness Equipment
Skilled staff
Timelines
Resuscitations
Interventions
Mortality
Survival
Appropriateness Staff configuration
Staff level
Evidence base
Research activities
Time at scene
New knowledge
Adverse events
Safety Monitoring system Safety procedures
Quality of care
Accreditation
Complications
Capability Appropriate staff
Equipment
Protocols and standards
Preparedness for disaster
Impaired physiology
Alleviation of discomfort
Continuity Sustainability
Teamwork
Coordination
Collaboration
Limitation of disability
Accurate information
Accessibility & Equity Time to cases
Distance to cases
Resource allocation processes
Utilization rates
Availability
Demand for services
Acceptability Public participation
Ethical standards
Respect for patient autonomy
Accountability
Satisfaction
Complaints
Efficiency Staff to case ratios Response times Affordability
Cost-effectiveness
The major weaknesses of this or any other performance framework remains the poor
quality of the available data and the dearth of personnel who have the skills to analyse
and act on the information collected. As described in Chapter 6, most Australian
ambulance services are undertaking the technological and educational strategies to
overcome these shortcomings.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
254
An important issue that needs to be considered when introducing a performance
framework is whether performance monitoring is an internal or external activity. In both
Victoria and New South Wales, most of the publicly available information about
ambulance service operations and management have come via Auditor General and
parliamentary inquiry reports. Nationally, the major source of information comes from
the Commonwealth Steering Committee for the Review of Commonwealth/State
Service Provision. These accountability mechanisms provide an excellent source of
comparative data and analysis, which can have a continuing role for funders and the
community at large. However, it is also vital that ambulance services themselves
develop and use performance measurement activities at the strategic, managerial and
operational levels. In this way, the confidence of internal and external stakeholders in
the ambulance service will be maintained and enhanced.
Apart from the inherent characteristics of
the out-of-hospital environment already
mentioned, a number of other
epidemiological issues need to be
considered when adopting a performance
framework. Firstly, the population’s ability
to benefit from health care equals the
aggregate of individuals’ ability to benefit.
For most health problems this can be
deduced more readily from epidemiological data than from clinical records. One
characteristic of ambulance services’ clinical review mechanisms has been their
concentration on individual patient care. There has been little use made of existing
databases to establish overall trends in demand for specific clinical conditions or
efficacy of particular interventions.
Secondly, the ability to benefit does not mean that every outcome will be favourable,
but rather that need implies potential benefit, which is on average effective. At times,
ambulance services in Victoria have been the target of strong criticism in the media
when individual interventions fail, with the result that they have sometimes made
reactive decisions in response to media hype and political pressure.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
255
Thirdly, the benefit of pre-hospital interventions is not just a change in clinical status
but can include reassurance, supportive care, and the relief of carers. The list of
beneficiaries of care can extend beyond the patient to families and carers. In recent
years ambulance services and state and territory health authorities may have ignored
these more holistic performance criteria in favour of the more concrete outcomes such
as response times and resuscitation successes. The pre-hospital research literature is also
open to the same criticism, as it also concentrates on the more easily measurable
outcomes.
Finally, health care includes not just treatment but also prevention, diagnosis,
continuing care, rehabilitation, and palliative care. In the United States, Neely et al
(1997) have made the suggestion that the role of Emergency Medical Services may
change from what they describe as a single-option decision response to a multiple-
option (MODP) model. In this option, EMS systems direct callers and patients to other
appropriate resources though what they describe as ‘pathway management’. Similar
suggestions have been made in the United Kingdom. These suggestions are explored in
the next chapter looking at different models of ambulance service delivery for rural
Victoria.
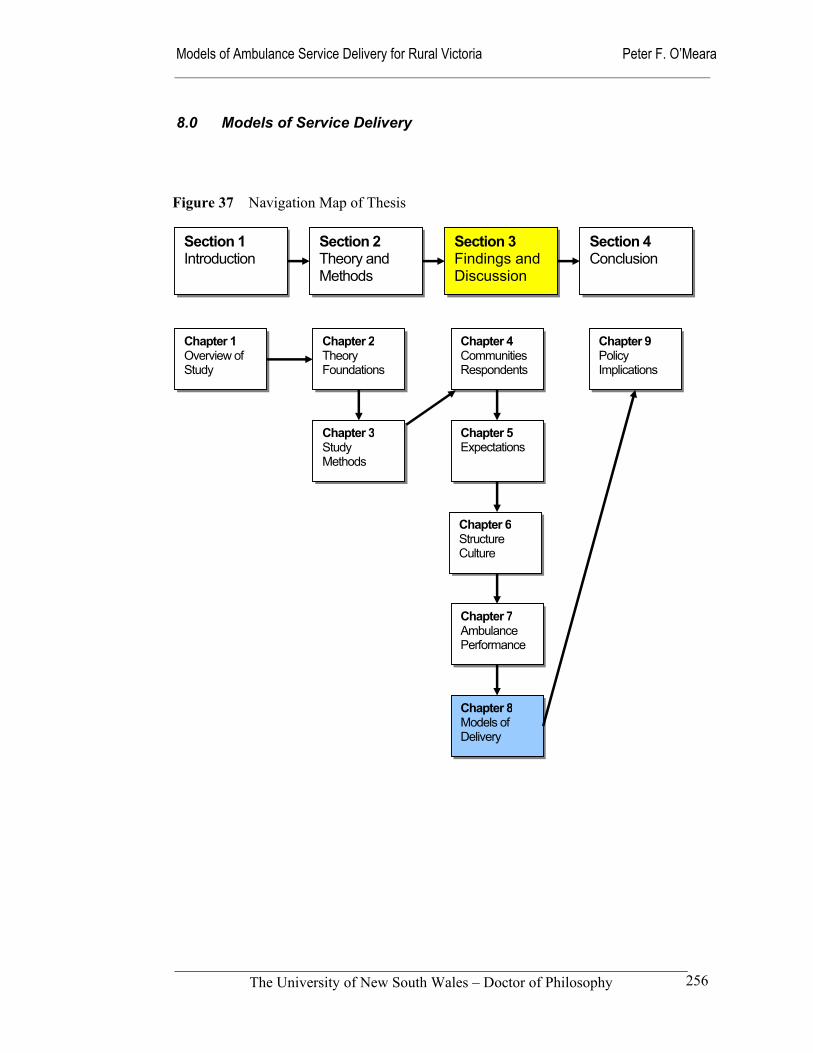
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
256
8.0 Models of Service Delivery
Section 1 Introduction
Section 2 Theory and Methods
Section 3 Findings and Discussion
Section 4 Conclusion
Chapter 1 Overview of Study
Chapter 2Theory Foundations
Chapter 4Communities Respondents
Chapter 5Expectations
Chapter 6Structure Culture
Chapter 7Ambulance Performance
Chapter 8Models of Delivery
Chapter 9 Policy Implications
Chapter 3Study Methods
Figure 37 Navigation Map of Thesis
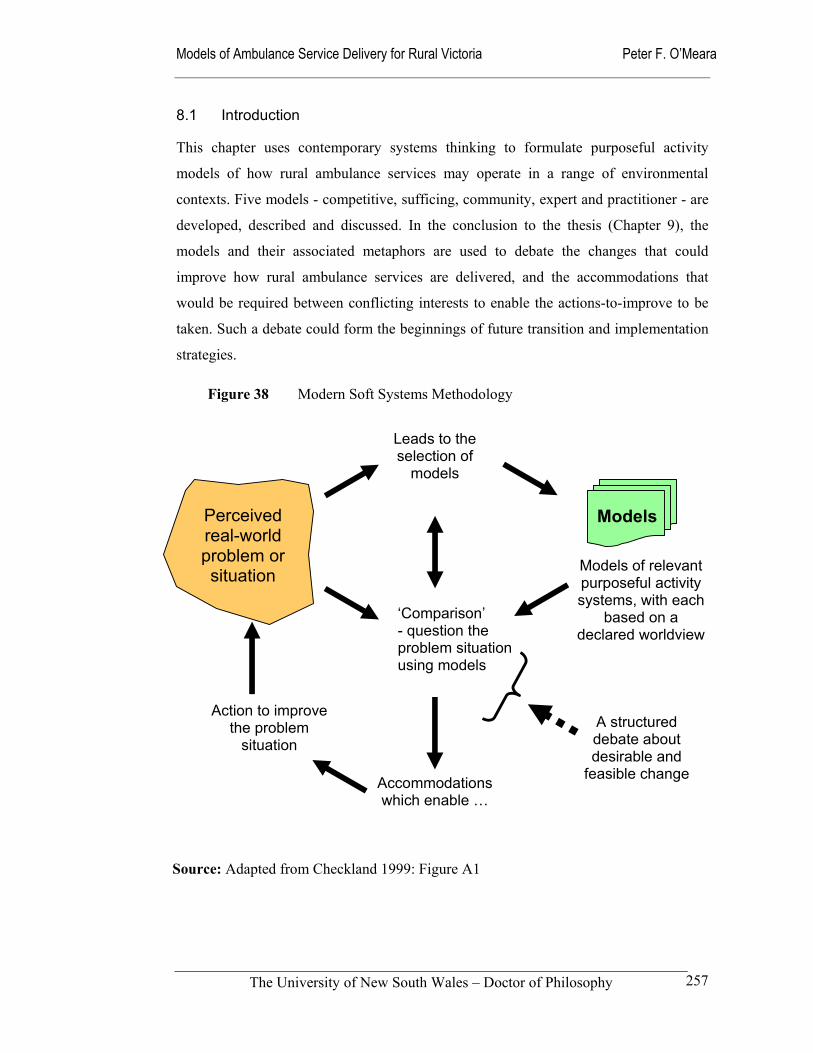
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
257
8.1 Introduction
This chapter uses contemporary systems thinking to formulate purposeful activity
models of how rural ambulance services may operate in a range of environmental
contexts. Five models - competitive, sufficing, community, expert and practitioner - are
developed, described and discussed. In the conclusion to the thesis (Chapter 9), the
models and their associated metaphors are used to debate the changes that could
improve how rural ambulance services are delivered, and the accommodations that
would be required between conflicting interests to enable the actions-to-improve to be
taken. Such a debate could form the beginnings of future transition and implementation
strategies.
Figure 38 Modern Soft Systems Methodology
Leads to the selection of
models
A structured debate about desirable and
feasible change Accommodations
which enable …
‘Comparison’ - question the problem situation using models
Action to improve
the problem situation
Perceived real-world problem or situation
Models
Models of relevant purposeful activity systems, with each
based on a declared worldview
Source: Adapted from Checkland 1999: Figure A1
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
258
A systems approach, namely SSM, was used to make sense of these data collected
because of its ability to deal with ill-structured or messy-problem contexts (Checkland
1999). This research approach was useful because it allowed an exploration of a
diversity of viewpoints as part of the decision-making and intervention process (Flood
& Jackson 1991). The significant advantage of this systems approach over classical
management approaches is its ability to take account of both the logic and the broader
cultural context of rural Australia. It incorporates mechanisms that allow for continuous
feedback loops between what is described as the ‘logic-based stream of analysis’ and
the ‘stream of cultural analysis’ (Checkland & Scholes 1990). These approaches have
been refined to a point where the two modes are integrated with each other and
constitute a non-linear process that is illustrated in Figure 38.
Model Building
At a practical level, the SSM model-building process is an iterative process that
incorporates four main stages:
i the selection of relevant systems;
ii the naming or describing of them;
iii their modelling; and
iv their comparison with real-world situations.
In the first instance, the identification of the tasks and issues associated with the
operation of rural ambulance services was a key research activity. It provided the
reasons for pursuing the research and the development of alternate approaches to the
provision of emergency ambulance services in rural Victoria.
The empirical research consisted of a review of the literature, collection of operational
and demographic data, and investigation of the cultural and political context. It included
both quantitative and qualitative information drawn from existing data sets and the
collection of ‘rich data’ through the use of questionnaires and interviews that have been
described in Chapter 3. Local community and professional experiences and satisfaction
levels were obtained from questionnaires. The policy responses of rural ambulance
services were obtained from documentation and directly through the conduct of a focus
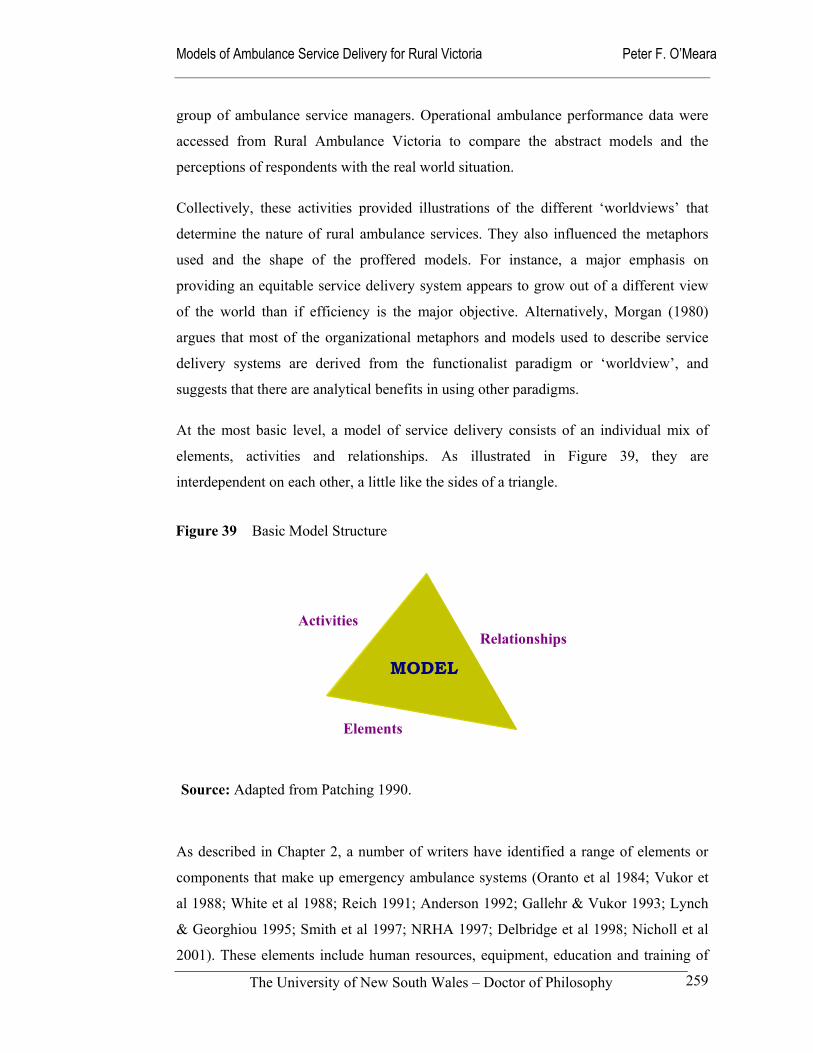
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
259
group of ambulance service managers. Operational ambulance performance data were
accessed from Rural Ambulance Victoria to compare the abstract models and the
perceptions of respondents with the real world situation.
Collectively, these activities provided illustrations of the different ‘worldviews’ that
determine the nature of rural ambulance services. They also influenced the metaphors
used and the shape of the proffered models. For instance, a major emphasis on
providing an equitable service delivery system appears to grow out of a different view
of the world than if efficiency is the major objective. Alternatively, Morgan (1980)
argues that most of the organizational metaphors and models used to describe service
delivery systems are derived from the functionalist paradigm or ‘worldview’, and
suggests that there are analytical benefits in using other paradigms.
At the most basic level, a model of service delivery consists of an individual mix of
elements, activities and relationships. As illustrated in Figure 39, they are
interdependent on each other, a little like the sides of a triangle.
As described in Chapter 2, a number of writers have identified a range of elements or
components that make up emergency ambulance systems (Oranto et al 1984; Vukor et
al 1988; White et al 1988; Reich 1991; Anderson 1992; Gallehr & Vukor 1993; Lynch
& Georghiou 1995; Smith et al 1997; NRHA 1997; Delbridge et al 1998; Nicholl et al
2001). These elements include human resources, equipment, education and training of
Figure 39 Basic Model Structure
Elements
Activities Relationships
MODEL
Source: Adapted from Patching 1990.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
260
staff, medical input, research, communication systems and planning. The list of
elements making up an ambulance service delivery model is hard to limit in any
meaningful sense. Partly, this is the result of the elements themselves being so disparate,
with some relating to the environment, others to personnel or infrastructure.
SSM and its related concepts provided a means of structuring these elements and the
relationships between them into meaningful metaphors and pictures that can be
understood for the purposes of analysis. The activities of a model describe how the
combination of the elements and relationships work together to achieve outputs in the
form of a service delivery model. These may include public education, disaster
planning, dispatch, clinical care and transport. Together they form the transformation
processes of each model of service delivery.
As useful as this approach was, it needs to be remembered that the systems and models
described and examined here are abstractions, with actual service delivery models being
more messy and imperfect. They do not always achieve their objectives when facing the
uncertainty and pressures of reality. Observation of the real world, illustrates that real
service delivery models may be amalgams of the difference models in response to their
local contexts.
Following the selection of relevant systems, the next component in the development of
purposeful models was to name the systems. In SSM, the names of the systems are
known as ‘root definitions’; they express the core or essence of the perception to be
modelled. That core purpose is always expressed as a transformation process in which
some entity is changed into some new form of that same entity according to a particular
‘worldview’ (Checkland & Scholes 1990: 33). The mnemonic used to formulate ‘root
definitions’ is CATWOE, which has already been described in Chapter 3. Each ‘root
definition’ describes what the model is setting out to achieve, how it is done and by
whom. That is, it is a system to do X by Y in order to achieve Z, where T will be the
means. The transformation process (T) describes the activities used to achieve the
objective, without the ‘clutter’ of describing the customers, actors (providers), the
owners, or the environmental constraints that are addressed separately within the
mnemonic.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
261
The five models were modelled using metaphors and pictures based on their root
definitions. Activity models were assembled that identified the activities required to
obtain the desired input, and its transformation into the desired output. This initially
resulted in drawings resembling flowcharts that in the language of SSM are called
‘holons’; these drawings describe the elements, relationships and activities existing
within the system (Hindle et al 1995). To make the models comprehensible to a wider
audience, each model is also presented as metaphors and ‘rich pictures’. This removed
much of the SSM jargon and allowed a free-hand approach to be taken when describing
the models.
Comparison with the real world, or reality testing, is the final component of the
purposeful activity development process. This step was undertaken in terms of the
elements of ambulance systems and the relationships between them. It drew on the
findings in Chapters 5 to 7 and inferred probable outcomes for each model. The
transformation processes or activities of each model are described in more detail in an
effort to provide a sense of how each model might operate in the real world; this is in
the form of ‘transformation processes’ and ‘patient pathways’.
However, it was appreciated throughout the model formulation process that the
sequential flow of activities is often little more than a logical demonstration of how
activities may interact. The reality is more likely to be made up of activities that occur
in random sequences depending on circumstances or chance. When comparing the
models, it is important to remember that each of the models is distinct and may not
necessarily be pursuing the same objectives. The contexts in which they may operate are
certainly different. For example, the survival rates of cardiac arrest patients may be the
key performance criteria for one model; while in contrast another model may be more
concerned with supplying a two-officer response within 30 minutes for all members of
the population. It is therefore important that any direct comparisons be validated and not
applied inappropriately.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
262
Linkages with Stakeholder Expectations
During the modelling stage, each of the models was tested against the generic
expectations or standards identified in Chapter 5, along with any other expectations
specific to each model. These stakeholder expectations that are looked for in rural
ambulance services are:
i. Accessibility
This involves the population served being able to contact the ambulance service easily
and reliably, request assistance and have their needs met. This calls for reliable
communications systems, availability of staff and equipment and some degree of
allocative efficiency within the catchment area. Supporting the provision of these
physical resources is an appropriate financial base and effective management systems.
ii Responsiveness
Rural people, institutions and insurers all expect ambulance services to respond quickly
and appropriately to emergency calls for assistance. While their expectations of what
constitutes an appropriate response in terms of time and level of response may vary, the
general value of responsiveness is universal.
iii Competency
Ambulance providers at the organizational and personal levels are expected to be
competent. From a legal standpoint, individual providers in the chain of care are
expected to perform at the standard of care expected for each individual’s level of
training (Plueckhahn 1983: 70-76). For instance, an ambulance officer trained at a basic
life support standard is not expected to perform as an officer trained at an advanced life
support level. Those trained at tertiary educational institutions and accredited through
registration mechanisms have even higher expectations placed on them.
iv Communication and Teamwork
This describes the ability and willingness of the ambulance service and its staff to work
with other members of the health and emergency service systems. In rural areas, the
crucial relationships are between ambulance officers, general practitioners and nurses.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
263
Having adequate information technology and radio communications are important
elements of effective communication and teamwork with kindred organizations.
v Ethical Behaviour
The basic ethical expectations of ambulance paramedics are consistent across all skill
levels whether they are volunteers trained at the level of a first-aider, or as an advanced
health professional undertaking highly invasive clinical procedures. Two examples of
the day-to-day ethical issues that ambulance paramedics face are ensuring that consent
to treatment and transport is obtained, and maintaining appropriate patient
confidentiality without compromising the safety of third parties (Plueckhahn 1983: 76-
86).
Overview of the Models Developed
The remainder of this Chapter develops and describes five alternate rural models of
ambulance service delivery in terms of their ‘worldviews’. Applying SSM principles,
metaphors, holons and rich pictures are as used as descriptive and analytical devices,
and critical path analysis is used to explore each models transformation processes. The
five models developed through the research process are: competitive; sufficing;
community; expert; and practitioner. Each is described here to provide an overview.
Competitive Model
This model is based on the recognition that the dominant ideological paradigm for the
previous Victorian state government was that espoused in the National Competition
Policy. It allows for the regulatory and purchasing roles to be separated from the
provider role, which can be provided through either the public or private sector. The
major risk to rural communities from the competitive model is market failure. For
instance, small or isolated communities may have insufficient catchment population to
ensure financial survival for the provider. This model’s reliance on population-ecology
theory puts weaker or more vulnerable communities at risk of being unable to sustain
their services.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
264
Sufficing Model
This model provides a minimum level of service as a ‘safety-net’ on the basis that all
citizens are entitled to basic services irrespective of socio-economic status, demographic
profile, or place of residence. It treats the provision of ambulance services as a ‘public
good’. The risk with this model is that it may fail to encourage ‘best practice’ systems
due to the lack of financial, community or professional incentives. Its critics also claim
that it is susceptible to ‘union capture’ with the domination of a conflict-driven culture
(Allen Consulting 1999).
Community Model
Under this model the community itself takes responsibility for the provision of
emergency pre-hospital care. This may be through the activation of health professionals
or community volunteers, who provide a viable service with or without active
government support. This ‘bottom up’ characteristic of the model makes it a strong and
resilient model in communities that are strong. However, it lacks strong professional
linkages between local ambulance personnel and those practicing elsewhere. Staff
working in this model may be volunteers, who often lack professional training and
education. As a result, there may be a lack of professional support for volunteer staff in
the same way that career paramedics are supported. Because of this weakness, the
community model needs strong standards frameworks built into it, with strong medical
audit mechanisms.
Expert Model
The expert model is characterized by the employment of full-time, professionally
trained personnel who have access to the latest bio-medical equipment and who practice
a high level of clinical intervention. This model is very expensive to establish and
maintain due to the level of technology required and its extensive education and training
needs. Ambulance service managers are also faced with the challenge of managing a
highly skilled and motivated workforce. There is a risk that the professional ambulance
paramedics may adopt a paternalistic attitude to the community and other health
workers, with the result that they could become estranged from the wider community
and health system.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
265
Practitioner Model
The practitioner model is flexible and provides either an emergency ‘safety-net’ system
or an advanced clinical care system, responding to emergency needs, combined with an
integrated public health role that is closely linked to the broader health system.
Ambulance officers and paramedics have a key role in promoting healthy lifestyles, and
preventing death and injury through public education programs. The two distinctive
characteristics of the practitioner model are the existence of a research and development
agenda, and the multiple decision-points that exist during the cycle of care. The
practitioner model has the potential to be more cost-effective than the expert model,
while providing an appropriate level of clinical care for any given community. It is
particularly suited to rural areas with high ambulance ‘down-time’ and a dearth of
public health workers. It also offers the possibility of multi-skilling health professionals.
Locating the Models of Service Delivery within Paradigms and Systems
The models developed tend toward two descriptions; they are either ‘primary task’
models that map existing organizational structures, or ‘issue-based’ models that move
into the informal structures that cut across organizational boundaries (Checkland 1999:
A21-A22). In Australia, there is a general consensus about the basic task of emergency
ambulance systems, which is reflected in organizational objectives and international
benchmarks. Examples of this are, the objectives of Rural Ambulance Victoria (RAV)
as set out in the amended Ambulance Services Act 1986: it explicitly addresses rapid
response, the provision of clinical care and transport.
It is less clear that other less empirical issues are as well understood or appreciated. For
example, an omission from RAV’s objectives is any explicit notion that the community
should have any say in determining the nature of the services provided or how
sometimes conflicting issues of expectations, and needs and efficiency are to be
managed. As already reported in Chapter 6, RAV has acknowledged the importance of
community input through the formation of a community reference group from members
of the public in rural Victoria (RAV 2000a). It is yet to be seen how much long-term
influence this group will have on policy formation and implementation.
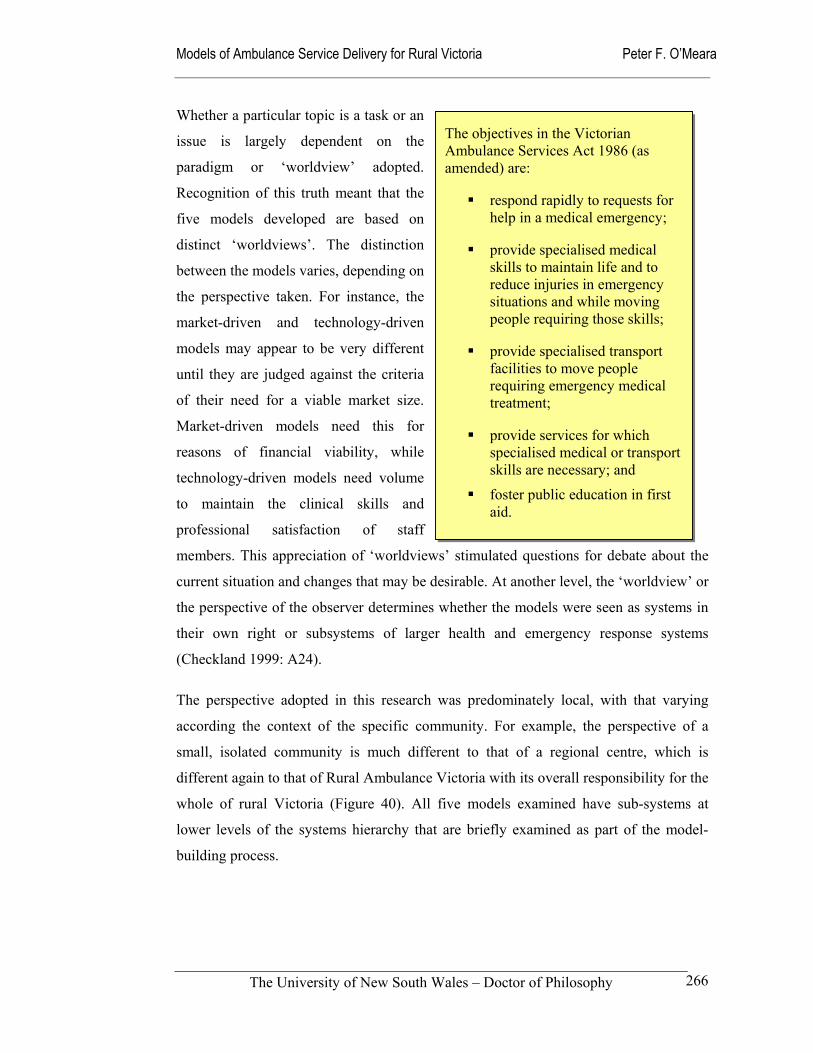
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
266
Whether a particular topic is a task or an
issue is largely dependent on the
paradigm or ‘worldview’ adopted.
Recognition of this truth meant that the
five models developed are based on
distinct ‘worldviews’. The distinction
between the models varies, depending on
the perspective taken. For instance, the
market-driven and technology-driven
models may appear to be very different
until they are judged against the criteria
of their need for a viable market size.
Market-driven models need this for
reasons of financial viability, while
technology-driven models need volume
to maintain the clinical skills and
professional satisfaction of staff
members. This appreciation of ‘worldviews’ stimulated questions for debate about the
current situation and changes that may be desirable. At another level, the ‘worldview’ or
the perspective of the observer determines whether the models were seen as systems in
their own right or subsystems of larger health and emergency response systems
(Checkland 1999: A24).
The perspective adopted in this research was predominately local, with that varying
according the context of the specific community. For example, the perspective of a
small, isolated community is much different to that of a regional centre, which is
different again to that of Rural Ambulance Victoria with its overall responsibility for the
whole of rural Victoria (Figure 40). All five models examined have sub-systems at
lower levels of the systems hierarchy that are briefly examined as part of the model-
building process.
The objectives in the Victorian Ambulance Services Act 1986 (as amended) are:
respond rapidly to requests for help in a medical emergency;
provide specialised medical skills to maintain life and to reduce injuries in emergency situations and while moving people requiring those skills;
provide specialised transport facilities to move people requiring emergency medical treatment;
provide services for which specialised medical or transport skills are necessary; and
foster public education in first aid.
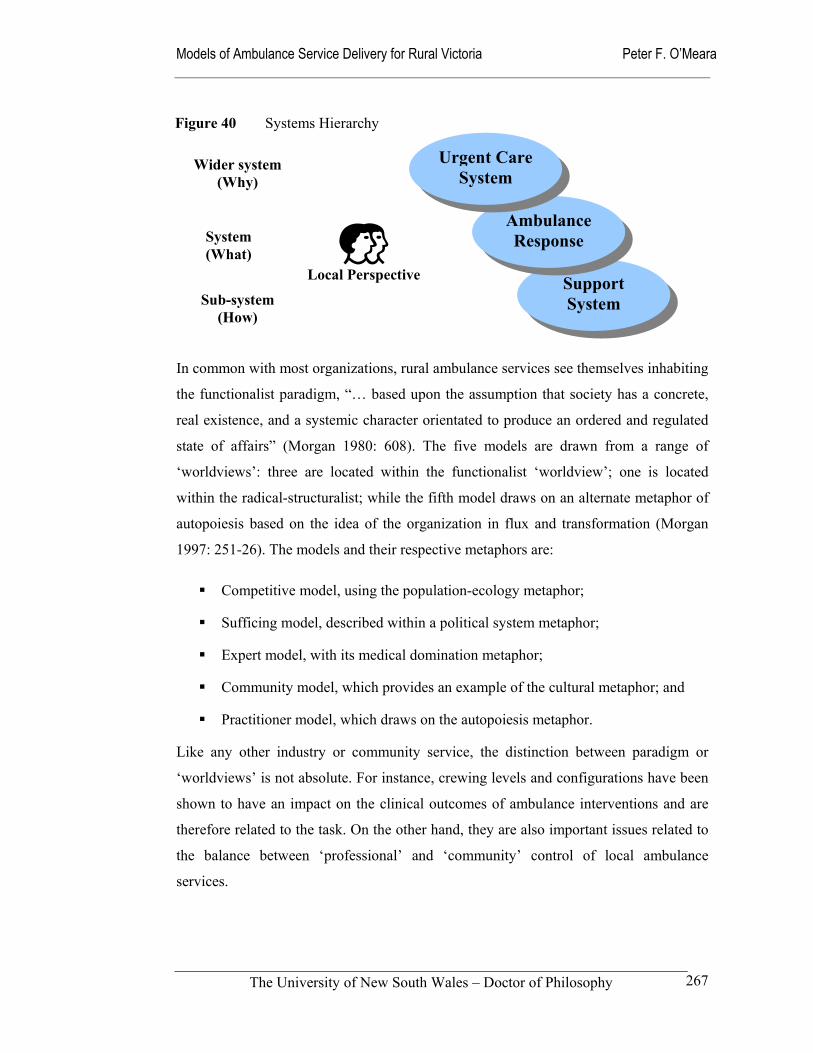
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
267
In common with most organizations, rural ambulance services see themselves inhabiting
the functionalist paradigm, “… based upon the assumption that society has a concrete,
real existence, and a systemic character orientated to produce an ordered and regulated
state of affairs” (Morgan 1980: 608). The five models are drawn from a range of
‘worldviews’: three are located within the functionalist ‘worldview’; one is located
within the radical-structuralist; while the fifth model draws on an alternate metaphor of
autopoiesis based on the idea of the organization in flux and transformation (Morgan
1997: 251-26). The models and their respective metaphors are:
Competitive model, using the population-ecology metaphor;
Sufficing model, described within a political system metaphor;
Expert model, with its medical domination metaphor;
Community model, which provides an example of the cultural metaphor; and
Practitioner model, which draws on the autopoiesis metaphor.
Like any other industry or community service, the distinction between paradigm or
‘worldviews’ is not absolute. For instance, crewing levels and configurations have been
shown to have an impact on the clinical outcomes of ambulance interventions and are
therefore related to the task. On the other hand, they are also important issues related to
the balance between ‘professional’ and ‘community’ control of local ambulance
services.
Support System
Ambulance Response
Urgent Care System
Figure 40 Systems Hierarchy
Wider system (Why)
System (What)
Sub-system (How)
Local Perspective

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
268
In Table 61 the relative strengths and weaknesses of five models are briefly compared
against the three performance criteria of access, effectiveness and efficiency. This
comparative device allowed these preliminary views to be subjected to the challenge of
verification during the research and evaluation process.
Table 61 Relative Strengths and Weakness of Abstract Ambulance Models
Model Patient Access Effectiveness Efficiency
Competitive Very weak Weak Strong
Sufficing Very strong Weak Very weak
Community Very strong Very weak Very strong
Expert Weak Very strong Very weak
Practitioner Strong Very strong Strong
Each of these five models of service delivery are formulated, described and then
analyzed against these three broad performance criteria in the remainder of this chapter.
In the final part of the chapter, it is recognized that all five can co-exist and meld with
each within the one system. As a result, the concept of an integrated system in rural
Victoria was explored through the application of a planetary metaphor based on the idea
of pushers and drivers that are a little akin to how gravity or magnetism operates in the
physical world. Using this metaphorical device, links the different models together into
a practical framework that explains how real ambulance systems develop and operate in
the rural environment.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
269
8.2 Competitive model
The competitive model of ambulance service delivery is located within the functionalist
paradigm and draws on the population-ecology metaphor described in Flood and
Jackson (1991) and Morgan (1980 & 1997). It is the model that closely matched the
political environment in Victoria during the reign of the former Kennett government in
the 1990s.
The ideology of the marketplace that was ascendant in the 1980s and 1990s under the
influence of the Reagan and Thatcher governments in the United States and the United
Kingdom respectively held that the power of the market would produce desired
outcomes (Krieger 1986). The competitive model is influenced by this big business and
capitalist view of the world. The population-ecology metaphor emphasizes the role of
the environment as the major force in organizational survival. In the ideal
environmental conditions of the ambulance free-marketeer, the market drives the
performance of ambulance service providers with financial incentives and penalties
linked to performance. The various competitive models proposed during the 1990s,
allowed for the regulatory and purchasing roles to be separated from the provider role
(Allen Consulting 1999). This policy environment was particularly strong in Victoria,
where free-market policies were followed with great vigour. As a result, the market
approach to the provision of ambulance services in Victoria more closely resembled the
situation in the United Kingdom than the situation in other Australian states (Mahony
2001).
Even though there has since been a change of state government, which is more
moderate in its language and approach, the value of examining this model remains.
Parts of the operation of the Metropolitan Ambulance Service, such as dispatch systems
and vehicle maintenance, continue for the time being to be operated privately on a
contract basis. A sizable portion of the routine inter-hospital transport market in both the
rural and metropolitan areas of Victoria also remain under the control of the private
ambulance providers. Another reason for the continued relevance of the competitive
model is the recognition that the political cycle may see a resurgence of market-driven
solutions at some time in the future.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
270
The major risk to rural and remote communities in the competitive model is market
failure. For instance, small or isolated communities may have insufficient catchment
population to ensure financial survival for the provider. The model’s reliance on
population-ecology theory puts weaker or more vulnerable communities at risk of being
unable to sustain their services. This has major implications for the equity of the
ambulance services provided; in some cases, the lack of a sustainable market may result
is no services being provided. The alternative approach is for governments or other
funding organizations to provide subsidies or regulate the market in a way that makes
the market viable. If this option were adopted, it would then no longer be a truly
competitive model.
From a theoretical perspective, the population-ecology view has been criticized for
being too environmentally deterministic to satisfactorily explain how organizations
actually evolve. For example, it negates the role of managers and decision-makers in
plotting the organizations strategic choices. Its one-sided view of the evolutionary
process also underplays the ability of organizations to collaborate as well as compete
(Morgan 1997: 63-65). Ambulance service examples of this include regular disaster
planning activities and the organisation of mutual aid from adjoining ambulance
services in the event of excessive demand or major system failure.
SSM is used to describe the competitive model through the application of the CATWOE
mnemonic to describe the competitive model root definition (Table 62); a holon (Figure
41) and a rich picture (Figure 42) provide the pictoral descriptions of the basic
competitive model. The abstract model formulated is then tested against the real world
situation. Figure 43 uses a patient pathway device to describe how a competitive model
may work. However, the two most important aspects of the model are the
‘Weltanchauung’ or ‘worldview’ that describes the underlying values and beliefs of the
system, and the transformation processes that deliver the contracted services. In this
case, the belief in the market is fundamental to the structure and processes used to
produce outcomes.
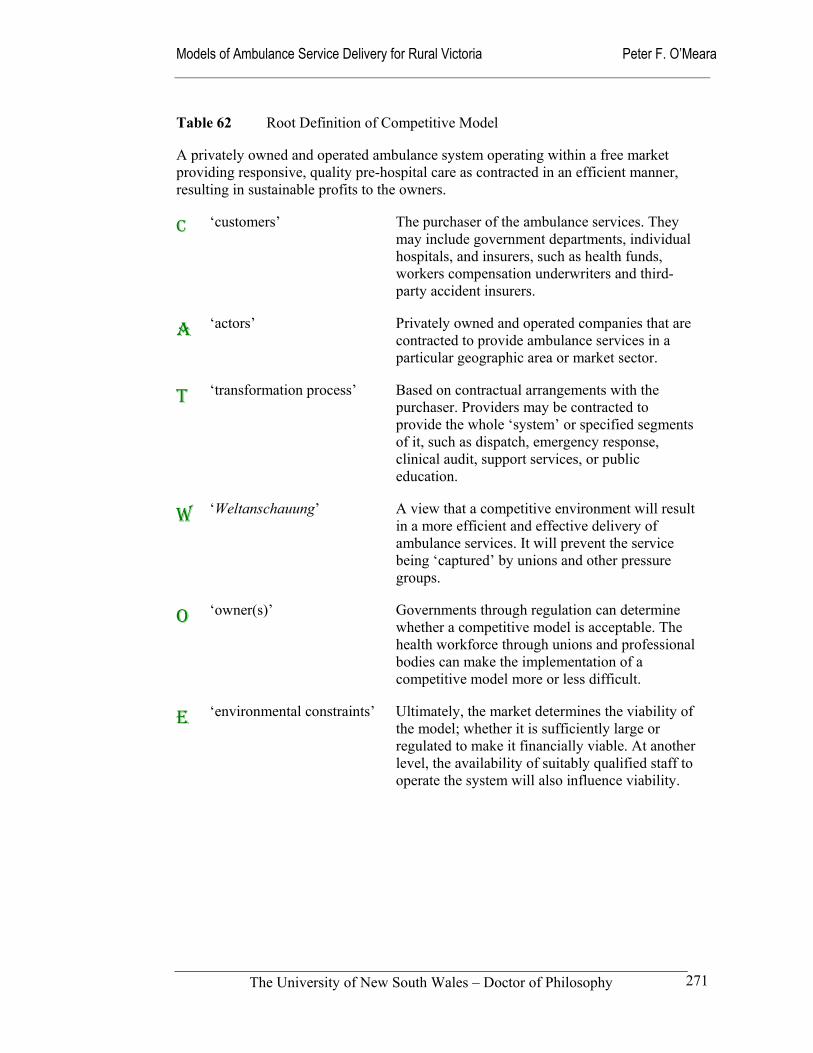
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
271
Table 62 Root Definition of Competitive Model
A privately owned and operated ambulance system operating within a free market providing responsive, quality pre-hospital care as contracted in an efficient manner, resulting in sustainable profits to the owners.
C ‘customers’ The purchaser of the ambulance services. They may include government departments, individual hospitals, and insurers, such as health funds, workers compensation underwriters and third-party accident insurers.
A ‘actors’ Privately owned and operated companies that are contracted to provide ambulance services in a particular geographic area or market sector.
T ‘transformation process’ Based on contractual arrangements with the purchaser. Providers may be contracted to provide the whole ‘system’ or specified segments of it, such as dispatch, emergency response, clinical audit, support services, or public education.
W ‘Weltanschauung’ A view that a competitive environment will result in a more efficient and effective delivery of ambulance services. It will prevent the service being ‘captured’ by unions and other pressure groups.
O ‘owner(s)’ Governments through regulation can determine whether a competitive model is acceptable. The health workforce through unions and professional bodies can make the implementation of a competitive model more or less difficult.
E ‘environmental constraints’ Ultimately, the market determines the viability of the model; whether it is sufficiently large or regulated to make it financially viable. At another level, the availability of suitably qualified staff to operate the system will also influence viability.
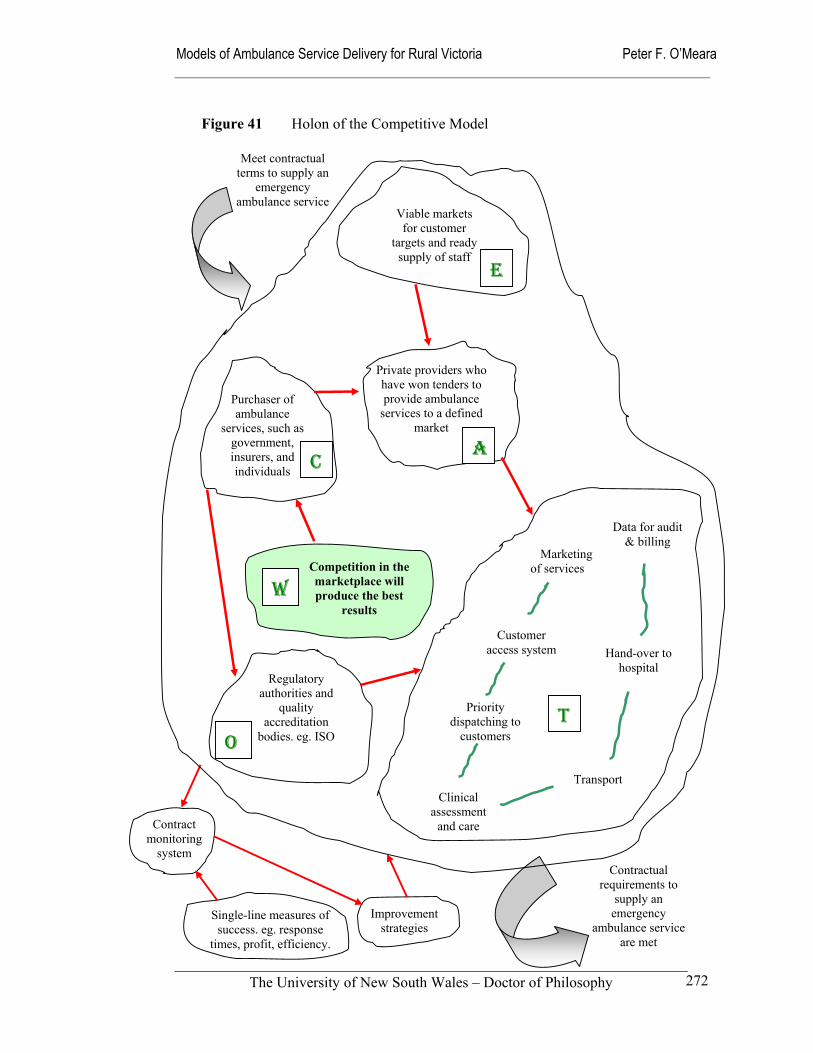
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
272
Single-line measures of success. eg. response
times, profit, efficiency.
Improvement strategies
Contract monitoring
system
Competition in the marketplace will produce the best
results
Marketing of services
Hand-over to hospital
Data for audit & billing
Customer access system
Priority dispatching to
customers
Clinical assessment
and care
Transport
Purchaser of ambulance
services, such as government, insurers, and individuals
Regulatory authorities and
quality accreditation
bodies. eg. ISO
Viable markets for customer
targets and ready supply of staff
Private providers who have won tenders to provide ambulance
services to a defined market
Contractual requirements to
supply an emergency
ambulance service are met
Meet contractual terms to supply an
emergency ambulance service
Figure 41 Holon of the Competitive Model
E
W
C A
O
T
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
273
Reality Testing of Competitive Model
It has already been argued that each model should be tested against its own inherent
standards and five generic standards. To do this, the competitive model was ‘unpacked’
and its distinctive characteristics examined in more detail. The holon and the rich
picture (Figures 41 and 42) provide pictoral representations of the competitive models
elements, activities and relationships. Aside from its philosophical basis in the
population-ecology metaphor, the major distinguishing features of the competitive
model are found in its management systems and its transformation processes. These
characteristics all impact on the model’s ability to deliver on its own aims and on the
generic expectations of the community that were identified in Chapter 5.
By definition, the market is said to be the ultimate judge of whether this model of
service delivery is successful. The biggest obstacle for the competitive model in the
rural and remote environment is its relatively low and sparse population base. A danger
is that funders and purchasers may apply simplified, single-line performance
requirements in a rural contract without an understanding of the complexities involved
or consideration of a higher contract price that recognises the greater degree of
difficulty in supplying a service that meets the same accessibility and responsiveness
standards of an urban ambulance service. For a competitive model to work effectively,
the performance indicators imbedded in its contractual arrangements need to reflect the
constraints of the rural and remote environment. For example, the greater distances
travelled in rural areas result in higher fuel costs, while the less frequent use of
advanced skills results in a greater need for skills maintenance programs (Ornato et al
1984). Undermining the competitive model is the weakness of the ambulance market in
rural areas. Unless the prices offered to providers are based on higher cost structures,
there are likely to be very few potential service providers in rural areas (Allen
Consulting 1999).
The market orientation of the competitive model may also impact on the service
delivery or transformation processes. While the activities carried out, and the
infrastructure and personal elements needed will be similar to other models, one
consequence may be the higher priority placed on the marketing of services than in the
case of public ambulance services. Staff may also be encouraged to project a positive
image of the ambulance service and avoid criticism; in other words, to be “… an
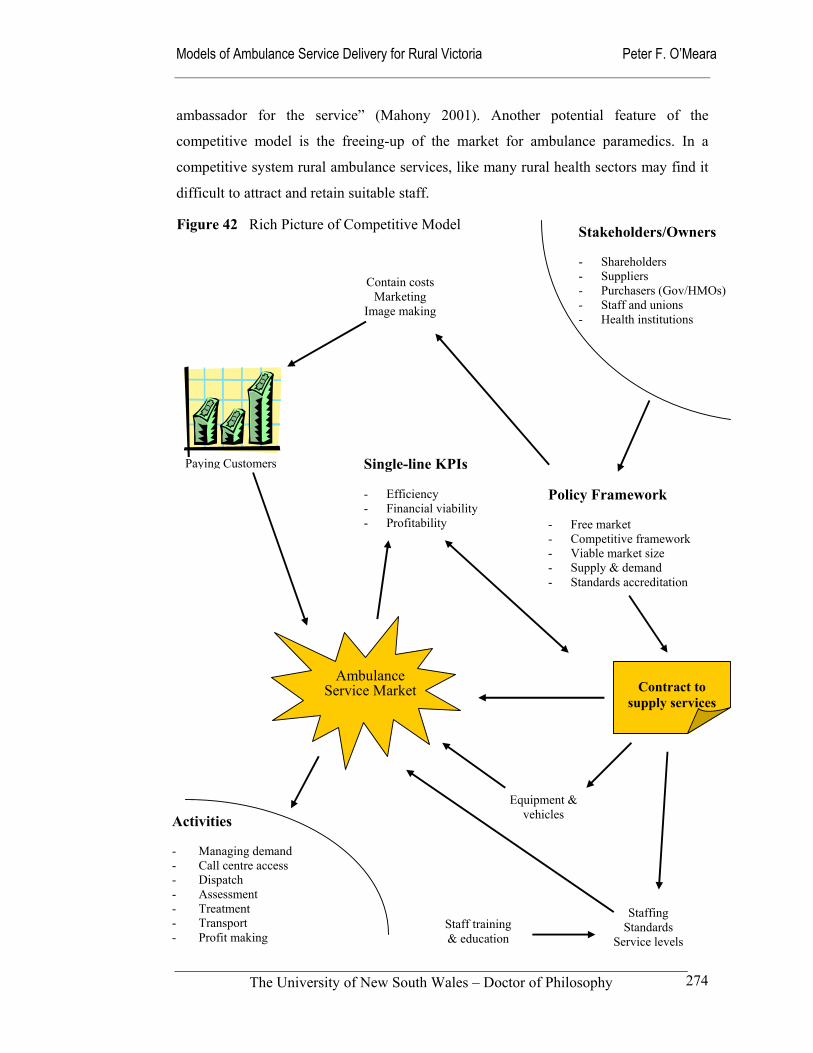
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
274
ambassador for the service” (Mahony 2001). Another potential feature of the
competitive model is the freeing-up of the market for ambulance paramedics. In a
competitive system rural ambulance services, like many rural health sectors may find it
difficult to attract and retain suitable staff.
Figure 42 Rich Picture of Competitive Model Stakeholders/Owners - Shareholders - Suppliers - Purchasers (Gov/HMOs) - Staff and unions - Health institutions
Policy Framework - Free market - Competitive framework - Viable market size - Supply & demand - Standards accreditation
Activities - Managing demand - Call centre access - Dispatch - Assessment - Treatment - Transport - Profit making
Contain costsMarketing
Image making
Paying Customers
Ambulance Service Market
Staffing Standards
Service levels Staff training & education
Equipment & vehicles
Contract to
supply services
Single-line KPIs - Efficiency - Financial viability - Profitability
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
275
Another potentially negative feature of the model is the reduced ability of providers to
use volunteer staff in the small remote communities that currently utilize the services of
community-minded members. The values of profit-driven ambulance services are
inconsistent with the values of volunteerism. However, a viable alternative for some
communities is to establish a non-profit competitive model on a similar basis to Charity-
owned private hospitals. In the larger regional centres private sector services may be in
a better position to offer more flexible appointment terms and conditions than public
sector providers; they could for example, offer equity within the company, enhanced
remuneration or more flexible work conditions. In the Australian context, ambulance
unions may see this as a threat to full-time work and a step toward ‘casualization’ of the
workforce. Union opposition to the Kennett government reforms of the Metropolitan
Ambulance Service support this view.
The major impact of the competitive model is the change in the relationships between
the provider and other health and emergency services. Where ambulance services and
their staff are generally seen as members of the health and emergency system teams, in
the competitive model the relationship is contractual. This changed relationship with
regulatory bodies and the other health and emergency professionals raises ethical and
professional issues that Australian ambulance paramedics have never faced before.
These ethical issues would appear to be no greater than other health professionals face,
with the solutions lying in the professional self-regulation of individual ambulance
paramedics through registration and quality accreditation of providers acting as
effective barriers against poor or unethical performance (Allen Consulting 1999).
The activities described in Figures 41 and 42 combine with the system elements and
relationships to achieve outputs in the form of transformation processes that address the
system’s tasks and issues. Table 63 links these, with sub-systems, activities and
performance indicators for the competitive model. This description of the model links
together the stakeholder expectations identified in Chapter 5, with the management
systems (Chapter 6) and performance indicators (Chapter 7). It is the basis of a
management system which identifies how each subsystem might operate and which part
of the organisation is responsible to achieve pre-determined levels of performance.
Figure 43 takes this further through the use of a patient pathway model based on the
idea of a patient flow diagram (Bissell et al 1999b). The notable feature of the
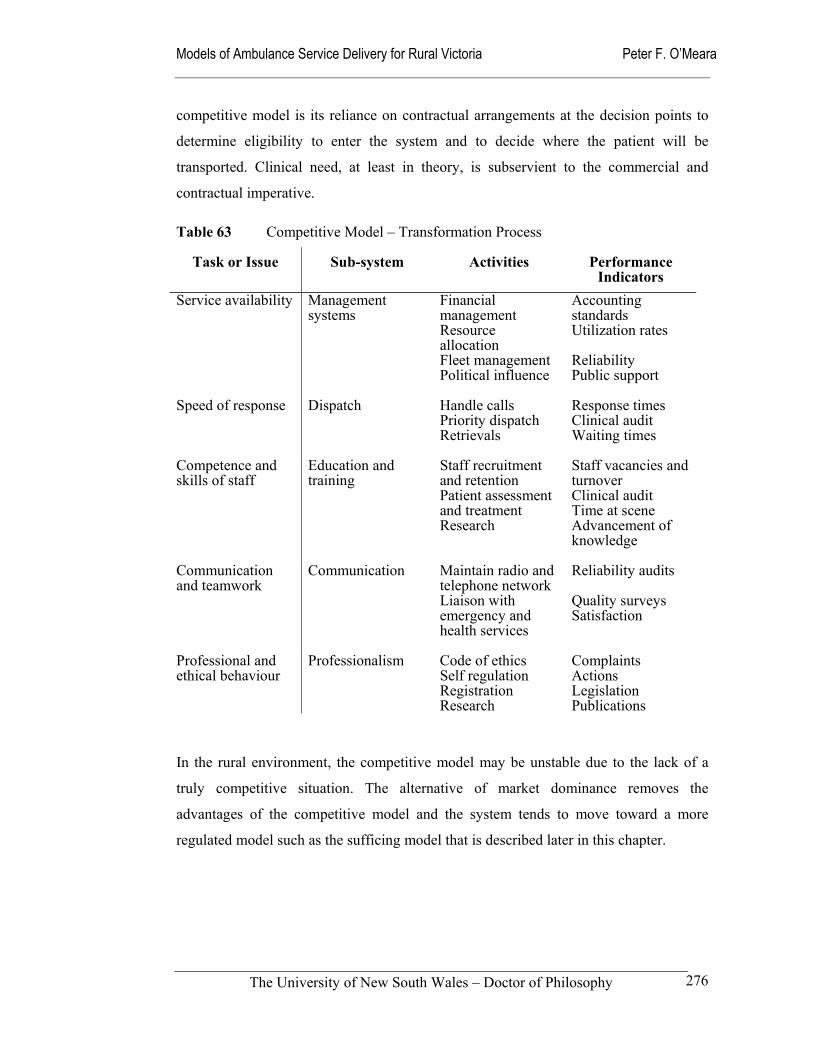
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
276
competitive model is its reliance on contractual arrangements at the decision points to
determine eligibility to enter the system and to decide where the patient will be
transported. Clinical need, at least in theory, is subservient to the commercial and
contractual imperative.
Table 63 Competitive Model – Transformation Process
Task or Issue Sub-system Activities Performance Indicators
Service availability
Management systems
Financial management Resource allocation Fleet management Political influence
Accounting standards Utilization rates Reliability Public support
Speed of response
Dispatch Handle calls Priority dispatch Retrievals
Response times Clinical audit Waiting times
Competence and skills of staff
Education and training
Staff recruitment and retention Patient assessment and treatment Research
Staff vacancies and turnover Clinical audit Time at scene Advancement of knowledge
Communication and teamwork
Communication Maintain radio and telephone network Liaison with emergency and health services
Reliability audits Quality surveys Satisfaction
Professional and ethical behaviour
Professionalism Code of ethics Self regulation Registration Research
Complaints Actions Legislation Publications
In the rural environment, the competitive model may be unstable due to the lack of a
truly competitive situation. The alternative of market dominance removes the
advantages of the competitive model and the system tends to move toward a more
regulated model such as the sufficing model that is described later in this chapter.
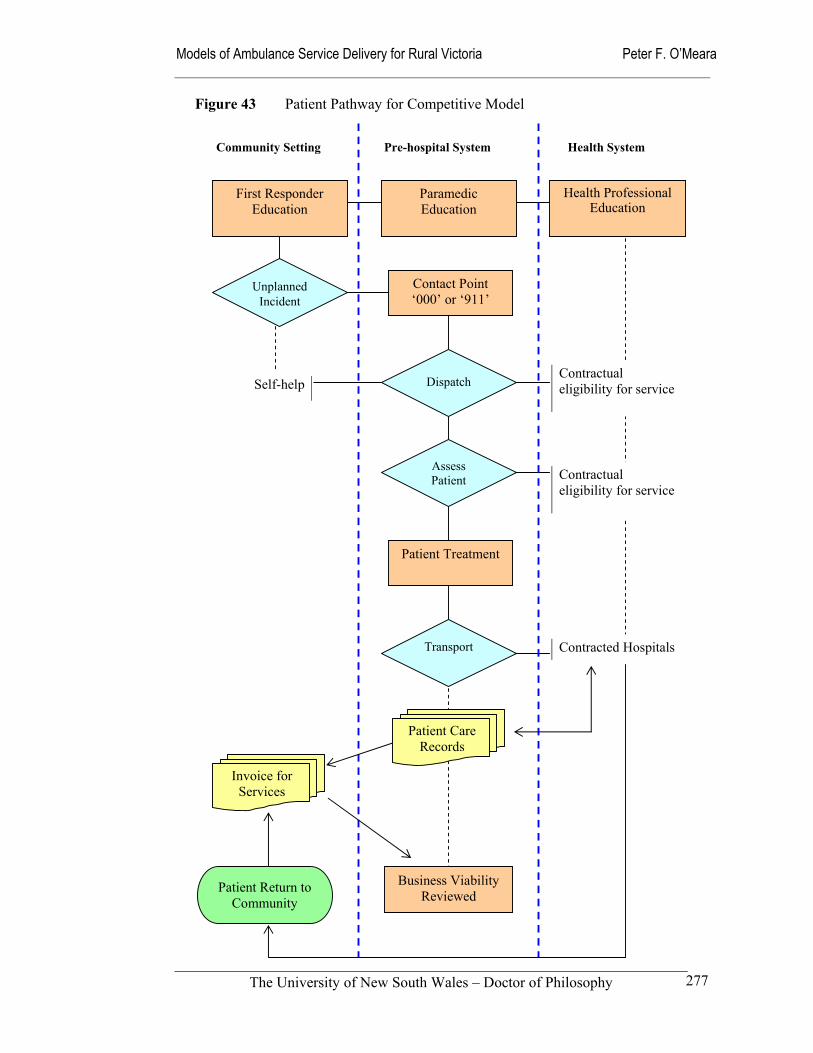
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
277
Community Setting Pre-hospital System Health System
Unplanned Incident
Dispatch
Assess Patient
Transport
First Responder Education
Paramedic Education
Health Professional Education
Patient Care Records
Business Viability Reviewed
Self-help Contractual eligibility for service
Contractual eligibility for service
Contracted Hospitals
Figure 43 Patient Pathway for Competitive Model
Invoice for Services
Contact Point ‘000’ or ‘911’
Patient Treatment
Patient Return to Community

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
278
8.3 Sufficing model
One of the curious features of organizational life is that although people know they are surrounded by organizational politics they rarely come out and say so. One ponders politics in private moments or discusses it off the record with close confidants and friends or in the context of one’s own political manoeuvrings with members of one’s coalition.
(Morgan 1997: 208)
The sufficing model is essentially a system for negotiating and managing the conflict
between competing interests who use their power bases to gain advantage for their
particular constituency. The model is best explained through the political metaphor that
encourages us to see all organizational activity as interest based. It places the role and
use of power at the centre of organizational analysis, challenging the notion that
organizational rationality is value free (Morgan 1997: 209).
In the ambulance service context, whole communities may use the established political
process to obtain more resources than rational planning processes may otherwise
allocate. In other cases ambulance unions may set the agenda through industrial action,
media scare campaigns or direct links with sympathetic governments. An example of
this political process in Victoria is the introduction of an Advanced Life Support
education program for almost all full-time rural paramedics.
Managers and Boards of Management also play the political game in their roles as
arbiters of resource allocation through their control of data and access to resources.
Some of the findings in Chapter 6 illustrate the outcomes of these political processes,
where some relatively small rural areas have managed to secure staffing levels that
support 24-hour rosters, while other similar-sized communities have been left with
minimal full-time staff, on-call rosters, and volunteer staff. These outcomes reflect
success in the political system, rather than rational responses to real need. With the
sufficing model so closely resembling the traditional operation of ambulance services in
Australia, it is difficult to remain detached from the reality of a system that espouses the
values of access and equity while operating as a highly political entity. Maintaining the
abstract nature of this model during the analysis was an ever-present challenge.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
279
The articulated mission of the sufficing model is to provide the minimum acceptable
level of service as a ‘safety-net’, on the basis that all citizens are entitled to basic
services irrespective of socio-economic status, demographic profile, or place of
residence. It treats the provision of ambulance services as a ‘public good’. From their
own perspective, practically all communities and pressure groups think they are in need
and deserve more resources and services. They enter the political arena to obtain what
they see as their right.
While the political metaphor encourages the recognition of how and why the actors
influence the operation of the service delivery system, it does have its limitations. One
of these is that concentrating on the political nature of the organization can dominate
and distort the operation of the system. The risk is that the model of service delivery
will become overly politicised.
We begin to see politics everywhere and to look for hidden agendas even where there are none. For this reason, the [political] metaphor must be used with caution. There is a very real danger that its use may generate cynicism and mistrust in situations where there was none before. … Under the influence of a political mode of understanding, everything becomes political. The analysis of interests, conflicts, and power easily gives rise to a Machiavellian interpretation that suggests everyone is trying to outwit and outmanoeuvre everyone else. Rather than use the political metaphor to generate new insights and understandings that can help us deal with divergent interests, we often reduce the metaphor to a tool to be used to advance our own personal interests.
(Morgan 1997: 212)
This political phenomenon is reported in Chapter 2, where the unsettled industrial
relations environment in which the Victorian rural ambulance services operated until the
formation of Rural Ambulance Victoria illustrated how the political processes can
overwhelm the capacity to plan and deliver appropriate emergency ambulance services
for the community. Throughout the 1980s and 1990s, managers and staff spent
enormous time and energy pursuing their goals through media stunts, industrial action
and reactive management strategies. These destructive activities have had a similar
impact on the NSW Ambulance Service in recent years (Audit Office NSW 2001;
Mahony 2001).
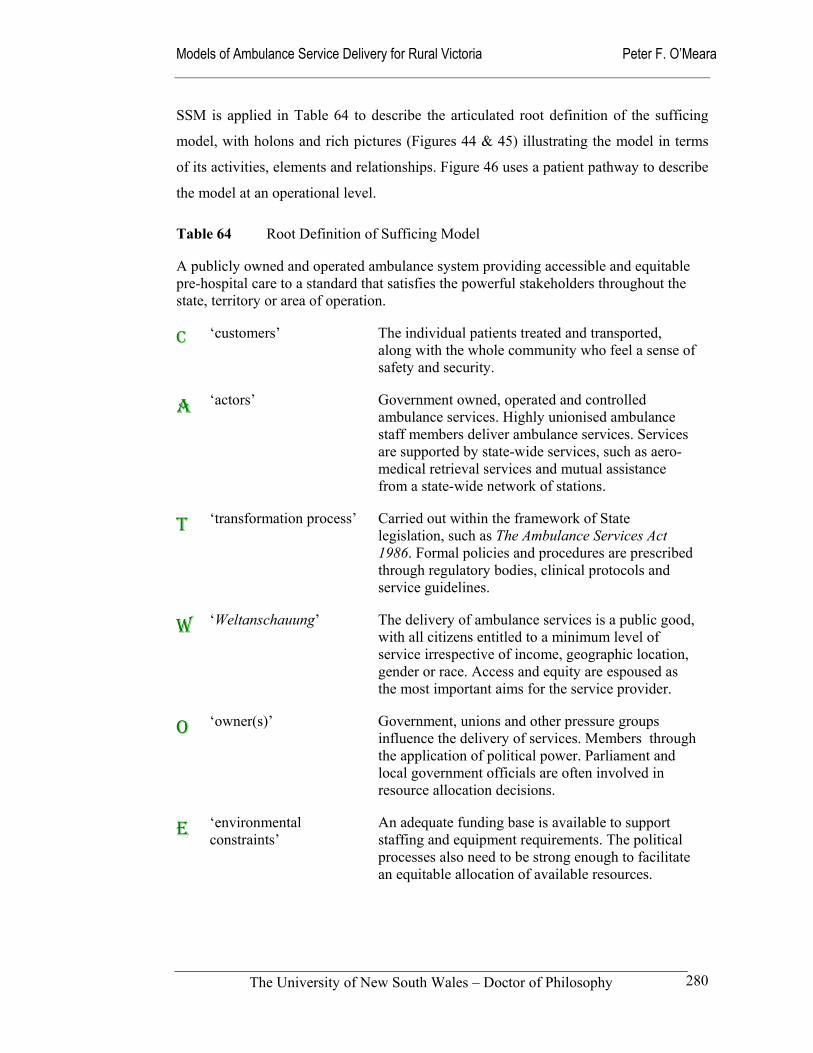
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
280
SSM is applied in Table 64 to describe the articulated root definition of the sufficing
model, with holons and rich pictures (Figures 44 & 45) illustrating the model in terms
of its activities, elements and relationships. Figure 46 uses a patient pathway to describe
the model at an operational level.
Table 64 Root Definition of Sufficing Model
A publicly owned and operated ambulance system providing accessible and equitable pre-hospital care to a standard that satisfies the powerful stakeholders throughout the state, territory or area of operation.
C ‘customers’ The individual patients treated and transported, along with the whole community who feel a sense of safety and security.
A ‘actors’ Government owned, operated and controlled ambulance services. Highly unionised ambulance staff members deliver ambulance services. Services are supported by state-wide services, such as aero-medical retrieval services and mutual assistance from a state-wide network of stations.
T ‘transformation process’ Carried out within the framework of State legislation, such as The Ambulance Services Act 1986. Formal policies and procedures are prescribed through regulatory bodies, clinical protocols and service guidelines.
W ‘Weltanschauung’ The delivery of ambulance services is a public good, with all citizens entitled to a minimum level of service irrespective of income, geographic location, gender or race. Access and equity are espoused as the most important aims for the service provider.
O ‘owner(s)’ Government, unions and other pressure groups influence the delivery of services. Members through the application of political power. Parliament and local government officials are often involved in resource allocation decisions.
E ‘environmental constraints’
An adequate funding base is available to support staffing and equipment requirements. The political processes also need to be strong enough to facilitate an equitable allocation of available resources.
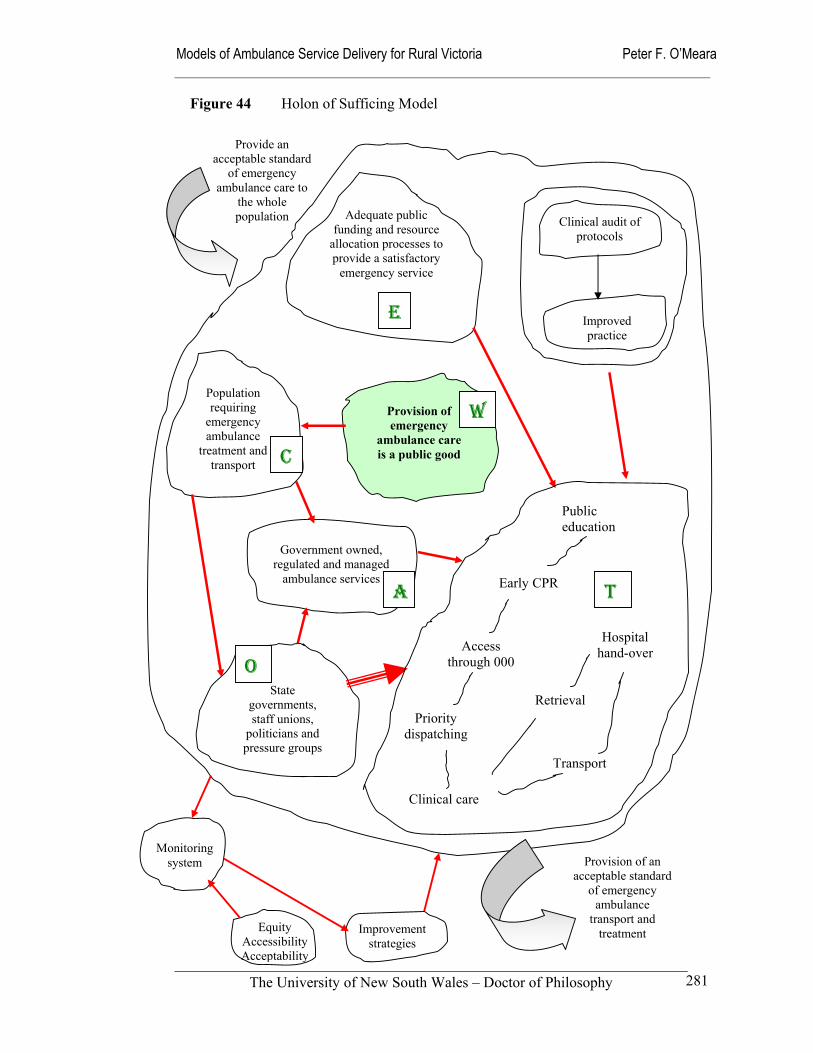
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
281
Government owned, regulated and managed
ambulance services
Population requiring
emergency ambulance
treatment and transport
State governments, staff unions,
politicians and pressure groups
Adequate public funding and resource
allocation processes to provide a satisfactory
emergency service
Provision of emergency
ambulance care is a public good
Provision of an acceptable standard
of emergency ambulance
transport and treatment
Provide an acceptable standard
of emergency ambulance care to
the whole population
Improved practice
Clinical audit of protocols
Public education
Early CPR
Access through 000
Priority dispatching
Hospital hand-over
Retrieval
Transport
Clinical care
Equity Accessibility Acceptability
Improvement strategies
Monitoring system
Figure 44 Holon of Sufficing Model
E
W
C
A
O
T
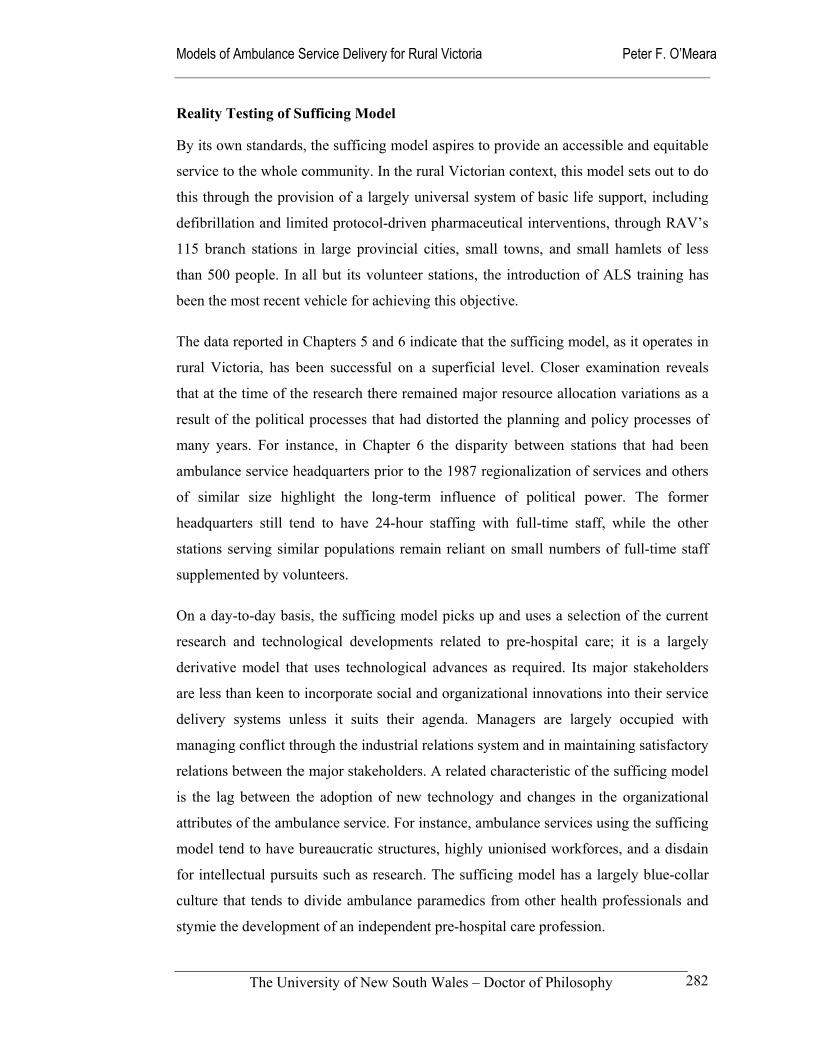
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
282
Reality Testing of Sufficing Model
By its own standards, the sufficing model aspires to provide an accessible and equitable
service to the whole community. In the rural Victorian context, this model sets out to do
this through the provision of a largely universal system of basic life support, including
defibrillation and limited protocol-driven pharmaceutical interventions, through RAV’s
115 branch stations in large provincial cities, small towns, and small hamlets of less
than 500 people. In all but its volunteer stations, the introduction of ALS training has
been the most recent vehicle for achieving this objective.
The data reported in Chapters 5 and 6 indicate that the sufficing model, as it operates in
rural Victoria, has been successful on a superficial level. Closer examination reveals
that at the time of the research there remained major resource allocation variations as a
result of the political processes that had distorted the planning and policy processes of
many years. For instance, in Chapter 6 the disparity between stations that had been
ambulance service headquarters prior to the 1987 regionalization of services and others
of similar size highlight the long-term influence of political power. The former
headquarters still tend to have 24-hour staffing with full-time staff, while the other
stations serving similar populations remain reliant on small numbers of full-time staff
supplemented by volunteers.
On a day-to-day basis, the sufficing model picks up and uses a selection of the current
research and technological developments related to pre-hospital care; it is a largely
derivative model that uses technological advances as required. Its major stakeholders
are less than keen to incorporate social and organizational innovations into their service
delivery systems unless it suits their agenda. Managers are largely occupied with
managing conflict through the industrial relations system and in maintaining satisfactory
relations between the major stakeholders. A related characteristic of the sufficing model
is the lag between the adoption of new technology and changes in the organizational
attributes of the ambulance service. For instance, ambulance services using the sufficing
model tend to have bureaucratic structures, highly unionised workforces, and a disdain
for intellectual pursuits such as research. The sufficing model has a largely blue-collar
culture that tends to divide ambulance paramedics from other health professionals and
stymie the development of an independent pre-hospital care profession.
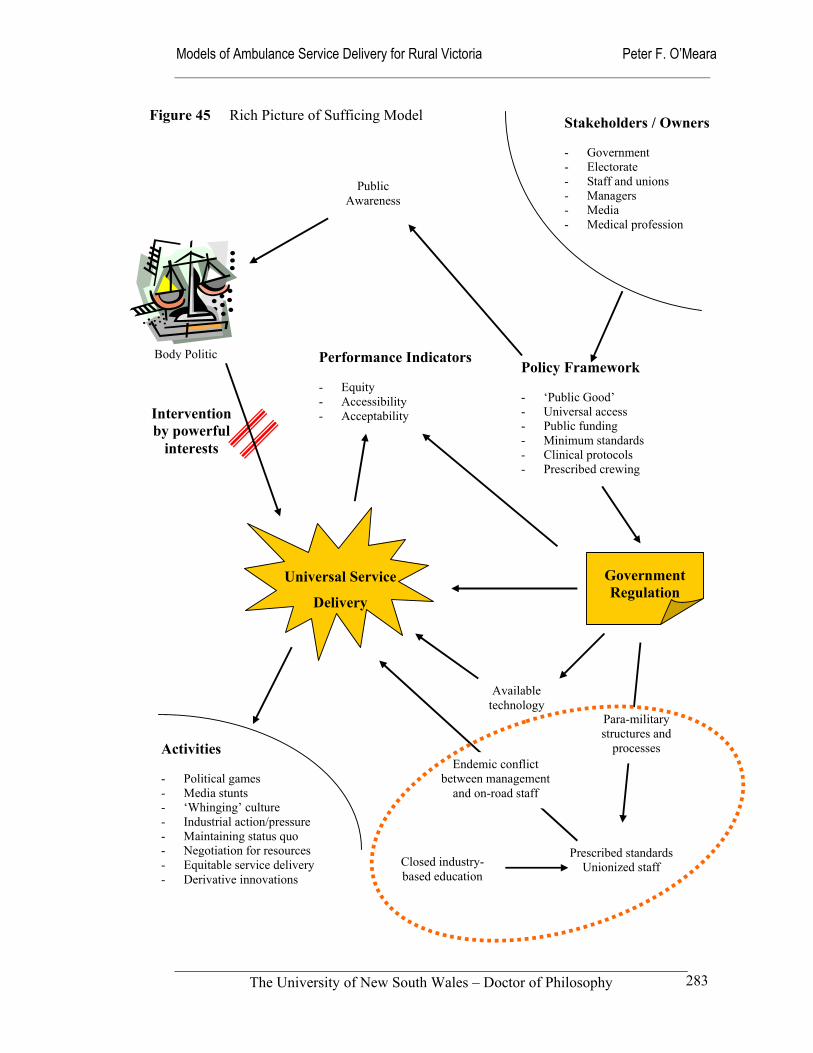
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
283
Stakeholders / Owners - Government - Electorate - Staff and unions - Managers - Media - Medical profession
Figure 45 Rich Picture of Sufficing Model
Policy Framework - ‘Public Good’ - Universal access - Public funding - Minimum standards - Clinical protocols - Prescribed crewing
Activities - Political games - Media stunts - ‘Whinging’ culture - Industrial action/pressure - Maintaining status quo - Negotiation for resources - Equitable service delivery - Derivative innovations
Public Awareness
Body Politic
Universal Service
Delivery
Prescribed standards Unionized staff
Closed industry-based education
Available technology
Government Regulation
Performance Indicators - Equity - Accessibility - Acceptability Intervention
by powerful interests
Para-military structures and
processes Endemic conflict
between management and on-road staff

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
284
At the clinical level, the sufficing model is highly reliant on strict medically endorsed
protocols to maintain standards, with little scope allowed for the exercise of clinical
judgement (Grantham 2001). This culture of non-questioning compliance with
established clinical protocols is also reflected in the absence of an independent research
culture (Jacobs 2000: Woollard et al 2000). An effect of this rather insular culture is that
many of the best and brightest practitioners either leave the organization or direct their
energies into the political games that are being played out.
As demonstrated earlier, a number of the rural communities examined in this study
receive inequitable shares of the available resources despite the operation of an
ambulance system that would describe itself as equitable. In those locations where
political power has been concentrated, high levels of staffing designed to meet any
possible emergency characterize the sufficing model; that is, 24-hour rosters with two-
officer crewing. Staff and their representative unions have considerable influence on the
shape and character of crewing policies and rosters, resulting in working conditions that
are often inflexible and better designed for staff convenience than service delivery. In
essence, the work processes of the ambulance service have been ‘captured’. Remedying
this situation has proved to be difficult where those forces with an interest in the status
quo ‘own’ the system, with neglected communities ‘locked out’ of the decision-making
processes of relatively large bureaucratic organizations. Mechanisms to give the less
powerful a voice have been often been characterised by ‘timid’ advisory committees
under the effective control of the senior managers, who can dominate the agenda
through their control of information flow and the provision of technical advice. The
inability to make timely changes to the sufficing model also limits its ability to be
responsive across its whole area of operation. This is manifested through variations in
resource allocation and utilization across the whole system. For example, the ambulance
utilization rates, reported in Chapter 7, demonstrate the link between higher utilization
and larger populations with more political power.
On a more positive note, the sufficing model’s ability to compromise and balance
internal and external demands, gives it an advantage when working in tandem with
kindred organizations in both the emergency services and health sectors. An example of
this cooperation is the growing trend toward co-location of ambulance stations with
other emergency and health services (Sinclair 2000; Audit Office NSW 2001: 102).

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
285
This co-operation may vary from complete integration to the physical sharing of sites
without any sharing of resources or professional interaction. Minimizing the capital cost
of building expensive physical assets is a tangible benefit of this approach, while more
effective teamwork and communication amongst professionals may also result from
closer proximity and more professional interaction.
However, the capacity of ambulance service personnel to act as members of teams in a
cooperative and collaborative manner is likely to be compromised by the overly
political culture that the sufficing model encourages. Ambulance paramedics within this
model, are close-knit, yet antagonistic toward ‘management’ and other outsiders – the
‘us versus them’ phenomenon is very much alive (Mahony 2001). In Chapter 5, tensions
between registered nurses and ambulance services were highlighted, with nurses and
some doctors reporting that communications centre staff are overly aggressive and at
times uncooperative. This is an example of ambulance service staff acting out their
political activities to external stakeholders through adversarial conduct that is the norm
within many ambulance services. Part of the reason for this overt aggression is the
insular and insecure nature of ambulance services, where staff have until relatively
recently been trained exclusively in industry-based, government sponsored education
centres. In Victoria, the former Hospitals and Charities Commission fulfilled this role
for many years. Formal links were rarely made between these training facilities and the
education systems of other health professionals. Thus collaboration or the transfer of
staff across professional divides was very difficult. As already reported in Chapter 6,
this situation is now changing in most parts of Australia with ambulance education and
training taking place in mainstream universities.
Standards in the sufficing model are maintained principally though a strong regulatory
framework and medical supervision. Appointed medical officers or Medical Advisory
Committees grant authority and accept ultimate responsibility for all aspects of the
clinical care provided by ambulance officers. In addition, medical officers have input
into many aspects of ambulance service delivery, including training, protocol
development, quality assurance, and relationships with the wider medical community to
ensure maintenance of accepted standards of medical practice (O’Meara et al 2001).
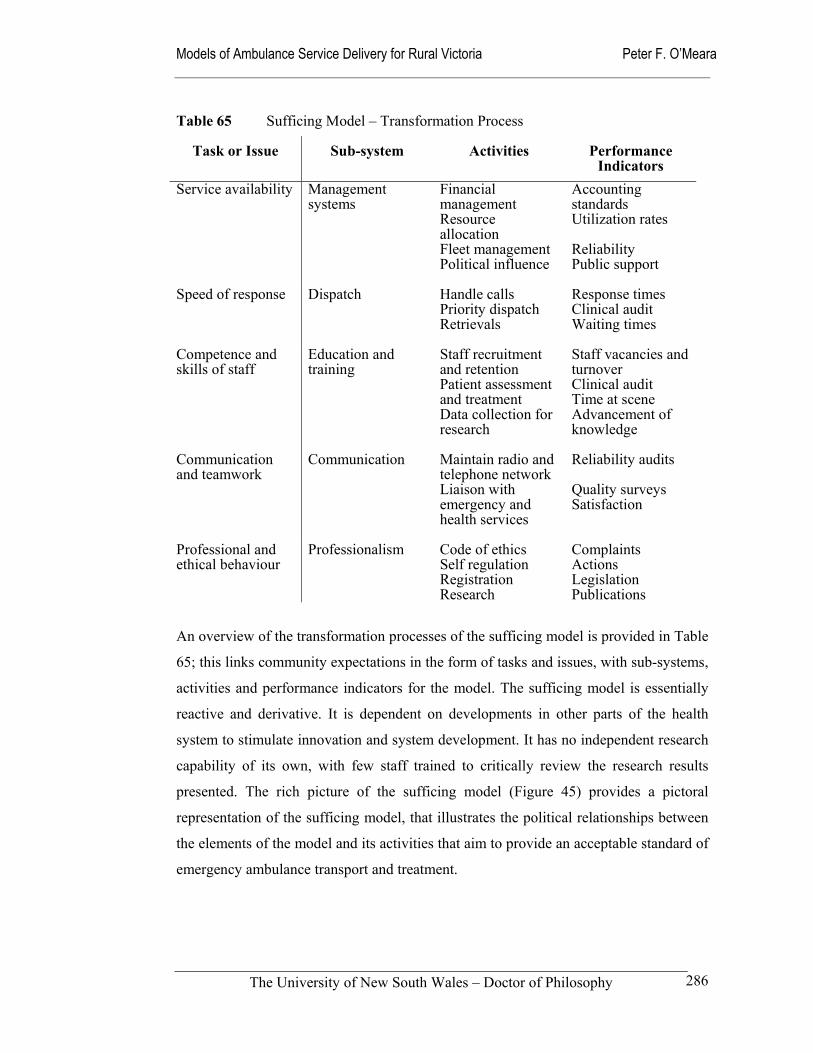
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
286
Table 65 Sufficing Model – Transformation Process
Task or Issue Sub-system Activities Performance Indicators
Service availability
Management systems
Financial management Resource allocation Fleet management Political influence
Accounting standards Utilization rates Reliability Public support
Speed of response
Dispatch Handle calls Priority dispatch Retrievals
Response times Clinical audit Waiting times
Competence and skills of staff
Education and training
Staff recruitment and retention Patient assessment and treatment Data collection for research
Staff vacancies and turnover Clinical audit Time at scene Advancement of knowledge
Communication and teamwork
Communication Maintain radio and telephone network Liaison with emergency and health services
Reliability audits Quality surveys Satisfaction
Professional and ethical behaviour
Professionalism Code of ethics Self regulation Registration Research
Complaints Actions Legislation Publications
An overview of the transformation processes of the sufficing model is provided in Table
65; this links community expectations in the form of tasks and issues, with sub-systems,
activities and performance indicators for the model. The sufficing model is essentially
reactive and derivative. It is dependent on developments in other parts of the health
system to stimulate innovation and system development. It has no independent research
capability of its own, with few staff trained to critically review the research results
presented. The rich picture of the sufficing model (Figure 45) provides a pictoral
representation of the sufficing model, that illustrates the political relationships between
the elements of the model and its activities that aim to provide an acceptable standard of
emergency ambulance transport and treatment.
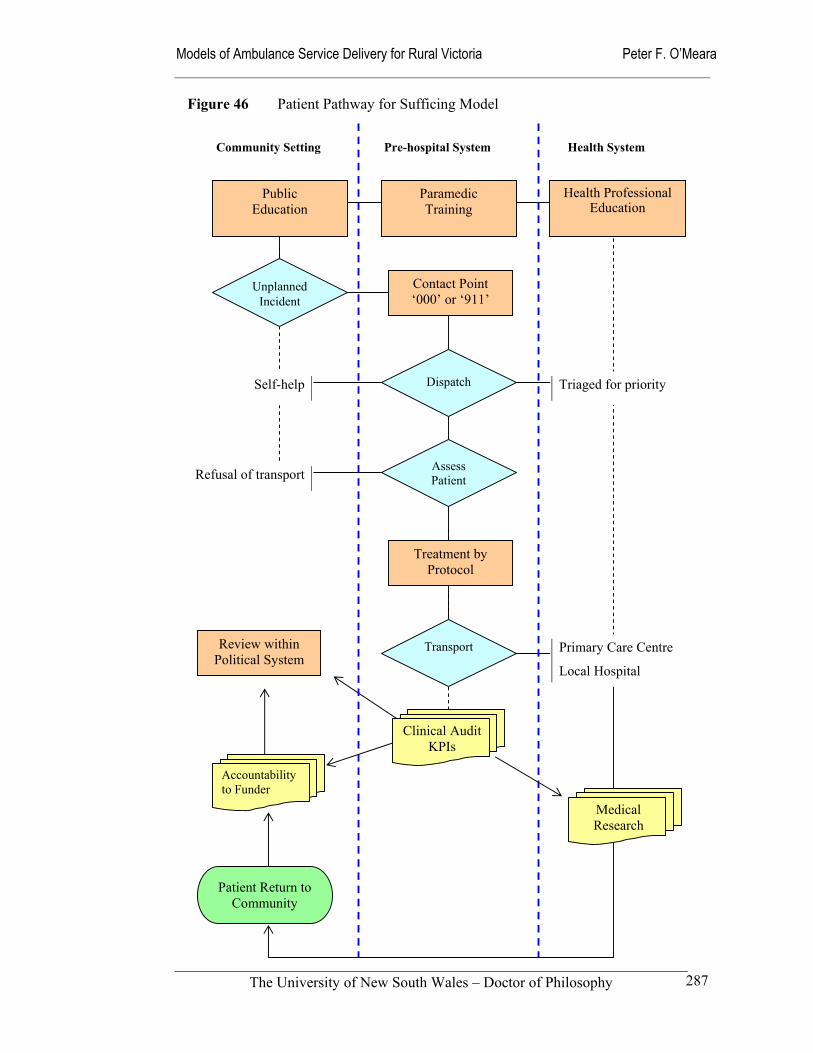
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
287
Community Setting Pre-hospital System Health System
Unplanned Incident
Dispatch
Assess Patient
Transport
Public Education
Paramedic Training
Health Professional Education
Clinical Audit KPIs
Medical Research
Review within Political System
Self-help Triaged for priority
Refusal of transport
Primary Care Centre
Local Hospital
Figure 46 Patient Pathway for Sufficing Model
Accountability to Funder
Contact Point ‘000’ or ‘911’
Treatment by Protocol
Patient Return to Community

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
288
From a more naive perspective, Figure 46 describes the model through the device of a
patient pathway. Unfortunately, the political nature of the sufficing model is hidden in
this description, thus reinforcing the value of using the political metaphor as a
descriptive and analytical device.
Despite the alienating characteristics of the sufficing model, the political nature of the
policy development and implementation processes will ensure that some elements of the
sufficing model will always exist in one form or the other. As will be seen in the
community model to follow, all ambulance models are subject to the disruptive impact
of the political games and the protection of the status quo that are part and parcel of the
sufficing model. Policy-makers, managers, ambulance paramedics, and members of the
community need to remain tuned into the political nature of all ambulance service
models, otherwise they will be swamped under the weight of powerful interests and the
political games played under the cover of the ‘public good’.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
289
8.4 Community model
The community model draws heavily from the cultural metaphor. Its strength is derived
from a belief that the community itself is taking responsibility for the provision of its
own emergency pre-hospital care. This may be through the activation of local health
professionals and/or community volunteers to provide a viable service, with or without
active government support. Local general practitioners provide one of the more
common sources of support for community ambulance services. And while they can
adopt a paternalistic relationship with the local ambulance service and its volunteer
staff, their support is vital to the maintenance of standards. The findings of this study
provide support for the continued existence of volunteer-based ambulance services; they
illustrate the sense of connection between small-town general practitioners, country
hospitals and their local ambulance services.
This ‘bottom up’ characteristic of the community model makes it a strong and resilient
model in communities where the relationship between the ambulance service and the
community is based on a socially constructed framework. Advanced technology, rules,
systems, procedures and policies are unable to sustain a community-based ambulance
service (Morgan 1997: 150). Where other models emphasize the importance of
organizational structures and processes, the community model is held together through
stories of the past, rituals and myths. It focuses on the human influences that create and
shape organized activity by influencing the ideologies, values, beliefs, language, norms,
ceremonies and other social practices that shape and guide organized action (Morgan
1997: 147).
The Country Fire Authority in Victoria (CFA), with 67,000 volunteer members, uses
this management approach very effectively. The CFA has identified the motivating
factors and disincentives amongst its volunteers, and makes a concerted effort to
account for them in their management practices (Reinholtd & Smith 1998: 41-44). Rural
Ambulance Victoria has only 370 Community Ambulance Officers, however the
Western Australian and South Australian ambulance services have respectively 1,687
and 1,477 volunteer staff, that constitute a large percentage of their total workforces
(Audit Office NSW 2001: 92). It is also well to note, that most existing ambulance
services in Australia can trace their origins back to voluntary organisations (Duffield et
al 2000).
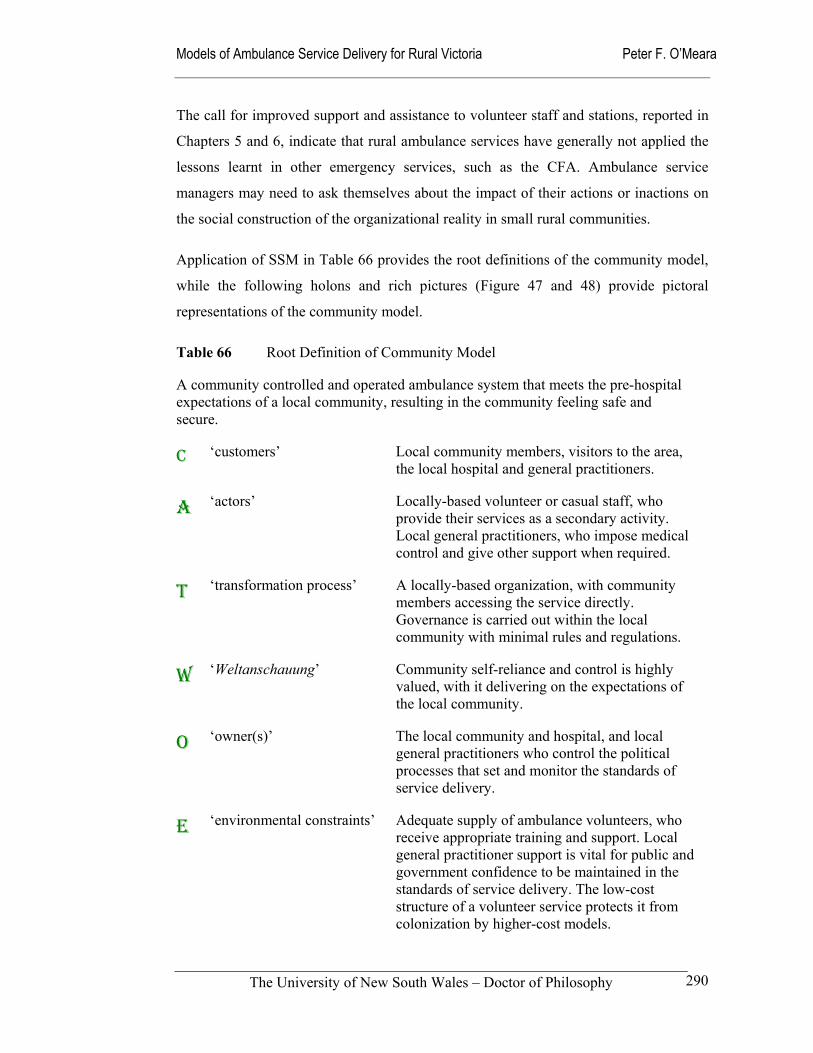
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
290
The call for improved support and assistance to volunteer staff and stations, reported in
Chapters 5 and 6, indicate that rural ambulance services have generally not applied the
lessons learnt in other emergency services, such as the CFA. Ambulance service
managers may need to ask themselves about the impact of their actions or inactions on
the social construction of the organizational reality in small rural communities.
Application of SSM in Table 66 provides the root definitions of the community model,
while the following holons and rich pictures (Figure 47 and 48) provide pictoral
representations of the community model.
Table 66 Root Definition of Community Model
A community controlled and operated ambulance system that meets the pre-hospital expectations of a local community, resulting in the community feeling safe and secure.
C ‘customers’ Local community members, visitors to the area, the local hospital and general practitioners.
A ‘actors’ Locally-based volunteer or casual staff, who provide their services as a secondary activity. Local general practitioners, who impose medical control and give other support when required.
T ‘transformation process’ A locally-based organization, with community members accessing the service directly. Governance is carried out within the local community with minimal rules and regulations.
W ‘Weltanschauung’ Community self-reliance and control is highly valued, with it delivering on the expectations of the local community.
O ‘owner(s)’ The local community and hospital, and local general practitioners who control the political processes that set and monitor the standards of service delivery.
E ‘environmental constraints’ Adequate supply of ambulance volunteers, who receive appropriate training and support. Local general practitioner support is vital for public and government confidence to be maintained in the standards of service delivery. The low-cost structure of a volunteer service protects it from colonization by higher-cost models.
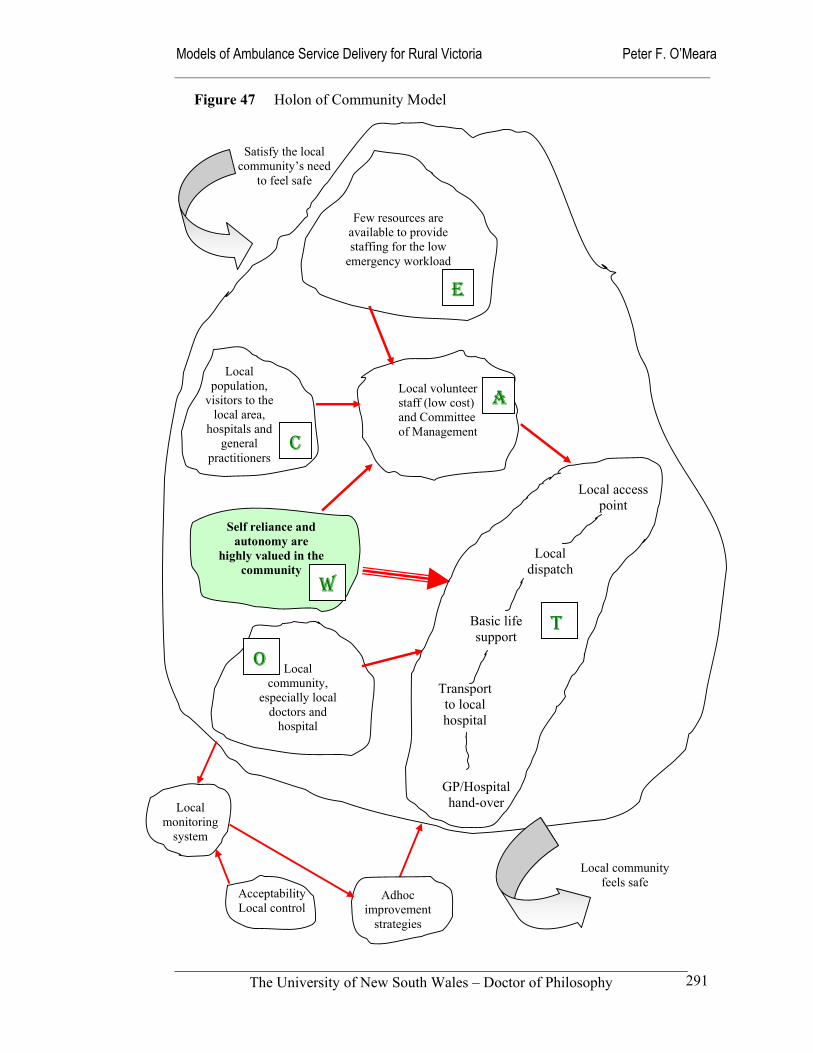
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
291
Self reliance and autonomy are
highly valued in the community
Local access point
Local dispatch
Basic life support
Transport to local hospital
GP/Hospital hand-over
Local population,
visitors to the local area,
hospitals and general
practitioners
Local community,
especially local doctors and
hospital
Few resources are available to provide staffing for the low
emergency workload
Local volunteer staff (low cost) and Committee of Management
Local community feels safe
Satisfy the local community’s need
to feel safe
Acceptability Local control
Adhoc improvement
strategies
Local monitoring
system
Figure 47 Holon of Community Model
E
W
C
A
O
T
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
292
Reality Testing of Community Model
The major practical departure between the community model and other models is in the
relatively uncomplicated transformation processes it uses to deliver services. Key
elements of the model are a knowledgeable and empowered community, a dispatch
system with local knowledge, adequate physical resources to meet community
expectations, a volunteer-based staffing system, and direct communication and
subservience to local health professionals. These relatively uncomplicated
characteristics are illustrated in the ‘rich picture’ provided in Figure 48.
The model operates most effectively in a viable community that has the scope to support
community organizations. Being able to draw on community members for
organizational support and for the supply of volunteer staff is an important attribute of
the model (Reich 1991). The ability of the community model to foster local autonomy
and community participation provides its greatest strength and potentially its greatest
threat. Local enthusiasts can be either driving forces behind the provision of good
services or the destroyers of service delivery systems through poor management. Reich
(1991) provides examples from North America, of how community-based ambulance
services have a tendency to fragment and disintegrate as a result of internally generated
strains and tensions. Without good management and a nurturing environment, they run
the risk of self-destructing. The lack of central support and a reliance on a narrow
section of the community to maintain and develop the service delivery system in an
essentially voluntary capacity is inherently risky, and a poor strategy for sustainability.
Successful community ambulance services, need to be integrated into a local urgent care
system that has the support of a broad coalition of stakeholders such as doctors, nurses,
emergency services workers, local government and a local hospital (Kelly et al 1999;
O’Meara et al 2002).
If a local community model lacks these local links with general practitioners, nurses and
hospital, the absence of strong professional linkages with other ambulance professionals
leaves it vulnerable to operating as a sub-standard system, using outmoded equipment
and professional practices. Poor community and professional linkages leave volunteer
staff with limited education and training exposed to excessive emotional and legal risks.
This is not to say that volunteer staff members are inherently inferior to full-time
professional staff. It has been demonstrated that successful volunteer systems recruit
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
293
members from the talented and successful members of the community (Reich 1991;
Norris et 1993). To overcome these weaknesses of limited education and training
opportunities for volunteers that results in a lack of a defined place in the occupational
framework the community model needs strong standards frameworks built into it,
including strong medical audit mechanisms. As already implied, effective community
models also need to have a strong sense of organizational strength, with community
members being proud to be members (Reich 1991).
Local governance and management is another distinctive characteristic of the
community model. Community-controlled committees of management can dominate the
tone and direction of the services provided through fund raising activities, the
recruitment and retention of staff, and extent of the monitoring and quality improvement
strategies they adopt. Both my direct experience of managing community models and
their theoretical basis supports the notion that community models can be either
innovative or very resistant to change (Reich 1991). Therefore, tapping into the cultural
essence of a community model to implement change can be a very powerful strategy.
However, it can also be a dangerous ploy if culture is reduced to a discrete set of
variables such as values, beliefs, stories, norms and rituals. Morgan (1997: 152) points
out that, culture is a lived experience and cannot be controlled in the sense that some
management writers advocate.
An understanding of organizations as cultures opens our eyes to many crucial insights that elude other metaphors, but they do not always provide the easy recipes for solving managerial problems that many managers and management writers hope for.
(Morgan 1997: 152)
In terms of the generic expectations established in Chapter 5, the report card of the
community model is mixed. For instance, its local focus opens it to the risk of
compromising access in the wider area or region. The model may not, for example,
develop linkages with adjoining ambulance services for the purposes of mutual aid
(Reich 1991; Norris et 1993). A Victorian example of the community models
isolationism was the reluctance of the Alexandra and District Ambulance Service to be
involved in this study through apparent fear of scrutiny from an ‘outsider’.
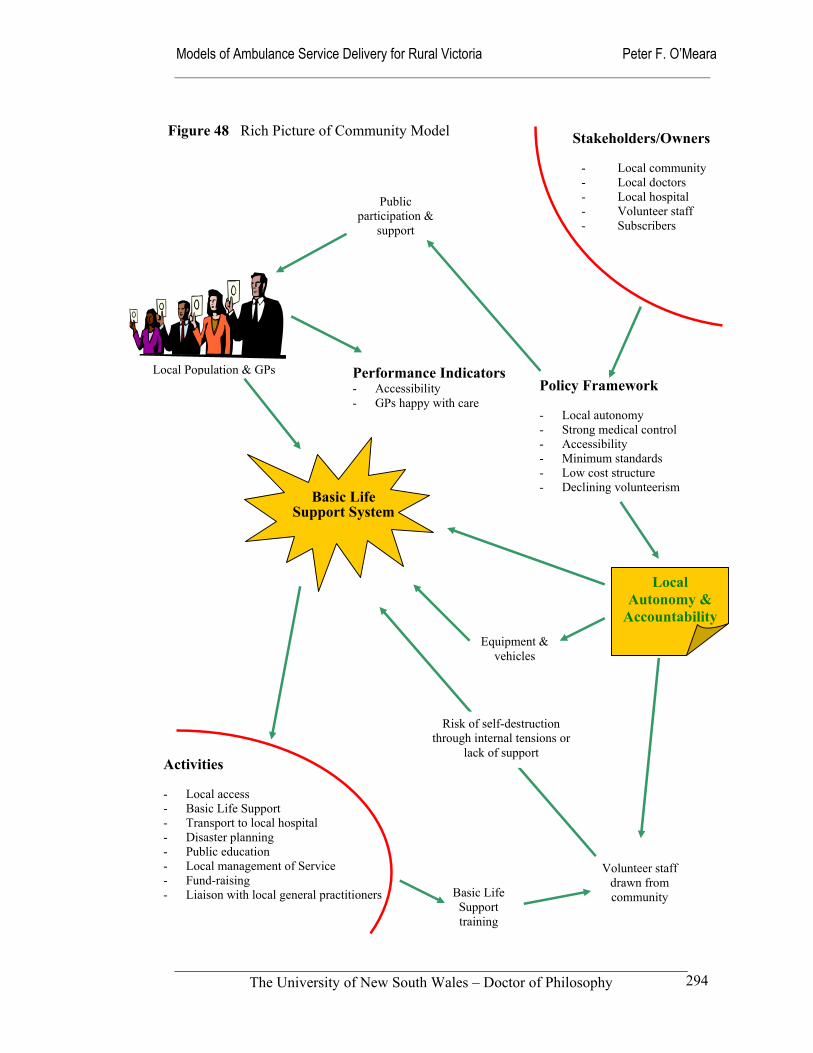
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
294
Basic Life Support System
Figure 48 Rich Picture of Community Model Stakeholders/Owners
- Local community - Local doctors - Local hospital - Volunteer staff - Subscribers
Policy Framework - Local autonomy - Strong medical control - Accessibility - Minimum standards - Low cost structure - Declining volunteerism
Activities - Local access - Basic Life Support - Transport to local hospital - Disaster planning - Public education - Local management of Service - Fund-raising - Liaison with local general practitioners
Public participation &
support
Local Population & GPs
Volunteer staff drawn from community Basic Life
Support training
Equipment & vehicles
Local Autonomy &
Accountability
Performance Indicators - Accessibility - GPs happy with care
Risk of self-destruction through internal tensions or
lack of support

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
295
The difficulty of recruiting and retaining volunteer staff in rural areas is of particular
concern to the community model because of its potentially adverse impact on the
responsiveness of the services offered. The challenge of recruiting and retaining staff is
particularly acute in volunteer systems where financial factors are irrelevant. Factors
that make staff recruitment problems more pressing are ageing populations in many
rural areas and higher workforce participation rates of spouses. These and other factors
mean that the ability to commit the time and energy for training and service is becoming
increasing limited for current and potential volunteer staff. Other factors impacting on
human resources include increased personal risks, perceptions of increased personal
liability, lack of enlightened leadership, inadequate medical participation, and limited
funding for training, equipment and supplies. Ensuring an adequate supply of trained
and motivated staff to volunteer-based systems is an ongoing challenge that is shared
with other emergency services. Positive factors that have been identified in this regard
include the provision of good management, training, recognition, organizational support
and activity, and internal communication networks (Reinholtd & Smith 1998). An
environmental factor that places pressure on the community model is, the growing
competition for volunteer staff amongst emergency services in rural areas; this
emerging factor may not always assist efforts to develop and maintain teamwork and
co-operation between kindred health and emergency services.
A related personnel issue is the maintenance of competency amongst volunteer staff,
who individually may have small caseloads and limited opportunity to maintain their
skills or develop satisfactory clinical judgement. In some locations in rural Victoria this
risk is minimized through the employment of fully qualified staff to take leadership and
training roles in those areas that would otherwise be totally reliant on volunteers or
Community Ambulance Officers. This strategy is particularly valuable in those
locations without general practitioners, who would ordinarily be expected to assume
leadership roles in relation to pre-hospital care. Although often criticized as
paternalistic, community models without links to regional ambulance services are
highly dependent on local general practitioners for support and advice. Local general
practitioners act as role models and advisors for volunteers. For example, the findings in
Chapter 5 indicate that voluntary staff may lack adequate training in how to handle the
ethical problem of dealing with confidentiality in small communities.
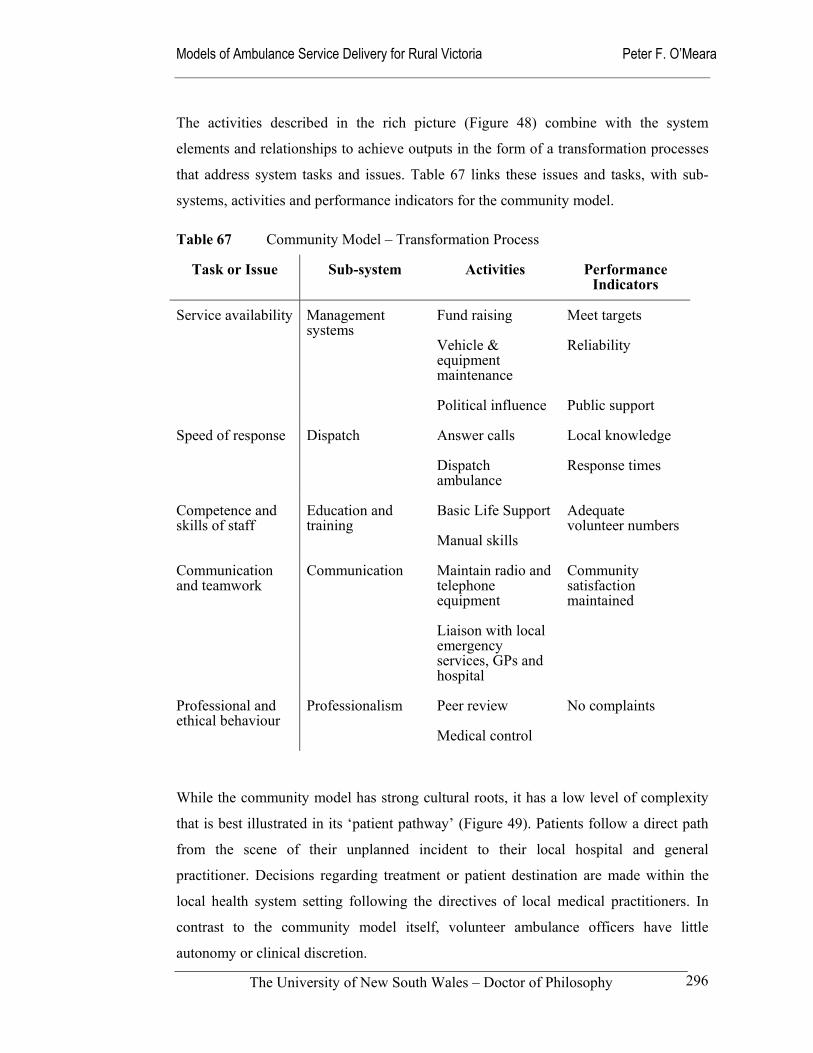
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
296
The activities described in the rich picture (Figure 48) combine with the system
elements and relationships to achieve outputs in the form of a transformation processes
that address system tasks and issues. Table 67 links these issues and tasks, with sub-
systems, activities and performance indicators for the community model.
Table 67 Community Model – Transformation Process
Task or Issue Sub-system Activities Performance Indicators
Service availability
Management systems
Fund raising
Vehicle & equipment maintenance
Political influence
Meet targets
Reliability
Public support
Speed of response
Dispatch Answer calls
Dispatch ambulance
Local knowledge
Response times
Competence and skills of staff
Education and training
Basic Life Support
Manual skills
Adequate volunteer numbers
Communication and teamwork
Communication Maintain radio and telephone equipment
Liaison with local emergency services, GPs and hospital
Community satisfaction maintained
Professional and ethical behaviour
Professionalism Peer review
Medical control
No complaints
While the community model has strong cultural roots, it has a low level of complexity
that is best illustrated in its ‘patient pathway’ (Figure 49). Patients follow a direct path
from the scene of their unplanned incident to their local hospital and general
practitioner. Decisions regarding treatment or patient destination are made within the
local health system setting following the directives of local medical practitioners. In
contrast to the community model itself, volunteer ambulance officers have little
autonomy or clinical discretion.
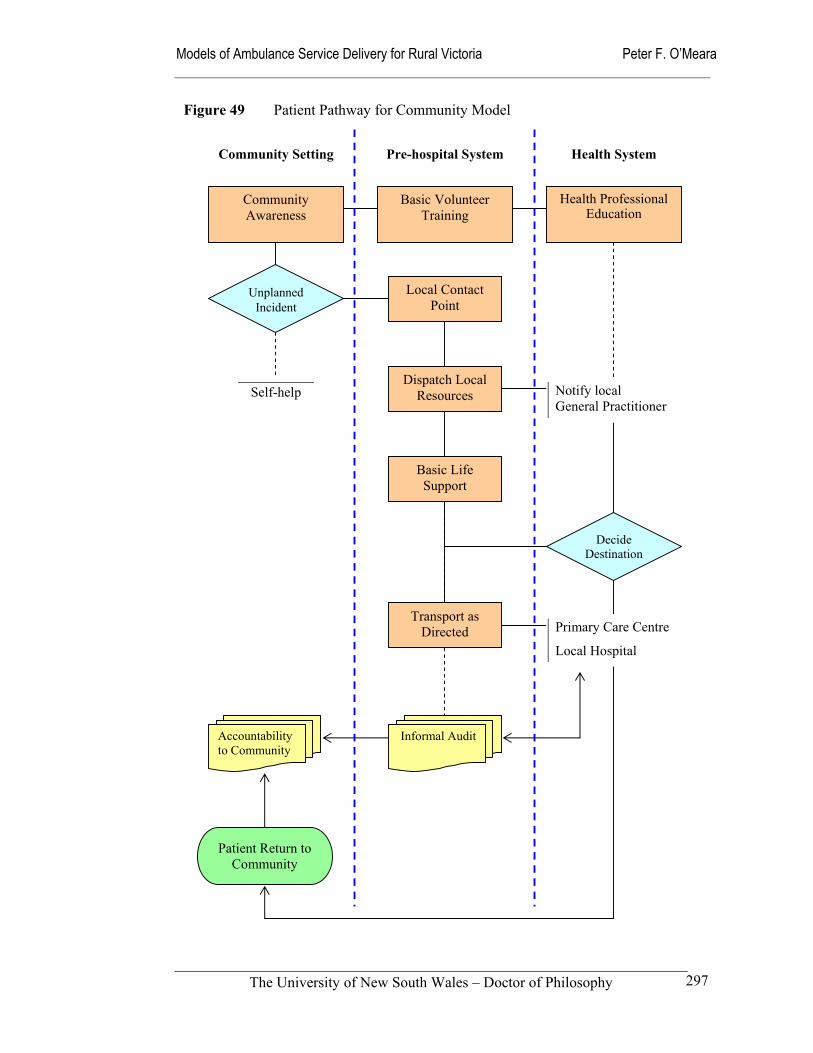
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
297
Community Setting Pre-hospital System Health System
Unplanned Incident
Decide Destination
Community Awareness
Basic Volunteer Training
Health Professional Education
Self-help Notify local General Practitioner
Primary Care Centre
Local Hospital
Figure 49 Patient Pathway for Community Model
Informal AuditAccountability to Community
Basic Life Support
Transport as Directed
Dispatch Local Resources
Local Contact Point
Basic Life Support
Patient Return to Community

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
298
Culturally, the community model has a very strong rural character, with ample
opportunity for health professionals, emergency workers and members of the local
community to be involved. This may be as a volunteer ambulance officer or as a
participant in the local governance of the service; all citizens have the opportunity to
influence the setting of organizational priorities and objectives. This attribute contrasts
with the expert model that follows, where priority setting is firmly in the hands of the
‘experts’.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
299
8.5 Expert model
The expert model is a professionally staffed and managed ambulance system providing
pre-hospital care based on the availability of advanced technology and technically
skilled staff. Its aim is to reduce the mortality and morbidity rates for trauma and other
acute illness, such as cardiac arrest. It purports to be based on clinical evidence of its
efficacy and effectiveness in treating patients suffering from acute injury or illness. The
employment of full-time, professionally trained personnel who have access to the latest
bio-medical equipment and practice a high level and standard of clinical intervention
within medically prescribed boundaries characterise the model. The medical dominance
metaphor is used here to describe the expert model. Willis and McCarthy (1986) made
the observation in the mid-1980s that in metropolitan Melbourne the MICA variation of
the expert model evolved from volunteer roots with the help and support of an active
medical community. Little has changed since, with medical dominance remaining a
potent force in Australia and elsewhere. An example is in the United Kingdom, where
paramedics have been recognised as a profession supplementary to medicine (Nicholl et
al 2001: 18). This phenomenon of medical domination is not confined to ambulance
paramedics; other health professionals such as nurses all tend to be defined through
their relationship to medicine (Hancock 1999: 42-47; Daniel 1993; Bates & Lapsley
1986: 207).
A feature of the expert model is its high cost structure. It is very expensive to establish
and maintain, due to the level of technology required and the extensive education and
training requirements for staff. Its idealistic nature results in a practitioner-level view
that consigns the challenges of running the service efficiently to ‘someone else’.
Ambulance service managers are faced with the challenge of managing a highly skilled
and motivated workforce within a system that is expected to respond to a largely
uncontrolled level of demand. Politically, they also have to contend with the power and
influence of emergency medicine physicians as the mentors and allies of ambulance
paramedics. The image of heartless managers and bureaucrats denying sick patients the
skills and expertise of the expert paramedic through cost-containment or out-dated rules
is a powerful image that has been used extensively in Australia and elsewhere to obtain
sympathy or public support for resource increases (Payne 2000; Hickey 2001a & 2001b;
Mahony 2001).
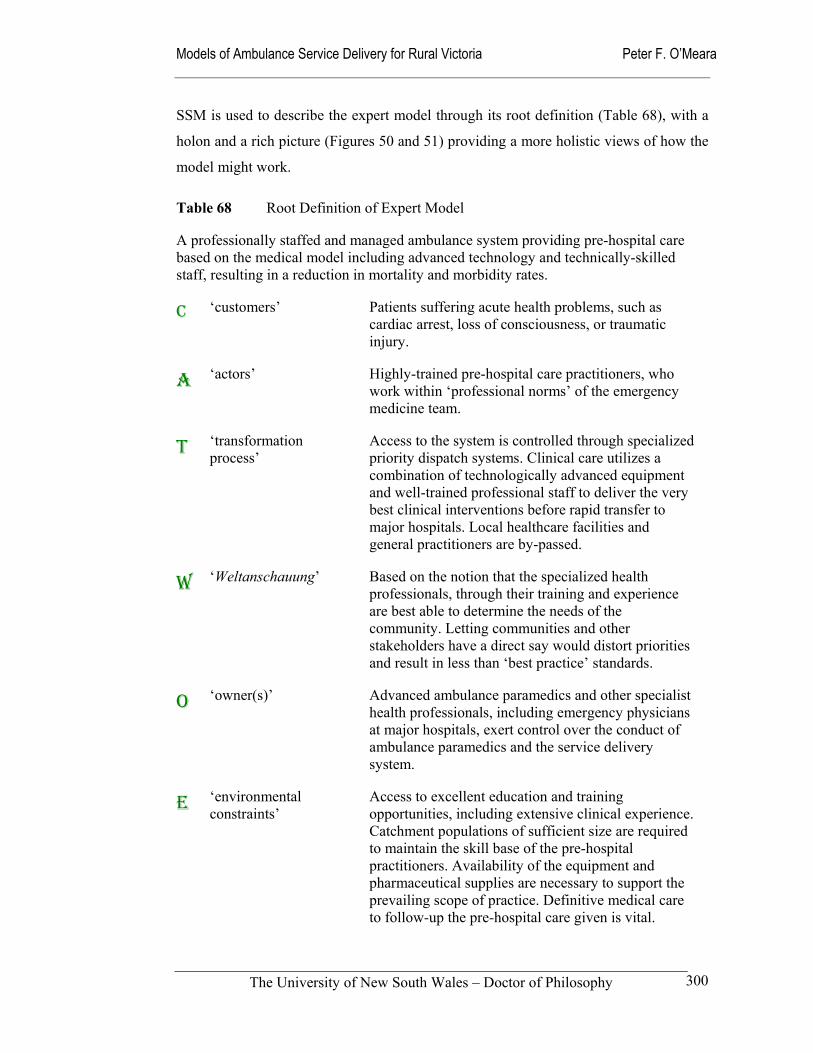
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
300
SSM is used to describe the expert model through its root definition (Table 68), with a
holon and a rich picture (Figures 50 and 51) providing a more holistic views of how the
model might work.
Table 68 Root Definition of Expert Model
A professionally staffed and managed ambulance system providing pre-hospital care based on the medical model including advanced technology and technically-skilled staff, resulting in a reduction in mortality and morbidity rates.
C ‘customers’ Patients suffering acute health problems, such as cardiac arrest, loss of consciousness, or traumatic injury.
A ‘actors’ Highly-trained pre-hospital care practitioners, who work within ‘professional norms’ of the emergency medicine team.
T ‘transformation process’
Access to the system is controlled through specialized priority dispatch systems. Clinical care utilizes a combination of technologically advanced equipment and well-trained professional staff to deliver the very best clinical interventions before rapid transfer to major hospitals. Local healthcare facilities and general practitioners are by-passed.
W ‘Weltanschauung’ Based on the notion that the specialized health professionals, through their training and experience are best able to determine the needs of the community. Letting communities and other stakeholders have a direct say would distort priorities and result in less than ‘best practice’ standards.
O ‘owner(s)’ Advanced ambulance paramedics and other specialist health professionals, including emergency physicians at major hospitals, exert control over the conduct of ambulance paramedics and the service delivery system.
E ‘environmental constraints’
Access to excellent education and training opportunities, including extensive clinical experience. Catchment populations of sufficient size are required to maintain the skill base of the pre-hospital practitioners. Availability of the equipment and pharmaceutical supplies are necessary to support the prevailing scope of practice. Definitive medical care to follow-up the pre-hospital care given is vital.
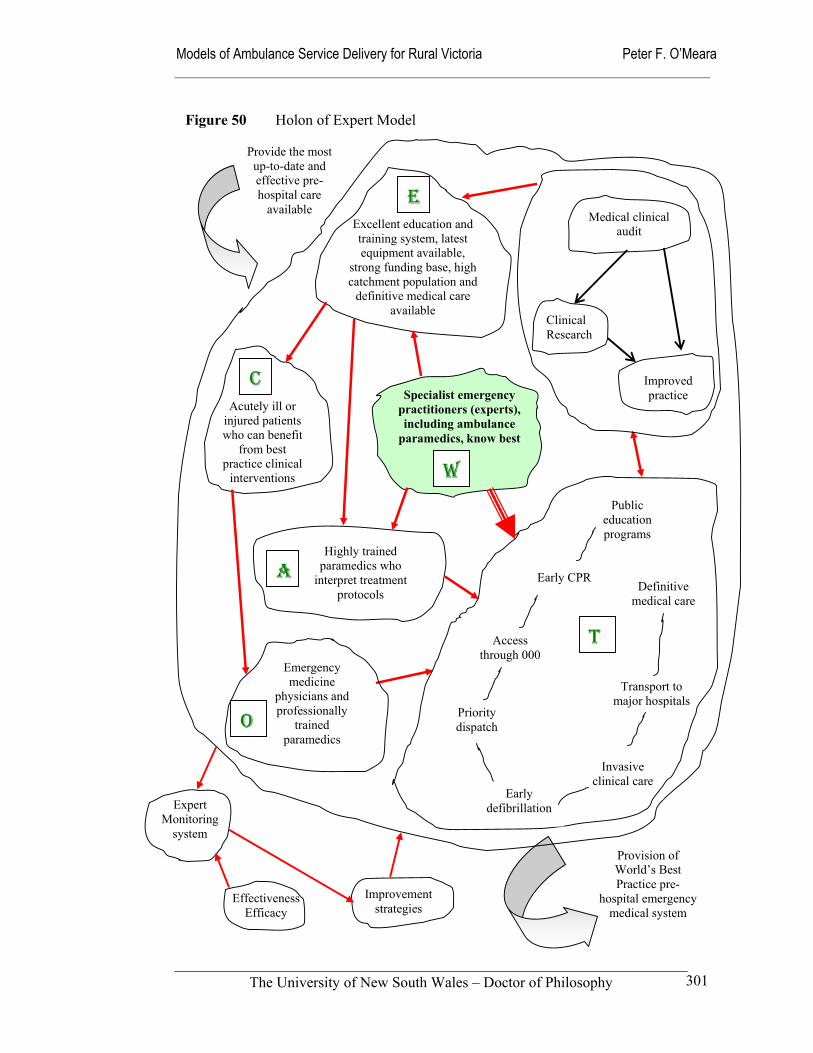
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
301
Highly trained paramedics who
interpret treatment protocols
Emergency medicine
physicians and professionally
trained paramedics
Excellent education and training system, latest equipment available,
strong funding base, high catchment population and
definitive medical care available
Provision of World’s Best Practice pre-
hospital emergency medical system
Provide the most up-to-date and effective pre-hospital care
available
Public education programs
Early CPR
Access through 000
Priority dispatch
Invasive clinical care
Definitive medical care
Transport to major hospitals
Early defibrillation
Improved practice
Clinical Research
Medical clinical audit
Effectiveness Efficacy
Improvement strategies
Expert Monitoring
system
Acutely ill or injured patients who can benefit
from best practice clinical
interventions
Specialist emergency practitioners (experts), including ambulance
paramedics, know best
E
W
C
A
O
T
Figure 50 Holon of Expert Model
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
302
Reality Testing of Expert Model
The domination of emergency medicine physicians and other related medical specialists
over the expert model is a cause for concern amongst other rural health professionals,
and to a lesser extent amongst members of the public. It adds to rural health
practitioners feeling they are being ‘deskilled’ through the bypass of local hospitals and
devaluing of their emergency skills (Somers & Drinkwater 1997; Somers 1999). One
outcome of the close association between ambulance paramedic and emergency
medicine specialists is that they sometimes adopt paternalistic attitudes toward local
general practitioners, nurses, volunteer staff and community members.
Indeed, this elitist attitude of advanced paramedics extends to relations with other
ambulance staff with less specialised training. In NSW for instance, the advanced
paramedics (Level 5 officers) have resisted attempts to have them work with ‘lesser’
qualified officers (Audit Office NSW: 91).
Competition to gain entry into the elite paramedic course in Service Oz [NSW] is intense, creating rivalry where there was once mateship. All Level 3 respondents commented that the process for entry was unclear, and that selection was unfair and smacked of favouritism and cronyism.
So few are trained as paramedics in Service Oz that competition has further split the service into two factions. … Whilst upskilling adds to the professionalism of the service, should provide more skills and autonomy for staff and is much better for the client, upskilling some members nearly always takes away some of the decision making and responsibility previously enjoyed by experienced staff.
(Mahony 2001: 140)
As a result of this tendency toward elitism, pre-hospital paramedics in the expert model
run the risk of becoming estranged from the wider community, other health system
components, and their peers. In the rural context, this attitude diminishes the
effectiveness and sustainability of the whole urgent care system (O’Meara et al 2002).
The counter argument is that this is a transitional stage of organizational development,
with improved education and training likely to enhance teamwork with other health
professionals as ambulance paramedics develop improved clinical assessment skills
(Cooke 1999).
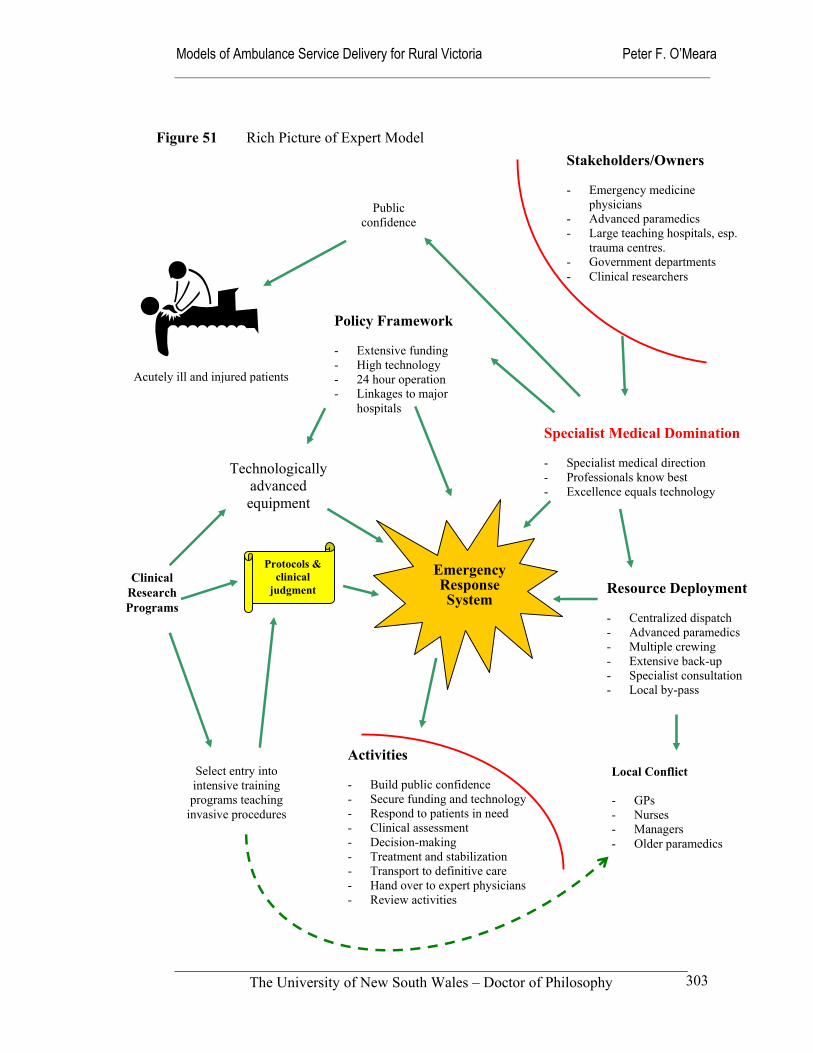
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
303
Protocols & clinical
judgment
Technologically advanced equipment
Clinical Research Programs
Figure 51 Rich Picture of Expert Model
Emergency Response System
Stakeholders/Owners - Emergency medicine
physicians - Advanced paramedics - Large teaching hospitals, esp.
trauma centres. - Government departments - Clinical researchers
Policy Framework - Extensive funding - High technology - 24 hour operation - Linkages to major
hospitals
Resource Deployment - Centralized dispatch - Advanced paramedics - Multiple crewing - Extensive back-up - Specialist consultation - Local by-pass
Public confidence
Specialist Medical Domination - Specialist medical direction - Professionals know best - Excellence equals technology
Activities - Build public confidence - Secure funding and technology - Respond to patients in need - Clinical assessment - Decision-making - Treatment and stabilization - Transport to definitive care - Hand over to expert physicians - Review activities
Select entry into intensive training programs teaching
invasive procedures
Local Conflict - GPs - Nurses - Managers - Older paramedics
Acutely ill and injured patients
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
304
These criticisms of the expert model are powerful, with ambulance services already
perceived to have communication and collaboration problems with other health
professionals in rural areas. As a result of these tensions, general practitioners and
nurses in smaller towns appear to be less willing to accept the rapidly changing status of
ambulance paramedics. For instance, as reported in Chapter 5, some rural general
practitioners are very keen to maintain the presence of volunteer staff, despite their
limited training and expertise. The ‘pay-off’ for GPs, is their ability to maintain control
of the emergency response system and retain their patients within the local health
system. Part of the problem with the expert model for local GPs and nurses, is that it has
direct links with major metropolitan referral hospitals through consultant level medical
advice, specialized patient retrieval systems, and advanced clinical training
opportunities. The rich picture (Figure 51) illustrates these external relationships
between the expert model and the metropolitan and regional health systems.
Expert paramedics such as MICA paramedics in Victoria, who may be dispatched from
larger and more distant regional centres to small rural centres, see themselves as the
controlling party when relating to rural health services and not under the supervision or
control of local general practitioners. Nurses are also uncomfortable with this newly
emerging health profession that is not yet subject to registration requirements in
Australia and is a recent entrant into the tertiary education system. The position of
ambulance paramedics therefore lacks these reference points to connect with the
profession of nursing. As a result of this late professional development and the
perceived arrogance of some ambulance paramedics, nurses may be inclined to ‘pick-
up’ on any mis-judgements that ambulance paramedics may make in the hospital
environment. Despite these concerns, it is clear that many ambulance paramedics are
deeply embedded in the life of their communities and have excellent professional
relationships with health institutions and professionals.
Although ambulance professionals are not yet a registered profession in Australia, they
have adopted many of the professional and ethical norms of their medical and nursing
colleagues. There have been limited calls for registration from the College of
Ambulance Professionals and industrial unions for a number of years. And as in other
countries, registration is likely to occur at some time in the not too distant future.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
305
More so than other pre-hospital models, the expert model is highly reliant on ambulance
paramedics who are very competent and technically skilled. This workforce
characteristic raises the issue of recruitment and retention that bedevils other health
professions in rural Australia. The ability of rural towns to maintain an expert pre-
hospital model depends on the existence of an advanced health system infrastructure
and the broader economic, social and cultural conditions within the local community.
Without strong and vibrant communities, the recruitment and retention of suitably
qualified staff will present many challenges. In common with other health professionals,
ambulance paramedics have aspirations for themselves and their families that may be
difficult to fulfil in isolated areas or stressed economic zones.
The development of the expert model throughout the world has been built on a narrow
educational base with little independent research to guide its implementation.
Innovations and operational advances have often been predicated on resource
availability, perceived needs and individual personalities. What little research has taken
place has lacked funding and been limited by a shortage of academic interest and
education amongst ambulance personnel. This lack of research effort is even greater in
rural areas, where limited resources are often more acute than in urban areas. Without
substantial outside support, rural ambulance services lack the resources required to
pursue promising research agendas. This weakness offers an important opportunity for
regionally located universities to nurture and develop a pre-hospital research culture
amongst rural ambulance paramedics.
On a broader scale, the expert model suffers because of its narrow scope of practice and
its need for relatively large catchment populations to ensure paramedics maintain their
complex skill base. Populations with high levels of trauma and other acute medical
conditions that are amenable to emergency interventions are particularly attractive to the
expert model. This requirement makes it very difficult to successfully introduce and
sustain the expert model in rural areas. A positive innovation that has improved the
accessibility of the expert model in the rural areas of Victoria has been the introduction
of airborne MICA paramedics, where highly trained staff can be flown in by rotary-
wing aircraft to the patient or incident. The experience in the Gippsland region of
Victoria has been that the community has embraced this variation of the model with
gusto; local communities continue to raise large sums of money for equipment, and led
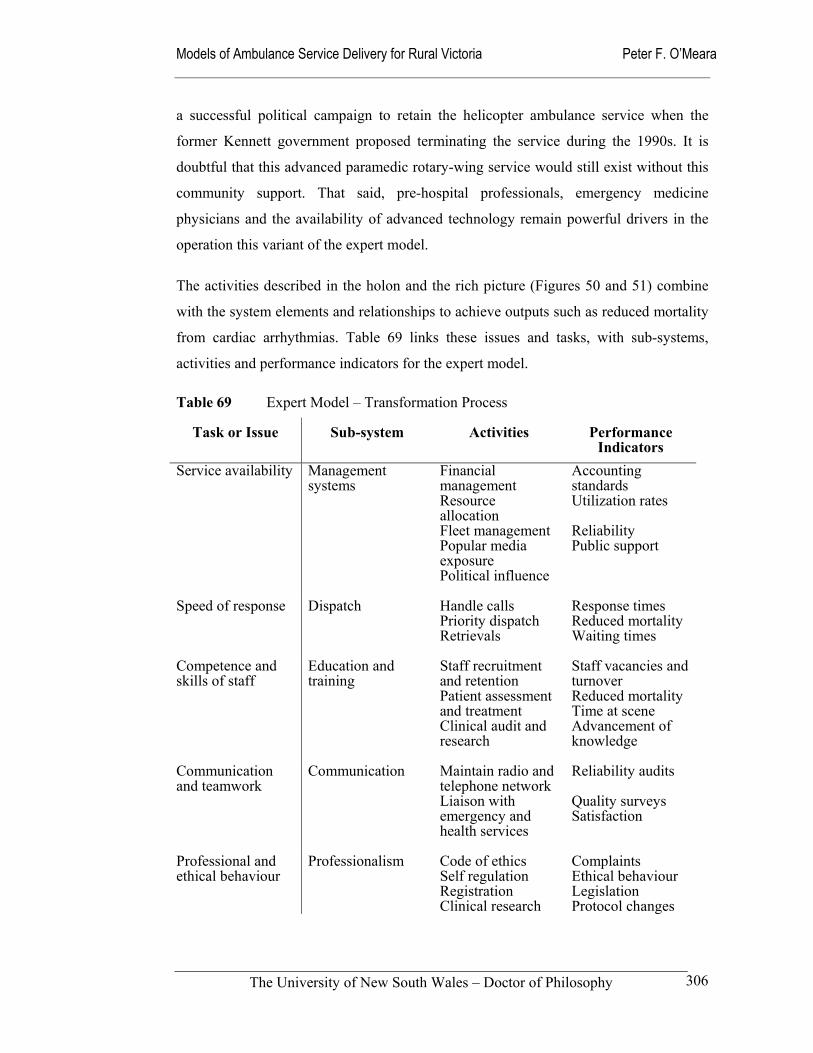
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
306
a successful political campaign to retain the helicopter ambulance service when the
former Kennett government proposed terminating the service during the 1990s. It is
doubtful that this advanced paramedic rotary-wing service would still exist without this
community support. That said, pre-hospital professionals, emergency medicine
physicians and the availability of advanced technology remain powerful drivers in the
operation this variant of the expert model.
The activities described in the holon and the rich picture (Figures 50 and 51) combine
with the system elements and relationships to achieve outputs such as reduced mortality
from cardiac arrhythmias. Table 69 links these issues and tasks, with sub-systems,
activities and performance indicators for the expert model.
Table 69 Expert Model – Transformation Process
Task or Issue Sub-system Activities Performance Indicators
Service availability
Management systems
Financial management Resource allocation Fleet management Popular media exposure Political influence
Accounting standards Utilization rates Reliability Public support
Speed of response
Dispatch Handle calls Priority dispatch Retrievals
Response times Reduced mortality Waiting times
Competence and skills of staff
Education and training
Staff recruitment and retention Patient assessment and treatment Clinical audit and research
Staff vacancies and turnover Reduced mortality Time at scene Advancement of knowledge
Communication and teamwork
Communication Maintain radio and telephone network Liaison with emergency and health services
Reliability audits Quality surveys Satisfaction
Professional and ethical behaviour
Professionalism Code of ethics Self regulation Registration Clinical research
Complaints Ethical behaviour Legislation Protocol changes
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
307
Variations of the expert model continue to influence the development of ambulance
systems throughout the world. Initially, this was through the introduction of intensive
care ambulance systems in larger cities such as Seattle, Belfast, Melbourne and Sydney
(Eisenberg et al 1996). Despite its detractors, the expert model is well suited to larger
regional centres and variations can operate effectively in medium-sized rural centres
where local medical and health infrastructure can support it. In Figure 52, patient
pathways are used to describe how the expert model operates; in particular, it illustrates
the role of specialist medical control over the system of pre-hospital care.
The feasibility of introducing the expert model in smaller centres or those without larger
hospitals is more problematical. Apart from being very expensive to establish and
operate, major workforce recruitment and retention problems are likely to develop along
the same lines as those experienced in medicine and nursing. In the rural context, the
pre-hospital expert model of service delivery is a narrow and inflexible approach when
contrasted with the promise that some of the expanded-scope models offer. The
following pre-hospital practitioner offers an alternative to this; unlike the expert model,
its foundation rests on a broad educational base, increased clinical autonomy,
independent research, and improved links with local health professionals when dealing
with out-of-hospital incidents.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
308
8.6 Practitioner model
In rural settings ambulances often transport patients long distances to health care
facilities that are not closely affiliated with their local health care resources. In some
cases this is appropriate, due to a requirement that some emergency patients -
particularly severely injured trauma patients - receive sophisticated tertiary care.
However, this long distance transportation may simply reflect the traditional separation
of the ambulance service from local primary care providers, public health and social
service agencies that might be able to deal effectively with the needs of the patient.
In either case, the ability to provide integrated health services is often impeded by the
geographic separation of health system components and the lack of regular
communication or organizational networking between them. This observation is
reflected in suggestions to co-locate ambulance services with rural hospitals and to
encourage greater involvement of ambulance staff in public health activities during their
down-time (Sinclair 2000). It is in rural areas that ambulance services have a unique
opportunity to demonstrate the capacity of the ambulance system to fulfil broader public
health and primary care outreach roles for traditionally under-served communities.
The proposed pre-hospital practitioner model has strong foundations within the
established health professions where ambulance paramedics see themselves as an
emerging health profession. While it conceptually incorporates the well-known chain of
survival system, which nests within it, the practitioner model addresses many of the
shortcomings of the expert model. The practitioner model extends its interest both
before and beyond the chain of survival’s seven links of the emergency event,
discovery, access, notification, triage and dispatch, care and transport, and definitive
treatment. It does this through, an extension of the depth of treatment and clinical
decision-making, and the inclusion of primary care activities both before and after the
chain of survival as an extension of ambulance practice. The extension and deepening of
ambulance roles and practice is illustrated in Figure 53 that shows how the chain of
survival concept nests within the practitioner model.
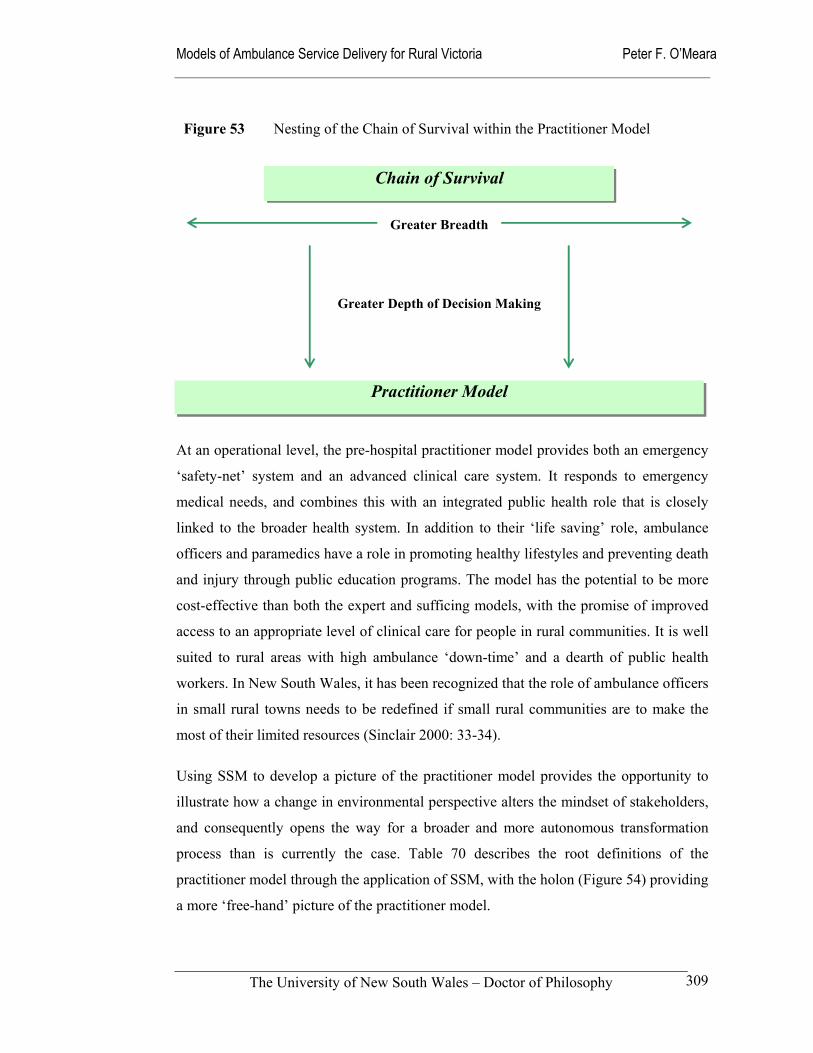
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
309
At an operational level, the pre-hospital practitioner model provides both an emergency
‘safety-net’ system and an advanced clinical care system. It responds to emergency
medical needs, and combines this with an integrated public health role that is closely
linked to the broader health system. In addition to their ‘life saving’ role, ambulance
officers and paramedics have a role in promoting healthy lifestyles and preventing death
and injury through public education programs. The model has the potential to be more
cost-effective than both the expert and sufficing models, with the promise of improved
access to an appropriate level of clinical care for people in rural communities. It is well
suited to rural areas with high ambulance ‘down-time’ and a dearth of public health
workers. In New South Wales, it has been recognized that the role of ambulance officers
in small rural towns needs to be redefined if small rural communities are to make the
most of their limited resources (Sinclair 2000: 33-34).
Using SSM to develop a picture of the practitioner model provides the opportunity to
illustrate how a change in environmental perspective alters the mindset of stakeholders,
and consequently opens the way for a broader and more autonomous transformation
process than is currently the case. Table 70 describes the root definitions of the
practitioner model through the application of SSM, with the holon (Figure 54) providing
a more ‘free-hand’ picture of the practitioner model.
Chain of Survival
Practitioner Model
Greater Breadth
Greater Depth of Decision Making
Figure 53 Nesting of the Chain of Survival within the Practitioner Model
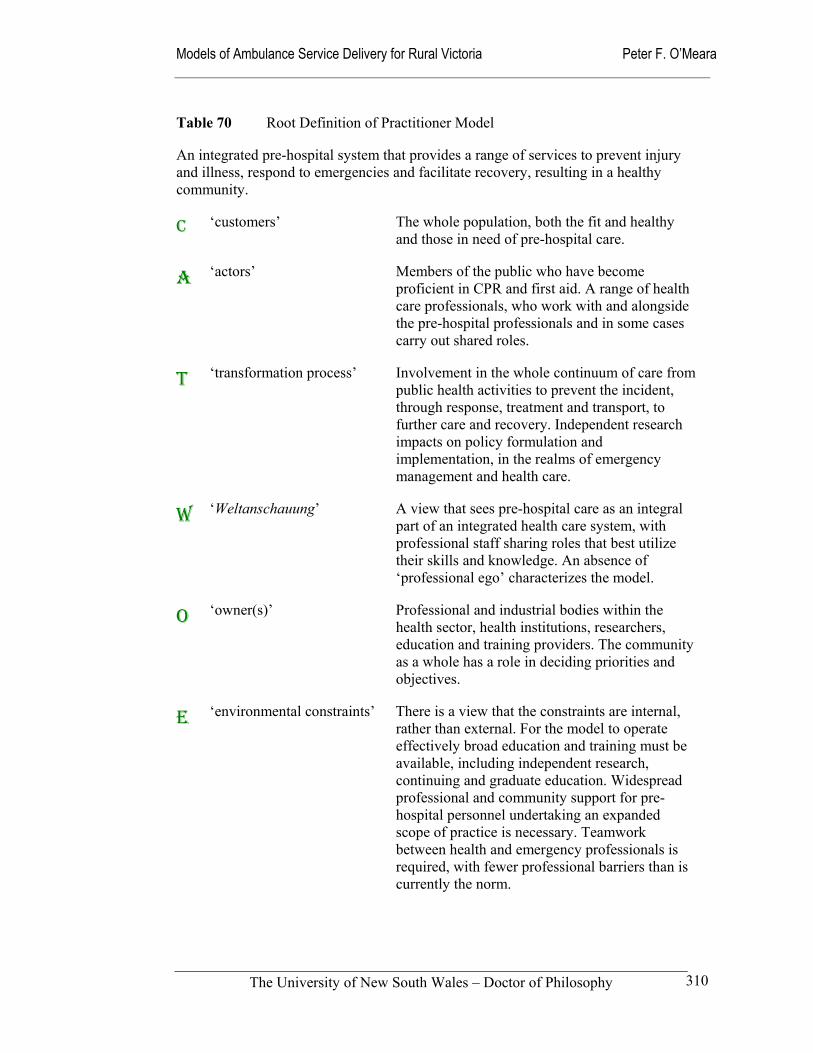
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
310
Table 70 Root Definition of Practitioner Model
An integrated pre-hospital system that provides a range of services to prevent injury and illness, respond to emergencies and facilitate recovery, resulting in a healthy community.
C ‘customers’ The whole population, both the fit and healthy and those in need of pre-hospital care.
A ‘actors’ Members of the public who have become proficient in CPR and first aid. A range of health care professionals, who work with and alongside the pre-hospital professionals and in some cases carry out shared roles.
T ‘transformation process’ Involvement in the whole continuum of care from public health activities to prevent the incident, through response, treatment and transport, to further care and recovery. Independent research impacts on policy formulation and implementation, in the realms of emergency management and health care.
W ‘Weltanschauung’ A view that sees pre-hospital care as an integral part of an integrated health care system, with professional staff sharing roles that best utilize their skills and knowledge. An absence of ‘professional ego’ characterizes the model.
O ‘owner(s)’ Professional and industrial bodies within the health sector, health institutions, researchers, education and training providers. The community as a whole has a role in deciding priorities and objectives.
E ‘environmental constraints’ There is a view that the constraints are internal, rather than external. For the model to operate effectively broad education and training must be available, including independent research, continuing and graduate education. Widespread professional and community support for pre-hospital personnel undertaking an expanded scope of practice is necessary. Teamwork between health and emergency professionals is required, with fewer professional barriers than is currently the norm.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
311
The possibility of an expanded role for ambulance paramedics has received limited
attention in Australia. What little interest there has been in this concept has been
generally confined to dialogue about whether ambulance paramedics should be trained
in the style of a tradespersons or educated as health professionals (Wellard 1994; Field
1994; Field et al 1999). The latter implies a more holistic approach to preparing
paramedics for practice, with a greater emphasis on the social sciences and preparation
for independent practice and research (Lord 1998; Grantham 2001).
In spite of this limited discussion about the changing role of ambulance paramedics in
Australia a version of the practitioner model has been evolving in South Australia. The
model developed there is philosophically anchored in the linkages between knowledge,
trust and outcomes. It addresses some of the clinical and organizational frustrations that
Australian paramedics complain about; principally, a lack of autonomous decision
making and a perceived lack of trust from ambulance service management (Mahony
2001).
In this model [in SAAS] the role of the medical input is to educate, providing the most appropriate current medical management of the situation and the underlying rationale behind that management. The actual implementation is … the responsibility of the pre-hospital professional, but the pre-hospital professional is working within a fully integrated medical care system.
(Grantham 2001)
The concept of expanding the ambulance paramedics’ scope of practice is not novel in
other countries, where it has been widely discussed and debated (Garza 1994; Neely et
al 1997; Martinez 1998; Roberts 1998; Cooke 1998; Delbridge et al 1998; O’Connor et
al 1999; Hunt et al 1999; Meade 1999; Lendrum et al 2000; Schmidt et al 2000).
Internationally, the most influential document is the United States National Highway
Traffic Safety Administrator’s Agenda for the Future, which articulates a vision for the
future of EMS in the United States (NHTSA 1996). Martinez (1998) also sets out a
vision for an expanded role in the United States, where existing EMS has been criticized
for being isolated from other health services, reactive to acute illness and injury,
focused on service to individuals care and failing to fully use utilize the available
communications technology.
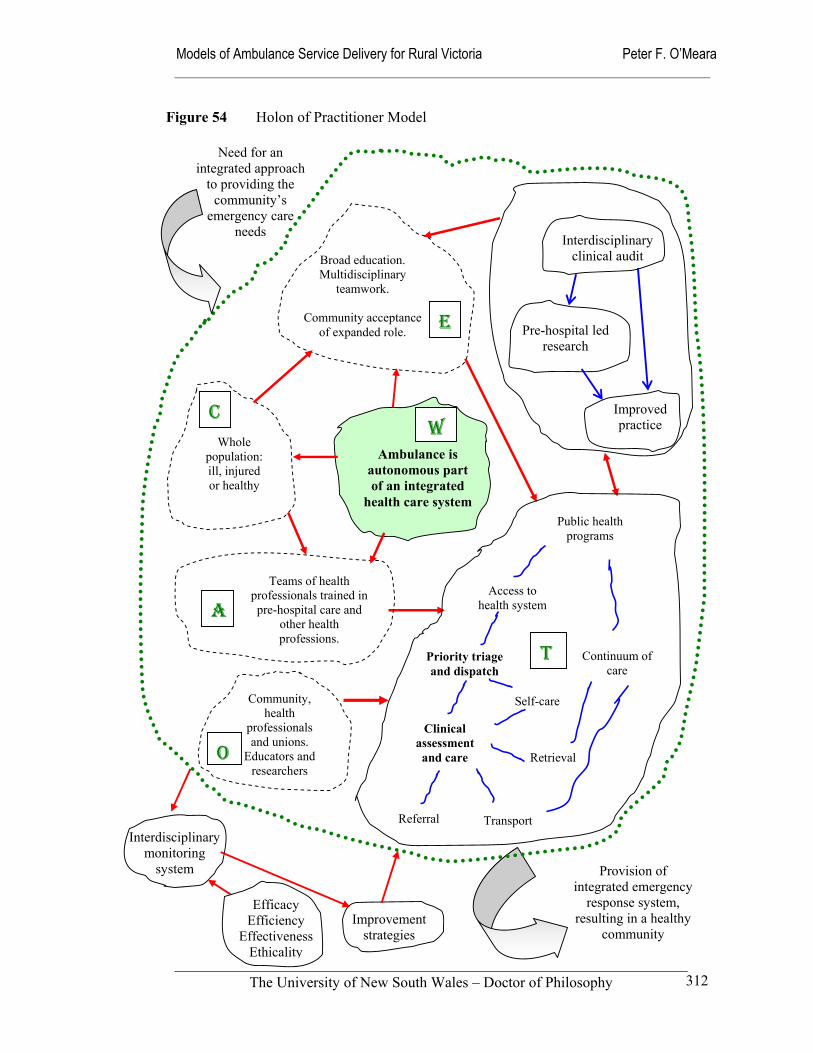
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
312
Whole population: ill, injured or healthy
Broad education. Multidisciplinary
teamwork.
Community acceptance of expanded role.
Ambulance is autonomous part of an integrated
health care system
Provision of integrated emergency
response system, resulting in a healthy
community
Need for an integrated approach
to providing the community’s
emergency care needs
Improved practice
Pre-hospital led research
Interdisciplinary clinical audit
Efficacy Efficiency
Effectiveness Ethicality
Improvement strategies
Interdisciplinary monitoring
system
Figure 54 Holon of Practitioner Model
E
WC
Community, health
professionals and unions.
Educators and researchers
O
Teams of health professionals trained in pre-hospital care and
other health professions.
A
Public health programs
Access to health system
Priority triage and dispatch
Clinical assessment and care
Referral
Continuum of care
Retrieval
Transport
T
Self-care
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
313
The American College of Emergency Physicians has suggested that for any expansion
of pre-hospital scope of practice to be successful, seven principles must be met:
Close medical supervision by physicians with experience and an understanding of the roles and capabilities of EMS personnel is mandatory.
Education programs with quality-assurance mechanisms to ensure maintenance of standards established for these programs must be in place before implementing an expanded scope for EMS providers.
Expanded roles for prehospital providers must adhere to legal requirements. Physician oversight of any such expanded roles for prehospital providers is a necessity.
The existing emergency response system must not suffer for the sake of an expanded-scope program.
Access to emergency care must not be compromised by efforts to alter the basic emergency response system as a part of medical care integration.
A community plan and needs assessment with physician input must guide the development of any expanded-scope program.
Attempts to expand the scope of paramedic practice without the support of all involved parties and adequate medical oversight are not in the best interest of good patient care. (ACEP 1997: 364)
In the United Kingdom the report of the Joint Royal Colleges and Ambulance Liaison
Committee on the future role and education of paramedics has set the agenda (JRCALC
2000). Nichol et al (2001) have expanded on this discussion, with a suggestion to
develop a new profession called a Practitioner in Emergency Care. While Roberts
(1998) has suggested that rather than extend the education and training of ambulance
paramedics, it may be more appropriate to develop a generic health worker called a
Paramedic Practitioner who can move between a variety of community and hospital
settings. Also in Britain, Lendrum et al (2000) have examined the match between
existing workload and training of ambulance paramedics. They found a strong training
emphasis on potentially life threatening conditions and comparatively little training in
minor injuries that represent a large proportion of workload. They concluded that more
training would be required in those areas if more responsibility is to be taken for
discharge of patients at the scene of the incident or event.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
314
Utilizing a more free-market perspective, O’Connor et al (1999) make similar
suggestions, where expanded-scope paramedics would form part of an integrated health
care system. Bissel et al (1999a & 1999b) caution that expanding the scope of practice
needs to be closely scrutinized to ensure that any changes have positive public health
outcomes.
Neely et al (1997) and Schmidt et al (2000) have looked at the option of a multiple-
option decision point (MODP) model, which uses protocols to place patients into four
action categories. Hunt et al (1999) has tested a similar concept in Kansas to determine
whether paramedics can accurately determine the necessity for transport to hospital.
Through the use of pictures, the holon (Figure 54) shows the idea of multiple decision
points within the transformation process of the practitioner model. Later, the patient
pathway (Figure 56) provides a clearer understanding through the use of flowcharting.
Neely and Schmidt’s four action categories are:
Patient would require ambulance transport to emergency department;
Patient is thought to need emergency department evaluation, but may safely go by alternative means;
Patient may be referred to his or her primary care provider within 24 hours; or
Patient would require field assessment and treatment only.
Meade (1999) attempts to define expanded-scope practice and examines more broadly
what it would mean to expand ambulance paramedic roles. He argues, that such a
paradigm shift would result in changes in the areas of:
Equipment and technology;
Policies and procedures;
Education and research;
Legislation and organization; and
Mission and attitude.
Along with Garza (1994), Meade sees Emergency Medical Services (EMS) in future at
the intersection of public safety, public health, and health care. Locating EMS at this
junction ignites a debate about how much education a pre-hospital provider needs to

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
315
competently render patient care in the out-of-hospital environment (Meade 1999). This
debate cuts to the core of the question about whether pre-hospital practice is a health
profession or a skilled artisan (Field et al 1999). Australian contributions to this debate
from ambulance paramedics have varied from the thoughtful to others that are stronger
on rhetoric than substance (Sweet 1997; Bailey 1996 &1997; Butson 1999; DeWitt
1997). Mahony (2001) picked up this tendency amongst Australian ambulance
paramedics to ‘whinge’ about the management, rather than take personal responsibility
for initiating positive change.
Reality Testing of Practitioner Model
The unique characteristics of the pre-hospital practitioner model are derived from its
view of the world. Its adherents see pre-hospital care as an actor within the overall
health system, with influence over its own destiny and that of others.
When the model is unpacked (‘decomposed’ to use the SSM terminology) in Table 70
and in the holon and rich picture (Figures 54 and 55), a major area of interest
highlighted is the existence of a research and development agenda that is at once
interdisciplinary and independent of the dominant medical paradigm. This characteristic
drives a transformation process that is evidence-based, rather than one that stands on
myths and traditional ways of doing things. Another characteristic of the transformation
process is the centrality of teamwork between pre-hospital providers of all professional
disciplines, and other emergency service and health care providers. To do this, open
channels of communication are established through co-location of facilities, combined
education and training, and the establishment of interdisciplinary clinical and
operational audit systems.
Morgan (1997) provides a means of expressing the basis of the pre-hospital practitioner
model through four processes that he calls the ‘logics of change’. Each provides a
metaphorical frame for explaining how the life of organizations is formed and
transformed.
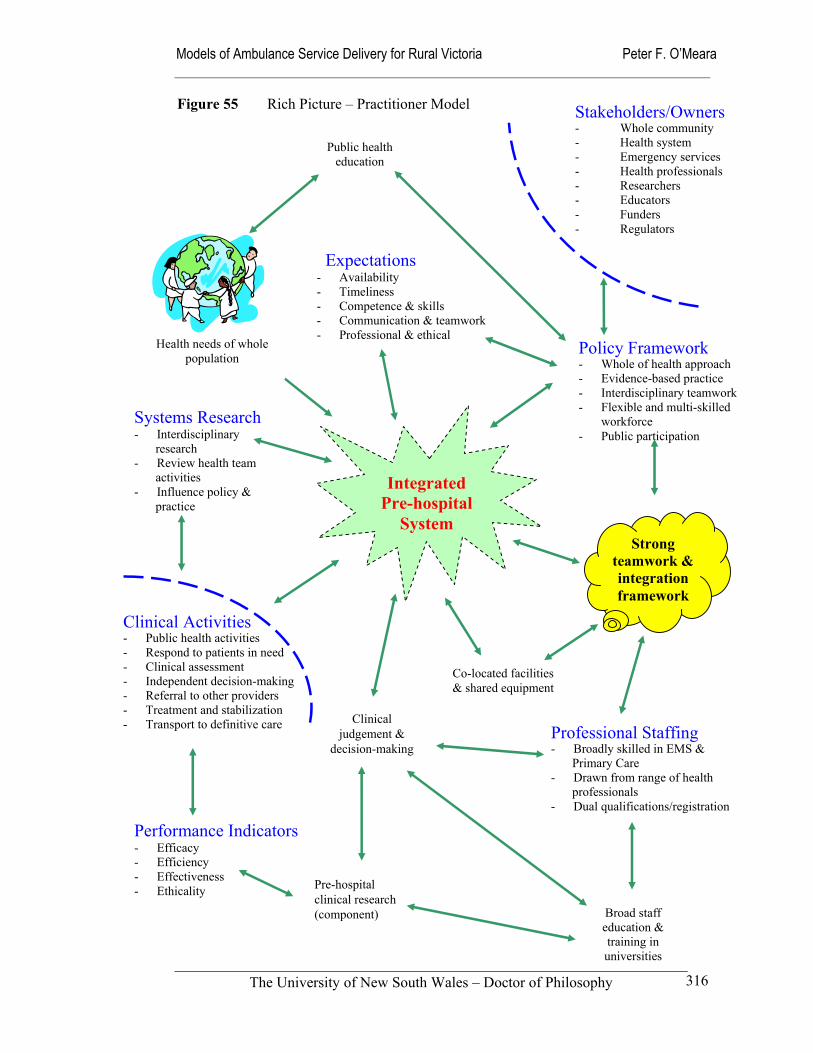
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
316
Figure 55 Rich Picture – Practitioner Model Stakeholders/Owners
- Whole community - Health system - Emergency services - Health professionals - Researchers - Educators - Funders - Regulators
Integrated Pre-hospital
System
Co-located facilities & shared equipment
Policy Framework- Whole of health approach - Evidence-based practice - Interdisciplinary teamwork - Flexible and multi-skilled
workforce - Public participation
Public health education
Pre-hospital clinical research(component)
Professional Staffing- Broadly skilled in EMS &
Primary Care - Drawn from range of health
professionals - Dual qualifications/registration
Broad staff education & training in universities
Strong teamwork & integration framework
Clinical judgement &
decision-making
Expectations - Availability - Timeliness - Competence & skills - Communication & teamwork- Professional & ethical
Clinical Activities - Public health activities - Respond to patients in need - Clinical assessment - Independent decision-making - Referral to other providers - Treatment and stabilization - Transport to definitive care
Performance Indicators - Efficacy - Efficiency - Effectiveness - Ethicality
Systems Research - Interdisciplinary
research - Review health team
activities - Influence policy &
practice
Health needs of whole population
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
317
The four theoretical perspectives of the ‘logics of change’ process are:
Autopoiesis; which rethinks the relationships between systems and their environment.
Chaos and complexity; which explains how order can emerge from spontaneous self-organization.
Mutual causality; draws on cybernetic ideas suggesting that change is enfolded in the strains and tensions found in circular tensions.
Dialectical change; suggests that change is the product of tensions between opposites. (Morgan 1997: 252)
While all four perspectives provide valuable insights, autopoiesis strikes the most useful
link with the soft systems approach as it intimately connects the ambulance system with
its environment. Metaphorically, the pre-hospital practitioner model can be described as
a symbiotic system, where it forms an interdependent relationship with the environment.
In this model, the environment is not seen as a threat to survival or an opportunity to
exploit, but as an integral part of the whole that can be influenced and shaped for the
common good. Each part of the environment affects the whole through its actions and
inaction. While other parts of the health system and the community have two-way
relationships with the pre-hospital system both giving and receiving inputs that change
the way health care is provided. The rich picture in Figure 55 illustrates these two-way
relationships between the environment, customers, actors and owners of the model. An
evolving example may be how independent pre-hospital research could influence the
practice of emergency medicine and nursing in the same way that these two disciplines
currently influence the provision of pre-hospital care.
Achieving the introduction of the practitioner model is likely to be an aspirational
objective in many parts of rural Australia. Whether it is widely adopted, or not, there are
many aspects of the model that are well worth pursuing. In particular, the aims of
improving teamwork with other health professionals and developing a mature research
culture. The most powerful reason for considering the model is that it places pre-
hospital systems within a symbiotic relationship with the health care system and the
broader community it services. The rich picture in Figure 55 tries to capture this
metaphorical relationship between the practitioner model and the environment.
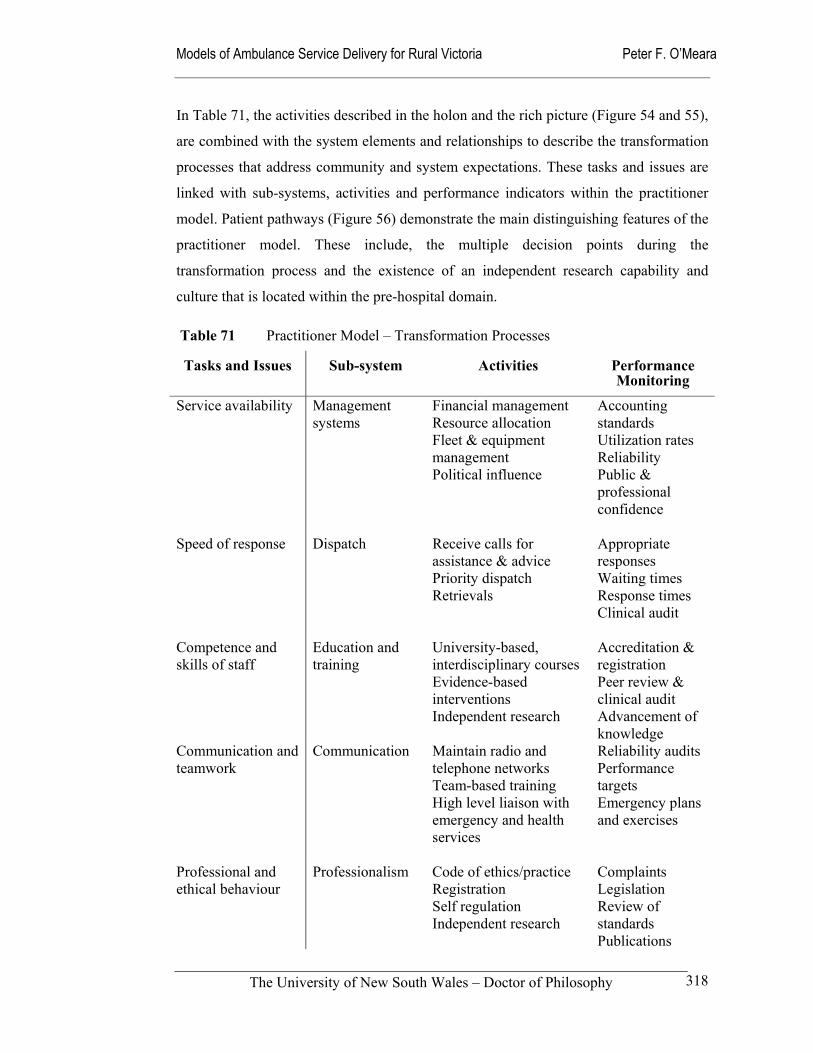
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
318
In Table 71, the activities described in the holon and the rich picture (Figure 54 and 55),
are combined with the system elements and relationships to describe the transformation
processes that address community and system expectations. These tasks and issues are
linked with sub-systems, activities and performance indicators within the practitioner
model. Patient pathways (Figure 56) demonstrate the main distinguishing features of the
practitioner model. These include, the multiple decision points during the
transformation process and the existence of an independent research capability and
culture that is located within the pre-hospital domain.
Table 71 Practitioner Model – Transformation Processes
Tasks and Issues Sub-system Activities Performance Monitoring
Service availability
Management systems
Financial management Resource allocation Fleet & equipment management Political influence
Accounting standards Utilization rates Reliability Public & professional confidence
Speed of response
Dispatch Receive calls for assistance & advice Priority dispatch Retrievals
Appropriate responses Waiting times Response times Clinical audit
Competence and skills of staff
Education and training
University-based, interdisciplinary courses Evidence-based interventions Independent research
Accreditation & registration Peer review & clinical audit Advancement of knowledge
Communication and teamwork
Communication Maintain radio and telephone networks Team-based training High level liaison with emergency and health services
Reliability audits Performance targets Emergency plans and exercises
Professional and ethical behaviour
Professionalism Code of ethics/practice Registration Self regulation Independent research
Complaints Legislation Review of standards Publications
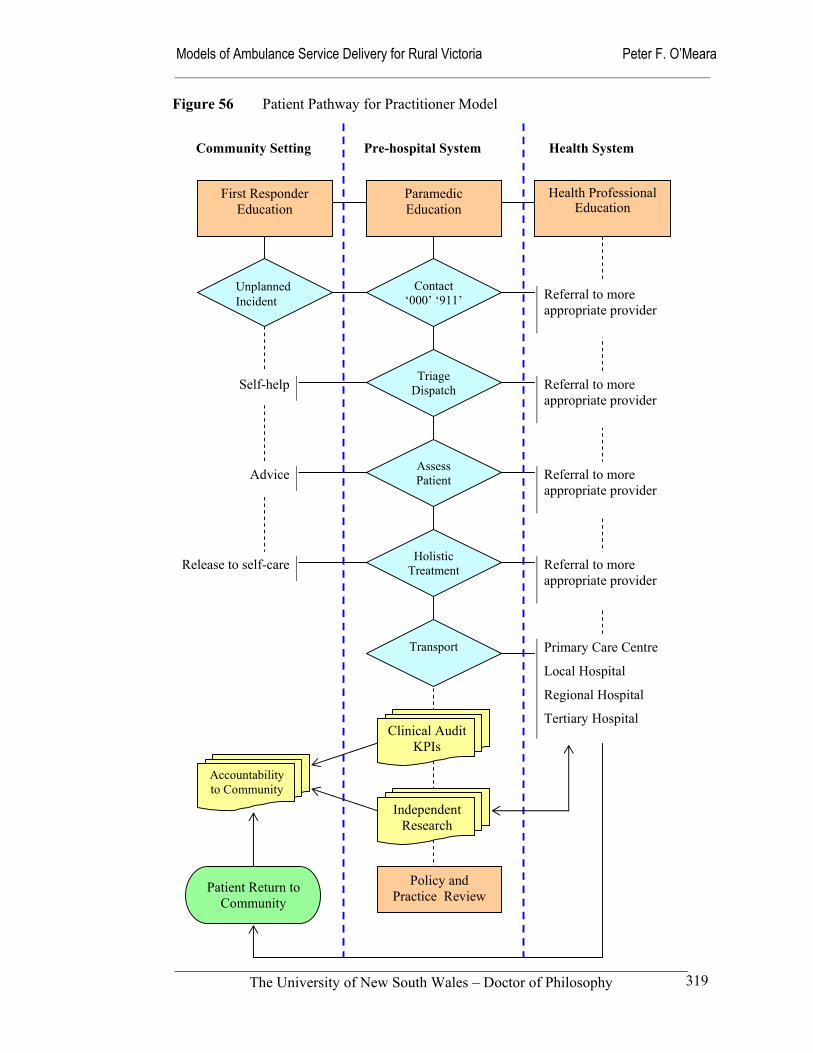
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
319
Community Setting Pre-hospital System Health System
Unplanned Incident
Contact ‘000’ ‘911’
Triage Dispatch
Assess Patient
Holistic Treatment
Transport
First Responder Education
Paramedic Education
Health Professional Education
Clinical Audit KPIs
Independent Research
Policy and Practice Review
Self-help
Referral to more appropriate provider
Advice
Release to self-care
Referral to more appropriate provider
Primary Care Centre
Local Hospital
Regional Hospital
Tertiary Hospital
Figure 56 Patient Pathway for Practitioner Model
Accountability to Community
Referral to more appropriate provider
Referral to more appropriate provider
Patient Return to Community

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
320
The practitioner model is speculative and builds on the dialogue taking place in the
United States and the United Kingdom about expanding the scope of ambulance
practice (Nicholl et al 2001; NHTSA 1996). It balances its performance against the
criteria of access, effectiveness, efficiency and ethicality; it is integrated within the
broader health system; and uses multi-skilled and adaptable staff to improve clinical
outcomes. The unique characteristics of the practitioner model are derived from its
philosophy or view of the world; its advocates place it within the larger health system,
with influence over its own destiny. It does not see itself as a ship on the ocean at the
mercy of the winds. With educational and organizational developments in the United
States, the United Kingdom and Australia, the development of the pre-hospital
practitioner model may be more likely to occur than was ever imagined in the recent
past.
The pre-hospital practitioner
model proposed here is broad
enough to account for
different perspectives across
rural Australia and from both
sides of the Atlantic. It is a
response to the need for pre-
hospital providers, in common
with other health
professionals such as nursing,
to review the way they practice and to re-evaluate their roles and functions (Duffy
1998). The model has the capacity to integrate existing ambulance services with public
health and social service agencies, primary care providers and other health care facilities
to ensure that patients are referred to or transported to the most appropriate and cost-
effective facility. This theoretical strength can ensure that pre-hospital care occurs as
part of a seamless system that provides patients with well-organized and high-quality
care. To succeed the pre-hospital practitioner model requires the cooperation and
availability of each component of the emergency medical system. This includes access
to medical officers trained in emergency medicine, health care facility staff, system
planners and others.
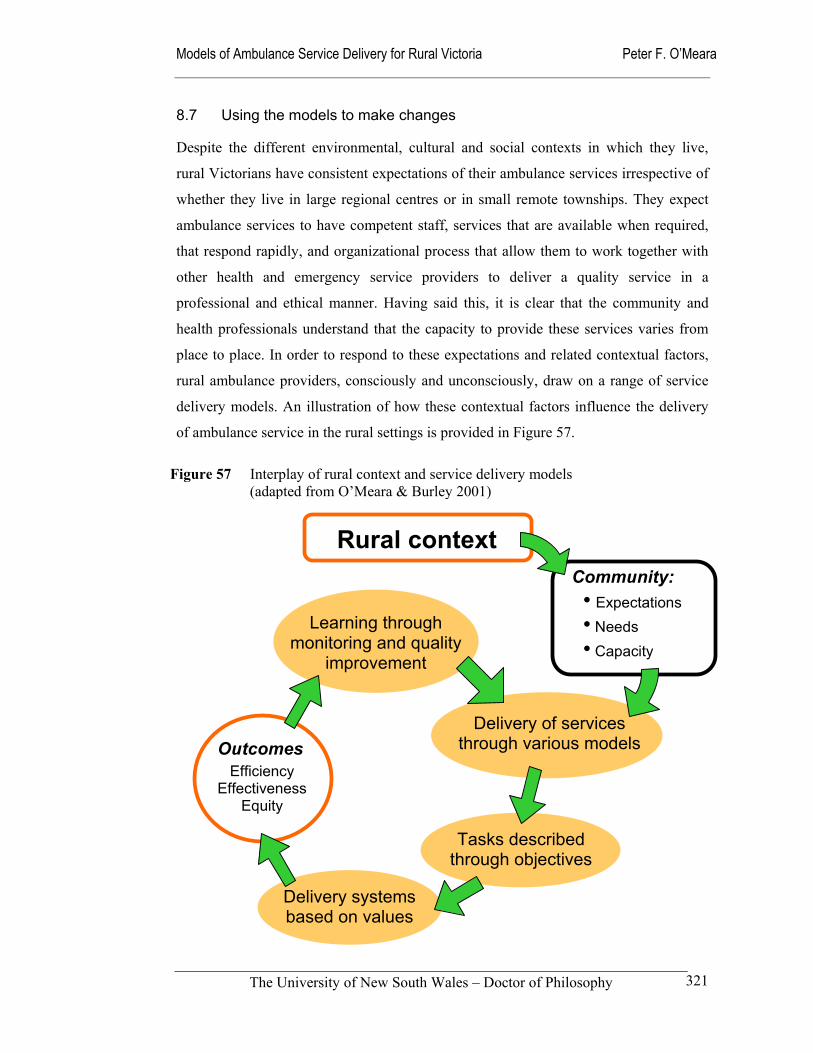
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
321
8.7 Using the models to make changes
Despite the different environmental, cultural and social contexts in which they live,
rural Victorians have consistent expectations of their ambulance services irrespective of
whether they live in large regional centres or in small remote townships. They expect
ambulance services to have competent staff, services that are available when required,
that respond rapidly, and organizational process that allow them to work together with
other health and emergency service providers to deliver a quality service in a
professional and ethical manner. Having said this, it is clear that the community and
health professionals understand that the capacity to provide these services varies from
place to place. In order to respond to these expectations and related contextual factors,
rural ambulance providers, consciously and unconsciously, draw on a range of service
delivery models. An illustration of how these contextual factors influence the delivery
of ambulance service in the rural settings is provided in Figure 57.
Rural context
Delivery of services through various models
Tasks described through objectives
Learning through monitoring and quality
improvement
Delivery systems based on values
Outcomes Efficiency
Effectiveness Equity
Community: • Expectations• Needs • Capacity
Figure 57 Interplay of rural context and service delivery models (adapted from O’Meara & Burley 2001)

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
322
The great challenge for rural ambulance services in Victoria is the heterogeneous nature
of the Victorian environment. Although Victoria has few areas that can be described as
extremely remote, the geographical, demographic, epidemiological and socio-economic
circumstances of rural Victorians vary enormously. In many larger provincial centres
the expectations and needs of potential ambulance users are little different to those
living and working in large metropolitan cities. Nor do the services currently offered
vary greatly from those found in capital cities. However, the services provided in
smaller rural centres, rural areas and remote areas, that often lack easy access to hospital
and medical services, vary greatly in accessibility and quality.
Rural ambulance services in Victoria, with one notable exception, operate under one
system. However, it is clear that a number of service delivery models are in operation.
The rural ambulance system is in some ways a mixture or complex weave of these
models, with stakeholders holding to some aspects of the different models at different
times, places and across different circumstances. The range of options and
configurations offered here are likely to be useful to rural communities and policy
makers. Each model has its own strengths and weaknesses that need to be taken into
consideration. This concept of choice is particularly relevant for rural communities,
where successive governments have imposed urban ‘solutions’ on rural people. It needs
to be understood that “… solutions to rural health concerns must be tailor-made to the
existing situation – a simple nostrum but one which can be lost in a policy framework
which tries to impose a ‘one-fits-all’ philosophy” (Best 1999). The lesson is that while
each of the models formulated have a contribution to make, no one model is suitable for
all rural areas. The rural context varies too much for that; there are variations in their
demography and economic performance, degree of isolation from essential services, and
the nature of their needs and expectations. Each rural community needs to make its own
decisions or exercise its own influence based on its own values, priorities and capacity
to provide the resources for its preferred model of pre-hospital service delivery.
At the most basic level, models consist of an individual mix of elements, activities and
relationships. Our understanding of how these characteristics interact is enhanced
through the use of SSM with its twin approach of building logical models and
subjecting the abstract creations to cultural analysis. While the five models presented
here – competitive, equity, community, expert and practitioner – can be seen in various
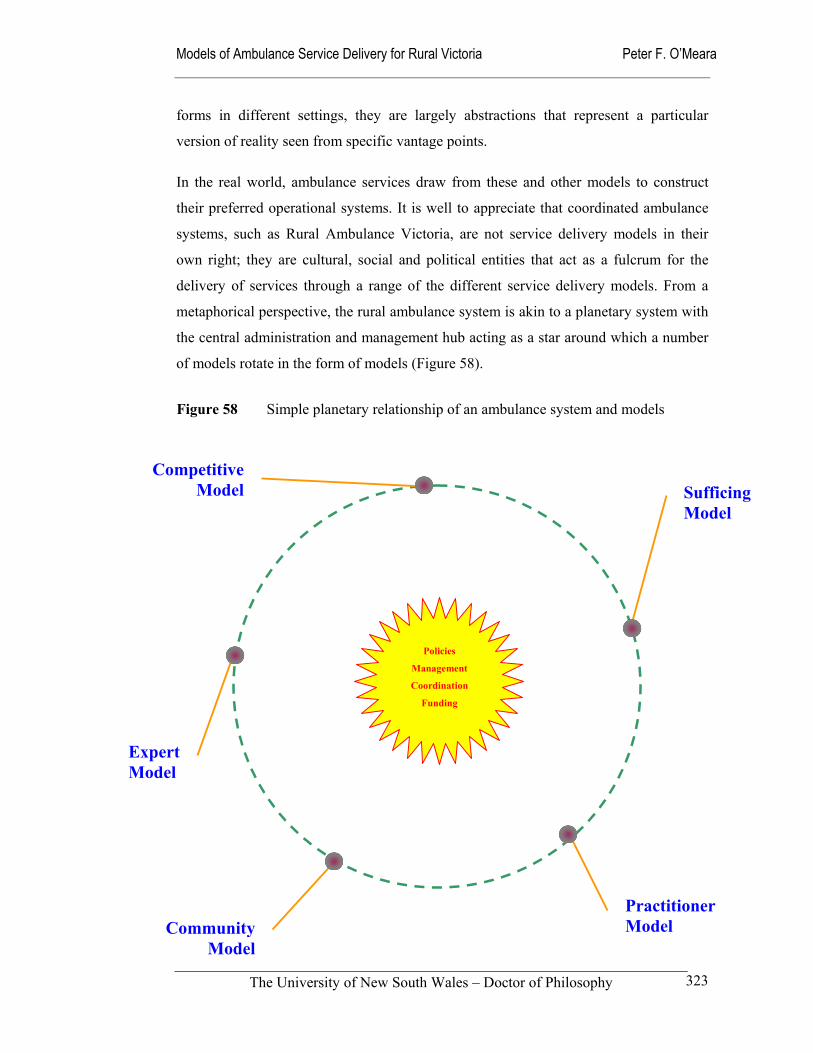
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
323
forms in different settings, they are largely abstractions that represent a particular
version of reality seen from specific vantage points.
In the real world, ambulance services draw from these and other models to construct
their preferred operational systems. It is well to appreciate that coordinated ambulance
systems, such as Rural Ambulance Victoria, are not service delivery models in their
own right; they are cultural, social and political entities that act as a fulcrum for the
delivery of services through a range of the different service delivery models. From a
metaphorical perspective, the rural ambulance system is akin to a planetary system with
the central administration and management hub acting as a star around which a number
of models rotate in the form of models (Figure 58).
Figure 58 Simple planetary relationship of an ambulance system and models
Policies
Management
Coordination
Funding
Community Model
Expert Model
Practitioner Model
Competitive Model Sufficing
Model
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
324
Each model operates more strongly in some environmental conditions than others
depending on the political, economic, social, cultural and technological climates. In
practice, the relative strength and influence of each model varies through time and
space. Sometimes specific features of one kind of model emerge, dominate or are
imposed. As we saw during the time of the Kennett government, the influence of the
competitive model was very strong, only for it to lose its attraction to policy makers and
service providers following the change of state government.
The other pre-hospital models also vary in their impact on the policy environment,
according to the ascendancy of particular worldviews. While the community model has
long been a useful description of how rural ambulance services operate, in recent years
it has been overtaken in importance by both the sufficing and expert models. These are
characterized respectively by industrial relations difficulties and medical dominance,
which are identifiable examples of the political and medical dominance metaphors.
Environmental factors such as education and technology, cultural and social trends, and
the general economic and political climate influence the life cycles of these service
delivery models. As a result, rational planning has much less influence on the strategic
choices made than is often imagined. The reality is that these other contextual factors
are very powerful forces, which need to be taken into account during the policy
development and implementation processes. Because the five models presented here
have been developed from distinct philosophical perspectives they offer an opportunity
to make a link between the logical but abstract approach to the planning of ambulance
services, and the messy world of competition, community, power, conflict, and
teamwork that is found in the real world.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
325
SECTION 4 CONCLUSION
9.0 Policy Implications of the Models
Section 1 Introduction
Section 2 Theory and Methods
Section 3 Findings and Discussion
Section 4 Conclusion
Chapter 1 Overview of Study
Chapter 2Theory Foundations
Chapter 4Communities Respondents
Chapter 5Expectations
Chapter 6Structure Culture
Chapter 7Ambulance Performance
Chapter 8Models of Delivery
Chapter 9 Policy Implications
Chapter 3Study Methods
Figure 59 Navigation Map of Thesis
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
326
9.1 Summary of thesis
This thesis is significant, because unlike earlier work in this field it is empirically
grounded and is located within a consistent theoretical framework. To the extent
possible, the analyses are based on information from various sources, sound
methodology and objective analysis. Triangulating data from various sources increased
the richness of the analysis and provided support for the discussions and models that
followed.
Using a systems approach was significant for its novelty in this area of study. Its
strength was its ability to examine problems and issues from the perspectives of
ambulance officers (paramedics and voluneers), registered nurses, general practitioners
and lay members of the rural community. Other attempts to study ambulance services
and emergency medical services have touched on the use of systems concepts.
However, they have been generally limited in their scope (Anderson 1992; Brown et al
1994; Narad 1998; O’Connor et al 1999; Kelly et al 1999; Holliman et al 2000).
My findings and analysis showed that rural communities, whether they are in regional
centres, small rural areas, or remote areas, expect adequately resourced ambulance
services that are able to respond quickly to their needs with well-trained staff who
behave in a professional manner. People in small or isolated communities expect similar
standards of service to their peers in larger centres. The real question is how can this be
achieved, not if it is expected?
Associated issues of concern to the principal stakeholders are the number and skills of
staff, the degree of local management autonomy, and the future roles of the ambulance
service. These themes flowed into my examination of the structure and culture of
Victorian rural ambulance services. This came at an interesting time, for not only were
rural ambulance services in Victoria dealing with widespread educational and
technological developments within pre-hospital care, they were being amalgamated into
a single rural-focused provider of ambulance services.
The opportunity to use this major organizational shift as a focus helped bring the
historical and cultural dimensions of ambulance services to the fore. My findings
highlighted the confused place of the ambulance service, located as it is on the boundary

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
327
of the public safety and health systems. The structural and cultural characteristics of
ambulance services throughout Australia and other comparable countries vary from
traditional systems based on rigid hierarchies in the style of paramilitary organizations,
to open knowledge-based systems that encourage independent clinical practice. In
between these two extremes are many variations of community models and
entrepreneurial systems.
The agreed location of ambulance services across the health, emergency service, and
business sectors is important. Expressed through a tacit philosophical position or value
statement, the ‘place’ of the ambulance service influences the range and scope of the
services offered, who and how they are delivered, and the approach taken to measuring
success. This is precisely the reason that I used SSM to formulate a range of alternate
models of service delivery based on distinct worldviews. To recap, the five pre-hospital
models that have been formulated, and their respective metaphors are:
Competitive model, using the population-ecology metaphor;
Sufficing model, described within a political system metaphor;
Expert model, with its medical domination metaphor;
Community model, which provides an example of the cultural metaphor; and
Practitioner model, which draws on the autopoiesis metaphor.
While the five models can be seen in various guises, reflected in the real world, they are
largely abstractions that represent the reality seen from specific vantage points. In
reality, ambulance services draw from these and other models to construct their
actualised operational models. Ambulance systems such as Rural Ambulance Victoria
are not service delivery models in their own right. They are cultural, social and political
entities that act as fulcrum for the delivery of pre-hospital services through different
models and combinations of models.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
328
9.2 Future directions
The main issues or concerns that became evident during the course of the research were
adequate staffing, local management and control, and the future role of ambulance
services. Each of the models presented address one or more of these issues from the
perspective of their dominant value systems or worldviews.
Transferring these separate models into real situations across different rural settings
presents an interesting set of challenges. Implementation of any model, organizational
approach or structure is almost always more difficult than imagined. Individual rural
communities have access to different levels of infrastructure, economic resources and
political power that influence the style and sophistication of its pre-hospital services.
The ‘unplanned event model’ that conceptually integrates the technological and cultural
capacity of societies across the emergency medical system, potentially provides one
very effective way of accounting for the variations in the levels of care provided in
different settings throughout the cycle of care (Turner et al 2000). It provides an
excellent means of describing and analysing the differing levels of model sophistication,
based on financial capacity, education and training of providers and differing levels of
technology.
The weakness of the unplanned health event model is its inability to incorporate the
importance of a society’s dominant worldview or ‘Weltanschauung’, and the other
cultural and environmental factors that act as the backdrop to the development of policy
and changes in practice. SSM provides the opportunity to explain the influence of these
strong background forces, along with the means of showing the linkages between the
different elements and activities that constitute an integrated pre-hospital system within
rural settings. A modified holon is used in Figure 60 to demonstrate these relationships
across the pre-hospital system. Some of the activities and environmental issues, such as
disaster planning and the political processes, are embedded in the background while the
key components of the system are shown as sub-systems in their own right. For
instance, the allocation of resources is represented at the top of the holon, and is then
linked to the measurement of performance, thus picking up the socio-political decisions
that are part-and-parcel of the health and emergency service systems.
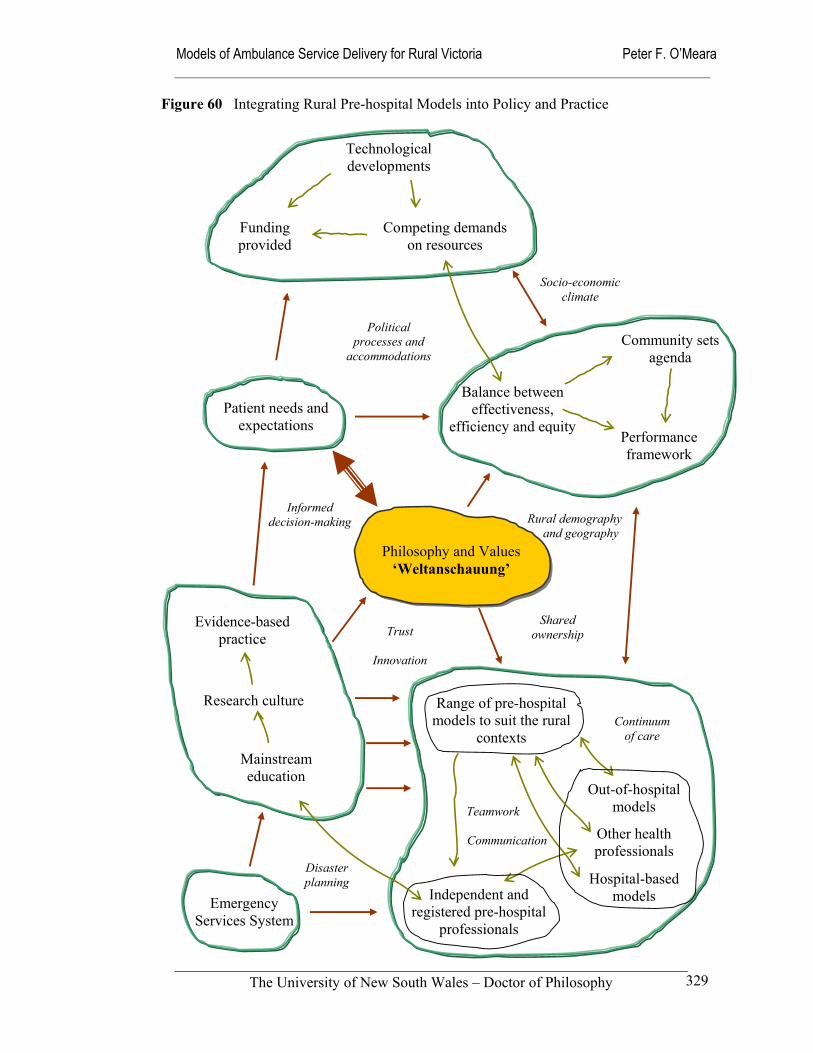
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
329
Community sets agenda
Technological developments
Funding provided
Competing demands on resources
Evidence-based practice
Research culture
Mainstream education
Balance between effectiveness,
efficiency and equity Performance framework
Patient needs and expectations
Political processes and
accommodations
Informed decision-making
Independent and registered pre-hospital
professionals
Range of pre-hospital models to suit the rural
contexts
Other health professionals
Hospital-based models
Out-of-hospital models Teamwork
Communication
Philosophy and Values ‘Weltanschauung’
Figure 60 Integrating Rural Pre-hospital Models into Policy and Practice
Continuum of care
Shared ownership Trust
Innovation
Disaster planning
Rural demography and geography
Socio-economic climate
Emergency Services System

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
330
The holon incorporates my own explicit worldview, based on the preceding analysis and
my own experience in conducting the research program, that pre-hospital care is located
within the health system, with the emergency services system of relatively less
importance than has been traditionally the case. The very strong link between the
patients’ needs and expectations, and the dominant philosophy and values of the system
is illustrated through the bold link between them in the holon (Figure 60). This is
consistent with the prominent place of patient pathways in each of the five models I
have formulated.
Once all these and other models are acknowledge within a unified system, it is possible
to combine and meld them into practical and acceptable models for the rich diversity of
rural settings. For example, it is possible to combine the community model with the
practitioner model in remote communities, using a combination of community volunteer
staff and dual registered nurse/paramedic practitioners. In the real world, there will be
formidable barriers to the successful translation of creative and innovative ideas. These
restraints on change and innovation cannot be lightly dismissed as merely the products
of self-interest and political manoeuvres. They are the outcome of shared histories and
existing systems that have not always been characterized by trust or informed decision-
making. A well-developed education and research base will allow a vigorous debate to
be initiated and sustained within a mature professional framework that is both
autonomous and inclusive of other health professionals, emergency service
professionals and the broader rural community. Change is difficult, but we may well be
advised to remain optimistic.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
331
The future of rural pre-hospital care will include much of the ‘old’, as suggested in the
community and sufficing models, and something of the ‘new’, drawn from the expert
and practitioner models. Metaphorically and logically, each provides a different
perspective that is valuable and worth holding onto: the community model brings home
the importance of maintaining local community links; the sufficing model reminds us of
the central place that politics occupies; the expert model highlights the centrality of
clinical excellence; and the practitioner model provides hope of an integrated
emergency health system where patients and the community are paramount. Doubtless,
the market-orientated elements of the competitive model will be called upon to promote
change when the efficiency or responsiveness of other models is under challenge or
stress.
These five pre-hospital models can be used as catalysts for policy development and
changes in the practice of pre-hospital service delivery in rural Victoria. The theoretical
frameworks developed here can form a solid foundation for dialogue, debate and
discussion about alternative ambulance service delivery models for rural Victoria within
an atmosphere of mutual respect and understanding amongst the principal stakeholders
with the shared aim of improving ambulance services for rural people.
As a result of the research and reflection undertaken the four main recommendations that have emerged from this study are:
1. Policy makers need to provide sufficient resources to ensure that ambulance services are able to meet the needs and expectations of rural communities on an equitable basis (Chapter 5).
2. The organizational structure and culture of rural ambulance services needs to evolve in a way that will accommodate a more independent paramedic profession that is integrated into the health system (Chapter 6).
3. Rural ambulance services should adopt a coherent performance framework based on the National Health Performance Committee’s framework (Chapter 7).
4. Models of rural ambulance service delivery need to be based on the values, priorities and capacity of the communities that they serve, while being firmly located within an integrated health system (Chapter 8).
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
332
Bibliography Adams, JD. (Ed.) (1986) Transforming Leadership: From Vision to Results. Miles River Press, Alexandria.
Aday LA. Begley CE. Lairson DR. and Slater CH. (1998) Evaluating the Healthcare System: Effectiveness, Efficiency and Equity. AHSR, Chicago.
Aday, LA. (2001) ‘Establishment of a conceptual base for health services research’. Journal of Health Services Research and Policy. 6(3): 183-185.
Abbadi, S. Abdallah, AK. and Holliman, C. (1997) ‘Emergency medicine in Jordan’. Annals of Emergency Medicine. 30(3): 319-321.
Aitken, A. (2000) ‘Identifying key issues affecting the retention of emergency service volunteers’. Australian Journal of Emergency Management. Winter 2000.
Albrecht, GL. Fitzpatrick, R. and Scrimshaw, SC. (Editors) (2000) Handbook of Social Studies in Health and Medicine. SAGE Publications, London.
Alderfer CP. and Cooper CL. (1980) Advances in Experiential Social Processes, Volume 2. John Wiley & Sons, Brisbane, Chapter 11.
Aldrich, CA. Hisserich, JC. and Lave, LB. (1971) ‘An analysis of the demand for emergency ambulance service in an urban area’. American Journal of Public Health. 61(6): 1156-69.
Alexander K. and Hicks N. (1998) ‘Sailing without radar: An excursion in resource allocation’. Australian Health Review. 21(2): 76-99.
Alford, R. (1993) ‘Health policy, politics and power’, in Study Guide in Health Policy and Administration. Deakin University.
Allen Consulting Group. (1999) Review of the Ambulance Services Act 1986: Final Report. Department of Human Services.
Alonso-Serra, HM. Delbridge, TR. Auble, TE. Mosesso, VN. and Davis, EA. (1997) ‘Law enforcement agencies and out-of-hospital emergency care’. Annals of Emergency Medicine. 29(4): 497-503.
Ambulance Service of New South Wales. (1992a) Future Directions: A Report to the Minister for Health Services Management. Rozelle.
Ambulance Service of New South Wales. (1992b) A Resource Allocation Formula for the NSW Ambulance Service. NSW Health Services Research Group.
Ambulance Service of New South Wales. (1994) Resource Allocation Formula for the NSW Ambulance Service. Rozelle.
Ambulance Services Act 1986. Version No. 020. Version incorporating amendments as at 1 December 1999.
American College of Emergency Physicians. (1997) ‘Expanded Roles of EMS Personnel’. Annals of Emergency Medicine. 30(3): 364.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
333
Anderson, PB. (1992) 'Rural EMS System Development: Innovative Technological Approaches', in Straub, La Vonne & Walzer, Norman (Eds.). Rural Health Care: Innovation in a Changing Environment. Praeger, London.
Arnold, JL. (1999) ‘International Emergency Medicine and Recent Developments of Emergency Medicine Worldwide’. Annals of Emergency Medicine. 33(1): 97-103.
Arreola-Risa C. Mock CN. Lojero-Wheatly L. de la Cruz O. Garcia C. Canavati-Ayub F. and Jurkovich GJ. (2000) ‘Low-cost improvements in prehospital trauma care in a Latin American city’. The Journal of Trauma: Injury, Infection and Critical Care 48(1): 119-124.
Asplin, BR. (1997) ‘Access, Quality, and Cost Control in Emergency Medicine: Can We Have All Three?: A Resident’s Perspective on the Future of Emergency Medicine’. Annals of Emergency Medicine. 30(6): 779-781.
ASV - South Eastern Region. (1992a) South Eastern Region's Response to the Report of the Victorian Ambulance Services Review - 1992. Ref Type: Unpublished Work
ASV - South Eastern Region. (1992b) Submission to the Victorian Ambulance Board from South Eastern Region Concerning the Future Structure and Management of Ambulance Service Victoria. Ref Type: Unpublished Work.
ASV - Western Region. (1992) Submission into Review of Ambulance Services. Ref Type: Unpublished Work.
ASV - North Western Region. (1992) Review of the Future Structure and Management of Victoria's Ambulance Services. Ref Type: Unpublished Work.
ASV - Metropolitan Ambulance Service. (1992) Submission to Victorian Ambulance Review. Ref Type: Unpublished Work.
Audit Office of New South Wales. (2001) Performance Audit Report: Ambulance Service of New South Wales: readiness to respond. The Audit Office of New South Wales.
Auble, TE. Menegazzi, JJ. and Paris, PM. (1995) ‘Effect of Out-of-Hospital Defibrillation by Basic Life Support Providers on Cardiac Arrest Mortality; A Metaanalysis’. Annals of Emergency Medicine. 25(5).
Audit Commission. (1998) A Life in the Fast Lane: Value for Money in Emergency Ambulance Services. NHS, United Kingdom.
Australian College of Ambulance Professionals. (2001a) Minutes of Board Meeting, 16 June 2001. www.acap.org.au/minrep/bm160601.doc [accessed 31/12/01]
Australian College of Ambulance Professionals. (2001b) Code of Ethics, www.acap.org.au/codoeth.html [accessed 31/12/01]
Australian Health Ministers’ Conference. (1994) National Rural Health Strategy.
Australian Industrial Relations Commission. (1994) 'Interim Order, AEAV and ASV, 22 March 1994'.
Australian Labor Party. (2000) ‘A Better Ambulance System: Labor’s Plan’. www.vic.alp.org.au/policy/health/ambul.html [accessed 10/3/00]
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
334
Bailey, P. (1996) ‘Developing ambulance models for practice’. Australian Journal of Emergency Care. 3(1): 26-28.
Bailey, P. (1997) ‘Ambulance Paramedics – An Endangered Species?’. Australasian Journal of Emergency Care. 4(2): 12-14.
Baragwanath CA. (1997a) Metropolitan Ambulance Service: Fulfilling a vital community need. Special Report No. 50, Auditor-General of Victoria.
Baragwanath CA. (1997b) Victorian Rural Ambulance Services: Fulfilling a vital community need. Special Report No. 51, Auditor-General of Victoria.
Barrett, B. and Guly, HR. (1999a) ‘How accurate are the times held by the ambulance control computer’. Pre-hospital Immediate Care. 3: 206-208.
Barrett, B. and Guly, HR. (1999b) ‘How long to intravenous cannulation and drug administration add to the on scene time?’ Pre-hospital Immediate Care. 3: 219-223.
Barrett, B. and Guly, HR. (2000) ‘How long does it take to perform procedures on scene?’ Pre-hospital Immediate Care. 3: 25-29.
Bates, E. and Lapsley, H. (1985) The Health Machine: The Impact of Medical Technology. Penguin Books, Melbourne.
Battersby, D. (1999) ‘The future of ambulance officer education and training in the UK’. Pre-hospital Immediate Care. 3: 113-114.
Baum, F. (1998) The New Public Health: an Australian perspective. Oxford University Press, Melbourne.
Baume, P. (1995) ‘Towards a health policy’. Australian Journal of Public Administration. 54(2): 196-204.
Beaulieu, JE. and Berry, DE. (Eds.). (1994) Rural Health Services: A Management Perspective. Aupha Press/Health Administration Press, Michigan.
Berwick, DM. (1996) ‘A primer on leading the improvement of systems’. British Medical Journal. 312: 619-622.
Best, J. (1999) ‘Taking Stock’. Regional Australia Summit. Canberra.
Billittier, AJ. Lerner, EB. Tucker, W. and Lee, J. (2000) ‘The lay public’s expectations of prearrival instructions when dialing 9-1-1’. Prehospital Emergency Care. 4: 234-237.
Bilton, T. Bonnett, K. Jones, P. Sheard, K. Stanworth, and M. Webster, A. (1993) 'Professionalisation: an occupational strategy', in Reader in Health Policy and Administration. Deakin University.
Bird, PH. (Ed.) (1999). A History of Ambulance Services in Country Victoria. Victorian Ambulance Services Association, Bendigo.
Birk HO. and Henriksen LO. (2000) ‘How much to do at the scene?: prehospital interventions prolong prehospital time’. British Medical Journal 320(7240): 1005.
Birnbauer, B. (1994) 'Tehan's intensive care: The Problems', The Age, 2 June 1994.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
335
Bissell, RA. Seaman, KG. Bass, RR. Racht, E. Gilbert, C. Weltage, AF. Doctor, M. Moriarity, S. Eslinger, D. and Doherty, R. (1999a) ‘Change the scope of practice of paramedics? An EMS/public health policy perspective’. Prehospital Emergency Care. 3(2): 140-149.
Bissell, RA. Seaman, KG. Bass, RR. Racht, E. Gilbert, C. Weltage, AF. Doctor, M. Moriarity, S. Eslinger, D. and Doherty, R. (1999b) ‘A medically wise approach to expanding the role of paramedics as physician extenders’. Prehospital Emergency Care. 3(2): 170-173.
Blaskett B. (1993) ‘Rural health policy and the accidental tourist’, Regional Journal of Social Issues, 27: 43-46.
Bouma, GD. (1993) The Research Process. Oxford University Press, Melbourne.
Braithwaite, J. Hindle, D. Iedema, R. and Westbrook, JI. (2002) ‘Introducing SSM plus (SSM+): why we need it and what it can contribute.’ Australian Health Review. 25(2): 195-202.
Brazier, H. Murphy, AW. Lynch, C. and Bury, G. ‘Searching for the evidence in pre-hospital care: a review of randomised controlled trials. On behalf of the Ambulance Response Time Sub-Group of the national Ambulance Advisory Committee’. Journal of Accident and Emergency Medicine. 16(1): 18-23.
Brearley, P. Gibbons, J. Miles, A. Topliss, E. and Woods, G. (1978) The Social Context of Health Care. Blackwell & Robertson, London.
Breen, N. Woods, J. Bury, G. Murphy, AW. and Brazier, H. (2000) ‘A national census of ambulance response times to emergency calls in Ireland’. Journal of Accident and Emergency Medicine. 17: 392-395.
Brennan, D. (1996) ‘Geographic location and provision of dental services in Australia’, Australian Health Review. 19(2 1): 138-140.
Brice, JH. Garrison, HG. and Evans, AT. (2000) ‘Study design and outcomes in out-of-hospital emergency medicine research: a ten-year analysis’. Prehospital Emergency Care. 4: 144-150.
Bridgeman, P. and Davis, G. (1998) Australian Policy Handbook. St Leonard's N.S.W. : Allen and Unwin
Briskman, L. (1999) ‘ Setting the scene: Unravelling rural practice’ in Challenging rural practice: human services in Australia. Eds. Briskman, L. and Lynn, M. Deakin University Press, Geelong. pp. 3-14.
Broadhead, P. (1991) 'Approaches to public funding of Australia's health care', Australian Health Review. 14(3).
Brodsky, H. (1992) ‘Delay in ambulance dispatch to road accidents’. American Journal of Public Health. 82(6): 873-875.
Brown, D. (1999) ‘The Challenges of Rural Health’. Australian Health Executive, Spring 1999.
Brown, LH. Prasad, H. and Grimmer, K. (1994) ‘Public Perceptions of a Rural Emergency Medical Service System’, Prehospital and Disaster Medicine. 9(4).
Bryant, L. and Strasser, R. (1999) ‘The delivery of sustainable rural and remote health services’. Regional Australia Summit, Canberra.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
336
Buchan, H. (1998) ‘Different countries, different cultures: convergent or divergent evolution for healthcare quality?’. Quality in Health Care. 7(Supplement): S62-S67.
Burke, D. (1990) Casuals/Volunteers in the Ambulance Service. Ambulance Officers' Training Centre. Ref Type: Unpublished Work
Burgess, S. (1998) ‘An analysis of ambulance service response times and service delivery in Melbourne’. Australia. Australasian Journal of Emergency Care. 5(3): 8-12.
Butler, JRG. and Doessel, DP. (Eds.) (1989) Health Economics: Australian Readings. Australian Professional Publications, Sydney.
Butson, M. (1999) ‘Ambulance officer as a professional occupation’. Response. 11(1): 19-22.
Button, V. (1998) ‘Firemen get to the heart of the matter’. The Sunday Age. 14 September 1998.
Cadigan, RT. and Bugarin, CE. (1989) 'Predicting Demand for Emergency Ambulance Service', Annuals of Emergency Medicine, 18: 618-621.
Callaham, M. (1997) ‘Quantifying the Scanty Science of Prehospital Emergency Care’ Annals of Emergency Medicine. 30(6): 785-790.
Callaham, M. and Madsen, CD. (1996) ‘Relationship of Timeliness of Paramedic Advanced Life Support Interventions to Outcome in Out-of Hospital Cardiac Arrest Treated by First Responders With Defibrillators’. Annals of Emergency Medicine. 27(5): 638-648.
Campbell D. Strasser R. and Kirkbright S. (1996) Survey of Victorian Rural General Practitioners in Towns without a Hospital. Monash University, Centre for Rural Health, Moe.
Capewell, S. MacIntyre, K. Stewart, S. Chalmers, JWT. Boyd, J. Finlayson, A. Redpath, A. Pell, JP. and McMurray, JJV. (2001) ‘Age, sex, and social trends in out-of hospital cardiac deaths in Scotland 1986-95: a retrospective cohort study’. The Lancet. 358: 1213-1217.
Capp, S.(Chairman) (1992) The Victorian Ambulance Services Review. The Victorian Ambulance Board. Melbourne.
Carrington, DJ. (1997) ‘Review of emergency ambulance performance standards’. Care of the Critically Ill. 13(1): 19-20.
Carson, N. (1998) Profile of Rural Victorians’ Health. Department of Human Services, Victoria.
Cayten CG. Murphy JG. and Stahl WM. (1993) ‘Basic life support versus advanced life support for injured patients with an injury severity score of 10 or more.’ Journal of Trauma. 35(3): 460-466.
Checkland, P.B. (1981) Systems thinking, systems practice. John Wiley & Sons, Chichester.
Checkland, P.B. and Scholes, J. (1990) SSM in Action. John Wiley & Sons, Chichester.
Checkland, P.B. (1999) SSM: a 30-year retrospective. John Wiley & Sons, Chichester.
Clancy, CM. and Eisenberg, JM. (1997) ‘Emergency Medicine in Population-Based Systems of Care’, Annals of Emergency Medicine, 30(6): 800-803.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
337
Clark, MJ. Purdie, J. Bischoff, NG. Fitzgerald, GJ. and O’Rourke, PK. (1998) Emergency Pre-hospital Ambulance Services: an evaluation of unmet demand. Queensland Ambulance Service.
Clark, M. and Fitzgerald, G. (1999) ‘Older people’s use of ambulance services: A population based analysis’, Journal of Accident and Emergency Medicine. 16(2): 108-111.
Clark, MJ. Purdie, JG. and Fitzgerald, G. (2000) ‘Determinants of pre-hospital care non-usage for patients with emergency care needs’. Pre-hospital Immediate Care. 4: 90-96.
Clegg, C.R. Hardy, C. and Nord, W.R. (Eds.) (1996) Handbook of Organization Studies. Sage, London.
Coats, TJ. And Goode, A. (1999) ‘Opportunity to improve pre-hospital care in the UK’, The Lancet. 353(9161): 1292.
Community Services and Health Training Australia. (2000) Ambulance Industry Forum, 26 June 2000, Record of Meeting. DRAFT REPORT.
Conners, A-M. (1994) ‘Patient classification system in a rural emergency department’, Accident and Emergency Nursing. 2: 7-20.
Cooke MW, Wilson S, Allan T, Bridge P, Edwards S, Morrell R. (1998) Safety and effectiveness of criteria based dispatch in the prioritisation of 999 calls. The University of Birmingham.
Cooke, M. (1999a) ‘How much to do at the accident scene?: spend time on essentials, save lives’. British Medical Journal. 319(7218): 1150.
Cooke, MW. (1999b) ‘How much to do at the accident scene?’ Journal of Accident and Emergency Medicine. 16(5): 339-341.
Cooke, M. and Wilson, S. (1999a) Organisation of emergency healthcare in Norway: lessons for the UK system. EmeRG. University of Warwick.
Cooke, M. and Wilson, S. (1999b) ‘Obstacles to research in pre-hospital care’. Pre-hospital Immediate Care. 3: 149-151.
Cooper, DJ. McDermott, FT. Cordner, SM. and Tremayne, AB. (1998) ‘Quality Assessment of the Management of Road Traffic Fatalities at a Level 1 Trauma Center Compared with other Hospitals in Victoria, Australia’. The Journal of Trauma. 45(4): 772-779.
Coopers & Lybrand Consultant. (1997) Review of issues relating to options for reorganising rural ambulance services. Victorian Ambulance Services Association, Melbourne.
Country Fire Authority. (2001). CFA Website. www.cfa.org.au [accessed 31/12/01]
Courtney, Mary D. (Ed.) (1992) Issues in Rural Health. Association of Rural Nurses.
Cullen, T. Dunn, P. and Lawrence, G. (Eds.) (1989) Rural Health and Welfare in Australia. Centre for Rural Welfare Research, Charles Sturt University.
CSIRO Mathematical and Information Sciences. (2001) ‘Measuring service performance tells the SA Ambulance Service if it is effective’. www.cmis.csiro.au/opm/CaseStudies/SAAS.htm [accessed 9/01/02]
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
338
Danaher, G. Schirato, T. and Webb, J. (2000) Understanding Foucault. Allen & Unwin, Sydney.
Daniel, A. in Colquhoun, D. and Kelleher, A. (Eds.). (1993) Health Research in Practice: Political, ethical and methodological issues. Chapman & Hall, Melbourne.
Danne, P. Brazenor, G. Cade, R. Crossley, P. Fitzgerald, M. Gregory, P. Kowal, D. Lovell, L. Morley, P. Smith, M. Taylor, R. and Walker, S. (1998) “The major management study: an analysis of the efficacy of current trauma care’, Aust N.Z. J. Surg. 68: 50-57.
Davies, L. and Ledington, P. (1991) Information in Action: SSM. MacMillan, London.
Davis, A. and George, J. (1988) States of Health: Health and Illness in Australia. Harper & Row, Sydney.
Davis, G. Wanna, J. Warhurst, J. and Weller, P. (1993) Public Policy in Australia. Allen & Unwin, Sydney.
Deakin University. (1996) AIP 741: Social Policy Study Guide and Readings.
Dean, JM. Vernon, DD. Cook, L. Nechodom, P. Reading, J. and Suruda, A. ‘Probabilistic Linkages of Computerized Ambulance and Inpatient Hospital Discharge Records: A Potential Tool for Evaluation of Emergency Medical Services’. Annals of Emergency Medicine. 37(6): 616-626.
Delbridge, TR. Baily, B. Chew, JL. Conn, AKT. Krakeel, JJ. Manz, D. Miller, DR. O’Malley, PJ. Ryan, SD. Spaite, DW. Stewart, RD. Suter, RE. And Wilson, EM. (1998) ‘EMS Agenda for the Future: Where We Are … Where We Want to Be’. Annals of Emergency Medicine. 31(2): 251-263.
DeMello, S. and Gardner, BH. (1990) ‘Systems Thinking: A powerful tool for healthcare management’, Healthcare Forum Journal.
Demetriades, D. Chan, L. Cornwell, E. Belzberg, H. Berne, TV. Asensio, Juan, Chan, D. Eckstein, M. and Alo, K. (1996) ‘Paramedic vs Private transportation of Trauma patients: Effect on Outcome’. Archives of Surgery. 131: 133-138.
Department of Health and Human Services, Tasmania. (1999) Tasmanian Medical Emergency Services Plan for Rural and Remote Areas. Hobart.
Department of Health and Social Security – UK. (1990) Review of Ambulance Services Standards, Emergency and Urgent Targets: Final Report.
Department of Human Services, Victoria. (1993) Epidemiology and Public Health.
Department of Human Services, Victoria. (1996) The MPS Option: Health & Aged Care in Rural Communities.
Department of Human Services, Victoria. (1997) Multi Purpose Services Development and Design Guidelines: Health & Aged Care in Rural Communities.
Department of Human Services, Victoria. (1996) Efficiency in Health - Resource Allocation: A Discussion Paper.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
339
Department of Human Services, Victoria. (1998a) Review of Ambulance Services Act 1986: Discussion Paper.
Department of Human Services, Victoria. (1998b) Review of Health Act 1958: Discussion Paper.
Department of Primary Industries and Energy, and Department of Human Services and Health. (1994) Rural, Remote and Metropolitan Areas Classification 1991 Census Edition, AGPS, Canberra.
Dewdney, J. (1993) 'Australia's health system: a brief description'. Study Guide in Health Policy and Administration. Deakin University.
De Witt, A. (1997) ‘Against the odds: Tertiary education for ambulance paramedics in Victoria, Australia’. Australasian Journal of Emergency Care. 4(3): 19-22.
Diagnosis Pty. Ltd. (1992) 'Report on Terms of Reference 2, 3 and 4', The Victorian Ambulance Services Review. The Victorian Ambulance Board. Ref Type: Unpublished Work
Dickinson, G. (1998) ‘EMS: The Canadian Perspective’. 1st Pan-American Congress on Disaster and Emergency Medicine, San Juan, Costa Rica, March 1998. www.medicine.wisc.edu/sections/em/pdm/dickinson.htm [accessed 12/01/2000]
Doherty, J. and Price, M. (1998) ‘Evaluation of rural ambulance services.’ World Health Forum. 19(3): 315-319.
Donabedian, A. (1980) ‘The definition of quality and approaches to its assessment’. In Explorations in Quality Assessment and Monitoring. Vol 1, Ann Arbor, MI: Health Administration Press.
Drummond, MF. (1985) Principles of economic appraisal in health care. Oxford University Press, Melbourne.
Duck, J. and Ord, J. (1999) First Responder Scheme Pilot Project – Evaluation Report Part 1. Essex Ambulance Service. United Kingdom.
Duckett, S. (1999) ‘Policy challenges for the Australian health care system’. Australian Health Review. 22(2): 130-147.
Duffy, E. (1998) ‘Advanced Rural Nurse Practitioner: an alternative health service delivery model’. 6th International Nurse Practitioner Conference, 5-8 February 1998, Melbourne.
Duffield, C. Macneil, F. Bullock, C. and Franks, H. (2000) ‘The role of the Advanced Casualty Management Team in St John Ambulance Australia (New South Wales District)’. Australian Health Review. 23(1): 90-99.
Dunham, RB. and Pierce, JL. (1989) Management. Scott, Foresman and Company, London.
Dunne, P. Patterson, C. Kilkartin, M. and Sladden, M. (1994) ‘Health service provision in rural and remote areas: a needs analysis’. The Medical Journal of Australia. 161(2): 160-162.
Dyas, J. Ayres, P. Airey, M. and Connelly, J. (1999) ‘Management of major trauma: changes required for improvement’. Quality in Health Care. 8: 78-85.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
340
Eckstein, M. and Alo, K. (1999) ‘The effect of a quality improvement program on paramedic on-scene times for patients with penetrating trauma’. Academic Emergency Medicine. 6(3): 191-195.
Edwards, ND. (1998) ‘B Med Sci degree course in paramedical studies at the University of Sheffield’. Pre-hospital Immediate Care. 2: 224-226.
Eisenberg, MS. Pantridge, JF. Cobb, LA. and Geddes, JS. (1996) ‘The Revolution and Evolution of Prehospital Cardiac Care.’ Archives of Internal Medicine. 156: 1611-1619.
Eisenberg, MS. (2000) ‘Is it time for over-the-counter defibrillators?’ JAMA. 284(11): 1435-1438.
Epstein, IE. Kazananjian, A. and MacAulay, D. (1999) Health Professions Council Emergency Medical Assistants Scope of Practice Report. Government of British Columbia, Ministry of Health Planning.
Erich, J. (2001) ‘The State of EMS: “Three simple digits” face complex challenges’. The Journal of Emergency Care, Rescue and Transportation. www.emsmagazine.com/issues/state.html [accessed 21/05/2001]
Esposito, TJ. Maier, RV. Rivara, FP. Pilcher, S. Griffith, J. Lazear, S. and Hogan, S. (1995) ‘The impact of variation in trauma care times: urban versus rural’. Prehospital Disaster Care Med. 10: 161-167.
Evans, T. (1998) ‘Cardiac arrests outside hospital’. British Medical Journal. 316: 1031-1032.
Evans, F. and Hoodless, M. (1999) ‘Using Evidence Based Needs Assessment to lead Change in a Small Rural Community’. 5th National Rural Health Conference, Adelaide. www.ruralhealth.org.au/fifthconf/evanspaper.htm [accessed 22/10/01]
Field, J. and Lord, B. (1999) ‘An undergraduate, pre-employment program in pre-hospital care: the first year experience at Charles Sturt University.’ Response. 11(3): 22-26.
Field, J. (1994) ‘Establishment of ambulance education in a University context’. Australasian Journal of Emergency Care. 1(1): 13-15.
Field, J. Battersby, D. and Hodge, D. (1999) ‘Professional qualifications for Ambulance Officers: A case study’. Australian Journal of Emergency Care. 6(2): 11-16.
Flinders University. (2001) Courses and programs: Bachelor of Health Sciences (Ambulance Studies). www.flinders.edu.au/courses/ugrad/bachelor/bhscas.htm [accessed 13/11/01]
Flood, RL. and Jackson, MC. (1991) Creative Problem Solving: Total Systems Intervention. John Wiley & Sons, Brisbane.
Forbes, M. (1999) ‘Break the union, was the chief’s brief’. The Sunday Age. 12 September 1999.
Forrester, JW. (1969) Urban Dynamics. MIT Press, Massachusetts.
Forrester, JW. (1980) Principles of Systems. MIT Press, Massachusetts.
Fragar, LJ. Gray, EJ. Franklin, RJ. and Petrauskas, V. (1997) A picture of health: a preliminary report of the health of country Australians. Australian Agricultural Health Unit, Moree, NSW.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
341
Gaffney, R. (Winter 84/Spring 85) ‘Systems Thinking in Business: An Interview with Peter Senge’, in Revision. 7(2).
Gallehr, JE. and Vokov, LF. (1993) ‘Defining the benefits of rural emergency medical technician-defibrillation’. Annals of Emergency Medicine. 22(10): 108-112.
Gardner, H. (Ed.) (1992) Health Policy: Development, Implementation, and Evaluation in Australia. Churchill Livingstone, Melbourne.
Gardner, H. (Ed.) (1997) Health Policy in Australia. Oxford University Press, Melbourne.
Garside, P. (1998) ‘Organisational context for quality: lessons from the fields of organisational development and change management’. Quality in Health Care. Volume 7 Supplement: S8-S15.
Garza, MA. (1994) ‘Rethinking EMS after Sand Key, things will never be the same’. J Emerg Med Ser. 19(5): 103-7.
Georgetown Linguistics. (1996) Web Chi Square Calculator. www.georgetown.edu.cball/webtools/web_chi.html [accessed 03/05/02]
Gilbert, R. Gibberd, B. and Stewart, J. (1992) 'The New South Wales Resource Allocation Formula: a method for equitable health funding'. Australian Health Review. 15(1): 6-21.
Gilligan, JE. Griggs, WM. Jelly, MT, Morris, DG. Haslam, RR. Matthews, NT. Everest, ER. Bryce, RL. Marshall, PB. and Peisach, RA. ‘Mobile intensive care services in rural South Australia’. Med J Aust. 171: 617-620.
Gippsland Research and Information Bank. (1993) Gippsland Region: Quarterly Profile, Number 39.
GISCA. (1999) Accessibility/Remoteness Index of Australia (ARIA). Department of Health and Aged Care, Occasional Paper Series No. 6.
Graham, JC. and Vinen, J. (1992) Management of seriously injured patients. Royal Flying Doctor Service of Australia.
Grantham, H. (2001) ‘New Paradigm Paramedics’. South Australian Ambulance Service. www.saamabulance.com.au/publicweb/para.html [accessed 10/01/02]
Greenfield, T. (Ed.). (1996) Research Methods: Guidance for postgraduates. Arnold, Sydney.
Grossman, DC. Hart, LG. Rivara, FP. Maier, RV. and Rosenblatt, R. (1995) ‘From roadside to bedside: the regionalization of trauma care in a remote rural county’. The Journal of Trauma: Injury, Infection and Critical Care 38(1): 14-21.
Grossman, DC. Kim, A. Macdonald, SC. Klein, P. Copass, MK. and Maier, RV. (1997) ‘Urban-rural differences in prehospital care of major trauma’. The Journal of Trauma: Injury, Infection and Critical Care 42(4): 723-729.
Guly, UM. Mitchell, RG. Cook, R. Steedman, DJ. and Robertson, CE. (1995) ‘Paramedics and technicians are equally successful at managing cardiac arrest outside hospital’. British Medical Journal. 310(6987): 1091-1094.
Guppy, L. and Woollard, M. (2000) ‘Emergency ambulance services: performance management and review’. Pre-hospital Immediate Care. 4: 40-45.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
342
Hancock, L. (Ed.) (1999) Health Policy in the Market State. Allen & Unwin, Sydney.
Handmer, J. (2000) ‘Are Emergency Services becoming private?’ Australian Journal of Emergency Management. Spring 2000.
Harrison, H. (1997) Trends in the delivery of rural health, education and banking services. NFF Research Paper Volume 11.
Harrison, JF. and Cooke, MW. (1999) ‘Study of early warning of accident and emergency departments by ambulance services’. Journal of Accident and Emergency Medicine. 16: 339-341.
Harvey, D. Strasser, R. Kelleher, S. Sandhu, G. McQuillen, M. Burley, M. and Kelly, H. (1995) Health and Health Service Needs in Small Rural Communities. Monash University Centre for Research in Health Education and Social Science.
Hay, R. Hughes, J. Kellehear, A. Kellow, A. Muetzelfeldt, M. and Williams, P. (1993) Study Guide in Health Policy and Administration: Reader in Health Policy and Administration. Deakin University.
Haynes, DF. (1989) Report of the Staffing Resources Sub-Committee to the Regional Committee of Management. Ambulance Service Victoria - South Eastern Region. Ref Type: Unpublished Work
Haynes, BE and Pritting, J. (1999) ‘A rural emergency medical technician with selected advanced skills’. Prehospital Emergency. 3(4): 343-346.
Health Office Circular HSC (IS)67/WHSC(IS)57. (1974) Organisation of Ambulance Services: Standards and Incentive Bonus Schemes. Department of Health and Social Security/Welsh Office.
Health Solutions Pty. Ltd. (1992) 'Ambulance Services Review'. The Victorian Ambulance Services Review. The Victorian Ambulance Board. Ref Type: Unpublished Work
Hickey, N. (2001a) ‘RAV stands by proposal’. Latrobe Valley Express. 20 September 2001.
Hickey, N. (2001b) ‘Ambo move may place lives at risk’. Latrobe Valley Express. 20 September 2001.
Hill, G. (2001) ‘Beyond the Trails Proceedings Report’. After Hours Primary Medical Care National Workshop. 22-23 March 2001, Sydney.
Hill, M. (1997) The Policy Process in the Modern State. Prentice Hall, Sydney.
Hindle, T. Checkland, P. Mumford, M. and Worthington, D. (1995) ‘Developing a methodology for multidisciplinary action research: a case study.’ Journal of the Operational Research Society. 46(4): 453-464.
Hindle, D. Frances, M. and Pearse, J. (1998) ‘Casemix funding in rural NSW: Exploring the effects of isolation and size’. Australian Health Review. 21(4).
Hindle D. and Braithwaite, J. (2001) SSM: a guide for Australian health professionals. Centre for Clinical Governance Research, University of New South Wales, Sydney.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
343
Hodge, G. (2000) ‘Good governance and the privatising state: some international lessons’. Privatisation and Good Governance Conference, Melbourne, 8 September 2000.
Holliman, CJ. VanRooyen, MJ. Green, GB. Kirsch, TD. Delooz, HH. Clem, KJ. Thomas, TL. Davis, MA. Wang, E. and Wolfson, AB. (2000) ‘Planning recommendations for international emergency medicine and out-of-hospital care system development’. Academic Emergency Medicine. 7(8): 911-917
Holman, P. (1997) Community Based Emergency Response Teams - A trend for the future. Ref Type: Unpublished Work
Hospitals and Health Services Commission. (1976a) Health Transport Policies for Australia. AGPS, Canberra.
Hospitals and Health Services Commission. (1976b) Rural Health in Australia. AGPS, Canberra.
Hugo, G. (1999) ‘Putting People back into the Planning Process: The changing role of Geographic Information Systems’. University of Adelaide.
Humphreys JS. and Rolley, F. (1991) Health and Health Care in Rural Australia: A Literature Review. Department of Geography and Planning, University of New England, Armidale.
Humphreys, JS. and Weinand, HC. (1991) ‘Health care preferences in a country town’, The Medical Journal of Australia, Vol 154: 733-737.
Humphreys, J. Rolley, F. and Weinand, H. (1992) ‘How Healthy is Life in the Bush? Problems Associated with the Assessment of Health Status in Rural Australia’, The Australian Journal of Rural Health. 1(1): 17-27.
Humphreys, JS. (1993) ‘Planning for services in rural Australia’, Regional Journal of Social Issues, No 27: 10-19.
Humphreys, JS. Mathews-Cowey, S. and Rolley, F. (1996) Health Service Frameworks for Small Rural and Remote Communities: Issues and Options. University of New England.
Humphreys, JS. (1998) Rural Health and the Health of Rural Communities. Latrobe University, Bendigo.
Humphreys, JS., and Mathews-Cowey, S. (1999) Models of Health Service Delivery for Small Rural and Remote Communities. La Trobe University, Bendigo.
Hunt, JD. Gratton, MC. and Campbell, JP. (1999) ‘Prospective determination of medical necessity for ambulance transport by on-scene paramedics’. Academic Emergency Medicine. 6(5): 447.
Jacobs, IG and Oxer, HF. (1990) ‘A review of pre-hospital defibrillation by ambulance officers in Perth, Western Australia’. Medical Journal of Australia. 153(11-12); 662-664.
Jacobs, I. (2000) ‘Prehospital care: A plea for more research’. Emergency Medicine. 12: 175-176.
Jacobs, I. (2001) ‘Personal communication’, 20 November 2001.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
344
Jacobs, I. Callanan, V. Nichol, G. Valenzuela, T. Mason, P. Jaffe, AS. Landau, W. and Vetter, N. (2001) ‘The Chain of Survival’. Annals of Emergency Medicine. 37(4): S5-S16).
Jermyn, BD. (2000) ‘Cost-Effectiveness Analysis of a Rural/Urban First-responder Defibrillation Program’. Prehospital Emergency Care. 4(1): 43-47.
Jewkes, R. and Murcott, A. (1996) ‘Meanings of Community’. Soc. Sci. Med. 43(4): 555-563.
Johnson, DB. (1995) ‘Delivering high-quality rural emergency medical services: Issues and options’ Top Emerg Med, 17(3): 14-21.
Johnson, GS and Guly, HR. (1995) ‘The effect of pre-hospital administration of intravenous nalbuphine on on-scene times’. Journal of Accident and Emergency Medicine. 12(1): 20-2.
Johnson, JC. (1991) ‘Prehospital Care: The Future of Emergency Medical Services.’ Annals of Emergency Medicine. 20(4):426-30.
Joint Royal Colleges Ambulance Liaison Committee. (2000) The future role and education of paramedic ambulance service personnel (emerging concepts). Ref. www.asancep.org.us/JRCALC/pec_concepts.htm [accessed 04/08/2000]
JoÓ, S. (2000) ‘Emergency medical services (EMS) in the Federal Republic of Germany: roadside accidents’. Pre-hospital Immediate Care. 4: 86-89.
Jordan, J. Dowswell, T. Harrison, S. Lilford, RJ. and Mort, M. (1998) ‘Whose priorities? Listening to users and the public’, British Medical Journal, 316: 1668-1670.
Karlsten, R. and Sjöqvist, BA. (2000) ‘Telemedicine and decision support in emergency ambulances in Uppsala’. Journal of Telemedicine and Telecare. 6: 1-7.
Kauffman, DL. (1980) Systems 1: an introduction to systems thinking. Future Systems, Minneapolis.
Kaweski, SM. Sise, MJ. and Virgilio, RW. (1990) ‘The Effect of Prehospital Fluids on Survival in Trauma Patients’. The Journal of Trauma. 30(10): 1215-1219.
Kelleher, A. (1993) 'Country health: another side of the rural crisis'. Reader in Health Policy and Administration. Deakin University.
Kelly, H. O’Meara, P. and Burley, M. (1999) Urgent care in Victorian rural towns: Final Report. Monash University, Traralgon.
King, JA. (2000) ‘NHTSA Notes Commentary: EMS Education Agenda for the Future: Flexner Revisited’. Annals of Emergency Medicine. 35(6): 624-625.
Kinglake and District Community News. (2001) Mountain Monthly. September 2001.
KPMG Management Consulting. (1997) Review of ambulance services. Victorian Ambulance Services Association, Melbourne.
Kramer, FA. (1975) ‘Policy Analysis as Ideology’. Public Policy Review. Sept/Oct 1975.
Krieger, J. (1986) Reagan, Thatcher and the Politics of Decline. Polity Press, Cambridge.
Kurowski, R. (2002) ‘Boost for ambo teams’. Latrobe Valley Express. 7 January 2002.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
345
Langford, S. (1992) Preparation of patients for transport. Royal Flying Doctor Service of Australia.
Lawrence, G. and Share, P. (1993) ‘Rural Australia: current problems and policy directions’, Regional Journal of Social Issues, No 27: 3-9.
Ledington, P. and Donaldson, J. (1997) ‘Soft OR and management practice: a study of the adoption and use of SSM.’ Journal of the Operational Research Society. 48(3): 229-240.
Le Grand, J. (1993) 'Equality', Study Guide in Health Policy and Administration. Deakin University.
Lendrum, K. Wilson, S. and Cooke, MW. (2000) ‘Does the training of ambulance personnel match the workload seen?’ Pre-hospital Immediate Care. 4: 7-10.
Levit, LK. (2001) ‘Use it or Lose it: Is de-skilling evidence-based?’ Rural and Remote Health 1. http://rrh.deakin.edu.au [accessed 31/12/01]
Lilienfeld, R. (1978) The Rise of Systems Theory: an ideological analysis. John Wiley, Brisbane.
Lord, B. (1998) ‘Re-confirming the role of paramedics in prehospital care’. Australasian Journal of Emergency Care. 5(4): 10-14.
Lyle, DM. Thomson, PC. Deane, SA. and Coulon, LA. (1991) ‘Regionalization of trauma services in western Sydney: predicted effect on ambulance and hospital utilization rates’. Australian and New Zealand Journal of Surgery. 61(8): 589-96.
Lynch, TG. and Georghiou, PF. (1995) ‘Managing rural emergency medical services: Doing more with less’. Top Emerg Med, 17(3): 1-13.
Mackay, CA. Burke, DP, and Bowden, DF. (1997) ‘Effect of paramedic scene time on patient outcome’. Pre-hospital Immediate Care. 1: 4-7.
Macklin, J. (1991) The Australian Health Jigsaw: Integration of Health Care Delivery. National Health Strategy, Issues Paper No. 1.
Mahony, K. (2000) ‘Faith in the ‘cultural fix’: limits to a planned cultural change program in a rural health service’. Australian Health Review. 23(4): 187-196.
Mahony, K. (2001) ‘Management and the creation of occupational stressors in an Australian and a UK Ambulance Service’. Australian Health Review. 24(4): 135-145.
Maio, RF. and Spaite, D. (1995) ‘Using Epidemiological Methods to Evaluate Out-of Hospital care: The Ecologic Study’, Annals of Emergency Medicine. 26(2): 153-157.
Maio, RF. Garrison, HG. Spaite, DW. Desmond, JS. Gregor, MA. Cayten, CG. Chew, JL. Hill, EM. Joyce, SM. MacKenzie, EJ. Miller, DR. O’Malley, PJ. and Stiell, IG. (1999) ‘Emergency medical services outcomes project 1 (EMSOP 1): prioritizing conditions for outcomes research’. Annals of Emergency Medicine. 33(4): 423-32.
Marcum, L. and Callaham, M. (1998) ‘The not-so-scientific value of EMS’. Annals of Emergency Medicine. 32(5): 634-636.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
346
Marshall, C. and Rossman, GB. (1987) Designing Qualitative Research. SAGE Publications, London.
Martinez, R. (1998) ‘New vision for the role of emergency medical services’. Annals of Emergency Medicine. 32(5): 594-599.
Mason, J. (1995) ‘Maintaining standards in a time of change’. Response. 7(1): 18-19.
Mayski, W. (1999) ‘The influence of culture on the Metropolitan Ambulance Service, Melbourne, Australia’. Australasian Journal of Emergency Care. 6(1): 18-27.
McCallum, AL. and Rubes, CR. (1996) ‘Prehospital interventions’. Emergency Medicine Clinics of North America. 14(1): 1-12.
McCoy, J. (1996) ‘Ambulance Service Victoria, A partnership to achieve quality performance’. Australian Journal of Emergency Care. 3(3): 30-31.
McCoy, J. Garside, A. Eichler, G. and Austin, T. (1997) ‘A case study in health care: Ambulance Service Victoria’. The Quality Magazine. 6(1): 24-28.
McDermott, FT. Cordner, SM. and Tremayne, AB. (1996) ‘Evaluation of the medical management and preventability of death in 137 road traffic fatalities in Victoria, Australia: an overview’. The Journal of Trauma. 40(4): 520-535.
McDonell, A. Edwards, D. and Harries, R. (2000) ‘Paramedic education: flexible learning delivered via an Internet based classroom’. Response. 13(4): 28-33.
McKie, J. Richardson, J. Singer, P. and Kuhse, H. (1998) The Allocation of Health Care Resources: An Ethical Evaluation of the ‘QALF’ Approach. Ashgate Dartmouth, Sydney.
McWhinney, IR. (1998) ‘Core values in a changing world’, British Medical Journal. 316: 1807-1809.
Meade, DM. (1999) ‘Expanded-Scope Practice: EMS at the Crossroads of Care’. EMS Magazine. www.emsmagazine.com/articles/emsarts/meade [accessed 07/02/1999]
Meislin, HW. Conn, JB. Conroy, C. and Tibbitts, M. (1999) ‘Emergency medical service agency definitions of response intervals’. Annals of Emergency Medicine. 34(4): 453-458.
Meyer, ADMcR. Cameron, PA. Smith KL. and McNeil, JJ. (2000) ‘Out-of-hospital cardiac arrest’. Medical Journal of Australia. 172: 73-84.
Miller, R.(Chairman) (1986) Report of the Ambulance Services Implementation Advisory Committee to the Minister of Health.
Mingers, J. and Taylor, S. (1992) ‘The use of SSM in practice’. Journal of the Operational Research Society. 43(4): 321-332.
Ministerial Taskforce on Trauma and Emergency Services. (1998) Education & Training for an integrated Trauma and Emergency System in Victoria. DRAFT 2.
Ministerial Taskforce on Trauma and Emergency Services and Department of Human Services Working Party on Emergency and Trauma Services. (1999) Review of Trauma and Emergency Services Victoria.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
347
Monash University. (2001) Ambulance & Paramedic Studies. www.med.monash.edu.au/paramedic/ [accessed 13/11/01]
Mooney, G. and Scotton, R. (Eds.) (1998) Economics and Australian Health Policy. Allen and Unwin, Sydney.
Moore, L. (1999) ‘Measuring quality and effectiveness of prehospital EMS’. Prehospital Emergency Care. 3(4): 325-31.
Morgan, G. (1980) ‘Paradigms, metaphors, and puzzle solving in organization theory’. Administrative Science Quarterly. 25(4): 605-622.
Morgan, G. (1997) Images of Organization. Sage Publications, Thousand Oaks, Calif.
Morrisey, MA. Ohsfeldt, RL. Johnson, V. and Treat, R. (1995) ‘Rural Emergency Medical Services: patients, destinations, times and services’. J. Rural Health. 11(4): 286-294.
Morrisey, MA. Ohsfeldt, RL. Johnson, V. and Treat, R. (1996) ‘Trauma patients: an analysis of rural ambulance trip reports’. J. Trauma. 41(4): 741-746.
Moss, J. (1993) 'Health economics and health policy issues'. Study Guide in Health Policy and Administration. Deakin University.
Napthine, D. (Chairman) (1994) Small Rural Hospitals Task Force Report. H. & C.S.
Neergaard, L. (2001) ‘Ambulance-ER video link may speed stroke care’. www.star-telegram.com [accessed 27/07/01]
Narad, RA.. (1998) ‘Coordination of the EMS system: an organizational theory approach’. Prehospital Emergency Care. 2(2): 145-52.
Narad, RA. and Driesbock, KR (1999) ‘Regulation of ambulance response times in California.’ Prehospital Emergency Care. 3(2): 131-135.
Narad, R. (2000) ‘Emerging organizational structures in the ambulance industry in the United States’. Prehospital and Disaster Medicine. 15(1): 57-64.
National Health Ministers’ Benchmarking Working Group. (1998) Second National report on health sector performance indicators. Australian Health Ministers’ Conference.
National Health Performance Committee. (2000) Measuring performance in the Australian health system: towards a national performance assessment framework. Discussion Paper. Sydney.
National Highway Traffic Safety Administrator. (1996) Emergency Medical Services Agenda for the Future. www.nhtsa.dot.gov/people/injury/ems/agenda/emsman.html [accessed 1/12/2000]
National Rural Health Alliance. (1995) 3rd National Rural Health Conference Handbook.
National Rural Health Alliance.(1995) Strategies for Change: A Summer Statement to Shareholders.
National Rural Health Alliance. (1999) The National Rural Health Strategy Mid-Term Review and Update.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
348
National Rural Health Alliance. (1999) Health Horizons: A Framework for Improving the Health of Rural, Regional and Remote Australians.
National Rural Health Association (USA). (1997) Rural and Frontier Emergency Medical Services Toward the Year 2000.
National Rural Health Association (USA). (1998) A Vision for Health Reform Models for America’s Rural Communities. www.nrharural.org/dc/issuepapers/ipaper11.html [accessed 01/14/99]
National Rural Health Policy Forum and National Rural Health Alliance. (1998) DRAFT Healthy Horizons 1999-2003: A Health Strategy for Regional, Rural and Remote Australian. Australian Health Ministers’ Conference, Canberra.
Navein, J. and Driscoll. P. (2000) ‘Telemedicine and the future of pre-hospital care’. Pre-hospital Immediate Care. 4: 46-50.
Neely, KW. Drake, MER. Moorhead, JC. Schmidt, TA. Skeen, DT. and Wilson, EA. (1997) ‘Multiple Options and Unique Pathways: A New Direction for EMS?’, Annals of Emergency Medicine. 30(6): 797-799.
NHS Executive. (1999) The NHS Performance Assessment Framework. NHS.
Nikkanen, HE. Pouges, C. and Jacobs, LM. (1998) ‘Emergency Medicine in France’, Annals of Emergency Medicine . 31(1): 116-120.
Nicholl, J. and Turner, J. (1997) ‘Effectiveness of a regional trauma system in reducing mortality from major trauma: before and after study’. British Medical Journal 315(7119): 1349-1354.
Nicholl J. and Willoughby J. (1998) ‘Effects of ambulance response times are being evaluated’. [letter; comment]. British Medical Journal . 317(7159): 684.
Nicholl, J. Hughes, S. Dixon, S. Turner, J. and Yates, D. (1998) ‘The costs and benefits of paramedic skills in pre-hospital trauma care’. Health Technology Assessment. 2(17): i - iv.
Nicholl, J. and Munro, J. (2000) ‘Systems for emergency care: Integrating the components is the challenge’. British Medical Journal 320: 955-956.
Nicholl, J. Turner, J. and Martin, D. (2001) The Future of Ambulance Services in the United Kingdom. Ambulance Service Association.
Norris, DF. Mandell, MB. and Hathaway, WE. (1993) ‘Volunteers in Emergency Medical Service: A Case Study from Rural America’. Public Productivity and Management Review. 16: 257-69.
NSW Ministerial Advisory Committee on Quality in Health Care. (1999) A Framework for Managing the Quality of Health Services in New South Wales. NSW Health.
O’Connor, RE. Cone, DC. De Lorenzo, RA. Domeier, RM. Moore, WE. Taillac, PP. Verdile, VP. Zachariah, BS. and Davidson, SJ. (1999) ‘EMS systems: foundations for the future’. Academic Emergency Medicine. 6(1): 46-53.
O’Meara, P. (1995) Resource Allocation for Gippsland Ambulance. Ambulance Service Victoria -South Eastern Region. Ref Type: Unpublished Work
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
349
O’Meara, P. and Somers, G. (1999) ‘Ambulance Service Delivery in Emerald: a pilot study’, Health Services Research Conference, Sydney, 8-11 August 1999.
O’Meara, P. (2000) ‘Ambulance Service Delivery in Emerald: a pilot study’, 5th Biennial Australian Rural and Remote Health Scientific Conference, Toowoomba, 24-26 February 2000.
O’Meara, P. Strasser, R. Marrow, A. and Le Leivre, P. (2001) ‘An integrated approach to the role of the Ambulance Medical Officer in rural Australia’, Pre-hospital Immediate Care. 5(1): 24-26.
O’Meara, P. (2001) ‘Professional and community expectations of rural ambulance services in Australia’, Pre-hospital Immediate Care. 5(1): 27-30.
O’Meara, P. and Boyle, M. (2001) ‘From Roadside to Hospital: An investigation of the factors influencing the time taken to deliver trauma patients to a regional hospital’. Monash Rural Health Bulletin. 8(1). www.med.monash.edu.au/mrh/education/cpe/v8n1-bulletin.html [accessed 7/01/02].
O’Meara, P. Burley, M. and Kelly, H. (2002) ‘Urgent care systems: what are they made of? Australian Journal of Rural Health. [accepted for publication in 10(1)].
Ord, J. (1999) First Responder Scheme Pilot Project – Evaluation Report Part 2. Essex Ambulance Service.
Ornato, JP. McNeill, SE. Craren EJ. and Nelson, NM. (1984) ‘Limitation on effectiveness of rapid defibrillation by emergency medical technicians in a rural setting’. Annals of Emergency Medicine. 13(12): 1096-1099.
Ortenwall, P. (1999) ‘ ‘’Load and go” or “stay and play”? Measures at the accident site must be adapted according to the needs of the injured’. Lakartidningen. 96(37): 3862-4.
Ohsfeldt, RL. Morrisey, MA. Johnson, V. and Treat, R. (1996) ‘Simplifying the Assessment of Rural Emergency Medical Services Trauma Transport’, Medical Care, 34(12): 1180-1187.
Osborne, D. and Gaebler, T. (1993) Reinventing Government: How the entrepreneurial spirit is transforming the public sector. Plume, New York.
O’Toole, K. (1993) ‘Changing the focus from “rural” to “local” state’, Regional Journal of Social Issues. No 27: 20-31.
O’Toole, K. (1999) ‘Competition and marketisation: a small town responds’. in Challenging rural practice: human services in Australia. Eds. Briskman, L. and Lynn, M. Deakin University Press, Geelong. pp. 64-76.
Palmer, GR. and Short, SD. (1994) Health Care & Public Policy: An Australian Analysis. McMillan, Melbourne.
Palmer, GR. and Short, SD. (2000) Health Care & Public Policy: An Australian Analysis. McMillan, Melbourne.
Patching, D. (1990) Practical Soft Systems Analysis. Pitman, London.
Payne, D. (2000) ‘Poor ambulance response causes 700 deaths annually in Ireland’. British Medical Journal, 321: 1176.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
350
Peach, HG. Pearce, DC. and Farish, SJ. (1998) ‘Age-standardised Mortality and Proportional Mortality Analyses of Aboriginal and Non-Aboriginal Deaths in Metropolitan, Rural and Remote Areas.’ Australian Journal of Rural Health, 6: 36-41.
Pegram, R. (2001) After Hours Primary Medical Care Services in Australia. General Practice Strategic Policy and Development Unit, DHAC, Canberra.
Pepe, PE. (2000) ‘Controversies in the prehospital management of major trauma'. Emergency Medicine 12: 180-189.
Performance Indicators Implementation Committee. (1992) Report of Recommendations. Ambulance Service Victoria. Ref Type: Unpublished Work
Peters, J and Hall, GB. (1999) ‘Assessment of ambulance response performance using geographic information system’. Social Science and Medicine. 49(11): 1551-66.
Peters, TJ. and Waterman, RH Jr. (1982) In Search of Excellence: Lessons from America’s Best-Run Companies. Harper & Row, Sydney.
Pettingill, L. (1990) ‘Public policy – power – professionalism’. Journal – Australian College of Midwives. 3(3): 23-28.
Plsek, PE. and Greenhalgh, T. (2001) ‘The challenge of complexity in health care’. British Medical Journal. 323; 625-628.
Plsek, PE. and Wilson, T. (2001) ‘Complexity, leadership, and management in healthcare organisations’. British Medical Journal. 323; 746-749.
Plueckhahn, VD. (1983) Ethics, Legal Medicine and Forensic Pathology. Melbourne University Press.
Powar, M. Nguyen-Van-Tam, J. Pearson, J. and Dove, A. (1996) ‘Hidden impact of paramedic interventions’. Journal of Accident and Emergency Medicine. 13(6): 383-385.
Public Bodies Review Committee. (1984) Final Report on Victoria's Ambulance Services. Parliament of Victoria.
Public Bodies Review Committee. (1993) Summary of Initial Findings: Metropolitan Fire Brigades Board. Parliament of Victoria.
QEMS Secretariat. (1998) Queensland Emergency Medical System (QEMS) Strategic Plan 1999 to 2002. DRAFT July 1998.
Reich, J. (1991) ‘The rural route to success: Comparing EMS in three Alabama counties’. Journal of Emergency Medical Services. 16: 53-56.
Reid, M. and Solomon, S. (1992) Improving Australia’s Rural Health and Aged Care Services. National Health Strategy, Background Paper No. 11.
Ricketts, TC. Johnson-Webb, KD. and Taylor, P. (1998) Definitions of rural: a handbook for health policy makers and researchers. US DHHS.
Reinholtd, S. and Smith, P. (1998) Directions in volunteer development in Australian emergency services. Country Fire Authority, Victoria.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
351
Reinholtd, S. (1999) ‘Managing change within the emergency services to ensure the long-term viability of volunteerism’. Australian Journal of Emergency Management. Summer 1999-2000.
Roberts, G. Duck, J. and Ord, J. (1999) ‘Community volunteers as first responders’. Pre-hospital Immediate Care. 3(4): 186-190.
Roberts, G. (1998) ‘Paramedics: should we be creating a new profession?’ Ambulance UK. 13: 7-8.
Robbins, SP. and Barnwell N. (1994) Organisation Theory in Australia. Prentice Hall, Sydney.
Robinson JS. Davies MK. Johns BM. and Edwards SN. (1998) ‘Out-of-hospital cardiac arrests treated by the West Midlands Ambulance Service over a 2-year period’. European Journal of Anaesthesiology. 15(6): 702-709.
Rogers, FB. Shackford, SR. Hoyt, DB. Camp, L. Osler, TM. Mackerise, RC. and Davis, JW. (1997) ‘Trauma Deaths in a Mature Urban vs Rural Trauma System’. Archives of Surgery. 123: 376-382.
Rogers, FB. Shackford, SR. Osler, TM. Vane, DW. and Davis, JW. (1999) ‘Rural trauma: the challenge for the next decade’. The Journal of Trauma: Injury, Infection, and Critical Care. 47(4): 802.
Rourke, J. (1997) ‘In search of a definition of rural’, Canadian Journal of Rural Medicine. 3(3).
Rowan S. (1998) ‘Provider and consumer perceptions of allied health service needs’. Australian Health Review. 21(1).
Rucker, DW,. Edwards, RA. Burstin, HR. O’Neil, AC. and Brennan, TA. (1997) ‘Patient-specific predictors of ambulance use’. Annals of Emergency Medicine. 29(4): 484-91.
Rural Ambulance Victoria. (2000a) ‘Ambulance to seek community input’. Media Release.
Rural Ambulance Victoria. (2000b) Rural Ambulance Victoria Annual Report 2000.
Rural Committee of the Canadian Association of Emergency Physicians. (1997) Recommendations for the Management of Rural, Remote and Isolated Emergency Health Care Facilities in Canada. Canadian Association of Emergency Physicians. Ontario, Canada.
Rutledge, R. Ricketts, TC. and Bell, E. (1992) ‘Emergency Medical Services in Rural Areas’, in Gesler, M. and Ricketts, TC. (Eds.). Health in rural North America: the geography of health care services and delivery. Rutgers, pp. 226-247.
Sargent, LT. (1972) Contemporary Political Ideologies. Dorsey Press, Homewood, Ill.
Schmidt, T. Atcheson, R. Federiuk, C. Mann, NC. Pinney, T. Fuller, D. and Colbry, K. (2000) ‘Evaluation of protocols allowing emergency medical technicians to determine need for treatment and transport’. Academic Emergency Medicine. 7(6): 663-669.
Schoenman, JA. Mohr, PE. and Mueller, CD. (1999) ‘EMS initiatives under the Medicare Rural Hospital Flexibility Program’, Chapter 7 Rural Hospital Flexibility Program Tracking Project. Rural Policy Research Institute.
Senge, PM. (1990) The Fifth Discipline: the art and practice of the learning organization. Doubleday Currency, Sydney.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
352
Senge, Peter M. (1998) ‘A Brief Walk into the Future: Speculations About Post-Industrial Organizations’. The Systems Thinker. 9(9).
Senge, P. Kleiner, A. Roberts, C. Ross, R. Roth, G. and Smith, B. (1999) The Dance of Change: The Challenges of Sustaining Momentum in Learning Organizations. Nicholas Brealey, London.
Shapiro, SE. (2000) ‘Outcomes of prehospital care: do we really make a difference?’ Journal of Emergency Nursing. 26(3): 239-241.
Sheldon, T. (1998) ‘Promoting health care quality: what role performance indicators?’. Quality in Health Care. 7(Supplement): S45-S50.
Short, C. (1986) ‘Equal pay: what happened?’ Journal of Industrial Relations. 28(3): 315-335.
Shortell, SM. and Kaluzny, AD. (1994) Health Care Management: Organization Design and Behaviour. Delmar Publishing.
Shuster, M. and Chong, J. (1989) ‘Pharmacologic Intervention in Prehospital Care: a Critical Appraisal’. Annals of Emergency Medicine. 18: 192-196.
Simeon R. (1976) ‘Studying public policy’. Canadian Journal of Political Science. 9(4).
Sinclair Report. NSW Ministerial Advisory Committee on Health Services in Smaller Towns. (2000) Report to the NSW Minister for Health: A Framework for Change. NSW Government.
Skelton, R. (1994) 'Tehan's intensive care: The profile'. The Age, 2 June 1994.
Smith, GA. Thompson, JD. Shields, BJ. Manley, LK. and Haley, KJ. (1997) ‘Evaluation of a Model for Improving Emergency Medical and Trauma Services for Children in Rural Areas’. Annals of Emergency Medicine. 29(4): 504-510.
Snooks H. Wrigley H. George S. Thomas E. Smith H. and Glasper A. (1998) ‘Appropriateness of use of emergency ambulances’. Journal of Accident and Emergency Medicine. 15(4): 212-215.
Somers, GT. Drinkwater, EJ. and Torcello, N. (1997) ‘The GP as first responder in a major medical emergency’. Australian Family Physician. 26(12): 1406-1409.
Somers, GT. (1999) ‘GP-based Emergency Response in Rural Areas: Is there a need?’ Aust. Journal Rural Health. 7: 104-108.
Sosnin, M. Young, D. and Dunt, DR. (1989) ‘A study of emergency utilisation’. Australian Family Physician. 18(3) 233-238.
Spaite, DW. Valenzuela, TD. Meislin, HW. et al ‘Prospective validation of a new model for evaluation of EMS systems by in-field observation of specific time intervals in prehospital care’. Annals of Emergency Medicine. 22: 638-645.
Spaite, DW. Criss, EA. Valenzuela, TD. and Guisto, J. (1995) ‘Emergency Medical Service Systems Research: Problems of the Past, Challenges of the Future’, Annals of Emergency Medicine. 26(2): 146-152.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
353
Spaite, DW. Criss, EA. Valenzuela, TD. and Harvey W. (1997) ‘Developing a Foundation for the Evaluation of Expanded-Scope EMS: A Window of Opportunity That Cannot Be Ignored’. Annals of Emergency Medicine. 30(6): 791-796.
Spaite, D. (1998) ‘Intubation by Basic EMT’s: Lifesaving Advance or Catastrophic Complication?’ Annals of Emergency Medicine 31(2): 276-277.
Spaite, DW. Maio, R. Garrison, HG. Desmond, JS. Gregor, MA. Stiell, IG. Cayten, CG. Chew, JL. MacKenzie, EJ. Miller, DR. and O’Malley, PJ. (1999) ‘Emergency Medical Services Outcomes Project (EMSOP) II: Developing the Foundation and Conceptual Models for Out-of-Hospital Outcomes Research’. Annals of Emergency Medicine. 37(6): 657-663.
Sutherland, K. and Dawson, S. (1998) ‘Power and quality improvement in the new NHS: the roles of doctors and managers’. Quality in Health Care. 7(Supplement): S16-S23.
Stapczynski, J. Svenson, JE. and Stone, CK. (1997) ‘Population Density, Automated External Defibrillator Use, and Survival in Rural Cardiac Arrest’. Academic Emergency Medicine. 4(6): 552-558.
State Emergency Service. (1989) Road Accident Rescue in Victoria - A New Era. Ministry for Police and Emergency Services, Victoria.
Steering Committee for the Review of Commonwealth/State Service Provision. (2000) Report on Government Services 2000. AusInfo, Canberra.
Stevens, A. and Gillam, S. (1998) ‘Needs assessment: from theory to practice’, British Medical Journal. 316: 1448-1452.
Stiell, IG. (1993) ‘Cardiac Arrest in Your Community: Are There Weak Links in the Chain of Survival?’ Canadian Medical Association Journal. 149(5): 563-565.
Stiell, IG. Hebert, PC. Wells, GA. Laupacis, A. Vandemheem, K. Dreyer, JF. Eisenhauer, MA. Gibson, J. Higginson, LA. Kirby, AS. Mahon, JL. Maloney, JP. and Weitzman, BN. (1996) ‘The Ontario trial of active compression-decompression cardiopulmonary resusitation for in-hospital and prehospital cardiac arrest’. JAMA. 275(18): 1417-1423.
Stiell, IG. Wells, GA. Spaite, DW. Lyver, MB. Munkley, DP. Field, BJ. Dagnone, E. Maloney, JP. Jones, GR. Liuinstra, LG. Jermyn, BD. Ward, R. and DeMaio, V. (1998) ‘The Ontario Prehospital Advanced Life Support (OPALS) Study: Rationale and Methodolgy for Cardiac Arrest Patients’. Annals of Emergency Medicine. 32(2): 180-190.
Stiell, IG. Wells, GA. DeMaio, VJ. Spaite, DW. Field, BJ 3rd. Munkley, DP. Lyver, MB. Liuinstra LG. and Ward, R. (1999a) ‘Modifiable factors associated with improved cardiac arrest survival in a multicenter basic life support/defibrillation system: OPALS Study Phase I results. Ontario Prehospital Advanced Life Support’. Annals of Emergency Medicine. 33(1): 44-50.
Stiell, IG. Wells, GA. Field, BJ. Spaite, DW. DeMaio, VJ. Ward, R. Munkley, DP. Lyver, MB. Liuinstra LG. Campeau, T. Maloney, J. and Dagnone, E. (1999b) ‘Improved out-of-hospital cardiac arrest survival through the inexpensive optimization of an existing defibrillation program: OPALS Study Phase II. Ontario Prehospital Advanced Life Support. JAMA. 281(13): 1175-1181.
Stout, J. Pepe, PE. and Mosesso, VN. (2000) ‘All-Advanced Life Support vs Tiered-response Ambulance Systems’. Prehospital Emergency Care. 4(1): 1-6.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
354
Strattan, S. and Niemann, JT. (1998) ‘Effects of Adding Links to “The Chain of Survival” for Prehospital Cardiac Arrest: A Contrast in Outcomes in 1975 and 1995 at a Single institution’, Annals of Emergency Medicine. 30(4): 471-477.
Strasser, RP. Harvey, D. and Burley, M. (1994) 'The health service needs of small rural communities'. The Australian Journal of Rural Health. 2(2): 7-13.
Strasser, R. Worley, P. Hays, R. Togno, J. (1999) ‘Developing Social capital: Community participation in Rural Health Services’. 5th National Rural Health Conference, Adelaide. www.ruralhealth.org.au/fifthconf/strasserpaper.htm [accessed 22/10/01]
Stripe, SC. and Susman, J. (1991) ‘A Rural-Urban Comparison of Prehospital Emergency Medical Services in Nebraska’. Journal of the American Board of Family Practice. 4(5): 313-318.
Strong, K. Trickett, P. Titulaer, I. and Bhatia, K. (1998) Health in rural and remote Australia: The first report of the Australian Institute of Health and Welfare on rural health. Australian Institute of Health and Welfare, Canberra Cat. No. PHE 6.
Sweet, G. (1997) ‘A history of advanced life support programs for ambulance paramedics in Victoria, Australia’. Australasian Journal of Emergency Care. 4(4): 25-28.
Tanberg, D. Tibbetts, J. and Sklar, DP. (1998) ‘Time series forecasts of ambulance run volume’. American Journal of Emergency Medicine. 16(3): 232-237.
Tehan, M. and Knowles, R. (1994) Ministerial Responses to Small Rural Hospitals Task Force Report. H. & C.S.
Thompson, AM. (1993) ‘Rural emergency medical volunteers and their communities: a demographic comparison’, Journal of Community Health, 18(6): 379-392.
Titulaer, I. Trickett, P. and Bhatia, K. (1998) The health of Australian’s living in the rural and remote areas: preliminary results. - Discussion paper. Australian Institute of Health and Welfare.
Townsend, M. Hallebone, E. and Mahoney, M. (1999) ‘The Role Of Volunteerism In Maintaining Emergency Services In Small Rural Communities’. 5th National Victorian Rural Health Conference. Adelaide. www.ruralhealth.org.au/fifthconf/townsendpaper.htm [accessed 22/10/01]
Turner, J. Judge, TP. Ward, ME. Johns, BM. Wilby, J. Roberts, G. and Trautner, S. (2000) ‘A new worldwide systems model for emergency medical services: statement from the Cape Town EMS summit, South Africa, January 1998’. Pre-hospital Immediate Care. 4: 183-188.
Victor, CR. Peacock, JL. Chazot, C. Walsh, S. and Holmes, D. (1999) ‘Who calls 999 and why? A survey of the emergency workload of the London Ambulance Service’. J Accid Emerg Med. 16: 174-178.
Victorian Ambulance Services' Association. (1992) 'A Submission of the Victorian Ambulance Services Association to the Victorian Ambulance Board'. Ref Type: Unpublished Work
Victorian Ambulance Superintendents' Council. (1992A) 'Submission to the Victorian Ambulance Review'. Ref Type: Unpublished Work
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
355
Victorian Ambulance Superintendents' Council. (1992B) 'Response to the Victorian Ambulance Review 1992'. Ref Type: Unpublished Work
Vukov, LF. White, RD. Bachman, JW. and O’Brien, PC. (1988) ‘New perspectives on rural EMT defibrillation’. Annals of Emergency Medicine. 17(4): 318-321.
Wadsworth, Y. (1991) Everyday Evaluation on the Run. Action Research Issues Association, Melbourne.
Wainer, J. Strasser, R. Harvey, D. and Kelly, H. (1997) ‘Health Service Delivery in Small Rural Communities: The Process of Change’. 3rd Biennial Australian Rural and Remote Health Scientific Conference, Perth.
Wardman, KT. (1992) ‘No More Band-Aids for Healthcare Reform’, The Systems Thinker. 3(6).
Warwick, J. (2000) ‘Paramedic agrees with most of comments about prehospital care’. British Medical Journal. 320: 1005.
Watson, R. and Smith, R. (1988) ‘Applications of the Lancaster SSM in Australia’. Journal of Applied Systems Analysis. 15: 3-26.
Wears, RL. (1989) ‘Predicting the demand for emergency medical services’. Annals of Emergency Medicine. 18(6): 705-6.
Wellard, R. (1995) ‘Directions in ambulance officer education’. Response. 7(3): 43-44.
Weston, CF. and McCane, MJ. (1992) ‘Audit of an emergency ambulance service: impact of a paramedic system’. Journal of Royal College of Physicians. 26(1): 86-89.
White, RD. and Vukov, LF. (1990) ‘Benefits of early defibrillation’. Annals of Emergency Medicine. 19(5): 613-614.
White, RD. Vukov, LF. and Bugliosi TF. (1994) ‘Early defibrillation by police: initial experience with measurement of critical time intervals and patient outcome’. Annals of Emergency Medicine. 23(5): 1009-1013.
White, RD. Asplin, BR. Bugliosi, TF. and Hankins, DG. (1996) ‘High Discharge Survival Rate After Out-of-Hospital Ventricular Fibrillation With Rapid Defibrillation by Police and paramedics’ Annals of Emergency Medicine. 28(5): 480-485.
White, RD. Hankins, DG. and Bugliosi, TF. (1998) ‘Seven years experience with early defibrillation by police and paramedics in an emergency medical services system’. Resuscitation. 39(3): 145-151.
Wilkinson, JR. and Murray, SA. (1998) ‘Assessment in primary care: practical issues and possible approaches’. British Medical Journal. 316: 1524-1528.
Williams, R. and Wright, J. (1998) ‘Epidemiological issues in health needs assessment’. British Medical Journal. 316: 1379-1382.
Williams, JM. Ehrlich, PF. and Prescott, JE. (2001) ‘Emergency Medical Care in Rural America’. Annals of Emergency Medicine. 38(3): 323-327.
Willis, E. and McCarthy, L. (1986) ‘From first aid to paramedical: ambulance officers in the health division of labour’. Community Health Studies. 10(1): 57-67.

Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
356
Willis, E. (1989) Medical dominance: the division of labour in Australian health care. Allen & Unwin, Sydney.
Willis, E. (1994) Illness and social relations: issues in the sociology of health care. Allen & Unwin, Sydney.
Wood, I. (2000) ‘Practitioners in emergency care: generic workers of skilled professionals?’ Pre-hospital Immediate Care. 4: 132-135.
Woollard, M. and Ellis, D. (1999) ‘Pre-hospital care five years hence’. Pre-hospital Immediate Care. 3:102-107.
Woollard, M. Leaves, S. Charters, K. Pitt, K. Bottell, J. and Donnelly, P. (2000) ‘Learning the alphabeta: developing a research capability in the Welsh Ambulance Service’. Pre-hospital Immediate Care. 4: 100-101.
Wright, J. Williams, R. and Wilkinson, JR. (1998) ‘Development and importance of health needs assessment’. British Medical Journal, Vol 316: 1310-1313.
Wright, J. and Walley, J. (1998) ‘Assessing health needs in developing countries’ British Medical Journal. 316; 1819-1823.
Wright, SW. Stack, LB. McMurray, BR. and Bolyukh, S. (2000) ‘Emergency medicine in Ukraine: challenges in the post-Soviet era’. Am J Emerg Med. 18(7): 828-832.
Zachariah, BS. (1999) ‘The problem of ambulance misuse: whose problem is it, anyway?’ Academic Emergency Medicine. 6(1): 2-5.
Zhang, W. Bowman, A. and Mueller, KJ. (2000) Rural/urban definitions: alternatives and numbers by State. Nebraska Center for Rural Health Research, Omaha.
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
357
Appendices
Approval No:..98202..........
THE UNIVERSITY OF NEW SOUTH WALES
SUBJECT INFORMATION STATEMENT AND CONSENT FORM
(Title of project: Ambulance service delivery models in rural Australia)
Subject selection and purpose of study
You are invited to participate in this study of Victoria’s rural ambulance services. The study aims to develop rural models of ambulance service delivery that satisfy the needs of local rural communities. You were selected as a participant in this study because your perspective as an ambulance service manager is considered to be of value.
Description of study
If you decide to participate, you will be asked to participate in a focus group estimated to last 60 minutes. The proceedings of the focus group will be taped and transcribed for analysis.
The organizational restructure of Victorian rural ambulance services provides a unique opportunity to view rural ambulance services as a distinct discipline or area of study. Rural ambulance service are most often seen as a subset of a State-wide system in which rural issues and concerns are potentially subsumed into an urban-orientated view of the world.
The primary aim of the study is to develop conceptual models that stimulate debate about models of ambulance service delivery that may be suitable for rural Australia. This is in response to the dearth of pre-hospital research in Australia. Soft systems methodology is being used to develop five models of service delivery that can potentially operate in rural environments. The specific objectives are to:
1. Identify the professional and community expectations of rural ambulance services in Victoria, and to suggest improvements in how they operate;
2. Describe the structure and organization of rural ambulance services within their socio-political climate, along with the educational and technological changes that continue to shape their evolution;
3. Compare the perceived and actual performance of rural ambulance services in different geographical areas in terms of utilization rates, time intervals and resource allocation with a view to developing a useful performance framework for rural ambulance services; and
4. Develop models of ambulance service delivery from different philosophical perspectives to stimulate debate about models that may be most suitable for rural Australia.
page 1 of 3
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
358
THE UNIVERSITY OF NEW SOUTH WALES
SUBJECT INFORMATION STATEMENT AND CONSENT FORM (continued)
Confidentiality and disclosure of information
Any information that is obtained in connection with this study and that can be identified with you will remain confidential and will be disclosed only with your permission or except as required by law.
If you give us your permission by signing this document, I plan to publish the results in a PhD Thesis and in professional journals. The conclusions of the research may also be shared with Australian Ambulance Services. In any publication, information will be provided in such a way that you cannot be identified.
Complaints may be directed to the Ethics Secretariat, University of New South Wales, SYDNEY 2052 AUSTRALIA (phone 9385 4234, fax 9385 6648, email [email protected] ).
Your consent
Your decision whether or not to participate will not prejudice your future relations with the University of New South Wales. If you decide to participate, you are free to withdraw your consent and to discontinue participation at any time without prejudice.
If you have any questions, please feel free to ask me. If you have any additional questions later, Mr Peter O’Meara on 03 51441019 (A.H.) or 03 51738200 (B.H.) will be happy to answer them.
You will be given a copy of this form to keep.
******************************************************************************************* Contact Details (optional)
Name: Postal Address:
Telephone:
page 2 of 3
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
359
THE UNIVERSITY OF NEW SOUTH WALES
SUBJECT INFORMATION STATEMENT AND CONSENT FORM (continued)
(Title of project: Ambulance service delivery models in rural Australia)
You are making a decision whether or not to participate. Your signature indicates that, having read the information provided above, you have decided to participate.
Signature of subject Signature of witness
Please PRINT name Please PRINT name
Date Nature of Witness
Signature of investigator
PETER O’MEARA
Please PRINT Name
page 3 of 3
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
360
Instructions This questionnaire will take about fifteen minutes to complete. Please fill in your answers in the space provided. For the multiple-choice questions mark your answer with an ‘X’ in the boxes provided. In some questions more than one positive answer is possible. All questions relate to the situation in 1996. 1. Ambulance Branch Station?
2. Main localities in primary catchment area? (ie. include only those areas of primary cover for emergencies)
3. Distance to the next nearest ambulance station?
4. How would you describe the area the branch station services?
Remote Area Remote Centre Rural Area Small Rural Centre Large Rural Centre
Questionnaire
Models of ambulance service delivery in Rural Australia You are invited to participate in this study of Victoria’s rural ambulance services, which aims to develop rural models of ambulance service delivery that satisfy the needs of local rural communities. The research focuses on 40 sample branch stations throughout Victoria using 1996 as the benchmark. Any information that is obtained in connection with this study and that can be identified with you will remain confidential and will only be disclosed with your permission or except as required by law. In any publication, information will be provided in such a way that you cannot be identified.
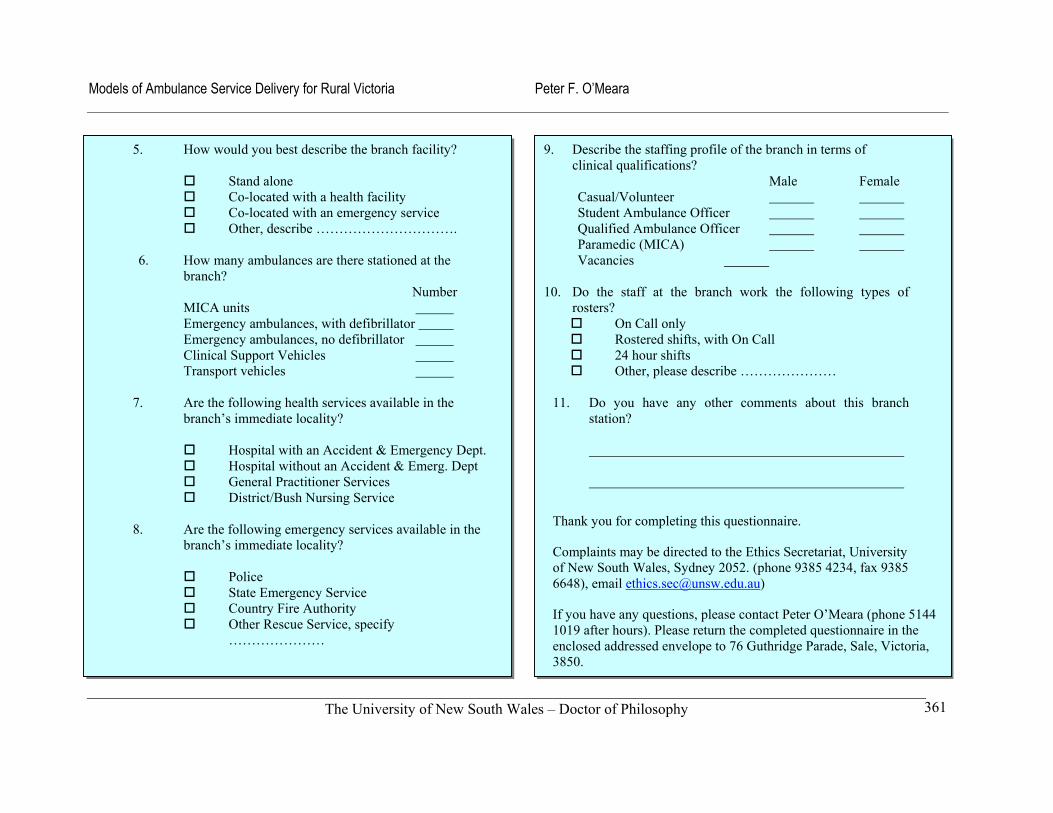
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
361
5. How would you best describe the branch facility?
Stand alone Co-located with a health facility Co-located with an emergency service Other, describe ………………………….
6. How many ambulances are there stationed at the
branch? Number
MICA units Emergency ambulances, with defibrillator Emergency ambulances, no defibrillator Clinical Support Vehicles Transport vehicles
7. Are the following health services available in the
branch’s immediate locality?
Hospital with an Accident & Emergency Dept. Hospital without an Accident & Emerg. Dept General Practitioner Services District/Bush Nursing Service
8. Are the following emergency services available in the
branch’s immediate locality?
Police State Emergency Service Country Fire Authority Other Rescue Service, specify
…………………
9. Describe the staffing profile of the branch in terms of clinical qualifications? Male Female Casual/Volunteer Student Ambulance Officer Qualified Ambulance Officer Paramedic (MICA) Vacancies
10. Do the staff at the branch work the following types of rosters?
On Call only Rostered shifts, with On Call 24 hour shifts Other, please describe …………………
11. Do you have any other comments about this branch station?
Thank you for completing this questionnaire.
Complaints may be directed to the Ethics Secretariat, University of New South Wales, Sydney 2052. (phone 9385 4234, fax 9385 6648), email [email protected])
If you have any questions, please contact Peter O’Meara (phone 5144 1019 after hours). Please return the completed questionnaire in the enclosed addressed envelope to 76 Guthridge Parade, Sale, Victoria, 3850.
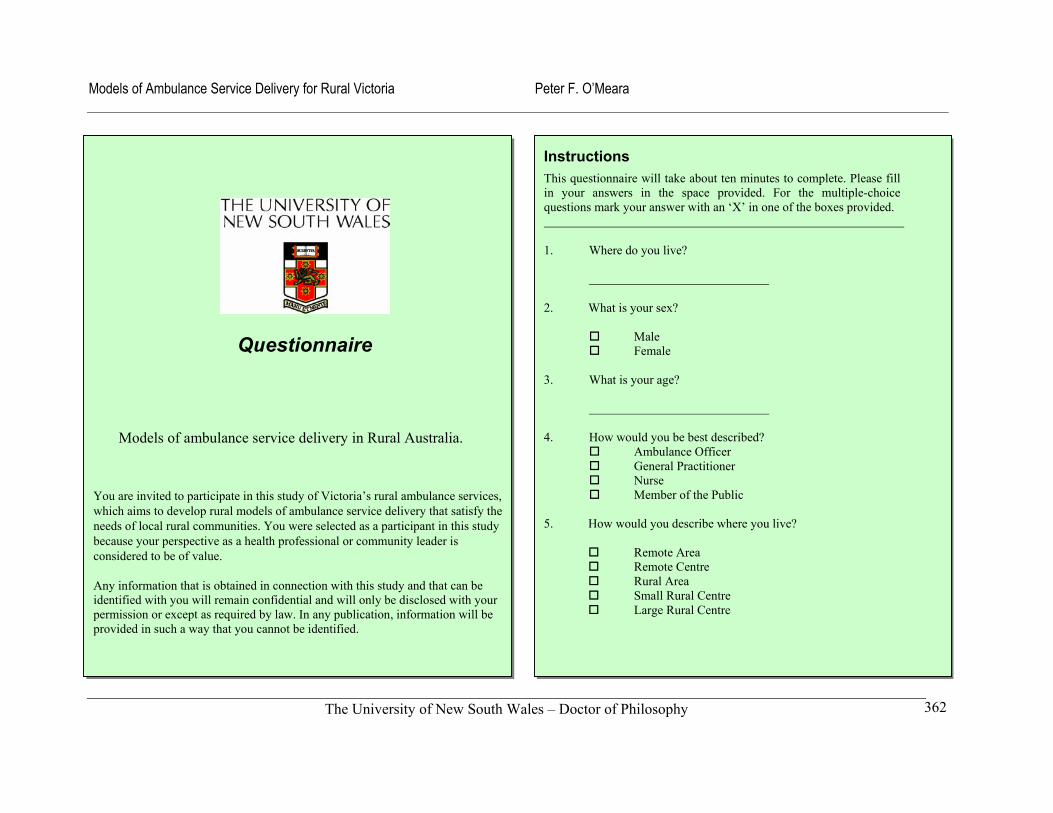
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
362
Questionnaire
Models of ambulance service delivery in Rural Australia.
You are invited to participate in this study of Victoria’s rural ambulance services, which aims to develop rural models of ambulance service delivery that satisfy the needs of local rural communities. You were selected as a participant in this study because your perspective as a health professional or community leader is considered to be of value.
Any information that is obtained in connection with this study and that can be identified with you will remain confidential and will only be disclosed with your permission or except as required by law. In any publication, information will be provided in such a way that you cannot be identified.
Instructions This questionnaire will take about ten minutes to complete. Please fill in your answers in the space provided. For the multiple-choice questions mark your answer with an ‘X’ in one of the boxes provided. 1. Where do you live?
2. What is your sex?
Male Female
3. What is your age?
4. How would you be best described? Ambulance Officer General Practitioner Nurse Member of the Public
5. How would you describe where you live?
Remote Area Remote Centre Rural Area Small Rural Centre Large Rural Centre
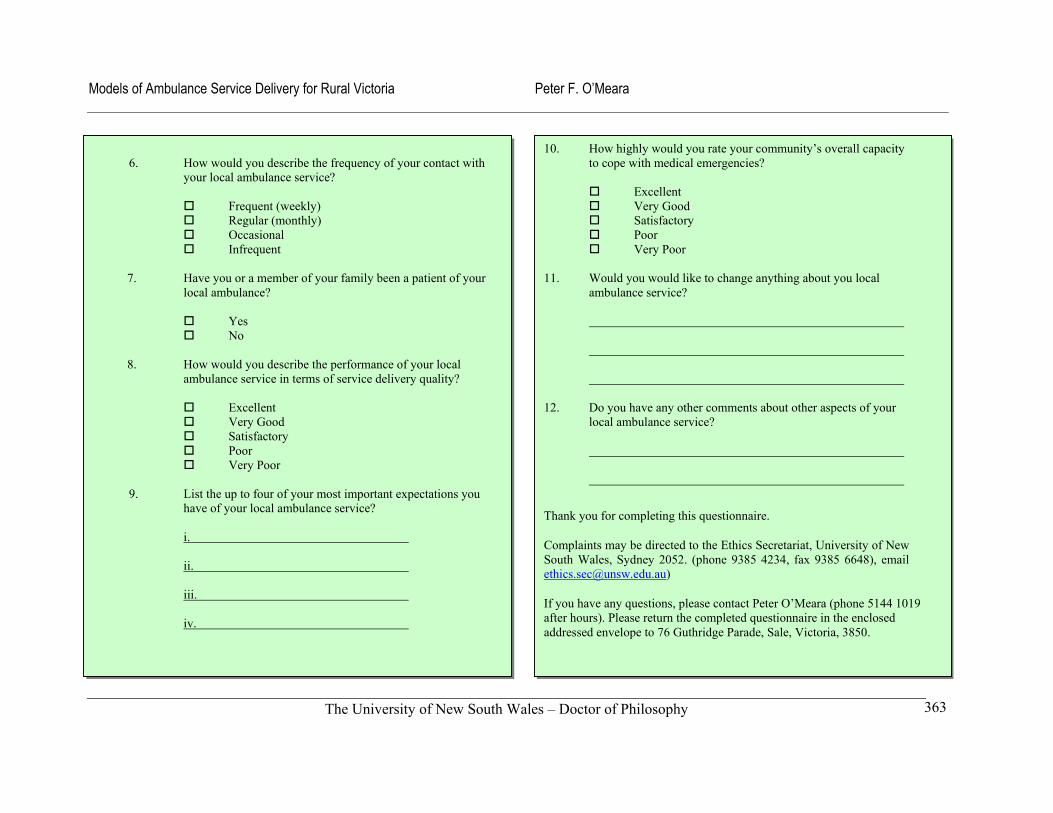
Models of Ambulance Service Delivery for Rural Victoria Peter F. O’Meara
The University of New South Wales – Doctor of Philosophy
363
6. How would you describe the frequency of your contact with your local ambulance service?
Frequent (weekly) Regular (monthly) Occasional Infrequent
7. Have you or a member of your family been a patient of your
local ambulance?
Yes No
8. How would you describe the performance of your local
ambulance service in terms of service delivery quality?
Excellent Very Good Satisfactory Poor Very Poor
9. List the up to four of your most important expectations you have of your local ambulance service?
i.
ii.
iii.
iv.
10. How highly would you rate your community’s overall capacity to cope with medical emergencies?
Excellent Very Good Satisfactory Poor Very Poor
11. Would you would like to change anything about you local
ambulance service?
12. Do you have any other comments about other aspects of your local ambulance service?
Thank you for completing this questionnaire.
Complaints may be directed to the Ethics Secretariat, University of New South Wales, Sydney 2052. (phone 9385 4234, fax 9385 6648), email [email protected])
If you have any questions, please contact Peter O’Meara (phone 5144 1019 after hours). Please return the completed questionnaire in the enclosed addressed envelope to 76 Guthridge Parade, Sale, Victoria, 3850.





























