Embed Size (px)
Citation preview

Myopic Picosecond Laser Keratomileusis with the Neodymium-Yttrium Lithium Fluoride Laser in the Cat Cornea
Omar E. Hanuch, MD, a Vinay B. Agrawal, MD, n Sharon Bassage, MS, I Manuel del Cerro, MD, 2 James V. Aquavella, MD I
Objective: The study aimed to evaluate the effects of myopic picosecond laser keratomileusis (PLK) in the feline model with follow-up of up to 6 months.
Design: The study design was a case-controlled, feline animal model. Participants: The procedure was completed in 1 eye each of 12 cats divided into 3 groups (group 1, sham
operation; group 2, 100-#m lenticle thickness; and group 3, 150-/~m lenticle thickness). The second eye of each cat was used as a control.
Intervention: Picosecond laser keratomileusis, a new intrastromal laser technique with the neodymium-yttrium lithium fluoride picosecond laser, was presented. The procedure, analogous to laser keratomileusis in situ, consists of two lamellar ring cuts and one vertical ring-shape cut that define a 4-mm-diameter intrastromal lenticle.
Main Outcome Measures: Corneal pachymetry, topography, tonometry, and biomicroscopic examination were performed before and after surgery at scheduled intervals for 6 months. • Results: The mean (_+standard deviation) diopter change for group 2 was 5.4 _+ 3.2 diopters at 1 month and
remained stable during the 6-month period. For group 3, the change was 8.1 _+ 0.22 diopters at 1 month and 6.8 +__ 1.5 diopters at 6 months. Group 1 (sham operation) did not show significant diopter change compared with that of control eyes at any timepoint. Pachymetry results for group 1 showed no significant difference in the thickness of the cornea at any timepoint (P >0.05). For groups 2 and 3, the corneal thickness was reduced significantly by 1 month (P <0.05), but it regressed to nearly preoperative values at 3 months. At 6 months, the corneas were clear with no grossly visible scar. With the slit-lamp examination, a faint, thin line of haziness barely was visible in the periphery of the flap. The histologic examination results showed no significant collagen disruption, inflammation, or endothelial irregularities comparing the control with the postoperative corneas.
Conclusion: Myopic intrastromal PLK produces a refractive effect on the cornea that depends on the thickness of the lenticle removed and persists after 6 months with minimal stromal haze and no surgical complications. The authors' results, although encouraging, indicate the need for further studies to confirm the efficacy of PLK as a valid refractive procedure. Ophthalmology 1998; 105:142-149
The introduction of laser technology with the capability to selectively remove intrastromal corneal tissue t'2 has opened a new frontier for the modification of the refrac- tive power of the cornea to treat myopia, hyperopia, and astigmatism. This.advance is possible using the neodym-
Originally received: October 28, 1996. Revision accepted: August 22, 1997.
Cornea Research Laboratory, University of Rochester Medical Center, Rochester. New York.
-" Department of Ophthalmology, University of Rochester Medical Cen- ter, Rochester, New York.
Presented in part as a poster at the Annual Meeting of the Association for Research in Vision and Ophthalmology, Fort Lauderdale, Florida. April 1996.
Supported in part by Intelligent Surgical Lasers, Inc., San Diego, Cali- fornia.
The authors have no financial or proprietary interests in any procedures or devices used in this article.
Address correspondence to James V. Aquavella, MD, Genesse Valley Eye Institute, 919 Westfall Road, Rochester, NY 14618.
ium-yttrium lithium fluoride (Nd:YLF) laser. 3"4 This is a 1053-nm, solid-state laser with a mode-locking system that can produce pulses with a duration in the picosecond range (10 -~2 second). Because laser power is defined as energy/time, 5 a reduction in the laser pulse duration from the standard 6-nanosecond range to the 20- to 40-pico- second range decreases the energy required for corneal photodisruption to 6 to 21 #j,3 allowing for less thermal and acoustic damage to the surrounding tissue. 6 The pi- cosecond pulse laser- t issue interaction is characterized by photodisruption or plasma-mediated ablation and is composed of three major phenomena: ( l ) plasma forma- tion; (2) shock wave generation; and (3) gas bubble cavi- tation. 7 These events are entirely limited to the corneal stroma without epithelial or Bowman membrane dam- age, thus avoiding complications related to corneal wound healing, such as superficial stromal opacification or regression of refractive effect, that occur with surface refractive procedures. 8'9
After the introduction of keratomileusis by Barraquer, '° a broad base of experience has been acquired in the effect of
142

H a n u c h et al • Picosecond Laser Keratomileus is
subtraction lamellar refractive surgery and the nonempirical calculation of the resection required for correcting v,'u'ious types of ametropia) ~ However, this procedure has not been widely accepted because of the complexity of equipment (microkeratome) and technique and the potential for vision- threatening complications principally involving re-epitheliali- zation and wound healing, p--~4
We introduce picosecond laser keratomileusis (PLK), an intrastromal laser technique analogous to laser keratomileusis in situ that eliminates the need for a microkeratome and minimizes the epithelial and Bowman involvement, thus avoiding wound-healing complications.
The feline model was chosen for its similarities in curva- ture, diameter, and thickness to the human cornea and because this model has been used previously in refractive sur~cal studies? 5.16
This study presents the biomicroscopic, pachymetric, topo- ~aphic, and histologic effects of myopic PLK in the feline model with follow-up of up to 6 months.
Materials and Methods
Laser D e s c r i p t i o n
The instrument used in this study was a Model 4000 Nd:YLF picosecond laser (Intelligent Surgical Lasers, Inc., San Diego, CA). This is a solid-state, mode-locked, regeneratively ampli- fied Nd:YLF laser that generates pulses at 1053 nm with a repetition rate of I kHz and a pulse duration of 40 picoseconds. The energy ranges from 5 to 350 /.tJ with a 15-pro spot size and a 5- to 100-/~.m adjustable spot separation. The beam cone angle is 32 °. The delivery system is through a modified moler operating microscope equipped with a removable quartz contact lens cone for cornea applanation and a limbal suction ring for eye fixation. The system allows placement of the formed beam in the x-, y-, and z-directions. Different three-dimensional pat- terns can be defined using the supplied computer software pro- gram. A focal offset function enables the operator to program the laser photodisruption to start at a different depth from the helium/neon aiming beam focal point in the Z-axis. Thus, a focus of the visible heliunv'neon beam on the epithelium with a focal offset of 300/.zm will cause the initial point of ablation to be located 300 #m within the stroma. The energy output of the Nd:YLF laser is calibrated before and periodically through- out testing to ensure energy stability using a Field Master energy meter (Coherent Inc., Palo Alto, CA).
P i c o s e c o n d Laser K e r a t o m i l e u s i s P r o c e d u r e
The intrastromal PLK procedure consists of two lamellar ring cuts and one vertical ring-shape cut that define a 4-mm-diame- ter intrastromal lenticle. The depth of these cuts varies de- pending on the thickness of the desired lenticle. A second ring pattern connects the lenticle to the corneal surface along an arc that can be varied from 45 ° to 360 °, defining a parallel-faced corneal flap that is not open to the surface. The flap is open to the surface through a 45 ° to 90 ° manual microblade incision. Blunt dissection with a 0.5-mm lens spatula is performed from the surface to allow access to the lenticle, which finally is re- moved from the stroma with a micro forceps (Fig 1).
S t u d y P r o t o c o l
Twelve short-hair, adult, male cats weighing 5 to 6 kg originally were involved in this study. The cats were divided randomly into three groups: group 1 underwent laser photodisruption in the right eye programmed for a 100-,urn thick lenticle, but the lenticle was not removed (sham operation); group 2 underwent PLK in the right eye with the removal of a 100-/,zm thick len- ticle; and group 3 underwent PLK in the right eye with the removal of a 150-#m thick lenticle. The left eye of each cat was used as a control. Because of nonsurgical-related infections, two cats were removed from the study within 1 month of incep- tion. All previous data from these cats were omitted from the study. To accommodate for the loss, two cats already involved in the study were selected randomly to receive the PLK proce- dure in the left eye (one was included in group 1 and the other in group 3). In summary, the study was comprised of 10 cats in which a total of 12 eyes were included in the surgical groups and 8 eyes were regarded as control specimens. The cats were anesthetized with intramuscular ketamine (10 mg/kg) and xylaz- ine (0.5 mg/kg). Topical tetracaine was instilled in the conjunc- tiva before every surgical and measurement procedure. Before surgery, bilateral topography (Model TMS-I; Tomey Technol- ogy, Cambridge, MA), ultrasonic pachymetry (Model Pachette; DGH Technology, Inc., Exton, PAL tonometry (Model Tono- PenXL; Mentor O&O, Inc., Norwel, MA), and biomicroscopy examinations were performed.
For corneal topography, the anesthetized cats were positioned prone on an adjustable table. The body and head of the cat were supported by two assistants to align the eye to be examined with the topography light cone. The eye was maintained open with gentle, manual traction of the eyelids from the frontal bone. The investigator operating the topography centered the pupil in the real-time video- keratoscope image. Alignment was checked by observing the limbus at the 12-, 3-, 6-, and 9-o'clock positions.
The laser PLK procedure was performed with the Model 4000 motor-driven operating microscope delivery system of the Nd:YLF laser. It consists of an applanating cone containing a convex-concave quartz contact lens with a posterior curvature of 7.8 mm that applanates the cornea. Then, the pupil is cen- tered, sighting through the operating microscope. To align the central cornea with the cone's lens, the cats were positioned supine on a molded vacuum pillow and the heads were stabi- lized. Fixation of the globe was obtained with two 5 - 0 silk sutures placed at the 12- and 6-o'clock positions in the episclera 2 to 3 mm from the limbus. The laser parameters were the same for each study group with the exception of the depth of the initial lamellar disk, which varied depending on the thickness of the lenticle desired. For the 100-#m and 150-,urn lenticle, it was placed at 300 #m and 350 #m depth, respectively, in the central cornea. Complete parameters are shown in Figure 1.
After the laser pattern was completed, the cats were placed under a surgical microscope, the lenticle was removed as de- scribed previously, and the eye was bandaged with a collagen corneal shield (Bio-Cor; Bausch and Lomb, Rochester, NY). Postoperative medications consisted of tobramycin 0.3% solu- tion (Tobrex; Alcon, Ft. Worth, TX) three times per day in both eyes for 1 week after treatment. A randomly selected group of four cats (two from group 2 and two from group 3) received 1% prednisolone acetate (Pred-Forte; Allergan Pharmaceutical, Irvine, CA) three times per day in the treated eye for 2 weeks.
After surgery, corneal topography, ultrasonic pachymetry, tonometry, and slit-lamp biomicroscopy were performed at 1, 3, and 6 months, in all groups. The refractive effect of treatment was measured comparing the preoperative and postoperative topographic map with the same absolute color scale obtained
143
Ophthalmology Volume 105, Number I, January 1998
A
Surface of Comea
,n Outer Diameter 5mm m I 7
1 . . . . . . . . . . . . . 7 . . . . . . .
Stroma !°Lenticle Diameter 4mm ~
Pattem: Lens Lenticule thickness: 100/1501am
Energy: 301~1. Offset: 300/3501xm
Spot Sep: 30Otto Lenticule diameter: 4ram
Rep.Rate: 1000Hz Outer diameter:, 5mm
Total Pattern Time: 150 seconds
B
C
D x.
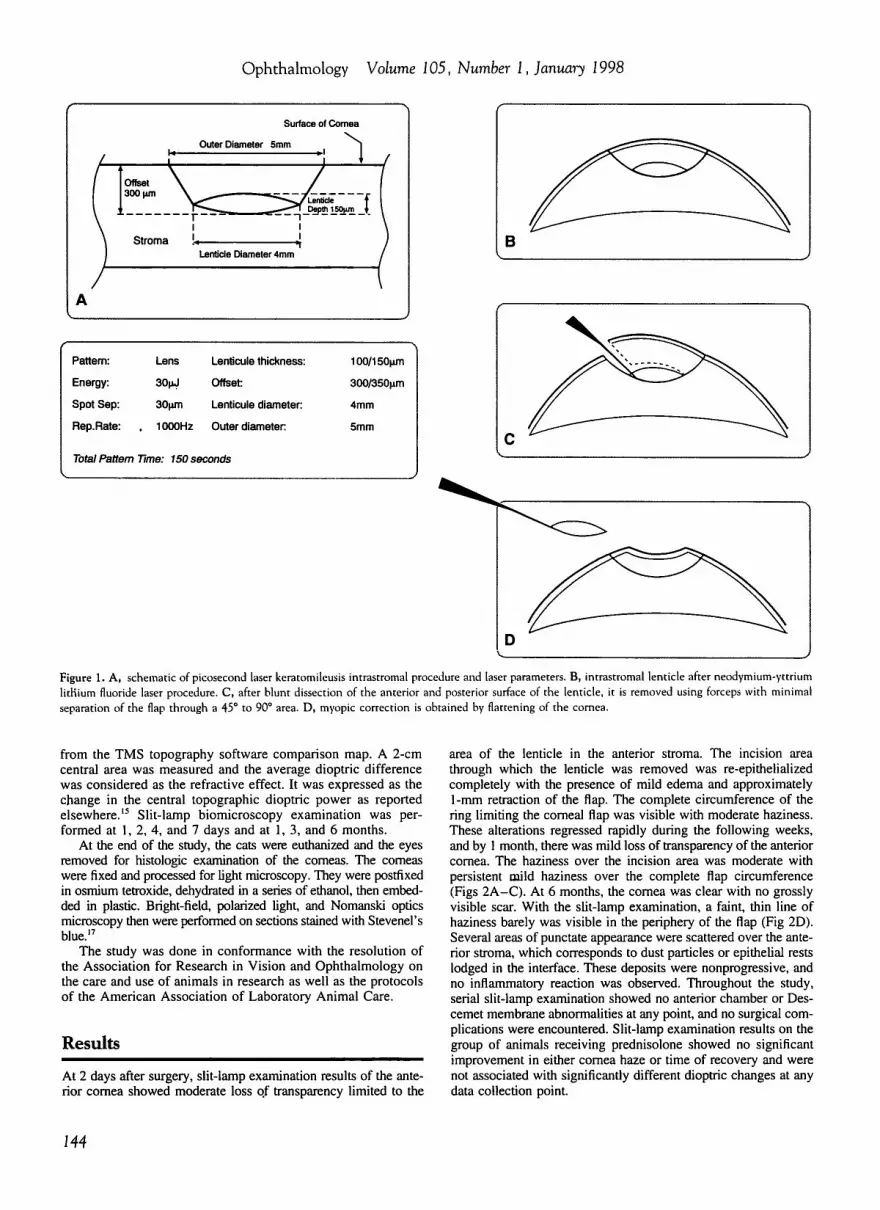
Figure 1. A, schematic of picosecond laser keratomileusis intrastromal procedure and laser parameters. B, intrastromal lenticle after neodymium-yttrium lidlium fluoride laser procedure. C, after blunt dissection of the anterior and posterior surface of the lenticle, it is removed using forceps with minimal separation of the flap through a 45 ° to 90 ° area. D, myopic correction is obtained by flattening of the cornea.
from the TMS topography software comparison map. A 2-cm central area was measured and the average dioptric difference was considered as the refractive effect. It was expressed as the change in the central topographic dioptric power as reported elsewhere, t5 Slit-lamp biomicroscopy examination was per- formed at 1, 2, 4, and 7 days and at 1, 3, and 6 months.
At the end of the study, the cats were euthanized and the eyes removed for histologic examination of the corneas. The comeas were fixed and processed for light microscopy. They were postfixed in osmium tetroxide, dehydrated in a series of ethanol, then embed- ded in plastic. Bright-field, polarized light, and Nomanski optics microscopy then were performed on sections stained with Stevenel's blue? 7
The study was done in conformance with the resolution of the Association for Research in Vision and Ophthalmology on the care and use of animals in research as well as the protocols of the American Association of Laboratory Animal Care.
Results
At 2 days after surgery, slit-lamp examination results of the ante- rior cornea showed moderate loss o.f transparency limited to the
area of the lenticle in the anterior stroma. The incision area through which the lenticle was removed was re-epithelialized completely with the presence of mild edema and approximately l -mm retraction of the flap. The complete circumference of the ring limiting the corneal flap was visible with moderate haziness. These alterations regressed rapidly during the following weeks, and by 1 month, there was mild loss of transparency of the anterior comea. The haziness over the incision area was moderate with persistent mild haziness over the complete flap circumference (Figs 2A-C) . At 6 months, the cornea was clear with no grossly visible scar. With the slit-lamp examination, a faint, thin line of haziness barely was visible in the periphery of the flap (Fig 2D). Several areas of punctate appearance were scattered over the ante- rior stroma, which corresponds to dust particles or epithelial rests lodged in the interface. These deposits were nonprogressive, and no inflammatory reaction was observed. Throughout the study, serial slit-lamp examination showed no anterior chamber or Des- cemet membrane abnormalities at any point, and no surgical com- plications were encountered. Slit-lamp examination results on the group of animals receiving prednisolone showed no significant improvement in either cornea haze or time of recovery and were not associated with significantly different dioptric changes at any data collection point.
144

H a n u c h et al • Picosecond Laser Keratomileusis
~ PRTIEN1: 008 , GE CLINIC~: S. ~
-lO. SO -9,40 -e .30 -7. =*'0 -~,~. I 0 -6.00 -1~0 -; m m
s . o o ~ ~o~,~ I z .a z~;=-z
8: .~ ] 4.1
40.~ ¢..0
~;,.~, I;,.~ lel 4/..o ;'.3 44.5 I ?.6 4~0 I 7.g 0 ~
4O.0 ~4
=~J.O
14.0 24.1 O.o I~t%s
GENESEE VRLLEY S$#:
-- B (Difference) r~ ,~:=
H ] I E S C a p e k e g J o r ~ l e r n I l e n u .
~ ~RTIENT: 002, GENESEE VRLLEY ;LINIC#: SS#:
IGI.5 ~-3 Z#~3-1 ~SOOTH -
m . 5 3 . ; ,
~ . D 4 . ! z ~ g 4.4 ~ . w 4 .7
{$ .1 L 5 ~ s ~ O
IO.0 ~ 9
43-0 ;'.8 I b m
~ L e
:;:O. o t l . 6
14.0 ~ . l
Figure 2. Biomicroscopic pictures of cat cornea after picosecond laser kemtomileusis procedure. A, 2 days after surgery. Note the anterior stromal haze over the flap area with increase density over the incision area (arrow). The double line (arrowhead) depicts the flap (outer) and lenticle (inner) laser incision. B, 1 month after surgery. The haze over the whole flap area persists. C, 3 months after surgery. Note resolution of the anterior stromal haze over the flap area with persistence of peripheral ring. D, at 6 months after surgery, a barely perceptible ring of haze is seen with maximal slit-lamp illumination.
Figure 3. Topographic changes in the cat cornea after picosecond laser keratomileusis procedure. Difference map showing changes between preoperative and postoperative examinations in group 2 (100 ~*m), left, and group 3 (150/~m), right. Preoperative picture (B) is subtracted from the postoperative picture (A) comparing both examinations with an absolute color scale (left scale). The difference map displays a normalized color scale (top scale).
145

Ophthalmology Volume 105, Number I, January 1998
Table 1. Picosecond Laser Keratomileusis Topographic and Pachymetric Results
Group No. of Eyes Time CTDP (D) CTDP (difference) Pachymetry (/*m)
1 (sham) 3 Preoperative 40.0 _+ 0.0 NA 603 + 14.0 3 1 mo 38.7 + 1.0 -1.35 _+ 1.0 595 -+ 57.4 3 3 mos 40.0 + 1.3 -1.00 + 0.4 580 + 30.0 1 6 mos 37.5 - 0.0 -2.50 + 0.0 615 + 0.00
2 (100/zra) 4 Preoperative 42.3 -+ 1.2 NA 617 + 2.60 4 1 mo 36.5 -+ 2.0 -5.18 -+ 3.5 569 - 15.1 4 3 raos 37.6 +- 2.5 -5.25 + 2.5 606 -+ 46.9 4 6 mos 36.7 + 2.4 -5.38 -+ 1.3 568 + 38.8
3 (150 ~,n) 5 Preoperative 42.1 - 2.0 NA 596 -+ 49.3 5 1 mo 33.8 -+ 1.7 -8.2 +- 0.4 520 + 55.3 5 3 mos 34.7 + 2.9 -7.3 + 1.4 566 + 39.6 4 6 mos 35.9 - 2.0 -6.8 +- 1.5 566 +- 43.8
CTDP = central topographic dioptric power; NA = not applicable.
The analysis of the topographic changes at 1,3, and 6 months after surgery is presented in Table 1. Group 1 (sham operation) did not show significant diopter change compared with that of control eyes at any timepoint. For group 2, the mean (__+standard deviation) diopter change was 5.4 __. 3.2 diopters at 1 month and remained stable during the 6-month period. For group 3, the mean (__.standard deviation) diopter change was 8.1 ___ 0.22 diopters at 1 month. At 6 months, the mean (___standard devia- tion) diopter change was 6.8 +- 1.5 diopters. One of the eyes in this group underwent a 3-diopter regression of refractive effect at 6 months. The other eyes remained stable. Figure 3 shows preoperative and postoperative topographic map changes for corneas of groups 2 and 3.
Pachymetry and tonometry results were evaluated using the Student's t test for paired data. For pachymetry (Table 1), group 1 showe~l no significant difference in the thickness of the cornea at any timepoint (P >0.05). Both groups 2 and 3 showed sig- nificant changes in the thickness of the cornea at the 1-month postoperative evaluation (P <0.05). By 3 months, both groups regressed to near-preoperative values.
The tonometric measurements did not show significant changes over the course of the study in any group (P >0.05), as listed in Table 2. No significant change in the central corneal thickness or topographic dioptric power was noted in the control eyes at any timepoint during the study (Table 3).
The histologic analysis of the corneas with bright-field, po- larized light, and Nomanski optics microscopy at 6 months after s'urgery showed no. significant collagen disruption, inflamma- tion, or endothelial irregularities comparing the control with the postoperative corneas (Fig 4).
Discuss ion
The potential of using a laser "sca lpe l" for ocular micro- surgery to achieve tissue dissection rather than tissue dis-
ruption has been contemplated heavily. This currently is possible with the use of picosecond optical breakdown with generation of small amounts of plasma by a laser pulse energy as low as 15/.tJ. ~8 Because the damage range increases with the cube root of the laser pulse energy, the use of low energy implies the subsequent reduction of the disruptive side effects when compared with that of the nanosecond lasers. 4'7 A high degree of picosecond laser spatial confinement has been shown with the re- moval of single cell lines, ~9 and animal experiments with intrastromal ablation refractive surgery have proved promising, t5 However, previous attempts to produce re- fractive changes with a pure intrastromal ablation in hu- mans have produced variable results. 2° With PLK, we showed the possibility of changing the refractive power of the cornea by selectively removing a lenticle created intrastromally with the picosecond laser with a technique analogous to keratomileusis. We applied principles used in keratomileusis and photorefractive keratectomy to cal- culate the thickness and diameter of the removed lenticle to obtain different refractive correct ions] ~'= In PLK, only a small area of the laser demarcated flap is dissected through the epithelium with the lenticle removed through the opening. This limits the wound-heal ing process to a small area of the epithelium, usually 45 ° to 90 ° . Although we were able to remove the lenticle in one piece in eight of ten eyes, the procedure was moderately difficult, and a great deal of blunt dissection was needed to release the lenticle. This was especially noted on dissection of the anterior surface of the lenticle, that is, the second layer (disk) ablated by the laser. We consider that this difficulty is related to irregularities in the ablation, possibly related to the effect of cavitation bubble accumulation. When the
Table 2. Intraocular Pressure (mmHg)
Group Preoperative 1 mo 3 mos 6 mos
1 (sham) 13.0 -+ 2.0 18.0 -+ 3.0 20.0 -+ 2.0 16.0 -+ 0.0 2 (100 #m) 14.0 -+ 1.2 23.0 -+ 6.0 16.0 +_ 2.0 19.0 +- 4.0 3 (150 #m) 16.0 -+ 2.0 21.0 -+ 4.0 17.0 -+ 1.3 18.0 -+ 5.0
146

Hanuch et al • Picosecond Laser Keratomileusis
Table 3. Picosecond Laser Keratomileusis Topographic and Pachymetric Results of Control Group
No. of Eyes Time CTDP CTDP (difference) Pachymetry (/xm)
8 Preoperative 40.7 -+ 1.9 NA 612.2 + 36.5 8 1 mo 41.0 -+ 1.9 0.79 + 0.82 628.0 +- 33.1 8 3 mos 40.9 + 1.8 0.56 -+ 0.34 617.0 + 47.1 8 6 mos 41.0 -+ 2.5 0.47 +- 1.10 610.0 -+ 39.2
CTDP = central topographic dioptric power; NA = not applicable.
laser pulse hits inside an existing cavitation, it does not remove tissue but increases the size of the cavitation through heat transfer to the gas. 2° To avoid this, the next pulse must hit the tissue outside the bubble. Therefore, in an optimum case, the ratio of the cavitation diameter at the moment of the arrival of the next pulse to the plasma diameter should approach unity. 23'24 Conse- quently, moderate pulse energies must be used to generate small cavitation, coupled with optimum spot separation to avoid overlapping. 25 Failure to find optimal parameters may lead to cavitation bubble accumulation and inade- quate photodisruption. Currently, studies are being con- ducted for the development of femtosecond laser pulses. These are pulses 1000 times shorter than the picosecond pulses, allowing for plasma formation at even lower ener- gies with significant reduction of the cavitation effect.
Another difficulty is the length and precise placement of the different ablations that configure the lenticle. It takes 150,000 laser pulses to complete the pattern. At 1- kHz repetition rate, it represents 150 seconds of laser exposure. These factors make the procedure extremely
vulnerable to unwanted movements. The delivery system of the laser has been improved recently, allowing the stabilization of the cornea and eliminating the need for a tracking system. However, improvement of the applana- tion system and limbal suction together with stabilization of the laser system to allow the use of 2-kHz repetition rate to decrease procedure time would reduce these com- plications significantly.
The average corrections obtained were moderate but consistent in each group. For group 2, the average was 5.25 __. 2.5 diopters at 3 months. For group 3, the average was 7.35 _ 1.43 diopters at 3 months. The method of analyzing the diopter difference (central topographic di- optric power) reflects the average change of the whole area and not the area of maximum change. Note that the diopter change was irregular over the treatment area, with well-localized zones of flattening of up to -12.25 diop- ters, as measured by the difference map absolute scale (Fig 3). Nevertheless, these corrections are below that expected for keratomileusis, considering the thickness of the lenticle removed. Several reasons can explain this
t~_{ ~.': =:: ~. ,: : / ; ~ : : " " . ;';~:: ~ " , " , " . ~ - . ' ~ } W - * ~ . ~
Figure 4. Bright-field micros- copy of control (left) and group 2 (right) corneas. The typical collagen arrangement and kera- tocytes are seen in the control cornea. The group 3 cornea shows no inflammatory cells or significant disruption of the col- lagen structure. The vertical compression lines (arrowheads) in the stromal tissue most likely represent dehydration during the processing procedure (origi- nal magnification, x66; stain, toluidine blue).
147

Ophthalmology Volume 105, Number I, January 1998
surgical undercorrection. First, the animal model chosen has its limitations. Even though the curvature and diame- ter of the cat cornea are similar to those of the human cornea, there are significant differences in the thickness of Bowman membrane. In cats, it is 0 to 4 ~zm compared to 12 /zm in humans? 5 The influence of this difference in the effect of flattening needs further investigation. Also related with the animal model is the fact that we could not apply the previously tested PLK laser settings used in human donor eyes and in European studies with blind human eyes because they were ineffective in our animal model. The laser settings used were significantly different. The different collagen composition of the cat cornea may account for the technical difficulties encountered. Com- parative studies between human and cat cornea threshold energies for plasma formation using the Nd:YLF are needed, and the laser parameters and the energies and spot separation used in o.ur study may need further adjustment, specifically for the cat cornea. Second, the topographies of the cat cornea are difficult to obtain because of anatomic differences (e'.g., the long snout limits the centration of the eye). Furthermore, because the extreme accuracy of the TMS requires consistent image quality, the optics, video gain, and image-processing parameters are all cali- brated in the human cornea surface reflectance image and not in that of the cat. This leads to irregularities in the topographic maps and difficulties in the interpretation. Third, there is a lack of one-to-one relationship between change in corneal curvature and change in refractive error, which has been noted in radial keratotomy and orthokera- tology. 26.27
The absence of significant diopter change in the control and sham operation group suggests that the effect is caused mainly by the thickness of the lenticle removed and is not influenced substantially by maturation factors or wound heal- ing: Furthermore, there was no significant difference in the group treated with topical steroids for 2 weeks.
Regression of the corneal thickness measured by pachyme- try to the preoperative values was noted at 2 months. This was coincident with regression of subepithelial haziness but was not accompanied by diopter power regression. Remodel- ing of the stroma to preoperative appearance, as noted in the histologic analysis, seems to account for these changes. The absence of damage to the endothelium and anterior chamber corroborates previous observations about the safety of the picosecond laser when used at a distance of more than 150/zm from the endothelium.15'19"28 Nevertheless, with the prolonged exposure in our study, endothelial damage might explain the return to normal corneal thickness measured in all groups without regression of refractive changes. Further studies, per- haps with serial specular microscopy, are necessary to con- template this possibility. Our results, although encouraging, indicate the need for further studies to confirm the efficacy of PLK as a valid refractive procedure.
References
1. Remmel RM, Dardenne CM, Bille JF. Intrastromal tissue removal using an infrared picosecond Nd:YLF ophthalmic
laser operating at 1053 nm. Lasers and Light in Ophthal- mology 1992;4:169-73.
2. Frueh BE, Bille JF, Brown SI. Intrastromal relaxing exci- sions in rabbits with a picosecond infrared laser. Lasers and Light in Ophthalmology 1992;4:165-8.
3. Fankhauser F, LOrtscher H, Van der Zypen E. Clinical stud- ies on high and low power laser radiation upon some struc- tures of the anterior and posterior segments at the eye. Int Ophthalmol 1982;5:15-32.
4. Vogel A, Schweiger P, Frieser A, et al. Intraocular Nd:YAG laser surgery: light-tissue interaction, damage range, and reduction of collateral effects. Fortschritte der Ophthalmo- Iogie 1990; 87:675-87.
5. Mainster MA, Sliney DH, Belcher CD III, Buzney SM. Laser photodisruptors. Damage mechanisms, instrument design and safety. Ophthalmology 1983;90:973-91.
6. Stern D, Schoenlein RW, Puliafito CA, et al. Corneal abla- tion by nanosecond, picosecond, and femtosecond lasers at 532 and 625 nm. Arch Ophthalmol 1989; 197:587-92.
7. Zysset B, Fujimoto JG, Puliafito CA, et al. Picosecond optical breakdown: tissue effects and reduction of collateral damage. Lasers Surg Med 1989; 9:193-204.
8. Lin CP. Laser-tissue interactions: basic principles. Ophthal- mology Clinics at North America 1993;6:381-91.
9. Stern D, Puliafito CA, Dobi ET, Reidy WT. Infrared laser surgery of the comea. Studies with a Raman-shifted neo- dymium:YAG laser at 2.80 and 2.92 micron. Ophthalmol- ogy 1988;95:1434-41.
10. Barraquer JI. Keratomileusis for the correction of myopia. Ann Inst Barraquer 1964;5:209-29.
11. Slade SG, Updegraff SA. Advances in lamellar refractive surgery. Int Ophthalmol Clin 1994;34:147-62.
12. American Academy at Ophthalmology. Keratophakia and keratomileusis: safety and effectiveness. Ophthalmology 1992; 99:1332-41.
13. DelPero RA, Gigstad JE, Roberts AD, et al. A refractive and histopathologic study of excimer laser keratectomy in primates. Am J Ophthalmol 1990; 109:419-29.
14. Tuft SJ, Zabel RW, Marshall J. Corneal repair following keratectomy. A comparison between conventional surgery and laser photoablation. Invest Ophthalmol Vis Sci 1989; 30:1769- 77.
15. Habib MS, Speaker MG, Kaiser R, Juhasz T. Myopic intras- tromal photorefractive keratectomy with the neodymium- yttrium lithium fluoride picosecond laser in the cat cornea. Arch Ophthalmol 1995; 113:499-505.
16. Climenhaga H, Macdonald JM, McCarey BE, Waring GO III. Effect of diameter and depth on the response to solid polysulfone intracorneal lenses in cats. Arch Ophthalmol 1988; 106:818-24.
17. del Cerro M, Cogen J, del Cerro C. Stevenel's Blue, an excellerrt stain for optical microscopical study of plastic embedded tissues. Microsc Acta 1980;83:117-21.
18. Vogel A, Busch S, Jungnickel K, Birngruber R. Mecha- nisms of intraocular photodisruption with picosecond and nanosecond laser pulses. Lasers Surg Med 1994; 15:32-43.
19. Vogel A, Capon MR, Asiyo-Vogel MN, Birngruber R. Intraocular photodisruption with picosecond and nanosec- ond laser pulses: tissue effects in cornea, lens, and retina. Invest Ophthalmol Vis Sci 1994;35:3032-44.
20. Gimbel HV, Willerscheidt AB, Beldays RA. Nd:YLF abla- tion of epikeratophakia lenticules: early case results. Euro- pean Journal at Implant and Refractive Surgery 1994;6:64- 73.
21. Pureskin N. Weakening ocular refraction by means of par-
148

H a n u c h et al • Picosecond Laser Keratomileusis
tial stromectomy of cornea under experimental conditions. Vesmik Oftalmologii 1967; 80: I.
22. Munnerlyn CR, Koons S J, Marshall JM. Photorefractive keratectomy: a technique for laser refractive surgery. J Cat- aract Refractive Surg 1988; 14:46-52.
23. Juhasz T, Hu XH, Turi L, et al. Dynamics of shock waves and cavitation bubbles generated by picosecond laser pulses in corneal tissue and water. Lasers Surg Med 1994; 15:91- 8.
24. Niemz, Klancnik E, Bille JF. Plasma-mediated ablation of corneal tissue at 1053 nm using a Nd:YLF oscillator/regen- erative amplifier laser. Lasers Surg Med 1991;11:426-31.
25. Fujimoto JG, Lin WZ, lppen EP, et al. Time-resolved stud-
26.
27.
28.
ies of Nd:YAG laser-induced breakdown. Plasma forma- tion, acoustic wave generation and cavitation. Invest Oph- thalmol Vis Sci 1985;26:1771-7. Binder PS, May CH, Grant SC. An evaluation of orthokera- tology. Ophthalmology 1980;87:729-44. Arrowsmith PN, Sanders DR, Marks RG. Visual, refractive, and keratometric results of radial keratotomy. Arch Oph- thalmol 1983; 101:873-81. Habib MS, Speaker MG, McCormick SA, Kaiser R. Wound healing following intrastromal phot0refractive keratectomy with the Nd:YLF picosecond laser in the cat. J Refract Surg 1995; 11:442-7.
MEMORANDUM
To: Time-limited Certificate Renewal Diplomates From: Denis M. O'Day, MD, Executive Director Date: September 1997 Re: Certificate Renewal Process Update
As the implementation of Time-limited Certificate Renewal draws near and the pathways become more defined, we are now able to provide you with more information concerning the renewal process. We hope the following information will help in keeping you informed.
Annual Assessment Fee/Certificate Renewal F e e - - A n annual $I00 assessment fee request form for all 1992 through 1995 Time-limited Certificate holders may be requested from the ABO office. This assessment fee is used to support the development and implementation of the entire certificate renewal process and will apply toward the $1000 Certificate Renewal fee. The annual fee is first assessed for the year following your certification and is collected in all subsequent years until you make application, at which time the balance of the $1000 Certificate Renewal fee is due.
T i m e f r a m e - - T h e Knowledge and Practice Assessment components for Certificate Renewal are designed to be completed within a 2-year period. Three years prior to the expiration of a certificate, candidates will be notified that they may make application. Even though the first ~oup of 1992 Time-limited Certificate holders does not need to make application until the January 1 through June 1, 2000 filing period, applications may be made beginning in January 1998.
App l i ca t i on - -The application filing period runs from January through June 1 ~' each year. All eligible Time-limited Certificate Renewal holders will be notified when it is appropriate to make application. Please keep the Board office informed of your current address so you will be assured of receiving all ABO updates and mailings. Ultimately, it is the Diplomate's responsi- bility to obtain an application. Submitting your application indicates that you are ready to initiate the Knowledge and Practice Pathway Examinations.
C M E - - T h o s e Diplomates wishing certificate renewal are to attain 500 Continuing Medical Education (CME) credits from an Accreditation Council for Continuing Medical Education (ACCME) approved institution. At least 60% of these hours should be in Category I, and 40% may be from Category II. It is recommended that you have an average of 50 CME hours per year. A (CME) tracking form will be enclosed with applications for you to itemize category, name of the course, sponsor, location and dates. It will not be necessary to submit certificates of CME attendance when you make application.
L i c e n s u r e - - T h e Board requires that a valid and unrestricted license to practice medicine in the United States, its territories or Canada be held during the entire Certificate Renewal process. A copy of this registration to practice medicine is to be submitted with your application.
Knowledge and Practice Assessments--Registrat ion forms for both the Knowledge and Practice Assessments will be enclosed with the application approval letter. With submission of your application, you will be ~lsked to select one of the three Knowledge Assessment pathways in which to be examined. The Knowledge Assessments are offered once a year. The Practice Assessment is offered twice yearly.
149





























