Embed Size (px)
Citation preview

A
eht
ow
1d©
K
1
dn(
ST
0d
Neurobiology of Aging 31 (2010) 1903–1911
Myocardial 123I-MIBG scintigraphy for differentiationof Lewy bodies disease from FTD
Fabiana Novellino a, Antonio Bagnato b, Maria Salsone a, Giuseppe Lucio Cascini c,Giuseppe Nicoletti a,d, Gennarina Arabia a,d, Pierfrancesco Pugliese d, Maurizio Morelli a,
Sandra Paglionico a, Stefania Cipullo c, Ida Manna d, Elvira Valeria De Marco d,Francesca Condino d, Carmelina Chiriaco a, Letterio Morgante e,
Mario Zappia f, Aldo Quattrone a,d,∗a Institute of Neurology, University Magna Graecia, Catanzaro, Italy
b Department of Nuclear Medicine, Azienda Ospedaliera, Cosenza, Italyc Institute of Radiology, University Magna Graecia, Catanzaro, Italy
d Institute of Neurological Sciences, National Council, Mangone, Cosenza, Italye Department of Neurosciences, Psychiatry and Anesthesiology, University of Messina, Messina, Italy
f Department of Neurosciences, University of Catania, Catania, Italy
Received 3 September 2008; received in revised form 24 November 2008; accepted 25 November 2008Available online 9 January 2009
bstract
Clinical distinction between Lewy bodies disease (LBD) and frontotemporal dementia (FTD) is sometimes difficult. Nigrostriatal dopamin-rgic degeneration occurs in both LBD and FTD, limiting helpfulness of DAT imaging to differentiate these forms of dementia. Several studiesave emphasized the usefulness of myocardial scintigraphy with 123Metaiodobenzylguanidine (123I-MIGB) in assessing the sympathetic nerveerminals in LBD demonstrating that cardiac 123I-MIGB uptake is decreased in patients with this disease.
We investigated the role of cardiac 123I-MIBG scintigraphy in differentiating patients with LBD from those with FTD. Clinical diagnosisf LBD and FTD was determined according to established consensus criteria. Nine patients with LBD (1 possible and 8 probable), 6 patientsith FTD, and 16 control subjects were involved in the study.
The heart to mediastinum ratio (H/M) of 123I-MIBG uptake was markedly reduced in all patients with LBD (H/M early: 1.25 ± 0.12; delayed:.14 ± 0.13) whereas it was normal in patients with FTD (H/M early: 1.86 ± 0.20; delayed: 1.80 ± 0.23) and in controls (H/M early: 1.91 ± 0.17;elayed: 1.99 ± 0.19), suggesting that cardiac 123I-MIBG scintigraphy can help distinguish patients with LBD from those with FTD.
2008 Elsevier Inc. All rights reserved.
ccf
eywords: Lewy body disease; Frontotemporal dementia; Cardiac MIBG
. Introduction
Dementia with Lewy bodies (LBD) and frontotemporal
ementia (FTD) are the second most common cause of senileeurodegenerative dementia following Alzheimer’s disease.McKeith et al., 2004; Ratnavalli et al., 2002). Although the∗ Corresponding author at: Institute of Neurology, Department of Medicalciences, University Magna Graecia, Catanzaro, Italy.el.: +39 0961 3647075; fax: +39 0961 3647177.
E-mail address: [email protected] (A. Quattrone).
twwedeap
197-4580/$ – see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1016/j.neurobiolaging.2008.11.009
linical profile of these forms of dementia is different in mostases, in some patients symptoms may overlap making dif-erential diagnosis difficult. A recent study has emphasizedhat visual hallucinations and early memory impairmenthich characterize LBD can also occur up in 30% of patientsith FTD carrying progranulin (PGRN) mutations (Le Ber
t al., 2007). On the other hand, LBD with a family history of
ementia and language disorders has been reported (Bonnert al., 2003). Cerebral SPECT and PET improve diagnosticccuracy in both diseases but are not useful to distinguishatients with LBD from those with FTD on an individual
1 logy of
boi
dednir
2
2
wiwtPPiMGAMsAc1(ecCe(cMtDiws
ui(
n(sdbd
1
in
Eadtup
2
Wi
gfiaptDmaitectflbTtatwwa
diwksgmgco
w
904 F. Novellino et al. / Neurobio
asis. Moreover, nigrostriatal dopaminergic degenerationccurs in both LBD and FTD, limiting helpfulness of DATmaging to differentiate these forms of dementia.
There is evidence that patients with LBD show a markedecrease in cardiac 123I-MIBG uptake, indicating the pres-nce of cardiac sympathetic denervation in this form ofementia. Myocardial 123I-MIBG scintigraphy, however, hasot been investigated in FTD. The aim of this study was tonvestigate the usefulness of myocardial 123I-MIBG scintig-aphy for differentiation of LBD from FTD.
. Materials and methods
.1. Patients
Our study involved 9 patients with LBD and 6 patientsith FTD. All patients were interviewed and clinically exam-
ned. McKeith et al. (2005) and Neary et al. (1998) criteriaere used to establish diagnosis of LBD and FTD, respec-
ively. Extrapyramidal signs were assessed using the Unifiedarkinson’s Disease Rating Scale motor score (UPDRS-ME).atients underwent an accurate neuropsychological exam-
nation. Global cognitive decline was assessed with Miniental State Examination (MMSE) (Folstein et al., 1975).lobal executive functions were screened through Frontalssessment Battery (FAB) (Dubois et al., 2000) and theodified Card Sorting Test (MCST) (Nelson, 1976). Verbal,
hort and long term memory were evaluated through the Reyuditory-Verbal Learning test (RAVL) (Rey, 1958) and Bab-
ock Story Recall Test (Babcock, 1930; Babcock and Levy,940). Visuo-spatial function through Clock Drawing TestShulman et al., 1986) and Copy drawing test (Carlesimot al., 1996). Attention was rated with Attentive Matri-es (Carlesimo et al., 1996). Logical thinking with Raven’soloured Progressive Matrices (Raven, 1947) and word flu-ncy with COWAT (Controlled Oral Word Association Test)Benton et al., 1994). Language was also rated with neuropsy-ological examination for aphasia (E.N.P.A.) (Capasso andiveli, 2001). Patients who were not able to run the full bat-
ery of tests were evaluated with M.O.D.A. (Milan Overallementia Assessment) (Brazzelli et al., 1994). The result-
ng scores were corrected for age and education and patientsere considered to have a deficit in a cognitive domain if they
cored below the 5th percentile on the test.Routine laboratory tests of blood and urine were also eval-
ated. All patients were investigated for genetic mutationsn microtubule associated protein tau (MAPT), progranulinPGRN) and glucocerebrosidase (GBA) genes.
Neuroimaging studies included brain Magnetic Reso-ance Imaging (MRI), 123Ioflupane (123I-FP-CIT) SPECTDAT scan), and myocardial 123I-MIBG scintigraphy. No
ubjects had any history of cerebrovascular diseases, otheregenerative neurological diseases or intracranial lesions inrain MRI. None of them had cardiovascular diseases, thyroidiseases or diabetes mellitus, which may affect myocardiala
su
Aging 31 (2010) 1903–1911
23I-MIBG uptake. No subject was taking drugs known tonterfere with 123I-MIBG uptake in sympathetic nerve termi-als.
Sixteen control subjects also participated in our study.xclusion criteria for patients and controls were: diabetes,history of dementia and neuropathy, previous relevant car-iac disease, or any other medical condition that could affecthe autonomic nervous system or the myocardial 123I-MIBGptake. Written informed consent was obtained from eacharticipant in the study.
.2. Genetic testing
Genomic DNA was extracted from whole blood usingizard Genomic DNA purification kit according to the
nstructions of the supplier (Promega, Madison, WI).Non-coding exon 0, and coding exons 1–12 of PGRN
ene and coding exons 1–13 of MAPT gene were ampli-ed using specific primers, as previously described (Gass etl., 2006; Baker et al., 2006; Spillantini et al., 1998). Weerformed MAPT and PGRN mutation analysis using dena-uring high-performance liquid chromatography (DHPLC).HPLC analysis was carried out on a WAVETM DNA Frag-ent Analysis System (TRANSGENOMIC). After PCR
mplification, 10 �l of each sample was denatured by heat-ng to 95 ◦C for 10 min, followed by reannealing at roomemperature over a period of 30 min, to maximize het-roduplex formation. Products were loaded onto a DNAsepolumn (TRANSGENOMIC) and using a linear acetoni-rile gradient were eluted from the column at a constantow rate of 0.9 ml/min. The gradient was created by com-ining 0.1 M triethylammonium acetate buffers (TEAA,RANSGENOMIC), pH 7.65 with both 0.025% (v/v) ace-
onitrile (Buffer A, TRANSGENOMIC) and 25% (v/v)cetonitrile (Buffer B, TRANSGENOMIC). The elution ofhe PCR products was monitored by a UV detector. Samplesere then analyzed by DHPLC at the melting temperatureshich were determined using the Wavemaker software pack-
ge (TRANSGENOMIC).Sequence differences of amplified fragments were
etected as a pattern of more than two peaks. Direct sequenc-ng of the exons with heterozygous profiles was performedith a BigDye terminator cycle sequencing ready reactionit (Applied Biosystems, Foster City, CA) on the ABI 3130equencer (Applied Biosystems). Those samples initiallyenotyped as homozygous (one peak) were repeated afterixing of 10 �l of sample with 10 �l of a known homozy-
ous control, which was confirmed by DNA sequencing. Thisould then be used to determine whether homozygotes weref a wild type or variant genotype.
The presence of the Ser111Phe mutation in PGRN geneas verified in 400 cognitively healthy controls matched for
ge, sex, and ethnicity.The presence of the N370S and L444P substitutions was
creened in the GBA gene. Genotyping was performed bysing PCR amplification followed by restriction enzyme

logy of
dt
2
sBoT(eSafntvat(u0
suorcmfwsu
wav
2
rdcBirmuwaRrsmtsalw
2
TC
C
ASADHPU
G
H
LcL
*
F. Novellino et al. / Neurobio
igestion with XhoI for the N370S mutation and NciI forhe L444P mutation (Toft et al., 2006).
.3. 123I-FP-CIT studies
All patients received perclorate (1000 mg) 30 min beforecanning to block thyroid uptake free radioactive iodine.rain imaging was performed 3 h after the administrationf 200 MBq of 123I-FP-CIT (GE-Amersham, Eindhoven,he Netherlands) using a dual-headed gamma camera
Infinia Hawkeye, General Electric, Milwaukee, WI, USA)quipped with a low-energy, high-resolution collimators.cans were acquired with a photopeak window centeredround 159 keV ± 10% with a 128 × 128 image matrix (zoomactor: 1.5, 40 s per view and 2 × 64 views). The slice thick-ess was 2.95 mm. Patients had been carefully positioned inhe gamma camera, with their meato-orbito axis in a trans-erse plane to reduce reorientation during reconstruction, inspecial head-holder that allowed a minimal rotation dis-
ance. Images were reconstructed using a Butterworth filtercut-off 0.5 and order 6). Chang’s correction method’s wassed to compensate for attenuation using a coefficient, μ, of.11 cm−1.
Qualitative and semi-quantitative analysis were performedelecting three consecutive slices with the highest striatalptake. Fixed size regions of interest, were bilaterally drawnver the striatum and the occipital cortex, as the referenceegion. All medications which may affect DAT binding wereurtailed prior to scanning in accordance with the DaT-SCANanufacturer’s instructions. Qualitative analysis was per-
ormed by two experienced nuclear medicine physicians whoere blind to patients’s clinical data. The striatal to non-
pecific uptake ratio, the caudate nucleus to non-specificptake ratio, and the putamen to non-specific uptake ratio
wupf
able 1haracteristics and H/M ratio in patients and controls.
linical characteristic LBD (n = 9) F
ge (mean ± SD) 72.67 ± 3.57 6ex (n, %male) 5 (55.6)ge at onset (mean ± SD) 68.11 ± 4.31 6uration of disease (mean ± SD) 4.33 ± 1.87allucinations (n, %) 9 (100)arkinsonism (n, %) 9 (100)PDRS-ME (mean ± SD) 24.22 ± 13.05 3
enetic mutations (n, %)GBA gene 0 (0.00)MAPT gene 0 (0.00)PRGN gene 0 (0.00)
/M ratio (mean ± SD)Early image 1.25 ± 0.12Delayed image 1.14 ± 0.13
BD, Lewy Bodies Disease; FTD, Frontotemporal dementia; H/M ratio, heart toorrected according to Bonferroni). H/M ratio: LBD versus controls (early: p < 0.0BD versus FTD (early: p < 0.001; delayed: p < 0.001; unpaired t-test corrected acc* One-way ANOVA.
** Monte Carlo exact test.** Unpaired t-test.
Aging 31 (2010) 1903–1911 1905
ere evaluated in all subjects, and values were consideredbnormal if they were 2 SDs below the respective controlalues.
.4. 123I-MIBG scintigraphy
Myocardial 123I-MIBG scintigraphy was performed atest. A total of 111 MBq of 123I-MIGB (Amersham, Ein-oven, NL) was injected intravenously in 60 s. Data wereollected using a dual head gamma camera (Axis, Picker,edford, OH) at 10 min (early image) and 240 min (delayed
mage) after the isotope injection. Static planar imaging andegional 123I-MIBG uptake were obtained with 128 × 128atrix. Only planar images in thoracic anterior view were
sed for quantitative evaluation. Regions of interest (ROI)ere drawn around the whole heart and mediastinum of the
nterior image, and tracer uptake was measured within eachOI to calculate the heart/mediastinum (H/M) ratio. The H/M
atio from early and delayed images was evaluated in allubjects, and values were considered abnormal if they wereore than three standard deviations below the respective con-
rol mean. Regional 123I-MIBG uptake was assessed usingingle-photon emission tomography (SPECT) on the threexes display (short axis, vertical long axis, and horizontalong axis). Images were evaluated by an investigator whoas blinded to the patients’s diagnosis.
.5. Statistical analysis
The difference in mean age and H/M ratio among groups
ere assessed using one-way analysis of variance followed bynpaired t-test corrected according to Bonferroni for multi-le comparisons. Monte Carlo exact test was used to comparerequencies distributions of discrete variables among groups.TD (n = 6) Controls (n = 16) p-Value
4.83 ± 11.30 63.37 ± 4.67 0.004*
4 (66.7) 8 (50.0) 0.892**
1.00 ± 10.82 – 0.096***
3.83 ± 1.47 – 0.592***
2 (33.3) – 0.011**
6 (100) –6.50 ± 17.10 – 0.138***
0 (0.00) –0 (0.00) –2 (33.3) – 0.143
1.86 ± 0.20 1.91 ± 0.17 <0.001*
1.80 ± 0.23 1.99 ± 0.19 <0.001*
mediastinum ratio. Age: LBD versus controls (p = 0.004; unpaired t-test01; delayed: p < 0.001; unpaired t-test corrected according to Bonferroni);ording to Bonferroni).

1906F.N
ovellinoetal./N
eurobiologyofA
ging31
(2010)1903–1911
Table 2Clinical data of patients.
Sex/age atonset (y)
Duration ofdisease (y)
Familialhistory
Sign and symptoms UPDRS-ME(score)
Visualhallucinations
Gene mutations MIBG H/M ratio
Early Delayed
LBD1. M/67 8 S Parkinsonism with early freezing-gate. Progressive
cognitive impairment42 + − 1.35 1.10
2. M/62 5 S Depression, apathy, anxiety, irritability. Fluctuatingcognition. Memory and language impairment.Parkinsonism. Neuroleptic sensitivity
16 + − 1.27 1.30
3. M/65 5 S Loss of empathy, deficit on attention and memoryimpairment. Systematized delusions. Parkinsonism.Fluctuating cognition with pronounced variations inalertness
38 + − 1.36 1.17
4. F/66 3 S Spontaneous features of Parkinsonism. Memory impairmentand loss of empathy
35 + − 1.32 1.28
5. M/72 2 S Moderate loss of memory and attention. Mild Parkinsonism 14 + − 1.30 1.116. F/76 3 S Parkinsonism. Systematized delusions. Irritability and
aggressivity. Fluctuating cognition and neurolepticsensitivity
30 + − 1.39 1.31
7. M/65 4 S Psichotic disorders with systematized delusions, paranoidideation and episodic delirium of jealousy. Inappropriatesocial behaviour. Very slight bradikinesia. Vivid dreams
2 + − 1.05 1.00
8. F/71 3 S Parkinsonism. Depression, apathy. Progressive cognitiveimpairment. Fluctuating cognition
18 + − 1.16 1.01
9. F/75 6 S Parkinsonism. Prominent memory impairment 23 + − 1.13 1.05
FTD10. F/62 2 S Depression, apathy. Poor concentration, loss of empathy.
Impairment of occupational function. Progressive cognitiveimpairment. Hesitant speech. Parkinsonism. Uurinaryincontinence
18 − − 1.69 1.42
11. M/73 5 S Apathy, impulsivity depression, apathy. Hyperorality.Ecolalia, stuttering speech. Parkinsonism
63 − − 1.96 1.97
12. F/53 2 S Inappropriate social behaviour. Disinhibition. Hyperoralitywith abnormal eating behaviour. Decreased quantity ofspeech up to mutism. Parkinsonism. Uurinary incontinence
29 + PRGNSer111Phe
1.64 1.68
13. M/45 5 F Depression, loss of empathy. Inappropriate social behaviour.Decreased quantity of speech. Hypersomnolence.Systematized delusions, aggressivity. Parkinsonism
42 + − 1.74 1.79
14. M/72 5 F Progressive memory impairment. Impulsivity anddisinhibition. Hypersomnolence. Decreased quantity ofspeech, palilalia. Parkinsonism
46 − PGRNArg139Cys
2.01 1.92
15. M/61 4 S Impulsivity, depression, anxiety, obsession. Parkinsonism 21 − − 2.06 2.07
LBD: Lewy Bodies Disease; FTD: Frontotemporal dementia; y: years; PGRN: progranulin; S: sporadic; F: familial.

F. Novellino et al. / Neurobiology of Aging 31 (2010) 1903–1911 1907
Table 3Neuropsychological features.
Patients MMSE(score)
Executivefunctions
Short term verbalmemory
Long term verbalmemory
Visuo-constuctivepraxis
Attention Logicalthinking
Verbalfluency
Word comprehension
LBD1. M/67 20 + + + + + + + +2. M/62 9 + + + + + + + +3. M/65 12 + + + + + + + +4. F/66 n.a. + + + + + + + −5. M/72 13 + + + − + + − −6. F/76 26 + + − + + − + +7. M/65 27 + + − + + + + −8. F/71 11 + + + + + + + +9. F/75 20 − + + + − − − −
FTD10. F/62 23 + − − + + + + −11. M/73 15 + + + + + − + +12. F/53 n.a. + + + + + + + +13. M/45 8 + + + + + + + +14. M/72 n.a. n.a. n.a. n.a. n.a. n.a. n.a. n.a. n.a.15. M/61 28 + − − − − − + −
L mentaln
Udg
3
ip
bacwii
mflnGcs
mAdfpe
Fs
BD: Lewy Bodies Disease; FTD: Frontotemporal dementia; MMSE: minieuropsychological testing; −: absence of impairment; n.a.: not applicable.
npaired t-test was calculated to compare age at onset,isease duration and UPDRS-ME between LBD and FTDroups.
. Results
Characteristics and clinical data, including H/M ration early and delayed images in 123I-MIBG scintigraphy ofatients and controls are listed in Tables 1 and 2.
LBD group included 9 patients (1 possible and 8 proba-le; 5 males and 4 females; mean age: 72.67 ± 3.57; meange at onset: 68.11 ± 4.31). Cognitive impairment and psy-
hotic disorders were the initial presentation in 4 patientshile Parkinsonism was the initial symptom in the remain-ng 5 patients. All patients developed visual hallucinationsn the first years of illness, according to 1-year rule recom-
mpTp
ig. 1. Cardiac 123I-MIBG scintigraphy in a patient with LBD. Myocardial 123I-Mevere decrease of the cardiac 123I-MIBG uptake.
state examination; +: presence of scores at or below the 5th percentile on
ended in diagnostic criteria. Four of 9 LBD patients haductuation in cognitive symptoms and 2 had sensitivity toeuroleptics drugs. None of LDB patients had mutations inBA, MAPT, and PGRN genes. Brain MRI showed diffuse
ortical atrophy in all patients, and DAT-SPECT showed aeverely decreased bilateral striatal uptake in 8 of 9 patients.
FTD group included 6 patients (4 males and 2 females;ean age: 64.83 ± 11.30; mean age at onset: 61.00 ± 10.82).ll patients had prominent behavioural changes at onset ofisease with decline in social interpersonal conduct, thatulfilled clinical diagnostic criteria for FTD. Two of thisatients had hyperorality, one of them had echolalia andmpty spontaneous speech, and four had language impair-
ent with impaired repetition and economy of speech. Allatients developed Parkinsonism and cognitive impairment.wo patients had early visual hallucinations. None of FTDatients had mutations in GBA and MAPT genes. Two
IBG planar anterior view 10 min p.i. (A) and 240 min p.i. (B) showed a

1 logy of
pafrmclp
p
1
imTniwp1
Fr
908 F. Novellino et al. / Neurobio
atients carried heterozygous variants in the PGRN gene:patient (p12) carried the Ser111Phe variant which was not
ound in 400 healthy subjects from the same geographicalegion, while the other patient (p14) carried the Cys139Argutation in the PGRN gene. MRI showed in all patients a
ortical atrophy mainly evident in the frontal e/o temporalobes, while DAT-SPECT showed a reduced uptake in 5 of 6atients.
Neuropsychological features of both LBD and FTPatients are summarized in Table 3.
In the control group, the H/M ratio (mean ± SD) was.91 ± 0.17 in the early and 1.99 ± 0.19 in the delayed
apuc
ig. 2. Cardiac 123I-MIBG scintigraphy in a patient with FTD. Myocardial 123I-Madiolabeled 123I-MIBG uptake 240 min p.i. (C), all showing a normal 123I-MIBG a
Aging 31 (2010) 1903–1911
mages, and the lower normal limit of the ratio (meaninus three SDs) was set at 1.40 and 1.42, respectively.he early and delayed cardiac 123I-MIBG uptake was sig-ificantly decreased in patients with LBD (H/M ratio in earlymage: 1.25 ± 0.12; in delayed image: 1.14 ± 0.13) comparedith FTD patients (H/M ratio in early image: 1.86 ± 0.20,< 0.001; in delayed image: 1.80 ± 0.23, p < 0.001) and with6 age-matched control subjects (8 men and 8 women; mean
ge 63.37 ± 4.67; early image, p < 0.001; delayed image,< 0.001). All patients with LBD had a cardiac 123I-MIBGptake values which was lower than 3 SDs from those of theontrol subjects. The H/M ratio of the FTD patients was notIBG planar anterior view 10 min p.i. (A) and 240 min p.i. (B) and regionalctivity in all regions of the heart.
logy of
s1
F
4
wa
wrdaitPilvcthestswtiec
ihpfPffraknharwip
hdam
imhm
it1tteMPwiK
cssui2
uwwspudhfhuaiecpctmesmuAbdNF
F. Novellino et al. / Neurobio
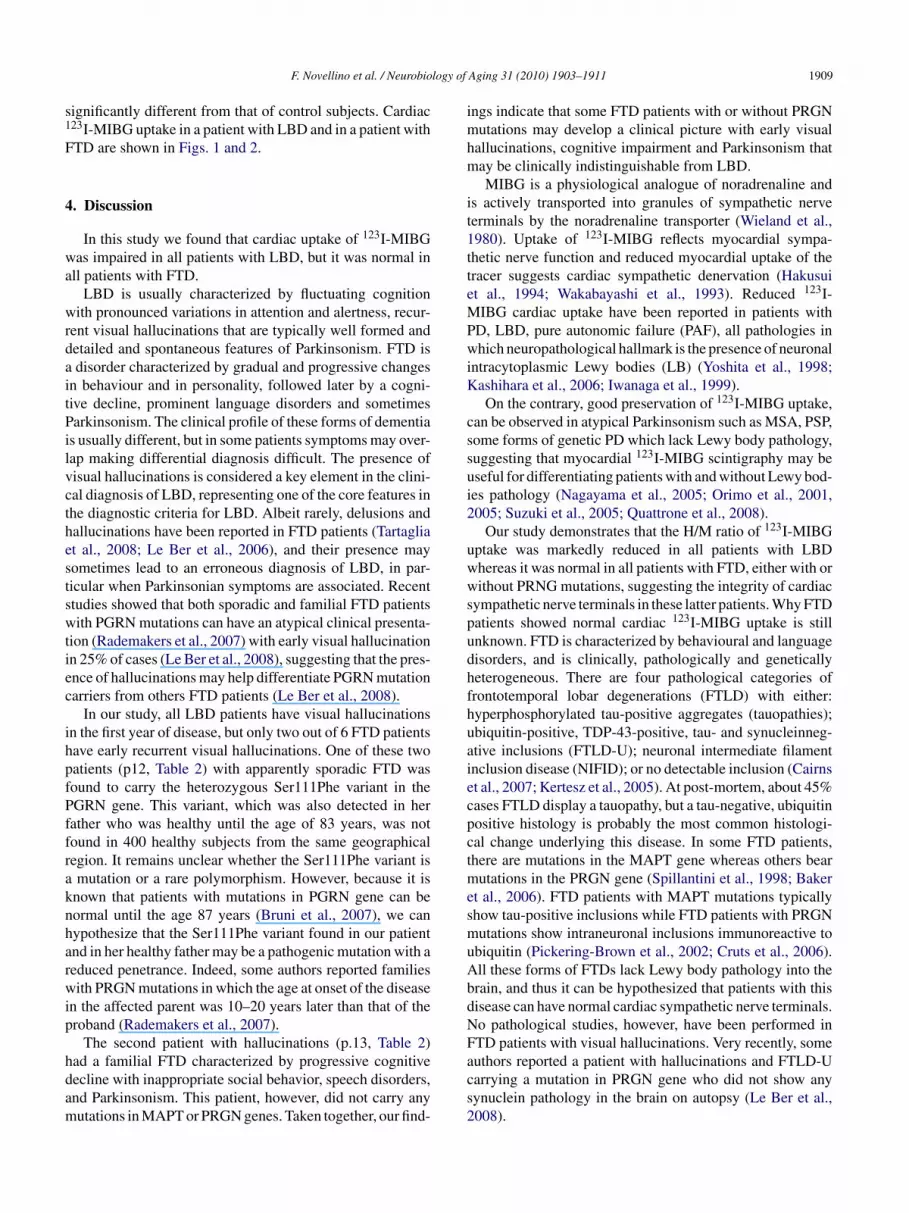
ignificantly different from that of control subjects. Cardiac23I-MIBG uptake in a patient with LBD and in a patient withTD are shown in Figs. 1 and 2.
. Discussion
In this study we found that cardiac uptake of 123I-MIBGas impaired in all patients with LBD, but it was normal in
ll patients with FTD.LBD is usually characterized by fluctuating cognition
ith pronounced variations in attention and alertness, recur-ent visual hallucinations that are typically well formed andetailed and spontaneous features of Parkinsonism. FTD isdisorder characterized by gradual and progressive changes
n behaviour and in personality, followed later by a cogni-ive decline, prominent language disorders and sometimesarkinsonism. The clinical profile of these forms of dementia
s usually different, but in some patients symptoms may over-ap making differential diagnosis difficult. The presence ofisual hallucinations is considered a key element in the clini-al diagnosis of LBD, representing one of the core features inhe diagnostic criteria for LBD. Albeit rarely, delusions andallucinations have been reported in FTD patients (Tartagliat al., 2008; Le Ber et al., 2006), and their presence mayometimes lead to an erroneous diagnosis of LBD, in par-icular when Parkinsonian symptoms are associated. Recenttudies showed that both sporadic and familial FTD patientsith PGRN mutations can have an atypical clinical presenta-
ion (Rademakers et al., 2007) with early visual hallucinationn 25% of cases (Le Ber et al., 2008), suggesting that the pres-nce of hallucinations may help differentiate PGRN mutationarriers from others FTD patients (Le Ber et al., 2008).
In our study, all LBD patients have visual hallucinationsn the first year of disease, but only two out of 6 FTD patientsave early recurrent visual hallucinations. One of these twoatients (p12, Table 2) with apparently sporadic FTD wasound to carry the heterozygous Ser111Phe variant in theGRN gene. This variant, which was also detected in herather who was healthy until the age of 83 years, was notound in 400 healthy subjects from the same geographicalegion. It remains unclear whether the Ser111Phe variant ismutation or a rare polymorphism. However, because it is
nown that patients with mutations in PGRN gene can beormal until the age 87 years (Bruni et al., 2007), we canypothesize that the Ser111Phe variant found in our patientnd in her healthy father may be a pathogenic mutation with aeduced penetrance. Indeed, some authors reported familiesith PRGN mutations in which the age at onset of the disease
n the affected parent was 10–20 years later than that of theroband (Rademakers et al., 2007).
The second patient with hallucinations (p.13, Table 2)
ad a familial FTD characterized by progressive cognitiveecline with inappropriate social behavior, speech disorders,nd Parkinsonism. This patient, however, did not carry anyutations in MAPT or PRGN genes. Taken together, our find-acs2
Aging 31 (2010) 1903–1911 1909
ngs indicate that some FTD patients with or without PRGNutations may develop a clinical picture with early visual
allucinations, cognitive impairment and Parkinsonism thatay be clinically indistinguishable from LBD.MIBG is a physiological analogue of noradrenaline and
s actively transported into granules of sympathetic nerveerminals by the noradrenaline transporter (Wieland et al.,980). Uptake of 123I-MIBG reflects myocardial sympa-hetic nerve function and reduced myocardial uptake of theracer suggests cardiac sympathetic denervation (Hakusuit al., 1994; Wakabayashi et al., 1993). Reduced 123I-IBG cardiac uptake have been reported in patients with
D, LBD, pure autonomic failure (PAF), all pathologies inhich neuropathological hallmark is the presence of neuronal
ntracytoplasmic Lewy bodies (LB) (Yoshita et al., 1998;ashihara et al., 2006; Iwanaga et al., 1999).On the contrary, good preservation of 123I-MIBG uptake,
an be observed in atypical Parkinsonism such as MSA, PSP,ome forms of genetic PD which lack Lewy body pathology,uggesting that myocardial 123I-MIBG scintigraphy may beseful for differentiating patients with and without Lewy bod-es pathology (Nagayama et al., 2005; Orimo et al., 2001,005; Suzuki et al., 2005; Quattrone et al., 2008).
Our study demonstrates that the H/M ratio of 123I-MIBGptake was markedly reduced in all patients with LBDhereas it was normal in all patients with FTD, either with orithout PRNG mutations, suggesting the integrity of cardiac
ympathetic nerve terminals in these latter patients. Why FTDatients showed normal cardiac 123I-MIBG uptake is stillnknown. FTD is characterized by behavioural and languageisorders, and is clinically, pathologically and geneticallyeterogeneous. There are four pathological categories ofrontotemporal lobar degenerations (FTLD) with either:yperphosphorylated tau-positive aggregates (tauopathies);biquitin-positive, TDP-43-positive, tau- and synucleinneg-tive inclusions (FTLD-U); neuronal intermediate filamentnclusion disease (NIFID); or no detectable inclusion (Cairnst al., 2007; Kertesz et al., 2005). At post-mortem, about 45%ases FTLD display a tauopathy, but a tau-negative, ubiquitinositive histology is probably the most common histologi-al change underlying this disease. In some FTD patients,here are mutations in the MAPT gene whereas others bear
utations in the PRGN gene (Spillantini et al., 1998; Bakert al., 2006). FTD patients with MAPT mutations typicallyhow tau-positive inclusions while FTD patients with PRGNutations show intraneuronal inclusions immunoreactive to
biquitin (Pickering-Brown et al., 2002; Cruts et al., 2006).ll these forms of FTDs lack Lewy body pathology into therain, and thus it can be hypothesized that patients with thisisease can have normal cardiac sympathetic nerve terminals.o pathological studies, however, have been performed inTD patients with visual hallucinations. Very recently, some
uthors reported a patient with hallucinations and FTLD-Uarrying a mutation in PRGN gene who did not show anyynuclein pathology in the brain on autopsy (Le Ber et al.,008).
1 logy of
sLnhd
chpsnFMwLLu
assdtms
D
atntc
ut
A
S
R
B
B
B
B
B
B
B
C
C
C
C
D
F
G
H
I
910 F. Novellino et al. / Neurobio
Taken together, these findings suggest that FTD patientshow normal cardiac 123I-MIBG uptake because they lackewy body pathology into the brain and cardiac sympatheticerve terminals, differently from patients with LBD whoad severe sympathetic cardiac denervation and a markedecrease of cardiac MIBG uptake.
There are some limitations to this study. We used clini-al criteria for the diagnosis of the diseases, and we did notave pathologic confirmation. Thus it is possible that in someatients the clinical diagnosis may be in error. However, thiseems unlikely because the specificity of the clinical diag-ostic criteria that we applied in our patients for DLB andTD is high (McKeith et al., 2000; Mendez et al., 2007).oreover, our sample of patients with FTD was small, ande cannot exclude that a subset of FTD patients with anBD-like phenotype or hallucinations may prove to haveBD-pathology on autopsy, and an altered cardiac MIBGptake.
In conclusion, we demonstrate that FTD patients showednormal cardiac 123I-MIBG uptake, indicating that cardiac
ympathetic nerve terminals are normal in this disease. Ourtudy suggests that myocardial MIBG scinthigraphy can helpistinguish LBD from FTD. This finding may be of impor-ance especially in FTD patients with hallucinations who
ay have a clinical picture resembling that of LBD. Furthertudies in a larger cohort of patients are warranted.
isclosure
The authors have no conflict of interest to disclose. Nouthor has contracts relating to this research. The data con-ained in the manuscript have not been previously published,or submitted elsewhere. All authors have reviewed the con-ents of the manuscript being submitted, and approved itsontents and validated the accuracy of the data.
All procedures required for human subjects’ research weresed and all participants provided informed consent for par-icipation in the study.
cknowledgement
This work was supported by the Institute of Neurologicalciences, National Research Council, Cosenza, Italy.
eferences
abcock, H., 1930. An experiment in the measurement of mental deteriora-tion. Arch. Psychol. 117, 105.
abcock, H., Levy, L., 1940. Test and Manual of Directions: The RevisedExamination for the Measurement of Mental Functioning. Ch. Stoelting,
Chicago.aker, M., Mackenzie, I.R., Pickering-Brown, S.M., Gass, J., Rademakers,R., Lindholm, C., Snowden, J., Adamson, J., Sadovnick, A.D., Rollinson,S., Cannon, A., Dwosh, E., Neary, D., Melquist, S., Richardson, A.,Dickson, D., Berger, Z., Eriksen, J., Robinson, T., Zehr, C., Dickey, C.A.,
K
Aging 31 (2010) 1903–1911
Crook, R., McGowan, E., Mann, D., Boeve, B., Feldman, H., Hutton,M., 2006. Mutations in progranulin cause tau-negative frontotemporaldementia linked to chromosome 17. Nature 442, 916–919.
enton, A.L., Hamsher, K., Sivan, A.B., 1994. Multilingual Aphasia Exam-ination. AJA Associates, Iowa City.
onner, L.T., Tsuang, D.W., Cherrier, M.M., Eugenio, C.J., Du Jennifer,Q., Steinbart, E.J., Limprasert, P., La Spada, A.R., Seltzer, B., Bird,T.D., Leverenz, J.B., 2003. Familial dementia with Lewy bodies with anatypical clinical presentation. J. Geriatr. Psychiatry Neurol. 16, 59–64.
razzelli, M., Capitani, E., Della Sala, S., Spinnler, H., Zuffi, M., 1994. Aneuropsychological instrument adding to the description of patients withsuspected cortical dementia: the Milan Overall Dementia assessment. J.Neurol. Neurosurg. Psychiatr. 57, 1510–1517.
runi, A.C., Momeni, P., Bernardi, L., Tomaino, C., Frangipane, F., Elder,J., Kawarai, T., Sato, C., Pradella, S., Wakutani, Y., Anfossi, M., Gallo,M., Geracitano, S., Costanzo, A., Smirne, N., Curcio, S.A., Mirabelli,M., Puccio, G., Colao, R., Maletta, R.G., Kertesz, A., St George-Hyslop,P., Hardy, J., Rogaeva, E., 2007. Heterogeneity within a large kindredwith frontotemporal dementia: a novel progranulin mutation. Neurology69, 140–147.
airns, N.J., Bigio, E.H., Mackenzie, I.R., Neumann, M., Lee, V.M., Hatan-paa, K.J., White 3rd, C.L., Schneider, J.A., Grinberg, L.T., Halliday, G.,Duyckaerts, C., Lowe, J.S., Holm, I.E., Tolnay, M., Okamoto, K., Yokoo,H., Murayama, S., Woulfe, J., Munoz, D.G., Dickson, D.W., Ince, P.G.,Trojanowski, J.Q., Mann, D.M., Consortium for Frontotemporal LobarDegeneration, 2007. Neuropathologic diagnostic and nosologic criteriafor frontotemporal lobar degeneration: consensus of the Consortium forFrontotemporal Lobar Degeneration. Acta Neuropathol. 114, 5–22.
apasso, R., Miveli, M., 2001. Esame Neuropsicologico per l’Afasia.Sprinter, Milano.
arlesimo, G.A., Caltagirone, C., Gainotti, G., 1996. The Mental Deteri-oration Battery: normative data, diagnostic reliability and qualitativeanalysis of cognitive impairment. The group for the standardization ofthe Mental Deterioration Battery. Eur. Neurol. 36, 378–384.
ruts, M., Gijselinck, I., van der Zee, J., Engelborghs, S., Wils, H., Pirici, D.,Rademakers, R., Vandenberghe, R., Dermaut, B., Martin, J.J., van Duijn,C., Peeters, K., Sciot, R., Santens, P., De Pooter, T., Mattheijssens, M.,Van den Broeck, M., Cuijt, I., Vennekens, K., De Deyn, P.P., Kumar-Singh, S., Van Broeckhoven, C., 2006. Null mutations in progranulincause ubiquitin-positive frontotemporal dementia linked to chromosome17q21. Nature 442, 920–924.
ubois, B., Slachevsky, A., Litvan, I., Pillon, B., 2000. The FAB: a FrontalAssessment Battery at bedside. Neurology 55, 1621–1626.
olstein, M.F., Folstein, S.E., McHugh, P.R., 1975. Mini-mental state. Apractical method for grading the cognitive state of patients for the clini-cian. J. Psychiatr. Res. 12, 189–198.
ass, J., Cannon, A., Mackenzie, I.R., Boeve, B., Baker, M., Adam-son, J., Crook, R., Melquist, S., Kuntz, K., Petersen, R., Josephs,K., Pickering-Brown, S., Graff-Radford, M., Uitti, N., Dickson, R.,Wszolek, D., Gonzalez, Z., Beach, J., Bigio, T.G., Johnson, E., Wein-traub, N., Mesulam, S., White, M., 3rd, C.L., Woodruff, B., Caselli,R., Hsiung, G.Y., Feldman, H., Knopman, D., Hutton, M., Rademakers,R., 2006. Mutations in progranulin are a major cause of ubiquitin-positive frontotemporal lobar degeneration. Hum. Mol. Genet. 15,2988–3001.
akusui, S., Yasuda, T., Yanagi, T., Tohyama, J., Hasegawa, Y., Koike, Y.,Hyrayama, M., Takahashi, A., 1994. A radiological analysis of heartsympathetic functions with meta-(123I)iodobenzylguanidine in neuro-logical patients with autonomic failure. J. Auton. Nerv. Syst. 49, 81–84.
wanaga, K., Wakabayashi, K., Yoshimoto, M., Tomita, I., Satoh, H.,Takashima, H., Satoh, A., Seto, M., Tsujihata, M., Takahashi, H., 1999.Lewy body-type degeneration in cardiac plexus in Parkinson’s disease
and incidental Lewy body diseases. Neurology 52, 1269–1271.ashihara, K., Ohno, M., Kawada, S., Okumura, Y., 2006. Reduced cardiacuptake and enhanced washout of 123I-MIBG in pure autonomic fail-ure occurs conjointly with Parkinson’s disease and dementia with Lewybodies. J. Nucl. Med. 47, 1099–1101.

logy of
K
L
L
L
M
M
M
M
N
N
N
O
O
P
Q
R
R
R
R
S
S
S
T
T
W
W
adrenomedullary imaging with [123I]Metaiodobenzylguanidine. J. Nucl.Med. 21, 349–353.
F. Novellino et al. / Neurobio
ertesz, A., Mcmonagle, P., Blair, M., Davidson, W., Munoz, D.G., 2005.The evolution and pathology of frontotemporal dementia. Brain 128,1996–2005.
e Ber, I., Guedj, E., Gabelle, A., Verpillat, P., Volteau, M., Thomas-Anterion, C., Decousus, M., Hannequin, D., Véra, P., Lacomblez, L.,Camuzat, A., Didic, M., Puel, M., Lotterie, J.A., Golfier, V., Bernard,A.M., Vercelletto, M., Magne, C., Sellal, F., Namer, I., Michel, B.F.,Pasquier, J., Salachas, F., Bochet, J.; French research network onFTD/FTD-MND., Brice, A., Habert, M.O., Dubois, B., 2006. Demo-graphic, neurological and behavioural characteristics and brain perfusionSPECT in frontal variant of frontotemporal dementia, Brain 129,3051–3065.
e Ber, I., van der Zee, J., Hannequin, D., Gijselinck, I., Campion, D., Puel,M., Laquerrière, A., De Pooter, T., Camuzat, A., Van den Broeck, M.,Dubois, B., Sellal, F., Lacomblez, L., Vercelletto, M., Thomas-Antérion,C., Michel, B.F., Golfier, V., Didic, M., Salachas, F., Duyckaerts,C., Cruts, M., Verpillat, P., Van Broeckhoven, C., Brice, A.; FrenchResearch Network on FTD/FTD-MND, 2007. Progranulin null muta-tions in both sporadic and familial frontotemporal dementia. Hum. Mutat.28, 846–855.
e Ber, I., Camuzat, A., Hannequin, D., Pasquier, F., Guedj, E., Rovelet-Lecrux, A., Hahn-Barma, V., van der Zee, J., Clot, F., Bakchine, S.,Puel, M., Ghanim, M., Lacomblez, L., Mikol, J., Deramecourt, V., Leje-une, P., de la Sayette, V., Belliard, S., Vercelletto, M., Meyrignac, C.,Van Broeckhoven, C., Lambert, J.C., Verpillat, P., Campion, D., Habert,M.O., Dubois, B., Brice, A.; French research network on FTD/FTD-MND, 2008. Phenotype variability in progranulin mutation carriers:a clinical, neuropsychological, imaging and genetic study. Brain 131,732–746.
cKeith, I.G., Ballard, C.G., Perry, R.H., Ince, P.G., O’Brien, J.T., Neill, D.,Lowery, K., Jaros, E., Barber, R., Thompson, P., Swann, A., Fairbairn,A.F., Perry, E.K., 2000. Prospective validation of consensus criteria forthe diagnosis of dementia with Lewy bodies. Neurology 54, 1050–1058.
cKeith, I., Mintzer, J., Aarsland, D., Burn, D., Chiu, H., Cohen-Mansfield,J., Dickson, D., Dubois, B., Duda, J.E., Feldman, H., Gauthier, S., Halli-day, G., Lawlor, B., Lippa, C., Lopez, O.L., Carlos Machado, J., O’Brien,J., Playfer, J., Reid, W.; International Psychogeriatric Association ExpertMeeting on DLB, 2004. Dementia with Lewy Bodies. Lancet Neurol. 3,19–28.
cKeith, I.G., Dickson, D.W., Lowe, J., Emre, M., O’Brien, J.T., Feldman,H., Cummings, J., Duda, J.E., Lippa, C., Perry, E.K., Aarsland, D., Arai,H., Ballard, C.G., Boeve, B., Burn, D.J., Costa, D., Del Ser, T., Dubois, B.,Galasko, D., Gauthier, S., Goetz, C.G., Gomez-Tortosa, E., Halliday, G.,Hansen, L.A., Hardy, J., Iwatsubo, T., Kalaria, R.N., Kaufer, D., Kenny,R.A., Korczyn, A., Kosaka, K., Lee, V.M., Lees, A., Litvan, I., Londos,E., Lopez, O.L., Minoshima, S., Mizuno, Y., Molina, J.A., Mukaetova-Ladinska, E.B., Pasquier, F., Perry, R.H., Schul, J.B., Trojanowski, J.Q.,Yamada, M.; Consortium on DLB, 2005. Diagnosis and managementof dementia with Lewy bodies: third report of the DLB Consortium.Neurology 65, 1863–1872.
endez, M.F., Shapira, J.S., McMurtray, A., Licht, E., Miller, B.L., 2007.Accuracy of the clinical evaluation for frontotemporal dementia. Arch.Neurol. 64, 830–835.
agayama, H., Hamamoto, M., Ueda, M., Nagashima, J., Katayama, Y.,2005. Reliability of MIBG myocardial scintigraphy in the diagnosis ofParkinson’s disease. J. Neurol. Neurosurg. Psychiatry 76, 249–251.
eary, D., Snowden, J.S., Gustafson, L., Passant, U., Stuss, D., Black,S., Freedman, M., Kertesz, A., Robert, P.H., Albert, M., Boone, K.,Miller, B.L., Cummings, J., Benson, D.F., 1998. Frontotemporal lobardegeneration: a consensus on clinical diagnostic criteria. Neurology 51,1546–1554.
Y
Aging 31 (2010) 1903–1911 1911
elson, H.E., 1976. A modified card sorting test sensitive to frontal lobedefects. Cortex 12, 313–324.
rimo, S., Ozawa, E., Oka, T., Nakade, S., Tsuchiya, K., Yoshimoto,M., Wakabayashi, K., Takahashi, H., 2001. Different histopathologyaccounting for a decrease in myocoardial MIBG uptake in PD and MSA.Neurology 57, 1140–1141.
rimo, S., Amino, T., Yokochi, M., Kojo, T., Uchihara, T., Takahashi, A.,Wakabayashi, K., Takahashi, H., Hattori, N., Mizuno, Y., 2005. Preservedcardiac sympathetic nerve accounts for normal cardiac uptake of MIBGin PARK2. Mov. Disord. 20, 1350–1353.
ickering-Brown, S.M., Richardson, A.M., Snowden, J.S., McDonagh,A.M., Burns, A., Braude, W., Baker, M., Liu, W.K., Yen, S.H., Hardy,J., Hutton, M., Davies, Y., Allsop, D., Craufurd, D., Neary, D., Mann,D.M., 2002. Inherited frontotemporal dementia in nine British familiesassociated with intronic mutations in the tau gene. Brain 125, 732–751.
uattrone, A., Bagnato, A., Annesi, G., Novellino, F., Morgante, L., Savet-tieri, G., Zappia, M., Tarantino, P., Candiano, I.C., Annesi, F., Civitelli,D., Rocca, F.E., D’Amelio, M., Nicoletti, G., Morelli, M., Petrone, A.,Loizzo, P., Condino, F., 2008. Myocardial 123Metaiodiobenzylguanidineuptake in genetic Parkinson’s disease. Mov. Disord. 23, 21–27.
ademakers, R., Baker, M., Gass, J., 2007. Phenotypic variability associ-ated with progranulin haploinsufficiency in patients with the common1477C → T (Arg493X) mutation: an international initiative. Lancet Neu-rol. 6, 857–868.
atnavalli, E., Brayne, C., Dawson, K., Hodges, J.R., 2002. The prevalenceof frontotemporal dementia. Neurology 58, 1615–1621.
aven, J.C., 1947. Progressive Matrices. Sets A. Ab, B: Board and BookForms. Lewis, London.
ey, A., 1958. Memorisation d’ une serie de 15 mots en 5 repetitions. In:Rey, A. (Ed.), L’ Examen Clinique en Psycologie. Presses Universitairesdes France, Paris.
hulman, K.I., Shedletsky, R., Silver, I., 1986. The challenge of time: clockdrawing and cognitive funcition in the elderly. Int. J. Geriatry Psychiatry1, 135–140.
pillantini, M.G., Murrell, J.R., Goedert, M., Farlow, M.R., Klug, A., Ghetti,B., 1998. Mutation in the tau gene in familial multiple system tauopathywith presenile dementia. Proc. Natl. Acad. Sci. U.S.A. 95, 7737–7741.
uzuki, M., Hattori, N., Orimo, S., Fukumitsu, N., Abo, M., Kono, Y.,Sengoku, R., Kurita, A., Honda, H., Inoue, K., 2005. Preserved myocar-dial Metaiodiobenzylguanidine uptake in autosomal recessive juvenileParkinsonism: first case report. Mov. Disord. 20, 634–636.
artaglia, M.C., Kertesz, A., Ang, L.C., 2008. Delusions and hallucina-tions in frontotemporal dementia: a clinicopathologic case report. Cogn.Behav. Neurol. 21, 107–110.
oft, M., Pielsticker, L., Ross, O.A., Aasly, J.O., Farrer, M.J., 2006. Gluco-cerebrosidase gene mutations and Parkinson disease in the Norwegianpopulation. Neurology 66, 415–417.
akabayashi, K., Takahashi, H., Ohama, E., Takeda, S., Ikuta, F., 1993.Lewy bodies in the visceral autonomic nervous system in Parkinson’sdisease. In: Narabayashi, H., Nagatsu, N., Yanagisawa, N., Mizuno,Y. (Eds.), Advances in Neurology. Lippincott-Raven, New York, pp.609–612.
ieland, D.M., Wu, J.L., Brown, L.E., Mangner, T.J., Swanson, D.P., Beier-waltes, W.H., 1980. Radiolabeled adrenergic neuron-blocking agents:
oshita, M., Hayashi, M., Hirai, S., 1998. Decreased myocardial accumu-lation of 123I-metaiodiobenzylguanidine in Parkinson’s disease. Nucl.Med. Commun. 19, 137–142.



![Membrane type 1 matrix metalloproteinase detection in tumors, using the iodinated endogenous [123I]-tissue inhibitor 2 of metalloproteinases as imaging agent](https://img.pdfslide.net/doc/110x75/63286f7664795e54c206f3fa/membrane-type-1-matrix-metalloproteinase-detection-in-tumors-using-the-iodinated.jpg)



![Quantitation of benzodiazepine receptor binding with PET [11C]iomazenil and SPECT [123I]iomazenil: preliminary results of a direct comparison in healthy human subjects](https://img.pdfslide.net/doc/110x75/63586e4fa90bb46f52085f25/quantitation-of-benzodiazepine-receptor-binding-with-pet-11ciomazenil-and-spect.jpg)
![Double-blind olanzapine vs. haloperidol D2 dopamine receptor blockade in schizophrenic patients: a baseline-endpoint [ 123I]IBZM SPECT study](https://img.pdfslide.net/doc/110x75/631d2a55665120b3330c3641/double-blind-olanzapine-vs-haloperidol-d2-dopamine-receptor-blockade-in-schizophrenic.jpg)
![Double-blind olanzapine vs. haloperidol D2 dopamine receptor blockade in schizophrenic patients: a baseline-endpoint [123I]IBZM SPECT study](https://img.pdfslide.net/doc/110x75/63483e5af5483db9d306e0c1/double-blind-olanzapine-vs-haloperidol-d2-dopamine-receptor-blockade-in-schizophrenic-1699673912.jpg)




![Striatal amphetamine-induced dopamine release in patients with schizotypal personality disorder studied with single photon emission computed tomography and [123I]iodobenzamide](https://img.pdfslide.net/doc/110x75/635eb6ef2dc9f5f89b06e3e1/striatal-amphetamine-induced-dopamine-release-in-patients-with-schizotypal-personality-1701677425.jpg)





![Midbrain binding of [123I]nor-β-CIT in atypical depression](https://img.pdfslide.net/doc/110x75/6347e6047442d262850ebe4c/midbrain-binding-of-123inor-v-cit-in-atypical-depression.jpg)
![Imaging of serotonin transporters with [123I]FP-CIT SPECT in the human hypothalamus](https://img.pdfslide.net/doc/110x75/6334b5d92532592417003033/imaging-of-serotonin-transporters-with-123ifp-cit-spect-in-the-human-hypothalamus.jpg)


