Embed Size (px)
Citation preview
NeurosurgicalTreatments forPsychiatric Disorders
Bomin Sun · Antonio De Salles Editors
Neurosurgical Treatments for PsychiatricDisorders
Bomin Sun • Antonio De SallesEditors
NeurosurgicalTreatments forPsychiatric Disorders
123
EditorsBomin SunRuijin Hospital, Center for Functional
NeurosurgeryShanghai Jiao Tong UniversityShanghaiChina
Antonio De SallesNeurosurgeryUniversity of CaliforniaLos AngelesUSA
and
HCor NeuroscienceSao PauloBrazil
ISBN 978-94-017-9575-3 ISBN 978-94-017-9576-0 (eBook)DOI 10.1007/978-94-017-9576-0Springer Dordrecht Heidelberg New York London
Library of Congress Control Number: 2014953249
Jointly published with Shanghai Jiao Tong University Press
© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business MediaDordrecht 2015This work is subject to copyright. All rights are reserved by the Publishers, whether the wholeor part of the material is concerned, specifically the rights of translation, reprinting, reuse ofillustrations, recitation, broadcasting, reproduction on microfilms or in any other physical way,and transmission or information storage and retrieval, electronic adaptation, computer software,or by similar or dissimilar methodology now known or hereafter developed. Exempted from thislegal reservation are brief excerpts in connection with reviews or scholarly analysis or materialsupplied specifically for the purpose of being entered and executed on a computer system, forexclusive use by the purchaser of the work. Duplication of this publication or parts thereof ispermitted only under the provisions of the Copyright Law of the Publishers’ locations, in itscurrent version, and permission for use must always be obtained from Springer. Permissions foruse may be obtained through RightsLink at the Copyright Clearance Center. Violations areliable to prosecution under the respective Copyright Law.The use of general descriptive names, registered names, trademarks, service marks, etc. in thispublication does not imply, even in the absence of a specific statement, that such names areexempt from the relevant protective laws and regulations and therefore free for general use.While the advice and information in this book are believed to be true and accurate at the date ofpublication, neither the authors nor the editors nor the publishers can accept any legalresponsibility for any errors or omissions that may be made. The publishers make no warranty,express or implied, with respect to the material contained herein.
Printed on acid-free paper
Springer is part of Springer Science+Business Media (www.springer.com)

Foreword I
Modern Psychiatric Surgery and Old FearsAlthough it is acceptable to prescribe medication to patients, damping braincircuitry, to a point that the patients’ cognition, sexual function, balance, andmotor function are impaired, surgical procedures to improve brain function,guided to a specific disturbance detected by functional imaging are still intheir infancy, chiefly for established psychiatric diseases. It is important thatthe specificity of these procedures bypass at large the systemic side effectsrelated to medications. The effectiveness, safety, and reversibility of novelsurgical procedures directed to psychiatric symptoms, for example, contin-uous electrical stimulation, or nonreversible novel lesion-making techniques,such as high frequency ultrasound and gamma knife surgery, which does noteven violate the skull, are attractive for highly suffering patients.
Functional imaging is bringing to light previous studies of neurosurgeons,psychiatrists, and neurologists working together to understand brain circuitryand the consequences of structural modification of this circuitry, either sec-ondary to structural diseases or iatrogenic. While at the birth of behavioralsurgery the procedures were massively aggressive to the brain and practicedindiscriminately, now the multidisciplinary approach, institutional reviewboards, and improved methods of diagnosis of psychiatric disorders make thepossibility of poor practice of behavioral surgery very remote. Moreover,some of the current procedures are reversible, such as deep brain stimulation.
The association of functional imaging to structural imaging based onrobust software for imaging analysis and device development to influencebrain function is the center of the novel “Why Fly Over the Cuckoo’s Nest,Psychosurgery in My Brain Please,” by Antonio De Salles (Ref. [28] of theChap. 19), challenging the outdated control by civil authorities of the so-called “psychosurgery.” To what degree are civil authorities and the generalpublic aware of the important differences between current behavioral/psy-chiatry neurosurgery, psychiatry and neuroscience, and the stereotypesevoked by the controversial figures of the past exemplified by Dr. WilliamFriedman, who performed lobotomies indiscriminately and without respect toevent the most basic surgical practices of asepsis and hemostasis?
While tight control of surgical procedures modifying the human brain fortherapeutic reasons seems to be outdated, the hideous use of such practices tochange the individual minds due to disagreement of political and cultural
v

views has fortunately been abolished from “medical” practice. The confusionbetween patient’s need for surgery and the malpractice of medicine for profitin disregard to patient’s interest is still a matter of worry though. On the otherhand, thousands of helpless patients with intractable psychiatric symptoms(by currently available noninvasive treatments) remain without access tosurgical procedures that have been proven to be both safe and effective. Towhat degree is the psychosurgery stigma guarding us from old fears ormerely precluding the access of needy patients to treatment?
Lincoln FriasRicardo de Oliveira
Jorge MollD’Or Institute for Research and Education (IDOR)
Rio de JaneiroBrazil
vi Foreword I

Foreword II
Functional Imaging and developments in pacemakers for the brain, as well asthe acceptance of the psychiatric community of medical therapy’s failure tohelp a substantial number of patients with psychiatric diseases has broughtback the interest in Psychiatric Surgery.
“Surgical Treatment for Psychiatric Disorders”: Is there a chance to havesociety broadly agreeing to the renaissance of what was in the past called“Psychosurgery,” the terrible invasion of the human mind? Are we preparedto undertake this controversial field ahead and avoid the terrible wounds ofthe past from being reopened, as described by a lobotomized patient in 1960?
“I am a bus driver. I am a survivor: In 1960, when I was twelve years old,I was given a transorbital, or “ice pick” lobotomy. My stepmother arrangedit. My father agreed to it. Dr. Walter Freeman, the father of Americanlobotomy, told me he was going to do some “tests.” It took ten minutes andcost two hundred dollars. The surgery damaged me in many ways. But itdidn’t “fix” me, or turn me into a robot. So my family put me into aninstitution. I spent the next four decades in and out of insane asylums, jails,and halfway houses. I was homeless, alcoholic, and drug-addicted. I was lost,I knew I wasn’t crazy. But I knew something was wrong with me. Was it thelobotomy? Was it something else? I hadn’t been a bad kid. I hadn’t ever hurtanyone. Or had I? Was there something I had done, and forgotten – some-thing so horrible that I deserved a lobotomy? I asked myself that question formore than forty years. I thought about my lobotomy all the time, but I nevertalked about it. It was my terrible secret. What had been so wrong with me?”
My LobotomyHoward Dully
vii
Preface
This now over 50 year-old man was hurt for life by the abuse of a Psychi-atrist, a luminary of the “Surgical Treatment of Psychiatric Disorder” field atthat time.
While these kinds of stories are examples that come from that dark past,patients were also helped by surgery, otherwise it would not have arrived asfar as it did during those years, when it was even a reason for a Nobel prize,at a time when the psychiatrists did not see the brain structure and function ina living patient as we can see today. Therefore, surgery was performed basedon the subjective decision of a doctor, influenced by the desire of mal-intentioned people (this 12-year-old boy’s story exemplifies this influence),by doctors’ vanity and greediness, and by the financial pressure of publicadministrators dealing with the burden of overcrowded psychiatric hospitals.Unfortunately, the field was victim of the later reasons, since the mostimportant tool supporting a surgical indication and precision was not avail-able at that time, i.e., the visualization of the diseased brain and itsfunctioning.
Presented in the pages of this textbook, written by specialists in Psychi-atry, Neurosurgery, Neurology, Neuroanatomy, Neuroradiology, and Ethics,the reader will decide by himself if he is prepared to assume the heavyresponsibility to help patients suffering from the most terrible suffering that ahuman can suffer, the suffering of the mind. They are not understood by theirfamily members and society, and are therefore discriminated and doped sothey do not participate and do not disturb normal lives. They becomedepressed to a point of not having the drive to work, date, and enjoy life. Thisleads to a very high addiction and suicidal rate, so high that it accounts as oneof the diseases that kills most humans, close to the death rate of cancer,stroke, or heart disease. It also represents a terrible economical burden tosociety on jobs loss, absenteeism, and expenses with the care for thesepatients.
The first three chapters of the book bring the reader updated with theneuroanatomy and pathophysiology of the Psychiatric Disorders based onmodern imaging, including connectivity and functional changes in specificareas of the brain. Following, come three chapters bringing lessons learnedfrom the past, when the poor practice of this important field reigned and norules existed. The ways lesions were made in the brain and the consequencesof these lesions are stressed. These historical lessons are employed to discuss
ix
the ethical meanders of the Psychiatric Surgery practice. Once these issuesare settled, the patients are prepared for surgery in a chapter dedicated topreoperative issues. At this point the reader is ready to learn and judgeapplications of novel techniques for modifying brain function, comparingthem to the older approaches used for specific diseases. Further, applicationsin development, expanding the horizons of the field, are presented in the lastsix chapters.
This book is to be seen as an update of anatomical, ethical, and indicationsof “Surgery for Psychiatric Disease,” opening the mind of the reader to thefuture of this promising field. It is expected that the reader acquire under-standing of the surgical anatomy, the surgical techniques at hand, and ethicaljudgment of the power of this field, with the knowledge that this practice is infrank evolution and therefore controversial.
Bomin Sun Antonio De Salles
x Preface
Acknowledgments
After I graduated from medical school, I trained in Psychiatry. There, Iunderstood that there were so many psychiatric patients who did not respondto psychological therapy and neuroleptics. There was really a need for analternative treatment for these refractory patients. In 1986, by chance, I hadbeen involved in a group performing stereotactic surgical treatment formental disorders; at that time we only used ventriculography-guided surgery.Since then, I became very interested in surgical treatment for psychiatricdisorders and I started training in neurosurgery including stereotactic andfunctional neurosurgery.
At UCLA medical center, I trained with Prof. Antonio De Salles as afellow in stereotactic and functional neurosurgery and learned many basicknowledge and skills. During that period, I had the chance to meet manyworld class experts and discussed with them surgical treatment for psychi-atric disorders. I remember that during a meeting of the ASSFN in 1999, Dr.Marwan Hariz taught me how to do capsulotomy in a swimming pool in SaltLake city.
Since there are too many debates and misunderstandings on surgicaltreatment for psychiatric disorders, I was thinking that we needed a book thatsystematically and comprehensively discusses surgical treatment for mentaldisorders. My friend Prof. Keith Matthews, Psychiatrist from Dundee,Scotland provided many suggestions. Dr. Ree Cosgrove in Boston alsoprovided detailed and constructive help toward this book.
I would like to express a special word of gratitude to my two greatmentors. Dr. Jian-ping Xu, a pioneer of surgical treatment for psychiatricdisorders in China, who triggered and stimulated my interest in stereotacticand functional neurosurgery while I was a resident in psychiatry. And toProf. Antonio De Salles, who taught me advanced stereotactic and functionalneurosurgery and opened my view to worldwide functional neurosurgery.Furthermore, he encouraged me to go back to China to establish a functionalneurosurgery center after my training in UCLA, so that I had my platform tomake effort toward stereotactic and functional neurosurgery.
xi

Finally, I would also like to express a special word of gratitude to mycolleagues, residents and fellows who over the years have contributed somuch to the development of neurosurgical treatment for psychiatric disordersand their contributed to this book.
Bomin Sun
xii Acknowledgments
Contents
1 Related Circuitry and Synaptic Connectivityin Psychiatric Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . 1Jean-Jacques Lemaire
2 High-angular diffusion MRI in reward-based psychiatricdisorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Wenwen Yu, Qiming Lv, Chencheng Zhang,Zhuangming Shen, Bomin Sun and Zheng Wang
3 Neuroimaging in Psychiatry . . . . . . . . . . . . . . . . . . . . . . . 35Chuantao Zuo and Huiwei Zhang
4 DBS in Psychiatry and the Pendulum of History . . . . . . . . 47Marwan I. Hariz
5 Ablative Surgery for Neuropsychiatric Disorders:Past, Present, Future. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53Yosef Chodakiewitz, John Williams, Jacob Chodakiewitzand Garth Rees Cosgrove
6 Legal Issues in Behavioral Surgery . . . . . . . . . . . . . . . . . . 69Sam Eljamel
7 Preoperative Evaluation and Postoperative Follow-upof Deep Brain Stimulation for Psychiatric Disorders. . . . . . 77Loes Gabriëls, Hemmings Wu and Bart Nuttin
8 Ablative Surgery for Depression . . . . . . . . . . . . . . . . . . . . 87Sam Eljamel
9 Deep Brain Stimulation for the Managementof Treatment-Refractory Major Depressive Disorder . . . . . 95Nir Lipsman, Peter Giacobbe and Andres M. Lozano
10 Ablative Surgery for Obsessive-Compulsive Disorders . . . . 105Roberto Martinez-Alvarez
xiii
11 DBS for Obsessive-Compulsive Disorder . . . . . . . . . . . . . . 113Mayur Sharma, Emam Saleh, Milind Deogaonkarand Ali Rezai
12 Focused Ultrasound for the Treatmentof Obsessive-Compulsive Disorder . . . . . . . . . . . . . . . . . . . 125Young Cheol Na, Hyun Ho Jung and Jin Woo Chang
13 Deep Brain Stimulation for Tourette Syndrome . . . . . . . . . 143Jianuo Zhang, Yan Ge and Fangang Meng
14 Stereotactic Neurosurgery for Drug Addiction . . . . . . . . . . 161Guodong Gao and Xuelian Wang
15 Surgical Treatments for Anorexia Nervosa. . . . . . . . . . . . . 175Bomin Sun, Dianyou Li, Wei Liu, Shikun Zhan,Yixin Pan and Xiaoxiao Zhang
16 Neurosurgery for the Treatment of RefractorySchizophrenia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 189Bomin Sun, Wei Liu, Shikun Zhan, Qianqian Hao,Dianyou Li, Yixin Pan, Yongchao Li and Guozhen Lin
17 Surgical Management for Aggressive Behavior. . . . . . . . . . 203Wei Wang and Peng Li
18 Deep Brain Stimulation in Aggressive Behavior . . . . . . . . . 211Giuseppe Messina, Giovanni Broggi, Roberto Cordellaand Angelo Franzini
19 Radiosurgery for Psychiatric Disorders . . . . . . . . . . . . . . . 217Antônio De Salles and Alessandra A. Gorgulho
Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 227
xiv Contents

1Related Circuitry and SynapticConnectivity in Psychiatric Disorders
Jean-Jacques Lemaire
Abstract
Deciphering the connectivity supporting brain function in psychiatricdisorders is one of the major challenges in clinical neurosciences. Neuralcorrelates of psychiatric disorders are not well-known because experimentalresearch is extremely difficult to carry on facing the complexity of biological,medical and socio-psychological concepts. Although far from an extensiveknowledgeof suchcomplex issue, one can summarizemostmainmacroscopicor microscopic circuits known in human and higher species, but also inrodents. After a reminder of scales and functionality of neurobiologicalcircuits, anatomo-functional correlates of the executive-behavioral systemandpsychiatric disorders are exposed, focusing on most frequent domains ofpsychiatry, anxiety, mood, substance disorders and memory.
1.1 Network Scalesand Functionalityof Neurobiological Circuits
The functionality of circuits involved in psychi-atric disorders can be described from the molec-ular to the connectomics scales. The molecularscale is the neuronal transmission of information,still not extensively mastered, which can be splitinto two main types [2]: wiring transmissionrelying on synapses, neurotransmitters, excitatory
such as the glutamate or inhibitory such as thegamma-amino-butyric acid (GABA), and gatedion channels; volume transmission relying onneuromodulators within the extracellular spaceand cerebrospinal fluid, such as dopamine andserotonin monoamine circuits, affecting largepopulation of neurons through G protein-coupledreceptors. Neurons can release several neuro-transmitters, fast such as the glutamate andGABA, and modulatory, such as the dopamine[9]; typically within the striatum, medium-sizedspiny neurons contain GABA and either sub-stance P or enkephalin (see [32, 65]). Within thecortex, the complex distribution of neuromodu-lator and neurotransmitter receptors makes diffi-cult the analysis of functionality of circuitriesaccounting molecular transmission of informa-tion, in particular in the context of psychiatricdisorders (see e.g. [86]). At microscopic level,the study of structural microanatomy still relies
J.-J. Lemaire (&)Image-Guided Clinical Neuroscience andConnectomics, Auvergne University,Clermont-Ferrand, Francee-mail: [email protected]
J.-J. LemaireService of Neurosurgery, University Hospitalof Clermont-Ferrand, Clermont-Ferrand, France
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0_1© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
1
on ex vivo histologic sampling; axonal tracinghaving harvested a lot of data on micro connec-tivity in humans and other species, however stillcomplex to extrapolate at large scale. Molecularimaging using Petscan could explore in vivocomponents of neuronal signaling process, suchas dopaminergic neurotransmission [105]. Nanocircuitry of inter and intra cellular signaling (seee.g. [74]) is beyond the purpose of chapter, lim-ited to microcircuits, i.e. inter neuronal connec-tivity. Ongoing researches tackling the challengeof mastering brain function based on bio-molec-ular controls should help in the near future [12,14, 63, 111]. On the other hand, the connecto-mics scale, meso-macroscopic or millimetric,relies on segregation of brain function and par-cellation of gray matter (GM); it is very close tothe size of circuit elements described at thefunctional anatomy scale currently used in clinicsfor reasoning, and should likely be suitable fordeciphering, at least partially, psychiatric disor-der pathophysiology. Recent advances in opto-genetic [75] rise hopes that future technologiesmix electrical and pharmacological modulation,tuning finely neuromodulation at the core ofneural circuits. Diffusion tensor imaging (DTI)fiber tracking (FT) enables in vivo analysis of themacroscopic connectivity of brain, probing whitematter (WM) structures connecting cortical areasand deep GM regions. DTI is a fast magneticresonance imaging (MRI) sequence exploringwater molecule movements sequentially in sev-eral directions, usually from 6 to 20. The mainorientation of water motion is resolved withineach MRI voxel, resulting, after fiber trackingcomputational post processing, in colored fibersdisplayed in 3D within the whole MRI voxel dataset. It is assumed that the anisotropic organizationof WM due to nerve fiber (or axon) bundlesexplains the fibers resulting of DTI FT analysis.WM organization was explored by pioneeringneuro-anatomists using brain hardening tech-niques of anatomic specimen [16, 50], introduc-ing the term WM fascicle, later defined asmicroscopically delimitated bundle of nervefibers [89]. Tractus and pathways referred tobundles of nerve fibers subserving functions and
systems [89]: tractus or tract defined groups offibers, such as the cortico-spinal tract subservingthe motor system; pathway or path define chainsof neurons, such as the visual pathway. Practi-cally the macroscopic WM bundles, as thosedisplayed by DTI FT, are structural, whereastractus or pathways are related to known func-tion; however the terms are often mixed up. Withrecent advances of functional connectivity andconnectomics in vivo analysis, these differencescould be of importance, connectomics referringto structure and functional connectivity to func-tion, which are still not explored at the same time,at least with the same technique: functional MRI(fMRI; at rest and activation), 3D electroen-cephalography, molecular imaging, and magnetoencephalography explore function; structuralMRI is the most precise in vivo imaging tech-nique to explore the brain meso- and macro-architecture. Exploration of macro connectivityof psychiatric disorders using DTI could facilitatethe understanding of abnormalities [41].
Fill the gap between micro and meso-macroconnectivity is of upmost importance, and chal-lenging, in psychosurgery, as we do not masterthe full functionality of the executive-behavioralsystem. Consequently we must deal with macroand micro approaches of pathologies and relatedcircuits: topography of anatomo-functional ele-ments of macro circuits, and molecular func-tionality of micro circuits. The tremendousknowledge of biochemical neuromodulation andtransmission within the executive-behavioralsystem, enables the integration of micro andmacro connectivity, which is however far to beextensively mastered. Among the circuits of theexecutive-behavioral system, the mesocortico-limbic circuitry, involved in reward [44] andmood disorder [86], is emblematic of the longway covered and also the considerable distancestill to cover. Schematically the mesocorticolim-bic system corresponds to the efferent connectionof the ventral tegmental area (VTA) with neo andtransitional cortices, such as the sensorimotorcortex, medial prefrontal cortices and the insula,and with limbic structures, such as the accumbensnucleus, the septal region, the cingulate and the
2 J.-J. Lemaire
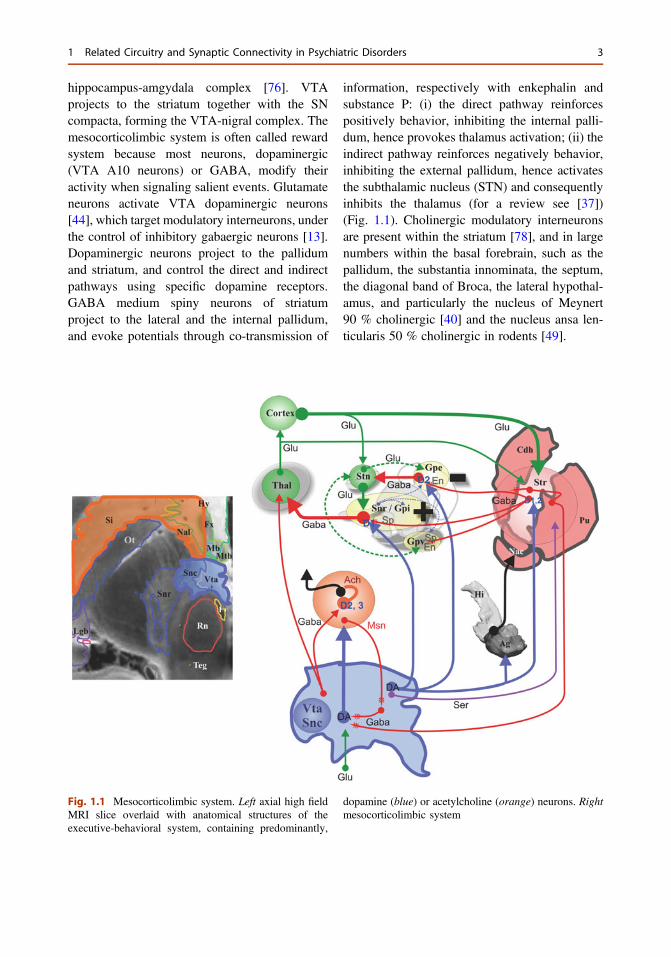
hippocampus-amgydala complex [76]. VTAprojects to the striatum together with the SNcompacta, forming the VTA-nigral complex. Themesocorticolimbic system is often called rewardsystem because most neurons, dopaminergic(VTA A10 neurons) or GABA, modify theiractivity when signaling salient events. Glutamateneurons activate VTA dopaminergic neurons[44], which target modulatory interneurons, underthe control of inhibitory gabaergic neurons [13].Dopaminergic neurons project to the pallidumand striatum, and control the direct and indirectpathways using specific dopamine receptors.GABA medium spiny neurons of striatumproject to the lateral and the internal pallidum,and evoke potentials through co-transmission of
information, respectively with enkephalin andsubstance P: (i) the direct pathway reinforcespositively behavior, inhibiting the internal palli-dum, hence provokes thalamus activation; (ii) theindirect pathway reinforces negatively behavior,inhibiting the external pallidum, hence activatesthe subthalamic nucleus (STN) and consequentlyinhibits the thalamus (for a review see [37])(Fig. 1.1). Cholinergic modulatory interneuronsare present within the striatum [78], and in largenumbers within the basal forebrain, such as thepallidum, the substantia innominata, the septum,the diagonal band of Broca, the lateral hypothal-amus, and particularly the nucleus of Meynert90 % cholinergic [40] and the nucleus ansa len-ticularis 50 % cholinergic in rodents [49].
Fig. 1.1 Mesocorticolimbic system. Left axial high fieldMRI slice overlaid with anatomical structures of theexecutive-behavioral system, containing predominantly,
dopamine (blue) or acetylcholine (orange) neurons. Rightmesocorticolimbic system
1 Related Circuitry and Synaptic Connectivity in Psychiatric Disorders 3
1.2 Anatomo-FunctionalCorrelates of the Executive-Behavioral System
The frontal, the temporal and the limbic lobes,coupled with basal ganglia, thalamus, hypothal-amus, and upper midbrain nuclei are the mainstructures modulating behavioral phenotypes, andare all or part linked with psychiatric disorders.The cerebellum could be involved in psychiatricsymptoms, through the cerebello-thalamo-cortico-pontine loop, in the posterior a fossa, andthe cerebellar cognitive affective syndromes andothers cognitive and affective disorders [15, 69].
The core system supporting neural correlatesof psychiatric disorders is the executive-behav-ioral system involving the prefrontal and thecingulate cortices, and the rest of the limbicsystem, which includes the limbic lobe (Fig. 1.2).From the clinical experience, the whole frontallobe could be involved in the executive-behav-ioral system, however this has to be interpretedcautiously [4], even though recent data showsthat the supplementary motor area of medial
motor cortex could participate to action-moni-toring system, adjusting behavior according tothe result of action [8]. Functional imagingshould help to segregate functionalities support-ing executive-behavior functions within thefrontal lobe [102].
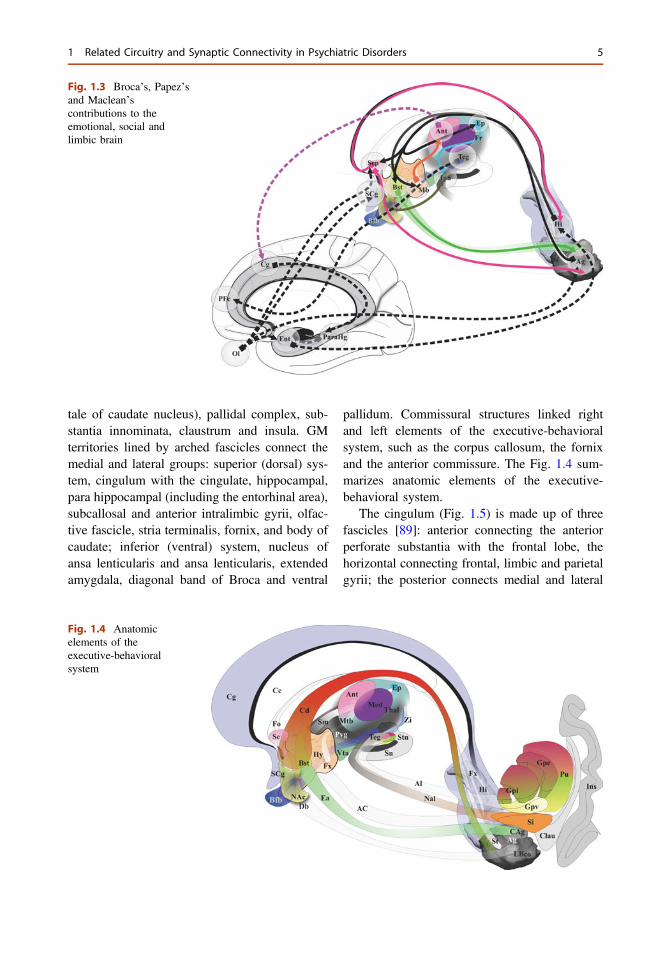
The executive-behavioral system supports theso-called “emotional brain” and “social brain”[24, 52], coming from pioneering works of Brocaintroducing the term “grand lobe limbique” [11],Papez [79] proposing the concept of corticotha-lamic correlate of emotions, and MacLean [58]extending Papez’s work with the visceral brain(Fig. 1.3). A lot of connections between thesestructures are known, although the functionality,physiologic and pathophysiologic, of circuits isnot fully mastered.
Broadly elements of executive-behavioralsystem are pushed aside by WM fascicles of theinternal capsule, separating two groups: (i) themedial group, hypothalamus, subthalamus, thal-amus, head of caudate nucleus, accumbensnucleus; (ii) the lateral group, hippocampus-am-gydala complex, lateral striatum (putamen and
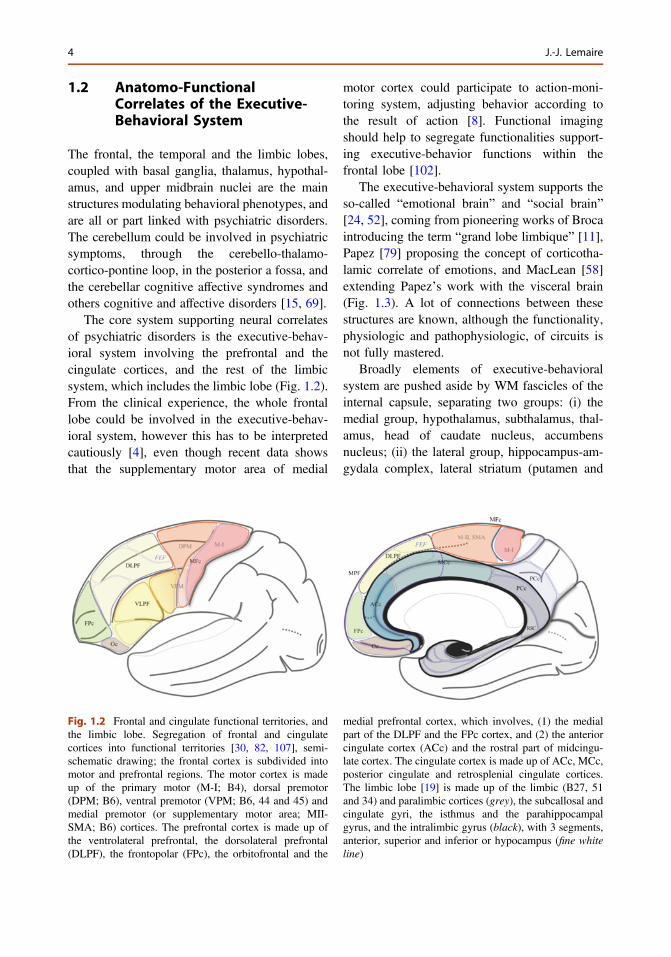
Fig. 1.2 Frontal and cingulate functional territories, andthe limbic lobe. Segregation of frontal and cingulatecortices into functional territories [30, 82, 107], semi-schematic drawing; the frontal cortex is subdivided intomotor and prefrontal regions. The motor cortex is madeup of the primary motor (M-I; B4), dorsal premotor(DPM; B6), ventral premotor (VPM; B6, 44 and 45) andmedial premotor (or supplementary motor area; MII-SMA; B6) cortices. The prefrontal cortex is made up ofthe ventrolateral prefrontal, the dorsolateral prefrontal(DLPF), the frontopolar (FPc), the orbitofrontal and the
medial prefrontal cortex, which involves, (1) the medialpart of the DLPF and the FPc cortex, and (2) the anteriorcingulate cortex (ACc) and the rostral part of midcingu-late cortex. The cingulate cortex is made up of ACc, MCc,posterior cingulate and retrosplenial cingulate cortices.The limbic lobe [19] is made up of the limbic (B27, 51and 34) and paralimbic cortices (grey), the subcallosal andcingulate gyri, the isthmus and the parahippocampalgyrus, and the intralimbic gyrus (black), with 3 segments,anterior, superior and inferior or hypocampus (fine whiteline)
4 J.-J. Lemaire
tale of caudate nucleus), pallidal complex, sub-stantia innominata, claustrum and insula. GMterritories lined by arched fascicles connect themedial and lateral groups: superior (dorsal) sys-tem, cingulum with the cingulate, hippocampal,para hippocampal (including the entorhinal area),subcallosal and anterior intralimbic gyrii, olfac-tive fascicle, stria terminalis, fornix, and body ofcaudate; inferior (ventral) system, nucleus ofansa lenticularis and ansa lenticularis, extendedamygdala, diagonal band of Broca and ventral
pallidum. Commissural structures linked rightand left elements of the executive-behavioralsystem, such as the corpus callosum, the fornixand the anterior commissure. The Fig. 1.4 sum-marizes anatomic elements of the executive-behavioral system.
The cingulum (Fig. 1.5) is made up of threefascicles [89]: anterior connecting the anteriorperforate substantia with the frontal lobe, thehorizontal connecting frontal, limbic and parietalgyrii; the posterior connects medial and lateral
Fig. 1.3 Broca’s, Papez’sand Maclean’scontributions to theemotional, social andlimbic brain
Fig. 1.4 Anatomicelements of theexecutive-behavioralsystem
1 Related Circuitry and Synaptic Connectivity in Psychiatric Disorders 5

occipito-temporal gyrii with the temporal gyrus.Recent advances have added new insights intothe cingulum bundle, showing the multiple con-nection fibers merged [46]. In monkeys the cin-gulum also contains fibers connecting theprefrontal dorsolateral cortex and the hippocam-pal formation [31]. The distal, rostral, anteriorcingulate is a part of the sub cingulo-callosalregion that includes also the subcallosal (orsubcallosal cingulate) gyrus and the carrefourolfactif of Broca (paraolfactory area). The gyrusrectus merges with the anterior cingulate and thesubcallosal gyrus within the carrefour olfactif[89]. The organization of the WM of the subcingulo-callosal region illustrates the complexityof connections, allowing the prefrontal cortex toconnect with the lateral and the medial groups ofelements of the executive-behavioral system(Fig. 1.6). The fornix connects the hypothalamus(mammillary and tubero mammillaris), the sep-tum, and the habenula, with the Amon horn(alveus; medial) and the gyrus dentatus (fimbria;
lateral). The olfactive fascicle connects the pos-terior septum and cingulate through the corpuscallosum, with the anterior septal nuclei andthe anterior perforate area, and continues to theamygdala, the substantia innominata and theuncus, through the diagonal band of Broca [89].The stria terminalis connects the septal and par-aseptal region (or bed of the stria terminalis) withthe amygdala; the extended amygdala, a networkof sparse cells and connections within the rostralmediobasal forebrain, located laterally to thehypothalamus and below the lenticular nucleus,bridges the bed nucleus of stria terminalis and thecentromedial amygdala [27, 26]. The hypothal-amus, made of 11 nuclei, had a large connectivitywith the cortex and the deep brain [55] (Fig. 1.7),some features seems specific: dorsomedialnucleus mostly connected with the medial thal-amus and the midline gray substance; ventro-medial area (ventromedial nucleus and theadjacent tuberomamillaris nucleus) stronglyconnected with the prefrontal cortex; preoptic
Fig. 1.5 Cingulum. Left fascicles of the cingulum. RightDTI tractography of the cingulum showing differentcomponents; note that anterior commissural fibers of the
beak of callosum (yellow) merge with anterior fibers ofthe cingulum
6 J.-J. Lemaire
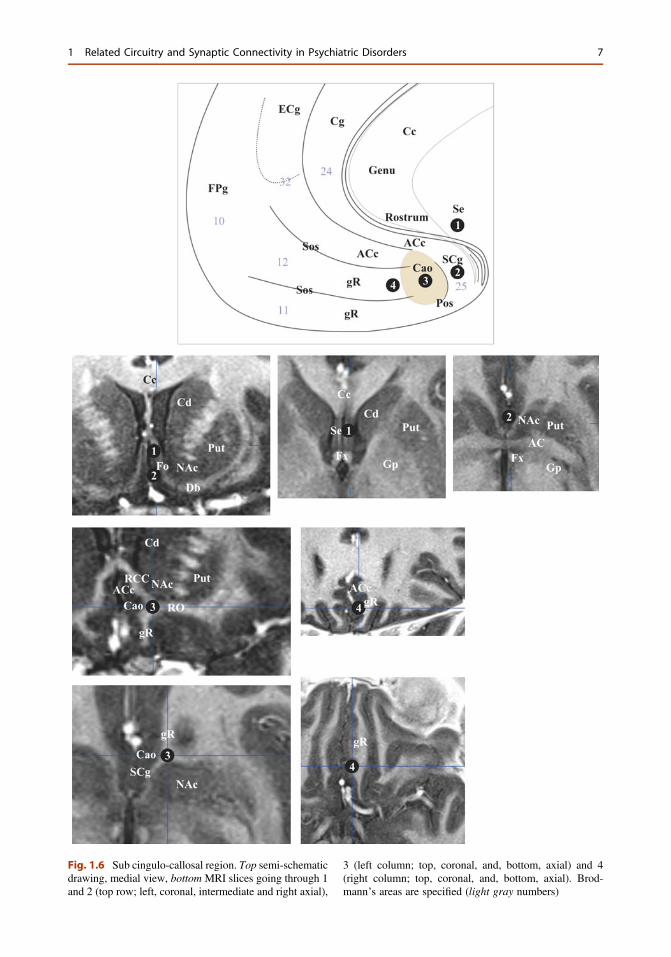
Fig. 1.6 Sub cingulo-callosal region. Top semi-schematicdrawing, medial view, bottom MRI slices going through 1and 2 (top row; left, coronal, intermediate and right axial),
3 (left column; top, coronal, and, bottom, axial) and 4(right column; top, coronal, and, bottom, axial). Brod-mann’s areas are specified (light gray numbers)
1 Related Circuitry and Synaptic Connectivity in Psychiatric Disorders 7
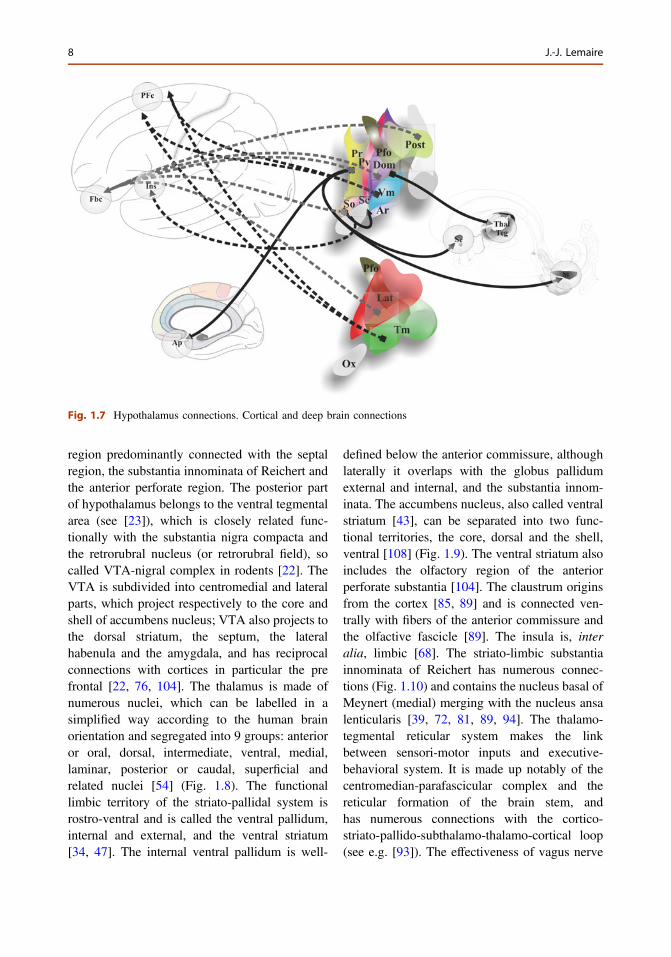
region predominantly connected with the septalregion, the substantia innominata of Reichert andthe anterior perforate region. The posterior partof hypothalamus belongs to the ventral tegmentalarea (see [23]), which is closely related func-tionally with the substantia nigra compacta andthe retrorubral nucleus (or retrorubral field), socalled VTA-nigral complex in rodents [22]. TheVTA is subdivided into centromedial and lateralparts, which project respectively to the core andshell of accumbens nucleus; VTA also projects tothe dorsal striatum, the septum, the lateralhabenula and the amygdala, and has reciprocalconnections with cortices in particular the prefrontal [22, 76, 104]. The thalamus is made ofnumerous nuclei, which can be labelled in asimplified way according to the human brainorientation and segregated into 9 groups: anterioror oral, dorsal, intermediate, ventral, medial,laminar, posterior or caudal, superficial andrelated nuclei [54] (Fig. 1.8). The functionallimbic territory of the striato-pallidal system isrostro-ventral and is called the ventral pallidum,internal and external, and the ventral striatum[34, 47]. The internal ventral pallidum is well-
defined below the anterior commissure, althoughlaterally it overlaps with the globus pallidumexternal and internal, and the substantia innom-inata. The accumbens nucleus, also called ventralstriatum [43], can be separated into two func-tional territories, the core, dorsal and the shell,ventral [108] (Fig. 1.9). The ventral striatum alsoincludes the olfactory region of the anteriorperforate substantia [104]. The claustrum originsfrom the cortex [85, 89] and is connected ven-trally with fibers of the anterior commissure andthe olfactive fascicle [89]. The insula is, interalia, limbic [68]. The striato-limbic substantiainnominata of Reichert has numerous connec-tions (Fig. 1.10) and contains the nucleus basal ofMeynert (medial) merging with the nucleus ansalenticularis [39, 72, 81, 89, 94]. The thalamo-tegmental reticular system makes the linkbetween sensori-motor inputs and executive-behavioral system. It is made up notably of thecentromedian-parafascicular complex and thereticular formation of the brain stem, andhas numerous connections with the cortico-striato-pallido-subthalamo-thalamo-cortical loop(see e.g. [93]). The effectiveness of vagus nerve
Fig. 1.7 Hypothalamus connections. Cortical and deep brain connections
8 J.-J. Lemaire
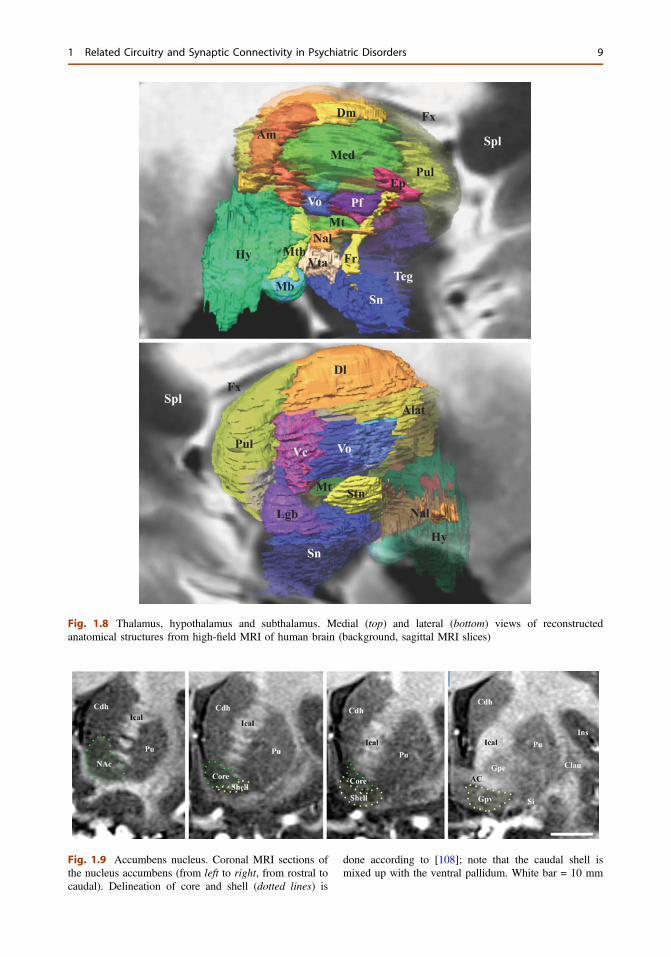
Fig. 1.8 Thalamus, hypothalamus and subthalamus. Medial (top) and lateral (bottom) views of reconstructedanatomical structures from high-field MRI of human brain (background, sagittal MRI slices)
Fig. 1.9 Accumbens nucleus. Coronal MRI sections ofthe nucleus accumbens (from left to right, from rostral tocaudal). Delineation of core and shell (dotted lines) is
done according to [108]; note that the caudal shell ismixed up with the ventral pallidum. White bar = 10 mm
1 Related Circuitry and Synaptic Connectivity in Psychiatric Disorders 9
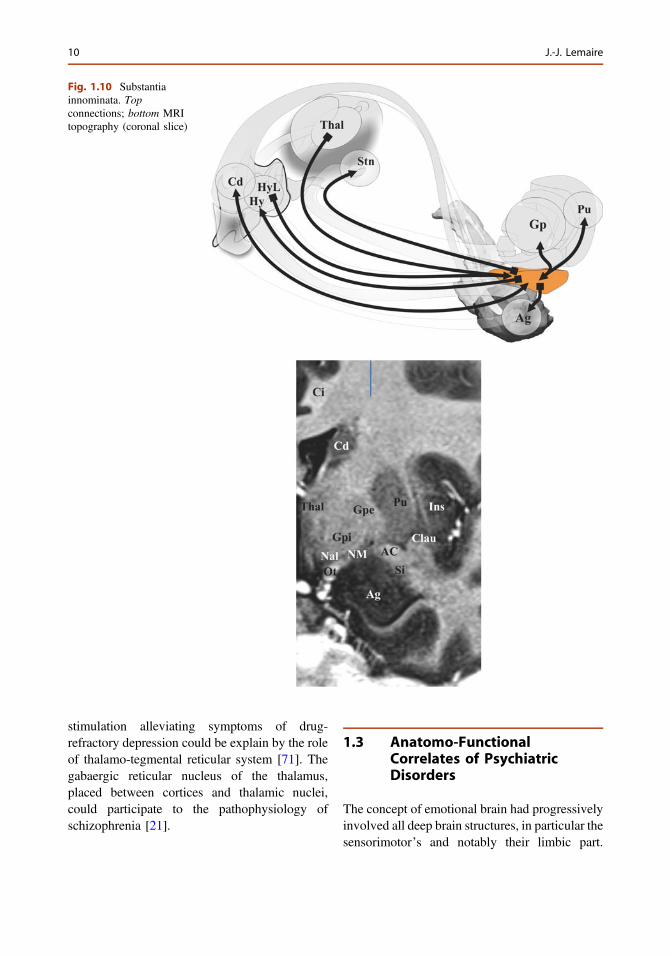
stimulation alleviating symptoms of drug-refractory depression could be explain by the roleof thalamo-tegmental reticular system [71]. Thegabaergic reticular nucleus of the thalamus,placed between cortices and thalamic nuclei,could participate to the pathophysiology ofschizophrenia [21].
1.3 Anatomo-FunctionalCorrelates of PsychiatricDisorders
The concept of emotional brain had progressivelyinvolved all deep brain structures, in particular thesensorimotor’s and notably their limbic part.
Fig. 1.10 Substantiainnominata. Topconnections; bottom MRItopography (coronal slice)
10 J.-J. Lemaire
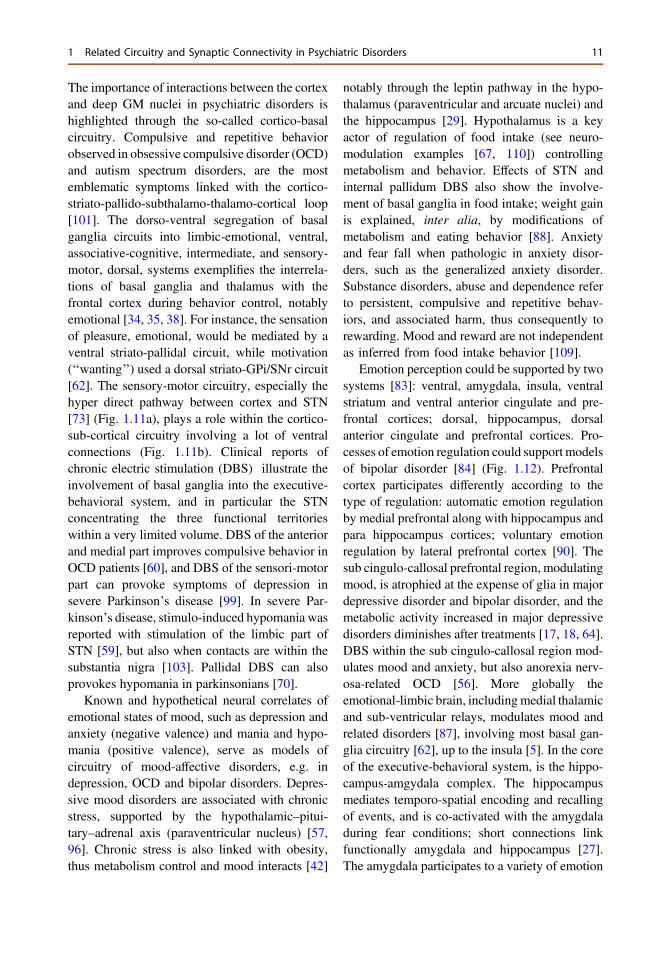
The importance of interactions between the cortexand deep GM nuclei in psychiatric disorders ishighlighted through the so-called cortico-basalcircuitry. Compulsive and repetitive behaviorobserved in obsessive compulsive disorder (OCD)and autism spectrum disorders, are the mostemblematic symptoms linked with the cortico-striato-pallido-subthalamo-thalamo-cortical loop[101]. The dorso-ventral segregation of basalganglia circuits into limbic-emotional, ventral,associative-cognitive, intermediate, and sensory-motor, dorsal, systems exemplifies the interrela-tions of basal ganglia and thalamus with thefrontal cortex during behavior control, notablyemotional [34, 35, 38]. For instance, the sensationof pleasure, emotional, would be mediated by aventral striato-pallidal circuit, while motivation(‘‘wanting’’) used a dorsal striato-GPi/SNr circuit[62]. The sensory-motor circuitry, especially thehyper direct pathway between cortex and STN[73] (Fig. 1.11a), plays a role within the cortico-sub-cortical circuitry involving a lot of ventralconnections (Fig. 1.11b). Clinical reports ofchronic electric stimulation (DBS) illustrate theinvolvement of basal ganglia into the executive-behavioral system, and in particular the STNconcentrating the three functional territorieswithin a very limited volume. DBS of the anteriorand medial part improves compulsive behavior inOCD patients [60], and DBS of the sensori-motorpart can provoke symptoms of depression insevere Parkinson’s disease [99]. In severe Par-kinson’s disease, stimulo-induced hypomania wasreported with stimulation of the limbic part ofSTN [59], but also when contacts are within thesubstantia nigra [103]. Pallidal DBS can alsoprovokes hypomania in parkinsonians [70].
Known and hypothetical neural correlates ofemotional states of mood, such as depression andanxiety (negative valence) and mania and hypo-mania (positive valence), serve as models ofcircuitry of mood-affective disorders, e.g. indepression, OCD and bipolar disorders. Depres-sive mood disorders are associated with chronicstress, supported by the hypothalamic–pitui-tary–adrenal axis (paraventricular nucleus) [57,96]. Chronic stress is also linked with obesity,thus metabolism control and mood interacts [42]
notably through the leptin pathway in the hypo-thalamus (paraventricular and arcuate nuclei) andthe hippocampus [29]. Hypothalamus is a keyactor of regulation of food intake (see neuro-modulation examples [67, 110]) controllingmetabolism and behavior. Effects of STN andinternal pallidum DBS also show the involve-ment of basal ganglia in food intake; weight gainis explained, inter alia, by modifications ofmetabolism and eating behavior [88]. Anxietyand fear fall when pathologic in anxiety disor-ders, such as the generalized anxiety disorder.Substance disorders, abuse and dependence referto persistent, compulsive and repetitive behav-iors, and associated harm, thus consequently torewarding. Mood and reward are not independentas inferred from food intake behavior [109].
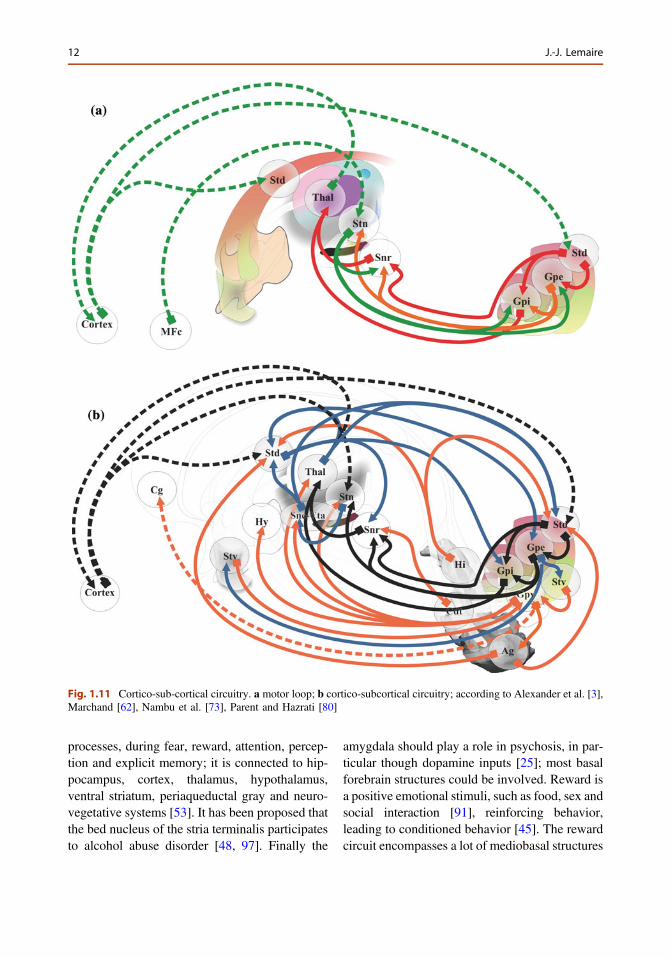
Emotion perception could be supported by twosystems [83]: ventral, amygdala, insula, ventralstriatum and ventral anterior cingulate and pre-frontal cortices; dorsal, hippocampus, dorsalanterior cingulate and prefrontal cortices. Pro-cesses of emotion regulation could support modelsof bipolar disorder [84] (Fig. 1.12). Prefrontalcortex participates differently according to thetype of regulation: automatic emotion regulationby medial prefrontal along with hippocampus andpara hippocampus cortices; voluntary emotionregulation by lateral prefrontal cortex [90]. Thesub cingulo-callosal prefrontal region, modulatingmood, is atrophied at the expense of glia in majordepressive disorder and bipolar disorder, and themetabolic activity increased in major depressivedisorders diminishes after treatments [17, 18, 64].DBS within the sub cingulo-callosal region mod-ulates mood and anxiety, but also anorexia nerv-osa-related OCD [56]. More globally theemotional-limbic brain, includingmedial thalamicand sub-ventricular relays, modulates mood andrelated disorders [87], involving most basal gan-glia circuitry [62], up to the insula [5]. In the coreof the executive-behavioral system, is the hippo-campus-amgydala complex. The hippocampusmediates temporo-spatial encoding and recallingof events, and is co-activated with the amygdaladuring fear conditions; short connections linkfunctionally amygdala and hippocampus [27].The amygdala participates to a variety of emotion
1 Related Circuitry and Synaptic Connectivity in Psychiatric Disorders 11
processes, during fear, reward, attention, percep-tion and explicit memory; it is connected to hip-pocampus, cortex, thalamus, hypothalamus,ventral striatum, periaqueductal gray and neuro-vegetative systems [53]. It has been proposed thatthe bed nucleus of the stria terminalis participatesto alcohol abuse disorder [48, 97]. Finally the
amygdala should play a role in psychosis, in par-ticular though dopamine inputs [25]; most basalforebrain structures could be involved. Reward isa positive emotional stimuli, such as food, sex andsocial interaction [91], reinforcing behavior,leading to conditioned behavior [45]. The rewardcircuit encompasses a lot of mediobasal structures
Fig. 1.11 Cortico-sub-cortical circuitry. a motor loop; b cortico-subcortical circuitry; according to Alexander et al. [3],Marchand [62], Nambu et al. [73], Parent and Hazrati [80]
12 J.-J. Lemaire
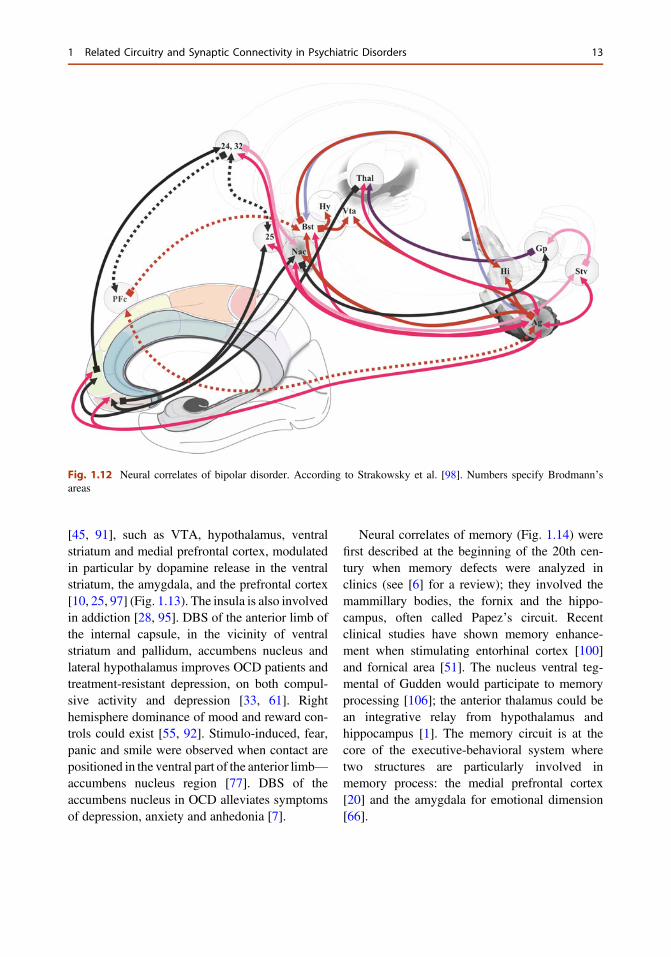
[45, 91], such as VTA, hypothalamus, ventralstriatum and medial prefrontal cortex, modulatedin particular by dopamine release in the ventralstriatum, the amygdala, and the prefrontal cortex[10, 25, 97] (Fig. 1.13). The insula is also involvedin addiction [28, 95]. DBS of the anterior limb ofthe internal capsule, in the vicinity of ventralstriatum and pallidum, accumbens nucleus andlateral hypothalamus improves OCD patients andtreatment-resistant depression, on both compul-sive activity and depression [33, 61]. Righthemisphere dominance of mood and reward con-trols could exist [55, 92]. Stimulo-induced, fear,panic and smile were observed when contact arepositioned in the ventral part of the anterior limb—accumbens nucleus region [77]. DBS of theaccumbens nucleus in OCD alleviates symptomsof depression, anxiety and anhedonia [7].
Neural correlates of memory (Fig. 1.14) werefirst described at the beginning of the 20th cen-tury when memory defects were analyzed inclinics (see [6] for a review); they involved themammillary bodies, the fornix and the hippo-campus, often called Papez’s circuit. Recentclinical studies have shown memory enhance-ment when stimulating entorhinal cortex [100]and fornical area [51]. The nucleus ventral teg-mental of Gudden would participate to memoryprocessing [106]; the anterior thalamus could bean integrative relay from hypothalamus andhippocampus [1]. The memory circuit is at thecore of the executive-behavioral system wheretwo structures are particularly involved inmemory process: the medial prefrontal cortex[20] and the amygdala for emotional dimension[66].
Fig. 1.12 Neural correlates of bipolar disorder. According to Strakowsky et al. [98]. Numbers specify Brodmann’sareas
1 Related Circuitry and Synaptic Connectivity in Psychiatric Disorders 13
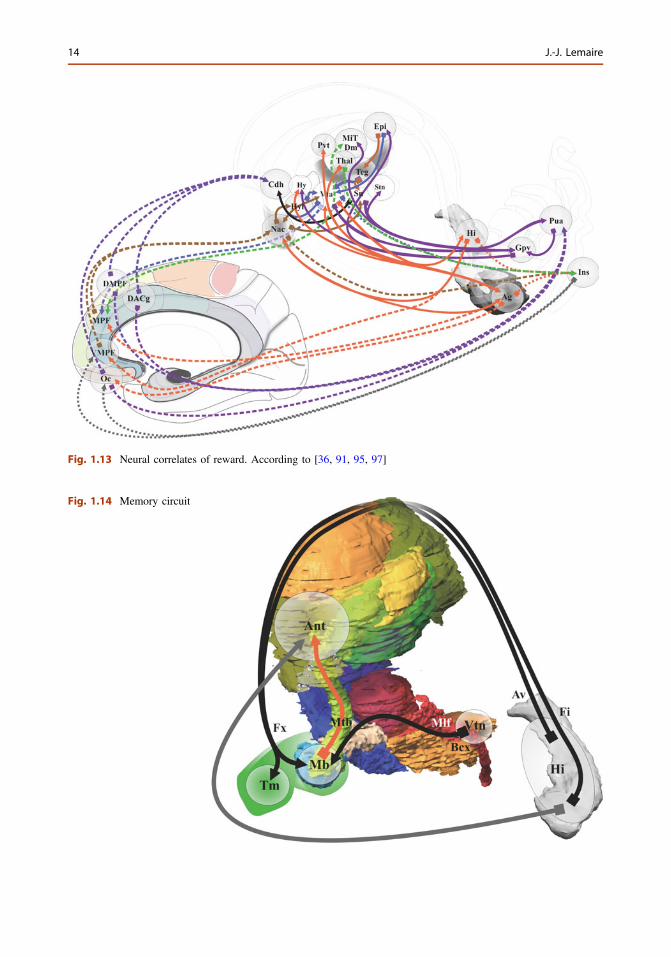
Fig. 1.13 Neural correlates of reward. According to [36, 91, 95, 97]
Fig. 1.14 Memory circuit
14 J.-J. Lemaire
List of Abbreviations Used in Figures
AC Anterior commissure
ACc Anterior cingulate cortex
Ach Acetylcholine
Ag Amygdala
Al Ansa lenticularis
Alat Anterolateral nucleus (Thalamus)
Am Anteromedial nucleus (Thalamus)
Ant Anterior thalamus
Ap Anterior perforate region
Ar Arcuate nucleus (hypothalamus)
Av Alveus
Bfb Basal forebrain bundle
Bst Bed of stria terminalis
CAg Centromedial amygdala
Cc Corpus callosum
Clau Claustrum
Cd, h, t Caudate nucleus, head, tale
Cg Cingulate (gyrus)
Ci Cingulum (longitudinal fascicleof the gyrus limbici)
Cao Carrefour olfactif of Broca (para-olfactory area)
Cs Cingulate sulcus
D1, 2 Dopamine receptor: types 1 and 2
DA Dopamine neuron
DACg Dorsal anterior cingulate
Db Diagonal band of Broca
Dl Dorsolateral nucleus (thalamus)
DLPF Dorsolateral prefronal cortex
DMPF Dorsomedial prefronal cortex
Dm Dorsomedial nucleus (thalamus)
Dom Dorsomedial nucleus(hypothalamus)
DPM Dorsal premotor cortex
Ea Extended amygdala
ECg External cingulate gyrus
Ep Epithalamus
Epl Lateral habenula
Ent Entorhinal cortex
Fa Fascicle angularis
Fbc Fronto-basal cortex
FEF Frontal eye field
Fi Fimbria
Fo Fascicle olfactorius, diagonalband of Broca
FPc Frontopolar cortex
Fr Fascicle retroflexus
Fx Fornix
Gaba Gamma-aminobutyric acidneuron
Glu Glutamate
gR Gyrus rectus
Gp, e, i, v Globus pallidum extern, intern,ventral
Hi Hippocampus
Hy, l Hypothalamus, lateral
Ical Internal capsule anterior limb
Ida Insular dysgranular area
Ifs Inferior frontal gyrus
Ins Insula
Ipn Interpeduncular nucleus
Isth Isthmus
Lat Lateral nucleus (hypothalamus)
Lgb Lateral geniculate body
LBco Laterobasal complex of amygdala
M-I Primary motor area
M-II,SMA
Supplementary motor area
Mb Mammilary body
MCc Midcingulate cortex
MFc Motor frontal cortex
1 Related Circuitry and Synaptic Connectivity in Psychiatric Disorders 15
MiT Midline thalamus
MPF Medial prefrontal cortex
Msn Medium spiny neuron
Mtb Mamillo-thalamic bundle
Nac (c, s) Nucleus accumbens (core, shell)
Nal Nucleus ansa lenticularis
NM Nucleus of Meynert
Mt Mammillo-tegmental fascicle
Oc Orbitofrontal cortex
OFg Orbitofrontal gyri
Ol Ofactive system
Ot Optical tract
Ox Optic chiasma
ParaHg Parahypoccampal gyrus
PCc Posterior cingulate cortex
PCs Paracingulate sulcus
Pf Parafascicular nucleus (thalamus)
Pfo Perifornical nucleus(hypothalamus)
PFc Prefrontal cortex
Pol Temporo-polar region
Pos Paraolfactive or subcallosal sulcus
Post Posterior nucleus (hypothalamus)
Pr Preoptic nucleus (hypothalamus)
PreCuneus Pre cuneus of the medial parieto-cingulate region
Pu, a Putamen, anterior
Pul Pulvinar
Pv Periventricular nucleus(hypothalamus)
Pvg Paraventricular grey matter
Pvt Paraventricular thalamus
RCc Radiation of the corpus callosum
RSC Retrosplenial cingulate cortex
Ro Olfactive radiation
Rn Red nucleus
Rrn Retrorubral nucleus or field
Sc Suprachiasmatic nucleus(hypothalamus)
SCg Subcallosal gyrus
Se Septum (nuclei)
Ser Serotonine or5-hydroxytryptamine
Si Substantia innominata
Sm Stria medullaris
So Supraoptic nucleus(hypothalamus)
Sos Supraorbitaris sulci
Spl Splenium of the corpus callosum
Sq Substance Q
St Stria terminalis
Stn Subthalamic nucleus
Std Dorsal striatum
Stv Ventral striatum
Sn, c, r Substantia nigra, compacta,reticulata
Teg Tegmentum
Thal Thalamus
Tm Nucleus tuberomammillaris(hypothalamus)
Trg Transverse gyri
VLPF Ventrolateral prefrontal cortex
VMPF Ventromedial prefrontal cortex
Vc Thalamus ventro-caudal
Vm Ventromedial nucleus(hypothalamus)
Vo Thalamus ventro-oral
VPM Ventral premotor cortex
Vta, L,CM
Ventral tegmental area, lateral andcaudo-medial parts
Zi Zona incerta
16 J.-J. Lemaire
References
1. Aggleton JP. Multiple anatomical systemsembedded within the primate medial temporallobe: Implications for hippocampal function.Neurosci Biobehav Rev. 2012;36:1579–96.
2. Agnati LF, Guidolin D, Guescini M, Genedani S,Fuxe K. Understanding wiring and volumetransmission. Brain Res Rev. 2010;64:137–59.
3. Alexander GE, DeLong MR, Strick PL. Parallelorganization of functionally segregated circuitslinking basal ganglia and cortex. Annu RevNeurosci. 1986;9:357–81.
4. Andrés P. Frontal cortex as the central executive ofworking memory: time to revise our view. Cortex JDevoted Stud Nerv Syst Behav. 2003;39:871–95.
5. Avery JA, Drevets WC, Moseman SE, Bodurka J,Barcalow JC, Simmons WK. Major depressivedisorder is associated with abnormal interoceptiveactivity and functional connectivity in the insula.Biol Psychiatry. 2013.
6. Barbizet J. Defect of memorizing of hippocampal-mammillary origin: A review. J Neurol NeurosurgPsychiatry. 1963;26:127–35.
7. Bewernick BH, Hurlemann R, Matusch A, KayserS, Grubert C, Hadrysiewicz B, Axmacher N, LemkeM, Cooper-Mahkorn D, Cohen MX, Brockmann H,Lenartz D, Sturm V, Schlaepfer TE. Nucleusaccumbens deep brain stimulation decreases ratingsof depression and anxiety in treatment-resistantdepression. Biol Psychiatry. 2010;67:110–6.
8. Bonini F, Burle B, Liégeois-Chauvel C, Régis J,Chauvel P, Vidal F. Action monitoring and medialfrontal cortex: Leading role of supplementary motorarea. Science. 2014;343:888–91.
9. Borisovska M, Bensen AL, Chong G, WestbrookGL. Distinct modes of dopamine and GABA releasein a dual transmitter neuron. J Neurosci Off J SocNeurosci. 2013;33:1790–6.
10. Britt JP, Bonci A. Optogenetic interrogations of theneural circuits underlying addiction. Curr OpinNeurobiol. 2013;23:539–45.
11. Broca P. Sur la circonvolution limbique et lascissure limbique. Bull Société Anthr Paris.1877;12:646–57.
12. Brüstle O. Developmental neuroscience: miniaturehuman brains. Nature. 2013;501:319–20.
13. Creed MC, Ntamati NR, Tan KR. VTA GABAneurons modulate specific learning behaviorsthrough the control of dopamine and cholinergicsystems. Front Behav Neurosci. 2014;8:8.
14. Dani A, Huang B, Bergan J, Dulac C, Zhuang X.Superresolution imaging of chemical synapses in thebrain. Neuron. 2010;68:843–56.
15. De Smet HJ, Paquier P, Verhoeven J, Mariën P. Thecerebellum: its role in language and related cognitiveand affective functions.Brain Lang. 2013;127:334–42.
16. Dejerine J. Anatomie des centres nerveux (Tomes 1and 2), Rueff et Cie. ed. Paris; 1901.
17. Drevets WC, Price JL, Simpson JR Jr, Todd RD,Reich T, Vannier M, Raichle ME. Subgenualprefrontal cortex abnormalities in mood disorders.Nature. 1997;386:824–7.
18. Drevets WC, Savitz J, Trimble M. The subgenualanterior cingulate cortex in mood disorders. CNSSpectr. 2008;13:663–81.
19. Duvernoy H, Cabanis E-A, Iba-Zizen M-T, TamrazJ, Guyot J. Le cerveau humain: surfaces, coupessériées tridimentionelles et IRM. Paris: Springer;1992.
20. Euston DR, Gruber AJ, McNaughton BL. The roleof medial prefrontal cortex in memory and decisionmaking. Neuron. 2012;76:1057–70.
21. Ferrarelli F, Tononi G. The thalamic reticularnucleus and schizophrenia. Schizophr Bull. 2011;37:306–15.
22. Ferreira JGP, Del-Fava F, Hasue RH, Shammah-Lagnado SJ. Organization of ventral tegmental areaprojections to the ventral tegmental area-nigralcomplex in the rat. Neuroscience. 2008;153:196–213.
23. Fontaine D, Lanteri-Minet M, Ouchchane L,Lazorthes Y, Mertens P, Blond S, Geraud G, FabreN, Navez M, Lucas C, Dubois F, Sol JC, Paquis P,Lemaire JJ. Anatomical location of effective deepbrain stimulation electrodes in chronic clusterheadache. Brain J Neurol. 2010;133:1214–23.
24. Fossati P. Neural correlates of emotion processing:from emotional to social brain. Eur Neuropsychopharmacol. 2012;22:S487–91.
25. Fudge JL, Emiliano AB. The extended amygdalaand the dopamine system: another piece of thedopamine puzzle. J Neuropsychiatry Clin Neurosci.2003;15:306–16.
26. Fudge JL, Haber SN. Bed nucleus of the striaterminalis and extended amygdala inputs to dopaminesubpopulations in primates. Neuroscience. 2001;104:807–27.
27. Fudge JL, deCampo DM, Becoats KT. Revisitingthe hippocampal–amygdala pathway in primates:association with immature-appearing neurons.Neuroscience. 2012;212:104–19.
28. Garavan H. Insula and drug cravings. Brain StructFunct. 2010;214:593–601.
29. Ge J-F, Qi C-C, Zhou J-N. Imbalance of leptinpathway and hypothalamus synaptic plasticitymarkersare associated with stress-induced depression in rats.Behav Brain Res. 2013;249:38–43.
30. Geyer S, Luppino G, Rozzi S. Motor cortex. In: MaiJK, Paxinos G, editors. The human nervous system;3rd ed. Elsevier: London; 2012. p. 1012–1035.
31. Goldman-Rakic PS, Selemon LD, Schwartz ML.Dual pathways connecting the dorsolateralprefrontal cortex with the hippocampal formationand parahippocampal cortex in the rhesus monkey.Neuroscience. 1984;12:719–43.
32. Govindaiah G, Wang Y, Cox CL. Substance Pselectively modulates GABA(A) receptor-mediatedsynaptic transmission in striatal cholinergicinterneurons. Neuropharmacology. 2010;58:413–22.
1 Related Circuitry and Synaptic Connectivity in Psychiatric Disorders 17
33. Greenberg BD, Malone DA, Friehs GM, Rezai AR,Kubu CS, Malloy PF, Salloway SP, Okun MS,Goodman WK, Rasmussen SA. Three-year outcomesin deep brain stimulation for highly resistant obsessive-compulsive disorder. Neuropsychopharmacol OffPubl Am Coll Neuropsychopharmacol. 2006;31:2384–93.
34. Haber SN. The primate basal ganglia: parallel andintegrative networks. J Chem Neuroanat.2003;26:317–30.
35. Haber SN, Calzavara R. The cortico-basal gangliaintegrative network: the role of the thalamus. BrainRes Bull. 2009;78:69–74.
36. Haber SN, Knutson B. The reward circuit: Linkingprimate anatomy and human imaging.Neuropsychopharmacology. 2009;35:4–26.
37. Haber SN, Adler A, Bergman H. The basal ganglia.In: Mai JK, Paxinos G, editors. The human nervoussystem. 3rd ed. Amsterdam: Academic Press; 2011.p. 678–738.
38. Haynes WIA, Haber SN. The organization ofprefrontal-subthalamic inputs in primates providesan anatomical substrate for both functionalspecificity and integration: implications for BasalGanglia models and deep brain stimulation.J Neurosci Off J Soc Neurosci. 2013;33:4804–14.
39. Heimer L. Basal forebrain in the context ofschizophrenia. Brain Res Brain Res Rev.2000;31:205–35.
40. Heimer L, Harlan RE, Alheid GF, Garcia MM, deOlmos J. Substantia innominata: a notion whichimpedes clinical-anatomical correlations inneuropsychiatric disorders. Neuroscience. 1997;76:957–1006.
41. Heng S, Song AW, Sim K. White matterabnormalities in bipolar disorder: insights fromdiffusion tensor imaging studies. J Neural Transm.2010;1996(117):639–54.
42. Hryhorczuk C, Sharma S, Fulton SE. Metabolicdisturbances connecting obesity and depression.Front Neurosci. 2013;7:177.
43. Ikemoto S. Dopamine reward circuitry: twoprojection systems from the ventral midbrain to thenucleus accumbens-olfactory tubercle complex.Brain Res Rev. 2007;56:27–78.
44. Ikemoto S, Wise RA. Mapping of chemical triggerzones for reward. Neuropharmacology. 2004;47(1):190–201.
45. Ikemoto S, Bonci A. Neurocircuitry of drug reward.Neuropharmacology. 2014;76:329–341.
46. Jones DK, Christiansen KF, Chapman RJ, AggletonJP. Distinct subdivisions of the cingulum bundlerevealed by diffusion MRI fibre tracking:implications for neuropsychological investigations.Neuropsychologia. 2013;51:67–78.
47. Karachi C, François C, Parain K, Bardinet E, TandéD,Hirsch E, Yelnik J. Three-dimensional cartography offunctional territories in the human striatopallidalcomplex by using calbindin immunoreactivity.J Comp Neurol. 2002;450:122–34.
48. Kash TL. The role of biogenic amine signaling inthe bed nucleus of the stria terminals in alcoholabuse. Alcohol. 2012;46:303–8.
49. Kha HT, Finkelstein DI, Pow DV, Lawrence AJ,Horne MK. Study of projections from theentopeduncular nucleus to the thalamus of the rat.J Comp Neurol. 2000;426:366–77.
50. Klingler J. Erleichterung des makroskopischenpraeparation des gehirns durch den gefrierprozess.Schweiz Arch Neurol Psychiatr. 1935;36:247–56.
51. Laxton AW, Tang-Wai DF, McAndrews MP,Zumsteg D, Wennberg R, Keren R, Wherrett J,Naglie G, Hamani C, Smith GS, LozanoAM.A phaseI trial of deep brain stimulation of memory circuits inAlzheimer’s disease. Ann Neurol. 2010;68:521–34.
52. LeDoux J. The emotional brain, fear, and theamygdala. Cell Mol Neurobiol. 2003;23:727–38.
53. LeDoux J. The amygdala. Curr Biol. 2007;17:R868–74.
54. Lemaire J, Sakka L, Ouchchane L, Caire F,Gabrillargues J, Bonny J. Anatomy of the humanthalamus based on spontaneous contrast andmicroscopic voxels in high-field magneticresonance imaging. Neurosurgery. 2010;66:161–72.
55. Lemaire J-J, Frew AJ, McArthur D, Gorgulho AA,Alger JR, Salomon N, Chen C, Behnke EJ, DeSalles AAF. White matter connectivity of humanhypothalamus. Brain Res. 2011;1371:43–64.
56. Lipsman N, Woodside DB, Giacobbe P, Hamani C,Carter JC, Norwood SJ, Sutandar K, Staab R, EliasG, Lyman CH, Smith GS, Lozano AM. Subcallosalcingulate deep brain stimulation for treatment-refractory anorexia nervosa: a phase 1 pilot trial.Lancet. 2013;381:1361–70.
57. Lucassen PJ, Pruessner J, Sousa N, Almeida OFX,Van Dam AM, Rajkowska G, Swaab DF, Czéh B.Neuropathology of stress. Acta Neuropathol (Berl).2014;127:109–35.
58. MacLean PD. Psychosomatic disease and thevisceral brain; recent developments bearing on thePapez theory of emotion. Psychosom Med.1949;11:338–53.
59. Mallet L, Schüpbach M, N’Diaye K, Remy P,Bardinet E, Czernecki V, Welter M-L, Pelissolo A,Ruberg M, Agid Y, Yelnik J. Stimulation ofsubterritories of the subthalamic nucleus reveals itsrole in the integration of the emotional and motoraspects of behavior. Proc Natl Acad Sci USA.2007;104:10661–6.
60. Mallet L, Polosan M, Jaafari N, Baup N, WelterM-L, Fontaine D, du Montcel ST, Yelnik J, ChéreauI, Arbus C, Raoul S, Aouizerate B, Damier P,Chabardès S, Czernecki V, Ardouin C, Krebs M-O,Bardinet E, Chaynes P, Burbaud P, Cornu P, DerostP, Bougerol T, Bataille B, Mattei V, Dormont D,Devaux B, Vérin M, Houeto J-L, Pollak P, BenabidA-L, Agid Y, Krack P, Millet B, Pelissolo A. STOCStudy Group. Subthalamic nucleus stimulationin severe obsessive-compulsive disorder. N Engl JMed. 2008;359:2121–34.
18 J.-J. Lemaire
61. Malone DA Jr, Dougherty DD, Rezai AR, CarpenterLL, Friehs GM, Eskandar EN, Rauch SL,Rasmussen SA, Machado AG, Kubu CS, TyrkaAR, Price LH, Stypulkowski PH, Giftakis JE, RiseMT, Malloy PF, Salloway SP, Greenberg BD. Deepbrain stimulation of the ventral capsule/ventralstriatum for treatment-resistant depression. BiolPsychiatry. 2009;65:267–75.
62. Marchand WR. Cortico-basal ganglia circuitry: areview of key research and implications forfunctional connectivity studies of mood and anxietydisorders. Brain Struct Funct. 2010;215:73–96.
63. Markram H. The blue brain project. Nat RevNeurosci. 2006;7:153–60.
64. Mayberg HS, Lozano AM, Voon V, McNeely HE,Seminowicz D, Hamani C, Schwalb JM, KennedySH. Deep brain stimulation for treatment-resistantdepression. Neuron. 2005;45:651–60.
65. McCollum LA, Roche JK, Roberts RC.Immunohistochemical localization of enkephalin inthe human striatum: a postmortem ultrastructuralstudy. Synapse. 2012;66:204–19.
66. McGaugh JL. The amygdala modulates theconsolidation of memories of emotionally arousingexperiences. Annu Rev Neurosci. 2004;27:1–28.
67. Melega WP, Lacan G, Gorgulho AA, Behnke EJ, DeSalles AAF. Hypothalamic deep brain stimulationreduces weight gain in an obesity-animal model.PLoS One. 2012;7:e30672.
68. Menon V, Uddin LQ. Saliency, switching, attentionand control: a network model of insula function.Brain Struct Funct. 2010;214:655–67.
69. Mignarri A, Tessa A, Carluccio MA, Rufa A, StortiE, Bonelli G, Marcotulli C, Santorelli FM, LeonardiL, Casali C, Federico A, Dotti MT. Cerebellum andneuropsychiatric disorders: insights from ARSACS.Neurol Sci. 2013.
70. Miyawaki E, Perlmutter JS, Tröster AI, Videen TO,Koller WC. The behavioral complications of pallidalstimulation: a case report. Brain Cogn.2000;42:417–34.
71. Mohr P, Rodriguez M, Slavíčková A, Hanka J. Theapplication of vagus nerve stimulation and deepbrain stimulation in depression. Neuropsycho-biology. 2011;64:170–81.
72. Naidich TP, Duvernoy HM, Delman BN, SorensenAG, Kollias SS, Haache EM. Duvernoy’s atlas ofthe human brain stem and cerebellum. Austria:Springer; 2009.
73. Nambu A, Tokuno H, Takada M. Functionalsignificance of the cortico-subthalamo-pallidal“hyperdirect” pathway. Neurosci Res. 2002;43:111–7.
74. Niciu MJ, Kelmendi B, Sanacora G. Overview ofglutamatergic neurotransmission in the nervoussystem. Pharmacol Biochem Behav. 2012;100:656–64.
75. Nieh EH, Kim S-Y, Namburi P, Tye KM.Optogenetic dissection of neural circuits
underlying emotional valence and motivatedbehaviors. Brain Res. 2013;1511:73–92.
76. Oades RD, Halliday GM. Ventral tegmental (A10)system: neurobiology. 1. Anatomy and connectivity.Brain Res Rev. 1987;12:117–65.
77. Okun MS, Mann G, Foote KD, Shapira NA, BowersD, Springer U, Knight W, Martin P, Goodman WK.Deep brain stimulation in the internal capsule andnucleus accumbens region: responses observedduring active and sham programming. J NeurolNeurosurg Psychiatry. 2007;78:310–4.
78. Oldenburg IA, Ding JB. Cholinergic modulation ofsynaptic integration and dendritic excitability in thestriatum. Curr Opin Neurobiol. 2011;21(3):425−432.
79. Papez JW. A proposed mechanism of emotion. ArchNeurol Psychiatry. 1937;38:725–43.
80. Parent A, Hazrati LN. Functional anatomy of thebasal ganglia. I. The cortico-basal ganglia-thalamo-cortical loop. Brain Res Rev. 1995;20:91–127.
81. Perry RH, Candy JM, Perry EK, Thompson J,Oakley AE. The substantia innominata and adjacentregions in the human brain: histochemical andbiochemical observations. J Anat. 1984;138(Pt4):713–32.
82. Petrides M, Pandya DN. The frontal cortex. In: MaiJK, Paxinos G, editors. The human nervous system,3rd ed. London; 2012. p. 988–1011.
83. Phillips ML, Drevets WC, Rauch SL, Lane R.Neurobiology of emotion perception I: the neuralbasis of normal emotion perception. Biol Psychiatry.2003;54:504–14.
84. Phillips ML, Ladouceur CD, Drevets WC. A neuralmodel of voluntary and automatic emotionregulation: implications for understanding thepathophysiology and neurodevelopment of bipolardisorder. Mol Psychiatry. 2008;13(829):833–57.
85. Pirone A, Cozzi B, Edelstein L, Peruffo A, Lenzi C,Quilici F, Antonini R, Castagna M. Topography ofGng2- and NetrinG2-expression suggests an insularorigin of the human claustrum. PLoS One. 2012;7:e44745.
86. Price JL, Drevets WC. Neurocircuitry of mooddisorders. Neuropsychopharmacol: Neuropsycho-pharmacol Off Publ Am Coll; 2009.
87. Price JL, Drevets WC. Neural circuits underlying thepathophysiology of mood disorders. Trends CognSci. 2012;16:61–71.
88. Rieu I, Derost P, Ulla M, Marques A, Debilly B, DeChazeron I, Chéreau I, Lemaire JJ, Boirie Y, LlorcaPM, Durif F. Body weight gain and deep brainstimulation. Sci: J Neurol; 2011.
89. Riley H. An atlas of the basal ganglia, brain stemand spinal cord. Williams & Wilkins: Baltimore;1953.
90. Rive MM, van Rooijen G, Veltman DJ, Phillips ML,Schene AH, Ruhé HG. Neural correlates ofdysfunctional emotion regulation in majordepressive disorder. A systematic review ofneuroimaging studies. Neurosci Biobehav Rev. 2013.
1 Related Circuitry and Synaptic Connectivity in Psychiatric Disorders 19
91. Russo SJ, Nestler EJ. The brain reward circuitry inmood disorders. Nat Rev Neurosci. 2013;14:609–25.
92. Rück C, Karlsson A, Steele JD, Edman G, MeyersonBA, Ericson K, Nyman H, Asberg M, Svanborg P.Capsulotomy for obsessive-compulsive disorder:long-term follow-up of 25 patients. Arch GenPsychiatry. 2008;65:914–21.
93. Sadikot AF, Rymar VV. The primate centromedian-parafascicular complex: anatomical organizationwith a note on neuromodulation. Brain Res Bull.2009;78:122–30.
94. Schaltenbrand G, Bailey P, editors. Introduction tostereotaxis with an atlas of the human brain, GeorgThieme: Stuttgart; 1959.
95. Sinha R. Disgust, insula, immune signaling, andaddiction. Biol Psychiatry. 2014;75:90–1.
96. Solomon MB, Furay AR, Jones K, Packard AEB,Packard BA, Wulsin AC, Herman JP. Deletion offorebrain glucocorticoid receptors impairs neuroen-docrine stress responses and induces depression-likebehavior in males but not females. Neuroscience.2012;203:135–43.
97. Stamatakis AM, Sparta DR, Jennings JH, McElligottZA, Decot H, Stuber GD. Amygdala and bed nucleusof the stria terminalis circuitry: implications foraddiction-related behaviors. Neuropharmacology.2014; 76:320–328.
98. Strakowski SM, Adler CM, Almeida J, AltshulerLL, Blumberg HP, Chang KD, DelBello MP,Frangou S, McIntosh A, Phillips ML, Sussman JE,Townsend JD. The functional neuroanatomy ofbipolar disorder: a consensus model. BipolarDisord. 2012;14:313–25.
99. Strutt AM, Simpson R, Jankovic J, York MK.Changes in cognitive-emotional and physiologicalsymptoms of depression following STN-DBS for thetreatment of Parkinson’s disease. Eur J Neurol Off JEur Fed Neurol Soc. 2012;19:121–7.
100. Suthana N, Haneef Z, Stern J, Mukamel R, BehnkeE, Knowlton B, Fried I. Memory enhancement anddeep-brain stimulation of the entorhinal area. N EnglJ Med. 2012;366:502–10.
101. Ting JT, Feng G. Neurobiology of obsessive-compulsive disorder: insights into neural circuitrydysfunction through mouse genetics. Curr OpinNeurobiol. 2011;21:842–8.
102. Tsuchida A, Fellows LK. Are core componentprocesses of executive function dissociable within
the frontal lobes? Evidence from humans with focalprefrontal damage. Cortex. J Devoted Stud NervSyst Behav. 2013;49:1790–800.
103. Ulla M, Thobois S, Llorca P-M, Derost P, LemaireJ-J, Chereau-Boudet I, de Chazeron I, Schmitt A,Ballanger B, Broussolle E, Durif F. Contactdependent reproducible hypomania induced bydeep brain stimulation in Parkinson’s disease:clinical, anatomical and functional imaging study.J Neurol Neurosurg Psychiatry. 2010.
104. Van Domburg PH, ten Donkelaar HJ. The humansubstantia nigra and ventral tegmental area.A neuroanatomical study with notes on aging andaging diseases. Adv Anat Embryol Cell Biol.1991;121:1–132.
105. Van Wieringen J-P, Booij J, Shalgunov V, ElsingaP, Michel MC. Agonist high- and low-affinity statesof dopamine D2 receptors: methods of detection andclinical implications. Naunyn Schmiedebergs ArchPharmacol. 2013;386:135–54.
106. Vann SD. Gudden’s ventral tegmental nucleus isvital for memory: re-evaluating diencephalic inputsfor amnesia. Brain J Neurol. 2009;132:2372–84.
107. Vogt BA, Palomero-Gallagher N. Cingulate cortex,In: Mai JK, Paxinos G, editors. The human nervoussystem. 3rd ed. Elsevier: London; 2012. p. 943–987.
108. Voorn P, Brady LS, Berendse HW, Richfield EK.Densitometrical analysis of opioid receptor ligandbinding in the human striatum—I. Distribution of μopioid receptor defines shell and core of the ventralstriatum. Neuroscience. 1996;75:777–92.
109. Weltens N, Zhao D, Van Oudenhove L. Where is thecomfort in comfort foods? Mechanisms linking fatsignaling, reward, and emotion. NeurogastroenterolMotil Off J Eur Gastrointest Motil Soc. 2014;26:303–15.
110. Whiting DM, Tomycz ND, Bailes J, de Jonge L,Lecoultre V, Wilent B, Alcindor D, Prostko ER,Cheng BC, Angle C, Cantella D, Whiting BB, MizesJS, Finnis KW, Ravussin E, Oh MY. Lateralhypothalamic area deep brain stimulation forrefractory obesity: a pilot study with preliminarydata on safety, body weight, and energy metabolism.J Neurosurg. 2013;119:56–63.
111. Zhou Y, Chen C-C, Weber AE, Zhou L, Baker LA,Hou J. Potentiometric-scanning ion conductancemicroscopy for measurement at tight junctions.Tissue Barriers. 2013;1:e25585.
20 J.-J. Lemaire
2High-angular diffusion MRIin reward-based psychiatric disorders
Wenwen Yu, Qiming Lv, Chencheng Zhang,Zhuangming Shen, Bomin Sun and Zheng Wang
Abstract
The structural mapping of the complex brain networks under healthy anddiseased states is of great importance to understand the workingmechanism of the brain function. Diffusion weighted magnetic resonanceimaging and its derivative methods are currently the only way to measuremacroscopic axonal organization in nervous system tissues, in vivo andnon-invasively. Nevertheless, it has revealed tremendous unprecedenteddetails about the brain architecture and inspired unlimited expectation onits future development. In this chapter, we first explain the basic principlesof diffusion tensor imaging (DTI), and then discuss the strategies forresolving multiple fibers within one voxel, in particular on the diffusionspectrum imaging (DSI) method. We further introduce the pipeline of dataanalysis including quantification of whole brain white matter andvisualization of specific microstructural tracts, and conclude with theirrecent applications in psychiatric disorders.
Keywords
Magnetic resonance imaging � Diffusion tensor imaging � Diffusionspectrum imaging � Tractography � Fiber crossing � Neuroanatomy
2.1 Introduction
Diffusion-weighted magnetic resonance imaging(DW-MRI) is an emerging magnetic resonanceimaging (MRI) method ever since the mid-1980s[7, 37, 62], which allows the detecting of thediffusion process of water molecules in biologi-cal tissues, in vivo and non-invasively. By cal-culating the biophysical trajectory of waterdiffusion to infer the architecture of the whitematter, diffusion tensor imaging (DTI) hasbecome one of the most valuable MRI techniques
W. Yu � Q. Lv � Z. Shen � Z. Wang (&)Institute of Neuroscience, Shanghai Institutes forBiological Sciences, Chinese Academy of Sciences,320 Yueyang Road, Shanghai 200031, Chinae-mail: [email protected]
C. Zhang � B. SunDepartment of Functional Neurosurgery, RuijinHospital, School of Medicine, Shanghai JiaotongUniversity, Shanghai 200025, China
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0_2© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
21
of pursuing the working mechanism of brainarchitecture [26, 33, 43, 56]. Furthermore,assessment of the microstructural integrity of theaxonal fibers using a variety of diffusion indiceshas absorbed an increasing attention in the studyof neurological diseases or psychiatric disorders[4, 5, 13, 25, 32, 45].
This chapter starts from some theoreticalbackground of diffusion derived MRI methodsincluding the widely-accepted DTI and newly-developed diffusion spectrum imaging (DSI), andintroduces some popular algorithms available forin vivo constructing tractography, as illustratedwith some classic white matter (WM) fiber tracts.Finally it concludes with short summary of theircurrent clinical applications in a wide range ofpsychiatric disorders. It is reasonably expectedthat such kind of discussion could catalyze thetechnological development in the light of meet-ing the clinical needs, and vice versa foster morepotential applications for various categories ofdiagnostic purposes.
2.2 How DTI Works
The human body is made up of over 70 % water,in which the incessant random motion of watermolecules is influenced by distinct kinds ofrestricted factors such as cell membranes, cyto-skeleton, and macromolecules [26]. Becausediffusional processes are influenced by the geo-metrical structure of the biological environment,diffusion MRI, has been successfully demon-strated to characterize diffusion displacement ofwater molecules and reveal the underlyingmicrostructure in vivo [14, 16, 53, 66]. In spite ofits recent introduction to brain imaging, tensor-based diffusion MRI has inspired a rising waveof biomedical applications of quantifying thediffusional characteristics of a wide range ofspecimens. In particular, for brain diseasesdiagnostics, DTI has been successfully used todemonstrate subtle abnormalities in a variety ofneurological diseases (including stroke, multiplesclerosis, dyslexia, schizophrenia, and Alzhei-mer’s disease) and is currently becoming an
indispensable part of many routine clinical pro-tocols [4, 13, 25, 32, 34, 40, 48, 50, 63]. Thediffusion pattern of water molecules can besimplified by the diffusion tensor model, whichmakes it feasible to show the gross fiber orien-tation and provide quantitative descriptions suchas fractional anisotropy (FA) and diffusivity [54].As such, more unique insights into tissuemicrostructure can be gained through the use ofthese indices: diffusion anisotropy as a usefulindex of white matter integrity and estimatedorientation of the principal direction of axonfibers to enable tractography [21, 23]. Theseunprecedented information obtained from DTIstudies are hence increasingly invaluable to bothclinical physicians and scientific researchers.
Here we present a brief overview of the basicprinciples of DTI method and the readers canconsult to the literature for more in-depth tech-nical details [10, 26]. In essence, diffusion MRImeasures the dephasing of spins of protons in thepresence of a spatially-varying magnetic field(‘gradient’), which changes their Larmor fre-quency [37, 59, 62]. The intuitive mechanismhere is the phase change resulting from compo-nents of incoherent displacement of spins alongthe axis of the applied field gradient. For sta-tionary (non-diffusing) molecules, the phasesinduced by both gradient pulses will completelycancel so as to lead the maximally coherentmagnetization and there will be no signal lossfrom diffusion [27]. In the case of coherent flowin the direction of the applied gradient, the bulkmotion will cause the signal phase to change bydifferent amounts regarding to each pulse so thatthere will be a net phase difference. Therefore, inthe presence of diffusion gradients, water mole-cules will accumulate different phases, and thephase dispersion from diffusion will cause signalattenuation, S.
S ¼ S0e�bD ð2:1Þ
where S is the DW signal, S0 is the signalwithout any DW gradients (but otherwise iden-tical imaging parameters), D is the apparent dif-fusion coefficient, and b is so-called “b-factor”.MRI signals are proportional to the sum of
22 W. Yu et al.
magnetization components from all water mole-cules in a voxel, which is closely associated withthe area of the diffusion gradient pulses definedby the amplitude of the magnetic field gradientpulses, G, and the temporal duration, δ, and thetemporal spacing between the pulses, Δ. Theeffects of all these parameters are indeed ascribedto a coarse term “b-factor” as below:
b ¼ c2G2d2ðD� d=3Þ ð2:2Þwhere γ is the gyromagnetic ratio.
By applying the appropriate magnetic fieldgradients, MR imaging may be sensitized to therandom, thermally driven motion (diffusion) ofwater molecules in the direction of the fieldgradient. Diffusion is anisotropic (directionallydependent) in WM fiber tracts, as axonal mem-branes and myelin sheaths present barriers to themotion of water molecules in directions notparallel to their own orientation. The direction ofmaximum diffusivity has been shown to coincidewith the orientation of WM fiber tracts [44].
In short, the fundamental concept behind DTIis that water molecules diffuse differently in thetissues heavily depending on its type, integrity,architecture, and presence of barriers, generatinginformation about its orientation and quantitativeanisotropy embodied by the diffusion tensors [9,14, 44]. DTI may be used to map and charac-terize the three-dimensional diffusion pattern as afunction of spatial location, which can further betaken advantage of estimating the connectivityproperties of the whole brain WM networks,using the diffusion anisotropy and the principaldiffusion directions [23].
Undoubtedly, DTI holds a unique andunparalleled sensitivity to water movements ofpainting the blueprint of brain architecture [26,33, 43, 56], as uses existing MRI technologywithout the necessity of investing new equip-ment, contrast agents, or even radiochemicaltracers. However, there remain many technicalissues with regard to the performance of the tool,practical considerations of working on biologicalspecimens, and the interpretation of DTI trac-tography images. For instance, within each voxelof diffusion-encoded images, it can only resolve
the single (the most dominant) fiber direction andcannot differentiate the kissing/crossing/branch-ing fibers in the complex cerebral regions [1, 71].Consequently it estimates the fiber orientation tobe the mean of the underlying fiber directions,even though the mean direction will not be rep-resentative of the true fiber directions [3]. Nev-ertheless, it is not capable of determining withaccuracy the origin and destination of fibers,which requires further comprehensive evidenceto corroborate, even in combination withemploying other advanced technologies [5, 58].
2.3 Diffusion Spectrum MRI (DSI)
Recent technological development of MRImethods has been devoted to solving the afore-mentioned issues, so as to better characterize thecomplicated fiber patterns and discern fiber ori-entations. As matter of a fact, either model-basedor model-free methods have been acknowledgedthat have the capacity to resolve heterogeneity offiber orientations in each resolved volume oftissue (voxel) [65, 68], and provide detailedviews into the precise organization of cerebralwhite matter tracts [69]. Here we will focus onthe model-free derivations of diffusion MRItechnique.
Model-free methods, also called q-spaceimaging methods [11, 16, 59], measure themicroscopic diffusion function directly withoutany assumptions on the form of the underlyingdiffusion function, even though they still have tocount on the Fourier transform relation betweenthe diffusion MR signals and the underlying dif-fusion displacement [31]. Firstly the probabilitydensity function (PDF) or orientation distributionfunction (ODF) of the diffusion displacement inthe three biophysical dimension are obtained.One can then calculate a common quantitativescalar measure, generalized fractional anisotropy(GFA) in DSI, physiologically equivalent toFA [19], so as to implicate the microstructureproperty. Worthy to mention, FA, an indexderived from the diffusion tensor that reflects thedegree of directional coherence, myelination, and
2 High-angular diffusion MRI in reward-based psychiatric disorders 23
diameter of axonal fibers has been widely used toexamine the integrity of white matter tracts in DTI[4, 26]. Simply put, higher FA or GFA valuesimply higher coherence of fiber directions, moremyelination or larger axonal diameters in thewhite matter at the microstructural level.
More frequently the connections of each ODFwill be explored to infer the underlying linkingpatterns of the fibers [22]. Here in after, webriefly discuss two commonly used q-space(diffusion-encoding space) reconstruction meth-ods to estimate the ODF from the acquired dif-fusion MR signals, with particular emphasis onthe DSI method.
Q-ball imaging (QBI): Tuch and his co-workers introduced q-ball imaging (QBI) [64],which usually used the Funk–Radon transform(also known as the spherical Radon transform) toreconstruct ODF at the cost of large pulsed fieldgradient and time-intensive sampling. It is alsofeasible to resolve intravoxel fiber crossingthrough using a high angular resolution diffusionimaging (HARDI) scheme, which samples dataon a shell in the diffusion encoding space. TheFunk–Radon transform relation forms the corebasis of the QBI reconstruction method to avoidany assumptions on the diffusion process likeGaussianity or multi-Gaussianity and to achievebetter accuracy and efficiency [17].
Diffusion spectrum imaging (DSI): Wedeenand his colleagues proposed to acquire the dif-fusion MR signals by using the grid samplingscheme, and then applied the Fourier transformon the q-space data to estimate the underlyingdiffusion displacement pattern for further calcu-lation of the ODF [15, 21, 31, 61, 65, 68–70, 72].The sampling scheme of DSI produces a clusterof grid points distributed on a sphere in the q-space. Each grid point corresponds to a specificvalue of diffusion sensitivity (b-value) anddirection, and the b-value increases incrementallyfrom 0 to a maximal b-value (b-max). When allthe diffusion-encoding samples in the q-spacehave been collected, the Fourier transform (FT)is performed to obtain the PDF as the diffusion-encoding samples S(q) and their correspondingPDFs constitute a Fourier pair [10]. In sum, DSImeasures the ODF by acquiring hundreds of
diffusion-weighted images (DWI) with differentdiffusion-encoding gradients, each with differentstrength and direction [5, 21]. In this manner, it ispossible to infer the number of fiber-compart-ments and their relative amplitude as well asspatial orientations by reconstructing the ODFlocal maxima. It enables DSI to resolve kissingor crossing or bending fiber orientations at singlevoxel-based level, as shown in Fig. 2.1.
Bear in mind, though, some precautionsshould be carefully exercised when implement-ing these two q-space imaging methods to derivediffusion ODF. One caveat of the QBI method isthat the acquired diffusion MR signal is in factcontributed by the diffusion displacements in alldirections, not just the displacements perpendic-ular to the diffusion gradient vector. Conse-quently the q-ball ODF can only be deemed asgood approximation since it doesn’t consider alldiffusion displacements in the three-dimensionalspace [62]. On the other hand, DSI is able tocharacterize the diffusion probability densityfunction by applying the Fourier transform to theMR signals in the q-space; however, it still relieson numerical estimation to calculate the ODF.The mathematical estimation often encountersthe truncation artifacts in the Fourier transform,as entails additional treatment like a Hanningfilter smoothing on the PDF [22, 31].
Generalized-sampling imaging (GQI):Recently the spin distribution function (SDF) hasbeen defined to quantitatively describe a distri-bution of the spins undergoing diffusion on thevoxel basis, which is unlike the diffusion ODFrepresenting a probability distribution of thediffusion displacement [72]. This relation leadsto an imaging method named generalizedq-sampling imaging (GQI) which is readilyapplicable to a wide range of q-space datasetsincluding those acquired by the shell or gridsampling schemes. Taking a closer look at thereconstruction equations of GQI and DSI, theyshare the same theoretical basis. Hence GQI andDSI reconstruction could result in similar diffu-sion patterns. Note that the reconstruction pro-cess of GQI does not require deconvolutionprocedures and the SDF values can be comparedacross voxels [72].
24 W. Yu et al.
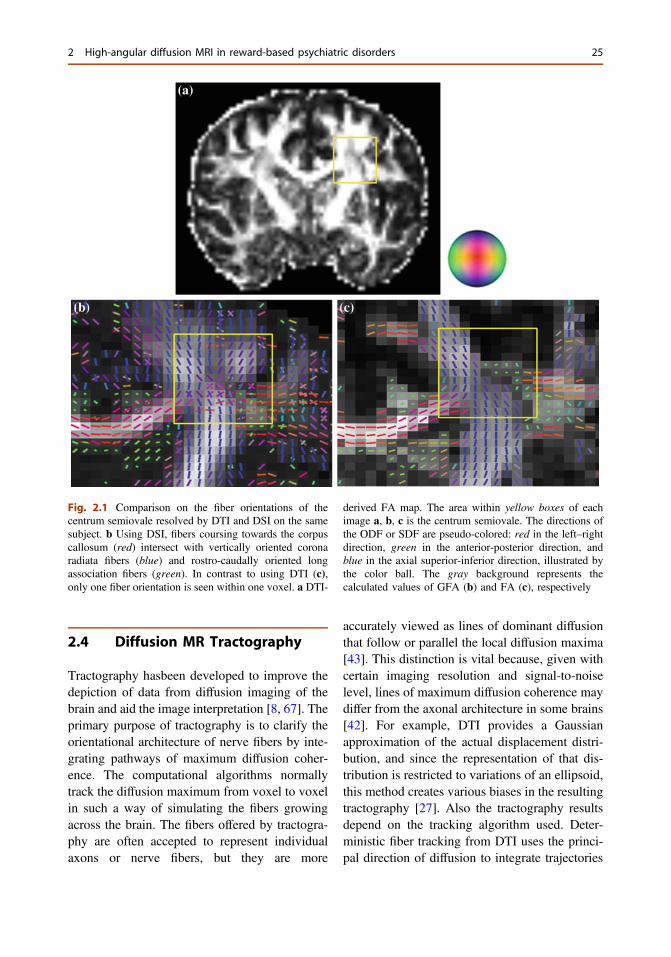
2.4 Diffusion MR Tractography
Tractography hasbeen developed to improve thedepiction of data from diffusion imaging of thebrain and aid the image interpretation [8, 67]. Theprimary purpose of tractography is to clarify theorientational architecture of nerve fibers by inte-grating pathways of maximum diffusion coher-ence. The computational algorithms normallytrack the diffusion maximum from voxel to voxelin such a way of simulating the fibers growingacross the brain. The fibers offered by tractogra-phy are often accepted to represent individualaxons or nerve fibers, but they are more
accurately viewed as lines of dominant diffusionthat follow or parallel the local diffusion maxima[43]. This distinction is vital because, given withcertain imaging resolution and signal-to-noiselevel, lines of maximum diffusion coherence maydiffer from the axonal architecture in some brains[42]. For example, DTI provides a Gaussianapproximation of the actual displacement distri-bution, and since the representation of that dis-tribution is restricted to variations of an ellipsoid,this method creates various biases in the resultingtractography [27]. Also the tractography resultsdepend on the tracking algorithm used. Deter-ministic fiber tracking from DTI uses the princi-pal direction of diffusion to integrate trajectories
Fig. 2.1 Comparison on the fiber orientations of thecentrum semiovale resolved by DTI and DSI on the samesubject. b Using DSI, fibers coursing towards the corpuscallosum (red) intersect with vertically oriented coronaradiata fibers (blue) and rostro-caudally oriented longassociation fibers (green). In contrast to using DTI (c),only one fiber orientation is seen within one voxel. a DTI-
derived FA map. The area within yellow boxes of eachimage a, b, c is the centrum semiovale. The directions ofthe ODF or SDF are pseudo-colored: red in the left–rightdirection, green in the anterior-posterior direction, andblue in the axial superior-inferior direction, illustrated bythe color ball. The gray background represents thecalculated values of GFA (b) and FA (c), respectively
2 High-angular diffusion MRI in reward-based psychiatric disorders 25
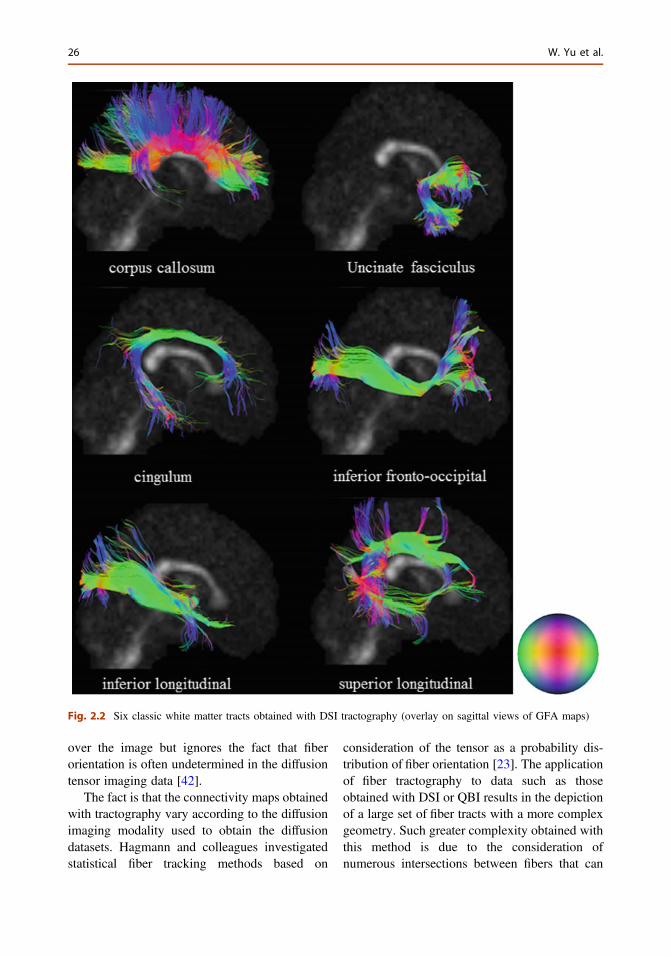
over the image but ignores the fact that fiberorientation is often undetermined in the diffusiontensor imaging data [42].
The fact is that the connectivity maps obtainedwith tractography vary according to the diffusionimaging modality used to obtain the diffusiondatasets. Hagmann and colleagues investigatedstatistical fiber tracking methods based on
consideration of the tensor as a probability dis-tribution of fiber orientation [23]. The applicationof fiber tractography to data such as thoseobtained with DSI or QBI results in the depictionof a large set of fiber tracts with a more complexgeometry. Such greater complexity obtained withthis method is due to the consideration ofnumerous intersections between fibers that can
Fig. 2.2 Six classic white matter tracts obtained with DSI tractography (overlay on sagittal views of GFA maps)
26 W. Yu et al.

be resolved or differentiated. In such sense, DSItractography overcomes some above biases andallows more realistic mapping of connectivity[21, 31, 69, 70]. Figure 2.2 presents typicalexamples of six major white matter tractsreconstructed by DSI.
Nonetheless, tractography provides moreinteresting and valuable information for depict-ing the human neuroanatomy in vivo.
2.5 Procedure of Data Analysis
Here we used the DSI image dataset collected byFunctional Brain Imaging Platform (FBIP) atInstitute of Neuroscience, Chinese Academy ofSciences, Shanghai, to demonstrate the procedurewidely-used in the analysis of the diffusion MRIdata. It will lend the support to those who areinterested in applying these neuroimaging tech-niques to solve those clinically-driven problemsduring diagnostics and therapy of psychiatricdisorders. A schematic workflow diagram of dif-fusion MRI processing is illustrated in Fig. 2.3.
The detailed imaging protocol will be descri-bed in other places and summarized shortlyhere. T1-weighted structural MRI imageswere acquired on a 3T MR imaging system(Magnetom Trio; Siemens, Erlangen, Germany)using a 12-channel phased array head coil(TR = 2,300 ms, TE = 3 ms, TI = 1,000 ms, flipangle = 9°, FOV = 256 × 256 mm2, voxelsize = 1.0 × 1.0 × 1.0 mm3, 176 slices, no slicegap). Earplugs were used, and movement wasminimized by stabilizing the head with cushions.Diffusion spectrum imaging was acquired using atwice-refocused spin-echo EPI pulse sequence[55]. The diffusion-encoding scheme used inthis study followed the framework of DSIin which diffusion-weighted images wereacquired with diffusion gradients of different bvalues corresponding to the grid points filledwithin a sphere in the 3D diffusion-encodingspace (q-space) [68]. TR = 9,500 ms,
TE = 152 ms, flip angle = 90°, FOV = 80 ×80 mm2, voxel size = 2.4 × 2.4 × 2.4 mm3,b-max = 7,000 s/mm−2. To reduce the scan time,we only recorded half-sphere DSI data [20, 21].Specifically, the DSI data were acquired with 128diffusion-encoding directions corresponding togrid points filled in the half sphere of the q-space.Acquisition time for the half-scheme acquisitionwas 21 min. To correct for image distortionresulting from magnetic susceptibility, field mapswere acquired using a GRE sequence with twoTEs (acquisition time, 91 s, TR/TE = 500/3.38and 5.84 ms). The matrix size and FOV of thefield maps were the same as those used in theDSI dataset.
The half-sphere data were extrapolated to theother half of the sphere based on the symmetryproperty of the data in the q-space, and the eightcorners of the cube that were unsampled werezero-filled. The susceptibility-induced distortionon each DSI image was first corrected using theacquired field maps [24], and then subjected tothe motion correction and eddy current com-pensation using the software based on FSL(http://www.fmrib.ox.ac.uk/fsl). The followingDSI data reconstruction was conducted throughusing the generalized q-sampling imagingapproach available in the software of DSI Studio(http://dsi-studio.labsolver.org) [15]. The ODFswere reconstructed to 162 discrete samplingdirections (corresponding to the vertices of a4-fold regularly tessellated icosahedron projectedonto the sphere). The diffusion deconvolutionwas then applied to the diffusion ODFs generatedfrom GQI to increase the angular resolution ofthe resolved fiber. Having obtained the ODF, theGFA (similar to FA) was derived to quantify thedirectionality of the diffusion on a scale fromzero (when the diffusion was totally random) toone (when the diffusion was along one directiononly). The formula of deriving the value of GFAis defined as the ratio of the standard deviation ofODF and its root mean square [64]. Like FA,GFA has been used to infer microstructureintegrity of the white matter fiber tracts.
2 High-angular diffusion MRI in reward-based psychiatric disorders 27
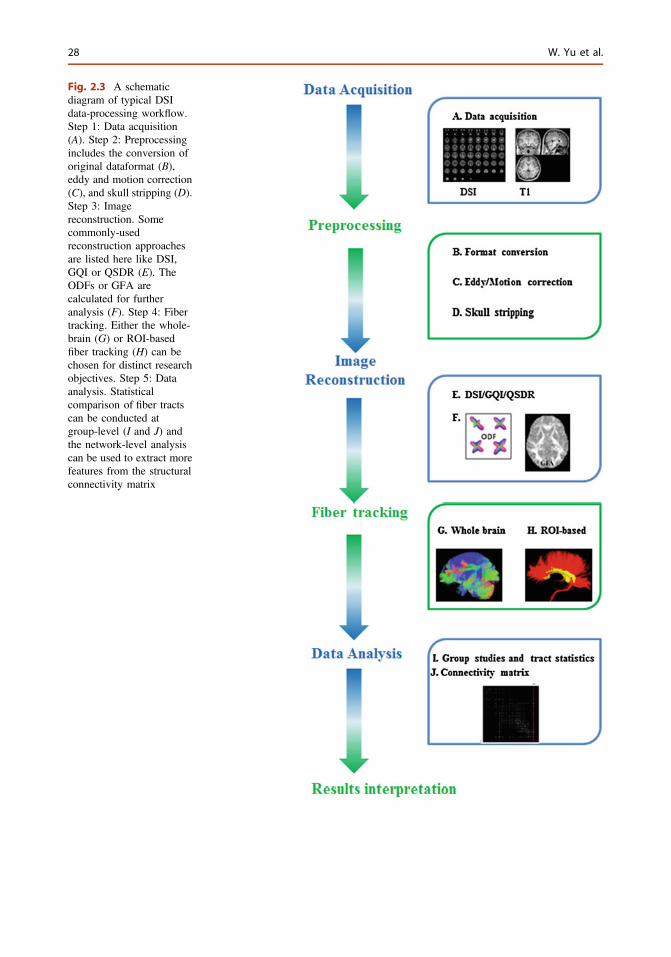
Fig. 2.3 A schematicdiagram of typical DSIdata-processing workflow.Step 1: Data acquisition(A). Step 2: Preprocessingincludes the conversion oforiginal dataformat (B),eddy and motion correction(C), and skull stripping (D).Step 3: Imagereconstruction. Somecommonly-usedreconstruction approachesare listed here like DSI,GQI or QSDR (E). TheODFs or GFA arecalculated for furtheranalysis (F). Step 4: Fibertracking. Either the whole-brain (G) or ROI-basedfiber tracking (H) can bechosen for distinct researchobjectives. Step 5: Dataanalysis. Statisticalcomparison of fiber tractscan be conducted atgroup-level (I and J) andthe network-level analysiscan be used to extract morefeatures from the structuralconnectivity matrix
28 W. Yu et al.
In addition to subject-specific reconstructionapproach, we also reconstructed the DSI data inMNI-152 space (a standard space introduced bythe International Consortium for Brain Mapping,http://www.bic.mni.mcgill.ca/ServicesAtlases/ICBM152NLin2009) using q-space diffeomor-phic reconstruction (QSDR) [15], which providesa direct approach to analyze the group differenceand also facilitates the comparison using fibertracking. QSDR is the generalization of GQI thatallows users to construct ODFs in any giventemplate space (e.g. MNI space). DSI Studio firstcalculates the quantitative anisotropy (QA)mapping and then normalizes it to the NTU-90QAmap. The NTU-90 atlas is the average of thenormalized subject data in the MNI-152 space.
For the fiber-tracking datasets, all fiber trackingwas performed using the DSI Studio. In most ofclinical studies, an ODF-streamlined region ofinterest (ROI)-based approach are frequentlychosen to discern the difference between thepatient and control groups [15]. Depending onvarious kinds of research objectives, there areseveral ways available to define the ROIs of thesubjects. In QSDR reconstruction approach, weused the normalized ROIs from the JHU WhiteMatter tractography atlas provided by DSI studio[67]; In GQI reconstruction approach, we used theselected ROIs from the JHU atlas and warped it tothe subject T1-weighted image space by linearregistration. Tracts were generated using an ODF-streamline version of the FACT deterministictractography algorithm [8, 15], and left and righthemispheres were investigated separately. If anODF had more than one peak orientation, theinitial direction was the primary fiber from theresolved orientations. The advantage of “primary”is the stableness and consistency of the results.Trilinear interpolation was used to estimate thepropagation direction. Fiber progression contin-ued with a certain step size like 1 mm (half thespacing for QSDR reconstruction approach),minimum fiber length like 40 mm, and turningangle threshold (usually set at 40°–70°). Tosmooth each track, the next moving directionalestimate of each voxel was weighted by a com-bination of the previous incoming direction andthe nearest fiber orientation. Once tracked, all
streamlineswere saved in the TrackVis file format.Segmentation of the fiber tracts was performedwith TrackVis software (http://trackvis.org).
2.6 Diffusion MRI Applicationsin Psychiatric Disorders
Diffusion MRI has been becoming an indis-pensable tool to investigate a variety of psychi-atric disorders such as schizophrenia, majordepressive disorder, eating disorders, attentiondeficit disorder and addictions and so on. It hasshed insightful light on our understanding ofneural connectivity and how abnormalities inconnectivity may contribute to the pathogenesisof psychiatric illnesses. This section will con-cisely summarize recent applications on thosepsychiatric diseases with DTI/DSI techniques,specifically restricting our attention to thereward-circuitry based brain disorders.
Obsessive-Compulsive Disorder (OCD):Alterations in the WM tracts within the classiccortico-striato-thalamo-cortical (CSTC) circuitry,which has long been implicated in the patho-genesis of OCD [39], were always observed inthe literature with DTI method. There have beenreported that alterations of FA were observed inmany brain regions of OCD patients, such as theanterior cingulate [12, 60], internal capsule [12,73], white matter in the area superolateral to theright caudate [73], corpus callosum [57, 73], andthe right inferior parietal and medial frontalregions [36], the bilateral semiovalcenterextending to the subinsular white matter [45].However, the conclusions drawn from thesecurrent studies have been inconsistent. Forexample, findings in the FA of the anterior cin-gulate were particularly mysterious, showinghigher values [12], lower values [60], or nochanges [36, 45, 73] in OCD patients in com-parison to normal subjects.
Findings concerning the anterior thalamicradiations (ATR) seem to be inconsistent as well.Cannistraro et al. [12] reported an increased FAvalue in the left anterior limb of the internal-capsule, whereas Yoo et al. [73] found increases
2 High-angular diffusion MRI in reward-based psychiatric disorders 29

in FA in the superolateral area of the right cau-date that were penetrated by the ATR. Thesedivergent observations by the DTI could becaused by the notoriously complicated structureof the brain network, in which the presence ofcrossing fibers has been robustly demonstratedby the DSI-based tractography in both nonhumanprimate and human [21, 58, 69]. Therefore, Chiuand his co-workers applied the GFA value todescribe the microstructural integrity of the whitematter tracts [15]. They found significantly lowermean GFA in the right ATR and the left theanterior segment of cingulum bundles in OCDsubjects compared to the ATRs and cingulumbundles of normal controls. In addition to theGFA measure, asymmetry of the mean GFAbetween the left and right tracts was also calcu-lated [15], which might provide a parsimoniousexplanation to the above discrepancy observed indifferent reports. Notwithstanding the new evi-dence, it requires further research to fully eluci-date those apparent contradictory results. Besidesthat, more widespread WM abnormalities like themicrostructural alterations in the fronto-basalpathways targeting the orbitofrontal cortex andthe anterior cingulate cortex have been proposedto be involved in OCD [39]. Menzies and col-leagues reported that the anatomical connectivitybetween lateral frontal and parietal regions wasaltered as well as microstructural abnormalities inintra-hemispheric bundles linking distinctiveareas of the prefrontal cortex to posterior parietaland occipital association cortices [36].
Major depressive disorder (MDD): Decreasein FA was found in the right middle frontalgyrus, left occipitotemporal gyrus, and the sub-gyral and angular gyri of the right parietal lobe inmedication-free young adults with MDD [2].Lower FA in regions lateral to the anterior cin-gulate was associated with lower occurring ratesof remission in geriatric depression [4]. Olderpatients with MDD have been shown to dem-onstrate lower FA in the dorsolateral prefrontalcortex and anterior cingulate cortex [6], anddiffuse frontal [2, 47, 63] and temporal lobe [47].Interestingly, after electroconvulsive therapy(ECT), depressed geriatric patients had anincrease in frontal FA associated with the
improvement of their clinical symptoms [46], butnot in the temporal WM regions. Diminished FAin white matter regions including anterior cin-gulate and dorsolateral frontal pathways inpatients with late life depression was found to bea strong predictor of poor response to theantidepressant Citalopram [4]. In the futuregrowing psychiatric research with diffusionMRI that points to predicting the disease risksand response factors (ultimately for early inter-vention or prevention) can be much of transla-tional utility [2].
Eating Disorder (ED): Eating disorder is asevere psychiatric disorder associated with self-driven food refusal and emaciation, altered bodyperception and preoccupations with weight,which generally includes three major categories:Anorexia Nervosa (AN), Bulimia Nervosa (BN)and Eating Disorder Not Otherwise Specified(EDNOS) [29]. In AN patients, Kim and Whalenfound that left ventral amygdala responses tofearful versus neutral faces were positively cor-related with local FA values along the whitematter fibers located within the amygdala-ven-tromedial prefrontal cortex pathway. Intriguingly,these significantly correlated voxel clustersextended into the left ventral striatum and termi-nated at the left medial orbitofrontal cortex [30].The abnormal WM integrity of the limbic andassociation pathways in AN patients has beenfound to account for disturbed feeding, emotionprocessing and body perception. Moreover,changes of FA in the left and right fimbria-fornixwere allowed to predict the harm avoidancebehavior of AN patients, which suggested that thefimbria-fornix WM pathway is possibly involvedin high anxiety level of AN [28]. Frieling and hiscoworkers identified disturbances of associationaland commissural fibers in the bilateral occipito-temporal white matter, suggesting that the dis-tortion of self-body image could be related tomicrostructural alterations of white matter tractsconnecting the extrastriate visual cortex with otherbrain regions involved in body perception [18].Moreover, they identified in AN patients bilateralreductions of FA maps in the posterior thalamicradiation including the optic radiation and the leftmediodorsal thalamus [18]. On the other hand,
30 W. Yu et al.
widespread decrease in FA values of BN patientswere observed in the bilateral corona radiataextending into the posterior limb of the internalcapsule, the corpus callosum, the right subinsularWM, and right fornix. The result suggested thatthe integrity ofWM fiber tracts was largely alteredin BN, especially in the corona radiata which wasdeemed to account for taste and brain rewardprocessing [38].
Substance Dependence (SD): Compared withnormal controls, both men and women withchronic alcoholism show a decrease in FA in thegenu of the CC and the centrum semiovale[48–52]. FA decreases in the splenium of the CCwas also found in male subjects [48, 51]. Thedecrease in FA in the genu was associated withdecreased volume of both the genu and the bodyof the CC, and decreases in FA have been shownto correlate with the amount of alcohol con-sumption and with comorbid human immuno-deficiency syndrome infection [50]. Men withalcohol dependence showed lower generalizedFA values on all segments of the corpus callo-sum. The segment interconnecting the bilateralorbitofrontal cortices was the most affected [15].
Another major SD in our daily life is cocaineuse, which can result in a number of neurologicalcomplications including headaches, seizures, andstrokes. There is evidence that cocaine adverselydisrupted the myelin sheaths [41]. DTI studies ofcocaine abuse patients reveal a decrease in frontalFA and the genu and rostral body of the CC, andthe FA measures in the CC were inversely corre-lated with impulsivity [35, 36, 40, 70].
2.7 Conclusion
The high sensitivity of diffusion MRI techniqueenables its rising popularity in the diagnosis ofpsychiatric illnesses and the monitoring of thebrain response to therapeutic interventions. Oneattractive perspective is to follow subjects lon-gitudinally to determine how the microstructuralproperties of the tissue change over time if eachsubject serves as their own baseline reference. In
this way, the abnormality at different stage can bewell characterized and the therapeutic effects arereadily predicted. Diffusion image-based prog-nostic indicators of disease course and responseto therapy would be extremely valuable to assessthe responsiveness of patients to specific thera-pies, since predictive imaging measures wouldenable earlier interventions. Up to date, there areonly a handful of DSI studies to examine thebrain architecture and connectivity in psychiatricdisorders. Due to differences in methodologies,scanner sequences, and image processing algo-rithms, it requires more cautions to interpret thephysiological meaning of results obtained by thediffusion MRI methods in clinical psychiatricresearch.
Acknowledgments This work was partially supportedby The Hundred Talent Program (Technology), ChineseAcademy of Sciences (ZW). We thank Franz Schmitt,Renate Jerecic, Thomas Benner, Kecheng Liu, IgnacioVallines, and Hui Liu for their help and contribution tothe construction of our custom-tuned gradient-insert MRIfacility.
References
1. Alexander AL. Analysis of partial volume effects indiffusion-tensor MRI. Magn Reson Med. 2001;45:770–80.
2. Alexander AL, Lee JE, Lazar M, Field AS. Diffusiontensor imaging of the brain. Neurotherapeutics.2007;4:316–29.
3. Alexander DC, Barker GJ. Optimal imagingparameters for fiber-orientation estimation indiffusion MRI. Neuroimage. 2005;27:357–67.
4. Alexopoulos GS, Kiosses DN, Choi SJ, Murphy CF,Lim KO. Frontal white matter microstructureand treatment response of late-life depression:a preliminary study. Am J Psychiatry. 2002;159:1929–32.
5. Ardekani BA, Nierenberg J, Hoptman MJ, Javitt DC,Lim KO. MRI study of white matter diffusionanisotropy in schizophrenia. Neuroreport. 2003;14:2025–9.
6. Bae JN, MacFall JR, Krishnan KR, Payne ME,Steffens DC, Taylor WD. Dorsolateral prefrontalcortex and anterior cingulate cortex white matteralterations in late-life depression. Biol Psychiatry.2006;60:1356–63.
7. Basser PJ, Mattiello J, LeBihan D. MR diffusiontensor sepctroscopy and imaging. Biophys J.1994;66:259–67.
2 High-angular diffusion MRI in reward-based psychiatric disorders 31
8. Basser PJ, Pajevic S, Pierpaoli C, Duda J, AldroubiA. In vivo fiber tractography using DT-MRI data.Magn Reson Med. 2000;44:625–32.
9. Beaulieu C. The basis of anisotropic water diffusionin the nervous system—a technical review. NMRBiomed. 2002;15:435–55.
10. Callaghan PT. Principles of Nuclear MagneticResonance Microscopy. Oxford: Oxford UniversityPress; 1993.
11. Callaghan PT, Eccles CD, Xia Y. NMR microscopyof dynamic displacements—K-Space and Q-SpaceImaging. J Phys E: Sci Instrum. 1988;21:820–2.
12. Cannistraro PA, Makris N, Howard JD, Wedig MM,Hodge SM, et al. A diffusion tensor imaging study ofwhite matter in obsessive-compulsive disorder.Depress Anxiety. 2007;24:440–6.
13. Catani M. Diffusion tensor magnetic resonanceimaging tractography in cognitive disorders. CurrOpin Neurol. 2006;19:599–606.
14. Chenevert TL, Brunberg JA, Pipe JG. Anisotropicdiffusion in human white matter: demonstration withMR techniques in vivo. Radiology. 1990;171:401–5.
15. Chiu CH, Lo YC, Tang HS, Liu IC, Chiang WY,et al. White matter abnormalities of fronto-striato-thalamic circuitry in obsessive-compulsive disorder: astudy using diffusion spectrum imaging tractography.Psychiatry Res. 2011;192:176–82.
16. Cory DG, Garroway AN. Measurement oftranslational displacement probabilities by NMR—an indicator of compartmentation. Magn Reson Med.1990;14:435–44.
17. Descoteaux M, Angelino E, Fitzgibbons S, DericheR. Regularized, fast, and robust analytical Q-ballimaging. Magn Reson Med. 2007;58:497–510.
18. Frieling H, Fischer J, Wilhelm J, Engelhorn T, BleichS, et al. Microstructural abnormalities of the posteriorthalamic radiation and the mediodorsal thalamicnuclei in females with anorexia nervosa—a voxelbased diffusion tensor imaging (DTI) study.J Psychiatr Res. 2012;46:1237–42.
19. Gorczewski K, Mang S, Klose U. Reproducibility andconsistency of evaluation techniques for HARDI data.MAGMA. 2009;22:63–70.
20. Granziera C, Schmahmann JD, Hadjikhani N, MeyerH, Meuli R, et al. Diffusion spectrum imaging showsthe structural basis of functional cerebellar circuits inthe human cerebellum in vivo. PLoS One. 2009;4:e5101.
21. Hagmann P, Cammoun L, Gigandet X, Meuli R,Honey CJ, Wedeen VJ. Mapping the structural coreof human cerebral cortex. PLoS Biol. 2008.
22. Hagmann P, Jonasson L, Deffieux T, Meuli R, ThiranJP, Wedeen VJ. Fibertract segmentation in positionorientation space from high angular resolutiondiffusion MRI. Neuroimage. 2006;32:665–75.
23. Hagmann P, Thiran JP, Jonasson L, Vandergheynst P,Clarke S, et al. DTI mapping of human brainconnectivity: statistical fibre tracking and virtualdissection. Neuroimage. 2003;19:545–54.
24. Hsu YC, Hsu CH, Tseng WYI. Correction forsusceptibility-induced distortion in echo-planarimaging using field maps and model-based pointspread function. IEEE Trans Med Imaging.2009;28:1850–7.
25. Johansen-Berg H. Behavioural relevance of variationin white matter microstructure. Curr Opin Neurol.2010;23:351–8.
26. Johansen-Berg H, Behrens TEJ. Diffusion MRI: fromquantitative measurement to in-vivo neuroanatomy.In: Johansen-Berg H, Behrens TEJ, editors. DiffusionMRI. San Diego: Academic Press; 2009.
27. Jones DK, Knosche TR, Turner R. White matterintegrity, fiber count, and other fallacies: the do’s anddon’ts of diffusionMRI. Neuroimage. 2013;73:239–54.
28. Kazlouski D, Rollin MD, Tregellas J, Shott ME,Jappe LM, et al. Altered fimbria-fornix white matterintegrity in anorexia nervosa predicts harm avoidance.Psychiatry Res. 2011;192:109–16.
29. Keel PK, Brown TA, Holland LA, Bodell LP.Empirical classification of eating disorders. AnnuRev Clin Psychol. 2012;8:381–404.
30. Kim MJ, Whalen PJ. The structural integrity of anamygdala-prefrontal pathway predicts trait anxiety.J Neurosci. 2009;29:11614–8.
31. Kuo LW, Chen JH, Wedeen VJ, Tseng WY.Optimization of diffusion spectrum imaging and q-ball imaging on clinical MRI system. Neuroimage.2008;41:7–18.
32. Kyriakopoulos M, Frangou S. Recent diffusion tensorimaging findings in early stages of schizophrenia.Curr Opin Psychiatry. 2009;22:168–76.
33. Le Bihan D. Looking into the functional architectureof the brain with diffusion MRI. Nat Rev Neurosci.2003;4:469–80.
34. Le Bihan D, Breton E, Lallemand D, Grenier P,Cabanis E, Laval-Jeantet M.MR imaging of intravoxelincoherent motions: application to diffusion andperfusion in neurologic disorders. Radiology.1986;161:401–7.
35. Lim KO, Wozniak JR, Mueller BA, Franc DT,Specker SM, et al. Brain macrostructural andmicrostructural abnormalities in cocaine dependence.Drug Alcohol Depend. 2008;92:164–72.
36. Menzies L, Chamberlain SR, Laird AR, Thelen SM,Sahakian BJ, Bullmore ET. Integrating evidence fromneuroimaging and neuropsychological studies ofobsessive-compulsive disorder: the orbitofronto-striatal model revisited. Neurosci Biobehav Rev.2008;32:525–49.
37. Merboldt K-D, Hanicke W, Frahm J. Self-diffusionNMR imaging using stimulated echoes. J MagnReson. 1985;64:479–86.
38. Mettler LN, Shott ME, Pryor T, Yang TT, Frank GK.White matter integrity is reduced in bulimia nervosa.Int J Eat Disord. 2013;46:264–73.
39. MiladMR, Rauch SL. Obsessive-compulsive disorder:beyond segregated cortico-striatal pathways. TrendsCogn Sci. 2012;16:43–51.
32 W. Yu et al.
40. Moeller FG, Hasan KM, Steinberg JL, Kramer LA,Dougherty DM, et al. Reduced anterior corpuscallosum white matter integrity is related to increasedimpulsivity and reduced discriminability in cocaine-dependent subjects: diffusion tensor imaging.Neuropsychopharmacology. 2005;30:610–7.
41. Moeller FG, Hasan KM, Steinberg JL, Kramer LA,Valdes I, et al. Diffusion tensor imaging eigenvalues:preliminary evidence for altered myelin in cocainedependence. Psychiatry Res. 2007;154:253–8.
42. Mori S, van Zijl PCM. Fiber tracking: principles andstrategies—a technical review. NMR Biomed.2002;15:468–80.
43. Mori S, Zhang J. Principles of diffusion tensorimaging and its applications to basic neuroscienceresearch. Neuron. 2006;51:527–39.
44. Moseley ME, Cohen Y. Diffusion-weighted MRimaging of anisotropic water diffusion in cat centralnervous system. Radiology. 1990;176:439–45.
45. Nakamae T, Narumoto J, Shibata K, Matsumoto R,Kitabayashi Y, et al. Alteration of fractionalanisotropy and apparent diffusion coefficient inobsessive-compulsive disorder: a diffusion tensorimaging study. Prog Neuropsychopharmacol BiolPsychiatry. 2008;32:1221–6.
46. Nobuhara K, Okugawa G, Minami T, Takase K,Yoshida T, et al. Effects of electroconvulsive therapyon frontal white matter in late-life depression: adiffusion tensor imaging study. Neuropsychobiology.2004;50:48–53.
47. Nobuhara K, Okugawa G, Sugimoto T, Minami T,Tamagaki C, et al. Frontal white matter anisotropyand symptom severity of late-life depression: amagnetic resonance diffusion tensor imaging study.J Neurol Neurosurg Psychiatry. 2006;77:120–2.
48. Pfefferbaum A, Adalsteinsson E, Sullivan EV.Dysmorphology and microstructural degradation ofthe corpus callosum: interaction of age andalcoholism. Neurobiol Aging. 2006;27:994–1009.
49. Pfefferbaum A, Adalsteinsson E, Sullivan EV.Supratentorial profile of white matter microstructuralintegrity in recovering alcoholic men and women.Biol Psychiatry. 2006;59:364–72.
50. Pfefferbaum A, Rosenbloom MJ, Adalsteinsson E,Sullivan EV. Diffusion tensor imaging withquantitative fibre tracking in HIV infection andalcoholism comorbidity: synergistic white matterdamage. Brain. 2007;130:48–64.
51. Pfefferbaum A, Sullivan EV. Microstructural but notmacrostructural disruption of white matter in womenwith chronic alcoholism. Neuroimage. 2002;15:708–18.
52. Pfefferbaum A, Sullivan EV. Disruption of brainwhite matter microstructure by excessive intracellularand extracellular fluid in alcoholism: evidence fromdiffusion tensor imaging. Neuropsychopharmacology.2005;30:423–32.
53. Pierpaoli C. Diffusion tensor MR imaging of thehuman brain. Radiology. 1996;201:637–48.
54. Pierpaoli C, Basser PJ. Toward a quantitativeassessment of diffusion anisotropy. Magn ResonMed. 1996;36:893–906.
55. Reese TG, Heid O, Weisskoff RM, Wedeen VJ.Reduction of eddy-current-induced distortion indiffusion MRI using a twice-refocused spin echo.Magn Reson Med. 2003;49:177–82.
56. Roberts RE, Anderson EJ, Husain M. White mattermicrostructure and cognitive function. Neuroscientist.2013;19:8–15.
57. Saito Y, Nobuhara K, Okugawa G, Takase K,Sugimoto T, et al. Corpus callosum in patients withobsessive-compulsive disorder: diffusion-tensorimaging study. Radiology. 2008;246:536–42.
58. Schmahmann JD, Pandya DN, Wang R, Dai G,D’Arceuil HE, et al. Association fibre pathways of thebrain: parallel observations from diffusion spectrumimaging and autoradiography. Brain. 2007;130:630–53.
59. Stejskal EO, Tanner JE. Spin diffusion measurements:spin echoes in the presence of a time-dependent fieldgradient. J Chem Phys. 1965;42:288–292.
60. Szeszko PR, MacMillan S, McMeniman M, Lorch E,Madden R, et al. Amygdala volume reductions inpediatric patients with obsessive-compulsive disordertreated with paroxetine: preliminary findings.Neuropsychopharmacology. 2004;29:826–32.
61. Tang PF, Ko YH, Luo ZA, Yeh FC, Chen SH, TsengWY. Tract-specific and region of interest analysis ofcorticospinal tract integrity in subcortical ischemicstroke: reliability and correlation with motor functionof affected lower extremity. Am J Neuroradiol.2010;31:1023–30.
62. Taylor DG, Bushell MC. The spatial-mapping oftranslational diffusion-coefficients by the NMRimaging technique. Phys Med Biol. 1985;30:345–9.
63. Taylor WD, MacFall JR, Payne ME, McQuoid DR,Provenzale JM, et al. Late-life depression andmicrostructural abnormalities in dorsolateralprefrontal cortex white matter. Am J Psychiatry.2004;161:1293–6.
64. Tuch DS. Q-ball imaging. Magn Reson Med.2004;52:1358–72.
65. Tuch DS, Reese TG, Wiegell MR, Makris N,Belliveau JW, Wedeen VJ. High angular resolutiondiffusion imaging reveals intravoxel white matterfiber heterogeneity. Magn Reson Med. 2002;48:577–82.
66. Tuch DS, Reese TG, Wiegell MR, Wedeen VJ.Diffusion MRI of complex neural architecture.Neuron. 2003;40:885–95.
67. Wakana S, Caprihan A, Panzenboeck MM, Fallon JH,Perry M, et al. Reproducibility of quantitativetractography methods applied to cerebral whitematter. Neuroimage. 2007;36:630–44.
68. Wedeen VJ, Hagmann P, Tseng WY, Reese TG,Weisskoff RM. Mapping complex tissue architecturewith diffusion spectrum magnetic resonance imaging.Magn Reson Med. 2005;54:1377–86.
2 High-angular diffusion MRI in reward-based psychiatric disorders 33

69. Wedeen VJ, Rosene DL, Wang R, Dai G, MortazaviF, et al. The geometric structure of the brain fiberpathways. Science. 2012;335:1628–34.
70. Wedeen VJ, Wang RP, Schmahmann JD, Benner T,Tseng WY, et al. Diffusion spectrum magneticresonance imaging (DSI) tractography of crossingfibers. Neuroimage. 2008;41:1267–77.
71. Wiegell MR. Fiber crossing in human brain depictedwith diffusion tensor MR imaging. Radiology.2000;217.
72. Yeh FC, Wedeen VJ, Tseng WY. Generalized q-sampling imaging. IEEE Trans Med Imaging.2010;29:1626–35.
73. Yoo SY, Jang JH, Shin YW, Kim DJ, Park HJ, et al.White matter abnormalities in drug-naive patientswith obsessive-compulsive disorder: a diffusiontensor study before and after citalopram treatment.Acta Psychiatr Scand. 2007;116:211–9.
34 W. Yu et al.

3Neuroimaging in Psychiatry
Chuantao Zuo and Huiwei Zhang
3.1 Introduction
Psychiatric disorders are generally defined by acombination of how a person feels, behaves,thinks, or perceives. The disorders may beassociated with particular brain regions or func-tional units or with the nervous system as awhole, and are often diagnosed within a partic-ular social context. In the past few decades,neuroimaging modalities have been developed toinvestigate specific brain regions thought to beinvolved in particular disorders. Neuroimaginghas been applied in the differential diagnosis ofneuropsychiatric syndromes and disorders,especially in otherwise difficult clinical contexts.Neuroimaging methodologies can also provideinformation about neural mechanisms andabnormal neural circuitry involved in variouspsychiatric disorders. Additionally, neuroimag-ing is an important tool for drug discovery anddevelopment.
With the advancement of neuroimaging tech-niques and softwares, it is now possible to reli-ably segment the brain into gray matter (GM),white matter (WM), and cerebrospinal fluid(CSF) with little effort. Imaging studies can bedivided into structural gray matter studies, stud-ies examining the white matter connectivity,
functional magnetic resonance imaging (fMRI)studies, and studies measuring neurotransmitterand neurotransmitter receptor changes. Structuralbrain imaging studies can be broadly divided intoregion of interest (ROI) studies and voxel-basedmorphometric (VBM) analyses. In the former, abrain region is chosen and using specific tracingguidelines, the region is then demarcated withsubsequent volume calculation and comparison,for example, between patients with schizophreniaand healthy subjects. The latter (i.e., VBM) ismore automated with easier methods for seg-mentation and volume comparisons. The basicprinciple underlying diffusion tensor imaging(DTI), which is used to assess white matterintegrity, is that the diffusion of water moleculesis restricted equally in all directions in the CSF(isotropic diffusion) but not in the white and greymatter; water exhibits strong anisotropic diffu-sion in the white matter, whereas in gray matter,it exhibits weak anisotropic diffusion. There hasbeen a rapid increase in the number of fMRIstudies on psychiatric disorders. fMRI helps inunderstanding the relationship between brain andbehavior. An essential aim of a study using fMRIis to show how a failure to stimulate a neuralsystem (as evidenced by reduced blood flow intest subjects during attempts to stimulate thesystem relative to control patients) leads tobehavioral deficits in patients. Magnetic reso-nance spectroscopy (MRS) is a non-invasiveanalytical technique that has been used to studymetabolic changes in the brain. This technique isused to study metabolites that reflect specific
C. Zuo (&) � H. ZhangPET Center, Huashan Hospital, Fudan University,Shanghai, Chinae-mail: [email protected]
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0_3© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
35
brain functions. In addition, the introduction oftechniques such as positron emission tomogra-phy (PET) and single photon emission tomog-raphy (SPECT) has allowed direct in vivoexamination of neurotransmitter functioning inthe brain. PET/SPECT have been employed inmany studies to quantify metabolism or bloodflow in different brain regions, measure neuro-transmitter receptor binding potential, quantifyregional density of receptors of a given type,determine receptor binding displacement duringpharmacological or physiological challenge, aswell as to quantify neurotransmitter release.
3.2 Schizophrenia
Magnetic resonance imaging (MRI) studies haveexamined various aspects of schizophrenia rang-ing from establishing structural brain deficits tobrain connectivity impairments down to the levelof functional impairment apart from neurotrans-mitter and receptor changes. Structural MRIrepresents a useful tool in understanding thebiological underpinnings of schizophrenia and inplanning focused interventions, thus assistingclinicians especially in the early phases of theillness [1]. The current concept of pathophysiol-ogy of schizophrenia has shifted towards abnor-malities in pathways rather than a region-specificlesion, even though it is difficult to definitivelystate that a specific pathway is affected. Theneuropsychological deficits consistently reportedin schizophrenia are executive function impair-ments in tests such as rule set shifting, responseinhibition, and selective attention. Deficits inprocessing speed, language abilities, workingmemory, and verbal and visual memory are alsoreported. The diversity of symptoms could alsoreflect multiple brain region involvement [2].
Studies using VBM or other quantitativestructural MRI techniques have shown thatpatients with first-episode schizophrenia (FES)have significant regional gray matter reduction inthe prefrontal cortex, temporal cortex, and hip-pocampus, as well as in the anteromedial thala-mus [3–5]. Similar structural changes can be
effected by the use of antipsychotic medication[6]. A VBM study on patients with schizophreniaand their unaffected siblings revealed that theymight share decreases in the gray matter volumeof the left middle temporal gyrus. This regionalreduction might be a potential endophenotype ofschizophrenia [5]. However, a meta-analysesstudy argued that the GM changes in patientswith schizophrenia and their unaffected relativesare largely different, although there is subtleoverlap in some regions [7].
fMRI has been utilized to evaluate manyaspects such as cognition [8], emotional pro-cessing [9], and social cognition [10] in schizo-phrenia, in addition to identifying substrates ofpsychopathology [11]. fMRI studies haveexamined and demonstrated functional brainabnormalities at rest and during various postu-lated cognitive aberrations due to schizophrenia.They have also been able to provide insightsregarding the neural basis of some important andclassical schizophrenia-related symptoms such asauditory hallucinations [12]. In addition, byexamining the relationship between specific eyemovement and neuropsychological measures,antisaccade errors were suggested to be a sign ofa generalized neuropsychological deficit inpatients with schizophrenia [13]. fMRI and H2
15OPET scans have revealed abnormal activation inthe prefrontal and cingulate cortex and the medialtemporal lobe in these patients as well asabnormal interaction between these structures[14, 15]. Decreased suppression of the restingstate brain network during stimulation paradigmshas also been reported in schizophrenia [16].
Structural volumetric MRI studies havefocused on a priori relevant brain regions inschizophrenia. VBM studies have also identifiedthe areas implicated in the cortico-cerebello-thalamo-cortical circuit. This circuit and itscomponents have been implicated in monitoringand coordinating the smooth execution of mentalactivity. Disruption in this circuit has been pro-posed as to cause “cognitive dysmetria” leadingto disordered cognition and symptoms of schizo-phrenia. DTI studies have provided evidence forcortico-cortical and cortico-subcortical discon-nectivity in schizophrenia. These changes appear
36 C. Zuo and H. Zhang
to be widespread, and structural data supplementthe evidence of extensive abnormalities in corticalareas demonstrated by VBM studies.
Neurotransmitters, including dopamine (DA),serotonin, gamma-aminobutyric acid (GABA)and glutamate, have been evaluated in the contextof schizophrenia. DA function has been studied atseveral levels: (1) at a presynaptic level, neuro-imaging studies investigating DOPA uptakecapacity clearly show increased DA synthesis inpatients with schizophrenia (meta-analysisshowed consistently increased striatal dopaminesynthesis capacity in schizophrenia, with a 14 %elevation in patients compared with healthycontrols [17, 18]; (2) at a synaptic level, neuro-imaging studies investigating dopamine trans-porter availability (DAT) do not show anyevidence of dysfunction; (3) at a DA receptorlevel, neuroimaging studies investigating DAreceptor density show a mild increase of dopa-mine D2 receptor density in basic condition and ahyper-reactivity of the DA system in dynamicconditions. Striatal DA abnormalities are nowclearly demonstrated in patients with schizo-phrenia as well as the at-risk population and couldconstitute an endophenotype of schizophrenia.Subtle sub-clinical striatal DA abnormalities inthe at-risk population could be a biomarker oftransition from a vulnerability state to theexpression of frank psychosis [19]. A significantreduction of 18F-MPPF, a labeled PET ligand for5-HT1A receptors, was found in treated patientswith schizophrenia compared to age- and sex-matched healthy subjects. These alterations weremainly localized to the frontal and orbitofrontalcortex and may reflect either the pathophysiologyof schizophrenia or medication effects [20].18F-FFMZ PET was recently used to measureGABA-A/BZ receptor binding potential. Indi-viduals at ultra-high risk demonstrated signifi-cantly reduced binding potential of GABA-A/BZreceptors in the right caudate [21]. PET/SPECTstudies testing the effects of NMDA blockade ondopaminergic indices in healthy subjects usingketamine alone found mixed results in the stria-tum but significant effects in the cortex, consistentwith prior rodent data. However, strikingly sim-ilar results for amphetamine-induced dopamine
release in individuals with schizophrenia andhealthy subjects given acute ketamine provideinitial support for the glutamate/NMDA hypoth-esis of schizophrenia. Nevertheless, directlyin vivo measurements of glutamatergic indicesare necessary to translate preclinical and clinicalfindings into effective therapies. Although thedevelopment of PET/SPECT imaging of theglutamate system has lagged behind that of thedopamine system, MRI-based technologies havebeen effectively utilized to measure glutamatergicindices in vivo [22].
3.3 Depression
Clinical depression affects 7–18 % of the popu-lation on at least one occasion during their life.Major depression is certainly the most prevalentpsychiatric disorders and results in the largestnumber of disability adjusted life years. In con-trast to some of the neurodegenerative disordersthat mimic depression and are accompanied bydecreased frontal lobe metabolism, majordepression is associated with elevated metabo-lism but reduced volume in the subgenual regionof the medial frontal lobe. In addition, the acti-vation pattern on fMRI can be used to distinguishthese disorders. Orbitofrontal and cingulate acti-vation are greater in patients with depression thanin those with AD and healthy controls. Geno-typic variants are likely to influence both thelikelihood of developing major depression andaccompanying imaging findings. For instance, indepression, increased activity of the amygdala inresponse to negative stimuli appears to be mod-ulated by the 5-HT transporter gene (SLC6A4)promoter polymorphism (5-HTTLPR). Hippo-campal volume loss is characteristic of elderlysubjects and of patients with chronic illness anddepression and may be impacted by the V66Mbrain-derived neurotrophic factor gene variantand the 5-HTTLPR SLC6A4 polymorphism[16]. 3D-MRI studies reported higher perfusionin the ventral anterior cingulate/basal cingulate ofresponders compared to non-responders, andperfusion measurements are correlated with
3 Neuroimaging in Psychiatry 37
changes in the Hamilton depression rating scale[23–25].
PET/SPECT studies have shown an abnor-mally high serotonergic binding potential inpatients with more severe pessimism, suggestingthat extracellular serotonin relates to severity ofpessimism [26]. Other studies have shown thathigher-than-normal dopamine binding potentialduring depressive episodes worsened in patientswith motor slowing, suggesting that dopamineplays a role in motor aspects of depression. Thesehigher binding potentials for serotonin anddopamine are linked to lower extracellular con-centration in these neurotransmitters; thus,depression is often said to be due to low sero-tonin and dopamine levels and treated withmedications that inhibit active transport of theseneurotransmitters from the extracellular space tointracellular locations, subsequently increasingextracellular levels [27]. PET imaging alsoprovides an important contribution towardunderstanding the pathophysiology of majordepressive disorders (MDDs), identifying endo-phenotypes and vulnerability traits, as well asassessing therapeutics and identifying newopportunities for prevention. Neuroreceptor PETimaging has associated major depression withdecreased 5-HT1A binding potential in the raphenuclei, medial temporal lobe, and medial pre-frontal cortex. Facilitated by the development ofsuitable radio ligands for monoaminergic recep-tors such as the 5-HT1A, 5-HT2A, and D2receptors; reuptake transporters such as theserotonin transporter (SERT/5-HTT), dopaminetransporter (DAT), and norepinephrine trans-porter (NET); and catabolic enzymes (MAO-Aand -B), PET imaging has had a considerableimpact on the monoamine theory of MDD. Giventhat MAO-A is an enzyme that metabolizesmonoamines, such as serotonin, norepinephrine,and dopamine, elevated MAO-A density is pro-posed as the primary mechanism of the multiplemonoamine reduction observed in MDD. An80 % occupancy of the 5-HTT by serotonin re-uptake inhibitors distinguishes medications fromplacebo in clinical trials on the treatment ofmajor depressive episode [28]. Low 5-HTTbinding activity was found in the dorsolateral
prefrontal cortex of healthy twins of patients withmood disorders, indicating a genetic vulnerabil-ity that may contribute to the pathophysiology ofdepression [29]. Moreover, 18F-fluoro-2-deoxy-glucose (FDG) PET imaging showed distinctregional cerebral patterns of glucose metabolismthat may be serotonin-sensitive biomarkers ofsuicide risk [30].
3.4 Anxiety
MRI has been used in studies on anxiety disor-ders. Relative to controls, patients with general-ized anxiety disorder (GAD) have larger volumesof the amygdala and dorsomedial prefrontal cor-tex (DMPFC). Moreover, patients with GADshowed localized gray matter volume differencesin brain regions associated with anticipatoryanxiety and emotion regulation [31]. The obser-vation of alterations in pre-frontal regions andreduced activity observed in the striatal andparietal areas have shown that much remains to beinvestigated within the complexity of socialanxiety disorder (SAD). Interestingly, follow-upstudies have observed a decrease in perfusion inthese same areas after either pharmacological orpsychological treatment. The medial prefrontalcortex provides additional support for a cortico-limbic model of SAD pathophysiology, being apromising area of investigation [32]. Although ina fMRI study, patients with SAD showed acti-vation patterns similar to that of the HC group,they showed comparatively decreased activationin the left cerebellum, left precuneus, and bilateralposterior cingulate cortex [33]. DTI can be usedto examine the structural integrity of regionalwhite matter and to map white matter tracts. Formost anxiety disorders, the results of DTI studiesare in line with other structural and fMRI findingsand can be interpreted within the frameworks ofexisting models for the neurocircuitry of variousdisorders. DTI findings could further enrichneurobiological models for anxiety disorders,although replication is often warranted, andstudies in pediatric populations are laggingbehind remarkably [34].
38 C. Zuo and H. Zhang
In addition, PET/SPECT studies haveobserved reductions in 5-HT1A availability inanxiety disorders. Interestingly, 5-HTT reduc-tions observed in patients with MDD correlatedin magnitude with the severity of co-occurringanxiety, rather than depressive symptoms.A recent meta-analysis found decreased striatalD2 receptor and mesencephalic 5-HTT bindingin obsessive compulsive disorder (OCD) andreduced GABA-A receptors in frontocorticalregions in panic disorder as well as temporo-cortical areas in generalized anxiety disorder.When all anxiety disorders were pooled, reduc-tions in midbrain 5-HTT and 5-HT1A receptorsand striatal D2 and GABA-A receptors wereobserved, indicating a major role for dopamine,5-HT, and GABA neurotransmission in anxietydisorders [35].
3.5 Eating Disorders
Eating disorders (EDs) include anorexia nervosa(AN) and bulimia nervosa (BN). Functional brainimaging is commonly performed in conjunctionwith paradigms and tasks designed to identifyareas of brain activation that might be specific forAN pathophysiology. Visual high-calorie pre-sentation elicited high anxiety in individuals withAN, together with left mesial temporal as well asleft insular and bilateral anterior cingulate cortex(ACC) activity. The prefrontal cortex could beactive to appropriately or inappropriately restrictfood, possibly via heightened fear related acti-vation and anxiety followed by related decisionmaking such as food restriction. Heightened brainresponse to randomly applied pleasant and aver-sive taste stimuli have been observed in the insulaand striatum of recovered individuals with AN,suggesting an overly sensitive taste reward sys-tem. Moreover, body image distortion is an inte-gral part of AN pathophysiology and is part of itsdiagnostic criteria. Perceptual alterations may berelated directly to the mechanisms of body imageconstruction. Cingulate and prefrontal activity is
frequently different between patients with AN andcontrols. Those regions may be over-activatedwhen confronted with anxiety-provoking food-related stimuli. Such a heightened vigilance isprobably related to anxiety and fear-of-fatnesscognitions, followed by actions to avoid weightgain. On the other hand, individuals with AN mayrespond less to taste and other reward stimuli,which may help to restrict food intake, especiallyof neurobiologically “rewarding” foods. It furtherappears that individuals with AN do have alteredself-perception-related brain activation and thissuggests incorrect processing, and maybe abnor-mal proprioceptive feedback, which, in turn, mayallow over-valued ideas of thinness to control theself-image [36]. In BN, insula activation repre-sents emotional arousal by the image of food,whereas ACC activation acts as a counterbalanceto that response, as the ACC is implicated inselection of emotional attention and control ofsympathetic autonomic arousal [37, 38]. BN isassociated with reduced response in the tastereward circuitry, which may indicate rewardpathway desensitization in response to excessivefood, possibly similar to that observed in modelsof substance use. Similarly to AN, BN is associ-ated with reduced lateral fusiform gyrus activa-tion and, compared to AN, high aversion ratingsto any body shape. Thus, reduced brain activationin BNmay be an aversion-driven restraint in brainresponse [39].
A 18F-FDG PET study of AN showed hyper-metabolism in the frontal lobe, the limbic lobe,lentiform nucleus, left insula, and left subcallosalgyrus. It also showed hypometabolism in theparietal lobe. The hypermetabolism in frontallobe, hippocampus, and lentiform nucleusdecreased after deep brain stimulation [40](Figs. 3.1 and 3.2). PET studies of monoaminefunction in AN and BN have focused on 5-HT1A
receptor, 5-HT2A receptor, 5-HT transporter(5-HTT), and dopamine. Individuals with ANhave a 50–70 % increase in 11C-WAY100635 BPin the subgenual, mesial temporal, orbitofrontal,and raphe brain regions as well as in the pre-frontal, lateral temporal, anterior cingulate, and
3 Neuroimaging in Psychiatry 39
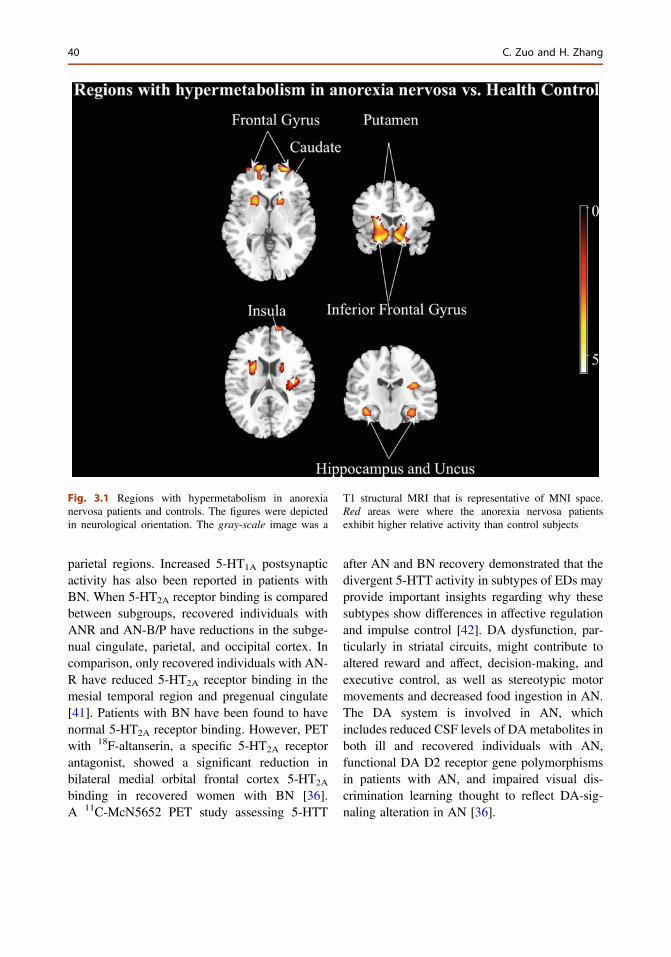
parietal regions. Increased 5-HT1A postsynapticactivity has also been reported in patients withBN. When 5-HT2A receptor binding is comparedbetween subgroups, recovered individuals withANR and AN-B/P have reductions in the subge-nual cingulate, parietal, and occipital cortex. Incomparison, only recovered individuals with AN-R have reduced 5-HT2A receptor binding in themesial temporal region and pregenual cingulate[41]. Patients with BN have been found to havenormal 5-HT2A receptor binding. However, PETwith 18F-altanserin, a specific 5-HT2A receptorantagonist, showed a significant reduction inbilateral medial orbital frontal cortex 5-HT2A
binding in recovered women with BN [36].A 11C-McN5652 PET study assessing 5-HTT
after AN and BN recovery demonstrated that thedivergent 5-HTT activity in subtypes of EDs mayprovide important insights regarding why thesesubtypes show differences in affective regulationand impulse control [42]. DA dysfunction, par-ticularly in striatal circuits, might contribute toaltered reward and affect, decision-making, andexecutive control, as well as stereotypic motormovements and decreased food ingestion in AN.The DA system is involved in AN, whichincludes reduced CSF levels of DA metabolites inboth ill and recovered individuals with AN,functional DA D2 receptor gene polymorphismsin patients with AN, and impaired visual dis-crimination learning thought to reflect DA-sig-naling alteration in AN [36].
Fig. 3.1 Regions with hypermetabolism in anorexianervosa patients and controls. The figures were depictedin neurological orientation. The gray-scale image was a
T1 structural MRI that is representative of MNI space.Red areas were where the anorexia nervosa patientsexhibit higher relative activity than control subjects
40 C. Zuo and H. Zhang
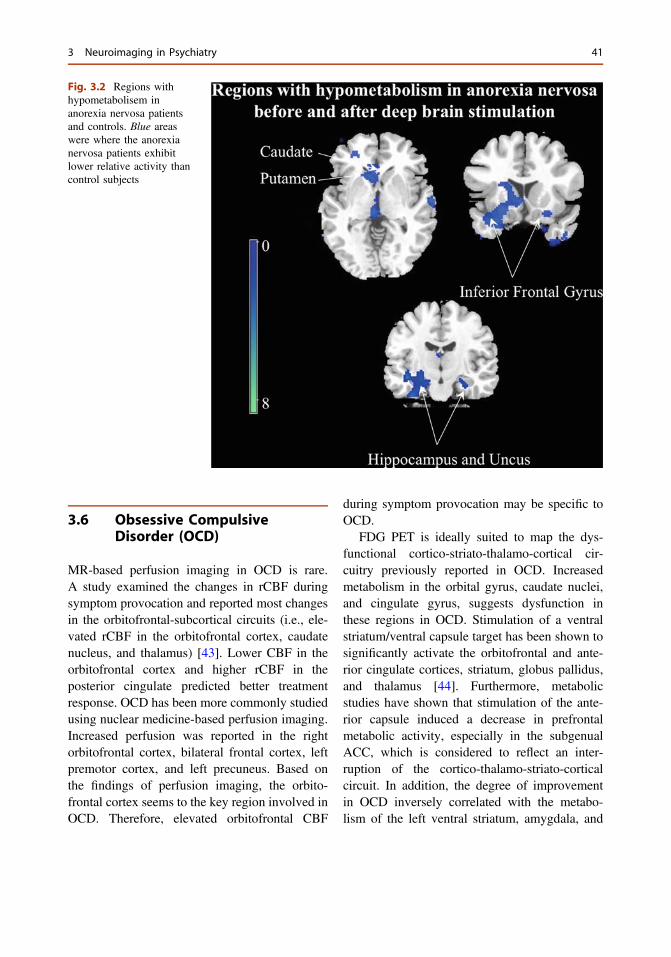
3.6 Obsessive CompulsiveDisorder (OCD)
MR-based perfusion imaging in OCD is rare.A study examined the changes in rCBF duringsymptom provocation and reported most changesin the orbitofrontal-subcortical circuits (i.e., ele-vated rCBF in the orbitofrontal cortex, caudatenucleus, and thalamus) [43]. Lower CBF in theorbitofrontal cortex and higher rCBF in theposterior cingulate predicted better treatmentresponse. OCD has been more commonly studiedusing nuclear medicine-based perfusion imaging.Increased perfusion was reported in the rightorbitofrontal cortex, bilateral frontal cortex, leftpremotor cortex, and left precuneus. Based onthe findings of perfusion imaging, the orbito-frontal cortex seems to the key region involved inOCD. Therefore, elevated orbitofrontal CBF
during symptom provocation may be specific toOCD.
FDG PET is ideally suited to map the dys-functional cortico-striato-thalamo-cortical cir-cuitry previously reported in OCD. Increasedmetabolism in the orbital gyrus, caudate nuclei,and cingulate gyrus, suggests dysfunction inthese regions in OCD. Stimulation of a ventralstriatum/ventral capsule target has been shown tosignificantly activate the orbitofrontal and ante-rior cingulate cortices, striatum, globus pallidus,and thalamus [44]. Furthermore, metabolicstudies have shown that stimulation of the ante-rior capsule induced a decrease in prefrontalmetabolic activity, especially in the subgenualACC, which is considered to reflect an inter-ruption of the cortico-thalamo-striato-corticalcircuit. In addition, the degree of improvementin OCD inversely correlated with the metabo-lism of the left ventral striatum, amygdala, and
Fig. 3.2 Regions withhypometabolisem inanorexia nervosa patientsand controls. Blue areaswere where the anorexianervosa patients exhibitlower relative activity thancontrol subjects
3 Neuroimaging in Psychiatry 41
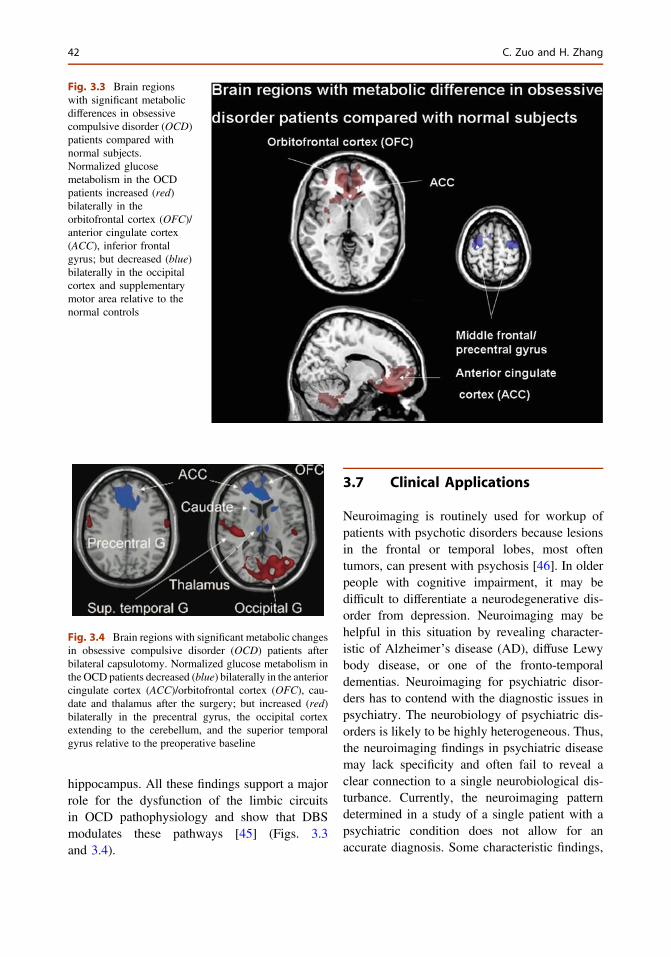
hippocampus. All these findings support a majorrole for the dysfunction of the limbic circuitsin OCD pathophysiology and show that DBSmodulates these pathways [45] (Figs. 3.3and 3.4).
3.7 Clinical Applications
Neuroimaging is routinely used for workup ofpatients with psychotic disorders because lesionsin the frontal or temporal lobes, most oftentumors, can present with psychosis [46]. In olderpeople with cognitive impairment, it may bedifficult to differentiate a neurodegenerative dis-order from depression. Neuroimaging may behelpful in this situation by revealing character-istic of Alzheimer’s disease (AD), diffuse Lewybody disease, or one of the fronto-temporaldementias. Neuroimaging for psychiatric disor-ders has to contend with the diagnostic issues inpsychiatry. The neurobiology of psychiatric dis-orders is likely to be highly heterogeneous. Thus,the neuroimaging findings in psychiatric diseasemay lack specificity and often fail to reveal aclear connection to a single neurobiological dis-turbance. Currently, the neuroimaging patterndetermined in a study of a single patient with apsychiatric condition does not allow for anaccurate diagnosis. Some characteristic findings,
Fig. 3.3 Brain regionswith significant metabolicdifferences in obsessivecompulsive disorder (OCD)patients compared withnormal subjects.Normalized glucosemetabolism in the OCDpatients increased (red)bilaterally in theorbitofrontal cortex (OFC)/anterior cingulate cortex(ACC), inferior frontalgyrus; but decreased (blue)bilaterally in the occipitalcortex and supplementarymotor area relative to thenormal controls
Fig. 3.4 Brain regions with significant metabolic changesin obsessive compulsive disorder (OCD) patients afterbilateral capsulotomy. Normalized glucose metabolism inthe OCD patients decreased (blue) bilaterally in the anteriorcingulate cortex (ACC)/orbitofrontal cortex (OFC), cau-date and thalamus after the surgery; but increased (red)bilaterally in the precentral gyrus, the occipital cortexextending to the cerebellum, and the superior temporalgyrus relative to the preoperative baseline
42 C. Zuo and H. Zhang

however, have been derived from samples ofpatients with each of the psychiatric diagnosticgroupings [16].
3.8 Drug Discoveryand Development
Neuroimaging can be helpful at several levels ofdrug discovery and development [47]: (1) char-acterizing preclinical models; (2) conductingearly clinical studies to show that targetengagement by the new drug induces the bio-logical changes expected to give clinical benefit;(3) evaluating patients in clinical trials to dem-onstrate proof of concept. In other words,engaging a particular target can be shown to belinked to a meaningful change in a clinical end-point observable via neuroimaging, thus provid-ing evidence supporting the treatment beingstudied. Since neuroimaging can likely enablein vivo observation of brain structure and func-tion, it could potentially provide ideal biomarkersfor therapeutic intervention development. Con-sidering the definition of biomarker [47], mostneuroimaging methods do not meet the bio-marker standards for now. However, somemethods have the potential to be used as bio-markers or pre-biomarkers because they allowfor identification of therapy-relevant characteris-tics of the disease. For instance, by examiningstriatal DA D2 receptors in a [11C]raclopridePET scan, a link was found between D2 receptoroccupancy by a drug and a reduction in thepositive symptoms in schizophrenia; ascendingdoses of up to 80 % receptor occupancy wereprogressively more effective in relieving delu-sions and hallucinations [48].
In a conclusion, neuroimaging is beingincreasingly applied for the development of psy-chiatric therapies. Neuroimaging is clinically rel-evant for diagnosis and differential diagnosis. Itcan yield further insights into the mechanisms ofpsychiatric diseases. Neuroimaging provides thepre-clinical researcher a relatively easy method totest whether a potential drug target shows an
abnormality in a psychiatric disorder and whether,therefore, its correction may be therapeutic.Finally, by identifying the individuals who man-ifest the expected pharmacological action of thedrug, neuroimaging can aid in personalized med-icine by selecting individuals most likely to ben-efit from a particular treatment in a clinical trial.
References
1. Perlini C, Bellani M, Brambilla P. Structural imagingtechniques in schizophrenia. Acta Psychiatr Scand.2012;126(4):235–42.
2. Narayanaswamy JC, Venkatasubramanian G,Gangadhar BN. Neuroimaging studies inschizophrenia: an overview of research from Asia.Int Rev Psychiatry. 2012;24(5):405–16.
3. Sun D, et al. Elucidating a magnetic resonanceimaging-based neuroanatomic biomarker forpsychosis: classification analysis using probabilisticbrain atlas and machine learning algorithms. BiolPsychiatry. 2009;66(11):1055–60.
4. Meisenzahl EM, et al. Structural brain alterations atdifferent stages of schizophrenia: a voxel-basedmorphometric study. Schizophr Res. 2008;104(1–3):44–60.
5. Hu M, et al. Decreased left middle temporal gyrusvolume in antipsychotic drug-naive, first-episodeschizophrenia patients and their healthy unaffectedsiblings. Schizophr Res. 2013;144(1–3):37–42.
6. Thompson PM, et al. Time-lapse mapping of corticalchanges in schizophrenia with different treatments.Cereb Cortex. 2009;19(5):1107–23.
7. Xiao Y, et al. Similar and different gray matter deficitsin schizophrenia patients and their unaffectedbiological relatives. Front Psychiatry. 2013;4:150.
8. Vago DR, et al. Identification of neural targets for thetreatment of psychiatric disorders: the role offunctional neuroimaging. Neurosurg Clin N Am.2011;22(2):279–305.
9. Sorg C, et al. Increased intrinsic brain activity in thestriatum reflects symptom dimensions inschizophrenia. Schizophr Bull. 2013;39(2):387–95.
10. Ebisch SJ, et al. Altered brain long-range functionalinteractions underlying the link between aberrant self-experience and self-other relationship in first-episodeschizophrenia. Schizophr Bull. 2013.
11. Tu PC, et al. Schizophrenia and the brain’s controlnetwork: aberrant within- and between-networkconnectivity of the frontoparietal network inschizophrenia. Schizophr Res. 2013;147(2–3):339–47.
12. Mou X, et al. Voice recognition and alteredconnectivity in schizophrenic patients with auditoryhallucinations. Prog Neuropsychopharmacol BiolPsychiatry. 2013;44:265–70.
3 Neuroimaging in Psychiatry 43
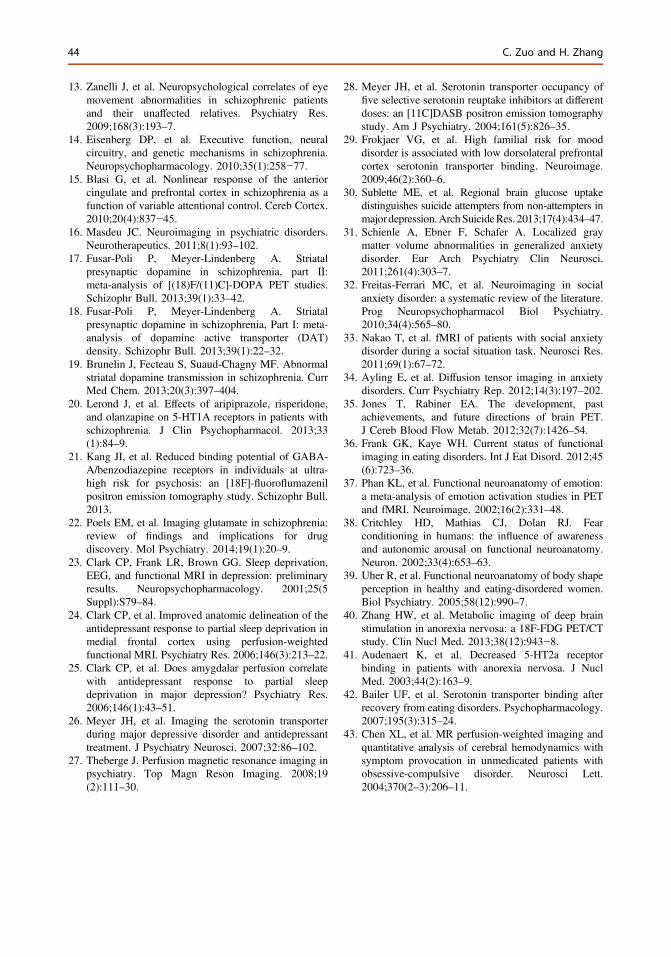
13. Zanelli J, et al. Neuropsychological correlates of eyemovement abnormalities in schizophrenic patientsand their unaffected relatives. Psychiatry Res.2009;168(3):193–7.
14. Eisenberg DP, et al. Executive function, neuralcircuitry, and genetic mechanisms in schizophrenia.Neuropsychopharmacology. 2010;35(1):258−77.
15. Blasi G, et al. Nonlinear response of the anteriorcingulate and prefrontal cortex in schizophrenia as afunction of variable attentional control. Cereb Cortex.2010;20(4):837−45.
16. Masdeu JC. Neuroimaging in psychiatric disorders.Neurotherapeutics. 2011;8(1):93–102.
17. Fusar-Poli P, Meyer-Lindenberg A. Striatalpresynaptic dopamine in schizophrenia, part II:meta-analysis of [(18)F/(11)C]-DOPA PET studies.Schizophr Bull. 2013;39(1):33–42.
18. Fusar-Poli P, Meyer-Lindenberg A. Striatalpresynaptic dopamine in schizophrenia, Part I: meta-analysis of dopamine active transporter (DAT)density. Schizophr Bull. 2013;39(1):22–32.
19. Brunelin J, Fecteau S, Suaud-Chagny MF. Abnormalstriatal dopamine transmission in schizophrenia. CurrMed Chem. 2013;20(3):397–404.
20. Lerond J, et al. Effects of aripiprazole, risperidone,and olanzapine on 5-HT1A receptors in patients withschizophrenia. J Clin Psychopharmacol. 2013;33(1):84–9.
21. Kang JI, et al. Reduced binding potential of GABA-A/benzodiazepine receptors in individuals at ultra-high risk for psychosis: an [18F]-fluoroflumazenilpositron emission tomography study. Schizophr Bull.2013.
22. Poels EM, et al. Imaging glutamate in schizophrenia:review of findings and implications for drugdiscovery. Mol Psychiatry. 2014;19(1):20–9.
23. Clark CP, Frank LR, Brown GG. Sleep deprivation,EEG, and functional MRI in depression: preliminaryresults. Neuropsychopharmacology. 2001;25(5Suppl):S79–84.
24. Clark CP, et al. Improved anatomic delineation of theantidepressant response to partial sleep deprivation inmedial frontal cortex using perfusion-weightedfunctional MRI. Psychiatry Res. 2006;146(3):213–22.
25. Clark CP, et al. Does amygdalar perfusion correlatewith antidepressant response to partial sleepdeprivation in major depression? Psychiatry Res.2006;146(1):43–51.
26. Meyer JH, et al. Imaging the serotonin transporterduring major depressive disorder and antidepressanttreatment. J Psychiatry Neurosci. 2007;32:86–102.
27. Theberge J. Perfusion magnetic resonance imaging inpsychiatry. Top Magn Reson Imaging. 2008;19(2):111–30.
28. Meyer JH, et al. Serotonin transporter occupancy offive selective serotonin reuptake inhibitors at differentdoses: an [11C]DASB positron emission tomographystudy. Am J Psychiatry. 2004;161(5):826–35.
29. Frokjaer VG, et al. High familial risk for mooddisorder is associated with low dorsolateral prefrontalcortex serotonin transporter binding. Neuroimage.2009;46(2):360–6.
30. Sublette ME, et al. Regional brain glucose uptakedistinguishes suicide attempters from non-attempters inmajordepression.ArchSuicideRes.2013;17(4):434–47.
31. Schienle A, Ebner F, Schafer A. Localized graymatter volume abnormalities in generalized anxietydisorder. Eur Arch Psychiatry Clin Neurosci.2011;261(4):303–7.
32. Freitas-Ferrari MC, et al. Neuroimaging in socialanxiety disorder: a systematic review of the literature.Prog Neuropsychopharmacol Biol Psychiatry.2010;34(4):565–80.
33. Nakao T, et al. fMRI of patients with social anxietydisorder during a social situation task. Neurosci Res.2011;69(1):67–72.
34. Ayling E, et al. Diffusion tensor imaging in anxietydisorders. Curr Psychiatry Rep. 2012;14(3):197–202.
35. Jones T, Rabiner EA. The development, pastachievements, and future directions of brain PET.J Cereb Blood Flow Metab. 2012;32(7):1426–54.
36. Frank GK, Kaye WH. Current status of functionalimaging in eating disorders. Int J Eat Disord. 2012;45(6):723–36.
37. Phan KL, et al. Functional neuroanatomy of emotion:a meta-analysis of emotion activation studies in PETand fMRI. Neuroimage. 2002;16(2):331–48.
38. Critchley HD, Mathias CJ, Dolan RJ. Fearconditioning in humans: the influence of awarenessand autonomic arousal on functional neuroanatomy.Neuron. 2002;33(4):653–63.
39. Uher R, et al. Functional neuroanatomy of body shapeperception in healthy and eating-disordered women.Biol Psychiatry. 2005;58(12):990–7.
40. Zhang HW, et al. Metabolic imaging of deep brainstimulation in anorexia nervosa: a 18F-FDG PET/CTstudy. Clin Nucl Med. 2013;38(12):943−8.
41. Audenaert K, et al. Decreased 5-HT2a receptorbinding in patients with anorexia nervosa. J NuclMed. 2003;44(2):163–9.
42. Bailer UF, et al. Serotonin transporter binding afterrecovery from eating disorders. Psychopharmacology.2007;195(3):315–24.
43. Chen XL, et al. MR perfusion-weighted imaging andquantitative analysis of cerebral hemodynamics withsymptom provocation in unmedicated patients withobsessive-compulsive disorder. Neurosci Lett.2004;370(2–3):206–11.
44 C. Zuo and H. Zhang

44. Zuo ct, et al. Metabolic imaging of bilateral anteriorcapsulotomy in refractory obsessive compulsivedisorder: an FDG PET study. J Cereb Blood FlowMetab. 2013;33(6):880−7.
45. Ballanger B, et al. PET functional imaging of deepbrain stimulation in movement disorders andpsychiatry. J Cereb Blood Flow Metab. 2009;29(11):1743–54.
46. Bunevicius A, et al. Brain lesions manifesting aspsychiatric disorders: eight cases. CNS Spectr.2008;13(11):950–8.
47. Wong DF, Tauscher J, Grunder G. The role ofimaging in proof of concept for CNS drug discoveryand development. Neuropsychopharmacology.2009;34(1):187–203.
48. Grunder G, et al. The striatal and extrastriatal D2/D3receptor-binding profile of clozapine in patients withschizophrenia. Neuropsychopharmacology. 2006;31(5):1027–35.
3 Neuroimaging in Psychiatry 45

4DBS in Psychiatry and the Pendulumof History
Marwan I. Hariz
Abstract
Recent published statements on Deep brain stimulation (DBS) bypsychiatrists and ethicists claim that DBS was developed first formovement disorders and is now applied in psychiatry; that it was thebehavioural and psychiatric side-effects of DBS in subthalamic nucleus(STN) in Parkinsonian patients that prompted investigation of DBS inpsychiatry; and that neurosurgeons should not act alone in this field, butshould be within multidisciplinary teams in order not to repeat abuses ofthe past. The present author conducted a review of old literature since thebirth of human stereotactic neurosurgery in 1947 and establishedthe following: (1) The first applications of DBS in the early 1950s werein the field of psychiatry, and promoted mainly by neurologists andpsychiatrists without involvement of neurosurgeons. (2) Some of these oldpsychiatric applications of DBS were found to be dubious and precariouseven by yesterday’s ethical standards. (3) Modern DBS for psychiatricillness started in 1999 on the initiative of neurosurgeons who had involvedfrom the beginning psychiatrists, and it had nothing to do with non-motorside-effects of STN DBS. (4) A recent consensus meeting on psychiatricDBS insisted in its guidelines on multidisciplinarity and included30 panelists none of whom a neurosurgeon.
Keywords
Deep brain stimulation � Psychosurgery � History � Ethics
M.I. Hariz (&)UCL Institute of Neurology, Box 146, QueenSquare, London WC1N 3BG, UKe-mail: [email protected]
M.I. HarizDepartment of Clinical Neuroscience, UmeåUniversity, Umeå, Sweden
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0_4© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
47
Hegel remarks somewhere that all great world-historic facts and personages appear,so to speak, twice. He forgot to add: the first time as tragedy, the second time as farce.
Karl Marx, 1852: The 18th Brumaire of Louis Bonaparte, (Chap. 1).
4.1 Introduction
Deep brain stimulation (DBS) is an establishedmethod for surgical treatments for movementdisorders. Today, most of the investigationalapplications of DBS are in the field of Neuropsy-chiatry, especially for Obsessive compulsive dis-orders (OCD), Gilles de la Tourette syndrome andmajor depressive disorder. It is a common beliefthat DBS in psychiatry follows upon DBS inmovement disorders; for example, Kopell et al.wrote in 2004: “Over the last decade, deep brainstimulation (DBS) has revolutionized the practiceof neurosurgery, particularly in the realm ofmovement disorder. It is no surprise that DBS isnow being studied in the treatment of refractorypsychiatric diseases” [13]. Also, Stelten et al. [22]wrote: “The DBS procedure was originally intro-duced for the treatment of movement disorders,but nowadays it is being studied as a possibletreatment option for intractable states of neuro-psychiatric conditions.” It is also common beliefthat DBS in psychiatry stemmed from observationon psychiatric and behavioural side effects of DBSin the STN in PD patients. Schläpfer and Bewer-nick [20] wrote: “The observation of inducedpsychiatric side effects (e.g., changes in mood,hypomania, reduction of anxiety) gave theimpulse to try DBS also for psychiatric disorders.”Finally, it is assumed that the old stereotacticsurgery for psychiatry illness was not enoughmultidisciplinary with neurosurgeons actingalone, many time without consulting the psychi-atrists. As an example of this statement one canread the followingwritten by ethicist Fins et al. in apaper published 2006 in Neurosurgery [9]: “It isethically untenable for this work to proceed byneurosurgeons in isolation without psychiatristsdetermining the diagnosis and suitability ofpatients for treatment. The mere fact that elec-trodes can be placed is not amoral warrant for their
insertion… Such errant behavior is especiallyinappropriate because it represents a recapitula-tion of the excesses associated with psychosur-gery… If this generation of neuroscientists andpractitioners hope to avoid the abuses of thatearlier era, and avoid conflation of neuromodula-tion with psychosurgery, it is critical that neuro-modulation be performed in an interdisciplinaryand ethically sound fashion” [9].
The aim of the present paper is to scrutinizethese statements that are representative of leadingopinions in contemporary literature, in the lightof available historical literature on the subject.
4.2 Materials and Methods
The author has attempted to trace, through liter-ature search in scientific journals, as well as inpublished books and proceedings from scientificmeetings, the origins of chronic deep brainstimulation to find out which were its firstapplications in humans, and who were involvedin practice of early DBS.
4.3 Results
4.3.1 Origins of DBS
Stereotactic functional neurosurgery started witha co-operation between a neurologist Spiegel, anda neurosurgeon Wycis [21]. They introduced thestereotactic technique in humans with the explicitaim to avoid the side effects of lobotomy bymaking very focal lesion in pertinent pathwaysand nuclei in psychiatric patients. Indeed, in theirseminal paper published in Science in 1947 [21],they wrote: “This apparatus is being used forpsychosurgery… Lesions have been placed in
48 M.I. Hariz
the region of the medial nucleus of the thalamus(medial thalamotomy)…”. Soon after, neuro-physiologist and neuropsychiatrist José Delgadodescribed in 1952 a technique of implantation ofelectrodes for chronic recording and stimulationto evaluate its value in psychotic patients [4]. In1953, in the proceedings of the Mayo Clinic, in anarticle about depth stimulation of the brain onecould read the following [3]: “An observation thatmay have some practical significance was thatseveral of our psychotic patients seem toimproved and become more accessible in thecourse of stimulation studies lasting severaldays”. The authors thought that a likely expla-nation for this phenomenon “was that the localstimulation was having a therapeutic effect com-parable to that of electroshock”. They wrote fur-ther: “This aspect of localized stimulation studiesrequires further investigation since it may lead toa most specific, less damaging, and more thera-peutically effective electrostimulation technicthan can be achieved by the relatively crudeextracranial stimulation methods in use at pres-ent” [3]. Meanwhile, Delgado continued toinvestigate the use of deep brain stimulation anddevised a technique of “radio communicationwith the brain” through chronically implantedelectrodes attached to a subcutaneously implantedreceiver in the scalp, that he called “stimoceiver”,specifically for use in psychosurgical patients[5, 6]. In parallel, a group at Tulane University inNew Orleans led by psychiatrist Robert Heathwas heavily involved during three decades,starting in the early fifties, in studies of chronicdepth stimulation in patients with schizophreniaand in search for the brain’s “pleasure center” [1].Some of Heath’s work related to studies of“rewarding” and “aversive” subcortical structures[10], to surgical control of behavior and initiationof heterosexual behavior in a homosexual male[16], and other aspects of modulation of emotionthrough deep brain stimulation in order to find atreatment for intractable psychiatric illness [12].The Tulane experience in this field was analysedin 2000 by Alan Baumeister and published in theJournal of the History of the Neurosciences underthe title: “The Tulane Electrical Brain Stimulation
Program. A historical case study in medical eth-ics” [1]. Baumeister wrote: “The central conclu-sion of the present review is that the Tulaneelectrical brain stimulation experiments had nei-ther a scientific nor a clinical justification… Theconclusion is that these experiments were dubiousand precarious by yesterday’s standards”. Longbefore Baumeister’s verdict, neurosurgeon LauriLaitinen wrote in 1977, in his paper on “EthicalAspects of Psychiatric Surgery” [14] a commentabout one of Heath’s papers published in 1972[11]: “There is no doubt that in this study allstandards of ethics had been ignored. The ethicalresponsibility of the editors who accept reports ofthis kind for publication should also be dis-cussed” [14].
In view of the above, it is difficult to give anycredit to the claim of some ethicists that “It isethically untenable for this work to proceed byneurosurgeons in isolation” [9], when historyshows that when somebody was conducting suchwork “in isolation”, and disclosing such an“inappropriate”… “errant behavior”, it was someneuropsychiatrists and not neurosurgeons whowere to blame. It is interesting in that context tonote the historical ignorance of some of today’spsychiatrists who recently published a paper inAdvances in Neurology [15] entitled “BehavioralNeurosurgery” and wrote: “One of the mostnotable surgeons was the American neurosur-geon Walter Freeman… Freeman began to applyhis relatively untested procedure, the prefrontallobotomy, in which he transorbitally inserted anice pick into the frontal cortex” [15]. In factFreeman was a neuropsychiatrist and the truth isthat he was abandoned by his neurosurgeonJames Watts, following Freeman’s increasinglyuncritical attitude to lobotomy [7]. When neu-rosurgeons are made scapegoats by some, whoremembers that the Norwegian psychiatrist Or-nulf Odegård, who was director of Norway’smain psychiatrist hospital during more than30 years, wrote in 1953 in the Norwegian Med-ical Journal [18]: “Psychosurgery can be easilyperformed by the psychiatrist himself with thetool he might have in his pocket, and strangelyenough it may be harmless and effective.”
4 DBS in Psychiatry and the Pendulum of History 49
Coming back to the DBS of the early days,this method continued well into the seventies tobe rarely tested primarily for behavioural disor-ders [8]. Meanwhile, in that same decade,Bechtereva et al. [2] from Leningrad pioneeredchronic stimulation of thalamus and basal gan-glia in treatment of Parkinson’s disease.
4.3.2 “Modern” Applications of DBSin Psychiatry
The first use of modern era DBS in psychiatricdisorders had nothing to do with the observationof psychiatric and behavioural side effects ofSTN DBS, as claimed by some [20]. WhenVandewalle et al. [23] pioneered DBS for Tou-rette, and Nuttin et al. [17] DBS for OCD, both in1999, these workers were simply targeting thevery same brain structures that were stereotacti-cally lesioned in the past for same disorders.
4.4 Discussion
A review of the old scientific literature about DBSbears witness to the inaccuracy of several con-temporary statements, in which neurosurgeons areerroneously blamed for (mal)practices of the past,and criticised for neglecting multi-disciplinarityand ethical rules. How ironic and hollow theseaccusations are is evidenced by a recent publica-tion in the September 2009 issue of the Archive ofGeneral Psychiatry entitled “Scientific and EthicalIssues Related to Deep Brain Stimulation forDisorders of Mood, Behavior, and Thoughts”[19]. This paper summarises the results of a 2-dayconsensus conference held to examine scientificand ethical issues in the application of DBS inpsychiatry in order to “establish consensus amongparticipants about the design of future clinicaltrials of deep brain stimulation for disorders ofmood, behavior, and thought” and to “developstandards for the protection of human subjectsparticipating in such studies” [19]. Among the
30 participants at the meeting, 19 of which areauthors of the paper, there was not one singleneurosurgeon, although the authors insisted onmultidisciplinarity in relation to this neurosurgicalprocedure, but without including a single neuro-surgeon on the panel.
4.5 Conclusions
(a) DBS was not “originally introduced for thetreatment of movement disorders”. DBSstarted from the very beginning as a tool tostudy and eventually treat psychiatric illness.
(b) The first application of modern DBS inpsychiatric illness tried to mimic lesionalsurgery by implanting electrodes in the sametargets that were lesioned before for the sameconditions.
(c) While “It is ethically untenable for this workto proceed by neurosurgeons in isolationwithout psychiatrists determining the diag-nosis and suitability of patients for treat-ment” [9], it was indeed psychiatrists andneurologists who were working in isolation.Some of today’s self-promoted experts in thefield need to read history instead of accusingneurosurgeons as scapegoats. It is a scandalethat a consensus meeting on DBS in psy-chiatry with 30 participants insisting onmultidisciplinarity did not include a singleneurosurgeon.
(d) Multidisciplinarity in functional neurosur-gery, including psychosurgery is not new; ithas been the rule rather than the exceptionssince the very beginning and when therewere exceptions to multidisciplinarity it wasoften the psychiatrists and the neurologistswho chose to work alone. This pattern ofbehavior is unfortunately risking to repeatitself today.
Conflict of Interest Statement The author has occa-sionally received from Medtronic reimbursement for tra-vel expenses and honoraria for speaking at meetings.
50 M.I. Hariz
References
1. Baumeister AA. The Tulane Electrical BrainStimulation Program. A historical case study inmedical ethics. J Hist Neurosci. 2000;9:262–78.
2. Bechtereva NP, Kambarova DK, Smirnov VM,Shandurina AN. Using the brain’s latent abilities fortherapy: chronic intracerebral electrical stimulation. In:Sweet BW, Obrador S, Martín-Rodrígez JG, editors.Neurosurgical treatment in psychiatry, pain and epilepsy.Baltimore: University Park Press; 1977. p. 581–613.
3. Bickford RG, Petersen MC, Dodge HW Jr, Sem-Jacobsen CW. Observations on depth stimulation ofthe human brain through implanted electrographicleads. Mayo Clin Proc. 1953;28:181–7.
4. Delgado JM, Hamlin H, Chapman WP. Technique ofintracranial electrode implacement for recording andstimulation and its possible therapeutic value inpsychotic patients. Confin Neurol. 1952;12:315–9.
5. Delgado JM, Mark V, Sweet W, Ervin F, Weiss G,Bach-y-Rita G, Hagiwara R. Intracerebral radiostimulation and recording in completely freepatients. J Nerv Ment Dis. 1968;147:329–40.
6. Delgado JMR, Obrador S, Martín-Rodriguez JG.Two-way radio communication with the brain inpsychosurgical patients. In: Laitinen LV, LivingstoneKE, editors. Surgical approaches in psychiatry.Lancaster: Medical and Technical Publishing CoLtd; 1973. p. 215–23.
7. El-Hai J. The lobotomist. Hoboken: Wiley; 2005.8. Escobedo F, Fernández-Guardiola A, Solís G. Chronic
stimulation of the cingulum in humans with behaviourdisorders. In: Laitinen LV, Livingstone KE, editors.Surgical approaches in psychiatry. Lancaster: Medicaland Technical Publishing Co Ltd; 1973. p. 65–8.
9. Fins JJ, Rezai AR, Greenberg BD. Psychosurgery:avoiding an ethical redux while advancing atherapeutic future. Neurosurgery. 2006;59:713–6.
10. Heath RG. Electrical self-stimulation of the brain inMan. Am J Psychiatry. 1963;120:571–7.
11. Heath RG. Pleasure and brain activity in man: deepand surface electroencephalograms during orgasm.J Nerv Ment Dis. 1972;154:3–18.
12. Heath RG. Modulation of emotion with a brainpacemaker. Treatment for intractable psychiatricillness. J Nerv Ment Dis. 1977;165:300–17.
13. Kopell BH, Greenberg B, Rezai AR. Deep brainstimulation for psychiatric disorders. J ClinNeurophysiol. 2004;21:51–67.
14. Laitinen LV. Ethical aspects of psychiatric surgery.In: Sweet WH, Obrador S, Martín-Rodríguez JG,editors. Neurosurgical treatment in psychiatry, painand epilepsy. Baltimore: University Park Press; 1977.p. 483–8.
15. Malone DA Jr, Pandya MM. Behavioralneurosurgery. Adv Neurol. 2006;99:241–7.
16. Moan CE, Heath RG. Septal stimulation for theinitiation of heterosexual behavior in a homosexualmale. J Behav Ther Exp Psychiat. 1972;3:23–30.
17. Nuttin B, Cosyns P, Demeulemeester H, Gybels J,Meyerson B. Electrical stimulation in anterior limbsof internal capsules in patients with. Lancet.1999;354:1526.
18. Odegård O. Nye framsteg i psychiatrien. Tidskrift forden Norske Laegeforening. 1953;123:411–4.
19. Rabins P, Appleby BS, Brandt J, DeLong MR, DunnLB, Gabriëls L, Greenberg BD, Haber SN,Holtzheimer PE 3rd, Mari Z, Mayberg HS, McCannE, Mink SP, Rasmussen S, Schlaepfer TE, VawterDE, Vitek JL, Walkup J, Mathews DJ. Scientific andethical issues related to deep brain stimulation fordisorders of mood, behavior, and thought. Arch GenPsychiatry. 2009;66:931–7.
20. Schläpfer TE, Bewernick BH. Deep brain stimulationfor psychiatric disorders—state of the art. Adv TechStand Neurosurg. 2009;34:37–57.
21. Spiegel EA, Wycis HT, Marks M, Lee AS.Stereotaxic apparatus for operations on the humanbrain. Science. 1947;106:349–50.
22. Stelten BM, Noblesse LH, Ackermans L, Temel Y,Visser-Vandewalle V. The neurosurgical treatment ofaddiction. Neurosurg Focus. 2008;25(1):E5.
23. Vandewalle V, van der Linden C, Groenewegen HJ,Caemaert J. Stereotactic treatment of Gilles de la byhigh frequency stimulation of thalamus. Lancet.1999;353:724.
4 DBS in Psychiatry and the Pendulum of History 51

5Ablative Surgery for NeuropsychiatricDisorders: Past, Present, Future
Yosef Chodakiewitz, John Williams, Jacob Chodakiewitzand Garth Rees Cosgrove
5.1 Historical Perspective
The history of surgical intervention for psychi-atric disorders is a long, complex, and contro-versial one. The original use of surgical methodsto treat symptoms of the mind occurred in theprescientific era as far back as antiquity. Theancient practice of trephination involved using acylindrical saw to perform craniotomy. Literaturedating back to 1500 BC can be found describingtrephination to relieve psychiatric symptoms,including affective and psychotic disorders [1]. Itcan further be surmised that surgical trephinationwas occurring as far back as 5100 BC, based oncarbon dating of a trephined skull, which showedevidence of proper healing to suggest a surgicalwound origin rather than a traumatic origin,found at the Enshisheim burial site in France [2].
The modern scientific era of psychosurgerycan find its origins in the 19th century, whenstrong correlates between brain and behaviorwere starting to be drawn. Much of this work wasdone through clinicopathologic correlates ofparticular neurological insults leading to partic-ular cognitive dysfunction, as seen in the lan-guage aphasias described by Broca and Wernicke
from patient autopsy studies [3, 4]. The case in1848 of Phineas Gage, a railroad worker whosuffered an accident involving a sharp rodpiercing his skull and his brain’s frontal lobe, isanother famous example [5]. In Gage’s case,physically, he recovered surprisingly well.However, he was noted by those who knew himto have an undergone an obvious and significantpersonality change.
It was in this environment of brain-behaviorcorrelative science in the mid-late 1800s thatpresent day psychosurgery came into being, withthe Swiss psychiatrist Gottlieb Burckhardt per-forming the first procedures in 1888. Working toclinically apply the developing theories of neuro-psychiatric correlations, he performed bilateraltopectomy, which involved selective excision ofcortex from multiple foci [1, 6]. These earlyattempts were not clearly successful, and psy-chosurgery (a term not yet coined was notparticularly accepted by the neuropsychiatriccommunity. Years later in the 1930s, Fulton andJacobson demonstrated calming behavioral chan-ges, along with some changes in overall cognition,in chimpanzees as a result of surgical bilateralfrontal lobe lesions [7, 8]. This work by Fulton andJacobson particularly influenced the Portugueseneurologist Egas Moniz, who subsequently beganproposing the idea that an efficacious psychosur-gical procedure to relieve anxiety states in peoplewould involve interruption of afferent and efferentfibers of the frontal lobe [9, 10]. Furthermore, itwas in fact Moniz who coined the term “psycho-surgery” [10, 11]. Together with his neurosurgical
Y. Chodakiewitz (&) � J. Williams � G.R. CosgroveDepartment of Neurosurgery, Alpert MedicalSchool, Brown University, Providence, USA
J. ChodakiewitzDepartment of Neurosurgery, David Geffen Schoolof Medicine, UCLA, Los Angeles, USA
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0_5© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
53
colleague Almeida Lima, Moniz and Limadeveloped the procedure that came to be known asthe prefrontal leukotomy or lobotomy for psychi-atric disease [12].
Moniz’ and Lima’s original procedureinvolved the injection of alcohol into frontal lobewhite matter to sever connections apparentlygiving rise to mental illness [13]. Their firstpatient was a 63 year old woman suffering fromparanoid delusions, anxiety and melancholia; theoperation was deemed an overall success interms of ridding the patient of her psychosis andanxiety, though she remained with significantapathy and a blunted affect after the procedure [8,13]. Moniz and Lima continued to refine theirprefrontal leukotomy procedure, devising aninstrument known as the leukotome to make theirlesions rather than their original use of alcoholinjections, which otherwise often required sev-eral procedures for repeat injections. The leuko-tome consisted of a rod with a retractable wireloop that could be inserted into the white matterand rotated to create series of small circularlesions within the frontal lobe white matter tracts[8, 10, 13]. This procedure for psychiatric diseasewas now becoming much more accepted by thecommunity and resulted in Moniz receiving theNobel Prize in Medicine/Physiology for thiswork in 1949 [14].
Starting already in 1936, the neurologistWalter Freeman and the neurosurgeon JamesWatts began adapting Moniz’ and Lima’s pre-frontal leukotomy in the US. The Freeman-Wattsprefrontal lobotomy was performed via bilateralposterior frontal burr holes through which asmooth, blunt, calibrated blade was inserted tothe midline and then swept up and down to dis-connect the frontal lobes at the level of the genuof the corpus callosum [15].
At the time in the US, there were still noeffective psychoactive drugs available and psy-chiatric disease posed a particularly significantpublic health problem. In the late 1930s and early1940s, there were 477 American psychiatricinstitutions housing over 400,000 patients andtreatment of psychiatric illness was costing$1.5 billion annually [16, 17]. It had been arguedthat more widespread use of prefrontal
leukotomies would save American taxpayer$1 million per day, by relieving the heavy costs offunding the asylums [18]. Within this context ofthe great burden posed to society by mental ill-ness, Freeman further evolved the procedure andfervently promoted it in a mass-market fashion.
By 1948, Freeman began promoting his ownmodified surgical technique using a transorbitalapproach [19]. Before this modification, theprefrontal leukotomies had to be carried out byexperienced neurosurgeons under operatingroom conditions to gain appropriate intracranialaccess; these were conditions not widely avail-able in the psychiatric institutions. Freemanintended his transorbital leukotomy to be simpleand quick enough so that the procedure could beperformed in the office-setting by non-surgeons.The modified procedure involved using an ice-pick-like instrument, known as an orbitoclast,inserted underneath the upper eye-lid but overthe eye globe and then driven by a mallet throughthe orbital roof to a desired distance of 7 cminto the frontal lobe white matter. At that point,the orbitoclast would be swept side to side with adeft wrist movement to complete the lesionbefore being removed. The need for an anesthe-tist was also eliminated, as the procedure wasperformed on the patient in the immediate post-ictal phase after an electroconvulsive treatment[8, 10, 13, 19]. Freeman fervently popularizedthis procedure, opening up an infamous chapterin the history of psychosurgery in which histechnique was so enthusiastically received thatpsychosurgery was at times abused and indis-criminately applied. Complications arose relatedto its practice by unqualified practitioners inunsterile conditions using crude instruments withpoor anesthesia care and perioperative monitor-ing. Furthermore, the morbidity and neurologicsequelae from the procedure became more evi-dent over time, patient selection criteria werequestioned, and the procedure’s actual efficacywas questioned more criticially.
Freeman’s procedure (which also came to beknown as “the icepick lobotomy” [20]) quicklyfell out of favor with the neurosurgical estab-lishment, including with Watts, leading the twoformer collaborators to part ways soon thereafter
54 Y. Chodakiewitz et al.
[13]. Nevertheless, given the public health crisisregarding the mass management of psychiatricillness in the population before the introduction ofeffective psychotropic medications with chlor-promazine in 1954, the Freeman lobotomy con-tinued to be widely performed, with an estimated60,000 procedures performed between 1936 and1956 [15]. However, with the rejection of Free-man’s procedure by neurosurgeons, and thecontinuing social recognition of its excessivelyexuberant application, along with the availabilityof effective neuroleptic drugs, the notorious era ofthe Freeman frontal lobotomy mostly came to anend in the late 1950s [1, 8, 13, 21].
At the same time that Freeman was over-zealously promoting his transorbital leukotomy,more responsible practitioners of the day wereemploying a safer and more restricted approachto psychosurgery [13]. William Beecher Scoville,a neurosurgical contemporary of Freeman, wasthe first to introduce the concept of minimalismin psychosurgery, which very much divergedfrom Freeman’s industrial scale concept. Theidea was to maximize therapeutic efficacy, whileminimizing unnecessary morbidity and undesir-able sequelae to the patient. In the late 1940s,Scoville developed the technique of orbitalundercutting to selectively ablate orbitofrontalcortex in a more anatomically localized mannerthrough bifrontal trephinations [13, 22, 23].Other more precise open surgical procedureswere also described during this time period andincluded bilateral inferior leucotomy, bimedialfrontal leucotomy and anterior cingulectomies,all guided by the most current understanding atthat time, of the neuroanatomic pathwaysunderlying psychiatric illness.
The goal of making small, accurate andeffective lesions in psychiatric patients withoutserious mortality and morbidity was the majorimpetus for the development of stereotactic neu-rosurgery [10, 13, 20]. All intracranial psycho-surgery today stems from the stereotactic school,including both contemporary ablative techniquesand deep brain stimulation techniques [20].
In stereotactic neurosurgery, the brain is ref-erenced against a fixed frame of reference,assigning a specific coordinate system to define
any point in the brain in Cartesian three dimen-sional space [24]. Stereotactically guided neuro-surgical procedures were first devised for use inhumans in 1947 by Ernst Spiegel and HenryWycis, who designed a stereotactic system ref-erenced by X-ray ventriculography to performdorsomedial thalamotomy, representing the firstattempt at a minimally invasive subcorticalablative procedure [13, 24]. Various other ste-reotactic systems were developed for clinical useand lesioning of deep brain structures for treat-ment of psychiatric disease began. Jean Talairachfirst described ablation in the anterior internalcapsule to treat psychiatric disease in 1949 [25,26], and Leksell began using his stereotacticsystem to further study and develop methods toperform minimally invasive anterior capsulot-omy to treat a variety of psychiatric disorders.
Soon after introducing his stereotactic frame in1951, Leksell envisioned the concept of radio-surgery to improve upon the minimally invasivenature of stereotactic procedures [25]. Open ste-reotactic procedures still required a scalp incision,boney access through the cranial vault and apenetrating needle trajectory through the brainparyenchyma to the target, but Leksell imaginedthat sharply focused radiation beams from exter-nal radiation sources could summate at the ste-reotactic target, to create the desired lesioncompletely non-invasively. Leksell’s concept ofstereotactic radiosurgery laid the groundwork forthe eventual development of the gamma-knifetechnology, which became commercially avail-able in the 1980s [13]. In the present day, both“traditional open” stereotactic surgery and mini-mally invasive stereotactic radiosurgery are pur-sued as options in psychosurgery. In particular,gamma knife is being investigated for carrying outanterior capsulotomy in a double blind random-ized control trial in Brazil, the first study of its kindfor a psychiatric lesion procedure [8, 26, 27].
The mortality and morbidity associated withthe imprecise methods and risky approaches ofthe Freeman lobotomy era and other earlierpsychosurgical practices were largely erased withthe advent of modern stereotactic techniques.A variety of targets were subsequently exploredincluding the anterior cingulate gyrus, anterior
5 Ablative Surgery for Neuropsychiatric Disorders: Past, Present, Future 55
limb of the internal capsule and the subcaudateregions. Much of our best contemporary under-standing of the neurophysiologic basis of psy-chiatric disease focuses on the limbic system andits neural circuitry connecting with the frontallobes and basal ganglia. Consequently, nearly allcurrent psychosurgical interventions place theirtarget in one or more aspect of the limbic systemand its connections.
5.2 Relevant Anatomyand Physiology
An understanding of the frontal-subcortical cir-cuitry involved in psychiatric diseases is neces-sary for understanding target selection inpsychosurgical lesioning. Executive dysfunction,apathy, and impulsivity are hallmarks of frontal-subfrontal circuit dysfunction, and the psychiat-ric illnesses treated by psychosurgery, such asdepression and obsessive-compulsive disorder(OCD), are associated with dysfunctional neuralsubstrates in these circuits as well [28].
To understand the importance of the frontal-subcortical circuits of interest, a review of sub-cortical targets is essential. All three circuitsconnect through the basal ganglia. The basalganglia are a group of nuclei situated at the baseof the forebrain and include the striatum (caudatenucleus and putamen), the globus pallidus, thesubstantia nigra, the nucleus accumbens, and thesubthalamic nucleus, each with its own complexinternal anatomical and neurochemical organi-zation. These nuclei are involved in variedfunctions, including voluntary motor control,procedural learning, including those involved inbehavior and habits, eye movements, as well ascognitive and emotional functions [29]. The mostunified, current theory relating the varied nucleisuggests that they are all involved in actionselection or the decision of which of severalpossible behavioral actions to take at any giventime [30]. Experimental evidence indicates thebasal ganglia inhibit a number of motor systems,wherein discontinuation of this inhibition allowsa given motor system to become active. The
action selections by the basal ganglia are heavilyinfluenced by input from the prefrontal circuitrydescribed [31, 32]. Lesions in the circuitry con-necting the frontal lobes to the basal ganglia cangenerate disorders closely resembling frontallobe lesions. These “striatal” syndromes have notbeen extensively studied, but disinhibition andexecutive dysfunction are documented conse-quences [32].
Lesions in basal ganglia structures are impli-cated as the major substrate for a number ofneurological conditions. Movement disorders,including Parkinson’s and Huntington’s disease,are associated with the degeneration of dopa-mine-producing cells in the substantia nigra parscompacta and damage to the striatum, respec-tively [30, 33]. Parkinson’s patients exhibitdepression, dementia and confusional states.Dysfunction in the basal ganglia are also impli-cated in disorders of behavior control, includingTourette’s syndrome, hemiballismus, and obses-sive-compulsive disorder (OCD) [34]. Addition-ally, positron emission tomography studies ofpatients with OCD show increased metabolicfunction in the frontal lobes, cingulum, andcaudate nucleus [34].
Arguably, more critical to the success ofpsychosurgery are the functions and neuroanat-omy of the limbic system. The system wasnamed by Paul Broca, with limbic originatingfrom the Latin limbus, meaning “border”, as itlies between two functionally different portionsof the brain; the neocortex, which mediatesexternal stimuli, and the brainstem, whichmediates internal stimuli [35, 36]. The limbiclobe is an intricate set of brain structures, broadlyconsisting of the arcuate convolution of the cin-gulate and parahippocampal gyri of the medialaspect of the cerebral hemispheres [37, 38].These arcuate structures are situated around thethalamus bilaterally, composed of a conglomer-ate of structures from the telencephalon, dien-cephalon, and mesencephalon. The limbicsystem also includes the olfactory bulbs, hippo-campus, amygdala, anterior thalamic nuclei,fornix, column of fornix, mammillary body,septum pellucidum, habenular commissure, cin-gulate gyrus, parahippocampal gyrus, limbic
56 Y. Chodakiewitz et al.
cortex and limbic midbrain regions [39]. Thesestructures have myriad functional capacities,including memory, emotion, behavior, motiva-tion, long-term memory, and olfaction. It is bestknown as the central system for human emotionand memory formation, and includes the famedPapez circuit [37–39].
The location and role of the limbic system asmediator between internal and external stimuli asreported by the neocortex and primitive brainallow it to regulate the complex processes ofsubjective, somatic, visceral, and behavioralstimuli integration and modulation necessary foremotional experience. Reciprocal connectionsconverge in the amygdala, symmetric almondshaped nuclei positioned at the anterior end ofthe hippocampi, which are critically important inemotional processing and memory [40]. Lesionsin the amygdala in rhesus monkeys results in theKluver-Bucy syndrome, characterized by limitedemotional arousal regardless of presence orabsence of threatening stimuli, hypersexuality,hyperorality, hyperphagia, amnesia andagnosia [41].
The origins of the frontal-subcortical circuitsare all located within the frontal lobe. A simpli-fied model of frontal lobe circuitry consists offive major pathways. Two of the pathways arethe motor and oculomotor circuits, which origi-nate in the frontal eye fields and drive eyemovement, but will not be discussed in detailhere. The remaining three circuits are behavior-ally relevant with origins in the prefrontal cortex;a dorsolateral prefrontal circuit, which is regar-ded as the mediator of executive function; theanterior cingulated circuit, which governs moti-vational functions; and the orbitofrontal circuit,which has two subdivisions: the lateral andmedial [28]. All five circuits share commonstructures and are both parallel and contiguous,yet they are distinctly partitioned anatomically.Brain regions linked by these circuits are func-tionally related; those governing limbic functionsynapse heavily with other limbic structures andthose related to executive function have diverseconnections to higher cortical areas involved incognition [42–45].
The dorsolateral prefrontal circuit begins inthe dorsolateral region of the frontal lobe inBroadmann’s areas 9 and 10. Neurons from thislocus project to the head of the dorsolateral headof the caudate nucleus and medial putamen of thebasal ganglia, and the projections communicateinformation regarding “executive” function [45].Executive function integrates anticipation, goalselection, planning, observation and incorpora-tion of external and internal feedback in taskperformance [46]. The clinicopathological corre-lation between lesions in this circuit and psychi-atric illness is elucidated by dorsolateralprefrontal syndrome. Individuals affected by thiscondition have defects in executive functionmarked by marked perseveration, often measuredwith the Wisconsin Card Sort Test, designed togauge test-takers’ ability to shift strategies [47].Other features include impaired verbal and designfluency, memory search strategy, motor pro-gramming, and organizational and constructionalstrategies during learning and copying tasks. Aswith all frontal circuits, similar syndromic fea-tures have been reported with lesions to efferentbasal ganglia regions [48, 49]. Psychiatric syn-dromes including schizophrenia, depression andOCD display impaired executive function, sug-gesting that this circuit is involved [28].
The orbitofrontal circuit consists of the medialand lateral divisions. The lateral division has itsorigin in the lateral orbital gyrus of Brodmann’sarea 11 as well as the medial inferior frontal gyrusof areas 10 and 47 [50]. Lateral division projec-tions lead to the ventromedial caudate [51]. Themedial division originates in the inferomedialprefrontal cortex in the gyrus rectus and medialorbital gyrus of Brodmann’s area 11, projecting tothe medial nucleus accumbens [50, 52]. As theorbitofrontal cortex is considered to be the neo-cortical representation of the limbic system, itfunctions in calculating appropriate strategy,timing, and place for behavioral responses toenvironmental stimuli [53]. Thus, lesions in thecircuit sever the frontal monitoring and modula-tion mechanisms necessary to curb impulses fromthe limbic system, resulting in orbitofrontal syn-drome with characteristic disinhibition, lability,
5 Ablative Surgery for Neuropsychiatric Disorders: Past, Present, Future 57

and irritability [54]. Affected patients appeartactless and may exhibit inappropriate jocularity,improper sexual remarks or gestures. Patientsmay also display transient irritable outbursts,inattention, distractibility, and increased motoractivity along with hypomania or mania [55, 56].Extreme changes in personality are typically inthe setting of bilateral insults to the orbitofrontalregions, however unilateral lesions result in sim-ilar changes with lesions to the right hemispheredemonstrating disproportionately greater loss ofinhibition [57, 58]. Similarly, patients withlesions to the ventral caudate have been docu-mented exhibiting disinhibition, euphoria,impulsivity, and inappropriate social behaviors,showing the reciprocal relationship between theefferent and afferent ends of the circuit [59].
The anterior cingulate circuit originates in theanterior cingulate gyrus (Broadmann’s area 24)and projects to the ventral striatum, including theventromedial caudate, ventral putamen, nucleusaccumbens, and olfactory tubercle, all of whichare referred to collectively as the limbic striatum[60]. Anterior cingulate syndrome at its worstcan result in profound apathy and akinetic mut-ism, a waking state of profound apathy, absenceof motor and psychic initiative with a lack ofspontaneous movement; indifference to pain,thirst, and hunger; absent verbalization; andfailure to respond to commands [61, 62]. Thiscondition has been documented in bilaterallesions to the anterior cingulate cortex and vas-cular and neoplastic lesions involving the ventralstriatum, as well as and obstructive hydroceph-alus in the region of the third ventricle and [28,61]. A less severe form of this condition termed“abulia” involves similar psychomotor qualities,including lack of spontaneity, apathy, anddecreased speech and movement. These behav-ioral syndromes highlight the importance of thefrontal lobe pathways in regulating executive andsocial function as well as mood and motivation[61, 63].
5.3 Contemporary Psychosurgery
5.3.1 Established PsychosurgicalProcedures and Indicationsin the Modern Era
With the application of stereotactic techniques inpsychosurgery, several minimally invasive tech-niques were developed to treat psychiatric illnesswith impressive results. There are currently fouraccepted psychosurgical techniques, each withvaried targets but all performed bilaterally understereotactic guidance for optimal precision intargeting. They have evolved to a level ofsophistication and critical appraisal far beyond theprimitive operations performed by non-expertphysicians in the Freeman era of frontal lobotomy.
Anterior Cingulotomy In 1947, Fulton pub-lished evidence that stimulating the anteriorcingulate in monkeys resulted in significantlyless fearful but more aggressive subjects withautonomic responses that mimicked those ofheightened emotion [59]. Fulton postulated thatmodulation of the anterior cingulated cortexcould mitigate psychiatric disease, and in theearly 1950s, a British group first performed theprocedure [64]. The procedure was popularizedby the American surgeon Ballantine in the 1960s,who subsequently conducted research over dec-ades [65].
The procedure is currently employed to treatrefractory major affective disorder, severechronic pain, chronic anxiety states and OCD[66]. The cingulate plays a crucial role in thePapez circuit, and OCD studies have shownincreased metabolism in the anterior cingulate inindividuals affected by the disorder [37, 38, 67].The procedure is not performed until patients areaccepted through a rigorous multidisciplinaryscreen, after which bilateral stereotactic thermo-coagulation lesions are placed bilaterally in thecingulum [68]. Retrospective studies have shownthat 25–30 % of medically refractory OCD
58 Y. Chodakiewitz et al.
patients were considered improved post-opera-tively, where treatment success was consideredto be improvement of 35 % or greater on theYale-Brown OCD Scale [69]. Furthermore, thestudy highlighted the relative safety of the pro-cedure: no surgery-related deaths were reported,the only complications reported in the post-operative period were seizures responsive tomedication. In the first prospective study, asimilar success rate of 25–30 % for medically-refractory OCD patients was reported to achievethe same level of improvement [69]. Anotherprospective study showed 32 % met criteria forresponse to treatment and an additional 14 %were found to be partial responders at an averageof 32 months follow-up. Complications wereagain limited: one patient reported increasedurinary incontinence, one had drug responsiveseizures, and one committed suicide. The mostrecent study of response to anterior cingulotomyby those with medically refractory OCD showedfull response (35 % or more severity reduction onthe Yale-Brown Scale) rates of 47 % of fullresponse and 22 % partial response (24–35 %reduction on the Yale-Brown Scale) at a meanfollow-up of 63.8 months, the most impressiveresults yet [70]. Additionally, comorbid majordepressive disorder severity decreased by 17 %in the same study.
Anterior Capsulotomy This technique wasdeveloped by Talairach in France in the 1940s.Indications for this procedure initially included awide range of conditions, including schizophre-nia, depression, chronic anxiety and obsessionalneurosis [66]. It uses thermocoagulation orgamma knife to lesion the fronto-limbic fibersthat pass between caudate and putamen in theinternal capsule of the basal ganglia [71]. WhenLeksell initially operated on patients with psy-chiatric disease, he reported a 50 % satisfactoryresponse with “obsessional neurosis” and 48 %with depression, while lower rates of 20 and 14 %satisfactory response were observed with “anxi-ety neurosis” and schizophrenia, respectively[72]. When compared to anterior cingulotomy,studies have reported a higher index of efficacywith anterior capsulotomy, and success rates ashigh as 70 % have been published. Unfortunately,
the procedure is also associated with the highestfrequency of complications and morbidity, mostnotably weight gain, confusion, nocturnal incon-tinence and cognitive dysfunction [72].
Subcaudate Tractotomy Designed in Eng-land by Geoffrey Knight in 1964, this approachtargets fibers from the frontal lobes to subcorticalstructures in the limbic system, including theamygdala [73]. The procedure was created as amethod of reducing the extent of frontal lobelesioning, and has been more popular in the UKthan the US since its advent. Like the anteriorcingulotomy, the procedure is indicated foraffective and anxiety disorders, including severe,refractory OCD and depression. However, it isnot indicated for cognitive disorders. The precisetarget of the subcaudate tractotomy is the sub-stantia innominata, directly inferior and adjacentto the head of the caudate nucleus [10]. Origi-nally, the procedure involved the placement ofradioactive seeds in the frontal lobes, but iscurrently performed with stereotactic thermoco-agulation. In the first major assessment of theefficacy of the procedure in the 1970s, over 60 %of patients with depression or anxiety showedimprovement with nearly 50 % of patientsaffected by obsessive-compulsive disordershowing improvement [74]. A subsequent retro-spective study reported a response rate of 34 % inpatients undergoing the procedure from 1979 to1991 [74, 75]. Like the anterior capsulotomyprocedure, these high rates of efficacy come at ahigher cost than is associated with anterior cin-gulotomy. Approximately 1.6 % of patients suf-fered from seizures after surgery, and just under7 % reported negative personality changes post-operatively [74]. However, a psychometric studyperformed on 23 patients pre-operatively and attwo intervals post-operatively showed no majorcognitive deficits [76].
Limbic Leucotomy This technique combinesthe lesions of the anterior cingulotomy and sub-caudate tractotomy, thereby disrupting orbital-frontal-thalamic pathways. The intervention wasintroduced by a group lead by Kelley andMitchell-Heggs, and it involves lesioning targetswith a cryoprobe or thermocoagulation [77]. Thatgroup’s first assessment of the procedure was a
5 Ablative Surgery for Neuropsychiatric Disorders: Past, Present, Future 59

retrospective follow-up study after 16 monthsusing a 5-point global rating scale. Of 66 patientswith a variety of illnesses, 89 % of those withOCD, 66 % of those with chronic anxiety, and78 % of those with depression reportedimprovement [77].
The most substantive review of the procedurefrom the Massachusetts General Hospital reports36–50 % of patients with refractory OCD andmajor depressive disorder responded to thetreatment [78]. Additionally, 4 of 5 patientstreated with limbic leucotomy for medicallyrefractory OCD or schizoaffective disorder whoengaged in self-mutilation showed sustainedreduction in injurious behavior and 2 of 3 inassaultive behavior after a mean follow-up of31.5 months [78]. Though the procedure inher-ently calls for more lesions than either the ante-rior cingulotomy or subcaudate tractotomy alone,few adverse post-operative effects were reported.
Each of these interventions has shown suffi-cient evidence for efficacy without significantharm to justify their continued practice despitepsychosurgery’s sordid past. Any medicaltreatment that demonstrated the level of efficacyin the treatment of profound, refractory mentalillness that these four procedures have, couldwell be considered a “miracle intervention”.However, these studies are largely retrospective,and prospective studies with better efforts tocoordinate outcome assessment measures will benecessary to truly establish the success rates ofany current or future form of psychiatric neu-rosurgery along with continued longitudinalfollow-up studies to assess long-term outcomesin those that have already undergone existingoperations. Efforts to train surgeons outside ofmajor surgical centers will also be necessary toreduce surgical center bias and unify outcomemeasures to allow for meta-analyses of theseprocedures.
5.3.2 Future Potential PsychosurgicalIndications and Targets
As the field of neuroscience continues to expand,so will theoretical targets for ablation in the
treatment of psychiatric illness. President Oba-ma’s BRAIN Initiative with its 3 billion dollarbudget should provide the awareness and fundingto elucidate the circuitry and substrates underlyingpsychiatric disease on an order never seen before.Furthermore, advances in the understanding of thephysiologic alterations underlying the efficacy ofdeep brain stimulation will provide more insightinto the viability of psychosurgical procedureswith the same targets as DBS. This evolution willbe necessary as pharmacologic treatmentsadvance, making refractory illness more and morechallenging to treat.
One of the most promising areas of progressin psychosurgery may be the combination ofsurgical intervention with electroconvulsivetherapeutic techniques. Electroconvulsive ther-apy (ECT), formerly known as “shock therapy”,is another somatic or physical treatment forpsychiatric illness. Transcranial magnetic stimu-lation (TMS) may achieve similar micro-electri-cal changes as electroconvulsive therapy. TMSinvolves the placement of a magnetic coil againstthe scalp, through which pulses of electricalcurrent are sent, generating a magnetic field thatcan depolarize superficial cortical neurons [79].Neural responses vary in accordance to theintensity of pulses, regions targeted, and numberof sites targeted, and neurochemical changesaffected are similar to those found with phar-macologic treatments and ECT [80–82]. Analy-ses of TCM in depression have been equivocal,but convincing evidence has been accumulatingsuggesting that 10 Hz rTMS over the left dor-solateral prefrontal cortex can improve depres-sion in a specific subset of patients [83].
ECT and TMS are relatively non-specific intheir delivery of electrical pulses to the brain.A combination of electrical stimulation withsurgical placement of electrodes for better deliv-ery may have additional benefits. Implantableelectrodes have been used widely for focal mod-ulation of the vagal nerve for epilepsy treatmentwith good results [84, 85]. The vagus nerve is animportant conduit for information relay from thebody to the brain and serves to cover much of thedistance of autonomic feedback loops. The nervedelivers input to the forebrain via the parabrachial
60 Y. Chodakiewitz et al.

nucleus and locus ceruleus, which connect tocentral structures in the limbic system, such as theamygdala and hypothalamus [86]. Vagal nervestimulation (VNS) has been explored withincreasing reports of long-term success in thetreatment for refractory depression [87]. Researchhas demonstrated VNS has a role in increasingserotonergic and noradrenergic activity in thebrain with evidence that it increases perfusion oflimbic structures [88, 89]. VNS implantation isrelatively minimal in invasiveness with an elec-trode placed on the nerve in the carotid region ofthe neck and a battery typically placed subcuta-neously over the pectoralis major. Complicationsin the post-operative period are likely related tointra-vagal cross talk phenomena with primaryadverse effects being pain, cough, vocal cordparalysis, hoarseness, nausea, and concerning buttransient and rare, reports of asystole and dyspnea[90, 91]. The procedure has been generally welltolerated in epilepsy patients, and there ismounting evidence to suggest that it is a viableextra-cranial surgical intervention that can pro-vide relief for refractory depression without theneed for attempts at more invasive procedures.
Advances in genetics and bioengineering haveopened an entirely new subfield in the arena ofpsychosurgery: constructive psychosurgery.Lesioning has been the mainstay of psychosur-gery since its advent, and even less destructivemanipulations of neural function such as deepbrain stimulation (discussed below) are predi-cated in functional strategies. Psychosurgery,thus far, has been limited to strategies that pro-mote desirable behavior by inhibiting activitythat either promotes undesirable behavior orinhibits desirable behavior. With constructivepsychosurgery, there is promise for techniquesthat augment positive function as opposed toablating the negative. If and when geneticmarkers for psychiatric illness are elucidated,targeted gene therapy could offer lasting relief.Progress in the understanding of the intersectionsof infectious, neoplastic, and inflammatorydisease processes could shed light on howinflammatory chemical factors modulate electro-chemical equilibria in the brain and potentiatepsychiatric illness [92]. Evidence is mounting to
support the idea that microglia play a significantrole in the development of the brain andinflammatory processes that may contribute tothe pathogenesis of psychiatric illness [93].Implanting genetically modified host immunecells to dampen inflammatory processes or usingestablished gene therapy techniques to deliverviral vectors that will alter the genetic expressionof inflammatory molecules could be the keytherapeutic advances in mental illness [92, 93].Delivery of cellular products such as stem cells todegenerated or dysregulated parenchyma couldenhance regeneration and recovery, promotinghealthier behavior and psychiatric states. Stemcell research has already shown success in otherneurologic disease and holds great promise inpsychiatric disease [94, 95].
5.3.3 Established Ablative Methodsin Psychosurgery
In addition to the choosing optimal stereotactictarget for specific psychosurgical candidate, thesurgeon must decide on the instrument for cre-ating the desired lesion. Methods of stereotacti-cally creating precisely focused CNS lesionscontinue to be investigated today [96]. Spiegeland Wycis made electrolytic lesions for theiroriginal stereotactic procedures [96–98]. Overthe years other modalities using focused heat,cold, alcohol, radiofrequency and ultrasoundhave also been attempted. Various ablatingmodalities continue to be used today in psycho-surgery, and the particular modality used willdepend on what has been used historically in thegiven psychosurgical procedure.
Thermocoagulation for lesioning is an accep-ted option in several of the traditional psycho-surgical procedures, including anteriorcingulotomy, limbic leukotomy, and anteriorcapsulotomy [8, 27, 99]. For anterior capsulot-omy, Gamma-knife is another relatively neweraccepted modality; it has been used to performcapsulotomy for over 18 years. Gamma-knifeanterior capsulotomy appears similar to the effi-cacy of thermocoagulation [8, 100], while elim-inating the need for craniotomy and open
5 Ablative Surgery for Neuropsychiatric Disorders: Past, Present, Future 61

surgery. It also produces comparatively smallerlesions and can be performed as an outpatientprocedure [27]. However, despite the less inva-sive nature of gamma-knife radiosurgery overtraditional invasive stereotactic surgery, radio-surgery still includes serious side-effects such asradiation-induced edema and necrosis anddelayed cyst formation [8].
Gamma-knife anterior capsulotomy forrefractory OCD is currently being investigated ina double-blind control study, a first study of thiskind for any ablative psychosurgical procedure[8, 26, 27]. In limbic leukotomy, lesions made byfreezing with a cryoprobe have also been used asan alternative to thermocoagulation [77, 99].
In stereotactic subcaudate tractotomy, aunique ablative modality was originally used.Small rod-shaped seeds of radioactive yttrium-90are placed at the stereotactic targets. Beta-radia-tion emitted from the implanted seeds destroysthe surrounding white matter up to 2 mm fromthe surface of the seed, producing lesion volumesof approximately 2 cm3 [8, 10, 27, 101, 102].However, in 1995 yttrium-90 was no longeravailable and so a modified version of the ori-ginal procedure now makes the lesion usingthermocoagulation instead [8, 103].
5.3.4 Ablation Versus Stimulation
While the practice of psychosurgery has contin-ued to develop and become more refined over theyears, it has done so on a much smaller scale inthe aftermath of the Freeman lobotomy era of the1940s and 1950s. While there have been decadesof experience and demonstrated efficacy of theablative psychosurgical procedures describedabove, the practice of psychosurgery remainedlimited to very few centers throughout the world.This restricted development is likely largely aresult of the notoriety of the Freeman lobotomy,which created a stigma for psychosurgery and itsassociated methodology of surgical lesioning.However, in recent years, with the demonstratedsuccess of deep brain stimulation technology inthe neurosurgical treatment of disorders such asessential tremor and Parkinson’s disease, there is
now resurgent enthusiasm in psychosurgeryresearch and practice using DBS for neuromod-ulation, rather than the historical practice of le-sioning in psychosurgery.
From its applications in the treatment ofmovement disorders, the early experience withDBS suggested that it worked functionally tomimic a lesion, but was reversible. This lesion-mimicry theory was based on the clinical obser-vations that the motor effect of high-frequencystimulation of the subthalamic nucleus (STN) orVIM-Thalamus resembled those followinglesions of those nuclei [104]. DBS is thus a moreforgiving technology to the neurosurgeon andserves as a more palatable concept for psycho-surgical intervention to the general public. Inaddition, DBS offers particular advantages as aninvestigational tool: (i) it is amenable to studyunder blinded placebo-controlled conditions withthe ability to turn the stimulator on and off at will,and (ii) its non-destructive and reversible naturefacilitates safer and ethical exploration of newbrain targets [105]. For these reasons, manyassume that DBS is inherently superior to lesion-ing and argue that the future of psychosurgicalpractice lies with DBS, while lesioning will berelegated to history. However, DBS is extremelyexpensive and time intensive requiring continuousprogramming and replacements. It is important torecognize that the respective roles of both DBSand lesioning in the future of psychosurgery arestill being debated, with separate benefits anddrawbacks to each modality in their present states.Despite the excitement surrounding DBS in psy-chosurgery, lesioning still warrants strong con-sideration for continued study and practice.
Despite the early DBS clinical experiencesuggesting that DBS functioned in lesion-mim-icking fashion, the precise therapeutic mecha-nism of DBS remains poorly understood to thisday. While DBS target selection to date has lar-gely been based on prior lesioning experience[105], it is clear that the previous analogybetween DBS and lesioning is overly simplistic.The two modalities are actually quite far frombeing functionally or clinically equivalent, astheir clinical effect can diverge depending onseveral factors.
62 Y. Chodakiewitz et al.
Experience from use of DBS in treatment forParkinson’s disease (PD) and essential tremor(ET) showed that, even at the same target nucleus,clinical effects did not always mimic lesions andin fact opposite clinical effects on motor symp-toms could be seen depending on stimulationfrequency. In PD, high frequency stimulation([130 Hz) at the STN improved motor symp-toms, while some low frequency stimulationlevels (10 Hz) actually worsened motor symp-toms, as compared to stimulation off [104]. Sim-ilarly, for ET, thalamic DBS at low frequency(\50 Hz) would fail to suppress tremor and couldeven be seen to worsen tremor as compared tostimulation off, while high frequency stimulation([90 Hz) did suppress tremor [105].
The functional non-equivalence between DBSand lesioning can also be seen in their differingeffects at particular targets. Studies carried out inParkinsonian monkeys found opposite effects onmotor symptoms when comparing GPe lesionsand GPe DBS. GPe lesions worsened motorsymptoms, while GPe DBS ameliorated motorsymptoms [105]. Furthermore, high-frequencystimulation (HFS) generally behaves oppositelydepending on whether it is stimulating greymatter or white matter. The effect of HFS cangenerally be said to be inhibitory and more“lesion-like” on grey matter, while it is generallyactivating on white matter [106]. The moleculareffects and neurophysiologic mechanism ofaction of DBS is clearly much more complicatedthan simple lesion-mimicry. While DBS some-times does appear to mimic lesions clinically, thecomparative clinical effects depend on specifictarget tissues and stimulation frequencies. Themechanism of DBS remains incompletelyunderstood, and it is clear we cannot assumeDBS and lesions in general to be clinicallyequivalent.
With the recognition that DBS and lesioningare neither physiologically nor always clinicallyequivalent, we ought to also recognize thatexperience with DBS in psychosurgery is still inits infancy and relatively minimal. In contrast,there is much experience with lesioning, span-ning decades, demonstrating its various indica-tions and efficacy, including in the long term.
Therefore, while investigational DBS targets forpsychiatric disease are mostly based on the his-torical lesioning targets, it is not quite the casethat DBS has supplanted lesioning techniques inpsychosurgery, nor is it obvious that it will do so.More experience with DBS as a psychosurgicalintervention will be required before such ajudgment can be made.
Beyond recognizing the physiologic andclinical non-equivalence between ablative tech-niques and DBS, there are practical factors toconsider which in the long run may continue tofavor ablative methods over DBS in developingpsychosurgery as a more standard option inpsychiatric treatment. For one, the clinical costsof DBS far outweigh the costs of its ablativecounterpart. With DBS, there is ongoing costsstemming from required multiple return follow-ups over the short-term and long-term. Theseinvolve follow-ups to adjust stimulation settings,as well as to repair or replace components of theimplanted hardware. In particular, given thehigh-frequency stimulation settings that aregenerally required to achieve clinical benefit forpsychiatric disorders, inevitable battery changesare currently required approximately every 10–-18 months [107]. The initial cost to have a DBSsystem implanted is between $50,000 and$120,000 and the cost to replace a battery isbetween $10,000 and $25,000 [108–110]. Thehigh cost of DBS systems and the dependence onhighly specialized multidisciplinary centers tomanage its long-term follow-up care limits use ofDBS as a psychosurgical modality to developednations. Since refractory psychiatric disease isalso prevalent in less developed countries, themore economical ablative techniques have avaluable role to play in these countries whereDBS will still not be available.
Another disadvantage of DBS systems, incomparison to ablative methods, stems from thevery nature of having implanted hardware andthe additional possible complications, such aselectrode lead fracture, increased risk of infec-tion, and patient compliance issues [105]. Elec-trode leads can migrate within the parenchyma,distancing them from their intended targets orcausing them to become disconnected from their
5 Ablative Surgery for Neuropsychiatric Disorders: Past, Present, Future 63
power source. Implanted metal is a contraindi-cation for MRI, meaning patients with DBSimplants would have to undergo surgical removalto accurately assess new onset focal neurologicaldeficits related to any etiology. Given the possi-bility of damaging the implanted hardware, DBSsystems may be contraindicated in certain con-ditions with certain behaviors, such in Tourette’ssyndrome with head-banging behaviors; ifinvestigations prove there to be a comparativelyefficacious target for either ablation or DBS inthese types of patients, they therefore may bebetter served by an ablative option.
A commonly touted feature DBS is the abilityto fine-tune stimulation parameters after implan-tation. Theoretically, this offers an advantage ofDBS over lesioning procedures, as it wouldfacilitate maximization of therapeutic benefit ofstimulation while minimizing side-effects to thepatient over time. While this feature is useful inthe movement disorder realm, where the thera-peutic effects are objectively observable, it maynot be clear how to tune DBS systems whenthere may be no overt effect of stimulation, as inpsychiatric disorders [104]. Therefore, it is notclear that this theoretic of advantage of DBS overablations is as strong in the psychosurgical realm,as it is in the movement disorder arena.
Finally, a tolerance effect to DBS has beenobserved to arise in some of the movement dis-order patients. In these patients, at given stimu-lation parameters, therapeutic effectiveness is lostover time. Consequently, such patients mayrequire progressively increasing current outputfor continued symptomatic control, leading tobattery failure and impractical number of batteryreplacements. In fact, in such cases, the DBSelectrodes themselves have sometimes been usedto produce therapeutic radiofrequency deliveredlesions before surgical removal of hardware[111]. The observed tolerance effect that occurs insome DBS cases may be due to development oftrue physiologic tolerance or due to loss of earlierplacebo effect. If tolerance were to develop in apsychosurgical patient treated with DBS, it ispossible such a patient may still benefit from alesioning procedure. Ablative psychosurgery
over the long term has shown increasing rates ofsuccessful responses as time goes on after theprocedure [70]. This observation from the abla-tive psychosurgical experience supports its long-term efficacy and argues against any placeboresponse producing the benefit from thismodality.
5.4 Conclusions
Surgical interventions for the treatment of psy-chiatric disease have a long history. Before theavailability of effective psychotropic drugs, thewidespread practice of psychosurgery reached adramatic peak in the mid 20th century, with thenotorious era of the Freeman lobotomy. Thepractice of psychosurgery continued on a muchsmaller scale for medically-refractory psychiatricpatients, continuing to develop with a concept ofminimalism out of the school of stereotaxy inneurosurgery. The modern era of psychosurgeryhas established four procedures with extensiveexperience supporting their indications and effi-cacies in properly selected patients. All of mod-ern intracranial psychosurgery is stereotactic innature, though historically interventions havebeen lesion-based. More recently, the idea ofpsychosurgery has been met with renewedenthusiasm, favoring DBS to avoid the historicdependence on lesioning. While there are someadvantages to DBS over ablative methods, it isimportant to keep in mind that the two modalitiesare neither functionally nor clinically equivalent.Furthermore, while DBS is a new and experi-mental modality with unproven long-term effects,there is extensive experience with lesioning thatsupports its benefit for carefully selected psy-chiatric patients. Furthermore, the theoretical andpractical aspects of each modality, warrant con-tinued consideration and research to determinetheir optimal roles in psychosurgical practice.However, it is clear that ablative methods play animportant role in the surgical management ofsevere, intractable psychiatric disease today andwill likely continue to do so in the future.
64 Y. Chodakiewitz et al.
References
1. Feldman RP, Goodrich JT. Psychosurgery: a historicaloverview. Neurosurgery. 2001;48(3):647–59.
2. Alt KW, Jeunesse C, Buitrago-Téllez CH, WächterR, Boës E, Pichler SL. Evidence for stone agecranial surgery. Nature. 1997;387(6631):360.
3. Broca P. Sur le siège de la faculté du langagearticulé. Bulletins de la Société d’anthropologie deParis. 1865;377–93.
4. Wernicke C. Der aphasische Symptomencomplex.1874.
5. Damasio H, Grabowski T, Frank R, Galaburda AM,Damasio AR. The return of Phineas Gage: cluesabout the brain from the skull of a famous patient.Science. 1994;264(5162):1102–5.
6. Manjila S, Rengachary S, Xavier AR, Parker B,Guthikonda M. Modern psychosurgery before EgasMoniz: a tribute to Gottlieb Burckhardt. 2008.
7. Fulton J, Jacobsen C. The functions of the frontallobes: A comparative study inmonkeys, chimpanzeesand man. Adv Mod Biol. 1935;4:113–25 (Moscow).
8. Patel SR, Aronson JP, Sheth SA, Eskandar EN.Lesion Procedures in psychiatric neurosurgery.World Neurosur. 2013; 80(3–4):S31.e39–S31.e16.
9. Bridges P, Bartlett J. Psychosurgery: yesterday andtoday. Brit J Psychiatry. 1977;131(3):249–60.
10. Mashour GA, Walker EE, Martuza RL.Psychosurgery: past, present, and future. Brain ResRev. 2005;48(3):409–19.
11. Kotowicz Z. Gottlieb Burckhardt and Egas Moniz-two beginnings of psychosurgery. Gesnerus.2005;62(1–2):77–101.
12. Moniz E. Prefrontal leucotomy in the treatment ofmental disorders. Am J Psychiatry. 1937;93(1379–85):1385.
13. Robison RA, Taghva A, Liu CY, Apuzzo ML.Surgery of the mind, mood, and conscious state: anidea in evolution. World Neurosurg. 2013;80(3–4):S2–26.
14. Tierney AJ. Egas Moniz and the origins ofpsychosurgery: a review commemorating the 50thanniversary of Moniz’s Nobel Prize. J HistNeurosci. 2000;9(1):22–36.
15. Anderson CA, Arciniegas D. Neurosurgicalinterventions for neuropsychiatric syndromes. CurrPsychiatry Rep. 2004;6(5):355–63.
16. Valenstein ES. Great and desperate cures: the rise anddecline of psychosurgery and other radical treatmentsfor mental illness. New York: Basic Books; 1986.
17. Deutsch A. The mentally ill in America. New YorkCity: Columbia University Press; 1949.
18. Fulton J. The frontal lobes: research publication forthe association for research in nervous and mentaldisease. Baltimore: Williams & Wilkins; 1948.
19. Freeman W. Transorbital leucotomy. Lancet.1948;252(6523):371–3.
20. Lapidus KA, Kopell BH, Ben-Haim S, Rezai AR,Goodman WK. History of psychosurgery: a
psychiatrist’s perspective. World Neurosurg. 2013;80(3–4):S27 e21–S27 e16.
21. Heller AC, Amar AP, Liu CY, Apuzzo ML. Surgeryof the mind and mood: a mosaic of issues in timeand evolution. Neurosurgery. 2006;59(4):720–39.
22. Scoville WB. Selective cortical undercutting as ameans of modifying and studying frontal lobefunction in man. J Neurosurg. 1949;6(1):65–73.
23. Scoville WB, Wilk EK, Pepe AJ. Selective corticalundercutting results in new method of fractionallobotomy. Am J Psychiatry. 1951;107(10):730–8.
24. Spiegel E, Wycis H, Marks M, Lee A. Stereotaxicapparatus for operations on the human brain.Science. 1947;106(2754):349–50.
25. Leksell L. The stereotaxic method and radiosurgeryof the brain. Acta Chir Scand. 1951;102(4):316.
26. Taub A, Lopes A, Fuentes D, et al.Neuropsychological outcome of ventral capsular/ventral striatal gamma capsulotomy for refractoryobsessive-compulsive disorder: a pilot study.J Neuropsychiatry Clin Neurosci. 2009;21(4):393–7.
27. Greenberg BD, Rauch SL, Haber SN. Invasivecircuitry-based neurotherapeutics: stereotacticablation and deep brain stimulation for OCD.Neuropsychopharmacology. 2009;35(1):317–36.
28. Bonelli RMCJ. Frontal subcortical circuitry andbehavior. DialoguesClinNeurosci. 2007;9(2):141–51.
29. Chakravarthy VSJD, Bapi RS. What do the basalganglia do? A modeling perspective. Biol Cybern.2010;103(3):237–53.
30. Stocco ALC, Anderson JR. Conditional routing ofinformation to the cortex: a model of the basalganglia’s role in cognitive coordination. PsycholRev. 2010;117(2):541–74.
31. Weyhenmeyer JA. Rapid review of neuroscience.Amsterdam: Mosby Elsevier. 2007.
32. Cameron IGWM, Pari G, Munoz DP. Executiveimpairment in Parkinson’s disease: responseautomaticity and task switching. Neuropsychologia.2010;48(7):1948–57.
33. Fix JD. Basal ganglia and the striatal motor system.Neuroanatomy (Board Review Series) 4th ed.Baltmore: Wulters Kluwer & Lippincott Williams &Wilkins; 2007. p. 274–81.
34. Robinson DWH, Munne LA, Ashtari M, Alvir JM,Lerner G, Koreen A, Cole K, Bogerts B. Reducedcaudate volume in obsessive compulsive disorder.Arch Gen Psychiatry. 1995;52:393–8.
35. Saunders RCRD. A comparison of efferent’s of theamygdala and the hippocampal formation in the rhesusmonkey: I. Convergence of the entorhinal, prorhinal, andperirhinal corticies. J Comput Neurol. 1988;271:153–84.
36. Saunders RCRD, Van Hoesen GW. A comparisonof efferent’s of the amygdala and the hippocampalformation in the rhesus monkey: II. Reciprocal andnon-reciprocal connections. J Comput Neurol.1988;271:185–207.
37. Pd M. Psychosomatic disease and the visceral brain:recent developments bearing on the Papez theory ofemotion. Psychosom Med. 1949;11:228–353.
5 Ablative Surgery for Neuropsychiatric Disorders: Past, Present, Future 65
38. Jw P. A proposed mechanism of emotion. ArchNeurol Psychiatry. 1937;38:725–43.
39. Sg W. The limbic system. In: Sg W, editor. Clinicalneuroanatomy. vol 26.NewYork:McGraw-Hill; 2010.
40. Dh Z. The human amygdala and the emotionalevaluation of sensory stimuli. Brain Res.2003;41:88–123.
41. Kluver HBP. An analysis of certain effects ofbilateral temporal lobectomy in rhesus monkeys.J Psychol. 1938;5:33–54.
42. Groenewegen HJ, Berendse HW. Connections of thesubthalamic nucleus with ventral striatopallidal partsof the basal ganglia in the rat. J Comput Neurol.1990;294:607–22.
43. Parent A. Extrinsic connections of the basal ganglia.Trends Neurosci. 1990;13:254–8.
44. Bonelli RM. KH, Pillay SS., Yurgelun-Todd DA.Basal ganglia volumetric studies in affectivedisorder: what did we learn in the last 15 years? JNeural Transmitters. 2006;113:255–68.
45. Salmon D. HW, Hamilton JM. Cognitive abilitiesmediated by frontal-subcortical circuits. In: LichterDG, Cummings JL, editors. Frontal subcorticalcircuits in psychiatric and neurological disorders.New York: Guilford Press; 2001. p. 114–50.
46. Alvarez JA, Emory E. Executive function and thefrontal lobes: a metaanalytic review. NeuropsycholRev. 2006;16:17–42.
47. Milner B. Effects of different brain lesions on cardsorting. Arch Neurol. 1963;9:90–100.
48. Jl C. Frontal-subcortical circuits and humanbehavior. Arch Neurol. 1993;50:873–80.
49. Cummings JL, Bogousslavsky J. Emotionalconsequences of focal brain lesions: an overview.Behavior and mood disorders in focal brain lesions.Cambridge: Cambridge University Press; 2000.
50. Mega MS, Cummings CJ, Salloway S, Malloy P.The limbic system: an anatomic, phylogenetic, andclinical perspective. J Neuropsychiatry ClinNeurosci. 1997;9:315–30.
51. Johnson TN, Rosvold HE. Topographic projectionson the globus pallidus and the substantia nigra ofselectively placed lesions in the precommissuralcaudate nucleus and putamen in the monkey. ExplorNeurol. 1971;33:584–96.
52. Haber SN. The primate basal ganglia: parallel andintegrative networks. J Chem Neuroanat.2003;26:317–30.
53. Lichter DG, Cummings JL. Introduction andoverview. New York: Guilford Press; 2001.
54. Macmillan MLM. Rehabilitating Phineas Gage.Neuropsychologic Rehab. 2010;20(5):641–58.
55. Stuss DT, Gow CA, Hetherington CR. “No longerGage”: frontal lobe dysfunction and emotionalchanges. J Consult Clin Psychol. 1992;60:349–59.
56. StarksteinSE,ManesF.Mania andmanic-like disoders.Cambridge: Cambridge University Press; 2000.
57. Meyers CA, Meyers SA, Scheibel RS, Hayman A.Case report: acquired antisocial personality disorder
associated with unilateral left orbital frontal lobedamage. J Psychiatry Neurosci. 1992;17:121–5.
58. Miller BL, Chang L, Mena I, Boone K, Lesser IM.Progressive right frontotemporal degeneration:clinical, neuropsychological and SPECTcharacteristics. Dement Geriatr Cogn Disord.1993;4:204–13.
59. Mendez MF, Adams NL, Lewandowski KS.Neurobehavioral changes associated with caudatelesions. Neurology. 1989;39:349–54.
60. Levy R, Dubois B. Apathy and the functionalanatomy of the prefrontal cortex-basal gangliacircuits. Cereb Cortex. 2006;16:916–28.
61. Ackermann H, Ziegler W. Akinetischer Mutismus-eine Literaturübersicht. Fortschr NeurologischerPsychiatr. 1995;63:59–67.
62. Mega MS, Cohenour RC. Akinetic mutism:disconnection of frontal-subcortical circuits.Neuropsychiatry Neuropsychol Behav Neurol.1997;10:254–9.
63. Nielsen JM, Jacobs LL. Bilateral lesions of theanterior cingulate gyri. Bull Los Angeles NeurolSoc. 1951;16:231–34.
64. Whitty CWM, Duffield JE, Tow PM, Cairns H.Anterior cingulectomy in the treatment of mentaldisease. Lancet. 1952;1:475–81.
65. Ballantine Jr HT, Cassidy WL, Flanagan NB,Marino Jr R. Sterotaxic anterior cingulotomy forneuropsychiatric illness and intractable pain.J Neurosurg. 1967;26:488–95.
66. Hayempour BJ. Psychosurgery: treatingneurobiological disorders with neurosurgicalintervention. J Neurol Disord. 2013;1(1):1–19.
67. Scarone S, Colombo C, Livian S, Abbruzzese M,Ronchi P, Locatelli M, Smeraldi E. Increased rightcaudate nucleus size in obsessive compulsivedisorder: detection and magnetic resonanceimaging. Psychiatry Res. 1992;45:115–21.
68. Martuza RL, Chiocca EA, Jenike MA, Giriunas IE,Ballantine HT. Stereotactic radiofrequency thermalcingulotomy for obsessive compulsive disorder.J Neuropsychiatry Clin Neurosci 1990;2:331–36.
69. Baer L, Rauch SL, Ballantine HT, Martuza R,Cosgrove R, Cassem E, Jenike MA. Cingulotomyfor intractable OCD: prospective long-term follow-up of 18 patients. Arch Gen Psychiatry.1995;52:384–92.
70. Sheth SA, Neal J, Tangherlini F, et al. Limbicsystem surgery for treatment-refractory obsessive-compulsive disorder: a prospective long-termfollow-up of 64 patients: clinical article.J Neurosurg. 2013;118(3):491–7.
71. Leksell LBE. Stereotactic gamma capsulotomy.New York: Elsevier/North Holland BiomedicalPress; 1979.
72. Bingley TLL, Meyerson BA, Rylander G. Long-term results of stereotactic capsulotomy in chronicobsessive-compulsive neurosis. Baltimore:University Park Press; 1977.
66 Y. Chodakiewitz et al.
73. Knight GC. The orbital cortex as an objective in thesurgical treatment of mental illness: the developmentof the stereotactic approach. Brit J Surg.1964;53:114–24.
74. Göktepe EO, Young LB, Bridges PK. A furtherreview of the results of stereotactice subcaudatetractotomy. Brit J Psychiatry. 1975;126:270–80.
75. Hodgkiss AD, Malizia AL, Bartlett JR, Bridges PK.Outcomes after the psychosurgical operation ofstereotactic subcaudate tractotomy. J NeuropsychiatryClin Neurosci. 1995;7:230–34.
76. Poynton AM, Kartsounis LD, Bridges PK.A prospective clinical study of stereotacticsubcaudate tractotomy. Psychol Med. 1995;25:763–70.
77. Mitchell-Heggs N, Kelly D, Richardson A.Stereotactic limbic leucotomy–a follow-up at 16months. Brit J Psychiatry. 1976;128(3):226–40.
78. Price BH, Baral I, Cosgrove GR, Rauch SL,Nierenberg AA, Jenike MA, Cassem EH.Improvement in severe self mutilation followinglimbic leucotomy: a series of 5 consecutive cases.J Clin Psychiatry. 2001;62:925–32.
79. Malhi GS, Sachdev P. Novel physical treatments forthe management of neuropsychiatric disorders.J Psychosom Res. 2002;53:709–19.
80. Cohen LG, Roth BJ, Nilsson J, Dang N, Panizza M,Bandinelli S, Friauf W, Hallett M. Effects of coildesign on delivery of focal magnetic stimulation.Electroencephalogr Clin Neurophysiol. 1990;75:350–57.
81. Ben-Shachar D, Belmaker RH, Grisaru N, Klein E.Transcranial magnetic stimulation inducesalterations in brain monoamines. J NeuralTransmitters. 1997;104:191–97.
82. Levkovitz Y, Grisaru N, Segal M. Transcranialmagnetic stimulation and antidepressive drugs sharesimilar cellular effects in rat hippocampus.Neuropsychopharmacology. 2001;24:608–16.
83. Aleman A. Use of repetitive transcranial magneticstimulation for treatment in psychiatry. ClinPsychopharmacol Neurosci. 2013;11(2):53–9.
84. Vagus Nerve Stimulation Study Group. A randomizedcontrolled trial of chronic vagus nerve stimulation fortreatment ofmedically intractable seizures. Neurology.1999;45:224–30.
85. Morris GL, Gloss D, Buchhalter J, Mack KJ,Nickels K, Harden C. Evidence-based guidelineupdate: vagus nerve stimulation for the treatment ofepilepsy: report of the Guideline DevelopmentSubcommittee of the American Academy ofNeurology.
86. Van Bockstaele EJ, Peoples J, Valentino RJ.Anatomic basis for differential regulation of therostrolateral peri-locus coeruleus region by limbicafferents. Biol Psychiatry. 1999;46:1352–63.
87. Mohr P, Rodriguez M, Slavíčková A, Hanka J. Theapplication of vagus nerve stimulation and deep brainstimulation in depression. Neuropsychobiology.2011;64(3):170–81.
88. Henry TR, Votaw JR, Pennell PB, Epstein CM,Bakay RAE, FaberTL, Grafton ST, Hoffman JM.Acute blood flow changes and efficacy of vagusnerve stimulation in partial epilepsy. Neurology.1999;52:1166–73.
89. Jobe PC, Dailey JW, Wernicke JF. A noradrenergicand serotonergic hypothesis of the linkage betweenepilepsy and affective disorders. Crit Rev Neurobiol.1999;13:317–56.
90. Charous SJ, Kempster G, Manders E, Ristanovic R.The effect of vagal nerve stimulation on voice.Laryngoscope. 2001;111:2028–31.
91. Schachter SC, Saper CB. Vagus nerve stimulation.Epilepsia. 1998;39:677–86.
92. Kay MA, Glorioso JC, Naldini L. Viral vecotrs forgene therapy: the art of turning infectious agents intovehicles of therapeutics. Nat Med. 2001;7:33–40.
93. Frick LR, Williams K, Pittenger C. Microglialdysregulation in psychiatric disease. Clin DevImmunol. 2013;2013:1–10.
94. Rossi F, Cattaneo E. Opinion: neural stem celltherapy for neurologic diseases: dreams and reality.Nat Rev Neurosci. 2001;3.
95. Kanno H. Regenerative therapy for neuronaldiseases with transplantation of somatic stem cells.World J Stem Cells. 2013;5(4):163–71.
96. Elias WJ, Khaled M, Hilliard JD, et al. A magneticresonance imaging, histological, and dose modelingcomparison of focused ultrasound, radiofrequency,and gamma knife radiosurgery lesions in swinethalamus: laboratory investigation. J Neurosurg.2013;1–11.
97. Spiegel EA, Wycis HT, Freed H.Stereoencephalotomy in thalamotomy and relatedprocedures. J Am Med Assoc. 1952;148(6):446–51.
98. Spiegel EA, Wycis HT, Marks M, LeeAJ. Stereotaxic apparatus for operations on thehuman brain. Science. 1947;106(2754):349–50.
99. Hayempour BJ. Psychosurgery: treatingneurobiological disorders with neurosurgicalintervention. J Neurol Disord. 2013;1(1).
100. Ruck C, Karlsson A, Steele JD, et al. Capsulotomyfor obsessive-compulsive disorder: long-termfollow-up of 25 patients. Arch Gen Psychiatry.2008;65(8):914.
101. Binder DK, Iskandar BJ. Modern neurosurgery forpsychiatric disorders. Neurosurgery. 2000;47(1):9–21 (discussion 21–23).
102. Newcombe R. The lesion in stereotactic subcaudatetractotomy. Brit J Psychiatry. 1975;126(5):478–81.
103. Malhi GS, Bartlett JR. A new lesion for thepsychosurgical operation of stereotactic subcaudate
5 Ablative Surgery for Neuropsychiatric Disorders: Past, Present, Future 67
tractotomy (SST). Brit J Neurosurg. 1998;12(4):335–39.
104. Birdno MJ, Grill WM. Mechanisms of deep brainstimulation in movement disorders as revealed bychanges in stimulus frequency. Neurotherapeutics.2008; 5(1):14–25.
105. Larson PS. Deep brain stimulation for psychiatricdisorders. Neurotherapeutics. 2008;5(1):50–8.
106. Bejjani BP, Arnulf I, Houeto JL, Milea D, DemeretS, Pidoux B, Agid Y. Concurrent excitatory andinhibitory effects of high frequency stimulation: anoculomotor study. J Neurol, Neurosurg Psychiatry.2002;72(4):517–22.
107. Malone DA Jr. Use of deep brain stimulation intreatment-resistant depression. Cleveland Clin JMed. 2010;77(3):S77–80.
108. Yount K. The brain electric: deep brain stimulationfor neurologic disorders. DukeMed Magazine. Vol
11. Durham: Duke University Office of Marketingand Communications; p. 28–35.
109. Hall W, Carter A. Science, safety and costs makedeep brain stimulation for addiction a low priority: areply to Vorspan et al. (2011) and Kuhn et al.(2011). Addiction. 2011;106(8):1537–38.
110. McIntosh E, Gray A, Aziz T. Estimating the costs ofsurgical innovations: the case for subthalamicnucleus stimulation in the treatment of advancedParkinson’s disease. Mov Disord: Off J Mov DisordSoc. 2003;18(9):993–9.
111. Oh MY, Hodaie M, Kim SH, Alkhani A, Lang AE,Lozano AM. Deep brain stimulator electrodes usedfor lesioning: proof of principle. Neurosurgery.2001;49(2):363–67 (discussion 367–9).
68 Y. Chodakiewitz et al.

6Legal Issues in Behavioral Surgery
Sam Eljamel
Abstract
Surgery for psychiatric illnesses (SPI) is still shrouded by ethical,governance and public concerns because of what happened in the past.There is a need to develop, agree and implement stringent guidelines andprotocols to manage patients referred for SPI appropriately. Theseconsensus guidelines are required to safe guard patients and surgeons.Patients considered for SPI must have failed adequate therapies: inobsessive compulsive disorders (OCD) failure of at least three adequatetrials of Serotonin reuptake inhibitors (SRIs) including clomipramine andaugmentation and behavioural therapies and in depression (MDD) failureof at least four adequate antidepressive therapies including antidepressivemedicines, psychotherapy, and electroconvulsive therapy (ECT). Patientsshould be assessed by psychiatrist-led multidisciplinary team of experi-enced healthcare professionals, who must confirm the diagnosis, adequacyof previous treatments, and the ability of patients to give informedconsent. Ability of patients to give informed consent and the diagnosismust be verified by an independent authority designated for this purposeunder jurisdiction of the state where SPI will be carried out, e.g. Mentalhealth welfare commission (MHWC) or Behavioural Surgery ReviewBoards. The independent body or authority must also decide whether thetreating team is adequately trained to perform the procedure and provideaftercare. These procedures should only be performed in adequatelyresourced centers subject to annual inspections and robust clinical andregulatory governance frameworks. Postoperative assessment should beblinded to avoid placebo effects and biases, i.e. the assessor should beblinded as to what procedure did the patient receive to avoid bias.Adhering to these principles will safe guard the return of SPI and protectthose who deliver it to patients.
S. Eljamel (&)Department of Neurosurgery, University of Dundee,Dundee, Scotland, UKe-mail: [email protected]
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0_6© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
69
6.1 Introduction
The majority of patients with psychiatric illnessescan be managed effectively by means of medi-cations and psychotherapy. However, 20–40 % ofpatients become chronic, refractory to standardtherapy or do not tolerate standards therapybecause of unacceptable side effects, leadingto increased demand on healthcare resources[1, 5, 19]. These patients would be candidatesfor further therapy such ablative surgery orneurostimulation for psychiatric illnesses [7].However, such therapeutic options are stillshrouded by uncertainties, controversy, skepti-cism and at times barefaced opposition [7]. Themain reason for these attitudes towards suchintervention in mental illnesses is that in the1960s crude ablative surgery was used at timesindiscriminately resulting into disrepute and legalban in some jurisdictions. As a result stringentprotocols specifically designed for this area ofsurgery must be developed and adopted to com-ply with local ethical and legal requirements. Thischapter will explore the ethical and legal issuesshrouding surgery for psychiatric illnesses (SPI).
6.2 Issues Leading to the Demiseof Psychosurgery
6.2.1 Lack of Scientific Basis
The most important concern that shrouded psy-chosurgery in the 1960s was lack of scientificevidence to justify targeted brain area and thepatient groups treated. The data upon which itwas introduced was at most inconclusive andcontradictory [3]. Furthermore, psychosurgeonsof the past were accused of using vague unveri-fiable preoperative diagnosis, vague controversialselection criteria, vague or invalid assessmentmethods, and extreme bias in postoperative out-come reporting. The procedures performed in thepast were very crude, imprecise, and inaccurate.Most of the procedures were carried out as part ofclinical practice without proper research protocolsapproved by ethics committees, independent
assessments of postoperative outcome, or precisecategorization of the psychiatric illness beingtreated [16]. The practice of psychosurgery in thepast was applied to humans after very few animalexperiments, which gave unreliable and unpre-dictable results [18].
6.2.2 Lack of Informed Consent
The second concern-shrouded psychosurgerywas informed consent or lack of it. Howinformed consent was obtained? Did patientsunderstand what they were going to have? Werethey aware of potential irreversible risks? Wherethey told or made aware of alternative manage-ment? e.g. Can an appropriate candidate forpsychosurgery give valid consent for the proce-dure or can a third party, family, or society whomight benefit from the procedure give consent onbehalf of a patient. Some argued that psycho-surgery may produce irreversible change inbehaviour, self, or mind of the individual on thesame bar as body mutilation [3].
6.2.3 Potential Misuseof the Procedure
Opponents and the general public have voicedtheir concern that psychosurgery had been, maybe, or will be used or abused as a social orpolitical tool to control and subdue those who areconsidered abnormal to justify controlling dissi-dents, ethnic minorities, political opponents,political opposition leaders or bothersome indi-viduals such prisoners or criminals [3, 7].
6.3 How can These ConcernsBe Overcome?
6.3.1 Informed Consent
Current surgical procedures applied to psychiatricillnesses include what is considered “established”techniques: i.e. thermal radiofrequency bilateral
70 S. Eljamel

anterior capsulotomy (BACA), thermal radiofre-quency bilateral anterior cingulotomy (BACI) andleft vagus nerve stimulation (VNS). In recent yearsa number of new techniques and procedures haveemerged e.g. deep brain stimulation (DBS) inmultiple brain targets: i.e. DBS in the subjenucingulum, DBS in nucleus accumbens, and othertargets. The level of evidence behind these pro-cedures is not robust to alley all criticism andbiases, at best the strength of scientific evidencebehind “established” procedures is level II.Therefore when consenting patients for such pro-cedures it is very important that patients are madeaware of alternative procedures and the degree ofevidence behind each procedure, its outcome andpotential risks, e.g. in the case of treatmentrefractory depression (TRMDD) the optionswould be either to continue with standard therapy,BACI, BACA, VNS or DBS. It is important to befamiliar with the evidence base behind each pro-cedure and what is considered accepted procedurein the jurisdiction under which the procedure isbeing carried out. For example in Belgium BACAis considered “established” ablative procedure forobsessive compulsive disorders (OCD) [13],while in Scotland BACI is considered “estab-lished” ablative procedure for TRMDD and OCD[6]. The importance of being familiar with allalternatives is very important for the purpose ofinformed consent as all neurostimulation proce-dures apart from VNS for TRMDD are still clas-sified as experimental procedures, thoughDBS forOCD does have regulatory approval in the USAand Europe. The reason for being familiar with allpossible alternative procedures is to give thepatient the choice, e.g. if a patient was offeredBACI without mentioning any other alternativese.g. in TRMDD, VNS, and the patient agrees toundergo the procedure, and later on the patientfinds out about VNS, the surgeons and psychiatristmight find themselves in an occult situation. Backin 2000, a three arm randomized controlled trialallocating patients with TRMDD to BACI, Cin-gulate DBS or VNS was designed and approved[6, 7]. When patients were offered the threetreatment options or continue as usual, no patientagreed to be randomized as patients choose BACIarguing that if it works, it is one-off treatment, no
hardware and continuous follow up or batterychanges and programming. Others however,elected VNS arguing VNS is an extracranial pro-cedure without exposure to risks of surgery on thebrain [7]. It is understandable patients’ choicesmight make it hard to recruit patients for newertreatments, but it is essential that patients are giveall the information to choose what they think isbest for them. Furthermore, what is called“established” procedures for SPI is thermalradiofrequency lesioning with level II scientificevidence. Newer techniques such as stereotacticradiosurgery (SRS) and MRI guided high fre-quency ultrasound (MgHFUS) do not have thislevel of evidence behind them [13]. Any “non-established” or unapproved procedures shouldonly be offered within a clinical trial protocolapproved by the local ethics committee (LREC),institutional research board (IRB) and local regu-latory bodies.
6.3.2 Allaying the Fearsof the General Publicand Satisfying RegulatoryAuthorities
Because of the bleak history of surgery for psy-chiatric illnesses, it is paramount that any pro-gramme offering surgery for psychiatric illnesses(SPI) to develop stringent protocols that satisfyand comply with ethical standards and regulatoryauthorities. For example in Scotland, patients areassessed by a group of specialized psychiatricteam to establish the diagnosis, assess adequacyof previous trials of therapies, and assess thecapacity of the patient to give informed consent.Patients, who pass these stringent criteria, willthen be referred to a Mental Health WelfareCommission (MHWC), an independent authorityestablished by the Scottish Government. TheMHWC then visits the patient to confirm thediagnosis, adequacy of previous trials of therapyand assesses the ability of the patient to giveinformed consent to the proposed procedure.Furthermore, the MHWC or the National Ser-vices Division receives six-monthly detailedreport about activities, outcomes and morbidity
6 Legal Issues in Behavioral Surgery 71
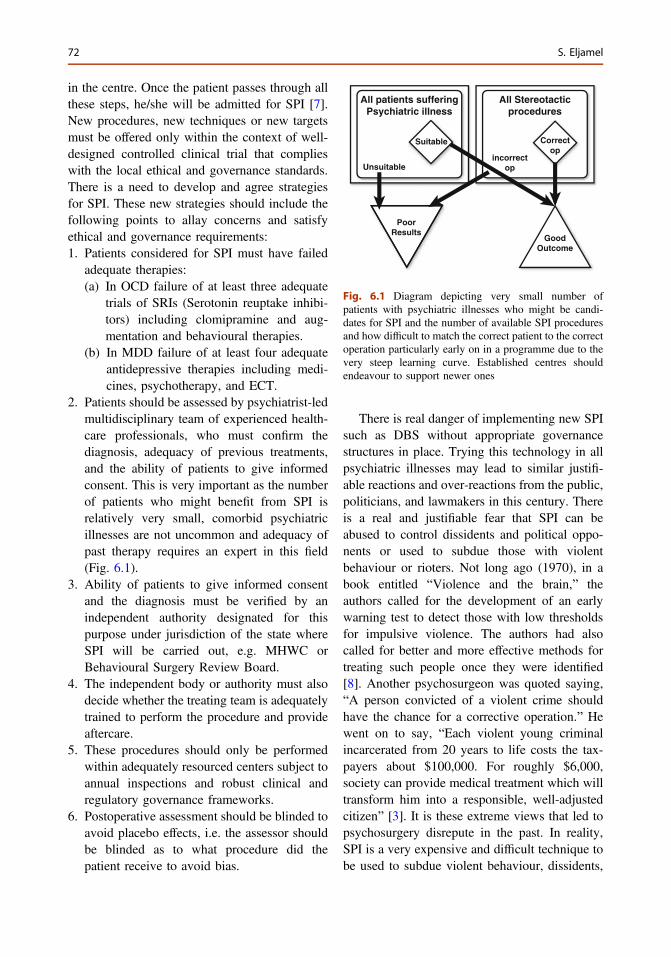
in the centre. Once the patient passes through allthese steps, he/she will be admitted for SPI [7].New procedures, new techniques or new targetsmust be offered only within the context of well-designed controlled clinical trial that complieswith the local ethical and governance standards.There is a need to develop and agree strategiesfor SPI. These new strategies should include thefollowing points to allay concerns and satisfyethical and governance requirements:1. Patients considered for SPI must have failed
adequate therapies:(a) In OCD failure of at least three adequate
trials of SRIs (Serotonin reuptake inhibi-tors) including clomipramine and aug-mentation and behavioural therapies.
(b) In MDD failure of at least four adequateantidepressive therapies including medi-cines, psychotherapy, and ECT.
2. Patients should be assessed by psychiatrist-ledmultidisciplinary team of experienced health-care professionals, who must confirm thediagnosis, adequacy of previous treatments,and the ability of patients to give informedconsent. This is very important as the numberof patients who might benefit from SPI isrelatively very small, comorbid psychiatricillnesses are not uncommon and adequacy ofpast therapy requires an expert in this field(Fig. 6.1).
3. Ability of patients to give informed consentand the diagnosis must be verified by anindependent authority designated for thispurpose under jurisdiction of the state whereSPI will be carried out, e.g. MHWC orBehavioural Surgery Review Board.
4. The independent body or authority must alsodecide whether the treating team is adequatelytrained to perform the procedure and provideaftercare.
5. These procedures should only be performedwithin adequately resourced centers subject toannual inspections and robust clinical andregulatory governance frameworks.
6. Postoperative assessment should be blinded toavoid placebo effects, i.e. the assessor shouldbe blinded as to what procedure did thepatient receive to avoid bias.
There is real danger of implementing new SPIsuch as DBS without appropriate governancestructures in place. Trying this technology in allpsychiatric illnesses may lead to similar justifi-able reactions and over-reactions from the public,politicians, and lawmakers in this century. Thereis a real and justifiable fear that SPI can beabused to control dissidents and political oppo-nents or used to subdue those with violentbehaviour or rioters. Not long ago (1970), in abook entitled “Violence and the brain,” theauthors called for the development of an earlywarning test to detect those with low thresholdsfor impulsive violence. The authors had alsocalled for better and more effective methods fortreating such people once they were identified[8]. Another psychosurgeon was quoted saying,“A person convicted of a violent crime shouldhave the chance for a corrective operation.” Hewent on to say, “Each violent young criminalincarcerated from 20 years to life costs the tax-payers about $100,000. For roughly $6,000,society can provide medical treatment which willtransform him into a responsible, well-adjustedcitizen” [3]. It is these extreme views that led topsychosurgery disrepute in the past. In reality,SPI is a very expensive and difficult technique tobe used to subdue violent behaviour, dissidents,
All patients sufferingPsychiatric illness
Suitable
Unsuitable
GoodOutcome
incorrectop
All Stereotacticprocedures
PoorResults
Correctop
Fig. 6.1 Diagram depicting very small number ofpatients with psychiatric illnesses who might be candi-dates for SPI and the number of available SPI proceduresand how difficult to match the correct patient to the correctoperation particularly early on in a programme due to thevery steep learning curve. Established centres shouldendeavour to support newer ones
72 S. Eljamel
or political opponents. There are much easier,cheaper, and effective ways of mass control,including the use of media, television, medicines,and education systems. Historically, psychosur-gery was not based on proper scientific studies; itstarted by Ego Moniz who turned to psychosur-gery as a means to be in the limelight and forfame to obtain a Nobel Prize. Ego Moniz usedlobotomy on patients after hearing of Fulton’scase report of a single chimpanzee lobotomizedby Jacobsen where the agitated chimp becamecalm [7]. There has been no verification of theexact location of the lesion or report of itspotential serious side effects [3]. Almost every-one at the time ignored these important ethicalissues because they felt they were morallyobliged to help thousands of incarcerated men-tally ill patients. They were blinded by the hugeunmet need and the greed for wealth and fame.After the introduction of Moniz’s lobotomy inthe USA, it spread like wildfire and was practicedin smaller and less-equipped hospitals [17]. Itwas the actions of Walter Freeman, who wasneither a neurosurgeon nor a psychiatrist, whichbrought psychosurgery to disrepute. Recognizingpsychosurgery was a “Catch 22” situation; whilepsychosurgery relieved symptoms of psychosis,it was very costly in terms of loss of affect andcreativity. Despite this fact, Walter Freemancontinued the procedure and introduced thetransorbital lobotomy (today’s equivalent ofminimally invasive procedure) instead ofreflecting and auditing his results [17].
It is comforting to know that the way SPI ispracticed today is very different from that ofpsychosurgery of the past; today’s SPI is accu-rate and precise, and it can allay most of theconcerns encountered in the past in this field ofneurosurgery. However, a review of the literatureon DBS for OCD and MDD uncovers a plethoraof articles in recent years; a total of 90 publica-tions during 2009–2011 compared to only 17articles between 2002 and 2005 [7]. The vastmajority of these publications reported unblindedoutcomes of small selected study patients withfavourable outcome, which was not verifiedwhen larger multicentre controlled studies wereconducted. My own concern is that many
psychiatric patients are being treated in smallgroups outside multicenter, controlled, prospec-tive trials. In a survey of North AmericanFunctional Neurosurgeons published in 2011,50 % of the responders were engaged in somesort of SPI, mainly DBS for OCD or MDD, andsaw SMI as a growing field of business [9].Although, DBS and VNS are neither destructivenor irreversible and give sufferers the option todiscontinue the stimulation if they wished to doso, these procedures should not be used outsideproperly designed clinical protocols because ofthe large placebo effect and inherent biases [7].Although DBS had Food and Drug Administra-tion (FDA) approval for OCD under Humani-tarian Device Exemption (HDE) rules and VNShad FDA approval for MDD, some concerns hadbeen raised regarding their use. These concernsare based on lack of strong scientific evidence ontheir safety and efficacy in the long run, thenumerous conflicts of interests held by investi-gators such as holding patents for certainprocedures, and the ambiguity and lack oftransparency of research sponsored by commer-cial partners [8]. However, recent studies onablative, VNS-, and DBS-SPI were carried outwithin stringent protocols that stood the heat ofscientific rigor and scrutiny of peer reviewers[4, 6, 10–12, 16]. The outcomes reported in thesestudies were objective and based on objectiveassessments. Reduction of YBOCS score of35 % is considered a clinical response in OCD,while a reduction of 50 % on MADRS or HDRSis considered a worthwhile response in MDD.However, careful observation and further studiesof SPI procedures are required to establish theirlong-term efficacy, longevity, and side effects.Nevertheless, there remain ethical and socialchallenges facing SPI and consensus guidelines,workshops, and public engagement are just a fewthings that need to be done to overcome thesechallenges [2]. SPI must be approached withcaution and commitment for long-term care. SPIis complicated by issues such as patient catego-rization, selection criteria, long-term manage-ment of these patients, and the different patternsof potential benefits and burdens [15]. There is aneed for stringent ethical, governance, and
6 Legal Issues in Behavioral Surgery 73
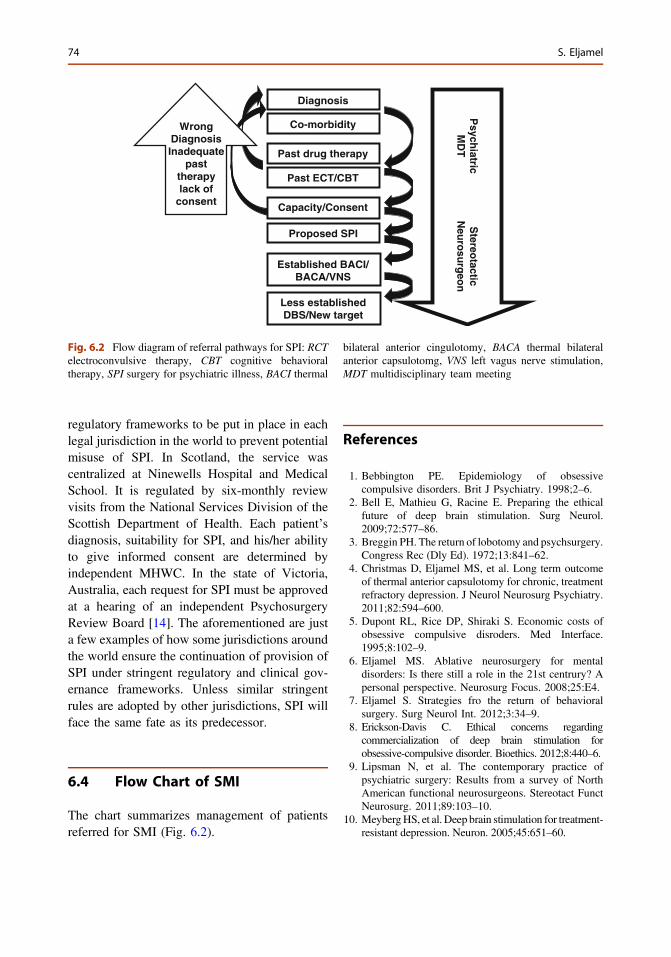
regulatory frameworks to be put in place in eachlegal jurisdiction in the world to prevent potentialmisuse of SPI. In Scotland, the service wascentralized at Ninewells Hospital and MedicalSchool. It is regulated by six-monthly reviewvisits from the National Services Division of theScottish Department of Health. Each patient’sdiagnosis, suitability for SPI, and his/her abilityto give informed consent are determined byindependent MHWC. In the state of Victoria,Australia, each request for SPI must be approvedat a hearing of an independent PsychosurgeryReview Board [14]. The aforementioned are justa few examples of how some jurisdictions aroundthe world ensure the continuation of provision ofSPI under stringent regulatory and clinical gov-ernance frameworks. Unless similar stringentrules are adopted by other jurisdictions, SPI willface the same fate as its predecessor.
6.4 Flow Chart of SMI
The chart summarizes management of patientsreferred for SMI (Fig. 6.2).
References
1. Bebbington PE. Epidemiology of obsessivecompulsive disorders. Brit J Psychiatry. 1998;2–6.
2. Bell E, Mathieu G, Racine E. Preparing the ethicalfuture of deep brain stimulation. Surg Neurol.2009;72:577–86.
3. Breggin PH. The return of lobotomy and psychsurgery.Congress Rec (Dly Ed). 1972;13:841–62.
4. Christmas D, Eljamel MS, et al. Long term outcomeof thermal anterior capsulotomy for chronic, treatmentrefractory depression. J Neurol Neurosurg Psychiatry.2011;82:594–600.
5. Dupont RL, Rice DP, Shiraki S. Economic costs ofobsessive compulsive disroders. Med Interface.1995;8:102–9.
6. Eljamel MS. Ablative neurosurgery for mentaldisorders: Is there still a role in the 21st centrury? Apersonal perspective. Neurosurg Focus. 2008;25:E4.
7. Eljamel S. Strategies fro the return of behavioralsurgery. Surg Neurol Int. 2012;3:34–9.
8. Erickson-Davis C. Ethical concerns regardingcommercialization of deep brain stimulation forobsessive-compulsive disorder. Bioethics. 2012;8:440–6.
9. Lipsman N, et al. The contemporary practice ofpsychiatric surgery: Results from a survey of NorthAmerican functional neurosurgeons. Stereotact FunctNeurosurg. 2011;89:103–10.
10. MeybergHS, et al. Deep brain stimulation for treatment-resistant depression. Neuron. 2005;45:651–60.
Diagnosis
Co-morbidity
Past drug therapy
Past ECT/CBT
Capacity/Consent
Proposed SPI
Established BACI/BACA/VNS
Less establishedDBS/New target
Psych
iatricM
DT
Stereo
tacticN
euro
surg
eon
WrongDiagnosisInadequate
pasttherapylack of
consent
Fig. 6.2 Flow diagram of referral pathways for SPI: RCTelectroconvulsive therapy, CBT cognitive behavioraltherapy, SPI surgery for psychiatric illness, BACI thermal
bilateral anterior cingulotomy, BACA thermal bilateralanterior capsulotomg, VNS left vagus nerve stimulation,MDT multidisciplinary team meeting
74 S. Eljamel
11. Nuttin BJ, et al. Long-term electrical capsularstimulation in patients with obsessive-compulsivedisorder. Neurosurgery. 2003;52:1263–74.
12. Nuttin BJ, et al. Long-term electrical capsularstimulation in patients with obsessive-compulsivedisorder. Neurosurgery. 2008;62(Suppl 3):966–77.
13. Nuttin B, et al. Consensus on guidelines forstereotactic neurosurgery for psychiatric disorders.J Neurol Neurosurg Psychiatry. 2014;85(9):1003−8.doi: 10.1136/jnnp-2013-306580.
14. Psychosurgery Review Board of State of Victoria,Australia (Home page). http://government-state.goaus.net/melbourne/psychosurgery-review-board-of-victoria/. Accessed 03 Jan 2014.
15. ReadCN, et al. Psychiatric neurosurgery 2009; Reviewand perspective. Semin Neurol. 2009;29:256–65.
16. Steele JD, et al. Anterior cingulotomy for majordepression: clinical outcome and relationship to lesioncharacteristics. Biol Psychiatry. 2008;63:670–7.
17. Sterling P. Ethics and effectiveness of psychosurgery.In: Brady B, editor. Controversy in psychosurgery.Philadelphia: W B Saunders Co.; 1978.
18. Valenstein ES. The practice of psychosurgery: asurvey of the literature (1971–1976). Report toNational Commission on the Protection of HumanSubjects in Biomedical and Behavioural Research.US Dept HEW 1976.
19. World Health Organization (WHO). Chapter 2, Burdenof mental and behavioral disorders, in mental health,new understanding, New hope. WHO report 2001.
6 Legal Issues in Behavioral Surgery 75
7Preoperative Evaluationand Postoperative Follow-up of DeepBrain Stimulation for PsychiatricDisorders
Loes Gabriels, Hemmings Wu and Bart Nuttin
Abstract
Deep brain stimulation (DBS) is under investigation as a new treatmentfor an increasing number of psychiatric conditions. Candidates for DBSare treatment refractory, severely incapacitated and have a very lowquality of life. Patient selection should identify candidates that obtain andretain the greatest benefit. In psychiatric care, it is evident that apsychiatric disorder does not affect patients alone, but has a profound anddevastating impact on those around them. These caregivers cannot beneglected in the follow-up process, since the impact of DBS on thepsychiatric symptoms of the patient will reflect on the relationships. Aftersurgery, the search for adequate stimulation parameters and the optimi-zation process with fluctuations in symptom severity may be burdensome.Patients may not be abandoned once the DBS procedure is performed.With improvement of symptoms, patients are less stuck in their chronicpsychiatric disorder and may need help in the definition of new goals andnew purposes in life.
7.1 Introduction
Despite conscientious compliance and adherenceto treatment according to internationally acceptedevidence based treatment algorithms, somepatients with psychiatric disorders do notrespond to pharmacotherapy and psychotherapytreatment. Such patients are treatment refractoryand are severely incapacitated and have a verylow quality of life.
Deep brain stimulation (DBS) is underinvestigation as a new treatment for an increasingnumber of psychiatric conditions. Pilot studies inrecent years have begun to demonstrate efficacyof DBS as a possible novel therapeutic modality
L. Gabriëls (&)UPC KU Leuven, Herestraat 49, 3000 Leuven,Belgiume-mail: [email protected]
H. Wu � B. NuttinLaboratory of Experimental Neurosurgeryand Neuroanatomy, KU Leuven, Leuven, Belgium
B. NuttinUniversity Hospitals Leuven, Leuven, Belgium
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0_7© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
77

for patients suffering from a severe form of thesepsychiatric disorders.
DBS for psychiatric disorders has evolvedfrom a history of stereotactic ablative neurosur-gery. If research of DBS proves non-inferiority incomparison to ablative techniques, DBS may bemore acceptable than brain lesioning for patientand general public due to its adjustability andreversibility.
Obsessive compulsive disorder (OCD) wasthe first psychiatric disorder where the use ofDBS was investigated, and sustained beneficialeffects were documented by several researchgroups worldwide [3, 7, 11, 14]. Increasingly,DBS becomes a focus of research for otherpsychiatric indications such as major depressivedisorder [9, 12, 16], addiction [13], eating dis-orders [8] and impulse control disorders [10].
In this developing domain of DBS for psy-chiatric disorders, it is of crucial importance todefine and accept guidelines that respect thecultural and religious diversity and heterogeneityof healthcare environments of internationallycollaborating partners. Such guidelines state a setnorms at a given time but can and will evolve inan iterative process, taking into account theevolution of scientific findings, the continuingtechnical developments and the clinical experi-ence gathered from patients living with DBS.They are meant to guide ethical and effectiveresearch and represent an international multidis-ciplinary consensus on best ethical practices,norms and professional behaviors, both in clini-cal and research settings [15].
Due to the stringent inclusion criteria, the yearprevalence of DBS in psychiatric disorders dur-ing the last decade is low [6]. Patients that arecandidates for DBS trials have a longstandingcourse of impairment and are disappointed bymany failed treatments.
The DBS process in order to optimize treat-ment outcome can be divided in sequential pha-ses: ethics of the clinical decision makingprocess, selection procedure of appropriate can-didates and preoperative evaluation, surgicalintervention, post-surgery treatment and longterm follow-up. Problems can emerge at each
phase and a patient’s progress through this DBSprocess requires careful monitoring and adequateinterventions from multidisciplinary team.
7.2 Ethical Challengesand the Clinical DecisionMaking Process for DBSin Psychiatric Disorders
According to the World Health Organization [19]it is a patient’s right to be offered a treatment thatcan alleviate suffering and permits improvementin quality of life. If there is enough evidence thatDBS can lead to significant relief of symptomsand improvement of quality of life, it seemsunethical not to consider the issue of DBS forcarefully selected patients.
The protection of the human rights and dig-nity of psychiatric patients is a major issue andprovides the frame to discuss the ethical princi-ples of this ultimate therapeutic approach. Spe-cific normative problems have to be consideredsuch as safety concerns, the best interest of thepatient, questions of patient’s autonomy andability to give free informed consent.
The risk/benefit ratio of the surgical inter-vention should be favorable Expectations andvalues of the patient and significant others areconsidered against the potential benefits of theprocedure, as established in the context and at thetime of the DBS procedure.
The compliance of patients to former treat-ment plays a role in the decision-making processas a good follow-up after the neurosurgical pro-cedure is a crucial factor. Not only the symptomrelief, but transformation of symptom relief intoimprovement in general wellbeing and amelio-ration in quality of life depends on thiscompliance.
The clinical decision making process needs tobe considered in the context of a given era andsociety, with its specific role definitions, cus-toms, moral views and laws. Knowledge oftreatment efficacy, risks and alternative treat-ments and ethical status of DBS may change over
78 L. Gabriels et al.

time. The perspective of the patient, his/her val-ues, quality of life and consent to treatment needto be taken into account. Regular accuratereviews of available literature on targets, indi-cations, results and adverse events are crucial inthis developing field. Honest and solid scientificreporting on the effectiveness and burden ofthese invasive procedures are an ethical duty ofresearch centers who engage themselves in DBSfor psychiatric disorders. To improve benefitsand reduce risks, research into the precise defi-nition of the brain target may help. Improve-ments in the field of technology and biomedicalengineering may make interventions less inva-sive and less destructive. Advances in structuraland functional neuroimaging and anatomic andelectrophysiological studies, along with micro-electrode technology, allow for more precisecharacterization of the neural pathways involvedin certain disease states. However, microelec-trode recording may increase the risk for brainhaemorrhage, especially when approaching newbrain areas via new trajectories, and thisincreased risk should be weighed against thepossible advantage of its use.
DBS influences signal transduction and brainactivity. The intention of “ideal” DBS is to nor-malize pathological brain signals without impacton non-pathological brain activity. The preciseneurophysiologic mechanisms of psychiatricdisorders and mechanism(s) of action of DBS arenot yet fully understood. At the current level ofknowledge, we have no strict delineationbetween pathological and non-pathological brainactivity for psychiatric disorders. Knowledge onelectrophysiological biomarkers is only verypreliminary. DBS is under investigation in sev-eral different brain targets and for different psy-chiatric indications. DBS is not ultimatelyaccurate. It does not only modulate pathologicalbrain circuits. It may also influence other areaswhich cause unwanted effects. Furthermore, abrain circuit may dysfunction only intermittently.DBS in that circuit may at certain moments bebeneficial for the patient, and at other momentshave no influence, or even provoke unwantedeffects.
The concept of autonomy in this chronicallyill, severely impaired patient population needsfurther development and differentiation [1].Respect for self-determination is undeniablyimportant, but the intense chronic suffering andvulnerability influence the patients’ decision-making process. Some patients want to be fullyinvolved in the deliberative consent process,others defer decision-making to significant othersor the physician in charge [18]. A psychiatricdisorder does not affect patients alone, but canhave a profound and devastating impact on thosearound them. The involvement of significantothers and caregivers in medical decision-makingprocess needs to be acknowledged [2]. Patientsdepend on these caregivers. Assessment of theexpectations and values of both patient and sig-nificant others is crucial. Caregivers and patientsmay have divergent values and priorities, influ-enced by the burden created by patient’s disor-der. This can represent an additional, largelyunrecognized, source of vulnerability in psychi-atric patients. The influence of caregivers orclose thirds can potentially translate into takingon additional ‘involuntary’ risks, including clin-ical trial enrollment. A dependent relation mayresult in undesirable pressure on the patient toadopt the caregivers preferences, and theirinvolvement can counter patient autonomy andbest interests. An acceptable approach is toconsider the psychiatric disorder as a problem ofa particular patient as well as to bear in mind thedisruptive effects of the patient’s psychiatricdisorder on significant others. Conceivable sec-ondary gains and expectations from caregiversneed clarification before the patient decides toundergo DBS [4]. The effects of DBS reach(indirectly) beyond effects on disease symptomsand not only the patient but also these significantothers will have to adapt to a new situation.
Although in psychiatric disorders cognitivedistortions and biases may be present, carefullyinstructed patients (eventually with the aid of afamily member, trusted counselor and/or legalguardian) are able to consent to complex, high-risk treatment or research proposals. Patientswith treatment refractory psychiatric disorders
7 Preoperative Evaluation and Postoperative … 79
often initiate the plea for DBS themselves. Thevery strong and demanding claim for surgerylooks in fact closer to a desire than to a statementfor informed consent. They may request dispro-portionate treatments and their desperation mayimpair their ability to rationally weigh the ben-efits against the risks. It is this paradoxical easeof securing consent in these patients that requiresa higher degree of responsibility from DBSteams in the informed consent process. Thepatient must fully understand the risks and pos-sible benefits and special attention regarding theconcept of therapeutic misconception in the caseDBS is required. This concept needs to beactively addressed, without withdrawing everyhope the patient has put in the intervention.Furthermore, we want to emphasize the ethicalrequirement that individuals, participating in tri-als on DBS for psychiatric disorders, should notbe used merely as a mean to increase our scien-tific knowledge, but always as an entity of theirown. The aim of research on therapeutic inno-vations such as DBS for psychiatric disordersgives priority to the patient, who’s safety exceedsthe stringent application of the research protocol.
DBS is an intracranial neurosurgical procedurethat comes with limited but significant risks.Aside from multidisciplinary assessment todetermine suitability for the procedure, the patientmust be able to give informed consent. Patientsshould also be counselled for the possibility thatthey may derive no benefit from DBS or not tol-erate it well, necessitating the devices to be eitherswitched of, or even their complete removal.
Even when a patient is judged to be anappropriate candidate to undergo DBS, the rightto decline this treatment proposal remains obvi-ous. The decision to decline can be linked to thepsychopathological features of the disorder.Symptoms such as pathological anxiety inherentto anxiety disorders, apathy or indifference ordisinterest in mood disorders, contaminationfears or obsessive doubting may prevent thepatient from making the decision to proceed withthe intervention. Regardless the arguments andunderpinnings of the patient’s refusal, the deci-sion is respected.
7.3 Selection Procedurefor Appropriate Candidatesand Preoperative Evaluation
Carefully identifying good candidates for DBSfor psychiatric disorders is of fundamentalimportance and must be based on sound ethicsand scientific evidence, when available. In thecurrent stage, patients must meet criteria forseverity and functional impairment, must dem-onstrate adequate treatment refractoriness, andmust be able to consent to their participation inthe research trial. During patient selection doc-tors should aim to identify candidates who willobtain and retain the greatest benefit from a DBSintervention. Patients must be able to tolerateDBS surgery and participate not only in researchprotocols, but adhere to the requirements ofpostoperative care and actively take part in it.Poorly selected patients may obtain less benefitalthough they are subject to the same risks of theDBS procedure, and thus the risk/benefit ratio inthese patients becomes more unfavorable. Pres-ently and under conditions of the investigationalstatus of DBS for psychiatric disorders, there areno standardized criteria for choosing appropriatecandidates. Nevertheless establishment of patienteligibility criteria seems of fundamental impor-tance both in optimizing efficacy and safety.Pooling the data of the different research centersis strategically important to discover prognosticfactors of poor or good outcome and to incite thecontinuous optimization of selection criteria.
A formal request for DBS for psychiatricdisorders starts with a thorough, scrutinizedreview of the complete patient file, coveringdemographic features, family history, present andpast illness history and treatment survey. Anexperienced multidisciplinary DBS team screenspotential candidates and each discipline contrib-utes with its specific expertise to the profit of thepatient and the whole team. Patients are assessedduring several introductory meetings at the out-patient clinic, to complete missing data in the fileand to provide general information about DBS. Afocus on failing or inadequate information andlacunas in the available records, especially
80 L. Gabriels et al.

regarding comorbidities or patient compliance isadamant. Comorbid conditions are frequent inpsychiatric patients. In this stage, significantothers often accompany the patient. The oftendesperate patients and their equally desperatefamilies may tend to hide facts, in order to getaccess to DBS, not realizing that this missinginformation may compromise the outcome.Family support, commitment, and expectationmay play an important role in the DBS processant its outcome and thus it seems wise to assesstheir role early in the screening process. Indi-vidual realistic and unrealistic expectations ofboth the patient and the caregiver must be con-sidered before including the patient in a study.The use of qualitative data obtained by semistructured or open in-depth interviews of patientand caregiver(s) may be necessary to detectsubjective perception and expectations of DBS.Probing the expectations of DBS outcome inboth parties enables the clinician to discuss val-ues, to re-explain possible benefits and to correctunrealistic expectations.
7.4 Inclusion Criteria for DBSin Psychiatric Disorders
Applicants for DBS should meet all defined cri-teria for severity, chronicity, disability, andtreatment refractoriness, and must have the abil-ity to give informed consent. The criteria forseverity, chronicity and treatment refractorinesswill depend on the psychiatric disorder underinvestigation. Severity can be measured withdisease specific, properly validated, standardizedoutcome scales, and in this stage of research, thethreshold for severity may be defined to justifythe use of an invasive treatment technique. Thislimits the number of candidates that participate inresearch on DBS for the psychiatric disorderunder investigation, and restricts the generaliz-ability of the research findings to a restrictedgroup of patients.
Moreover, a quality of life scale and assess-ment of functioning should be included toquantify the disruption of the psychiatric symp-toms in activities in many life domains. For everyindication, a proper, state-of-the-art, evidencebased treatment algorithm (pharmacologic, psy-chotherapeutic, less invasive neuromodulationtechniques), must be defined to allow for dem-onstration of treatment refractoriness.
Patients in less severe or earlier stages of thedisorder may show a better response to investi-gational DBS, but in this early phase of researchthe desire to do no harm justifies restricting thisexperimental procedure to those with severepsychiatric indication who have failed otherforms of treatment. There are no trials conductedin less severe, less chronic, less treatmentrefractory trial, and until now, reviews and meta-analysis of available data do not demonstratecorrelations between specific patient or illnesscharacteristics and outcome, so data to argue forthe implementation of DBS in a less severe orearlier stage of the psychiatric disorder are cur-rently lacking.
Participating in DBS research for psychiatricdisorders places a high demand on patients andtheir family or caregivers. They must agree tocome frequently to the research center for ade-quate follow-up and evaluation of specificsymptoms of the disorder under investigation, ofside effects and adverse events. Moreover there isthe follow-up on specific DBS aspects, such asthe parameter optimization and replacements ofthe neurostimulator in case of battery failure.Besides these DBS and research related visits, itis important that patients after surgery remain infollow-up with their treating psychiatrist or psy-chologist, to guide them through the (sometimesabrupt) changes in symptoms and in many lifedomains (occupational, social and relational). Wetend to discuss this and ask for a formal accep-tance on this counseling task.
Patients must be able to understand, complywith instructions and provide their own writteninformed consent. A significant other is frequently
7 Preoperative Evaluation and Postoperative … 81
involved in the process of extensive informationon available treatment options. Patients and sig-nificant others are encouraged to ask questionsand clarifications.
7.5 Exclusion Criteria
Exclusion criteria depend again on the psychiat-ric indication under investigation. Depending onthe psychiatric disorder a variety of psychiatriccomorbidities may be listed as contraindications.Personality disorders that may increase the riskof impulsive behavior or non-compliance aftersurgery are evaluated on a case-by-case basis.Surgical contraindications comprehend inabilityto undergo presurgical MRI (cardiac pacemaker,pregnancy, …), infection, coagulopathy or, sig-nificant cardiac or other medical risk factors forsurgery and possibly labeled contraindicationsfor DBS.
While the delineation of disease severity,chronicity and treatment refractoriness is not themajor problem for most psychiatric disorders, thetoxic effect on the brain of chronic alcohol ordrug consumption in addiction, or chronic star-vation in the case of anorexia nervosa maychallenge another important mandatory aspect ofenrolling a patient as a research subject: it mayhave an important impact on their competence toprovide informed consent since altered mentalfunctioning may disrupt their ability to carefullyevaluate the risks and benefits of the procedure.Moreover, even in the case of improvement ofprimary symptoms of the disorder under inves-tigation, irreversible brain damage as a sequel ofthe psychiatric disorder may become a seriousburden for the patient and cause other unwantedcognitive or behavioral challenges.
7.6 Outcome Evaluation
DBS first of all should be effective in reducing thesymptoms of the psychiatric disorder in a stableand long-lasting manner. To evaluate this primary
outcome, the use of well validated scales,designed specifically for the psychiatric indicationunder investigation, is indispensable. This doesnot mean that the aim of DBS is to get fullremission of the psychiatric disorder, or thatsymptoms should be completely suppressed, orthe patient completely cured. Many patients con-tinue to live with clinically significantly reducedsymptoms, that still may be obviously present.
To provide an actual benefit to the very indi-vidual patient, DBS not only has to improvesymptoms scores in rating scales, but it alsoneeds tobe demonstrated that these reduced scores areassociated with an actual improvement for theindividual patient. DBS-induced improvement insymptom scores, or in cognitive and physicalfunctions does not necessarily mean that the patientis better off. In other words, statistically significantefficacy is only a necessary, but not a sufficientcondition for true effectiveness, and might, in cer-tain cases, present an invalid surrogate parameterfor the patient’s true well-being [17]. To ascertainthat DBS treatment allows the patient to live a moresatisfying life, other variables (re-establishing asocial life and work, general well-being and mul-tifaceted quality of life) are needed. Assessment ofmore general psychiatric pathology, neurocogni-tive status and a comprehensive evaluation of short-and long-term adverse eventsmust complement theprimary outcome evaluation. Especially, theincorporation and dependence on the implanteddevicemay not only influence body image, butmaybe considered as a constant reminder of thecontinuing psychiatric disorder.
7.7 Surgical Intervention,Post-surgery Treatmentand Long Term Follow-up
DBS involves the stereotactic implantation ofelectrode leads into specific neuroanatomicalstructures where (in most cases) continuousstimulation is applied. Implanted leads are routedsubcutaneously and connected to an implantedneurostimulator fixed onto the pectoral fasciabelow the clavicle or onto the rectus abdominis
82 L. Gabriels et al.
fascia in the abdominal region. This neurostimu-lator delivers electrical pulses through one orseveral of the four stimulation contacts. Choice ofstimulation contacts and other stimulationparameters (amplitude, pulse width, frequency)can be modulated using an external electromag-netic programming device. Multiple adjustmentsin association with alteration in medical therapymay be required before stable stimulationparameters are achieved. DBS is non-ablative andtherefore reversible in the sense that the stimula-tion can be switched off should the patient wantso, or in case of intolerable side effects.
DBS has both acute and long-term effects, andstimulation parameters can and should be adjus-ted to attain an optimal therapeutic effect in everyindividual patient. For patients, the stageencompassing the surgical intervention is oftenmarked by emotional instability and insecurity.They go from despair to a state of hope, but at thesame time, they react often in a black and white,“now or never” or “all or nothing” manner. Thepresence of the psychiatrist in the operatingtheater is not a must, but for patients, this givesrise to trust and reassurance.
Postoperatively, patients must have access toa standardized, frequent follow-up in a multi-disciplinary team. A close collaboration withinthis multidisciplinary team between a psychiatristwith special expertise in the psychiatric disorderunder investigation, a neurosurgeon with ampleexpertise in the field of stereotactic and func-tional neurosurgery and a neuropsychologist isvital. Moreover, this team must have access toother specialties (neurology, social worker,neuro-imaging specialist, …) for consultationson an ad hoc basis. Adequate psychiatric andpsychotherapeutic post-surgery treatment andfollow-up must be available, not only for thor-ough assessment of research outcome, but also tohelp patients to resume their lives.
After DBS surgery, there is the time-con-suming search for adequate stimulation parame-ters with sometimes unexpected side-effects andfluctuations in symptom severity. Ultimately thefeeling of being dependent on a foreign devicemay require extra attention from the clinician.The process of programming the leads after DBS
surgery is complicated and time/labor-intensive.Nevertheless optimization of possible settings,with thoughtful changes to the configuration ofthe active electrodes, pulse widths, frequencies,amplitudes and configuration of anodes andcathodes, is critical for therapeutic success orfailure. Acute stimulation effects are sometimesdisturbing for the patients and may fade awayafter some days. They are not always predictivefor the long-term outcome. The time involved toobserve clinical effects after a programmingchange is sometimes very short (seconds tominutes), and the changes may appear veryabrupt, but it often takes longer to obtain a stablesymptom reduction. This contributes to the manymonths, with several sessions of optimization ofstimulation parameters, necessary to obtain thefull clinical benefit from DBS. The person whoprograms must know the patient well enough toread changes in symptoms associated withchanges in parameters. The use of standardizedself-rated and observer-rated instruments andblinded DBS adjustments is only a partial aid.
Patients may not be abandoned or left withoutprofessional after-care once the DBS procedureis performed. With improvement of symptoms,patients are less stuck in their chronic psychiatricdisorder and sometimes need help in the defini-tion of new goals and new purposes in life andwith the development of new intentions and newplans. They often go through a mourning processfor the years and life options lost in the disorderdue to the formerly severe psychiatric symptoms.In the follow-up period, guidance should focuson the development of new abilities in the eventof major therapeutic benefits, and on the accep-tance of limitations if residual symptoms remain.Over the extended period of follow-up, signifi-cant others are interested in providing the bestguidance, but they require instruction in theirexpectations as well [5]. Patient and familiesoften have a lot of questions about living withDBS. Since DBS gives mostly symptomaticrelief, they feel dependent on the optimal func-tioning of the hardware and dread a malfunction.
Patients may need help to adjust to their greaterdegree of independence and autonomy.Moreover,postoperative psychiatric and psychotherapeutic
7 Preoperative Evaluation and Postoperative … 83

care are important since sometimes postoperativepsychiatric problems may be related to emergenceof previously existing disorders that had not beennoted preoperatively, or were covered by the verysevere primary psychiatric disorder for whichDBS was indicated.
When patients change as a consequence ofsymptom reduction, meaningful relationshipswith caregivers may need redefinition. Patientsmay become less dependent or even independenton their caregivers. Partners need to switch fromthe role of a caregiver to more equality in therelationship. They may need help to cope withthe changed balance, and sometimes partnersneed training in coping and communicationskills. Moreover, patients and caregivers need tolearn to live with the technical aspects of DBSand need close monitoring for re-appearance ofpsychiatric symptoms due to battery depletion oraccidental deactivation.
Since one of the purposes of current researchon DBS for psychiatric disorders is to test effi-cacy, patients need to be aware that there is acertain possibility of failure, hitherto unknownadverse events and an insufficient understandingof the reasons why some patients respond well toDBS treatment and others don’t. If the patientexpects full remission of the psychiatric symp-toms in the context of a trial, but turns out to beeither a partial responder or non-responder, theresulting disappointment needs to be dealt with.Occasionally, although the multidisciplinaryDBS team may be satisfied with the outcome ofDBS treatment, patient or family do not neces-sarily share this opinion. In optimal circum-stances adequate pre-operative educationregarding reasonable and unreasonable expecta-tions would have prevented such discrepancy,but patients may still fail to appreciate the com-plexity of symptom relief on the one hand andsatisfaction and general quality of life on theother. Patients may show dissatisfaction withsymptom control, or with the emergence of newor worsening symptoms and adverse effects.Often, the residual symptoms they complainabout include both symptoms of the psychiatricdisorder that were expected to benefit from DBSas well as symptoms for which DBS was not
intended in the first place (e.g. they want moreenergy, a better relationship, less headache, …),but hoped to obtain. The need of repetitivepre-operative education to reinforce realisticexpectations is once-more crucial to preventdisappointment with the outcome.
References
1. Agich GJ. Reassessing autonomy in long-term care.Hastings Cent Rep. 1990;20:12–7.
2. Anita H. Relational autonomy or undue pressure?Family’s role in medical decision-making. Scand JCaring Sci. 2008;22:128–35.
3. Denys D, Mantione M, Figee M, et al. Deep brainstimulation of the nucleus accumbens for treatment-refractory obsessive-compulsive disorder. Arch GenPsychiatry. 2010;67:1061–8.
4. Donchin A. Understanding autonomy relationally:toward a reconfiguration of bioethical principles.J Med Philos. 2001;26:365–86.
5. Gabriëls L, Cosyns P, Nuttin B. Clinical guidance inneuromodulation: keeping track of the process and thepatient. Neuromodulation. 2007;10(2):179–80.
6. Gabriëls L, Nuttin B, Cosyns P. Applicants forstereotactic neurosurgery for psychiatric disorders:role of the Flemish advisory board. Acta PsychiatrScand. 2008;117(5):381–9.
7. Greenberg B, Gabriels L, Malone DA Jr, et al. Deepbrain stimulation of the ventral internal capsule/ventralstriatum for obsessive-compulsive disorder: worldwideexperience. Mol Psychiatry. 2008;15(1):64–79.
8. Israël M, Steiger H, Kolivakis T, et al. Deep brainstimulation in the subgenual cingulate cortex for anintractable eating disorder. Biol Psychiatry. 2010;67(9):e53–4.
9. Lozano AM, Mayberg HS, Giacobbe P, et al.Subcallosal cingulate gyrus deep brain stimulationfor treatment-resistant depression. Biol Psychiatry.2008;64(6):461–7.
10. Maley JH, Jorge E, Alvernia JE, et al. Deep brainstimulation of the orbitofrontal projections for thetreatment of intermittent explosive disorder.Neurosurg Focus. 2010;29(2):E11.
11. Mallet L, Polosan M, Jaafari N, et al. Subthalamicnucleus stimulation in severe obsessive-compulsivedisorder. N Engl J Med 2008;359(20):2121–34.
12. Malone DA Jr, Dougherty DD, Rezai AR, et al. Deepbrain stimulation of the ventral capsule/ventralstriatum for treatment-resistant depression. BiolPsychiatry. 2009;65(4):267–75.
13. Müller UJ, Sturm V, Voges J, et al. Successfultreatment of chronic resistant alcoholism by deepbrain stimulation of nucleus accumbens: firstexperience with three cases. Pharmacopsychiatry.2009;42:288–92.
84 L. Gabriels et al.

14. Nuttin B, Gabriëls L, Cosyns P, et al. Long-termelectrical capsular stimulation in patients withobsessive-compulsive disorder. Neurosurgery.2003;52(6):1263–74.
15. Nuttin B, Wu H, Mayberg H, et al. Consensus onguidelines for stereotactic neurosurgery for psychiatricdisorders. J Neurol Neurosurg Psychiatry. 2014.doi:10.1136/jnnp-2013-306580.
16. Schlaepfer TE, Cohen MX, Frick C, et al. Deep brainstimulation to reward circuitry alleviates anhedonia inrefractorymajor depression.Neuropsychopharmacology.2008;33(2):368–77.
17. Synofzik M, Schlaepfer TE. Electrodes in the brain—ethical criteria for research and treatment with deepbrain stimulation for neuropsychiatric disorders.Brain Stimul. 2011;4(1):7–16.
18. Waterworth S, Luker KA. Reluctant collaborators: dopatients want to be involved in decisions concerningcare? J Adv Nurs. 1990;15:971–6.
19. World Health Organization: Health for all by the year2000: strategies. Geneva, Switzerland, 1980. WHOofficial document 173.
7 Preoperative Evaluation and Postoperative … 85
8Ablative Surgery for Depression
Sam Eljamel
Abstract
Treatment refractory depression (TRMDD) is not uncommon despiteadequate anti-depressive treatment trials. Patients who failed adequate trialsof anti-depressive therapy including electroconvulsive therapy (ECT) arecandidates for stereotactic surgery for mental illnesses. Ablative neurosur-gery for TRMDD is performed in 21st century in highly specialized centers,where stereotactic surgeons teamed up with specialized psychiatristsworking within stringent governance and ethical guidelines specificallydesigned for this purpose. The most commonly used procedures today arestereotactic bilateral anterior cingulotomy (BACI) or capsulotomy(BACA). Both thermal coagulation and stereotactic radiosurgery are usedto ablate the desired targets. These procedures are safe with good trackrecord. Forty to sixty percent of carefully selected patients with TRMDDare expected to respond or remit within a year of follow up. Response isdefined as at least 50 % improvement on validated depression scales, whileremission is defined as returning to normal mood and behavior.
8.1 Introduction
The World Mental Health Survey conducted in17 countries found that on average about one intwenty people reported having an episode ofdepression [17], with a lifelong prevalence ofmajor depression disorder (MDD) of 6.7 % [28].Up to 20 % of MDD becomes chronic lastingmore than two years and treatment resistant [14].The management of patients with treatment
resistant MDD (TRMDD) is very challengingwith only 13 % or less remit after four adequateantidepressant trials [22].
Ablative surgery was first used to treat chronicneuropathic pain and during surgery somepatients reported changes in mood during theprocedures, particularly in patients with co-mor-bid symptoms of depression or anxiety leading toits use in TRMDD for several decades. Foltz andWhite described cingulotomy in 1962 [6], whilestereotactic anterior capsulotomy was describedby Leksell in 1978 [16]. Several other targets inthe limbic system circuits were used to treatTRMDD. This chapter summarizes the differentablative surgery for TRMDD.
S. Eljamel (&)Department of Neurosurgery, University of Dundee,Dundee, Scotland, UKe-mail: [email protected]
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0_8© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
87
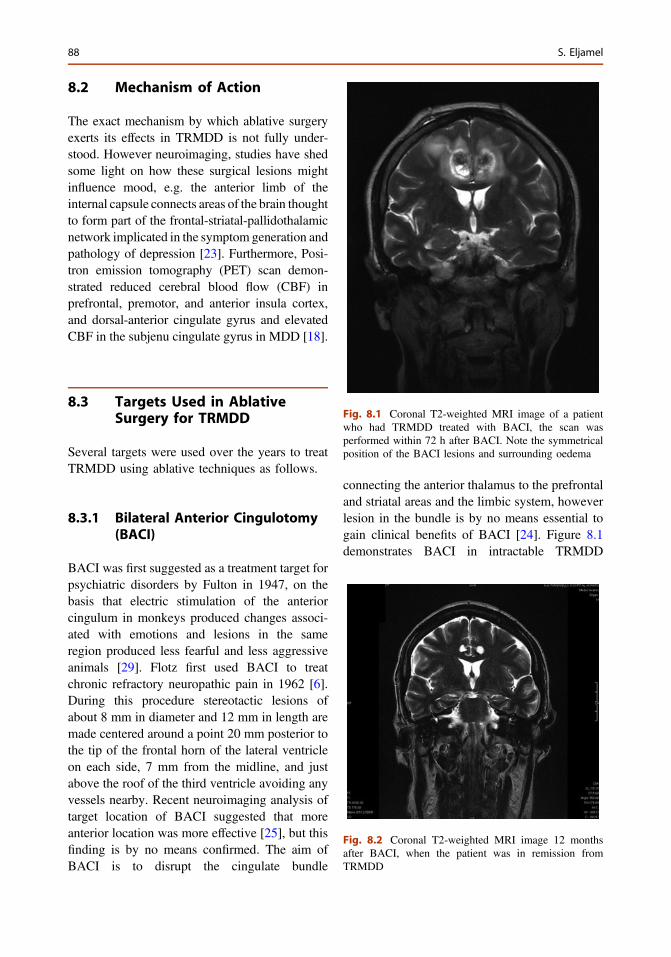
8.2 Mechanism of Action
The exact mechanism by which ablative surgeryexerts its effects in TRMDD is not fully under-stood. However neuroimaging, studies have shedsome light on how these surgical lesions mightinfluence mood, e.g. the anterior limb of theinternal capsule connects areas of the brain thoughtto form part of the frontal-striatal-pallidothalamicnetwork implicated in the symptom generation andpathology of depression [23]. Furthermore, Posi-tron emission tomography (PET) scan demon-strated reduced cerebral blood flow (CBF) inprefrontal, premotor, and anterior insula cortex,and dorsal-anterior cingulate gyrus and elevatedCBF in the subjenu cingulate gyrus in MDD [18].
8.3 Targets Used in AblativeSurgery for TRMDD
Several targets were used over the years to treatTRMDD using ablative techniques as follows.
8.3.1 Bilateral Anterior Cingulotomy(BACI)
BACI was first suggested as a treatment target forpsychiatric disorders by Fulton in 1947, on thebasis that electric stimulation of the anteriorcingulum in monkeys produced changes associ-ated with emotions and lesions in the sameregion produced less fearful and less aggressiveanimals [29]. Flotz first used BACI to treatchronic refractory neuropathic pain in 1962 [6].During this procedure stereotactic lesions ofabout 8 mm in diameter and 12 mm in length aremade centered around a point 20 mm posterior tothe tip of the frontal horn of the lateral ventricleon each side, 7 mm from the midline, and justabove the roof of the third ventricle avoiding anyvessels nearby. Recent neuroimaging analysis oftarget location of BACI suggested that moreanterior location was more effective [25], but thisfinding is by no means confirmed. The aim ofBACI is to disrupt the cingulate bundle
connecting the anterior thalamus to the prefrontaland striatal areas and the limbic system, howeverlesion in the bundle is by no means essential togain clinical benefits of BACI [24]. Figure 8.1demonstrates BACI in intractable TRMDD
Fig. 8.1 Coronal T2-weighted MRI image of a patientwho had TRMDD treated with BACI, the scan wasperformed within 72 h after BACI. Note the symmetricalposition of the BACI lesions and surrounding oedema
Fig. 8.2 Coronal T2-weighted MRI image 12 monthsafter BACI, when the patient was in remission fromTRMDD
88 S. Eljamel
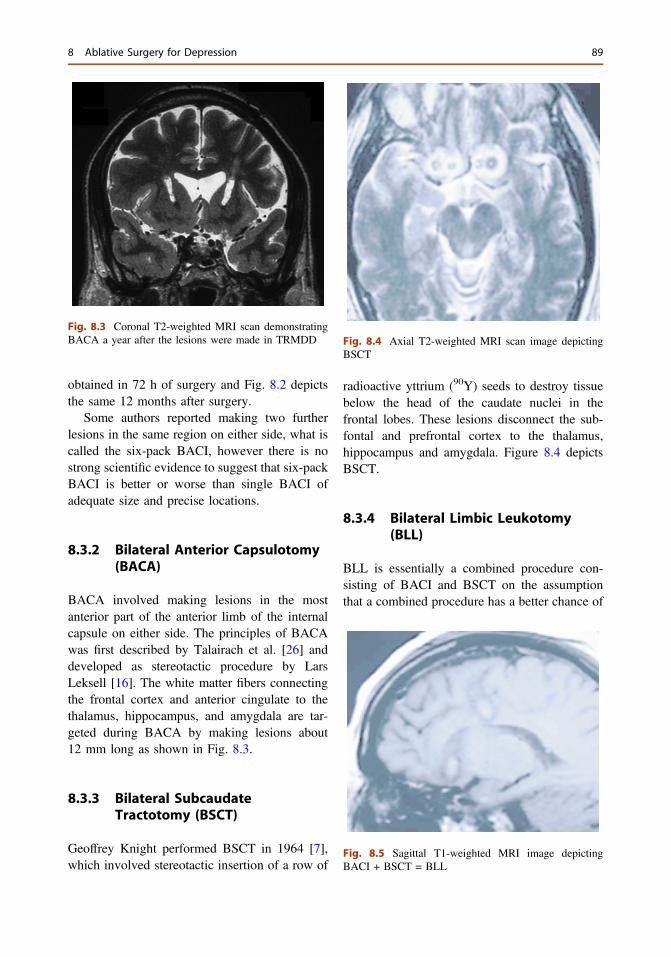
obtained in 72 h of surgery and Fig. 8.2 depictsthe same 12 months after surgery.
Some authors reported making two furtherlesions in the same region on either side, what iscalled the six-pack BACI, however there is nostrong scientific evidence to suggest that six-packBACI is better or worse than single BACI ofadequate size and precise locations.
8.3.2 Bilateral Anterior Capsulotomy(BACA)
BACA involved making lesions in the mostanterior part of the anterior limb of the internalcapsule on either side. The principles of BACAwas first described by Talairach et al. [26] anddeveloped as stereotactic procedure by LarsLeksell [16]. The white matter fibers connectingthe frontal cortex and anterior cingulate to thethalamus, hippocampus, and amygdala are tar-geted during BACA by making lesions about12 mm long as shown in Fig. 8.3.
8.3.3 Bilateral SubcaudateTractotomy (BSCT)
Geoffrey Knight performed BSCT in 1964 [7],which involved stereotactic insertion of a row of
radioactive yttrium (90Y) seeds to destroy tissuebelow the head of the caudate nuclei in thefrontal lobes. These lesions disconnect the sub-fontal and prefrontal cortex to the thalamus,hippocampus and amygdala. Figure 8.4 depictsBSCT.
8.3.4 Bilateral Limbic Leukotomy(BLL)
BLL is essentially a combined procedure con-sisting of BACI and BSCT on the assumptionthat a combined procedure has a better chance of
Fig. 8.3 Coronal T2-weighted MRI scan demonstratingBACA a year after the lesions were made in TRMDD Fig. 8.4 Axial T2-weighted MRI scan image depicting
BSCT
Fig. 8.5 Sagittal T1-weighted MRI image depictingBACI + BSCT = BLL
8 Ablative Surgery for Depression 89
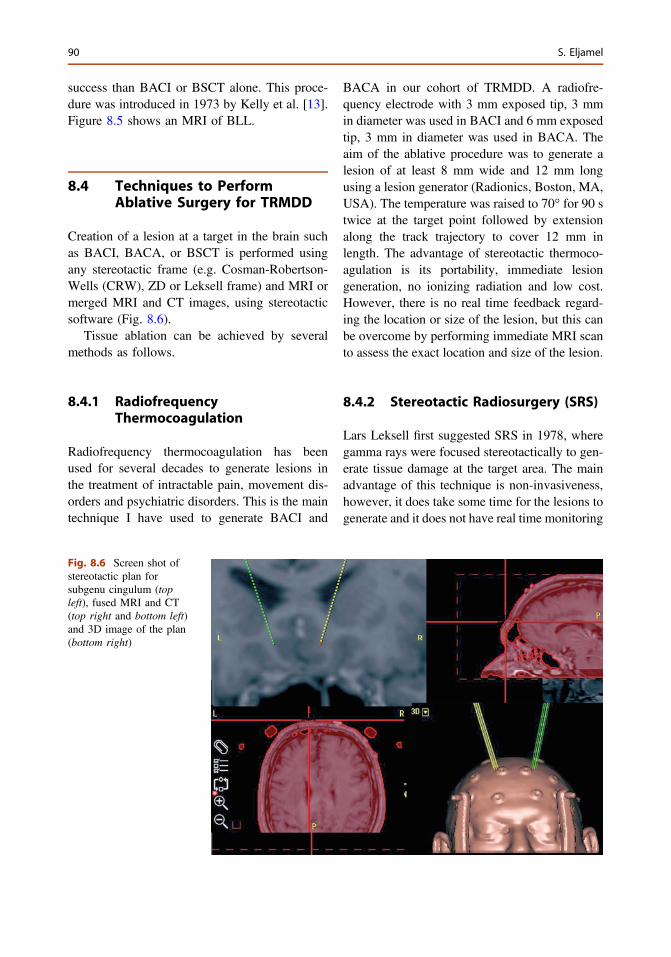
success than BACI or BSCT alone. This proce-dure was introduced in 1973 by Kelly et al. [13].Figure 8.5 shows an MRI of BLL.
8.4 Techniques to PerformAblative Surgery for TRMDD
Creation of a lesion at a target in the brain suchas BACI, BACA, or BSCT is performed usingany stereotactic frame (e.g. Cosman-Robertson-Wells (CRW), ZD or Leksell frame) and MRI ormerged MRI and CT images, using stereotacticsoftware (Fig. 8.6).
Tissue ablation can be achieved by severalmethods as follows.
8.4.1 RadiofrequencyThermocoagulation
Radiofrequency thermocoagulation has beenused for several decades to generate lesions inthe treatment of intractable pain, movement dis-orders and psychiatric disorders. This is the maintechnique I have used to generate BACI and
BACA in our cohort of TRMDD. A radiofre-quency electrode with 3 mm exposed tip, 3 mmin diameter was used in BACI and 6 mm exposedtip, 3 mm in diameter was used in BACA. Theaim of the ablative procedure was to generate alesion of at least 8 mm wide and 12 mm longusing a lesion generator (Radionics, Boston, MA,USA). The temperature was raised to 70° for 90 stwice at the target point followed by extensionalong the track trajectory to cover 12 mm inlength. The advantage of stereotactic thermoco-agulation is its portability, immediate lesiongeneration, no ionizing radiation and low cost.However, there is no real time feedback regard-ing the location or size of the lesion, but this canbe overcome by performing immediate MRI scanto assess the exact location and size of the lesion.
8.4.2 Stereotactic Radiosurgery (SRS)
Lars Leksell first suggested SRS in 1978, wheregamma rays were focused stereotactically to gen-erate tissue damage at the target area. The mainadvantage of this technique is non-invasiveness,however, it does take some time for the lesions togenerate and it does not have real time monitoring
Fig. 8.6 Screen shot ofstereotactic plan forsubgenu cingulum (topleft), fused MRI and CT(top right and bottom left)and 3D image of the plan(bottom right)
90 S. Eljamel
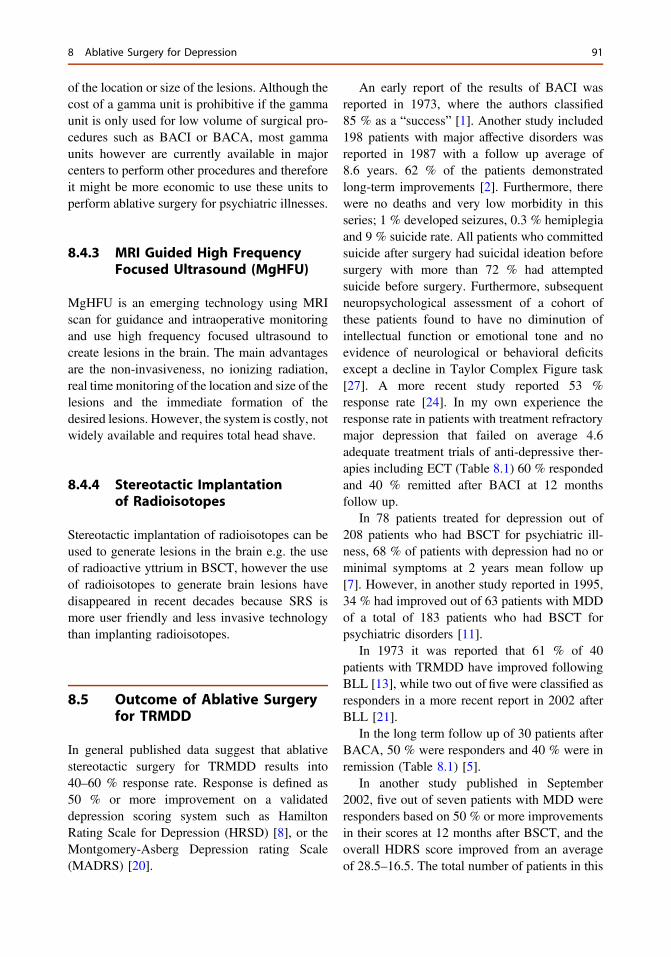
of the location or size of the lesions. Although thecost of a gamma unit is prohibitive if the gammaunit is only used for low volume of surgical pro-cedures such as BACI or BACA, most gammaunits however are currently available in majorcenters to perform other procedures and thereforeit might be more economic to use these units toperform ablative surgery for psychiatric illnesses.
8.4.3 MRI Guided High FrequencyFocused Ultrasound (MgHFU)
MgHFU is an emerging technology using MRIscan for guidance and intraoperative monitoringand use high frequency focused ultrasound tocreate lesions in the brain. The main advantagesare the non-invasiveness, no ionizing radiation,real time monitoring of the location and size of thelesions and the immediate formation of thedesired lesions. However, the system is costly, notwidely available and requires total head shave.
8.4.4 Stereotactic Implantationof Radioisotopes
Stereotactic implantation of radioisotopes can beused to generate lesions in the brain e.g. the useof radioactive yttrium in BSCT, however the useof radioisotopes to generate brain lesions havedisappeared in recent decades because SRS ismore user friendly and less invasive technologythan implanting radioisotopes.
8.5 Outcome of Ablative Surgeryfor TRMDD
In general published data suggest that ablativestereotactic surgery for TRMDD results into40–60 % response rate. Response is defined as50 % or more improvement on a validateddepression scoring system such as HamiltonRating Scale for Depression (HRSD) [8], or theMontgomery-Asberg Depression rating Scale(MADRS) [20].
An early report of the results of BACI wasreported in 1973, where the authors classified85 % as a “success” [1]. Another study included198 patients with major affective disorders wasreported in 1987 with a follow up average of8.6 years. 62 % of the patients demonstratedlong-term improvements [2]. Furthermore, therewere no deaths and very low morbidity in thisseries; 1 % developed seizures, 0.3 % hemiplegiaand 9 % suicide rate. All patients who committedsuicide after surgery had suicidal ideation beforesurgery with more than 72 % had attemptedsuicide before surgery. Furthermore, subsequentneuropsychological assessment of a cohort ofthese patients found to have no diminution ofintellectual function or emotional tone and noevidence of neurological or behavioral deficitsexcept a decline in Taylor Complex Figure task[27]. A more recent study reported 53 %response rate [24]. In my own experience theresponse rate in patients with treatment refractorymajor depression that failed on average 4.6adequate treatment trials of anti-depressive ther-apies including ECT (Table 8.1) 60 % respondedand 40 % remitted after BACI at 12 monthsfollow up.
In 78 patients treated for depression out of208 patients who had BSCT for psychiatric ill-ness, 68 % of patients with depression had no orminimal symptoms at 2 years mean follow up[7]. However, in another study reported in 1995,34 % had improved out of 63 patients with MDDof a total of 183 patients who had BSCT forpsychiatric disorders [11].
In 1973 it was reported that 61 % of 40patients with TRMDD have improved followingBLL [13], while two out of five were classified asresponders in a more recent report in 2002 afterBLL [21].
In the long term follow up of 30 patients afterBACA, 50 % were responders and 40 % were inremission (Table 8.1) [5].
In another study published in September2002, five out of seven patients with MDD wereresponders based on 50 % or more improvementsin their scores at 12 months after BSCT, and theoverall HDRS score improved from an averageof 28.5–16.5. The total number of patients in this
8 Ablative Surgery for Depression 91
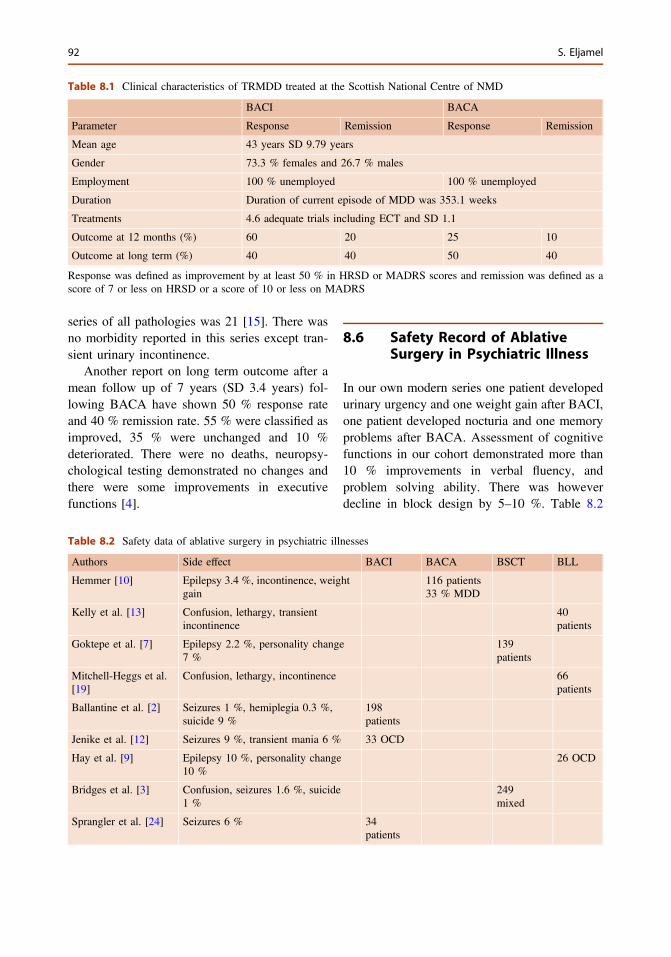
series of all pathologies was 21 [15]. There wasno morbidity reported in this series except tran-sient urinary incontinence.
Another report on long term outcome after amean follow up of 7 years (SD 3.4 years) fol-lowing BACA have shown 50 % response rateand 40 % remission rate. 55 % were classified asimproved, 35 % were unchanged and 10 %deteriorated. There were no deaths, neuropsy-chological testing demonstrated no changes andthere were some improvements in executivefunctions [4].
8.6 Safety Record of AblativeSurgery in Psychiatric Illness
In our own modern series one patient developedurinary urgency and one weight gain after BACI,one patient developed nocturia and one memoryproblems after BACA. Assessment of cognitivefunctions in our cohort demonstrated more than10 % improvements in verbal fluency, andproblem solving ability. There was howeverdecline in block design by 5–10 %. Table 8.2
Table 8.1 Clinical characteristics of TRMDD treated at the Scottish National Centre of NMD
BACI BACA
Parameter Response Remission Response Remission
Mean age 43 years SD 9.79 years
Gender 73.3 % females and 26.7 % males
Employment 100 % unemployed 100 % unemployed
Duration Duration of current episode of MDD was 353.1 weeks
Treatments 4.6 adequate trials including ECT and SD 1.1
Outcome at 12 months (%) 60 20 25 10
Outcome at long term (%) 40 40 50 40
Response was defined as improvement by at least 50 % in HRSD or MADRS scores and remission was defined as ascore of 7 or less on HRSD or a score of 10 or less on MADRS
Table 8.2 Safety data of ablative surgery in psychiatric illnesses
Authors Side effect BACI BACA BSCT BLL
Hemmer [10] Epilepsy 3.4 %, incontinence, weightgain
116 patients33 % MDD
Kelly et al. [13] Confusion, lethargy, transientincontinence
40patients
Goktepe et al. [7] Epilepsy 2.2 %, personality change7 %
139patients
Mitchell-Heggs et al.[19]
Confusion, lethargy, incontinence 66patients
Ballantine et al. [2] Seizures 1 %, hemiplegia 0.3 %,suicide 9 %
198patients
Jenike et al. [12] Seizures 9 %, transient mania 6 % 33 OCD
Hay et al. [9] Epilepsy 10 %, personality change10 %
26 OCD
Bridges et al. [3] Confusion, seizures 1.6 %, suicide1 %
249mixed
Sprangler et al. [24] Seizures 6 % 34patients
92 S. Eljamel
summarizes the safety record of ablative surgeryin psychiatric illnesses.
In summary ablative surgery fro TRMDD issafe, the risk of seizures is the same as any otherstereotactic procedure 1–2 %, which can beabolished by using non-invasive techniques topreform the lesions e.g. SRS or MgHFUS.Transient confusion or transient incontinence arenot common and they resolve within days toweeks, and the risk of permanent neurologicaldeficit is less than 1 %.
8.7 Conclusions
The most commonly used ablative procedures forTRMDD in the 21st century are BACI andBACA, they carry very low risk of seizures orpermanent neurological deficit. 40–60 % ofTRMDD respond to ablative surgery. Theseprocedures however, should only be performedunder stringent protocols by qualified multidis-ciplinary teams consisting of a stereotactic neu-rosurgeon, specialized psychiatrists, specializedneuropsychologists, specialist psychiatric nursesand supportive staff.
References
1. Bailey H, Dowling J, Davies E. Studies in depressionIII. Med J Aus. 1973;2:366–71.
2. Ballantine HT, et al. Treatment of psychiatric illnessby stereotactic cingulotomy. Biol Psychiatry.1987;22:807–19.
3. Bridges PK, et al. Psychsurgery: stereotacticsubcaudate tractotomy, an indispensible treatment.Brit J Psychiatry. 1994;165:599–613.
4. Christmas D, Eljamel S, et al. Long term outcome ofthermal anterior capsulotomy for chronic treatmentrefractory depression. JNNP. 2011;82:594–600.
5. Eljamel S. Strategies fro the return of behavioralsurgery. Surg Neurol Int. 2012;3:34–9.
6. Foltz EL, White LE. Pain relief by frontalcingulotomy. J Neurosurg. 1962;19:89–94.
7. Goktepe EO, Young LB, Bridges PK. A furtherreview of the results of stereotactic subcaudatetractotomy. Brit J Psychiatry. 1975;128:270–80.
8. Hamilton A. A rating scale for depression. JNNP.1960;23:56–63.
9. Hay P, et al. Treatment of obsessive compulsivedisorder by psychosurgery. Acta Psychiatr Scand.1995;87:197–207.
10. Hemmer T. Treatment of mental disorders withfrontal stereotactic thermo-lesions: a follow up of116 cases. Acta Psychiatr Scand. 1961;153:36.
11. Hopkins AD, et al. Outcome after the psychosurgicaloperation of stereotactic subcaudate tractotomy1979–1991. J Neuropsychiatry Clin Neurosci.1995;7:230–4.
12. Jenike MA, et al. Cingulotomy for refractoryobsessive compulsive disorder: a long term followup in 33 patients. Arch Gen Psychiatry.1991;48:548–55.
13. Kelly D, et al. Stereotactic limbic leucotomy: apreliminary report on forty patients. Brit J Psychiatry.1973;123:141–8.
14. Kennedy N, et al. Remission and recurrence ofdepression in the maintenance era: long term outcomein a Cambridge cohort. Psychol Med.2003;33:927–38.
15. Kim M-C, Lee T-K, Choi C-R. Review of long termresults of stereotactic psychosurgery. Neurol MedChir (Tokyo). 2002;42:365–71.
16. Leksell L, et al. Radiosurgical capusolotomy—aclosed surgical method for psychiatric surgery.Lakartidningen. 1978;75:546–7.
17. Marcus M, et al. Depression: a global public healthconcern. http://www.who.int/mental_health/management/depression/who_paper_depression_wfmh_2012.pdf. Accessed on 29 Dec 2013.
18. Meyberg HS, et al. Deep brain stimulation fortreatment resistant depression. Neuron.2005;45:651–60.
19. Mitchell-Heggs N, Kelly D, Richardson A.Stereotactic limbic leucotomy: a follow up at 16months. Brit J Psychiatry. 1976;128:226–40.
20. Montgomery SA, Asberg M. A new depression scaledesigned to be sensitive to change. Brit J Psychiatry.1979;134:382–9.
21. Montoya A, et al. Magnetic resonance imagingguided stereotactic limbic leucotomy for treatmentof intractable psychiatric disease. Neurosurg.2002;50:1043–52.
22. Rush AJ, et al. Acute and longer-term outcomes indepressed patients requiring one or several treatmentsteps. Am J Psychiatry. 2006;163:1905–17.
23. Siminowicz DA, et al. Limbic-frontal circuitry inmajor depression, a path modeling metanlysis.Neuroimage. 2004;22:409–18.
24. Spangler WJ, et al. Magnetic resonance image-guidedstereotactic cingulotomy for intractable psychiatricdisease. Neurosurgery. 1996;38:1071–6.
25. Steele JD, et al. Anterior cingulotomy for majordepression: clinical outcome and relationship to
8 Ablative Surgery for Depression 93
lesion characteristics. Biol Psychiatry. 2008;63:670–7.
26. Talairach J, et al. Lobotomie prefontale limitee parelectrocoagulation des fibres thalamo-frontalisemergence du bras anterior de la capsule interne.Proceedings of the 4th Congress NeurologiqueInternationale. 1949;41.
27. Teuber HL, Corkin SH, Twitchell TE. Study ofcingultomy in man. In: Sweet WH, Obradar S,
Martin-Rodriguez JG, editors. Neurosurgicaltreatment in psychiatry, pain and epilepsy.Baltimore: University Park Press; 1977. p. 355–62.
28. Waraich P, et al. Prevalence and incidence studies ofmood disorders, a systematic review of the literature.Can J Psychiatry. 2004;124:0706–7437.
29. Ward AA. The cingular gyrus, area 24. J Neurophysiol.1948;11:13–23.
94 S. Eljamel
9Deep Brain Stimulationfor the Managementof Treatment-Refractory MajorDepressive Disorder
Nir Lipsman, Peter Giacobbe and Andres M. Lozano
Abstract
Major Depressive Disorder (MDD) is among the most common psychiatricconditions, and is responsible for substantial human morbidity worldwide.The last two decades have seen significant progress in our understanding ofthe neural circuits driving MDD, which is now increasingly understood as adisorder of neural circuitry. The success of deep brain stimulation (DBS) asa modulator of circuit dysfunction in motor disorders such as Parkinson’sDisease has generated interest in it’s use in other circuit-based conditions,including MDD. The result has been resurgence in interest in surgery forrefractory mood disorders, where advances in functional imaging havehelped identify key anatomic targets as critical notes in the circuit. Thischapter reviews the history of surgery for major depression, the rationalefor focal neuromodulation in the condition, and provides a summary of theclinical experience of DBS in MDD to date.
9.1 Background
Major Depressive Disorder (MDD) is among themost common psychiatric conditions, with apopulation lifetime prevalence of 14–17 % [1–3].The costs of MDD are substantial, and representone of society’s most significant sources of lostwages and productivity [4]. Other costs are more
difficult to measure, and relate to the humansuffering wrought by an illness that has chal-lenged clinicians for centuries [5]. The last twodecades, however, have seen much progress inelucidating the brain circuits driving depressedmood, and offer hope that a better understandingof the illness may lead to new and improvedtherapeutic options.
MDD is highly heterogeneous. Althoughsadness is a defining feature, other brain systemssuch as reward, cognition, and vegetative func-tions, are involved, suggesting a more complexpicture of disease etiology and maintenance. Forexample, patients with MDD report high degreesof anhedonia, or lack of pleasure with previouslypleasurable activities, which implicates dysfunc-tion in reward circuitry. Basal vegetative func-tions, such as sleep, sexual arousal and appetite,
N. Lipsman (&) � A.M. LozanoDivision of Neurosurgery, Toronto WesternHospital, University Health Network, University ofToronto, Toronto, Canada
P. GiacobbeDepartment of Psychiatry, Toronto General Hospital,University Health Network, University of Toronto,Toronto, Canada
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0_9© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
95
are often disturbed, implicating dysfunction inautonomic and regulatory circuits. Further,symptoms such as rumination, agitation, patho-logic crying, and suicidality, all support thenotion that MDD is more than merely a ‘deficit’state [6]. MDD, therefore, cannot be ascribed to asingle anatomic structure or circuit, and is likelya manifestation of network wide dysfunctionaffecting multiple circuits and involving multipleneurotransmitter systems.
The mainstays of treatment for MDD arepsychopharmacologic and psychotherapeutic,and are most effective when used in tandem.Medical treatments are aimed at restoring con-centrations of key neurotransmitters, most nota-bly serotonin, dopamine and norepinephrine,while psychosocial treatments attempt to identifyand correct maladaptive cognitive biases influ-encing behavior. A large study in nearly 3,000patients with MDD found that response andremission rates with a single serotonin-reuptakeinhibitor (SRI) were 47 and 28 %, respectively[7]. Subsequent studies found that even aftercontinued dose and drug escalations remissionrates improved to only 60 % [8, 9]. Such resultsshow that despite optimal medical management,at least one-third of MDD patients remainsymptomatic. For these patients neuromodulationoptions are available [8].
Neuromodulation for MDD can be dividedinto non-invasive and invasive. The advantagesof non-invasive approaches, such as electrocon-vulsive therapy (ECT) and repetitive transcranialmagnetic stimulation (rTMS), are the absence ofsurgical risk as well as their relatively low-costand widespread availability. Although effectivein some patients, it may be difficult to maintainefficacy in long-term follow-up, and in someinstances, such as with ECT, repeated use may beassociated with deleterious effects on cognitivefunctioning [10]. Nevertheless, ECT is highlyeffective in the management of some types ofrefractory MDD, and remains the ‘gold-standard’for neuromodulation in this patient group [8].Invasive approaches are typically reserved forpatients who have failed non-invasive attempts,and provide a permanent or chronic means ofadjusting dysfunctional neural circuitry. Next, we
review the rationale and experience for invasiveneuromodulation in MDD, focusing specificallyon the development of DBS.
9.2 Rationale for DBS in MajorDepression
Several factors led to the investigation of DBSfor MDD. First, was the establishment of DBS asa safe and effective procedure for a range ofneurologic, typically motor, diseases [11–14]. Asa result, over 100,000 patients world-wide haveundergone DBS, most commonly for Parkinson’sDisease, essential tremor, and dystonia [11]. Thisability to focally modulate neural circuits moti-vated the investigation of DBS in other circuit-based disorders, including psychiatric conditions.An additional development has been structuraland functional imaging, which have helpedidentify key nodes in limbic circuitry drivingpathologic mood. fMRI and PET helped estab-lish hypothesis-driven models of neural circuitdysfunction, and suggested anatomic targets forDBS procedures. Finally, the existence of a coregroup of patients, up to a third with MDD, whohave no available treatment options, has spurredclinicians to search for novel, safe and effectivetreatment options (Fig. 9.1).
9.2.1 Neurosurgery for Depression
Surgery for depression is among the oldest pro-cedures in neurosurgery, with reports of limbicleucotomy, and prefrontal lobotomy, extendingback to the early 1940s [15–17]. Early attempts,however, were crude with targeting aided onlyby surface landmarks, and involving broad dis-connections of frontal white matter tracts[16–18]. The introduction of stereotactic tech-niques, whereby lesions could be generatedanywhere in the brain with millimeter-scaleaccuracy, led to the development of cingulotomyand capsulotomy, which specifically tackleddisorders of mood. Cingulotomy involves bilat-erally lesioning the anterior cingulate cortex
96 N. Lipsman et al.
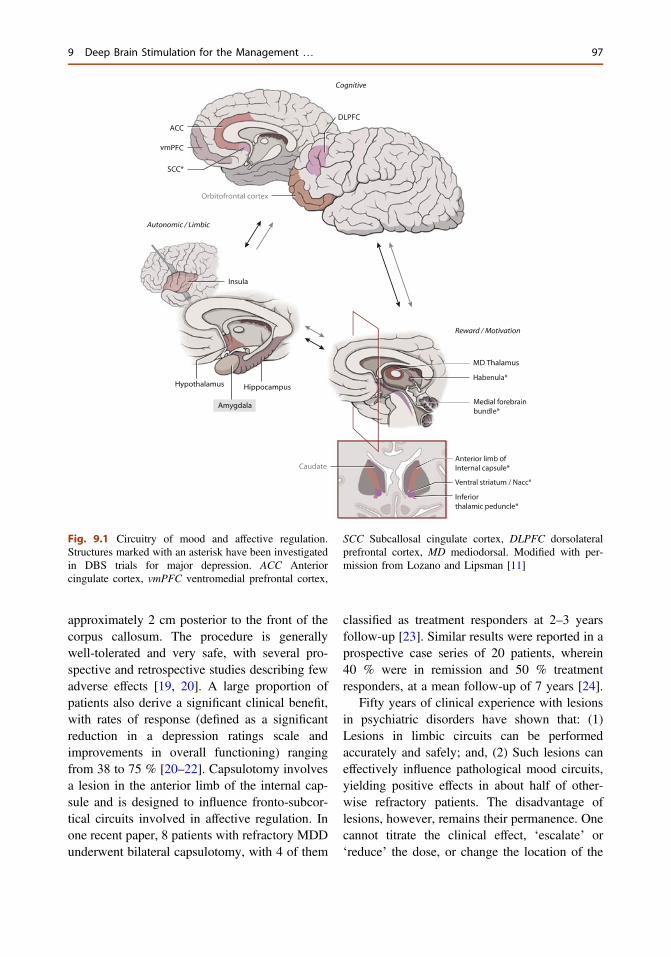
approximately 2 cm posterior to the front of thecorpus callosum. The procedure is generallywell-tolerated and very safe, with several pro-spective and retrospective studies describing fewadverse effects [19, 20]. A large proportion ofpatients also derive a significant clinical benefit,with rates of response (defined as a significantreduction in a depression ratings scale andimprovements in overall functioning) rangingfrom 38 to 75 % [20–22]. Capsulotomy involvesa lesion in the anterior limb of the internal cap-sule and is designed to influence fronto-subcor-tical circuits involved in affective regulation. Inone recent paper, 8 patients with refractory MDDunderwent bilateral capsulotomy, with 4 of them
classified as treatment responders at 2–3 yearsfollow-up [23]. Similar results were reported in aprospective case series of 20 patients, wherein40 % were in remission and 50 % treatmentresponders, at a mean follow-up of 7 years [24].
Fifty years of clinical experience with lesionsin psychiatric disorders have shown that: (1)Lesions in limbic circuits can be performedaccurately and safely; and, (2) Such lesions caneffectively influence pathological mood circuits,yielding positive effects in about half of other-wise refractory patients. The disadvantage oflesions, however, remains their permanence. Onecannot titrate the clinical effect, ‘escalate’ or‘reduce’ the dose, or change the location of the
Fig. 9.1 Circuitry of mood and affective regulation.Structures marked with an asterisk have been investigatedin DBS trials for major depression. ACC Anteriorcingulate cortex, vmPFC ventromedial prefrontal cortex,
SCC Subcallosal cingulate cortex, DLPFC dorsolateralprefrontal cortex, MD mediodorsal. Modified with per-mission from Lozano and Lipsman [11]
9 Deep Brain Stimulation for the Management … 97
lesion once performed. Repeat procedures, par-ticularly with cingulotomy, are routinely donebut expose patients to additional surgical risk.
9.2.2 Neurocircuitry of MDD
Several structures have been implicated in circuitmodels of MDD, including the medial and dor-solateral prefrontal cortex (mPFC; DLPFC),anterior cingulate cortex (ACC), nucleus ac-cumbens/ventral striatum (NAcc/VS), as well asthe amygdala. Neuroimaging has been the primerdriver of progress in the investigation of moodcircuitry, and both structural and functionalabnormalities have been found in MDD patients.For example, ACC and hippocampal volumes areboth diminished in patients with acute depres-sion, with additional studies finding diffuse graymatter volume reductions. Pre-clinical modelshave further established a direct link betweenactivity in the nucleus accumbens and both theenjoyment of reward (“liking”) as well as it’spursuit (“wanting”) [25–27]. Imaging studieshave linked activity in reward pathways to boththe mPFC and the ventral tegmental area (VTA),a key brainstem dopaminergic center. The abilityof VTA to influence both ‘top-down’ corticalcenters, via mesocortical pathways, and ‘bottom-up’ regulatory centers, via mesolimbic pathways,has been proposed as a key maintenance systemfor depressed mood, and anhedonia specifically.For example, dysfunction in both or either mes-olimbic or mesocortical systems can result infailure to anticipate or expect a rewarding out-come. Hypoactivation of NAcc in response tootherwise rewarding stimuli has been shown inconditions where reward deficits are well estab-lished, such as anorexia nervosa, further linkingactivity of this structure to affect-laden decisions[28, 29].
Studies performed in healthy subjects andunmedicated MDD patients have shown thatactivity in the ventral PFC, and subcallosal cin-gulate (SCC) specifically, is increased inresponse to sad stimuli in the former, and in theresting state in the latter [30]. This activity isattenuated with medical treatment of depression
as well as with DBS in otherwise refractorypatients [31, 32]. This has been found in bothpatients with unipolar depression as well as thosewith anorexia nervosa with comorbid MDD [33].Such results have suggested that depression maybe linked to a functional ‘decoupling’ of cortical-amygdalar projections, whereby increased activ-ity in both regions leads to a failure of brainhomeostatic control over affect [6]. Neurophysi-ological studies involving recordings directlyfrom neurons are also informing the mechanismsof mood disturbance and the function of keylimbic regions. For example, our group hasshown using microelectrode recordings fromsingle neurons in the SCC, that neurons in thisregion fire preferentially to negative picturescompared to neutral or positive ones [34].Additional work in bipolar depression patientsfound that SCC neuronal populations undergosynchronization of firing immediately prior tomaking an emotional decision [35]. These resultssuggest that this region may be ‘programmed’ torespond to sad and depression-maintainingstimuli.
9.3 Clinical Experience of MDDDBS to Date
Several targets are currently under investigationfor DBS in major depression (Table 9.1). Theseinclude structures involved in reward (nucleusaccumbes/ventral striatum), affective regulation(subcallosal cingulate), and pathways that bridgetop-down and bottom-up mood processing(medial forebrain bundle, inferior thalamicpeduncle, habenula). Although the global expe-rience with DBS for MDD is growing, all ofthese trials remain investigational. Below wereview the rationale and results to date with themost commonly investigated DBS targets.
9.3.1 Subcallosal Cingulate (SCC)
The target with the most experience to date is thesubcallosal cingulate cortex (SCC). The SCC is a
98 N. Lipsman et al.
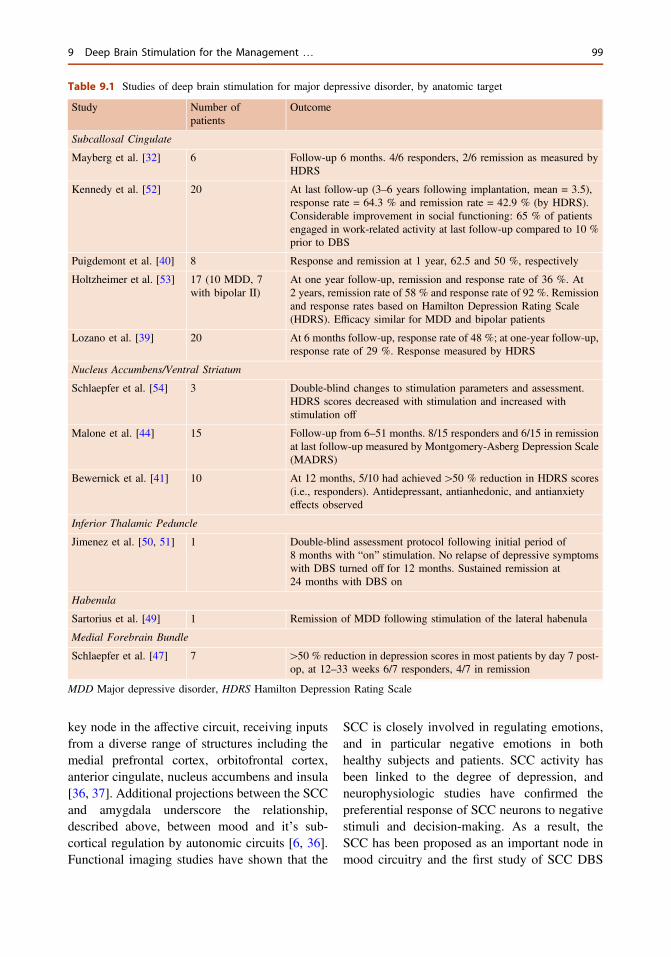
key node in the affective circuit, receiving inputsfrom a diverse range of structures including themedial prefrontal cortex, orbitofrontal cortex,anterior cingulate, nucleus accumbens and insula[36, 37]. Additional projections between the SCCand amygdala underscore the relationship,described above, between mood and it’s sub-cortical regulation by autonomic circuits [6, 36].Functional imaging studies have shown that the
SCC is closely involved in regulating emotions,and in particular negative emotions in bothhealthy subjects and patients. SCC activity hasbeen linked to the degree of depression, andneurophysiologic studies have confirmed thepreferential response of SCC neurons to negativestimuli and decision-making. As a result, theSCC has been proposed as an important node inmood circuitry and the first study of SCC DBS
Table 9.1 Studies of deep brain stimulation for major depressive disorder, by anatomic target
Study Number ofpatients
Outcome
Subcallosal Cingulate
Mayberg et al. [32] 6 Follow-up 6 months. 4/6 responders, 2/6 remission as measured byHDRS
Kennedy et al. [52] 20 At last follow-up (3–6 years following implantation, mean = 3.5),response rate = 64.3 % and remission rate = 42.9 % (by HDRS).Considerable improvement in social functioning: 65 % of patientsengaged in work-related activity at last follow-up compared to 10 %prior to DBS
Puigdemont et al. [40] 8 Response and remission at 1 year, 62.5 and 50 %, respectively
Holtzheimer et al. [53] 17 (10 MDD, 7with bipolar II)
At one year follow-up, remission and response rate of 36 %. At2 years, remission rate of 58 % and response rate of 92 %. Remissionand response rates based on Hamilton Depression Rating Scale(HDRS). Efficacy similar for MDD and bipolar patients
Lozano et al. [39] 20 At 6 months follow-up, response rate of 48 %; at one-year follow-up,response rate of 29 %. Response measured by HDRS
Nucleus Accumbens/Ventral Striatum
Schlaepfer et al. [54] 3 Double-blind changes to stimulation parameters and assessment.HDRS scores decreased with stimulation and increased withstimulation off
Malone et al. [44] 15 Follow-up from 6–51 months. 8/15 responders and 6/15 in remissionat last follow-up measured by Montgomery-Asberg Depression Scale(MADRS)
Bewernick et al. [41] 10 At 12 months, 5/10 had achieved[50 % reduction in HDRS scores(i.e., responders). Antidepressant, antianhedonic, and antianxietyeffects observed
Inferior Thalamic Peduncle
Jimenez et al. [50, 51] 1 Double-blind assessment protocol following initial period of8 months with “on” stimulation. No relapse of depressive symptomswith DBS turned off for 12 months. Sustained remission at24 months with DBS on
Habenula
Sartorius et al. [49] 1 Remission of MDD following stimulation of the lateral habenula
Medial Forebrain Bundle
Schlaepfer et al. [47] 7 [50 % reduction in depression scores in most patients by day 7 post-op, at 12–33 weeks 6/7 responders, 4/7 in remission
MDD Major depressive disorder, HDRS Hamilton Depression Rating Scale
9 Deep Brain Stimulation for the Management … 99

for refractory MDD was performed in 2005. Thisstudy included 6 patients and found that at 6-months follow-up, 4 were in remission, and thatSCC perfusion, measured using PET, was sig-nificantly lower compared to baseline [32]. Alarger study, published in 2008 in 20 patientsfollowed to 1-year, found a 50 % response rate[defined as a [50 % reduction in HamiltonDepression Rating (HAMD) Scale scores] [38].A multicenter study utilizing the same targetfound a more modest response rate of 29 % at 1-year, which increased to 62 % if treatmentresponse was defined as an improvement in theHAMD by at least 40 % [39]. These resultsindicated that the majority of patients were eitherfull or partial responders. Similar results wereobtained by another group who reported a 50 %response rate with SCC DBS in otherwiserefractory patients [40].
9.3.2 Nucleus Accumbens/VentralStriatum (NAcc/VS)
Given the prominence of anhedonia and deficitsin reward processing, there is much interest inmodulating reward circuits in MDD. The nucleusaccumbens exists at the interface between thestriatum and caudate at it’s infero-lateral border.There is a robust pre-clinical and human litera-ture linking activity within the NAcc to virtuallyevery element of the reward experience, fromanticipation to enjoyment [25–27]. Dopaminer-gic pathways predominate in the NAcc and it’skey mesolimbic afferent projections, namelyfrom the ventral tegmental area, via the medialforebrain bundle (MFB). Modulating thesepathways to address pathological anhedonia isthe goal of NAcc and ventral striatum (VS) DBS.In one early report, authors found a 50 %response rate following DBS when patients werefollowed to 1-year, with key metabolic changesin the brain mirroring those detected with SCCDBS [41, 42]. Whether DBS at reward pathwayshas an influence on dopaminergic transmission
remains to be seen and investigated, althoughsuch a symptom-based approached to MDDmanagement could be promising.
An additional target that has been explored isthe ventral caudate/ventral striatum, a region thatis sometimes used interchangeably with NAcc,given the anatomic location of the latter. VC/VShas previously shown promise as a target inrefractory OCD, and further allows the DBSelectrode to influence regions close to the ante-rior limb of the internal capsule, which is thetraditional capsulotomy target [43]. In open-labelstudies to date, results from VC/VS stimulationhave been positive, with rates of response andremission at 6-months of 53 and 20 %, respec-tively [44]. Results from a placebo-controlled,randomized trial of VC/VS DBS in MDD havenot yet been published.
9.3.3 Medial Forebrain Bundle (MFB)
Another DBS target in the reward system is themedial forebrain bundle (MFB). The MFB con-tains both ascending and descending fibers and isa prominent component of the mesolimbicpathway connecting brainstem dopaminergiccenters, such as the VTA, with limbic basalganglia structures, such as NAcc [45]. In animalmodels, the MFB is most closely associated withthe septal nuclei, which were the subject ofclassic experiments by Olds and Milner, whodemonstrated the rewarding effects of intracranialself-stimulation of these structures in rats [46].One recent paper investigated MFB stimulationin 7 patients with severe, long-standing MDD,and found rapid anti-depressant effects withstimulation [47]. Within 7 days of stimulationonset, 6 patients were treatment responders. Thiswork is currently being expanded to a largerpatient cohort, but such results are neverthelesspromising and suggest a potentially differentanti-depressant mechanism than either SCC orNAcc stimulation, where treatment response isexpected to take weeks to months.
100 N. Lipsman et al.

9.3.4 Habenula (Hab) and InferiorThalamic Peduncle (ITP)
Other targets that have been investigated includethe habenula and the inferior thalamic peduncle,both components of the brain’s reward system.The habenula is a collection of cells in the pinealregion divided into medial and lateral compo-nents. The lateral habenula has generally beenassociated with reward processing and receiveshippocampal as well as thalamic and Nacc pro-jections [48]. Accordingly, the lateral habenulahas been proposed as a DBS target for depres-sion, with at least one case report showing sig-nificant improvements in mood following DBS atthis target [48, 49].
The inferior thalamic peduncle (ITP), similarto MFB is a reward pathway, suggested to havean important role in both mood and anxietydisorders, such as OCD. The ITP is closelyassociated with the mediodorsal thalamus, withprojections to orbitofrontal regions as well as theamygdala. The first report of ITP DBS in apatient with MDD was published in 2007, anddescribed significant clinical benefit in onepatient [50]. An additional paper describedresults in a mixed population of OCD and MDDpatients, and found significant effects on bothrefractory anxiety and mood, with the MDDpatient experiencing a clinical remission [51].
9.4 Future Directions
Results of DBS studies for depression have thusfar been promising, but the field’s enthusiasmshould be tempered by the limited amount ofavailable data and the lack of published blinded,randomized trials. Several of these are currentlyin progress, and may yet shed light on the rolethat DBS may play, if any, in the management ofthe severely depressed patient. There remain,further, many open questions regarding themechanisms of DBS in MDD, as well whichtypes of patients would benefit from the proce-dure. Work is currently ongoing to identify bio-markers of depression, whether radiologic,
serologic or genetic, that may portend more orless favourable outcomes with neuromodulation.Further, it may be that different regions of thebrain may be influencing the same anatomiccircuit, supported by the roughly similar rates ofresponse in trials at different targets. Alterna-tively, it may be that stimulation of some regions,even within the same structure, may yield dif-ferential effects, as it is still unclear which stim-ulation parameters are optimal for which patient.
The future of DBS for MDD will see bothtechnical and conceptual advances. Technicaladvances will see a miniaturization of the tech-nology, improved battery life, and more stream-lined programming, which may make theprocedure more efficient, and hence, moreattractive for clinicians and patients. Emergingtechnologies such as optogenetics, nanomedicineand focused ultrasound may further offer alter-native means of modulating mood circuits.Conceptual advances will see an improvedcharacterization of the clinical response such thatthe procedure can be tailored to the patient’sclinical picture and anatomy. Such work willhelp improve the safety and tolerability of DBS,enhance patient outcomes, and provide a clearerpicture of the circuitry of major depression.
References
1. Bromet E, Andrade LH, Hwang I, Sampson NA,Alonso J, de Girolamo G, de Graaf R, DemyttenaereK, Hu C, Iwata N, Karam AN, Kaur J, KostyuchenkoS, Lepine JP, Levinson D, Matschinger H, Mora ME,Browne MO, Posada-Villa J, Viana MC, WilliamsDR, Kessler RC. Cross-national epidemiology ofDSM-IV major depressive episode. BMC Med.2011;9:90. doi:10.1186/1741-7015-9-90.
2. Kessler RC, Berglund P, Demler O, Jin R, Koretz D,Merikangas KR, Rush AJ, Walters EE, Wang PS. Theepidemiology of major depressive disorder: resultsfrom the National Comorbidity Survey Replication(NCS-R). J Am Med Assoc. 2003;289(23):3095–105.doi:10.1001/jama.289.23.3095.
3. Kessler RC, Petukhova M, Sampson NA, ZaslavskyAM, Wittchen HU. Twelve-month and lifetimeprevalence and lifetime morbid risk of anxiety andmood disorders in the United States. Int J MethodsPsychiatric Res. 2012;21(3):169–84. doi:10.1002/mpr.1359.
9 Deep Brain Stimulation for the Management … 101
4. Sobocki P, Lekander I, Borgstrom F, Strom O,Runeson B. The economic burden of depression inSweden from 1997 to 2005. Eur Psychiatry: J AssocEur Psychiatrists. 2007;22(3):146–52. doi:10.1016/j.eurpsy.2006.10.006.
5. Berrios GE. Melancholia and depression during the19th century: a conceptual history. Brit J Psychiatry: JMental Sci. 1988;153:298–304.
6. Giacobbe P, Mayberg HS, Lozano AM. Treatmentresistant depression as a failure of brain homeostaticmechanisms: implications for deep brain stimulation.Exp Neurol. 2009;219(1):44–52. doi:10.1016/j.expneurol.2009.04.028.
7. Trivedi MH, Rush AJ, Wisniewski SR, NierenbergAA, Warden D, Ritz L, Norquist G, Howland RH,Lebowitz B, McGrath PJ, Shores-Wilson K, BiggsMM, Balasubramani GK, Fava M. Evaluation ofoutcomes with citalopram for depression usingmeasurement-based care in STAR*D: implicationsfor clinical practice. Am J Psychiatry. 2006;163(1):28–40. doi:10.1176/appi.ajp.163.1.28.
8. Lipsman N, Sankar T, Downar J, Kennedy SH,Lozano AM, Giacobbe P. Neuromodulation fortreatment-refractory major depressive disorder. CanMed Assoc J. 2013. doi:10.1503/cmaj.121317.
9. McGrath PJ, Stewart JW, Fava M, Trivedi MH,Wisniewski SR, Nierenberg AA, Thase ME, Davis L,Biggs MM, Shores-Wilson K, Luther JF, NiedereheG, Warden D, Rush AJ. Tranylcypromine versusvenlafaxine plus mirtazapine following three failedantidepressant medication trials for depression: aSTAR*D report. Am J Psychiatry. 2006;163(9):1531–41 (quiz 1666). doi:10.1176/appi.ajp.163.9.1531.
10. Sackeim HA, Prudic J, Fuller R, Keilp J, Lavori PW,Olfson M. The cognitive effects of electroconvulsivetherapy in community settings. Neuropsycho-pharmacology. Off Publ Am Coll Neuropsycho-pharmacol. 2007;32 (1):244–54.
11. Lozano AM, Lipsman N. Probing and regulatingdysfunctional circuits using deep brain stimulation.Neuron. 2013;77(3):406–24. doi:10.1016/j.neuron.2013.01.020.
12. Deuschl G, Schupbach M, Knudsen K, Pinsker MO,Cornu P, Rau J, Agid Y, Schade-Brittinger C.Stimulation of the subthalamic nucleus at an earlierdisease stage of Parkinson’s disease: concept andstandards of the EARLYSTIM-study. ParkinsonismRelat Disord. 2013;19(1):56–61. doi:10.1016/j.parkreldis.2012.07.004.
13. Follett KA, Weaver FM, Stern M, Hur K, Harris CL,Luo P, Marks WJ Jr, Rothlind J, Sagher O, Moy C,Pahwa R, Burchiel K, Hogarth P, Lai EC, Duda JE,Holloway K, Samii A, Horn S, Bronstein JM, StonerG, Starr PA, Simpson R, Baltuch G, De Salles A,Huang GD, Reda DJ. Pallidal versus subthalamicdeep-brain stimulation for Parkinson’s disease.N Engl J Med. 2010;362(22):2077–91. doi:10.1056/NEJMoa0907083.
14. Weaver F, Follett K, Hur K, Ippolito D, Stern M.Deep brain stimulation in Parkinson disease: ametaanalysis of patient outcomes. J Neurosurg.2005;103(6):956–67. doi:10.3171/jns.2005.103.6.0956.
15. Birley JL. Modified frontal leucotomy: a review of106 cases. Brit J Psychiatry: J Mental Sci.1964;110:211–21.
16. Freeman W, Watts JW. Prefrontal lobotomy: thesurgical relief of mental pain. Bull NY Acad Med.1942;18(12):794–812.
17. Freeman W, Watts JW. Psychosurgery. ProgressNeurol Psychiatry. 1946;1:649–61.
18. Freeman W, Watts JW. Prefrontal lobotomy; surveyof 331 cases. Am J Med Sci. 1946;211:1–8.
19. Cosgrove GR, Rauch SL. Stereotactic cingulotomy.Neurosurg Clin N Am. 2003;14(2):225–35.
20. SpanglerWJ, Cosgrove GR, Ballantine HT, Jr, CassemEH, Rauch SL, Nierenberg A, Price BH. Magneticresonance image-guided stereotactic cingulotomy forintractable psychiatric disease. Neurosurgery. 1996;38(6):1071–76 (discussion 1076–1078).
21. Shields DC, Asaad W, Eskandar EN, Jain FA,Cosgrove GR, Flaherty AW, Cassem EH, Price BH,Rauch SL, Dougherty DD. Prospective assessment ofstereotactic ablative surgery for intractable majordepression. Biol Psychiatry. 2008;64(6):449–54.doi:10.1016/j.biopsych.2008.04.009.
22. Steele JD, Christmas D, Eljamel MS, Matthews K.Anterior cingulotomy for major depression: clinicaloutcome and relationship to lesion characteristics.Biol Psychiatry. 2008;63(7):670–7. doi:10.1016/j.biopsych.2007.07.019.
23. Hurwitz TA, Honey CR, Allen J, Gosselin C, HewkoR, Martzke J, Bogod N, Taylor P. Bilateral anteriorcapsulotomy for intractable depression.J Neuropsychiatry Clin Neurosci. 2012;24(2):176–82. doi:10.1176/appi.neuropsych.11080189.
24. Christmas D, Eljamel MS, Butler S, Hazari H,MacVicar R, Steele JD, Livingstone A, MatthewsK. Long term outcome of thermal anteriorcapsulotomy for chronic, treatment refractorydepression. J Neurol Neurosurg Psychiatry. 2011;82(6):594–600. doi:10.1136/jnnp.2010.217901.
25. Carelli RM. Nucleus accumbens cell firing and rapiddopamine signaling during goal-directed behaviors inrats. Neuropharmacology. 2004;47(1):180–9. doi:10.1016/j.neuropharm.2004.07.017.
26. Martin PD, Ono T. Effects of reward anticipation,reward presentation, and spatial parameters on thefiring of single neurons recorded in the subiculum andnucleus accumbens of freely moving rats. BehavBrain Res. 2000;116(1):23–38.
27. Nicola SM, Yun IA, Wakabayashi KT, Fields HL.Firing of nucleus accumbens neurons during theconsummatory phase of a discriminative stimulus taskdepends on previous reward predictive cues.J Neurophysiol. 2004;91(4):1866–82. doi:10.1152/jn.00658.2003.
102 N. Lipsman et al.
28. Frank GK, Bailer UF, Henry SE, Drevets W, MeltzerCC, Price JC, Mathis CA, Wagner A, Hoge J, ZiolkoS, Barbarich-Marsteller N, Weissfeld L, Kaye WH.Increased dopamine D2/D3 receptor binding afterrecovery from anorexia nervosa measured by positronemission tomography and [11c]raclopride. BiolPsychiatry. 2005;58(11):908–12. doi:10.1016/j.biopsych.2005.05.003.
29. Kaye WH, Wierenga CE, Bailer UF, Simmons AN,Bischoff-Grethe A. Nothing tastes as good as skinnyfeels: the neurobiology of anorexia nervosa. TrendsNeurosci. 2013;36(2):110–20. doi:10.1016/j.tins.2013.01.003.
30. Mayberg HS. Limbic-cortical dysregulation: aproposed model of depression. J NeuropsychiatryClin Neurosci. 1997;9(3):471–81.
31. Kennedy SH, Konarski JZ, Segal ZV, Lau MA,Bieling PJ, McIntyre RS, Mayberg HS. Differences inbrain glucose metabolism between responders to CBTand venlafaxine in a 16-week randomized controlledtrial. Am J Psychiatry. 2007;164(5):778–88. doi:10.1176/appi.ajp.164.5.778.
32. Mayberg HS, Lozano AM, Voon V, McNeely HE,Seminowicz D, Hamani C, Schwalb JM, KennedySH. Deep brain stimulation for treatment-resistantdepression. Neuron. 2005;45(5):651–60. doi:10.1016/j.neuron.2005.02.014.
33. Lipsman N, Woodside DB, Giacobbe P, Hamani C,Carter JC, Norwood SJ, Sutandar K, Staab R, Elias G,Lyman CH, Smith GS, Lozano AM. Subcallosalcingulate deep brain stimulation for treatment-refractory anorexia nervosa: a phase 1 pilot trial.Lancet. 2013. doi:10.1016/S0140-6736(12)62188-6.
34. Laxton AW, Neimat JS, Davis KD, Womelsdorf T,Hutchison WD, Dostrovsky JO, Hamani C, MaybergHS, Lozano AM. Neuronal coding of implicitemotion categories in the subcallosal cortex inpatients with depression. Biol Psychiatry. 2013.doi:10.1016/j.biopsych.2013.03.029.
35. Lipsman N, Kaping D, Westendorff S, Sankar T,Lozano AM, Womelsdorf T. Beta coherence withinhuman ventromedial prefrontal cortex precedesaffective value choices. Neuroimage. 2013. doi:10.1016/j.neuroimage.2013.05.104.
36. Hamani C, Mayberg H, Stone S, Laxton A, Haber S,Lozano AM. The subcallosal cingulate gyrus in thecontext of major depression. Biol Psychiatry. 2011;69(4):301–8. doi:10.1016/j.biopsych.2010.09.034.
37. Price JL, Drevets WC. Neurocircuitry of mooddisorders. Neuropsychopharmacol: Off Publ AmColl Neuropsychopharmacol. 2010;35(1):192–216.doi:10.1038/npp.2009.104.
38. Lozano AM, Mayberg HS, Giacobbe P, Hamani C,Craddock RC, Kennedy SH. Subcallosal cingulategyrus deep brain stimulation for treatment-resistantdepression. Biol Psychiatry. 2008;64(6):461–7.doi:10.1016/j.biopsych.2008.05.034.
39. Lozano AM, Giacobbe P, Hamani C, Rizvi SJ,Kennedy SH, Kolivakis TT, Debonnel G, Sadikot AF,
Lam RW, Howard AK, Ilcewicz-Klimek M, HoneyCR, Mayberg HS. A multicenter pilot study ofsubcallosal cingulate area deep brain stimulation fortreatment-resistant depression. J Neurosurg. 2012;116(2):315–22. doi:10.3171/2011.10.JNS102122.
40. Puigdemont D, Perez-Egea R, Portella MJ, Molet J,de Diego-Adelino J, Gironell A, Radua J, Gomez-Anson B, Rodriguez R, Serra M, de Quintana C,Artigas F, Alvarez E, Perez V. Deep brain stimulationof the subcallosal cingulate gyrus: further evidence intreatment-resistant major depression. Int JNeuropsychopharmacol. 2011;1–13. doi:10.1017/S1461145711001088.
41. Bewernick BH, Hurlemann R, Matusch A, Kayser S,Grubert C, Hadrysiewicz B, Axmacher N, Lemke M,Cooper-Mahkorn D, Cohen MX, Brockmann H,Lenartz D, Sturm V, Schlaepfer TE. Nucleusaccumbens deep brain stimulation decreases ratingsof depression and anxiety in treatment-resistantdepression. Biol Psychiatry. 2010;67(2):110–6.doi:10.1016/j.biopsych.2009.09.013.
42. Bewernick BH, Kayser S, Sturm V, Schlaepfer TE.Long-term effects of nucleus accumbens deep brainstimulation in treatment-resistant depression: evidencefor sustained efficacy. Neuropsychopharmacol: OffPubl Am Coll Neuropsychopharmacol. 2012;37(9):1975–85. doi:10.1038/npp.2012.44.
43. Aouizerate B, Cuny E, Martin-Guehl C, Guehl D,Amieva H, Benazzouz A, Fabrigoule C, Allard M,Rougier A, Bioulac B, Tignol J, Burbaud P. Deepbrain stimulation of the ventral caudate nucleus in thetreatment of obsessive-compulsive disorder and majordepression. Case report. J Neurosurg. 2004;101(4):682–6. doi:10.3171/jns.2004.101.4.0682.
44. Malone DA Jr, Dougherty DD, Rezai AR, CarpenterLL, Friehs GM, Eskandar EN, Rauch SL,Rasmussen SA, Machado AG, Kubu CS, TyrkaAR, Price LH, Stypulkowski PH, Giftakis JE, RiseMT, Malloy PF, Salloway SP, Greenberg BD. Deepbrain stimulation of the ventral capsule/ventralstriatum for treatment-resistant depression. BiolPsychiatry. 2009;65(4):267–75. doi:10.1016/j.biopsych.2008.08.029.
45. Coenen VA, Honey CR, Hurwitz T, Rahman AA,McMaster J, Burgel U, Madler B. Medial forebrainbundle stimulation as a pathophysiological mechanismfor hypomania in subthalamic nucleus deep brainstimulation for Parkinson’s disease. Neurosurgery.2009;64(6):1106–14 (discussion 1114–1105). doi:10.1227/01.NEU.0000345631.54446.06.
46. Olds J, Milner P. Positive reinforcement produced byelectrical stimulation of septal area and other regionsof rat brain. J Comp Physiol Psychol. 1954;47(6):419–27.
47. Schlaepfer TE, Bewernick BH, Kayser S, Madler B,Coenen VA. Rapid effects of deep brain stimulationfor treatment-resistant major depression. BiolPsychiatry. 2013;73(12):1204–12. doi:10.1016/j.biopsych.2013.01.034.
9 Deep Brain Stimulation for the Management … 103

48. Sartorius A, Henn FA. Deep brain stimulation of thelateral habenula in treatment resistant majordepression. Med Hypotheses. 2007;69(6):1305–8.doi:10.1016/j.mehy.2007.03.021.
49. Sartorius A, Kiening KL, Kirsch P, von Gall CC,Haberkorn U, Unterberg AW, Henn FA, Meyer-Lindenberg A. Remission of major depression underdeep brain stimulation of the lateral habenula in atherapy-refractory patient. Biol Psychiatry. 2010;67(2):e9–11. doi:10.1016/j.biopsych.2009.08.027.
50. Jimenez F, Velasco F, Salin-Pascual R, Velasco M,Nicolini H, Velasco AL, Castro G. Neuromodulationof the inferior thalamic peduncle for major depressionand obsessive compulsive disorder. Acta NeurochirSuppl. 2007;97(Pt 2):393–8.
51. Jimenez F, Nicolini H, Lozano AM, Piedimonte F,Salin R, Velasco F. Electrical stimulation of theinferior thalamic peduncle in the treatment of majordepression and obsessive compulsive disorders. WorldNeurosurg. 2012. doi:10.1016/j.wneu.2012.07.010.
52. Kennedy SH, Giacobbe P, Rizvi SJ, Placenza FM,Nishikawa Y, Mayberg HS, Lozano AM. Deep brainstimulation for treatment-resistant depression: follow-up after 3 to 6 years. Am J Psychiatry. 2011;168(5):502–10. doi:10.1176/appi.ajp.2010.10081187.
53. Holtzheimer PE, Kelley ME, Gross RE, FilkowskiMM, Garlow SJ, Barrocas A, Wint D, Craighead MC,Kozarsky J, Chismar R, Moreines JL, Mewes K,Posse PR, Gutman DA, Mayberg HS. Subcallosalcingulate deep brain stimulation for treatment-resistant unipolar and bipolar depression. Arch GenPsychiatry. 2012;69(2):150–8. doi:10.1001/archgenpsychiatry.2011.1456.
54. Schlaepfer TE, Cohen MX, Frick C, Kosel M,Brodesser D, Axmacher N, Joe AY, Kreft M,Lenartz D, Sturm V. Deep brain stimulation toreward circuitry alleviates anhedonia in refractorymajor depression. Neuropsychopharmacol: Off PublAm Coll Neuropsychopharmacol. 2008;33(2):368–77. doi:10.1038/sj.npp.1301408.
104 N. Lipsman et al.

10Ablative Surgeryfor Obsessive-Compulsive Disorders
Roberto Martinez-Alvarez
Abstract
Intractable OCD and depression cause tremendous suffering. An estimated20 % of patients remain severely affected in spite of the best availablemedication and behavioural therapies. Existing data suggest that lesionprocedures can benefit a large proportion (ranging from about 60 to 80 %)of patients with medically intractable OCD. Long-term serious adverseevents are very infrequent. Functional neuroimaging studies play anextremely important role in understanding the mechanisms of diseasedevelopment and therapeutic action. Our experience over the past 10 yearsprovides evidence that the most recent lesion procedures are even safer,alleviate suffering, and improve the quality of life of patients with thesedisabling disorders.
10.1 Introduction
Obsessive-compulsive disorder (OCD) affects2–3 % of the population; there are some sixmillion patients in the United States alone [36].Prevalence is similar in other countries and cul-tures [39]. Features of the disorder are recurringnotions, termed “obsessions”, that are a source ofdistress and can result in patients’ being unableto function; “compulsions”, described as theineluctable need to carry out actions that gratifythe obsessions, commonly associated with guiltand anxiety; and “rituals”, i.e., performing
repetitive, mechanical actions likewise related tothe obsessions. Onset of this disorder takes placein the first few decades of life, commonly startingin adolescence. Symptoms gradually increaseand can prevent patients from being able to carryout activity of any kind at all [1]. In the past20 years OCD has been the tenth cause of dis-ability worldwide, according to statistics releasedby the World Health Organization. There is agenetic component to the disorder, with thelikelihood that a first-degree relative of a patientwill have the disorder being three times greaterthan the reported incidence [12].
Current behavioural and pharmacologicaltherapies are far from universally effective.Selective serotonin reuptake inhibitors (SSRIs) arethe mainstays of pharmacological treatment. Clo-mipramine, a tricyclic antidepressant and a potentbut non-serotonin reuptake inhibitor, is a second-line agent. Typical and atypical neuroleptics have
R. Martinez-Alvarez (&)Functional Neurosurgery and RadiosurgeryDepartment, Ruber International Hospital,Madrid, Spaine-mail: [email protected]
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0_10© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
105
been effective in controlled studies but impose theadditional burden of unwanted secondary effects.Even when effective, undesirable effects maysubstantially limit the treatment compliance usu-ally required for ongoing relief of symptoms.An estimated 20 % of patients remain severelyaffected, even when the best available medicationand behavioural therapies are brought to bear[16, 17, 38]. This group suffers from intractableOCD, a source of tremendous suffering [1] andoverall functional impairment. For this group,surgical treatment is the next step.
10.2 Historical Background
Surgical techniques for treating psychiatric ill-nesses by creating lesions in the frontal lobeshave been around since the 1930s. These lesionsproduced in patients a certain disconnect fromtheir milieu and their inhibitions, typical of largefrontal lobe lesions. Dr. António Egas Moniz wasawarded the Nobel Prize for developing the“frontal leucotomy” procedure [5]. In the 1940svarious groups of neurosurgeons and psychia-trists developed more refined methods of pro-ducing lesions at different sites in the frontallobe. Specifically, Freeman and Watts launched a“crusade” advocating Freeman’s leucotomy pro-cedure, with dire consequences that still hauntthe memories of some psychiatrists even today[14]. At the present time these procedures havebeen abandoned, and they are unrelated to thetreatments discussed in this chapter.
10.3 Current Concepts
The purpose of neurosurgical procedures used totreat psychiatric disorders is to improve a series ofspecific symptoms caused by mental illnesses, thesame purpose that informs their use in treatmentsin response to other functional disorders, such aspain and abnormal movements. This type of sur-gery involves making specific lesions to
disconnect the limbic system circuits related to thedifferent psychiatric disorders [13, 18]. Blockingcertain interconnecting pathways enhances brainfunction, with patients experiencing relief of cer-tain symptoms without undergoing alterations intheir personalities, and their cognitive functionsordinarily improve [6, 37].
10.3.1 Neuroanatomy, BrainConnectivity, and NeurosurgicalTechniques
Functional neuroimagingfindings relating toOCDhave laid the theoretical foundation for surgicalprocedures intended to alleviate OCD. Thesestudies constitute the groundwork for the nowwell-established identification of anatomical pro-jections reaching into the caudate nucleus from theorbitofrontal cortex and the cingulum [4, 44].Patients in a resting state examined using PET andSPECT show heightened metabolic activity in theorbitofrontal cortex, cingulate cortex, and caudatenucleus. Furthermore, metabolic activity in theseregions has been observed to return to normallevels in patients who improve in response topharmacological or behavioural therapy.
Functional MR neuroimaging has alsorevealed hyperactivity in the cortical-striatal-thalamic circuit, including the orbitofrontal cor-tex and caudate nucleus [8]. These findingsindicate that the basal ganglia are not functioningproperly, giving rise to changes in other struc-tures. Combining neuropsychology and func-tional MRI has improved our understanding ofthese alterations and allows us to select the mostsuitable targets for surgery [32].
Modern procedures enabling functional MRIand tractography guided stereotactic ablation andthe use of special computer software for guidancemake it possible to create lesions in the pathwaysinterconnecting the limbic system with evergreater precision and safety (Fig. 10.1) [15, 18].The lesions currently effected by our team, whichhas gained extensive experience over the past20 years, are:
106 R. Martinez-Alvarez
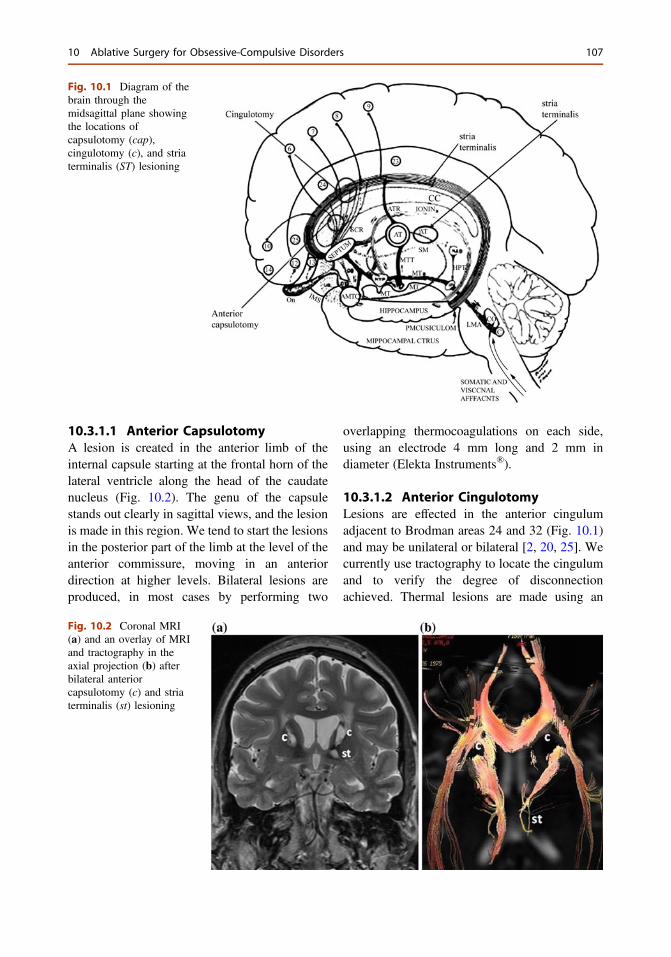
10.3.1.1 Anterior CapsulotomyA lesion is created in the anterior limb of theinternal capsule starting at the frontal horn of thelateral ventricle along the head of the caudatenucleus (Fig. 10.2). The genu of the capsulestands out clearly in sagittal views, and the lesionis made in this region. We tend to start the lesionsin the posterior part of the limb at the level of theanterior commissure, moving in an anteriordirection at higher levels. Bilateral lesions areproduced, in most cases by performing two
overlapping thermocoagulations on each side,using an electrode 4 mm long and 2 mm indiameter (Elekta Instruments®).
10.3.1.2 Anterior CingulotomyLesions are effected in the anterior cingulumadjacent to Brodman areas 24 and 32 (Fig. 10.1)and may be unilateral or bilateral [2, 20, 25]. Wecurrently use tractography to locate the cingulumand to verify the degree of disconnectionachieved. Thermal lesions are made using an
Fig. 10.1 Diagram of thebrain through themidsagittal plane showingthe locations ofcapsulotomy (cap),cingulotomy (c), and striaterminalis (ST) lesioning
Fig. 10.2 Coronal MRI(a) and an overlay of MRIand tractography in theaxial projection (b) afterbilateral anteriorcapsulotomy (c) and striaterminalis (st) lesioning
10 Ablative Surgery for Obsessive-Compulsive Disorders 107
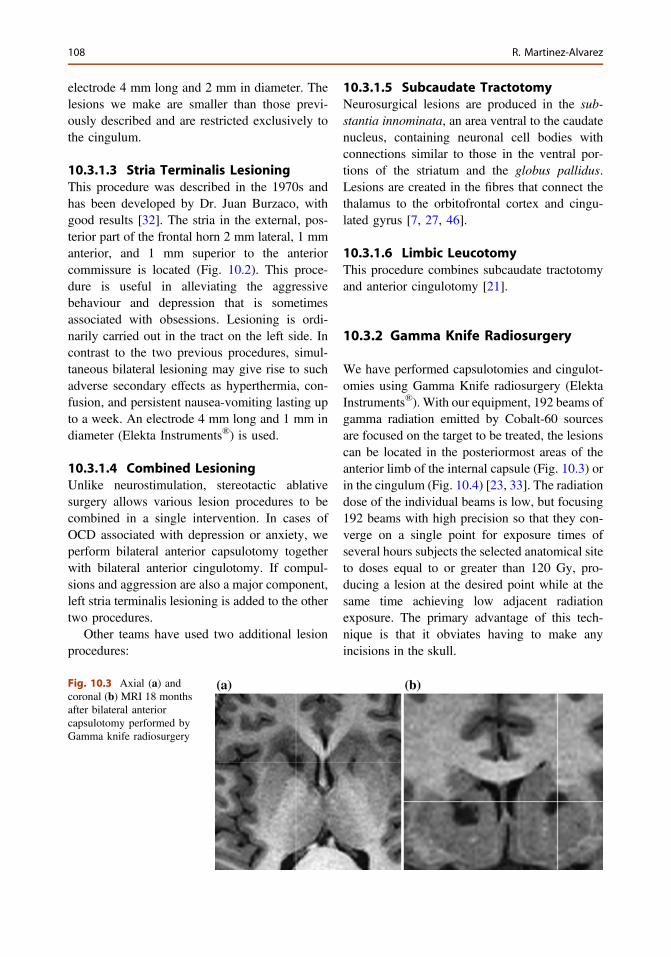
electrode 4 mm long and 2 mm in diameter. Thelesions we make are smaller than those previ-ously described and are restricted exclusively tothe cingulum.
10.3.1.3 Stria Terminalis LesioningThis procedure was described in the 1970s andhas been developed by Dr. Juan Burzaco, withgood results [32]. The stria in the external, pos-terior part of the frontal horn 2 mm lateral, 1 mmanterior, and 1 mm superior to the anteriorcommissure is located (Fig. 10.2). This proce-dure is useful in alleviating the aggressivebehaviour and depression that is sometimesassociated with obsessions. Lesioning is ordi-narily carried out in the tract on the left side. Incontrast to the two previous procedures, simul-taneous bilateral lesioning may give rise to suchadverse secondary effects as hyperthermia, con-fusion, and persistent nausea-vomiting lasting upto a week. An electrode 4 mm long and 1 mm indiameter (Elekta Instruments®) is used.
10.3.1.4 Combined LesioningUnlike neurostimulation, stereotactic ablativesurgery allows various lesion procedures to becombined in a single intervention. In cases ofOCD associated with depression or anxiety, weperform bilateral anterior capsulotomy togetherwith bilateral anterior cingulotomy. If compul-sions and aggression are also a major component,left stria terminalis lesioning is added to the othertwo procedures.
Other teams have used two additional lesionprocedures:
10.3.1.5 Subcaudate TractotomyNeurosurgical lesions are produced in the sub-stantia innominata, an area ventral to the caudatenucleus, containing neuronal cell bodies withconnections similar to those in the ventral por-tions of the striatum and the globus pallidus.Lesions are created in the fibres that connect thethalamus to the orbitofrontal cortex and cingu-lated gyrus [7, 27, 46].
10.3.1.6 Limbic LeucotomyThis procedure combines subcaudate tractotomyand anterior cingulotomy [21].
10.3.2 Gamma Knife Radiosurgery
We have performed capsulotomies and cingulot-omies using Gamma Knife radiosurgery (ElektaInstruments®). With our equipment, 192 beams ofgamma radiation emitted by Cobalt-60 sourcesare focused on the target to be treated, the lesionscan be located in the posteriormost areas of theanterior limb of the internal capsule (Fig. 10.3) orin the cingulum (Fig. 10.4) [23, 33]. The radiationdose of the individual beams is low, but focusing192 beams with high precision so that they con-verge on a single point for exposure times ofseveral hours subjects the selected anatomical siteto doses equal to or greater than 120 Gy, pro-ducing a lesion at the desired point while at thesame time achieving low adjacent radiationexposure. The primary advantage of this tech-nique is that it obviates having to make anyincisions in the skull.
Fig. 10.3 Axial (a) andcoronal (b) MRI 18 monthsafter bilateral anteriorcapsulotomy performed byGamma knife radiosurgery
108 R. Martinez-Alvarez
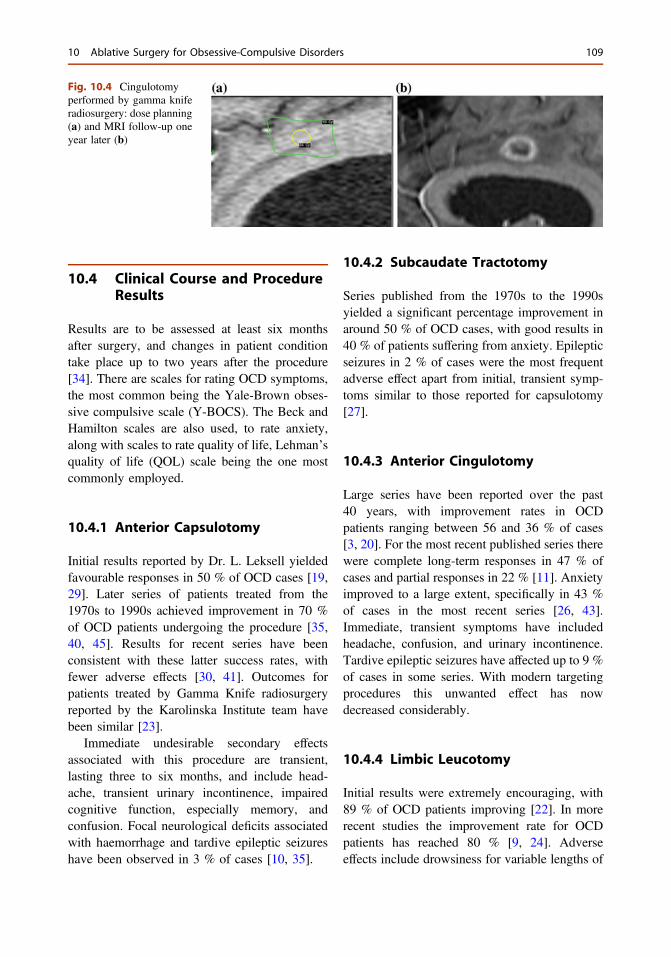
10.4 Clinical Course and ProcedureResults
Results are to be assessed at least six monthsafter surgery, and changes in patient conditiontake place up to two years after the procedure[34]. There are scales for rating OCD symptoms,the most common being the Yale-Brown obses-sive compulsive scale (Y-BOCS). The Beck andHamilton scales are also used, to rate anxiety,along with scales to rate quality of life, Lehman’squality of life (QOL) scale being the one mostcommonly employed.
10.4.1 Anterior Capsulotomy
Initial results reported by Dr. L. Leksell yieldedfavourable responses in 50 % of OCD cases [19,29]. Later series of patients treated from the1970s to 1990s achieved improvement in 70 %of OCD patients undergoing the procedure [35,40, 45]. Results for recent series have beenconsistent with these latter success rates, withfewer adverse effects [30, 41]. Outcomes forpatients treated by Gamma Knife radiosurgeryreported by the Karolinska Institute team havebeen similar [23].
Immediate undesirable secondary effectsassociated with this procedure are transient,lasting three to six months, and include head-ache, transient urinary incontinence, impairedcognitive function, especially memory, andconfusion. Focal neurological deficits associatedwith haemorrhage and tardive epileptic seizureshave been observed in 3 % of cases [10, 35].
10.4.2 Subcaudate Tractotomy
Series published from the 1970s to the 1990syielded a significant percentage improvement inaround 50 % of OCD cases, with good results in40 % of patients suffering from anxiety. Epilepticseizures in 2 % of cases were the most frequentadverse effect apart from initial, transient symp-toms similar to those reported for capsulotomy[27].
10.4.3 Anterior Cingulotomy
Large series have been reported over the past40 years, with improvement rates in OCDpatients ranging between 56 and 36 % of cases[3, 20]. For the most recent published series therewere complete long-term responses in 47 % ofcases and partial responses in 22 % [11]. Anxietyimproved to a large extent, specifically in 43 %of cases in the most recent series [26, 43].Immediate, transient symptoms have includedheadache, confusion, and urinary incontinence.Tardive epileptic seizures have affected up to 9 %of cases in some series. With modern targetingprocedures this unwanted effect has nowdecreased considerably.
10.4.4 Limbic Leucotomy
Initial results were extremely encouraging, with89 % of OCD patients improving [22]. In morerecent studies the improvement rate for OCDpatients has reached 80 % [9, 24]. Adverseeffects include drowsiness for variable lengths of
Fig. 10.4 Cingulotomyperformed by gamma kniferadiosurgery: dose planning(a) and MRI follow-up oneyear later (b)
10 Ablative Surgery for Obsessive-Compulsive Disorders 109

time, confusion, urinary incontinence, and cog-nitive impairment lasting longer than in otherprocedures.
10.5 Our Results
Over the past 10 years our team has operated on100 OCD patients with suitable follow-up ofcases; current mean follow-up is six years.Obsessions and compulsions underwent signifi-cant improvement in 71 % of the OCD casestreated. Improvement was evidenced by a sus-tained decrease of more than 50 % in the Y-BOCSscore. Overall, quality of life in these patientsimproved in 75 % of cases as measured by Leh-man’s quality of life (QOL) scale in late follow-up, with scores increasing by 50 % or more [32].
Transient symptoms observed for time periodsof between two and six months have includedconfusion, some degree of cognitive impairment,urinary incontinence, fever of central origin,nausea-vomiting, hallucinations, heightenedresponse to psychotropic medication, and tardivedepression. Haemorrhagic lesions were observedin 5 % of cases, requiring intervention in twocases (40 % of the patients with bleeding),infections were recorded in 2 % of cases, andepileptic seizures were observed in 4 % of for-merly seizure-free patients.
Results are attained gradually over the course ofthe two years following surgery, as confusion andcognitive impairment improve. In 30 % of casespatient condition worsened, making a secondsurgery necessary. In the cases that underwent asecond surgical intervention, improvement wassimilar to the rate achieved after thefirst procedure.
10.6 Gamma Knife Radiosurgery
10.6.1 Bilateral Anterior Capsulotomy
There have been few published series since the1960s [23, 28, 29, 31, 33, 42]. With improve-ments in imaging definition, the precision of
lesion localization has increased, with less dam-age to more posterior areas of the thalamus.Symptoms improve without collateral effects tothe extent that surgery succeeds in cutting off onlythe anterior limb of the internal capsule bylocating the target in the area that includes themedial connections of the internal capsulebetween the thalamus and the basal frontal regionvisualized by functional MRI. For cases with theproper indications, outcomes are similar to thoseattained using open ablative procedures, that is,significant improvement in 70 % of cases.Changes appear in patients from between sixmonths to a year after treatment, and our team hasnot observed any adverse effects, though cogni-tive impairment and other disorders such as apa-thy (indifference towards one’s surroundings)have been reported in a significant number ofcases in earlier series with long-term follow-up[9]. These effects have been related to the pres-ence of lesions in the posterior and basal regionsof the thalamus.
Our series includes five patients suffering fromOCD treated by capsulotomies carried out using aGamma Knife and followed up for from one to sixyears. We observed better than 50 % improve-ment in the Y-BOCS score in all cases one yearafter the procedure without adverse effects, whilefollow-up MRI visualized the lesions withoutdisclosing any damage to peripheral structures.Our team stands out for its use of a maximumdose (120 Gy) lower than previously reporteddoses and for employing tractography in theplanning stage in all cases [33].
10.7 Conclusions and FutureOutlook
Optimum indications for performing these pro-cedures are conditions suitable for the creation oflocalized lesions capable of disconnecting thelimbic system circuits related to a variety ofpsychiatric disorders. We have made appreciableprogress along this path, and both stimulation ofdifferent brain centres and disconnection of thepathways interconnecting them hold out the
110 R. Martinez-Alvarez
potential of solving a significant proportion ofpsychiatric illnesses that do not respond topharmacological therapy. Specifically, for OCDthere is sufficient evidence to support the viewthat stereotactic surgery using ablation or radio-surgery is a safe, efficacious option for treatingcases refractory to medication and cognitivetherapy.
As is the case with other surgical procedures,adverse effects and complications have beengradually decreasing, and these lesioning tech-niques are gaining increasing acceptance by thepsychiatric profession. The outcomes achieved,in particular the improved quality of life ofpatients, have amazed recent cohorts ofpsychiatrists.
The objective of our work is to unsettle psy-chiatrists, psychologists, neurophysiologists, andradiologists more and more and thereby toencourage them to form multidisciplinary teamsthat will work together to make this type ofsurgery progressively more efficacious, safe, wellknown, and commonplace in all sectors of thepsychiatric profession.
References
1. Alonso P, Segalas C, Real E, Pertusa A, Labad J,Jiménez-Murcia S, Jaurrieta N, Bueno B, Vallejo J,Menchón JM. Suicide in patients treated forobsessive-compulsive disorder: a prospective follow-up study. J Affect Disord. 2010;124:300–8.
2. Ballantine HT. Stereotactic anterior cingulotomy forneuropsychiatric illness and intractable pain.J Neurosurg. 1967;26:488–95.
3. Ballantine HT Jr, Bouckoms AJ, Thomas EK,Giriunas IE. Treatment of psychiatric illness bystereotactic cingulotomy. Biol Psychiatry.1987;22:807–19.
4. Baxter LR Jr, Schwartz JM, Bergman KS, Szuba MP,Guze BH, Mazziotta JC, Alazraki A, Selin CE, Huan-Kwang F, Munford P, Michael P. Caudate glucosemetabolic rate changes with both drug and behaviortherapy for obsessivecompulsive disorder. Arch GenPsychiatry. 1992;49:681–9.
5. Berrios GE. The origins of psychosurgery: Shaw,Burckhardt and Moniz. Hist Psychiatr. 1997;8:61–81.
6. Binder DK, Iskandar BJ. Modern neurosurgery forpsychiatric disorders. Neurosurgery. 2000;47:9–21.
7. Bridges PK, Bartlett JR, Hale AS, Poynton AM,Malizia AL, Hodgkiss AD. Psychosurgery:
stereotactic subcaudate tractomy. An indispensabletreatment. Brit J Psychiatry. 1994;165:599–611.
8. Cannistraro PA, Makris N, Howard JD, Wedig MM,Hodge SM, Wilhelm S, Kennedy DN, Rauch SL. Adiffusion tensor imaging study of white matter inobsessive-compulsive disorder. Depress Anxiety.2007;24:440–6.
9. Cho DY, Lee WY, Chen CC. Limbic leukotomy forintractable major affective disorders: a 7-year follow-up study using nine comprehensive psychiatric testevaluations. J Clin Neurosci. 2008;15:138–42.
10. D’Astous M, Cottin S, Roy M, Picard C, Cantin L.Bilateral stereotactic anterior capsulotomy forobsessive-compulsive disorder: long-term follow-up.J Neurol Neurosurg Psychiatry. 2013;84:1208–13.
11. Dougherty DD, Baer L, Cosgrove GR, Cassem EH,Price BH, Nierenberg AA, Jenike MA, Rauch SL.Prospective long-term follow-up of 44 patients whoreceived cingulotomy for treatment-refractoryobsessive-compulsive disorder. Am J Psychiatry.2002;159:269–75.
12. Eisen JL, Goodman WK, Keller MB, Warshaw MG,DeMarco LM, Luce DD, Rasmussen SA. Patterns ofremission and relapse in obsessive-compulsivedisorder: a 2 year prospective study. J ClinPsychiatry. 1999;60:346–52.
13. Feldman RP, Alterman RL, Goodrich JT.Contemporary psychosurgery and a look to thefuture. J Neurosurg. 2001;95:944–56.
14. Freeman W, Watts J, Hunt TC. Psychosurgery:intelligence, emotion and social behavior followingprefontal lobotomy for mental disorders. Springfield:Bailliére, Tindall & Cox; 1942.
15. Gaviria M, Ade B. What functional neurosurgery canoffer to psychiatric patients: a neuropsychiatricperspective. Surg Neurol. 2009;71:337–43.
16. Greenberg BD, Price LH, Rauch SL, Friehs G, NorenG, Malone D, Carpenter LL, Rezai AR, RasmussenSA. Neurosurgery for intractable obsessive-compulsive disorder and depression: critical issues.Neurosurg Clin N Am. 2003;14:199–212.
17. Greenberg BD, Rauch SL, Haber SN. Invasivecircuitry-based neurotherapeutics: stereotacticablation and deep brain stimulation for OCD.Neuropsychopharmacology. 2010;35:317–36.
18. Heller AC, Amar AP, Liu ChY, Apuzzo ML. Surgeryof the mind and mood: a mosaic of issues in time andevolution. Neurosurgery. 2006;59:720–39.
19. Herner T. Treatment of mental disorders with frontalstereotactic thermolesions: a follow-up of 116 cases.Acta Psychiatrica Scand. 1961;58(36):1–140.
20. Jenike MA, Baer L, Ballantine T, Martuza RL, TynesS, Giriunas I, Buttolph ML, Cassem NH.Cingulotomy for refractory obsessive-compulsivedisorder. A long-term follow-up of 33 patients.Arch Gen Psychiatry. 1991;48:548–55.
21. Kelly D, Richardson A, Mitchell-Heggs N.Stereotactic limbic leucotomy: neurophysiologicalaspects and operative technique. Brit J Psychiatry.1973;123:133–40.
10 Ablative Surgery for Obsessive-Compulsive Disorders 111
22. Kelly D, Richardson A, Mitchell-Heggs N, GreenupJ, Chen C, Hafner RJ. Stereotactic limbic leucotomy:a preliminary report on forty patients. Brit JPsychiatry. 1973;123:141–8.
23. Kihlström L, Hindmarsh T, Lax I, Lippitz B, MindusP, Lindquist C. Radiosurgical lesions in the normalhuman brain 17 years after gamma knifecapsulotomy. Neurosurgery. 1997;41(2):396–401.
24. Kim MC, Lee TK, Choi CR. Review of long-termresults of stereotactic psychosurgery. Neurol MedChir (Tokyo). 2002;42:365–71.
25. Kim CH, Chang JW, Koo MS, Kim JW, Suh HS,Park IH, Lee HS. Anterior cingulotomy for refractoryobsessive-compulsive disorder. Acta PsychiatricaScand. 2003;07:283–90.
26. Kim MC, Lee TK. Stereotactic lesioning for mentalillness. Acta Neurochir Suppl. 2008;101:39–43.
27. Knight G. Further observations from an experience of660 cases of stereotactic tractotomy. Postgrad Med J.1973;49:845–54.
28. Kondziolka D, Flickinger JC, Hudak R. Resultsfollowing gamma knife radiosurgical anteriorcapsulotomies for Obsessive Compulsive Disorder.Neurosurgery. 2011;68:28–33.
29. Leksell L. Modern concepts in pshchiatric surgery.Amsterdam: Elsevier; 1979.
30. LiuK, ZhangH, LiuCh,GuanY,LangL, ChengY, SunB, Wang H, Zuo Ch, Pan L, Xu H, Li S, Shi L, Qian J,Yang Y. Stereotactic treatment of refractory obsessivecompulsive disorder by bilateral capsulotomy with3 years follow-up. J Clin Neuros. 2008;15:622–9.
31. Lopes AC, Greenberg B, Norén G, Montes CanterasM, Busatto G, Mathis ME, Taub A, Chaubet C,Queiroz M, Sauerbronn F, Cecconi J, Gentil A,Arzeno Y, Fuentes D, Campi de Castro C, Leite C,Salvajoli J, Duran F, Rasmussen S. Treatment ofresistant obsessive-compulsive disorder with ventralcapsular/ventral striatal gamma capsulotomy: a pilotprospective study. J Neuropsychiatry Clin Neurosci.2009;21:381–92.
32. Martínez R. Psicocirugía ablativa. In: García de SolaR, García Navarrete E, editors. NeurocirugiaFuncional y Estereotáctica. Viguera, Barcelona; 2011.
33. Martínez R, Cruz MA. Radiocirugía en trastornospsiquiátricos In: Samblas J, Sallabanda K, MartinezR, Calvo FA, editors. Radiocirugia: Fundamentos,avances tecnológicos, indicaciones y resultados.Aran, Madrid; 2012.
34. Mindus P, Rasmussen SA, Lindquist C.Neurosurgical treatment for refractory obsessive-compulsive disorder: implications for understandingfrontal lobe function. J Neuropsychiatry ClinNeurosci. 1994;6:467–77.
35. Mindus P, Meyerson BA. In: Schmideck HH, SweetWH, editors. Operative neurosurgical tecniques.Indications, methods and results, 3rd edn. WBSaunders: Philadelphia; 1995. p. 1443–54.
36. Narrow WE. Revised prevalence estimates of mentaldisorders in the United States: using a clinicalsignificance criterion to reconcile surveys stimates.Arch Gen Psychiatry. 2002;59:115–23.
37. Nyman H, Andreewitch S, Lundback E, Mindus P.Executive and cognitive functions in patients withextreme obsessive-compulsive disorder treated bycapsulotomy. Appl Neuropsychol. 2001;8:91–8.
38. Pallanti S, Quercioli L. Treatment-refractoryobsessive-compulsive disorder: methodologicalissues, operational definitions and therapeutic lines.Prog Neuropsychopharmacol Biol Psychiatry.2006;30:400–12.
39. Rasmussen SA, Eisen JL. The epidemiology andclinical features of obsessive compulsive disorder.Psychiatr Clin North Am. 1992;15:743–58.
40. Rück C, Karlsson A, Steele JD, Edman G, MeyersonBA, Ericson K, Nyman H, Asberg M, Svanborg P.Capsulotomy for obsessive-compulsive disorder:long-term follow-up of 25 patients. Arch GenPsychiatry. 2008;65:914–22.
41. Ruck C, Larsson KJ, Mataix-Cols D. Predictors ofmedium and long-term outcome followingcapsulotomy for obsessive-compulsive disorder: onesite may not fit all. Eur Neuropsychopharmacol.2012;22:406–14.
42. Sheehan JP, Patterson G, Schlesinger D, Xu Z.Gamma knife surgery anterior capsulotomy for severeand refractory obsessive-compulsive disorder.J Neurosurg. 2013;119(5):1112–8.
43. Sheth SA, Neal J, Tangherlini F, Mian MK, Gentil A,Cosgrove GR, Eskandar EN, Dougherty DD. Limbicsystem surgery for treatment-refractory obsessive-compulsive disorder: a prospective long-term follow-up of 64 patients. J Neurosurg. 2013;118:491–7.
44. Vago DR, Epstein J, Catenaccio E, Stern E.Identification of neural targets for the treatment ofpsychiatric disorders: the role of functionalneuroimaging. Neurosurg Clin N Am. 2011;22:279–305.
45. Waziri R. Psychosurgery for anxiety and obsessive-compulsive disorders. In: Burrows GD, Noyes Jr R,Roth M, editors. Handbook of anxiety: the treatmentof anxiety. Amsterdam: Elsevier;1990. p. 519–35.
46. Woerdeman PA, Willems PW, Noordmans HJ,Berkelbach van der Sprenkel JW, van Rijen PC.Frameless stereotactic subcaudate tractotomy forintractable obsessive-compulsive disorder. ActaNeurochir (Wien). 2006;148:633–7.
112 R. Martinez-Alvarez
11DBS for Obsessive-CompulsiveDisorder
Mayur Sharma, Emam Saleh, Milind Deogaonkarand Ali Rezai
Keywords
Neuromodulation � Deep brain stimulation � Obsessive-compulsivedisorder � PsychosurgeryAbbreviations
DBS Deep brain stimulationOCD Obsessive-compulsive disorderY-BOCS Yale-Brown obsessive compulsive scalefMRI Functional magnetic resonance imagingPET Positron emission tomographyNAcc Nucleus accumbensSTN Subthalamic nucleusALIC Anterior limb of internal capsuleVc/Vs Ventral capsule and ventral striatumITP Inferior thalamic peduncleGpi Globus pallidus internus
11.1 Introduction
According to Diagnostic and Statistical Manualof Mental disorders, fifth edition (DSM-V),Obsessive compulsive disorder (OCD) is char-acterized by persistent obsessions with intrusivethoughts leading to severe generalized anxietyand/or compulsions in the form of repetitivetasks to relieve this distress. OCD is often asso-ciated with depression and other co-morbidities[1]. There is also an increase in the incidence ofsuicidal ideation and suicide among patients withOCD [2, 3]. OCD is a chronic and severe dis-abling heterogeneous disorder that has a signifi-cant impact on the life of patients and theirfamilies with public health consequences. Itaffects approximately 2–3 % of population in theUnited States and worldwide and is the 10th
M. SharmaCenter of Neuromodulation, Wexner MedicalCenter, The Ohio State University, 410 W 10th Ave,Room 1047, Columbus, OH 43210, USAe-mail: [email protected]
E. Saleh � M. DeogaonkarDepartment of Neurosurgery, Center ofNeuromodulation, Wexner Medical Center,The Ohio State University, 480 Medical CenterDrive, Columbus, OH 43210, USAe-mail: [email protected]
M. Deogaonkare-mail: [email protected]
A. Rezai (&)Neuroscience Program and Center forNeuromodulation, Wexner Medical Center,The Ohio State University, 480 Medical CenterDrive, Columbus, OH 43210, USAe-mail: [email protected]
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0_11© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
113
leading cause of disability worldwide [1, 4–8].OCD affects both genders equally [7, 8]. Phar-macological [Selective Serotonin reuptakeinhibitors (SSRIs)] and non-pharmacologicaltherapies such as cognitive behavior therapy(CBT) are the first line treatment options inpatients with medical refractory OCD [9, 10].These modalities are effective in approximately50 % of patients with 40–60 % reduction in OCDsymptoms [6, 11]. However, 10–25 % of theserefractory patients have persistent OCD symp-toms despite aggressive pharmacotherapy andbehavior therapy [5, 9, 12, 13].
Neurosurgical management of various psy-chiatric disorders including OCD can be datedback to the origin of this specialty. However,availability of effective pharmacotherapy with ahigher incidence of surgical morbidity/mortalityand limited understanding of the pathophysiologyof these disorders, led to the rapid fall of psy-choneurosurgery. Technological advances andevolution of neuroimaging techniques revivedinterest in the neurosurgical management ofpatients with medical refractory psychiatric dis-orders. Integration of stereotaxis, neuroimagingand electrophysiology not only improved ourunderstanding of OCD pathophysiology but alsomade it possible to aim different target or targetswith submillimetric accuracy. Ablative (capsu-lotomy, cingulotomy, subcaudate tractotomy andlimbic leucotomy) or neuromodulation (DBS)techniques have been utilized in the surgicalmanagement of patients with refractory OCDwith varied success. Reversibility, adjustability,adaptability and ability to blind the stimulationfor research studies are the advantages of DBStherapy over ablative surgeries. Till now over100 patients underwent DBS implantation sur-gery for medical refractory OCD and DBS forOCD has been granted a humanitarian deviceexemption (HDE) status by FDA in 2009[14–17]. In this chapter, we have focused on theDBS therapy for OCD, historical aspects of psy-choneurosurgery, pathophysiology and involvedcircuits, surgical techniques, different anatomicaltargets for OCD and ethical consideration with anoverview of the pertinent literature.
11.2 Deep Brain Stimulation (DBS)for OCD
DBS is a reversible, adjustable and a well-accepted surgical therapy for patients with med-ical refractory movement disorders. The successof DBS therapy in movement disorders with over100,000 implants in the last couple of decades ledclinicians to explore this treatment option forpatients with medical refractory OCD. Psycho-surgery has evolved over the years following atorment past. Surgery for psychiatric disorderswas first presented in a scientific meeting in 1889.Talairach first presented the stereotactic guidedtargeting of the frontothalamic fibers in theinternal capsule at the 4th international neurologycongress in Paris in 1943. In 1950s, variousresearchers performed experimental DBS inpatients with refractory psychiatric disorders withan intent to reduce the severity of clinical symp-toms [18, 19]. Stimulation of the area near theparafascicular complex and cerebellar vermis hasbeen shown to ameliorate OCD symptoms bytargeting neural circuits in patients with refractoryOCD [16, 20]. These initial studies fostered withadvances in imaging and technology pushed thefrontiers of psychosurgery. Subsequently in 2009,DBS for OCD has been granted a humanitariandevice exemption status by FDA [14–17]. Theadvantages of DBS in terms of reversibility,adjustability as per patient’s requirements,excellent safety profile and ability to enrollpatients in cross over blinded research studies todetermine the efficacy of DBS, made neurosti-mulation surgery an attractive treatment optionfor patients with severe medical refractory OCD.Till date, over 100 patients underwent DBSimplantation surgery for OCD. However, resultsfrom these studies need to be cautiously inter-preted due to challenges such as heterogeneouscohort of patients with medical refractory OCD,non-uniform assessment criterion, prolongedtitration intervals and practical implication forpatients travelling from far-off places for titration.
The exact mechanism of action of DBS ther-apy is still elusive. It is widely believed that DBStherapy works similar to ablation therapy by
114 M. Sharma et al.
inducing neuronal inhibition by depolarizingneurons in the vicinity of a stimulating electrode[21]. Contrary to this, recent studies supportedthat high frequency stimulation results in axonalexcitation which subsequently blocks the patho-logical bursting and oscillatory activity [21].Synaptic inhibition, synaptic depression, depo-larization blockade and stimulation-inducedmodulation of pathological network activity arethe putative mechanisms underlying the efficacyof DBS [22, 23]. DBS therapy has also beenshown to improve the fidelity of thalamocorticalneurons and to modulate the pathological cog-nitive-behavior-emotional circuit [24].
Advances in neuroimaging, Neuronavigationtechniques coupled with improved understandingof the intricate neural circuits implicated in thepathophysiology of OCD, enabled neurosur-geons to target various nodal points to modulatethese pathological neural circuits. Anterior limbof internal capsule (ALIC), Ventral Capsule/Ventral striatum (Vc/Vs), Nucleus accumbens(Nu Acc), subthalamic nucleus (STN) and Infe-rior thalamic peduncle have been investigated aspotential DBS targets in various research studiesto benefit patients with medical refractory OCD.
11.2.1 Anterior Limb of InternalCapsule (ALIC)
Based on the beneficial effects of anterior cap-sulotomy in patients with refractory OCD, ALICwas the first target to be selected for DBS therapy[25, 26]. The fibers connecting the orbitofrontal,subgenual anterior cingulate cortex, medialdorsomedial and anterior thalamic nuclei coursesthrough the anterior limb of the internal capsuleand therefore ALIC could be a potential surgicalnode to modulate this neural circuit. This targetwas first explored by Nuttin et al. [25] in 1999 in4 patients with medical refractory OCD with thetarget coordinates similar to that used for cap-sulotomies. In this controlled study, 75 % ofpatients (3 out of 4) experienced reduction intheir obsessive compulsive symptoms. However,this improvement was not quantified using clin-ical scales and 1 patient experienced 90 %
improvement in her OCD symptoms following2 weeks of stimulation in this study. In 2003 and2008, same group published significantimprovement in Y-BOCS and GAF scales in6 patients with medical refractory OCD whounderwent bilateral ALIC-DBS [27, 28]. In thisdouble blind controlled study,[35 % reductionin Y-BOCS score compared to baseline wasconsidered as a “responder” criterion. 3 of4 patients who entered the assessment phase inthis study, reported significant improvement inmean Y-BOCS (DBS off: 32.2; on: 19.8) andclinical global severity scores (DBS off: 5;on: 3.3) following DBS stimulation whichworsened in the DBS “off” state [27, 28]. Thisreduction in core OCD symptoms following DBSwas observed 21 months after surgery in patientswith medical refractory OCD. Of note, DBSelectrode contacts 0 was located in the nucleusaccumbens, contacts 1 and 2 in the anterior limbof the internal capsule and contact 3 was locateddorsal to the internal capsule. This study alsoreported increased metabolism in pons on fMRIand decreased metabolism in the frontal lobe onPET scans following 10 days and 3 months ofcontinuous bilateral stimulation [27]. Mild cog-nitive and behavior disinhibition was noted athigher voltages in this study, which improvedwith changes in programming parameters. Nosignificant complications related to the DBSimplantation surgery was reported in this study[27]. Abelson et al. [29] in a double blindcontrolled study reported 19.8 % decrease inY-BOCS score in DBS “ON” state followingbilateral ALIC DBS in 4 patients with medicalrefractory OCD. In the blind phase of the study,1 patient experienced [35 % improvement inY-BOCS score, another one reported 17 %reduction in Y-BOCS score and other 2 patientshad no impact on their OCD symptoms follow-ing DBS stimulation. During the open phase ofthe study, 2 out of 4 patients (50 %) repor-ted[35 % reduction in Y-BOCS score followingstimulation [29]. Another study reported a27 point decrease in Y-BOCS score followingbilateral ALIC-DBS stimulation at 10 months inan isolated patient with medical refractoryOCD [30].
11 DBS for Obsessive-Compulsive Disorder 115
11.2.2 Ventral Capsule and VentralStriatum (Vc/Vs)
The ventral portion of the caudate nucleus andnucleus accumbens together forms the ventralstriatum and are considered to be the rewardcenters of the brain [31, 32]. Following thesuccess of both ablative and DBS surgeriesinvolving the anterior limb of anterior capsule,ventral striatum in combination with ventralcapsule was explored as the potential DBS targetin patients with medical refractory OCD [33].Greenberg et al. [34] reported complete ([35 %reduction in Y-BOCS score) and partial(25–35 % reduction in Y-BOCS scores) responsein 40 and 20 % of patients respectively, follow-ing bilateral Vc/Vs DBS in 10 patients withmedical refractory OCD. In this uncontrolledstudy, there was 12.3 points decrease in Y-BOCSscore with improvement in symptoms such asanxiety, depression, independent living and self-care at 36 months of DBS stimulation as com-pared to baseline [34]. Asymptomatic hemor-rhage, seizure, superficial infection, hypomaniaand worsening of depression were reported inthis study [34]. In 2010, Greenberg et al. [35]reported a response rate of 62 % followingbilateral ALIC-Vc/Vs DBS in 26 patients withmedical refractory OCD across three centers inUnited States (Butler Hospital/Brown MedicalSchool, Cleveland Clinic and University ofFlorida) and one center in Europe (Leuven/Antwerp). This open study over 8 years reporteda 13.1 points decrease in Y-BOCS score fol-lowing neurostimulation as compared to baselineat 3–36 months follow up [35]. They also notedincreased responsiveness on stimulating DBSelectrode contacts closer to the ventral caudate ornucleus accumbens than otherwise. A total of23 adverse events in 11 patients related to DBSimplantation surgery (asymptomatic intracerebralhemorrhage in 2 patients, seizure in 1 patient,superficial wound infection in one case and onecase each of stimulating lead and extension wirebreakage) and 9 adverse events (increaseddepression in 4 patients, three events of increasedOCD symptoms, one case of hypomania and onereport of domestic problems/irritability) related
to stimulation was reported in this study [35].Goodman et al. [36] in a randomized controlledstudy reported response rate of 67 % followingbilateral Vc/Vs DBS in 6 patients with refractoryOCD at 1 year follow up. There was 15.7 pointsdecrease in Y-BOCS score following bilateralVc/Vs DBS as compared to baseline in this study[36]. No significant adverse effects related toimplantation and hypomania in 4 of 6 patientsrelated to chronic stimulation was reported in thisstudy [36]. Tsai et al. [37] investigated the rela-tionship between stimulation induced smile/laughter and long term DBS outcome in 4patients, who underwent bilateral Vc/Vs DBS formedical refractory OCD. They reported thatacute Vc/Vs DBS was associated with moodchanges, hemodynamic, sensory, or motor effectsthat were transient and tend to adapt over time[37]. In this study, they noticed that the stimu-lation induced smile/laughter was significantlycorrelated with the reduction in Y-BOCS score at15 months of stimulation [37].
11.2.3 Nucleus Accumbens (NAc)
Nucleus accumbens is one of the components ofventral striatum located at the junction of the endof the anterior limb of the internal capsule, headof caudate nucleus and anterior portion of puta-men. NAc is considered the “reward center” ofbrain [38, 39]. In 2003, Sturm et al. [40] reporteda response rate of 75 % (3 of 4 patients) fol-lowing DBS implantation in the shell region ofright NAc in patients with medical refractoryOCD and anxiety disorders at 24–30 monthsfollow up. In this study, PET imaging performedin one of the patients during stimulation alsosupported the role of nucleus accumbens inmodulating the limbic loop [40]. However,clinical assessment tools such as Y-BOCS orother scoring systems were not used to quantifypost-operative improvement in this study.Another study reported remission of OCD (Y-BOCS\16) with 13 points decrease in Y-BOCSscore compared to baseline following DBS of theventral caudate nucleus in an isolated patientwith intractable severe OCD and associated
116 M. Sharma et al.
depression at 12–15 months [41]. Similarly,another study reported sustained improvement ofOCD symptoms in an isolated patient withresidual schizophrenia following right ALIC-NAc DBS at 24 months [42]. This patient did notmeet the criteria for “responder” ([35 % reduc-tion in Y-BOCS scale) in this study [42]. In2010, an open study reported a response rate of50 % (1 of 2 patients) with a 13 point decrease inY-BOCS score compared to baseline followingbilateral NAc DBS in patients with medicalrefractory OCD at 24–27 months follow up [43].In 2010, Huff et al. [44] in a double blind con-trolled study reported that 10 % of patients(n = 10) were complete responders ([35 %reduction in Y-BOCS score) and 50 % werepartial responders ([25 % reduction in Y-BOCSscore) following right NAc-DBS for medicalrefractory OCD. The mean Y-BOCS scoredecreased from 32.2 at baseline to 25.4 followingDBS with alleviation in depression, globalfunctioning, quality of life and no changes inanxiety, global symptom severity and cognitivefunction at 12 months [44]. Implantation relatedmild adverse effects such as dysesthesia in thesubclavicular region in 1 patient with no othersignificant adverse events reported in this study[44]. Stimulation related side effects such ashypomania, agitation/anxiety, weight gain, con-centration difficulties with failing memory, sui-cidal thoughts, headache, and insomnia werereported following stimulation [44]. Denyset al. [45] reported[35 % reduction in Y-BOCSscore in 9 out of 16 patients (56 % responders)following bilateral NAc-DBS for medicalrefractory OCD at 21 months follow up. Overall,there was 17.5 points decrease in Y-BOCS scorefollowing stimulation with a difference of8.3 points between 2 weeks DBS On and2 weeks DBS off phases [45]. In addition, therewas significant improvement in symptoms suchas depression and anxiety following stimulationin this study. Mild side effects related toimplantation and stimulation such as superficialwound infection, numbness at the incision site,feeling of extension leads, word finding prob-lems, mild forgetfulness, hypomania, werereported in this study [45].
11.2.4 Subthalamic Nucleus (STN)
STN is one of the preferred targets to amelioratemotor symptoms in patients with Parkinson’sdisease. Researchers have noticed improvementin mood, anxiety and other neuropsychologicalsymptoms in patients who underwent STN DBSfor PD [46–51]. In addition, psychologicalsymptoms such as transient acute depression,episodes of hypomania/mania or mirthful laugh-ter following STN stimulation at supra thresholdlevels have been reported in literature [51–54].STN is one of the components of dorsolateralprefrontal, orbitofrontal and limbic neural cir-cuits and thus can be modulated to improvesymptoms in patients with medical refractoryOCD. Specifically, medial/ventromedial portionsof STN and structures in close proximity to STNsuch as lateral hypothalamus, ventral tegmentalarea, substantia nigra and zona incerta have beenimplicated in the neuropsychological effects ofSTN stimulation. An uncontrolled study repor-ted [35 % reduction in Y-BOCS score in2 patients with PD and severe OCD whounderwent bilateral STN DBS at 6 months ofstimulation [49]. In this study, electrodes wereimplanted either in the anteromedial portion ofSTN, between anteromedial portions of STN/zona incerta, or in the anterior portion of zonaincerta and reported 20 points decrease inY-BOCS score compared to baseline followingstimulation [49]. In 2004, Fontaine et al. [55]reported a 31 points decrease in Y-BOCS scorecompared to baseline following bilateral STN-DBS in an isolated patient with refractory OCDat 12 months. Subsequently, in a randomizedmulticenter controlled study, Mallet et al. [56]reported a response rate of 75 % (12 of16 patients) with[25 % reduction in Y-BOCSscore compared to baseline following bilateralSTN DBS for refractory OCD. Overall, there wasan improvement in global assessment of functionscale with no effect on neuropsychologicalparameters such as depression or anxiety fol-lowing stimulation in this study. Adverse eventssuch as intracerebral hemorrhage (n = 1), andserious infections leading to explantation ofhardware (n = 2) were reported in this study.
11 DBS for Obsessive-Compulsive Disorder 117
Chabardes et al. [57] reported[70 % reductionin Y-BOCS score in 3 out of 4 patients (75 %response rate) who underwent bilateral STNDBS for refractory OCD at 6 months.
11.2.5 Inferior Thalamic Peduncle (ITP)
There is only one open study investigating theefficacy of inferior thalamic peduncle as apotential DBS target to alleviate symptoms inpatients with medical refractory OCD. ITP pro-vides a route to the white fibers connectingthalamus to the orbitofrontal cortex and thereforeITP can be explored as a potential nodal point forneuromodulation [58]. In 2009, Jimenez-Ponceet al. [59] reported a significant response ([35 %reduction in Y-BOCS score) in all 5 patients(100 % responders) who underwent bilateral ITPDBS for medical refractory OCD. In this openstudy, there was 17.2 points decrease in Y-BOCSscore following stimulation at 12 months followup compared to base line. The mean globalassessment of functioning scale (GAF) improvedfrom 20 to 70 % following stimulation in thisstudy [59]. Neither significant adverse effectrelated to implantation surgery/chronic stimula-tion or changes in neuropsychological functionsfollowing stimulation reported in this study [59].Although the results of this study are instigating,randomized controlled studies are needed tosubstantiate the efficacy of ITP as potential DBStarget in patients with medical refractory OCD.
11.2.6 Globus Pallidus Internus (Gpi)
In 2013, Nair et al. [60] reported 100 and 85 %improvement in Obsessive-compulsive inventoryscale (OCI) in 2 patients each following bilateralanteromedial (limbic) globus pallidus internus(Gpi) DBS for Tourette’s syndrome and severeOCD at 3–26 months follow up. In this study,bilateral Gpi was targeted to mitigate the motorsymptoms associated with Tourette’s syndromeand they noted that this target also alleviated thesymptoms associated with OCD [60]. Therefore,
Gpi can be explored as a potential DBS target formedical refractory OCD and necessitates furthercontrolled studies to validate its efficacy.
11.3 Patient Selection, TeamApproach and Ethicsin Psychosurgery
In 1977, the National Commission for the Pro-tection of Human subjects was formed under thenational research act to avoid indiscriminate useof psychosurgery in patients with psychiatricdisorders in both clinical and research settings[61]. According to the guidelines laid down bythis commission, patients who are being consid-ered for psychosurgery, should meet the criterionfor chronic and medical refractory OCD [Diag-nostic and Statistical Manual V (DSM-5)] [62].The team involved in care of these patients con-sists of psychiatrist, neurologist, functional neu-rosurgeon, neuropsychologist, bioethicist and laypersonnel to ensure appropriate selection of sur-gical candidates. Patients should be educated andcounselled regarding surgery, possible risksinvolved and expected benefits. Patients shouldalso be able to understand the procedure and havethe ability to take decisions including opting outof the study. A written informed valid consent isthen obtained from the patient or patient’s legalguardian. Quantitative scales such as Yale-Brownobsessive-compulsive scale (Y-BOCS) or obses-sive-compulsive inventory (OCI) must be used byan experienced psychiatrist to quantify theseverity of disease before and after the procedureas well as to ensure uniformity across differentresearch studies. Following approval of the studyprotocol and procedure by the Institutional reviewboard (IRB), the procedure is carried out by anexperienced team of functional neurosurgeons,psychiatrists and neurologists [15]. It is crucial tofollow a series of protocols, safety measures andethical considerations to avoid mimicking thetorment history of psychosurgery and to helppatients with these complex disorders [63]. Fur-thermore, psychosurgery should not be used in
118 M. Sharma et al.
pediatric patients, to enhance memory functions,to modify one’s behavior/identity or enforced bylegal or political causes [15, 64]. With appropriatepatient selection, strict adherence to safety pro-tocols and consideration to ethical issues, we arelikely to push the frontiers of psychosurgery andto benefit patients with this clinical conundrum.
11.4 Surgical Techniques of DBSImplantation
Operative set up and technique of DBS leadplacement for OCD is similar to that establishedfor movement disorders. An outline of the pro-cedure as it is performed in our institution isdescribed below. The procedure is usually per-formed in two stages 7–10 days apart.Stage 1: Involves stereotactic guided implanta-
tion of DBS electrode into deep ana-tomical targets. The procedure is doneaccording to the following steps:(a) Frame placement: Patient’s head is
shaved and stereotactic Leksellframe (Elekta Inc., Atlanta, GA) isattached to the patient’s head undersedation and local anesthesia. Thisis followed by head CT scan usingstealth protocol (1-mm contiguouscuts). These stealth images are thenexported to the stealth station andfused to the stealth CT scan toacquire the coordinates of the tar-get. The target is localized usingeither indirect targeting method inreference to the coordinates of mid-commissural point or by directvisualization of the nucleus on T-2weighted MRI. A safe surgical tra-jectory to the target avoiding thecortical sulci, intracranial vesselsand ventricular walls is planned onthe stealth station.
(b) Neurophysiological mapping usingmicroelectrodes: On the day ofStage 1 surgery, the location of the
burr hole is defined by the Leksellframe coordinates acquired from thestealth station and the surgical site isprepared and draped in a standardmanner. With the patient in supineposition, a burr hole is made at thepredetermined location according tothe Leksell coordinates. Followingburr hole, the Navigus Stimloc™Burr Hole Cover system (Medtron-ic, Minneapolis, MN, USA) isattached over the burr hole and fixedto the skull with screws, to securethe DBS lead following implanta-tion. The underlying dura is coagu-lated and opened at the entry pointof the cannula providing adequateroom to avoid hitting the duraledges. Piamater is coagulated andopened using no. 11 blade at theentry point of cannula. A cannula(length = 177 mm) is insertedthrough the pial opening to 15 mmabove the target. The burr hole isthen covered with surgicel andsealed using Tisseal glue to preventCSF loss. The inner stylet of can-nula is removed and a platinum-iridium or platinum/gold platedtungsten microelectrode withimpedance range of 0.6–1.0-mega-ohm is introduced into the cannulafor microelectrode recording. Themicroelectrode is then advancedthrough the brain matter using amotorized Microdrive system insubmillimetric steps in an awakepatient. The neuronal activitieswithin the target are evaluated bypassive manipulation and activemovements of the extremities ororofacial structures every 1–2 mmalong the length of the nucleus.The neuronal activity is amplified,filtered, displayed and recordedusing a high-quality audio monitor,computer display and digital
11 DBS for Obsessive-Compulsive Disorder 119
oscilloscopes [65]. Based on themicroelectrode recordings and kin-esthetic responses the borders andvolume of the intended target isdefined using either single or mul-tiple parallel trajectories separatedby 2–3 mm. Each neuronal structurehas characteristic electrophysiologi-cal properties which assist in delin-eating the entry and exit pointsthrough that that structure such asSTN neurons had a lower mean fir-ing rate (37 Hz) and irregular patternas compared to SNr (mean firingrate of 71 Hz and regular pattern)[66]. Following satisfactory electro-physiological recordings, themicroelectrode is withdrawn into theguide tube (≥3 mm) and macrosti-mulation is performed to delineatethe thresholds of surrounding struc-tures such as internal capsule, med-ial leminiscus, occulomotor nervefibers and hypothalamus.
(c) Final electrode implantation: Thedata regarding location, character-istics of microelectrode recordingsand the effects of macrostimulationare then evaluated and discussed bythe whole team. Based on thisevaluation, a “best-fit” to theSchaltenbrand and Bailey [67] atlasis created and final location of theDBS implantation is decided.
Stage 2: (Implantable pulse generator place-ment) is an outpatient procedure doneunder general anesthesia and involvesconnecting the distal end of electrodeto the extension cable which is sub-sequently tunneled under the scalp andskin of neck into the subclavicular/abdominal area. Usually a linear inci-sion in made below the clavicle and asubcutaneous pocket is dissected toaccommodate the pulse generator. Theextension cable is connected to thepulse generator.
We start deep brain stimulation 1 month afterthe second stage to allow adequate time for thesurgical site to heal and for edema to subside.Chronic stimulation parameters are adjusted by aneurologist who is familiar with the patientcondition. Usually the neurologist is part of thepatient management team and participated in theevaluation, patient selection before surgery andintraoperative physiological mapping.
11.5 Conclusion
Unlike surgery for movement disorders, DBSsurgery for OCD requires targeting multipleneural circuits to alleviate clinical symptoms inpatients with medical refractory OCD. Techno-logical advances and increased understanding ofthe OCD pathophysiology made it possible todelineate specific nodes for surgical interventionto maximize the clinical benefits associated withDBS. Furthermore, advances in imaging, neuro-navigation and targeting techniques hasimproved the precision and safety profile of thisminimally invasive surgery and made it a favoredtherapeutic option in patients with medicalrefractory OCD. DBS is now a FDA approvedtherapy under Human device exemption (HDE)status for patients with medical refractory OCD.DBS for OCD requires a close collaborationbetween expert group of multidisciplinaryspecialists such as psychiatrists, functionalneurosurgeons, neurologist, neuropsychologist,neuroradiologist, biomedical engineers and bio-ethicist to manage these complex patients. Thenext generation DBS smart devices in the form ofadaptive and responsive closed loop feedbackdevices based on chemical and electrical signals,add to the utility of this therapy for refractoryOCD. Newer ablative techniques such as gammaknife, high intensity focused ultrasound orradiofrequency can be non-invasive alternativeoptions in these complex patients. The rapidlyadvancing field of neuromodulation is likelyto offer hope and benefit patients withmedical refractory OCD. However, long-term
120 M. Sharma et al.
randomized controlled studies are warranted tovalidate the efficacy of DBS therapy in patientswith this clinical conundrum.
References
1. Ruscio AM, Stein DJ, Chiu WT, Kessler RC. Theepidemiology of obsessive-compulsive disorder in theNational Comorbidity Survey Replication. MolPsychiatry. 2010;15:53–63.
2. Alonso P, Segalas C, Real E, Pertusa A, Labad J,Jimenez-Murcia S, Jaurrieta N, Bueno B, Vallejo J,Menchon JM. Suicide in patients treated forobsessive-compulsive disorder: a prospective follow-up study. J Affect Disord. 2010;124:300–8.
3. Kamath P, Reddy YC, Kandavel T. Suicidal behaviorin obsessive-compulsive disorder. J Clin Psychiatry.2007;68:1741–50.
4. Rasmussen SA, Eisen JL. The epidemiology andclinical features of obsessive compulsive disorder.Psychiatr Clin North Am. 1992;15:743–58.
5. Bjorgvinsson T, Hart J, Heffelfinger S. Obsessive-compulsive disorder: update on assessment andtreatment. J Psychiatr Pract. 2007;13:362–72.
6. de Koning PP, Figee M, van den Munckhof P,Schuurman PR, Denys D. Current status of deep brainstimulation for obsessive-compulsive disorder: aclinical review of different targets. CurrentPsychiatry Rep. 2011;13:274–82.
7. Blomstedt P, Sjoberg RL, Hansson M, Bodlund O,Hariz MI. Deep brain stimulation in the treatment ofobsessive-compulsive disorder. World Neurosurg.2013;80:e245–53.
8. Robison RA, Taghva A, Liu CY, Apuzzo ML.Surgery of the mind, mood, and conscious state: anidea in evolution. World Neurosurg. 2013;80:S2–26.
9. Denys D. Pharmacotherapy of obsessive-compulsivedisorder and obsessive-compulsive spectrumdisorders. Psychiatr Clin North Am. 2006;29:553–84, xi.
10. Math SB, Janardhan Reddy YC. Issues in thepharmacological treatment of obsessive-compulsivedisorder. Int J Clin Pract. 2007;61:1188–97.
11. Abudy A, Juven-Wetzler A, Zohar J.Pharmacological management of treatment-resistantobsessive-compulsive disorder. CNS Drugs.2011;25:585–96.
12. Rasmussen SA, Eisen JL. Treatment strategies forchronic and refractory obsessive-compulsive disorder.J Clin Psychiatry. 1997;13:9–13.
13. Pallanti S, Quercioli L. Treatment-refractoryobsessive-compulsive disorder: methodologicalissues, operational definitions and therapeutic lines.Prog Neuropsychopharmacol Biol Psychiatry.2006;30:400–12.
14. Lapidus KA, Kopell BH, Ben-Haim S, Rezai AR,Goodman WK. History of psychosurgery: a
psychiatrist’s perspective. World Neurosurg.2013;80:S27–e21–16.
15. Kopell BH, Greenberg B, Rezai AR. Deep brainstimulation for psychiatric disorders. J ClinNeurophysiol. 2004;21:51–67.
16. Lapidus KA, Kopell BH, Ben-Haim S, Rezai AR,Goodman WK. History of psychosurgery: apsychiatrist’s perspective. World Neurosurg.2013;80:e1–S27.
17. Goodman WK, Alterman RL. Deep brain stimulationfor intractable psychiatric disorders. Annu Rev Med.2012;63:511–24.
18. Heath RG, Monroe RR, Mickle WA. Stimulation ofthe amygdaloid nucleus in a schizophrenic patient.Am J Psychiatry. 1955;111:862–3.
19. Bickford RG, Petersen MC, Dodge HW Jr., Sem-Jacobsen CW. Observations on depth stimulation ofthe human brain through implanted electrographicleads. In: Proceedings of the staff meetings. MayoClinic. 1953;28:181–7.
20. Heath RG, Dempesy CW, Fontana CJ, Fitzjarrell AT.Feedback loop between cerebellum and septal-hippocampal sites: its role in emotion and epilepsy.Biol Psychiatry. 1980;15:541–56.
21. Johnson MD, Miocinovic S, McIntyre CC, Vitek JL.Mechanisms and targets of deep brain stimulation inmovement disorders. Neurother: J Am Soc ExpNeurother. 2008;5:294–308.
22. McIntyre CC, Savasta M, Kerkerian-Le Goff L, VitekJL. Uncovering the mechanism(s) of action of deepbrain stimulation: activation, inhibition, or both.Clinical Neurophysiol: Official J Int Fed ClinNeurophysiol. 2004;115:1239–48.
23. McIntyre CC, Grill WM, Sherman DL, Thakor NV.Cellular effects of deep brain stimulation: model-based analysis of activation and inhibition.J Neurophysiol. 2004;91:1457–69.
24. Guo Y, Rubin JE, McIntyre CC, Vitek JL, Terman D.Thalamocortical relay fidelity varies acrosssubthalamic nucleus deep brain stimulationprotocols in a data-driven computational model.J Neurophysiol. 2008;99:1477–92.
25. Nuttin B, Cosyns P, Demeulemeester H, Gybels J,Meyerson B. Electrical stimulation in anterior limbsof internal capsules in patients with obsessive-compulsive disorder. Lancet. 1999;354(9189):1526.
26. Mindus P, Rasmussen SA, Lindquist C.Neurosurgical treatment for refractory obsessive-compulsive disorder: implications for understandingfrontal lobe function. J Neuropsychiatry ClinNeurosci. 1994;6:467–77.
27. Nuttin BJ, Gabriels LA, Cosyns PR, Meyerson BA,Andreewitch S, Sunaert SG, Maes AF, Dupont PJ,Gybels JM, Gielen F, Demeulemeester HG. Long-term electrical capsular stimulation in patients withobsessive-compulsive disorder. Neurosurgery.2003;52:1263–72.
28. Nuttin BJ, Gabriels LA, Cosyns PR, Meyerson BA,Andreewitch S, Sunaert SG, Maes AF, Dupont PJ,Gybels JM, Gielen F, Demeulemeester HG. Long-term
11 DBS for Obsessive-Compulsive Disorder 121
electrical capsular stimulation in patients withobsessive-compulsive disorder. Neurosurgery.2008;62:966–77.
29. Abelson JL, Curtis GC, Sagher O, Albucher RC,Harrigan M, Taylor SF, Martis B, Giordani B. Deepbrain stimulation for refractory obsessive-compulsivedisorder. Biol Psychiatry. 2005;57:510–6.
30. Anderson D, Ahmed A. Treatment of patients withintractable obsessive-compulsive disorder with anteriorcapsular stimulation. Case report. J Neurosurg.2003;98:1104–8.
31. Knutson B, Adams CM, Fong GW, Hommer D.Anticipation of increasing monetary rewardselectively recruits nucleus accumbens. J Neurosci:Official J Soc Neurosci. 2001;21(16):Rc159.
32. Schultz W. Neural coding of basic reward terms ofanimal learning theory, game theory, microeconomicsand behavioural ecology. Curr Opin Neurobiol.2004;14:139–47.
33. Ruck C, Karlsson A, Steele JD, Edman G, MeyersonBA, Ericson K, Nyman H, Asberg M, Svanborg P.Capsulotomy for obsessive-compulsive disorder:long-term follow-up of 25 patients. Arch GenPsychiatry. 2008;65:914–21.
34. Greenberg BD, Malone DA, Friehs GM, Rezai AR,Kubu CS, Malloy PF, Salloway SP, Okun MS,Goodman WK, Rasmussen SA. Three-year outcomesin deep brain stimulation for highly resistant obsessive-compulsive disorder. Neuropsychopharmacol: OfficialPubl Am Coll Neuropsychopharmacol. 2006;31:2384–93.
35. Greenberg BD, Gabriels LA, Malone DA Jr, Rezai AR,Friehs GM, Okun MS, Shapira NA, Foote KD, CosynsPR, Kubu CS, Malloy PF, Salloway SP, Giftakis JE,Rise MT, Machado AG, Baker KB, Stypulkowski PH,Goodman WK, Rasmussen SA, Nuttin BJ. Deep brainstimulation of the ventral internal capsule/ventralstriatum for obsessive-compulsive disorder: worldwideexperience. Mol Psychiatry. 2010;15:64–79.
36. Goodman WK, Foote KD, Greenberg BD, Ricciuti N,Bauer R, Ward H, Shapira NA, Wu SS, Hill CL,Rasmussen SA, Okun MS. Deep brain stimulation forintractable obsessive compulsive disorder: pilot studyusing a blinded, staggered-onset design. BiolPsychiatry. 2010;67:535–42.
37. Tsai HC, Chang CH, Pan JI, Hsieh HJ, Tsai ST, HungHY, Chen SY. Acute stimulation effect of the ventralcapsule/ventral striatum in patients with refractoryobsessive-compulsive disorder—a double-blindedtrial. Neuropsychiatric Dis Treat. 2014;10:63–9.
38. Knutson B, Wimmer GE, Kuhnen CM, WinkielmanP. Nucleus accumbens activation mediates theinfluence of reward cues on financial risk taking.NeuroReport. 2008;19:509–13.
39. Liu X, Hairston J, Schrier M, Fan J. Common anddistinct networks underlying reward valence andprocessing stages: a meta-analysis of functionalneuroimaging studies. Neurosci Biobehav Rev.2011;35:1219–36.
40. Sturm V, Lenartz D, Koulousakis A, Treuer H,Herholz K, Klein JC, Klosterkotter J. The nucleusaccumbens: a target for deep brain stimulation inobsessive-compulsive-and anxiety-disorders. J ChemNeuroanat. 2003;26:293–9.
41. Aouizerate B, Cuny E, Martin-Guehl C, Guehl D,Amieva H, Benazzouz A, Fabrigoule C, Allard M,Rougier A, Bioulac B, Tignol J, Burbaud P. Deepbrain stimulation of the ventral caudate nucleus in thetreatment of obsessive-compulsive disorder and majordepression. Case report. J Neurosurg. 2004;101:682–6.
42. Plewnia C, Schober F, Rilk A, Buchkremer G,Reimold M, Wachter T, Breit S, Weiss D, KrugerR, Freudenstein D. Sustained improvement ofobsessive-compulsive disorder by deep brainstimulation in a woman with residual schizophrenia.IntJ Neuropsychopharmacol/Official Sci J CollegiumInt Neuropsychopharmacol (CINP). 2008;11:1181–3.
43. Franzini A, Messina G, Gambini O, Muffatti R,Scarone S, Cordella R, Broggi G. Deep-brainstimulation of the nucleus accumbens in obsessivecompulsive disorder: clinical, surgical andelectrophysiological considerations in twoconsecutive patients. Neurol Sci: Official J Ital NeurolSoc Ital Soc Clin Neurophysiol. 2010;31:353–9.
44. Huff W, Lenartz D, Schormann M, Lee SH, Kuhn J,Koulousakis A, Mai J, Daumann J, Maarouf M,Klosterkotter J, Sturm V. Unilateral deep brainstimulation of the nucleus accumbens in patients withtreatment-resistant obsessive-compulsive disorder:outcomes after one year. Clin Neurol Neurosurg.2010;112:137–43.
45. Denys D, Mantione M, Figee M, van den MunckhofP, Koerselman F, Westenberg H, Bosch A,Schuurman R. Deep brain stimulation of the nucleusaccumbens for treatment-refractory obsessive-compulsive disorder. Arch Gen Psychiatry. 2010;67:1061–8.
46. Alexander GE, DeLong MR, Strick PL. Parallelorganization of functionally segregated circuitslinking basal ganglia and cortex. Annu RevNeurosci. 1986;9:357–81.
47. Ardouin C, Pillon B, Peiffer E, Bejjani P, Limousin P,Damier P, Arnulf I, Benabid AL, Agid Y, Pollak P.Bilateral subthalamic or pallidal stimulation forParkinson’s disease affects neither memory norexecutive functions: a consecutive series of 62patients. Ann Neurol. 1999;46:217–23.
48. Woods SP, Fields JA, Troster AI. Neuropsychologicalsequelae of subthalamic nucleus deep brainstimulation in Parkinson’s disease: a critical review.Neuropsychol Rev. 2002;12:111–26.
49. Mallet L, Mesnage V, Houeto JL, Pelissolo A, YelnikJ, Behar C, Gargiulo M, Welter ML, Bonnet AM,Pillon B, Cornu P, Dormont D, Pidoux B, Allilaire JF,Agid Y. Compulsions, Parkinson’s disease, andstimulation. Lancet. 2002;360:1302–4.
50. Temel Y, Kessels A, Tan S, Topdag A, Boon P,Visser-Vandewalle V. Behavioural changes after
122 M. Sharma et al.
bilateral subthalamic stimulation in advancedParkinson disease: a systematic review. ParkinsonRelat Disord. 2006;12:265–72.
51. WittK,DanielsC,Reiff J,KrackP,Volkmann J, PinskerMO, Krause M, Tronnier V, Kloss M, Schnitzler A,Wojtecki L, Botzel K, Danek A, Hilker R, Sturm V,Kupsch A, Karner E, Deuschl G. Neuropsychologicaland psychiatric changes after deep brain stimulation forParkinson’s disease: a randomised, multicentre study.Lancet Neurol. 2008;7:605–14.
52. Krack P, Kumar R, Ardouin C, Dowsey PL,McVicker JM, Benabid AL, Pollak P. Mirthfullaughter induced by subthalamic nucleusstimulation. Mov Disord. 2001;16:867–75.
53. Bejjani BP, Damier P, Arnulf I, Thivard L, BonnetAM, Dormont D, Cornu P, Pidoux B, Samson Y,Agid Y. Transient acute depression induced by high-frequency deep-brain stimulation. N Engl J Med.1999;340:1476–80.
54. Tommasi G, Lanotte M, Albert U, Zibetti M, CastelliL, Maina G, Lopiano L. Transient acute depressivestate induced by subthalamic region stimulation.J Neurol Sci. 2008;273:135–8.
55. Fontaine D, Mattei V, Borg M, von Langsdorff D,Magnie MN, Chanalet S, Robert P, Paquis P. Effect ofsubthalamic nucleus stimulation on obsessive-compulsive disorder in a patient with Parkinsondisease. Case report. J Neurosurg. 2004;100:1084–6.
56. Mallet L, Polosan M, Jaafari N, Baup N, Welter ML,Fontaine D, du Montcel ST, Yelnik J, Chereau I, ArbusC, Raoul S, Aouizerate B, Damier P, Chabardes S,Czernecki V, Ardouin C, Krebs MO, Bardinet E,Chaynes P, Burbaud P, Cornu P, Derost P, Bougerol T,Bataille B, Mattei V, Dormont D, Devaux B, Verin M,Houeto JL, Pollak P, Benabid AL, Agid Y, Krack P,Millet B, Pelissolo A. Subthalamic nucleus stimulationin severe obsessive-compulsive disorder. N Engl JMed. 2008;359:2121–34.
57. Chabardes S, Polosan M, Krack P, Bastin J, KrainikA, David O, Bougerol T, Benabid AL. Deep brainstimulation for obsessive-compulsive disorder:subthalamic nucleus target. World Neurosurg.2013;80:S31–e31–38.
58. Greenberg BD, Rauch SL, Haber SN. Invasivecircuitry-based neurotherapeutics: stereotactic
ablation and deep brain stimulation for OCD.Neuropsychopharmacol: Official Publ Am CollNeuropsychopharmacol. 2010;35:317–36.
59. Jimenez-Ponce F, Velasco-Campos F, Castro-FarfanG, Nicolini H, Velasco AL, Salin-Pascual R, Trejo D,Criales JL. Preliminary study in patients withobsessive-compulsive disorder treated with electricalstimulation in the inferior thalamic peduncle.Neurosurgery. 2009;65:203–9; discussion 209.
60. Nair G, Evans A, Bear RE, Velakoulis D, Bittar RG.The anteromedial GPi as a new target for deep brainstimulation in obsessive compulsive disorder. J ClinNeurosci: Official J Neurosurg Soc Australas.2013;21(5):815–21.
61. Protection of Human Subjects. Use of psychosurgeryin practice and research: report and recommendationsof National Commission for the Protection of HumanSubjects. Fed Reg. 1977;42:26318–32.
62. American Psychiatric Association. Diagnostic andstatistical manual of mental disorders. Washington,DC: American Psychiatric Association; 2013.
63. Nuttin B, Gybels J, Cosyns P, Gabriels L, MeyersonB, Andreewitch S, Rasmussen SA, Greenberg B,Friehs G, Rezai AR, Montgomery E, Malone D, FinsJJ. Deep brain stimulation for psychiatric disorders.Neurosurg Clin N Am. 2003;14(2):xv–xvi.
64. Grant RA, Halpern CH, Baltuch GH, O’Reardon JP,Caplan A. Ethical considerations in deep brainstimulation for psychiatric illness. J Clin Neurosci:Official J Neurosurg Soc Australas. 2013;18:00251–8.
65. Baker KB, Lee JY, Mavinkurve G, Russo GS, WalterB, DeLong MR, Bakay RA, Vitek JL. Somatotopicorganization in the internal segment of the globuspallidus in Parkinson’s disease. Exp Neurol.2010;222:219–25.
66. Hutchison WD, Allan RJ, Opitz H, Levy R,Dostrovsky JO, Lang AE, Lozano AM.Neurophysiological identification of the subthalamicnucleus in surgery for Parkinson’s disease. AnnNeurol. 1998;44:622–8.
67. Schaltenbrand G, Bailey W. Introduction tostereotaxis with an atlas of the human brain.Stuttgart: Thieme; 1959.
11 DBS for Obsessive-Compulsive Disorder 123
12Focused Ultrasound for the Treatmentof Obsessive-Compulsive Disorder
Young Cheol Na, Hyun Ho Jung and Jin Woo Chang
Obsessive-compulsive disorder (OCD) is a dis-abling neuropsychiatric disorder characterized byrecurrent and intrusive thoughts, desires, and/orimages (obsessions) that lead to repetitivebehavior aimed at reducing the associated anxi-ety (compulsions). Typical symptoms of OCDinclude fear of being contaminated by the envi-ronment, which patients try to ease by compul-sively washing their hands until they becomesore and chapped. Despite this effort, obsessivethoughts and the resulting behavior persist. Epi-demiologic studies have revealed that about1–2 % of the general population meet the diag-nostic criteria for OCD at some time in theirlives, with a lifetime prevalence of 2–3 % [4, 24,27]. Despite the best available treatmentsincluding cognitive-behavioral therapy andmedications, 10–20 % of patients with OCDremain refractory to conservative treatments [54].
Various neurosurgical approaches such asablative procedures, deep brain stimulation(DBS), and gamma knife radiosurgery (GKRS)have been used for treating refractory OCDpatients. Recently, transcranial magnetic reso-nance-guided focused ultrasound (MRgFUS) hasbeen introduced as a novel thermal ablationmethod that is performed without opening thecranium [12, 26, 32, 36]. The appropriate targets,
surgical procedures, technical considerations,advantages, potential risks, and clinical results ofMRgFUS for OCD, will be discussed here.
12.1 Contemporary Neural Circuitsin Obsessive-CompulsiveDisorder
Although contemporary understanding of theneural circuits involved in psychiatric disorders isadvancing rapidly, the exact neural circuits rela-ted to OCD are yet to be fully elucidated. Manyearlier studies have revealed increased activitywithin the orbitofrontal cortex, anterior cingulategyrus, and caudate nucleus [2, 45], whereasdecreased activity has been observed in the dor-solateral prefrontal cortex [52]. A correlation hasalso been reported between decreased metabo-lism in the caudate nucleus and improvements inOCD symptoms after medical treatment [23].Dysregulation of basal ganglia circuits has beendemonstrated in the motor and OCD symptomsof Tourette syndrome. These circuits and some ofthe clinical features of OCD are also related tothose of Parkinson’s disease [30, 38]. Thesefindings support the hypothesis that cortico-stri-ato-thalamo-cortical (CSTC) loop functions arestrongly implicated in the pathogenesis of OCD[3, 30]. Decreased frontal-striatal control oflimbic structures such as the amygdala results inan inadequate fear response in patients with OCD
Y.C. Na (&) � H.H. Jung � J.W. ChangDepartment of Neurosurgery, Brain ResearchInstitute, Yonsei University College of Medicine,Seoul, Korea
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0_12© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
125
and may also be responsible for the fear of con-tamination [52].
With this understanding of neural circuitry,three interconnected neural circuits have beenproposed in the pathogenesis of OCD: the circuitof Papez, the basolateral circuit, and the CSTCloop [3]. The anterior nucleus of the thalamusprojects to the cingulate gyrus through the ante-rior limb of the internal capsule (ALIC) in thecircuit of Papez [25]. The dorsomedial nucleus ofthe thalamus projects to the orbitofrontal cortexvia the ALIC in the basolateral circuit [3]. Thethalamus also projects to the cerebral cortex viathe ALIC in the CSTC loop, and these anatom-ical locations, together with the anterior cingulategyrus and nucleus accumbens, are the most fre-quent targets in surgical treatments for OCD.Thus, knowledge of these interconnected neuralcircuits is critical for understanding the rationalebehind the choice of certain targets for surgicalintervention.
12.2 Surgical Strategiesfor Obsessive-CompulsiveDisorder
Surgical strategies can be divided into two cate-gories: ablation and neuromodulation. Variousanatomical targets have been proposed for eitherapproach. However, there are still controversiesin the application of surgical procedures to ana-tomical targets in patients with OCD.
Ablative procedures offer benefits to about45–65 % of patients with intractable OCD [21].Anatomical targets include the anterior cingulategyrus and anterior limb of the internal capsule.Considering the major role of the anterior cingu-late gyrus in the neural circuits described above,neurosurgeons can target this structure for abla-tive therapy in patients with OCD. We havepreviously reported that bilateral anterior cingu-lotomy resulted in a mean improvement of 36 %in the Yale-Brown obsessive-compulsive scale(Y-BOCS). Among 14 cingulotomy patients,6 met the criteria for responders, with a 35 %or higher improvement rating on Y-BOCS
12 months postoperatively. Most importantly,there was no significant cognitive dysfunctionafter cingulotomy [28]. Similar results have beenreported after anterior capsulotomy, with a meanimprovement in Y-BOCS of 33 % and no adversecognitive effects [40, 42]. The invasive nature ofablative procedures means they can inevitably beassociated with surgical complications such asintracerebral hemorrhage, epilepsy, and hydro-cephalus. In addition, the operator cannot alwaysestimate the exact size and location of the lesionsuntil they are visualized in postoperative images.The development of GKRS has provided a non-invasive and accurate method for locating lesionswithout the need for invasive surgery. However,the use of a high dose of radiation is associatedwith an unpredictable risk of adverse effects[48, 49].
Several deep brain structures including theALIC, nucleus accumbens (NAc), caudatenucleus, subthalamic nucleus (STN), and dorso-medial thalamus have been proposed as DBStargets. Nuttin et al. [39] reported a double-blinded study that achieved an improvement inY-BOCS score of at least 35 % in 50 % ofpatients after bilateral anterior capsular DBS. Themean Y-BOCS score was 19.8 ± 8.0 duringstimulation compared with 32.3 ± 3.9 with thestimulator turned off, and this stimulation-induced effect was maintained for at least21 months after anterior capsular DBS. Alongwith the improvements seen after DBS of theanterior capsule, the ventral caudate nucleus [1]and NAc [50] have also been proposed aseffective DBS targets in treatment-refractorypatients with OCD and have yielded improve-ments in OCD symptoms. Unlike ablative pro-cedures, DBS is reversible and adjustable basedon symptoms or disease progression. However,DBS requires permanent implantation of at leastone multi-contact electrode, lead extensions, andan implantable pulse generator (IPG). Thismeans that the patient must be followed closelyfor device management, and undergo replace-ment of the IPG every 3–5 years. Furthermore,DBS devices are sensitive to high-energy elec-trical fields, which can switch them off or evencause a reset of the device. Despite the relatively
126 Y.C. Na et al.
effective outcomes described above, these limi-tations have urged investigators to find less-invasive and more precise methods.
12.3 Transcranial MagneticResonance Guided FocusedUltrasound
12.3.1 Brief History
The earliest applications of ultrasound in medi-cine were therapeutic. Initial reports on the bio-logical effects of ultrasound appeared early in1928 when Harvey and Loomis reported thathigh-intensity high-frequency ultrasound couldbring about changes in living biological tissues[43, 51]. Although a few studies reported suc-cessful treatment outcomes using ultrasound [13,47], therapeutic applications were hampered untilthe late 1990s, especially due to safety issues.With the development of improved ultrasoundtechniques and greater understanding of theeffects of ultrasound on cells and tissues, such asthe damage mechanisms, thresholds, and propa-gation properties through tissues, the therapeuticapplication of ultrasound has been realized [43].
Transcranial ultrasound has been used inpediatric neurosurgery to detect hydrocephalusand midline shifts in the brain. In adults, bloodvelocity in the carotid arteries may be monitoredthrough the intact skull using the Doppler effect.Lynn et al. [34, 35] reported the earliest inves-tigation of focused ultrasound for non-invasiveablation in 1942. Since the 1950s, the use offocused ultrasound to produce focal thermallesions deep within the brain has been demon-strated in several studies [16–18]. Fry et al. [14]demonstrated that low-frequency (around0.5 MHz) ultrasound could be focused throughthe skull. Later, this group also demonstrated theacoustic parameters and histological features offocal brain lesions produced in 10 craniectom-ized cats using intense focused ultrasonic beams[15]. Because the histological appearance ofthese lesions compared with previous thermallesions was similar without the intervening skull,
they predicted the application of transcranialultrasound in the clinical field.
Until the 1990s, the major obstacle to the useof transcranial focused ultrasound was the skullitself. Its deflecting effects and variable thicknessaffect wave propagation to such an extent thatultrasound could not produce a focal lesion. Thegeneration of high temperatures within the skullwas also a major concern due to energy absorp-tion, which could damage the scalp, bone, andadjacent brain parenchyma. For this reason,previous focused ultrasound treatment of thebrain required removal of the skull for energydelivery, resulting in an invasive procedure withadditional risks and costs [14, 15, 17, 22]. As aresult, many researchers agreed that therapeuticultrasound energy could not be delivered throughan intact skull. However, the development ofphased array transducers compatible with mag-netic resonance, which is the most progressivetechnological advancement, has rekindled inter-est in transcranial focused ultrasound. Combinedwith the utilization of temperature-dependentproton resonance frequency shift, which allowsMR thermometry, these advances have yieldedMRgFUS technology, which enables non-inva-sive, image-guided, and temperature-monitoredMRgFUS interventions [29].
12.3.2 Biological Effects of Ultrasound
It was originally believed that diagnostic ultra-sound would never produce biological damage.However, in the early 1990s, Child et al. [6]reported that diagnostic ultrasound could pro-duce significant damage in mice. Two mainbiological effects are demonstrated when highintensity acoustic waves propagate through tis-sues: thermal, and non-thermal or mechanicaleffects [41, 43].
12.3.2.1 Thermal EffectsThe principle of focused ultrasound is that a beamof ultrasound is brought to a focus on the target.As ultrasound waves propagate into attenuatingmaterials such as tissue, the wave amplitudedecreases with distance. This attenuation is
12 Focused Ultrasound for the Treatment of Obsessive-Compulsive Disorder 127
caused by wave absorption and scattering.Whereas absorption is thought of as a mechanismthat converts some portion of the ultrasonic waveinto heat, scattering can be thought of as changesto the direction of the wave. Wherever absorptiontakes place in tissues, the temperature willincrease as long as the rate of heat production isgreater than the rate of heat removal [41]. Thethermal mechanism is relatively well understoodbecause the increase in temperature produced byultrasound can be calculated using the widelyused bio-heat transfer equation [43]. With thisequation, it is possible to estimate the thermaldose and evaluate whether the dose is high enoughto destroy the tissue. Injurious effects in vitrogenerally occur at temperatures of 39–43 °C aftera sufficient time period; at higher temperatures(≥44 °C) coagulation of proteins can occur [41].Dickson and Calderwood [11] reported thatexposures of long duration (5–100 h) wererequired for thermally induced cell death at 40 °Cand no irreversible adverse effects were detectedat temperatures below 40 °C.
The temperature of the focused volume mayrise rapidly by more than 20 °C. Although thevolume of destroyed tissue is small (typically0.5 mL) for a single ultrasound beam, a moreclinically relevant volume can be obtained fromcontiguous arrays of focused ultrasound lesionsthroughout the volume of interest [51].
12.3.2.2 Non-thermal or MechanicalEffects
Of the non-thermal effects, acoustically gener-ated cavitation has received the most attention,and results principally from microbubbles inultrasound contrast agents. Radiation forces canalso be produced by the non-thermal effects ofultrasound.
Acoustic cavitation refers to ultrasonicallyinduced activity occurring in a liquid or liquid-like material containing microbubbles that areeither formed spontaneously or are presentnaturally. Under ultrasonic stimulation, thesemicrobubbles oscillate and can collapse at suffi-ciently high ultrasonic pressure levels. Thisphenomenon is termed inertial cavitation becausethe bubble motion is dominated by the inertia of
the liquid [41]. In general, inertial cavitationresults when microbubbles expand during theacoustic cycle and then collapse rapidly due tooscillations and the rapid growth of the cavity[43]. This cavitation can generate a temperatureincrease, mechanical stress, and reactive freeradicals [41]. Microbubble oscillation itself alsoproduces mechanical stress due to the viscosityof the surrounding fluid, which opposes theoscillation, creating what are known as radiationforces [43]. The occurrence of cavitation andradiation forces depends precisely on the type oftissue being exposed, making it difficult to obtaina consistent response.
12.3.3 The MRgFUS System
For non-invasive, non-ionized thermal ablationwith real time imaging and thermal feedback,MRgFUS is an attractive modality. This tech-nique addresses the limitations described aboveby combining a large phased array, active water-cooling, an acoustic aberration correction algo-rithm, and computed tomography (CT) data forskull-thickness registration.
The large phased array transducer used inMRgFUS is composed of numerous transducerelements. It has been proven that large hemi-spherical phased arrays can deliver adequateenergy through human skulls to ablate brain tis-sue in vivo without an excessive elevation oftemperature on the skull surface [7, 8]. CurrentMRgFUS systems employ 1,024 hemisphericalphased array transducers operating at a frequencyof 650 kHz. The interface between the subject’shead and the transducer is also filled with waterto provide the acoustic path. The MRgFUS sys-tem includes a chiller (refrigeration unit) thatkeeps the water chilled to a constant temperatureso that the skull-bone temperature remains withinsafe limits.
Acoustic aberration is created mostly byvariations in the bony structure of the skull. Thedegree of compensation necessary for eachtransducer element is based on predicting theaberration along the acoustic path from eachelement to the target and calculating the relative
128 Y.C. Na et al.

phase and amplitude correction necessary for thatelement. The result of this compensation is thatthe acoustic energy contribution from each ele-ment will arrive at the focal point in phase. Thephase/amplitude correction algorithm, based onray acoustic methods, relies on an input thatprovides the bone density profile along a ray castbetween each acoustic element and the targetpoint. This information is extracted from a three-dimensional CT image of the skull.
The MRgFUS system combines a focusedultrasound delivery system with a conventionaldiagnostic 1.5 T or 3 T MRI scanner. This systemprovides a real-time therapy planning algorithm,thermal dosimetry, and closed-loop therapy con-trol. The treatment process for MRgFUS is notvery different conceptually from the system that iscurrently in clinical use for other soft tissueapplications. The treatment begins with a series ofstandard diagnostic MR images to identify thelocation and shape of the area to be treated. Theworkstation uses the physician’s designation ofthe target volume to plan the best way to cover thetarget volume with small spots called “sonica-tions”. These treatment spots are cylindrical inshape. Their size depends on the sonicationpower and duration. During the treatment, aspecific MR scan, which can be processed toidentify changes in tissue temperature, provides athermal map of the treatment volume to confirmthe therapeutic effect [53]. The thermal map isused to monitor the treatment in progress, andconfirm that the ablation is proceeding accordingto plan, thus closing the therapy loop.
Before delivering a therapeutic dose ofacoustic energy to the target site, confirmation ofthe alignment of the thermal spot within thetarget site is necessary. Therefore, several sub-threshold sonications (low power and shortduration, usually 10–20 s) should be performedfor which the peak tissue temperature (39–42 °C)is below the threshold for ablation but can still bevisualized on MR thermography images. Afterthis targeting confirmation procedure, sequentialsonications of incremental acoustic energy levelscan be applied to the site to induce tissue abla-tion, as indicated by peak temperatures of53–60 °C.
12.3.3.1 Advantages of MRgFUSAs a non-invasive, non-ionized MR-guided pro-cedure with real time imaging and thermalfeedback, MRgFUS has several advantages. Thetreatment can be monitored in real-time usingMRI and MR-thermography. This allows forimmediate confirmation of the targeting process.Thermal lesioning can be performed discretelyand accurately, and can be evaluated immedi-ately. Unlike stereotactic radiosurgery, MRgFUSdoes not use ionizing radiation and does not carrythe risk of radiation-induced tumorigenesis.Because the MRgFUS procedure is non-invasive,there is no scalp incision, no burr hole, and noelectrode penetrating the brain, unlike radiofre-quency lesioning. Thus, MRgFUS reduces therisk of hemorrhagic complications and this non-invasive procedure also eliminates the risk ofinfectious complications. Compared with DBStreatment, there is no implanted hardware, noconcern about interference with external sourcesof electromagnetic noise, no need for extensivefollow-up for programming, and no need forperiodic battery replacement. This represents amuch simpler treatment plan for all patients, andwill save hours of clinic time for DBS devicemanagement and replacement. Additionally,health care costs will be greatly reduced. It willbe possible to re-treat a patient who develops arecurrence after other surgical treatments.
12.3.3.2 Potential Risks of MRgFUSAlthough ultrasound techniques have advancedenough to overcome many former issues, skullheating may still be sufficient to damage boneand/or adjacent soft tissues. The sonication timesshould be calculated to keep skull temperaturesbelow dangerous levels, and a minimum of10 min assigned for skull cooling will providetime for the skull to return to normal tempera-tures before any additional heating takes place.Tissues along the path to the target (scalp, dura,arachnoid) and brain tissues adjacent to the tar-get, also can become heated to the point wheretissue damage or a burn might occur. This heat-ing can be caused directly by improper treatmenttargeting, irregularities on the skin surface,treatment volumes of tissue that are too close to
12 Focused Ultrasound for the Treatment of Obsessive-Compulsive Disorder 129

the skin or bone, or the conduction of sufficientheat to cause a burn at the surface. The presenceof microcalcification in the brain tissue maycreate additional heating effects along the beampath. By utilizing the CT data, the ultrasoundbeam can be prevented from passing throughthese calcified areas.
Secondary hot-spot formation at bone-tissueand air-tissue interfaces is also a major concern,especially at the base of the skull. Pulkkinenet al. reported [44] that therapeutic ultrasounddevices can produce potentially dangerous heat-ing of the base of the skull. They determinedsafety limits, which apply for the thermal treat-ments operating at a frequency of 230 kHz.
Blood brain barrier (BBB) disruption, edema,swelling, and hemorrhage outside and remotefrom the targeted area also can occur. Theoreti-cally, these events may be due to heating effectsand/or to the pressure wave of the ultrasoundbeam. An increased rate of cerebral hemorrhagehas been reported in stroke patients concomi-tantly treated with intravenous tissue plasmino-gen activator (tPA) [10].
High-field MR-induced vertigo is oftenobserved in users of high-field (≥2 T) MRIscanners who experience disorientation or thesubtle perception of movement when workingclose to or within the bore tube of the magnet, andthis can also torment patients during the proce-dure. The patients will manifest symptoms suchas nausea, vomiting, and dizziness. Althoughthese symptoms may be temporary in most casesand disappear when the subject moves out of themagnet, the sensation of vertigo may accompanylonger exposure. In our experiences of treatingessential tremor using MRgFUS, half of thepatients (5 among 11 patients) suffered from MR-induced vertigo [5]. Three main hypotheses wereproposed for this effect: induced currents, whichmodulate the firing rate of the vestibular haircells, magneto-hydrodynamics, and tissue mag-netic susceptibility differences [19].
There is a risk associated with subject motionduring a sonication or between sonications. Thiscould cause a movement of the tissue relative tothe planned treatment volume on the system, andin extreme cases could result in the treatment of a
point outside the planned treatment volume.Because the skull functions as a defocusing lens,the phase correction map computed for the targetspot, will also become ineffective if the subjectmoves.
If the CT andMR volumes are not well alignedwith each other, the tuning of the ultrasonic ele-ments will be suboptimal and distortion will makeit difficult to achieve an exact volume of heating.The protocols for image fusion are well-estab-lished and will be visually confirmed by cliniciansexperienced in stereotactic targeting. Observationof the location, size and pattern of areas heatedby the low-power sonication trials will also pro-vide direct confirmation of the accuracy of theMRgFUS focus. MR thermography allows for theconfirmation of accuracy before the process oftherapeutic sonications begins.
12.3.3.3 Treatment Procedurefor MRgFUS
The patient’s hair is carefully removed and thescalp examined for existing scars or any otherlesions before the day of treatment. Just beforeapplying head fixation, the patient’s hair isshaved again to prevent thermal injury to thehair. Overall steps in the treatment proceduresteps are performed as follows (Fig. 12.1).1. The patient’s head is placed in a MR-com-
patible stereotactic frame (similar to thoseused in stereotactic radiotherapy headfixation).
2. The patient is positioned supine and head-first on the MRgFUS therapy table.
3. A hemispherical helmet containing the trans-ducer elements is positioned on the patient’shead in the treatment position (this should bedone according tomeasurements taken duringthe pre-operative imaging session).
4. A rubber diaphragm is attached to thepatient’s head and to the transducer to allowacoustic coupling between the ultrasoundtransducer and the scalp.
5. The immobilization system is secured overthe patient’s head to maintain a fixed posi-tion between the patient’s head and theultrasonic transducer.
130 Y.C. Na et al.

6. A localizer scan (quick T1) and a T2 fastspin echo (T2-FSE) MR scan is obtained toallow further refinement of the transducerfocal point with respect to the targeted zone.
7. Then, the interface within the rubber dia-phragm is completely filled with degassedwater to avoid air bubbles between thetransducer and the scalp (active circulation,degassing, and cooling of this water is con-tinuously maintained throughout the proce-dure to avoid undesired heating of the scalpand skull).
8. A series of MR images will be acquired toidentify the target area, and plan the actualtreatment:a. T2 Weighted imaging is examined along
at least 2 axes: Axial and Sagittal.b. Other MR imaging series may also be
acquired.
9. The pre-treatment MRI and CT image data-sets are registered to the T2 weighted MRimages acquired in the previous steps. Thisimage fusion of pre-operative MR assists inthe accurate delineation of the target areaand determination of a safe sonicationpathway:a. The fusion of the CT data is required for
the computation of phase correction val-ues to correct for skull aberration, andidentification of intracranial calcifications.
b. Scars on the scalp are designated toensure the ultrasound beam avoids thesespecific areas.
10. The treating physician defines the treatmentvolume and plan. A commercial workstationautomatically computes the number ofsonications, and the phase and amplitudecorrections (per sonication spot) necessary
Fig. 12.1 Overall procedure of MRgFUS
12 Focused Ultrasound for the Treatment of Obsessive-Compulsive Disorder 131
for the system to produce a focal spot at eachof the desired locations.
11. A central point in the targeted area is tar-geted by a low-dose sonication with a sub-lethal energy level to confirm the targetingaccuracy on the MR images. Focal pointposition and/or transducer location areadjusted as necessary.
12. To enhance the procedure safety and toreduce some of the inherent risks of thermallesioning of brain tissue:a. MRgFUS treatment is performed as a
series of sonications with small incre-ments in power within the designatedtarget volume in the conscious patient.
b. The patient is examined by the clinicalteam during and after each sonication forneurologic signs and symptoms.
c. Sonication starts with low energy prior topermanent thermal ablation. Low-energysonication non-destructively warms thetarget. The warming is captured by theMR thermometry and the MR thermalimages are displayed to the treating phy-sician in real time. The physician thenverifies that the warming is centered onthe anatomical target. This allows thecentering of the permanent thermal lesionin the correct location.
d. The titration of escalating focal sonica-tions continues up to 60 °C within a 5 mmdiameter centered on the target point, oruntil side effects are reported by the sub-ject or observed by the clinical team.
13. After MRgFUS treatment, a series of MRimages is acquired to assess the treatmenteffects.
12.4 Capsulotomy Using MRgFUSfor Obsessive-CompulsiveDisorder
There are no previous clinical reports on MRg-FUS for OCD, and the world’s first clinical trialwas conducted in our institute. This will be dis-cussed below.
12.4.1 Patient Selection
Details about inclusion and exclusion criteria arelisted in Table 12.1. Using these criteria,4 patients with OCD were selected and treatedwith MRgFUS. OCD was diagnosed by a psy-chiatrist according to the criteria of the Diag-nostic and Statistical Manual of MentalDisorders, 4th edition (DSM-IV). All patientswere refractory to medications and cognitivebehavioral therapy (CBT), had suffered fromOCD for at least 3 years, and their Y-BOCSscores were more than 28, as listed in Table 12.1.Refractoriness to medication was defined as alack of improvement after taking more than twodifferent types of serotonin reuptake inhibitors atthe maximum tolerable dose for more than12 weeks. Refractoriness to CBT was defined asa lack of response after one year of therapy, orafter 20 sessions. Before MRgFUS, all patientstook medication stably, and medication doseswere not changed during the entire follow-upperiod. The patient demographics and clinicalcharacteristics are presented in Table 12.2.
12.4.2 Procedures
The fundamental procedures are described aboveand have also been described in detail in ourprevious papers. The MRgFUS was performedusing a 3 T MRI system (GE Medical System,Milwaukee, WI), and the ExAblate 4000 (In-Sightec, Haifa, Israel), which features a 30-cmdiameter, hemispherical 1,024 element phased-array transducer operating at 650 kHz and heldby a mechanical positioner. The patient’s scalpwas closely shaved and the head was fixed with aCosma-Roberts-Wells stereotactic frame (Rad-ionics, USA) after injection of local anesthetic. Acircular flexible silicone membrane with a centralhole was stretched around the patient’s head andsealed to the outer face of the transducer tocontain the degassed and chilled (15–20 °C)water that was circulated between the head andthe transducer. After the patient entered the MRIroom, the stereotactic frame was fixed to thetable, which was part of the ExAblate 4000
132 Y.C. Na et al.
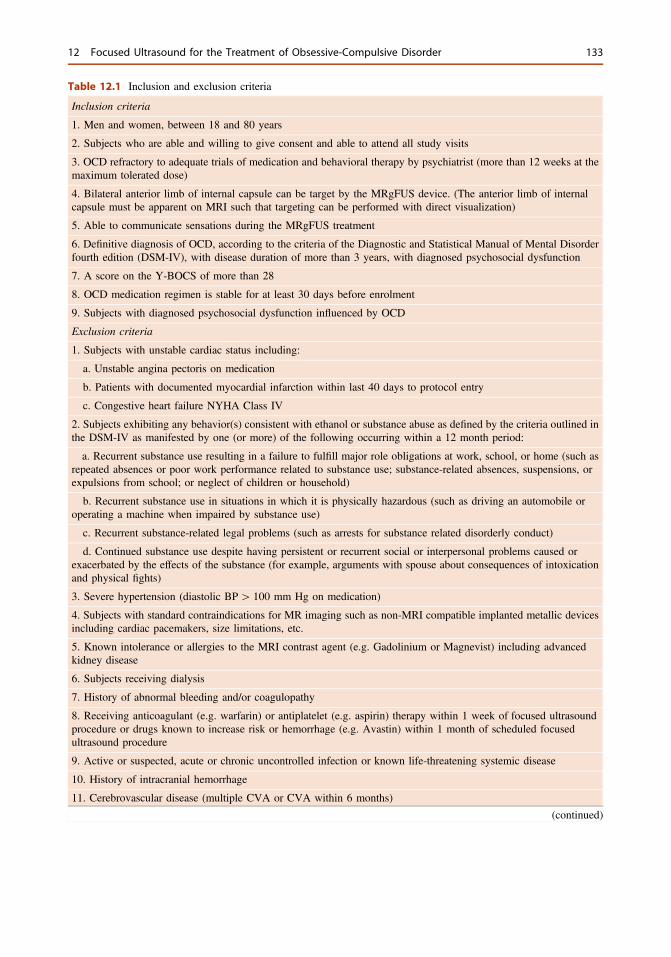
Table 12.1 Inclusion and exclusion criteria
Inclusion criteria
1. Men and women, between 18 and 80 years
2. Subjects who are able and willing to give consent and able to attend all study visits
3. OCD refractory to adequate trials of medication and behavioral therapy by psychiatrist (more than 12 weeks at themaximum tolerated dose)
4. Bilateral anterior limb of internal capsule can be target by the MRgFUS device. (The anterior limb of internalcapsule must be apparent on MRI such that targeting can be performed with direct visualization)
5. Able to communicate sensations during the MRgFUS treatment
6. Definitive diagnosis of OCD, according to the criteria of the Diagnostic and Statistical Manual of Mental Disorderfourth edition (DSM-IV), with disease duration of more than 3 years, with diagnosed psychosocial dysfunction
7. A score on the Y-BOCS of more than 28
8. OCD medication regimen is stable for at least 30 days before enrolment
9. Subjects with diagnosed psychosocial dysfunction influenced by OCD
Exclusion criteria
1. Subjects with unstable cardiac status including:
a. Unstable angina pectoris on medication
b. Patients with documented myocardial infarction within last 40 days to protocol entry
c. Congestive heart failure NYHA Class IV
2. Subjects exhibiting any behavior(s) consistent with ethanol or substance abuse as defined by the criteria outlined inthe DSM-IV as manifested by one (or more) of the following occurring within a 12 month period:
a. Recurrent substance use resulting in a failure to fulfill major role obligations at work, school, or home (such asrepeated absences or poor work performance related to substance use; substance-related absences, suspensions, orexpulsions from school; or neglect of children or household)
b. Recurrent substance use in situations in which it is physically hazardous (such as driving an automobile oroperating a machine when impaired by substance use)
c. Recurrent substance-related legal problems (such as arrests for substance related disorderly conduct)
d. Continued substance use despite having persistent or recurrent social or interpersonal problems caused orexacerbated by the effects of the substance (for example, arguments with spouse about consequences of intoxicationand physical fights)
3. Severe hypertension (diastolic BP[ 100 mm Hg on medication)
4. Subjects with standard contraindications for MR imaging such as non-MRI compatible implanted metallic devicesincluding cardiac pacemakers, size limitations, etc.
5. Known intolerance or allergies to the MRI contrast agent (e.g. Gadolinium or Magnevist) including advancedkidney disease
6. Subjects receiving dialysis
7. History of abnormal bleeding and/or coagulopathy
8. Receiving anticoagulant (e.g. warfarin) or antiplatelet (e.g. aspirin) therapy within 1 week of focused ultrasoundprocedure or drugs known to increase risk or hemorrhage (e.g. Avastin) within 1 month of scheduled focusedultrasound procedure
9. Active or suspected, acute or chronic uncontrolled infection or known life-threatening systemic disease
10. History of intracranial hemorrhage
11. Cerebrovascular disease (multiple CVA or CVA within 6 months)
(continued)
12 Focused Ultrasound for the Treatment of Obsessive-Compulsive Disorder 133
device. Presonication MRI was performed, andimages were fused with computed tomography(CT) and other MR sequences to determine thetarget coordinates. We targeted the bilateralALIC (7 mm anterior to the anterior margin ofthe anterior commissure in the same anteriorcommissure-posterior commissure (AC-PC)plane, extending 2–3 mm along the capsule in acoronal view). Several sub-threshold heatingswith low-power sonications of 10 s duration were
applied to induce peak temperatures of 40–42 °C.This allowed us to visualize the exact positionand size of the thermal spot and the overall safetyprofile of the applied sonication parameters.Then, high-power sonications were applied withstepwise increases in acoustic power and energyto achieve a peak temperature in the target regionof 51–56 °C for more than 3 s duration. All thesesonication processes were guided by MRI andMR thermometry. The goal was to make 10-mm
Table 12.1 (continued)12. Individuals who are not able or willing to tolerate the required prolonged stationary supine position duringtreatment (can be up to 4 h of total table time)
13. Symptoms and signs of increased intracranial pressure (e.g. headache, nausea, vomiting, lethargy, andpapilledema)
14. Subjects unable to communicate with the investigator and staff
15. Presence of any other neurodegenerative disease like Parkinson-plus syndromes suspected on neurologicalexamination. These include:
a. Multisystem atrophy
b. Progressive supranuclear palsy
c. Dementia with Lewy bodies
d. Alzheimer’s disease
16. Subjects diagnosed with idiopathic Parkinson’s disease
17. Presence of significant cognitive impairment as determined with a score ≤24 on the Mini Mental StatusExamination (MMSE)
18. History of immunocompromise, including patient who are HIV positive
19. Subjects with a history of seizures within the past year
20. Subjects with risk factors for intraoperative or postoperative bleeding:
a. Platelet count less than 100,000 mm−3
b. PT[ 14 s
c. PTT[ 36 s
d. INR[ 1.3
e. Documented coagulopathy
f. Patients receiving medications that are known to induce or contribute to Hemorrhages
21. Subjects with any types of brain tumors, including metastases
22. Any illness that in the investigator’s opinion preclude participation in this study
23. Pregnancy or lactation
24. Subjects with history of aneurysms, including newly diagnosed condition
25. Subjects who have had deep brain stimulation or a prior stereotactic ablation of anterior cingulated gyrus
26. OCD medication regimen is not stable for at least 30 days before enrolment
27. Legal incapacity or limited legal capacity
28. Subjects with remarkable atrophy and poor healing capacity of the scalp ([30 % of the skull area traversed by thesonication pathway)
29. Are participating or have participated in another clinical trial in the last 30 days
134 Y.C. Na et al.
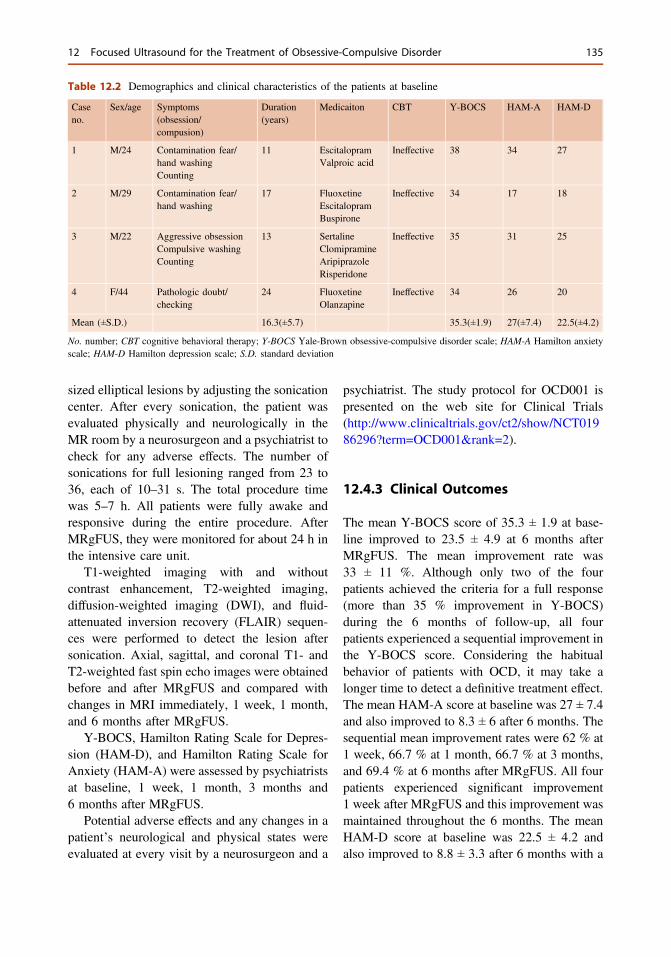
sized elliptical lesions by adjusting the sonicationcenter. After every sonication, the patient wasevaluated physically and neurologically in theMR room by a neurosurgeon and a psychiatrist tocheck for any adverse effects. The number ofsonications for full lesioning ranged from 23 to36, each of 10–31 s. The total procedure timewas 5–7 h. All patients were fully awake andresponsive during the entire procedure. AfterMRgFUS, they were monitored for about 24 h inthe intensive care unit.
T1-weighted imaging with and withoutcontrast enhancement, T2-weighted imaging,diffusion-weighted imaging (DWI), and fluid-attenuated inversion recovery (FLAIR) sequen-ces were performed to detect the lesion aftersonication. Axial, sagittal, and coronal T1- andT2-weighted fast spin echo images were obtainedbefore and after MRgFUS and compared withchanges in MRI immediately, 1 week, 1 month,and 6 months after MRgFUS.
Y-BOCS, Hamilton Rating Scale for Depres-sion (HAM-D), and Hamilton Rating Scale forAnxiety (HAM-A) were assessed by psychiatristsat baseline, 1 week, 1 month, 3 months and6 months after MRgFUS.
Potential adverse effects and any changes in apatient’s neurological and physical states wereevaluated at every visit by a neurosurgeon and a
psychiatrist. The study protocol for OCD001 ispresented on the web site for Clinical Trials(http://www.clinicaltrials.gov/ct2/show/NCT01986296?term=OCD001&rank=2).
12.4.3 Clinical Outcomes
The mean Y-BOCS score of 35.3 ± 1.9 at base-line improved to 23.5 ± 4.9 at 6 months afterMRgFUS. The mean improvement rate was33 ± 11 %. Although only two of the fourpatients achieved the criteria for a full response(more than 35 % improvement in Y-BOCS)during the 6 months of follow-up, all fourpatients experienced a sequential improvement inthe Y-BOCS score. Considering the habitualbehavior of patients with OCD, it may take alonger time to detect a definitive treatment effect.The mean HAM-A score at baseline was 27 ± 7.4and also improved to 8.3 ± 6 after 6 months. Thesequential mean improvement rates were 62 % at1 week, 66.7 % at 1 month, 66.7 % at 3 months,and 69.4 % at 6 months after MRgFUS. All fourpatients experienced significant improvement1 week after MRgFUS and this improvement wasmaintained throughout the 6 months. The meanHAM-D score at baseline was 22.5 ± 4.2 andalso improved to 8.8 ± 3.3 after 6 months with a
Table 12.2 Demographics and clinical characteristics of the patients at baseline
Caseno.
Sex/age Symptoms(obsession/compusion)
Duration(years)
Medicaiton CBT Y-BOCS HAM-A HAM-D
1 M/24 Contamination fear/hand washingCounting
11 EscitalopramValproic acid
Ineffective 38 34 27
2 M/29 Contamination fear/hand washing
17 FluoxetineEscitalopramBuspirone
Ineffective 34 17 18
3 M/22 Aggressive obsessionCompulsive washingCounting
13 SertalineClomipramineAripiprazoleRisperidone
Ineffective 35 31 25
4 F/44 Pathologic doubt/checking
24 FluoxetineOlanzapine
Ineffective 34 26 20
Mean (±S.D.) 16.3(±5.7) 35.3(±1.9) 27(±7.4) 22.5(±4.2)
No. number; CBT cognitive behavioral therapy; Y-BOCS Yale-Brown obsessive-compulsive disorder scale; HAM-A Hamilton anxietyscale; HAM-D Hamilton depression scale; S.D. standard deviation
12 Focused Ultrasound for the Treatment of Obsessive-Compulsive Disorder 135
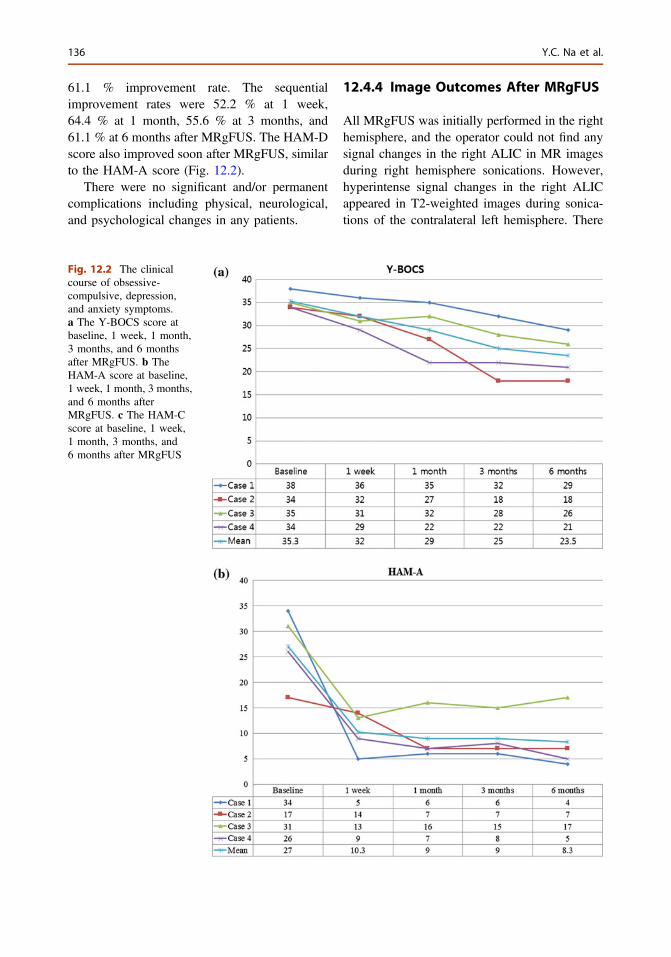
61.1 % improvement rate. The sequentialimprovement rates were 52.2 % at 1 week,64.4 % at 1 month, 55.6 % at 3 months, and61.1 % at 6 months after MRgFUS. The HAM-Dscore also improved soon after MRgFUS, similarto the HAM-A score (Fig. 12.2).
There were no significant and/or permanentcomplications including physical, neurological,and psychological changes in any patients.
12.4.4 Image Outcomes After MRgFUS
All MRgFUS was initially performed in the righthemisphere, and the operator could not find anysignal changes in the right ALIC in MR imagesduring right hemisphere sonications. However,hyperintense signal changes in the right ALICappeared in T2-weighted images during sonica-tions of the contralateral left hemisphere. There
Fig. 12.2 The clinicalcourse of obsessive-compulsive, depression,and anxiety symptoms.a The Y-BOCS score atbaseline, 1 week, 1 month,3 months, and 6 monthsafter MRgFUS. b TheHAM-A score at baseline,1 week, 1 month, 3 months,and 6 months afterMRgFUS. c The HAM-Cscore at baseline, 1 week,1 month, 3 months, and6 months after MRgFUS
136 Y.C. Na et al.
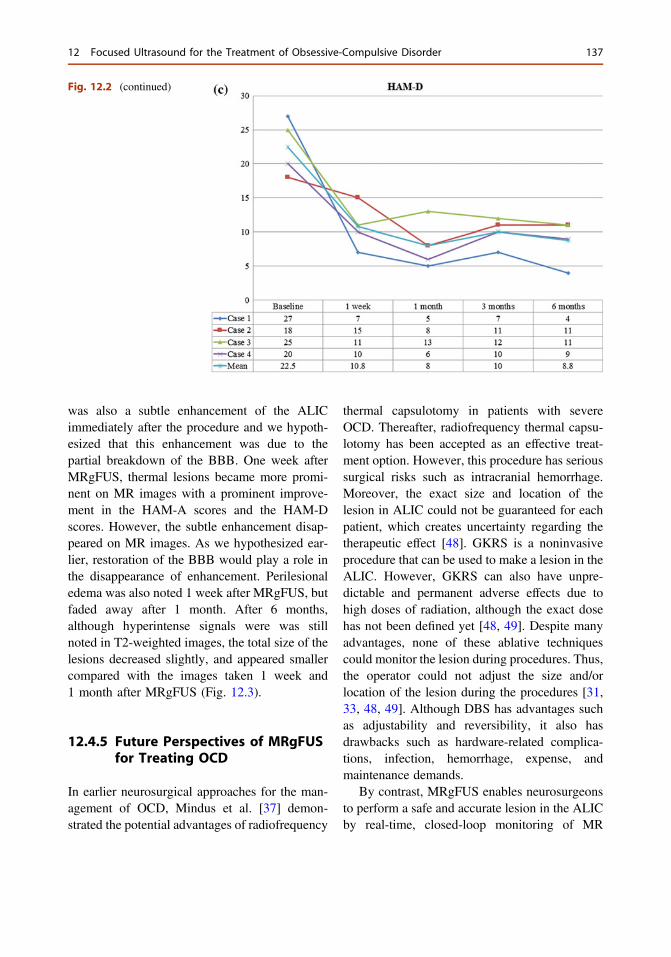
was also a subtle enhancement of the ALICimmediately after the procedure and we hypoth-esized that this enhancement was due to thepartial breakdown of the BBB. One week afterMRgFUS, thermal lesions became more promi-nent on MR images with a prominent improve-ment in the HAM-A scores and the HAM-Dscores. However, the subtle enhancement disap-peared on MR images. As we hypothesized ear-lier, restoration of the BBB would play a role inthe disappearance of enhancement. Perilesionaledema was also noted 1 week after MRgFUS, butfaded away after 1 month. After 6 months,although hyperintense signals were was stillnoted in T2-weighted images, the total size of thelesions decreased slightly, and appeared smallercompared with the images taken 1 week and1 month after MRgFUS (Fig. 12.3).
12.4.5 Future Perspectives of MRgFUSfor Treating OCD
In earlier neurosurgical approaches for the man-agement of OCD, Mindus et al. [37] demon-strated the potential advantages of radiofrequency
thermal capsulotomy in patients with severeOCD. Thereafter, radiofrequency thermal capsu-lotomy has been accepted as an effective treat-ment option. However, this procedure has serioussurgical risks such as intracranial hemorrhage.Moreover, the exact size and location of thelesion in ALIC could not be guaranteed for eachpatient, which creates uncertainty regarding thetherapeutic effect [48]. GKRS is a noninvasiveprocedure that can be used to make a lesion in theALIC. However, GKRS can also have unpre-dictable and permanent adverse effects due tohigh doses of radiation, although the exact dosehas not been defined yet [48, 49]. Despite manyadvantages, none of these ablative techniquescould monitor the lesion during procedures. Thus,the operator could not adjust the size and/orlocation of the lesion during the procedures [31,33, 48, 49]. Although DBS has advantages suchas adjustability and reversibility, it also hasdrawbacks such as hardware-related complica-tions, infection, hemorrhage, expense, andmaintenance demands.
By contrast, MRgFUS enables neurosurgeonsto perform a safe and accurate lesion in the ALICby real-time, closed-loop monitoring of MR
Fig. 12.2 (continued)
12 Focused Ultrasound for the Treatment of Obsessive-Compulsive Disorder 137
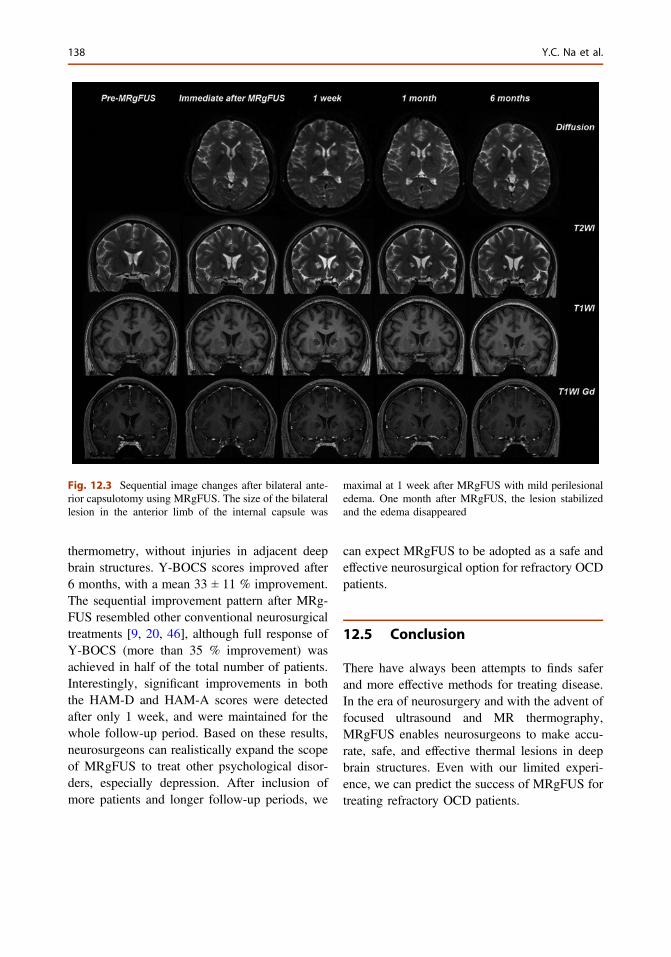
thermometry, without injuries in adjacent deepbrain structures. Y-BOCS scores improved after6 months, with a mean 33 ± 11 % improvement.The sequential improvement pattern after MRg-FUS resembled other conventional neurosurgicaltreatments [9, 20, 46], although full response ofY-BOCS (more than 35 % improvement) wasachieved in half of the total number of patients.Interestingly, significant improvements in boththe HAM-D and HAM-A scores were detectedafter only 1 week, and were maintained for thewhole follow-up period. Based on these results,neurosurgeons can realistically expand the scopeof MRgFUS to treat other psychological disor-ders, especially depression. After inclusion ofmore patients and longer follow-up periods, we
can expect MRgFUS to be adopted as a safe andeffective neurosurgical option for refractory OCDpatients.
12.5 Conclusion
There have always been attempts to finds saferand more effective methods for treating disease.In the era of neurosurgery and with the advent offocused ultrasound and MR thermography,MRgFUS enables neurosurgeons to make accu-rate, safe, and effective thermal lesions in deepbrain structures. Even with our limited experi-ence, we can predict the success of MRgFUS fortreating refractory OCD patients.
Fig. 12.3 Sequential image changes after bilateral ante-rior capsulotomy using MRgFUS. The size of the bilaterallesion in the anterior limb of the internal capsule was
maximal at 1 week after MRgFUS with mild perilesionaledema. One month after MRgFUS, the lesion stabilizedand the edema disappeared
138 Y.C. Na et al.
References
1. Aouizerate B, Cuny E, Martin-Guehl C, Guehl D,Amieva H, Benazzouz A, Fabrigoule C, Allard M,Rougier A, Bioulac B, Tignol J, Burbaud P. Deepbrain stimulation of the ventral caudate nucleus in thetreatment of obsessive-compulsive disorder and majordepression. Case report. J Neurosurg. 2004;101:682–6.
2. Baxter LR. Brain imaging as a tool in establishing atheory of brain pathology in obsessive compulsivedisorder. J Clin Psychiatry. 1990;51 Suppl 22–25;discussion 26.
3. Bear RE, Fitzgerald P, Rosenfeld JV, Bittar RG.Neurosurgery for obsessive-compulsive disorder:contemporary approaches. J Clin Neurosci: OfficialJ Neurosurg Soc Australas. 2010;17:1–5.
4. Bjorgvinsson T, Hart J, Heffelfinger S. Obsessive-compulsive disorder: update on assessment andtreatment. J Psychiatr Pract. 2007;13:362–72.
5. Chang WS, Jung HH, Kweon EJ, Zadicario E,Rachmilevitch I, Chang JW. Unilateral magneticresonance guided focused ultrasound thalamotomyfor essential tremor: practices and clinicoradiologicaloutcomes. J Neurol Neurosurg Psychiatry. 2014.
6. Child SZ, Hartman CL, Schery LA, Carstensen EL.Lung damage from exposure to pulsed ultrasound.Ultrasound Med Biol. 1990;16:817–25.
7. Clement GT, Sun J, Giesecke T, Hynynen K. Ahemisphere array for non-invasive ultrasound braintherapy and surgery. PhysMed Biol. 2000;45:3707–19.
8. Clement GT, White J, Hynynen K. Investigation of alarge-area phased array for focused ultrasoundsurgery through the skull. Phys Med Biol. 2000;45:1071–83.
9. D’Astous M, Cottin S, Roy M, Picard C, Cantin L.Bilateral stereotactic anterior capsulotomy forobsessive-compulsive disorder: long-term follow-up.J Neurol Neurosurg Psychiatry. 2013;84:1208–13.
10. Daffertshofer M, Gass A, Ringleb P, Sitzer M, SliwkaU, Els T, Sedlaczek O, Koroshetz WJ, Hennerici MG.Transcranial low-frequency ultrasound-mediatedthrombolysis in brain ischemia: increased risk ofhemorrhage with combined ultrasound and tissueplasminogen activator: results of a phase II clinicaltrial. Stroke; J Cereb Circ. 2005;36:1441–6.
11. Dickson JA, Calderwood SK. Temperature range andselective sensitivity of tumors to hyperthermia: acritical review. Ann N Y Acad Sci. 1980;335:180–205.
12. Elias WJ, Huss D, Voss T, Loomba J, Khaled M,Zadicario E, Frysinger RC, Sperling SA, Wylie S,Monteith SJ, Druzgal J, Shah BB, Harrison M,Wintermark M. A pilot study of focused ultrasoundthalamotomy for essential tremor. N Engl J Med.2013;369:640–8.
13. Field SB, Bleehen NM. Hyperthermia in the treatmentof cancer. Cancer Treat Rev. 1979;6:63–94.
14. Fry FJ, Barger JE. Acoustical properties of the humanskull. J Acoust Soc Am. 1978;63:1576–90.
15. Fry FJ, Goss SA, Patrick JT. Transkull focal lesionsin cat brain produced by ultrasound. J Neurosurg.1981;54:659–63.
16. Fry WJ. Intense ultrasound in investigations of thecentral nervous system. Adv Biol Med Phys.1958;6:281–348.
17. Fry WJ, Barnard JW, Fry EJ, Krumins RF, BrennanJF. Ultrasonic lesions in the mammalian centralnervous system. Science (N Y, NY). 1955;122:517–8.
18. Fry WJ, Barnard JW, Fry FJ, Brennan JF.Ultrasonically produced localized selective lesionsin the central nervous system. Am J Phys Med.1955;34:413–23.
19. Glover PM, Cavin I, Qian W, Bowtell R, GowlandPA. Magnetic-field-induced vertigo: a theoretical andexperimental investigation. Bioelectromagnetics.2007;28:349–61.
20. Greenberg BD, Gabriels LA, Malone DA Jr, RezaiAR, Friehs GM, Okun MS, Shapira NA, Foote KD,Cosyns PR, Kubu CS, Malloy PF, Salloway SP,Giftakis JE, Rise MT, Machado AG, Baker KB,Stypulkowski PH, Goodman WK, Rasmussen SA,Nuttin BJ. Deep brain stimulation of the ventralinternal capsule/ventral striatum for obsessive-compulsive disorder: worldwide experience. MolPsychiatry. 2010;15:64–79.
21. Greenberg BD, Price LH, Rauch SL, Friehs G, NorenG, Malone D, Carpenter LL, Rezai AR, RasmussenSA. Neurosurgery for intractable obsessive-compulsive disorder and depression: critical issues.Neurosurg Clin N Am. 2003;14:199–212.
22. Guthkelch AN, Carter LP, Cassady JR, Hynynen KH,Iacono RP, Johnson PC, Obbens EA, Roemer RB,Seeger JF, Shimm DS, et al. Treatment of malignantbrain tumors with focused ultrasound hyperthermiaand radiation: results of a phase I trial. J Neurooncol.1991;10:271–84.
23. Hansen ES, Hasselbalch S, Law I, Bolwig TG. Thecaudate nucleus in obsessive-compulsive disorder.Reduced metabolism following treatment withparoxetine: a PET study. Int J NeuropsychopharmacolOfficial Sci J Collegium Int Neuropsychopharmacologi-cum (CINP). 2002;5:1–10.
24. Hollander E. Obsessive-compulsive disorder: thehidden epidemic. J Clin Psychiatry. 1997;58(Suppl12):3–6.
25. Jang SH, Yeo SS. Thalamocortical tract betweenanterior thalamic nuclei and cingulate gyrus in thehuman brain: diffusion tensor tractography study.Brain Imaging Behav. 2013;7:236–41.
26. Jolesz FA. MRI-guided focused ultrasound surgery.Annu Rev Med. 2009;60:417–30.
27. Karno M, Golding JM, Sorenson SB, Burnam MA.The epidemiology of obsessive-compulsive disorderin five US communities. Arch Gen Psychiatry.1988;45:1094–9.
28. Kim CH, Chang JW, Koo MS, Kim JW, Suh HS,Park IH, Lee HS. Anterior cingulotomy for refractoryobsessive-compulsive disorder. Acta Psychiatr Scand.2003;107:283–90.
12 Focused Ultrasound for the Treatment of Obsessive-Compulsive Disorder 139
29. Kyriakou A, Neufeld E, Werner B, Paulides MM,Szekely G, Kuster N. A review of numerical andexperimental compensation techniques for skull-induced phase aberrations in transcranial focusedultrasound. Int J Hyperth: Official J Eur Soc HyperthOncol, N Am Hyperth Group. 2014;30:36–46.
30. Lapidus KA, Kopell BH, Ben-Haim S, Rezai AR,Goodman WK. History of psychosurgery: apsychiatrist’s perspective. World Neurosurg.2013;80:S27–e21-16.
31. Lippitz BE, Mindus P, Meyerson BA, Kihlstrom L,Lindquist C. Lesion topography and outcome afterthermocapsulotomy or gamma knife capsulotomy forobsessive-compulsive disorder: relevance of the righthemisphere.Neurosurgery. 1999;44:452–58; discussion458–60.
32. Lipsman N, Schwartz ML, Huang Y, Lee L, SankarT, Chapman M, Hynynen K, Lozano AM. MR-guided focused ultrasound thalamotomy for essentialtremor: a proof-of-concept study. Lancet Neurol.2013;12:462–8.
33. Lopes AC, Greenberg BD, Noren G, Canteras MM,Busatto GF, de Mathis ME, Taub A, D’Alcante CC,HoexterMQ,Gouvea FS, Cecconi JP,Gentil AF, FerraoYA, Fuentes D, de Castro CC, Leite CC, Salvajoli JV,Duran FL, Rasmussen S, Miguel EC. Treatment ofresistant obsessive-compulsive disorder with ventralcapsular/ventral striatal gamma capsulotomy: a pilotprospective study. J Neuropsychiatry Clin Neurosci.2009;21:381–92.
34. Lynn JG, Zwemer RL, Chick AJ. The biologicalapplication of focused ultrasonic waves. Science (NY, NY). 1942;96:119–20.
35. Lynn JG, Zwemer RL, Chick AJ, Miller AE. A newmethod for the generation and use of focusedultrasound in experimental biology. J Gen Physiol.1942;26:179–93.
36. Martin E, Jeanmonod D, Morel A, Zadicario E,Werner B. High-intensity focused ultrasound fornoninvasive functional neurosurgery. Ann Neurol.2009;66:858–61.
37. Mindus P, Nyman H. Normalization of personalitycharacteristics in patients with incapacitating anxietydisorders after capsulotomy. Acta Psychiatr Scand.1991;83:283–91.
38. Muller N, Putz A, Kathmann N, Lehle R, Gunther W,Straube A. Characteristics of obsessive-compulsivesymptoms in Tourette’s syndrome, obsessive-compulsive disorder, and Parkinson’s disease.Psychiatry Res. 1997;70:105–14.
39. Nuttin BJ, Gabriels LA, Cosyns PR, Meyerson BA,Andreewitch S, Sunaert SG, Maes AF, Dupont PJ,Gybels JM, Gielen F, Demeulemeester HG. Long-term electrical capsular stimulation in patients withobsessive-compulsive disorder. Neurosurgery2003;52:1263–72; discussion 1272–64.
40. Nyman H, Andreewitch S, Lundback E, Mindus P.Executive and cognitive functions in patients withextreme obsessive-compulsive disorder treated bycapsulotomy. Appl Neuropsychol. 2001;8:91–8.
41. O’Brien WD Jr. Ultrasound-biophysics mechanisms.Prog Biophys Mol Biol. 2007;93:212–55.
42. Oliver B, Gascon J, Aparicio A, Ayats E, RodriguezR, Maestro De Leon JL, Garcia-Bach M, Soler PA.Bilateral anterior capsulotomy for refractoryobsessive-compulsive disorders. Stereotact FunctNeurosurg 2003;81:90–5.
43. Phenix CP, Togtema M, Pichardo S, Zehbe I, CurielL. High intensity focused ultrasound technology, itsscope and applications in therapy and drug delivery.J Pharm Pharm Sci: Publ Can Soc Pharm Sci, SocCan Sci Pharm. 2014;17:136–53.
44. Pulkkinen A, Huang Y, Song J, Hynynen K.Simulations and measurements of transcranial low-frequency ultrasound therapy: skull-base heating andeffective area of treatment. Phys Med Biol.2011;56:4661–83.
45. Rauch SL, Jenike MA, Alpert NM, Baer L, BreiterHC, Savage CR, Fischman AJ. Regional cerebralblood flow measured during symptom provocationin obsessive-compulsive disorder using oxygen15-labeled carbon dioxide and positron emissiontomography. Arch Gen Psychiatry. 1994;51:62–70.
46. Roh D, Chang WS, Chang JW, Kim CH. Long-termfollow-up of deep brain stimulation for refractoryobsessive-compulsive disorder. Psychiatry Res.2012;200:1067–70.
47. Rubin D, Kuitert JH. Use of ultrasonic vibration inthe treatment of pain arising from phantom limbs,scars and neuromas; a preliminary report. Arch PhysMed Rehabil. 1955;36:445–52.
48. Ruck C, Karlsson A, Steele JD, Edman G, MeyersonBA, Ericson K, Nyman H, Asberg M, Svanborg P.Capsulotomy for obsessive-compulsive disorder:long-term follow-up of 25 patients. Arch GenPsychiatry. 2008;65:914–21.
49. Sheehan JP, Patterson G, Schlesinger D, Xu Z.Gamma knife surgery anterior capsulotomy for severeand refractory obsessive-compulsive disorder.J Neurosurg. 2013;119:1112–8.
50. Sturm V, Lenartz D, Koulousakis A, Treuer H,Herholz K, Klein JC, Klosterkotter J. The nucleusaccumbens: a target for deep brain stimulation inobsessive-compulsive- and anxiety-disorders. J ChemNeuroanat. 2003;26:293–9.
51. ter Haar G. Intervention and therapy. Ultrasound MedBiol. 2000;26(Suppl 1):S51–4.
52. van den Heuvel OA, Veltman DJ, Groenewegen HJ,Dolan RJ, Cath DC, Boellaard R, Mesina CT, vanBalkom AJ, van Oppen P, Witter MP, LammertsmaAA, van Dyck R. Amygdala activity in obsessive-
140 Y.C. Na et al.

compulsive disorder with contamination fear: a studywith oxygen-15 water positron emission tomography.Psychiatry Res. 2004;132:225–37.
53. Vykhodtseva N, Sorrentino V, Jolesz FA, BronsonRT, Hynynen K. MRI detection of the thermal effectsof focused ultrasound on the brain. Ultrasound MedBiol. 2000;26:871–80.
54. Zhang QJ, Wang WH, Wei XP. Long-term efficacy ofstereotactic bilateral anterior cingulotomy andbilateral anterior capsulotomy as a treatment forrefractory obsessive-compulsive disorder. StereotactFunct Neurosurg. 2013;91:258–61.
12 Focused Ultrasound for the Treatment of Obsessive-Compulsive Disorder 141
13Deep Brain Stimulation for TouretteSyndrome
Jianuo Zhang, Yan Ge and Fangang Meng
13.1 Instruction
Tourette syndrome (TS) is a chronic neurobe-havioral disorder characterized by waxing andwaning motor and phonic tics that persist for atleast 12 months [1]. It is also a multifactorialneurodevelopmental disorder that affects up to1 % of children as well as many adults worldwide.The first clear description of this condition, pub-lished by Georges Albert Édouard Brutus Gillesde la Tourette in 1885 [2], noted childhood onsetof stereotyped, abnormal movements and vocal-izations (called tics), heritability, coprolalia (theutterance of obscene or socially offensive words),echolalia (repeating other people’s words), andwaxing and waning of symptoms; this descriptionremains accurate and relevant today.
Tics generally occur in episodes and are pre-ceded by premonitory sensations in themajority ofpatients. Asmany as 90%of patients with TS havecomorbid psychiatric conditions, such as obses-sive compulsive behavior (OCB), attention deficithyperactivity disorder (ADHD), or exhibit self-injurious behavior (SIB), depression and anxiety[3]; of these, OCB and ADHD are the most com-mon, each occurring in up to 50 % of patients [4].
Once thought to be relatively rare, the preva-lence of TS may in fact be as high as 50/10,000in the general population [5]. The condition is
approximately 10-fold more common in childrenthan in adults, with a prevalence of up to 299/10,000 in 13- to 14-year-old children. In addi-tion, TS is approximately 3 times more commonin males than females. The onset of tics occurs ata mean age of 5–7 years, and severity appears topeak around age 10 years [5]. Symptoms mayimprove or even remit over time without treat-ment, and this tends to occur in the 3rd decade.However, no patient or clinical characteristicspredictive of spontaneous resolution have beenfound [4].
13.2 Diagnosis
Instruments used to diagnose TS include theDiagnostic and Statistical Manual, 4th edition(DSM-IV) [6], the World Health OrganizationInternational Classification of Disease and Rela-ted Health Problems, 10th edition (ICD-10) [7]and the Tourette’s Syndrome ClassificationStudy Group (TSCSG) criteria [8]. According tothe TSCSG, a diagnosis of definite Tourette’ssyndrome requires motor and/or phonic tics to bewitnessed by a reliable examiner or to be cap-tured in a video recording [8]. A patient may beconsidered to have Tourette’s syndrome by his-tory if a family member or close friend witnessesthe tics and is able to provide a description to areliable examiner that is accepted as indicative ofTS. A diagnosis of TS is made when multiplemotor tics and at least one vocal tic are present
J. Zhang (&) � Y. Ge � F. MengDepartment of Neurosurgery, Beijing TiantanHospital, Capital Medical University, Beijing, China
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0_13© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
143
(not necessarily concurrently), develop before theage of 18 years, and last for more than 1 yearfrom their onset, although the intensity and fre-quency of tics may wax and wane during thisperiod. Other potential causes of tics, includingdirect physiological effects of drugs (such ascocaine), or medical conditions (such as stroke,Huntington disease, or postviral encephalitis),should also be excluded. Moreover, tics cansometimes resemble choreic, myoclonic move-ments and stereotypies, but the presence of pre-monitory urges and the ability to temporarilysuppress tics can help to distinguish TS fromother movement disorders, where ADHD, OCB,SIB, or non-obscene socially inappropriatebehaviors are also present.
13.3 Course of the Syndrome
The natural history of TS is fairly well under-stood. Tics usually emerge in childhood betweenthe ages of 4 and 6 years and then increase inseverity, peaking between the ages of 10 and12 years. Motor tics generally precede thedevelopment of vocal tics, and onset of simpletics often predates that of complex tics. Tics tendto decline in severity during adolescence and, byearly adulthood, most individuals experiencemarkedly reduced numbers of tics or are free oftics. Tics that appear during adulthood are oftenattributable either to reemergence of childhoodtics or to other factors, such as drugs, trauma, andstroke or brain infection. Onset of psychiatricconditions, especially ADHD, can precede thedevelopment of tics, present concurrently, oremerge after the appearance of tics. Thesecomorbidities sometimes follow a similar clinicalcourse to the tics, but in other cases they differgreatly. Some features of psychiatric conditions,such as mood disorders and SIB, often persist orworsen during adulthood, irrespective of ticseverity. Certain factors and events, such asstress, anxiety, and fatigue, can increase theoccurrence of tics, whereas others, such as tasksrequiring concentration and motor skills,including musical and athletic performances and/
or physical exercise, can reduce or even tempo-rarily halt tics. In addition, some individuals canvoluntarily delay or suppress their tics for a shorttime; however, tics often reemerge withincreased intensity and/or frequency.
The severity of tics and psychiatric disordersin patients with TS ranges from mild to severe. Insome individuals, severe tics (for example, of theneck) can lead to self-inflicted pain, injury, anddisability. However, for many patients with TS,the psychiatric comorbid disorders are moreproblematic than the tics, and can have a pro-foundly negative effect on quality of life. Theseindividuals often live with various degrees ofimpairment in their academic and professionaldevelopment, as well as reduced psychosocialwellbeing. Nonetheless, many individuals withTS lead successful lives, and can be unusuallygifted and highly creative.
13.4 Pathophysiology
Anatomical and neurochemical changes thatunderlie the clinical manifestations of TS areunclear [9]. However, several studies provideevidence that both functional and structuralalterations in the basal ganglia and other neuro-nal systems have a role in the complex symp-tomatology of the disorder. These changes couldlead to alterations in filtering or sensorimotorgating mechanisms, resulting in urges to performmotor and vocal activities that are inappropriate,poorly timed, excessive, and/or very frequent [9].
Neuropathological studies in patients with TSdemonstrate a reduction of up to 60 % in thenumber of fast-spiking γ-aminobutyric acid-releasing (GABAergic) and cholinergic inter-neurons in the caudate nucleus and putamen.Such individuals also demonstrate a decreasednumber of parvalbumin-positive GABAergicneurons in the globus pallidus externa (GPe),whereas the number of these neurons is markedlyincreased in the globus pallidus interna (GPi).These findings need to be confirmed in futurestudies, but they raise the possibility that defectsin neuronal migration occurring during CNS
144 J. Zhang et al.

development lead to altered basal ganglia cir-cuitry and function [10, 11].
Brain imaging studies in patients with TShave produced inconsistent and sometimesconflicting results. Magnetic resonance imaging(MRI), for example, reveals considerable alter-ations in the volumes of certain neuroanatomicalstructures, including a notable reduction in thevolume of the caudate nucleus and an increasein the volume of the hippocampus, amygdala,and thalamus. Similar studies have also reportedthinning of sensory and motor cortical areas inindividuals with this disorder. Functional MRIstudies of patients with TS who were perform-ing tasks to control their tics demonstratedalterations in the activity of various cortical,limbic, and basal ganglia areas. These observa-tions might reflect either how the brain isaffected by TS or how it seeks to compensatefor the illness.
Overall, patients with TS seem to exhibithypoactivity in the basal ganglia and hyperac-tivity in motor and/or premotor areas, consistentwith the structural neuroimaging findings.Exactly how the above-mentioned neuroana-tomical changes are related to TS is not clear,although an increasing body of evidence suggeststhat alterations in basal ganglia function, specif-ically within the corticostriatal–thalamocorticalcircuitry and perhaps also the dopaminergicnigrostriatal pathway, play a role in the patho-physiology of this disorder. Ablation or electricalstimulation of the globus pallidus internal seg-ment or thalamic nuclei has been reported toreduce the severity of tics. Similarly, dopamineD2 receptor antagonists, such as haloperidol andpimozide, and dopamine-depleting agents, suchas tetrabenazine, are effective in alleviating themotor symptoms of TS. By contrast, drugs thatincrease dopamine levels and/or activity in thebrain, such as levodopa, also increase the fre-quency of tics. Notably, other neuronal path-ways, including noradrenergic, serotoninergic,histaminergic, glutaminergic, GABAergic, andcholinergic systems, have been implicated in TS,perhaps because drugs that target these systemscan improve some symptoms of the disorder.
13.5 Therapy
The early attempts to treat individuals with TS areconsidered, by today’s standards, bizarre, inven-tive, and largely ineffective. These approachesincluded application of leeches to the skin, coolingof the body, static electricity, hydrotherapy, spinalelongation, and the use of various chemical agents,such as herbs. To date, no cure exists for TS, butseveral rational approaches are now available formanagement of the disorder, although they are notuniversally effective. Importantly, the complexpresentation of motor dysfunction, psychiatricfeatures, and psychosocial impairments in indi-viduals with TS clearly require a multifactorialapproach to management of the disorder.
After a diagnosis is obtained, educating thepatient, their parents, and other interested parties(for example, a child’s teachers) about TS canhelp to define appropriate expectations for theseindividuals, as well as to optimize the patient’streatment strategy. Indeed, for most children withTS, addressing the many popular misconceptionsabout the disorder among their peers often leadsto informed and improved relationships and cansubstantially reduce the burdens associated withthis condition. Medication is not necessary formany individuals with TS, especially those withonly mild tics. However, for those with moderateto severe tics or psychiatric comorbidities, whichare often more problematic than the tics, severalpharmacological agents are available, althoughsuch treatments frequently produce ineffectiveresults, whereby the risks associated with treat-ments outweigh the benefits. Some patients withTS find that professional counseling, guidance,and psychotherapy sessions are invaluable,whereas others, such as children with learningimpairments, might benefit from access to spe-cialist educational and disability services.Behavioral and surgical approaches to TS arealso currently being investigated and are expec-ted to become accessible treatment options in thefuture for some people with this disorder.Treatment for TS is, therefore, highly personal-ized, and optimization requires effort from boththe care provider and the patient.
13 Deep Brain Stimulation for Tourette Syndrome 145
13.6 Pharmacological Therapy
During the 1960s and 1970s, researchers showedthat the dopamine D2 receptor blocker haloperi-dol could reduce tic severity in patients with TS.These findings led to the investigation of manyother potential drug treatments for the disorder.Notably, none had been specifically developed totreat TS; instead, these agents were all in use forother indications, both neurological (such asschizophrenia) and non-neurological (such ashypertension), before they were found to beeffective in the treatment of TS. Haloperidol andpimozide are currently the only FDA-approvedmedications for this syndrome. These two drugsand other medications can be used to reduce ticseverity, as well as some of the psychiatriccomorbidities associated with TS.
Physicians typically follow a sequentialapproach to treating tics in people with TS.α-Adrenergic agonists, such as guanfacine andclonidine, are the usual first-line treatment. Thesetwo drugs are recommended for individuals withmild tics, since these medications are associatedwith fewer adverse effects than are other classesof drugs. Second-line treatment (used owing tolack of efficacy of α-adrenergic agonists) consistsof antipsychotic agents, which are the mosteffective drugs for treating TS. However, theseagents are associated with serious adverse effects.Antipsychotic drugs are classified as either typi-cal or atypical; the typical agents are dopamineD2 receptor antagonists (such as haloperidol,pimozide and fluphenazine), whereas the atypicalantipsychotic drugs are dopaminergic and sero-tonergic receptor antagonists (such as risperidoneand aripiprazole). Atypical antipsychotic drugsare preferred over typical ones as the atypicalagents carry a lower risk of extrapyramidal andother adverse effects (such as tardive dyskine-sias). In addition, atypical antipsychotic drugsimprove behavioral comorbidities, as well as tics,in patients with TS.
Other medications beneficial for treating TSinclude benzodiazepines, such as clonazepam,topiramate, and injections of botulinum toxin intothe muscle groups associated with bothersome or
disabling tics (for example, those of the eyelids,neck, or larynx). Some case reports suggest thattetrabenazine, a dopamine-depleting agent, canreduce tic severity in patients with TS, but double-blind studies are required to define its efficacy[3, 5, 12].
As previously mentioned, psychiatric comor-bidities often pose a greater problem than tics forpeople with TS. The stimulant drug methylphe-nidate, the α-adrenergic agonists guanfacine andclonidine, and the selective norepinephrine re-uptake blocker atomoxetine, can improve ADHDin patients with TS. Initial concerns that stimulantdrugs could worsen tics and other features of TShave been refuted by the results of further studies.Cognitive behavioral therapy, selective serotoninreuptake inhibitors such as fluoxetine, and bothtypical and atypical antipsychotic drugs have allbeen used to treat OCB in patients with TS.
13.7 Behavioral Therapy
Behavioral therapies for patients with TS aim toteach the individual how to modify the environ-mental factors that influence their tic severity, aswell as offer skills that can be used by the indi-vidual to optimize their management of thesymptoms of the disorder. The therapeuticpotential of these approaches, such as habitreversal training and exposure with responseprevention, has long been known, but theseapproaches have not been investigated as exten-sively as pharmacological interventions for TS. Inrecent years, however, major advances have beenmade in behavioral therapies for TS. A random-ized controlled trial in children and adolescentswith TS or chronic tic disorders showed thatcomprehensive behavioral intervention for tics(CBIT), an enhancement of the widely used habitreversal training method for treating behavioraldisorders, significantly reduced tic severity inalmost 50 % of patients. CBIT is a promisingtherapy that should be further developed andtested in future studies, and will probably becomeaccessible to many people with TS.
146 J. Zhang et al.

13.8 Surgical Therapy
Although it is frequently self-limited, some patientsremain symptomatic and require chronic treatment.The standard treatment is pharmacologic involvingmainly neuroleptics, 2-adrenergic agonists, andsometimes benzodiazepines. In some cases,behavioral treatment may provide temporary con-trol of symptoms but certain patients prove medi-cally untreatable or experience unbearable sideeffects from the medication. It is these patients whoare potential candidates for neurosurgical inter-ventions. During the past few decades, manyablative procedures have been performed in anattempt to treat intractable TS. In total, 65 patientsunderwent ablative surgery varying from “tailored”stereotactic operations to more rigorous prefrontallobotomies, which were lobotomy, limbic leucot-omy, leucotomy, cingulotomy, campotomy, thala-motomy, dentatotomy, coagulation, ablativesurgery, and stereotactic surgery.
In 1962, Baker [13] described TS as an“involuntary paroxysmal hyperkinesis involvingthe entire skeletal musculature” and reported thefirst leucotomy for TS. The procedure wascomplicated by a frontal lobe abscess, which wasaspirated. In the same year, Cooper [14] pub-lished the case of a 16-year-old girl, and a rightchemothalamectomy was performed, followedby a left chemothalamectomy 1 year later. Coo-per reported that after the surgery, the patientexperienced substantial tic reduction and wasfully functional. Two years later, Stevens [15]published long-term follow-up results of a37-year-old man who had undergone the firstprefrontal lobotomy, carried out by James Wattsin 1955. In 1970, Hassler and Dieckmann [16]reported the results of bilateral thalamotomies in3 patients with intractable TS. They performedmore than 10 coagulations of the intralaminarand medial thalamic nuclei, and, in case of facialtics, in the ventro-oralis internus (Voi). Only theeffects with respect to tics were reported, whichimproved after surgery by 100 % in Patient 1,90 % in Patient 2, and 70 % in Patient 3. Nodetails regarding the tic-rating method wereprovided. Nadvornik and associates [17]
described a case of stereotactic dentatotomy andbilateral frontal leucotomy. Beckers [18] pub-lished the outcome of neurosurgical treatment in3 TS patients. Two stereotactic operations (targetunclear) were performed on Patient 1 (female)with a interval of 1 year between surgeries.Patient 2 (male) underwent a bilateral campoto-my and prefrontal leucotomy in two surgicalsessions. A bilateral leucotomy was performedon the third patient (female). The authorobserved that these stereotactic interventionsresulted in partial tic reduction. Nevertheless,surgery was not advocated as a good treatmentoption for intractable TS because of the sideeffects, which were not specified. In 1978,Wassmann and associates [19] briefly mentioneda female patient who had undergone a prefrontallobotomy but they did not provide any informa-tion regarding the outcome. Asam and colleagues[20] provided a brief (and incomplete) review ofthe literature on surgical interventions for TS andreported their experience with two TS patients.The patients were male, 14 and 15 years old,with a disease duration of 5 and 11 years,respectively. Their first patient underwent ste-reotactic surgery (target unclear) with temporaryrelief of tics. Postoperatively, this patient devel-oped a spastic hemiplegia. Coagulation of the leftzona incerta (ZI) was performed in the secondpatient, who also experienced a postoperativehemiplegia. The same patient was operated on15 months later, for unclear reasons, in the con-tralateral ZI. Postoperatively, this patient devel-oped hemiplegia of the left side and becamequadriplegic. According to the authors, tempo-rary relief of symptoms was achieved in thispatient. Later, tics reoccurred in combinationwith complex dystonic movements. They con-cluded that surgical intervention in TS mayproduce temporary improvement of tics but thatsurgery can be accompanied by severe sideeffects. In 1982, Hassler [21] updated the mate-rial on stereotaxic surgery for psychiatric distur-bances in Schaltenbrand’s textbook and brieflymentioned his experience with thalamic surgeryin 15 patients suffering from intractable TS. Nodetails were provided about the outcome.
13 Deep Brain Stimulation for Tourette Syndrome 147

In 1987, Cappabianca and coworkers [22]published the long-term results of 3 patientsdescribed initially by de Divitiis and associates[23], and of 1 new patient. In addition, theyprovided a review of (all) operated patients. Theiroperation was based on stereotactic coordinatesproposed by Hassler and Dieckmann. The intra-laminar and dorsomedian nuclei of the thalamuswere coagulated bilaterally in 1 patient and uni-laterally in 3 patients. The authors reported tem-porary tic improvement in 2 patients lasting a fewmonths, a slight reduction in compulsive symp-toms in 1 patient, and almost complete ticregression in the fourth. Follow-up examinationsof these patients were several years earlier thanone would expect when considering the publica-tion year. Robertson and associates [24] reportedon a 19-year-old man with disease onset at the ageof 5.5 years, presenting with a variety of verbaland motor tics. The tics were treated successfullywith the D2 receptor antagonist, sulpiride; how-ever, compulsions could not be treated. Stereo-tactic limbic leucotomy was performed involvingbilateral lesions in the lower medial quadrants ofthe frontal lobes and separate lesions in theanterior cingulum (limbic leucotomy). Postoper-atively, compulsions disappeared within 6 weeks.Side effects consisted of apathy, general intel-lectual impairment, organizational problems, anddifficulties in concentration. After 2 years, thepatient was socially independent and free fromSIB. Robertson and colleagues concluded thatlimbic leucotomy should be considered an effec-tive treatment in TS patients with severe self-injurious behavior, but emphasized that long-termeffects on tics required further assessment. Again,the authors did not mention the method of ticevaluation, the impact or the time course of sideeffects, or criteria for the diagnosis of TS. In1993, Sawle and colleagues reported on theresults of bilateral limbic leucotomy in a 45-year-old man suffering from TS. The symptoms con-sisted of severe SIB, obsessions and compulsions[25], and vocal and motor tics. Long-term trials ofpharmacologic and behavioral therapy had failed.During limbic leucotomy, bilateral coagulationswere performed on the anterior hypothalamus andcingulate gyrus. In a personal communication to
Rauch and coworkers [26], Sawle remarked thatthe actual targets were those of conventionallimbic leucotomy (cingulotomy plus thermoco-agulation of the frontothalamic fibers). Accordingto the authors, the surgery had no direct effect ontics whereas the compulsions were reduced.Nineteen months after surgery, however, therewere no longer any signs of tics and the patientreported excellent improvement with regard to hisobsessions. Leckman and associates [27] in 1993reported on a 40-year-old man suffering from TSand OCB who underwent surgery. Disease onsetwas at the age of 3 years with motor tics. Vocaltics appeared later, and checking and cleaningcompulsions were present, as was SIB. Symp-toms failed to respond to medication trials. Thepatient underwent bilateral stereotactic infratha-lamic lesioning and anterior cingulotomy. Post-operatively, the obsessions and compulsionsimproved, but the patient continued to experiencesevere motor and vocal tics. Three weeks later,the left infrathalamic and cingulated lesions wererepeated. During this second surgical session, theinfrathalamic lesion was extended more inferiorlywithin the borders of the red nucleus and a sub-sequent coagulation was performed in the H fieldsof Forel. The patient experienced severe neuro-logical deficits postoperatively including dysar-thria, dysphagia, handwriting and gait problems,mild hemiparesis, abnormal extraocular move-ments, axial rigidity, and bradykinesia. Theauthors suggested that these side effects were dueto extension of the infrathalamic lesion. Long-term, tics and OCB returned. The authors con-cluded that brain lesioning not only influencespathological symptoms, but also damages physi-ological functioning.
One year later, Baer and coworkers [28]reported on the effects of cingulotomy in apatient with TS and OCB. The patient was a35-year-old man with OCB and associated TSwith onset at age 5 years. He failed to respond toeither behavioral therapy or medication. Thepatient underwent two cingulotomies with aninterval of 18 months between procedures. Afterthe first and second operation, there was no cleareffect on his tics. This procedure, however,resulted in an improvement in OCB. The authors
148 J. Zhang et al.

concluded that cingulotomy alone was not aneffective treatment for TS. In 1995, Rauch andcolleagues [28] published a comprehensivereview of neurosurgical treatments for TS. Theyprovided detailed information regarding the dif-ferent neurosurgical approaches by summarizingthe available literature. In their report, emphasiswas placed on the rationale for the different tar-gets. Mention was made, however, regarding3 patients who underwent bilateral anterior cin-gulotomies and infrathalamic lesioning, whichhad not been published previously. The firstpatient was a 34-year-old woman with severe TS,OCB, and bipolar disorder. The patient under-went an anterior cingulotomy plus infrathalamiclesioning. Tic counting using videotapes, per-formed by Rauch and co-workers, revealed adecrease in the number of tics from 18 to 2 tics/min. The second patient was a 40-year-old mansuffering from self-injurious motor tics, copro-lalia, and OCB. The third patient was notdescribed in detail. The latter 2 patients under-went the same procedure as the first, with a pooroutcome. Furthermore, the second patient expe-rienced dysarthria and swallowing, handwriting,and gait problems, postoperatively. Only amoderate improvement in tics and OCB wasobserved. The third patient experienced noimprovement in symptoms at all. In addition,Rauch and associates noted a case published inthe Russian literature by Korzenin in 1991. Thisinvolved a 19-year-old man with TS and asso-ciated OCB who underwent bilateral cryotha-lamotomy (ventrolateral nuclei) with good resultsobserved at a 1-year follow-up. Several yearslater, Korzenev and colleagues [29] publishedresults of their surgical treatment of 4 intractableTS patients. They concluded that stereotacticsurgery was an effective method of treatment forsevere incurable TS. However, in their article nodescription of the TS patients was provided withrespect to patient characteristics, tics, surgicaltarget, or method of evaluation.
Many different lesioning procedures havebeen performed in TS throughout the history ofsurgical treatment of this disorder. Frontal lobeoperations included prefrontal lobotomies andbimedial frontal leucotomies. The limbic system
was targeted during limbic leucotomy and ante-rior cingulotomy. Thalamic operations includedlesioning of the medial, intralaminar, and ven-trolateral thalamic nuclei. Infrathalamic lesionswere performed at the level of Forel’s fields(campotomies) and the zona incerta, and cere-bellar surgeries included dentatotomies. In anattempt to achieve total control of symptoms,more complex operations have been performed,such as combined anterior cingulotomies andinfrathalamic lesioning.
13.9 Deep Brain Stimulation
Deep brain stimulation (DBS) is a reversible andadjustable neurosurgical technique involving theimplantation of stimulating electrodes that sendcontinuous electrical impulses to specific targetareas in the brain. Following implantation of theelectrodes, the stimulator settings are adjusted atfollow-up endpoints to achieve optimal resultswith minimal adverse effects.
In 1999, the first DBS was performed forintractable TS, with the target for thalamicstimulation based on the thalamotomies descri-bed by Hassler [30]. Since then, different targetshave been used. While DBS is a well-establishedtreatment option for different neurological dis-orders, including Parkinson’s disease, dystonia,and tremor, its use in TS is still experimental.
13.10 Deep Brain Stimulationin Tourette Syndrome
Although DBS has shown potential in the treat-ment of refractory TS, there are numerous issuesstill to be resolved: (1) The proper indications forDBS and the definition of ‘refractoriness’ toconventional treatments, (2) the choice of targetarea on the basis of the clinical picture, (3) thesuitability of general anesthesia during DBS, (4)postoperative issues, such as follow-up evalua-tion techniques, and (5) optimization of pulsegenerator settings.
13 Deep Brain Stimulation for Tourette Syndrome 149
13.10.1 Patient Selection
Useful recommendations for patient selectionhave been provided by the Tourette SyndromeAssociation (TSA) [4]. However, on the basis ofthe waxing and waning nature of the clinicalpicture of TS and considering the rather frequentbehavioral comorbidities that limit patient com-pliance, indication for DBS can be difficult.Moreover, the widespread view that DBS shouldbe considered an adjunctive therapy for conser-vative or noninvasive/nonsurgical treatments(such as botulinum toxin infiltration) is the mostuncertain issue as criteria for the definition of‘refractoriness’ are still not clearly defined.
DBS is used on the basis of a documentedlack of response or presence of unbearableadverse effects over a minimum of 6 months’treatment with conventional (typical and atypicalneuroleptics) or innovative treatments (includingdopamine depletors such as tetrabenazine), whileselective serotonin reuptake inhibitors (fluvox-amine 25–100 mg) are also administered forobsessive-compulsive comorbidity, alone or inassociation with clorimipramine 25–100 mg/day.ADHD is treated with clonidine 75–150 mg/dayor guanfacine 5 mg or higher/day, while nonre-sponsive isolated tic manifestations can be trea-ted with botulinum toxin infiltration at theinvolved districts (including the cricoarythenoidmuscles for phonic tics) [31, 32].
Patients were selected from our specialty clinicof thousands of TS patients and all potential sub-jects were screened by a multidisciplinary teamincluding a neurologist, neurosurgeon, neuro-psychologist, psychiatrist, and ethicist, and werealso required to have followed a psychobehavioralapproach for at least 6 months without clinicalsuccess. Surgery should be considered if a patientcontinues to demonstrate clinical signs incom-patible with normal social functioning, or if thesymptoms are life threatening. A study by Serv-ello et al. reported that 2 of 18 patients underwentDBS because their refractory neck twisting ticscaused cervical myelopathy requiring spinal sur-gery. Following DBS, the neck torsion boutsdecreased significantly, motor impairment was
stabilized and a motor rehabilitation program wasestablished [33].
Moreover, in order to be eligible for DBS,patients should demonstrate compliance withprevious treatments. Compliance should beassessed in terms of (1) adherence to pharma-cological protocols, (2) completion of follow-upvisits, and (3) adherence to psychobehavioraltraining programs. The rational to use differenttargets is that all targets belong to the ventralstriatal-thalamo-cortical circuitries which arethought to be dysfunctional in TS.
13.10.2 Target Choice
In TS patients, the most often used targets ofstimulation are the thalamus (centromedian-para-fascicular complex; CM–Pf) and the globus pal-lidus internus (GPi). In the literature, however,seven different targets have been described so farin patients with chronic tics: thalamus (CM–Pf)and CM–Spv [substantia periventricularis/nucleusventralis oralis intermedius (Voi)], GPi (postero-ventrolateral and anteromedial part), nucleusaccumbens (NA), anterior limb of the internalcapsule (AIC), and subthalamicus nucleus (STN).
One of the most commonly used targets forDBS in the treatment of TS, the CM-Pf, part ofthe intralaminar nucleus of the thalamus, isinvolved in sensorimotor basal ganglia circuitry[34, 35]. The anterior CM-Pf is able to influencecells involved in tremor generation located in awide area including the ventral oral anterior andposterior (VoA and VoP) nuclei [36]. Theintralaminar nuclei and CM-Pf convey multi-modal stimulatory signals to the striatum, and arethus involved in attention and arousal in responseto stimulation. Stimulation of the CM-Pf andVoA complex has proved to be effective in thetreatment of behavioral aspects of TS as well asalleviation of tics [33]. In a study of 18 patientsreported by one center treated with DBS of theCM-Pf and VoA, all patients responded wellwith significant, although varied, reductions inseverity and frequency of tics and in behavioralcomorbidities after DBS. The mean total Yale
150 J. Zhang et al.
Global Tic Severity Scale (YGTSS) scores werereduced from 41.1 (SD 8.3) prior to DBS to 28.6(SD 17.5) post-DBS (p < 0.001) and similarreductions were seen in YGTSS motor, phonic,and social impairment scores (all p < 0.001 vs.baseline) [33]. In a recent case report, a womanwith severe refractory TS despite DBS of theanterior internal capsule achieved significantimprovement in tic control at 3 months followingbilateral centromedian thalamic stimulation(reduction in total tic score: 42 % compared withpre-DBS baseline and 27 % compared with DBSof the postinternal capsule) and a reduction inpsychiatric side effects such as altered mood andimpulse control compared with internal capsulestimulation [38].
Although the CM-Pf is often thought to be thepreferred target for DBS [33, 35], alternativelocations such as the nucleus accumbens and theGPi are not to be excluded; favorable outcomesin patients with TS have been reported with DBSof both the nucleus accumbens and the GPi.
The anteromedial part of the GPi acts as alimbic relay for output pathways of the basalganglia, and continuous high frequency stimula-tion of this region has been shown to amelioratedystonia. Stimulation of the GPi is able tomodify the neuronal activity of the VoA nucleus.The VoA nucleus is involved in initiating plan-ned movement and suppressing unwantedmovement, whereas the VoP nucleus plays a rolein the sensations of touch, itching, temperature,taste and arousal, in addition to body position.Recently, in a double blind, randomized study in3 patients with severe, refractory TS, bilateralstimulation of the GPi produced a significant andgreater reduction in tic severity (assessed usingthe Yale Global Tic Severity Scale; YGTSS) thanstimulation of the CM-Pf [38].
The nucleus accumbens is presumed to have amodulatory activity on amygdaloid basal gan-glia-prefrontal cortex circuitry and, as the activityof its neurons is modulated by dopamine and ahigh proportion of cells have high concentrationsof dopamine D1 and D3 receptors, the nucleusaccumbens is believed to also be involved inaddiction and OCB [39]. The effectiveness of
DBS of the nucleus accumbens has been dem-onstrated in patients with severe OCB and anx-iety disorder. In a 37-year-old woman withsevere refractory TS, DBS administered to theanterior limb of the internal capsule (electrodeterminating in the nucleus accumbens) providedsignificant reduction in tic frequency and severityat 18 months after surgery [12]. Tic reductionwas also shown following DBS of the nucleusaccumbens in a 26-year-old male patient withsevere tics and SIB; coprolalia and tics involvingself-harm were almost completely resolved [40].
The optimal area for the final DBS electrodeimplantation within the chosen target nucleuswas studied with intraoperative microrecordingsin at least two monopolar electrode tracks,acquired at steps of 1–0.5 mm from 8–10 mmabove to 1 mm below the neuroradiologicallyestimated position of the target nucleus. Under-going studies are evaluating firing patterns inorder to characterize a neurophysiological targetthus increasing DBS precision.
We retrospectively assessed long-term clinicaloutcomes of 13 TS patients, who were refractoryto pharmacological and psychotherapeutic treat-ment, and underwent DBS targeting the GPi,using data from Beijing Tiantan Hospital data-base from January 1 2006 to May 31 2013. Theprimary outcome was a change in tic severity asmeasured by the YGTSS and the secondaryoutcome was a change in associated behavioraldisorders and mood as measured by the TouretteSyndrome–Quality of Life Scale (TSQOL)assessment. The results showed that the averagereduction in the total YGTSS scores at last fol-low-up (mean 43 months, range 13–80 months)compared with those at baseline were reduced by52 % (range 4–84 %), and mean improvementrates at 1, 6, 12, 18, 24, 30, and 36 months rel-ative to baseline were 13, 22, 29, 34, 42, 47, and55 %, respectively. We noticed significantimprovements in tic symptoms after 6 months ofDBS programming (p < 0.05), as assessed bypaired t-test. TSQOL scores improved by anaverage of 46 % (range 11–77 %). Our studyprovides the largest reported GPi DBS case seriesof 13 treatment-refractory TS patients with the
13 Deep Brain Stimulation for Tourette Syndrome 151
longest follow-up. Our results support thepotential beneficial effect of GPi DBS forreducing disabling tics and improvement inquality of life. The details are as follows.
Totally, thirteen patients (12 males and1 female) with TS were selected to undergo GPiDBS (Tables 13.1 and 13.2) due to the severedisability arising from their tics. All patientsfailed treatment with α-adrenergic agonists, ≥2dopamine receptor antagonists, benzodiazepine,and behavioral therapy. Preoperatively, each ofthese patients was evaluated by a specialist andidentified to fulfill Diagnostic and StatisticalManual of Mental Disorders (Fourth Edition) [6]criteria for TS. The DBS procedure wasapproved by the Neuromodulation Committee atBeijing Tiantan Hospital. Preoperatively, andagain after optimization of DBS parameters, eachpatient was tested with the YGTSS, as detailed insupplementary materials. A YGTSS score of 35/50 (motor and vocal tic severity on a 0–50 scale)or higher for 1 year is a marker of diseaseseverity sufficient to warrant consideration forDBS. All patients had severe tic disorders withfunctional impairment and YGTSS > 35/50(motor and vocal tic severity on a 0–50 scale). Inaddition, tics were the major symptom causingdisability in all patients and their comorbidconditions were stably treated.
In brief, patients were fixed with a Leksell Gstereotactic head frame (ElektaAB, Stockholm,Sweden) on the morning of surgery and trans-ferred to an MRI suite to obtain MRI (3.0 T)scans. Image data were then transferred to aSurgiplan Workstation (Elekta, Sweden) in theoperation room to visualize the individual palli-dal target [41–43]. The target was the GPi loca-ted on fused MRI images with the followingcoordinates: GPi was 3 mm anterior to the mid-commissural point, 18–21 mm lateral to themidplane of the third ventricle, and 4–6 mmbelow the intercommissural line. Target coordi-nates were adapted according to the width of thethird ventricle and anterior commissure-posteriorcommissure (AC-PC) length. During planning,visible vessels were avoided in the planned tra-jectory. A Leksell stereotactic frame was used,
with microelectrode recording to documentelectrode location in relation to the patient’sindividual anatomy. Full details of the neuro-surgical procedure were published previously.After placement of a burr hole, in line with theplanned trajectory, extracellular single-unitmicroelectrode recordings were performed.Recording started 15 mm above target and con-tinued until 4 mm beneath target (LeadPoint,Medtronic, Minneapolis, MN, USA) in0.5–1 mm steps. In all 13 patients, microelec-trode recordings clearly showed GPi electricalsignals. The signals demonstrated a high fre-quency and high amplitude firing pattern withhigh background noise. Electrical activity wasrhythmic and in some cases “tremor cells” couldbe detected. Tentative stimulation usually mildlyrelieved the hypertension of muscles, while theinvoluntary movement seldom improved. Sub-sequently, the quadripolar electrode (model3387; Medtronic) with the deepest contact (con-tact 0) at the level of the GPi target wasimplanted, and a temporary test stimulation wasperformed below the best electrical signal (0–3+,frequency 185 Hz, pulse width 90 μs) to assessstimulation-induced side effects. Stimulus inten-sity was gradually increased in steps of 0.1 mA,until unwanted side effects occurred or until amaximum stimulus intensity of 5.0 mA. Finally,this definite electrode was fixed in the burr holewith acrylic cement, and connected to an exter-nalized extension cable. DBS was always per-formed bilaterally. CT scans were performed onthe operative day to evaluate electrode positionand detect asymptomatic hemorrhage. MRI wasalso performed on the next day of the operationto evaluate the electrode position. Once agree-ment between the neurologist, the neurosurgeon,and the psychiatrist was obtained regardingpotential beneficial effects, an implantable pulsegenerator (IPG) was implanted as a separateprocedure, under general anesthesia, within1 week (Kinetra model 7428, Medtronic).
After the second procedure, stimulationparameters were adjusted during a 4-weekunblinded period to determine the most effectiveparameters on tics with the lowest amplitude.
152 J. Zhang et al.
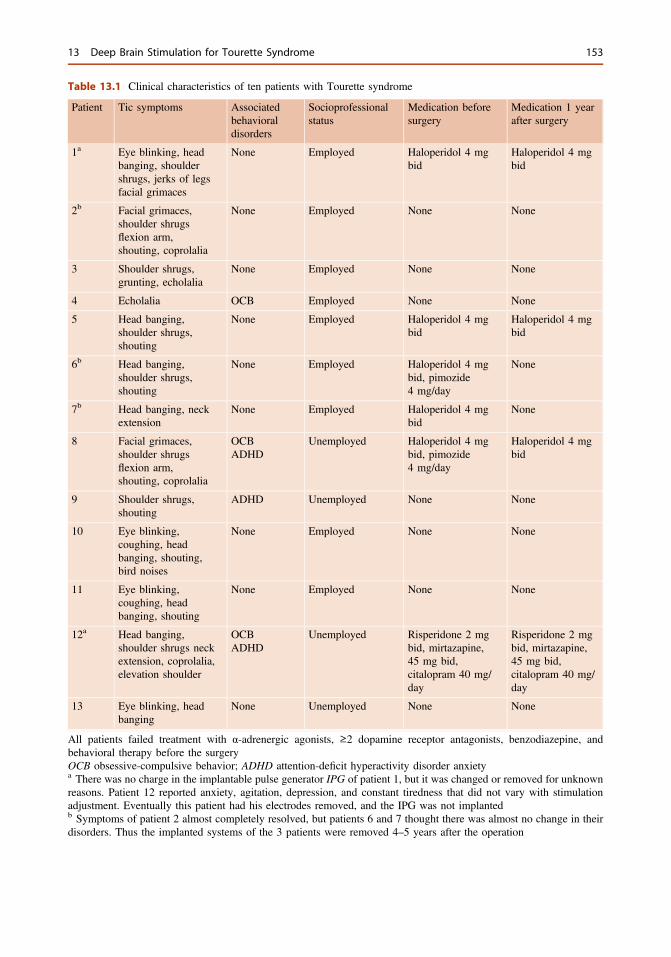
Table 13.1 Clinical characteristics of ten patients with Tourette syndrome
Patient Tic symptoms Associatedbehavioraldisorders
Socioprofessionalstatus
Medication beforesurgery
Medication 1 yearafter surgery
1a Eye blinking, headbanging, shouldershrugs, jerks of legsfacial grimaces
None Employed Haloperidol 4 mgbid
Haloperidol 4 mgbid
2b Facial grimaces,shoulder shrugsflexion arm,shouting, coprolalia
None Employed None None
3 Shoulder shrugs,grunting, echolalia
None Employed None None
4 Echolalia OCB Employed None None
5 Head banging,shoulder shrugs,shouting
None Employed Haloperidol 4 mgbid
Haloperidol 4 mgbid
6b Head banging,shoulder shrugs,shouting
None Employed Haloperidol 4 mgbid, pimozide4 mg/day
None
7b Head banging, neckextension
None Employed Haloperidol 4 mgbid
None
8 Facial grimaces,shoulder shrugsflexion arm,shouting, coprolalia
OCBADHD
Unemployed Haloperidol 4 mgbid, pimozide4 mg/day
Haloperidol 4 mgbid
9 Shoulder shrugs,shouting
ADHD Unemployed None None
10 Eye blinking,coughing, headbanging, shouting,bird noises
None Employed None None
11 Eye blinking,coughing, headbanging, shouting
None Employed None None
12a Head banging,shoulder shrugs neckextension, coprolalia,elevation shoulder
OCBADHD
Unemployed Risperidone 2 mgbid, mirtazapine,45 mg bid,citalopram 40 mg/day
Risperidone 2 mgbid, mirtazapine,45 mg bid,citalopram 40 mg/day
13 Eye blinking, headbanging
None Unemployed None None
All patients failed treatment with α-adrenergic agonists, ≥2 dopamine receptor antagonists, benzodiazepine, andbehavioral therapy before the surgeryOCB obsessive-compulsive behavior; ADHD attention-deficit hyperactivity disorder anxietya There was no charge in the implantable pulse generator IPG of patient 1, but it was changed or removed for unknownreasons. Patient 12 reported anxiety, agitation, depression, and constant tiredness that did not vary with stimulationadjustment. Eventually this patient had his electrodes removed, and the IPG was not implantedb Symptoms of patient 2 almost completely resolved, but patients 6 and 7 thought there was almost no change in theirdisorders. Thus the implanted systems of the 3 patients were removed 4–5 years after the operation
13 Deep Brain Stimulation for Tourette Syndrome 153
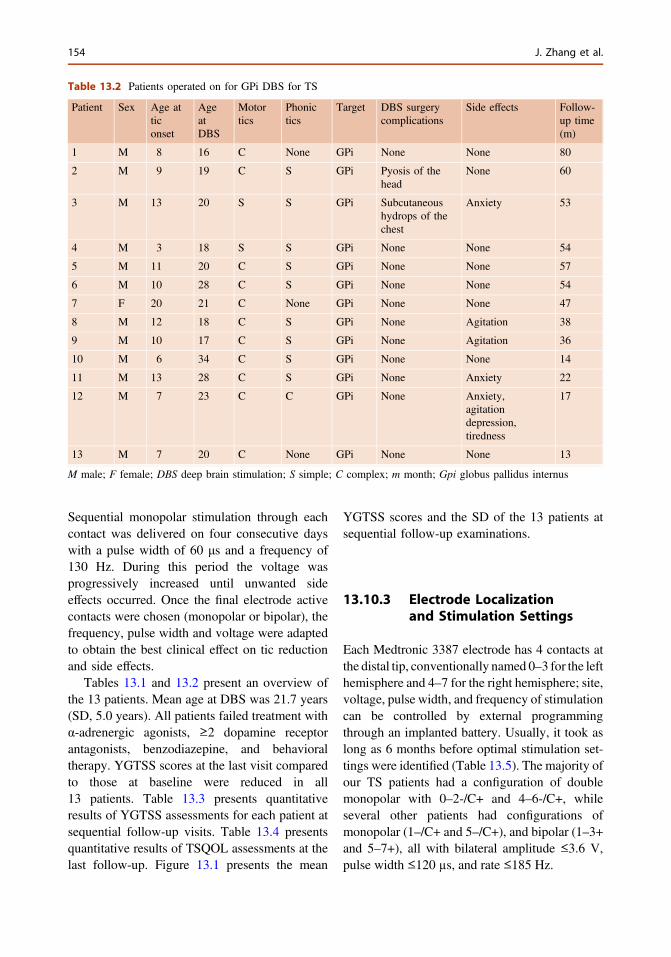
Sequential monopolar stimulation through eachcontact was delivered on four consecutive dayswith a pulse width of 60 μs and a frequency of130 Hz. During this period the voltage wasprogressively increased until unwanted sideeffects occurred. Once the final electrode activecontacts were chosen (monopolar or bipolar), thefrequency, pulse width and voltage were adaptedto obtain the best clinical effect on tic reductionand side effects.
Tables 13.1 and 13.2 present an overview ofthe 13 patients. Mean age at DBS was 21.7 years(SD, 5.0 years). All patients failed treatment withα-adrenergic agonists, ≥2 dopamine receptorantagonists, benzodiazepine, and behavioraltherapy. YGTSS scores at the last visit comparedto those at baseline were reduced in all13 patients. Table 13.3 presents quantitativeresults of YGTSS assessments for each patient atsequential follow-up visits. Table 13.4 presentsquantitative results of TSQOL assessments at thelast follow-up. Figure 13.1 presents the mean
YGTSS scores and the SD of the 13 patients atsequential follow-up examinations.
13.10.3 Electrode Localizationand Stimulation Settings
Each Medtronic 3387 electrode has 4 contacts atthe distal tip, conventionally named 0–3 for the lefthemisphere and 4–7 for the right hemisphere; site,voltage, pulse width, and frequency of stimulationcan be controlled by external programmingthrough an implanted battery. Usually, it took aslong as 6 months before optimal stimulation set-tings were identified (Table 13.5). The majority ofour TS patients had a configuration of doublemonopolar with 0–2-/C+ and 4–6-/C+, whileseveral other patients had configurations ofmonopolar (1–/C+ and 5–/C+), and bipolar (1–3+and 5–7+), all with bilateral amplitude ≤3.6 V,pulse width ≤120 µs, and rate ≤185 Hz.
Table 13.2 Patients operated on for GPi DBS for TS
Patient Sex Age atticonset
AgeatDBS
Motortics
Phonictics
Target DBS surgerycomplications
Side effects Follow-up time(m)
1 M 8 16 C None GPi None None 80
2 M 9 19 C S GPi Pyosis of thehead
None 60
3 M 13 20 S S GPi Subcutaneoushydrops of thechest
Anxiety 53
4 M 3 18 S S GPi None None 54
5 M 11 20 C S GPi None None 57
6 M 10 28 C S GPi None None 54
7 F 20 21 C None GPi None None 47
8 M 12 18 C S GPi None Agitation 38
9 M 10 17 C S GPi None Agitation 36
10 M 6 34 C S GPi None None 14
11 M 13 28 C S GPi None Anxiety 22
12 M 7 23 C C GPi None Anxiety,agitationdepression,tiredness
17
13 M 7 20 C None GPi None None 13
M male; F female; DBS deep brain stimulation; S simple; C complex; m month; Gpi globus pallidus internus
154 J. Zhang et al.
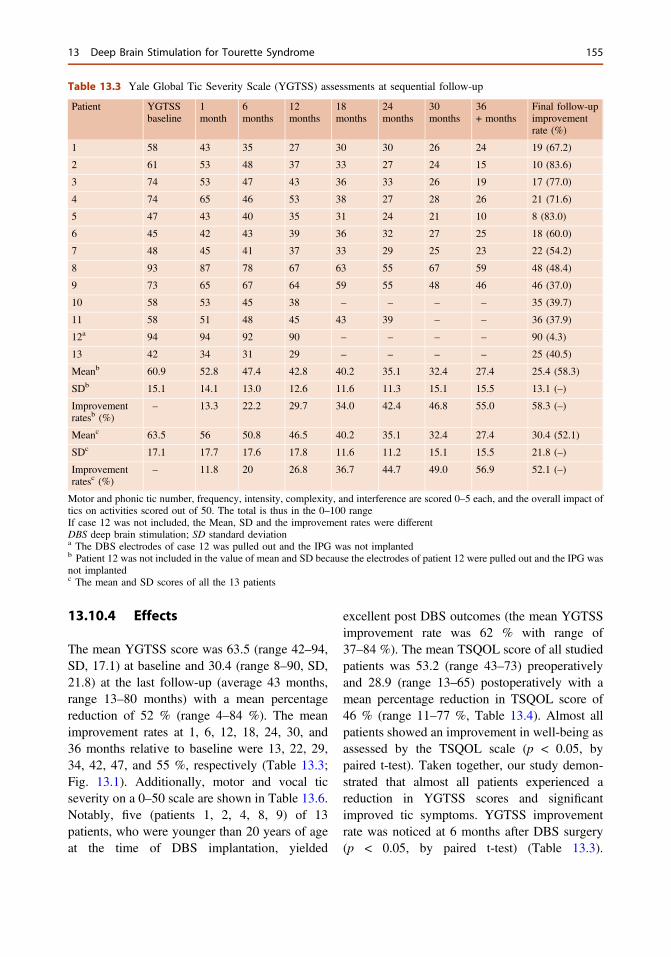
13.10.4 Effects
The mean YGTSS score was 63.5 (range 42–94,SD, 17.1) at baseline and 30.4 (range 8–90, SD,21.8) at the last follow-up (average 43 months,range 13–80 months) with a mean percentagereduction of 52 % (range 4–84 %). The meanimprovement rates at 1, 6, 12, 18, 24, 30, and36 months relative to baseline were 13, 22, 29,34, 42, 47, and 55 %, respectively (Table 13.3;Fig. 13.1). Additionally, motor and vocal ticseverity on a 0–50 scale are shown in Table 13.6.Notably, five (patients 1, 2, 4, 8, 9) of 13patients, who were younger than 20 years of ageat the time of DBS implantation, yielded
excellent post DBS outcomes (the mean YGTSSimprovement rate was 62 % with range of37–84 %). The mean TSQOL score of all studiedpatients was 53.2 (range 43–73) preoperativelyand 28.9 (range 13–65) postoperatively with amean percentage reduction in TSQOL score of46 % (range 11–77 %, Table 13.4). Almost allpatients showed an improvement in well-being asassessed by the TSQOL scale (p < 0.05, bypaired t-test). Taken together, our study demon-strated that almost all patients experienced areduction in YGTSS scores and significantimproved tic symptoms. YGTSS improvementrate was noticed at 6 months after DBS surgery(p < 0.05, by paired t-test) (Table 13.3).
Table 13.3 Yale Global Tic Severity Scale (YGTSS) assessments at sequential follow-up
Patient YGTSSbaseline
1month
6months
12months
18months
24months
30months
36+ months
Final follow-upimprovementrate (%)
1 58 43 35 27 30 30 26 24 19 (67.2)
2 61 53 48 37 33 27 24 15 10 (83.6)
3 74 53 47 43 36 33 26 19 17 (77.0)
4 74 65 46 53 38 27 28 26 21 (71.6)
5 47 43 40 35 31 24 21 10 8 (83.0)
6 45 42 43 39 36 32 27 25 18 (60.0)
7 48 45 41 37 33 29 25 23 22 (54.2)
8 93 87 78 67 63 55 67 59 48 (48.4)
9 73 65 67 64 59 55 48 46 46 (37.0)
10 58 53 45 38 – – – – 35 (39.7)
11 58 51 48 45 43 39 – – 36 (37.9)
12a 94 94 92 90 – – – – 90 (4.3)
13 42 34 31 29 – – – – 25 (40.5)
Meanb 60.9 52.8 47.4 42.8 40.2 35.1 32.4 27.4 25.4 (58.3)
SDb 15.1 14.1 13.0 12.6 11.6 11.3 15.1 15.5 13.1 (–)
Improvementratesb (%)
– 13.3 22.2 29.7 34.0 42.4 46.8 55.0 58.3 (–)
Meanc 63.5 56 50.8 46.5 40.2 35.1 32.4 27.4 30.4 (52.1)
SDc 17.1 17.7 17.6 17.8 11.6 11.2 15.1 15.5 21.8 (–)
Improvementratesc (%)
– 11.8 20 26.8 36.7 44.7 49.0 56.9 52.1 (–)
Motor and phonic tic number, frequency, intensity, complexity, and interference are scored 0–5 each, and the overall impact oftics on activities scored out of 50. The total is thus in the 0–100 rangeIf case 12 was not included, the Mean, SD and the improvement rates were differentDBS deep brain stimulation; SD standard deviationa The DBS electrodes of case 12 was pulled out and the IPG was not implantedb Patient 12 was not included in the value of mean and SD because the electrodes of patient 12 were pulled out and the IPG wasnot implantedc The mean and SD scores of all the 13 patients
13 Deep Brain Stimulation for Tourette Syndrome 155
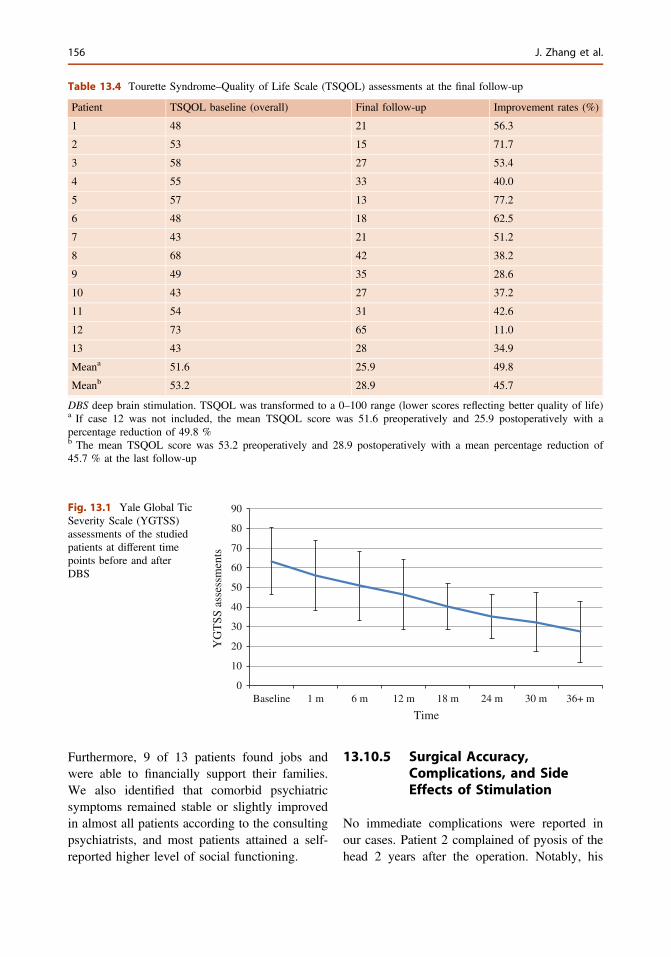
Furthermore, 9 of 13 patients found jobs andwere able to financially support their families.We also identified that comorbid psychiatricsymptoms remained stable or slightly improvedin almost all patients according to the consultingpsychiatrists, and most patients attained a self-reported higher level of social functioning.
13.10.5 Surgical Accuracy,Complications, and SideEffects of Stimulation
No immediate complications were reported inour cases. Patient 2 complained of pyosis of thehead 2 years after the operation. Notably, his
Table 13.4 Tourette Syndrome–Quality of Life Scale (TSQOL) assessments at the final follow-up
Patient TSQOL baseline (overall) Final follow-up Improvement rates (%)
1 48 21 56.3
2 53 15 71.7
3 58 27 53.4
4 55 33 40.0
5 57 13 77.2
6 48 18 62.5
7 43 21 51.2
8 68 42 38.2
9 49 35 28.6
10 43 27 37.2
11 54 31 42.6
12 73 65 11.0
13 43 28 34.9
Meana 51.6 25.9 49.8
Meanb 53.2 28.9 45.7
DBS deep brain stimulation. TSQOL was transformed to a 0–100 range (lower scores reflecting better quality of life)a If case 12 was not included, the mean TSQOL score was 51.6 preoperatively and 25.9 postoperatively with apercentage reduction of 49.8 %b The mean TSQOL score was 53.2 preoperatively and 28.9 postoperatively with a mean percentage reduction of45.7 % at the last follow-up
0
10
20
30
40
50
60
70
80
90
Baseline 1 m 6 m 12 m 18 m 24 m 30 m 36+ m
YG
TSS
ass
essm
ents
Time
Fig. 13.1 Yale Global TicSeverity Scale (YGTSS)assessments of the studiedpatients at different timepoints before and afterDBS
156 J. Zhang et al.
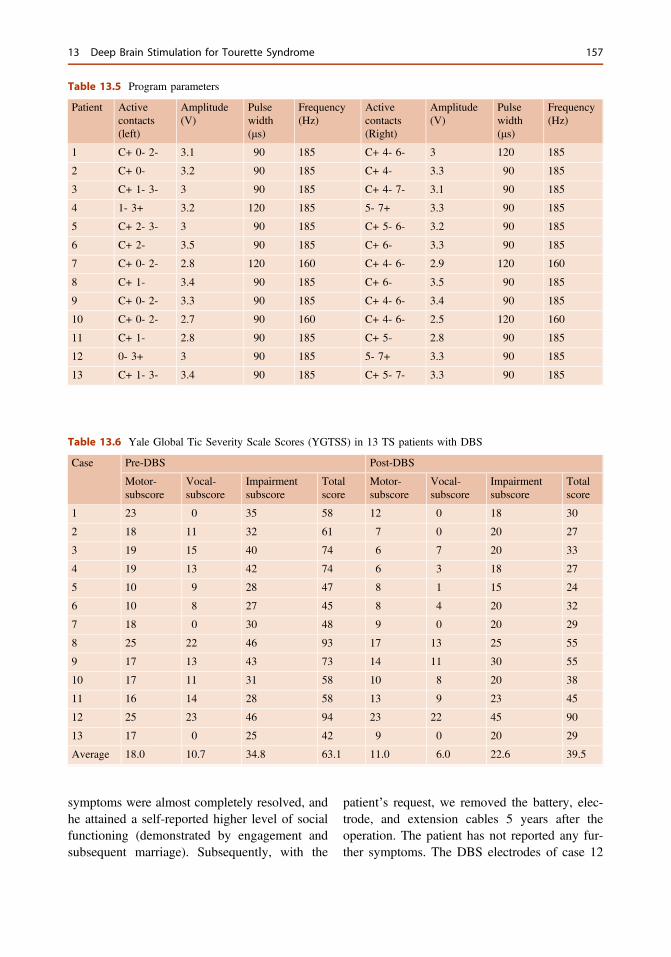
symptoms were almost completely resolved, andhe attained a self-reported higher level of socialfunctioning (demonstrated by engagement andsubsequent marriage). Subsequently, with the
patient’s request, we removed the battery, elec-trode, and extension cables 5 years after theoperation. The patient has not reported any fur-ther symptoms. The DBS electrodes of case 12
Table 13.5 Program parameters
Patient Activecontacts(left)
Amplitude(V)
Pulsewidth(μs)
Frequency(Hz)
Activecontacts(Right)
Amplitude(V)
Pulsewidth(μs)
Frequency(Hz)
1 C+ 0- 2- 3.1 90 185 C+ 4- 6- 3 120 185
2 C+ 0- 3.2 90 185 C+ 4- 3.3 90 185
3 C+ 1- 3- 3 90 185 C+ 4- 7- 3.1 90 185
4 1- 3+ 3.2 120 185 5- 7+ 3.3 90 185
5 C+ 2- 3- 3 90 185 C+ 5- 6- 3.2 90 185
6 C+ 2- 3.5 90 185 C+ 6- 3.3 90 185
7 C+ 0- 2- 2.8 120 160 C+ 4- 6- 2.9 120 160
8 C+ 1- 3.4 90 185 C+ 6- 3.5 90 185
9 C+ 0- 2- 3.3 90 185 C+ 4- 6- 3.4 90 185
10 C+ 0- 2- 2.7 90 160 C+ 4- 6- 2.5 120 160
11 C+ 1- 2.8 90 185 C+ 5- 2.8 90 185
12 0- 3+ 3 90 185 5- 7+ 3.3 90 185
13 C+ 1- 3- 3.4 90 185 C+ 5- 7- 3.3 90 185
Table 13.6 Yale Global Tic Severity Scale Scores (YGTSS) in 13 TS patients with DBS
Case Pre-DBS Post-DBS
Motor-subscore
Vocal-subscore
Impairmentsubscore
Totalscore
Motor-subscore
Vocal-subscore
Impairmentsubscore
Totalscore
1 23 0 35 58 12 0 18 30
2 18 11 32 61 7 0 20 27
3 19 15 40 74 6 7 20 33
4 19 13 42 74 6 3 18 27
5 10 9 28 47 8 1 15 24
6 10 8 27 45 8 4 20 32
7 18 0 30 48 9 0 20 29
8 25 22 46 93 17 13 25 55
9 17 13 43 73 14 11 30 55
10 17 11 31 58 10 8 20 38
11 16 14 28 58 13 9 23 45
12 25 23 46 94 23 22 45 90
13 17 0 25 42 9 0 20 29
Average 18.0 10.7 34.8 63.1 11.0 6.0 22.6 39.5
13 Deep Brain Stimulation for Tourette Syndrome 157
were removed 1 week after implantation due tothe absence of clinical benefit during program-ming and persistent requests from the patient andhis family members. In addition, the electrodes ofpatients 6 and 7 were removed 4 years after theoperation, and both patients obtained substantialbenefit from the DBS and returned to normal life.Patient 3 experienced subcutaneous hydrops ofthe chest and signs of infection 3 years aftersurgery. Unsurprisingly, some patients com-plained of mood disorders, for instance, patients3 and 11 reported anxiety; patients 8 and 9experienced agitation. However, these symptomswere resolved by careful programming. Patient12 complained of anxiety, agitation, depression,and constant tiredness that was not amenable tostimulation adjustment, and eventually, his elec-trodes were removed.
Our recommendations are given against thebackground that up to now there are no ran-domized controlled studies available including asufficiently large number of patients. Hence, itcannot entirely be excluded that at least in someof the patients beneficial effects following DBSwere related to placebo effects or to the waxingand waning course of the symptomatology.Therefore, the aim in the near future must beconduct blinded controlled trials including asufficient number of patients and/or to sharedatabases to combine samples to obtain a suffi-ciently large sample size. This is best establishedby collaborating among centers and sharingdatabases.
13.11 Complementaryand Alternative Therapies
Some individuals with TS assert that acupunc-ture, hypnosis, dietary supplements, and/orhomeopathic remedies reduce both the fre-quency and severity of tics to various degrees.Although these approaches could be beneficialfor some individuals, their effectiveness has notyet been confirmed in well-designed, largeclinical trials.
References
1. Bloch MH, Leckman JF. Clinical course of Tourettesyndrome. J Psychosom Res. 2009;67(6):497–501.
2. de la Tourette GG. Étude sur une affection nerveusecaractérisée par de l’incoordination motriceaccompagnée d’écholalie et de coprolalie (French).Arch Neurol. 1885;9:158–200.
3. Robertson MM. Tourette syndrome, associatedconditions and the complexities of treatment. Brain.Mar 2000;123(3):425–62.
4. Mink JW, Walkup J, Frey KA, et al. Patient selectionand assessment recommendations for deep brainstimulation in Tourette syndrome. Mov Disord.2006;21(11):1831–8.
5. Leckman JF. Tourette's syndrome. Lancet. 2002;360(9345):1577–86.
6. DSM-IV-TR. Diagnostic and Statistical Manual ofMental Disorders. 4th ed. Washington: AmericanPsychiatric Association; 2000. p. 111–4.
7. ICD-10. International Classification of Disease andRelated Health Problems. Classification of mental andbehavioural disorders: clinical descriptions anddiagnostic guidelines. 10th ed. Geneva: WorldHealth Organization; 1992, p. 284–6.
8. TSCS Group. Definitions and classification of ticdisorders. The Tourette Syndrome ClassificationStudy Group. Arch Neurol. 1993;50:1013–16.
9. Jankovic J. Tourette’s syndrome. N Engl J Med.2001;345:1184–92.
10. Peterson BS, Skudlarski P, et al. A functionalmagnetic resonance imaging study of tic suppressionin Tourette syndrome. Arch Gen Psychiatry. 1998;55:326–33.
11. Singer HS, Minzer K. Neurobiology of Tourette’ssyndrome: concepts of neuroanatomic localizationand neurochemical abnormalities. Brain Dev. 2003;25(Suppl 1):S70–84.
12. Flaherty AW, Williams ZM, et al. Deep brainstimulation of the anterior internal capsule for thetreatment of Tourette syndrome: technical case report.Neurosurgery. 2005;57(suppl 4):E403.
13. Baker EFW. Gilles de la Tourette syndrome treatedby bimedial leucotomy. Can Med AssocJ. 1962;86:746–7.
14. Cooper IS. Dystonia reversal by operation in the basalganglia. Arch Neurol. 1962;7:64–74.
15. Stevens H. The syndrome of Gilles de la Tourette andits treatment. Med Ann District Columbia. 1964;36:277–9.
16. Hassler R, Dieckmann G. Stereotaxic treatment of ticsand inarticulate cries or coprolalia considered asmotor obsessional phenomena in Gilles de laTourette’s disease. Rev Neurol (Paris). 1970;123:89–100.
17. Nadvornik P, Sramka M, Lisy L, Svicka I.Experiences with dentatotomy. Confin Neurol. 1972;34:320–4.
158 J. Zhang et al.
18. Beckers W. Gilles de la Tourette’s disease based onfive own observations. Arch Psychiatr Nervenkr.1973;217:169–86.
19. Wassman ER, Eldridge R, Abuzzahab S Sr, Nee L.Gilles de la Tourette syndrome: clinical and geneticstudies in a midwesterncity. Neurology. 1978;28:304–7.
20. Asam U, Karrass W. Gilles de la Tourette syndromeand psychosurgery. Acta Paedopsychiatr. 1981;47:39–48.
21. Hassler R. Stereotaxic surgery for psychiatricdisturbances. In: Schaltenbrand G, Walker AE,editors. Stereotaxy of the human brain. New York:Thieme-Stratton Inc.; 1982. p. 570–90.
22. Cappabianca P, Spaziante R, Carrabs G, de Divitiis E.Surgical stereotactic treatment for Gilles de laTourette’s syndrome. Acta Neurol (Napoli).1987;9:273–80.
23. de Divitiis E, D’Errico A, Cerillo A. Stereotacticsurgery in Gilles de la Tourette syndrome. ActaNeurochir (Wien) 1977; (Suppl. 24):73.
24. Robertson M, Doran M, Trimble M, Lees AJ. Thetreatment of Gilles de la Tourette syndrome by limbicleucotomy. J Neurol Neurosurg Psychiatry.1990;53:691–4.
25. Sawle GV, Lees AJ, Hymas NF, Brooks DJ,Frackowiak RS. The metabolic effects of limbicleucotomy in Gilles de la Tourette syndrome.J Neurol Neurosurg Psychiatry. 1993;56:1016–9.
26. Rauch SL, Baer L, Cosgrove GR, Jenike MA.Neurosurgical treatment of Tourette’s syndrome: acritical review. Compr Psychiatry. 1995;36:141–56.
27. Leckman JF, de Lotbiniere AJ, Marek K, Gracco C,Scahill L, Cohen DJ. Severe disturbances in speech,swallowing, and gait following stereotacticinfrathalamic lesions in Gilles de la Tourette’ssyndrome. Neurology. 1993;43:890–4.
28. Baer L, Rauch SL, Ballantine HT Jr, et al.Cingulotomy for intractable obsessive compulsivedisorder. Prospective long-term follow-up of 18patients. Arch Gen Psychiatry. 1995;52:384–92.
29. Korzenev AV, Shoustin VA, Anichkov AD,Polonskiy JZ. Nizkovo- los VB, Oblyapin AV.Differential approach to psychosurgery of obsessivedisorders. Stereotact Funct Neurosurg. 1997;68:226–30.
30. Vandewalle V, van der Linden C, Groenewegen HJ,Caemaert J. Stereotactic treatment of Gilles de laTourette syndrome by high frequency stimulation ofthalamus. Lancet. 1999;353:724.
31. Porta M, Maggioni GR, Ottaviani F, Schindler A:Treatment of phonic tics in patients with Tourette’ssyndrome using botulinum toxin type A. Neurol Sci.2003;24:420–3.
32. Porta M, Sassi M, et al. Tourette’s syndrome and roleof tetrabenazine: review and personal experience.Clin Drug Investig. 2008;28:443–59.
33. Servello D, Porta M, et al. Deep brain stimulation in18 patients with severe Gilles de la Tourettesyndrome refractory to treatment: the surgery andstimulation. J Neurol Neurosurg Psychiatry. 2008;79:136–42.
34. Priori A, Giannicola G, Krauss JK, Simpson RK Jr,et al. Concepts and methods in chronic thalamicstimulation for treatment of tremor: technique andapplication. Neurosurgery. 2001;48:535–43.
35. Houeto JL, Karachi C, et al. Tourette’s syndrome anddeep brain stimulation. J Neurol Neuro surgPsychiatry. 2005;76:992–5.
36. Katayama Y, Kano T, et al.: Difference in surgicalstrategies between thalamotomy and thalamic deepbrain stimulation for tremor control. J Neurol2005;252 (suppl 4):IV17–IV22.
37. Welter ML, Mallet L, et al. Internal pallidal andthalamic stimulation in patients with Tourettesyndrome. Arch Neurol. 2008;65:952–7.
38. Sturm V, Lenartz D, et al. The nucleus accumbens: atarget for deep brain stimulation in obsessivecompulsive and anxiety-disorders. J ChemNeuroanat. 2003;26:293–9.
39. Kuhn J, Lenartz D, et al. Deep brain stimulation of thenucleus accumbens and the internal capsule intherapeutically refractory Tourette syndrome.J Neurol. 2007;254:963–5.
40. Hirabayashi H, Tengvar M, Hariz MI. Stereotacticimaging of the pallidal target. Mov Disord. 2002;17(Suppl 3):S130–4.
41. Hu W, Klassen BT, Stead M. Surgery for movementdisorders. J Neurosurg Sci. 2011;55:305–17.
42. Schiefer TK, Matsumoto JY, Lee KH. Movingforward: advances in the treatment of movementdisorders with deep brain stimulation. Front IntegrNeurosci. 2011;5:69.
13 Deep Brain Stimulation for Tourette Syndrome 159

14Stereotactic Neurosurgery for DrugAddiction
Guodong Gao and Xuelian Wang
Drug addiction is also known as drug depen-dence. A committee of experts from WHOdefined drug addiction as a mental, and some-times a physical, state caused by the interactionof the drug with the organism. Individualsaddicted to a drug exhibit a compulsive andcontinuous drug-taking behavior along withother reactions. The aim of these reactions iseither to experience euphoria or to avoid thediscomfort caused by drug withdrawal. The corefeature of addiction is that the addicts know thatthe behavior is pernicious but they cannot controltheir intake. Drug addiction includes two parts,physiological dependence (physical dependence)and psychological dependence (psychic depen-dence). Physiological dependence is a physio-logical adaptation state caused by repeated drugconsumption and displays drug tolerance andwithdrawal syndrome. Psychological dependenceis the euphoria caused by drug consumption andunderlies the need for continuous consumption toexperience the euphoria repeatedly. It is the maincause for relapse into drug addiction.
The survey results announced by the UnitedNations Office of Drug-inspection and Crime-defense (UNODC) on June 25, 2007 indicate thataround 200 million people (equivalent to 5 % ofthe world population at that time) showed
drug-taking behavior in 2006. Each year, amongdrug addicts, about 100 thousand people die and10 million people become incapacitated world-wide. The investigation of Substance Abuse andMental Health Services Administration indicatedthat about 22.3 million above-12-year-old people(equivalent to 8.9 % of the whole population atthat time) had used drugs at least once in 2010.The data announced by National Ban DrugCommission and Ministry of Public Security ofChina showed that by the end of 2010, therewere 15.45 million registered drug addicts andamong them, there were 10.65 million (69 %)were heroin addicts. By November of 2011, therewere 17.8 million registered drug addicts under35 years, which amount to 87 % of all addicts,and the actual total may be far higher.
At present, the methods for treating drugaddiction in China mainly include replacementtherapy, non-replacement therapy, Chineseherbs therapy, acupuncture, and electro-acupunc-ture therapy.Replacement therapy uses drugs withpharmacologic actions similar to opioids toreplace the addiction drugs. In this method, con-sumption of the replacement drugs are graduallyreduced over time until addiction ceases to exist.Methadone and buprenorphine are representativesof replacement drugs. Non-replacement therapyemploys central-acting α2 receptor agonist todecrease withdrawal symptoms. Clonidine andlofexidine are representative non-replacementdrugs. Withdrawal symptoms for these drugs areweaker than those for replacement drugs. Chineseherbs, acupuncture, and electro-acupuncture
G. Gao (&) � X. Wang4th Military Medical University, Tang Du Hospital,Xi an 710038, Shan Xi, Chinae-mail: [email protected]
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0_14© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
161

therapy can cause withdrawal within a short timebut cannot efface the psychological dependencecaused by addiction drugs, and therefore, cannotprevent relapse effectively. This problem exists forall noninvasive treatment methods available atpresent. Addicts fall into the vicious circle of drugtaking,withdrawal, and relapse. The relapse rate ofwithdrawal within a half year is 97–100 %.Therefore, relapse prevention is a problem thatdefies a solution by these methods and poses achallenge, to both the medical community andhuman society.
Following the development of experimentalstudies and stereotactic and functional surgery, itis possible to reduce the psychological depen-dence on drugs effectively by intervening in keycerebral nuclei for drug addiction used minimalinvasive surgery and adjust the function ofaddictive cycle in the brain. Stereotactic andfunctional surgery is an important branch ofmodern neurosurgery that can be regarded as afrontier discipline. During several decades ofdevelopment, stereotactic surgery has beenwidely applied to non-organic brain diseaseswhose main symptoms are characterized bymovement disorders, psychiatric diseases, andseveral types of pain and seizure disorders. Thissurgical procedure has gradually become acomponent of integrated treatment strategies thatmay include pharmacotherapy and other conser-vative therapies. Over the years, some neuro-surgeons with expertise in functional braindisease have attempted to treat drug addiction bytargeting brain lesions with stereotactic technol-ogy. From 2000 to 2004, such operations wereperformed in several hospitals in China, but thiscaused widespread public concern and extensivedebate. In November of 2004, China’s Ministryof Public Health subsequently banned theseoperations as a clinical service, but continues tosupport this technology as part of clinicalresearch projects. This chapter will describe thehistory of stereotactic surgery for the treatment ofdrug addiction, the neurological basis of thismethod, the surgical techniques involved, theassessment of outcomes, and the prospects forthe use of this technique in the future.
14.1 History of Stereotactic Surgeryfor Drug Addiction
Stereotactic technology had been applied topsychosurgery since the late 1950s. It enablesaccurate localization of target sites and reducesthe operation wound size and subsequent com-plication rate. Since the 1960s, published papershave reported that the cingulate gyrus, hypothal-amus, and frontal white matter could be treatmenttargets for opioid and alcohol addiction [1–3]. AnIndian scholar, Kanaka, reported in 1978 [3] that73 drug addicts had undergone stereotactic abla-tion of anterior cingulate gyrus lesions, with anefficacy rate of 60–80 %. Medvedev et al., fromthe Human Brain Research Institute of theRussian Academy of Sciences, has com-pleted 348 cases of bilateral stereotactic cingu-lotomy to treat drug addiction since 1998. Hefollowed-up 187 of these cases over 2 years anddetermined that 62 % of the patients did notrelapse, while 13 % of patients had dramaticallyreduced the levels of drug-taking; some had beenable to resume work, and only minor operativecomplications were recorded in this series [4].However, due to lack of long-term follow-upresults, this study’s focus can be applied to onlypsychosurgery rather than drug addiction. Forexample, Medvedev considered that bilateralstereotactic cingulotomy can help addicts choosethe right selection when faced to the drugs by thetreatment results of reduced the compulsive drug-taking behavior in addicts. Therefore, this reportdid not raise much interest.
Guodong Gao from the NeurosurgeryDepartment of Tangdu Hospital, the Fourth Mil-itary Medical University, Xi’an, China, usedstereotactic surgery to create bilateral lesions inthe nucleus accumbens (NAc) to treat patientswith opioid addiction in 2000 [5, 6]. He reportedthat 45 % of the 42 patients had not relapsed1 year postoperatively with only rare adversereactions [5, 6]. Subsequently, more than 10 hos-pitals performed this operation in China until2004, which sharply increased the number ofpatients who received this therapy to over 1,000.However, due to varying equipment quality,
162 G. Gao and X. Wang

technologies, and practice experience in thesehospitals, it has been difficult to objectivelyevaluate this huge case series. In addition,increasing numbers of scholars realized that therapid spread of this surgical method was notsuitable as it was still in the clinical researchphase. Their major concerns were that the neuralmechanisms of drug addiction remain unknown,and unforeseen long-term complications mayoccur since the areas targeted in such operationsare involved in many advanced brain functions,such as reward, cognition, behavioral decision-making, and learning-memory. It is true that thepotential for such risks are unknown, and theoperation could carry high risks. In addition, thissurgical technique has other potential negativefactors, including its intrinsic aggressive nature,controversial efficacy rates, and unknown long-term outcomes and complications. Based on thesefactors, China’s Ministry of Public Health bannedsuch operations from clinical services inNovember 2004, and has only permitted thistechnology to be applied as part of clinicalresearch projects. For similar reasons, Russianofficials had previously banned this therapeuticmethod in 2002.
14.2 Pathophysiology of DrugAddiction
The pathophysiology mechanism is extremelycomplex. Although different addiction drugs arequite different in their chemical structure, acutetarget sites, and pharmacological effect, themajor common features resulting in drug abuse,and finally drug addiction, are the effects ofreward and reinforcement. There is sufficientevidence to show that the NAc and cerebralcortex are the final neural substrates producingthe reinforcement effect of opioid. Olds andMilner discovered a mesencephalon-limbicdopamine (DA) system, which is composed of amesencephalon-protocerebrum-extrapyramidalcircle with the NAc as the center of this circle.The cerebral nucleus related to rewarding systeminvolves the ventral tegmental area (VTA), NAc,
arcuate nucleus, amygdaloid nucleus, locus coe-ruleus, and periaqueductal gray, and so on.
Although there are other independent rein-forcement pathways of opiates addiction, themain mechanism is that opioids act on dopami-nergic neuron via opiate receptor to inducereinforcement. The other independent reinforce-ment ways may include the following: (i) Opi-oids directly spur increased DA release andprevent DA reabsorption; (ii) Opioids restrain theaction of gamma-aminobutyric acid (GABA) byacting on the μ receptors on GABAergic inter-neurons thereby removing the inhibitory effect ofGABA on DA neurons in the VTA and increaseDA release in its target region; (iii) Opioidsdirectly spur increased DA release, which thenexcites related neurons, inducing euphoria. Theopioids-opiates receptor-dopaminergic neuronpathway is the specific cycle responsible for DAinvolvement in the rewarding process. The drugconsumption/stimulation, DA release, rewardingeffect, and drug-seeking behavior show a mutu-ally promoting relationship. Blocked DA recep-tors can weaken this reinforcement. In opiateaddiction, DA level increases in the brain and isadaptively balanced at a high level. Once thedrug intake ceases, DA content decreases grad-ually and then withdrawal symptoms and drug-seeking behavior emerge. Among the DAreceptors, D2 particularly functions in therewarding effect. In opiate-addiction rats withoutthe D2 receptor gene, the drug-seeking behaviorand conditioned place preference still exist, butare restrained. These results reinforce that the DAsystem has an important role in the psychologicaldependence in opiates addiction.
Acute administration of most of the addictiondrugs can activate the DA neurological circuitswithin the NAc and cerebral cortex, which arepart of the rewarding system, and can inducereward and reinforcement effects. Cocaine andDA transporter act together to prevent DAreabsorption. As a result, DA concentration inthe synaptic spaces of NAc neurons increases.Benzedrine specifically increases monoamineneurotransmitter release and simultaneouslyaccelerates DA release in NAc neurons. There-fore, benzedrine and cocaine have similar
14 Stereotactic Neurosurgery for Drug Addiction 163
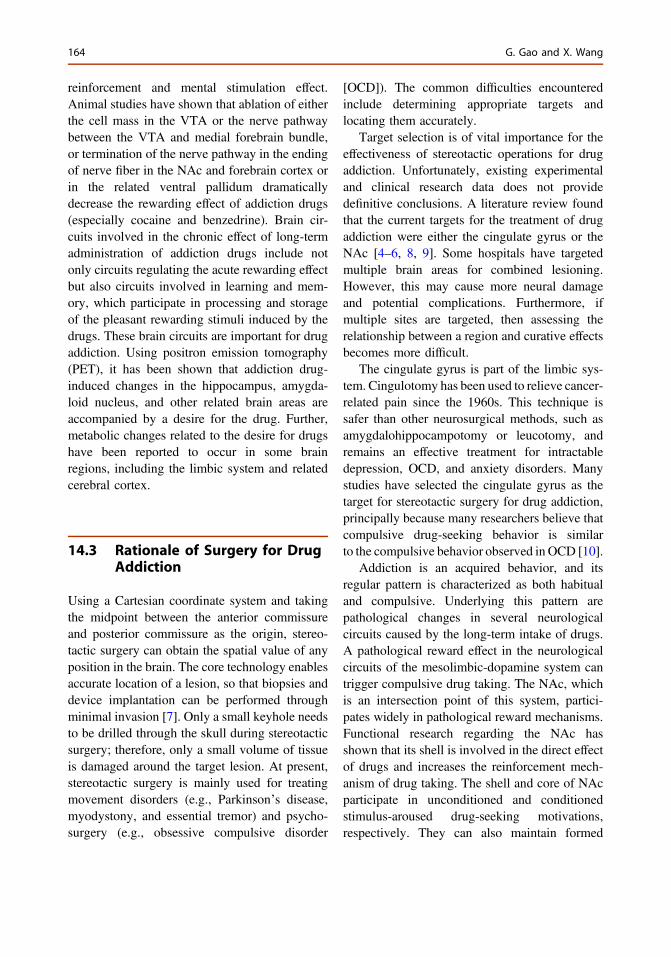
reinforcement and mental stimulation effect.Animal studies have shown that ablation of eitherthe cell mass in the VTA or the nerve pathwaybetween the VTA and medial forebrain bundle,or termination of the nerve pathway in the endingof nerve fiber in the NAc and forebrain cortex orin the related ventral pallidum dramaticallydecrease the rewarding effect of addiction drugs(especially cocaine and benzedrine). Brain cir-cuits involved in the chronic effect of long-termadministration of addiction drugs include notonly circuits regulating the acute rewarding effectbut also circuits involved in learning and mem-ory, which participate in processing and storageof the pleasant rewarding stimuli induced by thedrugs. These brain circuits are important for drugaddiction. Using positron emission tomography(PET), it has been shown that addiction drug-induced changes in the hippocampus, amygda-loid nucleus, and other related brain areas areaccompanied by a desire for the drug. Further,metabolic changes related to the desire for drugshave been reported to occur in some brainregions, including the limbic system and relatedcerebral cortex.
14.3 Rationale of Surgery for DrugAddiction
Using a Cartesian coordinate system and takingthe midpoint between the anterior commissureand posterior commissure as the origin, stereo-tactic surgery can obtain the spatial value of anyposition in the brain. The core technology enablesaccurate location of a lesion, so that biopsies anddevice implantation can be performed throughminimal invasion [7]. Only a small keyhole needsto be drilled through the skull during stereotacticsurgery; therefore, only a small volume of tissueis damaged around the target lesion. At present,stereotactic surgery is mainly used for treatingmovement disorders (e.g., Parkinson’s disease,myodystony, and essential tremor) and psycho-surgery (e.g., obsessive compulsive disorder
[OCD]). The common difficulties encounteredinclude determining appropriate targets andlocating them accurately.
Target selection is of vital importance for theeffectiveness of stereotactic operations for drugaddiction. Unfortunately, existing experimentaland clinical research data does not providedefinitive conclusions. A literature review foundthat the current targets for the treatment of drugaddiction were either the cingulate gyrus or theNAc [4–6, 8, 9]. Some hospitals have targetedmultiple brain areas for combined lesioning.However, this may cause more neural damageand potential complications. Furthermore, ifmultiple sites are targeted, then assessing therelationship between a region and curative effectsbecomes more difficult.
The cingulate gyrus is part of the limbic sys-tem. Cingulotomy has been used to relieve cancer-related pain since the 1960s. This technique issafer than other neurosurgical methods, such asamygdalohippocampotomy or leucotomy, andremains an effective treatment for intractabledepression, OCD, and anxiety disorders. Manystudies have selected the cingulate gyrus as thetarget for stereotactic surgery for drug addiction,principally because many researchers believe thatcompulsive drug-seeking behavior is similarto the compulsive behavior observed in OCD [10].
Addiction is an acquired behavior, and itsregular pattern is characterized as both habitualand compulsive. Underlying this pattern arepathological changes in several neurologicalcircuits caused by the long-term intake of drugs.A pathological reward effect in the neurologicalcircuits of the mesolimbic-dopamine system cantrigger compulsive drug taking. The NAc, whichis an intersection point of this system, partici-pates widely in pathological reward mechanisms.Functional research regarding the NAc hasshown that its shell is involved in the direct effectof drugs and increases the reinforcement mech-anism of drug taking. The shell and core of NAcparticipate in unconditioned and conditionedstimulus-aroused drug-seeking motivations,respectively. They can also maintain formed
164 G. Gao and X. Wang
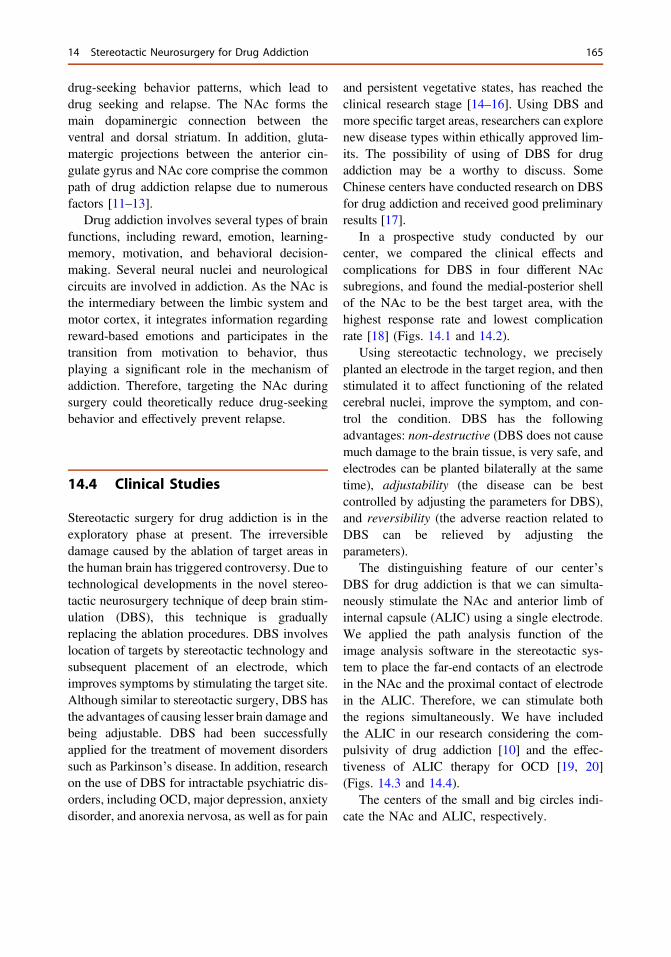
drug-seeking behavior patterns, which lead todrug seeking and relapse. The NAc forms themain dopaminergic connection between theventral and dorsal striatum. In addition, gluta-matergic projections between the anterior cin-gulate gyrus and NAc core comprise the commonpath of drug addiction relapse due to numerousfactors [11–13].
Drug addiction involves several types of brainfunctions, including reward, emotion, learning-memory, motivation, and behavioral decision-making. Several neural nuclei and neurologicalcircuits are involved in addiction. As the NAc isthe intermediary between the limbic system andmotor cortex, it integrates information regardingreward-based emotions and participates in thetransition from motivation to behavior, thusplaying a significant role in the mechanism ofaddiction. Therefore, targeting the NAc duringsurgery could theoretically reduce drug-seekingbehavior and effectively prevent relapse.
14.4 Clinical Studies
Stereotactic surgery for drug addiction is in theexploratory phase at present. The irreversibledamage caused by the ablation of target areas inthe human brain has triggered controversy. Due totechnological developments in the novel stereo-tactic neurosurgery technique of deep brain stim-ulation (DBS), this technique is graduallyreplacing the ablation procedures. DBS involveslocation of targets by stereotactic technology andsubsequent placement of an electrode, whichimproves symptoms by stimulating the target site.Although similar to stereotactic surgery, DBS hasthe advantages of causing lesser brain damage andbeing adjustable. DBS had been successfullyapplied for the treatment of movement disorderssuch as Parkinson’s disease. In addition, researchon the use of DBS for intractable psychiatric dis-orders, including OCD, major depression, anxietydisorder, and anorexia nervosa, as well as for pain
and persistent vegetative states, has reached theclinical research stage [14–16]. Using DBS andmore specific target areas, researchers can explorenew disease types within ethically approved lim-its. The possibility of using of DBS for drugaddiction may be a worthy to discuss. SomeChinese centers have conducted research on DBSfor drug addiction and received good preliminaryresults [17].
In a prospective study conducted by ourcenter, we compared the clinical effects andcomplications for DBS in four different NAcsubregions, and found the medial-posterior shellof the NAc to be the best target area, with thehighest response rate and lowest complicationrate [18] (Figs. 14.1 and 14.2).
Using stereotactic technology, we preciselyplanted an electrode in the target region, and thenstimulated it to affect functioning of the relatedcerebral nuclei, improve the symptom, and con-trol the condition. DBS has the followingadvantages: non-destructive (DBS does not causemuch damage to the brain tissue, is very safe, andelectrodes can be planted bilaterally at the sametime), adjustability (the disease can be bestcontrolled by adjusting the parameters for DBS),and reversibility (the adverse reaction related toDBS can be relieved by adjusting theparameters).
The distinguishing feature of our center’sDBS for drug addiction is that we can simulta-neously stimulate the NAc and anterior limb ofinternal capsule (ALIC) using a single electrode.We applied the path analysis function of theimage analysis software in the stereotactic sys-tem to place the far-end contacts of an electrodein the NAc and the proximal contact of electrodein the ALIC. Therefore, we can stimulate boththe regions simultaneously. We have includedthe ALIC in our research considering the com-pulsivity of drug addiction [10] and the effec-tiveness of ALIC therapy for OCD [19, 20](Figs. 14.3 and 14.4).
The centers of the small and big circles indi-cate the NAc and ALIC, respectively.
14 Stereotactic Neurosurgery for Drug Addiction 165
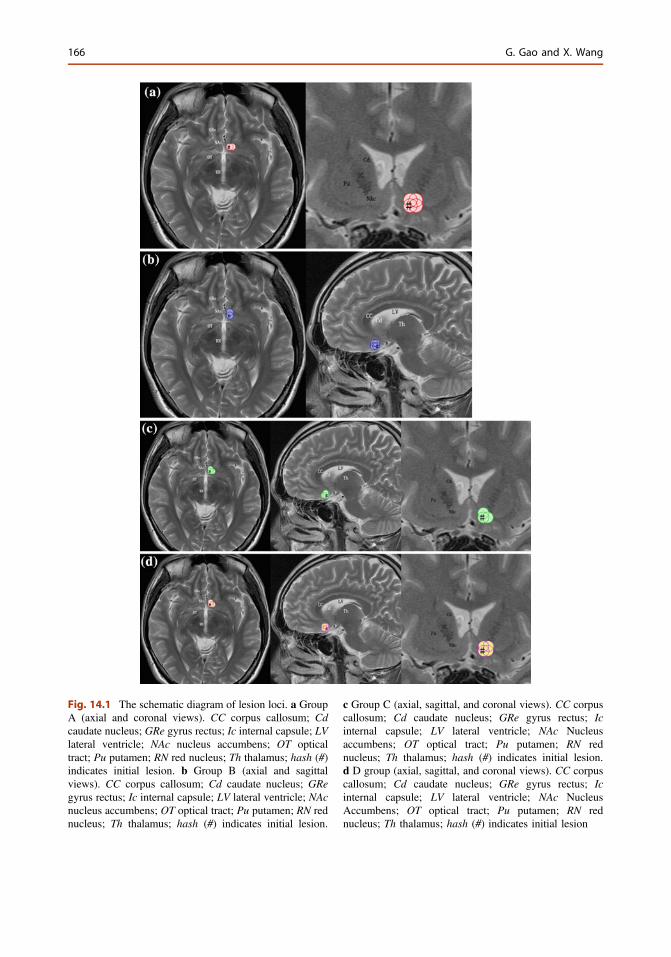
Fig. 14.1 The schematic diagram of lesion loci. a GroupA (axial and coronal views). CC corpus callosum; Cdcaudate nucleus; GRe gyrus rectus; Ic internal capsule; LVlateral ventricle; NAc nucleus accumbens; OT opticaltract; Pu putamen; RN red nucleus; Th thalamus; hash (#)indicates initial lesion. b Group B (axial and sagittalviews). CC corpus callosum; Cd caudate nucleus; GRegyrus rectus; Ic internal capsule; LV lateral ventricle; NAcnucleus accumbens; OT optical tract; Pu putamen; RN rednucleus; Th thalamus; hash (#) indicates initial lesion.
c Group C (axial, sagittal, and coronal views). CC corpuscallosum; Cd caudate nucleus; GRe gyrus rectus; Icinternal capsule; LV lateral ventricle; NAc Nucleusaccumbens; OT optical tract; Pu putamen; RN rednucleus; Th thalamus; hash (#) indicates initial lesion.d D group (axial, sagittal, and coronal views). CC corpuscallosum; Cd caudate nucleus; GRe gyrus rectus; Icinternal capsule; LV lateral ventricle; NAc NucleusAccumbens; OT optical tract; Pu putamen; RN rednucleus; Th thalamus; hash (#) indicates initial lesion
166 G. Gao and X. Wang
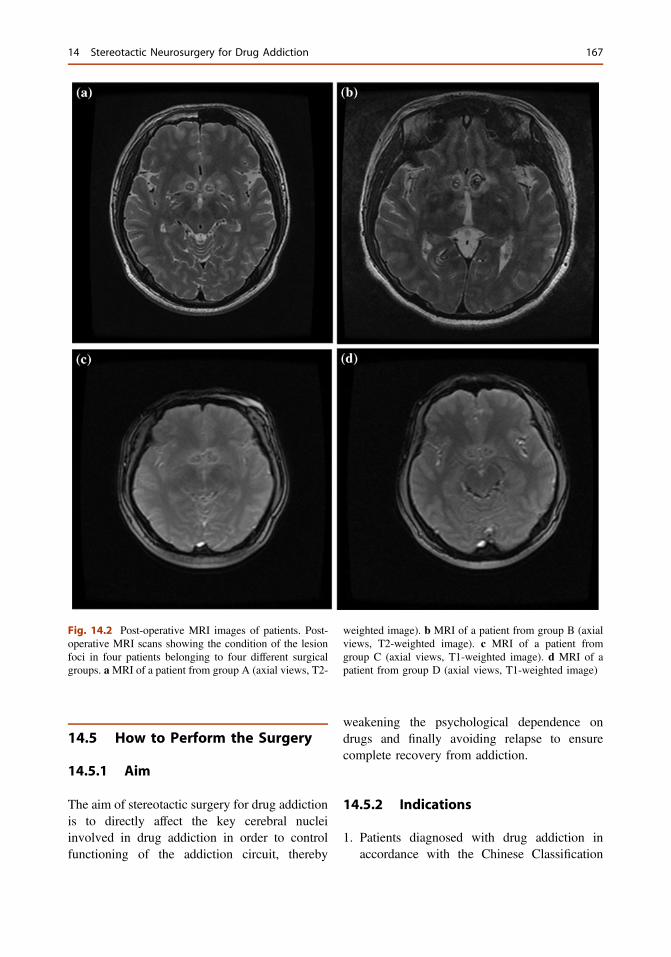
14.5 How to Perform the Surgery
14.5.1 Aim
The aim of stereotactic surgery for drug addictionis to directly affect the key cerebral nucleiinvolved in drug addiction in order to controlfunctioning of the addiction circuit, thereby
weakening the psychological dependence ondrugs and finally avoiding relapse to ensurecomplete recovery from addiction.
14.5.2 Indications
1. Patients diagnosed with drug addiction inaccordance with the Chinese Classification
Fig. 14.2 Post-operative MRI images of patients. Post-operative MRI scans showing the condition of the lesionfoci in four patients belonging to four different surgicalgroups. aMRI of a patient from group A (axial views, T2-
weighted image). b MRI of a patient from group B (axialviews, T2-weighted image). c MRI of a patient fromgroup C (axial views, T1-weighted image). d MRI of apatient from group D (axial views, T1-weighted image)
14 Stereotactic Neurosurgery for Drug Addiction 167
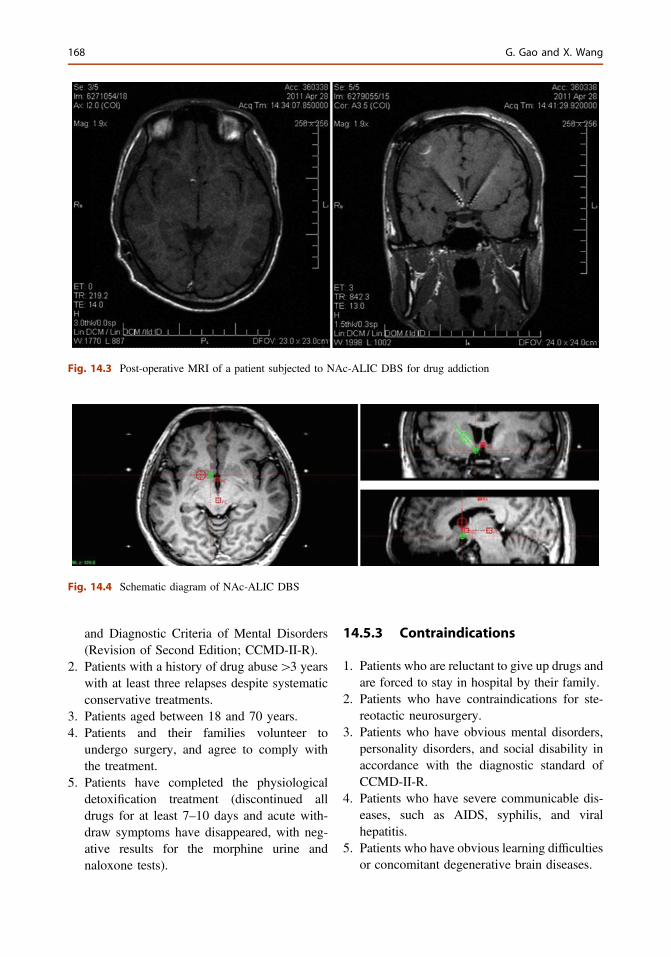
and Diagnostic Criteria of Mental Disorders(Revision of Second Edition; CCMD-II-R).
2. Patients with a history of drug abuse[3 yearswith at least three relapses despite systematicconservative treatments.
3. Patients aged between 18 and 70 years.4. Patients and their families volunteer to
undergo surgery, and agree to comply withthe treatment.
5. Patients have completed the physiologicaldetoxification treatment (discontinued alldrugs for at least 7–10 days and acute with-draw symptoms have disappeared, with neg-ative results for the morphine urine andnaloxone tests).
14.5.3 Contraindications
1. Patients who are reluctant to give up drugs andare forced to stay in hospital by their family.
2. Patients who have contraindications for ste-reotactic neurosurgery.
3. Patients who have obvious mental disorders,personality disorders, and social disability inaccordance with the diagnostic standard ofCCMD-II-R.
4. Patients who have severe communicable dis-eases, such as AIDS, syphilis, and viralhepatitis.
5. Patients who have obvious learning difficultiesor concomitant degenerative brain diseases.
Fig. 14.3 Post-operative MRI of a patient subjected to NAc-ALIC DBS for drug addiction
Fig. 14.4 Schematic diagram of NAc-ALIC DBS
168 G. Gao and X. Wang
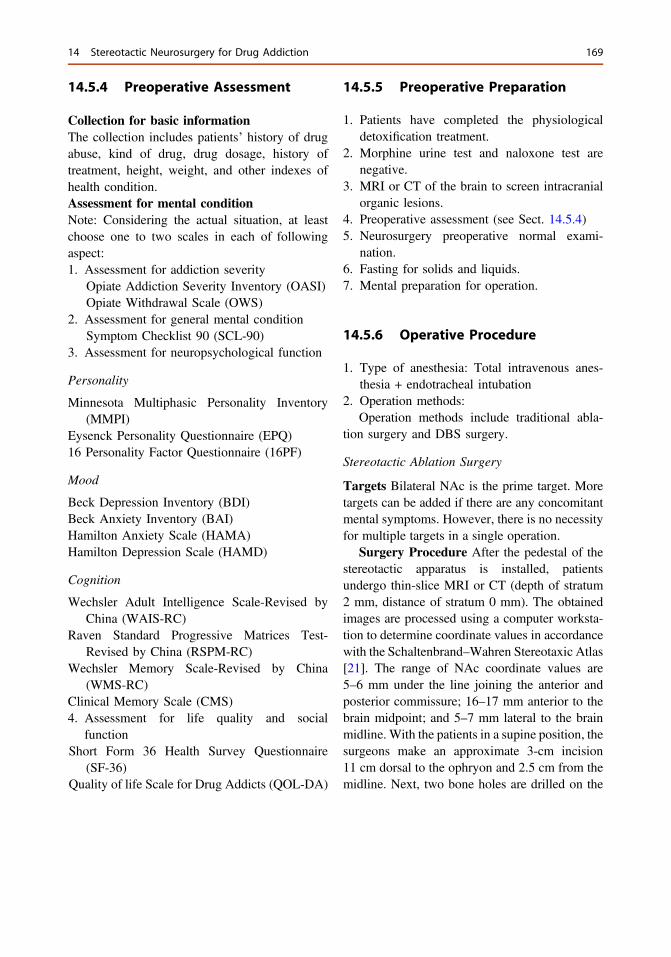
14.5.4 Preoperative Assessment
Collection for basic informationThe collection includes patients’ history of drugabuse, kind of drug, drug dosage, history oftreatment, height, weight, and other indexes ofhealth condition.Assessment for mental conditionNote: Considering the actual situation, at leastchoose one to two scales in each of followingaspect:1. Assessment for addiction severity
Opiate Addiction Severity Inventory (OASI)Opiate Withdrawal Scale (OWS)
2. Assessment for general mental conditionSymptom Checklist 90 (SCL-90)
3. Assessment for neuropsychological function
Personality
Minnesota Multiphasic Personality Inventory(MMPI)
Eysenck Personality Questionnaire (EPQ)16 Personality Factor Questionnaire (16PF)
Mood
Beck Depression Inventory (BDI)Beck Anxiety Inventory (BAI)Hamilton Anxiety Scale (HAMA)Hamilton Depression Scale (HAMD)
Cognition
Wechsler Adult Intelligence Scale-Revised byChina (WAIS-RC)
Raven Standard Progressive Matrices Test-Revised by China (RSPM-RC)
Wechsler Memory Scale-Revised by China(WMS-RC)
Clinical Memory Scale (CMS)4. Assessment for life quality and social
functionShort Form 36 Health Survey Questionnaire
(SF-36)Quality of life Scale for Drug Addicts (QOL-DA)
14.5.5 Preoperative Preparation
1. Patients have completed the physiologicaldetoxification treatment.
2. Morphine urine test and naloxone test arenegative.
3. MRI or CT of the brain to screen intracranialorganic lesions.
4. Preoperative assessment (see Sect. 14.5.4)5. Neurosurgery preoperative normal exami-
nation.6. Fasting for solids and liquids.7. Mental preparation for operation.
14.5.6 Operative Procedure
1. Type of anesthesia: Total intravenous anes-thesia + endotracheal intubation
2. Operation methods:Operation methods include traditional abla-
tion surgery and DBS surgery.
Stereotactic Ablation Surgery
Targets Bilateral NAc is the prime target. Moretargets can be added if there are any concomitantmental symptoms. However, there is no necessityfor multiple targets in a single operation.
Surgery Procedure After the pedestal of thestereotactic apparatus is installed, patientsundergo thin-slice MRI or CT (depth of stratum2 mm, distance of stratum 0 mm). The obtainedimages are processed using a computer worksta-tion to determine coordinate values in accordancewith the Schaltenbrand–Wahren Stereotaxic Atlas[21]. The range of NAc coordinate values are5–6 mm under the line joining the anterior andposterior commissure; 16–17 mm anterior to thebrain midpoint; and 5–7 mm lateral to the brainmidline. With the patients in a supine position, thesurgeons make an approximate 3-cm incision11 cm dorsal to the ophryon and 2.5 cm from themidline. Next, two bone holes are drilled on the
14 Stereotactic Neurosurgery for Drug Addiction 169
skull and the dura mater is incised. After arrestingthe bleeding and fulguratively incising the cortex,using the stereotactic device, the surgeons guidethe electrode to the target site and ablate it. Afterablation is completed and the bleeding hasstopped, the incision on the scalp is sutured.
Parameters of Ablation Temperature: 80 °F;Time: 60 s; Specification of radio frequencystylus: 1.6 × 4.0 mm or 1.6 × 5.0 mm; Volume oflesion: 2 × 2 × 8 mm3.
Stereotactic DBS Surgery
Targets The prime targets are bilateral NAc orbilateral NAc + ALIC.
Surgery Procedure Up until the step oflocation, DBS surgery and stereotactic ablationsurgery are the same. After affirming NAc’scoordinate values, the surgeon can set and con-firm the “skull approach” using the path analysisfunction of the image analysis software in thestereotactic system in order to place the far-endcontacts of the electrode in the NAc and theproximal contact of the electrode in the ALIC. Inthis skull approach, a bilateral, small-disc-shapedincision is made on the scalp, two bone holes aredrilled in the skull, and the dura mater incised.Used the guide bow of the stereotactic apparatus,the electrodes are guided to the targets and fixed.The guide bow of stereotactic apparatus areremoved, the bleeding is stopped, and the inci-sion in the scalp is sutured. After recovery fromgeneral anesthesia, the temporary stimulator canbe turned on. The instant effect and side reactioncan then be observed. If there are no obvious sidereactions within 1 week postoperatively and thereview MRI shows no deviation in the locationof electrodes, the subskin impulsator can beplanted in the pre-thoracic skin under localanesthesia.
Stimulating electrode and stimulation’srelated parameters Stimulating ElectrodeMedtronic model 3387 (Medtronics, Inc., Min-neapolis, Minnesota), four-contact electrode,contact length 1.5 mm, and the space betweencontacts length is 1.0 mm. Stimulation mode:monopolar or bipolar stimulation mode, single ormultiple contact stimulation mode, continuous
stimulation mode, high frequency and fixed pulsewidth, gradually increased voltage. Stimulationparameter 130 Hz, 90 µW, 4.0–7.0 V.
14.5.7 Operative Response Evaluation
The standard for successful rehabilitation fromdrug addiction is that the patients can refrainfrom consuming any kind of drug for 1 year, andthat within the first year, the morphine urine andnaloxone tests are negative at any given time.The evaluative criteria for the curative effect arebased on the occurrence of relapse and with-drawal duration as follows: (1) Good: Refrainedfrom all kinds of drugs over 12 months postop-eratively; (2) Improvement: Refrained from allkinds of drugs 6–12 months postoperatively; (3)Ineffective: Consumed any kind of drug within6 months postoperatively.
14.5.8 Postoperative Follow-Up
Face-to-face follow-up is conducted at postop-erative months 1, 3, 6, 12, 18, and 24, respec-tively. The scope of examination is as follows:1. Effectiveness: Relapse, retention rate and time
of drug addiction, dose and frequency of drugrelapse, and changes in the levels of cravingand euphoria.
2. Safety: Changes in e general physiologicalparameters (e.g., blood pressure, temperature,weight), appetite and sexual desire; compari-son of the preoperative and postoperativevalues of multiple indexes for psychologicalassessment (memory, intelligence, personal-ity, etc.); incidence of nonspecific complica-tions (e.g., bleeding and infection); andincidence of specific neurological complica-tions (e.g., central high fever, aconuresis,anterograde amnesia, and dysfunction inmotivation-forming).
3. Verification of lesion targeting: A repeatedthin-slice MRI conducted within 6 monthspostoperatively in order to verify the locationof the targeted lesion.
170 G. Gao and X. Wang
14.5.9 Complications
1. Non-specific complications: Include compli-cations not related to functions of the targetarea and related closely to the wound itself.These mainly include fever, infection, head-ache, incontinence of urine, and epilepsy. Theoccurrence rate of non-specific complicationsis 10 %, and these complications are usuallytransient and mild and can disappear afterappropriate handling.
2. Specific complications: Refers to complica-tions related closely to the function of thelesion target. These mainly include personal-ity changes, aprosexia, memory complaints,interest changes, mild affective disorder, hy-posphraesia, and parasexuality. The occur-rence rate of specific complications is 10 %,and these complications usually disappeargradually after appropriate handling.
14.5.10 Unresolved Questions
1. Stereotactic surgery is more than a surgicalmethod to treat drug addiction; it also con-cerns about psychotherapy and social support.It is a holistic treatment model and canovercome psychological dependence, reducethe relapse rate post-operatively. However,this surgery treatment is not the only approachto drug addiction. It is only adopted whenother conservative treatment methods failedrepeatedly.
2. For success of this surgical treatment,patients’ cooperation is the most importantfactor. Patients and their family realizing theharmful effects of drug addiction and volun-teering to receive the treatment are the primepremise and guarantee the success of thissurgical treatment.
3. At our institute, this method yielded goodresults, in that the patients received detoxifi-cation for 7–10 days and waited until allwithdrawal symptoms disappeared (Themorphine urine and naloxone tests were neg-ative.), before the stereotactic operation was
performed. The reasons for this stringentcondition is that the interaction betweenphysiological and psychological dependencecan easily lead to relapse.
4. Some patients still report chronic protractedwithdrawal symptoms, which include refrac-tory insomnia, anxiety, and pain in the limbjoints and muscles, after completion of thedetoxification treatment and attainment ofnegative results for morphine urine and nal-oxone tests. For such cases, some medicationcan be used. However, Chinese medicinesfree of risk of addiction are preferred over“easy-to-cause addiction” Western medicineslike adanon, tramagetic, dilantin, and triazo-lam. If a Western medicine has to be selected,the medications daily decreasing principle ismore helpful.
5. Postoperative specific and non-specific com-plications are mainly related to brain edemaaround the target. The complications can beprevented by precise stereotactic technologyand apparatus, abundant clinical experience,and timely symptomatic treatment.
14.6 Follow-up Results:A Multicenter Study in China
Most clinical reports have indicated that stereo-tactic surgery can effectively prevent relapse indrug addiction [4–6, 8, 9]. After this treatment,over half of patients show no relapses and, amongthose who relapse, intake dose and drug-takingfrequency is markedly dropped [4–6, 8, 9]. Theincidence of nonspecific complications, such asbleeding and infection, is low [4–6, 8, 9]. Amongspecific complications, central high fever andaconuresis are common shortly after the opera-tion, but these resolve after symptomatic treat-ment is applied. These complications may arisedue to edema around the targeted lesion [6]. Somepatients have been reported to shown anterogradeamnesia and dysfunction in motivation-forming,which is characterized by silence, apathy, lack ofinterest, lack of proactive behaviors, idleness, and
14 Stereotactic Neurosurgery for Drug Addiction 171

social withdrawal [22]. These patients usuallyrecover after some months of rehabilitation.
Most researchers who have applied stereo-tactic surgery for treating drug addiction considerit to be safe and effective. Although evidence-based medical evidence to support this opinion islacking, pilot studies have indicated that thissurgery is effective in terms of short-term out-comes. However, regrettably, most pilot studiesdid not verify the location and volume of thetargeted lesion and did not analyze the relation-ship between the lesion location, targeted vol-ume, and treatment effectiveness. Most pilotstudies only reported follow-up results within1 postoperative year, and gave no indicationabout the long-term effects of this treatment.
In contrast to these positive reports, manyexperts have raised questions about the safety andefficacy of this surgery. Furthermore, the ethicalissues concerning this surgery have become amatter of contention [23, 24]. The Chinese “11thFive Years” scientific support plan project, enti-tled the “Clinical reevaluation of current pre-vention of relapse” (No. 2007BAI0703), wascompleted in 2010. An independent third-partycommittee of experts evaluated the safety andefficacy of stereotactic surgery comprehensivelyand scientifically, with the aim of reaching animpartial and compelling conclusion.
The follow-up results showed that 17 centersin China had adopted stereotactic surgery fordrug addiction, and 1,167 patients had undergonethis surgery until November of 2004. From them,8 centers participated in the follow-up study, and769 patients were included in the study. Thestudy selected 150 patients by applying a com-pletely random digital method. After completionof follow-up, of the 150 patients, 122 patientsagreed for a face-to-face interview, and28 patients were either lost during follow-up orrefused for a face-to-face interview. Non-relapsewas judged by the conformity of patients andtheir families’ denial of drug-taking behavior,negative results for both morphine urine andnaloxone tests, and negative results for hair drug-content detection. The conservative non-relapserate of this follow-up study was 50 % (75/150),
and the longest non-relapse time was 8 years.And among the 47 cases of patients whorelapsed, 34 relapsed within 1 year postopera-tively. The study identified that the following asmain reasons for relapse in this sequence: nega-tive events in life, lack of social and family care,drug traffickers’ lure, psychological dependencefor drugs, and body discomfort caused by chronicprotracted withdrawal symptoms. The occurrencerate of non-specific complications was 9.0 % (11/122), and all of them were resolved within6 months post-operatively. The occurrence rate ofspecific complications was 7.4 % (9/122), andmost of them improved gradually with time.Among the 122 patients, 75.4 % had differentkinds of regular work, and 84.6 % patients werefinancially independent. Compared with patientswho did not undergo the surgery, patients whodid lived a better life postoperatively. Moreover,quality of life for patients who did relapse for 5 ormore years postoperatively was similar to that ofnormal people.
In conclusion, drug treatment should consti-tute a system that includes the following threecontinuous processes: detoxification, relapseprevention, and societal return. In this chapter, wehave summarized our successful clinical experi-ence at achieving a curative effect through pre-operative physiological detoxification, accurateand appropriate ablation of the NAc, and positivecognitive behavior modification. In addition toother treatment methods, a standardized stereo-tactic technique can help humans overpower thedemon of drug addiction in the future.
References
1. Dieckmann G, Schneider H. Influence of stereotactichypothalamotomy on alcohol and drug addiction.Appl Neurophysiol. 1978;41(1–4):93–8.
2. Jansson B, Nystrom S. Lobotomy as a therapeuticalternative in drug addiction. Lakartidningen. 1968;65(24):2444–5.
3. Kanaka TS, Balasubramaniam V. Stereotacticcingulumotomy for drug addiction. ApplNeurophysiol. 1978;41(1–4):86–92.
4. Medvedev SV, Anichkov AD, Polyakov YI.Physiological mechanisms of the effectiveness of
172 G. Gao and X. Wang
bilateral stereotactic cingulotomy against strongpsychological dependence in drug addicts. HumPhysiol. 2003;29(4):492–7.
5. Gao G, Wang X, He S, et al. Clinical study foralleviating opiate drug psychological dependence by amethod of ablating the nucleus accumbens withstereotactic surgery. Stereotact Funct Neurosurg.2003;81(1–4):96–104.
6. Wang X, He S, Heng L et al. Follow-up of nucleusaccumbens lesion for treatment of drug dependence.Chinese Journal of Neurosurgery. 2005;10.28;21(10).
7. Fu X, Niu C. Stereotactic and FunctionalNeurosurgery Anhui Science and TechnologyPublishing House. 2004
8. Xu M, Wang C, Jiang C. Bilateral cingulotomy forthe treatment of heroin dependence. Chinese Journalof Minimally Invasive Neurosurgery. 2005;10(4):162–3.
9. Yang K, Xi S, Wang K et al. Stereotactic bilateralnucleus accumbens lesion for the treatment of opioiddependence. Chinese Journal of Stereotactic andFunctional Neurosurgery. 2005;18(3):135–9.
10. Orellana C. Controversy over brain surgery for heroinaddiction in Russia. Lancet Neurol. 2002;1(6):333.
11. Everitt BJ, Robbins TW. Neural systems ofreinforcement for drug addiction: from actions tohabits to compulsion. Nat Neurosci. 2005;8(11):1481–9.
12. Belin D, Everitt BJ. Cocaine seeking habits dependupon dopamine-dependent serial connectivity linkingthe ventral with the dorsal striatum. Neuron. 2008;57(3):432–41.
13. Kalivas PW, McFarland K. Brain circuitry and thereinstatement of cocaine-seeking behavior.Psychopharmacology. 2003;168(1–2):44–56.
14. Bittar RG, Kar-Purkayastha I, Owen SL, et al. Deepbrain stimulation for pain relief: a meta-analysis.
J Clin Neurosci: Official J Neurosurg Soc Australas.2005;12(5):515–9.
15. Wichmann T, Delong MR. Deep brain stimulation forneurologic and neuropsychiatric disorders. Neuron.2006;52(1):197–204.
16. Yamamoto T, Katayama Y. Deep brain stimulationtherapy for the vegetative state. NeuropsychologicalRehabil. 2005;15(3–4):406–13.
17. Zhou H, Xu J, Jiang J. Deep brain stimulation ofnucleus accumbens on heroin-seeking behaviors: acase report. Biol Psychiatry. 2011;69:e41–2.
18. Li N, Wang J, Wang XL, Chang CW, Ge SN, Gao L,et al. Nucleus accumbens surgery for addiction.World Neurosurg. 2012. pii:S1878–8750(12)01106–0, doi:10.1016/j.wneu.2012.10.007.
19. Greenberg BD, Gabriels LA, Malone DA Jr, RezaiAR, Friehs GM, Okun MS, et al. Deep brainstimulation of the ventral internal capsule/ventralstriatum for obsessive-compulsive disorder:worldwide experience. Mol Psychiatry. 2010;15(1):64–79.
20. Anderson D, Ahmed A. Treatment of patients withintractable obsessive-compulsive disorder withanterior capsular stimulation: case report.J Neurosurg. 2003;98:1104–8.
21. Schaltenbrand G, Wahren W. Atlas for stereotaxy ofthe human brain. Stuttgard: Thieme; 1977.
22. Heng L, Wang X, He S, et al. Complications ofnucleus accumbens leasions for the treatment of drugdependence. Chinese Journal of Stereotactic andFunctional Neurosurgery. 2006;19(1):5–8.
23. Hang J. Reflections on neurosurgery detoxification.Chinese Journal of Pain Medicine. 2005;11(1):45–6.
24. Qu X, Qiu Z. Our views for the treatment of drugaddiction by neurosurgery. Medicine and Philosophy.2004;25(12):32.
14 Stereotactic Neurosurgery for Drug Addiction 173

15Surgical Treatments for AnorexiaNervosa
Bomin Sun, Dianyou Li, Wei Liu, Shikun Zhan, Yixin Panand Xiaoxiao Zhang
Abstract
Anorexia nervosa (AN) is a severe psychiatric disorder with high rates ofmorbidity and mortality. An estimated 21 % of patients experience a chroniccourse despite treatment with the best available medications and behavioraltherapies. Existing data suggest that lesioning and deep brain stimulation canbenefit a large proportion (ranging from60 to 80%)of patientswithmedicallyintractable AN. Long-term serious adverse events are very infrequent.Functional neuroimaging studies have increased our understanding of themechanismsofdisease development and therapeutic action.At our institution,we gradeANon a four-point scale based on patient clinical characteristics andour surgical experience over the past 8 years. This scale is particularly usefulfor guiding the selection of surgical procedures. Such treatment optionsinclude deepbrain stimulation or lesioning of the nucleus accumbens, anteriorcapsulotomy, and anterior cingulotomy. Data suggest that surgical treatmentis a viable option for intractable AN, and can alleviate suffering and improvethe quality of life of patients with these disabling disorders.
Keywords
Anorexia nervosa � Surgery � Deep brain stimulation � Capsulotomy �Cingulotomy
15.1 Introduction
Anorexia nervosa (AN) is one of the most chal-lenging psychiatric disorders which usuallybegins in adolescence and is characterized by arefusal to maintain body weight at or above aminimally normal weight for age and height, anintense fear of gaining weight, a relentless drivefor thinness, and a disturbance in the way one’sbodyweight and shape experienced. Amenorrhea
B. Sun (&) � D. Li � W. Liu � S. Zhan � Y. Pan �X. ZhangDepartment of Stereotactic and FunctionalNeurosurgery, Ruijin Hospital, Shanghai JiaotongUniversity School of Medicine, 197 Ruijin Er Road,Shanghai 200025, Chinae-mail: [email protected]
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0_15© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
175
is also often present in female patients. Otherfeatures include disturbed body image, heighteneddesire to lose more weight, and pervasive fear offatness [1, 2]. The average point prevalence rate ofAN is 0.3–1 % in young females and approxi-mately one tenth of that rate in males. Lifetimeprevalence is 2.2 % among females [3, 4].
Anorexia nervosa, which has one of the highestexcessive mortality rates of all psychiatric disor-ders, causes remarkable agony for the patients andtheir families. Suicide or medical complicationsare themajor causes ofmortality for thosewithAN[5, 6]. Long-lasting malnutrition can lead tonumerous severe physical complications, includ-ing osteoporosis, gastrointestinal and cardiaccomplications, liver damage, electrolyte distur-bances, and eventually multiple organ failure [7].AN psychiatric comorbidities include majordepressive disorder (MDD; 50–70 % of ANpatients), anxiety disorder ([60 %), obsessive-compulsive disorder (OCD;[40 %) [8, 9]. Per-sonality disorders and alcohol or substance abusemay also be present (12–27 %) among those withthe binging-purging subtype of AN, in whom therate of impulsive behavior is also higher than in therestricting subtype of AN [10].
In an extensive literature review, it reportedthat less than half (46.9 %) of surviving patientsrecover from AN, one-third (33.5 %) improvepartially, and in 20.8 % (0–79 %) the diseasetakes on a chronic course [11, 12]. AN patientswith a duration of illness longer than 10 years arevery unlikely to recover [11, 13, 14]. Besides,linkage studies further confirmed that AN, majordepressive disorder(MDD), anxiety, OCDs andaddictive disorders shared about a third of geneticrisk factors [15]. And there is evidence indicatesthat the presence of depressed mood may be a riskfactor for AN, which could lead to worse out-comes and greater rates of relapse in AN patients[5, 16]. These psychotic disorders may havesignificant overlap in the anatomic structures.
15.2 Neurocircuitry of AnorexiaNervosa
The neurocircuitry underlying food intake iscomplex and the precise mechanism of AN isstill unclear. Since no single factor has beenshown to be either necessary or sufficient fordevelopment of AN, a multifactorial thresholdmodel is likely the most appropriate explanatorymodel of illness [14]. The biology and neuralcircuitry of AN are research “hotspots”, withmost disease models focusing on factors thatunderlie pathological mood, anxiety, reward,body perception, inhibition, alexithymia, andappetite [17]. Much of this work on AN is drivenby neuroimaging, which has been used exten-sively to show both structural and functionaldifferences between patients with AN, thoserecovered from AN, and healthy controls.
Individuals with AN typically exhibit distinc-tive temperament and personality traits, whichoften first occur in childhood before the onset ofAN, may even contribute to the development ofAN, and often persist after recovery [18]. Manyof these traits are likely encoded in neural circuits,for example, characteristic harm avoidance ispositively associated with dopamine (DA) D2/D3receptor binding in the dorsal caudate [19], andperfectionism and obsessive personality traits areassociated with exaggerated cognitive control bythe dorsolateral prefrontal cortex (DLPFC). TheDLPFC may become excessively involved ininhibitory processes to dampen information pro-cessing through reward pathways [20]. The anx-ious temperament of patients with AN leads to avariety of dysfunctional behaviors thought toserve as a means of coping with adverse mood.Functional brain imaging demonstrates thatdecreased activation of fronto-striatal circuits,including the ventral striatum, anterior cingulatecortex (ACC), and supplementary motor area(SMA), may underlie the impaired cognitive
176 B. Sun et al.
flexibility in patients with AN, which results inthe stereotypical and ritualistic behaviors to con-trol eating and weight [21].
Considerable data indicate that individualswith AN exhibit disturbances in DA and sero-tonin (5-HT) systems. 5-HT might play a role inaltered satiety, impulse control, and mood,whereas DA is implicated in motivation, execu-tive functions (i.e. inhibitory control, salienceattribution, and decision-making), and the aber-rant reward effects of food. Recent studies of AN,using positron emission tomography (PET) andsingle photon emission computed tomography(SPECT) with 5-HT-specific radio ligands, con-sistently show alterations in 5-HT1A and5-HT2A receptor and 5-HT transporter activity incortical and limbic structures, which may berelated to anxiety, behavioral inhibition, andbody image distortions [17]. Depletion of 5-HTlevels reduces anxiety in acutely ill patients andthose recovered from AN [22]. Starvation mayreduce pathologically increased DA levels thatare associated with anxious temperament [20].
The processing of food reward is complex andmodulated by cognitive, emotional, and biologi-cal factors involving learned behaviors andgenetic predispositions. The motivation to eat andapproach food is a critical part of the rewardpathway and is particularly disturbed in AN. It ispossible that food has little reward value in AN,and thus may be associated with correspondingresponses in the orbitofrontal cortex (OFC) or thestriatum [19]. Recent imaging studies provideevidence for disturbed gustatory processing inpatients with AN, which involves the anteriorinsula as well as striatal regions [18]. Genetic,pharmacological, and physiological data showthat individuals with AN and those recoveredfrom AN exhibit altered striatal DA function [23,24]. DA disturbances could contribute to alteredmodulation of appetitive behaviors as well assymptoms of anhedonia, dysphoric mood, ascet-icism, and increased motor activity [25]. Theseresults raise the possibility that individuals withAN have altered appetitive mechanisms that mayinvolve either sensory, interoceptive, or rewardprocesses. These disturbances in the modulationof reward and emotion may increase vulnerability
to dysregulated appetitive behaviors. Individualswith AN may be able to inhibit appetite and haveextraordinary self-control due to exaggerateddorsal cognitive circuit function [17].
In addition to the reward pathway, severalother neural circuits contribute to AN. The insularcortex serves to integrate processing from manyof the structures relevant to AN, and thus may becritical for AN. It has therefore been hypothesizedthat a rate limiting dysfunction of neural circuitryintegrated by the insula may account for theclinical phenomena of AN [26]. However, theexact neural circuitry of anorexia remains unclear.Neuroimaging, neurophysiological, and lesionstudies implicate the ventral (limbic) and dorsal(cognitive) neural circuits, which may be of par-ticular relevance for understanding behavior inAN. The ventral neurocircuitry consists of theamygdala, insula, ventral striatum, ventral regionsof the ACC and OFC, and mediates identificationof and responses to stimuli. By contrast, thedorsal circuitry consists of the hippocampus,dorsal regions of the ACC, DLPFC, and parietalcortex, and may be involved in the modulation ofselective attention, planning, and effortful regu-lation of affective states [27, 28].
Key regions involved in fear perception includethe amygdala, hippocampus, insular cortex, ACC,striatum, and prefrontal cortex (PFC) [29]. Inresponse to visual food cues, patients with ANdisplay stronger activation of the bilateral amyg-dala, medial PFC, ACC, and striatum than healthycontrols. Thus, food cues trigger arousal, fear, andavoidance in patients with AN [30]. Fear circuitryis also involved in the extinction of fearful mem-ories. Furthermore, inhibitory projections from themedial PFC/OFC to the amygdala are importantfor this extinction. In this regard, individuals suf-fering from eating disorders exhibit faster fearlearning and heightened resistance to the extinc-tion of conditioned responses [21].
In a recent 18F-FDG PET/CT study ofpatients with AN, we observed that hyperme-tabolism in the frontal lobe, hippocampus, andlentiform nucleus decreases after deep brainstimulation of the nucleus accumbens (NAcc-DBS) [31]. Lipsman et al. [32] also reporteddecreased hypermetabolism of the anterior
15 Surgical Treatments for Anorexia Nervosa 177
cingulate, insular, and parietal lobes after sub-callosal cingulate-DBS, together with substantialimprovements in body mass index (BMI) andmood. These results demonstrate the importanceof these brain regions for AN.
It remains unknown whether disturbances inneural circuits occur prior to or secondary tomalnutrition. It has been proposed that structuraland functional alterations in the insula and frontalcortex, including areas that contribute toreward and anxiety processing, such as orbito-frontal and cingulate regions, could predisposeindividuals to developing EDs and that the adap-tive changes in these circuits may occur inresponse to malnutrition [33]. Thus, structural andfunctional alterations in specific brain regions,together with neurotransmitter-mediated changes,are implicated in the etiopathology of AN. Addi-tional studies are required to further elucidate theetiopathology and neurocircuitry of AN.
15.3 Non-invasive Treatments
Anorexia nervosa is usually a chronic illnesswhich could annoyed one’s whole lifetime.Current psychotherapeutic interventions andpharmacological therapies for AN are far fromuniversally effective. Surprisingly, there is nohigh-level evidence [category A, according toNational Institute for Health and Clinical Excel-lence (NICE) guidelines] regarding the efficacyof pharmacological or psychotherapeutic inter-ventions. Furthermore, only family interventionsmeet category B criteria (well-conducted studiesbut no randomized controlled trials) [34, 35].Variants of family therapy are effective in ado-lescents but there is little evidence regarding theirefficacy in adults [36].
Selective serotonin reuptake inhibitors(SSRIs) are the main stay of pharmacologicaltreatment for AN symptoms or weight restora-tion; however, the American Psychiatric Asso-ciation does not support the use of SSRIs in themanagement of underweight patients with AN[37]. There are only limited data available foratypical antipsychotics; olanzapine may help
increase weight and decrease obsessive symp-toms in chronic severe AN outpatients, butpractice guidelines do not recommend routineuse [38–40].
Although there are many available treatmentsfor AN, almost 20 % of the patients are refractoryto all current medical treatments and at risk forpremature death. The standardized mortality ratioover the first 10 years is about 10 % [11, 12, 41].For treatment-refractory AN, surgical manage-ment may be an alternative therapy.
15.4 Neurosurgical Managementof Anorexia Nervosa
15.4.1 History of Neurosurgeryin Anorexia Nervosa
Experimental neurosurgical approaches for ANhave been proposed for over half a century. Thefirst case report of a prefrontal leucotomy forthe treatment of AN was published in 1950 [42].The patient was a 21-year-old female andreceived a transorbital leucotomy, followed by afull prefrontal leucotomy as a result of diseaserelapse. Two months after the second surgery,the patient experienced significant weight gainand increased appetite. In the next 20 years,16 patients with AN who underwent prefrontalleucotomies were evaluated and reported[43–49]. In a similar manner to the first publi-cation, most patients experienced significantweight gain and greater interest in food; how-ever, a number developed complications. Forexample, 3 patients experienced continued psy-chiatric symptoms including depression, anxiety,and panic disorder. In addition, 1 patient com-mitted suicide approximately 4 months after theoperation [43, 44, 46]. A study in 1976 reviewedthe management of AN patients who underwentstereotactic limbic leucotomies [50–53]. Allpatients reported significant weight gains andimprovements in other psychiatric disorders.
Modern stereotactic psychosurgery for AN hasexperienced are naissance over the past 10 years.The approaches of modern procedures have
178 B. Sun et al.
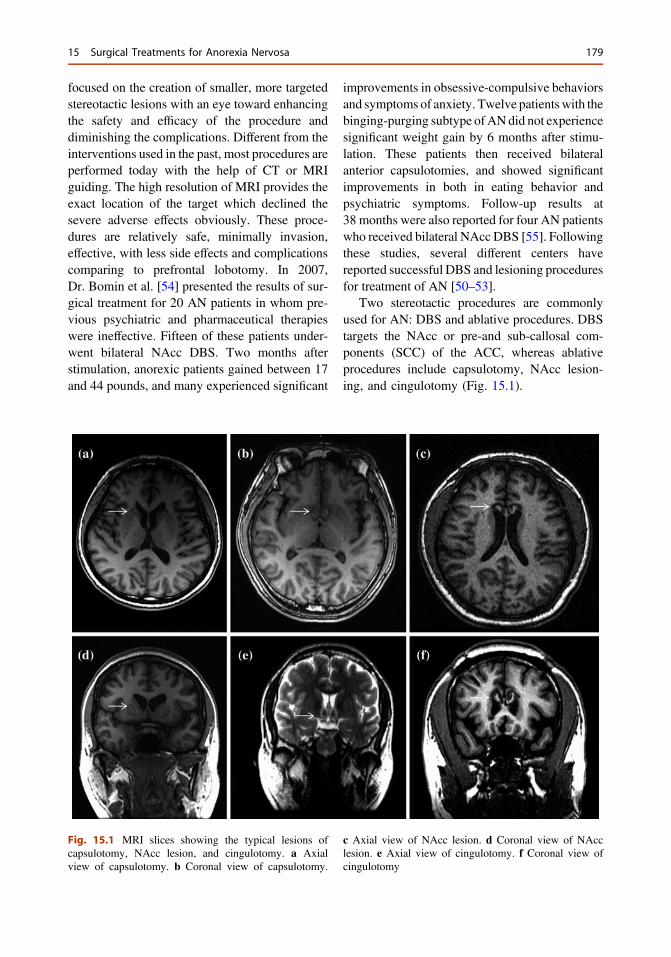
focused on the creation of smaller, more targetedstereotactic lesions with an eye toward enhancingthe safety and efficacy of the procedure anddiminishing the complications. Different from theinterventions used in the past, most procedures areperformed today with the help of CT or MRIguiding. The high resolution of MRI provides theexact location of the target which declined thesevere adverse effects obviously. These proce-dures are relatively safe, minimally invasion,effective, with less side effects and complicationscomparing to prefrontal lobotomy. In 2007,Dr. Bomin et al. [54] presented the results of sur-gical treatment for 20 AN patients in whom pre-vious psychiatric and pharmaceutical therapieswere ineffective. Fifteen of these patients under-went bilateral NAcc DBS. Two months afterstimulation, anorexic patients gained between 17and 44 pounds, and many experienced significant
improvements in obsessive-compulsive behaviorsand symptoms of anxiety. Twelve patientswith thebinging-purging subtype ofANdid not experiencesignificant weight gain by 6 months after stimu-lation. These patients then received bilateralanterior capsulotomies, and showed significantimprovements in both in eating behavior andpsychiatric symptoms. Follow-up results at38 months were also reported for four AN patientswho received bilateral NAcc DBS [55]. Followingthese studies, several different centers havereported successful DBS and lesioning proceduresfor treatment of AN [50–53].
Two stereotactic procedures are commonlyused for AN: DBS and ablative procedures. DBStargets the NAcc or pre-and sub-callosal com-ponents (SCC) of the ACC, whereas ablativeprocedures include capsulotomy, NAcc lesion-ing, and cingulotomy (Fig. 15.1).
Fig. 15.1 MRI slices showing the typical lesions ofcapsulotomy, NAcc lesion, and cingulotomy. a Axialview of capsulotomy. b Coronal view of capsulotomy.
c Axial view of NAcc lesion. d Coronal view of NAcclesion. e Axial view of cingulotomy. f Coronal view ofcingulotomy
15 Surgical Treatments for Anorexia Nervosa 179

15.4.2 Deep Brain Stimulation
Deep brain stimulation (DBS) has been consid-ered as an effective treatment for a variety ofneurological and psychotic disorders refractoryto normal therapy, including Parkinson’s disease(PD), dystonia, tremor, and obsessive-compul-sive disorder (OCD) [56–59]. Deep brain stim-ulation (DBS) is a neurosurgical treatmentinvolving implantation of electrodes that sendelectrical impulses to specific locations in thebrain. Unlike ablative procedures, DBS is areversible intervention that causes less damage toneural tissue. Furthermore, most side effects arereversible and can be managed by adjustingstimulation parameters.
DBS is an innovative and promising approachfor the treatment of patients with treatment-refractory reward-related psychiatric disorders,DBS targets, such as the NAcc, the ventral cap-sule/ventral striatum (VC/VS), and SCC, havebeen used in the treatment of OCD, addiction,MDD, and AN. We demonstrated the efficacy ofDBS for AN, as DBS targeting the NAcc reducedexcessive hypermetabolism in the frontal lobe,hippocampus, and lentiform nucleus. Thesefindings suggest that DBS can reduce maladap-tive activity and connectivity in the stimulatedregion and restore diseased neural networks to ahealthy state [31].
To date, there are few publications regardingthe effects of DBS on AN. The first study (a caseseries) of DBS in AN was conducted by Wu et al.[55] in Shanghai. Four adolescent patients withAN treated with DBS of the NAcc exhibited anaverage 65 % increase in body weight (averagebaseline BMI: 11.9 kg/m2; average follow-upBMI: 19.6 kg/m2) at a 38-month follow-upexamination, and menstrual cycles were restoredwithin 11 months for all these patients. At thefinal follow up, where DBS systems are ex-planted 1 year after the battery has fully dis-charged, no recurrence of symptoms wasobserved; thus patients were in remissionaccording to Diagnostic and Statistical Manual ofMental Disorders-IV (DSM-IV) criteria. Wanget al. [60] report that ablation (6 AN patients) orDBS (2 patients) of the NAcc resulted in
restoration of menstruation within 9 months ofsurgery, and a recovery in BMI to within a nor-mal range ([18 kg/m2) within 12 months. Thesetwo preliminary studies demonstrate that DBS isa viable option for weight restoration in AN.
Recently, Lipsman et al. [32] published theresults of a phase 1 pilot trial of subcallosalcingulate (ACC) DBS in 6 adult patients withtreatment-refractory AN. They observed thatDBS was relatively safe in this population andresulted in improvements in mood, anxiety,affective regulation, and anorexia-related obses-sions and compulsions in 4 patients. At 9-monthfollow-up examinations, only 3 patients exhib-ited improved BMI’s relative to estimated his-torical baselines; menstruation status was notnoted.
Given the similarities in symptomatology andassociated neurocircuitry between OCD and AN,and the established efficacy of DBS for OCD[50, 51], we hypothesize that DBS of the NAccand other areas associated with reward, might beeffective in patients with chronic, treatmentrefractory AN, providing not only weight resto-ration, but also significant and sustainedimprovements in core AN symptoms and asso-ciated comorbidities and complications.
15.4.3 Ablative Procedures
As mentioned previously, not all treatment-refractory AN patients experience beneficialeffects from DBS, especially the binging-purgingsubtype, and those with long term ([10 years)AN. In these cases, lesion procedures, such ascapsulotomy and cingulotomy, should be con-sidered, as discussed below.
15.4.3.1 Anterior CapsulotomyAnterior capsulotomy is a stereotactic ablativeprocedure that involves specific lesions to dis-connect limbic circuits involved in differentpsychiatric disorders, such as OCD, MDD, andaddiction. Most patients exhibit relief of certainsymptoms and improved cognitive function,without experiencing alterations in personality[61–64].
180 B. Sun et al.
Anterior capsulotomy involves ablation of theanterior limb of the internal capsule to disconnectthe prefrontal cortex and subcortical nuclei(including the dorsomedial thalamus), and is awidely used psychosurgical procedure. Ablationsare performed by thermal coagulation or focalgamma radiation guided by computed tomogra-phy (CT) or magnetic resonance imaging (MRI).MRI is considered the best modality for locatingthe anterior capsule because of the large inter-individual differences in this structure. Targetsare first identified by visualization of the internalcapsule on stereotactic MRIs. Two bilateraltrepanations are then performed immediatelybehind the coronal suture and a lesion is createdby thermo-coagulation using radiofrequencyprobes reaching 80 °C for approximately 60 s.Lesions are typically 4 mm in diameter and10 mm in length along the contoured target.
A recent study reported the results of 1 patientwith OCD comorbid with AN who receivedbilateral anterior capsulotomy. The patientexperienced significant weight gain andimprovement in OCD symptoms at a 3 monthfollow-up examination [53]. In our institution, ofthe 150 patients who underwent capsulotomiesduring October 2005 to December 2013, 85 %experienced an improvement in symptoms, andmenstruation resumed in all female patients. Theresults suggest that this is a very promisingprocedure for treatment of AN. In contrast toDBS, bilateral capsulotomy can cause short-termside effects including incontinence, disorienta-tion, sleep-disorders, and refeeding syndrome.These symptoms usually resolve within 1 monthof the operation. A few patients (\5 %) experi-ence long-term side effects including memoryloss, fatigue, excessive weight gain, and per-sonality changes.
15.4.3.2 Anterior CingulotomyAnterior cingulotomy is one of the most popularpsychosurgical procedures currently performed inthe US [65, 66]. Clinicians based atMassachusettsGeneral Hospital have significant experience withcingulotomies for treatment of OCD orMDD, and
report very positive outcomes [66, 67]. Typicallylesions are created by thermo-coagulation throughradiofrequency probes reaching 80–85 °C for 90 s.The electrode is then withdrawn by 1.0 cm and thelesion is enlarged superiorly using the same lesionparameters. These steps are repeated for theopposite hemisphere. This produces symmetricalbilateral lesions of the ACC.
Cingulotomy is a relatively safe procedure witha lower incidence of adverse events than anteriorcapsulotomy. Immediate, transient symptomsinclude headache, confusion, and urinary incon-tinence. In our institution, anterior cingulotomiesare performed on AN patients only after a bilateralcapsulotomy has failed for at least 1 year, andapproximately half of these patients experiencepositive clinical outcomes with this procedure.
15.4.3.3 Lesioning of the NucleusAccumbens
Dysfunctions of the primary reward system are acentral feature of AN. The NAcc is a key com-ponent of this reward system, and may beimportant for progression of AN. NAcc DBS hasbeen successfully used for treatment of OCD,drug addiction, MDD, and AN. Wang et al. [60]reported the results of 6 AN patients treated withNAcc lesioning. One year after the operationpatients exhibited improved basic vital signs andBMI, restoration of menstruation, and improve-ments in the symptoms of depression, anxiety,and OCD. Although data were obtained from alimited number of cases, considering the suc-cessful reports of NAcc DBS, lesioning of theNAcc should be considered as a potential pro-cedure for treatment of refractory AN.
15.4.3.4 Combined Surgical ProceduresAs stated above, the majority of AN patientspresent with psychiatric comorbidities includingOCD, MDD, or anxiety disorders. Personalitydisorders and alcohol or substance abuse may alsobe present among those with the binging-purgingsubtype of AN. These parallel symptoms indicatethat there is a considerable overlap in rewardsystem neurocircuitry between these psychiatric
15 Surgical Treatments for Anorexia Nervosa 181
disorders and eating disorders. For some chronic,refractory AN patients, if the first surgical proce-dure has failed, a second surgery targeting areasincluding the NAcc, the anterior internal capsule,and the ACC, should be considered, which canlead to improvements in both core AN symptomsand associated comorbidities and complications.
NAcc DBS Combined with Anterior
Capsulotomy
Animal experiments suggest thatDBSof theNAccis a potential treatment option for AN either aloneor in combination with an anterior capsulotomy[68]. In our first series, of 15 AN patients treatedwith NAcc DBS, 12 cases experienced treatmentfailure and thus bilateral anterior capsulotomieswere performed at a second surgery. All thesepatients achieved a significant improvement inboth eating behaviors and psychiatric symptoms[54]. NAcc DBS combined with a bilateral orunilateral anterior capsulotomy is therefore a via-ble treatment option for severe, treatment-refrac-tory AN patients.
Anterior Capsulotomy Combined with
Anterior Cingulotomy
Given the successful results of anterior cingu-lotomy in OCD and anxiety, this procedureshould be considered as a potential second sur-gery for AN patients experiencing symptoms ofOCD, depression, or anxiety, following failure ofthe initial bilateral anterior capsulotomy. Nota-bly, of 12 patients at our institution in whombilateral anterior capsulotomies failed, an addi-tional anterior cingulotomy resulted in furtherimprovements in about half of these patients.
15.5 Grading of Anorexia Nervosaand Surgical Options
Patients with AN have elevated rates of lifetimediagnoses of anxiety disorders, MDD, OCD, per-sonality disorders, and substance abuse disorders.Severe comorbidities and longer disease durationcontribute to less favorable outcomes for AN.Based on data obtained from 180 cases of surgical
treatment for AN, we categorize AN into 4 gradesdepending on clinical characteristics, which inturn guide the selection of treatment options.
15.5.1 Grading of AN Accordingto Clinical Features
Grade I: Dieting and/or excessive exercise.Grade II: Dieting and at least one psychiatric
symptom such as OCD, anxiety, ordepression.
Grade III: Binge-eating and/or purging behaviors(self-induced vomiting or the misuse of lax-atives, diuretics), accompanied by psychiatricsymptoms including OCD, anxiety, ordepression.
Grade IV: Binge-eating and/or purging behaviors,accompanied by at least one of the followingsevere psychiatric disorders: substance abuse,kleptomania, promiscuity, self-injuriousbehavior, or a personality disorder.Note that if AN disease duration is longer than
6 years, the patient will be graded one levelhigher.
15.5.2 Selection of Surgical Treatment
Patient treatment options depend on the grade ofAN, as follows.Grade I: Psychotherapeutic interventions and
pharmacological therapies.Grade II: Psychotherapeutic interventions/phar-
macological therapies or/and bilateral NAccDBS.
Grade III: Bilateral anterior capsulotomy orbilateral NAcc ablation.
Grade IV: Bilateral anterior capsulotomy com-bined with bilateral anterior cingulotomy.
15.6 Indications and PatientSelection Criteria
Since there are few publications regarding patientselection criteria and limited data are available,
182 B. Sun et al.
there are no definite guidelines on AN patientselection criteria. However, the general consen-sus regarding selection criteria for surgery in ourinstitution is as follows:1. Patients must exhibit a consistent diagnosis of
AN, either the restricting or binge-purgingsubtype, as defined by DSM-IV criteria andbased on a psychiatric interview.
2. Patients must be confirmed as treatment-refractory AN. In our center, treatment-refractory AN is defined as follows. Firstly,patients must have been treated with anappropriate therapy for more than 3 years.Secondly, at least two types of therapy(including pharmacological treatment, behav-ioral therapy, and psychotherapy) must havebeen applied with no response. Lastly,patients must have experienced a rapiddecrease in body weight over a short timeperiod, which could be life threatening with-out effective intervention.
3. AN must be of disabling severity with sub-stantial functional impairment according toDSM-IV criterion C, and patients must exhi-bit a global assessment of functioning (GAF)score of 45 or less for at least 2 years.
4. Patient weight must be\85 % of ideal bodyweight (and/or BMI\ 17.5).
5. Patients or their representatives must bewilling to give informed consent for treatmentand any subsequent follow-up study.Exclusion criteria are as follows:
1. Unstable physical condition (severe electrolytedisturbances, cardiac failure, or other physicalcontraindications for surgery/anesthesia).
2. Patients with obvious encephalotrophy causedby Alzheimer’s disease, tumor, or trauma, asconfirmed by MRI.
3. Patients with any contraindication to MRI(pregnancy, pacemakers, or metal implantscontraindicated for MRI, not including theDBS implant and the stimulator itself).
4. Patients with severe heart disease or otherorganic problems contraindicated forneurosurgery.
5. Patients younger than 14 years.6. Refusal to sign the patient information and
consent form.
15.7 Perioperative PatientManagement
Considering the wide range of physiologicalabnormalities observed in AN, careful perioper-ative management is required.
15.7.1 Preoperative Management
As a result of long-term malnutrition, most ANpatients have an unstable physical conditionwhichis contraindicated for surgery or anesthesia. Theseconditions include severe electrolyte disturbances,cardiac failure, abnormal liver function, andcoagulation abnormalities, amongst others.Therefore, more detailed preoperative screeningexaminations such as electrocardiograms andappropriate blood tests (disseminated intravascu-lar coagulation tests, blood biochemical examin-ations, routine blood tests, blood glucose tests) areessential to assess potential medical risks.
According to our experiences, hypokalemiaand hypoalbuminemia are the most commonelectrolyte disorders, which should be restored tonormal conditions before surgery. In addition,most patients with AN exhibit comorbiditiessuch as OCD, depression, and anxiety. Themental status of AN patients is often unstable andpatients frequently present with irritation anddeep depression. Thus, patients must be closelymonitored throughout the entire procedure.
15.7.2 Intraoperative Management
Local anesthesia is recommended during the le-sioning procedure to avoid hypervolemia andexcessive dilution of electrolytes. For AN patientsreceiving DBS treatment, local and general anes-thesia are required. Considering the potentialanesthetic complications, a thorough preoperativeanesthetic assessment and evaluation is required.In addition, doses of most (anesthetic) drugsshould be adjusted for weight, and during theoperation, electrocardiographic changes andpotassium levels should be monitored carefully tominimize the risk of arrhythmias.
15 Surgical Treatments for Anorexia Nervosa 183
Specific caution must be taken during the burrhole procedure because the skull of AN patients isusually very thin; excessive pressure to the duramay cause epidural hematomas. To avoid cerebro-spinal fluid overflow during the operation, fibringlue should be applied immediately after openingthe dura. Furthermore, a warm air blower is nec-essary during the operation to maintain normalbody temperature. Lastly, the operation should becompleted in a timely manner and appropriate softmats should be applied to avoid bedsores.
15.7.3 Postoperative Management
Since patients with AN exhibit a very low bodyweight, strict control of rehydrationfluids should beobserved after surgery. According to our experi-ence, mannitol should not be administered consid-ering the risk of intracranial hemorrhage. Bloodtests should also bemonitored closely to avoid fluidand electrolyte disturbances. Pharmacologicaltherapies should be administered on the second dayafter surgery, but dosage should be adjusted basedon the patients’ symptoms; psychotherapeuticinterventions can be initiated 2 weeks after surgery.
15.8 Adverse Events Associatedwith Surgery for AnorexiaNervosa
Complications of stereotactic surgery in ANpatients can be classified into the followingsubtypes.
15.8.1 Operative Complications
Intracranial hematomas are a severe complicationof stereotactic surgery. In 216 cases of stereo-tactic surgery at our institution, four cases ofepidural hematoma were observed; three recov-ered after surgery and 1 patient died as a result ofdisseminated intravascular coagulation. Hemato-mas occur more frequently in AN patients than in
other disorders treated with stereotactic surgery,such as Parkinson’s disease, dystonia, OCD, andothers, likely as a result of the serious conditionof patients with AN.
Wound infections are more common afterDBS treatment than lesioning procedures as aresult of subcutaneous hydrops and subcutaneoushematomas in DBS. In our center, the rate ofwound infections is about 2 %, which is similarto other medical centers.
15.8.2 NeuropsychologicalComplications
Neuropsychological complications can be divi-ded into short-term and long-term complications.Short-term side effects include incontinence,disorientation, sleep disorders, and headache.These symptoms usually resolved within 1 or2 months of the operation. A number of patientsexperience long-term side effects includingmemory loss, fatigue, excessive weight gain, andpersonality changes.
15.8.3 DBS System-AssociatedComplications
In addition to surgical complications, hardwareproblems with the DBS system, including lead orwire fracture, hardware rejection, malfunction ofthe implantable pulse generator, and leadmigration, can occur. Bhatia et al. reviewed atotal of 191 patients who received 330 electrodeimplants and found that the overall incidence ofhardware-related problems was 4.2 %, based onthe total number of systems implanted. The meanduration between implantation and complicationwas 1.8 years [69]. Similar results were observedin our institution.
15.9 Conclusions and FutureOutlook
AN is a complex and severe, sometimes life-threatening, psychiatric disorder with a high rateof relapse under current therapies. Stereotactic
184 B. Sun et al.

surgery provides a viable option for treatment ofrefractory AN. Although positive outcomes havebeen reported for psychosurgery of refractoryAN, limited data on the surgical management ofAN patients are available, particularly in thecontext of experimental trials, and the safety andefficacy of psychosurgery remains under inves-tigation. Several concerns must be addressed tofurther the application of stereotactic surgery forAN. First, a deeper understanding of the exactetiology and neural circuit of AN must be elu-cidated. Second, a continuing evolution of ste-reotactic and functional techniques should bemaintained to reduce the unnecessary damage tothe brain. Finally, more specific psychometrictesting methods should be used to better definethe disorder and evaluate surgical outcomes.
Optimum indications for performing theseprocedures are conditions suitable for the creationof localized lesions capable of disconnectingspecific limbic system circuits. We have madeappreciable progress along this path, and bothstimulation of different brain centers and discon-nection of interconnecting pathways hold greatpotential for solving a significant proportion ofpsychiatric illnesses that do not respond to phar-macological therapy. Specifically, for OCD thereis sufficient evidence to support the view that ste-reotactic surgery via ablation or radiosurgery is asafe and efficacious option for treating casesrefractory to medication and cognitive therapy. Asis the case with other surgical procedures, adverseeffects and complications are gradually decreas-ing, and these lesioning techniques are gainingincreasing acceptance in psychiatry. The out-comes achieved, in particular the improved qualityof life of patients, are especially noteworthy.
Conflict of Interest Statement The authors declare thatthere are no conflicts of interest.
References
1. Steiner H, et al. Risk and protective factors forjuvenile eating disorders. Eur Child AdolescPsychiatry. 2003;12(Suppl 1):i38–46.
2. Yager J, Andersen AE. Clinical practice. Anorexianervosa. N Engl J Med. 2005;353(14):1481–8.
3. Keski-Rahkonen A, et al. Epidemiology and course ofanorexia nervosa in the community. Am J Psychiatry.2007;164(8):1259–65.
4. Hoek HW, van Hoeken D. Review of the prevalenceand incidence of eating disorders. Int J Eat Disord.2003;34(4):383–96.
5. Berkman ND, Lohr KN, Bulik CM. Outcomes ofeating disorders: a systematic review of the literature.Int J Eat Disord. 2007;40(4):293–309.
6. Forcano L, et al. Suicide attempts in anorexia nervosasubtypes. Compr Psychiatry. 2011;52(4):352–8.
7. Norrington A, et al. Medical management of acutesevere anorexia nervosa. Arch Dis Child Educ PractEd. 2012;97(2):48–54.
8. Herpertz-Dahlmann B. Adolescent eating disorders:definitions, symptomatology, epidemiology andcomorbidity. Child Adolesc Psychiatr Clin NorthAm. 2009;18(1):31–47.
9. Treasure J, Claudino AM, Zucker N. Eating disorders.Lancet. 2010;375(9714):583–93.
10. Bulik CM, et al. Alcohol use disorder comorbidity ineating disorders: a multicenter study. J ClinPsychiatry. 2004;65(7):1000–6.
11. Strober M, Freeman R, Morrell W. The long-termcourse of severe anorexia nervosa in adolescents:Survival analysis of recovery, relapse, and outcomepredictors over 10–15 years in a prospective study. IntJ Eat Disord. 1997;22(4):339–60.
12. SteinhausenHC.Theoutcomeof anorexia nervosa in the20th century. Am J Psychiatry. 2002;159(8):1284–93.
13. Herzog DB, et al. Recovery and relapse in anorexia andbulimia nervosa: a 7.5-year follow-up study. J AmAcadChild Adolesc Psychiatry. 1999;38(7):829–37.
14. Connan F, et al. A neurodevelopmental model foranorexia nervosa. Physiol Behav. 2003;79(1):13–24.
15. Clarke TK, Weiss AR, Berrettini WH. The genetics ofanorexia nervosa. Clin Pharmacol Ther. 2012;91(2):181–8.
16. Noordenbos G, Seubring A. Criteria for recoveryfrom eating disorders according to patients andtherapists. Eat Disord. 2006;14(1):41–54.
17. Kaye WH, et al. Neurocircuity of eating disorders.Curr Top Behav Neurosci. 2011;6:37–57.
18. Kaye WH, Fudge JL, Paulus M. New insights intosymptoms and neurocircuit function of anorexianervosa. Nat Rev Neurosci. 2009;10(8):573–84.
19. Frank GK, et al. Increased dopamine D2/D3 receptorbinding after recovery from anorexia nervosameasured by Positron emission tomography and[11C] raclopride. Biol Psychiatry. 2005;58(11):908–12.
20. Kaye WH, et al. Nothing tastes as good as skinnyfeels: the neurobiology of anorexia nervosa. TrendsNeurosci. 2013;36(2):110–20.
21. Friederich HC, et al. Neurocircuit function in eatingdisorders. Int J Eat Disord. 2013;46(5):425–32.
22. Kaye WH, et al. Abnormalities in CNS monoaminemetabolism in anorexia nervosa. Arch GenPsychiatry. 1984;41(4):350–5.
15 Surgical Treatments for Anorexia Nervosa 185
23. Bergen AW, et al. Association of multiple DRD2polymorphisms with anorexia nervosa.Neuropsychopharmacology. 2005;30(9):1703–10.
24. Friederich HC, et al. Differential motivationalresponses to food and pleasurable cues in anorexiaand bulimia nervosa: a startle reflex paradigm.Psychol Med. 2006;36(9):1327–35.
25. Halford JC, Cooper GD, Dovey TM. Thepharmacology of human appetite expression. CurrDrug Targets. 2004;5(3):221–40.
26. Nunn K, et al. The fault is not in her parents but in herinsula–a neurobiological hypothesis of anorexianervosa. Eur Eat Disord Rev. 2008;16(5):355–60.
27. Phillips ML, et al. Neurobiology of emotionperception II: Implications for major psychiatricdisorders. Biol Psychiatry. 2003;54(5):515–28.
28. Phillips ML, et al. Neurobiology of emotionperception I: the neural basis of normal emotionperception. Biol Psychiatry. 2003;54(5):504–14.
29. Shin LM, Liberzon I. The neurocircuitry of fear,stress, and anxiety disorders. Neuropsycho-pharmacology. 2010;35(1):169–91.
30. Giel KE, et al. Attentional processing of food picturesin individuals with anorexia nervosa–an eye-trackingstudy. Biol Psychiatry. 2011;69(7):661–7.
31. Zhang H-W, et al. Metabolic imaging of deep brainstimulation in anorexia nervosa: a 18F-FDG PET/CTstudy. Clin Nucl Med. 2013;38(12):943–8.
32. Lipsman N, et al. Subcallosal cingulate deep brainstimulation for treatment-refractory anorexia nervosa:a phase 1 pilot trial. Lancet. 2013;381(9875):1361–70.
33. Frank GK. Altered brain reward circuits in eatingdisorders: chicken or egg? Curr Psychiatry Rep.2013;15(10):396.
34. Focker M, Knoll S, Hebebrand J. Anorexia nervosa.Eur Child Adolesc Psychiatry. 2013;22:S29–35.
35. Guarda AS. Treatment of anorexia nervosa: insightsand obstacles. Physiol Behav. 2008;94(1):113–20.
36. Wade TD, Treasure J, Schmidt U. A case seriesevaluation of the Maudsley model for treatment ofadults with anorexia nervosa. Eur Eat Disord Rev.2011;19(5):382–9.
37. Bulik CM, et al. Anorexia nervosa treatment: asystematic review of randomized controlled trials. IntJ Eat Disord. 2007;40(4):310–20.
38. Brewerton TD. Antipsychotic agents in the treatmentof anorexia nervosa: neuropsychopharmacologicrationale and evidence from controlled trials. CurrPsychiatry Rep. 2012;14(4):398–405.
39. McKnight RF, Park RJ. Atypical antipsychotics andanorexia nervosa: a review. Eur Eat Disord Rev.2010;18(1):10–21.
40. Wilson GT, Shafran R. Eating disorders guidelinesfrom NICE. Lancet. 2005;365(9453):79–81.
41. Couturier J, Lock J. What is recovery in adolescentanorexia nervosa? Int J Eat Disord. 2006;39(7):550–5.
42. Drury MO. An emergency leucotomy. Br Med J.1950;2(4679):609.
43. Crisp AH, Kalucy RS. The effect of leucotomy inintractable adolescent weight phobia (primary anorexianervosa). Postgrad Med J. 1973;49(578):883–93.
44. Morgan JF, Crisp AH. Use of leucotomy forintractable anorexia nervosa: a long-term follow-upstudy. Int J Eat Disord. 2000;27(3):249–58.
45. Birley JL. Modified frontal leucotomy: a review of106 cases. Br J Psychiatry. 1964;110:211–21.
46. Carmody JT, Vibber FL. Anorexia nervosa treated byprefrontal lobotomy. Ann Intern Med. 1952;36(2:2):647–52.
47. Kay DW. Anorexia nervosa: a study in prognosis.Proc R Soc Med. 1953;46(8):669–74.
48. Sargant W. Leucotomy in psychosomatic disorders.Lancet. 1951;2(6673):87–91.
49. Sifneos PE. A case of anorexia nervosa treatedsuccessfully by leucotomy. Am J Psychiatry.1952;109(5):356–60.
50. Zamboni R, et al. Dorsomedial thalamotomy as atreatment for terminal anorexia: a report of 2 cases.Acta Neurochirurgica. 1993;34–35.
51. Kelly D, Mitchell-Heggs N. Stereotactic limbicleucotomy—a follow-up study of thirty patients.Postgrad Med J. 1973;49(578):865–82.
52. Mitchell-Heggs N, Kelly D, Richardson A.Stereotactic limbic leucotomy–a follow-up at 16months. Br J Psychiatry. 1976;128:226–40.
53. Barbier J, et al. Successful anterior capsulotomy incomorbid anorexia nervosa and obsessive-compulsivedisorder: case report. Neurosurgery. 2011;69(3):E745–51; discussion E751.
54. Bomin S, Li D, Zhan S (2007) DBS for anorexianervosa. The eighth world congress of InternationalNeuromodulation Society. Acapulco, Mexico.
55. Wu H, et al. Deep-brain stimulation for anorexianervosa. World Neurosurg. 2012;80(3-4):S29 e1–10.
56. Deuschl G, et al. A randomized trial of deep-brainstimulation for Parkinson’s disease. N Engl J Med.2006;355(9):896–908.
57. Mueller J, et al. Pallidal deep brain stimulationimproves quality of life in segmental and generalizeddystonia: results from a prospective, randomized sham-controlled trial. Mov Disord. 2008;23(1):131–4.
58. O’Sullivan D, Pell M. Long-term follow-up of DBSof thalamus for tremor and STN for Parkinson’sdisease. Brain Res Bull. 2009;78(2–3):119–21.
59. Goodman WK, Alterman RL. Deep brain stimulationfor intractable psychiatric disorders. Annu Rev Med.2011;63:511–24.
60. Wang J, et al. Treatment of intractable anorexianervosa with inactivation of the nucleus accumbensusing stereotactic surgery. Stereotact FunctNeurosurg. 2013;91(6):364–72.
61. Zhan S, et al. Long-term follow-up of bilateralanterior capsulotomy in patients with refractoryobsessive-compulsive disorder. Clin NeurolNeurosurg. 2014;119:91–5.
62. Zuo C, et al. Metabolic imaging of bilateral anteriorcapsulotomy in refractory obsessive compulsive
186 B. Sun et al.

disorder: an FDG PET study. J Cereb Blood FlowMetab. 2013;33(6):880–7.
63. Christmas D, et al. Long term outcome of thermalanterior capsulotomy for chronic, treatment refractorydepression. J Neurol Neurosurg Psychiatry. 2011;82(6):594–600.
64. Hurwitz TA, et al. Bilateral anterior capsulotomy forintractable depression. J Neuropsychiatry ClinNeurosci. 2012;24(2):176–82.
65. Cosgrove GR, Rauch SL. Stereotactic cingulotomy.Neurosurg Clin N Am. 2003;14(2):225–35.
66. Dougherty DD, et al. Prospective long-term follow-upof 44 patients who received cingulotomy for
treatment-refractory obsessive-compulsive disorder.Am J Psychiatry. 2002;159(2):269–75.
67. Baer L, et al. Cingulotomy for intractable obsessive-compulsive disorder. Prospective long-term follow-upof 18 patients. Arch Gen Psychiatry. 1995;52(5):384–92.
68. van der Plasse G, et al. Deep brain stimulation reveals adissociation of consummatory and motivated behaviourin the medial and lateral nucleus accumbens shell of therat. PLoS One. 2012;7(3):e33455.
69. Bhatia S, et al. Surgical complications of deep brainstimulation. Stereotact Funct Neurosurg. 2008;86(6):367–72.
15 Surgical Treatments for Anorexia Nervosa 187

16Neurosurgery for the Treatmentof Refractory Schizophrenia
Bomin Sun, Wei Liu, Shikun Zhan, Qianqian Hao,Dianyou Li, Yixin Pan, Yongchao Li and Guozhen Lin
Abstract
Schizophrenia is a chronic, severe, and disabling psychiatric disease that ischaracterized by perturbations in cognition, affect, and behavior. Of themany available treatments, pharmaceutical interventions remain as firstchoice-treatments. However, about 20 % of patients with schizophreniaexhibit refractory schizophrenia that does not respond well to pharma-ceutical treatments. As a result, neurosurgery performed for the treatmentof refractory schizophrenia, also called psychosurgery, is an alternativetreatment that has a long history. With the refinement and improvedaccuracy of neuroimaging techniques, modern psychosurgery has greatersuccess with fewer risks. Nevertheless, these procedures are still invasivemethods and the resulting lesions are irreversible. Therefore, we mustkeep in mind that surgical therapy should only be considered as asupplementary part of the comprehensive treatment of schizophrenia andthe inclusion criteria for surgery must be strict.
16.1 Introduction
Schizophrenia, which was also called “dementiapraecox” by Emil Kraepelin, a German psychia-trist in the late nineteenth and early twentiethcentury, is a chronic, severe, and disabling mental
disorder characterized by perturbations in cogni-tion, affect, and behavior. It is diagnosed on thebasis of a series of clinical psychiatric symptomssuch as auditory hallucinations, paranoia, or dis-organized speech and thinking. Symptoms ofschizophrenia typically emerge in adolescenceand early adulthood, with a global lifetime prev-alence of about 0.30–0.66 % [1]. Schizophreniadoes not only affect mental health, but also neg-atively impacts physical health, shortening thelife expectancy of patients with schizophrenia by12–15 years compared to the general population;this gap has also widened over recent decades [2].Therefore, schizophrenia causes more loss of lifethan most cancers and physical illnesses. Fur-thermore, it is one of the most burdening andcostly illnesses worldwide [3–5].
B. Sun (&) � W. Liu � S. Zhan � Q. Hao � D. Li �Y. PanDepartment of Functional Neurosurgery, RuijinHospital, School of Medicine, Shanghai Jiao TongUniversity, Shanghai, China
Y. Li � G. LinDepartment of Psychiatry, Ruijin Hospital, School ofMedicine, Shanghai Jiao Tong University, Shanghai,China
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0_16© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
189
The exact mechanisms underlying schizo-phrenia are still unclear. However, scientists havelong known that genetic factors play an impor-tant role in the development of schizophrenia.The illness occurs in less than 1 % of the generalpopulation, but, interestingly, it occurs in about10 % of people who have a first-degree relativewith the disorder. Monozygotic twins have aconcordance rate of about 50 % [6]. Besidesgenetic susceptibility, many environmental fac-tors may be involved in the development ofschizophrenia, such as exposure to viruses, dif-ficulties during birth, and other unknown psy-chosocial factors. Therefore, most researchersbelieve that interactions between genes and theenvironment are necessary for the developmentof schizophrenia.
There are many hypotheses to explain theunderlying mechanisms of schizophrenia. Ros-sum [7] first presented the dopamine (DA)hypothesis of schizophrenia based on the obser-vation that antipsychotics may block DA recep-tors. Subsequently, accumulating evidencesupported the idea that schizophrenia is associ-ated with frontal-subcortical neuronal circuits,especially the orbito-frontal and anterior cingu-late circuits [8–11]. The orbito-frontal circuitprojects to the ventromedial caudate nucleus andthe anterior cingulate circuit sends fibers to theventral striatum, which includes the ventromedialcaudate, ventral putamen, nucleus accumbens,and olfactory tubercle. These circuits primarilyuse DA as a neurotransmitter, and process cor-tical-subcortical emotional information. Disrupt-ing these circuits can thus trigger the onset ofschizophrenia’s positive symptoms. Besides theDA hypothesis, it was reported that the seroto-ninergic system plays an important role in thenegative symptoms of schizophrenia. Serotonin-ergic neurons from the dorsal and median raphenucleus project to the prefrontal cortex (PFC),and the PFC sends projections back to the raphenuclei providing feedback control of corticalserotonin release. Serotonin could stimulate 5-HT2A receptors in the PFC that inhibits theactivity of dopaminergic neurons in this area.
At present, pharmaceutical treatment is the firstoption pursued in schizophrenia. The first-linedrugs used in schizophrenia include: Haloperidol,Perphenazine, Chlorpromazine, Risperidone,Aripiprazole, Clozapine, and Olanzapine. Amongthese drugs, Haloperidol, Perphenazine, andChlorpromazine are first-generation antipsychot-ics, while the remainder are second-generationantipsychotics. Although controversy remainsover the higher rate of effectiveness of second-generation antipsychotics, the use of drugs such asClozapine and Olanzapine has grown due to theirinducing fewer side effects. Medication usuallyshows good results in the treatment of positivesymptoms of schizophrenia while negativesymptoms are generally less receptive to similartreatment. Besides medication, family therapy,supported employment, skills training, and otherpsychosocial interventions may be helpful in thetreatment of schizophrenia [12–15]. However,approximately 20 % of schizophrenics remainnon-responsive to any of the aforementionedtreatments [16]. For refractory schizophrenia,psychosurgery, also called neurosurgery formental disorders, is considered as a last resort. Inthis chapter, we briefly introduce the history,indications, optimal surgical target, surgical pro-cedure, and surgical results of psychosurgeryapplied in schizophrenia.
16.2 A Brief Historyof Psychosurgery
Psychosurgery, including the lesion and stimu-lation techniques, has a long and storied historywhich can be traced back to ancient times. Askull with a trepanation hole identified in Francehas been carbon dated to the Neolithic period ofthe Stone Age, or approximately 5100 BC [17].Signs of healing in the skull indicate a surgicalrather than a traumatic origin of the wound.Literature on trephination for the relief of neu-ropsychiatric symptoms stemming from mentaldisorders can be dated back to 1500 BC [18].
190 B. Sun et al.
In the modern era, the links between the brainand behavior was brought into cultural awarenessthrough the famous account of Phineas P. Gage,a railroad worker in Vermont. Gage experienceda terrible explosion that caused severe headtrauma. He miraculously survived, but his per-sonality was profoundly altered [19]. The firstpsychosurgical procedure was performed in 1888by Swiss psychiatrist Gottlieb Burckhardt, whocontributed widely to the birth of modern psy-chosurgery. The process involved the excision ofcerebrum at multiple foci in frontal, parietal, andtemporal cortices. The results of six cases rangedfrom success (in three patients) to failure (in onefatal case) [20]. Almost 50 years later, the Por-tuguese neurologist Egas Moniz, who is oftenregarded as the founder of psychosurgery, per-formed the first prefrontal lobotomy in 1935 withthe help of neurosurgeon Almeida Lima. Differ-ent from the psychosurgical interventions per-formed by Burckhardt, Moniz’s surgery focusedon the white matter of the brain and garneredgreat attention worldwide. He won the NobelPrize for Medicine in 1949, which is still highlycontroversial today. In the United States, Free-man and Watts introduced the prefrontal lobot-omy in 1942. There was an upsurge in surgicalinterventions between 1943 and 1954 because ofthe lack of effective psychopharmacologicalagents and the large social and financial burdensof psychiatric illness.
However, with the introduction of newer psy-chotropic medications, such as chlorpromazine,and the growing realization of severe surgical sideeffects, psychosurgery lost its popularity as atreatment [21]. Although stereotactic and func-tional neurosurgery for alleviating psychiatricdisorders was maturing due to the development ofstereotactic neurosurgical devices and neuroim-aging, it is approved only in specific circum-stances and performed only in a few specializedcenters across the globe, largely as a precautionagainst widespread abuse similar to that of theprefrontal lobotomy. Several procedures includ-ing anterior capsulotomy, anterior cingulotomy,amygdaloidotomy, subcaudate tractotomy, and
limbic leucotomy have been sparingly applied inschizophrenia patients [18, 22–26]. Different fromthe interventions used in the past, most procedurestoday are performed with the help of CT or MRIguidance. The high-resolution of MRI providesthe exact location of the target, which has reducedthe severe adverse effects. These procedures arerelatively safe, minimally invasive, effective, andhave fewer side effects and complications com-pared to the prefrontal lobotomy.
16.3 Patient Selection Criteria
Patient selection criteria are strict for treatingrefractory schizophrenia (TRS). A general con-sensus about the selection criteria for TRS sur-gery in our center is summarized below:1. Patients diagnosed with schizophrenia in the
Department of Psychiatry by independentpsychiatrists according to the DSM-IV.
2. Refractory schizophrenia patients confirmedby a team of psychiatrists, neurosurgeons, andneurologists and proposed for neurosurgicaltreatment. In our center, refractory schizo-phrenia is defined as follows:(I) Illness severity with a score of ≥35 on
the 18-item Brief Psychiatric RatingScale (BPRS, scored 1–7) and a clinicalglobal impression (CGI)[4.
(II) At least three periods of treatment in thethree preceding years with neurolepticagents (at least two different chemicalclasses) at dosages equivalent to orgreater than 500 mg/d of Chlorproma-zine for a period of 8 weeks, eachwithout significant symptomatic relief.
(III) Duration of mental disorder[3 yearsand no period of good function.
3. Patients or their representatives must be ableand willing to give informed consent and havethe support of their family.
4. Patients are between the ages of 18 and60 years old.
5. Pregnant women are excluded.
16 Neurosurgery for the Treatment of Refractory Schizophrenia 191
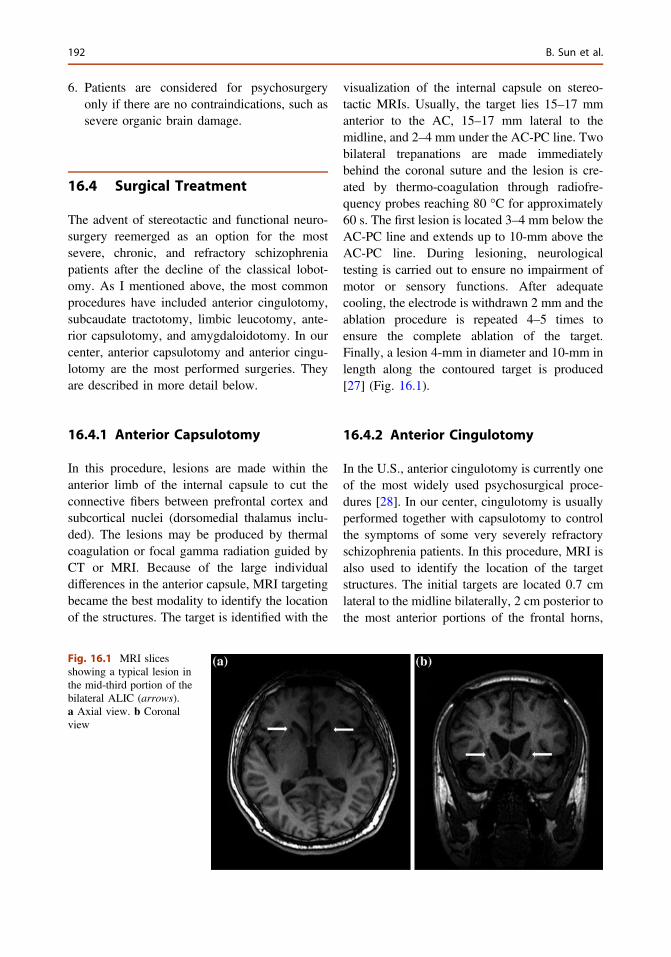
6. Patients are considered for psychosurgeryonly if there are no contraindications, such assevere organic brain damage.
16.4 Surgical Treatment
The advent of stereotactic and functional neuro-surgery reemerged as an option for the mostsevere, chronic, and refractory schizophreniapatients after the decline of the classical lobot-omy. As I mentioned above, the most commonprocedures have included anterior cingulotomy,subcaudate tractotomy, limbic leucotomy, ante-rior capsulotomy, and amygdaloidotomy. In ourcenter, anterior capsulotomy and anterior cingu-lotomy are the most performed surgeries. Theyare described in more detail below.
16.4.1 Anterior Capsulotomy
In this procedure, lesions are made within theanterior limb of the internal capsule to cut theconnective fibers between prefrontal cortex andsubcortical nuclei (dorsomedial thalamus inclu-ded). The lesions may be produced by thermalcoagulation or focal gamma radiation guided byCT or MRI. Because of the large individualdifferences in the anterior capsule, MRI targetingbecame the best modality to identify the locationof the structures. The target is identified with the
visualization of the internal capsule on stereo-tactic MRIs. Usually, the target lies 15–17 mmanterior to the AC, 15–17 mm lateral to themidline, and 2–4 mm under the AC-PC line. Twobilateral trepanations are made immediatelybehind the coronal suture and the lesion is cre-ated by thermo-coagulation through radiofre-quency probes reaching 80 °C for approximately60 s. The first lesion is located 3–4 mm below theAC-PC line and extends up to 10-mm above theAC-PC line. During lesioning, neurologicaltesting is carried out to ensure no impairment ofmotor or sensory functions. After adequatecooling, the electrode is withdrawn 2 mm and theablation procedure is repeated 4–5 times toensure the complete ablation of the target.Finally, a lesion 4-mm in diameter and 10-mm inlength along the contoured target is produced[27] (Fig. 16.1).
16.4.2 Anterior Cingulotomy
In the U.S., anterior cingulotomy is currently oneof the most widely used psychosurgical proce-dures [28]. In our center, cingulotomy is usuallyperformed together with capsulotomy to controlthe symptoms of some very severely refractoryschizophrenia patients. In this procedure, MRI isalso used to identify the location of the targetstructures. The initial targets are located 0.7 cmlateral to the midline bilaterally, 2 cm posterior tothe most anterior portions of the frontal horns,
Fig. 16.1 MRI slicesshowing a typical lesion inthe mid-third portion of thebilateral ALIC (arrows).a Axial view. b Coronalview
192 B. Sun et al.
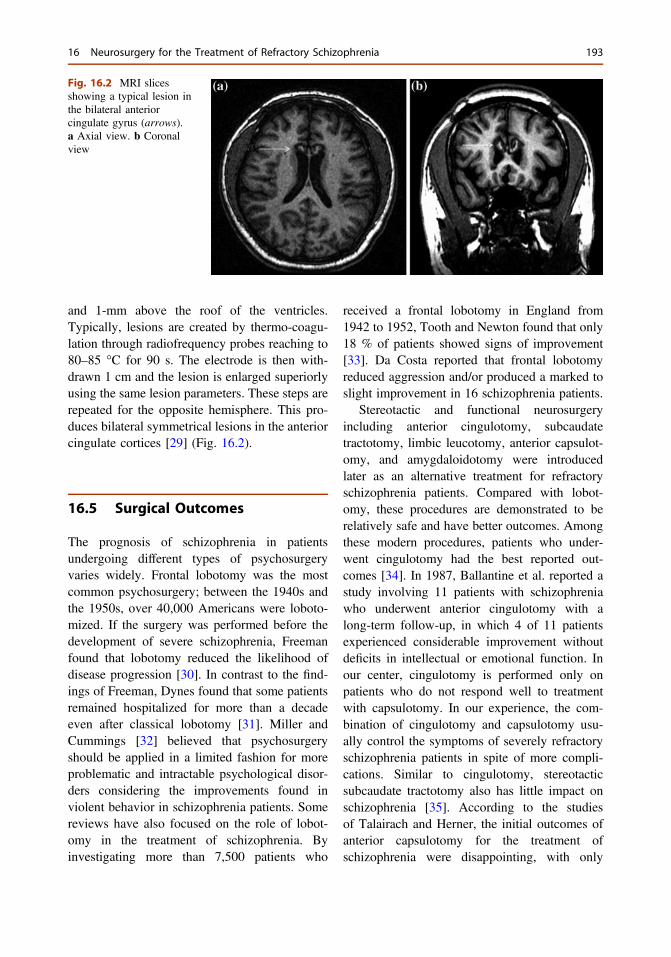
and 1-mm above the roof of the ventricles.Typically, lesions are created by thermo-coagu-lation through radiofrequency probes reaching to80–85 °C for 90 s. The electrode is then with-drawn 1 cm and the lesion is enlarged superiorlyusing the same lesion parameters. These steps arerepeated for the opposite hemisphere. This pro-duces bilateral symmetrical lesions in the anteriorcingulate cortices [29] (Fig. 16.2).
16.5 Surgical Outcomes
The prognosis of schizophrenia in patientsundergoing different types of psychosurgeryvaries widely. Frontal lobotomy was the mostcommon psychosurgery; between the 1940s andthe 1950s, over 40,000 Americans were loboto-mized. If the surgery was performed before thedevelopment of severe schizophrenia, Freemanfound that lobotomy reduced the likelihood ofdisease progression [30]. In contrast to the find-ings of Freeman, Dynes found that some patientsremained hospitalized for more than a decadeeven after classical lobotomy [31]. Miller andCummings [32] believed that psychosurgeryshould be applied in a limited fashion for moreproblematic and intractable psychological disor-ders considering the improvements found inviolent behavior in schizophrenia patients. Somereviews have also focused on the role of lobot-omy in the treatment of schizophrenia. Byinvestigating more than 7,500 patients who
received a frontal lobotomy in England from1942 to 1952, Tooth and Newton found that only18 % of patients showed signs of improvement[33]. Da Costa reported that frontal lobotomyreduced aggression and/or produced a marked toslight improvement in 16 schizophrenia patients.
Stereotactic and functional neurosurgeryincluding anterior cingulotomy, subcaudatetractotomy, limbic leucotomy, anterior capsulot-omy, and amygdaloidotomy were introducedlater as an alternative treatment for refractoryschizophrenia patients. Compared with lobot-omy, these procedures are demonstrated to berelatively safe and have better outcomes. Amongthese modern procedures, patients who under-went cingulotomy had the best reported out-comes [34]. In 1987, Ballantine et al. reported astudy involving 11 patients with schizophreniawho underwent anterior cingulotomy with along-term follow-up, in which 4 of 11 patientsexperienced considerable improvement withoutdeficits in intellectual or emotional function. Inour center, cingulotomy is performed only onpatients who do not respond well to treatmentwith capsulotomy. In our experience, the com-bination of cingulotomy and capsulotomy usu-ally control the symptoms of severely refractoryschizophrenia patients in spite of more compli-cations. Similar to cingulotomy, stereotacticsubcaudate tractotomy also has little impact onschizophrenia [35]. According to the studiesof Talairach and Herner, the initial outcomes ofanterior capsulotomy for the treatment ofschizophrenia were disappointing, with only
Fig. 16.2 MRI slicesshowing a typical lesion inthe bilateral anteriorcingulate gyrus (arrows).a Axial view. b Coronalview
16 Neurosurgery for the Treatment of Refractory Schizophrenia 193
27 % of patients having a positive response.However, we find better results with anteriorcapsulotomy in our schizophrenia patients. In ourcenter, 100 refractory schizophrenia patients whomet the inclusion criteria (see Patient SelectionCriteria above) were treated with capsulotomyguided by MRI; 74 % of such patients demon-strated improvements. The accurate target local-ization with the help of MRI greatly contributesto the improved outcomes of capsulotomy. Am-ygdaloidotomy is usually used in schizophreniapatients with severely aggressive behavior and alarge percentage of cases showed a markedreduction in aggressive behavior [36]. In ourcenter, amygdaloidotomy is restricted to refrac-tory schizophrenia patients with severelyaggressive behavior. The results are consistentwith the aforementioned study. Besides ourcenter, many neurosurgeons in China have alsoapplied stereotactic surgery in schizophreniapatients (see Table 16.1).
16.6 Complications
The classical lobotomy had a high rate of com-plications [18, 37–39]. The short-term compli-cations included confusion, frailty, and languor.The long-term sequelae, which were known as“frontal lobe syndrome”, included inertia, apa-thy, social withdrawal, and attention deficits.Furthermore, some patients developed epilepsypostoperatively and hemorrhage was anotherseverely adverse effect, which was sometimesfatal. As a consequence, most neurosurgeonsagreed that frontal lobotomy was not a beneficialintervention. With the introduction of stereotacticand functional neurosurgery, complications havebeen greatly reduced and capsulotomy is con-sidered the safest procedure. Rare complicationsincluding fatigue, loss of initiative, memorydeficits, weight gain, and intracranial hemorrhagehave been reported following anterior capsulot-omy. In our experience, fatigue, loss of initiative,and memory deficits are observed postopera-tively and recover in a few months, while intra-cranial hemorrhage and epilepsy are rarely seen
after the surgery. Cingulotomy is also quite safeand no severe complications such as hemiplegia,aphasia, or death directly caused by cingulotomyhave been reported [40]. Teuber et al. [41]reviewed the results of cingulotomy in a widerange of patients and found a small incidence ofpermanent cognitive deficits. Similar to cingu-lotomy, stereotactic subcaudate tractotomy doesnot produce deficits in intellectual or emotionalfunction [42, 43].
16.7 New Developments
Deep brain stimulation (DBS) is a new form ofneurosurgery that was originally developed totreat Parkinson’s disease (PD) and is emerging asa potential treatment for some mental disorders.Compared to ablative neurosurgery, DBS has theadvantage of reversibility and adjustability; theparameters of the stimulation can be changed andthe electrodes can be removed from the brain.DBS has been applied in obsessive and com-pulsive disease (OCD), and major depression[44–48]. To the best of our knowledge, there areno published articles focused on the applicationof DBS in schizophrenia patients. Importantly,DBS testing using schizophrenia animal modelsis increasing. Perez et al. [49] provided initialpreclinical evidence demonstrating the feasibilityof hippocampal DBS as a potential novelapproach for the treatment of schizophrenia byimplanting the electrodes in the ventral hippo-campus in a rodent model of schizophrenia.Similar results were found by Ewing et al. [50].Besides the hippocampus, the mediodorsal tha-lamic nucleus and nucleus accumbens are alsoconsidered potential targets of DBS in the treat-ment of schizophrenia [51, 52]. Furthermore, aclinical study of DBS application in schizophre-nia in humans aimed at the nucleus accumbens/ventral striatum and ventral tegmental area hasalready been registered (ClinicalTrials.gov Iden-tifier: NCT01725334). As in the development ofneuroimaging, the improved targeting efficiencyof DBS in schizophrenia now deserves increasedattention.
194 B. Sun et al.
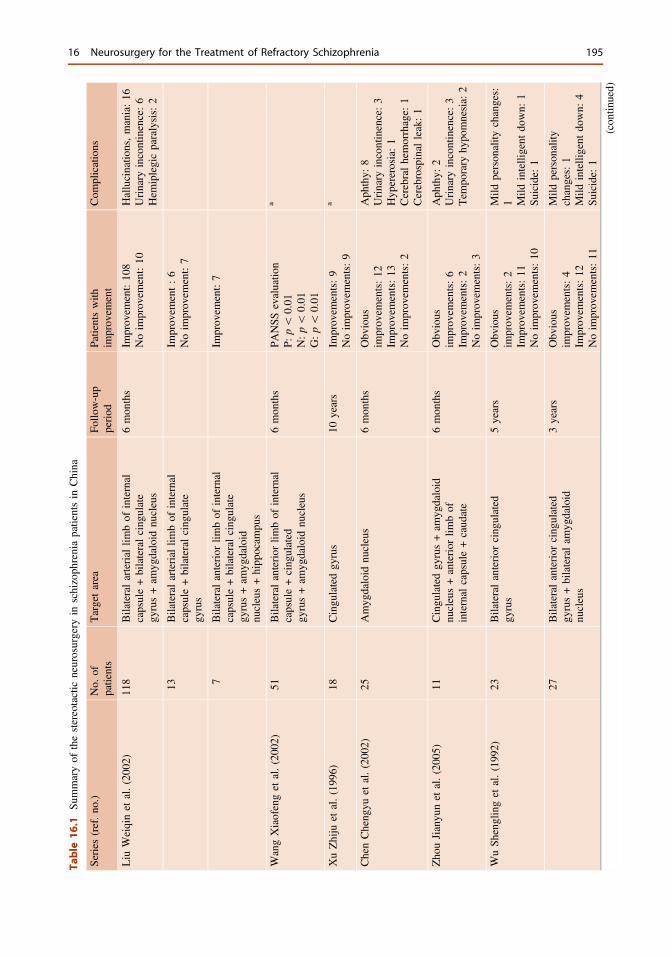
Table
16.1
Summaryof
thestereotactic
neurosurgery
inschizoph
reniapatientsin
China
Series
(ref.no
.)No.
ofpatients
Targetarea
Follo
w-up
period
Patientswith
improv
ement
Com
plications
Liu
Weiqinet
al.(200
2)11
8Bilateralarterial
limbof
internal
capsule+bilateralcing
ulate
gyrus+am
ygdaloid
nucleus
6mon
ths
Improv
ement:10
8Noim
prov
ement:10
Hallucinatio
ns,mania:16
Urinary
incontinence:6
Hem
iplegicparalysis:2
13Bilateralarterial
limbof
internal
capsule+bilateralcing
ulate
gyrus
Improv
ement:6
Noim
prov
ement:7
7Bilateralanterior
limbof
internal
capsule+bilateralcing
ulate
gyrus+am
ygdaloid
nucleus+hipp
ocam
pus
Improv
ement:7
WangXiaofenget
al.(200
2)51
Bilateralanterior
limbof
internal
capsule+cing
ulated
gyrus+am
ygdaloid
nucleus
6mon
ths
PANSS
evaluatio
nP:
p\
0.01
N:p\
0.01
G:p\
0.01
a
XuZhiju
etal.(199
6)18
Cingu
latedgy
rus
10years
Improv
ements:9
Noim
prov
ements:9
a
ChenCheng
yuet
al.(200
2)25
Amyg
daloid
nucleus
6mon
ths
Obv
ious
improv
ements:12
Improv
ements:13
Noim
prov
ements:2
Aph
thy:
8Urinary
incontinence:3
Hyp
ererosia:1
Cerebralhemorrhage:
1Cerebrospinal
leak:1
Zho
uJianyu
net
al.(200
5)11
Cingu
latedgy
rus+am
ygdaloid
nucleus+anterior
limbof
internal
capsule+caud
ate
6mon
ths
Obv
ious
improv
ements:6
Improv
ements:2
Noim
prov
ements:3
Aph
thy:
2Urinary
incontinence:3
Tem
porary
hypo
mnesia:
2
WuSh
englinget
al.(199
2)23
Bilateralanterior
cing
ulated
gyrus
5years
Obv
ious
improv
ements:2
Improv
ements:11
Noim
prov
ements:10
Mild
person
ality
changes:
1 Mild
intelligent
down:
1Su
icide:
1
27Bilateralanterior
cing
ulated
gyrus+bilateralam
ygdaloid
nucleus
3years
Obv
ious
improv
ements:4
Improv
ements:12
Noim
prov
ements:11
Mild
person
ality
changes:1
Mild
intelligent
down:
4Su
icide:
1
(con
tinued)
16 Neurosurgery for the Treatment of Refractory Schizophrenia 195
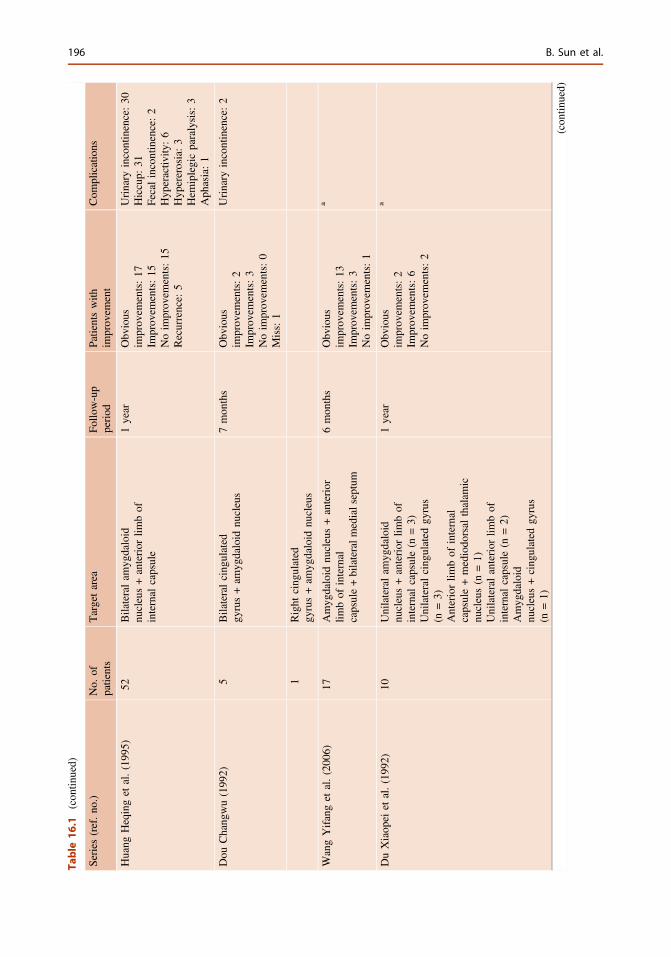
Table
16.1
(con
tinued)
Series
(ref.no
.)No.
ofpatients
Targetarea
Follo
w-up
period
Patientswith
improv
ement
Com
plications
Huang
Heqinget
al.(199
5)52
Bilateralam
ygdaloid
nucleus+anterior
limbof
internal
capsule
1year
Obv
ious
improv
ements:17
Improv
ements:15
Noim
prov
ements:15
Recurrence:
5
Urinary
incontinence:30
Hiccup:
31Fecalincontinence:2
Hyp
eractiv
ity:6
Hyp
ererosia:3
Hem
iplegicparalysis:3
Aph
asia:1
Dou
Chang
wu(199
2)5
Bilateralcing
ulated
gyrus+am
ygdaloid
nucleus
7mon
ths
Obv
ious
improv
ements:2
Improv
ements:3
Noim
prov
ements:0
Miss:1
Urinary
incontinence:2
1Right
cing
ulated
gyrus+am
ygdaloid
nucleus
WangYifanget
al.(200
6)17
Amyg
daloid
nucleus+anterior
limbof
internal
capsule+bilateralm
edialseptum
6mon
ths
Obv
ious
improv
ements:13
Improv
ements:3
Noim
prov
ements:1
a
DuXiaop
eiet
al.(199
2)10
Unilateralam
ygdaloid
nucleus+anterior
limbof
internal
capsule(n
=3)
Unilateralcing
ulated
gyrus
(n=3)
Anteriorlim
bof
internal
capsule+mediodo
rsal
thalam
icnu
cleus(n
=1)
Unilateralanterior
limbof
internal
capsule(n
=2)
Amyg
daloid
nucleus+cing
ulated
gyrus
(n=1)
1year
Obv
ious
improv
ements:2
Improv
ements:6
Noim
prov
ements:2
a
(con
tinued)
196 B. Sun et al.
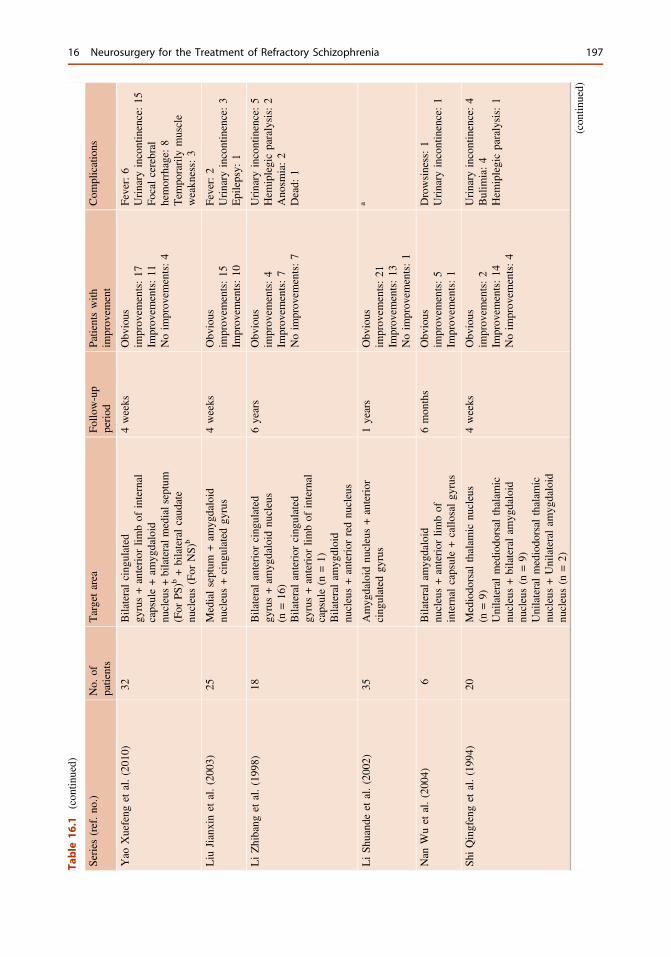
Table
16.1
(con
tinued)
Series
(ref.no
.)No.
ofpatients
Targetarea
Follo
w-up
period
Patientswith
improv
ement
Com
plications
Yao
Xuefeng
etal.(201
0)32
Bilateralcing
ulated
gyrus+anterior
limbof
internal
capsule+am
ygdaloid
nucleus+bilateralm
edialseptum
(For
PS)b
+bilateralcaud
ate
nucleus(For
NS)
b
4weeks
Obv
ious
improv
ements:17
Improv
ements:11
Noim
prov
ements:4
Fever:6
Urinary
incontinence:15
Focalcerebral
hemorrhage:
8Tem
porarily
muscle
weakn
ess:3
Liu
Jianxinet
al.(200
3)25
Medialseptum
+am
ygdaloid
nucleus+cing
ulated
gyrus
4weeks
Obv
ious
improv
ements:15
Improv
ements:10
Fever:2
Urinary
incontinence:3
Epilepsy:
1
LiZhibang
etal.(199
8)18
Bilateralanterior
cing
ulated
gyrus+am
ygdaloid
nucleus
(n=16
)Bilateralanterior
cing
ulated
gyrus+anterior
limbof
internal
capsule(n
=1)
Bilateralam
ygdloid
nucleus+anterior
rednu
cleus
6years
Obv
ious
improv
ements:4
Improv
ements:7
Noim
prov
ements:7
Urinary
incontinence:5
Hem
iplegicparalysis:2
Ano
smia:2
Dead:
1
LiSh
uand
eet
al.(200
2)35
Amyg
daloid
nucleus+anterior
cing
ulated
gyrus
1years
Obv
ious
improv
ements:21
Improv
ements:13
Noim
prov
ements:1
a
Nan
Wuet
al.(200
4)6
Bilateralam
ygdaloid
nucleus+anterior
limbof
internal
capsule+callo
salgy
rus
6mon
ths
Obv
ious
improv
ements:5
Improv
ements:1
Drowsiness:1
Urinary
incontinence:1
ShiQingfenget
al.(199
4)20
Mediodo
rsal
thalam
icnu
cleus
(n=9)
Unilateralmediodo
rsal
thalam
icnu
cleus+bilateralam
ygdaloid
nucleus(n
=9)
Unilateralmediodo
rsal
thalam
icnu
cleus+Unilateralam
ygdaloid
nucleus(n
=2)
4weeks
Obv
ious
improv
ements:2
Improv
ements:14
Noim
prov
ements:4
Urinary
incontinence:4
Bulim
ia:4
Hem
iplegicparalysis:1
(con
tinued)
16 Neurosurgery for the Treatment of Refractory Schizophrenia 197
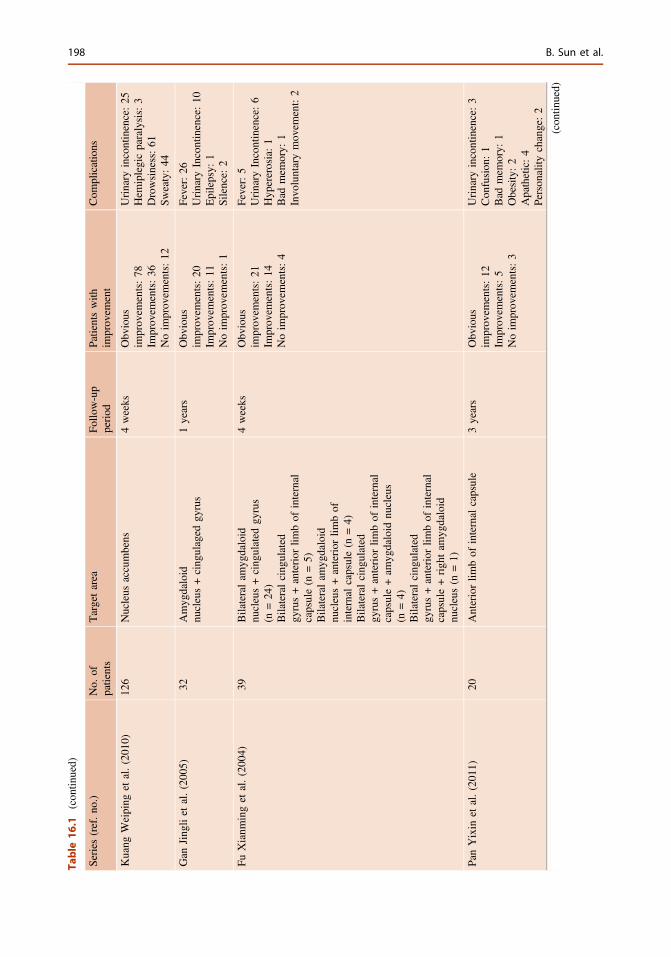
Table
16.1
(con
tinued)
Series
(ref.no
.)No.
ofpatients
Targetarea
Follo
w-up
period
Patientswith
improv
ement
Com
plications
Kuang
Weiping
etal.(201
0)12
6Nucleus
accumbens
4weeks
Obv
ious
improv
ements:78
Improv
ements:36
Noim
prov
ements:12
Urinary
incontinence:25
Hem
iplegicparalysis:3
Drowsiness:61
Sweaty:44
Gan
Jing
liet
al.(200
5)32
Amyg
daloid
nucleus+cing
ulaged
gyrus
1years
Obv
ious
improv
ements:20
Improv
ements:11
Noim
prov
ements:1
Fever:26
Urinary
Incontinence:10
Epilepsy:
1Silence:
2
FuXianm
inget
al.(200
4)39
Bilateralam
ygdaloid
nucleus+cing
ulated
gyrus
(n=24
)Bilateralcing
ulated
gyrus+anterior
limbof
internal
capsule(n
=5)
Bilateralam
ygdaloid
nucleus+anterior
limbof
internal
capsule(n
=4)
Bilateralcing
ulated
gyrus+anterior
limbof
internal
capsule+am
ygdaloid
nucleus
(n=4)
Bilateralcing
ulated
gyrus+anterior
limbof
internal
capsule+righ
tam
ygdaloid
nucleus(n
=1)
4weeks
Obv
ious
improv
ements:21
Improv
ements:14
Noim
prov
ements:4
Fever:5
Urinary
Incontinence:6
Hyp
ererosia:1
Bad
mem
ory:
1Invo
luntarymov
ement:2
PanYixin
etal.(201
1)20
Anteriorlim
bof
internal
capsule
3years
Obv
ious
improv
ements:12
Improv
ements:5
Noim
prov
ements:3
Urinary
incontinence:3
Con
fusion
:1
Bad
mem
ory:
1Obesity:2
Apathetic:4
Person
ality
change:2
(con
tinued)
198 B. Sun et al.
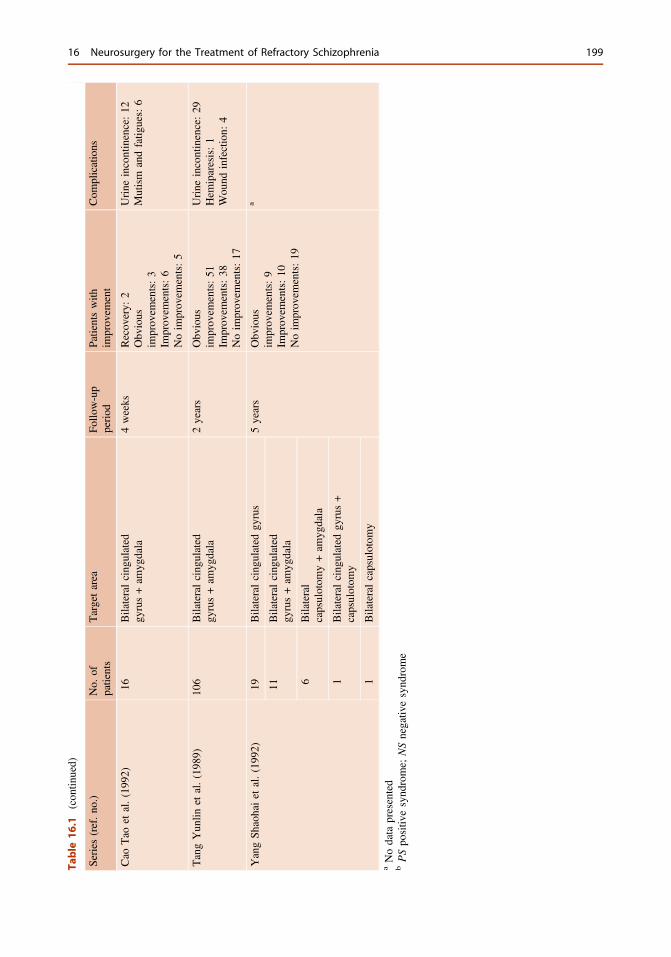
Table
16.1
(con
tinued)
Series
(ref.no
.)No.
ofpatients
Targetarea
Follo
w-up
period
Patientswith
improv
ement
Com
plications
Cao
Tao
etal.(199
2)16
Bilateralcing
ulated
gyrus+am
ygdala
4weeks
Recov
ery:
2Obv
ious
improv
ements:3
Improv
ements:6
Noim
prov
ements:5
Urine
incontinence:12
Mutism
andfatig
ues:6
TangYun
linet
al.(198
9)10
6Bilateralcing
ulated
gyrus+am
ygdala
2years
Obv
ious
improv
ements:51
Improv
ements:38
Noim
prov
ements:17
Urine
incontinence:29
Hem
iparesis:1
Wou
ndinfection:
4
YangSh
aohaiet
al.(199
2)19
Bilateralcing
ulated
gyrus
5years
Obv
ious
improv
ements:9
Improv
ements:10
Noim
prov
ements:19
a
11Bilateralcing
ulated
gyrus+am
ygdala
6Bilateral
capsulotom
y+am
ygdala
1Bilateralcing
ulated
gyrus+
capsulotom
y
1Bilateralcapsulotom
yaNodata
presented
bPSpo
sitiv
esynd
rome;
NSnegativ
esynd
rome
16 Neurosurgery for the Treatment of Refractory Schizophrenia 199

16.8 Conclusion
Schizophrenia is usually accompanied by signif-icant social or occupational dysfunctions thatcause a heavy economic burden for both thepatient’s family and society as a whole. In the U.S., the cost of schizophrenia was estimated to be$62.7 billion in 2002 [4]. Therefore, there is a veryurgent need to find a newmethod for the treatmentof refractory schizophrenia. We propose thatmodern stereotactic neurosurgery (includingcapsulotomy and cingulotomy) may be a potentialmethod for such treatment. However, these pro-cedures are still invasive and the lesions createdare irreversible. Therefore, we must keep in mindthat surgical therapy should only be considered asa supplementary part of the comprehensive treat-ment of schizophrenia and the inclusion criteriamust be strict. Close psychiatric follow-up isnecessary not only to monitor improvement ofsymptoms, but also to assess potential adversepsychiatric consequences. Finally, to help thepatients recover, surgery should be accompaniedby an appropriate psychological rehabilitationplan and family-social support program.
References
1. Saha S, Chant D, McGrath J. A systematic review ofmortality in schizophrenia: is the differential mortalitygap worsening over time? Arch Gen Psychiatry.2007;64:1123–31.
2. van Os J, Kapur S. Schizophrenia. Lancet.2009;374:635–45.
3. Goeree R, Farahati F, Burke N, Blackhouse G,O’Reilly D, Pyne J, Tarride JE. The economic burdenof schizophrenia in canada in 2004. Curr Med ResOpin. 2005;21:2017–28.
4. Wu EQ, Birnbaum HG, Shi L, Ball DE, Kessler RC,Moulis M, Aggarwal J. The economic burden ofschizophrenia in the united states in 2002. J ClinPsychiatry. 2005;66:1122–9.
5. Zhai J, Guo X, Chen M, Zhao J, Su Z. Aninvestigation of economic costs of schizophrenia intwo areas of china. Int J Ment Health Syst. 2013;7:26.
6. Cardno AG, Gottesman II. Twin studies ofschizophrenia: from bow-and-arrow concordances tostar wars Mx and functional genomics. Am J MedGenet. 2000;97:12–7.
7. van Rossum JM. The significance of dopamine-receptor blockade for the mechanism of action of
neuroleptic drugs. Arch Int Pharmacodyn Ther.1966;160:492–4.
8. Goldman-Rakic PS, Selemon LD. Functional andanatomical aspects of prefrontal pathology inschizophrenia. Schizophr Bull. 1997;23:437–58.
9. Tekin S, Cummings JL. Frontal-subcortical neuronalcircuits and clinical neuropsychiatry: an update.J Psychosom Res. 2002;53:647–54.
10. Volk DW, Lewis DA. Prefrontal cortical circuits inschizophrenia. Curr Top Behav Neurosci. 2011;4:485–508.
11. Laviolette SR. Dopamine modulation of emotionalprocessing in cortical and subcortical neural circuits:evidence for a final common pathway inschizophrenia? Schizophr Bull. 2007;33:971–81.
12. Rodrigues MG, Krauss-Silva L, Martins AC. Meta-analysis of clinical trials on family intervention inschizophrenia. Cad Saude Publica 2008;24:2203–18.
13. Pharoah F, Mari J, Rathbone J, Wong W. Familyintervention for schizophrenia. Cochrane DatabaseSyst Rev. 2006;CD000088(12).
14. Medalia A, Choi J. Cognitive remediation inschizophrenia. Neuropsychol Rev. 2009;19:353–64.
15. McGurk SR, Twamley EW, Sitzer DI, McHugo GJ,MueserKT.Ameta-analysis of cognitive remediation inschizophrenia. Am J Psychiatry. 2007;164:1791–802.
16. Smith T, Weston C, Lieberman J. Schizophrenia(maintenance treatment). Am Fam Physician. 2010;82:338–9.
17. Alt KW, Jeunesse C, Buitrago-Tellez CH, Wachter R,Boes E, Pichler SL. Evidence for stone age cranialsurgery. Nature. 1997;387:360.
18. Mashour GA, Walker EE, Martuza RL.Psychosurgery: past, present, and future. Brain ResBrain Res Rev. 2005;48:409–19.
19. Damasio H, Grabowski T, Frank R, Galaburda AM,Damasio AR. The return of Phineas gage: clues aboutthe brain from the skull of a famous patient. Science.1994;264:1102–5.
20. Joanette Y, Stemmer B, Assal G, Whitaker H. Fromtheory to practice: the unconventional contribution ofGottlieb Burckhardt to psychosurgery. Brain Lang.1993;45:572–87.
21. Feldman RP, Goodrich JT. Psychosurgery: ahistorical overview. Neurosurgery 2001;48:647–57;discussion 649–57.
22. Kelly D, Mitchell-Heggs N. Stereotactic limbicleucotomy–a follow-up study of thirty patients.Postgrad Med J. 1973;49:865–82.
23. Jimenez-Ponce F, Soto-Abraham JE, Ramirez-TapiaY, Velasco-Campos F, Carrillo-Ruiz JD, Gomez-Zenteno P. Evaluation of bilateral cingulotomy andanterior capsulotomy for the treatment of aggressivebehavior. Cir Cir 2011;79:107–13.
24. da Costa DA. The role of psychosurgery in thetreatment of selected cases of refractory schizophrenia:a reappraisal. Schizophr Res. 1997;28:223–30.
25. Goktepe EO, Young LB, Bridges PK. A furtherreview of the results of stereotactic subcaudatetractotomy. Br J Psychiatry. 1975;126:270–80.
200 B. Sun et al.
26. Vaernet K, Madsen A. Stereotaxic amygdalotomy andbasofrontal tractotomy in psychotics with aggressivebehaviour. J Neurol Neurosurg Psychiatry.1970;33:858–63.
27. Sun B, Krahl SE, Zhan S, Shen J. Improvedcapsulotomy for refractory Tourette’s syndrome.Stereotact Funct Neurosurg. 2005;83:55–6.
28. Ballantine HT Jr, Bouckoms AJ, Thomas EK, GiriunasIE. Treatment of psychiatric illness by stereotacticcingulotomy. Biol Psychiatry. 1987;22:807–19.
29. Dougherty DD, Baer L, Cosgrove GR, Cassem EH,Price BH, Nierenberg AA, Jenike MA, Rauch SL.Prospective long-term follow-up of 44 patients whoreceived cingulotomy for treatment-refractoryobsessive-compulsive disorder. Am J Psychiatry.2002;159:269–75.
30. Freeman W. Frontal lobotomy in early schizophrenia.Long follow-up in 415 cases. Br J Psychiatry.1971;119:621–4.
31. Dynes JB. Lobotomy–twenty years later. Va MedMon. 1918;1968(95):306–8.
32. Miller BL, Cummings JL. The human frontal lobes:functions and disorders. New York: Guilford Press;2007. p. 505–17.
33. Tooth GC, Newton MP. Leucotomy in England andWales 1942–1954. Reports on Public Health andMedical Subjects, No 104 Ministry of Health,London, UK: 1961; Her Majesty’s Stationery Office.
34. Leiphart JW, Valone FH III. Stereotactic lesions forthe treatment of psychiatric disorders. J Neurosurg.2010;113:1204–11.
35. Bridges PK, Bartlett JR, Hale AS, Poynton AM,Malizia AL, Hodgkiss AD. Psychosurgery:stereotactic subcaudate tractomy. An indispensabletreatment. Br J Psychiatry. 1994;165:599–611;discussion 593–612.
36. Kiloh LG, Gye RS, Rushworth RG, Bell DS, White RT.Stereotactic amygdaloidotomy for aggressive behaviour.J Neurol Neurosurg Psychiatry. 1974;37:437–44.
37. Elias WJ, Cosgrove GR. Psychosurgery. NeurosurgFocus. 2008;25:E1.
38. Robison RA, Taghva A, Liu CY, Apuzzo ML.Surgery of the mind, mood, and conscious state: anidea in evolution. World Neurosurg. 2013;80:S2–26.
39. Miller A. The lobotomy patient—a decade later: afollow-up study of a research project started in 1948.Can Med Assoc J. 1967;96:1095–103.
40. Cosgrove GR, Rauch SL. Psychosurgery. NeurosurgClin N Am. 1995;6:167–76.
41. Teuber JL, Corkin S, Twitchell TE. Study ofcingulotomy in man: a summary. Neurosurgical
treatment in psychiatry, pain, and epilepsy.Baltimore: University Park Press; 1977.
42. Poynton AM, Kartsounis LD, Bridges PK. Aprospective clinical study of stereotactic subcaudatetractotomy. Psychol Med. 1995;25:763–70.
43. Ramamurthi B. Thermocoagulation for stereotacticsubcaudate tractotomy. Br J Neurosurg. 1999;13:219.
44. Dettling M, Anghelescu IG. Subthalamic nucleusstimulation in severe obsessive-compulsive disorder.N Engl J Med. 2009;360:931 (Author reply 932).
45. Kapoor S. Subthalamic nucleus stimulation in severeobsessive-compulsive disorder. N Engl J Med.2009;360:931–2 (Author reply 932).
46. Mallet L, Polosan M, Jaafari N, Baup N, Welter ML,Fontaine D, du Montcel ST, Yelnik J, Chereau I,Arbus C, Raoul S, Aouizerate B, Damier P,Chabardes S, Czernecki V, Ardouin C, Krebs MO,Bardinet E, Chaynes P, Burbaud P, Cornu P, DerostP, Bougerol T, Bataille B, Mattei V, Dormont D,Devaux B, Verin M, Houeto JL, Pollak P, BenabidAL, Agid Y, Krack P, Millet B, Pelissolo A.Subthalamic nucleus stimulation in severeobsessive-compulsive disorder. N Engl J Med.2008;359:2121–34.
47. Saleh C. Are the anterior internal capsules and nucleusaccumbens suitable DBS targets for the treatment ofdepression? Prog Neuropsychopharmacol BiolPsychiatry. 2010;35:310 (Author reply 311).
48. Cusin C, Dougherty DD. Somatic therapies fortreatment-resistant depression: ECT, TMS, VNS,DBS. Biol Mood Anxiety Disord. 2012;2:14.
49. Perez SM, Shah A, Asher A, Lodge DJ. Hippocampaldeep brain stimulation reverses physiological andbehavioural deficits in a rodent model ofschizophrenia. Int J Neuropsychopharmacol. 2012;16:1331–9.
50. Ewing SG, Grace AA. Deep brain stimulation of theventral hippocampus restores deficits in processing ofauditory evoked potentials in a rodent developmentaldisruption model of schizophrenia. Schizophr Res.2013;143:377–83.
51. Ewing SG, Porr B, Pratt JA. Deep brain stimulation ofthe mediodorsal thalamic nucleus yields increases inthe expression of zif-268 but not c-fos in the frontalcortex. J Chem Neuroanat. 2013;52:20–4.
52. Ewing SG, Grace AA. Long-term high frequencydeep brain stimulation of the nucleus accumbensdrives time-dependent changes in functionalconnectivity in the rodent limbic system. BrainStimul. 2013;6:274–85.
16 Neurosurgery for the Treatment of Refractory Schizophrenia 201

17Surgical Management for AggressiveBehavior
Wei Wang and Peng Li
The etiology of human aggressive behavior hasnot been elucidated. In clinical practice, thedefinition of aggressive behavior is as follows:attack to property, others, or oneself with thedeliberate intention of destruction. Organicpsychosis, schizophrenia, mental retardation,emotional disorders, and personality disorderscan be associated with aggressive behavior, andmost frequently occur in the acute phase ofmental illness [1]. In 1990, a regional epidemi-ological investigation for violent psychosis in theUnited States showed that the incidence ofaggressive behavior in patients with psychiatricdisorders was five times that of normal people.Moreover, 50 % of the patients with psychiatricdisorders and 10 % of patients with schizophre-nia have histories of making threats, agitation,and aggressive behavior [2]. This aggressivebehavior causes serious threat to the safety ofmedical staff, the whole society, and even topatients themselves.
A variety of drugs have been recommendedfor the treatment of aggressive behavior, includ-ing typical and atypical antipsychotic drugs suchas benzodiazepines, mood stabilizing drugs, betablockers, selective 5-HT re-uptake inhibitors, etc.These drugs have different effects on brain neu-rotransmitter systems. At present, the knowledgeof the etiology of aggressive behavior is limited.
Several chemical compounds are supposed tohave influence to the aggressive behavior such as5-HT, dopamine, y-aminobutyric acid (GABA),norepinephrine and other neurotransmitters [1].However, the detailed mechanism underlyingaggressive behavior is still unclear. Currentneurophysiological research on the managementof large numbers of patients with schizophreniaaccompanied by agitated and aggressive behav-iors is limited. Although improvement ofaggressive behaviors with medication can beobserved, the efficacy is still not ideal in manycases. Thus, surgical management may be apossible choice for carefully selected patients.
From 1935 to 1937, Moniz and Lima firstreported successful results of bilateral frontallobe lobotomies for the treatment of mentaldisorders. The main purpose of the treatment wasto improve impulse, violence, and difficultlycontrolled behaviors. Based on their results, theyproposed the “psychosurgical method” for treat-ing certain cases of mental disorders [3, 4]. In1947, with the help of the stereotactic technique,the mediodorsal thalamotomy was successfullycompleted by Wycis and Spiegel to treat patientswith serious mental disorders. This new surgicalapproach resulted in smaller regions of damage,which helped to reduce the side effects ofsurgery. Moreover, patient disabilities and thenumber of mortalities were significantly reduced.In recent years, along with the development ofclinical psychiatry, neurophysiology, neuroanat-omy, imaging techniques, and functionalW. Wang (&) � P. Li
West China Hospital of Sichuan University,Chengdu, China
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0_17© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
203

neurosurgery, more attention has been paid topsychosurgery by clinicians [5].
Mental and behavioral disorders associatedwith aggressive behavior can be observed inpatients with schizophrenia, schizoaffective dis-order, mental retardation, personality disorders,and other psychiatric illnesses. For seriousmedically refractive patients with aggressivebehavior, inclusion criterion for surgical man-agement may be suggested as: (1) confirmeddiagnosis by more than two psychiatrists, (2) atleast 6 weeks of failed medication with more thanthree kinds of drugs with normalized psycho-logical management that cannot relievesymptoms, (3) more than 5 years of diseasehistory, (4) patients between 18 and 75 years old(for stereotactic surgery or radiosurgery treat-ment). However, for patients with severe mentalretardation, considering the serious influence ondaily life and with behavioral training beingconducted soon after the operation, surgery canbe carefully considered when the patient is morethan 10 years old. (5) Behavior has seriouslyinfluenced the patient’s ability to lead a normallife and does harm to the patient and his/herfamily members, (6) families and patients canaccept the risk of operation, and can keep upsubsequent treatment and long-term follow-up.
The following patients should be excludedfrom receiving psychosurgery: (1) patients whoseage does not conform to the inclusion criteria,(2) those with disease duration of less than5 years, (3) those with lack of normativemedication, psychological treatment, and/orhospitalization, (4) patients with some accom-panying bodily disease such as: infectiousdisease, metabolic disease, frailness, seriouslyhigh blood pressure, heart disease, and/or severepathological brain disease, (5) patients whosepsychosurgical targets have been damaged, (6)those with other bodily reason that impedesproper implementation of the surgery, (7) thoserefusing treatment (with the exception of mentaldisorder without self-knowledge), (8) lack ofgood family support, since postoperative follow-up would not be guaranteed and post-surgicalmanagement would be difficult, (9) conflicts withthe law, ethics, politics, and/or religion [6, 7].
For patients that meet the standards ofpsychosurgery, psychiatrists and neurologicalsurgeons should again carefully evaluate the con-dition of the patients before the operation. Thisshould include assessments of a patient’s diagno-sis and previous drug and psychological behaviortreatment, judgment of patient and family expec-tations, status of support and supervision, andwhether the procedure would comply with thecountry’s ethics and laws. Relevant preoperativeexamination, neural electrophysiological, imageand psychological measurement are also impor-tant for preparation of the operation. Good coop-eration between doctors, patients, and theirfamilies helps to have better disease improvement.
The theoretical basis of modern psychosur-gery considers that human mental processes areextremely complex. Although the specificanatomical structure related to mental disordersis yet to be clarified, the limbic system and itsconnected structures are thought to have closerelationship with a human’s mental activities.The anatomy and theoretical basis of modernpsychosurgery mainly concentrate on threecircuits of the human limbic system: the internaland lateral circuits, and the defense reaction cir-cuit. These structures have complex connectionsto the basal ganglia and frontal lobe, which areclosely related to mental activities such as emo-tion and motivation [8].(1) The internal circuit of the limbic system,
which was first reported by Papez in 1937,begins at the septal area and passes throughthe cingulate gyrus to the hippocampus, viathe mammillary body. It then runs againfrom the mammillary body-thalamus accessto the anterior nucleus of the thalamus, andthen back to the cingulate gyrus.
(2) The lateral circuit of the limbic system,which was first reported by Yakovlev in1948, contains fiber tracts that originate inthe orbitofrontal cortex, the insular lobe,frontal temporal lobe, and amygdala. Thesefiber tracts project to the mediodorsal tha-lamic nucleus, and then run back to theorbitofrontal cortex.
(3) The defense reaction circuit of the limbicsystem, which was reported by Kelly,
204 W. Wang and P. Li
originates from the hypothalamus via thestria terminalis and runs from the septal areato the amygdala before returning to thehypothalamus [5].Lesions to the structures of these three circuits
and related structures may change brain neuro-transmitters, thus achieving the purpose ofimproving and controlling psychiatric disorders.Operations can be completed under local orgeneral anesthesia. Stereotactic radiofrequencythermocoagulation, stereotactic radiosurgery, anddeep brain stimulation are the most popularsurgical procedures used to treat psychiatricdisorders.
Common surgical targets include the anteriorlimb of the internal capsule, amygdaloid nucleus,and medial septal area [8–10].(1) The anterior limb of the internal capsule
contains the efferent fiber tracts of the ante-rior nucleus of the thalamus and frontal lobe,the frontopontine tract, and the tractsbetween the orbitofrontal cortex and hypo-thalamus. Lesions to the anterior limb of theinternal capsule aim to cut off the fiber tractsbetween the thalamus and the prefrontalcortex, which serve to partially interruptcommunication between the nucleus media-lis thalami and the frontal lobe. An anteriorinternal capsulotomy has been reported to bean effective treatment option for obsessive-compulsive disorder, anxiety, and phobia inselected patients.
(2) The amygdaloid nucleus, also known as theamygdala complex, receives afferent fibersfrom the olfactory bulb and anterior olfactorynucleus, via the lateral olfactory stria. Thefibers from the piriform area and dienceph-alon end in the basolateral amygdaloidnucleus. In addition, the amygdaloid nucleusreceives fibers from the hypothalamus, thal-amus, brainstem reticular formation, andneocortex. The afferent fibers of the amyg-daloid nucleus pass through the terminal striaand septal area, medial preoptic nucleus,anterior part of the hypothalamus, preopticarea, and the anterior commissure. Thus, aportion of the fibers end in the hypothala-mus, dorsomedial nucleus of the thalamus,
and the midbrain reticular formation, whilethe other fibers end in the rein nuclear via thestria terminalis. The amygdaloid nucleus stillhas complex connection to the prefrontalcortex, cingulate gyrus, anterior part of thetemporal lobe, and ventral insula. Thus,lesions to the amygdaloid nucleus result inbehavior that is mild and calm, with lack ofinitiative and will. Obvious improvement hasbeen reported following amygdalohippo-campectomy for the treatment of mania,aggressive and destructive behavior, andimpulsive mood.
(3) Medial septal area: The nucleus accumbensis located in the septal area, which is dividedinto interior and lateral part. The interior partis located anterior to the anterior commissureand the lateral part is located posterior to theanterior commissure. The nucleus accum-bens is a key part of the Papez circuit andcomprises the lateral circuit of the basallimbic system. It is considered by manyresearchers to be a “relay station” of thelimbic system, and has close fiber connec-tions with many structures such as thehypothalamus, mammillary bodies, cingulategyrus, amygdala, and hippocampus. Lesionsto the interior part of the nucleus accumbenshave been used to treat behaviors associatedwith vandalism, associability tension, irrita-bility, and other symptoms. The optimaltargets for patients with psychiatric disordersassociated with mania, impulsiveness,aggression, self-injury, compulsion, anddestruction, are the amygdaloid nucleus,anterior limb of the internal capsule, andmedial septal area. Additionally, for theabove target behaviors, the nucleus accum-bens, cingulate gyrus, and caudate nucleuscan be targeted in select patients.Multiple bilateral target lesions are commonly
used during operation. According to the condi-tion of the individual patient and the experienceof the surgeons, optimal basic targets and addi-tional targets can be used. Secondary operationcould be considered to expand the lesion foci oradd new targets if the first surgery has failed.However, a second operation should be
17 Surgical Management for Aggressive Behavior 205
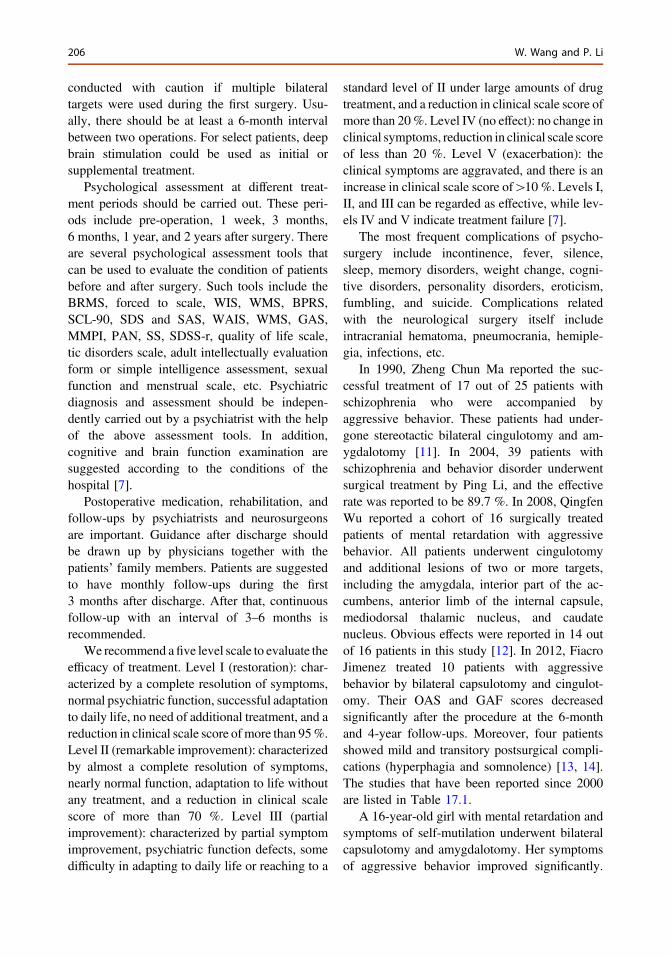
conducted with caution if multiple bilateraltargets were used during the first surgery. Usu-ally, there should be at least a 6-month intervalbetween two operations. For select patients, deepbrain stimulation could be used as initial orsupplemental treatment.
Psychological assessment at different treat-ment periods should be carried out. These peri-ods include pre-operation, 1 week, 3 months,6 months, 1 year, and 2 years after surgery. Thereare several psychological assessment tools thatcan be used to evaluate the condition of patientsbefore and after surgery. Such tools include theBRMS, forced to scale, WIS, WMS, BPRS,SCL-90, SDS and SAS, WAIS, WMS, GAS,MMPI, PAN, SS, SDSS-r, quality of life scale,tic disorders scale, adult intellectually evaluationform or simple intelligence assessment, sexualfunction and menstrual scale, etc. Psychiatricdiagnosis and assessment should be indepen-dently carried out by a psychiatrist with the helpof the above assessment tools. In addition,cognitive and brain function examination aresuggested according to the conditions of thehospital [7].
Postoperative medication, rehabilitation, andfollow-ups by psychiatrists and neurosurgeonsare important. Guidance after discharge shouldbe drawn up by physicians together with thepatients’ family members. Patients are suggestedto have monthly follow-ups during the first3 months after discharge. After that, continuousfollow-up with an interval of 3–6 months isrecommended.
We recommend afive level scale to evaluate theefficacy of treatment. Level I (restoration): char-acterized by a complete resolution of symptoms,normal psychiatric function, successful adaptationto daily life, no need of additional treatment, and areduction in clinical scale score ofmore than 95%.Level II (remarkable improvement): characterizedby almost a complete resolution of symptoms,nearly normal function, adaptation to life withoutany treatment, and a reduction in clinical scalescore of more than 70 %. Level III (partialimprovement): characterized by partial symptomimprovement, psychiatric function defects, somedifficulty in adapting to daily life or reaching to a
standard level of II under large amounts of drugtreatment, and a reduction in clinical scale score ofmore than 20%. Level IV (no effect): no change inclinical symptoms, reduction in clinical scale scoreof less than 20 %. Level V (exacerbation): theclinical symptoms are aggravated, and there is anincrease in clinical scale score of[10 %. Levels I,II, and III can be regarded as effective, while lev-els IV and V indicate treatment failure [7].
The most frequent complications of psycho-surgery include incontinence, fever, silence,sleep, memory disorders, weight change, cogni-tive disorders, personality disorders, eroticism,fumbling, and suicide. Complications relatedwith the neurological surgery itself includeintracranial hematoma, pneumocrania, hemiple-gia, infections, etc.
In 1990, Zheng Chun Ma reported the suc-cessful treatment of 17 out of 25 patients withschizophrenia who were accompanied byaggressive behavior. These patients had under-gone stereotactic bilateral cingulotomy and am-ygdalotomy [11]. In 2004, 39 patients withschizophrenia and behavior disorder underwentsurgical treatment by Ping Li, and the effectiverate was reported to be 89.7 %. In 2008, QingfenWu reported a cohort of 16 surgically treatedpatients of mental retardation with aggressivebehavior. All patients underwent cingulotomyand additional lesions of two or more targets,including the amygdala, interior part of the ac-cumbens, anterior limb of the internal capsule,mediodorsal thalamic nucleus, and caudatenucleus. Obvious effects were reported in 14 outof 16 patients in this study [12]. In 2012, FiacroJimenez treated 10 patients with aggressivebehavior by bilateral capsulotomy and cingulot-omy. Their OAS and GAF scores decreasedsignificantly after the procedure at the 6-monthand 4-year follow-ups. Moreover, four patientsshowed mild and transitory postsurgical compli-cations (hyperphagia and somnolence) [13, 14].The studies that have been reported since 2000are listed in Table 17.1.
A 16-year-old girl with mental retardation andsymptoms of self-mutilation underwent bilateralcapsulotomy and amygdalotomy. Her symptomsof aggressive behavior improved significantly.
206 W. Wang and P. Li
The follow-up magnetic resonance (MR) imagesare shown in Figs. 17.1, 17.2, 17.3, 17.4, 17.5,17.6 and 17.7.
Based on the limited results of previousstudies, psychosurgery for patients with positiveclinical psychiatric symptoms such as aggressive
behavior could not only effectively alleviate apatient’s symptoms, but could also facilitatepost-surgical behavioral therapy. On the otherhand, effective surgical procedures could preventpatients from doing harm to themselves andothers.
Table 17.1 Studies in recent years
Year Authors Numberof cases
Follow-uptime
Treatment approach Improvedcases
2012 [13] Fiacro Jiménez 10 4 years Bilateral capsulotomy andcingulotomy
–
2008 [15] Kim MC 2 8 years Bilateral amygdalotomy andsubcaudate tractotomy
1
2007 [16] Fountas KN 1 – Bilateral amygdalotomy 1
2005 [17] Franzini A 2 1 year Posterior hypothalamus stimulation 2
2001 [18] Price BH 5 31.5 months Limbic leucotomy 4
2009 [19] Yang KJ 1 – Bilateral nucleus accumbens lesion 1
2007 [20] WangLianzhong
3 – Bilateral capsulotomy,cingulotomy, and amygdalotomy
3
2008 [12] Wu Qingfen 16 18 months Bilateral capsulotomy, cingulotomyamygdalotomy, nucleus accumbenslesion, and subcaudate tractotomy
14
Fig. 17.1 Coronal MR image 1 week after bilateralcapsulotomy
Fig. 17.2 Coronal MR image 3 months after bilateralcapsulotomy
17 Surgical Management for Aggressive Behavior 207
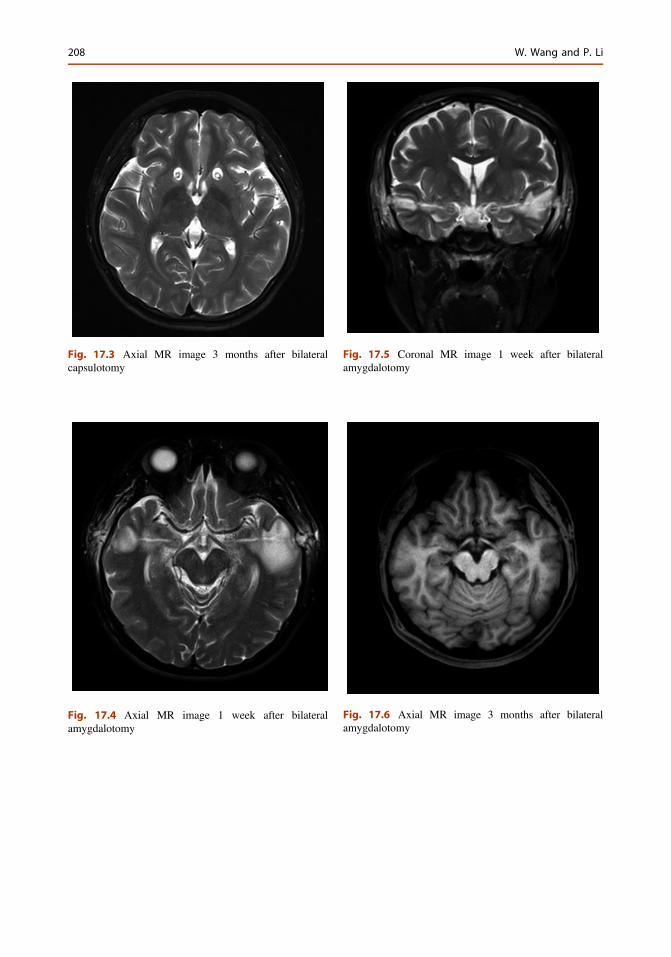
Fig. 17.4 Axial MR image 1 week after bilateralamygdalotomy
Fig. 17.5 Coronal MR image 1 week after bilateralamygdalotomy
Fig. 17.6 Axial MR image 3 months after bilateralamygdalotomy
Fig. 17.3 Axial MR image 3 months after bilateralcapsulotomy
208 W. Wang and P. Li

References
1. Campbell M, Gonzalez NM, Silva RR. Thepharmacologic treatment of conduct disorders andrage outbursts. Psychiatr Clin North Am. 1992;15(1):69–85.
2. Sramka M, Pogady P, Csolova Z, et al. Long-termresults in patients with stereotaxic surgery forpsychopathologic disorders. Bratisl Lek Listy.1992;93(7):365–6.
3. Kopell BH, Rezai AR. Psychiatric neurosurgery: ahistorical perspective. Neurosurg Clin N Am. 2003;14(2):181–97.
4. Diering SL, Bell WO. Functional neurosurgery forpsychiatric disorder: a historical persoective.Stereotact Funct Neurosurg. 1991;57(4):175–99.
5. Fedlman RP, Alterman RL, Goodrich JT.Contemporary psychosurgery and a look to thefuture. J Neurosurg. 2001;95(6):944–56.
6. Li P, Fu X, Wang Y. Targets, mechanism, efficacy andfuture expectation of stereotactic psychosurgery. ChinJ Stereotact Funct Neurosurg. 2007;20(5):313–7.
7. Neurosurgery Branch of Chinese Medical DoctorAssociation. Clinical guidelines of psychosurgery.Chin J Nerv Psychiatr Dis. 2009;35(8):449–50.
8. Byrum J, Ahearn EP, Krishnan KR. A neuroanatomicmodel for depression. Prog NeuropsychopharmacolBiol Psychiatry. 1999;23:175–93.
9. Modell JC, Mountz JM, Curtis GC, et al.Neurophysiologic dysfunction in basal ganglia/limbic striatal and thalamocortical circuits as apathogenetic mechanism of obsessive compulsivedisorder. Clin Neurosic. 1989;1(1):27–9.
10. Li J, Wang X. The role of different intracranialstructures in stereotactic surgery. Chin J StereotactFunct Neurosurg. 2009;22(1):55–7.
11. Ma Z, Dou Y, Sun Y, et al. Preliminary observationof 25 patients with schizophrenia treated bystereotactic surgery. Chin J Stereotact FunctNeurosurg. 2004;17(6):321–4.
12. Wu Q, Liu C, Zhang W. Multi-target treatment ofmental retardation by stereotactic techniques-a studyof 16 cases. J Xinjiang Med Univ. 2008;31(11):1578–9.
13. Jiménez F, Soto JE, Velasco F. Bilateral cingulotomyand anterior capsulotomy applied to patients withaggressiveness. Stereotact Funct Neurosurg.2012;90:151–60.
14. Jimenez-Ponce F, Soto-Abraham JE, Ramirez-TapiaY, Velasco-Campos F, Carrillo-Ruiz JD, Gomez-Zenteno P. Evaluation of bilateral cingulotomy andanterior capsulotomy for the treatment of aggressivebehavior. Cir Cir. 2011;79(2):107–13.
15. Kim MC, Lee TK. Stereotactic lesioning for mentalillness. Acta Neurochir Suppl. 2008;101:39–43.
16. Fountas KN, Smith JR, Lee GP. Bilateral stereotacticamygdalotomy for self-mutilation disorder. Casereport and review of the literature. Stereotact FunctNeurosurg. 2007;85:121–8.
17. Franzini A, Marras C, Ferroli P, Bugiani O, Broggi G.Stimulation of the posterior hypothalamus formedically intractable impulsive and violentbehavior. Stereotact Funct Neurosurg. 2005;83:63–6.
18. Price BH, Baral I, Cosgrove GR, Rauch SL,Nierenberg AA, Jenike MA, Cassem EH.Improvement in severe self-mutilation followinglimbic leucotomy: a series of 5 consecutive cases.J Clin Psychiatry. 2001;62(12):925–32.
19. Kaijun Y, Songtao Q, Kewan W, et al. Operativetechnique and electrophysiologic monitoring ofstereotactic accumbensotomy. Chin J StereotactFunct Neurosurg. 2009;22(3):129–33.
20. Wang LZ, Yin ZM, Wen H, Jiang XL, Wang L.Stereotactic multi-target operation for patients withaffective disorder. Chin J Surg. 2007;45(24):1676–8.
Fig. 17.7 Coronal MR image 3 months after bilateralamygdalotomy
17 Surgical Management for Aggressive Behavior 209
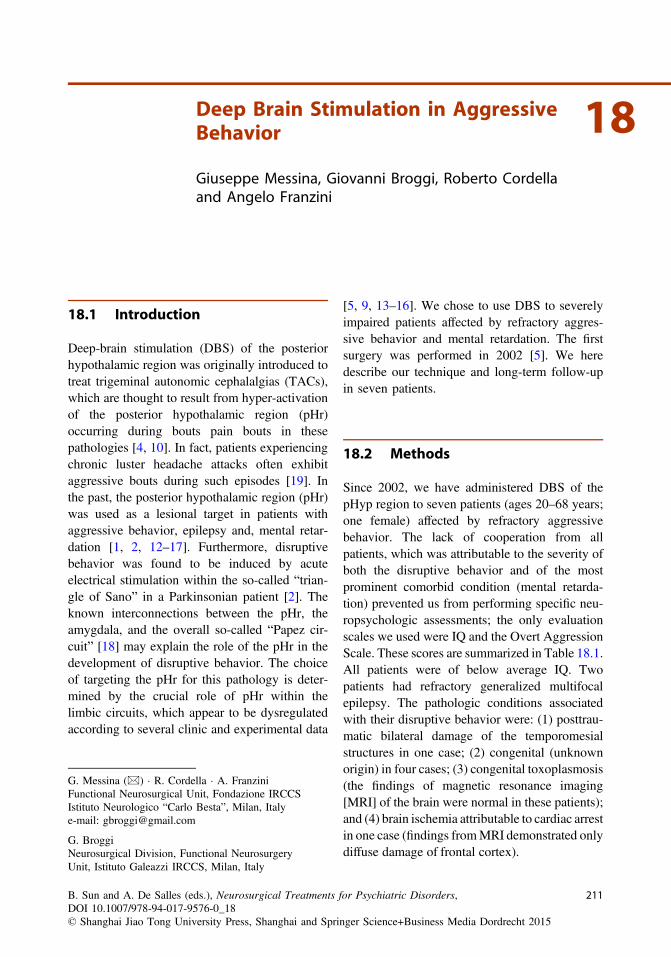
18Deep Brain Stimulation in AggressiveBehavior
Giuseppe Messina, Giovanni Broggi, Roberto Cordellaand Angelo Franzini
18.1 Introduction
Deep-brain stimulation (DBS) of the posteriorhypothalamic region was originally introduced totreat trigeminal autonomic cephalalgias (TACs),which are thought to result from hyper-activationof the posterior hypothalamic region (pHr)occurring during bouts pain bouts in thesepathologies [4, 10]. In fact, patients experiencingchronic luster headache attacks often exhibitaggressive bouts during such episodes [19]. Inthe past, the posterior hypothalamic region (pHr)was used as a lesional target in patients withaggressive behavior, epilepsy and, mental retar-dation [1, 2, 12–17]. Furthermore, disruptivebehavior was found to be induced by acuteelectrical stimulation within the so-called “trian-gle of Sano” in a Parkinsonian patient [2]. Theknown interconnections between the pHr, theamygdala, and the overall so-called “Papez cir-cuit” [18] may explain the role of the pHr in thedevelopment of disruptive behavior. The choiceof targeting the pHr for this pathology is deter-mined by the crucial role of pHr within thelimbic circuits, which appear to be dysregulatedaccording to several clinic and experimental data
[5, 9, 13–16]. We chose to use DBS to severelyimpaired patients affected by refractory aggres-sive behavior and mental retardation. The firstsurgery was performed in 2002 [5]. We heredescribe our technique and long-term follow-upin seven patients.
18.2 Methods
Since 2002, we have administered DBS of thepHyp region to seven patients (ages 20–68 years;one female) affected by refractory aggressivebehavior. The lack of cooperation from allpatients, which was attributable to the severity ofboth the disruptive behavior and of the mostprominent comorbid condition (mental retarda-tion) prevented us from performing specific neu-ropsychologic assessments; the only evaluationscales we used were IQ and the Overt AggressionScale. These scores are summarized in Table 18.1.All patients were of below average IQ. Twopatients had refractory generalized multifocalepilepsy. The pathologic conditions associatedwith their disruptive behavior were: (1) posttrau-matic bilateral damage of the temporomesialstructures in one case; (2) congenital (unknownorigin) in four cases; (3) congenital toxoplasmosis(the findings of magnetic resonance imaging[MRI] of the brain were normal in these patients);and (4) brain ischemia attributable to cardiac arrestin one case (findings fromMRI demonstrated onlydiffuse damage of frontal cortex).
G. Messina (&) � R. Cordella � A. FranziniFunctional Neurosurgical Unit, Fondazione IRCCSIstituto Neurologico “Carlo Besta”, Milan, Italye-mail: [email protected]
G. BroggiNeurosurgical Division, Functional NeurosurgeryUnit, Istituto Galeazzi IRCCS, Milan, Italy
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0_18© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
211
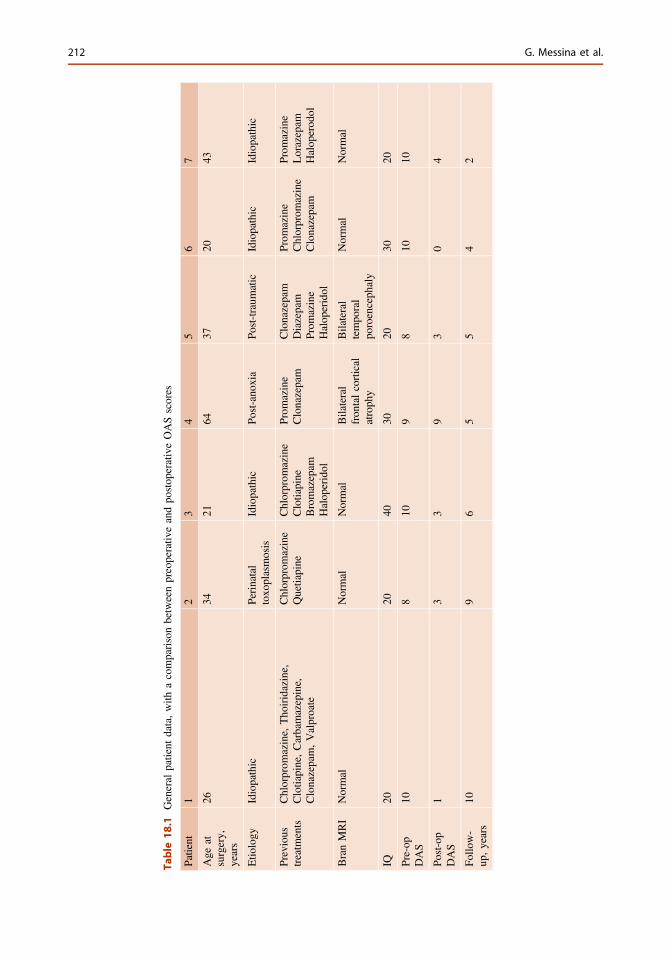
Table
18.1
General
patient
data,with
acomparisonbetweenpreoperativ
eandpo
stop
erativeOASscores
Patient
12
34
56
7
Age
atsurgery,
years
2634
2164
3720
43
Etio
logy
Idiopathic
Perinatal
toxo
plasmosis
Idiopathic
Post-ano
xia
Post-traum
atic
Idiopathic
Idiopathic
Previous
treatm
ents
Chlorprom
azine,
Tho
iridazine,
Clotiapine,Carbamazepine,
Clonazepam,Valproate
Chlorprom
azine
Quetiapine
Chlorprom
azine
Clotiapine
Bromazepam
Halop
eridol
Prom
azine
Clonazepam
Clonazepam
Diazepam
Prom
azine
Halop
eridol
Prom
azine
Chlorprom
azine
Clonazepam
Prom
azine
Lorazepam
Halop
erod
ol
BranMRI
Normal
Normal
Normal
Bilateral
fron
talcortical
atroph
y
Bilateral
tempo
ral
poroenceph
aly
Normal
Normal
IQ20
2040
3020
3020
Pre-op
DAS
108
109
810
10
Post-op
DAS
13
39
30
4
Follo
w-
up,years
109
65
54
2
212 G. Messina et al.

The Ethical Committee of our institutionapproved the surgical procedure in all of thepatients, taking into account the chronicity andseverity of the condition, the related burden tofamilies, and the refractoriness to conservativetreatments. The relatives of all of the patientsprovided their written consent after a detailedexplanation of its hypothetical rationale and ofthe surgical risks was given. The stereotacticimplantation was performed with the Leksellframe (Eleckta, Stockholm, Sweden) under gen-eral anesthesia in all patients. Preoperative anti-biotics were administrated to all patients. Apreoperative MRI (brain axial volumetric fastspin echo inversion recovery and T2 images) wasused to obtain high-definition images for theprecise determination of both anterior and pos-terior commissures and midbrain structuresbelow the commissural plane, such as the mam-millary bodies and the red nucleus. MRIs werefused with 2-mm thick computed tomography(CT) slices that were obtained under stereotacticconditions by the use of an automated techniquethat is based on a mutual-information algorithm(Frame-link 4.0, Sofamor Danek Steathstation;Medtronic, Minneapolis, Minnesota, USA).
The workstation also provided stereotacticcoordinates of the target: 3 mm behind the mid-commissural point, 5 mm below this point, and2 mm lateral from the midline.
A possible error in this intervention could beattributable to the anatomical individual variabilityof the angle between the brainstem and the com-missural plane. To correct this possible error, weintroduced a third anatomical landmark, whichallowed final target registration. We called thislandmark the “interpeduncular nucleus” or “inter-peduncular point,” and it is placed in the apex ofthe interpeduncular cistern 8 mm below the com-missural plane at the level of the maximumdiameter of the mammillary bodies [6]. TheY value of the definitive target (anteroposteriorcoordinate to the mid-commissural point in theclassical mid-commissural reference system) wascorrected in our patients, and the definitive targetcoordinate was chosen 2 mm posterior to theinterpeduncular point instead of 3 mm posterior tothe mid-commissural point. A dedicated program
and atlas has been developed and is freely avail-able on the internet to get the proper coordinates ofthe target (www.angelofranzini.com/BRAIN.htm).
During the surgical session, all patientsreceived general anesthesia. Target control infu-sion was used. This method of intravenous infu-sion of anesthetic drugs has been studied for itsability to achieve targeted blood or effect-siteconcentration for selected drugs. Maintaining aconstant plasma or effect compartment concen-tration of an intravenous anesthetic requires con-tinuous adjustment of the infusion rate accordingto the pharmacokinetic properties of the drugs,which can be achieved by commercially availabletarget controlled infusion pumps (in our study, weused Injectomat Agilia, Fresenius Kabi, France).
A rigid cannula was inserted through a 3-mm,coronal, paramedian twist-drill hole and placedup to 10 mm from the target. This cannula wasused as both a guide for microrecording and forthe placement of the definitive electrode(Quad 3389; Medtronic).
As far as microrecording is concerned, in twopatients spontaneous neuronal activity wasrecorded along four trajectories (two in eachpatient). Along the trajectories, it was possible toidentify several types of firing discharge rates andpatterns. Of the several recorded neurons, a totalof 14 cells located within the posterior hypo-thalamus were further analyzed. None showedeither activation or inhibition after tactile andpinprick stimulation. The average firing rate forthese cells was 13 Hz, although nine cells (64 %)showed a low-frequency discharge at around5 Hz, and the remaining five cells (36 %) dis-charged at greater frequencies (26 Hz). Severalfiring patterns have been noticed: four cellsexhibited tonic regular discharge, four cellsexhibited tonic irregular discharge, four exhibiteda bursting discharge, and two had a sporadicfiring. Periodicity was described in five units(four bursting and one regular), but the remainingone randomly fired [3]. Microrecordings withinthe pHyp were performed within 2 mm of thestereotactic coordinates (specifically, as statedpreviously, 2 mm lateral to the commissural line,3 mm posterior to the mid-commissural point,and 5 mm below the commissural line).
18 Deep Brain Stimulation in Aggressive Behavior 213

It is important to note that there is no clearevidence of the neurophysiologic characteristicsof either the superior or inferior borders of thenucleus. However, the presence of greater firingrates more than 5 mm from the target may sug-gest that the microelectrode is passing throughthe thalamus, whereas the lack of neuronalactivity at the target site and beyond may indicatethat the microelectrode is not in the pHyp but inadjacent structures (that is, the interpeduncularcistern at the inferior border).
No vegetative responses or cardiovasculareffects were elicited by intraoperative macrosti-mulation at therapeutic parameters (185 Hz,80 μs, from 1 to 3 V). At increasing chargedensity above this level, internal gaze deviationwas observed in all cases. When side effects wereruled out at the standard parameters of stimula-tion, the guiding cannula was removed and theelectrode secured to the skull with microplates.
Postoperative stereotactic CT was performedto assess the positioning of the electrode and ruleout complications (Fig. 18.1).
A bilateral implantable pulse generator (IPG;Soletra; Medtronic.) was placed in the subcla-vicular pocket and connected to the brain elec-trode for chronic electrical stimulation.
The parameters of chronically delivered elec-trical currents were 185 Hz, 60–90 μs, and 1–3 Vin unipolar configuration with case positive. Thecurrent amplitude was progressively increaseduntil the impairment of ocular movements, asside effect, was reached in all cases.
18.3 Results
Follow-up cases ranged from 1 to 9 years of age.Case 1’s self-aggression promptly stopped, andbursts of uncontrolled violence became less fre-quent, disappearing completely within 3 weeks.The patient returned to family and began to attenda therapeutic community for mentally impairedpatients. Generalized epileptic seizures disap-peared, and partial seizures and absences werereduced 50 %. Antiepileptic drug therapy wascontinually checked and was reduced to 30 %.
Case 2 had an immediate disappearance ofviolence bursts and was discharged from theinstitution where he had been hospitalized for along time. Forced bed contention was withdrawn,and he was charged to a therapeutic communityfor mentally disabled patients. Three years later,after the IPG was temporary turned off for kneesurgery, the patient’s violent behavior relapsed,and when the chronic stimulation was restored,the therapeutic effect resulted considerablyreduced despite the increase in current amplitude,which could not be set greater than 2 V becauseof the appearance of side effects. The psychia-trists who had the patient in their charge sug-gested a possible evolution of the original diseaseto explain the loss of the therapeutic effect.
With the IPG turned on, the burst of violenceare still less frequent and less intense than in theabsence of stimulation. And duration of theviolence attacks only when the amplitude ofstimulation was set to 1.8 V few months aftersurgery. This patient is still quiet, and her socialactivities have improved consistently. Now she isable to attend a psychiatric rehabilitation centerand her family integration is good. Violencebursts may appear only if the patient is provokedby adverse events.
Fig. 18.1 Postoperative computed tomography scanshowing the electrode tips at the level of the posteriorhypothalamic region, bilaterally
214 G. Messina et al.

Case 4 had only an improvement in sleephabits (before surgery, he slept only 2 h pernight, and after surgery he sleep more than 6 hper night). His behavior was not affected by thestimulation despite the electrical currentincreased to 2 V’ amplitude.
Two years after surgery, the stimulator wasturned off but the improvement of sleep was notreverted to the preoperative condition, and at3 years follow-up, the patient still sleeps morethan 6 h per night. The same patient had a stabledecrease of arterial pressure, and all antihyper-tensive drugs could be withdrawn; this effect isstill persists despite the IPG being turned off.
Case 5 had a prompt, marked improvement ofaggressive behavior, and care by the familybecame consistently easier. The therapeutic effectpersisted at 1-year follow-up, but when bothIPGs were turned off, the violent behavior reap-peared within a few hours. The left IPG had beenremoved because of skin erosion (but has beensubsequently reimplanted) and the therapeuticeffects seemed to be sustained only by the right-side stimulation of the pHyp; the reimplantationof the left IPG anyway led to further reduction ofthe frequency of violent outbursts.
At 1-year follow-up, in case 6 the rate ofepileptic seizures decreased to 50 % of the pre-operative condition just during the early post-operative weeks. In this patient the insertion ofthe second electrode at the target was immedi-ately followed by the disappearance of interictalepileptic activity from the scalp electroencepha-logram (EEG) [7]. During this intervention,infusion of a constant concentration of propofolwas maintained, thus excluding the role ofintraoperative anesthetics in the change in EEGactivity. Anyway, no postoperative EEG wasperformed for this patient. The aggressivebehavior has completely disappeared.
Case 7 had prompt disappearance of overalldisruptive behavior; aggressive bouts now occuronly episodically (about once every 2 months),but their duration and intensity is remarkablyreduced (from about 9–10 episodes per day to2–3 episodes per month). This improvement ispresent at the last follow-up, conducted 2 yearsafter the intervention.
18.4 Discussion
This series shows that patients affected by mentalretardation in whom violent and aggressivebehavior is associated could consistently benefitfrom high-frequency stimulation of the pHyp. Nopatient worsened after surgery, and no patientdeveloped newneurologic symptoms in our series.The patients affected by drug-refractory epilepticsyndromes also showed a marked decrease of fre-quency of epileptic episodes, and in both cases thepharmacologic therapy was consistently reduced.This observation was reported also by Espinosaet al., who used high-frequency stimulation to thepHyp to treat a patient with aggressive behaviorand epileptic seizures (personal communicationand poster presentation at the meeting of theAmerican Society for Stereotactic and FunctionalNeurosurgery held in Boston, June 2006). Exper-imental data are also available on this topic [11].
Besides our series, two other cases treated withposterior hypothalamic DBS have been reportedin the literature; Hernando et al. [8] reported thecase of a 22-year-old patient with drug-resistantaggression and comorbid mental retardation whopresented a significant improvement at a18 months’ follow-up; low-frequency stimulationwas used in this case. Kuhn et al. [9] reported thecase of a 22-year-old woman with self-mutilatingbehavior after severe traumatic brain injury. Thispatient experienced a resolution of symptoms4 months after beginning DBS.
18.5 Conclusions
In conclusion, the reversibility and the positiveeffects of pHyp chronic stimulation make thisprocedure ethically acceptable in mentally retar-ded patients with violent aggressive behavior. Ourknowledge about the mechanisms that underliepathologic aggressive and impulsive behavior isstill incomplete; nonetheless, it has become clearfrom previous experimental studies that somespecific structures play a role in the pathogeneticmechanism. Our group in the first article pub-lished on this topic [5] pointed out the role playedby structures connected to the posterior
18 Deep Brain Stimulation in Aggressive Behavior 215

hypothalamus (amygdala, dorsomedial thalamus,and orbito-frontal cortex) through loops rever-berating within the limbic circuit; in 1988 Sanoand Mayanagi [14] hypothesized the causativerole of an imbalance between the “ergotropic” andthe “trophotropic” circuits in favor of the former,thus justifying the use of a lesion in the “ergo-tropic” posterior hypothalamus to treat thesepatients. Kuhn et al. [9] also considered the role ofzona incerta cells and their connections with thethalamus, superior colliculus, and pontome-sencephalic tegmentum in the regulation of moodand circadian rhythms, given the proximity of thisstructure to the posterior hypothalamic area.
The possible adjunctive benefits of stimula-tion may include the control of refractory epi-lepsy, which sometimes is associated with thesecomplex syndromes. At any rate, the reportedmethodology is the only neuromodulation pro-cedure available to treat disruptive and aggres-sive behavior, and it is still the only alternative toclassical lesional surgery; furthermore, it shouldbe emphasized that DBS is a reversible treatmentthat may help patients chronically isolated inmental institutions to be integrate into society.
References
1. Arjona VE. Stereotactic hypothalamotomy in hereticchildren. Acta Neurochir. 1974;21(Suppl):185–91.
2. Bejjani BP, Houeto JL, Hariz M, Yelnik J, Mesnage V,Bonnet AM, Pidoux B, Dormont D, Cornu P, Agid Y.Aggressive behavior induced by intraoperativestimulation in the triangle of Sano. Neurology. 2002;12(59):1425–7.
3. Cordella R, Carella F, Leone M, Franzini A, BroggiG, Bussone G, Albanese A. Spontaneous neuronalactivity of the posterior hypothalamus in trigeminalautonomic cephalalgias. Neurol Sci. 2007;28:93–5.
4. Franzini A, Ferroli P, Leone M, Broggi G.Stimulation of the posterior hypothalamus fortreatment of chronic intractable cluster headaches:first reported series. Neurosurgery. 2003;52:1095–9.
5. Franzini A, Marras C, Ferroli P, Bugiani O, Broggi G.Stimulation of the posterior hypothalamus for
medically intractable impulsive and violentbehavior. Stereotact Funct Neurosurg. 2005;83:63–6.
6. Franzini A, Marras C, Tringali G, Leone M, Ferroli P,Bussone G, Bugiani O, Broggi G. Chronic highfrequency stimulation of the posteromedialhypothalamus in facial pain syndromes and behaviourdisorders. Acta Neurochir. 2007;97(Suppl):399–406.
7. Franzini A, Messina G, Marras C, Villani F, CordellaR, Broggi G. Deep brain stimulation of twounconventional targets in refractory non-resectableepilepsy. Stereotact Funct Neurosurg. 2008;86:373–81.
8. Hernando V, Pastor J, Pedrosa M, Peña E, Sola RG.Low-frequency bilateral hypothalamic stimulation fortreatment of drug-resistant aggressiveness in a youngman with mental retardation. Stereotact FunctNeurosurg. 2008;86:219–23.
9. Kuhn J, Lenartz D, Mai JK, Huff W, Klosterkoetter J,Sturm V. Disappearance of self-aggressive behavior ina brain-injured patient after deep brain stimulation ofthe hypothalamus: technical case report. Neurosurgery.2008;62:E1182.
10. May A, Bahra A, Büchel C, Frackowiak RS, GoadsbyPJ. Hypothalamic activation in cluster headacheattacks. Lancet. 1998;352:275–8.
11. Nishida N, Huang Z-L, Mikuni N, Miura Y, Urade Y,Hashimoto N. Deep brain stimulation of the posteriorhypothalamus activates the histaminergic system toexert antiepileptic effect in rat pentylenetetrazolmodel. Exp Neurol. 2007;205:132–44.
12. Ramamurthy B. Stereotactic operation in behaviourdisorders. Amygdalotomy and hypothalamotomy.Acta Neurochir. 1988;44(Suppl):152–7 (Wien).
13. Sano K. Sedative neurosurgery. NeurolMedicochirurgica. 1962;4:224b–5b.
14. Sano K, Mayanagi Y. Posteromedial hypothalamotomyin the treatment of violent, aggressive behaviour. ActaNeurochir. 1988;44(Suppl):145–51 (Wien).
15. Sano K, Yoshioka M, Ogashiwa M. Stimulation anddestruction of the hypothalamus. NeurolMedicochirurgica. 1963;5:169–70.
16. Sano K, Yoshioka M, Ogashiwa M, Ishijima B, OhyeC. Upon stimulation of human hypothalamus. NeurolMed Chir. 1965;7:280.
17. Schvarcz JR, Driollet R, Rios E, Betti O. Stereotactichypothalamotomy for behaviour disorders. J NeurolNeurosurg Psychiatry. 1972;35:356–9.
18. Tarnecki R, Mempel E, Fonberg E, Lagowska J.Some electrophysiological characteristics of thespontaneous activity of the amygdala and effect ofhypothalamic stimulation on the amygdalar unitsresponses. Acta Neurochir. 1976;23(Suppl):135–40.
19. Torelli P, Manzoni GC. Pain and behaviour in clusterheadache. A prospective study and review of theliterature. Funct Neurol. 2003;18:205–10.
216 G. Messina et al.

19Radiosurgery for Psychiatric Disorders
Antônio De Salles and Alessandra A. Gorgulho
19.1 Introduction
Behavioral surgery, previously know as Psy-chosurgery initiated with lesions disconnectingpathways in the brain. The infamous FrontalLobotomy proposed by Moniz [1], designed tointerrupt the pathways of the frontal lobesevolved to more elegant disconnections with theuse of the stereotactic technique by Spiegel andWicys interrupting the thalamo-connections tothe frontal lobe through lesions the anteriorthalamus. Indeed, the collaboration of the Aus-trian Neurologist Spiegel with the NeurosurgeonWicys in Philadelphia led to the first stereotacticsurgery in humans. It was an anterior thalamot-omy to modify behavior [2]. The progressiverefinement of the understanding of the frontallobe, know them to control behavior, called forprecise lesions in strategic areas, instead of themassive initial lesions in the frontal lobe. Dr.Leksell from Karolinska University in Stock-holm, living that era envisioned the necessity of anon invasive way to treat functional diseases of
the brain, i.e. realizing precise lesions in specificbrain pathways without opening the skull toavoid the unacceptable complications, as psy-chiatric patients were then being brutally violatedby the trans orbital frontal lobectomy [3]. Theideas of radiosurgery matured during the 1950sand 1960s to culminate with the development ofthe Gamma Knife which was suitable andpromptly applied to treat psychiatric diseases, theone chosen then was obsessive-compulsive dis-order (OCD) [4].
The evolution of radiosurgery initiated with theidea to focus external beam radiation to concen-trate dose to the pathology and spare the periph-eral structures appeared in the literature in 1906. Itwas described by Kohl only 18 years after thediscovery of X-rays. During the following yearsfocus radiation progressed with spiral convergingbeams, pendulum beams and finally rigid hemi-spheric attached beam directed with stereotacticprecision [5]. Leksell attached an X-ray tube to hisstereotactic frame and delivered radiosurgery tothe first patient submitted to the technique. Thetrigeminal ganglion was the target for treatment oftrigeminal neuralgia. The term “radiosurgery”wascoined [6]. This was actually the first applicationof photon radiosurgery. Radiosurgery was used tomake thalamic lesions for cancer pain control,giving the first autopsy generated appearance ofthe lesions in the gray matter of humans asreported in 1955 [7]. Already in 1983, 26 patientshad been submitted to radiosurgery for treatmentof malignant obsessive-compulsive disorders(OCD) [4]. In 1985, Dr. Leksell et al. reported for
A. De Salles (&) � A.A. GorgulhoDepartment of Neurosurgery and Departmentof Radiation Oncology, David Geffen Schoolof Medicine, University of California,10495 Le Conte Ave, Suite 2120, Los Angeles,CA 90095, USAe-mail: [email protected];[email protected]
A. De Salles � A.A. GorgulhoHCor Neuroscience, Sao Paulo, Brazil
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0_19© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
217
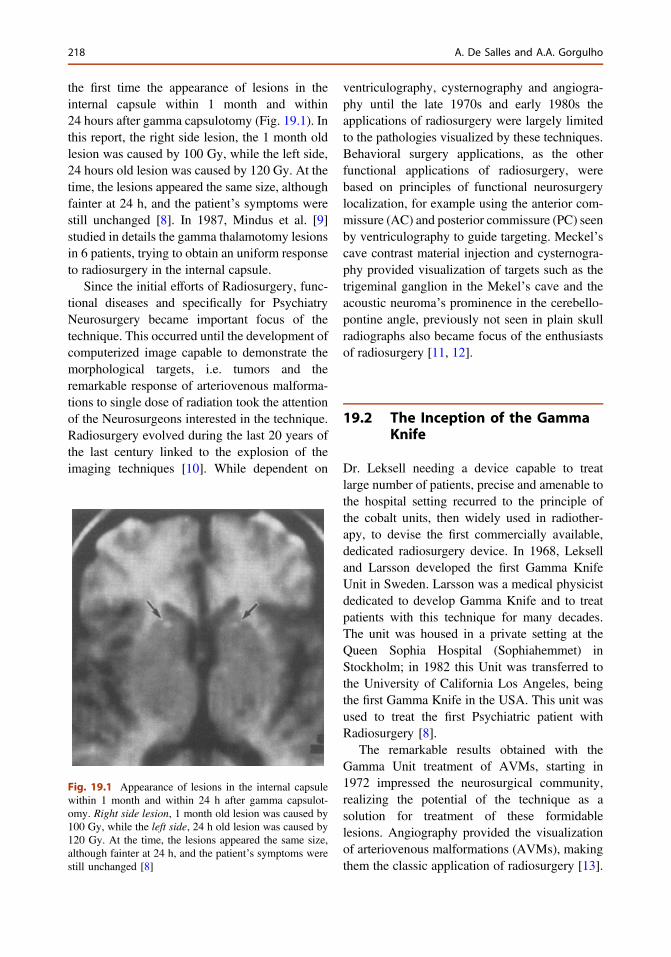
the first time the appearance of lesions in theinternal capsule within 1 month and within24 hours after gamma capsulotomy (Fig. 19.1). Inthis report, the right side lesion, the 1 month oldlesion was caused by 100 Gy, while the left side,24 hours old lesion was caused by 120 Gy. At thetime, the lesions appeared the same size, althoughfainter at 24 h, and the patient’s symptoms werestill unchanged [8]. In 1987, Mindus et al. [9]studied in details the gamma thalamotomy lesionsin 6 patients, trying to obtain an uniform responseto radiosurgery in the internal capsule.
Since the initial efforts of Radiosurgery, func-tional diseases and specifically for PsychiatryNeurosurgery became important focus of thetechnique. This occurred until the development ofcomputerized image capable to demonstrate themorphological targets, i.e. tumors and theremarkable response of arteriovenous malforma-tions to single dose of radiation took the attentionof the Neurosurgeons interested in the technique.Radiosurgery evolved during the last 20 years ofthe last century linked to the explosion of theimaging techniques [10]. While dependent on
ventriculography, cysternography and angiogra-phy until the late 1970s and early 1980s theapplications of radiosurgery were largely limitedto the pathologies visualized by these techniques.Behavioral surgery applications, as the otherfunctional applications of radiosurgery, werebased on principles of functional neurosurgerylocalization, for example using the anterior com-missure (AC) and posterior commissure (PC) seenby ventriculography to guide targeting. Meckel’scave contrast material injection and cysternogra-phy provided visualization of targets such as thetrigeminal ganglion in the Mekel’s cave and theacoustic neuroma’s prominence in the cerebello-pontine angle, previously not seen in plain skullradiographs also became focus of the enthusiastsof radiosurgery [11, 12].
19.2 The Inception of the GammaKnife
Dr. Leksell needing a device capable to treatlarge number of patients, precise and amenable tothe hospital setting recurred to the principle ofthe cobalt units, then widely used in radiother-apy, to devise the first commercially available,dedicated radiosurgery device. In 1968, Lekselland Larsson developed the first Gamma KnifeUnit in Sweden. Larsson was a medical physicistdedicated to develop Gamma Knife and to treatpatients with this technique for many decades.The unit was housed in a private setting at theQueen Sophia Hospital (Sophiahemmet) inStockholm; in 1982 this Unit was transferred tothe University of California Los Angeles, beingthe first Gamma Knife in the USA. This unit wasused to treat the first Psychiatric patient withRadiosurgery [8].
The remarkable results obtained with theGamma Unit treatment of AVMs, starting in1972 impressed the neurosurgical community,realizing the potential of the technique as asolution for treatment of these formidablelesions. Angiography provided the visualizationof arteriovenous malformations (AVMs), makingthem the classic application of radiosurgery [13].
Fig. 19.1 Appearance of lesions in the internal capsulewithin 1 month and within 24 h after gamma capsulot-omy. Right side lesion, 1 month old lesion was caused by100 Gy, while the left side, 24 h old lesion was caused by120 Gy. At the time, the lesions appeared the same size,although fainter at 24 h, and the patient’s symptoms werestill unchanged [8]
218 A. De Salles and A.A. Gorgulho
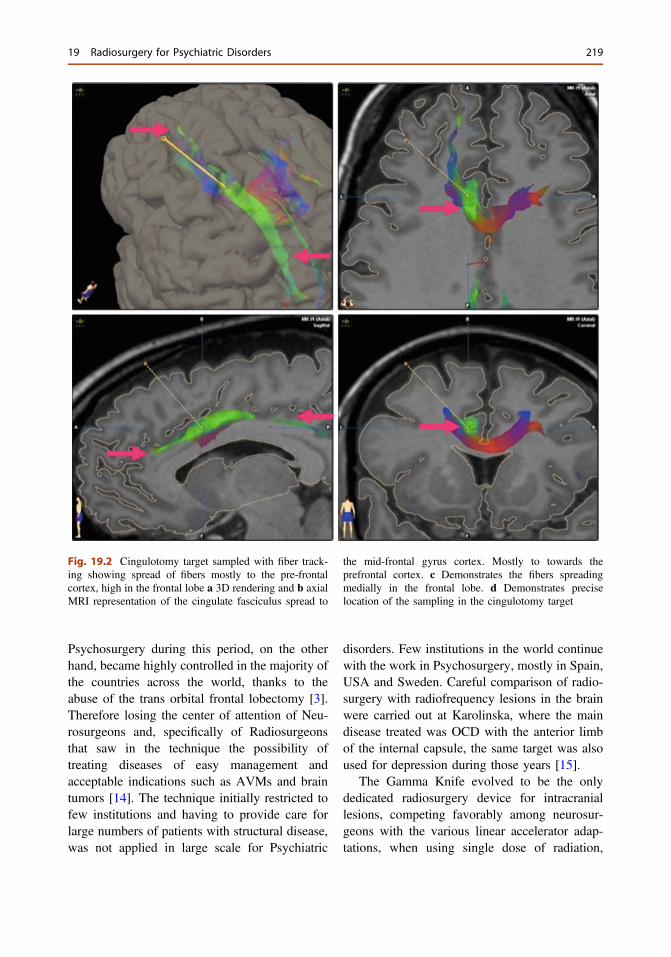
Psychosurgery during this period, on the otherhand, became highly controlled in the majority ofthe countries across the world, thanks to theabuse of the trans orbital frontal lobectomy [3].Therefore losing the center of attention of Neu-rosurgeons and, specifically of Radiosurgeonsthat saw in the technique the possibility oftreating diseases of easy management andacceptable indications such as AVMs and braintumors [14]. The technique initially restricted tofew institutions and having to provide care forlarge numbers of patients with structural disease,was not applied in large scale for Psychiatric
disorders. Few institutions in the world continuewith the work in Psychosurgery, mostly in Spain,USA and Sweden. Careful comparison of radio-surgery with radiofrequency lesions in the brainwere carried out at Karolinska, where the maindisease treated was OCD with the anterior limbof the internal capsule, the same target was alsoused for depression during those years [15].
The Gamma Knife evolved to be the onlydedicated radiosurgery device for intracraniallesions, competing favorably among neurosur-geons with the various linear accelerator adap-tations, when using single dose of radiation,
Fig. 19.2 Cingulotomy target sampled with fiber track-ing showing spread of fibers mostly to the pre-frontalcortex, high in the frontal lobe a 3D rendering and b axialMRI representation of the cingulate fasciculus spread to
the mid-frontal gyrus cortex. Mostly to towards theprefrontal cortex. c Demonstrates the fibers spreadingmedially in the frontal lobe. d Demonstrates preciselocation of the sampling in the cingulotomy target
19 Radiosurgery for Psychiatric Disorders 219
which was dedicated mostly to structural dis-eases. The appearance of computerized imagingin the 1970s and 1980s amplified the radiosur-gery applications, making the demand for dedi-cated devices for radiosurgery throughout theworld [10]. Several models of Gamma Kniferepresent the evolution of the machine to its statenow called commercially Perfexion®. During theevolution of the gamma knife technique lesionsin the internal capsule were carried out withsearching doses and many times having to adaptto new models, leading to surprises on the size oflesions obtained in the internal capsule, believedto be due to differences in dosimetry between themodels of Gamma Knife (Table 19.1).
19.3 Technical Aspectsof Radiosurgery
19.3.1 The Energy and CollimationSystem
60Cobalt decays to 60Ni leading to a half-life of5.26 years to the cobalt sources powering theGK. The gamma rays resulting from this decayare collimated to the target to achieve the bio-logical effect. Gamma rays of 1.17 and 1.33 MeVare grouped by three different collimation sizesavailable in the GK Perfexion to automatically
take advantage of modulation and shapingcapabilities [16]. The previous collimation sys-tem of the models U, B and C (Table 19.1),which was dependent on four exchangeablehelmets with 4 different sizes of apertures (4, 8,14, 18 mm) was replaced by a single dynamicconic helmet. This new collimation system iscapable of movement throughout three differentapertures (4, 8, 16 mm), as well as plugging themstrategically to modulate and shape the dosedistribution, as desired to optimize the intensityconformity and intensity. The cumbersome pro-cess of hoisting the collimators every time thatsize of the isocenter was changed, serving todelay and bring possible errors to the procedure,is now bypassed in the GK Perfexion [17].
19.4 Flow of Patient Treatment
The psychiatric patient is treated as outpatientsafter acquisition of the MRI dedicated for thetreatment. They are recommended to come to theGamma Knife department fasting. The daybefore the procedure they are advised to washtheir heads with an antiseptic shampoo. They areadvised of the risks of the procedure and sign theinformed consent understanding the implicationsof the radiation, including immediate, delayedand long-lasting effects, as well as the purpose of
Table 19.1 Evolution of gamma unit models—technical and economical demands
Gamma Knife U I. Pioneer: functional neurosurgery (60Co 179 sources)
II. Initial applications for morphological radiosurgery
Gamma Knife B I. Initial worldwide demand: devices for large-scale treatment and diversity of histology andapplications
II. Economical pressure: replacement of sources at ±7 years interval (60Co 201 sources)became possible
Gamma Knife C I. Computer integration allowing initial efforts of robotization
II. Computerized treatment plan—replacement of Kula planning—expediting the number ofpatients treated daily
Gamma Knifeperfexion
I. Full robotization decreasing possibility of human error
II. Maximization of collimator interplay for conformality and treatment speed. Replacement of4 hemispherical helmets of apertures in mm (4, 8, 14, 18) each by one conical helmet withapertures in mm (4, 8, 16) capability, sectors accepting exposure of different number of the60Co 192 sources available. The GK Perfexion plus brings imaging check capabilities at thetime of the treatment
220 A. De Salles and A.A. Gorgulho
the procedure, i.e. slow and long lasting effect ofradiation in the brain tissue. Therefore thedelayed nature of any effect of the procedure intheir disease and advised to continue taking theirusual medication.
19.5 Placement of the StereotacticFrame
They are prepared sterile in the forehead andoccipital region with topical anesthetic creamfollowed by injection of 5 cc of mixed Lidocaine/Marcaine and sodium bicarbonate in each ste-reotactic frame pin site. The frame is appliedstrategically with the care of including the ante-rior limb of the internal capsule, i.e. the centralpart of the brain, AC and PC, central in the ste-reotactic space. The compatibility of the stereo-tactic frame placement with all hardwareattachments of the Gamma Knife is checked.Measurements of the head surface are acquiredwith a plastic stick helmet, as well as the mea-surements of the stereotactic hardware for inputin the Gamma Plan for calculation of beamattenuation. The patient is transferred to the CTscan for the stereotactic image acquisition to bemerged to the previously obtained MRI. Thecontour of the patient’s head obtained based onthe CT can be used instead of the manual mea-surements previously obtained to calculate theattenuation of the beams.
19.6 Targeting and TreatmentPlanning
The target for anterior gamma capsulotomy hasbeen perfected over the years, as well as the dose.Studies are still ongoing to determine whetherthe most ventral portion of the capsule is mosteffective or even if there is a lateralization on thebrain, which could lead to need of only one sidelesion. Now that lesions can be seen, as well asthe fibers interrupted by the these lesions can beidentified with MRI fiber tracking techniques,
understanding may improve on the effects spe-cific lesion localization with consequent optimi-zation of the results (Fig. 19.2).
The initial targets for capsulotomy as descri-bed by Mindus et al. [9] was 10 mm in front ofthe AC, 8 mm above the inter-commissural lineand on average 17 mm lateral to the mid-plane.This target was chosen when the first GammaUnit was available in Stockholm. It was applied across-firing of 179 gamma beams precisely col-limated with 3 × 5 mm beams. On the basis ofexperience gained from post-mortem observa-tions on patients subjected to gamma thalamot-omy for cancer pain, it was used a centralirradiation dose of 160 Gy. The treatment plan-ning now available, the Gamma Plan, takesadvantage of full computerized system which canoptimize the shape of the lesion, even usingdifferent sizes of collimators to reach most ven-tral portions of the internal capsule in an elon-gated shape, it has been suggested doubleisocenters of 4 mm (Fig. 19.3).
19.7 Functional LesionConsiderations
19.7.1 Prescribing to a Point
Sharp and well-circumscribed lesion to discon-nect pathways or ablate nuclei are the goals ofthis application. The prescription dose for func-tional neurosurgery is by convention and bytradition to the isocenter since the initial work ofLeksell in psychiatric surgery [9]. This meansthat 100 % of the dose (=maximal dose) is pre-scribed to a target point, i.e. prescribed to theisocenter. The radiation prescription dose is thesame as the maximal dose, when prescribing tothe maximum [18]. The fall off distance, i.e. thevolume of tissue receiving at least 50 % of thedose is proportional to the diameter of the aper-ture. The application of this concept is nicelyseen during the targeting of the root entry zone intrigeminal neuralgia with the 4 mm field. Thediameter of the 50 % isodose line is 4 mm. Theplacement of the isocenter while planning
19 Radiosurgery for Psychiatric Disorders 221
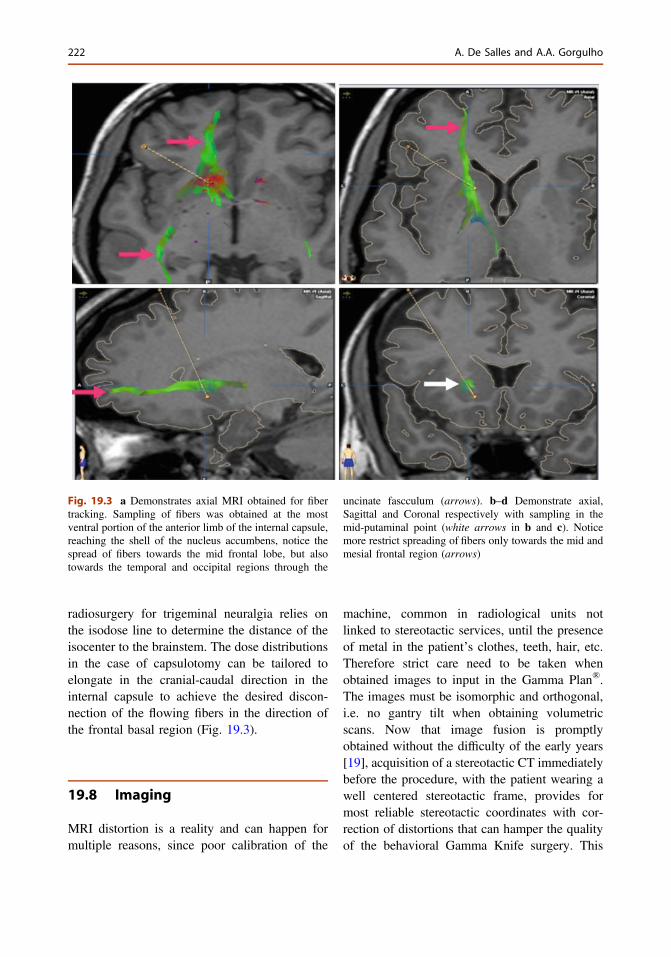
radiosurgery for trigeminal neuralgia relies onthe isodose line to determine the distance of theisocenter to the brainstem. The dose distributionsin the case of capsulotomy can be tailored toelongate in the cranial-caudal direction in theinternal capsule to achieve the desired discon-nection of the flowing fibers in the direction ofthe frontal basal region (Fig. 19.3).
19.8 Imaging
MRI distortion is a reality and can happen formultiple reasons, since poor calibration of the
machine, common in radiological units notlinked to stereotactic services, until the presenceof metal in the patient’s clothes, teeth, hair, etc.Therefore strict care need to be taken whenobtained images to input in the Gamma Plan®.The images must be isomorphic and orthogonal,i.e. no gantry tilt when obtaining volumetricscans. Now that image fusion is promptlyobtained without the difficulty of the early years[19], acquisition of a stereotactic CT immediatelybefore the procedure, with the patient wearing awell centered stereotactic frame, provides formost reliable stereotactic coordinates with cor-rection of distortions that can hamper the qualityof the behavioral Gamma Knife surgery. This
Fig. 19.3 a Demonstrates axial MRI obtained for fibertracking. Sampling of fibers was obtained at the mostventral portion of the anterior limb of the internal capsule,reaching the shell of the nucleus accumbens, notice thespread of fibers towards the mid frontal lobe, but alsotowards the temporal and occipital regions through the
uncinate fascculum (arrows). b–d Demonstrate axial,Sagittal and Coronal respectively with sampling in themid-putaminal point (white arrows in b and c). Noticemore restrict spreading of fibers only towards the mid andmesial frontal region (arrows)
222 A. De Salles and A.A. Gorgulho
also allows for the convenience of obtaining theMRI days before the procedure to study thepatients’ brain in detail with functional andmorphological images, including fiber tracking tounderstand which pathways will be interrupted(Table 19.2).
The CT, a faster acquisition image, with fewerissues of claustrophobia, movement issues andpossible distortions is the ideal imaging modalityto obtain in a psychiatric patient in the day of theprocedure. To improve quality of the fusion, aCT post contrast is recommended, using thevascular structures seen on the CT and MRI [20].
19.9 Clinical Applications
Gamma Knife radiosurgery is indicated for allpsychiatric disorders already treated with lesionand that the effectiveness is proven. This is how-ever still under study, as much of the literatureexistent for lesions involving the limbic systemdate before the advent of computerized imaging.For example, lesions for depression in the cingu-lum, the limbic leucotomy, subcaudate tractot-omy, the anterior thalamotomy [21], all lack ofstudies with modern scientific methodology cor-relating the location of the lesions and the clinicaleffects. More recently, it has been suggested thatplacing the lesions lower in the internal capsulehas led to better control of obsessive symptoms.The body of literature involving Gamma Knife inPsychiatric surgery concentrates on the treatmentof OCD having as target the anterior limb of theinternal capsule, as early developed by Leksell incollaboration with Talairach in the 1950s [4],further perfected by the studies at KarolinskaUniversity, Brown University and University of
Sao Paulo, where sham randomized procedureswhere performed [22].
19.10 Penetration Worldwide
The patients’ appeal for a more comfortabletreatment, avoidance of large surgeries and reli-ability of the treatment and prognosis was met byradiosurgery. Progressively the treatment of thepatient does not depend on the manual skills of aperson, but on the intellectual and mathematicalexpertise of a team of specialists dedicated toprovide the most reliable and comfortable carefor the patient. This development worldwidebased on the mushrooming of the computertechnology permitted the introduction of robot-ized medicine and the Gamma Knife is a proto-type of this approach, relying exclusively incomputer capability to deliver treatment. Thispromises uniformity of treatment for psychiatricpatients suggesting it will have a progressivenumber of patients undergoing Gamma Knifesurgery to relieve their suffering. The indicationand the management of the patient are stilldependent on the doctor expertise, mostly whenthe medical therapy is unable to provide thecomfort and/or cure. As Gamma Knife providesthis immediate population need, it receivedimmediate acceptance in the developed worldand marches progressively through the countriesin development, as resources become availableoffering hope for psychiatric patients needing aminimally invasive surgical procedure.
Table 19.2 Minimal quality of imaging and sequences for treatment planning
Functionalprocedures
T2—volumetric fast spin echo recovery through basal ganglia axial T1 v/a—1 mm tck, n/g, w/c,w/fs, whole brain
Stereotactic CT Axial a/q, 1 mm tck, n/c and w/c, whole brain
tck thickness, n/g no gap, n/c no contrast, w/c with contrast, w/fs with fat saturation, v/a volumetric acquisition, a/q acquisition
19 Radiosurgery for Psychiatric Disorders 223

19.11 Obsessive CompulsiveDisorder
The target for obsessive-compulsive disorder(OCD) has been in anterior limb of the internalcapsule, as determined by the head of the caudatemedially and the putamen laterally [8, 23]. It hasevolved from the midpoint of the internal capsuleas one sees it in the coronal MRI scan to the mostinferior portion of the capsule in the proximity ofthe nucleus accumbens [24]. It became apparentover the years of experience by the groups ofKarolinska University and Brown University thatas the target was brought ventrally the resultsimproved [15, 25]. Sheehan et al. [24] suggestplacement of the 50 % IDL at the most ventralportion of the internal capsule. Recently a ran-domized trial performed by the Brazilian Groupshowed that indeed this rational might hold true[26]. Studies are under way to confirm thishypothesis.
The GK capsulotomy calls for a 4-mm colli-mator aimed to the anterior limb of the internalcapsule on each side. It is planned to be located19–21 mm anterior to the AC on the intercom-missural plane. This approximately correspondedto the mid-putaminal point. T1 and T2 weightedMRI demonstrates precisely the mid-putaminalpoint of the anterior limb of the capsule. Themost ventral portion of the 50 % isodoselinereaches the most ventral portion of the internalcapsule. Doses in the literature have varied from140 to 200 Gy [24–26], therefore 70–100 Gyreaches the shell of the accumbens at the base ofthe IC (Fig. 19.1). Kondziolka et al. [27] showedconsistent lesions in the internal capsule usingtwo isocenters of 4 mm, trying to obtain an ovalshaped lesion of 48 mm3 with its most inferiorextension in the ventral portion of the internalcapsule. The dose used in his study was 140 and150 Gy.
19.12 Conclusion
Modern Gamma Knife radiosurgery offers easi-ness of treatment planning and delivery with
patient’s comfort as an important goal. It is anexcellent choice as an instrument of lesionmaking for patients with Psychiatric diseases, asit is non-invasive, its effect is slow settingallowing for re-adaptation of the patient to itsnew therapeutic condition, facilitating rehabili-tation and permitting the caring physicianobserve the patient closely to adjust medicationin a progressive and sensible work frame.
References
1. Moniz E. How I came to perform prefrontalleucotomy. J Med (Oporto). 1949;14(355):513–5.
2. Gildenberg PL. Spiegel and Wycis—the early years.Stereotact Funct Neurosurg. 2001;77(1–4):11–6.
3. De Salles A. Evolution of radiosurgery. In: De SallesAAF, Agazaryan A, Selch M, Gorgulho AA, SlotmanB, editors. Shaped beam radiosurgery. Berlin:Springer; 2011. p. 3–10.
4. Leksell L. Stereotactic radiosurery. J NeurolNeurosurg Psychiatry. 1983;46:797–803.
5. Holly FE. Radiosurgery equipment: physicalprinciples, precision, limitations. In: De Salles AAF,Goetsch SJ, editors. Stereotactic surgery andradiosurgery. Madison: Medical Physics PublishingCorporation; 1993. p. 185–200.
6. Leksell L. The stereotaxic method and radiosurgery ofthe brain. Acta Chir Scand. 1951;102:316.
7. Leksell L, Herner T, Liden K. Stereotaxicradiosurgery of the brain. Report of a case. KunglFysiograf Sallsk Lund Forhandl. 1955;25(17):1–10.
8. Leksell L, Herner T, Leksell D, Persson B, LindquistC. Visualisation of stereotactic radiolesions bynuclear magnetic resonance. J Neurol NeurosurgPsychiatry. 1985;48(1):19–20.
9. Mindus P, Bergström K, Levander SE, Norén G,Hindmarsh T, Thuomas KA. Magnetic resonanceimages related to clinical outcome afterpsychosurgical intervention in severe anxietydisorder. J Neurol Neurosurg Psychiatry. 1987;50(10):1288–93.
10. De Salles AAF, Gorgulho A, Agazaryan N. Linearaccelerator radiosurgery: technical aspects. In:Youmans neurologic surgery, vol. 3. 67th ed.Amsterdam: Elsevier; 2011. pp. 2622–32.
11. Gorgulho AA, Ishida W, De Salles AAF. Generalimaging modalities: basic principles. In: Lozano AM,Gildenberg PL, Tasker RR, editors. Text book ofstereotactic and functional neurosurgery. Berlin:Springer; 2009.
12. De Salles AA, Gorgulho AA, Pereira JL, McLaughlinN. Intracranial stereotactic radiosurgery: concepts andtechniques. Neurosurg Clin N Am. 2013;24(4):491–8.doi:10.1016/j.nec.2013.07.001.
224 A. De Salles and A.A. Gorgulho
13. Steiner L, Leksell L, Greitz T, Forster DMC,Backlund EO. Stereotaxic radiosurgery for cerebralarteriovenous malformations. Report of a case. ActaChir Scand. 1972;138:459–64.
14. de Lunsford DL, Flickinger J, Lindner G, Maitz A.Stereotactic radiosurgery of the brain using the firstUnited States 201 cobalt-60 source gamma knife.Neurosurgery. 1989;24(2):151–9.
15. Lippitz BE, Mindus P, Meyerson BA, Kihlström L,Lindquist C. Lesion topography and outcome afterthermocapsulotomy or gamma knife capsulotomy forobsessive-compulsive disorder: relevance of the righthemisphere. Neurosurgery. 1999;44(3):452–8;discussion 458–60.
16. Bhatnagar JP, Novotny J Jr, Huq MS. Dosimetriccharacteristics and quality control tests for thecollimator sectors of the Leksell Gamma Knife(®)Perfexion(TM). Med Phys. 2012;39(1):231–6.
17. Régis J, Tamura M, Guillot C, Yomo S, Muraciolle X,Nagaje M, Arka Y, Porcheron D. Radiosurgery withthe world’s first fully robotized Leksell Gamma KnifePerfeXion in clinical use: a 200-patient prospective,randomized, controlled comparison with the GammaKnife 4C. Neurosurgery. 2009;64(2):346–55.
18. Leksell L.Cerebral radiosurgery. I.Gammathalanotomyin two cases of intractable pain. Acta Chir Scand.1968;134(8):585–95.
19. De Salles AAF, Asfora WT, Abe M, Kjelberg RN.Transposition of target information from the magneticresonance and CT-scan images to the conventional X-ray stereotactic space. Appl Neurophys.1987;50:23–32.
20. JonkerBP. Image fusionpitfalls for cranial radiosurgery.Surg Neurol Int. 2013;4(Suppl 3):S123–8.
21. Hazari H, Christmas D, Matthews K. The clinicalutility of different quantitative methods for measuringtreatment resistance in major depression. J AffectDisord. 2013;150(2):231–6.
22. Cecconi JP, Lopes AC, Duran FL, Santos LC,Hoexter MQ, Gentil AF, Canteras MM, Castro CC,Norén G, Greenberg BD, Rauch SL, Busatto GF,Miguel EC. Gamma ventral capsulotomy fortreatment of resistant obsessive-compulsive disorder:a structural MRI pilot prospective study. NeurosciLett. 2008;447(2–3):138–42.
23. Leksell L, Backlund EO. Radiosurgicalcapsulotomy–a closed surgical method forpsychiatric surgery. Lakartidningen. 1978;75(7):546–7 (Swedish. No abstract available).
24. Sheehan JP, Patterson G, Schlesinger D, Xu Z.Gamma Knife surgery anterior capsulotomy forsevere and refractory obsessive-compulsive disorder.J Neurosurg. 2013;119:1112–8.
25. Ruck C, Karlsson A, Steele D, et al. Capsulotomy forobsessive-compulsive disorder. Long-term follow-upof 25 patients. Arch Gen Psych. 2008;65(8):914–22.
26. Lopes A, Greenberg B, Noren G, et al. Treatment ofresistant obsessive-compulsive disorder with ventralcapsular/ventral striatal gamma capsulotomy: a pilotprospective study. J Neuropsych Clin Neurosci.2009;21(4):381–92.
27. Kondziolka D, Flickinger JC, Hudak R. Resultsfollowing gamma knife radiosurgical anteriorcapsulotomies for obsessive compulsive disorder.Neurosurgery. 2011;68(1):28–32; discussion 23-3.
19 Radiosurgery for Psychiatric Disorders 225
Index
AAblation, 55, 60, 62, 64, 90, 106, 111, 114, 125–129, 132,
134, 145, 164, 165, 169, 170, 172, 181, 182, 192Ablative neurosurgery, 78, 87, 194Aggressive behavior, 194, 203, 204, 206, 207, 211, 215,
216Anorexia nervosa, 11, 30, 39–41, 82, 98, 165, 175, 176,
184Anterior capsulotomy, 55, 59, 61, 62, 87, 107, 109, 115,
126, 180–182, 191–194Anterior limb of internal capsule, 115Antipsychotic, 146Antipsychotic drugs, 146, 203Autonomy, 78, 79, 83
BBasal ganglia, 4, 11, 50, 56, 57, 59, 100, 106, 125, 144,
145, 150, 151, 204, 223Behavioral surgery, 217, 218Bilateral anterior cingulotomy, 71, 74, 87, 88, 108, 126,
182Bilateral limbic leukotomy, 89–92Brain neurotransmitter systems, 203
CCapsulotomy, 61, 96, 97, 100, 107, 109, 114, 132, 137,
179, 180, 192–194, 200, 205, 221, 222, 224Caudate nucleus, 4, 5, 41, 56, 57, 59, 106–108, 116, 125,
126, 144, 145, 166, 190, 197, 205, 206Cerebello-thalamo-cortico-pontine loop, 4Cingulate cortex, 4, 36, 106Cingulotomy, 58–61, 87, 96, 98, 107–109, 114, 126,
147–149, 162, 164, 179–182, 191–194, 200, 206, 207,219
Cognitive-behavior-emotional circuit, 115Compulsion, 105, 108, 110, 113, 125, 148, 180, 205Cortical-striatal-thalamic circuit, 106Corticostriatal–thalamocortical circuitry, 145
DDeep brain stimulation, 11, 39, 47–50, 55, 60–62, 71, 77,
95, 114, 120, 125, 134, 149, 165, 175, 177, 180, 194,206
Diffusion spectrum imaging, 21, 22, 24, 27
Diffusion tensor imaging, 2, 21, 26, 35Dopamine, 1, 3, 12, 37–39, 56, 146, 151, 152, 163, 176,
190Doppler effect, 127Drug addiction, 161–165, 167, 168, 170–172, 181
FFiber crossing, 24Functional magnetic resonance imaging, 2, 35–38, 96,
115
GGamma capsulotomy, 218, 221Gamma knife, 55, 59, 108–110, 120, 125, 217–224
HHippocampus-amgydala complex, 3, 5, 11
LLesions, 42, 48, 53–58, 60–64, 88–91, 93, 96, 97,
106–108, 110, 126, 127, 130, 135, 137, 138, 148, 162,179, 181, 189, 192, 193, 205, 217–221, 223, 224
Limbic leucotomy, 59, 60, 96, 108, 109, 114, 147–149,191–193, 207, 223
MMagnetic resonance imaging, 2, 21, 36, 145, 181, 211Major depressive disorder, 11, 29, 30, 38, 48, 59, 60, 78,
95, 176Medial forebrain bundle, 98–100, 164MRI guided high frequency focused ultrasound, 91
NNetwork, 1, 6, 21, 23, 28, 30, 36, 88, 96, 115, 180Neural circuits, 2, 95, 115, 117, 125, 126, 176–178Neuroanatomy, 27, 56, 106, 203Neurobiological circuits, 1Neuroimaging, 27, 35, 37, 42, 43, 79, 88, 98, 105, 106,
114, 115, 145, 175–177, 189, 191, 194Neuromodulation, 2, 11, 48, 62, 81, 95, 96, 101, 114,
118, 120, 126, 152, 216
B. Sun and A. De Salles (eds.), Neurosurgical Treatments for Psychiatric Disorders,DOI 10.1007/978-94-017-9576-0© Shanghai Jiao Tong University Press, Shanghai and Springer Science+Business Media Dordrecht 2015
227
Nucleus accumbens, 9, 56–58, 71, 98–100, 115, 116, 126,150, 151, 162, 166, 175, 177, 181, 190, 194, 205, 207,222
OObsession, 105, 108, 110, 113, 125, 135, 148Obsessive compulsive disorder, 11, 29, 39, 41, 42, 48, 56,
69, 71, 78, 105, 113, 125, 126, 132, 164, 176, 180,205, 217, 224
Orbital frontal cortex, 40Orbitofrontal circuit, 57
PPapez’s circuit, 13Patient selection, 54, 77, 80, 118–120, 132, 150, 182,
183, 191, 194Physiological dependence, 161Positron emission tomography, 36, 38, 39, 88, 96, 100,
106, 115, 116, 164, 177Psychiatric comorbidities, 82, 145, 146, 176, 181Psychiatric disorder, 1, 2, 4, 10, 22, 27, 29–31, 35, 37, 42,
43, 48, 50, 53, 55, 63, 64, 77–84, 88–91, 97, 106, 110,114, 118, 125, 144, 165, 175, 176, 178, 180, 182, 184,191, 203, 205, 219, 223
Psychosurgery, 49, 61, 74, 114, 190, 217, 219
QQuality of life, 77–79, 81, 82, 84, 105, 109–111, 117,
144, 152, 169, 172, 175, 185
RRadiosurgery, 55, 62, 71, 87, 90, 108–111, 125, 129, 185,
204, 205, 217, 218Refractory psychiatric disorders, 79, 114
Refractory schizophrenia, 191Region of interest, 28, 29, 35Replacement therapy, 161
SSchizoaffective disorder, 60, 204Serotonin, 69, 72, 190Serotonin reuptake, 38, 69, 72, 105, 113, 114, 132, 146,
150, 178Stereotactic surgery, 48, 55, 62, 87, 91, 111, 147, 149,
162, 164, 165, 167, 171, 172, 184, 185, 194, 204, 217Subcaudate tractotomy, 59, 60, 62, 108, 109, 114,
191–194, 207, 223Substantia innominata, 3, 5, 6, 8, 10, 59, 108Surgery, 42, 50, 59, 62, 70, 71, 80–83, 87, 89, 91
TThalamotomy, 49, 55, 147, 203, 217, 218, 221, 223Thermocoagulation, 58, 59, 61, 62, 90, 148, 205Tourette syndrome, 48, 125, 143, 149–151Tractography, 6, 22, 23, 25–27, 29, 30, 106, 107, 110Transcranial magnetic resonance-guided focused ultra-
sound, 125, 127–130, 132, 133, 135–138Treatment refractory depression, 71, 87
VVentral capsule and ventral striatum, 100, 115, 116, 180Violent psychosis, 203Voxel-based morphometric analyses, 2, 23–25, 29
228 Index





























