Embed Size (px)
Citation preview
ii | Page NPHCDA/2019 ANNUAL REPORT
NATIONAL PRIMARY HEALTH
CARE DEVELOPMENT AGENCY
2019 ANNUAL PROGRAMME REPORT
COVER PAGE
iii | Page NPHCDA/2019 ANNUAL REPORT
2019
PROGRAMME ANNUAL REPORT
COMPILED
BY
DEPARTMENT OF PLANNING, RESEARCH &STATISTICS
JANUARY, 2020
NATIONAL PRIMARY HEALTH
CARE DEVELOPMENT AGENCY

iv | Page NPHCDA/2019 ANNUAL REPORT
ACKNOWLEDGEMENT
The 2019 Annual Report of the National Primary Health Care Development Agency
(NPHCDA) was compiled through a collaborative process involving all departments,
divisions, ED’s office and Six (6) Zonal Offices of the Agency. This Annual Report was
prepared based on the National Strategic Health Development Plan (NSHDP) II Pillars as it
relates to NPHCDA - Enabled Environment For Attainment of Sector Outcomes, Increased
Utilization of Essential Package of Health Care Services, Strengthened Health System for
Delivery of Package of Essential Health Care Services and Predictable Financing and Risk
Protection. The tremendous supports of the Executive Director/Chief Executive Officer of
the Agency, Dr. Faisal Shuaib, all the Directors and the top management staff of the Agency
is highly appreciated. Dr. Abdullahi Bulama Garba, Dr. O. Olayinka, Mr. Remi Joseph, Dr.
Nneka Onwu, Mr. Steven Yusuf, Mr. Yibis Gotar, Hajia Iyabo Daradara, Dr. Joseph Oteri and
the Zonal Directors were also very supportive in the Course of preparing the 2019 Annual
Report of the Agency. The collection, compilation and summary of the Annual Report by the
Heads of Division of Planning, Research and Statistics including Dr. Usman Gana Abdulkadir,
Analyst Dare Jimoh, Mr. Rotimi Oyewole, Mr. Olalekan Runmonkun, and all members of Staff
of the Planning, Research and Statistics Department of the Agency who were part of the
process of developing this Annual Report are highly appreciated. We cannot end this piece
without recognizing and appreciating the role of Mrs. Maureen Gopep, Mr. Philip Tanko, Mr.
Mohammed Kamal Rabiu, Dr. Aliyu Muhammad Sabiu, Mrs. Juliet Amuche and Susan Magaji
who are members of the Policy, Planning and Partnership Coordination Division of PRS, and
all other staff of the PRS Department who were involved throughout the process of
developing and finalizing this Annual Report. I must sincerely commend the efforts of the
Clean Up and Finalization Team (Dr. Usman Gana Abdulkadir, Analyst Dare Jimoh, Mr. Rotimi
Oyewole, Mr. Olalekan Runmonkun, Mrs. Maureen Gopep, Mr. Philip Tanko, Mr. Mohammed
Kamal Rabiu, Dr. Aliyu Muhammad Sabiu and Mrs. Juliet Amuche) who worked tireless to
see that this report is ready and on time. Finally, the NPHCDA is profoundly grateful to all
those, too numerous to mention, who contributed to the laudable achievements recorded in
the past year and pray that the Almighty God will Bless and Reward all for their efforts.
Dr. Abdullahi Bulama Garba
Ag. Director Planning Research and Statistics. NPHCDA, Abuja
v | Page NPHCDA/2019 ANNUAL REPORT
Table of Contents NATIONAL PRIMARY HEALTHCARE DEVELOPMENT
AGENCY ................................................................................................................................. ii
NATIONAL PRIMARY HEALTH CARE DEVELOPMENT
AGENCY ................................................................................................................................ iii
ACKNOWLEDGEMENT ......................................................................................................... iv
Table of Contents ...................................................................................................... v
ACRONYMS .......................................................................................................................... x
Our Purpose ....................................................................................................................... xiii
Our Vision ........................................................................................................................... xiv
Mission Statement............................................................................................................... xv
Our Mandate ...................................................................................................................... xvi
Our Motto ......................................................................................................................... xvii
EXECUTIVE SUMMARY...................................................................................................... xviii
INTRODUCTION ............................................................... 1
1.0 INTRODUCTION ............................................................................................................... 2
1.1 OPERATIONAL AND FINANCIAL REPORTS ........................................................................ 3
OPERATIONAL REPORTS ............................................... 4
2.0 ENABLED ENVIRONMENT FOR ATTAINMENT OF
SECTOR OUTCOMES ........................................................ 5
2.1 Leadership & Governance ................................................................................................ 6
2.1.1 Governing Board Meetings .......................................................................................................... 6
2.1.2 Executive Secretaries SPHCBs Quarterly Review Meetings with Executive Director of
NPHCDA ................................................................................................................................................ 6
2.1.3 Technical Assistance Delivery and Leadership Development Academy (LDA) ........................ 7
2.1.4 62nd National Council on Health (NCH) Meeting in Asaba, Delta State .................................. 10
vi | Page NPHCDA/2019 ANNUAL REPORT
2.1.5 Staff Retreat/Succession Planning Workshop .......................................................................... 11
2.1.6 Programmes Implementation Monitoring and Compliance Committee (PIMCC) ................. 11
2.2 Partnership for Health................................................................................................... 13
2.2.1 Engagement with Partners ........................................................................................................ 13
2.2.2 2019 Seattle Declaration ............................................................................................................ 13
2.3 Health Promotion and Social Determinants of Health (Environmental Health) ............. 13
2.3.1 Supplemental Immunization Activities For Polio Eradication ................................................. 13
2.3.2 Routine Immunizations ............................................................................................................. 16
2.3.3 Nigeria Immunization Technical Advisory Group (NGI-TAG)................................................... 22
2.3.4.Other Disease Control Activities .............................................................................................. 26
2.4 Strengthening Primary Health Care Services and Service Delivery ............................... 36
2.4.1 Standard Guidelines for PHC Practice in Nigeria ...................................................................... 36
2.4.2 National Primary Health Care Under One Roof (PHCUOR) Scorecard 5 Assessment in 36
States and FCT. ................................................................................................................................... 36
2.4.3 NSHIP/Additional Funding States (AF States) ......................................................................... 39
2.4.4 Conduct of First Lots Quality Assessment Survey (LQAs) for Ondo State; by World Health
Organization ....................................................................................................................................... 39
2.5 Community Participation .............................................................................................. 41
2.5.1 Northern Traditional Leaders Committee (NTLC) on Primary Health Care Delivery Meetings
............................................................................................................................................................ 41
2.5.2 Orientation training of State Health Educators on Communication for VDPV2 .................... 41
2.5.3 CHIPS Programme Retreat ....................................................................................................... 42
3.0 INCREASED UTILIZATION OF ESSENTIAL PACKAGE
OF HEALTH CARE SERVICES .......................................... 45
3.1 Reproductive, Maternal, Newborn, Child, Adolescent Health Services & Nutrition .... 46
3.1.1 National Emergency Maternal and Child Health Intervention Center (NEMCHIC) ................. 46
3.1.2 First Consultative Retreat .......................................................................................................... 47
3.1.3 Categorization of States ............................................................................................................ 48
3.1.4 First State engagement (Bauchi and Kebbi) ............................................................................ 48
4.0 STRENGTHENED HEALTH SYSTEM FOR DELIVERY
OF PACKAGE OF ESSENTIAL HEALTH CARE SERVICES 54
vii | Page NPHCDA/2019 ANNUAL REPORT
4.1 Human Resources for Health ......................................................................................... 55
4.1.1 Staff Recruitment and Training ................................................................................................. 55
4.1.2 Ongoing/Outstanding Activities for the Year: .......................................................................... 55
4.1.3 N-Power Health Initiative .......................................................................................................... 55
4.2 Health Infrastructure .................................................................................................... 55
4.2.1 Health Facility Assessment for the Southern States ............................................................... 55
4.2.2 2019 Conditional Assessment/Survey for Project under the 2018 Appropriation .................. 57
4.2.3 Health Facility Dashboard ......................................................................................................... 57
4.2.4 Renovation of HQ, Annex, Zonal and State Offices ................................................................ 58
4.2.5 Upgrade of NPHCDA Internet Facilities ................................................................................... 59
4.2.6 Other achievements: ................................................................................................................ 59
4.3 Medicines, Vaccines and Other Health Technologies and Supplies ............................ 60
4.3.1 State Engagements and 2020 Vaccines States Specific Forecast. .......................................... 60
4.3.2 Vaccine and Related Commodities Physical Stock Count in Nigeria from 10th – 23rd June,
2019 ..................................................................................................................................................... 62
4.3 Research for Health ...................................................................................................... 80
4.3.1 Post Campaign Coverage Surveys (PCCS) ................................................................................ 80
4.3.2 Preston Leadership Associates Survey .................................................................................... 81
4.3.3 International Standard Book Number (ISBN) Workshop ....................................................... 81
4.3.4 Health Management Information Systems ............................................................................. 81
4.3.5 Health Informatics Conference (HELINA Conference) in Botswana. ..................................... 84
5.0 PREDICTABLE FINANCING AND RISK PROTECTION
....................................................................................... 86
5.1 Health Financing ........................................................................................................ 87
5.1.1The Basic Health Care Provision Fund (BHCPF) ......................................................................... 87
B. Financial Report ....................................................... 96
B. Financial Report .............................................................................................................. 97
REVENUE: ........................................................................................................................................... 97
EXPENDITURE .................................................................................................................................... 97
viii | Page NPHCDA/2019 ANNUAL REPORT
STAFF PRODUCTIVITY AWARDS/SEND FORTH FOR
RETIRED OFFICERS; NPHCDA ANNUAL SPORTS
COMPETITION AND GIVING BACK TO THE COMMUNITY
....................................................................................... 98
7.0 STAFF PRODUCTIVITY AWARDS/SEND FORTH FOR RETIRED OFFICERS; NPHCDA
ANNUAL SPORTS COMPETITION AND GIVING BACK TO THE COMMUNITY ......................... 99
7.1 Staff Productivity Awards and Send Forth for Retired Officers ................................................. 99
7.1.1 NPHCDA Annual Sports Competition ...................................................................................... 100
7.1.2 Giving Back to the Community ................................................................................................ 101
LIST OF FIGURES
Figure 1 Pictures of Executive Secretary Quarterly Review Meeting ........................................................ 6
Figure 2 Flag Off of Technical Support Programme by HMH Prof. Isaac F. Adewole .............................. 9
Figure 3 Distribution of cVDPV2 in Nigeria .................................................. Error! Bookmark not defined.
Figure 4 National Flag-off of Men A Vaccine .......................................................................................... 120
Figure 5 Showing Cholera CFR in States affected .................................................................................... 28
Figure 6 Reported Cholera Cases by Week .............................................................................................. 29
Figure 7 Error! Bookmark not defined. Preliminary Results of 2019 National PHCUOR Scorecard 5 ....... 37
Figure 8 Conferment of CHIPS Champion Award on the Sultan of SokotoError! Bookmark not defined.
41
Figure 9 Scenes of CHIPS agents in Actions ............................................................................................... 44
Figure 10 Declaration of State of Public Concern on MNCH Death by ED, NPHCDA .............................. 46
Figure 11 Categorization of States based on MCH Indices ........................ Error! Bookmark not defined.8
Figure 12 Health Facility Dash Board .......................................................... Error! Bookmark not defined.8
Figure 13 New NPHCDA Looks ................................................................................................................. 519
Figure 14 Map of States that have Graduated to the DHIS2 Platform .................................................... 61
Figure 15 Disbursement of BHCPF Programmatic Funds through NPHCDA Gateway ........................... 92
LIST OF TABLES
Table 1: Status of TA requests from SPHCBS and their Spread across the PHC Building Blocks ............. 8
Table 2: List of Council Memos Presented by NPHVDA at the 62nd NCH in Asaba, Delta State ............. 10
Table 3: Summarizes SIAs Conducted in 2019 .......................................................................................... 14
Table 4: Summarizes cVDPV2 Isolation from different Sources in 2019. ................................................ 15
Table 5: List of Inaugurated NGI-TAG Members ....................................................................................... 23
ix | Page NPHCDA/2019 ANNUAL REPORT
Table 6: Cholera Outbreaks, Year to Date Comparison Between 2018 and 2019 (Nigeria) ................... 29
Table 7: Outcome of the OCV Campaign .................................................................................................. 30
Table 8: Showing National Cholera Hotspots ........................................................................................... 31
Table 9: Results of Round One MNTE Campaigns Conducted from September to December 2019 .... 36
Annexures:
Annex I: Communique from 62nd NCH in Asaba, Delta State………………………………...103
Annex II: 2019 Seattle Declaration…………………………………………………………………….106
x | Page NPHCDA/2019 ANNUAL REPORT
ACRONYMS
ACTU Anti- Corruption and Transparency Unit
AIDSTAR AIDS Support and Technical Assistance Resources
CHESTRAD Centre for Health Sciences Training Research and Development
CHEW Community Health Extension Worker
CHIPS Community Health Influencers and Service
CHP Child Health Packs
CHSD Community Health Services Department
CMD Chief Medical Director
DHIS2 District Health Information System 2
DPT Diphtheria Pertussis Tetanus
DQA Data Quality Assurance
ELSS Expanded Life Saving Skills
ENC Essential Newborn Care
ERC Expert Review Committee
FCT Federal Capital Territory
FMoH Federal Ministry of Health
GAVI Global Alliance for Vaccines and Immunizations
GF HSS Global Fund Health Systems Strengthening
GIS Geographic Information System
HBV Hepatitis B Vaccine
HCWM Healthcare Waste Management
HERFON Health Reform Organization of Nigeria
HF Health Facility
HMIS Health Management Information System
HSS Health Systems Strengthening
IMCI Integrated Management of Childhood Illnesses
IPDs Immunization Plus Days
IPT Intermittent Preventive Therapy
ISS Integrated Supportive Supervision
LERICC Local Government Emergency Routine Immunization Coordination Centre
LGAs Local Government Areas
LLIN Long Lasting Insecticide Treated Nets
LSS Life Saving Skills
MADEX Mobile Application Data Exchange
xi | Page NPHCDA/2019 ANNUAL REPORT
MCH Maternal and Child Health
MCHIP Maternal and Child Health Integrated Programme
MDA Ministries, Departments and Agencies
MDG Millennium Development Goals
M&E Monitoring and Evaluation
MHGAP Mental Health Gap Action Plan
MMCHIT Mobile Maternal Child Health Information Technology
MNCHW Maternal Newborn and Child Health Week
MNTE Maternal Neonatal Tetanus Eradication
MOU Memorandum of Understanding
MSS Midwives Service Scheme
MTSS Mid-Term Sector Strategy
NBS National Bureau of Statistics
NCZ North Central Zone
NERICC National Emergency Routine Immunization Coordination Centre
NEZ North – East Zone
NGO Non – Governmental Organizations
NICS National Immunization Coverage Survey
NPC National Population Commission
NPHCDA National Primary Health Care Development Agency
NPHCDASP National Primary Health Care Development Agency Strategic Development
Plan
NSHDP National Strategic Health Development Plan
NSIPSS Nigeria Strategy for Immunization and PHC Systems Strengthening
NSMWG National Social Mobilization Working Group
NSHIP Nigeria State Health Investment Project
NTLC Northern Traditional Leaders Committee
NWZ North – West Zone
OPV Oral Polio Vaccine
ORT Oral Rehydration Therapy
RBME Results Based Monitoring and Evaluation
PBF Performance Based Financing
PHC Primary Health Care
PLA Participatory Learning Activity
PMTCT Prevention of Mother to Child Transmission
POA Plan of Action
xii | Page NPHCDA/2019 ANNUAL REPORT
PPH Post-Partum Hemorrhage
PPP Public Private Partnership
PRRINN Partnership for Reinforcing Routine Immunization in Northern Nigeria
RBF Results-Based Financing
RI Routine Immunization
RH Reproductive Health
SC State Coordinator
SERICC State Emergency Routine Immunization Coordination Centre
SEZ South – East Zone
SOP Standard Operating Procedure
SSZ South – South Zone
SWZ South – West Zone
TL Traditional Leaders
TOT Training of Trainers
TT Tetanus Toxoid
UNFPA United Nations Population Fund
VAS Vitamin A Supplementation
VPD Vaccine Preventable Diseases
WCBA Women of Child Bearing Age
WDC Ward Development Committee
WFP Ward Focal Person
WHC Ward Health Centre
WMHCP Ward Minimum Health Care Package
WPV Wild Polio Virus
YFV Yellow Fever Vaccine
ZD Zonal Director
ZTOs Zonal Technical Officers
xiii | Page NPHCDA/2019 ANNUAL REPORT
Our Purpose
To Provide Technical directions for the development of
Primary Health Care in Nigeria
xiv | Page NPHCDA/2019 ANNUAL REPORT
Our Vision
To make PHC Services available to all in Nigeria
xv | Page NPHCDA/2019 ANNUAL REPORT
Mission Statement
To Provide Technical and Programmatic Support to States,
LGAs, and other Stakeholders in the Functioning, Planning,
Implementation, Supervision and Monitoring of PHC Services
in Nigeria
xvi | Page NPHCDA/2019 ANNUAL REPORT
Our Mandate
Providing support to the National Health Policy for the development
of Primary Health Care
Providing technical support for planning, management and
implementation of Primary Health Care
Mobilizing resources nationally and internationally for the
development of Primary Health Care
Providing support for monitoring and evaluation of the National
Health Policy
Promoting health manpower development needed for Primary
Health Care through orientation and continuing education
Providing support to the Village Health System by training Village
Health Workers
Promoting Health System Research by promoting and supporting
problem-oriented health system research
Promoting technical collaboration by stimulating Universities, NGOs
and International Agencies
Providing annual reports on the status of Primary Health Care
implementation nationwide
xvii | Page NPHCDA/2019 ANNUAL REPORT
Our Motto
Making Nigerians Healthy
xviii | Page NPHCDA/2019 ANNUAL REPORT
EXECUTIVE SUMMARY
The 2019 Annual Report Summaries all the various activities and innovative initiatives taken
by the NPHCDA in Conjunction with Partners, to Provide needed support to States, LGAs and
Communities in the Country in the delivery of qualitative Primary Health Care Services, as well
as address various Challenges that confronted the Organization.
The report is in line with the National Strategic Health Development Plan (NSHDP) II Pillars as
it relates to NPHCDA.
• Enabled Environment For Attainment of Sector Outcomes
• Increased Utilization of Essential Package of Health Care Services
• Strengthened Health System for Delivery of Package of Essential Health Care Services
• Predictable Financing and Risk Protection
• In the year under review,the Agency introduced an initiative the National Emergency Maternal
and Child Health Intervention Center (NEMCHIC) following the declaration of a State of Public
Health Concern on Maternal and Child Health in Nigeriaon 8th April, 2019.The Center is a
Coordination Platform on Reproductive, Maternal, Neonatal, Child and Adolescent Health +
Nutrition (RMNCAH + N) activities at Primary Health Care (PHC) and Community levels, with
the goal of reducing Preventable Maternal and Child Mortality in Nigeria by 50% in 2021. With
a VISION of a Country where no Woman or Child dies from Preventable causes and a MISSION
to promote awareness and ensure effective Emergency Response to Maternal and Child
Mortality that addresses the Four (4) delays to care through integrated approach.
Polio Eradication Initiative in Nigeria made remarkable Progress in 2019 with no reported case of Wild Polio Virus (WPV) in the Country since 2016. There was an increase in vaccination and Surveillance reach in inaccessible areas in the Northeast especially in Borno and Yobe States. Despite many successes observed in 2019, there were major challenges encountered. One
such challenge was the sporadic outbreaks of circulating Vaccine Derived Polio Virus type 2
(cVDPV2). The country experienced several outbreaks of cVDPV2 and several cases of AFP
cases of cVDPV2 were reported; 18 AFP cases , 59 cases from enviromental samples, and 9
fromhealthy contacts and a total of 21 cVDPV AFP cases reported, 7 from AFP, 4 from Human
contacts and 10 from enviromental samples. In addition to the several outbreak responses
(OBRs, two NIPDs were planned, but the country implemented one due to resource ramp
down and BMGF sponsored one National Sub-immunizations Plus Days (SIPDs) which has
almost same visibility with a National round. Three Sub-national Immunization Plus Days
(SIPDs) were conducted. Sustaining the gains made through Polio Campaigns was also
threatened by potential immunity gaps as revealed by the upsurge in cVDPV2 cases and low
xix | Page NPHCDA/2019 ANNUAL REPORT
coverages based on Community Surveys and Routine Immunization Lot Quality Assurance
Sampling (LQAS) data. As at December, 2019, the Classification in the database, the total no
of AFP cases was (7129), total no discarded (6743), no of cVDPV2 (18), aVDPV2 (7), WPV (0),
not true AFP (122), Pending Classification (234), Compatible case (5), Ready for NPEC review
(7), Pending adequate AFP cases(171),Pending Inadequate cases (63), inadequate AFP <60
days (21), Inadequate AFP 60-90 days 28. There were also challenges of the non-accessibility
with the estimated Children of 34,845 ,000 unreached in Borno State (Abadan and Marte
LGAs), including settlements along some Islands on the Lake Chad Basin. These Challenges
are due to insurgency, insecurity from kidnapping, Communal Clashes, armed banditry, Cattle-
rustling. Also, other States like Benue, Zamfara, Kaduna were affected.
The year 2019 saw a lot of Outbreaks of Measles, Meningitis, Yellow Fever and cVDPV2 but
these were all contained.
The African Regional Certification Commission (ARCC) Verification Team visited Nigeria from
9th to 20th December 2019, where the team reviewed the National complete documentation,
made corrections to the document, and were posted to Six States – Lagos, Oyo, Abia, Edo,
Ebonyi and Delta States to review State, LGA and health facility level documentation for
Polio Certification.
The NERICC Center made a lot of Progress from 4th July 2017 to date as a Coordination Center.
The first activity in 2019 was the Independent Review Committee meeting that was conducted
on the 7th of January 2019.The Critical Success of the meeting was all the 5 Proposals
Presented to the IRC members were approved making it the first time in the history of Gavi
that 5 Proposals were presented by One Country and all the five proposals were approved.
In February 2019, the NERICC team conducted the Joint Reporting form (JRF) and the National
ToT for the PCV Switch from 2 dose vial to 4 dose vial and all the 36 +1 States participated in
the training in March 2019, all the 36+1 States successfully implemented the PCV Switch
implementation and was completed in the second Quarter of 2019.
NERICC also introduced into the Routine Immunization Schedule Meningitis Serotype A in
August 2019 and Successfully trained HCWs on Men A introduction into RI across the 36+1
States, 774 LGAs and 9565 Political Wards. Over 58,700 HCWs’ Capacity was built. National
Flag-off was done on the 9th August 2019 and State level introductions were completed in all
the 36+1 States. Measles Second Dose was introduced in the4th Quarter of 2019.
Also, in the year under Review, a High-Level Mission by the Gavi Delegation Led by the Gavi
CEO took place in Nigeria. After the renewed engagement with 8 Gavi States, the Country,
Partners and Gavi made a Commitment for a high-level engagement meeting at least once in

xx | Page NPHCDA/2019 ANNUAL REPORT
a year and ended their visit with Ceremonial Launch/Flag-Off of the Cold Chain Equipment
Optimization Platform (CCEOP) support from Gavi to Nigeria.
It is said that “All Day Work without Play Makes Jack a Dull Boy” – on this note, the year 2019
ended with a Staff Productivity Award/Send Forth for Retired Officers/Departmental Talent
Show and Annual Sports Competition in December which has been institutionalized since
2018.
1 | Page NPHCDA/2019 ANNUAL REPORT
INTRODUCTION
2 | Page NPHCDA/2019 ANNUAL REPORT
1.0 INTRODUCTION
The National Primary Health Care Development Agency (NPHCDA) is a Parastatal of the
Federal Ministry of Health, established by Decree 29 of 1992 to guide and Sustain the
Implementation of Primary Health Care through Federal assistance to States and Local
Governments in the provision of essential health care particularly at the grassroots where
majority of Nigerian lives. The Agency is to support the States and Local Governments in
developing a sustainable system of PHC services that are accessible, affordable and
acceptable, and of good quality through the participation of individuals, families and
communities in partnership with government and non- governmental organizations.
The Agency is charged with the following statutory responsibilities (Functions):
• To provide support to the National Health Policy through reviews and implementation processes;
• To provide technical support to the planning, management and implementation of primary health care in Nigeria; promoting manpower development;
• To mobilize resources, nationally and internationally, for the development of primary healthcare in Nigeria;
• To provide support to the monitoring and evaluation of the national health policy
• To promote health manpower development;
• To provide support for the village health system;
• To promote health system research;
• To promote technical collaboration with universities, non-governmental organizations, international agencies in support of LGAs
• To promote primary health care through advocacy, conferences/ seminars, case-studies, resource centres and reviews, among others.
• With a Motto of “Making Nigerians Healthy”, the Agency has Seven Goals:
• Control Preventable Diseases
• Improve Access to Basic Health services
• Improve Quality of Care
• Strengthen Community Engagement
• Develop high performing Health Workforce
• Strengthen Partnerships
• Strengthen the Institution.
The development Projects of the Agency are all targeted towards achieving the above goals
and contributing to actualizing the health-related Sustainable Development Goals (SDGs).
3 | Page NPHCDA/2019 ANNUAL REPORT
The Agency’s structure is made up of ten (10) Departments, Six Zonal Offices and the office
of the Executive Director. The Departments are: Planning, Research and Statistics (PRS),
Primary Health Care Systems Development (PHCSD), Community Health Services (CHS),
Disease Control and Immunization, Administration and Human Resources (AHR), Advocacy
and Communication (AC), Logistic and Health Commodities (LHC), Special Duties, Audit,
Finance and Accounts. The Zonal Offices are: North West (Kano), North East (Bauchi), North
Central (Minna), South West (Ibadan), South East (Enugu) and South-South (Benin).
1.1 OPERATIONAL AND FINANCIAL REPORTS
The report will have two components (Operational and Financial Reports) based on the
various activities that were carried out in the Agency in year 2019 and is here presented
according to the Pillars of NSDHP II.
4 | Page NPHCDA/2019 ANNUAL REPORT
OPERATIONAL REPORTS
5 | Page NPHCDA/2019 ANNUAL REPORT
2.0 ENABLED ENVIRONMENT
FOR ATTAINMENT OF SECTOR
OUTCOMES
6 | Page NPHCDA/2019 ANNUAL REPORT
2.1 Leadership & Governance
2.1.1 Governing Board Meetings During the year 2019, emergency and regular Board Meetings took place where issues of the
Agency were discussed and approvals sought. The Governing Board during those meetings
deliberated and made resolutions on Appointment, Promotion & Discipline Matters rand
also received and reviewed Financial Reports.
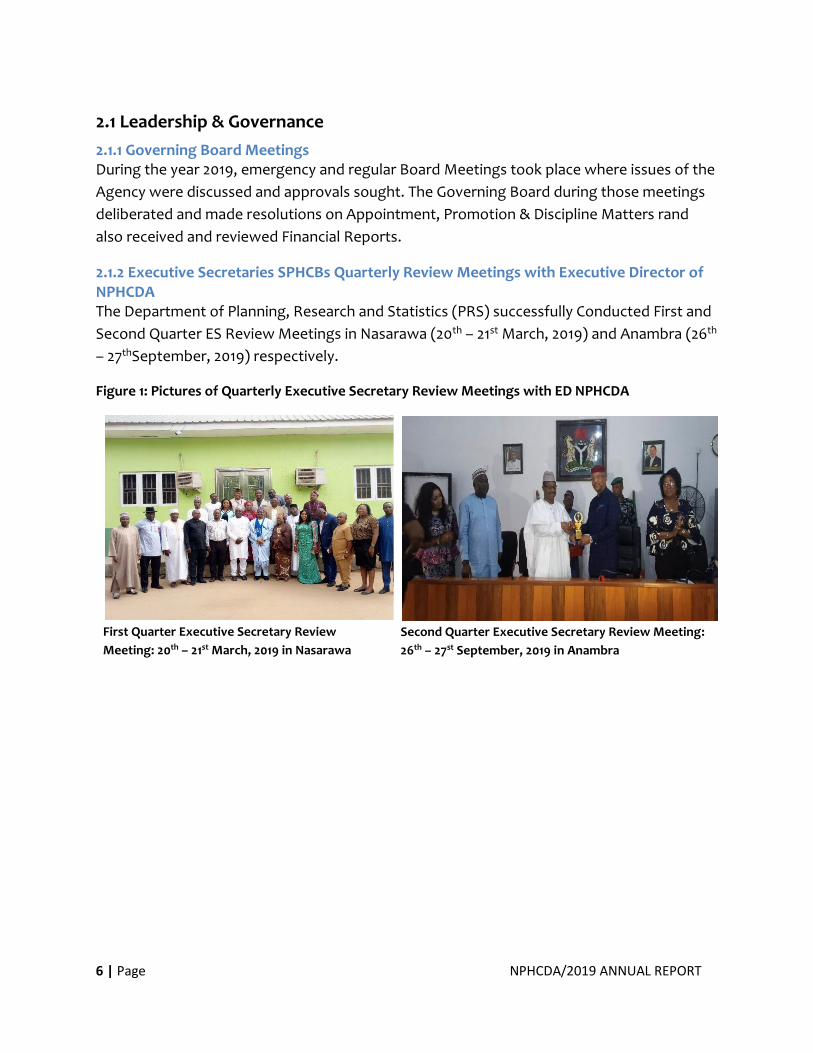
2.1.2 Executive Secretaries SPHCBs Quarterly Review Meetings with Executive Director of NPHCDA The Department of Planning, Research and Statistics (PRS) successfully Conducted First and
Second Quarter ES Review Meetings in Nasarawa (20th – 21st March, 2019) and Anambra (26th
– 27thSeptember, 2019) respectively.
Figure 1: Pictures of Quarterly Executive Secretary Review Meetings with ED NPHCDA
First Quarter Executive Secretary Review
Meeting: 20th – 21st March, 2019 in Nasarawa Second Quarter Executive Secretary Review Meeting:
26th – 27st September, 2019 in Anambra
7 | Page NPHCDA/2019 ANNUAL REPORT
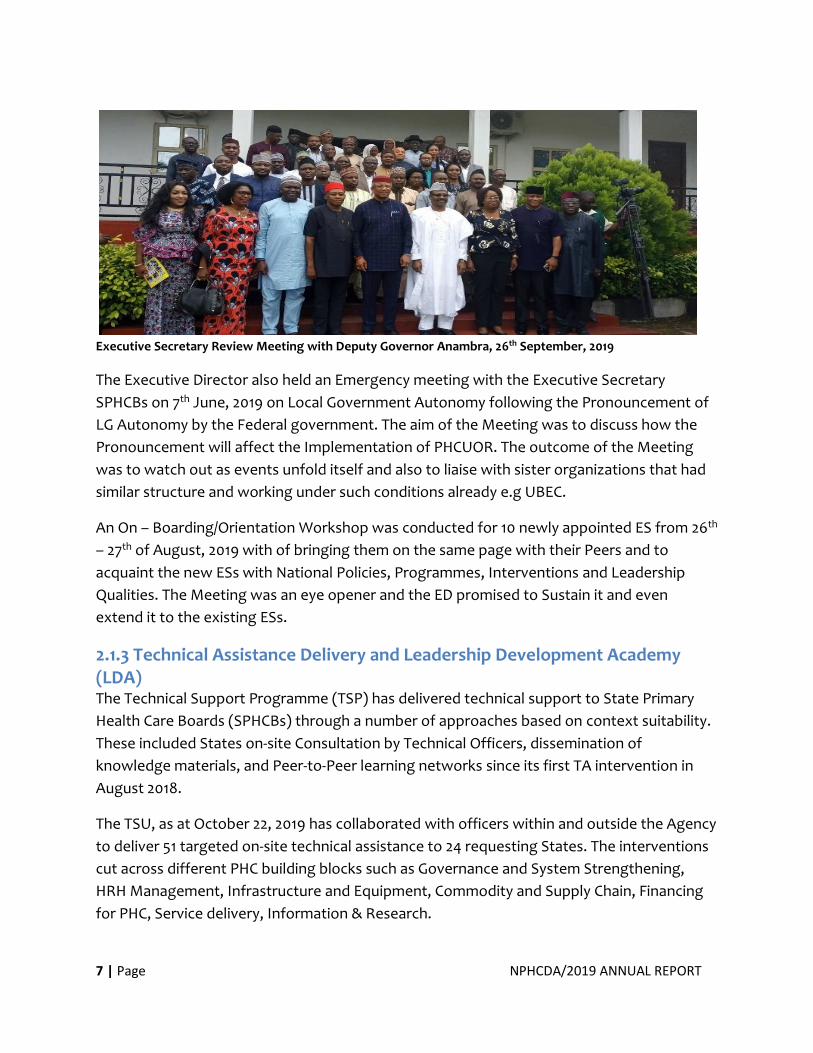
Executive Secretary Review Meeting with Deputy Governor Anambra, 26th September, 2019
The Executive Director also held an Emergency meeting with the Executive Secretary
SPHCBs on 7th June, 2019 on Local Government Autonomy following the Pronouncement of
LG Autonomy by the Federal government. The aim of the Meeting was to discuss how the
Pronouncement will affect the Implementation of PHCUOR. The outcome of the Meeting
was to watch out as events unfold itself and also to liaise with sister organizations that had
similar structure and working under such conditions already e.g UBEC.
An On – Boarding/Orientation Workshop was conducted for 10 newly appointed ES from 26th
– 27th of August, 2019 with of bringing them on the same page with their Peers and to
acquaint the new ESs with National Policies, Programmes, Interventions and Leadership
Qualities. The Meeting was an eye opener and the ED promised to Sustain it and even
extend it to the existing ESs.
2.1.3 Technical Assistance Delivery and Leadership Development Academy (LDA) The Technical Support Programme (TSP) has delivered technical support to State Primary
Health Care Boards (SPHCBs) through a number of approaches based on context suitability.
These included States on-site Consultation by Technical Officers, dissemination of
knowledge materials, and Peer-to-Peer learning networks since its first TA intervention in
August 2018.
The TSU, as at October 22, 2019 has collaborated with officers within and outside the Agency
to deliver 51 targeted on-site technical assistance to 24 requesting States. The interventions
cut across different PHC building blocks such as Governance and System Strengthening,
HRH Management, Infrastructure and Equipment, Commodity and Supply Chain, Financing
for PHC, Service delivery, Information & Research.
8 | Page NPHCDA/2019 ANNUAL REPORT
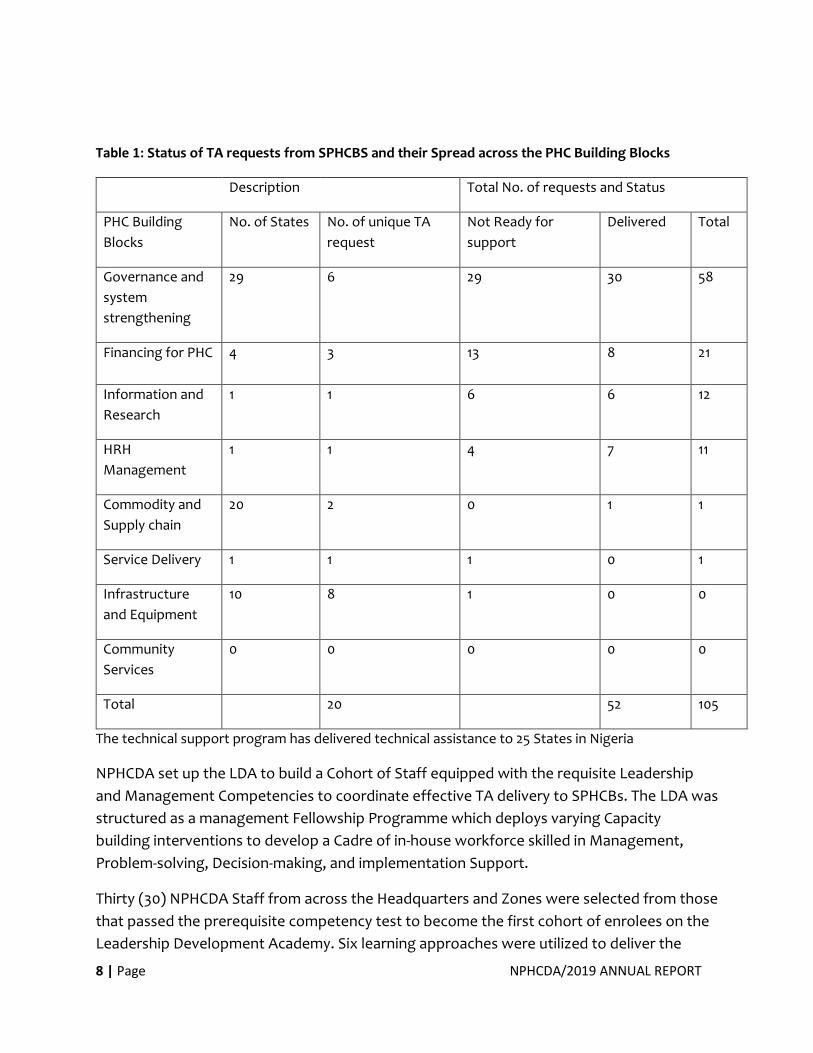
Table 1: Status of TA requests from SPHCBS and their Spread across the PHC Building Blocks
Description Total No. of requests and Status
PHC Building
Blocks
No. of States No. of unique TA
request
Not Ready for
support
Delivered Total
Governance and
system
strengthening
29 6 29 30 58
Financing for PHC 4 3 13 8 21
Information and
Research
1 1 6 6 12
HRH
Management
1 1 4 7 11
Commodity and
Supply chain
20 2 0 1 1
Service Delivery 1 1 1 0 1
Infrastructure
and Equipment
10 8 1 0 0
Community
Services
0 0 0 0 0
Total 20 52 105
The technical support program has delivered technical assistance to 25 States in Nigeria
NPHCDA set up the LDA to build a Cohort of Staff equipped with the requisite Leadership
and Management Competencies to coordinate effective TA delivery to SPHCBs. The LDA was
structured as a management Fellowship Programme which deploys varying Capacity
building interventions to develop a Cadre of in-house workforce skilled in Management,
Problem-solving, Decision-making, and implementation Support.
Thirty (30) NPHCDA Staff from across the Headquarters and Zones were selected from those
that passed the prerequisite competency test to become the first cohort of enrolees on the
Leadership Development Academy. Six learning approaches were utilized to deliver the

9 | Page NPHCDA/2019 ANNUAL REPORT
curriculum, which include: in-class sessions, external rotations, mentorship, e-learning,
learning tour and a culminating Capstone Project.
Figure 2: Flag Off of Technical Support Programme (TSP) by HMH Prof. Isaac F. Adewole
Having gone through all the learning approaches designed for the LDA, the enrolees
successfully graduated in November 4, 2019. Also, the capacity of the enrolees has been built
to be able to support the SPHCBs in delivering Technical Assistance.
First Cohort Leadership Development Academy
Grandaunts
Executive Director, Dr. Faisal Shuiab
Making Speech at Graduation of First
Cohort of the Leadership Development
Academy
10 | Page NPHCDA/2019 ANNUAL REPORT
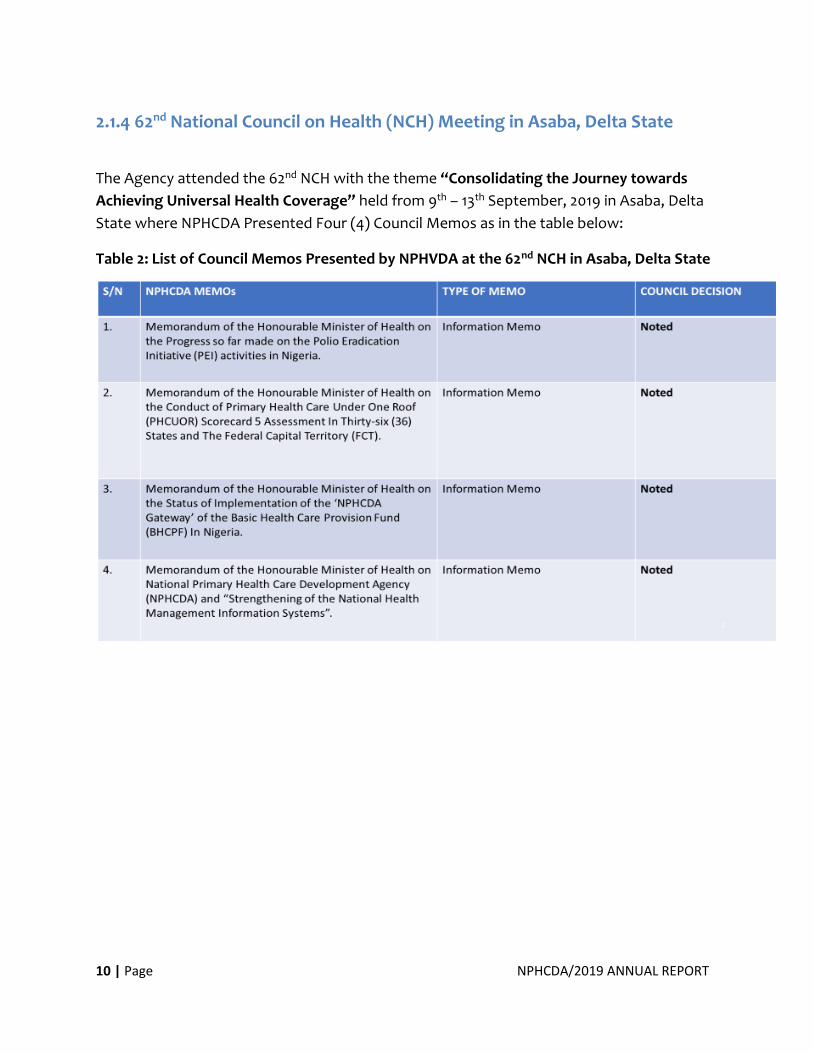
2.1.4 62nd National Council on Health (NCH) Meeting in Asaba, Delta State
The Agency attended the 62nd NCH with the theme “Consolidating the Journey towards
Achieving Universal Health Coverage” held from 9th – 13th September, 2019 in Asaba, Delta
State where NPHCDA Presented Four (4) Council Memos as in the table below:
Table 2: List of Council Memos Presented by NPHVDA at the 62nd NCH in Asaba, Delta State
11 | Page NPHCDA/2019 ANNUAL REPORT
Honourable Minister and State Minister of Health
and Other Dignitaries at 62ND NCH Meeting Asaba,
Delta State; 9th – 13th September, 2019
Ag. Director PRS Presenting NPHCDA Council
Memos at NCH Meeting Asaba, Delta State; 9th –
13th September, 2019
Communique of 62nd NCH Resolutions (See annex I)
2.1.5 Staff Retreat/Succession Planning Workshop In the year under review, a retreat for all Agency Staff both in the Headquarters and the
Zones took place from January - May 2019.
Due to the large number of retirees and the Vacuum created, management in its wisdom
conducted a Workshop on Succession Planning for Staff in August, 2019.
Also, a 2-day retreat for Senior Management Staff of the agency took place in Abuja on 30th
October, 2019. The engagement provides an opportunity to appraise and align on the
agency’s vision. The staff also brainstormed on key Strategies to Strengthen & Optimize the
agency’s programmes and priorities and address barriers to optimal program effectiveness.
2.1.6 Programmes Implementation Monitoring and Compliance Committee (PIMCC) In a bid to forestall accountability in the Agency especially as regards Staff participation in
Programmes, the ED inaugurated the PIMCC on the 17th of September, 2019 to serve as a Watch Dog
over Programme Officers and Staff. The Committee has the mandate to ensure that all Programmes
are carried out as at when due and track Staff postings on the field of assignment.
12 | Page NPHCDA/2019 ANNUAL REPORT
Their ToR included the followings:
TERMS OF REFERENCE (ToR)
1. To ensure that appropriate calibre of staff are deployed for all field activities
2. To ensure Equity, Fairness, Transparency and Accountability in the execution of field
activities
3. To ensure appropriate and timely Reporting of program performance including individuals
ODK report and the general programmatic report.
4. To ensure that only authorized staff members participate in field activities except where
partner’s involvement or other experts are required.
5. To ensure proper monitoring of all staff participation in field activities with the aim of
recommending sanction for non-compliance.
6. To ensure committee submit monthly Report to the Executive Director / CEO
Membership included Union members, all Union Chairmen and Admin Officers of the Zonal Offices
and a legal officer.
Executive Director Dr. Faisal Shuiab, some Directors with Members of the Programmes Implementation Monitoring and Compliance Committee at their Inauguration: Abuja; 17th September, 2019
13 | Page NPHCDA/2019 ANNUAL REPORT
2.2 Partnership for Health
2.2.1 Engagement with Partners During the year under review, NPHCDA had several engagements with development and
Donor Partners – WHO, UNICEF, BMGF, CDC/AFENET/NSTOP, SOLINA, CHAI, EU–SIGN, e-
HEALTH AFRICA, Gavi, UNFPA etc. The Objective of the various engagements were to Support
NPHCDA to achieve its Mandates and were fruitful and led to series of Collaborations.
2.2.2 2019 Seattle Declaration A 2-day meeting on Human Capital Development (HCD) with focus on Primary Health Care
(PHC) was convened by the Aliko Dangote Foundation (ADF), Bill & Melinda Gates
Foundation (BMGF) and the Nigeria Governors’ Forum (NGF) on 12th and 13th November 2019
in Seattle, Washington, USA. The meeting was aimed at fostering deeper understanding of
States government’ development agenda within the context of the HCD and PHC
framework and to harvest Perspectives to better inform joint Strategies for Prioritization of
PHC for greater Impact and Progress in meeting the Sustainable Development Goals (SDG)
by 2030.
At the end of the meeting, Governors and the two Foundations made commitments aimed
at Promoting Stronger Collaboration between the Governors, the NPHCDA, Federal Ministry
of Health and Development Partners to move the needle and transform Primary Health Care
(PHC) at the subnational level.
The Outcome of the meeting led to the 2019 SEATTLE DECLARATION with 9 Commitments
towards improving HCD for PHC.
Seattle Declaration (See Annex 2)
2.3 Health Promotion and Social Determinants of Health (Environmental
Health)
2.3.1 Supplemental Immunization Activities For Polio Eradication
2.3.1.1 Immunization Plus Days (IPDs)
The 36th Expert Review Committee on Polio and Routine Immunization (ERC) Calendar,
approved a total of 5 Supplemental Immunization Activities (SIAs) - all were conducted in
2019 using bivalent Oral Polio Vaccine (bOPV). Management Support Team (MSTs), Senior
Supervisors and Crack Teams were deployed for each of the Campaigns to give technical
support to the States and LGAs of posting and to ensure close supervision of vaccination
teams for high quality coverage to be achieved. However, some of the SIA States surveyed
achieved >=90% Coverage as shown in the LQAS results of 2019.
14 | Page NPHCDA/2019 ANNUAL REPORT
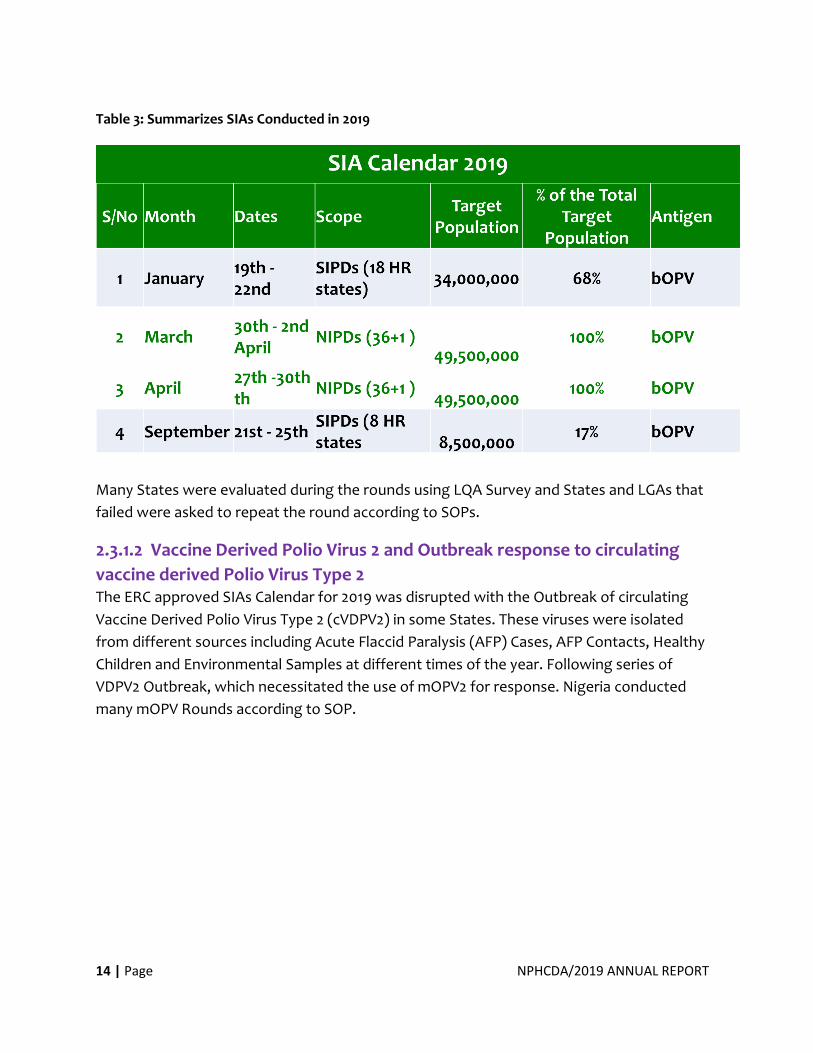
Table 3: Summarizes SIAs Conducted in 2019
Many States were evaluated during the rounds using LQA Survey and States and LGAs that
failed were asked to repeat the round according to SOPs.
2.3.1.2 Vaccine Derived Polio Virus 2 and Outbreak response to circulating
vaccine derived Polio Virus Type 2 The ERC approved SIAs Calendar for 2019 was disrupted with the Outbreak of circulating
Vaccine Derived Polio Virus Type 2 (cVDPV2) in some States. These viruses were isolated
from different sources including Acute Flaccid Paralysis (AFP) Cases, AFP Contacts, Healthy
Children and Environmental Samples at different times of the year. Following series of
VDPV2 Outbreak, which necessitated the use of mOPV2 for response. Nigeria conducted
many mOPV Rounds according to SOP.
15 | Page NPHCDA/2019 ANNUAL REPORT
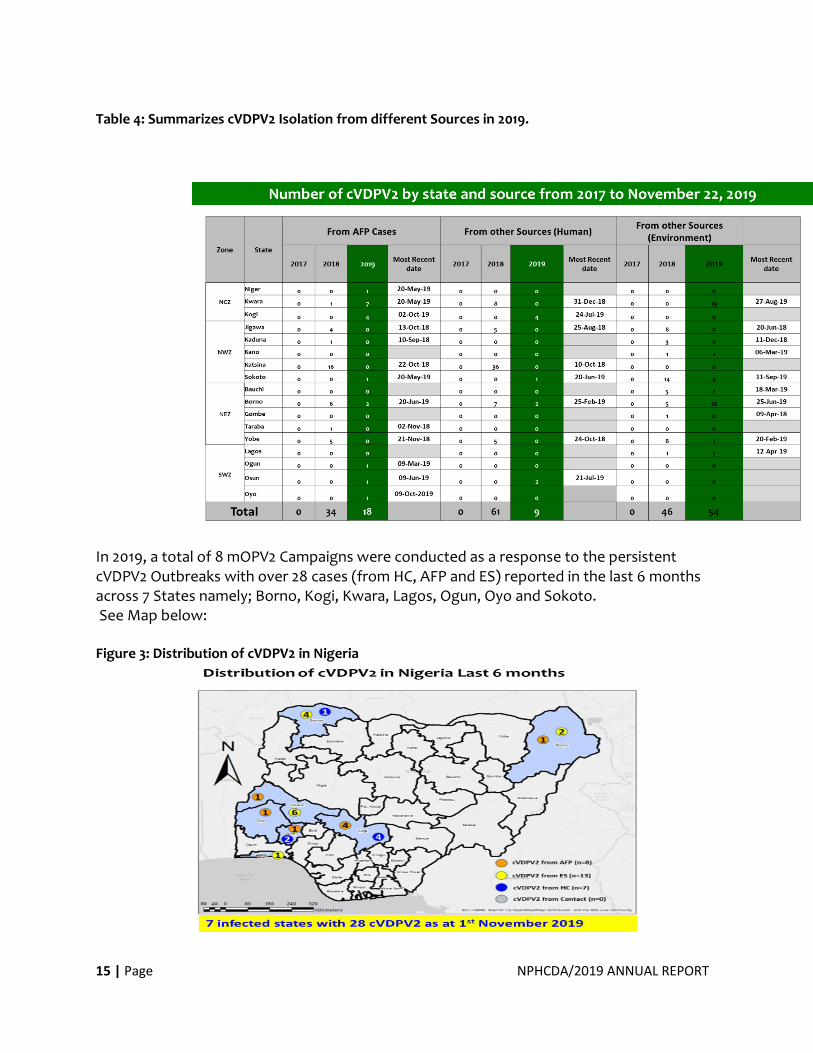
Table 4: Summarizes cVDPV2 Isolation from different Sources in 2019.
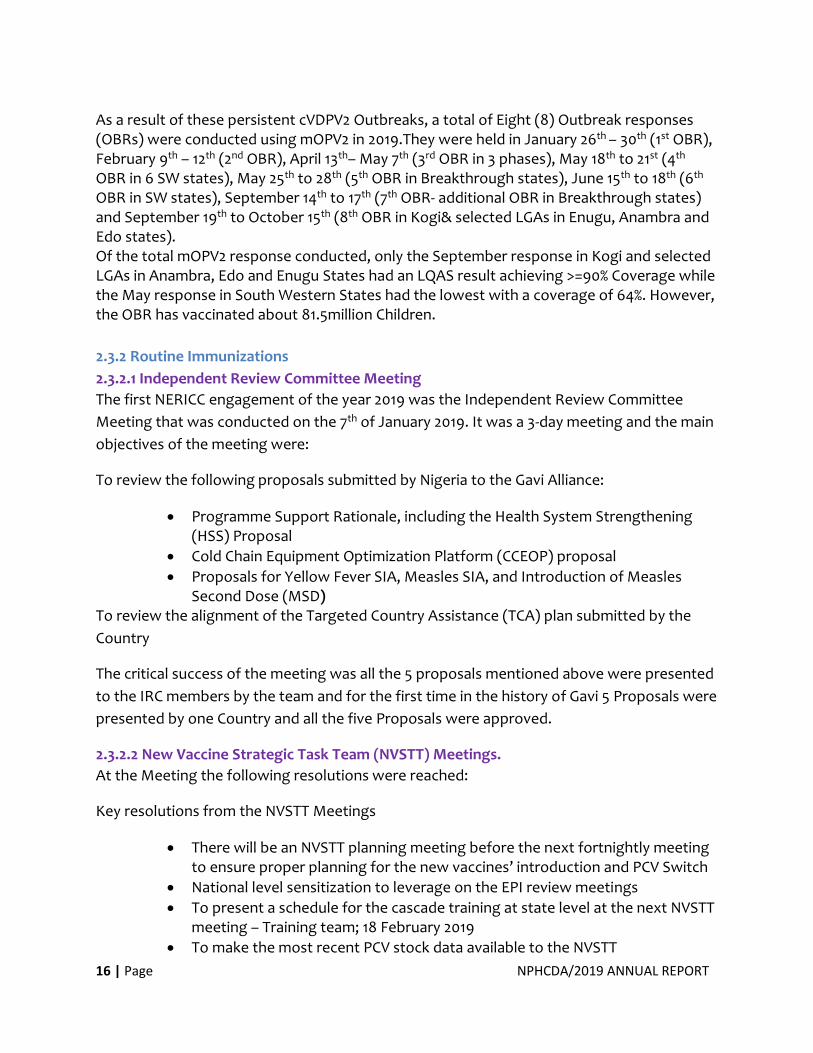
In 2019, a total of 8 mOPV2 Campaigns were conducted as a response to the persistent cVDPV2 Outbreaks with over 28 cases (from HC, AFP and ES) reported in the last 6 months across 7 States namely; Borno, Kogi, Kwara, Lagos, Ogun, Oyo and Sokoto. See Map below: Figure 3: Distribution of cVDPV2 in Nigeria
16 | Page NPHCDA/2019 ANNUAL REPORT
As a result of these persistent cVDPV2 Outbreaks, a total of Eight (8) Outbreak responses (OBRs) were conducted using mOPV2 in 2019.They were held in January 26th – 30th (1st OBR), February 9th – 12th (2nd OBR), April 13th– May 7th (3rd OBR in 3 phases), May 18th to 21st (4th OBR in 6 SW states), May 25th to 28th (5th OBR in Breakthrough states), June 15th to 18th (6th OBR in SW states), September 14th to 17th (7th OBR- additional OBR in Breakthrough states) and September 19th to October 15th (8th OBR in Kogi& selected LGAs in Enugu, Anambra and Edo states). Of the total mOPV2 response conducted, only the September response in Kogi and selected LGAs in Anambra, Edo and Enugu States had an LQAS result achieving >=90% Coverage while the May response in South Western States had the lowest with a coverage of 64%. However, the OBR has vaccinated about 81.5million Children.
2.3.2 Routine Immunizations
2.3.2.1 Independent Review Committee Meeting
The first NERICC engagement of the year 2019 was the Independent Review Committee
Meeting that was conducted on the 7th of January 2019. It was a 3-day meeting and the main
objectives of the meeting were:
To review the following proposals submitted by Nigeria to the Gavi Alliance:
• Programme Support Rationale, including the Health System Strengthening (HSS) Proposal
• Cold Chain Equipment Optimization Platform (CCEOP) proposal
• Proposals for Yellow Fever SIA, Measles SIA, and Introduction of Measles Second Dose (MSD)
To review the alignment of the Targeted Country Assistance (TCA) plan submitted by the
Country
The critical success of the meeting was all the 5 proposals mentioned above were presented
to the IRC members by the team and for the first time in the history of Gavi 5 Proposals were
presented by one Country and all the five Proposals were approved.
2.3.2.2 New Vaccine Strategic Task Team (NVSTT) Meetings.
At the Meeting the following resolutions were reached:
Key resolutions from the NVSTT Meetings
• There will be an NVSTT planning meeting before the next fortnightly meeting to ensure proper planning for the new vaccines’ introduction and PCV Switch
• National level sensitization to leverage on the EPI review meetings
• To present a schedule for the cascade training at state level at the next NVSTT meeting – Training team; 18 February 2019
• To make the most recent PCV stock data available to the NVSTT
17 | Page NPHCDA/2019 ANNUAL REPORT
• To hold further discussions and decide on the modalities for the pre-switch spot check
• To send communication to the states on the switch plans.
• To present the demand generation plan for the PCV switch in the next meeting
• The call for materials to be sent out for the collection to be done immediately after the meeting.
• Create an email for the NVSTT ([email protected])
• Follow up on mapping of partners to activities for the funding of Men A introduction.
2.3.2.3 Optimized Integrated Routine Immunization Services (OIRIS)
OIRIS visit from 28th January to 1st February 2019and March 17th to 21st 2019 to 18 NERICC
Priority States (Jigawa, Kebbi, kano, Sokoto, Katsina, Kaduna, Zamfara, Borno, Yobe,
Adamawa, Bauchi, Gombe, Taraba, Plateau, Niger, Kogi, Nasarawa and Bayelsa States).
OIRIS visits to 18 NERICC priority states (Jigawa, Kebbi, kano, Sokoto, Katsina Kaduna,
Zamfara, Borno, Yobe, Adamawa, Bauchi, Gombe, Taraba, Plateau, Niger, Kogi, Nasarawa
and Bayelsa states). The first and the 2nd quarter visits were jointly conducted with NPHCDA
Staff from the Southern States and it serves as a learning visit. The idea was for them to
domesticate the concept in their States.
2.3.2.4 Mini EPI Review Meetings
Mini EPI Reviews were conducted by NERICC team in Bayelsa, Gombe and Katsina supported
by CDC/AFENET/NSTOP.
2.3.2.5 Joint Reporting form (JRF) and the National ToT for the PCV Switch from 2 dose vial
to 4 dose Vial
In February 2019 the main activities conducted by the NERICC team were the Joint Reporting
form (JRF) and the National ToT for the PCV Switch from 2 dose vial to 4 dose vial and all the
36 +1 States participated in the training and in March 2019 the main activity conducted by the
Centre was the State level training on PCV switch that started in the second week of March
2019.
Objectives of the PCV switch included:
• To update the knowledge of State EPI managers and health workers on Pneumococcal Diseases and Pneumococcal Conjugate Vaccine (PCV) 4-dose vial presentation.
• To train state EPI managers & health workers on vaccines accountability (proper PCV 4-dose storage, safe handling, administration, AEFI and waste management).
18 | Page NPHCDA/2019 ANNUAL REPORT
• To build the capacity of state EPI managers and health workers on the application of the Multi Dose Vial Policy (MDVP).
• To improve knowledge and skills of state EPI managers & health workers on how best to communicate with caregivers and community leaders, and improve demand for immunization and PHC services.
Key achievements:
All the 36+1 States successfully implemented the PCV switch based on the above objectives
and the PCV switch implementation was completed in the second Quarter of 2019.
2.3.2.6 Engagement Meeting with Low Performing LGAs
This took place in Kaduna in the month of May from 13thto 24thMay 2019. Over 40 LGAs and
290 participants from the States were engaged.
The goal of the engagement was Primarily to identify the Specific Challenges of the poor
performing States and design interventional strategies aimed to address the identified
challenges and improve the overall performance of the LGAs.
The Meeting had the following Objectives:
• To provide feedback from National to states on RI performance using the results of the RI LQAS (Q4 2017 – Q1 2019)
• To share lessons learned and best practices from good performing LGAs
• To understand LGA specific challenges responsible for poor RI performance and proffer solutions to address identified challenges
• To develop LGA specific actionable solutions detailing KPI’s, responsible persons and timelines to improve RI performance
• To provide feedback on functionality of LERICCs including RIOs, review ToRs and chart way forward
• To obtain a renewed commitment on improving RI from poor performing LGAs
19 | Page NPHCDA/2019 ANNUAL REPORT
Cross section of Participants at the Engagement Meeting in Kaduna; May 2019
2.3.2.7 Engagement Meeting with Medium and High Performing States of NERICC
Strategies – 19 States (3 from NCZ and 16 from the South) were engaged in July in Awka
Anambra State.
Over 150 Senior Officials from the States were engaged and NERICC concepts and Strategies
were presented to them. Three States (Oyo, Kwara and Benue) were mandated to
inaugurate SERICC in their States, while others were given an option to consider
establishment of SERICCs in their States.
2.3.2.8 Introduction of Men A into RI Schedule
In August 2019, Meningitis serotype A was introduced into Routine Immunization Schedule.
Objective:
To update knowledge of immunization officers at all levels on Meningitis disease and its
surveillance, build their capacity on handling and administration of MenA Vaccine
Achievement:
Successful training of HCWs on MenA introduction into RI across the 36+1 States, 774 LGAs
and 9,565 political wards.
Over 58,700 HCWs’ capacity was build based on the above objectives

20 | Page NPHCDA/2019 ANNUAL REPORT
National Flag-off was done on the 9th August 2019 and State level introductions were
completed in all the 36+1 States.
Figure 4: National Flag off of Men A Vaccine
Executive Director and Traditional Rulers during Men-A
National flag-off in FCT: 9th August 2019 Dr. Faisal Shuaib ED NPHCDA Administering of
Men A Vaccine
2.3.2.9 Joint Appraisal Report (JAR)
Approach to Gavi Joint Appraisal for 2020 has been developed and presented to NERICC
2.3.2.10 Measles Second Dose introduction into RI Schedule
On 14th of November, 2019, the Federal Government Successfully through NPHCDA
introduced Measles Containing Vaccine (MCV2) Second Dose at 15 Months into the Routine
Immunization Schedule. Apart from the usual first dose of Measles at nine (9) months old,
all Children will be vaccinated at 15 months with a Measles Vaccine SECOND DOSE. The
SECOND DOSE of Measles Vaccination is given to every Child at 15 months as a Second
opportunity to fully protect Children against the deadly Measles disease.
2.3.2.11 RI-RMNCH Programme Assessment for Performance management & Action (PAPA)
Planning meeting, NToT and implementation have been successfully executed in all the Q3
PAPA States and findings disseminated to all the relevant stakeholders. PAPA LQAS for first
to 3rd Quarters were successfully conducted and disseminated.
21 | Page NPHCDA/2019 ANNUAL REPORT
2.3.2.12 JAR development
The draft JAR has been completed and to be shared with core Group members for
comments and inputs before presenting to ICC for endorsement.
2.3.2.13 Gavi Programme Capacity Assessment
This simply refers to assessment of the Country’s capacity to implement and oversee Gavi-
supported programmes. It is a periodic assessment and is in line with the Gavi’s
Transparency and Accountability Policy.
Key areas of this assessment included:
In-country Financial Mechanism for receiving Gavi support.
Structures that oversee the use of Gavi support
• Engagement meeting with Gavi 8 States.
The 8 States were selected by Gavi for an extended support in the form of HSS, the States
are currently developing their HSS Proposals. The States are: Kebbi, Katsina, Zamfara,
Jigawa, Taraba, Gombe, Niger and Bayelsa.
Mock review meeting in Kano was concluded successfully and proposals submitted to Gavi
and endorsed by ICC. Now awaiting IRC review proposed for 2020.
• High Level Mission by the Gavi Delegation led by Gavi CEO After the renewed engagement, the Country, Partners and Gavi made a commitment for a
high-level engagement meeting at least once in a year.
The aims included:
• Appreciate the effort the FGoN is making in increasing the funding for Immunization and PHC System based on the agreed commitment between Gavi and FGoN
• Reiterate the Commitment of Gavi on the implementation of the agreed accountability framework between FGoN and Gavi.
The key activities during the visit included but not limited to the following:
Courtesy visit to the Honourable Minister of Health (HMH)
Meeting of the Inter-Agency Coordination Committee (ICC)
Meeting with Honourable Ministers of Health, Finance, Budget and National Planning
22 | Page NPHCDA/2019 ANNUAL REPORT
Courtesy visit to Mr President
Ceremonial Launch/flag-off of the Cold Chain Equipment Optimization Platform (CCEOP)
The meeting was successfully executed as planned and the expected outcomes achieved.
2.3.3 Nigeria Immunization Technical Advisory Group (NGI-TAG)
2.3.3.1 NGI-TAG General Meeting on Introduction of HPV Vaccine into RI
NPHCDA, in July of 2017 requested the advice of the NGI-TAG on the introduction of HPV
Vaccine into the RI System as well as the type of vaccine to use if it were to be introduced.
The HPV disease working group was then formally inaugurated to gather all evidence
required to come to a decision. After over 8 DSWG meetings, the group finally presented it
findings to the general house on the 10th of April 2019 at the NGI-TAG General meetings and
the following were recommended to the FMoH/NPHCDA:
Nigeria should introduce the HPV Vaccine in its immunization programme in line with the
proposed 2021 timelines in the Nigeria Strategy for Immunization and PHC System
Strengthening 2018 – 2028. The HPV introduction should target age group 9 – 14years.
The Country should consider introduction of the HPV Vaccine in both sexes (Boys and Girls)
with a phased approach initially targeting Girls - this is due to the burden of Cancer of Cervix.
In the medium to long term, the Country should improve on its immunization financing
status and consider inclusion of HPV schedules for boys.
Based on the appraisal of the Vaccine products on efficacy, prevalence of serotypes in
Nigeria, added protection against genital warts and duration of protection; cost per fully
immunized and cold chain capacity, it is recommended thatQuadrivalent HPV Recombinant
Vaccine should be the vaccine of choice
The Nigeria Immunization Programme should use the following Strategies for HPV
introduction:
• Facility based
• Outreaches (in Schools and out of Schools)
2.3.3.2 Inauguration and Orientation of the new and returning NGI-TAG
members (15th October 2019) The members were formally inaugurated by the Minister of Health, Dr. Osagie Ehanire on
the 15th -17th of October 2019. In addition, orientation of all members was conducted on the
16th and 17th of October 2019.
23 | Page NPHCDA/2019 ANNUAL REPORT
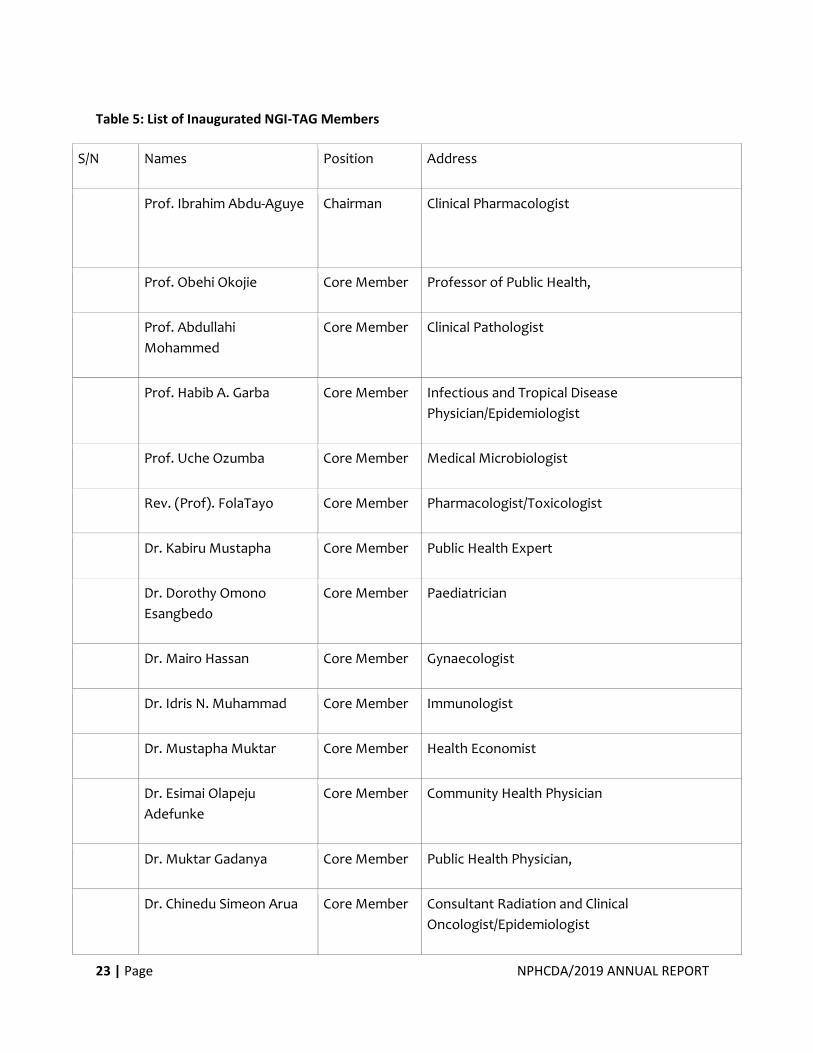
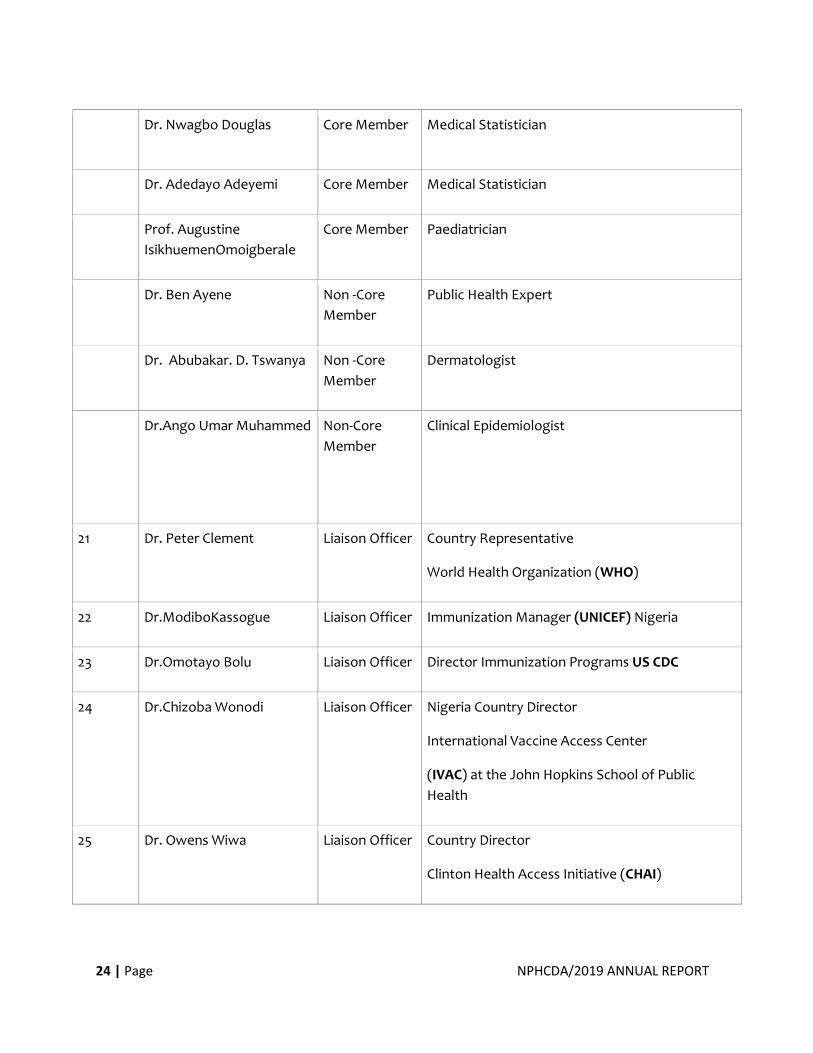
Table 5: List of Inaugurated NGI-TAG Members
S/N Names Position Address
Prof. Ibrahim Abdu-Aguye Chairman Clinical Pharmacologist
Prof. Obehi Okojie Core Member Professor of Public Health,
Prof. Abdullahi
Mohammed
Core Member Clinical Pathologist
Prof. Habib A. Garba Core Member Infectious and Tropical Disease
Physician/Epidemiologist
Prof. Uche Ozumba Core Member Medical Microbiologist
Rev. (Prof). FolaTayo Core Member Pharmacologist/Toxicologist
Dr. Kabiru Mustapha Core Member Public Health Expert
Dr. Dorothy Omono
Esangbedo
Core Member Paediatrician
Dr. Mairo Hassan Core Member Gynaecologist
Dr. Idris N. Muhammad Core Member Immunologist
Dr. Mustapha Muktar Core Member Health Economist
Dr. Esimai Olapeju
Adefunke
Core Member Community Health Physician
Dr. Muktar Gadanya Core Member Public Health Physician,
Dr. Chinedu Simeon Arua Core Member Consultant Radiation and Clinical
Oncologist/Epidemiologist
24 | Page NPHCDA/2019 ANNUAL REPORT
Dr. Nwagbo Douglas Core Member Medical Statistician
Dr. Adedayo Adeyemi Core Member Medical Statistician
Prof. Augustine
IsikhuemenOmoigberale
Core Member Paediatrician
Dr. Ben Ayene Non -Core
Member
Public Health Expert
Dr. Abubakar. D. Tswanya Non -Core
Member
Dermatologist
Dr.Ango Umar Muhammed
Non-Core
Member
Clinical Epidemiologist
21 Dr. Peter Clement Liaison Officer Country Representative
World Health Organization (WHO)
22 Dr.ModiboKassogue Liaison Officer Immunization Manager (UNICEF) Nigeria
23 Dr.Omotayo Bolu Liaison Officer Director Immunization Programs US CDC
24 Dr.Chizoba Wonodi Liaison Officer Nigeria Country Director
International Vaccine Access Center
(IVAC) at the John Hopkins School of Public
Health
25 Dr. Owens Wiwa Liaison Officer Country Director
Clinton Health Access Initiative (CHAI)
25 | Page NPHCDA/2019 ANNUAL REPORT
2.3.3.3 NGI-TAG General Meeting on Introduction of Rotavirus vaccine into RI (18th October
2019)
Objectives of the meeting:
To deliberate on the NPHCDA request on a new Rotavirus recommendation
To review the previous Rotavirus Vaccine Introduction recommendations
To review new evidence and data on Rotavirus vaccine products and proffer
recommendations
The group met on the 18th of October 2019 to deliberate on the request sent by the FMoH/
NPHCDA on the need to review its previous recommendation on the type of Rotavirus
Vaccine to be introduced into RI considering new information on the different product types
now available. The Rota Disease Working Group was then formally inaugurated to gather
and review all the new information on the different product type to enable the group make
a final decision.
2.3.3.4 NGI-TAG Emergency Meeting on Rotavirus vaccine introduction into RI (28th
November 2019)
Objective of the meeting:
To review the Rota Disease working Group draft recommendation on Rotavirus vaccine
introduction into RI
To proffer a recommendation to the FMoH/NPHCDA on the type of Rotavirus vaccine to be
introduced into RI
To draft the recommendation, note to Honourable Minister of Health
After 2 meetings held by the Rotavirus Disease Working Group, a general meeting was held
on the 18th of November 2019 at Valencia Hotel, Abuja, with 16 members present including
the Chairman of the group, and the following recommendations were made concerning
Rotavirus vaccine and submitted to the FMoH:
It was the decision of the NGI-TAG to resubmit the previous recommendation of Rota Vac as
the preferred Rotavirus vaccine choice for Nigeria.
To introduce Rota Vac vaccine into the expanded program on immunization
To establish a Surveillance mechanism to determine the background rate for intussusception
and monitor post introduction
26 | Page NPHCDA/2019 ANNUAL REPORT
To avoid delays of forwarding NGI-TAG recommendations in the future
To improve the sanitation practices and treatment of diarrheal diseases
ACHIEVEMENTS OF THE GROUP
NGI-TAG is one of the globally recognized and functional NITAGs.
•Despite the challenges, the group achieved all its objectives of setting it up.
•Training and Improvement of skills to ensure evidence-based decision making
•Development of Green book and Strategic Plan
•Provision of recommendations based on various Questions posed by FMoH/NPHCDA
CHALLENGES
•Permanent and equipped NGI-TAG office
•Paid access to scientific literature and journals
2.3.4. Other Disease Control Activities
2.3.4.1 Meningitis A
Neisseria Meningitidis is the leading cause of bacterial Meningitis and other serious
infections worldwide. Nigeria has Twenty-Six of its Thirty-Six States and the FCT along the
Meningitis Belt. So far, the Country has conducted 4-phased Meningitis Campaign to control
CSM using Men Afri Vac from 2011 to 2014 targeting persons aged 1 to 29 years of age.
Due to the high burden of the disease amongst under five children and following the WHO
recommendation of conducting Campaign after introduction of Meningococcal - A
Conjugate Vaccine into the Routine Childhood immunization, Nigeria planned to implement
a follow up Campaign targeting children 1 to 5 years (North West and North East States) and
1 to 7years to reach the cohort of children that were born after the completion of previous
Campaigns.
The overall goal of the 2019/2020 Men A Campaign was to eliminate epidemics of
Meningococcal Meningitis due to Sero Type A from Nigeria by vaccinating at least 95% of
Children in States with high disease burden.
27 | Page NPHCDA/2019 ANNUALREPORT
Other activities:
Supportive Supervision to Measles/Yellow Fever Laboratories in Gaduawa and Maitama. 8th
– 9th August 2019
Participated at the Integrated Disease Surveillance and Response (IDSR) review and update:
August 25th -31st 2019 in Lagos
Short Term, Medium Term and Long-Term Prospects for Cholera Control in Nigeria review by
Global Task Force on Cholera Control (GTFCC) - November 2019
Meeting of National Committee for the Verification of Measles Elimination in Ilorin- 7th – 9th
October 2019
Northern AEFI cluster training involving 19 Northern states in Kano - 26th – 30th October 2019
New Vaccines surveillance meeting in Abuja- 14th – 16th October 2019.
National Expert Committee meeting on AEFI in Rivers - 18th – 20th November 2019
Participated Mid- term Joint External Evaluation on Nigeria health security - 18th – 22nd
November 2019
28 | Page NPHCDA/2019 ANNUALREPORT
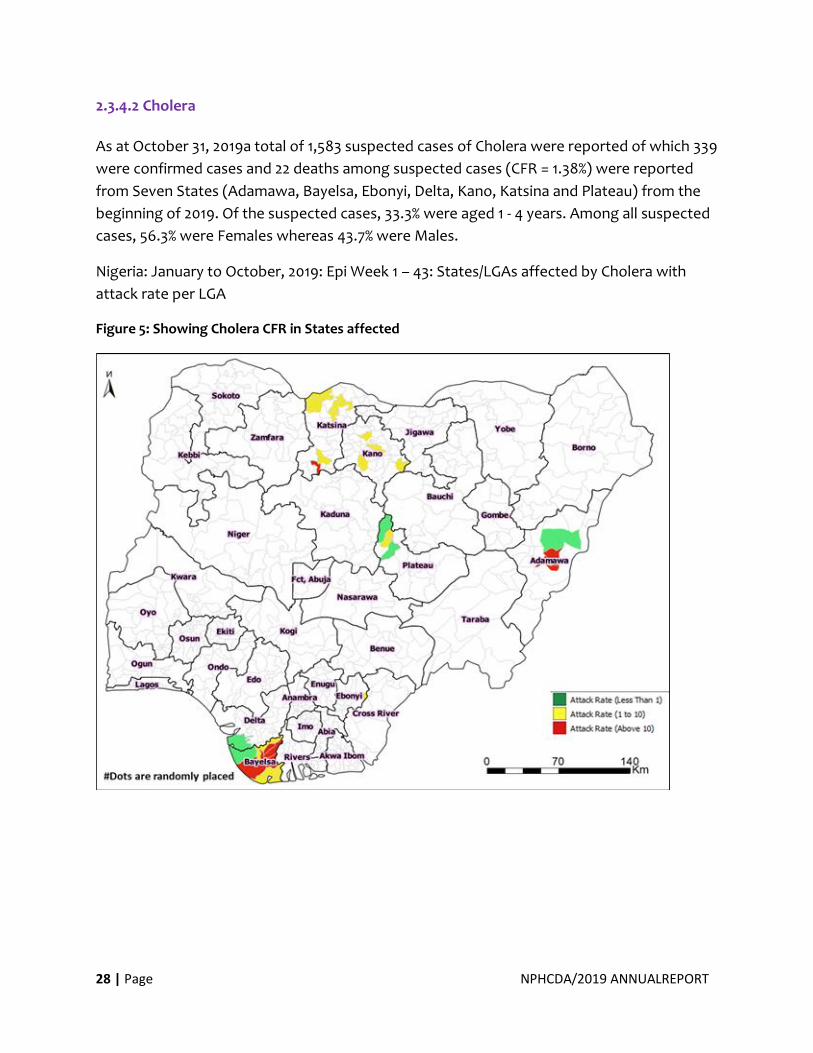
2.3.4.2 Cholera
As at October 31, 2019a total of 1,583 suspected cases of Cholera were reported of which 339
were confirmed cases and 22 deaths among suspected cases (CFR = 1.38%) were reported
from Seven States (Adamawa, Bayelsa, Ebonyi, Delta, Kano, Katsina and Plateau) from the
beginning of 2019. Of the suspected cases, 33.3% were aged 1 - 4 years. Among all suspected
cases, 56.3% were Females whereas 43.7% were Males.
Nigeria: January to October, 2019: Epi Week 1 – 43: States/LGAs affected by Cholera with
attack rate per LGA
Figure 5: Showing Cholera CFR in States affected
29 | Page NPHCDA/2019 ANNUALREPORT
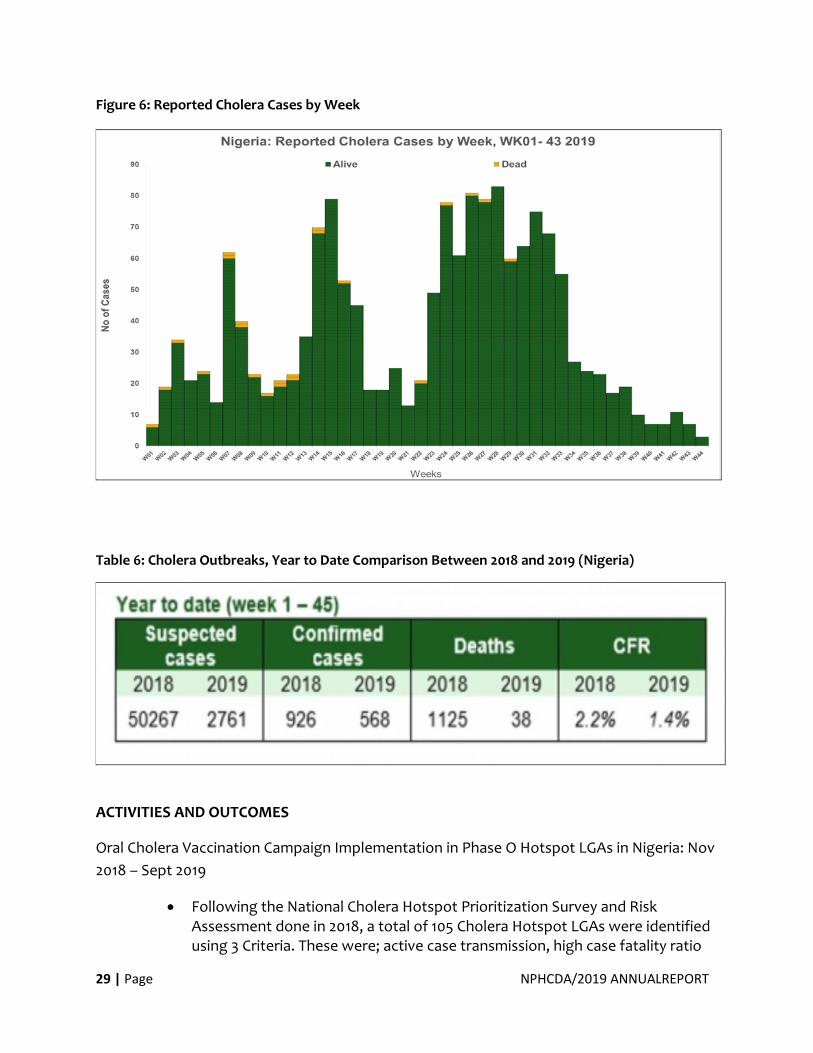
Figure 6: Reported Cholera Cases by Week
Table 6: Cholera Outbreaks, Year to Date Comparison Between 2018 and 2019 (Nigeria)
ACTIVITIES AND OUTCOMES
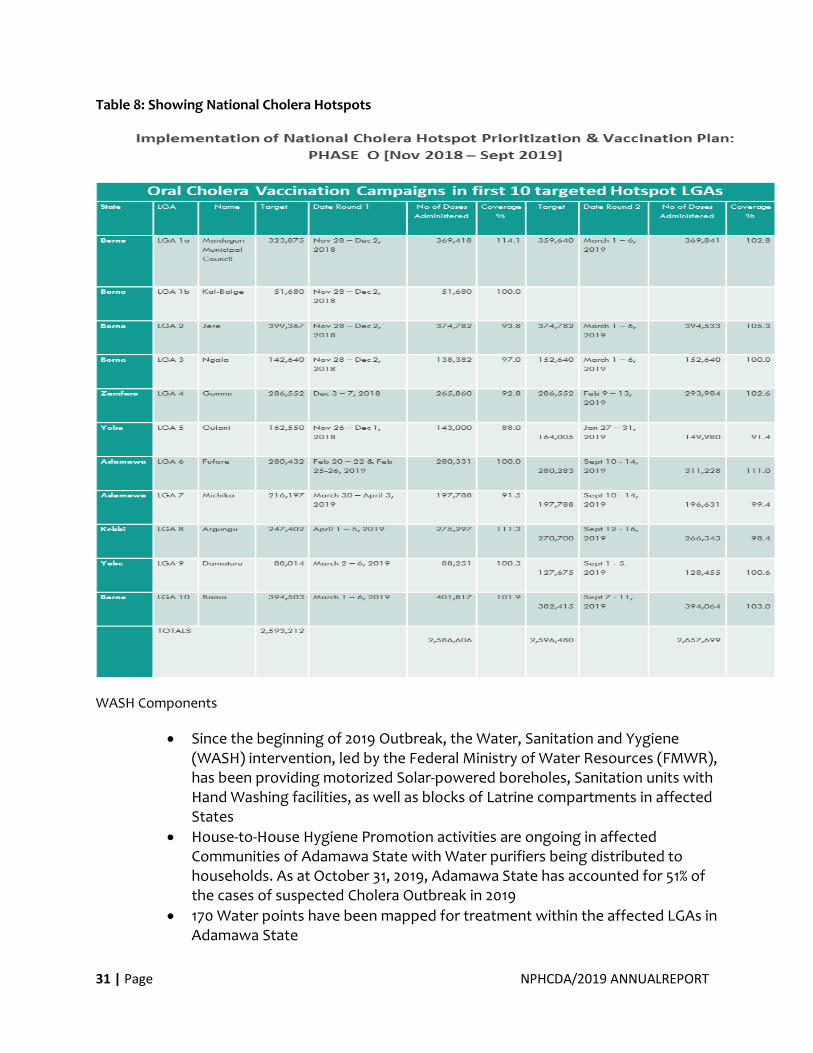
Oral Cholera Vaccination Campaign Implementation in Phase O Hotspot LGAs in Nigeria: Nov
2018 – Sept 2019
• Following the National Cholera Hotspot Prioritization Survey and Risk Assessment done in 2018, a total of 105 Cholera Hotspot LGAs were identified using 3 Criteria. These were; active case transmission, high case fatality ratio
30 | Page NPHCDA/2019 ANNUALREPORT
and vulnerability index. The LGAs were grouped as High Risk, Moderate Risk and Low Risk and targeted for interventions in the medium term-as part of a multi-sectoral Cholera control plan, with a vaccination plan in 9 phases.
• This proposal is still under consideration by the Global Task Force on Cholera Control (GTFCC) and was due for review in November 2019. However, the urgent situation presented by the then ongoing outbreak in 4th Quarter of 2018 had necessitated the selection of 10 affected LGAs for urgent intervention by Global Task Force on Cholera Control (GTFCC), including the use of OCV (Phase 0).
• The 2 rounds of the Campaigns were conducted between Nov 2018 and Sept 2019 and witnessed massive turn-out in each case. There was high acceptability level of Oral Cholera Vaccine in Nigeria. In most of the LGAs vaccinated, part of the logistics challenges observed was the influx of Community members from non-targeted and nearby LGAs to targeted LGAs.
Table 7: Outcome of the OCV Campaign
Total Population
Targeted
Total Population
Vaccinated
National Coverage
5,189,692
5,244,305
101 %
• Coverage Survey: The aggregated weighted coverage for the 2 LGAs included in the survey in Borno State was 87%
• AEFI was of negligible significance in all the Campaigns
• At present, impact evaluation is yet to be conducted. However, there has not been any reported cases of suspected Cholera Outbreak in any of the LGAs that have been Vaccinated since 2017 except in Maiduguri Municipal Council where there was a high influx of unvaccinated IDPs from other parts of Borno State affected by crises.
31 | Page NPHCDA/2019 ANNUALREPORT
Table 8: Showing National Cholera Hotspots
WASH Components
• Since the beginning of 2019 Outbreak, the Water, Sanitation and Yygiene (WASH) intervention, led by the Federal Ministry of Water Resources (FMWR), has been providing motorized Solar-powered boreholes, Sanitation units with Hand Washing facilities, as well as blocks of Latrine compartments in affected States
• House-to-House Hygiene Promotion activities are ongoing in affected Communities of Adamawa State with Water purifiers being distributed to households. As at October 31, 2019, Adamawa State has accounted for 51% of the cases of suspected Cholera Outbreak in 2019
• 170 Water points have been mapped for treatment within the affected LGAs in Adamawa State
32 | Page NPHCDA/2019 ANNUALREPORT
• At least 510,663 litres of Water have been Chlorinated in 39 of the mapped water points and this was being carried out daily
• Distribution of Water Purification Tablets were being carried out in some affected Communities of Adamawa and Katsina States.
Others
• Nigeria is also working with other Lake Chad Basin Countries to Strengthen Cross-
border Collaboration for Cholera Control
Challenges
• Inadequate global Oral Cholera Vaccine stockpile which sometimes results in delayed reactive Vaccination Campaigns to contain Outbreaks
• In case of preventive OCV campaigns as planned in the Hotspot Prioritization, it was expected that the 1st and 2nd doses should be concluded in the targeted LGAs and Communities before the onset of the Season. Conversely, due to the limited global OCV stockpile, achievement of this outcome has been a major challenge
• Other identified challenges included personnel and staffing inadequacies especially at subnational levels, security concerns as well as other sundry issues that may be associated with vaccination and mass Campaigns generally
Way Forward
• In addition to the hotspot prioritization which has been planned for review in January 2020, and in response to a call for a multi-sectoral long-term plan for the Cholera Control in Nigeria, a 5-year National Strategic Plan of Action for Cholera Control has been developed. This is to drive a coordinated approach to Cholera Control in Nigeria and this plan currently forms the basis for all cholera control interventions in the country.
• Seven (7) Strategic areas of interventions have been identified as complementary tools for achieving the medium-term goal. These are; Leadership and coordination, Epidemiologic surveillance, Laboratory surveillance, Case Management and Control, Social Mobilization/Risk Communication, Improvement in the Supply of Safe Water, Sanitation and Hygiene and the use of Oral Cholera Vaccine.
• A Critical part of the goal plan was to reduce the incidence and mortality due to Cholera by 67% by the year 2023. This medium-term goal forms part of a larger framework of eliminating cholera in Nigeria by 2030 as part of global target
• Measurable indicators and annual targets have been set for the monitoring and evaluation of each sphere of activity contained in the plan
• Efforts were being made to identify relevant partnerships to conduct impact evaluation on the various Cholera Control Strategies so far deployed as well define research priorities for strengthening cholera control in Nigeria
33 | Page NPHCDA/2019 ANNUALREPORT
• Implementation of the 2020 agenda of the just concluded 6thGlobal Task Force on Cholera Control - OCV Working Group meeting held on December 3-4, 2019 in
• Geneva, Switzerland
2.3.4.3 Yellow Fever
Nigeria has aligned with the Eliminating Yellow Fever Epidemics (EYE) strategy to eliminate
Yellow fever from Nigeria by 2026. In furtherance of this and because of the reduced
availability of yellow fever vaccines, Nigeria is staggering its preventive campaigns over the
next 5 years to cover the entire country while also responding to outbreaks.
Activities conducted in 2019 included:
Conduct outbreak investigation together with NCDC and WHO on suspected yellow fever
reported cases including entomology studies
Katsina implemented YFPMVC from 28th sept – 9th oct 2019 (27th sept 2019 in Dan-
musa&Kankara due to the YF outbreak)
YF Preventive mass vaccination campaign in 3 LGAs in Borno state- 11th to 20th December
2019
Yellow Fever outbreak response
Edo (13 LGAs), Delta (1 LGA) and Ondo (6 LGAs) – June/July 2019
Ebonyi (Abakaliki, Izzi and Ebonyi LGAs) and Cross River (Yala LGA) – 8th -18th September
2019
Benue (Ado and Oju LGAs) – 18th – 28th September 2019
Bauchi (Alkaleri LGA)- 13th -17th September 2019
Together with NCDC and Partners, a Yellow Fever risk assessment was done to prioritize
highest risk states for Preventive Campaigns to forestall outbreaks
Preventive Mass Vaccination campaigns planned for Anambra, Ekiti and Rivers in 2020.
34 | Page NPHCDA/2019 ANNUALREPORT
2.3.4.4 Measles
2.3.4.4.1 Integrated Measles and Meningitis A Mass Vaccination Campaign
Meningitis A and Measles Mass Vaccination Campaign was integrated in 18 States of the Northern
Zone except Kano and Yobe. Kano had stand alone for Measles and Meningitis A while Yobe had only
Measles Campaign. The target for Measles was 9 – 59 months, while the target for Meningitis A
varied from 1 -5 years and 1-7 years across 25 States. The Campaigns began on the 31st October 2019 in
Kano.
Stand-alone Meningitis A vaccination campaign started on the 6th December 2019 in Imo and Enugu
states. Oyo, Ebonyi, Cross Rivers, Anambra will conduct their Men A mass vaccination Campaign in
2020.
2.3.4.4.2 2019 Measles Outbreak and Responses
Nigeria conducted a measles follow up campaign targeting children 9 months to 59 months between
November 2017 and April 2018. This was in response to the low Routine Immunization coverage and
the suboptimal SIA coverages. Campaign was conducted in four streams. The operational target
population for the campaign was 37,412,277 (GIS for the North and House Hold enumeration
Walkthrough for the South). At the end of the exercise from the administrative data (tally sheet), a
total of 40,044,875, representing 107% of children 9-59 months were given measles vaccine. A total of
5, 391,435 (15.9%) of children received their first MCV during the campaign (zero dose). The post
campaign coverage survey put the national coverage at 87.5%. For the first time, in a measles
campaign 19 States got more than 90% vaccine coverage, among a higher proportion of rural children
36.2% received their first measles dose during the campaign against 26.8% urban children. No marked
gender difference in those receiving the vaccine for the first time.
2.3.4.4.3 Post 2017/2018 Measles Vaccination Campaign
According to the measles situation report for 2018 and 2019, a total of 1,610 and 1,638 suspected
measles cases occurred respectively.
The NPHCDA has supported most of the affected states in responding to these outbreaks through
providing the states with vaccines. The NPHCDA zonal and state offices were leveraged upon to
provide technical support to the states. However, the NPHCDA has conducted some reactive
vaccination in some very high prone areas: The Measles OBR took place in the following States viz;
Yobe, Ogun, Benue, Lagos, Borno, Igabi LGA of Kaduna and Hong in Adamawa.
Conclusion:
Most of the Outbreaks that have occurred were areas where vaccination could not take place due to
security challenges - IDP camps and their host communities. The agency through its vaccine
forecasting for the year 2020 has planned to prioritize preposition of vaccines in these vulnerable
areas.
35 | Page NPHCDA/2019 ANNUALREPORT
2.3.4.4.4 Maternal Neonatal Tetanus Elimination (MNTE) Activities in Nigeria 2018/2019
The global Maternal Neonatal Tetanus Elimination (MNTE) target is 2020 and activities are
ongoing towards ensuring the country meets this target. In October 2017, MNTE was
validated in the South-East zone. A pre-validation assessment was conducted in the South-
west zone in May,2017, findings from the assessment identified seven LGAs as high risk in
Oyo state namely Saki west, Saki east, Ibarapa north, Oyo west, Iwajowa, Itesiwaju and
Atisbo. In Ogun state, Itapa community in Remo North LGA was also identified as high risk.
Three rounds of SIAs were recommended in these LGAs. These rounds were implemented
with administrative coverages of 130%, 122%, 133% for Td1, Td2, and Td3 respectively. In Itapa
community, administrative coverages of 185%, 99% and 109% for Td1, Td2 and Td3 was
attained. The high coverage above 100% can be attributed to influx of people from
neighbouring LGAs, Communities, and denominator issues as projected 2006 census was
used. Following implementation of recommended activities in 2018, MNTE was validated in
the South-west zone in May 2019.
A high-risk assessment conducted in the South-South zone identified 94 LGAs in the six
States as high risk. One round was recommended for 94 LGAs in the six states, 2 rounds for
56 LGAs in five states, then 3 rounds for 8 LGAs in one state. NPHCDA with support of
Partners has implemented two rounds as recommended reaching an administrative
coverage as follows; Akwa-Ibom (Td 1 - 112% ; Td 2 - 84%),Bayelsa (Td1 - 95% ; Td 2 72%),Cross-
river(Td 1 – 118% ;Td 2 - 91%),Delta (Td 1 - 97%),Edo(Td 1 - 80% ; Td 2 - 56%)and Rivers(Td 1 -
102%).
A high-risk assessment was conducted for Northern States in March 2019 and 136 LGAs were
identified as high risk in 16 states namely: Kano (3), Katsina (14), Kaduna (3), Kebbi (10),
Sokoto(6), Zamfara (6), Benue (18), Kogi (15), Kwara (10), Niger (7), Plateau (16), Taraba (4),
Yobe (3) ,Borno (19), Bauchi (1) and Adamawa (1). Three rounds of SIAs were implemented
as recommended for these LGAs. National MNTE Northern States (North-West and North-
Central zones) implementation training was conducted on the 9-10th September 2019.
A National workshop with South-East and South-West Zones was conducted to develop Plan
of Action to sustain elimination of Maternal Neonatal Tetanus (5 - 9 September 2019).
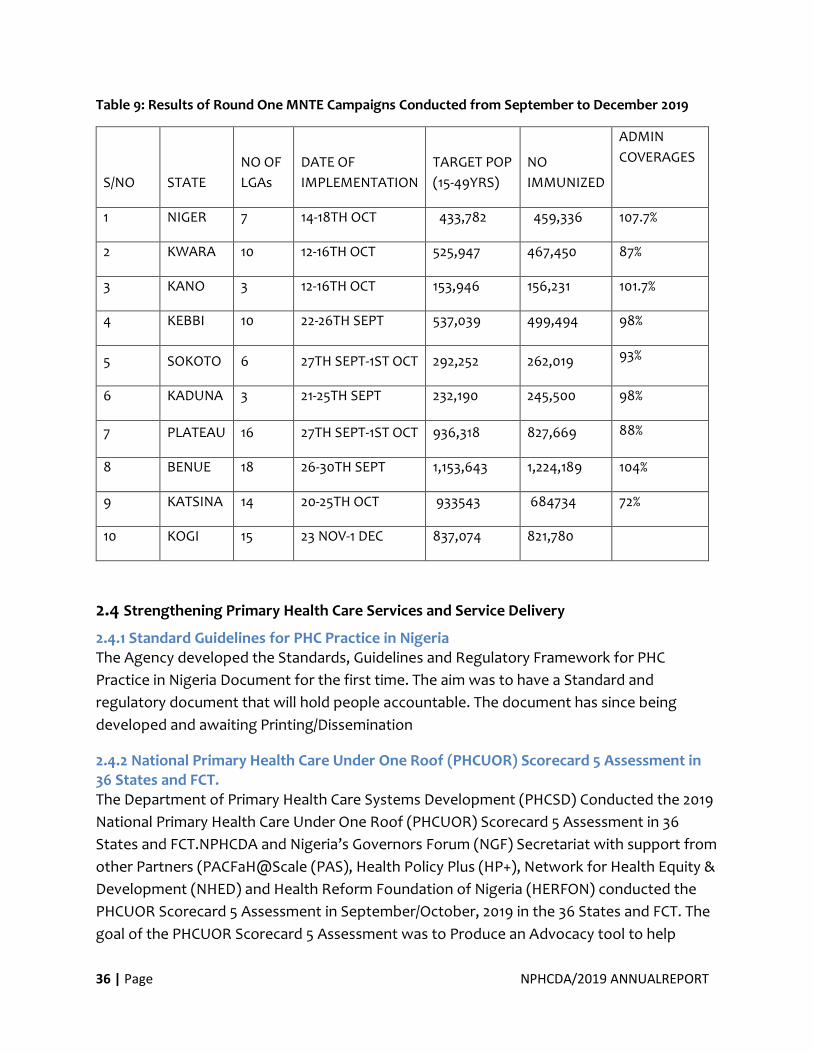
36 | Page NPHCDA/2019 ANNUALREPORT
Table 9: Results of Round One MNTE Campaigns Conducted from September to December 2019
S/NO STATE
NO OF
LGAs
DATE OF
IMPLEMENTATION
TARGET POP
(15-49YRS)
NO
IMMUNIZED
ADMIN
COVERAGES
1 NIGER 7 14-18TH OCT 433,782 459,336 107.7%
2 KWARA 10 12-16TH OCT 525,947 467,450 87%
3 KANO 3 12-16TH OCT 153,946 156,231 101.7%
4 KEBBI 10 22-26TH SEPT 537,039 499,494 98%
5 SOKOTO 6 27TH SEPT-1ST OCT 292,252 262,019 93%
6 KADUNA 3 21-25TH SEPT 232,190 245,500 98%
7 PLATEAU 16 27TH SEPT-1ST OCT 936,318 827,669 88%
8 BENUE 18 26-30TH SEPT 1,153,643 1,224,189 104%
9 KATSINA 14 20-25TH OCT 933543 684734 72%
10 KOGI 15 23 NOV-1 DEC 837,074 821,780
2.4 Strengthening Primary Health Care Services and Service Delivery
2.4.1 Standard Guidelines for PHC Practice in Nigeria The Agency developed the Standards, Guidelines and Regulatory Framework for PHC
Practice in Nigeria Document for the first time. The aim was to have a Standard and
regulatory document that will hold people accountable. The document has since being
developed and awaiting Printing/Dissemination
2.4.2 National Primary Health Care Under One Roof (PHCUOR) Scorecard 5 Assessment in 36 States and FCT. The Department of Primary Health Care Systems Development (PHCSD) Conducted the 2019
National Primary Health Care Under One Roof (PHCUOR) Scorecard 5 Assessment in 36
States and FCT.NPHCDA and Nigeria’s Governors Forum (NGF) Secretariat with support from
other Partners (PACFaH@Scale (PAS), Health Policy Plus (HP+), Network for Health Equity &
Development (NHED) and Health Reform Foundation of Nigeria (HERFON) conducted the
PHCUOR Scorecard 5 Assessment in September/October, 2019 in the 36 States and FCT. The
goal of the PHCUOR Scorecard 5 Assessment was to Produce an Advocacy tool to help
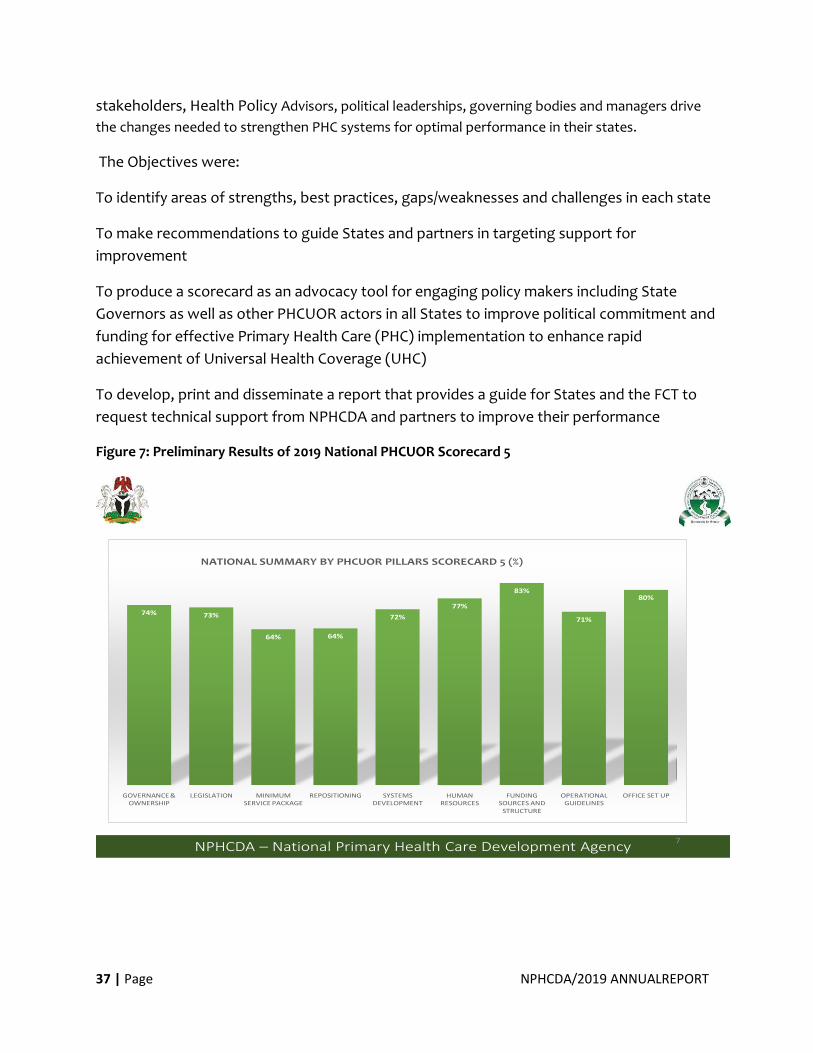
37 | Page NPHCDA/2019 ANNUALREPORT
stakeholders, Health Policy Advisors, political leaderships, governing bodies and managers drive
the changes needed to strengthen PHC systems for optimal performance in their states.
The Objectives were:
To identify areas of strengths, best practices, gaps/weaknesses and challenges in each state
To make recommendations to guide States and partners in targeting support for
improvement
To produce a scorecard as an advocacy tool for engaging policy makers including State
Governors as well as other PHCUOR actors in all States to improve political commitment and
funding for effective Primary Health Care (PHC) implementation to enhance rapid
achievement of Universal Health Coverage (UHC)
To develop, print and disseminate a report that provides a guide for States and the FCT to
request technical support from NPHCDA and partners to improve their performance
Figure 7: Preliminary Results of 2019 National PHCUOR Scorecard 5
NPHCDA – National Primary Health Care Development Agency7
74% 73%
64% 64%
72%
77%
83%
71%
80%
GOVERNANCE & OWNERSHIP
LEGISLATION MINIMUM SERVICE PACKAGE
REPOSITIONING SYSTEMS DEVELOPMENT
HUMAN RESOURCES
FUNDING SOURCES AND
STRUCTURE
OPERATIONAL GUIDELINES
OFFICE SET UP
NATIONAL SUMMARY BY PHCUOR PILLARS SCORECARD 5 (%)
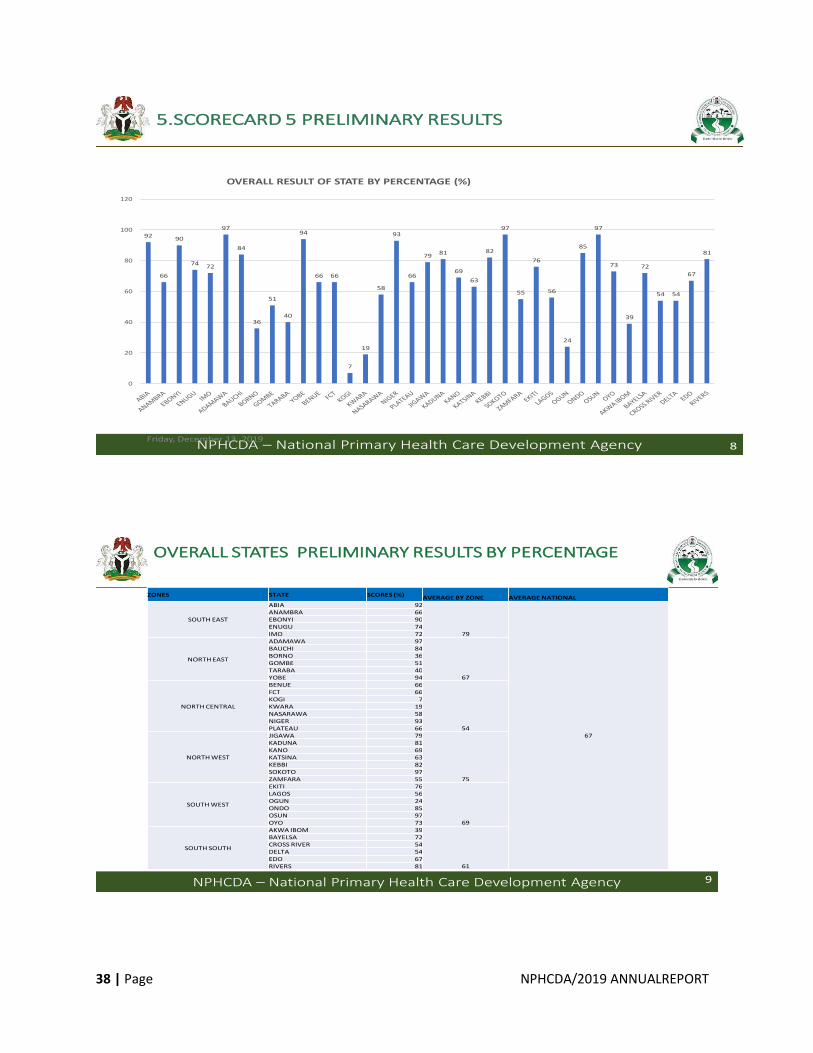
38 | Page NPHCDA/2019 ANNUALREPORT
NPHCDA – National Primary Health Care Development AgencyFriday, December 13, 2019
5.SCORECARD 5 PRELIMINARY RESULTS
8
92
66
90
7472
97
84
36
51
40
94
66 66
7
19
58
93
66
7981
69
63
82
97
55
76
56
24
85
97
73
39
72
54 54
67
81
0
20
40
60
80
100
120
OVERALL RESULT OF STATE BY PERCENTAGE (%)
NPHCDA – National Primary Health Care Development Agency
OVERALL STATES PRELIMINARY RESULTS BY PERCENTAGE
9
ZONES STATE SCORES (%) AVERAGE BY ZONE AVERAGE NATIONAL
SOUTH EAST
ABIA 92
79
67
ANAMBRA 66EBONYI 90ENUGU 74IMO 72
NORTH EAST
ADAMAWA 97
67
BAUCHI 84BORNO 36GOMBE 51TARABA 40YOBE 94
NORTH CENTRAL
BENUE 66
54
FCT 66KOGI 7KWARA 19NASARAWA 58NIGER 93PLATEAU 66
NORTH WEST
JIGAWA 79
75
KADUNA 81KANO 69KATSINA 63KEBBI 82SOKOTO 97ZAMFARA 55
SOUTH WEST
EKITI 76
69
LAGOS 56OGUN 24ONDO 85OSUN 97OYO 73
SOUTH SOUTH
AKWA IBOM 39
61
BAYELSA 72CROSS RIVER 54DELTA 54EDO 67RIVERS 81
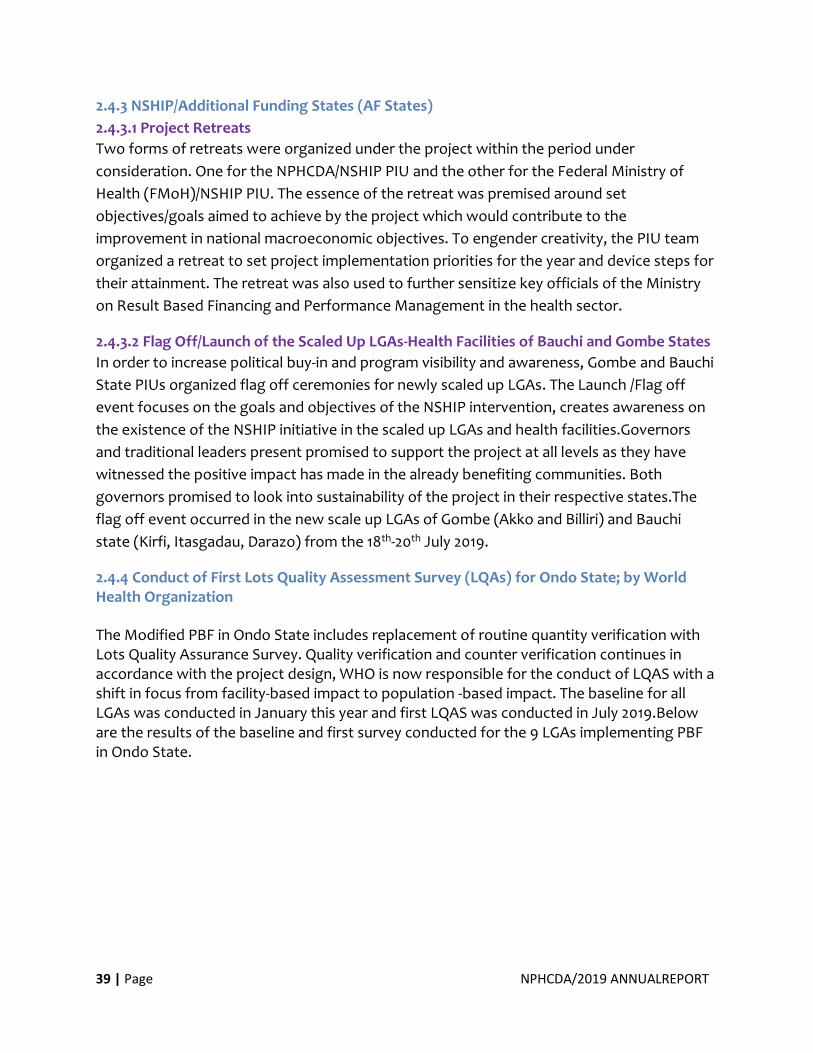
39 | Page NPHCDA/2019 ANNUALREPORT
2.4.3 NSHIP/Additional Funding States (AF States)
2.4.3.1 Project Retreats
Two forms of retreats were organized under the project within the period under
consideration. One for the NPHCDA/NSHIP PIU and the other for the Federal Ministry of
Health (FMoH)/NSHIP PIU. The essence of the retreat was premised around set
objectives/goals aimed to achieve by the project which would contribute to the
improvement in national macroeconomic objectives. To engender creativity, the PIU team
organized a retreat to set project implementation priorities for the year and device steps for
their attainment. The retreat was also used to further sensitize key officials of the Ministry
on Result Based Financing and Performance Management in the health sector.
2.4.3.2 Flag Off/Launch of the Scaled Up LGAs-Health Facilities of Bauchi and Gombe States
In order to increase political buy-in and program visibility and awareness, Gombe and Bauchi
State PIUs organized flag off ceremonies for newly scaled up LGAs. The Launch /Flag off
event focuses on the goals and objectives of the NSHIP intervention, creates awareness on
the existence of the NSHIP initiative in the scaled up LGAs and health facilities.Governors
and traditional leaders present promised to support the project at all levels as they have
witnessed the positive impact has made in the already benefiting communities. Both
governors promised to look into sustainability of the project in their respective states.The
flag off event occurred in the new scale up LGAs of Gombe (Akko and Billiri) and Bauchi
state (Kirfi, Itasgadau, Darazo) from the 18th-20th July 2019.
2.4.4 Conduct of First Lots Quality Assessment Survey (LQAs) for Ondo State; by World Health Organization
The Modified PBF in Ondo State includes replacement of routine quantity verification with Lots Quality Assurance Survey. Quality verification and counter verification continues in accordance with the project design, WHO is now responsible for the conduct of LQAS with a shift in focus from facility-based impact to population -based impact. The baseline for all LGAs was conducted in January this year and first LQAS was conducted in July 2019.Below are the results of the baseline and first survey conducted for the 9 LGAs implementing PBF in Ondo State.
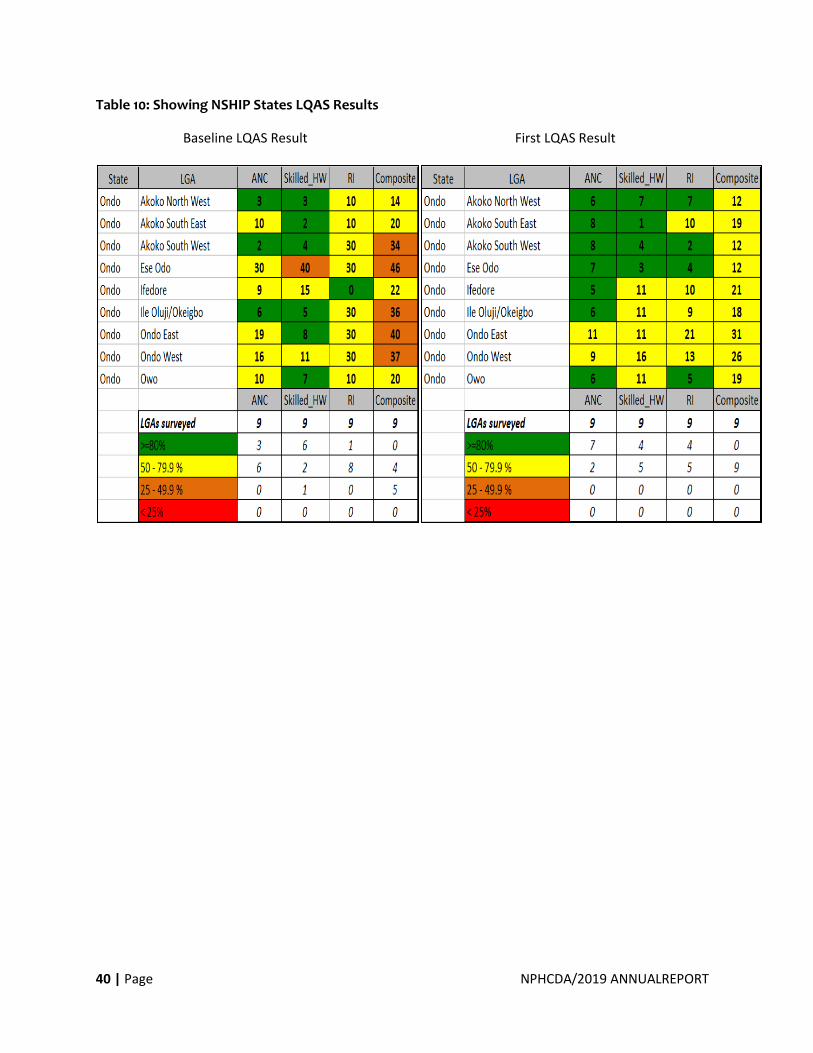
40 | Page NPHCDA/2019 ANNUALREPORT
Table 10: Showing NSHIP States LQAS Results
Baseline LQAS Result First LQAS Result
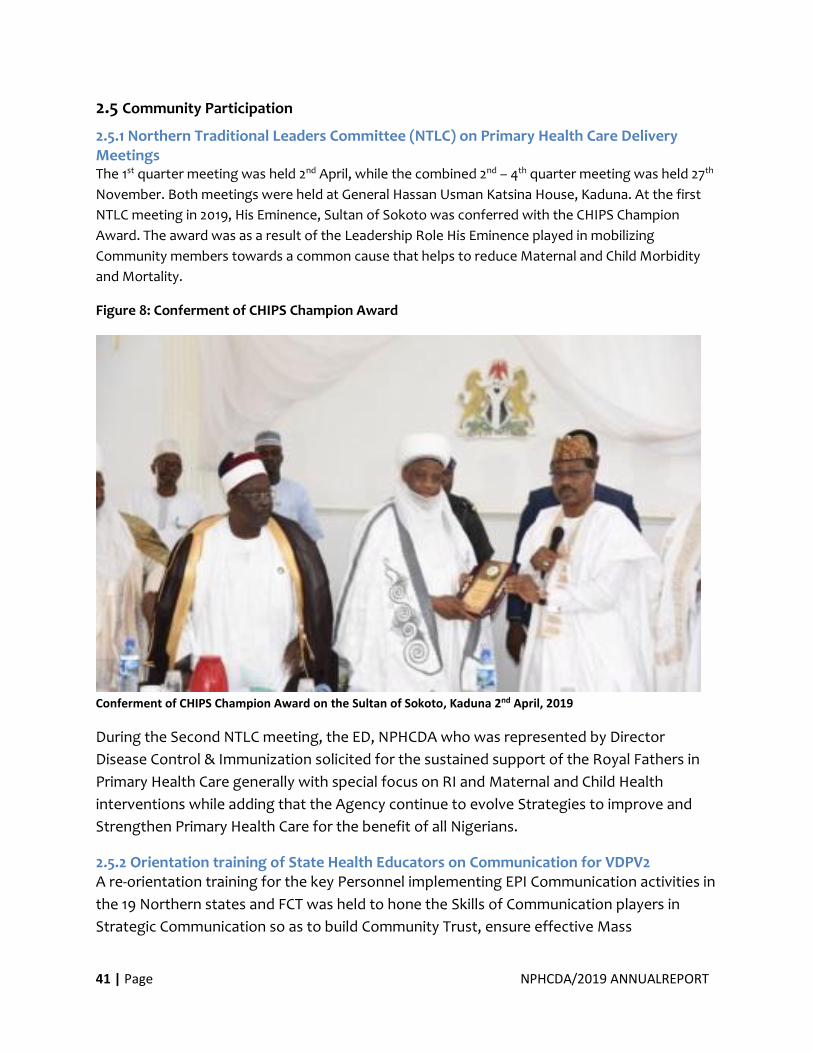
41 | Page NPHCDA/2019 ANNUALREPORT
2.5 Community Participation
2.5.1 Northern Traditional Leaders Committee (NTLC) on Primary Health Care Delivery Meetings The 1st quarter meeting was held 2nd April, while the combined 2nd – 4th quarter meeting was held 27th
November. Both meetings were held at General Hassan Usman Katsina House, Kaduna. At the first
NTLC meeting in 2019, His Eminence, Sultan of Sokoto was conferred with the CHIPS Champion
Award. The award was as a result of the Leadership Role His Eminence played in mobilizing
Community members towards a common cause that helps to reduce Maternal and Child Morbidity
and Mortality.
Figure 8: Conferment of CHIPS Champion Award
Conferment of CHIPS Champion Award on the Sultan of Sokoto, Kaduna 2nd April, 2019
During the Second NTLC meeting, the ED, NPHCDA who was represented by Director
Disease Control & Immunization solicited for the sustained support of the Royal Fathers in
Primary Health Care generally with special focus on RI and Maternal and Child Health
interventions while adding that the Agency continue to evolve Strategies to improve and
Strengthen Primary Health Care for the benefit of all Nigerians.
2.5.2 Orientation training of State Health Educators on Communication for VDPV2 A re-orientation training for the key Personnel implementing EPI Communication activities in
the 19 Northern states and FCT was held to hone the Skills of Communication players in
Strategic Communication so as to build Community Trust, ensure effective Mass
42 | Page NPHCDA/2019 ANNUALREPORT
Communication of the Outbreak and increase demand for immunization Services. This was in
line with the 36th ERC recommendation that the Programme convenes a Strategic meeting
to address the emerging mass Communication challenges related to VDPV2 Outbreak.
Outcome:
Some of the Outcomes of the meeting were:
• Improved knowledge of Participants in Polio epidemiology, especially VDPV2
• Improved knowledge and Skill of Participants in rumour management and Mass Communication of VDPV2
• State Specific Strategic Communication Plans to address key challenges were developed.
2.5.3 CHIPS Programme Retreat The National Primary Health Care Development Agency (NPHCDA) in Collaboration with
UNICEF organized a two – day CHIPS Programme Retreat in Transcorp Hotel, Abuja from
29th- 30th April, 2019 to review Progress made so far since the commencement of the
Programme in 2018.
Objectives of the Retreat were:
• To review programme activities conducted during the year 2018 challenges encountered and lessons learnt
• To identify and develop strategies for harmonisation and transitioning of existing community health interventions in focus states
• To discuss and brainstorm on scaling up and sustainable implementation in States.
43 | Page NPHCDA/2019 ANNUALREPORT
Scenes from the Retreat
Following the development of the CHIPS Programme Information, Education and
Communication (IEC) materials, a two day Photoshoot Session was conducted in Kokona
LGA of Nasarawa State from Tuesday 6th to Wednesday 7th August, 2019 for the materials
with the following Objectives:
• To do a photoshoot with the real CHIPS Agents for the IEC material
• To get appropriate pictures for each scenerio
• To have available pictures for the CHIPS Programme Unit Various Scenarios were discussed and agreed on by the National level team before the
activity. Some of which included CHIPS Agent Counselling a Womanwho is holding a baby
inside a house;A CHIPS Agent trying to teach a mother proper positioning and attachment of
her baby during breastfeeding; A CHIPS Agent completing her data tools; A CHIPS Agent
escorting a Caregiver to the Health Facility etc.

44 | Page NPHCDA/2019 ANNUALREPORT
Figure 9: Scenes of CHIPS agents in Actions
A CHIPS Agent escorting a Caregiver to the
Health Facility CHIPS Agent Counselling a Woman
who is holding a baby inside a house A CHIPS Agent completing her
data tools

45 | Page NPHCDA/2019 ANNUALREPORT
3.0 INCREASED UTILIZATION
OF ESSENTIAL PACKAGE OF
HEALTH CARE SERVICES
46 | Page NPHCDA/2019 ANNUALREPORT
3.1 Reproductive, Maternal, Newborn, Child, Adolescent Health Services &
Nutrition
3.1.1 National Emergency Maternal and Child Health Intervention Center (NEMCHIC) The National Emergency Maternal and Child Health Intervention Center (NEMCHIC) was
established by National Primary Health Care Development Agency (NPHCDA) following the
declaration of State of Public Health Concern on Maternal and Child Health in Nigeria by the
Agency on 8th April 2019. The Center is a Coordination Platform on Reproductive, Maternal,
Neonatal, Child and Adolescent Health + Nutrition (RMNCAH + N) activities at Primary Health
Care (PHC) and Community levels, with the goal of Reducing Preventable Maternal and Child
Mortality in Nigeria by 50% in 2021.NEMCHIC operated only within the last three quarters
(Q2,Q3, Q4) of 2019. The Followings are highlight on the major activities carried out by the
Center in the 2019 Operational Period:
• Operationalization of NEMCHIC
• Consultative Retreat
• Categorization of States based on RMNCAH+N key Indicators
• Development of state engagement tools
• Development of NEMCHIC operational guideline
• Engagement of RMNCAH+N stakeholders
• Development of Monitoring & Evaluation (M&E) framework
• First state engagement (Bauchi and Kebbi)
• Harmonization of state engagement visits and tools under the Optimized Integrated RMNCAH+N and Immunization Supportive Supervision (OIRISS)
• Second state engagement (Katsina, Combe and Taraba)
• Engagement with partners:
• REAKTHROUGH ACTION – NIGERIA for harmonization and standardization of community engagement and WDC tools
• e-Health Africa
47 | Page NPHCDA/2019 ANNUALREPORT
Figure 10: Declaration of State of Public Concern on MNCH Deaths
Executive Director, NPHCDA declaring a State of Public Health Concern on Maternal and Child Deaths with some Traditional Rulers; Abuja, April 8th 2019
3.1.2 First Consultative Retreat The first consultative retreat successfully held on 8-10th May 2019 at Ajuji Hotel, Abuja. The
retreat was the most immediate step taken after the emergency declaration to secure the
buy-in of stakeholders and partners across RMNCAH+N space into NEMCHIC objectives and
goals.
The Objectives of the Retreat were:
• To appraise the situation of Maternal and Child Health for each state including a review of the progress and status of the states’ RMNCAH +N operational plan in line with SSHDP and NSHDP
• To identify enablers and bottle necks to reducing maternal and child mortality in the different states
• To align on priority interventions and stakeholder’s ownership of interventions.
• To introduce the concept of National Emergency Maternal and Child Health Intervention Centre (NEMCHIC) and develop Terms of Reference for State coordinated platform.
• To facilitate peer to peer learning amongst the high and low performing states towards reduction of maternal and child mortality.
• To plan for the conduct of NEMCHIC technical and advocacy visit to states in the low category of RMNCH+N performance
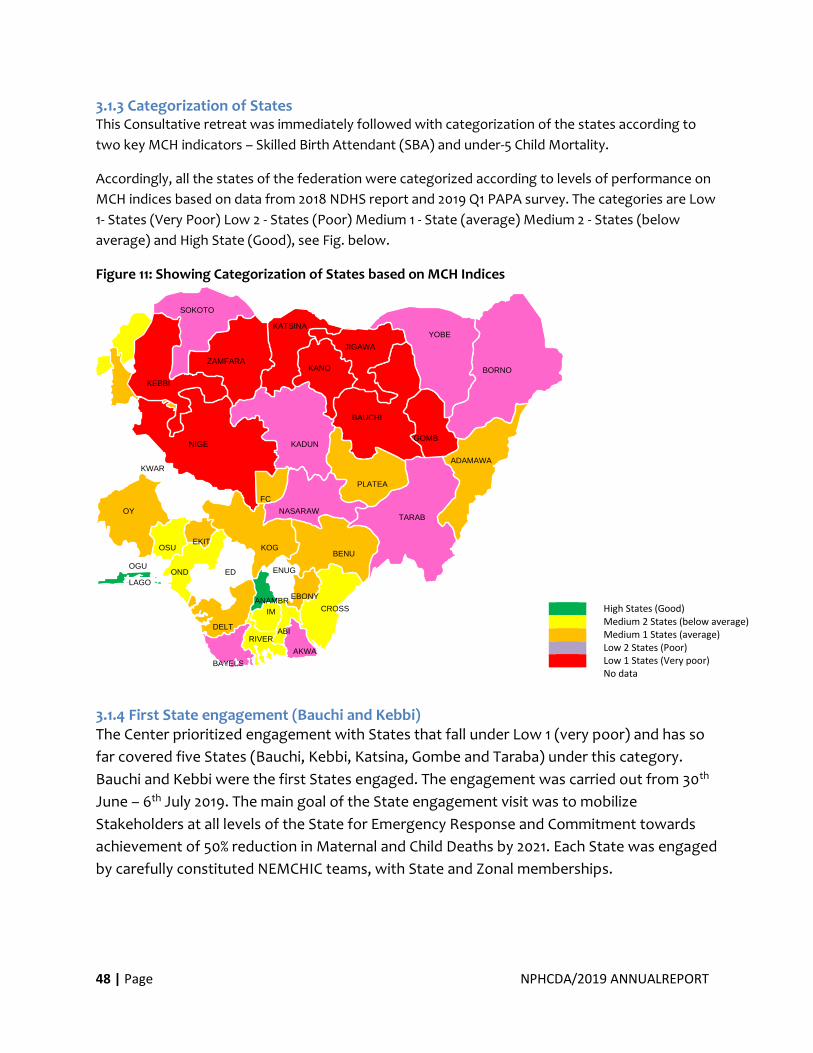
48 | Page NPHCDA/2019 ANNUALREPORT
3.1.3 Categorization of States This Consultative retreat was immediately followed with categorization of the states according to
two key MCH indicators – Skilled Birth Attendant (SBA) and under-5 Child Mortality.
Accordingly, all the states of the federation were categorized according to levels of performance on
MCH indices based on data from 2018 NDHS report and 2019 Q1 PAPA survey. The categories are Low
1- States (Very Poor) Low 2 - States (Poor) Medium 1 - State (average) Medium 2 - States (below
average) and High State (Good), see Fig. below.
Figure 11: Showing Categorization of States based on MCH Indices
3.1.4 First State engagement (Bauchi and Kebbi) The Center prioritized engagement with States that fall under Low 1 (very poor) and has so
far covered five States (Bauchi, Kebbi, Katsina, Gombe and Taraba) under this category.
Bauchi and Kebbi were the first States engaged. The engagement was carried out from 30th
June – 6th July 2019. The main goal of the State engagement visit was to mobilize
Stakeholders at all levels of the State for Emergency Response and Commitment towards
achievement of 50% reduction in Maternal and Child Deaths by 2021. Each State was engaged
by carefully constituted NEMCHIC teams, with State and Zonal memberships.
High States (Good) Medium 2 States (below average) Medium 1 States (average) Low 2 States (Poor) Low 1 States (Very poor) No data
RIVERS
FCT
ANAMBRA
ENUGU
AKWA IBOM
ADAMAWA
ABIA
BAUCHI
BAYELSA
BENUE
BORNO
CROSS RIVER
DELTA
EBONYI
EDO
EKITI
GOMBE
IMO
JIGAWA
KADUNA
KANO
KATSINA
KEBBI
KOGI
KWARA
LAGOS
NASARAWA
NIGER
OGUN OND
O
OSUN
OYO
PLATEAU
SOKOTO
TARABA
YOBE
ZAMFARA
49 | Page NPHCDA/2019 ANNUALREPORT
Key Successes recorded from Kebbi State:
• Establishment of SEMCHIC in the State, partners in Kebbi state also pledged technical support to the SEMCHIC
• Establishment of LEMCHIC
• Setting up of a Commission on revitalization of PHCs
• Flag off of distribution of delivery and other lifesaving equipment for 361 PHCs in 361 Wards in line with the upgrade of one functional PHC per Ward.
• Kebbi state government committed to ending preventable maternal and under- five mortality in the State
• The traditional institutions support towards ending preventable maternal and under- five mortality in the state through aggressive community engagement and sensitization
• Commencement of implementation of community engagement strategy for improving ANC, SBA and care of Under 5 children
Advocacy Visit to Deputy Governor Kebbi State Advocacy visit to HRH Emir of Argungu(Kebbi State)
50 | Page NPHCDA/2019 ANNUALREPORT
Advocacy Visit to Dep. Gov. Kebbi State Director Advocacy Visit to HRH Emir of Arugugun
Kebbi State
Key successes recorded from Bauchi State:
• Establishment of SEMCHIC
• High level commitment and support from the traditional council on implementation of SEMCHIC interventions
• PHC facilities provided with Mama and delivery kits
• On the job training on Data Management and Infection control/hygiene
• WDC understands the need to include RMNCAH+N Issues in meeting agenda
• Development of SEMCHIC work plan Other State engagements were Bauchi, Taraba, Katsina
Dr Nwosu Presenting Mama Kits to Gov Taraba First Lady Bauchi State Decorated as NEMCHIC Ambassador
51 | Page NPHCDA/2019 ANNUALREPORT
First Lady Katsina State Being Decorated as
Patroness Katsina NEMCHIC
Dr. Onwu Presenting Mama Kits to ES, Katsina
SPHCB
2.1 Figure 1
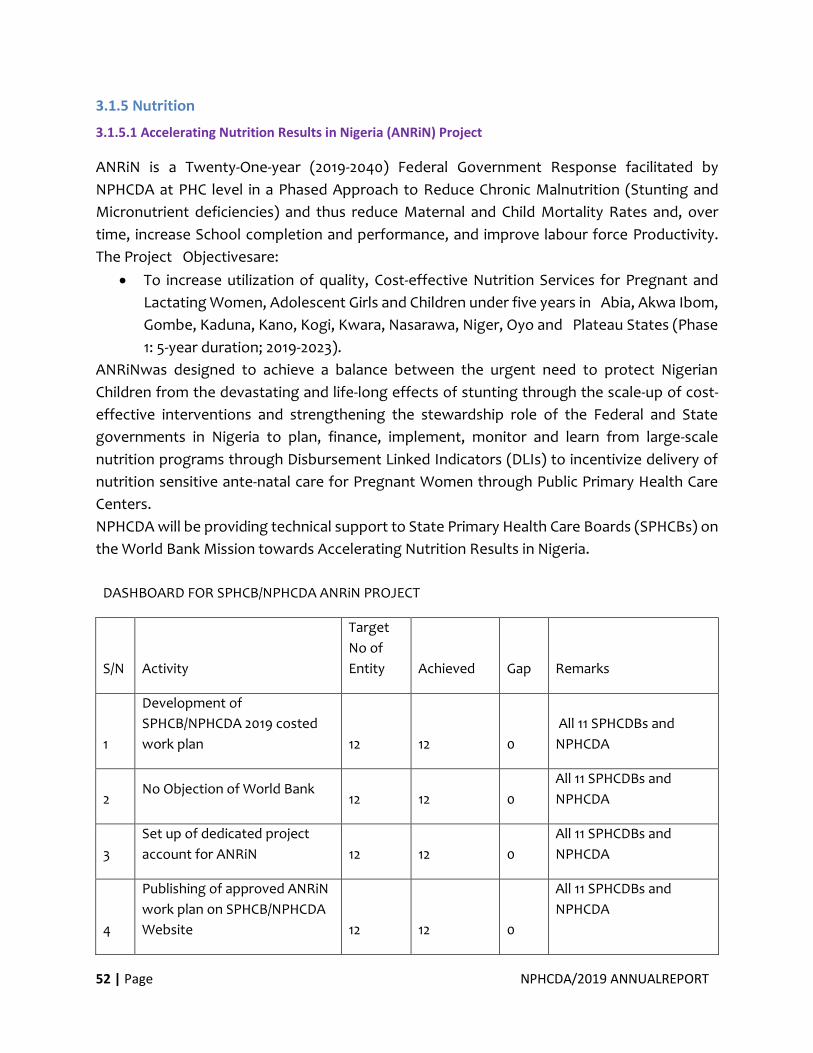
52 | Page NPHCDA/2019 ANNUALREPORT
3.1.5 Nutrition
3.1.5.1 Accelerating Nutrition Results in Nigeria (ANRiN) Project
ANRiN is a Twenty-One-year (2019-2040) Federal Government Response facilitated by
NPHCDA at PHC level in a Phased Approach to Reduce Chronic Malnutrition (Stunting and
Micronutrient deficiencies) and thus reduce Maternal and Child Mortality Rates and, over
time, increase School completion and performance, and improve labour force Productivity.
The Project Objectivesare:
• To increase utilization of quality, Cost-effective Nutrition Services for Pregnant and
Lactating Women, Adolescent Girls and Children under five years in Abia, Akwa Ibom,
Gombe, Kaduna, Kano, Kogi, Kwara, Nasarawa, Niger, Oyo and Plateau States (Phase
1: 5-year duration; 2019-2023).
ANRiNwas designed to achieve a balance between the urgent need to protect Nigerian
Children from the devastating and life-long effects of stunting through the scale-up of cost-
effective interventions and strengthening the stewardship role of the Federal and State
governments in Nigeria to plan, finance, implement, monitor and learn from large-scale
nutrition programs through Disbursement Linked Indicators (DLIs) to incentivize delivery of
nutrition sensitive ante-natal care for Pregnant Women through Public Primary Health Care
Centers.
NPHCDA will be providing technical support to State Primary Health Care Boards (SPHCBs) on
the World Bank Mission towards Accelerating Nutrition Results in Nigeria.
DASHBOARD FOR SPHCB/NPHCDA ANRiN PROJECT
S/N Activity
Target
No of
Entity Achieved Gap Remarks
1
Development of
SPHCB/NPHCDA 2019 costed
work plan 12 12 0
All 11 SPHCDBs and
NPHCDA
2 No Objection of World Bank
12 12 0
All 11 SPHCDBs and
NPHCDA
3
Set up of dedicated project
account for ANRiN 12 12 0
All 11 SPHCDBs and
NPHCDA
4
Publishing of approved ANRiN
work plan on SPHCB/NPHCDA
Website 12 12 0
All 11 SPHCDBs and
NPHCDA
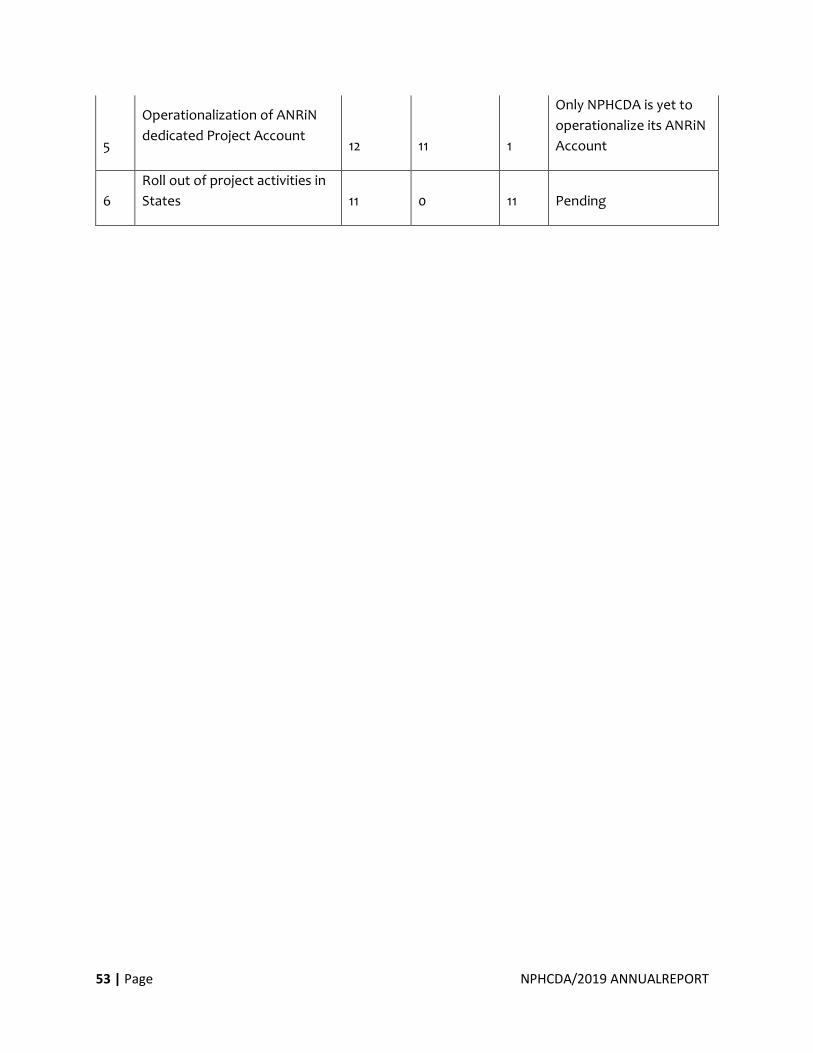
53 | Page NPHCDA/2019 ANNUALREPORT
5
Operationalization of ANRiN
dedicated Project Account 12 11 1
Only NPHCDA is yet to
operationalize its ANRiN
Account
6
Roll out of project activities in
States 11 0 11 Pending
54 | Page NPHCDA/2019 ANNUALREPORT
4.0 STRENGTHENED HEALTH
SYSTEM FOR DELIVERY OF
PACKAGE OF ESSENTIAL
HEALTH CARE SERVICES
55 | Page NPHCDA/2019 ANNUALREPORT
4.1 Human Resources for Health
4.1.1 Staff Recruitment and Training Recruitment and Documentation of Programme and Operation officers: August, 2019
Enrolment of thirty (31) officers who will be retiring in 2020 into the PENCOM database: July-
August, 2019.
Update of the 2019 promotion on the IPPIS portal: August, 2019
• Orientation workshop for newly recruited officers: August, 2019
• Workshop on Efficient Service Delivery through Discipline in the work
• Training on Work Ethics and Attitudinal Change (GL 15 - 16) and Improving Personal Effectiveness (GL 13 - 14), March, 2019.
• 2019 Promotion exercise: June-July, 2019
• Orientation workshop for Corp members and IT students: July, 2019
• Entrepreneurship Development Training for officers that will retire in 2020.
4.1.2 Ongoing/Outstanding Activities for the Year:
• Staff Audit exercise.
• Capturing of newly recruited officers on the IPPIS portal.
• Staff Training
4.1.3 N-Power Health Initiative The N-Power Health Initiative (2 years programme) is one of the four pillars of N-Power
Volunteers Corps; a Social Investment Programme of the Federal Government of Nigeria
designed to address high unemployment rate in the Country for the population (18 and 35
years). The initiative also seeks to strengthen the entrepreneurial and technical skills of the
volunteers with view to enhancing their employability after the programme. Since
November 2016, about 50,000 volunteers for health to work in their various Local
Government Areas of residence have been concluded, engaged and deployed to States to
work in the Primary Health Care Space.
The key activities conducted includes the review and update of training materials for the
volunteers and sub-national planning meetings.
4.2 Health Infrastructure
4.2.1 Health Facility Assessment for the Southern States As part of PHC re-vitalization, the National Primary Health Care Development Agency
(NPHCDA) conducted a nationwide Health Facility assessment with the following Objectives:
• To Provide a Comprehensive Database and Directory of Primary Health Care (PHCs) facilities in Nigeria
• To Validate the Primary Health Care facilities and Update the National HF List
• To Assess the Functionality of the PHC facilities
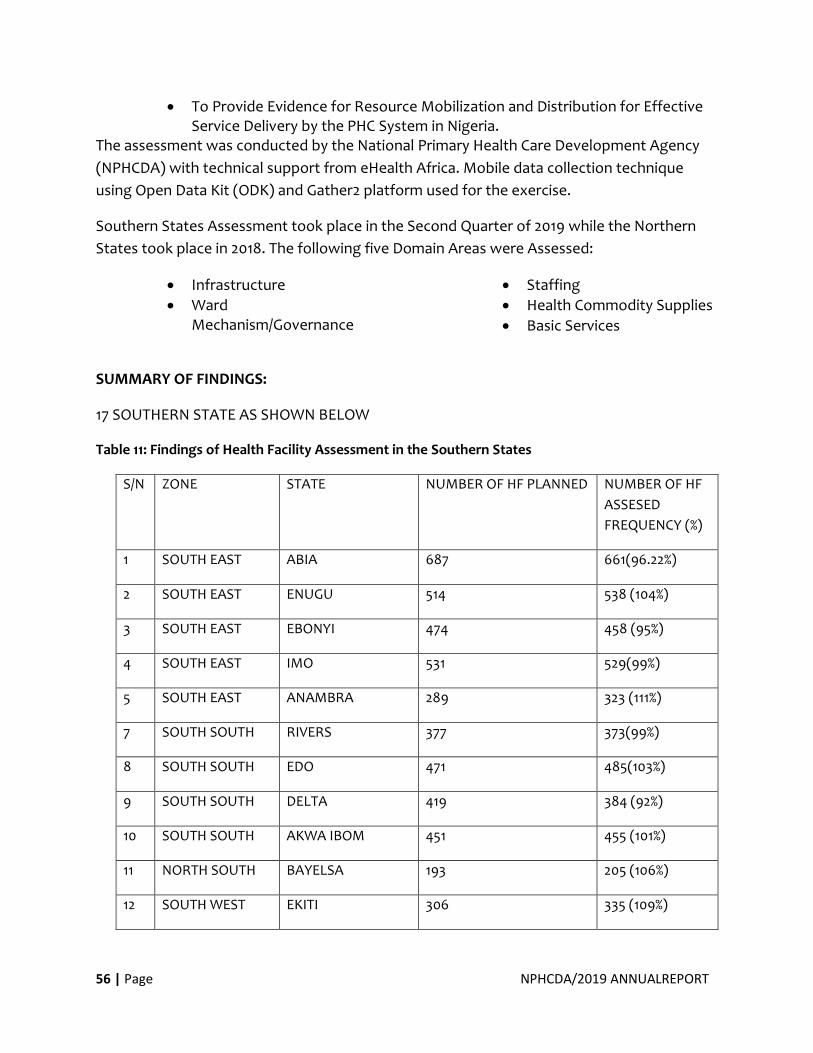
56 | Page NPHCDA/2019 ANNUALREPORT
• To Provide Evidence for Resource Mobilization and Distribution for Effective Service Delivery by the PHC System in Nigeria.
The assessment was conducted by the National Primary Health Care Development Agency
(NPHCDA) with technical support from eHealth Africa. Mobile data collection technique
using Open Data Kit (ODK) and Gather2 platform used for the exercise.
Southern States Assessment took place in the Second Quarter of 2019 while the Northern
States took place in 2018. The following five Domain Areas were Assessed:
• Infrastructure
• Ward Mechanism/Governance
• Staffing
• Health Commodity Supplies
• Basic Services
SUMMARY OF FINDINGS:
17 SOUTHERN STATE AS SHOWN BELOW
Table 11: Findings of Health Facility Assessment in the Southern States
S/N ZONE STATE NUMBER OF HF PLANNED NUMBER OF HF
ASSESED
FREQUENCY (%)
1 SOUTH EAST ABIA 687 661(96.22%)
2 SOUTH EAST ENUGU 514 538 (104%)
3 SOUTH EAST EBONYI 474 458 (95%)
4 SOUTH EAST IMO 531 529(99%)
5 SOUTH EAST ANAMBRA 289 323 (111%)
7 SOUTH SOUTH RIVERS 377 373(99%)
8 SOUTH SOUTH EDO 471 485(103%)
9 SOUTH SOUTH DELTA 419 384 (92%)
10 SOUTH SOUTH AKWA IBOM 451 455 (101%)
11 NORTH SOUTH BAYELSA 193 205 (106%)
12 SOUTH WEST EKITI 306 335 (109%)
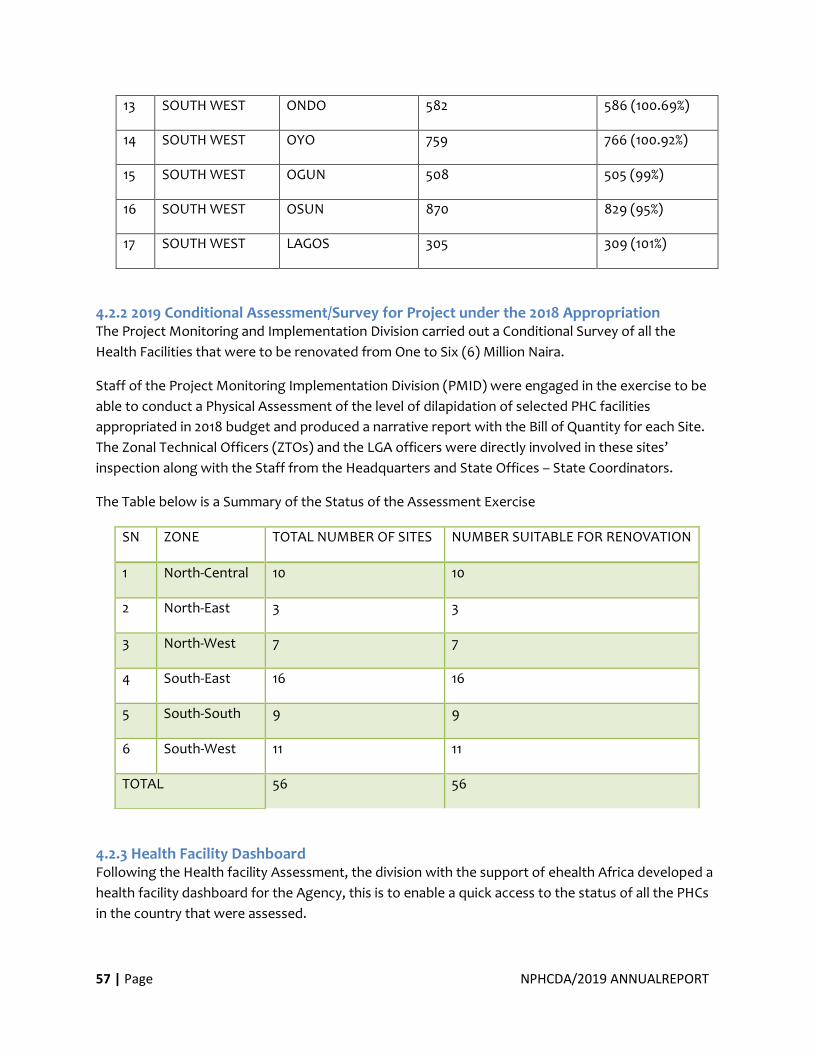
57 | Page NPHCDA/2019 ANNUALREPORT
13 SOUTH WEST ONDO 582 586 (100.69%)
14 SOUTH WEST OYO 759 766 (100.92%)
15 SOUTH WEST OGUN 508 505 (99%)
16 SOUTH WEST OSUN 870 829 (95%)
17 SOUTH WEST LAGOS 305 309 (101%)
4.2.2 2019 Conditional Assessment/Survey for Project under the 2018 Appropriation The Project Monitoring and Implementation Division carried out a Conditional Survey of all the
Health Facilities that were to be renovated from One to Six (6) Million Naira.
Staff of the Project Monitoring Implementation Division (PMID) were engaged in the exercise to be
able to conduct a Physical Assessment of the level of dilapidation of selected PHC facilities
appropriated in 2018 budget and produced a narrative report with the Bill of Quantity for each Site.
The Zonal Technical Officers (ZTOs) and the LGA officers were directly involved in these sites’
inspection along with the Staff from the Headquarters and State Offices – State Coordinators.
The Table below is a Summary of the Status of the Assessment Exercise
4.2.3 Health Facility Dashboard Following the Health facility Assessment, the division with the support of ehealth Africa developed a
health facility dashboard for the Agency, this is to enable a quick access to the status of all the PHCs
in the country that were assessed.
SN ZONE TOTAL NUMBER OF SITES NUMBER SUITABLE FOR RENOVATION
1 North-Central 10 10
2 North-East 3 3
3 North-West 7 7
4 South-East 16 16
5 South-South 9 9
6 South-West 11 11
TOTAL 56 56
58 | Page NPHCDA/2019 ANNUALREPORT
The data of the assessment included Pictures of the facilities as submitted on the server by the
individuals was used for analysis, ranking and report for each State using data on the above domain
areas. Over 21,000 health facilities were captured on the dashboard showing the pictures and status
of each facility. This is still yet to be made accessible to the public because the data collected from
the Health Facility assessment is still being validated.
Figure 12: The Health Facility Dashboard
4.2.4 Renovation of HQ, Annex, Zonal and State Offices
• During the year under Review, Management of NPHCDA renovated, furnished and equipped with
State-of-the-Art Equipment her Offices at the HQ, Zones and States. The Offices are now having a
new look and comparable with Standards in other Sister organizations.
Comprehensive renovation of the Headquarter (August-December, 2019)/Annex (January-August,
2019)/State offices (September- December, 2019).
Furnishing of the Annex office (October-November, 2019).
Provision of 300KVA generator set for the Annex office (October-November, 2019).
Routine maintenance of the office facilities/furniture and equipment.

59 | Page NPHCDA/2019 ANNUALREPORT
Figure 13: New NPHCDA Looks
New look of NPHCDA HQ at Gimbiya Street, Garki Abuja
4.2.5 Upgrade of NPHCDA Internet Facilities In order to deliver better internet experience to Staff and to prepare for deployment of fast-internet-
demanding solutions, the internet service provision contract was reviewed. Glo was selected as the
preferred Service Provider of STM-1 Capacity. This was fully deployed in March, 2019. Prior to
deployment, infrastructural updates were done on existing devices which included routers, switches,
antennas and access points. These are all functioning well. The ICT Unit also deployed an Enterprise
Internet Security: ESET Endpoint Security was approved at the close of 2018 for 500 users as a result
of the inventory of ICT equipment of Staff carried out by the ICT team. This was deployed to provide
protection to Agency Staff.
4.2.6 Other achievements:
• Distribution of 400 units of USB drives of varied Capacities (4GB: 200; 8GB: 100 & 16GB: 100). These were meant to be distributed to staff that responded to the online inventory form that was sent through the official email platform to encourage use of the official email. Distribution was concluded with the completion of the last set of Zonal Retreats.
• Deployment of fire suppression Systemin the Server Room to take care of any incidence of fire outbreak in the ICT Office. The System automatically quenches fire through a delicate Smoke Detection System and is Serviceable every Six Months. The first Servicing due Six Months Post-deployment has already been paid for.
• Installation and Configuration of Server Procured for NPHCDA by AFENETand ready for use and already functioning.
• Procurement and activation of Office 365 E3 License
• Deployment of Office 365 E3 P Solution has commenced and is still ongoing.
• Installation of Clock-in devices for two locations: Asokoro and Sahad Stores junction Offices. Configuration and installation would be completed.
60 | Page NPHCDA/2019 ANNUALREPORT
• Security door, CCTV cameras and access control systems have already been deployed in the office to guarantee the integrity of information housed in the server.
Challenges:
• Inadequate Personnel The ICT Unit, with the quantum of responsibilities being taken up and solutions proposed currently lacks the requisite personnel. This is slowing down the deployment of available solutions and the response time to issues, particularlytroubleshooting. The Unit is in dire need of personnel with competencies in database/software management, hardware management, network administration etc.
• Office Space Sequel to the enlargement of the server room, the remaining space in the ICT Office can no longer accommodate the staff, including NYSC and IT personnel attached to the Unit. The proposed movement of critical databases from Partners to the NPHCDA server would also mean that access to the server room must be restricted.
4.3 Medicines, Vaccines and Other Health Technologies and Supplies
4.3.1 State Engagements and 2020 Vaccines States Specific Forecast. The Department of Logistics and Health Commodities (LHC) Conducted the Second States
Specific Vaccine Forecasting in 2019 based on the result of 2018 NDHS.
The Objectives of the exercise were as follows:
• To Review the Current 2019 Forecast and its Performance for the States
• Conduct the Forecast considering the new trend of coverage per vaccine antigens
• Review consumption on coverage data for preceding year to guide the forecast assumptions
• Determine target and activities for the coming year including new vaccine introduction campaigns and expected coverage projections
• Forecast quantities for the year 2020 using the just concluded nationwide physical stock count of immunization supplies
• Prepare a shipment plan for vaccine and devices based on our storage capacity
Summary of Findings
Following the Physical Count exercise across the Country, the following findings were made:
61 | Page NPHCDA/2019 ANNUALREPORT
Quantitative Findings:
• Huge disparity in quantities of vaccines and diluents e.g high volumes of vaccines in VVM Stage II
• Sustained disparity in quantities of vaccines and diluents for BCG, Measles and Yellow Fever vaccines
• High volumes of bOPV and Pentavalent vaccines in VVM Stage II
• High volumes of nearly expiring vaccines
• PCV2 is still in circulation
• Overstock of some vaccines, including bOPV and Pentavalent vaccines, at a number of LGA stores
• Stock-on-hand is disproportional to target population of the LGA cold store
Qualitative Findings:
• Non-recording of stock transactions related to vaccine diluents and injection devices in the Vaccines/Diluents/Injection Equipment ledger across all levels
• Limited/no reporting of vaccines/diluents damage and expiry across all levels
• Disparity between physical stock count, ledger entries and LMIS’ at appropriate levels
• Multiplicity of data tools that are not in compliance with nationally approved data tools
Communique Issued at the States-Specific Vaccines Forecasting For 2020 Held at Barcelona
Hotels, Blantyre Crescent Wuse 2, Abuja
The following Recommendations/Resolutions were adopted:
• Physical Stock Count should be conducted monthly at State level and Weekly at LGA and Facility levels by the cold chain officers at all levels with regular effective Supportive Supervision by the SLWG
• The National Logistics Working Group (NLWG) to agree on more reliable denominator to be used by states for vaccine forecasting
• High doses containing vaccines like BCG should be reduced by the manufacturers, immunization sessions and SIAs properly monitored, improve the capacity of vaccine stakeholders across all levels and revamp cold chain infrastructures
• States should provide budget line and release funds timely for vaccine logistics to all levels in the State
• Establish/Reactivate SLWG, provide budget line to fund the LWG and monitor the implementation of Continuous Improvement Plan (CIP)
• National and States to provide data tools, States to improve capacity of stakeholders on DHIS2 usage by training and retraining and National to improve the functionality of the DHIS2 platform by allowing the State to have full access and control facilities on the platform
62 | Page NPHCDA/2019 ANNUALREPORT
4.3.2 Vaccine and Related Commodities Physical Stock Count in Nigeria from 10th – 23rd June, 2019 As part of the drive to improve Vaccine Accountability and Stock Management, the NPHCDA
through the National Logistics Working Group (NLWG) conducted a nationwide Physical
Stock Count (PSC) Exercise from the National level to the Service delivery points. The
Purpose of this exercise was to provide Strategic and actionable insight into the volume of
Vaccines and related Commodities available ahead of the 2020 Vaccines and devices forecast
exercise.
The Objectives were:
• To Conduct a Physical Stock Count of all Antigens and devices at the National, Zonal, State and Local Government Area (LGA) Cold and Dry Stores, Health Facilities (HFs) with Cold Chain Equipment and other Storage points across the Country;
• To determine the actual quantity of Vaccines and related Commodities in Country
• To verify the accuracy and completeness of stock records at all levels in compliance with best practices
• To obtain selected indicators that provide insight into performance of Nigerian iSC and its alignment with the Dashboard for Immunisation Supply Chain (DISC) indicators
• To support stores to arrange products according to Earliest Expiry FirstOut (EEFO) principle
• To identify gaps and recommend strategies for improving stock and inventory management practices per EVM Standards.
FINDINGS
The following were some of the findings from the various Zones and their corresponding
States, LGAs and HFs.
SOUTH WEST ZONE FINDINGS
• Results of the PSC at the SW Zonal Store revealed that all the assessed vaccines and diluents were available in the store. The most stocked vaccines and devices were bivalent oral polio vaccine (bOPV) and 0.5ml syringe respectively while the least stocked vaccine and devices were Yellow fever vaccine and 2ml syringe respectively.
• PSC results from the Six SW State stores revealed that the most stocked vaccines were monovalent oral polio vaccine type 2 (mOPV2) with the highest stock found in Lagos State store, Yellow fever with the highest stock found in Ondo State store, and bOPV with the highest stock found in Lagos State store.
63 | Page NPHCDA/2019 ANNUALREPORT
Meningococcal ACWY vaccine (MenACWY) was found only in Lagos State store, Inactivated polio vaccine - 10 (IPV10) was only found in Ekiti and Ogun State stores while Pneumococcal conjugate vaccine – 2 (PCV2) vaccine was found only in Ekiti State store.
• Across all the stores visited, the most stocked device was 0.5ml syringe while the least stocked was 2ml syringe. Also, there was no expired vaccine at the zonal and State stores, but expired devices were found only at the zonal and Lagos State stores. However, ‘soon-to expire’ vaccines were found at the zonal and State stores.
• It is worthy of note that there was no Trivalent oral polio vaccine (tOPV) vaccine found in any of the stores visited in the SW zone. However, mOPV2 vaccines were found, at all the levels of the supply chain.
• All WICRs in the State stores were functional. However, in Lagos State Store, one of the compartments of the dual WICR was not functional. Further analysis showed that about 83% of the deep freezers in Lagos State Store and 47% of deep freezers in Ekiti were functional. Additionally, no deep freezer was reportedly found in Ogun and Ondo State cold stores.
• SOUTH EAST ZONE FINDINGS
Total stock of vaccines, diluents, devices, data tools and asset – including diluents (in vials
and doses) segregated by batch number, expiry date and VVM status.
The Tables below showed the sums of the Vaccines counted at each Zonal, State and LGA
Cold Stores.
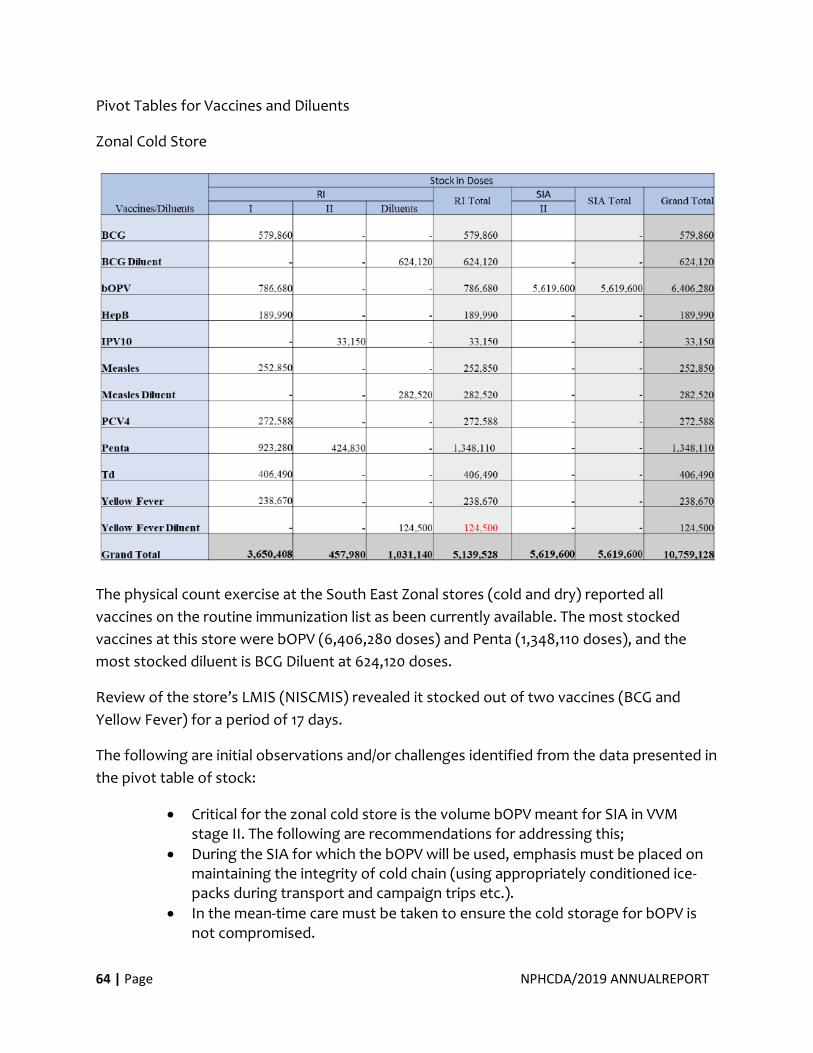
64 | Page NPHCDA/2019 ANNUALREPORT
Pivot Tables for Vaccines and Diluents
Zonal Cold Store
The physical count exercise at the South East Zonal stores (cold and dry) reported all
vaccines on the routine immunization list as been currently available. The most stocked
vaccines at this store were bOPV (6,406,280 doses) and Penta (1,348,110 doses), and the
most stocked diluent is BCG Diluent at 624,120 doses.
Review of the store’s LMIS (NISCMIS) revealed it stocked out of two vaccines (BCG and
Yellow Fever) for a period of 17 days.
The following are initial observations and/or challenges identified from the data presented in
the pivot table of stock:
• Critical for the zonal cold store is the volume bOPV meant for SIA in VVM stage II. The following are recommendations for addressing this;
• During the SIA for which the bOPV will be used, emphasis must be placed on maintaining the integrity of cold chain (using appropriately conditioned ice-packs during transport and campaign trips etc.).
• In the mean-time care must be taken to ensure the cold storage for bOPV is not compromised.
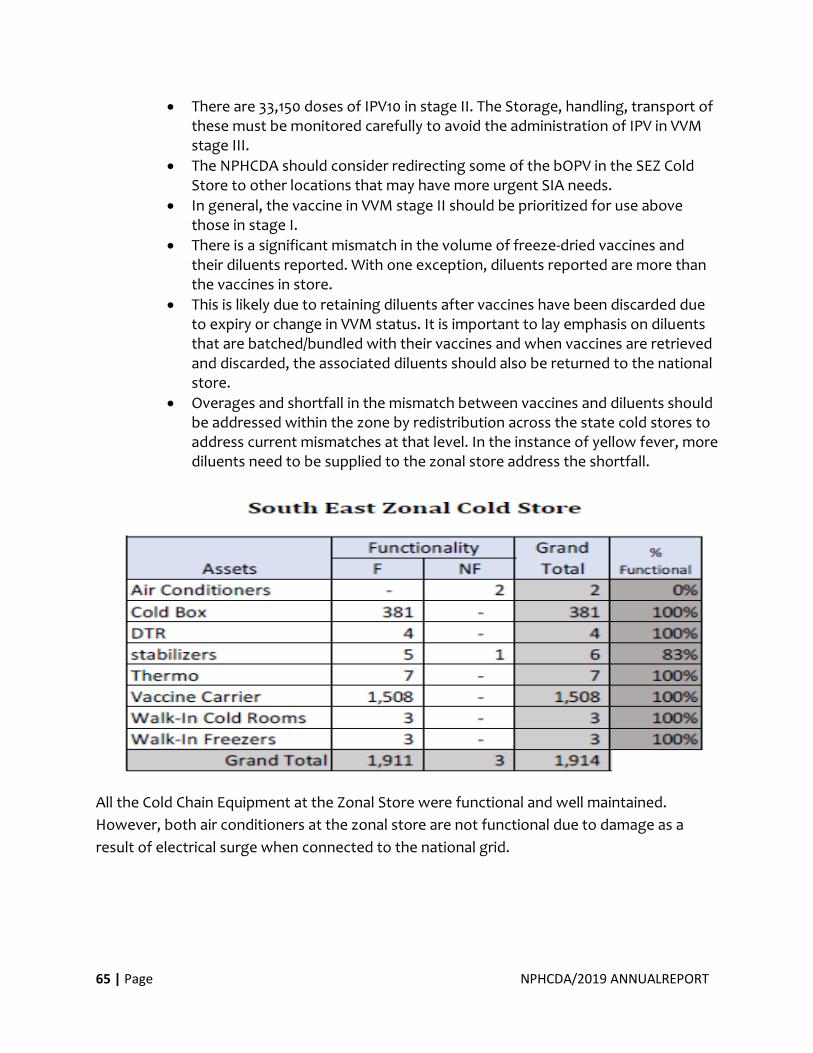
65 | Page NPHCDA/2019 ANNUALREPORT
• There are 33,150 doses of IPV10 in stage II. The Storage, handling, transport of these must be monitored carefully to avoid the administration of IPV in VVM stage III.
• The NPHCDA should consider redirecting some of the bOPV in the SEZ Cold Store to other locations that may have more urgent SIA needs.
• In general, the vaccine in VVM stage II should be prioritized for use above those in stage I.
• There is a significant mismatch in the volume of freeze-dried vaccines and their diluents reported. With one exception, diluents reported are more than the vaccines in store.
• This is likely due to retaining diluents after vaccines have been discarded due to expiry or change in VVM status. It is important to lay emphasis on diluents that are batched/bundled with their vaccines and when vaccines are retrieved and discarded, the associated diluents should also be returned to the national store.
• Overages and shortfall in the mismatch between vaccines and diluents should be addressed within the zone by redistribution across the state cold stores to address current mismatches at that level. In the instance of yellow fever, more diluents need to be supplied to the zonal store address the shortfall.
All the Cold Chain Equipment at the Zonal Store were functional and well maintained.
However, both air conditioners at the zonal store are not functional due to damage as a
result of electrical surge when connected to the national grid.
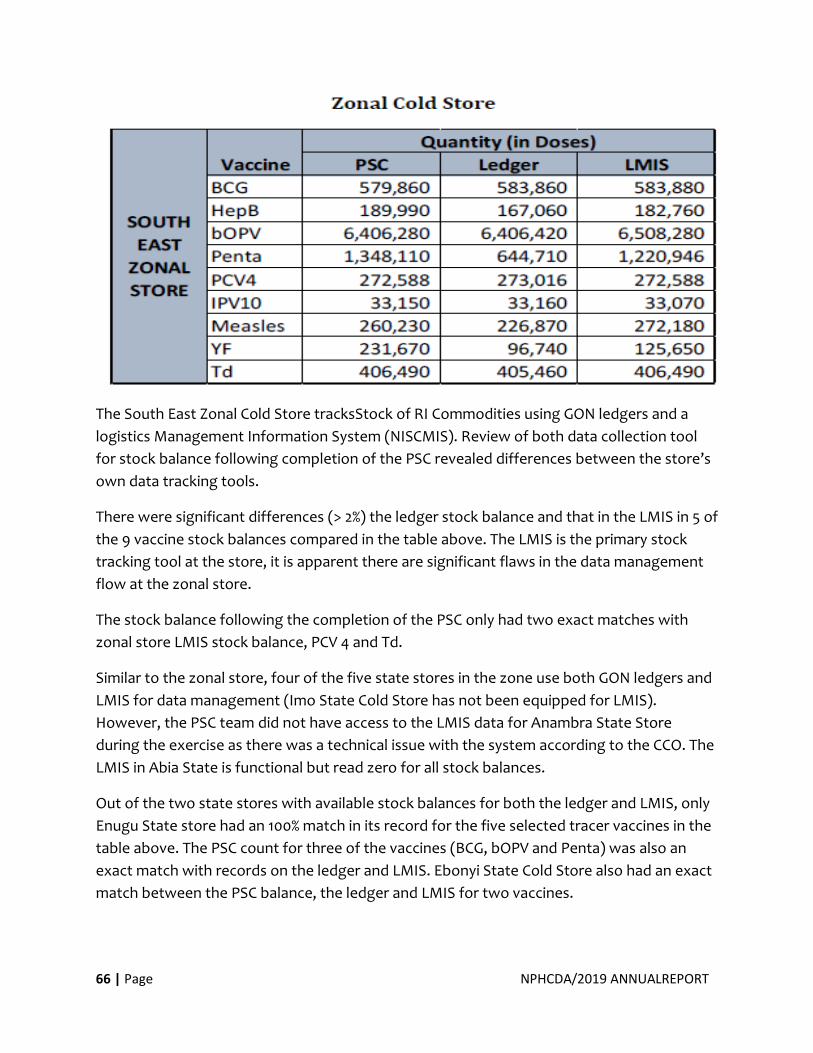
66 | Page NPHCDA/2019 ANNUALREPORT
The South East Zonal Cold Store tracksStock of RI Commodities using GON ledgers and a
logistics Management Information System (NISCMIS). Review of both data collection tool
for stock balance following completion of the PSC revealed differences between the store’s
own data tracking tools.
There were significant differences (> 2%) the ledger stock balance and that in the LMIS in 5 of
the 9 vaccine stock balances compared in the table above. The LMIS is the primary stock
tracking tool at the store, it is apparent there are significant flaws in the data management
flow at the zonal store.
The stock balance following the completion of the PSC only had two exact matches with
zonal store LMIS stock balance, PCV 4 and Td.
Similar to the zonal store, four of the five state stores in the zone use both GON ledgers and
LMIS for data management (Imo State Cold Store has not been equipped for LMIS).
However, the PSC team did not have access to the LMIS data for Anambra State Store
during the exercise as there was a technical issue with the system according to the CCO. The
LMIS in Abia State is functional but read zero for all stock balances.
Out of the two state stores with available stock balances for both the ledger and LMIS, only
Enugu State store had an 100% match in its record for the five selected tracer vaccines in the
table above. The PSC count for three of the vaccines (BCG, bOPV and Penta) was also an
exact match with records on the ledger and LMIS. Ebonyi State Cold Store also had an exact
match between the PSC balance, the ledger and LMIS for two vaccines.
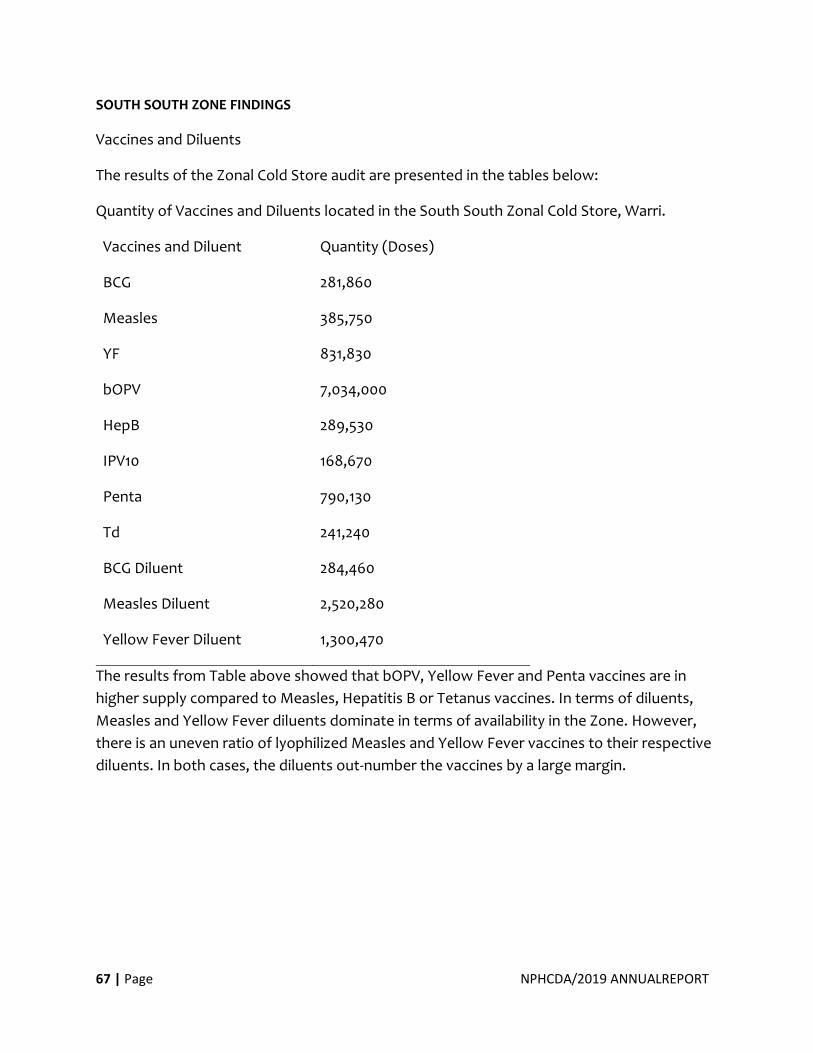
67 | Page NPHCDA/2019 ANNUALREPORT
SOUTH SOUTH ZONE FINDINGS
Vaccines and Diluents
The results of the Zonal Cold Store audit are presented in the tables below:
Quantity of Vaccines and Diluents located in the South South Zonal Cold Store, Warri.
Vaccines and Diluent Quantity (Doses)
BCG 281,860
Measles 385,750
YF 831,830
bOPV 7,034,000
HepB 289,530
IPV10 168,670
Penta 790,130
Td 241,240
BCG Diluent 284,460
Measles Diluent 2,520,280
Yellow Fever Diluent 1,300,470
The results from Table above showed that bOPV, Yellow Fever and Penta vaccines are in
higher supply compared to Measles, Hepatitis B or Tetanus vaccines. In terms of diluents,
Measles and Yellow Fever diluents dominate in terms of availability in the Zone. However,
there is an uneven ratio of lyophilized Measles and Yellow Fever vaccines to their respective
diluents. In both cases, the diluents out-number the vaccines by a large margin.
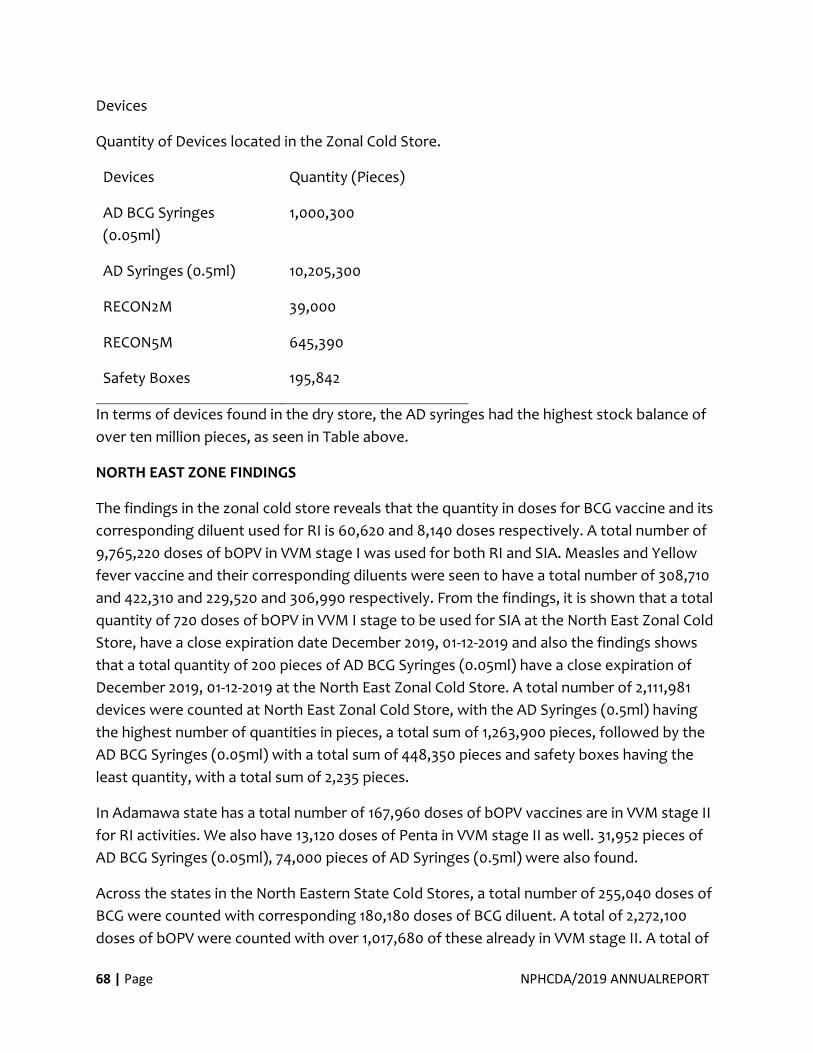
68 | Page NPHCDA/2019 ANNUALREPORT
Devices
Quantity of Devices located in the Zonal Cold Store.
Devices Quantity (Pieces)
AD BCG Syringes
(0.05ml)
1,000,300
AD Syringes (0.5ml) 10,205,300
RECON2M 39,000
RECON5M 645,390
Safety Boxes 195,842
In terms of devices found in the dry store, the AD syringes had the highest stock balance of
over ten million pieces, as seen in Table above.
NORTH EAST ZONE FINDINGS
The findings in the zonal cold store reveals that the quantity in doses for BCG vaccine and its
corresponding diluent used for RI is 60,620 and 8,140 doses respectively. A total number of
9,765,220 doses of bOPV in VVM stage I was used for both RI and SIA. Measles and Yellow
fever vaccine and their corresponding diluents were seen to have a total number of 308,710
and 422,310 and 229,520 and 306,990 respectively. From the findings, it is shown that a total
quantity of 720 doses of bOPV in VVM I stage to be used for SIA at the North East Zonal Cold
Store, have a close expiration date December 2019, 01-12-2019 and also the findings shows
that a total quantity of 200 pieces of AD BCG Syringes (0.05ml) have a close expiration of
December 2019, 01-12-2019 at the North East Zonal Cold Store. A total number of 2,111,981
devices were counted at North East Zonal Cold Store, with the AD Syringes (0.5ml) having
the highest number of quantities in pieces, a total sum of 1,263,900 pieces, followed by the
AD BCG Syringes (0.05ml) with a total sum of 448,350 pieces and safety boxes having the
least quantity, with a total sum of 2,235 pieces.
In Adamawa state has a total number of 167,960 doses of bOPV vaccines are in VVM stage II
for RI activities. We also have 13,120 doses of Penta in VVM stage II as well. 31,952 pieces of
AD BCG Syringes (0.05ml), 74,000 pieces of AD Syringes (0.5ml) were also found.
Across the states in the North Eastern State Cold Stores, a total number of 255,040 doses of
BCG were counted with corresponding 180,180 doses of BCG diluent. A total of 2,272,100
doses of bOPV were counted with over 1,017,680 of these already in VVM stage II. A total of
69 | Page NPHCDA/2019 ANNUALREPORT
380,660 doses of mOPV2 were also found. From findings, Bauchi State has a total number of
824,720 doses of bOPV vaccines which are in VVM stage II cutting across both RI and SIA
activities. Borno state has a total of 480,000 doses of bOPV vaccine and a total number of
6,530 PCV4 vaccines which are VVM Stage II. Gombe state has a total number of 25,000
doses of bOPV in stage II, 17,100 doses of IPV10 in stage II and 61,410 doses of Penta in stage
II. From the finding, more BCG vaccines can be found in the Taraba state cold store without
the matching number of diluents. The State also has a total of 315,120 doses of bOPV. Yobe
state has a total number of 5,200 doses of IPV5 in VVM stage II. During the stock count
exercise, 33,100 doses of bOPV were counted. No tOPV was found in the North East Zone.
From the findings, it was shown that in Adamawa state, Gombi LGA Cold store and Song LGA
Cold store had IPV10 and Penta vaccines in VVM stage III. Also, Hong LGA Cold store was
seen to have 220 doses of bOPV in VVM stage IV. Additionally, in Michika LGA cold store of
Adamawa state, Hep B vaccine used for RI programme expired on the 1st of April 2019 and in
Damaturu Satellite Cold Store, Yobe state, mOPV2 was seen to have expired on 01/09/2018.
Findings also shows the vaccine/diluent that had expired in the Zonal cold store. Measles
diluent of batch number 9912414 and 03-1674 expired in 01/05/2019 and 01/08/2018
respectively. Furthermore, Yellow fever diluent with batch number 46 and M8003-1 was
found to have expired on 01/04/2019 and 01/01/2018 respectively. Td was also seen to have
expired on 01/01/2018.
Across State cold stores in the North East Zone, findings showed that there were less than
1% (<1%) closed vial wastage of vaccine and diluents.
At the North East Zonal Cold Store level, most of the storage points had full stock availability
of over 80% for the resupply period. Analysis of findings from the physical stock count also
revealed that at the state cold store level, 94.9% of the state cold stores had full stock
availability over the resupply period. In the North East zone three states (Bauchi, Borno,
Yobe) have state satellite cold store. The state satellite cold store supplies stock to the LGA
cold store. Very few states satellite cold stores experienced stock out over the specified
resupply period. 94.7% of the satellite cold store had full stock availability. Findings also
showed that 89.40% of the LGA cold store across the North East zone had full stock
availability of vaccines and devices across. At the Health Facility Level, Majority 92.7% of
health facilities had full stock availability over the specified however, only 5.9% of the health
facilities in the North East Zone experienced stock out of vaccines and devices over the
specified resupply period.
Significant non-functional cold chain equipment as shown in the table 48 include 2 walk-in
cold room in Taraba and 1 walk in freezer also in Taraba. All walk-in cold rooms at the North
70 | Page NPHCDA/2019 ANNUALREPORT
East State Satellite cold stores are functional. There was however a single unit of Ice pack
Freezer found at the Borno Central State Satellite cold store which was non-functional.
In calculation of the DISC indicator stocked according to plan (SATP) requests over a
specified period were used to calculate the average monthly consumption (AMC) and the
stock on hand which was obtained during the physical stock count exercise was then used
to calculate the months or weeks of stock. The estimates from Bauchi, Adamawa, and Yobe
state cold stores show that these stores are understocked while the Borno state cold store
is overstocked.
Compliance with best storage and record keeping practices seemed to decline significantly
down the supply chain as it was observed that the LGA separated and documented expiries
better than the health facilities. Comparison across the states showed that Gombe state
health facilities had a poor compliance to best storage and record keeping practices. 14% and
10% of the health facility in Bauchi and Adamawa were seen to document damages and
expiries following best storage and record keeping practices. More than 60% of the LGA cold
stores across the 6 north eastern states observe EEFO principle and store vaccine under the
right temperature. LGA cold stores especially in Bauchi and Borno did not seem to have
shelves and pallets to properly store their dry stock items. Separation and documentation of
expiries seemed to be a common challenge at the health facilities and LGA cold stores. All
the state cold stores in the NEZ including the zonal cold store observe the EEFO principle in
vaccine/diluent and devices storage except the Borno state. Shelves and pallets can be
found in the dry store of the NEZCS and that of the six states cold stores in the zone. All the
state cold stores seem to separate expiries from the usable products. Finding also shows
that these expiries are documented and properly recorded into a designated checklist.
Data Accuracy was determined using the WHO’s validated standard methodology for
immunisation Data Quality Audit (DQA). This methodology was adopted to compare stock
balances across physical count quantity, ledger balance and LMIS balance at the Zonal, State
and Health Facility Cold Stores. An Accuracy Ratio of between ≥ 0.95 to ≤ 1.05 indicates
consistent data and AR of < 0.95 or >1.05 indicates data over reported or under reported.
The figure below shows that some satellite stores still have challenges with data accuracy
and records are not transferred adequately into the ledgers and the LMIS system available.
At the State level similar documentation challenges exist across board except in Bauchi state
where adequate records are kept and transferred across the physical count conducted,
ledgers and LMIS available.
71 | Page NPHCDA/2019 ANNUALREPORT
NORTH CENTRAL FINDINGS
Vaccines and diluents were taken stock of and recorded at the National Strategic Cold Chain
Store. All vaccines and diluents counted were in the VVM stage I and were used for both
Routine Immunization and Supplementary Immunization activities. The quantity in doses for
BCG vaccine and its corresponding diluent used for RI is 2,358,480 and 2,451,140 doses
respectively. The total number of bOPV is 12,222,760 doses as seen in the table shown above.
Measles vaccine and its corresponding diluents used for RI have a total number of 4,937,040
and 3,576,900 while Yellow fever vaccine and its diluent was seen to have 2,732,360 and
4,824,460 quantities in doses respectively. At the National Strategic Cold Chain Store AD
BCG Syringes (0.05ml) and AD Syringes (0.5ml) have a total number of 4,167,660 and
1,045,953 pieces respectively. The 2ml and 5ml RUP Reconstitution Syringes were 3,592 and
665,558 pieces respectively. 5L safety boxes were 34,106 pieces in quantity.
The North Central Zonal Cold store, the team found disparities between BCG vaccine and its
corresponding diluent at 2,284,480 and 631,020 doses respectively as well as Measles
vaccine and its diluent with a total number of 252,660 and 343,100 doses respectively. The
table above also shows that Yellow Fever vaccine and its diluents are 151,300 and 206,550
doses respectively. 1,565,600 doses of bOPV were found to be in VVM II. Other vaccines
counted include IPV 10, Penta and Td with 346,000, 352,360 and 188,660 doses respectively.
A total of 992,990 pieces AD Syringes (0.5ml), 45,730 pieces of AD Syringes (5ml) and
143,225 pieces of Safety boxes (5L) were counted in the zonal cold store.
At the National and North Central Zonal Cold Store there were no historical expired and
damage vaccines found over the specified period. Across facilities and cold store in the
North Central Zone, findings showed that there were less than 1% (<1%) closed vial wastage
of vaccine and diluents. With exception of Kwara State where Penta vaccine was found to
have 4.96% Closed Vial wastage rate.
At the National and Zonal Cold Store level, no stock out was recorded, as they both had a
100% full stock availability over the resupply period. Analysis of findings from the physical
stock count also revealed that at the state cold store level, 87.50% of the state cold store had
full stock availability over the resupply period. Findings also showed that at the Local
Government Area Cold Store level, 92.50% of the LGA cold store across the North Central
zone had full stock availability of vaccines and devices over the resupply across. At the
Health Facility Level, Majority 93.6% of health facilities had full stock availability over the
specified period.
A further analysis was done at the state level and findings showed that health facilities and
cold store in Kwara State did not have any stock out of vaccines and diluents within the

72 | Page NPHCDA/2019 ANNUALREPORT
period of review (100% full stock availability). However, facilities and Cold stores in Niger and
Nasarawa State, had the lowest (85.1% and 85.3% respectively) full stock availability when
compared to other states in the zone.
A DISC indicator (functional Status of cold chain equipment) was determined in combination
with other cold chain assets by estimating the ratio between the quantities of functional and
non-functional items. Vaccine carriers, walk in cold rooms and freezers were 100% functional
at the National Strategic Cold Store. The Store had just one non-functional domestic freezer.
The walk-in freezer room, refrigerator rooms and cold boxes were 100% functional at the
NCZCS.
NORTH WEST ZONE FINDINGS
Analysis of the Proportions of Vaccines/Diluents at the Facilities Level
The chart below depicts the proportion of all vaccines and their corresponding diluents at
each supply chain level in all the seven (7) states. 32.9% BCG was at the zonal cold store. Also
at the zonal store, was bOPV at 87.0%, mOPV at 86.4%, and PCV4 at 44.1%, Penta at 48.3%, Td
at 50.5% and YF at 55.7%.
In addition, them OPV2 was mostly available at the zonal cold store (86.4%) as it is only been
used on an outbreak basis.
Antigens like IPV10 (83.6%), Men ACW (92.3%), Men A Diluent (96.8%), and PCV (49.0%) were
mostly found in the state cold stores pending distribution to the satellite, LGA and health
care facilities.
Proportion of vaccines/diluents at the facilities levels

73 | Page NPHCDA/2019 ANNUALREPORT
Analysis of Vaccines/Diluents Expiry in the North-West Zone
The chart below shows the total doses of all vaccines expiring in July 2019 up to December
2020. There are relatively large number of vaccines that will be expiring in 2019 like the Penta
with 1,176,922 doses, Measles 68,320 doses, Hep B 1810 doses, and Yellow Fever 7270 doses.
While, most of the vaccines, will expire in 2020 like the BCG with 1,258,377, bOPV 16,160,296,
Men A 14, IPV 3660, and PCV with 220 doses.
Analysis of vaccines/diluents expiry
The table below shows the total number of vaccines at each supply chain level and their year
of expiry for 2019, 2020 and 2021 and above.
While twenty million, one hundred and six thousand, three hundred and fifty-eight
(20,106,358) doses of vaccines will be expiring by 2020, six million, nine hundred and sixty-
one thousand, five hundred and seven (6,961,507) will expire 2021 and above.
By the end of 2019, one million, two hundred and eighty-six thousand, six hundred and four
(1,286,604) doses of vaccines would have expired.
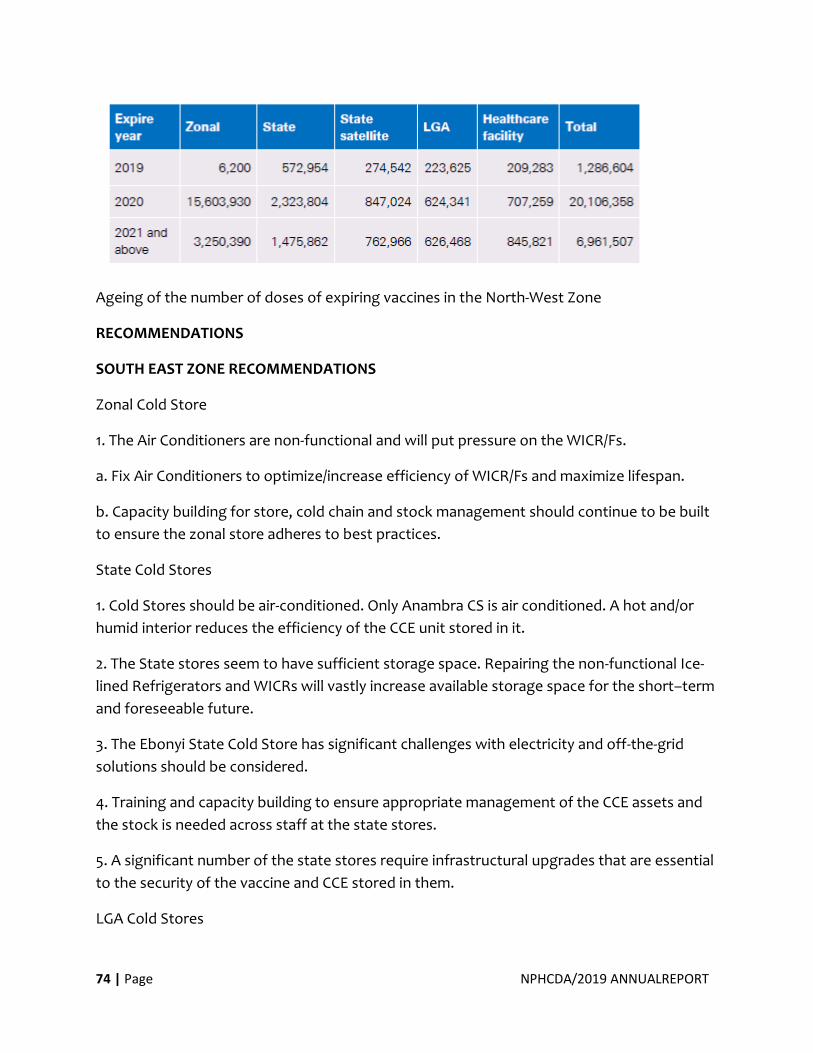
74 | Page NPHCDA/2019 ANNUALREPORT
Ageing of the number of doses of expiring vaccines in the North-West Zone
RECOMMENDATIONS
SOUTH EAST ZONE RECOMMENDATIONS
Zonal Cold Store
1. The Air Conditioners are non-functional and will put pressure on the WICR/Fs.
a. Fix Air Conditioners to optimize/increase efficiency of WICR/Fs and maximize lifespan.
b. Capacity building for store, cold chain and stock management should continue to be built
to ensure the zonal store adheres to best practices.
State Cold Stores
1. Cold Stores should be air-conditioned. Only Anambra CS is air conditioned. A hot and/or
humid interior reduces the efficiency of the CCE unit stored in it.
2. The State stores seem to have sufficient storage space. Repairing the non-functional Ice-
lined Refrigerators and WICRs will vastly increase available storage space for the short–term
and foreseeable future.
3. The Ebonyi State Cold Store has significant challenges with electricity and off-the-grid
solutions should be considered.
4. Training and capacity building to ensure appropriate management of the CCE assets and
the stock is needed across staff at the state stores.
5. A significant number of the state stores require infrastructural upgrades that are essential
to the security of the vaccine and CCE stored in them.
LGA Cold Stores
75 | Page NPHCDA/2019 ANNUALREPORT
1. Dry Stores should be equipped with shelves and pallets to enable efficient storage of the
dry goods.
2. LGA cold Stores should be air-conditioned to extend the lifespan on the Ice-lined
refrigerators and increase the efficiency of the storage devices kept there.
3. Stores should be encouraged to institute the Early Expiry, First Out (EEFO) stock
management principle.
4. A significant proportion of CCE at the LGA and State stores are non-functional, with
number of LGA stores having to store their vaccines at nearby facilities. Nearly half of the
CCE in Abia are non-functional. States need to develop a Preventive Maintenance Plan to
routinely service functional CCE as well as identify and fix non-functional yet repairable ones
within a reasonable time. This should be preceded by an obsolescence analysis to identify
CCE that should be discarded – using environmentally responsible and safe techniques -and
not counted as part of the state cold chain asset. Obsolescence analysis (and performance
testing) also needs to be conducted for passive devices to ensure they are still viable and
functional.
5. A significant number of the state stores require infrastructural upgrades that are essential
to the security of the vaccine and CCE stored in them.
Additional LGAs without storage capacity
1. Oguta local government area cold store, in Imo State, stored their vaccines at Egbeoma
health center.
2. 500 doses of expired vaccines (Penta) were retrieved during counting at Egbeoma health
center
3. One functional freezer belonging to Oguta local government Area is at Imo state Cold
store.
4. Owerri West LGA stock their vaccines at Obinze health centre
General
The NPHCDA should pursue certain best practices to achieve the required safety standards
1. Air conditioning rooms/stores that house CCE significantly improves their efficiency and
this should be pursued as a best Practice.
76 | Page NPHCDA/2019 ANNUALREPORT
2. Providing a reliable power source for State/LGA cold stores (a sustainable mix between
national grid access and a supplementary power generation equipment).
3. Capacity building on skills on the organization of stores - dry or cold – (EEFO, the use of
pallets and shelves, etc.) is critical to appropriate record keeping and proper management of
stock and assets.
4. Activity should not be conducted during the rainy season as it was difficult to access some
areas it also increased the hours spent on the road consequently increased the number of
days for completion of the exercise.
SOUTH WEST ZONE RECOMMENDATIONS
The 2019 PSC presents comprehensive findings on the total physical stock of all vaccines,
diluents and devices available at the SWZ cold store, six State stores (Ekiti, Lagos, Ogun,
Ondo, Osun and Oyo State), all LGA stores and all HFs with cold chain equipment, with key
indicators that provide insight into the performance of the supply chain across the SW zone.
It is worthy of note that all the stores across all levels of the supply chain have a system to
run the store. This however should be in full compliance with the effective vaccine
management (EVM) standard at every level of the supply chain. This audit has provided
strategic and actionable insight into the volume of vaccines and related commodities
available insomuch as to guide the NLWG in the 2020 vaccines and devices forecast exercise.
Based on the presented survey findings, some recommendations are: (a) use of electronic
data tools for record keeping at the lower supply levels; (b) development of vaccines and
diluents redistribution protocol; (c) deployment of technically sound store keepers; (d)
continuous professional training of the stores technical officers so as to catch up with the
industry global best practice. Others are: (i) incentivizing best practices in EVM standards at
every level of the supply chain system; (ii) investment in store structures and equipment; (iii)
monitoring of performance of stores and supportive supervision; (iv) effective waste
management practice of cold chain waste; (v) questions on EVM compliance should be part
of subsequent PSC paper checklist; and (vi) vendor’s data manager should be granted access
to the server, alternatively, ODK input file should be shared with the vendors.
SOUTH SOUTH ZONE RECOMMENDATIONS
Vaccine to Diluent Ratio
▪ The Zonal Cold Store should distribute more Yellow Fever diluents from its large stock
(see Table 4.1), to stores or facilities lacking this commodity. This will also help to utilize
vaccines and devices which are close to expiry.
77 | Page NPHCDA/2019 ANNUALREPORT
Staffing
▪ The Zonal Cold Store and Some State Cold Stores appear to be understaffed. While there
may be sufficient security guards in these facilities, it is recommended that more staff
trained in vaccine management are required to carryout the essential duties of the Zonal and
State Vaccine Cold Stores.
Record Keeping
▪ The data provided in this report should be used to assist Cold Chain Officers (CCO) to
update their stock records.
▪ Optimize the use of the web-based stock recording tool. The maintenance of accurate
stock records is critical for effective management of the stock. The use of the web-based
LMIS tool should be effected at all levels of the supply chain. It is also recommended that
the users of the LMIS be well trained vis a vis their roles.
▪ In order to maintain the drive for accurate and updated records at various supply chain
levels, the Physical Stock Count exercise should be conducted annually.
▪ Also, routine supportive supervision systems should be strengthened to ensure
continued reporting of stock levels by CCOs.
EEFO Compliance
▪ The vaccine stores at Zonal, State and LGA levels should ensure strict compliance with
EEFO principles. Store managers should ensure that all the stock movements are recorded in
the stock record tool (LMIS).
NORTH CENTRAL ZONE RECOMMENDATIONS
1. Identify and redistribute excess stock of vaccines at all levels of the supply chain.
2. Improve on stock distribution and transportation systems.
3. Ensure stock availability at all levels of the supply chain
4. Ensure continuous performance improvement on Effective Vaccine Management
Practices.
5. Separate and properly document of all damaged and expired stock.
6. Invest in store infrastructure like pallets, shelves, lighting, heat and ventilation equipment.
78 | Page NPHCDA/2019 ANNUALREPORT
7. Continue Routine Monitoring and Evaluation of the vaccine supply chain system.
NORTH EAST ZONE RECOMMENDATIONS
1. Identify and redistribute excess stock of vaccines at all levels of the supply chain.
2. Improve on stock distribution and transportation systems.
3. Ensure stock availability at all levels of the supply chain
4. Ensure continuous performance improvement on Effective Vaccine Management
Practices.
5. Separate and properly document of all damaged and expired stock.
6. Invest in store infrastructure like pallets, shelves, lighting, heat and ventilation equipment.
7. Continue Routine Monitoring and Evaluation of the vaccine supply chain system.
NORTH WEST ZONE RECOMMENDATIONS
Poorly arranged stores
OIC should ensure that stores are properly arranged. All Inventory item arrangement should
be based on EEFO principle. Further to this, vaccine and diluents should be stored according
to the following:
• Vaccine type
• Vaccine manufacturer
• Vaccine Vial Monitor (VVM) stage
• Date of expiry Where the VVM stage of the vaccine has progressed, the OIC should be knowledgeable
enough to make an exception.
Facilities with near-expiry stock should liaise with the LGA or State Store to initiate the
process of having the affected stock moved to other facilities that may be in need.
A demarcated area marked “PRODUCTS FOR DISPOSAL” should be designated for holding
expired stock before proper disposal.
There should be an increase in the interaction between lower cadre staff and senior staff to
improve supervision, knowledge transfer, coaching, and training. Particularly, lower cadre
staff should be sensitized on the benefits of the EEFO principle of stock management.
Inadequate/no inventory record keeping
79 | Page NPHCDA/2019 ANNUALREPORT
• All inventory records should be updated immediately.
• Periodic stock count of inventory should be initiated across all facilities. This stock count should be observed by the staff of a superior store. For instance, a LGA staff should observe the stock count of a primary health care facility.
• Facilities that accommodate the inventory of other facilities should maintain records of the inventory. Furthermore, the inventory should be segregated from that of the host-facility.
• Adequate inventory record can be considered as control responsibilities that could form part of the performance appraisal of the OIC.
• Also, vaccines for campaigns should be recorded separately from vaccines used in routine immunization. Combining records can give a false representation of stock levels.
Poor controls over inventory levels
The facilities should define their stock level including, maximum, minimum and re-order
levels. The stock level can be determined using the facilities’ daily/weekly stock consumption
rate as the basis for definition.
The OIC should regularly review stock levels to ensure compliance.
Poor physical controls over inventory
• The timely renovation of the affected facilities should be initiated to prevent exposure of the inventory to the elements and to protect the facilities’ buildings.
• The dry stores should be relocated from open spaces to secure places in the facilities. The facilities that are experiencing space constraints should consider relocating their open/unsecured dry stores to the OIC offices.
80 | Page NPHCDA/2019 ANNUALREPORT
Permanent Secretary FMoH, Executive Secretary NPHCDA and Partners at Scenes of Launching Cold
Chain Equipment in ALEYITA PHC, Lugbe FCT Abuja.
4.3 Research for Health
4.3.1 Post Campaign Coverage Surveys (PCCS) Sequel to the Various Campaigns Conducted in 2019 on Yellow Fever, Measles, Meningitis, a PCCS
was Conducted to ascertain the Coverages, Card Retention of all antigens used. The Survey is still on
and Results are expected in early 2020.
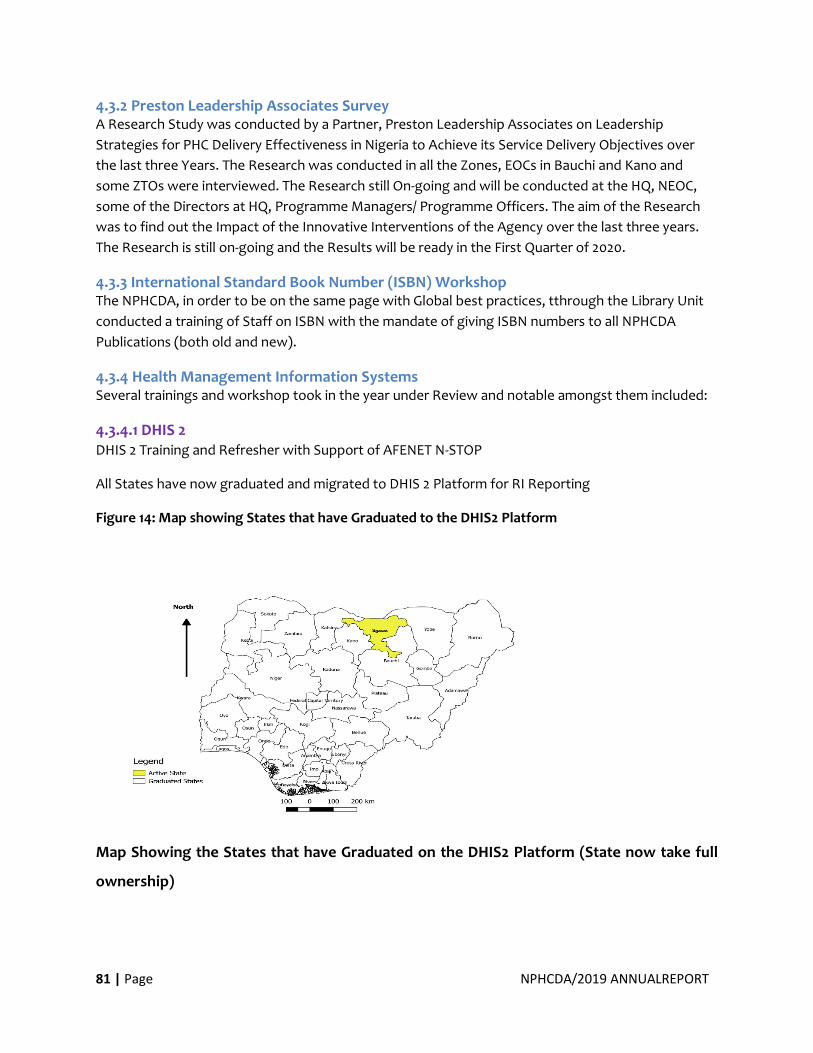
81 | Page NPHCDA/2019 ANNUALREPORT
4.3.2 Preston Leadership Associates Survey A Research Study was conducted by a Partner, Preston Leadership Associates on Leadership
Strategies for PHC Delivery Effectiveness in Nigeria to Achieve its Service Delivery Objectives over
the last three Years. The Research was conducted in all the Zones, EOCs in Bauchi and Kano and
some ZTOs were interviewed. The Research still On-going and will be conducted at the HQ, NEOC,
some of the Directors at HQ, Programme Managers/ Programme Officers. The aim of the Research
was to find out the Impact of the Innovative Interventions of the Agency over the last three years.
The Research is still on-going and the Results will be ready in the First Quarter of 2020.
4.3.3 International Standard Book Number (ISBN) Workshop The NPHCDA, in order to be on the same page with Global best practices, tthrough the Library Unit
conducted a training of Staff on ISBN with the mandate of giving ISBN numbers to all NPHCDA
Publications (both old and new).
4.3.4 Health Management Information Systems Several trainings and workshop took in the year under Review and notable amongst them included:
4.3.4.1 DHIS 2 DHIS 2 Training and Refresher with Support of AFENET N-STOP
All States have now graduated and migrated to DHIS 2 Platform for RI Reporting
Figure 14: Map showing States that have Graduated to the DHIS2 Platform
Map Showing the States that have Graduated on the DHIS2 Platform (State now take full
ownership)
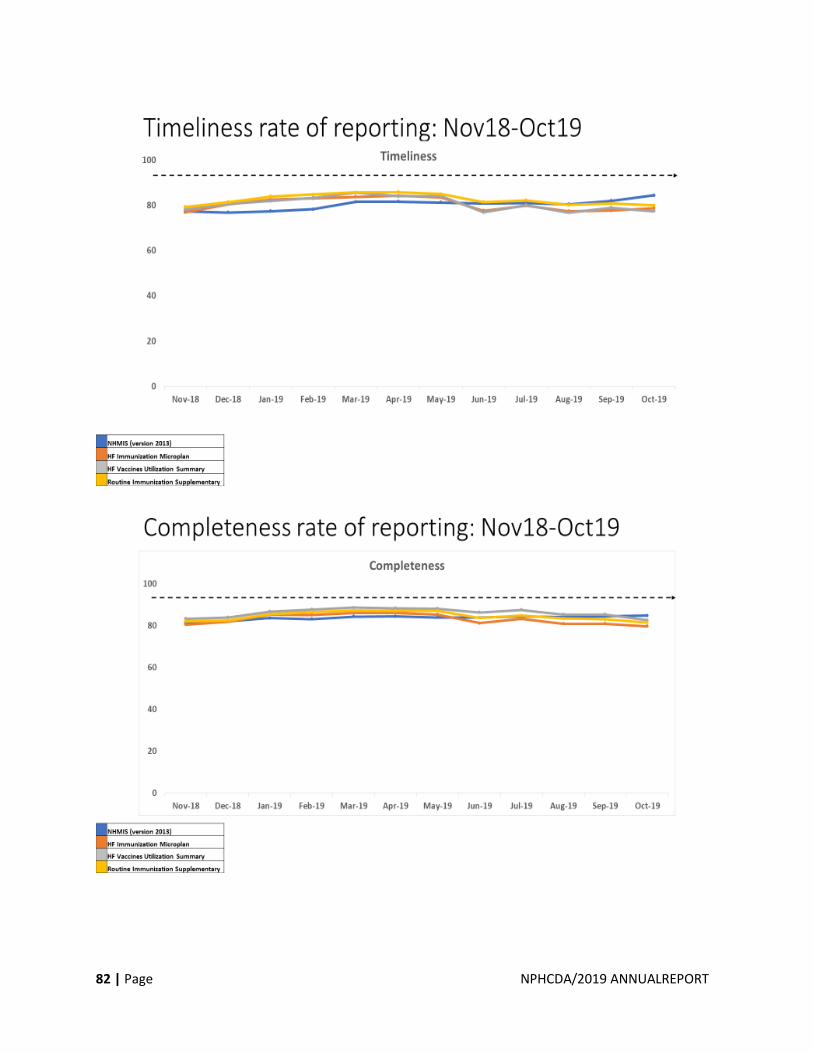
82 | Page NPHCDA/2019 ANNUALREPORT
83 | Page NPHCDA/2019 ANNUALREPORT
Advocacy and Communication during Final Transition Visits
4.3.4.2 Data Quality Use Supportive Supervision) DQUSS
Conducted DQUSS in Delta July and Anambra States in August the last week of July to improve
the data quality, provide on the job mentoring and review RI data quality job aids and DQUSS
checklist. This exercise was also supported by AFENET-STOP in collaboration with FMOH.
On the job mentoring During Supportive Supervision (DQUSS and ISS)
4.3.4.3 Supportive Supervision
Conduct of Integrated Supportive Supervision in Bauchi, Kano, Sokoto, Anambra, Kwara,
Ogun and Ebonyi States between July and August, 2019 in collaboration with FMoH and MSH-
RSSH GF.
84 | Page NPHCDA/2019 ANNUALREPORT
4.3.4.4 Monthly RI Feedback
RI Monthly Feedback has now been institutionalized and feedbacks given monthly.
4.3.5 Health Informatics Conference (HELINA Conference) in Botswana. In the last week of November, Staff from the M & E Division attended the HELINA
Conference for Health Informatics in Botswana.
Specific objectives of the conference were included:
• Instil a culture of digital health interventions that will generate data from evidence to
practice
• Build a data ecosystem in Africa for data health expert
• Outline strategies to institutionalize data health in respective countries to ensure efficient
health care delivery
Four posters were submitted by the CDC/NSTOP/NPHCDA GEEKS project and the GEEKS
fellows for each poster provided further explanations in the various sub project topics to
participants during the conference. A key outcome from the conference was the emphasis
on development of a public health informatics workforce through capacity building within
the continent. The established education working group within HELINA promised to bridge
this gap and collaborate with institutions in setting up public health informatics curriculum.
The next country to host the conference will be selected through a bidding process and
interested countries were encouraged to participate in the process. The HELINA board will
continue to engage participants via emails post conference and strengthen collaboration
with agencies e.g Africa CDC.
85 | Page NPHCDA/2019 ANNUALREPORT
At the HELINA Conference Communique
86 | Page NPHCDA/2019 ANNUALREPORT
5.0 PREDICTABLE
FINANCING AND RISK
PROTECTION
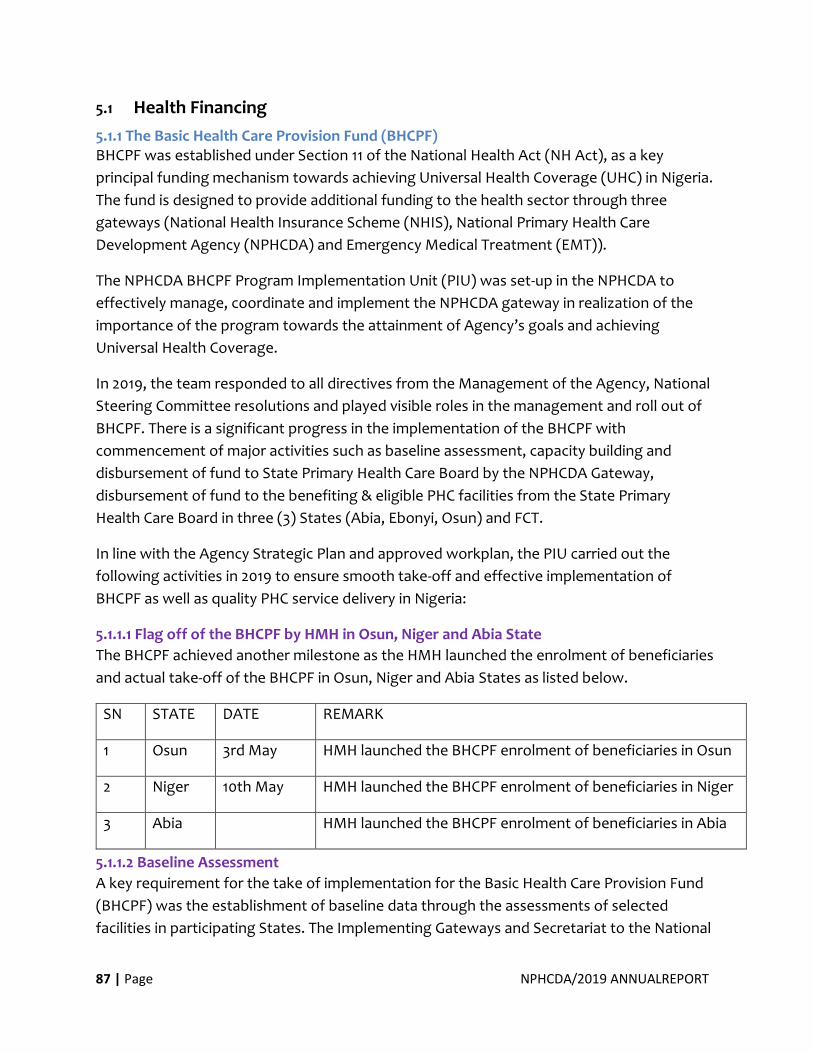
87 | Page NPHCDA/2019 ANNUALREPORT
5.1 Health Financing
5.1.1 The Basic Health Care Provision Fund (BHCPF) BHCPF was established under Section 11 of the National Health Act (NH Act), as a key
principal funding mechanism towards achieving Universal Health Coverage (UHC) in Nigeria.
The fund is designed to provide additional funding to the health sector through three
gateways (National Health Insurance Scheme (NHIS), National Primary Health Care
Development Agency (NPHCDA) and Emergency Medical Treatment (EMT)).
The NPHCDA BHCPF Program Implementation Unit (PIU) was set-up in the NPHCDA to
effectively manage, coordinate and implement the NPHCDA gateway in realization of the
importance of the program towards the attainment of Agency’s goals and achieving
Universal Health Coverage.
In 2019, the team responded to all directives from the Management of the Agency, National
Steering Committee resolutions and played visible roles in the management and roll out of
BHCPF. There is a significant progress in the implementation of the BHCPF with
commencement of major activities such as baseline assessment, capacity building and
disbursement of fund to State Primary Health Care Board by the NPHCDA Gateway,
disbursement of fund to the benefiting & eligible PHC facilities from the State Primary
Health Care Board in three (3) States (Abia, Ebonyi, Osun) and FCT.
In line with the Agency Strategic Plan and approved workplan, the PIU carried out the
following activities in 2019 to ensure smooth take-off and effective implementation of
BHCPF as well as quality PHC service delivery in Nigeria:
5.1.1.1 Flag off of the BHCPF by HMH in Osun, Niger and Abia State
The BHCPF achieved another milestone as the HMH launched the enrolment of beneficiaries
and actual take-off of the BHCPF in Osun, Niger and Abia States as listed below.
SN STATE DATE REMARK
1 Osun 3rd May HMH launched the BHCPF enrolment of beneficiaries in Osun
2 Niger 10th May HMH launched the BHCPF enrolment of beneficiaries in Niger
3 Abia HMH launched the BHCPF enrolment of beneficiaries in Abia
5.1.1.2 Baseline Assessment
A key requirement for the take of implementation for the Basic Health Care Provision Fund
(BHCPF) was the establishment of baseline data through the assessments of selected
facilities in participating States. The Implementing Gateways and Secretariat to the National
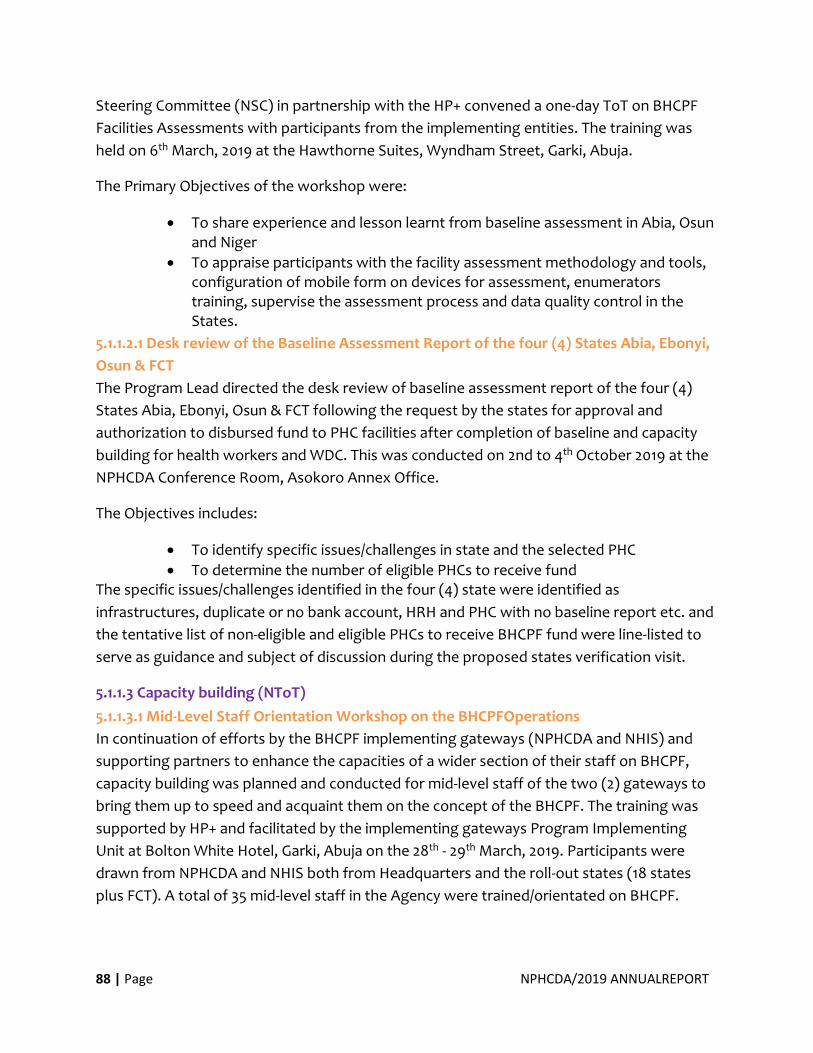
88 | Page NPHCDA/2019 ANNUALREPORT
Steering Committee (NSC) in partnership with the HP+ convened a one-day ToT on BHCPF
Facilities Assessments with participants from the implementing entities. The training was
held on 6th March, 2019 at the Hawthorne Suites, Wyndham Street, Garki, Abuja.
The Primary Objectives of the workshop were:
• To share experience and lesson learnt from baseline assessment in Abia, Osun and Niger
• To appraise participants with the facility assessment methodology and tools, configuration of mobile form on devices for assessment, enumerators training, supervise the assessment process and data quality control in the States.
5.1.1.2.1 Desk review of the Baseline Assessment Report of the four (4) States Abia, Ebonyi,
Osun & FCT
The Program Lead directed the desk review of baseline assessment report of the four (4)
States Abia, Ebonyi, Osun & FCT following the request by the states for approval and
authorization to disbursed fund to PHC facilities after completion of baseline and capacity
building for health workers and WDC. This was conducted on 2nd to 4th October 2019 at the
NPHCDA Conference Room, Asokoro Annex Office.
The Objectives includes:
• To identify specific issues/challenges in state and the selected PHC
• To determine the number of eligible PHCs to receive fund The specific issues/challenges identified in the four (4) state were identified as
infrastructures, duplicate or no bank account, HRH and PHC with no baseline report etc. and
the tentative list of non-eligible and eligible PHCs to receive BHCPF fund were line-listed to
serve as guidance and subject of discussion during the proposed states verification visit.
5.1.1.3 Capacity building (NToT)
5.1.1.3.1 Mid-Level Staff Orientation Workshop on the BHCPFOperations
In continuation of efforts by the BHCPF implementing gateways (NPHCDA and NHIS) and
supporting partners to enhance the capacities of a wider section of their staff on BHCPF,
capacity building was planned and conducted for mid-level staff of the two (2) gateways to
bring them up to speed and acquaint them on the concept of the BHCPF. The training was
supported by HP+ and facilitated by the implementing gateways Program Implementing
Unit at Bolton White Hotel, Garki, Abuja on the 28th - 29th March, 2019. Participants were
drawn from NPHCDA and NHIS both from Headquarters and the roll-out states (18 states
plus FCT). A total of 35 mid-level staff in the Agency were trained/orientated on BHCPF.
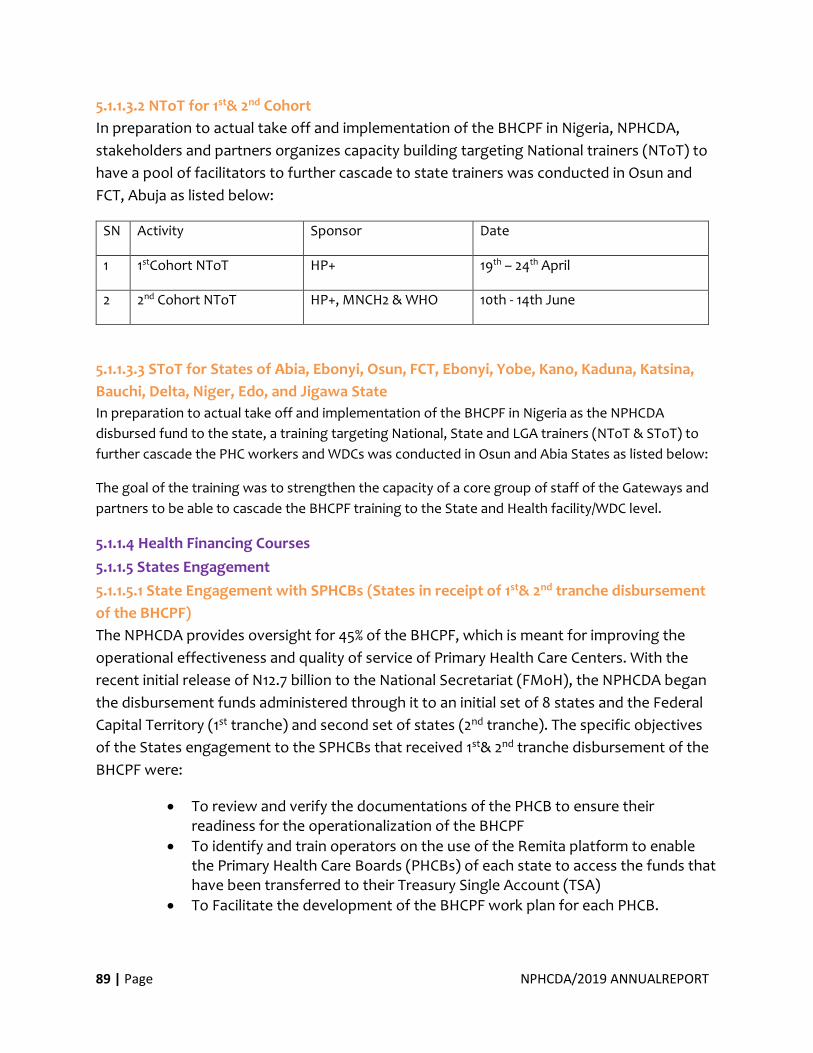
89 | Page NPHCDA/2019 ANNUALREPORT
5.1.1.3.2 NToT for 1st& 2nd Cohort
In preparation to actual take off and implementation of the BHCPF in Nigeria, NPHCDA,
stakeholders and partners organizes capacity building targeting National trainers (NToT) to
have a pool of facilitators to further cascade to state trainers was conducted in Osun and
FCT, Abuja as listed below:
SN Activity Sponsor Date
1 1stCohort NToT HP+ 19th – 24th April
2 2nd Cohort NToT HP+, MNCH2 & WHO 10th - 14th June
5.1.1.3.3 SToT for States of Abia, Ebonyi, Osun, FCT, Ebonyi, Yobe, Kano, Kaduna, Katsina,
Bauchi, Delta, Niger, Edo, and Jigawa State
In preparation to actual take off and implementation of the BHCPF in Nigeria as the NPHCDA
disbursed fund to the state, a training targeting National, State and LGA trainers (NToT & SToT) to
further cascade the PHC workers and WDCs was conducted in Osun and Abia States as listed below:
The goal of the training was to strengthen the capacity of a core group of staff of the Gateways and
partners to be able to cascade the BHCPF training to the State and Health facility/WDC level.
5.1.1.4 Health Financing Courses
5.1.1.5 States Engagement
5.1.1.5.1 State Engagement with SPHCBs (States in receipt of 1st& 2nd tranche disbursement
of the BHCPF)
The NPHCDA provides oversight for 45% of the BHCPF, which is meant for improving the
operational effectiveness and quality of service of Primary Health Care Centers. With the
recent initial release of N12.7 billion to the National Secretariat (FMoH), the NPHCDA began
the disbursement funds administered through it to an initial set of 8 states and the Federal
Capital Territory (1st tranche) and second set of states (2nd tranche). The specific objectives
of the States engagement to the SPHCBs that received 1st& 2nd tranche disbursement of the
BHCPF were:
• To review and verify the documentations of the PHCB to ensure their readiness for the operationalization of the BHCPF
• To identify and train operators on the use of the Remita platform to enable the Primary Health Care Boards (PHCBs) of each state to access the funds that have been transferred to their Treasury Single Account (TSA)
• To Facilitate the development of the BHCPF work plan for each PHCB.
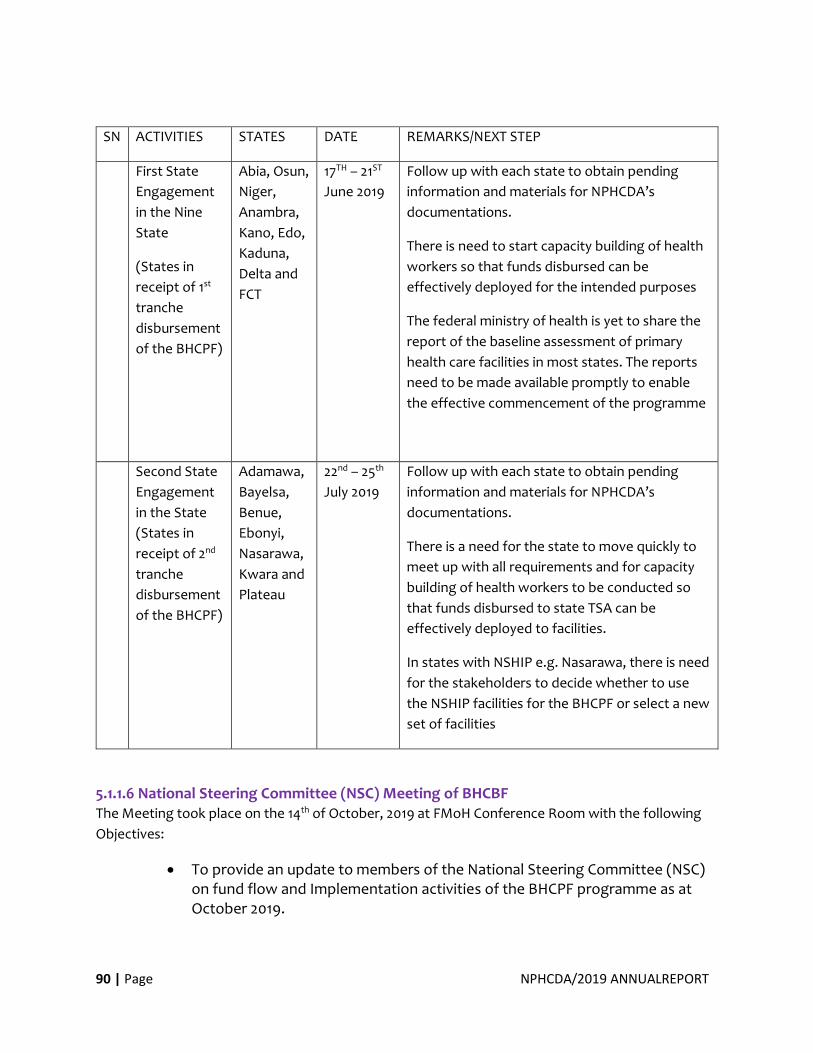
90 | Page NPHCDA/2019 ANNUALREPORT
SN ACTIVITIES STATES DATE REMARKS/NEXT STEP
First State
Engagement
in the Nine
State
(States in
receipt of 1st
tranche
disbursement
of the BHCPF)
Abia, Osun,
Niger,
Anambra,
Kano, Edo,
Kaduna,
Delta and
FCT
17TH – 21ST
June 2019
Follow up with each state to obtain pending
information and materials for NPHCDA’s
documentations.
There is need to start capacity building of health
workers so that funds disbursed can be
effectively deployed for the intended purposes
The federal ministry of health is yet to share the
report of the baseline assessment of primary
health care facilities in most states. The reports
need to be made available promptly to enable
the effective commencement of the programme
Second State
Engagement
in the State
(States in
receipt of 2nd
tranche
disbursement
of the BHCPF)
Adamawa,
Bayelsa,
Benue,
Ebonyi,
Nasarawa,
Kwara and
Plateau
22nd – 25th
July 2019
Follow up with each state to obtain pending
information and materials for NPHCDA’s
documentations.
There is a need for the state to move quickly to
meet up with all requirements and for capacity
building of health workers to be conducted so
that funds disbursed to state TSA can be
effectively deployed to facilities.
In states with NSHIP e.g. Nasarawa, there is need
for the stakeholders to decide whether to use
the NSHIP facilities for the BHCPF or select a new
set of facilities
5.1.1.6 National Steering Committee (NSC) Meeting of BHCBF The Meeting took place on the 14th of October, 2019 at FMoH Conference Room with the following
Objectives:
• To provide an update to members of the National Steering Committee (NSC) on fund flow and Implementation activities of the BHCPF programme as at October 2019.
91 | Page NPHCDA/2019 ANNUALREPORT
• To update the National Steering Committee on the activities carried out to date in engaging Independent Verification Agents (IVA) and the External Auditor (EA) for the programme.
• To seek the approval of the National Steering Committee to disburse funds to states that are yet to receive funds under the programme.
Outcomes:
The HMH and Steering Committee members ruled and installed the 25% Counterpart Fund by
the State Governments through SPHCB for infrastructure and HRH development as Stated in
the NHAct 2014.
The NSC was updated on fund flow and Implementation activities of the BHCPF programme
as at October 2019. Specifically, the NSC is invited to note that:
• A total sum of N13.8bn has been disbursed to NHIS, NPHCDA, DHS and NCDC TSA accounts following the approved criteria by the National Steering Committee
• The NPHCDA Gateway has further disbursed N5.55bn and N100.2m as programme and operational funds respectively for the next four (4) quarters to the TSA accounts of sixteen (16) SPHCBs.
The disbursement was made in two tranches as highlighted below:
• 1st tranche - N3.85bn (N3.79bn being programmatic and N61.99m being operational) disbursed on the 23rd May 2019 to nine (9) States namely: Abia, Anambra, Delta, Edo, Kaduna, Kano, Niger, Osun and FCT.
• 2nd tranche - N1.81bn (N1.76bn being programmatic and N48.21m being operational) disbursed on the 28th June 2019 to seven (7) states namely: Adamawa, Bayelsa, Benue, Ebonyi, Kwara, Nasarawa and Plateau.
• These States are divided into two (2) categories: I. States that have received funds from just one of the implementing gateways. These states are Bauchi, Benue, Imo, Katsina, Lagos, Oyo, Yobe, Nasarawa, and Kwara. II. Other states that have recently met or on the path to meeting the disbursement criteria.
The members were updated on processes and status of engaging Independent Verification
Agents (IVA) and the External Auditor (EA) for the programme:
• The ToR, Procurement approach and other relevant documents have been developed for the engagement of the IVA and EA, with a NO objection obtained.
• Funds for the professional fees of the IVA and the EA will be sourced from the Government of Nigeria, the World Bank, and Bill & Melinda Gates Foundation
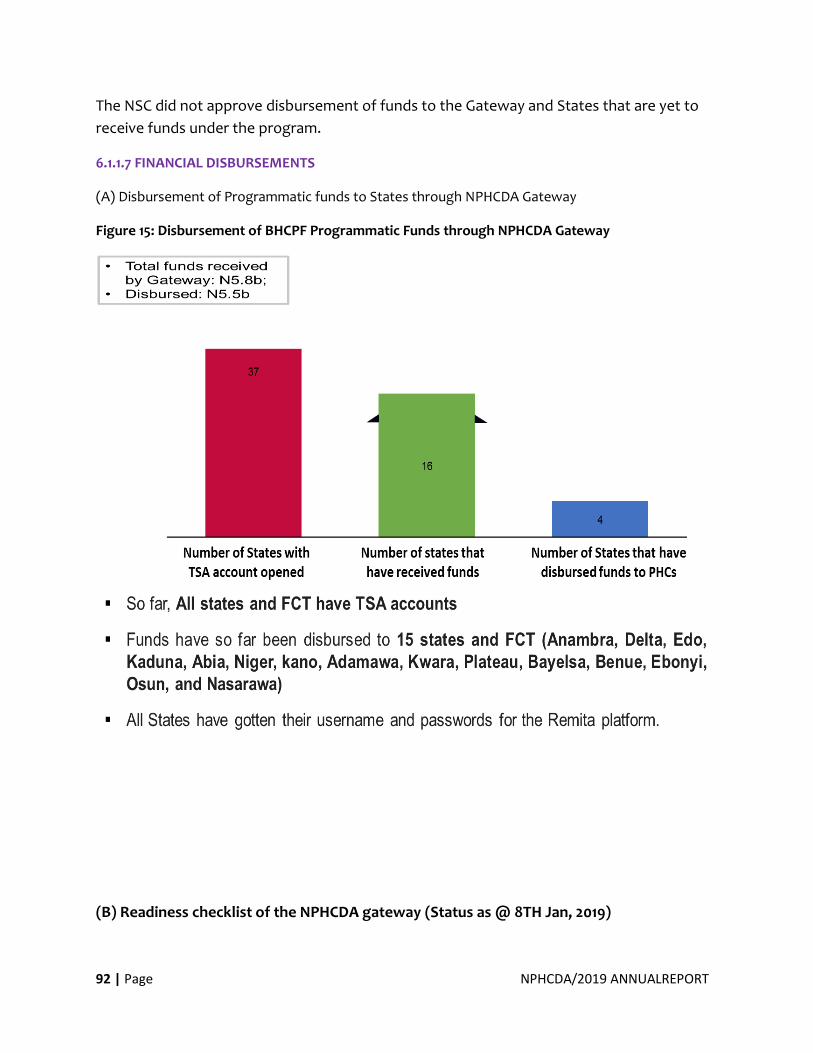
92 | Page NPHCDA/2019 ANNUALREPORT
The NSC did not approve disbursement of funds to the Gateway and States that are yet to
receive funds under the program.
6.1.1.7 FINANCIAL DISBURSEMENTS
(A) Disbursement of Programmatic funds to States through NPHCDA Gateway
Figure 15: Disbursement of BHCPF Programmatic Funds through NPHCDA Gateway
(B) Readiness checklist of the NPHCDA gateway (Status as @ 8TH Jan, 2019)
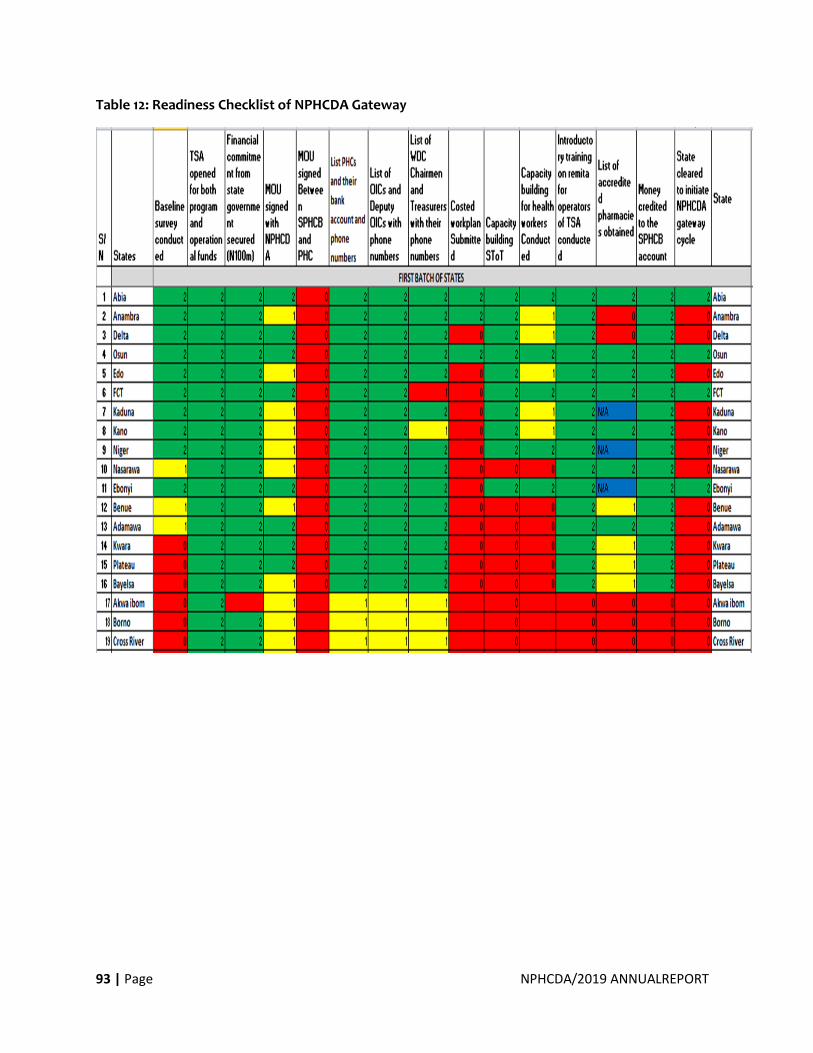
93 | Page NPHCDA/2019 ANNUALREPORT
Table 12: Readiness Checklist of NPHCDA Gateway
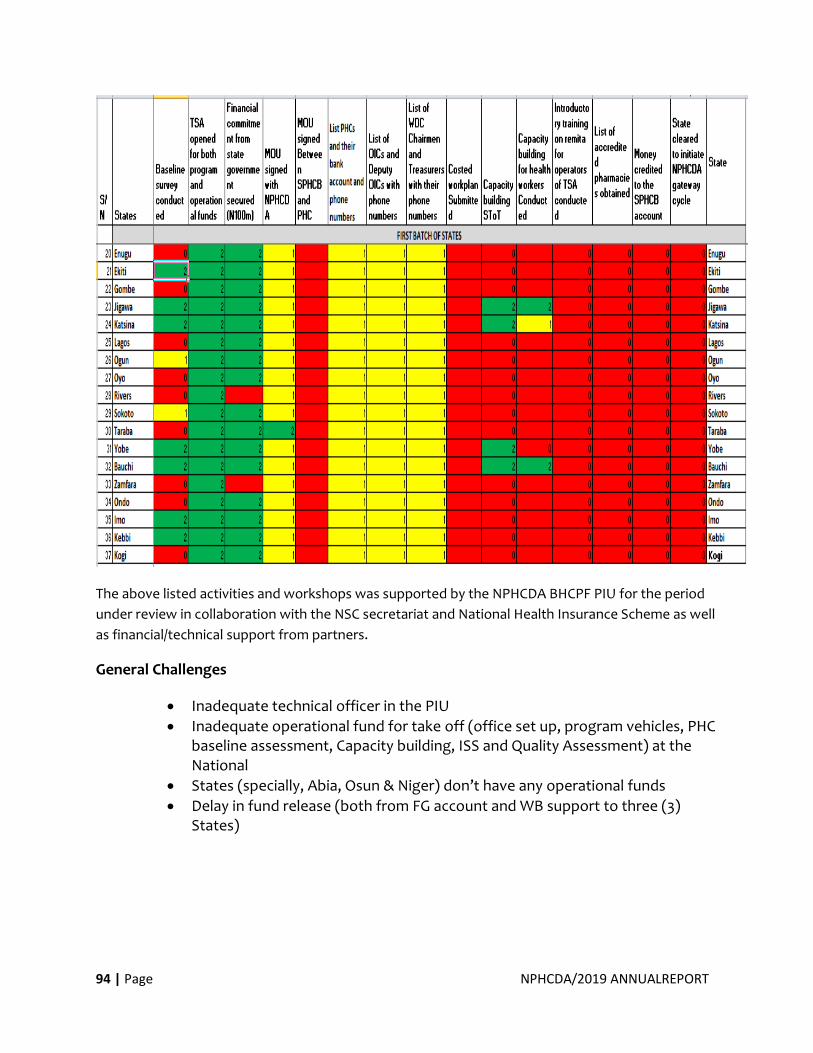
94 | Page NPHCDA/2019 ANNUALREPORT
The above listed activities and workshops was supported by the NPHCDA BHCPF PIU for the period
under review in collaboration with the NSC secretariat and National Health Insurance Scheme as well
as financial/technical support from partners.
General Challenges
• Inadequate technical officer in the PIU
• Inadequate operational fund for take off (office set up, program vehicles, PHC baseline assessment, Capacity building, ISS and Quality Assessment) at the National
• States (specially, Abia, Osun & Niger) don’t have any operational funds
• Delay in fund release (both from FG account and WB support to three (3) States)
95 | Page NPHCDA/2019 ANNUALREPORT
Recommendations
• Deployment of technical officer to the PIU
• Advocacy for partner support and increase operational fundingEarly release of funding
• Needs to advocate to Partners (WB) to release operational funds for Abia, Osun & Niger.
Executive Director NPHCDA, HMH, HMSH at FMoH
at NSC Meeting in 2019
HMH Giving BHCPF Cheque to the Deputy Gov. of
Niger State
96 | Page NPHCDA/2019 ANNUALREPORT
B. Financial Report
97 | Page NPHCDA/2019 ANNUALREPORT
B. Financial Report
In year 2019 under review, NPHCDA continues the implementation of the recommendation of KPMG
in conjunction with the restructuring of Finance and Accounts Department in Ministries, Department
and Agencies as stipulated by the office of the Accountant general of the Federation (OAGF) leading
to the newly created divisions of the department included:
• Expenditure Division
• Budget Division
• Financial and Fiscal Reporting Division
• Revenue and External Assistance Division
REVENUE:
The total revenue received for the first three quarters of the Year 2019 (January-Sept 2019)
was N122,109,737.75which was mainly from the receipt for Recurrent/Overhead. From the
2018 Capital release, the sum of N17,667,668,538.46 was for 2018 rolled-over to the year
2019. These forms part of the entire release for the year 2018 as the Appropriation for 2019
fund was partly received in the fourth quarter of 2019 amounting to 3.3 Billion Naira.
EXPENDITURE:
The total expenditure of the Agency for the first three quarters of 2019 was N91,526,467.23
for the recurrent expenditure while that of Capital Expenditure isN17,641,746,994.63.
Other key achievements are as follows:
• Audit of 2018 Financial Statement for the Agency as concluded as copies of the has been submitted the relevant/statutory stakeholders
• Stock Verification and Stock taking Exercise was successfully carried out for the mid-year 2019
• Prompt Compilation and Preparation of the Agency Budget for year 2020
• Assets Verification and Tagging Exercises for the Agency Assets as successfully completed within the year
• Successful Retrieval of GAVI Funds Retirements documents and Fund Balances in Abia, Anambra, Kano, Ondo, Oyo and Rivers State respectively.
• Prompt submission of interim financial reports (IFR) and IPSAS Accrual Trial Balance (TB) on the Agencies World Bank funded projects to then bank and other stakeholders.
• Early Procurement of treasury Non-Security Documents, Accounting forms, Journals, Registers etc for ease documentation of the Agencies financial transactions.
98 | Page NPHCDA/2019 ANNUALREPORT
STAFF PRODUCTIVITY
AWARDS/SEND FORTH FOR
RETIRED OFFICERS; NPHCDA
ANNUAL SPORTS
COMPETITION AND GIVING
BACK TO THE COMMUNITY
99 | Page NPHCDA/2019 ANNUALREPORT
7.0 STAFF PRODUCTIVITY AWARDS/SEND FORTH FOR RETIRED OFFICERS;
NPHCDA ANNUAL SPORTS COMPETITION AND GIVING BACK TO THE
COMMUNITY
The NPHCDA Leadership has institutionalized Staff Productivity Awards/Send Forth for
Retired Officers and also the Annual PHC Sports Competition. The 2019 Edition of the Staff
Productivity Award was the third following the Maiden Edition in 2017. Similarly, the 2019
annual Sports was the Second edition after the first in 2018. Dr Faisal Shuiab, the Executive
Director NPHCDA promised to sustain these activities and true to his words it happened for
the third and Second time in 2019 after the Maiden edition of 2018.
7.1 Staff Productivity Awards and Send Forth for Retired Officers
Scenes from Staff Productivity Awards and Send Forth of Retired Officers, Abuja; 2019
100 | Page NPHCDA/2019 ANNUALREPORT
7.1.1 NPHCDA Annual Sports Competition
Scenes from NPHCDA Annual Sports Competition, Abuja; 2019
101 | Page NPHCDA/2019 ANNUALREPORT
7.1.2 Giving Back to the Community The NPHCDA family were in Gboko, Benue State on the 12th of October, 2019 to Commission
the renovated and equipped Maternity Centre in honour of Dr. Eugene Ivase, former
Director, Advocacy and Communication Department, as recipient of the 2018 Executive
Director/CEO’s award – tagged “Giving Back to the Community”. On the 5th of December,
2019 they were in Kano to honour Dr Laila Umar of the Department of CHS for a similar
event.
Scenes of “Giving Back To the Community” Gboko, Benue State; 12th October, 2019
102 | Page NPHCDA/2019 ANNUALREPORT
Scenes of “Giving Back to the Community” Kano, Kano State; 5th of December, 2019
103 | Page NPHCDA/2019 ANNUALREPORT
ANNEXURES:
Annex I: Communique from 62nd NCH Asaba, delta State
1. Following extensive deliberations, the Council considered a total of 65 memoranda,
approved 26, noted 24 and stepped-down/withdrew 15.
The following resolutions were approved:
I. Federal, 36 states, FCT and health stakeholders should adopt the National Council
on Health handbook as a guide on all National/State council on health matters in
Nigeria.
II. The Federal Ministry of health should continuously build the capacity of relevant
officers at all levels on NCH matters including writing of good quality NCH/SCH
memoranda;
III. The ten-year compendium on NCH resolutions should be used as a score card for
evaluating the impact of NCH meetings
IV. All Departments, Agencies and Parastatals of the Federal and State Ministries of
Health should develop Annual Operations Plans (AOPs) on or before 3rd quarter each
year to inform annual budget development and to demonstrate the
operationalisation of the NSHDP II;
V. Federal Ministry of Health to continue monitoring the implementation of the
NSHDP II at all levels and report progress to Council at every council meeting;
VI. Federal, 36 states and FCT should ensure Development Partners supporting the
implementation of the NSHDP II key into the AOP regime as part of their support;
VII. Federal, 36 states and FCT should adopt and commence implementation of the
National Health Promotion Policy (2019);
VIII. All Development partners and Civil Society Organisations to endorse the Country
Compact committing to the implementation of the National Strategic Health
Development Plan II;
IX. The FMOH to commence provision of technical support to all states for the adoption
and implementation of the National Roadmap for accelerating reduction of
Maternal and Neonatal mortality in Nigeria at all levels and the designation of Desk
Officers at both the Federal and State levels;
X. Federal, 36 states and FCT should adopt and commence implementation of the
National Noma Policy and three-year Noma action plan for Nigeria (2019 – 2021) and
identify more centres for establishment;
XI. Federal, 36 states and FCT should adopt and commence implementation of the
National Policy and Strategic Plan for Ear and Hearing Care (EHC) at all levels;
XII. State Coordinators for EHC activities should be appointed in all 36 State Ministries of
Health and FCT to work with the Desk Officers on EHC at the Federal Ministry of
104 | Page NPHCDA/2019 ANNUALREPORT
Health;
XIII. Federal, 36 states and FCT should adopt and commence implementation of the
National Quality of Care Strategy for the reduction of Maternal and Neonatal
mortality at all levels;
XIV. The NHREC should establish an electronic platform (e-platform) for protocol
submission and review;
XV. The NHREC should commence charging of 0.5% of grant value as fees for submission
and review of protocols from researchers;
XVI. Federal, 36 states and FCT should observe World Food Safety Day (WFSD)
celebration and activities at all levels;
XVII. All 36 States and FCT should establish Traditional, Complementary and Alternative
Medicine Department/Boards to enhance coordination, regulation and control of
TCAM practice and its products in Nigeria;
XVIII. Federal, 36 states and FCT should ensure appropriation of adequate funds for polio
eradication and routine immunization to enable the polio eradication
programme sustain its high impact interventions to finally achieve certification and
a polio free status;
XIX. 36 states and FCT should establish or reactivate State/LGAs Task Forces on
Immunization (STFI/LGTFIs) to provide the needed coordination and oversight at the
state and LGA levels as well as for Council to interface with Governors and Chairmen
of LGAs with identified low commitment;
XX. Federal, 36 states and FCT should engage with development partners working in
states to develop a transition mechanism by end of 1st quarter 2020 to cushion the
effects of the global ramp down of polio resources which inevitably leads to lay off
of several development partners agencies’ members of staff, as we move closer to
certification;
XXI. Federal, 36 states and FCT should adopt and commence implementation of the
National Eye Health Policy at all levels and the designation of Eye Health desk officer
to interface with the National Eye Health Programme;
XXII. Federal, 36 states and FCT should adopt and commence implementation of
Treatment Guideline for Child Eye Health at all levels of government by all
stakeholders in the Nigerian Health Sector;
XXIII. All 36 states and FCT should establish State DR-TB treatment compliance teams;
XXIV. Federal, 36 State Ministries of Health and FCT Health Secretariat should create Legal
Units where none exists and create and institutionalize a MEDICO-LEGAL WEEK to
create awareness on legal issues in health;
XXV. FMOH should repurpose of the national coordination architecture for health sector
response to humanitarian crisis to provide normative guidance for processes
105 | Page NPHCDA/2019 ANNUALREPORT
geared towards improving health outcomes for populations within fragile settings;
XXVI. Federal, 36 States and FCT to improve health outcomes within fragile setting by
strengthening and scaling up present response modalities;
XXVII. FMOH in collaboration with states and other relevant stakeholders should develop
a national policy document for the health of refugees, migrants and internally
displaced persons;
XXVIII. FMOH should set up and operationalise systems to collaborate with the Ministry of
Humanitarian Affairs, Disaster Management and Social Development in the
provision of relevant technical support for health in humanitarian crisis, and
disaster management;
XXIX. Federal and State Ministries of Health to prioritize the provision of Water,
Sanitation and Hygiene services in health facilities across the country by creating a
budget line or increasing budgetary allocation for Water, Sanitation and Hygiene;
XXX. Federal Ministry of Health should develop a policy that will guarantee free
treatment for all Leishmaniasis patients, the inclusion of Leishmaniasis treatment
into procurement plan/budget of the Ministry of Health for the purchase of drugs on
annual basis and that development partners working in the State support the
initiative;
XXXI. All State Ministries of Health and Agriculture and Rural Development, Departments
and Agencies to create budget lines for training of staff as field epidemiologists in
the Nigerian Field Epidemiology and Laboratory Training Programme;
XXXII. All tertiary and specialist hospitals in Nigeria should procure and ensure a continuous
supply of basic antidotes in their hospitals;
XXXIII. All tertiary and specialist hospitals should establish functional poison centres in all
satellite hospitals or clinics that are affiliated to tertiary hospitals and in all states
of the federation to improve access to medical management of poisoning;
XXXIV. All states and FCT should establish data quality “control rooms” domiciled in their
Primary Health Care Boards (PHCBs) for stakeholders to address challenges relating
to service delivery on DHIS2 for the enhancement of decision making through the use
of quality data;
XXXV. FMOH should disseminate the report of the 2017 NHA as validated by stakeholders
from the 36 States and FCT;
XXXVI. 36 States and FCT should adopt Workload Indicator of Staffing Needs (WISN) tool
for the assessment of Human Resource for Health needs and distribution at all levels
of the health sector;
2. Council noted that 35 States of the Federation and FCT were represented.
106 | Page NPHCDA/2019 ANNUALREPORT
3. Council appreciated the support and hospitality extended to it by the Government and
people of Delta State.
4. Council further appreciated the role of Development Partners in health, Civil Society
Organisations, the media and other stakeholders for their contribution towards the
success of the meeting.
5. Council agreed that the 63rd NCH will hold in Ondo State in June 2020.
CONCLUSION
6. A motion for adjournment was moved by the Honourable Commissioner for Health,
Borno State and seconded by the Honourable Commissioner for Health, Cross River
State.
7. The 62nd Session of the NCH was formally closed by the Chairman of Council
following the vote of thanks by the Director, Health Planning, Research and Statistics,
Federal Ministry of Health, Dr Meribole.
Annex II: 2019 Seattle Declaration
107 | Page NPHCDA/2019 ANNUALREPORT
1. Clear commitments to fully implement Primary Health Care Under One Roof (PHCUOR) – per the recommended actions defined in the PHCUOR scorecard 2019, e.g. stronger workforce planning through the initial step of the transfer of PHC staff from LGAs, SMOH, MLG&CA, LGSC etc to State Primary Health Care Boards (SPHCBs). NPHCDA should provide technical assistance in support of processes leading to the full implementation of PHCUOR.
2. Understand the need for a fully costed minimum service package (MSP) tailored to
state realities (e.g. fiscal space, number of workers, number of facilities) as a way of attaining the ward minimum health care package – then develop and implement such an MSP
3. Fulfil all associated Basic Health Care Provision Fund (BHCPF) state requirements
(e.g. state counterpart funding)
4. Governors commit to review state PHC performance on a quarterly basis in State Executive Council meetings
5. Attend Q1 2020 summit to discuss PHC action plan – with the goal of articulating a
compelling vision for sustainable PHC investment in Nigeria
In addition, we commit to the following asks for Polio and Routine Immunization (RI):
6. As listed in Abuja Commitment, active leadership and commitment of Governors re: immunization programs
o Be personally and actively involved o Release counterpart funding on time – at least 1 week prior to start of
campaign o Make sure the LGA chairman is accountable e.g. ensuring that they chair
daily evening review meetings during campaigns
7. Strong state task force on PHC and immunization; should involve regular meetings chaired by Deputy Governors, driving and tracking on quality of RI services and campaigns, and reporting out each quarter at a minimum
8. Engagement of traditional and religious leaders around PHC – endeavor to motivate
and mobilize around PHC
9. National Economic Council (NEC) should have polio and RI as specific agenda items each month between now and June 2020. NEC should monitor aggressively and identify gaps, keeping the pressure on and driving the program to a successful conclusion.

108 | Page NPHCDA/2019 ANNUALREPORT





























