Embed Size (px)
Citation preview

Int J Biumed Compur. 30 (1992) 21-42 Elsevier Scientific Publishers Ireland Ltd.
27
MULTI CENTRE SYSTEMS ANALYSIS STUDY OF PRIMARY HEALTH CARE: A STUDY OF SOCIO-ORGANIZATIONAL AND HUMAN FACTORS
K. MOIDU”.h, 0. WIGERTZ” and E. TRELL
(Received July 16th. 1991) (Revision received October 1st. 1991) (Accepted October 15th. 1991)
The information management systems to support health programmes are inadequate. As computers become cheaper and more powerful. their application in the strengthening of the information infrastruc- ture becomes more feasible. However. the high cost of specialized applications software limits their poten- tial, especially in developing countries. A multi-centre systems analysis, (a descriptive study using a questionnaire). was made of District Health Sites in developing countries to analyse whether a common specialized application software design for implementation at a primary health care centre was feasible. Responses to the questionnaires by physicians at the primary health centres were compared between district health sites using contingency tables. Significant inter-site differences in social factors existed. respondents had no prior experience. but with near unanimity (98%) accepted the idea of computer assis- tance in their work. However, general reservations (31%) and fears (26%) about computer interference in the doctor-patient relationship were expressed. The human factor must be considered in interface design and training before implementation.
Kqwwclst Computers; Developing country: End-users: Information systems; Primary health care; Physi- cians; Systems analysis study
Introduction
If solutions to basic public health problems are known, what then is lacking in the drive to attain the goal of health for all? As Bertrand [I] states ‘it is the socially ac- ceptable and economically viable delivering capability’ that requires research. Health Systems Research (HSR) focuses on the means to strengthen the health care organization’s infrastructure, and on strengthening Primary Health Care (PHC) de- livery. Favourable results have been reported [2,3]. In one case, the objective of &creasing the demand for higher levels of health services was achieved [2].
Information systems in many health care organizations are inadequate, and this is emphasized by the World Health Organization’s (WHO) global review report of 1987. It states that ‘a major constraint reported by practically all countries is inade-
Corr~.~ponhwce to: K. Moidu, Department of Medical Informatics. Linkoping University. Linkoping S-581 83. Sweden.
0020-7101/92/%05.00 0 1992 Elsevier Scientific Publishers Ireland Ltd. Printed and Published in Ireland

28 K. Moidu et al.
quate information support for the managerial process’ [4]. Research is needed to strengthen the information infrastructure of computer technology in primary health care delivery. The application of computers in a health care organization demands caution and a well defined strategy, particularly in the case of developing countries [5]. Successful implementation of computers depends on the applications software, which is costly to develop [6] and constitutes one of the major constraints of im- plementation in developing countries.
As research in Medical Informatics, a descriptive study for systems analysis was made of district health sites in developing countries. With a focus on PHC centres, the goal was to analyse whether a common basis existed to design specialized ap- plications software for computer-based primary health care information systems. Results relating to social factors (human and infrastructural issues) are reported here and show inter-site differences. Despite a near unanimous acceptance, the respond- ents also expressed some reservations. There is a lack of commonality in the socio- organizational factors which are recognized to be the most difficult to deal with [6]. The apprehensions and aspirations of potential end-users need to be considered in any systems design and addressed prior to implementation.
Information link in primary health care delivery A PHC organization has an administrative team, organized in a hierarchy, that
manages
0 policy formulation 0 pohcy implementation 0 policy monitoring
and for this they require an efficient flow of information. At the peripheral PHC centres located close to the community, are teams of care
providers who:
?? Provide health care to the community, produce the reports i.e the data for management action from their records of encounters, and require information for decision making.
?? As part of their administrative duties collate and transmit data about the health status of the community, actions taken and resources utilized. Management of finances and personnel may also be included.
At all levels action is based on information, and this information links the organization together. The routine source of administrative data needs is the PHC centre, although data may occasionally be collected directly by special census studies (Fig. 1).
A computer-based information system at a PHC could improve information management and thus the delivery of care, and in addition support the administra- tion at no extra effort., For example, there is a drop-out problem in the expanded immunization programme. According to a WHO report this ranges between 20% and 40% [7], with higher drop-out rates in developing countries [4,7]. Genuine suc-

29
Fig. I. Primary health care administration - data need and source.
cess can only be achieved by the monitoring and follow-up of the target group by the PHC team. A computer-based information system to support the care providers in these tasks would provide lists for follow-up and reports for the administration. Data from a system that is routinely utilized by the care provider would have greater accuracy [8,9] and would improve programme management.
Medical informatics A committee of the Association of American Medical Colleges defines medical in-
form,&tics as ‘... a body of knowledge and a set of techniques concerning the organizational management of information in support of medical research, educa- tion and patient care.... Medical informatics combines medical science with several technologies and disciplines in the information and computer sciences and provides

30 K. Moidu ef ul.
methodologies by which these can contribute to better use of the medical knowledge base and ultimately to better patient care’ [lo]. Results of research in medical infoz- matics are implemented at the PHC level in developed countries [I l-131. A status report on the computerized PHC information systems in Scandinavian countries was published by the Nordic Medico-Statistical Committee [ 141.
In medical informatics education, trainees at higher levels are involved in the development and/or maintenance of medical information systems [ 151, especially in evolving methods for developing tools, as in this research project.
In developing countries the care providers spend 40% of their work time collating data by manual methods [S]. To alleviate this drudgery, revision of existing informa- tion systems to support health care delivery has been instituted [16], and computer- based systems have been implemented [ 171. They often have external assistance [ 17,181 and instances of mismatch are .reported [ 18,191. These occur due to poor planning and inadequate effort in systems analysis, though a recommendation that has been made for developing countries is that ‘careful planning of needed software is the most important first step in application design’ [I]. As a prerequisite and also for purposes of systems analyses [9], a study both of how information flows, and of the opinions of those who will be involved is needed [19]. To build a common ap- plications software would require a method in systems analysis that covers more than one organization and thus in this study a multi-centre approach was taken.
Aims of the Study
An international multi-centre study was undertaken to study the feasibility of a common applications software design. The main objective in systems analysis was to identify the shared characteristics that could provide the foundation for a com- mon applications software design and the level for deployment. The assessment of information flow, from data collection to reporting has been reported elsewhere [20]. In this paper we present the assessment of social and organizational factors which could be of influence, such as:
?? the profile of potential end-users and their work loads at the PHC centres; ?? the potential end-users’ attitudes to computers; ?? the PHC environmental infrastructure and coverage; ?? the technological facilities and maintenance in the organization.
Methods and Materials
Letters of invitation describing the study, along with nomination forms, were sent to 35 health care organizations in 15 developing countries, mainly the Ministries of Health in these countries, and some non-government organizations (based on earlier contact). The organizations were asked to designate a District Health Site (DHS) for the study. A DHS was defined as comprising a secondary care centre such as a hospital, including all the PHC centres manned by physicians in the catchment area of the hospital, like the model advocated by WHO.
Applications were received from three countries. The applications involved 11

district health sites covering 70 PHC centres, with a total of 130 physicians. These were the target sample for this study. For each DHS, a secondary care centre (hospital) and an administrative coordinator were indicated by name on the appli- cation.
Traditional systems analysis takes an approach where the investigation is of a single organization, and the design is based on deductive logic from the qualitative descriptive variables collected i.e. the perceptions and descriptions or direct quota- tions following a visit. A multi-centre study which included a visit to all sites would be difficult and expensive, hence an empirical base for analysis, to build the ques- tionnaire was designed. The present study may be described as a non-experimental, one-time cross-sectional study, primarily descriptive, to compare the participating district health sites.
The data collection tool was a questionnaire with quantitative variables that were classified and ordered. The questions were about physicians’ working environments, facilities, their work load, their information records and reporting patterns, their in- formation needs for decision making, and their attitudes. The questionnaire design was based on experiences from an earlier study in a developing country [21], a study in Sweden to evaluate the decision support information needs of primary care physi- cians [13], and a book on the art of framing questions [22]. Simple language and familiar terms were used. The questions were mainly binary logical questions to ascertain the position of the respondents on the issues, with a mix of close-ended questions, close-ended with unordered, or partially ordered responses, plus open- ended questions. Measures were taken to avoid bias either in linguistic phrasing or in the order of questions. There were built-in checks for validating data, and a pre- test was done on physicians with developing country backgrounds.
Distance required that mailed questionnaires were used for data collection. The questionnaires were sent directly to the sites at the addresses provided by the par- ticipating health authorities. A covering letter was sent which was carefully compos- ed so as to make each respondent feel that his opinion was important to the design process [23]. A detailed set of directions for answering the questionnaires was also sent. In cases in which the questions were not applicable, or in which there was uncertainty, participants were asked to leave the questions unanswered. To ensure follow-up of non-respondents, each questionnaire had a unique number which was maintained in a register with the address of the site to which it had been sent. After each 3-month period, a polite reminder and a questionnaire set with the same number, identifying it as ‘duplicate’ or ‘triplicate’ was sent. A list of PHC centres with non-respondents was sent to the respective DHS administrative coordinators to keep them informed and seek their assistance. A card for listing reasons for non- participation was sent along with the third reminder.
A DHS with a 100% response was to be treated as a ‘site’ and respondents from PHC centres within a DHS which did not have a 100% response were grouped under ‘others’ for site comparisons. The data analysis was done on a microcomputer with a statistical package STATVIEWO (Abacus Concepts, Inc. 1986). Response dis- tribution between sites was compared by contingency tables (chi-squared Test), and overall analyses were made to study frequency distribution and to seek significant correlations.
TAB
LE
I
RES
PON
DEN
TS’
PRO
FILE
S
GP.
G
ener
al
Prac
titio
ners
; PG
, Po
st
Gra
duat
e;
CM
E.
Con
tinui
ng
Med
ical
Ed
ucat
ion;
P(
U)H
C.
Prim
ary
(Urb
an)
Hea
lth
Cen
tre;
Res
p.
Res
pond
ent;
Acc
ept,
Ac-
ce
pt
com
pute
r as
sist
ance
in
the
ir w
ork;
R
eser
vat.,
H
ave
som
e re
serv
atio
ns
to
use
of c
ompu
ters
.
Seria
l D
istri
ct
No.
he
alth
si
te
in
Res
pond
ent
at
PHC
in
se
x is
Com
pute
rs
Perio
d Y
ear
of
Yea
r of
at
PH
C
grad
uatio
n bi
rth
used
A
ccep
t R
eser
v.
I 2 3 4 5 6 7 8 9 IO
II
12
I3
14
Mah
rash
tra
Loni
M
ale
GP
Loni
M
ale
GP
Rah
ata
Fem
ale
GP
Rah
ata
Mal
e G
P K
olha
r M
ale
GP
Prav
ara
Mal
e G
P Ta
lega
on
Mal
e G
P A
shw
i M
ale
GP
Nim
gaon
jali
Mal
e G
P N
imga
onja
li M
ale
GP
Pond
iche
rry
Met
tupa
laya
m
Fem
ale
GP
Met
tupa
laya
m
Mal
e G
P Th
aval
kupp
am
Fem
ale
GP
Thav
alku
ppam
M
ale
GP
I5
I6
I7
18
I9
20
Cal
cutta
U
HC
C
hetla
M
ale
PG
No
Yes
No
Y
ears
<I
19
61
1935
U
HC
C
hetla
M
ale
PG
No
Yes
No
Y
ears
>3
19
73
1948
U
HC
C
hetla
Fe
mal
e G
P No
Y
es
No
Yea
rs
>3
I969
I9
46
UH
C
Che
tla
Fem
ale
GP
No
Yes
No
Y
ears
>3
19
62
1931
U
HC
C
hetla
M
ale
GP
No
Yes
No
Y
ears
>3
19
74
1948
U
HC
C
hetla
M
ale
PG
No
Yes
No
Y
ears
>3
19
60
1938
No
No
- No
No
No
No No
No
No
No
No No
Yes
No
Y
ears
<I
19
78
Yes
No
Y
ears
l-3
19
85
Yes
No
Y
ears
l-3
19
83
Yes
No
Y
ears
>3
19
70
Yes
No
Y
ears
l-3
19
86
Yes
No
Y
ears
l-3
19
84
Yes
No
Y
ears
l-3
19
81
Yes
No
Y
ears
>3
I9
82
Yes
No
Yea
rs
<I
1982
Y
es
No
Yea
rs
<I
1982
Yes
No
Y
ears
<I
19
85
1962
Y
es
No
Yea
rs
<I
1974
19
47
Yes
No
Y
ears
<I
19
86
1958
Y
es
No
Yea
rs
<I
1981
19
58
1953
19
57
1962
19
44
1962
19
58
3 19
52
1956
%
1958
$
1958
2 9
Mea
n 19
81
1956
R
ange
l9
70-
I986
19
44-1
962
Mod
e 19
82
1958
Mea
n R
ange
M
ode
1981
I9
74-
I986
19
55
1947
-196
2 I9
58

21
UH
C
Che
tla
Fem
ale
PG
No
Yes
No
Y
ears
>3
19
55
1932
22
U
HC
C
hetla
M
ale
PG
No
Yes
No
Y
ears
l-3
19
66
1938
23
U
HC
C
hetla
Fe
mal
e PC
No
Y
es
No
Yea
rs
<I
1984
19
61
24
UH
C
Che
tla
Mal
e PC
No
Y
es
No
Yea
rs
l-3
1961
19
39
25
26
21
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
Oth
ers
Com
bine
d pr
ofile
of
re
spon
dent
s (a
ll gr
oups
) Pe
riod
at
PHC
Mal
e Fe
mal
e Fe
mal
e M
ale
Mal
e M
ale
Mal
e M
ale
Fem
ale
Fem
ale
Mal
e M
ale
Mal
e M
ale
Mal
e Fe
mal
e M
ale
Mal
e
GP
No
Yes
No
Y
ears
<I
19
77
GP
No
No
Yes
Y
ears
<I
19
80
GP
No
Yes
No
Y
ears
<I
I9
63
PC
Yes
Y
es
No
Yea
rs
l-3
1979
PG
Y
es
Yes
No
Y
ears
>3
19
51
GP
No
Yes
N
o Y
ears
l-3
19
85
PG
No
Yes
No
Y
ears
>3
19
55
GP
No
Yes
No
Y
ears
1-
3 19
68
GP
No
Yes
Y
es
Yea
rs
>3
I974
GP
No
Yes
No
Y
ears
<
I 19
80
GP
No
Yes
Yes
Y
ears
>3
19
76
GP
No
Yes
No
Y
ears
>3
19
83
GP
No
Yes
No
Yea
rs
>3
1983
GP
Yes
Y
es
No
Yea
rs
< I
1981
G
P Y
es
Yes
N
o Y
ears
<I
19
81
GP
No
Yes
Y
es
Yea
rs
>3
1967
G
P N
o Y
es
Yes
Y
ears
l-3
19
84
GP
No
Yes
N
o Y
ears
>3
I9
75
GP
No
Yes
No
Y
ears
>3
19
75
Sex
Res
pond
ents
w
ere
Atte
nd
CM
E
Mea
n 19
66
Ran
ge
1955
” I9
84
Mod
e 19
61
Mea
n R
ange
M
ode
I974
19
51-1
985
-
1941
19
31-1
961
I948
19
52
1936
19
54
I926
19
54
1928
19
38
1951
19
48
I960
19
60
I956
19
56
I942
19
54
1952
19
52
I948
19
26-
1960
Mal
e 31
G
Ps
32
Yes
27
Fe
mal
e I I
PC
s IO
N
o I6
<I
ye
ar
I5
Mea
n l-3
ye
ars
II
Ran
ge
>3
year
s I7
M
ode
1974
I9
49
1951
-198
6 19
26-1
962
1981
19
58
:

34 K. Moic

Results
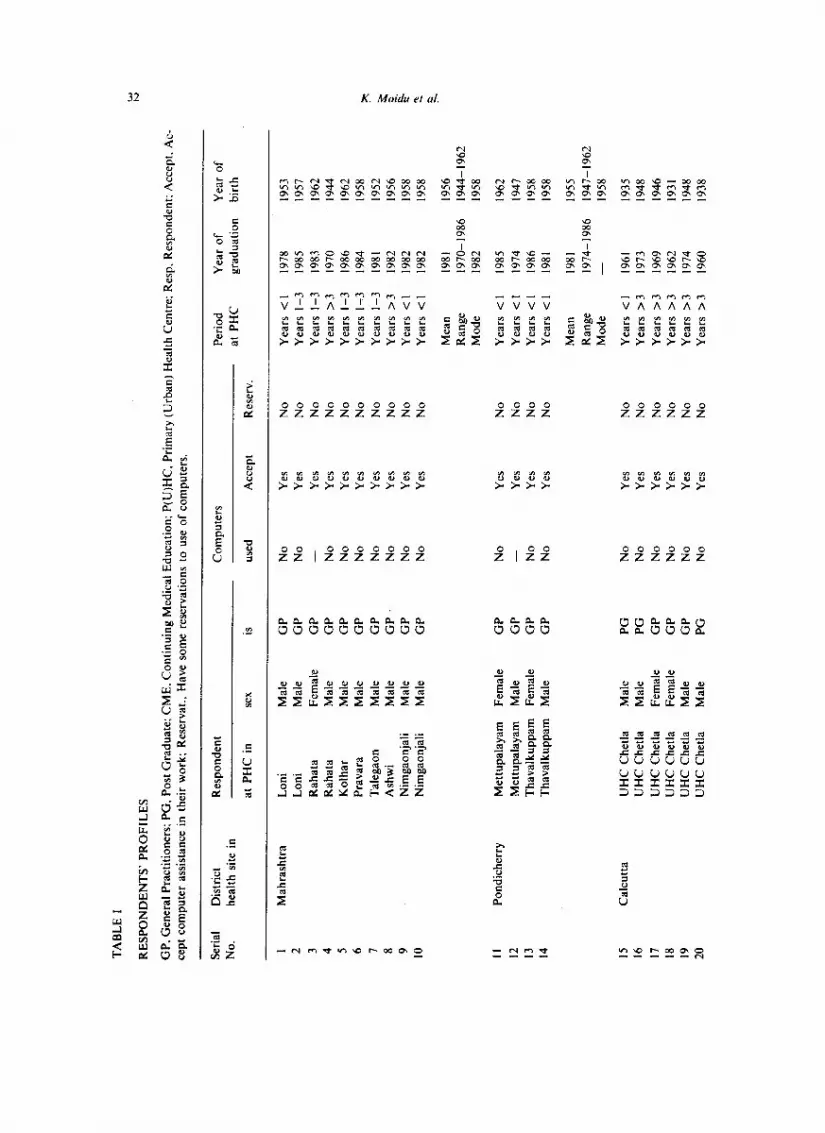
Responses were received from 32% of the target group, and there was a 100% response from only three district health sites, all of which were in India. The respon- dent profile of the 43 respondents is presented in Table 1. In the respondent group taken as a whole (across all sites), only four persons had previously used computers, but a unanimous majority (98%) were nevertheless ready to accept computer assis- tance in their work environment. A fair turnover of personnel at PHC centres was observed.
From an organizational perspective, when the work loads of respondents at dif-’ ferent sites were compared (Table II), significant differences were found in the total working hours per week, and also for the hours spent on administrative chores (P < 0.001). However, on further analysis longer working hours had no association to the populations served or the organizational affiliation, nor did it correlate to the number of patients seen per month.
The first preference of the respondents for the area in which they expected com- puters to assist them in was in health management (Table III). It was observed that of these respondents, 61% had felt the impact of computers in their daily life from encounters at banks and offices. There were no significant differences between sites, although it appears that the respondents under ‘others’ chose medical education rather than patient care as their second preference.
The positive attitudes expressed were not without some reservations about com- puters (31’%,), and fears were expressed (26%) that computers might interfere with the doctor-patient relationship (Table IV). A statistically significant difference was noted between the sites in reference to reservations and fears. The fears were voiced mainly from one site. The respondents at this site were located in a semi-rural area and had no prior computer experience.
Significant inter-site differences were observed with respect to PHC locations,
TABLE III
ORDER OF PREFERENCE FOR COMPUTER ASSISTANCE
Preference
Health management Patient care
I St 2nd 3rd I st 2nd 3rd
Medical education
I St 2nd 3rd
Maharashtra 6 2 2 1 8 I 3 7 Pondicherry 4 _ _ _ 4 4 Calcutta” 8 0 I 0 I 2 I 2 6 Others” 7 5 5 6 4 x 5 7 5 Total 25 7 8 I 23 II Y Y 22
“Calcutta: I missing: others: 2 missing

36 K. Moidu ct ul.
TABLE IV
RESERVATIONS TO COMPUTERS
Have someC Feel the use OF Computers may interfereC reservations to computers may in patient-doctor
the use of computers dehumanize medicine relationship
Yes No Yes No Yes No
Maharaashtra 8 2 9 I 9 I Pondicherry - 4 4 4
Calcutta IO IO IO Others 5” 12 2 I7 2h I6
“Missing 2. ‘Missing I.
‘P < 0.001.
number of staff and the population coverage (Table V). Interestingly, post graduate respondents were found only at urban locations.
Table VI shows that no uniform pattern of support facilities existed at the PHC centres. Electricity was not available to six respondents around the clock. However, except for X-ray facilities, differences in facilities were not significant between sites. No uniform protocol was followed for repair of electro-mechanical devices, and there were variations in terms of time even within district health sites. Fifteen respondents were able to obtain local help.
Detailed analyses to determine whether there were any statistically recognizable patterns correlating the respondents’ acceptance or reservations with other factors mentioned above did not reveal any differences.
Discussion
In developing countries, the reasons for failure of the public health programmes are attributed to many causes, such as lack of resources, dependence on poorly train- ed manpower, illiteracy and poor community participation. These problems are identified due to comparison of the situation in the developing countries to those in the developed world. However, a point often missed is the immense use of informa- tion for strategic planning and action in the developed countries. In the developing countries there are poor information systems and even those that exist are not used, the latter being ascribed to the lack of validity of the data. The foundation of all scientific decisions is based on information. In the delivery of health care, informa- tion on the extent of a disease in a community is required by the administrators so that they can mobilize appropriate resources, and information on the pattern, spread and control of the disease is vital to the care providers. Inadequate information im- poses constraints on both the administrators and the care providers. A WHO global

TAB
LE
V
LOC
ATI
ON
A
ND
C
OV
ERA
GE
OF
THE
PHC
C
ENTR
ES
Dire
ct
Hea
lth
site
s
Res
pond
ent
Dis
tanc
e of
PH
C
*PH
C
site
s lo
cate
d in
*S
taff
at
PH
C’s
*P
opul
atio
n co
vere
d af
filia
tions
fro
m
hosp
ital
Gov
t. N
on
govt
. c5
0 <5
0 U
rban
Se
mi
Sem
i R
ural
<2
0 <5
0 >5
0 <2
5000
<5
0000
>5
0000
ur
ban
urba
n
Mah
aras
htra
9
I IO
-
I 9
- IO
I
9 Po
ndic
herry
4
- 4
- 2
2 4
- 4
Cal
cutta
10
-
IO
IO
- 10
-
- 10
O
ther
s I3
6
I6
2 IO
3
6 8
9 I
6 5
5 9 r
*P <
0.
001.
2 2
TAB
LE
VI
FAC
ILIT
IES
AN
D
MA
INTE
NA
NC
E SU
PPO
RT
OF
THE
PHC
C
ENTR
ES
(a)
Clin
. la
bora
tory
; (b
) O
bser
vatio
n be
ds;
(c)
Ope
ratin
g fa
cilit
ies;
(d
) A
mbu
lanc
e;
(e)
Elec
trici
ty
24 h
rs;
ffI
Tele
phon
e:
(g)
X-ra
y.
*P
< 0.
001;
(h
) EC
G.
Dis
trict
he
alth
si
tes
Faci
litie
s at
PH
C
cent
res
(a)
fb)
(c)
fd)
k)
tg)*
(h
)
Rep
air
time
for
elec
tro-m
echa
nica
l de
vice
s(da
ys)
<7
< I4
<3
0 >3
0
Loca
l he
lp
avai
labl
e
Mah
aras
htra
4
8 I
I 9
4 0
0 2
0 2
I 3
Pond
iche
rry
4 4
4 4
4 4
0 0
0 0
0 2
0 C
alcu
tta
IO
3 IO
IO
IO
IO
IO
0
2 1
I 3
7 O
ther
s I2
9
I8
1 I4
I4
5
9 I
4 4
3 5
2

38 K. Moiciu et 01.
report has identified it as a serious lacuna [4]. The problem in respect to developing countries has been well documented [ 1,17,19,24].
Existing management information systems in developing countries are often designed to support the administration and are thus report oriented, i.e. they convey head counts from the care providers to higher levels of administration. In their sup- port of bureaucracy these systems tend to be ‘biased more towards procedure than performance’ 1251. This approach in information systems is criticized, by those in the field who are working to develop primary health care in developing countries. As Chabot warns, ‘the culture of data dependency is an imposition of western values,’ and further adds that ‘data collection becomes a preoccupation to a level of distrac- tion, so much so that the process of primary health care implementation is ignored’ [26]. It was noted that the health information systems emerge into a separate entity from the delivery of care.
This distraction with data handling is known to take up nearly 40% of a care pro- vider’s work time [8], which should primarily be spent in delivery of care. This could be reduced with the application of computer assistance in information management. In a document prepared by Mandil et al. for WHO with the health organization deci- sion maker in mind, the potential of informatics in support of health care has been comprehensively described, including for PHC centres [6]. While the health sciences are information intensive, computers have been available as tools and the price of computers has been falling. Nevertheless, the level of computer adoption and utiliza- tion is not as high as expected even in developed countries. A study of the technology dispersion in Sweden at the primary health care centre reports that only 5% of PHC centres had computers to support their clinical activities [27]. The success of any computer implementation depends on the applications software. In view of the high costs of specialized applications software development, the use of off-the-shelf general purpose applications packages is recommended [6]. This is a partial solution, and the premise of the present research is to determine the basis of a common design for applications software to support the care providers at multiple sites that could be implemented within the framework of any organization. Then by the principle of ‘economies of scale’, computer-based primary health care information systems could perhaps be affordable even in developing countries.
An innovative method was required to design an applications package for multi- centre usage. From the 35 sites originally invited a few declined as they were not following the model of a district health site as described. Others were either not in- clined to participate as they were already involved in a similar activity, and a few did not respond at all. The aim was to evolve a method and the smaller group may be considered as appropriate for the purpose.
The standard systems analysis takes an approach where the investigation is of a single organization, thus many features incorporated in the resultant design do not fit the needs of others. The questionnaire was designed to collect data as quantitative variables in order to base the design not just on deductive logic but on an empirical basis. The quantitative empirical approach is often employed in computer science to study human computer interactions; it was also applied to study decision making in- formation needs [13]. The use of such methods is recommended [28]. With question- naires one is faced with a problem of low response. As for the non-respondents they

did not respond even to the cards sent, the site coordinators were unable to assist. It must be emphasized here that the comparison was between the district health sites taken as groups, and the three sites representative of the urban, semi urban and rural situation in a developing country.
Before any implementation of a computer application in a developing country can take place, an analysis of the attitudes of people involved must be conducted [19]. This recommendation is applicable not only to developing countries, but also to other situations as well [20].
There are several formal studies on physician attitudes in the developed world context, and a selection with related issues has been published on the impact of com- puters in clinical medicine [29]. The papers concur that physician’s attitudes have been positive, but with reservations in regard to automated decision making, the depersonalizing nature of computers and interference in the patient-doctor relation- ship. The lag has been attributed by one author to a mismatch between the aspira- tions of the system developers, policy makers and those of the intended users. These studies were carried out in an era prior to the advent of microcomputers, and were mainly from hospital settings [29]. In a previous study prior to the current study, that was also conducted on developing country physicians, human factors were dealt with extensively. The findings were similar to those of the present study. Only respondents with computer experience and/or those who had read information about computers, had accepted computers as decision support tools [21].
In the present study group, the majority (86%) had no prior experience in comput- er use, yet they all (98%) wanted computer assistance in their work. It is important to remember that the response was low, and that only those who were positive may have replied. The reservations expressed by such a positive group must be considered seriously, though this is not unusual and also seen in an earlier user-attitude- appraisal study done in a developing country [21]. Similar reservations were express- ed in a recent report from the United States of an informal study [30]. The fact that the reservations were primarily voiced at a DHS emphasizes the role of the physician network in dispersion and adoption of technology [29].
In the design of information systems, end-user awareness and acceptance are im- portant in ensuring a suitable design and in identifying areas of resistance that must be addressed. It is best to determine these with an attitude study, either as part of the organizational analysis or before implementation of a package, as they constitute the most important component of the system. Shortliffe advises that a sensitivity to these issues must be reflected in system design, in the way in which the tools are described, and in educating care providers about the use of the tools [30]. Training is a crucial factor for dispelling fears in the transfer of technology [3 I], particularly when the end-users have high interest but a low awareness and level of information.
Health organization decision makers who are responsible for initiating computer systems development must consider these reservations. In their dialogue with the system developers they should first make provisions to address this problem. This can be done by requesting exposure and training for potential end-users. There is also a high turnover of manpower at PHC centres, and provisions therefore must be made for continuous training of new employees.
The priority accorded to acceptance of computers in management as compared to

40 K. h4oidu et (I/.
patient care must not be ignored. Care providers must be made to recognize that the source of information for management is primarily generated at patient encounters. Intelligent end-users will provide a feedback to system developers that will enhance the system’s design to meet their needs. Such studies may help chart areas of overlap in the aspirations of system developers, policy makers and potential end-users.
Other socio-organizational factors such as work load patterns, location, facilities available and population coverage have technical implications and influence the design of a common applications systems package. For example, the population size in a community based health care delivering PHC would mandate a record for each individual. To maintain a permanent record would make a demand on secondary memory storage, and it would also necessitate an exact definition of the volume of data to be stored. This would influence both the applications software development and the hardware selection, but there is often a solution, either through technology or management re-organization.
The absence of facilities such as X-Ray and ECG machines at a PHC centre raises the question of economy. Can a PHC organization in a developing country afford an investment in a computer-based PHC information system? The answer lies in the priorities of the PHC organization. As a point of argument, information is required for all the patient-doctor encounters, and not all patients require an ECG or an X- ray. A computer could also reduce the drudgery of collating administrative reports and provide information for management action. However, there is a cost involved, and a common applications package may only reduce the high costs of a vital com- ponent in the implementation of computers.
The capability of a health care organization to handle, maintain and repair the computers must be evaluated in order to make provisions for technical support in the implementation plan. The modular architecture of microcomputers simplifies trouble shooting. Bertrand, with extensive experience in different developing coun- tries, considers it feasible that a good television-repair person with a little training could carry out the maintenance and care with replaceable parts [23], provided the microcomputer is locally produced or is popular on the market. Otherwise problems could be experienced as the difficulties faced in getting parts for a microcomputer that was not supported locally in a recent report from Nigeria [32].
Conclusion
If information inadequacy is an identified constraint, then computers as tools of information management would not only enhance the properties of information, but also support primary health care delivery [33]. Computers have been installed in PHC centres in developing countries. Some have attained their objectives [ 181, while others have been outright failures 1191. The purpose of such field studies is not only for research and the systems analyst, but also so that health care professionals and administrators can gain insights into the issues and avoid the risk of failure, particu- larly in developing countries [1,19]. The position of being for or against computer applications in developing countries is’often based on subjective personal experience, and not on an objective field study. To formulate a scientific judgment would require a framework for evaluation, and that should be applied after a period of implemen- tation (331.

41
The level at which a computer-based support could be implemented in delivery of primary care and the shared characteristics were identified in the second part of the systems analysis (the study of information flow). The site was a PHC centre with a physician. It was concluded that the applications software could be developed with the core data set required by the care providers to deliver and administrators to manage a vertical health programme [20]. There is a need for consensus on limiting the quantity of core data that must be available in a computer-based information system of a health care organization. Thus the concept of an essential data set has been described, and a set to support the Maternal Health Services programme detin- ed. Its applicability has been tested in software (Moidu et al., unpublished).
Differences between sites in regard to human and organizational issues are bound to exist. Social factors are more difficult issues to address than the technical issues [6] in the design of an applications software. The organizational differences in in- frastructure could be rectified through reorganization and technology. The aspira- tions and apprehensions of the potential end-users need consideration. They need to be assuaged by interaction, sensitization, education and training. They are the most important link in a system and to ignore them is one sure path to failure.
References
I
2
3
4
5
6
7 8
Bertrand WE: Use of microcomputers in health and social service applications in developing nations, CRC Crir Rev Ma/ It& I (3) (1987) 229-240 Sjijnell G: Relution.ship hetwwn use of increu.wtl primury Iwulth cure uncl other our-puiicnr cuw in u Snvdish urhun urea. Doctoral Dissertation, Department of Social Medicine, Karolinska Institute, Sundyberg. 1985. Westman G: Pkmningprimury heul~h cure provision. Doctoral Dissertation No. 180.. Umez Universi- ty. Department of Social Medicine. Ume& 1986. World Health Organization. Assessment of Achievement. In Eruluution 01 I/W S/rurc:q.v ./or Ilw//h
,Jiw u/l hy the ywr 2000. Seventh report on the World Health situation. Global Review, World Health Organization. Geneva, I ( 1987) 109-I 16. Mandil S: Present trends in health informatics in developing countries. In Hw//h In/ormu/ics in Developing Countries (Eds: AFP DeTalens, EM Ravetto. DB Shires), North Holland. Amsterdam. 1982, pp. 37-39. Mandil S. Beck R, Chaves EOC. Kaihara S, Khalid bin Sahan A, Peel V. Protti D. Sabbatini RME and Towle WI: Irzfiwmurics untl T&mutic.s in Health, Prcwnr untl Polenriul U.W. World Health Organization, Geneva, 1988. WHO Notes and News: EPI-Success but no complacency. W&l Hrul/h Forun~. 8 (4) (1987) 551-52. Helfenbein S. Sawyer H, Sayer P and Wijesinghe S: Improving management effectiveness and cffi- ciency. In Tdmolc~gic~s ,Ji~r Munugcment Infinmurion SWUIIS in Primurv Hwlth Curt (Eds: M. Favin, C. Dunn. D. Rajasingham) World Federation of Public Health Association, Washington DC. 1987. pp. 52-57. Moidu K: Anulysis of’prc,rryuisi/rs to inrroclucr compurw-hu.vetl infinwution ,swrcwr.v in hcwl~h cure. A dewloping country SO&. Studies in Health Sciences Thesis no. I, Department of Medical Infor- matics. Linkoping University, Linkoping, 1989. Association of American Medical Colleges, Washington, D.C. Medical lnformatics in the Informa- tion Age. Proc Swp Md InJ' Murch 1985. Washington DC, Assoc Am Med Coil. 1985. Hosia P and Finstar A: Comprehensive information system for primary care. Sccrncl J Primury Herr/r/~ Cure, 2 (4) (1984) 163-66.
Barnett GO, Cimino JJ, Hupp JA and Hoffer EP: DXplain: an evolving diagnostic decision-support system, J Ant Ma/ Assoc. 258 (I) (1987) 67-74. Timpka T: Design ofu computer-howl tlwision support ,Ji)r gcwerul pructitiomw. Doctoral Disserta-

42 K. Moidu ei al.
14
15
16
17
18
19
20
21
22 23
24
25
26 27
28
29
30
31 32
33
tion No 298, Faculty of Health Sciences. Department of Medical lnformatics and Department of Social Medicine, Linkiiping. 1989. Nordic Medico-Statistical Committee: Con~purerized /nfi,rmation Systm~rs ./iv Prinrar.~ Hcwl~h Cuw in the Nordic Cuunfries, Copenhagen, Nordic Medico-Statistical Committee. Report No 27. 1988. Zimmerman JL, van Bemmel. JH and Rienhoff 0: Medical lnformatics Education, J Am .%c III/’ Sci, 39 (2) (1988) 138-41. Ministry of Health and Family Welfare: &ernntent c$ India Munagcwen/ /~/~nwttr/icm S.~em Health fir All Strategy, Primary Health Care Scheme. Training Manual, Ministry of Health and Family Welfare. Government of India. New Delhi, 1989. Kholy AE and Mandil SH: The relevance of microcomputers to health improvement in developing countries, fnf Manage. 8 (1984) 177-82. Nabarro D. Annett H. Graham-Jones S and Nabeta E: Microcomputers in developing country pro- grammes: valuable tools or troublesome toys? Experience from Uganda and Nepal. In Munagcwent
Informution Systems und Microcc~tirputurs in Primary Health Care (Eds: RG Wilson. BE Echols. JH Bryant and A Abrantes). Aga Khan Foundation, Geneva, 1988. pp. 41-52. Schware R and Trembour A: Rethinking microcomputer technology transfer to third world coun- tries, Sci Puh Policy 12. (I) (1985) 15-20. Moidu K. Wigertz 0 and Trell E: Information flow in delivery and management of primary health care. A multi centre study, J Med Sr.s/, (1991) in press. Moidu K and Wigertz 0: Computers and physicians: an appraisal study. Mcd /TV/; I4 (I) (1989) 63-70. Payne, SL: The Art qf Asking Quevrions. Princeton University Press, Princeton. NJ, 1954. McKillip. J and Lockhart, DC: The effectiveness of cover letter appeals, J .%c P.s~cho/, 122 (1984) 85-91. Bertrand WE: Information as a primary health care intervention: the impact of new technology on improving health for all. In Management Itzformation Systems and Microcomputers in Primary Health
Care (Eds: RG Wilson. BE Echols. JH Bryant, A Abrantes). Aga Khan Foundation. Geneva. 1988. pp. 27-37. Chen LC: Primary health care in developing countries: overcoming operational. technical. and social barriers. kncet, (1986) 1260-65. Chabot HTJ: Primary health care will fail if we do not change our approach, Lrrncer. (1984) 340-41. Persson J. Borgquist L and Debourg C: Medical Technology in Primary Health Care: u Quevriomwire Study Directed at Primury Health Centres and Mediwl Technology Departmenrs. CMT Report no. 7, Center for Medical Technology Assessment, Linkiiping University, Linkiiping. 1987 (in Swedish). Mitchell J and Welty C: Experimentation in computer science: an empirical view. /n/J Morn-Mrrclrine Stud. 29 (1988) 613-624. Anderson JG and Jay SJ: Use und Impucr of Computers in Clinical Medicine. Compurer in Mcdicinc
Series. Springer-Verlag. New York. 1987. Shortliffe EH: Testing reality: the introduction of decision-support technologies for physicians. Merhods fnf Med. 28 (1989) l-5. Lassere P: Training: key to technological transfer. Long Range Plann, IS (3) (1982) 51-60. Korpela M: The IFE Project, Computing Centre, University of Kupio. Kupio. 1990. Moidu K and Wigertz 0: Computer-based informations systems in primary health care - why ? J Medical Syst. I3 (2) (1989) 59-65.





























